Hinduja newsletter Golden hour1-Dt.07-09-06.pmd
20
Volume 21, No.1
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Hinduja newsletter Golden hour1-Dt.07-09-06.pmd

Volume 21, No.1

2
GUEST EDITORIAL
EDITORIAL TEAMEditorDr. V. R. Joshi
Guest EditorDr. Khusrav Bajan
Editorial BoardDr. Philip Abraham Dr. C.BalakrishnanDr. Tester F. Ashavaid Dr. Sudeep ShahDr. Reeta Dalal Dr. Gauri MankekarDr. Soonu UdaniPhotographyPramod Tandel
Cover Page SourceSynergy Creations
FROM THE EDITOR’S DESK
In today’s world, the chances of an emergencysituation striking an individual are on the rise.
Emergency Medicine as a specialty is arelatively recent phenomenon even in the USA.In 1960s, the public in USA started demandingimproved quality of care in hospitalemergency departments. As a result manyphysicians got involved in the practice ofEmergency Medicine. Over time it lead to theformation of the American College of Emergency Physicians andthe Society for Academic Emergency Medicine. In the late seventiesEmergency Medicine was recognized as a board certified specialty.
Emergency Medicine in India has been brought into awarenesssince the past two decades but has picked up momentum in privateand more so in public hospitals since last five years.
few Emergency Medicine and Trauma centres of repute in India sofar are Trauma centre at Sion Hospital Mumbai, St. Johns HospitalBangalore, CMC Vellore, Hinduja Hospital Emergency Unit, just toname a few.
The Hinduja Hospital Emergency department was formulated sincethe inception of the hospital in the year 1986, but has been upgradedto a Fully Equipped Emergency Unit since 2001. Since its inception,it has attended to approximately 50-100 patients per day. The mainfunction is to quickly assess the problem, its severity and stabilizethe patient before transfer to an ICU. As a rule the patients do notspend more than 24 hours in this section. At present the Emergencydepartment has 6 Acute beds and 5 Emergency Critical care beds.
An emergency department should have a support system readily
Dr. Khusrav Bajan
‘Golden Hour’ is a concept and not a fixedtime-frame. It defines the period, during which,if prompt and efficient action(s) is taken, manylives can be saved and serious complicationsavoided. Originally introduced to treat victimsof road accidents, the concept now embracesalmost all acute emergencies. A day to dayexample would be cardiopulmonaryresuscitation.In this issue our guest editor Dr. Khusrav Bajan has put togethermanagement of such emergencies.Obviously a small communication like the Newsletter cannot covereverything. The idea is to spread awareness. Surely, readers willfind the information useful.
Contd. on page 4
Dr. V. R. Joshi
• From the Editor’s Desk
Dr. V. R. Joshi
• Guest Editorial
Dr. Khusrav Bajan
• Anaphylactic and Anaphylactoid
Reactions: Initial Emergency
management
Dr. Farhad N. Kapadia
• Management of Poisoning
Dr. Ashit V. Hegde
• Role of a Poison Centre
Dr. T. F. Ashavaid, Dr. Alpa J. Dherai.
• Snake and Scorpion Bites
Dr. Neeraj Uttamani
• The Unconscious Patient
Dr. R. Gursahani
• Out-of-Hospital Cardiopulmonary
Resuscitation
Dr. Khusrav Bajan
• Newer 2005 Cardiopulmonary
Resuscitation Guidelines
• Approach to Fever
Dr. Rajeev Soman
• Acute Breathlessness
Dr. Simran Singh
• From the corridors of
Hinduja Hospital
C O N T E N T S

3
Introduction
Anaphylactic and anaphylactoid reactions (AR) areacute life-threatening reactions to a wide variety ofexternal stimuli. The external stimuli set off a cascadeof mediator release with subsequent adversephysiological sequel. The respiratory and circulatorysystems are most affected, resulting in tissuehypoperfusion and hypoxia. The commonestmanifestations of a severe AR are dyspnoea andhypotension. Prompt recognition and treatment is vitalas the AR may rapidly progress to death. Managementconsists of ensuring a secure airway, administeringoxygen (O2), replenishing the depleted circulation withfluids, stabilizing the circulation with adrenaline, andpreventing a late-phase reaction with corticosteroids.
Clinical manifestations
The hallmark of AR is the rapid onset of dyspnoea orhypotension following exposure to an allergen. Thereaction usually takes place in 20 minutes but maybe delayed up to 6 hours. A biphasic reaction mayoccur and the second reaction may be more severethan the first one. The severity of the reaction dependson several factors including the site of entry of theantigen, the rate of antigen absorption, the antigenload, the degree of sensit ization, the use ofmedication like beta-blocking drugs, and the presenceof any underlying cardiorespiratory disease. In itsmilder forms AR may present only with a fewsymptoms such as nasal congestion, hoarseness ofvoice, a scratchy sensation in the throat, a chokingsensation, rhinorrhoea, excess lacrimation, pruritus,and urticaria. Food allergens often present withnausea, vomiting, abdominal cramps, or diarrhoea.Wheezing, stridor, tachypnoea, tachycardia, anddyspnoea suggest significant pulmonary involvement.Periorbital oedema and swelling of the lips and tonguefrequently occur. Tachycardia, hypotension, cyanosis,respiratory fatigue, and unconsciousness are signsof a severe AR and an impending cardiorespiratoryarrest is the commonest circulatory manifestationof an AR.
Diagnosis
The diagnosis of anaphylaxis should be entertainedin any patient who develops dyspnoea, wheeze,stridor, or hypotension after exposure to a potentialallergen. Milder forms which present with orbital,lip, and tongue oedema are easily diagnosed.The absence of facial swelling may make thediagnosis less apparent. The presence of the abovementioned symptoms occurring rapidly (usually in afew minutes) after exposure to an allergen is the mostuseful clue to the diagnosis of an AR.
Management
The basics of management are given below and theguidelines are shown in the figure
The major points to note are:
• Early recognition is important as a reaction canrapidly become life-threatening
• Rest lessness, agi tat ion, tachycardia,tachypnoea, dyspnoea, and al tered l imbperfusion suggest a severe reaction and thepatient should be promptly transferred to ahospital
• Adrenaline is the mainstay of treatment. It shouldbe used intramuscularly in moderate reactionsand may be used intravenously in severereactions.
General measures (for all degrees of AR)
• Stop antigen exposure
• Supplemental oxygen
• Establish intravenous access
• Observe for progress of reaction
• Call for anaesthetist and ENT assistance
ANAPHYLACTIC ANDANAPHYLACTOID REACTIONS:
INITIAL EMERGENCY ANAGEMENT– Dr. Farhad N. Kapadia

4
Figure. Treatment of anaplylaxis
For all severe orrecurrent reactions and
patients with asthmagive hydrocortisone100-500 mg IM or
lowly IV
If clinical manifestations ofshock do not respond to drug
treatment, give 1-2 litres IVfluid. (Rapid infusion of 1 litre )
Repeat dose may benecessary
In addition
Antihistamine(chlorpheniramine)
10-20 mg IM / or slow IV
Repeat in 5 minutes if noclinical improvement
Adrenaline (Epinephrine)1:1000 solution 0.5 ml
(500 µg) IM
Oxygen treatmentwhen available
Stridor, wheeze,respiratory distress, orclinical signs of shock
Consider when compatible history of severe allergic typereaction with repiratory difficulty and/or hypotension,
especially if skin changes present
Figure. Resuscitation Council Guidelines, UK. EmergencyMedical Journal: 2001:18:393-395
• Arrange for transfer to ICU or nearest casualtydepartment (last two are optional in very mildreactions)
Mild reaction
• IV steroid and antihistamine agents
• Bronchodilators
Moderate reaction
• Adrenaline 0.5 mg or 0.5 ml of a 1:1000 solution(intra-muscular preferred to subcutaneous)
• Adrenaline (nebulized)
• Intravenous fluids
• Other supplemental therapy
Severe reaction
• Secure airway (endotracheal tube ortracheostomy)
• Adrenaline (intravenous)
• Intravenous fluids; rapid infusion
• Adrenaline or dopamine infusion
• Mechanical ventilation (rarely required)
• Other supplemental therapy
GUEST EDITORIAL (Contd.)
Dr. Khusrav Bajan
available such as blood Bank, Radiology, 24 hours OT facility, Super-specialty surgeons, ICU facilitieswith ventilators. All these facilities are available at Hinduja Hospital.
It is hoped that this very important facet of medical service attracts attention both of physicians and thepowers that be.
This bulletin is aimed at providing a step wise approach to the management of medical emergencies inthe pre-hospital phase by the general practitioner (GP), and also to provide guidelines to be followedwithin the Golden Hour, in the emergency room.

5
Poisoning-accidental, suicidal, or homicidal-iscommon. Most of the patients are young, otherwisehealthy and if treated properly can go back to a longand normal life. Most (though not all) who haveconsumed a poison with suicidal intent, do so on animpulse and are unlikely to repeat the attempt. Promptand efficient treatment of the poisoned patient cantherefore be a very rewarding experience.
Poisoning should be one of the differential diagnosesin a patient with any of the following :
• Unexplainable stupor, coma, or agitation(especially in the young)
• Unexplained cardiac arrhythmia, hyper-orhypotension
• Unexplained respiratory, liver, or renal failure
• A prior suicide attempt
• A history of psychiatric illness (especially withsuicidal ideation)
If poisoning is suspected and if the patient is unableor unwilling to give more details,the patient’s family,friends, and colleagues should be interviewed (Thisshould be done only after the patient has beenstabilized).
Initial supportive measures
Care of the ABC (airway, breathing, and circulation)take precedence over anything else. In a deeplyunconscious patient, endotracheal intubation may beneeded. If the patient is hypotensive an initial rapidbolus of fluids is indicated in most cases. Ionotropesmay have to be administered for refractoryhypotension.
Prevention of further absorption of toxin
Toxin can enter the body via skin, eyes, stomach,intestines (GI), lungs, or parenterally. The patient’sclothing may serve as a source of continuousabsorption of the poison and should be carefullyremoved. The skin should be cleaned thoroughly withsoap and water. The eyes, if affected, need to beirrigated with large volumes of saline.
The majority of toxins however are absorbed throughthe GI tract. Attempts to limit absorption through theGI tract (especially more than one hour after thepoisoning) probably do more harm than good.
Induced emesis
There is no evidence that induced emesis altersoutcome in patients who are stable and fully awakewhen they reach hospital, and induced emesis canbe dangerous in an unstable unconscious patient(high risk of aspiration). This form of therapy shouldprobably be done away with altogether.
It is virtually never indicated after hospital admission.(because of its questionable efficacy > I hr afteringestion). Contraindications to emesis includepoisoning with corrosives, petroleum products, andin situations where there is a high risk of seizuresand altered consciousness.
Gastric lavage
The efficacy of this procedure (especially if donethrough a narrow-lumen tube and if done more thanone hour after ingestion) is being questioned. The risksassociated with this procedure include aspiration,arrhythmias, and stomach perforation. Because ofthese risks and its doubtful efficacy, gastric lavageshould not be performed in patients who have ingesteda nontoxic substance, a nontoxic amount of a toxicsubstance, or when the toxin is no longer expectedto be present in the stomach. Gastric lavage shoulddefinitely be avoided in patients who have ingestedcaustic or volatile liquids.
There is also a concern that gastric lavage may propelmaterial into the duodenum, increasing the chancesof drug absorption.
Gastric lavage is therefore another popular butprobably useless and probably dangerous procedureand should be used only sparingly.
Activated charcoal
Activated charcoal is a powerful, inert, nontoxic, andnonspecific adsorbent that irreversibly binds drugsand interferes with their absorption. It is particularlyeffective in binding high-molecular-weightcompounds and is usually well tolerated. It is usuallyadministered along with a cathartic like mannitol orsorbitol.
In summary activated charcoal along with a catharticgiven as early as possible is more effective and saferthan the more popular methods of limiting absorptionof the poison.
MANAGEMENT OF POISONING - Dr Ashit V. Hegde

6
Enhancement of elimination
Enhanced elimination of toxins
Multiple doses of activated charcoal (MDAC) enhanceelimination of drug. This is recommended only forpoisoning with carbamazepine, dapsone,phenobarbital, quinine, and theophylline.
Forced diuresis by administration of large volumesof isotonic fluids and diuretics to increase renalexcretion of drug or metabolite is of limited clinicalvalue. It is not recommended because of potentialvolume overload and electrolyte abnormalities. Urinaryalkalinization to enhance excretion of weak acids isbeneficial only for salicylates, phenobarbital, andprimidone.
Invasive techniques such as haemodialysis andhaemoperfusion are reserved for elimination ofspecific life-threatening toxins. Haemodialysis can beconsidered for poisoning with methanol, ethyleneglycol, salicylates, and lithium. Haemoperfusioninvolves the passage of blood through an absorptive-
containing cartr idge (usually charcoal). Thistechnique removes substances that have a highdegree of plasma protein binding. Charcoalhaemoperfusion may be indicated for intoxication withcarbamazepine, phenobarbital, phenytoin, andtheophylline.
Administration of specific antidote
Very few poisons have a specific antidote e.g. atropineand PAM for organophosphorous poisoning, N-aetylcysteine for paracetamol poisoning, naloxone foropiate poisoning, etc. It is therefore very important tomake all efforts to identify the specific poison.Thiamine and glucose are also administeredempirically to all patients though the value of thispractice is dubious.
Most poisons however do not have any antidote andtreatment is supportive .
The one take-home message is : In our enthusiasmto treat the poisoned patient, it is quite likely that wemay do more harm than good – think twice.
To provide information on management of various poisonings and treatment protocols all over the country,a National Poisons Information Centre has been set up in the Department of Pharmacology at AIIMSwhich provides round-the-clock, 7 days-a-week, 365 days service on telephone
Tel. No.: (011) 26859391, (011) 26593677. Email: [email protected]
The mission of a poison centre is to preventpoisonings and to reduce or eliminate the associatedmorbidity and mortality. This implies that manyfunctions and roles must be played by the centre, e.g.poison prevention education, professional education,and specialized services to the business and industrysection and governmental agencies.
The traditional responsibilities of a poison centre are:
• Provide a 24-hour hotline service
• Provide poison information, telephoneconsultation
• Poison identification and diagnosis
• Provide education to lay public and medicalprofessionals
• Co-ordination of antidotes
• Develop a network of poison control centres
• Maintain toxicosurveillance
Fig. 1 : Types of agent involved in poisoning
House hold pdct
47%4% 5.3% 1.5% 3.20%
9%
8%
22%
DrugsIndustrialproduct
Agriculturalpesticides
Bites and stings Plants Miscelloneousproduct
Unknownproduct
ROLE OF A POISON CENTRE - Dr. T. F. Ashavaid, Dr. Alpa J. Dherai

7
In the US, there are around 61 poison centres whichparticipate in a “Poison Help” toll-free telephonenumber programme. The centres are organized intoan electronic telephone grid and calling the number(1-800-222-12222 in US) routes the call automaticallyto the nearest poison centre. In India there is no suchnational electronic system as very few poison centresexist namely, NPIC, AIIMS (New Delhi), NationalInstitute of Occupational Health (Ahemdabad), AIMS(Cochin). Toxicology and IMCU Unit, GovernmentGeneral Hospital (Chennai), and Industrial ToxicologyResearch Centre (Lucknow).
Acute poisoning is a common paediatric emergencymainly due to the innovative and exploratory natureand mouthing tendencies of the children. Theintroduction of a whole range of new and complexchemicals in the form of pesticides, householdcleaners, medicines, etc. has widened the spectrumof toxic products to which children may get exposed.The elderly are also not immune to poisoning, drugsbeing the most common agents. The exposure iseither intentional or accidental (overdose due toforgetfulness, mistaken identity, incorrect route ofadministration, and improper storage). Occupationalaccidents are an important cause of poisoning in theyoung.
A retrospective analysis of three-year data at AIIMS,New Delhi, suggests that the most vulnerable agegroup included children between 0 and 6 years andhad a highest exposure to household productsfollowed by drugs and others (fig 1).
The poison information centre plays a vital role in themanagement of poisoning. The specially trainednurses, pharmacists, and physicians who staff these24-hour emergency telephone services assess the
severity of the pesticide exposure, make treatmentrecommendations, and often provide valuableinformation for spill containment and cleanup. Whenhospitalization is required, the poison centre contactsthe receiving hospital and provides the emergencydepartment with the most current treatmentinformation available. During large-scale pesticideaccidents (hazardous material incidents), manypoison centres assist first responders with selectionof proper protective gear, determination of properdecontamination techniques, and development oftriage guidelines for victims.
The poison centres have an aggressive poisoneducation programme that focuses on education ofthe public and health-care professionals. Publicpoison prevention initiatives include the developmentof brochures that address specific problem areassuch as paediatric poisonings, senior cit izenpoisonings, adverse drug reactions, terrorism, plants,carbon monoxide, inhalant abuse, food poisoning,activity books for children, etc. Magnets, pencils,posters, and stickers are used extensively to promotepoison centre awareness.
There is no charge for using a poison centre. Usuallythe state, country, or city supports this service. Insome places private hospitals or industries sponsorthe programme.
In summary, the functions of a poison centre are
• Free service to inquiries about poisoningemergencies
• Prevent poisonings through education
• Conduct research, participate actively withgovernment to insure the safety of the residentsof the region.
Less than 1/10th of the known species of snake arevenomous. Commonly found in India are king cobra,krait, and pit viper.
The venom of snakes is a mixture of toxic proteinsand enzymes like cobra neurotoxin, haemolysin,cardiotoxin, cholinesterases, and also inhibitors ofcytochrome oxidase.
Death in most of the snake-bite cases is preceded
by circulatory collapse associated with marked fall incirculatory blood volume, haemolysis, abnormalitiesof coagulation, and respiratory paralysis.
Factors affecting severity
• Age, size, and health of patient
• Size of snake, condition of fangs, condition ofvenom glands
SNAKE AND SCORPION BITES - Dr. Neeraj Uttamani

8
• Location of bite : bites on extremities and adiposetissues are less dangerous than those on thetrunk, face, or directly into a blood vessel. Even athin layer of clothing may afford great protection
• Presence of bacteria especially clostridia andother anaerobic bacteria in mouth of snake.
• Exercise or exertion immediately after bite speedssystemic absorption
Clinical features
Local : Severe burning pain, swelling spreading inall directions, serosanguinous fluid discharge fromthe puncture wound. Later gangrene of skin andsubcutaneous tissue may develop.
Cobra bites do not have local oedema but cause localnecrosis and sloughing.
Latent period is 15 minutes to 8 hours
Generalised : Nausea, vomiting, circulatory collapse,bleeding into the skin and all body orifices, musclecramping, delirium, and convulsions.
Complications include acute renal failure (ARF), ARFsecondary to DIC or tubular necrosis, circulatorycollapse, and death.
Venom is neurotoxic and myotoxic especially toskeletal muscles.
Late complications : Leucocytosis, progressiveanaemia, disordered coagulation profi le,hypoproteinaemia, and azotaemia.
Treatment
Reassure the patient that most of the bites are non-poisonous.
Absence of distinct fang puncture and failure of localpain and oedema, numbness and weakness to appearwithin 20 min strongly sugggest bite of nonpoisonoussnake.
Removal of the poison from the tissues
Patient is placed at rest and the bitten extremityimmobil ised. If anatomically feasible a wideconstriction band should be placed to impede lymphflow. If patient is seen within 5 min and he or she ismore than 30 min from the hospital, 1.0 cm linear
incision (about 0.3 cm deep) should be made througheach fang mark and suction done by rubber bulb orbreast pump. Mouth suction should be done only ifno oral ulcers are present. Suction for up to 1 hourmay remove 50% of subcutaneously injected venom.During transportation the bitten part is immobilisedby splinting.
Hospital care includes treatment of shock andrespiratory failure, antivenom, antibiotics, and generalsupportive care. Polyvalent antivenin is a lyophilisedpowder of refined horse serum reconstituted bydiluting with water to 10 ml. Prior hypersensitivitytesting needs to be carried out. Local infiltration ofantivenom does not help much. For moderateenvenomation 5-10 vials are required, or more in caseof severe envenomation.
Tetanus toxoid or tetanus immune globulin antibiotics(covering gram–ve organisms), fasciotomy, surgicaldebridement, management of shock, respiratoryfailure are part of the management.
SCORPION STING
Scorpions often get into shoes and clothing and eveninto bedding. Scorpion bite is rarely fatal exceptsometimes in children or the elderly.
Clinical features
Local oedema and ecchymosis with burning pain,paraesthesia, hyperaesthesia, numbness, neurologichyperexcitability, lacrimation, rhinorhoea, salivation,nausea, vomiting may develop.
The poison is CNS stimulant and can cause anautonomic storm manitested with techycordia,hypertension etc, and secondary cardiotoxicity dueto both and to receiptor stimulation. This leads topulmonary oedema and death.
Treatment is with cold compresses and mildanalgesics. Specific antivenom from goat serumshould be considered if victim develops signs of CNSor cardiac involvement.
Cardiotoxiaty is treated prozocin + dobutomine.This theropy has led to a significant reduction inmortality.
Supportive care includes shock management.Diazepam is useful in reducing restlessness.

9
‘Found unconscious’ is an uncommon but not a rareopening line in emergency ward case histories. TheHinduja Hospital Intensive Care Units have, at anygiven point in time, approximately 20%-30% patientsin altered states of sensorium, which can range fromdelirium, obtundation, stupor’ to coma.
This article is limited to that subset of patients whoare first seen in a comatose state where the diagnosisand immediate responses are based on circumstantialevidence.
Immediate management
• ABC assessment to diagnose or exclude cardiacevent
• Administration of glucose especially in knowndiabetics and alcoholics without waiting for bloodsugar report. If possible a blood sample toestimate blood sugar should be collected beforeadministering glucose
• For seizure persisting beyond 10 minutesdiazepam 10 mg IV (adult dose) or lorazepam 4mg IV (SC or IM) should be administered
• If above are not applicable or helpful, the patientshould be shifted to a hospital
Clinical examination
The clinical examination of an unconscious patientcan be completed fairly quickly. As in other neurologicsituations, localization is the key to diagnosis. Fiveitems need assessment:
i) Level of sensorium: This needs to be assessedand recorded formally because of its obviousimplications for the required speed of interventionand prognosis. Obtunded and delirious patientscan be roused verbally. Stuporous patientsrespond to deep pain only, while coma is definedby the absence of any response.
ii) Pattern of respiration: Breathing is a fairly complexfunction with representation at multiple levels. Atthe lowest (medullary) level a slow gaspingbreathing is often pre-terminal but some patientsmay have ataxic breathing wheredeep and shallow breaths occur in an irregularpattern with irregular pauses. Cheyne-Stokes’respiration is a poorly localized version in which
phasic hyperpnoea and apnoea alternate with asmooth crescendo and decrescendo. Centralneurogenic hyperventilation is a marker ofhypothalamic-midbrain impairment and occursearly in brain herniation.
iii) Pupil size and reactions: The pupils are controlledby the autonomic nervous system and theconcerned pathways in the brainstem are in closeproximity to the structures concerned withconsciousness. Mid-brain lesions produce mid-position fixed pupils while pontine lesions producebilaterally small pupils by damaging descendingsympathetic fibres. Asymmetrical pupil dilatationmay signify impending herniation. Severehypoxaemia (after cardiac arrest for instance) canproduce bilaterally fixed and dilated pupils. Thepupillary pathways are relatively resistant tometabolic encephalopathies and hencepreservation of this reflex is an important sign inan unconscious patient.
iv) Ocular movements: The pathways for theoculomotor reflexes too pass in proximity to thereticular activating system. Here too, preservationof these reflexes in an unconscious patient impliesmetabolic dysfunction. Conversely, loss,especially if asymmetric, signifies structuraldamage. At the bedside the easiest test is thedolls’ eye head manoeuvre in which the examinerholds the eyelids open and briskly rotates the headfrom side to side and then completes the test withflexion-extension. A positive response, that is,conjugate eye deviation to the opposite side ofhead movement means that the brainstempathways are intact.
v) Motor response: The most appropriate method ispressure with a pen across a finger nail bed.A normal response consists of a brisk withdrawaland may include pushing the stimulus away ormoving the body away. Abnormal responses tendto be stereotyped and consist of abnormal flexionand extension. The ‘decorticate rigidity’ responseconsists of slow flexion and adduction of the upperlimbs with extension and internal rotation of thelower limbs. In the ‘decerebrate rigidity’ the upperlimbs are also extended and adducted. Theseresponses can be asymmetrical and should beassessed independently on both sides. Both imply
THE UNCONSCIOUS PATIENT - Dr. R. Gursahani

10
History
Peter Safar is known as the ‘father of moderncardiopulmonary resuscitation (CPR)’. In 1958adequate rescue ventilation became possible with thedevelopment of mouth-to-mouth techniques by Safaret-al and by Elam et-al. In the 1960s. Kowenhoven etal described closed chest compressions, thusintroducing the modern era of CPR. Between 1950and 1960, Zoll et-al described the technique ofdefibrillation. The technique of sternal compressionwith mouth-to-mouth ventilation was developed asbasic CPR.
Cardiac arrest
Cardiac arrest is a terminal event or a natural end formany people suffering from prolonged ailments. Butit can strike a substantial number of humans early inlife, thus leading to a loss of productive life, a hugeloss to the family, and to the society.
Cardiac arrest is defined as complete cessation ofcardiac mechanical activity manifested byunresponsiveness, apnoea or absent breathing, andundetectable or absent pulse. The attempt andmeasures adopted to maintain an airway and support
upper brainstem impairment but are less severeand more likely to be reversible in case of theformer. No response or flaccidity signifies deepcoma and in structural disease usually meansinvolvement up to the mid-pons.
Investigations
Two parallel sets of investigations must be organizedsimultaneously: clinical laboratory investigations andneuroimaging.
In an unconscious patient the following blood testsare sent off immediately: CBC, ESR, blood sugar,BUN/creatinine, liver function tests, and serumelectrolytes. Optional tests include ammonia, calcium,CPK, blood gases, and a toxic screen for drugoverdose.
If the diagnosis is clearly suggested by the historyand circumstances, neuroimaging may be deferred.In all other situations a plain CT scan of the headshould be performed immediately or as soon as thepatient is stable enough to be moved to radiology. MRIis an inappropriate investigation for an unconsciouspatient because it takes longer and the patient cannoteasily be monitored during the study. Also most ofthe information required in an unconscious patient,except in unusual situations such as brainsteminfarction, is available on the CT.
Diagnosis, prognosis, and triaging
With the information available from clinicalexamination and the investigations as detailed above,
further management can be decided.
Three groups of problems can be identified:
1. Supratentorial mass lesions: this includesmassive infarction, haemorrhage, abscess, andtumours in the cerebral hemispheres. The initialpresentation is dominated by asymmetric motorimpairment and hemiplegia. Since these lesionsevolve less rapidly, surgical or medical interventionmay be possible.
2. Infratentorial lesions: Destructive lesions of thebrainstem such as infarction may be difficult toreverse although thrombolysis offers an option inpatients who come in time to medical attention.Cerebellar mass lesions, whether infarct, bleed,or infective, can often be tackled surgically withvery good results.
3. Metabolic encephalopathies and other diffusedisorders: In most metabolic encephalopathiesprognosis and treatment depend on the underlyingcause. Patients with meningitis and sub-arachnoidhaemorrhage can also present with abrupt or rapidloss of consciousness without focal signs andneed emergent assessment and management.
At the end of this assessment the clinician shouldalso be able to judge the likely prognosis of theindividual patient. End-of-life issues need to behandled sensitively so that the level of care andintervention is appropriate and commensurate withthe patient’s and family’s wishes.
OUT-OF-HOSPITALCARDIOPULMONARY RESUSCITATION
- Dr. Khusrav Bajan
11
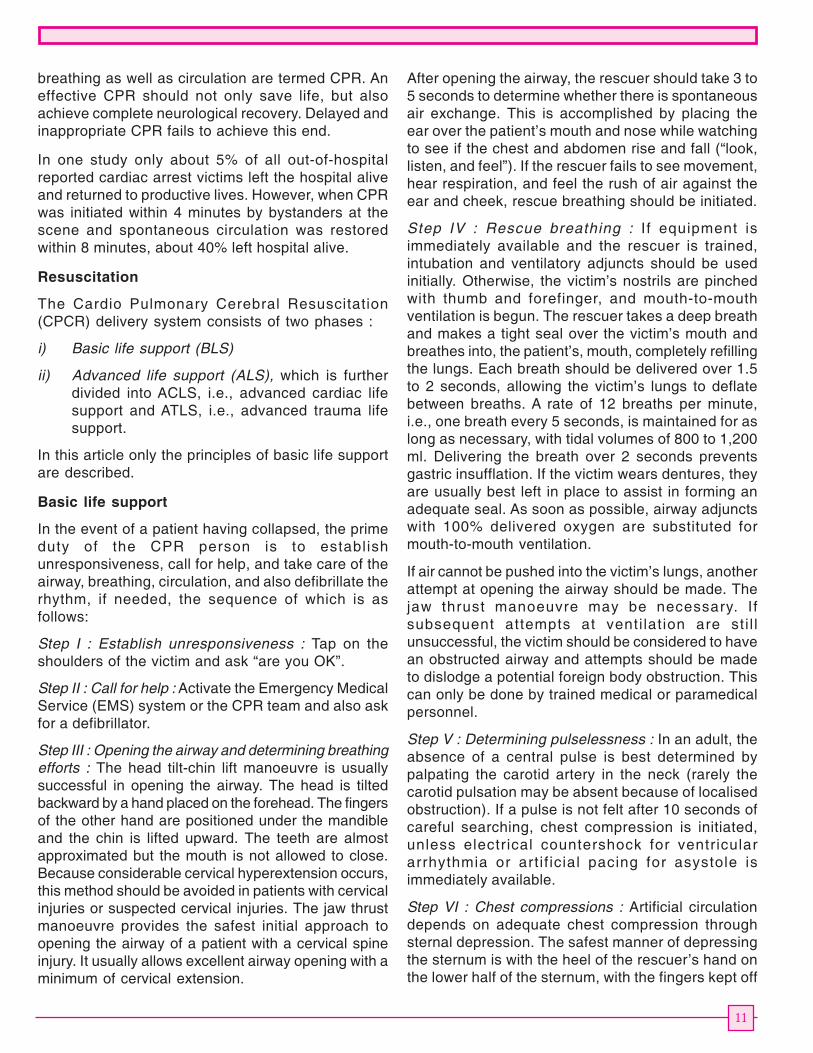
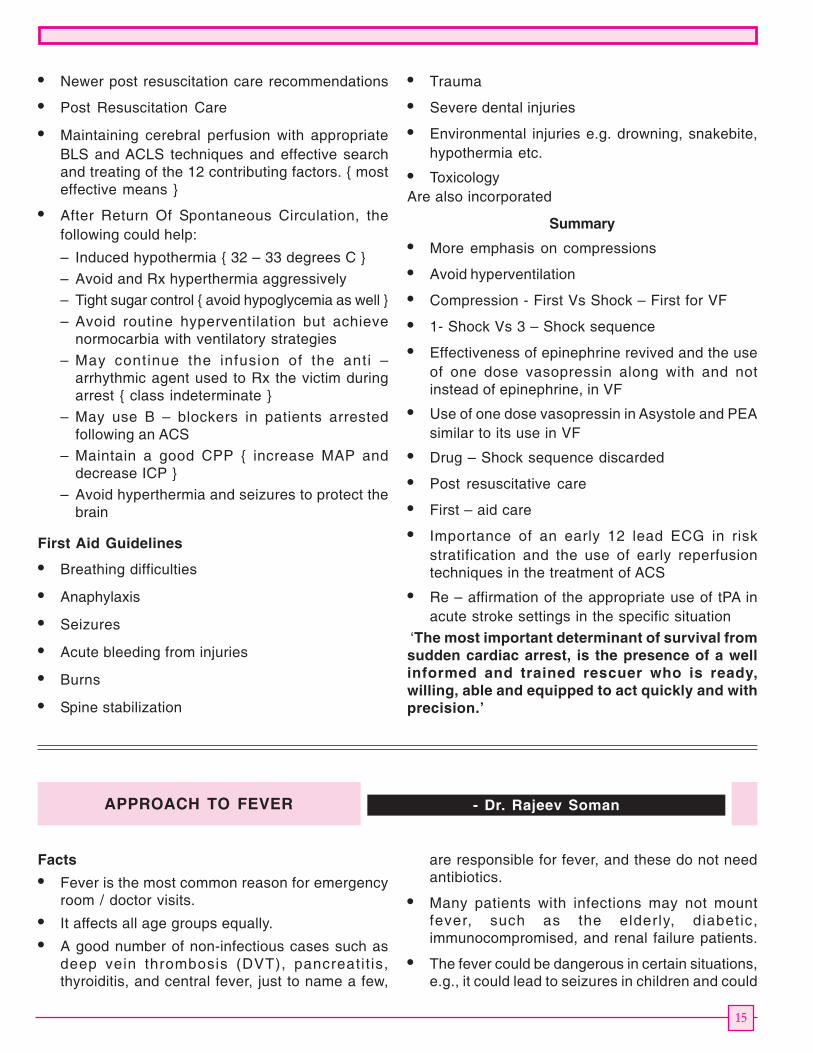
breathing as well as circulation are termed CPR. Aneffective CPR should not only save life, but alsoachieve complete neurological recovery. Delayed andinappropriate CPR fails to achieve this end.
In one study only about 5% of all out-of-hospitalreported cardiac arrest victims left the hospital aliveand returned to productive lives. However, when CPRwas initiated within 4 minutes by bystanders at thescene and spontaneous circulation was restoredwithin 8 minutes, about 40% left hospital alive.
Resuscitation
The Cardio Pulmonary Cerebral Resuscitation(CPCR) delivery system consists of two phases :
i) Basic life support (BLS)
ii) Advanced life support (ALS), which is furtherdivided into ACLS, i.e., advanced cardiac lifesupport and ATLS, i.e., advanced trauma lifesupport.
In this article only the principles of basic life supportare described.
Basic life support
In the event of a patient having collapsed, the primeduty of the CPR person is to establishunresponsiveness, call for help, and take care of theairway, breathing, circulation, and also defibrillate therhythm, if needed, the sequence of which is asfollows:
Step I : Establish unresponsiveness : Tap on theshoulders of the victim and ask “are you OK”.
Step II : Call for help : Activate the Emergency MedicalService (EMS) system or the CPR team and also askfor a defibrillator.
Step III : Opening the airway and determining breathingefforts : The head tilt-chin lift manoeuvre is usuallysuccessful in opening the airway. The head is tiltedbackward by a hand placed on the forehead. The fingersof the other hand are positioned under the mandibleand the chin is lifted upward. The teeth are almostapproximated but the mouth is not allowed to close.Because considerable cervical hyperextension occurs,this method should be avoided in patients with cervicalinjuries or suspected cervical injuries. The jaw thrustmanoeuvre provides the safest initial approach toopening the airway of a patient with a cervical spineinjury. It usually allows excellent airway opening with aminimum of cervical extension.
After opening the airway, the rescuer should take 3 to5 seconds to determine whether there is spontaneousair exchange. This is accomplished by placing theear over the patient’s mouth and nose while watchingto see if the chest and abdomen rise and fall (“look,listen, and feel”). If the rescuer fails to see movement,hear respiration, and feel the rush of air against theear and cheek, rescue breathing should be initiated.
Step IV : Rescue breathing : If equipment isimmediately available and the rescuer is trained,intubation and ventilatory adjuncts should be usedinitially. Otherwise, the victim’s nostrils are pinchedwith thumb and forefinger, and mouth-to-mouthventilation is begun. The rescuer takes a deep breathand makes a tight seal over the victim’s mouth andbreathes into, the patient’s, mouth, completely refillingthe lungs. Each breath should be delivered over 1.5to 2 seconds, allowing the victim’s lungs to deflatebetween breaths. A rate of 12 breaths per minute,i.e., one breath every 5 seconds, is maintained for aslong as necessary, with tidal volumes of 800 to 1,200ml. Delivering the breath over 2 seconds preventsgastric insufflation. If the victim wears dentures, theyare usually best left in place to assist in forming anadequate seal. As soon as possible, airway adjunctswith 100% delivered oxygen are substituted formouth-to-mouth ventilation.
If air cannot be pushed into the victim’s lungs, anotherattempt at opening the airway should be made. Thejaw thrust manoeuvre may be necessary. Ifsubsequent attempts at venti lat ion are sti l lunsuccessful, the victim should be considered to havean obstructed airway and attempts should be madeto dislodge a potential foreign body obstruction. Thiscan only be done by trained medical or paramedicalpersonnel.
Step V : Determining pulselessness : In an adult, theabsence of a central pulse is best determined bypalpating the carotid artery in the neck (rarely thecarotid pulsation may be absent because of localisedobstruction). If a pulse is not felt after 10 seconds ofcareful searching, chest compression is initiated,unless electrical countershock for ventriculararrhythmia or art i f icial pacing for asystole isimmediately available.
Step VI : Chest compressions : Artificial circulationdepends on adequate chest compression throughsternal depression. The safest manner of depressingthe sternum is with the heel of the rescuer’s hand onthe lower half of the sternum, with the fingers kept off

12
the rib cage. It is usually most effective to cover theheel of one hand with the heel of the other, the heelbeing parallel to the long axis of the sternum. Theexact location of the hand placement is determinedby keeping two fingers above the xiphisternum andthen placing the heel of the palm on the centre of thesternum. If the rescuer’s hands are placed either toohigh or too low on the sternum, or if the fingers areallowed to lie flat against the rib cage, broken ribsand organ laceration can result.
The rescuer’s elbows should be kept locked and thearms straight, with the shoulders directly over thepatient’s sternum. This position allows the rescuer’supper body to provide a perpendicularly directed forcefor sternal depression. The sternum is depressed1.5 to 2 inches (3.75 – 5.0 cm) at a rate of more than100 per minute. At the end of each compression,pressure is released and the sternum is allowed toreturn to its normal position, without removing thehand from the sternum. Equal time should be allottedto compression and relaxation, with smoothmovements, avoiding jerking or bouncing thesternum. Manual and automatic chest compressorsfor fatigue-free sternal compression are used by someemergency medical services crews and emergencyroom and ICU personnel. An experimental deviceusing a suction plunger-like device may improveflows by facilitating sternal rebound and thoracicvascular filling. This has been referred to as activecompression-decompression CPR.
Ventilation and sternal compression should not beinterrupted for longer than 7 seconds to check on thereturn of a pulse, except under special circumstances.Warranted interruptions include execution of ACLSprocedures such as endotracheal intubation. Even inthese limited circumstances, CPR should not beinterrupted longer than 30 seconds.
The recommendation for CPR sequence is 15:2 forchest compression to ventilation in case of anunsecured airway victim, irrespective of the numberof CPR rescuers. Once the airway is secured, thereis no need to synchronize the compressions withventilations and one can adopt the simultaneousventilation compression (SVC) technique, at acompression rate of more than 100 / min. and aventilation rate of 12 / min.
Step VII : Defibrillation : 95% of out-of-hospital cardiacarrests are due to ventricular fibrillation. Defibrillationis not discussed as it needs specific equipment andtrained personnel.
In conclusion, when a cardiac arrest is encounteredin out-of-hospital setting, the rescuer should first sendout message for proper help and then carry out theBLS until the CPR team arrives on the scene. Thisneeds proper training. It is essential that all laypersons get trained in BLS. Such trainingprogrammes are regularly held at Hinduja Hospital.
NEWER 2005 CARDIOPULMONARYRESUSCITATION GUIDELINES
Why Newer guidelines by the AHA in the year 2005These Guidelines have been updated as per changingevidence.
They are easy to remember and streamlinedguidelines, across all age groups.
They limited to the most important and specific skillsthat the rescuer needs to perform
The guidelines have to keep changing with time,experience and evidence to make it lucrative andtempting for rescuers like us all over the world toaccept, practice and disseminate these guidelines
Aim of the Newer Guidelines in Basic LifeSupport are to
• Simplify CPR instructions
• Increase the number of chest compressionsdelivered per min
• Reduce the interruptions in chest compressions
Newer Guidelines in Basic Life Support
• The lay rescuer should not assess signs ofcirculation, but start chest compressionsimmediately after delivering 2 rescue breaths to anon-breathing unresponsive victim
• For HCP, the child group is now extended from1yr to adolescent age rather than 8 yrs as stillmaintained for lay rescuers
• B : All breaths with or without O2 or with anyinterface, should be given over 1 second withsufficient volume to achieve visible chest rise
• B : ~ 10 – 12 breaths / m for adults and ~ 12 – 20breaths for infant and child. Once Intubated : then~ 8 – 10 breaths / m across all age groups andgive uninterrupted chest compressions
• C : Pulse check : carotid for adult and child andfemoral / brachial for infants

13
• C : Compression Landmarks : Lower half ofsternum between nipples for adult and child andjust below nipples for infant
• C : Compression Technique : two hands for adult.One or two hands for child. 2- 3 fingers for layrescuers and 2 encircling thumbs for HCP forinfants.
• C : A universal single rescuer compression – to –ventilation
– A ratio of 30 : 2 across all age groups acceptin newborn infants
– A ratio of 15 : 2 is still recommended for 2 ormore rescuers { HCP }, in 2 age groups i.e.infant and child
• C : Each rescuer should complete five 30 : 2cycles within 2 min before asking for a switch.Check pulse every 2 mins.
BLS – Newer Guidelines
• Chest Compressions
– Push hard, push fast
– Rate ~ 100/m across all age groups
– Allow complete chest recoil
– Minimize interruptions in chest compressions
• D : Automated External Defibrillator (AED)
– Adult : only adult pads
– Child :
• Lay rescuers or Emergency Medical Team (EMT)for un-witnessed arrest more than 5 min, give 5cycles of CPR before use of AED
• HCP for witnessed out – of hospital arrests andfor all in – hospital arrests, use AED / defibrillatorAs Soon As Possible
What happened to thePrimary and Secondary Surveys ??
• It revolves around three steps
– Assessment of the problem
– Management of the problem
– Evaluate the Response to therapy
• It is divided into the 5 “QUADRADS” or “PHASES”
Quadrad 1 { Primary Survey : A –D }
• A : Open airway , if trauma suspected – immobilizecervical spine
• B : If not breathing — give 2 breaths over 1 sec each
• C : If Pulse absent – Chest compressions{as specified}
• D : Defibrillation – attach AED and check rhythm.
– If VF : deliver shock fol lowed by chestcompressions
– If PEA / Asystole : check pulse and resumeCPR
Quadrad 2 { Secondary survey : A – H }
• A : Airway
– relieve obstruction, suction
– Insert oral or nasal airway
– Advanced airway if needed
• B : Breathing
– Intubate, confirm,secure
– Oxygenate
– Now perform CC at ~100/m and deliver breathsone every 6 – 8 seconds, unsynchronized.
• C : Circulation
– Establish IV / (Intra osseous) IO access,
– Rhythm specific drugs
– Check BP and use vasopressors if needed
– Send blood for group and type
– Pregnant lady should be kept 15 – 30 degress(L) lateral
• D :
– Differential Diagnosis { 6 H’s and 6 T’s }
– Disability
• Mental status
• Rule out stroke
• E : Expose extremities and examine skin
– Identify and stabilize injuries
– Compress bleeding sites
• F : Fingers . Foleys . Flip
– PR / PV
– Catheterise
– Flip to examine back
• G : Gastric aspiration
– Rx toxins / bleeding if any
• H : History
– Documentation

14
Quadrads 3, 4, 5
• Quadrad 3 : O2 – IV – Monitor
• Quadrad 4 : Temp – HR – BP – Resp
• Quadrad 5 : Tank (volume) – Tank (SVR) – Pump–Resp
– Fluids / Vasopressors / Inotropes / Ventilation
Advanced Cardiac Life Support (ACLS) – Newerguidelines
• Do not check pulse / rhythm immediately after ashock is delivered, but instead resume five cyclesof CPR for 2 min and then check rhythm / pulse.
• Insert an advanced airway, administermedications and reassess patient ASAP but in amanner where interruptions in chestcompressions are minimized.
Pulseless Arrest{ Pulseless Electrical Activity and Aystole }
Search & Rx possible factors { 6 H’s and 6 T’s }
• Hypovolemia
• Hypoxia
• H+ ion acidosis
• Hypo / Hperkalemia
• Hypoglycemia
• Hypothermia
• Toxins
• Tamponade – cardiac
• Tension Pneumothorax
• Thrombosis – coronary
• Thrombosis – pulmonary
• Trauma
(VF) Ventricular Fibrillation / Pulseless VT :SHOCK
• Deliver only one shock instead of the initial 3stacked shocks
• Always follow a shock with a 2 min five cycle ofCPR before checking the rhythm or pulse
• ONE SHOCK
• Manual Biphasic { device specific or 200Joules if unknown device }
• Manual Monophasic { 360 J }
• AED : { device specific }
• ONE SHOCK : Why ?
– High first shock success rate with newerbiphasic defibrillators
– More aggressive and less interrupted chestcompressions improve O2 and substratedelivery to the myocardium, making it moreprone to respond to the next single shock
ACLS Drugs
• VF / PEA / Asystole
– Epinephrine 1 mg , repeat every 3 min
OR
– May give one 40 U vasopressin dose insteadof the 1st or 2nd dose of epinephrine.
– In VF : deliver vasopressors IV / IO after2nd shock { do not time it with the shock}
• VF
– Consider anti – arrhythmics after the 3rd shock
• Amiodarone 300 mg and later 150mg or
• Lignocaine 1st dose 1.5 mg/kg , second and thirddose 0.5 - 0.75 mg/kg { max 3 mg / kg }
• For Torsades de pointes Consider Magnesium1 to 2 g loading.
• In Asystole and slow PEA
– Atropine 1 mg , repeat every 3 – 5 min upto 3doses max.
Things to avoid in ACLS management
• Pacing in Asystole
• Procainamide in VF
• Nor-epinephrine instead of Epinephrine
• Precordial thump for VF or pulseless VT
• Magnesium accept in Torsades de pointes( class II a )
• Routine administration of IV fluids accept inproven hypovolemic arrests
What else is new ?
• Re affirmation on the use of tPA for stroke in theappropriate setting
• Newer first aid recommendations
15
• Newer post resuscitation care recommendations
• Post Resuscitation Care
• Maintaining cerebral perfusion with appropriateBLS and ACLS techniques and effective searchand treating of the 12 contributing factors. { mosteffective means }
• After Return Of Spontaneous Circulation, thefollowing could help:
– Induced hypothermia { 32 – 33 degrees C }
– Avoid and Rx hyperthermia aggressively
– Tight sugar control { avoid hypoglycemia as well }
– Avoid routine hyperventilation but achievenormocarbia with ventilatory strategies
– May continue the infusion of the anti –arrhythmic agent used to Rx the victim duringarrest { class indeterminate }
– May use B – blockers in patients arrestedfollowing an ACS
– Maintain a good CPP { increase MAP anddecrease ICP }
– Avoid hyperthermia and seizures to protect thebrain
First Aid Guidelines
• Breathing difficulties
• Anaphylaxis
• Seizures
• Acute bleeding from injuries
• Burns
• Spine stabilization
• Trauma
• Severe dental injuries
• Environmental injuries e.g. drowning, snakebite,hypothermia etc.
• ToxicologyAre also incorporated
Summary
• More emphasis on compressions
• Avoid hyperventilation
• Compression - First Vs Shock – First for VF
• 1- Shock Vs 3 – Shock sequence
• Effectiveness of epinephrine revived and the useof one dose vasopressin along with and notinstead of epinephrine, in VF
• Use of one dose vasopressin in Asystole and PEAsimilar to its use in VF
• Drug – Shock sequence discarded
• Post resuscitative care
• First – aid care
• Importance of an early 12 lead ECG in riskstratification and the use of early reperfusiontechniques in the treatment of ACS
• Re – affirmation of the appropriate use of tPA inacute stroke settings in the specific situation
‘The most important determinant of survival fromsudden cardiac arrest, is the presence of a wellinformed and trained rescuer who is ready,willing, able and equipped to act quickly and withprecision.’
Facts
• Fever is the most common reason for emergencyroom / doctor visits.
• It affects all age groups equally.
• A good number of non-infectious cases such asdeep vein thrombosis (DVT), pancreatit is,thyroiditis, and central fever, just to name a few,
are responsible for fever, and these do not needantibiotics.
• Many patients with infections may not mountfever, such as the elderly, diabetic,immunocompromised, and renal failure patients.
• The fever could be dangerous in certain situations,e.g., it could lead to seizures in children and could
APPROACH TO FEVER - Dr. Rajeev Soman

16
lead to coning in cases of reduced intra-cranialpressure.
• In family practice fever is the most commonreason for the overuse, misuse, and abuse ofantibiotics thus leading to antibiotic resistance.
Infectious causes of fever (salient features)
The most common ones are
Viral fever : It is usually associated with mild upperrespiratory tract and gastrointestinal symptoms.There is also fatigue, severe myalgia, and leucopenia.
Dengue fever : Fever is usually associated with glove-and-stocking rash, i.e. rash over palms and feet, withintense itching, headche, severe thrombosis,cytopenia, and increased haemoglobin concentration,due to haemoconcentration.
Malaria : Malarial fever is usually associated withchills or rigors, abdominal pain, vomiting, severeheadache, and pancytopenia. Patient is usuallynormal in between fever spikes. One has to watchout for the development of ARDS in the second weekof the illness.
Enteric fever (Typhoid) : The fever is usually low-grade, of indolent course, with some gastrointestinalsymptoms. The patient usually appears toxic even inbetween fever spikes. There may be low or normalWBC counts.
Important differential diagnosis
• DVT• Pancreatitis• Subacute thyroiditis• Pulmonary embolism• Drug fever• Central fever• Myocardial infarction• Vasculitis• Malignancy
Common causes of fever in special situations
• Diabetes Urinary tract infectioncellulitis (UTI)
• Elderly patients UTI, pneumonia
• Children Viral infection
• Traveler Malaria,acute gastroenteritis
• Immunocompromised TB,patients lymphoma
Pneumocystiscariini pneumonia
Specific treatment• Viral Just observe• Vivax malaria Chloroquine• Falciparum malaria Artesunate
compounds• Enteric fever Ceftriazone• Respiratory tract infection Ceftriaxone +/-
Quinolone• Meningitis Ceftriaxone +/-
Vancomycin
Stepwise approch to fever
i) Is the case infectious or not
NO
ii) Investigate for non-infectious cause such asDVT, thyroiditis, pancreatitis, etc.
YES
iii) Is he low risk or high risk patient
Low risk - young patient, stable patient, consciouspatient
High risk - extremes of age, tachycardia, tachypnoea,drowsiness
Low risk
• Look for site of infection
- Urinary tract (UT)
- Lower respiratory tract (LRT)
- Gastro - intestinal tract (GIT)
• Start appropriate empirical antibiotics
• Observe
High risk
• Refer patient to hospital and admit.
• Appropriate labs + give supportive treatment,i.e., oxygen, IV fluids, etc.
• Start appropriate IV antibiotics
PUO (pyrexia of unknown origin)
I f fever persists for more than three weeksconsider :
• Cellulitis• Enteric fever• TB• HIV infection• Subacute thyroiditis• Pancreatitis• Autoimmune system diseases• Malignancy

17
Respiratory difficulty is a common presentingcomplaint in the outpatient setting. Most clinicianshave no difficulty in recognizing the signs of potentialrespiratory failure such as tachypnoea, dyspnoea,stridor, wheezing, accessory muscle recruitment,abdominal paradox, intercostal retractions, alteredmentation, and tachycardia. Sometimes establishinga diagnosis may be difficult because dyspnoea is acommon symptom for multiple aetiologies. The initialgoal in the patient management is to determine theseverity of dyspnoea with regard to the need foroxygenation and venti lat ion and accordinglyhospitalizing the patient for the same. Subsequentmanagement depends upon the diagnosis, which isestablished by taking a proper history, physicalexamination, and carrying out relevant investigations.
Initial assessment
Assess airway patency and listen to lungs for wheeze,stridor, and crepitations. Observe the breathingpattern, including the use of accessory muscles,tracheal shift. Traditionally, respiratory rate has beenshown to be a good index of respiratory compromise.However it is an imprecise measurement and is alsoa poor index of hypoxaemia.
• Check the JVP and look for peripheral oedema
• Monitor cardiac rhythm
• Monitor vital signs and pulse oxymetry
• Obtain history of cardiac, pulmonary disease, ortraumaq
• Evaluate the mental status
Investigations
This should include basic investigations like
• X-ray chest
• Arterial blood gas analysis
• ECG
• Peak expiratory flow rate
• Complete blood count, renal and liver profile
• Sputum for gram stain and culture sensitivity
Specific investigations
• 2D ECHO
• D-dimer
• V/Q scan
• Chest computed tomography
• Bilateral lower limb venous Doppler
Differential diagnosisPulmonary diseases
Airway diseases
Foreign body obstruction
Epiglottitis/ epiglottic abscess
Airway trauma
Obstructive diseases
Asthma
COPD
Pleural effusion
Empyema
Pneumothorax
Thromboembolism
Trauma
Flail chest
Infectious diseases
Community–aquired pneumonia
Bronchitis
Bronchiolitis
Inflammatory diseases
Acute lung injury
ARDS
Pleural diseases
Systemic diseases
Sepsis
Hypovolaemia
Shock
Neuromuscular dysfunction
Metabolic dystunction
Diabetic Ketoacidosis
Central and peripheral nervous system Causes
Cerebrovascular accidents, Drugs like opiates
Brainstem or spinal cord trauma
Guillan Barre syndrome
Myasthenia gravis
ACUTE BREATHLESSNESS - Dr. Simran Singh

18
Cardiovascular causes
Congestive heart failure
Valvular heart disease
Ischemic heart disease
Aortic dissection
Initial management
Patients should be rapidly assessed and stabilized,first with regard to airway, breathing, and circulation,as sometimes there may not be adequate time to,carry out the relevant investigations.
He/she should be immediately connected to the pulseoximeter and cardiac monitor.
Supplemental oxygen should be given using theappropriate device-nasal prongs, plain mask, venturimask, or a non-rebreathing mask. Intravenous accessshould be obtained immediately.
If the patient is unconscious or obtunded and isunable to maintain the airway then the triplemanoeuvre, which consists of head tilt jaw thrust orchin lift, should be carried out or alternatively anoropharyngeal or nasopharyngeal airway should beinserted.
Non-invasive ventilation can be tried initially if thepatient is conscious.
Endotracheal intubation and mechanical ventilationis considered in case of respiratory muscle fatigue,increased work of breathing, haemodynamicinstability, and altered sensorium.
Discussing the clinical presentation and managementof the different aetiologies of acute dyspnoea isbeyond the scope of this art icle. Hence, themanagement in brief of the common respiratoryconditions that one encounters in the emergencydepartment or the outpatient are discussed.
Acute left ventricular failure
There is usually a history of coronary artery disease/rheumatic heart disease, history of paroxysmaldyspnoea with pink frothy sputum, and basilarcrepitations. Also there is ECG evidence of cardiacischaemia , positive troponin T/I and elevated cardiacenzymes. X-ray chest wil l show evidence ofpulmonary oedema.
Specif ic treatment measures would beadministeration of oxygen, diuretics, opiates,nitroglycerin, and ionotropic support if the systolicblood pressure is less than 100 mmHg. Also specificcardiac medications, e.g. antiplatelet agents shouldbe commenced.
Noninvasive ventilation, which is the delivery ofmechanical ventilation without the placement of anendotracheal tube, can also be applied to patients withacute cardiogenic pulmonary oedema in order toreduce the work of breathing and to providesymptomatic relief.
Pulmonary thromboembolism (PE)
The main clinical presentation in acute PE isdyspnoea, hypoxaemia, pleuritic chest pain, andtachycardia. Sudden collapse, hypotension, andsyncopal attacks can be seen in major pulmonaryembolism. Investigations would include X-ray chestwhich would show oligaemic lung fields, d-dimerassay, which would be elevated, arterial blood gasanalysis, and a ventilation-perfusion scan showing amismatched defect. A spiral chest CT or CTpulmonary angiography also has good sensitivity andspecificity for central and segmental thrombus but isless accurate for sub-segmental embolism. 2D echois an invaluable investigation which can be easily doneat the bedside. In case of a PE there would be rightventricular (RV) dilatation, RV hypokinesia, pulmonaryartery enlargement, and tricuspid regurgitation.A 2D-echo also helps in excluding other possiblecauses of acute dyspnoea like acute myocardialinfarction, aortic dissection, and pericardial tamponade.
Management of PE would be anticoagulation withlow-molecular-weight heparin, followed by warfarintherapy for 6 months. Intravenous thrombolysis withstreptokinase or tissue plasminogen activator isindicated for haemodynamically unstable patients withPE. Inferior vena caval filters can be inserted in thosein whom anticoagulation is a contraindication.
Community-acquired pneumonia (CAP)
Patients present with upper respiratory symptomsand fever with radiological evidence of a lung infiltrate.Complete blood count, sputum for gram stain andculture, blood for atypical serology and culture, andX-ray chest is the initial workup. “Typical” organismsin the immunocompetent host include Streptococcuspneumoniae, H.influenzae, and Staphylococcousaureus. “Atypical” refers to pneumonia caused byLegionella species, Mycoplasma pneumoniae andChlamydia pneumoniae. Bacteraemia accompaniesthe pneumonia in 20%-30% of the cases only.
Cefotaxime and ceftriaxone are the preferredantibiotics for the treatment of CAP caused bypneumococc. The American Thoracic Society andInfectious Diseases Society of America consensuson community acquired pneumonia recommends

19
azithromycin or levofloxacin (as a part of combinationtherapy or monotherapy) for patients with CAP whorequire hospitalization.
Acute exacerbation of bronchial asthma andCOPD
The common precipitating events for an asthmaticor COPD exacerbation could be an upper or a lowerrespiratory tract infection, pneumothorax, pleuraleffusion, pulmonary embolism, heart failure, andfailure to comply with bronchodilator therapy. Theclassic signs of wheezing correlate poorly with thedegree of airflow limitation.
The initial treatment is administration of oxygen, beta2 agonist nebulization every 15-20 min followed by1-4 hourly, methylprednisolone 60 mg 6 hrly, andipratropium bromide nebulization 2-4 hourly havesynergistic bronchodilatory activity with beta2agonists
Upper airway obstruction :
Acute upper airway obstruction may result fromfunctional or mechanical causes. Functional causesinvolve central nervous system or neuromusculardysfunction. Mechanical causes may be due to
Hinduja Hospital rated 9th best hospital in India by Week
In February issue of ‘The Week, Hinduja Hospital was rated as the 9th best hospital in the country,according to the results of the 2006 week - TNS Survey’
The Hospital was also recognized in the following specialities: neurology, gastroenterology, and oncologyby the medical fraternity across 20 cities.
The general practitioners and specialists of Mumbai rated Hinduja Hospital as the number 1 hospital inthe city. We are proud of this achievement and will continue our dedication in providing world-classmedical services to patients.
foreign body aspiration, epiglottitis, retropharyngealabscess, Ludwig’s angina, laryngeal oedema,orpharyngeal or laryngeal neoplasms. In case of aforeign body, expulsion manoeuvre can be tried at thescene if the patient is awake. Otherwise the patienthas to be shifted to a hospital for management ofupper airway obstruction, which could includesecuring the airway with an endotracheal tube orsurgically by doing a cricothyroidotomy, or anemergency tracheostomy.
Conclusion
Acute breathlessness is thus a combination ofmultiple signs and symptoms rather than a specificdisease process. Evaluation of a patient in acuterespiratory distress sometimes poses a complexproblem to the treating physician. There is aheterogeneous population that can present withacute respiratory distress. The emergencyphysician should become aware of the benefits ofnon-invasive positive pressure ventilation in themanagement of respiratory failure. Essential to themanagement of these patients is the ability toanticipate a difficult airway and the formulation ofalternative airway strategy.
GOLDEN PEACOCK GLOBAL AWARD FOR PHILANTHROPY IN EMERGING ECONOMICS 2006
Hinduja Hospital was presented the prestigious ‘GOLDEN PEACOCK GLOBAL AWARD FOR PHILANTHROPYIN EMERGING ECONOMICS 2006’, the inaugural ceremony of the Global Conference on Social Responsibility,at which was held at Vilamoura, Portugal from 16th -18th February 2006.
It is award is globally recognized as benchmark of corporate excellence in different areas such as businessleadership, corporate governance, corporate social responsibility, and environment management.
It’s awarded to organizations and individuals that have contributed significantly by providing funds andmanagerial skills to provide a better quality of life to the less fortunate and deprived section of society.

20
FROM THE CORRID0ORS OF HINDUJA HOSPITAL
Papers published / presented
• Thrombophil ia in non cirrhotic portal veinthrombosis. Indian Gastroenterol: Dr. Sudeep Shahyr-vol-pg
• Does the organism causing abdominaltuberculosis differ from pulmonary tuberculosis:Dr. Sudeep R. Shah, Dr. Shubhada Shenai, MinalDeshmukh, Dr. Devendra Desai, Dr. Anand Joshi,Dr. Phil ip Abraham, Dr. Ajita Mehta,Dr. Camilla Rodrigues 46th Annual Conferenceof the Indian Society of Gastroenterology:place-yr-dates
• A family with MENI syndrome; sequencing thegenetic mutation: 46th Annual Conference of theIndian Society of Gastrology: place-yr-datesDr. Sudeep R. Shah, Rani Raghavan,Dr. Murad Lala, Dr. Devendra Desai, Dr. PhulrenuChauhan, Dr. Tester Ashavaid
Achievements
• Dr. Ashok Mahashur has been awarded the‘Fellowship of the Royal College of Physicians(FRCP)’ by the Royal College of Physicians andSurgeons, U.K.
• Dr. Ashok Mahashur has been elected President,Indian Chest Society for the year 2006.
Dr. Vinod A. Chandiramani became a Fellow ofthe American College of Surgeons during theconvocation of the College’s 91st Annual ClinicalCongress in San Francisco.
1. Antibasal ganglia antibodies (ABGA)
Indications :
Movement disorders, chorea, tics, dystonia,post streptococcal acute, disseminatedencephalomyelitis, behavioural disturbances
2. Brain derived neurotropic factor (BDNF)
Indications :
Mood disorders, Alzheimer’s disease, learningand memory disorders, bipolar disorders,obsessive compulsive disorder, epilepsy anddepression.
3. Acetylcholine receptor antibodies (ACHR-Abs)
Indications :
Diagnosis, follow-up and prognosis of patientswith myasthenia gravis.
4. Muscie-specific receptor tyrosine kinase autoantibodies (MUSK Abs)
Indications :
Generalized myasthenia gravis negative for actylcholine receptor antibodies.
The research students who have been awarded MSc in 2005 are:
– Ms Betsy Joseph for her study “Detection of theetiological agents in endopthalmit is usingmicrobiological and molecular methods”.
– Ms Sudha Srinivasan for her study “Diagnosis ofherpes virus encephalitis”.
Printed and Published by Marketing Department, P. D. Hinduja National Hospital & Medical Research Centre, Veer Savarkar Marg,Mahim, Mumbai - 400 016 at SYNERGY CREATIONS, for free and private circulation. Editor : Dr. V. R. Joshi. Registered.
(The Publisher cannot be held responsible for errors or for any consequences arising from the use of the informationcontained in this newsletter.)