Alcoholic liver disease: A current molecular and clinical ...
Upload
independentCategory
view
4download
0
Ha
MJR
*C
BafihwAwelsCteEsvlmanvtwsCcnlansyocspm
Alb
GASTROENTEROLOGY 2009;136:1639–1650
epatic Expression of CXC Chemokines Predicts Portal Hypertensionnd Survival in Patients With Alcoholic Hepatitis
ARLENE DOMINGUEZ,* ROSA MIQUEL,‡ JORDI COLMENERO,* MONTSERRAT MORENO,*OAN–CARLES GARCÍA–PAGÁN,* JAIME BOSCH,* VICENTE ARROYO,* PERE GINÈS,* JUAN CABALLERÍA,* andAMÓN BATALLER*
Liver Unit, ‡Pathology Unit, Hospital Clínic, Institut d’Investigacions Biomèdiques August Pi i Sunyer, CIBER de Enfermedades Hepáticas y Digestivas, Barcelona,
atalonia, SpainshCtuwaAda
iacadts6tfm
CEmmaGfd
AsfGdpfa
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
ackground & Aims: Alcoholic hepatitis (AH) is char-cterized by hepatocellular damage, inflammation, andbrosis. We performed a prospective study to associateepatic expression of the CXC subfamily of chemokinesith histology findings and prognosis of patients withH. Methods: Liver biopsy samples from 105 patientsith AH and 5 normal liver samples (controls) were
valuated for steatosis, inflammation, fibrosis, and cho-estasis. Computer-based morphometric analysis as-essed the numbers of infiltrating CD3� T cells andD15� cells (neutrophils); terminal deoxynucleotidyl
ransferase–mediated deoxyuridine triphosphate nick-nd labeling staining was used to quantify apoptosis.xpression of CXC and CC chemokines and selectedignaling components were assessed by quantitative re-erse-transcription polymerase chain reaction; proteinevels of interleukin (IL)-8 and Gro-� also were deter-
ined by immunohistochemistry. Serum levels of IL-8nd Gro-� were measured by enzyme-linked immu-osorbent assay. The Cox regression model identifiedariables associated with mortality. Results: Most pa-ients (75%) had severe AH; their 90-day mortality rateas 21.9%. In AH liver samples, expression of the CXC
ubfamily members IL-8, Gro-�, CXCL5, CXCL6,XCL10, and platelet factor 4 was up-regulated and
ompared with controls. The CC chemokine CCL2, butot CCL5, also was up-regulated. Higher expression
evels of IL- 8, CXCL5, Gro-�, and CXCL6 were associ-ted with worse prognosis. Expression of CXC compo-ents correlated with neutrophil infiltration and theeverity of portal hypertension. In the multivariate anal-sis, IL-8 protein levels were an independent predictorf 90-day mortality. IL-8 and Gro-� serum levels did notorrelate with prognosis. Conclusions: Hepatic expres-ion of CXC components correlates with prognosis ofatients with AH. Reagents that target CXC chemokinesight be developed as therapeutics.
lcoholic hepatitis (AH) occurs in patients with heavyalcohol intake and it is characterized by hepatocel-
ular damage; inflammatory cell infiltrate, predominantly
y neutrophils; and rapidly progressive fibrosis.1 Theevere forms are associated with liver failure and portalypertension, leading to a short-term poor prognosis.2,3
urrent therapies for this condition fail in many pa-ients. Prognosis of patients with AH has been assessedsing the Maddrey’s Discriminant Function.4 Recently,e described the ABIC score, a new scoring system thatllows prognostic stratification of these patients.5 TheBIC score identifies patients with low (�6.71), interme-iate (6.71– 8.99), and high risk (�9) of death at 90 daysnd 1 year.
The pathogenesis of AH is poorly understood. Annteraction between neutrophils and cytokines may play
role.6 Patients with chronic alcohol abuse have in-reased endotoxin serum levels leading to Kupffer cellctivation, neutrophil recruitment, and increased pro-uction of cytokines.6,7 The degree of neutrophil infiltra-ion as well as serum levels of proinflammatory cytokinesuch as tumor necrosis factor �, and interleukins (ILs) 1,, and 8, are associated with disease severity.7–9 However,he use of monoclonal antibodies against tumor necrosisactor � in patients with severe AH is associated with
ore severe infections and a higher mortality rate.10,11
Chemokines are classified into 4 subfamilies: CC, CXC,X3C, and C. CXC chemokines can be subclassified intoLR� or ELR� based on the presence of a tripeptideotif ELR (Glu-Leu-Arg) at the NH2 terminus. The ELRotif appears to be important in ligand/receptor inter-
ctions on neutrophils. IL-8, CXCL5, CXCL6, CXCL7,ro-�, Gro-�, and Gro-� are members of the ELR� CXC
amily. In contrast, ELR� CXC chemokines have a re-uced ability to induce neutrophil chemotaxis. This sub-
Abbreviations used in this paper: ALD, alcohol-induced liver disease;H, alcoholic hepatitis; HR, hazard ratio; HVPG, hepatic venous pres-ure gradient; IL, interleukin; CXCR, chemokine receptor; PF4, plateletactor 4; ENA-78, epithelial-derived neutrophil-activating peptide 78;CP-2, granulocyte chemotactic protein 2; �IP-10, interferon-�–in-uced protein 10; IFN, interferon; MCP-1, monocyte chemoattractantrotein 1; STAT-1, signal transducer and activator of transcriptionactor 1; RANTES, regulated upon activation, normally T-expressed,nd presumably secreted.
© 2009 by the AGA Institute0016-5085/09/$36.00
doi:10.1053/j.gastro.2009.01.056

gak�
Etfimampwpteala
ppps
tuafaMtif�aea(adoptnh�wcmt
mf
psi(dmb(m(s(mdszfisls
4os
ttbtawiiArApcCCacbrwLw
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1640 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
roup includes interferon-�–induced protein (�IP-10)nd PF4 (platelet factor 4). Importantly, ELR� chemo-ines bind CXC receptor 1 (CXCR1) and CXCR2, whereasIP-10 and PF4 interact with CXCR3.12,13
We hypothesize that CXC chemokines, in particularLR� CXC chemokines, may play an important role in
he pathogenesis of AH. This assumption is based on theollowing data. First, the CXC family of chemokinesncludes a number of ligands and receptors that play a
ajor role in neutrophil infiltration of chronically dam-ged tissues.14 –16 Second, neutrophil infiltration is a hall-ark histologic finding in patients with AH and has
rognostic significance.17–23 Third, livers from patientsith AH have overexpression of IL-8 and Gro-� com-ared with normal livers.23,24 Moreover, studies in pa-ients with AH have shown that IL-8 is present in vascularndothelium, inflammatory cells, intrahepatic bile ducts,nd in fibrous septa.25 Fourth, it is likely that the bio-ogical effects of CXC chemokines on liver cells may play
role in AH.2
The current study was undertaken to investigate theathogenic role of CXC chemokines in AH. For thisurpose, we investigated the impact of hepatic gene ex-ression of CXC chemokines on disease severity andurvival in patients with AH.
Materials and MethodsPatientsWe prospectively included patients admitted to
he Liver Unit (Hospital Clínic, Barcelona) between Jan-ary 2000 and September 2007 with clinical, analytic,nd histologic features of AH. Inclusion criteria were asollows: patients with active alcohol abuse were definedccording to the Diagnostic and Statistical Manual ofental Disorders IV26 and excessive ethanol consump-
ion (�60 g/day) for at least 3 months before admission;ncreased aminotransferase levels (aspartate aminotrans-erase [AST] � alanine aminotransferase [ALT]), high-glutamyl transpeptidase and bilirubin serum levels,nd histologic diagnosis of AH characterized by the pres-nce of hepatocellular damage (hepatocellular ballooningnd presence of Mallory bodies), inflammatory infiltrateneutrophils), and pericellular fibrosis. Patients with hep-tocellular carcinoma or any other potential cause of liverisease were excluded from the study. Liver biopsy wasbtained using a transjugular approach because mostatients with AH have severe coagulation disorders, ando measure portal pressure gradient. All patients receivedutritional and psychological support for achieving alco-ol abstinence. Patients with severe AH (ABIC score,6.71) were treated with 40 mg/day prednisone for 4eeks followed by a 2-week taper, unless they had any
ontraindication (severe bacterial infection or diabetesellitus with poor metabolic control) to corticosteroid
reatment. The study was approved by the Ethics Com- 7
ittee of the Hospital Clínic and all patients gave in-ormed consent.
Histologic Analysis and HepaticHemodynamic MeasurementsLiver biopsy specimens were formalin-fixed and
araffin-embedded. Liver specimens (3-�m thick) weretained with H&E and Masson’s trichrome. Biopsy spec-mens were assessed blindly by the same pathologistR.M.). Histologic analysis was performed as follows: (1)egree of hepatocellular damage/ballooning (0, none; 1,ild; 2, moderate or severe) and presence of Mallory
odies, giant mitochondria, and cholestasis (0, no; 1, yes);2) degree of lymphocytic infiltration (0, none; 1, mild; 2,
oderate; 3, severe); (3) degree of neutrophil infiltration0, none; 1, mild; 2, moderate; 3, severe); (4) degree ofteatosis (0, �10%; 1, 10%–33%; 2, 33%– 66%; 3, �66%);5) steatosis type (0, macrovesicular; 1, microvesicular; 2,
ixed); (6) steatosis distribution (0, focal; 1, diffuse); (7)egree of lobular fibrosis (0, none; 1, mild; 2, moderate; 3,evere); (8) lobular fibrosis distribution (0, zone 3; 1,ones 2 and 3; 2, panlobular); (9) fibrosis stage (0, nobrosis; 1, portal; 2, portal fibrosis and few septa; 3,eptal fibrosis without cirrhosis; 4, cirrhosis), (10) cho-estasis type (0, canalicular; 1, mild hepatocellular; 2,evere hepatocellular; 3, canalicular and hepatocellular).
Hepatic hemodynamic assessment was performed within8 hours of admission. The portal pressure was estimatedn the hepatic venous pressure gradient (HVPG), as de-cribed in detail previously.27
Hepatic Gene Expression AnalysisHepatic gene expression was evaluated in 49 pa-
ients. In the remaining patients, the amount of liverissue obtained only allowed histologic analysis. Liveriopsy specimens were submerged in an RNA stabiliza-ion solution (RNAlater; Ambion, Austin, TX) and storedt �20°C until RNA extraction. Total RNA was extractedith TRIzol (Life Technologies Inc, Rockville, MD). RNA
ntegrity and concentration was assessed with a microflu-dic glass chip platform (Bioanalyzer 2100; Agilent, Palolto, CA). Five hundred micrograms of total RNA were
etrotranscribed with a high-capacity complementary DNArchive Kit (Applied Biosystems, Foster City, CA). Elevenredesigned Taq-Man assays for target genes of CXChemokine family were assessed in patients with AH:XCL1 or Gro-�, CXCL2 or Gro-�, CXCL3 or Gro-�,XCL4 or PF4, CXCL5 or epithelial-derived neutrophil-ctivating peptide 78 (ENA-78), CXCL6 or granulocytehemotactic protein 2 (GCP-2), CXCL7 or proplateletasic protein, IL-8, CXCL10 or �IP10, CXCR1 or IL-8eceptor A, and CXCR2 or IL-8 receptor B. These genesere selected and distributed into a 384-well Taq-Manow Density Array cards (Applied Biosystems). Samplesere analyzed for quadruplicate using an ABI PRISM
900 (Applied Biosystems) as described in detail else-
wsCpt[n(rEpemf
e(lmdsoonardw
iaAtveomasuEg
tmmLma
tcuSoilisnb
opbpGtshnatfindc
bg4alNsgac
mt(ctUw
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 CXC CHEMOKINES IN ALCOHOLIC HEPATITIS 1641
here.28 In addition, genes encoding CC chemokinesuch as monocyte chemoattractant protein 1 (MCP-1 orCL2) and regulated on activation, normally T-ex-ressed, and presumably secreted (regulated upon activa-ion, normally T-expressed, and presumably secretedRANTES] or CCL5), interferon gamma (IFN-�) and sig-al transducer and activator of transcription factor 1
STAT- 1) were assessed by quantitative polymerase chaineaction. Taq-Man reactions were performed in duplicate.xpression levels of target genes were normalized to ex-ression of 18S ribosomal RNA (endogenous gene). Genexpression values were calculated based on the ��Ctethod.29 The results were expressed as 2-��Ct referred as
old in relation with mean normal livers.
Selection of Control LiversNormal livers were obtained from optimal cadav-
ric liver donors (n � 3) or resection of liver metastasesn � 2). All controls had normal serum aminotransferaseevels and normal liver histology. Criteria to obtain nor-
al livers were as follows: (1) no past history of liverisease, alcohol abuse, or metabolic syndrome; (2) ab-ence of maintained arterial hypotension before laparot-my; (3) normal serum aminotransferase levels; (4) timef brain death to laparotomy less than 12 hours; (5)ormal liver histology; (6) no use of vasodilator drugs;nd (7) liver specimens obtained immediately after lapa-otomy and before vascular clamp. The samples acquireduring surgical liver resection for secondary liver cancerere obtained at a minimum of 5 cm from the tumor.
Assessment of IL-8 Hepatic Gene Expressionin Patients With Chronic Hepatitis CHepatic gene expression of IL-8 also was evaluated
n patients with chronic hepatitis C. Patients with detect-ble serum RNA hepatitis C virus (HCV) and increasedLT level underwent a percutaneous liver biopsy. Pa-
ients with HCV genotype 1 and without previous anti-iral treatment were included (n � 35). Patients withvidence of excessive alcohol intake (�20 g/day) andther causes of liver disease were excluded. Liver speci-ens were analyzed by an expert pathologist (R.M.) andpart of the biopsy specimen was submerged into a RNA
tabilization solution (RNAlater) and stored at �20°Cntil RNA extraction. The protocol was approved by thethics Committee of the Hospital Clinic and all patientsave informed consent.
Immunohistochemical StudiesParaffin-embedded sections were incubated with
he following primary antibodies: anti-human CD15onoclonal mouse (DakoCytomation, Glostrup, Den-ark), anti-human CD3 monoclonal mouse (Novocastra
aboratories Ltd, Newcastle, UK), an anti-human IL-8onoclonal mouse (Endogen, IL), anti-human ENA-78
nd anti-human Gro-� monoclonal mouse (R&D Sys- m
ems, MN). The number of lymphocytes (CD3-positiveells) and neutrophils (CD15-positive cells) was assessedsing an image-analysis system (AnalySIS; Soft-Imagingystem, Münster, Germany). Twenty fields, using a 200�bjective, were chosen randomly and the number of pos-
tive cells was counted in each specimen. The number ofabeled cells with IL-8, ENA-78, and Gro-� was identifiedn 20 random high-power fields (objective, 200�). Aemiquantitative analysis was performed as follows: 0,one; 1, mild; 2, moderate; and 3, severe. All studies werelindly performed by the same observer (M.D.).
Identification of Cell Apoptosis by TerminalDeoxynucleotidyl Transferase–MediatedDeoxyuridine Triphosphate Nick-EndLabelingApoptotic cells were identified by the terminal de-
xynucleotidyl transferase–mediated deoxyuridine triphos-hate nick-end labeling technique. Briefly, paraffin-em-edded liver slices were incubated with 20 �g/mLroteinase K (Roche Diagnostics GmbH, Mannheim,ermany) and labeled using the In Situ Cell Death De-
ection Kit (POD; Roche, Mannheim, Germany). Finally,ections were stained with 3,3’-diaminobenzidine tetra-ydrochloride and counterstained with hematoxylin. Theumber of terminal deoxynucleotidyl transferase–medi-ted deoxyuridine triphosphate nick-end labeling–posi-ive cells was counted using a 400� objective. Twentyelds were chosen randomly and the number of termi-al deoxynucleotidyl transferase–mediated deoxyuri-ine triphosphate nick-end labeling–positive cells wasounted in each specimen.
Serum IL-8 and Gro-� DeterminationSerum samples obtained from peripheral venous
lood were analyzed in the subset of patients in whomene expression was studied. Blood was extracted within8 hours from admission. Serum concentrations of IL-8nd Gro-� were measured in duplicate by an enzyme-inked immunosorbent assay (BioSource Europe S.A.,
ivelles, Belgium; and R&D Systems, respectively). IL-8erum levels greater than 15 pg/mL and Gro-� levelsreater than 118 pg/mL were considered abnormally highccording to data from healthy controls obtained in ourenter.
Statistical AnalysisResults of quantitative variables are expressed as
ean � SE, unless otherwise specified. Differences be-ween groups were analyzed using nonparametric testsMann–Whitney U test) for continuous variables and thehi-square test for categoric variables. Correlations be-ween variables were evaluated using the Spearman rho.nivariate and multivariate analysis using Cox regressionas used to identify variables associated with 90-day
ortality of AH. Variables with a P value of less than .1
isc.cad
itcalt9Sci(ip
Ttn
mwmCtw
fcreiu
mtwse
T
AMMMASA9GCSAAGBAHPLNIH
NGa
b
T
CL
SS
S
I
B
C
CCTI
NTt
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1642 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
n the univariate model were entered into a backwardtepwise elimination variable selection procedure. Theriterion for retaining predictors was a P value less than05. Survival curves by the Kaplan–Meier method werereated and compared using the log-rank test. Statisticalnalysis was performed using SPSS version 14.0 for Win-ows (SPSS Inc, Chicago, IL).
ResultsGeneral Characteristics of PatientsWe prospectively identified 146 patients with clin-
cal and analytical characteristics of AH. Forty-one pa-ients did not meet all inclusion criteria and were ex-luded from the final analysis. Finally, 105 patients metll criteria and were included in the study. Clinical, ana-ytical, and hepatic hemodynamic variables of these pa-ients are shown in Table 1. The main causes of death at0 days were sepsis (24.3%) and liver failure (43.2%).eventy-six patients (73.1%) developed at least one majoromplication during hospitalization, including bacterialnfection (44.2%), ascites (18.3%), hepatic encephalopathy20.2%), renal failure (18.3%), and gastrointestinal bleed-ng (8.7%). The majority of patients had severe sinusoidalortal hypertension (median HVPG, 20 mm Hg).Hepatic histologic characteristics are shown in Table 2.
he median length of the biopsy specimens was 6 mm,he median number of fragments was 5, and the medianumber of portal spaces was 7.
able 1. Clinical, Analytical, and Hepatic HemodynamicCharacteristics of Patients With AH Included in theStudy
Variables Value
ge, y 49.10 � 0.8ale, % 66.7addrey’s DFa 56.6 � 3.65ELD scoreb 22 � 0.7BIC score 7.69 � 0.15evere AH, % 75lcohol intake, g/day 118 � 6.440-day mortality, % 21.9lucose level, mg/dL 114 � 4.7reatinine level, mg/dL 1.09 � 0.11odium level, mEq/L 133 � 0.51ST level, U/L 152 � 9.9LT level, U/L 62 � 4.42GT level, U/L 629 � 81.09ilirubin level, mg/dL 12.6 � 0.9lbumin level, mg/dL 26.9 � 0.5ematocrit, % 31.55 � 0.64latelet count, �109 139 � 9eukocyte count, �109/L 10.4 � 0.5eutrophil count, % 74 � 0.14
NR 1.80 � 0.05VPG, mm Hg 19.37 � 0.6
OTE. Mean � SE or percentage shown.GT, �-glutamyl transpeptidase; INR, international normalized ratio.Maddrey’s discriminant function.
AModel for end stage liver disease.
Hepatic Gene Expression StudiesWe first analyzed the hepatic gene expression of
ost components of the CXC chemokine family in liversith AH compared with normal livers. For this purpose,essenger RNA was obtained from a subset of patients.linical, analytical, histologic, and hemodynamic charac-
eristics of this subgroup of patients were similar to thehole series (data not shown).Among all studied genes, we found 7 genes of the CXC
amily that were regulated differentially in livers with AHompared with control livers (Table 3). IL-8, the mostepresentative component of this family, was found over-xpressed by 14-fold compared with normal livers. Sim-larly, ENA-78, Gro-�, GCP-2, PF4, and �-IP10 also werep-regulated in patients with AH.We also studied the gene expression of IL-8, the hall-ark component of the CXC chemokine family, in pa-
ients with chronic hepatitis C. Interestingly, patientsith chronic hepatitis C showed reduced hepatic expres-
ion of IL-8 compared with normal livers (0.54 � 0.09xpressed as 2^-��CT; P � .038). Moreover, patients with
able 2. Histologic Characteristics of Patients With AHIncluded in the Study
Variables Value
irrhosis, % 59.6obular fibrosisFibrosis in zone 3, % 23.8Fibrosis in zones 2 and 3, % 40.6Panlobular fibrosis, % 33.7
teatosis, % 50 � 2.69teatosis typeMacrovesicular, % 22.2Mixed, % 76.8
teatosis distributionFocal, % 8.1Diffuse, % 91.9
nflammatory gradeMild, % 68.3Moderate, % 8.9Severe, % 22.8
allooningMild, % 41Marked, % 59
holestasisAbsent, % 31.4Canalicular, % 26.5Mild hepatocellular, % 10.8Severe hepatocellular, % 2Canalicular � hepatocellular, % 29.4
D3� cells/field 69 � 4.5D15� cells/field 74 � 6.5UNEL� cells/field 6 � 0.6L-8 staining
None/mild, % 61Moderate/marked, % 39
OTE. Mean � SE or percentage shown.UNEL, terminal deoxynucleotidyl transferase–mediated deoxyuridineriphosphate nick-end labeling.
H showed increased hepatic gene expression of IL-8

(t
cMwcpew.
tia.(�GsesaEks
whptp
roGCa
pst(m(iCd
a6d..rltrwEPSeaHope
hflaattlshs(mC
T
D
U
U
Nl
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 CXC CHEMOKINES IN ALCOHOLIC HEPATITIS 1643
14.01 � 2.57 expressed as 2^-��CT) compared with pa-ients with chronic hepatitis C (P � .00002).
Next, we explored hepatic gene expression of 2 CChemokines (MCP-1 and RANTES). We found that
CP-1 was up-regulated in patients with AH comparedith controls (fold expression, 3.40 � 0.39; P � .008). In
ontrast, RANTES was not found up-regulated (fold ex-ression, 1.62 � 0.15; P � .23). Finally, hepatic genexpression of IFN-� and STAT-1 did not differ in patientsith AH from controls (fold expression, 1.84 � 0.23; P �
57; and 2.01 � 0.22; P � .12, respectively).
Relationship Between Hepatic GeneExpression and Short-Term Prognosis,Histologic Data, and Hemodynamic DataWe studied hepatic gene expression according to
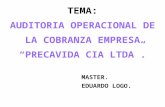
he short-term prognosis, as indicated by 90-day mortal-ty. We found 4 genes overexpressed in patients who diedt 90 days compared with those who survived: IL-8 (P �
042), ENA-78 (P � .008), Gro-� (P � .046), and GCP-2P � .02) (Figure 1). Patients with severe AH (ABIC score,
6.71) showed up-regulation of Gro-� (P � .006) andro-� (P � .036). Interestingly, patients with an ABIC
core obtained at 7 days of 6.71 or greater showed over-xpression of 3 genes that previously were associated withhort-term mortality: ENA-78 (P � .05), Gro-� (P � .023),nd GCP-2 (P � .04). In contrast, hepatic expression ofLR� CXC chemokines (PF4 and �-IP10) and CC chemo-ines (MCP-1 and RANTES) was not associated withurvival or severity disease.
We next correlated expression of CXC chemokinesith histologic findings. The median value of 52 cells/igh-power field was used as the cut-off value to defineatients with low and high hepatic neutrophil infiltra-ion. Patients with marked hepatic infiltration of neutro-
able 3. Hepatic Gene Expression of the CXC ChemokineFamily in Patients With AH Versus Controls
Genes NCBInumber Fold
AH vs controls,Mean � SE P
own-regulatedGro-� (CXCL2) Hs00236966_m1 0.17 � 0.06 .00001
p-regulatedIL-8 (CXCL8) Hs00174103_m1 14.02 � 2.58 .00009ENA-78 (CXCL5) Hs00171085_m1 112.50 � 21.29 .000004Gro-� (CXCL1) Hs00236937_m1 762.76 � 133.95 .00001GCP-2 (CXCL6) Hs00237017_m1 110.21 � 21.31 .00001PF4 (CXCL4) Hs00236998_m1 47.32 � 16.38 .00005�-IP-10 (CXCL10) Hs00171042_m1 7.25 � 3.31 .022
nchangedPPBP (CXCL7) Hs00234077_m1 6.73 � 2.30 .37Gro-� (CXCL3) Hs00171061_m1 1.03 � 0.19 .69IL-8RA (CXCR1) Hs00174146_m1 0.91 � 0.22 .068IL-8RB (CXCR2) Hs00174304_m1 1.12 � 0.25 .131
CBI, National Center for Biotechnology Information; PPBP, proplate-et basic protein; IL-8RA, IL-8 receptor �; IL-8RB, IL-8 receptor �.
hils (CD15� staining), which is the main pathogenic 1
ole of this family of chemokines, showed up-regulationf 6 genes (Figure 2): IL-8 (P � .02), ENA-78 (P � .048),ro-� (P � .02), Gro-� (P � .009), CXCR1 (P � .006), andXCR2 (P � .008). Lymphocyte infiltrate did not associ-te with gene expression.
In addition, we investigated whether hepatic gene ex-ression correlated with the severity of portal hyperten-ion, which is a hallmark clinical feature of these pa-ients. Patients with more severe portal hypertensionHVPG greater than the median value of the series, 20
m Hg) showed up-regulation of IL-8 (P � .01), ENA-78P � .007), and Gro-� (P � .032) (Figure 3). These resultsndicate that expression of key components of the ELR�XC chemokine subfamily correlates with clinical, hemo-ynamic, and histologic findings.
Systemic Serum Levels of IL-8 and Gro-� inPatients With AHSerum levels of IL-8 and Gro-� were increased in
ll patients with AH (208 � 44.6 pg/mL and 351.79 �7.48 pg/mL, respectively). Serum IL-8 and Gro-� levelsid not correlate with 90-day mortality (P � .06 and P �
49, respectively) or with disease severity (P � .9 and P �75, respectively). Interestingly, serum levels of IL-8 cor-elated with Gro-� levels (r � 0.96, P � .0001). Serumevels of IL-8 did not correlate with clinical complica-ions, histologic, analytical, or hepatic hemodynamic pa-ameters. However, serum IL-8 was correlated weaklyith hepatic gene expression of IL-8 (r � 0.44, P � .019),NA-78 (r � 0.45, P � .016), Gro-� (r � 0.38, P � .048),F4 (r � 0.45, P � .015), and CXCR1 (r � 0.39, P � .041).erum levels of Gro-� did not correlate with hepatic genexpression of CXC chemokines, MCP-1, RANTES, IFN-�,nd STAT-1 or with clinical complications. Patients withVPG greater than 20 mm Hg showed high serum levels
f Gro-� (P � .048). These results indicate that intrahe-atic expression of IL-8, rather than systemic serum lev-ls, correlate with disease prognosis.
Prognostic Value of Hemodynamic andHistologic Parameters IncludingImmunohistochemistry StudiesWe finally investigated the prognostic value of
istologic parameters such as steatosis, cholestasis, in-ammatory infiltration (lymphocytes and neutrophils),poptosis, protein expression (IL-8, ENA-78, and Gro-�),s well as hepatic hemodynamic parameters (HVPG) inhe whole series of patients with AH (n � 105). We foundhat livers with AH contain significant neutrophil andymphocyte infiltration (Figure 2A and B). Protein expres-ion of IL-8, Gro-�, and ENA-78 was localized in bothepatocytes and nonparenchymal cells. Univariate analy-is showed that moderate/marked expression of IL-8hazard ratio [HR], 2.11; 95% CI, 0.91– 4.89; P � .08),
oderate/marked expression of ENA-78 (HR, 3.14; 95%I, 1.00 –9.95; P � .049), HVPG (HR, 1.08; 95% CI, 1.01–
.15; P � .035), the presence of cholestasis (HR, 3.49; 95%
C(we1P5pM
mImhn.et
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1644 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
I, 1.04 –11.75; P � .04), and none/mild hepatic steatosisHR, 0.98; 95% CI, 0.96 – 0.99; P � .018) were associatedith 90-day mortality. In the multivariate analysis, mod-
rate/marked expression of IL-8 protein (HR, 2.9; 95% CI,.21– 6.99; P � .017), HVPG (HR, 1.12; 95% CI, 1.04 –1.22;� .004), and the presence of hepatic cholestasis (HR,
.74; 95% CI, 1.47–22.44; P � .012) were associated inde-endently with 90-day mortality (Table 4). A Kaplan–
eier survival analysis was performed to compare 90-day oortality according to the degree of protein expression ofL-8 and ENA-78. As shown in Figure 4, patients with
oderate/marked protein expression of IL-8 or ENA-78ad lower rates of survival at 90 days than patients withone/mild protein expression of IL-8 or ENA-78 (P �
041 and P � .038, respectively). The hepatic proteinxpression of Gro-�, the degree of inflammatory infiltra-ion, either by lymphocytes or neutrophils, or the degree
Figure 1. (A–D) Identification ofcomponents of the CXC chemo-kine family that correlate with 90-day mortality in patients withAH. Gro-�, ENA-78, GCP-2, andIL-8 hepatic gene expressionwas higher in patients who diedat 90 days. *P � .05. (E) Kaplan–Meier curve showing 90-daysurvival according to IL-8 geneexpression (fold expression re-spect to controls). A value of9.33 (fold expression) was iden-tified as the cut-off value withbetter sensitivity and specificityto define patients with low andhigh IL-8 gene expression. (F)Kaplan–Meier curve showing 90-day survival according to ENA-78gene expression (fold-expressioncompared to controls). A valueof 88 (fold expression) was iden-tified as the cut-off value with bet-ter sensitivity and specificity to de-fine patients with low and highENA-78 gene expression.
f apoptosis did not correlate with short-term mortality.

Ftw(pcokgloufipEapwt
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 CXC CHEMOKINES IN ALCOHOLIC HEPATITIS 1645
igure 2. (A and B) Represen-ative photomicrographs of liversith AH stained with anti-CD15
neutrophils) and anti-CD3 (lym-hocytes), respectively (magnifi-ation, 200�). (C–H) Identificationf components of CXC chemo-ines that correlated with the de-ree of neutrophil infiltration in
ivers with AH. The median valuef 52 cells/high-power field wassed as the cut-off value to de-ne patients with low and high he-atic neutrophil infiltration. IL-8,NA-78, Gro-�, Gro-�, CXCR1,nd CXCR2 hepatic gene ex-ression was higher in patientsho had severe neutrophil infil-
ration. *P � .05.

Tm
pwcotlhoiwCAcs
apefApicc
4FrohIp
T
U
M
C
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1646 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
aken together, these data indicate that IL-8 and ENA-78ay play a role in the pathogenesis of severe AH.
DiscussionThe current study investigated the potential
athogenic role of the CXC chemokine family in patientsith biopsy-proven AH. We provide evidence that key
hemokines of this family including IL-8 and ENA-78 areverexpressed markedly in the livers with AH. Impor-antly, hepatic expression of some of these genes corre-ates with short-term prognosis and the severity of portalypertension. These results are in keeping with previ-usly published data indicating that neutrophil-attract-
ng chemokines such as Gro-� are increased in patientsith AH.15,24 Because the biological properties of ELR�
XC chemokines include events found in the livers withH such as infiltration by neutrophils, fibrogenesis, andell death, our results suggest a potential role for thisubfamily of cytokines in this clinical condition.
Most studies performed to date to identify the medi-tors of alcohol-induced liver disease (ALD) have beenerformed in experimental models in rodents.30 –32 How-ver, such models do not exactly mimic the histologiceatures of severe ALD including AH.33 In patients withH, the main clinical consequences are related to theresence of hepatocellular injury and severe fibrosis.34 It
s therefore not surprising that clinical trials targetingytokines identified in rodents with ALD (eg, tumor ne-rosis factor �) have not yielded positive results.10,11,35
™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™™igure 3. Identification of components of CXC chemokines that cor-
elate with severe portal hypertension. The median value of 20 mm Hgf HVPG was used as the cut-off value to define patients with lower andigher degrees of portal hypertension. (A) Gro-�, (B) ENA-78, and (C)
L-8 hepatic gene expression was higher in patients with more severe
able 4. Factors Associated With 90-Day Mortality in theUnivariate and Multivariate Analyses in the WholeSeries of Patients (n � 105)
Variables90-day
mortality, HR 95% CI P
nivariate analysisHVPG, mm Hg 1.08 1.01–1.15 .035IL-8 protein expression,
moderate/marked2.11 0.91–4.89 .081
ENA-78 protein expression,moderate/marked
3.14 1.00–9.95 .049
Cholestasis 3.49 1.04–11.75 .044Steatosis 0.98 0.96–0.99 .018ultivariate analysisIL-8 protein expression
(moderate/marked)2.9 1.21–6.99 .017
Cholestasis 5.74 1.47–22.44 .012HVPG, mm Hg 1.12 1.04–1.22 .004
I, confidence interval.
ortal hypertension. *P � .05.

TtpHCApdtfbpst
haltpocsoate
FtweIKdptwaw2sismem
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 CXC CHEMOKINES IN ALCOHOLIC HEPATITIS 1647
herefore, we think that there is a clear need to performranslational studies with human samples to uncover theathogenesis of AH to identify new targets for therapy.ere, we prospectively analyzed the expression of theXC chemokine family in patients with biopsy-provenH. Two main reasons prompted us to choose theseotential targets: previous data from our laboratory in-icating that some chemokines are overexpressed in pa-ients with AH, and that the biological properties of thisamily may participate in ALD.7,19,24 Ethanol metabolismy hepatocytes may have influenced CXC chemokineroduction. In fact, acetaldehyde increases tumor necro-is factor �–induced synthesis of IL-8 in cultured hepa-
igure 4. Representative pho-omicrographs of livers with AHith (A) none/mild and (B) mod-rate/marked staining with anti–
L-8 (magnification, 200�). (C)aplan–Meier curve showing 90-ay survival according to IL-8 liverrotein expression. Representa-ive photomicrographs of liversith AH with (D) none/mildnd (E) moderate/marked stainingith anti–ENA-78 (magnification,00�). (F) Kaplan–Meier curvehowing 90-day survival accord-
ng to ENA-78 liver protein expres-ion. Patients with moderate/arked IL-8 and ENA-78 protein
xpression had higher 90-dayortality.
ocytes.15 t
To show a pathogenic role for these chemokines inuman beings, we performed 2 types of analysis. First, wessessed the gene expression of these chemokines in theiver and analyzed the correlation of this expression withhe main clinical and histologic characteristics of theatients. By showing that several CXC chemokines wereverexpressed in livers with AH and that their expressionorrelated with short-term mortality, we provide evidenceuggesting a pathogenic role for these substances. Sec-nd, we showed that hepatic protein expression of IL-8 isn independent predictor of short-term mortality inhese patients. In contrast, we found that hepatic genexpression of Gro-� was up-regulated markedly in pa-
ients with AH, yet it was not associated with prognosis
oahfo
ecctmsi
cwiAncitspE�n
lpIsspc
ipntcodkkwcwslmtsII
ii
asKpuIdktc
etathgasTa
EwsktcasIafit
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1648 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
r disease severity. Gro-� is a less powerful neutrophilctivator than IL-8, suggesting that IL-8 may be a morearmful inflammatory mediator in these patients.15 This
act could explain why Gro-� has no impact on survivalr disease severity.
An important finding of our study is that hepaticxpression of IL-8 and other ELR� CXC chemokinesorrelate with the degree of portal hypertension. Thelinical relevance of portal hypertension is indicated byhe fact that HVPG is an independent predictor of 90-day
ortality. This result is in keeping with previous studieshowing that HVPG correlates with in-hospital mortalityn patients with AH.34
Our results suggest that increased CXC chemokinesould contribute to neutrophil infiltration in patientsith AH. We have found a heterogeneous inflammatory
nfiltrate (neutrophils and lymphocytes) in livers withH. However, the degree of lymphocyte infiltration didot correlate with clinical outcomes in our series. On theontrary, patients with severe AH had higher neutrophilnfiltration in liver tissue. These results suggest that neu-rophils, rather than lymphocytes, contribute to diseaseeverity. We also found that patients with higher neutro-hil infiltration had overexpression of 3 genes of theLR� CXC chemokine subfamily (IL-8, GCP-2, and Gro-), suggesting that these mediators contribute to attracteutrophil to the damaged liver.Other findings of our study are that systemic serum
evels of IL-8 and Gro-� do not correlate with diseaserognosis. Instead, both gene and protein expression ofL-8 correlated with short-term mortality. Our resultsuggest that intrahepatic expression of IL-8, rather thanystemic serum levels, plays a pathogenic role. However,reviously published data suggest that serum IL-8 asso-iates with severe AH.36,37
The results of the current study may have pathophys-ologic implications. First, increased CXC chemokine ex-ression may play a major role in the recruitment ofeutrophils, which is a hallmark biological property ofhis family of cytokines. Neutrophils are supposed toontribute to liver injury by releasing high amounts ofxygen reactive species and sensitizing hepatocytes to celleath.38 Second, hepatic overexpression of CXC chemo-ines may directly induce hepatocellular injury. It isnown that IL-8 and Gro-� stimulate intracellular path-ays involved in parenchymal cell death.15,16 Third, CXC
hemokines may induce endothelial dysfunction in liversith AH. CXC chemokines are expressed in endothelial
inusoidal cells and participate in endotoxin-inducediver injury.39 Finally, chemokines may participate in pro-
oting liver fibrogenesis, leading to severe disruption ofhe hepatic architecture and subsequent portal hyperten-ion.39,40 Activated stellate cells release large amounts ofL-8 in response to vasoactive agents. It is possible that
L-8 acts on these cells in an autocrine manner promot-ng collagen synthesis.41 Other chemokines (eg, MCP-1)nduce fibrogenic signals in these cells.16
Previous studies have found that serum levels of IFN-�re increased significantly in patients with AH.42 IFN-�timulate hepatocytes, sinusoidal endothelial cells, andupffer cells via STAT/interferon regulatory factor 1 toroduce multiple chemokines.43 IFN-� and STAT-1 werenchanged in patients with AH compared with controls.
nterestingly, hepatic expression of IFN-� and STAT-1id not correlate with hepatic expression of CXC chemo-ines, but with CC chemokines. These data suggest thathe IFN–STAT axis may influence the expression of CChemokines, rather than CXC chemokines, in AH.
Our study had several limitations. First, hepatic genexpression analysis only was performed in nearly half ofhe patients. This was owing to ethical concerns. Genenalysis was performed only when the amount of liverissue obtained in transjugular biopsies allowed bothistologic analysis and RNA extraction. Second, the de-ree of IL-8, Gro-�, and ENA-78 protein expression wasssessed semiquantitatively because the staining was ob-erved in both hepatocytes and nonparenchymal cells.his type of pattern does not allow a clear selection ofreas with positive staining by computer analysis.
In conclusion, we found that liver gene expression ofLR� CXC chemokines are overexpressed in patientsith AH and correlate with disease severity. These results
uggest a potential role for IL-8 and other CXC chemo-ines in the pathogenesis of AH. The next step would beo investigate whether drugs that interfere with thesehemokines (ie, of CXCR1 and CXCR2 antagonists) havebeneficial effect in rodents with experimental alcoholic
teatohepatitis. In a model of ischemia-reperfusion, anL-8 –receptor blocker prevents neutrophil infiltrationnd attenuates liver injury.44 Further studies should con-rm if this beneficial effect also is observed in experimen-ally induced ALD.
References
1. Pares A, Caballeria J, Bruguera M, et al. Histological course ofalcoholic hepatitis. Influence of abstinence, sex and extent ofhepatic damage. J Hepatol 1986;2:33–42.
2. Purohit V, Russo D. Cellular and molecular mechanisms of alco-holic hepatitis: introduction and summary of the symposium.Alcohol 2002;27:3–6.
3. Walsh K, Alexander G. Alcoholic liver disease. Postgrad Med J2000;76:280–286.
4. Maddrey WC, Boitnott JK, Bedine MS, et al. Corticosteroid ther-apy of alcoholic hepatitis. Gastroenterology 1978;75:193–199.
5. Dominguez M, Rincon D, Abraldes JG, et al. A new scoring systemfor prognostic stratification of patients with alcoholic hepatitis.Am J Gastroenterol 2008;103:2747–2756.
6. Ramaiah SK, Jaeschke H. Role of neutrophils in the pathogenesisof acute inflammatory liver injury. Toxicol Pathol 2007;35:757–766.
7. Tilg H, Diehl AM. Cytokines in alcoholic and nonalcoholic steato-
hepatitis. N Engl J Med 2000;343:1467–1476.
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
R
Hb
A
eUt
C
CLI
NIC
AL–
LIV
ER,
PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
May 2009 CXC CHEMOKINES IN ALCOHOLIC HEPATITIS 1649
8. Taieb J, Mathurin P, Elbim C, et al. Blood neutrophil functions andcytokine release in severe alcoholic hepatitis: effect of cortico-steroids. J Hepatol 2000;32:579–586.
9. Taieb J, Chollet-Martin S, Cohard M, et al. The role of interleu-kin-10 in severe acute alcoholic hepatitis. Clin Biochem 2001;34:237–238.
0. Naveau S, Chollet-Martin S, Dharancy S, et al. A double-blind ran-domized controlled trial of infliximab associated with prednisolone inacute alcoholic hepatitis. Hepatology 2004;39:1390–1397.
1. Boetticher NC, Peine CJ, Kwo P, et al. A randomized, double-blinded, placebo-controlled multicenter trial of etanercept in thetreatment of alcoholic hepatitis. Gastroenterology 2008;135:1953–1960.
2. Belperio JA, Keane MP, Arenberg DA, et al. CXC chemokines inangiogenesis. J Leukoc Biol 2000;68:1–8.
3. Bizzarri C, Beccari AR, Bertini R, et al. ELR� CXC chemokines andtheir receptors (CXC chemokine receptor 1 and CXC chemokinereceptor 2) as new therapeutic targets. Pharmacol Ther 2006;112:139–149.
4. Graves DT, Jiang Y. Chemokines, a family of chemotactic cyto-kines. Crit Rev Oral Biol Med 1995;6:109–118.
5. Maltby J, Wright S, Bird G, et al. Chemokine levels in human liverhomogenates: associations between GRO alpha and histopatholog-ical evidence of alcoholic hepatitis. Hepatology 1996;24:1156–1160.
6. Marra F. Chemokines in liver inflammation and fibrosis. FrontBiosci 2002;7:d1899–914.
7. Bautista AP. Neutrophilic infiltration in alcoholic hepatitis. Alcohol2002;27:17–21.
8. Bird G. Interleukin-8 in alcoholic liver disease. Acta GastroenterolBelg 1994;57:255–259.
9. Ciecko-Michalska I, Szczepanek M, Cibor D, et al. Serum cytokineconcentration as prognostic factor in patients with alcoholic liverdisease. Przegl Lek 2006;63:249–252.
0. Hill DB, Marsano LS, McClain CJ. Increased plasma interleukin-8concentrations in alcoholic hepatitis. Hepatology 1993;18:576–580.
1. Huang YS, Chan CY, Wu JC, et al. Serum levels of interleukin-8 inalcoholic liver disease: relationship with disease stage, biochem-ical parameters and survival. J Hepatol 1996;24:377–384.
2. Huang YS, Wu JC, Chang FY, et al. Interleukin-8 and alcoholicliver disease. Zhonghua Yi Xue Za Zhi (Taipei) 1999;62:395–401.
3. Ishii K, Furudera S, Kumashiro R, et al. Role of serum interleu-kin-8 and intercellular adhesion molecule-1 in the severity ofalcoholic hepatitis. Alcohol Alcohol Suppl 1994;29:81–85.
4. Colmenero J, Bataller R, Sancho-Bru P, et al. Hepatic expression ofcandidate genes in patients with alcoholic hepatitis: correlation withdisease severity. Gastroenterology 2007;132:687–697.
5. Afford SC, Fisher NC, Neil DA, et al. Distinct patterns of chemo-kine expression are associated with leukocyte recruitment inalcoholic hepatitis and alcoholic cirrhosis. J Pathol 1998;186:82–89.
6. Hasin D. Classification of alcohol use disorders. Alcohol ResHealth 2003;27:5–17.
7. Bosch J, Garcia-Pagan JC, Berzigotti A, et al. Measurement ofportal pressure and its role in the management of chronic liverdisease. Semin Liver Dis 2006;26:348–362.
8. Asselah T, Bieche I, Laurendeau I, et al. Liver gene expressionsignature of mild fibrosis in patients with chronic hepatitis C.Gastroenterology 2005;129:2064–2075.
9. Livak KJ, Schmittgen TD. Analysis of relative gene expressiondata using real-time quantitative PCR and the 2(-delta delta C(T))method. Methods 2001;25:402–408.
0. Iimuro Y, Gallucci RM, Luster MI, et al. Antibodies to tumor
necrosis factor alfa attenuate hepatic necrosis and inflammationcaused by chronic exposure to ethanol in the rat. Hepatology1997;26:1530–1537.
1. Ponnappa BC, Israel Y, Aini M, et al. Inhibition of tumor necrosisfactor alpha secretion and prevention of liver injury in ethanol-fedrats by antisense oligonucleotides. Biochem Pharmacol 2005;69:569–577.
2. Saito H, Ishii H. Recent understanding of immunological aspectsin alcoholic hepatitis. Hepatol Res 2004;30:193–198.
3. Siegmund S, Spanagel R, Singer MV. Role of the brain-gut axis inalcohol-related gastrointestinal diseases—what can we learnfrom new animal models? J Physiol Pharmacol 2003;54(Suppl4):191–207.
4. Rincon D, Lo IO, Ripoll C, et al. Prognostic value of hepaticvenous pressure gradient for in-hospital mortality of patients withsevere acute alcoholic hepatitis. Aliment Pharmacol Ther 2007;25:841–848.
5. Spahr L, Rubbia-Brandt L, Frossard JL, et al. Combination ofsteroids with infliximab or placebo in severe alcoholic hepatitis: arandomized controlled pilot study. J Hepatol 2002;37:448–455.
6. Gonzalez-Quintela A, Campos J, Gude F, et al. Serum concentra-tions of interleukin-8 in relation to different levels of alcoholconsumption. Cytokine 2007;38:54–60.
7. Swiatkowska-Stodulska R, Bakowska A, Drobinska-Jurowiecka A.Interleukin-8 in the blood serum of patients with alcoholic liverdisease. Med Sci Monit 2006;12:CR215–CR220.
8. Jaeschke H. Neutrophil-mediated tissue injury in alcoholic hepa-titis. Alcohol 2002;27:23–27.
9. Bautista AP. Chronic alcohol intoxication primes Kupffer cells andendothelial cells for enhanced CC-chemokine production andconcomitantly suppresses phagocytosis and chemotaxis. FrontBiosci 2002;7:a117–a125.
0. Tsukamoto H. Cytokine regulation of hepatic stellate cells in liverfibrosis. Alcohol Clin Exp Res 1999;23:911–916.
1. Bertolani C, Sancho-Bru P, Failli P, et al. Resistin as an intrahe-patic cytokine: overexpression during chronic injury and inductionof proinflammatory actions in hepatic stellate cells. Am J Pathol2006;169:2042–2053.
2. McClain CJ, Barve S, Deaciuc I, et al. Cytokines in alcoholic liverdisease. Semin Liver Dis 1999;19:205–219.
3. Jaruga B, Hong F, Kim WH, et al. IFN-gamma/STAT1 acts as aproinflammatory signal in T cell-mediated hepatitis via inductionof multiple chemokines and adhesion molecules: a critical role ofIRF-1. Am J Physiol Gastrointest Liver Physiol 2004;287:G1044–G1052.
4. Cavalieri B, Mosca M, Ramadori P, et al. Neutrophil recruit-ment in the reperfused-injured rat liver was effectively attenu-ated by repertaxin, a novel allosteric noncompetitive inhibitorof CXCL8 receptors: a therapeutic approach for the treatmentof post-ischemic hepatic syndromes. Int J Immunopathol Phar-macol 2005;18:475–486.
Received August 05, 2008. Accepted January 29, 2009.
eprint requestsAddress requests for reprints to: Ramón Bataller, MD, Liver Unit,
ospital Clínic, Villarroel 170, 08036 Barcelona, Spain. e-mail:[email protected]; fax: 34 934515522.
cknowledgmentsThe authors thank Cristina Millán and Elena Juez for their
xcellent technical support, the personnel of the Liver Hemodynamicnit, Xavier Forns and Stella Martínez for collaboration in obtaininghe samples, and Roser Casamitjana for technical support.
onflicts of interest
The authors disclose no conflicts.
F
Tf0
(dFg
CLIN
ICA
L–LIVER
,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
1650 DOMINGUEZ ET AL GASTROENTEROLOGY Vol. 136, No. 5
undingThis work is supported by grants from the Ministerio de Ciencia y
ecnología, Dirección General de Investigación (SAF 2005-06245),rom the Instituto de Salud Carlos III (FIS 05/050567, FIS PI
60085, and PI 080237), and from the European Community SV2006-CE036644). Dr Dominguez received a grant from the Institut’Investigacions Biomèdiques August Pi i Sunyer and from theundación Banco Bilbao Vizcaya Argentaria. Dr Moreno received arant from the Institut d’Investigacions Biomèdiques August Pi i
unyer.Copyright © 2022 FDOKUMEN