
Platelet-derived growth factor-D expression in developing and mature human kidneys

High CXCL10 Expression in Rejected Kidneys andPredictive Role of Pretransplant Serum CXCL10 for
Acute Rejection And Chronic Allograft Nephropathy
Elena Lazzeri,1 Mario Rotondi,1 Benedetta Mazzinghi,1 Laura Lasagni,1 Andrea Buonamano,1
Alberto Rosati,2 Fabio Pradella,3 Vittorio Fossombroni,3 Giorgio La Villa,4 Mauro Gacci,5
Elisabetta Bertoni,2 Mario Serio,1 Maurizio Salvadori,2 and Paola Romagnani1,6
Background. Several experimental models have shown that CXCL10 is required for initiation and development of graftfailure caused by both acute and chronic rejection.Methods. CXCL10 expression and distribution was investigated in tissue specimens obtained from 22 patients sufferingfrom acute rejection (AR) or chronic allograft nephropathy (CAN) by using in situ hybridization. Furthermore,pretransplantation sera of 316 cadaveric kidney-graft recipients were tested retrospectively for serum CXCL10 levels bya quantitative sandwich immunoassay.Results. Bioptic specimens obtained from patients with CAN were characterized by wide CXCL10 expression not only at levelof infiltrating inflammatory cells but also of vascular, tubular, and glomerular structures. In addition, assessment of pretrans-plant serum CXCL10 levels in 316 graft recipients and stratification of patients in three groups according to serum CXCL10levels (�100 pg/mL, n�163; 100–150 pg/mL, n�69; �150 pg/mL, n�84) showed highly significant differences in 5-yearsurvival rates for the two extreme groups (95.7% vs. 79.7%, P�0.0002). Accordingly, patients who developed severe, early AR(277.14�65.08 p�0.004) and those who developed CAN also showed increased pretransplant serum CXCL10 levels(193.2�36.9, P�0.03). Multivariate analysis demonstrated that among the analyzed variables, CXCL10 (relative risk [RR]2.801) and delayed graft function (RR 3.728) had the highest predictive power of graft loss.Conclusions. These results suggest that pretransplant serum CXCL10 levels greater than 150 pg/mL confer an increasedrisk of early, severe, AR and subsequent CAN, finally resulting in renal-allograft failure. This finding might be used forthe individualization of immunosuppressive therapies.
Keywords: CD30, Rejection, Chronic allograft nephropathy, CXCR3.
(Transplantation 2005;79: 1215–1220)
Growing evidence suggests that the chemokine CXCL10may be particularly important for the immune response
to transplant. Indeed, in knockout models of the CXCL10gene or of its receptor gene, called CXC chemokine receptor 3(CXCR3), cardiac transplant undergoes permanent engraft-ment (1–3). Furthermore, neutralization of CXCL10 withmonoclonal antibodies prolongs the allograft survival in both
cardiac and small-bowel allograft rejection (3, 4). Of particu-lar importance, the intragraft expression of CXCL10 has beenreported in association with clinical rejection of acute renal(5), lung (6), and cardiac (7, 8) allografts. Thus, CXCL10-CXCR3 interactions appear to play an important role in thepathogenesis of graft failure caused by rejection in multiorganmodels. Recent evidence indicates that CXCR3 and CXCL10are also highly expressed in conjunction with the develop-ment of transplant vasculopathy in cardiac allografts (9) andthat glomerular infiltration by CXCR3� T cells is associatedwith transplant glomerulopathy (10).
In the present study, we investigated CXCL10 expres-sion and distribution in tissue specimens obtained from pa-tients suffering from acute rejection (AR) or chronic allograftnephropathy (CAN). In AR, CXCL10 was expressed by infil-trating monocytes/macrophages, whereas CAN was charac-terized by wide CXCL10 expression not only at level of infil-trating inflammatory cells but also of vascular, tubular, andglomerular structures. Furthermore, as assessed on 316 ca-daveric kidney recipients, pretransplant quantitation ofCXCL10 serum levels were able to predict the recipient’s riskof severe AR, CAN, and transplant failure. The comparisonwith a number of variables that have all been proposed aspossible predictors of transplant failure, including solubleCD30 (sCD30) (11), showed that high pretransplant serumCXCL10 levels have a high predictive power in identificationof subjects with high risk of allograft failure, a finding thatmight be used for the individualization of immunosuppres-sive therapies.
Selected as one of the top abstracts for presentation at the XX InternationalCongress of The Transplantation Society (ICTS) held in Vienna, Septem-ber 5–10th, 2004; the invited manuscript was peer-reviewed and acceptedfor publication in the special issue dedicated to the XX Congress.
Elena Lazzeri and Mario Rotondi contributed equally to this work.The experiments reported in this article were supported by funds from the
Azienda Ospedaliera Careggi of Florence (Finalized Program of the Tus-cany Region on “Pleiotropic Effects of Glitazones, TRESOR”), and fromthe Italian Ministry of University and Scientific Research (MIUR).
1 Center for Research, Transfer and High Education MCINDENT, Florence,Italy.
2 Center for Nephrology, Dialysis and Transplantation, Florence, Italy.3 Immunogenetics Unit, Azienda Ospedaliera di Careggi, Florence, Italy.4 Department of Internal Medicine, University of Florence, Florence, Italy.5 Department of Urology, University of Florence, Florence, Italy.6 Address correspondence to: Dr. Paola Romagnani, Interdepartmental Lab-
oratory of Cellular and Molecular Nephrology, University of Florence,Viale Pieraccini 6, 50139, Firenze, Italy.
E-mail: [email protected] 1 October 2004. Accepted 14 December 2004.Copyright © 2005 by Lippincott Williams & WilkinsISSN 0041-1337/05/7909-1215DOI: 10.1097/01.TP.0000160759.85080.2E
Transplantation • Volume 79, Number 9, May 15, 2005 1215

MATERIALS AND METHODS
PatientsA total number of 316 cadaveric kidney transplants
were carried out at the Florence Transplant Center betweenJanuary 1991 and June 2001, had pretransplant sera available,and were tested retrospectively for CXCL10 and sCD30 con-tent levels. All patients were on hemodialysis before trans-plant and underwent measurements of main hematochemi-cal parameters every 6 months. Samples were collected on themorning before dialysis. An aliquot was obtained from theserum sample that was used for final cytotoxic cross-matchperformed within 1 month before the date of transplantation.The other aliquot was randomly selected from all availablesamples obtained from the same patients at least 6 monthsbefore. In addition, 48 age- and sex-matched controls weretested. All the recipients were white. The demographic char-acteristics of the recipients were the followings: age46.33�6.4 years; sex M/F 209/107; dialytic age 38.3�2.1months; and original disease glomerulopathies 43.3%, AD-PKD 21.5%, interstitial nephritis 12%, nephroangiosclerosis11.5%, and others 11.7%. Ninety-three percent of the pa-tients received cyclosporine-based immunosuppression,whereas the remaining 7% received a FK-based immunosup-pression. Only one patient had more than one transplant.Human leukocyte antigen (HLA) typings and panel reactivelymphocytotoxic antibody (PRA) determinations were per-formed at the Tissue Typing Laboratory of Azienda Osped-aliera Careggi of Florence, Italy. Patients with 5% or greaterantibody reactivity against a randomly chosen lymphocytetest panel were categorized as sensitized and represented 13%of all subjects. HLA-A�B�DR mismatches were three or lessin 44% and three or more in 56% of patients. Donor age was45.5�0.93 years, and cold ischemia time was 20.2�0.36hours. Information on graft function and patient survival wasdocumented at 1, 3, and 6 months and at 1, 2, 3, 4, and 5 years.Death with a functioning graft was not counted as graft failurein this analysis. The median follow-up time after transplantwas 39 months. Delayed graft function was defined as theneed of at least one session of dialysis during the first 7 daysafter transplantation (12). The procedures used in this studywere in accordance with the Regional Ethical Committee onhuman experimentation.
Renal-biopsy specimens from a total number of 22 sub-jects were used throughout the study. Biopsy specimens wereobtained from 10 patients suffering from AR and from 12patients affected by CAN. Only biopsy proved AR were usedfor statistical analysis. AR episodes were classified accordingto Banff classification (13) and treated with steroids. AR epi-sodes showing vascular components at biopsy (grade II or III)and failure to reverse after a course of steroids were treatedwith rabbit anti-human thymocyte globulin (ATG).
ImmunohistochemistryImmunohistochemical staining was performed as pre-
viously described (14). For double label immunohistochem-istry, the anti-CXCL10 (Peprotech, Rocky Hill, NJ) pAb wasapplied first, and AEC was used as peroxidase substrate. Sec-tions were subsequently exposed to anti-CD68 (EBM11;Dako, Glostrup, Denmark), anti-von Willebrand factor(vWf) (rabbit anti-human polyclonal antibody; Dako), anti-
cytokeratin (CK, C-11; Sigma, Saint Louis, MO), and anti-�-smooth muscle actin (SMA; 1A4; Sigma), and Vector SG(Vector Laboratories, Burlingame, CA) was used as a chro-mogen. No counterstain was applied.
In Situ HybridizationCloning and sequencing of the CXCL10 probe and in
situ hybridization were performed as previously described(14). For combined in situ hybridization and immunohisto-chemistry, after hybridization with the CXCL10 probe,RNAse digestion and appropriate washings, sections werestained with anti-vWf or anti-�-SMA Abs and then subjectedto autoradiography, as reported earlier (14).
Serum AssaysSerum CXCL10 (R&D Systems, Minneapolis, MN) and
sCD130 levels were assayed by a quantitative sandwich im-munoassay using commercially available kits, as describedpreviously (11, 15).
Statistical AnalysisStatistical analysis was performed using SSPS software
(SPSS, Inc., Evanston, IL). Because of nonparametric distri-bution, comparisons of serum CXCL10 and sCD30 levelsamong different groups were performed by Mann-WhitneyU test for unpaired data. Correlation between two variableswas ascertained by linear regression analysis and Spearman’scorrelation test as appropriate. To test the independent effectsof different variables on renal-allograft survival, multiple re-gression analysis was used, and partial correlation coefficientswere computed. Kaplan-Meier estimates were used to gener-ate an overall survival curve for transplanted grafts, and dif-ferences among groups were assessed by log-rank test.P�0.05 was considered statistically significant. Results areexpressed in the text as mean�SEM unless otherwise stated.
RESULTS
CXCL10 is Highly Expressed in Kidney ofSubjects with AR and CAN
CXCL10 mRNA appeared to be highly expressed in bi-opsy specimens from kidneys of patients affected by AR (Fig.1, A to C), as assessed by in situ hybridization. In kidneysfrom patients with AR, positive cells were mainly identifiableas infiltrating inflammatory cells, which in many cases sur-rounded both vessels and tubular structures (Fig. 1, A and C).Sections hybridized with a sense CXCL10 RNA probe showedvirtually no signal (Fig. 1B). Double immunostaining forCXCL10 and �-SMA, CK, vWf, and CD68 confirmed that inAR, monocytes/macrophages were the main source of thischemokine (Fig. 1C).
Biopsy specimens from kidneys of patients affected byCAN were also examined. High CXCL10 mRNA (Fig. 1, D toH) expression was consistently found even in these speci-mens, but the signal was not only localized to infiltrating in-flammatory cells but also to proximal and distal tubules, aswell as to medullary collecting ducts (Fig. 1, D and E). More-over, some resident glomerular cells and vascular structuresexpressed CXCL10 mRNA (Fig. 1, F to H).
Combined in situ hybridization and immunohisto-chemistry or double immunostaining for CXCL10 and
1216 Transplantation • Volume 79, Number 9, May 15, 2005
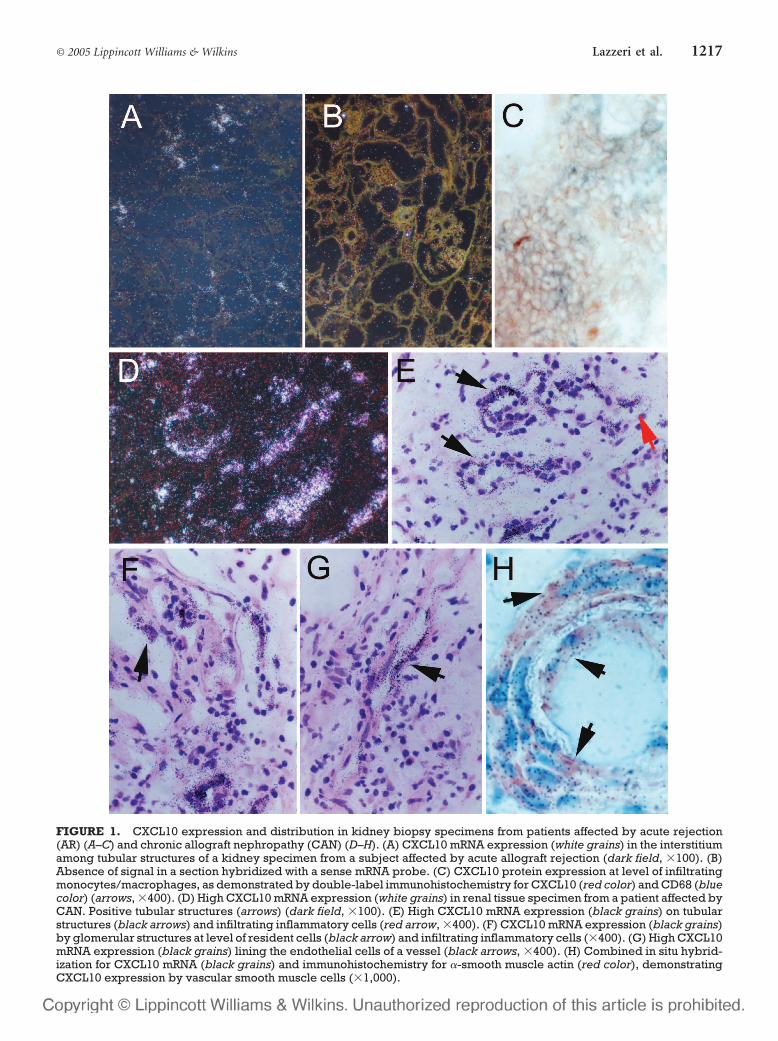
FIGURE 1. CXCL10 expression and distribution in kidney biopsy specimens from patients affected by acute rejection(AR) (A–C) and chronic allograft nephropathy (CAN) (D–H). (A) CXCL10 mRNA expression (white grains) in the interstitiumamong tubular structures of a kidney specimen from a subject affected by acute allograft rejection (dark field, �100). (B)Absence of signal in a section hybridized with a sense mRNA probe. (C) CXCL10 protein expression at level of infiltratingmonocytes/macrophages, as demonstrated by double-label immunohistochemistry for CXCL10 (red color) and CD68 (bluecolor) (arrows, �400). (D) High CXCL10 mRNA expression (white grains) in renal tissue specimen from a patient affected byCAN. Positive tubular structures (arrows) (dark field, �100). (E) High CXCL10 mRNA expression (black grains) on tubularstructures (black arrows) and infiltrating inflammatory cells (red arrow, �400). (F) CXCL10 mRNA expression (black grains)by glomerular structures at level of resident cells (black arrow) and infiltrating inflammatory cells (�400). (G) High CXCL10mRNA expression (black grains) lining the endothelial cells of a vessel (black arrows, �400). (H) Combined in situ hybrid-ization for CXCL10 mRNA (black grains) and immunohistochemistry for �-smooth muscle actin (red color), demonstratingCXCL10 expression by vascular smooth muscle cells (�1,000).
© 2005 Lippincott Williams & Wilkins 1217Lazzeri et al.
�-SMA, CK, vWf, and CD68 provided direct evidence thatvascular smooth muscle cells (SMC) (Fig. 1H), in addition toendothelial cells, tubular epithelial cells, and monocytes/macrophages (data not shown), were the main sources ofCXCL10.
CXCL10 Pretransplant Serum Levels PredictRecipient’s Risk of Early, Severe AcuteRejection, Chronic Allograft Nephropathy, andGraft Failure
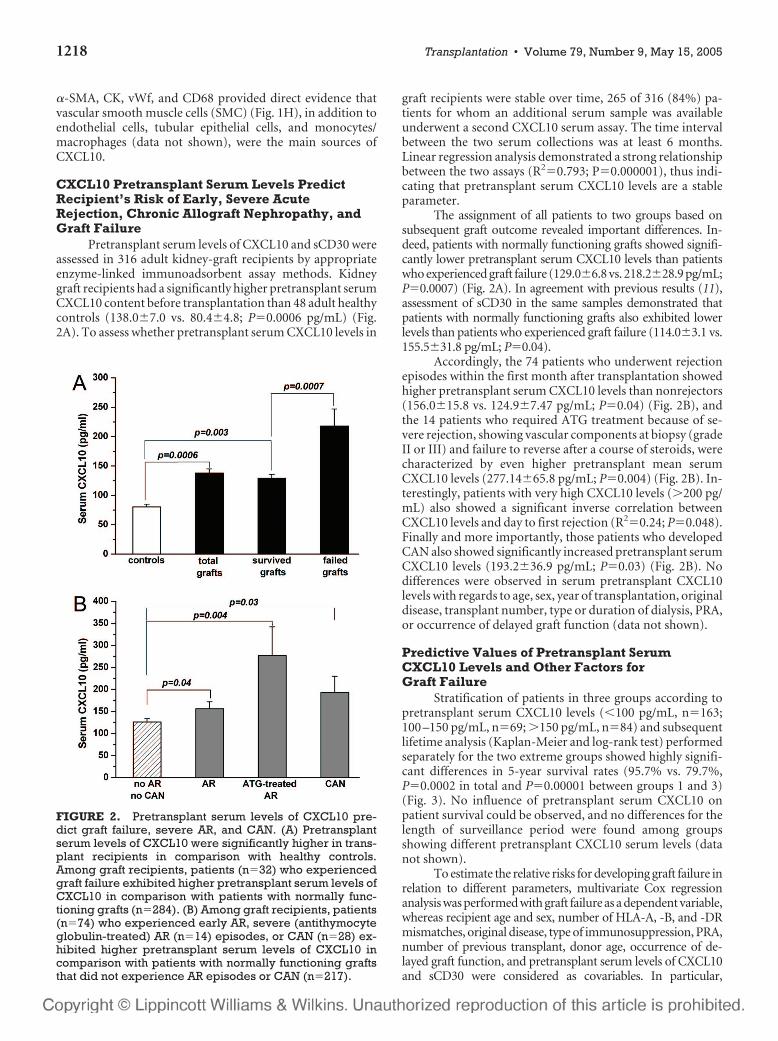
Pretransplant serum levels of CXCL10 and sCD30 wereassessed in 316 adult kidney-graft recipients by appropriateenzyme-linked immunoadsorbent assay methods. Kidneygraft recipients had a significantly higher pretransplant serumCXCL10 content before transplantation than 48 adult healthycontrols (138.0�7.0 vs. 80.4�4.8; P�0.0006 pg/mL) (Fig.2A). To assess whether pretransplant serum CXCL10 levels in
graft recipients were stable over time, 265 of 316 (84%) pa-tients for whom an additional serum sample was availableunderwent a second CXCL10 serum assay. The time intervalbetween the two serum collections was at least 6 months.Linear regression analysis demonstrated a strong relationshipbetween the two assays (R2�0.793; P�0.000001), thus indi-cating that pretransplant serum CXCL10 levels are a stableparameter.
The assignment of all patients to two groups based onsubsequent graft outcome revealed important differences. In-deed, patients with normally functioning grafts showed signifi-cantly lower pretransplant serum CXCL10 levels than patientswho experienced graft failure (129.0�6.8 vs. 218.2�28.9 pg/mL;P�0.0007) (Fig. 2A). In agreement with previous results (11),assessment of sCD30 in the same samples demonstrated thatpatients with normally functioning grafts also exhibited lowerlevels than patients who experienced graft failure (114.0�3.1 vs.155.5�31.8 pg/mL; P�0.04).
Accordingly, the 74 patients who underwent rejectionepisodes within the first month after transplantation showedhigher pretransplant serum CXCL10 levels than nonrejectors(156.0�15.8 vs. 124.9�7.47 pg/mL; P�0.04) (Fig. 2B), andthe 14 patients who required ATG treatment because of se-vere rejection, showing vascular components at biopsy (gradeII or III) and failure to reverse after a course of steroids, werecharacterized by even higher pretransplant mean serumCXCL10 levels (277.14�65.8 pg/mL; P�0.004) (Fig. 2B). In-terestingly, patients with very high CXCL10 levels (�200 pg/mL) also showed a significant inverse correlation betweenCXCL10 levels and day to first rejection (R2�0.24; P�0.048).Finally and more importantly, those patients who developedCAN also showed significantly increased pretransplant serumCXCL10 levels (193.2�36.9 pg/mL; P�0.03) (Fig. 2B). Nodifferences were observed in serum pretransplant CXCL10levels with regards to age, sex, year of transplantation, originaldisease, transplant number, type or duration of dialysis, PRA,or occurrence of delayed graft function (data not shown).
Predictive Values of Pretransplant SerumCXCL10 Levels and Other Factors forGraft Failure
Stratification of patients in three groups according topretransplant serum CXCL10 levels (�100 pg/mL, n�163;100 –150 pg/mL, n�69; �150 pg/mL, n�84) and subsequentlifetime analysis (Kaplan-Meier and log-rank test) performedseparately for the two extreme groups showed highly signifi-cant differences in 5-year survival rates (95.7% vs. 79.7%,P�0.0002 in total and P�0.00001 between groups 1 and 3)(Fig. 3). No influence of pretransplant serum CXCL10 onpatient survival could be observed, and no differences for thelength of surveillance period were found among groupsshowing different pretransplant CXCL10 serum levels (datanot shown).
To estimate the relative risks for developing graft failure inrelation to different parameters, multivariate Cox regressionanalysis was performed with graft failure as a dependent variable,whereas recipient age and sex, number of HLA-A, -B, and -DRmismatches, original disease, type of immunosuppression, PRA,number of previous transplant, donor age, occurrence of de-layed graft function, and pretransplant serum levels of CXCL10and sCD30 were considered as covariables. In particular,
FIGURE 2. Pretransplant serum levels of CXCL10 pre-dict graft failure, severe AR, and CAN. (A) Pretransplantserum levels of CXCL10 were significantly higher in trans-plant recipients in comparison with healthy controls.Among graft recipients, patients (n�32) who experiencedgraft failure exhibited higher pretransplant serum levels ofCXCL10 in comparison with patients with normally func-tioning grafts (n�284). (B) Among graft recipients, patients(n�74) who experienced early AR, severe (antithymocyteglobulin-treated) AR (n�14) episodes, or CAN (n�28) ex-hibited higher pretransplant serum levels of CXCL10 incomparison with patients with normally functioning graftsthat did not experience AR episodes or CAN (n�217).
1218 Transplantation • Volume 79, Number 9, May 15, 2005

CXCL10 was entered as a dichotomous variable for valuesgreater than 150 pg/mL and because previous studies demon-strated an increased risk of graft failure only when sCD30 levelsare greater than 100 U/mL (14), sCD30 was analyzed as a cate-goric variable for values below and above 100 U/mL. The resultsconfirmed a significant increased risk (risk ratio 2.801; confi-dence interval 1.201–6.536; P�0.017) for developing graft fail-ure in such patients (Table 1). In agreement with previous results(12), multivariate analysis confirmed the importance of twoother variables, donor age and delayed graft function, that had asignificant predictive power for graft failure (Table 1).
DISCUSSIONDespite the administration of immunosuppressants,
allograft rejection remains the primary cause of human renal-transplant failure. AR is particularly frequent in the earlyposttransplant period and despite the graft loss in only a smallpercentage of subjects represents a leading cause of morbilityand hospitalization and predisposes renal allografts to thedevelopment of CAN (16). Large experimental evidence em-phasizes the important role of CXCL10 in the initiation andamplification of host alloresponses that lead to AR. CXCL10not only mediates leukocyte recruitment to rejecting allo-grafts but is also a critical initiator of alloimmune response tothe antigen (17); inasmuch, CXCL10 drives T-cell prolifera-tion to allogenic and antigenic stimulation and interferon-�secretion in response to antigenic challenge (17). Accord-ingly, CXCL10-deficient mice have impaired T-cell re-sponses, impaired contact hypersensitivity response, limitedinflammatory cell infiltrates, and are unable to control viralinfections (17). In addition to its powerful effects within im-mune responses (17), CXCL10 also alters vascular cell func-tions (18 –24). Indeed, CXCL10 can induce SMC (19) andmesangial cell proliferation (14, 19, 20) and also acts as apowerful angiostatic factor (21, 22) on activated endothelium(22–24). The dual targets of CXCL10 suggest a possible rolefor this chemokine, not only in the pathogenesis of AR butalso of CAN. Indeed, CAN is characterized by endothelial cellinjury, vascular SMC proliferation, and mesangial expansion(1).
In this study, we demonstrate that CXCL10 is highlyexpressed not only in the kidney of subjects with AR but alsowith CAN. In AR, the main sources of CXCL10 were infiltrat-ing inflammatory cells, particularly macrophages. More im-portantly, we demonstrate for the first time that the source ofCXCL10 in CAN are several cell types, including not only
FIGURE 3. Association of pretransplant serum CXCL10levels with cadaver kidney-graft survival. Better graft sur-vival rate in recipients with very low serum CXCL10 levels(�100 pg/mL; n�163) than in recipients with intermediateserum CXCL10 levels (100–150 pg/mL; n�69) or very highserum CXCL10 levels (�150 pg/mL; n�84) (P�0.0002).Death with a functioning graft was not counted as graft fail-ure in this analysis.
TABLE 1. Multivariate analysis showing the relative risk of graft failure according to selected risk factors
P value Relative risk
95.0% CI
Lower Upper
Cold ischemia time 0.247 1.036 0.975 1.101
CXCL10 �150 pg/mL 0.017 2.801 1.201 6.536
Recipient gender 0.476 0.719 0.290 1.783
Original disease 0.382 1.047 0.945 1.160
Type of dialysis 0.860 1.095 0.397 3.022
Transplant no. 0.728 1.370 0.233 8.055
MMA 0.599 0.850 0.463 1.559
MMB 0.969 0.986 0.498 1.954
MMDR 0.409 1.427 0.614 3.316
Donor sex 0.314 1.524 0.672 3.456
PRA 0.669 0.752 0.204 2.777
Recipient age 0.178 0.971 0.931 1.013
Type of immunosuppression 0.263 3.670 0.377 35.771
Donor age 0.004 1.053 1.016 1.091
CD30 �100 U/mL 0.603 1.267 0.519 3.089
Delayed graft function 0.003 3.728 1.565 8.884
CI, confidence interval; MMA, HLA-A mismatches; MMB, HLA-B mismatches, MMDR, HLA-DR mismatches.
© 2005 Lippincott Williams & Wilkins 1219Lazzeri et al.

infiltrating mononuclear cells but also vascular and tubularstructures. These findings provide clear evidence that persis-tent CXCL10 expression can be found in CAN, and this ob-servation provides a further possible link between AR andCAN. In a previous study, we suggested that pretransplantserum CXCL10 might predict the long-term success of renaltransplantation (15). Furthermore, Hu et al. (25) found thatCXCL10 is increased in the urine of patients with AR and is amore sensitive and predictive parameter than serum creati-nine in terms of monitoring the response to antirejectiontherapy. On the basis of this experimental evidence, we alsoinvestigated whether pretransplant determination ofCXCL10 serum levels may predict the recipient’s risk of se-vere, early AR and CAN.
It has been a primary goal of transplant immunologiststo develop tests for assessing the pretransplant risk of patientsfor immunologic rejection and graft failure. Various risk fac-tors— including recipient age and sex, number of HLA-A, -B,and -DR mismatches, original disease, type of immunosup-pression, PRA, number of previous transplant, donor age,delayed graft function and pretransplant serum levels ofsCD30 greater than 100 U/mL— have all been proposed asmeans for differentiating between patients with a goodchance of long-term survival of a renal allograft and thosewith a poor chance. However, at least in our patients, onlypretransplant serum CXCL10 levels greater than 150 pg/mLand the occurrence of delayed graft function had a predictivepower of allograft loss. Accordingly, pretransplant quantita-tion of CXCL10 serum levels were also able to predict therecipient’s risk of early, severe AR and CAN. Interestingly,patients with very high CXCL10 levels also showed a signifi-cant inverse correlation between CXCL10 levels and day tofirst rejection, suggesting that the highest CXCL10 levels cor-respond with the least days for occurrence of AR.
Therefore, it is reasonable to speculate that patientswith high serum CXCL10 pretransplant levels develop severeAR episodes because of increased immune activation but arealso more prone to generation of intimal hyperplasia, chronicendothelial cell damage, and vascular necrosis that result inCAN and finally in graft failure (17–24). Finally, the demon-stration that pretransplant serum CXCL10 levels are a clini-cally useful parameter for the identification of subjects exhib-iting high risk of AR, CAN, and graft failure suggests thatthese subjects may require heavier posttransplant immuno-suppressive regimens.
REFERENCES1. Rossi D, Zlotnik A. The biology of chemokines and their receptors.
Annu Rev Immunol 2000; 18: 217.2. Hancock WW, Gao W, Csizmadia V, et al. Donor-derived IP-10 ini-
tiates development of acute allograft rejection. J Exp Med 2001; 193(8):975.
3. Hancock WW, Lu B, Gao W, et al. Requirement of the chemokinereceptor CXCR3 for acute allograft rejection. J Exp Med 2000; 192(10):1515.
4. Zhang Z, Kaptanoglu L, Haddad W, et al. Donor T cell activation ini-tiates small bowel allograft rejection through an IFN-�-inducible pro-tein-10-dependent mechanism. J Immunol 2002; 168(7): 3205.
5. Segerer S, Cui Y, Eitner F, et al. Expression of chemokines and chemo-kine receptors during human renal transplant rejection. Am J KidneyDis 2001; 37(3): 518.
6. Agostini C, Calabrese F, Rea F, et al. CXCR3 and its ligand CXCL10 areexpressed by inflammatory cells infiltrating lung allografts and mediatechemotaxis of T cells at sites of rejection. Am J Pathol 2001; 158(5):1703.
7. Melter M, Exeni A, Reinders ME, et al. Expression of the chemokinereceptor CXCR3 and its ligand IP-10 during human cardiac allograftrejection. Circulation 2001; 104(21): 2558.
8. Fahmy NM, Yamani MH, Starling RC, et al. Chemokine and chemo-kine receptor gene expression indicates acute rejection of human car-diac transplants. Transplantation 2003; 75(1): 72.
9. Zhao DX, Hu Y, Miller GG, et al. Differential expression of the IFN--inducible CXCR3-binding chemokines, IFN-inducible protein 10,monokine induced by IFN, and IFN-inducible T Cellchemoattractant in human cardiac allografts: association with cardiacallograft vasculopathy and acute rejection. J Immunol 2002; 169(3):1556.
10. Akalin E, Dikman S, Murphy B, et al. Glomerular infiltration byCXCR3� ICOS� activated T cells in chronic allograft nephropathywith transplant glomerulopathy. Am J Transplant 2003; 3(9): 1116.
11. Susal C, Pelzl S, Dohler B, et al., for the Collaborative Transplant Study.Identification of highly responsive kidney transplant recipients usingpretransplant soluble CD30. J Am Soc Nephrol 2002; 13: 1650.
12. Perico N, Cattaneo D, Sayegh MH, et al. Delayed graft function inkidney transplantation. Lancet 2004; 364: 1814.
13. Solez K, Benediktsson H, Cavallo T, et al. Report of the Third BanffConference on Allograft Pathology (July 20 –24, 1995) on classificationand lesion scoring in renal allograft pathology. Transplant Proc 1996;28: 441.
14. Romagnani P, Lazzeri E, Lasagni L, et al. IP-10 and Mig production byglomerular cells in human proliferative glomerulonephritis and regu-lation by nitric oxide. J Am Soc Nephrol 2002;13:53.
15. Rotondi M, Rosati A, Buonamano A, et al. High pretransplant serumlevels of CXCL10/IP-10 are related to increased risk of renal allograftfailure. Am J Transplant 2004; 4(9): 1466.
16. Kahan BD, Ponticelli C, eds. Principles and practice in renal transplan-tation. London, Martin Dunitz Ltd 2000, p. 846.
17. Dufour JH, Dziejman M, Liu MT, et al. IFN-gamma-inducible protein10 (IP-10;CXCL10)-deficient mice reveal a role for IP-10 in effector Tcell generation and trafficking. J Immunol 2002; 168(7): 3195.
18. Lazzeri E, Romagnani P. CXCR3-binding chemokines: multifacetedtherapeutic targets. Curr Drug Targets Immune Endocr Metabol Disord2005; 5: 109.
19. Wang X, Yue TL, Ohlstein EH, et al. Interferon-inducible protein-10involves vascular smooth muscle cell migration, proliferation, and in-flammatory response. J Biol Chem 1996; 271: 24286.
20. Romagnani P, Beltrame C, Annunziato F, et al. Role for interactionsbetween IP-10/Mig and their receptor (CXCR3) in proliferative glo-merulonephritis. J Am Soc Nephrol 1999; 10: 2518.
21. Bonacchi A, Romagnani P, Romanelli RG, et al. Signal transduction bythe chemokine receptor CXCR3: activation of Ras/ERK, Src, and phos-phatidylinositol 3-kinase/Akt controls cell migration and proliferationin human vascular pericytes. J Biol Chem 2001; 276: 9945.
22. Romagnani P, Annunziato F, Lasagni L, et al. Cell cycle-dependentexpression of CXC chemokine receptor 3 by endothelial cells mediatesangiostatic activity. J Clin Invest 2001; 107: 53.
23. Romagnani P, Lasagni L, Annunziato F, et al. CXC chemokines: theregulatory link between angiogenesis and inflammation. Trends Immu-nol 2004; 25(4): 201.
24. Lasagni L, Francalanci M, Annunziato F, et al. An alternatively splicedvariant of CXCR3 mediates the IP-10, Mig and I-TAC induced-inhibi-tion of endothelial cell growth and acts as functional receptor for PF-4.J Exp Med 2003; 197: 1537.
25. Hu H, Aizenstein BD, Puchalski A, et al. Elevation of CXCR3-bindingchemokines in urine indicates acute renal-allograft dysfunction. Am JTransplant 2004; 4(3): 432.
1220 Transplantation • Volume 79, Number 9, May 15, 2005
Copyright © 2022 FDOKUMEN




















