
History of Cholera in Latin America
24
Final Draft December 17, 2006 Historical Analysis of Cholera in Latin America By Ivan J. Ramirez Department of Geography, Michigan State University Epidemiology 805 Dr. Michael Rip
Transcript of History of Cholera in Latin America

Final Draft
December 17, 2006
Historical Analysis of Cholera in Latin America
By Ivan J. Ramirez
Department of Geography, Michigan State University
Epidemiology 805
Dr. Michael Rip
2
I. Introduction In 1991 the seventh pandemic of cholera reached the shores of Peru. This would
mark the reemergence of the disease in Latin America for the first time in the 20th
century (CDC, 1991). Outbreaks would follow in neighboring countries like
Ecuador and Colombia, and by the year’s end 15 countries in the region
including the U.S. would be afflicted. Although the fatality rate (<1%) of cholera
was dramatically less so than in the past, its morbidity remained high. Almost
400,000 cases were reported in 1991 of which 80% was in Peru (PAHO, 1996).
Since then, more than 1.2 million cases have been documented in Latin America
(PAHO, 2004). The scourge returned to the western hemisphere.
The outbreak was attributed to an Asian ship that docked in several ports
throughout the coast of Peru. It is hypothesized that the waste of infected
passengers was dumped into the sea and contaminated shellfish and the waters.
Contamination was possible because of Peru’s inadequate water and sanitation
services, which were in decline (PAHO, 1998). Another theory which has recently
gained support is one where multiple pathways via marine life that host the
cholera bacteria contributed to the outbreak. Furthermore, it is posited that these
bacteria and its host populations were increased and spread through climatic and
environmental mechanisms (Huq et al., 2001; Lipp et al., 2002; Rode et al.,
2002; Pascual et al., 2002; Pascual et al., 2000; Seas et al., 2000). While
these studies are not yet conclusive, they have spurred interest among the
climate science, public health, geography and many other disciplines.
How did cholera breach South American borders and regain a foothold in the
western hemisphere? Why after so many years? What is the history of cholera in
Latin America? Most historical accounts provide extensive details of epidemics in
Asia and Europe. A historical synthesis of Latin American accounts of epidemics
is lacking, at least from authors in the Northern Hemisphere (Politzer, 1959; De,
1961; Barua & Greenough, 1992; Hays, 2005; Ackerrnecht, 1965).

3
Understanding the past may help us to shed some light on the present and
future.
The paper attempts to historically synthesize cholera epidemics in Latin America
from as far back as the 17th century to the present status. I describe the series of
epidemics in Latin America within the context of the global pandemics and refer
to them as ‘waves’. It also attempts to provide some insight to how the
understanding of cholera may have affected epidemics in Latin American
countries. Of course, this will be provided when data or reports are available. Did
Snow and Koch’s discoveries diffuse to these states? How have recent
discoveries of cholera ecology changed our perception of transmission in the
region? Following this introduction I present some background on cholera. I
describe the disease, the causative agent of cholera, transmission, prevention,
treatment and describe some historical context of discoveries in relation to each
topic. The next section briefly describes the history of the term cholera and the
pandemics. It excludes Latin American epidemics since I will be describing them
in the next section. The fourth section discusses the ‘waves’ of cholera epidemics
as they occurred overtime in Latin America and the reemergence of cholera in
1991. The final section is conclusions.
II. Cholera Background
Cholera is a diarrheal disease caused by the bacterium Vibrio cholerae, which
infects the small intestine of humans (Rabbini & Greenough III, 2001; WHO,
2000; De, 1961). In 1953, De discovered that vibrios release toxins within one to
five days, which sets off the course of the disease (Barua, 1992; WHO, 2000). It
typically proceeds in several stages, and begins with acute watery diarrhea and
vomiting that becomes continuous, and can lead to severe dehydration, uraemia,
and eventually death (WHO, 2000; De, 1961). By the mid-stage cholera victims
experience a rapid fall in blood pressure and radial pulse disappears; the eyes
shrink in and the skin becomes clammy and wrinkled (De, 1961). The disease
can spread without notice because the bacterium can be present for up to 14
days before any symptoms arise (WHO, 2000).
4
Snow’s seminal work in London in 1854 had found that cholera was a water-
borne disease, but the agent or mechanism for transmission was not yet
understood (Huq et al., 2001, Vinten-Johansen et al., 2003). Although the
causative agent or mechanism was not yet known, it was beneficial for public
health. This finding led to many sanitary initiatives to prevent cholera. That same
year in December of 1854, a Florentine microscoptist named Pacini would
discover that agent, but could not demonstrate convincingly its etiology (Barua,
1992; Vinten-Johansen et al., 2003). Moreover, he published the findings in a
small journal during a time when contagion of cholera was being disputed (Lipp
et al., 2002; Barua, 1992). In 1883 Koch discovered the causative agent while
examining cholera in Egypt and India. He named it Vibrios cholerae (Barua,
1992; Lipp et al., 2002). Cholera could now be identified microbiologically.
Approximately 200 types of the Vibrio cholerae have been identified, but so far
two been associated with epidemics. The serogroup 01 is associated with
pandemics one through seven, and 0139, which emerged in 1992 in Bangladesh,
is believed to be the beginning of the eighth pandemic. This was the first time two
groups were present during global cholera outbreaks. Serogroup 0139 appears
to be a mutation of the 01 group and a non-01 group (as cited in Lipp et al.,
2002; Huq et al., 2001). Serogroup 01 consists of two biotypes: classical and El
Tor. The latter type was isolated from dead cholera victims in 1904 during
quarantine in Egypt. It is not clear why El Tor did not emerge as the primary
biotype until the seventh pandemic. But it was found in cholera epidemics in
Indonesia during the 1930s through forties (Barua, 1992). Cholera is normally transmitted through the ingestion of contaminated water, but
infection can also occur through the consumption of food such as seafood and
beverages (Glass & Black, 1992; Lipp et al., 2002). The vibrios are found in the
feces of humans, which are passed into water when evacuations take place.
There have also been studies which postulate that transmission may possibly
occur through flies (landing on infected species), fomites (inanimate objects), and
person-to-person (sweat). However these pathways are contentious and have
not been documented empirically (Glass & Black, 1992).

5
In 1977 Colwell et al. found that humans were not the only reservoirs for the
cholera bacterium. Vibrios existed in natural marine and estuarine environments
such as those coastal inlands of Bangladesh (as cited in Lipp et al., 2002; Huq
et al., 2001; WHO, 2000). They attach themselves to phytoplankton, which are
eaten by zooplankton and crustaceans (shrimp and lobster). This finding could
possibly explain many sporadic outbreaks and those which emerged in “virgin”
environments such as Peru. Furthermore, it illustrated that solely poor hygiene
and cultural behaviors were not responsible for risk exposure (Huq et al., 2001).
Prevention methods could now look for vibrios in the environment and in the
laboratory specimens from humans (Huq et al., 2001; Barua & Greenough III,
1992).
This environmental aspect of the vibrio is actively being researched, particularly
in the context of a warmer world. Marine reservoirs are sensitive to changes in
the environment such as seas surface temperatures (Huq et al., 1992; Lipp et
al., 2002). So then what would be the implications if temperatures increased?
They are also sensitive to salinity. The right combination of factors may create a
habitat where the reservoir populations are able to thrive, and hence, vibrios may
increase. This hypothesis is being investigated and has been put forth to partially
explain the emergence in Peru (Lipp et al., 2002; Hug et al., 2001). I will
elaborate on this further when I discuss the Fifth wave of epidemics in Latin
America.
Adequate water and sanitation systems are the best methods to prevent cholera
and other diarrheal disease outbreaks. This means a safe mechanism for the
disposal of human feces and treatment of polluted water so it does not
contaminate the water supply. Public education is also important such as
informing of hygienic practices especially during times of outbreaks (WHO,
2000). Another prevention tip to avoid using waste water for irrigation. This can
infect crops and increase risk exposure (Barua, 1992). However, if water supply
is scarce and sanitation systems are inadequate, behaving appropriately will be
6
difficult and in some cases not possible. How can you boil water or wash your
hands when there is no water to boil? Or avoid seafood when it is the cheapest
food available? These factors were largely attributed to the widespread
outbreaks in Latin America (Tickner & Gouveia-Vigeant, 2005; Witt & Reiff, 1991).
Lastly it is important to correctly identify cases of cholera and identify an
outbreak, and therefore surveillance is necessary and technology to clinically id
the disease. It was argued that in many cases in the Latin American countries,
cholera was not clinically identified (Barua, 1992). Therefore in some places the
number of cases may have been over reported and in others there may have
been less. However PAHO does report that generally in Latin America,
underreporting of cholera is approximately 50% (PAHO, 2004). I understand this
to mean that the cholera outbreak in 1991 may have been worse than statistics
illustrate.
There are several treatment methods that include oral rehydration therapy (ORT)
composed of a solution of salts and glucose, antibiotics, intravenous fluids, and
vaccines. ORTS have been the most effective in terms of cost and recovery.
According to the WHO (2000), this method can sufficiently treat up to almost 90%
of cholera victims unless the conditions are severe (lost too many fluids). In such
cases, a combination of ORT with intravenous fluids may help. Although
antibiotics are available, increasing resistance to them has been documented. If
effective they help to minimize the amount of fluids evacuated (WHO, 2000).
Vaccines are also available but they may create false security. Protection can
last up to several months. However its effectiveness requires more research.
III. History of Cholera The Term The scourge of cholera can be traced as far back as 500 – 400 B.C. in India,
where it is thought to have originated. There it was known as visuchika meaning
a disturbance of the stomach (Barua, 1992: 1). The word “cholera” is believed to
have originated from the Greek words chole (bile) and reins (flow) and first used
7
by the Greek philosopher Hippocrates (470 – 377 B.C.). He described it as a flow
of bile (De, 1961: 4) and attributed cholera and all diseases to an imbalance of
humors (fluids) within the body (Thagard, 1996). Asclepiads, a follower of
Hippocrates, thought cholera as a flow of humor rather than bile (De, 1961: 4). In
Ancient China, it was called fok lun and was described as “something huddled up
in a confused manner inside the body…expressed by vomiting and purging.”
(quoted in Barua, 1992: 2). The present Chinese term is huo lon, which means
gastrointestinal infections (Barua, 1992: 2). In Latin writings around the third and
fourth centuries, cholera was referred to as “bitter”, a violent anger (De, 1961: 4)
It was known in Tibetan writings around A.D. 802 as nja, something which afflicts
the body and empties it of water (cited in Politzer, 1959: 11). Haida meaning
shattered was the word for cholera in Arabic around 900 A.D. and in Bengal it
was called olautha, purging and vomiting (Barua, 1992: 4). In the middle of the
17th century, Thomas Sydeham, the father of English Medicine, introduced the
term cholera morbus to distinguish it from anger (Barua, 1992).
The various terms found across cultures overtime have made it quite difficult for
researchers to accurately understand the history of cholera (Barua, 1992). Were
these recorded accounts of cholera as we currently know it or just severe
gastrointestinal infections? Each place or region described it as they observed
and experienced it. It was also difficult because sporadic forms of the disease
were being documented and the understanding throughout time changed; until
Koch’s discovery, cholera had been attributed to the environment or atmosphere
(as cited in Barua, 1992: 6).
Pandemics Although cholera outbreaks were recorded in India during the 14th and 15th
centuries, it wasn’t until the 16th century that widely documented accounts began
appearing. Portuguese settlers in Goa reported cholera epidemics with high
mortalities in the springtime of 1503 and 1543. Outbreaks in this same region
were also documented by the Dutch, French, and British (as cited in Politzer,
8
1959: 12-13). Throughout Europe several reports of cholera epidemics were
found in places like London (1667 and 1669) Montpellier (1649), Nuremberg
(1689), Ghent (1665), Nimes (1654), and Vienna (1768). There were even
reports of outbreaks as far away as Brazil (1658) (as cited in Barua, 1992: 4-5;
Dubos, 1976).
It was not until the 19th century that the first pandemic (1817-1829) would take
course. According to Politzer, the year 1817 appeared to be a turning point in the
virulence of cholera. The spread of cholera became quick and severe covering
almost 200,000 square miles in three months across India (as quoted in
Politzer, 1959: 18). Interestingly it was also a year of heavy rains, floods, and
crop failures. Cholera found its way by land and sea to Southeast Asian countries
including Nepal (1818), Ceylon (1818), Burma (1819), and Siam (1820), which
was reportedly devastated (as cited in Barua, 1992: 8; Politzer, 1959: 19). By
1821, it reached the shores of Oman and was likely imported by Indian
expeditionary troops from Bombay. China was invaded by land in 1817 and by
sea in 1820. Outbreaks would last until 1824 and follow the caravan route along
the Great Wall. In the Persian Gulf and Mediterranean (1821), cholera would
affect the ongoing war between Persia and Turkey. In less than three weeks,
more than 15,000 people were killed in the port city of Basra in Persia. It reached
Russian shores via the Caspian Sea in 1823, but was not so severe due to
severe winter conditions. It is suspected that these infections were recrudescent
(as cited in Barua, 1992: 8; Politzer, 1959: 19-20). Japan (1822) would be
invaded via the sea from Java and Mauritius (1819) via Ceylon (Barua, 1992: 8).
By the second pandemic (1829-1851) cholera would reach the New World. It
would arrive in the summer of 1832 via infected Irish immigrants in Quebec and
the east coast cities of New York and Philadelphia. Quarantine measures were
implemented but not all incoming ships could be inspected. It made its way
through to the south and New Orleans, where several importations and
exportations of cholera and other infectious diseases were reported. “Mass
burials were held” and outbreaks continued until 1835 and resurged in 1848. In
9
South America, Peru and Chile were the first countries to be afflicted. It would
later spread to the Caribbean and Central America. Spain, Portugal, and
Morocco reported outbreaks from 1833 – 1834. A ship from England was
responsible for the Iberian epidemics (Barau, 1992). England itself had
experienced its first outbreak during this pandemic in 1830 and cholera
“seemingly took advantage of the new conditions of industrialized England—
entering through the seaports…new highways and railroads, and attacking first
the most densely populated and…the desperately poor” (Winton-Johansen et
al., 2003: 170). Sweden, Denmark (1850), Southern France and parts of Central
Europe experienced cholera outbreaks and for some it was the first time. Cholera
would subside from 1839 until 1846 in Europe and then reemerge. Researchers
are not sure whether these outbreaks in Europe were recrudescent or
importations. The same questions arose during a major outbreak at a Mecca
pilgrimage in 1835. China (1835) would again be afflicted and cholera was again
found in the Mediterranean (1835-1837), northern Africa (1835, 1850), and now
in Sudan and Ethiopia (Barua & Greenough, 1992; Politzer).
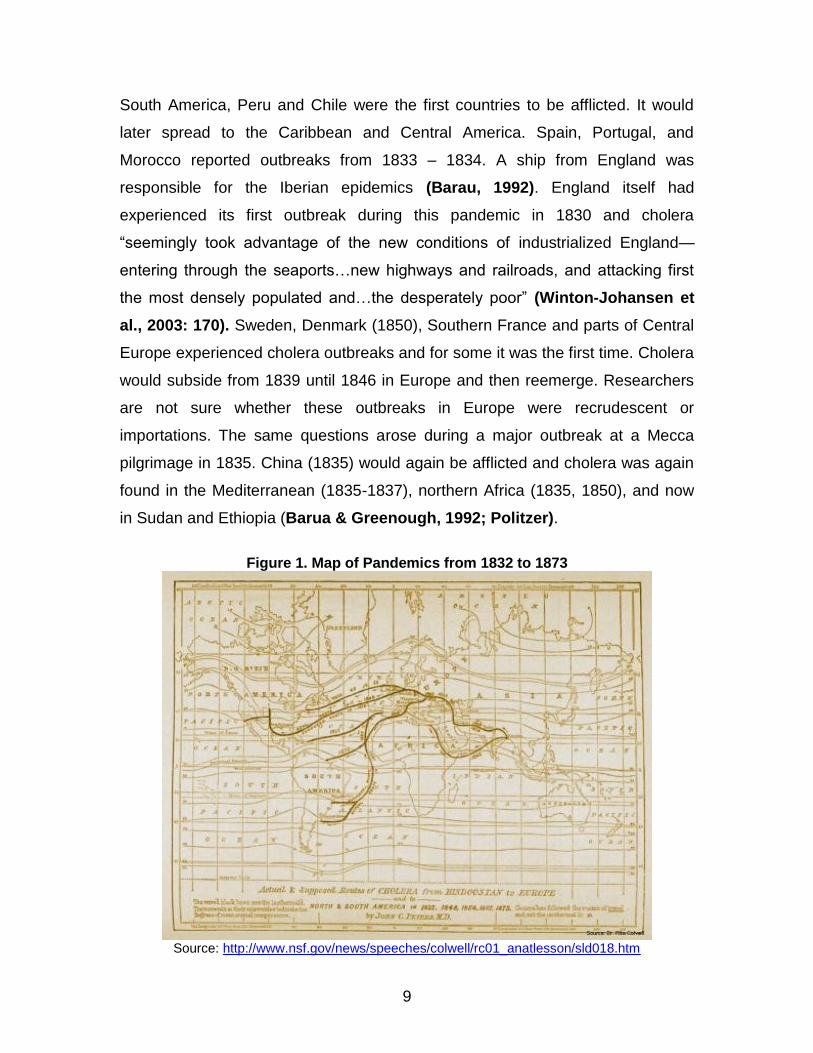
Figure 1. Map of Pandemics from 1832 to 1873
Source: http://www.nsf.gov/news/speeches/colwell/rc01_anatlesson/sld018.htm

10
At this time, it was still believed that cholera was attributable to miasma. The fear
of cholera and the spread via unhygienic behavior was so prevalent that a
national conference on sanitary measures was held in Paris in 1851 and would
meeting many times until 1938 (Barua, 1992).
The next four pandemics would strike many new places for the first time (i.e.
Southern cone in South America) and many old places continuously. Pilgrimages
in Mecca reported several outbreaks in 1865, 1881, and 1902. The 1865 would
claim one-third of the visitors. In 1866, some of the worst epidemics were
experienced throughout Western Europe in countries such as Austria, Hungary,
and Germany. It was likely exacerbated by an ongoing war in the region (Barua,
1992). That same year in New York City, it is believed that the first public health
board was created in direct response to cholera (as cited in Huq et al., 2001).
Snow’s discovery of the water connection would strongly influence public health
measures. However, bad air and filth was still blamed for the cause of cholera.
By the sixth pandemic which began in 1899, bacteriology was at work. Koch had
found the causative organism of cholera. However many cases and outbreaks
would continue in many parts of the world. In Leningrad about 800,000 lives were
lost to cholera from 1893-94. Cholera was no longer present in Latin America
after the 1890s and would not see the disease until the seventh pandemic
reached its shores in 1991 (Barua, 1992).
The seventh pandemic is illustrated in Figure 2 (below). Until that time, the
classical biotype of cholera was responsible for the pandemics. Furthermore,
cholera was mainly confined to Asian countries. In 1961, cholera spread out of
Asia and again cholera would return to Africa, the Mediterranean, Soviet Union,
the Middle East, and eventually the western hemisphere. The number of cases
would spike in 1971; the largest number of cases ever reported in that pandemic
occurred that year of which Bangladesh claimed one-third. Until that time El Tor
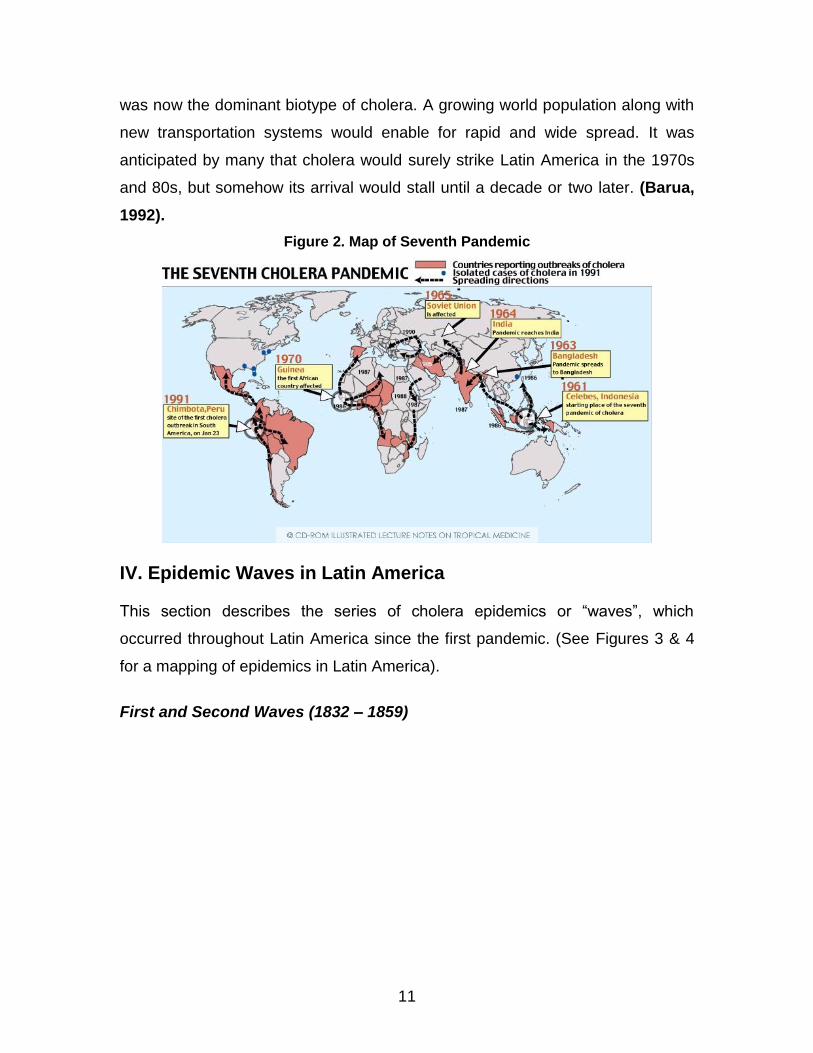
11
was now the dominant biotype of cholera. A growing world population along with
new transportation systems would enable for rapid and wide spread. It was
anticipated by many that cholera would surely strike Latin America in the 1970s
and 80s, but somehow its arrival would stall until a decade or two later. (Barua,
1992).
Figure 2. Map of Seventh Pandemic
IV. Epidemic Waves in Latin America This section describes the series of cholera epidemics or “waves”, which
occurred throughout Latin America since the first pandemic. (See Figures 3 & 4
for a mapping of epidemics in Latin America).
First and Second Waves (1832 – 1859)

12
________________________________________________________________ The colored dots represent epidemics in each respective country. Please note they do not refer to the specific location of the epidemic. Please refer to the bibliography section for sources. Map by Ivan Ramirez.
The First Wave (1832-1851) of cholera began not long after the independence of
many South American countries and during the second pandemic (1829-1851).
The Second Wave (1853-1859) would take place during the third pandemic
(1852-1859) and Snow’s discovery (1854).
In 1832 Peru and Chile were the first to encounter cholera in the Latin American
region. These first two accounts have been contested and the pathways in which
they arrived were not clear, but they have been cited in many literatures (Barua,
1992; Politzer, 1959; Hays, 2005). The cholera accounts in the Caribbean are
well documented.
In February or March of 1833, Cuba would experience its first of several
outbreaks (Politzer, 1959: 24; Kipple, 1985). The disease apparently came via
13
Spain and the U.S. The consequences would be severe and by September of
that year, more than 22,000 Cubans would be dead (Kipple. 1985). According to
Kipple (1985), cholera “raged in white-hot fashion” and overwhelmed Havana’s
two cemeteries. He also notes that blacks (free and slaves) were affected the
most and died at three times the rates of whites. At the time, Cuba under Spain’s
rule harbored a large population of slaves. It was also found in the poorest
sections of cities like El Barrio of San Lazaro in Havana, where sanitation was
significantly inadequate. Again in 1850, cholera would resurge in Havana even
though stringent quarantine measures were taken. From 1850 to 1854,
approximately 32,000 cases were reported with a case fatality rate of 53%
(Kipple, 1985).
Cholera would visit the island of Jamaica for the first time in 1850. According
reports in Kingston, it created a “terrible rate of mortality…such that husbands
refused to lift dead wives into their coffins and mothers deserted their children”
(cited in Kipple, 1985). This was not uncommon as was evident in Brazil, which
I will describe later, and more recently in the 1992-93 outbreak in the Delta
Amacuro in Venezuela. The disease would subside in Jamaica by 1852, but
close to 30,000 deaths were documented and in some reports it closer to 50,000.
Puerto Ricans were anxious during this time, and averted invasion through strict
quarantines of ships until 1855. A weary public resorted to church and faith for
support. According to Kipple, churches were overwhelmed and a “marathon” of
prayers were hoped would appease God’s wrath on the people (1985). Finally in
the fall of 1855, the first cases were reported in the eastern city of Naguabo,
apparently “sneaking in” from St. Thomas. Draconian measures of cordon
sanitaire were implemented including the disinfection of incoming mail with
vinegar. There were even measures to scatter the bad air by “firing guns on the
heavens”. In the end, almost 25,000 were recorded (Kipple, 1985).
Snow’s discovery in 1854 had not yet influenced authorities in the Caribbean to
act—in time— based on this new knowledge of water transmission. However, the
14
events did prompt them to take some preventive measures, mostly in the form of
sanitary improvements, for future epidemics (Kipple, 1985).
Accounts of outbreaks in Mexico’s coasts and higher plateaus were widely
documented. In some accounts cholera arrived in the spring of 1833 and others
believed it was in 1834 (cited in Politzer, 1959; Guzman et al., 1999).
According to Guzman, 14,000 lives were lost from August to November of that
year. Cholera would return in 1848, 1850 (via trade from Europe and New
orleans), and from 1853-1854 (as cited in Politzer, 1959; Guzman et al., 1999;
Barua, 1992).
In Central America, Nicaragua and Guatemala were struck in 1837. Reportedly
the former’s outbreak was more severe (Politzer, 1959: 24). Cholera would not
reach Panama until 1849 via a ship from New Orleans en route to the Chagres
River. Epidemics were also documented in various parts of the Central America
in 1856 (Barua, 1992).
Outbreaks in South America’s Colombia and Ecuador were reported in the early
1850s; however, these accounts have been debated like those earlier in Peru.
According to Politzer an outbreak took place on the northernmost coast of
Colombia. Guyana experienced an outbreak in its coast in 1837 and 1857
(Politzer, 1959). In Venezuela, outbreaks were found in 1853-1854 and again in
1857 (Politzer, 1959; Barua, 1992; Colmenares, 2002).
Cholera invaded Brazil in 1853 and remained until 1856. This account was well
documented in a study by Cooper (1986). In the 1855-56 epidemic, Belem was
the first city to encounter the disease. Located at the mouth of the Amazon River
in the North, it was an entry/exit point for trade. Apparently cholera came in the
infected bowels of sailors and passengers. It soon spread to 13 provinces and
afflicted the worst on the populations in Northeast Brazil. In the Bahia province,
almost 36,000 people had died. According to the British Consul in Belem, 4% of
the population in that town had perished; these were mostly Blacks and Indians.

15
Samuel Vines of the Consul reports: “the sick were abandoned, and the dead
went unburied…entire crews of canoes were carried off and small villages were
depopulated” (as cited in Cooper, 1986). Dr Santa Rosa of Belem diagnosed
the first cases of cholera. He documented the classic symptoms of sunken eyes,
severe diarrhea and vomiting. His recommendations for a strict quarantine were
ignored; and in fact he was told he was wrong in his analysis. Such measures
would have been detrimental to trade and Brazil’s economy. Furthermore, the
medical commission, mostly comprised of anti-contagionists, believed what was
occurring in Belem was a local phenomenon and could not have possibly been
transmitted from person-to-person. In Rio de Janeiro, the same thought persisted
and it was believed to have been a malady due to “overindulgence in food, drink,
or…sex”. However, the rapid spread to neighboring and far away towns could not
be explained considering that atmospheric conditions had not been any different
from those in the past. A Dr. Rego from the Central Board of Public Health notes
“it seems that reason is on the side of the advocates of importation” (as cited
and quoted in Cooper, 1986). By 1856, Cholera had taken almost 200,000
lives.
Third and Fourth Waves (1861 – 1895)
16
________________________________________________________________
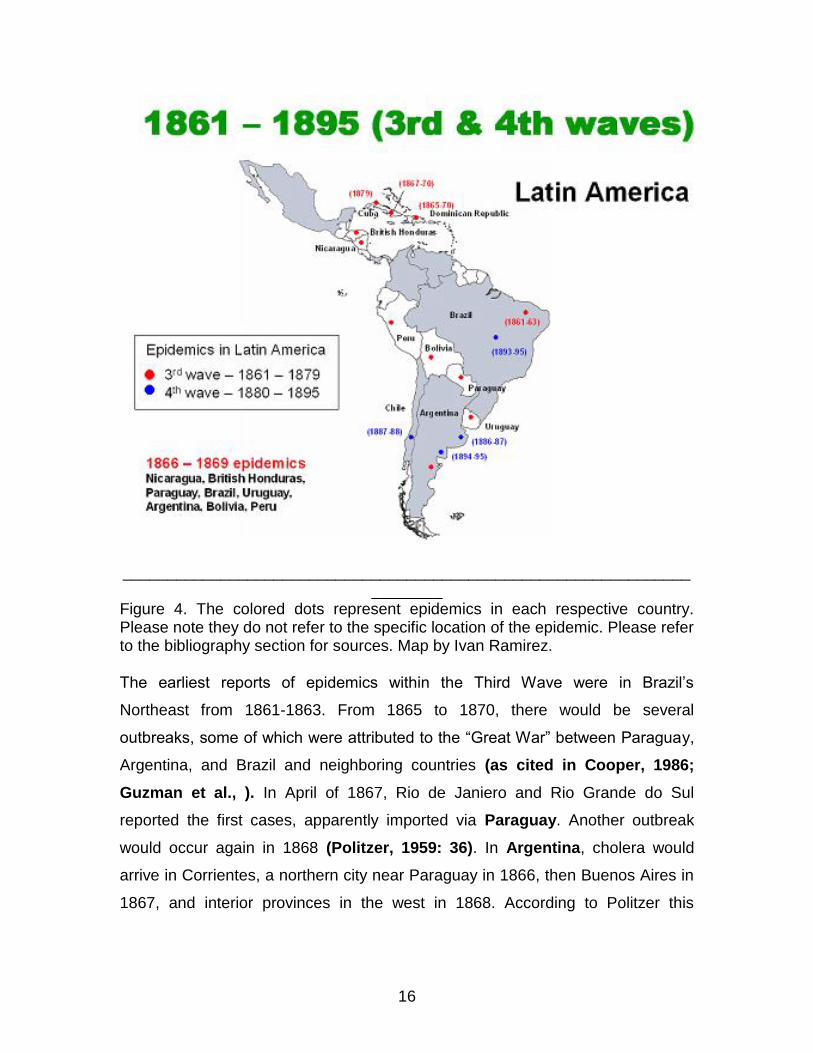
________ Figure 4. The colored dots represent epidemics in each respective country. Please note they do not refer to the specific location of the epidemic. Please refer to the bibliography section for sources. Map by Ivan Ramirez. The earliest reports of epidemics within the Third Wave were in Brazil’s
Northeast from 1861-1863. From 1865 to 1870, there would be several
outbreaks, some of which were attributed to the “Great War” between Paraguay,
Argentina, and Brazil and neighboring countries (as cited in Cooper, 1986;
Guzman et al., ). In April of 1867, Rio de Janiero and Rio Grande do Sul
reported the first cases, apparently imported via Paraguay. Another outbreak
would occur again in 1868 (Politzer, 1959: 36). In Argentina, cholera would
arrive in Corrientes, a northern city near Paraguay in 1866, then Buenos Aires in
1867, and interior provinces in the west in 1868. According to Politzer this
17
allowed entry to Peru and Bolivia. Outbreaks in Uruguay via the Parana River
were reported in 1868 (Politzer, 1959: 36).
Caribbean accounts were found in Cuba and now the Dominican Republic.
Cholera would return to Havana in October of 1867. Again Black slaves were
affected the most and it was believed that they were racially susceptible to the
disease. Although the amount of cases (~ 8,000) from 1867-68 was considerably
lower than past epidemics, the case fatality remained high at 85% in 1867 and
50% in 1868. Snow’s discovery as mentioned earlier, had prompted officials to
improve sanitation and this was believed to reduce the morbidity on the island
(Kipple, 1985). In the Dominican Republic, an outbreak took place in 1866
(Politzer, 1959: 32).
In Central America (1866-1868), there were reports of outbreaks in Nicaragua
and the British Honduras via ships from New Orleans (Politzer, 1959: 36).
The Fourth Wave (1880-1895) would strike South America in 1886 and makes its
last impression in that century in 1895. Argentina and Chile were invaded from
1886 to 1888. Uruguay in 1895 and Argentina its last cholera outbreak in 1894-
1895 (Politzer, 1959: 39). Brazil reported its final outbreaks in 1893-1895.
According to Stepan (1981), several outbreaks were reported at the Hotel of
Immigrants in the summer of 1893. It likely imported and thrived due to poor
water sanitation conditions. Dr. Alfredo Lutz investigated and confirmed the
diagnosis of cholera through bacteriological analysis in several instances at that
same location. However there was much resistance from the medical community
in Brazil, the same resistance that Dr. Rosa experienced in 1855. Many believed
the “cases were only diarrhea” and denied the existence of cholera in Brazil. Lutz
effectively proved his case by disproving an alleged cholera outbreak, where
2,000 people became sick; this time is was simply food poisoning. Although
Koch’s discovery of the cholera bacterium was now known, the Brazilian
authorities may have found the disease threatening to its.

18
Fifth Wave: Reemergence in Peru (1990 – Present) In October of 1990 on the northern coast of Peru, cholera would resurface for the
first time in the twentieth century in Latin America (PAHO, 2003). The Fifth Wave
had begun and cholera moved rapidly through its neighboring countries. (See
Figure 5 for the initial outbreak trail in South America). It affected most of
South America, Central America, and reached the U.S. The widely accepted date
of the outbreak is in late January of 1991 in the coastal city of Chimbote. Latin
America would now face the El Tor biotype and participate in the Seventh
Pandemic (as cited in Huq et al., 2001).
By March of 1991, cholera had reached Ecuador and Colombia. In April it was in
Brazil. By the summer, Mexico, Guatemala, Bolivia, Honduras, Panama, and
Nicaragua reported outbreaks (Guzman, ). At the end of 1991, 391,724 cases
across 14 countries were reported in Latin America (Geography Department,
University of Colorado at Boulder, 2001). Although the case fatality rate of 1%
was considerably low, the morbidity remained high.
Figure 5. Map of Initial outbreaks in Latin America
19
Many believe it was imported via the waste of infected passengers from an Asian
ship that docked along the coast of Peru. However multiple outbreaks were
reported in several places within Peru and outside of Peru where importation
could not be explained. A case of multiple pathways that consist of social and
environmental factors has gained much support. Specifically the climate
variability patter known as El Nino and global change were attributed to the
spread in the western hemisphere (Patz, 2002; Seas et al., 2000; Pacual et al.,
2000;2002).
Figure 6.
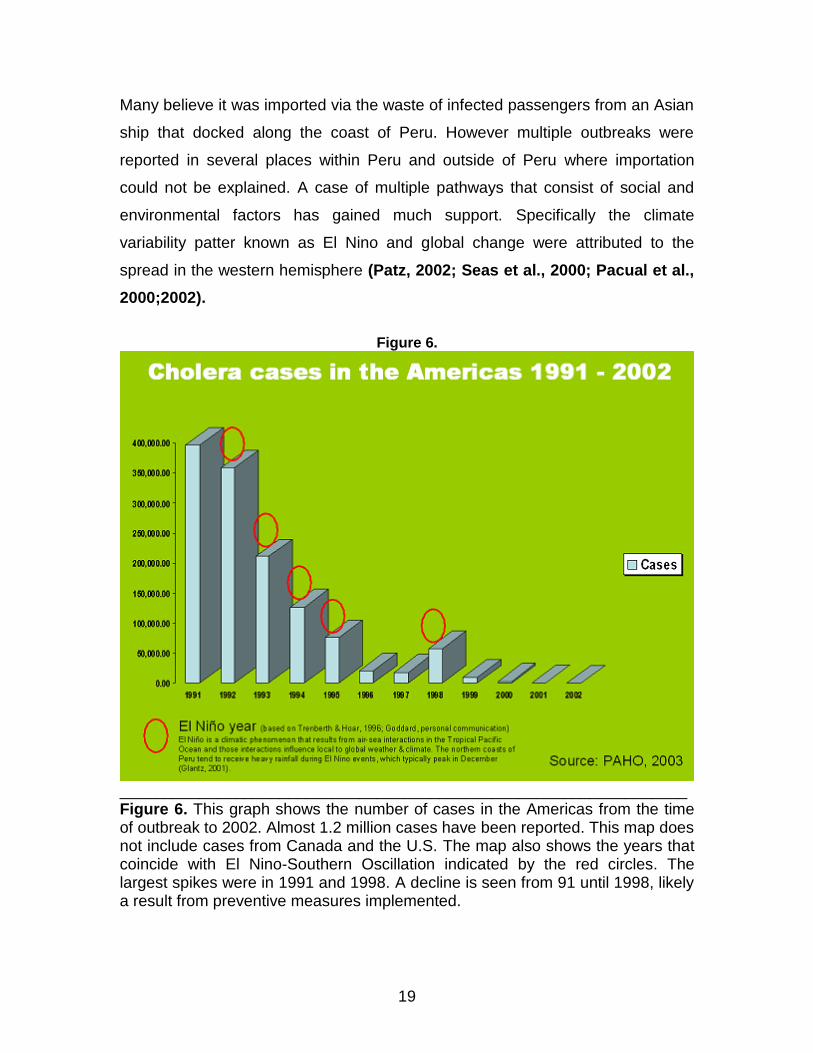
________________________________________________________________ Figure 6. This graph shows the number of cases in the Americas from the time of outbreak to 2002. Almost 1.2 million cases have been reported. This map does not include cases from Canada and the U.S. The map also shows the years that coincide with El Nino-Southern Oscillation indicated by the red circles. The largest spikes were in 1991 and 1998. A decline is seen from 91 until 1998, likely a result from preventive measures implemented.
20
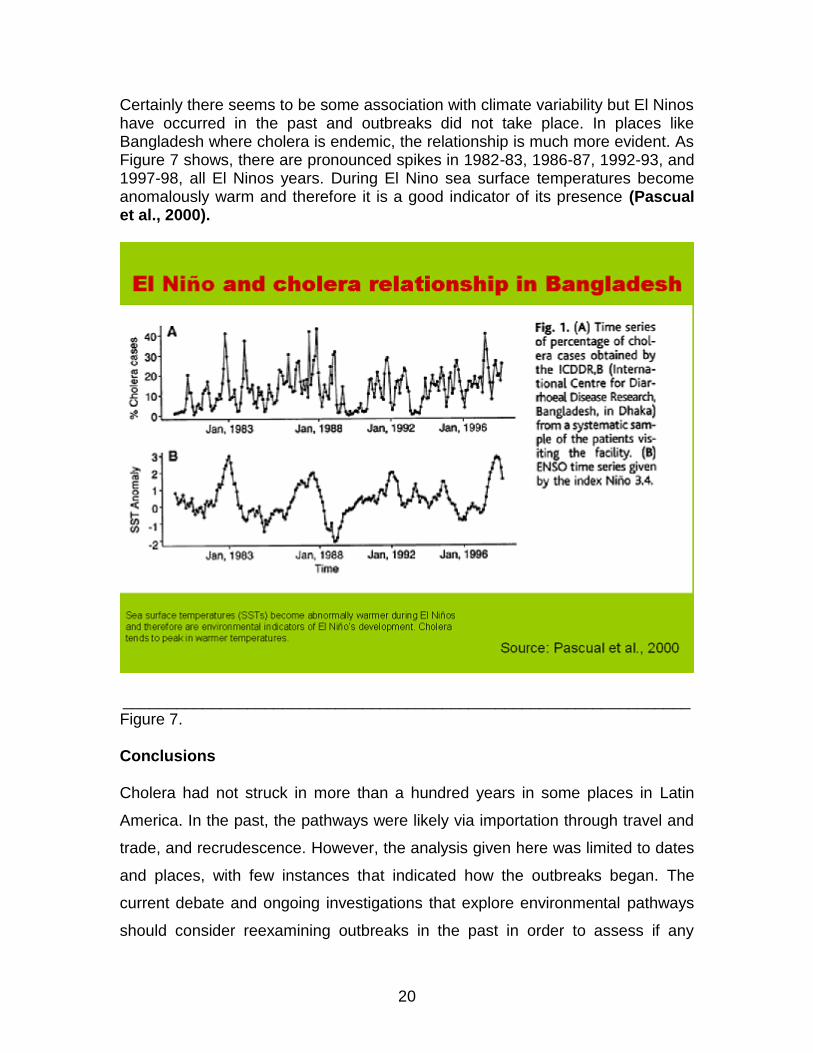
Certainly there seems to be some association with climate variability but El Ninos have occurred in the past and outbreaks did not take place. In places like Bangladesh where cholera is endemic, the relationship is much more evident. As Figure 7 shows, there are pronounced spikes in 1982-83, 1986-87, 1992-93, and 1997-98, all El Ninos years. During El Nino sea surface temperatures become anomalously warm and therefore it is a good indicator of its presence (Pascual et al., 2000).
________________________________________________________________ Figure 7. Conclusions Cholera had not struck in more than a hundred years in some places in Latin
America. In the past, the pathways were likely via importation through travel and
trade, and recrudescence. However, the analysis given here was limited to dates
and places, with few instances that indicated how the outbreaks began. The
current debate and ongoing investigations that explore environmental pathways
should consider reexamining outbreaks in the past in order to assess if any

21
unexplained outbreaks may have relationships with anomalous sea
temperatures. Of course, these are only correlations, but they may prove useful
in early warning systems for cholera. This may be of crucial importance as sea
surface temperatures continue to warm. How will that affect the current pandemic
and future pandemics if any? Lastly it should not be ignored that social factors
are instrumental in the sustainability of outbreaks and possibly their initial
outbreaks as may have been evident in Peru and Latin America.
References Ackerrknecht, E.H. (1965). History of geography of the most important diseases. New York: Hafner Publishing. Anderson, R.M. (1982). The population dynamics of infectious diseases: Theory and applications. New York: Chapman and Hall Huq, A., R.B. Sack, R.R. Colwell (2001). Cholera and global ecosystems. Eds. Aron, J.L., J.A. Patz. Ecosystem change and public health: a global perspective. Baltimore, London: Johns Hopkins University. Pp 325-347. Barua, D., Greenough III, W.B. (1992). Cholera. New York: Plenum Medical. Barua, D., M.H. Merson (1992). Prevention and control of cholera. Eds. Barua, D., Greenough III, W.B. Cholera. New York: Plenum Medical. Pp 329-347 Beard, J.H. The contribution of cholera to public health. Scientific Monthly. 515 – 520 Briggs, A. (1961). Cholera and society in the Nineteenth Century. Past and Present. 19: 76 – 96. Cholera Factsheet (2000). World Health Organization. Homepage. March 2000 http://www.who.int/mediacentre/factsheets/fs107/en/print.html (accessed 1 December 2006). Colmenares, G.Y. (2002). Modernizacion, medicina, enfermedades y salud publica en la ciudad de Caracas (1870-1877). Historia, Ciencias, Saude—Manguinhos. 9 (supplement): 89-109. http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-59702002000400005 (accessed 10 October 2006). Cooper, D.B. (1986). The new “Black Death”: Cholera in Brazil, 1855 – 1856. Social Science History. 10 (4): 467 – 488. De, S.N. (1961). Cholera: Its pathology and pathogenesis. Edinburgh, London: Oliver and Boyd.

22
Department of Geography at University of Colorado-Boulder. Medical Geography and cholera in Peru. 28 September 2001http://www.colorado.edu/geography/gcraft/warmup/cholera/cholera.html (accessed 10 October 2006) Dubos, R. (1976). Louis Pasteur: Free lance of science. New York: Charles Scribner’s Sons Epidemiological notes and reportscholera –New York, 1991 (1991). Morbidity and Mortaality Weely Report. Center for Disease Control and Prevention. 40 (30): 516-518. http://www.cdc.gov/mmwr/preview/mmwrhtml/00014926.htm 2 May 1998 (accessed 10 October 2006). Gangarosa, E.J., R.V. Tauxe (1992). Epilogue: the Latin American cholera epidemic. Eds. Barua, D., Greenough III, W.B. Cholera. New York: Plenum Medical. Pp 351-357. Glantz, Michael H. Currents of Change. Cambridge, UK: Cambridge University Press Glass, R.I., M. Claeson, P.A. Blake, R.J. Waldman, N.F. Pierce (1991). Cholera in Africa: lessons on transmission and control for Latin America. The Lancet. 338: 791-795. Glass, R.I., R.E. Black (1992). The epidemiology of cholera. Eds. Barua, D., Greenough III, W.B. Cholera. New York: Plenum Medical. Pp 129-150. Goddard, Lisa, et al. Current Approaches to Seasonal-To-Interannual Climate Predictions. International Journal of Climatology. 21 (2001): 1111-1152 Guzman, V.T. Montes, P.B. (1999). Historia del colera en el mundo y Mexico. Ciencia ergo sum. http://ergosum.uaemex.mx/julio00/colera.html (accessed 30 September 2006). Hays, J.N. (2005). Epidemics and pandemics: Their impacts on human history. Santa Barbara: ABC-CLIO. Kipple, K.F. (1985). Cholera and race in the Caribbean. Journal of Latin American Studies. 17 (1): 157-177. Lipp, E.K., Huq, A., Colwell, R.R. (2002). Effects of global climate on infectious disease: the cholera model. Clinical Microbiology Reviews. 15 (4): 757 – 770 Mahalanabis, A., A.M. Molla, D.A. Sack (1992). Clinical management of cholera. Eds. Barua, D., Greenough III, W.B. Cholera. New York: Plenum Medical. Pp 253-281. Mekalanos, J.J., Sadoff, J.C. (1994). Cholera vaccines: Fighting an ancient scourge. Science. 265: 1387 – 1389. Murdock, C.J. (1995). Physicians, the state and Public Health in Chile. Journal of Latin American Studies. 27 (3): 551-567.
23
Cholera (2003). Pan American Health Organization. Homepage. http://www.paho.org/english/ad/dpc/cd/cholera.htm (accessed 10 October 2006). Pascual, M., Bouma, M.J., Dobson, A.P. (2002). Cholera and climate: revisiting the quantitative evidence. Microbes and Infection. 4: 237 – 245 Pascual, M., Rodó, X., Ellner, S.P., Colwell, R.R., Bouma, M.J. (2000) . Cholera Dynamics and El Niño-Southern Oscillation. Science. 289: 1766 – 1769. http://www.sciencemag.org/cgi/content/abstract/289/5485/1766 (accessed 14 October 2006) Patz, J. (2002). A human disease indicator for the effects of recent global climate change. Proceedings of the National Academies of Science. 99 (20): 12506 – 12508). http://www.pnas.org/cgi/doi/10.1073/pnas.0601277103 (accessed 1 October 2006). Pollitzer, R. (1959). Cholera. Geneva: World Health Organization Rita Colwell’s powerpoint on cholera http://www.nsf.gov/news/speeches/colwell/rc01_anatlesson/sld016.htm Rodó, X., M. Pascual, G. Fuchs, and S. Faruque. 2002. ENSO and cholera: a nonstationary link related to climate change? Proceedings of the National Academy of Sciences 99(20): 12901-12906. (See commentary, J. Patz, PNAS 2002: 99: 12503-12505). Seas, C., Miranda, J., Gil, A.I., Leon-Barua, R., Patz, J., Huq, A., Colwell, R.R., Sack, R.B. (2000). New insights on the emergence of cholera in Latin America during 1991: the Peruvian experience. The American Journal of Tropical Medicine and Hygiene. 62 (4): 513 - 517 Snow, J. (1854). Mode of communication of cholera, 2nd edition. London: John Churchhill Stepan, N. (1982). Beginnings of Brazilian Science. New York: Science History Publications. Thagard, P. (1996). The concept of disease: structure and change. Communication and Cognition. 29: 445-478. Tickner, J., Gouveia-Vigeant, T. (2005). The 1991 cholera epidemic in Peru: Not a case of precaution gone awry. Risk Analysis. 25 (3): 495 – 501. Under the weather: Climate, ecosystems, and infectious disease (2001). National Research Council. Washington DC: National Academy Press Vinten-Johansen, Brody, Paneth, Rachmanm, Rip, M. (2003). Cholera, chloroform, and the science of medicine. New York: Oxford Press Witt, V.M., F.M. Reiff (1991). Environmental health conditions and cholera vulnerability in Latin America and the Caribbean. Journal of Public Health Policy. 12 (4) Winter: 450-463.

24
WHO, Cholera, and El Nino. World Health Organization. Homepage. http://www.who.int/csr/don/1998_03_31/en/index.html (accessed 10 October 2006)




















