Horizontal space misrepresentation in unilateral brain damage: II. Eye-head centered modulation of...
11
Neuropsychologia 40 (2002) 1118–1128 Horizontal space misrepresentation in unilateral brain damage II. Eye-head centered modulation of visual misrepresentation in hemianopia without neglect Fabrizio Doricchi a,b,∗ , Alessandra Onida a , Paola Guariglia a a Centro Ricerche di Neuropsicologia, Fondazione Santa Lucia, IRCCS—Laboratorio Europea di Neuroscienze dell’Azione (L.E.N.A.), Via Ardeatina 306-00179 Rome, Italy b Dipartimento di Psicologia, Universita’ degli Studi di Roma, La Sapienza, Rome, Italy Received 6 April 2001; received in revised form 19 December 2001; accepted 4 January 2002 Abstract We used a visual distance reproduction task (endpoint task) to evaluate horizontal space representation in two left brain damaged (LBD) and three right brain damaged (RBD) patients with contralateral homonymous hemianopia and no neglect. All patients were examined in the chronic phase of the stroke and were aware of their visual field defect. Along with contralesional deviation in the line bisection task, all patients estimated size (Landmark task) and distances in the contralesional space as being longer than equivalent size and distances located in the ipsilesional space. Misreproduction of distances was abolished or reduced when the task was performed in the ipsilesional head-centred space with the head turned contralesionally. This finding points out that misrepresentation of horizontal space linked to hemianopia can be modulated by combined proprioceptive input from eye and neck muscles. The pattern of misrepresentation found in chronic hemianopic patients is opposite to the one described in chronic neglect patients with concomitant hemianopia. These different patterns of space misrepresentation are the likely consequence of the presence, in hemianopics, and the absence, in neglect patients with hemianopia, of compensatory strategies based on the non-retinotopic and multimodal coding of spatial positions falling in the retinotopically organised blind field. © 2002 Elsevier Science Ltd. All rights reserved. Keywords: Hemianopia; Neglect; Size; Space; Proprioceptive 1. Introduction In humans, unilateral neglect is frequent after right brain damage encroaching the parietal lobe and is characterized by defective representation and attention to stimuli posi- tioned in the contralesional space [43]. One of the most typical clinical features of the syndrome, is the ipsilesional deviation showed by neglect patients when marking the centre of horizontal lines [43]. It was suggested [5,28,34] that the bisection performance of neglect patients depends on a basic pathological representation or perception of hori- zontal stimuli, with contralesional stimuli being considered shorter than equivalent ipsilesional ones. This hypothesis is based on the finding that when forced to compare the length of an horizontal line segment positioned in the contrale- sional body-centered space with that of an adjacent iden- tical segment positioned in the ipsilesional space, neglect patients consistently judge the contralesional segment as ∗ Corresponding author. Tel.: +39-6-5150-1509; fax: +39-6-5150-1366. E-mail address: [email protected] (F. Doricchi). being shorter [28,34]. Similarly, neglect patients may set the contralesional endpoint of a remembered horizontal line too far from its physical centre (i.e. overextension) and the ipsilesional endpoint too close from the same centre (i.e. underextension; [5,37] ). Using a visuomotor task in which patients were asked to reproduce an horizontal distance between a central mark and a dot located in the contrale- sional or in the ipsilesional body-centered space by setting another pen dot in the opposite space (the “endpoint task”; [5,37]), Doricchi and Angelelli [17] found that horizon- tal space misrepresentation (contralesional overextension/ ipsilesional underextension) is consistent and severe only in patients with concomitant neglect and hemianopia and slight in neglect patients with posterior lesions and no hemi- anopia. These findings led these authors to hypothesize that misrepresentation of horizontal space in neglect patients is due to the failure of framing a correct representation of the horizontal dimension of stimuli falling in a retinotopically organized blind field during combined eye, head and arm movements. This failure should be functionally consequent to damage, in one hemisphere, of both visual retinotopic and 0028-3932/02/$ – see front matter © 2002 Elsevier Science Ltd. All rights reserved. PII:S0028-3932(02)00011-8
-
Upload
mariatomarchio -
Category
Documents
-
view
2 -
download
0
Transcript of Horizontal space misrepresentation in unilateral brain damage: II. Eye-head centered modulation of...

Neuropsychologia 40 (2002) 1118–1128
Horizontal space misrepresentation in unilateral brain damageII. Eye-head centered modulation of visual misrepresentation
in hemianopia without neglect
Fabrizio Doricchia,b,∗, Alessandra Onidaa, Paola Guarigliaaa Centro Ricerche di Neuropsicologia, Fondazione Santa Lucia, IRCCS—Laboratorio Europea di Neuroscienze dell’Azione (L.E.N.A.),
Via Ardeatina 306-00179 Rome, Italyb Dipartimento di Psicologia, Universita’ degli Studi di Roma, La Sapienza, Rome, Italy
Received 6 April 2001; received in revised form 19 December 2001; accepted 4 January 2002
Abstract
We used a visual distance reproduction task (endpoint task) to evaluate horizontal space representation in two left brain damaged (LBD)and three right brain damaged (RBD) patients with contralateral homonymous hemianopia and no neglect. All patients were examined inthe chronic phase of the stroke and were aware of their visual field defect. Along with contralesional deviation in the line bisection task,all patients estimated size (Landmark task) and distances in the contralesional space as being longer than equivalent size and distanceslocated in the ipsilesional space. Misreproduction of distances was abolished or reduced when the task was performed in the ipsilesionalhead-centred space with the head turned contralesionally. This finding points out that misrepresentation of horizontal space linked tohemianopia can be modulated by combined proprioceptive input from eye and neck muscles. The pattern of misrepresentation found inchronic hemianopic patients is opposite to the one described in chronic neglect patients with concomitant hemianopia. These differentpatterns of space misrepresentation are the likely consequence of the presence, in hemianopics, and the absence, in neglect patients withhemianopia, of compensatory strategies based on the non-retinotopic and multimodal coding of spatial positions falling in the retinotopicallyorganised blind field. © 2002 Elsevier Science Ltd. All rights reserved.
Keywords:Hemianopia; Neglect; Size; Space; Proprioceptive
1. Introduction
In humans, unilateral neglect is frequent after right braindamage encroaching the parietal lobe and is characterizedby defective representation and attention to stimuli posi-tioned in the contralesional space [43]. One of the mosttypical clinical features of the syndrome, is the ipsilesionaldeviation showed by neglect patients when marking thecentre of horizontal lines [43]. It was suggested [5,28,34]that the bisection performance of neglect patients dependson a basic pathological representation or perception of hori-zontal stimuli, with contralesional stimuli being consideredshorter than equivalent ipsilesional ones. This hypothesis isbased on the finding that when forced to compare the lengthof an horizontal line segment positioned in the contrale-sional body-centered space with that of an adjacent iden-tical segment positioned in the ipsilesional space, neglectpatients consistently judge the contralesional segment as
∗ Corresponding author. Tel.:+39-6-5150-1509; fax:+39-6-5150-1366.E-mail address:[email protected] (F. Doricchi).
being shorter [28,34]. Similarly, neglect patients may setthe contralesional endpoint of a remembered horizontal linetoo far from its physical centre (i.e. overextension) and theipsilesional endpoint too close from the same centre (i.e.underextension; [5,37] ). Using a visuomotor task in whichpatients were asked to reproduce an horizontal distancebetween a central mark and a dot located in the contrale-sional or in the ipsilesional body-centered space by settinganother pen dot in the opposite space (the “endpoint task”;[5,37]), Doricchi and Angelelli [17] found that horizon-tal space misrepresentation (contralesional overextension/ipsilesional underextension) is consistent and severe onlyin patients with concomitant neglect and hemianopia andslight in neglect patients with posterior lesions and no hemi-anopia. These findings led these authors to hypothesize thatmisrepresentation of horizontal space in neglect patients isdue to the failure of framing a correct representation of thehorizontal dimension of stimuli falling in a retinotopicallyorganized blind field during combined eye, head and armmovements. This failure should be functionally consequentto damage, in one hemisphere, of both visual retinotopic and
0028-3932/02/$ – see front matter © 2002 Elsevier Science Ltd. All rights reserved.PII: S0028-3932(02)00011-8

F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128 1119
multimodal non-retinotopic coding of space integrating vi-sual input with proprioceptive and vestibular cues signallingthe position of the eye in the orbit and the position of thehead and the arms with respect to the the trunk. In the samestudy, Doricchi and Angelelli [17] found that the asymme-try between contralesional overextension and ipsilesionalunderextension was positively and significantly correlatedwith the ipsilesional shift in the line bisection task.
When compared to neglect patients, hemianopic patientswithout neglect have a well documented opposite bias in theperformance of the line bisection task, showing a compen-satory contralesional deviation toward the blind hemifield[3,15,31,47]. Accordingly, patients with pure hemianopiashould perceive or represent the size of contralesional hori-zontal stimuli (or an equivalent distance between two stim-uli) as being longer than an identical ipsilesional one. Here,we document with purely visual tasks this very “reversed”pattern of horizontal space misrepresentation in two leftbrain damaged (LBD) and in three right brain damaged(RBD) patients with contralesional full post-chiasmatichemianopia and no neglect. Separated and combined exper-imental manipulation of eye and neck position also allowedus to define the influence of eye and neck proprioceptiveinput on the evaluation and reproduction of horizontaldistances in these patients.
In accordance with the terminology used in the mostrecent literature [5,17,21], in the present paper the term“underestimation” will be used to indicate that a size or areproduced distance is subjectively judged as being shorterthan it objectively is (the term is therefore synonymous of“overextension”). The term “overestimation” will be usedin the opposite case (as synonymous of “underextension”).Both terms will be used in the relative sense, that is to say inrelationship to the comparison between contralesional andipsilesional distance reproduction within each of the groupof patients considered in the study.
2. Methods
2.1. Patients
All hemianopic patients (see clinical data in Table 1) wereright handed, free from psychiatric disorders or dementia
Table 1Individual clinical data of hemianopic patients and performance scores in the letter cancellation, line bisection and Landmark task (with relativebinomialprobabilities)a
Patient Age(year)
Stroke onset(month)
Letter cancellation Line bisection (20 cm),deviation (mm)
Landmark task
Left Right Ipsilesional half shorter p (binomial test)
LBD1 74 3 53/53 51/51 −4.3 10/12 0.01LBD2 76 3 53/53 51/51 −14 12/12 0.0002
RBD1 74 3 51/53 48/51 −3 10/12 0.01RBD2 60 6 51/53 50/51 −2.6 9/12 0.07RBD3 65 17 52/53 51/51 −21 11/12 0.003
a Negative values in the line bisection task indicate contralesional deviation.
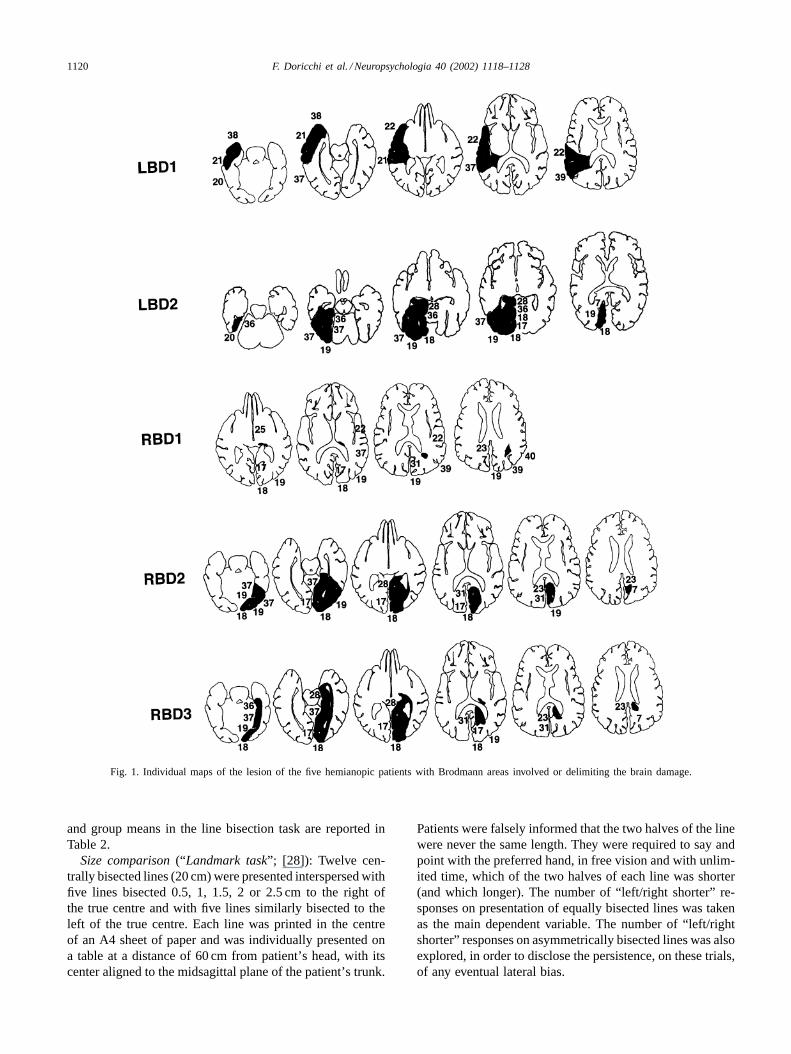
and suffered contralesional complete homonymous hemi-anopia without macular sparing after unilateral stroke. Thevisual field defect was assessed with Humphreys perime-try in patients RBD1, RBD2, RBD3 and with Goldmannperimetry in patients LBD1 and LBD2. All patients wereexamined in the chronic phase of the illness and all of themwere aware of their visual field defect. According to theclassification of unawareness of visual loss in the affectedfield proposed by Critchley [13,10] patients LBD2, RBD1and RBD3 were classified as type 5 (i.e. awareness of thedefect which is erroneously interpreted as being a “prob-lem in one eye”); patients LBD1 and RBD2 were classifiedas type 6 (i.e. awareness that the deficit is due to a cere-bral lesion). None of the patients had tactile extinction onclinical examination. The brain damage was documentedby MRI scans. The maps of the lesions on the templatesby Damasio and Damasio [14] are shown in Fig. 1. Inpatients LBD2, RBD2, and RBD3 the damage involvedthe medial–ventral occipital–temporal area irrigated by theposterior cerebral artery. In RBD3 there was also an in-volvement of the posterior thalamus. In patient RBD1 therewas a posterior thalamic lesion and another lesion in theparaventricular white matter. LBD1 developed hemianopiaafter deep haemorragic infarction in the temporal lobe.
2.2. Neglect evaluation in hemianopics
Line bisection task: On six trials patients marked the sub-jective midpoint of a 20 cm× 2 mm line, printed centrallyon a horizontally oriented A3 sheet of paper. On each trialthe sheet was placed on a table with its center aligned to themidsagittal plane of the patient’s trunk. The performanceof the group of hemianopics (N−H+) was compared: (a)to the performance of four samples of RBD patients (pa-tients with no neglect or hemianopia, N−H−; patients withneglect and no hemianopia, N+H−; patients with neglectand hemianopia, N+H+; patients with neglect and inferiorquadrantanopia, N+Q+) and of a group of healthy con-trols (C) not participating in the experimental “visual end-point task” of the present study; (b) to the performance ofthe control samples of RBD N+H− and N+H+ performingthe experimental “visual endpoint task” in the present study.In all control patients the presence of neglect was assessedwith a standardised screening battery [38]. Clinical data
1120 F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128
Fig. 1. Individual maps of the lesion of the five hemianopic patients with Brodmann areas involved or delimiting the brain damage.
and group means in the line bisection task are reported inTable 2.
Size comparison(“Landmark task”; [28]): Twelve cen-trally bisected lines (20 cm) were presented interspersed withfive lines bisected 0.5, 1, 1.5, 2 or 2.5 cm to the right ofthe true centre and with five lines similarly bisected to theleft of the true centre. Each line was printed in the centreof an A4 sheet of paper and was individually presented ona table at a distance of 60 cm from patient’s head, with itscenter aligned to the midsagittal plane of the patient’s trunk.
Patients were falsely informed that the two halves of the linewere never the same length. They were required to say andpoint with the preferred hand, in free vision and with unlim-ited time, which of the two halves of each line was shorter(and which longer). The number of “left/right shorter” re-sponses on presentation of equally bisected lines was takenas the main dependent variable. The number of “left/rightshorter” responses on asymmetrically bisected lines was alsoexplored, in order to disclose the persistence, on these trials,of any eventual lateral bias.

F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128 1121
Table 2Clinical data of groups examined in the line bisection task and of groups performing the “visual endpoint” taska
Control samples (line bisection task) Hemianopics Control samples (visual endpoint task)
C N−H− N+H− N+H+ N+Q+ N−H+ C N+H+ N+H−n 10 9 20 19 5 5 5 4 10
Age (year) 65.9 55.6 66.6 66 67.8 69.8 60.6 55 71.4S.D. 7.6 15.2 11.1 10.3 10.5 6.6 9.4 6.2 7.4
Stroke onset (month) – 7 4.6 9 4.5 6.2 – 2.4 3.1S.D. – 10.4 3.5 13.2 2.3 6.1 – 0.82 1.3
Line bisection (mm) +0.49 +1.3 +9.3 +32.6 +9.2 −8.9 – +54.5 +6.3S.D. 3.1 5.4 7 23 5.1 8.1 – 17 10
a Positive values in the line bisection task indicate ipsilesional deviation (rightward deviation in the C group), negative values indicate contralesionaldeviation (leftward deviation in the C group; deviations are indicated in mm). C, healthy controls; N−H−, RBD patients without neglect or hemianopia;N+H−, occipital–temporal patients with neglect and no hemianopia; N+H+, RBD patients with both neglect and hemianopia; N+Q+, RBD patientswith both neglect and inferior quadrantanopia; N−H+, hemianopics.
Letter cancellation task[16]: One hundred and four targetletters (“H”) were interspersed with 208 distractor lettersalong six rows of 52 letters each, on a horizontally orientedA3 sheet of paper. Fifty-three target letters were on the leftside of the sheet and 51 on the right side. The sheet ofpaper was presented on a table with its center aligned tothe midsagittal plane of the patient’s trunk. Patients had
Table 3Performance of groups examined in the visual endpoint taska
Group Bar position
CP(bar side)
HC(bar side)
HI(bar side)
BC(bar side)
BI(bar side)
Leftcontra
Rightipsi
Leftcontra
Rightipsi
Leftcontra
Rightipsi
Leftcontra
Rightipsi
Leftcontra
Rightipsi
CMean 9.89 9.87 10.2 10 9.96 10 10 9.89 9.94 10.1S.D. 0.34 0.24 0.26 0.37 0.17 0.4 0.27 0.48 0.22 0.37
N−H+Mean 9.76 10.7 10.4 10.66 9.80 11.1 9.9 11.12 9.86 10.7S.D. 0.89 0.49 0.46 0.59 0.61 0.51 0.57 0.25 0.55 0.52
N+H+Mean 11.66 10.07 11.28 9.8 11.17 10.07 11.23 10.57 11.12 9.9S.D. 0.72 1.31 0.4 0.99 1.33 1.46 0.72 1.2 0.36 0.98
N+H−Mean 9.85 10.04 10.4 9.69 9.61 10.18 9.69 10.26 10.39 9.41S.D. 0.75 0.92 0.82 0.63 0.78 0.83 0.76 0.70 0.67 1.17
a Average distance reproduced by the groups (with R.S.D.) are in cm. Task conditions for RBD, LBD and healthy controls (C) are depicted at thebottom of the corresponding columns in the table. CP, central position; HC, head rotated contralesionally; HI, head rotated ipsilesionally; BC, barin thecontralesional head–body space; BI, bar in the ipsilesional head–body space.
unlimited time to cancel all target letters with a pen. Thescore was the number of cancelled targets on each side ofthe sheet.
Copying figures: Patients were required to copy the linedrawing of a street scene containing eight items (two in eachquadrant [45]). The model was presented on a horizontallyoriented A4 sheet of paper, immediately above another sheet

1122 F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128
where the patient had to copy the model. The center of bothsheets was aligned to the midsagittal plane of the patient’strunk.
3. Experimental task
Distance reproduction task(visual “endpoint task”[5,37]): Three coloured vertical marks (green, red and yel-low; 2 mm×5 mm) were mounted on a horizontal bar (1 m).The red mark was placed at the center of the bar, the yellowmark could be moved rightward and the green mark leftward(patient’s viewpoint). The bar was positioned on a table at adistance of 60 cm from the patient’s eyes. The centre of thebar (see Table 3) could be: (a) aligned to the head–body mid-sagittal plane (central position, CP); (b) aligned to the bodymidsagittal plane but positioned in the ipsilesional (HC)or contralesional head hemispace (HI) (head turn= 30◦ ineach case); or (c) placed in the contralesional (BC) or ip-silesional (BI) head–body hemispace. In each condition sixleftward and six rightward trials were performed. On left-ward trials, the yellow mark was placed in a fixed position10 cm (approximately, 10◦ of the visual angle) to the rightof the red mark and the green mark immediately adjacent tothe left of the red one. On rightward trials, the green markwas placed 10 cm to the left of the red mark and the yellowmark immediately adjacent to the right of the red one. Theexperimenter moved the green mark leftward or the yellowmark rightward. The patients’ heads were restrained andthey were required to stop the movement when the distancebetween the moving mark and the central red mark sub-jectively equalled the standard 10 cm distance between thecentral mark and the fixed mark on the other side of thebar. The patients then had unlimited time to adjust the markposition and check the standard distance. During testing,patients were allowed to move their eyes freely. The averagedistance (cm) between the moving mark and the central redmark was considered as the dependent variable. The perfor-mance of the group of N−H+ was compared to that of asample of ten N+H−, to that of a sample of four N+H+ andto that of a sample of five age-matched healthy control sub-jects (C). In patients LBD1, LBD2 and RBD3 we were ableto test the effect of contralesional or ipsilesional 30◦ trunkturns with the bar remaining aligned to the head midsagittalplane as well. Their performance was compared to that of C.
4. Results
4.1. Neglect evaluation in hemianopics
Line bisection task: Mean individual shifts (mm) from theobjective midline were considered for statistical analysis.Ipsilesional shifts (or rightward ones in the case of healthycontrols) were treated as positive values, contralesional shifts(or leftward ones in the case of healthy controls) as negative
ones. All hemianopic patients displayed contralesional devi-ation when bisecting horizontal lines (see individual data inTable 1). A series of one way between ANOVAs comparingthe performance of the group of N−H+ with that of each ofthe control samples not participating in the “visual endpointtask” (see group means in Table 2) showed that N−H+ hada significant contralesional shift when compared to N+H−(F = 25, P < 0.001), to N+H+ (F = 14, P < 0.001),to N+Q+ (F = 17, P = 0.002), to N−H− (F = 8, P =0.01) and that the performance of N−H+ also differed fromthat of C (F = 10.8,P = 0.005). These samples of subjectsdid not differ in age (F = 1.9,P = 0.1). Time elapsed fromstroke-onset was not different among the groups of braindamaged patients (F < 1).
The performance of N−H+ was also compared to thatof the groups of N+H− and of N+H+ performing the “vi-sual endpoint task” (see group means in Table 2). The con-tralesional deviation of N−H+ was different both from theipsilesional deviation showed by N+H− (F = 8.6, P =0.01) and from that of N+H+ (F = 53.9, P < 0.001).Time from stroke onset was not different among these threegroups of patients (F = 1.9,P = 0.17;P > 0.1 in each sin-gle between groups comparison). The mean age of groupsparticipating to the “visual endpoint task” was comparedthrough a one way between ANOVA. N+H+ were youngerthan N−H+ and N+H− (F = 5.6, P = 0.005; P < 0.01in each planned comparison). There was no age differencebetween N−H+ and C (P not significant).
Letter cancellation task[16]: In all hemianopic patients(see individual data in Table 1) the difference between thenumber of target letters cancelled in the ipsilesional half ofthe sheet minus the number of target letters cancelled in thecontralesional half (see Table 1) was below the cut-off dif-ference (4), thus indicating the absence of contralesional ne-glect. This cut-off score was defined on a normative sampleof 104 unilateral brain damaged patients [38,48].
Size comparison(Landmark task): Every hemianopic pa-tient consistently judged as “shorter” the ipsilesional halvesof a centrally bisected bar (see individual data and relatedprobabilities of the binomial test in Table 1). This pattern ofperformance is exactly the opposite to the one originally de-scribed by Milner and co-workers [28,34] in unilateral braindamaged patients with contralesional neglect. On asymmet-rical trials the performance of hemianopics was flawless,with the only exception of LBD2 who still considered theipsilesional section of the line as being shorter on two trialswhen objectively this section was longer.
Copying figures: None of the hemianopic patients showedomissions in the copy of the line drawing.
4.2. Experimental task
Distance reproduction task(visual “endpoint task”): Theperformance of the group hemianopics (N−H+) in the dif-ferent bar side× bar position conditions was compared tothat of the control groups of N+H−, N+H+ and C through

F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128 1123
a group×bar position(CP, HC, HI, BC, BI)×bar side (con-tralesional, ipsilesional) ANOVA performed on the averagedindividual distance reproductions (group means are reportedin Table 3). This ANOVA showed significant group×bar side(F = 12.6,P < 0.0001) and group×bar position×bar side(F = 2.6,P = 0.004) interactions. Separated bar position×bar side ANOVAS were performed on each group. In N+H−there was only a significant bar position×bar side interaction(F = 8.6, P < 0.0001). Planned comparisons, showed thatno lateral difference was present in the CP condition (P =0.4) whereas there were relative contralesional overexten-sion in the HC (P = 0.006) and BI conditions (P = 0.0003)and relative ipsilesional overextension in the HI (P = 0.02)and BC (P = 0.02) conditions. In N+H+ there was a sig-nificant bar side effect (F = 11.8, P = 0.04) but no barposition×bar side interaction (F < 1). Planned comparisonsshowed that in all bar positions there was relative contrale-sional overextension (P ≤ 0.02 in all contra versus ipsi sidecomparisons). In the group of N−H+ there was significantrelative ipsilesional overextension (bar side effect:F = 33,P = 0.004; contra 9.9 cm (S.D. 0.62 cm), ipsi 10.8 cm (S.D.0.49 cm)). However, a significant bar side× bar position in-teraction (F = 6, P = 0.003) showed that in N−H+ theside difference disappeared when the bar was positionedin the ipsilesional head hemispace and was aligned to thebody midsagittal plane (HC condition,P > 0.1; all barside comparisons in the other conditions,P < 0.001). No
Fig. 2. Individual averaged distances reproduced by the five hemianopic patients on the contralesional and ipsilesional side of the bar in the differenttask conditions of the visual endpoint task. The dark grey abscissa placed at 10 cm on theY-axis indicates perfect distance reproduction: LBD, left braindamaged; RBD, right brain damaged.
significant effect, interaction or side comparison in any ofthe bar position conditions was present in C subjects.
Analysis of individual data in hemianopics: Bar position(CP, HC, HI, BC, BI)×bar side (contra, ipsi) ANOVAs wereperformed on the data of each individual patient. These anal-yses showed that all hemianopic patients had relative con-tralesional underextension (overestimation) and ipsilesionaloverextension (underestimation) when reproducing standarddistance (bar side effect,P < 0.05 in LBD1 and RBD1,P < 0.002 in LBD2 and RBD3). The only exception wasRBD2 in which the lack of side difference both in the HCand BI condition (i.e. when the bar was positioned in theipsilesional head centred space, see below) reduced the sig-nificance of the bar side effect to theP = 0.08 level. Atthe individual level (see Fig. 2) the bar side× bar positioninteraction was present in RBD2 and RBD3 (P < 0.01),approached significance in LBD2 (P = 0.1) and was notsignificant in LBD1 and RBD1 (P > 0.2). Planned com-parisons showed that in the HC condition the side differ-ence was not significant in any patient with the exception ofLBD2 (planned comparison,P = 0.03); however, in the lat-ter patient the asymmetry was at its lowest level comparedto all other conditions (see Fig. 2).
Effect of trunk turns in hemianopics: The performance ofN−H+ was compared to that of C through a group× trunkposition (central, contra-turn, ipsi-turn) × bar side (contra,ipsi) ANOVA. Only a significant group×bar side interaction

1124 F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128
Table 4Effect of trunk turns on the visual endpoint taska
Group Trunk position
Central(bar side)
Contra(bar side)
Ipsi(bar side)
Left contra Right ipsi Left contra Right ipsi Left contra Right ipsi
CMean 9.92 9.88 9.91 9.87 9.93 9.97S.D. 0.34 0.23 0.08 0.15 0.14 0.17
N−H+Mean 9.75 10.86 9.99 10.83 10.14 11.15S.D. 1.2 0.67 0.51 0.72 0.34 0.23
a Only C and three N−H+ (LBD1, LBD2 and RBD3) participated in this experiment. Task conditions are depicted at the bottom of the correspondingcolumns in the table. Distances reproduced (with R.S.D.) are in cm.
was found (F = 39.1, P = 0.0007). Contralesional or ip-silesional trunk turns did not influence both the asymmetricalperformance of N−H+ (P < 0.01 in all trunk position×barside comparisons) and the symmetrical performance of C (Pnot significant in all trunk position×bar side comparisons).Means and S.D. are reported in Table 4.
5. Discussion
5.1. Main findings and previous evidences
The present study documents asymmetrical reproduc-tion of horizontal distances, with relative overestimation(underextension) of contralesional distances (and size) andcorresponding relative underestimation (overextension) ofipsilesional ones in patients with postchiasmatic hemianopiaand no neglect. This finding was observed in two purelyvisual tasks and was present in each hemianopic patient,independent of the side of the lesion. In the baseline condi-tion (CP) of the distance reproduction task, N+H+ patientsshowed relative contralesional underestimation and ipsile-sional overestimation whereas N+H− patients had no lateralasymmetry. These two latter findings replicate the resultsof a previous study by Doricchi and Angelelli [17] wherea visuomotor version of the endpoint task was used. Ferberand Karnath [21] recently reported relative underestimationof horizontal bars presented in the contralesional space andoverestimation of bars presented in the ipsilesional spacein five hemianopic patients. These authors interpreted thefailure of Doricchi and Angelelli’s study [17] in detectingasymmetrical performance in hemianopics, as being due tothe use of a visuomotor version of the endpoint task (and the
possible influence of untested impairments of visuomotorcoordination) and to the fact that four out of the five hemi-anopic patients considered in the same study had left braindamage (whereas all neglect patients had right brain dam-age). The results of the present study point out that when themotor component of the endpoint task is removed chronichemianopic patients aware of their visual field defect showan asymmetrical performance opposite to the one found byFerber and Karnath [21] and that this is so, independentof the side of the lesion. Therefore, the objections raisedby Ferber and Karnath [21] appear not to hold and theirresults are not replicated. Our interpretation of Ferber andKarnath’s findings is that they arise from the spurious in-fluence of two relevant and inter-related factors which werenot controlled in their study. First, virtually all Ferber andKarnath’s patients with neglect and hemianopia or with purehemianopia were studied in the acute phase of the illnesswithin 1 month from stroke onset (N+H+, mean= 25.2days; N−H+, mean= 20.6 days), some of them even 3or 4 days after stroke onset. It is well known that confusedmental states compromise awareness and management ofthe visual field defect in the acute phase [46] and that lack offull awareness of the visual field defect can persist well afterthe end of the acute phase in a high percentage of patients(60–70%; [10,46]). Ferber and Karnath [21] reported notesting of the awareness of the visual field defect. We notethat in their group of hemianopics the influence of unaware-ness could have been enhanced by the age of the patients,since three of them (out of five) were 80 years old or more.Second, and even more unfortunately, is the failure to report(as in a previous study [20]; see comment by Halligan [27])the performance of hemianopic patients in the line bisectiontest. This could have provided both an index of awareness

F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128 1125
and attention to the section of the line falling into the blindhemifield and a more accurate evaluation of neglect. Evalu-ation of neglect through multi-item cancellation or drawingtasks (as those administered by Ferber and Karnath) is in-sufficient because it has been convincingly documented thatdefective performance of neglect patients in line bisection (atask depending on the simultaneous and parallel visuospatialanalysis of the entire length of the line) can be dissociatedfrom the performance of tasks requiring the sequential anal-ysis of an array of separated and spatially distributed items[4]. Thus, the possibility that the hemianopic patients exam-ined by Ferber and Karnath had signs of neglect on the linebisection task cannot be excluded. Similarly, the contrale-sional underestimation of size found by Ferber and Karnathin their hemianopic patients [21] is totally incompatiblewith the well established contralesional deviation of hemi-anopics in the line bisection test [3,15,31,47] a finding thatwas further corroborated by the results of the present study.Contralesional deviation predicts overestimation (not under-estimation) of contralesional horizontal size and our studyfully confirmed this prediction. Ferber and Karnath’ findingof mild contralesional underestimation in acute or subacuteN+H− seems also not in agreement with the results froma previous study by Karnath and Ferber [30] in which nohorizontal space misrepresentation was found in a purelyvisual task in seven patients with neglect but no hemianopia;however, this latter result could be linked to the location ofthe lesion, since Doricchi and Angelelli [17] showed thatmild contralesional underestimation of horizontal distancescan be present in neglect patients with no hemianopia andposterior damage, no misrepresentation seems present inthose with anterior damage and severe misrepresentation ispresent in neglect patients with hemianopia and lesion over-lapping in the occipital cortical and subcortical structures(BA 17 and 18, see Fig. 2 [17]). This last anatomical corre-late of horizontal space misrepresentation was subsequentlyfully replicated by Ferber and Karnath [21]. Looking ret-rospectively at the findings by Doricchi and Angelelli [17],Ferber and Karnath [21] and at the results of the present andthe joint study [18], some conclusions can be drawn. First,taking into account that the absence of line bisection testingin Ferber and Karnath’ study does not allow to unequivo-cally assume that their acute hemianopic patients sufferedno neglect when analyzing the horizontal size of a stimulussimultaneously extending both in the contralesional andipsilesional space, it could be still tentatively hypothesizedthat both patients with neglect and hemianopia and patientswith pure hemianopia can show relative underestimation ofcontralesional horizontal distances and overestimation ofipsilesional ones in the acute phase of the stroke. In thisphase both groups of patients could not have developedstrategies aimed at the management of their visual field de-fect yet. However, second and most importantly, the sameset of data clearly suggests that in the chronic phase of thestroke horizontal space misrepresentation is consistentlypresent in neglect patients with concomitant hemianopia
whereas it disappears or even reverses in hemianopics. Insupport of this conclusion is a recent study by Kerkhoff [32]who found no visual misrepresentation of horizontal sizeor distance in RBD patients with pure contralesional hemi-anopia (with a central sparing of 2◦) studied 5 or 7 monthsafter the stroke. Also in keeping with the same conclu-sion are less recent findings by Zihl and von Cramon [47].These authors asked chronic hemianopic patients (studied 2months to 7 years after the stroke) to judge whether two vi-sual targets presented in total darkness along an horizontalperimeter, one in the contralesional and one in the ipsile-sional hemified, were at the same distance with respect tothe centre of the perimeter. The centre of the perimeter wasaligned to the restrained head–body midsagittal plane of pa-tients. In each block of trials the position of one target wasmaintained fixed whereas that of the target in the oppositehemifield was varied. Exactly as in the baseline condition(CP) of the present study, hemianopic patients underex-tended the distance between the central reference and thevariable-position target in the contralesional hemifield andoverextended the same distance in the ipsilesional hemifield(i.e. considered a contralesional target and an ipsilesionalone as being at the same distance from the centre when thedistance between the contralesional target and the centrewas objectively shorter than the distance between the ipsile-sional target and the centre). In the same study, all patientsshowed contralesional deviation both in the estimation ofthe subjective “straight ahead” and, as in the present study,in the line bisection task. It is worth noting that, contraryto the terminology adopted in more recent studies, Zihl andvon Cramon used the term “underestimation” as synony-mous of “underextension” and the term “overestimation”as synonymous of “overextension”. The different terminol-ogy adopted by Zihl and von Cramon, probably inducedFerber and Karnath [20,21] to erroneously conclude thattheir findings in acute hemianopics (overextension in thecontralesional hemifield and underextension in the ipsile-sional hemifield) were compatible with those by Zihl andvon Cramon. This statement should be corrected: Ferberand Karnath’ findings [21] are opposite and incompatiblewith those reported by Zihl and von Cramon [47].
5.2. Interpreting misrepresentation in hemianopiaand neglect
The whole of these results reinforce the hypothesis thatunderestimation of contralesional horizontal size and dis-tances and overestimation of ipsilesional ones in chronicneglect patients with hemianopia (as initially reported byMilner and co-workers [28,34] in six out of their seven pa-tients and by Bisiach et al. [5] in both of their two pa-tients; see also the case study by Halligan and Marshall [26])is not a simple effect of the retinotopic visual field defectas proposed by Ferber and Karnath [21]. Horizontal spacemisrepresentation in these patients rather seems to dependon the lack, difficulty or impossibility of compensating for

1126 F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128
a visual retinotopic deficit, due to concomitant damage ofnon-retinotopic multimodal representations of space, as orig-inally proposed by Doricchi and Angelelli [17]. Undam-aged multimodal representations could still allow the effec-tive coding of spatial positions falling in the blind field byintegrating residual visual information from the intact fieldwith proprioceptive and vestibular cues from the eyes, thehead and the arms. As an example, the spatial position of astimulus falling in the seeing hemifield before the start of ahorizontal eye/head movement bringing the stimulus in theblind hemifield, can be still effectively coded, after the endof the movement, by taking into account the changes oc-curred in the proprioceptive inputs from the eye and neckmuscles and in the vestibular inputs from the labirynths. Thelack of multimodal compensation of a retinotopic visual fielddeficit seems chronically suffered by neglect patients withhemianopia and, hypothetically, could be also suffered byneglect patients with a damage to retinotopically organizedvisual areas outside the primary visual cortex [42] and in-complete or no visual field defects. The same deficit couldbe only transitorily present in acute patients with neglectand no damage to retinotopical representations of space orin hemianopics who have not yet developed awareness andcompensatory management of their visual field defect.
When compared to the pattern of horizontal space mis-representation of chronic neglect patients with concomi-tant hemianopia [5,17,18,26,28,34], the reversed patternfound in chronic hemianopic patients without neglect canbe explained by the presence of compensatory strategiesdepending on head and body centred [1] representationsof contralesional space. These representations, which canbe disrupted in neglect patients [43], may contribute toawareness of the visual field defect [10,46], favouring inhemianopic patients the development of a representationalovercompensation of sectors of horizontal space falling inthe blind hemifield. We hypothesise that this overcompen-sation could have influenced the performance of the visualendpoint task in the following way: when foveating thelocation where the ipsilesional endpoint is being set, hemi-anopics are aware that the space between the central refer-ence mark and the subjective endpoint position entirely fallsin the blind field (this also as a consequence of the previousfree inspection of the array with the intact visual hemifield).In this case, hemianopics tend to boost their attention to thisblind space, overcompensate the representation of the samespace and set the endpoint at a relatively larger distancecompared to contralesional distance reproduction. In thislatter case overcompensation is absent because the blindfield can be shifted away contralesionally and the space be-tween the fovea on the subjective endpoint and the centralreference can be made to fall entirely in the seeing hemifield.
5.3. Eye–head centered proprioceptive modulation
In the distance reproduction task, overcompensation ofthe blind field in hemianopics was tempered by combined
contralesional head and ipsilesional eye turning (i.e. by con-comitant tonic modification of neck and eye proprioceptiveinput). In accordance with this result, during the clinicalexamination all patients informally reported that contrale-sional head turning and re-centring of the seeing hemifieldon the sagittal body midline was a compensatory strategyfrequently and spontaneously adopted in many everyday lifesituations. Hemianopia is generally considered a retinotopicdeficit. However, gaze position modulates the dischargeof neurones both in early retinotopically organised visualareas (with a clear hemispheric lateralised increase of dis-charge for contralateral gaze deviations in V1 and V3a[23,25]) and in thalamic [39,41], occipital–temporal [9],occipital–parietal [24], temporal [8] and frontal areas [6,7].These mechanisms could underlie the reduction of the con-tralesional visual field defect produced by ipsilesional gazedeviation originally described in a hemianopic patient byNadeau and Heilman [36] and the reduction of horizontalspace misrepresentation documented in the present study.Vuilleumier et al. [44] observed that ipsilesional gaze de-viation reduced the horizontal extent of hemianopia in twoneglect patients. One of the patients had damage involv-ing the medial occipitotemporal region and the posteriorthalamus; the other patient had a frontoparietal and basalganglia lesion. In both patients selective contralesional (oripsilesional) head deviation had no effect on the visual fielddefect and the influence of combined contralesional headand ipsilesional eye turning was not investigated. Amongour five hemianopic patients, only one (RBD2) showedremission of horizontal space misrepresentation when onlythe eyes were deviated ipsilesionally (BI condition). Thedifferent tasks used in our study and in the case reports ofNadeau and Heilman [36] and of Vuilleumier et al. [44] canprobably explain the slightly different results among thesestudies that, nonetheless, all emphasise similar beneficialeffects of ipsilesional gaze deviation. In the present study,selective modification of neck proprioceptive inputs (i.e.trunk turns) providing important cues for the coding of thebody-centered position of stimuli had no influence on theperformance of the distance reproduction task. This findingshows, as also pointed out by Vuilleumier et al. [44], thatthe coding of the body-centered position of visual stimulicould be relevant for tasks requiring manual reaching or theexplicit coding of extrapersonal positions with respect to thebody but not for visual comparison among distances or size.
Hemianopic patients with concomitant neglect showed noeye–head centered modulation of contralesional overexten-sion and ipsilesional underextension. Compared with theirsymmetrical performance in the baseline condition (CP), ne-glect patients without hemianopia showed relative overex-tension in the direction opposite to the shift of the bar (withrespect to head-centered coordinates) and independent of theside of the shift. These findings could suggest that in neglectpatients without hemianopia the modulation of the activityof retinotopic representations of space could be still rela-tively modulated by gaze shift whereas neglect patients with

F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128 1127
hemianopia suffer a severe and multi level deficit of spacerepresentation that prevents or makes difficult the effectivemanagement of their visual field defect.
5.4. Objections and conclusions
Two possible objections to our interpretation of the resultsof the present study must be considered. First, the contrale-sional deviation in the line bisection task and the pattern ofmisrepresentation of horizontal size and distances found inour hemianopic patients could be attributed to ipsilesionalneglect or contralesional visual grasp. In our opinion thishypothesis is hardly tenable because all available evidenceshows that ipsilesional neglect is linked to frontal–basal gan-glia lesions and none of our patients suffered this type ofbrain damage. In a series of 53 patients Kim et al. [33,35]found ipsilesional neglect in five patients only with unilateralfrontal–basal ganglia lesions, explicitly stating that ’no pa-tients with ipsilesional neglect were seen with lesions limitedto the posterior association areas’. Barrett et al. [2] describeda patient with a left medial thalamic lesion, contralesionalattentional bias in far space (but not in near space), nocontralesional bias in the line bisection task and no hemi-anopia. In the present study the only patient with thalamicinvolvement (RBD3) had a medial occipital and a posteriorthalamic lesion, hemianopia and a clear contralesional bias(21 mm) when bisecting lines in near space. All these evi-dences seems to clearly indicate that Barrett et al.’s patientand our RBD3 case are clinically different with no anatom-ical, functional or clinical overlaps. The second objectionconcerns the possible role of dysmetropsia in space misrep-resentation. Some authors [29,30] suggested that manifes-tation of space misrepresentation in neglect patients mightdepend on dysmetropsia. We think that this hypothesis couldapply to some cases of patients with neglect and no visualfield defect (although these patients seem to show no or mildsigns of space misrepresentation), but less likely applies toneglect patients with hemianopia or to hemianopics. Con-tralateral dysmetropsia, whether micro or macropsia, was re-ported in patients with unilateral damage of the retrosplenialregion [19] or of ventrolateral occipital–temporal extrastri-ate visual cortex [11,12,22,40] with no or with very limitedcontralateral visual field defects (i.e. paracentral scotomas;[40]). As noted by different authors [11,12] complete hemi-anopia simply prevents the processing of visual stimuli inthe extrastriate cortex of the damaged hemisphere and theclinical expression of disorders of size perception. There-fore, hypothesing a role of dymetropsia in the pathogene-sis of space misrepresentation of patients with contralateralhemianopia (with or without concomitant neglect) seemsequivalent to formulating the unlikely hypothesis that dys-metropsia is due to some altered functional processing inthe intact hemisphere.
In conclusion, the results of the present study providespecific cues on the functional relationships linking neu-ral representations of space, compensatory strategies and
awareness of visual sensory and attention impairments inunilateral brain damaged patients.
Acknowledgements
We thank Prof. Guido Gainotti, Prof. Luigi Pizzamiglioand two anonymous reviewers for useful suggestions. Wealso wish to thank Dr. Elena Natale, Dr. Marta Panella,Dr. Michele Tinazzi and Dr. Giandaniele Zannino for theirhelp. The first author (FD) wishes to thank H.O. Karnathfor kindly providing copies of papers from the less recentGerman literature. The data from the present study werepresented in preliminary form at the EuroConference on“Cognitive and neural bases of spatial neglect” (organiz-ers: Hans-Otto Karnath, David Milner and Giuseppe Val-lar), Como (Italy), 14–19 September 2000. This work wassupported by a grant from the Fondazione Santa Lucia toFabrizio Doricchi.
References
[1] Andersen RA, Snyder LH, Bradley DC, Xing J. Multimodalrepresentations of space in the posterior parietal cortex and its use inplanning movements. Annual Review of Neuroscience 1997;20:303–30.
[2] Barrett AM, Schwartz RL, Crucian GP, Kim M, Heilman KM.Attentional grasp in far extrapersonal space after thalamic infarction.Neuropsychologia 2000;38:778–84.
[3] Barton JJS, Black SE. Line bisection in hemianopia. Journal ofNeurology Neurosurgery and Psychiatry 1998;64:660–2.
[4] Binder J, Marshall R, Lazar R, Benjamin J, Mohr JP. Distinctsyndromes of hemineglect. Archives of Neurology 1992;49:1187–93.
[5] Bisiach E, Rusconi ML, Peretti VA, Vallar G. Challenging currentaccounts of unilateral neglect. Neuropsychologia 1994;32:1431–4.
[6] Boussaud D, Barth TM, Wise SP. Effects of gaze on apparent visualresponses of frontal cortex neurons. Experimental Brain Research1993;93:423–34.
[7] Boussaud D, Jouffrais C, Bremmer F. Eye position effects on theneuronal activity of dorsal premotor cortex in the macaque monkey.Journal of Neurophysiology 1998;80:1132–50.
[8] Bremmer F, Ilg UJ, Thiele A, Distler C, Hoffman KP.Eye, Eye position effects in monkey cortex. I. Visual andpursuit-related activity in extrastriate areas MT and MST. Journal ofNeurophysiology 1997;77:944–61.
[9] Bremmer F. Eye position effects in macaque area V4. Neuroreport2000;11:1277–83.
[10] Celesia GG, Brigell MM, Vaphiades MS. Hemianopic anosognosia.Neurology 1997;49:88–97.
[11] Ceriani F, Gentileschi V, Muggia S, Spinnler H. Seeing objectssmaller than they are: micropsia following right temporo-parietalinfarction. Cortex 1998;34:131–8.
[12] Cohen L, Gray F, Meyrignac C, Dehaene S, Degos JD. Selectivedeficit of visual size perception: two cases of hemimicropsia. Journalof Neurology Neurosurgery and Psychiatry 1994;57:73–8.
[13] Critchley M. The problem of awareness or non-awareness ofhemianopic field defects. Transations of the OphthalmologicalSociety UK 1949;69:95–109.
[14] Damasio H, Damasio AR. Lesion analysis in neuropsychology. NewYork: Oxford University Press, 1989.
1128 F. Doricchi et al. / Neuropsychologia 40 (2002) 1118–1128
[15] D’Erme P, De Bonis C, Gainotti G. Influenza dell’emi-inattenzionee dell’emianopsia sui compiti di bisezione di linee nei pazienticerebrolesi. Archivio di Psicologia Neurologia e Psichiatria1987;48:193–207.
[16] Diller L, Ben-Yishay Y, Gerstman LJ, Goodkin R, Gordon W,Weinberg J, et al. Studies in cognition and rehabilitation inhemiplegia, vol. 50. Rehabilitation Monograph, New York: UniversityMedical Center, 1974.
[17] Doricchi F, Angelelli P. Misrepresentation of horizontal space in leftunilateral neglect: role of hemianopia. Neurology 1999;52:1845–52.
[18] Doricchi F, Galati G, De Luca L, Nico D, D’Olimpio F.Horizontal space misrepresentation in unilateral brain damage. I.Visual and proprioceptive—motor influences in unilateral neglect.Neuropsychologia 2002;40:1107–17.
[19] Ebata S, Ogawa M, Tanaka Y, Mizuno Y, Yoshida M. Apparentreduction in the size of one side of the face associated with a smallretrosplenial haemorrhage. Journal of Neurology Neurosurgery andPsychiatry 1991;54:68–70.
[20] Ferber S, Karnath HO. Parietal and occipital lobe contributionsto perception of straight ahead orientation. Journal of NeurologyNeurosurgery and Psychiatry 1999;67:572–8.
[21] Ferber S, Karnath HO. Size perception in hemianopia and neglect.Brain 2001;124:527–36.
[22] Frassinetti F, Nichelli P, di Pellegrino G. Selective horizontaldysmetropsia following prestriate lesion. Brain 1999;122:339–50.
[23] Galletti C, Battaglini PP, Fattori P. Eye position influence on theparieto-occipital area PO(V6) of the macaque monkey. EuropeanJournal of Neuroscience 1995;7:2486–501.
[24] Galletti C, Battaglini PP. Gaze-dependent visual neurons in area V3aof monkey prestriate cortex. Journal of Neuroscience 1989;9:1112–25.
[25] Guo K, Li C. Eye position-dependent activation of neurones in striatecortex of the macaque. Neuroreport 1997;8:1405–9.
[26] Halligan PW, Marshall JC. Spatial compression in visual neglect: acase study. Cortex 1991;27:623–9.
[27] Halligan P. Hemianopia and visual neglect: a question of balance?Journal of Neurology Neurosurgery and Psychiatry 1999;67:565–6.
[28] Harvey M, Milner AD, Roberts RC. An investigation of hemispatialneglect using the Landmark task. Brain and Cognition 1995;27:59–78.
[29] Irving-Bell L, Small M, Cowey A. A distortion of perceived spacein patients with right-hemisphere lesions and visual hemineglect.Neuropsychologia 1999;37:919–25.
[30] Karnath HO, Ferber S. Is space representation distorted in neglect?Neuropsychologia 1999;37:7–15.
[31] Kerkhoff G. Displacement of the egocentric visual midline inaltitudinal postchiasmatic scotomata. Neuropsychologia 1993;31:261–5.
[32] Kerkhoff G. Multiple perceptual distortions and their modulation inleftsided visual neglect. Neuropsychologia 2000;38:1073–86.
[33] Kim M, Na DL, Kim MG, Adair JC, Lee KH, Heilman KM, et al.Ipsilesional neglect: behavioural and anatomical features. Journal ofNeurology Neurosurgery and Psychiatry 1999;67:35–8.
[34] Milner AD, Harvey M, Roberts RC, Forster SV. Line bisectionerrors in visual neglect: misguided action or size distortion?Neuropsychologia 1993;31:39–49.
[35] Na DL, Adair JC, Choi SH, Seo DW, Kang Y, Heilman KM, etal. Ipsilesional versus contralesional neglect depends on attentionaldemands. Cortex 2000;36:455–67.
[36] Nadeau SE, Heilman KM. Gaze-dependent hemianopia withouthemispatial neglect. Neurology 1991;41:1244–50.
[37] Nico D, Galati G, Incoccia C. The endpoints’ task: an analysisof length reproduction in unilateral neglect. Neuropsychologia1999;37:1181–8.
[38] Pizzamiglio L, Antonucci G, Judica A, Montenero P, RazzanoC, Zoccolotti P, et al. Cognitive rehabilitation of the hemineglectdisorder in chronic patients with unilateral brain damage. Journal ofClinical and Experimental Neuropsychology 1992;14:901–23.
[39] Robinson DL, McClurkin JW, Kertzman C. Orbital position and eyemovement influences on visual responses in the pulvinar nuclei ofthe behaving macaque. Experimental Brain Research 1990;82:235–46.
[40] Safran BA, Achard O, Duret F, Landis T. The “thin man”phenomenon: a sign of cortical plasticity following inferiorhomonymous paracentral scotomas. British Journal of Ophthalmo-logy 1999;83:137–42.
[41] Schlag J, Schlag Rey M, Peck CK, Joseph JP. Visual responses ofthalamic neurons depending on the direction of gaze and the positionof targets in space. Experimental Brain Research 1980;40:170–84.
[42] Tootell BH, Hadjikani NK, Mendola JD, Marrett S, Dale AM. Fromretinotopy to recognition: fMRI in human visual cortex. Trends inCognitive Sciences 1998;2:174–83.
[43] Vallar G. Spatial hemineglect in humans. Trends in CognitiveSciences 1998;2:87–96.
[44] Vuilleumier P, Valenza N, Mayer E, Perrig S, Landis T. To see betterto the left when looking more to the right: effects of gaze directionand frames of spatial coordinates in unilateral neglect. Journal of theInternational Neuropsychological Society 1999;5:75–82.
[45] Walker R, Findlay JM, Young AW, Lincoln NB. Saccadic eyemovements in object based neglect. Cognitive Neuropsychology1996;13:569–615.
[46] Zihl J. Rehabilitation of Visual Disorders after Brain Injury. Hove(East Sussex): Psychology Press, 2000.
[47] Zihl J, von Cramon D. Zerebrale Sehstörungen. Stuttgart:Kohlhammer, 1986.
[48] Zoccolotti P, Antonucci G, Judica A, Montenero P, Pizzamiglio L,Razzano C, et al. Incidence and evolution of the hemineglect disorderin chronic patients with unilateral right brain damage. InternationalJournal of Neuroscience 1989;47:209–16.