i 1 i I I I I i I I I I I I I I I I
246
I i 1 i I I I I i I I I I I I I I I I THE SOCIETY OF PERINATAL ANNUAL CLINICAL, SCIENTIFIC & BUSINESS MEETING FEBRUARY 2-4, 1984 Hyatt Regency Hotel San Antonio, Texas
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of i 1 i I I I I i I I I I I I I I I I

I i 1 i I I I I i I I I I I I I I I I
THE SOCIETY OF PERINATAL
ANNUAL CLINICAL, SCIENTIFIC &
BUSINESS MEETING
FEBRUARY 2-4, 1984
Hyatt Regency Hotel San Antonio, Texas

I I I I
4th Annual
Society of
I I I
In accordance with the wishes of the majority of the SPO membership, we ask that our members and guests refrain from smoking in the meeting room. This conforms to the spirit of our society and the written procedures of our parent organization.
I I

I I I
PROCEEDINGS OF THE
FOURTH ANNUAL SCIENTIFIC MEETING
I SOCIETY OF PERINATAL OBSTETRICIANS
I I I
FEBRUARY 2-4, 1984 SAN ANTONIO, TEXAS
HYATT REGENCY
I I I I I I I I I
OFFICERS
President Robert H. Hayashi
Vice-President/ President-Elect
Roy H. Petrie
Secretary-Treasurer Amelia C. Cruz
PAST PRESIDENTS
William N. Spel]acy ’71 Roy M. Pitkin ’78 James A. O’Leary ’79 Donald M. Sherline ’80 Loren P. Petersen ’81 Bruce A. Work, Jr. ’82 Robert H. Hayashi ’83 Roy H. Petrie ’84
HONORARY MEMBERS ELECTED 1984
Donald Barron Charles Hendricks
Edgar Makowski Giacomo Meschia
BOARD OF DIRECTORS
Bruce A. Work, Jr. ’84 Amelia C. Cruz ’84 John I. Fishburn ’84 Robert H. Hayashi ’84 jeffrey Lipshitz ’85 Richard H. Paul ’85 Robert J. Sokol ’85 Steven Gabbe ’86 Tom Garite ’86 John C. Morrison ’86
Publication of these Proceedings has been made possible through the support of Beckman Instruments, Inc. We gratefully acknowledge their contribution to the success of this meeting.
I I I

I I I I I I I I I I I I I I I
Table of Contents
Welcome
Proceedings
Table of Contents
Acknowledgements
Award Papers
Meeting at a Glance
Map of the Hyatt Regency Hotel
Detailed Program
Scientific Session I
Scientific Session II
Scientific Session III
Poster Session A
SPO Business Meeting
Scientific Session IV
Scientific Session V
Poster Session B
Author Index
Subject Index
Membership Roster
Critique Sheet
Future Meetings
Page 1
Page 2
Page 3
Page 4
Pages 5- 6
Page 7
Page 8
Pages 9- 16
Pages 17- 20
Pages 21 - 26
Pages 27- 32
Pages 33-104
Pages 105-106
Pages 107-112
Pages 113-118
Pages 119-194
Pages 195-199
Pages 200-206
Pages 207-225
Page 226
Page 227
I
I I

I i
ACKNOWLEDGEMENTS
The Society of Perinatal Obstetricians would like to express its deepest appreciation to the following organizations for their generous support of our Annual Meeting:
I I I
Astra Pharmaceutical Products, Inc. Beckman Instruments, Inc. Corometrics Medical Systems, Inc. Mead Johnson Pharmaceutical Division Ortho Pharmaceutical Corporation Institute of Perinatal Biology, Inc. Perinatal Resources, Inc. Ross Laboratories Savage Laboratories, Division of Byk-Gulden, Inc.
I I I I i I ! ! I I I !
I would also like to recognize several individuals, without whose assistance, this meeting would not have been possible. These are the persons responsible for the superior quality of this annual meeting.
The Program Committee: Doctors Steven Gabbe, Thomas Garite, Jeffrey Lipshitz, Frank Miller, Robert Sokol and Sze-ya Yeh, as well as their junior faculty and fellows, for their helpful suggestions and the exhaustive review of 180 abstracts for the meeting.
Last year’s program chairman, Dr. Richard Paul for sharing his experience in program preparation and preventing my mistakes of omission and commission.
The officers of the Society: Dr. Robert Hayashi, President, Dr. Roy Petrie, President Elect, and Dr. Amelia Cruz, Secretary-Treasurer, for their support and flexibility in allowing me to develop this year’s program.
Dr. Roger Wallace for all of his skills and diligence in the local arrangements.
Doctors James Martin, Sue Palmer and Bill Roberts for their review of the abstracts and active participation in the development of the syllabus.
Ms. Wanda Cockrell, my Administrative Assistant, who is responsible for all of the organizational aspects of the meeting and the majority of the work involved.
Rita Morrison, for not leaving me during this hectic year.
Good Luck to Fr~k Miller
~/~C. MorNson, M.D.
( ~r~o~r~am Chairman \~ociety of Perinatal Obstetricians
i

! I I ! I I I i i I I
AWARDS
The Society of Perinatal Obstetricians is pleased to designate the following awards for outstanding research by our members presented during this Annual Meeting.
SOCIETY OF PERINATAL OBSTETRICIANS AWARDS
First Place - $1,000
The Dublin Fetal Monitoring Trial Peter Boylan, Dermot MacDonald, Adrian Grant, Margaret Pereira and lan Chalmers The National Maternity Hospital, Dublin and The National Perinatal Epidemiology Unit, Oxford.
Second Place - $500
The Association Between Nonspecific Vaginitis and Adverse Pregnancy Outcome Michael G. Gravett, H. Preston Nelson, David A. Exchenbach, King K. Holmes Departments of Obstetrics and Gynecology and Medicine, University of Washington, Seattle, Washington
Third Place - $500
Monitoring the Neonatal Brain Uma L. Verma, Frank Archblad, Nergesh Tejani, and Sara Mittelmann-Handwerker Health Sciences Center, State University of New york at Stony Brook; Nassau County Medical Center, Department of Obstetrics and Gynecology
! I I I
PERINATAL RESOURCES INC.
Outstanding Work by a Fellow in Training - $1,000
Baseline Lymph Flow Rate in the Nearterm Pregnancy Sheep and Effect of Terbutaline G.A. Valenzuela, L.L. Woods and R.A. Brace Department of Obstetrics and Gynecology and Division of Perinatal Biology, Loma Linda University, Loma Linda, California
i ! !
5

I I I I I I I I
ASTRA PHARMACEUTICAL PRODUCTS, INC.
Best Poster (Session A) - $500
Paradoxical Heart Rate Response to the Valsalva Maneuver in Preeclampsia Micki L. Cabaniss, C. Daniel Cabaniss, and Patricia C. Wagner Department of Obstetrics and Gynecology (Division of Maternal-Fetal Medicine) and Department of Internal Medicine (Division of Cardiology), University of South Alabama, Mobile, Alabama
Best Poster (Session B) - $500
Immunoglobulin G (IgG) Subclasses and Neonatal Outcome in Pregnancies Complicated by Isoimmunization M. Mark Taslimi, Baha M. Sibai, John V. Dacus and James M. Mason Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
I I I I
INSTITUTE OF PERINATAL BIOLOGY, INC.
Best Research Idea - $500
Nicardipine Tocolysis of Preterm Labor in the Pregnant Rabbit R. Harold Holbrook, Michel Lirette and Michael Katz Department of Obstetrics and Gynecology, and Reproductive Sciences and the Cardiovascular Research Institute, University of California at San Francisco
I I I I
I I

Meeting at a Glance Society of Perinatal Obstetricians
Location Thursday, February 2, 1984 Friday, February 3, 1984 Saturday, February 4, 1984
200pm 400pm 600pm 80Opm 630am 800am lOOOam 12 00pm 1 30pm 300pm 530pm 700pm 800pro 63Oam 800am 1OOOam 12 O0 noon
Med=na I SPO Board
Meet=ng
Guadaloupe I Program D~rector’s
Meeting
Nueces t Armed Forces Meeting
Los R~os Foyer I Registration I
Garden Terrace I Cocktails
Corometncs
Regency Foyer Reg=stratlon I I Cocktads I I Registration I
East Regency Ballroom
Meeting I Sc=ent=fic Sessions
IV and V
R~o Grande Ballroom
West Regency Ballroom
Annual
Banquet
Opemng Cocktad Recept=on Thursday, February 2, 1984 Garden Terrace (Corometncs)
Board of D~rector’s Meeting Thursday, February 2, 1984 Med=na Room
Annual Banquet Friday, February 3, 1984 West Regency Ballroom
Cocktad Recept=on Friday, February 3, 1984 Regency Foyer (Savage Laboratories)
SPO Business Meeting February 3, 1984 East Regency Ballroom

I ! I I I I I I I I I I I I I I I BALLROOM
I

I I DETAILED PROGRAM
SOCIETY OF PERINATAL OBSTETRICIANS
I I I
THURSDAY, FEBRUARY 2, 1984
2:00- 4:00 p.m. 4:00- 5:00 p.m. 4:00- 6:00 p.m. 4:30- 6:00 p.m. 6:00- 8:00 p.m. 8:00
Board of Director’s Meeting Program Director’s Meeting Registration Armed Forces Meeting Cocktail Reception (Corometrics) Dinner on your own
Medina Guadaloupe Los Rios Foyer Neuces Garden Terrace
I I I ! ! I I I I I I I I I
FRIDAY, FEBRUARY 3, 1984
6:30- 8:00 a.m. Continental Breakfast Garden Terrace
7:00-12:00 noon
8:00- 8:15 a.m.
Registration
Welcome, Announcements Dr. John C. Morrison, Program Chairman
Regency Foyer
East Regency Ballroom
8:15- 8:30 a.m.
8:30- 9:00 a.m.
Introduction of Honorary Members Dr. Robert Hayashi, President
Current Status: Maternal/Fetal Medicine Boards (Questions&Answers), Dr. Gloria Sarto
East Regency Ballroom
East Regency Ballroom
9:00-10:00 a.m. SCIENTIFIC SESSION I (Award Papers) MODERATOR: Dr. Robert Hayashi
East Regency Ballroom
9:00 a.m. Award for Outstanding Research by a Fellow in Training (Perinatal Resources, Inc. 1. Baseline Lymph Flow Rate in the Near-term
Pregnant Sheep and Effect of Terbutaline. G.A. Valenzuela, L.L. Woods and R.A. Brace. Department of Obstetrics & Gynecology, Loma Linda University, Loma Linda, California.
9:10 a.m. Discussion
9:15 a.m. Society of Perinatal Obstetricians First Place Award for Outstanding Research 2. The Dublin Fetal Monitoring Trial.
P. Boylan, D. MacDonald, A. Grant, M. Pereira and I. Chalmers. The National Maternity Hospital, Dublin and The National Perinatal Epidemiology Unit, Oxford.
9:25 a.m. Discussion

I I I I I ! I I ! I I I ! I ! I I
9:30 a.m.
9:40 a.m.
9:45 a.m.
9:55
10:00-10:30 a.m.
10:30-12:00 noon
10:30 a.m.
10:40 a.m.
10:45 a.m.
10:55 a.m.
11:00 a.m.
11:10 a.m.
Society of Perinatal Obstetricians Second Place Award for Outstanding Research 3. The Association Between Nonspecific Vaginitis
and Adverse Pregnancy Outcome. M. Gravett, H.P. Nelson, D.A. Exchenbach and K.K. Holmes. Departments of Obstetrics and Gynecology and Medicine, University of Washington, Seattle, Washington.
Discussion
Society of Perinatal Obstetricians Third Place Award 4. Monitoring the Neonatal Brain. U.L. Verma,
F. Archblad, N. Tejani and S. Mittelmann- Handwerker. Health Sciences Center, State University of New York at Stony Brook, Nassau County Medical Center, Department of Obstetrics & Gynecology, East Meadow, N.Y.
Discussion
Break Regency Foyer
SCIENTIFIC SESSION II MODERATOR: Dr. Donald Barron East Regency Ballroom
5. The Natural History of Genital Herpes Complications. Z. Brown, L. Vontver, D. Hickok, J. Benedetti and S. Berry. Departments of Obstetrics & Gynecology and Microbiology, Univ. of Washington, Seattle.
Discussion
Antithrombin Ill Activity in Hypertensive Pregnant Women. C.P. Weiner, H. Kwann, F. Duboe, M. Paul, M. Antiel and W. Hauck Northwestern University, Prentice Women’s Hospital, Chicago, Illinois.
Discussion
o Ritodrine Disposition in Parturient and Preterm Neonate. B.R. Kuhnert, T.L. Gross, P.M. Kuhnert. Department of Ob/Gjn~ and the Perinatal Clinical Research Center, Cleveland Metropolitan General Hospital/ C.W.R.U., Cleveland, Ohio.
Discussion
I 10

11:15 a.m.
11:25 a.m.
11:30 a.m.
11:40 a.m.
11:45 a.m.
11:55 a.m.
12:00- 1:30 p.m.
1:30- 3:00 p.m.
1:,30 p.m.
1:40 p.m.
1:45 p.m.
1:55 p.m.
o The Effect of Myo-lnositol on the Glycerophos- pholipid Composition of Adult and Fetal Rat Lung Tissue and Surfactant. J.G. Quirk, J.E. Bleasdale. Departments of Obstetrics & Gynecology and Biochemistry and Cecil H. Ida Green Center for Reproductive Biology Sciences University of Texas Southwestern Medical School, Dallas.
Discussion
go Effects of Diuretics on Plasma Volume in Preg- nancies Complicated by Chronic Hypertension. B. Sabai, R. Grossman, H. Grossman, T. Abdella and G. Anderson. Division of Maternal/Fetal Medicine, Department of Ob/Gyn, University of Tennessee College of Medicine, Memphis.
Discussion
10. Cardiovascular Alterations in Severe Pregnancy- Induced Hypertension: Effects of Magnesium Sulfate and Hydralazine. D.B. Cotton, B. Gonik and K. Dorman. Department of Obstetrics and Gynecology, University of Texas Medical School at Houston, Houston, Texas.
Discussion
Lunch On Your Own
SCIENTIFIC SESSION Ill MODERATOR: Dr. Charles Hendricks East Regency Ballroom
11. First Trimester Prenatal Diagnosis by Chorionic Villus Sampling (CVS). R.J. Wapner, L.G. Jackson, M. Barr and E. Grebner. Jefferson Medical College of Thomas Jefferson University, Philadelphia, Pennsylvania.
Discussion
12. Head Out Immersion In Treatment of Pregnancy Associated Edema. R.C. Goodlin, K.L.E. Hoffman and N.E. Williams. Department of Obstetrics and Gynecology, University of Nebraska Medical Center, Omaha, Nebraska.
Discussion
I !

! ! ! ! ! ! ! ! ! !
!
!
2:00 p.m.
2:10 p.m.
2:15 p.m.
2:25 p.m.
2:30 p.m.
2:40 p.m.
2:45 p.m.
2:55 p.m.
3:00- 3:30 p.m.
3:30- 5:30 p.m.
13. A Prospective, Controlled Analysis of Silastic Obstetrical Vacuum Cup Deliveries. M.D. Berkus, R. Ramamurthy, P. O’Connor, K. Brown and R.H. Hayashi. Departments of Ob/Gyn and Pediatrics, Ophthal, UTHSC at San Antonio.
Discussion
14. Disposition of Ritodrine in the Mother and Fetus. T.L. Gross, P.M. Kuhnert, B.R. Kuhnert, M.G. Rosen and T. Williams. Department of Ob/Gyn and the Perinatal Clinical Research Center, Cleveland Metro General Hospital/Case Western Reserve University.
Discussion
15. Glycosylated Hemoglobin and Plasma Protein in Newborns of Normal and Diabetic Women. M.M. Elsweidy, H.E. Fadel and E.C. Abraham. Department of Cell and Molecular Biology and Department of Obstetrics and Gynecology, Maternal-Fetal Medicine Section, Medical College of Georgia, Augusta.
Discussion
16. Study of Silent Amniotic Fluid Infections and Evaluation of Their Relationship to Failure of Tocolysis. C. Hameed, U.L. Verma and N. Tejani. Health Sciences Center, State University of New York at Stony Brook; Nassau County Medical Center, Department of Ob/Gyn, East Meadow, N.Y.
Discussion
Break Regency Foyer
POSTER SESSION A (Numbers 29 through 100) Rio Grande Ballroom
Astra Pharmaceutical Company Award for Best Poster -Session A -
29. Paradoxical Heart Rate Response to the Valsalva Maneuver in Preeclampsia. M.L. Cabaniss, C.D. Cabaniss, and P.C. Wagner. Department of Obstetrics and Gynecology (Division of Maternal/Fetal Medicine) and Department of Internal Medicine (Division of Cardiology), Univ. of South Alabama, Mobile.
12

5:30- 6:30 p.m.
7:00- 8:00 p.m.
8:00-10:00 p.m.
Institute of Perinatal Biology Award for Best Research Idea - Session A -
100. Nicardipine Tocolysis of Preterm Labor in the Pregnant Rabbit. R.H. Holbrook, M. Lirette, M. Katz. Department of Obstetrics and Gynecology and Reproductive Sciences. The Cardiovascular Research Institute, University of California at San Francisco.
SPO Business Meeting (Members Only) Dr. Robert Hayashi, Presiding
Cocktail Reception (Savage Laboratories)
Annual Banquet
East Regency Ballroom
Regency Foyer
West Regency Ballroom
I I I ! I I I ! I
SATURDAY, FEBRUARY 4, 1984
6:30- 8:00 a.m. Continental Breakfast
8:00-10:00 a.m. Registration
8:00- 8:15 a.m. Announcements - Dr. John Morrison
8:15- 9:45 a.m. SCIENTIFIC SESSION IV MODERATOR: Dr. Edgar Makowski
8:15 a.m. 17. Premature Rupture of Membranes Occurring in Pregnancy Prior to Fetal Viability. T.J. Garite, and J. Taylor. Women’s Hospital, Memorial Medical Center of Long Beach, CA and The University of California, Irvine Medical Center, Irvine, California.
8:25 a.m. Discussion
8:30 a.m. 18. Dietary Sodium Manipulation, Angiotensin II, and Blood Pressure Regulation in Pregnancy. M.I. Lee, H. Todd and R.J. Sokol. Department of Ob/Gyn, Hutzel Hospital/Wayne State University and St. Louis University.
8:40 a.m. Discussion
Garden Terrace
Regency Foyer
East Regency Ballroom
East Regency Ballroom

I
I
I
I
I
8:45 a.m.
8:55 a.m.
9:00 a.m.
9:i0 a.m.
9:15 a.m.
9:25 a.m.
9:30 a.m.
9:40 a.m.
9:45-10:15 a.m.
10:15-11:45 a.m.
10:15 a.m.
10:25 a.m.
19. Prostaglandins Play a Role in the Anti- hypertensive Effect of Pregnancy in the Spontaneously Hypertensive Rat? R.A. Ahokas, G.D. Anderson, S.L. Reynolds and J. Lipshitz. Division of Maternal/Fetal Medicine, Department of Obstetrics and Gjmecology, University of Tennessee Center for the Health Sciences, Memphis.
Discussion
20. The Disposition of Meperidine and Nor- meperidine in Mother, Fetus and Neonate Following Multiple Doses of Meperidine During Labor. B.R. Kuhnert, E.H. Philipson, P.M. Kuhnert and C.D. Syracuse. Cleveland Metropolitan General Hospital/ CWRU, Cleveland, Ohio.
Discussion
21. Penicillin Allergy and Desensitization in Serious Maternal/Fetal Infections. G.D. Wendel, Jr., B.J. Stark, R.B. Jamison and T.J. Sullivan. Departments of Ob/Gyn and Internal Medicine, Univ. of Texas Southwestern Medical School, Dallas, Texas.
Discussion
22. Biparietal Diameter Femoral Length Growth in Normal Twin Pregnancies. D. Graham, Y. Shah, S. Moodley, F.J. Yannuzi and S. Logghe. University of Rochester Medical Center, Department of Ob/G~, Rochester, N.Y.
Discussion
Break Regency Foyer
SCIENTIFIC SESSION V MODERATOR: Dr. Roy Petrie East Regency Ballroom
23. Continuous Long-Term Intravenous Betamimetic Tocolysis. W.C. Hill, M. Katz, J.L. Kitzmiller and P.J. Gill. Department of Obstetrics and Gynecology, Children’s Hospital of San Francisco, San Francisco, California.
Discussion
I 14

I I I I I I I i
I I I I I I I
10:30 a.m.
10:40 a.m.
10:45 a.m.
10:55 a.m.
ii:00 a.m.
ii:i0 a.m.
11:15 a.m.
11:25 a.m.
11:30 a.m.
11:40 a.m.
11:45-12:00 noon
24. Lidocaine for Episiotomy. E.H. Philipson, B.R. Kuhnert, C.D. Syracuse. Cleveland Metropolitan General Hospital, Perinatal Clinical Research Center, Case Western Reserve University, Cleveland, Ohio.
Discussion
25. Preterm Labor Managed Without Tocolysis P. Boylan. The National Maternity Hospital,Dublin.
Discussion
26. Emergency Hysterectomy and Hypogastric Artery Ligation in the Control of Obstetric Hemorrhage. S.L. Clark, S. Yeh, S. Bruce and R.H. Paul. Department of Obstetrics and Gynecology, University of Southern California School of Medicine and Women’s Hospital, Los Angeles County/USC Medical Center, Los Angeles.
Discussion
27. Multiple Gestation: Time Interval Between Delivery of the First and Second Twin. W. Rayburn, J. Lavin, M. Miodovnik, and M. Varner. Department of Obstetrics and Gynecology, University of Michigan, Akron City Hospital, University of Cincinnati and University of Iowa.
Discussion
28. Effect of Maternal Smoke Exposure on Ultrastructure of Fetal Peripheral Blood Vessels in the Mouse. R.C. Kaufmann, K.S. Amankwah and A.D. Weberg. Southern lllinois University School of Medicine, Department, of Ob/Gyn, Springfield, lllinois.
Discussion
Break Regency Foyer
I I I I

I I I I i I I I I I I I I I I I i I I
12:00- 2:00 p.m.
2:00 p.m.
POSTER SESSION B (Numbers 101 through 178) Rio Grande Ballroom
Astra Pharmaceutical Award for Best Poster -Session B-
101. Immunoglobulin G (IgG) Subclass and Neonatal Outcome in Pregnancies Complicated by Isoimmunization. M.M. Taslimi, B.M. Sibai, J.V. Dacus and J.M. Mason. Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis.
ADJOURN

SCIENTIFIC SESSION I
AWARD PAPERS
Moderator: Dr. Robert Hayashi
Friday, February 3, 1984
9:00 - i0:00 a.m.
East Regency Ballroom
I I I I I I I I I I I I I I I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#1 February, 1984
9:00 a.m.. February 3rd
~ASELINE LYMPH FLOW RATE IN THE NEAR-TERM PREGNANT SHEEP AND EFFECT OF TERBUTALINE. G.J. Valenzuela*, L.L. Woodsx and RoA. Bracex, Department of Obstetrics and Gynecology and Division of Perinatal Biology, Loma Linda University, Loma Linda, California.
Normal human pregnancy is characterized by many cardiovascular changes includ- ing an increase in blood volume, interstitial fluid volume, and frequent edema. This edema occurs even in nondependent extremities (Chesley, Hypertensive Disorders in Pregnancy, Appleton Century Croft, NY, 1978). One of the possibilities in explaining the edema is a change in lymph flow rate during pregnancy secondary to a decrease in lymph vessel contractility similar to the pregnancy induced vasodilation. Although sheep have a minimal increase in blood volume during pregnancy (Ueda et al, SGI Abstract #196, Washington DC, March~ 1983) and inter- stitial pressure (Brace et al, Am. J. Physiol. 1981), they do have a decrease in vascular contractility as measured by the response to angiotensin II infusion (Rosenfeld et al, J. Clin. Invest. 67:486) at doses similar to those required by pregnant women. Another related question that interested us was to study a possible lymph flow decrease in the genesis of pulmonary edema in pregnant women when a 8 mimetic drug is utilized. Previous animal experiments have failed to demonstrate an effect of ~ mimetic drugs upon capillary permeability (Hauth et al, Am, J. Obstet. Gynecol. 146:916, 1983). A recent work by the same group described a greater increase in interstitial volume in an animal treated with ritodrine as compared to control. We used a chronic sheep model in which the thoracic duct was catheterized under general anesthesia and connected to a catheter placed on the superior vena cava. The connection remained exteriorized over the animal’s neck (this approach allows multiple checking of the catheter patency). In the sheep the thoracic duct drains approximately 80% of the body. Measurements of the lymph flow were done between 4 days and 2 weeks after surgery. The lymph £1ow rate was measured by draining the lymph into a weighed container. The derivative of the weight change constitutes the lymph flow rate and about every 15 rain the lymph was returned to the sheep. Protein determinations were carried on in plasma and lymph. The lymph flow rate in the pregnant animal during a 30 rain observation period was 0.0776 + 0.0226 (SD) (n = 5) cc/min/kg vs 0.0783 + 0.025 (SD) (n = 7) cc/min/kg in nonpregnant chronically catheterized sheep (~ > 0.05). The plasma protein concentrations (+ SD) w~re 5.83 + 0.4 and 6.16 + 0.802 in the pregnant and nonpregnant animals respectively. The lymph protein concentrations were 3.4 + 0.88 and 4.07 + 0.61 (p > 0.05). Thus there appears _ _ to be little evidence for changes in whole body lymph flow rate or lymph protein concentrations during pregnancy in the sheep. To the best of our knowledge this is the first report of lymph flow measurements in pregnant animals. The acute administration of terbutaline as a bolus did not have a significant effect on lymph flow rate of the thoracic duct, in spite of having a dilating effect on systemic blood vessels. Therefore, the present results suggest only a minimal role for the lymph system in the genesis of edema during pregnancy or of pulmonary edema secondary to 8 mimetic administration if the fluid administered is iso-osmotic.
17

I Society of Perinatal Obstetricians "= Annual Meeting
San Antonio, Texas ¯ #2 February, 1984
9:15 a.m. - February 3rd
I THE DUBLIN FETAL MONITORING TRIAL
Peter Boylanx+, Dermot MacDonaldX+, Adrian Grantx°, Margaret Pereira×÷ Ian Chalmersx°
+The National Maternity Hospital, Dublin and °The National Perinatal Epidemiology Unit, Oxford.
There is continuing controversy about the relative merits of continuous electronic fetal heart rate monitoring (E.F.M.) versus intermittent auscultation (I.A.} as the method of choice ofI fetal monitoring in labor. In an attempt to resolve this controversy a prospective randomized controlled trial of E.F.Mo versus I.d. was undertaken at the National Maternity Hospital, from March 1981 to March 1983. Before the trial 5% of patients, in whom liquor was absent, or there was significant meconium staining, in labor, were monitored by EFM and scalp pH. All other patients were monitored by I.A. Eligibility criteria for inclusion in the trial were: gestation > 28 weeks; a diagnosis of labor made; demonstration of l~quor without significant meconium staining. 13,025 women met thes entry criteria; 99.5% (12,960) were allocated at random, by opening a sealed envelope, to either EFM or IA. All subsequent analyses are based on unbiased comparisons between the two randomized groups.
Randomization achieved comparability in respect of maternal age, marital status, parity, gestation, birthweight, induction of labor, an~ presence of maternal risk factor. 98% of those allocated to I.A
received I.A., 80% allocated E.F.M. received it (10% delivered too quickly, 6% refused, 4% did not receive E.F.M. for a variety of
reasons}. Scalp pH was measured in~2.7% E.F.M. patients and~.~_of I.A. patients (p<O.O01). C.S. ~and ~orc~ rates in the E.F.M. and I.A. groups were 2.4% and 2.2% (N.S.}, and 8.2% and 6.2% (p<O.051 respectively. Duration of labor was shorter (3.9 hours) among E.F.M patients than I.A. patients (4.2 hours}, p<O.05. There were B intrapartum fetal deaths in the E.F.M. group and 2 in the I.A. group: these are analyzed in detail. Convulsions occurred in 12 infants in the E.F.M. group and 27 in the I.~. group (p<O.05); 3 ~.F.M. infants subsequently died while 6 I.A. died. There was a total of ii NND in the I.A. group and 9 in the E.F.M. group. The trial results show that E.F.M. significantly reduces the incidence o~ neonatal convulsions but does not influence the rate of intrapartum death: these conclusions are discussed.
I I I I I I I I I I I I I
18

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#3 February, 1984
9:30 a.m. - February 3rd
THE ASSOCIATION BETWEEN NONSPECIFIC VAGINITIS AND ADVERSE PREGNANCY OUTCOME. Michael G. Gravett, M.D., H. Preston Nelson, M.D., David A. Eschenbach, M.D., King K. Holmes, M.D., Ph.D. (Departments of Obstetrics and Gynecology and Medi- cine, University of Washington, Seattle, Washington.) Sponsored by T. J. Benedetti, M.D.
Microorganisms, especially anaerobic bacteria, produce phospholipase A~. Pre- mature labor may be stimulated when phospholipase A2 stimulates prostagla~din pro- duction through the generation of free arachidonic acid. We have demonstrated a l,O00-fold increase in the quantitative concentration of vaginal anaerobes among women with nonspecific vaginitis (NSV) compared to control women without vaginitis This concentration of anaerobes represents a potentially rich source of phospholi- pase A2. To investigate the hypothesis that NSV may be associated with premature labor, we conducted a matched cohort study of NSV in pregnancy. A total of 740 consecutively seen patients in labor and delivery underwent multiple cervical-vag- inal cultures and gas-liquid chromatography (GLC) of vaginal secretions was per- formed to detect NSV. NSV was identified in 102 (13.8%) patients. Each patient with NSV was matched with two patients without NSV for maternal age, race, parity, welfare status, marital status, and gestational age at the time of entry. Multi- ple gestations were excluded. Successful matching was accomplished for 75 patient~ with NSV and 150 patients without NSV. Analysis revealed no differences between patients currently with and th~ewithout NSV in past reproductive losses, antepar- tum hemorrhage, medical or prior obstetrical complications. Significant differ- ences were found between those with NSV and those without NSV in: premature labor < 34 weeks, 22.7% vs 11.3% (p<O.05); birthweight < 2500 grams, 29.3% vs 16% (p < 0.025); and PROM < 36 weeks, 26.7% vs 14% (p<O.Ol). Differences were also found in amniotic fluid infection (9.3% vs 4.0%), and in recovery of cervical C~mgdx]z XpLachom~ut~L~ (Ct)(lO.7% vs 6.7%) but neither of these later differences were sta- tistically significant. However, because Ct has been associated both with NSV and adverse pregnancy outcomes, a further restrictive analysis was performed among only CZ negative patients with and without NSV to eliminate this potential con- founder. Data for this restrictive analysis are shown below. Significant differ- ences persisted in premature labor and birthweight < 2500 grams.
Premature labor < 34 weeks Birthweight < 2500 grams PROM < 36 weeks Amniotic fluid infection
Women With Women With- p NSV (60) out NSV (120) value
17 (28.3%) 13 (10.8%) <0.01 14 (23.3%) 16 (13.3%) .07
7 (11.7%) 5 (4.2%) 0.I0
Odds Ratio (95% C.I.)
3.83 (I.42-I0.31) ...... 2.23 (1.40- 8.19) 2.71 (0.92- 8.02) 3.25 (0.77-13.78)
We conclude: I) NSV occurs frequently during pregnancy, and 2) the risks of prema- ture labor and low birthweight infants were 3.8 times and 2.2 times greater among patients with NSV in our population.
I I I I I I I I I I I I I I I I
19
I

I I I I

I Society of Perinatal Obstetricians -- Annual Meeting
I San Antonio, Texas
#4 February, 1984
9:45 a.m. - February 3rd
MONITORING THE NEONATAL BRAIN. Uma L. Verma, M.D.x .... , Frank Archbald, M.D., Nergesh Tejani, M.D. and Sara Mittelmann-Handwerker, M.D. Health Sciences Center, State University of New York at Stony Brook; Nassau County Medical Center, Department of Obstetrics and Gynecology, East Meadow, N.Y.
Continuous monitoring of neonatal brain function is urgently needed for early detection and prevention of hypoxic-ischemic brain injury. The cerebral function monitor (CFM), a new concept of integrated EEG, was used in this study to monitor the neonatal brain. In the initial phase of the study, 49 normal neonates were monitored and normal patterns were defined for various gestational ages. These patterns were evaluated on the basis of their general form, level of activity during quiet sleep (SI), active sleep ($2), and response to stimuli ($6). CFM patterns correlated well with simultaneously obtained EEG. In the latter part of the study, a group of 31 asphyxiated neonates were evaluated. CFM patterns were of three types: (i) normal pattern (20 cases); all but two of these were dis- charged in good condition. The two demises were due to extreme prematurity and sepsis. (2) A flat, low voltage and nonreactive pattern (8 cases); all of these died of hypoxic-ischemic injury and/or intraventricular hemorrhage. (3) Matura- tional delay (3 cases); all three have neurological deficits. CFM patterns seen in these 31 neonates correlated well with EEG, CAT scan, fontanelle scanning and clinical outcome. The CFM monitor seems to be an accurate, reliable and easy to interpret monitoring modality in neonates at risk for hypoxia.
I I I I I I I I I I I I I I I I
2O I

SCIENTIFIC SESSION II
Moderator: Dr. Donald Barron
Friday, February 3, 1984
10:30 - 12:00 noon
East Regency Ballroom
I I I ! i I I ! I I I ! I I I ! I I I

Society of Perinatal Obstetricians Annual/Vleeting
San Antonio, Texas
#5 February, 1984
10:30 a.m. - February 3rd
THE NATURAL HISTORY OF GENITAL HERPES COMPLICATING PREGNANCY X X X X
Z. Brown, L. Vontver, L. Corey, D. Hickok, J. Benedetti, and S. Berry. Depts. of Obstetrics and Gynecology and Microbiology, Univ. of Washington, Seattl~
Studies in the past have suggested that certain viral infections increase in severity with advancing gestation. Though this relationship has been suggested for genital herpes, careful prospective studies of the natural history of genital herpes complicating pregnancy have not been performed. In a study group of 163 pregnant patients, 148 had recurrent disease antedating pregnancy and 15 had the first episode during pregnancy. Cervical and vulvar cultures were obtained week- ly from entry until delivery. During a recurrence cultures were obtained at least every third day until healing. With asymptomatic shedding, cultures were repeated as soon as the positive cultures were identified. Infants were examined by a single observer until 6 months of age.
Of the 148 patients with recurrences antedating pregnancy, 109 registered prio to 26 weeks. For these patients, recurrence rates were computed from the obser- ved plus the historical account of recurrences. There was a progressive and highly significant increase in the recurrence rates as pregnancy progressed.
ist 2nd 3rd 2nd & 3rd p = .06 n = 109 .352 .390 .496 ist & 3rd p = .003
The duration of the lesions did not demonstrate significant changes with advanc- ing gestation. Of the total study group (n=163), 26 had asymptomatic viral shedding at least once during pregnancy. Fifteen were from labia only, 6 from cervix only and 5 from cervix and labia concomitantly. Although numbers were small, there was no apparent trend in asymptomatic shedding with gestational age. Asymptomatic shedding in patients with a first episode of genital herpes in pregnancy (5/15) was much more frequent than with recurrent genital herpes ante- dating pregnancy (21/148) (p=.01). Furthermore, of the five patients with asymptomatic viral shedding from both the cervix and labia, 3 were in patients with their first episode of genital herpes in early pregnancy. Demographically, asymptomatic shedding occurred in younger, single patients, with less oral herpes and a shorter duration of genital herpes (p=.05). None of the 148 pts. delivered prior to 36 weeks and none demonstrated major anomalies on follow up until 6 months of age. Thirty one percent delivered by C-Section of which ~alf were for the indication of active genital herpes at the onset of labor.
In summary, we have shown that the frequency of recurrences of genital herpes but not the duration of the lesions increase with advancing gestation. Asympto- matic viral shedding occurs much more commonly from the external genitalia and is more common in younger, single patients with less oral herpes and a shorter duration of genital disease. In patients with first episode disease during preg- nancy, asymptomatic viral shedding is more frequent than with recurrent disease antedating pregnancy and is more likely to involve both the cervix and labia concomitantly.
I I I I I I I I I I I I I I I
21
I I

I Society of Perinatal Obstetricians -- Annual Meeting
1 San Antonio, Texas
#6 February, 1984
10:45 a.m. - February 3rd
ANTITHROMBIN III ACTIVITY IN HYPERTENSIVE PREGNANT WOMEN C.P. Weanerx, H. Kwaanx, F. Duboex, M. Paulx, M. Antielx and W. Hauckx Northwestern University, Prentice Women’s Hospital, Chicago, IL 60611
Differentiating preeclampsia from either renal or essential hypertension remains
¯ problematic. Antithrombin III (AT III), the major naturally occurring coagulation inhibitor, has been reported to be reduced in patients with preec]ampsia. We
sought to investigate the use of AT III as an aid in the differential diagnosis of
third trimester hypertension. A prospective study of functional, plasma AT III
activity in women with hypertension in the third trimester was conducted over an 18 month period at Prentice Women’s Hospital. One hundred twenty-seven patients, of
which 53 had hypertension, were sampled once within 4 weeks of delivery. Normal
controls were free of clinical complications. The diagnoses of attending physi-
cians were used to divide the patients into four groups - normal (N), preeclampsia
(~), chronic hypertension (CH) and chronic hypertension with superimposed ~reeclampsia (CHP). Proteinuria was present in 90% of preeclamptic (P and CHP) 3atients. Th~eean % AT III activity ± i SD by categories were N=85±~5, CH---~±I3,
~=60±15 and CHP=68±16. If an AT III activity of less than 70% is arbitrarily selected as a dividing line, the number of women in each group is:
AT III< 70%
N CH P CHP
8 0 22 i0
AT III> 70% 66 ii
sensitivity = 76%
specificity = 91%
predictive value of preec]ampsia if AT III< 70% = 80%
predictive value of no preec]ampsia if AT III> 70% = 88.5%
The sensitivity was greatly diminished in the CHP patients in comparison to the P
9atients (59% vs. 88%). This could represent errant diagnosis. The mean g.a. in ~reec]amptic women whose AT III was > 70% (n=32) was similar to those < 70% (n=10)
35 weeks) as was the serum uric acid level (6.8±0.9 vs 7.5±1.1 mg%). Preeclamptic
romen whose AT III activity was < 70% had lower birthweight infants and a greater
percent less than the 10th percentile for birthweight (16% vs 10%) than those whose
AT III> 70%. However, two women in the control group delivered infants less than
the 10th percentile for weight. The AT III values were above 80% in each. There
were three patients classified as severe P or CHP with an AT III> 70%: 70, 72 and
74%. There was no evidence of uteroplacenta] insufficiency as manifest by late
decelerations in those patients whose AT III exceeded 70%, but late decelerations
were noted in three patients whose AT III was less than 70% (p<0.05). We conclude
that, in the absence of other factors known to decrease AT III ~n pregnancy, an AT
III< 70% in a hypertensive woman is consistent with the diagnosis of either P or ZHP. When the AT III is > 80% in a preterm patient, delay of delivery and a ~ria] 0’f oral antihypertensives may be helpful.
I I I I I I I I I I I I I I
I 22 I

#7 11:00 a.m. - February 3rd
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
RITODRINE DISPOSITION ~ PARTURI~ A~D P~ ~ONATE
Betty R. Kuhnert, Ph.D.,x Thomas L. G, oss, M.D., Paul M. Kuhnert, Ph.D.,x Dap~. Cb/~ and the Perinatal Clinical Researoh Center, Cleveland Metropolitan General Hospital/C.W.R.U., Cleveland, Ch.
Ritodrine is the only approved tocolytic agent. However, there is little information regarding its pharmacology in the peripar- t~m period ~hen treatment fails and labor is not inhibited. Pre- vious studies here provided basic pharmacological data from men and other nonpregnant vol~mteers, or on fetal/m~cernal plasma ratios at term following short infusions of ritodrine prior to repeat Cesarean section. The latter study also suggested that the term infant could not excrete ritodrine in a conjugated form. The purpose of this study was to determine the disposition of ritodrine in parturients and preterm neonates. Ei~ parturients and 5 of their infants were studied. ~he mothers had received intravenous infusions of ritodrine and/or combinations of intravenous and oral ritodrine prior to delivery. The infants were 30.4 + 0.9 weeks gestation by Dubowitz exmn. Plasma samples from 3 mothers were obtained imnediately prior to cessation of intravenous ritodrine infusion -end delivery, and periodically for 25 hours after infusion. Mater~al and neonatal urine samples were collected from 5 mothers and infants for 36 hours and from one mother for 72 hours. Plaars and urine ritodrine (free and conjugated) ~as deten~ined using high performance liquid chromatography with electrochemical detection. The results show that in maternal plsama, disappearance of ritodrine was biphasic: A rapid disappearance phase with a half life of 40-63 minutes was followed by a prolonged disappearance phase with a half life ranging from 16-~8 hours. In maternal urine, 79% of the ritodrine was excreted in the first 6 hour col- lection period (figure); 9~% had been excreted by 24 hours. The average excretion rate was 0.14 milligrans/hr. Rito~rine was detectable in maternal urine for 72 hours and most (67-83%) of the rito- drine was excreted in the form of a glucuronide conjugate. In neonatal urine, only 10 percent of the ritodrine was excreted in the first 6 hour collection period (figure); 78% had been excreted by 24 hours. The average excretion rate was 0.044 micrograms/hour. Most of the ritodrine excreted by the neonate was also excreted in the form of a glucuronide conjugate; the percent of conjugated ritodrine (80-95%) was higher than in maternal urine. Two infants ~hose mother received oral ritodrine for pro- longed periods (up to 25 days)prior to delivery excreted significantly less ritodrine than the 3 infants ~hose mothers had received intravenous inD~_sions of ritodrine the day prior to delivery. ~he results show that the disappearance of ritodrine is prolonged in both mother and neonate and that conju- gates can be formed by both. This study provides basic pharmacological data and suggests that the potential for adverse effects may be prolonged, particularly in the neonate.
I ! I I I I I I I I I ! I I I I
23

Society of Pednatal Obstetricians Annual Meeting
San Antonio, Texas
#8 February, 1984
11:15 a.m. - February 3rd
I
THE EFFECT OF MYO-INOSITOL ON THE GLYCEROPHOSPHOLIPID COMPOSITION OF ADULT AND FETAL RAT LUNG TISSUES AND SURFACTANT. J. Gerald Quirk* and John E. Bleasdale , Departments of Obstetrics and Gynecology and ~ochemistry and Cecil H. & Ida Green Center for Reproductive Biology Sciences, University of Texas Southwestern Medical School, Dallas.
In many species, including man, the second most abundant lipid in lungsurfactant is phosphatidylglycerol (PG) which may comprise 10% of the total lipid in surfac- tant from mature lungs. Interest in surfactant PG was stimulated by the finding that surfactant obtained from tracheal aspirates of full-term infants contained significant amounts of PG while this lipid was absent from the surfactant of pre- mature infants. Regulation of the PG content of lung surfactant is not understood completely, but the reciprocal changes in the amount of PG and phosphatidyl- inositol (PI) in surfactant are suggestive of regulation at the level of their common precursor, CDP-diglycerideo It has been observed in several species that the enzymes that synthesize PI and PG compete for the limited amount of CDP- diglyceride and this competition is influenced by the availability of myg-inositol The ratio of PG to PI in lung surfactant increases during a period in fetal lung development when the concentration of myo-inositol in fetal serum is declining. We have proposed that the developmental decline in fetal serum myo-inositol con- centration restricts m_~_9_-inositol availability to the fetal lungs and favors PG biosynthesis at the expense of PI biosynthesis. The objective of the present investigation was to alter the concentrations of myo-inositol in the serum of pregnant rats and to examine the effect on the PG:PI ratio in surfactant of the dams and their fetuses. For 5 days, pregnant rats received twice daily I.P. injections of myo-inositol while being given free access to food and drinking wate containing myo-inositol (7% w/v). Myo-inositol administration increased signi- ficantly the concentration of~yo-inositol in maternal serum (0.06 mM to 0.67 mM on d 18 or d 21) and in fetal serum (0.36 mM to 1.17 mM on d 18, and 0.23 mM to 0.52 mM on d 21). M¥o-inositol treatment decreased the PG:PI ratio in maternal lung tissue and lung lavage material (p .01) without affecting the relative amount of phosphatidylcholine present. The normal increase in the PG:PI ratio in fetal rat lung, which occurs between d 18 and d 21, failed to occur in fetuses whose mothers receive myo-inositol (p .05). These findings are supportive of the hypothesis that m_~_9_-inositol availability influences the PG:PI ratio of surfactant in both adult and fetal rat lungs.
I I
24

I I I I I I I I I I I ! ! I I I I I I

Society of Perinatal Obstetricians
Annual M. eeting San Antonio, Texas
#9 February, 1984
11:30 a.m. - February 3rd
EFFECTS OF DIURETICS ON PLASMA VOLUME IN PREGNANCIES COMPLICATED BY CHRONIC HYPER- TENSION: Baha Sibai, M.D., Robert Grossman, M.D.x, Hannah Grossman, M.D.x, Thomas Abdella, M~d D. Anderson, M.D., Division Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medi- cine, Memphis, Tennessee
The purpose of this randomized, prospective study was to determine the rela- tionship between diuretic therapy and plasma volume changes during the course of pregnancy. The study group consisted of 20 pregnant women with a documented his- tory of chronic hypertension. All patients were in their first trimester and were receiving diuretics at time of entry into the study: each patient was randomly assigned to one of 2 groups. Patients assigned to the first group were allowed to continue taking their diuretic medication throughout the course of pregnancy. For patients in the second group, diuretics were discontinued immediately. Alpha- methyldopa was added when necessary to keep blood pressure below 160 mm Hg, systo- lic and/or below ii0 mm Hg diastolic levels. Using the Evan’s Blue dye-dilution technique apparent plasma volume was serially measured throughout pregnancy. The relationship of plasma volume to clinical course, perinatal outcome, and other maternal laboratory findings was subsequently analyzed. The average age, parity, and height of the 2 groups were similar. There were no significant differences in mean arterial blood pressure, duration of hypertensive disease, number of patients requiring ~-methyldopa or incidence of superimposed preeclampsia. There were no significant differences in serially measured serum creatinine, creatinine clear- ance, or proteinuria. The table below summarizes the plasma volume findings in the 2 groups of patients at various gestational ages. These results suggest that in hypertensive pregnancies, diuretics prevent normal plasma volume expansion. This finding might have clinical significance since low plasma volume is associat- ed with poor perinatal outcome.
~ COMPRRISOH OF PLRSNR UOLUMES
~ ~eee1 ~ ~ ~
2~58~ .......
P<.04
2088"
I I I I I ! I I I ! I I I I I
25
I I

I I I I ! I I I I I
I I I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 10 February, 1984
11:45 a.m. - February 3rd
CARDIOVASCULAR ALTERATIONS IN SEVERE PREGNANCY-INDUCED HYPERTENSION: EFFECTS OF MAGNESIUM SULFATE AND HYDRALAZINE. D~vid B. Cotton~ M.D., Bernard Gonik, M.D.*, Karen Dorman, R.N.x, Department of Obstetrics and Gynecology, University of Texas Medical School at Houston, Houston, Texas.
Magnesium sulfate (MgS04) and Hydralazine (HZ) are two of the most commonly utilized agents in the treatment of severe Pregnancy-induced hypertension (PIH). While many studies have evaluated their clinical efficacy, there exists a paucity of reports on their central hemodynamic effects. We therefore initiated this
investigation on the acute cardiovascular effects of MgSO$ infusion and HZ administration. Material and Methods: Six patients with severe PIH were entered into this study. The effects of MgSO4 infusion were studied in 5 patients and the HZ bolus effects were studied in 6 patients. After informed consent, Swan-Ganz and radial artery catheterization were performed. A 4 gm I.V. loading dose of MgSO4 was given followed by a 1.5 gm/hr continuous infusion. Hemodynamic and oxygen related variables were measured at baseline; 15 min., 30
min., and one hour post loading dose. Two to 4 hours after MgSO4 had been initiated, I0 mg I.V. bolus of HZ was given. Hemodynamic and oxygen related variables were again measured every 15 minutes for one hour and then hourly for two hours. Results (M_~_~4): The mean arterial pressure (MAP) was significantly (p ~ 0.01) decreased 30 minutes after the 4 gm loading dose, but had returned to baseline values by 1 hour. There were no other significant changes in heart rate (HR), right atrial pressure (RAP), mean pulmonary arterial pressure (MPAP), pulmonary capillary wedge pressure (PCWP), cardiac output (CO), cardiac index (CI), stroke volume index (SVI), systemic vascular resistance index (SVRI), pulmonary vascular resistance index (PVRI), left ventricular stroke work index (LVSWI), oxygen availability index (02AVI), and oxygen consumption index (V02). Results (HZ): Post I0 mg I.V. bolus, the HR was increased by 13.8% from baseline and remained significantly (p 4 0.05) elevated until 1 hour post bolus. There was an initial 19.2% increase in CI 15 minutes post bolus, and the CI remained significantly (p < 0.05) elevated until 45 minutes post infusion. The MAP significantly (p 4 0.01) decreased by 15 minutes following the bolus and averaged a I0 mmHg decrease until 2 hours post infusion. The SVRI dropped significantly (p K 0.01) by 15 minutes and remained depressed throughout the study period. There were no significant changes in the other hemodynamic or oxygen related variables described above. Conclusions: I) MgSO4’s primary effect was a transient lowering of MAP. 2) MgSO4’s hypotension effect was dependent on being given rapidly and was not maintained by a continuous infusion. 3) Clinical
doses of MgSO4 did not appear to depress myocardial work as evidenced by a stable LVSWI. 4) HZ bolus resulted in a significant increase in fiR and CI that returned to baseline values by 2 hours. 5) HZ bolus resulted in a significant lowering of MAP and SVRI throughout the study period.
I I I I I i I I I I
I I I I I I
26 I

SCIENTIFIC SESSION Ill
Moderator: Dr. Charles Hendrlcks
Friday, February 3, 1984
1:30 - 3:00 p.m.
East Regency Ballroom

I Society of Perinatal Obstetricians !
Annual/~eeting I
San Antonio, Texas i # |1 February, 1984 1
] :30 p.m. - February 3rd
FIRST TRIMESTER PRENATAL DIAGNOSIS BY CHORIONIC VILLUS SAMPLING (CVS)
Ronald J. Wapner, Laird G. Jacksonx, Marie Barrx, Eugene Grebnerx, Jefferson Medical College of Thomas Jefferson University, Philadelphia, PA 19107
Attempts at first trimester prenatal diagnosis of genetic diseases have been made over the past i0 years. Recently European centers have shown that direct sampling of chorionic villi under ultrasound guidance is a feasible and accurate way to diagnose both cytogenetic and biochemical fetal disorders prior to I0 weeks gestation. We have performed over 60 chorionic villus biopsies on pregnancies tha were to be terminated and 19 samplings on continuing gestations. Chorionlc villus sampling was performed using a "Portex catheter" (18ram long x 1.5mm diameter) with an aluminum trocar. Under ultrasound guidance the chorion frondosum was located in gestations 7 to 12 weeks from the last menstrual period, and the cannula was inserted extra-amnioticlly to an area just beneath the placental edge. A 20cc syringe was attached, and suction was applied, and 5 to 30mg of chorionic villi were obtained. In pregnancies at risk for a cytogenetic disorder, a direct prep- aration of the villi was performed, and a karyotype was available within 24 hours. Appropriate biochemical and DNA analysis was performed on the villi when indicated Indications for cytogenetic sampling in continuing pregnancies were: maternal age (8), previous trisomy 21 (4), parental translocation carrier (I), and obligate he- mophiliac carrier (I). Biochemical analysis was performed for Tay-Sachs disease (2), =-I antitrypsin deficiency (i), Gaucher disease (I), and metachromatic leuko- dystrophy (I). Of the 19 continuing pregnancies sampled, adequate samples were obtained in 17. Of the 2 with no samples, one was not obtainable because of large uterine fibroids, and in the other a uterine contraction and poor visualization of the actual placental site in an obese patient hampered retrieval. The only com- plication of sampling was minimal spotting lasting less than 24 hours. A positive diagnosis of triploidy (69XX¥) was made in one pregnancy and was confirmed by anal. ysis of cultured placental, fetal, and amnion specimens at termination. Villi from a pregnancy at risk for Tay-Sachs disease demonstrated no hexosaminidase A. The positive diagnosis was confirmed by amniocentesis and fetal tissue at termi- nation. ~7ne results of the arylsulfatase A assay for metachromatic leukodystrophy was suspicious but not conclusive of an affected fetus, and an amniocentesis will be done at 16 weeks. All other results were normal. At present 17 pregnancies are continuing normally.
We conclude that CVS is a feasible technique for obtaining pure fetal tissue appropriate for first trimester prenatal diagnosis of cytogenetic and biochemical abnormalities with a low incidence of early complications. More work is still needed for detection of possible long-term sequelae and risks.
I I I ! I I I I I I I I I I
27

I Society of Perinatal Obstetricians I
Annual Meeting San Antonio, Texas 1
# 12 February, 1984
1:45 p.m. - February 3rd
1
HEAD OUT IMMERSION IN TREATMENT OF PREGNANCY ASSOCIATED EDEMA Robert C. GoodlinT M.D., Kristen L, Engdahl Hoffman, M.D. & Nathan E. Williams, M,D.
Department of Obstetrics & Gynecology, University of Nebraska Medical Center #2nd and Dewey Avenue, Omaha, Nebraska 68105
In males submerged to their necks in water, plasma volume expansion occurs at a rate
comparable to an intravenous infusion of a ~iter per hour of balanced salt solution. Cardiac reflexes then initiate a significant diuresis. Fifty pregnant women in the last trimester of pregnancy were immersed to their necks while exercising for one hour, one to three times per week. At fifteen minutes post-immersion, in 92%, mean blood pressure decreased, even in those with mild hypertension. Urine output increased 73 + 12% and pulse rate declined a mean of 12 +- #%. Subsequent urine output following the immersion was directly related to degree of dependent edema. Urinary sodium increased approximately #0%. The diuresis often continued for 36 hours. Preliminary analysis suggests that the prolonged diuresis is
enhanced in pregnant women by performing ca!~sthenics in standing position while immersed in water whose temperature is between 30-32 C. It may be that "head out~’ immersion for brief periods (one hour 2-3 times per week) is comparable to bed rest for pregnancy
abnormalities associated with edema. SincF the many previous studies failed to consider the effects of leg exercises while immersed we are continuing to study the definition of optimal physical activity and water temperature for maximum diuresis. Subjects responded enthusiastically to such an exercise "immersed" program, and its possible ability to assure normal plasma volume expansion needs to be explored.
R....eference: I. Epstein, M.: Renal effects of head-out water immersion in man: Implications for an
understanding of volume homeostasis. Physiological Reviews 58:529, 1978.
1 1 1 1 1 1 1 I 1 1 1 1 1 1
28
1 1

#13 2:00 p.m.. February 3rd
Society of Perinatal Obstetricians ,annual Meeting
San Antonio, Texas February, 1984
A PROSPECTIVE, CONTROLLED ANALYSIS OF SILASTI OBSTETRICAL VACUUM CUP DELIVERIES. M.D. Berkus*, R. Ramamurthyx, p. O’Connor, K. Brownx, R.H. Hayashi, Dept. of Ob/Gyn Peds, Ophthal, UTHSC @ San Antonio.
In a prospective analysis of 301 term deliveries at the University of Texas Health Science Center at San Ant6nio between November 1982 and July 1983, (84) consecutive vacuum extraction deliveries (VE) using a Silastic~cup were compared to matched groups of (88) spontaneous vaginal deliveries (SVD), (84) forceps deliveries (FD), and (45) cesarean sections after labor (C/S), to determine the effects of delivery method on maternal and neonatal morbidity; including retinal hemorrhage, ultrasonic evidence of intracranial injury, detailed neurological assessment (encephalopathy scoring), and neurobehavioral status using the:method of Scanlon. The study showed no significant increase of maternal trauma for VE vs SVD, but a significantly greater incidence (p<.01) for FD or C/S vs VE; i.e. lacerations and episiotomy extensions (60 vs 0 vs 37%); Hg loss > 2 gm (40.5 vs 43.5 vs 27.4%); transfusions (1.2 vs 6.5 vs 0%); and post partum fever (13.1 vs 52.2 vs 3.6%). These findings are consistent with the existing literature on the Malmst~o~ vacuum extractor. However, unlike theMalmstr~m VE, there is no significant increase in neonatal morbidity compared to FD Or in serious morbidity over SVD. Specifically for VE vs FD there was no statistical difference in i and 5 minute Apgar scores; extent of resuscitation; birth trauma including cephalhematomas; neonatal jaundice; retinal hemorrhage; and mean NICU or hospital stay. SVD was associated with less morbidity(p<.05) for these categories. Noticeably, there was no mortality related to delivery method, but there were 3 unrelated deaths. There were no cases of
intracranial or subgaleal hemorrhage, but one case of subarachnoid hemorrhage secondary to a coagulation defect. Finally, there was no significant difference in encephalopathy scoring or Scanlon Neurobehavioral assessment between SVD, FD, and VE. Based on these findings, soft-cup vacuum extraction delivery is a safe delivery method for the infant and a significantly less morbid procedure for the mother than forceps delivery.
I I I I I I I I I I I I I I I I I I I

#14 2:15 p.m. o February 3rd
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
DISPOSITION OF RITODRINE IN T~ MOTHER AND FETUS
Thomas Gross, ~D, PM K~hnert, PhD,x B~ K~hnert, PnD,x MG Rosen, MD, T Williams, MA,x Dept Ob/Gyn ~nd the Perinatal Clinical Research Center, Cleveland Metro Ge~ Hospital/Case Western Reserve University
Beta-adrenergic agents such as ritodrine are important in the treatment of premature labor.. However, previous studi,es with isox- suprine show that if the treatment fails and the patiehts deliver shortly after the beta-adrenergic drug is discontinued there is a direct correlation between the neonatal drug concentration an4 morbi- dity. Although ritodrine is the only drug approved for the treatment of premature labor, studies evaluating the perinatal disposition of ritodrine are not available. The purpose of the present study was to exmnine the relationship between mate~n%al ritodrine dose and drug discontinuance to delivery interval (DDDI) and the disposition of ritodrine in the mother and fetus. Plasma ritodrine levels were determined using high performance liquid chromatography with electro- chemical detection as described elsewhere. The disposition was stu-
60
40
DDDI HOURS
died by measuring the drug concentration at delivery in 28 mother and infant pairs in whom the mother had received intravenous ritod-ine within the preceding 17 hours. Results were analyzed by t test and stepwise multilinear regression. Ritodrine was infused according to the package insert at rates varying frcm 6 to 21 rag/hour. The mean total dose administered was 261 + 233 mg (range 22-764 rag). The mean fetal to maternal ratio, (unbilical vein concentration/mate~ vein concentration) for 25 patients was I. 17 _+ 0.48. Both u~bilical artery and vein ritodrine levels were obtained in a subset of 13 patients. When the infusion of ritodrine was prolonged beyond six hours the Lm~bilical artery concentration was significantly higher than the ~r~bilical vein (19.0 _+ 6.3 versus 12.3 _+ 4.0 ng/ml (p<.02, paired t). Previous studies in pregnamt animals have suggested fetal ritod~ine levels are approximately 20% of maternal; the present study shows that in humans, the fetal level consistently approaches 100% or more of that of the concentration in maternal peripheral vein. In order to determine the rapidity of rito- drine disappearance in the maternal-fetal pair, the u~bilical and maternal vein concentrations at delivery were each correlated with the length of time the drug was discontinued p~ior to delivery (DDDI) (figure). ~qe concentration of ritodrine in the nmternal vein varied inversely with the DDDI (r=-.56; p<.01). A stepwise multilinear regression was used to examine the relative importance of the maternal ritodrine dose in the 24 hours prior to delivery (24 H PTD dose), and (DDDI) for predicting ~ilical vein ritodrine concentration. ~he (24 H PTD) dose and the (DDDI) are linearly related to cord vein ritodrine concentration (partial correlations of +.60 and -.51, respectively. When the (24 H PTD) dose and (DDDI) are combined the relationship improves, multiple R=.74 (p<.01); the n~iltiple R2 indicates that together these t~o variables can explain 55% of the variance in the uebilical vein ritodrine con-
centration. The results of the present study provide new knowledge regarding perinatal ritodrine phar- maeokinetics. First, the fetal level approaches 100% of m~ternal concentration and the drug may concen- trate in fetal tissue following prolonged infusions. Second, u~bilical vein levels of ritodrine are higher than those fouqd in studies of similar drugs. Third, the internal dose of drug and the (DDDI) are both importm~ dete~nminants of Lm~bilical vein drug concentration. Further studies correlating neo- natal morbidity_with .drug levels are indicated.
I I I I I i I I I I I I I I I I I
30

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas # 15 February, 1984
2:30 p.m. - February 3rd
GLYCOSYLATED HEMOGLOBIN AND PLAS~MA PROTEIN IN NEWBORNS OF NORMAL AND DIABETIC WOMEN. ~ohamed M. Elsweidy, MD", Hossam E. Fadel, MD and Edathara C. Abra- ham, MD", From< the Department of ~n-~ ~la-~-Biology and Department of Obstetrics and Gynecology, Maternal -Fetal Medicine Section, Medical College of Georgia, Augusta, GA 30912
A new affinity chromatographic technique allows one to measure the total glycosylated portion of plasma proteins (Glyco PR), and hemoglobin (Glyco Hb). The latter includes products of glycosylation of both the echain amino terminus as well as~-amnio groups of certain lysyl residues in both ~ and ~:hains that are normally not separated by the previously used method, i.e., cation exchange chromatography. All glyco-HbA can be quantitated even in the presence of HbF and various abnormal hemoglobins. Furthermore, in contrast with cation exchange chromatography, affinity chromatography will measure all glycosylated HbF components while excluding the acetylated component of HbFl~. Using this new technique we measured glyco Hb and glyco PR in maternal and cord blood of 20 normal (Group I), 20 class A diabetic (Group II), and 8 insulin-dependent diabetic (Group III) mothers. Maternal HbA~, was also measured using cation exchange chromatography. Maternal HbA~, and glycoPR levels were slightly but insignficantly higher in Group IIIithan in Group I mothers, indicating that adequate metabolic control was achieved. However, the mean maternal glyco Hb level in Group Ill mothers (8.9 + 0.9%) was significantly higher than in Group I mothers (7.0 + 0.6%), p = ~ 0.005. This indicates that this technique (affinity chromatography) is more sensitive in identifying patients with slightly increased mean levels of blood glucose. The difference in the mean maternal HbAl, glyco Hb, and glyco PR between Group II and Group I mothers were all insignificant indicating strict metabolic control in these patients. The cord blood glyco Hb and glyco PR in Group ii neonates (4.4 + 1.2% and 9.0 + 1.9% respective- ly) were not significantly different from those in Group-~ (4.7 + 0.7% and 15.~5 + 1.6% respectively). On the other hand in Group III neonate~ the cord bloo~F glyco Hb (6.2 + 0.7%) and glyco PR (13.4 + 3.7%) were significantly higher than in Group- I neonates, P = < 0.005. TI~is confirms our previous report that fetuses of insulin diabetic mothers are hyperglycemic in utero even when good metabolic control is achieved. This also supports the relation of fetal hyperglycemia to overgrowth of the fetus and may explain why there is still high incidence of LGA and macrosomic babies delivered of diabetic mothers in spite of good metabolic control.
I I I I I I I I I I I I I I I I I

I Society of Perinatai Obstetricians 1
Annual Meeting San Antonio, Texas 1
#16 February, 1984
2:45 p.m. o February 3rd
STUDY OF SILENT AMNIOTIC FLUID INFECTIONS AND EVALUATION OF THEIR RELATIONSHIP TO FAILURE OF TOCOLYSIS. Chaudhry Hameed, M.D.x*, Uma L. Verma, M.D. and Nergesh Tejani, M.D. Health Sciences Center, State University of New York at Stony Brook; Nassau County Medical Center, Department of Obstetrics and Gynecology, East Meadow N.Y.
We evaluated the relationship of silent amniotic fluid infections as a possible etiologic factor in preterm labor and as a cause of failure of tocolysis. Thirty- two patients with singleton pregnancies between 24-34 weeks’ gestation with un- complicated preterm labor and intact membranes were studied. After obtaining blood for routine work-up, C-reactive protein and a clean-catch specimen of urine for culture, all patients were tocolysed with Ritodrine substituted by magnesium sulfate where Ritodrine was contraindicated. Under sonographic control, trans- abdominal amniocentesis was performed 4-12 hours after initiation of tocolytic therapy. A cell count, gram stain, aerobic and anaerobic culture of amniotic fluid were done immediately. After delivery, cord blood was obtained for aerobic/ anaerobic cultures, and placentas were examined histopathologically. Neonatal mortality and maternal/neonatal morbidity was studied. Based on the outcome of tocolytic therapy, patients were divided into two groups. Failed tocolysis (F) was diagnosed if delivery occurred within seven days of initiation of tocolysis. Tocolysis was considered successful (S) if delivery occurred after seven days. Significant differences were found in the outcome of these two groups. (Table i)
Table i. F (6) S (26) "P" Value
Amniotic Fluid (a) Bacterial growth (b) WBC > 100/min.
Positive CRP (Maternal blood) Chorioamnionitis Neonatal Mortality Nursery Stay > 7 Days Mean Birth Weight in Grams + SD
*NS = Not Significant
3 1 < 0.025 5 1 < 0.0005 4 2 < 0.01 5 2 < 0.01 1 0 NS* 6 0 < 0.0005
1481 + 2846 + < 0.001 565 579
We conclude that silent amniotic fluid infection is an important cause of un- complicated preterm labor and is a major cause of failed tocolysis.
1 I I 1 I 1 1
1 ! I I I 1
i I
32
I

! !
I I I I I I ! I ! I I ! I I I I

POSTER SESSION A
3:30 - 5:30 p.m.
Friday, February 3, 1984
Rio Grande Ballroom
I I ! I I I I I I I i I I ! I I I I I

#29
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
~ARADOXICAL HEART RATE RESPONSE TO THE VALSALVAMANEUVER IN PREECLAMPSIA Micki L. Cabaniss, M.D., C. Daniel Cabaniss*, M.D. and Patricia C. Wagner*, R.N.C. Department of Obstetrics and Gynecology (Division of Maternal/Fetal Medicine) and Department of Internal Medicine (Division of Cardiology), University of South
Alabama, Mobile, Alabama.
The Valsalva maneuver is a simple, measurable and reproducible test for investi- gating cardiac autonomic reflexes. It has been used to demonstrate autonomic dys- function in a variety of conditions including mitral valve prolapse, diabetes and congestive heart failure. Previous study by the principal investigators explored the heart rate response to the Valsalva maneuver in 282 pregnant subjects. The study provided experience that the recorded beat-to-beat pattern of the heart rate response in normal pregnant patients was usually similar in configuration to that o5 nonpregnant controls, although the Valsalva ratio declined with advancing pregnancy through 29-32 weeks. Because hypertensive disorders in pregnancy may be expected to alter pressure and volume sensitive cardiac reflexes, study of heart rate response
to the Valsalva maneuver was next undertaken in this group of patients. Methodology The Valsalva maneuver is performed as a sustained expiration against a fixed re- sistance followed by an abrupt release. A standard fetal monitor is utilized for studying the rapidly changing heart rate. Fifty-three patients with hypertensive disorders associated with pregnancy have been included thus far in an ongoing study Results: The recordings of heart rate response to a Valsalva maneuver in hyper- tensive pregnant patients fall into 3 categories: i. those with a rising heart rate of normal configuration, usually followed by a period of bradycardia upon re- lease of the Valsalva, 2. those with a rising heart rate but abnormal in config- uration and 3. those with a paradoxical fall in heart rate, followed by a rise upon release of the Valsalva. The paradoxical heart rate response was seen almost ex- clusively in patients with a diagnosis of preeclampsia. In contrast, patients with a heart rate change of normal configuration were predominantly chronically hyper- tensive without superimposed preeclampsia. The group of patterns consisting of a rise in heart rate, but abnormal in its configuration, was comprised of patients with mild preeclampsia, some with chronic hypertension, and chronic hypertensive )atients in whom the presence of superimposed preeclampsia was inconclusive. Con- :lusion: The finding of a paradoxical heart rate response to the Valsalva maneuver in some patients with preeclampsia provides opportunity for further exploration of the role of the autonomic nervous system in this disorder.
[. normal ~onfiguration
abnormal onfiguration
3. paradoxical response S - Strain R Release
--i
I I
I I I
I I I i
I I I
I !
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#30 February, 1984
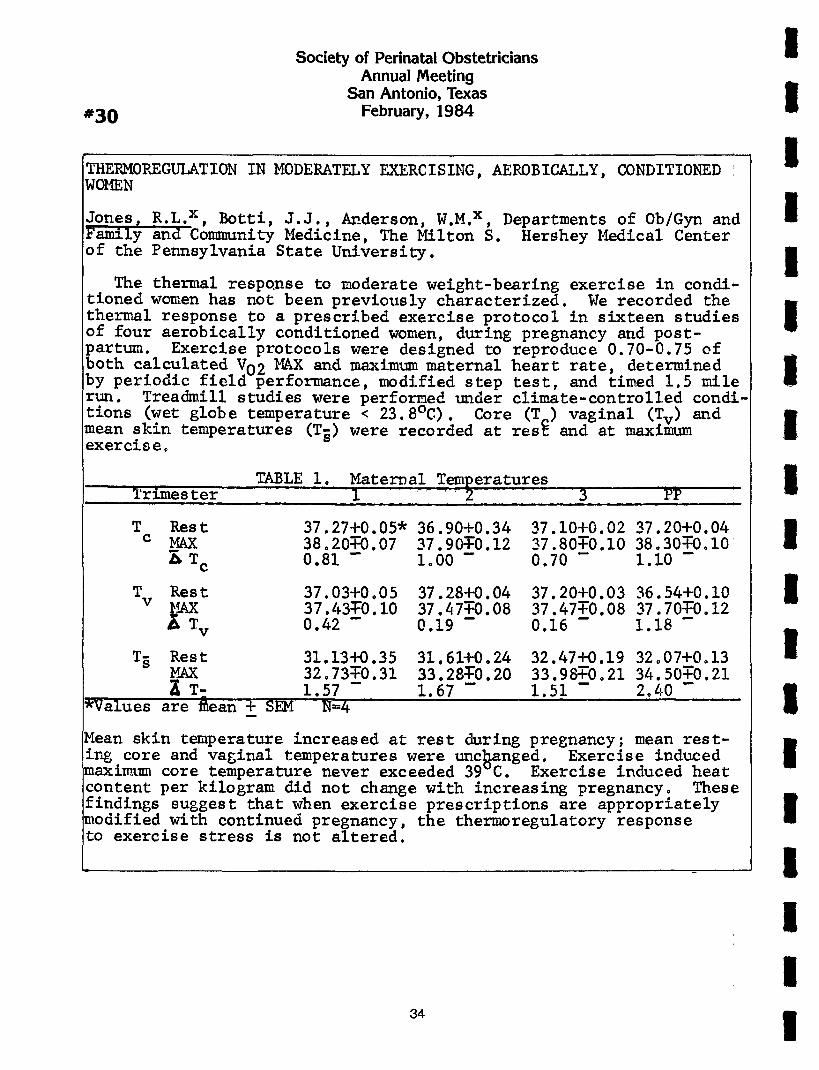
THERMOREGULATION IN MODERATELY EXERCISING, AEROBICALLY, CONDITIONED WOMEN
Jones~ R.L.x, Botti, J.J., Anderson, W.M.x Departments of Ob/Gyn and Family ~nd Community Medicine, The Milton ~. Hershey Medical Center of the Pennsylvania State University.
The thermal respo~nse to moderate weight-bearing exercise in condi- tioned women has not been previously characterized. We recorded the thermal response to a prescribed exercise protocol in sixteen studies of four aerobically conditioned women, during pregnancy and post- partum. Exercise protocols were designed to reproduce 0.70-0.75 of both c.alc.u.lated V.O2 MAX and maximum maternal heart rate, determined by perlodlc field performance, modified step test, and timed 1.5 mile run. Treadmill studies were performed under climate-controlled condi- tions (wet globe temperat.ure < 23.8°C). Core (To) vaginal (T~v) and mean skin temperatures (Ts) were recorded at res~ and at maximum exercise o
TABLE I. MaterDal Temperatures Trimes ter I .... 3 PP
T Rest c MAX
37.27+0.05* 36.90+0.34 38.20~0.07 37.90~0.12 0.81 -- io00 --
37.10+0.02 37.20+0.04 37.80;0.I0 38 o30~0oI0 0.70 - 1.10 --
T Rest 37.03+0.05 37.28+0.04 v ~AX 37.43;0.I0 37.47~0.08 ~ Tv 0.42 - 0.19 -
37.20+0.03 36.54+0. I0 37.47;0.08 37.70~0o 12 0.16 - 1.18 -
T§ Rest 31.13+0.35 31.61+0.24 MAX 32.73~0.31 53.28~0.20 ~ T- 1.57 - 1.67 -
*Values are ~ean + SEM N=4
32.47+0.19 32o07+0o13 33.98/0.21 34.50~0.21 1.51 - 2.40 -
Mean skin temperature increased at rest during pregnancy; mean rest- ing core and vaginal temperatures were unchanged. Exercise induced maximum core temperature never exceeded 39~C. Exercise induced heat content per kilogram did not change with increasing pregnancy° These findings suggest that when exercise prescriptions are appropriately modified with continued pregnancy, the thermoregulatory response to exercise stress is not altered.
I I I ! i I I I i I i I ! I I
34
I I

#31
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
PROSPECTIVE ASSESSMENT OF A DYNAMIC AEROBIC EXERCISE PROTOCOL FOR PREGNANCY.
Botti~. J.J., Jones, R.L.x, Anderson, .W.M.X, Departments of Ob/GyrL and Family and Community Medicine, The Milton S. Hershey Medical Center of the Pennsylvania State University, Hershey, PA 17033.
Previous studies of maternal exercise response have not taken maternal conditioning or exercise environments into account. The con clusions of ~eny of these acute studies are that exercise stress during pregnancy evokes abnormal cardiopulmonary responses. We con-. ducted sixteen studies of four aerobically conditioned women to evaluate individual response to continued weight-bearing exercise during pregnancy. Exercise protocols were designed to approach daily individual oxygen consumption and maximum heart rate in the field, derived from patients logs, observation, modified step test, and timed 1.5 mile run. Maz.imum laboratory exercise stress was set at 0.70-0.75 calculated V02 MAX and 0.75 maternal heart rate MAX. Pre- study maximum limits were set for core temperature (Tc), maternal heart rate (HR), respiratory quotient, (RQ), multiples of resting oxygen consumption, and EKG changes. Fetal response to maternal exercise was recorded by ultrasonographic and electronic heart rate monitoring methods° Laboratory exercise was modified once in sixteen studies because of transient EKG changes and maternal heart rate exceeding the predetermined target rate in a first trimester study. Daily exercise activity did not change in any patient during the first two trimesters but gradually diminished by 20-30% in the third trimester. Individual changes were variable. Laboratory documenta- tion of ~mternal exercise response of ten appropriate modification of thee exercise prescription showed similar maximum levels of Tc (< 39vC), HR (158 + 6/rain), P,Q (0.94 + 0°06) and multiples of resting V~2 (7.9 + 1.4) ~xercise induced change in oxygen pulse (.Vo~/Hr.) decreased-from ~.9 + 0.6 ml in the first trimester to 6.4 ml in the third trimester, indicating an increased cardiovascular cost of exercise stress with increasing pregnancy° The recorded fetal bio- physical profile was not altered by maternal exercise stress. These findings suggest that moderate exercise stress is associated with normal maternal and fetal physiologic responses during much of preg- nancy but, because of individual variation in exercise response and gradually diminished exercise tolerance in late pregnancy, periodic re-evaluation and modified exercise prescriptions may be necessary for maternal and fetal health.
I
I I I i I I I I I I ! I i I ! I !

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#32 February, 1984
PLACENTAL MICROBIOLOGY: CORRELATION WITH PLACENTAL HISTOLOGY
AND CLINICAL COURSE
Robert P. Lorenz, M.D., Glen A. Pankucho B.S.X, Peter C. Applebaum, M.D. Ph.D.X, Jonn J. Botti, ~i.6., Julius Schachter, Ph.D.x*, and Richard Naeye, M.D.X’
Department of Obstetrics and Gynecology and Department of Pathology, The Milton S. Hershey Medical Center, The Pennsylvania State University, Hershey, Pennsylvania 17033 and *Department of Laboratory Medicine, San Francisco General Hospital, University of California, San Francisco, San Francisco, California
Seventy-seven placentas from 70 patients with normal and abnormal pregnancies were examined to compare microbiologic findings with placental histology and clinical factors. Placentas were processed to optomize yields of aerobic and anaerobic bacteria, and to avoid vaginal contamination. Placental cultures yielded growth in 37.5% and placental histology demonstrated infection in 39% of cases not associated with antibiotic use (n = 64). Culture results and hist- ology were strongly correlated (p ~ .005). Anaerobes/microaerophils were found in 61% of placentas with growth. Cultures and serology for Chlamydia tracho- matis were uniformly negative. Cultures for genital mycoplasmas were negative, Positive cultures were not related to gestational age, length of labor, mode of delivery, but were related to interval from rupture of membranes to delivery. Findings from ten patients with clinical chorioamnionitis supported the asso- ciation between histologic chorioamnionitis, placental microbiology, and clinical infection. However, many placentas showed histologic chorioamnionitis and positive cultures without clinical signs of infection in the mother or infant. Six of the nine perinatal deaths had positive placental cultures; five of these had clinical chorioamnionitis. This study clearly establishes a posi- tive correlation between placental microbiologic findings and histologic evi- dence of chorioamnionitis, but impact on clinical decision-making is limited. Further studies may verify our impression that patterns of infection vary be- tween the preterm labor and normal patient.
I I I
! !

#33
Society of Perinatai Obstetricians Annual/Vleeting
San Antonio, Texas February, 1984
PURIFICATION AND COMPARISON OF LAMELLAR BODIES FROM MATURE AND FETAL RABBIT LUNG
LAVAGE. ~alph L. Cavalieri, M.D., Ph.D.* and Sonja Woodling.* The Johns Hopkins University School of Medicine, Johns Hopkins Hospital, Baltimore, Maryland 21205.
Deficiency of pulmonary surfactant is a major cause of respiratory distress syndrome in the neonate. Lamellar bodies are believed to be a Form of pulmonary surfactant which is secreted by Type IT alveoIar pneumocytes. In anticipation of studying the ontogeny of lamellar bodies we have developed a method For the purification of these structures. Mature New Zealand white rabbits were sacri- ficed and the lungs lavaged with Tris buffer. The fluid was centrifuged at I00 x g to remove cellular debris and the supernatant was applied to a molecular sieve column made from 5ephacryl 5-300. Foliowing chromatography, diphenylhexa- triene (DPH), a hydrophobic Fluorescent probe, was added to each elution Fraction and the Fluorescence at 435 nm measured with excitation at 357 rim. One peak of Fluorescence activity (peak I) was identified which had an anisotropy (~) of 0.194±0.007 (mean ±S.D.) which is consistent with DPH located in a lipid bilayer. Peak I and some of the original supernatant From the I00 x g centri- Fugation were centrifuged separateiy at 15,000 x g. Electron microscopy revealed that each pellet contained lamellar bodies. Sucrose gradient (5%-20%) centrifug- ation of both pellets showed a single peak at the same mid position in the gradient indicating a similar density. The protein to phospholipid ratio of peak I was determined to be 0.7. Fetal rabbits of 25 days gestation were aIso sacrificed, the Iungs iavaged, and the fluid studied. The ratio of the concen- tration of lecithin to sphingomyelin was 2.8±0.9. In contrast to the adult lavage, purification of the fetal lavage Fluid by SephacryI chromatography resulted in two peaks of Fluorescence activity. Peak I From the adult and Fetal rabbit was in the same fractions. The ~ of peak I From Fetal rabbit was always higher than peak I From adult rabbit indicating that the bilayer core of the Fetal lamelIar bodies is less fluid. Furthermore, the ~ of peak I was always lower than For peak II, which is consistent with the hypothesis that peak I contains structures which are more mature than in peak II. The structures in peak I ave apparently larger than those in peak IT because peak I elutes First from the molecular sieve column, peak I scatters Iight and peak II does not, and the structures in peak I but not peak IT could be peiIeted and visualized easily with electron microscopy. Peak I may represent mature surgactant, and peak II a precursor in the developing Fetus.
I
I I I I I I i I I I I ! ! I
37

I Society of Perinatai Obstetricians i
Annual Meeting San Antonio, Texas 1
#34 February, 1984
EVALUATION OF THE USE OF CONTINUOUS LUMBAR EPIDURAL ANESTHESIA FOR HYPERTENSIVE GRAVIDAS IN LABOR. T.R. Moore*, T.C. Key, and R. Resnik. Department of Reproductive Medicine, University of California, San Diego School of Medicine, San Diego, California.
The safety of continuous lumbar epidural (CLE) anesthesia for laboring women wi~h pregnancy-induced hypertension (PIH) remains a controversial issue.
Accordingly, we retrospectively reviewed the hospital charts of all women with a diagnosis of pregnancy-induced hypertension delivered at UCSD Medical Center from January, 1980 through December, 1982. Of the 285 women with this diagnosis, 185 (65%) were delivered vaginally and 100 (33%) required cesarean delivery. Comparing the type of anesthetic utilized (CLE vs. local/none) in vaginally and abdominally-delivered women, numerous maternal and fetal/neonatal outcome characteristics were evaluated, including the pertinent observations in the following table:
Vaginally-Delivered Patients
CLE (n=l16) Local/None (n=69)
Highest BP during labor*
Lowest BP during labor*
Abnormal FHR tracings
5-Minute Apgar score*
Umbilical artery pH*
Ist stage of labor (hrs)*
2nd stage of labor (hrs)*
155±18/97±13 156!13/i00!9 NS
154118/79112 125±15/78±12 NS
7 5 NS
8.6!0.6 8.710.6 NS
7.281.06 7.28±.11 NS
13.7!7.9 9.215.1 p= <.001
1.56!I.19 .79!.69 p= <.001 *~ +SD
Of those patients undergoing cesarean delivery, 85 received CLE anesthesia, and 15 had general anesthetics with a pentothal, nitrous oxide, succinylcholine
technique. The latter group experienced significantly higher mean systolic and diastolic pressures, lower 5-minute Apgar scores and umbilical artery pH. However, the incidence of severe PIH and fetal distress prior to delivery was greater among those receiving a general anesthetic. These data demonstrate that CLE anesthesia is safe for the mother and fetus in the presence of PIH, for both vaginal and abdominal deliveries.
I I I I I I I I I I ! I I !
38

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #35 February, 1984
COMPARATIVE STUDY OF PROSTAGLANDIN El, LAMINARIA, AND MINIDOSE OXYTOCIN FOR RIPENING THE UNFAVORABLE CERVIX PRIOR TO INDUCTION OF LABOR. W.E. Roberts* J.E Speedx, J.B. Harrisx, J.C. Morrison, Division of Maternal-Fetal Medicine Department of Obstetrics/Gynecology, Univ. of Miss. Med. Cntr., Jackson Mississippi.
Induction of labor in the high risk parturient forms an integral part of moder~ obstetrics. When the cervix is unfavorable, attempts at induction of labor by oxy- tocin and/or amniotomy are associated with long labor and its sequellae of infec- tious morbidity, midforcep delivery and cesarean birth. A prospective, randomized study comparing prostaglandin El, minidose oxytocin, and laminaria as cervical ripening agents versus untreated patients was performed. Although there was a trend toward a shortened labor, improvement in the Bishop Score, and the ability to achieve successful induction for all the cervical ripening agents studied, sta- tistical significance was not achieved. This most likely was due to the small num- bers in each study group. Since the trend was identical in the three cervical ripening groups, a log likelihood heterogenity test was performed and allowed for pooling of the cervical ripening groups. With the larger numbers in the combined group, statistical significance was obtained in the ability of the agents to suc- cessfully induce a patient (P<.O01) and in its ability to promote a change in the Bishop Score (P<.05). Although there was no statistical significant difference in the incidence of cesaran delivery in the cervical ripening group versus control, there were 5 out of 14 patients in the control group whose induction of labor was unsuccessful. If, instead of a return visit and a repeat attempt at induction in one week as was the plan per protocol, cesarean section had been performed after the failed induction then the incidence of decrease of cesarean section in the cer- vical ripening group would have been significantly lower than that in the control group (P<.05). There was no untoward maternal and/or fetal effects from any of the cervical ripening agents studied.
39
I I

I Society of Perinatal Obstetricians 1
Annual/Vieeting San Antonio, Texas 1
#36 February, 1984
ANTEPARTUM EXTERNAL CEPHALIC VERSION UNDER TOCOLYSIS: REPORT OF 154 PATIENTS WITH AN ANALYSIS OF FACTORS DETERMINING SUCCESS J E. Ferguson II M.D *, Donald C. Dyson, M.D. , Candace W. Weinstein, D.O.x, Paul A. Hensleigh, M.D., Ph.D., Department of Gynecology and Obstetrics, Stanford University School of Medicine and Santa Clara Valley Medical Center, and the Department of Obstetrics and Gynecology, Kaiser Hospital, Santa Clara, California.
Antepartum external cephalic version with tocolysis (A-ECV-T) has been reported to be successful in reducing breech presentation at confinement and reducing the rate of cesarean sections. To date the issues of safety, efficacy and applica- bility surrounding the use of this procedure remain unresolved. Further, there has been no analysis of maternal or fetal factors that could effect success. This report describes our A-ECV-T protocol experience in 154 selected patients con- sidered for version at gestational ages > 37 weeks. Two patients declined and lO were excluded for a variety of maternal ~r fetal indications. One-hundred forty-two patients underwent attempted version and success was achieved in I09 (77%). In no successful version did the vertex revert to breech; conversely in no failed version did the breech spontaneously convert to a vertex. In the suc- cessful version group (N=109), 96 patients experienced vaginal delivery (cesarean section rate 12%). Indications for the 13 cesarean sections were CPD (lO instances), failed induction for PIH (l instance) and two episodes of fetal distress. In the 33 patients with failed versions, vaginal delivery of the breech occurred in only 3 patients (cesarean section rate 91%). Analysis of maternal factors likely to influence success revealed that versions were successful in "functional" primaparas in 47/76 (62%) versus 62/66 (94%) in "multiparas." The type of breech appeared to be important as well. Only 59/90 frank breeches (66%) were successfully verted, whereas, success was achieved in 44/46 (96%) and 6/6 (I00%) of complete and footling breeches, respectively. Placentation appeared to be important as well; however, the influence of gestational age is uncertain. There were no perinataI deaths. Eight episodes of intraversion bradycardia occurred (decreased FHR to IO0 beats per minute for greater than 60 seconds) and none required immediate delivery. One patient with bradycardia was induced 24 hours later due to variab}e decelerations on a post-version NST. She required a cesarean section for severe variables during induction and delivered an Apgar 6/9 outborn infant. In summary, it appears in selected patients A-ECV-T can safely and successfully reduce the incidence of breech presentation and cesarean sections when performed within strict protocol guidelines by experienced individ- uals. Further, there appear to be important maternal and fetal factors that influence ultimate success; these will be discussed in-more detail.
I I ! I I I I I I I ! I I I I
4O
I I

I Society of Perinatai Obstetricians -- Annual Meeting
I San Antonio, Texas
#37 February, 1984
I ~NTEPARTUM SINUSOIDAL FETAL HEART RATE PATTERNS Kenneth C. Manfre, MDXand Albert M. Haverkamp, ~ID*
Denver General Hospital~ Denver Colorado
The prevention of antepartum fetal demise remains a vexln~ perinatal problem. A number of unexplained stillbirths may be due to undlagnosed fetal maternal bleeding. Two cases are presented in which the diagnosis of fetal-maternal bleeding was aided by the recognition of a sinusoidal fetal heart rate pattern, and in which the amount of bleeding was ~uantified by the use of the Kleihauer-Betke test on the maternal blood. Emergency cesarean section resulted in the delivery of two profoundly ianemic (Hct.< 15) infants, both of whom survived and did well. A plan for the evaluation of antepartum slnusoidal fetal heart rate patterns, using the Kleihauer-Betke test to establish the presence, and to eval- uate the amount, of fetal-maternal bleeding is presented. The s~gnlf- icance of s~nusoidal heart rate patterns is discussed, as are the rea- sons for the lack of other ominous findln~s on antepartum feta! heart rate tracings despite the presence of profound fetal anemia.
I I I I I I I I I I I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
VARIABLE DEGREE OF HEMOLYTIC DISEASE IN RHESUS SENSITIZED TWIN GESTATION: DINESH M. SHAH, M.D., VANDERBILT UNIVERSITY SCHOOL OF MEDICINE, NASHVILLE, TENNESSEE, ROBERT A. KNUPPEL, M.D., M.P.H., UNIVERSITY OF SOUTH FLORIDA COLLEGE OF MEDICINE, TAMPA, FLORIDA.
The incidence of Rh-sensitized twin gestation is extremely low. There are several perinatal risks inherent to twinning and erythroblastosis further increases .the hazards of such a compromised gestation. We recently reported three cases of Rhesus isoimmunization in twin gestations. It is generally accept- ed that the fetuses of a twin gestation may be affected to a different degree with hemolytic disease. We have retrospectively analysed the cord hemoglobin and bilirubin data of appropriately selected twin pairs from published reports to evaluate the intra-pair difference in the severity of hemolytic disease. Data about the number of exchange transfusions in these pairs and factors responsible for occurrence of hydrops fetalis in one of the twin amongst remaining twin pairs have been examined. Based on these, we conclude that there are no factors unique to_twin gestation other than expected sibling differences that explain a disparity in degree of hemolytic disease within a twin pair.
I I I I I I I I I I I I I I
42

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#39 February, 1984
ASSOCIATION OF INTRAPARTUM FACTORS AND INTRAVENTRICULAR HEMORRHAGE (IVH) IN VERY LOW BIRTH WEIGHT (VLBW) INFANTS: PRELIMINARY REPORT
.Kirz*,A.Strauss,H.Modanlou,and R.Freeman. Division of Perinatal Medicine, iMiller Children’s and Women’s Hospital, Long Beach, University of California Irvine
112 neonates (BW<I5OOg) with fetal heart rate (FHR) monitoring were prospectivel~ studied for intrapartum factors in relation to the development of IVH documented by" real-time ultrasonography. Ultrasound of the head was performed at a mean + ISD a~ of 27.3 + 17.1 hours. Of the 112 infants, 27 (24%) had IVH at the initial study (20 Grad~ I, 2 Grade II, 2 Grade III and 3 Grade IV). Mean BW for the non-IVH group was 1087 + 268 vs. 1029 + 276g for those with IVH. Male sex accounted for 48% of the non-TVH and 63% of t-he IVH group (NS). Umbilical cord pH was performed
n 81 neonates; 5 (9%) of the non-IVH and 3 (14%) of the IVH group had a pH <7.20 NS). The incidence of uncorrected fetal distress was 12% in the non-IVH and 22% ~f the IVH group (NS). All five of the neonates with major IVH (Grades III and IV)
had abnormal FHR patterns. Of six vaginal breech deliveries, there was only one with IVH (Grade I). The incidence of PROM was 40% in non-IVH vs. 63% in IVH group with increased incidence of amnionitis in the latter group (II.I vs. 4.7%), (NS). Fetal presentation, duration of labor, type of delivery and incidence of RDS were similar in the two groups. Volume expansion was required by 34% of the non-IVH and 52% of the IVH group (NS). Due to insufficient number of neonates with major IVH, no definite conclusion can be made, but the data suggest that the IVH group may have been compromised during the intrapartum period, as manifested by increased incidence of abnormal RHT pattern and acidosis at birth. Early correction/intervention of fetal distress in VLBW infants may lessen the incidence of major IVH.
I I I I I I I I I I I I I I
43

#40
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
COMPARISON OF CONCURRENT VS NONCONCURRENT ULTRASOUND USE IN GENETIC AMNIOCENTE- SIS, John V. Dacus, M.D., Robert S. Wilroy, M.D.x, George S. Flinn, M.D.x, et al, Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
The first 2000 patients undergoing genetic amniocentesis at our institution were analyzed for the incidence of abnormal findings, the safety, and the accu- racy of the procedure. Most of the diagnostic amniocentesis procedures were per- formed by members of the full-time university faculty ("staff cases"). A de- creasing number of procedures has been performed by physicians in other facili- ties. For comparative purposes, this group will subsequent|y be referred to as "other or non-staff cases." The further subdivision of cases into the recent and previous experience categories was based on procedural changes instituted in January of 1980. At that time, the non-staff physicians began to routinely per- form real-time ultrasonography immediately prior to each diagnostic amniocentesis but not concurrently. Also early in 1980, two significant changes were made in the procedure for staff cases. First, we began using concurrent, real-time scan- ning during all amniocenteses. Second, we developed a special amniocentesis team consisting of an ultrasonographer and one faculty member, both of whom have spe- cial expertise in this procedure. The following table summarizes the experience in amniocentesis during the two time periods. During the latter part of our ex- perience, a reduction in blood tinged specimens from 15.0% to 5.2% was noted. One percent of the patients were found to have aneuploid fetuses and another one per cent were found to have elevated amniotic fluid concentrations of alpha-feto- protein. Advanced maternal age was the indication for amniocentesis in 84% of the women with aneuploid fetuses. Thirty-two (1.6%) of the pregnancies ended in spontaneous abortion and thirty-five (1.7%) were terminated due to abnormal re- ~sults of the prenatal diagnostic procedure. Our error rate was 0.15% and tissue iculture was successful in 97.7% of the procedures. In experienced hands, midtri- mester amniocentesis for the purpose of prenatal diagnosis of genetically deter- mined defects is a safe, accurate, and valuaO~e procedure for the ~dentificat~on of fetal abnormalities.
# of # Blood Stained Successful Cases Amniotic Fluid (%) Amniocenteses (%)* Time Period
Before 1980 Staff 487 74 (15.0) 447 (91.7) Unknown 29 5 (17.2) - Others 379 59 (15.5) 329 (86.8) Total s 895 138 776
1980-June 1982 Staff 923 48 (5.2) 847 (92.2) Others 195 22 (Ii.3) 156 (80.0) Tota I s I 118 70 1003
* On first insertion
I I I I I I I I I I I I I I I I

#41
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
EFFICACY AND SAFETY OF THE CONTRACTION STRESS TEST BY NIPPLE STIMULATION. S.M. Palmer, C.P. Poole, M.K. Sieh, J. Ewing, M. Moreland, J.C. Morrison, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Mississippi Medical Center, Jackson, Mississippi
Freeman et al in 1977 reported a collaborative study comparing the sensitivity and specificity of the non-stress test with the contraction stress test and showed a significant improvement in antenatal surveillance when both tests are combined. However, many centers are unable to provide the increase in nursing personnel, fetal monitors or individual patient cost that implementation of the normal perfor- mance of combined tests would necessitate. Between 1/1/82 - 10/31/82, 638 non- stress test were performed in our ambulatory unit with one fetal monitor utilizing one nurse. Utilizing the Huddleston technique of nipple stimulation, which does not require the patient to disrobe, we were able to significantly increase the num- ber of contraction tests performed in the same area with the identical monitor and nursing coverage without significantly reducing the number of tests. From 12/1/82- 9/30/83 we performed 646 non-stress tests, 320 nipple stimulations, 115 spontaneous and nipple stimulation augmented tests, and 17 oxytocin challenge test. The patien acceptance was 98%. This high acceptance, we feel, was a combination of nursing attitude, patient remaining clothed and fear of needles. There were no cases of hyperstimulation or other complications and only I0 failures with nipple stimula- tion requiring pitocin induced testing were noted. The average time necessary to obtain contractions with nipple stimulation was 8.4 min. + i.i (n=88). Spontaneous contractions with nipple stimulation augmentation to increase the frequency to ob- tain 3 contractions in i0 minutes was 34.8 + 2.2 min. (n=88) versus 37.5 + 1.3 min. (n=154) for the nonstress test alone. These are not statistically different. The time of the NST-nipple stimulation, (without spontaneous contractions) was 65 ! 1.5 min. (n=270) with a distinct trend to a decreasing duration of time with increased familiarity of the test in the unit. The time required for a classic OCT in 1982 was 99 + 36 min. (n=46) and is obtained at a cost for supplies only of $24.50; a cost oviated by our current protocol. In utilizing the nipple stimulation versus the OCT we have significantly decreased nursing time by 30 minutes (p<.01) and on an average of 5 tests per pregnancy, saved the patient $122.50 in supply cost for the testing. This does not place a value on the patients relief from not having venapuncture. In conclusion, we feel that we were able to improve the antenatal fetal surveillance testing program at our institution by the addition of the Hud- dleston technique of nipple stimulation for endogenous oxytocin release. We were safely able to augment or induce a uterine contraction pattern sufficient for per- ~ormance of a contraction stress test. This was accepted well by our patient popu- lation and decreased the nursing/patient time involvement necessary in starting intravenous solutions and increased the efficiency/cost effectiveness of the antenatal testing center.
I I I I I I I I I I I I I I I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#42 February, 1984
"CRITICAL ANALYSIS OF SONOGRAPHIC EVALUATION OF ECTOPIC PREGNANCY".
Stephen S. Kasparian: M.D.X, O’dell M. Owens, M.D.x, Menachem Miodovnik, M.D.X, Tariq A. Siddiqi, M.D.X, Harold B. Spitz, M.D.X, Departments of Obstetrics and Gynecology and Radiology, University of Cincinnati Medical Center, Cincinnati, Ohio 45267.
In clinically stable patients suspected of having an eetopie pregnancy, ultrasound examination of the pelvis has been widely advocated as a very useful diagnostic procedure. In practice however, ultrasonography has been helpful only in excluding the diagnosis of ectopic pregnancy by identifying an intrauterine pregnancy, since the co-existence of an ectopic pregnancy and an intrauterine pregnancy is very rare (l in 30,000). The sonographic diagnosis of ectopic pregnancy involves examination of the uterus (size and contents), adnexal structures, and the cul-de-sac (presence of free fluid). The present study was designed to evaluate the efficacy of ultrasound examination in the diagnosis of ectopic pregnancy. It was hoped that criteria could be developed for a directed and rigidly adhered to protocol which would increase the accuracy of diagnosis in these patients. The medical records of 298 patients admitted to the Gynecology Service of the University of Cincinnati Medical Center from 11-8-78 to 1-28-83 with the diagnosis of "rule-out ectopic pregnancy" were reviewed. In tabulating the data, the patients were divided into two major groups: those who had pelvic sonograms (I09), and those who were transferred directly to the operating room without pelvic sonograms (189). The original sonographic images were re- examined by one of the authors (H.B.S.) who was blinded to the actual diagnosis, using a rigidly adhered to protocol. One half (50%) of all patients admitted with a diagnosis of ectopic pregnancy actually had the diagnosis. It is interesting that 58% of the patients who were transferred directly to the operating room had ectopic pregnancies, while only 35% of the more stable patients who underwent sonographic evaluation had ectopic pregnancies. Comparison between the ultrasound diagnosis and the final discharge diagnosis showed a true positive diagnosis of 46% and a true negative diagnosis of 76%. This would seem to indicate that a negative diagnosis of ectopic pregnancy carries more significance than a positive diagnosis. No significant difference was found in uterine dimensions obtained from sonographic images of patients with and without ectopic pregnancies. Sixty-three percent of patients having an adnexal mass on ultrasound did not have ectopic pregnancies, while greater than 70% of patients with no adnexal mass did not have an ectopic pregnancy. Only 50% of patients found to have fluid in the cul-de-sac had ectopie pregnancies, while 75% of patients lacking fluid did not have ectopic pregnancies. Of those patients with fluid, 39% had unruptured ectopic pregnancies, while 79% of the ectopie pregnancies demonstrating fluid were unruptured. No significant increase in the diagnosis of ectopic pregnancy was found by adhering to a rigid protocol. Traditional sonographic criteria of uterine enlargement, pelvic mass, and presence of fluid in the cul-de-sac were not significant. Many of these criteria were more helpful in eliminating the diagnosis of ectopic pregnancy than in confirming the diagnosis. Our findings indicate that the use of ultrasound may hinder more than aid the physician in reaching the clinical diagnosis of ectopic pregnancy. In fact, significant sonographie findings may have no correlation with the pathologic diagnosis. Our study demonstrates that in the vast majority of patients, the clinician is best guided by the clinical signs and symptoms.
I I I I I I I I I I I I I I
46
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#43 February, 1984
IMPROVED FUEL OXIDATION IN INSULIN DEPENDENT DIABETICS DURING PREGNANCY WITH INSULIN THERAPY
Paul yon Oeyen, MD*, Milton Foss, MD, Fredricka Vlachokosta, MD, Donna Younger, MD John Kitzmiller, MD, Thomas Aoki, MD, Depts. of Ob-Gyn and Med., Brigham and Women’s Hospital and the Joslin Diabetes Center, Boston, MA
Normalization of glucose processing and not merely normalization of intermitten glucose measurements may be essential to the reduction of risks during diabetic pregnancy. Indirect calorimetry with determination of carbohydrate oxidation rate (CHO OX) was used in conjunction with blood sampling to assess competence of glucose processing in the fasting state and after a 50 gm oral glucose challenge in early pregnancy (I0 - 13 weeks) in 8 insulin dependent diabetic women on insulin pump therapy (IP), 9 comparable diabetic gravidas on intensive conventional insulin treatment (IC) and a control group of 7 normal pregnant (NOR) women. Values at 60’ for results are expressed below for the three groups (data mean + SEM) o --
CHO OX GLUCOSE GLUCOSE GLUCOSE (mg/m2/min) (mg/dl) OXIDIZED (g/2 hrs) STORED (g/2 hrs)
IP 65.4+6.6 147+12 11.2+0.9 29.1+2.1 IC 41.3+5.8 226+18 7.6+0.7 20.6+4.5 NOR 77.0+11.4 111+5 12.3+1.3 35.9+1.5
All groups had comparable baseline (fasting) values for CHO OX and total metabolic rate. The rise in CHO OX of the IP patients was similar to, but slightly less than that of the NOR control group. In contrast, the IC group had significantly lower CHO OX rates at 60’ when compared with normal pregnancy (p=.0044) or the IP group (p=.0361). Glucose processing calculations revealed that the IP patients oxidized more glucose (ii.2~0.9 g) than the IC patients (7.6+0.7 g; p=.0218) and stored more glucose in liver or muscle (29.1+2.1 g vs. 20.6+4.5 g; p=.0458). These findings indicate an improved capacity to oxidize and store glucose fuel in IP first trimester gravidas compared to women on IC therapy. Indirect calorimetry is a powerful tool in assessing competence of glucose processing in insulin dependent gravidas.
Presently at Baystate Medical Center in Springfield, Massachusetts
I ! I I I I I i
I I i
I I I i
47
! i

I Society of Perinatal Obstetricians Annual/Vleeting
San Antonio, Texas i February, 1984
DECELERATIONS IN NONSTRESS TEST Chang Y. Lee, M.D.,* Ann Conway-Harkins, R.N.C. Henry Ford Hospital, Detroit, Michigan
x
To determine the clinical significance of decelerations in NSTs, the authors correlated the different degrees and patterns of decelerations in both reactive and nonreactive NSTs with fetal outcome. The fetal outcome was measured by the incidence of FHR distress in labor, signs of IUGR, low 5 minute Apgar scores and perinatal mortality. Abnormal cord position at delivery and incidence of severe oligohydramnios were also evaluated. The study includes 119 NSTs obtained from ninety-seven patients. These were selected from 4,600 NSTs performed during a seven and a half year period from January i, 1976 to June 31, 1982. Eighty-five tests were reactive and thirty-five tests were nonreactive. Four or more vari- able decelerations of a mild degree were recorded in twenty minute periods in sixty-one reactive NSTs (43 patients). In this group, intrapartum complications and perinatal outcome were not significantly different from the control group. Moderate degree of variable decelerations were recorded in 19 reactive NSTs (16 patients). In this group, there were high incidences of severe variable decelerations (54.5%) in labor and abnormal cord positions (43.8%). Late decel- erations were recorded in five reactive NSTs (5 patients). In four cases, the recording appeared to be due to Poseiro effect. In one post date pregnancy, the baseline FHR was nonreactive with recording of persistant late decelerations in labor. A mild degree of variable decelerations were recorded in seven nonreactive NSTs. Repeated NSTs were reactive in all tests. A moderate degree of stressed (reassuring) pattern of variable decelerations were recorded in five nonreactive NSTs (4 patients). Severe oligohydramnios was~ found in three and abnormal cord position in one patient. All four fetuses revealed signs of IUGR. Distressed (nonreassuring) pattern of variable decelerations were recorded in five nonreactive NSTs (5 patients) and late decelerations were recorded in seventeen nonreactive NSTs (15 patients). In these groups, nonintervention or delayed intervention led to fetal death in five cases and perinatal mortality rate was 455/1000. Suggestions were made in the management of these cases on the basis of the present and previously reported study.
I ! ! I i I i I ! I ! I !
48

I Society of Perinatal Obstetricians -- Annual/~eeting
I San Antonio, Texas
#45 February, 1984
ULTRASONOGRAPHIC EVALUATION IN THE ~IANAGEMENT OF POSTPARTUM INFECTIONS
C~hhang Y. Lee, M.D., Beatrice L. Madrazo, M.D.,X Sheryl Parks, M.D.,X and Michael Sandler, M.D.x
Henry Ford Hospital, Detroit, Michigan
To evaluate the effectiveness of ultrasound in the management of postpartum problems, the authors performed ultrasonographic examination on ninety-eight patients with suspected postpartum infection. The study includes only those patients wo did not respond to antibiotic treatment for at least 48 hours and the patients who were readmitted to the hospital with suspected postpartum infection. Table 1 reveals the ultrasonographic findings of these patients. Utilization of these findings in the management of the cases with postpartum infection will be presented.
Table i. SONOGRAPHIC FINDINGS IN PATIENTS WITH SUSPECTED POSTPARTUM INFECTIONS
No. of Patients
Dilated uterine cavity with echogenic tissues Dilated uterine cavity with echogenic tissues and gas Dilated uterine cavity with fluid Dilated uterine cavity with fluid and gas Gas within the uterine cavity Fluid collection around uterine incision Gas within or around uterine incision Hematoma in broad ligament Hematoma or abscess formation in abdominal incision Normal uterine cavity with fluid in cul-de-sac Possible ovarian vein thrombophlebitis No abnormal findings
I0 2
22 2 5* 5 4**
2 ii 3 1
31
Total 98
* Two patients were found to have abscess formation in abdominal wall ** Three patients were found to have gas formation in uterine cavity
! I I I I I I I I I I I I I
49

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#46 February, 1984
FETAL PLASMA ESTROGENS IN NORMAL AND COMPLICATED PREGNANCIES. Gary D.V. Hankins, x
M.D.,* Pamela Drewry, R.N.,x Nanette Mitchell, B.S., and C. Richard Parker, Jr., Ph’D.,~ Dept. of Ob/Gyn, Univ. Texas Southwestern Med. Sch., Dallas, TX 75235. (Sponsored by F. Gary Cunningham, M.D.)
The relationship between maternal disease states and fetal estrone (El) and estradiol-17B (E2) was investigated in 106 pregnancies. To do so we quantified mixed umbilical cord plasma concentrations of E1 and E2 in normal newborns (N=45) and those delivered of women having diabetes (N=16), pregnancy-lnduced hypertension (N=20) and twins (N=13 sets). Umbilical cord plasma levels of El and E2 were significantly positively correlated in all groups of newborns. Within groups there were no significant differences in mean estrogen levels or in the El/E2 ratio when subdivided into gestations of less than or greater than 36 weeks. The highest E1 levels were found in infants of diabetic mothers (14.56±3.96 ng/ml). Conversely, infants of diabetic mothers had the lowest E2 levels (6.07±1.45 ng/ml). The highest E2 levels were in the hypertensive group (9.08±1.84 ng/ml). Twin gestations had lower El and E2 levels than did singleton pregnancies. Although certain trends appeared the only significant difference noted across groups was the disparity between El/E2 ratios of infants of diabetic vs. hypertensive pregnancies (p = .02). Since estrogens have been postulated to play a role in pulmonary maturation, the relationship between respiratory distress and fetal El and E2 levels was also analyzed. Although the mean E1 and E2 levels in infants who developed respiratory distress did not differ significantly from those without respiratory distress, the El/E2 ratio was lower (p < .001). These results are suggestive that maternal complications of pregnancy result in differential estrogenlzation of the growing fetus and that alterations in the relative proportions of estrogens in the fetal compartment may play a role in the genesis of respiratory problems in the newborn.
MEAN (± S.E.) ESTRONE AND ESTRADIOL LEVELS (ng/ml) AND ESTRONE-ESTRADIOL RATIOS FOR NORMAL AND COMPLICATED PREGNANCIES.
El (ng/ml) E2 (ng/ml) El/E2 Normal (N=45) 11.51 (± 1.47) 6.85 (± 1.14) 2.11 (± 0.18)
> 36 wks (N=31) 11.22 (± 1.74) 6.65 (± 1.39) 2.04 (± 0.17) < 36 wks (N=I4) 12.15 (± 2.83) 7.31 (± 2.03) 2.26 (± 0.46)
PIH (N=20) 13.34 (± 2.07) 9.08 (± 1.84) 1.65 (± 0.19) Diabetes mellitus
(N=I6) 14.56 (± 3.96) 6.07 (± 1.45) 2.49 (± 0.33) Twins (N=25) 9.28 (± 0.87) 5.7± (± 0.67) 1.88 (± 0.17)
I i I I I I I I I I ! I I I

#47
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
ANALYSIS OF THE POTENTIAL FOR TRANSFER OF LIPOPROTEIN-CHOLESTEROL ACROSS THE HUMAN PLACENTA. Gary D.V. Hankins, M.D.,* Timothy Deahl, B.S. x Pamela Drewry,
X -~ R.N., and C.R. Parker, Ph.D., Univ. Texas Southwestern Med. Sch., Dallas, TX 75235. (Sponsored by F. Gary Cunningham, M.D.)
We sought to determine to what extent maternal plasma cholesterol contributes to the fetal plasma cholesterol pool. Maternal lipoprotein-cholesterol levels at the time of delivery were significantly higher than those in mixed umbilical cord plasma. The maternal plasma levels of total-cholesterol, low-density lipoprotein (LDL)-cholesterol, and high-density lipoprotein (HDL)-cholesterol were not correlated to fetal plasma levels of these lipoprotelns. There was a weak, but statistically significant, positive correlation between maternal and fetal plasma levels of very low-density lipoprotein (VLDL)-cholesterol. Also, we found a highly significant difference between the levels of HDL-, LDL-, and total- cholesterol in umbilical venous and umbilical arterial plasma; venous levels being 7.7-12.8% higher than those in arterial plasma.
Lipoprotein-cholesterol (C) in umbilical arterial (UA) and umbilical venous (UV) sera. Lipoprotein-C (mg/dl)I
(uv) Total-C 51.5±0.71~
VLDL-C 5.~±0.~
HDL-C 20.3±0.49* LDL-C 25.9~0.65"
Data presented as the mean±SE
V/A Gradient (UA) V/A Gradient2 as % of (A)
47.9±0.75 +3.67±0.68 7.66% 6.4±0.44 -1.00±0.59 - 18.0±0.55 +2.30±0.57 12.78% 23.5±0.64 +2.44±0.68 10.38%
Computed from the V/A gradients in each individual pair Significantly higher (p<0.001) than in arterial plasma by paired t-test.
These data are suggestive that cholesterol derived from maternal plasma can be delivered across the placenta to the fetal compartment in normal pregnancies at term. The contribution of such cholesterol to the fetal plasma cholesterol pool, however, appears to be of minimal quantitative importance in newborns of women with uncomplicated pregnancies.
I I I I I I 1 I i I I
i I i I I I I
51
I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#48 February, 1984
PLASMAPHERESlS IN SEVERE Rh DISEASE. Chaudhry Ham~e~, M.D.x*, Uma L. Vel~na, M.D., Nergesh Tejani, M.D. and Avrum Golub, M.D. Health Sciences Center, State Univer- sity of New York at Stony Brook; Nassau County Medical Center, Department of Ob- stetrics and Gynecology and the Department of Pathology and Laboratories, Blood Bank/Transfusion Service, East Meadow, N.Y.
Intensive prenatal plasmapheresis was successfully utilized in the management of three consecutive patients with severe Rh isoimmunization. These patients were selected for plasmapheresis because of severe disease as assessed by a history of previous hydrops prior to 24 weeks in one patient, and amniotic fluid A OD at 450 in Liley’s upper zone 2 and zone 3 in the remaining two patients. Plasmapheresis was done using the Hemanetics Cell Separator Model 30 and was performed 2-3 times a week from 18-24 weeks until delivexy which was between 30 and 33 weeks. On each occasion, 3,000-4,000 cc. of blood was drawn off and the cells separated and re- transfused. The plasma was replaced by plasmanate and electrolyte solutions. There were no maternal complications secondary to the procedures. Antibody titers gradually diminished. Serial amniotic fluid A OD 450 in all three patients re- mained stable or decreased indicating a steady or decreasing rate of hemolysis. Sonography and fetal well-being tests were performed to assess fetal status. Patients were delivered between 30 and 33 weeks when ~ OD 450 suggested exacerba- tion of hemolysis. All three patients were delivered by cesarean section between 30-33 weeks after steroid therapy for lung maturity. The three neonates were born in a satisfactory condition, had moderate hemolytic disease requiring 2-3 exchange transfusions and were discharged home in satisfactory condition. The results of these cases indicate that plasmapheresis is effective in reducing hemolysis in the fetus with severe Rh disease in early pregnancy, and allows the pregnancy to be maintained to a gestational age when conventional modalities such as intrauterine transfusion or preterm delivery are more likely to result in neonatal survival. We also feel that it is a reasonable alternative to intrauterine transfusion.
I
I
I ! I I
I I ! I
52

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #49 February, 1984
7-9 YEAR EVALUATION OF CHILDREN EXPOSED TO RITODRINE IN UTERO. N@rgesh Tejani, M.~., Diane Polowczyk, Ph.D., Niels Lauersen, M.D., Alfred Cohen, Ph.D., and Foazia Siddiq, M.D. Health Sciences Center, State University of New York at Stony Brook; Nassau County Medical Center, Departments of Obstetrics and Gynecology and Pediatrics, East Meadow, N.Y.; New York Hospital-The Cornell Medical Center, De- partment of Obstetrics and Gynecology, New York, N.Y. and Hofstra University, De- partment of Psychology, Hempstead, N.Y.
Twenty children who had been exposed to Ritodrine between 24 and 34 weeks of intrauterine life in the management of preterm labor were examined at 7-9 years of life and compared with controls matched for gestational age, birth weight, race~ route of delivery and age at examination. No significant differences were detec- ted in factors of growth, neurological findings and psychometric testing. Test scores, however, were consistently but insignificantly higher in the control group and indicate the need for larger studies of this type.
! I I I I I I I I I I I ! i

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #50 February, 1984
EFFECT OF CONTINUOUS INFUSION OF MgS04 ON PULMONARY FUNCTION TESTS IN PREECLAMPTIC WOMEN IN LABOR Ja~/a Ramanathan, M.D.x, Baha M. Sibai, M.D., Vijaya Duggirala, M.D.x, Albert L. Maduska, M.D.x, Depar~ents of Anesthesiology and Obstetrics and Gynecology, Uni- versity of Tennessee College of Medicine, Memphis, Tennessee
Ten preeclamptic patients of comparable age, weight, height and gestational age were studied. Each patient acted as her own control and was treated with a 4 gram loading dose of magnesium sulfate (MgS04) that was followed by a maintenance dose of 1 g/dl/hour. Using a waterless direct displacement spirometer (Breon 2400), Forced Vital Capacity (FVC), Forced Expiratory Volume at one second (FEVl) and Maximum Voluntary Ventilation (MVV) were measured prior to, 2 hours and 6 hours after the start of the MgS04 infusion. All measurements were made between con- tractions with patients in sitting position. Blood pressure, respiratory rate and temperature were noted during each measurement. The mean serum magnesium level during the infusion was 3.66 +_ 0.44 mg/dl (range 3.0-4.1). Table I summarizes the mean FVC, FEVl, mean MVV, and FEVI/FVC ratio before, 2 hours and 6 hours after starting MgS04. The results indicate a decrease in pulmonary functions probably due to the action of magnesium ion at the myoneural junction. These changes may become clinically significant in patients with underlying pulmonary disease/or in cases where higher maternal serum Mg levels are utilized.
PULMONARY FUNCTIONS BEFORE AND DURING MgS04 INFUSION
FVC (liter)
Baseline 2 hours 6 hours Mean +_ ISD Mean +_ ISD Mean +_ ISD
a ab ac 3.05 +_ 0.41 2.67 +_ 0.50 2.71 +_ 0.42
FEVI (liter) a ab ac
2.50 _+ 0.41 2.25 _+ 0.45 2.75 _+ 0.37
MVV (liter) a ab ac
93.75 +_ 15.6 84.4 +_ 17.1 83.75 +_ 13.50
FEVI/FVC ratio (%) 82.4 _+ 11.1 b c
84.8 -+ 10.4 83.6 +_ 10.6
Values in the same row sharing a common superscript letter are significantly dif- ferent (P <0.01) by paired student T-test.
! I ! I ! I I I I I ! I I I !
54
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#51 February, 1984
THE USE OF CONTRACTION STRESS TESTS AND SERUM ESTRIOLS IN THE MANAGEMENT OF THE DIABETIC PREGNANCY
ohn D. Yeast*, Wendy Dorchester, Roger K. Freeman. Perinatal Division, Department of Obstetrics & Gynecology, Long Beach Memorial Hospital and the University of California Irvine, Orange, California.
Over the past decade significant improvement in perinatal outcome in the diabetic ,regnancy has occurred, largely due to improved metabolic control and stricter ante- ~artum assessment. Fetal well-being has usually been monitored with fetal heart ~ate testing, and biochemical evaluation of fetal-placental function by various methods. Beginning in 1976 at Memorial Hospital, Long Beach, a protocol for ante- partum testing in the diabetic pregnancy was established. Class A diabetic patient~ at no risk for placental insufficiency (No hypertension, intrauterine growth retard- ation ((IUGR)), etc.) began weekly contraction stress tests (CST) at 40 wks. Insuli~ dependent diabetic patients and high risk Class A patients began CST’s at 34 wks., or earlier if the clinical situation warranted. Daily serum Estriols (E3) began at the initiation of antepartum testing in the latter group of patients. If a signif- icant fall in E3 level was noted, a fetal nonstress test (NST) was done that day. CST’s and NST’s were carefully read and a positive CST or repeatively suspicious CST’s usually prompted delivery. A total of 409 Class A-R patients were tested from September 1976 through March 1983. 235 patients were insulin dependent and 174 patients were Class A. However, 58 Class A patients were tested prior to term, due to hypertension, IUGR, etc. were as follows:
The distribution of indications for intervention
CLASS A CLASS B-R
Maternal 13 (7.5%) 31 (13.2%)
Elective 57 (32.8%) 94 (40.4%)
Abnormal CST/NST 27 (15.5%) 24 (10.2%)
Abnormal Estriol 4 (2.3%) 26 (11.1%)
PROM 3 (1.7%) 19 (8.1%)
Prior to 38 wks. gestation only 14 patients demonstrated a drop in E~ that prompted delivery. 8/14 patients had evolving maternal complications; and 5/14 patients also had a suspicious or positive CST. A total of 17 patients less than 38 wks. were found to have a positive or repeatedly suspicious CST as the primary indica- tion for delivery. 6/17 patients had evolving maternal complications. Among these 31 patients with early intervention, 20/31 patients had mature amniotic fluid studies prior to delivery, and only 6/31 infants had respiratory distress syndrome (RDS), none considered severe. There was only one stillborn infant in the entire series; that death occurring in a Class B diabetic at 39 wks. gestational age. There were a total of 6 perinatal deaths for a perinatal death rate of 14.6/1000. Three infants died due to congenital malformations. It appears from this study that a protocol of carefully read CST’s and daily E3’s provides significant safety
in the management of the diabetic patient~ with minimal iatrogenic morbidity.
I !
I I I I I I I I I
55

#52
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
SERIAL NEPHELOMETRIC URINE IgG MEASUREMENT IN PREGNANCY-INDUCED-HYPERTENSION
x Robert D. Eden~ M.D. and Stanley A. Gall, M.D.* Duke University Medical Center, Durham, N. Carolina 27710
The purpose of this report is to investigate the response to treatment and correlation with maternal and fetal clinical course and outcome in Pregnancy- Induced-Hypertension (PIH) patients with serial nephelometric urine IgG concentrations. Urine samples were obtained from PIH patients at measured intervals throughout the antepartum, intrapartum and postpartum periods. Quantitative determination of IgG was performed by means of a nephelometric method with mono-specific antisera against IgG and appropriate reference standards. Patients were classified as having "Minimal" (~ 35 mg/liter) or "Significant" (> 35 mg/liter) i=~unoglobulinuria at the time of hospital admission. All PIH patients were treated with parenteral fluid and magnesium sulfate with reservation of intravenous hydralazine administration for significant hypertension. The "Significant" immunoglobulinuria patients were further classified by serial IgG urine concentrations following treatment and delivery. Patients excreting IgG concentrations in excess of 35 mg/liter despite treatment or delivery were classified as having "No Response" to treatment. Patients demonstrating minimal renal excretion of IgG (! 35 mg/liter) following treatment or delivery were classified as having a "Response" to treatment. Significant immunoglobulinuria (> 35 mg/liter IgG) develops prior to the onset of maternal azotemia, markedly diminished creatinine clearance, significant proteinuria (~ 3+ dipstick or ~ 5 grams per 24 hours) or oliguria. The nephelometrical~y determined IgG
urine concentration technique is rapid and appears to be helpful in determining clinical disease severity, the effect of treatment on renal function and the likelihood of postpartum maternal morbidity.
I I ! I ! I I I ! ! ! I I I I I

#53
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
Alloantibody Detection by an ELISA in a Case of Neonatal Alloimmune Thrombocytopenic Purpura and Review of the Literature John Deaver, M.D.x, Phyllis Leppert, M.D., and George Zaroulis, M.D. from Division of Perinatal Medicine, Columbia University, New York, New York and Department of Medicine, Mr. Sinai Medical School, New York, New York
Abstract
Maternal-fetal platelet antigen incompatibility, most commonly involving
the PLA 1 system, results in maternal sensitization and neonatal alloimmune
thrombocytopenic purpura (NAITP) in 1 - 2/10,000 pregnancies.
Routine antenatal screening is available. Fifty percent of cases
occur in nulliparous patients in whom the diagnosis is made at birth.
Recurrence of NAITP is a function of the gene frequency of the offending
allele, which for the PLA I antigen is 85%. Traditional methods of
alloantibody detection and quantitation have failed to reliably predict
the occurence or severity of the disease in subsequent pregnancies.
Recently, antihuman globulin methods have proven sensitive for
the postpartum detection of platelet alloantibody. Recentl~ in a case
of recurrent PLA 1NAITP, one such method, an EL%SA, demonstrated
alloantibody in early gestation with rising titers near term allowing
a decision to proceed with Cesarean Section at 35 weeks gestation.
There are 33 case reports of NAITP. The incidence of intracranial
hemorrhage and CNS sequelae was eleven cases in the literature (33%).
In four cases, in utero intracranial hemorrhage was suspected. The
mortality rate was 9.1%. Elective cesarean section, steroid therapy,
and maternal platelet transfusion appeared to be associated with an
improved prognosis. We advocate cesarean section as early as is
compatible with fetal pulmonary maturation to prevent some cases of
in utero intracranial hemorrhage.
!
I I
I

#54
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE EFFECT OF RITODRINE ON FETAL GROWTH. I. EXPERIMENTAL IUGR ~DEL IN RATS Chin-Chu Lin, L. Philip Riverx, Atef H. Moawadx. Department of Ob/Gyn, University of Chicago, Chicago, Illinois.
Ritodrine has been reported to increase maternal serum glucose level and ~lacental transfer of glucose to the fetus, but to decrease uteroplacental blood flow in experimental animals. However, its net impact on fetal growth has not been established. This study was to examine its possible effect in both normal and retarded fetal growth in rats. Intrauterine growth retardation (IUGR) was produced in the fetal rats inside one uterine horn by ligation of the proximal end of the uterine artery at the 17th day of gestation (Wigglesworth technique) while the fetal rats inside the other uterine horn constituted the control group. After recovery from the surgery, either Ritodrine hydrochloride 0.5 mgm/kg (n=7) or equal volume of isotonic saline (n=6) was given intraperitoneally every 12 hours to the mother for three days. Fetal rats were delivered on the 21st day by C-section, and fetal body weight, brain weight, liver weight, placental weight (mean + SEM in gms) were compared between the two different groups. Among the fetal rats from saline treated mothers, a significant difference was observed between the unligated (n=24) and ligated (n=22) group in fetal body weight (5.19 + 0.23 vs 4.21 + 0.28, 19% reduction, P<0.01), fetal liver weight (0.351 + 0.01~ vs 0.222 + 0.520, 37% reduction, P<0.001), and placental weight
(0.843 + 0.037 vs 0.691 + 0.033, 18% reduction, P<0.002), but there was no difference in fetal brain weight (0.169 ~ 0.006 vs 0.167 ! 0.009, 1.2% reduction) Similarily, among the fetal rats from Ritodrine treated mothers, a significant difference was observed between the unligated (n=36) and the ligated (n=14) group in fetal body weight (5.08 + 0.14 vs 3.80 + 0.22, 25% reduction, P<O.O01), fetal liver weight (0.333 + 0.011--vs 0.182 + 0.0~6, 45% reduction, P<0.001), and placental weight (0.82 ! 0~035 vs 0.65 ! 0.569, 22% reduction, P<0.01), but there was no difference in fetal brain weight (0.168 + 0.025 vs 0.164 + 0.007, 2.4% reduction). However, there was no difference between the two ligated groups nor between the two unligated groups treated with Ritodrine and saline respectively. These results indicate that no significant effect of Ritodrine in the range of therapeutic dosage on intrauterine fetal growth in either normal growth fetuses or retarded growth fetuses in rats.
I I I I I
I I
I I I I I I I I I

I Society of Perinatal Obstetricians 1
Annual Meeting 1
Antonio, Texas 1 #55 February, 1984
THE EFFECT OF RITODRINE ON FETAL GROWTH. II. LONG TERM ORAL MEDICATION OF RITODRINE IN HUMAN PREGNANCIES. Chin-Chu Lin, Jenny Riverx.
Department of Ob/Gyn, University of Chicago, Chicago, Illinois.
This study was designed to compare the effect of Ritodrine on intrauterine fetal growth in human pregnancies. In our previous study of amniotic fluid C-peptide (AFCP) in non-diabetic human term pregnancies, a significantly lower level of AFCP was associated with SGA infants and a significantly higher level of AFCP was associated with LGA infants (Am. J. Ob. Gyn. 139:390, 1981). Thirty patients who received Ritodrine (I0 to 20 mg q. 6 h. p.o.) treatment for at least 4 weeks after mid-pregnancy for threatened premature labor were compared to 107 control patients. All the patients in this study had amniocentesis between the 37th and the 39th week of gestation and delivered at the 37th week or beyond. After the delivery, fetal body weight, fetal length, and head circumference were measures and AFCP values were obtained. A statistical comparison was made between the two groups in these parameters. There was no difference in mean age, mean parity, or mean and distribution of gestational weeks, between the Ritodrine treated and the control group. However, the mean fetal weight (mean + SEM in gms) was significantly smaller in the Ritodrine- treated group (3005 + 73 vs 3146 + 37, P<0.05). This is due to a higher percentage of low growth percentile infants (defined as <50th percentile for gestational age) in the Ritodrine group compared to the control group (67% vs
46%, P<0.02). Among the low growth percentile infants, AFCP values (mean ~ SEM in pmol/ml) were significantly lower (P<0.002) in the Ritodrine-treated group (n=20, AFCP=0.45 + 0.059), than in the control group (n=54, AFCP=0.69 + 0.042). However, there was no difference between the two groups among the high growth percentile infants. Furthermore, a significant correlation (f=12, P< .O1) between the AFCP level with differenet weight groups (0.58 + 0.05 in > 2800 gms, 0.65 + 0.03 in 2801-3600 gms, and 0.99 + 0.11 in > 3601 gms) in the control population. This trend was not observed in the Ritodrine treated group, possibly due to the small case number. Ritodrine treatment was not associated with a significant change in either body length (49.8 ~ 0.57 cm vs 50.5 ~ 0.28 cm) or head circumference (33.7 + 0.23 cm vs 34.0 + 0.11 cm). These results suggest that Ritodrine is associated with production of a higher percentage of low growth profile infants, but not associated with a significant reduction in fetal body length or head circumference.
I I I I I I I I I I I I I
59

#56
Society of Perinatal Obstetricians ,~mnuai Meeting
San Antonio, Texas February, 1984
INTRAI~ER]~E FETAL D~MISE IN MULTIPLE GESTATIC~ .
D’Altcn, M.E. , ~etrulo, C.L., Newton, E.R., Feingold, M. Tufts University School of Medicine St. Margaret’ s Hospital for Women Boston, MA 02125
Seventeen cases were identified over a five year period with intrauterine demise of one member of a multiple gestation. Ten cases were mcnozygous twin pairs, four were dizygotic, and three were triplets. Gestational age ranged from 27 to 39 weeks. The initial management protocol for the first fifteen cases consisted of delivery in all cases after ccnfirmation of the diagnosis. In four cases delivery was inm~diate because of labor. Elective delivery was performed in eleven cases if gestational age was 37 weeks or greater (4) or if a~niocentesi~ revealed pulmonary maturity. Steroids were given if the Lecithin!Sphingomyelin (L/S) was inmature and delivery was performed 48 hours after initiation of steroid therapy. None of the mothers exhibited any clinical or laboratory evidence of disseminated intravascular coagulation (DIC). Using this protocol all of the co-twins or co-triplets survived. However, one survivor of a mcnozygous twin pail has ~iticystic eneephalcmalacia possibly inplicating perinatal arterial occlusio~ or in utero DIC. There was no evidence of antenatal cc~p~se in this fetus. On review of our experienee, our management protocol has been modified. Perinatal DIC if it occurs would appear to be an unusual and unpredictable event. Elective delivery is not reec~rended for the co-survivor of a maeerated stillbirth unless antenatal surveillance suggests fetal ccmprcmise.
I I I I I I I I I I I i I I I
6O I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#57 February, 1984
VARIABLE DECELERATIONS DURING NON-STRESS TESTS (NST): A SIGN OF FETAL COMPROMISE? x x Paul J. Meis~ John R. Ureda,x Melissa Swain,x Randall T. Kelly, Mary Penry, and
Penny Sharp, Department of Obstetrics and Gynecology and Department of Community Medicine, Bowman Gray School of Medicine of Wake Forest University, Winston- Salem, North Carolina 27103.
Variable decelerations (VDN) during an NST have been described by some as a sign of oligohydramnios, fetal growth retardation, significant cord problem, or fetal jeopardy and as an indication for immediate delivery. To examine the occurrence rate and significance of VDN we examined NST’s, intrapartum fetal heart rate (FHR) records, and neonatal outcome of 428 consecutive patients followed over an 18 month time span for a variety of high risk pregnancy indi- cations. VDN were defined as a deceleration of 20 beats per minutes or more below baseline. Duration of VDN was usually <10 seconds. One or more VDN occurred in one or more NST’s in 50.7% of the patients, and in 36% of the last NST’s before delivery. The presence and frequency of VDN in the last NST showed an association with nuchal cord location (p=0.01) and with absence of FHR accel- erations during labor (p=0.01). No association existed between VDN and mild, moderate or severe variable decelerations during labor, early or late decel- erations during labor, abdominal delivery, low I or 5 minute apgar score or birth weight. Conclusions: While VDN are often associated with a nuchal cord loca- tion, they do not portend a poor pregnancy outcome. This frequently encountered benign fetal response is not an indication for immediate delivery.
/00096
I I ! I I I I I I I I I I
61
I I

I Society of Perinatal Obstetricians " Annual/Vteeting
San Antonio, Texas ¯ #58 February, 1984
AMNIOTIC FLUID LAMELLAR BODIES AND FETAL PULMONIC MATURITY, O’Grady, J.P., M.D., Novy, M.J., M.D.x, Swanson, R., Ph.D.x, Reynolds, J., M.D.x, Ivie, W., Ph.D.~,
Bachus, ~., B.A.X
Obstetrical Special Studies Unit, Department of Ob/Gyn, The Oregon Primate Center, Clinical Pathology, OHSU, Pediatrics, OHSU, 3181 S.W. Sam Jackson Park Road Portland, Oregon 97201
Lamellar bodies in amniotic fluid contain phospholipid surfactant and an LB-PL*
assay could have advantage over standard surfactant tests. From 6/80 to 12/82, 194 samples of amniotic fluid were assayed for fetal lung maturity by the Lecithin-Sphingomyeolin (L/S) ratio, phosphotidylglycerol assay (PG), and LB-PL assay within 3 days of delivery. Samples were collected by amniocentesis. Neo- natal outcomes were observed closely. Lamellar bodies were isolated by ultra- centrifugation at 115,000 x G for 20 minutes, extracted with ChCI3:MeOH, and digested with 70% perchloric acid. Phospholipid phosphorus was measured by absorbance at 729 nm. The L/S ratio was a modification of the method of Gluck involving ChCI3/MeOH extraction, acetone precipitation, and chromotography with analysis by densitometry. PG was developed and detected by the L/S procedure without acetone precipitation. PG presence on chromotography was semi-quantitated by comparison to density controls. The RST added ethanol to fresh amniotic fluid followed by vigorous agitation and observation of bubble stability after 15 min- utes. Results: Meconium contamination (0.1-2.0%) showed no significant effect on LB-PL content. There was no significant difference in LB-PL content of paired samples analyzed before and after freezing at -20°C. Test results included blood/ meconium contaminated specimens. Correct
Correct Immature Predict.(HMD) Correct Mature Predict.(No HMD) TTN LB-PL(0)++ 13/16 (81.3Z) 151/168 (89.9%) 1/6 (16.7) L/S (5) 15/16 (81.3%) 121/163 (74.2%) 2/6 (23.4) PC (8) 14/16 (87.5%) 113/160 (70.6%) 1/6 (16/7) RST (24) ii/13 (84.0%) 94/147 (63.9%) 3/6 (50.0)
Test Results: Uncontaminated specimens+ LB-PL L/S
Sensitivity 90.0 80.0 Specificity 88.4 74.0 Predictive Value (Immature) 34.6 17.4 Predictive Value (Mature) 99.2 98.2 Efficiency 88.5 74.4
+ - N=156
PG RST 90.0 90.0 70.5 62.9 17.3 14.5 99.2 98.9 71.8 64.7
We conclude: I) The LB-PL assay has greater efficency and specificity than L/S, PG or RST tests and may be less affected by contamination; 2) Further clinical studies of LB-PL assay are indicated.
* - Lamellar Body/Phospholipid Assay
I I I I I I I I I I I I I I
62

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #59 February, 1984
EFFECTS OF EXERCISE ON UTERINE ACTIVITY IN THE THIRD TRIMESTER ~.C. Veille, M.D. x, R. Hohimer, Ph.D. x, Burry, K., R.N. x, and Speroff, L., M.D.x
Department of Obstetrics and Gynecology, Department of Medicine, Oregon Health Sciences University, 3181 S.W. Sam Jackson Park Road, Portland, Oregon 97201
The effects of exercise during pregnancy and reproduction has received recent, ~increased attention with the upsurge in physical fitness desires and practice. It
has been suggested that exercise may increase the incidence of uterine activity during two types of exercise: weight bearing (walking, running) and non-weight bearing (bicycling). Twenty tests were performed on seventeen patients who were recruited from antenatal exercise classes. Mean maternal age was 31±2 years, and !gestational age was 35±2 weeks. All volunteers exercised prior to pregnancy and were normal. A Hewlett-Packard external fetal monitor was applied to record for uterine contractions (UC), and fetal heart rate (FHR) during a 30 minute test period. Blood pressure (BP) and maternal heart rate (MHR) were ascertained by sphygmomanometry and palpation. Thereafter, patients were randomly assigned to a walking or to a bicycling group for a 15-30 minute period of exercise. ~Immediately after exercise the patients were again monitored for changes in FHR, MHR and UC’s. Results are expressed as means ± standard deviation. Significance was determined by student’s t test. RESULTS
N=20 Pre-Exercise Post-Exercise
BP (mmHg) 79±7 MHR (bpm) 78±9 FHR (bpm) 141±6
Uterine Activity = (square inches)
CONCLUSIONS
83± 5 NS 138±15" p< 0.001 149± 9 (ist 15 min.) NS 143± 7 (2nd 15 min.) NS
16 x 10-3 8 x 10-3 NS
(*During Maximum Exercise
o
o
Moderate prenatal exercise during the last eight weeks of pregnancy in a healthy, highly motivated population does not increase uterine activity.
Despite maternal tachycardia, FHR did not significantly increase following maternal exercise.
Maternal exercise in the third trimester during normal pregnancy is unlikely to promote uterine irritability and/or premature labor in a healthy population.
(Support by USPHS Program Project Grant HDI0034 is acknowledged)
I I I I I I I I I I I i
I I
63

I Society of Perinatal Obstetricians 1
Annual Meeting San Antonio, Texas 1
#60 February, 1984
-THE TAP TEST: A RAPID INDICATOR OF FETAL PULMONARY MATURITY. Michael L. Socol., Eric Slng,x O. Richard Depp, Northwestern University Medical School, Prentice Women’s Hospital, Chicago, lllfnofs.
The authors present a new rapid, inexpensive method to assess fetal pulmonary maturity called the tap test. Approximately i ml. of amniotic fluid (AF) is mixed with i drop of 6N HCI (concentrated HCI diluted i:i) and then approximately 1.5 ml of diethyl ether is added. The 16 X 150 mm test tube is briskly tapped 3-4 times which creates an estimated 200-300 bubbles in the ether (top) layer. In AF from a mature fetus the bubbles quickly rise to the surface and break down; in AF from an immature fetus the bubbles are stable or slowly break down. The tap test is read at 2, 5, and i0 minutes and is considered mature if no more than 5 bubbles persist in the ether layer. Borderline tests are performed in duplicate, relying on the second test if it is mature. One hundred forty-nine patients, 75% of whom were < 36 weeks, had a simultaneous phospholipid profile performed by the hospital ~hemistry laboratory (mature if L/S > 2.0 or phosphatidylglycerol present) and delivered within 3 days. Most AF spe--cimens were clear samples obtained by
amnlocentesis and these were not centrifuged prior to performing the tap test. AF that was obtained from a freely flowing vaginal pool or that was contaminated by blood, meconium, or large amounts of vernix was centrifuged. RDS was the clinical endpoint against which the tap test and phospholipld profile were compared.
True False True False Mature Mature Immature Immature
Tap Test 2 mfn. 82 0 26 41 5 min. I01 2 24 22 i0 mfn. 108 3 23 15
Phospholipid Profile 82 2 24 41
The predictive values for a mature tap test at 2, 5, and i0 minutes were 100% (82/82), 98% (101/103), and 97% (108/111), respectively. The predictive value for a mature phospholipfd profile was 98% (82/84). The predictive values for an immature tap test at 2, 5, and i0 minutes were 39% (26/67), 52% (24/46), and 61% (23/38), respectively. The predictive value for an immature phospholfpid profile was 37% (24/65). The 5 and i0 minute tap tests were better predictors of the absence of RDS than was the phospholipid profile (exact test, p <.01). These findings indicate that the tap test can be a valuable clinical aid. Advantages of this test are the time, cost, and small amount of AF required.
I I I I I I I I I I I I I I I
64
1 1

#61
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
VAGINAL VERSUS CESAREAN BIRTH FOR VERY LOW BIRTHWEIGHT INFANTS?
Newton ER, Kennedy J, Cetrulo CL, Hershel M, D’Alton M,* Feingold M.* Departments of Perinatology and Neonatology St. Margaret’s Hospital for Women Tufts University School of Medicine Boston, MA 02125
Several authors have advocated cesarean birth for all very low birthweight infants. As an initial step in deciding if this represents a reasonable posi- tion, the authors examined in a retrospective case-controlled manner the benefit of cesarean birth versus vaginal birth in non-compromised infants at <32 weeks.
From Jan. 1980-March 1983, five hundred and six infants<32 weeks wer[ deliver- ed. Case control was established by excluding all cases--suspected of antepartum fetal compromise. Exclusion criteria were the presence of abruptio placenta, placenta previa, diabetes, hypertension, multiple births, congenital abnormali- ties, small for gestational age, large for gestational age, and abnormal ante- partum testing. Two hundred and thirty three cases were eliminated. The remain- ing 273 were divided into 90 cesarean and 183 vaginal births. The most common indications for abdominal delivery were malpresentation and previous cesarean. The data was analyzed using the following variables: demographic, intrapartum, early/late neonatal morbidity, neonatal mortality, and maternal morbidity. The comparison of abdominally delivered infants and vaginally delivered infants with
these morbidity and mortality variables showed no significant benefit by cesarean birth in non-compromised infants at <32 weeks. Further stratifications of the data into the gestational ages above an"d below thirty weeks and by 500 grams birthweight increments were performed. A benefit of cesarean birth was shown to be significant (P<.OI) for the infant <i000 grams and less than 30 weeks gestation. The positive association is clS-~ded by significantly (P<.01) lower average birthweight in the vaginally delivered group <i000 grams an~-~29 weeks. Review of excess neonatal deaths (8 versus 3) in th~vaginally del{~vered
group revealed causes unrelated to method of delivery ie: late infection (2) and hypoplastic lungs from prolonged rupture of membranes (2). In conclusion,’ a prospectiv9 randomized trial should be started and evaluate non-compromised infants delivered at < 29 weeks gestation and 41000 grams estimated fetal weight.
I I I I I I I I I I I I I I I I I I
65 I

#62
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
TWINDELIVE~ ~A~RINAT~CENTEROVERAS~YEARPERI~
)’ Altcn, M. E. * ; Cetrulo, C.L. ; Feingold, M. * ; Newton, E.R. Tufts University School of Medicine St. Margaret’ s Hospital for W~men Boston, MA 02125
314 twin deliveries were reviewed between January I, 1976 to December 31, 1982. There was a steady increase in the number of twin deliveries over this tim~ period mainly due to the increasing numbers of maternal transfers. 142 (55%) delivered iprior to 37 %~eks; 103 (32%) delivered between 26 and 34 weeks and 21 (6.6%) delivered between 20 and 25 weeks. Excluding deaths less than 25 w~eks and major congenital anomalies incompatible with life, the perinatal mortality rate (PMR) was 85/1000. There ~ere no neonatal deaths after 31 weeks gestation with the single exception of a baby with a major congenital anomaly. Neonatal mortality and morbidity was closely examined in the group whose gestational age ranged frcm 26-34 w~eks (Table I). The Cesarean section rate in this group was 80%. With a few exceptions, patients were delivered abdominally if presentation was other than vertex/vertex. Presentation, mode of delivery, steroid use and plaeentation were correlated with mortality and morbidity; i.e., respiratory distress syndrome, intraventricular hemorrhage and days spent in the neonatal nursery. The PMR in this group conpares favorably with our singleton births in the same gestational age range. Developmental assessment at 1-3 years of age was correlated with the perinatal course.
Table I
Gestational Age Survivors % Survival
26 weeks 3/8 37% 27 " 3/8 37% 28 " 12/14 85% 29 " 20/22 90% 30 " 22/22 100% 31 " 9/14" 64% 32 " 29/30 97% 33 " 34/34 100% 34 " 51/54# 94%
* 2 conjoined twins 1 anencephalic
# 1 Potters 1 non-~e Hydrops
I I I I I I I I I I I i I i i
i i
66 i

#63
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
NONSTRESS AND CONTRACT{ON STRESS TESTS iN POSTDATE PREGNA~}CIES. Washington C. }1i11., M.D.*, Ramona Moenning, R.N.X,Michael Katz, H.D., and John L. Kitzmiller, M.D., Department of Obstetrics and Gynecology, Children’s Hospital of San Francisco, San Francisco, California.
The management of the postdate pregnancy remains a controversial clinical problem. Nonstress testing, contraction stress testing, ultrasound and estriol determinations have all been used in different protocols. Which of the antepartum fetal heart rate tests is more predictive of perinatal outcome remains an unanswer- ed question. Several authors have suggested that the nonstress test (NST) is a less sensitive indicator of fetal well-being or distress than the contraction stress test (CST) in the postdate pregnancy. The purpose of this study was to compare the predictive value of the NST wlth that of the CST in these pregnancies. NSTs follow- ed by CSTs were performed twice a week in pregnancies ~ 42 weeks gestation. A reac- tive NST required at least 2 accelerations in a 10 minute period 2 15 bpm lasting ~15 seconds. The patients were grouped according to their last tests’ results( ~
7 days antepartum). 88% of the 85 patients who qualify for evaluation had their contractions induced by breast stimulation, The clinical course and pregnancy out come for the NST and CST groups are presented in the tah]e:
R~IVE N~ATIVE REA~IVE EQUIV~AL NONR~A~IVE P~ITIVE
CST NST CST NST CST
NUMBER 70 84 ANTEPAR~OM FETAL DEAT~ I I CESAREAN SF~ITION FOR ANTEPARTUM 0 3
FETAL DISTRESS MECONIUM STAINED FLUID IN LABOR 22 24 ABNORMAL FHR PATTERN IN LABOR 10 15 CESAREAN SECTION FOR INTRAPAR~JM
FETAL DISTRESS 5 6 APGAR SCORE < 7 AT I MINUTE 5 6 APGAR SCORE < 7 AT 5 MINUTES I 1
12 0 1
0 1 0
I o o
o o o
3 0 2
1 0 0
NEGATIVE REACTIVE POSITIVE NONREACTIVE
CST (70) NST (8~) CST (3) NST (I)
ANTEPARTUM ANTEPARTUM FETAL DISTRESS 0 3 FETAL DISTRESS
INTRAPARTIJ~ INTRAPARTUM FETAL DISTRESS 10 15 FETAL DISTRESS
In spite of the limited number of patients included in this preliminary study the data tend to indicate that a negative CST is a better predictor of fetal well-being than a reactive NST. Similarly a positive CST tends to be a better predictor of ante- or intrapartum fetal distress than a non-reactive NST. Final conclusions about the predictive value of these tests will have to be drawn from a study includ- ing a larger patient sample currently continuing in this institution.
I I
I I I i I
I
I 67 I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#64 February, 1984
I HIGH RISK PREGNANCY ASSESSMENT WITH BIOCHEMICAL MARKERS (HPL AND FREE ESTRIOL) AND NONSTRESS TEST: A COMPLIMENTARY PACKAGE L. Zuidema, M.D., M. Gantes, R.N.x, and W. Spellacy, M.D. from the Dept. OB-GYN University of Illinois, College of Medicine, Chicago, Illinois.
The fetal heart rate nonstress test(NST) has become a primary method for
monitoring fetal well being in high-risk pregnancies. It takes time and there- fore is expensive and cannot be used for all pregnant women. Blood biochemical markers such as HPL and Estriol are less often used today but they have the advantage of being quick, easy and inexpensive. The purpose of this study was to see if the blood biochemical markers could be helpful in screening pregnant women to improve the yield of abnormal NST monitoring.
Fifty pregnant women with hypertension between 30 and 40 weeks gestation had 150 tests. At a test session, a blood sample was drawn for the determin- ation of HPL and free plasma estriol levels using radiolmmunoassay techniques. A NST was run and a segment of fetal heart rate tracing of 20 minutes was obtained. All of the tracings were later read independantly (L.Z.) to determine the number of heart rate accelerations of~15 bpm that lasted for ~15 seconds in the 20 minute strip. The abnormal NST results are given in the table.
Biochemical NST accelerations in 20 minutes Test
0 I
HPL
Normal(132)
Abnormal(18)
Free Estriol
Normal(98)
Abnormal(49)
5.3% (7/132)
22.2%*(4/18)
2.0% (2/98)
16.3%*(8/49)
*pC 0.01
14.4% (19/132)
33.3%*(6/18)
10.2% (10/98)
26.5%*(13/49)
In conclusion, the screening with blood biochemical test such as HPL and/or free estriol can significantly increase the yield of abnormal NST results and therefore aid in the selection of candidates for the testing.
I I I I I I I I I I I I I I I
68 I

| Society of Perinatal Obstetricians I
Annual Meeting San Antonio, Texas 1
#65 February, 1984
USE OF ABDOMINAL CI~CUMFERI~CE/FE~JR LENGTH (A.C./F.L. ) RATIO IN THE PRE- DICTION OF IARGE FOR G~STATIONAL A~E (LGA) FETUSES IN DIABETIC GRAVIDAS
Luis A. Bracero*, M.D., Laxmi V. Baxi, M.D., and Ming-Neng Yeh, M.D. (Section of Perinatal Obstetrics, Division of Perinatal Medicine, College of Physicians and Surgeons of Columbia University, New York, New York)
Diabetic pregnancies with increased mean blood sugar levels are associated with accelerated fetal growth. Fetal growth can be assessed by ultrasonograph- ic measurement of abdominal circ~m%ference amd femur length. In our institution the ultrasonographic measurement of the fes~r length has been found to be more reliable than the biparietal diameter in the determination of gestational age.
A retrospective aDmlysis of third trimester ultrasonographic findings in forty-four diabetic patients with known gestational age seen over a one year period was carried out. In order to minimize the error due to individual variation at different gestational ages a ratio of abdcminal circumference to femur length was obtained. In the present series twenty-four patients delivered LGA infants and twenty patients delivered average for gestational age ~AGA) infants. The mean value of A.C./F.L. ratio in the AGA group was 4.25-’0.19 and the mean value in the LGA group was 4.53-’0.29. These values were statistically significant (p< .001; two tailed or single tailed T-test). In nineteen out of twenty-four patients (80%) with LGA infants and in five out of twenty patients (25%) with AGA infants A.C./F.L. ratio values were above 4.35. The predictive value of A.C./F.L. ratio above 4.35 in the detection of LGA infants in diabetic patients was 80%. A prospective evaluation of this parameter with serial measurements in a larger series is being performed.
I I I I I I I I I I I I I
69

#66
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
RELIABILITY OF THE FOAM STABILITY INDEX TEST IN ASSESSING FETAL LUNG MATURATION WNP Herbert, MD, JF Chapman, PhD, and RC Cefalo, MD, PhD, of the Department of Obstetrics & Gynecology and Department of Pathology, UNC School of Medicine, Chapel Hill, North Carolina, and JC Hisley, MD, and S Maynard, MD, of the Department of Obstetrics & Gynecology and Department of Pathology, Charlotte Memorial Hospital, Charlotte, North Carolina
The foam stability index test (FSI) and its prepackaged version, the Lumadex- FSI, have recently been reported to be useful in evaluating fetal lung maturity.
I " Slnce 1979, a total of 486 uncontaminated amniotic fluid samples representing a variety of pregnancy complications have been subjected to both lecithin- Isphingomyelin (LS) determination and FSI testing in 2 tertiary care centers. More !recently, we have evaluated the Lumadex-FSI in 180 samples. The purpose of this presentation is to: i) compare the LS ratio and the FSI in assessing fetal lung maturity, 2) determine interlaboratory differences in performing these procedures; and 3) report our preliminary experience with the Lumadex-FSI.
Using 242 specimens submitted to both laboratories within 72 hours of delivery, a mature LS ratio (> 2.0) and a mature FSI (> 0.47) were reliable in "predicting the absence of respiratory distress syndrome--(RDS). However, neither an immature LS ratio (< 2.0) nor an immature FSI (< 0.47) consistently predicted the subsequent development of RDS.
LS FSI PREDICTIVE VALUE UNC CMH UNC CMH Positive Test 99.2% 100.0% 100.0% 100.0%
(no RDS)
Negative Test 23.8% 33.0% 37.5% 3.4% (RDS)
(UNC = University of North Carolina; CMH = Charlotte Memorial Hospital)
Interlaboratory variation was evaluated using test results trends with advancing gestational age and independent laboratory determination of the same amniotic samples. Despite using identical procedures for the FSI and similar procedures for the LS ratio, variation in test results occurred.
Our preliminary experience with the Lumadex-FSI suggests that this method compares favorably with the traditional FSI. Moreover, interlaboratory difference may be less with this prepackaged version.
In summary, the FSI appears to compare favorably with the traditional LS ratio in predicting fetal lung maturity. Although interlaboratory differences do exist, the ease and simplicity of the FSI may make this test preferable in many hospitals. Furthermore, the Lumadex-FSI results appear to be consistent with standard FSI tests and interlaboratory differences may be less using this prepackaged form.
I I I I I I I I i I I I I I I I I
70 I

#67
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
CLINICAL UTILITY AND CORRELATION OF THE LUMADEX-FSI TEST John A. Garbaciak~ M.D.~ and John J. Barton, M.D.x, F.A.C.0.G. Department of Obstetrics and Gynecology,Illinois Masonic Medical’ Center, University of Illinois College of Medicine, Chicago, Illinois.
The commercially available foam stability index test (R) is felt to be a rapid method to accurately determine functional pulmonary maturity. The aim of this study was to determine the sensitivity, specificity and efficiency of the Lumadex-FSI when used in a community hospital. A comparison between the L/S ratio results, phosphatidyl glycerol (PG) and FSI values when predicting neonatal outcome was made. RESULTS: Comparison between L/S ratio and neonatal outcome was made in 35 cases. The L/S ratio accurately predicted pulmonary maturity in 30 of 31 cases for a sensitivity of 96.2%. It accurately predicted hyaline membrane disease (NMD) in 2 of 4 cases for a specificity of 50%. Neonatal outcome was accurately predicted in 32 of 35 cases for an efficiency rate of 91.4%. The Lumadex-FSl (R) accurately predicted pulmonary maturity in 33 of 33 cases for a 100% sensitivity. It accurately predicted HMD in 2 of 4 cases for a 50% specificity. Neonatal outcome was accurately predicted in 35 of 37 cases for an efficiency rate of 94.6%. The presence of phosphatidyl glycerol (PG) accurately predicted pulmonary maturity in 17 of 18 cases for a 94.4% sensitivity. Its absence predicted HMD in 2 of 18 cases for an ll.l% specificity. Neonatal outcome was accurately predicted in 19 of 36 cases for an efficiency rate of 52.8%. CONCLUSIONS: l) The Lumadex-FSI test is as good as the L/S ratio in sensitivity~ specificity and efficiency of predicting neonatal outcome. 2) The Lumadex-FSI test is as good as the presence of PG when predicting pulmonary maturity. The Lumadex-FSI is better than the absence of PG when predicting HMD. The overall efficiency of the Lumadex-FSI in predicting pulmonary maturity is better than that of the PG determination. 3) The result of a Lumadex-FSI is quicker to obtain than either an L/S or PG determination and requires no sophisticated equipment or technology. 4) The cost of determining an FSI value is substantially less than that for either an L/S ratio or PG determination. 5) An FSI value can be obtained with less amniotic fluid than that required for an L/S ratio or a PG determination.
(R) Lumadex-FSl - Beckman Instruments, Brea, California 92621
I I I I I ! I I I I I ! I I I I
71
i

#68
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
ULTRASOUND AS THE PRIMARY SCREEN FOR UTERO-PLACENTAL INSUFFICIENCY Paul A. Hensleigh, M.D., Ph.D. and J. E. Ferguson II M.D., Department of Obstetrics and Gynecology, Santa Clara Valley Medical Center, San Jose, Ca. Stanford University Medical School, Stanford, Ca.
Evaluation of fetal well-being has been done by measuring the fundal height, biochemical tests on maternal serum, analyses of fetal heart rate, and most recently by ultrasound observations of amniotic fluid volume, fetal size and fetal activity. The facility and staff for obstetrical ultrasound scanning in our perinatal unit became operational in 1978. Since that time we have stopped using biochemical fetal testing with maternal serum estriols altogether based on a retrospective analysis which showed that essentially no clinical decisions were being influenced by them. During the last 2 years when we have provided obstetrical care for some 2000 high risk pregnancies, it has been apparent that the nonstress tests of fetuses at risk for utero-placental dysfunction were seldom abnormal unless there was decreased amnionic fluid or deviation below the 25th percentile in growth of the biparietal diameter and/or the abdominal circumference. During this time most of the patients thought to be at increased risk for fetal growth retardation have been scanned every 3 weeks and have had NSTs every week beginning at 30 to 34 weeks gestation. The data presented in the poster is the retrospective analysis of.these two studies done serially in about 400 pregnancies showing how seldom the NST became nonreactive before the ultrasound result was abnormal. Based on this review we will propose the obstetrical conditions in which it may be effective and possibly more efficient to use the ultrasound study as the primary screen for fetal jeopardy.
I I I I I ! I I I I I I
i I I
72
! I

#69
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
REACTING APPROPRIATELY TO THROMBOCYTOPENIA IN PREGNANCY, David A. Nagey, Carlyle Crenshaw, Jr.*, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Maryland School of Medicine and Hospital, Baltimore, Maryland 21201.
Normal non-pregnant adult platelet count is considered to be 150,000/mm3 to 450,000/mm3 based upon chamber count studies done prior to 1950. Because it is virtually impossible to rule out immune thrombocytopenia (ITP) and because one- third of all babies born to mothers with ITP with platelet counts above i00,000 have deppressed platelet counts (<50,000), the optimal mode of delivery for an asymptomatic mother with a platelet count of less than 150,000 is problematic. Insurmountable technical difficulties in obtaining accurate fetal scalp platelet counts led to a re-examination of platelet counts in pregnancy. All current ob- stetric files on a certain date (9/18/83) at the University of Maryland Hospital were reviewed, and the most recent platelet count recorded. Of the 345 patients, approximately one third were being followed in the High Risk Clinic for a variety of reasons. The mean platelet count considering the entire population was 258,600 with a standard deviation of 69,860. The distribution of platelet counts is sta- tistically indistinguishable from a normal distribution (P > 0.5), suggesting that the 13 patients being followed for thrombocytopenia with platelet counts below 150,000 were merely part of that distribution, not patients with ITP. Of the 1599 patients delivered at University of Maryland Hospital from 1/1/83 through 9/18/83, 14 (0.88%) had platelet counts less than 150,000/mm~. Only one of these patients did not experience a return to ’normal’ platelet count within days of delivery; this patient later underwent splenectomy when steroids failed to ameliorate her ITP. None of the neonates had thrombocytopenia. A platelet count of 100,000/mm~ is perhaps a more appropriate "alarm value".
I I I I I I I I I I I ! t i I I I

#70
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I I
CORRELATION OF THE INTERPRETATION OF FETAL HEART RATE RECORDS WITH CORD PLASMA ERYTHRO~OIETIN LEVELS J.A. Widnessx ¯ ~. , K.A. Teramox, G.K. Clemonsx, D.R. Coustan , R.L. Cavalieri~, W. Ohx, G.P. Welchx, and R.Schwartzx. Departments of Pediatrics and of Obstetrics and Gynecology, Brown Univ., Women and Infants Hospital of Rhode Island and Rhode Island Hospital, Providence, RI; Lawrence Berkeley Lab, Univ. of Calif., Berkeley, CA.
Plasma erythropoietin (Ep), which does not cross the placenta, has been shown to increase in response to tissue hypoxemia in fetal animal models. We have previously shown Ep values to be significantly lower in’cord plasma of term human infants born after elective C-sectlon compared to matched controls after labor (26±10 vs 46±34 mU/ml, M±SD, p<.Ol). The purpose of the present study was to evaluate the relationship of Ep measured in human cord blood at delivery to the degree of abnormality in the corresponding intrapartum fetal heart rate (FHR) record. A standardized scoring system for interpreting the FHR record was blindly applied to monitor tracings from 41 pregnancies >32 weeks gestation during the 8 hours preceeding birth. The FHR records were analyzed by 20 minute epochs and the sum of three successive epochs yielded a mean hourly FHR score. Of these 41 pregnancies, 34 were prospectively chosen because of the clinical impression of fetal distress, while 7 were presumably normal. Hourly FHR scores became more abnormal (increasing FHR score) as delivery approached (p<.001). An overall mean FHR score was determined for each patient by summing the available hourly FHR scores and dividing by the number of hours scored (range 4.2-16.2). The 41 cord blood Ep values were distributed in a non-parametric manner (median: 41; range: 16-3517 mU/ml). Significant differences were observed in the cord Ep values when the l0 fetuses manifesting the most normal overall mean FHR scores (Group I) were compared with the i0 having the worst overall mean FHR scores (Group II):
Overall Mean Cord Ep FHR Score (mU/ml)
N Mean Range Median Range Group I I0 6.2 4.2-7.4 ,~ 24 20-44 Group II I0 13.6 11.1-16.2 ~141 71-3517
*p<O.Ol (Wilcoxon rank sum test) The correlation of the individual hourly FHR scores with cord blood EP was significant (p<.05) for the ist to 4th hr before birth, but not the 5th to 8th. The highest Ep values and the most abnormal FHR scores were observed most often in growth retarded fetuses (p<.O01). We speculate that elevated cord blood Ep levels observed in fetuses after labor are the result of chronic and/or superimposed acute hypoxemia. The value of fetal plasma Ep as a clinical indicator of fetal hypoxemia requires further evaluation.
I I I
I I
I I I i ! I I I I I

#71
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE COST EFFECTIVENESS OF PROPHYLACTIC ANTIBIOTICS WITH CESAREAN SECTION
,... Hesser*, G. Briggs,S.Lang, R. Bohart, T. Garite, W. Dorchester, Dept. OBGYN, Perinatal Division, Women’s Hospital, Memorial Hospital Med. Ctr. of Long Beach,CA.
Hultiple previous studies have proven that the use of prophylactic antibiotics have decreased the incidence of endometritis following c/s but have not changed the ncidence of major complications. Hence the only real benefit of prophylaxsis woul( ~ppear to be cost savings. Therefore, we examined prospectively 866 sequential patients undergoing c/s, in order to determine what treatment regimen seemed most cost effective. These patients were managed by their private physician with respect to choice of antibiotic. The total dollar cost of therapy was computed by the Phar- macy Department. All obstetrical assessments regarding antepartum and postpartum complications were made by the private physician. No patient was admitted to the study who was felt to be infected prior to the c/s. Of the 866 patients, 429 re- :eived prophylaxsis and 437 did not. The 75/429 who received prophylaxsis developed ~ndometritis and 72/437 who were not prophylaxed developed endometritis. The foil- )wing risk factors were studied: age, gravity,parity, rupture of membranes, labor, ~uration of labor, Hg<10.5, and if the patient was considered high risk for any )ther reason. The only significant factor was whether or not the patient had rup- tured membranes. Therefore, the following graph: Only
Pts. Without ROM:518 No Prophylaxsis Any Prophylaxsis Handol Irrigation % Endometritis 12.8% 16.2% 15.2%
Pts. t’lith R01~:348 % Endometritis
No significant difference in any group.
No Prophylaxsis Any Prophylaxsis Only Mandol Irrigation 26.7% 18.5% 12.7%
~andol irrigation, therefore is effective (p<O.05) in preventing endometritis as :ompared to no prophylaxsis. As there appears to be no reason to give prophylactic intibiotic to a patient without ruptured membranes, we will only analyze the rup- tured membrane group by the individual drug, with respect to cost.
No Proph. Ampicillin Kefli.p. Other Ceph. Mandol Irrigation No. of Patients 116 68 20 31 63 No. Treated 33 68 20 31 63 Cost of Treated 89.45+117.63 80.54+ 153.50 114+187 48+110.94
175.29 +169 These are the actual costs to the patient, an~, as illustrated, ~andol irrigation s clearly more cost effective (p<O.05) than any of the other I.V. antibiotics. How- ~ver, if you include the 83 patients in the no prophylaxsis group who did not devel- op endometritis the average cost to the treated and untreated patients is $25.45. Therefore, we can demonstrate no cost savings by using prophylactic antibiotics.
I ! ! I I I ! I I I i I I I I I !
75

Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas
#72 February, 1984
CLINICAL UTILITY OF THE RELATIONSHIP BETWEEN FETAL FEMUR LENGTH AND BIPARIETAL DIAMETER R. William Quinlan, M.D., Gail Allen, R.N.~ Amelia C. Cruz, M.D., Depart- ment of Ob/Gyn, University of Florida College of Medicine, Gainesville, Florida
The relationship between fetal femur length and biparietal diameter on ultra- sound examination was evaluated in a large, unselected obstetrical population be- tween 12 and 40 weeks gestational age (n=I,128). The femur length to biparietal diameter ratio (FBR) was derived using computer-assisted linear modelling. The first-order linear model obtained (figure I) had a high coefficient of variation and was similar to previously published relationships. The relationship of FBR to femur length (F) was also determined by linear regression analysis. Unlike pre- viously published results, the FBR was found to vary with gestation; FBR = 54% at 12 weeks gestation and FBR = 85% at 40 weeks gestation. Ninety-fifth percent pre- diction limits were derived for the relationship of F to FBR. Fifty-three preg- nancies (4.7%) fell outside the prediction interval- (figure 2). Twenty-three percent (12/53) of the pregnancies with an abnormal FBR produced infants with ab- normal in utero growth or birth defects. Three infants were severely growth re- tarded; 5 were macrosomic infants weigh#ng more than 4300 gmso Four infants had anomalies whose discovery was aided by measurement of the FBR. Of these, two in- fants were hydrocephalic, one was microcephalic, and one had hypochondroplasia. The FBR is suggested as an additional parameter to be calculated in the performanc( of a basic ultrasound exam as it will aid in the detection of the fetus with asym- etric or abnormal growth an~ indicate those studies in need of supervised re-eval- uation. A prospective study is needed to evaluate the sensitivity of FBR deter- mination in predicting the growth retarded or macrosomic fetus.
/ /
/ / /
/ /
FEMUR LENGTH (turn)
Femur length as a function of biparietal diameter. Broken Line = 95’~ prmdiction interval.
FBR as function of F, Broken Line = 95% prediction interval. m- normal infants> 16 weeks,I--l- normal infants<16 weeks, ~- normal infants, abnormal cephalic index,~- anomalous infants, D- macrosomic infants, O- IUGR.
76

#73
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
DRAINAGE OF DANDY-WALKER CYST IN UTERO
Shashi Sharma, M.D.; Joseph V. McDonald M.D~ x x , Yogesh Shah, M.D.; Birgit Bader,
x x A.A.S., R.D.M.S~ ~argaret Steinbrecher, B.S., R.D.M.S.; Darla Kolb. The
University of Rochester, Strong Memorial Hospital, Rochester, New York, U.S.A.
Advances in prenatal diagnosis and management of neural tube defects have allowed accurate diagnosis of fetal hydrocephaly by the 17th gestational week and placement of ventriculoamniotic shunt in uncomplicated, rapidly progressive hydro- cephaly in immature fetuses. This report describes the drainage of a rapidly growing Dandy-Walker cyst by placement of a shunt in the cyst to drain into the amniotic cavity. A 25-year-old, white female was in the 27th week of her second pregnancy when an ultrasound revealed asymmetrical hydrocephaly, posterior fossa cyst (possibly Dandy-Walker), microcephaly, and lack of calvarium in occipital region. The parents were informed of the abnormalities and their implications, such as severe cerebellar deficit causing incoordination, difficulty in walking, possibly dysarthria, and scanning speech. The brain stem compression could produce some difficulties in swallowing, sucking, controlling pharyngeal secretions, and possibly some respiratory difficulties. The asymmetrical hydrocephaly and small size of cerebral hemispheres made it highly likely that some degree of mental retardation would be present. Motor difficulties and problems with vision could also be present. Irrespective of the handicaps mentioned above, the parents strongly desired that everything be done to give their unborn baby the very best care and the best chance to survive. TORCH titers, glucose tolerance test, and karyotyping of amniotic fluid cells were all promptly done and found to be normal. Serial ultrasounds showed rapid increase in size of the posterior fossa cyst as well as acute deterioration of hydrocephaly at the 32nd week when the fetal lungs were still immature, with L:S of 0.7 only. In accordance with the patient’s desire and consensus of the fetal therapy team, a shunt was placed under ultrasound guidance to drain the posterior fossa cyst into the amniotic cavity. Remarkable increase in fetal activity and growth of fetal brain occurred over the next five weeks. However, inspite of a complete resolution in hydrocephaly, the fetus remained microcephalic. The fetal lungs matured at 37 weeks gestation when L:S ratio was 2.4. A baby boy was delivered by cesarean section with the shunt in situ. He had Apgars of 5 and 6. The baby’s progress and the videotapes of ultra- sound done at 26, 28, 30, 32, 33, 34, 35, and 36 weeks will be presented.
!
I ! ! I I I I ! I I I I I ! I
77

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #74 February, 1984
ROLE OF ULTRASOUND DIAGNOSIS IN MANAGEMENT OF DISCORDANT TWINS
;hashi Sharma, M.D.; Yogesh Shah, M.D.’~ David Graham, M.D~ Birgit Bader~ Darla Kolb~ University of Rochester, Strong Memorial Hospital, Rochester,
New York, U.S.A.
Twins may be discordant from placental failure, twin-twin transfusion, genetic or structural abnormality. The discordancy for structural malformations are more severe and in excess in monozygotic twins. Ultrasound is most useful in early diagnosis of twins as well as their abnormalities. The presence of a membrane indicates diamniotic twins and eliminates the possibility of conjoined twinning tha! occurs in one percent of monozygotic twins. The dichorionic, diamniotic membrane is bright and easy to visualize except when one fetus is affected by severe growth retardation and oligohydramnios and has the membrane closely wrapped around its surface. The monochorionic, diamniotic membrane is faint and difficult to visualize with routine examination. However, with high resolution ultrasound, this fine membrane can be demonstrated. Failure to visualize a membrane raises high possibility of monozygotic, monoamniotic twins. Failure to demonstrate complete separation of the twins by intervening amniotic fluid raises suspicion of conjoined twinning. With high resolution ultrasound it is now possible to define the type of conjoined twinning encountered. The discordant growth of diamniotic twins can be followed by serial ultrasound to determine the optimal time for delivery for bes~ perinatal survival. The parent of twins with discordance for severe congenital malformations who desires selective birth of normal twin can be offered fetocide to cause demise of the abnormal fetus by fetal cardiac puncture and air embolizatior under ultrasound guidance. The presence of discordancy for anomalies such as acardia, primitive heart, or absence of head and upper extremities or presence of lymphatic edema indicates monozygotic twinning in which retrograde perfusion of the abnormal fetus via placental vascular anastomosis is maintained by the cardiac output of the normal fetus. The poor perfusion of upper part of abnormal fetus ~causes malformations mentioned above. Fetocide is contraindicated in these patient~ as the placental vascular anastomosis increases the risk of the surviving fetus to ;be affected by coagulation disorders generated by the thromboplastins liberated
from the dead fetus. A report of seven sets of abnormal monozygotic twins, five of which were discordant for major malformations and two sets of severe twin- twin transfusions will be presented.
I I
78 I

#75
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I I
VAGINAL FLORA IN THE SECOND TRIMESTER AND RISK FACTORS FOR PREMATURITY
Howard Minkoff,MD; xAmos N.Grunebaum,MD; William McCormack,MD;x William Crombleholme,MD;xMarcel Sierra,PhD;George Pringle,MD;X
Richard Schwarz ,MD. * Department of Obstetrics and Gynecology, Infectious Diseases,Microbiology. State University of New York, Downstate Medical Center. Brooklyn, New York.
Vaginal Cultures were obtained at the first antenatal visit in the early second trY, ester (average: 14 weeks) in 233 patients. Carriage of organisms was prospectively correlated with events related to preterm birth. Parame- ters of outcome included pren~ture rupture of membranes(PROM), preterm premature rupture of membranes, preterm labor, preterm delivery, and birth- weight. The distribution of the major pathogens among the 233 patients was the following: Non-specific vaginitis (NSV) 31.8%; Trichomonas 14.6%; M.Ho- minis 39.9%; Oreaplasma 65.2%, and Bacteroides species 25.8%. Relative risks (RR) were assessed for the association of carriage of organisms with events related to outcome: Trichomonas vaginalis (RR=2.0;p<0.05), M.hominis (RR=I.8;p<0.05), Bacteroides (RR=I.5), and non-hemolytic streptococci (RR=I.8) were more frequently seen in patients with PROM. Carriage of NSV (RR=I. 9) was significantly more often observed in patients with preterm labor. Bacteroides (RR=2.2;p<0.01) and NSV (RR=I.5) were more often observed in patients with preterm deliveries. The following combinations of organisms were significantly associated with morbid events: Bacteroides and NSV with PROM(p<0,001) and low birthweight(p<0.05), Bacteroides and M.hominis with PROM(p<0.05) ~id preterm delivery(p<0.05), ureaplasm and NSV with preterm labor(p<0.05), M.hominis and NSV with PROM(p<0.05), Trichomonas and M.homi- nis with PROM(p<0.01). This report suggests that the vaginal flora of the early second trimester may provide an important index of risk for prematuri- ty. No single organism was a highly specific predictor of risk. This may be related to the fact that prematurity secondary to infection is probably the result of a highly complex interaction of host defenses and offending orga- nisms. Organisms associated with an alkaline vaginal milieu were carried in a non-random fashion, and were related to events associated with prematuri- ty. Since the majority of deaths due to prematurity occur as a result of deliveries in the second trimester, intervention protocols ~ust be based on screening performed early in pregnancy. Subsequent screening later in preg- na~icy may be necessary to find microbiologic correlates of neonatal morbidi- ty, and to further elucidate the ecology of many of the organisms in the vaginal flora.
I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#76 February, 1984
THE ROLE OF EXTERNAL CEPHALIC VERSION IN THE INTRAPARTUM MANAGEMENT OF THE TRANSVERSE LIE PRESENTATION: A PRELIMINARY REPORT. Jeffrey P. Phelan, MD, Lucille E. Stine, MDx, Nancy B. Edwards, MDx, Steven L. Clark, MD*x, Departments of Obstetrics and Gynecology and Pediatrics, University of Southern CaliFornia School of Medicine and Women’s Hospital, Los Ange|es County/USC Medical Center, Los Angeles, California.
External cephalic version under tocolysis (ECV-T) has been shown to be an effective technique for the antepartum management of the term breech presentation. Based on our experience with the breech presentation, ECV-T was applied intrapartum and studied prospectively as an alternative to routine cesarean section in the transverse lie presentation in labor. After sonographic confirmation and informed consent, I0 patients with transverse lie presentation, back down - 5, back up - 5, and intact membranes agreed to participate in the current prospec’tive investigation. Of these I0 patients, 8 were successfully converted to a longitudinal lie (7 cephalic, I breech). Two remained transverse. Mean cervical dilatation at the time of attempted version was 3 cm with a range from 0-6 cm. Of the 8 patients successfully verted, 5 (63%) delivered vaginally while 3 (37%) required cesarean section. In the three patients requiring cesarean section, one was successfully converted from transverse to breech. Because of an estimated fetalwe~ghtin excess of 4000 grams, an elective cesarean de|ivery was done. In the second patient successfully converted to vertex, a cesarean section was done for failure to progress. At delivery, a short cord which measured 26 cm was noted, and the infant was later found to have craniosynostosis. The third patient required a cesarean ’ for failure to descend due to a compound presentation of vertex and elbow. Apgar scores for these 8 patients were all 7 or greater at 5 minutes. In two (20%) patients, external version was unsuccessful. The reasons for failure were an elbow lodged in the cervix and a small part caught in the pelvis and a funic presentation. Both patients were delivered by cesarean, Apgar scores at five mintues were greater than seven. While the findings of this preliminary report are encouraging, the clinical application of external cephalic version under tocolysis for the intrapartum management of transverse lie presentations with intact membranes still warrants further investigation and definition of the maternal and fetal risks.
! I I I I I I I I I I I I

I Society of Perinatal Obstetricians -- Annual Meeting
San Antonio, Texas ¯ #77 February, ] 984
A PORTABLE AUTOMATED PERINATAL DATA BASE Thomas A. Abdella, M.D., Garland D. Anderson, M.D., Baha M. Sibai, M.D. Division of Maternal/Fetal’ Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
The purpose of the project was to develop an economical, computerized perinata| data base which could be easily replicated at other facilities. This data base was designed to provide i.nformation useful for both research and administrative activities. The data set was comprised of 30 items, including all of the information normally recorded in the labor and delivery log-book. This information was obtained from the existing "hospital billing slip", thus obviating
.the need for any special data collection forms. All data storage and analysis was performed with an inexpensive (<$3,500) microcomputer system. The entire perinatal data system was designed and implemented within a two month period without the assistance of data processing professionals. In spite of the limited size of the data base, the system has been very productive. It generates resident case lists, monthly obstetrical statistics, and a variety of exception lists (eg. low Apgar infants, 4° lacerations, etc.). In addition, the system also supports a variety of clinical studies. The results of this project demonstrate the feasibility and usefu|ness of a simple, microcomputer-based obstetrical data system.
AUTOMATED
OBSTETRICAL
LOG-BOOK
REStDENT
CASE
LISTS
QUALITY
ASSURANCE
SYSTEM
CLINICAL
RESEARCH
SUPPORT
! I I I I I I I I I I I I I
81

#78
8ociety of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
INCREASED FIBRIN GENERATION DURING THE DIABETIC PREGNANCY
C.P. Weiner, M.D.x, H. Kwaan, M.D.x, M. Paul, M.D.x and F. Duboex, Northwestern University, Prentice Women’s Hospital, Chicago, IL 60611
We]] established complications of the diabetic pregnancy include an increased
risk of hypertension in the mother and sudden, unexplained fetal death. Each is
associated with an increased tendency for thrombosis. Fibrin catabolism has not
previously been examined ih the diabetic pregnancy. Fibrinopeptide A (FPA) is
the first peptide cleaved from fibrinogen during conversion to fibrin. With a
3-minute half-life, FPA levels reflect current fibrin generation. As part of a
general investigation into coagulation abnormalities found in the pregnant
patient, FPA was determined by RIA prospectively in 20 pregnant, insulin dependent diabetic patients, White’s classes B-F, between 26 and 38 weeks
gestation. Not all patients were sampled at each time period. The overall goal
of management was eug]ycemia. To this end, the patients received insulin two to
three times per day and blood sugars were monitored frequently at home with
dextrometers. The mean HbAIC was within normal limits in this population. The resulting values were compared to normal pregnancy by the Wi]coxan Rank Sum test.
GoAo
Normal Diabetes (N)
FPA FPA
ng/ml + 1 SD ng/m] + 1 SD
26 weeks 3.3 ± 0.7
28 weeks 3.9 ± 0.3
30 weeks 4.1 ± 2.1
32 weeks 4.7 ± 1.2
35 weeks 4.3 ± 1.3
36 weeks 4.6 ± 1.9
38 weeks 4.5 ± 1.6
* p < 0.05
3.9 ± 1.4 (12)
*7.0 ± 4.2 (9)
*5.8 ± 2.1 (13)
4.9 ± 1.9 (i0)
5.7 ± 2.8 (13)
*6.5 + 2.8 (14)
"9.0 ± 5.5 (6)
The level of FPA exceeded control at each gestational period and was signifi-
cantly higher in 4 of the 7 intervals. Because of the large SDs and the presence
of sampling errors, a prospective, expanded study controlling for White’s Class
is required. In the nonpregnant patient, FPA can be normalized with intensive
insulin therapy in the absence of vascular disease. If FPA remains elevated in
the pregnant diabetic despite euglycemia, it may be secondary to the unmasking of
underlying vascular disease.
I I I I I I I I I I I I I I I I
82

#79
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
FETAL MONITORING IN WESTERN GERMANY Roemer,V.M.,* BUhler,K., Kieback,D.G., Weller,Ch. and Hammacher,K. Dept.Obstetrics & Gynecology II, head: Prof.Dr.K.Hammacher, Universi- ty of Tuebingen, West-Germany.
In order to assess the situation of fetal surveillance during labor we send questionaires ~o all departments (N=1173) of obstetrics in Western Germany. 684 questionaires were returned (60.1%) and 675 were submitted to statistical analysis. Results: The median number of de- liveries per year was 525. The median cesarean section rate was 10%, the median rate of forceps deliveries 2% and the median rate of vacuu extractions 7.0%. The median duration of clinical use of cardiotoco- graphy was ten years. Nearly all deliveries (median=99%) are moni- tored. The median number of monitors per department was 3.0 and the median number of deliveries per year and per monitor was 178. Four categories of hospitals were created: According to the centiles of the empiric distribution of the number of deliveries per year the 25th, 50th and the 75th centile were used. The corresponding figures are 329, 525, 802 deliveries per year. Additional methods of fetal monitoring (e.g. fetal blood sampling, tcpO -measurements) are used i 16.3% in the small departments and in 40.4%2in the large ones. Thus FHR is the predominant method of fetal surveillance during labor in Western Germany. External methods in FHR-monitoring are used in 85%: This means in 72% ultrasound, in 15% phonocardiography and in 12% F-ECG. This distribution is quite constant throughout the four groups of hospitals differing in size. Telemetric devices are used in 27%. In the small hospitals (<25. centile) this figure is 9.8%, in the large departments it reaches 49.1%. Intrauterine catheters are used for labor-monitoring in 19% overall. In small hospitals however only in 7.4%, in the large ones 29.7%. Reasons of rejection of intrauterin labor-monitoring are: 9% felt that the method is too complicated, 32% mentioned the possibly increased infectious morbidity, 14% believed it handicaps the patient and 20% complained the need of early artifi- cial amniotomy. CTG-scores are used in 34%. Interpretation of FHR: 53% of all departments believe that the deceleration pattern is most suitable to detect severe fetal hypoxia. Other phenomena of FHR are mentioned less often: Variability 16%, amplitude 20% and basal FHR 12 There exists a significant association between the cesarean section- rate (as well as the rate of instrumental deliveries) and the number of deliveries per year and per monitor: Monitoring increases the ce- sarean section-rate.
I I I I I I I I I I I I I I I I I I I

#80
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
OW TO DELIVER PREMATURE INFANTS? oemer,V.M.*, BUhler,K., Kieback,D.G ept. Obstetrics & Gynecology II, head: Prof. Dr.K.Hammacher, Universit f Tuebingen, West-Germany
n the seven year period 1976 till 1982 we delivered 1387 babies in etween the 24th and 37th week of pregnancy. Reliable fetal ultrasound ~easurements were available in ~, 80%. If we look to birthweights we mad 1207 babies above 500 g up to 2500 g. This group of 1207 prematu- res contains a significant number of babies born beyond the 37th week )f pregnancy what means maturity but also hypotrophy to various de- ]rees: If we analyse the gestational age of 1112 premature infants ~eighting 500 - 2500 g we find that 29% are mature with regard to thei estational age. In babies weighting 2100 - 2500g this figure is 6,4%, in infants weighting 1001 - 1500 g it is still 5.8%, what means evere hypotrophy. Therefore, we prefer to analyse our data according
to the gestational age. our groups were chosen: 24th - 31th, 32th - 34th and 35th - 37th week f pregnancy. The neonatal mortality rates in these groups were: 46.8, 4.8, 5.8 and 1.8%. Our neonatal loss in 103 babies weighting 501 - 000 g was 49.5% and 11.5% in infants weighting 1001 - 1500 g. The aci otic risk (pH,UA<7,100) was stadily increased with the degree of im- naturity from 3.7% (35th - 37th week) to 10.7% (24th - 28th week). his means a five-to tenfold increase when compared with healthy matur~ nfants. The incidence of low I minute Apgar-scores (~ 3) was concomi- antly increased from 6.6% (35th - 37th week) to 55.5% (24th - 28th eek). ur cesarean section rate in the very low birthweight infant (501 - 500 g)was stadily increased from 24.2% (1977) to 79.7% (1982). In our eries cesarean section seems to have beneficial effect to the newborn: he neonatal mortality rate in babies (24th - 32th) born by the vaginal oute (n = 200) was 26%, in the cesarean section group (n = 122) 16% c( ~ 0.05). In liveborn singletons without malformations we had a neo- natal loss in the cesarean section group of 13.8%; 21.7% in the group )orn per vias naturales. The mean birthweights in the groups (24th - 32th week) were identical. Considering l iveborn singletons without mal- Formations presenting by the breech (24th - 32th week) neonatal loss in he vaginal group was 54% versus 4% in the group with cesarean section ~(,< 0.001). Therefore, cesarean section seems to be mandatory in the ery low birthweight infant presenting by the breech. In liveborn ingletons without malformations in cephalic presentation the correspon ing figures were 15.4% versus 12.7% again in favor of cesarean section Ot~ : n.s.).
I I I I I I I I I I I I I I I I I I I

#80
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
OW TO DELIVER PREMATURE INFANTS? oemer,V M * BUhler K Kieback D G ept. Obstetrics & Gynecology II, head: Prof. Dr.K.Hammacher, Universit f Tuebingen, West-Germany
n the seven year period 1976 till 1982 we delivered 1387 babies in etween the 24th and 37th week of pregnancy. Reliable fetal ultraso.und ~easurements were available in ~, 80%. If we look to birthweights we
~ad 1207 babies above 500 g up to 2500 g. This group of 1207 prematu- res contains a significant number of babies born beyond the 37th week )f pregnancy what means maturity but also hypotrophy to various de- ~rees: If we analyse the gestational age of 1112 premature infants ~eighting 500 - 2500 g we find that 29% are mature with regard to thei estational age. In babies weighting 2100 - 2500g this figure is 6,4%, in infants weighting 1001 - 1500 g it is still 5.8%, what means evere hypotrophy. Therefore, we prefer to analyse our data according o the gestational age. our groups were chosen: 24th - 31th, 32th - 34th and 35th - 37th week f pregnancy. The neonatal mortality rates in these groups were: 46.8, 4.8, 5.8 and 1.8%. Our neonatal loss in 103 babies weighting 501 - 000 g was 49.5% and 11.5% in infants weighting 1001 - 1500 g. The aci otic risk (pH,UA<7,100) was stadily increased with the degree of im- aturity from 3.7% (35th - 37th week) to 10.7% (24th - 28th week). his means a five-to tenfold increase when compared with healthy matur, nfants. The incidence of low I minute Apgar-scores (~ 3) was concomi- antly increased from 6.6% (35th - 37th week) to 55.5% (24th - 28th ’eek). ur cesarean section rate in the very low birthweight infant (501 - 500 g)was stadily increased from 24.2% (1977) to 79.7% (1982). In our eries cesarean section seems to have beneficial effect to the newborn he neonatal mortality rate in babies (24th - 32th) born by the vagina oute (n = 200) was 26%, in the cesarean section group (n = 122) 16% o( ~ 0.05). In liveborn singletons without malformations we had a neo- iatal loss in the cesarean section group of 13.8%; 21.7% in the group orn per vias naturales. The mean birthweights in the groups (24th - 2th week) were identical. Considering l iveborn singletons without mal ormations presenting by the breech (24th - 32th week) neonatal loss i he vaginal group was 54% versus 4% in the group with cesarean section ~(,<0.001). Therefore, cesarean section seems to be mandatory in the ery low birthweight infant presenting by the breech. In liveborn ingletons without malformations in cephalic presentation the correspon ing figures were 15.4% versus 12.7% again in favor of cesarean section Ot~ : n.s.).
I I I I I I I I I I I I I I I I I I I

#81
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
A COMPARISON OF THE LUMADEX FOAM STABILITY INDEX TEST WITH OTHER RAPID ASSESSMENTS OF FETAL ~ULMONARY MATURITY. ~*, N.S. WhitworthX, J.C. Morrison, J.B. Fiorio×, K.K. Bowersx U~-. Med. Cntr., Department of Ob/Gyn, Jackson.
The foam stability index (FSI) test provides a method for the rapid eva- luation of amniotic fluid fetal pulmonary surfactant. To further simplify this procedure, the BecRman Lumadex-FSI (L-FSI) test utilizes a standardized cassette and predispensed reagents. We have compared the performance charac- teristics of the L-FSI with other rapid tests of fetal maturity: 1) the ori- ginal Clements shake test (CST), 2) a modification of the CST based on the measurement of the percent ring (%R) of foam produced in the 1:1 dilution tube, and 3) the percent amniotic fluid fetal fat cells (FFC). Amniotic fluid samples (n=72) were collected between weeks 30 and 42 of gestation. The results are shown in Table I as the frequency of test results correctly pre- dicting the L/S ratio as mature or immature.
TABLE I
L-FSI CST %R FFC % Correct L/S Estimates 50% 39% 67% 68%*
*P <0.05 vs L-FSI or CST
The %R and FFC gave a significantly more accurate estimate of L/S ratio maturity than either the L-FSI or CST. The accuracy of the L-FSI was, however, at least comparable to that of the CST.
I I I I I I I I I I I I I I I I I
85
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#82 February, 1984
A RANDOMIZED COMPARISON OF THREE METHODS OF ADMINISTERING "PROPHYLACTIC" ANTIBIOTICS AT C-SECTION. John P. Elliott, M.D. and James F. Flaherty,x D.O., Letterman Army Medical Center, San Francisco, California.
Prophylactic antibiotics have been administered intravenously and more recently by intraoperative uterine lavage at the time of cesarean section in an effort to reduce the incidence of post- operative endomyometritis. Comparison of these two modes of deliv- ery of antibiotics was performed. Four treatment groups were defined: i) Control group - no antibiotic therapy; 2) I.V. anti- biotics - 2 gm. of cefoxitin q 6 hr. x 8 doses; 3) Irrigation - uterus irrigated with 2 gm. of cefoxitin in 1 liter of normal saline; 4) I.V. plus irrigation - combination of 2 + 3. Patients were randomized to the four treatment groups by a table of random numbers. Patients selected all had been in labor prior to the c-section. Results in 103 patients are as follows:
Treatment Group Pts Febrile Morbidity Control 29 ii (38%) I.V. 26 2 (8%) pc.06 Irrigation 8 3 (11%) p < . 07 I.V. + Irr 25 1 (4%) p< .05
There is no significant difference between the three treatment groups, but each treatment group approaches statistical signifi- cance when compared to the control group. There were no adverse drug reactions in any patient. Considering the costs of antibiotic administration, it would seem clinically appropriate and cost effective to administer one dose of antibiotic by uterine lavage at the time of c-section if prophylactic antibiotics are indicated.
I I I I I I I I I I I I I I I I
86

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#83 February, 1984
PREVENTION OF POST DATES PREGNANCY BY BREAST STIMULATION. John P. Elliott, M.D. and James F. Flaherty,x D.O., Capt., M.C., USA, Letterman Army Medical Center, San Francisco, California, 94129.
Post dates pregnancy (> 294 days) is a risk to both the mother and the fetus. We prospectively evaluated the effect of maternal self breast stimulation on the incidence of post dates pregnancy. Two hundred low risk patients at 39 weeks’ gestation or greater were randomized to a control group and a breast stimulation group. The treatment group was instructed in self breast stimulation to be performed at home. They were encouraged to stimulate their breasts for a minimum of three hours per day. The control group was instructed to avoid touching their breasts and they were followed weekly in the clinic. Success was defined as spontaneous labor prior to 42 weeks or a "ripe" cervix (Bishop score of > 8) at 42 weeks. In the control group, 15/100 patients reached 42 weeks with an unfavorable cervix for induction compared to 5/100 in the breast stimulated group, p <.01. There were no antepartum or intrapartum complications associated with breast stimulation. Results of this study are supportive of the conclusion that in low risk patients at term, breast stimulation will significantly decrease the number of patients at risk for the morbidity and mortality associated with post dates pregnancy.
I I I i I I I ! I ! I I I I
87
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#84 February, 1984
THE BIOCULAR DISTANCE: A NEW PARAMETER TO ESTIMATE FETAL A~E
P Oeanty MD ~., F Cantraine F:’hD * , R Romero MD * .~ ~;C Hobbins MD From Yale University School o~ Medic:ine I)ept of Ob.-..Gyr~ Ne~ l-~aven
The Free University c)f Brussels Computer Dept a n d
Introduction Previous reports (1-3) have correlated the size of the ocular parameters with the gestational age of the fetus and the fetal biparietal diaeeter. It has also been suggested that ocular biometry could be utilized as an additional parameter to predict gestational age (2,3}. However, an equation has not been derived to permit such a prediction, and the error in the estimation of gestational I
has not been established. I Material and Methods 177 normal pregnant patients were included in the study. The gestational age of the fetuses was derived from an early ultrasonic assessment of the crown-rump length (before 12 weeks), or the BPD (before 18 weeks). The correct plane was imaged according to the technique previously reported (I). The data were analyzed with the SPSS 15) on a Cyber 174 computer. Results I A nomogram (table If) has been constructed to allo~ easier use of the data. The left column indicates the size of the biocular distance, and the three columns on the riqht indicate the predicted gestational age and the 5th and I 95th confidence limits, ; 30 16+1 19+3 22+5
l 31 16+4 20+0 23+2 Discussion I 32 17+1 20+4 23+6 Three recent papers have stressed the interest of the I 33 17+~ 21+1 24+4 ocular biometry in the antenatal diagnosis of. conqenita] : 34 18+3 21+5 25+1 malformations (1-3), It has been the experience of the [ 35 19+0 22+2 25+5 authors that the most important parameter froa the ocular I 3~ 19+4 22+~ 2~+2 biometry is the biocular distance, Ne have chosen to ] 37 20+1 23+4 2b+& predict the age from the biocu]ar distance because it is t 38 20+~ 24+1 27+3 the largest of the ocular parameters, The biocular ~ 39 21+3 24+5 28+0 distance can be measured in the vast majority of the
Estimated qestationa] age from the biocular distance
BO Percentile in 5th 50th 95th
15 7+I 10+3 13+6 16 7+5 11+0 14+3 17 8+2 11+4 15+0 18 8+6 12+I 15+4 19 9+4 12+6 16+I
20 I0+I 13+3 16+5 21 10+5 14+0 17+2 22 11+2 14+4 17+6 23 11+6 15+I 18+4 24 12+4 15+6 19+I 25 13+I 16+3 19+5 26 13+5 17+0 20+2 27 I~+2 17+~ 20+6 28 14+6 18+I 21+4 29 15+4 18+6 22+I
BD Percentile in 5kh 50th 95th
40 22+0 25+2 28+4 41 22+4 25+b 29+1 42 23+I 26+4 29+~ 43 23+6 27+I 30+3 44 24+3 27+5 31+0 45 25+0 28+2 31+4 46 25+4 28+6 32+I 47 26+I 29+4 32+6 48 26+6 30+I 33+3 49 27+2 30+5 34+0
50 27+6 31+2 34+4 51 28+4 31+6 35+I 52 29+I 32+~ 35+b 53 29+5 33+0 36+3 54 30+2 33+4 37+0 55 30+6 34+I 37+4 56 31+4 34+6 38+I 57 32+I 35+3 38+5 58 32+5 3~+0 39+2 59 33+2 3b+4 39+6 ~0 33+~ 37+I 40+4 ~I 34+4 37+~ 41+I ~2 35+I 38+3 41+5 ~3 35+5 39+0 42+2 ~4 3~+2 39+4 42+~ ~5 36+~ 40+! 43+4
fetuses; the only instance in ,hich it cannot be obtained is when the head is in the occiput-anterior position. Although rare, some fetuses have congenita~ diseases in which both the cranial and the lonq bone parameters can b~ unreliable for the prediction of gestational age. Common e~aaples are thanatophoric dysplasia, and achondroplasti~ dwarfism. REFERENCES:I)J Benet Hum 29:395-407 1981 2)Radioloqy 143:513-517 1982 3)Am O Obstet Gynecol 144:289-293 1982
I I I I I I I I I I I I I I I I
88

m Society of Perinatal Obstetricians m Annual/Vleeting
San Antonio, Texas m #85 February, 1984
VA~c~CULAR ANATOMY OF’ THE FE’T’US
Jeanty P *., Romero R *., l’4obbi, r)s OC MD From the Dept of Ob-Gyn., Yale University., Sc:hool of Medi(~inc..,
INTRODUCTION: The normal anatomy of the fetus as observed with ultrasound has been the subject of numerous papers and review articles in recent years. The basic anatomy is now fairly ~ell kno#n, and more advanced details can now be described on the previously laid basis.
MATERIAL AND METHOD: All ultrasound scans were obtained by a physician (PJ) with the Toshiba SAL 50A whose 5 MHz transducer provides outstanding axial and lateral resolution. Only pregnancies bet.sen 25 and 32 weeks of qestation ~ere included in this report.
NORMAL ANATOMY: The CORONARY A.: In a basal section through the aortic cusps, the right coronary artery arises in front of the anterior semilunar valve, The left coronary arises in front of the left posterior semilunar valve. The COMMON CAROTIDS are roughly parallel and sIiqhtly posterior to the trachea in the neck. The JUOULAR V. can be seen lateral to the carotid arlery. The trachea is recognizable by its larqer diameter. The SUBCLAVIAN A. can be recognized by its ~ell defined relationship with the clavicle and can be observed at its lower and poslerior aspect. The DUCTUS ARTERIOSUS can be recognized between the aortic arch and the left pulmonary artery. The CELIAC AXIS is visible in transverse section below the heart. The celiac axis has the same typical ’seagull" shape that iL assumes in the adult but the ’legs of the seagull" (the celiac axis ilself) are better visible because of the horizontaliLy of the section The branch of the celiac axis easiest to image is the SPLENIC A. which is fairly straiqht in the fetus. The splenic artery can be differentiated from the SPLENIC V. by its course and smaller size. The splenic vein is joined by the SUPERIOR flESENTERIC V. and then forms the MAIN PORTAL V.. The more anterior position of the INFERIOR VENA CAVA (compared to the aorta) as it bends anteriorly to join the right atrium can be appreciated at this level. The HEPATIC A. makes a sharp bend to the right at the end of the celiac axis. Below the level of the celiac axis one can observe the origin of the SUPERIOR MESENTERIC A. (SMA). The SUPERIOR MESENTERIC V. can be differentiated from the SMA by its larger caliber, its anterior position, and because it courses to the right of the BMA. The RENAL V. is fairly easy to recognize. The bifurcation of the aorta and the COMMON ILIAC A. have also been demonstrated in the past. Nhen an oblique plane from the level of the bifurcation to the femoral head is selected , the COMMON ILIAC A. and its prolongation into the EXTERNAL ILIAC A., and finally into the FEMORAL A. can be demonstrated. The ILIAC V. is visible at the medial aspect of the artery. Even =ore medially one can recognize the inlraabdominal portion of the UMBILICAL A. as they travel along both sides of the fetal bladder. The anatomy of the intrahepatic circulation is best described by following the flow in the umbilical vein. The UMBILICAL V. enlers the abdominal wall and makes a sharp cephalic curve and travels along the free margin of the suspensory ligament of the liver to reach the transverse fissure. Hhen the umbilical vein penetrates the liver, it becomes the umbilical part of the left portal vein. From then on it can be recognized ultrasonically by the fact that VENA ADVEHENTES can be seen branching from it. The blood then flows either to the DUCTUS VENOSUS or to the portal system. The duckus venosus anastomoses the portal circulation ~ilh the ]eft hepatic vein or directly with the inferior vena tara. The main portal vein is composed of the confluence of the splenic and the SHY. Leaving the right ventric]e~ one can observe the PULMONARY A. and its bifurcation into its left and right branches. The terminal portions of the PULMONARY V. are visible in a four chamber view at their junction with the left atrium. In the same view the AZY60S V. is visible behind the rioht atrium.
! I I I i
I I I I I I I I
89
I I

#86
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
ULTRASOUND IN TWIN PREGNANCIES Jyotsna Gandhi, M.D., New York Medical College - Metropolitan Hospital Center, New York, N.Y.
It is common knowledge that perinatal mortality and morbidity in multiple ges- tations is several fold for that in singleton pregnancies. Prematurity, intra- uterine growth retardation and fetal anomalies are the most outstanding problems. This has prompted an intensive ultrasonic monitoring of twin pregnancies in most institutions. However, presently, we tend to consider growth profile of singleton babies as the standard for comparative purpose. The aim of this study is to high- ~light some of the differences between growth pattern in singleton and twin fetuses, and to point out the contribution of sonography in evaluation of twin pregnancies. A program of intensive care of multiple pregnancies has been in practice at Metro- politan Hospital and New York Medical College since 1979. This program includes an attempt to early diagnosis whenever possible, dietary and hematimic supplementa- tion, reduced maternal activity from time of diagnosis and hospitalized bedrest between 28 and 34 weeks of gestation. Fetal status is religiously monitored with intensive ultrasonic evaluations~ and electronic fetal heart rate monitoring, with an attempt to evaluate for presence of fetal anomaly, zygocity, head and body growth and status of each individual fetus. A total of 152 twin babies comprising 76 pairs of twins were delivered at Metropolitan Hospital Center between January, 1979 and December, 19820 Most of them were intensively monitored ultrasonically. Twenty-two (22) pairs were diagnosed during the first trimester, 32 pairs during the second trimester and the rest were seen during the third trimester of pregnancy Four pairs of twins delivered during the second trimester had not been prenatally diagnosed° Fifty-four (54) pairs of 108 twin fetuses were selected to be included
in the statistical study of ultrasonic vertex growth profile; excluding those with discordant growth demise of one or both twins and those with congenital anomalies. All of these babies weighed between 2000 gms. and 3800 gms. at birth and were de- livered after 34 weeks of gestation. Those 108 babies underwent 320 total ultra- sonic examinations including biparietal diameter (BPD). Ninety-eight (98) of these babies were scanned prior to 28 weeks of gestation, and in almost all, the last menstrual period was known, enhancing the validity of their gestational ages. A regression analysis of BPD and gestational age, was carried out and a 50th percen- tile, and 25th percentile value was calculated for each gestational age for twins. An increment value between each week of gestation was also computed° One hundred (i00) normal babies horn at term and of average height were considered as control, comprising a total of 320 BPD examinations and a normogram of head growth was de- veloped for them with similar statistical analysis. BPD’s of twins were comparable with those of the controls until the 21st week, thereafter, there was a consistent- ly lower BPD among twins. The weekly increment in BPD was similar to singletons° Results of this growth profile of twin infants and normal singleton infants will be presented, with an object to highlight differences between head growth of normal singleton and twin infants and to identify those twin infants with subnormal
growth in light of normogram for twin infants.
I I I I I I I I I I I I I i I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #87 February, 1984
ULTRASONIC ASSESSME~ OF FETAL PHYSIOLOGY-ITS IMPACT ON THE OUTC@~E OF THE POST- DATE PREGNANCY. Jyotsna Gandhi, M.D.~ and Camillo L. Gugliucci, M.D~, New York Medical College, Metropolitan Hospital Center., New York, N.Y.
Real time sonography has recently revolutionized the practice of perinatology in the management of the high risk fetus in general. This report attempts to demon- strate the impact of sophisticated sonographic evaluations on the overall outcome of a postdate fetus and frequency of operative delivery. A total of 385 patients with a fetal gestational age of 42 weeks and above were delivered at Metropolitan Hospital Center and New York Medical College between January, 1981 and June, 1983. Most of these patients were hospitalized and closely monitored from the end of 42 weeks until delivery. Serial nonstress tests (NST’s), maternal estriols, clin- ical and gross ultrasonic evaluation of intrauterine fluid and fetal biometry were used for monitoring purposes between January, 1981 to June, 1982. Oxytocin chal- lenge test (OCT) was used when NST was found to be nonreactive. Pregnancy was only terminated when specific signs of fetal hypoxia were detected by these parameters of fetal evaluation. Following availability of modern Real Time Equipment, fetal monitoring included serial NST’s~ fetal biometry, placental maturational status, imaging and measurements of amniotic fluid pockets for more accurate assessment, and fetal physiologic activity profile, using fetal motion, respiration, tone, NST and quantitative amniotic fluid. OCT was performed in cases of nonreactive NST’s when oligohydramnios was the only other abnormality on the activity profile. Preg- nancy was terminated only when definite fetal hypoxia or markedly reduced placental perfusion could be demonstrated. These two groups of patients were designated as group A (traditional monitoring) and group B (ultrasonically monitored). Maternal and perinatal outcome in terms of cesarean section rate, intrapartum meconium or fetal distress, low Apgar score or perinatal loss were analyzed in 220 patients in group A and 150 patients of group B and compared. There was significant difference in the perinatal profile between the infants who were ultrasonically monitored for assessment of intrauterine environment and those traditionally monitored. The cesarean section rate was likewise influenced. Sophisticated sonographic evalua- tion of postdate fetus has an agreeable impact on the overall management, opera- tive delivery and identification of the fetus at risk, in this entity with a wide individual variation in placental perfusion and its effect on the fetus.
I I I I i I I I I I I I I I I
91
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #88 February, 1984
THE ULTRASONIC DIAGNOSIS OF ALTERED FETAL GROWTH BY USE OF A NORMAL ULTRASONIC FETAL WEIGHT CURVE
William J. Ott, M.D.*, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Washington University School of Medicine, St. Louis, Missouri; Sue Doyle, R.N., Department of Perinatal Ultrasound, St. Mary’s Health Center, St. Louis, Missouri
Alterations in intrauterine growth are significant contributors to perinatal mortality and morbidity. There are a variety of techniques that are used ante- natally for the diagnosis of altered fetal growth. The current report presents the results of the use of a normal ultrasonic fetal weight curve for the antenatal diagnosis of altered fetal growth. A group of 595 patients who had undergone real- time ultrasound examination within 72 hours of birth were utilized in this study. Fetal weight was estimated using biparietal diameter and abdominal circumference, and plotted on a previously published normal ultrasonic fetal weight curve (Ott, W.J., Doyle, S.; Obstet. Gynecol. 59:603, 1982). The diagnosis of small gestation- al age (SGA) or large gestational age (LGA) was made on the basis of whether or not the ultrasonic weight fell below or above the normal limits. After delivery, infants were classified as SGA, LGA, or average gestational age (AGA) by birth weight based on the Altman-Coles nomogram; and the postnatal diagnosis was compared to the antenatal ultrasonic diagnosis. The accuracy of the ultrasonic diagnosis as compared to the postnatal diagnosis is presented in the table below:
DIAGNOSIS AT DELIVERY (by Weight-Centile) [columns]
Diagnosis at time of Ultrasound Examination [rows]
SGA AGA LGA SGA 99 67 0 AGA 12 347 13 LGA 0 21 34
The overall sensitivity of the technique for the diagnosis of SGA infants was 89.9% and for the diagnosis of LGA infants was 73.5%. The overall specificity of the technique was 79.8%. In infants who had severe intrauterine growth retardation (less than the third percentile), there was a 100% sensitivity for the diagnosis of SGA (all 39 of these severely growth retarded infants were correctly identified). This method of diagnosing altered fetal growth can also be utilized with other parameters of fetal growth and well-being, such as antenatal cardiotocometry or serial estriol determinations, and may prove to be a technique that can provide simple and accurate information for the diagnosis and management of altered fetal growth.
! I ! I I i I I I I I I ! I
92

#89
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE SIGNIFICANCE OF EXAGGERATED FETAL HEART RATE ACCELERATIONS DURING ACTIVE LABOR
~William J. Ott~ M.D.*, Department of Obstetrics and Gynecology, St. Louis University School of Medicine, St. Louis, Missouri
Accelerations of the fetal heart during the course of active labor have been identified by many authors as an appropriate response to the stress of labor and as a sign of fetal well-being. Exaggerated fetal heart rate accelerations (EFHRA) however, are felt to indicate fetal compromise or antecede the development of significant fetal distress. In order to further evaluate the significance of EFHRA during labor, patients with singleton pregnancies in the vertex presentation who began fetal heart rate monitoring prior to 4 cms. of dilatation and progressed in active labor to at least 5 cms. dilatation, and delivered infants weighing)1500 grams, were analyzed. One hundred fifty-three of 1289 patients monitored in active labor were identified as having EFHRA (11.9%), defined as accelerations of the fetal heart rate above the baseline of 30 beats per minute or greater, lasting at least 30 seconds. Comparisons of patients with and without EFHRA showed that the only significant difference between the two groups was a higher percentage of nulliparous patients in the EFHRA group. Comparisons of the intrapartum complica- tions between the two groups showed a decreased incidence of meconium staining and an increased percentage of abnormal labor patterns in the EFHRA group. Comparisons of neonatal outcome statistics showed a lower perinatal morbidity and a higher mean birth-weight in the EFHRA group. Though other investigators have felt that EFHRAs were a bad prognostic sign, the current study seems to indicate that not only are EFHRA during active labor not a sign of fetal compromise, but also indicate that the pattern is a reassuring one.
I I
I I I ! I I I ! I I !
! I

Society of Perinatal Obstetricians Annual/~leeting
San Antonio, Texas
#90 February, 1984
TERN NATERNALAND NEONATAL COHPLICATIONS OF ACUTE CHORIOAHNIONITIS. John C.
Hauth, Col, USAF, MC, Larry C. Gilstrap III, Lt Col, USAF, MC, Karen D.
Connorx, MEd.
Ninety-nine patients with acute chorioamnionltis at ~37 weeks gestation and with infants more than 2500 gm were reviewed. Diagnostic criteria included ~,terine tenderness (19%), maternal tachycardla (21%), mar~ed (50%) and mild
(32%) fetal tachycardia, and maternal fever (98.2%). Maternal complications
occurred in five of the 46 (II%) cesarean deliveries. Three required
secondary antibiotic coverage for aneroblc bacteria and two had a suprafascial
wound infection requiring drainage. Significant neonatal complications
occurred in 30% of the vaginal and 37% of the cesarean deliveries. Group B
streptococcus was the most common isolate from amnionic fluid or the neo~ates’
throat, gastric aspirate, or blood. Most importantly, our data could not
identify a critical time interval between 0 and I0 hours from the diagnosis of
chorloamnionitis to delivery with regard to either total or infectious
neonatal morbidity. In addition, no such trend was apparent within the r~,~ge
of 24 hours from amnion rupture to delivery. Hence, we cannot justify the
increased maternal morbidity associated with immediate operative delivery of
women with acute chorloamnionitis.
I I I ! I I I I I I I I I I
94
! I

#91
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
UMBILICAL CORD pH, pCO2, pO2, AND HCO~ FOLLO~-ING UNCOMPLICATED TERHVAGINAL D~LIV~RIES. Edward R. Yeomansx, Capt, USAF, MC, John C. Hauth, Col, USAF, MC,
Larry C. Gilstrap III, Lt Col, USAF, MC.
In f~ture studies of the management of the second stage of labor an
understanding of the normal values of pH, pC02, and HCO~ ~n umbilical artery and venous blood is essential. Previous reports of normal values were not
controlled for many variables including abnormalities of the FHR. We selected
115 term vaginal deliveries of which all patients had a normal baseline fetal
heart rate and normal variability for at least ten m~nutes preceding
expulsion. All patients with significant complications such as diabetes
mellltus, pre-eclampsia, twins, meconium or fetal growth retardation were
excluded. Arterial - The mean pH value was 7.28~.053 SD, mean pCO2 was
49.0+--8.2 SD, mean pO2 was 17.9+6.4_ SD, and mean HCO~ was 22.2+2.4_ SD. Venous - The mean pH value was 7.35~.051SD, mean pCO2 was 38.3+__5.8 SD, mean pO2 was
28.6+~.0 SD, and mean HCO~ was 20.4+__2.1SD. Recent interest in umbilical cord acid base and blood gas values as an assessment of intrapartum management
techniques and short and long term neonatal outcome, as well as the
limitations of the more nonspecific Apgar rating, make identification of
normal values of paramount importance.
i ! I I I ! I I I I I I I I I I
! I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#92 February, 1984
PREMATURE RUPTURE OF MEMBRANES IN PRETERM GESTATIONS. Valerie Rappaport, M.D. and Amelia C. Cruz, M.D., Department of Ob/Gyn, University of Florida College of Medicine, Gainesville, FL 32610.
Management of premature rupture of membranes remains controversial in preterm pregnancies. Improved neonatal intensive care technology has changed both the mortality and morbidity associated with premature birth, this is particularly true of the near term infants with gestations ranging from 32-36 weeks. In view of this, a retrospective review of 220 cases of premature rupture of membranes (PROM) ranging from 32-36 weeks of gestation was performed to evaluate the benefit of management. Cases included were delivered at Shands Hospital from January 1981 to December 1982. When the estimated gestational age was 32-35 weeks, no attempt at delivery was initiated unless a clinical diagnosis of chorioamnionitis was made. In the 36 week gestation group, delivery was usually effected within 24 hours of rupture. Results show that the incidence of maternal infection as defined by fever, leukocytosis and uterine tenderness increased after 24 hours of PROM. The number of infants treated with antibiotics increased with increasing length of PROM, however the incidence of culture positive disease was greatest at 24-72 hours of PROM, then decreased. The length of time from rupture to delivery had no effect on complications of prematurity, including respiratory distress syndrome. Similarly, length of rupture of membranes had no effect on the number of days of NICU care required. The peak incidence of chorioamnionitis and of fetal infection was in the group having 24-72 hours of ruptured membranes. Cervical and fetal culture results showed an increased incidence of Group B ~ hemolytic streptococcal isolates in this group. This suggests a positive correlation berween both maternal and fetal infections with colonization of ~ streptococcus prior to delivery. In summary, this retrospective study shows no fetal benefit in prolonging pregnancy greater than 24 hours once PROM has occurred, after 32 weeks of gestation. Maternal morbidity as defined by chorioamnionitis and need for antibiotic treatment on the other hand is increased by expectant management. In addition, colonization of Group B ~ strep was associated with increased maternal and fetal morbidity confirming the value of cervical culture when PROM occurs. Documentation of colonization and treatment prior to onset of clinical symptoms may decrease the associated morbidity. A prospective study addressing this issue should be done.
I I ! I I I I I I I I I I
96

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #93 February, 1984
Perinatal events leadi~ to handica~ in the very low birthweight infant.
Richard P. Perkins, M.D., Division of Maternal-Fetal Medicine, U. New Mexico School of Medicine, Albuquerque, I~ 87131
Perinatal events occurring in the pregnancies of 178 babies weighing less than 1501g. at birth were studied for their impact upon long-term morbidity. There were 5 babies 500-900g., 31 babies 901-1200g., and 42 babies 1201-1500g. available for follow-up evaluation over a period of up to 3 years. The re- mainder did not survive or were lost to follow-up except by report from elsewhere.
Those studied were subjected to DD~T evaluation and scored for mental and motor performmnce as well as being assessed for overall deficiency on a scor- ing system of 0-3 for abnornmlity. Maternal events as well as neonatal events were subj ected to con~uter statistical analysis for association with normml or abnormal outcome. The initial screening process involved the selection of individual events which achieved a "p" value of 0.20 or less with deficit. These factors were then combined in a stepwise discrimin~t analysis to deter- mine their specific and collective association with the observed outcome.
Collectively, the factors cited (out of 52 mmternal and 53 neonatal cate- gories) resulted in the selection of 16 mternal and 18 neonatal aspects for study.
Mental handicap correlated with BIRTHWEIGHT snd ABS~qCE OF ~.
Motor deficit correlated with RAPID DELIVERY and MECONIII~.
Overall score was found related to lABOR INTOT.k~ANCE, MECONII~, and ABSENCE of HYPOCALC~MIAo
The events cited could explain 80% of mental, 63% of motor, and 79% of low score observations.
Since all babies studied were at risk for abnormal outcome, it is felt that these observations may be of value in predicting handicap in future studies on similar populations managed similarly and could be of use in cur- rent programs of neonatal intensive care.
I I I I I I I I I I I I I I I
97
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#94 February, 1984
CERVICAL INCC~PETENCE: DIA6~OSIS AhD OUtCOmE. Donald A.G. Barford, M.D., ~.brtimer G. Rosen, M.D., Dept. OB/(XN Cleveland Metro Hosp/Case Western Reserve O., Cleveland, Ohio.
~le purpose of this study was to determine if there was a single or set of historical features associated with successful pregnancy outcon~ following cervical cerclage and if there was a specific time or set of findings beyond which cervical cerclage should not be perform. The gynecological and obstetrical histories of 147 patients who underwent cervical cerclage procedures for a diagnosis of cervical incorapetence were reviewed. Patients with a history of second trimester pregnancy loss or premature labor without the classical symptoms of painless cervical dilatation or rupture of the membranes were defined as having "discrepant" histories. Comparison was made with patients having "classical" histories of cervical incompetence in the second trimester. Pregnancy outcome was defined as successful if a gestation lasted 37 weeks or infant birthwelght exceeded 2500 gra~s. Of patients with discrepant histories (59.4%) had a successful pregnancy outcome following cerclage compared with (38%)of patients with classical histories (p < ~. 01). Pregnancies failing to achieve the criteria for successful outcon~ were divided into subgroups according to birth weight or gestational age at delivery. Analysis of tl~ subgroups of failed outcomes showed 30/47 (63.8%) patients with classical histories delivered infants weighing < 1500 grans conpared with 35/95 (36.8%) of those with discrepant histories (p < ~.ZI). Crude infant survival for all patients was 18.2% prior to, and 65.9% following cerclage. ~e mean gestation, gravidity, history of therapeutic abortion a~ the proportion of patients with abnormal cervices at the time of cerclage was si~dlar in both the successful and the failed outcome groups. Four patients required Cesarean section for cervical stenosis and eleven had cervical lacerations requiring repair following delivery. Patients with discrepant histories of cervical inconpetenoe had better pregnancy outcomes follo%~ing cervical cerclage than those with classical histories. Past reproductive performance was a better indicator of which patients are likely to have a successful pregnancy outcon~ following cervical cerclage than the classical s~ptomatology generally used to define these patients. The timing of the cerclage procedure and the anatomical stahe of the cervix at the time of cerclage were not predictive of the pregDmncy outcome following cerciage. Although non recurring etiologies nay account for the pregnancy losses° in the group with discrepant histories, the improvement in outcome following cerclage in this group and the poor correlation of a classical history with outcome following cerclage indicate the need for a prospective randomized study of the efficacy of cervical cerclage.
I I I I I I I I I I I I I I
98

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#95 February, 1984
INTRAUTERINE FETAL TRANSFUSION: SAFE AND EFFECTIVE David A. Luthy MD, Thomas J. Benedetti M D, Durlin E. Hickok MD, Jack H. Hirsch MD, Laurence Mack MD, and Roger Lenke MD Swedish Hospital Medical Center and Dept. Obstetrics and Gynecology University of Washington, Seattle, Washington
Intrauterine fetal transfusion (IUT) prior to 1980 has been reported to have a 10-20% operative mortality (fetal), and o~erall perinatal mortality of 30-60%. Since Jan. i, 1980, all IUTs have been performed by a transfusion team and have been performed exclusively with the use of real-time ultrasound. To study the impact of this change, all IUTs performed between Jan. i, 1980 and Sept. 30, 1983 were reviewed. All IUTs were performed using an ATL Mark 3 or Mark 600 with a 3
mHZ off-set transducer and disposable needle-biopsy guide. A 19-gauge thin-wall, short-bevel needle was used and the needle was left in the fetal abdomen during the transfusion. The entire IUT was observed under continuous ultrasonic guidance. An entry point in the fetal abdomen was selected in the left lower quadrant, if possible, and always below the level of the umbilical cord insertion and above the iliac crest. IUT volumes were calculated according to the formula of Bowman. A total of 48 IUTs were performed in 20 patients in the time period, with an average of 2.4 transfusions per patient (range 1-4). The first IUT was performed as early as 23 weeks and as late as 30 weeks; the last IUT was performed not later than 32 weeks. All women presented with an Anti-D titer 71/128. Fifteen of twenty fetuses
(75%) had an ~0D450 >0.3 at the time of first transfusion (6/15 AOD450 70.4, 8/15 AOD450 0.36-0.40). Two fetuses were hydropic at the time of initial IUT. There were no fetal deaths related to the procedure, and the overall perinatal survival was 95% (19/20). Both hydropic fetuses survived. The perinatal death occurred after an uncomplicated IUT at 30 weeks. (AOD450 0.23 and past history of hydropic stillborn with a ~OD450 of 0.25). The fetus did not absorb the intraperitoneal blood, and delivery was performed 14 days post-transfusion with ultrasonic evidence of hydrops. The infant died at 36 hours from cardiogenic shock. Delivery occurred by cesarean section in 14/20 patients (70%). Gestational age at delivery was 30- 35 weeks. There were no cases of hyaline membrane disease. Cord Hct ranged 20- 56%. Cord bilirubin levels ranged 4-10%. Cord Kleihauer-Betke smear averaged 95% adult cells (range 90-99%). There were no cases of peripartal asphyxia (cord pH 7.26-7.37). Neonatal hospital stay ranged from 5-35 days and 85% of neonates (17/20) required one or more exchange transfusions. Minor procedural complications occurred in 4 of 48 procedures (8%): The fetal colon was entered twice, and in two cases small retroperitoneal transfusions occurred without fetal sequelae. Ante- partum complications occurred in 3 patients (15%). There were 2 cases of PROM: one case at 31 weeks, i0 days post-IUT, and one case at 33 weeks, 3 weeks post-IUT. There was one case of premature labor and delivery at 30 weeks, 2 days post-IUT. All three infants survived. We conclude intrauterine transfusion is a safe and effective means of treating severe Rh-isoimmunization, and recent changes in tech- nique have greatly improved its safety and efficacy.
I I I I I I I I I I I I I I
99
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#96 February, 1984
AMBULATORY MANAGEMENT OF PREGNANT DIABETICS USING A MANUALLY OPERATED INSULIN INFUSION PUMP. LUIS B o CURET, M.D. MADISON GENERAL HOSPITAL
Eighty eight insulin dependent diabetics were managed following an ambulatory protocol during pregnancy with the use of a home monitoring device and a manual in- sulin infusor pump. The average 2 hours post prandial blood sugar was 130 mgm/dl and the average intrapartum blood sugar was 76.8 mgm/dl. Patients had a low inci-
dence of hypoglycemic reactions and the average HbAlc was 7.1%. Five infants died neonatally: Two with severe anomalies, two from prematurity and one from perinatal asphyxia. One fetal death from placental insufficiency occurred at 32 weeks after a normal O.C.T. The average neonatal blood sugar was 55.1 mgm/dl and i0 babies had mild hypoglycemia. There was no significant maternal nor neonatal morbidity. Patients’ tolerance of the system was great and most of them continued to use the system after pregnancy. Ambulatory management of pregnant diabetics with home mon- itoring and a manual infusor pump is a safe and successful alternative for )atients
I I I I I I I I I I I I I I I
tO0
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#97 February, 1984
THE CAUSE AND NATURAL HISTORY OF FETAL CYSTIC HYGROMA. FA Chervenakx G Isaccsonx K0 Blakemorex WR Bregx JC Hobbins* RL Berkowitz* M Tortorax K Maydenx MJ Mahoney.x Depts OB/GYN, Human Genetics, Pathology, Yale U.
Fetal cystic hygromas are thought to arise as part of the jugular lymphatic obstruction sequence and often progress to hydrops and fetal demise. To delin- eate better the etiology and natural history of this disorder, we studied a ser- ies of 15 consecutive nuchal hygromas detected antenatally by ultrasound. During a three-year period, 15 cases of fetal cystic hygroma were diagnosed in our peri- nata~ u±trasound unit. Gestational age at the time of diagnosis varied from 18 to 29 weeks. Fetal demise had occurred prior to the time of diagnosis in five cases, and bradycardia was present at the time of t~e scan in two instances. In 13 of the 15 cases, the masses were larger than the size of the fetal head. In fact, one lilled ~early all of the uterine cavity. All of these large hygromas were divided by septa. The two smaller masses were free of internal echoes. In 13 cases, including one with a small hygroma, there was evidence of fetal hydrops including massive skin edema, ascites~ and pleural or pericardial effusions. Amniotic fluid volume was decreased in eight cases, normal in three cases, and increased in four cases. Karyotypes were 45X in nine cases, 45X/46XX in one, 46XX in three, and 46XY in one. Amnion cells were X-chromatin negative in remaining case. All fetuses were phenotypically female. Amnlotic fluid AFP con- centration was elevated between 7 and 40 standard deviations above t~e mean in three of the eight cases where it was measured. A~hE activity was measured in two of the cases with an elevated AFP and was absent in both. In t~e one stance where fluid was aspirated from a cystic hygroma, AFP concentration was 250 standard deviations above the mean for amniotic fluid, and AChE activity was pre- sent. In i0 cases, the pregnancies were terminated based on the sonographic diagnosis. In two additional cases, spontaneous fetal death occurred within one week of sonographic evaluation. One pregnancy with a fetal demise was continued to term to permit delivery of a normal twin. Two other affected fetuses were delivered at 35 and 36 weeks; both had 46XX karyotypes. One of the babies, hy- dropic at birth, died at 12 hours of age of respiratory compromise. She had short limbs, ~ydronephrosis, and a diaphragmatic hernia. The other died at one month of age due to congestive heart failure secondary to an atrio-ventricular canal defect and coarctation of the aorta. In this last case~ a small cystic hygroma had been clearl~ visualized, and at birth, mild neck webbing was present in the corresponding position. Once a cystic hygroma is detected, a careful search for fetal skin edema, ascites, pleural and pericardia± effusions, as well as cardiac and renal anomalies is indicated. If a hygroma is associated with hydrops, the chance of survival is small. There is scant information, however, about prognosis in the absence of hydrops. Also of prime importance, especially for genetic counseling, is determination of the karyotype. Our data emphasize that Turner syndrome is not the only cause of cystic hygromas. Monitoring of future pregnancies wit~ ultrasound and possibly with a fetal karyotype should be offered and will often provide reassurance to the family.
I I I I I I I I I I I I I I I
101
I I

#98
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THIRD TRIMESTER PREGNANCY TERMINATION -- A MORALLY JUSTIFIABLE PROCEDURE? FA Chervenakx MA Farleyx L Weltersx JC Hobbins* MJ Mahoney.x Dept OB/GYN, Mt Sinai Sch Med; Yale U Divinity Sch; Kennedy Inst Ethics Georgetown U; Dept OB/GYN Yale U Sch Med; Dept Human Genetics, Yale U Sch Med. New York, New Haven, Washington D.C.
Selective abortion because of serious fetal disease or defect is currently practiced in many hospitals during the first and second trimesters of pregnancy. However, after 24 weeks of gestation, when the probability of extrauterine sur- vival increases, termination of pregnancy is often denied, even though third- trimester pregnancy termination was not proscribed by the landmark Roe vs. Wade decision of the US Supreme Court. The authors argue that termination of preg- nancy during the third trimester is a morally justifiable procedure if two ~condi- tions are fulfilled: i) the fetus is afflicted with a condition that is either a) incompatible with postnatal survival of more than a few weeks or b) charac- terized by the total or virtual absence of congitive function; and 2) highly re- liable Oiagnostic procedures are available for determining prenatally that the fetus fulfills either condition la or lb. Currently, one entity, anencephaly, clearly fulfills both conditions. We present our experience with the antenatal diagnosis and obstetrical management of this condition and discuss ethical con- siderations in third-trimester abortion for this and several other fetal diseases and defects. Our intention is to provide a theoretical justification for selec- tive termination of pregnancy under s~ecified conditions which are currently ful- filled by one major fetal defect, and which may, in the future, include a small number of additional fetal defects, but exclude most such defects. During a five-year period, fetal anencephaly was diagnosed in 28 cases at our perinatal ultrasound unit. In i8 of the 28 cases of fetal anencephaly, the gestationai age at the time of diagnosis was less than 24 weeks. In all of these cases, termina- tion o2 pregnancy was elected by the pregnant woman, and the diagnosis of anen- cephaly was confirmed after the abortions. In i0 cases, fetal anencephaly was diagnosed after 24 weeks of gestation. The gestational age was 25-28 weeks in three cases, 29-32 weeks in four cases, and 33-36 weeks in three cases. In each instance, the fetus was alive at the time of diagnosis, and there was no maternal complication necessitating delivery. In all i0 cases, termination of pregnancy was elected by the pregnant women and was induced by prostaglandin E2 supposi- tory (seven cases), oxytocin induction (two cases), or elective cesarean section due to previous cesarean section with vertical uterine incision (one case). In no instance was fetal monitoring utilized. In eight cases, a stillbirth re- suited, and in two cases, neonatal death occurred spontaneously within an hour of birth. In all i0 third-trimester cases, anencephaly was confirmed after birth. There were no maternal complications in this series. Ethical considerations in third-trimester pregnancy termination for anencephaly and other fetal defects including trisomy 21, renal agenesis, holoprosencephaly, trisomy 13, Tay-Sachs disease are discussed.
I I I I I I I I I I I I I I I I
102

| Society of Perinatal Obstetricians ¯
Annual t4eeting San Antonio, Texas
#99 February, 1984
Title:
Authors:
Location:
INFLUENCE OF ROUTE OF DELIVERY AND ANESTHESIA ON INTRAPARTUM TO POSTPARTUM COLLOID OSMOTIC PRESSURE CHANGES
Bernard Gonik~. M.D.* David Cotton, M.D. Tom Spillman, Ph.D.X Karen Dorman, R.N.x
University of Texas Medical School at Houston Houston, Texas
A study was undertaken to determine the effects of route of delivery and anesthetic choice on plasma colloid osmotic pressure (COP). Plasma COP was measured on a~mission to the hospital and 8 to 24 hours postpartum in 72 patients at term with uncomplicated prenatal histories. Thirty-six patients underwent uncomplicated vaginal deliveries (18 - local anesthesia, 18 - conduction anesthesia) and 36 patients had cesarean sections (18 - conduction anesthesia, 18 - general anesthesia). The mean (+ SD) intrapartum COP of the overall group was 21.0 + 2.1 and declined significantly (p ~ 0.01) to 15.4 + 2.1 -.,Hg postpartum. A comparison of the reduction in COP that occurre~ intrapartum to postpartum between those undergoing vaginal delivery and those undergoing cesarean section revealed no significant differences. Furthermore, the mean reduction in COP when all four groups were compared by type of anesthesia was not significantly different. Fifteen patients (20.8%) in the study had a postpartum COP of less than 13.6 um~Hg and five (6.9%) had a postpartum COP of less than 12.5 ,~,Ng. Our results indicate that for normal pregnancy COP is uniformly lowered in the postpartum period and, in some cases, to levels that have been reported to be dangerously low. Although all patients studied had written orders for intravenous fluids to run between 125 - 150 ml/hr, a review of the charts demonstrated excessive crystalloid a~-inistration during the intrapartum and postpartum periods. Since COP changes are related to crystalloid ac~inistration, care should be taken to carefully control fluids in patients at risk for pulmonary edema during labor.
I ! ! I I I i I I I i i i
I i

#100
Society of Perinatal Obstetricians Annual/qeeting
San Antonio, Texas February, 1984
I I I
NICARDIPINE TOCOLYSIS OF PRETERM LABOR IN THE PREGNANT RABBIT
R. Harold Holbrook, Jr.,M.D., Michel Lirette, M.D.,x Michael Katz, M.D. Department of Obstetrics,Gynecology, and Reproductive Sciences, and the Cardiovascular Research Institute, University of California at San Francisco.
The effect of tocolysis with Nicardipine hydrochloride (NIC) on induced preterm labor was studied in 20 pregnant New Zealand white rabbits. On day 27 of gestation, extraovular microballoons, electromyographic electrodes, and an extraovular infusion catheter were implanted. After a 48-hour recovery period, prostaglandin F2-alpha was infused in a stepwise manner into the extraovular space to induce preterm uterine contractions. NIC was then admin- istered intravenously as follows: A) 7.3 mcg/kg/min through 36.2 mcg/kg/min in equal steps; B) 36.2 mcg/kg/min continuously; C) 73 mcg/kg/min through 362 mcg/kg/min in equal steps. Stepwise incre- ments were administered over 20 minutes and the uterine activity
recorded for an additional 20 minutes at the final dose in each group. A fourth group received only saline infusion. Frequency of contractions(FRC), Montevideo Units(MU), frequency of electrical bursts (FRE), and Myoelectrical Index (MI) were recorded and expressed as percent of baseline activity before NIC. GROUP FRC MU
A 78.3+18.6 46.3+17.2 B 37.7~16.9 19.1~ 6.8 C 8.95 9.5 5.35 6.2
saline 86.0+ 7.0 71.9+18.0 baseline i00.0 100.0
FRE MI N
74.9+23 45.8+20.0 5 46.25~23. i 28.8+14.4 5 6.57 5.6 2.0+ 1.7 5
87.7~ 7.8 82.2+ 8.1 5
100.0 I00.0 5
We conclude that NIC has potent tocolytic activity upon PgF2-alpha induced preterm labor in the rabbit. The tocolytic effect is dose- dependent and is apparent in both myoelectrical and mechanical uterine activity. These findings suggest that NIC deserves further
investigation as an agent for inhibition of preterm uterine activ- ity.
I I I I I I I I I I ! i I
104

I I I I I I i I i I I ! I I I I I I I
SPO BUSINESS MEETING
Dr. Robert Hayashi, Presiding
5:30 - 6:30 p.m.
Friday, February 3, 1984
East Regency Ballroom
105

I I I I i I I I I I I I I I I I I ! I
Notes

SCIENTIFIC SESSION IV
Moderator: Dr. Edgar Makowski
Saturday, February 4, 1984
8:15 - 9:45 a.mo
East Regency Ballroom
I ! I ! I, i I ! I i ! I I I I I i I I

#17
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I
8:15 a.m. o February 4th
! PREMATURE RUPTURE OF MEMBRANES OCCURRING IN PREGNANCY PRIOR TO FETAL VIABILITY Thomas J. Garite, M.D. and Jo Taylor, M.D. Women’s Hospital, Memorial Medical Center of Long Beach, CA and The University of California, Irvine Medical Center,
Irvine, CA.
I I I I I I I I I I I I
Premature rupture of membranes (PROM) during the early gestational ages of pregnancy 616-25 wks) often results in the immediate termination of a pregnancy by the clinician. This approach is apparently taken because maternal risks from infection are thought to be too high to justify continuation of pregnancy given a presumed low likelihood of achieving a viable infant. However, data regarding risk of infection or likelihood of neonatal survival within this gesta- tional age group is unavailable. A retrospective review of all deliveries at Long Beach Memorial Women’s Hospital for the four year period of 1979 through 1982 was undertaken. A total of 109 patients were found with PROM between 16 and 25 weeks of pregnancy. Of these, 53 cases which were managed expectantly were found. The median gestational age at the time of the PROM was 23 weeks. Length of time from rupture of membranes until delivery ranged from 5 hours to 87 days with a mean of 16.8 days; 62% of patients delivered within one week, 71% within 2 weeks and 77% within a month. Eighteen patients carried their pregnancies to at least 26 weeks. Indications for delivery included spontaneous labor in 37 patients, 13 of which had clinical infections; 9 patients were induced because
of infection and the remainder were delivered for fetal demise, fetal distress or vaginal bleeding. Forty-two patients were delivered vaginally and II required cesarean section. Overall 22 patients (41%) deve!oped amnionitis prior to delivery. The risk of infection did not increase with longer duration of rupture of membranes. Four patients had prolonged postpartum hospital stays (>7 days) because of sepsis, thrombophlebitis or endometritis. Twenty-two mothers (42%) had no complications following expectant management. There were 53 deliveries, 7 twins, for a total of 60 babies. Sixteen (27%) of the fetuses were stillborn, all born prior to 26 weeks. There were 31 neonatal deaths. Of the neonatal survivals, half had ruptured membranes prior to 23 weeks and half had ruptured after that point. Thirteen infants with birthweights ranging from 740 grams to 2170 grams survived the neonatal period and went home alive. Follow-up data was available on 9 of the 13 surviving infants. One died at 9 months, 3 had mild to moderate neuro- muscular morbidity and 5 were developing normally at 6 months to 2 years. In considering whether or not expectant management of the patient with PROM prior to viability is reasonable, the above data may help one make that decision. Without expectant management, the perinatal mortality rate would be close to 100%. With expectant management the maternal morbidity rate was nearly 60~. However, there were no permanent sequelae in these mothers and serious complications were few. The 25~ survival rate with reasonable long-term follow-up of these surviving newborns would suggest that conservative management of patients with early PROM with immediate delivery for infection may be a reasonable alternative for mothers who understand and are willing to take the risks.
I
107 I

#18
Society of Perinatal Obstetricians Annual/Vieeting
San Antonio, Texas February, 1984
! !
8:30 a.m.- February4th
DIETARY SODIUM MANIPULATION, ANGIOTENSIN II, AND BLOOD PRESSURE REGULATION IN PREGNANCY
lilton I. Lee, MD, Herbert Todd, BS, and Robert J. Sokol, MD-Hutzel Hospital/Wayne State University, and St. Louis University - Departments of OB/GYN.
The renin-angiotensin system and dietary sodium have been repeatedly implicated in the pathogenesis of pregnancy induced hypertension (PIH). Mechanisms responsibl~ for increased vascular responsiveness to angiotensin II (A-II) observed in PIH are not completely understood. Plasma A-II levels and blood pressure are functions of sodium balance in the non-pregnant state, but less is known about their relationshil during gestation. A-II levels increase in normal pregnancy, but the reported level~ of this pressor substance circulating in subjects with PIH are in conflict. The pregnant rabbit demonstrates several conditions similar to those found in pregnant human subjects. We used this model to study the effeCts of dietary sodium manipula- tion on plasma levels of A-II and BMAP during late pregnancy in 22 chronically pre- pared New Zealand white rabbits. The animals were 24 to 28 days gestation (term 30 ± 1 day). All animals were maintained on 1 of 3 diets for 8 days prior to opera- tion and for the duration of the investigation: 7 were fed Purina regular chow (0.4% sodium), and permitted to drink 0.9% saline; 7 were fed trace-sodium diet (Purina 5881-R) and deionized water ad libitum; and 8 were continued on tap water and regular rabbit chow (0.4% sodium) and served as controls. Urines were collectec for 24 hours prior to surgery for sodium determination. An indwelling catheter was )laced in the carotid artery and connected to a 8805 C Hewlett-Packard recorder, vi~ a transducer. After a 20 minute stabilization period, BMAP was repeatedly recorded for 1 minute and 4 ml of blood were obtained from the indwelling catheter and suit. ably preserved for determination of A-II levels and sodium concentration. Plasma A-II was determined by RIA methods described by Goodfriend, Ball and Farley.
Urinary and serum sodium levels were also determined. All data are reportedI as means ± S. E. and analyzed using one-way analysis of variance. ,
Salt Loaded (n=7)
Salt Restricted (n=7)
Controls (n=8)
Urine Na Serum Na BMAP (mM/L) (mM/L) (mm 237 + 30 142 +- 2 83 + 3
5 ± 2 133 + 2 72 + 3
26 + 6 139 +- 0.4 67 ± 3
F = 46.26 10.30 5.97
A-II (pg/ml)
32 ± 19
325 ± 79
135 ± 25
4.96
.025 P < .005 .005 .025
As shown in the table above dietary sodium manipulation significantly alters urinar and serum sodium concentrations. The level of Plasma A-II is a function of sodium balance and can be manipulated by dietary means. If this is also true in PIH, the state of sodium balance in these hypertensive subjects may in part be responsible for the conflicting reports on plasma levels of A-II. Further studies of this relationship in humans suffering from this disease are needed.
I ! i I ! I
I I I I I i
108
I! !

#19 8:45 a.m. - February 4th
Society of Pefinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
~0 PROSTAGLANDINS PLAY A ROLE IN THE ANTIHYPERTENSIVE EFFECT OF PREGNANCY IN THE ,SPONTANEOUSLY HYPERTENSIVE RAT? Robert A. Ahokas,x Garland D. Anderson, Sam L. Reynoldsx and Jeffrey Lipshitz, Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee Center for the Health Sciences, Memphis, Tennessee.
Pregnancy has a profound antihypertensive effect in the spontaneously hyper- tensive (SHR) rat. Blood pressure falls progressively during the last week of gestation until it is in the normotensive range just before term. Since blood levels of PGE2 increase coincident with the decline in blood pressure, it has been suggested that prostaglandin (PG) may play a role in this antihypertensive effect. As an entry into a study of the mechanisms involved, we measured maternal cardiac output (CO) and organ blood flow in conscious 21 day pregnant (N=IO), and age- matched nonpregnant (N=61, SHR with 15 ~m diameter radioactive labeled microspheres. To test the hypothesis that PG are involved in the fall in blood pressure, the pregnant rats were subsequently given the PG synthetase inhibitor Indomethacin (2-10 mg/kg IV.), and CO and organ blood flow was measured again 30 min. later with differently labeled microspheres. Mean arterial blood pressure (MAP) was reduced in the pregnant rats as compared with the nonpregnant rats, while CO was increased (see Table). Thus total peripheral resistance (TPR) was reduced in pregnancy. Blood flow to the pancreas, small intestine, and ovaries was increased, while that to the kidneys, spleen, and uterine tissue was decreased in pregnancy. Heart, adrenal, hepatic arterial, stomach, large intestine and skeletal muscle blood flow was unchanged. Vascular resistance was significantly reduced in the heart, pancreas, gastrointestinal tract, ovaries, and skeletal muscle of the pregnant rats, and increased only in the uterine tissue itself. While MAP was slightly, but significantly, lower following Indomethacin, neither CO nor TPR were signifi- cantly affected (see Table). Except for a small decrease in adrenal and hepatic arterial resistance, Indomethacin had no effect on the vascular resistance of the measured organs. The results indicate that the decrease in MAP that occurs during pregnancy is the result of a reduction in TPR due to a generalized decrease in the vascular resistance of most body organs and the carcass (skeletal muscle). Since their inhibition did not increase TPR, it appears that PG do not play a role in the pregnancy-induced reduction of vascular resistance, at least at term. Additional work is necessary to determine which factors are involved in the antihypertensive effect of pregnancy.
Preqnant Nonpregnant Before Indomethacin After Indomethacin
MAP (mmHg) 160.0 + 3.6 112.0 + 6.3* 103.0 + 6.5 + CO (ml/min) 70.0 ¥ 6.6 I05.0 ¥ 13.1" 102.9 ¥ 11.6 TPR (R units/9.) 2.42 ¥ 0.14 1.58 ¥ 0.17" 1.52 ¥ 0.26
* Significantly different from nonpregnant (~<0~’05) + Significantly different from pregnant before Indomethacin (P<O.05).
I
I !
! I
I I ! I I 1 i
109

#2O 9:00 a.m. - February 4th
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
B.R_. Kuhnert, ~.D.,x E.H. Philipson, iM.D.x, P.M. Kuhnert,x Metropolitan General Hospital/OalRU, Cleveland, Ohio.
Ph.D. and C.D. Syracuse, B.s.,X Cleveland
Normeperidine, the active meperidi~e metabolite, has been impli- cated in the adverse neonatal effectS that may follow the a@ministra- tion of meperidine. However, r~nt Studies have suggested that nor- meperidine levels are not high enough to have adverse effects follow- ing single low doses of meperidine. It is not known if nonneperidine reaches clinically significant levels following m_~Itiple injections of maperidine over several hours. ~herefore, the ~urpose of this study was to docunent the disposition of meperidine an~ normeperidine in
mother, fetus-and neonate following imultiple doses of meperidine. Twelve mothers who received multiple doses of mepe-idine intravenously and their infants were Studied. Mate~al blood was collected intra- part,m, umbilical cord blood at delivery, and maternal and neonatal blood and neonatal urine s~les were: collected postpartum. Meperi- dine and normeperidine were analyzed using gas chrcmatographyhnass spectrometry techniques. In the mother, the data show that both mepe~idine and normeperidine acctm~late in plasma following mlltiple injections (Figure). The half life of normeperidine averaged 20.6 hours. Since neither drug decreases in plasma, there is a continued dif- fusion gradient frcm mother to fetus. In the fetus, high concentrations of both meperidine and nor- meperidine were found in unbilical cord blood at delivery; the meperidine levels were oomperable to those found in maternal plasma shortly after a 25rag intravenous injection. The fetal data also show that the anount o~ normeperidine increased with time in u~bilical cord blood, that the ratio of nor- meperidine to meperidine increased with time, and that the t,nbilical artery to vein ratio of meperidine (but not normeperidine) was greater t~ one following long drug to delivery intervals; these data sug- gest that both meperidine and normeperidine are continuously accumulating in fetal tissues after multi- ple doses. Additional findings were that ion trapping of meperidine can occur if the fetus is acidotic, and that normeperidine levels of 60% Or more of the total active drug oculd be present in fetal blood at delivery. In the neonate, normeperidlne plasma and urine levels increased as meperidine decreased and elimination of both cc~unds wasi prolonged. Mean plasna half lives were 13.2 and 62.6 hours for meperidine and normeperidine, respectively. The study suggests that multiple doses of meperidine to the mother over long periods of time ’esult in maximun exposure of the fetus to both mepe~idine and nor- meperidine.
I I ! I ! !
I ! ! ! I ! ! I I I
110

#21
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I
9:15 a.m. - February 4th !
I
! ! I I I I i
! I I I
PENICILLIN ALLERGY AND DESENSITIZATION IN SERIOUS MATERNAL/FETAL INFECTIONS. Georg~ D. Wendel, Jr., M.D.,* Barbara J. Stark, M.D.,x, Richard B. Jamison, M.D.,~ and Timothy J. Sullivan, M.D.,x Depts. of Ob/Gyn & Internal Medicine, Univ. Texas Southwestern Med. Sch., Dallas, TX 75235 (Sponsored by F. Gary Cunningham, M.D.)
Selection of a drug of choice for therapy of antepartum systemic infections involves consideration of maternal/fetal pharmacokinetics, organism susceptibility and drug allergy. In infections complicated by penicillin allergy, the second choice antimicrobial often is less efficacious in curing infection and may have adverse fetal effects. Five cases of maternal infections with potential for direct and indirect fetal morbidity are reported in which allergy to penicillin complicated selection of antibiotic therapy. Three women had syphilis and one had listeriosis, both of which, if untreated, may cause abortion, premature labor, stillbirth, congenital infection, or neonatal death. The other woman had endocarditis due to Strep. viridans complicated by mitral regurgitation and septic cerebral embolization. All five patients related a history of allergic reactions to penicillin, four of which were systemic in nature, including one that occurred during skin testing. Each woman manifested immediate wheal and flare skin test reactions to the major determinant antigen of penicillin, benzylpenicilloyl- polylysine. Every patient showed sensitivity to at least one of the minor determinant antigens: 3 of 5 were reactive to penicilloic acid and all five were reactive to penicillin G. These five women underwent a total of six acute desensitizations using a protocol with oral benzylpenicillin. The initial dose administered was 100-200 units which then was doubled every fifteen minutes to a total of over i million units prior to giving parenteral therapy. There were no serious acute allergic reactions, but three patients experienced mild urticaria or pruritis in the first 24 hours of desensitization and therapy. Only one patient, who experienced urticaria, warranted antihistamines for relief of pruritis. Maternal response to antibiotics has been satisfactory in all five cases. Fetal therapy has been effective in both infants delivered from the syphilitic mothers to date; one is still pregnant. In the woman with listeriosis, pregnancy was complicated by vaginal bleeding at the i,~itiation of therapy; and the gestation ultimately aborted. The infant born to the woman with endocarditis is normal. We conclude that acute penicillin desensitization for the pregnant woman appears to be free of serious allergic reactions and permits the use of penicillin in specific infections in which alternative antimicrobials may be unsatisfactory.
I I
111

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #22 February, 1984
9:30 a.m. - February 4th
BIPARIETAL DIAMETER FEMORAL LENGTH GROWTH IN NORMAL TWIN PREGNANCIES X X * X X
D. Graham, M.D.; Y. Shah, M.D.; S. Moodley, M.D.; F.J. Yannuzi; S. Logghe
The relationship of biparietal diameter and femoral length to gestational age has been well evaluated in the normal and abnormal singleton pregnancy. Published series of biparietal diameters in twin pregnancies have produced conflicting re- sults with studies showing identical growth, persistently decreased growth or late slowing of growth of twins compared to singletons. These conflicting results are in part due to the small series sizes used and in part due to the inclusion of twin pairs in which growth of one or both twin had significant growth retardation. (e.g. due to twin-twin transfusion) The present study was designed to determine the relationship of biparietal diameter and femoral length to gestational age in a group of twins with good clinical dating, delivery after 36 weeks and non-dis- cordant growth. The biparietal diameter and femoral length measurements were ob- tained on 2,304 singleton pregnancies and 104 twins who had delivered after 36 weeks, had good correlation of clinical gestational age, early sonographic eval- uation of gestational age, and Dubowitz assessment at birth consistent with gest- tational age at birth. Biparietal diameter was seen to increase linearly with gestational age until approximately 28 to 30 weeks when there was a slowing in BPD growth. A similar curve was obtained for femoral length against gestational age. Linear and long regression fits were obtained for these parameters for both the singleton and twin pregnancies and almost indentical results were obtained. It is concluded that under normal circumstances fetal growth, as assessed by BPD and femoral length, is identical in singleton and twin pregnancies and that pre- vious studies showing a decreased growth in twins have resulted from inclusion of twin pairs with significant discordant growth.
The University of Rochester Medical Center Department of Obstetrics and Gynecology Rochester, New York 14642
!
I
I
112
I I

SCIENTIFIC SESSION V
Moderator: Dr. Roy Petrie
10:15 - 11:45 a.m.
February 4, 1984
East Regency Ballroom
I I I I I I I I I ! I I I I I I I !

#23 10:15 a.m. - February 4th
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
CONTINUOUS LONG-TERM INTRAVENOUS BETAMIMETIC TOCOLYSIS. Washing.ton C. Hill, M.D.*, Michael Katz, M.D., John L. Kitzmiller, M.D., and Pamela J. Gill, R.N., M.S,N.X, Department of Obstetrics and Gynecology, Chi]dren~s Hospital of San Francisco, San Francisco, California.
Serious maternal cardiovascular complications have occurred with the use of the beta-adrenergic agonist tocolytic agents. These side effects have usually been diagnosed after 24-96 hours of parentera] treatment. It has therefore been recom- mended that parenteral tocolysis be replaced by oral medication within 24 hours. Such a therapeutic protocol is efficacious, but our experience has shown that in 2-4% of patients undergoing tocolysis, oral therapy could not effectively control preterm labor. In these patients, the choice is either continuous long-term parenteral tocolysis or preterm delivery. This preliminary report concerns the clinical course and outcome of 16 patients treated by continuous long-term intra- venous betamimetic tocolysis (~ 1 week intravenous therapy). Half of the patients were on therapy for at least 5 weeks. Infusion rate was adjusted so that uterine activity did not exceed 4-6 contractions/hour and that pulse rate was not ~ 120- 130 bpm ~ 2 hours; BP not less than 90/40 torr. This mode of therapy was continued (n=ll) unless clinical condition necessitated the addition of intravenous magnesium sulfate MgSO4 (n=5). Parenteral tocolysis was continued until there was either a successful transition to oral therapy or fetal maturity or maternal/fetal indica- tion for delivery. Our data indicate that the cardiovascular and metabolic effects were pronounced mostly during the first 3-4 days of therapy and then returned toward pre-treatment values. The clinical course and outcome are presented in the following table:
(mean ~
MAXEANAL AGE (Y~) 30 ~
PRIMIPARA II TH[RAPY WITH ADDITION OF HDS04 (WK)
HULTIPARA 5 GESTATIONAL AGE WHEN IV THERAPY STARTED (WK)
SINGLETON 12 GESTATIONAL AGE WHEN IV THERAPY STOPPED (WK)
TWINS 3 DURATION IV THERAPY (RANGE: 1-12 WKS)
TRIPLETS I GESTATIONAL AGE AT DELIVERY (WK)
Cx DILATION ONSET IV THERAPY (CH) .7 ~ .6 PATIENTS AEHIEVINE TRANSITION TD ORAL THERAPY
£~ EFFACEMENT ONSET IV THERAPY (~) 56 ~ 19 PATIENTS ACHIEVING ~ 36 WEEKS GESTATIONAL AGE
In none of the study patients was the treatment discontinued because of drug re-
lated problems, EKG changes, chorioamnionitis or fever. In summary, our experience indicates that in a selected group of patients and under close supervision, con- tinuous long-term intravenous betamimetic tocolysis may be considered a safe thera- peutic modality able to prolong pregnancy with a more desirable outcome.
I
I
I
I I I
I I
113 I

#24 10:30 a.m. - February 4th
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I I
LIDOCAII~] FOR EPISIUIL~[f: Ei±iot H. Philipson~ M.D. Betty R. Kuhnert,x Ph.D., Caro± D. Syracusex, B.S., Clevei~u%d Met~-opolitan General Hospita±, Pe~’inatal Clinical Resea~ch Center, Case Weste~’n Resetre Univel-sity, Cleve!~!]d, Oi~io
An eplsiotomy is generally pe~forr~d afte~ infiltrating the pe~ineu~ %~ith a .local anesthetic agent. A small ~ount of local anest~etic agent c~n be administered quickly ~nd accurately ho the parturient just to vagJ!~al delivery ~d unDiiical cord c!~.ping. As a resui~ of the s~Drt d~’ug to delive£y interval, ve£-y little ±oca! ~esthetic agenh was thought to reach the fetus. However, the [~ternal and neonata± disposlt~on of a co~ly used local anesthetic agent n~ not beei~ studie~] folio%.;ing local perineal infiltration fo~ episioto,ly. ~_~!~.-gose of this study was to docu~%h p!ac ~ental t[-ansfe~ o~~ non tr~nsfe~ of ±idoca~ne following local perlneal infiltration. Fifteen no~~al parturients ~d their infants were studied. After local per±heal infiltration, hhe conc~ntrations of iidoca~ne and two ~taboJ.ites and ~X) we£e deter-mined in ~ternai plasma, in u~i~ilical cord vein a~ deiivery~ in materna! and neonaUal piasr~ or urine for t%.~ days posbpartum. Lidocaine and its metaboiihes were [~%titated by gas chromatography/mass spectrometry. The phar~cologic results indicated the fo±~owing: First, lidocaine is detected in [~ternai pias~a a~ early as one minute post injection and pe~ plasma c~centrations occur 3-15 minutes. Second, the£e is rapid placental trar~fer of lidocaine; the me~ fetal [~ternal ratio of 1.32 %~;as significant±y higl~r than tlmt found foiio%.;ing c-pidurai anesthesia. Third, lidocaine and ~ts active ~taboiites persisted in neonatal urine for at least 48 ~u~s post delivery. This study suggests tl]ah local perineal infiltration with lidocaine for episioton[f should be considered similar to any other ~,esthetic tecl’mique in tlmt it may ~esult in significant neonatal drug ~posure.
I I I I I I I I I I I I I I I
114

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#25 February, 1984
10:45 a.m.. February 4th
i PRETERM LABOR MANAGED WITHOUT TOCOLYSIS.
X Peter Boylan
The National Maternity Hospital, Dublin.
Tocolytic agents are not used in any circumstances at the National Maternity Hospital, Dublin. A progressive fall in perinatal mortality attributed to spontaneous preterm labor over the past fifteen years, despite lack of tocolytic therapy, has been reported previously (Boylan and O’Driscoll, Am. J. Obstet Gynecol. 145: 781, 198B). This report presents the results of a prospective analysis of the perinatal outcome of al! patients who presented to the hospital in 1981 with a presumptive diagnosis of preterm labor. The study was done so that contemporary figures for the outcome of untreated preterm labor might be available to units already using tocolytics, or contemplating their introduction. All births were analysed prospectively from January 1st thru December 31st 1981. By definition a preterm birth occurred between 20 weeks (140 days} or 500 g. birthweight and 37 weeks (259 days). Detailed analysis was confined to patients who presented with a presumptive diagnosis of preterm labor. Outcome was measured by perinatal death, including neonatal death up to 28 days, and incidence of respiratory distress syndrome (R.D.S.). during the year 8996 infants were born; 332 (3.7%) were preterm. Birth was attributed to spontaneous preterm labor in 265 instances; 67 infants were delivered electively, 51 by caesarean section and 16 by induction of labor. 295 women presented with a presumptive diagnosis of preterm labor; 240 delivered and 55 proceeded to term; 265 infants were born to the 240 w~men who delivered preterm: there were B3 perinatal deaths among these 265 infants: 2- fetal deaths, no death in labor, 12 neonatal deaths and 2 deaths due to malformation. Causes of death and details of labor are analyzed. There was a 10% incidence of R.DoS. among the 2BB normally formed live-born infants. There were no deaths among the 55 patients who proceeded to term. The results demonstrate that the perinatal outcome of preterm labor, managed without tocolytic agents is no worse, or better, than outcome where there have been attempts at inhibition of labor. This conclusion is discussed.
I I I I I I I I I I I I I
115

#26 11:00 a.m. - February 4th
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
EMERGENCY HYSTERECTOMY AND HYPOGASTRIC ARTERY LIGATION IN THE CONTROL OF OBSTETRIC HEMORRHAGE, Steven L. Clark, MD~ Sze-Ya Yeh, MD~ Sanuel Bruce, MD~ Richard H. Paul, MD~ Department of Obstetrics & Gynecology, University of Southern California School of Medicine and Women’s Hospital, Los Angeles County/USC Medical Center, Los Angeles California
From 1978 to 1982, 70 cases of emergency hysterectomy were performed for obste- tric hemorrhage at our institution. Sixty hysterectomies followed cesarean section and I0 were performed electively or for sterilization. The most common indication for hysterectomy was atony (43%) followed by placenta accreta (30%), uterine rupture (13%), extension of a low transverse incision (10%) and fibroids making uterine closure and hemostasis impossible (4%). Hysterectomies performed for atony had a significant association with the following factors when compared to hysterectomies ,performed for other indications: age, parity, amnionitis, cesarean section for ilabor arrest, oxytocin augmentation of labor, MgSO4 infusion and fetal weight. Fifty. seven percent of hysterectomies performed for placenta accreta were associated with a previous cesarean section. During this study period, 53% of all patients pre- senting at term with both a placenta previa and one or more previous cesarean sec- tions subsequently underwent hysterectomy for placenta accreta. Patients undergoing !cesarean section for arrest disorders in the face of amnionitis, oxytocin augmenta-
ition of labor, MgSO4 infusion or fetal macrosomia, and patients presenting at term with the combined diagnosis of placenta previa and one or more previous cesarean section will account for two-thirds of all patients who subsequently undergo emer- gency hysterectomy. Sub-total hysterectomy is not associated with decreased blood loss, operating time or post-operative infection when compared to total abdominal hysterectomy. However, this is a function of the clinical situation in which each type of operation is employed. Although STH remains the procedure of choice in the face of massive blood loss, this operation may be ineffective in’cases of placenta previa-accreta. In 24 patients, estimated blood loss at the time of the decision for hysterectomy was recorded and averaged 2125 ml. This subgroup of patients lost, on the average, an additional 2183 ml prior to termination of the surgery. During this 5 year period, hypogastric artery ligation for control of hemorrhage was succ- essful in 8 of 19 cases (42%), Mean blood loss and operating time were increased in patients undergoing hypogastric artery ligation. Two of three intraoperative cardiac arrests: and two of three ureteral injuries occurring in this entire series occurred in patients undergoing unsuccessful hypogastric artery ligation. Hypo- gastric artery ligation for the control of obstetric hemorrhage should be restricted .to hemodynamically stable individuals of low parity in whom future childbearing is fan overwhelming concern.
I I I I I I I I I I I I I I I I I I
116 I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#~.7 February, 1984
11:15 a.m. - February 4th
MULTIPLE GESTATION: TIME INTERVAL BETWEEN DELIVERY OF THE FIRST AND SECOND TWIN William Rayburn, Justin Lavin, Menachem Miodovnik, and Michael Varner Departments of Obstetrics and Gynecology, University of Michigan, Akron City Hospital, University of Cincinnati, and University of Iowa.
An intrapartum dilemma unique to twin gestations is the time interval that should be allowed between the deliveries of the first and second fetuses. The temptation to perform an expedient extraction is great, since uterine inertia, umbilical cord prolapse, placental abruption, fetal hypoxia, and stillbirth are concerns. An accepted view for many years has been that the interval between the delivery of the twin infants should be preferably within 15 minutes and not certainly beyond 30 minutes.
This guideline may not be applicable to the present standard of obstetric practice, since these time restraints were recommended initially when continuous intrapartum fetal and uterine monitoring and intensive care nurseries were either unavailable or in the early stages of development. The delivery of the second twin in the least traumatic manner is an especially major concern today and may not be accomplished easily within the previously proposed time interval. The present study was therefore undertaken to test the authors’ clinical impression that the second twin may be delivered safely beyond this commonly accepted time limit. Methods
The perinatal outcomes of twin pregnancies delivering during 1981 and 1982 were compared at four regional perinatal centers. Protocols at each institution for the anticipated delivery of twins were essentially the same. The study group consisted of pregnancies in which vaginal delivery at 34 weeks gestation or beyond was undertaken if the first fetus was in a cephalic presentation. Results
During the two year period, 21,420 patients were delivered at the four institutions. Of the 294 (1.4%) twin gestations, 115 qualified for this investigation. The time interval between vaginal delivery of the first and second twin averaged 21 minutes (range 1-134 minutes). The elapsed time interval was within 15 minutes in 70 (61%) cases, within 16-30 minutes in 28 (24%) cases, and more than 30 minutes in 17 (15%) cases. The maternal ages, race, parity, gestational ages at delivery, and form of anesthesia were similar regardless of whether the delivery occurred within the first 15 minutes, 15-30 minutes, or more than 30 minutes.
Excluding conditions associated primarily with prematurity, all second twins that delivered beyond 15 minutes did well despite the delay and had no signs of excess trauma or low five minute Apgar scores. Total breech extraction of 11 second twins occurred Within the first 15 minutes, in contrast to spontaneous or assisted extraction of the other 34 breech fetuses which occurred in a less hurried manner.
Extensive lacerations of the cervix or vagina, halothane anesthesia for delivery of the second twin, retained placental fragments requiring re-exploration, and postpartum anemia requiring transfusion were uncommon and not more frequent in those patients delivering the second twin vaginally after the initial 15 minutes. Combined vaginal-abdominal delivery in 10 (9%) of the 115 cases were significantly more common after the initial 15 minutes (8/45 vs 2/70, p<0.02). Conclusion
We conclude that if there is continuous fetal and uterine monitoring, a time restriction for the delivery interval between the first and second twin is not necessary at or beyond 34 weeks gestation.
I I I I I I I I I I I I I I I
117
I I

#28 11:30 a.m. - February 4th
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
EFFECT OF MATERNAL SMOKE EXPOSURE ON ULTRASTRUCTURE OF FETAL PERIPHERAL BLOOD VESSELS IN THE MOUSE Robert C.Kaufmann, M.D., Kofi S. Amankwah, M.D., Aruna D. Weberg* Southern lllinois University School of Medicine, Department of OB/GYN, Springfield, Illinois
Ultrastructural changes have been found in umbilical blood vessels, placental blood vessels, and peripheral blood vessels in human fetuses whose mothers smoked during pregnancy. This study was undertaken to determine if similar changes could be found in peripheral blood vessels in mice fetuses whose mothers were exposed to cigarette smoke during pregnancy. Breeding mice of the C57BL/KsJ strain were placed in a smoking box and exposed to cigarette smoke as we have previously described. This produces carbon monoxide levels in the adult mice similar to that found in human adults smoking one pack of cigarettes per day. Similarly caged mice of the same strain were used as controls. The female mice were not removed from their cage from the pre-conception time until after delivery. After delivery each pup was sacrificed via neck fracture and the entire pup was immersed in a solution of 2.5% gluteraldehyde in O.1M cacodylate buffer at pH 7.3. While still under solution, the rear leg muscles were dissected free, sliced, and immersed in the same preservative for four to five hours. They were then placed in fresh 2.5% gluteraldehyde mixture overnight. The tissues were post-fixed in Osmium ferro-cyanide and enblock stained with uranyl acetate in a graded series of alcohol. The tissues were infiltrated and embedded in Spurr. Sections were taken via an ultramicrotome and post-stained with uranyl acetate and lead citrate. The sections were examined in a Phillips 201 electron microscope at 60VK. In the peripheral vessels of the fetuses from smoke-exposed mothers, endothelial blebbing (both surface-type and vacuole-type) was seen. In addition, dilated rough endo- plasmic reticulum was found in these vessels. These findings were not demon- strable in the control fetuses. Surface-type blebs, dilated RER, thickened basal lamina, and collagen changes have been found in the umbilical blood vessels of human fetuses whose mothers smoked during pregnancy. Vacuole-type endothelial blebs have been seen in the aortas of adult rats exposed to cigarette smoke. Carbon monoxide exposure alone has produced similar vacuole-type endothelial blebs in the rat aorta. In all of the previous studies the vascular changes were seen in vessels that initially received the blood that was exposed to noxious effects of cigarette smoking (umbilical vessels and adult aortas). This is the first known report of finding changes in vessels far-removed from the point of noxious transfer in fetuses of smoke exposed mothers.
I I I I I I I I I I I I I I I I I I
118 I

POSTER SESSION B
12:00 - 2:00 p.m.
February 4, 1984
Rio Grande Ballroom
I I I I I I I I I I I I I I I I I I I

m Society of Perinatal Obstetricians m Annual Meeting
San Antonio, Texas m #101 February, 1984
IMMUNOGLOBULIN G (IgG) SUBCLASSES AND NEONATAL OUTCOME IN PREGNANCIES COMPLICATED BY ISOIMMUNIZATION M. Mark Taslimi, M.D.*, Baha M. Sibai, M.D., John V. Dacus, M.D. and James M. Mason, Ph.D.x Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
Removal of IgG sensitized cells by macrophages in the spleen is probably the major mechanism of red cell destruction in hemolytic disease of newborn (HDN). Most blood group antibodies have at least a portion of the immunoglobulin molecule belonging to an IgG subclass. Identification of the IgG subclass is important in HDN, because of differences in the rate of placental transport and ability of the IgG subclass to interact with macrophage receptor. IgG 3 is the most efficient antibody at binding to macrophages and therefore potentially the most destructive to fetal red blood cells. Sixteen antepartum patients with positive indirect Coombs’ test were studied. Patient evaluation included antibody identification, maternal antibody titer and score, IgG subclass of such antibody, 0D450 analysis of amniotic fluid, cord blood Coombs’ test and neonatal outcome. The findings in thirteen such cases are summarized below. Our primary findings suggest that HDN does not occur in the absence of IgG 3 subclass in maternal circulation.
Patient Antibody Indirect Score IgG a OD Cord Blood Neonatal Outcome Identified Coombs Sub 450 Direct Antibody
Ttter Class Coombs
W.L. Anti Jsb 1:2024 80 1 Zone 1 + Anti Jsb Good
V.L. Anti S 1:256 61 1 Zone Ix3 + Anti S Good
S.E. Anti Kell 1:256 50 l&2 Zone Ix3 + Anti Kell Good
C.H. Anti Fya 1:32 39 l Zone Ix2 + Anti Fya Good
L.E, Anti D 1:32 39 l&3 Zone 2 + Anti D Hyperbilirubinemia - Photo Therapy
L.A. Anti ~ 1:16 17 4 N/A + Anti ~ Good
B.C. Anti D 1:256 85 2&4 N/A + Anti D Good
B.M. Anti D 1:1000 95 l&3 Zone Ill + Anti D Intra Uterine Trans- fusion x l-Exchange Transfusion x 6
G.C. Anti u 1:64 51 1&3&4 N/A Neg None Good
F.R. Anti Jsb 1:32 N/A 1 N/A + Anti Jsb Good
L.(j)E. Anti S 1:32 27 l&2 Zone 1 N/A N/A Good. Delivered Out- side. No Cord Blood Available
Anti D 1:128 75 l&2&4 Zone 1 + No Anti D Good B.L. Anti Jsb 1:132" 47 4 Anti Jsb
H.R. Anti Kel] 1:512 70 l&2&3 Zone II Still Pregnant
Anti Jka 1:4 26 2
I I i I I I I I I I I i ! i
119
I !

#102
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
BREAST STIMULATION CONTRACTION STRESS TEST: ABSENCE OF OXYTOCIN SURGE. Michael G. Ross,x Rosemary D. Leake,X M. Gore Ervin,x James Simon,x and Delbert A. Fisher.X Harbor-UCLA Medical Center, UCLA School of Medicine, Torrance, CA
The Breast Stimulation (BS) Contraction Stress Test (CST) has been advocated for evaluation of fetal well-being. The criteria for test interpretation has been identical to that of the oxytocin challenge test (OCT). Although oxytocin (OT) is released in response to BS in postpartum women, this response may be suppressed during pregnancy. In an attempt to elucidate the mechanism of BSCST we measured plasma OT levels by RIA in 9 pregnant women at term. Venous blood (6 ml) was collected at 5 minute intervals during a 15 min basal period before BS, during the first uterine contraction, during the third contraction of 3 within a 10 min period, and 5 minutes following BS. There was no significant change in mean (± SEM) plasma OT (3.0 ± 0.4 to 3.2 ± 0.3 uU/ml; basal to 3rd contraction values, respectively). Conclusions: 1. Uterine contractions occur without significant increases in plasma OT during BSCST, and 2. The mechanism of uterine contraction during BSCST is different from that during OCT. Since the uterine response and the fetal reaction thereto during the BSCST may differ from the responses to OCT, it is recommended that uterine contractility, fetal heart rate response, and fetal outcome criteria be separately established for the BSCST.
I ! I I I I I I I I I I I I I I ! I
120 I

#103
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I I
AN ANIMAL MODEL TO EVALUATE THE FETAL EFFECTS OF DIABETES. S.M. Palmer, W.E. Roberts, J.N. Martin, K. Sullivan, J.C. Morrison, University of Mississippi Medical Center, Jackson, Mississippi
Despite the prevalence of significant maternal/fetal/neonatal morbidity, investigators evaluating the effects of maternal hyperglycemia on the fetus have been hampered due to the lack of a suitable animal model. Spontaneous diabetes occurs in the animal kingdom infrequently and is usually associated with infertility. Although an innate state of diabetes in the animal is preferred, it is prohibited by the above factors as a reliable research source. We have performed initial studies on the production of a maternal hyperglycemic state in sheep through the use of intravenous streptozotocin (STZ) administration during pregnancy. Streptozotocin, an antibiotic drug cytotoxic to the ~-islet cells of the pancreas, is available commercially and reliably produces a hyperglycemic state with normal blood levels of ketones and free fatty acids. Streptozotocln, administered to the pregnant ewe intravenously, produces a consistent pattern of alteration in insulin secretion and carbohydrate metabolism occurring with 5-12 days depending on the degree of clinical severity desired. Though administered during pregnancy, this drug has no demonstrable placental passage in the monkey with a hemochorial placenta. The sheep have a desmochorial placentation and are also, therefore, more unlikely to have placental passage. Utiliz- ing a single administration dose in 4 pregnant ewes, we established a consistent elevation of fasting glucose 79 + 8 mg/dl vs 47 + 5 mg/dl control gestational ewes, associated with an elevated glucose metabolic response to a standard intravenous tolerance test. In this group, there was an exaggerated insulin response to glucose load in a pattern similar to adult onset diabetes. In the two dose regime, an elevation of fasting blood sugar to 193 + ii was noted in 4 ewes with little or no endogenous insulin release to glucose or tolbutamide challenge. The fetal progeny of these ewes showed an increase in total body weight 3629 ~ 180 gms versus 2830 + 56 gms in control animals. The fetal pancreatic response to various stimuli was explored and revealed an altered response. Histo- togically, the fetal pancreatic tissue of the diabetic progeny showed an increase in number of ~-islet cells compared to gestational control using an insulin-anti-insulin i~unoperoxidase technique. In conclusion, we feel we have developed a large animal diabetic model which simulates the diabetic disease process that occurs clinically in humans.
I
121
I !

#104
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE RELATIONSHIP OF ARGININE-VASOPRESSIN TO FETAL DISTRESS, S.M. Palmer, W.E. Roberts, K. Sullivan, J.N. Martin, J.B. Harris, R. Leake, J.C. Morrison, Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, University of Mississippi Medical Center, Jackson, Mississi
The release of arginine vasopressin (AVP) by the posterior pituitary is initiated by various stimuli but predominantly in response to oxygen deprivation, hemorrhage and change in fetal or maternal plasma osmo- lality at least in fetal sheep. The physiologic role of fetal AVP secre- tion is not clearly elucidated but its effect on the adenyl cyclase of the renal tubules to conserve urine excretion and on vasculature to maintain central blood flow suggest a stress response. Clearance studies in chronically catheterized fetal sheep indicate a slow clearance of amniotic fluid AVP by placental vasopressinases in contrast to plasma levels of AVP. To determine if AVP levels in human amniotic fluid and fetal plasma might be indicators of acute and long term fetal distress, we collected, at the time of cesarean birth, amniotic fluid and mixed umbilical cord blood from nine term fetuses. The primary criterion for inclusion in the study was non-emergent repeat cesarean birth (n=7) or abdominal delivery for fetal distress (n=6). Each parturient had the onset of labor less than 6 hours prior to delivery. Samples for AVP
were analyzed by radioimmunoassay and cord blood pH, pO2 and pCO2 were determined. A significant correlation between plasma AVP and pO2 levels (r=0.75, p<0.05) was noted by regression analysis. Correlation of cord pH with plasma AVP almost achieved statistical significance (r=0.57,
p=0.05); pCO2 levels did not correlate. Amniotic fluid AVP levels did not correlate with the presence of meconium although the numbers were small. Amniotic levels of AVP were significantly related to the presence, either of a nuchal cord(s) or a "cord pattern", on fetal heart rate monitoring. There was also a significant relationship between elevated amniotic fluid AVP and neonatal hypoglycemia. Plasma levels in the discordant twin B (1.09 ~U) were not elevated dramatically in comparison
to twin A (0.95 ~U) but the amniotic fluid was 5.62 ~U in this twin. Neonatal weights were in twin A 2810 gms versus twin B 2480 gms, both having 9,10 apgars at time of delivery and acceptable cord gases. Amniotic AVP as a predictor of long standing stress is extremely exciting but only speculative. Long term prospective evaluation of amniotic AVP are presently being initiated at our institution.
I I I ! ! ! I I I I i I I I I I I !
122 I

#105
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE UNRELIABILITY OF PLACENTAL GRADINGS AS AN INDICATOR OF LUNG MATURITY IN THE PRE-TERM FETUS
D. Hills, M.D.,x S. Tuck, M.D.x, G.A.L. Irwin, M.D.x
Research performed at: Nassau Cmmty Medical Center East Meadow, New York
The 188 high risk and normal patients undergoing amniocentesis for L/S ratio done under ultrasound control were reviewed. Only 151 patients were found suitable for analysis and were evaluated comparing L/S ratio and placental grade. Of the 131 cases, 83 were ful! term (greater than 37 weeks) and 48 were pre-term (less than 27 weeks). A 20% incident of grade III placentas were found in both the term and pre-term populations.
I II III
TERM 52.5% 45.8% 20.5% PRE-TERM 50 % 29.2% 20.8%
In our laboratory a L/S ratio greater than 2 is considered to correlate with fetal lung maturity. In the term gvoup, 100% of the grade III placenta cases were associated with L/S ratios greater than 2 (lung maturity). The cases in the pre-term group did not exhibit this correlation between L/S ratio and grade III placental changes.
% L!S greater I
than 2, TERM 63%
II III
76% 100%
%L/S greater than 2, PRE-TERM 13% 56% 50%
We had hoped that early maturational changes (premature aging) of the placenta might signal lung maturation but our data did not support this correlation.
It is our opinion, therefore, that the presence of a grade III placenta in the pre-term pregnancy does not necessarily correlate with fetal lung maturity (L/S greater than 2).
I I I I ! I I I I I ! I i I I I I I
123

#106
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
PLACENTAL GRADE AS A PREDICTOR OF BIRTHWEIGHT PERCENTILE
D. HIIIs, M.D.X~ S. Tuck~ M.D.x, G.A.L. Irwln,M.D.x
Research performed at: Nassau County Med(cal Center East Meadow~ New York
A group of 142 hlgh r~sk grav~das~ who had undergone amn~ocentes~s and uttra- sound evaluatlon w~th(n a week of del(very~ were evaluated and contrasted w~th 62 normal gray, alas, They were d~v~ded ~nto three groups according to b~rthwe(ght,
A. Less than 25th percent~le~ (41 pat~ents)~ (low b~rthwelght).
B. Greater than 75th percentile, (63 pat~ents}~ (h~gh b(rthwe~ght) o
C.I 26th - 7/~th percent~le~ (38 pat~ents)~ (average blrthwe~ght).
The normal grav~das a11 gave b~rth to bab(es of average b~rthwe~ght. The d~str~butlon of placental grades were deterndned for each group and subdivided lnto term and pre-term groups.
NORMAL GROUP (62 patients)
Placental Grade Distrlbut~on Grade D~str~bution ii " iii ~ .... ii
3~ 3~ 23% 14 Pre-term 5~ 29% 21% 48 Term 3~ 42% 25%
HIGH RISK GROUP (142 patlents)
LOW BIRTHWEIGHT: 41 pat(ents GFade D(stribut(on I II III
14 Pre-term 29% 21% 50% 27 Term 2~ 3T~ 41%
!I, HIGH BIRTHWEIGHT: 61 pat(ents Grade D(stribut(on ¯ I II III
19 Pre-term 47°~ 47°~ ~ Ll!+Term 43% 50% ~
m ! I I ! I ! I ! ! ! !
! I m
124

#106
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
PLACENTAL GRADE AS A PREDICTOR OF BIRTHWEIGHT PERCENTILE - Continued
AVERAGE BIRTHWE IGHT: 38 Patient~ Grade O~stribution ii
15 Pre-term 73% 20% 13%
23 Term 30°/0 /+/+% 26~o
From this prelin~inary study we have concluded that a grade llI placenta~ while not pred(ct(ve of SGA~ suggests that the neonate wll! be in a low birthwe(ght group, This ls partlcularly true when found (n the pre-term fetus, Pre-term low b(rthwe(ght infants were more commonly associated w(th Grade III placentas than were average or high b(rthwelght infants,
I ! 1 I ! I
!
I I
I
124a

#107
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
CHANGES IN PLACENTAL GRADE DISTRIBUTION WITH INCREASING GESTATIONAL AGE AND ITS RELATIONSHIP TO FETAL LUNG MATURITY.
D. Hills, M.D.x, S. Tuck, "M.D.x, GoA.L, Irwin, M.D,x
Research performed at: Nassau County Hedlcal Center, East Meadow, New York
To develop a better understanding of the changes that take place in the placenta as gestation progresses, we reviewed 313 sonograms of high risk obstetrlcal patients. The patients selected for this study had amn~ocentesis performed for lung maturity of placental grading. Gestational ages, at the time of sonograms, were assigned retrospectively on the basis of the neurologic gestatlonal age at birth. The patients were d~vlded into the f911owing grpup@, based on gestational age: (a) 28-32 wks. (75), (b) 32-34 wks. (58), (c) 34-36 wks, (64), (d) 36-42 wks. (t16). The groups were deliberately overlapped to better
represent the true gestat~onal age. ~ach group was evaluate~ for d~strtbut~on of the placental grade and lung meturlty (L/S)2). Those patients delivering with- ~n one week of the ultrasound exam were also analyzed w~th respect to development of RDS. The results are tabulated below:
Placental Grade ,~ I II IIl ~8-32 7~ ’1~ 32-34 57/0 28°/0 16% 34-36 52% 30% 36-42 33% b~% 23%
Mean L/S % L/S 2 % +RDS I II Ill I II Ill I II III 1.2 1.3 2.1 I~% 27 25 67% ~5~o o% 1o0 2.2 2.8 8 64 73 0% 40°/0 0% 1.9 2.3 3.1 t~ 67 93 0% 0% 0% 2=8 2.9 3.5 68 75 96 ~/0~:~ 2.4%* 0%
*This group contained a h~gh percentage of diabetic patients
In our group of high r(sk patients the d~stribution of placenta! grades changed ~n a progressive linear fashion w~th gestat(onaI age. L/S ratio progressively ~ncreased with gestationaI age in all placenta! grade groups~ w~th 6~/0 of grade placenta at term hav(ng L/S ratios greater than~ 2. For each gestationaI age, however, there were s~gnificant differences in mean L/S ratios and percentage with L/S ratios greater than 2 between each placenta! grade group. At any gestationaI age a h~gher grade placenta was associated with a h~gher L/S ratio. A grade III placenta ~s associated in feta! |ung maturity to a different degree at each gestational age,
28-32 wkso 25% 32-34 wks. 73% 34-36 wks. 9~/0
Therefore, ~f a grade III placenta is seen, the chances are good that the baby will have lung maturity if the gestational age is greater than 32 weeks.
I I I I i I I I I I I i I I I I
125
i I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# | 08 February, ~1984
’USE OF HEXOPRENALINE IN THE MANAGEMENT OF FETAL DISTRESS IN LABOR Jeffrey, Lipshitz, M.B. and David C. Shaver, M.D.XDivision of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
Fetal distress in labor is an obstetric emergency which results in significant short- and long-term fetal and maternal morbidity. Late and variable fetal heart rate (FHR) decelerations result from interference with feto-placental blood flow by uterine contractions. If not corrected, progressive fetal asphyxia and acidosis may result. Inhibition of uterine contractions should remove the aggravating cause of the impaired blood flow and allow intra-uterine resuscitation of the fetus. Thus, the use of a tocolytic drug prior to delivery for fetal distress, if successful, will have the following advantages: prevent the delivery of a compromised baby; prevent further decompensation due to unavoidable delays; allow sufficient time to adequately prepare the pat.lent for surgery; allow time to use correct sterile procedures and unhurried surgical technique. Methodology: Twelve patients with fetal distress related to uterine contractions, as evidenced by severe FHR abnormalities associated with a fetal scalp blood pH of less than 7.20, were entered into the study. Meconium was present in eight of the patients. Late decelerations, or severe variable decelerations with a late component, were present in II of the 12 patients. Beat-to-beat variability was decreased in i0 patients. After failure to respond to traditional treatment, each patient was given a I0 pg intravenous bolus of hexoprenaline followed by an I.V. infusion, which was titrated to inhibit uterine contractions. Cervical dilatation was between 4 and I0 cm. The patients were delivered by cesarean section after approximately 40 minutes of treatment. Results (see table): Mean venous cord blood pH was 7.31. Only one baby had a value of less than 7.25. No 5-minute Apgar score was less than 8. A single I-minute Apgar score was less than 6. All the babies left hospital in good condition. Maternal heart rate, measured one minute after the I.V. bolus injection, increased by a mean of 17 bpm.
GESTATIONAL AGE (WKS)
FETAL SCALP pH
CORD BLOOD PCO2 pH PO2
39.4 + 2.9 7.17 + .02 7.31 + .06 41.33 + 8.96 30.56 + 7.42 16.8 + 13.0
Results expressed as mean + standard deviation
MATERNAL PULSE INCREASE
Conclusion: Hexoprenaline, a selective ~2-sympathomimetic drug, appears to be a promising new modality in the management bf fetal distress in labor.
I
126
I I I

Society of Perinatai Obstetricians Annual/Vteeting
San Antonio, Texas # 109 February, 1984
THE EFFICACY OF AMBULATORY REFLECTANCE METER USE FOR MANAGEMENT OF THE INSULIN-REQUIRING DIABETIC GRAVIDA. O, Phillipsx, P.G. Blakex, J.N. Martin,Jr.x, W.E. Roberts*, S.M. Palmerx, J. SherrillX, J.C. Morrison. Division of Maternal-Fetal Medicine, Department of Ob/Gyn, Univ. of Miss. Med. Cntr., Jackson.
Maintenance of a euglycemic state in the insulin-requiring pregnant diabetic is a cornerstone of the contemporary management of this disorder. The achievement of glucose control correlates well with significantly improved maternal and perinatal statistics. Recently ambulatory glucose monitoring via reflectance meter has been reported to be efficacious for blood glucose control. From July I, 1979 to September 30, 1983, management of the insulin dependent gravida in our institution has been standardized on a protocol of glucose control utilizing ambulatory reflec- tance meter for determinations of fasting blood glucose (FBG) and 2 hour postpran- dial blood sugar values (2hPP). Euglycemic control was considered to be a FBG < lOOmg/dl and a 2h PP < 150md/dl. The 2hPP assessment was chosen rather than ~ preprandial test or a ~xture of several glucose values since it represents a sta- bilized means of comparison and a physiologic response to glycemic excursion after a glucose load. The present report details our experience with 64 insulin- dependent gravidas (Class B-42, Class C-14, Class D-8) who were managed by protocol (Group I) and compares their course and outcome with 67 contemporary nonprotoco] insulin-dependent diabetic gravidas (Class B-46, Class C-17, Class D-4) from our general patient populace (Group 2). Utilizing reflectance meters on an ambulatory basis to maintain a euglycemic state, Group I gravidas achieved a mean FBG of 99mg/dl and a mean 2hPP value of 138mg/dl. The incidence of diabetic ketoacidosis, infection, intrauterine fetal death, hydramnios and neonatal morbidity (LGA babies, RDS, macrosomia, neonatal hypoglycemia and hyperbilirubinemia) was significantly greater in the Group 2 parturients. The concurrent gestational complication of pregnancy-induced hypertension or the incidence of congenital malformations and first trimester losses were not significantly different between groups. Considerably improved maternal and perinatal outcomes for Group 1 patients suggest that the maintenance of a euglycemic state via ambulatory reflectance meter use is an important ingredient in the optimal care of these high risk parturients.
I ! ! I ! I I I I I I I I I
127
! I

Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas
#110 February, 1984
TREATMENT OF SEVERE PREGNANCY-INDUCED HYPERTENSION REMOTE FROM TERM BY THERAPEUTIC PLASMAPHERESIS/EXCHANGE. J.N. Martin Jr.x, P. Normanx, P.G. Blakex, F.S. Morrisonx, and J.C. Morrison. Divlslon of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, and the Departments of Medicine (Hematology) and Anesthesia.
The antihypertensive effect of plasmpheresis/exchange for patients with hyper- tension and renal disease suggests to us a potential role for this therapeutic moda- lity in the treatment of severe pregnancy-induced hypertension(PIH) Plasmapheresis and plasma exchange have recently been shown to be effective therap, for thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, disorders which share similar pathophysiologic characteristics with PIH and which might be expected to respond positively to similar therapy. The definitive management of severe, fulminating PIH is pregnancy termination. The most common cause of perina- tal loss associated with PIH is prematurity associated complications. A therapeutic modality to safely ameliorate or reverse progressively worsening PIH especially in the gestation remote from term with immature fetal lungs might be attended with a significant improvement in overall perinatal morbidity and mortality. In this report we describe our initial experience with three study subjects as part of an extensive ongoing project to evaluate (a) the clinical usefulness of therapeutic apheresis/exchange to safely prolong preterm gestation associated with significant PIH; and (b) to assess the impact of this treatment modality upon the feto-maternal unit. The continuous, automated IBM 2997 mechanical cell separator was utilized to effect a safer, more rapid and more easily managed apheresis procedure for mother and fetus. Strenuous exclusion criteria for patient selection included the absence of labor, infection, ruptured membranes, difficult vascular access, extre- mes of maternal weight, severe IUGR, overt fetal distress, severe oligohydramnios, severe thrombocytopenia, emotional instability, epigastric pain, severe headache or other critical medical conditions. Maternal cardiovascular function was con- tinuously monitored via a flow directed pulmonary artery catheter before, during and for 24 hours following each procedure. Concurrent electronic fetal monitoring was )erformed. Blood and urine samples were collected at selected intervals to help guide obstetric/medical care as well as evaluate the impact and potential mecha- nisms of action of this therapeutic maneuver upon the feto-maternal unit. Clinical resolution of the PIH disease process in the first study subject followed two sequential apheresis procedures with 5% Albumin and crystalloid fluid replacement. Less dramatic improvement in clinical parameters was observed in the second and third study subjects with more severe disease who underwent a single apheresis pro- cedure each. The impact of apheresis upon maternal cardiovascular parameters, )ulmonary and renal function, the renin-angiotensin-aldosterone system, electrolyte/fluid balance, fetal biochemical/biophysical assessment as well as related maternal hormonal coagulation and immunologic parameters revealed signifi- cant changes. Cautions and preliminary conclusions for future investigations are offered.
I
I
I I
I I
128
I I

#111
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
hORRELATION OF THE ONE-MINUTE APGAR SCORE AND UMBILICAL CORD ACID BASE STATUS Frank H. Boehm, M.D., Lisa M. Fields, R~N., B.S.N., Stephen S. Entman, M.D. William K. Vaughn, Ph.D., Vanderbilt University Medical Center, Nashville, TN
The one minute Apgar score is often poorly correlated with other indicators of fetal well-being. Since fetal asphyxia is directly associated with neonatal acido- sis, a low Apgar score in the face of normal pH and base deficit does not, there- fore, indicate an asphyxiated infant. A study was performed at Vanderbilt Univer- sity Hospital to ascertain the feasibility of combining umbilical arterial acid- base status with the one minute Apgar score for neonatal assessment. Umbilical arterial pH and Apgar scores were obtained on 212 singleton pregnancies. When the Apgar score was less than 7, over half (60%) the neonates had normal acid-base status. Fifty-one percent of this group had undergone intubation and nasopharyn- geal suctioning, procedures known to be associated with lowered Apgar scores. When reviewing the umbilical arterial gases and base deficit in those neonates with a pH ( 7.20, it was noted that of the eight patients with an Apgar score of 7 or greater, seven (87.5%) were classified as having metabolic acidosis with only one having respiratory acidosis. In those neonates with Apgar scores of ~ 7, approxi- mately two-thirds were noted to have blood gases compatibl@ with metabolic acidosis while the remaining displayed respiratory acidosis. It is recommended, therefore, that neonates with a one minute Apgar score less than 7 be further evaluated with umbilical arterial pH to confirm the presence or absence of acidosis. When the pH is less than 7.20 it is also recommended that a complete set of gases be evaluated with that specimen. More precise co~f±rmation of the diagnosis of fetal distress and neonatal asphyxia for treatment and medicolegal purposes and more reliable follow-up data, is POssible with this information.
I I ! I I I I I I I I I ! I I I I
129

Society of Perinatal Obstetricians 1 Annual Meeting
San Antonio, Texas 1 #112 February, 1984 1
CLINICAL EVALUATION OF A RAPID SLIDE AGGLUTINATION TEST FOR AMNIOTIC FLUID PHOSPHATIDYLGLYCEROL
Ph___il_~ Halvorsen, M.D.,X Thomas L. Gross, M.D., Perinatal Clinical Research Center and Department of Obstetrics and Gynecology, Cleveland Metro General Hospital/Case Western Reserve University
Amniostat-FLMtm (AFLM) is a new rapid immunologic agglutination test for amni- otic fluid (AF) phosphatidylglycerol (PG). To our knowledge, there is only one previous study correlating PG determined by two-dimensional thin-layer chromatog- raphy (TLC) and AFLM, and a 91% concordance between the two techniques was noted. In this previous study, PG was not quantitated and thus there was no discussion of results when low levels of PG were present. There is some disagreement in the literature as to what level of AF PG is needed to predict maturity. Most investi- gators feel that any level of PG, including a trace (defined as I-2% of total phospholipids) can be considered positive, but other studies report that >2% PG is considered a positive result. The purpose of the present study was to compare PG quantified by two-dimensional TLC (PG-TLC) with PG determined by Amniostat- FLMtm (AFLM). One hundred seventy-nine samples of AF were tested for L/S ratio and PG by two-dimensional TLC. A separate technician, blind to the TLC results, performed AFLM tests on these same samples. If any level of PG-TLC, including a trace, was considered positive, then PG-TLC and AFLM were concordant in 170/179 (95%) cases. Both were positive in 123 and both negative in 47. The 9 AF’s with discrepant results were as follows: 5 negative AFLM’s were associated with trace PG-TLC (I- 2% of total phospholipids), I negative AFLM was associated with 3% PG-TLC , and 3 positive AFLM’s were associated with negative PG-TLC. There were 14 patients with trace PG-TLC; of these, there were 9 positive and 5 negative AFLM’s. If >2% PG- TLC was considered positive, concordance between the two tests was 93% (166/179). From these samples, 119 neonates were delivered within 72 hours of amniocentesis. In this group hyaline membrane disease (HMD) was diagnosed by one neonatologist using strict clinical and radiographic criteria. There were 100 positive AFLM and all were associated with the absence of HMD; of the 19 negative AFLM, 5 developed }]MD. We conclude that (I) AFLM is a simple slide agglutination test that can be performed in 15 minutes (2) the overall correlation of PG-TLC with AFLM is very high (95%), (3) over 50% of the discrepancies are associated with trace amounts of PG-TLC and (4) when trace amounts of PG-TLC are present, AFLM is positive in up to
2/3 of the cases. Based on these results, it appears that Amniostat-FLMtm may represent a simple, rapid test for PG that can be used alone or in combination with other AF maturity tests.
130 ! !

#113
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
~AUDITORY STIMULATION OF THE FETUS--HEART RATE AND STARTLE RESPONSE CORRELATION WITH GESTATIONAL AGE AND NEUROLOGIC OUTCOME
Michael Crade,M.D.x, John D. Yeast, M.D., Roger K. Freeman, M.D. and Dennis S. McQuown, M.D. Memorial Medical Center of Long Beach, CA.
Recent studies have emphasized the possible role that careful monitoring of fetal movements may have in evaluation of fetal well being. In order to further expand our understanding of normal fetal neurologic development we studied fetal "startle response" to external sound stimuli. A series of 205 fetuses ranging in biparietal diameter (BPD) measurement of 4.0 to 9.6 (17.5 wks to 40.0 wks) was studied. Each was stimulated by sound, utilizing a hand held artificial laryny pressed against the maternal abdomen near the location of the fetal ear as deter- mined by ultrasound. Each fetus was observed at the time of stimulation by real time ultrasound. The pregnant mothers were also asked to indicate if they felt a strong kick at the time of the fetal auditory stimulation. Normal as well as high risk pregnancies were evaluated. The "BPD threshold" was established at which time virtually all normal fetuses demonstrated a "startle" type response. Those fetuses not responding to auditory stimulation were often at risk for placen- tal insufficiency or congenital anomaly. The non-responders were also evaluated by standard antepartum fetal heart rate testing, usually with the use of the con- traction stress test (CST). During the CST, auditory stimulation was applied to the maternal abdomen in an attempt to produce fetal heart rate accelerations. The correlation between the absence or presence of a startle response during ultra- sound and an inability to demonstrate fetal heart rate accelerations will be discussed. The outcome of these pregnancies will also be discussed. A BPD "gray zone" of fetal response was noted when a normal response may be either startle or no startle, to the sound stimuli. Below a certain BPD measurement, no fetuses responded to auditory stimulation as monitored by ultrasound or fetal heart rate testing. It is speculated that these fetuses may not yet have adequate higher cortical development to process and respond to auditory stimulation. It is hoped, therefore, that these data may further expand our understanding of the normal and stressed fetal development. In addition, the ability of the fetus to respond to auditory stimulation may serve as a marker of fetal viability, since responsive- ness seems to develop during the 26-28 week gestational period.
I I ! ! I ! I I I I I I
I I I
131

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 114 February, 1984
! INTRAUTERINE FETAL DEATH IN TWINS AFTER THIRTY-TWO WEEKS OF GESTATION. Rattan~ P. K., Knuppel, R. A., and O’Brien, W. F. Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, University of South Florida College of Medicine, Tampa, Florida, 33606.
Intrauterine fetal death after 31 to 32 weeks of gestation has been reported to be a major contributor towards total perinatal mortality in twin pregnancies. Between January 1, 1975 to July 31, 1979, out of a total of 14,210 deliveries, 153 were twins. In this historical control group there were seven intrauterine fetal deaths that occurred after 32 weeks of gestation (23/thousand). From January I, 1980, management protocol in twins included routine non-stress tests once a week after 31 to 32 weeks of gestation. Whenever non-stress tests were non-reactive, it was followed by a contraction stress test either spontaneous or oxytocin induced. Between January 1, 1980 to July 31, 1983, there were 160 twin deliveries out of a total of 14,215 deliveries. There were six pregnancies where contraction stress tests were either positive or two consecutive equivocal contraction stress tests were noted in one or both twins. Delivery was preferred in these patients.
Case # Twin NST CST GA Apgar Scores ~eight in grams I A R neg 38 8/10 3416
B NR + CST 9/10 2211
A NR Eq 33 9/9 1644 B NR Eq 9/9 1531
A NR Eq 35 5/8 2268 B NR + CST 4/7 2013
4 A R neg 32 7/9 2013 B NR + CST 2/4 1899
5 A R neg 38 8/9 3175 B NR + CST 5/7 2126
A R neg 36 9/9 2268 B NR + CST 1/2 1475
There were no intrauterine fetal deaths that occurred after 32 weeks of gestation in the protocol group. We consider routine use of non-stress tests coupled with contraction-stress tests to be a major contributor towards this outcome.
I I
132 !

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
#115 February, 1984
AMNIOCENTESIS IN THE TWIN GESTATION. Knuppel, R. A., Rattan, P. K., Tedesco, T., and Hager, J. Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, and the Department of Human Genetics, University of South Florida College of Medicine, Tampa, Florida, 33612.
The first report of amniocentesis in twin gestation was published less than ten years ago. Since then, data has been presented with vastly differing conclusions. Risks mentioned vary from minimal to a six-fold increase in abortion rate in detected twins. Most of these reports included patients before 1980, when the use of ultrasound was not universal as evidenced by a detection rate of only 62% in the largest series published. The aim of our review was to evaluate the out- come of twin pregnancies which underwent amniocentesis since 1980 and where all twins were detected by ultrasound. Out of a total of 1,902 amniotic fluid samples for genetic evaluation, 14 were from twin pregnancies. Both sacs were successfully tapped in 13 of the 14 (92%) and maternal cell contamination compli- cated a second twin pregnancy. The number of taps varied between two to five. There were no cases of vaginal leakage of fluid, bleeding or spontaneous abortion within 30 days of amniocentesis. Significant outcome other than normal karyotype include: one patient where the second twin was anencephalic, but both twins had normal female karyotypes; one case where the second twin had posterior urethral valve obstruction, but both twins had normal karyotypes, and one set of twins where both were translocation Down’s in a young mother. When amniocentesis is performed under ultrasound, we find no increase in complication rate. The complexity of genetic counseling in twin gestation is underscored by varying outcomes.
133

#116
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
OUTCOME OF PREGNANCY IN THE PRESENCE OF UTERINE FIBROID
Author: Shailaja M. Didolkar, M.D., Union Memorial Hospital, Baltimore, Maryland
To evaluate the outcome of pregnancy and suggest guidelines for its management in the presence of uterine fibroids, thirty seven pregnant patients with uterine fibroids were studied. These patients were diagnosed by ultrasound during their pregnancy. Seventy percent of the patients were over thirty years of age, one fifth were over thirty five years of age; none were under twenty years of age. Twenty five percent of the patients had a prior history of prolonged infertility. Five patients had prior poor obstetrical histories. Diameter of fibroids ranged from 3-15 centimeters. Out of the thirty seven patients, eight had elective termination of their pregnancy. Of the remaining twenty nine patients, seven- teen had full term uncomplicated pregnancies. Twelve had complications. The most common complications were abdominal pain in nine patients, followed by bleeding in five, premature labor in five, sponteneous abortion in four, and intrauterine growth retardation with fetal distress in one patient. Ten out of these twelve complicated pregnancies had partial implantation of the placenta on the fibroid. Two most significant complications; premature labor and bleeding during pregnancy were influenced by presence of fibroid in lower uterine segment and or implantation of placenta on fibroid. Of twenty nine patients, twenty two (85 %) had full term deliveries. Ten (38 %) were delivered by cesarean section; prior cesarean section (4 patients); failure to progress (3 patients); prior myomectomy (2 patients); fetal distress and breech ( 1 patient) respective- ly. Three had spontaneous abortions and one had immature delivery at twenty two weeks. Thus the outcome of pregnancy was significantly influenced by: a) placental implantation on fibroid; b) presence of fibroid in lower uterine segment; and c) largest diameter of fibroid I0 cm. or more. This accounted for eighty three percent of the complications. The number of fibr6ids did not influence the outcome. Spontaneous misscarriage rate (14%) was not increased due to fibroids. Therefore it is suggested that exact localization of placenta in relation to fibroid should be done. Those with placental implantation on fibroid should be carefully monitored for premature labor. Patients without these above factors can be reassured regarding pregnancy outcome.
I I I I I I I I I I I I I I I I
i 134

I Society of Perinatal Obstetricians -" Annual Meeting
San Antonio, Texas I
# | 17 February, 1984
CONTINUOUS FETAL TISSUE pH MONITORING DURING MATERNAL POSITION CHANGE USING A F~BEROPTIC PROBE
Steven H. Swersky, M.D., and Harold E. Fox, M.D. College of Physicians and Surgeons Columbia University, New York, N.Y.(-suppoFted in part by NICH-Grant #HD-13063)
The effect of position on maternal circulatory hemodynamics have been well- documented. We have used a newly designed flexible fiberoptic tissue pH (TpH) probe system to investigate changes in fetal TpH associated with maternal positiona] changes in labor. The TpH probe is attached to the fetal scalp using a system similar to the standard fetal heart-rate monitoring electrode.
Eighteen patients who elected to participate in an approved evaluation of the fiberoptic probe system participated in this study. All patients were in labor with membranes ruptured. During labor the patients were moved from either the supine (S) to the l.lateral (L) position, or from the L position to the S position. Maternal vital signs were taken before and after each position change. Tissue pH was continuously monitored during the maternal po~ition changes. One patient demon- strated a classic supine hypotensive syndrome and is considered separately.
A total of 63 positional changes were observed in our 17 patients. 41 of the trials were observed in the S÷L position change, 23 from the L÷S position. In 37 of the 41 trials from S÷L (90%) there was an average increase in tissue pH of 0.032 (S.D.+.O2)(range 0.001-0.b72). In the trials from L S, 18 of the 22 (82%) had an average ~ecrease in fetal pH, of 0.039 (S.D.+.O2)(ranae O.O04-O.lOl).It was found that maternal positional effects on fetal tissu~ pH were noted for each patient. 50% of patients had a TpH increase over .030 when moved to the left lateral position (Table I). 39% of patients had a TpH decrease more than 0.030 when
I
moved to the supine position (Table II).
TABLE I. S~t Trials .010 to .020 to .030 to
TDH Chanqe <.OlO .019 .029 .035 >.040
Tof tri-~ia~s so I0 5 l~ -8- ~ of trials 27 27 It ll 21
~ of pts.~ith values < ~l ~ SO ~|
TABLE II. L-’~ Trials -.OlO to -.020 to -.030 to
~pH Change <~010 -.01~ -.02~ -.0~ >-.Old)
i of trials 2 2 ~ ] 5
~ of trials I! II 33 17 28
t of pts.with values < 8 23 61 ~
One patient experienced a classical symptomatic supine hypotensive syndrome. This patient’s blood pressure changed from 120/80 in the lateral position to 80/55 in the supine position. In this clinical setting a decrease in tissue pH of 0.173 units was noted. Therapeutic intervention (S÷L) was associated with a tissue pH l~ncrease of 0.255 and a return to normal blood pressure.
L These observations demonstrate the application of a new technique to measure
fetal tissue pH during labor. The results are consistent with our current under- standing of maternal positional effects on the intrauterine environment. Evaluation of the TDH changes leads to the conclusion that the lateral position is preferred
r th~ ]~hnring pmtient~
I I I I I I I I I I I I I I I
135 I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #1 |8 February, ~1984
DOES CESAREAN DELIVERY IMPROVE THE SURVIVAL OF THE VERY LOW BIRTH WEIGHT (VLBW) INFANTS?, Sze-ya Yeh, M.Do, Louise Sipos, R.N.x, Richard H. Paul, M.D., Department of Obstetrics and Gynecology, University of Southern California School of Hedicine, Los Angeles, California
The survival rate of VLBW infants (B.W. < 1,500 gms) has improved markedly during the last decade due to improvement in neonatal resuscitation and aggressive obstetric management. However, there remains a question regarding the effect related to mode of delivery. Host of the published data equate cesarean delivery in the non-vertex VLBW infants with better neonatal survival. The purpose of this study is to investigate the role of cesarean delivery in the survival of the vertex VLBW infants. During a one-year period from 7/82 through 6/83, 186 liveborn infants who weighed 500-1500 gms were delivered at LAC/USC Medical Center. Of these, 119 (64%) infants survived beyond 28 days. Ninety-six patients were se- lected for this study. The selection criteria were vertex presentation, no major congenital anomaly and medical information available for study. Sixty-three ~atients had vaginal delivery, 47 infants survived (75%); 33 had cesarean delivery, and 29 (88%) survived (p > .05). In the cesarean group four neonates died of RDS and H~.ID. There were 19 non-sterile unexpected vaginal deliveries, and 12 (63%) survived. This survival rate was lower than that of controlled vaginal deliveries (80%) (p > .05). The type of uterine incision and the interval between incision and delivery was not associated with a different survival. Fifty-eight patients were admitted with cervical dilatation < 4 cm, 25 (43%) had cesarean delivery, 23 (92%) survived; and 25 of 33 (76%) vaginal deliveries survived (p > .05). Of the remaining 28 patients with a cervix 4 cm or more dilated, only 3 had cesarean section, and 2 survived. The number of infants with low Apgar scores (<7) was not significantly different in the vaginal delivery group as compare’d to the cesarean section group. In summary, VLBW infants delivered by cesarean section had slightly higher survival rates, yet the data from this study did not show a statistical difference. To answer this question properly, a prospective, randomized study on a larger patient population will be necessary.
I I I I I I I I I I I I I !
136
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 11 9 February, ! 984
~IRTH-ASSOCIATED MECHANICAL INJURIES (BI): A CONTEMPORARY REVIEW, Yonekura, M.L., M.D., Teberg, Ax, Nandino, Nx, Wallace, T~ Depts. of Ob-Gyn and Pediatrics, University o{Southern California School of Medicine, Los Angeles, California
To determine the impact of current obstetrical approaches on the incidence of BI, a prospective study of all BI was performed at Women’s Hospital, a tertiary care center serving a predominantly Hispanic indigent population. 16,067 deliveries with 15,918 live births occurred during the one-year study period. All patients were cared for by housestaff and graphic labor records utilized to guide management. Trial of labor (TOL) following previous cesarean section (CS) was offered to quali- fying parturients. Moreover, laboring patients with breech presentation and ade- quate pelvimetry were offered a TOL if the EFW was 2500-3800 gm with a flexed fetal head. During the study period there were 107 neonates with BI which included: 76 fractured clavicles (FC), 38 Erb’s palsies (EP), 1 facial nerve injury, 1 phrenic nerve palsy, i fractured humerus, I sprained knee, 1 scrotal hematoma, and I cepha- lohematoma., i0 neonates had both an FC and an EP. Pertinent demographic data re- garding patients with FC and EP are shown in Table I.
Fractured Clavicle (N=76) Hispanic Gravidity (% nulliparous) Gestational age, wks Birthweight, gms Side of birth injury: Left/Right Sex of infant: Male/Female
Erb’s Pal.sy (N:38) 71 (93%) 38 (100%)
3.25+1.85(20%) 3.16+2.17(32%) 40.10+1.6 39.50+2. !
3935.40+551.4 3917.40+634.9 34/42 20/18 43/33 18/20
The majority of injuries occurred in term neonates; 42% of neonates with FC and 43% with EP weighed > 4000 gin. Approximately half of the injured neonates were LGA by California growth-curves. 73% of injured neonates were delivered by housestaff, 10% by medical students, and 17% by nurse midwives. 5 FC and 2 EP occurred in neonates delivered vaginally after a successful TOL in women with previous CS. The incidence of FC and EP were 4.8 and 2.4 per I000 live births respectively. The incidence of FC and EP by method of delivery is shown in Table II; the highest incidence of both types of BI was associated with midforceps delivery (p < .00005).
Incidence by Method of Delivery Method of Delivery No.
NSVD 13,043 Outlet forceps 673 Mi dforceps 161 Vacuum 61 Breech 330
Fx. Clavicle Erb’s Palsy
O. 5 I% O. 2% O. 3% O. 15% 4.3% 4.3% 1.6% 0 0 0.6%
8% of the FC and 47% of the EP were associated with a shoulder dystocia (p<.O0005). One case of EP following vaginal delivery of a breech was associated with a nuchal arm. In summary, 0.67% of live births were associated with BI. In spite of a liberal policy with respect to breech deliveries, the incidence of BI was only 1.6 times more common with a breech than with a vertex presentation delivered vaginally.
I I I I I I I I I I I I I I I I
137
I

#120
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
USE OF OXYTOCIN IN PREVIOUS CESAREAN SECTION TRIAL OF LABOR PATIENTS, Janet M. Horenstein, M.D.*X, Jeffrey P. Phelan, M.Dx, Gary S. Eglinton, M.D.x, Mona P. Tahilramaney*x, Marc Boucher, M.D., FRCS(C)*x, Department of Obstetrics and Gynecology, University of Southern California School of Medicine and Women’s Hospital, Los Angeles County/USC Medical Center, Los Angeles, California
In patients with a previous cesarean section, the use of oxytocin during a trial of labor remains controversial. In order to better delineate the risks associated with oxytocin usage in patients with prior cesarean section undergoing a trial of labor, a retrospective investigation was undertaken. During the study period, I January 1980 to 31 December 1980, 308 previous cesarean section patients underwent a trial of labor. Of these, oxytocin was used in 58 (18.8%) patients for either induction (12) or augmentation (46). In those patients who received oxytocin, vaginal delivery was accomplished in 31 (53.4%). In 292 patients who labored spontaneously, vaginal delivery was accomplished in 196 (83.8%). Patients who had no vaginal deliveries after their previous cesarean section and required oxytocin were at a significant increased risk of cesarean section. There was no statistically significant difference among the oxytocin versus non-oxytocin groups with regards to instrumental vaginal delivery, uterine scar dehiscence, transfusions, birth trauma or neonatal outcome. In patients with a previous cesarean section who undergo a trial of labor, the use of oxytocin in a judicious manner appears to be safe. However, additional studies are required to corroborate these findings.
I I I I I I I I I I I I I I I I I I
138 I

| Society of Perinatal Obstetricians m
Annual Meeting San Antonio, Texas
i # 121 February, 1984 ¯
THE EFFECT OF INDICATION FOR PREVIOUS CESAREAN SECTION ON SUBSEQUENT DELIVERY OUTCOME IN PATIENTS UNDERGOING TRIAL OF LABOR, Steven L. Clark, MD,x Jeffrey P. Phelan, MDx, Gary S. Eglinton, MDx, Marie H. Beall, .MDx, Department of Obstetrics and Gynecology, University of Southern California School of Medicine and Women’s Hospital, Los Angeles County/USC Medical Center, Los Angeles, California
During a one year period in 1980, 308 patients with a previous cesarean section underwent a trial of labor. Hospital records of these patients were examined in an effort to correlate delivery outcome with the indication for the prior uterine incision. Patients with a previous cesarean section for breech had the highest incidence of subsequent vaginal delivery (81 of 94 patients or 86%), and patients with a previous cesarean section for cephalopelvic disproportion or failure to progress had the lowest incidence of subsequent vaginal delivery (22 of 64 patient:. or 64%). However, the lower rate of vaginal delivery among the latter group is found only among that sub-population who had never delivered vaginally. The incidence of oxytocin induction or augmentation of labor, use of forceps or vacuum: incidence of delivery complications, birth trauma, intraoperative blood transfusior and intraoperative complications were not significantly different between any groups undergoing trial of labor, regardless of the indication for previous cesarean section. Fetal distress does not appear to be a significant recurring factor in patients given a trial of labor after a cesarean section. The presence of a uterine scar per se does not appear to significantly influence the likelihood of a successful vaginal breech delivery. Exclusion of patients from a trial of labor after a previous cesarean section for CPD/FTP does not appear to be justified.
I I I I ! I i
i i
I i
I i i i
139
i !

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas # 122~ February, 1984
FETAL BREATHING AND SHORT TERM HEART RATE VARIABILITY, Michael Y. Divon~ MDx, Lawrence D. Platt, MD,*Eitan Z. Zimmer, MD~ Eitan Paldi, MD,*University of Southern California School of Medicine and Women’s Hospital, Los’Angeles County/USC Medical Center, Los Angeles, CA and Rambam Medical Center, Haifa, Isarel
The assessment of fetal heart rate variability and its significance relative to the state of the fetus have received increased attention in recent years. Yet, there have been few quantitative investigations of mechanisms responsible for such variations. It has been known for a long time that during extrauterine breathing, variations in heart rate occur simultaneously with respiration. In order to quantify changes in short term heart rate variability that occur with fetal breathing, we ha~ monitored 16 healthy women w~th uncomplicated pregnancies at 38-41 weeks of gesta- tion. Fetal breathing movements were monitored by an observer using a real time ultrasound scanner (ADR-2130). The fetal electrocardiogram was obtained via a scalp electrode, amplified and fed into a microcomputer (Compucolor II). Information regarding fetal breathing activity was simultaneously fed into the microcomputer (cessation o.f respiration of more than 6 seconds was defined as "apnea"). Short term heart rate variability was defined as the standard deviation of (Tn -’T(n-~))/ (Tn + T(n-l)), where Tn = The nth interbeat interval. Short term variability during breathing and apnea were compared using the Wilcoxon’s matched pairs signed rank test. Heart rate variability was 4.48 + 1.71 (Mean + SD) during apnea, and it rose to 5.80_ + 2.20 during breathing. This difference was found to be significant: p<0.01. The significan~ association between fetal breathing movements and short term fetal heart rate’variability may prove useful.~n evaluation of fetal weil being
I I I I I I I I I I I I I I I I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 123 February, 1984
GESTATIONAL AGE DETERMINATION IN THE FETUS OF THE DIABETIC MOTHER: I. BIPARIETAL DIAMETER AND FEMUR LENGTH, Steven H. Golde~ M.D. and Lawrence D. Platt, M.D., Department of Obstetrics and Gynecology, University of Southern California School of Medicine, Los Angeles, California
Previous dat~ on the relationship of biparietal diameter (BPD) with gesta- tional age in fetuses of diabetic mothers have suggested that BPD’s are larger in this population. These early studies used bistable imaging and technique at variance with standards currently employed in most ultrasound labs. More re- cently, cross-sectional data, derived from normal populations, either excluded diabetic women or-included only small numbers in a much larger study population. Femur length (FL) measurements have not previously been described in a diabetic population. We have studied the relationship of BPD and FL to gestational age in a series of 511 scans employing standardized technique on 323 fetuses of diabetic women. This data base allowed us to define such relationships in both a cross- sectional and a longitudinal manner and to make comparisons of growth rates with previously established, nondiabetic populations. The longitudinal data base con- sisted of ll6 patients undergoing an average of 2.5 scans. Multiple regression analysis showed that the rate of BPD growth correlated to gestational age with an r2=0.975 (t statistic=30.4; p>0.001). A similar analysis for FL values revealed an r2 of 0.9h9 (t statlstic=2~.8; p<0.001). Cross-sectional curve means corre- lated well with previously published values from a normal population for both BPD and FL (r=0.995; p<0o001 and r=0.981; p<0.001 respectively). Slight variations in both BPD and FL values between our diabetic and previously established non- diabetic populations could be attributed solely to the greater variation in ges- tational dating of our diabetic population. Analysis of longitudinal data showed parallel growth of fetuses of both diabetic and nondiabetic populations. Conclusion: Currently available growth curves for both BPD and FL calculated from a normal population can be directly applied to fetuses of diabetic preg- nancies.
I I I I ! I I I I I I I I I
141
I I

Society of Perinatal Obstetricians Annual Meeting mm
San Antonio, Texas
# 124 February, 1984
A PROSPECTIVE STUDY ON THE USE OF FETAL FEMUR LENGTH A~ A PREDICTOR OF PULMONARY MATURITY, Mona TahilramaneF~ M.D.~*, Steven H. Golde, M.D. and Lawrence D. Platt, M.D., Department of Obstetrics and Gynecology, University of Southern California School of Medicine, Los Angeles, California
Elective delivery in the third trimester requires confirmation of fetal lung maturity to reduce the incidence of hyaline membrane disease (HMD). Since amnio- centesis has a known, albeit small, risk, we have previously reported our prospec- tive experience using ultrasound markers of fetal maturity in a population screened for maternal diabetes. These markers, the presence of a standard plane biparietal diameter (BPD) or the existence of a grade III placenta circumvented the need for an amuiocentesis in 60 percent of our population at risk. We now report our preliminary experience with an additional marker, a femur length >7.3 cm (FL), as an adjunct to our previously established sonographic criteria. Fifty- seven patients presented in the third trimester with unconfirmed dates requiring elective operative delivery. All were found free of diabetes upon screening with a 100 gm glucose load. Ultrasound criteria of the existence of a BPD >--9.2 cm, a grade III placenta, or a FL >7.3 cm were present in 46 (81%). A FL of 7.3 or more was present in 32 of 46--(70%) of patients meeting criteria and was asso- ciated with a BPD >_9.2 cm in 13 instances (41%). An association of mature FL values with a placental grade of III occurred in 5 patients (15.7%), and all three criteria were positive in 3 patients (9.4%). Maturity was predicted solely on the basis of FL size in 17 of 32 patients with fetal femurs of 7.3 cm or more (53%). The mean FL for the population was 7.38 cm ±0.32 (SD). No patient delivered an infant with HMD. The mean scan to delivery interval was 4.8 days. Conclusion: A femur length of 7.3 cm in a nondiabetlc patient indicates little risk for the development of HMD. Its incorporation with our previously de- scribed ultrasound criteria obviated the need for amniocentesis in 81 percent of our patients.
I I I I I I I I ! I I I I I I
142

Society of Perinatal Obstetricians Annual/Vleeting
San Antonio, Texas
#125 February, 1984
I FETAL GROWTH SUSTAINED BY PARENTERAL NUTRITION IN PREGNANCY: Manuel E. Rivera- Alslna~ M.D., Luis R. Saldana, M.D., and C. Allen Stringer, MoD.X: Division of Maternal-Fetal Medicine, University, of Texas Medical School at Houston, Houston, Texas
Total Parenteral Nutrition (TPN) has rarely been reported in the management of pregnancy complicated by severe maternal nutritional deprivation and intrauterine growth retardation. These entities are associated with premat,lre labor and increased perinatal mortality and morbidity. We have managed four patients where TPN was used successfully to support fetal growth in such diverse complications as twin pregnancy with maternal jejunoileal bypass, regional enteritis~ and acute pancreatitis. TPN included intralipids, amino acids, vitamins, trace metals, albumin and dextrose. Maternal serum electyolytes~ glucose~ amino acids~ vitamins, liver function and renal function studies were monitored during TPN. Fetal growth was assessed using sonography and antenatal fetal well being was evaluated using the biophysical profile. These patients demonstrate the successful use of TPN in gravida suffering from fetal-maternal nutritional deprivations from diverse etiology. In three of these four women~ fetal growth was sustained as evidence by increasing BPD growth in serial ultrasound and the birth weight of the infants. Fetal growth was even sustained in a patient where demands of multiple gestation were superimposed on a fatty liver secondary frem intestinal bypass. Both women with previous jejunoileal bypass had significant metabolic sequela. They had a maximum weight loss six months after surgery, had severe cachexia as long as five years after the bypas s. One of our patients developed a Wernicke-Korsakoff encephalopathy caused by thiamine deficiency which has been reported with the use of TPN. We have confirmed the usefullness of TPN in supporting fetal growth where other modalities have failed. Maintanence of fetal growth evidenced by serial sonographic examination allows achievement of fetal lung maturization prior to delivery. In all four cases there was no perinatal mortality or morbidity. Most important the largest deviation frem ideal birth weight for gestational age was the twin gestations studied in which the infant deviated 160 grams from ideal body weight for their gestational weight. The main clinical implication for our report is the possible application of TPN to maintain adequate fetal growth in small for gestational fetuses due to nutritional deprivation.
I I I I I I i
I I I I I I I I I

Society of Perinatal Obstetricians Annual/~eeting
San Antonio, Texas
# 126 February, 1984
CONTRACTION STRESS TESTING BY INTERMITTENT NIPPLE STIMULATION PRIOR TO 34 WEEKS’ GESTATION
Cynthia G. Brumfield, M.D.*, John F. Huddleston, xM.D., Gail Sutliff Williams, B.S.N.^, Doris Robinson
D epartm ent of 0 bstetrics and Gynecology The University of Alabam a in Birmingham
Birmingham, Alabam a 35294
Nipple stimulation (NS) previously has been shown to result in uterine activity sufficient for performing a contraction stress test (CST). 827 CSTs by intermittent NS were performed on 372 patients from September 1, 1981 through August 31, 1983. Antepartum complications for which CSTs were used for primary fetal surveillance included insulin-dependent diabetes m ellitus, fetal growth retardation, chronic! hypertension, and oligohydramnios; CSTs were also used to follow-up abnormalities found during nonstress testing. All tests were successfully completed without the use of intravenous oxytocin. The mean time required to complete the tests was 43 min. 81% of all tests were completed after only 1 or 2 NS cycles (2 min of unilateral NS followed by 5 min rest per cycle). In reviewing these data, we were curious as to whether uterine response to NS varied with maternal age, parity, or race and whether this response in the early third trimester differed from that near term. 717 CSTs by NS were performed at_>34 weeks’ gestation; 110 tests were performed prior to 34 weeks, the earliest testing being at 26 weeks. In comparing the numbers of NS cycles and the total time required for testing, no differences were found with respect to these maternal factors or to gestational age 634 weeks versus <34 weeks). Our data indicate that uterine activity sufficient to achieve a successful CST can be elicited as early as 26 weeks’ gestation. A]so, no more intermittent NS is required to obtain, a CST prior to 34 weeks’ gestation than subsequent to this time. Despite the observation of others that the gravid uterus is less responsive to exogenous oxytocin in early gestation, we have found that regular uterine contractions can be obtained easily by intermittent NS (and thus CSTs by NS can be performed) in the early third trimester when antepartum conditions of the patient so indicate.
I I I I I I I I I I I i i I
144

Society of Perinatai Obstetricians Annual/Vteeting
San Antonio, Texas #127 February, 1984
FETAL CARDIAC FUNCTION AND GEOMETRY MEASURED BY REAL-TIME ULTRASOUND
Milo B. Sampson, M.D. University of lllinois, Chicago lllinois 60612
OBJECTIVE: The normal geometry of the fetal heart is to be measured in systole and diastole and cardiac function derived indirectly from these measurements.
METHODS: Cardiac images from a 3 MHz 90°sector scanner were recorded on 60 patients at 32 frames per second and later played back on a 19"TV monitor in the frame by frame mode. Systolic and diastolic dimensions were measured in i0 consecutive cardiac cycles and averaged. Adequate data was obtained in 60% of patients whose gestational ages ranged from 3 to 39 weeks with a mean birthweight of 3200 grams. In utero weights were estimated ultrasonically. Ventricular volumes were calculated from the formula ~/6(transverse axis)2.(longitudinal axis). Fractional shortening ~asodeflned by~ (end diastolic-end sysolic dlmension)/(end diastolic dimension)-iO0%. Output for eachventricle was derived from the calculated systolic and° diastolic volumes and normalized for weight and heart rate.
RESULTS: Ventricle diameter transverse 8.6 / 16 +2mm systole/~ia~tole longitudinal
Ventricle Wa~l ~hickness (trans&long)
L~R Ventricle Ratio
5mm all dimensions left wall oSmm greater late preK p<.05
increased larger infants p<.05
Fractional Shortening 30%indep wt/gest age
Ratio Systole/Diastole 1.25@]25bpm 1.35@150bpm
Cardiac Output L: 136 R: 131 ml/min indep of gest age/wt !80ml/min variance
CONCLUSIONS:
i. The length of systole decreases absolutely but increases relative to systole with increasing heart rate.
2. Cardiac outputs from both ventricles were equal and independent of gestational age or birthweight over the range of the study. However, measurements varied greatly.
3. Left/Right ventricle ratios were greater lor large birthweight infants and left ventricular wall thickness increased with gestational age.
I I I I I I I i
I i I I
145

I Society of Perinatal Obstetricians 1
Annual Meeting San Antonio, Texas 1
# 128 February, 1984 |
A PROSPECTIVE RANDOMIZED CONTROLLED TRIAL OF AMNIOCENTESIS FOR PREMATURE RUPTURE OF THE MEMBRANES
Sidney F. Bottoms, MD, David B. Cotton, MD, Karen F. Dorman, RN, Bernie G. Gonik, MD Glen M. Tse, MBA. University of Texas Medical School at Houston and Wayne State University, Detroit, Michigan.
Amniocentesis to guide the management of preterm pregnancies complicated by pre- mature rupture of the membranes (PROM) has been adopted at several centers. The purpose of this study is to evaluate this practice prospectively among comparable groups of patients, which has not previously been reported. In this study, 44 patients with PROM at 26-34 weeks of gestation and an accessible pocket of amniotic fluid on ultrasound examination were randomly assigned to an Amniocentesis Group (N=24) or to a No Amniocentesis Group (N=20). Amniocentesis results were utilized when making clinical decisions regarding tocolytics, steroids and effecting delivery in the Amniocentesis Group. These decisions were made on a clinical basis alone in the No Amniocentesis Group. The Mann-Whitney U test, chi-square and Fisher’s exact test were used as appropriate, with p~0.05 considered statistically significant. The efficacy of the randomization was evaluated by comparing several potentially confounding variables. No significant differences were detected in age, parity, number of previous premature births, cervical dilatation, labor prior to randomiza- tion, malpresentation, or biparietal diameter between the two groups. The proportior of patients receiving tocolytics and steroids were similar in the Amniocentesis Group (71% and 17% respectively) and the No Amniocentesis Group (60% and 20 % respectively Likewise, gestational age at time of randomization, as calculated from modified Dubowitz examination of the infant after delivery, was similar in the two groups. There were no antepartum fetal deaths and one neonatal death in each group. Fetal distress, as judged by the fetal monitor tracing, was more frequent in the No Amniocentesis Group (p = 0.02). The number of days the infant remained in the hospital after discharge of the mother was significantly less in the Amniocentesis Group (median = 8.5 days, range 2-88 days) than in the No Amniocentesis Group (median = 22 days, range 6-104 days, p = 0.01). This difference in neonatal hospital days appeared to be mainly due to a reduced combined frequency of respira- tory disease and intracranial hemorrhage, although no significant differences In these complications were demonstrated individually. No differences in antepartum hospital days, postpartum hospital days, postpartum endometritis or sepsis were apparent between the two groups. We conclude that amniocentesis appears to be an effective diagnostic adjunct to aggressive pharmocologic management of PROM (as in this study). A similar study comparing this management approach to strictly conservative management without amniocentesis, tocolytics or steroids is badly needed.
I
I 1 1 1 I ! 1 I I I I I 1 I
146
1 I

#129
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
PROBABILITY (F SK)NTANEOUS CONVERSION OF BREECH TO VERTEX PP~ATION DURING T~ THIRD TRIMESTER
Wolfson, R.N. and Hertz, R.H. Department of Cbstetrics an~ Gynecology/Perinatal Clinical Research Center; Clevela~d Metropolitan General Hospital/Case Western Reserve University
Exterrml cephalic version with tocolysis has been proposed as a meens of r~ucing the incidence of breech presentation at the onset of term labor. The procedure is not without potential maternal and fetal m~rbidity and mortality. Therefore, one of the considerations in attempting and timing version must be the spontaneous conversion rate of breech to vertex presentation. The purpose of this study was to describe the probability of delivering vertex or breech at term depending on the gestational age at which breech presentation was diagnosed. Data were obtained fram 1938 consecutive p~tients referred for ultrasound exanination between 26 and 42 weeks’ gestation, with a singleton intrauterine pregnancy, intact membranes and a sonographically non~ appearing fetus, in when fetal presentation on ultraso~qd (vertex, breech, shoulder, o~ transverse lie) could he cc[~mred with presentation on delivery at term (> 38 weeks). Patients with oligohydramnios or polyhydra~nios were excluded. Gestational age at ultrasound examination and at delivery was based on the modifie4 Dubowitz estimate of gestational age at birth. %he results are mm~narlzed in the Table below. ~qe probability of spontaneous conversion from breech to vertex progressively decreased from 95% at 26- 29 weeks to 24% at term ~hile tD~ chance of breech delivery progressively increased from 5% to 76% over the sane interval (not all percentages su~ to 100% since sa~e patients presented at term with shoulder presentation). A spontaneous conversion p~obability of 4/23 = 17% at or beyond 37 weeks was previously reported*; for our data 31% of breech presentations spontaneously converted to vertex presentation at or beyond 37 weeks (p<_0.~2). These data suggest that the probability of spontaneous conversion, and, therefore, the p~obability of vertex delivery after identification of breech presentation may be higher than previously anticipated. Knowing these probabilities may also prove helpful in co~qseling patients and in electing and timing the mode of intervention, if any, for breech presentation.
~ (F PATIENTS BREECH ON ULTRASOUND
PROPORTIONS DELIVERED BREECH DELIVF/~D VERqEX
26-29 84 5% 95% 30-33 49 22% 78% 34-37 33 36% 58%
>_38 17 76~ 245
*Van Dorsten, J.P. et al., Am. J. Cbstet. Gynecol. 141:147, 1981.
I I I j
I
I I I i I I I I I I
147

#130
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
BEYOND RESPIRATORY DIS~BESS SYNDRO~ (RDS): AVOIDING IATROGENIC PR~TURITY IN TFE INFANT OF %1£ DIABETIC MOTHER
Ka-en M. Ferroni, M.D.,x ~Ix~as L. Gross, M.D., Depa-tment of Obstetrics and Gynecology "and the Perina- tal Clinical Research Center., Cleveland Metropolitan General Hospital/Case Western Reserve University
Previous studies of diabetic pregnancies have disagreed as to ~hether the lecithin to sphingomyelin ratio (L/S) or phosphatidylglycerol (K]) should be used to predict fetal maturity. These previous stu- dies have looked at the frequency of BI%B as a measure of neonatal outcome. We have found that in a group of diabetic pregnancies, RZB was uncomrgn (<2%); but, despite this low frequency of RDS, there was significant neonatal morbidity, including transient tachypnea of the newborn (TfN), hype.-bili~ubinemia, and feeding difficulties, even when the L/S was mature. Although there were no neonatal deaths, this morbidity resulted in many admissions to the neonatal intensive are ~qit (NICU), and neonatal discharge home after their mothers (HAM). The purpose of the present study was to determine whether anniotic fluid (AF) PG was useful in predicting this less severe, yet costly morbidity. A group of 101 diabetic pregnancies (30 A, 58 B and C, and 13 D-R) were evaluated. Management was based on a one dimensional L/S (>--3.0 mature). On a second portion of amliotic fluid L/S and PG were determined using a two- dimensional technique. These results were not available to the clinician, and are reported here. RDS and Tll~ were diagnosed by a neonatologist using strict clinical and radiographic criteria. Admission to the NICU for > 24 hours and discharge H~M were used as general measures of neonatal morbidity. Results were analyzed using chi-square or t tests. Patients were included in the analysis only if the L/S was mature (>2.0) and the amniocentesis was performed within one week of delivery. In this g~oup of patients, the mean obstetric estimate of gestational age (GA) was 38.4 + 1.5. With this late inte.-ven~on in preg- nancy, no neonatal deaths or RDS oecurred. Twenty-three i--nfants, h~wever, were admitted to the NICU, 12 were discharged HAM, 8 developed T~N, 57 had hyperbilirubinemia, and 17 required pbototherapy. Of the 86 patients, 70 had PG present in their anniotic fluid. The PG negative patients were more likely than l the PG positive group to ~ire a~nission to the NICU [9/16 (56%) vs 14/70 (20%) p<.0005]. The PG negative patients were also more likely to be discharged HAM [6/16 (38%) vs 6/70 (~) p<.005]. The mean CA of the infants admitted to the NICU was significantly lower than those admitted to the normal nursery! (37.0 _+ 1.7 versus 38.9 _+ 1.7 weeks, p<.001). Likewise, the mean GA of those sent H~4 was significantly lower than those discharged with their mothers (37.5 _+ 1.7 versus 38.5 _+ 1.9 weeks, p<.05). This sug- gests that some of the non-RDS neonatal morbidity may be related to relative prematurity. It has been suggested that increasing the mature level for an L/S to 3.0 may be used to predict a positive PG. With an L/S of 2.0, 70/86 patients (81%) had PG present. With an L/S of >3.0, 60/68 (88%) patients would be positive for PG. This would misclassify 10 patients (14%) with positive PG into the PG negative group. Eight of the 16 patients with negative PG (50%) had an L/S of 3.0, and thus would have been misclassi- fled to the PG positive group. In the present study when the L/S was mature R~ did not oecur, but sig- nificant morbidity ~s still common. FLrthermore, it appears that some of this morbidity is related to mild p~aturity. This relative pr~naturity may explain scme of the neonatal morbidity previously t}Dught to be due to an effect of maternal diabetes itself. Because PG appears later in gestation than a mature L!S, it is a better indicator of term gestaticn and that the ccmplications of mild prematurity’ may be decreased. Our findings suggest that ~hen planning the elective delivery of the diabetic patient, awaiting the onset of a positive R] may reduce the incidence of this previously unrecognized source of neonatal morbidity....
I I I I I I I I I I ! I I ! I ! ! ! I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 131 February, 1984
CENTRIFUGATION SPEED AND FALSE ~GATIVE RESULTS C~ AMNIOTIC FLUID PHOSPHATIDYLGLYCEROL
Sharon Patrick,x T~ L. Gross, M.D., Paul M. Kub~mrt, Fn.D.,x Department of Cbstetrics and Ghynecology and the Perinatal Clinical Research Center, Cleveland Metropolitan General Hospital, Case Western Reserve University
It has become increasingly co,mon to use a~niotic fluid (AF) phosphatidylglycerol (PG) to p~edict fetal pulmonary maturity. The presence of AF PG has been shown to accurately predict fets1 maturity. However, a negative PG is frequently followed by a mature neonate, ~esulting in a high false negative rate for predicting respiratory distress synd~ne. A modification in the centrifugation technique has been proposed ~hich may allow PG to be detected at lower concentrations and thus result in a lower false negative rate (Bent, et al., ~ J Obstet Gynecol 139:259, 1981). The ~/~ is centrifuged at ~0,000 x g, a speed proposed to separate all PG out of solution, then the phospholipids are extracted frcm the pellet at the bottom of the tube. In the p~esent study, the standard method of centrifuging AF at 750 x g and extracting the lipids from the supernatant was compared to the technique of centrifugation at 10,000 x g ~ ~ssaying the lipids in the pellet at the bottom of the tube. AF specimens obtained for clinical indications in 70 patients were centrifuged at 750 x g for 5 minutes. The supernatant from each patient was then divided into two 5 ml aliquots. The first was set aside for phospholipid extraction. The second was re-centrifuged at 10,000 x g for 20 minutes in a refrigerated centrifuge (Sorvall, RC-5 Superspeed); the supernatant was discarded and the pellet re-suspended in 3 ml 0.85% NaC1 and set aside’ for phospholipid extraction. For each of the 70 AF samples, phopholipids were extracted from both of the aliquots and then separated by two-dimensional thin layer chromatography. PG was visually estimated to be positive, present in trace amounts or negative. PG results determined by the two different methods ware ccmpar%4 in each of the 70 patients. In 39 of the AF sables PG was absent in the aliquot centrifuged at 10,000 x g, as well as that centrifuged at 750 x g. PG was present following both rates of centrifugation in 26 of the samples. Therefore, there was agreement between the two methods in 65 patients, 93% of those studied. In all 5 of t~ AF specimens with discrepant results PG was present only in trace a~D~Its. In 4 of these patients PG was present in the aliquot spun at 750 x g, but absent when I0,000 x g was used; one AF s~le was PG negative in the aliquot centrifuged at 750 x g, but posi- tive following 10,000 x g. In order to determine if PG is consistently localized in the pellet at the bott~n of the tube following centrifugation at I0,000 x g, a subset of AF samples was centrifuged at 10,000 x g, and the phospholipids assayed in both the supernatant and the centrifuged pellet. Both the supernatant and the centrifuged pellet in this g-oup consistently contained the major phospholipids, including PG. Results of the p~esent study indicate that the initial rate of cent~ifUgation of AF had no effect en the PG results in 93% of samples tested. Only one patient was AF negative for PG by the stan- dard method (centrifugation at 750 x g and extraction of the supernatant), but positive when extracted from the 10,000 x g centrifuged pellet. Also, several patients with trace PG determined by the standard method had negative PG ~hen the lipids were extracted from the 10,000 x g pellet. In addition, both lecithin and PG were found in appreciable amounts in the supernatant of AF samples centrifuged at 10,000 x g. These findings suggest that detection of sm~ll anounts of PG will not be improved and trace amounts of PG may even be discarded if the technique of centrifugation at 10,000 x g and assaying the centrifuged pellet is implemented for the determination of AF phospholipids.
I I I I I I I I I i
I
I ! I
149 I I

I Society of Perinatal Obstetricians 1
Annual Meeting San Antonio, Texas 1
# | 32 February, 1984
Thomas J. ~i~lin, M.D.,x Thomas L. Gross, M.D., Robert N. Wolfson, M.D., Ph.D.,x Department of Cbstetrics and Gynecology and the Perinatal Clinical Research Center, Cleveland Metropolitan General Hospi -tal/Case Western Reserve University
Ultrasot~d (U/S) examination of fetal biparietal diameter (BID) _>~ and placental grading have been correlated with fetal lung maturity. These observations are accurate in predicting fetal lung maturity when positive, but the false negative rate is high. It is known that a~niotic fluid (A/F) changes fr~ clear to turbid as gestation progresses. The occurrence of free-floating particles (FFP) in AF on U/S examination has been associated with increasing particulate matter floating in suspension and increasing
AF turbidity. These particles, when seen at term, my represent vernix and may be associated with fetal~ maturity. This laboratory has already reported that the presence of FFP’s in the AF on U/S examination is associated with a mature lecithin to sphingc~yelin (L/S) ratio. This study was undertaken to test if finding FFP’s on U/S examination could enhance the prediction of fetal lung maturity beyond that already achievable by observation of the BID alone. Frcm Jure, 1981 to June, 1983 213 consecutive patients undergoing aTniocentesis for fetal 1Lng maturity determination, and who also had an U/S performed. within three days of a~liocentesis, were evaluated for the ability of a BID > 9~ (BPD-POS) or the l
presence of FFP’s in AF (FFP-PRESENT) to predict a m~ture L/S ratio. Cc~lications included 73 repeat C-sections, 21 class A and 34 class B-R diabetics, 38 pre-eclamptics, 8 chronic hypertensives, 6 pla- centa previas, 6 post-dates and 27 other. Respiratory distress syndrome (RDS) is uncomnon in patients undergoing fetal hmg maturity testing. The L/S ratio was used as the outcome variable similar to other investigations correlating ultrasound findings with fetal lung maturity. The L/S ratio was determined by a method for which a value of 3.0 is associated with RDS in < 0.5% of patients. Examination of the data was by contingency table and X2 analysis. Of 189 patients with a mature L/S ratio, 65 had FFP- PRESENT (sensitivity = 65/189 = 34%); and of 66 patients with FFP-PRESENT, 65 had a positive L/S ratio [(true positive rate = 65/66 = 98%) p<.01]. The BID could be obtained in only 164 patients. Of 144 patients with a mature L!S, 55 had BPD-POS (sensitivity = 55/144 = 38%); and all with BPD-POS had a mature L/S ratio [(true positive rate = 55/55 = 100%) p<.01]. When combining the two U/S paraneters so that an U/S screen is positive (U/S-POS) with either FFP-PRF~ or BPD-POS, or both, the following was seen. Of 144 patients with a mature L/S ratio, 79 were U/S-PCS (sensitivity = 79/144 = 55%), and of 80 U/S-POS patients, 79 had a mature L/S ratio [(true positive rate = 79/80 = 99%) p<.05]. Additional analysis also explained the reason for the increase in sensitivity. When patients were not BID-PCB, the FFP-PRESENT finding predicted an additional 26% (35/134) mature L/S ratios. Conversely, for patients not FFP-PRESENT, a BPD-PCS finding predicted an additional 20% (25/124) mature L/S ratios. Thus, FFP’s and BPD > ~ occur equally in the face of a mature L/S (sensitivity)and ~hen used alone are equivalent--predictors of fetal lung maturity (true positive rate); h~wever, when either parameter is considered, the sensitivity to predict a mature L/S ratio is increased. The BPD is not often obtained in late pregnancy due to fetal position. ~hen considered singly, a BID > 9~ or the presence of FFP’s on U/S exanination, occur in only I/3 of pregnancies with a mature L/S ratio. However, when either cri- teria is used, a mature L/S ratio is foond in over I/2 of the anniocenteses performed. Therefore, if these results are prospectively confirmed, it may be possible to avoid over I/2 of the amniocenteses now being performed for fetal maturity. This significantly improves upon observation of the BID alone.
I
i
150
I I

#133
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
ASSESSmeNT OF THYROID FUNCTION IN PREGNANCY: A Comparison of Serum Free Thyroxine Measurements by Radioimmunoassay and Equilibrium Dialysis with the Ratio of Total Thyroxine to Thyroxine Binding Globulin. P.M. Hays, M.D., D.P. Cruikshank, M.D., and M.J. Fratkin, M.D., Departments of Obstetrics/Gynecology and Nuclear Medicine, Medical College of Virginia, Richmond, Virginia, and M.R. Pandian, Nichols Insti- tute, San Juan Capistrano, California.
The diagnosis and management of thyroid disease during pregnancy is largely dependent on the laboratory assessment of thyroid function. These parameters are altered in the normal pregnant woman because of the estrogen induced doubling of thyroid binding globulin (TBG) concentration. Free thyroxine (FT4) concentration determined by the equilibrium dialysis technique (EDT) is the only method which compensates for these increases in TBG levels. Radioimmunoassay (RIA) of FT4 are being introduced with increasing frequency, but some evidence suggests that eleva- tion of TBG concentration adversely effects the results of these assays by falsely lowering the measured FT4 concentration. In order to indentify which, if any, of the readily available thyroid function tests best correlate with the FT4 by EDT, serum concentrations of FT4 were measured by equilibrium dialysis and by the one and two step RIA techniques in 21 patients between 34-40 weeks gestation, in whom no thyroid dysfunction existed. The concentrations of total thyroxine (TT4) by RIA and of TBG by RIA were also measured in these same patients and the total thyroxine thyroid binding globulin (TT4:TBG) ratio was calculated.
thyroid function test FT4 one step RIA (ng/dl) FT4 two step RIA (ng/dl) FT4 by EDT (ng/dl) TT4:TBG ratio
observed observed mean _~ S.D. range non-pregnant range 0.81 ± 0.15 0.5 - I.i 1.0 - 2.4 0.99 ± 0.12 0.7 - 1.2 1.0- 2.4 2.68 ± 0.38 2.1 - 3.8 1.3 - 3.8 1.93 ~ 0.21 l.S - 2.5 2.0 - 4.8
As can be seen, both the one step and two step RIA methods seriously under- estimated the FT4 concentration in pregnancy. FT4 by EDT correlated best with rT4:TBG ratio (r=0.82, p=0.0001), less well with the two step FT4 RIA (r=01.61, p=0.04), and did not correlate with FT4 values obtained by the one step RIA (r=0,41, p=0.07). These results indicated that the TT4:TBG ratio provides a more accurate reflection of actual thyroid status than either of the RIA techniques. Clinical use of TT4:TBG ratio is the most accurate assessment of thyroid function during pregnancy. Reliance upon RIA determination of FT4 may be seriously ~isleading in pregnancy.
I I
I I I I I I i I I
I I I I I
151
I I

Society of Perinatal Obstetricians Annual/Vleeting
San Antonio, Texas # 134 February, 1984
A COMPARISON OF SCREENING METHODOLOGIES FOR GESTATIONAL DIABETES Robert C. Kaufmann, M.D., Kofi S. Amankwah, M.D., Southern lllinois University School of Medicine, Department of OB/GYN, Springfield, lllinois
Gestational diabetes can cause significant perinatal morbidity and mortality if it is unrecognized and untreated. Various methods have been used to attempt to determine which women are gestational diabetics. The most accepted definition is based upon O’Sullivan’s criteria whereby if two values of a three-hour Glucose Tolerance Test (GTT) are greater than two standard deviations above the mean the person is a gestational diabetic. Various screening procedures have been employed to determine which pregnant patients should have a GTT. The screening procedures must have a high sensitivity (not miss any gestational diabetes) and a high specificity (not have too many patients that have to have GTTs and are not gestational diabetics) to be useful in clinical practice. In this study two different screening procedures were used on similar patient populations. In both groups, pregnant patients, 28 to 32 weeks, were given a 50 gm glucose load after an overnight fast. In group I, the plasma glucose was drawn at one hour after ingestion, and in group II the plasma glucose was drawn at two hours after ingestion. In both groups a blood glucose level of > 130 mg/dl was used as the cutoff as to whether a three-hour GTT should be done~ The results are tabulated below:
Total Positive Gestational Normal Patients Screen Diabetics GTT
Group I 4,340 995(22.9) 215(4.9) 780(18.0%) Group II 21.3 20(9.4) 11(5.2) 9(4.2)
The percentage of patients requiring a GTT in Group II was > 50% less than that in group I (p<O.O01). The percentage of diabetics was essentially unchanged (4.95 vs 5.2%). However, the percentage of individuals who required a GTT but were not diabetic was dramatically less in group II (4.2%) as compared to group I (18.0%) (p<O.O01). The specificities for the one hour screen (group I) and the two hour screen (group II) are 81% and 96% respectively. The sensitivities for the two screening criteria cannot be computed from this data. However, in a previous stud the percentage of gestational diabetes in a similar population was found to be 5.1%. Since, in both groups I and II the gestational diabetic population was approximately 5%, the sensitivities of the two screening procedures must be very near 100%. Based upon these data, it seems that the use of a two-hour blood sugar_> 130 mg/dl after a 50 gm glucose load as a cutoff value is a more specific and sensitive screening test for gestational diabetes.
I
152
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 13 5 February, 1984
THE RELATIONSHIP BETWEEN NONSTRESS TEST REACTIVITY AND GESTATIONAL AGE: IMPLICATIONS FOR TESTING IN THE PRETERM PERIOD
JUSTIN P. LAVIN, JR., M.D., MENACHEM MIODOVNIK, M.D. AND TOM P. BARDEN, M.D.
From the Divisions of Maternal-Fetal Medicine, University of Cincinnati Medical Center, Cincinnati, Ohio: and Akron City Hospital, Akron, Ohio
The relationship between gestational age and reactivity during the nonstress test was evaluated in 297 high-risk patients. When the incidence of nonreactive tests at gestational a~es of 28 to 44 was evaluated week-by-week either on the basis of tests performed or patients tested, there was no statistically significant relationship between reactivity and gestational age (P = .184tests P = .222 patients). Four grouped gestational-age intervals were evaluated. Interval A consisted of the period from 28 to 32 weeks- gestation, interval B consisted of the period from 33 to 36 weeks , interval C consisted of the.period from 37 to 41 weeks gestation and interval D consisted of the period from 42 to 44 weeks gestation. The incidences of nonreactive tests were 15.3, 3.9, 2.5 and 5.9% in intervals A, B, C, and D, respectively. The differences in the incidences of nonreactive tests between those performed in intervals A and B and intervals A and C were highly statistically significant (P < .001). Differences in the incidences between other intervals did not reach statistical significance. The incidences of patients who experienced a nonreactive test were 10.2, 2.4, 2.8, and 4.7% in intervals A, ~, C, and D, respectively. The differences in the incidences of patients who experienced a nonreactive test in interval A and B and intervals A and C were highly statistically significant (P < .001). Differences in the incidences between other intervals did not reach statistical significance.
Four of 108 (3.7%) of the fetuses tested in the period, from 28 - 32 weeks exhibited a nonreactive nonstress test followed by a positive contraction s[ress test. All of these infants developed fetal distress in labor and/or were asphyxiated or SGA age at birth. There were 2 (1.4%) cases of RDS among the infants tested prior to 32 weeks. Delivery of one of these infants was necessitated by episodes of prolonged fetal bradycardia. The second infant was severely SGA,and oligohydramnios precluded amniocentesis. Although the mothers tested in the interval from 28 - 32 weeks were selected because their pregnancies were considered to be at extreme risk for utero-placental insufficiency, no perinatal mortality occurred in thi~ group.
The results of the current study combined with published reports suggest that in certain high-risk patients it is reasonable to extend the testing period to include less advanced gestational ages than have traditionally been included in antepartum fetal heart rate testing programs. However, it should be anticipated that the number of nonreactive tests will be higher than observed whez
patients are tested at more traditional ~estatlonal ages.
I
I
153
I I

I Society of Perinatal Obstetricians 1
Annual Meeting San Antonio, Texas ¯
# 136 February, 1984
FETAL LUNG MATURITY ASSESSMENT BY MODIFIED A-650 DETERMINATION
Michael F. Koszalka, Jr., M.D.x
Charles H. Blomquist, Ph.D.x
David J. Lakatua M.D.x
St. Paul-Ramsey Medical Center Department of Obstetrics and Gynecology
Department of Anatomical and Clinical Pathology University of Minnesota Medical School
St. Paul, Minnesota 55101
Although many biochemical methods have been proposed for deter-
mination of fetal lung maturity, most are tec~nically complex and time consuming. A-650 development by Sbarra,- suggests utility in the biophysical measurement of absorbance at 650 nanometers follow- ing centrlfugation at 2,000 x g x i0 minutes. Refinement of this methodology was developed utilizing differential centrifugation. Absorbance determination of lamellar body fraction was performed and the contribution of the non-sedimentable fraction determined. Three hundred thirty samples of amniotic fluid of varying gestational ages were subjected to two-step centrifugation. Fluid was first centrifuged at 250 x g for 20 minutes and then absorbance at 650 nanometers determined (A-650). A second centrifugation at i0,000 x g was used to sediment lamellar bodies. The absorbance at 650 nano- meters of the supernatant was used as a blank. Three parameters were extracted from the data to form an A-650 battery. Initial ana- lyses suggest that maturity estimates based on the A-650 battery compare favorably with estimates based on L/S ratios, A-2000 and neonatal outcome.
i. Sbarra, A.J.0 et.al. J. Reprod. Med. 27:34, 1982.
I I I I I I I I I I I I I 1 1
154
I I

Society of Perinatal Obstetricians Annual/Vieeting
San Antonio, Texas
# 137 February, 1984
~REAL-TIME ULTRASOUND ESTIMATIONS OF WEIGHT IN FETUSES OF DIABETIC GRAVIDAS Ralph K. Tamura, M.D., Rudy E. Sabbagha, M.D.,x Sharon L. Dooley, M.D., Michael L. Socol, M.D., Naomi Vaisrub, PH.D.x and Richard Depp, M.D. Northwestern University, Chicago, Illinois, 60611
In this report the applicabity of equations used to estimate fetal weight is examined in a group of suspect large for gestational age (LGA) fetuses. Real-time ultrasound measurements of fetal biparietal diameters (BPD) and abdominal circumferences (AC) were obtained on 34 fetuses of diabetic mothers. Descriptive statistics for study infants (mean and S.D.) are: fetal age 38.6 + 1.19 wks., BPD=9.36 + 0.45cm, AC=38.74 + 2.3cm, ABW=4143.5 + 506.4grams and scan to delivery interval of seven days or less. In the first phase of the study, the accuracy in the prediction of weight was assessed using two known equations. The first was designed for preterm fetuses by Thurnau et. al. AJOG 145:557, 1983 and the second was formulated for fetuses of any gestatlonal age by Shepard et. al. AJOG 136:45, 1982. Using the BPD & AC data of the suspect LGA fetuses in the study, the estimated fetal weights (EFW) were calculated and then compared to the actual birthweights (ABW). Computerized data analysis by the Statistical Package for the Social Sciences program provided means and standard deviations for the EFW, ABW and differences ie. ABW-EFW. The 95% confidence interval for the mean difference was calculated and the two tailed students t-test for null hypothesis of mean difference equal to 0 was conducted (p <.05, significant). The results are as follows:
STUDY BY: EFW Mean S.D.
Thurnau et. al. 3089.5 284.56 Shepard et. al. 4276.4 608.65 * T33 = 17.26, p<.001, + T33 = 1.77, NS
ABW-EFW Mean S.D.
1054.05 356.10 -132.8 436.62
95% CI FOR ABW-EEW
+929.80 to +1178.31" -285.2 to +19.5+
In the second phase, BPD, AC and ABW data of the 34 study fetuses were used as in- dependant variables to determine the best fitting equation for relating EFW to BPD and AC; this equation is: log (EFW) = .02597 AC + .2161 BPD - (ACxBPD2)/IO00.
The standard deviation of differences = 322.29g and multiple R = .781. The data presented suggest that in suspect LGA fetuses of diabetic mothers weight
estimates calculated at or near term may be enhanced if predictive equations are formulated specifically from such fetuses. In addition, the large standard deviation values of the mean difference (ABW-EFW) imply that assessment of additional fetal parameters may further improve weight predictions.
I I I I I I I I I I I I I
155
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# | 38 February, 1984
COMPARATIVE CLINICAL EVALUATION OF TICARCILLIN AND CLAVULENIC ACID WITH CLINDAMYCIN-GENTAMICIN IN THE TREATMENT OF POST-CESAREAN SECTION ENDOMYOMETRITIS. Joseph J. Apuzzio, M.D.,* Vijaya Ganesh, M.D.x IrwinLandau, M.D.,x Donald Louria, M.D.,x Department of Obstetrics and Gynecology, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark, New Jersey 07103.
A new combination of ticarcillin and clavulenic acid was compared with clindamycin-gentamicin for the treatment of post-cesarean section endomyometritis.
The two antibiotic regimens were compared in the treatment of post-cesarean endomyometritis: Ticarcillin plus clavulenic acid 3.1 grams IV every 4 hours; or clindamycin 600 mg q h IV plus gentamicin 3-5 mg/Kg/day IM. Each regimen was given for 4-5 days. The prospective randomized schedule was calculated to divide half the patients into each group. The diagnosis of endomyometritis was based upon an elevated oral temperature of lO0.4°F or higher on any two occasions excluding the first 24 hours postpartum, and uterine tenderness, and the absence of other foci of infection. Lochial discharge was foul in most but not all cases. Thirty-six patients were treated. Treatment failure rates were: clindamycin-gentamicin 0 of 20; Ticarcillin-clavulenic acid 2 of 18 (If%). Treatment failures did not appear to be different from successes demographically or in risk factors for endomyometritis. The differences between the treatment failure rates were not statistically significant. The study suggests that ticarcillin plus clavulenic acid is effective in the treatment of post-cesarean endomyometritis when compared to our usual standard therapy of clindamycin and gentamicin.
156
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 139 February, 1984
SONOGRAPHIC SCREENING FOR GESTATIONAL DIABETES. Manuel E. Rivera-AlsinaL M.D_._I., Jeam, arie K. Salinas, M.A.x and Jeanne Holland, E.N., E.D.M.S.x~ Division of Maternal-Fetal Medicine, University of Texas Medical School at Houston, Houston, Texas.
Glucose intolerance during pregnancy exerts a deleterious influence on both mother and fetus. Patients at risk for gestational diabetes are screened with a one hour 50g glucose challenge test (GCT). If the results of the GCT are above a threshold, patients are tested further with a 3 hour, 100g oral glucose tolerance test (GTT). Even with early screening some gravidae with negative GCT and GTT will develop gestational diabetes later in pregnancy. Sixteen patients, at risk for developing gestational diabetes, with negative GCT and GTT were referred to the Antenatal Testing and Ultrasound Unit. Sonographic scans for gestational dating were performed using a linear-array real-time scanner (ADR Industries, Tempe, Arizona), with the use of a 3.5 MHz transducer. These tests were repeated every week and subsequently they developed gestational diabetes. All patients scanned had singleton pregnancies. Mean age was 27.3 years with a range of 18-40. Five patients were Mexican-Americans, 4 were black and 7 were caucasians. Our study population consisted of 4 nulliparous patients and 12 multiparous patients. A "diabetic halo" (DH) was first observed between 27-29 weeks of gestation. At the time of initial visualization of the DH there was no evidence of polyhydramnios~ fetal ascites or fetal congenital anomalies. Initial screening test with a 50g GCT or a 100g 3 hour GTT were negative in all patients. Weekly serial GTTs later became positive in all patients during gestation. In 8 of these patients maternal and fetal circulating nonsuppressible insulinlike activity (NSILA) and both fetal and maternal growth hormone (GH) were measured. All of these fetuses had increased amounts of GH levels as well as increased NSILA. In conclusion, the fetal DH may precede overt metabolic derangements in the mother. A normal GTT does not protect against metabolic and anatomic changes consistent with diabetes mellitus. The DH may be the initial finding in patients that will eventually develop gestational diabetes. Correlation between sonographic par~,eters, maternal GTT and fetal GH as well as NSILA~ substantiates that a DH can be the earliest manifestation of gestational diabetes as evidenced by these 16 women presented.
I I I i I I I I I I I I I I I I
157

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas # 140 February, 1984
~’URINARY ESTRIOLS IN DIABETIC PREGNANCY: A REAPPRAISAL USING FETAL HEART RATE TESTING AS THE STANDARD OF FETAL WELL-BEING. Sharon L. Dooley, M.D., Richard Depp, M.D., Michael L. Socol, M.D., Ralph K. Tamura, M.D., Naomi Vaisrub, Ph.D.x Section on Maternal-Fetal Medicine, Northwestern University Medical School, Chicago, Ii.
Daily 24 hour urinary estrlols (E3) were obtained from 138 hospitalized insulin-dependent diabetics in order to assess: i) the clinical usefulness of serial E3 in detecting fetal compromise; and 2) the relationship of absolute levels of E3 excretion to measures of fetal and placental mass. E3 was assayed by gas chromatography, and urinary creatinine by the alkaline plcric acid technique. An E3 drop of >40% was considered significant only if confirmed by a >40% drop in E3-creatin~ne ratio (E3/C). An E3/C drop of >40% did not alter management if a reactive non-stress test (NST) and/or negative contraction
stress test (CST) occurred within 24 hours of the drop. A >40% E3/C drop was denoted a false positive if I) E3 subsequently returned to baseline levels or 2) the E3 drop occured the day before delivery of a healthy neonate. A total of 3085 E3 were obtained (mean 22.4/patient). A >40% E3 drop
occurred 49 times in 38 patients. In 27 of these E3/C was < 40% and no action was taken. The E3/C drop was >40% on 22 occasions. One was asssoclated with antibiotic therapy. Two were associated with fetal compromise, both also
identified by NST/CST. The remaining 19 E3/C drops of >40% (range 40-82%) in 17 patients were designated false positives. Three patients delivered healthy neonates (Apgar5 = 9, cord arterial pH>7.20) the day after the drop. In the remainder E3 returned to baseline and delivery occurred a mean of 20 days later (range 2-53 days). In 7 additional patients mean E3 excretion was <12 mg/24 hour at 36 weeks. None had evidence of fetal compromise and all had favorable outcomes. Total patient billing for E3 assays in 1983 dollars was ~284,591 (mean ~2062/patlent). The cost of identifying each distressed fetus was ~142,296.
Mean E3 for i week prior to delivery was compared by linear regression to birthwelght (BW), placental weight (PW), and fetal abdominal circumference by ultrasound (AC). With all three independent variables there was a significant positive correlation as follows:
variable_r ~ BW 0.499 <.0001 PW 0.462 <.0001 AC 0.443 <.001
We conclude: i) urinary E3 in well-controlled diabetics add considerably to patient care costs without supplementing the information provided by NST/CST; 2) both E3 drops and chronically low E3 excretion are poor indicators of fetal jeopardy; and 3) there is a positive correlation of E3 with blrthweight, placental weight, and fetal abdominal circumference.
I I I I I I I I I I I I I
i i !

i Society of Perinatal Obstetricians m Annual Meeting
San Antonio, Texas ¯ #141 February, 1984
A SPECTRUM OF HEART FAILURE IN ASSOCIATION WITH THYROTOXICOSIS AND PREGNANCY. Thomas W. Lowe, M.D.,* Gary D.V. Hanklns, M.D.,*, George D. Wendel, Jr., M.D.,* and F. Gar~ Cunnln~ham, M.D., Dept. Ob/Gyn, Univ. Texas Southwestern Med. Sch., Dallas, TX 75235
The adverse effect untreated thyrotoxlcosls has on perinatal outcome is well documented. This report emphasizes that significant maternal morbidity may also occur in this setting. During an 11 year period 101 gravldas with thyrotoxlcosis were managed at Parkland Memorial Hospital. In 5 of these women pregnancy was complicated by heart failure associated with untreated thyrotoxlcosls. Two women developed heart failure in the second trimester, three developed it in the third trimester. Two pregnancies were compllcated by fetal deaths: one at 20 weeks gestation, the other at 34 weeks gestation. Two healthy infants were delivered: one at 36 weeks gestation, the other at 38 weeks gestation. One woman was lost to follow-up prior to dellvery. All women were clincally and chemlcally hyperthyroid with the following findings:
Tachy- Hyper- Cardio- Thyro- Exoph- cardla tension Anemia Fever megaly megaly thalmus (p>100) (MAP>I00) (Hct<30Z) (T>38°C) on x,ra7
+ -- + + -- -- --
2 3 4 5
+ + + + + + +
+ + + + + + - + +
In addition to thyrotoxicosis, factors predisposing to heart failure in these five women included increased cardiac workload secondary to pregnancy, anemia, infection, chronic hypertension, and induction of general anesthesia. Each woman received specific treatment for thyrotoxicosis. Management of heart failure was individualized and included preload reduction, afterload reduction, efforts to increase myocardial contractility, rate reduction, supplemental oxygen, ventilatory support, and decreased physical activity. All women experienced resolution of heart failure once thyrotoxicosis and other factors were appropriately treated.
! I ! I I
I I i i I I I i
159
i i

¯ Society of Perinatal Obstetricians
¯ Annual Meeting
~n Antonio, Texas ¯ # 142 February, 1984
A COMPARISON OF THREE METHODS OF PREDICTING FETAL OVERGROWTH Frederick A Korndorffer, IIIx, Joseph M. Miller, Jr. and Harvey A. Gabert, Depart- ment of Obstetrics and Gynecology, Louisiana State University Medical Center, New Orleans, Louisiana
Macrosomic infants are at increased risk for birth trauma if delivered vaginally Cesarean section is advised if the fetus is greatly overgrown. Several predictive models using data obtained by ultrasonograms have attempted to identify the ex- cessively large fetus. This study compares three methods: (i) estimated fetal weight from tables from Shepard et al Am J Obstet Gynecol 142:47, 1982; (2) esti- mated fetal weight from the normogram of Hansmann, Gynaekol 9:133, 1976; and (3) the macrosomic index = transthoracic diameter - the biparietal diameter (TTD - BPD) ~ 1.4 cm of Elliott et al, Obstet Gynecol 60: 159, 1982. Twenty liveborn singleton infants with birth weights 3500 grams constitute the study group. All had a real time ultrasound (Toshiba SAL-38) within 4 (18 of 20 within 2 and 15 within i) weeks of delivery. To correct for interval growth, the fetus was assumed to follow its centile growth unitl delivery occurred. The birth weight curves of Brenner et al, Am J Obstet Gynecol 126:555, 1976 were used. The estimated fetal weight obtained using the tables from Shepard (EFW-Yale) was statistically significantly correlated with the actual birth weight (ABW). ABW = 193 + 0.84 (EFW-Yale), r = .48, p < .05. Individual weights were not well predicted, with a mean absolute error of 612 ~ 255 grams and an average error of -435 ± 507 grams. The normogram of Hansmann (EFW- Norm) yielded similar results. ABW = 1389 + 0.55 (EFW-Norm), r = .53, p < .05, with a mean absolute error of 446 ± 257 and an average error of -390 ± 340. Of the i0 infants weighing ~ 4000 grams at birth, 4 were identified by the method of Shepard, 2 by the normogram of Hansmann and 5 by the macrosomic index.
, EFW-Yale* EFW-Norm* Macrosomic Index
PREDICTED WlEGHT ~ 4000 < 4000 ~ 4000 4 4000 ~ 4000 ~ 4000
~ 4000 4 6 2 8 5 5 ACTUAL WEIGHT
< 4000 1 9 1 9 2 8
*p=N.S., exact test
We are currently developing a model for predicting the weight of the large fetus and will test this prospectively.
I ! I ! I I I I I i I I I
160
I i

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas #143 February, 1984
THE SECOND TWIN. Michael Schellpfeffer, M.D.x and Amelia C. Cruz, M.D., Depart-
ment of Obstetrics and Gynecology, University of Florida College of Medicine, Gainesville, Florida 32610.
The perinatal mortality for the second twin is considerably higher than the first twin. The excess perinatal loss is primarily related to neonatal mortality in all weight groups. Neonatal mortality for the second twin is almost twice that of the first twin when weight above i000 grams is considered. Whether the outcome could be improved by delivering twins by cesarean section especially when the second twin is in abnormal presentation has been debated. A retro- spective study of 157 twin gestations delivered between 1977 and 1981 was done. During this time 43.3% of those deliveries were accomplished by cesarean section with 11.8% of these cesarean sections being performed exclusively for the second twin. A cesarean section was performed in the majority of cases (61.8%) for an abnormal fetal presentation. Fifty-six and seven tenths percent of the remaining deliveries were accomplished vaginally with 36% of these deliveries involving a breech extraction and/or internal podalic version. Fifty percent of nonvertex second twins were delivered as a part of a cesarean section and 50% were delivered vaginally by breech extraction and internal podallc version. Poor outcome (low Apgar score) of the second twin, when compared to the first twin, was closely associated with prematurity by birth weight and gestational age. Thirty-two (97%) of second twins with low Apgar scores were by definition premature. Sixty-seven (42.7%) of second twins as opposed to 49 (31.2%) of first twins experienced morbidity (not significant). Thirteen (8.3%) of second twins as opposed to 8 (5.1%) of first twins experienced mortality (not significant). With regard to the method of delivery there was no significant difference in the number of second twins with depressed Apgar scores or with poor neonatal outcomes accepting a greater than 40% cesarean section rate done for prematurity and presentations.
I I I I I I I I I I I I I I
161 i I

I Society of Perinatal Obstetricians " Annual/~leeting
San Antonio, Texas ~
#144 February, ~1984
MATERNAL SERUM ALPHA FETOPROTEIN (AFP) AND INTRAUTERINE GROWTH
F. G. Mariona,,,M.D., X*M.M. Hassan, M.D., XF.N. Syner, Ph.D. xL.C. Chik, Ph.D., R.J. Sokol, M.D.
From The Department of 0bstetrics/Gynecology Division of Maternal-Fetal Medicine C.S. Mott Center for Human Growth and Development and; Medical Database Informatics Wayne State University/Hutzel Hospital Detroit, Michigan
Early second trimester screening of maternal serum AFP for the detection of ~eural tube defects is becoming a routine part of obstetric care. Even in the absence of fetal anomalies, high levels have been variably related to low infant birthweight (BW) and adverse perinatal outcome; low levels have also been related to adverse outcome. However, the overall relationship, if any, of maternal serum AFP to infant birthweight has not previously been characterized. In ii0 viable singleton pregnancies seen for genetic consultation in the early second trimester 16.8_+ 1.2 weeks), without fetal anomalies or chromosomal abnormalities, maternal :erum AFP was determined by radioimmunoassay and expressed as multiples of the median (MOM, range 0.19 - 3.11). At 39.6 + 2.0 weeks (range 30.5 - 42.5), the infants weighed 3436_+ 654 grams (range 964---4990). Using polynomial regression, it was found that BW = -332 AFP + 3748 (r = .234, p < .02) -- for an increase of one MOM, BW decreased 322 grams. The fit was not improved beyond the linear. To determine the relative contribution of gestational duration and intrauterine growth to this relationship, gestational age (GA) at birth and BW adjusted for GA were related to AFP using multilinear regression. AFP was related to BW adjusted for GA(R2 = 6.3%, p < .01) about I0 times more strongly than to GA (R2 = 0.6%, NS). These results indicated that second trimester maternal serum AFP levels relate linearly and significantly to continuing fetal growth, but not pregnancy duration. Although the explanation for this relationship remains speculative, the utility of routine AFP screening for the antenatal detection of intrauterine growth retarda- tion deserves further study.
I I I I I I I I
I !
162

#145
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
IMPLEMENTATION OF A MICROCOMPUTERIZED PERINATAL DATABASE
H. Frank Andersen, M.D.*
University Hospitals Case Western Reserve University
Cleveland, Ohio
A number of perinatal database systems have been described in the past several years. Most of these systems depend on medium to large computers which are generally beyond the resources and expertise of small to medium- sized hospitals. However, there is interest in some of these hospitals to more carefully record and evaluate their obstetrical experience. New micro- computers have the power and capacity to store and manipulate moderate sized databases. A perinatal database has been developed using DBASE II (a popular database manager and programming language for microcomputers) which can operate on a variety of microcomputers ("personal computers") for an initial hardware and software cost of under $15,000. The data captured includes the major components of the minimal perinatal database which has been described plus specific prenatal and intrapartum problems. The system provides "user-friendly" menus to select operations and screens for data-entry from standardized obstetric record forms. The majority of data-entry and report generation tasks can be performed by a secretary after i to 2 hours of training and require about i0 hours of personnel time per i00 deliveries per month. Reports generated include OB statistics, activity reports for individual MD’s, delivery log, and individual patient summaries. In addition, it is possible to retrieve information on patients with specific obstetric problems, specific delivery modes, etc. for use in clinical studies. The database has been in operation since January i, 1983 at Mt. Sinai, a medium-sized private hospital (800
deliveries recorded as of October I, 1983) and has been used as an interim system at University Hospitals (694 deliveries recorded as of October I, 1983). Physician response and interest in the system has been good, although problems with completeness of the standardized record forms persist. The data are adequate for necessary reporting functions of the hospital and have provided the bas~s for studies of specific problems such as breech and forceps deliveries. Additionally, there has been interest at Mt. Sinai Hospital to expand the database to include neonatal outcome information. This system provides an effective tool for recording and organizing perinatal data and is within the cost and personnel requirements of most hospitals, expanding their ability to evaluate effectiveness of perinatal care.
I I ! ! ! I I l I ! i I I I I I
i 163

#146
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
BRACHIAL PLEXUS INJURY: A REVIEW OF THE JOHNS HOPKINS HOSPITAL EXPERIENCE~
1972-1982. John T. Repke~ M.D.~* Jennifer R. Niebyl~ M.D., Theodore M. King~*
M.D.~ Ph.D.~ The Johns Hopkins University School of Medicine~ The Johns Hopkins
Hospital, Baltimore, Maryland 21205. Injury to the brachial plexus is a serious and relatively uncommon obstet£ical
complication. A review of the deliveries at the Johns Hopkins Hospital from 1972-1982 was undertaken in an effort to better understand the possible events leading to this injury. Seventeen documented cases of Erb’s palsy occurred in this time period For an incidence of 0.725/1000. Patient profiles were obtained For each case, including parity, duration of labor, use of oxytocin and epidura[ anesthesia. Antepartum and delivery parameters were also assessed as were the trends in cesarean section and Forceps delivery rates. Over the study period the incidence of Erb’s palsy remained the same despite an increasing cesarean section rate. Of the seventeen cases of Erb’s palsy~ there were three cases wlth birth weights greater than 4,000 grams. Eight of the 17 cases had shoulder dystocia present. Four of the l? cases were mid forceps deliveries. There were three cases of prolonged second stage of labor, two of which were delivered by mid Forceps. Shoulder dystocia accompanied two of these three cases. Epidural anesthesia was used in seven of the i? cases of Erb’s palsy. Five of our patients were screened For diabetes with Four of the Five having a normal GTT. Two of the 17 patients delivering children with Erb’s palsy had a pregnancy weight gain in excess of 30 [bs. There were three cases of persistent neurologic deficits. Two of these three cases were simple uncomplicated Erb’s paralyses diagnosed at delivery. The other case was complicated by diaphragmatic paralysis and a partial Homer’s syndrome. Our series demonstrated that mid forceps operations are associated with an increased risk of brachial plexus injury. Dysfunctional labor and macrosomia could not be specifically associated with the development of a brachiaI plexus injury. Reliable predictors For those patients at highest risk For delivering a child with an Erb’s palsy are difficult to identify. Our data would suggest that the nul~iparous patient with a large baby would be at greatest risk particula£1y if a mid Forceps operation is performed. The data would also suggest that although cesarean section is not absolutely protective against the development of an Erb’s palsy, abandonment of mid Forceps operations may aid in reducing the incidence of this complication.
I I I

#147
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE VALIDITY OF LEUKOCYTE ESTERASE AND NITRITE REAGENT STRIPS FOR THE DETECTION OF ASYMPTOMATIC BACTERIURIA. Gerald P. Marquette, M.D.*, Todd W. Dillard,x Jennifer R. Niebyl, M.D., The Johns Hopkins University School of Medicine, The Johns Hopkins Hospital, Baltimore, Maryland 21205
To analyze the use of leukocyte esterase (L.E.) and nitrite reagent strips as screen tests For asymptomat£c bacteriuria, the cleancatch mid-stream urine specimens of 245 consecutive registering obstetrical patients were studied. After each specimen was collected, a Chemstrip 9, containing both L.E. and nitrite reagents was used following exact manufacturer’s directions. Although the nitrite reagent reaction on the Chemstrip 9 is graded as either 0 or +, the leukocyte esterase is graded as O, trace, +, or ++. For the purpose of analysis, any positive reaction on these strips was considered a positive test. The specimens were immediately sent to the bacteriology laboratory where they were all processed within one hour of collection for culture and sensitivity. There were 54 positive urine cultures that were not considered contaminated. The validity of testing For asymptomatic bacteruria by only L.E., only nitrite or £f either test is positive is summarized in the following table: ~
Sensitivity Specificity Negative Predictive Value
L.E. 85,% 47,~ 95,4 Nitrite 18% 98% 88% Either 94% 46,~ 98,~
We conclude that the combination of results derived From the L.E. and nitrite reagent strips is a sensitive screening technique for asymptomatic bacteriuria and is more cost effective than universal screening by urine culture.
I I I I I I I ! I ! I I i I I I I I
165
I

#148
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
I I I
EXTERNAL VERSION
F. B~guin x, Ph. Extermann x
Department of Obstetrics and Gynecology, University Hospital, Geneva, Switzerland
A successful external version offers a better prognosis for both mother and fetus at the time of delivery by decreasing morbidity and mortality associated with breech delivery and cesarean section. In the present study we have fol- lowed the proposition outlined by Saling, in 1974, carrying out the procedure at 37 weeks under close cardiotocographic and ultrasonic surveillance while intra-venous tocolytic drugs were being administered. Forty-five of 82 breech presentations treated in this fashion were converted to a vertex presentation. Of these, 40 subsequently had a vaginal delivery, (11% were delivered by cesa- rean section). Failure of a successful conversion occurred in 37 of the 82 patients. Of these, only 15 delivered vaginally (60% cesarean section). The following ccmplications had to be noted : 2 cases of minimal vaginal bleeding, 1 asymptomatic retro-placental hematoma, 7 cases of transient fetal bradycardia. There was no perinatal mortality. There was no evidence of feto-maternal trans- fusion. Only in one instance there was spontaneous reversal to a breech presen- tation after a completed external podalic version. In the failure group, there was no spontaneous version to a vertex presentation. There were thus for the entire group of 82 patients 27 (33%) who were delivered by cesarean section. This represents a reduction by 50% of the cesarean section rate encountered for breech presentation in our service. In conclusion, we feel that an attempt at external podalic version presents a worthwhile procedure associated, under the present safeguards, with little risk and offering a better outlook at the time of delivery for mother and fetus.
I I I i I I I ! I I I
I ! I I
166 !

#149
Society of Pednatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
PREDICTIVE VALUE OF BACTERIAL CULTURES DURING CESAREAN BIRTH W. F. O’Brien, I. A. Abbasi*, C. C. Coddingtonx Uniformed Services University, Bethesda, Maryland
Postoperative endometritis is the most frequent complication of cesarean birth. Although prompt antibiotic treatment usually results in a favorable outcome, such infections prolong hospital stay and may result in significant morbidity. Intra- operative bacterial cultures have been suggested as a method for prediction of patients at high risk for subsequent infection. We obtained cultures of amniotic fluid, lower uterine segment swab, and endomyometrial biopsy in 41 women under- going cesarean birth. Predictive value was compared to a simple clinical risk assessment in which women in labor with rupture of the membranes for greater than three hours were considered at high risk. None of the women were treated pro- phylactically and nine (22%) developed endometritis. All of the women in the endometritis group had at least one culture yielding mixed flora or a probable pathogen compared to 44% in the non-endometritis group. As noted below, however, none of the culture sites were superior to clinical assessment in the prediction of endometritis. We conclude that intra-operative bacterial cultures are not cost-effective in the prediction of post cesarean endometritis.
Criterion Fluid Swab Biopsy Clinical
Sensitivity 55 89 64 89 Specificity 78 62 56 72 Pred Val Pos 48 40 33 47 Pred Val Neg 86 95 90 96
! I I I I I i I ! I ! I I I I ! I
167

Society of Perinatal Obstetricians Annual/Vleeting
San Antonio, Texas
# 150 February, 1984
THE EFFECTS OF MATERNAL HYPEROXlA ON FETAL BREATHING MOVEMENTS IN THIRD TRIMESTER PREGNANCIES
, Lawrence D. Devoe, M.D.; Hassan Abduljabbar, M.D.; Lesley Carmichael, B.Sc.; Carol P~obert, B.Sc.; John Patrick, M.D. Department of Obstetrics and Gynecology, Medi- cal College of Georgia, Augusta, Ga.; Department of Obstetrics and Gynecology and of Physiology, MRC Group in Reproductive Biology, University of Western Ontario, London, Ontario, Canada.
Fetal breathing movements (FBM) may reflect both extrauterine and intrauterine influences. The state of maternal oxygenation, as studied in animal experiments, may alter the incidence of FBM: Maternal hypoxia, producing chronic fetal hypox- emia, may reduce FBM incidence, while acute fetal hypoxemia may ablate FBM. Mater- nal hyperoxia, in these experiments, usually restores FBM to normal but does not change the incidence of FBM in normoxemic fetuses. In humans, induction of mater- nal hypoxia has proven too dangerous to the fetus, while maternal hyperoxia, as a probe for placental respiratory function, has been inadequately studied. The pres- ent study examined the influence of maternal hyperoxia with a respect to the incid- ence, rate, and variability of FBM in a population of 14 healthy, pregnant women at
:term with normal fetal outcomes. Studies were conducted, 90 minutes after a stan- dard 800 calorie meal and consisted of a 30-minute baseline observation period, a 15-minute hyperoxia period induced by a 50% oxygen mixture, and a 45-minute period of continued observation. FBM as observed with a realtime B-scanner was analyzed on line by a PDP 11/40 computer using a previously developed and validated program. Analyses of FBM, fetal movement (GFBM), apneic episodes and fail time were deter- mined for each fetus during 5-minute and 15-minute epochs. Maternal hyperoxia was validated by transcutaneous (Tc) pO~ measurements. Results: Mean incidences of FBM and GFBM for the group were 58728 + 3,74% and 7~ ~ ]86%, respectively. Mean breathing rate for the entire study group was 46.32 + 2.~4 breaths/min. Hyperoxia did not produce any significant changes in incidence~of FBM, GFBM, breathing rate, breath-to-breath intervals, or breath-interval variability. Conclusion: Maternal hyperoxia can be achieved easily and safely. Under uniform study conditions, nor- mal fetuses, supported by adequate placentas, exhibit a cyclical pattern of breath- ing activity which is unaffected by maternal hyperoxia. The observation of FBM, in the presence of transient maternal hyperoxia, may provide a useful tool for evalu- ating compromised placental function or suspected cases of intrauterine hypoxia.
I I I i i ! I I I I ! I I !

#151
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
UMBILICAL ARTERY VELOCITY WAVES IN TWIN PREGNANCIES.
.X, * G. Farmakides, M.D H .... Schulman, M.D , A Fleischer, M.D x, and L. Bracero, M.D.x. Albert Einstein College of Medicine of Yeshiva University, Department of Obstetrics and Gynecology, Bronx, New York, 10461.
Umbilical velocity waveforms (UVW) were measured in twin preg- nancies to test the hypothesis that they would detect fetal dis- cordant growth, and diagnose the twin transfusion syndrome. In i0 pregnant women between 30-36 weeks gestation, the UVW were measured with a continuous wave Doppler probe. Umbilical arteries are recognized by pattern analysis and easily differentiated from fetal aortic and cardiac signals. The UVW has a high end diastolic component, a characteristic of a low resistance vessel. Calcula- tions were carried out by dividing the systolic peak by the diastolic trough, the S/D ratio. This calculation overcomes angle dependency. The ratios obtained ranged between 2.1 to 4.1, and are comparable to those described in singleton pregnancies. The ~UVW was compared to the ~birth weight revealing an Dvalue of 0.82. ~Biparietal diameter measurements did not correlate with ~UVW or ~birth weights. Two cases of twin transfusion were diagnosed when UVW ratios were markedly divergent.
The UVW appears to be a promising modality for the recognition and diagnosis of normal and abnormal twin pregnancies.
169
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 152 February, 1984
MEASUREMENT OF C-REACTIVE PROTEIN USING LATEX AGGLUTINATION. J. Mac Ernest, Melissa Swain,x Christos G. Hatjis, Paul J. Mels, Department of Obstetrics and Gynecology, Bowman Gray School of Medicine of Wake Forest University, Winston- Salem, North Carolina 27103.
Maternal serum C-reactive protein (CRP) has been used as an early maker of infection in patients at risk for preterm delivery. The most widely used recent method of determining CRP has been laser nephelometry (LN). However, LN requires special equipment and training. We have evaluated a latex agglutination test (RAPI/TEX - CRP Test, Calbiochem-Behring) as a simple, inexpensive alternative. This test is read as positive or negative, a positive indicating a CRP level ~ 0.8 mg/dl. Twenty-two patients between 20-34 weeks gestation with preterm labor or premature rupture of membranes had a total of 91 simultaneous latex agglutination and laser nephelometric determinations prior to delivery. Ninety- five percent of the 37 positive latex tests were reported > 0.8 mg/dl by LN whereas 80% of the 54 negative latex tests were < 0.8 mg/dl by~LN.
Latex Agglutination 37 tests positive
(~ 0.S mg/dl)
54 tests negative (< 0.8 mg/dl)
> LN -- 0.8 mg/dl LN < 0.8 mg/.dl
35 2
Ii
(5/11 were < 0.9; mean of 1.2 ~g/dl)
43
Of the 22 patients, 13 had all negative latex tests, 8 had at least one positive latex CRP, and i had a single sample reported +/- by latex.
O.posltive latex tests 13 patients
> > 0 LN tests -- 0.8 mg/dl -- 1LN tests > 0.8 mg/dl
8 5 (3/5 were < 0.9 mg/dl)
1-12 positive latex tests 8 patients 0
+/- latex tests 1 patient
A preliminary review of patients to date suggests an association between clinical morbidity and a positive latex test. Eight/eight patients with at least one positive latex test evidenced clinical morbidity, and only 3/13 patients with no positive latex tests showed clinical morbidity. The latex agglutination test for CRP determination shows promise as a rapid inexpensive method to screen patients at risk for preterm delivery for signs of inflammatory complications.
I I I I ! I I I I I
I
I
170

#153
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
FETAL BIOPHYSICAL PROFILE VERSUS NONSTRESS TEST- IMPACT ON MANAGEMENT OF HIGH RISK PREGNANCY. Jyotsna Gandhi, M.D., New York Medical College-Metropolitan Hospital, New York, N.Y.
Assessment of fetal status in high risk pregnancy has traditionally been done with fetal heart rate monitoring tests either as one or as a combination of two tests, eg. nonstress test (NST) and oxytocin challenge test (OCT). With the arrival of Real Time sonography, several parameters of fetal physiology and intra- uterine environment can be assessed. It is the aim of this report to evaluate the impact of this sophisticated multifactorial approach to fetal evaluation on peri- natal outcome and the need for active intervention in a group of high risk pregnan- cies, when in the past, perinatal outcome and opportunity for conservative manage- ment have been adversely affected. A total of 850 fetal physiologic activity pro- file tests were performed on 410 high risk patients at Metropolitan Hospital Cen- ter and New York Medical College. Several parameters of fetal status; including differential fetal motion, respiration, tone, quantitative amniotic fluid and NST were used for assessment. Each individual activity was allotted a score of two when observed to be completely satisfactory, a score of one when present but not satisfying the set criteria, a perfect score being ten. Testing done within one week of the delivery was considered in the evaluation of the outcome of the test for its predictive value for the ultimate perinatal outcome in terms of associa- tion with intrapartum growth retardation (IUGR), intrapartum fetal distress, low five minute Apgar score and perinatal death. Four (4) parameters of fetal activ- ity other than NST were individually and collectively evaluated in light of the outcome of the nonstress test for their predictive ability. When nonstress test was reactive, absence of anyone of the parameters did not alter the ultimate peri- natal outcome. There were no babies with more than one other parameter absent. However, when nonstress test was nonreactive, presence or absence of these activ- ities markedly affected the ultimate perinatal outcome. Over 40% of the nonre- active NST’s were false positive. When NST was accompanied by at least three other normal parameters of physiologic fetal existence; the perinatal outcome of these babies was not adversely affected. However, when more than one other para- meter was absent, there was a perceptible disadvantage in the ultimate perinatal performance. This approach was accompanied by a primary cesarean section rate comparable to the general population, and demonstrated a decrease in the primary cesarean sections for each category of high risk situations at our institution. Biophysical profile of fetal physiologic activities is helpful in assessment of a high risk fetus when NST is nonreactive and can help to differentiate between fe- tuses with false positive and true positive nonreactive NST. This approach could help to better identify a compromised fetus and prevent unnecessary and even op- erative intervention in other normal fetuses where a nonreactive NST has indicated otherwise.
I I I I I I I ! I I I ! ! I ! I
171
! I

#154
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE SYLVIAN FISSURE: A COMMONLY MISLABELED CRANIAL LANDMARK
aeanty P *, Chervenak FA *, Romero R *, Hobbins aC MD From the Dept o÷ Ob-Gyn, Yale University, School o.F Medicine
INTRODUCTION Correct sonographic identification of fetal anatomy, besides its intrinsic interest, is necessary Lo define standard planes for consistent fetal biometry (1-31. Because of the lack of fetal sonographical-anatolical correlations, fetal and neonatal scans are often colpared to anatolical sections of adults (4-b). The clinical pediatric dictum !that: ’An infant is not a small adult’ is even ~ore applicable for the fetus.! Failure to recoqnize anatomical differences bet#men fetuses and adults have led Lo the mislabeling of such structures as the cavum of the sepLum pellucidul being named the third ventricle (71. We demonstrate in this presentation that the structure that is commonly labeled as the ’Sylvian fissure’ in the sonoqraphy literature (4,8-101, in fact~ corresponds Lo the insular region of the cortex, also called the ’insula.’
MATERIAL AND NETHODS A fetus of 20 ,eats of gestation, after fixation in formalin, ,as scanned in a ,ater bath. The calvariue, the dura mater, and the arachnoid ~ere removed, and the fetus ~as scanned at each step of the dissection. In addition, sonographic images of cranial anatomy ~ere obtained of normal intrauterine fetuses. All scans ~ere produced ~ith the Toshiba 8AL 50~, using a 5 BHz transducer. Both sonographic images ~ere compared ~iLh anatomical sections of a 23 ~eek old abortus obtained ~ith microcryoscopy.
RESULTS Sonographic i,ages obtained both of intrauterine fetuses and extrauterine abortuses clearly demonstrate a high amplitude echo that is approximately concentric Lo the fetal skull in the peripheral part of the distal hemisphere, in the living fetus, pulsation of the middle cerebral artery is visible at this level. Macroscopic vie~ of the head as ~ell as obsrevation of the anatomical sections demonstrate that ~hile the Sylvian fissure does not yet exist, the insula is ,ell identified and corresponds to the location of the ultrasonic echo.
DISCUSSION The above findings demonstrate that because the Sylvian fissure does not exist during the second trimester, it cannot be responsible for the observed echo. The clearly demonstrab]e insula is lost likely responsible for this echo. The
apposition of the opercula is a developmenta~ event late in gestation. In the latter part of the third trimester~ although the Sylvian fissure may be anatomically present~ it is physically unlikely that it is responsible for the generation of this echo. When the fetal head is in occiput transverse position, the 8ylvian fissure is parallel to the ultrasonic beam~ and subsequently ~ould be poorly reflective. However, the insula is perpendicular Lo the beae~ and its surface produces a brightly echogenic interface.
~EFERENCES:I) ~UM h145-150 1982, 21~3R 138: 871-874 1982, 3)Rad 144: 15~ 1982, 41A3R 136:IT3-137 1981, 5)A3R 13b: 265-270 19B1, &)RCNA IS: 117-131 1980, 7)B~OG 89: 165-174 1982, 8)Rad 131:781-787 1979, 9)RCNA 20: 285-29b 1982, IO)OCU 8: 311-31B 1980~ ll)"The Developi~q Human: Clinically Oriented Elbryology’ WB Saunders 1982 pp 393-400, 12)’Human embryology’ p 274-276 Williams ~ Wilkins Co 1972 pp 474-483
I
I I I I I I I I I I I I
172
! I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 155 February, 1984
"FUNGAL CHORIOAMNIONITIS DIAGNOSED AT AMNIOCENTESIS WITH SUBSEQUENT FETAL INFECTION. John P. Elliott, M.D., Joseph P. Bruner,XM.D., Capt., M.C., USA, Howard W. Kilbride,XM.D., Thomas J. Garite, M.D., Arthur T. Evans,XIII, M.D. and G. Eric Knox, M.D., Letterman Army Medical Center, San Francisco, California, Memorial Hospital Medical Center, Long Beach, California and Abbott-Northwestern Medical Center, Minneapolis, Minnesota.
Candida albicans vaginitis occurs frequently in pregnancy with an incidence of 31 to 46%. Intrauterine infection caused by candida or other fungi in pregnancy is relatively rare with only 80 cases reported in the literature, all diagnosed after delivery. We report six cases of fungal chorioamnionitis diagnosed by amnio- centesis associated with premature labor and delivery of five viable infants. Three of these six patients had intrauterine contraceptive devices in situ. Three infants had a diagnosis of congenital cutaneous candidiasis and two congenital systemic can- didiasis, one with monilial pneumonia and one with meningitis and septicemia. All viable neonates were treated and survived. One very immature infant died shortly after delivery. Candida albicans represents a potential pathogen which may cause chorioamnionitis and is associated with significant mortality (95%) in infants weighing less than 1500 gm. The use of amniocentesis in patients with premature labor or premature preterm rupture of membranes may allow early detection of subclinical fungal chorioamnionitis, thus guiding appropriate perinatal management.
I I I I I I I I I I I I I I I I
173
I

~156
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
SERIAL ELECTROENCEPHALOGRAPHIC FINDINGS FOLLOWING ECLAMPSIA Baha M. Sibai, M.D., Joseph A. Spinnato, M.D.*, Dottle L. Watson, M.D.*, Gar|and D. Anderson, M.D., Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee The purpose of this prospective investigation is to report the neuro|ogic and: electroencephalographic (EEG) abnormalities in eclamptic patients. Sixty-five such patients were studied regarding EEG findings (n=65), computerized axial tomo- graphy (CT) (n=20) and cerebral arteriogram (n=3). Initial EEG’s were obtained during the first 48 hours of hospitalization and were serially obtained during the subsequent 6 months. CT scans and arteriograms were obtained when convulsions were multiple, EEG abnormalities were marked, or the clinica| course was consider- ed atypical. The EEG was abnorma| in 75% (n=49) of patients at the initial asses- sment. Observed abnormalities were both local and diffuse. Table I summarizes the initial and follow-up EEG data. The EEG returned to norma| in a|| observedi patients. CT scans were obtained within 96 hours of admission and all were nor- mal. The cerebral arteriograms were normal in each case. None of the patients had neurologic deficits at time of discharge or upon follow-up (3 months - 3 years). No patients were noted to have persistent convulsive disorder. Twenty- nine patients had one or more subsequent pregnancies without recurrent eclampsia. These findings suggest that the neurologic events of eclampsia are acute and tran- sient. Long term neurological deficit is rare in the properly managed ec|amptic patient. CT scans and EEGs are rarely indicated in the management of ec|amptic patients and long term ant~convulsant therapy seems unwarranted.
TABLE I
EEG FINDINGS
TIME EEG DONE NORMAL ABNORMAL # (~) # (~)
Initial (n=65) 16 (25) 49 (75) I Week (n:46) 15 (33) 31 (67) 6 Weeks (n=30) 23 (77) 7 (23) 3-6 Months (n=6) 6 (100) 0
I I I I I I I I I I I I I I I I
174

#157
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
COMPARISON OF THE LUMADEX(TM)*-FSI TEST WITH L/S RATIO. L.J. Zuidema and B.A. Work, Jr.,~Dept of OB-GYN, University of Illinois, Chicago, Illinois
The Lumadex(TM)-Foam Stability Index test is designed to be used as an indic- ator of fetal lung maturity to aid in the management of high-risk pregnancies. The cassette contains seven standardized wills, six of which contain ethanol of appropriate volume such that addition of 480 microliters of amniotic fluid to each well will produce a range of ethanol volume fraction equivalent to the range of 44% to 50%. The seventh control well produces an example of a stable foam endpoint. Clinical studies have shown that for an FSI level 47, the probability of respiratory distress syndrome(RDS) is very low. We compared the Lumadex-FSl test versus the lechithin:sphingomyelin ratio (L/S)on 102 pregnant women undergo- ing amniocentesis for assessment of fetal lung maturity. Medical indications included diabetes, hypertension, previous cesarean section with an unknown scar, and premature labor. The Lumadex-FSl test was performed on an aliquot of amniotic fluid after centrifugation for 5 minutes at lO00rpm. The remainder of the amn~tic fluid was analyzed for L/S, phosphatidylglycerol, and phosphatidylinnositol. Thirty-nine of the amnicentesis were performed within 72 hours of the delivery. Of the 39 patients, 3 had an FSl value~--46. Two out of the 3 developed RDS. Thirty-six patients had an FSI ~47, none of whom developed RDS (p K .004). Seven patients had an L/S~2. Two of those 7 patients (28%) developed RDS. The false positive rate for the L/S was 72% whereas the false positive rate for the FSI test was 33%. It is concluded that the Lumadex-FSl test is a reliable method of predicting fetal lung maturity with fewer false positives than the L/S.
*Beckman Instruments, Inc.
I I I I I I I I I I I I I I I I I I
175 I

I Society of Perinatal Obstetricians I
Annual/Vleeting San Antonio, Texas 1
# 158 February, 1984
CAUSES OF PERINATAL DEATH
Newton ER, Kennedy J, Louis F, Cetrulo CL, Hershel M, D’Alton M,* Feingold M.* Department of Perinatology, Neonatology, and Pathology St. Margaret’s Hospital for Women Tufts University School of Medicine Boston, MA 02125
All perinatal deaths from Jan. i, 1978 - Jan. I, 1983 at St. Margaret’s Hospital are examined by chart review and autopsy report. A total of 447 cases are examined. The causes of infant death are stratified by clinical obstetric diagnosis. Population demographics are: 15477 total deliveries, 10% black or other races, 67% private insurance, 16% 20 Y/O, 12.9% 36 weeks gestation, total
maternal transfer 1515. Perinatal statistics are: PNM rate 28.9, corrected PNM for maturity and congenital abnormalities 17.9, NND rate 18.9, still birth rate 10.1.
PNM BY GESTATIONAL AGE Gest. Age 26 28 30 32 34 36 38 40 42 PNM 750 180 160 60 60 25 16 2.4 32 Corrected PNM 740 150 150 50 40 14 6 1.4 31 Clinical obstetric diagnosis were assigned by responsible obstetricians and infant diagnosis by responsible neo~atalogist. 83 cases had 2 or more obstetric diagnoses. 47 cases had 2 or more infant diagnoses.
OB DIAGNOSIS Infant Other Post Dates Preme. Diagnosis FD Abrupt. TTB PROM IUGR ~ BP Labor Anoxia (%) 52 32 33 11 85 44 II Infection 0 4 ii 18 0 3 15 Cong. Abnl. 40 4 16 6 15 18 9 Immature 0 23 16 39 0 13 33 Respiratory 40 22 6 14 0 15 15 Hypoplastic Lung 0 3 0 6 0 0 2 NEC 0 0 0 2 0 0 4 IUH 0 6 16 6 0 6 9 Conclusions: I. There is better than 85% survival at 28 weeks or greater gesta- tion. 2. Death from congenital abnormality was most frequent in mothers with diagnosis of fetal distress. All mothers had C/S with diagnoses of congenital abnormalities and fetal distress. 3. Hypoplastic Lung is a significant risk to conservative management of ROM at 26-30 weeks. 4. Stratification of infant diagnoses by gestational age reveals an increase in diagnosis of congenital abnor- malities and anoxia with an increase in gestational age. The contribution of these diagnoses are 57% at 29-32 weeks, 77% at 33-36 weeks, 94% at <37 weeks.
! I I I I I I I I I I I I I 1 I
176
1

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 159 February, 1984
MATERNAL LEFT VENTRICULAR SIZE AND INTRAUTERINE GROWTH RETARDATION C Veille, M,D.* ¯ ¯ , M.J. Morton, M.D.X, J.P. O’Grady, M.D.,
~.L. Briggs, R.N.x, C. Toomey, R.N.X, Department of Ob/Gyn, (Special tudies), and Department of Medicine (Cardiology), Oregon Health ciences University, Portland, Oregon 97201
aternal heart size measured by radiographs correlates with fetal 3ize at birth. It has been suggested that a small maternal heart nay be related to intrauterine growth retardation (IUGR). We ~valuated maternal left ventricular (LV) size near end of gestation in 31 consecutive patients with suspected IUGR to further test this lypothesis. M-mode echocardiography was performed in lateral ~ecumbancy to measure LV end diastolic dimension (EDD) and cardiac )utput (CO). Birthweights were plotted on a standard curve (Ref. J. of Ped. 77:11, 1970) against the Gestational Age (GA) at delivery. )f the 31 newborns, I0 were between ~ean and i S~D. (Group I), i0 ~ere between the ist and 2nd S.D. (Group II) and ii were between 2 .D. (Group III = True IUGR).
iaternal Age (Yrs) ;.A. at Delivery (Wks) ~t. of Babies (gm) ~aternal Surface Area (m2) EDD (cm) SO (£.min-I)
Group I Group II Group III (m = i0) (N = i0) (N = ii)
23±7 23±6 22±4 38±2 38±2 3614
29771517 2436±337 17771660 1.7±0.2 1.6!0.I 1.6±0.2 5.0±0.3 4.910.4 5.0±0.5 5.911.2 6.0±1.5 6.412.8
LVEDD and cardiac output were not statistically different in the ~hree groups. LVEDD does not appear related to IUGR. Discordance ~ith previous studies may be due to different technique to posture.
~upport by USPHS Grant HD 10034 is acknowledged.
I I I I I I I I I I I I I I
177

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas # 160 February, 1984
EXTERNAL CEPHALIC VERSION: A CLINICAL EXPERIENCE J.P. O’Grady, M.D., J.C. Veille, M.D.x , R.L. Holland, Ph.D.x, K.A. Burry, R.N.x Department of Ob/Gyn, Special Studies, Oregon Health Sciences University, Portland, Oregon 97201 Breech presentation increases perinatal risks and often results in Cesarean delivery. However, a fetus may be manipulated from breech to cephalic presenta- tion by external cephalic version (ECV), thus eliminating the risks of vaginal delivery. In an outpatient setting aided by tocolytics, real time ultrasound (U/S) screening and external cardiotocography, between 10/27/81 and 9/1/83, we performed ECV on 84 patients between 34 and 41 weeks gestation (~ = 37.6 = 1.58) as estimated by LMP and U/S dating criterion. Terbutaline, 0.25 mg., s.c. was given in 41 instances at the clinical discretion of the operator. Normal patients from private and university services were selected for ECV if in breech presentation at > 35 weeks gestation. Version was performed with the patient supine in steep Trendelenberg’s position. A head-over-heels technique was preferred. Rh- patients were routinely given 300 mcg of anti-D immunoglobulin following manipuations. Pregnancy outcomes were subsequently reviewed. RESULTS:
84 Patients Attempted
*+ 31 Failures ~
12 Vaginal Del. 14 C/S
3 Vertex 9 Breech
53 Successful~-~
44 Vaginal Del. 3 C/S: °Failed Induction
PROM °Reverted to Breech
2 Days After Version
°Failure to Progress (*2 lost to followup); (+3 not yet delivered); (++6 not yet delivered) No clinically important complications could be attributed to ECV. Transient, but innocuous bradycardia (10-15 bpm) was often observed. No emergent deliveries or return versions were required. One neonatal death occurred in a previously verted infant due to aortic atresia which was not diagnosed antenatally. One marginal placental separation occurred i0 days post version. Except for the anomalous infant, successfully verted cases with vaginal delivery, all had 5 minute Apgar scores which were greater than 7. CONCLUSIONS: i) 53 of 84 third trimester patients (63%) underwent successful version; 2) no significant fetal or maternal complications occurred; 3) third trimester ECV is safe and can reduce the incidence of breech presenta- tion and Cesarean section rate for malpresentation at term.
I I I I I I I il I I I I I I I
178
I I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 161 February, 1984
PREGNANCY ALTERS TIME OF DAY INFLUENCE ON GLUCOSE METABOLISM. Paul J. Meis X X ¯
James C. Rose, Melissa Swain, Department of Obstetrics and Gynecology, Bowman Gray School of Medicine, Wake Forest University, Winston-Salem, North Carolina
Circadian (time of day) variation characterizes many features of carbohydrate metabolism in nonpregnant humans, but little is known of these phenomena in human pregnancy. To examine circadian variation in glucose metabolism we performed intravenous glucose tolerance tests (IVGTT) on pregnant women at 0800 and 1600 on separate days after an 8 hour fast. The results were compared with pairs of IVGTT’s performed on nonpregnant (NP) volunteers under identical conditions.
Fasting Glucose Concentration Glucose Clearance Rate Pregnant NP Pregnant NP
0800 78.1 ± 3.5 80.6 ± 1.6 1.71 ± 0.20 2.07 ± 0.16 1600 68.7 ± 3.1 80.0 ± 2.0 1.50 ± 0.16 1.23 ± 0.12
p < 0.01 NS NS < 0.005
(i) The circadian variation of glucose clearance rate found in NP women is not demonstrable in human pregnancy. (2) In contrast to NP women, pregnant women do not maintain afternoon plasma glucose concentration at 0800 levels after a similar length of fast. (3) To maintain optimal glucose availability to the fetus, pregnant women should not skip the mid-day meal.
I I I I I I I I I I I I I I
179
I I

#162
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
TREATM~ OF PREMATURE LABOR WITH NIFEDIPINE: A PRELIMINARY REPO~
* X, D’ Alton, M.E. , Hou, S. Cetrulo, C.L.
Tufts University School of Medicine St. Margaret’ s Hospital for Wc~en Boston, MA 02125
Seven patients in premature labor were treated with Nifedipine. The reasons for premature labor were n~itiple pregnancy (I case), degenerating fibroid (i case), inconpetent cervix (2 cases), and undiagnosed (3 cases). Thi indica- tions for Nifedipine were (a) chest pain and ischemic EKG changes on Ritodrine followed by failure of magnesium sulphate (3 patients) , (b) failure of both Ritodrine and magnesium sulphate (4 patients). The gestational age at initiation of therapy ranged from 24 to 27 weeks in six of the seven cases. In the seventh case, the gestational age was 32 weeks. Oervical dilatation ranged from 1 to 3 cm. Nifedipine was administered orally as a loading dose of 30 mg. every 3-4 hours to a maximum daily dose of 80 mg. Decadron was administered simultaneously. The maximum duration of therapy was ten days. Labor was successfully stopped in 6 of the 7 patients. The seventh patient was found to have an abruptio placentae at delivery. With the exception of this single patient who delivered within 24 hours, pregnancy was prolonged for at least 4 weeks. Fetal growth was assessed by ultrasound and was normal. Gestational age at delivery ranged from 26 to 40 weeks. All birth weights were appropriate for gestational age. The infants were evaluated closely at the time of delivery and no adverse effects were found. Follow up is ongoing in all infants. Maternal side effects were minimal : 2 patients reported facial flushing after the initial bolus; there were no hypotensive episodes. Preliminary work suggests that Nifedipine is safe and effective in premature labor.
I I I I I I I I I I I I I I I I I I
180 I

| Society of Perinatai Obstetricians ¯
Annual Meeting San Antonio, Texas
i # 163 February, 1984
Analysis of Residual Low Birth Weight in an Intensive, Comprehensive Prenatal Care Program Alexander Blackwoodx, Doris Barker~ and Phyllis C. Leppert College of Physicians and Surgeons, Columbia University, New York, New York
A comprehensive and intensive care program has reduced the prevalence
of low birth weight babies by a five-fold factor delivered to young women in an
urban multiethnic and poor community. Since extensive preventive methodologies
are utilized to achieve this result it becomes important to ascertain the
characteristics of the residual gravidas who deliver low birth weight (LBW)
infants in spite of intensive preventive efforts. A retrospective study of 809
women followed in this program over fifteen months (Jan ’82 - Mar ’83) was
conducted . 69 low birth weight infants were born (8.6%).
The average age of the mothers of these LBW babies was 18 years. The
average height was 61" (< l~ercentile for 18 year olds). The average pre-
pregnant weight was 113.4 Ibs. and weight gain was 21.5 ibs. There were no
significant differences in obstetrical complications among these mothers.
Infant weight and gestational age by Dubowitz were analysed by weight chart.
All preterm infants, although technically appropriate weight for age were
slightly and progressively growth retarded as indicated by the following table:
SGA PRETERM
< 10th percentile 25 percentile 50 percentile
Maternal 18.8 yrs. 18.1 yrs. 18.3 Age ± 2.23 ± 2.22 ± 1.63
Gestational 38.3 weeks* 35.0* 32.4* Age ± 1.76 ± 1.66 ± 2.81
* Statistically significant (p <.01)
Developmentally there may be an insult which arrests growth; in some in-
stances leading to preterm birth and in others to term but small infants in this
population. In a previous ultrasound study, diminished intrauterine growth
revealed a predicted term diminished weight of preterm infants ~
4Weiner, CP et al Society of Per±natal Obstetricians, San Antonio, Texas 1983
I I I I I I I I i I I ! I i i
181
i i

#164
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
ORAL GLUCOSE TOLERANCE TESTING CRITERIA AND FAMILY HISTORY OF DIABETES MELLITUS
Joanne Piscitelli, M.D.x, Robert D. Eden, M.D.x, Frederick R. Jelovsek, M.D.x, Arnold S. Grandis, M.D.x and Stanley A. Gall, M.D.* Duke University Medical Center, Durham, N. Carolina 27710
A review of one-hundred-eighty-five patients, having a family history of Diabetes Mellitus without medical history of glucose intolerance in the non- pregnant state, was conducted. A 3-hour, i00 gram oral glucose tolerance test was performed on all patients between twenty and thirty-four weeks gestation. According to O’Sullivan criteria for glucose tolerance testing, normal glucose tolerance occurred in 89.7% while Class A diabetes was identified in 10.3% of the patients. Overt diabetes, requiring insulin treatment, occurred in 3.8% of the patients tested, yet was found to occur only in patients initially classified as having Class A diabetes. Duke University has traditionally defined the abnormal glucose tolerance test at a lower level than the widely established criteria of O’Sullivan. This intermediate group, termed "Carbohydrate Intolerance", having abnormal glucose values by Duke criteria, yet normal values by O’Sullivan criteria, comprised 32.4% of the patients tested. Furthermore, Carbohydrate Intolerance and O’Sullivan Class A patients were managed identically. Analysis of perinatal outcome, indication for and mode of delivery, incidence of macrosomia, birth trauma and neonatal morbidity revealed that Carbohydrate Intolerance patients have outcomes distinct from the O’Sullivan Class A patients while being more similar to patients with clearly normal test results. The data suggest that Carbohydrate Intolerance patients may be managed as normal patients, not requiring the increased antepartum surveillance and early intervention that characterizes the usual management of O’Sullivan Class A diabetes patients. Retrospective review of perinatal outcome statistics for the entire obstetrical population suggest that the study population, having a family history of diabetes mellitus, were at significant risk for the development of macrosomia, cesarean delivery, fetal distress in labor and low five-minute apgar score regardless of the degree of abnormal glucose tolerance test results or the number of risk factors for untoward perinatal outcome present.
I I i I I I I I ! I ! ! i I I i
i 182
i

#165
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
THE RISKS OF AMNIOCENTESIS IN THE MANAGEMENT OF PREMATURE RUPTURE OF MEMBRANES
John D. Yeast*, Thomas J. Garite, Wendy Dorchester. Perinatal Division, Department of Obstetrics & Gynecology, Long Beach Memorial Hospital and the University of California Irvine, Orange, California.
Amniocentesis has proven to be a useful tool in the management of preterm patient~ with premature rupture of the membranes (PROM). Concern has been expressed, however= regarding possible risks of amniocentesis to mother or fetus. A review was performe( of maternal transports referred due to PROM between 28 and 34 weeks gestation. Man- agement followed a prospective protocol which included an attempt at ultrasound- directed amniocentesis to rule out amnionitis. A total of 137 patients were entered in this review, and amniocentesis was successfully performed in 91 patients (66%). Patients not candidates for amniocentesis due ~o clinical findings at admission (e.g~ active, labor, fetal distress) were excluded. Patients intervened upon based on the results of amniocentesis and patients requiring intervention prior to the onset of spontaneous labor were also not included. The remaining patients having successful amniocentesis and then entering spontaneous labor were statistically compared to the group of patients with unsuccessful amniocentesis who entered spontaneous labor.
AMNIO NO AMNIO
Interval Sono. to Spont. Labor Total No. Patients Range (Hours) Mean (Hours) S.D. (Hours) W* (Wilcoxon Rank Sum)
35 28
0.5 - 1801 0.25 - 240 I14.2 27.4
327.3 46.1 1.35 (N.S.)
Interval Sono. to Spont. Labor (>4 Hrs. <72 Hrs. after Sono.)
Total No. Patients Range (Hours) Mean (Hours) S.D. (Hours)
W* (Wilcoxon Rank Sum)
21 18
5 - 72 4 - 54.5 28.4 28.3 20.5 19.4
o.o4 (N.S.)
The above analysis of the time interval from amniocentesis to labor failed to show evidence that amniocentesis might induce labor. Refining each study group by elim- inating those patients laboring less than 4 hours or greater than 72 hours after amniocentesis again yielded no significant difference between each study group. A review of neonatal records revealed no evidence of neonatal trauma or morbidity due
to amniocentesis. In addition, no maternal morbidity was apparent in those patients undergoing amniocentesis. This study demonstrates the safety of ultrasound-directed amniocentesis in the management of the preterm patient with PROM.
I I I I ! i ! I i I I I I I i i ! i
183
I

#166
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
~YOCARDIAL INFARCTION DURING PREGNANCY - MANAGEMENT PRINCIPLES. Gary D.V. Hanklns, M.D.,* George D. Wendel, Jr., M.D.,* and Kenneth J. Leveno, M.D., Dept. of Ob/Gyn, Univ. Texas Southwestern Med. Sch., Dallas, TX 75235.
Myocardial infarction (MI) during pregnancy was first reported by Katz in 1922. Subsequently, there have been 68 well documented cases of MI during pregnancy with an overall maternal mortality of 38%. Mortality was directly related to occurrence of the MI during the third trimester (47% mortality), delivery within 14 days of infarction (53% mortality), or reinfarction during parturition (75% mortality). Route of delivery did not alter maternal mortality rates.
We now report a management approach and its results in two women who had Ml’s during pregnancy. This approach included route of delivery based on obstetrical indications, conduction anesthesia to lessen hemodynamic stresses during parturition, intravenous nitroglycerine to improve myocardial perfusion, and invasive hemodynamic monitoring. Both women were successfully delivered vaginally without incident, however, during each uterine contraction ventricular filling pressures were noted to increase acutely (central venous and pulmonary capillary wedge pressures increasing to 24-25 mm~g). This inability to effectively handle the 300-500 ml bolus of blood accompanying each uterine contraction was felt to reflect a relative ventricular dysfunction which, if further stressed, could have resulted in overt heart failure. We conclude that an approach designed to minimize hemodynamlc stress, while maximizing coronary perfuslon, should be used in the pregnant patient who has an MIo Further, invasive hemodynamic monitoring is of value both for diagnosis of dysfunction as well as its treatment.
I I ! I ! i
I i
I I I I I i I I I ! I

Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas
# 167 February, 1984
MATERNAL, FETAL, NEONATAL AND INFANT OUTCOMES WITH EXPECTANT MANAGEMENT OF PRETERM RUPTURE OF MEMBRANES (PROM). Gary D.V. Hankins, M.D.,* Kenneth J. Leveno, M.D., Peggy J. Whalley, M.D.,x Ralph T. DePalma, M.D., ,x M. Lynne Williams, R---~.,x and Sheryl Nelson, R.N., Dept. of Ob/Gyn, Univ. Texas Southwestern Med. Sch., Dallas, TX 75235
One hundred seventy-six women with rupture of fetal membranes at 34 weeks estimated gestational age or less, and who did not enter labor within 12 hours of admission, were managed conservatively. Management was purely clinical with no attempt to recover amniotic fluid to evaluate for fetal maturity or infection, no tocolysis and no steroid administration. Median duration from PROM to delivery was 3.6 days with a range of 12 hours to 160 days. Duration of latency was inversely proportional to length of gestation and subsequent development of neonatal sepsis was unrelated to the length of the latent period. There were 3 stillbirths and 23 neonatal deaths (28 days) for a perinatal mortality rate of 148/1000. The combination of respiratory distress (52%) and intracranial hemorrhage (26%) accounted for 78% of the neonatal deaths, sepsis accounting for only 13%. The 173 liveborn infants utilized 5,104 hospital days (13.98 years) at a cost of $2,228,895 just for bed space in the Intensive and Acute Care Nurseries from birth through discharge. Additionally, four more deaths occurred prior to one year of age. Of the remaining 146 infants, 41 have been lost to follow-up; however, follow-up ranging from 3 to 48 months was available for the remaining 105 children. Of these 88 (84%) are normal while 17 (16%) have long-term sequelae in the form of developmental delay or cerebral palsy.
Maternal morbidity was minimal and there were no maternal deaths. Chorioamnionitis was diagnosed in 20% and metritis in 10% of these women. Cesarean delivery was performed in 21%. Although 30% of the women delivering vaginally and 46% of those delivering by cesarean section had a postpartum hospital stay that exceeded that of the normal patient, only 5% exceeded 7 days. One woman required a blood transfusion and none required a second operative procedure.
We thus conclude that although conservative management posed little risk to the mother, it yielded poor results for her fetus with 30 (17%) ultimately dying and 17 (9.7%) suffering long-term sequelae. This obtained primarily due to prematurity and points out that attention must be directed toward identification of the cause of PROM and its prevention. These fetal, neonatal and infant results serve to emphasize that simple expectant management of preterm ruptured membranes by no means abolishes morbidity and mortality.
I i
185
I i

#168
Society of Perinatal Obstetricians Annual Meeting
~an Antonio, Texas February, 1964
ASSESSMENT OF ROUTINE PROPHYLACTIC EXCHANGE TRANSFUSION IN THE MANAGEMENT OF PREG- NANT WOMEN WITH SICKLE CELL DISEASE David C. Shaver, M.D., Joseph A. Spinnato, M.D., Baha M. Sibai, M.D., Garland D. Anderson, M.D., Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee Co|lege of Medicine, Memphis, Tennessee
The use of prophylactic exchange transfusion in the management of pregnant wo- men with sickle cel| disease is highly controversial. Previous reports from this institution suggested a definite improvement in maternal-perinatal outcome in such pregnancies managed by prophylactic exchange transfusion. This study reports on the recent pregnancy outcomes uti|izing the same protocol. Between April I, 1979 and June 30, 1982, forty-one pregnancies were entered into the exchange transfuion protocol recommended by Morrison. Thirty-one patients received transfusions, two patients developed chorioamn~onitis and delivered prior to receiving transfusions
.because of Anti-Jsb antibodies developed from previous transfusions. The remain- ~ng seven patients were excluded because of failure to present for prenatal care. There was no maternal mortality in patients managed by protocol, but maternal mor- bidity was frequent. Several complications were directly related to transfusion; four patients developed hepatitis and five patients had isoimmunization (two clinically significant). Other frequent complications included eclampsia (three patients), chorioamnionitis (four patients), pneumonia (two patients), and pyelo- nephritis (two patients). Six patients required exchange transfusion prior to 28 weeks because of infection or crisis. Perinatal outcome was complicated by three neonatal deaths and two fetal deaths. Six infants (18%) were small for gestation- al age. Our findings suggest that: I) the risk from exchange transfusion may not justify its routine use; 2) if exchange transfusion is beneficial its benefit may- be maximized by earlier initiation of therapy, and 3) neonatal outcome remains poor in patients treated by this protocol.
I I I I I I I I I I I I I I I I I I I

#169
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
NUTRITIONAL INTERVENTION IN PREGNANT DIET-RESTRICTED RATS J.A. ~pinnato, M.D.*, R.A. Ahokas, Ph.D.X, S.L. Reynolds, M.S.X, and G.D. Anderson, M.D., Department of Obstetrics and Gynecology, Division of Maternal/ Fetal Medicine, University of Tennessee College of Medicine, Memphis, Tennessee.
The perinatal literature is replete with investigations of post-natal nu- tritional support of the growth retarded newborn. However, little concrete data is available regarding antenatal nutritional resuscitation of the malnourished gravida. In pursuit of this concern, the effects of early gestational mal- nutrition that was allowed to persist throughout gestation was compared to three regimens of nutritional supplementation in the third trimester, and to control gestations in Sprague-Dawley rats. Thirty-seven (37) pregnant rats were re- stricted, from the beginning of gestation, to a diet providing 50% of the nu- tritional requirements of gestation and were compared to I0 rats fed ad libitum throughout gestation. The diet restricted rats were divided into 4 groups: (I) 50% restricted diet throughout gestation, (2) fed from day 15 to day 21 with 100% of daily carbohydrate requirements, (3) fed day 15-21 with 125% daily protein re- quirements, and (4) ad libitum feeding day 15-21.
Dietary restriction throughout gestation resulted in a significant reduction in birthweight when compared to control (P<.OOl) and to each of the refed groups. No significant difference in birthweight was noted among the refed groups. Birth- weight in the refed groups was significantly less than control only in those re- fed with carbohydrate. (P<O.03). A significant reduction in placental weight occurred in restricted throughout and carbohydrate refed group when compared to control. The restricted group ha~ smaller fetal brains than the control (P<O.02) and the refed groups had brainweights intermediate between the control and re- stricted groups. Determinations of fetal brain protein and DNA were performed. Total brain DNA was unchanged from control in any group. Although the Protein/DNA ratio was decreased in the restricted throughout group when compared to control or refed groups, statistical significance was not demonstrated.
It is concluded that nutritional deprivation reduces fetal birthweight. Nu- tritional intervention in the third trimester can restore near-control fetal growth. Fetal brain cellularity is not altered by dietary restriction and a tendency to reduced brain cell size was observed in dietary restricted animals, as evidenced by the reduced brainweight observed.
I I I I I I I ! I I
I
I
I
187
I I

#170
Society of Pefinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
SUBSTANCE ABUSE IN PREGNANCY. Jack [itzSimmons, Sandra TunisX, Joseph Izesx, Ronald Wapner, Donna Websterx, Lorretta Finneganx. Jefferson Medical College Philadephia, Pa.
Substance abuse during pregnancy is a serious health risk for both mother and fetus. Attempts at improving perinatal outcome by prov%ding care for drug- dependent women at special centers has met with some success. The Family Center has been operating at this institution since 1976, with comprehensive pre- and postnatal care provided by a team of physicians, nurses and social workers. From January i, 1981 to July 31, 1983, i01 women on methadone maintenance and 55 women with a history of non-opiate drug abuse delivered through this program. A
retrospective review of their charts forms the basis for the present study. The mean age of the women was 28 years, and 63% were black, 35% were white, and 2% hispanic. Only 7.8% were primigravid, but 22% were nulliparous, largely due to the frequent use of therapeutic abortion (38%). The number of women with previous premature deliveries (9%) and spontaneous abortions (22%) differed little from that reported for the general population. Women with a history of opiate abuse were maintained on methadone (mean daily dose 38.5 mg.) throughout their pregnancies, while in-hospital detoxification with subsequent abstinence was employed in abusers of non-opiate substances. Regular urine toxicologies confirmed continued, albeit reduced, use of illicit substances in both groups. Obstetrical complications (31%) and medical complications (15%) were common in both groups. Mean gestational age at delivery was 38 weeks in both groups by obstetrical and neonatal assessment, with 32% delivering at less than 37 completed weeks. The overall Cesarean section rate was 14.8%. A summary of the data appears below.
Methadone maintenance Poly-drug abuse Clinic visits (mean) Birth weight (mean, S.D.) Infants less than 2500 gm. 5 minute APGAR APGAR less than 7 (5 min.) Neonatal complications Neonatal abstinence syndrome Stillbirths Neonatal deaths Maternal deaths
6.5 3.5 2885 gm., 541 2768 gm., 472
23% 33% 8.4 8.9 7% 2%
48% 33% 72% 31% 5% 4% 2 0 2 0
Thus, despite intensive perinatal care, substance abuse during pregnancy remains an extremely high-risk condition for both mother and fetus.
I i I I I I I I I I I I I I I I I I I

#171
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
UTILITY OF AMNIOTIC FLUID GRAM STAIN AND CULTURE IN THE EXPECTANT MANAGEMENT OF PREMATURE RUPTURE OF MEMBRANES AND PRETERM LABOR. Kathleen Kuhlman, M.D.x James Smeltzer, M.D.x and R. Depp, M.D. Northwestern University Med. School, Chgo., Ii.
This study was performed to assess the utility of an "amniotic fluid microbiologic profile" (gram stain for bacteria, WBC, and cultures) in deliberatin a proper course of action for the patient with premature rupture of membranes (PROM). Patients were excluded if: i) there was overt amnionitis; 2) delivery was anticipated within 24 hours; and 3) the gestational age by best estimate was < 26 weeks or > 34 weeks. Amniocentesis was attempted in 155 patients with PROM, and 29 preterm labor (PTL) patients, who served as controls for background amnlotic fluid (AF)findings. AF was immediately gram stained, and aerobic and anaerobic cultures initiated. AF gram stain results were not used in prospective patient management. Amnlocentesis was successful in 80 (52%) PROM and 27 (93%) PT] patients. Both the presence of bacteria (Table i) on gram stain (GS) and positive cultures (not shown) were predictive of a later clinical diagnosis of amnionitis. Further, a positive GS was predictive of culture results (Table 2). Only 7 (11%) of 65 negative GS were associated with positive cultures; in three of the seven, labor ensued spontaneously and delivery occurred within 48 hours of PROM.
Table i CORRELATION OF GRAM STAIN BACTERIA
AND AMNIONITIS
Table 2 CORRELATION OF GRAM STAIN BACTERIA
AND CULTURES - + - +
Amnionitis Amnionitis Cultures Cultures (-) Bacteria 52 (80) 13 (20) (-) Bacteria 58 7 (ii)
(N = 65) (N = 65) (+) Bacteria 4 (27) ii (73) (+) Bacteria i 14 (93)
(N = 15) (N = 15) 80 56 24 p <.001 80 59 21 p<.001
Twelve (80%) of 15 patients with a positive GS labored spontaneously and delivered within 48 hours of amniocentesis. Cultures could not be used prospectively, as results were incomplete by 48 hours. In contrast, when there was a negative GS only 32/65 (49%) delivered < 48 hours. Patients with PTL (no PROM) had negative GS and cultures, except two cases, in which a diagnosis of amnionitis was strongly suspected. Endometritis occurred more often in patients with amnionitis (13%) versus no amnionitis (5%), but the microbiologic profile (MP) was not predictive. Neither MP nor amnionitis was predictive of subsequent serious neonatal infection. In summary, AF GS is clinically useful; it is predictive of both culture results and subsequent amnionitis. A negative MP does not eliminate the risk of subsequent amnionitis, as 20% eventually developed amnionitis. Most importantly, culture results are not clinically useful when a positive GS is obtained, as most patients with positive cultures and GS labor spontaneously and deliver within 48 hours of amniocentesis. Amniocentesis for microbiologic study cannot be recommended in PTL. unless there is strong clinical suspicion of amnionitis.
I
I I
189 I

#172
Society of Perinatai Obstetricians Annual Meeting
San Antonio, Texas February, 1984
COMPARISON OF INTRAVENOUS AND INTRAMUSCULAR MAGNESIUM SULFATE IN PREECLAMPSIA, James M. Graham, M.D.x, Baha M. Sibai, M.D., and Jack H. McCubbin, M.D., Division of Maternal/Fetal Medicine, Department of Obstetrics and Gynecology, University of Tennessee College of Medicine, Memphis, Tennessee
A prospective study of continuous intramuscular (IM) magnesium sulfate (MgSO4.7H20 UPS) compared to continuous intravenous (IV) MgSO4.7H20 UPS was per- formed in 32 preeclamptic patients. Eighteen patients received the IM regimen for mild or severe preeclampsia as recommended by Pritchard. The remaining four- teen patients received a continuous IV regimen consisting of a 4 gm IV loading dose over 15 minutes followed by a maintenance dose of 1 gm/hr (n=7) or 2 gm/hr (n=7). All groups were very similar with respect to age, height, weight and ges- tationa] age. There was no significant difference after 3 hours of therapy bet- ween the mean Mg levels achieved with the IM protocol as compared to the continu- ous IV regimen using a maintenance dose of 2 gm/hr. However, this same IM regi- men produced mean serum Mg levels that were significant|y higher than those levels obtained with a continuous IV regimen using a maintenance dose of 1 gm/hr (P<O.O01). Both methods were uncomplicated and safe. We question the uti|ity of the I gm/hr maintenance dose in a patient with norma| renal function.
2
INTRAMUSCULAR MgSO4./H20 USP
O-~ Severe (n-B) ~ M~Id (n-t0)
Time In Hours
INTRAVENOUS MgSO4-7H20 UPS
(n,7)
T~ne Zn Flours After Looding Dose
I i I ! I I i I i ! i
I I
190

#173
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
SURVIVAL AND SHORT TERM MORBIDITY 0¥ ~IMAT[WJ~ VERSUS VERY PR]~iATDRE NEONATES Larry C. Gilstrap, Ill, Lt Col, USAF, MC,, John C. Hauth, Col, USAF, MC, Richard E. Bellx, Capt, USAF, MC, Neel B. Ackerman, Jr.x, Capt, USAF, MC, Bradley A. Yoderx, Capt, USAF, MC, Robert A. DeLemosx, Col, USAF, MC, Wilford Hall USAF, Medical Center, Lackland AFB, TX
Obstetrical decisions regarding immature and very premature infants must be based on gestational age. However, most premature and immature survival data is based on birth weight. The present report related neonatal survival to accurate obstetrical gestational age criteria of between 23-34 weeks. There were 105 neonates between 23 and 34 weeks gestation delivered at Wilford Hall Medical Center over three years. Gestational age was based on at least four obstetrical criteria including LMP, early exam, FHT’s, fundal height and sonographic evaluation. Six (40%) of 15 neonates, 23 to 26 weeks gestational age survived. Of the six survivors, two had significant intracranial hemorrhage, five had broncho-pulmonary dysplasia, and two had severe retrolenticular fibroplasia. Fourteen of 16 neonates, gestational age 27 to 29 weeks, survived. Of the 14 Survivors, three had significant intracranial hemorrhage, three had bronco-pulmonary dysplasia, and three had mild retrolenticular fibroplasia. Of the 74 neonates from 30 to 34 weeks gestational age, 72 (97%) survived. Only one had an intracranial hemorrhage and none had broncho-pulmonary dysplasia or significant retrolenticular fibroplasia. Thus 11/20 (55%) of survivors between gestational ages of 24 to 29 weeks were discharged with significant morbidity versus only 1/72 (1.4%) survivors between 30 to 34 weeks (p <0001). Of the 31 neonates <--29 weeks, I/6 (17%) delivered by cesarean section survived compared to 19/25 (76%) delivered vaginally. Of the 74 neonates 30 to 34 weeks gestational age, 30/32 (94%) delivered via cesarean section and 41/42 (98%) delivered vaginally survived.
191
I

#174
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
Susan C. Robinson, M.D. x and Curtis L. Cetrulo, M.D. * Tufts University School of Medicine St. Margaret’s Hospital for Women Boston, MA 02125
"I Dcn’t Feel Good" is a program for an Apple II+ or Apple IIE or other Apple compatible cc~puter designed to aid in the study of obstetrical and .gynecological problems. It is a sophisticated quiz giver which guides a student through actual cases 9~nerated by experienced practitioners. The program is designed to be as "friendly" as possible requiring a minimum of computer experienee on the part of the teacher and none at all on the part of the student. Cases are presented beginning with the introduction followed by questions presented in three formats:
Multiple Choiee True/False Fill In The Blanks
A correct answer brings a congratulatory response keeping the students interest levels up. The case closes with pertinent final comments. Program Operation: The program is organized with two major modules--the Patient Module which is used by the student and the Teacher Input M~dule. The modules are on separate disks and the student does not have access to the teacher disk. Cases are stored on the patient disk ready for use by the student. After a student cc~pletes a patient disk, the student is allow~d to play a computer game. To date the program has had limited exposure to n~dical students and residents but b~s been received enthusiastically. We believe that this represents an exciting and innovative approach to a standardized reproducible method to educate medical students in obstetrics.
192
I !

#175
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
FETAL LACTIC ACIDOSIS AND FETAL OUTCOME Joseph S. Suidan* and Bruce K. Young, New York University Medical Center and Bellevue Hospital, New York, New York.
Umbilical arterial lactate, pH, pOp, pCO~, and base deficit were studied in 468 liveborn infants. The correlation between ~he I-minute Apgar score and lactate (r = -0.34) was not significantly stronger than the correlation between the l-min Apgar score and the pH (r = 0.30). The multiple correlation coefficient between the l-min Apgar score and all five parameters combined (lactate, pH, pO~, pCOp, and base deficit) was 0.36. This was not significantly higher than the:simpl~ correlation coefficient for pH alone (0.30). The correlation between the 5-minute Apgar score and lactate (r = -0.34) was not significantly stronger than the corre- lation between the 5-min Apgar score and the pH (r = 0.31). Also, the multiple correlation coefficient between the 5-min Apgar score and all five parameters combined (0.38) was not significantly higher than the simple correlation coeffi- cient for pH alone (0.31). The dividing point between normal and pathologic lactate levels was calculated to be 3.70 mM/L. A pH<7.20 and a lactate~3.70 mM/L had the same incidence in the general population, and had the same sensitivity, specificity, and positive and negative predictive values for low Apgar scores (see table below). Assuming that the capillary scalp blood values would not be more strongly correlated with the Apgar scores than the umbilical values, the measure- ment of multiple fetal parameters during labor would probably not improve our capability to predict neonatal depression over that already available by measurement of fetal pH alone. Furthermore, either pH or lactate measurements alone may be used. This suggests that lactate is the metabolic component which is most significant in fetal acidosis and neonatal depression.
Comparison of a low pH to a high lactate as predictors of a low 1-min Apgar score (<7)
Comparison of a low pH to a high lactate as predictors of a low 5-min Apgar score (<7)
- Proportion of all fetuses with abnormal values
- Sensitivity
- Specificity
- Positive predictive value
- Negative predictive value
pH<7.20 Lactate~3.70 mM/L pH< 7.20 Lactate~3.70 mM/L
20% 19% 20% 19%
49% 45% 50% 50%
83% 84% 81% 82%
8.4% 8.9% 26% 26%
93% 93% 98% 98%
19,3

~#176
Society of Perinatal Obstetricians Annual Meeting
San Antonio, Texas February, 1984
FETAL ACIDOSIS AhD 2-CHLOROPROCAINE: E.H. Philipsonx, M.D., B.R. Kuhnertx, Ph.D. and C.D. Syracuse,x B.S., Cleveland Metropolitan General Hospital, Per±natal Clinical Research Center, Case Western Reserve University, Cleveland, Ohio.
Placental transfer of drugs ada%inistered to the mother can be influenced by fetal acidosis. For exanple, elevated fetal and neonatal levels of ~mide- linked iocai anesthetic agents such as lidocaine and mepivacaine, ~ve been reported in acidotic infants. ~ese local anesthetics become "trapped" in their ionized form on t~ fetal side of the placenta, and tic!s, net placental transfer increased. In contrast, ester-linked local anesthetic agents such as 2-ch~oroprocaine are rapidly metabolized and placental transfer is limited. However, the n~tabolism of 2-chloroprocaine by fetal plasma is slower tlk~n in maternal piaster. Therefo,-e, in theory, the potential for ion trapping exists. The pu~l~ose of this study was ho determine i~ the disposition of 2-chloroprocaine and its metabo±ite, chlo~oaminobenzoic acid (CABA) is influenced by the acid base status of the fetus at delivery. Forty-four women at term from the obstetrical population at Cleveland Metropolitan General [bspitai }~re studied. Lumbar epidurai anesthesia with 2 or 3 percent 2-chioroprocaine was administered pr’ior to cesarean section. At delivery, the levels of 2-chloroprocaine and CABA in nmterna± plas~m and u~ilicai cord vein were quantitated by r~ss spectrometry and gas chromatograpl~y, respectively. ~,e umbilical cord vein pH at delivery was measured with an automatic blood gas system. Neonates were divided into t}~) groups; tl~)se with a pH less than or equal to 7.25 %~re considered acidotic, timse wl~)se pH was 9rea~er tlmn 7.25 were considered non-acidotic. Ten of the forty-four patients, delivered acidotic neonates while thirty- four delivered non-acidotic neonates. The n~an ur~Dilicai cord vein pH in the acidotic and non-acidotic groups ~re 7.22 -+ 0.03 and 7.32 _+ 0.03, respectively (p<0.001). There %~re no differences between ~:mternal and neonatal clinical characteristics. There were also no diffe~-ences between the grou~s in the total dose of 2-chloro~l~rocaine administered or the drug to delivery interval. The plmr]~mcologic results demonstrated placental t~’ansfer of 2-cnloroprocaine with no statistical differences in the concentration of 2- ch,oroproca~_ne or CABA in the maternal vein or ur~ilical cord vein at delivery between the two groups. The results of this study demonstrate that placental transfer of 2-chloroprocaine is not affected by fetal acidosis. These results are clinically relevant because elevated or toxic levels of ram±de-linked local m~estbetic agents may be detrimental to the fetus and neonate. Feta± acidosis or fetal distress occurs during labor and local anesthetic agents are often used during delivery. As a result, 2-chloroprocaine should be the drug of choice when fetal acidosis or distress is anticipated. ~ese results may also be relevant for local anesthe-&ic agents given by other routes of adn~inistration.
! I ! ! I ! I I I I ! I I I I
i I I
194

I I I
I
i ! I I ! i
I I I I I I I
AUTHOR INDEX

I I I I I I I I I I I I I I I I I
AUTHOR INDEX
(Note: Numbers refer to abstract numbers.)
Abbasi, I.A., 149 Abdella, T., 9, 77 Abduljabbar, H., 150 Abraham, E.C., 15 Ackerman, N.B., 173 Ahokas, R.A., 19, 169 Allen, G., 72 Amankwah, K.S., 28, 139 Andersen, H.F., 145 Anderson, G.D., 9, 19, 77, 156
168, 169 Anderson, W.M., 30, 31 Antiel, M., 6 Aoki, T., 43 Applebaum, P.Co, 32 Apuzzio, J.J., 138 Archbald, F., 4
Bachus, K., 58 Bader, B., 73, 74 Barden, T.P., 135 Barford, D.A.G., 94 Barker, D., 163 Barr, M., ii Barton, J.J., 67 Baxi, L.V., 65 Beall, M.H., 121 Beguin, F., 148 Bell, R.E., 173 Benedetti, J., 5, 95 Berkowitz, R.L., 97 Berkus, M.D., 13 Berry, S., 5 Blackwood, A., 163 Blake, P.G., 109, ii0 Blakemore, K.J., 97 Bleasdale, J.E., 8 Blomquist, C.H., 136 Boehm, F.H., iii Bohart, R., 71 Botti, J.J., 30, 31, 32 Bottoms, S.F., 128 Bowers, K.K., 81 Boylan, P., 2, 25 Boucher, M., 120 Brace, R.A., 1
Bracero, L.A., 65, 151 Breg, W.R., 97 Briggs, G., 71 Brown, K., 13 Brown, Z., 5 Bruce, S., 26 Brumfield, C.G., 126 Bruner, J.P., 155 Buhler, K., 79,80 Burry, K.A., 59, 160 Cabaniss, C.D., 29 Cabaniss, M.L., 29 Cantraine, F., 84 Carmichael, L., 150 Cavalieri, R.L., 33, 70 Cefalo, R.C., 66 Cetrulo, C.L., 56, 61, 62, 158,
162, 174 Chalmers, I., 2 Chapman, J.F., 66 Chervenak, F.A., 97, 98, 154 Chik, L.C., 144 Connor, K.D., 90 Conway-Harkins, A., 44 Cotton, D.B., 10, 99 Cotton, D.M., 128 Coustan, D.R., 70 Clark, SOL., 26, 121 Crenshaw, C., 69 Crombleholme, W., 75 Cruickshank, D.P., 133 Cruz, A.C., 72, 92, 143 Cunningham, G.F., 141 Curet, L.B., 96
Dacus, J.V., 40, 101 D’Alton, M.E., 56, 61, 62, 158, 162 Deahl, T., 46 Deaver, J., 53 Delemos, R.A., 173 DePalma, R.T., 167 Depp, O.R., 60 Depp, R., 137, 140, 171 Devoe, L.D., 150 Dillard, T.W., 1147 Divon, M.Y., 122
I I 195

I i i I
i ! I
I ! I i ! I I I I I !
Dooley, S.L., 137, 140 Dorman, K., 10, 99, 128 Dorchester, W., 51, 71, 165 Drewry, P., 46, 47 Duboe, F., 6, 78 Duggirala, V., 50 Dyson, D.C., 36
Eden, R.D., 52, 164 Edwards, N.B., 76 Eglinton, G.S., 120, 121 Elliott, J.P., 82, 83, 155 Elsweidy, M.M., 15 Entman, S.S., 111 Ernest, J.M., 152 Erwin, M.G., 102 Eschenbach, D.A., 3 Evans, A.T., 155 Ewing, J., 41 Extermann, P., 148
Fadel, H.E., 15 Farley, M.A., 98 Farmakides, G., 151 Feingold, M., 56, 61, 62, 158 Ferguson, J.E., 36, 68 Ferroni, K.M., 130 Fields, L.M., iii Finnegan, L., 170 Fiorio, J.B. 81 Fisher, D.A., 102 Fitzsimmons, J., 170 Flaherty, J.F., 82, 83 Fleischer, A., 151 Flinn, G.S., 40 Foss, M., 43 Fox, H.E., 1117 Fratkin, M.H., 133 Freeman, R., 39, 51, 113
Gabert, H.A., 142 Gall, S.A., 52, 164 Gandhi, J., 86, 87, 153 Ganesh, V., 138 Gantes, M., 64 Garbaciak, J.A., 67 Garite, T.J., 17, 71, 155, 165 Gill, P.J., 23 Gilstrap, L.C., 90, 91, 173
Golde, S.H., 123, 124 Golub, A., 48 Gonik, B., 10, 99, 128 Goodlin, R.C., 12 Graham, D., 22, 74 Grant, A., 2 Gravett, M.G., 3 Grebner, E., 11 Gross, T.L., 14, 7, 130, 131, 132
112 Grossman, H., 9 Grossman, R., 9 Grunebaum, A.N., 75 Gugliucci, C.L., 87
Hager, J., 115 Hameed, C., 16, 48 Hammacher, K., 79 Handwerker, 4 Hankins, G.D.V., 46, 47, 141, 166, 167 Harris, J.B., 35, 104 Harvorsen, P., 112 Hassan, M.M., 144 Hatjis, C.G., 152 Hauck, W., 6 Hauth, J.C., 90, 91, 173 Haverkamp, A.M., 37 Hayashi, R.H., 13 Hays, R.M., 133 Hensleigh, P.A., 36, 68 Herbert, W.N.P., 66 Hershel, M., 61, 158 Hertz, R.H., 129 Hesser, J., 71 Hickok, D.E., 5, 95 Hill, W.C., 23, 63 Hills, D., 105, 106, 107 Hirsch, J.H., 95 Hobbins, J.C., 84, 85, 97, 98, 154 Hoffman, K.L.E., 12 Hohimer, R., 59 Holbrook, R.H., 100 Holland, J., 139 Holland, R.L., 160 Holmes, K.Ko, 3 Horenstein, J.M., 120 Hou, S., 162 Huddleston, J.F., 126
196

I I I I
I I I I I I
I I I I I I
Isaacson, G., 97 Irwin, G.A.L., 105, 106, 107 Ivie, W., 58 Izes, J., 170
Jackson, L.G., 11 Jamison, R.B., 21 Jeanty, P., 84, 85, 154 Jelovsek, F.R., 164 Jones, R.L., 30, 31
Kasparian, S.S., 42 Katz, M., 23, 63, 100 Kaufmann, R.C., 28, 134 Keily, R.T., 57 Kennedy, J., 61, 158 Key, R.C., 34 Kieback, D.G., 79, 80 Kilbride, H.W., 155 King, T.M., 146 Kirz, D., 39 Kitzmiller, J., 23, 43, 63 Knox, G.E., 155 Knuppel, R.A., 114, 115 Kolb, D., 74, 75 Korndorffer, F.A., 142 Koszalka, M.F., Jr., 136 Kuhlman, K., 171 Kuhnert, B.R., 7, 14, 20
24, 176 Kuhnert, P.M., 7, 14, 20,
131 Kwaan, H., 78
Lakatua, 136 Landau, E., 138 Lang, S., 71 Lauersen, N., 49 Lavin, J., 27, 135 Leake, R.D., 102, 104 Lee, C.Y., 44, 45 Lee, M.I., 18 Lenke, R., 95 Leppert, P., 53, 163 Leverno, K.J., 166, 167 Lin, C.C., 54, 55 Lipshitz, J., 19, 108 Lirette, M., 100
Logghe, S., 22 Lorenz, R.P., 32 Louira, D., 138 Louis, F., 158 Lowe, T.W., 141 Luthy, D.A., 95
MacDonald, D., 2 Mack, L., 95 Madrazo, B.L., 45 Maduska, A.L., 50 Mahoney, M.J., 97, 98 Manfre, K.C., 37 Marlona, F.G., 144 Marquette, G.P., 147 Martin, J.N., Jr., 103, 104, 109,
110, Mayden, K., 97 Mason, J.M., 101 McCormack, W., 75 McCubbin, J.H., 172 McDonald, J.V., 73 McQuown, D.S., 113 Meis, P.J., 57, 152, 161 Miller, J.M., Jr., 142 Minkoff, H., 75 Miodovnik, M., 27, 135 Mitchell, N., 46 Mittlemann, S., 4 Moawad, A.H., 54 Modanlou, H., 39 Moenning, R., 63 Moodley, S., 22 Moore, T.R., 34 Moreland, M., 41 Morrison, F.S., 110 Morrison, J.C., 35, 41, 81, 103
104, 109, 110 Morton, M.J., 159 Mul]in, T.J., 132
Naeye, R., 32 Nagey, D.A., 69 Nandino, N., 119 Nelson, P., 3 Newton, E.R., 56, 61, 62, 158 Niebyl, J.R., 146, 147 Norman, P., 110 Novy, M.J., 58
197

I I I I I I I I I I I I I I I I I I I
O’Brien, W.F., 114, 194 O’Connor, P., 13 Oeyen, P.V., 43 O’Grady, J.P., 58, 159, 160 Oh, W., 70 Owens, O.M., 42
Paldi, E., 122 Palmer, S.M., 41, 103, 104, 109 Pankuch, G.A., 32 Parker, C.R., 46, 47 Parks, S., 45 Patrick, J., 150 Patrick, S., 131 Paul, M., 6, 78 Paul, R.H., 26, 118 Penry, M., 57 Pereira, M., 2 Perkins, R.P., 93 Phelan, J.P., 76, 120, 121 Philipson, E.H., 20, 24, 176 Phillips, 0., 109 Piscitelli, J., 164 Platt, L.D., 122, 123, 124 Polowczyk, D., 49 Poole, C.P., 41 Pringle, G., 75 Probert, C., 150
Quinlan, R.W., 72 Quirk, J.G., 8 Ramamurthy, R., 13 Ramanathan, J., 50 Rappaport, V., 92 Rattan, P.K., 114, 115 Rayburn, W., 27 Repke, J.T., 146 Resnik, R., 34 Reynolds, J., 58 Reynolds, S.L., 19, 169 River, P., 54, 55 Rivera-Alsina, M.E., 138, 139 Roberts, W.E., 35, 81, 103,
104, 109 Robinson, D., 126 Robinson, S.C., 174 Roemer, V.M., 79, 80 Romero, R., 85, 154 Rose, J.C., 161
Rosen, M., 14, 94 Ross, M.G., 102 Sabbagha, R.E., 137 Saldana, L.R., 125 Salinas, J.K., 139 Sampson, M.B., 127 Sandler, M., 45 Sanson, R., 58 Schauchter, J., 32 Schellpfeffer, M., 143 Schulman, H., 151 Schwartz, R., 70 Schwartz, R., 75 Shah, D.M., 38 Shah, Y., 22, 73, 74 Sharma, S., 73, 74 Sharp, P., 57 Shaver, D.C., 108, 168 Sibai, B.M., 9, 50, 77, 101,
156, 168, 172 Siddig, F., 49 Siddigqi, T.A., 42 Sieh, M.K., 41 Sierra, M., 75 Simon, J., 102 Sing, E., 60 Sipos, L., 118 Smeltzer, J., 171 Socol, M.L., 60, 137, 140 Sokol, R.J., 18, 144 Speed, J.E., 35 Spellacy, W., 64 Speroff, L., 59 Spillman, T., 99 Spinnato, J.A., 156, 168, 169 Spitz, H.B., 42 Stark, B.J., 21 Steinbrecher, M., 73 Stine, T.E., 76 Strauss, A., 39 Stringer, C.A., 124 Suidan, J.S., 175 Sullivan, K., 103, 104 Sullivan, T.J., 21 Swain, M., 57, 152, 161 Swersley, S.H., 117 Syner, F.N., 144 Syracuse, C.D., 20, 24, 176
198

I I I I I I I I I I I I I I I I I I I
Tahilramaney, M.P., 120, 124 Tamura, R.K., 137, 140 Taslami, M.M., 101 Taylor, J., 17 Teberg, A., 119 Tedesco, T., 115 Tejani, N., 4, 16, 48, 49 Teramo, K.A., 70 Todd, H., 18 Tortora, M., 97 Tse, G.M., 128 Tuck, S., 105, 106, 107 Tunis, S., 170
Ureda, J.R., 57
Vaisrub, N., 131, 140 Valenzuela, G.J., 1 Varner, M., 27 Vaughn, W.K., 111 Veille, J.C., 59,159,160 Verma, U.L., 4, 16, 48 Vlachokosta, F., 43 Vontver, L., 5
Wagner, P.C., 29 Wallace, T., 119 Walters, L., 98 Wapner, R.J., 11, 170 Watson, D.L., 156 Weberg, A.D., 28 Webster, D., 11, 170 Weiner, C.P., 6, 78 Weinstein, C.W., 36 Welch, G.P., 70 Weller, C.H., 79 Wendel, G.D., 21, 141, 166 Whalley, P.J., 167 Whitworth, N.S., 81 Widness, J.A., 70 Williams, G.S., 126 Williams, M.L., 167 Williams, N.E., 12 Williams, T., 14 Wolfson, R.N., 129, 132 Woodling, S., 33 Woods, L.L., 1 Work, B.A., 157
Yannuzi, F.J., 22 Yeast, J.D., 51, 113, 165 Yeh, S., 26, 118 Yoder, G.A., 173 Yonekura, M.Lo, 119 Young, B.K., 175 Younger, D., 43
Zaroulis, G., 53 Zimmer, E.Z., 122 Zuidema, L., 64, 157
199

I I I I I I I I I I I I I I I I I I I
SUBJECT INDEX

I I I
SUBJECT INDEX
(Note: Numbers refer to abstract numbers.)
SUBJECT ABSTRACT NUMBER
I I I I I I I I I I I I I I I
Accelerations, exaggerated fetal heart rate in labor Acidosis, fetal lactic and outcome Alpha fetoprotein, serum and fetal growth Amniocentesis, genetic Amniocentesis, risks with PROM Amniocentesis, chorioamnionitis Amniocentesis, PROM & preterm labor Amniocentesis, PROM Amniocentesis, Twins Amniotic fluid, infections Amniotic fluid, fetal lung maturity Amniotic fluid, PROM and preterm labor Amniotic fluid, phosphatidylglycerol Analgesia, meperidine disposition Analgesia, lidocaine for episiotomy Amalgesia, fetal acidosis and 2-chloroprocaine Analgesia, epidural for laboring hypertensives Angiotensin II, blood pressure Antibiotics, prophylaxis and C/Section Antibiotics, C-Section endomyometritis Antithrombin Ill activity, hypertension Apgar score, correlation acid-base status Arginine-Vasopressin, fetal stress Asymptomatic bacteriuria detection Auditory stimulation of fetus
Biochemical, fetal assessment Biocular distance, ultrasound Biophysical, fetal profile Birth trauma, brachial plexus Birth trauma, review Brachial plexus injury Breast stimulation, post-dates pregancy Breast stimulation, CST testing Breathing, fetal and maternal hyperoxia Breathing, fetal and short term heart rate variability Breech, external cephalic version Breech, spontaneous third trimester conversion
to vertex
Cardiac, infarction Cardiac, function and IUGR Cardiac, failure and thyrotoxicosis Cardiac, fetal evaluation by ultrasound Cardiovascular alterations, severe PIH Cesarean section, antibiotics
89 175 144 40
165 155 171 128 115 16 58
171 112, 131 20 24
176 34 18 71, 82
138 6
111 104 147 113
64 84 153 146 119 146 83 41, 102, 126
150 122 36, 148, 160
129
166 159 141 127 10 71, 82, 138
I

I I I I I I I I I I I I I I I I I I
SUBJECT
Cesarean Section, bacterial cultures for infection predictability
Cesarean Section, previous and oxytocin use Cervical incompetence Cervical ripening Chorioamnionitis, fungal Chorioamnionitis, complications Chorion biopsy, prenatal diagnosis Colloid osmotic pressure Computer, perinatal data base Computer, Apple Contraction stress tests (CST), diabetes mellitus Contraction stress tests (CST), postdate pregs Contraction stress tests (CST), nipple/breast
stimulation Cost effectiveness, antibiotics and C/Section C-Reactive protein
Dandy Walker cyst, drainage Death, perinatal causes of Decelerations, fetal and NST Demfse, fetal and multfple gestatfon Diabetes mellitus, gestational Diabetes mellitus, avoiding iatrogenic prematurity Diabetes mellitus, ambulatory management
with reflectance meter Diuretics Drug Abuse, pregnancy Dublin fetal monitoring trial
Eclampsia, EEG Ectopic pregnancy, ultrasound Edema, immersion for Electroencephalograms, eclampsia Epidural analgesia for laboring hypertensive gravidas Episiotomy, lidocaine for analgesia Erythropoetin, cord and fetal heart rate Estriols, serum and diabetes mellitus Estriols, free and HPL/NST Estriols, urinary and diabetes mellitus Estrogens, fetal plasma Ethics, third trimester pregnancy termination Exercise in pregnancy
Fetal acidosis, 2-chloroprocaine Fetal anatomy, ultrasound Fetal biophysical profile Fetal breathing and maternal hyperoxia Fetal breathing, short term heart rate variability Fetal cardiac function, ultrasound assessment Fetal cystic hygroma Fetal demise, twins
ABSTRACT NUMBER
149 120 94 35
155 90 11 99 77, 145
174 51 63
41, 102, 126 71
152
73 158 44, 57 56
134, 135 130
109 9
170 2
156 42 12
156 34 24 70 51 64 140 46 98 30, 31, 59
176 85, 154
153 150 122 127 97 56, 114
I 201

I I I I I I I I I I I I I I I I I I
SUBJECT
Fetal distress, hexaprenaline for Fetal distress, arginine-vasopressin relationship Fetal growth, ritodrine effect Fetal growth, parenteral nutrition Fetal heart rate, exaggerated accelerations in labor Fetal lactic acidosis, outcome Fetal lung maturation FSI, Lumadex (TM) & L/S Ratio Fetal maturity, expanded ultrasound screening Fetal maturity, fetal femur length Fetal maturity, placental grading Fetal monitoring, continuous pH Fetal monitoring, Western Germany Fetal monitoring, Dublin trial Fetal surgery, hydrocephaly Fetal surveillance, CST Fetal Surveillance, HPL Fetal Surveillance, Estriol Fetal Surveillance, Diabetic pregnancy Fetal weight, ultrasound diagnosis of altered
fetal growth Fibrin generation, diabetic pregnancy Fibroids in pregnancy
Genetic amniocentesis Gestational age determination, BPD & Femur
(See Ultrasound) Glucose metabolism Glucose tolerance testing, oral Glycerophospholipids, fetal lung Growth, fetal and Ritodrine Growth, retardation & maternal cardiac size Growth, fetal and ultrasound Growth, fetal and serum AFP Growth, fetal overgrowth detection Growth, fetal and parenteral nutrition
Hemoglobin, glycosylated in newborns from normal and diabetic gestations
Hemolytic disease of newborn Hemorrhage, Intraventricular Hemorrhage, hypogastric artery ligation
and hysterectomy Herpes, genital and pregnancy Hexaprenaline, fetal distress HPL, fetal surveillance Hydralazine, severe PIH Hydrocephaly, Dandy Walker cyst Hygeralimentation, fetal growth Hyperoxia, maternal and fetal breathing Hypertension, analgesia in labor by epidural
ABSTRACT NUMBER
108 104 54, 55
125 89
175 8, 33
66, 67, 157 132 124 107 117
79 2
73 41, 126 64 51, 64
140
88 78
116
4O
22, 72, 123 161 164
8 54, 55
159 88
144 142 125
15 38 39
26 5
108 64 10 73
125 150
34
I 2O2

I I I I I I I I I I I I I I I I I I
SUBJECT
Hypertension, chronic with diuretics and plasma volume
Hypertension, cardiovascular alternations in severe PIH
Hypertension, antithrombin III activity Hypertension, agiotensin II and dietary sodium Hypertension, prostaglandins Hypertension, plasmapheresis/exchange Hypogastric artery ligation, hemorrhage Hysterectomy, emergency for hemorrhage
IgG, subclass Rh disease IgG, nephelometric and PIH Immersion, head out Infections, fungal chorioamnionitis Infections, acute chorioamnionitis and complications Infections, cesarean birth and cultures Infections, penicillin allergy and desensitization Insulin pump, ambulatory Insulin therapy, diabetes mellitus Intraventricular hemorrhage, factors
Labor, premature and Nifedipine Labor, fetal distrss and hexaprenaline Labor, ripening cervix for induction of Lamellar bodies, fetal Laminaria, cervical ripening Lipoprotein cholesterol placental transfer Low birth weight analysis Low birth weight, IVH Low birth weight, delivery method Low birth weight, handicap & Perinatal events L/S Ratio, Lumadex (TM)-FSI Lung, fetal maturation Lung, fetal maturity testing
Lymph flow rate, effect of tocolysis
Magnesium sulfate, treatment regimens Magnesium sulfate, cardiovascular Magnesium sulfate, pulmonary function testing Meperidine disposition in labor Monitoring, fetal hart rate sinusoidal pattern Monitoring, cord erythropoetin Monitoring, accelerations Myocardial infarction Myo-lnositol, fetal lung
Nacardipine, premature labor Neonate, glycosylated hemoglobin in normal and
diabetic gestations
ABSTRACT NUMBER
10 6
18 19
Ii0 26 26
101 52 12
155 9O
149 21 96 43 39
162 108
35 33, 58 35 47
163 39 61, 118 93 66, 67, 81, 157 8, 33, 58
60, 66, 67, 81, 112, 131, 136
i, 81
172 10 5O 2O 37 70 89
166 8
i00
15
I

I I I I I I I I I I I I I I I I I I
SUBJECT
Neonate, low birthweight and IVH Neonate, Alloimmune thrombocytopenic purpura Neonate, brain monitoring Neonate, morbidity and mortality of immature/very
premature Neonate, meperidine disposition Nifedipine, premature labor Nipple stimulation CST Normeperidine disposition in labor NST, decelerations NST, postdate pregnancies NST vs. fetal biophysical profile NST and gestational age Nutrition, pregnancy
Oxytocin, pre-induction ripening Oxytocin, previous C/Section and Oxytocin, absence of surge with nipple
stimulation CST
Penfc~]lin, allergy testing Perinatal data, portable automated Perinatal death, causes Phosphatidylglycerol, amniotic fluid PIH/Preeclampsia, MgSO4
PIH/Preeclampsia, pulmonary function PIH/Preeclampsia, urine IgG PIH/Preeclampsia, EEG & eclampsia PIH/Preeclampsia, valsalva maneuver PIH/Preeclampsia, plasmaapheresis/exchange Placenta, histology Placenta, transfer of lipoprotein-cholesterol Placenta, insufficiency and ultrasound Placenta, grading by ultrasound Placenta, microbiology Plasma volume Plasmapheresis/Exchange, Rh Plasmaphresis/Exchange, severe PIH Postdates pregnancy, prevention Postdates pregnancy, NST Postdates pregnancy, Ultrasound Pregnancy termination, third trimester Premature labor, amniocentesis Premature labor, Nifedipine Premature labor, without tocolysis Premature labor, Nacardipine Premature labor, long term tocolysis Prematurity, vaginal flora Prematurity, delivery method Prematurity, PROM Prematurity, Avoiding in diabetes mellitus
ABSTRACT NUMBER
39 53
4
173 20
162 41, 102, 126 20 44, 57 63 153 135 169
35 120
102
21 77
158 112, 131 172
50 52
156 29
110 32 47 68 105, 106, 107 32 9
48 110 83 63 87 98
171 162 25 100 23 75 80 17, 92
130
I 204

I I I I I I I I I I I I I I I I I I
SUBJECT
Prenatal diagnosis, chorion biopsy Prenatal diagnosis, amniocentesis PROM
Prostaglandins, hypertension Prostaglandins, cervical ripening Pulmonary function tests, preeclampsia Purpura, neonatal allolTP
Rh Disease, twins Rh Disease, plasmapheresis Rh Disease, IgG subclass Rh Disease, IUT Risk Assessment, Pregnancy Risk Assessment, prematurity and second trimester
vaginal flora Risk Assessment, gestational diabetes Ritodrine, pediatric outcome Ritodrine, fetal growth (rat) Ritodrine, fetal growth (human) Ritodrine, disposition in mother, Ritodrine, fetus and neonate
Sickle cell disease, transfusion Sinusoidal pattern Smoking, effect on fetus Sodium, dietary and blood pressure Sylvian Fissure, ultrasound
Tap Test Terbutaline, lymph flow Thrombocytopenia, neonatal allo ITP Thrombocytopenia, pregnancy definition Thyroid function, pregnancy Thyrotoxicosis and heart failure Tocolysis, amniotic fluid infections Tocolysis, Nacardipine Tocolysis, Longterm IV betamimetic Tocolysis, terbutaline and lymph flow rate Transfusion, sickle cell disease Transverse lie, external version Trauma, birth and brachial plexus injury Twins, rhesus sensitization Twins, intrauterine fetal demise Twins, review Twins, discondance diagnosis and ultrasound Twins, ultrasound Twins, time between deliveries Twins, umbi|ical artery velocity waves Twins, the second twin Twins, ultrasound BPD & femur length
ABSTRACT NUMBER
Ii 40 17, 92, 165, 167
128, 171 19 35 5O 53
38 48
101 95 64
75 134
49 54 55
7 14
168 37 28 18
154
60 1
53 69
133 141
16 100
23 1
168 76
146 38 56, 114 62 74 86 27
151 143
22
I 205

i I I I I I I I I I ! I I I I
SUBJECT
Ultrasound, genetic amniocentesis Ultrasound, femur length & pulmonary maturity Ultrasound, fetal overgrowth Ultrasound, ectopic pregnancy Ultrasound, puerperal infections Ultrasound, prediction of LGA Ultrasound, abdominal circum/femur length ratio Ultrasound, uteroplacental insufficiency Ultrasound, BPD/femur length ratio Ultrasound, twins and discordance Ultrasound, biocular distance Ultrasound, fetal vascular anatomy Ultrasound, sylvian fissure Ultrasound, twins Ultrasound, postdates pregnancy Ultrasound, growth retardation diagnosis
by fetal weight Ultrasound, Fetal weight and growth curve Ultrasound, fetal cystic hygroma Ultrasound, gestational diabetes Ultrasound, fetal weight estimation and diabetes Ultrasound, fetal maturity Ultrasound, fetal cardiac function Ultrasound, placental grading Umbilical artery velocity waves, twins Umbilical cord, erythropoetin Umbilical cord, pH, pCO2, HCO3
Urine, nephelometric IgG and PIh Uterine fibroids, pregnancy outcome Uteroplacental insufficiency, ultrasound
Vacuum cup deliveries Vaginitis, pregnancy effect Valsalva maneuver, pre-eclampsia Version, external cephalic (breech) Version, external cephalic (transverse lie) Very low birth weigh, delivery method
(see low birthweight)
ABSTRACT NUMBER
40 124 142 42 45 65 65 68 22, 72, 123 74 84 85 154 22, 74, 153 87
88 88 97
139 137 124, 132 127 105, 106, 107 151 70 91, 111
52 116 68
13 3
29 36, 148, 160 76 61, 118
i i

I I I I I I I I I I I I I I ! I I I I
MEMBERSHIP ROSTER

I I I I I I I I I I I I I I I I I I I
SOCIETY FOR PERINATAL 09STETRICI~S
HORPITAL #IFFILIATION ikM)RESS
DF.PT OF O)/GYII UNIVERSITY OF TENNESSEE
800 ~ISON AVENUE ~HFI’{IS, TEWW 38163
]~.PT OF O]~/I;YN, ~UITE 501 720 HAII~ISON ~ BOSTON UIIIV S~II)OL OF HE~ICINE IOSTON ~.88 02118
142 JI]RALEIMM STREET Ill001(LYIb N,Yo 11201
LOYOLA UNIVERSITY HEIIIC~d. ~ 2160 SOUTH FIRST AVEHME ~YiROI{, ILL 601~
EPI, OF ~IGYN UNIU° OF IIARYL~N~ SCHOOL liE),
5902 WILik~RY LANE gN.TIItORE, ~° 21210
APT, 510, 321 NORTH KUMINI ST
~EPT ooF O~/GYN, SiAIIHERN ILLINOIS UNIV°
800 N° RUTLEI~ P.O.)QX 3926 SPRIII~FIELI~, ILL. 62708
]XEPT OF OB/GYN ~IV° OF NORIII CAROLINA
214 II~NI~ 111~1., ~ L’IIAP~ Hilt., N.C. 27514
~EPT, OF OI)/GYN CASE WESTERN RESERVE IJNIV+
2105 A~gEL]~T ~VELA}~, OH 44106
~PT.OF OB/GYN. 800 I~ISON AU~UE UNIU° OF TFJ. COLL. OF t~l). l~l~HIS, TENN. 38163
]XEPT.OF OS/GYN. BOX B442, ~ ~ ~HAHR~, SAUi~I
~PT. OF OB/GYN 2451 FILLINQIH UNIV, OF S, ALA]~.~ SOIOOL ~ i~ILE kLA~ 36~17
])EPTo OF I))/I;YN 530 FIRSt NEW YORK UNIV, HE])IC~L IEIffER IEW YOR~, N,Y° 10016
~PT. OF O81GYN 100 IERGEN STREET NEW JERSEY HEI~I~AL S(IXOOL }E}{ARX, N,J. 07103
I~EPT OF O~GYN IIA~HINGTON UNIV./]~IES HORP°
4911 ~ HORPIT~. PL#~ ST. LOUIS, ~ 6~110
)M.LAS, TEXAS 7520~
~EPT.OF OiV’GYN LAC/USCI~°CTR.WONEN’SHOSPo
1240 N. HISSloNRO#~ LOS~S, ~4LIF~#033
UPSTATE ~I~.~TT~R 750 EAST ~AHS S~, N.Y. 1~210
I~T. OF O~/~N° JEWISH HILLSI{E HI~,CTR, lIEg HY]E PARK, N°Yo 11042
D[{:’T.~ O~/GYH, STONY BRDOK tEALTH~. CTR, STATE UNIV,OF N,Yo Sl’Ol~ ~ STONY N~O(M(, N.Y. 11794
~ OF GOOD 5AIIN(ITNI II05PITAL
~217 CLIFTON ~ CINCINNATI, OHIO 45220
I)EPT. OF O)/GYN 211 )ETHESDA M~E, ~ ,ill5 UNIV OF CINCIMMTI IIIDIC~L CTR CINCINW~TI, I0110 15267
]~T. OF O~/GYN CLEVF.LAN) IETRO IfN, IIO~PITAL
Z395 SCRANTON ROW~ CLEVEL~, ONIO 66109
~EPT,OF O~/G~ 9klI~ER~ILI UHI9. HEg,CTR, NASTILY, 1t3N. ]72,~2
207
HEI~IP
A
A
A
A
A

I I
I I I I I I I I I I I I I I I I
12-21-8~
26
2~
29
42
~I]~E’I"E I!~ LIST
SOCIETY FOR PER]NATAL O~TETRICIAHS
HO~IT~L AFFILIATION A~RES8
])EPT.OF O~GYN ~ IE~ 168 ~rREET. COLU~IA"PI~YTERIAH HE]I.CTR. NBI YORK, N.¥. 10032
.OF O]~/GYN, UNIV.OF UTAIt
50 N, tti~ICAL SALT LAKE CITY, UTAH 84132
UIIITI~ & CHILgi~’S HOSPITAL
~F’T. OF 08/GYN IUt-~ UIIIVERI~Y OF Wt~ill~"l"ON ~ATll.E
i~’F’T,OF OB/GYHo SINAI I~ICAL CENTER
I~PT. OF OB/GYH. UNIV. OF itlAltI SCHOOL IIEDICINE
~PT. OF O~/GYN, TOLE~ HOSP.~D.COLLG~ OF OHIO
I GUS"TA~JE ~UY ~ IEW YOig~, H,Y. 10029
P,O, ~OX 016960 ltlAiiI, FL~. ~101
2142 H, ~ 81.V9, TOLE~, OHIO
ll~ NORTH HIGIIL~ APSP~ AURORA, ILL ~
~£PT. OF ~IGYN NAIS~ FOI~I~ATION II08PIT~
4647 ZION A~. BAH DIE~O, ~
TEXAS TECH.~IV, liEALTH CTR. .4800 ALBERTA EL PASO, TEXAS 79905
~EPT.I)F O8/GYN. VANi~U{DILT UINV, HOSPITAL
21ST AVENUE SOUTH NA~IIlE, TENN. ;]7232
~ ~ OIU’GYN 829 ~ ~ FT~NHS~U~INIA ~IT~ IqIILAI~FJ.FIIIA, PA 19107
I~T OF O~GYN 500 UNI~I~ITY ~ HILTOl! S. HERSHEY II~ICAL CTR ~Y, i~cHH 17033
DEPT, OF ~IGYN IPJVZEL i~)SPITAL
t707 S’T. AiIIOINE I~, DETROIT, HIC’h 48201
~£PT. OF Og/GYN 1240 N, HISSlOH ROA9 HOBEN’S HOSP. LAC/OSC ~9 CTR LOS ANGUS, CA 90033
]~PT, OF IB/GYN 214 HACPI~]~R ~LIXG, 202H UNC’CH UNIU. OF NORTH CAROLINA CItAPEL HILL, NC 27514
EPT, OF OB,/GYN. UNIV. OF
9~PT. OF Og/GYH 2~2-£ PACES VIEW EllORY UNIV. SilO01. OF HEDICINE ATLAHTA, GA ~03~9
~PT,OF O~/GYN, ~IVERSITY OF IIASItlilGTOii
~PT ~ O~GYN HOLLYWO~ PRESBYTERIAN
UHIV. OF ~A~HA IN BIi~tlHGHAH
~EMTLE, Wt~, ~81~5
245 SOUTH Ga~ ~ WEST CO~INA, CA 91791
])EPT. OF O~/GYN LONG BEACH llOltEN’5 HO~/UCI
I056 TERR#’.,E LONG ]~EACH, CA 90807
I)EPT, OF ~/GYH ItAR~R/UCLA ltE~ICAL CENTER
~ RA~NSPUR ~R, 110t RANCHO P V£RDES CA 90274
~PT, OF OB/GYN UNIV. OF 80UTH ALA]~AHA I~O~ILE, ALA. 36608
2O8
A
A
H
H
A
H
A
A
A

I I I I I I I I I I I I I I I I I I I
NO,.
,51
52
53
5+.
6O
6t
65
70
+72
NAliE
WII~TON Ao
NICHAEL S, C~DWELL,
STEVE N. CI~ITIS
RO~RT C. C:EF~O~N.Do
CURTIS CETRULO~Hol),
PRAS~TA C. CHANI)RA,H.D.
PRAJAKS CitNtTARATHERAKITTI,H D
HOLLY S, CHATTERJEG, N.D.
FRANCIS A. CI~RVENAK,I~.D.
RUNLAII CHEZ
USHA CIIIIKARA,
CHARLES R,
CLYDE li.
PHILIP K.
FRANCIS J. CIOFFI,H.I).
DANIEL. CLEHENT,H.D.
ARNOLII M,
JO’~PH V. COLLEA,H,D.
DAVID B, COTTON,ll.D.
LARkY COUSINS,IS,B,
CUNPLETE ~ LIST
SOCIETY FOR PERIMATAL ODST£TRICIANS
DEPT. OF OB/GYH UNIV. OF CONN I{~TX CENTER
22~ CAig~.E’WYC~ ~RI~ NEWINGTUN CONN. 0~111
~PTo OF OD/GYN IAYLOR COLJ.EGE OF liI~ICINE
DEPT. OF OB/GYH. MGEE WUN~’S HOSPITAL
ll.,PT OF OS/G~ WO#EN ~ INFW~TS HO~ITN.
2515 AD~)WT #ISSOURI CITY, TX 77459
FORGES MD HACKET STREET PITT~I~RI;H, PElith 15213
50 HAUBE STREET PROVIDENCE, RI 02908
BEPTo OF IB/GYN 1200 liOURSUND ~YLOR UNIV, SCliOOL OF liED. HOUSTON TX llOZO
BEPT.OF OB/GYH. UNIV, OF NORTH CAROLINA
214 ltACHI]~R ~L~G., CMPB. HILL, N,C, 2/514
SEPT,OF OB/GYH. TUFT UNIV/ST, HARGARET HOSP.
DEPT OF O~STETRII~ HAHNEEAi,IN lIED COLLEGE & XOSP.
~0 CUSHIm m IOST~, HASS. 02125
163 BRI~WOOD ROAD liT. LAUREl., N.J, 08051
RA~ARIRANA ROAg, IWIGPAKOK I~N~KOK 6 TWII- I.~,~
IIPT OF O~/GYll NEW JERSEY WEBICAL COLLE~
100 RERGEH STREET, E506 ~EIk~, NJ 07103
BEPT,OF ODIGYN, YALE UNIV, SCNOOL OF IEDICIIE
HEALTH LEARNING SYSTEiS, INC,
DEPT OF fiT. SIWAI l~.Bl~i. CENTER
3,T4 CE~,R STREET NEW H#,~M, COWN, 06510
2~0 ~.DACI~S ~RI~ )LOO~B.B, NJ 07003
1176 FIFTH AVE, 2N~ FLOOR NEW YORIb H,Y. 10029
BEPT OF OB/GYN 1 WYOIIING STREET lII~l VI~.LEY IIO~PITAL DAYTON, OHIO 45409
ASSOCIATES 180 N. 795O TUN IIALL ROAD I~ FALLS WISC 53051
BEPT OF O9/GYN SOUTHERH ILLINOIS UNIVERSITY
SEPT,OF OIS’GYtl CHDNJ-RLITGER HEDICAL SCHOOL
P. O. mx 3~26 SPRIIg;FIELD, ILL 62708
~ E~RGREEN L~ SO, PI.~INFIELn, N.J. 07080
2/5 WEST %TH STREET,20-C liBI YORK, H.Y. 10025
BEPT. OF O~IGYH YORE ~ TADOR ~ ALBERT EINSTEIN IBICN. CF~TIER PHILAIE~PHIA, PBBIA 19141
DF.PT OF O]~IGYN ~ORGETOWN |IV. ~ OF ItD
BEPT.II ODIGYN. UNIV,TEXAS i~.SCNOOL HOUSTOH
3BOO ilL3ERVOIR ROAD,li.ll. iiASHIHGTOH,D,C. 20<)07
6431 FANNIH, R~ 32/0 HOUSTON, TEY~ 770~0
SEPT OF ODIGYN UNIV. OF ~J~LIF, .£~ DIEGO
225 DIEINSON ST, S~N ])1EGO, CALIF ~103
SEPT,OF OB/GYN. WOH£N’S & INF~Ff HOSP OF R.I.
50 HAUBE STREET PEOVI]t~E R,I. 02908
BEPT.OF OBIGYN, 1480 liOFFITT UNIV, OF CALIF., ~ FRANCISCO S~ FRANCISCO, CALIF 941+.3
209
~P
A
A
H
li
k
A
A
A
A
A
A
li
It
H

74
I I
76 WARREN H, CROS~Y~H.D.
77 ~WIGHT P. CRUIK~IIANI(,
78 t~HELI~Z~
I I
79 JEANNE A. CULLINAN,
81 LUIS ~. ~LIRET,,D.
I m
82 LAR~Y J, D’ANGF.LO,H,Do
WALTER C, IXANIEL.L,
I I 87 EZRA C.
I I
88 RICHAR~ O. DAUIS~
B~ SOLON [,
?0 ISAAC 9B.I(E~
m m
92 ROBERTA H, ]IEREGT~ H.Jo
i I
9~ STEPHEN J, DEVOE~H,B.
95 GRE~GORY R, ~VORE~
i
CONPLETE ~ LIST
SOCIETY FUR PERIflATAL OISIEIRICI~NS
HOSPITAL N:FILIATIUN
22 SOUTH ~ STREET ~ilLTIHONI ~ HI}, 21201
102 PHYSICIAN OF’FIE 1928 ~LCO~ HIGHWAY IOIOXVILLE, IIIIN ]Jg’~
~PT OF ~/~11 tOOt POTRERO ~ FR/II~I~O GEIEY~ ItOSPITAL ~1 FRN~I~1~O OIl.IF 94110
~.PT. OF ODIGYNo
DI[P1 OF O~/GYN i~ICAL COLLEGE OF VIRGINIA
IIPT,OF OIVGYN. ONlY OF FLONI~ COLLEGE
BEPT, OF ~IGYH STRONG itEItORIAL IiO~PITAL
PEPT.~ 08/GYH. UNIV OF TEXAS HEALTH S~][ CTR
P.O, ~gx 26307 Oltt.AHO~ CITY, OKLA. ~126
1111{ Ai~ ~ 5"T., iBX 34 RICltHOID~ VA 2L:~98
~6X J-294~ J.H.HILLER HEALTH GAIIIESVILLE, FLA~ 37.610
P,O, ~ 668, 601 B.JO0~ AV[, ROCHESTER, N.Y. 14642
5123 HARRY HIHES BLVg.
~1". OF ~/GYN UNIV. OF WISCONSIN
202 SOUTH PtW( ~TREET
Jf~PT.OF OIVGYN. 6161 8. YALE, 1Z228 "rUL~ i.F..Bo COLLEGE 11JLSk, OIg~, 74177
DEPT.OF OD/GYH, it@I~wNI ARflY ~l~I~t. CEHTER
NO HA~I~ON ~PHIS, TENN, 38163
1600 LEE TRE~I#0, ~IITE IH EL P~O, TEX~ 79F’,,6
938 ~IG~ ~ lIED, CTR, TACOHA, WA~. ~31
~£PT. OF OB/GYH
~PT.~ 09/GYN. HAl{TIN LUlt{R KI~ H£N, HOSP,
12O21 WlL~Im AVL LOS AiI~ELES, CALIF 90059
~PT. OF O]L/GYit UNIV, 6F ALADANA IN DIRIIINGHAH |IRHIIiQHAH
DEPT.OF O8/GYH. NATIONAL NAVAL iii[DI{J~L ~
450 CLAi~SON AU£HU£ DROOI(LYH N.Y.
~£PT.OF 08/GYN. HORTHHE~IER# UNIV.
9EPT. OF 09/GYH 9UNY ]N)HNSTAT£ ~.I)I~L ~NTER
~EPT. BF IEI)ICAL COLLEGE OF
III ~ AUEW, JE IIANt~:,~, NY 110]0
AUGUSTA, GA }0912
BEPT.~ O~/GYN. OSU RIVERSID£ IL’IHODI~T HO~.
DEPT OF OB/GYH LA~ itEB. CTR,WOilBI’S HO~.
1244) H. tlISSI0~ R0~I), RII 5K’22 LO~ AH~ELES, CALIF 90033
DEPT.OF O~/GYH, 201 E, ONIV~RSITY PARI~Y THE UNION I~HRIAL HOSPT, BILTIilORE ~. 21218
210
HI~IP
A
#
H
A
H

I I I I I I I I I I I I I I I I I I I
I~IPI.ETE ilEH~:R LIST
SOCIETY FOR PERINkTAL OBSTETRICIANS
HOSPITAL ~FILI~TIiM
~EPT OF O]~GYN
]~PT OF I~/GYN STATE IM]~,OF N,Y, AT ~’FIV.O
])EPT,OF UN]V OF TENNESSEE COLL. OF ~
W:IMI~Y IIEDICAL COLLEGE
~EPT OF O~/GYN NORTHk~STERN gNIVo
IIEPT.OF 69/GYW, HEW YORK HO~P-CORflELL ~D CTR
DEPT. OF OB.GYN ~SE ~STEI~RESERVE Ikl]P°
DEPT.OF OB/GYH, ~’YLWAIA HOSPITAL
I~PT, OF O~/GYH ON~ODHi]~ITAL
NJ~ ooF O]~GYN, WESTCHESTER COlJIITY BE~IC~L CTR
D£PTo OF~/GYN ST. PAUL-RNtSEYI~ICALCENTER
~P"T °OF OiVGYH, LETTERI~ ARHY i~,CTR,
~EPT. OF OB/GYH ilOUNT SINAI HI]$~ITAL~ ~ICAGO
3395 8CRANTI~ RON) CLEVELANd, OHIO 44109
I~OHO~E STREET WFFALO, H.Y, 14222
IlEHPHIS~ ~ ~8163
1005 NkSINILLE, TN Z7208
2617 N,W, 58THPLACE OKI.~O~CITY, OK 73112
~3 EAST SIJIT.RIOR ST,, I~ 440 CHICAGO, ILL 6#611
3~1 LN~ON A~, ilIUIETTE ILL,
525 EAST 6BTH STI[ET NEW YORI(, N°Y. 10021
2105 #k~EL~RT ROAD CLEVELAND, OH 44105
205 15TH PUY~J.I~,
STH AWO SPRIJC£ STR£ET RtILN)ELP!iIA, I~, 19107
18101 ~ DLVD.
~EI~T.OF OB~YN, ilORTH ~ UNIV. IIO~PIT~L
IIPT,OF 0~, LIWIT~
9i~PT. OF OB/GYN ALBERT EINSTEIN HED. CgLLEGE
IIORTH Ill.IN. NED° CTR.
211
HAHii~T, N,Y. 11030
675 WINF.M~ ~LYI~OOTH, H~I, 55441
JACO~I HO~P/PEIJW~.EASTCHESIER N.Y. 104~1
2620 ~ORIA LAH~ J~J.LHO~E N.Y. 11710
N
A
A
A
A
A
A
A

I I I I I I I I I I I I I I I I I I I
12-21-4~
NO,
121
122
123
125
128
129
130
132
I33
135
138
140
141
143
COUPLETE ~ LIST
SOCIETY FOR PERIHATAL OSSTETRICIAHS
HOSPITAL AFFILIATIOH
IF~.PT, OF ~IGYH ~EUELA#41) HETRO, ~H, ~ITAL
DEPT,OF 08/GYH, UItlVo OF OKLAHOI~ HEALTH SCI,
EPT,OF OBII;YN° COLUflBIA"PRES~YTERIAN XO~o
~.PT ooF O]FGYN, DANIH.IRY ~PITAL
DEPT ,OF OS/GYH. HOSPIT~ OF ~IV, OF PA.
9EPT.OF OB/GYN. L.S.U. i¢~ICAI. CENTER
~I~ °OF OB/GYN, UNIV. HEI), CTR,
DEPT,OF OB/GYN, UlllP° OF TEXAS IF.ALTH ~, CTR,
I)EPT OF OR/GYN ILLINOIS P4~OW~ HE~° CEHTER
VOitEH’ S XOSPTIAL
~EPT,OF $1o FiL411CIS HOSPT° If3o CTR°
DEPT,OF O]B/GYH, UNIV,TEXAS IEALTH SC° CTRo
~EPT,OF OS/GYN, TEXAS TECH° UNIV, W,.ALTH CTRo
212
55 OCEAN A~TNOE, APT, 7"F ilOl~TH H[ACH, H,,.lo 07750
1728 SI~LIG LM£ LOS ALTOS, CALIF 94022
P, O, 90X 26901 Ol6..AHOi~ CITY, Off.A, ~190
630 IE~ 16~TH ST, NBI YORK, NoY, 10032
20 ~LAN AVe, ~I~JRY, O~NN, 06B10
333 E, 91.,mERIOR CRICAGO, ILL 60611
280! ATI.A~ITIC A~,~ ~X 1428 LONO ~.ACH, ~I.IF 90801
221 LOHGNOO9 AVE, ~TON, HASS 02215
7725 KEHTHOOD ~E, LOS ANGUS, CALIF 90045
4554 SYLVAN ~RIUE ALLISON PARK, I~NN 15101
3400 SPRU~ STREET P~ILAi)ELPHIA, P~, 19104
1542 TIJLAi4E AVE, WEB ORLEANS, LA, ~0112
DUKE UNIV, i~, CTR,~X,~I3 N,.C° 27710
241 8EVF..qLY ROAD ~ALE, N,Yo 1051~
5323 HARRY HIHES ~LVL ~q.LAS, T~XAS 752Z5
~ W. WELLINGTON ILL
2B01 ATLANTIC LOUG )EACH~ ~3~I.IF 90~01
73~ KIIlG~IRY ST. LOUIS, NO, 63130
900 W, PLYNOUTH N~LANO, FLA. 32720
2160 S, FIHT A~E. ~AYHOUg, ILL, d415Z
|J4 WOO~AN~ STi~ET
770.1 FLOY9 CIRL I~]VE SAH AHTOHIO, TEXAS 78284
4TH AH9 INOI~4A LUBBOCK, TEXAS 7!N30

I I I I I I I I I I I I I I I I I I
12-21-83 I~"TE HEELER LIST
~OCIETY FOR ~RINAT~ OI~ST~ICIAN~
NOSIqTAL AFI:ILIATI~ ANXRES~
DEPT,0F OB/GYH, WII.LFOU HALl. ~ I’B, CTR,
~PT. IX: ~IGYN NIIIIlZ HBORIN. ~IIAL
EPT OF OIUGYN J~S I(]@I(I~ NII@IT~
EPT,OF O~/GYN, ~ N~, CTR,ll)~’S HOSP.
7206 FOE~ SAN ANTONIO, TE~ 7E40
5~14) NOITH HI)Jkl)WAY, HI~ 3H H.TIHRE, ~ 21205
1240 NIRTH itIEI| ~ LOS ~LES, ~I.IF ~
EPT, OF OBIG~ ~I~L:RSITY ~ATI~ UNIV. OF ~ ~IHINGI~, ~A ~5294
flATERi~-F’ETAL ~ICI~ Sl~I HOSPIT~ OF ETROIT
6767 Y OUTER ET~IT, HI~. 492~5
~3’T.OF I~GYN. 101 CITY ~IVE ~OUTlt UNIV, ~ CALIF, IRUINE, ~, CALIF 926~
EPT,OF OIUGYN. SINAI I(]f~P,OF BAI.TI~,I~,
EPT OF ~IGYN INDIANA UNIVERSITY
~LEE~ ~ GI~NSPRIt; ~, H.TII~E, I~. 2%215
II00 ~ST NICIIIG~N STIIEET INDI~:t]LIS I~, U~23
~F’T. OF ~/GYN UNIV. TEXAS lB. SCHOOL
I~:PI.OF UNIg,0F ~ I(D. ~NTER
~PT,OF OBIGYN, UNIV.OF IOWA
~31 FN~NIN ~IT~O~
SI~ I~N~ITI]A STREET, 12 PLAYA lB. REY~ CALIF 90291
42ND STREET L EWi[YAH~E ONANA, ~ ~I05
IUN~ CITY, IO~ 5224,2
EPT.OF 0]UGYN° ETA ~ATE8 HOSPT.
~X)l COLSY ~EET N~EL~, CALIF 94705
]~:’T. OF ~/GYN LOltk LINNA UNIV. SCHDOL OF HED LOHA LIN~,
I)EPT OF OD/GYH, W. VIRGINIA UNIVo IB, ENTER
N}’T ~ IIlUG~ YN.J[ UNIV, SCHgOL OF HE)ICII[
NORG~0H, W,VA. 26.506
333 I~ STREET COLIN 0~I0
EPT OF Oi~G’/N 3O0 COI~ITY BRIVE ~T, N,Y, I00~0
EPT, OF ~IGYN ~RI~ i WO(N’S HO]~PIT~
]EFT OF OBIGYN ST, PETER’S IB%~ ~NTER
EPT, OF OI~YN D.EI/ELAN~ (TROI%IT~ BOSP.
~ FNA~I~IS ST, H~TH, ~ 02115
(WI~I~ICK, g,J, oBgoz
EPT.OF O~/GYN. 21.50 PENNSYLVANIA #WE. GEORGE W~IW{;TUN HIVJ~.CTR lt~!IINGTON,9..C. 20037
~PT OF 0~GY# Hill ~ IIOHN.L ~ ST, LUES IEPIT~ ~ CITY H0 Mlll
EPT. OF I~/GYN 210,5 AELERT ~ CA~ WESTERN R@ERgE ~IP° I:LEELk~, OH 4410~
N
A
N
A
fl
N
A
N
fl
A
A
A
A
fl
il
A
H
I 213

I I I I I I I I I I
I I I I !
COIIPLETEHEIIIERLIST
SOCIETY FOR PERINATAL O~TETRICIiMIS
HOSPITAL ~FILIATI~ APDRESS
~EPT, OF OB/GYN
THE ffRINATALCENTER SLITTER #EIIORIAL IIOSPITAL
RO0~ CJ-24~ AUGUSTA, G~ 30912
52N!) AHI) F STREET ~0, CALIF 9~19
~ I{UCI(IHI;H~BRIV[ BIX HILLS, N.Y, 1174~
IEPT.~ OB/GYN. 950 R. 12TH ST~ET UNIV. WISCONSIN HEB. ~CHOOL HILWAUKEE, WISC. 53201
~{PT ~ OBIG~ ~ J-~4 JhW£ ~IU,OF FL~I~ ~IHESVILt.E, FLA, ~2610
EPT,OF 08/GYN. fl~EE-W6HEN’SHOSPITAL
FBRIES ~VE AN~ I;~LILrl ST, PITTB~R~, ~#d, 15213
IfcPT.OF OB/GYil. 254 EASTOIq AVE. RUTER8 IIEIICAL ~CHOOL NEW JICK, N,J, 08~3
~{PT,OF UNIV. OF
~>T. OF O~/GYH il~YgE STATE UiilV, ~l~.t CTR,
@NIV,OF ~IV.STA. {IR}~INGH~, ALA+ 352~4
31340 J~ R+’-AF{ G liADISON ~S, HI~, 48071
1705 E~T 19 ST. ST,. JOHH’S BOCTDRS li.I~, # 707 TULSA, OKLA. 74104
IfPT OF 08/GYN 300 S, HAWTHORNE ROAD WINSTON-SALB N,C, 27103
7215 TRACE i)UCELE SAN AHTOHIO, TEXAS 78240
IiEPT.OF OE/GYH, BF.H~ER GENERAL I, IO~’T.
820 CLERltOWT ST., ~IT£ 120 BENV~, COLO, 80220
BEPT.OF OBIGYN. IIARBOR GEHERAL-,r_,LA HED. CTR,
1000 g. ~SO!l SIIEEI T~#~/]Z, ~ Wr’~W)9
IfPT, OF OB/GTH, DAYLOR COL.LGEG OF lg’~ICIHE
])EPT,OF OD/GYH. UNIV. OF WI~CONBIN"M~ISON
KPT.OF GB/GYN. SliltTA CLARA VALLEY HE9. CTR.
~PT OF OBIGYH UNIV, OF NORTH CAROLIII~
1200 HOUSTON, TEXAS 77030
2O2 SOUTH P~K STREET BIBISON, WISC. 53715
751 SO, S~! J~, ~IF 95128
214 lY~l]IR m.~. ~ CIIAPEL HILL H.C. 27514
BEPI.OF OD/GYN, CLEVELAND ~ITAN XOSPT.
UNIFORP:J ER~ICE8, UNIV+ OF HEALTH ~CI.,~ETHESI~A
~_PI, OF 08/GYN UNIV+ CALIF, IRUIHE NEg, CTR,
101 CITY BRI~ ORANg, CA ~2~8
DEPT.OF O]L/GYN. POLYCLIHIC HOSPITAL PENN. 17105
I~/GYN ST~FF 200 FIRST STREET CLINIC RSCHF~TER,
]fPT OF CHILIX~N’8 HOSP. SAH FRAHCISCO CALIF 94605
214
HEI~J~IP
k
A
A
H
A
H
A
A
H
k
H
A
A

I I I I I I I I I I I I I I I I I I I
12-21-83 CglIPLETE ~ LIST
SOCIETY FOR PEi~14ATALOBSTE~ICI~
HOSPITAL kFFILIAHOH ~
DEPT,OF OS/GYH, 1200 ~ ST, LUKE’S EPISCOPAL/’DAYL.OR HOU~TOH, TiET.A8 77630
~.PT OF 68/GYH EVAHSTOH HI~ITAL E1/AHSTOH~, ILL ~20!
DEFT OF 08/GYH 7~’53 ~ STREET YALE 1~I9, ~ OF HE~ICINE ~ INi4/EN~ CONN
[email protected] 08/GYN, I000 HEST CARSON HARBOR-IJCLA HE~CAL CEIfI’ER TORRANCE~ C~.,IF
]~PT~ OF OB/~Y14 ~ gEST ~ ST, JOfiEPH’S HOSPITAL HB.. CTR PttOEt!ZX~ ~ 852~
II~"T, OF ~/GYit 140 gkllT~ lg]~IC~ IgtY UgIV. OF CALIF. ~ F’RkNCXSCO ~ FRt4tCIS~O, C~ 94127
gl3>To OF Og,~Y14 12~ It, ILTSSIOH IIOHEH’S HOSPo,I.~CAISC HE~ CTR LOS I~IgEI.E’S~ C~
~EPT.OF OS/GYH, 171 klIiEY A~E. 14EgICAL UNIV,OF S.CAROLINA CIIARLESTOH. S.C*
142 JORALEN]N STREET ]~OKLYIt. Nolo 11201
APT. 508, 6008 IIESTRIgGE FORT itORTH~ TEXAS 7~I1~
IPT.OF O~IGY14o UItlVERSITY STkTION OltlV. OF kLkl~]tk SCliOOL OF ~ ~]Rfl114Gl~, ALA,
ST. ELIZABETH 14BICAL CENTER ~IYTON, OHIO 45408
])EPT, OF 08/GYN 445 EAST 68TH STI~H~ APT, 8~ CORNELL UHZV, 14EgICAL CENTER HL~ YORK H,Y, 104)21
~EPT,OF O)k/GYN ~ g, I~ STREET COLLH~IA"PRESBYTERIAN HE]hCTR, lIEU YOl~ H,Y, 10032
DEFT,OF 08/GYN, ’ 4~I0 NEST TENTH A~E, H"~5 THE OHIO STATE OHIV, HO~T, CILlaliH~, OHIO
COLLEGE HOSHTAL IIEHARK~, H,J,
4,7 TALL TIII~ER8 LAH£ GLASTOIGHJRY ~ COiOl, Od, OZ3
C/O ARAitCO, P,O,90X I~7
KPT, OF O~/GYH 374, E, 9~TH ST, UH]V, OF ZLLIHOIS HEg, CTR, CHICAGO, ILL d~19
9EPT,OF OB/GYH, INIVERSITY CIRCLE ~ HOUSE UNIV.H.OF CLV9 CLEVELk~, OHIO
PL~O TEXAS 75O75
v’lg~, OHIV. OF FLORISt GAIIESVILLE, FLA.. 32~t0
ALE~IA~ VA 22307
~PT, OF G~JGYH i£gARK E’TH ISi~L ~ CEIg~
201 LYgNS AVEHLE NE"i~ ~ g,J, 0711:2
215
14
A
A
A
A
14
k
A
A
k
A
A
#
#
A

I I I I I I I I I I I I I I I I I I I
12-21-83
NO,
218
~0
231
2~
BOCIETY FOR PERINATAL O~STETRICIAHS
NOII~ITAL ~FILIATION ~
D~T. OF OWGYH LOYOLA UNIV. IEDICAL CENTER
N~F’T OF ~/I;YN SOUTHERN ILLINOIS UiIIQ~RISTY
~EPT. OF OB/GYN NOTZEL HOSPIWAYIE STATE UNIV.
~£PT OF OIVQYN ~ISER FOUNDATION I#~PIT~
D£PT OF O8/GYN U. C. IRVINE I~I)ICAL ~
]~.PT OF O~/GYN UNI~RISTY OF FLORIM
D£PT.OF Oi/GYII. HARICIIPA COUNTY ~ HOS~.
itPT OF OB/GYH ~IV. OF TEXA~ ~ICAL ~
9EPT OF OB/GYH ~IP, OF HEll HEXICO HE]). CTR,
B£PT. OF OB/GYN U, C. ~ DIEGO IEI)IC~L ~HTI[R
~F.PT. OF OWGYN 91JKIZ UNI~RSITY ~ICAL ~IrlER
~EPT OF OWGYN CIIIL]Rdt’S Ii0~, ~N FRA#ICI~CO
~EPT.OF ~/I;YH, EJIORY UNIV.I~Y HEH. HOB~.
I)£PT.OF O~/GYN. HOSPITAL
|£PT,OF O~/GYH. UNIV.OF SOUTH FLORIDA
~EPT,OF OB/G~rl~, UNIV. OF UTAH SCllOOL OF
I£PT. OF ARCAIJIA IETHO~IST NO~IIAL
])EFT OF O~/GYN NIIIX [ UNIV. NOSPIT~
8 BEICHWO6~ ROAB BiST HILLS~ N.Y. 11~76
216
HI~P
A
A
H
A
A
#
H
A

CUNPLETE ~ LIST
I i i I I I I ! I i ! I ! I I I
~EPI. OF 09JGYN HIV. CALIFo IRVINE HEB. CIR.
DEPT. OF OB/GYH UNIP, HI~II~IA~KSOW N], HOOP.
~EPT.OF OR/GYN. HIP.OF CALIF. NED. CENTER
BEPT.OF O~/GYN. GEORGE WYJ;IINGTUN UNIV.
~I oOF O])/GYN, UNIV. OF LOOISVILLIZ
IIPT OF OlPGYH AKRON CITY HOSPITAL
P..OoIOX 14~8,~80I ATLANTIC LONG BE~CH, CA
4298 iOniA CII~LE I])~WUT I;REEK, FLA Z30&~
1480 14OFFITT SAN FRANCIS(O, CALIF 74143
2150 PI~IlS"YLWOIIA AU£. H,M. MA~14114GTOfl,]).C. ~7
323 BST CNESTNOT 8TNEET LOUISVILLE, I(Y. 40202
AER~,~ FJ~T lkI~I(ETOH]oS"TR~ET4¢z~)?
BEPT.OF O])/GYHo 27~7 lEST GRA~ HENRY FOR]) HOSPT. 9ETROIT, 14II}io ~"202
D£PT OF OB/GYN STATE UNIUER~ITY OF NEW YOl~
~4~ STACY PLACE LANE OLIVETII£, HO. ~ZlZ2
l~O F.I~E STR£ET ~JFFALO, N.Y. 14222
BEPT, OF OB/GYW RH 20 UNIV, OF WABIflNGT014 ~ CENER ~TTLE,
4465 DOUGLAS A~., 7H RIV£R])AL£, N.Y. 10471
])EPT.OF O~IGYN. 2~1 I~TNE~ AVE. ~.,1560 UNIV. OF CINCINI~ITI HEB.CTRo CINCINNATI, OHIO �5267
~PT Of O])/GYH 600 I}ESHAH ~IVE EASTERN VIRGINIA NED. ~ l!ORFOLI(, VA 23~07
~EPI.OF OBIGYH. 5~11 S, HARY~ AVE. UNIV,OF ~]CAGO LYING-IN 140~PT C141CJM;O, ILL. 60637
DEPT. OF OB/GYH UNIV, OF CINCINNATI 14F.~. CIR. CINCINNATI, OHIO
242~ ~OOLII~ MO~EN’ S ltO~PIIAL
~PT.OF O~/GY14o UNIQ,OF ~SEE
~I~T OF OR/GYN ~ILT~ S, ~Y ~IC#W. ~
I~T,OF OIL/GYN. ALTA DA~S HO~ITAL
DEPT. OF ~IGYH UNIV. OF CINCINNATI HE~. CIR,
CALIF 92667
500 IJWIVEI~ITY lltI~E, IIEI~3NEY, PENN 17033
I COL~ PLAZA AT ASI~Y DI~I~EY, CA ?4705
1600 A. ~ ~I~TS CINCIN14ATI, ~I0 4,’~3
BEPT OF O~/GY14 RH-20 UNIV. OF WA,,°HINGTUN Bl"n.E,
PEPT, OF {BIGYN TULANE UNIU. SCHOOl. OF NED.
])£PT.~ O~GYN. ~TIN-LUI}ER KING, ~° HOSP.
~T, ~F O]~IGYH 14#d~TIN LUTNER KING HOSPITAL
14ETAIRIE, ~ 70003
12021 S. WlUflNGTUN ~ LOS ANGELES, C.~ 90059
1785~ CAIIE~AL PL~E E~CINO, CALIF 71,116
A
A
14
A
A
A
A
14
A
H
A
14
A
217

I I I I I I I I I I I I I I I I I I I
t2-21-8~
KPT, OF ~/GYN ONIUERSIIY OF COLONABO
9EPT.OF OD/GYH, HOIZEL HO~./IIAYIE STAII ONIV,
EPT. OF Ol~GYil JOIHR H6PKIN~ HOSPITAL
~t?T,OF SlNI RAIIO~IIEKI]~I8
DIVISION OF PERIKATAL If.), NORTH SHORE UNIV,HOBPITAL
KPT ,OF ODIGTN, ~NIV, OF TSi~. ~L.OF HE~.
BEPT, OF ~GYH ~ GRAY H OF 8ICIHE
~EPT,OF OBIGYN, H@~P,OF THE ONIVo OF PEW#,
Ia~PT.OF l~/GYIh #4.BERT EIHBTEIH COLL, OF
KPT.0F 0WGYW,
~d~ OF I~GYN LSU SCHOOL OF IBEIIE
IIPI. OF KAISER F@U~DATION HOSPITAL
~PI, OF O91GYN U.C, IRVIHE flF.DICAL CENTER
KPT OF OB/GYH UNIV. OF CINCINNATI ~ CTR
~(PT, OF ~YH CHICA~O LYIMG-Ill/ONIV, CHICd~O
~EPT,OF OB/GYH. UHIU,i~IGSI~BIPPI HE9. CTR.
DEPT.OF O8/GYN, Ig~EE WBHE)i’ HOSPIT~
~PT OF OB/GY# ~IV, OF HARY~ HO~PIT~
218
|-1~, 42gg ~ HI#TN ~ ~ ~2~2
~07 P~ 4WE, HEW YORK, N,Y. IW’~I
4707 ~T, ANTOINE RWROIT, HICH, 4~201
~00 CONHONITY ~IVE ~N~T[, N.Y, 114)30
~IS, TEHN ~8~d~
300S, StWTHOI~Kt~ IINSFolFS~dt H.C. 27103
PHI~IA, PEi~, 19104
I3k) l!!~IS P~RK AUBtIJE
4301 i. HARI~ ~ LITTLE RO(X, AR~. 72205
1~42 TULME NEW ORLEkNS LA, 70112
26 lfl’, WI~F.N~JRQ ~I’, ~ R~AEL, ~A 9~3
I01 CITY ~IVE ~b~, K~ 25
196 D 123 STRE~ 61J{Ei~ H,Y. 11694
231 ~IHES~I ~AfJ~ CIiRIHIVITI, i}ll{i 4~/
5841 S, MRYLNtB A~, ONICN;O, IL, ~6]~
~ITE 611, O~ kWIS~LVI), TAHPA FLA 33609
~93 STgHE ROAD PITT~$~, N.Y.
250~HORTHSTAT£STRR’r J~(XSON, ~I~B ~16
F$~f.S A~.~, H~ ST, PIT~, PEHII, 15213
HE#PONT RV~., ~0X Y
22 SOUm GRF~NE ~ ~tLTIHOR~ ~ 21201
H
H
H
A
A
H
H
A
H
A
A

I I ! I I I I I ! I I I I I ! I I I !
12-21-83
2%
2~
2~
302
311
CgOIPLET£ HEHIER LIST
~OCIETY FOR PERINATAL OBSTETRICIIV!8
HOGPITAL ~FILIATION
D£PT. OF O]~GYN ~ GRAY SCHOOL OF HEBICIHE
TIFTS UNIV.-ST.HARGARET’8 HOgP
IPT,O~ OD/GYH. J.HOPKINS UNIV.SOIOOL OF HE~).
DEPToOF O~GYH.
300 S. IIAUTID~£ ROAD #IHST~OI N,C, 2710~
90 CUSHIIIG AV£. DOSTOH, HASS. 02125
~01 #. BRI~Y~ HAirY 108 MII.TIIIOI~ i~. 21205
2041 GEORGIA AUE, N,W. IIAOHIIIGTOH,9.C, 200~
]~EPT. OF ~/I;YN, 3181 S,W, ~ JACI~SOH UIII9,OF OREGON HEALTH tiC, CTR. PORTLAND, ORE,
~.PT, ~ O~/GYN MIU. OF S. FLORIDA lIED. CTR.
9EPT. OF ~/~N ~IV, ~ O~GOfl i~C
~,PT. OF OB/GYN GOO~ GAffARITAN ltEDICAL CENTER
~£PT, 6F OB/GYH LINIU. HOSP, 6~ JACK$OINILLE
~PT,OF tIB/GYH TI~ OHIO STATE UNIV. HOSPT.
THE PERINATAL i~.NTER
DEPT.OF O9/GYN. UNIV OF WISC.CTR.FOR HEALTH
DEPT.OF INDIANA UNIV. HELICAL CENTER
I DAUIS IU;~., SUITE 611 TAHPA, FLIiA
3161 S.#. S~ JAl~Sgll PK. ROAD PO~TLAID, 01~ 97201
IIII E, ~ ROAD PIiOEHIX, A~ 850d2
~5 ~ 8TH STREET JACKSOH~ILLE, FL
410 ~ TE#TH C~l.Ui~, OHIO 4;]210
I000 6, CARSOH ST. T~, CALIF 9q)502
52?5 F STREH SACRAHEHTO, CA 95819
600 HIGHLAND AUI[, M~I~OH, WI~C, 5~792
POINT COU~T LIAIIS, Hi]. 631;~1
9~ HEST HICHIGAH INglAHAPOLI6, liD, ’1~23
])EPT, OF ~/GYH 2~,~0 H. STATE ST. U#IU. OF HISSISSIPPI i~9. CTR. JAi~Oll, HISS. 37216
DEPT. OF O8/GYH, UNIV. OF CLIAF. HEg. CTR.
D£PT, OF OB/GYH itADISOH GEHERAL IIO~PITAL
I)EPT OF OB/GYH U#IVERSITY OF ILLINOIS
.OF OD/GYN, LAC/USC H£1),CTR,WOHEH’S HOSP.
DEPT ~ ~IU, 6F PITTSDIJGH
DEPT.O~ OD/GYNo lJlU.OF HEW i¢:Xl~O HE). CTER.
H[PT. ~ O~/QYN TULAH£ U#IV. SCHOOL OF liED,
219
1480 ilOFFITT SdSt FRANCISCO, CALF 9~143
202 SOUTH PAR~ STi~ ltADI5OH, HI 53715
84O S, ~ STREET CHICAGO, ILL ~12
1240 #, IilSSION LOS ANGELESr CALIF
HAGEE~’ S HOOP, PITT53tlRGH, PA 15213
2211 LOI~ ~@. N,E, ALSUglJERI~ ~ N,H. 87131
1430 TIL4NE ~ ~ ORLEAIE, LA 70112
H£HgI~HIP
A
H
H
A
H
A
A
A
A
A
H
H

i I ! I
12-21-83
I l
31~ ROT Bo PITKIN,Ho{.
318 JOEL I. POLIN,
I I I I I I
P~HAN K, RATTAN,
KATHLEEN ~,
KEITHFRANCISRAWLINSUN,H,9,
I WILLI~ Fo RAY~LIRN,H,9.
JOHN A.~Ag,LTC,IIC,IJSk
KHTHRYN L. REED,
I I
ALEXANDER
JOHN T. REPKE~
ROBERT
I I
DANIEI. A, RI~THIRE, H,9,
I
DEPT. OF OBIGYN. UfllU,OF TEX, XEHLTX tRI.CTR.
~.PT,.OF OD/GYH GEORGETOWN IJNIVoSCHOOL OF
~.PT,OF HNIU, OF CALIFI~I~ ~DCTR
I~.PT, OF OB/GYN UNIV. OF ALAI~A, BIR14INGlt~
~PT OF Og/GYN
9EPT.OF 6D/GYN I~RLEH ~ITAL ~E#TER
I~PT,OF O~’GTN, UNIV, OF 141CHIGM
Ii~PT, OF OD/GYN ~IGAN AHNY ~ICAL ~
~PT OF O~/GYN
~EPT. OF OB/GYH ~ HI)PILIHS HO~ITAL
Dial’.OF OS/GYH, UNIV,, OF CALIF.
I~’PT OF OS/GYH GLENIN~L£ ADVENTIST HOSPITAL
~.PT OF ODv’GYN LSIJ~
EPT.OF 09/GYN, UNIV.TEXAS I~.SCH~ HOt~N
220
63O M, 168TH, ST, H.Y, 10032
UINVo OF IOl~ IOHA CITY, IOHA 52L~2
3900 RESERUOIR R~ #,#, ii~IHGTON,D,C, 200#7
0~t~, CALIF 92668
UNIV£R~ITY STATION
4301 W, HARKH~ STtEET LITTLE RO0(, ARK.
~UITE 611, ON~ ~AVI$, ~L~I, TAHi’A FLA " 2~I09
135 ~,~ ~ 4WE. NEd YORK, N,,Y+ 1009
9102 LAKE S~ POINT TACOMA, HA 98~98
11802 ]]EI.LFERN HOUSTON, IX 770~5
108 HARg~Y, ~00 #, lil]I.FE ST. ~M.TINI~E, 14~ 21205
HI3, 225 l~l~lifliON b’llIEi[T SAN I)IEGg, ~ALIF 92103
GLENI~LE C~4.1~ 912~
P,O, ~X 33932 ~REUEI~RT, LA 711~
NE~B~P
H
A
14
A
#
H
A
A
A
A
A
14
A
A

I I I I I I I !
I ! I I I ! I I I I
339 BRU~D.
340 ~ETO ROHE~,H,~o
3~0
~LTE~ C. ~EN~H.~.
~57 ~I~D H. ~Z,~.9.
358 ~kHIEL ~T,~,~.
359
~0 JO~PH
COIOq.ETE ~ LIST
SOCIETY FOR PERIHATAL ODSTETRICIAHS
IIO~ITAL AFFILIATION
OlH~.OF CALIF. SAH FRANCISCO
~.PT.OF O9/GYH, I~ENIISTL~WIIA HOSPITAL
~EPT OF O8/G~ll BUFFALO CHILDI~N’S HOSPITAL
D£PT. OF OB/GYH° CASE UESTEI~ RESERVE UNIV.
~EPT.OF O8/GYN, D~YLO~ COLLEGE OF HEDICIflE
~PT° OF O91GYN MglGAIIARBY HEDICAL [~HIER
9£PT.OF 09/GYN, UHIU.OF TEXAS HEALTH SCI° CIR,
DEPT,OF OD/GYH, UHIU OF ILLIHOIS ~F.9, CENTER
DEPT.OF ODJGYN. UNIV. OF HIll R-136
DEPT OF 08/GYN ~IP. ~ CA, IRVINE NED CTR
~EPT° OF ~IGYN COLU~DIA PDEBY~RIAH II08PITAL
TIE ~RINATAL ~R
~cPT.OF O~/GYNo
DEPT. OF IB/GYN ALBERT EIHSTEIN COLL. HEDICIHE
I)EPT, OF ~/GYN I~)I#ISTMEflED, CENTER, ~HY
~£PT ,OF OWGYH. ~S~YTERIAN liOSP. OF I~LLA8
9EPT. OF ~/GYN ~IU, OF N. CAROLI~
]~,PT.OF OD/GYH. UNIV. TEXAS HEALTH 5CI.CTR+
221
ADDRESS
UINV.OF CALIF. SAH FRANCISCO S~ FRAI~ISCO, CALZF ~143
PHII.~DELIqlIA, PENH, 19107
2?30 ~IH b"IIIF.ET, N’T. 18 )SFFALO, HY 16214
222 OPTING HILL ROAi) NWIDFOItD, COIN 06405
33?5 SCRANTON RgkD CLEPELAfl9, OHIO 4410~
7507 N~"IF’TON HOI/STUN, TEIAS 77025
177 CEHTER ST.P.O,IOX 2810 JAC~5ON, WYO,, 830~1
303~ COPA DE ORE DRIVE LOS ALANTOS, CALIF ~07"kO
10427 LAKE STIH T,V~O~, HASH°
644)0 It~ST ClkLF~ HOUSTON, TE~ 770~0
840 SOUTH HOO~ CHICAGO ILL t~12
P.O.BOX 01~960 BIA~I, FLA+ 33101
SUITE 611, ~ DAUIS~.UD. TAHPA FLA 33d~
1519 RISING GLEN ROA9 LOS AHGELES, CALIF 90069
101 CITY DRIVE SOUTH OI~NGE, CA
622 14, I~A~TH STREET HEU YOlk, I~’ lO0~
~ ~ F STREEIS ~AI~BITO, CALIF 9"~819
33OO IIEDRY ~ ~ILAOFJ.IqiIA, PENN. 191~
¯ 2875 DRIARCLIFF ANN ~N]R, HICH. ~10~
~ U5ONIA ~ P~A,~NTVILL~, NoY, lO~.~O
3O WATERSI~ PLAZA
8200 ilALHUT HILL LAH£ D~LLAS, TEXAS 75231
21~ IkSD4IDER ILDG, 20214 ~ HILL, NC 27514
7703, FLOYD ~ DR~ ~ ~TUNIO, TEXAS 78~$4
H
A
A
A
H
H
H
H
H
A
A
H
A
A
H
H
H
k
H

12-21-8~ CUNPLETE ~ LIST
SOCIETY F61( PERINATAL O~TETRICIANS
HOSPITAL AFFILIATION Am~ HEHDEllSHIP
HAIERHAL-FETAL HE.DICIE ST, DAR14AD~HEDICAL CENTER
33 HIHDSOH ROAD SIH~IT, N,J. OP/OI
DE.PT, OF OIIGYN 9ANDERSILT UNI~ITY NASWILIEs, T14’
IE~T, OF ~/I;YN UNIV. ROCIEST£R/GTRONG NSI.
DEPT OF OD/GY14, ROCHESTER GENERAL HOSPITAL
1~5 I~ORTI..q~ A~. ROCIESTER, 14.Y~ 14t~.l
365 PAVID CORYIX)N SHAF,.R,H°D. I~PT.OF OD/GYNo 800 HADISOH AgE. A UNIV.OF TEHN.CTR,FOR IEALTH St:: H£HPHtS, TF,.HN. ~gIL~
l 3~ GEOFFREY 8HER,II.L H~PT.OF O~/GYN. ~ST SIXTH S~. ,~0~ A3 14 UNIV. OF EWd~F-REHO
I i ~9 TARI6 ~ SIBDIOI,14.D.
I£PT,OF OD/GYN. i{9ICAL COLLEGE OF GEOH;IA Ai.GUSTA GA. ~12
R.PT.OF HUGYH. ~O01~ISON g. UNIV, OF IIWNEI;IIE If.i~IS, THIN.
D£PT.OF 09/GYH. 2~I ETH£S~ A~o,Fd4.45~O CINCINNATI, OHIO
H
A
I I
370 G.fiILLARBSIIII40~,dR.,H.D,
371 JPa~ES S. St~LTZEV~ 14,D.
372 ALEXA~DERR° S~YIIE,II,14.D,
~TERNAL--FETAL 9ARTHOUTH-HITCHCOCK ig~i.CTR, HANO~R, N.H. 03755
~.PT, OF ~/;YN 4;8 PRENTICE,333 E SI~II~ ST IIORTH{SIERN UNIg~RSlTY OllLq;O, ILL
IEPT.OF O]L/GYN, U~ Si]OOL [F if[DICIHi[
332I 14B)ICAL PARK RO~, COLimlA S.C.. 29203
14
A
A
! I
373
374 kOB£RT
375 WILLI~N, ~PF.LLACY,H°D.
D£P’T.OF OD/GYN, NORTHIRSTERNUNIV, ~, 438
~.PT.OF ~/GYN. HUTZELHOSPITAL
gEPT,OF UNIV. OF ILL. HED. CIR.
~ E. SUPB(IOIt STIE£T CHICAGO, ILL. ~0~I1
4.707 ST. ANTOIIE1411t.i~D,48201 ILTROIT,
8~0 SOU114 WgOb ~ C14ICAG~ ILL. (~12
14
14
I I
376 ROGER ~I.LEN ~NCER,H,D.
377 dO~
378 CHARLES R. STAFFORD, 14.9.
DEPT OF 08/GYH UNIV. OF TENIESS[E
DEPT OF OBIG~II ~DIC~L COL-__L[~ OF GEORGIA
1317 PARKS HOHOUU HI 9~15’19
i~PHIS, TE~ ~163
AUGUSTA GA 30912
A
A
A
I I I I
379 KUWISJ. STAISI~,H°9o
~80 LAWRENCE ERIC STBfT.b 14,D.
3GI LUCILLE E, STINE, 14,D.
382 HOWARD T. STl~Semi~-R,fl°D.
~8~ STaY d. S~S,H.L
~PT.OF 08/G~ll. UL’LA ~ OF BEgCINE
h’T’T.~F 09/GYN TIE OHIO STATE UNIV.
D£PT, OF Og/gYH ilE]~ICAL COLLE{ OF ~I0
H[P1.0F OB/GYN, RUSH-PRESBYTERIAR-’ST, LUEE HOSP
DEPToOF Og/G~. UNIV.CINCIN~TI HEB, CIR,
BEPT. OF OB/GYN BELLE£qJE HO~IT~I.
I08~ LECOHTE AVE. LOS A14GilES, I~LIF fl)024
5~ FIRS"T A~IP~I ~g YORK N.Y. IH16
222

I I I I I I I I I I I I I I I I I I !
12-21-8~ COttPLETE HEBgER LIST
,SU~YIt~P~TAT£ I~E]IC~.~HIER 725 IRVING (~A~Eo, ~ITE 115
NY I~I0
D~PT,OF OBIGYN. GARFIELD HOSPITAL
~ N, GARFIILB AV{o~JIT£ HONTEREYPARK~ ~
~PT ~ OBIGYN ~ 4611~ A~B~E, A~’I. I~ COLlh~B~IA-PI~E~YT~RI~ HOSPIT~ ~YSIE, N.Y. 11~I
388 KHALIL H,A.TABASH,H.D. 91[PT.OF OD/GYH UCLA 81~OOL OF #EgICIN£
1006 NORTH KENTER AVE, LOS ~LF.~, CALIF 9004,9
~ XATSUHIKO TA~AHA~HI~H.D, I~T,OF ODIGYN, 29TH AMB B.I.IS A{, HICHAEL R££~ HOSP, CI~C~GO, ILL, 6~616
390 RALPH K. TA~URA~N,B. ~F.PT,OF O~/GYN, L!3 E, ~I~RIOR STIEtT NORTHWESTERN U. BEB,CTR,I~,438 I~ICAGO, ILL. 60611
391 NERG~HA. DEPT. OF OB/GYH 2201 HE~EAD TUR~KE HA5’GALI COiNTY HELICAL CEHTER EAST HEABOU~ HY 11554
392 FRAHZ 9F, PT OF OD/GYH WILLIAIt EAOHONT AHY Hi~ CTR EL Pt~O, ltXA~ 79920
39~ JE~l~ L. THOflASOfl~.Oo H~PT.OF O~/GYN, 840 S, WOOP 5’TR£ET UNIV.OF ILL. liD, CTR. CHICAGO, ILL,. 60612
9F.PToOF O9/GYH, 104) DERGEH STREET COLLEGE OF HED/gEH OF H, J. H£’~RK~ H,J. 07103
3?5 YVONNE S, THORNTON~i~,D, bEPT.OF O8/GYH. 525 E. 68TH STI~ NEll YORK HO~P-CgRNELL HED. CTR NEW YORK H.Y. 10021
396 G~RY R, B~PT.~ ~IGYH HIV.UT~ HEDI~L {~KIH
50 H. I~ICAL DR, Rfl, SDZ02 giLT LAKE CITY, UTAH 841Z2
DEPT OF OS/GYH 840 S* WO0~ CILICAGO I~ 60612
398 PAUL G. TOfllCHd%9. ~EPT.OF OB/GYN, 2160 8. FIRST AVE. LOYOLA LNIV. IIAY’WO~ ILL. 6~1~
3.o9 JAHES @. TORIIEY~JR.~H,D. 9EPT.OF O~/GYH. 2000 NORTH VILLAGE AVE. ilEi~Y ilO~.RYkit PY_]hARTS iLOG. ROCKVILLE CTR.~ N.Y. 11~0
~ PAHELA J. TROPPER~.D. [£PT.OF I~GYN, {Bt.~BIA-PRES~YTERIAN
6~g, 16STH ~ NEW YORK, N.Y,
~01 KENT UEI.,AN~, N,B, 9F.PT.O~ OB/GYH. A328 STANFOR9 UNIU, I~, CTR. STANFOi~, C~£1F
402 ~UILL[R~O ~-~’T ~F 08/STN LOHA LIN~A UNIV. ~ OF Hi~ LO#~ CALIF 92~H
~03 HI~AB. g~LIl~ VA~MEI~,N,D. ]~7.PT .OF OD/GYN. UNIV,OF IOWA HO~ITAL lOgA CITY, IOgA
CLAUDE L. V£1LL~, H.D. ~.PT. ~F 08/GYH OREGON IEALTH ~CIF, H~S UNI.
3181 SW PORTLAND, OREG 9720t
405 UflA L. U~HA, H.D. ~.PT. OF ~/I;YN NkSSAU COUNTY Hi~ICkL GNTER
4~6 ~OREN JOHN VIN~ILI~ ~.~. ~"PT. OF OB/GYH L~IV. OF TEXAS, HOUSTON
H~OIJ~3! F~gNIH, ~JI~770]0 TOH,
~07 PAUL T. ~.PTo OF{~B/GYN ~Y STAlt H~I~ICALCB{IB
759 CHESTNUT STREET ~RIJ~I:IB.i), ~, 01107
608 GAEL P. WAGE~, ~ ~RI~T~ CENTER ~I~)TT-.NORTHWE~II~RN HOBPIT~
2/2701ICAGOAV£, HINNEAPOLIS HINN 55401
223
HEHB{R~IP

~ HEIIDER LIST
SOCIETY FOR PERINATAL OBSTETRICIANS
NOo HAHE IlgSPITAL AFFILIATION
I I I i I I
40~ ROI;ER
410 STEVT.H L,
411 ~IE L. ~T~
412
413
415 ~ B. ~I~H.~.
fl Mil INIlJ6TON, TEX~ 78214
DEPT OF I~/GYH I~IV. OF TEHESSE
9[P! OF O~/GYN IIi{LT.O~ IEALIH ~CI UNI9
~80! W. Ge, NTEN~IN PORTLANI), gRI[ 97227
~EPT,OF OB/GYN 33~ E. 9I~ERIOR ST. NORTHWESTERN U.Rtl.438 PRENTICE I~IICAGO, ILL,
~EPT, OF OB/GYN, I~NSYL~IlA HOSPITAL
SPRUCE STR~:T PHILASB.PHIA~ PEIIH 19107
~(PT.OF OB/GYII. 2150 PEIIN$YLVANIA AVE’N°W’72003 GEO.WASHINGTON UNIV.IIEB.CEIITER IIASHINGTON~D.C.
~EPT.OF OIVGYN. IIASfd~ COUTY i[~, CTR.
2201 IIEIIPETE~ TUIUlPIKE. FAST HEADI]M, N.Y* 11~54
417 ~ELI~ IL BELI,H.B, KPT. OF O8/GYN P.O. ~0~ 19~70-41 EASTERN TENN STATE UNIV. ,JOHNSON CITY, TEHN
I I
421 PREST~WILLIAiB,H.B.
~22 DONALD C, WILLIS,
42~ 51EPHEN JAY WILSON,H,D.
~.OF OD/GYH. HAYO IIBIORIE ILE. ~OX 395
~EPT. OF OB/GYH UNIV. OF FLORIgA COIL OF IEB.
9EPT.OF OiVGYH OIEENS II~J;PITAL CBfTER
420 ]IiAWARE ST, ltlNNF.N~LIS, HIIlN. 55455
Ik~ILLE, FLA 3~10
2O CAmERmJRY ROAO GREAT NECK, N,Y. 11021
I I
424 FRAi~ R. HITTER,
425 ROH[RT H. i~LF~OIh
~EPT, OF OB/GYH ~IOHNS HOPKINS UiilV. lIED, CTR,
~EPT, OF 08/GYN CLEVELAN9 IETRO. GEN, HOSPITAL
DEPT.OF O~/GYN, UNIV, OF CIHCINHATI HE~.CTR.
110 IIEST 39TIt 9T, APT, M.TIHORE, ~ 21210
3395 Sa~TON RO~ CLE~’LAI~, OHIO’ 44109
231 ~E~ CINCINNkTI, OHIO ~5,?,67
I I
427 ~UCE A. WORK,JR.,lt,D.
428 PELVIS IIORTHIHGTON, ll.D.
42’/ JAHET ilYG~L,
D£PT.OF UNIV. ILLINOIS COLLEGE OF BED,
EPT. OF OD/GYll
9L’PT. OF 08/GYN UNIV. OF LOUISPlLLE i~P CTR
84O SOgTH ~ICAGO~ ILL. L~tl2
8700 il£ST WISCONS~ AUi[iOJE BTLHAUKEE WISC 5Z226
550 S, ,IACKSI]N STREET LOUISPILL£
I I
JOHW D, YE~SI~ H,D.
SEPT OF TEXAS TECiiU, 14ENL.TH SCIEN(~
OF.PT.OF O~/GYN, COLUII~IA-PRES~YTEILI~ HEg,CTR.
224
k
A
A
A
it
H
H
A
A
A
H
A
A
A
A
H
A
H
A
A

I 435
CImPLETE HEII~ER LIST
SOCIETY FOR PERIHATAL OBSTETRICIANS
HO~’ITAL AFFILIATION
H~I’.OF OB/GYH. LAC/UGC H£D CTR, UO#£H’S HOSP,
O£PT, OF OB/GYH LAC/U~ HEglCAL CBITER
]~l’.6F OD/GYH. O!tlO STATE UNIVERSITY HO~ITAL
1244) H. HIS~IOH ROAg. LOS ANGI~,.E8 CALZF 900~
FIRST AVENUE & 27TH STREET ~ YOIIK, H.Y. lO01t~
28 ARBO~ LANE ROi~.YH HEIGHTS N.Y. 11577
840 8011TII tlOIB CIIICAGO ILL 1~12
410 H, IOTH AVE, , ~I.II~I~S, 6HIO 4~I0
k
A
H
i
225

I I I I I I I I I I I
CRITIQUE SHEET
MEETING:
Length: Longer
Oral Presentations: More
Poster Presentations: More
Time for Presentations/Posters:
Plenary Session: yes
Formal Discussant: yes
Session on MF Boards: Good
More Spouse Activity: Yes
Shorter Same
Less Same
Less Same
Longer Shorter Same
No WGASA
no WGASA
Bad WGASA
No WGASA
HOTEL:
Rooms Food Beverage Rates Service AV
Excellent Good Average
Comments:
Poor
I I I I I I I
OTHER:
Cocktail Parties Banquet Entertainment Syl I abus Brochure
Excellent Good Average Poor
Comments:
Name(optional ):
Category (Member, Assoc. Member, Fellow, Guest, Resident): - Check all that apply-
I 226

FUTURE MEETINGS
1985 - Las Vegas, Nevada Hilton Hotel
1986 - San Antonio, Texas Hilton Placio Del Rio
1987 - Orlando, Florida
1988 - To be Selected
227

I I I I I I I I
I ! I