Predictive action in infancy: tracking and reaching for moving objects
Heterogeneity in disease severity in a family with a novel G68V GCK activating mutation causing...
7
© 2007 The Authors. Journal compilation © 2007 Diabetes UK. Diabetic Medicine , 24 , 1393–1399 1393 DIABETIC Medicine DOI: 10.1111/j.1464-5491.2007.02285.x Blackwell Publishing Ltd Original Article: Treatment Original article Heterogeneity in disease severity in a family with a novel G68V GCK activating mutation causing persistent hyperinsulinaemic hypoglycaemia of infancy M. Wabitsch, G. Lahr, M. Van de Bunt*, C. Marchant*, M. Lindner†, J. von Puttkamer, A. Fenneberg, K. M. Debatin, R. Klein‡, S. Ellard§, A. Clark* and A. L. Gloyn* Paediatric Endocrinology, Department of Paediatrics, University of Ulm, Ulm, Germany, *Diabetes Research Laboratories, Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford, UK, †Department of Paediatrics, University of Heidelberg, Heidelberg, Germany, ‡Department of Forensic Medicine, University of Ulm, Ulm, Germany, §Institute of Biomedical Science and Clinical Medicine, Peninsula Medical School, Exeter, UK Accepted 19 June 2007 Abstract Background/aim Glucokinase ( GCK )-activating mutations cause persistent hyperinsulinaemic hypoglycaemia of infancy (PHHI). GCK-PHHI patients have regulated insulin secretion and can usually be treated with diazoxide. The six reported cases suggest that the severity of the mutation predicts the clinical phenotype. The aim of this study was to relate genotype to phenotype [clinical phenotype, glucose-stimulated insulin release (GSIR) and GCK functional analysis] in a large pedigree with eight affected individuals. Methods The genes encoding B-cell GCK and the K ATP channel subunits ( ABCC8 and KCNJ11 ) were sequenced to identify mutations for functional analysis. Genetic variants influencing B-cell function were genotyped in affected individuals. Islet secretory capacity was determined by oral glucose tolerance test Results A novel GCK mutation (G68V) co-segregating with hypoglycaemia was identified in eight family members. Kinetic analysis revealed that G68V-GCK activity is ~16 times more than wild-type-GCK with an increased affinity for glucose [concentration at half maximal activation (S 0.5 ) 1.94 ± 0.16 vs. 7.43 ± 0.12, mutant vs. wild type, mean ± SEM ]. Mathematical modelling predicted a threshold for GSIR of 1.9 mmol/l in the mutant. Oral glucose tolerance tests showed regulated insulin secretion. The severity of hypoglycaemia and related symptoms in affected subjects were heterogeneous. Clinical presentations were asymptomatic ( n = 1), extreme hunger ( n = 3), seizures ( n = 2) and loss of consciousness ( n = 2); 7/8 were managed with diet but the proband was treated with diazoxide and octreotide. Phenotypic modification by a second mutation in the K ATP channel genes ( ABCC8, KCNJ11 ) or by common genetic variants in KCNJ11 , GCK and TCF7L2 was excluded. Conclusion The novel activating GCK mutation G68V is associated with variable phenotypic severity, supporting modification of GSIR by genetic and/or environmental factors. Diabet. Med. 24, 1393–1399 (2007) Keywords diazoxide, genetics, glucokinase, octreotide, persistent hyperinsulinaemic hypoglycaemia of infancy Abbreviations GCK, glucokinase; GSIR, glucose-stimulated insulin release; GST, glutathionyl S-transferase; PHHI, persistent hyperinsulinaemic hypoglycaemia of infancy; T2DM, Type 2 diabetes; WT, wild type Introduction Activating glucokinase ( GCK ) mutations are a rare cause of persistent hyperinsulinaemic hypoglycaemia of infancy (PHHI). Five mutations have been reported in six families and studies have shown that insulin secretion is regulated but the threshold for glucose-stimulated insulin release (GSIR) is reduced [1–5]. Early studies suggested that GCK-PHHI is a relatively mild Correspondence to : Dr Anna L Gloyn, Diabetes Research Laboratories, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, Old Road, Headington, Oxford, OX3 7LJ, UK. E-mail: [email protected]
Transcript of Heterogeneity in disease severity in a family with a novel G68V GCK activating mutation causing...

© 2007 The Authors.Journal compilation © 2007 Diabetes UK.
Diabetic Medicine
,
24
, 1393–1399
1393
DIABETIC
Medicine
DOI: 10.1111/j.1464-5491.2007.02285.x
Blackwell Publishing Ltd
Original Article: Treatment
Original article
Heterogeneity in disease severity in a family with a novel G68V
GCK
activating mutation causing persistent hyperinsulinaemic hypoglycaemia of infancy
M. Wabitsch, G. Lahr, M. Van de Bunt*, C. Marchant*, M. Lindner†, J. von Puttkamer, A. Fenneberg, K. M. Debatin, R. Klein‡, S. Ellard§, A. Clark* and A. L. Gloyn*
Paediatric Endocrinology, Department of Paediatrics, University of Ulm, Ulm, Germany, *Diabetes Research Laboratories, Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford, UK, †Department of Paediatrics, University of Heidelberg, Heidelberg, Germany, ‡Department of Forensic Medicine, University of Ulm, Ulm, Germany, §Institute of Biomedical Science and Clinical Medicine, Peninsula Medical School, Exeter, UK
Accepted 19 June 2007
Abstract
Background/aim
Glucokinase (
GCK
)-activating mutations cause persistent hyperinsulinaemic hypoglycaemia ofinfancy (PHHI). GCK-PHHI patients have regulated insulin secretion and can usually be treated with diazoxide. The sixreported cases suggest that the severity of the mutation predicts the clinical phenotype. The aim of this study was to relategenotype to phenotype [clinical phenotype, glucose-stimulated insulin release (GSIR) and GCK functional analysis] in alarge pedigree with eight affected individuals.
Methods
The genes encoding B-cell GCK and the K
ATP
channel subunits (
ABCC8
and
KCNJ11
) were sequenced to identifymutations for functional analysis. Genetic variants influencing B-cell function were genotyped in affected individuals. Isletsecretory capacity was determined by oral glucose tolerance test
Results
A novel
GCK
mutation (G68V) co-segregating with hypoglycaemia was identified in eight family members. Kineticanalysis revealed that G68V-GCK activity is ~16 times more than wild-type-GCK with an increased affinity forglucose [concentration at half maximal activation (S
0.5
) 1.94
±
0.16 vs. 7.43
±
0.12, mutant vs. wild type, mean
±
SEM
].Mathematical modelling predicted a threshold for GSIR of 1.9 mmol/l in the mutant. Oral glucose tolerance tests showedregulated insulin secretion. The severity of hypoglycaemia and related symptoms in affected subjects were heterogeneous.Clinical presentations were asymptomatic (
n
=
1), extreme hunger (
n
=
3), seizures (
n
=
2) and loss of consciousness(
n
=
2); 7/8 were managed with diet but the proband was treated with diazoxide and octreotide. Phenotypic modificationby a second mutation in the K
ATP
channel genes (
ABCC8, KCNJ11
) or by common genetic variants in
KCNJ11
,
GCK
and
TCF7L2
was excluded.
Conclusion
The novel activating
GCK
mutation G68V is associated with variable phenotypic severity, supportingmodification of GSIR by genetic and/or environmental factors.
Diabet. Med. 24, 1393–1399 (2007)
Keywords
diazoxide, genetics, glucokinase, octreotide, persistent hyperinsulinaemic hypoglycaemia of infancy
Abbreviations
GCK, glucokinase; GSIR, glucose-stimulated insulin release; GST, glutathionyl S-transferase; PHHI,persistent hyperinsulinaemic hypoglycaemia of infancy; T2DM, Type 2 diabetes; WT, wild type
Introduction
Activating glucokinase (
GCK
) mutations are a rare cause ofpersistent hyperinsulinaemic hypoglycaemia of infancy (PHHI).Five mutations have been reported in six families and studieshave shown that insulin secretion is regulated but the thresholdfor glucose-stimulated insulin release (GSIR) is reduced [1–5].Early studies suggested that GCK-PHHI is a relatively mild
Correspondence to
: Dr Anna L Gloyn, Diabetes Research Laboratories, Oxford Centre for Diabetes, Endocrinology and Metabolism, Churchill Hospital, Old Road, Headington, Oxford, OX3 7LJ, UK. E-mail: [email protected]
dme_2285.fm Page 1393 Tuesday, November 13, 2007 7:20 PM
DIABETIC
Medicine Novel G68V activating
GCK
mutation causing PHHI •
M. Wabitsch et al.
© 2007 The Authors.
1394
Journal compilation © 2007 Diabetes UK.
Diabetic Medicine
,
24
, 1393–1399
disorder that can be treated with diazoxide and managed byeating regularly to avoid hypoglycaemic symptoms [1–3,5].However, as further cases are reported it is becoming clear thatthe phenotype can be severe, unresponsive to diaxozide andmay result in severe brain damage [4]. Characterization of
GCK
mutations suggests a correlation between clinical features andfunctional severity [6]. To examine this relationship, we studiedthe largest pedigree to date with eight affected individuals tofirstly establish the mutational mechanism for the hypoglycaemia,secondly to determine the variability in phenotype within a familyand finally to explore the natural history of GCK-PHHI.
Subjects, materials and methods
Subjects
The female proband was born at term to non-consanguineousparents. Because of loss of a previous child at 4 months old[recorded as sudden infant death syndrome (SIDS) of unknowncause], the proband was monitored (breathing/apnoea control)and apnoea was frequent. This resulted in extensive diagnostic
tests. Symptomatic recurrent hypoglycaemia was documented at7 months (fasting plasma glucose levels ~1.7 mmol/l) associatedwith hyperinsulinaemia. Associated symptoms of trembling,extreme crying and sweating were observed and several hypogly-caemic seizures occurred. Regular glucose monitoring wasperformed from infancy. Capillary blood glucose measurementswere taken every 2 h. Complex carbohydrates (commerciallyavailable parental nutrition enriched with starch) were givenorally during the day and via an intestinal tube during periodsof low glucose at night, allowing normal neurological develop-ment to be achieved. Liver and pancreas needle biopsies wereperformed. The diagnosis of an activating
GCK
mutation wasestablished at the age of 7 years. The patient is currently treatedwith diazoxide (3 mg/kg/day) and octreotide (17
μ
g/kg/day).Higher doses of diazoxide were not accepted by the proband’smother because of hypertrichosis in the proband. However, thiscombined treatment regime has resulted in very stable glucosevalues.
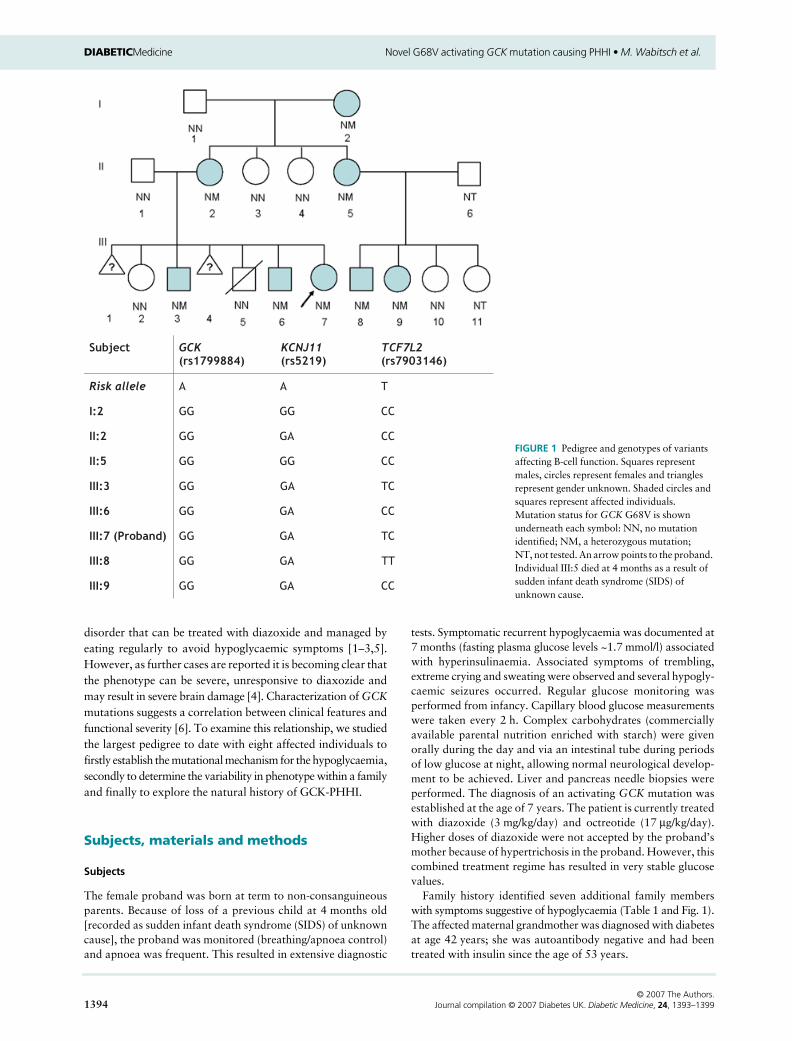
Family history identified seven additional family memberswith symptoms suggestive of hypoglycaemia (Table 1 and Fig. 1).The affected maternal grandmother was diagnosed with diabetesat age 42 years; she was autoantibody negative and had beentreated with insulin since the age of 53 years.
FIGURE 1 Pedigree and genotypes of variants affecting B-cell function. Squares represent males, circles represent females and triangles represent gender unknown. Shaded circles and squares represent affected individuals. Mutation status for GCK G68V is shown underneath each symbol: NN, no mutation identified; NM, a heterozygous mutation; NT, not tested. An arrow points to the proband. Individual III:5 died at 4 months as a result of sudden infant death syndrome (SIDS) of unknown cause.
dme_2285.fm Page 1394 Tuesday, November 13, 2007 7:20 PM

Original article
DIA
BETIC
Medicine
© 2007 The A
uthors.Journal com
pilation © 2007 D
iabetes UK
.
Diabetic M
edicine
,
24
, 1393–1399
1395
Table 1
Clinical characteristics of patients with G68V
GCK
mutation
Patient
III:9 proband III:7 I:2 II:2 III:3 III:6 II:5 III:8
Age at onset Infancy NA NA Infancy Infancy NA Infancy InfancyAge at genetic diagnosis (years) 7 64 40 18 15 35 9 7Gender (M/F) F F F M M F M FGestational week 40 NA 40 40 42 NA 40 36Birthweight (kg) 3.66 NA 3.24 3.17 3.77 NA 2.92 1.87BMI (kg/m
2
) 16.8 36.3 25.2 20.7 18.7 23.7 12.0 13.6BMI-SDS 0.35 3.30 1.25 –0.33 –0.49 0.85 –3.45 –1.37FPG (mmol/l) 1.6 ND 3.0 2.5 2.9 3.3 3.2 3.1Plasma insulin (pmol/ l) 45.5 ND 17.5 18 24.5 12 6.3 7.7C-peptide (nmol/ l) ND ND 49.9 33.3 40.0 46.2 16.7 36.6Proinsulin (pmol/ l) ND ND 2.5 3.0 1.6 2.4 2.0 5.2Lipid profile Normal Abnormal* Normal Normal Normal Normal Normal NormalClinical symptoms Trembling, extreme
crying, sweating, hypoglycaemic seizures
Diabetes since age 42 years, insulin dependent since age 53 years
Extreme hunger, occasional sweatiness, loss of consciousness
Extreme hunger, occasional sweatiness, seizures of unknown origin in childhood, dyslexia
Extreme hunger, occasional sweatiness
Learning difficulties, occasional loss of consciousness during childhood
Extreme hunger, learning handicap
Extreme hunger
Management and treatment Blood glucose monitoring, intestinal carbohydrate application; medication: diazoxide, octreotide
No specific treatment for hypoglycaemia
Diet Diet Diet Diet Diet Diet
BMI, body mass index; FPG, fasting plasma glucose; M/F, male/female; NA, not available; ND, not determined; SDS, standard deviation score.*LDL cholesterol 3.9 mmol/ l, triglycerides 195.5 mmol/ l.
dme_2285.fm
Page 1395 Tuesday, N
ovember 13, 2007 7:20 PM

DIABETIC
Medicine Novel G68V activating
GCK
mutation causing PHHI •
M. Wabitsch et al.
© 2007 The Authors.
1396
Journal compilation © 2007 Diabetes UK.
Diabetic Medicine
,
24
, 1393–1399
Genetic analysis
Genomic DNA was isolated from peripheral blood lymphocytesor archival formalin-fixed paraffin section (post-mortem specimenof the deceased brother III:5) using the QIAamp Flexi GeneDNA kit (Qiagen, Hilden, Germany).
GCK
sequencing wasperformed using standard protocols (primer sequences avail-able on request). Genotyping of the DNA sample from III:5 wasperformed by minisequencing of short GCK-PCR ampliconsusing the SNaPshot kit (Applied Biosystems, Darmstadt,Germany). SNaPshot products were analysed on an ABI310capillary sequencer. Sequencing of the
ABCC8
and
KCNJ11
genes were performed as previously described [7,8].
TCF7L2
genotyping (rs7903146, rs4506565, rs12255372, rs12243326)was performed using a KASPar based assay on the ABI 3900HT(details available on request). The four
TCF7L2
single nucleotidepolymorphisms (SNPs) are in strong linkage disequilibrium(LD;
r
2
>
0.7) allowing genotype quality control to be ascertainedby genotype concordance.
Biochemical characterization of G68V glucokinase
Recombinant human islet wild-type (WT) enzyme and mutantG68V GCK were generated and expressed in the form ofglutathionyl S-transferase (GST) fusion proteins as previouslydescribed with the following modifications [3]. The
Escherichiacoli
cell line BCL2 was used to improve protein yield, and thepurity of WT and mutant GST-GCK was assessed on the 2100Bioanalyser (Agilent Technologies, Wokingham, UK). Structuralanalysis was performed using a homology model based on theWT-GCK crystal structure [9].
Clinical investigations
Commercially available assays were used to determine insulinand C-peptide [electrochemiluminescence immunoassay(ECLIA), Modular Analytics E 170, Roche Diagnostics,Mannheim, Germany], proinsulin (enyzme immunoassay;IBL, Hamburg, Germany), and triglycerides and cholesterol(Dimension RxL Max; Dade Behring, Liederbach, Germany).The glucose concentration was determined in haemolysates(glucose oxidase, Ecomatic; Care Diagnostica, Voerde, Germany).Regulation of insulin secretion was examined in affected subjectsby oral glucose tolerance (1.75 g/kg body weight glucose—maximum 75 g) following an overnight fast (17 h). Blood glucose,insulin and proinsulin were determined in samples taken atintervals for up to 2 h (0, 30, 60, 90 and 120 min). All clinicalinvestigations were approved by the ethical committee of theUniversity Hospital of Ulm.
Histological examination
Sections were cut from formalin-fixed, wax-embedded biopsyspecimens of pancreas and liver of the proband for immuno-cytochemistry: insulin- and glucagon-positive cells were identifiedin adjacent sections using specific polyclonal antibodies andimmunoperoxidase. In hepatic and islet cells, glucokinasewas identified using polyclonal antiserum to glucokinase (C-terminal; Abgent, San Diego, CA, USA) and immunoperoxidase.
Distribution of islet cells in the proband was compared with asimilarly labelled, pancreatic specimen from an age-matchedcontrol subject who died from unknown causes.
Results
Genetic analysis
A novel heterozygous missense mutation (c.203G
>
T; p.Gly68Val)was identified in the proband. This G68V mutation co-segregated with hypoglycaemia (Fig. 1) but was not present inthe deceased sibling nor was it identified in 200 chromosomesfrom unrelated normal subjects. No mutations in
KCNJ11
or
ABCC8
were identified in the proband. The genotype of theislet promoter
GCK
-30 G
>
A (rs1799884: G
>
A), the
KCNJ11
E23K (rs5219: G
>
A), and the
TCF7L2
rs7903146: C
>
T,rs4506565: T
>
A, rs12255372: G
>
T, rs12243326: T
>
C variantswere also investigated in the G68V mutation carriers. Allindividuals were homozygous WT for the common
GCK
isletpromoter variant rs1799884 G allele. Individuals I:2 and II:5were homozygous (GG) for
KCNJ11
E23K whilst all otheraffected individuals were heterozygous (GA). For the
TCF7L2
variants, all genotypes for individuals were concordant. Anumber of affected individuals (I:2, II:2, II:5, III:6, III:9) werehomozygous for the WT allele, whilst two individuals, includingthe proband (III:7 and III:3), were heterozygous. One individual(III:8) was homozygous for the risk allele. The genotypingresults are illustrated in Fig. 1.
Biochemical and structural characterization of G68V
Purified mutant GCK showed a significant increase in affinityfor glucose indicated by a ~4-fold reduction in glucose con-centration at half maximal activation (S
0.5
; 1.94
±
0.16 vs.7.43
±
0.12 G68V and WT, respectively). The Hill numberwas slightly decreased (1.25
±
0.02 vs. 1.49
±
0.04 G68V andWT, respectively) whilst the maximal specific activity (K
cat
)was slightly increased (67.99
±
4.80 vs. 57.11
±
7.15 G68V andWT, respectively). Concentration at half maximal activation(K
m
) for ATP was decreased (0.28
±
0.04 vs. 0.45
±
0.05 forG68V and WT, respectively). The effective activation ofmutant GCK is expressed by the increased activity index of ~16compared with WT extrapolating to a marked enhancement ofB-cell glucose usage [6]. Structural analysis of G68V showedthat the mutated residue localizes to the allosteric activator site.The physiological consequences of the kinetic characteristicsof G68V on GSIR, and therefore glucose homeostasis, wasinvestigated using the published mathematical model whichtakes into account the impact of blood glucose levels on GCKexpression of both alleles [6]. Using this model, a predictedthreshold of 1.9 mmol/l was obtained.
Response to an oral glucose tolerance test
The oral glucose tolerance test in individuals with the G68Vmutation showed considerable variation. Insulin response was
dme_2285.fm Page 1396 Tuesday, November 13, 2007 7:20 PM

Original article
DIABETIC
Medicine
© 2007 The Authors.Journal compilation © 2007 Diabetes UK.
Diabetic Medicine
,
24
, 1393–1399
1397
regulated, with fasting insulin levels in the normal range(
<
70 pmol/l) and only inappropriately high for the measuredglucose concentrations. One subject (III:3) had elevatedglucose and insulin levels at 1 h (Fig. 2a and b).
Histology
Pancreatic islet morphology in the proband was not differentto an age-matched control pancreas: islet size and distributionof cell types was normal with some hormone-positive cellsfound adjacent to ductal cells; islet cells were insulin andglucokinase positive (Fig. 3). The density of glucokinase labellingwas heterogeneous in hepatocytes.
Discussion
The identification of
GCK
-activating mutations has increasedour understanding of the glucose sensor model for insulinsecretion. However, only five different mutations have beenreported and detailed phenotypic data is available for just 11patients [1–5]. We report a novel mutation (G68V) which co-segregates with hypoglycaemia in the largest reported pedigreeto date (eight affected individuals). The spectrum of clinicalphenotypes ranges from low blood glucose levels and extremehunger as the only clinical symptom to individuals with hypogly-caemia and seizures. The proband is the only individualrequiring pharmacological treatment.
Variability in phenotype is not uncommon in monogenicdisorders of B-cell function; there is variability in the age ofonset of diabetes with both
KCNJ11
and
HNF1A
/
TCF1
muta-tions within a family [7,10] and with other
GCK
-activatingmutations [1–3]. In previous reports, the spectrum of ages of
FIGURE 3 Pancreatic distribution of islets and islet cells. Distribution of insulin-positive cells in islets (Is) and adjacent to ducts (arrows) in a pancreas from (a) a control (aged 10 years) was similar to that in the proband (b). Adjacent pancreatic sections from the proband demonstrated normal distribution of insulin-positive cells (c). Glucokinase was present in a large proportion of islet cells (d), whereas a smaller, but normal, proportion of cells were glucagon positive (e). Scale bars: (a, b) = 100 μm; (c, d, e) 50 μm.
FIGURE 2 (a) Blood glucose levels (mmol/l) during an oral glucose tolerance test (OGTT) in affected individuals. Blood glucose levels during an oral glucose tolerance test in patients carrying the G68V GCK mutation are shown. (b) Insulin levels (pmol/l) during an oral glucose tolerance test in affected individuals. Blood insulin levels during an oral glucose tolerance test in patients carrying the G68V GCK mutation are shown.
dme_2285.fm Page 1397 Tuesday, November 13, 2007 7:20 PM

DIABETIC
Medicine Novel G68V activating
GCK
mutation causing PHHI •
M. Wabitsch et al.
© 2007 The Authors.
1398
Journal compilation © 2007 Diabetes UK.
Diabetic Medicine
,
24
, 1393–1399
diagnosis have ranged from birth to 30 years [1–3]. Pheno-typic modification might result from other genetic and/orenvironmental factors. In order to address this question, weexcluded an additional mutation in one of the K
ATP
channelgenes (
ABCC8
and
KCNJ11
) and modification by geneticvariants in
GCK
,
TCF7L2
and
KCNJ11
which influencepancreatic B-cell function [11–14]. If we hypothesize that thephenotypic variation seen in this family is influenced bycommon genetic variants which affect pancreatic B-cell function,one would anticipate that the proband with the severe clinicalphenotype would harbour the protective alleles of the variantswhich predispose to B-cell dysfunction. It would be temptingto speculate that individuals with the G68V mutation who alsohave the GCK-30 risk allele on their normal chromosomecould have a less severe phenotype, as it has been shown thatthis variant results in an average increase in fasting plasmaglucose of 0.06 mmol/l [11,15]. However, our results wouldsuggest this is unlikely as, firstly, none of the affected individualshas the GCK-30 variant and, secondly, the proband is hetero-zygous for the risk allele for the genetic variant with the largesteffect size described to data (
TCF7L2
). The genotype profile ofthe proband for the variants tested is not distinguishable fromthe rest of the family members (Fig. 1). Given the limited sizeof this study and our knowledge of the numbers required todetect such genetic modifications [16], the study of furtherreplicated and established genetic variants influencing glucosehomeostasis in this, and other families, with GCK-HI will benecessary to establish if common genetic variants whichinfluence B-cell function play a role in phenotypic modification.
There has been debate as to whether patients with neonatalhyperinsulinism are more likely to develop Type 2 diabetes(T2DM) later in life as a result of B-cell exhaustion. A previousstudy in a Finnish family has illustrated that mutations in the
ABCC8
gene can present as hypoglycaemia during infancy anddiabetes in adulthood [17]. More recently, Pearson andcolleagues have described cases of transient hypoglycaemia inthe neonatal period followed by maturity-onset diabetes inearly adulthood as a result of
HNF4A
mutations [18]. It remainsunclear from the current literature whether this is the case for
GCK
-activating mutations. Two of the six pedigrees reportedto date have at least one family member with T2DM [1,2],whilst the other reported cases were either sporadic [4] or theeldest affected generation were still under 40 years of age [3].It is noteworthy in our current study that the affected maternalgrandmother of the index patient had early onset of T2DMat 42 years of age and has been insulin dependent since age53 years. It is of course possible that the diabetes in the grand-mother is just coincidental and associated with her elevatedbody mass index (BMI; 36.3 kg/m
2
), but the early onset couldbe exacerbated by B-cell exhaustion. Her elevated triglyceridesand low-density lipoprotein cholesterol are consistent withdiabetes associated with obesity and insulin resistance. Anotherpotential point of interest is that one could hypothesize thatpatients with GCK-PHHI could be protected from developingT2DM because of their mildly elevated insulin levels, which
could compensate for insulin resistance. This would after allbe analogous to patients with impaired glucose tolerance orimpaired fasting glucose being treated with GCK activators[9,19,20] in order to prevent their progression to diabetes.Given the increasing prevalence of T2DM in the population,further longitudinal studies of patients with GCK-PHHI willbe required to tease out whether B-cell exhaustion is part of theclinical course of GCK-PHHI.
A previous study suggested that
GCK
-activating mutationscan result in abnormal pancreatic histology [4]. This is not thecase for all
GCK
-activating mutations as a histological examina-tion of the pancreas of a patient with the GCK T65Imutations demonstrated normal histology with no hyperplasia,no hypertrophied insulin cells, and regular-sized islets ofLangerhans [3]. Recently, mice with the A456V
GCK
mutationhave also been shown to have normal islet morphology andinsulin content [21]. In this current study, we also had theopportunity to perform a histological examination of theproband’s pancreas. We found no evidence to support abnormalpancreatic histology, as islet size and pancreatic proportion andislet-cell distribution were not different in the proband com-pared with an age-matched control; glucokinase was identifiedin the B-cells. This raises the question of whether abnormalpancreatic histology is a feature of GCK-PHHI or if it is onlyassociated with severe (threshold for GSIR
<
1.0 mmol/l)
GCK
mutations [4]. It remains possible that additional genetic and/or environmental factors contributed to the abnormal histologyreported in the patient with the Y214C mutation [4]. The iden-tification and study of further cases of GCK-PHHI is necessaryto determine if there is a direct consequence of
GCK
-activatingmutations on pancreas development and architecture.
The lipid profile of the individuals with the G68V mutationwere in the normal range except for the slightly elevated levelsof low-density lipoprotein cholesterol and triglycerides inthe maternal grandmother. As previously shown in otherindividuals, this finding does not support the association of anabnormal lipid profile with an activating
GCK
mutation as hasbeen suggested by findings in an animal model [3,22–24]. Thegrowing number of subjects with GCK-PHHI who demon-strate a normal lipid profile is relevant because of the existenceof small molecular
GCK
activators which are currently in develop-ment by a number of pharmaceutical companies [9,19,20].The fact that the described naturally occurring mutationsreported to date are not associated with lipid abnormalitiessuggests that the earlier work in animals reporting thatenhancement of
GCK
activity could have detrimental side-effects is less likely to be problematic when the first humanstudies commence.
Functional characterization of the G68V GST–GCKdemonstrated an increase in activity driven by an increase inaffinity for the substrate glucose. Functional severity wassimilar to the previously reported A456V mutation (predictedthreshold for GSIR 1.45 mmol/l) [6]. Both result in an increasein affinity for glucose with little effect on the maximal specificactivity. Both mutations result in a moderate decrease in the
dme_2285.fm Page 1398 Tuesday, November 13, 2007 7:20 PM

Original article
DIABETIC
Medicine
© 2007 The Authors.Journal compilation © 2007 Diabetes UK.
Diabetic Medicine, 24, 1393–1399 1399
affinity for the second substrate ATP. In keeping with theprevious reports of activating mutations, residue G68 is locatedin the allosteric activator site.
In conclusion, we report phenotypic heterogeneity in thelargest reported pedigree to date with a novel activating GCKmutation. We demonstrate the difficulty in predicting theseverity of the clinical phenotype from functional analysis ofthe mutant protein. Further studies are required to elucidateother genetic and environmental factors that modify thephenotype.
Competing interests
None to declare.
Acknowledgements
ALG is a Diabetes UK RD Lawrence Research Fellow and thiswork was funded in Oxford by Diabetes UK and the OxfordUniversity Press John Fell Research Fund. This work wasfunded in Ulm by the University of Ulm and Aventis PharmaDeutschland GmbH. The authors thank Dr Peter Moellerand Dr Erich Miltner, Department of Pathology and ForensicMedicine, University of Ulm for helpful discussion.
References
1 Glaser B, Kesavan P, Haymen M, Davies E, Cuesta A, Buchs A et al.Familial hyperinsulinism caused by an activating glucokinasemutation. N Engl J Med 1998; 338: 226–230.
2 Christesen HB, Jacobsen BB, Odili S, Buettger C, Cuesta-Munoz A,Hansen T et al. The second activating glucokinase mutation (A456V):implications for glucose homeostasis and diabetes therapy. Diabetes2002; 51: 1240–1246.
3 Gloyn AL, Noordam K, Willemsen MA, Ellard S, Lam WW,Campbell IW et al. Insights into the biochemical and genetic basisof glucokinase activation from naturally occurring hypoglycemiamutations. Diabetes 2003; 52: 2433–2440.
4 Cuesta-Munoz AL, Huopio H, Otonkoski T, Gomez-Zumaquero JM,Nanto-Salonen K, Rahier J et al. Severe persistent hyperinsulinemichypoglycemia due to a de novo glucokinase mutation. Diabetes2004; 53: 2164–2168.
5 Dullaart RP, Hoogenberg K, Rouwe CW, Stulp BK. Family withautosomal dominant hyperinsulinism associated with A456Vmutation in the glucokinase gene. J Intern Med 2004; 255: 143–145.
6 Gloyn A, Odili S, Buettger C, Njolstad PR, Shiota C, Magnuson Met al. Glucokinase and the regulation of blood sugar: a mathematicalmodel predicts the threshold for glucose-stimulated insulin releasefor GCK gene mutations that cause hyper- and hypoglycaemia.In: Magnuson, M, F Matschinsky, eds. Glucokinase and GlycemicDiseases: From the Basics to Novel Therapeutics: Basel: Karger,2004: 92–109.
7 Gloyn AL, Diatloff-Zito C, Edghill EL, Bellanne-Chantelot C, NivotS, Coutant R et al. KCNJ11 activating mutations are associated withdevelopmental delay, epilepsy and neonatal diabetes syndrome andother neurological features. Eur J Hum Genet 2006; 14: 824–830.
8 Proks P, Arnold AL, Bruining J, Girard C, Flanagan SE, Larkin B
et al. A heterozygous activating mutation in the sulphonylureareceptor SUR1 (ABCC8) causes neonatal diabetes. Hum Mol Genet2006; 15: 1793–1800.
9 Kamata K, Mitsuya M, Nishimura T, Eiki J, Nagata Y. Structuralbasis for allosteric regulation of the monomeric allosteric enzymehuman glucokinase. Structure (Camb) 2004; 12: 429–438.
10 Stride A, Shepherd M, Frayling TM, Bulman MP, Ellard S, HattersleyAT. Intrauterine hyperglycemia is associated with an earlier diagnosisof diabetes in HNF-1α gene mutation carriers. Diabetes Care 2002;25: 2287–2291.
11 Weedon MN, Clark VJ, Qian Y, Ben-Shlomo Y, Timpson N, EbrahimS et al. A common haplotype of the glucokinase gene alters fastingglucose and birthweight: association in six studies and population-genetics analyses. Am J Hum Genet 2006; 79: 991–1001.
12 Gloyn AL, Weedon MN, Owen K, Turner MJ, Knight BA, HitmanGA et al. Large-scale association studies of variants in genes encodingthe pancreatic beta-cell K-ATP channel subunits Kir6.2 (KCNJ11)and SUR1 (ABCC8) confirm that the KCNJ11 E23K variant isassociated with Type 2 diabetes. Diabetes 2003; 52: 568–572.
13 Helgason A, Palsson S, Thorleifsson G, Grant SF, Emilsson V,Gunnarsdottir S et al. Refining the impact of TCF7L2 gene variantson type 2 diabetes and adaptive evolution. Nat Genet 2007; 39: 218–225.
14 Grant SF, Thorleifsson G, Reynisdottir I, Benediktsson R, ManolescuA, Sainz J et al. Variant of transcription factor 7-like 2 (TCF7L2)gene confers risk of type 2 diabetes. Nat Genet 2006; 38: 320–323.
15 Weedon MN, Frayling TM, Shields B, Knight B, Turner T, MetcalfBS et al. Genetic regulation of birthweight and fasting glucose by acommon polymorphism in the islet cell promoter of the glucokinasegene. Diabetes 2005; 54: 576–581.
16 Lango H, Ellard S, Colclough K, Frayling TM, Hattersley AT,Weedon MN. Modifying effect of common Type 2 diabetes associatedvariants on MODY age of onset. Diabet Med 2007; 24: 39.
17 Huopio H, Otonkoski T, Vauhkonen I, Reimann F, Ashcroft F,Laakso M. A new subtype of autosomal dominant diabetes attributableto a mutation in the gene for the sulphonlyurea receptor 1. Lancet2003; 361: 301–307.
18 Pearson ER, Boj SF, Steele AM, Barrett T, Stals K, Shield JP et al.Macrosomia and hyperinsulinaemic hypoglycaemia in patients withheterozygous mutations in the HNF4A gene. PLoS Med 2007; 4:e118.
19 Grimsby J, Sarabu R, Corbett W, Haynes N, Bizzarro F, Coffey Jet al. Allosteric activators of glucokinase: potential role in diabetestherapy. Science 2003; 301: 370–373.
20 Brocklehurst KJ, Payne VA, Davies RA, Carroll D, Vertigan HL,Wightman HJ et al. Stimulation of hepatocyte glucose metabolismby novel small molecule glucokinase activators. Diabetes 2004; 53:535–541.
21 Pino MF, Kim KA, Shelton KD, Lindner J, Odili S, Li C et al.Glucokinase thermolability and hepatic regulatory protein bindingare essential factors for predicting the blood glucose phenotype ofmissense mutations. J Biol Chem 2007; 282: 13906–13916.
22 Ferre T, Pujol A, Riu E, Bosch F, Valera A. Correction of diabeticalterations by glucokinase. Proc Natl Acad Sci USA 1996; 93: 7225–7230.
23 Jackerott M, Baudry A, Bucchini D, Jami J, Joshi RL. Improvedmetabolic disorders of insulin receptor-deficient mice by transgenicoverexpression of glucokinase in the liver. Diabetologia 2002; 45:1292–1297.
24 Desai UJ, Slosberg ED, Boettcher BR, Caplan SL, Fanelli B, Stephan Zet al. Phenotypic correction of diabetic mice by adenovirus-mediatedglucokinase expression. Diabetes 2001; 50: 2287–2295.
dme_2285.fm Page 1399 Tuesday, November 13, 2007 7:20 PM




















