Human Papillomavirus Vaccine Policy and Delivery in Latin America and the Caribbean
8
Vaccine 26S (2008) L80–L87 Contents lists available at ScienceDirect Vaccine journal homepage: www.elsevier.com/locate/vaccine ICO Monograph Series on HPV and Cervical Cancer: Latin America and the Caribbean Regional Report Human Papillomavirus Vaccine Policy and Delivery in Latin America and the Caribbean Jon Kim Andrus a,∗ , Merle J. Lewis a , Sue J. Goldie b , Patricia J. García c , Jennifer L. Winkler d , Cuauhtémoc Ruiz-Matus a , Ciro A. de Quadros e a Immunization Unit, Pan American Health Organization, Washington DC, USA b Program in Health Decision Science, Department of Health Policy and Management, Harvard School of Public Health, Boston, MA, USA c Universidad Peruana Cayetano Heredia, Peruvian National Institute of Health, Lima, Peru d PATH, Seattle WA, USA e International Health Programs, Albert B. Sabin Vaccine Institute, Washington DC, USA article info Keywords: Latin America Caribbean Policy HPV Vaccines Cervical cancer abstract Cervical cancer caused by human papillomavirus (HPV) is a major preventable public health problem. Two vaccines are now available for primary prevention of HPV infection and their introduction offers new opportunities to enhance comprehensive cervical cancer prevention and control. Currently, HPV vaccine price is a significant barrier to rapid vaccine introduction and access. Therefore, making evidence- based decisions about whether and how to introduce HPV vaccine into the immunization schedule in the countries of Latin America and the Caribbean (LAC) requires a rigorous analysis of several factors. These include: estimates of disease burden, cost-effectiveness, operational feasibility of reaching a population of adolescent females and other key analyses that have been used in recent years to support the introduction of other vaccines, such as rotavirus and pneumococcal conjugate vaccines. Given the large number of public health priorities that are competing for limited public resources, developing and using a sound evidence base is of particular importance for vaccines, like HPV, which are currently available only at prices higher than other vaccines now in use. HPV vaccination provides the opportunity to dramatically improve women’s health and partnerships must also be broad-based and effectively coordinated. This can be achieved by developing programs based on the lessons learned from vaccination strategies used to eliminate rubella and neonatal tetanus and for scaling up influenza vaccination in countries of LAC. © 2008 Published by Elsevier Ltd. 1. Introduction With the availability of new vaccines to prevent premature deaths caused by cervical cancer, several issues arise that neces- sitate an accelerated human papillomavirus (HPV) vaccine policy in Latin America and the Caribbean (LAC). These issues include, but are not limited to the following: (1) extent of disease burden; (2) the framework for policy development; (3) extensive experience with immunization in LAC; (4) development of effective vaccination strategies; (5) access to vaccines; and (6) procurement and finance mechanisms. Here we describe the early experiences of the Pan American Health Organization (PAHO) in strengthening national capacity to make evidence-based, informed decisions in the con- text of the introduction of new and under-utilized vaccines, and summarize a strategy to address future challenges for sustaining ∗ Corresponding author. Tel.: +1202 974 3510; fax: +1202 974 3635. E-mail address: [email protected] (J.K. Andrus). programs, when vaccines being introduced are orders of magnitude more expensive than traditional vaccines. 2. Background The World Health Organization (WHO) and the International Agency for Research in Cancer (IARC) estimate that cervical cancer is responsible for approximately one percent of all causes of female mortality worldwide, killing more than 273,000 women per year [1,2]. Greater than 80% of those deaths occur in women living in developing countries, highlighting the fact that cervical cancer is a disease of poverty [3]. Cervical cancer results in premature loss of approximately 3.02 million potential years of life every year and accounts for 3.28 million disability adjusted life years (DALYs) [4,5]. Based on 2002 estimates, nearly 33,000 preventable cervical cancer deaths occur in LAC. Based on projected estimates in the year 2030, this figure will rise close to 70,000 deaths [2]. Marked dispari- ties exist between the sub-regions of the Americas as age-adjusted mortality rates of 16.0, 15.0 and 12.9 cervical cancer deaths per 0264-410X/$ – see front matter © 2008 Published by Elsevier Ltd. doi:10.1016/j.vaccine.2008.05.040
Transcript of Human Papillomavirus Vaccine Policy and Delivery in Latin America and the Caribbean

Vaccine 26S (2008) L80–L87
Contents lists available at ScienceDirect
Vaccine
journa l homepage: www.e lsev ier .com/ locate /vacc ine
ICO Monograph Series on HPV and Cervical Cancer: Latin America and the Caribbean Regional Report
Human Papillomavirus Vaccine Policy and Delivery in Latin America andthe Caribbean
Jon Kim Andrusa,∗, Merle J. Lewisa, Sue J. Goldieb, Patricia J. Garcíac, Jennifer L. Winklerd,Cuauhtémoc Ruiz-Matusa, Ciro A. de Quadrose
a Immunization Unit, Pan American Health Organization, Washington DC, USAb Program in Health Decision Science, Department of Health Policy and Management, Harvard School of Public Health, Boston, MA, USAc Universidad Peruana Cayetano Heredia, Peruvian National Institute of Health, Lima, Peru
d PATH, Seattle WA, USAe International Health Programs, Albert B. Sabin Vaccine Institute, Washington DC, USAhumailablance
nt barethera andse bu
her krota
at arularaccinand p
a r t i c l e i n f o
Keywords:Latin AmericaCaribbeanPolicyHPVVaccinesCervical cancer
a b s t r a c t
Cervical cancer caused byTwo vaccines are now avnew opportunities to enhvaccine price is a significabased decisions about whcountries of Latin Americinclude: estimates of diseaadolescent females and otof other vaccines, such aspublic health priorities thevidence base is of particprices higher than other vimprove women’s health
can be achieved by developingto eliminate rubella and neona1. Introduction
With the availability of new vaccines to prevent prematuredeaths caused by cervical cancer, several issues arise that neces-sitate an accelerated human papillomavirus (HPV) vaccine policyin Latin America and the Caribbean (LAC). These issues include, butare not limited to the following: (1) extent of disease burden; (2)the framework for policy development; (3) extensive experiencewith immunization in LAC; (4) development of effective vaccinationstrategies; (5) access to vaccines; and (6) procurement and financemechanisms. Here we describe the early experiences of the PanAmerican Health Organization (PAHO) in strengthening nationalcapacity to make evidence-based, informed decisions in the con-text of the introduction of new and under-utilized vaccines, andsummarize a strategy to address future challenges for sustaining
∗ Corresponding author. Tel.: +1202 974 3510; fax: +1202 974 3635.E-mail address: [email protected] (J.K. Andrus).
0264-410X/$ – see front matter © 2008 Published by Elsevier Ltd.doi:10.1016/j.vaccine.2008.05.040
an papillomavirus (HPV) is a major preventable public health problem.e for primary prevention of HPV infection and their introduction offerscomprehensive cervical cancer prevention and control. Currently, HPV
rier to rapid vaccine introduction and access. Therefore, making evidence-and how to introduce HPV vaccine into the immunization schedule in thethe Caribbean (LAC) requires a rigorous analysis of several factors. Theserden, cost-effectiveness, operational feasibility of reaching a population of
ey analyses that have been used in recent years to support the introductionvirus and pneumococcal conjugate vaccines. Given the large number ofe competing for limited public resources, developing and using a soundimportance for vaccines, like HPV, which are currently available only ates now in use. HPV vaccination provides the opportunity to dramaticallyartnerships must also be broad-based and effectively coordinated. Thisprograms based on the lessons learned from vaccination strategies used
tal tetanus and for scaling up influenza vaccination in countries of LAC.© 2008 Published by Elsevier Ltd.
programs, when vaccines being introduced are orders of magnitudemore expensive than traditional vaccines.
2. Background
The World Health Organization (WHO) and the InternationalAgency for Research in Cancer (IARC) estimate that cervical canceris responsible for approximately one percent of all causes of femalemortality worldwide, killing more than 273,000 women per year[1,2]. Greater than 80% of those deaths occur in women living indeveloping countries, highlighting the fact that cervical cancer isa disease of poverty [3]. Cervical cancer results in premature lossof approximately 3.02 million potential years of life every year andaccounts for 3.28 million disability adjusted life years (DALYs) [4,5].
Based on 2002 estimates, nearly 33,000 preventable cervicalcancer deaths occur in LAC. Based on projected estimates in the year2030, this figure will rise close to 70,000 deaths [2]. Marked dispari-ties exist between the sub-regions of the Americas as age-adjustedmortality rates of 16.0, 15.0 and 12.9 cervical cancer deaths per

ccine
J.K. Andrus et al. / Va100,000 population have been estimated for the Caribbean, CentralAmerica and South America, respectively. These rates are also sub-stantially higher than 2.3 cervical cancer deaths per 100,000 popu-lation in North America [2]. Although cervical cancer contributes asmaller proportion to overall female morbidity and mortality whencompared with ischemic heart disease, diabetes mellitus and evenbreast cancer, its public health importance hinges on the fact thatthis disease is eminently preventable and is a significant cause ofpremature deaths of women living in resource poor countries.
In resource wealthy countries where cervical cancer screen-ing strategies using the Papanicolaou cytology technique (Pap test)are accessible and of high-quality with guaranteed treatment andfollow-up services, reduction in cervical cancer mortality has beensubstantial. Prior to 1950, when screening was not performed in theUnited States of America (USA), invasive cervical cancer incidenceranged from 35 to 40 new cases per 100,000 women, annually. Withthe implementation of screening and aggressive follow-up, by 1990invasive cervical cancer incidence had dropped to approximately 10cases per 100,000 women annually, representing an approximate75% reduction and certainly one of the greatest success stories incancer prevention [6].
In LAC, cervical cancer screening systems are challenged with
large client loads that need to be managed adeptly to ensure thatreturn visits and re-testing occur every 2–3 years [7]. Quality ofservices, access, socio-cultural and gender issues further compli-cate the challenge of improving secondary prevention strategiesthrough Pap smear screening [8]. In some communities womenmay actually be afraid of the gynecological examination, or theymay think that a positive result is a death sentence warranting noneed for follow-up. In other cases women may have the Pap test butare not told of the results or the woman considers the procedureitself to be curative. No one explains the importance of returningfor follow-up and treatment depending upon the results. Screen-ing programs that have been proven to be remarkably successful inindustrialized countries have failed to reduce substantially cervicalcancer incidence in most developing countries.2.1. Current realities
Against this backdrop of the challenges of secondary prevention,the availability of two vaccines to prevent cervical cancer providesunique opportunities to accelerate prevention and control of cervi-cal cancer. Prophylactic HPV vaccines containing oncogenic types
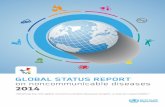
Fig. 1. Rubella vaccination coverage in selected countries oCountry reports to PAHO.
26S (2008) L80–L87 L81
HPV-16 and 18 can prevent up to 65–70% of the premature cervicalcancer deaths. However, to date they are generally only availablein industrialized countries and have yet to become accessible topoorer countries where the greatest burden of disease exists. Cur-rently, the price per dose of less than US$121 is prohibitive for usein most countries of LAC, and even more so when the schedulerequires three doses.
This situation is extremely disappointing because the expe-rience of resource poor countries of LAC has demonstrated thatvaccination programs have been very effective. Technical coop-eration among countries, coupled with efforts to ensure safe,affordable supplies of vaccines have contributed to the success ofseveral accelerated disease control initiatives, including the rubellaelimination initiative [9]. In September 2003, the PAHO DirectingCouncil comprised of Ministers of Health of all the countries in theAmericas resolved to eliminate rubella and congenital rubella syn-drome by 2010 [10]. Such resolutions require and reflect the highpolitical commitment towards immunization.
The strategies to eliminate rubella and congenital rubella syn-drome consist of: (1) achieving high vaccination coverage withmeasles-mumps-rubella (MMR) containing vaccine in the child-hood immunization schedule; (2) rapidly reducing the pool ofpeople susceptible to rubella infection by conducting mass rubella
vaccination campaigns generally targeting all persons younger than40 years in the country with MMR vaccine; and (3) conductinghigh-quality surveillance to monitor the impact. In most coun-tries the mass vaccination campaigns were conducted over 6 to8 weeks, resulting in approximately 45% of the nation’s populationbeing vaccinated. The results of these mass vaccination campaignsdemonstrate that very high levels of coverage can be reached incountries with large target populations (Fig. 1).In 1998, countries of LAC reported 135,947 confirmed rubellacases. As a result of implementation of the strategies outlinedabove, by 2007 the number of reported rubella cases declined to342, representing over 98% reduction in rubella cases (Fig. 2). Bythe end of 2007, of the 872 suspect congenital rubella syndrome(CRS) cases reported, only six were confirmed as CRS [11]. Those sixcases were reported from Brazil where the mass rubella vaccinationcampaign did not include men, which increased the likelihood forsustained virus transmission, particularly among men who had notbeen vaccinated. PAHO estimates that more than 20,000 CRS caseswere reported annually prior to rubella vaccine introduction [12].This experience demonstrates that countries of LAC can reach and
f the Americas, 1997-2006.

L82 J.K. Andrus et al. / Vaccine 26S (2008) L80–L87
ategie
Fig. 2. Impact of rubella and measles elimination strCountry reports to PAHO.vaccinate adolescents, resulting in rather significant public healthgains in lives saved, and in quality of life.
For nearly 30 years PAHO’s Revolving Fund (RF) has helped toensure a reliable supply of safe and affordable vaccines. The RFacts on behalf of Member Countries to negotiate and purchase vac-cines through a bulk purchasing mechanism. This bulk purchasingmechanism results in more affordable vaccine prices for countries,compared to what countries could individually negotiate on theirown. Countries repay the RF for their purchase. With the intro-duction of new vaccines the RF is positioned to forge partnershipsgeared for negotiating more affordable vaccine prices and upscal-ing vaccine access more rapidly [13]. Prior to the formation of thefund, countries had faced frequent encounters with vaccines beingout of stock and vaccine supply failures.
The countries of LAC have accumulated substantial experiencein vaccinating adolescents in schools, largely through measles andrubella elimination initiatives. Most of these countries have someform of cervical cancer prevention and control programs, whichalso include screening. The introduction of HPV vaccines, withthe support of the RF, will provide an additional opportunity to
strengthen these programs and add impetus for the developmentof comprehensive programs that include both screening and vacci-nation. To that end, reducing inequities in the provision of strategiesto prevent cervical cancer, such as introducing HPV vaccines, whilestrengthening secondary screening programs, is a high priority forcountries [14].Financial resources to support these new initiatives, particu-larly at the onset, were derived from both internal and externalsources. Presently, only six countries in LAC - Bolivia, Cuba, Guyana,Haiti, Honduras and Nicaragua - qualify for support from theGAVI Alliance to introduce more expensive new products, such asrotavirus and pneumococcal vaccines. Most countries of LAC mustfind other means to secure funding for vaccination, delivery and theimprovement of secondary screening strategies.
Accordingly, the decision to introduce HPV vaccine will requirea more expanded and rigorous analysis of the national situation.This becomes even more apparent in the next section when wediscuss competing priorities. The relative value of HPV vaccineswill depend on the epidemiologic and economic burden of disease,vaccine cost-effectiveness and affordability, the current costs andeffectiveness of other preventive interventions and the available
s, the Americas, 1980–2007.
resources for introducing the vaccines into national immunizationprograms that will ensure sustainability of operations and systems,as well as financing. Because the burden of disease and resourcesavailable vary between countries and sub-regions, the decision tointroduce these vaccines must be based in a wider body of evi-dence that reflects national conditions. If national policymakersmake decisions for new vaccine introduction irrespective of the evi-dence available, that could undermine the long-term sustainabilityof programs.
3. Competing public health priorities for vaccines andimmunization
Each year, rotavirus is estimated to cause approximately 111 mil-lion episodes of gastroenteritis requiring only home care, 25 millionclinic visits, 2 million hospitalizations and approximately 440,000deaths in children younger 5 years of age worldwide. Children in thepoorest countries account for 82% of rotavirus deaths. An estimated16,000 deaths by rotavirus caused diarrhea occur annually in LAC[15]. Community-based longitudinal studies in Brazil demonstrated
an incidence rate of 2.5 episodes of diarrhea per child aged <5 yearsannually [16]. Although rotaviruses were responsible for 10% ofdiarrhea cases, the average annual number of rotavirus diarrheaper child aged less than 5 years was 0.25.In 2002, PAHO estimated that pneumococcal invasive diseasekilled 20,200 children every year in countries of LAC [17]. Inci-dence of invasive pneumococcal bacteremia has been documentedas high as 212.2 per 100,000 children less than 2 years of age annu-ally in Argentina [18]. These two childhood diseases (rotavirus andpneumococcal), for which vaccines are currently available, causesubstantial childhood morbidity and mortality in LAC. The use ofnew vaccines for these priority diseases presents opportunitiesto make substantial gains in health, thus bringing many coun-tries closer to achieving global disease mortality reduction targets.Because these vaccines are orders of magnitude more expensivethan the traditional vaccines used in childhood immunization, theevolving landscape may be appear to one of competition betweenthe use of one vaccine versus another. Health professionals - includ-ing epidemiologists, public health experts, and other scientists -may be champions of causes that contribute to these life-saving vac-cines. However, the causes they champion may end up competing

ccine
J.K. Andrus et al. / Vaagainst one another. This landscape cries for infrastructure sup-port so that decisions are made rationally, relying on a process thatsystematically and objectively evaluates all the available evidence.
In the past, it was less difficult for policymakers to introducecheaper vaccines addressing important public health prioritiessuch as measles, when the vaccines were deemed clinically effi-cacious. In addition, the decision making process for prioritizingpublic health interventions has been historically driven by regionalpriorities in immunization. Examples include elimination initia-tives such as polio, measles and rubella elimination, and theexpansion of routine childhood vaccinations to add Haemophilusinfluenza type b and hepatitis B vaccines into national immu-nization schedules in the Americas. Disease burden and clinicaltrial data were generally sufficient to convince countries to takecoordinated action for accelerated disease control and vaccineintroduction [19]. The financial and logistical burden of newer vac-cines on already constrained programs will require future decisionsto be established in more rigorous methodology.
Two recent country experiences in 2006 highlight our concernthat decisions are being made irrespective of the evidence available.One country introduced varicella-zoster virus vaccine, despite dis-ease burden data and preliminary economic analyses to suggestthat pneumococcal and rotavirus infections may be of far greaterpublic health significance. Another much poorer country decided tointroduce rotavirus vaccine without addressing the systems capac-ity for including such a vaccine. To date, countries have been ableto finance vaccines from national budgets making previous vaccineintroductions sustainable.
4. Guiding principles for policy development
The examples of rotavirus, pneumococcal and HPV vaccines setthe stage for a more rational approach for their introduction. Theprocess of deciding when and what vaccine(s) to introduce is nowmore essential than ever, because each of these vaccines are beingoffered at significantly higher prices (rotavirus vaccine less thanUS$8 per dose, pneumococcal vaccine less than US$36 per dose andHPV vaccine less than US$121 per dose). Efforts should avoid settingone vaccine against another. Systems and financial sustainabilityconsiderations must be in the forefront of this process.
The comparison of annual estimates of disease mortality inLAC of three important diseases - HPV (33,000 deaths per year),rotavirus (nearly 16,000 deaths per year) and pneumococcus
(20,200 deaths per year) - illustrates through another lens the com-plexity of choices facing countries, again making the case for agreater body of evidence to be provided policymakers [2,15,17].At first glance, it would seem to make sense that preventing childdeaths leading to more life years saved, as compared to preventingadult deaths, argues for prioritizing the childhood vaccines. But pre-venting cervical cancer can save the lives of relatively young womenwho have critical roles in caring for their children and dependents,maintaining the stability of the household and the stability of largercommunity. It does not make sense to evaluate these issues in iso-lation of each other. Simply put, it is illogical to put all efforts intosaving the life of a child, but not preventing the mother from dyingof cervical cancer.To ensure that future decisions for new vaccine introductionsachieve the greatest sustainable impact and that various life-savingvaccines are not pitted against each other, PAHO has been workingwith countries of LAC to address four essential guiding principles:
• Decisions should be nationally basedAs described above, the paradigm must be changed to transition
from primarily regional decisions to national-based decisions.
26S (2008) L80–L87 L83
These decisions must be supported by national or sub-regionalevidence. While the end-products will be distinctly nationalapproaches for new vaccines, in countries requesting assistanceregional technical cooperation will continue to play a critical rolein supporting the generation of essential evidence and developingsustainable immunization policies.
• Evidence used to support decisions must be broad-basedRegional immunization policy decisions have historically relied
primarily on the burden of disease and vaccine efficacy; how-ever, the higher cost of new vaccines will require a much broaderevidence base ranging from cost-effectiveness and financial sus-tainability to health systems concerns (see next section). Forexample, with specific reference to HPV vaccines, the costs of cur-rent cervical cancer prevention and control programs, the futurecosts for strengthening such programs and the costs related towomen’s lives lost would collectively constitute a critical part ofthe required evidence for informed decision making. Sole con-sideration of the upfront costs associated with an adolescentvaccination program would be insufficient to understand the truecost and the true benefits of a comprehensive national cervicalcancer prevention strategy. Organizational partners can play aninstrumental role in the gathering of new evidence, which willultimately enhance the decision making process. To that end,PATH is currently assisting the Ministry of Health of Peru.
• Infrastructure must be in place to support nationally basedprocess
In the transition to primarily country-based decisions, nationaldecision making bodies must have the necessary technical capac-ity to ensure decisions are reached through rigorous and informeddeliberations, drawing on the expertise of national advisoryboards. In the case of HPV vaccines, the decision making processmust include stakeholders from the areas of cervical cancer con-trol; adolescent, sexual and reproductive health; gender equity;and immunization. To that end, Ministries of Health working withpartners have the opportunity to establish or strengthen theseadvisory boards.
• Immunization programs must prioritize family healthRecognizing child health to be an essential goal, immunization
programs that prioritize family health would be more likely torealize the potential of improving both child and family health as awhole [9]. Operationally, this would mean establishing new deliv-ery alternatives such as more permanent school-based strategiesthat rely on the commitment and involvement of broader spec-trum of actors, including Ministers of Education, adolescent
health services, teachers, and community leaders. Currently, 12countries in LAC have school-based immunization programs tar-geting children ranging from ages 5–13 years. Expanding thisapproach to all countries should help with the eventual introduc-tion of future vaccines, such as human immunodeficiency virus(HIV).5. Framework for vaccine introduction decision making
To these guiding principles, PAHO has developed a frameworkfor country-based decision making. Ideally, when policymakers incountries make decisions they should account for all the criterialisted below [19].
5.1. Technical criteria
5.1.1. Disease burdenAs in the past for the less expensive vaccines such as for polio and
measles, disease burden documented to define an essential pub-lic health priority remains the sine qua non of the evidence-based

ccine
L84 J.K. Andrus et al. / Vadecision making process. This has certainly been amply docu-mented for invasive cervical cancer where age-adjusted mortalityrates in LAC are some of the highest in the world [2]. In addition,after vaccine is introduced HPV-related disease burden will need tobe continually assessed through surveillance. This will mean thatexisting screening approaches will need to be shaped to be able toinform surveillance. This would argue for HPV testing as a primarycervical screening test. Doing so would: (1) provide information onvaccine effectiveness and impact; and (2) allow for longer inter-vals between screening, thus reducing costs which are high andresource wasteful. This cost-savings would be realized immediatelywhen compared to the cost-savings from averting future cervicalcancer, which will require years to realize. Countries will need todecide and plan which strategy will be most useful, given the localsituation.
5.1.2. Characteristics of the vaccineVaccine characteristics to consider are: immunogenicity and
efficacy, duration of immunity and type-specific composition invaccines that have multiple possibilities. This is the case for thetwo types of HPV vaccine available. The antigens in these vaccinesprotect against oncogenic HPV types −16 and 18. Other oncogenicHPV types, perhaps accounting for the remaining 30% cervical can-cer disease burden, are not covered. Unlike the bivalent vaccine(CervarixTM, GlaxoSmithKline Biologicals, Rixensart, Belgium), thecurrently available quadrivalent vaccine (Gardasil®, Merck & Co.,Inc., Whitehouse Station, NJ USA) also provides protection againstgenital warts due to HPV types -6 and 11. Countries will need toassess the relative benefits of each vaccine based on such character-istics. Other characteristics include dosage, route of administration,thermostability and liquid versus lyophilized presentation. Bothvaccines are liquid and intramuscularly administered, requiringthree doses. They differ in scheduling of doses. The quadrivalentvaccine is administered at 0, 2, and 6 months, while the bivalentvaccine is administered at 0, 1, and 6 months. Some flexibility inthe rigidity of the timing of the second and third dose is expectedand is being evaluated. In the case of childhood immunization, newvaccine schedules that match the routine immunization scheduleare much more conducive for effective introduction. In the case ofHPV vaccine, once the country has indicated its vaccine preferenceschool-based programs will need to be shaped to align with therecommendations of one of these HPV vaccines.
5.1.3. Adverse events and post-marketing surveillance
Fortunately, in the case of HPV vaccine most adverse events aremild, limited to local swelling and soreness at the injection site.But, as with all vaccines, the rare, severe adverse events can be life-threatening and need to be rapidly identified and treated. Publicconfidence is at stake. If not well managed, the overall program maybe undermined with obvious future implications on effectiveness ofprogram delivery and acceptance for all cervical cancer preventionstrategies.
5.1.4. Cost-effectiveness and other economic evaluationsCost-effectiveness analysis addresses the question “how much
health improvement can be gained, dollar for dollar, compared toan alternative use of resources?”. The underlying principle behindcost-effectiveness analysis is that resources should be used as effi-ciently as possible in order to maximize the health benefits to thepopulation. While cost-effectiveness analysis provides informationon value for money, it is not equivalent to providing budgetary infor-mation on the affordability and upfront financial costs required ofthe government. It is critical that financial costs and affordabilityare distinguished from issues of cost-effectiveness and value formoney.
26S (2008) L80–L87
Public health interventions that are found to be “cost-effective”generally do not save financial costs in the short-term. They do,however, avert future costs and in this regard, may be cost-saving. When this occurs policy decisions are easy, but most publicinterventions are not cost-saving but can still be extremely cost-effective. One of the best examples of a cost-savings interventionin the Americas is the Caribbean experience with the eliminationof rubella and congenital rubella syndrome. Rubella eliminationrequires the vaccination of young adolescents, which is also thetarget group for HPV vaccination. In the Caribbean, data indicatedthat every US dollar spent on eliminating CRS would result in a 13dollar savings in terms of healthcare costs required for treating andcaring for babies born with this disease, all the countries adoptedthe initiative to eliminate CRS [20].
In recent work by Goldie et al., a cost-effectiveness analysis ofHPV-16/18 vaccination in 33 countries in LAC showed that if thecost per vaccinated women is US$10 (implied price per dose US$1-2), vaccination would be cost-saving relative to the status quo in 26of the 33 countries [21]. If the cost per vaccinated women is US$25(implied price per dose US$5), vaccination would be cost-savingin some countries but extremely cost-effective in all 33 countries,with cost-effectiveness ratios of less than 10% of per-capita grossnational product (GNP).
Other analyses have addressed the cost-effectiveness of com-prehensive cervical cancer prevention and control strategies thatinvolve both vaccination and screening. In Brazil, if HPV costscould be maintained at US$25 per women (includes vaccine pricefor three doses, wastage, delivery, and programmatic costs) andvaccination coverage achieved was 70%, a program focused on vac-cinating pre-adolescents would be cost-saving. In this scenario thevaccine price is approximately US$5 per dose. If this strategy wereto include cervical cancer screening three times per lifespan (start-ing at ages between 30–35, then repeated at 5-year intervals), thelifetime risk reduction of cervical cancer would be 60%, also result-ing in a cost per-year of life saved that is less than 10% per capitaGNP [21]. When considering cost-effectiveness, affordability andsustainability, these analyses showed that vaccination is not fea-sible at higher vaccination costs. In summary, higher costs wouldprevent the populations with the highest disease burden, and inmost need, from receiving the benefits of vaccination.
Generally, experience demonstrates that analyses showing thatcosts will be averted by preventing disease outcomes, in addition tohealth benefits (cost-saving) are much easier to justify, gain accep-tance, and mobilize commitment and necessary resources. These
kinds of data will prove to be enormously useful to the decisionmaking process and should also be useful in vaccine price negotia-tions.5.2. Programmatic and operational criteria for ensuring vaccinedelivery
5.2.1. Vaccine supplyMaintaining long-term vaccine availability may have inherent
difficulties. For pneumococcal vaccine the conjugation processis operationally and technically challenging, and in the past hasimpeded mass production of the vaccine. To date, there has onlybeen one supplier. In the case of HPV vaccine there will be atleast two manufacturers. The HPV vaccine production process issimilar to hepatitis B vaccine. Most experts agree that the HPV vac-cine production situation should not impose major impedimentsto maintaining a regional and global supply.
5.2.2. Logistical and operational issuesVaccine packaged in single dose vials has the potential to rapidly
consume cold chain capacity and impede the programs ability to go

ccine
J.K. Andrus et al. / Vato scale on delivery, thereby limiting access to population groups.The national program needs to map out a vaccine distribution andstorage plan to ensure no disruptions in supply at the local level. Inthe context of school-based programs, there would a clear need tonegotiate the availability of multi-dose vials because the deliverystrategies will most likely be modified mass vaccination campaigns.Such multi-dose vial interventions would also lend to more afford-able prices per dose.
5.2.3. Financing strategiesTo date, more than 26 countries in the Region of the Americas
have vaccine laws that require the nation to purchase introducedvaccines and mandate vaccines for the public good [22]. Such lawsalso help sustain the program. PAHO has been working with coun-tries to develop a model vaccine law that could be used in theirefforts to improve their existing legislation in countries that alreadyhave laws and to provide a template to create new laws in countriesthat currently do not have such legislation. Laws that require a bud-get line in the national budget for vaccine purchase has contributedenormously to the sustainability of existing national immunizationprograms. Other financial strategy issues are covered in more detailin Andrus et al. 2008 [23].
5.2.4. PartnershipsSupport of partners during the initial phases of new vac-
cine introduction has proven important in some countries withpoor or borderline economies. Partners, public and private, canplay a role in LAC by providing seed money and resources thatwill help accelerate HPV vaccine introduction when the decisionanalysis deems appropriate to do so. Such countries can thenassume responsibility for financing gradually over time. Honduras,a country with average annual per capita income of less thanUS$ 1000, was able to introduce the pentavalent vaccine - con-taining diphtheria-pertussis-tetanus-Haemophilus influenza typeB-hepatitis B antigens - as a result from an initial in-kind con-tribution of vaccine from the manufacturer. Within a few yearsthe Honduranian government then assumed costs of future vac-cine purchases. A similar project for rotavirus vaccine introductionis currently underway in Nicaragua. Partners for accelerated con-trol of cervical cancer should strengthen their efforts to forge suchcountry specific alliances for HPV vaccine introduction, such aswhat is currently being done by the Ministry of Health of Peru andPATH.
5.3. Social criteria
5.3.1. Perception of riskDespite a relatively rare occurrence, the perception of risk of
meningococcemia meningitis and sepsis may be substantial insome countries. This disease is capable of rapidly progressing todeath causing great fear among families. A perception of risk thatproduces societal fear could influence policy. From the client’s per-spective, the perception of risk for developing cervical cancer willneed further study. Thus far, the client’s perception of risk may bebased on personal knowledge of a family member, close friend, orneighbor with the disease. However, it is unclear whether currentlevels of perception of risk translate into action by the client forprevention or into additional evidence for policy decisions.
5.3.2. Political willMinisters, Presidents, and First Ladies can be mobilized to pro-
mote immunization, such as happened with the elimination ofneonatal tetanus [24]. In the early 1990’s, a group of First Ladiesof Latin America declared that neonatal tetanus was unacceptableand largely through their advocacy the goal was quickly achieved.
26S (2008) L80–L87 L85
Similar high-level political commitment will be vital for HPVvaccine introduction. To that end, in 2006 all the Ministers of Healthof LAC voted unanimously to urge all countries to create fiscal spacefor introduction of HPV, rotavirus, pneumococcus, and influenzavaccines. In addition, they urged all countries to fully realize theparticipation of PAHO’s RF (Fig. 3). Similarly, in January 2008 theEuropean Union endorsed technical guidance for the introductionof new vaccines in European countries.
Another striking example is the recent rapid scaling up ofinfluenza vaccination. Prior to 2005, only 13 countries had intro-duced seasonal influenza vaccination, a proven strategy to reduceassociated disease morbidity and mortality. PAHO developedtechnical recommendations which ultimately were presented topolitical leaders to accelerate seasonal influenza vaccine introduc-tion. As a result, 28 countries now have introduced this vaccine[25].
5.3.3. EquityMany vaccine preventable diseases disproportionately affect the
poor and immunization provides an opportunity to prevent diseasein underserved populations. This will also true for HPV vaccinebecause 80% of the women dying from invasive cervical cancerreside in developing countries. Therefore, vaccine delivery pro-grams must ensure all women in both the public and private sectorshave access to this technology.
To reach the best overall decision, all the factors describedabove need to be systematically and critically assessed. Feedbackfrom countries over the last three years indicates that they needexpanded support with the economic evaluations of the proposedinterventions. Iglesias et al. found that the use of economic eval-uation studies in the decision making process in health in LatinAmerica was deficient despite the increasing interest in introduc-ing economic evaluations as a formal tool to inform the decisionmaking processes. Their findings suggest that there is little evi-dence on the conduct and use of these evaluations in most countries[26]. In various fora, Ministers of Health of LAC countries haveexpressed that the absence of suitable economic analyses repre-sented a “weak link” in the development of immunization policy[19].
To strengthen national capacity for making evidence-baseddecisions in the context of new vaccine introduction, PAHO in col-laboration with its partners (WHO, Centers for Disease Controland Prevention (CDC), PATH, Pneumococcal vaccines AcceleratedDevelopment and Introduction Plan (Pneumo-ADIP) and the Bill
& Melinda Gates Foundation) organized the “ProVac Initiative” in2004. To date, all countries of LAC have participated in a series ofmeetings and workshops intended to give a “hands-on” experienceutilizing tools developed by PAHO and its partners for conduct-ing cost-effectiveness analyses of the following priority vaccines:pneumococcal, rotavirus, influenza and recently HPV vaccines [27].This work is intended to provide countries with practical, field-based tools for estimating cost-effectiveness that do not requirethe academic rigor for models utilized in research settings, but thatremain sufficiently robust to provide useful information.The work plan over the next five years for PAHO’s ProVacinitiative will aim to accomplish the following objectives: (1)strengthening public health infrastructure and process throughwell-functioning advisory boards of national experts for vaccinepolicy; (2) strategizing the use of sub-regional data to optimize theavailability and efficiency of data use for policy development; (3)using the analytic tools developed for estimating disease burden,program costs, and cost-effectiveness of interventions wheneverappropriate; (4) effectively planning for vaccine introduction whenthe evidence indicates; and (5) promoting partnerships which willbest serve the countries meet their health priorities.

L86 J.K. Andrus et al. / Vaccine 26S (2008) L80–L87
ing Co
Fig. 3. PAHO, 47th DirectAlso, as part of the Regional support for policy development,ProVac will be assisting countries to develop their strategic visionand strategies for vaccine introduction, often referred to as “WhitePapers”. These papers will be living documents that can be modifiedas needed and that will help balance the components of the frame-work for decision making. Although important, economic analysisis only one component of several. The development of these pol-icy papers should help countries determine what components ofthe decision framework critically require local data and analysis, asopposed to when regional or sub-regional data could suffice. Onceagain, the role of national expert oversight and partner support willbe essential.
6. The challenges ahead
As already mentioned, price is the single largest obstacle to HPVvaccine introduction. Even if systems and financial sustainabilityissues in countries are relatively well-grounded, vaccine price willcontinue to be an important impediment to address. Existing dis-ease burden and excellent vaccine efficacy data set the stage toovercome this challenge. Fortunately, in the Americas PAHO’s RF forvaccine purchase on behalf of countries exists and should continueto be highly effective for the introduction of HPV and other new vac-cines, like HIV, when they become available [28]. Because PAHO’s RFis the bulk purchasing mechanism through which PAHO negotiatesmore affordable prices among the manufacturers, the RF played acritical role in how hepatitis B, H. influenza type b, rubella, and morerecently seasonal influenza vaccines, were introduced and rapidlyscaled up in national immunization programs. With support fromthe RF, countries in LAC are poised to accelerate their collectiveefforts to achieve more affordable prices and ensure sustainabilityof introduction through vaccine laws.
Another critical question will be: “how will HPV vaccine get tothose who need it most?”. The rubella elimination and other diseasecontrol initiatives provide invaluable insight for countries of LAC intheir efforts to rapidly accelerate the prevention and control of cer-
uncil, September 2006.
vical cancer. The rubella elimination lessons include: (1) nationaldecisions to embark on an elimination initiative were supportedby the regional mechanisms of PAHO’s RF to ensure an affordablevaccine supply chain; (2) the PAHO Directing Council of Ministersof Health provided a mechanism for sustaining high level politi-cal commitment; and 3) the PAHO Technical Advisory Group forImmunization provided high quality technical oversight to ensuredisease reductions were realized [13]. Rapid scale-up of HPV vac-cination and access will require political commitment, expandedfiscal space for creating new revenue sources for vaccine purchaseand for addressing any remaining operational and systems barriers.This will help avoid situations where one life-saving intervention isset against another. School-based strategies and other complimen-tary outreach programs will be essential for effective introductionof HPV vaccines.
Supported by PAHO’s RF, new partnerships will need to be forgedthat will facilitate delivery and access of interventions to groupsthat are otherwise not traditionally targeted by routine immu-nization programs. However, experience with several accelerateddisease control initiatives such as rubella, neonatal tetanus andinfluenza provide ample evidence that it can be done. Ministers ofEducation, Finance, and Health, professional medical associations,families and community leaders will need to be actively involved,as their perspectives and influence will ultimately help to ensurethat vaccine delivery strengthens health services, including cervicalcancer screening programs.
Disclosed potential conflicts of Interest
CQ: Advisory Board (Merck and Co., Inc).
References
[1] World Health Organization (WHO). The World Health Report 2004 – chang-ing the history, Annex Table 2: Deaths by cause, sex and mortality stratumin WHO regions, estimates for 2002. Geneva: WHO, 2004. Available at:http://www.who.int/whr/2004/en/.(last accessed: April 2008).

ccine
[
[
[
[
[
[
[
[
J.K. Andrus et al. / Va
[2] Ferlay J, Bray F, Pisani P, Parkin DM. Globocan 2002: cancer incidence andmortality worldwide. IARC CancerBase No. 5, version 2.0. Lyon: IARC Press,2004.
[3] Parkin DM, Bray F. Chapter 2: The burden of HPV-related cancers. Vaccine2006;24(Suppl 3):S11–25.
[4] World Health Organization (WHO). Health Statistics and Health InformationSystems - Years of Life Lost by age, sex and cause for the year 2002. RevisedGlobal Burden of Disease 2002 estimates. Geneva: WHO, 2002. Availableat: http://www.who.int/healthinfo/bodgbd2002revised/en/index.html.(lastaccessed: April 2008).
[5] World Health Organization (WHO). Health Statistics and Health Informa-tion Systems - Disability Adjusted Life Years by age, sex and cause forthe year 2002. Revised Global Burden of Disease 2002 estimates. Geneva:
WHO, 2002. Available at: http://www.who.int/healthinfo/bodgbd2002revised/en/index.html.(last accessed: April 2008).[6] Katz IT, Wright AA. Preventing cervical cancer in the developing world. N EnglJ Med 2006;354(11):1110.
[7] Denny L. The prevention of cervical cancer in developing countries BJOG2005;112(9):1204–12.
[8] Lewis MJ. A Situational Analysis of Cervical Cancer in Latin America and theCaribbean. Washington DC: Pan American Health Organization (PAHO); 2004.
[9] Tambini G, Andrus JK, Fitzsimmons JW, Roses Periago M. Regional immuniza-tion programs as a model for strengthening cooperation among nations. PanAm J Public Health 2006;20(1):54–9.
10] Pan American Health Organization (PAHO). Resolution CD44/R1. Sus-taining immunization programs - elimination of rubella and congen-ital rubella syndrome (CRS). Washington DC: PAHO, 2003. Availableat: http://www.paho.org/english/gov/cd/cd44-r1-e.pdf.(last accessed: April2008).
[11] Pan American Health Organization (PAHO). Measles/Rubella Weekly Bul-letin 2007; 13(52):1. Available at: http://www.paho.org/english/ad/fch/im/measles.htm.(last accessed: April 2008).
12] Castillo-Solorzano C, Carrasco P, Tambini G, Reef S, Brana M, de QuadrosCA. New horizons in the control of rubella and the prevention of con-genital rubella syndrome in the Americas. J Infect Dis 2003;187(Suppl:1):S146–52.
13] Andrus JK, Dietz V, Fitzsimmons JW, Castillo-Solarzano C. Accelerating pol-icy, deployment, and access to new and underutilized vaccines in developingcountries. Harvard Health Policy Review 2006;7(2):91–101.
14] Agosti JM, Goldie SJ. Introducing HPV vaccine in developing countries – Keychallenges and issues. N Engl J Med 2007;356(19):1908–10.
[
[
[
[
[
[
[
[
[
26S (2008) L80–L87 L87
15] Parashar UD, Hummelman EG, Bresee JS, Miller MA, Glass RI. Global ill-ness and deaths caused by rotavirus disease in children. Emerg Infect Dis2003;9(5):565–72.
16] Linhares AC, Gabbay YB, Freitas RB. Travassos da Rosa ES, Mascarenhas JDP,Loureiro ECB. Longitudinal study of rotavirus infections among children fromBelém. Brazil Epidemiol Infect 1989;102(1):129–45.
[17] Pan American Health Organization (PAHO). Estimating Vaccine-preventableChild Mortality. Immunization Newsletter 2006; 28(3):5-6.
18] Garcia S, Levine OS, Cherian T, Gabastou JM, Andrus J. Pneumococcal disease andvaccination in the Americas: an agenda for accelerated vaccine introduction.Rev Panam Salud Publica 2006;19(5):340–8.
19] Andrus JK, Toscano CM, Lewis M, Oliveira L, Ropero AM, Davila M, et al. A modelfor enhancing evidence-based capacity to make informed policy decisions
on the introduction of new vaccines in the Americas. Public Health Reports2007;122(6):811–6.20] Irons B, Lewis MJ, Dahl-Regis M, Castillo-Solarzano C, Carrasco P, de Quadros CA.Strategies to eradicate rubella in the English-speaking Caribbean. Am J PublicHealth 2000;90(10):1545–9.
21] Goldie SJ, Diaz M, Constenla D, Alvis N, Andrus JK, Kim SY. Mathematical Mod-els of Cervical Cancer Prevention in Latin America and the Caribbean. Vaccine2008;26.(Suppl 11):L59–72.
22] Pan American Health Organization (PAHO). Analysis of vaccine-related legisla-tion in the Americas. Immunization Newsletter 2006; 28(2)5-6.
23] Andrus JK, Sherris J, Fitzsimmons J, Kane M, Aguado T. Introduction of HumanPapillomavirus Vaccines into Developing Countries-International Strategies forFunding and Procurement. Vaccine 2008;26(Suppl 10):K87–92.
24] Pan American Health Organization (PAHO). First ladies support elimination ofneonatal tetanus. EPI Newsletter 1992; 14(6):8.
25] Pan American Health Organization (PAHO). Update on influenza vaccination inthe Americas. Immunization Newsletter 2007; 29(1):1-3.
26] Iglesias CP, Drummond MF, Rovira J. NEVALAT Project Group. Health-care deci-sion making processes in Latin-America: Problems and prospects for the use ofeconomic evaluation. Int J Technol Assess Health Care 2005;21(1):1–14.
27] Pan American Health Organization. Multiyear project proposal for the promo-tion of evidence-based policy decisions for new vaccine introduction in LatinAmerica and the Caribbean (ProVac). Immunization Newsletter 2006; 28(5):1-3.
28] Andrus JK, de Quadros CA. Global access to vaccines: Deployment, use, andacceptance. In: Khan P, Gust I, Koff W, editors. Accelerating AIDS vaccine devel-opment: Challenges and opportunities. Norfolk: Horizon Scientific Press; 2007,February.