Hospital Volume and Quality of Care: Selective-referral or Practice-makes-perfect?
36
Hospital Volume and Quality of Care: Selective-referral or Practice-makes-perfect? Gabriel Picone 1 Department of Economics University of South Florida Justin G. Trogdon School of Economics University of Adelaide James Jollis Duke University Medical Center Duke University March 2005 Abstract Physicians in hospitals that treat a large number of patients will gain experience about the most effective treatment methods. One would expect this expertise to be reflected in better health outcomes for these patients (practice-makes-perfect hypothesis). However, using observational data, a selection bias arises since patients prefer the perceived “better” quality hospital, creating a spurious correlation between volume and outcomes (selective-referral hypothesis). In this study, using data from the Cooperative Cardiovascular Project (CCP), we estimate the effect of hospital volume on quality of care for patients with acute myocardial infarction (AMI). Our main instrument is the differential distance between the closest hospital to the patient and the nearest high volume hospital. Hospital volume is measured by the number of AMI patients admitted to the hospital in the year prior to the patient’s admission. We conclude that after controlling for selective-referrals admission to a higher hospital volume leads only to small reductions in mortality and higher readmission rates for urban patients. JEL classification: I1, L1 Key Words: Volume-outcome relationship, practice-makes-perfect, selective-referrals. 1 Corresponding author: Gabriel Picone, University of South Florida, 4202 E. Fowler Ave., BSN 3403, Tampa, FL 33620, [email protected] . We would like to thank participants at 2004 the Latin American Meetings of the Econometric Society and seminar participants at ANU for helpful comments. This research was supported by a grant from the Agency for Healthcare Research and Quality, “Hospital Volume and Quality of Care,” (1R03-HS013386-01A1). 1
Transcript of Hospital Volume and Quality of Care: Selective-referral or Practice-makes-perfect?

Hospital Volume and Quality of Care: Selective-referral or Practice-makes-perfect?
Gabriel Picone1
Department of Economics University of South Florida
Justin G. Trogdon
School of Economics University of Adelaide
James Jollis
Duke University Medical Center Duke University
March 2005
Abstract
Physicians in hospitals that treat a large number of patients will gain experience about the most effective treatment methods. One would expect this expertise to be reflected in better health outcomes for these patients (practice-makes-perfect hypothesis). However, using observational data, a selection bias arises since patients prefer the perceived “better” quality hospital, creating a spurious correlation between volume and outcomes (selective-referral hypothesis).
In this study, using data from the Cooperative Cardiovascular Project (CCP), we estimate the effect of hospital volume on quality of care for patients with acute myocardial infarction (AMI). Our main instrument is the differential distance between the closest hospital to the patient and the nearest high volume hospital. Hospital volume is measured by the number of AMI patients admitted to the hospital in the year prior to the patient’s admission. We conclude that after controlling for selective-referrals admission to a higher hospital volume leads only to small reductions in mortality and higher readmission rates for urban patients. JEL classification: I1, L1 Key Words: Volume-outcome relationship, practice-makes-perfect, selective-referrals.
1 Corresponding author: Gabriel Picone, University of South Florida, 4202 E. Fowler Ave., BSN
3403, Tampa, FL 33620, [email protected]. We would like to thank participants at 2004 the Latin American Meetings of the Econometric
Society and seminar participants at ANU for helpful comments. This research was supported by a grant from the Agency for Healthcare Research and Quality, “Hospital Volume and Quality of Care,” (1R03-HS013386-01A1).
1

I. Introduction
Physicians in hospitals that treat a large number of patients with similar
conditions will gain experience about the most effective treatment methods. One would
expect this expertise to be reflected in better health outcomes for patients admitted to
high volume hospitals (practice-makes-perfect hypothesis). However, using observational
data, a selection bias arises since patients prefer the perceived “better” quality hospital,
creating a spurious correlation between volume and outcomes (selective-referral
hypothesis). Thus, it is not surprising that a large literature has established a positive
relationship between hospital or physician volume and better clinical outcomes for a large
number of ailments and procedures. For example, this relationship has been shown for
percutaneous transluminal coronary angioplasty (PTCA) (Jollis et al 1994, Hannan 1997,
and Canto et al 2000), coronary artery bypass grafts (CABGs) (Showstack et al 1987,
Grumbach et al 1995, Gregory et al 2000, and Birkmeyer et al 2002), heart transplant
(Laffel et al 1992), pancreatic cancer surgery (Begg et al 1998, Lieberman et al 1995, and
Birkmeyer et al 2002), breast cancer surgery (Roohan et al 1998), and hip fracture
surgery (Taylor et al 1997 and Hamilton and Hamilton 1998) among other procedures.
See Luft et al (1990) for a detailed review of this literature.
Knowing if there is a causal relationship between hospital volume and health
outcomes has important policy implications. First, federal and state regulators face a
considerable number of decisions involving mergers and entry into markets where a
certificate of need is required. Market advocates oppose mergers and certificate of need
legislation because they believe that competition results in lower cost and enhanced
quality. However, the practice-makes-perfect hypothesis, if correct, challenges the
2

efficiency of free-markets. If competition increases the number of hospitals it may lead to
a less than optimal utilization of some procedures in hospitals by spreading procedures
across more low volume hospitals. In addition, the existence of learning-by-doing for the
treatment of many classes of patients is considered a barrier to entry in the hospital
industry; it has been shown that hospitals in markets where the threat of entry is higher
increase their volume to deter entry (Dafny 2003). Second, insurers like Medicare and
Medicaid could lower mortality and costs by encouraging selective contracting of some
procedures like PTCA and CABG. Third, for many patients the probability of survival
may improve by being directed to a high volume hospital.
Few studies have tried to control for bias due to selective referrals. Exceptions are
Luft (1980); Luft, Hunt, and Maerki (1987); Hughes et al (1988); Farley and
Ozminkowski (1992); Hamilton and Hamilton (1998); Norton et al (1998); and Ho
(2002). Two approaches have been used to account for selective referrals. One approach
is to use instrumental variables methods, which depend crucially on the quality of the
instruments (Staiger and Stock 1997). The other approach is to use longitudinal data with
hospital fixed effects. Studies using longitudinal data with hospital fixed effects have the
drawback that in most cases there is not enough within-hospital variation to identify the
effects of changes in hospital volume on changes in outcomes. As a whole, these studies
have been inconclusive about the importance of selective referrals in explaining the
positive relation between outcomes and volume.
In this study, using data from the Cooperative Cardiovascular Project (CCP)
merged with the American Hospital Association’s (AHA) annual survey of hospitals and
the National Inpatient Survey (NIS), we estimate the effect of hospital volume on quality
3

of care for patients with acute myocardial infarction (AMI) controlling for selective
referrals.2 The CCP is a sample of over 180,000 Medicare patients who were admitted
for AMI during 1994-95. Our data has several advantages in studying the volume-
outcome relationship: 1) it is a large and nationally representative sample; 2) it contains
information on post-hospital mortality and readmissions; 3) it contains very detailed
information on the severity of illness at admission, which mitigates the omitted variable
bias of previous studies; 4) It contain better measures of hospital quality than previous
studies; and 4) it contains the patient’s zip code, which allows us to create better
instruments (differential distance) than previous studies.
Because of the sudden nature of heart attacks, which require immediate and
complex treatment, heart attacks are a very suitable case study to assess the importance of
practice-makes-perfect effects in medical care. First, selective referrals are not likely to
be as important compared to non-emergency ailments. Second, the differential distance
between the closest hospital and the closest high volume hospital is a plausible
instrument for a heart attack. AMI patients are less likely to travel far away just to be
admitted into a high quality hospital. At the margin, however, a patient may be willing to
travel a few extra miles in order to be admitted into a high quality hospital creating a
spurious correlation. Testing the selective-referral and practice-makes-perfect hypothesis
is much more difficult for non-emergency ailments (e.g., cancer or brain surgery) where
distance to the nearest high quality facility is not as important and it is not a plausible
instrument.
2 Heart disease is the leading cause of mortality in the United States and most of these deaths involve AMI (or heart attack).
4

Our main dependent variables are 30-day mortality, one-year mortality, and 30-
day readmission. Hospital volume is measured by the number of AMI patients admitted
to the hospital a year before the patient was admitted to that hospital. We conduct
separate analysis for hospitals in metropolitan statistical areas and hospitals in non-
metropolitan statistical areas. The results indicate that hospital volume is positively
correlated with all of our measures of quality of care for urban patients (even after we
control for hospital characteristics and severity of illness). As expected, the effect of
hospital volume decreases substantially once we control for hospital characteristics.
Controlling for endogenous selective-referrals does not affect the coefficients of hospital
volume in the mortality equations, but it appears to affect the readmission probability.
For rural patients we find a much weaker relation between volume and outcomes, which
disappears after we control for hospitals characteristics.
The rest of the paper is organized as follows. Section II develops the conceptual
framework. Section III describes the data and presents the descriptive statistics. Section
IV discusses the econometric strategy. Section V presents the empirical specification.
Section VI discusses the results and Section VII concludes the paper.
II. Conceptual Framework
The primary explanation of a positive effect of hospital volume on quality of care
and outcomes is learning-by-doing. This is known as the practice-makes-perfect
hypothesis. Most physicians agree that it takes many patients and some mistakes to
achieve a high level of expertise in their fields. Thus, physicians in hospitals that treat a
5

large number of patients with similar conditions will improve at treating these conditions
compared to those in low volume hospitals.3
However, hospital volume could also be a sign of quality. If so, patients and
emergency medical services will be attracted to high volume hospitals. Using the analogy
of restaurants, if we are driving through a town and observe two restaurants with similar
prices and locations, we expect the one with more customers to be the one of higher
quality. However, it is not the volume of the restaurant that creates the higher quality, but
the higher quality attracts the higher volume of customers.
Without loss of generality assume that a patient can go to two different hospitals,
A and B. The hospitals have different volumes of patients (HVA and HVB). The patients
have an indirect utility associated with each hospital (UA and UB) and the observed
hospital volume for a particular patient is:
( ) ( )( ) BBAABA HVUUHVUUHV >−+>= 111
By the time that a patient has his/her heart attack the volume of the hospitals in his/her
market area (HVA and HVB) are already predetermined and can be treated as exogenous in
our econometric analysis.4 However, the hospital volume of the admitting hospital, the
observed HV, depends on the patients’ preferences for higher quality creating a reverse
causation when studying the effect of the admitted hospital volume on quality of care.
Several factors affect preferences for a given hospital including the travel distance, price
(for some patients), perceived quality, and severity of the health shock. The patient
prefers the closer hospitals, but also prefers the higher quality hospitals. If volume is a
3 Another causal explanation is economies of scale. This scale may be due to the fact that hospitals that treat a large number of similar patients can purchase better and more expensive equipment compared to low volume hospitals. 4 Hospital volume for each hospital in a given area depends on market population and other demographics, number of competitors, hospital quality, and volume negotiated with managed care insurance companies.
6

sign for quality, the patient may be willing to forgo a few extra minutes in travel time in
order to be admitted into a high volume hospital. Moreover, this trade-off between
distance and hospital volume that patients are willing to make may depend on the severity
of the shock.
III. Data and descriptive statistics
The primary source of data is the Cooperative Cardiovascular Project (CCP). The
CCP sample consists of randomly selected patient records for Medicare patients admitted
to nonfederal acute-care hospitals in the US with a primary diagnosis of acute myocardial
infarction (AMI), or heart attack, (ICD-9-CM 410, excluding a fifth digit of 2) over an
eight-month period. All of the sampling occurred between February 1994 and July 1995.
The sample includes all hospitals in the US that had not participated in a four-state pilot
phase (Alabama, Connecticut, Iowa, and Wisconsin). Medical records for each sampled
hospitalization were forwarded to clinical abstraction centers. Altogether, charts were
abstracted for approximately 180,000 AMI patients. The CCP took steps to ensure
consistent data collection including comparison of randomly selected records across two
independent data abstraction centers. The results indicate a high degree of consistency in
data abstraction. See Marciniak et al (1998) for a detailed description of CCP goals,
sampling, and data collection methods.
In this study we restrict our sample to patients who were admitted from home. We
exclude inter-hospital transfers and admissions from nursing homes. This ensures that the
differential distance instruments are measured correctly. We also exclude patients that
were admitted to hospitals that have less than five AMI admissions the previous year.
These hospitals are unlikely to be in the AMI treatment market and are likely to be
7

outliers. The data is linked with Medicare claims data and with the national death index.
Thus, we know how long the patient survives after the index admission and if he/she is
readmitted to the hospital. This creates a unique data set that provides very detailed
information on the patients’ coexisting conditions, severity of illness, and treatments
received.
We complement the CCP data set with hospital variables from two sources. First,
we obtain information on hospital ownership; cardiac intensive care beds; total number of
beds; availability of facilities for cardiac catheterization, angioplasty, and open-heart
surgery at the hospital; the number of full time registered nurses; and the ratio of full-
time residents to beds from the American Hospital Association’s (AHA) annual survey of
hospitals for different years. Second, we calculate hospital volume from the Nationwide
Inpatient Sample (NIS), which is part of the Healthcare Cost and Utilization Project
(HCUP). NIS contains all discharge data from approximately 1,000 hospitals located in
22 states between 1988 and 1998. NIS includes primary and secondary diagnoses and
procedures, which allows us to measure the number of AMI patients that a hospital
admits each year. Using NIS to measure hospital volume, rather than measuring hospital
volume directly from CCP like in Thiemann et al. (1999) and McClellan and Noguchi
(2001), has two advantages: 1) it includes all AMI patients admitted to the hospitals,
rather than only Medicare fee-for-service patients, and 2) it allows us to measure hospital
volume for the year before the patient was admitted.
Because not all hospitals from CCP are included in NIS, our preferred AMI
hospital volume measure is missing for many hospitals. We use multiple imputation
methods to “fill in” the missing volume information using the following strategy. First,
8

we sample with replacement from the set of hospitals with both NIS and CCP volume
information. Then we regress the NIS volume on the Medicare hospital volume as
measured in the CCP, a metropolitan statistical area dummy, the percentage of the
population in the county over 65 and interaction terms among the regressors. The R-
squared is over 60 percent for the imputation equation. Next, we use these coefficients to
predict the total AMI hospital volume for the full sample of hospitals and define our low
and high volume cut-offs (see below). This process is repeated fifteen times to generate
fifteen data sets with imputed AMI hospital volume for all hospitals.5 Finally, we run the
empirical models for each of the imputed data sets and combine the estimates using
standard multiple imputation aggregation formulas (Rubin 1987). In particular, the
aggregation formula for the estimated standard errors accounts for both the variation
within each imputed sample and the variation between the imputed samples.
We conduct separate analysis for patients who lived in metropolitan statistical
areas (77,824 admissions) and patients who lived in non-metropolitan statistical areas
(22,193 admissions). A metropolitan statistical area (MSA) is a core area containing at
least one urbanized area of 50,000 or more inhabitants, together with adjacent
communities having a high degree of economic and social integration with that core.
Hereafter we denote a metropolitan statistical area a “urban” area and a non metropolitan
statistical area as a “rural” area.
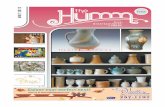
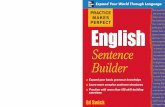
Figure 1.a presents kernel density estimates of hospital AMI volume for patients
in urban areas for the fifteen imputed samples. Figure 1.b presents the same kernel
5 The number of imputations needed is given by the relative efficiency (1 + λ/m)-1, where λ is the fraction of missing information and m is the number of imputations (Mander and Clayton 1999). Given the fraction of hospitals with missing NIS volume (83%), fifteen imputations provide a relative efficiency of approximately 95%.
9

estimates for rural areas. The observational unit in these figures is the hospital. There are
2,178 hospitals in the urban sample and 1,268 hospitals in the rural sample. Although
both distributions are unimodal and right skewed, urban hospitals are much larger. The
median hospital in an urban area admits approximately 220 patients a year, while a
hospital with this number of admissions would be in the top ten percent of admissions for
a rural hospital. For the urban sample the inter-quartile range is approximately 150 to 335
admissions per year; for the rural sample the inter-quartile range is approximately 90 to
140. Figure 1.c and 1.d contain the same kernel densities (rural and urban) of actual
(rather than imputed) AMI hospital volume using only those hospitals that are in both
NIS and CCP. The distributions of the imputed and non-imputed samples have the same
shape for both urban and rural patients, but the imputed samples have a higher mode and
less weight on the right tail.
IV. Econometric Strategy
Let HV be the hospital volume where the individual is admitted and Y* be the
health outcome of interest. We assume that the following model determines health
outcomes:
2
13221*
'
'
vZHV
vmmXY
i
i
+=
+++=
δ
γγβ (1)
where m2=1(HVL<HV< HVH ) and m3=1(HV> HVH ). In our specification, m2 is a binary
variable indicating whether the admitting hospital is a medium volume hospital and m3
indicates whether the admitting hospital is a high volume hospital. X represents a vector
of exogenous covariates that affect outcomes. X includes both patient and hospital
characteristics. Z represents covariates that affect the admitting hospital volume. Z
includes X and variables reflecting preferences for a given hospital like differential
10

distance. We do not observe Y*; instead we observe m1=1(Y*>0), for example 30-day
mortality. (v1,v2) are independent of (X ,Z) and follow a bivariate normal distribution with
mean zero, unit variance, and ρ=Corr(v1,v2). Our goal is to estimate the average treatment
effects of a patient being admitted to a high and medium volume hospital versus an
admission to a low volume hospital conditional on X. Given our model the average
treatment effects are given by: 1) medium versus low volume (E[Φ(X’β+γ1)- Φ(X’β)]),
and 2) high versus low volume (E[Φ(X’β+γ2)- Φ(X’β)]).
Standard probit methods allow us to consistently estimate these average treatment
effects only when ρ equals zero. This assumption will be violated if some hospital quality
is unobserved to us, but not to patients (or their provider such as emergency personnel).
We address this problem in two ways. First, we test for endogeneity using the two-step
method proposed in Rivers and Vuong (1988). The first step is to estimate a linear
projection for hospital volume and save the residuals. The second step is to estimate a
standard probit using the predicted residual as an additional regressor. A significant t-test
for the residuals is an indication of endogeneity. Second, we implement a maximum
likelihood estimator that will jointly estimate the admitted hospital volume equation and
the health outcome equation in (1).
The maximum likelihood estimator is implemented as follows: m2 and m3 are
mutually exclusive (but not exhaustive) binary variables and there are three plausible
outcomes: (0,0), (1,0), and (0,1). The probabilities that m2 and m3 take on each of these
values are given by
( ) ( ) ( )δδ 'PrHV'Pr0,0Pr 2L232 ZHVvvZmm L −<=<+===
11

( ) ( ) ( ) ( )δδδ 'Pr'Pr'Pr0,1Pr 22232 ZHVvZHVvHVvZHVmm LHHL −<−−<=<+<=== and
( ) ( )δ'Pr11,0Pr 232 ZHVvmm H −<−===
Because the outcome variable, m1, can only take the values of 0 and 1, there are six
possible combinations of m1, m2, and m3 that we can observe in our model. The log-
likelihood function for the ith individual is given by:
ln l i
ln 1i, 2i; 4i if m 1i 1 , m 2 i 0 , m 3 i 0 ln 1 i , 2 i 3 i ; 4i 1i, 2i; 4i if m 1i 1 , m 2 i 1 , m 3 i 0
ln 1 i , 2i 3i; 4i if m 1i 1, m 2 i 0 , m 3 i 1 ln 1i, 2i; 4i if m 1i 0, m 2 i 0 , m 3 i 0
ln 1 i , 2 i 3 i ; 4i 1i, 2i; 4i if m 1i 0, m 2 i 1 , m 3 i 0 ln 1 i , 2i 3i; 4i if m 1i 0, m 2 i 0 , m 3 i 1
where θ1i=X’β+γ1m2i+γ2m3i, θ2i= HVL -Z’δ, θ3i= HVH, and θ4i=ρ. Using the above
individual log-likelihood function, we construct the sample log-likelihood function (lnL)
and apply maximum likelihood methods (MLE) by maximizing lnL with respect to
(β,γ1,γ2,δ,ρ). We implement this method in STATA using the ML command.
This approach has several advantages: 1) it is straightforward to calculate, 2) it
has desirable statistical properties including asymptotic efficiency, under some
conditions, 3) it allows for a likelihood ratio test of the identification assumptions, and 4)
it provides a direct estimate of the correlation coefficient between the disturbances, which
serves as a test for endogeneity. The main disadvantage is that if the disturbances v1 and
v2 do not follow a bivariate normal distribution, the results will not be consistent and may
be misleading.6 As a robustness check we also estimate the model using two-stage least
6 An alternative likelihood function that accounts for the continuous nature of the hospital volume variable in the second equation is likely to give more efficient estimates of the parameters in the second equation,
12

squares (TSLS). TSLS is only consistent if we assume a linear probability model, but
provides a good estimate of the average treatment effect around the center of the
distribution of the index X’β (Angrist 2001).
As with any other method to control for endogeneity using instrumental variables,
the performance of our approach depends on the quality of our instruments in Z. We use
the differential distance between the nearest high volume and the nearest hospital to the
patient’s residence and the average hospital volume in the patient area as our main
instrumental variables. Our main identification assumption is that patients who live
farther from a high volume hospital are less likely to be admitted into a high volume
hospital, but this distance does not affect health outcomes once we control for the
admitting hospital characteristics and severity of illness at admission.7 McClellan,
McNeil, and Newhouse (1994) introduce differential distance as an instrument for
assessing the impact of catheterization on mortality. They show that the differential
distance to the nearest catheterization hospital and the nearest non-catheterization
hospital satisfies the requirements of a good instrument for their application: it is highly
correlated with treatment (catheterization) and uncorrelated with severity of illness. In
recent years differential distance has been widely used in health economics as an
instrumental variable. For example, McClellan and Newhouse (1995 and 1997) use
differential distance as an instrument to measure the effectiveness of different medical
treatments and Gowrisankaran and Town (1999) use differential distance as an
instrument to estimate the quality of care in hospitals.
but it is more complex to implement computationally. Because of this reason we did not pursue this likelihood function. 7 Because nursing homes are likely located close to high volume hospitals we exclude admissions from nursing homes in our analysis.
13

We also use the average hospital volume of all hospitals within a 50-mile radius
of the patient as an instrumental variable. As discussed in our conceptual framework, at
the time of the patient’s health shock the hospital volume of the hospitals in his/her area
is predetermined and uncorrelated with the severity of the shock. If the average hospital
volume in the patient’s area is larger, he/she will be more likely admitted to a high
volume hospital. A potential problem with this instrument is that some individuals may
locate into areas where there is at least one high quality hospital causing these areas to
have larger populations and higher hospital volume. If this is the case the average
hospital volume in the area will be caused by preferences for high hospital quality of
those patients, introducing reverse causality and making the patient area hospital volume
an invalid instrument. We exclude average hospital volume from our set of instruments in
some runs and obtain similar results.
V. Empirical Specification
Dependent Variables: The main dependent variables are binaries indicating mortality at
one month and one year following AMI. We also define a binary variable indicating
readmission for ischemic heart disease at one month following the date of the hospital
discharge for the original AMI admission.8
Hospital Volume: The key explanatory variable is hospital volume. As explained above,
we use a categorical specification for hospital volume. We define a high volume hospital
as one in the top quartile of admissions per year and medium volume hospital as one in
the second and third quartiles of admissions per year. The hospital volume dummies are
calculated separately for urban and rural areas in each imputed sample. For an urban area
a hospital is considered high volume if it has over 364 admissions per year on average 8 Ischemic heart disease, a broader term than AMI, refers generally to a loss of arterial blood flow to tissue.
14

across imputed samples (sd=6.8) and it is considered a medium volume hospital if it has
between 169 (sd=3.2) and 363 admissions per year. For rural hospitals the thresholds are
152 for high volume and 93 to 151 for medium volume. In preliminary research (not
reported) we use a quadratic specification and the conclusions are similar.
Sociodemographic characteristics: Sociodemographic variables include age at the time of
the admission, gender, and race.
Hospital characteristics: We also control for the following hospital characteristics that
may affect hospital quality and outcomes: the number of beds; the number cardiac
intensive care beds; and binary variables for catherization lab, cardiac surgery, teaching
status (non-teaching hospitals do not have medical residents, minor teaching hospitals
have resident-to-bed ratios below the national median, and major teaching hospitals have
resident-to-bed ratios above the national median), and ownership status (government, for
profit, or nonprofit). These characteristics are likely to be correlated with hospital volume
creating an omitted variable biased if we do not account for them.
Some of these measures have their own effects on health outcomes and may
reflect economies of scale, better equipment, or different managerial organizations.
Ideally, these hospital characteristics should not be correlated with practice-makes-
perfect effects. Unfortunately, we cannot rule out a reverse effect from past hospital
volume that led the hospital to acquire some of these facilities. For example, a high
volume of AMI patients might cause the hospital to open a catheterization lab, but after
the catheterization lab is open it may have a separate effect on health. We estimated the
model with and without these hospital characteristics. We only report results using
15

hospital characteristics, because once we control for severity of illness the effects of
hospital volume on outcomes are very similar with or without hospital characteristics.
Finally, some of our hospital characteristics, such as catheterization lab or cardiac
surgery facilities, are also correlated with perceived hospital quality and will control for
selective referrals. If we measure severity of illness and perceived hospital quality
perfectly, then we could argue that hospital volume should be treated as exogenous in our
outcome equations.
Severity of illness and coexisting conditions: An advantage of CCP compared to
Medicare claims data and standard surveys is that it contains very detailed information on
patients’ coexisting conditions (co-morbidities) and severity of illness. We use the results
of Krumholz et al (2001) and Thiemann et al (1999) to select our measures of severity of
illness and co-existing conditions. We summarize all co-existing conditions by the
Charlson index (Charlson et al. 1987) and binaries for lack of mobility and incontinence.
This is a weighted sum of co-morbidities, where the weights are proportional to the risk
of death from each co-morbidity. Higher values of the Charlson index indicate worse
health. Lack of mobility and incontinence are among the most important predictors of
one-year mortality (Krumholz et al 2001).
Severity of illness conditions include log mean arterial pressure, pulse, time since
the start of chest pains to admission, anterior myocardial infarction, ST elevation on
admission electrocardiogram, Killip class, left ventricular ejection fraction, congestive
heart failure, cardiac arrest, shock on arrival, hemorrhage, and renal function. All of these
variables were shown to be important determinants of health outcomes for AMI patients.
16

Killip class, a measure of severity at admission, is used as the initial assessment of
the severity of the heart attack. Using a method developed by Killip and Kimbal (1967),
heart attack patients are classified into one of four classes: those with no evidence of
congestive heart failure (CHF) (1), those with mild to moderate CHF (2), those with overt
pulmonary edema (3), and those in cardiogenic shock (4). Thus, a higher classification
indicates a more severe heart attack. Left ventricular ejection fraction (LVEF) measures
the relative output of blood per contraction and is grouped into three categories: <20%,
20% to 39%, and >39%. Low values of LVEF are associated with higher mortality. Renal
dysfunction is also associated with higher mortality and it is defined as creatinine > 2.5
mg/dl or blood urea nitrogen > 40 mg/dl.
Instruments: We include the differential distance between the nearest hospital and the
nearest medium volume hospital, and between the nearest hospital and the nearest high
volume hospital. We calculate the distance from patients’ residences to hospitals as the
linear distance from the center of the patient’s five-digit zip code to the center of the
hospital’s five-digit zip code. We use the same thresholds (250 and 500 admissions per
year) to define medium and high volume hospitals for urban and rural patients.9 Finally,
we also include the average hospital volume for all hospitals in a 50-mile radius of the
patient’s residence as an additional instrument.
VII. Results
The average 30-day mortality is 17.2% for urban areas and 17.6% for rural areas
(Table 1). We also observe a slightly lower average one-year mortality (30.1% vs.
30.7%) and 30-day readmission (13.6% vs 14.7%) for patients in urban areas compared
9 Ideally, we would have liked to use the same thresholds as in our main explanatory variable in the health equations, which vary by imputed sample, but it was not possible because of data restrictions.
17

to patients in rural areas. The average age of a patient admitted to a hospital is 75.9 for
patients from urban areas and 76.0 for rural areas. Roughly half the patients are females
(47.5% and 48.5%) and 6.8% (4.8%) of patients are black.
Not surprisingly, rural patients are more likely to be admitted to smaller hospitals
as measured by the number of beds (178.6 vs 346.8), less likely to be admitted to a
hospital with major teaching status (5.5% vs 21.6%), less likely to be admitted to a
hospital with cardiac catheterization lab facilities (41.9% vs 75.7%) and cardiac surgery
facilities (18.3% vs 53.5%) and more likely to be admitted to a hospital owned by the
government.
Around 12% of patients (urban and rural) have a Charlson index of 4 or above,
1.5% of patients are not mobile, and 4.5% are incontinent. For some important predictors
of severity of illness urban patients are marginally sicker at admission. Patients from
urban areas are more likely to have an anterior myocardial infarction (46.2% vs 45.7%),
more likely to have a higher Killip class (35.2% for III and 2.4% for IV vs. 34.5% and
1.8%) and more likely to have a lower left ventricular ejection fraction (20.8% for LVEF
between 20 and 39 vs 15.1%). One potential explanation for the relative healthiness of
rural patients compared to urban patients is that, given the higher distance, many of the
sicker patients in rural areas may never get admitted to a hospital.
Without controlling for other factors, medium volume hospitals (25th to 75th
percentile of AMI admissions per year) and high volume hospitals (over 75th percentile
of AMI admissions per year) have lower mortality and readmission rates compared to
low volume hospitals for urban patients (Table 2). For rural patients, high volume
hospitals have lower mortality rates than low volume hospitals, but medium volume
18

hospitals have higher readmission rates than low volume hospitals (significant at the ten
percent level for medium volume hospitals). The average treatment effects between
medium versus low hospital volume and between high versus low hospital volume are -
0.011 and -0.022 respectively for 30-day mortality for urban patients, -0.011 and –0.022
for one-year mortality, and –0.011 and –0.012 for 30-day readmissions. Adding
sociodemographic characteristics does not reduce the significance or magnitude of the
coefficients for urban patients, but the effect of high volume hospitals on one-year
mortality for rural patients is no longer significant. Given the average values of the
dependent variables, admission to a high volume hospital for an urban patient reduces 30-
day mortality by 12.7%, one-year mortality by 9.9%, and 30-day readmissions by 8.8%
after we control for sociodemographic characteristics. These are important effects and if
causal, policies that redirect patients to high volume hospitals would have significant
benefits on health outcomes.
Adding hospital characteristics reduces considerably the average treatment effects
for all of our measures of health outcomes. For example, for urban patients the effect of
an admission to a high AMI volume hospital on 30-day mortality is reduced from –0.022
to –0.015, for one-year mortality the effect goes from –0.030 to –0.019, and for 30-day
readmission the effect goes from –0.012 to –0.004. This latter effect is no longer
significant at conventional statistical levels. Controlling for coexisting conditions and
severity of illness for urban patients does not affect the average treatment effects, but the
significance of the associated coefficients is lower. Admission to a high volume hospital
reduces 30-day mortality by 5.8%, one-year mortality by 6.3%, and 30-day readmissions
by 4.4% compare to low volume hospitals. Thus the potential benefits due to better health
19

outcomes from redirecting patients away from low volume hospitals appears to be
modest. However, we should be cautious in interpreting these results since we are
holding important technological characteristics of the hospital constant.
For rural patients, controlling for hospital characteristics, severity of illness and
coexisting conditions makes the estimates imprecise and not significant. Due to this lack
of precision we do not discuss the specifications for rural patients in detail.10 For these
patients it is probably more important to have a hospital with decent AMI facilities within
a manageable distance than to be triaged to a high AMI volume hospital.
The Rivers and Vuong test for endogeneity is negative for all of the
specifications, suggesting that that v1 and v2 are negatively correlated, which is consistent
with selective-referrals. However, the tests are only significant for 30-day and one-year
mortality for rural patients. We find no strong evidence of endogeneity and selective
referrals for urban patients based on these tests. A RESET test of a correct functional
form is rejected for 30-day mortality for urban patients and one-year mortality for urban
and rural patients. This is likely due to non-linear effects of some of our controls other
than hospital volume, which we incorporate using a non-linear specification.
Our maximum likelihood estimates (Table 3) produce similar results for the
average treatment effect of the probit estimates after controlling for coexisting conditions
and severity of illness for the mortality equations. However, the coefficients of the
volume binaries are no longer significant at conventional levels, except for admission to a
medium volume hospital in the one-year mortality equation (at the 10% level). The
correlation coefficient is not significant in any of the mortality specifications, which
10 Because we use a relative measure of hospital volume (quartiles) it is possible that hospital volume has an effect on outcomes at higher thresholds.
20

implies that we cannot reject the null hypothesis that after controlling for coexisting
conditions and severity of illness, hospital volume is exogenous in the mortality
equations (a result consistent with the Rivers and Vuong test). We do find evidence of
endogeneity for 30-day readmission; the correlation coefficient is negative and significant
and the binaries describing hospital volume are positive and significant at the 10% level
for high volume. This implies that patients admitted to a high volume hospital have a
higher probability of readmission. A plausible explanation for this result is that high
volume hospitals lower mortality but create, at the margin, patients more likely to be
readmitted now that they have barely survived.
The most important determinants of 30-day mortality, one-year mortality, and 30-
day readmission for all patients are age (+ on mortality and – on readmissions) and many
of the variables grouped as coexisting conditions and severity of illness (Table 3). This
group includes high Charlson index (+), lack of mobility (+), incontinence (+), log mean
arterial pressure (-), number of hours since chest pain started (+), anterior myocardial
infarction (+), higher Killip class (+), low left ventricular ejection fraction (+), and renal
function problem (+). In contrast, very few hospital characteristics are significant at
conventional levels (the main exception is major teaching which has a negative effect on
mortality and positive on re-admission). In many instances variables have opposite signs
in the mortality and readmission equations (e.g. age, major teaching, immobile, and
incontinence). This is due to the fact that the most severely ill patients are more likely to
die and thus are less likely to be readmitted.
The most important determinants of the admitting hospital AMI volume are the
differential distances between the closest hospital and the closest medium, and high
21

volume hospitals (Table 4). For the urban (rural) sample the further a patient lives from a
high (medium) volume hospital the less likely the observed hospital volume will be high
(medium). Mean hospital AMI volume in a 50-mile radius is also positively correlated
with the observed hospital AMI volume at admission. All of our instruments are highly
significant and using likelihood ratio tests we reject the null hypothesis of no joint
significance of our instruments with p-value of 0.000.
Additional determinants of hospital volume are the number of beds (+), cardiac
catheterization lab (+), cardiac surgery (+), minor teaching (+), major teaching (-),
nonprofit (+), and for-profit status (+). The effect of major teaching may seem surprising,
but it is important to remember that we are controlling for cardiac technology capabilities
and number of beds. Interestingly, very few coexisting conditions and severity of illness
variables are significantly correlated with admission to high volume hospitals. Exceptions
are log mean arterial pressure (-), ST elevation on admission electocardiogram (+),
anterior myocardial infarction (-), and several indicators for missing variables such as
LVEF missing (-) and unable to determine the time since the start of chest pain (-).
VIII Discussion and Conclusion
A large literature has found a positive correlation between hospital volume and
health outcomes for a large number of medical conditions and procedures including heart
attacks (AMI). This relationship could be due to practice-makes-perfect or selective
referrals, or both. Based on these findings, many groups argue in favor of creating
regional centers for excellence to treat AMI patients. Creating these regional centers will
imply closing low volume hospitals and directing those patients to the regional centers.
For example, the Leapfrog group (a very influential coalition of more than 150 public and
22

private organizations that provide health care benefits) recommends directing patients to
hospitals that admit a certain threshold level of patients. However, if selective-referrals
explain most of the association between hospital volume and outcomes, then measures
that close hospitals based on required minimum thresholds levels may have unintended
consequences, like closing good hospitals while not improving outcomes. In this case
policies that help patients better assess hospital quality will be more effective in the long
run.
In this study, we revisit this important question with improved data and
econometric methods. Our large and nationally representative data set has two main
advantages. First, information from hospital charts allows for detailed measures of
coexisting conditions and severity of illness, the lack of which plagued previous studies.
Second, it allows calculating the patient’s distance to different hospitals, which provides
us with better instrumental variables than past studies. We find that higher hospital
volume is correlated with lower mortality even after controlling for selective-referrals
and hospital characteristics. However, the average treatment effects are small and only
marginally significant for urban patients. The potential reductions in 30-day mortality and
one-year mortality for admission to a medium volume hospital versus a low volume
hospital are 1.7% and 4.9%. The same effects for admission to a high volume hospital
versus a low volume hospital are 5.8% and 6.3%.
We only find evidence that hospital volume is endogenous for the 30-day
readmission specification for urban patients. An interesting result is that our MLE
method reverses the sign of the effect of hospital volume on readmission from a negative
effect into a positive effect implying that higher volume increases readmissions. We also
23

find a negative correlation between the disturbance in the hospital volume equation and
the disturbance in the 30-day readmission equation. This result is consistent with
selective referrals combined with practice-makes perfect and it can arise if there two
groups of hospitals with different unmeasured quality to the researcher, but not the
patient. For example, consider hospital A that has the following effects of volume on
mortality and re-admission: 1) if it is high volume the mortality rate is 0.20 and re-
admission rate is 0.14, 2) if it is low volume the mortality rate is 0.22 and the re-
admission rate is 0.12. For hospital B, the mortality and re-admission rates are 0.21 and
0.17 if it is high volume and 0.23 and 0.15 if it is low volume. For both hospitals high
volume causes a reduction in mortality, but at the cost of higher readmission rates.
Hospital A has better quality and a patient will always prefer hospital A to hospital B
provided he/she is willing to make the distance-quality trade-off. Suppose that patients
are equally distributed around both hospitals. However, a group of patients will have
equal distance between both hospitals. These patients will choose hospital A, which will
be the high volume hospital in this market and hospital B will be the low volume
hospital. The observed effects of hospital volume on mortality and re-admission rates are
-0.03 (0.20 for high volume A minus 0.23 for low volume B) and –0.01 (0.14 for high
volume A minus 0.15 for low volume B), but the causal effects are –0.02 (0.20-0.22 for
A or 0.23-0.21 for B) and 0.02 (0.14-0.12 for A or 0.17-0.15 for B).
Two weaknesses of this study should be acknowledged. First, our sample is
restricted to AMI admissions and we do not study the effects of the specific treatment
that the patient received. For example, after surviving a heart attack, a patient may have
surgery or angioplasty to open the blocked arteries. It is possible that the practice-makes-
24

perfect hypothesis is more important when performing procedures like surgery compared
with treating patient with similar conditions right after a health shock. Second, our
sample contains only those individuals with AMI that survived long enough to be
admitted to a hospital. Policies that close low volume hospitals, which are often the
closest hospital for a (potential) patient, would increase the number of individuals who
die before reaching a hospital. Thus, our results that find modest benefit from
regionalization likely overstate the benefits to that type of policy.
References ANGRIST, J.D. “Estimation of LimitedDependent Variable Models with Dummy Endogenous Regressors: Simple Strategies for Empirical Practice.” Journal of Business and Economic Statistics Vol. 19 (2001), pp. 2-16. BEGG, C.B. AND CRAMER, L.D., ET AL. “Impact of Hospital Volume on Operative Mortality for Major Cancer Surgery.” JAMA Vol. 280 (1998), pp. 1747-51. BIRMEYER, J.D., SIEWERS, A.E., AND FINLAYSON, E.V., ET AL. “Hospital Volume and Surgical Mortality in the United States.” NEJM Vol. 346 (2002), pp. 1128-37. CANTO, J., EVERY, N.R., AND MAGID, D.J., ET AL. “The Volume of Primary Angioplasty Procedures and Survival after Acute Myocardial Infarctions.” NEJM Vol. 342 (2000), pp.1573-1582. CHARLSON, M.E. AND POMPEI, P, ET AL. “A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. Journal of Chronic Diseases 40 (1987):373-383. DAFNY, L. “Entry Deterrence in Hospital Procedure Markets: A Simple Model of Learning-by-Doing.” NBER Working Paper no. 9871, 2003. FARLEY, D.E. AND OZIMINKOWSKI, R.J. “Volume-Outcome Relationships and In-Hospital Mortality: The Effect of Changes in Volume Over Time.” Medical Care Vol. 30 (1992), pp. 77-94. GOWRISANKARAN, G. AND TOWN, R. “Estimating the Quality of Care in Hospitals Using Instrumental Variables.” Journal of Health Economics Vol. 18 (1999), pp. 747-767.
25

GREGORY, P.M., ET AL. “Impact of Geographic Proximity to Cardiac Revascularization Services on Service Utilization.” Medical Care Vol. 38 (2000), pp. 45-57. GRUMBACH, K., ANDERSON, G.M., AND LUFT, H.S., ET AL. “Regionalization of Cardiac Surgery in The U.S. and Canada.” JAMA Vol. 274 (1995), pp. 1282-8. HAMILTON, B. and HAMILTON, V.H. “Estimating Surgical Volume-Outcome Relationships Applying Survival Models: Accounting for Frailty and Hospital Fixed Effects.” Health Economics Vol. 6 (1998), pp. 383-95. HANNAN, E.L. AND RACZ, M., ET AL. “Coronary Angioplasty Volume-Outcome Relationships for Hospitals and Cardiologists.” JAMA Vol. 277 (1997), pp. 892-8. HO, V. “Learning and the Evolution of Medical Technologies: The Diffusion of Coronary Angioplasty.” Journal of Health Economics Vol. 21 (2002), pp. 873-885. HUGHES, R., GARNICK, D., LUFT, H.S., ET AL. “Hospital Volume and Patient Outcomes: The Case of Hip Fracture Patients.” Medical Care Vol. 26 (1988), pp. 1057-67. JOLLIS, J.G. AND PETERSON, E.D., ET AL. “The Relation Between the Volume of Coronary Angioplasty Procedures at Hospitals Treating Medicare Beneficiaries and Short Term Mortality.” NEJM. Vol. 334 (1994), pp. 1625-1629. JOLLIS, J.G. AND ROMANO, P. S. “Volume-Outcome Relationship in Acute Myocardial Infarction: the Balloon and the Needle.” JAMA Vol. 284 (2000), pp. 3169-71. KILLIP, T. AND KIMBAL J.T. ” Treatment of Myocardial Infarction in a Coronary Care Unit.” American Journal of Cardiology Vol. 20 (1967), pp457-464. KRUMHOLZ, H.M., CHEN, J., AND CHEN, Y.T., ET AL. “Predicting One-Year Mortality Among Elderly Survivors of Hospitalization for an Acute Myocardial Infarction: Results from the Cooperative Cardiovascular Project.” Journal of the American college of Cardiology Vol. 38 (2001), pp. 453-9. LAFFEL, G. AND BARNETT, S., ET AL. “The Relation Between Experience and Outcome in Heart Transplantation.” NEJM Vol. 327(1992), pp. 1220-25. LIEBERMAN, M.D., KILBURN, H., AND LINDSEY, M., ET AL. “Relation of Perioperative Deaths to Hospital Volume Among Patients Undergoing Pancreatic Resection for Malignancy.” Ann Surg. Vol. 222 (1995), pp. 638-645. LUFT, H.S. “The Relationship between Surgical Volume and Mortality: An Exploration of Causal Factors and Alternative Models.” Medical Care Vol.18 (1980), pp 940-59.
26

LUFT, H.S., GARNICK, D., MARK, D., AND McPEAH, S. “Hospital Volume; Physician Volume and Patient Outcomes: Assessing Evidence.” Ann Arbor, MI: Health Administration Press Perspectives, 1990. LUFT, H.S., GARNICK, D., MARK, D., ET AL. “Does Quality Influence Choice of Hospital?” JAMA Vol. 263 (1990), pp. 2899-906. LUFT, H.S., HUNT, S., AND MAERKI, S. “The Volume Outcome Relationship: Practice Makes Perfect or Selective Referral Patterns?” Health Service Research Vol. 22 (1987), pp. 157-182. MANDER, A. AND CLAYTON, D. ”Weighted Hotdeck Imputation.” Stata Technical Bulletin Vol. 51 (1999), pp. 32-4. MARCINIAK, T.A., ELLERBECK, E.F., AND RADFORD, M.J., ET AL. ”Improving the Quality of Care for Medicare Patients with Acute Myocardial Infarction: Results from the Cooperative Cardiovascular Project” JAMA Vol. 287 (2002), pp. 1269-1276. McCLELLAN, M. AND NEWHOUSE, J.P. “The Marginal Benefits of Medical Technology: Acute Myocardial Infarction in the Elderly.” Journal of Econometrics Vol. 77 (1997), pp. 39-64. McCLELLAN, M. AND NEWHOUSE, J.P. “The Marginal Cost-Effectiveness of Medical Technology: A Panel Instrumental-Variables Approach.” Journal of Econometrics Vol. 77 (1997), pp. 39-64. McCLELLAN, M., McNEIL, B., AND NEWHOUSE, J.P. “Does More Intensive Treatment of Acute Myocardial Infarction Reduce Mortality.” JAMA Vol. 272(1994), pp. 859-866. McCLELLAN, A. AND NOGUCHI, H. “Validity and Interpretation of Treatment Effect Estimates: Using Observational Data.” Stanford University, Unpublished Manuscript, 2001. McCLELLAN, M., AND STAIGER, D. “The Quality of Health Care Providers.” NBER working paper no. 7327, 1999. NORTON, E.C., AND GARFINKEL, S.A., ET AL. “The Effect of Hospital Volume on the In-Hospital Complication Rate in Knee Replacement Patients.” Health Services Research Vol. 33 (1998), pp. 1191-1210. RIVERS, D. AND VUONG, Q.H. “Limited Information Estimators and Exogeneity Tests for Simultaneous Probit Models.” Journal of Econometrics Vol. 39 (1988), pp. 347-66 ROOHAN, P.J., BICKELL, N.A., ET AL. “Hospital Volume Differences and Five-year Survival from Breast Cancer.” AJPH Vol. 88 (1998), pp. 454-457.
27

28
RUBIN, D. “Multiple Imputation for Nonresponse in Surveys.” J. Wiley & Sons, 1987. SHOWSTACK, J. ET AL. “Association of Volume with Outcomes of Coronary Artery Bypass Graft Surgery.” JAMA, 1987. STAIGER, D. AND STOCK, J. “Instrumental Variables Estimation with Weak Instruments.” Econometrica. Vol. 65 (1997), pp. 557-586. TAYLOR, H.D., DENIS, D.A., AND CRANE, H.S. “Relationship Between Mortality Rates and Hospital Patient Volume for Medicare Patients Undergoing Major Orthopedic Surgery of the Hip, Knee, and Femur.” J. Arthroplasty Vol. 12 (1997), pp. 235-42. THIEMANN, D.H., CORESH, J., AND OETGEN, W. ET AL. “The Association Between Hospital Volume and Survival After Acute Myocardial Infarction in Elderly Patients.” NEJM Vol. 340 (1999), pp. 1640-1648.

Figure 1: Imputed and Non-Imputed Hospital Volume Kernel Densities Urban Patients Rural Patients Figure 1.a Figure 1.b
0.0
01.0
02.0
03.0
04D
ensi
ty
0 500 1000 1500Regression-Imputed AMI Volume
Gaussian Kernel DensityHospital AMI Volume
0.0
05.0
1.0
15.0
2D
ensi
ty
0 200 400 600 800Regression-Imputed AMI Volume
Gaussian Kernel DensityHospital AMI Volume
Figure 1.c Figure 1.d
0.0
01.0
02.0
03D
ensi
ty
0 500 1000 1500 2000AMI Volume
Gaussian Kernel DensityHospital AMI Volume
0.0
02.0
04.0
06D
ensi
ty
0 200 400 600 800 1000AMI Volume
Gaussian Kernel DensityHospital AMI Volume

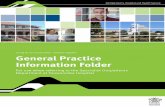
Table 1. Descriptive Statistics by Metropolitan Statistical Area--mean (standard deviation)
Metropolitan Statistical Non-Metropolitan StatisticalArea Area
Variable (N=77,824) (N=22,193)Outcomes
30-day mortality 0.172 0.176(0.377) (0.381)
1-year mortality 0.301 0.307(0.458) (0.461)
30-day readmission 0.136 0.147(0.343) (0.354)
Sociodemographic characteristicsAge 75.9 76.040
(7.130) (7.083)Female 0.475 0.485
(0.499) (0.499)Race
Black 0.068 0.048(0.251) (0.215)
Other 0.036 0.011(0.186) (0.107)
Hospital characteristicsCardiac intensive care beds 7.798 2.591
(9.665) (4.679)Cardiac intensive care beds missing 0.098 0.138
(0.298) (0.345)Bed total 346.856 178.645
(220.063) (133.880)Cardiac catheterization lab 0.757 0.419
(0.428) (0.493)Cardiac surgery 0.535 0.183
(0.498) (0.387)Teaching status
Minor teaching 0.212 0.102(0.409) (0.303)
Major teaching 0.216 0.055(0.411) (0.228)
OwnershipFor profit 0.109 0.090
(0.312) (0.287)Nonprofit 0.806 0.696
(0.395) (0.459)Hospital data missing 0.003 0.001
(0.060) (0.034)
Coexisting conditions
Charlson = 1 0.273 0.279(0.445) (0.448)
Charlson = 2 or 3 0.350 0.349(0.477) (0.476)
Charlson >= 4 0.122 0.119(0.328) (0.324)
Immobile 0.018 0.015(0.133) (0.121)
Incontinent 0.043 0.048

(0.203) (0.214)
Severity of illnessLog mean arterial pressure 4.498 4.532
(0.757) (0.698)Log mean arterial pressure missing 0.025 0.020
(0.157) (0.143)Pulse 87.648 87.645
(25.725) (25.804)Pulse missing 0.003 0.004
(0.061) (0.068)Chest pain
6 to 12 hours 0.088 0.090(0.284) (0.286)
> 12 hours 0.125 0.126(0.330) (0.332)
Unable to determine or none 0.215 0.208(0.410) (0.406)
Anterior myocardial infarction 0.462 0.457(0.498) (0.498)
ST elevation on admission electrocardiogram 0.426 0.421(0.494) (0.493)
Killip classII 0.118 0.122
(0.323) (0.328)III 0.352 0.345
(0.477) (0.475)IV 0.024 0.018
(0.156) (0.135)Left ventricular ejection fraction
< 20 0.018 0.015(0.133) (0.122)
20 to 39 0.208 0.151(0.406) (0.358)
Left ventricular ejection fraction missing 0.302 0.473(0.459) (0.499)
Congestive heart failure 0.288 0.278(0.453) (0.448)
Cardiac arrest 0.038 0.032(0.192) (0.176)
Hemorrhage 0.030 0.026(0.171) (0.159)
Renal function: BUN>40 or creatinine>2.5 0.093 0.081(0.290) (0.273)
InstrumentsDifferential distance
Nearest 250-500 admission hospital - nearest hosp. 11.046 10.535(28.674) (25.313)
Nearest 500> admission hospital - nearest hosp. 10.108 42.079(47.451) (63.455)
Mean hospital AMI volume in 50 mile radius 279.555 195.234(86.491) (86.333)

Table 2. Health Outcomes: Probit
30-Day Mortality 1-Year Mortality 30-Day Readmission 30-Day Mortality One-Year Mortality 30-Day ReadmissionVariable Coefficient Coefficient Coefficient Coefficient Coefficient CoefficientVolumeMedium volume (25%-75% of AMI admissions) -0.043** -0.071*** -0.051** -0.049 -0.044 0.064*
(0.019) (0.017) (0.020) (0.031) (0.028) (0.034)[-0.011] [-0.011] [-0.011] [-0.013] [-0.015] [0.015]
High volume (>75% AMI admissions) -0.085*** -0.090*** -0.056*** -0.109*** -0.063** 0.014(0.019) (0.017) (0.020) (0.031) (0.028) (0.034)[-0.022] [-0.022] [-0.022] [-0.028] [-0.022] [0.003]
Add sociodemographic characteristicsMedium volume (25%-75% of AMI admissions) -0.044** -0.069*** -0.052** -0.027 -0.014 0.061*
(0.020) (0.017) (0.020) (0.032) (0.029) (0.034)[-0.011] [0.024] [-0.011] [-0.007] [-0.005] [0.014]
High volume (>75% AMI admissions) -0.089*** -0.087*** -0.057*** -0.083*** -0.025 0.007(0.019) (0.017) (0.020) (0.032) (0.029) (0.034)[-0.022] [-0.030] [-0.012] [-0.021] [-0.009] [0.002]
Add hospital characteristicsMedium volume (25%-75% of AMI admissions) -0.028 -0.049*** -0.030 -0.014 -0.006 0.046
(0.021) (0.018) (0.021) (0.033) (0.030) (0.035)[-0.007] [-0.017] [-0.007] [-0.004] [-0.002] [0.011]
High volume (>75% AMI admissions) -0.060*** -0.056*** -0.020 -0.040 0.003 -0.020(0.022) (0.020) (0.023) (0.039) (0.035) (0.041)[-0.015] [-0.019] [-0.004] [-0.010] [0.001] [-0.004]
Add Coexisting conditions and severity of illnessMedium volume (25%-75% of AMI admissions) -0.013 -0.046** -0.036* -0.002 -0.006 0.032
(0.022) (0.020) (0.021) (0.035) (0.032) (0.035)[-0.003] [-0.015] [-0.008] [0.000] [-0.002] [0.007]
High volume (>75% AMI admissions) -0.045* -0.059*** -0.030 0.001 0.016 -0.047(0.024) (0.021) (0.023) (0.042) (0.037) (0.041)[-0.010] [-0.019] [-0.006] [0.000] [0.005] [-0.011]
River and Vuong Endogeneity test -0.699 -1.468 -0.962 -2.817 -2.247 -1.339(t-value)RESET test 3.692 -5.54 -0.384 1.152 -3.798 -1.761(t-value)
N 77,824 77,824 77,824 22,193 22,193 22,193
Standard error in parentheses, Marginal effect in bracketsSignificant at the 1% level (***)Significant at the 5% level (**)Significant at the 10% level (*)
Metropolitan Statistical Area Non-Metropolitan Statistical Area

Table 3. Health Outcomes: Multivariate Probit
30-Day Mortality One-Year Mortality 30-Day Readmission 30-Day Mortality One-Year Mortality 30-Day ReadmissionVariable Coefficient Coefficient Coefficient Coefficient Coefficient CoefficientVolumeMedium volume -0.029 -0.061 * 0.047 0.013 0.042 -0.005(25%-75% of AMI admissions) (0.042) (0.037) (0.040) (0.061) (0.054) (0.059)High volume -0.079 -0.090 0.145 * 0.032 0.120 -0.128(>75% AMI admissions) (0.078) (0.070) (0.076) (0.115) (0.102) (0.111)
Sociodemographic characteristicsAge 0.025 *** 0.035 *** -0.002 ** 0.024 *** 0.033 *** -0.004 ***
(0.001) (0.001) (0.001) (0.002) (0.001) (0.002)Female 0.046 *** 0.026 ** 0.039 *** 0.065 *** -0.003 -0.021
(0.012) (0.011) (0.012) (0.022) (0.020) (0.021)Black -0.131 *** -0.042 * 0.013 -0.099 * -0.029 -0.096 *
(0.028) (0.024) (0.026) (0.052) (0.045) (0.051)Other -0.028 -0.037 0.010 -0.126 -0.073 -0.074
(0.033) (0.030) (0.032) (0.102) (0.090) (0.100)
Hospital characteristicsCardiac intensive care beds 0.000 0.000 0.000 0.001 -0.002 -0.001
(0.001) (0.001) (0.001) (0.003) (0.002) (0.003)Cardiac intensive care beds missing -0.039 * -0.003 0.038 * 0.033 0.020 -0.132 ***
(0.022) (0.020) (0.021) (0.038) (0.034) (0.038)Bed total 0.000 0.000 0.000 *** 0.000 0.000 0.000
(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)Cardiac catheterization lab 0.061 *** 0.033 -0.003 0.062 0.031 0.015
(0.023) (0.020) (0.022) (0.038) (0.033) (0.036)Cardiac surgery -0.034 ** -0.039 *** -0.077 *** -0.048 -0.045 -0.010
(0.016) (0.014) (0.015) (0.036) (0.032) (0.034)Minor teaching -0.019 -0.010 -0.014 -0.038 -0.040 0.033
(0.016) (0.015) (0.016) (0.039) (0.034) (0.037)Major teaching -0.080 *** -0.040 *** 0.053 *** -0.176 *** -0.116 ** 0.051
(0.017) (0.015) (0.017) (0.058) (0.049) (0.053)For profit 0.020 0.012 -0.010 0.059 0.060 0.038
(0.028) (0.025) (0.027) (0.042) (0.038) (0.042)Nonprofit -0.031 -0.025 -0.030 -0.033 -0.021 0.035
(0.025) (0.022) (0.025) (0.029) (0.026) (0.029)Hospital data missing 0.020 -0.032 -0.146 -0.268 -0.200 0.093
(0.104) (0.092) (0.100) (0.318) (0.282) (0.294)
Coexisting ConditionsCharlson IndexCharlson = 1 0.012 0.128 *** 0.071 *** 0.058 * 0.149 *** 0.050 *
(0.017) (0.015) (0.016) (0.031) (0.028) (0.029)Charlson = 2 or 3 0.040 ** 0.260 *** 0.160 *** 0.051 * 0.278 *** 0.102 ***
(0.016) (0.014) (0.015) (0.030) (0.026) (0.028)Charlson >= 4 0.136 *** 0.478 *** 0.202 *** 0.066 * 0.453 *** 0.186 ***
(0.020) (0.018) (0.020) (0.039) (0.034) (0.037)Immobile 0.278 *** 0.378 *** -0.067 0.334 *** 0.529 *** -0.191 **
(0.039) (0.038) (0.045) (0.078) (0.077) (0.097)Incontinent 0.082 *** 0.135 *** -0.063 ** 0.038 0.146 *** -0.112 **
(0.026) (0.024) (0.029) (0.048) (0.043) (0.053)
Severity of illnessLog mean arterial pressure -1.001 *** -0.791 *** 0.151 *** -0.992 *** -0.833 *** 0.135 ***
Metropolitan Statistical Area Non-Metropolitan Statistical Area

(0.027) (0.025) (0.028) (0.050) (0.046) (0.051)Log mean arterial pressure missing -4.047 *** -3.173 *** 0.568 *** -4.029 *** -3.430 *** 0.372
(0.129) (0.118) (0.135) (0.238) (0.221) (0.253)Pulse 0.001 *** 0.003 *** 0.000 0.001 ** 0.003 *** 0.001
(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)Pulse missing 0.305 *** 0.491 *** -0.197 0.344 ** 0.659 *** -0.093
(0.093) (0.093) (0.136) (0.161) (0.169) (0.237)Chest pain
6 to 12 hours 0.128 *** 0.111 *** 0.004 0.120 *** 0.098 *** -0.001(0.021) (0.019) (0.020) (0.038) (0.034) (0.037)
> 12 hours 0.187 *** 0.157 *** -0.004 0.158 *** 0.136 *** -0.082 **(0.018) (0.016) (0.018) (0.033) (0.030) (0.033)
Unable to determine or none 0.194 *** 0.224 *** -0.107 *** 0.194 *** 0.216 *** -0.147 ***(0.015) (0.013) (0.015) (0.027) (0.025) (0.029)
Anterior myocardial infarction 0.233 *** 0.174 *** -0.010 0.220 *** 0.151 *** -0.002(0.012) (0.011) (0.012) (0.022) (0.020) (0.021)
ST elevation on admission electrocardiogr 0.094 *** 0.072 *** -0.012 0.141 *** 0.119 *** 0.007(0.012) (0.011) (0.012) (0.022) (0.020) (0.021)
Killip classII 0.121 *** 0.157 *** 0.054 *** 0.092 *** 0.101 *** 0.099 ***
(0.019) (0.017) (0.018) (0.035) (0.031) (0.033)III 0.291 *** 0.349 *** 0.080 *** 0.293 *** 0.346 *** 0.138 ***
(0.021) (0.019) (0.022) (0.039) (0.035) (0.039)IV 0.947 *** 0.841 *** -0.296 *** 0.867 *** 0.761 *** -0.350 ***
(0.036) (0.036) (0.050) (0.075) (0.077) (0.110)Left ventricular ejection fraction
< 20 0.701 *** 0.777 *** 0.015 0.836 *** 0.786 *** -0.149(0.038) (0.037) (0.043) (0.075) (0.075) (0.092)
20 to 39 0.366 *** 0.372 *** 0.053 *** 0.324 *** 0.384 *** 0.028(0.016) (0.014) (0.015) (0.034) (0.029) (0.032)
Left ventricular ejection fraction missing 0.609 *** 0.472 *** -0.064 *** 0.556 *** 0.431 *** -0.073 ***(0.014) (0.012) (0.014) (0.028) (0.024) (0.025)
Congestive heart failure -0.046 ** 0.038 ** 0.013 -0.016 0.057 -0.083 **(0.021) (0.019) (0.022) (0.039) (0.036) (0.041)
Cardiac arrest 0.827 *** 0.626 *** -0.297 *** 0.848 *** 0.666 *** -0.285 ***(0.028) (0.028) (0.038) (0.057) (0.058) (0.079)
Hemorrhage 0.061 ** 0.113 *** -0.140 *** -0.055 0.020 -0.010(0.031) (0.029) (0.036) (0.063) (0.057) (0.067)
Renal function: BUN>40 or creatinine>2.5 0.367 *** 0.553 *** 0.047 ** 0.398 *** 0.559 *** 0.083 **(0.018) (0.017) (0.020) (0.035) (0.034) (0.039)
Year 1994 -0.019 0.024 ** -0.012 -0.048 ** -0.031 0.042 *(0.012) (0.011) (0.012) (0.023) (0.020) (0.022)
Constant 0.816 *** -0.756 *** -1.738 *** 0.754 *** -0.487 ** -1.419 ***(0.145) (0.132) (0.149) (0.268) (0.244) (0.275)
rho 0.012 0.011 -0.063 ** -0.011 -0.038 0.030(0.027) (0.024) (0.026) (0.040) (0.035) (0.038)
N 77,824 77,824 77,824 22,193 22,193 22,193
Significant at the 1% level (***)Significant at the 5% level (**)Significant at the 10% level (*)
Results are the combination of 15 imputed samples.

Table 4. Volume Equation from Multivariate Probit
30-Day Mortality One-Year Mortality 30-Day Readmission 30-Day Mortality One-Year Mortality 30-Day ReadmissionVariable Coefficient Coefficient Coefficient Coefficient Coefficient CoefficientInstrumentsDifferential distance
Nearest 250-500 adm. hosp. - nearest hosp. 0.002 *** 0.002 *** 0.002 *** -0.010 *** -0.010 *** -0.010 ***(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)
Nearest 500> adm. hosp. - nearest hosp. -0.002 ** -0.002 ** -0.002 ** 0.000 0.000 0.000(0.001) (0.001) (0.001) (0.000) (0.000) (0.000)
Mean hospital AMI volume in 50 mile radius 0.003 *** 0.003 *** 0.003 *** 0.003 *** 0.003 *** 0.003 ***(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)
Sociodemographic characteristicsAge -0.001 -0.001 -0.001 -0.003 ** -0.003 ** -0.003 **
(0.001) (0.001) (0.001) (0.001) (0.001) (0.001)Female -0.023 ** -0.023 ** -0.023 ** 0.000 0.000 0.000
(0.009) (0.009) (0.009) (0.018) (0.018) (0.018)Black -0.690 *** -0.690 *** -0.690 *** -0.244 *** -0.245 *** -0.244 ***
(0.018) (0.018) (0.018) (0.040) (0.040) (0.040)Other -0.557 *** -0.557 *** -0.557 *** -0.013 -0.014 -0.014
(0.029) (0.029) (0.029) (0.081) (0.081) (0.081)
Hospital characteristicsCardiac intensive care beds 0.011 *** 0.011 *** 0.011 *** 0.024 *** 0.024 *** 0.024 ***
(0.001) (0.001) (0.001) (0.002) (0.002) (0.002)Cardiac intensive care beds missing -0.092 *** -0.092 *** -0.092 *** -0.451 *** -0.450 *** -0.451 ***
(0.017) (0.017) (0.017) (0.031) (0.031) (0.031)Bed total 0.003 *** 0.003 *** 0.003 *** 0.005 *** 0.005 *** 0.005 ***
(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)Cardiac catheterization lab 0.668 *** 0.668 *** 0.668 *** 0.802 *** 0.802 *** 0.802 ***
(0.017) (0.017) (0.017) (0.025) (0.025) (0.025)Cardiac surgery -0.106 *** -0.106 *** -0.106 *** -0.122 *** -0.122 *** -0.122 ***
(0.016) (0.016) (0.016) (0.032) (0.032) (0.032)Minor teaching 0.125 *** 0.125 *** 0.125 *** 0.211 *** 0.211 *** 0.211 ***
(0.013) (0.013) (0.013) (0.033) (0.033) (0.033)Major teaching -0.188 *** -0.188 *** -0.188 *** -0.445 *** -0.445 *** -0.445 ***
(0.021) (0.021) (0.021) (0.051) (0.051) (0.051)For profit 0.158 *** 0.158 *** 0.158 *** -0.070 ** -0.070 ** -0.070 **
(0.028) (0.028) (0.028) (0.033) (0.033) (0.033)Nonprofit 0.631 *** 0.631 *** 0.631 *** 0.277 *** 0.277 *** 0.277 ***
(0.021) (0.021) (0.021) (0.022) (0.022) (0.022)Hospital data missing 1.378 *** 1.378 *** 1.379 *** -0.334 -0.333 -0.333
(0.091) (0.091) (0.091) (0.234) (0.234) (0.234)
Coexisting ConditionsCharlson IndexCharlson = 1 -0.003 -0.003 -0.003 -0.009 -0.009 -0.009
(0.012) (0.012) (0.012) (0.024) (0.024) (0.024)Charlson = 2 or 3 0.013 0.013 0.013 0.038 0.038 0.038 *
(0.012) (0.012) (0.012) (0.023) (0.023) (0.023)Charlson >= 4 0.019 0.019 0.019 0.024 0.024 0.024
(0.016) (0.016) (0.016) (0.031) (0.031) (0.031)Immobile -0.069 ** -0.069 ** -0.069 ** 0.125 * 0.125 * 0.126 *
(0.034) (0.034) (0.034) (0.073) (0.073) (0.073)Incontinent -0.023 -0.023 -0.023 -0.028 -0.029 -0.028
(0.022) (0.022) (0.022) (0.041) (0.041) (0.041)
Metropolitan Statistical Area Non-Metropolitan Statistical Area

Severity of illnessLog mean arterial pressure -0.050 ** -0.050 ** -0.050 ** -0.048 -0.048 -0.048
(0.022) (0.022) (0.022) (0.041) (0.041) (0.041)Log mean arterial pressure missing -0.272 *** -0.272 *** -0.271 *** -0.118 -0.118 -0.117
(0.105) (0.105) (0.105) (0.200) (0.200) (0.200)Pulse 0.000 0.000 0.000 0.000 0.000 0.000
(0.000) (0.000) (0.000) (0.000) (0.000) (0.000)Pulse missing 0.080 0.080 0.079 0.127 0.127 0.128
(0.078) (0.078) (0.078) (0.144) (0.144) (0.144)Chest pain
6 to 12 hours -0.019 -0.019 -0.019 0.076 ** 0.076 ** 0.076 **(0.016) (0.016) (0.016) (0.031) (0.031) (0.031)
> 12 hours -0.048 *** -0.048 *** -0.048 *** -0.024 -0.024 -0.024(0.014) (0.014) (0.014) (0.027) (0.027) (0.027)
Unable to determine or none -0.011 -0.011 -0.011 -0.070 *** -0.070 *** -0.070 ***(0.012) (0.012) (0.012) (0.023) (0.023) (0.023)
Anterior myocardial infarction -0.042 *** -0.042 *** -0.042 *** -0.085 *** -0.086 *** -0.085 ***(0.009) (0.009) (0.009) (0.018) (0.018) (0.018)
ST elevation on admission electrocardiogram 0.021 ** 0.021 ** 0.021 ** 0.056 *** 0.056 *** 0.056 ***(0.009) (0.009) (0.009) (0.018) (0.018) (0.018)
Killip classII -0.033 ** -0.033 ** -0.034 ** 0.053 * 0.053 * 0.053 *
(0.015) (0.015) (0.015) (0.028) (0.028) (0.028)III 0.000 0.000 0.000 0.094 *** 0.094 *** 0.094 ***
(0.017) (0.017) (0.017) (0.033) (0.033) (0.033)IV -0.026 -0.026 -0.026 -0.029 -0.029 -0.029
(0.032) (0.032) (0.032) (0.070) (0.070) (0.070)Left ventricular ejection fraction
< 20 0.060 * 0.060 * 0.060 * -0.052 -0.053 -0.052(0.035) (0.035) (0.035) (0.076) (0.076) (0.076)
20 to 39 -0.011 -0.011 -0.011 -0.005 -0.005 -0.005(0.013) (0.013) (0.013) (0.028) (0.028) (0.028)
Left ventricular ejection fraction missing -0.066 *** -0.066 *** -0.066 *** -0.220 *** -0.221 *** -0.220 ***(0.011) (0.011) (0.011) (0.020) (0.020) (0.020)
Congestive heart failure 0.024 0.024 0.024 -0.029 -0.029 -0.030(0.018) (0.018) (0.018) (0.035) (0.035) (0.035)
Cardiac arrest -0.010 -0.010 -0.010 0.056 0.058 0.056(0.025) (0.025) (0.025) (0.055) (0.055) (0.055)
Hemorrhage -0.030 -0.030 -0.030 0.096 * 0.096 * 0.096 *(0.027) (0.027) (0.027) (0.055) (0.055) (0.055)
Renal function: BUN>40 or creatinine>2.5 0.021 0.021 0.021 0.019 0.019 0.019(0.016) (0.016) (0.016) (0.033) (0.033) (0.033)
Year 1994 -0.001 -0.001 -0.001 0.087 *** 0.087 *** 0.087 ***(0.010) (0.010) (0.010) (0.018) (0.018) (0.018)
Constant -0.595 *** -0.595 *** -0.594 *** 0.301 0.303 0.299(0.128) (0.128) (0.128) (0.219) (0.219) (0.219)
N 77,824 77,824 77,824 22193 22193 22193
Significant at the 1% level (***)Significant at the 5% level (**)Significant at the 10% level (*)
Results are the combination of 15 imputed samples.