
HIV/AIDS among youths in rural communities: role of opinion leaders
78
39 HIV/AIDS AWARENESS AMONG YOUTHS IN IGBAJA COMMUNITY: THE ROLE OF OPINION LEADERS BY OYAFEMI , Andrew Babatola 10/52HN021 BEING A PROJECT RESEARCH SUBMITTED IN PARTIAL FULFILLMENT OF THE AWARD OF BACHELOR OF SCIENCE (B.SC) DEGREE IN MASS COMMUNICATION, FACULTY OF COMMUNICATION AND INFORMATION SCIENCE. UNIVERSITY OF ILORIN, ILORIN, NIGERIA JULY, 2014.
Transcript of HIV/AIDS among youths in rural communities: role of opinion leaders

39
HIV/AIDS AWARENESS AMONG YOUTHS IN IGBAJA COMMUNITY:
THE ROLE OF OPINION LEADERS
BY
OYAFEMI , Andrew Babatola
10/52HN021
BEING A PROJECT RESEARCH SUBMITTED IN PARTIAL FULFILLMENT OF
THE
AWARD OF BACHELOR OF SCIENCE (B.SC) DEGREE IN MASS
COMMUNICATION, FACULTY OF COMMUNICATION AND INFORMATION
SCIENCE.
UNIVERSITY OF ILORIN, ILORIN, NIGERIA
JULY, 2014.

40
Abstract
In the last two decades since HIV/AIDS was first identified, the body of research into the
disease had been steadily growing. Today this research covers a wide a range of topics ranging
from strictly medical studies to the social and demographic implication of the study as well as
to research into interventions and best practices that may help to halt the spread of the disease.
The study explored the role opinion leaders play in creating or influencing the youths on
HIV/AIDS, particularly in rural communities, with Igbaja community as the focus.
Using the survey technique, an aggregate sample of 100 respondents were drawn from the
community in order to identify the various categories of opinion leaders determine the
effectiveness of the HIV/AIDS messages youths receive from opinion leaders and ways in
which opinion leaders engage in the creation of HIV/AIDS awareness.
this study reveal that, opinion leaders play the role of creating awareness on the deadly disease-
HIV/AIS, but there is a misconception among youths, as many of them still believe it has a
cure.
Based on the research findings, Opinion leaders should not just create awareness the disease
but should create a perfect understanding of the disease among youths, making understand that
it a medical phenomenon that can be managed medically and not cured with prayer.
By and large, findings from this study revealed that opinion leaders vary from person to person
ranging from community opinion leaders to motivational leaders and religious leaders.

41
CERTIFICATION
This research project by OYAFEMI, Andrew Babatola has been read and approved by the
Department of Mass Communication, Faculty of Communication and Information Sciences
for meeting the requirements of the award of a B.Sc. Degree in Mass Communication.
_________________________ _________________
Mrs. A. I. Omoloso Date
Project Supervisor
_________________________ _________________
Mr. Mahmud Abdulraheem Date
HOD Mass Communication
______________________ _________________
External Supervisor Date

42
DEDICATION To God Almighty, my Dad, my Mum and the other B Boys.

43
ACKNOWLEDGEMENT
I give all praise and adoration to God almighty – the author and finisher of our faith who has guided me
through my course of study in this noble higher institution. My final year project is the most
earthshattering of all the academic challenges I have ever had to face. Without the support – physical
and spiritual –, patience and guidance of the following people, this research would have only remained
a dream. It is to God almighty and these people I owe my sincerest gratitude.
Chief and Mrs. Oyafemi, my parents, who have given me all the support I needed and had encouraged
and believed in me, in all my endeavours. Not to forget the B.Boys –Bernard, Benedict and Babade –
who have always been there – physically, spiritually and morally.
Mrs. Aisha Omoloso, my project supervisor, who despite her many other academic, family and
professional commitments gave me sufficient, generous and ample attention, supervision and guidance.
Her wisdom, commitment and preference for attention to details continually inspired and motivated me.
One could not wish for a better or more committed supervisor.
Dr. A. L Azeez, who helped with resources for this study’s review of literature and notable for the
experience he exposed me to during my mini research project in 300 level also inspired this research
with reference to all the courses he taught me since 100 Level. Not to forget is Dr. S.S. Abdulbaqi who
did a similar topic for her Ph.D. who was humble enough to share from her repertoire of knowledge and
experience.
Next, my special friends, Akinyele Omolola, Durowaiye Gbemishola, Akerele Oluwakemi whose
belief in my competence at carrying out this research inspired my final efforts to put this report together.
The Department of Mass Communication, my very supportive HOD, Mr. Mahmud Abdulraheem, who
has played the role of a father, guide and instructor, his outstanding humility, character and intelligence
are incomparable. My principled, friendly and tireless level adviser, Mr. Patrick Udende and the other
staff members who guided me through my course of stay with their rare experience.
Worthy of mention are my course mates, it’s been a wonderful four years together. I appreciate everyone
of them for their love, care, faithfulness, night classes and care during the programme. Notable among
them are: Emeribe, Jimoh, Ahmed, Omooba, Feesh, Edith, Tosin, Tola, Aisha, Bukky, Abulatan,
Nsikak, Gbemi , Medulla, Ibk, Habolaji, Yacoubou, Elizabeth, Matthew, Safu, Omonoju and above all
Selowo and Shamsudeen.
It was indeed nice to have met all of you in my in my life and academic endeavour.
Thank you.

44
Table of Content
Title Page......................................................................................................................................i
Abstract........................................................................................................................................ii
Certification................................................................................................................................iii
Dedication...................................................................................................................................iv
Acknowledgements.....................................................................................................................v
Table of Content..........................................................................................................................vi
List of Tables...............................................................................................................................ix
List of Figures...............................................................................................................................xi
CHAPTER ONE
1.1 Background to the Study ................................................................................................1
1.2 Statement of the Problem .............................................................................................5
1.3 Objectives of the Study ..................................................................................................5
1.4 Research Questions .......................................................................................................6
1.5 Rationale of the study ................................................................................................... 6
1.6 Significance of the Study .............................................................................................. 6
1.7 Scope of the Study ........................................................................................................6
1.8 Definition of terms……………………...................................................................................7
REFERENCES .............................................................................................................................8
CHAPTER TWO
2.0 LITERATURE REVIEW
2.1 Introduction ................................................................................................................9
2.2 Conceptual Framework ................................................................................................9
2.2.1 HIV/AIDS IN NIGERIA: Causes and government intervention .....................................9
2.2.2 HIV/AIDS and Nigerian Youths...................................................................................13

45
2.2.3 Information impact on HIV/AIDS awareness among rural dwellers ......................15
2.2.4 Consequences of inadequate HIV/AIDS awareness ...............................................16
2.2.5 Opinion leaders and HIV/AIDS awareness creation ...............................................17
2.2.6 Characteristics of opinion leaders ...........................................................................19
2.2.7 Importance of opinion leaders in awareness creation ...........................................19
2.2.8 The role of the media …………………………………………………………………………………………21
2.3 Theoretical framework ............…………………………………………………………………………..22
2.3.1 Two step flow theory………………………………………………………………………………………………22
2.3.2 Social cognitive theory……………………………………………………………………………………………..24
2.4 review of empirical studies………………………………………………………………………………………...26
References…………………………………………………………………………………………………………………….…29
CHAPTER THREE METHODOLOGY
3.1 Introduction……………………………………………………………………………………………………..35
3.2 Research design………………………………………………………………………………………………..35
3.3 Research method………………………………………………………………………………………………35
3.4 Population of the study…………………………………………………………………………………….35
3.5 Sample size……………………………………………………………………………………………………….36
3.6 Sampling technique………………………………………………………………………………………..…36
3.7 Data collection instrument………………………………………………………………………………..36
3.8 Data collection method……………………………………………………………………………………..36
3.9 Data analysis……………………………………………………………………………………………………..36
3.10 Validity and reliability…………………………………………………………………………………………37 3.11
Ethical concerns…………………………………………………………………………………………………37
References…………………………………………………………………………………………………………………….38

46
CHAPTER FOUR
DATA ANALYSIS AND INTERPRETATION
4.1 Introduction……………………………………………………………………………………………………..39
4.2 Demographics of respondents…………………………………………………………………………39
4.3 Presentation and analyses of data based on research questions………………………42
4.4 Discussion of finding ………………………………………………………………………………………..53
Reference…………………………………………………………………………………………55
CHAPTER FIVE
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
5.1 Summary ..............................................................................................................56
5.2 Conclusion………………………………………………………………………………………………………….56
5.3 Limitations…………………………………………………………………………………………………………57
5.4 Recommendation……………………………………………………………………………………………….57
5.4.1 Recommendation based on findings of the study……………………………………………….57 5.4.2
Suggestion for further studies…………………………………………………………………………...58
Bibliography........................................................................................................................59
Appendix.........................................................................................................................64
List of Tables
Table 1 – sex of respondent
Table 2 – Age group of the respondent
Table 3 – occupation of respondent
Table 4 – respondents’ awareness about HIV/AIDS
Table 5 – HIV/AIDS is a dangerous disease
Table 6 – HIV/AIDS can be cured
Table 7 – How HIV/AIDS can be cured

47
Table 8 – Respondents’ first exposure to HIV/AIDS messages
Table 9- which media exposes respondents to HIV/AIS messages
Table 10 – how often are respondents exposed to HIV/AIDS messages
Table 11 – effectiveness of the HIV/AIDS messages respondents are exposed to
Table 12 – categories of opinion leaders respondents are exposed to
Table 13 - on what occasion do opinion leaders speak on HIV/AIDS
Table 14 – perception of respondents about opinion leaders
Table 15 – through which medium do opinion leaders speak on HIV/AIDS Table
16 – extent of effectiveness of opinion leaders on respondents.
List of figures
Figure 1 – a pie chart showing the sex of respondents
Figure 2 – a bar chart showing the age distribution of respondents
Figure 3 – a bar chart showing the occupation of the respondents
Figure 4 – a bar chart showing the respondents view on how HIV/AIDS can be cured
Figure 5 – a bar chart showing the respondents first exposure to HIV/AIDS message
Figure 6 – a bar chart showing the medium that exposes respondents to HIV/AIDS messages
Figure 7 – a pie chart showing the categories of opinion leaders youths are exposed to

48
Figure 8 – a pie chart showing occasions when opinion leaders talk about HIV/AIDS

49
CHAPTER ONE
1.1 Background of the study
Human life on earth started as a simple and modest one. As human kind started to explore
ways of making that life easier, greater discoveries and inventions were made. But along with
its many achievements, mankind also confronted serious diseases.
HIV/AIDS one of such diseases is a complex and incurable one which has engendered fear
and helplessness throughout the world Millions of children, men and women all over the world
are dying as a result of HIV/AIDS related causes.
The HIV/AIDS pandemic has evoked a wide range of reactions from individuals,
communities and even nations. These reactions range from sympathy and caring to silence,
denial, fear anger and even violence. (Malcolm et al. 1998). We know much less about the level
and reasons for silence and denial than we know about violent, hostile or isolationist reactions.
HIV stands for Human Immune Deficiency Virus. This is a virus which attacks and destroys
the defence system of the human body. After a period of time, HIV weakens the body to the
extent that it cannot defend itself against even minor diseases. Eventually symptoms of the
disease appear in the infected person. These collective symptoms are called AIDS (Andriote,
2000).
AIDS on its part, stands for Acquired Immune Deficiency Syndrome; which means symptoms
of deficiency in the body’s defence system. When a person contracts AIDS, any disease can
easily attack such person and this may cause death.
Globally, 751 percent of people living with HIV/AIDS have being infected through sexual
intercourse, while more than 2.2 million people have died of AIDS. Also half of those suffering
from HIV/AIDS are young people between the ages of 15 – 24 years, with twice as many girls

50
as boys infected. In some countries, five times as many boys are infected between the ages of
15 and 19(UNAIDS, 2008).
There are 1.43 million children under the age of 15 who have become orphans due to AIDS.
These children suffer malnutrition, drop out of school and become homeless and are forced
into labour or prostitution. They often suffer drink and drug addiction. In the absence of parents
and guardian, they are highly vulnerable to physical violence and abuse.
HIV/AIDS remains incurable and devastates the communities and nations. Since the first
reported case in the United States in 1981, it has spread unremittingly to virtually every country
in the world. The number of people living with the virus has risen from 10 million in 1991 to
33 million in 2007. In 2007, there were 2.7 million new infections and 2 million HIV related
deaths. Globally, about 45% of new infections occurred among young people aged 15-24
(NACA, 2001).
Africa remains the most affected region in the world. Sub-Saharan Africa, which has just 10%
of the world’s population, is home to two-thirds of all people living with HIV and three quarter
of all AIDS death (1.5 million deaths) in 2007 (Erica, 2008).
In the absence of pharmacological, immunological and medical interventions, the change in
behaviour and attitude of the public may only be considered a possible way for the prevention
and cure for HIV/AIDS (UNAIDS-WHO 1998, 10). Although the Human Immune-deficiency
Virus (HIV) has been identified as the etiological agent causing AIDS, transmission of this
virus depends largely on human behaviour and related to sexuality and drug use. The fact that
there has been an increase in Hepatitis B and C is alarming as modes of transmission are similar
to that of HIV/AIDS.
HIV/AIDS awareness initiative is a collective responsibility that is not limited to the health
sector only but to all and sundry. It could be termed “a global crisis” with victims all around

51
the entire globe. Inadequate information regarding the spread of this global disease could pose
a devastating effect on economic growth and social sustainability of the entire world. Therefore,
creativity, synergy and collaboration from all sectors of society are required to defining solution
to mitigate and curb the widespread (UNAIDS, 2008).
Information is indispensable for human development. Losce (1990) describes information as
the knowledge communicated or received concerning particular circumstances. In the opinion
of Okwilagwe (2000) information is an input, which reduces the level of uncertainty in any
decision process. It is the crucial factor for a healthy life. Access to quality health and
information is therefore critical to many facets of health care design and delivery.
Health information is published and unpublished knowledge on all aspects of health and
healthcare. Individuals seek healthcare information for reasons ranging from curiosity to
selfdiagnosis and treatment. (World Health Organization Report, 2008). This is particularly
true for People Living with HIV/AIDS (PLWHA). Nigeria has an estimated 3.5 million infected
persons (Federal Ministry of Information and National Orientation Report, 2007). It is
imperative that they be adequately empowered with information to make the right decision
pertaining to their health.
The role of people living with HIV/AIDS cannot be ignored. Information is vital to relive pain
and discomfort, both physical and mental. As posited by Peterson and Obileye (2002),
information helps extend and improve the quality of life by reducing viral load. The absence
of information can lead to interrupted treatment and self-modification (Colebunder, et al,.
1997). Access to quality healthcare information and knowledge by PLWHA is very essential.
In a survey carried out by Erica (2008) on barriers to equitable access to information, major
barriers were lack of political support, information infrastructure and workforce capacity, and
high cost of accessing up to date, timely and relevant information.

52
In Nigeria, HIV/AIDS was first identified in 1985 and reported at an international conference
in 1986(Adeyi et al., 2006). It is a significant barrier to development as 170,000 Nigerians died
from AIDS in 2007 alone (UNAIDS, 2008). The country has already surpassed the 5 percent
explosive prevalence. Thus far, this disease has killed more than 1.3 million and orphaned more
than I million children (Federal Ministry of Information and National Orientation Report,
2007). The infection rate in Nigeria varies across states and communities. The main mode of
HIV transmission in Nigeria is largely through unprotected heterosexual sex (NACA, 2001).
Factors such as poverty, Sexually Transmitted Infections (STIs), social and religious norms and
political and social changes (e.g. labour migration) contribute to increasing rates of HIV in
Nigeria (National AIDS/STD control programme /FMOH, 2001). There has been efforts geared
at halting the spread of HIV/AIDS by governmental and Non-Governmental Organizations
NGOs), Community Based Organisation (CBOs), faith-based and media organizations and
other international agencies such as USAID, PEPFAR, Bill and Melinda Gates Foundations,
CIDA, DFID, etc.
In spite of research and intervention efforts for prevention and treatment, access to appropriate
health information for PLWHA in Nigeria constitutes a great barrier (NACA, 2005). To halt
the spread of HIVAIDS, access to quality health information needs to be provided not only by
health officials but also by influential people who are referred to as opinion leaders who are
capable of effectively influencing the lives of people around them. The focus of this research
therefore is to carefully examine the various opinion leaders and determine the effectiveness of
the influence of such leaders not only on people living with HIV/AIDS, but other members of
the community in general.

53
1.2 Problem statement Information, no doubt makes a person more aware or educated about specific issues. It is
generally agreed by all stake holders in the HIV/AIDS campaign that education based on
factual information, remains one of the viable options to check the spread of the disease.
In Nigeria, due to the peoples’ respect for elders and cultural heritage, opinion leaders are
usually accorded a lot of respect and credibility by members of various communities.
It is therefore expected that such leaders, given their roles in the society should be in a position
to educate or influence members of their community positively on issues regarding HIV and
AIDS.
Several studies have focused on awareness about HIV/AIDS but this study examines what roles
opinion leaders play in the HIV/AIDS awareness campaign. With specific focus on Igbaja, a
community in Ifelodun local government area of Kwara state, this study evaluates the role of
community leaders on HIV/AIDS awareness creation among youths in the community.
1.3 Objective of the study The research work has the following objectives
1. To examine Igbaja community youths’ awareness about HIV/AIDS
2. To examine the effectiveness of HIV/AIDS messages among youths in Igbaja
community.
3. To determine the types of opinion leaders youths in Igbaja communities are exposed to
4. To determine the roles of opinion leaders in HIV/AIDS awareness among youths in
Igbaja community
5. To examine the effectiveness of the various opinion leaders in Igbaja community on
HIV/AIDS awareness creation among youths in the area.
1.4 Research questions
1. What is the level of awareness about HIV/AIDS among youths in Igbaja?

54
2. Through which sources are youths in Igbaja exposed to information on HIV/AIDS?
3. How effective are the HIV/AIDS messages youths’ are exposed to?
4. What categories of opinion leaders are youths in Igbaja community exposed to?
5. In what ways do opinion leaders in Igbaja community engage in HIV/AIDS awareness
creation?
6. To what extent have the opinion leaders effectively influenced the Igbaja community
youths’ awareness of HIV/AIDS?
1.5 Significance of the study
This research will be of importance to individuals and parents in knowing their status and
taking the right precautions to guide against the spread of HIV/AIDS. It will be of immense
benefit to the various opinion leaders (religious leaders, influencers in small communities
and the nation at large) in helping them to know how to play their role more effectively. It
will also be of benefit to various NGOs and to other researchers who will want to
investigate deeper about the effectiveness of HIV/AIDS messages.
1.6 Scope of the study
While the study deals with HIV/AIDS which is a major health concern, the focus or scope
of the study is from the informative perspective, with less emphasis on other areas such as
medical aspects. Thus awareness creation will be the focus of the study.
1.7 Rationale of the study
There is a gap in communication, there are many campaigns in urban areas and there are
only few campaigns in rural areas. As such, this research is carried out to determine ways
by which opinion leaders can bridge the gap.
1.8 Definition of terms
HIV- Human Immune Virus is the virus that causes or leads to Acquired Immune
Deficiency Syndrome. (AIDS)

55
AIDS – Acquired Immune Deficiency Syndrome is a viral disorder marked by severe loss
of resistance to information symptoms of persons affected with person’s natural defence
against illness.
Awareness – Having or showing realization, perception or knowledge about something
Youths – Individuals (either male or female) between the age bracket of 18 – 25
Igbaja – A community in Ifelodun local government area of Kwara state
Role – A function or part performed especially in a particular operation or success.
Opinion leaders – Opinion leaders here refer to people or leaders who have the ability to
influence others based on their wealth of experience, knowledge or charisma. In this case,
they are pastors, Imams, Political/youth leader, fellowship leaders, teachers etc.

56
REFERENCES
National Action Committee on AIDS (2001). HIV/AIDS emergence plan. Nigeria technical
report.
Okwilagwe, A.O (2000). Information capacity theory. Mimeograph, University of Ibadan.
UNAIDS (2008). Report on the global AIDS epidemic. Retrieved January 13, 2009, from
http://www.avert.org
Nelson E, (2010) “Access to health information by people living with HIV/AIDS in
Nigeria.” Library philosophy and practice.
Federal ministry of information and national orientation (2007). The Obasanjo reforms
HIV/AIDS response. Abuja, Federal ministry of information and national orientation,
Losce, R.M. (1990) society development and libraries. Centre for external studies; university
of Ibadan.
WHO (2008). Access to health information and knowledge sharing: an overview. Retrieved
January 17 2007, from http://e-health.org/articles.html.
Peterson K. & Obileye O. (2002). Access to drugs and related opportunistic infections in
Nigeria. Policy Project. Nigeria: Centre for Development and Population Activities
(CEDAP)
Colebunders R., et al (1987). Antiretroviral treatment in Africa. AIDS II (suppl.B): S 107-
113
Erica C (2008). Barriers to equitable access to quality health information. Journal of
medicine (5): 117 – 123. Retrieved January 17 2009 from http://e-
health.org/articles.html

57
CHAPTER TWO
2.1 Introduction
A literature review is a critical and an evaluative summary of the themes, issues and arguments
of a specific clearly defined research topic obtained from the published and unpublished
researches and studies in relation to the research topic. It aims at identifying what is already
known about an area of study to evaluate the similarities and differences, consistencies and
inconsistencies and draw up conclusions based on a prepared questionnaire or question guide.
The researcher in this work intends to examine how opinion leaders create awareness about
HIV/AIDS in rural areas and also to examine the extent to which the opinion leaders influence
the youths.
2.2 Conceptual framework
2.2.1 HIV/AIDS in Nigeria: Causes and government interventions
HIV/AIDS is one of the greatest natural challenges that has given humans concern in recent
times. Idoko (2004) calls it a disease starting as a single infection at the point of contact and
then progressing to a wasting disease known as AIDS. The pandemic is on a rapid global march.
Some of the world's most populous countries are severely affected. Kanki and Adeyi (2006)
observe that Nigeria has been devastated with an HIV/AIDS epidemic, with nearly a million
people dead and more than two million children orphaned. According to them, the National
Intelligence Council in 2002 identified Nigeria as one of the five countries expected to bear the
heaviest burden of an HIV/AIDS epidemic. The number of people living with this virus was
projected to be ten to 15 million by 2010.
The National Economic Empowerment and Development Strategy (NEEDS) (2004) shows
that more than 2.7 million Nigerians are presently living with the virus. Ejeagwu et al. (2007)
assert that mere mention of the name conjures fear in the minds of people. Those at risk include
those with multiple sex partners, commercial sex workers, people that need blood transfusions,
such as accident victims, sickle cell patients, and people who engage in tattooing and tribal
marks. The devastating effects of the disease are numerous, ranging from cost of HIV screening
and economic loss to an increased burden on communities, psychological trauma, disruption

58
of community life, the cost of preventive measures, increased number of AIDS orphans, and
so on.
The emergence of HIV AIDS has caused a whole world wide campaign to stop the disease,
cure it or at least control it. According to Encyclopaedia Britannica “In 1981 investigators in
New York and California reported the first official case of AIDS. Initially, most cases of AIDS
in the United States were diagnosed in homosexual men, who contracted the virus primarily
through sexual contact, and in intravenous drug users, who became infected mainly by sharing
contaminated hypodermic needles. In 1983 French and American researchers isolated the
causative agent, HIV. (In 2008 French virologists Françoise Barré-Sinoussi and Luc
Montagnier were awarded the Nobel Prize for Physiology or Medicine for their discovery of
HIV.) By 1985 serological tests to detect the virus had been developed. According to the 2007
United Nations report on AIDS, an estimated 33.2 million people were living with HIV,
approximately 2.5 million people were newly infected with HIV, and about 2.1 million people
died of AIDS. Relative to previous years, the statistics for 2007 reflect a decrease in the annual
number of new infections and deaths from AIDS and an increase in the overall number of
people living with AIDS. Some 25 million people have died of the disease since 1981.”
The first two cases of HIV/AIDS in Nigeria were identified in 1985 and were reported at an
international AIDS conference in 1986. (Adeyi et al., 2006).
However, the prevalence of the virus in developing countries is rather alarming with people
living in sub-Saharan Africa accounting for about 70 percent of all infections, and in some
countries of the region the prevalence of HIV infection of inhabitants exceeds 10 percent of the
population. Consequently, Nigeria as the most populated country in Africa has about 3.4
million people living with HIV AIDS (UNAIDS, 2012) and also the country has the second
highest number of new infections reported each year.
The statistics about the impact of HIV/AIDS world-wide are overwhelming. Estimates of the
United Nations Agency for AIDS (UNAIDS, 2012) indicate that over 40 million people were
living with HIV/AIDS in 2001, that nearly 25 million people have died of AIDS since the
disease was first discovered in the early 1980’s, and that more than 15.6 million children under
15, have lost either their mother, their father, or both parents as a direct result of AIDS
(UNAIDS, 2001).

59
While every nation has in some way been affected by this pandemic, it is in Africa that the grip
of HIV and AIDS has been, by far, the deadliest. 28 million people in Africa are living with
HIV/AIDS and Southern Africa has the highest HIV adult prevalence in the world. Well over
two thirds of the HIV/AIDS related deaths (18 million, or 72%) are from Africa (World Bank,
2002) and almost one in every ten adults in sub-Saharan Africa are HIV positive
(UNESCO,2002), although infection rates in individual countries such as South Africa,
Botswana, Malawi, and Swaziland are much higher.
Concurrently, there are three major ways of acquiring the HIV/AIDS infection, they include
the following:
1. Heterosexual sex: Approximately 80 percent of HIV infections in Nigeria are a result
of heterosexual sex (Global AIDS Response Progress Report, 2012). Women are
particularly affected by HIV; in 2011 an estimated 1.7 million women were living with
HIV and prevalence was 3 percent among young women aged 15-24 (UNAIDS, 2012).
Factors contributing to this include a lack of information about sexual health and HIV,
low levels of condom use, and high levels of sexually transmitted diseases. However,
gender inequality among women has been identified as a key driver of the HIV
epidemic among women( Global AIDS Response Progress Report, 2012)
2. Blood transfusions: HIV transmission through unsafe blood accounts for the second
largest source of HIV infection in Nigeria (Global AIDS Response Progress Report,
2012). Not all Nigerian hospitals have the technology to effectively screen blood and
therefore there is a risk of using contaminated blood. The Nigerian Federal Ministry of
Health has responded by backing legislation that requires hospitals to only use blood
from the National Blood Transfusion Service, which has far more advanced
bloodscreening technology (Global AIDS Response Progress Report, 2012).
3. Mother-to-child transmission: Most children infected with HIV acquire it from their
mothers. An estimated 69,400 children were newly infected with HIV in 2011
(UNAIDS, 2012)

60
Like the proverbial smoke, the upward rise of which is unstoppable, cases of HIV/AIDS
infection continue to rise in Nigeria, creating “deep moral chasm” for which the “desperate and
clearly misguided campaigners” are held responsible (Ejinkeonye, 2004:A16).
Like other parts of Africa, the HIV/AIDS scourge has affected virtually every stratum of
national life. There are impacts of HIV/AIDS on the health sector, the household, the economy,
education, life expectancy and total development (Shabani and Okebukola, 2004)
According to Madu (2004:16), in his newspaper article, quoting an undisclosed source:
There have been reports that so far an estimated 6.5
million people in Nigeria have been infected by HIV/AIDS
in Nigeria while researchers predict that over 75 million
people would be infected worldwide by 2010, with a loss
of human life totalling 100 million by 2010.
As of 2007, 33 million people were thought to be living with HIV; 2.5 million new infections
and 2.1 million deaths occur every year (UNAIDS, 2007:1). A report of the National Action
Committee on AIDS (NACA) in 2005 showed that Kwara State has the lowest HIV/AIDS
prevalence in the North Central geopolitical zone of Nigeria as at 2003. However, according to
NACA (2005) there are evidences to the fact that some part of the state had a greater
vulnerability to HIV/AIDS because of a number of factors including insufficient knowledge
about HIV/AIDS and the keeping of multiple sexual partners. An estimated 3.1 percent of adult
between ages 15-49 are living with HIV/AIDS, approximately 170,000 people died from AIDS
in 2007 alone (UNAID 2008).
HIV/AIDS represents not only a tragedy at a human level but also heavily affects the economic
development of countries, many of which are already severely strained for resources. The
weight on the health system is tremendous and the loss of productive workforce has
implications for the economy. Cross country analyses conducted by the World Bank suggest
that the region of Southern Africa is losing an estimated 0.7 to 1.0 percent per capita growth
per year as a direct result of HIV and AIDS and that by the year 2010 it may have reduced the
aggregate output by between 15 to 20 percent (World Bank, 2002)

61
The 2005 HIV/AIDS/syphilis sentinel survey shows that 4.4% are living with HIV/AIDS of
the total adult population aged 15-49 years who are still sexually active. The sentinel survey
was compiled from data collected at antenatal clinics across the country.
The median HIV/ AIDS prevalence among antenatal clinics has levelled off at around 4%
(Federal Ministry of Health Report, 2003). However, such a report is a guideline and cannot be
considered conclusive.
The reason is simple, most Nigerian mothers do not deliver in clinics and not all of them do
allow themselves to be tested for HIV/AIDS test (Afolabi and Adesina, 2005).
It is important to note however, that the Nigerian government has not folded its arms. In 1987,
the Nigerian health sector established the National AIDS Advisory Committee (NAAC) which
was shortly followed by the establishment of the National Expert Advisory Committee on
AIDS (NEACA) (Adeyi et al., 2006)
The Nigerian government was slow to respond to the increasing rates of HIV transmission and
it was in 1991 that the Federal Ministry of Health made its first attempt to Nigeria's AIDS
situation (Kanki and Adeyi 2006). The result then showed that 1.8 percent of the Nigerian
population was infected with the deadly disease. However, when Olusegun Obasanjo became
the president in 1999, HIV prevention, treatment and care became one of the government
primary concerns. The National Action Committee on AIDS (NACA) was created in 2001. The
government set up a three-year HIV/AIDS Emergency Action Plan (HEAP). Subsequently, the
president hosted the organization of Africa Unity's first African summit on HIV/AIDS,
Tuberculosis and other related infection diseases (Adeyi et al., 2006). A recent report from the
Director General of the National Agency for the Control of AIDS (NACA) during a stake
holders meeting with the National Steering Committee on Orphans and Vulnerable Children
(OVC), revealed that about one thousand (1,000) fresh cases of Human Immune Virus (HIV)
is being recorded daily in Nigeria and that it was prevalent among the youths. (NACA, 2010)
2.2.2 HIV/AIDS and Nigerian Youths
The definition of a youth varies from country to country and region to region. Generally,
according to the United Nations (UN), a youth is anybody between the ages of 15 to 24.

62
However this definition is not all encompassing as each member of the body is allowed to
define the concept “youth” based on different criteria such as politics, history and other
socioeconomic factors. That is why nations use different parameters and variables in defining
their youth. Consequently, the Nigeria National Youth Development Policy (2001) defines
youths
“as all young persons of ages 18-35. It represents the most active, most volatile and yet the
most vulnerable segment of the population socio-economically, emotionally and in other
respects.”
The HIV/AIDS pandemic poses a serious threat to all nations especially those of sub-Saharan
Africa including Nigeria. According to UNAIDS recent estimation, almost 16,000 new
infections occur every day in the world, 90% of which occur in Africa. Among these new cases,
50-60% is young people (UNAIDS 2012).
More importantly is the threat of this disease to the life of young persons in Nigeria. The
prevalence rate of HIV/AIDS in Nigeria rose steadily from 1.8% in 1992 to 2.2% in 1994, 4.5
in 1996, 5.4% 1999, and 5.8% in 2001. The figure for 2003 and 2005 were 5.0% and 4.4%
respectively (NACA 2010)
Recent findings of the UNAIDS show that youths are the most infected in Nigeria, with rates
higher than 4.4% obtained in the general population. For example, 4.7% percent for those aged
20-24 years and 4.9% for those aged 25-29 years. (UNAIDS 2012)This shows that youths are
a vulnerable group. They also constitute the highest percentage of the populations.
Youths still remain the focus of major researches on the HIV/AIDS epidemic in terms of rates
of infection, vulnerability, impact, and potential for change because they are the most sexually
active age group. Of the 1.7 billion young people worldwide, 5.4 million are estimated to be
living with HIV, youths are vulnerable to HIV for social, political, cultural, biological and
economic reasons. (UNFDP, 2007). HIV/AIDS is mostly transmitted through sex that is why
this research is focusing on the youths rather than the elderly.
Of the youths within the age group of 18 - 35, 47% of the men infected acquired HIV through
sex with other men. Regarding the women within the age group of 18 – 35, 51% were infected
through heterosexual sex (Rangel MC et al. 2006)

63
In 2007, people aged 13-29 accounted for the largest proportion (28%) of new HIV cases in
the world (CDC, 2007; 2009:12).
Additionally, data that estimate HIV infection show that even though new AIDS cases are
declining among young people (because of more effective treatment), there is no decline in
newly diagnosed cases of HIV (NACA, 2010)
In the absence of cure to HIV/AIDS, the most effective way remains prevention. The first step
for prevention of HIV/AIDS is awareness. Without being aware, one would not be able to take
any preventive step. The level of awareness is very important to design strategies to help
prevent diseases.
HIV spreads fastest and farthest in conditions of poverty, powerlessness and lack of
information, the condition in which many young people especially in rural areas live (FMOH,
2003). Adolescents tend to experiment with little awareness of danger. In fact, risky sexual
behaviours often are part of a larger pattern of adolescent behaviours (Hoffman & Futterman,
1996). Most young people have only limited knowledge about HIV/AIDS especially in the
suburban areas (Otte et al, 2008).
Billions of Dollars is spent yearly by both national and international organizations towards
educating people about the prevention of HIV/AIDS since the infection doesn’t have any cure
presently. Newer strategies are evolving everyday to keep the scourge at bay.
2.2.3 Information Impact on HIV/AIDS Awareness Among Rural Dwellers
Creating awareness about HIV/AIDS among rural dwellers has posed challenges. Though they
tap the natural resources of the nation, they are often starved of information relevant to their
well-being. A closer look at rural areas reveals that communities are seriously marginalized in
terms of the requirements for development such as education, health care, and leisure activities.
Bond (2007) states that they are disadvantaged in many areas of life, as reflected in the clinical
statistics surrounding AIDS, especially in developing countries.
Information increases the level of certainty in any human decision process; little wonder,
Edewor (2010) posits that information is indispensable for human development. Likewise ,
Nwafor-Orizu (2003) while describing sources of information dissemination in the rural areas
in Nigeria, avers that, oral sources like face-to-face interaction, radio, television, traditional
institutions, associations, and written sources like newspapers and magazines aims to facilitate
rural information transfer as a way of eliminating ignorance and superstition. The present

64
information and education campaign to forestall the spread of the disease should be pursued
with vigour but some energy has to be generated to the care of people already afflicted.
(Akanmu and Akinsete 2006)
Mooko and Aina (2007) opine that every individual, whether literate or illiterate, needs
information for a variety of issues essential for his or her survival. It is therefore, not surprising
that information is needed for awareness, increased productivity, health and so on. They further
assert that users of information are complex, while some are homogenous such as professionals,
students, policy makers, researchers, some could be heterogeneous like rural inhabitants,
artisans and so on. Kanki and Adeyi (2006) in their own opinion, submit that information is the
most potent weapon available for the prevention and cure of HIV & AIDS.
HIV is a recurrent theme in the health sector. In order to control the HIV epidemic, we all need
to learn as much as possible about the disease. As for those living with HIV, comprehensive
and up-to-date information is an essential part of a healthy life. There is no better place to start
the education than at the beginning.
2.2.4 Consequences of inadequate HIV/AIDS awareness
While young ladies claim they want to make ends meet by engaging in commercial sex, young
men resort to selling their blood and engaging in careless sexual behaviour due to financial
constraints (Mooko and Aina 2007)
Many myths and misconceptions about HIV/AIDS are in currency in Nigeria. Some of them
include notions that sharing food with and hugging infected persons lead to infection; sex is
the only means through which HIV/AIDS is contracted; AIDS is a phantom imperialist concept
to discourage sex (American Invention to Discourage Sex); sitting with or being in close
contact with an infected person leads to infection; it is better not to go for an HIV test because
what a person does not know does not kill him, etc. (Adedimeji, 2004)
Stigmatizing attitudes about HIV is yet another product of inadequate HIV/AIDS awareness.
We cannot actually talk about HIV/AIDS without making mention of the word stigma.
Stigma is ‘‘the identification that a social group creates of a person (or group of people) based
on some physical, behavioural, or social trait perceived as being divergent from group norms’’

65
(Goffman, 1963 cited in Castro and Farmer, 2005). According to Goffman stigma is an
attribute, behaviour or reputation that is related to a discredited stereotype. Essentially, it is
separating one’s real social identity from their virtual identity thereby leading to discrimination
A rigorously developed measure of stigma included three dimensions (shame, blame, and social
isolation; perceived discrimination; and equity) (Genberg et al., 2008), although Deacon,
(2006) explicitly distinguishes discrimination from stigma.
Thus, those fearful of stigma may attempt to reduce the visibility of their condition, internalize
their stigma, and may be held responsible for the cause of the stigma (Heatherton, et al 2000).
According to Hong et al. (2008) stigmatizing attitudes include denial, indifference, labelling,
separation, rejection, status loss, shame, hopelessness, and fear. Broader factors that influence
HIV/AIDS stigma, include higher HIV/AIDS-related risk behaviour, and lower development,
in one’s community (Chen, et al, 2005).
Furthermore, People living with HIV (PLHIVs) who expect stigma and discrimination may fail
to take advantage of healthcare and economic opportunities available to them, including
counselling, or public assistance (Reece et al. 2007).
Because of stigma fears and inaccurate knowledge, many self-treat, use traditional remedies,
obtain inappropriate treatments from local pharmacies, or go to local unlicensed private
physicians with little evaluation or follow-up (Guan et al., 2009).
According to the meta-analysis carried by Logie and Gadalla, between 2000 and 2007 they
found that high HIV stigma was related to low social support, poor physical health, poor mental
health, older age, and lower income (Logie & Gadalla, 2009).
Most of the Mass Media coverage involves general HIV/AIDS news, rather than knowledge or
stigma reduction education, which accounts for less than 4% of all coverage (Bu & Liu, 2004).

66
2.2.5 Opinion leaders and HIV/AIDS awareness creation
‘‘When spoken words of advice concerning HIV prevention and personal examples come from
persons who one already knows and likes, the impact of the messages will be stronger’’ (Kelly,
2004, p. 143).
Opinion leaders are those limited few in the community with a higher level of education,
exposure to idea and are sources of advice and knowledge. Opinion leaders exhibit prestige,
higher social status, cosmopolitanism, and mass media exposure (Rosario, 1971). These
characteristics provide the basis for how and why opinion leaders occupy and maintain their
role and have influence within their social network.
Thompson et al. (2006) reviewed roles similar to opinion leaders, including facilitators,
champions, linking agents, and change agents. They identified two similarities across each of
these roles: the assumption that interpersonal contact increases the availability of knowledge,
which in turn leads to behaviour change, and that all these roles function as change agents.
Several techniques exist for identifying opinion leaders for campaigns, each with advantages
and disadvantages (Valente & Pumpuang, 2007).
Opinion leaders perform better and faster when they are perfectly matched with the intended
audience. They perform a lot of functions which include providing access to information,
provide feedback to their community, act as role models and influence others through increased
awareness and persuasion.
Opinion leaders can exert their influence by speaking, writing, or modelling behaviour that
is copied by others. According to the two step flow theory by Rogers (1975), formal opinion
leaders are those in positions such as elected public officials or individuals chosen to head
unions, special-interest groups, or non-profit organizations. Journalists often ask them to
comment on issues in the news. Informal opinion leaders are those people who are not in elected
or appointed positions, but are able influence others because of personal characteristics such as
charisma or assertiveness.
Opinion leaders can be male or female and are found in every racial, ethnic, social, and
political group. (Lazarsfeld in Idoko, 2004) estimated that one in every five persons is an
opinion leader in some respect. During one of Lazarsfeld's studies, he asked people who their
opinion leaders were and why they listened to them. One waitress in a coffee shop described

67
to Lazarsfeld her opinion leader as "a customer who sounded like he knew what he was talking
about."(Idoko 2004)
2.2.6 Characteristics of opinion leaders.
According to Idoko (2004), Opinion leaders in today's society typically share five
characteristics. The first is that they tend to possess a higher degree of education than people
around them. The second characteristic is that they consume more media than other individuals
and are usually more informed about current events and social trends. They do so for the
purposes of information rather than entertainment.
The third characteristic is that opinion leaders tend to be active in politics and community
affairs. The majority attend public meetings, work for special-interest groups, and serve on the
boards of community associations and non-profit organizations. The fourth characteristic is that
they are early adopters of new ideas. Within a list of friends, co-workers, or other persons
considered to be members of a peer group, the first individual on that list to use electronic mail,
own a cellular telephone, or design his or her own website is also likely to be the group's opinion
leader.
The fifth and perhaps most important characteristic is that opinion leaders have the ability to
influence people around them, either because of position {such as in the case of parents,
employment supervisors, or union stewards) or personal qualities such as charisma or
assertiveness (Idoko 2004).
2.2.7 Importance of Opinion Leaders in Awareness Creation
The absence of education and media literacy in rural areas calls strongly for opinion leaders.
The opinion leader has the responsibility of effecting behavioural changes in reference to
HIV/AIDS. They have the pivotal role of creating interactive processes with members of the
community to develop positive behaviours; promote and sustain individual, community and
societal behaviour change; and maintain appropriate behaviours. (Ejeawu et al., 2007) In the
case of HIV/AIDS, the goal is to inform and educate youths about HIV/AIDS prevention and
management. The Opinion leaders serve as the chief or main actors in creating a change in
behaviour among youths towards HIV/AIDS in rural areas. This is elucidated by chief (2000)

68
that opinion leaders can cause behaviour change by partnering with government and doing the
following things:
1. Promote a better understanding of the interactions between gender dynamics, HIV/AIDS
and food security/rural development;
2. Create awareness among leaders at all levels of these interactions and about the need to
incorporate them into all prevention and mitigation activities;
3. Ensure the political commitment necessary to undertake an integrated effort to combat
AIDS and to sustain that effort over time;
4. Create awareness of the processional nature of the necessary interventions and make
available the means to implement them and follow them through the process;
5. Ensure that every rural development and food security policy is gender- and HIV/AIDS
sensitive;
6. Develop appropriate indicators for the monitoring and evaluation of interventions,
including both process and impact indicators.
According to Ejeagwu et al., 2007) the National Policy on HIV/AIDS in 2005 emphasises on
the following constraints that inhibit the success of opinion leaders in effecting behavioural
change among youths in rural areas:
• Non-acceptance of proven methods of HIV prevention by some social and religious
groups;
• Cultural ideologies that deny the known methods of transmission in order to maintain
cultural practices;
• Subjugation and subordination of women in the country which limits their ability to
decide when and how and with whom they have sex,;
• Lack of appropriate sex/family life education available in social and educational
institutions;
• Ineffective treatment methods used to treat sexually STIs in the both orthodox and
alternate health institutions and, and the wide spread practice of self-medication by
the infected.
The nature of the disease is such that open discussion is tremendously important

69
(Kelly, 2004) since it is the silence about the disease and its effects that facilitates its spread
and leads to stigmatization. Some researchers therefore argue that education about HIV/AIDS
and related areas should therefore not be seen as an “optional extra ... (but as) ...a matter of life
and death” (Kelly, 2004, p. 11).
2.2.8 The Role of The Mass Media
Chukwuma and Atelhe (2007) are of the view that “the media enables diffusion of ideas and
public awareness, which are indispensable for a progressive societal living.
The media, the print and electronic, include newspapers, magazines, newsletters etc. and radio,
television and cinematography films (Akinfeleye, cited in Adedimeji (2002). That the media
are powerful agents as agenda setter and “always an indispensable institution for social control”
(Anyim cited in Adedimeji, 2002:107) compels their significant role in the anti-HIV/AIDS
drive. The power and functions of the media as well as the language they use in stabilizing and
destabilizing have well been documented (Thomborrow, 1999). Thus, information will be
passed through the media through press releases, reports and features articles. They will also
be made to realize the effects of promoting the cause and course of HIV/AIDS through the
celebration of half -nude models and exploitative pornographic materials Adedimeji (2004).
To a far extent, attitudes to sexuality especially among the youth are formed through what they
read in newspapers and magazines, watch on televisions and films (often transmitted by the
media) and hear on radio. Thomborrow (1999:57), in reference to the media, submits that once
something has been represented in a particular way, it becomes more difficult to talk ‘around’
or ‘outside’ that representation, “to find an alternative of describing people and events; and as
such the media are a possible site for change”. In furtherance of the goals of preventive
intervention, interactions will be established between the implementers and media associations’
especially Nigerian Union of Journalists (NUJ) and its affiliate associations
Kayode and Jimoh (2007) were of the opinion that the media can help in educating people to
reduce every misconception that is associated with HIV/AIDS. They further said that people
who are well informed are likely to understand better and at least learn to live with others who
are even AIDS infected.

70
Okunnu (2002) clearly pointed out the role of the media in the following ways “The information
function of the media is all encompassing and essential for the existence of members of the
society. Through their various contents, the mass media collect, store, process and disseminate
news, data, pictures, facts, messages, opinions and comments which members of the public
need in order to react knowledgably to personal, environmental, natural and international
conditions as well as to be in a position to take appropriate decisions.”
2.3 Theoretical Framework
2.3.1 The Two Step Flow Theory.
The two step flow theory asserts that information from the media moves in two distinct stages.
First, individuals (opinion leaders) who pay close attention to the mass media and its messages
receive the information. Opinion leaders pass on their own interpretations in addition to the
actual media content (Bond, 2007).
The term ‘personal influence’ was coined to refer to the process intervening between the
media’s direct message and the audience’s ultimate reaction to that message. Opinion leaders
are quite influential in getting people to change their attitudes and behaviours and are quite
similar to those they influence.
The two step flow theory as propounded by Rogers in 1975 cited in Bond (2007) has been
successfully and contextually applied in many studies of information in developing countries
that include Nigeria, India and Middle East countries. Simply put, the theory states that in any
mass communication effort (such as in an information campaign) messages usually flow from
the mass media to opinion leaders, who then pass them on to others whom they unavoidably
influence in doing this.

71
In other words, media information influence is indirect and usually takes place in a cross- fire
of interpersonal connections or communications. Lazarsfeld et al. cited in Idoko (2004) in
presenting this theory, also highlighted the fact that families, friends, co-workers, churches and
similar social institutions while helping to play the media information influence role, can and
do also have their own independent influences.
Opinion leaders can exert their influence by speaking, writing, or modelling behaviour that
is copied by others. Formal opinion leaders are those in positions such as elected public officials
or individuals chosen to head unions, special-interest groups, or non-profit organizations.
Journalists often ask them to comment on issues in the news. Informal opinion leaders are those
people who are not in elected or appointed positions, but are able influence others because of
personal characteristics such as charisma or assertiveness.
Lazarsfeld estimated that one in every five persons is an opinion leader in some respect.
People tend to select their opinion leaders based on different characteristics, as such, during
one of Lazarsfeld's studies, he asked people who their opinion leaders were and why they
listened to them. One waitress in a coffee shop described to Lazarsfeld her opinion leader as "a
customer who sounded like he knew what he was talking about."
While the Two step flow is a social science theory, there are behavioural theories that also place
emphasis on the use of opinion leaders to bring about behavioural change in their communities,
which is similar to the tenets of the Two Step flow theory. For example, Social Learning Theory
asserts that people serve as models of human behaviour and that some people (significant
others) are capable of eliciting behavioural change in certain individuals, based on the
individual’s value and interpretation system (Bandura, 1986).
The Theory of Reasoned Action states that one of the influential elements for behavioural
change is an individual’s perception of social norms or beliefs about what people who are
important to the individual do or think about a particular behaviour (Fishbein & Ajzen, 1975).
The Diffusion of Innovation Theory posits that certain individuals (opinion leaders) from a
given population act as agents of behavioural change by disseminating information and
influencing group norms in their community (Rogers, 1983).
Also, the Intermedia theory posits that “An individual's opinions, beliefs, attitudes, values, and
behaviours are anchored in his/her social network of family, friends, and acquaintances.” The

72
social network according to the Intermedia theory refers to opinion leaders, for instance people
tend to rely on opinions of opinion leaders to validate their attitudes belief, and behaviour.
2.3.2 Social cognitive theory
The Social Cognitive Theory is relevant for designing health education and health behaviour
programs. This theory explains how people acquire and maintain certain behavioural patterns.
The theory can also be used for providing the basis for intervention strategies
The social cognitive theory explains how people acquire and maintain certain behavioural
patterns, while also providing the basis for intervention strategies (Bandura, 1997). Evaluating
behavioural change depends on the factors environment, people and behaviour. SCT provides
a framework for designing, implementing and evaluating programs.
Environment refers to the factors that can affect a person’s behaviour. There are social and
physical environments. Social environment include family members, friends and colleagues.
Physical environment is the size of a room, the ambient temperature or the availability of
certain foods. Environment and situation provide the framework for understanding behaviour
(Parraga, 1990). The situation refers to the cognitive or mental representations of the
environment that may affect a person’s behaviour. The situation is a person’s perception of the
lace, time, physical features and activity (Glanz et al, 2002).
The three factors environment, people and behaviour are constantly influencing each other.
Behaviour is not simply the result of the environment and the person, just as the environment
is not simply the result of the person and behaviour (Glanz et al, 2002). The environment
provides models for behaviour. Observational learning occurs when a person watches the
actions of another person and the reinforcements that the person receives (Bandura, 1997). The
concept of behaviour can be viewed in many ways. Behavioural capability means that if a
person is to perform a behaviour he must know what the behaviour is and have the skills to
perform it.
The premise of the Social Cognitive Theory (SCT) states that new behaviours are learned either
by modelling the behaviour of others or by direct experience.
Social learning theory focuses on the important roles played by vicarious, symbolic, and
selfregulatory processes in psychological functioning and looks at human behaviour as a

73
continuous interaction between cognitive, behavioural and environmental determinants
(Bandura, 1977).
Central tenets of the social cognitive theory are:
•self-efficacy – the belief in the ability to implement the necessary behaviour (“I know I can
insist on condom use with my partner”)
•outcome expectancies - beliefs about out -comes such as the belief that using condoms
correctly will prevent HIV infection.
Programmes built on SCT integrate information and attitudinal change to enhance motivation
and reinforcement of risk reduction skills and self-efficacy
Specifically, activities focus on the experience people have in talking to their partners about
sex and condom use, the positive and negative beliefs about adopting condom use, and the
types of environmental barriers to risk reduction.
From the above theories, it can be deduced that media messages have the best chance of
changing people's opinions, beliefs, attitudes, values, and behaviours if those messages receive
promotive support within social networks. Simply put, this means the best way to influence
individuals, opinions, belief and behaviour about an issue is if the issue is positively receive by
the opinion leaders. Therefore for HIV/AIDS awareness among youths in rural areas, youths
in rural areas can easily be influenced in they are positively exposed to their opinion leaders.
In short, what youths believe to be true is in a large way determined by what their opinion
leaders believe to be true.
To sum up, these theories and models are extensively used in health communication campaigns.
While the effectiveness of these theories and models is sometimes questioned in the light of
the growth of the HIV/AIDS epidemic in Africa, Asia and Latin America; their value as
important theories and models remains unchanged.
On the basis of the above mentioned theories and models the following steps can play an
important role in behaviour change for HIV/AIDS prevention.
(1) Knowledge: understanding about disease or issue and ability to recall the messages.

74
(2) Perception: respond favourably to campaign message and discuss issue/ campaign or
disease spread or effects with personal networks for instance, family, friends, spouse and
with co-workers and to get approval or to organize public opinion on campaign contents.
(3) Intention: recognizes the effects or usefulness of the campaign and intends to consult a
service provider to learn new techniques and willingness to practice it despite cost or
inconvenience (for instance, use of condoms).
(4) Practice: goes to provider of information/supplies /services and selection of method or
technique to prevent from spread of disease and consistency in practices.
(5) Advocacy: advocate practices to others on the basis of personal experiences, practices and
support programs in community (“U.S. Department of Health”, 2000, p. 3). To sum up, a
fair understanding and treatment of these five factors is crucial and pivotal in designing an
effective awareness campaign for the prevention of HIV/AIDS spread. (Ejeagwu et al 2007)
The major reason for reviewing the above theory is to explore its practical utility and
application in the creation of HIV/AIDS awareness among youths by opinion leaders.
2.4 Review of Empirical Studies
Though many researches have been conducted on this topic, while many of them focused on
the creation of information and knowledge, others focused on creation of awareness among
youths in cities, there is no empirical study in which individuals have been shown to influence
over 100 others directly Duncan and peter (2007).
In a study on the appraisal of the methods of disseminating HIV/AIDS information in
NnewiSouth Local Government Area of Anambra state, Nigeria conducted by Ejeagwu et al.,
(2007), they are of the view that one of the best ways of disseminating HIV/AIDS information
is to increase the use of rural-based sources like women's associations, churches, age grades,
town unions, etc. In the Nigerian rural setting, town criers serve as important communication
links between the opinion leaders of the town and the rest of the people. Government and

75
nongovernment agencies can pass their HIV/AIDS message through the town crier, because
citizens believe in his message.
Akunyili (2005) states that the methods of disseminating HIV/AIDS information in rural areas
is not efficient and results in poor awareness; however, the provision of the right information
at the right time can avert an epidemic and save lives.
Chukwuma and Atehe (2007) stated that “mass media is principally an agent of information
dissemination. The mass media also plays the following important roles, education and
enlightenment, socialization and cultural transmission, entertainment, agenda setting and
public advocacy.” From the above it can be understood that the use of one or a combination of
these medium of communication to inform, educate, entertain and enlighten the audience about
any aspect of preventing HIV/AIDS would help in no small measure to reduce or prevent the
spread of the disease. This agrees with Muluh (2009) who observed that “the mass media has
a great contribution to make in the fight against HIV/AIDS. Besides delivering direct
information, they have the potential to influence attitudes, behaviours and even policy-making
through their coverage of the epidemic in news, drama, documentation and discussion.” Since
the early 80s when HIV/AIDS was first noticed in Nigeria and in many other countries, both
government and non-governmental organizations have realized that the disease cannot be
fought successfully without the involvement of the media especially the broadcast media. They
are perceived to be an effective and powerful organ of communication. In the words of Kofi
Anan as quoted by Singh (2009; p. 1) “broadcast media have tremendous reach and influence,
particularly with young people who represent the future and who are the key to any
successful fight against HIV/AIDS, We must seek to engage these powerful organizations as
full partners in the fight to halt HIV/AIDS through awareness, prevention and education.”
The media has the unparalleled ability to save lives by providing vital information in electronic
and printed form on HIV/AIDS. The information so provided has the potential to change
people’s behaviour “as well as their culture. This corroborates the words of Pandey (2005 p.
211), where he said “to prevent HIV/AIDS effectively, people need to change their
behaviours... it is believed that mass media especially newspaper has the potential to change
individual behaviour as well as culture.”
Education is one of the key roles performed by the media in the society. Therefore, educating
the people on the danger of being infected by HIV/AIDS will save millions of lives. Taboos
and myths associated with HIV/AIDS will also be eliminated or reduced to the barest minimum.

76
Singh (2009 P. 7) observed that “media combats the disease through public education and
awareness as the disease is not only a battle against a virus but also a battle against the stigma,
discrimination, cultural taboo and the ideas.”
Mainstreaming is another method the message of HIV/AIDS can be spread to the people. This
way, HIV/AIDS issues are broadcast across a number of programmes. The report of the
conference on Global Media Strategies for HIV/AIDS held in Kuala Lumpur, agrees with this,
when it stated that “all section of the society need to be reached... to broadcast HIV/AIDS
messages and programmes across the programming schedule, including prime time, to produce
and broadcast programmes, related to HIV/AIDS in all genres and formats including news,
current affairs, documentaries, talk shows, game-shows drama and other entertainment
formats” (Mahdu 2007 P. 49).

77
References
Adedimeji, M.A.2002. “Language as Missiles: A Pragma-semiotic Study of the Press
Fireworks against Military Rule in Nigeria (1989-1999)” Unpublished M.A Thesis,
University of Ilorin, Ilorin
Adedimeji, M.A.2004. “The Effects of HIV/AIDS Education Programme on the Cognition
and Attitudes of Selected Tertiary Institution Students in Ilorin, Nigeria”. VIHEAP
Module 1 Project.
Afolabi, O. A., & Adesina, A. A. (2005). HIV/AIDS: Psychosocial and therapeutic issues in
the disclosure of diagnosis. Iroro: A Journal of
Arts, 10 (1&2), 140-153
Adeyi, S. (2006). AIDS in Nigeria: A nation on the threshold. In Adeyi S., & Ademo J.
(Eds.). The epidemiology of HIV/AIDS in Nigeria . USA: Centre for Population and
Development Studies.
AIDS. (2012). Encyclopaedia Britannica. Encyclopaedia Britannica Ultimate Reference
Suite. Chicago: Encyclopaedia Britannica.
Akanmu, A. S., Akinsete, A., and Njoku, O. S., (1999). Prevalence of hepatitis B surface
antigen among women of child bearing age in Lagos, Nigeria. African Journal of
Reproductive Health 3(1): 45-50
Akinfeleye, R.A. (1988). “The Youth, Education, Mass Media, and Nation Building”, In
Nnolim, C.E. (Ed.) the Role of Education in Contemporary Africa. New York:
Professors World Peace Academy. pp. 117-133
Akunyili, D. (2005). Fake drugs are more dangerous than HIV/AIDS. Daily Sun (April 12):
12.
Bond, V. (2007). Stigma when there is no other option: Understanding how poverty fuels
discrimination toward people living with HIV in Zambia. In S. Gillespie (Ed.), AIDS,
poverty, and hunger: Challenges and responses (Chapter 10, pp. 181–197).Washington
DC: International Food Policy Research Institute

78
Bu,W., & Liu, X. (2004). Zhongguo dazhong meijie zhong de aizibing baodao yanjiu
[Research on HIV/AIDS-related coverage in Chinese mass media]. Retrieved March 31,
2008, from http://antiaids.home.sunbo.net/show_hdr.php?xname=O26NL01&
dname=AJ9NL01&xpos=2
Castro A, Farmer P. (2005), Understanding and addressing AIDS-related stigma: From
anthropological theory to clinical practice in Haiti. Public Health Matters. (1):53–59
CDC. HIV/AIDS Surveillance Report,2007; 2009:12.
Chief M.V. (2000), A gender perspective on the impact of HIV/AIDS on food security and
labour supply: Leadership challenges. Gender and HIV/AIDS: leadership roles in social
mobilization. UNFPA. Addis Ababa.
Chen J, Choe MK, Chen S, Zhang S.(2005) Community environment and HIV/AIDSrelated
stigma in China. AIDS Education and Prevention. 17(1):1–11
Chukwuma A, and Atelhe A. (2007).The role of the mass media in the fight against
HIV/AIDs in Nigeria (Unpublished)
Duncan J.W. and Peter S.D. (2007), influential, networks and public opinion formulation,
journal of consumer behaviour. 441-458.
Egesie J. & Egesie E. (2011) 'Seroprevalence of Human Immunodeficiency Virus (HIV)
Among Blood Donors in Jos - Nigeria' cited in Barros E. (2011) 'HIV-infection: Impact,
Awareness and Social Implications of living with HIV/AIDS', InTech
Hoffman, N.D. & Futterman, M.D. (1996). 'Youth and HIV/AIDS' in J.Mann & D. Tarantola
(eds.) AIDS in the World II: Global Dimensions, Social Roots and Responses. New
York: Oxford University Press
Nwafor-Orizu, U.E., (2007). An appraisal of the methods of disseminating of HIV/AIDS
information in Nnewi-South Local Government Area of Anambra state, Nigeria.

79
Ejinkeonye, U. 2004. “Campaign Deadlier than AIDS”.Daily Independent. Lagos.June 2.
Pp.E16/back page
Federal Ministry of Health (FMOH), 2003. National HIV/AIDS and Reproductive Health
Survey. Lagos: Federal Ministry of Health, 2004. 2003 National HIV Sero-prevalence
Sentinel Survey, Abuja. Retrieved from www.synergyaids.com/documents/Nigeria on
December, 2007.
Federal Republic of Nigeria (2012) ‘Global AIDS Response Progress Report’
Genberg BL, Kawichai S, Chingono A, Sendah M, Chariyalertsak S, Konda KA, Celentano
DD. (2005) Assessing HIV/AIDS stigma and discrimination in developing countries.
AIDS and Behaviour; 12(5):772–780
Guan J, Wu Z, Rotheram-Borus MJ, Li L, Detels R, Wu S,(2009) NIMH Collaborative
HIV/STD Prevention Trial Group. Self-reported sexually transmitted disease symptoms
and treatment seeking behaviours in China. AIDS Patient Care & STDs. 23(6):443–448.
Heatherton, T. F., Klecik, R. E., Hebl, M. R., & Hull, J. G. (2000). The social psychology of
Stigma. New York, NY: Guilford Press
Hong, Y., Li, X., Stanton, B., Fang, X., Lin, D., Wang, J. (2008). Expressions of HIV-
related stigma among rural-to-urban migrants in China. AIDS Patient Care and STDs, 22,
823–831.
Idoko, J.A. (2004). An overview of HIV/AIDS diagnosis and antiretroviral therapy in
doctor's diary, Abuja: Nigeria Medical Association: 84-85
Kayode J and Jimoh J (2007). Newspaper coverage of HIV/AIDs stigma: An analysis of the
average of the Guardian and the Vanguard (Unpublished).

80
Kanki, P.J., & Adeyi O. (2006). Introduction. In: Adeyi, O., et al. (Eds.). AIDS in Nigeria:
A nation at the threshold. Cambridge, MA: Harvard Centre for Population and
Development Studies.
Kelly J. A. (2004) popular opinion leaders and HIV prevention peer education: Resolving
discrepant findings, and implications for the development of effective community
programmes. AIDS Care; 16(2):139–150
Logie, C., & Gadalla, T. M. (2009). Meta-analysis of health and demographic correlates of
Stigma towards people living with HIV. AIDS Care, 2, 742–753.
Madu, M.C. 2004. “HIV/AIDS: Wear Abstinence, not Condom”. The Punch. Lagos.
March 3. p.16
Mooko, N. P. and Aina, L.O. (2007) Information Environment of Artisans in Botswana.Libri
57 (1) 27-34
Otte, W.M., van der Mass, F. & der Boer, A. (2008). Comparison of knowledge and
accessibility to information sources of HIV/AIDS between blind and sighted population
in Nigeria. AIDS Care, 20(9): 1093-1097
Mahdu, K. P. (2007). Conference on global media strategies for HIV/AIDs and
associated competition and media festival. Geneva: UNAIDS
Muluh, H. (2009). The Challenge of HIV/AIDs: The role of the Cameroon Media
. Accessed online at www.findarticles.com
NEEDS (2004). Sustainable development. Abuja: National Planning Commission.
Okunnu, C. (2002). Teaching Mass Communication: A multi-dimensional approach .
Enugu: New Generation Books

81
Pandey, P. K. (2005) “Trends of HIV/AIDs reporting in the newspaper of Bangladesh: A
study of selected dailies” in Abstracts of the 14th International Conference on HIV and
STIs in Africa Abuja: ICASA
Rangel MC, Gavin L, Reed C, Epidemiology of HIV and AIDS among adolescents and
young adults in the United States. J Adolescent Health 2006; 39:156 –163.
Reece, M., Tanner, A. E., Karpiak, S. E., & Coffey, K. (2007). The impact of HIV-related
Stigma on HIV care and prevention providers. Journal of HIV/AIDS & Social Services, 6,
55–73.
Rogers, E. M. (2003). Diffusion of innovations (5th ed.). New York, NY: Free Press
Rosario, F. Z. (1971). The leader in family planning and the two-step flow model.
Journalism Quarterly 48(2):288-297, 303
Thompson, G. N., Estabrooks, C. A., & Degner, L. F. (2006). Clarifying the concepts in
knowledge transfer: A literature review. Journal of Advanced Nursing, 53, 691–701.
Singh, J. (2009). HIV/AIDs prevention and creating awareness, role of media.
Accessed online at http://www.boloji.com/society
Shabani, J. and P. Okebukola (Eds.) 2004. “HIV/AIDS Education Training Programme”.
UNESCO’s www.viheaf.net. Between March 1 and May 25.
Thomborrow, J. 1999. “Language and the Media” In Thomas, L and S. Wareing (Eds.).
Language, Society and Power: An Introduction. London and New York: Routledge. pp.
4963
UNAIDS, 2002. Global HIV/AIDS Epidemic, Retrieved from
www.unaids.org/publication/fact-sheets on June8, 2007
UNAIDS (2012) ‘Global Report: Annexes'

82
UNAIDS (2012) 'World AIDS Day Report - Results'
UNAIDS. Report on the global HIV/AIDS epidemic, 2002 update. Geneva: UNAIDS; 2002
(available at: www.UNAIDS.org).
UNICEF, UNAIDS, WHO. Youths and HIV/AIDS: opportunity in crisis. New York and
Geneva: UNICEF, UNAIDS, WHO: 2002.
Valente, T. W., & Pumpuang, P. (2007). Identifying opinion leaders to promote behaviour
change. Health Education & Behaviour, 34, 881–896. Quarterly, 48, 288–297
Edewor N. (2010), “Access to health information by people living with HIV/AIDS in
Nigeria.” Library philosophy and practice.

83
CHAPTER THREE
METHODOLOGY
3.1 Introduction
In this project, the following processes were undergone in conducting the research to gather
and analyse data that formed the core of the resolutions of the research work. The chapter deals
with the methods, techniques and procedures used in carrying out the investigation for the
study. It consists of the following sections:
3.2 Research Design The design of a research is the framework, which specifies the type of information to be
gathered including the source of data and the procedure used in collecting them. (Ezeja & Ogili,
2005).
Based on this, the design ensures that the researcher collects the right information from the
right sources.
The design for this research is the descriptive design. The aim is to describe frequencies of the
pattern of response from the respondents. According to Ogunjimi (2001:73), “it is concerned
with the collection of data for the purpose of describing and interpreting existing conditions,
prevailing practices, beliefs, attitudes, on-going process.”
3.3 Research Method This study used quantitative method in an effort to increase the validity of research findings by
comparing multiple forms of data and seeking convergence in the findings.
Quantitative research focuses on numbers and figures. According to Edmonds and Kennedy
(2012), “the emphasis of the researcher is on collecting scores that measures distinct attributes
of the population”. In this research, the survey was the techniques through which data was
obtained from respondents.
3.4 Population of the Study The population of a study is the animate or inanimate objects on which a study is focused
(Edmonds and Kennedy, 2012)

84
According to Ogunjimi (2001:79), population covers all members or elements of a well-defined
group. The population for this research included all the youths in Igbaja community, Ilorin.
3.5 Sample Size A sample is a subset of a population selected to meet specific research objectives (Olayiwola,
2007).This is the segment of population, which is of interest and relevance to the researcher.
For this research, a sample 100 respondents was drawn Igbaja community, Ilorin, Kwara State.
3.6 Sampling Technique In the selection of youths, a non-probability sampling technique – the purposive sampling
method was adopted in the selection of youths in Igbaja community of Ilorin, Kwara state. The
purposive sampling technique was adopted because it is a direct way of obtaining samples as
it afforded the researcher the opportunity of considering typical cases which quickly and easily
provided the required information (Ogunjimi, 2001).
For the quantitative survey, a simple random sampling technique was employed. The simple
random sampling technique was based on probability in which case all the elements of a
population stood equal chance of being a respondent. The administration of questionnaires
ceased immediately the questionnaire covered the benchmark of the total.
3.7 Data Collection Instrument In view of the fact that the study used the survey method to examine quantitatively, objectively
and systematically, a structured questionnaire was administered to the respondents.
3.8 Data Collection Method The questionnaire was self-administered to the respondents who constituted youths in Igbaja
community within the period of one month.
3.9 Data Analysis Descriptive statistics was employed by using data distribution method. With the employment
of descriptive statistics, tables of frequency, charts and percentages were also used to give

85
quantitative analysis of the facts gathered from the questionnaires administered on the
respondents.
3.10 Validity and Reliability In every research in general and social science research in particular, reliability and validity of
instrument(s) used are of major concern. Osuala (2005), contends that the subject of validity is
complex and controversial but of great importance in research.
Rosenbery and Vicker (2009: 22) define validity as the degree to which the instrument actually
measures what it is supposed to measure and can be extended to cases outside the test set.
Tejumaiye (2003:158) corroborates this describing validity “as the degree to which a measuring
instrument measures what is designed to measure”. Summarily, validity is the ability of a
measuring device to measure what it has been designed to measure with no visible limitation
in the case population extension.
On another but similar premise, the main concern of reliability is consistency, precision and
accuracy, which are important qualities in any research measurement. According to Amusan
(2004:70), a measuring instrument is said to be reliable if it measures consistently, under
varying conditions and at different times a person’s performance or trait. Reliability according
to Tejumaiye (2003: 155) “is a matter of whether a particular technique applied repeatedly to
the same people or object would yield the same result each time”. We can assume therefore,
that the greater the degree of consistency and stability in an instrument, the greater the
reliability. To ensure reliability in the first instrument – questionnaire, it was pilot-tested on ten
youths-respondents to ensure that they sufficiently know what they were expected to do with
the questionnaires; the necessary amendments were then effected. And to ensure that the
instruments truly measured what they were designed to measure; questions were formulated
within the purview of the research questions and the research objectives. The pilot test was
carried using two methods: the test retest and expert opinion.
3.11 Ethical Concerns As a way of avoiding ethical issues, the researcher was conscious to approach every aspect of
the research to include data collection and analyses with objectivity, truth, and honesty.
Plagiarism which constitutes a serious ethical issue in any field of study was also avoided. The
researcher provided proper acknowledgments when other people’s work or opinions were used.

86
REFERENCES
Amusan, A. (2004). Fundamentals of Research Methods in Education. Oluponna: Ola
Ayediran Publishers.
Edmonds, E., & Kennedy, T. D. (2012). An applied reference guide to research designs:
quantitative, qualitative and mixed methods. Thousand oaks, CA: Sage.
Ezeja, E., & Ogili, D. (2005). Project writing. Enugu: Providence Press (Nig) Ltd.
Fawole, M. (2006). Definition, spectrum and types of research. In A. Olayinka, V. Taiwo,
A. Raji, & I. Farai (Eds.), Methodology of Basic and Applied Research (2nd ed.),
pp. 1 - 17. Ibadan: University of Ibadan Post - Graduate School.
Ogunjimi, M. (2001). Introduction to research method and data processing. Surulere:
Raytel Communications Ltd.
Olayiwola, A. (2007). Procedures in educational research. Kaduna: Hanijam
Publications.
Osuala, E. (2005). Introduction to research methodology. Enugu: Africana First
Publishers Limited.
Rosenbery, J., & Vicker, L. (2009). Applied mass communication theory – A guide for
media practitioners. Boston: Pearson.
Tejumaiye, J. A. (2003). Mass communication research (An Introduction). Ibadan:
Scepters Prints Limited.

87
CHAPTER FOUR
DATA ANALYSIS AND INTERPRETATION
4.1 Introduction
This chapter is an analysis of all the data gathered in the course of this study. Survey was the
primary method of data gathering. The study assessed the level of awareness of HIV/AID
among youths in Igbaja community, the effectiveness of the messages youths are exposed to
the categories of opinion leaders the youths are exposed to, ways by which opinion leaders
create awareness and determine the effectiveness of the opinion leaders on youths.
A total of one hundred (100) copies of questionnaires were administered by the researcher to
the respondents and the one hundred (100) copies were retrieved. The analysis therefore is
based on the 100 questionnaires
4.2 Analysis of Demographics of Respondents
The table and chart below shows the sex of respondents, it can be seen that 67% (n=67) are
while 33% (n=33) are female.
Table 1: sex of respondent
Response Percent
Male 67 67%
Female 33 33%
Total 100 100%
Source: Researcher’s field work (2014)
Frequency

88
Figure 1: a pie chart showing the sex of respondent.
The table and chart below shows the age group of the respondents, it can be deduced that 75%
(n=75) of the respondent are between the age group of 18 -26, 25% (n=25) of the respondent
are between the age group of 27- 35.
Table 2: Age group of the respondent
Response Frequency Percent
18-26 75 75%
27-35 25 25%
Total 100 100%
Source: Researcher’s field work (2014)
male 67 %
female 33 %
sex of respondent
male female

89
Frequency
Figure 2: a bar chart showing the age distribution of respondents.
From the table below it can be said while majority of the respondents 42% (n=42) are students,
38 % (n=38) are traders and 20% (n=20) are artisans.
Table 3: occupation of respondents.
Response Percent
Student 42 42%
Trader 38 38%
Artisan 20 20%
Total 100 100%
Source: Researcher’s field work (2014)
18-26 27-35
A ge
Series1 75 25
0
10
20
30
40
50
60
70
80
Age of respondent

90
Figure 3: a bar chart showing the occupation of the respondents
4.3 presentation and analyses of data based on research questions.
RQ1: What is the level of awareness about HIV/AIDS among youths in Igbaja?
This question is answered by analysing variables 1, 2, 3, 4, 9, 10 and 11 of the survey data.
From the Table .2 displayed below, it can be deduced that 100% (all 100 respondents) of the
total respondents have heard about HIV/AIDS
Table 4: Respondents awareness about HIV/AIDS
Response Frequency Percent
Yes 100 100%
Total 100 100%
Source: Researcher’s field work (2014)
The Table 5 displayed below shows the level to which respondents believe HIV/AIDS can be
cured. It can be seen that the respondents are aware of the fact that HIV/AIDS is a dangerous
disease because 88% (n=88) strongly agreed and 12% (n=12) simply agreed to the fact that it
is a dangerous disease.
student trader artisan
42 38
20

91
Table 5: HIV/AIDS is a dangerous disease
Response Frequency Percent
Strongly Agree 88 88%
Agree 12 12%
Total 100 100%
Source: Researcher’s field work (2014)
From the table 6 and chart below, when respondents were asked if HIV/AIDS can be cured,
while 27% (n=27) strongly agreed that HIV/AIDS can be cured, 41% (n=41)of the respondents
simply agreed that it can be cured, 26% (n=26) of the respondents strongly disagreed that
HIV/AIDS can be cured and only 6% (n=6) disagreed that HIV/AIDS has a cure.
Table 6: HIV/AIDS can be cured
Response Frequency Percent
Strongly Agree 27 27%
Agree 41 41%
Disagree 6 6%
Strongly Disagree 26 26%
Total 100 100%
Source: Researcher’s field work (2014)
From Table 7, while 27% (n=27) strongly agreed that HIV/AIDS can be cured, 41% (n=41)
simply agreed that it can be cured, as a result the table 7 will be based on 68 rather than 100.
The Table 7 and chart below shows the various ways 68 respondents believe HIV/AIDS can
be cured. From the table and chart below, it can be said that 26% (n=18) believe it can cured
through prayer, 62% (n=42) believe that it can be cured medically, while the remaining 12%
(n=8) believe that it can be cured through further research.

Table
92
7: How HIV/AIDS be cured.
Response Frequency Percent
Prayer 18 26%
Medically 42 62%
Further research 8 12%
Total 68 100
Source: Researcher’s field work (2014)
Figure 4: a bar chart showing respondents view on how HIV/AIDS can be cured.
RQ 2: Through which sources are youths in Igbaja exposed to Information on
HIV/AIDS
For the purpose of answering the above research question, questions 9, 10 and 11 of the
questionnaire will be analyzed.
The Table 8 and chart below displays the various means by which respondents first got to hear
of HIV/AIDS. It can be seen that 63% (n=63) first heard it on the mass media, 17% (n=17)
first heard it from family and friends, 12% (n=12) first heard about HIV/AIDS from religious
institutions 4% (n=4) heard from Schools while the reaming 4% (n=4) heard from opinion
leaders.
26 %
62 %
12 %
Chart Title
Prayer Medically Further research

93
Table 8: Respondents’ first exposure to HIV/AIDS messages
Responses
Mass media 63 63%
Family and friends 17 17%
Religious institution 12 12%
School 4 4%
Opinion leaders 4 4%
Total 100 100%
Source: Researcher’s field work (2014)
Figure 5: a bar chart showing the respondents’ first exposure to HIV/AIDS message
From the table 9 below and chart, it can be said that 78% (n=78) became aware of HIV/AIDS
through the radio, 4% (n=4) gained awareness through the television, 10% (n=10) gains
awareness through newspaper while only 8% (n=8) gains awareness through the social media.
9: which media exposes respondents to HIV/AIDS messages?
Response Frequency Percent
Frequency Percent
0
10
20
30
40
50
60
70
Mass media Family and friends
Religious institution
School Opinion leaders
First exposure to HIV/AIDS messages

Table
94
Radio 78 78%
Television 4 4%
Newspaper 10 10%
Social media 8 8%
Total 100 100%
Source: Researcher’s field work (2014)
Figure 6: a bar chart showing the medium that exposes respondents to HIV/AIDS
messages
Table 10 shows how often respondents are exposed to HIV/AIDS messages, it can deduced
that 72% (n=72) of the respondents are exposed every day, 26% (n=26) are exposed to
HIV/AIDS messages about twice a week and only 2% (n=2) are exposed weekly.
0 10 20 30 40 50 60 70 80 90
Radio
Television
Newspaper
Social media
Media that exposes respondents to HIV/AIDS messages

Table
95
10: how often are respondents exposed to HIV/AIDS messages?
Response Frequency Percent
Everyday 72 72%
About twice a week 26 26%
Weekly 2 2%
Total 100 100%
Source: Researcher’s field work (2014)
RQ 3: how effective are the HIV/AIDS messages youths are exposed to?
For the purpose of answering research question 3, variables 5, 6, 7 and 8 of the questionnaire
will be analyzed.
The table 11 uses a Likert scale to analyze the effectiveness of HIV/AIDS messages youths are
exposed to. From the table, it can be that while 94% (n=94) strongly agreed to the fact
abstinence from casual sex can prevent HIV/AIDS, 6% (n=6) strongly disagree that abstinence
can prevent contracting HIV/AIDS. Also while 94% (n=94) strongly agreed that condoms can
prevent HIV/AIDS, 6% (n=6) simply disagreed that condoms can prevent HIV/AIDS.
For the third message, the question sought to know if sharing of sharp object can lead to
HIV/AIDS. All the respondents 100% (N=100%) strongly agreed that sharing of sharp objects
can lead to contracting HIV/AIDS. Along the same line, when asked if giving or receiving
blood can lead to HIV/AIDS, 84% (n=84) of the total respondent strongly agreed that giving
or receiving blood can lead to HIV/AIDS while 16% (n=16) simply disagreed that giving or
receiving blood can lead to HIV/AIDS.

Table
96
11: Effectiveness of the HIV/AIDS messages respondents are exposed to.
HIV/AIDS messages Responses Frequency Percent
Abstinence from casual sex can prevent
HIV/AIDS Strongly Agree 94 94
Agree 6 6
Neutral 0 0
Disagree
Condoms can be used to prevent
HIV/AIDS Strongly disagree 94 94
Strongly agree 6 6
Agree 0 0
Neutral 0 0
Disagree 0 0
Strongly Disagree 0 0
Sharing of sharp objects can lead to
HIV/AIDS Strongly Agree 100 100
Agree 0 0
Neutral 0 0
Disagree 0 0
Strongly Disagree 0 0
Giving or receiving blood can lead to
HIV/AIDS Strongly Agree 84 84
Agree 0 0
Neutral 0 0
Disagree 0 0
Strongly Disagree 16 16
Source: Researcher’s field work (2014)

97
RQ 4: What categories of opinion leaders are youths in Igbaja community exposed to?
To answer this question variable 13 will be considered.
The table below shows the different categories of opinion leaders that youths in Iguana
community are exposed to. It can be seen that 72% (n=72) of youths are exposed to religious
leaders, 26% (n=26) are exposed to motivational leaders and 2% (n=2) are exposed to
community leaders.
Table 12: Categories of opinion leaders respondents are exposed to
Response Frequency Percent
Religious leader 72 72%
Motivational leaders 26 26%
Community Leaders 2 2%
Total 100 100%
Source: Researcher’s field work (2014)
Figure 7: a pie chart showing the categories of opinion leaders youths are exposed to
72 %
26 %
2 %
Categories of opinion leaders youths are exposed
Religious leader Motivational leaders Community Leaders

Table
98
RQ 5: In what ways do opinion leaders in Igbaja community engage in HIV/AIDS
awareness creation?
In order to answer this research question, variables 16 and 17 will be considered.
From the Table .14 and chart below, it can be said that majority of the opinion leaders 57%(
n=57) engage in the creation of HIV/AIDS awareness during religious gatherings, 23% (n=23)
create awareness during informal gathering, 12%( n=12) during community events and the
remaining 8% (n=8) during socially organized events to create awareness about HIV/AIDS.

99
Table 13: On what occasion do opinion leaders speak on HIV/AIDS?
Responses Frequency Percent
During community events 12 12%
specially organized events to create
awareness about HIV/AIDS
8 8%
religious programme 57 57%
informal gatherings 23 23%
Total 100 100%
Source: Researcher’s field work (2014)
Figure 8: a pie chart showing occasions when opinion leaders talk about HIV/AIDS Table
14: perception of respondents about opinion leaders.
Response Frequency Percent
They are knowledgeable among the educated 36 36%
12 %
8 %
57 %
23 % During community events
specially organized events to create awareness about HIV/AIDS
religious programme
informal gatherings

100
They are widely exposed and experienced 44 44%
They are older and respectable 2 2%
They have access to the media than other members of the
community
8 8%
They have access to relevant information about HIV/AIDS 10 10%
Total 100 100%
Source: Researcher’s field work (2014)
From the Table 17 provided below, 35% (n=35) o the respondent said opinion leaders create
HIV/AIDS based on personal communication, 21% (n=21) said creation of awareness was
through group discussion, 18% (n=18) said it is done through one-to-many communication and
26% (n=26) said it is done through mass communication.
Table 15: Through which medium do opinion leaders speak on HIV/AIDS?
Response Frequency Percent
Personal communication/one on one
35 35%
Group Discussion 21 21%
One-to-many communication 18 18%
Mass Communication 26 26%
Total 100 100%
Source: Researcher’s field work (2014)
RQ 6: To what extent have the opinion leaders effectively influenced the youths in Iguana
community?
In order to answer the above research questions, variables 22 and 24 will be analyzed.
The table below is the result of a Likert scale that shows the level of respect and believe that
respondents that have for their opinion leaders. From the table it can be said, 78% (n=78)
strongly agree that they respect their opinion leaders and believe the things they hear from them
while 28% (n=22) simply agreed that to the fact. From the table below, it can also be deduced
that 60% (n=60) of the population strongly agree that they take note of the things their opinion
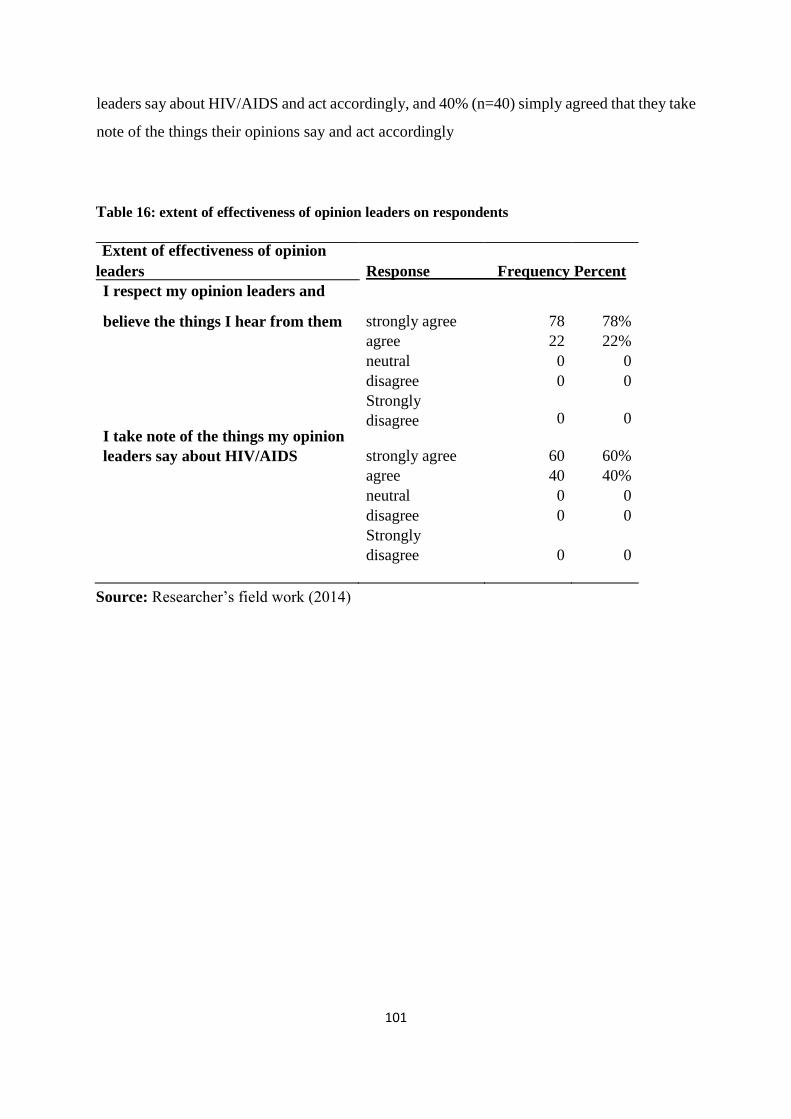
101
leaders say about HIV/AIDS and act accordingly, and 40% (n=40) simply agreed that they take
note of the things their opinions say and act accordingly
Table 16: extent of effectiveness of opinion leaders on respondents
Extent of effectiveness of opinion
leaders Response Frequency Percent
I respect my opinion leaders and
believe the things I hear from them strongly agree 78 78%
agree 22 22%
neutral 0 0
disagree 0 0
I take note of the things my opinion
Strongly
disagree 0 0
leaders say about HIV/AIDS strongly agree 60 60%
agree 40 40%
neutral 0 0
disagree 0 0
Strongly
disagree 0 0
Source: Researcher’s field work (2014)

102
4.4 Discussion of findings.
The primary objective of this research is examining the role the opinion leaders play in creating
or influencing the youths on HIV/AIDS, particularly in Igbaja community, while identifying
the various categories of opinion leaders determining the effectiveness of the HIV/AIDS
messages youths receive from opinion leaders and ways in which opinion leaders in Igbaja
community engage in the creation of HIV/AIDS awareness.
By and large, findings from this study revealed that opinion leaders vary from person to person
ranging from community opinion leaders to motivational leaders and religious leaders.
The study also found out the perception of youths about their opinion leaders.
As revealed in Table 2, it can deduced that all the youths in Igbaja are aware about HIV/AIDS.
However in Table 4, majority of youths believe that HIV/AIDS is a curable disease because
27% strongly agreed that HIV/AIDS is curable and 41% simply agreed that HIV/AIDS is
curable, of the 68% of youths that believe that HIV/AIDS is curable, 26% of them believe it
can cured by praying, 62% believed that it can cured medically and 12% believed that further
researches will help find a cure. This implies that they are not well informed about the disease.
The role of the media cannot be undermined as majority of youths who participated in this
study as seen in Table 7 first heard of HIV/AIDS via the radio and according to Table 8, 72%
of the youths are exposed to HIV/AIDS messages weekly. This implies that the media also
plays a pivotal role in creating awareness.
Regarding the influence of opinion leaders on youths, Nigerian youths are exposed to different
categories of opinion leaders as in Table .13, this range from religious leaders to motivational
leaders and community leaders.
Summarily:
a) Opinion leaders speak at different occasions such as community events, specially
organized events about HIV/AIDS, religious programmes and informal gatherings.
b) 78% of youths respect their opinion leaders and believe the things they hear from them
generally.
c) 60% of youths take notes of the things their opinion leaders say about HIV/AIDS.

103
Edewor (2010) posits that information is indispensable for human development. Likewise ,
Nwafor-Orizu (2003) while describing sources of information dissemination in the rural areas
in Nigeria, avers that, oral sources like face-to-face interaction, radio, television, traditional
institutions, associations, and written sources like newspapers and magazines aims to
facilitate rural information transfer as a way of eliminating ignorance and superstition. This
study correlates with the view of Nwafor_Orizu (2003) as Opinion leaders create awareness
through personal communication, group discussion, one-to-many communication and mass
communication.
Similarly, in the word of Rosario (1971), opinion leaders, are limited few in the community
with a higher level of education, exposure to idea and are sources of advice and knowledge.
They exhibit prestige, higher social status, cosmopolitanism, and mass media exposure.
Findings from this study can be related to the words of Rosario as majority of the youths in
Igbaja believe their opinion leaders are knowledgeable among the educated, are widely
exposed, are older and respectable and have access to relevant information about HIV/AIDS.

104
References
Edewor N.. (2010), “Access to health information by people living with HIV/AIDS in Nigeria.”
Library philosophy and practice
Nwafor-Orizu, U.E., (2007). An appraisal of the methods of disseminating of HIV/AIDS
information in Nnewi-South Local Government Area of Anambra state, Nigeria.
Rosario, F. Z. (1971). The leader in family planning and the two-step flow model. Journalism
Quarterly 48(2):288-297, 303,

105
CHAPTER FIVE
SUMMARY, CONCLUSIONS AND RECOMMENDATIONS
5.1 Summary This study set out to establish a framework that can explain the creation of HIV/AIDS
awareness among youths in rural areas. It focused on identifying the various categories of
opinion leaders and determining the level of their effectiveness of the opinion leaders on the
youths in rural communities.
Armed with responses from 100 youths in Igbaja communities, Ilorin, the researcher set out
to investigate the role opinion leaders’ play in the creation of HIV/AIDS awareness and
identifying youth’s perception about these opinion leaders. The research also hunted for the
effectiveness of the messages youths are exposed to.
This study used quantitative method in an effort to increase the validity of research findings
by analysing the data from the survey conducted with a sample size of one hundred (100)
youths in a rural community.
The researcher also found that there is a misconception about the cure of HIV/AIDS as some
youths believe it can be cured through prayer while others believe it can be cured medically
with the use of drugs and injections.
Findings generated from the survey revealed that youths in Igbaja community are aware of
HIV/AIDS, rely majorly on religious and motivational opinion leaders and believe and take
note of everything their opinion leaders say particularly about HIV/AIDS.
5.2 Conclusion Apparently, the concept of HIV/AIDS is indispensable to all, the respondents agree
HIV/AIDS is dangerous disease that can be prevented through abstinence from casual sex,
use of condoms, not sharing of sharp objects and avoiding blood transfusion.
In addition, the researcher found a high level of misconception about of the cure of
HIV/AIDS, this was a question asked to test the level of awareness of the youths in rural.

106
Furthermore, based on the research findings, the conclusion is that, though there is a good
understanding of the deadly disease, HIV/AIDS, there is a misconception about the cure.
This to a large shows a lapse in the role opinion leaders in rural communities play in the
creation of HIV/AIDS, it is tantamount to saying the role of opinion leaders in rural
communities is very unprofessional and tragically ordinary.
5.3 Limitations Aside the ever present financial and time constraints, youths were very difficult to come
across in the community, as many of the residents in the rural community are parents who
rely on their children who live in urban areas.
With regard to the external validity of this study, another limitation of this study is that the
number of samples was relatively small. This small sample size is a result of the poor number
of youths the researcher came across during the process of testing and retesting the pilot test.
5.4 Recommendations This section of the project suggest solutions to the problems studied based on research
findings and also make suggestions for future researchers who will be interested in
developing on this study or conducting research on related issues.
5.4.1 Recommendations based on findings of the study The findings from this research suggest several courses of action. Based on the findings of
this study, it is recommended that opinion leaders pay more attention to the creation of
awareness on methods of contracting HIV/AIDs among youths in rural communities.
Though the research found out that opinion leaders regularly speak on HIV/AIDS, but then
opinion leaders should make their discussions more succinct, explicit, and in depth
Besides this, the researcher recommends that opinion leaders should inform youths about
prevention of HIV/AIDS, make youths understand that HIV/AIDS is a scientific
phenomenon and can only be cured scientifically not spiritually.

107
5.4.2 Suggestions for further studies This research has thrown up many questions in need of further investigation. First, what is
the rationale behind gatherings where HIV/AIDS is discussed is just creation of awareness
of public relations activities is in Nigerian corporate organizations.
In addition, more research with a more representative sample is needed to better understand
the information role of opinion leaders in rural communities and the country at large. A
research of this scale is advised to be backed sufficiently by bodies, such as NACA, FMOH
to ensure ease of access of the research on HIV/AIDS awareness, prevention and
maintenance.
Another possible research avenue is to explore the role of opinion leaders such as community
opinion leaders and youth leaders.
The researcher hopes the study will spur more research on role of opinion leaders, impact of
Opinion Leaders as well higher level of understanding of HIV/AIDs in rural communities.

108
BIBLIOGRAPHY
Books Adeyi, S. (2006). AIDS in Nigeria: A nation on the threshold. In Adeyi S., & Ademo J.
(Eds.). The epidemiology of HIV/AIDS in Nigeria . USA: Centre for Population and
Development Studies.
Akinfeleye, R.A. (1988). “The Youth, Education, Mass Media, and Nation Building”, In
Nnolim, C.E. (Ed.) The Role of Education in Contemporary Africa. New York:
Professors World Peace Academy. pp. 117-133
Andriote J (1999) victory deferred: How AIDS changed gay life in America. University of
Chicago, Chicago.
Bond, V. (2007). Stigma when there is no other option: Understanding how poverty fuels
discrimination toward people living with HIV in Zambia. In S. Gillespie (Ed.), AIDS,
poverty, and hunger: Challenges and responses (Chapter 10, pp. 181–197).Washington
DC: International Food Policy Research Institute
Chief M.V. (2000), A gender perspective on the impact of HIV/AIDS on food security and
labour supply: Leadership challenges. Gender and HIV/AIDS: leadership roles in social
mobilization. UNFPA. Addis Ababa.
Heatherton, T. F., Klecik, R. E., Hebl, M. R., & Hull, J. G. (2000). The social psychology of
stigma. New York, NY: Guilford Press
Hoffman, N.D. & Futterman, M.D. (1996). 'Youth and HIV/AIDS' in J.Mann & D. Tarantola
(eds.) AIDS in the World II: Global Dimensions, Social Roots and Responses. New
York: Oxford University Press
Losce, R.M. (1990) Society development and libraries. Center for external studies;
University of Ibadan
Kanki, P.J., & Adeyi O. (2006). Introduction. In: Adeyi, O. (Eds.). AIDS in Nigeria: A
nation at the threshold. Cambridge, MA: Harvard Centre for Population and
Development Studies
Okunnu, C. (2002). Teaching mass communication: A multi-dimensional approach .
Enugu: New Generation Books
Okwilagwe, A.O (2000). Information capacity theory. Mimeograph, University of Ibadan

109
Thomborrow, J. 1999. “Language and the media” In Thomas, L and S. Wareing (Eds.).
Language, society and power: An introduction. London and New York: Routledge. pp. 4963
Journals/Journal articles. Afolabi, O. A., & Adesina, A. A. (2005). HIV/AIDS: Psychosocial and therapeutic issues
in the disclosure of diagnosis. Iroro: A Journal of Arts, 10 (1&2), 140-153
Akanmu, A. S., Akinsete, A., and Njoku, O. S., (1999). Prevatence of hepatitis B surface
antigen among women of child bearing age in Lagos, Nigeria. African Journal of
Reproductive Health 3(1): 45-50
Castro A, Farmer P. (2005), Understanding and addressing AIDS-related stigma: From
anthropological theory to clinical practice in Haiti. Public Health Matters. (1):53–59
Chen J, Choe MK, Chen S, Zhang S.(2005) Community environment and HIV/AIDSrelated
stigma in China. AIDS Education and Prevention. 17(1):1–11
Deacon H. Towards a sustainable theory of health-related stigma: Lessons from the
HIV/AIDS literature.(2006) Journal of Community & Applied Social Psychology
16:418–425
Duncan J.W. and Peter S.D. (2007), Influential, networks and public opinion formulation.
Journal of consumer behaviour. 441-458.
Erica C (2008). Barriers to equitable access to quality health information. Journal of
medicine(5): 117 – 123. Retrieved January 17 2009
Genberg BL, Kawichai S, Chingono A, Sendah M, Chariyalertsak S, Konda KA, Celentano
DD. (2005) Assessing HIV/AIDS stigma and discrimination in developing countries.
AIDS and Behavior ;12(5):772–780
Guan J, Wu Z, Rotheram-Borus MJ, Li L, Detels R, Wu S,(2009) NIMH Collaborative
HIV/STD Prevention Trial Group. Self-reported sexually transmitted disease
symptoms and treatment seeking behaviors in China. AIDS Patient Care & STDs.
23(6):443–448.

110
Hong, Y., Li, X., Stanton, B., Fang, X., Lin, D.,Wang, J. (2008). Expressions of HIV-
related stigma among rural-to-urban migrants in China. AIDS Patient Care and STDs, 22,
823–831.
Idoko, J.A. (2004). An overview of HIV/AIDS diagnosis and antiretroviral therapy in
doctor's diary, Abuja: Nigeria Medical Association: 84-85
Logie, C., & Gadalla, T. M. (2009). Meta-analysis of health and demographic correlates of
stigma towards people living with HIV. AIDS Care, 2, 742–753.
Malcolm, A, Angleton, P, Bronfman, M, Galva, J, Purina, M, and Verrall, J.(1998).
HIVrelated stigmatization and Discrimination: its forms and contexts. Critical Public
Health, 8, 347-370.
Mooko, N. P. and Aina, L.O. (2007) Information Environment of Artisans in Botswana.Libri
57 (1) 27-34
Rangel MC, Gavin L, Reed C (2006) Epidemiology of HIV and AIDS among adolescents
and young adults in the United States. Journal of Adolescent Health; 39:156 –163.
Reece, M., Tanner, A. E., Karpiak, S. E., & Coffey, K. (2007). The impact of HIV-related
stigma on HIV care and prevention providers. Journal of HIV/AIDS & Social Services, 6,
55–73
Rosario, F. Z. (1971). The leader in family planning and the two-step flow model.
Journalism Quarterly 48(2):288-297, 303,
Thompson, G. N., Estabrooks, C. A., & Degner, L. F. (2006). Clarifying the concepts in
knowledge transfer: A literature review. Journal of Advanced Nursing, 53, 691–701.
Valente, T. W., & Pumpuang, P. (2007). Identifying opinion leaders to promote behaviour
change. Health Education & Behaviour, 34, 881–896. Quarterly, 48, 288–297
Broadcast and unpublished works. Adedimeji, M.A.2004. “The Effects of HIV/AIDS Education Programme on the Cognition
and Attitudes of Selected Tertiary Institution Students in Ilorin, Nigeria”. VIHEAP
Module 1 Project
Akunyili, D. (2005). Fake drugs are more dangerous than HIV/AIDS. Daily Sun (April 12):
12

111
Chukwuma A, and Atelhe A. (2007).The role of the mass media in the fight against
HIV/AIDs in Nigeria (Unpublished)
Edewor N. (2010), “Access to health information by people living with HIV/AIDS in
Nigeria.” Library philosophy and practice.
Ejeagwu O., Nwafor-Orizu, U.E., & Uhegbu, A. (2007). An appraisal of the methods of
disseminating of HIV/AIDS information in Nnewi-South Local Government Area of
Anambra state, Nigeria.
Ejinkeonye, U. 2004. “Campaign Deadlier than AIDS”.Daily Independent. Lagos.June 2.
pp.E16/back page
Federal ministry of information and national orientation (2007). The Obasanjo reforms
HIV/AIDS response. Abuja, Federal ministry of information and national orientation,
Federal Ministry of Health (FMOH), 2003. National HIV/AIDS and Reproductive Health
Survey. Lagos:.Federal Ministry of Health, 2004. 2003 National HIV Sero-prevalence
Sentinel Survey, Abuja. Retrieved from www.synergyaids.com/documents/Nigeria on
December, 2007.
Kayode J and Jimoh J (2007). Newspaper coverage of HIV/AIDs stigma: An analysis of the
average of the Guardian and the Vanguard.
Madu, M.C. 2004. “HIV/AIDS: Wear Abstinence, not Condom”. The Punch. Lagos. March
3. p.16
Mahdu, K. P. (2007). Conference on global media strategies for HIV/AIDs and associated
competition and media festival. Geneva: UNAIDS
Muluh, H. (2009). The Challenge of HIV/AIDs: The role of the Cameroon Media .
National Action Committee on AIDS (2001). HIV/AIDS emergence plan. Nigeria technical
report
National Agency for the control of AIDS (2005) national strategy for behavior change,
interventions and communication for HIV.
Nwafor-Orizu, U.E., (2007). An appraisal of the methods of disseminating of HIV/AIDS
information in Nnewi-South Local Government Area of Anambra state, Nigeria.
Peterson K. & Obileye O. (2002). Access to drugs and related opportunistic infections in
Nigeria. Policy Project. Nigeria: Center for Development and Population Activities
(CEDAP)

112
Pandey, P. K. (2005) “Trends of HIV/AIDs reporting in the newspaper of Bangladesh: A
study of selected dailies” in Abstracts of the 14th International Conference on HIV and
STIs in Africa Abuja: ICASA
Shabani, J. and P. Okebukola (Eds.) 2004. “HIV/AIDS Education Training Programme”.
UNESCO’s www.viheaf.net. Between March 1 and May 25.
UNAIDS,(1998) level and flow of international resources for the response of AIDS. Geneva
UNAIDS(2008). Report on the global AIDS epidemic. Retrieved January 13, 2009, from
http://www.avert.org
UNAIDS (2012) ‘Global Report: Annexes'
UNAIDS (2012) 'World AIDS Day Report - Results'
WHO (2008). Access to health information and knowledge sharing: an overview. Retrieved
January 17 2007, from http://e-health.org/articles.html

113
APPENDIX
University of Ilorin
Faculty of Communication and Information Sciences
Department of Mass communication
Questionnaire
Dear respondent,
I am Oyafemi Andrew Babatola, a student of the department of Mass Communication, Faculty
of Communication and Information Sciences, University of Ilorin. I am conducting a research
on the “HIV/AIDS awareness among youths in Igbaja Community: the role of opinion
leaders” as part of the requirement for the award of B.Sc. degree in Mass communication. This
study is purely an academic exercise and I will be grateful if you could sincerely respond to
the questions in this questionnaire. Your response will be strictly held in confidence and used
for the purpose for which it is designed.
Instruction: Please tick (√) in the boxes that correspond to your responses to the following
questions.
Section A
1. Are you aware of HIV/AIDS?
(a)Yes (b) No
S/N SA A N D SD
2. HIV/AIDS is a dangerous disease
3. HIV/AIDS can be cured
4. If you Strongly Agree or Agree, How can it be
cured………………………………………………………………………………
………………………………………………………………………………………
…………………………………………….........

114
9. Where did you first hear about HIV/AIDS?
(a) Through the mass media (b) through family and friends (c) through religious
institutions (d) through school (e) through opinion leaders
10. Which media exposes you to HIV/AIDS messages?(you can choose more than one)
(a) Radio (b) Television (c) Newspaper (d) Social Media
11. How often are you exposed to messages HIV/AIDS?
(a) Every day (b) about twice a week (c) weekly (d) fortnightly (e) monthly 12.
Do you have any opinion leader that you are exposed to? (a) yes (b) no
14. What are the categories of opinion leaders you are exposed to?
(a) Political leaders e.g. local government chairman (b) religious leaders e.g. imam,
pastor(c) motivational leaders e.g. youth leader (d) Community leaders e.g.
Mogaji (f) others, please specify………………….
15. How do you get information from your opinion leaders?
(a) Radio (b) television (c) bill boards (d) social media (e) face to face (f) others, please
specify………………….
16. Do opinion leaders in your community talk about HIV/AIDS? (a)Yes (b) no
Please rank from scale of 1-5, with 5 being the highest, the rate at which you get HIV related
information from the following categories of opinion leaders.
1
2
3
4
5
A Political Leaders
S/N SA A N D SD
5. Abstinence from casual sex can prevent HIV/AIDS
6. Condoms can be used to prevent HIV/AIDS
7. Sharing of sharp objects can lead to HIV/AIDS
8. Giving or receiving blood can lead to HIV/AIDS

115
B Religious leaders
C Motivational leaders
D Community leaders
17. On what occasion do opinion leaders speak about HIV/AIDS?
(a) During Community events (b) specially organized events to create awareness about
HIV/AIDS (c) during political campaigns (d) religious programmes (e) informal
gathering (f) others, please specify………………….
18. Through which medium do opinion leaders talk on HIV/AIDS?
(a) Personal communication/ One on One (b) Group Discussion (c) one –to-many
communication (d) Mass communication
19. What is your perception about opinion leaders in your community? (You can tick more
than one.)
(a) They are knowledgeable among the educated. (b) They are widely exposed and
experienced (c) They are older and respectable (d) They have access to the
media than other members of the community (e) They have access to relevant
information about HV/AID (f) Others, please specify…
………………………………….
20. Please give reasons for your choice in question 18
………………………………………………………………………………………
………………………………………………………………………………………
…………………………….
21. How has your exposure to HIV/AIDS messages influenced you?
(a) It informs me about the syndrome (b) It educates me about abstinence (C) I t
educates me about unprotected contact (d) It alerts me about the stigmatization of
victims. (e) The messages have no significant influence on me.
S/N Perception about opinion leaders SA A N D S

116
21 I get a lot of HIV/AIDS related information from opinion leaders in my
community
22 I respect my opinion leaders and believe the things I hear from them generally
23 I believe the HIV/AIDS information I get from opinion leaders in my
community
24 I take note of the things my opinion leaders say about HIV/AIDS and act
accordingly




















