High-Intensity Interval Training leads to reduced testosterone ...
12
Page 1/12 High-Intensity Interval Training leads to reduced testosterone and increased estrogen levels in young women Wael Ramadan ( [email protected] ) Mansoura University Chrysovalantou E. Xirouchaki Monash University Medhat Kasem Abdel Razek Umm al-Qura University Mariam Abu Alim Yarmouk University Research Article Keywords: Trophic hormones, Reproductive hormones, High-Intensity Interval Training Posted Date: June 1st, 2022 DOI: https://doi.org/10.21203/rs.3.rs-1639546/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of High-Intensity Interval Training leads to reduced testosterone ...

Page 1/12
High-Intensity Interval Training leads to reducedtestosterone and increased estrogen levels inyoung womenWael Ramadan ( [email protected] )
Mansoura UniversityChrysovalantou E. Xirouchaki
Monash UniversityMedhat Kasem Abdel Razek
Umm al-Qura UniversityMariam Abu Alim
Yarmouk University
Research Article
Keywords: Trophic hormones, Reproductive hormones, High-Intensity Interval Training
Posted Date: June 1st, 2022
DOI: https://doi.org/10.21203/rs.3.rs-1639546/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License

Page 2/12
AbstractBackground: Hormone levels can be determined according the prevalence of a balance betweengeneration metabolism and clearance rates. High-Intensity Interval Training (HIIT) can affect this balancethrough a variety of mechanisms, including competition-associated stress, diet, body composition, heatproduction and hypoxia.
Aims: The present study aimed to evaluate the impact of HIIT on the Health hormones of femininity andfertility in young women.
Methods: The study was comprised of Eighteen females aged 18.06 ± 0.128 years old. The participantswere subjected to an eight-week training program (3 sessions/week, two hours (h) after lunch).Participants underwent basal pre-and post-exercise intervention tests, such as reproductive and trophichormones.
Results: The results revealed that 143.16% increased estrogen levels and a 62.12% reduction intestosterone levels . No signi�cant differences were detected in Luteinizing hormone (LH) and Prolactin(PRL) between participants.
Conclusions: HIIT exercise training in young women decreases testosterone levels and increases estrogenlevels, with no effect on trophic hormones (LH, PRL).
IntroductionHigh-intensity interval training (HIIT) includes alternate bouts of high-intensity intensive exercise alongwith low-intensity recovery periods. It is considered one of the most effective methods to improvecardiorespiratory and metabolic health [1]. Women have avoided resistance training for many years outof fear of being masculinized due to heavyweights. However, researchers have demonstrated thatsigni�cant female strength could be observed with only minor degrees of muscle hypertrophy [2, 3].Currently, it is widely accepted that exercise training in young women is very bene�cial, as it can lead toreduced adiposity and increased cardiovascular �tness.
Nevertheless, even if the exercise volume exceeds the physiological limit, this causes adverse effects onthe skeletal and reproductive system, one of which is primary/secondary amenorrhea, induced by manyfactors such as inadequate nutrition and low body weight [3]. Primary and secondary amenorrhea arepatterns of follicle-stimulating and luteinizing hormone suppression. Additionally, it may involve thehypothalamic-pituitary-adrenal axis and hypothalamic-pituitary-gonadal axis.
Hypoestrogenism may have a negative effect on bone growth in athletes. Amenorrhea, eating disorders,and osteopenia are all symptoms of fatigue in female athletes. Women with delayed menarchedemonstrate elevated stress features, osteopenia, and incidence of scoliosis compared with girls withaverage menarche [4, 5]. The balance of clearance rates, metabolism, and production is essential for

Page 3/12
maintaining hormonal blood levels. This balance may be affected by intensive physical exercises orthrough some mechanisms like dieting, production of heat and hypoxia, stress related to competition, andreduction of body fat mass [6]. Women who engage in high-intensity exercise on a regular basis mayexperience menstrual disturbances such as oligomenorrhea, amenorrhea, or delayed menarche due tohormonal changes. Among the exercise-induced menstrual disturbance is the impaired production ofgonadotropins, which may lead to anovulation and luteal phase de�ciency [7].
Previous literature illustrated that prolonged and high-intensity training has a disadvantageous effect onfemale reproductive hormones. The hypothalamus-ovarian axis and the circulation of femininereproductive hormones are disrupted due to related fatigue associated with low energy, leptin levels, andhigh-stress hormone concentration following strenuous exercise. This imbalance could lead to missmenstrual cycle regulation associated with the luteal phase and anovulation de�ciency. Consequently,this study aims to investigate further the potential interventions of HIIT, which may be bene�cial to reduceor prevent the impacts on reproductive health among female athletes by assessing femininity and fertilityhormones.
Methods
ParticipantsThe current study assessed eighteen females, as depicted in (Table 1). The participants completed afamiliarization session before initiating the measurements, where participants were excluded if sufferingfrom any metabolic disease or renal, pulmonary, or cardiovascular pathological conditions. Before theonset of any testing or training session, it was required to obtain all participants' oral and writteninformed signed consent. The Institutional Review Board approved the Faculty of Physical Educationstudy, Mansoura University, Egypt. Table (1) illustrates the participants' physical characteristics.
Table 1The participants' Physical characteristics. Values are represented as mean
(± sem)Variables Age (years) Height (m) Body mass (kg) BMI (kg/m2)
Mean 18.06 1.65 63.35 21.35
sem .128 2.74 2.68 0.46
Insert Table 1.
Hormonal Assay:Trained laboratory technicians performed blood sampling at standardized laboratory conditions. Beforeobtaining a blood sample, participants were required to fast for at least 4 hours. Subsequently, the

Page 4/12
venous blood sample was collected on the third day of the spontaneous cycle. The collected sampleswere allowed to clot at room temperature for one hour and were then subsequently centrifuged at 8000rpm for 15 minutes at 4 oC. The serum samples were then stored at -20 oC until assayed. Clear non-hemolyzed sera were separated and used for the assay of testosterone, estrogen, follicle-stimulating(FSH), luteinizing hormone (LH), and prolactin (PRL) by solid-phase competitive chemiluminescentenzyme immunoassay through the utilisation of IMMULITE analyser purchased from DPC (DiagnosticProducts Corporation, USA).
Training ProgramNone of the participants had engaged in any form of an exercise training programme for at least twomonths prior to the study. The group carried out their HIIT exercise training program (3 sessions/week, 2 hafter lunch) for eight weeks on alternate days (Sunday, Tuesday, and Thursday). Each participant'srepetition maximum (1RM) was measured. Participants completed a warm-up set of 8–10 repetitions at50% of their estimated 1RM, before moving to a warm-up set of 3–5 repetitions at 85% of their estimated1RM. To determine squat 1RM, participants performed 1RM attempts over 4–5 trials separated by 3 minrest intervals. 1RM was measured again, and intensity was re-established after four weeks of HIITtraining. The detailed exercise training programme is presented in Table 2.

Page 5/12
Table 2High-Intensity Interval Training (HIIT) Program
S Exercise Week 1,2 Week 3,4 Week 5,6 Week 7,8
(time× sets) rest (time× sets) rest (time× sets) rest (time× sets) rest
1 High knees (10×3) 10 (15×4) 30 (20×4) 20 (30×3) 30
Squats (10×3) 10 (15×4) 30 (20×4) 20 (30×3) 30
Basic burpees (10×3) 10 (15×4) 30 (20×4) 20 (30×3) 30
Elbow plank (10×3) 10 (15×4) 30 (20×4) 20 (30×3) 30
Flutter kicks (10×3) 10 (15×4) 30 (20×4) 20 (30×3) 30
2 Plank (10×4) 20 (15×3) 30 (20×5) 40 (30×5) 60
Elbow plank (10×4) 20 (15×3) 30 (20×5) 40 (30×5) 60
Body saw (10×4) 20 (15×3) 30 (20×5) 40 (30×5) 60
Side bridges (10×4) 20 (15×3) 30 (20×5) 40 (30×5) 60
Crunches (10×4) 20 (15×3) 30 (20×5) 40 (30×5) 60
3 Sit-ups (10×5) 30 (15×5) 45 (20×3) 40 (30×4) 60
Jumping jacks (10×5) 30 (15×5) 45 (20×3) 40 (30×4) 60
Scissors chops (10×5) 30 (15×5) 45 (20×3) 40 (30×4) 60
Arm Scissors (10×5) 30 (15×5) 45 (20×3) 40 (30×4) 60
Climbers (10×5) 30 (15×5) 45 (20×3) 40 (30×4) 60
Session (S), Time, rest by seconds
Insert Table 2.
Statistical AnalysisStatistical Package for Social Sciences (SPSS) (version 23.0.) and GraphPad Prism (version 8.4.2.GraphPad Software 154 LLC, CA, USA) were used to perform all statistical analyses. Data included themean ± standard error of the mean (sem) and "T" value. The signi�cance level was set at p < 0.05.
ResultsThe results of the current experimental procedure are presented as mean ± standard error of the mean(sem) for the given number of participants, as shown below. Table 1 presents the anthropometric andphysical characteristics of the participants (age, height, body mass, body mass index).

Page 6/12
Figure 1–3 depicts the primary data of the current study. It was revealed that 8-week training had asigni�cant impact on estrogen, testosterone, and follicle-stimulating hormone (FSH) levels (Fig. 1–3). Inaddition, there was a 2-fold increase in estrogen levels post-exercise training compared to the basalmeasurement prior to the initiation of the exercise intervention (Fig. 1).
Insert Fig. 1.
Furthermore, there was around a 3-fold reduction in testosterone levels after the exercise- regimen (Fig. 2),highlighting the crucial role of chronic exercise regulating testosterone levels in young femaleparticipants. In addition, post-exercise training measurements demonstrated a slight reduction (around15%) in FSH levels (Fig. 2). In contrast, 8-week exercise training had no signi�cant impact on LH andprolactin (Fig. 2–3).
Insert Fig. 2.
Insert Fig. 3.
DiscussionThis study found that high-intensity interval training had a signi�cant effect on estrogen and testosteronehormones in young females. In contrast, no signi�cant changes were detected in the LH, Prolactin, andFSH hormones. However, this could be related to the small sample size of this study. Previous researchstudies have indicated that exercise has a positive effect on female hormones. Sex hormone levels areconsidered an objective marker for assessing the level and effectiveness of exposure to physical trainingand specifying the appropriate physical activity levels and doses, especially in women. In this study,hormonal estrogen levels showed a signi�cant increase. Estrogen plays a crucial role in promoting thedevelopment and effectiveness of female reproductive structure and female secondary sexcharacteristics [8]. Similar results have been reported by Hackney et al. (2020). They assessed sevenyoung women's hormonal responses on a moderate bicycle ergometer training for eight weeks in a �xedrelative intensity. The results of their study detected an increase in beta-endorphin, beta lipotropin cortisol,and reproductive hormone levels [9]. Copeland et al. (2002) [10] investigated the female hormonalendurance and resistance training responses. They found a signi�cant increase in estradiol levels inresponse to both training interventions in their study. In addition, the impact of physical activity onhormonal circulation has been con�rmed by previous research �ndings reporting elevated estradiolcirculation after resistance exercise and endurance exercise in female participants [11]. Vicissitudes infemales' estrogen levels have been reported to be in�uenced by exercise duration, intensity, menstrualphase, and status [3, 12].
In addition to the increase of estrogen, the current study reported a signi�cant increase in testosteronelevels related to the impact of this study's proposed high-intensity interval training. These results werecon�rmed by the analysis of Gharahdaghi et al. 2021. They reported that resistance exercise could induce

Page 7/12
a temporary rise in testosterone in young, healthy females. Additionally, the anthropometrical indicationsof adiposity have been found to be signi�cantly correlated with testosterone concentrations [13].
A study conducted by Kochańska-Dziurowicz et al. (2001) investigated the effect of a proposed acuteexercise intervention on a cycle ergometer on testosterone and prolactin levels in 13 young femalerunners. Their study results addressed a signi�cant elevation in the testosterone concentration, indicatedat the end of the exercise and 90 minutes past the completion of the test. In contrast, the testosteronelevel had returned to the base levels as pre-exercise [14].
On the contrary, literature results have concluded that exercising had no effect on testosteroneconcentration in trained young women and was not in�uenced by their menstrual cycle [9, 15]. In addition,it has been revealed that training status contributes to mediating the hormones' response to physicalactivities. After a six-month resistance training intervention, changes in testosterone levels have onlyoccurred in women [16].
In a study by Schmitz et al. (2007), other results were reported, as they found that physical activity levelwas inversely related to estrogen in late transition age. The adjusted means of estrogen reported were24.6 and 37.9; a relative difference of 54% in estrogen level was detected when comparing highest tolowest activity (P = 0.02). Similarly, it was shown that physical activity was inversely related totestosterone levels (a relative difference of 47% was detected when comparing the highest to lowestactivity [17].
The current study illustrated that the increase in estrogen hormone had been linked to a rise in LH andPRL. Despite the signi�cant elevation in estragon levels, no signi�cant changes have been indicated inthe study participants' levels of LH and PRL. This �nding could be explained by the conclusion of a recentmeta-analysis conducted by Ennour-Idrissi et al., 2015, on the effect of physical activity on sex hormonesin women. The meta-analysis results addressed that the impact of physical activity on circulating sexhormones is relatively modest and probably not clinically signi�cant. Also, the levels of sex hormones inthe blood may not represent their effects on target tissues. Physical activity may continue to affect sexhormone function by modulating target-tissue sensitivity to these hormones [18].
SummaryRegular exercise may induce changes in the levels of reproductive hormones in females, including anincrease in estrogen level and a decrease in test level. High-intensity interval training exercise is highlyrecommended for young women as it leads to increased estrogen levels and reduced testosterone levels,with no effect on trophic hormones (LH and PRL).
DeclarationsEthics approval and consent to participate and publication:

Page 8/12
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approvedby the Institutional Review Board approved the Faculty of Physical Education study, Mansoura University,Egypt. Written and oral and informed signed consent was obtained from all participants
Availability of data and materials:
The datasets used and/or analyzed during the current study are available from the corresponding authoron reasonable request.
Competing interests: The authors declare no con�ict of interest.
Funding: No �nancial support for the current study.
Authors' contributions:
Wael Ramadan contributed to Conceptualization, Formal analysis, Methodology, Supervision, Validation,Visualization, Writing-review & editing. Chrysovalantou E. Xirouchaki contributed to Investigation, dataextraction, data analysis and manuscript writing, results discussion. Medhat Abdel Razek and Mariam Abu Alim contributed to Supervision, Writing-original draft, Writing-review & editing. All authors read andapproved the fnal manuscript.
Acknowledgements:
The authors would like to thank all the participants that voluntarily agreed to participate in the currentstudy after signed informed consent.
References1. Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval
training (HIT) on �tness in adults: a meta-analysis of controlled and non-controlled trials. Sportsmedicine. 2014;44(7):1005-17.
2. Zanker C, Swaine I. Relation between bone turnover, oestradiol, and energy balance in womendistance runners. British journal of sports medicine. 1998;32(2):167 − 71.
3. Piasecki J, Ireland A, Piasecki M, Cameron J, McPhee J, Degens H. The strength of weight-bearingbones is similar in amenorrheic and eumenorrheic elite long‐distance runners. Scandinavian journalof medicine & science in sports. 2018;28(5):1559-68.
4. Bjørnerem As, Straume B, Midtby M, Fønnebø V, Sundsfjord J, Svartberg J, et al. Endogenous sexhormones in relation to age, sex, lifestyle factors, and chronic diseases in a general population: theTromsø Study. The Journal of Clinical Endocrinology & Metabolism. 2004;89(12):6039-47.
5. Hirschberg AL. Female hyperandrogenism and elite sport. Endocrine connections. 2020;9(4):R81-R92.

Page 9/12
�. McTiernan A, Tworoger SS, Rajan KB, Yasui Y, Sorenson B, Ulrich CM, et al. Effect of exercise onserum androgens in postmenopausal women: a 12-month randomized clinical trial. CancerEpidemiology and Prevention Biomarkers. 2004;13(7):1099 − 105.
7. Vislocky LM, Gaine PC, Pikosky MA, Martin WF, Rodriguez NR. Gender impacts the post-exercisesubstrate and endocrine response in trained runners. Journal of the International Society of SportsNutrition. 2008;5(1):1–10.
�. Mosavat M, Mohamed M, Mirsanjari MO. Effect of exercise on reproductive hormones in femaleathletes. International Journal of Sport and Exercise Science. 2013;5(1):7–12.
9. Hackney AC, Willett HN. Testosterone Responses to Intensive, Prolonged Endurance Exercise inWomen. Endocrines. 2020;1(2):119 − 24.
10. Copeland JL, Consitt LA, Tremblay MS. Hormonal responses to endurance and resistance exercise infemales aged 19–69 years. The Journals of Gerontology Series A: Biological Sciences and MedicalSciences. 2002;57(4):B158-B65.
11. Mannerkorpi K, Landin-Wilhelmsen K, Larsson A, Cider Å, Arodell O, Bjersing JL. Acute effects ofphysical exercise on the serum insulin-like growth factor system in women with �bromyalgia. BMCmusculoskeletal disorders. 2017;18(1):1–8.
12. Lebrun CM, Joyce SM, Constantini NW. Effects of female reproductive hormones on sportsperformance. Endocrinology of physical activity and sport: Springer; 2013. p. 281–322.
13. Gharahdaghi N, Phillips BE, Szewczyk NJ, Smith K, Wilkinson DJ, Atherton PJ. Links BetweenTestosterone, Oestrogen, and the Growth Hormone/Insulin-Like Growth Factor Axis and ResistanceExercise Muscle Adaptations. Frontiers in Physiology. 2021;11:1814.
14. Kochańska-Dziurowicz A, Gawel-Szostek V, Gabryś T, Kmita D. Changes in prolactin and testosteronelevels induced by acute physical exertion in young female athletes. Human Physiology.2001;27(3):349 − 52.
15. O’Leary C, Lehman C, Koltun K, Smith-Ryan A, Hackney A. Response of testosterone to prolongedaerobic exercise during different phases of the menstrual cycle. European journal of appliedphysiology. 2013;113(9):2419-24.
1�. Hakkinen K, Pakarinen A, Kraemer WJ, Newton RU, Alen M. Basal concentrations and acuteresponses of serum hormones and strength development during heavy resistance training in middle-aged and elderly men and women. Journals of Gerontology-Biological Sciences and MedicalSciences. 2000;55(2):B95.
17. Schmitz KH, Lin H, Sammel MD, Gracia CR, Nelson DB, Kapoor S, et al. Association of physicalactivity with reproductive hormones: the Penn Ovarian Aging Study. Cancer Epidemiology andPrevention Biomarkers. 2007;16(10):2042-7.
1�. Ennour-Idrissi K, Maunsell E, Diorio C. Effect of physical activity on sex hormones in women: asystematic review and meta-analysis of randomized controlled trials. Breast Cancer Research.2015;17(1):1–11.

Page 10/12
Figures
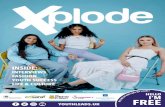
Figure 1
Estrogen levels (pg/ml) under basal and post-exercise training conditions.

Page 11/12
Figure 2
Testosterone levels (ng/ml) under basal and post-exercise training conditions.
Follicle Stimulating hormone (FSH) levels (mIU/ml) under basal and post-exercise training conditions.
Luteinizing hormone (LH) levels under basal and post-exercise training conditions.

Page 12/12
Figure 3
Prolactin levels (ng/ml) under basal and post-exercise training conditions.