(cDrI) - WHO | World Health Organization
14
, AFRICAN PROGRAMFOR ONCHOCERCIASIS CONTROL (APOC) YEAR 3 ANNUAL REPORT ON COMMUNITY DIRECTED TREATMENT WITH TVERMECTIN (cDrI) Legend I Oncho Endemic LGAs Not Oncho Endemic LGAs BORNO STATE, NIGERIA rl rfi/ trmor For lnformotion Tor ba r't- For Acu-,,. ,.ts To: brtr blo l4p LE{ <e5 CoP 0 7 A0IJT 2002 APOC/DIR RE CU 2002.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of (cDrI) - WHO | World Health Organization

,
AFRICAN PROGRAMFORONCHOCERCIASIS CONTROL (APOC)
YEAR 3 ANNUAL REPORT ON
COMMUNITY DIRECTED TREATMENTWITH TVERMECTIN
(cDrI)
LegendI Oncho Endemic LGAs
Not Oncho Endemic LGAs
BORNO STATE,NIGERIA
rlrfi/trmor
For lnformotion
Tor ba r't-
For Acu-,,.
,.ts
To:
brtrblol4p
LE{<e5CoP
0 7 A0IJT 2002
APOC/DIR
RE CU2002.

I
,
EXEC SUMMARY
Borno State of Nigeria is located at the northeastem part of the country and
shares international border with Cameroon, Chad and Niger. The State has
two vegetation zones, the arid - desert zone in the northem half and
grassland savannas in the south, suitable for breeding of the Black fly - the
vector for transmission of Onchocerciasis.
The State has a population of 3.5 million people (projected from 1991 National
Census figures), 27 Loeal Government Areas (LGAs) and traelve of these
LGAs are Onchocerciasis endemic (5 hyper and 7 meso). The total
population of the endemic LGAs is 669,655 people.
Prior to the commencement of Community Directed Treatment with lvermectin
(CDTI) three years ago, the State had been distributing Mectizan through the
Community Based Treatment with lvermectin (CBIT) approach in 8 out of the
twelve endemic LGAs. With the CDTI approach wtrich @mmenced in June
1999 following the inflow of financial assistance from the African Programme
for Onchocerciasis Control; coupled with the presence of the facilitating
NGDO - Helen Keller lnternational, the programme witnessed a desirable
degree of erpansion in treatment and geographic coverage.
More Health Workers and Community Distributors have been trained/re-
trained to meet the programme needs. Drugs are collected from designated
collection points by the endemic communities through their community
distributors.
The project is making increasing efforts to orientate the public and
stakeholders to support the programme. Three successful rounds of Mectizan
distributions have been carried out by the project and will soon commence
CDTI activities for the 4h treatment round. Through the support of the
collaborating NGDO, CDTI is being used as a vehicle for distribution of
Vitamin A in Onchocerciasis endemic areas of Borno State.
1

D
Lessons learnt is being documented and it may pave way for additional drugs
to be distributed in the target areas. The project is indeed conscious of the
repercussions of any possible overloading of the distributors. The treatment
figure for the cunent reporting year (April 2001 - May 2OO2) is 545,308
people.
With this, the project have achieved a treatment coverage of 81o/o afid 91o/o
geographical coverage.
The project has achieved 91o/o of the training objective (trained a total of 1,736
out of 1,905 CDTI personnel). These include: SOCTs 7; LOCTs 48; PHC
Staff 174; and 1,507 CDDs. Seven out of the twelve endemic LGAs have
contributed One Million, Seven Hundred and Fifty Thousand Naira
(N1,750,000.00) as counterpart funding.
The project has also employed Onchocerciasis Structure to deliver and
distribute Vitamin A Capsules to children of 6 - 59 months and Post Parteum
Mothers. As a result, 116,133 children and 32,933 mothers received Vitamin
A capsules during the period.
)

BORNO STATE
Year 3 Annual Reoorts on GDTI lmolementation in State
NI:
1. BACKGROUND INFORi'ATIONBorno State of Nigeria is located in the northeastern part of the country wherethe State shares lntemational Border with Niger and Chad in the north andCameroon in the east. lt shares borders with Adamawa State in theSoutheast, Gombe in the South and Yobe State in the West. The total landmass area of the State is 69,436.sq. km.
The State has two notable vegetational zones with the grassland savanna in
the southem half and Sahel desert zone in the northern half.Onchocerciasis is endemic in the southern half, wlrich is endoued withseasonal and perennial fast flowing rivers; that make the land suitable foragricultural activities, but are also breeding sites for black fly - (Simuliumdamnosum species), the vector for river blindness. The northern half isnotable for water scarcity with stunted - grasses and sparse trees,
The State has two seasons, the dry and wet seasons. The raining seasonbegins in Iate May and ends in early October when the dry seasoncommences until mid May. The average rainfall in the State is 760mm. Thewettest period is around August, September and the driest months beingJanuary, February and March with humidity as low as 12o/o.
The total population of Bomo State is 3.5 million people (projected from the1991 National Population Census results), with over 80% of the people livingin the rural communities. The State is divided into 27 Local Governmentareas (LGAs) and ten of these LGAs are Onchocerciasis endemic (5 Hyperand 5 Meso endemic). The endemic LGAs have a total population of 669,655people who are invariably at the risk of infection.
Before the commencement of Community Directed Treatment with Mectizan(CDTI) about three years ago, all but two endemic LGAs vvere already atdifferent rounds of Mectizan treatment based on Community-based lvermectinTreatment (CBIT) approach. With CBIT the Program was responsible for theselection of Community Distributors (CBDs) and delivery of Mectizan drug tothe beneficiaries without any community inputs. The aspect of programownership and sustainability by the "Communit/ and Governments was notvery much emphasized.
With the inflow of APOC financial assistance coupled with the presence ofHelen Keller lntemational (HKl) as the supporting NGDO and the encouragingsupport of the State Ministry of Health, CDTI took off in June 1999. Sincethen the project which initially covered 10 LGAs has now expanded to 12LGAs with the addition of tulo LGAs i.e. Kala Balge and Bama in the 3d yeartreatment cycle.
3

Before the commencement of CDTI in June 1999, the State OnchocerciasisControl Programme had covered only 523 communities with the Mectizandrug. Presently the programme has expanded geographically to a total of1,174 communities.
The LGAs with their respective communities are in different rounds ofMectizan treatment: Biu, Hawul, Kwaya Kusar, and Bayo have received sixrounds of Mectizan treatment, while Shani, Damboa, Chibok and Askira - Ubahave received their 5h round of Mectizan treatment. Dik\ ra and Gvroza are on
their 3'd round of Mectizan treatment. Kala Balge and Bama have receivedtheir first round of Mectizan treatment. Detail breakdown of the above is
provided in the table below.
Treatment rounds of endemic communities reflect the respective LGA'streatment cycle.
A community here is defined as a group of individuals sharing linguistic,geographic locations and socio-cultural similarities/lineage who are under adefined traditional h ierarchical structure.
4

L
SECTION 2:
IIIPLEUENTATION OF CDTI
Table l: Number of Endemic Communities
!t should be noted that the project have not reached all the endemiccommunities thus, there may be a change in the figures presented in the tableabove from the earlier one. Efforts are being made to cover all thecommunities.
Table ll CDTI IMPLEMENTATION
TRAINING OF THE DIFFERENT LEVELS OF STAFF INVOLVED IN CDTIIMPLEIIENTATION
5
S/n DistrictftGA Hy?er-Endecnic
tl/iesoErylemh
Conrnurf,ies underbeaEnert before
APOC
Communitiesinctded under
Remark
1 BIU 129 90 39 7
2 HAWUL 118 82 36 7
3 SHANI 116 50 66 7
4 I(A/AYA-KUSAR 66 53 13 7
5 BAYO 101 38 63 7
6 DAMBOA 90 66 24 67 GWOZA 130 17 113 48 CHIBOK 67 50 17 69 D[(\ /A 71 71 410 ASKIRA UBA 141 77 u 611 BAMA 83 83 1
12 KALA BALGE 62 62 1
TOTAL 530 64 523 651
SN LGA *ofComms.Mlh
ses
tofComm.Thd
selededCDDg
ilofConrns.VVhichcdleddrn
f of conms.That dccidedon the mefiodof disfrih.ilion
# of cornms.Which
decild onmonths ofhedrnerts
#ofoomm..
wififainedCDDs
#ofcomms.
Which paidCDDs in
cch or kind
1 BIU 129 129 129 119 119 129 902 HAWUL 118 118 118 112 112 118 993 SHANI 116 116 116 103 103 1't6 87
4 I(A/AYA-KUSAR 66 66 66 66 66 66 585 BAYO 101 101 101 101 101 101 506 DAMBOA 71 71 71 70 70 71 707 GWOZA 121 121 121 121 115 115 1008 CHIBOK 45 45 45 45 45 45 57
9 DII(VVA 70 70 70 70 70 70 6810 ASKIRA-UBA 141 141 141 136 136 136 101
11 BAMA 83 83 83 83 83 83 5612 KALA BALGE 62 62 62 6262 62 62 62
TOTAL 1,123 1,123 1,123 1,082 1,082 1,123 887
I
I
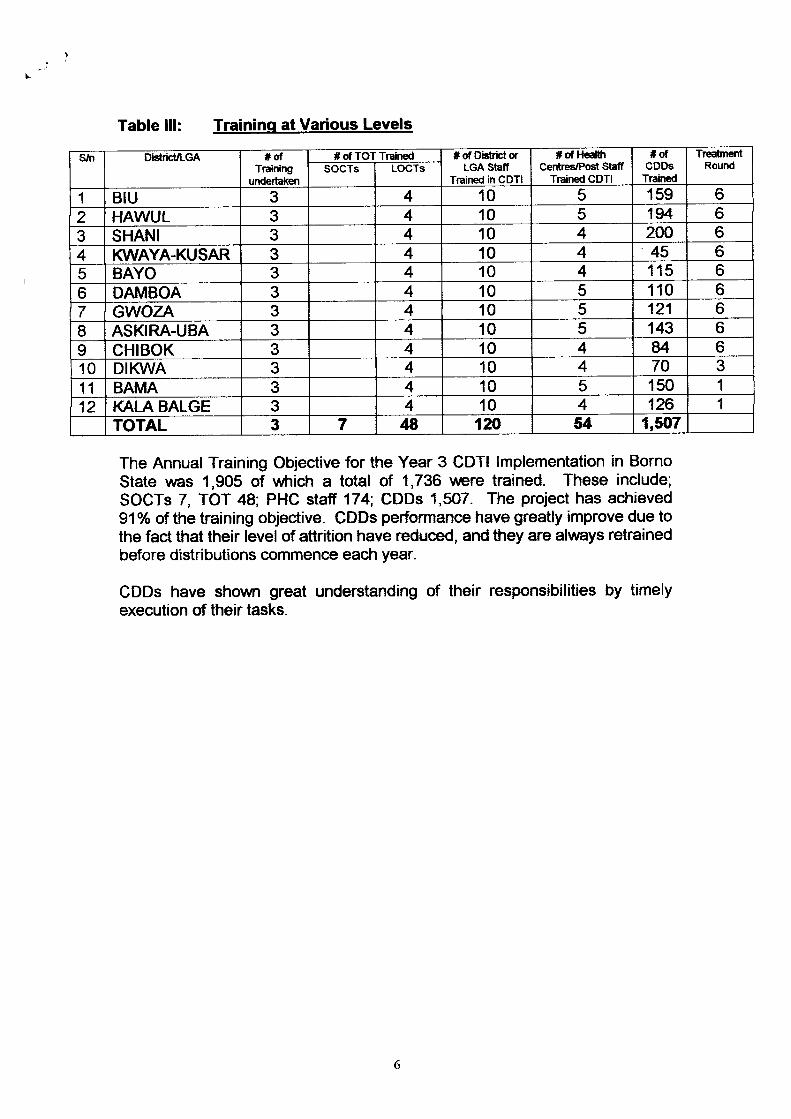
Table lll: Traininq at Various Levels
The Annual Training Objective for the Year 3 CDTI lmplementation in BornoState was 1,905 of wtrich a total of 1,736 vvere trained. These include;SOCTs 7, TOT 48; PHC staff 174; CDDs 1,507. The project has achieved91o/o of the training objective. CDDs performance have greatly improve due tothe fact that their level of attrition have reduced, and they are always retrainedbefore distributions commence each year.
CDDs have shown great understanding of their responsibilities by timelyexecution of their tasks.
SiTr Dis*rk rLGA *dTraining
urdertaken
*d # d Disfrict orLGA Staff
Trained in CDTI
# of H€atrtCentres/Po$ Staff
Trained CDTI
*olCDDs
Trained
TrcatmentRoundSOCTs LOCTs
1 BIU 3 4 10 5 159 6
2 HAWUL 3 4 10 5 194 63 SHANI 3 4 10 4 2N 64 IOVAYA.KUSAR 3 4 10 4 45 65 BAYO 3 4 10 4 115 6
6 DAMBOA 3 4 10 5 110 67 GWOZA 3 4 10 5 121 6I ASKIRA-UBA 3 4 10 5 143 6I CHIBOK 3 4 10 4 u 610 Dil( /A 3 4 10 4 70 3
11 BAMA 3 4 10 5 150 1
12 KALA BALGE 3 4 10 4 126 1
TOTAL 3 7 I 120 54 1,5O7
6
'Trahed

Table lV: Mobilization And Education Of Tarqet Communities
Mobilization and health education of the endemic communities have greatlyimproved. This was as a result of the following:
Production of more I.E.C. materials and distribution of same to theendemic communities.
o
o
a
Training of CDTI personnel on principles of effective mobilization
Having regular advocacy workshops with the stakeholders
lnvolvement of Community Based Organization and Religiousgroups in the mobilization of community members.
o
Sln Distrid/LGA *dComm/MlhgEs
tl/bbilized
# of CornmNilhgeswhich recei\red H.E.about importance ofExtended Treatment
# of ArlvocacyMslts to State
or RegionalDirectors of
Health
#of MOHslaff
involved inMobilization
,ofNGDOStaff
involved inttiobilized
# d Staffinvolved inMobilized
1 BIU 129 129 5 7 3 42 HAWUL 118 118 5 7 3 43 SHANI 116 116 5 7 3 44 ](A/AYA-KUSAR 66 66 5 7 3 45 BAYO 101 101 5 7 3 46 DAMBOA 71 71 5 7 3 47 GWOZA 121 121 5 7 3 4I ASKIRA-UBA 141 141 5 7 3 49 CHIBOK 45 45 5 7 3 410 Dil( /A 70 70 5 7 3 411 BAMA 83 83 5 7 3 412 KALA BALGE 62 62 5 7 3 4
TOTAL 1,123 1,123 60 84 36 48
7

,
SECTION 3:
ACHIEVEMENTS
TREATMENT SUMMARY FOR 2OO1
S'N LGAs Gonrnunith3
Tot lGcn:ur
Popnhtht
1.Io. otPcophE[ghlc
PcopleTrc.tcd
llo of TebletsUs.d
1 BIU 129 52,336 44,O23 41,080 111,2482 DAMBOA 71 50,372 45,288 44,069 118,4043 GWOZA 121 93,119 80,M0 75,477 201,7864 HAWUL 118 113,207 97,682 89,571 242,7155 SHANI 116 53,1il 4,578 40,900 105,791
6 I(A/AY-KUSAR 66 30,831 25,968 23,420 62,7827 CHIBOK 45 36,803 31,236 28,O45 80,1968 ASKIRA-UBA 141 69,746 u,4M 60,062 190,7729 BAYO 70 6,%2 41,489 38,256 1M,34710 Dil( /A 83 55,1|75 51,136 48,809 135,50211 BAT\,IA 62 62,071 43,650 42,145 120,39912 KALA BALGE u 15,879 14,248 13,474 38,344
TOTAL 1,123 669,655 583,802 545,308 1,512,286
a
o
o
The Annual Treatment Objective (ATO) for the year was to treat685,082.
A total number of people treated was 545,308 with 1,512,286Mectizan tablets.
Therapeutic coverage rate No. of People Treated x 100Total Population
95.308 x 100669,655
g10.h
Geographical coverage = No. of Communities Treated x 100Targeted Communities
1j23 x 1001,174
95.6%
a
8

Strengths Weakness SuggestionsLGAParticipation
Greater involvement of LGAauthorities in CDTI activities.Appreciable counterpart fi nancialcontributions from the LGAs
Some LGAs are not willing tosupport their staff whoparticipate in CDTI activities
- Need to intensify advocacYvisits to council authorities.
- Officials of Ministry for LocalGovemment and ChieftaincYAffairs should be contacted to beinvolved in advocacy visits toLGAs.
CommunityParticipation
Some communities haveimproved in their process ofCDDs remuneration.
- Few communities arereluctant to take decisions onthe time/mode of disfiribution
- Some communities still havedifficulties in supporting theirCDDs.
Frequent visits and alvarenesscampaign to the communities isnecessary to improve theiracceptability of the programme.
Sustainability The increased financialcontributions from the State andLGAs towards CDTI adivities
lnegular counterpart financialcontributions from the Stateand LGAs.
More advocacy visits to the Stateand LGAs is imperative to solicittheir financial supPort towardsustainability of the gogramme.
Logistics - NGDO continue to support theproject with logistics duringtreatment period.
- The State has purchasedadditional vehicle for the project.
- Communities are assisting theCDDs with transport when goingfor training and collection ofdruqs from collection centers.
- lnsufficient number ofmotorcycles to meet thelogistics needs at the LGAlevel.
- Minimal logistics support toLOCTs by the LGAs.
- The project will continue tosolicit for more logistics supportfrom the LGAs.
- Encourage collaboration withother programs at the LGA levelwhere they can assist in thedelivery and collec{ion of drug tothe communities.
9
,

I)
WEAKNESS NOW Ii'PROVED UPON
STATE GOVERNMENT GONTRIBUTION:The State Government through the MOH have made the followingcontributions to the project:
Provision of a Peugeot (505) Station Wagon.Supply of office equipment and fumitureRepairs of tulo old proiect vehicles.Renovation of Onchocerciasis Secretariat.Release of Three Million Naira (Il3 million) in the year 2000,
LOCAL GOVERNMENT GOUNGILS:. seven out of the tvrelve (12) endemic LGAs contributed One Million,
Seven Hundred and Fifty Thousand Naira (N1.750m) to the project.o The PHC Co-ordinators have indicated their willingness to be more
involved in CDTI activities by mobilizing community members andsoliciting for more LGA commitment.
CDDs PERFORMANCECDDs performance of tasks have continued to appreciate each year. Theirlevel of mobilization of community members; dosing; recording and reportinghave greatly improved.
This is so because of continuous training and retraining and the low CDDsattrition.
Weakness lmprovement MadeLGAParticipation
Some LGAs are not willing tosupport their staff thatparticipates in CDTI activities.
- The PHC Director in the Local Governmentand Chieftaincy Affair, Direstor of DiseaseControl in the Ministry of Health, and Director,Helen Keller lnternational nowfully involved inadvocacy visits to the LGAs, which have ledto LGA support to the programme financially.
- Worksho/Seminars on CDTIimplementation have been conducted for theLGAs PHC Coordinators to address themwith the activities and seek for their support.
CommunityParticipation
- Few communities are reluctantto take decision on thetime/mode of distribution.
- Some communities still havedifficulties in supporting theirCDDs.
Most communities have decided thetime/mode of distribution and are supportingtheir CDDs. They prefer Mectizan distributionbefore the rains set in.
Sustainability lnegular counterpart financialcontribution from the State andLGA.
lnvolvement of policy makers of the ministriesof health and Local Government ChiefiaincyAffairs have improved counterpartcontributions by both the State and LGAs.
l0

r- /'
NOCP INVOLVEMENTffre tlOCp (Zonal) office support and presence in regard to highJeveladvocacy visits, programme monitoring and supervision.
COMMUNITY PARTICIPATION :
The communities have embraced the principles and concepts of CDTI and arehighly interested in the program activities. This vnas evidenced by theirsupport to CDDs during training and distribution of Mectizan.
The religious and other Community Based Organizations are fully involved inthe mobilization of their members.
MAJOR ACHIEVEMENTS:o Mobilization/education of 1,123 communities for Mectizan uptake.o Training of 1,7fi programme personnel on CDTI.. Technical, Material and financial support by Helen Keller
lntemational.o Treatment of 545,308 out of 583,802 eligible population. An
increase ol 127,574 over year 2000 treatment figure of 417,734.. Successful integration of Vitamin A Supplementation along with the
Mectizan distributions.o A total of 116,131 children (6-59 months) (95.4%) and post parteum
mothers 32,933 (98.4%) vvere supplemented with Vitamin Asupplements. The supply of the supplements rnas along the healthsystems along with that of Mectizan tablets, from the State throughthe LGAs to the communities. The CDTI personnel uere trainedand re-trained to combine this task along with the Mectizandistributions.
GONSTRAINTS/CHALLENGEo Even though there is an appreciable increase of number of trainers,
the number is still inadequate. Efforts should be made to trainmore.
o lnadequate logistics and remuneration of LOCTs by some LGAso lncreased level of insecurity due to arm banditry in the project
areas.
ll

,t,t
BORNO STATE CDTI PROJECT
YEAR 4 P]AN OF ACTTVITIES (iTAY. 2OO2 - APRIL 2OO3I
SIn Actlvity M.y Jun Jul Aug Sept G lrlov Ilcc Jen Feb Mer April
1 State review meeting
2 Organization of Stakeholders meeting
3 Advocacy Meeting with LGA Officials
4 Training/Re-training of SOCTS, LOCTs &
PHC Workers
5 Community Mobilization/Public
Awareness Campaigns
o Selection/Fleplacement of CDDS
7 Procure & Delivery of Mectizan to
Project State
8 Training/Re'training of CDDs
I Update of Community Registration
(Census)
10 ZOTF Review Meeting
11 Drug (Mectizan) Distribution
12 Monitoring/Supervision of Mectizan
Distribution
13 Collection and Collation of Treatment
Reports
14 Analysis of the Reports
15 State Review Meeting
16 APOC Quarterly Reports
17 APOC Annual Reports
t2

o!maIoo@Lmo{m
| = ='<JE*Etj,; g 8enrO5- =.EEe3tao
i =.*I 96I rdoI rID r-lI (,|(,l jI OO-J
o-{oo-)+!,6qL-.d.oo<fo(XrKqroosBo'o
trlo€of
g<ioL.- o!+ F'9s_a. Joul o-
oodooro(t,
7oe.a,
o!=.of
AQoX=aur=re=
=
oUoo{lalot3l-t-t:l<alo
Ij
i\)oo
-{o5'loao0)UIo
=ofc3cto
o
8J33ogoffE: o.EE3'<rr 662vt
5'
No
hboatd6{r5o:<
$c
ogocto'fooao-o'foaoEoav,
{-l='oJo-l-6)o>dc)=oJ.iao-
ilrooa
=i(o
u)o Icd dtsP=';889 o=U'cl
*-9Lqd
Eo
3uoo
rn€ O
E*ErgE
q>o-o
x8y€
q aEB- J<=tt
fiil5oI6=;'o-ag
o=o<o)ooo9q
Es.4A5or=6UI
JG)iJ>to)
la .,loloIc,l-
iqEtio?':fr 6I t{+f
EF*gd-NC)=(fBr*
8SJT
=o-Jo,56=-o <riU,o
oaCLta
='=o
o{ooio5'ur=
GIo,)o-dIaol.:1.IGIo
='gd9ooloo'o=B.oof,o9+oof@55r
q, Ifoo-odd<.fo5'€
0,10
o)o=.=.og,
oIozE
EH-{{u, un'
z?oo0-o
o-ooI xrroo -IO4o=ooa
t-oo{U,
oooElJO3s,cf€ol
o-
T5oC)
J(l) ut'o,
t-A88{-lut ul'
aoo-{U'
z<oog-o
aoo{u,
<L<cofoox-ru$
=hofoox-sON
'ntl
==m
ctN g(ogtnf
SP(octof
=bESF9NN
{bEs-x6r ,\)
EholooF-tr$
oot,ciN
zosoN
6$x'xr$
eg=!8E=nimo
E=sao-QEilE]
EO=
q#=.fofO-O90c
ogf(o
-{NE.8f8-o
Et,o3.U'oa o
=89of;
d3H6 *9.OE
'Tl?lo-U'Eoo-oo-
p- ='0ori o
: id'o.q=gl-
9s\<oOfE
on-o=Eciofa6s>o-
ooCL
agBts-fi6'o- of=oEf; 3ll =ca;d=.
5\<
o>qo0.Peil_o- ili
7oooa
oogalr
+rO. -Nfoooo-
f<0r<5dcr=oo(D-)o;io-=J(D
=o-d(D3ro9Sln6
+>9.:lo++6
0laooo-
vtcEo3.oo-tn
8Pa<xorcaiQf
sfidat-o
9,old-f3Goflo
!
o>cO-ooo,o
v,='oroU'oo,3.(Do
=0o
ov
o->o=9o€gJOoffo6F3a)o5'o-<o
?oo-
3'
o{9aloJ+e=5ooU'
o
9l-
o=CLo3.o
o r-r'o9.o=.:I 6-.Loa.o9or3IOE-fa.<oouto
F'o=
='
oooo33=Eco1--
T'Io-oo
c){goU=tr 0t
ooo-ooco,ofc3ooo
3p_o3@
=!,=.of,
eo8b<o-Eoo-
ooo{8eo=<ze8 8eo<
i o
IElolnlzlolal{Elmloltr,l-rl!lvlolc-lmlol{