Hensley, Loren B., Jr., Ed. TITLE Health Education Teaching Ide
304
DOCUMENT RESUME ED 346 038 SP 033 760 AUTHOR Loyal Richard, Ed.; Hensley, Loren B., Jr., Ed. TITLE Health Education Teaching Ideas: Secondary. Revised Edition. INSTITUTION American Alliance for Health, Physical Education, Recreation and Dance. Reston, VA. Association for the Advancement of Health Education. REPORT NO ISBN-0-88314-529-4 PUB DATE 92 NOTE 304p. AVAILABLE FROM American Alliance for Health, Physical Education, Recreation and Dance. 1900 Association Drive, Reston, VA 22091. PUB TYPE Collected Works - General (020) -- Guides - Classroom Use - Teaching Guides (For Teacher) (052) EDRS PRICE MF01 Plus Postage. PC Not Available from EDRS. DESCRIPTORS *Class Activities; Curriculum Enrichment; *EducClional Games; *Health Education; Lesson Plans; Secondary Education; Substance Abuse; Teaching Guides; *Teaching Methods ABSTRACT Part I of this teaching guide contains teaching strategies which originally appeared in the "Journal of Health nucation" (JHE) and were included in the first edition of this guide, published in 1983. Part II includes teaching strategies published in JHE since 1983. The guide is designed to be a reference for those seeking workable ideas in teaching and delivering health education programs to junior and senior high school students. However, the material can be adapted for middle school through college level. Within each part, articles focus on two major areas: process and content. Examples of process-focused articles are: "Health Games"; "Health Science Fairs"; "The Writing Process in Health Class"; "Teaching about Authoring Systems: Instructional Design Tools for Health Education"; and "Using College Students as Senior Peer Teachers in Youth-to-Youth Health Education." EXamples of content-focuzed articles are: "Once upon a Synapse: A Drag Education Simulation in Three Acts"; "Teaching Abstinence to Today's Teens"; "Te ching the Four Cs of First Aid"; "Student-to-Student Teaching abaAt Tobacco Smoking"; and "Coping with Violence." (IAB) *********************************************************************** Reproductions supplied by EDRS are the best that can be made from the original document. ***********************************************************************
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Hensley, Loren B., Jr., Ed. TITLE Health Education Teaching Ide

DOCUMENT RESUME
ED 346 038 SP 033 760
AUTHOR Loyal Richard, Ed.; Hensley, Loren B., Jr., Ed.TITLE Health Education Teaching Ideas: Secondary. Revised
Edition.INSTITUTION American Alliance for Health, Physical Education,
Recreation and Dance. Reston, VA. Association for theAdvancement of Health Education.
REPORT NO ISBN-0-88314-529-4PUB DATE 92NOTE 304p.AVAILABLE FROM American Alliance for Health, Physical Education,
Recreation and Dance. 1900 Association Drive, Reston,VA 22091.
PUB TYPE Collected Works - General (020) -- Guides - ClassroomUse - Teaching Guides (For Teacher) (052)
EDRS PRICE MF01 Plus Postage. PC Not Available from EDRS.DESCRIPTORS *Class Activities; Curriculum Enrichment;
*EducClional Games; *Health Education; Lesson Plans;Secondary Education; Substance Abuse; TeachingGuides; *Teaching Methods
ABSTRACTPart I of this teaching guide contains teaching
strategies which originally appeared in the "Journal of Healthnucation" (JHE) and were included in the first edition of thisguide, published in 1983. Part II includes teaching strategiespublished in JHE since 1983. The guide is designed to be a referencefor those seeking workable ideas in teaching and delivering healtheducation programs to junior and senior high school students.However, the material can be adapted for middle school throughcollege level. Within each part, articles focus on two major areas:process and content. Examples of process-focused articles are:"Health Games"; "Health Science Fairs"; "The Writing Process inHealth Class"; "Teaching about Authoring Systems: InstructionalDesign Tools for Health Education"; and "Using College Students asSenior Peer Teachers in Youth-to-Youth Health Education." EXamples ofcontent-focuzed articles are: "Once upon a Synapse: A Drag EducationSimulation in Three Acts"; "Teaching Abstinence to Today's Teens";"Te ching the Four Cs of First Aid"; "Student-to-Student TeachingabaAt Tobacco Smoking"; and "Coping with Violence." (IAB)
***********************************************************************
Reproductions supplied by EDRS are the best that can be madefrom the original document.
***********************************************************************

A
t,
.L
kofr.'#.74.
Or
In NINCLUDING 69 NEW TEACHING IDEAS
U S DEPARTMENT OF EDUCATIONONIce of Educational Research and Improvement
EDUCATIONAL RESOURCES INFORMATIONCENTER (ERIC)
CI\ C Tnia document nos been reproduced astr\ retelved from the person or organization
originating ItC MinOr changes have been mad. to improve
reproduchon Quality
Points of view or OPoll0+4 $11110 in INS dOCumerit do not necessarily represent officialOERI position or policy
k
"PERMISSION TO REPROCUCE THISMATERIAL IN MICROFICHE ONLYHAS BEEN GRANTa) BY
TA
4114PeRp BEST COPY MAILZLETO THE EDUCATIO RESOURCESINFORMATION CENTER (ERIC1."

Purposes of the AmericanAlliance for Health, Physical Education,
Recreation and Dance
The American Alliance is an educational organization, structured for the purposes ofsupporting, encouraging, and providing assistance to member groups and their person-nel throughout the nation as they seek to initiate, develop, and conduct programs inhealth, leisure, and movement-related activities for the enrichment of human life.
Alliance objectives include:
1. Professional growth and development--to support, encourage, and provide guidancein the developmen and conduct of programs in health, leisure, and movement-relatedactivities which are based on the needs, interests, and inherent capacities of the indi-vidual in today's society.
2. Communication--to facilitate public and professional understanding and apprecia-tion of the importance and value of health, leisure, and movement-related activities asthey contribute toward human we'll-being.
3. Research--to encourage and facilitate research which will enrich the depth and scopeof health, leisure, and movement-related activities; and to disseminate the findings ..othe profession and other interested and concerned publics.
4. Standards and guidelines--to further the continuous development and evaluation ofstandards within the profession for personnel and programs in health, leisure, andmovement-related activities.
5. Public affairs--to coordinate and administer a planned program of professional,public, and governmental relations that will improve education in areas of health.leisure, and movement-related activities.
6. To conduct such other acti vities as shall be approved by the Board of Governors andthe Alliance Assembly provided that the Allianre shall not engage in any activity whichwould be inconsistent with the status of an educational and charitable organization asdefined in Section 501(c)(3) of the Internal Revenue Code of 1954 or any successorprovision thereto, and none of the said purposes shall at any time be deemed or con-strued to be purposes other than the public benefit purposes and objectives consistentwith such educational and charitable status.
Bylaws, Article 111

Health EducationTeaching Ideas:
SECONDARY
Revised EditionPart I, Richard Loya, Editor
Part II, Lorer B. Bens ley, Jr., Editor
Sponsored by theAssociation for the Advancement
of Health Education
an association of the
Ameri :an Alliance forHealth, F hysical Education,
Recreation and Dance
4
Nu-

Copyright © 1992American Alliance for Health,
Physical Education, Recreation and Dance1900 Association DriveReston, Virginia 22091
ISBN 0-88314-529-4
CON3 'NTSPART I
Foreword to Part I, Kathleen Middleton
Focus on Process
1 Stress on Reading, Elaine Ha ls 1
2 Affective Evaluation Techniques in School Health Education,Mary S. Sutherland 2
3 Five Cures for Dull Health Curriculums, Loren B. Bens ley, Jr. 54 Vary Your Teaching Methods, Glen G. Gilbert 75 Films for Effective Affective Teaching, James R. Mullen 96 Effective Teaching: Variety in the Classroom, Mary Sutherland and
William Hemmer 107 Health Science Fairs, Henry A. Lasch 148 The Open ContractA Program of Individualized Study, B.E. Pruitt 169 The Many Faces of Role Playing, Lynn Teper-Singer 1810 Extra Credit--Make It Meaningful, George F. Carter 2011 Promoting Fxperiential Learning, Michael Hamrick and Carolyn Stone 2112 The Hospital as Motivatoi for Health Learning, Saul Ross 2513 Field Trips, James H. Price 2714 Health Games 28iris) Health Games, Simulations, and Activities, David E. Corbin and
David A. Sleet 2916 Learning Games 3117 Horse Racing in the Classroom, Phillip Hossler 3318 Fantasy Games, Ratph Bates 3419 Choices, Lynn Teper-Singer 3520 Constructing an Educational Game, Sally L. Easierbrook 3621 Health 4 Fun: A Game of Knowledge, Raymond Nakamura 3722 School Health Bee, Bernard S. Krasnoui 3823 Not Merely Nostalgia, Ralph Edwardf, 3924 Health in Concert, Clay Williams and Judy Scheer 4025 Tuning in to Health Education, Warren L. Mc Nab 4126 Ideas for Successful Health Teaching, Loren B. Bens ley, Jr. 4227 The Student Interview Technique, Marc E. Meyer 4428 Positive Peer Influence: School-Based Prevention, Aida K. Davis,
Joan M. Weener, and Robert E. Shute 4529 Ernie, Lillian D. Fesperman 49

Focus on Content
Addictive Behaviors
30 Empathizing with Addicts, Peter Finn 53
31 How Much Can I Drink? H. Richard Travis 55
32 Senator Hogwash, Michael Young 58
33 Student-to-Student Teaching About Tobacco Smoking, Lorraine J. Henke 57
34 The Smoking Game, Ian Newman 59
35 Making Tobacco Education Relevant to the School-Age Child,John R. Seffrin 63
36 4\ Humanistic-Individualized Approach to Drug Education,Jerry L. G-eene and Phillip G. Huntsinger 68
37 Drug Use Situations, Bruce A. Uhrich 69
38 Chemically Dependent--But Only for One Week, Kathleen Fischer 70
39 Learning by Teaching, Elaine Ha Is 72
Aging
40 Aging: A Need for Sensitivity.. Kenneth A. Briggs41 Picnic in the Park: Humanizing an Aging Unit in a Personal Health Class.
Michael J. Gaeta
Consumer Health
73
75
42 Health Anagrams, Kathleen M. Siegwarth 78
43 Consumer Wellness, One School's Approach, Jon W. Hisgen 79
44 A Healthy Consumer Health Class, Tom McFarland and Ann Rudrauff 81
45 The Teenage Consumer, Lee Ann Larson 82
46 Crisis Hot Line Experience, Aloysius J. Jangl 84
47 Health Help Phone Numbers, Richard C. Hohn 86
48 Students Can Have a Say, Joan L. Bergy and Barney Hantunen 87
Death ane hung
49 A Unit for Independent Study in Death Education, Joan D. McMahon 89
50 Put a Little Life in Your Death, Charles R. O'Brien 94
51 Death Education: An Integral Part of School Health Education,Darrel Lang 95
52 A Teaching Strategy on I ragedy, Connie Jo Dobbelaere 97
Environmental Health
53 Health or Hazard? A Post-China Syndrome Game, Moon S. Chen, Jr. 99
54 Nuclear Power Debate, Bruce G. Morton 100
7
55 Health and Safety Education from the Trash Can, J. Clay Williams andJudith K. Scheer 101
56 Ecology Games, Ronald W. Hyatt 10357 Guidelines for a Recycling Project, George H. Brooks 105
Family Life
58 Easy Ways of Getting into Trouble When Teaching Sex Education,Glen G. Gilbert 107
59 Three Teaching Strategies, Florence J. Snarski and Cecilia A. Lynch 10960 The Implementation of Contraceptive Education, Warren L. McNab 11161 Pregnancy--A Gaming Technique, Edward T. Turner 11262 Contraception-Abortion Lifeline, Glenn E. Richardson 11463 Teaching Students About Their Future Role as Parents, Jan Young 11564 Ask the Students Themselves, A. Gordon Bennett 11765 Test Tube Considerations, Deborah A. Dunn 11866 Selected Impacts of Contraception on Man and/or Society,
Patrick Kidd Tow 119
Mental Health
70 On the Level, Gus T. Dalis 12671 Perceptions of Me, Jerrold S. Greenberg 12972 Enhancing Positive Self-Concept Through Creativity in the Classroom,
Barbara Beier 13173 Ideas from a Class in Interpersonal Relations, Caroll Kaiser 13274 Role Playing as a Tool in Mental Health Education, Lynn Teper 13475 The Mirror Game, Rosa Sullivan 13676 How to Cope with Stress in the Classroom, Charles C. Davis 13777 Coping with Violence, Elaine Hals 13978 Personality Spokes, Rosa Sullivan 14079 About Yourself, Ruth C. Engs 14180 A Lesson on Stress, Janet H. Shirreffs 14281 Mental Health Auctioning Strategy, Patrick Kidd Tow 14482 People Labeling Strategy, Patrick K. Tow and Hal Wingard 145
Nutrition
83 Creative Food Labels: Consumer Health Education, Moon S. Chen, Jr. 14684 Sensible Dieting, Marilyn Mudgett and Dorothy Culjat 147
S
pi

PART II
Foreword to Part II, Loren B. Bens ley
Focus on Process
150
85 The Writing Process in Health Class, Vicki Steinberg and Teresa M. Fry 153
86 Logo-Mania: Creative Health Art, Frank Calsbeek 155
87 Overcoming Xenophobia: Learning To Accept Differences,Judith A. Baker 157
88 Factors Important in Teaching Controversial Issues, Ansa Ojanlavnn 159
89 Teaching Ai)out Authoring Systems: Instructional Design Tools forHealth Education, Paul D. Sarvela and Marilyn J. Karaffa 161
90 Tic-Tac-Toe, Mary Lawler 163
91 Picture Charades: A Health Teaching Device, Richard T. Mackey 165
92 Drawing Interpretations of Health, Vicki L. Cleaver 166
93 Ur .ng Team Games to Teach Health, Mark A. Croson and Rose Ann Benson 167
94 The Concept of Health and Techniques of Conceptual Analysis,Joseph E. Balog 169
95 The Town Council Meeting: Decision Making Through a Large GroupRole Play, James D. Brown 172
96 The Health Reporter Pool, David Wiley 17397 Health Education Supermarket, Mary S. Sutherland 174
98 Health Education to the Third Power (Cubed?), Susan Cross Lipnickey 175
99 Junior High School Students as Facilitators of Elementary School HealthEducation Carnivals, David K. Hosick and Parris R. Watts 177
100 Thinking and Writing: A Strategy for Teaching Positive HealthDecision Making, Paul Villas 180
101 Personal Health Via Community Health, Linda Olasov 181
102 Using College Students as Senior Peer Teachers in Youth-to-YouthHealth Education, Anthony G. Adcock 183
103 Judgments Required from the Residency Coordinator, William N. Washington 185104 A Community Resource Class Assignment, Ansa Ojanlatva 188105 Evaluating Health News, Michele J. Hawkins 190
106 The Classics of Epidemiology: A Critical Thinking Approach,Wesley E. Hawkins 192
107 Discipline: A Parenting Dilemma, Patrick K. Tow and Warren L. Mc Nab 194
108 Counterbalancing Parental Concerns in Health Education,Lorraine G. Davis and Shirley Holder Hazlett 197
109 Incorporating Health Education Competencies into a Content Course:The Disease Guidebook Project, Joanna Hayden 199
110 Politics and Health, Randall R. Cottrell 201

Focus on Content
Addiction
111 Inoculating Students Against Using Smokeless Tobacco,Melody Powers Noland and Richard S. Riggs 205
112 The 12 Puffs of Christmas, Warren Mc Nab 208113 Drive-A-Teen--A Program to Prevent Drinking & Driving, Susan Willey Spa lt 209114 Analyzing Cigarette Smoke, David M. White and Linda H. Rudisill 211115 Promoting a Natural High, Catherine J. Paskert 213116 Alcoholics Anonymous: The Utilization of Social Experience in the
Classroom, Robert G Yasko 215117 "Can a Bike Run on Beer," Melvin H. Ezell, Jr. 217118 Once Upon a Synapse: A Drug Education Simulation in Three Acts,
William M. London 219119 Investigating the Social Aspects of Alcohol Use, Tom V. Savage 2221.7.(:; Drug Use, Misuse and Abuse as Presented in Movies, Kerry J. Redican,
Barbara L. Redican, and Charles R. Baffi 224121 Learning About Alcohol Drinking Attitudes and Motivations by
Examining the Vocabulary of Drunkenness, William M. London 226
Aging
122 Helping College Students Understand the Older Adult, Margaret J. Pope 228123 As Old as Trees, Glenn E. Richardson and Susan Bicknell 229
Chronic Diseases
124 Digging for Healthy Hearts: A Simulated Archaeological Dig for thePrevention of Cardiovascular Disease; Wesley E. Hawkins
125 Cancer: A Mini-Documentary, Stephen C. Corey
Consumer Health
126 Consumer Health: Medical Quackery, Carolyn E. Cooper
Enviromnental Health
127 Environmental Health Simulations: Island City and Production,Glenn E. Richardson, Alan Burns, and Janet Falcone
Family Life Education
230233
235
237
128 Reducing Anxiety About Teaching a Human Sexuality Program,Louise Row ling 239
1 0

129 Are You Ready for Prime Time Birth Control? Pamela Wild and Linda Berne 240130 "Hey! How Did That Baby Live in That Test Tube?" David A. Birch 242131 Actions Teach Better Than Words: Teen Life Theater and Role Play in
Sex Education, Peggy Brick 243132 Abortion Attitude Scale, Linda A. Sloan 247133 Marriage Yesterday and Today, Margaret J. Pope 249134 Teaching Abstinence to Today's Teens, Dee Gibbs Smalley 250135 Group Discussion on Contraceptive Issues, Barbara A. Rienzo 252136 Developing and Rejuvenating Relationships, Jane W. Lammers 254137 Courtesies and Rights Within Relationships, Bethann Cinelli and Robert Nye 256
First Aid and Safety
138 CPR Drilling Revisited, Mark J. Kittleson 258139 The Improvised ManikinHomemade CPR Equipment, Mardie E. Burckes 260140 Teaching the Four Cs of First Aid, Mark J. Kittleson 264141 Mock Disaster: An Effective Lesson in Preparation for the Real Thing,
Gary M. English and Cathie G. Stivers 263142 The Importance of Child Safety Seat Education, Karen D. Li ller 266
HIV-AIDS
143 AIDS "To Tell the Truth" Gaming Activity, Jon W. Hisgen 268144 AIDS/HIV Teaching Ideas, Barbara Beier, J. Leslie Oganowski,
Richard A. Detert, and Kenneth Becker 271
Mental and Emotional Health
145 Stress Manifestations Among Adolescents, Charles Regin 274146 An Introductory Activity for Adolescent Communication and Intimacy,
G. Greg Wojtowicz 276147 Show and Tell: Developing an Appreciation of Diversity, Kathryn Rolland 279148 Teaching Self-Awareness Through Idiosyncrasies, Patrick K. Tow,
Beverly Johnson, and Patricia N. Smith 280
Nutrition
149 Can You Name These Foods? Eileen L. Daniel 282150 "Digesting" Health Information, Richard A. Crosby 283151 Nutrition Is the Name of the Game, Paula R. Zaccone 284
Personal Health
152 Sun Smart: A Peer-Led Lesson on the Effects of Tanning and Sunning onthe Skin, Mary Elesha-Adams and David M. White
153 A Quick and Easy Check for Foot Problems, Dianne Boswell O'Brien288290

PART I

Foreword
Where is health taught at the secondary level? In the elementaryschool it is usually taught by the elementary teacher along with twentyor so other subjects. In the junior and senior high schools it can befound in many places: health classes; science classes; family livingclasses; social science classes; home economics classes; and drivers'education classes. In the school district where I taught, it was found inone high school in a class entitled "State Requirements." This uniqueclass included all the "loose end" topics that were required by the Stateof California to be covered before high school graduation.
Wherever health is taught in the schools, the ultimate success withstudents is not determined by the title of the class or placement withinthe curriculum. It is largely dependent upon the quality of the teach-ing. Health can be the most exciting, interesting, and meaningful classin the high school curriculum. Dedicated, energetic, caring teachers domake a difference. Teented teachers can motivate and positively affectthe lives of the most gifted students as well as the ones with specialproblems. This book, Health Education Teaching Ideas: Secondary, is forthose teachers. It includes innovative teaching strategies that are prac-tical and appropriate in the secondary classroom. The original articlesappeared in the "Teaching Ideas" column of Health Education and werecompiled by a high school health teacher. This book should be a usefuland exciting addition to the library of any instructor responsible forhealth education at the junior and senior high school levels.
Kathleen Middleton, DirectorSchool Health Programs
National Ce-ter for Health Educationid Contributing Editor to
"Teaching Ideas" column ofHealth Education

Focus on Process
1 4
1 TEACHNG IDEAS
Stress on Reading
ELAINE HALS is a teacher of health edu-cation at South Shore High School, Brook-lyn, New York 11236.
In the last few years large citiesthroughout the United States havebegun to put pressure on school dis-tricts to stress the "three R's" morereading, more math, and more writing.In New York City, where I teach, all ofthe principals have been instructed toincrease the number of periods perweek devoted to reading and other ba-sics in the elementary schools. The highschools have been instructed that allsubject areas give reading and writtenhomework several times weekly, andthat course curriculum should stress thebasics. Employers have also beenpressuring the schools to improve thereading ability of their graduates. Thepush is now on to raise the basic skillslevel of today's youth.
How does this push for basics affectus as health educators? Do we regress topredominantly cognitive teaching? Dowe return to stressing facts, and onlythose things that can be read, written,and tested? Ab.:nit tc.n years ago healtheducators began to realize the impor-tance of humanistic values and behav-ior modification that could be accom-plished in health teaching. Our fieldhas seen positive changes, and we haveshifted our emphasis into the affectivedomain. Health education has truly be-come learning for livingexaminationof values, decision making, and behav-ioral alternatives. If we help youngpeople become better, healthier, andmore aware, but do not help them toread better, are we in line with the edu-cational goals of the country? Should webe? The pendulum has swung back topre-1960s education. Should we ashealth educators re-evaluate our goals,and fall in line with other subject areas?Reading and writing are important; I donot mean to demean their significance.Yuuns people entering the job marketmust have basic skills in order to sur-vive.
Because both affective and cognitiveeducation are valuable, I feel that we ashealth educators must combine them inwir teaching. Following you will find afew suggestions.
1. Help stude, to explore new andcontroversial health issues by havingthem read and evaluate current news-paper and magazine articles on varioussubjectslaetrile, cloning, test tubebabies, food additives, new drugs, dis-ease cures.
2. Have students keep a written log(to be checked by the teacher periodi-cally) of feelings about the class, theirdaily decisions, new material learned,or anything the teacher feels is relevantto the class and the students.
3. Have students keep their own vo-cabulary list of new words learned inclass or from text, pamphlets or otherreading sources.
4. Have students write letters re-questing information, pamphlets, in-terviews.
5. Offer reading lists of novels, maga-zines, etc. for outside projects or justadditional information.
6. Give students controversial prob-lems for homework and have themwrite answers that can later be dis-cussed in class and even made into roleplaying situations.
Your parents catch you and yourfriends smoking grass in your room,what would you do?
You are caught cheating on an examand the teacher wants to see your par-ents
You find that you have venerealdiseaseyour boy or girl friend mayhave it, too-- what do you do?
Do the terminally ill have the right toknow they are dying?
You know something that could getyour best friend in trouble. You feel whatthis person did was wrong. You aregoing to be questioned about the situa-tion. What will you do?
. 'Jse pamphlets and current publi-cations instead of, or in addition to, textbooks.
8. Divide class into groups. Haveeach group research and investigate dif-ferent aspects of a subject and teach theclass.
9. Creative projects that combinereading and writing with other disci-plines such as art, photography, music.
10. Have class construct interviews orsurveys, then have students survey orinterview selected individuals andevaluate results.
Cognitive and affective can be madeto work well together. We do not haveto forsake our humanistic, affective ap-proach to health education in order tohelp our students read and write better.Instead of changing the educationalgoals we have for our students, weshould just add one morea betterknowledge of the basics and how theycan help our students live better,healthier lives.
1 5 1
2 TEACHING IDEAS
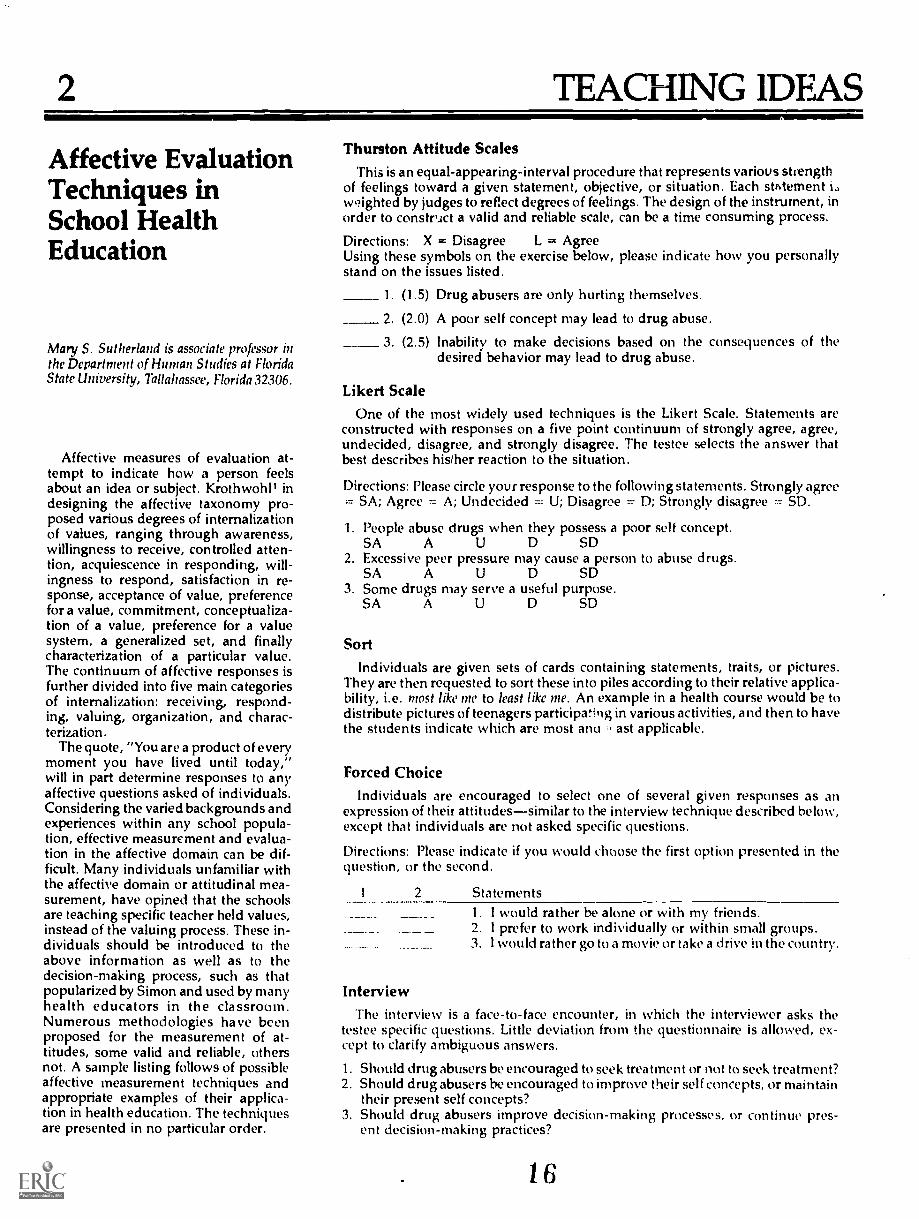
Affective EvaluationTechniques hiSchool HealthEducation
Mary S. Sutherland is associate professor inthe Department of Human Studies at FloridaState University, Tallahassee, Florida 32306.
Affective measures of evaluation at-tempt to indicate how a person feelsabout an idea or subject. KrothwohP indesigning the affective taxonomy pro-posed various degrees of internalizationof values, ranging through awareness,willingness to receive, controlled atten-tion, acquiescence in responding, will-ingness to respond, satisfaction in re-sponse, acceptance of value, preferencefor a value, commitment, conceptualiza-tion of a value, preference for a valuesystem, a generalized set, and finallycharacterization of a particular value.The continuum of affective responses isfurther divided into five main categoriesof internalization: receiving, respond-ing, valuing, organization, and charac-terization.
The quote, "You are a product of everymoment you have lived until today,"will in part determine responses to anyaffective questions asked of individuals.Considering the varied backgrounds andexperiences within any school popula-tion, effective measurement and evalua-tion in the affective domain can be dif-ficult. Many individuals unfamiliar withthe affective domain or attitudinal mea-surement, have opined that the schoolsare teaching specific teacher held values,instead of the valuing process. These in-dividuals should be introduced to theabove information as well as to thedecision-making process, such as thatpopularized by Simon and used by manyhealth educators in the classroom.Numerous methodologies have beenproposed for the measurement of at-titudes, some valid and reliable, othersnot. A sample listing follows of possibleaffective measurement techniques andappropriate examples of their applica-tion in health education. The techniquesare presented in no particular order.
2
Thurston Attitude ScalesThis is an equal-appearing-interval procedure that represents variovs strength
of feelings toward a given statement, objective, or situation. Each stAtementw9ighted by judges to reflect degrees of feelings. The design of the instrument, inorder to construct a valid and reliable scale, can be a time consuming process.
Directions: X = Disagree L = AgreeUsing these symbols on the exercise below, please indicate how you personallystand on the issues listed.
1 (1.5) Drug abusers are only hurting themselves.
2 (2.0) A poor self concept may lead to drug abuse.
3. (2.5) Inability to make decisions based on the consequences of thedesired behavior may lead to drug abuse.
Likert ScaleOne of the most widely used techniques is the Likert Scale. Statements are
constructed with responses on a five point continuum of strongly agree, agree,undecided, disagree, and strongly disagree. The testee selects the answer thatbest describes his/her reaction to the situation.
Directions: Please circle your response to the following statements. Strongly agree= SA; Agree = A; Undecided = U; Disagree = D; Strongly disagree = SD.
1. People abuse drugs when they possess a poor self concept.SA A U D SD
2. Excessive peer pressure may cause a person to abuse drugs.SA A U D SD
3. Some drugs may serve a useful purpose.SA A U D SD
Sort
Individuals are given sets of cards containing statenwnts, traits, or pictures.They are then requested to sort these into piles according to their relative applica-bility, i.e. most like me to least like me. An example in a health course would be todistribute pictures of teenagers participating in various activities, and then to havethe students indicate which are most any ast applicable.
Forced ChoiceIndividuals are encouraged to select one of several given responses as an
expression of their attitudessimilar to the interview technique described below,except that individuals are not asked specific questions.
Directions: Please indicate if you would choose the first option presented in thequestion, or the second.
2 Statements
^1. I would rather be alone or with my friends.2. I prefer to work individually or within small groups.3. I would rather go to a movie or take a drive in the country.
InterviewThe interview is a face-to-face encounter, in which the interviewer asks the
testee specific questions. Little deviation from the questionnaire is allowed, ex-cept to clarify ambiguous answers.
1. Should drug abusers be encouraged to seek treatment or not to seek treatment?2. Should drug abusers be encouraged to improve their self concepts, or maintain
their present self concepts?3. Should drug abusers improve decision-making processes, or continue pres-
ent decision-making practices?
1 6

Rating ScalesRating scales are similar to tne Likert Scale, except that instead of using a
standard set of options, specific adjective/verb describers are utilized:
D:rections: Circle your response about drug abuses on the continuum
DRUG ABUSERS
DRUG ABUSERS
DRUG ABUSERS
Possess noself concept.
Find it verydifficult tocommunicate.Find it verydifficult tomake adecision.
Possess apoor selfconcept.Find itdifficult tocommunicate.Find itdifficult tomake adecision.
Possess agood selfconcept.Find it easyto communicate.
Find it easyto make adecision.
Rating scales can be developed with three to seven responses, using describers orsingle adjectives. The final form should depend on the particular purpose for theutilization of the instrument.
Semantic DifferentialIn this instrument concepts are measured in terms of evaluation (good-bad),
potency (weak-strong), and activity (fast-slow). The respondent checks his re-sponse on the scale; the evaluation process assists in distinguishing differencesbetween concepts and individual responses.
Directions: Place an X or. the scale to indicate your feelings about each statementbelow.
GoodFoo:;shBeneficial
GoodFoolishBeneficial
ABUSING DRUGS IS:
DRUGS CAN BE:
BadWiseHarmful
BadWiseHarmful
Open-ended QuestionsThe open-ended question calls for the respondent to answer by writing state-
ments which reflect an attitude, belief, activity or value. It can assist in measuringattitude structure and socialization.
1. Drug abusers should be encouraged to
2. Drug abuse is
3. A positive self concept is
Projected TechniquesProjected techniques are designed to reveal information about a person's
deeper levels of feelings, and his reactions to a phenomenon via pictures. Gener-ally given are the beginning, middle, and ending of a situation related to thepictures, from which the testee must be able to write a complete story.
Projected BehaviorStudents are placed in a hypothetical situation arid are requested to determine
how they would behave under those circumstances.
Bob and Dan are friends of long standing. Bob tries to interest Dan in smoking ajoint. Dan should:a. Smoke the joint. c. Take the joint and later throw it away.b. Refuse to take the joint. ci. Take the joint and later smoke it in private.
1 7
Additional techniques to be utilizedinclude check lists and ranking sheets,classroom teacher observations, anec-dotal records (summaries of attitudes/behavior by the school staff), time sam-pling (what happened when), socio-grams, social distance scales, guess-whoquestionnaires, and autobiographicalsketches.
In contrasting and comparing the var-ious methods utilized for attitude as-sessment, it is most necessary to estab-lish a set and a setting for instrumentutilization. Each of the abovementionedinstruments can serve a valid and reli-able purpose if applied correctly in thesituation for which it was designed.
Affective measurement and evalua-tion techniques could be used for healthinstruction in many ways.
1. To determine student behavioral infor-mation to assist in the removal of barriers tothe efficientleffective functioning of the class-room educational process. Specifically withthe so-called behavioral problem stu-dent, cumulative records are useful toreinforce comments from anecdotal rec-ords and previous teacher time samplestudies. A sociogram exercise conductedwithin the class determines the problemstudent's social status within his peergroup; but more importantly, teachersand administrators should observe stu-dent attitude and behaviors for true indi-cators of causes of specific problems. Inaddition, a clue to behavioral problems isgained from a problem checklist and theprofessional psychological technique ofa Q Sort described above. However, inthe final analysis, the teacher must usu-ally sit down with the problem studentand communicate directly. The properleading questions should serve to flushout information related to the true causesof the problemis it lack of interest andmotivation, poor self-concept, poorcommunication skills, uncomfortableenvironment or what? The causes ofpoor behavior can trually be determinedby using one or a combination of affec-tive techniques. An appropriate plan ofaction should be developed by the stu-dent, to change his behavior to a moreacceptable level for the classroom.
2. Health Instruction . Many of theseattitudinal devices find their best use inthe area of classroom instruction. AThurstone attitude scale takes consider-able time to develop and field-test, butindicates most clearly differing degreesof feelings toward a topic or statement. Ifthe health educator has time tocomputer-score results, the Likert scalesare most useful to compare differences inattitudes. A modified version of the
3

14
Likert suits small group discussion ac-tivities, as do rating scales, rankingscales, checklists, open-ended sen-tences, projected behavior techniquesand closed sentences directed towardsspecific behavioral objectives. Activitiesshould be deliberately processed, so thatprinciples of communication, self-concept and decision-making may beapplied to specific health content areas.The abovementioned techniques aremarvelous ways in which the class andteacher can get to know and appreciateeach other, as well as marvelous step-ping stones to effective teaching/learning. In summary, an affective tech-nique can be a learning activity, a way ofreinforcing and applying specific contentcovered, and lastly, can be one of manytechniques to evaluate an effectivehealth education program.
3. Attitude Measurement. The meth-ods and techniques described above
4
measure changing attitudes, both shortterm and long term. Instruments mosthelpful in measuring attitudes includeThurstone scales, Likert scales, ratingscales, behavioral projected techniques,and behavioral pre ctices checklists.Great attention should be paid to fakabil-ity, wmantics, and criterion inadequacy.Is the student merely feeding to theteacher what the teacher wants to hear?Do the terms of questions and state-ments mean the same thing to the testerand the testee? Does the test really mea-sure what it is supposed to?
4. Evaluation of Classroom Learn-ing. Attitudinal devices such as open-ended sentences serve to indicate bothteacher effectiveness or learning effec-tiveness. Specific open-ended questionsmight include:
A. Today I learnedB. Today I relearnedC. Today, I wish
In this manner the health educator gainsinsight into the student's evaluation ofwhat is going on in the classroom.
In the final analysis, the setting as re-lated to health education should deter-mine the type of instrument used to ob-tain the most valid and reli:ble informa-tion possible for the most efficient/effective use of time and money for allconcerned parties and purposes.
1. Stanley and K. Hopkins. Educational andpsychological measurement and evaluation. En-glewood Cliffs, New Jersey, 1977, 229.

TEACHING IDEAS
Five Cures for DullHealth Curriculums
LOREN B. BENSLEY, IR., !S professor ofhealth education, Central MichiganUniversity, Mt. Pleasant, Michigan48858.
The health education philoso-phies, concepts, and attitudes of thepast are present in many of today'scurriculums and are breeding irrele-vant, dull, meaningless, distastefulclasses in health education.
We are in a time of educationalrevolutions. Students are question-ing our systems, curriculums, teach-er qualifications, and pedagogy.They find themselves trapped in aneducational system intent on turn-ing them into mechanical robots;irrelevant curriculums combinedwith poor teachers are forced onthem. Fortunately, educational sys-tems are trying to change, but muchof the change is no more than arattempt to refine the existing ma-chinery, making it ever more effi-dent in pursuit of obsolete goals.Alvin Toff ler, in his book FutureShock, suggests that "instead of as-suming that every subject taughttoday is taught for a reason iwelshould begin from the reverse prem-ise: nothing should be included ina required curriculum unless it canbe strongly justified in terms of thefuture. If this means scrapping a
substantial part of the formal cur-riculum, so be it."
Today millions of students are forcedthrough health classes and exposed tomeaningless experiences which will innoway result in favorable health behav-ior.
What evidence do we have to showthe public that we are accomplishingour objectives? Will a student be ahealthier citizen because of a course inhealth education?
It is time that we in health edu-cation produce results, not a collec-tion of meaningless philosophicalstatements and purposes. In orderto produce results two componentsmust be integrated: a relevant cur-
riculum and a creative and com-mitted health educator. When thesetwo components are plugged intoeach other, there will be generatedelectricity, excitement, enthusiasm,and vibrations in the student to turnhim on to health learning. Onlywhen the curriculum and the teach-er are united will there be an illu-rnination of the student. One with-out the other will result in totaldarkness. Unfortunately, much ofour school health education has nothad the proper electrical engineer-ing to illuminate proper health atti-tudes and behaviors of our students.
Health education may not be asbleak as the author has xesented it.Recent years have brought new in-sights and encouragement to cur-riculum development in health edu-cation. Approximately ten years agowe had a national school health ed-ucation study. From this was deviseda sophisticated curriculum based onthe conceptual approach. Aboutfour years ago, the state of Connec-ticut did a comprehensive study onthe health needs and interests ofschool children. Their documenttitled "Teach Us What We Want ToKnow" is extremely valuable in thehands of the health educator. Mostof us are familiar with the efforts ofNew York State in designing a cur-riculura for their public schools.Their most recent adventure in
computerized individualized in-struction is certainly encouraging.The State of Michigan is presentlydeveloping a curriculum K through14 in health education. From themost recent drug abuse crisis haveresulted ;ome excellent curriculumsin this specific subject matter.
Health in Three Grades OnlyThese new efforts are encourag-
ing; however, the relevance of someof the products that have been pre-pared are questionable. Take, forexample, the school health educa-tion study curriculum produced by
the 3M Company. The curriculumis so sophisticated and so compli-cated that 90% of our classroomteachers in Michigan are discour-aged from using it. It cannot be saidthat it isn't a good piece of work; itis in fact a product of excellence.Unfortunately, it's not realistic. Thisauthor questions how realistic theK-12 concept is without trainedhealth educators or health coordi-nators. Wouldn't it be better inhealth education to isolate threegrade levels where health could beemphasized? I suggest that possiblyhealth education be taught in thefourth, seventh, and eleventh grades.
I selected these grade levels be-cause these are the ages where wecan help our students develop de-sirable health behaviors. The nine-year-old has a keen interest in hisbody as well as in health in general.He shows excitement in learningabout the function of his total be-ing. The seventh-grader, on theother hand, is at the critical age indeveloping positive health behav-iors. At age 12 he is confronted withdecisions about whether or not heshould smoke or experiment withalcohol or drugs. At this age sec-ondary sex characteristics develop,which create a variety of physicaland mental problems. The eleventh-grade student has reached the ageof sophistication and needs informa-tion that will guide his behavior asan adult. He is now a health con-sumer and soon will be faced withhealth insurance decisions as wellas a multitude of other alternatives.We must also realize that withinthree years at least half of the girlswill be married.
New Names Can Be Magic
In a typical health course in thepublic schools, units have such ti-tles as Mental Health, First Aid, SexEducation, Alcohol, Tobacco, Drugsand Narcotics, etc. The titles ofthese units themselves are enough
5

to turn the students off to health.We were plagued for years with theterm "hygiene" until the 1920s,when Sally Lucas Jean came up withthe term "health education," indi-cating the change from hygieneteaching to behavior modification. Ithink the time has arrived when we,as health educators, can be morecreative and original in making theappearance of our curriculum excit-ing to the learner. Just a change intitles of the units may turn a stu-dent on to health learning ratherthan turn him off from what hewould anticipate as a dreadful ex-perience. For instance, instead ofcalling a unit First Aid, why not titleit Emergency Medical Care? Sex Ed-ucation could be called Human Sex-uality. A discussion of alcohol, to-bacco, and drugs could be titledMood Modifiers, or a mental healthunit Psychic Ecology. The title of aunit should arouse the student'scuriosity and create interest. A cre-ative and dynamic curriculum be-gins with exciting topics.
Are there other topics not in-cluded in the traditional health cur-riculum which could make thecourse more relevant and preparestudents to face future experiencesthat will affect their mental andphysical well-being? Could we in-troduce a unit, for instance, ondeath education and suicide preven-tion? Why not include a unit onpsychic phenomena, or one calledHealth in the Year 2000?
Try Micro-Courses
On the other hand, the presentcurriculum, based on a unit con-cept, may not be the proper way toteach health. A school using thisconcept may require a one-unithealth education course fo; gradua-tion. In such a school, ninth-gradestudents might attend health educa-tion classes five days a week for onesemester. I would like to propose astudent-centered rather than a
teacher-centered approach to cur-riculum offerings. Under this ap-
6
proach, a variety of micro-courseswould be offered in the curriculum.Students could meet the one-semes-ter requirement by selecting anythree 6-week micro-courses anytime between their freshman andsenior years. This approach is basedon the belief that we in healtheducation cannot accomplish all ofthe objectives for our courses in thelimited time allotted to us. What weend up with is 100% cognitivelearning, with no success in the af-fective domain or action domain. I
agree with Toff ler when he statesthat "children should be permittedfar greater choice than at presentlin selecting their curriculum]; theyshould be encouraged to taste a
wide ariety of short-term courses."'Such everiences should be basedon ivesent as well as future needs.
Certain courses based totally onbehavioral change can be offeredin school curriculums. I can con-ceive of short-term courses onweight control, smoking, abuse, orphysical fitness, and action pro-grams pertaining to ecology. Someof these experiences, if used as
micro-courses, could be offered inthe evening when students couldtake them with their parents. I canforesee parent-child courses inweight control, nutrition, or physi-cal fitness. It seems that there wouldhe a wealth of potential in this typeof cw riculum offering.
Get Involved in the CommunityAnother suggestion is for a prac-
ticum course in which studentswould be actively engaged in a
community project pertaining fo theimprovement of the health of theircommunity. Students should also begiven the opportunity to receivehealth education credit by workingin a local hospital as a candy striper,working with patients as a volunteerin a medical care facility, helpingwith cancer crusades, etc. Theselearning experiences under the su-pervision of qualified people, co-ordinated by the school health ed-
20
ucator, could be extremely relevantand educational for the student. An-other good idea would be to in-clude a course on ecology, or maybea reading class in health education.In addition, I would like to suggestthat an advanced course at thejunior or senior level be offered tostudents on an elective basis to ex-plore in depth a variety of health-related topics. This could be of-fered during the summer when theinstructor could take the class onweekend camping trips and in anoutdoor situation informally intro-duce and discuss ideas pertinent tothe health of both themselves andcodety.
Let Students Do the Teaching
Students can teach a health edu-cation course. Students learn in avariety of waysfrom teachers,from materials, from experiences,and from other students. Much ofwhat a student learns comes fromhis peer group; some of the mostmeaningful learning is from per-sonal experience. It is unfortunatethat many curriculums do not offeropportunities for these types oflearning experiences. In a coursecentered around students teachingstudents, the teacher could identifyfive or six students who have lead-ership abilities and work with themindividually to lead small groups oftheir peers. This gives students re-sponsibility and personalizes theinstruction. This approach could beespecially useful in large classes.
There are a number of opportuni-ties for creativity in health educa-tion curriculum design. The ideaspresented in this article are in-tended to stimulate some thinkingon the part ,of the reader. We haveonly scratched the surface in look-ing for innovations in health educa-tion curriculum development.
Alvin Toffler. Future Shock. NewYork: Bantam Books, 1970. p. 409.
Ibid., p. 412.

4
Vary Your Teaching
Methods
GLEN G. GILBERT is an assistant profes-sor of health education, P.O. Box 751, Port-land State University, Portland, Oregon97207.
Teachers of health education consis-tently ask two basic questions about thedesirability of using innovative teachingmethods. These questions have beenraised during numerous inservice work-shops over the last few years: (1) whyshould we provide a variety of teachingmethods? and (2) how can we providesuch a variety of teaching methods? Theanswers to both questions are extremelyimportant and any competent healtheducator should be able to answer bothquestions.
An answer to the first question can beproposed after referring to what the ex-perts in the field have to say about theneed for variety in teaching methods.These authorities draw conclusionsbased on research and personal experi-ence. They agree that providing a vari-ety of teaching methods is important ifwe are to enhance the learning settingand to overcome any stigma attached tohealth education as the result of histori-cal sins committed during the presenta-tion of health education information. Inaddition, the following are importantreasons for providing a variety of teach-ing methods.
1. An interesting methodology pre-vents many discipline problems. Stu-dents who are interested in what theyare doing are much less likely to act in-appropriately in the classroom. Thisholds true for adult students as well asyounger students.
2. It is a teacher's responsibility to pro-vide an educational environment. Thismeans teachers must do whatever isnecessary and within their capabilitiesto motivate students to favorably alterhealth behavior; experience indicatesthat it is not an easy task. If teachersmust stand on their heads to reach thestudents, then they should do it. Cer-tainly we cannot reach every student,but we can reach many. We cannot allbe showmen or great orators, but weshould do all we can to favorably alterhealth behavior.
TEACHING IDEAS
3. The performance of students is onereflection of teaching performance. Ifstudents are not performing well thenmuch of the responsibility must be as-sumed by the teacher involved. Cer-tainly it is a joint responsibility (studentand teacher), but a large part of it mustlie with the nature of the instruction.Utilizing appropriate methods is likelyto increase student performance.
4. You can make anything worth learn-ing interesting. If the material you arepresenting is truly worth learning thenyou should be able to develop a strategywhereby the worth becomes evident toyour students. Teachers must be willingto face the fact that they may be present-ing irrelevant information. If you can'treadily demonstrate that the informa-tion you are presenting is relevant, youhad better take another look at that in-formation and perhaps update or elimi-nate it.
How do we provide a variety of rele-vant teaching methods? Numerous textshave been written on the subject inhealth education, as well as in otherfields. One technique found very help-ful is to determine objectives to beachieved, then review the followingchart of strategies and make a decisionas to which might best facilitate theachievement of stated objectives.
21
This chart was developed by me foruse with pre-service and in-serviceteachers. Each method is rated as to thelikelihood of that particular method ac-complishing various types of objectives.The ratings listed in three columns tothe right of the method are: "Mr mean-ing most frequently; "0" meaning occa-sionally; or if blank, it is highly unlik*that it would be used in such a manner.
Objectives written in the cognitivedomain generally require recall of in-formation (e.g., the student will be ableto list the seven danger signs of cancer).Affective. objectives generally require ananalysis of feelings or perhaps result inan attitude modification (e.g., the stu-dent will indicate her willingness to as-sume her part of the responsibility forearly detection ot cancer by reportingany unusual findings to her doctor im-mediately without waiting for regularcheckups or pain). Psychomotor objec-tives require action (not just writing andthinking) during the activity or result inthe student carrying out a physical ac-tion (e.g., the student will be able todemonstrate on Resusci-Anne correctmouth-to-mouth resuscitation). Addi-tional information on objectives is read-ily available in any of the methodsbooks listed in the bibliography.
It is suggested that the reader or stu-dent keep clearly in mind the objectivesto be achieved by a class or course, thenreview the list, checking those methodswhich might achieve stated objectives.Faowing such an appraisal, considerhow each checked method might be im-plemented and then make a decisionbased on feasibility and likelihood ofsuccessful accomplishment of objec-tives. Following these guidelines shoulddiscourage selection based only on easeof use and will encourage innovation.
Using this system an appropriatetechnique should be located if the mate-rial being covered is useful and impor-tant. The reader may notice an over-abundance of available cognitive teach-ing methods. It generally requires morepreparation and thought on the part ofthe teacher in order to utilize techniqueswhich influence attitudes and stimulateaction.
This article has presented a rationalefor emp'oying a variety of teachingmethods and has presented a list ofmethods to achieve that end. If readersare unfamiliar with any of the teach-ing methods, they may wish to reviewsome of the sources in the bibliographyand/or correspond with the author.
7

Summary of teaching methods and strategies according to likelihood of meeting objectives incognitive, affective and psychomotor domains
Cogmtwe Affective PsychomotorKnowledge Attitude Action
1. Musk ME 0 02. Cartoons MF ME3. Brainstorming & buzz sessions MF 0 04. Stories with fill-in-the blanks ME 05. Interviews MF 06. l'antomimes ME 0 ME7. Self-appraisal 0 ME 08. Panel discussions ME 09. Visits to agencies 0 0
10. Field trips 0 011. Bulletin boards, displays,
flannel boards ME 012. Transparencies ME 013. Review bees MF14. Value clarification 0 MF 015. Mystery puzzles ME16. Word-o-games ME17. Anagrams ME18. Crossword puzzles ME19. Games ME 0 020. Simulated situations or critical
incidents ME ME ME21. Problem solutions
(a specific technique) ME22. Mock radio and T.V. ME ME 023. Personal health improvement
projects 0 MF ME24. Student produced movies, slides,
or videotapes ME 0 025. Debates ME 0 026. Skits ME 027. Plays MF 028. Role playing 0 Mr29. Self-tests ME30. Surveys 0 ME31. Oral reports
(individual or group) ME 0 032. Guest speakers ME MF33. Computer assisted instruction ME34. Programmed learning ME35. Experiments ME 0 ME36. Demonstrations MF 0 MF37. Mobiles ME38. Charts, transparencies
or graphs ME39. Models ME40. Slides ME ME 041. Videotapes ME 0 042. Auditory tapes or records ME 0 043. Films and film strips ME 0 0
ME= Most frequently0 z Occasionally
If blank, it is rarely or never used in this way.
8
22
5 TEACHING IDEAS
MMES R. MULLEN is a teacher ofEnglish at the Lower Cape MayCounty Regional High School, CapeMay, New jersey 08204.
One of the most significant edu-cational trends of the last decade isthe movement toward what is gen-erally known as affective or hu-manistic education. With roots inthe humanistic psychology of Abra-ham Maslow and human-potentialgrowth centers like the Esalen Insti-tute, humanistic and affective edu-cation (the terms are virtually inter-changeable) deals with the growthof the whole personthe develop-ment of sensory awareness, inter-personal relations, and, perhapsmost important, self-awareness andself-knowledge. Every board of edu-cation in every city and town in thecountly has some general statementof goals for the development of thewhole person (usually couched interms of encouraging "good citi-zenship" and "sound mind"). Butin most schools, these goals areempty pieties. Often the best a
teacher can do is to try to bring stu-dents up to grade, to advance stu-dents in basic skills, and maintaina semblance of order. Issues suchas drug abuse, lack of interest, dis-ruptive behavior, and poor retentionare increasing.
The time has come, more andmore educational reformers believe,for affective education to assume itsrightful place alongside the moretraditional curriculum. One of themain obstacles to this kind ofchange, howeve., is a dearth ofgood, proven materials. Teachers insearch of a geography book to usein their classes can choose fromhundreds, and huge film catalogsare readily available. But if a teach-er tries to find a text or film onaffective education, he'd better havesome inside information.
Films for EffectiveAffective Teaching
One illustration of how usefulmaterials on affective education canbe when they are available is a pro-gram developed by a small firm ofpsychologists and film make7:, inNew York City. The company, FilmModules Inc., is being funded bythe National Institute of MentalHealth, the New York State Depart-ment of Education, and the New
York State Narcotic Addiction Con-trol Commission under the um-brella title "Drug Abuse Self-Aware-ness." Four separate programs forschool-related use have been madeavailable.
Each program in the self-aware-ness series is based on a concept offilm usage which was developed byproducer-therapist Robert Rubin.The concept's first application wasa stress training program for policeofficers. It has been interposedwithin the training programs ofmore than 150 police departmentsthroughout the country since its re-lease in 1970.
The basic premise of Rubin'swork is that in most cases films donot elicit genuine involvement andfeedback, but rather make of theviewer a passive observer who ex-periences the film vicariously, atbest. Starting several years ago, Ru-bin began to explore ways of mak-
0 3
ing film a more directly involvingmedium. The "film modules," as
he calls his films, are structured todemand specific kinds of feedbackand interaction. The result is a re-markably efficient, yet gentle gener-ator of mature behavior.
The heart of each program is a
series of film modules that focus onsituations of tremendou:, emotionalintensity and which suddenly andunexpectedly stop, leaving the view-er so emotionally keyed up thathe or she is likely to have an al-most physical need for a discussionor a general exelange of feelingsand reactions v ith others. As anyteacher who has ever tried to ex-periment with group dynamicsknows, simply saying to students,"Well, what do you feeltell usabout your feelings" is likely toelicit dead silence more than anyother response. The iilm modules,on the other hand, make a verbalresponse a kind of necessary relief.
One indication of the success ofthis concept in forcing a genuineand often profound emotional feed-back from students was the responseto one of the drug abuse self-aware-ness films for high school stu-dents. A 17-minute module entitled"Fear" was tested with a group ofhigh school teenagers selected atrandom in a rural school. The stu-dents were so eager to talk abouttheir own experiences of fear in avariety of situations that the discus-sion became a kind of confessional."I felt like I was experiencing it my-self," said one boy referring to themodule. "My heart was beatingharder and I didn't know what todo. And I was breal:ing out in a
sweat right while Ads watching it.I had this feeling that everyone wastrying to escape and I was leftthere by myself." "But," added an-other, "if you show your fear allthe time as you feel it inside ofyou, then you're usually going to
9
get caught. As you go along andyou learn to deal with your fear,then it prepares you better for thenext time. But if you let your fearrun rampant, you go insane." Avideo tape was made of this dis-cussion and it was obvious from asingle viewing that the discussionincluded not only the recognitionthat the fei.r existed, but the moremature awareness that fear need notbe a mastering emotion, that being"in touch" with one's emotionshelps one to deal in a more realisticand aduh way than if one were lessaware.
As the title of the series implies,drug abuse is one target of thefilms. It is only an indirect target,however. Although each of the filmmodules in this series deals withteenagers using drugs in a peer-group situation, the emphasis ismore on the common emotions andexperiences of adolescent growththan on the usual sermonizing lec-ture so typical of drug preventionprograms everywhere. If you reallyknow who you are, the programsays, if you're in touch with your-self and behaving in a mature andsensible way, drugs won't troubleyou. It's only when your head getsmessed up (as happens at times tothe teenagers in the films) thatdrugs might cause you trouble. Thereal key to the drug problem, inshort, is not lecturing and punish-ment, but human self-understand-ing and self-concept.
A great deal of the success ofRubin'. film modules and the sup-portive material must be credited tohis talents as a filmmaker. The filmshave a quality of such completehonesty and spontaneity that it'sdifficult to believe they were madefrom written scripts and performedby teenage actors in New Jerseyand Long Islandthat they aren'treal-life documentaries. The scriptsand dialogue are based on hun-dreds of hours of taped groupprobes with teachers and youngpeople, often the same kids wholater performed in the films. It iseasy, therefore, for most teenagersin settings varying from urban tosemi-rural to identify strongly withthe experiences and feelings pre-sented.
10
Rubin sees his films as merelyone component in a totai educa-tional program, and there are ex-tensive teacher guides, intended tobe used in a package of twelve les-sons but adaptable to a number ofdifferent formats. The supportivewritten materials which guide theleader in the use of the films are soexplicit that a teacher (or peer lead-er) who has never had any experi-ence with group dynamics or affec-tive curriculum can follow themeasily. In line with the more proc-ess-oriented goals of affective edu-cation (as contrasted with the prod-uct-oriented goals of traditionaleducation), the introduction to theteacher's guide states: "The maintask for the leader . . . when usingthe film modules is to unlearn, orat least temporarily suspend, whatyou know about teaching. There isno knowledge which you canteach in this program." The instruc-tions proceed with such suggestionsas (in connection with "Fear")"Ask for volunteers to share per-sonal stories with the others aboutwhen they were 'conned into do-ing something they were afraid todo and did it anyway." Or (in con-nection with "Humiliation and An-ger") "Keep the discussion on tar-get: 'How would it feel if you wereturned in?"Did anything like thatever happen to you?'." The teach-er's guide includes a series of stu-dent work sheets which help stu-dents apply what they learn aboutthemselves to real life behavior.
Although the film modules aredefinitely not product-oriented,they do have specific educationalobjectives. The teacher's guide ex-plicitly states, for example, that it isdesirable to establish that "maturebehavior involves making a cleardistinction between a feeling andan action." The guide also stressesthe importance of peer-group pres-sure in shaping discussions to ex-amine feelings objectively and thenecessity of creating an open, hon-est, and relaxed classroom atmos-phere (with helpful suggestions onhow to do this). In various ex-perimental sessions with the films,students quickly realized many ofthese objectives by themselves. "Asyou go along and learn to deal withyour fear," one boy in a high school
24
in Schenectady said during a discus-sion of "Fear," "it prepares you bet-ter for the next time."
The films also open the way forsome benefits not mentioned in thespecific lesson plans. When oneteacher in a high school on LongIsland used the films, the most strik-ing result he noted was that for thefirst time the students who favoreddrugs and those who opposed themwere talking to each other andcommunicating. "Before, no matterwhat I did, they didn't want to com-municate with each other," theteacher said. "Many of the drugusers said they needed drugs tocommunicate, but it emerged dur-ing the discussion that they werecommunicating effectively in thediscussion without drugs. That reallysurprised them."
As for other specific results, theteacher couldn't be sure"It's stillin their minds," he commented sev-eral weeks after showing the films."I don't expect it to provoke per-manent change, but they keep re-ferring to the films in all kinds ofcontexts. It seems to have definitelyplanted seeds. I've used a great dealof audiovisual material, and this isby far the most effective."
"We spent a lot of time talkingabout feelings and emotions," com-mented another teacher who hasalso used the films. "For a largenumber of them it really hit home.Lots of kids get completely turnedoff when adults start discussingdrugsfor the last four or fiveyears that's all they've heard. Therewas none of that when we used thefilm modules; they could identifywith the kids completely."
Another unexpected benefitemerged in a mainly black andPuerto Rican school district in NewYork City, There are few minority-group teenagers in the filmstheywere intended mainly for a middle-class suburban audience, and theleader of this particular inner-citydrug program reports that studentswho had seen the films in her dis-trict were delighted to observe thatfor a change the poor and the mi-norities are not depicted as beingclosely associated with "the drugproblem." Seeing drug abuse not asa racial issue helped to calm the
defensiveness and hostility dis-played toward most drug programs.
In addition to the high school se-ries, the company has also produceda series on drug abuse self-aware-ness for teachers, another programfor parents, and a single film forstudents in elementary school thatclears up many common misconcep-tions and unreal fears.
Affective TeachingMany educators quite legitimately
question the role of schools inpsychological education. Affectivegains are difficult, if not impossible,to measure. Therefore, are suchmaterials safe when used by theaverage teacher? "Maybe affectiveeducation isn't much different froma bull sessionand shouldn'tschool be more than bull sessions?"
The film modules programs offeronly a brief immersion in intensivetechniques for developing self-awareness, and their positive effects,if left unsupported, will dissipatewith time. A learning system hasbeen devised as a follow-up, called"role modules." Here the studentsreenact (using role playing tech-niques) the situations presented inthe role modules. The goal is two-fold, first to reinforce the emo-tional awarenesses they had at-tained earlier from the films, andsecond, to present the many optionsavailable for mature behavior inreal life.
One could argue that the teacherwho would readily agree to use thefilm modules is probably someonealready inclined to favor affective
education and to encourage a re-laxed classroom atmosphere.
Whatever their emotional benefit,the programs are proving to be use-ful to a growing number of teach-ers. As one teacher put it, "Theyserved as a perfect trigger for dis-cussion; they helped to createa nonthreatening environment inwhich the kids felt free to talkabout things that they were reallyconcerned about." Rubin's filmmodules offer a workable alterna-tive to Clifton Fadiman's illustratedlectures of Dickens. As any teacherwho has watched his or her classesdrift off in a cloud of boredomknows too well, it's the kind ofalternative the schools desperatelyneed.
2 511

6 TEACHING IDEAS
Effective Teaching:Variety litheClassroomMARY SUTHERLAND is a master df pub-lic health student at the University of Ten-nessee, Knoxville, Tennessee 37916.WILLIAM HEMMER is an associate profes-sor in the Department of Health Science,State University College-Brockport,Brockport, New York 14420.
In developing an evaluation proce-dure for assessing student teacher com-petencies in a competency based teachereducation program, checklists of whatthe student teacher is expected to dousing a variety of techniques have beendeveloped by a consortium of teachers,administrators, and college supervisorsof the State University College atBrockport school health program. Thefield testing of this instrument was con-ducted with approximately 30 supervis-ing teachers and student teachers. Theparticipants provided many suggestionsfor the improvement of the assessmentinstrument, adding components andsubtracting others.
All the clues to the qualities of a goodlesson are provided for the studentteacher before the lesson is planned.Since the clues can be built into the les-son plan the lesson will be better than ifstudent teachers are left to their owndevices to develop a good lesson. There-fore, the Competency Evaluation Packethelps the student teacher preparesound, well-planned lessons which willsucceed in the classroom.
Supervising teachers found that theywere able to benefit by the checklists ofexpectations developed and found thatth?ir teaching improved because theywere conscious of the essential ingre-dients of a particular type of lesson. Achecklist of the qualities which thegroup felt would ensure success forthree types of lessons follows with adiscussion of the checklist items.
Demonstration Lesson
The teachers should demonstrate suc-cessfully, all of the following.
1. Arouse students' interest and at-tention before starting.
2. Explain the purpose of the demon-stration.
12
3. Demonstrate the steps in logicalorder.
4. Explain the purpose of the varioussteps.
5. Provide clarifying material to thestudents.
6. Hold the attention of the students.7. Provide sufficient opportunity for
student questions.8. Give clear answers to student
questions.9. Evaluate the success of the demon-
stration by eliciting student feed-back.
As in any lesson, the teacher mustbegin by catching the imagination of thestudents so they will begin to pay atten-tion. Students should know why thisidea is being demonstrated. Logicalorder is important so that students canfollow the procedure and understandthe reason for each step, as well as,what is happening at each state in thedemonstration, Thus, an explanation ofthe , 4 the steps as the demon-stration pru;eeds is helpful as are anyclarifying materials. Clarifying materialscan be anything from references tothings in the students' own textbook todefinitions written on the chalkboard.
The teacher should keep things mov-ing along so students' attention doesnot wander. This requires enthusiasm,showmanship, and ham acting.Another thing that breaks thPmonotony of the teacher's voice andhelps to hold interest is encouragingstudent questions as the demonstrationmoves along. There is nothing like clear,concise answers to encourage morequestions which means the teachermust be well prepared to field the typesof questions which may arise. At theend of the demonstration, the teacherwill want to elicit student feedback,probably with a few questions, such as:What do you think has happened here?Why? Do you agree with this explana-tion? Why do you suppose we did (this)instead of (that)? What might have hap-pened if we had done (this) at (step 1)?Why?
The teacher evaluates the success ofthe lesson by probing the depths of thestudents' understanding of what hashappened in the demonstration theyhave just seen.
Dramatization Lesson
Teachers should be able to demon-strate successfully, all of the following.
26
411.'
1. Aroue students' interests and at-tention before starting.
2. Select a relevant situation for stu-dent participation involving onemain idea or issue. This could in-volve personalities reiated to anindividual's beliefs, hopes, andaspirations.
3. Select students who are well in-formed on the issues and are self-confident in performing beforetheft peers.
4. Prepare the class in what to lookfor in the dramatization, e.g. be-haviors, feelings, etc.
5. Actively involve the students inthe dramatization, but maintainorderly direction toward fulfill-ment of the objectives.
6. Evaluate the dramatization as it re-lates to the objectives by means ofreview, discussions or question-a nswer sessions.
Again the teacher must have a devicefor getting students' attention beforestarting. If the situation to bedramatized is familiar and important tothe students, if somehow the studentscan relate to one or more of the characters, interest can be sustained. Usuallysituations or ideas which relate to theirvalues, beliefs, or hopes are .7onsideredrelevant topics by students.
In selecting the actors and actressesfor a dramatization, whether it be im-promptu or prepared ahead of time, it isimportant to use volunteers who areself-confident in front of their peers.Nothing kills a dramatization like a shystudent who mumbles a few words andquickly tries to sit down because hewould rather be almost anywhere ex-cept in front of the classroom. The par-ticipants in the demonstrattim shouldalso be those who are well informed onthe issues presented and who can easilyvisualize the situation to be dramatized.This is especially true in impromptu roleplaying.
Students in their seats should begiven a charge by the teacher to look forcertain behaviors, feelings, or whatever.The audience should be given an impor-tant evaluative or observer role so theywill not feel like passive observers, butco-participants in a class enterprise.
Objectives should be made clear tostudents so they will know why they aredoing this dramatization. At the end ofthe lesson, the teacher should evaluatethe dramatization in light of the objec-tives. Again, a five or ten minute dis-

cussion of what happened may be cru-cial in getting the main point of the les-son across to students. The teacher, forexample, might ask: Was the dramatiza-tion realistic? Why or why not? Do youthink (the protagonist) acted realisti-cally? Why? Would you have said (oracted) as (a character) did? Why? If not,how would you have acted in this situa-tion? How could the dramatization havebeen improved? Did you ever see any-thing like this happen in real life?1Vhere? flow?
Audiovisual Lesson
Teachers should be able to io all ofthe following.
I. Explain the purpose of using theaudiovisual material to the stu-dents.
2. Pose questions for students toseek answers to during the pre-sentation.
3. Use questions to get students tothink about material during orafter the presentation.
4. Select audiovisual material whichwill increase the students' depthof understanding and learning ofthe curriculum content.
5. Involve stuuents in the interpre-tation of the message presentedin the media.
6. Relate the media's message to thecurriculum objective.
7. Select media which present themessage in an effective manner.
8. Select media with appropriate vo-cabulary level for the students.
9. Help the children conceptualize.10. Summarize the main instructional
purposes of the media.Whether filmstrip, 16mm film, film
loop, slides or large poster pictures, the
teacher should first explain to the stu-dents why they are being asked to look/listen to it. In other words, the lessonobjectives should be made clear. To in-volve students and support the purposeexplained, ask students several ques-tions in advance, keyed into the objec-tive. One or two questions given in ad-vance are generally all that students cankeep in mind. An alternative is for theteacher to pose the questions one at atime during the presentation of the au-diovisual material.
The important thing is to get the stu-dents to think critically or to inquireabout the material being presented,both during the presentation processand afterward. Of course, for worth-while thinking to be stimulated, the au-diovisual material must be carefullyselected to focus the students' attentionon the objective desired and to fosterlearning of the ccntent of the cur-riculum.
The questions and the teaching pro-cedures used should be designed to in-volve the students in interpreting themedia's message. This involvementshould encourage creative solutionsto problems and interpretation ofphenomena and events depicted. Theopportunity to use creative abilitiessparks the interest and enthusiasm ofthe students in the project at hand. Ifpossible, the teacher must skillfullyallow the media's message to be relatedto the curriculum objective by the stu-dent instead of by the teacher.
The media which present the messageeffectively are usually best for stimulat-ing student interest through the use ofopen ended questions. A straight fac-tual presentation makes student in-volvement difficult since the media
2 7
seems to be saying, "Here it is folks, thisis the way it is, there's no argumentpossible with these facts." Students, notbeing subject matter experts, are usuallyin awe of straight factual presentationsand are not able to challenge this type ofpresentation effectively.
If the media has audio or printedcomponents, the teacher must makesure the vocabulary level is appropriatefor the studentsnot too simple or toohard.
The teacher will want to help the chil-dren conceptualize the main objective ofthe lesson, usually by folowup ques-tions that help students understand andevaluate what they have just seen.These followup questions will also helpto summarize the main instructionalpurpose of the media piesentation.
Conclusion
Teachers who wane to do demonstra-tion, dramatizations, or audiovisual les-sons for added variety in their class-rooms will find these checklists an aid inremembering all the fine points that areessential for making a lesson click with aclass of students. The checklists can beapplied profitably both before and afterthe lesson. Before the lesson, they canbe used as a guide in planning so that allnecessary components are built into thelesson. After the lesson a teacher canuse this same checklist as a thoughtfulmeans of evaluating his/her perform-ance in the classroom. In the light of thisevaluation technique, apparent weak-nesses can be shored up by extra effortin the planning stage the next time aparticular type of lesson is attempted.
13

7 TEACHING IDEAS
Health Science Fairs
HENRY A. LASCH is professor ofhealth science, Department of Phys-ical Education, New Mexico StateUniversity, Las Cruces, New Mexico88003.
Science fairs have been a tradi-tional project in many school dis-tricts throughout the United States,reaching a peak of interest after thespace-age touched off a fervor ofactivity in the mathematics and sci-ence curricula.
We are now on the threshold ofa new era in the health sciences. Thecrises brought on by drug abuse, thevenereal disease epidemic, smoking,alcoholism, destruction of the en-vironment, and other problems haveincreased public awareness in health.Although it is deplorable that mostschools and communities waited forcrises to develop before they real-ized the importance of a compre-hensive health program, we are onthe brink of one of the greatest ex-pansions in health in the history ofpublic education. Every possiblemeans must be employed to conveythe message of school health to thepublic.
14
The health science fair is one typeof activity that will add new dimen-sions to school health education. Itis similar to the traditional sciencefair except that it i hmited to proj-ects and exhibits which portrayhealth as the central theme. Schoolsthat may not want to .;ponsor sepa-rate health science fairs could desig-nate health as the main topic intheir regular science fair. Whateverroute is taker., the end results shouldbe worthwhile.
In organizing health science fairsit should be recognized that anytype of project can be included aslong as it pertains to health. It maycover anything ranging from per-sonal :Ind community heahh affairsto world-wide health problems. Spe-cial emphasis should be given toprojects related to health and medi-cal research and current, scientificdevelopments affecting man's healthand longevity.
Why Sponsor a Health pair?The health science fair presents
an unrivaled opportunity to promotegreater health awareness among stu-dents, school personnel, and the
community as a whole. Greater un-derstanding of the importance andscope of health in a changing worldcan be gained from this type of en-terprise. Students may discover newinterests and meaning in healn andunlimited opportunities exist forcreativity in all areas of health. Stu-dents who exhibit genuine interestand enthusiasm may show promisefor careers in one of the many alliedhealth and medical professions. It isquite conceivable that some of thecritical health manpower shortagecould be reduced if students wereprovided opportunities to developtheir interests and creative talents inthe field of health at an earlier age.
As plans take shape for a healthscience fair, students should becomeaware of the multitude of topics andprograms which comprise schoolhealth, public health, and interna-tional health. A health science fairpermits greater student involvementin current health affairs. It can alsoserve as a valuable tool to publicizehealth among all segments of thecommunity. Education must searchfor better ways to challenge andstimulate the minds of youth in thediversified fields of health.

The health science fair is an effec-tive way to gain respect for the en-tire discipline as well as a means ofsecuring more public support forhealth as a separate subject in thesecondary schools. Certain projectscan focus on health hazards and de-ficiencies in the community, thusproviding students with a challengeto assist in the solution of currenthealth problems.
Guidelines for Projects1. All projects entered in the fair
should center around some areaof health. The theme of the proj-ect should be clearly defined anddescribed.
2. Students should select their ownprojects as long as basic rulesand guidelines are followed.These should be clearly estab-lkhed by students and faculty.
3. Projects should be designed bythe students, who should be ex-pected to do their own construc-tion and assembling.
4. The general plan of the projectsshould be approved by a com-mittee of students and teachers.
5. Both individual and group proj-ects should be encouraged.
6. Participants in the fair should belimited to one project in orderto strengthen the quality of en-tries.
2 9
Organizational Committees
A health science fair will have agreater possibility of success if com-mittee responsibility is clearly de-fined and overlapping is avoided.The general administration of thefair can be handled by a steeringcommittee. Other suggested com-mittees are: publicity, design andconstruction, finance, facilities, andjudging Additional committees maybe added as deemed necessary.
Final success of a health sciencefair will depend upon the coopera-tion of all committees, the enthusi-asm of those who participate in theplanning, the motivation of studentand public interest, time allowed foradequate preparation of projects, se-lection of a desirable site, and thecontinuous publicity given the en-tire project.
15

8 TEACHING IDEAS
B. E. PRUITT is a staff member at LewisvilleHigh School, Lewisville, Texas 75067
A...M=111.1Y
As a multidisciplinary topic, healthethic ation can offer an exc client oppor-tunity to make classroom experiencesgermaine to individual life styles. Unlikemany other areas of study, health edu( a-tion is not obligated to concentrate onfragmented tools which may, or may not,be used to affect life quality. Instead,classroom health offers a cham e to ex-perience concepts of living--the "bigideas- of responsible personal health.
At Lewisville High School, we have re( -ognized this opportunity and are attempt-ing to offer classroom health to our stu-dents to not only provide them with in-formation about healthful living but to dothis in a learning environment which em-phasizes individual application of healthrelated information. We have developeda program of individual study, the "opencontract." The goal of the open contra( tprogram is to provide an environment inwhich each participant suc«,ssfully iden-tities topics or problems within spec di(health-related areas, acquires informa-tion about them, and, by analyzing thegathered information, proposes possiblemeans of dealing with suc h topic s orproblems. The ambiguity of this goal isnecessary if the vast range 01 individualdifferences and needs is to be «insid-ered.
Parti( ipants ri the open «ultra( t pro-gram are employed as student inves-tigators for 18 weeks. During that timethey are «msidered free citizens withinthe program. They assume three primaryresponsibilities: selection of topics orproblems for study, selection of meth-ods of investigation or investigationcategories, and selection of grades.
16
THE OPEN CONTRACTA PROGRAM OF
INDIVIDUALIZED STUDY
Selection of Topics
Participants in the open contract pro-gram are free to select topics for investiga-tion, but they are restricted in two ways.They must ( hoose topic s within the areasof study established at the beginning ofthe program, r :meragy corresponding tothe basic areas re«)mmended in theTexas 1. dt.1( ation Agent y's Bulletin 691,Se«mdary Sc hot)! Health I ducation Cur-ncuhun Guide. The se«md restri( ti(in isthat ea( h sele( tion must be appropriatelylimited to be elle( tively dealt w iththrough investigation pro( edures estab-lished by the investigation c ategories. Atopit such as "food- is obviously toobroad to be eftet tively investigated, bllt atopic suc h as -food tads" is more appro-priate. The tea( her never decides whattopic s are to be studied, for in doing so hewould risk losing the individual emphasisof the program. Rather, he establishesboundaries within whit h the student isenc ouraged to sele( t any topi«)r prob-lem of personal interest.
Selection ofInvestigation Categories
On( e a student has ( hosen a topic torstudy he must then sele( t a method ofinvestigation from the investigation cate-gories established by the teacher at thebeginning of the program. They must varyin degree ot diffic ulty arid value so thestudent has several choices. A more dif-fit ult ategory may be valued as mu( h as10 points while a simple category is worthonly S poil.(s. When selecting an investi-gation c ategory the student must wn-skier how muc h work he wishes to doss Oh the topic, how many points hewishes to earn, and whether the topic aridthe method of investigation are compati-ble.
f ollowing are several examples ot pos-siHe investigation ( ategories, designedtor the ninth grade level and c urrently apart of the program for Health I studentsat Lewisville High Sc hool. (With a moreadvanc('d student, more involved inves-tigation pro( edures would be appro-priate.) The six examples will beexplained in relation to the open «mtra( tdesign.
Position Paper: I ac h six-week periodInc ludes three opportunities tor the stu-dent investigator to express opinions onontroversial topics. This expression is
done in the form of a position paper.Suc h statements of personal opinionallow a student to re( eive ( redit tor inves-
BEST COPY AVAILABLE 3
Ugating his OW11 thinking in the areas ofstudv. The positirm papers are graded a( -
mrding to how well the selected topicrelates to the area ot study. the topic ismvered. the arguments are presented.and its general tidiness. The maximumvalue tor any position paper is list, points.
Critique: The ( ntique ( a tegors is pro-vided so the student investigator ( an re-«,ive t redit for analvzmg the varlets. (itintormation found in the health field.Newspaper and magazine arti( les, books.films, television programs, or personal in-terviews all provide opportunities for de-veloping 1 rniques. The student is en-couraged to produce a pie«, ot ( realm,evaluation DI b)th the intormation andthe information source. fat h ( ritiqu(' issalued at eight points and is graded acording to how the information relates to
the area of study, how a summary of theinformation is presented, how an analysisof the information is c arried out, how thesour«, is identified (usually through abibliographic note) and its neatness.
Correspondence: In eat h six-weekperiod, students have three opportuni-ties to ret eive credit for correspondingss ith various public health agencies orbusinesses concerning health-related in-formation. 1 his optional investigationategory exposes the student to the vari-
ety of agencies, businesses, and associa-tions whit h are concerned with thehealth of their clientele and helps thestudent encounter samples of literatureprovided by such service organizations.Students are provided with a list ofappropriate agencies with which theymay wrrespond. Each «mespondenc e isvalued at five points, ( redited when evi-dence of the wrresponde rice is pre-sented. As long as the information re-quested relates to the areas of study, full
redit is given.xamination : Three optional examina-
tions worth up to eight points eac h areprovided every six weeks. Questions areusually essay and deal with clavi ac-tivities, suggested readings, or general in-tormation to which the student may havebeen exposed. What might seem to be amisnomer in referring to examinations asone of the investigation ategories is notso when examinations are looked upon asindividual investigations of personalknowledge. Students are encouraged towrite examinations with this in mind.
Individual Project: The ( a tegory "indi-vidual prolecr gives the student inves-tigator a ( hance to express his ( reativity,expand his knowledge in a health-relatedtopic, and receive ( redit at the same time.

The design and means of development ofthe prole( t are entirely up to the student.Bulletin boards book reports, or spec ialnotebooks are wminon projects. Origi-nality, however, k encouraged. Up to tenpoints credit may be earned eac h six-week perioo by the completion of thisinvestigation c ategory.
Committee Pmjec t: If three or nloreudvnt investigators w is!) to work to-
gether on a projec t, they may c hoose toornplete the t ategory ommitttp pro-
le( t." Thy only restric !ions are that onlyone prole( t may he completed during anyUm. sixw eel( period and the selectedtopic must relate to the area of study.
h member ol a committee may rec eivea ma \imum ot ten poink tor prowt t.
Most, hut not all, points are earnedthrough investigation pro«%dures. Up to30 points may be earned eac h six-weekperiod through c lass partic ipation. Regu-lar tivities are planned whic h involvegroup work, role playing, or guest speak-ers so that intormation is provided overareas ot study. Many activities are de-sigcwd to help students with their investi-gations, or tor the sole purpose ot havingtun with health. The credit available en-courages students to take advantage ofthe activities or to make use of the classtime provided for investigating chosentopics.
A progress record is used to maintain arunning account of the number of pointsearned by each participant in the opencontract program. An official and an unof-ficial progress record is kept for each ofthe three six-week periods during theprogram. The unofficial record is kept upto date by each student investigator sothat he is always aware of where hestands. The official record is placed in afile and kept up to date by the teacher.Official credit is recorded at the time in-dividual investigations are placed on file.At the end of each six-week period, thetotal of all points recorded on the officialrecord is determined, and the resultingnumber is the six-week grade.
Selection of Grades
If a student investigator chooses tocomplete an invesogation option, hedoes not automatically receive full credit.But, points are never subtracted from astudent's grade. This evident contradic-tion leads us to one of the most importantaspects of the open contract programthe grading technique.
A major criticism of the traditionalclassroom environment involves the ex-tremely negative approach used in grad-ing. When averaginE, is used, one poorgrade may destroy all incentive. The open
contract program, on the other hand, in-volves a completely positive approach.When an investigation is graded it isawarded points for things done well; nopoints are subtracted 'or mistakes. Forexample, if a student completes the in-vestigation category "critique I," he mayreceive up to 8 points. When grading thepresentation the teacher notes any areasin which the critique may be improved. Ifthe teacher fe^!s that the paper is welldone then a full 8 points may be awarded.If the teacher sees ways for improvementhe may award 4 points or 2 points, de-
3 1
pending on the amount of improvementnecessary. Any time less than the max-imum number of points are awarded, thestudent has the option of accepting thepoints awarded by placing the paper onfile, or of rejecting the points, making theindicated improvements, and resubmit-ting the paper to be graded again. If astudent is not satisfied with this grade thepaper may be reworked once again.
Usually when students rework a cate-gory, they improve the number of pointsearned. If, however, a second presenta-tion receives a lower grade than the first,the student may ask that the first be filedand the original points awarded. Oncepoints are recorded they must not be sub-tiacted. The student is encouraged inevery way to earn the highest grade pos-sible.
Final grades are determined by the totalnumber of points accumulated during the18 week session. A student receives agood grade after completing a certainnumber of investigation categories well.A poor grade is given when the studentchooses to complete fewer investigationcategories. The option is available tocomplete no investigations and fail. Thistoo is considered a respectable choicebecause the student is held responsiblefor his decisions.
This totally positive grading techniqueis essential to the success of the opencontract program. The student must feelresponsible for his own grade and he canfeel that way only if he is allowed theoption of correcting and improving hiswork in each category to a point of per-sonal satisfaction.
Most participants in the open contractprogram have responded positively tothis individualized motivational ap-proach. They have become deeply in-volved in a variety of health-related areasand, in general, have increased under-standing of numerous concepts of health-ful living. Perhaps more importantly,however, participants have enjoyed theirhealth education experience.
17

9 TEACHING IDEAS
LYNN TEPLR-SINGER is an assistant pro-fessor in the Departments of Health Sci-ence, Physical Education, and Guidanceand Counseling at Long Island Univer-sityThe Brooklyn Center, Brooklyn,New York 11201.
Role playing as a classroom techniquehas provided a marvelous environmentfor the exploration of health concepts. Inthe February 1971 issue of School HealthReview a step by step procedure of thetraditional role playing situation waspresented in an article entitled, "RolePlaying as a Tool in Mental Health Educa-tion." Briefly the steps included:
1. Sensitizing the grouppresent asituation where the class discovers thateach person perceives a given situationdifferently based on past experience, as-sumptions, and expectations
2. The Warmupdescribe the roleplaying situation with limited information
3. The Enactmentspontaneous dra-matization
4. The Replaythe same peopleswitching roles
5. Student Observation--discussionby the students about their reactions
6. The Evaluationdraw conclusionsAt this time I would like to present
three alternative approaches to role play-ing. Although any area in mental healthcan be explored through these proce-dures, the following are examples for usein drug education.
Example I
Structure: The class is divided intogroups of four. Each group sits in a smallcircle within a large circle that the groupsform.
18
THE MANY FACES OFROLE PLAYING
X: x xrole players/ 7.x Ax N
x x
x F x
x x
x E x
x x
x D x
Situation: Student arrives home to afamily that has discovered a "stash" ofdrugs hidden away M his/her room.
Roles: Each group will enact the follow-ing roles spontaneously without prepara-tion other than deciding on a role.Mother and/or father, brother and/or sis-ter, student.
Procedure: In sequence each groupperforms their presentation of what theythink will happen. (Group A then B thenC, etc.) Generally e-n 1 oroup has a differ-ent approach. The r.lather may stop thegroup and go on t,) the next group at anypoint.
Discussion: After all groups haveenacted their presentation, the teacherwill have several options for proceedingwith the discussion depending upon thematerial presented. Some possibihtiesinclude:
1. The class may form new groupsbased on the behavior displayed by theparents. Students who think their parentswould behave as the role was played,would group together with the roleplayers. For example: parent who cries"How could you do this to me"; parentwho kicks child out; parent who ques-tions with concern; parent who lecturesand does not allow a response, etc.
Discussion questions may include:How do you feel when your parents ap-proach you in this manner when they dis-approve of your behavior? For what rea-sons do you believe your parents respondin this way? How would you approachyour child if you were the parent?
2. The class may discuss their reactionto each group's performance.
3. The teacher may present questionsfor the small groups to discuss based onthe diverse material that the teacher hasbeen jotting down during the differentpresentations. For example:
Describe the ways in which the personcaught responded.
For what reason do you believe peoplewould respond in this way?
What information about drugs do youbelieve was false, which was factual?
What are the penalties for breakingdrug laws?
What was your reaction when alcoholwas mentioned as alright for the adultsbut -pot" was put down?
Example II
Structure: Single group performancewith stop action directorship by the class.The performing group presents theirinterpretation of the situation in front ofthe class (the directors) who are sitting ina semi-circle around the classroom.
x- role players
o- directors000
0oX
X
oo000

Situation: One student is trying to con-vince three friends to smoke a joint.
Ro/es: Person who does the convinc-ing, person who refuses, person who isundecided, person who accepts.
Procedure: The group begins theirenactment. At any point any member ofthe class, as well as the teacher, may stopthe action by calling out "Stop Action"and
1. ask a question of a performer abouthow that performer feels at the moment.
2. assume the role of any of the playerswith a different approach.
3. ask the present players to switchroles.
Discussion: Questions for discussionmay involve aspects dealing with grouppressure and the decision-making proc-ess.
a. In what ways were the situationsrealistic or unrealistic?
b. How do you feel when someonetries to convince you to do somethingthat you really don't wish to do?
c. What feelings do you have when youwant to convince someone to do some-thing and they refuse?
Example III
Structure: One individual sitting on theedge of the circle who will enact two op-posing aspects of himself while the re-maining members of the class listen.
x- role playero- classmates
X 0 0 0O 0
O 0O 0
O 00 0 0
Situation: The forces (feelings and at-titudes) within the person that motivatehim to use drugs versus those that influ-ence him to refrain from using drugs.
Roles: The role is the dichotomy thatexists within us that determines our deci-sions.
Procedure: The student holds up twohands (puppets may be used if appropri-ate for the age group). One hand is firstused for emphasis "On the one hand whyshouldn't I use drugs, everyone is doingit?" The other hand is then used "But onthe other hand just because others do itdoesn't mean I have to follow their exam-ple." The alternation of hands is repeatedwith each feeling and thought for oragainst the use of drugs.
Discussion: Questions for discussionmay include:
1. In what ways are your feehngs simi-lar to and/or different from those pre-sented?
2. What is your response in other situa-tions wlwre a conflict exists between your
feelings, thoughts, and attitudes?
When teachers present role playingsituations it is most important for them tohave a facility for questioning so discus-sions are meaningful. The teacher's re-sponsibility in role playing is essentially tohelp students identify and define whatthey are experiencing, as well as to helpthem investigate their feelings and reac-tions. A non-judgmental setting is there-fore a must.
Suggestions for questioning:
1. Avoid questions that merely yield ayes or no response or that call for judg-ments such as good or bad, should orshouldn't.
2. Explore several ramifications ofquestions:
Clarify a point: If I understand you, yousaid. . . .
Seek additional information: Wouldyou tell us more about this?
Evaluate: What do you think this mightmean? How does the rest of the class feelabout this?
Conclude: What happened? Why isthis a problem? How could the outcordebe altered?
3. Provide an atmosphere where ques-tions arise from and between students aswell as from you.
19
10 TEACHING IDEAS
GEORGE F. CARTER is an instructor in theDepartment of Health and Physical Educa-tion, Triton College, River Grove, Illinois60171.
At one time or another most teachersfrom the elementary school through theuniversity are confronted by students de-siring to do an extra credit paper or proj-ect. Many times the student requestingthe opportunity has fallen behind hisclassmates in regular assignments andwould like to make amends through extraeffort. In other words, the extra creditbecomes a make-up which often causesproblems for the instructor at or near theclose of a term.
During the last nine years, many of mystudents at Triton College have requestedextra credit in Science of Personal Healthcourses. Reasons for the request varyfrom the desire to achieve an A ratherthan a B, to pass ra mer than fail. Mostrequests have been made in the last weekor two of the semester with little thoughtgiven to the learning experience. As ateacher, it is always encouraging to have astudent request to do something extrabut not under these circumstances. Onthe other hand, it is undesirable from aninstructional viewpoint to deny a studenta second opportunity, especially whenthey have requested the chance.
In the competition for grades, classrank, and as an opportunity to promotelearning, the extra credit assignmentshould be used as a teaching strategy andshould be open to all students. The na-ture of the assignment and appropriategrade compensation should be in keep-ing with the regular course evaluationprocedures. Everything pertaining toextra credit should be carefully explained
20
EXTRA CREDITMAKE IT MEANINGFUL
to the students so that misunderstandingis held to a minimum.
So students understand how they are tobe evaluated in health class, students aretold the objective criteria used in evaluat-ing their effort. Every effort is made topresent the student with the Opportunityto earn points toward his eventual grade.All assigned work is given a numericalvalue and students are made aware of thepoint value for tests, term projects,abstracts, oral reports, attendance, etc.
Extra credit is not used to replace regu-lar work but to increase opportunities forwilling students. The information given toeach student enrolled in Science of Per-sonal Health as a handout is shown here.Over the last several years this handouthas been revised and it will be continuallyrevised. There is no longer the urgentneed for an extra credit project; the extracredit must be carefully planned and con-tribute to the learning experience of thestudent.
EXTRA CREDIT OPPORTUNITIESScience of Personal Health
Dr. George F. Carter, InstructorStudeos who are interested in improv-
ing their information and skill level areinvited to submit extra credit projects. Allprojects must conform to the establishedguidelines for compensation. All pointsearned through extra effort will be addedto the previously earned point total. Gen-erally speaking, first come, first served ontopics. All work must be in good form tobe considered.1. Students may report informationgleaned from reading a newspaper ormagazine article which covers the subjectbeing dil,cussed in class. The studentmust have a copy of the article to presentto the instructor and give a brief accountof the information to the class. Art;clesnot pertaining to the day's lesson will notcount as extra credit. (2 pts.)2. Students may visit a local, county, orstate health agency and make an oral re-port to the class about the visit. In addi-tion, a one page summary of the visit,person visited, and other pertinent in-formation should be typed and turned in.(5 pts.)3. Students may visit a local, county, orstate health agency for the purpose ofexplaining the role of the agency. A briefreport to the class is required. (3 pts.)
4. Students may visit any health agencyor health related agency to get printedmaterial for distribution to the class. (2pts.)5. Students may bring a cassette, record,or other audio-vis.ial material to class thatpertains to the subject under class discus-sion. All arrangements for the presenta-tion must be made with the instructor oneweek prior to the presentation. (4 pts.)6. Students may review a film, cassette,videotape, or other medi? productionfrom the Triton College Learning Re-source Center collection. The studentmust make all the arrangements to reviewthe material and submit a one page sum-mary of the material in proper manuscriptstyle. (5 pts.)7. Students may make arrangements tohave a guest speaker come to class todiscuss the subject under study. Prior ap-proval must be granted a minimum of oneweek in advance of the presentation. Thestudent will introduce the speaker. (5pts.)8. Students may arrange an interviewwith some person involved in health careservice. A written summary of the inter-view with appropriate data must beturned in prior to the coverage of thematerial in class. (5 pts.)9. Students may make an oral report of aninterview with some person involved inthe health care delivery industry. This ma-terial must be useful to class discussionand approved by the instructor. (3 pts.)10. A student may submit a proposal forextra credit to the instructor. All pro-posals must be approved a minimum oftwo weeks prior to the due date. Pointtotals will range from 1-5. Suggestions forextra credit are: review a book, movie,play, or meeting; attend a seminar orclinic; critique a popular .ecord or tape, atelevision program on a health relatedsubject; visit a nursing home, mentalhospital; or send for health informationwhich would benefit the class or the per-son.
The handout has been of immense helpin answering questions and at-signingextra credit projects. Since my work is atthe community college level, these ac-tivities attract student involvement. Per-haps you might desire to adapt the guide-lines to your school environment but myexperience has been an increase of inter-est in extra credit.
r'r ST col' ""jaw tialg!

11 TEACHING IDEAS
Promoting Experiential
Learning
MICHAEL HAMRICK is associate profes-sor and head, Division of Health Scienceand Safety Education, Memphis StateUniversity and CAROLYN STONE is pa-tient education coordinator, City of Mem-phis Hospital, 860 Madison Avenue,Memphis, 'Tennessee .3810.3.
Getting students involved in healtheducation experiences outside thechssroomexperiential learning--continues to be a pressing need inhealth education. The purpose of thisarticle is to promote experiential learn-ing in health education by providing alist of projects to encourage out-of-the-classroom learning. While this list wasdeveloped for use in the personal healthcourse, similar lists can easily be devel-oped and implemented in courseswhere it is important to broaden stu-dents' experiences and to facilitateawareness of attitudes, behaviors, andlifestyles that are difficult to accomplishin the classroom.
These projects are designed for thestudent, not the teacher. Therefore, wesuggest that the list be duplicated anddistributed to students. These projectsshould be structured into course re-yuirements so that points or some kindof credit can be earned. Since the proj-ects vary in the amount of time, effort,and involvement required, possiblepoints/credits should also vary. Someprojects require several months tofinish while others may be completedin a 30 minute interview. Studentsshould be encouraged to pursue areasof personal interest and to take advan-tage of their talents. Some projects re-quire skill in journalism, photoa°raphy,movie production, art, research, etc.Students should be encouraged to selectonly those projects which offer a newexperience for them. Finally, guidelinesshould be developed which specifyhow and when projects are to be re-ported.
Experiential Learning Projects
L Do a film. Compile either an 8mm filmor 35mm slides focusing on some topic. This
display can be incorporated into a mul-timedia presentation using audio-tape orany other appropriate media. For example,you might produce a tape-slide show on eat-ing habits of college students, study habits,recreational habits, dating habits, marriagefrom the woman's point of view, people try-ing to make conversation, children's ideasabout death, etc.
2. Prepare an audio-tape collage. Tapemany songs, poems, readings or soundsaround a particular theme. The theme mightbe aging, drugs, self-identity, or sexuality.
3. Select one of the health habits/be-haviors that you are concerned about andwould like to work on. Develop a plan ofaction which focuses on the desired behav-ioral change. Use a behavioral modificationplan as described in class. Keep a log on thesuccess/failure of the plan. Follow up with ananalysis of the plan and the behavior andwhat you learned.
4. Pair up with someone else to form ahealth "therapy" dyad. The purpose of thepartnership is to have someone with whomthe health habit/behavior can be discussed.Meet with your partner several hours aweek. See if you can develop a plan forachieving desired behavioral change. Keep alog of your meetings. Use your partner bothas a sounding board and as a monitor tokeep you honest.
5. During the semester, keep a log of thebehaviors/habits you change or modify.Examine the circumstances of the changes.Can you identify a pattern to the changesmade? What did you learn? Report results.
6. Keep a journal. Record reactions to oc-currences related to some topic or activity.The journal could chronicle a physical fitnessregime or dietary pattern or an encountergroup experience running throughout thesemester.
7. Prepare and implement a research pro-posal. Some of you may have ideas for exper-iments such as the effects of various quan-tities of alcoholic beverages on reaction time,food tasting experiment, survey of attitudes.
8. Conduct a health demonstration. Sometopics may lend themselves to a
demonstration-- the effects of smoki -g onheart rate, blood pressure, body temperatureor how a medical test such as EEG or EKGworks and what it shows.
9. Go to the Health Department, VenerealDisease Clinic as if you were a client seekinghelp for V.D. You may use a false name ifyou prefer. Report what you learned. Hoe:were you treated? What did you observe inthe waiting room, the treatment rooms?How did you feel? What changes would you
3 5
suggest to make the experience less negativefor those who need their services?
10. Interview a person or persons whosmoke heavily (yourself if you fit the cate-gory). Get a profile on their smoking habits,when they smoke, for how long, how it af-fects them, why they think they smoke,comments of family and friends about thesmoker. Have they ever quit? Why? Why didthey resume smoking?
11. Go to a setting unfamiliar to your life-style and report your reactions, feelings, etc.Try a walk through an inner city neigh-borhood, attend church services of a dif-ferent religious group, go to an adult movieor bookstore, a gay bar, or shop at a smallcountry store.
12. Spend an evening in a local hospital'sintensive care waiting room. Listen, ob-serve. If you feel comfortable, talk with thefamilies waiting. Record your reactions,what you learned medically as well as emo-tionally.
13. Spend a morning making rounds witha public health nurse, food sanitation in-spector, rat control investigator, or environ-mentalist.
14. Go to a community health center andtake a seat in line. Examine the attitudes ofthe staff who work there. Talk to some of thepatients. Find out how adequate they thinktheir health care is, what problems they havegetting to see a doctor, etc.
15. Conduct a health campaign. Select ahealth topic and conduct an educationalcampaign such as anti-smoking, hyperten-sion, sickle cell anemia, cervical cancer de-tection, population control, human rela-tions.
16. Visit a health foods store and make alist of what you see. Intervi w personnelwho work there about their philosophies oneating. Compare prices of similar foods ingrocery stores or pharmacies.
17. Spend one weekend evening sitting ina public hospital's emergency room waitingarea. The same evening, spend the sameamount of time in a private hospital's E.R.Compare the two physical surroundings,personal attitudes of the staff, the patientsyou see, their families. How comfortable/un-comfortable would you be if you were a pa-tient?
18. Write a letter to a newspaper or maga-zine about a current health-related issue thatreally gets your dander up. Turn in a carboncopy.
21

19. Visit a health spa. What practicesseem valid? What claims are made whichseem unrealistic, unhealthy, deceptive, eva-sive? What do you get for how much money?
20. Go to a free lecture on transcendentalmeditation. How do you think it works?What are the benefits claimed? What sort ofimpression did you get from the whole expe-rience?
21. Talk with relatives who have planneda funeral. What were their impressions ofthe funeral business and the people who as-sisted them? What details must be attendedto when planning a funeral? What legal prob-lems did they run into?
22. Find out resources for contraceptiveinformation. Make a list and include costs, ifany, for the services and/or the contraceptivematerials. List at least ten resources.
23. Go to the local Unemployment Of-fices. Sit in the waiting room and listen tothe talk around you. Describe the place.Read the notices on the board. Describe anycontact with the employees. Wear oldclothes. As a variation two people can go to-gether, one dressed in old clothes and one inreally good clothes. Describe how individu-als differed in their reactions to you.
24. Go to any of the pregnancy counselingresources and ask to have a free pregnancytest. Describe the place, the people, howthey treated you. If you are male, you cancarry in a urine sample saying it is for yourgirl friend.
25. On a given night watch TV programsduring prime time hours and count the inci-dents which exploit sex, race, religion,minority groups, occupations, etc.
26. Look in the want ads for jobs whichroutinely hire only men or women. Call andinquire about the job if you are of the oppo-site sex. What attitudes did you perceive?Quote any remarks made about sex require-ments for the job. Sex discrimination is nowagainst the law in hiring practices. Variaton:Work with a person of the opposite sex Bothcall and inquire about the job and record theresults.
27. Interview a relative or family friendwho is retired. Find out how they spendtheir time, what they like about being re-tired, what they dislike. What attitudesabout being considered "old" do you pickup on?
28. Arrange for the class to "interview"you about a life crisis you have experiencedsuch as divorce, marriage, childbirth, etc.You do not have to answer any question youdon't want to. State any limitations beforethe interview begins.
29. Read an article in a health journal
22
which interests you. Write a two page typedreview of the major points of the article. In-clude your opinion.
30. Survey 5 "lay" magazines (Mc Calls,Ladies Home Journal, etc.) and write a de-scription of the ads which contradict goodhealth practices. You might want to look atmagazines such as Cosmopolitan, Playboy,Oui, which emphasize attractiveness andappeal. Include a synopsis of the ads' under-lying messages.
31. Attend lecture of guest speakers in-vited to a local university to discuss theirviews of heal'h related topics. Example: Lifeafter Life le e, rape prevention demon-stration. Sun the presentation.
32. Attend heL.in education meetings,fairs, programs sponsored by various com-munity agencies. Summarize presentation.
33. Send in health assessment from backof textbook. Summarize what you learnedabout your health status, risks and behav-iors. Takes about 4-6 weeks to get it back.
34. Get a test for diabetes through theHealth Department mobile unit, or get a Paptest. Bring. the results to class with a writtenreport of how it was done. Ask questions ofthe personnel as they perform the tests. Tryto find out how many people are detectedthrough this system.
35. Write a summary report on the relationship between personality, emotionalstate, and cancer .
36. Using a very large map of your city,designate the distribution of doctors in thecity. Which areas are heavily populated'Which have only a few? Which are under-supplied? You might want to use coloredpins to designate different types of physi-cians. Do the same with dentists. Write yourrecommendations.
37. Bring an advertisement to class. Listits claims. Analyze it for emotional appeal.Are its claims supported by facts? In whatways is the advertisement misleading? De-ceiving?
38. From the list of health products invest-igated by Consumer Reports and published inThe Medic-me Show, select one and sum-marize the findings of Consumer ReportsDoes the product render any medical orhealth benefit? What conditions, if any,must be met in its use? What brands are rec-ommended by Consumer Union?
39. Refer to the magazine, FDA Papers. amonthly publication of the Food and Drug
3 6
Administration and identify an example ofquackery. What is the claim of the product?What does the FDA say about the product?
40. Tape a radio or TV commercial andbring to class. What kind of propagandastrategy was used? How is it misleading?
41. Conduct a demonstration to test com-mercial claims of a health product.
42. Write a company for verification ofclaims made in advertising. Turn in carboncopy of letter and indicate company's re-sponse.
43. Write a brief summary report on thepublished article on chiropractics or a re-port on any other health related article in-cluded in the monthly publication of Con-sumer Reports.
44. Tell about the decisions a heart attackvictim or cancer victim makes in goingthrough treatment, surgery, rehabilitation.Comment on length of stay, financial as-pects, steps in rehabilitation, changes inlifestyles, etc.
45. Write a summary report on an articlepublished during the past calendar year on adisease. Compare the information with thatin the text and comment on the differences.
46. Develop a skit or role playing situationillustrating some attitudinal or behavioralaspect of a disease. For example, simulatethe typical reaction of a person observing adiabetic in insulin shock; the reaction ofsomeone to the news that he or she has achronic disease.
47. Write a position statement on somecontroversial aspect of various diseases andbe prepared to read to class. The positiondoes not necessarily have to be your ownA Epileptics should hay e limited L.r.ving
privileges.B. Medical science is going too far with
heart transplants.C Government restrictions in the form of
laws, penalties should be imposed onpersons with genetically related diseases.
D Marijuana should be legalized for use byglaucoma victims.
F. The government is restricting distribu-tion of laetrile because of loss of profitsand government grants in research.
48. Interview a person who by nature othis her job observes death and dying (policeofficer, mortician, war veteran, physician,nurse).
49 Develop a skit or role playing situationillustrating some aspect of death For exam-ple, how people act at a funeral home. a fam-ily making funeral arrangements.
50. Write a position statement on somecontroversial aspect of death and dying.A. Too much money is spent on funerals.B. Young children should be taken to
funerals.C. Being dead is more honorable than being
invalid.D. Burying bodies is a waste of good, pro-
ductive land.E. There is too much death in movies and on
TV.
51. Visit an Alcoholics Anonymous meet-ing and report your experience.
52. Write one page position statement ex-pressing an extreme point of view on al-cohol. The position does not have to be yourown. Read to class, time permitting.
53. Conduct a genetic experiment in classdemonstrating dominant-recessive traits.For example, obtain small crystals of phenyl-thiocarbamide or PTC test papers. Conduct araste experiment distinguishing betweenbitter tasters and non-tasters. What are theexpected results?
54. Write a case history or biographicalsketch on a person with a genetically relateddisease or condition. Describe the hfestyle ofthe person and how it differs from "normal-ity." Describe the effects on the family.
55. Find out what kind of genetic servicesand counseling are available locally, theconditions for service, prerequisites, costs,location, etc. Report to class.
56. Take a copy of the state penal codefrom the library and extract the basic crimi-nal statutes relating to sex offenses. Noteparticularly those describing such acts asrape, seduction, carnal abuse, cohabitation,adultery, indecent exposure, loitering,molesting, and vagrancy. Notice, too, lawsrelating to marriage, (consent, ceremony,verification) contraceptives, pregnancy,abortion, and venereal disease. Report toclass.
57. Develop a skit or role playing situationOn some aspect of sexuality or sexually re-lated behavior.
58. Select two newspapers (only one fromyour city), observe and rec rd for one weekthe newspapers' statistics on marriages, di-vorces, and annulment. Graph the results.Include in the graph a breakdown ongrounds for divorce.
59. Construct a sample marriage contractfor yourself with provisions for faccts of mar-ital life you consider particularly important.You may want to consider some of the morecommon features found in marriage con-tracts today.A. division of assets held pfior to marriageB. division of inconw after marriage
C. to have or not have childrenD. responsibilities of partners in child careE. obligations and rights regarding separate
careers
60. Conduct a survey on some aspect ofsexuality. For example, married couples ofdifferent ages could be asked to answer thefollowing questions.A. What do you see as the purpose of mar-
riage?B. Who controls the finances in your family?C. What effect has the women's movement
had on marriage today?D. What are your views on early marriage?
61. Write a story in the "true confession"style that deals with issues of reproduction,birth control, marriage, parenthood, sexroles, etc. The story may be discussed inclass.
62. IVrite a position paper on one of thefollowing statements.A. A couple should be encouraged to choose
the sex of their babyB. A single person or gay couple should be
allowed to raise a child.C. Men should assume the responsibility of
birth controlD. No one should have more than two chil-
drenE. Marriage contracts should become the
form of marriage lawF. A couple with hereditary disease should
not have childrenF. Abortion on demand is a basic human
rightH Unlimited availability of contraceptives
encourages promiscuity
63. Conduct an experiment/demonstra-tion in class which focuses on the effects ofair pollution, water pollution or noise pollu-tion.
64. Draw a cartoon series which illustratesany health-related topic for example:A. transmission of venereal diseaseB. use of contraceptivesC. access to medical care/physicianD. medical terminology or technologyDesign it to get a point across to college levelstudents.
65. Demonstrate in class how to test forblood type; how to test for sugar in urine;pregnancy test; T.B. skin test; test for sicklecell anemia. Be sure you understand thewhys and hows of what you are testing forand not just the procedure itself.
66. Interview several women who haveexperienced menopause. What were their at-titudes about it before they experienced it?After they experienced it? What myths aboutmenopause were true/untrue for them? Howdid it affect their families, their marital rela-tionship? Was any medical treatment given?What were the attitudes of their physidans?
3 7
67. Attend a meeting of the LaLecheLeague, the crganization that helps womenbreast-feed their children. Record what yousaw, heard, learned.
68. Compare costs of 15 common prescrip-tion drugs among several local pharmacies.Include a chain-owned pharmacy, a smallneighborhood one, and a hospital-ownedpharmacy. Include the attitudes of those youquestioned.
69. Compile a list of local psychiatrists.Call and ask for information on: fee scale,training, group or individual therapy, typeof therapy (psychoanalysis, primal therapy,gestalt, electroshock, etc.), hospital affilia-tion.
70. Contact the local organization for wifeabuse. What are their findings regardingwife abuse locally, their services, futureplans?
71. Interview someone who Byes in whatwould be considered an alternative lifestyle:communal setting, couple who chooses notto have children, unmarried couple livingtogether, homosexual couple living together.Question each person involved.
72. Collect drawings/paintings fromyoung, preschool children depicting theirimpressions of sexuality. Check with parentsfirst! These could include their concept ofanatomy, birth, sex roles, etc. Show these toclass with your observations and commentsmade by children. If you have small childrenyou may use their artwork.
73. Write a report on some new medical"gadget," such as mammography, CATscanners, fetal monitoring. Include any criti-cism the technique has received as well as itsbenefits.
74. Interview a couple who has experi-enced "natural childbirth" (the Lamazemethod).
75. Write a self-help guide to commonvaginal infections. Include symptoms,treatment, preventive measures, if any. Al-ternative topic: insomnia, urinary tract in-fections.
76. Give blood at one of the hospital bloodbanks. Bring proof of the donation. Includewritten report of how community blood do-nation plan works.
77. Visit a Weight Watchers meeting. Re-cord your experiences along with a descrip-tion of their program. Include a descriptionof "case histories" you might overhear orlearn about. How does their plan work?
78. Write an analysis of mibraine head-aches: what causes them, what happenswhen they occur, treatment, new ideas oftherapy.
23

79. Interview an acupuncturist or an os-teopath. Thoroughly document their train-ing programs and the usefulness of theirskills.
80. Put together a first aid kit designed fora specific purpose (camping, boat, work-room, etc.). Bring to class and explain whysof the contents you chose.
81. Find out and record 20 people's viewson raising the mandatory retirement age to70. Choose a mixture of ages for your sub-jects.
82. Design a sensitivity exercise to help agroup such as a new class break down initial
24
barriers of discomfort. The aims should be todecrease tension about being in a new,strange group and increasing knowledgeabout each other. Include factors such as:time needed, materials needed, goals,facilitators roles and responsibilities.
83. Collect at least five health pamphletsfrom community sources and critique themas to their usefulness, their appeal. Redesignthem to make them more "zingy," more ap-pealing.
84. Review filmstrip/tape on one of threeconsumer products (shampoo, acne treat-ments, aspirin) and write a critique of it. In-clude at least five ads for the product whichmake misleading statements.
38
85. Take the results of the health knowl-edge pretest which was administered inclass and complete a profile sheet and valida-tion exercise.
86. Preview health related films availableat local libraries and community agencies.Write a summary report.
87. If none of these projects grab you,think of another. Write a plan of action andturn in for approval. Points will be givenafter reading project description.

12 TEACHNG IDEAS
The Hospital as Motivatorfor Health Learning
Saul Ross is assistant professor of physical educa-tion, Schoo/ of Physical Education and Recreation,University of Ottawa, Ottawa, Canada. Previouslyhe was a teacher and physical education depart-ment head at Outremont High School in Mon-treal, Quebec, and instructor of health and physi-cal education at the High School of Commercein Ottawa, Ontario.
The problem confronting me was writtenclearly in the faces of the ninth grade boys star-ing up at me from behind their desks. A numberof factors were operating to produce those defiantlooks. Some of the boys were repeating grade 9,and almost everyone in the class had repeatedone or two school years previously, either in ele-mentary school or in junior high school. The agesof the pupils ranged from 13 years to 17 years.Their attitude also reflected the low status ofhealth education, confirmed by the fact that itwas assigned only one period per week. The lowopinion they had was also the result of someprosaic standardized teaching approaches to thissubject in their previous schooling.
The challenge was obvious. How could wechange their attitude to health education? Howwould we create interest and excitement? Whatnew method could we find that would involvethe students directly? What new area of the cur-riculum could we investigate that would meet thefollowing criteria: not covered before in previousgrades, interesting to all the boys, and somethingto which they could all relate readily?
Before relating how the challenge was met, itis important to describe the school setting. TheHigh School of Commerce is a beautiful newbuilding, constructed as part of an urban renewalproject to meet the needs of the people in theimmediate area. It is situated in a low-income,inner city area, amid government office buildings,and close to a large area that has been scheduledfor urban redevelopment for some time now. t3e-cause the curriculum is geared to commercial sub-jects, over 75% of the student population is fe-male. Few of the students aspire to university;most hope to land a good job after graduatingfrom high school, fairly confident that the com-mercial education they received will qualify themfor many office jobs. The boys aspire to jobs asoffice clerks, retail salesmen, management train-ees, or junior positions in advertising depart-ments; some hope to join the police force.,
My first step was to find out what parts of thehealth education curriculum had been covered.Each boy was invited to tell me and his classmateswhat areas he had studied or what he could re-call from previous years. The topics mentionedwere numerous, and the interest in each one var-ied. considerably. There did not seem to be aclear pattern, nor an exact core of subjects cov-ered, and this assessment applied equally to bothmy classes.
Pondering the problem, it occurred to me thatone area had been omitted completely; ..s anarea not covered in the textbooks used 4, healtheducation. The hospitalthe largest, most visiblehealth institutionwas a topic ignored complete-ly in their health education courses.
My next problem was how to present this topicto really motivate the students. One entire classperiod was devoted to having each boy relate hisexperience with a hospital, be it a visit to a friendor relative, a stay in the hospital, or contact withthe institution through service in the emergencydepartment or in one of the clinics. The fears, mis-conceptions, and negative feelings that emergedconfirmed my thinking about the importance ofdelving into this area.
After every pupil had talked, I asked them towrite as many questions as they could think upabout hospitals. This was something new to them,and after a few protests about not being able tothink up any questions, they set to work. Eachstudent was asked to prepare a list of 15 ques-tions for the next lesson. The assignment seemedtough, but the interest was there.
Plans for the next lesson called for dividing theclass into small groups of 4 or 5 boys. Each groupselected its own chairman and then set about thetask of analyzing the lists of questions to consoli-date them into one questionnaire. Questionscould be combined and, a:, discussion took place,new questions were added. Each class handed me5 question sheets, a process that lasted for twolessons. The questionnaires were mimeographed,with adequate space for answers, ready for usewell before our trip to the Ottawa Civic Hospital.
contacted the Ottawa Civic Hospital and ar-ranged for both classes to have a tour of the hos-pital. Copies of the questionnaires were sent tothe Hospital, to help the people there in planningour tour. The Hospital had never had such a largegroup (25-30 boys) take a tour, and so theyplanned an itinerary to take into account the largenumber as well as the interest of the group asindicated by our questionnaire.
3!)25

Arrangement; were made with the school officeto free the classes for the afternoon. The cost oftransportation was paid by the travel budget ofthe Physical and Health Education Departme
The tour included visiting the admissions office,records office, emergency department, furnaceand boiler rooms, laundry, kitchen, repair rooms,storage room, and underground passageways. Be-cause of the large lumbers of boys, laboratoriesand wards were omitted. The tour ended in a lec-ture theater where we heard two speakers. Thehead nurse of radiology explained the use ofX-rays and showed one of a clearly visible frac-ture. The supervisor of orderlies explained thefunctions of an orderly and detailed the trainingprogram he underwent. Each pupil had a ques-tionnaire with him as we toured the hospital andbusily wrote answers as they were provided byour guide. At the end of the tour the boys madetheir own way home from the hospital.
The next few lessons were devoted to follow-ing up what we had learned. The discussions thatwere held pertaining to the various functions ofthe hospital indicated that students had gainednew insights and attitudes. Heart transplants wasa subject of current interest and provided us witha natural and logical lead-in to the next topic--study of the heart and circulatory system.
In reviewing this unit in our health educationcourse, I felt the challenge had been well met.The students were involved. They made up aquestionnaire, which truly indicated what theywanted to know. By using the small group proc-ess to promote interaction, more questions ap-peared than with a simple compilation of all theoriginal questions. Interest was high and was sus-tained during the creation of the questionnaireand during the actual visit. There was consider-able excitement about visiting the hospital andbeing guided on a special tour. The interest re-
26
flected a real need. The boys explored a newworld on the tour of the hospital, a world fewpeople in the community had seen or eventhought about.
Two important questions need to be asked.Did students learn? What did they learn? Theycertainly learned about the operation of a hospi-tal and became aware of parts of the hospital thatmost people don't know exist. This new knowl-edge gave them new insight into the complexityof the institution and made them aware of manynew employment categories. They were affordedan opportunity to look into a world unto itself, acomplex and vital institution in our community.This new knowledge led to understanding whichin turn helped to change the negative feelingsthe boys had to the institution. Career possibili-ties in the hospital, specifically the position of anorderly, was important new information. Inciden-tally, the tour also pointed out to the hospitalstaff the need to embark on an educational andpublic relations program designed to modify thefeelings of people in the community about thehospital.
While attitude k difficult to measure, and cer-tainly no scientific effort was made to assess thisarea, I sensed a new interest 'n health educationon the part of the students. By using this experi-ence to launch the next topicheart and circula-tory systemthe progression was natural andlogical as compared to previous years where newsubjects were introduced artificially, merely be-cause they were listed next on the collrse of study.
Did they learn? What did they learn? By form-ing the questions they learned about the thingthey wa.ited to know, pinpointing the areas theywere most interested in. By constructing the ques-tionnaire, they learned to evaluate and discrimi-nate. Perhaps most important, they were directlyinvolved in the entire process.
4 0

13 TEACHNG IDEAS
Re id Trips
/.4.41ES H. PRICF assocrate profes:or ofAlhed Health Sciences at Kent State (Iniver-say, Kent, Ohio 44240.
Even though field trips are "old"teaching techniques, there arethousands of teachers who wver leavethe classroom. The community is filledwith health resources, and all healthteachers should make a 'ist o agenciesand places to visit which are related tohealth education.
The major objective of a field trip is togive students firsthand and accurate ex-periences not obtainable in the class-room. Trips should be taken only whenthey can contribute to the objectives ofthe course. The following questionsshouki be answered before the field tripis planned. Will the students begt.nuinely interested in the trip? Willcertain concepts be more clearly under-stood as a result of the trip? Vill thetinw and trouble be wortl A ti amountof learning produced? Is the trip trulyrepresentative ot the unit objectives?
Preliminary planning for a field triptakes considerable work and should bescheduled well in advance ot the trip.Anytime the class goes exploring in thecommunity there is the possibility of at:-cident, but caretul planning with atten-tion to details can help eliminat manyof the haiards ot a field trip. Properksuper-sed held trips, authonied by theappmpriate school authorities. usuallyinvolve the same legal habtlity condi-tions as anv classroom actr rt I eachershould find out it their state has specialrest ric how, Both administrative a nd pa-rental perm.ssion cc ill need to be ob-tained I he parents' permission slipshould identity the vs ho vs hat, vs hch,c, here. and %clic. ot the held trip andlarth ho i kga% repoh,ohle tor in-
surank e co\ erage ot the studenthe teacher should isit the site prior
tu the tr:p and plan the observationsand ak:R ities that vs ill best k ontribute tothe init obiectix t's Be sure that rest-100 ,s. eating accommodations. andtirst aid stations have been identihedI he development ot a route map withpoints ot interest marked can help in-
crease learning on the field trip. Ar-rangements for chaperones, transporta-tion, and finances must be made well inadvance of the trip.
Prepare the students for the trip byreviewing the objectives for taking thetrip, giving appropriate bak_kgrounci in-formation, identifying specific questions
the students should seek answers for,reviewing standards of conduct andsafety for traveling and while at the site,identifying any possible allergens orspecial problems students might en-counter (poison ivy, for example). in-form students of special needs, such asclothing, notebooks, expenses, lunch,etc.
Teachers should take along a first aidkit if the trip is going to be all day or ifthe visitation site does not have first aidsupplies. Other items for considerationto take along on the trip include: plasticbags in case someone gets carsick andbags for waste disposal (especially if thestudents take their lunches).
The group should be kept to a man-ageable size, by either limiting thenumber of students who can go or byincreasing the number of chaperonesand making subgroups. Take along a listof names of all students on the trip andcount heads frequently. Other aids areto assign partners for the trip and selecta place to meet if a student gets lost.Above alldon't panic! The trip willrequire a teacher who is enthusiastic,alert, and flexill/e!
Upon arriving at the site, if you are tohave a guide, introduce him or her andget the group moving along as quicklyas possible. Try to stick to the timeschedule while still answering all thestudents' questions. When leaving,check the class list, thank the guide. anddepart promptly. If a problem shouldarise which will cause the group to belate, telephone th school and let theprincipal know. I i reduces the anx-iety in principals and parents who maybe waiting for the returning students.
Plan for followup activities after thefield trip. Some ot the most importantlearning will come from sharing im-pressions and discussing events whichoccurred on the field trip. Further read-ing. cvriting, and class projects couldgrow out of the well-planned field trip.Followup classroom activities willlikely reveal to what extent your fieldtrip objectives were met. The classand/or the teacher should follow up andwrite a thank you letter to the visitationsite. A final evaluation of tlw trip shouldbe formallv cvritten and put on file in themain office. Then %Olen other teachersconsider visiting the same site, they willhave all objective evaluation by one ottheir colleagues.
27

14 TEACHNG IDEAS
HEALTH GAMESA recent publication presents learning games in several health education contentareas.' A drug game and an alcohol game from that source are presented here.
What's On My RackSlang terms for "street drugs" are
commonly used. However, the actualdrug, its action, its effect, and correctname are often not known. This game willfamiliarize students with the names, thetype, and the effects of drugs. Indexcards, felt tip pen and prizes are used.Place a slang term, correct name, andlong term effect on separate cards usingthe list r h own here.
i)P.,.ription for Playing: Pin one card onthe bad of each student without themseeing it.
Instruct the students that they must goto other students and ask for a clue as to
without a doctor's prescription?
DrinkingAlcohol consumption is a widespread
practice among all age groups. Alcoholeducation is one means of correcting themisconceptions many people currentlybelieve and/or practice. This game is de-signed to help students discriminate be-tween fact and fallacy about drinking.
Description for Playing: One story isgiven to each student. Intertwined in thisstory are misconceptions and/or falsestatements. Each sentence begins with anumber. Circle the number of thosestatements which are not true.
Name Slang NameAmphetamines bennies, dexies,
pep pills, uppers,hearts
Barbiturates barbs, blue devils,downers
Cocaine coke, snow, snuff
Codeine
Heroin
LSD
H., horse, scat,junk, smack,hard stuffacid, sugar,sunshine
Marijuana pot, grass,tea, M), weed
Methadone meth
Morphine white stuff,morph
"What's on n back" such as an effect,drug name, or slang term.
After a person correctly guesses whathis card says I e then finds the other stu-dents with the rest of the information per-taining to a certain drug. The first groupwith the correct cards wins a prize.
Discussion Questior.: 1. What are theimmediate effects of each drug?
2. What are stimulants, depressants orhallucinogens?
3. What is the legal, social, physicaldanger of many of these drugs taken
28
4ME
EffectAlertness, actively paranoid,loss of appetite, delusions,hallucinations.Euphoria, physical depend-ency with dangerous with-drawal symptoms.Excitation, sore nose,paranoia, depressive reboundon withdrawal.Euphoria, physical depend-ence, constipation, lossof appetite.Euphoria, physical depend-ence, constipation, lossof appetitu.Insightful experiences,distortion of senses, mayintensify existing psychosis,panic reactions, "flash-backs."Outside stimuli more vivid,relaxation, euphoria, physi-cal dependence.Constipation, loss ofappetite.Euphoria, physical depend-ence, constipation, lossof appetite.
'Woody, age 20, resides with his par-ents in Mt. Pleasant where he is a sopho-more at the university. 'The females oncampus find him very attractive; 6 feettall, 175 pounds, blond curly hair, andbright, blue eyes.
'Final exam week has brought aboutthe u,sual stress, and anxiety many collegestudents experience. 'In an effort to al-leviate the stress, Woody attended aweekend party. s It was the usual kind ofparty he attended with a lot of women,booze and loud music. Many of thefemales at the party were in constant pur-suit of him because his ability to drink
4 2
more than anyone else was viewed as asign of virility. 'This is partly due to thefact that the alcohol he consumed af-fected his muscles first. 'In Woody'scase, the alcohol also acted as an aph-rodisiac, as alcohol consumption usuallydoes. 'With these two factors contribut-ing to his virility, one can plainly see whyhe was pursued.
'°Woody is a fairly bright guy and hasestablished guidelines for his drinkingbehavior. " First, he always drinks vodkato prevent rapid absorption. "Second, heseldom eats any food before he drinksbecause it fills his stomach and he cannothold as many drinks. ''After all, if it's freebooze he wants to get all he can. "Third,he drinks slowly instead of gulping hisdrinks to prevent getting intoxicated.
's Since he is physically a big guy, he reallycan drink as much as he wants because hehas more body tissue and fluids to dilutethe alcohol.
'6As the evening progressed (3 hours),Woody collaumed six mixed drinks (11/2oz. alcohol per drink) and the only ob-servable sign he showed was a slight in-tensification of his talkative personality.
"As the party continued, he talked withfriends, danced and asked Joey, an attrac-tive girl clad in jeans, if he could drive herhome. "Of course, Joey answered yes,and they left the party.
" Should Joey have more carefully con-sidered the possible consequences ofleaving with Woody? 20After all, he wasonly drinking moderately and there areno risks if he drinks moderately. " Hewasn't acting "funny; " the alcohol hedrank stimulated himthat's the primaryeffect it has on a person. "And becauseboth his parents are alcoholics he proba-bly has inherited alcoholism from them."Oh well, why should she worry?
"The simple truth of this story is thatJoey is the alcoholic and not Woody.25 Everyone knows that there are morewomen alcoholics than men.
Questions: Which statements are false?(6, 7, 8, 11, 12, 15, 16, 20, 21, 22, 25).
Important Considerations: The instruc-tor should carefully explain why theabove statements are incorrect. Thisexercise can be used as a pretest prior todiscussion or as an evaluative tool afterdiscussion.
'Ruth C. Engs, ed., Eugene Barnes, andMolly Wantz, Health Games StudentsPlay (Indiana University: Bloomington,Indiana, 1974), pp. 13-23.

15 TEACHING IDEAS
lean Games,Widow andAchilles
DAVID E. CORBIN is in the School ofHPER, University of Nebraska, Omaha,Nebraska 68182 and DAVID A. SLEET isdirector of the Center for Health Games andSimulations, College of Human Services,San Diego State University, San Diego,California 92182.
Games and simulations are widelyused as teaching aids by classroomteachers across the country. We thinkthis attests to the potential of simulationand gaming activities in instruction. TheCenter for Health Games and Simula-tions at San Diego State Universityhouses the largest single collection ofhealth games and simulations andserves as a resource center for these ma-terials.
During the past five years, we havecollected, cataloged, and evaluatedgames in health for the benefit of con-sumers. We have found that materialsvary enormously in content, complex-ity, and priceranging from one-to-one patient education games for under$5.00, to computerized simulators forover $500.00.
The purpose of this article is to giveexamples of games which can be con-ducted with little cost or preparationtime. After experimenting with thesesuggestions, you can decide if you wantto pursue more formal and expensivecommercial products.
Drug Knowledge GamePrint the names of different drugs on
index cards, one per student. Be certainto use terms that are appropriate for thegrade level you are teaching. See the fol-lowing examples. Notice that groupnames, brand names, generic names,and common names are used.
Elementarycough syrupaspirinbeertobaccocoffeeTurnsRolaids
Middle SchoolmarijuananicotinecaffeineglueantacidsNytolSominexwhiskeyAnacinmilk of magnesia
High SchoolheroincodeineLSDginMidolEx-laxContacthashishwineBufferincocaineopium
Post High Schoolpsilocybinpenicillin'McmethadoneValiumLibriumhallucinogensmethedrinepeyotealcoholnitrous oxidePCPmorphineamphetaminesmescaline
Next, pin a drug card on the back ofeach student making sure the studentdoes not know what is written on thecard. The object of the game is for stu-dents to guess the name of the drug ordrug group pinned on their own backsby asking questions of fellow students.
Students should stand up and minglein a cleared area of the classroom.
The rules are as follows.1. Ask only yes or no questions.2. Limit questions to three per per-
son. This forces students to seek infor-mation from people other than theirfriends.
3. Approach the game cooperativelynot competitively. Once a person gues-ses his or her own drug card, pin thecard to the lapel. That student continuesto mingle answering questions for otherstudents. If time is a problem, set alimit.
Variation: Once the drug is guessed,pin a second card to the student's backfor the student to guess.
Use: This game can illustrate howmuch or how little students know aboutdrugs. Students will find they havebeen given conflicting information. Itwill also show some of the problems en-countered in the drug culture; forexample, buying drugs on the street isnot very reliable. A drug may be substi-tuted for another without the buyer'sknowledge. Sometimes the seller doesnot know the difference between drugs.This game can help reinforce the ideathat peers are not always reliablesources of information, nor are the sel-lers of drugs.
This game can also help improvequestioning skills and reasoning. If thequestions start out general and then be-come increasingly specific, students willbe more successful in guessing theircards. Here are some samplequestionsAm I an upper? Am I legal?Am I injected?
,1 3
Drug Grouping GameThis game is adapted from the game,
"Birds, Beasts, and Fowl," by GeorgeEnell, Kay Hardman, and Noreen Dres-ser (1977). It can be used as an offshootof the drug knowledge game or on itsown.
With a drug name card pinned totheir lapels, students group themselvesaccording to their cards without talkingto each other. The teacher should nottell the students how to group them-selves at this point.
After the students have settled intogroups, one student from each groupleaves the room. The teacher now asksmembers oi different groups what theirgroup is. After they are in agreement,the person outside the room returns andgives his or her perception of the groupto see if it is the same as that of the restof the group.
After this exercise is over you can givemore specific instrut tions for the nextsegment. For example: Group your-selves into two categorieslegal and il-legal; or five groupsstimulants, de-pressants, hallucinogens, narcotics, andothers. You can experiment with manypossibilities, all of which will help thestudents learn about drugs and variousclassifications.
After each grouping exercise, check tomake sure all students are in the propergroup. If they are not, ask tl class ifthey can find the person or persons whoshould change groups. Some can fit intomore than one group, for example if thegroups are legal and illegal then barbitu-rates could be in either, since they canbe prescribed or sold illegally.
Remember, students may not talkwhile grouping themselves, they mustrely on reading the drug cards and"body language" to determine wherethey belong.
Reproductive System Terms GameThis game is played in exactly the
same manner as the drug knowledgegame only cards with names of the maleand female reproductive system partsare pinned on the backs of the students.This is an excellent activity for teacherswho will be teaching sex education,s;nce it helps them to talk freely andopenly about terms having to do withreproduction. It is not recommended forgeneralized audiences. Like the drugknowledge game, it helps to illustratethe misinformation that abounds amongpeers.
29
Cards cal- include any of the follow-ing
hymen labia majoratestes Bartholin's
glandsepididymus urethraseminal vesicles glansfallopian tubes labia minoraovaries Graafian
follicleforeskin cervixuterus clitorisprostate seminiferousvas deferens tubules
vaginabulbou reth ral or
Cowper's glandspenis
Note: "urethra" is part of the maleand female anatomy, but, of course,only in the male's reproductivesystemthis may make it a more dif-ficult term for some.
Food Grouping Game
This game is very similar to the druggrouping game and is also adapted from"Birds, Beasts, and Fowl." Instead ofname tags cut out pictures of differentfoods from magazines. Be certain thatyou select different foods from all foodgroups and pseudo-foods such as al-coholic beverages, salt, pepper, condi-ments. Place all the pictures into a paperbag then have students remove onefood cutout without looking and pin iton their lapels. From this point on, theprogression is the same as the druggrouping game. Remember, studentsalways group themselves without talk-ing to each other.
Variations: Ask six people to leave theroom. Ask the rest of the class to re-group themselves according to theirtags this time according to a specific di-rection, such as foods high in sugar, abalanced meal, high protein foods.When the other students come back intothe room they try to guess upon whabasis the groups have been formed.
Ask all students to form the fourbasic food groups (or the basic seven).Make necessary corrections by asking
the class as a whole if everyone is in thecorrect group. If they don't know, helpthem.
30
Ask the students to group into foodsthat are high-risk for dental disease andfoods that are low-risk for dental dis-ease.
Ask the students to group into high-risk, neutral, and low-risk for cardiovas-cular disease.
Experiment with other groupings.After this exercise, students can easilysee that there are many different aspectsto consider in selecting foods. Just be-cause a food may be low-risk for dentaldisease, does not mean it is necessarilylow-risk for cardiovascular disease. Wealso like to add foods such as pizza orhamburger which don't fit neatly intoany single group.
"Drunk" Synonym GameThere are, reportedly, more
synonyms for the word "drunk" thanfor any other word in the English lan-guage. These words say somethingabout how ingrained and accepted al-cohol is in our society. To beglii thisgame open the floor to any and allsynonyms for the word "drunk." As thestudents call them out, write them onthe blackboard.
Examples:
juicedplasteredpollutedzonkedbiutedtight
inebriatedpickledunder the tablesmashedloadedintoxicated
To better see how our society viewsdrunkenness, make another list incategories. This cm be done as a class oras an assignmen: for each individual.The r ttegories could be: technical-
1) .1, funny-happy, tragic-sad, andtrAl. Discuss the implications. Invar-
..s. f the funny-happy category is the,hirgest.
'to extend this activity, students cartname plays, movies, comic strips, TVshows, and people in which (or whom)alcohol plays an integral part, thencategorize them the same way they didthe synonyms.
44
Examples:
Foster BrooksDean MartinAndy CappEd McMahonHagarJanis loptinW. C. Fields
"Lady Sings the Blues"Betty FordAlice Cooper"Streetcar Named Desire""All in the Family""Days of Wine and Roses"Wilbur Mills
After trying any of these games, youmay wish to try some of the other gameson file at the Center for Health Gamesand Simulations. For more informationon the use of games and simulations inhealth instruction, the reader is encour-aged to consult the suggested readings.
Originally presented at Association forAdvancement of Health Education Meeting,New Orleans, LA. March 1979.
16 TEACHING IDEAS
LEARNING GAMES
Getting To KnowOne Another
There are several interesting waysfor students to get to know oneanother better. Even though theyare in the same class, some studentsnever converse with or know muchabout many of their classmates. Thefollowing exercise provides for adiscussion of content within a proc-ess designed to expand communi-cation in the classroom; it therebyalso increases a sense of trustamong class members.
Each pupil is asked to selectanother pupil with whom to discussone of several listed topics. Thepartner selected, however, shouldbe someone whom the selectordoesn't know very well. Before dis-cussing the topic, each pair get'. toknow each other better by discuss-ing their aspirations, feelings aboutthe class, family history, or othermatters personal to their lives. Afterthis discussion is completed, thecontent topic is discussed. Twentyminutes should be allowed for thisphase of the exercise.
Possible topics for discussion are.
Foods that I like to eat. (Nutri-tion)
How to make our homes safe.(Safety education)
How girls are different from boys.(Sex education)
Next, each pair chooses anotherpair whom they don't know verywell, and the process k repeated.This time, however, each pupil in-troduces his partner to the otherpair and a general discussion ofpupil's backgrounds, etc. precedesthe content-related discussion. Thegroup of four can then be com-bined with another group of four tomake eights and eights can be com-bined to make sixteens, etc.
Listening PracticeStudents are formed into groups
of three for the purpose of discuss-ing a question. Questions may rangefrom "How does someone makefriends?" to "What's the safest wayto ride a bicycle?" During the en-suing discussion, in order for a
member of the group to communi-cate verbally, that member mustparaphrase, to the satisfaction ofthe previous speaker, what was lastsaid. If a paraphrase is attemptedbut is incorrect, the person who isbeing paraphrased repeats what hesaid and the paraphraser again at-tempts to paraphrase his comments.The purposes of this exercise are:
1. To provide a framework for class-mates to talk in small groups andget to know one another.
2. To emphasize that we are oftenthinking of what we want to sayand not listening to what othersare saying.
3. To discuss fully the topic at handin an interesting and effectivemanner.
4. To underline that communicationis often impeded by emotionalinvolvement in the topic, some-one who talks for a long periodof time, someone who presents alot of ideas all at once, seriousbiases, or a poor facility in whichto talk and listen. Any of theabove can, and often do, createdifficulties in hearing accuratelywhat is being communicated andcan cause difficulty in paraphras-ing.
If tHs exercise is conducted for atwenty minute period and then dis-cussed fully, pupils will becomeaware of their listening skills andattempt to sharpen them. A periodicrepeat of this exercise will providefeedback on progress in develop-ment of listening skills.
Family DrawingsOften children's insights into
their family lives are not such thatthe roles of the family members arereadily accessible to them. Percep-tions of family life are often re-pressed and hidden. An activity de-signed to bring to the surface a
child's feelings about his family isone in which he draws a picture ofhis family in a group activity orsome other context. At the conclu-sion of this activity, drawings areexchanged among all members ofthe class until each classmate hashad the opportunity to review eachdrawing. Pupils write a one sen-tence comment, which expressestheir reaction, on the back of eachdrawing they review. Commentsshould relate to the family as a
whole, or to individuals depicted.Next, drawings are returned to theartists with time provided to readthe comments of their classmates.A discussion follows of the objec-tives of this exercise.
Lost on the MoonThis activity helps children to
compromise and take part in con-sensual decision making processes.Each child is supplied with a copyof the following problem:
You are in a space crew originallscheduled to rendezvous with a
mother ship on the lighted surfaceof the moon. Mechanical difficulties,however, have forced your ship tocrash land at a spot some 200 milesfrom the rendezvous point The roughlanding damaged much of the eguiprnent aboard. Since Nurvival dependson reaching the mother ship, tlwmost critical items available must bechosen for the 200-mile trip. Thefifteen items left intact after the land-
are listed twIciw. Ycair task iN torank them in terms of their impor-tance to your crew in its attempt toreach the rendezvilus point Placenumber 1 by the most importantitem, number 2 by the second mostimportant, and so on through theleast important, number 15.
31
Box of matchesFood concentrates50 feet of nylon ropeParachute silkPortable heating unitTwo 45 caliber pistolsOne case dehydrated milk
_ Two 100-pound tanks of oxygenStellar map of the moon's con-stellation_ life raft containing CO2 bottles
_ Magnetic compass_ 5 gallons of water_ Signal flares
First-aid kit containing !nip( tionneedles
__ Solar-powered Fm receiver-trans-mitter
Below are the correct rankings asdetermined by National Aeronauticsand Space Administration:
15Box of matches (little or no useon the moon)
4Food concentrate (supply dailyfood required)
6-50 Feet of nylon rope (useful intying injured, help in ( limbing)
8Parachute silk (shelter againstsun's rays)
13Portable heating unit (useful onlyif party landed on dark side)
11Two .45 caliber pistols (self-pro-pulsion devices could be mad('for them)
12--One case dehydrated milk (food,mixed with water for drinking)
1Two 100-pound tanks of oxygen(fills respiration requirement)
3--Stellar map of the moon's con-stellation (one of the principalmeans of finding direction)
9Life raft (CO2 bottles for self-propulsion across chasms, etc.)
14Magnetic conlpass (probab:y nomagnetized poles; thus useless)
32
2-5 gallons of water (replenishesloss by sweating, etc.)
10Signal flares (distress call withinline of sight)
7--First-aid kit containing injectionneedles (ot.,' pills or injectionmedicine valuable)
5Solar-powered FM receiver-trans-mitter (distress signal transmitter,possible communication withmother ship).
Each child ranks the fifteenitems in terms of importance.Groups of six to eight students arethen formed to rank the fifteenitems as a group, utilizing con-sensual decision making rather thanvoting. No one group member'sopinion is allowed to override thegroup's decision. A comparison ofindividual and group opinions evi-dences the advantage of consensualdecision making. This analysis isconducted by computing the dif-ference between the NASA rank-ings and the individual rankingsfirstly, and the NASA rankings andthe group's rankings secondly. Thedifferences for the individual rank-ings are totaled, as are the differ-ences for the group rankings. Thelower the score, the more accuratethe rankings.'
Cognitive FootballA football field is drawn on the
blackboard, and the class is dividedinto two teams. A content area inhealth education is selected, forexample, nutrition. The teacher hasthree sets of cards which containquestions pertaining to the contentarea selected. One set of cards con-tains relatively easy questions, whichwhen answered correctly, result ina five-yard gain. Another set ofquestions, somewhat more difficult,
4 6
result in a ten-yard gain; and thelast set of questions is worth 15yards. The toss of a coin decideswhich team begins the game withthe ball on the fifty-yard line. Teammembers decide, previous to at-tempting to answer the question,from which set of cards the ques-tion should be selected and therebyhow much of a gain will be at-tempted. Teams alternate answeringquestions and the team that putsthe ball over the opponents' goalline is the winner. Only one teammember is allowed to answer thequestion and may not receive helpfrom his teammates.
Written ConversationsThis activity serves to correlate
language arts with health instruc-tion and, in particular, family living.The class is separated into pairs,one person assigned the role ofchild and the other the role of par-ent. A situation is described, e.g.,the child wants to play outdoorswith his friends while the parentinsists he stay indoors arid completehis homework. Each pair then en-gages in a written conversation re-corded on a sheet of paper. Noverbalizing is permitted. These pa-per and pencil conversations shouldlast approximately twenty minutesat which time pairs volunteer toread their conversations to the class.Each conversation read is analyzedwith access to "replays" since theconversation has been recorded onpaper.
Gene Stanford and Barbara Stanford,I earn, ng Disc uccion Skills 1hmugGames (New York: Citation Press, 1969,pp. 44-47.
17 TEACHING IDEAS
HORSE RACINGIN THECLASSROOM
PHILLIP HOSSL ER is a teaclwr of healthand physical educatum and trainer for allsports at the Madison Township HighSchool, Old Bridge, Net.% Jersey 08857.
One of the difficult problems faced byhigh school educators today is motivatingtheir students, especially in requiredcourses. The problem is convincing stu-dents that just because they have to be inthe class is no reason why they can't enjoyit and learn something at the- same time.Giving stars or lollipops for answering adifficult question or solving a problem isnot successful in high school, becauseolder students feel their performance de-serves a more beneficial reward, such asthe improvement of their grade. In manyrequired courses the students may onlydo that which is required to pass thecourse. Clearly what is needed is sonicsort of activity where the older studentsare able to feel they are properly reim-bursed for their endeavors and still learnsomething in the process.
I initiated an activity in my healthclasses wherein the students researched,in class, answers to questions and expla-nations to the notes that I planned tocover that day. This activity took the formof a horse race. To start class when I usethe horse race, I blow a whistle or ring abell. I have signs in the room saying "Sta-bles," "Race Tips," "Cashier," "Grand-stand," etc., and have long strings of col-ored flags hanging in the room to addauthenticity and show the class that I toohave enthusiasm and enjoy what I am do-ing.
Eac h group of tour students is a horse,so there are four joc keys to each horse,and each horse has a name. The first day Iput on the overhead projector the draw-ing of the oval track with the grandstands,flags, and finish line drawn in. In thecenter of the track I wrote "Hossler'sHappy Healthy Horse Sweepstakes."Next I showed on the overhead the ideas Iplanned to cover that day. For example,when the class starts the study of venerealdisease, the notes might look like:
Intro to VDVenusskin-to-skin contactpox, clapcausedamage to infected
__I
Then I give the class 10-15 minutes to lookthrough the books and pamphlets that I
have brought to class or ones they havegotten themselves to discover what I
mean by each of these short phrases.Each of the horses is questioned to ex-plain my own notes to me. I speak to adifferent jockey each time so thateveryone is involved at some point.
Each of the phrases is worth a certainpoint value, usually 1 point. If only onehorse gives the correct answer, that horsewould get the full point; if two horsesgive me equally correct answers theywould each get one-half point and soforth. The points that each horse receivesdetermine its position around the track. Ittakes a total of 12 points to run the lengthof the track.
For example, if horse #1, Sugar Daddy,tells me that skin-to-skin contact is themethod of transmission when speakingabout venereal disea3L, he would be cor-rect. If no other hcrse was able to give methis answer Sugar Daddy would receivethe full point. lf, however, horse #5,Carmel Corn, told me that skin-to-skincontact was the method of transmittingvenereal disease and that coitus was themost common form of skin-to-skin con-tact for transmitting VD, Carmel Cornwould receive three-fourths of a point orhe might even steal the full point awayfrom Sugar Daddy since Carmel Corngave me the more complete answer. Thestudents become involved with the racebecause of the constant advancing andfalling behind on each question. Aftertwo or three notes, I write the position ofthe horses on the track. The jockeys thenbegin to dig a little deeper the next timefor that bit of extra information that willgive them the edge over the rest of thepack.
I have also found that res?arc hing an-swers develops t .amwork arid prideamong the joc keys on eac h horse. They
BEST COPY AV:A:Z:1d 7
must researc h much material in a shortperiod of time, so the notes are delegatedto eacli of the jockeys on the horse so thatone might have the answer to a note thatthe other jockeys didn't have time to find.
After eac h horse has given me an an-swer explaining the note, I write thepoints awarded on the overhead next totheir horse's name amid cheers andgroans from the jockeys. Then I tell themexactly what I was looking for and givethem time to write it in their notebooksbefore going on to the next note. Theorder in whic h the horses respond varieseac h time so no one horse gains an advan-tage by being the last to answer eachtime.
The race continues until all the horseshave finished the course. If horse #1 tin-ished first the jockeys cannot sit back anddo nothing; they must still answer ques-tions to ensure that another one of thehorses doesn't earn more points and"nose them out at the wire."
If there are six horses running, the jock-eys on the winning horse each get sixpoints, the second place jockeys each getfive points, and sc forth. These bonuspoints are used at the end of the markingperiod when grades are determined.
This method of teaching requires moretime, because the amount of materialcovered each day may not be as much aswith the lecture method. It ?quires ateac her who is able to instruc t and stillmaintain control of the class amid mildchaos, much laughter, and student en-thusiasm. I have found that the grades onthe tests after using this method are thehighest grades of the marking period.
I personally enjoy using this method ofteac hing. I don't use it for the entire mark-ing period; instead I tell the class about itin the beginning and then save it untillast, This also helps to build enthusiasmtoward the ac tivity.
33

18 TEACHNG IDEAS
FANTASY GAMES
RALPH BATES is in the Department ofHealth, Physical Education and Recrea-tion, Ohio State University, Columbus,Ohio 43210.
I have used fantasy games with youngchildren, older children, and adults andhave found them to be very successful.Participants become more aware of howthey perceive themselves, what they arelike as people, their strengths and weak-nesses and, most important, they can be-come aware of emotions and deeper feel-ings which normally would not be dis-closed to individual or group members. Ihave also found that fantasy is relaxing,helps develop better listening skills, andleads to closer, more meaningful rela-tionships among participants.
In this paper I would like to share sev-eral of these games, to use with groups ofchildren as a means of relaxation and tohelp them learn more about themselves. Iwill indicate the method I use in present-ing these games, and the reader can adapteach one according to individual needs.The books and articles in the bibliographyare excellent resources for fantasy gamesas well as other communication skills forboth children and adults.
Make A Person
I have found this game to be effectivewith children to help you learn what theyare like as people.
1. Ask a group of children to think of aperson's name and write it on the board.
2. Using the general background of thegroup as a guide, and the age of thechildren you are dealing with, establishsame criteria for this person. Example:"Billy is 14 and lives at home with hismother, father, brother, and sister."
3. Ask the children the following: Withhelp from each one of you, I would like tofind out more about Billy. What is he likeas a person ?What is he like at home? Howdoes he do in school? What does he liketo do? How does he feel about himself?With these general questions as a guide,obtain several responses from eac h childand write them on the blackboard. If youlisten carefully, you will be surprisedabout how these children feel aboutthemselves, their peers, and theirfamilies. Follow this through with a groupdiscussion.
Rosebush and Object IdentificationThis game is directed more toward
older children. You may use the sameformat for younger children by substitut-ing a flower or animal for the rosebushand object.
34
1. Ask the participants to close theireyes and get as comfortable as possible.They may sit in their chairs or sit or lie onthe floor. Then say the following: I amgoing to take you on a fantasy trip. I wantyou to do exactly as I say and be aware ofnothing else but my voice.
2. The following questions can be usedfor the rosebush. You will have to adaptthese questions to the other games. Whatare you like as a rosebush (object)? Whatare your roots like . . . your stem . . . yourleaves . . . your thorns . . . your flowers?What are your surroundings like? Whatseason?
3. Now proceed with the following: Inseveral minutes I will ask you to openyour eyes then tell us what you are like asa rosebush. Have each member select agroup member after he has describedhimself to the group. The following ques-tions may be used for discussion.
1. What did you learn about yourself?2. What did the group learn?3. Nosy does this relate to disclosure,
listening, feedback, communication, andfantasy? (Adapted from Stevens, Aware-ness.)
Ocean TripObtain a record or tape of ocean
sounds such as Environmental Sounds, ora tape recording from a radio or TV com-munication center.
1. Have the group relax at their desksor lie on the floor.
2. Tell them the following: I am goingto take you on a fantasy ocean trip. I wantyou to close your eyes, relax, and concen-trate on what I say. Imagine yourself ap-proaching a beautiful vacated beach. . . .
You begin to walk in the sand. . . . Stopand take off your shoes. As you standthere, feel the sand on the bottom of yourfeet, the grains of sand sifting throughyour toes.. . . become aware of that feel-ing. Begin a stroll toward the water'sedge.. . As you continue your walk, be-come aware of the sun beating on yourface, smell the salty air, hear all thesounds around you. Find a spot ahead ofyou and sit down in the sand. . . . Holdsome sand in your hand. . . . Feel theindividual grains of sand sift through yourfingers. Stand up and continue your strolltoward the water's edge. . . . Before youreach the water, stand (and sit) in the wetsand. . . . Feel your feet sink into the wetsand. Grab a handful of wet sand. . . . Beaware of the difference between the wetsand and the dry sand. Stand by the wa-ter's edge. . . . Feel the water gently flow-ing under your feet and around yourankles.... Stand there and smell the saltyair, feel the wind blowing in your face,and be aware of all the sounds aroundyou. . . . (cont'd). . .
4 8
Use your own imagination with thisgame. After you are through give thegroup several minutes before they opentheir eyes and disclose their trip to thegroup.
The following questions may be usedfor discussion:
1. How was your fantasy trip?2. Where were you?3. What were your surroundings like?4. What were some of the feelings you
experienced?5. Could you feel the different textures
of sand?
Fantasy Dream (This exercise is also di-rected toward older groups of children.)
Close your eyes and become as relaxedas possible. I am going to take you back toyour early childhood to a recurring dreamthat you used to have then, a dream thatyou are going to have again.
Don't be afraid. Just concentrate onwhat I will tell you, and on your experi-ence as my words are spoken. At night,while you are asleep as a small child, thedream would occur over and over again.The dream would begin in the same way.You would get out of bed and walk acrossthe bedroom to the closet. There is now adoor behind the closet, a door which youcould never find while awake. As you ap-proach the door in your dream it nowopens.
As you stand in the door you look downan ancient looking stone staircase. In thedim light you begin to descend the stair-case, nOt at all afraid, down a step at atime. As you approach the bottom of thestaircase you stop and hear the gentlesound of water lapping against the rocksbelow. You approach the water's edge. Asmall boat is tied to the rocks. Sit in theboat and untie it. Just lie back in the bot-tom of the boat and let it take you where itwants to go. Sit there, relax, and listen tothe water lapping against the beat androcks, as you gently rock back and forth,back and forth, as the boat drifts downthe stream.
As you lie there enjoying your trip younotice a small opening ahead of you. Asyou approach the opening it becomeslarger and larger. You come out of theopening into a new environment whichyou will now experience. Continue tokeep your eyes closed and become awareof the new environment. Where are you?. . . What is it like? . . . What will you donext? . . . What sights, odors, sounds,and movements are you now experienc-ing? . . . etc.. . , Now open your eyes anddisclose your experiences to the group.(Adapted from Masters, Mind Games.

19 TEACHING IDEAS
CHOICES
LYNN TEPER-SINGER is an assistant pro-fessor in the Department of Health Sci-ence, Physical Education, and Guidanceand Counseling at Long IslandUniverstty----the Brooklyn Center, Brook-lyn, New York 11201.
One of my beliefs is that the way onefeels about oneself is reflected by thehokes one makes and the behavior that
follows these choices. Therefore, one ofthe ways I gain an understanding of theindividuals within my health classes is byobserving their behavior in here and nowsituations. Then, by exploring the motiva-tions behind their actions, the class takespart in understanding their decisions.
I have found that the following tech-nique arouses strong emotional re-sponses while dealing with making deci-sions:
Have your class stand in a cm le andlook around the room at their classmatespic king out one person they would like toknow better. At a signal from you, theirtask will be to go over to the person attheir choice and nonverbally show thatperson how they feel. Often no one willmove initially. It this occurs yen may wait,or you might em mirage them further bysaying. "You mean no one here wants toknow anyone better.- This may be metwith a display of discomfort or laughter,and at this point it is best to investigatewhat the students were feeling by dis-c ussing then objec lions to moving. f venit no one in the class responds to theinitial experiment, reactions are takingpla« within each person. Some mem-bers may he «in tused about Who theywould c house or how they would showtheir teelings and therefore nught not beable to make a decision. They may havethought it over and decided to do noth-ing. Sonie people might have hoped thatsomeone would make a dec ision to coineover to them, relies mg them of !lasing toinitiate the ac hon.
49
Questions ma% be raised tor classesthat will help students tie in their expen-em es to making c hoR es. The following INone way that this c an be explored.
I) What were your teelings: when I
told Yon what the initial task would he:while you were mos ing or antic loafingsomeone else s mme: alter the task w ascompleted?
(2) How did you decide': tat who youwould like to know better; (b) how youwould show that person how you feel; (c)whether or not you would act on yourteeling?
(3) Outside lite experiences m theclassroom: (recommended for smallgroups)
Under what other c irc umstances haveyou experienced similar feelings to thoseyou felt here today?
What decisions did you make underthose circumstances?
What correlations can you make thatwill help you understand the patterns ofyour choir es?
What other alternatn es do you believeare open to you?
How do you see your ability to makedec isions as a reflection ot your seltimage?
During experiences ot this sort withinclasses on both the high s hool arid al-lege level, I have tound that it is imma-terial whether or not the class moves atyour signal In both c ases, students havedisclosed feelings about: (1) being re-jectedthe feeling that the person theychoose may not be open to them. (2)Being nusunderstood--someone mightinterpret their action (to the same or op-posite sex) as one of sexual interest. (3)Being spec al --hoping sollIV011e wouldslmw them their feelings first. 141 Beingrisk-taker -in spite ot !lasing all the abovefeelings the person may dec ide to move.
Some students claim that they like theopportunits to let their feelings be knownand are more «mitortable showing theirfeelings than telling someone ,thoutthem.
This ter hnique is multilac eted. The«milu I that takes pia«, within ear h per-son mien deals with both the leelings theperson has about what he wants ordoesn't want to do and the f eel! ngs atmutw hat others want or expo( t of lum.Another area for disc ussion, thei (lore,c an inc luck's\ hal elle( I other people has eon the dec ision-mak rig pm( ess %%ohm
ll isms opinion that those tear heismake them own dec ision to us this tec ii
moues% ill mid it to be an excc'llent tool torhelping sludruts to dimmer and understand the dec ision-making pro( ess andtheir molls df ow. behind the c hon es theytnake
35
20 TEACHING IDE AS
Con Outing anEducationalGe
SALLY L. EASTERBROOK is an instructorof health education, Department of HealthSciences, Towson State University, Balti-more, Maryland 21204. This article isadapted from a presentation given to theMaryland AAHPER Convention in October1976, Largo, Maryland.
There are numerous types of gameswhich can be used in a classroom.Among these are the commercially pro-duced game, teacher adapted game,teacher made game, student adaptedgame, and student made game. The lastfour are the least expensive. An addi-tional advantage is that they can be con-structed to meet specific needs. Stepsfor developing an educational game forclassroom use follow.
1. First, it is essertial to know thecapabilities of the students who will beusing the gametheir abilities, atten-tion spans, and reading levds.
2. A prerequisite in game building is tooutline clearly the specific purpose ofthe game. The constructor should knowexactly how it will be used in the class-room.
Games can be used: to introduce newtopics, which creates a "sct" for thelearners; to illustrate an idea; or to re-view a unit. Some games may be usedas pretests and then adapted to serve asa posttest at the end of the unit.
3. Once the purpose of the game hasbeen formulated, the specific contentca n be outlined.
4. The constructor must then answersome questions concerning the class-room atmosphere during the game.
How quiet or disruptive should thegame be?How many st,identi will be directly
36
involved in game play?If not all students are involved, whatcan the rest do?How much competition should beencouraged through use of this par-ticular game?How much time needs to be set asidefor the playing of this game?
5. Next, the constructor needs to decidewhat type of game to createa boardgame, a word game, a team game, orsome other format? What types of ques-tions may be open-ended; based onchoice, or short answer? Some ques-tions may be opened ended; based onstudent answers, the players will haveto make certain decisions (branching).
6. Actual construction of the gamecomes next. Parts should be kept to aminimum to prevent the loss and neces-sary replacement of pieces. If a boardgame is being constructed, the boardshould be neat and colorful. All partsshould be safe and durable. Coveringparts with clear contact paper decreases"wear and tear."
5
'41I
rn.
4
oft__
I.
11..f/':1
X14`..f. .43_ r
The construction of directions fallsinto this step also. Directions should beas uncomplicated, clear, and concise aspocsible. The object of the game shouldbe stated and all possible situationsshould be included. If questions areasked during the game, an answerbooklet providing all acceptable re-sponses should be provided.
7. The last step in game construction isa trial run. A group of students shouldplay the game on their own. From ob-servations made during this session,modifications of time requirements,rules, directions, and wording of ques-tions can be made.
Development, construction, and useof an educational game can be bodi afun and profitable way to spend class-room time. Games can be pr6duced fora wide variety of purposes and to meetthe particular needs of students. If youhaven't yet used this technique, whynot give it a try?

21 TEACHING IDEAS
Health 4 Fun:A Game of Knott/ledge
RAYMOND NAKAMURA teaches in theprograms in physical education, School ofEducation, DePaul University, 1011 W. Bel-den Avenue', Chicago, Illinois 60614.
From time to time, as a diversion fromstandard methods, educational gamescan be excellent tools for learning."Health 4 Fun" has been a successfulgame because it requires a lot of knowl-edge and provides some fun. It can becooperative or competitive and can beused to develop research skills in dic-tionaries, encyclopedias, almanacs,textbooks, journals, etc
The purpose of the gdme is to fill inthe blanks of a play sheet with words orphrases that fit into pre-selected healthcategories. The filled-in words mustbegin with certain letters which are cho-sen at the beginning of the game.
The health categories chosen mustsuit the level of the class. Each one iswritten on a separate 3x5 index card.The cards are shuffled and placed facedown; four cards are drawn from thepile. As each selection is read, allplayers write them down in the fourcategory blanks on the play sheet.
Letters are written on another set ofindex cards, one per card. These areshuffled and four are drawn from thepile. The chosen letters are written inthe appropriate blanks on the playsheet.
The Game
Each player tries to think of a word orphrase in each of the 16 blanks on theplay sheet that fits the category at thetop of the column and begins with theselected letters. An example of a filled-in play sheet follows. To add excite-ment, a time limit of 2-5 minutes can beput on the game.
The game can be played as a form ofsolitaire or by the whole class. Teamscan be made for more competitive orcooperative games.
At the end of the game, playersshould research the answers they couldnot fill in. Discussions often developwhen students come up with words orphrases that the others are not familiarwith. Answers may be challenged; tlwnthey must be verified by research.
In competitive games the play sheetscan be scored by adding up the number
of correct answers in each column, hori-zontally and vertically for a maximumscore of 32.
Here are some suggested healthcategories.
1. Body systems, organs, and glands2. Bones or muscles3. Fniits and vegetables4. Meats, nuts or fish5. Dairy products6. Ice cream flavors7. American foods8. Foreign foods9. Diets
10. Fitness: names of sports11. Fresh and saltwater fish12. Types of transportation13. Types of fuel14. Pollutants: cigarette names15. Pollutants: automobile names16. Environmental pollutants17. Germs or bacteria18. Medical laboratory apparatus19. Human diseases20. Communicable dieases21. Non-communicable diseases22. Drugs, medicine tradenames23. Slang for drugs or medidnes24. Over the counter drugs25. Pollutants: detergents26. Wines27. Beer28. Soft drink tradenames29. Hospital names
30. Health related journals31. Health book titles32. Health authors33. Famous health people, past34. Famous health people, present35. Health organizations or societies36. Health agencies, offices or departments37. Health related professions38. Environment: mountains39. Environment: extinct animals or birds40. Environment: endangered species41. Environment: rivers and lakes42. Environment: national parks43. Bakery products44. Famous restaurants45. Kitchen utensils46. Health related household items47. Things commGnly found in the medicine
cabinet48. Health related words over seven letters49. Breakfast cereals50. Famous physicians51. Chemicals found in the body52. Articles of clothing53. Plant names54. Flower names55. Category of your choice
The degree of difficulty of thesecategories should be related to theacademic level of the class. Many a berefined to offer greater difficulty. Forexample, a generalized category likeprescription drugs can be limited tobarbiturates. However, I have found itnecessary to include some easycategories to ensure some success.
Ca19ory 11)+!4mbn, 62etse
Bohesand
Muse-Its
AtA+0Tieultt4 arrieS
Medial
sAirfal°4
16 r.Li P;f44`fria -1,e14o;e1
4
>clic Ii Wor
...1
1
XL_
t4kooriA3
Tibula r
.
rurs,
,n,i_61.t511
:D;seast
10 41)14 UYNC0111 Le-h5 .
5 1
czA
37

22 TEACHNG IDEAS
School Health Bee
Bernard S. Krasnow is assistant principal andsupervisor of health education at Arturo ToscaniniJunior High School in Bronx, New York.
Health education took a dramatic turn last yearat Toscanini Junior High School in Bronx, NewYork. Our school inaugurated its first annualhealth bee in order to stimulate greater partici-pation and interest in health education and incurrent health topics.
The project was created out of a desire tochange the traditional assembly program so thatan atmosphere of excitement would pervade theaudience. The health education department helda conference devoted to this idea and it wasdecided to promote a school-wide health knowl-edge quiz. This would culminate in a series ofgrade auditorium programs designed to dupli-cate the fun and excitement of television quizprograms.
The school's health instructor, Mr. Pluchik, wasdesignated as the teacher-in-charge for the proj-ect. He constructed a health knowledge test fromour own curriculum which was administered toall the students during their health or scienceperiods. The students who scored highest on thisinitial survey test were invited to a class winners'run-off. Fifty-five class winners appeared for therun-off test which was held after school. Thosewith five highest scores in each grade were thendesignated as finalists and invited to participatein the auditorium quiz programs the followingweek. They were given extra resources in the formof textbooks, pamphlets, etc., to study from inpreparation for the contest.
The auditorium program was modeled after atelevision panel quiz program. The industrial artsdepartment constructed an electrical responseboard so that a contestant who knew the answer38 5 2
was able to press a button to make a lightflash in front of him. Mr. Pluchik served as
moderator and asked the questions. Three otherteachers acted as judges. The questions for thefinal quiz were selected from among those in theinitial survey and the run-off examinations.
There was great anticipation on the part of thecontestants and the student body. Publicity hadbeen extensive through public address messages,posters, and class announcements so that most ofthe students were eagerly awaiting the program.The contests were well received by the audienceand seldom has there been more audience en-thusiasm. The excitement was, in fact, so greatthat many times the audience inadvertentlyshouted out the answer. (We did, in fact, throwthe questions to the audience if they were notanswered correctly by the contestants.) The scor-ing was conducted by awarding one point foreach question answered correctly. Each contest-ant had his own personal scoreboard that re-flected his current total. This kept the audienceposted on the current scores.
Each auditorium program was concluded byawarding a trophy to the health quiz winner ofeach grade, and the finalists received honor certifi-cates. The school photographer was there to takepictures of all the winners and we plan to displaythese for publicity purposes.
Our original idea in initiating this project wasto focus on health education and current healthtopics. We are sure that this school-wide programdid just that. We are, however, promoting follow-up activities so that our initial efforts are long-lasting. Some of these activities include: establish-ing a health information reference center in ourschool library, publicizing the health quiz in thecommunity, establishing a health award for gradu-ation, and promoting health topics to be taughtas part of the curriculum in other subjects.
We are also hoping that we can motivate otherschools in our district (District 9) to conduct theirown Health Bee and, perhaps, even a city-widecontest. We think that it is time to stimulatenationwide excitement for hedlth education. Whoknows, a National Health Education Bee maysomeday stand right alongside our National Spell-ing Bee.
23 TEACHNG IDEAS
Not Merely Nostalgia
RALPH EDWARDS is pmfessor of healtheducation and dean of adminiOratiini andplanning, Kingsborough Connnunity Col-lege, City University of New York, Brook-lynNlew Yorh 11235.
In moods of nostalgia, 1 am remindedof my elementary school days when westudied health heroes which, if memoryserves me, were offered us in pamphletspublished by Metropolitan Life Insur-ance Company. Tales of great exploitsby leaders of science and health, includ-ing Madame Curie, Louis Pasteur, Flor-ence Nightingale, and Walter Reed, setan example for a generation of youth forconcern for human wellbeing and asearch for truth, and ^.annot beminimized or ignored. Studying the lifehistory of famous individuals is a desir-able teaching tool and certainly well-known to our academic colleagues. Thefact that a famous Hollywood star or anathlete uses a particular deodorant,travels on a particular airline or dressesin a particular garment is valuable whereit counts heavily in this societyin thepocketbook. Health educators mightseriously consider turning back theclock, for at least part of their instruction,to the Charles Atlas, Babe Zaharias era,to get the attitudinal value and matura-tion for us in education.
Some may have seen a recent newsitem concerning Richard M. Eakin, Pro-fessor of Zoology at Berkeley, Dr. Eakin,in order to make his subject alive andmore interesting, has developed a tech-nique of dressing up in the costume offamous lecturers in areas of zoology.Gregor Mendel, William Beaumont,
. Charles Darwin, William Harvey, LouisPasteur are among "guests" that Eakinbrings to his students. While teacherscannot be expected to be actors, cer-tainly the impressions made by this in-structor and the favorable response ofthe students suggests a new slant on anold approach to content and impact.
For some time I have introducedcourses in health education with a his-torical perspective. Within these histori-cal perspectives, individuals were sin-
gled out for their contribution to under-standing health. Aesculapius and Hip-pocrates were the heroes of ancientGreece; Celsus and Galen of Greco-Rome; Rhazes, Avicenna, and MosesMaimonides of the Byzantine era;Paracelsus, Vesalius, Pare, Harvey, ofthe Renaissance; Lind, Hunter, Pinel,Rush, Bright, Braid were the 17th and18th century heroes of the Enlighten-ment. The 19th century was full of in-dividual efforts of Europeans as de-picted by Claude Bernard, John Snow,Ludwig lgnaz Semmelweis, Rudolf Vir-chow, Florence Nightingale, LouisPasteur, Joseph Lister, Richard Kraft-Ebbing, Robert Koch, Paul Ehrlich,Sigmund Freud, and Havelock Ellis.Americans are well placed in the healthhall of fame of the 19th century by suchluminaries as William Beaumont, Eph-raim McDowell, James Marion Sims,William Morton, Clara Barton, WilliamOs ler, William Welch, Walter Reed, Wil-liam Halsted, Simon Flexner, and Wal-ter Cannon.
American contemporaries of the 20thcentury do not pale when we mentionthem in comparison to earlier heroes.Howard A. Rusk spent a lifetime treat-ing the physically disabled and educat-ing the public about the importance ofrehabilitation; Will and Charles Mayodeveloped the model for cooperativegroup medical practice; Paul DudleyWhite, cardiologist, exercise proponentand physician to a president; BenjaminSpock, baby doctor, child care expert,social critic; Carl and William Men-ninger, advocates of psychiatric treat-
53
ment; Karl Landsteiner discoverer offour blood types; Jonas Salk and AlbertSabin, researchers and developers ofpolio vaccine; C. Walter Lillehi, ArthurDeBakey, Denton Cooley, pioneers inartificial heart devices; Linus Pau ling,chemist of molecular structure and ad-vocate of vitamin C; Rachel Carson,who in Silent Spring (1962) documentedthe effects on the environment of syn-thetic organic insecticides (DDT) andherbicides; John Rock and Gregory Pin-cus developed a synthetic fertility hor-mone; Rene Dubos, biochemist and ad-vocate of antibiotic therapy; and, HansSe lye, endocrinologist and exponent ofthe "stress theory" of disease.
We can add to the list above theyearly Nobel Prize winners in rhemis-try, medicine, and biology. We do havea large assembly of heroic figures whohave spent their professional lives work-ing to keep man healthy and fit. Theiraccomplishments can be recognized as ateaching device and as a technique forvaluable discussion. Their efforts de-mand applause even in an era whichglorifies the anti-hero in fiction, movies,and television. Acknowledging the con-tribution of real heroes and placingthem in a setting of everyday living is animportant contribution to the student ofhealth education and to the average citi-zen.
In bringing the heroes forward, it isnot so much a question of what we cancontribute to their memory, but ratherwhat remembering them can contributeto us and our teaching.
39

111111MIIIIIND
24WEN=
TEACHING IDEAS
Health in Concert
This article was submitted by the SeniorHealth Education Seminar, spring quarter1976, Bowling Green State University. Itwas edited by CLAY WILLIAMSissistantprofessor of health education, BowlingGreen State University, Bowfin.? Green,Ohio 43403 and JUDY SCHEER, ssistantprofessor of health education, L liversityof Toledo, Toledo, Ohio 43606.
What do "Puff the Magic Dragon,""Dead Babies," and "Junkfood Junkie"have in common? These and other suchpopular songs are a fantastic means oflearning about current health issues. A"health concert" is a means of develop-ing health concepts by capitalizing on apopular pastime of today's youth--music.
Music has much appeal for the youngand old alike. It can have a calming effectas well as an energizing effect. The topicrange is as diverse as the performersthemselves. Some approach life with sin-cerity and heartache while others em-phasize humor or entertainment. Listen-ing to music of entertainers like JohnDenver can create a greater understand-ing of human emotions, actions,philosophies, and lifestyles. By bringingmusic into the classroom students andteachers have the tools to elaborate uponthe relationship between music andhealth.
Songs can be used to introduce a unitcr to maintain interest during the courseof a unit. For example, by using a songlike "Junkfood Junkie" as a part of a nutri-tion unit, a teacher could easily developseveral followup activities relating to thetheme of the song. This song touches onthe sodal aspects of America's eatinghabitsthe fast food craze, health foods,junk foods, vitarnin supplements, andconvenience foods.
Using this song to introduce a unit,challenge students to see how miy nu-trition concepts are in the lyrics. Theirlists of concepts could then be used asguidelines to develop an overview of theunit. The song could also serve as aspringboard for group activities or indi-vidual projects to develop the practicalaspects of nutrition. Students may wantto survey local fast food chains to obtaindata enabling them to compare quantityand nutritional value for the consumerdollar. They could also research nu-tritional information about foods men-tioned in the song. Others may want toconstruct low calorie meal plans whichwould provide essential nutrients while
40
ailowing occasional indulgence in junkfoods without fear of weight gain.
Peter, Paul, and Mary's song "Puff theMagic Dragon," can be focused onmarijuana, mental health, value clarifica-tion, and understanding one's self andrelationship with others, creating an op-portunity for lively discussion as studentsare challenged to search for the numer-ous interpretations that are provided inthe lyrics. Interesting comparisons can bedrawn when students are asked to inter-pret these lyrics both before and afterappropriate health units. Students couldalso be encouraged to express their feel-ings and knowledge, individually or col-lectively, in song.
Another application would be to de-velop a mood chart based on the stu-dents' feelings after listening to the song.From this exposure, a discussion could befocused on using alternatives as a meansof achieving highs. After such dis-cussions, one could give the students avideo camera and allow them to expressvisually and to share various oppor-tunities for achieving natural highs.
Examples of additional health units andsome songs that might be used in eachcategory are as follows:Drugs"Mother's Little Helper" Rolling Stories"The No No Song" Ringo Starr
"Momma Told Me Not to Come" ThreeDog Night
"The Needle and the Damage Done" NeilYoung
Personal and Social Relations"At Seventeen" Janis Ian"Looking for the Right One" Elvis Presley"Everything I Own" David GatesDeath"Patches" Clarence Carter"Ode to Billy Jo""Run Johnny Ri 1"
Alcoholism"What Can A Family Say" America"Social Disease" Elton John"Another Try" AmericaSafety"Convoy" W. C. McCoy"Dead Man's Curve" CarpentersMental Health"Sweet Surrender" John Denver"Twisted" Joni Mitchell"Leave Me Alone" Helen Reddy"Brain Damage" Pink FloydEnvironment"Where Will the Children Play" Cat Ste-
vens"Big Yellow Taxi" Joni MitchellNutrition"Junk Food Junkie" Larry Grace"Savoy Truffle" BeatlesVenereal Disease"You Left Me Sore" Todd RungrenContraception"Unborn Child" Seals and Croft"The Pill" Loretta LynnSex Education"All the Girls Love Alice" Elton John"Sweet Painted Lady" Elton JohnAging"When I'm Sixty Four" Beatles."Old Folks" (from Jacques Brel is alive and
well and living in Paris'"Today is the First Day of the Rest of My
Life" John DenverSuggestions to help make your health
concert an effective learning experienceare:
1. Use quality audio equipment2. Screen the songs before they are
played to the class3. Make copies of the lyricis for the stu-
dents4. Be open to a variety of interpreta-
tions5. Be aware of miscomeptions that
may be conveyed in a song6. Try to use current or well-known
songs so the students can identify withthem
7. Do no overuse the strategy

25 TEACHING IDEAS
Tuning In To Health Education
WARREN L. McNAB is assistant professorof health education, Department ofHealth and Physical Education, Universityof Houston, 3801 Cullen Blvd., Houston,Texas 77004.
Music can be used effectively in healthteaching because today it incorporateswhat is taking place in "real life" andstimulates moods in both young and old.Lyrics tell of death, love, life, human rela-tionships, sorrow, happiness, and manyother emotional experiences.
In health education these particulartopics, as well as several others, are dealtwith in the physical, mental/emotional,and social makeup of health. Interpretingmusic in conjunction with the healtheducation discipiine requires students tocritically analyze and describe for them-selves, based upon their own interpreta-tion of the song and lyrics, what messageor mood is being conveyed.
One way in which we used music in.1 education was to have students
.-rpret a song sung by Melissa Man-( ester entitled "Midnight Blue." Beforep:aving the record divide the class intogrc, ips of four or five and give each stu-de,./ a copy of the lyrics to the song. Thegroups read along and listen carefully to'the lyrics and interpret what is said byapplying the song to a specific situation.
The three situations are: (1) A friend iscontemplating suicide .:nd is on a ledgeready to jumpyou .,e there trying topersuade this person to stop his/her at-tempt; (2) there has been a recent deathin your immediate family; (3) you andyour husbandrwife are contemplating, orare on the verge of getting a divorce. Eachgroup is given One of these situations.Based upon their 1. .rticular situation eachgroup is to relate and interpret what thesong's lyrics mean and how it can be tiedinto the topic of mental health. The songis played and the groups are given tenminutes to decide what the lyrics mean inrelation to their assigned topic and howeach situation deals with mental/emotional health. These ideas are thenshared in a class discussion.
The following lines from Melissa Man-chester's song "Midnight Blue" and thestudents interpretations serve as an
is.
example of how we applied and inter-preted the three situations to the song.
Line 1Whatever it isit'll keep till themorning
Suicide: Things right now seem unbeara-ble, but perhaps we can iron out theproblem tomorrow. Give it one morechance.
Death : If we can just get through todayssadness and grief, tomorrow will bebetter.
Divorce : Can't our differences be settledtomorrow? Let's sleep on it and we maychange our minds.
Line 2Haven't we both got better thingsto do?
Suicide: You have a purpose in life, youcan be somebody, you will hurt othersby what you are doing; there is muchmore in life to experience.
Death : One must go on in life; death ispart of living.
Divorce: Can't we try something else be.sides divorce ?
Line 3Midnight blueSuicide :Dark black, fearful, mysteriousDeath : time 'of one's lifeDivorce:
Line 4Even the simple things becomerough
Suicide: Everyone has problems in life. Atany one time we may think life is notworth living, but we can adjust to mostproblems. Suicide won't resolve theseproblems.
Death: Even though we know death iscoming, it is extremely difficult to ac-cept.
Divorce : Every little thing hurts at timeslike this; there is no simple solution.
This approach to teaching allows stu-dents to interpret the message stated inthe song and through individual and col-lective thinking apply their interpretationand feelings to a health related situation."Midnight Blue" is effective in looking atthe different, and yet similar, mental/
r
emotional problems that are dealt with ina crisis such as suicide, death, or divorce.Followup questions which are brought upcan be directly tied into their discussions,for example: How do you feel after listen-ing to the song? How do emotions affectone's life? How can emotions be benefi-cial in one situation and destructive inanother? Can music relieve or createstress and tension? Wha, emotions areelicited from you by this song in relationto suicide, death, divorce? How do emo-tions affect one's behavior? How doesone's mental/emotional health affectone's physical and social health?
These are basic questions that are dealtwith in the topic of mental health, but theuse of music allows students to relate tothis information and apply it in a relevantmanner. In addition, environmental in-fluences of one's mental health, and howmusic does indeed affect one's emotionalhealth in both positive and negative as-pects of life can be discussed.
Other song possibilities and their re-lated topics are "When I'm Sixty Four" (byJohn Lennon and Paul McCartney) for ag-ing, "Lighting Bar Blues" (by Arlo Guth-rie) for alcohol use, "I Love You" (byOlivia Newton John) for human relation-ships, "Poems, Prayers and Promises" (byJohn Denver) for mental health, and"Junkfood Junkie" (by Larry Grace) fornutrition.
Students can also be asked to bring in arecord which they feel has a health mes-sage or could be applied to a health topic.This particular method of teaching allowstor individual thinking, a sharing of ideas,and it stimulates students making healtheducation a fun, relevant and worthwhileexperience.
Permission for duphcation granted by RumanianPickleworks. Inc.. Ness York Times MusicRMI.
41

26 TEACHING IDEAS
Ideas for Successful HealthTeaching*
LOREN B. BENSLEY, IR. is associateprofessor of health education, Cen-tral Michigan University, Mt. Pleasant,Michigan 48858.
As a professor of teachingmethods, I am a great believer thathow you teach is just as importantas what you teach. Many times, weteach the way we were taught,rather than the way we were taughtto teach. In order for health teach-ing to be successful, it is of utmostimportance that the methods usedbe creative and original in everypossible way. By doing this, the sub-ject will be more interesting to thestudents and enhance the oppor-tunities for behavior change. It isimportant that the material pre-sented to the students be studentcentered rather than subject cen-tered.
in the past ten years of teachinghealth education to secondarychool and university students, I
have discovered four essentialpoints for successful health teach-ing. First, learning must be enjoy-able. If the students find that learn-ing health can be fun, it is thencorrect to assume that they willenter into the learning experiencewith a great deal of enthusiasm andexcitement. Second, students mustbecome emotionally involved in thelearning process. This can be donerather easily in teaching health edu-cation; one's health is a personalthing and to become involved emo-tionaHy in the subject matter isalmost automatic. The third pointto consider in teaching health edu-cation is that the student should begranted a degree of academic free-dom to explore his or her ownhealth needs and interests. By so do-ing, the student experiences healthlearning as something which be-comes relevant and has a purpose.
*The information in this article is basedon material which appeared originallyio a column entitled "Ideas for Success-ful Health Teaching" published in theJournal of the Michigan Association forHealth, Physical Education, 3nd Recrea-tion. The MAHPER Journal editor, JoanNelson, granted permission for its use.
42
For this to happen, it is necessaryfor the teacher to create an atmos-phere of freedom without externalthreats. The fourth essential pointin teaching health education is theneed for the teacher to know hisstudents. This point cannot bestressed enough. In order for a
health teacher to experience suc-cess to any degree, it is necessarythat he design the course with a fullunderstanding of the students'health needs and interests. Thehealth educator must gather dataon the personal health habits, atti-tudes, and behaviors of those stu-dents he is teaching at any onetime.
These four points are only a partof successful health teaching; theyare mentioned here because often-times teachers ovedook what mightbe considered the obvious items inteaching. With these points in mind,R is interesting to explore somedifferent ways to teach health edu-cation to secondary school students,such as the foHowing two methodsI have found to be successful.
Using Popular Music InTeaching Health
Much of today's popular musichas a great deal of meaning behindthe strange sounds and muddledvoices. By examining some of themusic subscribed to by today'syouth, the teacher will discoverthat much is written about drugabuse, human sexuality, environ-mental conditions, and mental andemotional heaRh. It is suggestedthat the teacher listen to some ofthe songs from the very popularand successful rock musical "Hair."The song "PoHution" is concernedwith air poHution, whereas the song"Sodomy" refers to human sex-uality. This topic is also discussedin the lyrics of music composed bycurrent popular artists such as MickJagger and the Rolling Stones, in"Live With M," or "Let's Spend theNight Together." The group calledThe Rare Earth also sings about sex-uality in their song titled "In Bed."Music about sexuality is extensive,and the health educator can be se-lective in choosing songs pertaining
5 6
to homosexuality, sexual inter-course, or fellatio.
Within the last few years the song "INever Promised You a Rose Garden"became very popular. This song couldbe played in class and discussed in rela-tion to mental and emotional health.The discussion could center around thefact that no one promises you every-thing and you must work for much thatyou receive in life. For a unit on mentalhealth the author has experienced suc-cess with a ninth grade health educationclass using some of Simon and Garfun-kel's work, notably, the songs "BridgeOver Troubled Water," "A Most Pecu-liar Man," and "Richard Cory." The lat-

ter two are pertinent to the topic ofsuicide. The students' favorite song per-taining to mental health, however, is"Walk a Mile in My Shoes" by JoeSouth.
The teacher can also talk about musi-cians or musical groups and center thediscussion around the use of drugs. Forexample, several years ago two verypopular musicians died of an overdoseof drugs. The class might discuss thequestions why Janis Joplin and JimmyHendrix used drugs and eventually tookan overdose.
The use of popular music as amedium to teach health has beenextremely interesting to me and mystudents. One reason is becausethe teacher is u 'ng a significantobject of the teenagers' lifehismusic. It is, in effect, a way ofreaching students through theirown medium.
Using Current and PopularLiterature in Teaching Health
Just as effective as using popularmusic in teaching health educationis the use of popular literature. Arethere any books you have read inthe past year which could be usedto teach about health? Often thereis a novel, fictional story, biography,or some piece of iiterature that con-tains information pertinent to a
health education class. When dis-cussing drug abuse, students mayread the book Valley of the Dolls,a story about barbiturate addictionand the eventual death of the main
rt)
character of the story. When dis-cussing the topic of love and per-sonal relationships, the ever popu-lar novel Love Story is suggested tothe students. This particular story,about two young people who fallin love and marry, is good becauseof the deep, meaningful feeling thecouple have toward each other. Itis essential when discussing emo-tions in regard to human sexualitythat mature love be understood.The boo!. Love Story brings this out.
There are hundreds of books thatcould be used for discussion pur-poses in a health education course.The important things when consid-ering this method are first, that theteacher select a book which is
suitable to the subject at hand and,second, that it has appeal to thestudents. It is both a real challengeand an enjoyable way of teaching.
43

27 TEACHING IDEAS
The StudentInterviewTechnique
MARC E. MEYER is a health educationteacher at North Rockland High School,Hammond Road, Thiells, New York 10984.
As health educators we are always look-ing for ways to encourage class participa-tion. One method seems to work quitewell within my health educationclassesthe "student interview tech-nique."
This technique works well hecause ithas certain qualities which help studentsin a variety ot ways. First, the technique isflexible, each teacher can use the inter-view for a particular unit or simply for achange of pace in daily routines. Second,it allows each student to communicatehis/her ideas to others. It helps develop
dents and the individuals who conductedthe interview will tell what they discov-ered.
I have found that there are a variety ofways one can use this technique. Eachteacher should choose that methodwhich best suits his/her situation. Theinterviev. can be specific, (drugs, alcohol,sex education, mental health) or general,asking questions as presented here,which explore a variety 01 ideas and val-ues.
By implementing activities such as the"student interview technique," studentscome away from class with a better feel-ing; most were eager to participate andmost had a p learning experiencewhich they will not soon forget.
Interview #1
Instructions:
Interview two individuals iii your class.You are not to give more than two in-terviews:
Interview #2
Instructions:Interview two individuals in your class.You are not to give more thanterviesvs,
t\v() in_
Questions:Name?What three things do you rrize most?It you could visit anywhere in the world,where would it be?If you could divide $5,000 between twoharities, what would they be?
When was the last time you werepunished?Why were you punished?Do you have many friends?What do you feel was the best mo,,ie youever saw?What is important to you?When was the last time yoll gave advice tosomeone?Did he.'she ask for your advice?
f 4PiN' filf N f .FPN. Is kpeot lir . 4 o- 4 6"1140,01b . WO% 4ir
qk"IIf . 144$61° qW.W.Sk./44704 0 471440. k A\IN 0.44
. -/o t / A r N ..-0,4,.iv rlio(%.do viigo, oflp
SINPVIZZZIAINVIRPIZZreiwel . gm 44 Quo is% (674 119Aft
dIrAvirr 4.1.4411Sm.(4.... (4.- "At. 111(411,
the ability to communicate and to listen,as well as to stimulate class discussion.
In speaking with my students, anumber of them have said that they findthe student' interview, "interesting,""makes time go faster," "gives us achance to learn more about our friends,"and it is "fun." Of the many activities andoptions available to my classes, the "stu-dent interview technique" allows for agreat range of communication and in-teraction within the classroom.
Below are examples of interviews usedat different times throughout the semes-ter. The interview sheet clearly tells eachstudent to interview two individualswithin the class. No student is to givemore than two interviews. Upon comple-tion, the teac her can simply call on stu-
44
Questions:
Name?What was the happiest time of your life?What do you like to do with your freetime?Favorite musicei group?Things you . best about being in highschool?Brothers and sisters ihow many)?Where do you like t,1 go with yourfriends?What is your favorite food?If you had a million dollars, how wouldvou spend it?What your favorite sport?
58
Interview #3
Instrt.ctions:Interview two individuals in your c lass.You are riot to give more than two in-terviews.
Questions:Name?What time do you get up ee.:1 day?What time do you go to sleep?Favorite .IV program?When was the last time you gave some-one a comphment?Is it difficult to give compliments?Is ''time" important to you?What was the most frightening movie youever saw?Which was the saddest movie you eversaw?

28 TEACHNG IDEAS
Positive Peer Influence:School-Based Prevention
AIDA K. DAVIS is a research assistant andJOAN M. WEENER is a project assistant inthe Addictions Preventimi Laboratory andROBERT E. SHUTE is assistant professorof health education. They are all at Pennsyl-vania State University, University Park,Pennsylvania 16802.
Peer pressure is often considered apsychological force--a direct attemptby a group to influence personal behav-iors of group members. However,Kies ler and Kies ler' have a somewhatbroader view which acknowledges un-planned, but nevertheless, highly con-trolling influences of groups: "All that isrequired is that the group expect theperson to act or believe in a certain way,or that the person think such things areexpected of him."
Whether peer influence is defined aspsychological forces or group sanctions,the mechanisms and effects are inextri-cably bound to the operations of socialinfluence, which include teaching,learning, imparting ideas and skills,generating enthusiasm and purpose,and even the application of force. Peerinfluence and the conformity it engen-ders is part of a much larger context ofcognitive and motivational processes re-lated to social learning.
While any social interaction is poten-tially influential the greatest power todispense social rewards and punish-ments to the individual member is at-tributed to peer group interactions. It iswithin the peer group that the effects ofsocial modeling and behavioral shapingtend to be most concentrated. Especiallyfor adolescent and college-aged people,the peer group is often cited as the pri-mary reference group for attitudes,values, and behaviors; it is within thepeel. group that outside influences (par-ents, the law, the schools, etc.) are dis-cussed, judged. and mediated. Ac-quiescence to direct or subtle pressuresin peer groups has been linked to someforms of juvenile delinquency, truancy,malicious mischief, sexual experimenta-tion, drug use, and other types of mis-behavior directed against self or society.
While the motivation for initiationand continuation of drug use and theconditions under which drug attitudes
and behaviors are learned are as variedas the social, religious, educational, oc-cupational, and psychological back-grounds of the user, many writers arenow emphasizing the critical role ofpeer influence as a variable which mayoverride many of these considerations.'
Researchers in high schools and col-leges have found that the likelihood ofpersonal drug use correlates highly Withthe drug-using activities of one's peergroup. This fact has influenced the de-velopment of a variety of school-basedpeer programs related to student per-formance and student attitude towardteachers, school, self, and others. Theunderlying assumption is that if stu-dents have a healthy self,concept, a fa-vorable attitude toward their teacherand schools, a number of satisfying andenhancing interpersonal relationshipswith family and friends, and are com-fortable about their values and abilitiesto make decisions, then they are muchless likely to succumb to pressureswhich encourage self-destructive be-haviors.
Several school-based programs haveevolved which draw on some of the pos-itive aspects of peer influence. Forexample, peer and cross-age tutoringand peer counseling, while not specifi-cally oriented toward prevention ofdrug and alcohol abuse, seek to reducebehavioral problems and bridge the gapbetween student and teacher (or par-ents) by providing individualized in-struction, personal interactions, andcounseling. The school can includeexercises which help students discussand understand the "mechanisms" ofpeer influence and help them developskills to deal with influential situations.All of these programs or strategies aremeant to develop the individual's senseof personal competence and responsibil-ity. Following are several workablestrategies and resources for involvingpeers in iirevention activities in theschool setting.
Peer/Cross-age TutoringPeer and cross-age tutoring has been
included in school programs for a longtime as a way cf meeting special educa-
tional needs. Historically pupils helpedor taught other children in order to al-leviate the resnonsibilities and timeconstraints of toe teacher in the one-room schoolhouse. Later, the idea ofstudents hs:lping each other proved to bea promising alternative in traditionalschools. The trained tutor was able toestablish a personal relationship withother students and could assist themwith their school work for both remedialand standard purposes. The learner wasable to receive help in a variety ofacademic areas, while the tutors foundthat the teaching provided a powerfullearning experience for themselves aswell.
Tutoring programs vary widely in re-lationship to the age differences whichexist between tutor and pupil. "Peertutoring" connotes that tutors are thesame age or are enrolled in the samecourse as the learners, whereas olderstudents or students who had com-pleted the course or were not enrolledin it at the same time as the pupils weredefined as "cross-tutors."3
Tutoring techniques have been pro-moted as a means of enhancing thelearning of both tutor and learner,though some researchers have urgedcaution in making this claim.4 Tutoringresponsibilitits and establishing a closepersonal relationship with the learnerare important affective gains for thestudent tutor. Opportunities for creat-ing constructive, social, and positiveroles, greatly enhance the tutor'sschool experience.5 The learner's gainsin academic skills and understandingseem to promote self-esteem.
Tutoring as a preventive approach todrug and alcohol abuse relies on theconcomitant de velopment of skillswhich ultimately enhance the student'spersonal satisfaction with life. Theseskills include intrapersonal aspects suchas improved self-concept, as well as in-terpersonal skills--effective communi-cation with others, sharing personal dif-ficulties, etc.
Resources. Many aspects involved indesigning and implementing a tutoringprogram are discussed in a variety oftraining guides available to schools. The
45

National Commission on Resources forYouth under the direction of MaryKohler has developed a tutoring projectcalled 'Youth Tutoring Youth." Severalhundred programs have been started inschools and by community agenciesacross the nation. Over 3,500 personshave been trained in the techniques oftutoring through this flexible programwhich can be adjusted to meet theneeds of school or community groups.6
The Ontario-Montclair School Districtin California has developed a cross-ageteaching manual designed to helpteachers or administrators organize andimplement a tutoring program. Thismanual describes agendas for trainingseminars and the matching procedurefor older and younger students as wellas describing scheduling, types of ac-tivities, and cost considerations.'
A further guide to tutoring is in-cluded in volume two of Balancing Headand Heart: Sensible Ideas for the Preventionof Drug and Alcohol Abuse. 8 These bookswere produced for Pennsylvania's Gov-ernor's Council on Drug and AlcoholAbuse and contain a general rationalefor primary prevention along with de-scriptions of eleven school-based ap-proaches to prevention of drug abuse,including peer tutoring and peer coun-seling. Sensible guidelines for imple-menting strategies and providing re-sources make this publication a handyreference guide.
Peer CounselingAnother activity, defined by M. G.
Sussman, which capitalizes on the posi-tive effects of peer influence, is peercounseling: "a process in which trainedand supervised students offer listening,support, and alternatives and otherverbal and non-verbal interaction, butlittle or no advice, to students who referthemselves."9 Peer counseling pro-grams are usually designed as suppor-tive programs which complement orsupplement existing guidance programsin the schools. While includingacademics, peer counseling programsare generally aimed at clarification offeelings, ideas, and valtfes in order toenhance personal decision-making andresolution. Trained students provide aclimate of acceptance for those fellowstudents who would rather share prob-lems with a peer than with an adult.
Junior and senior high school stu-dents are trained in reflective listeningskills, problem solving, and providinginformation or referral if needed, byschool counselors, teachers, or psychol-ogists. Training methods consist46
h.:
primarily of supervised seminars orworkshops for selected student volun-teers. In some schools the trainingcourses are given for credit, others pro-vide training on an extracurricular basis.A number of programs have establisheda general "rap room," "drop-in center"or "unwinding room" where studentsare welcome to come and talk abouttheir concerns. Appointments can alsobe made for private sessions with one ofthe peer counselors. This type of pro-gram expands available counseling re .sources and makes it easier for studentsto discuss problems on a less formalbasis. Counselors are trained to recog-nize and refer students with seriousproblems to professional counselors.
Resources. A variety of training mate-rials are available for help in implement-ing peer counseling programs. Samuelsand Sanniels' book is a thorough reviewof rationale, needs, organization, andevaluation of peer counseling.10 The au-
GO
thors provide a detailed account for in-terested administrators and partici-pants. The Balancing Head and Heartseries notes the benefits for both coun-selors and con nselees in com mu nicationskills, self-confidence, and self-esteem.
Newsletters such as the one distrib-uted by the National Resources forYouth" cover a number of projects inwhich teenagers counsel their peers. Aprevention resource bulletin, "Pyra-mid," sponsored by the PreventionBranch of the National Institute on DrugAbuse reviews and reports on peertutoring and counseling preventionprograms." A manual entitled Teen In-volvenwnt: A Teen Counselor TrainingManual by Gladys Conroy contains anumber of ideas for training teen coun-selors to work in the area of drug andalcohol abuse prevention.'3
Integrated Classroom ExperiencesMore informal, planned interventions
in the classrooms, which integrate nor-mal lessons with oppoi tunities for stu-dent growth in dealing with situationsinvolving peer and/or social influence,offer attractive, inexpensive startingpoints for peer prevention program-ming
*'
Peer Influence "Convince Me" Time: 35 minutes
Purpose: To have students develop an awareness of how they influence and are influenced bytheir peers.
Materials: One mimeographed sheet for each student in the class. Half of the sheets should havethe following written on them:
Role AYou' ve just left a home basketball game. Your older sister, who's obviously drunk,pulls over and says she wants to show you and your friend how fast her new car can go on aback road near town. You love the feel of speeding and are anxious to accept her offer, soalthough you think your friend is probably chicken, you try to convince him/her that he/shewould be a fool not to go along.
The other half of the sheets should have this written on them:
Role B You're a fairly shy person and don't want to have anything to do with what your friendsuggests.
Procedure1. Pass Role A out to half the class, Role B to the other half of the class, asking students to keep
their role secret.2. Have each student with a Role A sheet pair up with a student with a Role B sheet. if there is an
uneven number, have the extra student watch two others role play.3. Give students about five minutes to play their roles.4. Now have students trade roles and again spend about five minutes playing the opposite role.5. Ask students to return to their seats and have a class discussion about how they felt in each
role.6. Discussion hints:a. How did you feel in each role?b. What did your partner do to make you feel that way?c. What are some pros and cons of trying to get others to do things we want them to do?d. Under what circumstances would you try to convince a friend to do something?e. What do you gain when you give in? What do you lose?
Adaptations:1. Add more roles so that two or three students can try to convince classmates to do something
they do not want to do. Have the students rotate roles within the group.2. Have three students try to convince three other students to do something they do not want to
do. The activities can be modified e.g., taking drugs; going swimming in cold water; etc.
Integration Suggestions: Role playing is so versatile and enjoyable Phat you should find studentseager to participate and initiate suggestions. A few possibilities are:
1. MathematicsDevise roles for students so they may try to convince others of the "best" wayto invest $10,000. The setting could be a board of directors meeting for a small business.
2. ArtDevise roles for the artist, the merchant, the buyer, and the skeptic. Have the artist try toconvince the merchant to display his creation. Have the merchant try to convince the buyer tobuy it. Have the buyer try to convince a skeptical friend that he/she has made a wise purchase.A funny painting or sculpture would be an asset to the exercise. Discuss the motivation of eachperson in the role-play scene.
Contributed by Liz Kramer and Robert Shute
During the past year, a review of theresearch and existing curricular re-sources which relate directly to aspectsof peer pressure/peer influence wasconducted as a task of the Peer PressureProject (funded by the Addictions Pre-vention Laboratory and directed by Rob-ert E. Shute). The project staff will haveadapted a number of flexible lessonplans from existing resources or willhave created new ones when the projectis completed." These lesson plans willform one section of a teacher resourcepackage for integrating peer influencelessons into a classroom. A sample les-son with integration suggestions is pre-sented here.
We know of no other compilation otstrategies similar to the one being de-veloped for the Peer Pressure Project.Certainly, many excellent ideas for inte-grating peer influence study can befound in recent texts, curriculum guides,and audiovisual materials on relatedtopicsaffective education, humanisticeducation, developmental education,and confluent education. Several peer-rela ted exercises can be adapted from thevealth of existing materials which
schools can use to enhance learning, im-prove decision-making skills, clarifyvalues, etc., at all educational levels.Generally, these have come to be highlyregarded as valid enhancers of the edu-cational experience.
61
Alternative Peer-Related ActivitiesA number of other peer-related activi-
ties such as drop-in centers, alterna-tives-for-youth programs, vocationalskills training, and youth service pro-grams have been developed in bothschool and community settings. Theseprograms encourage activities whichprovide meaningful alternatives to drugand alcohol use. Program goals ma:,range from developing clearly definedskills, such as photography, macrame ordancing, to experiencing and sharing in-sight and ideas with peers and becominginvolved in service to others. The con-cept of service to others as a develop-mental goal for schools has been ac-knowledged by Kohler:
Our schools are no longer filling the needsof our children. A generation ago, livingitself provided opportunities foryoungsters to be with adults, to grasp thesatisfaction of work. Today we stick kids ina world of their own and tell them to staywhere they are until we need them. De-spite the increased number of "peopleneeds" in our complex society, adoles-cents aren't given a chance to "help out."We must link the teen-agers into the sys-temand give them opportunities to helpmeet human needs."
Alternative projects for peers, alongwith peer tutoring, peer counseling, andclassroom activities, draw strength asprevention activities by using positivepeer models rather than focusing on aspecific social/or health related problem.
Resources. For those who wish to be-come more familiar with alternative peerand prevention approaches the follow-ing publications are recommended. Al-ternative Pursuits for America's 3rd Centunj:A Resource Book on Alternatives to Drugsprovides a guide to possible projects.The section entitled "Alternatives" inthe Balancing Head and Heart series offersideas for teenage projects. Youth Alterna-tives, the monthly newsletter of the Na-tional Youth Alternatives Project, offersdescriptions of programs as well as fund-ing opportunities and legislative actionreports.16
The encouraging research and pro-gram evaluations point toward the effi-cier.cy of using peers as change agentsfor the prevention of drug and alcoholabuse. Likewise, the translation of the"positive peer influence" concept toother health related or social problemssuch as contraception behavior, smok-ing, reckless driving, etc., should beseriously considered when planningschool or community prevention pro-grams.
'Mester, C. and Kiesler, S. Conformity.Reading, Mass.: Addison Wesley Publ., 1969.
47

2Dumont, M. "Mainlining America: Whythe Young Use Drugs." Social Policy,November/December 1971, pp. 36-40.
3Deterline, W. A. Training .111 Managementof Student Tutors. ERIC Docunwnt Reproduc-tion Service, No. ED 048 133, 1970.
4Willis, J. and Crowder, J. "Does TutoringEnhance the Tutor's Academic Learning?"Psychology in the Schools, 1974, 11(1), pp.68-70.
sGartner, A.; Kohler, M. C.; andRiessman, F. "Every Child a Teacher,"Childhood Education, 1971, pp. 12-16.
6Youth Tutoring Youth: A Manual forTrainers. National Commission on Resourcesfor Youth, 36 West 44th St., New York, 1970.
7A Cross-age Teaching Resource Manual,Ontario-Montclair School District, 950 West
D St., Ontario, Calif., 1971.slialancing Head and Heart: Sensible Ideas for
the Prevention of Drug and Alcohol Abuse,Pacific Institute for Research and Evaluation,Suite 201, Quail Ct., Walnut Creek, Calif.,1975.
9Samuels, J. and Samuels, D. The CompleteHandbook of Peer Counseling, Miami, Fla.:Fiesta Publ., 1975, p. 41.
11Resources for Youth, National Commissionon Resources for Youth, 36 West 44th St.,New York.
"Pyramid, Pacific Institute for Researchand Evaluation, Walnut Creek, Calif.
48 6 2
"Conroy, G. Teen Involvement: A TeenCounselor Training Manual. New York: Holt,Rinehart and Winston, 1972.
14Shute, R. E. Explorations in Social and PeerInfluence: A Resource Manual for TeachersGrades 7 -10, 1977.
"Alternative Pursuits for America's 3rd Cen-tury: A Resource Book on Alternatives To Drugs,National Institute on Drug Abuse,Washington, D.C., 1974, p. 2.
,6Youth Alternatives, National Youth Alter-natives Project, Inc., 1346 Connecticut Ave.,NW, Washington, D.C.
29 TEACHING IDEAS
LILLIAN D. FESPERMAN is a graduakassWant in health and physical education,Miami University, Oxford, OhM 45056.
Are you tired of teaching digestion,respiration, drculation, the body sys-tems and functions the same way yearafter year, class after class? Or are youan inexperienced teacher looking for anew approach for old, unchanging yetvital material? In either case, here is asuccessful, exciting, beneficial solutionwhich can motivate your students
When I as teaching health at Alex-ander Graham Junior High School inCharlotte, North Carolina, I was a firstyear teacher willing to try just aboutanything that would motivate my stu-dents. I had to present a unit on thesystems of the body and wanted to try anew, creative approach. After evaluat-ing possibilities, I came up with the ideaof constructing a body in class.
Selling my idea to the students wasextremely easy and well-received;everyone wanted to "build a body." Wefirst got basic background informationon the systems of the body andgathered our ideas and materials forbuilding a body. We included fivesystemsdigestive, skeletal, respira-tory, circulatory, and nervouson ourbody. Since there were five seventhgrade health classes, each class contrib-uted one system to the body.
Information about systems was cov-ered in class by a series of handouts,lectures, discussions, pictures, andfilms. Students were required to keep anotebook related to the systems whichthey handed in at the end of the unit. Tofurther instill interest in the students, aswe discussed the systems I mentionedideas and suggestions about the bodythat we could try. We ail knew we wereworking to gather enough informationto construct a life-size body out of avariety of "raw" materials.
After completing the general back-ground information, a system was as-signed to each class and that class wasresponsible for bringing in any materialsrelated to their system. They were alsorequired to read books and study pic-tures and charts related to their sys-tems. Specific tasks were assigned tosmall groups, who worked together to
make their parhcular system fit into thebody.
The skeletal system included the pel-vic bone, upper and lower bones of thearms, finger bones, upper and lower legbones, the kneecap, the sternum, col-larbone, and back vertebrae. The ner-vous system had the brain and spinalcord, and nerves. Our digestive systemwas made up of the tongue andesophagus, spleen, liver, stomach,small intestine, large intestine, and therectum. The nasal cavity, trachea,bronchial tubes, and lungs (one openand one closed) with alveoli were the
"Ernie", created by seventh grade students.
parts of the respiratory system. The cir-culatory system consisted of the heart,aorta, large and small veins, and ar-teries.
We needed a base on which to mountour body parts. After considering thepossibilities of cardboard, wood andother hard material, we decided to use abig sheet of plywood so we could attachthe organs and have them stay in place.The plywood (about 5' by 3') wassupplied by one student's parents. Wecut out a body frame from paper, gluedit onto the plywood and started as-sembling organs and parts.
The materials brought in by theclasses for use included chicken bones,styrofoam of all sizes and shapes,sponges, thread of assorted colors, wireand plastic-coahzd wires of various col-ors and sizes, clay, newspaper, paints,cardboard cylinders, empty thread
63
spools, balloons, cloth scrap,glue, and toothpit s.
We made solve oc our bones out ofsticks covered papier mache, andothers with my roloam cut into theshapes of the banes we wanted. Thebones were. attached to the body framefirst along with the trachea, whichwe made from a cardboard cylinderwrapped in yarn for the cartilage, andthe bronchial tubes, which were madefrom clay. The digestive system was thenattached. The tongue was a small, semi-inflated balloon; the esophagus was asmall cardboard tube fitted inside thetrachea. The stomach and large intes-tines were papier mache wrapped overblown up balloons. The balloons werethen deflated and the papier mache or-gans cut in half to make a flat surface tomount on the plywood body. The smallintestine, liver, and spleen were madeout of clay which was dried and painted,then nailed or glued onto the frame. Thenasal cavity was cardboard cut intoshape, the bronchial tubes were clay,and the lungs were styrofoam. One lungwas painted as if it were closed, the otherlung was constructed as if it were open.The capillaries were drawn with magic
irker and little pieces of sponge gluedit to show the alveoli.
The heart was made by cutting theshape out of a thick sponge, with veinsand arteries drawn into it. The pulmo-nary vein and artery and the aorta wereinserted into the sponge with big redand blue wires. From the heart came redand blue arteries and veins made fromwire and thread. Veins and arteries notmade of wire or thread were drawn onthe body with red and blue pens. Thenervous system was done with variouscolored wires for the nerves leading allthroug:1 the body to the fingers andfeet. The spinal cord was made of yel-low yarn leading from the brain, whichwas a piece of plastic cauliflower sincethe bumps and shape were similar. Wecut the cauliflower to make a flat backsurface to fit onto the frame. It was defi-nitely an authentic-looking part of thebody.
An of the parts were eitlwr glued,taped, or nailed into place on the bodyframe. The bones were mounted firstwith the trachea, esophagus, andbronchial tubes. Then the lungs, heart,and digestive system was fitted intoplace. The veins, arteries, and nerveswere intertwined into place last, making
49

our body complete. The classes thennamed our project body "Ernie."
Other suggestions for materials thatwe did not include in our project thatcould be added to yours are a mop forhair, or maybe garden hose for intes-tines. Or how about bottle caps or
50
ping-pong balls for eyes? Other ideasmay be to use false teeth or plastic earsto make your body more complete.
The project was stimulating and in-teresting to the students. The studentsresponsible for making system partsand placing them onto the body also
had to explain the operations of theorgan or part. They benefited greatlyfrom this project by learning about thehuman body and working together andhad fun doing it. It is an excellent idea totry in your own classroom. Why notcreate your own "Ernie"?
Focus on Content
f ;

30 TEACHNG IDEAS
PETER FINN is senior Equiation and train-ing analyst at ABT Associates, Inc., 55Wheeler Street, Cambridge, Massachusetts02138.
Most people who have never experi-enced a major addiction such as, al-coholism, drug dependence, compul-sive eating, or cigarette smoking, havelittle understanding and often manymisconceptions about what it feels liketo have a persistent and irresistiblecraving for a substance or activity. Anaddiction is defined here as a craving fora substance or activity which a personcannot at the moment resist consistentlyor for a sustained period of time. In thefollowing learning exercise, s;:udentsgain insight into the nature of addic-tions by refraining for an agreed-uponperiod of time from an activity theyhave found extremely enjoyable forsome time. As a result of this period of"abstinence," students may be betterable to appreciate what an addicted per-son feels like and how they can besthelp relatives and friends who mayhave a dependency.
The exercise may also enable somestudents to realize that they have astrong and perhaps ungovernable urgefor a substance or activity and to con-sider whether their compulsive behav-ior is healthy and what causes it. Theexercise can foster insight into whyeveryone feels dependent on some ac-tivities and provide an inkling of howthe students may feel if they are someday deprived of a substance or activityto which they have become accustomedor addicted.
This exercise has been used manytimes by me at the junior and seniorhigh school level. However, it probablywould be successful with elementaryschool students and adult groups, aswell.
Procedure
Have students pick one or two ac-tivities which they would find verydifficultperhaps impossibleto stopdoing. Then have each student agree ina written contract with the rest of theclass to forego the activity for at least aweek, but preferably for a month. Itmigf-. be more enjoyable and educa-tional for students to experiment with afriend or small group, with each per-son renouncing the same activity.Depending on their "passions," stu-dents might:
use no salt or sugar in their foodgive up cigarettesstop sceing or talking with a close
friendnot kiss or touch their girlfriend,
boyfriend, husband, or wifenot make or answer any telephone
callsget up M 4:00 a.m. every morning (not
sleep late)stop watching television or listening
to the radiogive up Coke, coffee, or anotlwr fa-
vorite beveragegive up a favorite sport or other form
of recreationstop chewing gumIt may be helpful for the students to
keep a diary of their behavior and feel-ings during the experiment to jog theirmemory when they relate their experi-ences to the class. Students can also talkinto a tape recorder at the end of eachday and play back excerpts to the classat the conclusion of the experiment.
Follow-up Discussion
After students have refrained fromtheir activities for at least a week, havethe class recount their experiences, thenanswer the following questions.
1. How many of you succeeded in re-fraining from your activities for the en-tire period of time stipulated in yourcontracts? How soon did those whofailed give in? How do those of you whofailed give in? How do those of youwho failed feel about yourselvesdisappointed? angry? indifferent? re-lieved? How do those of you who suc-ceed feelsuperior? sympathetic? re-sentful? neutral?
Addictive Behaviors
2. What did not doing the activity feellike? Did you miss it badly? Did you getangry? frightened? miserable? grouchy?bored? frustrated?
3. Did your relationships with otherpeople change? For example, did youavoid certain people, or people in gen-eral, spend more time than usual withcertain people, or with people in gen-eral, or relate to people differently suchas, arguing more than normally?
4. Did talking or being with otherstudents who were refraining from thesame activity (or a different activity)help you resist the temptation to givein? Did you ask for, and get, help fromother people in your attempts to foregothe activity? How did they respond?How would you have liked them to re-spond?
5. Did other people change their be-havior, attitudes, or feelings toward youas a result of your experiment? How didyou feel about and react to that?
6. Did you start doing things that youdon't usually do, such as forget things,become less observant, overeat, or de-velop physical symptoms such as head-aches, stomach aches, tics, loss of appe-tite, insomnia, or unusual fatigue?
7. Did your other activities change atall? Did you compensate for the lack ofyour "forbidden" activity by partici-pating more in some other pursuit? Didthe substitute activity help take yourmind off the thing you wanted to do?Did your efforts at compensation affectany of the people around you?
8. Were you confronted with an op-portunity to "lapse," and did yourwillpower diminish in the presence ofthe forbidden activity or object? Wereother people considerate in not men-tioning the activity or substance, orhelpful in suggesting a substitute?
9. Did you go out of your way toavoid the activity or substance, or thingsthat might remind you of it? Did youravoidance behavior help reduce yourcraving?
10. Did you cheat at all? If so, did youtry to engage in your activity just a littleand find you couldn't resist resuming itcompletely? Did you bother to hide yourlapses from other people? If so, didanyone catch you cheating? How didthey react? How did you feel aboutbeing discovered?
53

11. When you finally did go back tothe activity, how did it feel? Did you tryto "make up for lost time"?
After the class has explored the issuesrelated to these questions, students candiscuss how their actions and feelingsmight be similar to those of an alcoholic,drug addict, cigarette smoker, compul-sive eater, or other addicted person. Thegroup should also consider how its ex-periences may have been different fromthose of truly addicted people. Forexample, the students knew they could
54
resume their activity with impunity atthe end of tlw test period, while an al-coholic, who has stopped drinking or anObese person who has begun dietingknows that to revert to their former be-havior is to court disaster.
Students may also erroneously con-clude, based on their own success, thataddicted people should be able %ith rel-ative ease to reject their self-destructivepractices. The students' experience mayhave misled them because their owncraving was a comparatively mild oneand made even more bearable by the
realization that it was only temporary.Finally, focus specifically on how the
students feel about addicted people. Dothey feel the same way about a 'coholicsor drug addicts as they felt about them-selves during their experiment? Shouldthey? Did they gain any new insightsinto what it feds like to have an addic-tion and how addicted people can bestbe helped to !;hake off their depen-dency? Were the students able to iden-tify any compulsive behaviors of theirOwn and gain a better understanding ofhow to evaluate and cope with them?
Ay/ ./////
:EST CCM AMBLE 6 7

31 TEACHNG IDEASWINNE
Now Much Can I Drink?
H. RICHARD TRAVIS is assistant profes-sor of health science, lanws Madison Uni-versity, Harrisonbuig, Virginia 22802.
I teach drug education courses andfrequently, when discussing alcohol,students will ask how much a personcan drink before being considereddrunk. I point out that there are manyvariables that influence the extent towhich an individual will be affected byalcohol.
1. Some people are affected more thanothers because of their biochemical make-up.
2. The attitude or mood of the individualat the time of drinking as well as the envi-ronment in which alcohol is drunk influencethe effect.
3. Food and liquid in the stomach dilutethe alcohol and slow down its absorption.
4. The carbon dioxide in carbonated al-coholic beverages tends to hasten the move-ment of the alcohol from the stomachthrough the pylorus to the small intestinewhere the majority of alcohol is absorbed.
5. The blood alcohol level reached in thebody is related to the individual's bodyweight. A larger person has more body fluidsand blood to dilute alcohol than a smallerperson. The more alcohol in the blood, themore that can diffuse into the cells of thebody. Most states set 0.1% as the blood al-cohol level at which a person is consideredlegally drunk.
A number of charts are available intextbooks or from state divisions ofmntor vehicles which relate the numberof drinks a person consumes to weight
and subsequent blood alcohol level. Iuse the following chart to have studentscalculate what their blood alcohol levelmight be after a certain number ofdrinks and the number of minutes b.ncethey first started drinking. Most stu-dents know their body weight, but ifnot, a scale can be brought into theroom for them. They follow these stepsto figure their blood alcohol level.
1. Emphasize that this chart is a guide andnot a guarantee. Remind the class of the vari-ables that have been listed.
2. If your weight is between two of thoseshown on the chart, use the lower weight.
3. On the chart, look up the blood alcohollevel associated with your weight and thenumber of drinks that would have beendrunk during a certain time period. Onedrink equals 12 ounces of beer, or 5 ounces ofwine, or 11/2 ounces of 80-100 proof whis-key.
4. Write down the blood alcohol level from
5. Write down the total number of min-utes that would have elapsed between start-ing to drink and leaving the party twohours or 120 minutes.
6. The liver is continuously metabolizingalcohol so we have to make a sut-tractionfrom the blood alcohol level from the chartdepending upon how long we have beendrinking. The correction factor is calculatedby first dividing the total number of drinkingminutes into 40 minute segments and thenmultiplying that answer by .01%. This is thecorrection factor for the alcohol that ismetabolized by the liver.
7. Subtract the correction figure from theblood alcohol level that we obtained from thechart in step three. This is the approximateBlood alcohol levels (percentage)
BodyWeir
Addictive Behaviorsblood alcohol level after a certain number ofdrinks in a certain time period.
8. Refer to the chart to see what the effectsof this bkxxl alcohol level might be.
The following example illustrates thesteps.
A 180-pound person consumes 4 drinks intwo hours.
Steps 3 & 4: .083 blood alcohol level from thechart.Step 5: 2 hours = 120 minutes.
Step 6: (a) total # of drinking minutes40 minutes
120 mi nutesa = .-..- 3
40
(b) a x .01% = correction figure for;iver metabolism of alcohol
3 x .01%
Step 7: .083 blood alcohol level from thechart
030 correction for livermetabolism for alcohol
= a
053 estimated blood alcohol levelfor 180- pound person drink-ing 4 drinks in 2 hours.
Step 8: The chart indicates that at .05 drivingbecomes increasingly dangerous.
This activity has been used in theclassroom and %vas also set up as abooth for a campus-wide alcoholawareness day. The students found thisa meaningful way to estimate howmany drinks they could have and therelationship this would have to theirblood alcohol level.
Drinks"1 2 3 4 5 6 7 8 9 10 11 12
---- - - - - --100 lbs. .038 .075 .113 .150 .188 .225 .263 .300 .338 .375 .413 .450120 lbs .031 .063 .094 .125 1,.,156_ .188 .219 .250 .281 .313 .344 .375140 lbs. .027 .054 .080 .107 .134 1 .161 .188 .214 .241 .268 .295 .321160 lbs. .023 .047 .070 .094 1.117 .141 1 .164 .188 .211 .234 .258 .281180 lbs. .021 .042 .063 .083 .104 .125 .146 L.1A7 .188 .208 .229 .250200 lbs. .019 .038 .056 .075 .0941 .113 .1131 .150 .169 .188 .206 .225220 lbs. .017 .034 .051 068 .085 L.102 .119 71_ .153 .170 .188 .205240 lbs. .016 .031 70:4-7-1 .063 .078 .094 j .109 .125 .141 1 .156 .172 .188
.-- - _ - -Under .05 .05 to 0.10 .10 to .15 Over .15
Driving is not seriously Driving becomesimpaired (although increasinglysome research indicates dangerousfine motor skills may beimpaired at .02 or .03 .08 is legallylevel) drunk in Utah
Driving is Driving isdangerous very dangerous
Legallv drunk Legallyin most states drunk in
any state
"One drink equals 1 ounce of 80-100 pro liquor or 12 ounces of beer or 5 ounces of wine.Reference: New Jersey Department of Law and Public Safety, Division of Motor Vehicles,Trenton, New Jersey.
455
32 TEACHNG IDEAS
Swathe Nogwash
MICHAEL YOUNG is at Auburn Univer-sity, Auburn, Alabama 36830.
With a little imagination educationalgames and activities can be used topromote learning that does get studentsinvolved. The objective of one activitymay be to introduce factual informationwhile another may promote discussionor enhance decision-making skills.Whatever the overall objective, educa-tional games and learning activities canprovide ways to make learning fun. Asimulation game designed especiallyfor smoking education is "SenatorHogwash and his tobacco advisorycommittee."
Simulation games can be used to helpclarify values or to introduce factual in-formation along with examining at-titudes and/or behaviors about a certainissue. "Senator Hogwash" can bringout not only the health hazards of smok-ing but can also show that there aremany economic, social, and politicalforces that make quick elimination ofcigarette smoking unlikely.
Game OverviewSt ,:or Hogwash is head of the Sen-
ate Committee on the Future of To-bacco. To obtain citizen .input, andmake points with the folks back home,he has appointed a citizen's advisorycommittee to make recommendations tothe Senate Committee. The committeemembers discuss the issues from theperspective of their assigned roles andprepart a verbal report.
Committee MembersSenator!. M. Hogwash ----From Horse
Kiss, Kentucky, the Senator serves as an"advisor" to the advisory committee.He has heard ugly rumors of the healthhazards of tobacco. He knows that to-bacco means money to Kentucky andother tobacco states. He wants to dowhat is best for all the people he repre-sents but is unclear as to what his posi-tion should be.
Medical DoctorThe good doctoronce smoked two packs a day bat quitsmoking abou, a year ago. He haskicked the habit for good, he hopes. Hehates to see anyone smoke because ofthe craving for a cigarette he still getswhenever he sees ,.neone light up.
56
Tobacco Company ExecutiveAsvice president of Brown and Jones to-bacco company this committee memberbelieves the claims of health hazardsdue to smoking are unproven. He is notreally concerned with health anyway,but with promoting tobacco sales. Hebelieves that government interferencein this area would be a blow to the entire free enterprise system of our na-tion.
Satisfied SmokerThis smoker en-joys his cigarettes and has no desire toquit. He proclaims that smoking is afundamental right guaranteed by theConstitution and wishes that folkswould just let him smoke in peace. Hefeels that smoking is probably not badfor his health, but even if it is harmful,everyone has to die from something.
Tobacco FarmerSince tobacco pro-vides this farmer with a major part ofhis income he is vitally concerned withgovernment plans in this area. Hewould like to see price supports andother government programs increased.He would hate to see anti-tobacco legis-lation passed. If that is what the futureholds, however, he hopes marijuanawill be legalized so he will have anothercash crop to take tobacco's place.
Nonsmoker's Rights AdvocateAnonsmoker whose father recently diedof lung cancer, this man has led thefight for nonsmoker's rights. He iscompletely against all forms of smokingand eels some type of government in-tervention is necessary.
Public Health EducatorThis healtheducator, a specialist in smoking andhealth, knows the hazards of smokingand is making every effort to turn usinto a nation of nonsmokers. He is forhigher taxes on cigarettes and feels thefunds raised should be earmarked forsmoking education and research.
How to PlayThe instructor assigns students to
play the roles of various committeemembers. Senator Hogwash, played bythe instructor or a student, introducescommittee members to each other(players may want to wear name tags)and outlines the committee's task. Thecommittee members discuss the variousaspects of the tobacco issue (healthhazards, smokers and nonsmokers'rights, economic impact of a possibletobacco prohibition, government's rolein tobacco research and promotion,etc.) from the perspective of their as-signed roles. Committee members may
69
Addictive Behaviorscompromise when necessary but theytry to push through their own idealswhenever possible in order to developrecommendations for the future of to-bacco in the United States.
OptionsStudents not assigned a committee
role may be members of the interestedpublic attending the committee meet-ing. They may wish to ask questions ofthe Senator and members of the advi-sory committee. The instructor maywish to appoint more than one advisorycommittee. These groups could presenttheir recommendations, which may bequite different from group to group.Students who are not members of anadvisory committee may be designatedSenators and appointed to the SenateCommittee on the Future of Tobacco.Advisory committees could presenttheir recommendations to the SenateCommittee. Senators could then discusswhich recommendations they wouldlike to see incorporated into futurelegislation.
Students should be introduced to thehealth aspects of smoking ankother is-sues through lecture material and/orreading assignments. They should notbe expected to begin play "cold." Fol-lowing play, which could run from 30minutes to one hour or more dependingupon the teacher and student interest, ateacher directed discussion pericd canbe of value in providing comments ongame play and in restating major is-sues.

33 TEACHING IDEAS
Addictive Behaviors
Student-to-Student TeachingAbout Tobacco Smoking
Lorraine J. Henke is a health educator at theEugene Burroughs Junior High School, Accokeek,Maryland.
For the past three years, the decision to smokeor not to smoke has been the subject of formaldiscussions between eighth grade health educa-tion students from Eugene Bui loughs Junior Highschool and elementary students in the fifth andsixth grades in various schools of Prince George'sCounty, Maryland. The project was designed toexplore the impact of presenting the smokingaspect of health education between students ofclose age groups. The assumption was that thefifth and sixth grade students would enthusias-tically accept and comprehend the presentationand interchange of health education informationwith their junior high school student contem-poraries. This assumption was proven to be valid.
A typical student-to-student teaching experi-!:nce consists of a group of seven or eight juniorhigh school health education students visiting afifth or sixth grade class (frequently a scienceclass). The eighth grade students first present thefacts of smoking as a panel, then each of themleads a small group of elementary students in adiscussion about the decision to smoke or not 'osmoke.
During the panel presentation, the junior h;ghschool students discuss the effects of tobaccosmoking on the body utilizing a machine (con .strur*ed by the students., which simulates theeff on the human respiratory system. A filtertip and nonfilter tip cigarette are both "smoked'.by the machine. The tar from each of the cig-arettes is passed through hollow glass rods repre-senting a person's mouth and throat. The tar thatdid not adhere to the glass rods then travels toglass test tubes constructed to represent a per-son's lungs. The presence of tar is always clearlyvisible, enabling succinct comparisons of tar con-tent to be made between th t! cigarettes, alongwith analyses of tar content regardless of the type
of cigarette. Safety precautions to prevent tobaccosmoking related fires, why people smoke, andhow to quit smoking are presented. The audienceis encouraged to join in the discussion and toask questions of the panel members.
Following the panel presentation, the elemen-tary students are diiiided into groups and eacheighth grader leads d group in discussing the ad-vantages and disadvantages of tobacco smoking.During these discussions, the eighth graders en-courage the elementary students to ask questions,to voice honest opinions, and to continue tokeep up-to-date regarding the facts about tobaccosmoking.
At the conclusion of each instruction program,the visiting junior high school students distributeleaflets stating the facts about tobacco smoking.These leaflets are contributed by the AmericanCancer Society, the Tuberculosis and RespiratoryDisease Association, and the U.S. Department ofHealth, Education, and Welfare. Also contributedby these organizations for use in the presentationsare posters, research data, and other printed ma-terials on tobacco smoking, including the book-let from HEW explaining how to construct themachine which the students used in their presen-tation.
Several points of interest, noted over the fewyears of being involved with the student-to-stu-dent teaching program, are as follows:
1. Elementary students who plan to attend thejunior high school represented by the panelgroup respond more enthusiastically than dothose who are not going to attend thatschool. Following this revelation, we haveencouraged elementary schook to seek theservices of the junior high school their stu-dents expect to attend.
2. Presentations made to large groups (over50) of elementary students are not as suc-cessful as those given to smaller groups.There appears to he less satisfaction for both
7 0 57
Eighth graders makeeffective teachers for
sixth graders--andespecially when they
come from the junior highschool their audience
will attend, when thereis a good mix of race,sex, and personality.
I.
Nr- :ft
taMe
71106;
the junior high school student teachers andthe elementary school students.
3. When the make-up of the panel of juniorhigh students includes a variety of students(in regard to sex, race, personality, and aca-demic achievements), there appears to be ahigher audience response (a ve.y good rap-port) than if these characteristics were notrepresented by the junior high school stu-dent teachers.
4. Parents of both the ele7untary and juniorhigh school students involved in the student-to-student teaching program have respondedto this form of health education in a veryfavorable manner.
5. Junior high school students involved in theprogram have repeatedly stated that theirexperience in teaching the facts about to-bacco smoking has reinforced thir decisionnot to smoke.
6. Repeated requests from the elementaryschools have been made to initiate a similarprogram for other aspects of health educa-tion, especially drug education.
58
Where do we go from here? We are constantlyseeking other effective teaching aids like thesmoking machine in an attempt to improve ourpresentations. We are investigating the student-to-student teaching of other aspects of healtheducation. The eighth grade student teachers areinvited back each year to relate their experiencesregarding tobacco smoking as thPy progress intothe higher school grades. We seek and evaluatethe suggestions of the elementary students andtheir junior high school student teachers. Mostimportant, since the program has been going onfor the past few years, we have been able to askthe eighth grade health students (who a few yearsago were elementary students attenlinF our stu-dent-to-stud,nt discussions) what ettect the dis-cussions had on their health itudes and be-havior. At this point suffici lata to make aconclusion have not been c ci and analyzed.The favorable responses ref:. .,u from those stu-dents who had attended the student-to-studentdiscussions, however, please us and spu us on tocontinue and improve.
71

TEACHING IDEAS
Addictive Behaviors
The Smoking Game
lan Newman is associate professor and chair-man, Division of Community Health Education, atthe University of Nebraska, Lincoln.
In 1964 a new rationale was published tojustify an old ethic. The surgeon general's reporton smoking and health reinforced the school'sposition that it should not allow youngsters tosmoke in the school building or on the schoolgrounds. Schools had traditionally forbiddensmoking, but now they had new medical evi-dence to support their nonsmoking stand. Need-less to say, smoking did not disappear from thehigh school, junior high school, or even the ele-mentary school. In an attempt to examine theschool's traditional stand on cigarette smoking byits students, a long-term examination was madeto document the actual smoking behavior con-ducted within the school. This paper describessomething of the behavior of the young peoplewho smoked in the school and the teachers whoattempted to prevent their smoking. Informationpresented here is based on data gathered over anine-month period of intensive participant ob-servation.
The General Setting of the GameThe events described in this pa:.er took place
in a Midwestern junior high school with 1,800students. It was assumed that while this schoolwas unique, it did have many aspects in commonwith other schools across the country and the stu-dents were, in fact, typical. The school in questionwas traditional and authoritarian. Discipline wasseen as a necessary requirement of efficient ad-ministration.
At the time of the study on which this report isbased, an important characteristic that distin-guished the act of smoking among junior high
* This material was originally presented to the workshopon educational programs influencing youth at the N3tionalConference on Smoking and Health, September 9, 1970,San Diego, California. The work on which this paper is
based was perfornwd pursuant to Contract numlwr PH10B-66192 of tlw United States Public Health Service, De-partment of Health, Education, and Welfare; William II. Cres-well, Jr., principal investigator; Warren I. IlLiffman andDonald B. Stone, research associates.
school pupils from smoking among the adult pop-ulation was its illegality, As one student put it,"When the teachers can't see the kids, the kidssmoke and when the kids can't see the teachers,the teachers smoke," This situation was furthercomphcated by the fact that machines dispensedcigarettes to any consumer, regardless of age. Ad-vertising enhanced the pleasures of smokingthrough subtle inferences. Adults openly violatedNo Smoking signs and ordinances. Even membersof the Board of Education disregarded the manyNo Smoking signs posted on the walls of theirconference room.
At school the rules against smoking appliedonly to the students. Faculty members smoked instaff rooms and in the locker room office. Theschool appeared to be the only place where smok-ing was prohibited only for minors. Students sawthis as a clear contradiction of principle. Theypointed out, however, that smoking was not theonly item of inconsistence. School regulation ap-plying to the length of hair, the color of girls hair,the length of skirts, and the behavior of athletesall represented inconsistencies of various typesclearly noted and described by many of the stu-dents. With these conditions existing, any actionon the part of the students appeared to them tohe justified, and activities related to cigarettesmoking took on all the dimensions of a game.Smokers played the game of attempting to out-smart the teachers, who for their part attemptedto enforce the school's rules and apprehend thesmoking students. Achievement in either role wasinterpreted as winning.
The ContestantsStudentsWhile smoking patterns differed with each sub-
ject, there appeared to be a general configurationwhich characterized the regular ninth-gradesmoker. This is illustrated by the following state-ment recorded during the course of the study.
After my dad goes to work I usually have onecigarette, then another one on the way to school.You can usually get one more outside the buildingbefore you come in and then after second houryou can get at least half a one if you hurry in thewashroom upstaiN. At lunch time I usually haveone outside and then after fifth hour I have
7 2 59

another one. There's usually a bunch of us whogo to the washrooms and there's always someonewho's willing to stand watch for the teachers.
The ContestantsTeachers
Smoking was illegal for students. Students wereencouraged to be like adults. However, whenyoungsters smokedlike adults--the heavy handof the school authority descended on them. It wasdifficult for students to see why 40% of their adultfaculty could smoke and they could not. Teachers,both smokers and nonsmokers, thought it theirduty to apprehend students who smoked. Stu-dents were better at avoiding the teachers thanthe teachers were at catching the students. Theharder the school authorities tried to catch thesmokers, the more fun it was for the smokers, andthe higher the status one achieved by foiling theauthorities' attempt to apprehend.
This set the ground rules for the game. Therisks were challenging. The payoff increased withthe teachers' increased efforts to catch the ciga-rette smokers. The teachers felt great frustration."If only we could cut down a few trees, they'dhave no place to hide and we could catch them,"lamented one counselor.
The reward to the students was expressed byone nonsmoker, who said:
You know, I get a kick out of it every time I see akid smoke and get away with it. It seems thereare still a few things around here that you can doand get away with. It's good to know we can stillbeat the teachers.
Strategks of the Game
Subjects and other informants reported thatsmoking occasionally took place in the lockerrooms, shower rooms, industrial arts shops,photographic dark room, and even in the class-rooms. However, tile majority of smoking in thisparticular school was limited to the washroornsand to a specific location adjacent to the schoolentrance but hidden from view by four small trees.Because both of these locations were essentiallywithin range of easy scrutiny by the faculty, nu-merous techniques were utilized to foil detection.Description of one of these will serve to illustratethe process of the game.
The majority of the smoking in the schoolbuilding was dorh? during the luncr hour and be-tween class periods. At lunch time swdents wentto the cafeteria in three shifts. During lunch theywere restricted to an area including the cafeteriaand the hallways immediately adjacent to it. Thisarea included boys and girls washrooms, whichbecame the centers for smoking activity. Becausethis location was heavily traveled by faculty going
60 73
to and from lunch, smoking required a well-coordinated team effort. To further complicatethe matter for the smokers, two counselors wereassigned to patrol this general area.
Those concerned about being caught posted"guards" outside the washroom to warn of ap-proaching faculty members. Methods utilized bythe guards to convey their warnings varied withthe urgency of the situation. The simp:est methodwas for the guard to go inside and tell the smok-ers that someone was approaching. However, thisendangered the guard as he then ran the risk ofbeing caught in the smoking setting. Another pro-cedure employed by the guard was simply to kickthe door with his heel to warn of the approachingfaculty member. Still another variation of this pro-cedure was to kick the radiator pipe which passedthrough the wall. On occasions when a teacherapproached too rapidly, or was unnoticed untilthe last moment, the student on guard wouldopen the door for the teacher and greet him byname in a loud voice so that those inside wouldget the warning. Nonsmokers often acted asguards, and it was reported that it was safer tohave a nonsmoker stand watch. They were lesslikely to leave their posts for a few puffs with therest of the group.
Inside the washroom the smokers took addi-tional precautions to avoid being caught. It was acommon practice for them to stand close to uri-nals, sinks, or toilet stools while smoking so thatit was an easy matter to get rid of the cigarettes.A wet paper towel was often kept ready to snuffout the cigarette as a last resort to avoid beingcaught if a teacher entered. Smokers would oftenstand on the toilet stools which enabled them toexhale smoke close to the air exhaust ducts on thewall. This cleared the smoke from the room. Thisalso provided for easy disposal of cigarette buttsby flushing them down the toilet.
While it was not possible to observe the smok-ing behavior of the girls as closely, informants re-ported similar practices in their washrooms; how-ever, fewer girls smoked and the necessity for anelaborate warning system was less important.While as many as fifteen boys might congregateto smoke cigarettes at any on,, time, it was un-usual for more than five girls to be present in asmoking situation. Girls were more likely to smokealone or with one or two classmates. They weremore apt to smoke when the washroom was emptyor they avoided smoking in school altogether.
Smoking outside the school building, but onthe school grounds, was le, But againstudents developed sophisticated systems to avoiddetection. The most popular location. adiacent to

the front entrance of the school and behind agroup of small trees, often produced a two-stepcommunication system to foil teachers' attemptsto apprehend smokers in the act.
Students found numerous ways to test theirskills of concealment against the teachers' skillsof detection. Students would smoke in the frontrows of the school movie theater on recreationnights. They smoked in the industrial arts shopswhere numerous odors aided in concealment andin shower and locker rooms which were usuallyunsupervised. On occasion, when faculty mem-bers supervised the loading of school buses,smokers would approach the supervising teacherto see how close they could get without beingcaught. Smokers and their friends appeared toenjoy the success of such ende6vors.
Chances of Changing the Came Plan
Throughout the year the garne varied in inten-sity. At times the facuRy would win out, severalsmokers would be caught and suspended, andsmoking would appear to subside. This reinforcedthe faculty's feeling that discipline did solve theproblem. In reality, the smokers had been forcedto regroup and utilize their most successful strat-egies. For awhile they were more careful andworked harder in maintaining the covert natureof their smoking behavior.
As in any game, learning took place. Studentsdecided on new ploys to outsmart teachers and altimes they even chose to quit the game com-pletely; they became nonsmokers. However, tochange roles and become a nonsmoker was diffi-cult.
Teachers s(..emed to react to smokers the same\vay they reacted to students who were failingacademically, prObably because they had ob-served that smoking and failing were often asso-ciated. Students who were grouped into eitherof these two categories tended to be treated dif-ferently by most teachers. On teachers' evalua-tions, for example, smokers were rated lower thantheir nonsmoking colleagues. Teachers expectedless of these students and tended to he suspiciousof them. As a result, students who were smokerstended to be offered little latitude within theschool. By comparison, nonsmokers w ho func-tioned successfully within the school were givenconsiderahle freedom, which they often ahused.
As one individual, a class monitor and foothallteam member, stated:
You know, I can do just ohout anything I pleasearound here. I get on real good with the teac hers.I can walk the halk whenever I want. 'leacherslet me out of class, monitor,. never ask me for my
7
pass; if they do, I just tell them so-and-so sent meon an errand and they never report me for nothaving a passit's rather bad actually.
By contrast, a student who was both a smokerand a poor student related the following inddent.He had been given a signed hall pass to visit theoffice. However, he was apprehended on his wayand finally escorted to his office by an assistantprincipal and a teacher, both of whom questionedthe authenticity of his pass. The student's explana-tion was as follows:
I gave my pass to the teacher and he made somecrack about getting out of his c isshe's a goodguy, however, y oil know. Then, as I was walkingdown the hall (this leacher) comes Out of hisclassroom and asks me for my pass. I shows it tohie and he makes some wise crack about forging
rie's always sticking his nose where it's notwanted. Then, I goes to the washroom and I cameout and (another teacher) asks for my pass. liesayti the pass \Vdti not for the toilet and that I
shouldn't woste time. Just as I came in the door, Istopped for a drink of \voter and she takes myposs and savs it don't look like your writing. I gaveher a NI of hp and whamo, the assrstont principaloppeors.
These incidents and others suggest that teach-ers' attitudes toward certain students became in-flexible. Consequently, any attempt by these stu-dents to mod:fy their own behavioral game planwas met with little recognition and considerableresistance. As one male smoker said:
I decided I was going 1l/ go good this year. I evenquit smoking. I tried real hard, but they (theteachers) just wouldn't give me a chance. I gaveup In the end . It seemed that whenever there
trorible they thought I was involved and evenwhen I wasn't they just viouldn't let me he good
The Observer's Perspective
!laving watched the game frorn the vantagepoint ot a participant observer, trusted by thestudents ancl the teachers and not required to takesides in the contest, I noted several points overthe duration of the year.
1. Cigarette smoking was not an end in itself.AI this age, it wasn't the taste or the associationwith coffee that encouraged the students tosmoke. Smoking was, in fact, just a symptom ofthe larger problem. The majority' of nonsmokingkids thought their friends smoked to "be big" orto achieve status. Smokers didn't admit to this,although their actions tended to confirm the mo-tivating forces of status, or at least compensatoryb eh avior.
2. Rec.ords showed that young people whosmoked at this early age were 011 Lir in IQ to
61

their nonsmoking contemporaries. While thesmokers knew what was expected of them, theyalso knew that they were often not meeting theseexpectations. School records showed that theywere correct in their recognition of low achieve-ment. They were more likely to be (ailing courses,truant, tardy, and suspended from school thanwere their nonsmoking contemporaries. Theydidn't participate in the extracurricular life of theschool and their fellow students tended to seethem as low social status individuals. They chosefriends who were hke themselves for supnort. Inother words, they tended to group tother as ar_?am--the peer group team.
3. Teachers tended to type individuals whosmoked and held lower expectations for them. Asa result, teachers tended to resist changes in ID(havior on the part of the smoker. Smokers hadgreat difficulty in casting off the smoking imageof low achievement and poor behavior if theychose to quit smoking.
4. As with all games, one left the scene of con-test wondering what would happen if other strate-gies had been employed by the contestants. Itappeared that the smokers had read the wrongsignals. While they still attended school, they hadalready dropped out. The school had providedthem with few rewards and they looked otherplaces, in other contests, for more meaningfulrewards.
What would have happened if the school had
62
stopped harissing the smokers and admitted to itsown hypocrisy, thereby removing the payoff fromthe game? If at the same time there had been al-ternative and meaningful activities available to thesmokers would they have found less encourage-ment to smoke?
Would new courses, interesting courses thatappealed to these early dropouts, have recapturedtheir restless spirits to a point where they wouldhave at least become a part of the educationalprocess?
What new methods could be used and whatnew ways could be made available to these youngsmokers to find status within the system ratherthan being forced to compete for status in thesmoking game?
How many poorly planned anti-smoking edu-cation campaigns actually enhance the status ofthe smoker by putting him in a position of braverisk takerwilling to stand fast against the sta-tistics, the true games player--willing to gambleagainst odds and possibly win?
Smoking has to be recognized as somethingmore than a dirty habit. It was a practice, complexand multidimensional in nature, even for the
rior high school student. Unfortunately, how-.'er, it appeared that the teachers had overlooked
this fact and thought they could win out with asingle strategy of firm discipline. It was apparentthat this single strategy game plan was not suc-cessful.

35 TEACHING IDEAS
Addictive Behaviors
Making Tobacco Education RelevantTo the School-Age Child
lohn R. Sef frith is professor and chairmanof Health and Safety Education and di-rector of Operation SmART at IndianaUniversity, Bloomington, IN 4740.5.
School health education is facedtoday with a number of challenging op-portunities to improve the quality oflife through effective instructional pro-grams. Whether it's sexually transmit-ted diseases, suicide, teenage drinking,illegitimacy or accidental deaths, mosthealth educators feel that our disciplinecan and should help ameliorate thesehealth problems through sound schoolhealth education programs.
Probably no greater challenge existsfor school health education today thanthat of cigarette smoking among youth.Although the per capita consumption ofcigarettes has dropped during the lastthree years, the estimated health-carecost to society because of cigarette-induced illness is fifteen billion dollarsannually. What is more important isthat at least 340,000 Americans die eachyear prematurely because they smokecigarettes.' In the words of Joseph A.Califano, former S:cretary of Health,Education and We'(are, the unadornedfacts clearly shov, that cigarette smok-ing is "public :s.ealth enemy numberone.''
The cigarette smoking dilemma is acomplex cultural problem with manyinteracting personal and social forces.However, the gross figures suggeststrongly that the school curriculum hasfailed to prevent children and teenagersfrom beginning to smoke. For example,although the percentage of adults whosmoke has gradually declined since1964, the percentage of children andteenagers who smoke has increased.The rate of increase among teenage girlsis particularly alarming.' All told, todaysix million children and teenagerssmoke.4 Past research and experienceclearly show that 1) the majority ofthese youngsters will continue to smokeregularly for life; and, 2) they will beless well and their livi -)rter becauseof their smoking habit.5.'
Finally, since the decision to smokeor not to sm, e is made very early in
life (almost always before age twentyand often by junior high school), therole of school health education, particu-larly during the primary and middleschool years, is of critical importance ifhealth educators are to reach studentsbefore they start smoking." Until andunless comprehensive efforts are madeto provide each school child with mean-ingful health instruction regardingcigarettes, the carnage in human healthand life is likely to continue.
Personal Choice and ResponsibilityEffectiveness of instruction is more
related to how we teach than to what weteach. In the area of personal lifestyle itis important for the health educator torecognize the pluralism in our society.With the contemporary emphasisplaced on personal rights and values,instructional strategies should be tail-ored accordingly. Therefore, carefulplanning by the teacher is necessary toprovide a balanced as well as scien-tifically accurate instructional program.For example, in addition to teachingabout the health consequences of smok-ing, instructional time should be usedto explore the reasons why some peoplechoose to smoke. In short. the teachershould develop an objective atmos-phere in which the pros and cons ofsmoking can be fully explored.
The therm should be: the student hasthe ultimate responsibility to decidewhether or not to smoke; therefore, thestudent must given the perhnentfacts in an objective setting. The goal isto provide the student with an oppor-tunity to make a decision based on factsand personal values. Attendant to thisapproach is the accompanying need forthe student to accept responsibility forhis or her decision. In an effort to de-velop an awareness of the full responsi-bility nivolved in such a decision, in-!Aructional time should be given to ex-plore a number of social issues such asaccuracy in advertising, special insur-ance rates for smokers, and non-smokers' rights.
In the past many working educationeftorts have been restricted to a narrow,
one-sided, health-facts unit whichcould be accurately described as a "thoushalt not" approach. Besides being a"turn-off" for many students, itsgreatest weakness was that, in omittingsubstantive socio-political issues, someof the strong persuasions against takingup smoking were never developed.Thus, millions of children and teenag-ers have decided to smoke, at least inpart, because the only disincentive wasan obscure threat to their health dec-ades in the future. To be truly respon-sive to student needs and to maximizethe relevancy and potential impact ofour teaching, we must go beyond thestatistical correlations associatingsmoking with age-onset diseases. Mor-bidity and mortality figures and factsare not enough.
Suggested Facts and ConceptsWith the knowledge explosion it is
impossible to teach all the facts in anyarea; thus the prcfessional responsibil-ity of the teacher to select appropriateinformation to develop valid concepts iscritical. Following are selected examplesof content and concepts which Lan bemade relevant to students.
Cigarette smoking is our natwn's leadingpreventable health problem. Consensusexists among medical scientists thatcigarette smoking is the greatest causeof preventable illness and prematuredeath in the United States."'" Thisyear, for example, over 122,000 peoplewill develop lung cancer in the UnitedStates; at least 80% of these cases aredue to cigarette smoking." Addi-tionally, thousands more will developcancers of the throat, oral cavity. pan-creas, esophagus and urinary bl. ,Iderbecause they smoke."." Heart dis-eases, our nation's leading cause ofdeath, will take the lives of smokers atleast twice as frequently as non-smokers.'4 Chronic obstructive !ungdisease, one of our nation's fastest-growing chronic diseases. is largelycaused by cigarette smoking.'5 In short,after 30,000 scientific studies over threedecades it is apparent that not onemeasure in preventive medicine could
63

abb._
do more to improve health and to pre-vent premature death than the controlof cigarette smoking.'"
Cigarette smoking is deletvrious to vowhealth now. The association of cigarettesmoking to the aforementioned dis-eases is well established and widelyrecognized. However, less well knownis that cigarette smoking is harmful tothe smoker's health immediately. headverse effects of smoking begin withthe first cigarette and get progressivelyworse as smoking continues.'' Im-media te negative physiological re-sponses to the smoker include in-creased heart rate, elevated bloodpressure, constriction ot blood vesselsand trachial irritation.'"" While per-manent, irreve .sible damage to thelungs does not occur immediMely,hyperplasia (overgrowth of cells andoverproduction of mucous) beginswithin weeks of regular cigarette smok-ing.2".21 Ciliary action is damaged andtrachial-mucosal velocity (TMV) is re-duced while one smokes.22-=' This, inpart, explains why smokers are moreprone to infectious diseases 01 the res-piratory tract.24
In recent years, s.ui..est Ilave shownbasic pulmonary dysfunction in teen-agers who have smoked for only a fewyears.25 Although some of the hara(uleffects of smoking are reversibl.- if aperson quits in time (e.g. smokers' lungcancer mortality rates return to non-smoker rates 10 to 15 years after smok-ing ceases),2" lung and respiratory tracttissue damage begins with the onset ofsmoking and becomes worse the longerone smokes.2' Some scar tissue will re-64
, dillow116goo
use
4ISO
11 4
f
lult after only a few months of regularsmoking.28
here is no such thing as safe smolons.Occasionally reports on smokingsuggest that "moderate or "light"smoking of low tar and nicotine cigaret-tes may be safe. This implication arisesfrom the well-established fact thatsmoking's impact on health is a doseresponse phenomenon.= The numberof cigarettes smoked, the frequency ofpuffing, and the depth of the inhale allrelate to increased risks."'
The inference, however, that theremay be a safe or threshold level belowwhich no harm occurs is unsubstan-tiated and invalid.'"2 As alreadypointed out, adverse effects begin earlyand grow progressively worse overtime." Further, although low tar andnicotine cigarettes are assumed to beless hazardous, no evidence existswhich would indicate that they are safe.On the contrary, certain harmful sub-Aances, such as carbon monoxide, arein greater concentration in the low tarand low nicotine brands." Scien-tifically, it is very difficult to makeblanket statements about the relativerisks of different brands because of in-dividual differences in smoking tech-nique. For example, some smokers whoswitch to a low tar and nicotine brandmay draw harder or inhale deeper andsmoke more cigarettes; thus, the rela-tive dosage of nicotiry: and other sub-stances may be about the same as be-fore.
In conclusion, if a person mustsmoke, a low tar and nicotine cigarette
7 7
may be the least harmful; however,from a health vantage point, any smok-ing is hazardous to one's health.
Cigarette smaing can be harmful toothers, and especially to fetuses. In addi-tion to the well-known irritation factor,which at least 60% of all people experi-ence, there are real health threats fromexposure to second-hand smoke.35-'"The most alarming threat is to personswho are already chronically ill with dis-eases like coronary artery disease,bronchitis, and chronic obstructivepulmonary disease." For example,people with existing heart disease willdevelop angina pectoris (chest pain)upon exertion sooner when breathingair polluted with tobacco smoke."Further, animal studies have shownsignificantly more malignant tumorsa in on g th ose an i m a Is brea th ingsecond-hand smoke on a daily basis.'"Finally, children exposed regularly tocigarette smoke have twice the respira-tory disease rate of other children .4" Al-though the smoker is affected most bysmoking, the non-smoker who breathesair polluted with cigarette smoke doe,,experience untoward physiological ef-fects.4 These unhealthy and immediateeffects include elevated blood pressure,increased heart rate, and abnormal car-hoxyhemaglohi n levels (carbonmonoxide in the blood).42 Recentstudies confirm that even healthy adultsdevelop marked small-airways dysfunc-tion from breathing secondhandsmoke.41
The most fearsome impact otsecond-hand smoke may be on the tetusof the pregnant smoker. Unless themother stops smoking before the fourthmonth of pregnancy, some untowardeffect can be expected in the baby.'Since carbon monoxide crosses the pla-cental bearier, the unborn fetus can beexpected to develop carboxyhemoglo-bin levels comparable to themother's:1c." Since it is known thatcarbon monoxide displaces oxygen inthe blood, it is obvious that the fetus isput at a distinct disadvantage duringthe most important period of its growthand development. For example, thehuman fetus' brain is growing at therate of one to two milligrams per min-ute at the time of delivery.4" Thus, anyoxygen deprivation is most critical. Inaddition to having more miscarriagesand stillbinhs, smoking mothers havebabies who weigh less at birth, alsotheir babies are more apt to die duringthe tirst year after birth, and, theirbabies have more respiratory diseaseduring childhood and adolescence.4"-4"One of the most discouraging findings

educationally has been the discoverythat children whose mothers smokedduring pregnancy do poorer onachievement tests in math and readingat ages 7 and
Regular cigarette smoking usually r-sults in a serlous th7,01thMt"1/ probh'm.Like any drug of abuse, tobacco has thepotential of causing serious depen-dency. Unlike users of other drugs ofabuse, however, research indicates thattobacco users will usually become de-pendent for life-- they will be less welland their lives shorter because of theirsmoking.'l For example, it is estimatedthat lbout 10-15"0 of the people alivetoday who ever used heroin are still de-pendent on it. However, 66",, of thosestill alive who ever smoked cigarettesare currently still dependent on cigaret-tes and smoke them daily."
While research to elucidate the mech-anisms of dependency continues, it issafe to say that cigarette smoking canand usually does result in strong dependency. The psychological factors as-sociated with habit formation and de-sire to smoke seem to be paramount;but, at least for some smokers, the de-velopment of a physical dependence tonicotine may also occur." These starkfacts should be included in educationalunits so that those deciding to smokeare aware, in advance, of the likelihoodot future dependency. It is known fromnational polls that at least 8 in 10 smok-ers would like to quit if there were aneasy way. Such informahon is particu-larly critical in view of the recent trendin children experimenting with tobaccoat earher ages. A 1%7 Britkh survey ofteenagers indicated that among thosewho smoked more' than one cigarette,80"o ultimately became regular smok-ers."
The //du/int/Nes ot not sntokin.g tin out-ieelgh the ildcantage, of :onolon,g. Chil-dren and teenagers who choose tosmoke do so for certain reasons. Al-though tht",e reasons may not be clearlyelucidated and evaluated, and just asimportantly, they may not be under-stood by the smoker, we must acknowl-edge that all behavior, healthy as wellas unhealthy, is caused h is a logicalassumption that many smokers findtheir habit enjoyable and somehow,reinforcing. For some youngsters,smoking may provide a way of emulat-ing adults; for others a way of rebelling;and for still others, simply a satisfactionof curiosity. 6' kducators should ex-plore with their students these andother possible reasons for smokmg. Inso doing, educators should avoid a
condescending attitude toward reasonsadvanced in favor of smoking. Sinceone's values relate intimately to one'srationale for behavior, it is inappropri-ate to label reasons as right or wrong.The merits and demerits of various rea-sons should be explored in an atmos-phere of respect with an emphasis onvalue clarification.
However, any comprehensiveanalysis of the pros and cons associatedwith smoking leads to one very criticalconclusion; that is, the advantages ofnot smoking far outweigh the advan-tages of smoking.
Issues for Class DiscussionSince the dedsion to smoke or not to
smoke is an individual one, much of theeducational strategy should focus onpersonalizing lessons. As stated, thereshould be adequate coverage of the var-ious values and motivations involved inchoosing a course of action.
However, to stop at the personal levelwould be remiss in light of the healthcare dilemma facing society today. In aneffort to explore the responsibility ofthe individual in society, a carefulexamination of social pohcies regardingcigarette smoking is important and rel-evant. Three examples follow of critical
vo"
doP
socio-political issues which should bedealt with in the secondary curriculom.
What should be our federal pohcy to-ward tobacco? Currently the federalgovernment is inconsistent and con-tradictory in its pohcy toward tobacco.Simultaneously, two cabinet-level de-partments pursue policies which haveantithetical objectives. The Departmentof Agriculture (USDA) continues tosupport and promote tobacco produc-tion. In 1977, for example, the U.S. De-partment of Agriculture spent approxi-mately 65 million dollars on the variousaspects of adrninistering the price-support program for tobacco." Further,the nM ion's lawmakers included to-bacco in Public Law 480, the "Food forPeace" program.'" Under this programmillions of dollars in tobacco have beensent to developing countnes around theworld.
On the other hand, the U.S. Depart-ment of Health and Human Services(DHHS) continues to battle cigarettesmoking in many ways. In 1964 the firstand landmark Surgeon General's Reporton SmokIng was published. Since then anumber of efforts have been institutedat the national level to combat smokingthrough school and public health edu-cation. In 1978, DHEW SecretaryCalifano established the Office on
-11111.
7S BEST COPY MAKE
1
65

Smoking and Health, and money con-tinues to be spent on anti-smoking pro-grams.6"
Who should pay the smoker's healthcare bill? The cost of medical care inAmerica continues to rise even fasterthan the inflation rate. This year,Americans will spend over 245 billiondollars on personal health serviceS,more than any other nation in the
world.61 With the trend toward someform of prepaid, social-health insuranceplan for all, greater emphasis needs tobe placed on the prevention of disease.For example, it is estimated that 350,000people will die this year from diseasescaused by cigarette smoking."' Prior totheir death many incurred large medicalbills resulting from expensive treatmentand lengthy stays in hospitals. Currentestimates are that each year at leastseven billion dollars are spent on thedirect medical costs of treating diseasescaused by cigarette smoking. If oneadds the lost productivity, the total costjumps to a staggering 20 billion dollarsannually." Presently, the direct healthcosts are borne primarily by private in-surance companies. Eventually, theymay all be paid through national healthinsurance. Regardless of the system,private or governmental, the consumerpaysall the consumers. Should non-smokers pay as much hi premiums ortaxes as the smoker?
What are the rights of smokers andnon-smokers? The spirit of this age isrights: rights for the handicapped,rights for Blacks, rights for the aged andrights for children. In all of the aboveexamples, one common denominatorexists. Each one of the above representsa minority group. In the case of non-smokers' rights, we are talking aboutthe majority. Most children and adults66
do not smoke. In spite of this fact, manywho are bothered by cigarette smokefeel as though they should not expresstheir discomfort, since it is the smoker'sright to smoke.
However, no one is proposing to takeaway the smoker's right to smoke. Onthe contrary, all major groups active inthe smoking and health controversymaintain that a person has the right todecide whether or not to smoke. How-
" 1
1101111.11"
111111111.MPIIIII
ever, a distinction needs to be made be-tween a right and a freedom. That is,although one has a right to choose tosmoke or not to smoke, one does nothave the freedom to engage in the prac-tice at will.
Since the beginning of our country,certain limitations have been placed onpersonal rights. Generally, these limita-tions are determined by two factors: thehealth and safety of the public; and therights that might be abridged by theunrestricted practice of the first right.The adoption of speed limits is anexample of protecting public safety. Agreat jurist once wrote, -My right toswing my fist ends when my fistreaches the end of your nose." Consis-tent with these principles and prece-dents, one's right to smoke should notbe total and unrestricted. For years, forsafety purposes, smoking has beenproperly disallowed in combustibleareas, and, smoking in bed is againstthe law.
We now know that ambient cigarettesmoke can be hazardous to the non-smoker's health, especially to childrenand persons with chronic illnesses.Since society should promote the publichealth, a new look at rights for smokersand non-smokers is justified and ap-propriate.
SummaryAmericans consume 615 billion
cigarettes annually.'4 Although the percapita consumption for adults hasdropped over the past fifteen years, theamount of cigarettes being smoked bychildren and teenagers has increased.The percent of teenage girls smokinghas nearly doubled during the last dec-ade." Because of this trend towardmore smoking among the young, andbecause of smoking's effect on humanhealth and life, educators must redou-ble their efforts. In spite of the diseasesexacted on humans as a result of smok-ing, cigarette smoking, as such, is not amedical problem; but rather, the realproblem lies in educating youngstersprior to the age at which the critical de-cision to smoke or not to smoke ismade.
Through careful planning and profes-sional discretion the school-health teamcan address this challenge in ways thatare meaningful and relevant to stu-dents. No longer do we need to threatenthe child with dread diseases in the dis-tant future; but rather, instructionalstrategies can be designed to respect thestudent's right to choose. However, inchoosing, it is imperative that the stu-dent grasp the profundity of the ded-sion. Through a comprehensive andbalanced instructional effort the studentcan better understand the personal aswell as social ramifications of cigarettesmoking. With an emphasis on the roleof values and motivations in decisionmaking the student can begin to ap-predate the words of Frost:
"Two roads diverged in a u'ood. and II took the one less traveled bu.And that has made all the difference..."
'American Cancer Society, Inc. A nationaldilemma: cigareit! f mokins oi the health ofAmericans - report of the. National Commissionon Smoking and Public Policy to Mc Board ofDirectors. 1978, 4.
=U.S. DHEW. limoking and health, reportof the Surgeon General, Washington, DC:USPHS. 1979, ii.
3U.S. DHEW. The smoking digest, NationelCancer Institute, 1977, 13.
4Horn, D. How much real progress havewe made in the Eight against smokMg? BullAm Lung Assoc. 1979, o3, n-9.
5Russell, M. A. H. Smoking problems: anoverview, in Research on smoking behavior,National institute on Drug Abuse ResedichMonograph 17, M. E. JaMk, J. W. Cullen,E. R. Gritz, T. M. Vogt, and L. J. West,(eds.), (U.S. Department of Health, Educa-tion and Welfare. Publication No. (ADM)78-581). Rockville, MD.: National Instituteon Drug Abuse, 1977, 13-33.
S. DHEW: The health consequences ofsmoking, report of the SUrgeoti Getieral, Office
79

on Smoking and Health, 1978.'American School Health Association. In-
troducing tobacco educatum in the elementaryschool K-4, Kent, OH American SchoolHealth Association, 1978, 2.
8W-10. Snwking and its effects on health,report of a WHO Expert Committee, Geneva,Switzerland; World Health Organization,1975, 29-33.
9Fletcher, C. M., & Horn, D. Smoking andhealth, WHO Chronicle, 1970, 24, 345-370.
'"U.S. DHEW. The health consequences ofsmoking, p. 2.
"American Cancer Society, Inc.: Cancerfacts and figure's 1981, New York, NY: Ameri-can Cancer Society, Inc., 1979, 9, 14.
p. 19."U.S. DHEW: The health consequence's of
smoking, ch. 5.'4Steinfeld, J. 1. Presentation at Opening
Plenary Session of the 3rd World Conferenceon Smoking and Health, in Proceedings of the.3rd World Conference on Smoking and Health,II. J. Steinfeld, W. Griffiths, K. Ball, & R. M.Taylor, (eds.), (U.S. Department of Health.Education and Welfare. Publication No. NIH77-1414). Washington, D.C. U.S. Govern-ment Printing Office, 1976, 21.
"U.S. DHEW. The health consequence's ofsmoking, 1975, (Publication No. CDC 76-8704). Washington, D.C.: U.S. GovernmentPrinting Office, 1975, 61.
"'Fletcher, C. M., & Horn, D. Smokingand health.
"Worick, W. W., and Schaller, W. E. Al-cohol, tobacco. and drugs. Englewood Cliffs,NJ: Prentice-Hall, Inc., 1977, 77-109.
19Dichl, H. S. Tobacco and your health. thesinoking controversy, New York, NYMcGraw-Hill, Inc., 1969, 47- 51.
=lay, S. J., Associate Professor ofMedicine, Indiana University School ofMedicine, Pulmonary Section, intervie.February 27, 1979.
'Essentials of life and health. New York,NY: Random House (CRM Books), 1977,86-87.
22American Lung Association. Chronicsmoking lowers rate at which the lungs clearmucus, Bull Am Lung Assoc., July-August,1977, 15.
"Newhouse, M. T. Effect of cigarettesmoking on muco-iliary clearance, in Pw.ceedulgs of the .3rd World Conference' on Smok-ing and Health. II. op. cit., pp. 131- 137.
24Diehl, Tobacco and your health, 87-95.25U.S. DHEW, The health consequences ot
smoking, 1978, ch. 6.26U.S. DHEW, The Smoking Digest, p. 28."Royal College of Physicians of London:
Snioking or health - the third report from theRoyal College of Physicians of London, Trent,England: Pitman Medical Publishing Co.LTD, 1977, 76-81.
'lay: op. cit.29U.S. DHEW. Report of the Surgeon Gen-
eral on smoking and health , 1964 through 1978."Diehl, Tobacco and your health, p. 202.
1160., 201-206.3 'Royal College of Physicians of London.
Smoking or health, pp. 121-122.33Worick and Schaller. Alcohol, tobacco and
drugs.14U.S. DHEW, The health consequences of
smoking, 1978, ch. 11."Speer, F. Tobacco and the nonsmoker,
Arch Eninron Health, 1968, lb, 443-446.36Burns, D. M. Consequences of smokingthe involuntary smoker, in Proceedings of
the .3rd World Conference on Smoking andHealth, II, 51 58.
'Tate, C. F. The effects of tobacco smokeon the non-smoking cardiopulmonary public, in Proceedings of the 3rd World Conferenceon Smoking and Health. II, 329-335.
38Aronow, W. S. Carbon monoxide andcardiovascular disease, in Proceedings of the3rd Wo-ld Conference on Smoking and Health,I. E. L. Wynder, D. Hoffmann, and G B.Gori, (eds.). (U.S. Department of Health.Education and Welfare Publication No. NIH76-1221). Washington, D.C.: U.S. Govern-ment Printing Office, 1976, 321-328.
39U.5. DHEW: The health consequences ofsmoking, a report of the' Surgeon General: 1972,(Publication No. HSM 72-7516).Washington, D.C.: U.S. Government Print-ing Office, 1972, 121-135.
"Colley, J. R. T., et al. Influence of pas-sive smoking and parental phlegm onpneumonia and bronchitis in early child-hood. Lancet, 1974, II, 1031- 1034 .
4 DHEW: The health consequences ofsmoking, 1975, 87- 106.
42White, J.R. & Frobe, H.F. Small-airwaysdysfunction in non-smokers chronically ex-posed to tobacco smoke. New England Journalof Medicine, 1980_302, 720-723.
'Turns, D. M. Consequences of snu.lk mg."Goldstein, H Smoking in pregnancy:
the statistical controversy and its resolution,in Proceedings of the .3rd World Conference onmoking and Health. 11, 201-210.45Longo, L. D. The biological effects of
ca rbon monoxide on the pregnant Worrhm,
71,!ST CUY Eir.:1:7,."
fetus, and newborn infant. Am 1 ObstetGym'col, 1977, 29, 69- 103.
47Dobbing, J. All flesh is grass, KaiserAluminum News: The World Food Crisis Man,Mind, Soul, 1%8, 2b, p. 13.
"Butler, N. I.., et al. Cigarette smoking inpregnancy: its influence on birth weight andprenatal mortality, Br Med I, 1972, 2, 127-30."Meyer, M. B., & Tonascia, J. A. Matemal
smoking, pregnancy complications and pre-natal mortality, Am I Obstet Gynecol, 1977,128, 494 -502.
"Butler, N. R., & Goldstein, H. Smokingin pregnancy and subsequent child devel-opment, Br Med I, 1973, 4, 573-575.
5 'U.S. DHEW: The health consequences ofsmoking, 1978. Preface, p. 5, ch. 1, 2, 3, 4, 6.
"Blair, G. Why Dick can't stop smokingthe politics behind our national addiction,Mother Ames, January 1979, 31-42.
Ro y a I College of Physicians of London;Smoking or health, pp. 43-44.
A4Olshavsky, R. W. No more butts - a psy-chologist's approach to quitting cigarettes,Bloomington, IN.: Indiana University Press,1977, 3.
"R oyal College of Physicians of London.Smoking or health, p. 89.
"U.S. DHEW: Teenage smoking-nationalpatterns of cigarette smoking, ages 12 through18, in 1972 and 1974. (l'ublication No. NIH76-931, Public Health Service) 1976.
"Seffrin, J. R. Risks, rewards and values,Health Values, SeptemberOctob.!r 1977, 1,197- 199.
" Eck holm, Cutting tobacco's toll, p. 19.p. 21.
"Califano Jr., J. A. A new commitment towellness, Bull Am Lung Assoc., November1978, 64, 5-.10.
"Health Insurance Institute, Sourcebook ofhealth insurance data, 1979-1980, Washing-ton, DC: Health Insurance Institute, 1979,47.
62Cancer facts and figures, 1981.p. 2.p. 1.
"Hill, H. Situational analysis: women andsmoking, in Proceedings of ..3rd World Con-ference on Smoking and 1 'h, 11, pp. 291-297.
"Frost, R. Complete poems of Robert Frost,New York, NY: Holt, Rinehart, andWinston, 1967, 131.
SO 67

36 TEACHING IDEAS
A Humanistic-IndividualizedApproach toDrug Education
JERRY L. GRE !NI is an assistant professorand PHIHIP C. HUNTSINGER is an as-sociate professor at health, physical edu-cationmd recreation at the LIniversitv ofXansas, Lawrence, 1sansas 660./5.
Many tea( hers individualize instruc-fion to sOille eXterlt ssith()1.11 realizing it bygiving spec al ulstrut tions to c edam stu-dents, by allowing Variety in student rolesin 0 lass, or by allowing work on ierentskills at ditterent times. this int !dualattention may he at the mpense I theother 51U dent 5 be( Just' the teat her's plandOeS not allow tor spe, LII pa( mg and in-volvement. 1 he problem Is to) mate anenvironment whit h will let the individualprogress thfinigh the learning programwith high degree oi selt-diret tion andinvolvement without impeding otherstudents.
the primary obi et IlVe ot thehumanistic-individualized approac h is toget the students involved in the learningprocess by doing and thinking with alltheir capabilities. It is up to the teac her tohelp students find the most produc tiveway to the student-tea( her agreed upongoals. This kind of approach should helpstudents learn the pro«.55 sell-education in addition to the sublet t mat-ter.
The following steps should be adheredto for implementing this teat hingstrategy:
Self-diagnosis: The teac her should de-velop this part ot the instruc tional unit sothat it is conducive to the student's modeof learning. See the diagnosis exert ises.
Prescribed a( in:ales: The leac her mustdetermine the kind and quantity ot inputand practice that students ()nip letebefore they c an Meet the desued oblec
Program ot learning c\perienc es: 1 his isthe total program ot ores( fibed experi-ences that the (eat her develops tor thestudents. It lin hides : Input these expe-rienct.2 allow the students to turther de-velop their competencies in areas shownto be weak by self-diagnosis. Output-these experiences will alto students todemonstrate the skills al knowledgedeveloped in weak areas af, strengthen-ing by input experiences.
Evaluation: The students and theteacher can determine if the learning ob-jective has been attained as a result of theinput and output experiences by analyz-ing specific performance objectives de-veloped for the unit.
68
We used this approach to teach drugeducation in the sixth grade, but it is eas-ily adaptable to a number of health educa-tion topics. In our class of about 30, thechildren had been exposed to qualityhealth education from grades 1 through5. The text used throughout the districtwas the Scott, foresman series. Thefour-week unit covered illegal drugs. Thelegal ones (alcohol, t affeine, nico(ine)were studied in other units.
Self-DiagnosisDirections: Read the questions and men-tally answer them. If you believe youknow the correct anFvver put a check inthe "yes- column. It you are not sure 01the answer or do not know, chec k the"no- c olumn. If you need to, check theat C uracy of your answers by comparingwith other students or with the teacher's
notes. It a question was answered in«ir-rec dr, hange your answer to the appro-priate
Can you-1 explain what the term "nart 061"means?2. define the term "halluc inogenic?"1. explain what the term "depressant-means?4, identity the meaning aSsmiated with astimulant drug?4. desc rihe a volatile substance?
c lassify the tollowing drug,: ltir), tran-quilizer, heroinwrosol sprays, "pep
7. dest rib(' how glue sniffing allec ts thebody?13. desc ribe the cliff eren«, between thephysical effects of stimulants and depres-sants?9. explain what effect a nart otit would
YUS NO
ha", on tbr, body?W. define drug abuse?I I. list ten reasons why people usedrugs?12. identify «munon household sub-stances that are ciangerous to the body?13. list ten slang terms assot rated withdrugs?
Prescribed ActivitiesDiret lions: Determine the number of
c het ks in the "yes" column. Now deter-
Addictive Behaviorsmine the percentages. To inc rease yourknowledge you may use the suggestedprogram of learning experiences recom-mended in the Input and Practu e col-
Results
More than 80%60 to 80%40 to 60%LPSS than 405.
Inputs
#1, 7, 8#1, 3. 7#1, 3, 5,#1, 2, 4,
7
5, 6, 7
Practices
#1, 7#1, 5, 6#2, 3, 4,#2, 3, 4,
65, 6
Progra.n of Learning ExperiencesDirections: The learner should follow
any or all suggestions in this program. Allof the experiences are designed to im-prove ability to motivate students for in-dividualized instruction.
Proposed lea rn i ng objec live : Thelearner will be able to develop a basicunderstanding of drugs and drug usage.
lnput1. Read Chapter 6, Health and Growth:I3ook 6 (Scott, Foresman series, 1974).2. Discuss why our culture is called a "pillculture.".3. Read a programmed learning unit ondri.gs and drug use.4. Discuss what role age should play indrug use.5. View the -Inside-Out" film series anddkcuss.6.Discuss the swpe of the lot al drugscene.7. Listen to a speaker troni a «mmt unityorganization that spec ialIzes in sonic' as-pect of drugs.8. Plan an input of your own,
Practice
. Write a report on drugs.2. Collect and post newspaper and maga-zine stories on drugs.3. Plan a role playing NO cm, showing howthe t harat ter Charlie Brown would de-so todav's drug users.4. Develop a bulletin board showingdangerous household substant es.5. Make a t roswvord pulzle using onlyslang drug terms.6. Draw something that would exhibitsymptoms of the influence of drugs.7. Develop a study guide on a t asWite torthe maim drug C Iassiti ahons.
Evaluationl'erforrname ObjecOses I he lea rner
will:I. Define the t lassification (it drugs.2. Understand the different ef fects of thevarious drugs.3. Understand the ditteren«, betweenthe use arid abuse of drugs.4. Know what common household sub-stances are dangerous to the body.5. Know the slang terms most often as-so( iated with drugs and drug use.

37 TEACHING IDEAS
Addictive Behaviors
r4P0PF
A
iambi
R\
W
Mg UseMations
BRUCE A. UHRICH is a former instructorin the Health Education Division at the Uni-versity of North Carolina at Greensboro. Heis currently a graduate student in the De-partment of Health Education at TempleUniversity, Philadelphia, Pennsylvania19122.
Under what conditions should theuse of a drug be regarded as acceptablebehavior in our society? To deal withthis question I have developed, over thepast two years, a series of statementswhich ,hallenge student values an,:stimulate classroom discussion I give.students a handout iNith the foliowingstatements and these directions: "Readeach statement carefully, then respondby rating each as an acceptable or unac-ceptable situation in which to use drugs.Be prepared to share each of your an .swers with the class, and to explainlyhyyou answered as you did."
Situation
1. Drinking an alcoholic beverage at aparty.
2. Drinking an alcoholic beverage afterwork to relax at home.
3. Drinking an alcoholic beverage be-
fore driving several hundred miles.4. Drinking an alcoholic beverage
alone after an argument.5. Drinking an alcoholic beverage at a
football game.6. Using a narcotic drug in a hospital
for relief of pain following an opera-tion.
7. Use of a narcotic drug by the headof a household in a lowersoc'oeconornic area.
S. Use of a narcotic drug by a physi-cian.Use of a narcotic drug by studentsin an upper class high school.
10 Use ot a narcotic drug as a cougnsuppressant.
1 Smoking tobacco in a high schoolrestroom.
12. Smoking tobacco after dinner.13. Smoking tobacco when meeting
new people at a reception.14. Smoking tobacco while riding in a
car pool.IS. Smoking tobacco in class.16. Using a sedative/tranquilizer to
commit suicide.17. lke of a sed ativelra nquilizer to
relax a neurotic personality.18. 1..!se of a sedativeitranquilizer to en-
courage sleep because of a loudroommate.Use of a sedativegranquilizer pre-scribed hy a physician and theodrinking heavily.
Q.
19.
2
20. Use of a sedative/tranquilizer torelax before having to make aspeech before a large group.
21. Utilizing marijuana at a dorm party.22. Using marijuana after work to relax
at home.23. Refusing when handed a ''joint" by
your best friend.24. Utilizing marijuana on a daily basis.25. Using marijuana before an in-
tramural softball game.26. Starting each day with a cup of caf-
feine, before anything else.27. Taking a "hit" of some stolen ni-
trous oxide28. Sniffing glue at a party.29. Taking aspirin every time vou feel
any pain.30. Reiving a patnlolling drug from a
paramedic for injuries at the sceneof the accident.
Because the choices are limited to theextremes of acceptable or unacceptable,most students are highly motivated toverbally ,luo:ity their feelings. This situ-ation allows the instrudor to act as atrue facilitator. For each ;tatement, allstudents indicate by snow of handswhich respcine *.hey chose. Severalstudents with acceptable and unacc.-pt-able rating are then asked to explaintheir i:hoice and supportive feelings.The result is class discussion, exposingail class members to a variety of opin-ions.
69

TEACHING IDEAS".111..
KAT! ft F I N HSCI IFR is a healthtea( her at the Orono Middle Sc hoot,long lake. Atinne,o1,1 She is nowit; her se, ond war of teaching andparticipat(1; m the program described here la,: summer
Haze/den (Center Citv. Minne-mtal. locatNl .10 miles northeast ofthe Twin Cities. is a treatment cen-ter for chemically dependent peoplc This was the setting for anin-service education program for 80educators this past Slimmer. Theprogram in cooperation with theMinnesota Departnwnt of Educa-tion, was funded by a grant fromthe Family Foundation Eightedit( alms per week welt, providedwith a "Ii\e in" exper;ence, par-ri:ipating in the full rehab.':tationProgram mth Patients and staffThe purposes Of the program wereto dev,gop a "gut le, al" feeling andattitude toward people with a de-pendency problem, to hecome moreaware of the causes of chemicaldependency problems, and to be-come aware that patients in treat-ment share the same basic needswith all men.
"God grant me the serenity toaccept the things I cannot change,the courage to change the things I,An. and the wisdom to know thedifference." These words have takenon a much greater significance forme now after having spent a weekat f.ta7eIden. The are words whichcan he found in every room the. ,
either inscribed on a wall ueor being verhaliied in group ses-sions. They ale one part of the re-habilitation program for the chemi-cally dependent person But what
' chemically dependent hereto a person who is dependent either onalcohol or drugs. Alcohol is ,:lso Con.sidered a drug. and it is cons dered inbe the. number one drug prob,ern in the(Ountty
70
Chemically Dependent
But Only for One Week
does this have to do with rehabili-tating chemically dependent peo-ple? During my "live in" experienceI was able to grasp the impact ofthat simple verse and its meaningto the entire program, and despitethe fact that I am not chemicallydependent, my experience wac real-istic in every other sense.
Eight of us, four women and fourmen, came to Hazelden as patient-observers. Our backgrounds in-cluded public school teachers, hihh¶;chool counselors, and psychiatricclinic: personnel. Each of us wasassigned a different unit as ourhome for the week, which wodldbe the essence of our experience.No two of us would have the sanwsituation, and yet we all would havegrappled with some intense feeling..at the end of our stay.
Hazelden is in a picturesque set-ting. The long driveway has a wayof quieting one's mind with a gen-tle peacefulness that all works for.,,r)od here. A patient's first con-tact with thz2 inside is the detoxifi-cation unit. Minimum stay in thisarea is at least one day, and mostpatients are eager to move to aunit as there is little to do here.
All of the treatment takes place inthe units, which are essentiallystructured in a home-like atmos-phere. There are three units fc:rmen and two for women. The onlytime all of the units are togetheris at meals and lectures, and thenno fraterni7ing is allowed. Thereason behind the no fraternizationpolicy is to prevent patients frombuilding up support groups whichwill set back their own rehabilita-tion. Our educator group, though,certainly appreciated the specialafternoon sessions we had together.It was the first time I had foundmyself in an environment where I
was the minority. And yet as theweek progressed we discovered wewere more alike than different.
83
Addictive Behaviors
Surprisingly enough, Hazelden isnot harboring a group of skid rowalcoholics. There is not a stereo-type for a chemically dependentperson. All of them are everydayreal people---many of the womenare housewives and mothers. Therewere young girls, quite a few olderwomen, and two nuns there at thattime. The number of older womensurprised me, but it was pointedout that today is as good a day asany to start living a better life.
Th2 day is rigidly scheduled forpatients; this is to in their treat-ment, for at some oint they mustagain start meeting these kinds ofresponsibilities. All three mealsmust be attended; each patient hasa work responsibility such as
vacuuming, cleaning the unit kitch-en, etc.; morning, afternoon, andevening lectures must be attended;and daily group therapy sessionsmust be participated in. The restof the day is spent reading assignedmaterials, meeting with staff, play-ing solitaire, sitting around the tabledrinking coffee and smoking ciga-rettes. (The cigarette consumptionincreases during a patient's stay atHazelden. This could be expectedsince they are attempting to alle-viate one problem at a time. Theever-present smoke, however, canbe quite overwhelming to non-smokers.) No recreational pursuitsare provided for patients. I foundthis confining for my usuMly inde-pendent nature, but the patient'spurpose for being there is not forhaving a fun time.
The entire program is based onthe Alcoholics Anonymous twelvesteps. These steps ba)ically requirea person to surrender control of hislife to a higher power (belief in Codper se is not a requirement), toconfess to oneself all one's fluitsand virtues, and to then confessthis to another person. When a pa-tient reaches the fifth step in theprogram he is then free to return

to the outside world. The staff de-termines when a patient is ready toproceed to the next step, and thiscan be anxiety-producing for somepatients who feel they are furtheralong than the staff thinks.
Upon arrival at Haze !den, pa-tients do not know how long theywill be staying there. The normalperiod of time is approximatelythree to Thur weeks, although somepatients may go into the extendedcare unit and remain up to a year.That unknowing fear can he a greatstress factor in the rehabilitation.Most of them want to make theirconfinement as short as possible,but occasionally one will find a pa-tient who has found Haze !den a
secure place away from reality andwould prefer to stay there. Few pa-tients fully realize the personaldepths to which their treatment willtake them. Within them are theanxieties, frustrations, worries andresentments which carried them tothe chemical escape they so desper-ately needed. Many of these peoplefor the first time in their lives arehaving to face feelings they havehidden for years.
Each patient is treateo accordingto his own personal needs. An es-sentia! part of recovery is learningto communicate feelings. Informalgroup therapy sessions aid in thistask. In these sessions, patients areforced through questioning by thegroup to open up about themselvesand get their true feelings out. 'Thegroup can become quite hard on aperson, and it is natural for peopleto avoid making responses that getat their feelings.
Patients do not nave a magicformula prescribed foi thern whenthey leave so that they will not goback to chemicals. But if treatmenthas been effective they have muchmore than magic, for they havegained a self-understanding whichcan lead to a fuller, happier life.The stresses and difficulties of dailyliving are always present, and this iswhere their belief in a higher powermust be strong.
The Haze !den experience is ex-tremely worthwhile in a personaland professional sense. All of us-.hould be given the opportunity tolook within ourselves. All who are
involved in the "helping" profes-sions deal with people every daywho are leading themselves to thebrink where they only have oncother out, and that may be chemi-cals. Each of us must t. P respon-sibility for sharing ou. own feel-ings and accepting these feelingsas real. In turn. thc process ofself-accepti. rice cLn then go forthto others. This nen will becomethe process we should use in pre-venting chemical dependency.
Our concern becomes that of the"feeling" life of people. Levi N.Larson, Education Director, NorthDakota State Department of Health,says the real hope of drug abuseprevention lies in meeting the emo-tional needs of peoplethe need tobe loved, to be heard, to be under-stood, the need to share feelings,the need to have meaningful com-munication with other people. Re-sponding to these needs is how weget people off drugs. In doing thksooner lies the hope of keepingthem from "getting on" drugs.
71

39 TEACHING IDEAS
Addictive Behaviors
Learning by Teaching
trv,m) st *uw.,iv$ t kt 0 .%1110,/ivIN)wr le-Aci/)hr \I)
A
\\14 ki k
Apr; eAri41(efr-lv"- IIINgiri....if, 4 4,4e1k- liort;
'1/47111*N:*q `it-6(17-k/ Nv!A 46, 411'-'*--e.:,..
ELAINE HALS is a teacher of healthand pi,ysical education at SouthShore High School in Brooklyn, NewYork. She is a new member of theSHR Editorial Board.
Drug education, an area of thehealth curriculum vital to highschool students, is an area that easilyturns young people off. They aretired of being preached to, moral-ized to, and lectured at. My dilem-ma was how to get the necessaryinformation across, without losingthe attention and interest of myhealth classes. I tried conventionallessons, contract teaching, and o(hermethods, but somehow still lostthem.
Last term I decided to let the stu-dents teach the unit to each other.I broke each of my classes into threecommittees and selected three ofthe most verbal members in eachclass to act as chairmen of the com-mittees. The committees were se-lected by me so that there would bean equal number of verbal peoplein each group.
The three committees were:1. Why drugs?2. The facts.3. Treatments available, includ-
ing overdoses and emergencyfirst aid.
In each class the committees hadone day in class and two days in thelibrary to organize their projects.72
The committees had complete lati-tude in handling their subject, know-ing that they had two days for theirpresentation. In cme class for ex-ample "the why" committee spentone day on adults and drugs, andone day on young..people and drugs.In the other clzess the committeedealt with drugs in advertising,sports, the school environment, andthe home. In both classes the com-mittee members asked questions ofthe class id involved them as partof the pres ?motion. When it becamenecessary I was able to add informa-tion, ask questions, or guide thecommittee and the class. The stu-dents made up and ran off their ownstelcils, some brought in music oftoday that concerns itself with drugs,and one group even made up a roleplaying situation (and used classmembers to act it out).
The role playing situation was asfollows: (a) parents waiting up forteenager to come home from party
young person comes homestoned; (b) reverse situation: teen-age boy or girl waiting for parentsto come home from a party--par-ents come home drunk.
This situation, and the discussicnthat followed, helped the studentslook at life for a moment from theirparent,' point of view, and to helpthem understand themselves interms of their tolerance for or.hers.The studenls listened to each other
anc1 were nonjudgmental. No valuejudgments were made, but the in-formation necessary for the studentsto make their own value judgmentsarid their own decisions was avail-able. This information was given tothem by a source that they werewilling to listen to--their classmates.
It was a worthwhile experiencefor the class, and for me. The stu-dents in my classes felt free to ex-press their opinions as well as theirknowledge. They had a chance tostep into the teacher's role for ashort while ano to see the class froma different point of view. The stu-dents received not only the neededinformation of the drug unit but ex-perience in working in a group andseeing their project through to com-pletion. The unit was more mean-ingful than if I had taught it.
After evaluation, the studentsfound some flaws: (a) people cameunprepared to give their reports and(b) people read long technical re-ports not meaningful to the class.In general, they favored this meth-od. As for me, I really got to hearabout and understand the drug"problem" from a young people'spoint of view.
This is an approach that I willuse again.
85

40 TEACHNG IDEAS
Aging: A Need
for Sensitivity
KENNETH A. BRIGGS is an assistant pro-fessor of lwalth education at the State Uni-veisity of New York, College at Cortland,Cortland, New York 13045.
With our culture's shift from reveringthe old t.) worshipping youth and thebreakdown of the extended family intoseparate nuclear units which usuallyexclude the elderly, a whole generationof young people are uneducated and in-sensitive to the eldedy and their needs.Comprehensive school health educa-tion, which seeks to improve the qualityof life through informed choices, is agood place to educate school age chil-dren about aging. It not only makesstudents more aware and sensitive tothe needs of the elderly; it also educatesthem for their own aging.
Following are some suggestions tohelp create an awareness and caring forthe elderly and their problems. Theseexercises help show students what it islike to old in a culture that treatssenior Lici lens the way we do.
Sensory DeprivationSimulation Exercises
The following simulation exercises tryto bring to the young and he a sen-sitivity to what it must be like to be Idand suffering from common sensory in-sults reported by the elderly.
Arthritis (reported by 33 out of RV el-derly)
Using cellophane tape, tape students'fingers together in various combina-tions, e.g., tape thumb and index fingertogether and the 4th and 5th fingers to-gether. Wrap elastic bandages aroundthe knees to simulate stiff knees. Havestudents perform simple tasks and thenshare their experitmces of what it mightbe like to be old and have arthritis.
Visual Handicaps (reported by 15 out of1(10 elderly)
Take sunglasses or laboratory protec-tive glasses and smear vaseline on themuntil you get your desired visual loss.Have students wear the glasses and per-form everyday things such as reading a
Aging
-aff:
4-'
menu or a newspaper, or look up thephone number of a pharmacy that willdeliver prescriptions to old people (ifthere is one). Have students record andshare their reactions.
Hearing Loss (reported by 22 out of 100elderly)
Place a cotton ball in the student's ex-terior ear canal. For a more pronouncedeffect, have them also wear headphonesor earmuffs. Have students listen to theTV or radio at a low level, or try to carryon a conversation with someone whohas no hearing loss and must shout at:hem to be heard. Again, have studentsshare their feelings.
Loss of Touch
Cover the students' fingers with rub-ber cement and after it dries, have themtry to thread a needle.
Loss of SmellHave students taste various foods
while pinching their nostrils shut.
Midtiphcity (polymorbidity)Certainly malc, elderly people suffer
from many ac,ing insults. They mayhave a hearing loss, arthritis, and a vis-ual handicar . To help students under-stand multiplidty and what it might belike, have several students performtasks with various combinations of the:above simulations. For example, onestudent can simulate finger arthritis,visual loss, and loss of touch and smell
F E
then go to the cafeteria and buy a cartonof milk. Upon returning, have the stu-dent share some of his feelings duringthe experience as an older person withsensory deprivation. Be sure to exercisenecessary safety precautions when stu-dents perform such simulations.
Songs and the Elderly
A lot of popular songs have been writ-ten recently that do a good job of devel-oping a caring sensitivity and awarenessof the elderly in listeners Following aresome examples of such songs and theirartists."Old Man" Neil Young"Old Friends" "Voices of OldPeople" Si111011 and Ga rfunkel"When I'm Sixty-Four" "EleanorRigby" The Beatles"Two Lonely Old People" Wings"Hello Old Friend" Eric Clapton"Lonely People" America"Good Company" Queen"Hello in There"Bette Midler"I Never Thought I'd Live to be 100""Travelin' Eternity Road" --MoodyBlues"Let Time Go Lightly" '.1arry Chapin"Father and Son" "But I Mighi DieTonight"--Cat Stevens
A nice touch to makc aging educationcome alive in the classroom is to addslides of old people to the music. It canbe quite powerful in creating sensitivityto aging.
73
Activities for Applicationand Discussion
Have students share some of theirfears about growing old.
Have students draw pictures of them-selves showing what they will be likewhen they are 100 years old. Whatlosses do they show?
Have students think of or photographthings in a grocery store that demon-;trate our insensitivity to the aged suchas, unit pricing numbers and prices thatare too small to read, bulk packaging,no carry out service.
Have someone in class carry on aconversation with another person inclass who has simulated speech prob-lems that follow a stroke by placing aping pong ball in his/her mouth.
Use the following opinionnaire togenerate discussion about the elderly.
Indicate to the right of each statementwhether vou agree or disagree.
1. Old people are better off living withother Old people.
2. Old people need rehabilitation.3. Rehabilitation is done best in a
nursing home.
74
4. .ixty-five is a good age at which toretire.
5. Old people live happier lives awayfrom the young, competitive world.
6. Old people should be kept active.7. Old people suffer a sense of loss
when their children leave home.8. Our society encourages old people
to be productive and useful.9. Old people should stay in their
own homes, if possible.10. Old people should le discouiaged
from dependent relationships withagency personnel.
11. Most older people are ready to restand don't want to be involved in "doingthings "
12. Old people cannot learn as well asyoung people because of deterioration ofthe brain associated with aging.
Take two pictures of, for example, astreet corner or the entrance steps to abus. One picture of your chosen sceneshould be in focus and the other shouldpurposely be out of focus. This willdramatically demonstrate the problemsencountered by those elderly who havea serious vision loss and the insensitiv-ity we have to these people by havingsuch things as "Do Not Walk" signs thatare too small to read.
We cannot overlook the most obviousand valuable resource of all the el-derly themselves. Bring the elderly tothe students or take the students to theelderly. Allow them to ask questions ofeach other, spend time together, andmost important of all, try to understandeach other.
Because of the nature of our modernsociety and quite often the insensitivityit carries with it for the elderly, healtheducation about and for aging that triesto reintroduce the elderly to those whomay be out of touch and insensitive totliii is imperative. Such education canbe valuable for the aged as well for allthose who may better understand theexigencies of the years to come.

41 TEACHING IDEAS
Picnic in the ParkHumanizing an Aging Unit in a
Personal Health ClassMICHAEL J. GAETA is a doctoral candidateand graduate teaching a sistant in the De-partment 4 Health Education, Oregon State
'niversity, Corvallis, Oregon 97330.
'-Audents in my Personal Health classht. d a ricnic in the park with 54 elderlyres'.ients from Heart of the Valley Re-t nent Center and Nursfitg Homet' ..p!ex in Corvallis, Oregor as the
1,itination of a unit on ar'ng. In plan-romg the aging unit I decided to design aprogram that would provide the stu-dents with an accurate knowledge baseof the biological, psychological, and so-ciological aspects of aging; and evenmore important, provide them with ex-periences that would sensitize them tothe realities of aging. At: of this was to beterminated in a picnic, a celebration oflife bringing the young together Mth theold.
"Ageism" is prejudice and disc;imina-tion leveled by one age group againstanother.' It is just as volatile and in; ust asother forms of bigotry such as racism andsexism. It is founded upon ignorance,myth, stereotypes, and fear. It results inalienation, despair, der ?.'vation, power-lessness, and even hL ,Llity. The onlyway to combat this prejudice is to meet ithead on with accurate information andexperiences that will demonstrate topeople of all ages how cruel it is to thinkof our elders as inhuman.
A total of six class periods were de-voted to the aging unit. We started thefirst class with Palmore's "Facts on Ag-ing" quiz,2 which covers basic facts andmisconceptions about aging. The quiztakes approximately 10 minutes to ad-minister, but stimulates much discus-sion about basic physical, mental, andsocial facts and most frequent mis-conceptions about aging. The quiz con-tains factual information documented byempirical data. This tool is an excellentresource that provides the students witha relevant vehicle for more clearly under-standing the multidimensional topic ofaging.
The second class was devoted to a cur-sory examination of the more commonand current biological theories of aging.The primary objective was to familiarizethe students with the present theory ofthe etiology of senescence. An excellentcornt rehensive review of the biological
.2ories of aging is found in the Handbookof the Biology of Aging. It provides an ex-cellent framework.3
In the third class session udents hadthe opportunity to discuss aging with a69-year-old senior activist. Several daysbefore the class students were instructedto write down any questions they hadabout any aspect of aging. The guestspeaker was given the questions a fewdays ahead of her scheduled talk so thatshe could more accurately ascertain theneeds and concerns of the students,
Sitting in a large circle with the class,the speaker answered questions and re-lated her philosophy of life so eloquentlythat the entire class was caught up in herbubbling enthusiasm for life. She sharedher feelings on everything from sexualityto death. After a standing ovation, thestudents without coercion lined up andone by one proceeded to hug and kissher as they left the class. R was obviousthat those students went away with amore positive and beautiful perspectiveon aging.
I.4111MMEIL-
,,z-.4-_
forewe
4,.--_
-
-c
Mow
vi
¶
8
Aging
The fourth class period consisted ofaging simulation games. With the helpand expertise of a gerontology professor,the students were divided into groups offive. Shoe boxes filled with parapher-nalia to simulate impairments broughton by the aging process were passed outto each group. Arthritir., visual, hearing,aphasic, and stroke impairments weresimulated as part of the exercise. Each"impaired individual" was given a taskto do alone. This was followed up by agroup task. These simulations enabledthe students to more realistically under-stand t;.e impairments and restrictionsthat many aged people live with ^achday. For an excellent review of agingsimulation games see Health EducationSeptember/October 1977.4
In clAss five a gerontological counseloraddressed the area of psychosocial needsof the elderly. The counselor em-phasized that we are all creatures ofneedto be fed, kept warm and dry, togrow and develop at our own pace, to beheld, caressed, recognized, loved andstimulated. While most people recognizethe importance of practicing and sub-scribing to these tenets in the early yearsof human development, many of usforget t :tat these needs must be met fromcradle to grave if we are to reach
111111Pan.
1". .0
14.0
cam. 413.
-111bp
4.
75

Gazette-Times PhotosBy Torn Warren
Laurence Garner, left. talks with studentMath Rabichaud.
Lunch in the parkThe 10 stir:lents in Michael Game's Personal Health class at Oregon State
had a special final examinationa box lunch in Chintimini Park with 40 resi .dents of Head of the Valley Center.
Jeanette Stoner. Rosemary Wick, Barbara Quinn and Cindy Miller enter-tained by singing to the senior citizens
Jeannette, who is a freshman preveterinarian student from Hood River,said students brought their own lunches and exchanged them with a senior.
"Ft was the neatest final I've ever taken," she said. "I used to be afraid ofgrowing old, but I learned from the seniors that they have a lot of fun, havehobb4s and really get around the community." She said she's also learnedhow they cope with arthritis, hearing and seeing problems.
.. 4,..1.1tirrOr 'XISle.._
M . rva,,,iii.
kf, ,..,
11111.111...-Youngsters and oldsters soak up the sunshine.
_
wrNWA
fro
On Friday, June 21978, the
; Gazette-Times ofCorvallis, Oregonran this picture storyabout the classdescribed by Gaetain this article. Thephotographs on thispage were taken byTom Warren.
oarrPo
Danita Ruzic, chats with Cora Warner, holdln-, cup. at the picnic in Chintimird ParkDanita has been spending each morning at Heart of the Valley Center and produceda term paper on her experiences.
76
Kimberly Koehler, lett, helps Marian Taylor 'Oh her picnic lunch
BEST COPY Ala.Z.E 9

optimum growth and ch elopment.This last session put the finishingtouches on preparing the students forthe picnic with the elderly.
Working in conjunction with the ac-tivities director from Heart of the ValleyRetirement Center and Nursing Homethe groundwork was laid fc,r the picnic.The picnic called for the exchange ofbox lunches with the elderly. The stu-dents were asked to prepare a lunchcomplete with treats not usually foundin an institution. Arrangements weremade through the administrator for theCenter cafeteria to pre-ide box lunchesfor the students plus lehionade and cof-fee tor the entire group.
The activities director took care ofpublicizing the event at the Center.Signs w placed in the elevator andon the bulletin boards notifying theresidents of the picnic. A list of poten-tial participants from the nursing sec-tion was compiled and these patientswere contacted and asked if they wouldlike to attend the event.
The park chosen for the picnic wacone block away from the Center so nobus transportation was necessary.However, since our group would haveto cross a busy str9et to get to the park,the Corvallis police were contacted andthey agreed to provide traffic directionand assistance.
The local newspaper was contactedand told of the picnic in the park. It wasthought that the publicity would begood for both the Heart of the ValleyCenter and the health education de-partment.
The day of the picnic was beautiful.The sky was blue, the sun was shiningand the temperature was pleasant. I ar-rived at the Center at 11:30 and foundpatients lined up in the lobby eagerlywaiting to depart. The police arrivedshortly thereafter and were given in-structions as to when we would departand what route we would traverse toreach the park. Within a matter of min-utes students started to arrive and webegan hooking them up with residentsfrom the Center. As I looked out of themain doors, the group of elders andstudents reminded me of a beautifulparade. A meeting of the young and theold. People with canes, some in wheel-chairs, all being escouted by students.Human beings that had been separatedby walls, not walls of wood or stone,but walls of ignorance and fear, weresharing love, food, talk, and compan-ionship. As I moved about the grouptaking pictures, I was amazed at the rateand quality of interaction that was hap-pening all around me.
Students with musical talents playedharmonica, guitar and sang to entertainthe group. Song sheets of old time fa-vorites printeu in large block type weredistributed and the whole group joinedin the merriment by singing songs,clapping hands, tapping feet, andlaughing.
After sharing lunch in the warm sun,gifts were handed out to the elderly bythe students. With the extra gifts stu-dents suggested that we have a contestand hand out gifts in descending orderfrom oldest to youngest. A 94-year-oldgrandmother won first prize.
f)U
Time seemed to fly by and before weknew it the time had come to leave thepark. On the way back to the Centertraffic was blocked up both ways onHarrison Boulevard, as students andresidents moved in a procession thatstretched from the park to the Center.Residents and staff from the Centerwere in the windows waving to ourgroup as we arrived.
The reactions from students and el-ders alike was unequivocally positive.No sooner did we get back to the Centerthan one elderly woman asked whenthe n xt picnic was to be scheduled.
Without any question, it was obviousthat many of the fears, myths, andstereotypes of aging were bashed downthat day. With a little bit of imagina-'ion, coordination, planning, and coop-eration, a picnic in the park on a sunnyday in May gave a group of personalhealth students the opportunity to learnfirst hand that aging is not all negativeand that old people are no differentfrom young people.
'Butler, Robert N. "Ageism: AnotherForm of Bigotry." Gerontologist, 1969, Vol. 9:243-46.
2Palmore, Erdman. "Facts or, AgingAShort Quiz." Gerontologist, 197', Vol. 17, No4.: pp. 315-20.
3Finch, Caleb E. and Leonard Hayflide(eds.) Handbook of the Rio;ogy of Aging, VanNostrand Reinhold Co., New York, 1977.
4Briggs, Kenneth. "Aging: A Need forSensitivity." tieatt'i Educatim.. Sept./Oct.1977, pp. 37-38.
77

42 TEACHNG IDEAS
HEALTHANAGaAMSKATHLEEN M. SIEGWARTH is instructor.Department of Health and Physical Educa-tion, Bowling Green State University,Bowling Green, Ohio 43403.
Health educato7s realize that the tech-niques used in teaching can serve ascatalysts to the material being presented.One way to help students learn abouthealth care specialists in the communityhealth unit of the health education curnculum is with anagrams. The procedureconsists of using handouts containinganagranns. which when properly un-scrambled spell out occupations n thehealth care profession. They are con-structed to read as names. Under the cap-tion "My Name Is" the anagrams arelisted in columns and opposite is a column headed by "My Occupation Is" withappropriate blanks. Periods are not to beconsidered in translation, but all lettersmust be used.
Example:My Name Is My Occupation Is1. Stu Coil 1.
The correct answer is ocuhst.Here are several ways this idea might be
used in class.1. Distribute the sheet one week priorto the scheduled lesson dav. Make it anindividual contest whereby the studentwith the most correct answers wouldreceive recognition as determined bYthe teacher. In case ot a tie. a 'playott-would be held in class. New wordswould be put forth and a time limit set.When time expires the one with themost correct answers is the winner.Hay'. the other students work the sameproblems. They then can offer any an-swers missed by the contestants andrate their own accomplishment.
78
2. Divide the class into two teams.Have each group elect a captain who isresponsible tor recording the solutionfor each anagram and serves as theirspokesman. Allow 30 minutes for eachteam to work. Validate the answers be-tween the two teams at the end of thetime limit. The team with the most cor-rect an<wers is the winner. Should a tieock. a playoff is held immediately,with a five minute time limit.
3. Group anagrams into similar cate-gories. For example, psychiatrist, psy.
chologrst, and analyst. This enables theteacher to distribute them during theunit in which they are pei tinent.
4. Release the anagrams in groups otfive or ten daily over a one to two weekperiod. Answers to the prooleins maybe turned in the next day and new onesdistributed. A winner is declared atterall answers have been submitted.
Consumer HealthFollowing is a list of 45 anagrams with
the appropriate answers.
1. Heston Sahsgole2. Les G. Trail3. Lenore Vut4. Sandie Sure5. Togol I. Scadir6. Hope Toast7. Lod N. Stouge8. Tobias T. Nicer9. Phil 0. Mostogoth
10. Patti Goolsh11. Nate I. Picidar12. Chris T. Stipay13. Sol Goitur14. Gail T. Sodoir15. Gib 0. Loist16. Tania M. Tornds17. Tad I. Porsit18. Seth Doorpit19. G. 0. Nurse20. Rod Ryle21. Ted Tins22. Thor Stondolt23. Ricator Porch24. Gipsy T. School25. T. S. Chime26. Tod Roc27. Unis T. Tortini28. Patricia Pylsthesh29 Nyle G. Gostico30. Thom Toilgoes31. Scott Golly32. Nat I. Eidic33. Stanlie Chet
Comlodig34. Caine Y. Xanchirt35. Peter Lance
Grantitoir36. Toni Pnceset37. Mort G. Sealdito38. Mic A. Prade39. Sy A. Lant40. I. N Rent41 I. C. Shypain42. R. E. Sun43. Pam C. H. Stair44. Mone T Topst45 Cher F. Raser
AnesthesiologistAllergistVolunteerNurse's AideCardiologistOsteopathNeurologistObstetricianOphthornologistPathologistPediatricianPwchiatristUrologistRadiologistBiologistAdministratorPodiatristOrthopedistSurgeonOrderlyDentistOrthodontistChuroprk torPsychologistChemistDoctorNutritionistPhysical TherapistGynecologistHemoh.iogistCytologistDieticianMedical
TechnologistX-ray TechnicianGeneral
PractitionerReceptionistDermatologistParamedicAnalystInternPhvsmanNursePharmacistOptometristResearcher

43 TEACHING IDEAS
Consumer Wellness,ONO School'sAPProach
ION W. HISGEN is a health instructor inwankee Public Schools, 210 Main
Street, Pewaukee, Wisconsin 53072 and aninstructor of consumer health for the Uni-versity of Wiseonsvi, Milwaukee.
Every year I instruct my consumerhealth units at the seventh and ninthgrade levels I am made acutely aware ofpeople's trusting nature. In this "creditcard culture" where we exist, instantpleasures are a signature away. There isno better example of this approach toconsumer decisions than in the world ofhealth products and services. Weblindly use hit or miss tactics in every-thing from wiping out those unsightlyblemishes with steam to strengtheningour rectus abdominus muscle with elec-tric belts.
The condition of wellness is a combi-nation of many interacting forces, in-cluding the individuals' environment,their reaction to it, associations, psy-chological background, Nicl ability toaccept attitudinal change. Today'shealth consumer is more likely to facethese forces after his/her health hasbeen threatened in some way. Con-sumer wellness is not an easily acquiredstatus but must be learned.
My initial seventh grade consumerhealth activity is to sell each student abottle of Dr. Lernke's Stomachic Dropsusing a stereotypical medicine man ap-proach. The following is an example ofthe pitch I use to convince the class theproduct works.
1. I tell students about a college assign-ment to recreate a medicine from an oldmedical text.
2. I chose Dr. Lemke's drops because ofits advertised ability to cure both acne prob-lems and split endb (7th grade concerns).
3. The mysterious ingredient is cap-sicum that must be inported from Africaand grown hydroponically.
4. I finished making the product in twomonths and successfully field tested it on myfriends and myself.
5. I unsuccessfully asked for supportfrom the AMA and Bristol Meyers.
6. I decided to market th2 productthrough magazines after receiving a patenton the product.
7. I bought a factory to grow capsicumand produce Dr. Lemke's drops.
.
8. Sales have increased each year for thelast three years.
9. Famous people have endorsed theproduct (the Osmonds, the Jackson Five).
10. A local newspaper is coming to takeadvertising pictures of students holding theproduct.
11. If the students bring the money nexttime we meet, I'll give them a special offer oftwo bottles for the price of one.
Over the past five years around 91%of the students have agreed to bring thecost of the product the next day while infact 70% actually did. When I tell thestudents that a cruel hoax was playedupon them the following responses canbe heard: "I'll never trust you again.""We thought you were above that.""Well, you certainly made me lookfoolish." "I was just playing along withyour little same."
The alarmingly high number of gulli-ble consume.-s pointed out the need for
1111111111111111111111°"111"41101W, 04.fr
M E S
00 5Piimaim:
Consumer Health
some direction in our consumer healthprogram. Out or this we instituted aconsumer health program entitled WISEMAN.
W iseI independentS afe/ef fectiveIi villuate
Aotivatewareotable
Each of the letters represented a com-petency we wanted our students tohave by the time they left our healthprogram.
1. The student will be able to ...rake wiseand careful decisiorc about the consumerproducts and services he/she uses (consumerhealth protection).
2. The student will be able to make deci-sions independent of outside influences (e.g.advertising, pseudo-science, etc.).
3. The student will be able to chooseproducts and services that are both safe andeffective.
j; F
4. The student will be able to evaluate newand existing health products and services(the work of government agencies, insuranceprograms, alternative medical practices,etc.).
5. The students will be able to niotivateothers in their present or future family tomake wise consumer health decisions (well-thought out family medicine chests and firstaid kits).
6. The student will be aware of pitfalls fac-ing the consumer of health products andservices (quackety, superstitions, fads, andfalla cies).
7. The students will be able to make nota-ble savings in their consumer health budgetand notable improvement in their overallwellness.
Our school's consumer health pro-gram is based on these competencies. Acopy of our consumer health curriculumand methods guide can be obtained bywriing the author.
79

44 TEACHING IDEAS
A HealthyConsumerHealth Class
TOM MO-ARLAND is a consumer educa-tion specialist at the family Life EducationCenter, Toledo Public Si hoo/s, Toledo,Ohio 43604. ANN RLIDRAIJI f is educativeservices specialist for tVGT1 -TV, Channel30, in Toledo.
Our experience has shown that themost succ essful way to teac h consumerhealth is to throw out traditional c lassesand have students learn by doing, usingthe community as a classroom. Most ofthe learning experiences we desc ribe areoriented toward high sc hool or collcgelevel but adaptations c an be made to sUitvarious sc hoof aged or «mini unitygroups.
Advertising
Thorough understanding of how ads er-Using works Is necessary for the con-sumer health student. Scum, suggestedat tivities are:
Ad substantiation campaign. Slifvevlocal media tor advertisements ot healthand beauty produc Is. Printed ads c an bebrought to c lass; radio and TV ads c an betaped tor disc ussion. Many ad agem ioand TV and radio stations throw awaytheir tapes and layouts and are hal,py tosee someone get sonw use I rom them.
Claims made in the ads aro sc rutinizedand some are selec ted tor analysis. `tu.dents write ompany president,- and asktor tactual substantiation ot the adver-tisement. lliis is examined to see it the
laim justified. lhe information gath-ered c an he shared with c lassmates andc an be made public .
Counter-xis Sinc e adwrtising is obvi-ously biased. «msumers deserve to hoarthe other side of the stor. prepare ounter-ads SIR h as. "aspirin Is allthe same, it may 0 ause internal bleed-ing." A visit to an ad agem y or asking anadvertising man in as guest instrut tor c anheft) students prepare their ads. Studentsshould then try to get Inc al media to usetheir counter-ads as public st.rvic e spots
fraudulent chanties. Most ol thefraudulent groups a..c. «mtered aroundrowan h in disease prevention and c tire,and they have bilked «msumers out otmillions of dollars. In this projec t to ex-
80
pose suc h operations, students paint andlabel empty coffee ans with "AmericanCancer Center. "National Sc hoot torI Newt( S'. or some other phony healthagency name. Working in pairs, the stu-dents take money and write downpledges. After c ounting the money, it isreturned to donors with an explanation.This activity should be widely public izedso that they can learn without being un-ne«.ssarily embarrassed. More peoplewill know they should check before giv-ing.
Health Insurance
Health insurance is a crucial issueabout which few con sunwrs have a work-ing knowledge. One way to identify andprobe health insurance issues is by valuesclarification tec hniques.
Voting an pertinent questions. Howmany of you have health insurance? Howmany are covered under a family policy?How many are covered under a grouppolicy? How many have Blue Cross-BlueShield? How many can list the exclusionsin their policy?
forced choice questions. These helpstudents decide which alternative theypret er: private medicine or socializedmedu me; unnecessary luxury or neces-sity? Students can vote hy moving toeither side of the room, then find some-one there to disc uss.t he reasons for theirdec ision. The teacher can design ques-tions to bring out important points to bedisc ussed.
Values continuums. Use to emcm ragepartic 'nation m discussion ot Ulrrent is-sues related to health insurance. Healthcosts are: too highjust right----too low.Medicine should be: socializedtotallyprivate. Health insurance is: a wasteallright cruc ial. I usually block out thec enter et the continuum to discouragestudents who ond it too easy to be indii-terent.
Rank order I) List motor exclusionstound in insuran«, pohc ws. Rank in orderof danger to «msomers. 12) list ways tolearn about health insurance and rank inorder ot preference. leo( hers c an useIlus list in planning c lasses. Ist typesot health insuranc e coverage, and rank inorder ot importance to the consumer orin order ot expense, suc h as: basic hospi-tal. major medical, dental rider, materiutybenefits. Students can share theirahonalvs tor rankings in groups of three.
Price Comparison Research
1 hese researc h results c an s'ied mu( hlight on luture buying prac ti«,s. A «,daintype ot prodmt is selected tor study by
9 3
Consumer Healthgroups ot students. Types of health prod-ucts good for study include: prescriptiondrugs, over-the-counter drugs, perisha-ble foods, cosmetics, or food sold in ahealth food store.
After groups are formed, students phnto visit a variety of stores such as a chainfood store, small pharmacy, and disc ountstoye. Pri.:.es may vary depending on loca-tion of the store, so encourage studentsto visit suburban, rural, and urban areas,it possible. Items to he price-chec kedshould be standardized by brand, size,weight, count, or whatever, so results willbe «wiparable and a« u rate.
Groups can make c harts to depict theirresults, analysis 01 data, and conclusions.Presentations to the whole c lass shouldhe made.
Health Practitioner Interviews
The teacher can assign job clasifica-tions or let students select the one theyare most interested in, t J go out andinterview someone in that area. Severalpossible candidates are listed under"guest speaker" later in the article.
Make sure students are aware of how tocontact people, set up in terviews, a nd askpertinent, interesting questions. Roleplaying in the classroom before the inter-view will give confidence to carry out theproject successfully.
Follow up activities inc;ude: oral re-ports, role play, group comparisons ofcategories, mock debates with studentsplaying the role of the person inter-viewed, and so 001.
General
Guest speakers. A wealth of informa-tion can be provided to students by out-side experts. This is especially helpful iftield trips are not within the budget.Tea( hers can call on a wide selection of«mimunity people inc luding:Health practitionersdoctors, pharma-o ists, paramedic s, nurses, public health()Moak, nutritionists.Governmental or voluntary agencies--Better Business Bureau, Consumer Pro-le( bon Agency, Post Ottic e. local healthdepartments, civic groups.ducators --university health staff , con-
sumer specialists. other teac hers f rumthe 5( hool.Businessinsurance agents, f ood pack-ers, advertising agencies, credit bureaus,health bond store owners, «)smetolo-gists, lawyers,
ft a speaker s time is limited, tape thepresentation for the rest of the classes.Invite several guest speakers at onc e to

form a panel or have a debate on a giventopi( . Preparing the speakers and stu-dents ahead ot time and following upmakes this more effec tive.
Pretest. Thk is a good way to assess thegroup's knowledge, mis«m«Ttions.ba( kground, values, and behavior. It ( anhe used to learn what the students wantto know or as a springboard tor disc us-sion. II the lest includes «mtent-hased
information covering the entire worse, it( an he used as tl posttest.
Some sample questions are:1. Content-based items (true or falso-1 oothpastes are necessary for good den-tal health; the best relict 01 arthritis painis p rest ription drugs; gargles or mouth-washes are not ettettive treatment iorsore throats. 2. Attitude and behavior-based items I see a do( ton and a dentist
at least Om e a year; I am adequately cov-ered by medical insuram e; I have a good( recto "4. 1. Unfinished sentencesIsp v.1 :ley loutishly on ;
,op around forsperiment with some (it the a( tivities
des( nhed here; adapt and appls them toour own teac hing situation. Remember,
an involved ( lass is a 'healthy"" lass.
9 4 81

45 TEACHING IDEAS
Consumer Health
The Teenage Consumer
LEE ANN LARSON is a 7th and 8th grade health teacher atthe Dexter McCarty Middle School, Gresham, Oregon.
The marketplace iswide open to today's teenage con-sumer. As the target of constant bombardment by adver-tisers, the teenager with access to money is in the posi-tion of making decisions with very little information.Health products, in particular, appeal to the teenagerwith their promises to beautify. Although informationfor the student in this vital area hard to find, I teach aunit with seventh and eighth graders to develop aware-ness of consumer health educati Dn.
To understand any new body of knowledge familiaritywith the terms that relate to that area is necessary. Thestudents' first task is to find definitions of appropriatewords. We use health books rather than dictionaries togive students specific subject definitions rather thangeneral definitions which they may have trouble apply-ing to topical situations. This list of words introduces theunit:
bait and switchcode-dating systemcomparison shoppingconsumercosmeticdentifricefraudindirect lic
medianostrumpatent medicineproductproprietary compoundquacktrademark
The students next investigate some far ts about theirrole as consumers. What is the history of health prod-ucts and services? What about the "medicine man" ofthe old west and his cure-all drugs? How are his claimsdifferent from or the same as advertising that we mighthear or see today? Students investigate how advertisingaffects the consumer and just how much advertising isdirected at their age group and why. They take a look athow Americans spend their health dollar, and of totalincome how many of their dollars are spent for healthproducts and services.
Middle-school students are still SN u re with thethought that if they get sick or hurt their parents or someother adult will make sure they are taken care of proper-ly. 'This unit's lessons present them with situations andfactual histories in which they must make sonie deci-sions of their own. What if their doctor tells them thatthey have a disease which cannot be cured, but theyread about a doctor who can cure the disease? What ifthey are told they have cancer of the leg and it must heamputated, but someone knows of a doctor who has acure for cancer? The possibilities are endless and the
82
cases do not even have to be so dramatic. This leads toan investigation of quackery and a realization that theyare one of the prime target groups because of theirsusceptibility. Mail-crder quackery traps them with itsglamour and seeming privacy of the postal system. Theyget involved with researching training, signs, and resultsof quackery.
Students can become pretty outraged about whatquacks are "getting away with." At this point, studentsinvestigate some of the organizations working in someway to protect the consumer from fraud. They study theFood and Drug Administration, Federal Trade Commis-sion, U.S. Postal Service, American Medical Association,Consumer's Union, and 1.:etter Business Bureau.Throughout the discussions, students are reminded thatthese organizations are handicapped by their de-pendence on consumer complaints to act. If the con-sumer is too ashamed, too af raid, or too lazy to report anincident or complaint, other unsuspecting consumerswill be subjected to the same treatment by a fraudulantperson or company.
Even if students have some information on quacks andthe groups which protect the consumer, they are still leftwith the problem of what to look for in good medicalservices. Investigation continues with some of theguidelines to follow in selecting a physician followed bya review of specialists (pediatrician, general prac-titioner, internist, surgeon, psychiatrist, etc.). Studentsneed to look for the physician best able to handle theirneeds at various stages in life. An increasingly importantaspect of medical service is that provided by hospitals.Students try to find out what kinds of hospitals exist andwhat questions should be answered before choosing ahospital.
The next project gets students involved in investigat-ing a product. With school funds, I purchased threebrands of several products from a discount store, addinganother price to the label from a regular grocery store ordrug store. The products used were aspirin, toothpaste,shampoo, deodorant, vitamin tablets, ready-to-eatcereal, arid acne preparations. Knowing seventh andeighth grade students, I emptied all of the containersbefore using them in the ( lassroom. The class arrangeditself in groups to provide an equal number to work oneach product. To make it somewhat fair, each groupdrew a number to indicate its turn at choosing a product.Once the preliminaries were settled, each group re-ceived a form on which to write the information to pre-sent to the class. The questions include:
1. What is the history of the product? (Where did itcome from? \Vho found it and how? How long has itbeen around?)
5

2. What are the ingredients as they are listed on thelabel of the product?
3. What are tne uses for the product as listed on thelabel?
4. Can this product cause any harm? (Not only theparticular brands they are investigating, but any otherbrand of the same product. In most cases this informa-tion is not on the label so they will have to do furtherreading.)
5. Is any brand of this product better than others?Where did yp(t. find that information? (Students have a
tendency to rely on advertising, written or word-of-mouth, to make this decision. Encourage them to useresource materials to see if they can find reliable infor-mation.)
6. What is the price comparison for the product?(Comparing the same brand at two different stores, dif-ferent brands at the same store, and different sizes of thesame brand. I purchased the products, as much as pos-sible in the same size, but students sometimes take itupon themselves to check on other sizes.
7. What is the latest information about this product ? (Icollected all the information I could--magazine andnewspaper articlesabout a product and let the stu-dents decide what is significant enough to report to therest of the class.)
KitfseteMINNIMP
8. What do advertisements for this product look orsound like? (Students can cut ads from magazines toshow or report Ones they have heard on the radio orfrom friends, or seen en television.)
The reports to the class c:In produce more questions anofurther research plus a wealth of basic information.
One of the common concerns to come from this in-vestigation is the inadequate information found on thelabeling standards and new ones currently under con-sideration. Included in the unit are not only the productsinvestigated, but any product which may in some wayrelate to health and safety, such as baby cribs and toys.Thic, is also an excellent time to get into nutrition label-ing. A fun exercise is for students to design a label for aproduct, including all of the information they think isimportant for the consumer.
Another way to get students thinking about healthproducts and selections is to have them collect adver-tisements abc ut many different brands of some product.
After students decide which brand of the woduct isbest, using only the advertisements, each will tell howconfident he feels in his decision. The students will alsoindicate other information they would like tG ha..emake an even better choice.
83
46 TEACHING IDEAS
Crisis Hot Line Experience
ALOYSIUS I. IANGL is health educationinstructor and subject area coordinator atArds ley Middle School, Ards ley, NewYork 10502.
The emergence and impact of two rela-tively new mental health concerns, deathand suicide education, can be viewed asoutgrowths of the education system at-tempting to ensure healthy personalitydevelopment. Nevel.theless, mentalhealth areas within the health educationcurriculum are often neglected or poorlypresent I. Why? Perhaps the curriculumis largt_r fact-oriented with little accom-modation for the bulk of affective contentinvolved in mental health. The wealth ofemotions and attitudes combined withinexperience and/or fear of affectiveteaching may make some health educa-tors apprehens. de about such vital healthareas.
With statistics climbing, suicide is nowthe third leading cause of death amongyoung people between the ages of 15 and19, and it ranks first or second on collegecampuses. The area of suicide and its pre-vention should be of vital concern to thehealth educator. Suicidology, the scien-tific study of suicide, investigates themany complex causes leading individualsto self-destructive behavior. Research hasshown that cuicides are not spontaneous.There are dues that foreshadow this be-havior to which both educator and stu-dent alike can become sensitized. Armedwith this awareness and sensitivity, pre-ventive and rein forcing steps can betaken to help the individual. It is errone-ous to assume that handling suicidal be-
84
havior or any "abnormal" behavior is thepsychiatrist's or psycholohist's provincealone. Suicide prevention is not exclu-sively a medical or psychiatric problem.Health educators can operate within cer-tain limits in teaching and counseling.Moreover, they can help shoulder theirmental health responsibility by present-ing the essential facts concerning crisisbehavior in a meaningful way to their stu-dents.
The following is an example of an in-structional strategy that has been used ina middie school mental health unit deal-ing with crisis prevention and interven-tion. It may encourage other healtheducators toward more effective affectiveteaching and the rewarding experience ofhumanistic health education.
Behavioral Objectives for Students1. Cite particular situations which have
the potential for critical or self-de-structive behavior.
Consumer Health
2. Devise a reference list of persons,groups, or agencies that deal withsuicide or attempted suicide.
3. Identify clues in the individual's be-havior that suggest a need for consul-tation with a professional specialist ora need for other forms of immediatehelp.
4. Identify and suggest various _onstruc-tive alternatives and psychological firstaid advice.
instructional Materials1. Battery operated walkie-talkie; 50 ft.
extension.2. Record player with microphone and
speaker jacks; speaker with 50 ft. ex-tension jack cord; microphone jackcord.
3. Thirty or more dittos of Crisis Hot LineEvaluation Sheet.
CRISIS HOT LINE EVALUATION SHEET
InstructionsPlace the name of the student who is the crisis hot line operator in the numbered boxatop each column. While listening carefully to the conversation, check off, in thevertical column under each operator's name, the psychological first aid advice hesuggests.
PSYCHOLOGICALFirst Aid
NAME OF OPERATOR
1. 2. 3. 4. 5.
Listens attentively
Takes complaints seriously
Evaluates seriousnessof intention
Examines intensity ofemotional disturbance
Assesses resources available
Does something tangible
Affirmative, yet supportive
Asks directly about suicidalthoughts and intent
Not misled by passingsecond thoughts
Suggests personal orprofessional assistance
Thus eviluation sheet has been formulated from the article. -Ecological Aspec ts of Self.Destruction: Some legal,Legislative and Behavioral Implicat ons,- by Calvin Frederic k m Health and Human Values by Allure ,efcoat (JohnWiley & Sons. Inc.. New York, 19.7) pp. 172-80.
9 7

Instructional ActivityInstruct each student in the class to
write out a critical situation which wouldwarrant a call to a local crisis hot linecenter. Next, distribute a Crisis Hot LineEvaluation Sheet to each student. Selectone student who wishes to be the crisishot line caller and another student to bethe crisis hot line operator. The hot linecaller will be stationed outside the class-room speaking into the microphone, thusrelating the incident tu the entire classwithin the room via the extension
speaker. Only the selected crisis hot lineoperator will be able to respond withquestions, advice, or "psycholog;cal firstaid" via the walkie talkie, while the otherclass members listen and evaluate theoperator's performance on their sheets.Five to seven minutes of dialogue is usu-ally sufficient.
Follow-Up ActivityAfter the hot line dialogue, the per-
formances of both students are discussed
S
by class members through their evalua-tions arid any additional comments by theteacher. Two different students areselected and the activity is repeated. Atthe end of the period, the assignment forthe next class is given: (1) to list all thepersons, groups or agencies mentioned,dealing with suicide or attempted suicide(2) to list any verbal or behavioral cluesthat indicated or implied any self-destructive behavior on the part of thecrisis hot line caller.
85
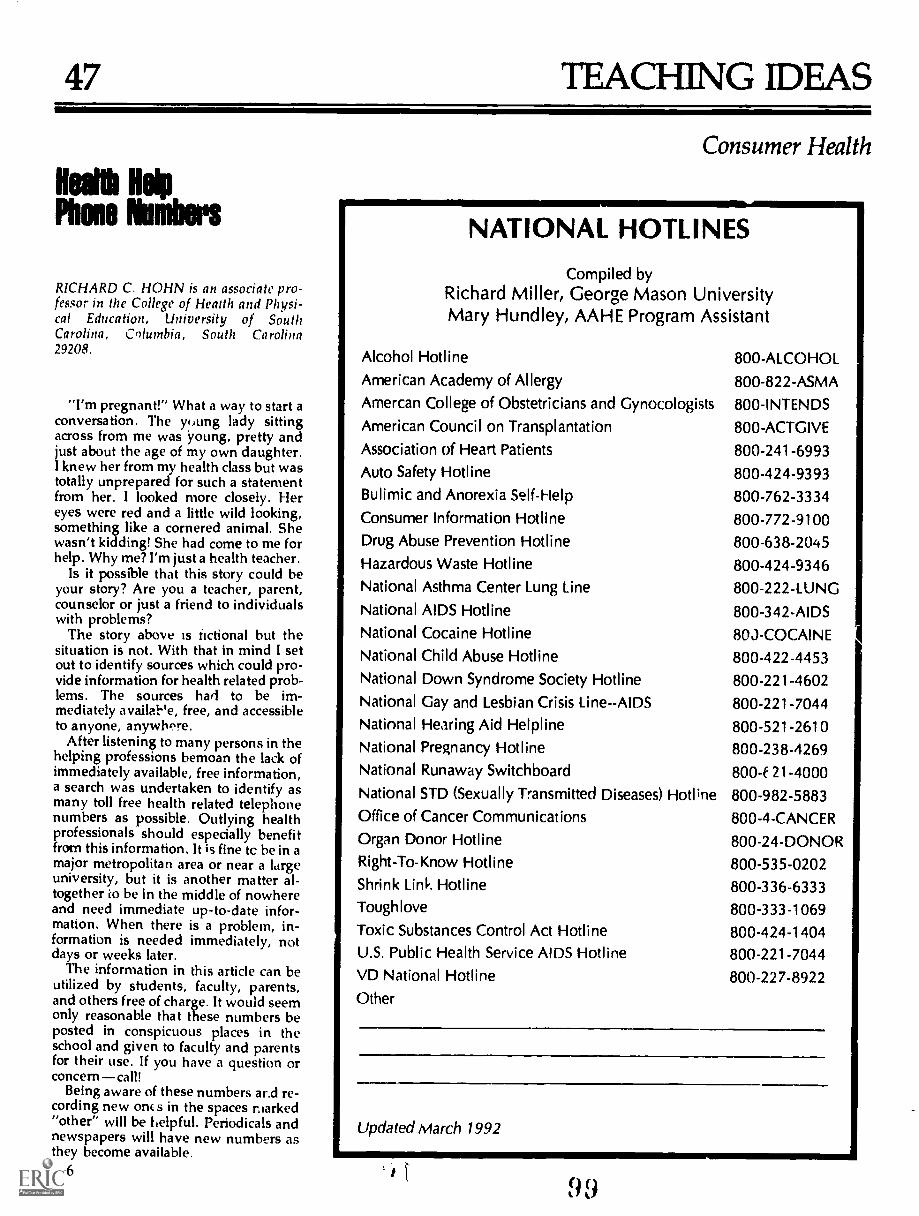
47 TEACHING IDEAS
Health HelpPhone Numbers
RICHARD C. HOHN is an associate pro-fessor in the College of Health and Physi-cal Education, University of SouthCarolina, Columbia, South Carolina29208.
"I'm pregnant!" What a way to start aconversation. The young lady sittingacross from me was young, pretty andjust about the age of my own daughter.I knew her from my health class but wastotally unprepared for such a statementfrom her. I looked more closely. Hereyes were red and a little wild looking,something like a cornered animal. Shewasn't kidding! She had come to me forhelp. Why me? I'm just a health teacher.
Is it possible that this story could beyour story? Are you a teacher, parent,counselor or just a friend to individualswith problems?
The story above is tictional but thesituation is not. With that in mind I setout to identify sources which could pro-vide information for health related prob-lems. The sources hart to be im-mediately availal-'e, free, and accessibleto anyone, anywhere.
After listening to many persons in thehelping professions bemoan the lack ofimmediately available, free information,a search was undertaken to identify asmany toll free health related telephonenumbers as possible. Outlying healthprofessionals should especially benefitfrom this information. It is fine tc be in amajor metropolitan area or near a ldrgeuniversity, but it is another matter al-together ko be in the middle of nowhereand need immediate up-to-date infor-mation. When there is a problem, in-formation is needed immediately, notdays or weeks later.
The information in this article can beutilized by students, faculty, parents,and others free of charge. It would seemonly reasonable that these numbers beposted in conspicuous places in theschool and given to faculty and parentsfor their use. If you have a question orconcerncall!
Being aware of these numbers ar.d re-cording new oncs in the spaces marked"other" will be helpful. Periodicals andnewspapers will have new numbers asthey become available.86
Consumer Health
NATIONAL HOTLINE;Compiled by
Richard Miller, George Mason UniversityMary Hundley, AAHE Program Assistant
Alcohol Hotline 800-ALCOHOLAmerican Academy of Allergy 800-822-ASMAAmercan College of Obstetricians and Gynocologists 800-INTENDS
American Council on Transplantation 800-ACTGIVE
Association of Heart Patients 800-241-6993Auto Safety Hotline 800-424-9393Bulimic and Anorexia Self-Help 800-762-3334Consumer Information Hotline 800-772-9100Drug Abuse Prevention Hotline 800-638-2045Hazardous Waste Hotline 800-424-9346National Asthma Center Lung Line 800-222-LUNGNational AIDS Hotline 800-342-AIDSNational Cocaine Hotline 803-COCAINENational Child Abuse Hotline 800-422-4453National Down Syndrome Society Hotline 800-221-4602National Gay and Lesbian Crisis Line--AIDS 800-221-7044National Hearing Aid Help line 800-521-2610National Pregnancy Hotline 800-238-4269National Runaway Switchboard 800-f 21-4000National STD (Sexually Transmitted Diseases) Hotline 800-982-5883Office of Cancer Communications 800-4-CANCEROrgan Donor Hotline 800-24-DONORRight-To-Know Hotline 800-535-0202Shrink Link Hotline 800-336-6333Toughlove 800-333-1069Toxic Substances Control Act Hotline 800-424-1404U.S. Public Health Service AIDS Hotline 800-221-7044VD National Hotline 800-227-8922Other
Updated March 1992

48.11.1111M.
TEACHING IDEAS
Consumer Health
Students Can Have a Say
JOAN L. BERGY, formerly a consumer specialistwith the U.S. Food and Drug Administration inSeattle, Washington, became on September 4,1973 the director of the Seattle Area Office of theU.S. Consumer Product Safety Commission.BARNEY HANTUNEN is the regional public infor-mation officer, Public Health Service, Departmentof Health, Education, and Welfare, Region X,Seattle.
A student voice in government rule-making? Aconsume, voice in government rule-making? Im-possible, you say?
Not rea::. if you look into a little known pub-licationthe Federal Register. Studentscon-sumerscan have an impact on, for example, theselection of the route for the proposed PacificCrest National Trail, the labeling of cosmetics, anda whole host of planned federal actions whichaffect all aspects of our daily lives, if they learnabout this publication and are willing to takeaction.
The Federal Register is a legal document pub-lished Monday through Friday by the Office ofthe Federal Register, National rchives and Rec-ords Service, GSA, Washington, D.C. 20402.
The Federal Register provides a uniform systemfor making available to the general public regu-lations and legal notices issued by the ExecutiveBranch of the federal government. Also includedare Presidential proclamations and ExecutiveOrders as well as various federal documents re-quired to be published by Act of Congress.
The format used to present regulations in theFederal Register includes:
... A preamble which reviews the background ofthe proposal
... A statement of the proposal
... Information on the procedure for submittingcomments
Where comments should be forwarded... The deadline date for receipt of comments
Following the expiration date the federal agencyconsiders all comments and takes action. The ac-tion may be in the form of a "final order" printed
in the Federal Register, including the effectivedate for the regulation.
A new requirement now makes it mandatorythat every "final order" is to include a summaryof the types of comments received and whetherthe "final order" includes, rejects, or modifiescomments received. In any case the "final order"must include the information on which the deci-sion was based.
The process of rule-making begins after Con-gress passes a law and the President signs it intolaw. Then, it is the responsibility of the federalagency charged with carrying out the law to pre-pare appropriate regulations to implement theiaw. Preparation of regulations is a complex andtime-consuming task. However, once that job isdone, the regulations are printed irl the FederalRegister.
This is the critical point. Usually 60 days areallowed for comment. This is the time when thestudent--the consumer--will have the opportu-nity for reacting to Ind commenting on the pro-posed set of regulations. It is also possible tochange current regulations by the rule-makingprocess. An individual or any group may petitiona federal agency to propose a change in regula-tions.
The system falls short, however, when con-sumers do not participate. More often than notthe number of comments received in response toFederal Register proposals is very limited.
In March 1973, as an example, FDA publishedin the Federal Regi.ster a proposed change in reg-ulations that would require cosmetic ingredientsto be listed in descending order of predominanceon labels attached to each cosinetic product. Thep.oposal specified details about the label design,language to be used, size of print, as well as fra-grances, coloring, and flavoring used in theproduct. As of May 1973, the sources of com-ments were as follows:
Cosmetic industry and associations--19
... Professional organizations-1
Universities-3... Other federal agencies-1
1 (4 87

... Organizations-5
... Individual consurners--267
A second example is the proposal to requirea warning statement on the labeling of aerosolcontainers, which wa. published in the FederalRegister during March 1973. One of the severalproposed warning statements was: "Warning:Do not inhale directly; deliberate inhalation ofcontents can cause death." As of May 1973, thefollowing summarizes comments received:
... Aerosol industry and associations-21
... Organizations-2Universities---5
... Consumers-1
It should be pointed out that the Federal Register is not the easiest document for the studentor the consumer to locate. It is available from theSuperintendent of Documents, Government Print-ing Office, Washington, D.C. 20202 at a cost of$3zi0.00 per year; single copiec cost $1.50 each.Mo libraries stock the publication. It is also gen-eraly available through libraries maintained byfedel.al agencies in the Regional Office cities ofBoston, New York, Philadelphia, Atlanta, Chicago,Dallas, Kansas City, Denver, San Francisco, andSeattle.
From time to time proposals published in theFederal Register are included as news items inlocal daily newspapers. However, more often thannot very little information .s included to guide thestudent or consumer in submitting timely com-ments to the appropriate place.
So how can students become involved? Howcan they gain access to the "system" of federal
88
rule-making? How can they gain a perception ofthe process which will stand them in good steadas they move from academic community into thecommunity at large?
A prerequisite, of course, is availability of theFederal Register in the classroom or the schoollibrary. A committee of students might review theFederal Register for a period of time in order toselect a proposal for class consideration.
Once the proposal is selected, the committeemight develop information and perhaps a demon-stration project to illustrate to the class what thepresent regulations are and what changes are con-templated in the proposal. In addition, the stu-dents might analyze proposed changes in theregulations and their effect upon industry, theconsumers, and others concerned with the sub-ject under consideration.
Upon reaching a consensus and having recon-ciled various points of view, the comments couldbe submitted to the agency, as indicated in theFederal Register, which has responsibility for pre-paring the "final order."
The stu dents would then need to develop afollow-up plan to assure continuity in their effortsto observe the final outcome of the process.When the "final order" does opear in the FederalRegister the wdents will be in the unique posi-tion of comparing their own experience and accu-mulated materials to the final outcome.
Most important of all, they would have seen,and shared in, the rule-makinl; process. Theywould, hopefully, have developed a heightenedconc:Tt nf their .igi-ts and responsibilities in theAmerican rule-making process.
1 01
49 TEACHING IDEAS
Death and Dying
A Unit forIndependent Studyin Death Education
JOAN D. McMAHON is a health educationteacher at Thomas Johnson Junior High Schoolin Lanham, Maryland.
The subject of death and dying is most oftenrojected by the conscious mind of the Americaneople. Our society is one aimed at the preserva-
t'on and enhancement of life; denying death andreducing its harshness have helped to cushion theAmerican people's fear of their eventual end.
In coming to grips with the dy.ng process anddeath, a person may have a better understandingof his own feelings and those of others who areactually experiencing dying and death. Death, formost people who are touched by it, presents acrisis state out of whkh coping with a new life-style becomes extraordinarily difficult. Too manypeople die suddenly and leave their families to-tally unprepared to rearrange their living patterns.Learning how to cope with a crisis, then, wouldappear to aid an individual in his adjustment tosuch a change as death brings.
A unit for independent study in death educa-tion has been prepared; this is an educationalmethod that allows progress at an individuallearning rate. It is the primary objective of theunit to help people come to grips with their ownfeelings and attitudes toward death and the dyingprocess so that life will be more rewarding andenjoyable and death will become less feared.1
The unit was compiled for advanced highschool or college students or thos professionalsinterested in improving their kno: ledge of thedying process and death. It was originally devel-oped from suggested course outlines by DanielLeviton of the University of Maryland, who is cur-
rently teaching a course on death education toover 300 students a semester. In an article in theJournal of the American College Health Associa-tion, Leviton outlined his topics and speakers forthe course. Some of the same general topics areincluded in this unit. It consists of behavioral ob-jectives, questions to be answered, activities to beperformed, and assessment tasks.
UNIT IN DEATH EDUCATION
Prerequisites: Any combination of the following: prac-ticum in counseling; work in crisis intervention centersor on hot lines; course utilizing techniques; course inthe psychology of adjustment.
Course Content:
Subunit A: The Taboo of DeathSubunit B: Definitions of Death Biological, Social,
and PsychologicalSubunit C: lite Crises of ManSubunit D: Views on Death and DyingSubunit E: Understanding the Dying Patient or Rela-
tiveSubunit F: The Funeral, Burial, and Bereavement:
Psychological ImplicationsSubunit G: Understanding Suicide and Self-desttuc-
tive Behaviors
Directions: Perform in the following order:
1. Read the behavioral objective2. Read the required readings3. Answet the questions listed4. Perform the activities5. Perform the assessment tasks
1 Leviton, Daniel, "A Course on Death Education and Sui-cide Prevention: Implications for Health Education," Journalof the American College Health Association, April 1971,pp. 217-20.
1 0289

Before beginning the course: Answer the followingquestionnaire and save your responses.
QUESTIONNAIRE I
1. When you were a child, how was death talked about inyour family?
a. Openly.b. With some sense of discomfort.c. Only when necessary and then with an attempt to
exclude the children.d. As though it were a taboo subject.e. Neser recall any discussion.
2. To what extent do you believe that psychological fac-tors can influence (or even cc use) death?
a. I firmly believe that they c6rl.b. I tend to believe that they cali.c. I am undecided or don't know.d. I doubt that they can.
3. What is your belief about the causes of most deaths?a. Most deaths result directly from the conscious ef-
forts by the persons who die.b. Most deaths have strong components of conscious
or unconscious participation by the persons whodie.
c. Most deaths just happen; they are caused by eventsover which individuals have no control.
d. Other.
4. Who died in your first personal involvement with death?a. Grandparerts or great-grandparents.b. Parents.c. Brother or sister.d. Other family member.e. Friend or acquaintance.f. Stranger.g. Public figure.h. Animal.
5. To the best of your memory, at what age were y JU firstaware of death?
a. Under three.b. Three to fivec. Five to ten.d. Ten or elder.
6. How religious ck ye, consider yourself to be?a. Very religious.b. Somewhat religious.c. Slightly religious.d. Not at all religious.e. Antireligious.
7. Which of the following best describes your childhoodconceptions of death?
a. Heaven-and-hell concept.b. After-life.c. Death as sleep.d Cessation of all physical and mental activity.e. Mysterious and unknowable.f. Other than ihe above.
g. No conception.h. Can't remember.
These questions are taken from the ''Death Question-naire" by Edwin S. Schneidman in Psychology Today maga-zine, @Communications/Research/Machines, Inc.
90
8. To what extent do you believe in a life after death?a. Strongly believe in it.b. Tend to believe in it.c. Uncertain.d. Tend to doubt it.e. Convinced it does not exist.
9. Regardless of your belief about life after death, what isyour wish about it?
a. I strongly wish there were a life after death.b. I am indifferent.c. I definitely prefer that there not be a life after
death.
10. If it were entirely up to you, how would you like tohave your body disposed of after you have died?
a. Burial.b. Cremation.c. Donation to medical school.d. I am indifferent.
11. How much of a role ha5 religion played in the develop-ment of your attitude toward death?
a. A very significant role.b. A rather significant role.c. Somewhat influeitial, but not a major role.d. A relatively minor role.e. No role at all.
12. Which of the following most influenced your presentattitudes toward death?
a. Death of someone close.b. Specific readings.c. Religious upbringing.d. Introspection and meditation.e. Ritual (e.g., funerals).f. TV, radio, or motion pictures.
g. Longevity of my family.h. My health or physical condition.i. Other.
13 Which of the following has influenced your present at-titudes toward your own death the most?
a. Pollution of the environment.b. Domestic violence.c. Television.d. Wars.e. The possibility of nuclear war.f. Poverty.g. Existential philosophy.h. Changes in health conditions and mortality statis-
tics.i. Other.
14. To what extent has the possibility of massive humandestruction by nuclear war influenced your present atti-tudes toward death or life?
a. Enormously.b. To a fairly large extent.c. Moderately.d. Somewhat.e. Very little.f. Not at all.
15. Have your attitudes toward death ever been affected bynarcotic or hallucinogenic drugs?
a. Yes.b. I have taken drugs but my attitudes toward death
have never been affected by them.c. I have never taken drugs.
103

16, What does death mean to you?a. The end; the final process of life.b. The beginning of a life after death; a transition; a
new beginning.c. A joining of the spirit with a universal cosmic con-
sciousness.d. A kind of endless sleep; rest and peace.e. Termination of this life but with survival of the
spirit,Don't know.Other,
f.
B.
17. What aspect of your own death is the most distastefulto you?
a. I could no longer have any experiences.b. I am afraid of what might happen to my body
after death,c. I am uncertain as to what might happen to me if
there is a life after death,d. I could no longer provide for my dependents.e. It would cause grief to my relatives and friends.f. All my plans and projects would come to an end.g. The process of dying might be painful.h. Other,
18. How often do you think about your own death?a. Very frequently (at least once a day).b. Frequently.c, Occasionall,.d. Rarely (no more than once a year).e. Very rarely or never.
19. When you think of your own death (or when circum-stances make you realize your own mortality), how doyou feel?
a. Fearful,b. Discouraged.c. Depressed.d. Purposeless.e. Resolved, in relation to life,f. Pleasure, in being alive,g. Other.
20. In your opinion, at what age are people most afraid ofdeath?
a, Up to 12 years.b, Thirteen to 19 years,c. Twenty to 29 years,d. Thirty to 39 years,e. Forty to 49 years,f. Fifty to 59 years.g. Sixty to 69 years.h. Seventy years and over.
21, If you could choose, when would you die?a. Iri vcurn.b. in the middle prime of life.c. Just after the prime of life.d. In old age.
22. When do you believe that, in fact, you will die?a. In youth.b. In the middle prime of life.c. Just after the prime of life.d. In old age.
23. If you had a choice, what kind of death would you pre-fer?
a, Tragic, violent death.b. Sudden, but not violent death.c. Quiet, dignified death,d. Death in the line of duty.
e. Death after a great achievement.f. Suicide.
g. Homicidal victim,h. There is no "appropriate" kind of death,
Other,
24, For whom or what might you be willing to sacrificeyour life?
a. For a loved une.b. For an idea or a moral principle.c. In combat or a grave emergency where a life
could be saved,d. Not for any reason,
25. What is your primary reason for the answer to question24?
a. To spare my spouse loneliness.b. To avoid loneliness for myself.c. To spare my spouse grief.d. To avoid grief for myself.e. Because the surviving spowe could cope better
with grief or loneliness,f. To live as long as possible.g. None of the above.h. Other,
26, Has there been a time in your life when you wantedto die?
a, Yes, mainly because of great physical pain.b. Yes, mainly because of great emotional upset.c. Yes, mainly to escape an intolerable social or in-
terpersonal situation.d. Yes, mainly because of great embarrassment.e. Yes, for a reaon other than above.f. No.
27. Suppose that you were to commit suicide, what reasonwould most motivate you to do it?
a. To get even or hurt someone.b. Fear of insanity.c. Physical illness or pain.d. Failure or disgrace.e. Loneliness or abandonment.f. Death or loss of a loved one.g. Family strife.h. Atomic war.i. Other.
28. Suppose you were to commit suicide, what methodwould you be most likely to use?
a. Barbiturates.b. Gunshot.C. Hanging.d. Drowning.e. Jumping.f. Cutting Or stabbing.
g. Carbon monoxide.h. Other.
Subunit A: The Taboo of DeathBehavioral Objective: The student will be able tofreely discuss and come to terms with his own feelingconcerning death,
104 91

Answer the following questions:1. Why do language barriers exist on the subject of
death and dying?2. How do you perceive death?3. What euphemisms can you think of to describe
death and dying?4. Do all persons have a negative attitude toward
dying?
Activities:Interview a person about his feeling toward death.
Assessment Tasks:1. Either talk with sz'meone about your ideas on death
or tape record your ideas and replay them.2. Save the responses that you made to the Schneid-
man questionnaire.
Subunit B: Definitions of Death: Biological,Social, and Psychological
Behavioral Objective: The student will be able to dif-ferentiate tictween the biological, social, and psycho-logical definitions of death.
An.swer the following questions:1. What is the biological definition of death?2. What constitutes social death?3. What constitutes psychological death?4. How do these definitions interrelate?
Activities
Upon reading all required readings for this subunit,make a chart depicting the interaction and separationof each definition of death.
Assessment Tasks:1. Define biological, social, and psychological death
as described by the various authors listed in therequired readings.Cite three case histories (can be hypothetical) thatdepict each type of death.
Subunit C: The Crises of ManBehavioral Objective: Upon identification of the dif-ferent stages of adjustment to a crisis, the student willapply these stages to death and dying.
Answer the following questions:1. What are Fink's stages to the adjustment of a crisis?2. What are Bow lby's stages to the adjustment of a
crisis?3. What are Kubler-Ross's stages of adjustment to a
crisis?4. Do the terminally ill adjust to death and dying ac-
cording to the stages above?
Activities:1. Write a story about a terminally ill person who
must cope with his own immediate death in termsof Bowlby's model (2 pages).
2. Examine a crisis in your life and determine whichmodel or combination of models approximatesyour crisis state.
92
Assessment Tasks:1. Correlate five patients in Kubler-Ross's book to
Bowlby's model as to the stages of adjustment theywent through during a crisis.
2. Read one of the following and write a two pageexplanation of how a character goes through anyof the stages mentioned by Fink:Death Be Not Proud, John GuntherA biography of Eleanor Roosevelt, any author
Subunit D: Views of Death and DyingBehavioral Objective: Upon examining the requiredreadings on the views of death and dying, the studentwill be abie to briefly explain how death and dyingare perceived from the viewpoint of children, adoles-cents and young adults, the middle aged, the elderly,and the terminally ill.
Answer the following questions:1. What are the developmental stagas in childhood
that lead to a mature concept of death?2. Name three adjustment mechanisms that affect the
elderly's attitudes toward death.3. Name four factors which influence the terminally
ill's adaptation or adjustment to their impendingdeath.
4. Do college students perceive death as threatening?Support or refute.
5. How do you feel the middle aged population feelsabout dying in their prime?
Activities:1. Create a hypothetical situation concerning a child's
reaction to the loss of a pet.2. Predict how you would react if a person in your
family was diagnosed as terminally ill. How do youthink they would want you to react?
3. Identify your feelings if you were suddenly facedwith the realization that you had a terminal illness.
Assessment Task:Plan a chart illustrating the various age groups, varia-bles affecting their death attitudes, the behavior thatshould or should not manifest itself on experiencinga situation involving death, and the views held by eachage group on the subject of death and dying.Subunit E: Understanding the Dying Patient or RelativeBehavioral Objective: Upon learning of the impendingdeath of an individual, the student will be supportiveand perceptive of their feelings and needs. The studentwill also be able to develop strategies for helping thedying patient or relotive to cope with death, dying,and bereavement.
Answer the following questions:1. What emotional and psychological needs should a
relative have fulfilled in order to cope with the im-pending death of a relative?
2. What emotional and psychological needs shouldthe patient have fulfilled in order to cope with hisown impending death?
3. Explain the reactions and emotions of those whoconfront dying daily, e.g., police officers, the mili-
105

tary, morticians, clergymen, physicians, nurses, etc.4. How would you feel in the presence of a dyil
person?5. Should a patient be permitted to return home to
die? Why or why not?6. Whose responsibdity is it to tell a person he is
going to die?
Activities:1. Interview any two of the following concerning their
reactions and emotions in observing death and thedying process: police officer, mortician, war vet-eran, physician, nurse.
2. Identify those factors which cause relatives to de-sert a dying patient. Do these apply to yourself?
Assessment Task:Eric is a 14 year old Negro with sickle cell anemia. Hisfamily has kept from him all mention of the disease,its symptoms, and its fatal outcome. He has been sleep-ing a great deal lately and his general condition hasbeen weakening. His teacher has been discussingbiology and disease causing organisms with him. Hehas been asking questions as to whether he has adisease. Eric has noticed that he has little energy andthinks he may have a serious disease but his familyhas not told him anything. You can perceive that hemay ask you what disease he has and what it will doto him.What needs and feeling do you suppose Eric has?Develop a strategy to cope with Eric's dying with himand his family on your visits.
Subunit F: The Funeral, Burial, and Bereavement:Psychological Implications
Behavioral Objective: This student will be able toevaluate the American grief process and foimulate con-structive plans for his or a relative's death.
Answer the following questions:1. Who should make the arrangements for the funeral?
Who should be responsible for the final decisionson place of burial, method of body disposal (cre-mation, burial, etc.)?
2. What constitutes a normal bereavement reaction?What constitutes an abnormal one?
3. What are the religious implications for burial?What are the psychological implications for burial?
4. What grief reactions can be expected upon learn-ing of the death of a child, a teenager or collegestudent, a middle aged individual, or an elderlyperson?
5. What happens to the family or perscns who con-tinue to live after a close friend or relative hasdied?
Activities: Choose two1. Consult a funeral director and/or visit his "lab."2. Decide what your role would be in the death or
dying process of mother or father; brother or sister;husband or wife; young child; close friend; ac-quaintance; and pet.
3. Write your will and go over the legal implicationswith a lawyer.
4. Plan a financial statement that would includemortgage, insurance policies, children's education,and funeral expenses.
Assessment Task:Prepare a detailed and operable plan to be used in theevent of your death. Include who should be notifiedof the death, expenses, settlement of the estate, dis-posal of personal possessions, etc. What is the ration-ale for your plans and did you account for the needsof the family who would be left?
Subunit G: Understanding Suicide andSelf-destructive Behaviors
Behavioral Objective: The student will be able to de-vise a reference list of persons, groups, or agenciesthat deal with suicide. He will also be able to identifyclues in the individual's behavior that suggest a needfor consultation with a professional specialist or a needfor other forms of immediate help.
Answer the following questions:1. Why do children commit suicide?2. Why do college students commit suicide?3. What are clues that a person may want to kill him-
self in the near future?4. What is crisis intervention and how can it be used
in suicide prevention programs?S. What can you do as a professional or nonprofes-
sional to help an individual cope with his prob-lem?
6. When should you recognize the necessity for pro-fessional psychological therapy for the individual?What persons or agencies are available for suchreferrals?
7. Does a person have the right to take his own life?
Activities:1. Visit a suicide prevention center or a crisis inter-
vention center that deals with suicide intervention.2. Contact the Center for Studies of Suicide Preven-
tion, National Institute of Mental Health, Rock-ville, Maryland 20852.
3. Interview two specialists on campus or in the com-munity who would be in contact with suicide prob-lems: health educator; clergy; sociologist; psy-chologist; counselor; or health service personnel.
Assessment Tasks:1. Make a list for your immediate reference of per-
sons, groups, or agencies that you could contact ifyou face a suicide case.
2. Identify those clues to suicide behavior that con-stitute immediate help, psychiatric help, or otherprofessional services.
3. Retake the Schneidman questionnaire and compareyour responses from your first attempt
REQUIRED READINGS
Readings from outside published sources are animportant part of the unit. Students should be en-couraged to make use of computerized on-line data-bases to locate appropriate materials.
C 93
50 TEACHING IDEAS
Put s Little Lifein tour both
CHARLES R. O'BRIEN is a graduate stu-dent in the Department of Health and Physi-cal Education at Bowling Green State Uni-versity, Bowling Green, Ohio 43403.
During the past years in health in-struction, there has been a major driveby educators to include the topic of deathand dying in the ruiriculum of their in-stitutions. One of the many reasons forthis impulse is because of the changes insociety. With these changes, death hasbeen taken out of the family structureand been replaced by "outsiders."
Years ago death was a significant as-pect in the foundation of the family. Anindividual was born, lived, and died atthe same location. Death at this time wasan experience which was cherished bythe family, friends, and individual reli-gious beliefs. At the present time how-ever, people tend to hide their childrenfrom the reality of death and pay othersto take the burden off their hands. Re-cently this factor has presented numer-ous mental problems for a number ofAmericans. Some of these problemshave resulted in child runaways, suicide,breakdown of religious beliefs, and haveforced changes in individual life pat-terns. Because of these and other rea-sons, the public and the education pro-fession think it is necessary for the topicof death to be included withal the educa-tional structure.
Since death education is beginning tobe included in many school systems, ithas created problems such as: what con-tent areas should be included in a deathunit and how are the content areas to betaught? Some major personal questionsshould be examined before you attemptto construct your unit on death. The firstquestion should be: do you know yourphilosophy on death?
Research indicates that there are twobasic philosophies dealing with death. Inboth of these philosophies the primaryconcern is awareness. The reason for thisis that by being aware of death the indi-vidual may be abie to see the full life cycle
94
and make the proper choice ofphilosophies to complement the indi-vidual's behavioral needs.
Philosophy 1 is death fear. In this phi-losophy people have such a fear of deaththat they change certain patterns in theirlife to accommodate this fear. By doingthis they minimize the risk of death andalso many of life's pleasures.
Philosophy 2 is'death acceptance. Inthis philosophy individuals understandand accept the reality of death. Throughacceptance of death within themselves,they lead their lives in whatever waythey wish, and accept the final outcomeof these actions.
The second personal question oneshould ask is: Do you fear death? If theanswer to this question is yes, takeanother look at this fear, determine ifyou fear death or if you fear dying. Theseare two terms which sometimes are usedsynonymously, but are they really?Death means the end of life whereas dyingis the process of death. There are manyways of dying such as through disease,aging, and accidents. With an individualthere is only one death. This death maycome in two speeds; slow as in disease,old age, and pollution; fast as in acci-dents, suicide, war, and domestic vio-lence.
Once you have gone through thisself-realization process, you should beable to see one of the basic reasons forteaching about death-the students'wellbeing. Death education could be animportant aspect of every individual'slife. Death as we know it now is some-thing which happens to everyone, but issomething we havo little control over.Individually we may be able to put offdeath through exercise, diets, and goodhealth practices, but death itself remainsthe same.
Now that you are aware of your viewson death you can start examining topicswhich will be included in the death unit.The following topics can be included.
1. Religious beliefs2. Rituals3. Stages of dying4. Types of funerals5. Insurance6. Attitudes toward death and dying7. Heaven-hell concept8. Death philosophies9. Euthanasia (direct-indirect)
10. Types of dying (physical-mental-social)
107
Death and Dying
Once you have your topics planned,find the teaching activities to comple-ment your lesson. Here are just a few.
1. Visit a cemetery2. Visit a funeral home3. Invite guest speakers (coroners,
doctors, lawyers)4. Make poems5. Make up tombstones and epitaphs6. Write an obituary7. Write out wills8. Make up a life inventory9. Role play
10. Interview students11. Look up laws on death (state and
taxes)12. Crossword puzzlesTo help with the classroom activities.
teaching techniques like small group dis-cussions, debates, and problem-solvingseem to be enhanced by the use of re-cordings. Below is a list of records whichpertain to death education and helpstimulate student participation.
1. "Ohio"-Neil Young2. "Life in the Bloodstream"-The
Guess Who3. "Unborn Child"-Seals and Crofts4. "Imagine"-John Lennon5. "Talisman"-The Guess Who6. "Fiddle in the Sky"-Seals and
Crofts7. "Changes IV"-Cat Stevens8. "Follow Me"-Seals and Crofts9. "Better off Dead"-Elton John
10. "Heaven Only Moved Once Yes-terday"-The Guess Who
In today's society we find it morbid todiscuss and think of our own death. Bynot discussing death, we place it in thecloset hoping it will not become a realitywe will have to face. A unit on deathwould make possible a needed discus-sion to help eliminate the problems dis-cussed earlier. It would also help stu-dents understand the full meaning ot lifeand bring out the necessity of . derstanding death.
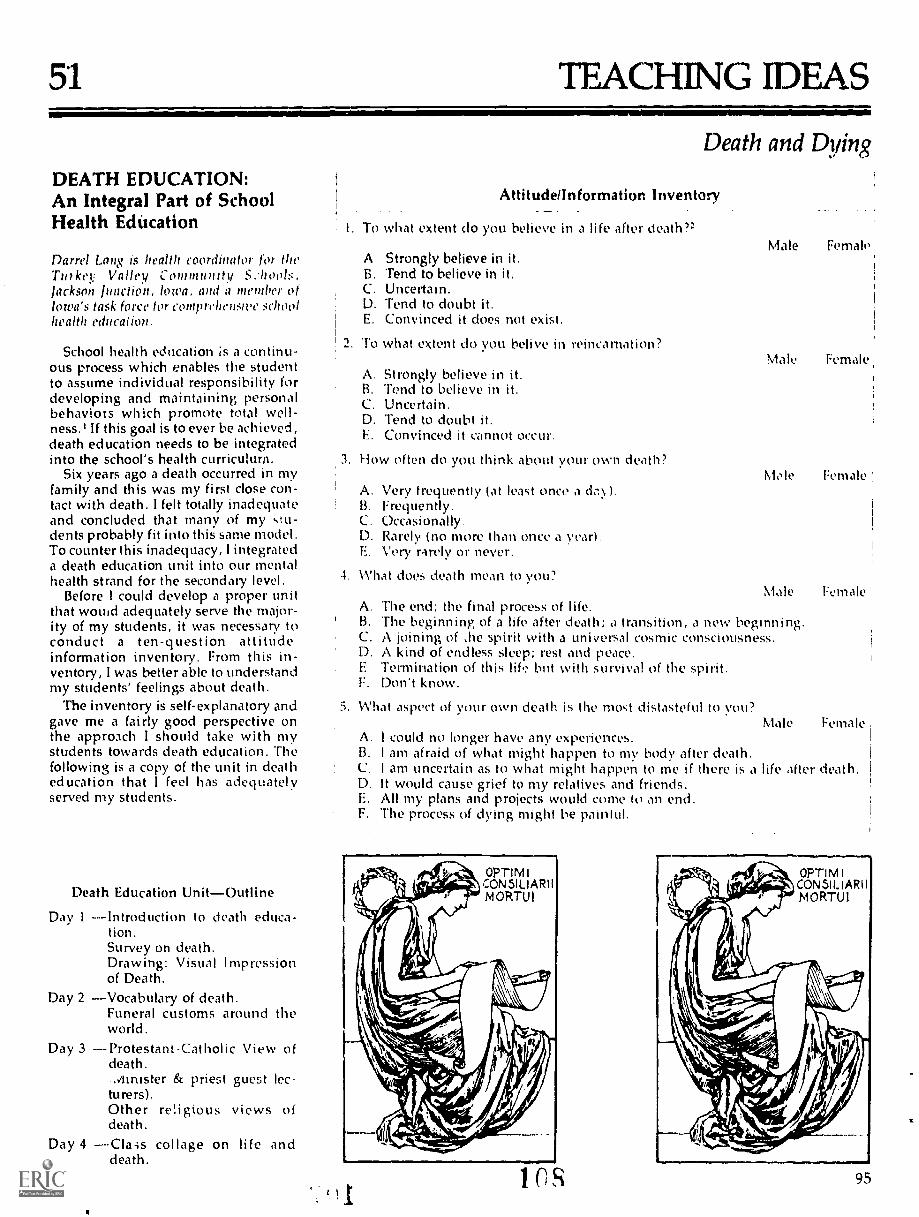
51 TEACHNG IDEAS
DEATH EDUCATION:An Integral Part of SchoolHealth Education
Darrel Lai is health coordinator for (heTurkey Valley Community S..hools,Iackson Inaction. town, and a member ofIowa's task force for comprehew;IN' SO1001lwalth education.
School health education is a continu-ous process which enables the studentto assume individual responsibility fordeveloping and maintaining personalbehaviors which promote total well-ness.' If this goal is to ever be achieved,death education needs to be integratedinto the school's health curriculum.
Six years ago a death occurred in mYfamily and this was my first close con-tact with death. I felt totally inadequateand concluded that many of my ,stu-dents probably fit into this same model.To counter this inadequacy, I integrateda death education unit into our mentalhealth strand for the secondary level.
Before 1 could develop a proper unitthat would adequately serve the major-ity of my students, it was necessary toconduct a ten-question attitudeinformation inventory. From this in-ventory, I was better able to understandmy students' feelings about death.
The inventory is self-explanatory andgave me a fairly good perspective onthe approach I should take with mystudents towards death education. Thefollowing is a copy of the unit in deatheducation that I feel has adequatelyserved my students.
Death Education UnitOutline
Day 1 ----Introduction to death educa-tion.Survey on death.Drawing: Visual Impressionof Death.
Day 2 Vocabulary of death.Funeral customs around theworld.
Day 3 ----Protestant-Catholic View ofdeath..Innister & priest guest lec-turers)Other religious views ofdeath.
Day 4 collage on life anddeath.
I. oAB.C.D.E.
Death and Dying
Attitudennformatkm Inventory
what extent do you believe in a life after death?=
Strongly believe in it.Tend to believe in it.Uncertain.Tend to doubt it.Convinced it does not exist.
2. To what extent do you belive in reincarnation?
A. Strongly believe in it.B. Tend to believe in it.C. Uncertain.D. Tend to doubt it.L. Convinced it cannot occur.
3. How often do you think about your own death?
A. Very frequently (at least once a &:),).B. Frequently.C. Occasionally.D. Rarely (no more than once a year).E. Very rarely or never.
4. What does death mean to you?
A.B.C.D.E.F.
Male Female.
Male Female
Mole Female
Male FemaleThe end; the final process of life.'Flw beginning of a life after death; a transition, a new beginning.A joining of .he spirit with a universal cosmic consciousness.A kind of endless sleep; rest and peace.Termination of this life but with survival of the spirit.Don't know.
5. What aspect of your own death is the most distasteful to you?Male Female
A. I could no longer have any experiences.B. I am afraid of what might happen to my body after death.C. I am uncertain as to what might happen to me if there is a life after death.D. It would cause grief to my relatives and friends.E. All my plans and projects would come to an end.F. The process of dying might be painlul.
ins 95

6. When you think of your own death (or when circumstances make you realizeyour own mortality), how ci ) you feeP
Male FemaleA. Fearful.B. Discouraged.C. Depressed.D. Purposeless.E. Resolved in relation to life.F. Pleasure in being alive.
7. If you had a choice, what kind of death would you prefer?
A. Tragic, violent death.B. Sudden but not violent death.C. Quiet, dignified death.D. Death in a line of duty.E. Death after a great achievement.F. Suicide.G. Homicidal victim.H. There is no "appropriate" kind of death.
8. What are your thoughts about leaving a will?
A. I have already made one.B. I have not made a will, but intend to do so some day.C. I am uncertain or undecided.D. I probably will not make one.E. I definitely won't leave a will.
9. To what extent do you belive in life insurance to benefit your survivors?Male Female
Male Female
A. Strongly believe in it; have insurance.B. Tend to believe in it; have or plan to get insurance.C. Undecided.D. Tend not to believe in it.E. Definitely do not believe in it.
10. What are your thoughts about funerals?
A. Feel they are very important for the bereaved.B. Tend to feel they are valuable.C. I am uncertain or undecided.D. Definitely do not believe in them.
96
Male Female
Male Female
109
Day 5 Filmstrip, Living with Dying,3on how America lives withdeath.
Day 6 Five stages of death, grief andbereavement.
Day 7 ----Film: "What Man Shall Liveand Yet See Death4, Part I.
Day 8 --Film: What Man Shall Live andYet See Death4, Part 11.Drawing students' owntombstone and writingepita phs.
Day 9 Pictorial report on epitaphstaken from cemeteries.Death-related music.
Day 10Group reports on death1) Life insurance2) Military view on death3) Medical examiner4) People who have been
brought back to life.Day 11Fantasy exercise on death.5Day 12Field trip to funeral home.Day 13Positive-negative euthanasia.Day 14Explaining death to children.
Death has been a fascinating subjectthat people have always questioned.Through a thorough unit on death edu-cation, many questions and thoughtsabout death may be answered. It ishoped this approach would better edu-cate our youth and eventually ovr soci-ety. We all should have a better under-standing of death, for we ALL will faceit some day.
1. Definition of Comprehensive SchoolHealth Education, Iowa's Task Force on Com-prehensive School Health Education.
2. Perspectives on Death Student ActivityBook, David W. Berg, George G. Daugherty,1972., p. 2-4, Arlington Press, 201 EighthAve. S., Nashville, Tenn. 37207.
3. Sunburst Communications, Pleas-antville, N.Y. 10570.
4. Area Educational Agency, Film's, Inc.,1972.
5. Psychology of Death & Dying, John C.Morgan, Richard L. Morgan, WestinghouseLearning Press, Sunnyville, CA.

52 TEACHING IDEAS
Death and Dying
A Teaching Strategyon Tragedy
CONNIE 10 DOBBELAERE is a graduateassistant at Bowling Green State Univer-sity, Department of Phu lth and PhysicalEducation, Bowling Green, Ohio 43402.
"Mary's life seemed to be at a perfectpoint! She was 16 years old, pretty, in-telligent, enthusiastic, a varsity cheer-leader, and had just been electedhomecoming queen for her high school.She had a happy home life, with twobrothers, four sisters, two parents, anda dog named Brownie. Mary loved lifeand had everything to live for. On aclear night in March, she was drivinghome from work, just getting ready tomake the left hand turn off of Highway617 into her driveway when fromnowhere a semi-truck started to passher on the left. Mary died on March 23,1976."
A similar tragedy may happen at anytime in your community or school sys-tem. The question is, how do we pre-pare our students to handle the death ofa friend or loved one properly? Is thereever a proper way to handle this situa-tion?" Death 40 to 50 years ago was ac-cepted as a natural culmination of life.However, today Americans try to coverit up and pretend that when death doesoccur they will be able to accept it. Thisidea has not proven to be valid in recentyears. There appears to be an inescapa-ble need to furnish our youth with amore comprehensive view of whatdeath really means, how they can copewith a death when it occurs, and why itis important for them to carry on andlive a more fulfilled life.
A death education unit taught in ahealth class needs to be implementedfor the benefit of each student. If deathis accepted as a natural part of life, aninevitable event in all existence, then wewill be able to stress the importance ofliving life to the utmost for today! Themain objective, it seems evident, is forthe death unit to emphasize the need todevelop in each individual a crisp zestfor every undertaking, day-to-day, thatone can. Life is rich in varied opportuni-ties and the mission is to find and per-ceive each and every advantage that
arises. We teach death in order to betterlive and understand the total process oflife!
A Tragedy Strategy
Once the need for a unit on deatheducation has been establislwd, the nextproblem a teacher faces is just exactlyhow to introduce the unit into the class-room. One teaching strategy, whichproved to be very functional in pasthealth instruction and upon which thisarticle is bised, used a questionnaire en-titled "You and Death," by EdwinShneidman.' It contains approximately72 questions which were condensed to40 for class purposes. In essence, it en-tails answering the questions in an at-tempt to identify and clarify students'feelings and conceptions on death. Thequestionnaire proved to be a thoughtprovoking and discussion stimulatingtechnique to introduce the death unit.
For a more complete and interestingdiscussion of the questionnaire, thestudents were instructed to mark a starby the most thought provoking ques-tions; an "S" by those which most sur-prised them; a "1" beside the questionsabout which they would really like totalk with someone; and an "MI" in frontof those questions they would like moreinformation on as they went throughthe test. These marks pinpointed theareas of most interest for the ensuingdiscussion. They also symbolized to the
1114
students where their ideals and valuesneeded to be researched and clarifiedfurther.
Four of the 40 questions that wereclarified at some length in the classroomare discussed here. They exemplify thetype of discussion that was carried on asa result of the questionnaire.
The first question seemed to influencethe way in which the students answeredthe rest of the questionnaire: to what ex-tent do you believe in a life after death?a. strongly believe in it; b. tend to be-lieve in it; c. uncertain; d. tend todoubt it; e. convinced it does not exist.
Some students were confused abouttheir feelings on the subject and there-fore seemed to have a great deal oftrouble completing the test. However,others answering the question eithercompletely affirmatively or completelynegatively had little trouble with thetest. By discussing the question ingreater detail it appeared thai most ofthe students felt more at peace withtheir own feelings towards the subjectand felt more open about their convic-tions because they found out that theywere not the only ones who had troublewith the subject.
A second question prompting interesttried to clarify situations in which onewould give up one's own life: For whomor what might you be willing to sacrificeyour life? a. a loved one; b. an idea ormoral principle; c. in combat or a graveemergency where a life could be saved;d. not for any reason.
Most of the students had a great dealof difficulty imagining sacrificing theirhves for anyone or anything. Most ofthe members enjoyed their presentlives. However, they all agreed thatthey would probably change theirminds if they were confronted with areal life situation involving one of thesechoices.
Another thought provoking questionhad to do with the actual date of one'sdeath: if it were possible, would youwant to know the exact date on whichyou are going to die?
The catalyst of this discussion wassupplied by one student's statementthat "if I were told that I was going to
97
live to be at least 40 years old, I would livelife to its fullest and try to experience allthat life affords and not wait for old age todo the things I've always dreamed of do-ing." Others responded that they woulddefinitely not like to know when theywere to die because it was a fearful subjectfor them and they would rather not thinkabout it. Still another response was sharedwith the class by a student stating that itreally doesn't matter to him whether ornot he knew because his religious faithwas so strong and he was so satisfied withhis present life that anytime death came hewould be ready.
Conclusions made from this questionhelped students to answer and discuss afourth question: What effect has this ques-tionnaire had on you? a. it has made mesomewhat anxious or upset; b. it hasmade me think about my death; c. it hasreminded me how fragile and precious lifeis; d. no effect at all; e. other effects(specify).
Most of the students responded to thequestion by either marking "b" or "e."The questionnaire did make them thinkabout their own death but it also madethem deliberate about their feelings onsuicide. It also brought suppressed feel-ings out into the open and helped them tobe more content with their ideas on deathand dying.
As we discussed the whole topic ofdeath once more in the summary, theyfelt also ,hat they could have responded"c" as well. The discussion of death didremind them of the pricelessness of afulfilled life and forced them to reevalu-ate their personal lives at the presenttime.
Strategy Evaluation
As a final evaluation of this experi-ence, the students filled out a sheet ofopen-ended statements. These evalua-tions proved even more valuable thanthe discussion. It helped ztudents to bemore understanding of each other'spersonal feelings and views on deathand the pricelessness of a fulfilled life.
The students were given no directionson the proper way to complete thestatements and thus were forced to an-swer them with their own unique per-ceptions of the total experience. In shar-ing some of their answers it is my hopethat each reader will see how successful
98
the strategy proved to be for each partic-ipant. me of the answers from thestudents 1ollow.
I learned that . . .
life, though often taken for granted istemporary, and protection of same, evenpromotion of same is of number one prior-ity.
"death education" can be an interestingtopic if tadght with the objective of livinglife better for now.
I am able to stand firmly convicted to thebelief in life after deathnot fearing deathas we know it here on earth.
I am satisfied with my life and death con-cept.
I want to . . .
find out more information about the stagesof life when one's attitudes toward deathchange.live what life is afforded me to its fullest,but regretfully must adjust to constraints(some of which may be unnecessarily self-imposed).
live my life to the fullest and when deathcomes, I hope to accept it gracefully and itaccept me the same way.
live daily with the attitude that today is myonly opportunity to tell others why I don'tfear death.
I hope that I . . .
can live life productively, yet joyouslyand never stray from the sense of perspec-tive that enables me to "always smell theflowers . ."
can develop sharper opinions on some ofthe questions I was unsure of.
if I discover I am scheduled to die soon, Ican lead exciting tinal days and not spendmy last days pouting and cursing my des-tiny.
live to be a ripe old age!!
I was surprised to see that . . .
--some people didn't want to give their livesfor others.
when confronted with the possibility thateven I might consider suicide, I reallycould not think of the way in which Iwould take my life.
I don't have very many strong convictionsabout my attitude toward death.
some refuse to seek the full life.
I was glad to see that . .
my religious faith is strong enough to an-swer most of these questions with ease.I was consistent in my thoughts on death.
I did have to think as a result of this ques-tionnaire about my feelings on death.
h 1 1
--others believe in God and put their trust inHis promise for eternal life.
Many treasure livingnot as solely basedon survival ethics, but on a fulfillingbasis . . . "I want all from life that is goodand beautiful."
I want h. remember that . . .
--today may be my lastI need to keep asmile on my face and a rainbow in myheart!
no matter what else I learn through myeducational career I am sure to remembertoday!
whatever I do with my lifethe only im-portant thing is to die with Jesus control-ing my heart.
death is not the end!life has order, peace, love and total appre-
ciation of nature."Death education can be a mind-
expanding unit if taught with the objec-tive of getting the students to learn toaccept and understand death and tothink of it as an inevitable end to life, aswe know it here on earth. When theycan accept this phenomenon, they candevelop a more meaningful opinionabout the necessity to live life to the ut-most and to instill in themselves a zealfor a more fulfilled life.
It is vitally important that One learnsthat one does not have to wait fortragedy before confronting the funda-mental and ineluctable questions relatedto death and dying with which one maybe confronted. The requirement here isfor one to be willing to participate andlearn to understand and accept death asa natural part of all life.
'Edwin Shneidman, Center for AdvancedStudy in the Behavioral Sciences, in consul-tation with Edwin Parker and C. R. Funk-houser of Stanford University, "You andDeath," Psychology Today. CommunicationsResearch Machines, Inc.; Del Mar, CA, Au-gust 1970, pp. 67-72.
53 TEACHNG IDEAS
Health orHazard?A Post-ChinaSyndrome Game
Moon S. Chen, Ir. is an assistant professor ofhealth education at Ohio State University,215 Pomerene Hall, 1760 Nkl Avenue. Col-umbus, Ohio 43210.
How important is it to teach aboutionizing radiation or noise protection orindustrial safety? For most students,these three topics seem remote and re-moved from the classroom. However,the movie, The China Syndrome,madethe Three Mile Island incident and thehazards of radiation hauntingly realistic.Students and teachers in the Harrison-burg area were undoubtedly affectedand students elsewhere certainly feltcuriosity and a need to know more facts.What better place to bring together thetopics of radiation and health hazards ofthe working environment than in an en-vironmental health course or in a unit onenvironmental health? And how betterto make learning more fun than with agame?
Fun and success with such a game,called "Health or Hazard?", are attrib-uted to proper orientation and to studentinvolvement and discovery. Orientationto the game consists of a cognitive intro-duction to the basic forms of radiation(e.g., ionizingalpha, beta, gammarays, and non-ionizingmicrowaves)and how to use time, distance, andshielding for protection. A cognitive in-troduction to health hazards of the work-ing environment should cover the det-rimental effects on humans of noise,dust, gases, and toxic liquids. Protectionmeasures would include environmentalmanipulation, medical surveillance,management decisions, and personalprotection. Students should be taught toadapt such principles to specific hazards(that is where much of the learning oc-curs).
Following cognitive input, the teachershould divide the class into three equal-sized and intellectually-matchedgroups. One group will be student re-ferees with respoosibility for awardingpoints and making decisions regardingdisagreenwnts between sides. Theirpreparation will consist of correctlymatching hazards with proper healthprotection methods.
The two other groups will be compet-
Enc ironmental Health
"1-4114.
- - - ,
'4Xisitakn" Ve,"S`Ammit4t;
,
1-'14*
ing teams. Each team should prepare it-self independently. Based on the cogni-tive information given in class, chteam should prepare an array of "oft-m-sive" hazards and an arsenal of "defen-sive" health protection measures. Es1chhazard and each health protection mea-sure should be written on a separateindex card large enough so that it can beread across a classroom.
The spirit of competition between thetwo sides fosters a spirit of cooperationon each side. Team members naturallyhelp each other in learning the associ-ations between hazards and the properhealth protection.
Competition begins after about fifteenminutes of preparation. Each side alter-nately chooses a player from the oppo-site team to "challenge." Each challengeis considered a "round." Each team al-ternately assumes an offensive and de-fensive position.
During the round the offensive playerchooses a hazard with which to "attack"the defensive player. The hazard is hid-den from view until the offensive anddefensive players face each other in thefront of the classroom. The defensiveplayer brings his arsenal of methods. Ona signal from the judge, the offensiveplayer flashes his hazard. The defensive
sa.
I
Jt.
player has fifteen seconds to respond byshowing the card with the correct healthprotection measure against that hazard.If the correct health protection measureis not on one of the defensive player'scards, the defensive player has the samefifteen second time limit to write theproper health protectiol: on a separateindex card. No coaching from teammatesis allowed.
A score results when either side wins a"round." Decisions regarding whichside wins will be made by the studentjudge for that particular round. The stu-dent judge must decide whether the de-fensive player's response is correct andmade within the fifteen-second limit.(The time should be kept by anotherjudge.) If the defensive player displaysthe correct response within the timelimit, the defensive side scores a point. Ifnot, the offensive side wins a point. Thefirst team to win a predeterminednumber of points wins.
For greater variety and excitement,more than one hazard can be introducedat one time, forcing the defensive playersto respond more quickly. This game canbe played at the pace of the students. It isfun, exciting, and a harmless way tolearn health protection measures againstradiation and hazards of the workingenvironment.
1 ? BEST COPY UWE99

54 TEACHING IDEAS=1.
Nuclear Power, Debate
Bruce G. Morton is an assistant professor ofhealth education, at Temple University,Philadelphia, PA 19122.
The nation is entering its second dec-ade of crisis over energy resources andenergy consumption. Gasoline has morethan doubled in price in the past twoyears. The rising price of home heatingoil threatens the health and welfare ofpoor people who are unable to pay theirbills. Congress is considering a proposalto relax environmental standards forstrip mining and air pollution emissionsfrom coal-burning power plants. Ram-pant inflation, partly caused by sky-rocketing energy costs, threatens publichealth as government slashes social pro-grams to balance the budget.
Concurrently, the long term commit-ment of the nation to the nuclear path-way to energy independence is being re-considered. The major accident at ThreeMile Island, together with the less pub-licized but nonetheless serious incidentsat Browns Ferry, Chalk River, RockyFlats, and Idaho Falls, have thrown apallor over the once rosy future of nuclearpower. At this writing only one state inthe country (Tennessee) is now willing toaccept radioactive wastes for storage anddisposal. Among the general public,concerns about radiation, the potentialfor sabotage and the contribution of nu-clear power technology to nuclear armsdevelopment, have grown dramaticallyin recent years. Among those who definethemselves as environmentalists, oppo-sition to nuclear fission power is virtuallyunanimous.
But there are two sides to each of thesequestions. Proponents point to the im-pressive safety record of nuclear plants.They argue that without nuclear power,electricity would be much more expen-sive than it is now and the air would bemore polluted from coal-fired powerplants. They contend that there are bene-fits and risks to every energy alternativeand nuclear benefits far outweigh therisks.
In a course I teach on health and theenvironment I attempted to broach theproblem of presenting the conflicting in-formation which clouds the nuclearquestior by organizing a debate inwhich the students assumed the roles ofvarious interested persons as describedbelow. The purpose of the exercise was100
to provide the students with the oppor-tunity to try on various viewpoints re-garding nuclear power in a simulatedreal life situation. First I provided thestudents with readings from a range ofperspectives; then I presented the prosand cons of each of the relevant issues inas unbiased a manner as possible. Ageneral discussion ensued. Emphasisthroughout was placed on determiningthe credibility of the information and onthe subsequent identification by stu-dents of the issues, facts and feelingssalient to their attitudes and values to-ward nuclear power. I found a plethoraof biases-4 materials written for the laypublic trom the local electric companyand from one of the local anti-nucleargroups active in my community. I aug-mented this with academically credible.sources. (A list of references is availableon written request).
The procedures for the debate that I
have found to be most valuable are asfollows:
1. During the class session prior to thescheduled debate, present or discuss theissues with reference to the articleswhich the students should already haveread. Next, break the students intogroups as per the directions below.
2. At the beginning of the secondclass, just before the debate, give eachgroup 10-15 minutes to compare notesand ideas, and select one person to serveon the panel.
3. Solicit a volunteer or assign some-one to be moderator. Charge this personwith the responsibility for limiting thetime for each presentation and facilitat-ing the democratic opportunity foreveryone who wants to speak at leastonce.
4. Ask those not on the panel to as-sume the roles of concerned citizens whohave the right, and who will be given theopportunity, to ask questions or makestatements.
5. Plan 30-40 minutcs for the debateincluding questions and comments fromconcerned citizens not on the panel.
6. After the debate, open up the classto general discussion and give people theopportunity through discussion and vot-ing to identify the issues, concerns andfeelings most important to them, and toclantv and affirm their personal valueswith respect to nuclear power.
Directions to Role PlayersYou are a participant in a discussion
among local residents and interestedpersons concerning the preposa I by theelectric company's directors to build a
1 1 3
Environmental Healthnuclear power plant in your neighbor-hood. Each of you may select one of thefollowing roles but there must be at leastone person for every role. For the pur-pose of the exercise attempt to assumethe arguments of the role assigned asyou perceive they would be. Each personon the panel will have a maximum of fiveminutes for an initial statement afterwhich there will be time for rebuttal andopen discussion.
ParticipantsSaliSally Slick is the electric company's
spokesperson. She:he is an outstandingproponent of nuclear power whose spe-cial talent is putting the levels of riskposed by nuclear power into perspectivewith other risks from automobiles, coalmining, natural disasters, cigarettesmoking, etc.
BertiBertha Booster is the Chamber ofCorn merce public relations person. Al-though this character may be either for oragainst nuclear power, she/he is inde-fatigable in boostering local business.
ConradCoirnie Cmicerned is a local resi-dent who is the parent of two childrenwho go to school in the vicinity of theproposed power plant.
Alan'Alice Academic is the local univer-sity scientist who is concerned with thebalanced presentation of the facts.She/he will often bring out the other sideof the argument so that everybody willbe apprised of all the facts. She'he likesto put things in the perspective of risksand benefits.
EdiEdna Ecolop, is a local environmen-tal ae tivist who is deeply concernedabout the ecology of the river on whichthe plant is proposed to be built as well asa number of other environmental prob-lems.
Be consci,mtious about limiting thetime tor each panel member to presentand rebut. The purpose of the exercise isto get a range of viewpoints out in theopen, not to resolve the issues or tojudge the presenters. The 10-15 minutesin groups before the debate assures thateach panelist will have a few good pointsto make, and is itself a good exercise ininformation sharing. However, you maywant to provide the moderator with afew leading questions just to get the dis-cussion going should it come to astandstill. Usually, the reverse occurs:: is hard to limit the debate. The roleplaying seems to provide many studentswith a comfortable vehicle ',II- interac-tion, and the instructor with a methodfor examining a controversial health con-cern.

55 TEACHNG IDEAS
Health and SafetyWaft from meTrash CanI. CLAY WILLIAMS is an associate profes-sor of lwalth education at Bowling GreenState University, Bowling Green, Ohio43402. JUDITH K. SCHEER is assistantprofessor of health education at the Uni-versity of Toledo, Toledo, Ohio 4.3606.
e
As educators, we constantly dream ofways to obtain effective visual aids tohelp us develop concepts; however, thedifficulty of getting school monies ap-propriated for visual aids to enhanceclassroom presentations too often con-fronts us. I am going to share a secret ofhow to cope with, even enjoy, two prob-lems of our everyday existenceteaching on a shoestring budget andtaking out the trash! The trash can of-fers unlimited potential for collecting anabundance of effective teaching aids.My recent practice of accumulating dis-carded items provides a wealth of in-valuable materials for the classroomthat we can use effectively to developimportant health and safety concepts.
In my collection is a necktie which isripped and tattered. It makes me thinkback to early spring, several years ago. Iwas itching to get my boat in the waterso, on returning home from church, Iannounced that anyone who wanted togo to the lake should be ready to leavein five minutes. My wife objected say-ing that I had promised to build somekitchen shelves for her and that I wasnot leaving the house until the job wasdone. Needless to say, I was in no moodto build kitchen shelves! Rushing like amadman, I started to cut a board withthe circular saw and the next thing Iknew, my tie was tangled in the sawblade which was rapidly approaching
my throat! Looking at the mutilated tieand thinking about the close call, I sud-denly realized what a perfect visual aidthis would make in teaching abouthazard potential of various items ofclothing. I saved the tie and it becamethe first of many items in my "trash cancollection."
A plastic cup brings to mind a per-sonal Lxample of how an accidentalpoisoning might occur. I wanted tomake a smoking machine out of a liquiddetergent bottle so I went into ourkitchen, grabbed the soap bottle, andpoured its contents into a plastic cup,placed the plastic cup on the windowsill and began making the smoking ma-chine.
About a week later, Tom was makinglemonade for the twins and found onlyone clean glass in the cupboard. Look-ing around, he spied the plastic cup onthe window sill and filled it withlemonade for Robby. Robby took a bigdrink and started to cough and choketearfully. His mother came running inand said, "What's the matter? Is yourlemonade too sour?" She took the glassfrom him and sampled it herself to seewhat was wrong, and she's been blow-ing bubbles ever since! This is an excel-lent example of how poisonings occurin the home! We are fortunate that theglass didn't contain drain cleaner, au-tomatic dishwasher detergent, or other
toxic substances which would havecaused extensive tissue damage. By thisexample, we can learn quite a lessona' sea proper storage.
Other trash that can be used to teachabout poisons is abundant. A paint canwith a "lead-free" label is an appropri-ate visual aid when teaching about leadpoisoning. A rusty, swollen or dentedfood can might be the focus of ques-tions designed to stimulate 'an aware-ness of food poisoning.
Once your trash collection becomeswell known, others will bring you itemsand stories to add.
i 1
Environmental Health
"I'd like to donate this to your trashcollection," said one of my students ashe handed me an old extension cord.The cord was peeling and cracked anddried out with wires exposed. He hadused this under the carpet for severalyears. Instead of just telling studentsnot to run extension co:ds under rugs,this cord can show how friction willbreak down the insulation. When stu-dents were asked to suggest ways thatthe cord might have become so abused,they told of pets which had chewedthrough extension cords and abouttimes when heavy duty appliances wereused on light duty extension cords caus-ing the cord to deteriorate. One of thevalues of utilizing items from the trashcan is that they act as discussionstimulators providing students withopportunities to share personal experi-ences.
One such experience involved ahandmade sweater which our twins de-cided to use as a replacement for theirlampshade when redecorating theirroom. The light bulb entrusted withcharred wool and the tiny sweater witha hole the size of a grapefruit tell therest of the story. Luckily, it was a woolsweater! Had it been made with syn-thetic yarn, it could have caused a fireinstead of smoldering as it did. Withthe sweater and light bulb or otherwearing apparel the concept of flamma-bility in clothing could be explored.
The topic of home fires is rich withbizarre stories. This past summer, Iheard a lot of commotion in the kitchen,so I came running in from the back yardand saw flames shooting out from be-hind the refrigerator. The coils on theback of the refrigerator had come intocontact with the plug; over a period oftime, vibrations had caused the coils tocut through the insulation. The meltedplug is a good reminder that we shouldregularly check oui electricalappliances.
In my trash collection I have a dishtowel that touched the lower heatingelement in the oven. A section of itburned away when it was being used asa pot holder and the unsuspecting cookhad a fire.
101
As a child, you probably enjoyedplaying with tape measures. Jeff was noexception. While watching TV, he wasreeling out a tape measure and watch-ing it spring back. As he reeled it out,the end dropped between a chair andthe far wall; Jeff flew out of his chair,eyes like saucers and hair standing onend. The metal tape had :ome into con-tact with the prong cat a lamp plugwhich was not all the way into the re-ceptacle. The other end hit thealuminum frame around the slidingglass patio door. At the contact points,the tape melted and charred. Jeff's tapeclearly illustrates how seemingly harm-less activities can be dangerous if theright conditions exist.
The average person can do little toprevent the unexpected; however, asafety conscious individual can takemeasures to guard against commonhazards. When purchasing electrical
appliances how careful are you to lookfor the Underwriters Laboratory (U.L.)label? When I found a battery charger atan unbelievably low price I looked onthe display card and found the U.L.label. It wasn't until sometime later thatI realized the U.L. approval appliedonly to the cord and plugnot the bat-tery, charger. I low often we have beenled into a false sense of security by notreading the fine print!
Items like the extension cord, swea-ter, refrigerator plug, tape measure, andU.L. labels are discarded daily. Alertyour friends and students to save thesetypes of items for you. It has been ourexperience that students are much morewilling to listen, share, and rememberexamples of home hazards than they areto memorize lecture notes of do's anddon'ts.
Hundreds of suffocations occur inhomes each year. Students become di-rectly involved when I introduce thesubject of suffocation by placing aplastic bag over my head. I demonstratewhen plastic bags are and are notdangerous. A plastic bag, tied in knots,will illustrate the p;oper method for i s
disposal.My mother-in-law receives shirts
from the cleaners in plastic bags which
102
she u. s for jobs around the house.When the twins were three, they dis-covered those bags in Grandmother'skitchen. They were just the right size toget over their heads. I happened to walkin just as Robyn pulled one down overher eyes and nose. Had she been moresuccessful, she would have been in
A
great danger of suffocation. A largerplastic bag in my collection was on arrib mattress at a hotel which couldhave tragic consequences if tired par-ents don't take time to check for suchhazards.
Many other household helpers can behazards. We all know that power to lsshould be handled with great respect,but often there is tendency to abuse orbe careless with "everyday" tools. Youprobably have a screwdriver with ablade that chipped because the cool wasused as a chisel, a crowbar, or some-thing else for which it wasn't designed.When there is finally an opportunity totighten a screw, there's not enoughblade. As you apply pressure, trying toturn the screw there is danger of per-
sonal injury as pressure causes the bro-ken blade to slip from the screw head.
Another example is my 98e bargainhammer which was designed for lightuse uch as driving tacks or small nailsWhen the kids decided to build a fort inthe back yard, they used my hammer todrive spikes. Half the spikes went incrooked so they tried to pull them out.All ot a sudden the claw bvoke, and therewas a tiving missile that might have putout an eye. These would-be-architectsalso damaged my hammer so that thehead would no longer fit. To avoid upset-ting me, they left it on the workbenchjust as they had found it, saying wrong.A week later, asl was working on a proj-ect the hammer head flew off and sailed
115
through the garage window onto thehood of my car. Are you saving yourplastic bags, broken screwdrivers andhammers as aids in developing conceptsrelating to hand tools and home safety?
Ar nually, hundreds of youngstersare tatally injured as a result of homefirearm accidents. Many of these acci-dents occur because youngsters don'tunderstand the danger of firearms. It isnot uncommon for children to consider.22 caliber guns as toys because of thesmall size of the cartridge. In an attemptto make students appreciate the de-structive capabilities of a small boregun, I showed them a soft drink canwhich was shot with a .22 hollow point.
This mutilated metal creates a lastingimpression when used to illustrate thedamage a .22 caliber bullet could inflicton a human body. Gunshot wounds canalso be explored with x-rays obtainedfrom a radiologist. My x-rav of a skullthat has been penetrated by BB clearlyillustrates the importance of safe gunhandling.
These items are examples of numer-ous objects that can be recycled fromthe trash to the classroom. As educatorsknow, the more we can do to allow stu-&tits to identify with our subject matterthe more we can enhance the learningprocess. By using common items ofsunk as a local point for discussing reallife situations, teachers can help stu-dents develop important concepts con-cerning their own health and safety.-Fight school budgets and rising infla-tion might be just the motivating fac-tors to encourage rummaging throughthe trash tor classroom stimulators.
56 TEACHING IDEAS
Ecology Games
RONALD W. HYATT is assistant profes-sor, Department of Physical Education,University of North Carolina, ChapelHill, North Carolina 27.519.
Ecology is currently a "hot" topic inhealth education courses in collegesand high schools. The topic is relevant,the subject matter is current, abundantresource material is available, the massmedia are active on the topic, publicand private agencies are concerned,and the students are involved in chang-
ing attitudes and legal approaches to-ward ecological matters. Still, the com-petent health education teacher, withall of this support, seeks fresh ideasin teaching ecology. Your departmenteditor has experimented with a learningapproach in ecology which is current,innovative, educationally sound, eco-nomical, appropriate to several schoollevels and allows for student creativity.This method is the game simulationtechnique, which allows students tocreate their own ecology games withecology problems and solutions pre-sented in the games.
The rationale for using this instruc-tional technique is, to some extent,based on the games theory which wasdeveloped in the 1960s at Johns H6p-kins University and other institutions.The games simulation theory, whichhas been used extensively in socialstudies, political science, and consumereducation, uses reproduced materials,
documents, historical events, and his-torical persons in a game setting withthe rules and regulations for the gamebased on the possibilities found withinthat game. Rules and regulations arebased on the many combinations whichhave or could occur in the interplay ofpeople, places, and events. Learningopportunities for the student are many,varied, and allied in theme. Creativesituations are different for each studentand each group. In brief, the game simu-lation method produces an excellentlearning situation. Granted, this ap-proach is rather a simple one, but it canbe modified for use on the college andLigh school levels and, perhaps, thejunior high school level merely by mak-;ng local classroom adaptations.
It is noted that several commercialgames are marketed in the area of ecol-ogy. SMOG, Litterbug, and Cleanup aregood examples of these. Pollution, acommerical product using game simu-lation, is suitable for use with juniorhigh school students through adults.The learning experiences describedhere are different from the commercialgames in several respects. Some of thesedifferences are as follows:1. The students provide the input andknowledge necessary to develop theirown game.2. The game conditions are current.3. The game situation can be scaled tolocal problems.4. The creative aspect is present.5. Small group work is educational andfun.6. Decisions must be made by theplayers which are relevant to theirneeds of the moment.
Materials NeededFew materials are needed, and they
are inexpensive. Six or eight pieces ofcardboard, scissors, felt tip pens orcrayons, glue, and scrap paper are suffi-cient. (Recycling is practicing what youteach!)
Class OrganizationGroup leaders are appointed, and six
to eight students are grouped in theareas of population, water, air, noise,and others as class size warrants. Anextensive bibliography is handed outseveral classes prior to this experience.Students are oriented as to the purpose
Environmental Healthof the class: to develop a game relatedto their area of interest. This game mustcontain rules and regulations, includechoices and chances, iod involve a de-cision-making process. Some of therules may be preplanned, or they maybe developed on the spot. The model ofmonopoly may be used where dice arerolled or number cards may be de-veloped .'s a means for the students totravel around the board, encounter thedifferent situations, and experiencelearning opportunities. Chance cardsare placed at appropriate areas, andstudents have to decide on a course ofaction. (For example: A student draws a
card and has the choice of additionalwaste controls in the company in whichhe owns stock, or he has an increaseddividend of two dollars. What willhe/she take?) Who wins the game andhow winners are declared are parts ofthe game which the group must estab-lish in their rules and regulations.
Starter Ideas
In case your students need kick offideas, here is an approach one classused.
NOISE POLLUTION: A playerstarts out with normal hearing. Hemoves and lands on a square of rock
103
music (3 decibels hearing loss), con-struction (-5 decibels), or sonicboom (-I- nervousness to your physi-cal conditi 1). Chance cards mightbe safety Jgislation, adding carpetsand drapes in house, etc.
The teacher can use starter ideasto get the groups rolling, but nor-mally a good introduction to theproblem is sufficient.
Desired OutcomesThe following teaching points are
among those that should be madeforcefully and vividly while ecologygames are being used.
1. The "random chance approach"to ecology matters, as expressed by
104
the dice or cards, is insufficient inreal life. Cooperative planning musttake place if we are to win the ecol-ogy game of life.
2. There is a total involvementneeded of legal methods, legislativeprocesses, citizenship practices andconcepts, industrial concerns, reli-gious beliefs and practices, and gen-uine concern about people and ourenvironment.
3. An understanding of the inter-relationships of ecology systems andsubsystems is a prerequisite to effec-tive action.
4. Careful selection in the me-nsof correcting the different ecology
117
problems, so as not to produce ad-ditional problems of ecology, is im-portant.
5. There should be a greater con-cern and knowledge about ecologywith its problems and promises.
The kind of game simulation andgame development outlined brieflyhere has worked for this teacher onthe college level. The students likeit, and its use creates an effectivelearning situation. Other healthteachers on different levels in otherlocales might well use this approachto help their students learn moreabout ecology.

57 TEACHING IDEAS
Environmental Health
Guidelines for a Recycling ProjectGeorge H. Brooks is assistant tothe dean of the University ofNorthern Colorado GraduateSchool and chairman of theGreeley Committee on Environ-ment,
Health educators and theirstudents may become involvedin local environmental action byhelping to establish a communitynewspaper recycling program.One such program has beensuccessfully operated since July1971 by the Greeley (Colorado)Committee on Environment. Thecommittee, appointed by the citycouncil in 1969, originally con-sisted of about a dozen mem-bersbusinessmen, housewives,teachers, and faculty members.Other members have beenadded, including a staff memberof the local newspapera recentjournalism graduate, keenly in-terested in the committee'swork, whose added publicity ef-forts have greatly helped thesuccess of the project.
The committee decided to un-dertake a newspaper recyclingproject after learning that 50% or
more of the volume of municipalsolid waste is made up of paperand paper products, and thatabout half of that volume con-sists of newspapers and maga-zines. They contacted a papersalvage company in Denver,which assured the committeethat they would purchase thepaper they collected.
A subcommittee was ap-pointed to find a building toserve as a untral collection cen-ter. In a ir g, unfruitful searchthey founL building owners re-luctant to permit storage ofnewspapers because of the po-tential fire hazard, or desiringto secure a long-term tenant.They investigated the possi-bility of securing a railroad caron a convenient siding, butlearned that a car couldn't bespared. A local trucking firm,learning of the project, offeredto spot a semi-trailer in a localshopping center parking lot oncollection day, then haul thetrailer to the paper salvage com-pany in Denver. Permission wasgotten to use the parking lot areafar enough away from the
dr 4
41111hrile."BEST COPY MAPLE
main parking lot traffic pattern,yet permitting smooth in-and-out traffic flow along both sidesof the trailer. Arrangements weremade with the local police de-partment for traffic control andwith the city street departmentfor portable barricades to chan-nel traffic flow along both sidesof the trailer.
The second Saturday of themonth was selected and publi-cized as collection day. TheCommittee on Environmentloaded the trailer that first Sat-urday, while a subcommitteesought volunteer groups to fur-nish labor for loading in subse-quent months. The first day'scollection yielded 27 tons. See-ing what the collection couldamount to, the committee de-cided to share the monetary re-turn from the sale of paper withthe groups which offered to help--one-third to the committee,one-third to the morning volun-teer group, and one-third to theafternoon group. The newsmedia carried the story of thecommittee's plans for continu-ing the paper collection on the
105

second Saturday of each month.Volunteer groups, wanting toearn money for their projects,were soon put on a waiting listas groups were assigned collec-tion days several months in ad-vance.
A telephone answering serviceagreed to receive calls from agedpersons and others unable tobring their papers to the collec-tion center. Trucks and stationwagons, furnished by membersof the groups working at thecollection center, collected pa-pers from callers. Most peoplewho wanted pick-up servicemade their calls ahead of the10 a.m. deadline on collectionday. There was little cause forconcern over abuse of the serv-ice.
The Committee on Environ-ment hopes that Greeley wilisoon combine its trash collectionwith recycling on a city-widebasis. However, though the tech-nology is available for such anundertaking, the market for re-cycled materials needs to be ex-panded. Even paper collectionalone is not yet feasible on acity-wide basis; the paper sal-vage company says it would beunable to handle all of Greeley'spaper along with all the otherpaper delivered to its docks.
Greeley's Commiuee on En-vironment can boast of a greatdeal of first-hand experiencewith what has become a widelyaccepted but not always prac-ticed dictum: man .riust live withhis environment, not despoil it.People will cooperate, if prop-erly informed and motivatedwith sound, well-pla.Ined proj-ects.
Here are some suggestions forthose who want to start theirown recycling project.
A market for the materials to herecycled is a must. The com-pany accepting secondary ma-
106
terials must be notified in ad-vance of the start of your proj-ect.
Have adequate transportationavailable. Greeley's first Satur-day collection filled a 40-footvan type semi-trailer. EverySaturday since, two trailershave been needed; in March1972 a third truck was partiallyfilled.
Advise city officials and thepolice department of yourproject.
Publicize each collection day,taking into account the differ-ent deadlines of daily andweekly newspapers and radioand television stations, An-nounce and adhere to open-ing and closing hours; remindpeople not to leave materialsat any other time. Includephone numbers of key com-mittee members and answer-ing service, if any. Give clearinstructions on how materialsare to be tied, bundled, orboxed.
liability insurance is a must.
Have adequate workers on handa minimum of 10 or 12during all collection hours. Attimes even that may not beenough, though at other timesit may be too many. Workersmay need gloves for handlingpaper bundles. Lifting bundlesby the heavy cord soon wearsblisters on tender hands.
Someone should be responsiblefor receiving the checks bymail from the company pur-chasing the papers or othermaterials. A home address orPost Office box may be used.The same person should beauthorized to write chi( cks tothe volunteer groups who fur-nish labor for your project,and should keep records ofnames and mailing addresses.
A=Ma.
119
I. IA
4 \'OW
II"
S.
58 TEACHING IDEAS
Family Life
Easy Ways of Getting into TroubleWhen Teaching Sex Education
GLEN G. GILBERT is associate professorof health education, Portland State thi-versity, School of Health and PhysicalEducation, P.O. Box 751, Portland, Ore-gon 97207.
During my career as a health educatorhave observed or have had related to
me numerous stories of problemsteachers have encountered while teach-ing sex education. Without exceptionthese teachers have been well meaningand have had the best interest of theirstudents at heart. Poor judgment ontheir part, however, has often resultedin placing their sex education programsin jeopardy; many supporters of sexeducation have become nonsupportersbecause of incidents involving poorjudgment. It is the hope of this articlethat such error can be minimized bycalling them to the attention of presentand future teachers of sex education.The list offered here is by no meanscomplete as teachers are constantlyfinding new ways to get into trouble.Here are a few easy ways of getting intotrouble teaching sex education.
1. Teaching sex education with in-adequate background. Sex education isone of the few areas where teachers are
:tually held accountable for what theyteach. Teachers of almost any other sub-ject area can have some poor days ofteaching and as long as they maintainorder it is unlikely they will ever bechastised for their teaching. Letteachers of sex education make an errorand you can bet they will hear of it. Itisn't that they shouldn't be held ac-countable, because they certainlyshould, but that such accountability israre in education and a major challengefor sex educators. There are few non-dedicated teachers teaching sex educa-tion for long, as it is a great deal of hardwork. It requires a thorough back-ground in the subject matteruniversity courses, seminars, and/or agreat deal of solid reading. Making con-tent errors in this subject will quicklyresult in lack of credibility with stu-dents, parents, colleagues, adminis-
trators, and will certainly draw the fireof the anti-sex education group.
2. Keeping your principal or adminis-trator in the dark. it is imperative thatyour principals and administrators beapprised of what is happening in yourclassroom. If you really wish to get intotrouble with administrators put themthrough a couple of late night phonecalls from irate parents concerning sexeducation material or projects whichthey know nothing about. It is highlylikely you will also be blessed with acall from that administrator. Keepingthe appropriate administrator up todate, for some, will mean just a state-ment that you are now studying sexeducation. For others it will mean de-tailed lesson plans from which you arenot to deviate.
3. Giving "secret" lessons. Anothersurefire way to get into trouble is tohave secret lessons with your students.Just make a statement such as "Today'slesson is just between you and me-- itis our little secret" and you can be cer-tain many parents will hear of it. Youhave no business teaching material thatyou cannot defend.
4. Violating district or school policy.This is clearly a violation of your re-sponsibility as a teacher. Curriculumguides are set up to give you paramet-ers to work in, and in a general sensereflect the wishes of the community.You should stay within those paramet-ers no matter what "you know is good"for your students. If you don't agreewith the curriculum you should cer-tainly work to change it, and a greatmany curricula need improvement.Until you get it changed, however, youare legitimately bound by contract to re-flect the existing curriculum.
5. Using poorly constructed home madematerials. Parents especially do not finda poorly constructed penis model or freehand drawings of genitalia amusing.Remember that you are dealing withtheir children. Giving a homework as-signment of freehand drawings of themale and female genitalia may seem in-nocuous, but many a parent has notedthat their daughter drew an erect penisape, wondered where she got her model
"lb f-1
image. Using anatomical drawings iscertainly a legitimate exercise, but havethem duplicated for your students.
6. Using questionable language. Slangterminology is often all students knowof reproductive anatomy and physiol-ogy. Students should not be re-primanded for using such terminologyunless they use it on purpose to create adisturbance, but they should be tact-fully taught the correct terminology.Teachers who feel they must use suchterms generally to "get on their level"may soon be on their level equally un-employed.
7. Not previewing films or materials.There should be a district committee toapprove films, and you are courtingdisaster if you use films not on the ap-proved list. It is always wise to previewfilms, but in sex education it is essen-tial. I will never forget an acquaintanceof mine who was not teaching healtheducation by choice, and consequentlyused a large number of films. He or-dered the district approved-for-high-school film, "The Story of Eric" (an ex-cellent film on Lamaze childbirth), forhis class. As the film progressed he wasnot prepared for the scene of actualchildbirth. He jumped in front of theprojector, and his class witnessed achildbirth in vivid color on his whiteshirt! He had not previewed his filmand was not trained or willing to dis-cuss childbirth.
8. Not being prepared for opposition.Most programs that are properly estab-lished suffer little opposition, as thevast majority of Americans support sexeducation, but numerous programshave been attacked. All teachers shouldbe able to verbalize the need for sexeducation when called upon and shouldanticipate such encounters. Do not re-spond with hostility or contempt. Par-ents will have honest questions andthey deserve sincere well-documentedanswers.
9. Teaching by the joke. Several in-structors have gotten into trouble bytelling or allowing students to tell "offcolor" jokes in the classroom. Teacherstelling inappropriate jokes can give thesex education classroom art improper
107

atmosphere for such an important sub-ject. One local high school teacher gotinto trouble by leaving his classroomfor a long distance phone call. In hisabsence a student leader was left incharge, who allowed jokes to be told. Itwas an all male class and the jokes soongot off color and deeper in raw sexualexpressiveness. One male not accus-tomed to hearing women discussed insuch terms left the room in tears.
10. Setting unrealistic goals. Manyprograms have been set up with goalsand objectives to eliminate VD, di-vorce, etc. Such programs are doomedto failure. A good example of this iswhen a program sets out to lower theVD rate. When a good sex educationprogram is established, the VD rateoften goes up! The reason for this in-crease is that people recognize signsand symptoms and go in for treatment.At a later date the rate may go down.
11. Forcing teachers to teach sex educa-tion. Mandating that all teachers shouldteach sex education is ludicrous. Forc-ing teachers to teach in any area theydon't wish to teach is unwise. Such ac-tion frequently leads to poor qualityeducation, and in sex education thatcan lead to disaster. Many teachers willnever be comfortable teaching sex edu-cation. Such unwilling or embarassedteachers can easily be turned to ananti-sex education position by suchforced compliance.
12. Letting personal bias overly influ-ence teaching. Everyone knows whatnormal sexual behavior is-- it is theway they behave. This erroneous beliefof major consequence is often carriedinto the classroom and can be devastat-ing. The advocate of open marriage,marriage at all costs, or any other par-
108
ticular lifestyle has no business preach-ing it in the classroom. We are allbiased. Recognize that bias and be care-ful not to try to convert your students.
13. Using inappropriate guest speakers.The selection of guest speakers must bedone with great care. Inviting right-to-life groups to class with brutal picturescan be a traumatic experience for stu-dents. Certainly the anti-abortiongroups should have the right to expresstheir point of view, but you as a teacherhave the right and the responsibility toscreen how it is done. Invitinghomosexuals to a junior high or highschool class is another example of aneasy way to get into trouble. Certainlythey should have the right to expresstheir opinion, but the problem thuscreated might jeopardize a total pro-gram.
14. Citing personal sexual eperience.It seems hard to believe that teachersneed to be reminded that this is notokay, but it still occurs. Do not let stu-dents push you into revealing your per-sonal life. It simply has no place in theclassroom.
15. Using nonapproved questionnairesof students sexual experiences or at-titudes. It may seem to you that findingout what is actually going on with yourstudents is a good place to start yourprogram, but your principal or ad-ministrator is likely to think differently.Remember that such questionnairesmay be construed as a reflection of theperformance of the school or district asa whole. Be certain to clear all suchquestionnaires beforehand. They mayprovide useful information, but be care-ful they don't cost you your job or hurtthe reputation of your school.
121
16. Leaving nonapproved reading mat-ter out for public view. It is of course ap-propriate for you as a teacher to readanything you wish, but remember thatthe district has approved materials foruse with students. Do not leave nonap-proved matter out where a studentmight pick it up or where an outsidermight view it. There is an excellentpaperback on birth control and STDs(sexually transmitted diseases) entitledIntercourse Without Getting Screwedwhich is a valuable resource. Many par-ents, however, may not find the titleamusing if they happen to walk by andview it on your derik.
Please ask yourself if you are un-necessarily endangering your sex edu-cation program. Sex education is far tooimportant to be eliminated or watereddown because of mistakes in judgment.Remember, sex education is one of thefew areas of education where teachersare truly held accountable for theirteaching. Making errors in teaching his-tory, English, or any other subject sel-dom results in chastisement, but makean error in teaching sex education andyou may be looking for a new line ofwork.
Readers are advised to review theNEA publication Suggestions for DefenseAgainst Extremist Attack: Sex Educationin the Public Schools, by the Commis-sion on Professional Rights and Re-sponsibilities, Washington, D. C.Readers might also wish to consult withlocal universitiel, the American Associ-ation of Sex Educators, Counselors andTherapists (AASECT) and the Sex In-formation and Education Council of theU.S. (SIECUS) for appropriate coursesin sex education in their locale.

59 TEACHING IDEAS
1-amily Life
Three Teaching StrategiesA soap opera, a silent walk, and apuzzlehelp present the faas about sexuality in a way
that is comfortable for both teacher and students
FLORENCE I. SNARSKI and CECEI IA A LYNCHare health educators teaching s cationcourses at Scotch Plains-Fanwood High School,Scotch Plains, New Jersey.
Prior to using any teaching method, the instruc-tor must carefully examine the philosophy of his/her course as well as the role of the teacher in theclassroom. Our basic philosophy is that sex edu-cation is the study of me-you-us. Sexuality cannotbe separated as a discrete, identifiable part of us.It permeates every aspect of our behavior. There-fore, as sex education teachers, our role is to helpour students learn more about themselves andothers. In our classroom, we consider three gen-eral areas of self: physical-psychological-societal.We do agree there is more to the total personthan these aspects; however, time and situationlimit content offerings.
As health educators, we have a part in thegrowth of our students in an area that is extreme-ly interesting to them and most humans. It couldbe so easy to slip into the same techniques forall our classes. Therefore, we strive to use differ-ent techniques to meet the needs of each studentand the different personalities of each class. Effec-tive teaching strategies can be as important in sexeducation as solid factual information.
In determining teaching strategies, we feel thereare basic questions to ask yourself:
What do my students want to learn?What do I want my students to learn at this
time?
How can I involve my students in this learning?How am I most comfortable dealing with this?Do I have limitations in this area?
Once these questions have beer ,:onsidered,the instructor can institute techniques that willdeal with the three areas mentioned: physical-psychological-societal.
YOUR OWN SOAP OPERA
Purpose: In sex education there is a need to explore,ocietal expectations versus individual values.
ObjectivesTo explore varied life style!To become aware of society's expectations for be-
havior.10 explore alternate modes of responses to life situa-
tions.To stimulate eative thinking.To illustrate the dynamics of day-to-day living experi-
ences as they influence our choice of behavior.
Procedure: Divide class into groups of four, providingfor male/female input in each group, if possible.
Each group is instructed to create a couple, givingbiographical structure to the couple, such as age, edu-cation, jobs, familial relationships, status of couple'srela`ionship, socioeconomic position, how did theyenter each other's life, etc.
After the groups are given about 20 minutes thefictitious couples are presented to the class with a
discussion of each couple as they relate to variabilitiesthat may influence their relationship, the future of therelationship, the permanency, and what kinds of needsthis relationship meets for each partner.
1 cl 109

AWARENESS WALK
Purpose: A relevant task of the sex education teacheris to provide for exploration of differing values amongthe students. An underlying factor in developing theseattitudes stems from previous learning experiences.Though we share some commonalities, we behaveindividually.
ObjectivesTo illustrate individual, divergent perceptions in reac-
tion to identical environments.To stimulate an understanding of One's own learning
processes.To provide insight into one's own responses or lack of
responses.To provide communication channels relevant to dif-
ferent attitudes about sexual behavior.
Materials
Paper/pencilsDitto slips reading: "We are on a classroom experi-
ment. We are not allowed to talk to you. Pleasecheck with my teacher (Name) for further informa-tion. We are timed so please do not delay us. Thankyou."
Procedure: Divide class into groups of four. Instructstudents they are to be nonverbal until further notice.
Each group is to take a walk in and around schoolenvirons deciding nonverbally where they are to goand planning to return to the classroom in 10 minutes.One member of the group will take a ditto explana-tion should 'anyone confront them in the halls. Theyare instructed to open their senses to everythingaround them on the walk.
Start the groups a minute or two apart so thatgroup moves out of sight before another begins.
Upon returning to the classroom, each student (stillnonverbal) is asked to write down all the things theybecame aware of on their walk.
When all groups have finished writing, allow fiveminutes for each group to share perceptions amongthe group and then form a large circle to discuss thedifferences in perceptions and translate the responsesto variances in behavior.
Conclusions: You will find yourself ref rring to thisexercise many times in subsequent classes lo explaindifferences in behavior. This exercise provides a subtlelearning experienre which requires teacher skill fortranslation into application.
One
LIFE PUZZLE
Purpose: A crucial building block for open communi-cation in sex education is the establishment of a"working vocabulary." An innovative review of anat-omy and physiology of the male and female reproduc-tive systems is through the LIFE puzzle.
110
e."i41
--`41-211
tip
Ohjectives:To display knowledge of terms and definitions of re-
productive systems----male and female.To provide student participation in general review.To determine areas requiring further clarification.
Materials:L a rge boxLIFE puzzle
To prepare WI. puzzle.1. Cut four letters-1 I f Iout ot large pie«s of con-
struction paper 124 x 36) _ For coding purposes and ease of!vision lion, a different mlor is used (or each.
2. 1)ivide eat h largo letter into segownts, sith each seg-ment containing 115o piec('s 55 )11( ii 11,1%1' hUVII ( into inter-im king irregular pieces. -Ihr numbei oi total segments ofall letters is determined hy usual class we so ia(h student
led'si one tw/lle part Also to he considered art' totalnumber ot terms anti definitions tom les ww.
On one hall of the segment Ow anatomical term is
written and on its interim king hall is placed the definition.4. Make a master layout designating \shot terms are on
the appropriate large letter tor instructor's reterence.5 Place all puzzle park into one large box
Procedure: Students select puzzle parts containing aterm or definition pertaining to the reproductive s 's-tems. Eac h student must find partner with correspond-ing term or definition. Partners present term/definitionto the class and then place their portion on the floorto put puiile together, eventually spelling out thelarge word LIFE.
Note- l)epending upon class si/e and 'Lime schedule,this c tivity may require more than one (lass periodto complete.
Com lo,ion: At the end of the lesson, the studentshave defined their terms. But this can also be used toillustrate the balance of Me, that all the,e terms to-gether "spell" life c reating as well as sustaining.
60 TEACHING IDEAS
The IofEducation
WARREN L. McNAB is an assistant profes-sor of health education at the University ofHouston, 3807 Cullen Blvd., Houston,Texas 77004.
Eleven million teenagers in theUnited States today are sexually active;'20% use contraceptives on a regularbasis 2 The unfortunate result of thisbehavior is .indicated by one millionunwanted pregnancies, higher fetal andmaternal death risk, increased numberof female school dropouts with a greaterrisk of unemployment, forced mar-riages, and a higher suicide rate amongexpectant teenage mothers, Thesestatements certainly indicate the needfor contraceptive education as a primarymeans of prevention.
Contraceptive education is not onlyproviding information and services toprevent teenage pregnancy. It is alsoeducation for young men and womenwho later in life may want a family andwill need to select a method of birth con-trol that will allow them to plan for awanted pregnancy. In addition, con-traceptive education teaches those whodo not want children to select a methodwhich will allow them the nonparentlife style they wish to live. It is impera-tive that we, as educators of sexuality,reinforce our cognitive objectives andprinciples through relevant learning ac-tivities which will enhance the total sex-uality and decision making skills of to-day's young people. With these con-cepts in mind the following learning ac-tivities are structured for three differenttarget groups--the junior high school
student, the senior high student, andthe parent.Don't Clown,Burst MisconceptionsGrades 7-9
This activity is effective as a cultnina-lion to a basic introduction of birth con-trol methods, functions, and knowledgedispelling misconceptions. in front ofthe class is a large, colored drawing of aclown. From his hands, strings projectto different colored balloons. Above hishead is the caption: Don't Clown, BurstMisconceptions! Inside each inflatedballoon is a misconception about con-traception; underneath each balloon onconstruction paper the same size as theballoon is the reason why the statementin the balloon is a misconception.
The activity is started when theteacher asks students of different teamsto correctly spell words related to con-traception. Examples are diaphragm,endometrium, intrauterine, lactation,gynecology, ovulation, etc. If the stu-dent spells the term correctly his teamreceives two points. If the student mis-spells the word he must come to theclown drawing, burst a balloon, and ex-plain why the statement in the balloonis false. A correct answer is worth twopoints. If the student cannot explainwhy the statement is a misconception,he opens the construction paper balloonand reads the correct answer to theclass. An example of a misconception is:A woman cannot become pregnantwhile lactating. The answer disprovingthis misconception is: 20% of nursingwomen who do not use a birth controlmethod become pregnant, and ovula-tion precedes menstruation. Reaching acertain point total can be the end of thegame.
Projected FutureGrades 10-12
Individually students are given thefollowing hypothetical situation: If youand your husband/wife have decidednot to have children for a while, or havedecided upon a nonparent lifestyle,what contraceptive method would youuse to prevent pregnancy? Justify yourchoice based upon the physical,mental'emotional, and social implica-tions of the contrac"ptive on yourhealth. For this exercise list the follow-ing he,dings in separate columns: prob-lem; alternatives; consequences; deci-sion.
The problem is selecting a contracep-tive. Individually the students fill in thecategories based upon knowledge re-
1 !)
Family Lifeceived in class and their own feelingsabout the different methods. There areseveral contraceptive choices or alterna-tives, and there are many different phys-ical, mental/emotional and social conse-qtwnces that will ultimately affect an in-dividual's decision. After individualselection,.groups of four or five studentscan share their contraceptive choicesand justify their selection with others inthe group. The teacher and class canthen identify similarities and differencesof contraceptive preference based uponthe physical, emotional, and social fac-tors influencing or prohibiting one'scontraceptive choice.
Dear WorldParents
This activity is to help facilitate com-munication between parents and theirsons and daughters. Parents individ.,-ally and'or collectively decide how theywould answer the following letter:
Dear World:I'm a parent with two beautiful teenagechildren. Torn is sixteen and Christine isfifteen, and both are dating regularly.While I certainly respect and trust them, Iwant to talk to them about the "facts oflife," contraception, and responsible be-havior. I know I am much too late, butthey seemed to grow up so fast! How canI go about talking to them and whatshould I say?
Signed Tongue Tied Parent
Following the parents' individual re-sponses they can collectively talk of theproblem, what their response would be,and how they would go about talking toa son or daughter. From this involve-ment parents can share ideas and dis-cuss other ways to open family com-munication channels about human sex-uality.
During our lives we are continuallymaking important decisions based uponwhat we as individuals feel is best forour own sexuality. Learning activitiesinvolving the cognitive and affectivedomains which help students make de-cisions based on their own perceptionof a given situation, reinforces indi-vidual responsibility which is para-mount to contraceptive education andpreventive health.
Bibliography
Guttmacher Institute, 11 Minim! Teenaga..,Planned l'arenthood Federation ofAmerica, New York, 1976.
Byrne, Donn. "A Pregnant Pause in the Sex-ual Revolution," II:yt-holoxy Today 11:2(July, 1977) pp. 67- 78.
111

61 TEACHING IDEAS
, sIA 1-
4,44
PregnancyA Gaming Technique
EDWARD T. TURNER is professorand the coordinator of graduatestudies, Health, Physical Educationand Recreation; and teacher of hu-man sexuality, Appalachian StateUniversity, Boone, North Carolina28608.
Gaming techniques are becomingmore and more a part of our educa-tional classroom teaching methods.With the greater use of games nu-merous companies have been man-ufacturing simulations and gamesfor use in the classroom. Thesegames are very good but they havetwo drawbacks: they are expensive;and they may not meet the specificneeds of a given teacher's class sit-uation. Games and simulations canbe easily thought out and con-structed by any interested teacherin order to meet his/her own indi-vidual classroom needs. Pregnancyis one such game which was de-signed for use in a senior graduatecollege class on human sexuality.The game has been quite success-ful in that it has greatly enhancedlearning through competition in a
fun sense. The largest problem inconstructing any game of this typeis getting your thoughts together onjust what you wish the game toencompass. The following construc-tion steps are helpful hints for put-ting together a board game, suchas Pregnancy.1. Select your topic or area.2. Collect ideas which you feel112
should be included on the topic.3. Select appropriate format for thephysical layout of the game.4. Place the needed information inthe appropriate places on yourboard.5. Construct your boards with col-ored tag board or poster board andcover them with clear contact paperin order to increase their longevity.6. Select equipment including mark-ers, dice, spinner, and decide onthe number of players.7. Select rules and interpretationsplay the game a number of times,revke your rules as needed.8. Mimeograph enough copies ofthe game and rules so that eachmember of the class has an indi-vidual copy.9. Revise rules and procedures andadjust game as necessary.
Pregnancy GameThe Layout (Seesample drawing and cards)
The Doctor Draw and Concep-tion cards are cut out of heavypaper, and stacked on the boardface down. On the back of eachcard is printed Doctor or Concep-tion.
Pregnancy RulesPlayers-2 to 5 players per board.Coed group preferred.Equipment board, markers andone die.1. Decide who is to go first.2. Each player rolls the die and
moves his/her marker, beginningon Start Fin.
1 9 ri
Family Life
3. When a player lands on a spacehe/she must read aloud the mes-sage written on that space. Dis-cussion among group membersensues. Thi., is an important partof the learning concept of thegame.
4. If a player lands on Conceptionor Doctor Draw he/she selectsthe top card, reads it aloud, andmakes the move. The group dis-cusses it.
5. Each player follows the sameprocedure.
6. The first person to reach thenewborn happy face is the win-ner. The exact number must berolled on the die in order toreach Baby Happy Face. Ifanother number is rolled theplayer must wait until the nextturn to complete the game.
7. Other players continue until allhave reached the end with thetotal group, including those al-ready finished, still responding inthe discussion.
This is just one type of boardgame that a teacher can constructat a minimum cost. Any otherhealth topic or any other area canlend itself to a similar game. Thetime and effort in formalizing theidea is well worth the positive learn-ing which ensues.

CONCEPTION CARDS
Abdomen begins to enlargeduring the third monthbuyloose fitting clothesTake anEXTRA TURN.
Morning sicknessnauseaduring the morning hours from6th to 14th weeks. MISS ONETURN.
More frequent urination. Uterusis pushing against bladderMISSONE TURN in order to buy extratoilet tissue.
GO BACK 4 SPACES
DOCTOR DRAW CARDS
Egg not implanted in uterusproperlygo back to nearestconception.
MiscarriageNatural abortionup until 6th month of pregnancygo to emergency roommissone turn then go to Start Fin.
Cesarean birth--incision in wallof abdornen in order to deliverbabystay still and miss threeturns.
Artificially induced laboroxytocintake two extra turns.
in\
EMERGENCYGo ToEmergency ROOM and misstwo turns
End of 1st monthEmbryo is 1/4"long, heartbeating 65/B/pm,eye, ears, & nosebegin to form, &(Doctors office)
End of 2nd monthEmbryo is 1"long. Large h-iad,nervous syst mfunctioning,embryo start tomove this pointon embryoknown as fetus
Rest.Doctor's
Office
EmergencyRoom
CONCEPTION CARD
4th weekFood passingfrom mother tn embryo
2nd week-2 membianesform around embryoaninner and outer. Fluidbetween them is amnioticfluidstructure is knownas bag of waters.
DOCTOR DRAW
Implantation of zygote inuterus wall--6th to 9th day
Float Trip in uterus forseveral days
Rapid Cell Division andZygote Becomes similar tos .iall hollow ball
Three day trip down thetube
Newly fertilized cell iscalled zygote
Da tors Offke
Doctor Draw
PREGNANCY
Labor Stage 3--immediately afterdelivery for 10 min.vigorously endswith passing ofplacenta (afterbirth)
One Sperm of 2-400 Breathing begins within oneminute, feet giasps and baby
1 21;
DOCTOR DRAW
End of 3rd lunar !nth--Fetus is 3" long, teethforming under gums, fingersand toes, bare thin nailsand sex is distinguishable.
End of 4th lunar mthFetus is 61/4" long, bodycovered with downy hair,skeleton is hardened, andmother may feel fetusmovement.
CONCEPTION CARD
End of 5th lunar mthFetus is 91/2" long, moremovement, heartbeat car'be heard with stethosco,
End of (Ah lunar mth--Fetus is 12" long, largehead, skin is very wrinkled,eyelids open and close
End of 7th lunar mth--Fetus is 14" long, thin andscrawny, reddish skin, ifborn po)r chance ofsurvival
End of 8th lunar maiFetus is 16" long, hair onhead more abundant, thinand wrinkled, if born thereis a good chance of survival
DOCTOR'S OFFICE
End of 9th lunar !nth--Fetus is 18" long, fatdevelops underskin givingphimper look, if bornexcellent chance of survival
10 lunar mth--Fetus is 20"long, fullterm 5'h to 11 lbs.average wt.
113

62 TEACHNG IDEAS
Contraception-Abortion Lifeline
Glenn E: Richardson is in the department ofhealth and physical edtaa lion at Tem sA&M University, College Station, Texas77843.
When using values clarification tech-niques, health educators often tend tooverlook valuable teaching opportuni-ties within the structure of the valueclarifying experience. The valuing expe-rience helps keep students' attentionwhile incorporating facts in an interest-ing manner. A technique that deals withthe sensitive issues of abortion and con-traception and yet integrates both teach-ing and valuing is what I call thecontraception-abortion life line. Thetechnique can be adapted to a 20-minuteperiod or continued for several hours ofdiscussion depending on age group, ob-jectives of the unit, and fadlitator skills.
MethodOn the chalk board or on a large piece
of paper, the instructor first draws alife-line with some key points labeled.
A values question is then asked,
"When does life begin?" Students re-spond independently until all who wantto respond, do. An "L" for life is placedon the continuum for each voluntary re-sponse.
Once the students have privately oropenly contemplated where life begins,a cognitive discussion of contraceptionand abortion methods can ensue. Foreach method of contraception dis-cussed, put a mark on the continuumabove the life line. The decision ofwhere to place the contraceptivemethod depends on the action of thecontraceptive method.
For example, the condom, foams, jel-lies, and diaphragm could be placed at apoint between 7 and 3 because theyprevent the sperm from reaching theegg. The IUD would be placed between4 and 5 because the IUD prevents im-planta ion of the fertilized egg. Vasec-tomies would be placed between 1 and 2since the sperm is never deposited. Thisallows for an interesting discussion ofthe contraceptive techniques and can beexplained in conjunction with the use ofcontraceptive kits.
Following the discussion of con-traceptive techniques, abortion tech-niques can be discussed and the periodsof most appropriate use be placed onthe lifeline. For example, D & C and
Contraception-Abortion Lifeline
cro
Ft-Suction
'2 E D&C
1 2 3 4 5
I I
6 7 8
InducedAbortion
L
L L L L
I I I 1 I I 1
9 10 11 12 13 14 15
L - Life begins
1 14 127
Family Life
.suclion techniques cover points 5through 10. Induced labor with salinesolution could cover points 10 through12.
After the cognitive portion of thetechnique is finished, then the valuingquestions begin. Questions such as thefollowing can be used:
1. Which, if any, of the contraceptivemethods is acceptable to you intellectu-ally? Spiritually? Emotionally? Socially?For what reasons?
2. Which, if any, of the abortionmethods is acceptable to you intellectu-ally? Spiritually? Emotionally? Sodally?For what reasons?
The final question in the technique isone that will reinforce personal valuesor promote the examination of personalvalues in a way that personal affectiveand cognitive value dissonance will beavoided or clarified. The question is: Isthe mark where you believe life beginson the right or left of your personallyaccepted contraceptive or abortivemethods? If the life mark is on the rightof the acceptable contraceptive andabortive techniques, then the preven-tive action of the methods occurs beforelife begins and no dissonance related toterminating life should be experienced.But if the life mark is on the left of .hemethods, then in the perception of theindividual, the method takes actionafter life has begun and potentiallycould be the source of mental and emo-tional guilt feelings if the methods areused.
The final question can lead to a dis-cussion of how to find peace of mindwhen using contraceptive methods, thatis, using appropriate methods (if any)which conform to one's own values. Ifstudents are unsure when life begins, asmany are, then the technique will prob-ably stimulate some pondering. It canalso lead to a discussion of the ease ofmodifying behaviors (use or non-use ofcontraceptive methods) versus the facil-ity of changing values. .
Other questions can be developed torelate the lifeline to other values, e.g.,questions regarding spontaneous abor-tion and life, therapeutic abortion ondvalues, and decisions to abort, keep thechild, or give it up for adoption.
The abortion-contraception lifeline, aconfluent education technique, places atraditional discussion of contraceptionand abortion methods within a valuingframework. The technique has beenused many times in university classesand has provided a stimulating, clarify-ing, and valuable experience for teacherand students.

TEACHNG IDEAS
Family Life
Teaching Students AboutTheir Future Role as Parents
JAN YOUNG is a health issues instructor in the MankatoPublic Schools, Mankato, Minnesota 56001.
Isn't it interesting, when we think of all of the time andeffort that is spent in curriculum development and cur-ricular changes, to realize that we have frequently madea complete circle to find ourselves back where westarted? This appears to be more and more evident in thetrend to go back to the "open school," to nongradedclassrooms, and to teachers working with students ofdifferent grades and certainly different interests andtalents.
In our attempts to concentrate on technical and scien-tific advances in knowledge, and our efforts to ensurethe proper sequential development of certain basicknowledge and skills, is it possible that sometimes weoverlook that which is the most obvious? Are we soconcerned about what we think the student shouldknow that we tend to overlook what they so desperatelyneed for their future mental and social happiness?
In my 11th grade health classes, whenever I pose thequestion or design an activity relating to future goals, atleast three-quarters of every class indicates that someday in their future they plan on being a parent. We givethem instruction in many other areas and subjects, buteducators neglect to spend much time on the subject of"how to be a better parent."
It is the "in thing" for many students in high schooltoday to talk about how their parents "just don't under-stand" and are really not "hip" or "in tune" with what isgoing on. We who work with students every day seemuch evidence of parent-teen conflicts.
Talk about "learning opportunities"! Let's start takingadvantage of these "teachable moments" in our healthclasses! For a perfect starter, the next time you hear anyof your students make a negative remark about theirparents, you can come back with the statement, "Well, Isuppose they have had little or no training in how to be aparent and so perhaps it would be nice to allow them tomake a few mistakes." This, or some similar statement,can get you off the ground into some very interesting"parent training" concepts.
Another interest getter is to write in large lettersacross the blackboardTODAY'S LESSON: HOW TOWIN AN ARGUMENT WITH YOUR PARENTS. I canguarantee you their undivided attention!
Recently, I was among the guest speakers at a confer-ence on "interpersonal relationships" at a local highschool. A variety of topics were offered simuitaneouslythroughout the day and students chose the five theywere most interested in. My assigned topic was "human
sexuality and transactional analysis," and for the firstsession not one student stopped by. They were attractedto the more obviously intriguing rooms labeled "vag-abond;ng Europe," "why you shouldn't get married,"and "medical aspects of abortion." Before the secondsession began, I put a new sign on the door that read:"How to win an argument with your parents!" For thatand the remaining sessions, I had a full house, withenthusiastic students. I covered the same material that Ihad intended to cover, but took a different approach.We discussed many of the concepts from the book byThomas Gordon, Parent Effectiveness Training, andThomas Harris's book, I'm OKYou're OK. By puttingmyself in their place and approaching parent-teen con-flicts from their view, the motivation was thereand thelearning outcomes were evidenced by their commentsand participation in role playing.
Many basic concepts included in a health class alsorelate to basic content areas in parenting.1. Growth and Development: A parent who understands
growth and development will be better prepared to adjust tochanges in offspring.
1 Attitudes and Habits: A parent who is knowledgeable aboutthe influence of the home in fostering healthy versus un-healthy attitudes will be more apt to convey positive healthattitudes and habits.
3. Communicative Skills: A parent who is aware of commoncommunication blocks and adept at using positive com-municating skills will have a better chance of fostering andmaintaining good family communication.
4. Decision Making Skills: Parents who allow their children tomake some choices will probably have teenagers d adultswho will be more responsible in making decisions that affecttheir health and welfare.
5. Coping with Crisis: Parents who understand that childrenlearn how to cope with crisis situations will be more likely toset a better example for the children in how they as a parentmeet a crisis in their family.
6. Parents' concern for their own development of maximumquality of physical, social, and mental health will hopefullydevelop a similar concern in their offspring.
These concepts are included in many health educa-tion programs, but those concerned with coMmunica-tive skills and decision-making skills are often over-looked. Therefore the remaining part of this article willdeal with methods to use these skills in teaching aboutparenting in a classroom.
The three main skills in parent effectiveness trainingthat I find myself using over and over again in my healthclasses are:1. Active Listening: this is the ability to understand what the
person is "feeling" as well as saying.2. Use of "/ Messages": An "I message" consists of three parts:
128115

(1) how you feel, (2) the situation or problem, and (3) theeffect or reason.
3. Who Owns the Problem: Sometimes a conflict resolves itselfwhen we decide whether it is really our problem or some-thing we are making our problem. If the problem is ownedby both parties involved, often a compromise is necessary.
Some examples of the three techniques and how theymight be used by a parent, a teacher, or a teenager aregiven below:SITUATION: A parent is totally frustrated by her daughter'sdisregard for house hours or policies established for schoolnights, weekends, etc.Positive Parent Responses:1. "You really seemed upset when I questioned you after you
came home late." (active listening response)2. "I feel bad that you came in so late since I thought we had
made an agreement on weekday hours." (I message.)3. They both own the problem. It is definitely a problem for the
mother, because of her concern for daughter's ability tokeep up in school. It is a problem for the daughter so long asshe is a member of the family living in the same household.
By using either active listening or an "I message" or both, theparent is taking some of the pressure off and may avoid a moreserious confrontation than using typical parent responses,which immediately put the person on the defensive, such as:"What is the matter with you anyway?" "When I was your age, ifI came in that late I would have been campused for a month.""How do you ever expect to amount to anything? You will neverbe able to keep a job if you can't obey some orders."
Classroom Strategies1 . Role play family-teenage conflicts in groups or
partners.2. Practice using "I messages" in response to cer-
tain situations with a partner.3. Conduct small group discussions about com-
mon teenage-parent conflicts and how tohandle them using active listening, "I mes-sages" and transactional analysis positions.
116
In role playing involving common conflicts, suggestrole playing using typical responses in contrast to re-sponses using active listening and "I messages" or prob-lem ownership.
SITUATION I: Jim and Father have frequent arguments over useof the car. Jim feels he should be able to use the car for his datesand his father feels that he should get a job and buy his own carbecause he thinks Jim does not take good care of the car.leaves it in a mess and uses too much gas.SITUATION 11: Mary, an 11th grader, has a continual hassle athome over her messy room. It has created a lot of frictionamong the entire family and many heated arguments betweenMary and her mother. Who owns this problem---Mary or hermother?
SITUATION 111: Jackie has a constant battle every time she datesJerome. She likes him and feels her parents are unfair andprejudiced because he has long hair and works in a servicestation. Jackie's parents want her to go to college and feel thather steady dating with Jerome will squelch this as Jerome isplanning on taking a one-year mechanics course at a vocationalschool.
Health teachers can gain an understanding of how touse the main methods which are explained in Gordon'sbook on parent effectiveness training (PET). There areother general communication strategies which can andshould be used, such as paraphrasing and receptivelistening. Courses are offered in communications andhuman relations. The PET classes which are offered inmany cities by certified instructors are an excellent wayto better understand the principles involved. Practicehelps and is really necessary to use the skills effectivelyand naturally in the classroom.
A common complaint of teenagers today revolvesaround conflicts with their parents. PET offers what isconsidered to be a no-lose method of solving conflicts.If you introduce these concepts to your high schoolstudents, they start to look at their own personal con-flicts with their parents and by putting themselves intheir parents' place they often gain much insight intohow complicated the job of being a parent can be. Theycould, as a result of some parent training, become moreresponsible parents in the future.
64 TEACHING IDEAS
Ask the Students Themselves
A. GORDON BENNE11 is supervisorof health, physical education, andrecreation in the flyria City Schools,Elyria, Ohio 44035.
In spite of a new liberation, in-cluding children, we are still Vic-torian in talking with our youngstersabout intimate personal hygienematters. Yet, they watch us act free-ly and without restraint; we drinkto excess, smoke too much, take toomany tranquillizers, eat too muchof the wrong things, exercise toolittle and let our children get hung-up on drugs. Adults are still overlyconcerned about "hush-hush" and"hidden" subjects, and when any-one mentions sex education in thepublic schools, everyone panics.
Despite the antiquated fears ofparents and the general public ahoutthe concept, Elyria High Sr hoolstudents overwhelmingly confirmedthat they want and need such a pro-gram in their city schools.
Students do not talk to their par-ents about the problem of venerealdisease, for instance, but they arevery much aware of it. Venereal dis-ease is a small part of the totalhealth education program, yet thestatistics in this area of the totalsubject show us the weakness of ourprograms in the public schools,
Elyria High School, Elyria, Ohiohas an enrollment of 2,734 students,tenth through twelfth grades. In No-vember, 1,767 students went to thegym to see the film "Quarter Mil-lion Teenagers," participated in dis-cussion, and were given names andaddresses where they could betested for VD by a health depart-ment official.
The next day, about three fourthsof the student hody were givensome form of education on venerealdisease. .1-he facts presented were
furnished by the State Board ofHealth and the State Board of Edu-cation. Examples of the stark anddismaying statistics furnished fol-low:
1 The U.S. is involved in the worstepidemic of venereal disease in his-tory.VD is second only to the commoncold in the communicable diseasefield.
3. In Elyria alone the reported casesjumped from 20 to 60 in one year.
4. In Lorain County, Ohiothetwelfth most affected in Ohio--there was an increase of over 25%.
5. In the state of Ohio, reported casesincreased over 20%.
6. Cleveland, Ohio had 73,880 newcases and is ranked 8th in the na-tion in venereal disease increase.
7. Ohio had 218,356 cases of gonor-rhea reported.
8 In the U.S. there were over fivemillion new cases of venereal dis-ease in one year.It is estimated by leading healthauthorities that only 1 out of 8Cases of venereal disease is everreported.
After being exposed to thosestatistics, the Elyria High School stu-dents participated in a county-wideVD Awareness Week. They madeposters, spent hours manning a
booth for the Lorain City HealthDepartment at the Midway Mall,and distributed literature contrib-uted by the State Boards of Healthand Education.
In an effort to determine, the atti-tude of students to health educa-iton in general, and to the inclusionof such topics as venereal diseasein health education, we asked about85'!1, of the student body to respondanonymously to questions such asthe following:
13U
Family Life
Do you think health educationshould be put into our course ofstudy? If so, when?
When did you first become inter-ested and adventurous in sex?
Do you think venereal disease edu-cation should be included in a
course in health education?
All the students responding feltthat health should be taught K-12;the majority favored a formalizedhealth education program beginningsometime between the fifth andninth grade. None suggested begin-ning such a program as late as theeleventh or twelfth grade. As onestudent remarked during the dis-cussion, "If we don't know it bythen, it will be too late!" The stu-dents wanted health education tocover such topics as personal hy-giene, grooming, VD, disease pre-vention, and dating.
In the area of VD education, ourstudents felt free to acknowkAgetheir need and lack of information.Adults are afraid to talk to their chil-dren about intimate physical sub-jects, but many refuse to allowknowledgeable professionals to doso. What kind of climate is it thatwill he all for permissiveness athome and in the school, but bealmost obsessively opposed to giv-ing young people necessary facts toprotect them from the results ofthis much touted premissiveness?
With the kind of positive re-sponse of high school students dem-onstrated in the brief survey con-duc ted at our high school, it ap-pears imperative that mmm Unitiesbegin to listen to young people aridhelp them get the health educationpmgram they feel they want aridneed.
117

65 TEACHING IDEAS
Test Tube
Considerations
DEBORAll A. DUNN is (issislant profes-sor and health specialist In the Departmentof Physical Education for Women,tvashiuNton Stale 1.Inivelsily, ,
tVashin:Oorr 9016.1.
The July 25, 1978 birth of LouiseBrown, the first so-called test-tubebaby, intensified an international de-bate over the ethical, legal, and societalimplications of in vitro fertilization(IVF) as a means of human reproduc-tion. With talk of cloning, surrogatemotherhood, and parthenogenesis, it'spossible that in the years to come, soci-ety's reproductive options may be in-
118
creased, thus placing additional deci-sion making demands on individuals.
Through health education experi-ences, students can be aided in comingto grips with moral issues which mayarise as a result of scientific advances inhuman reproduction. The following ac-tivity was designed to help college stu-dents identify a wide range of possibleimplications of WI'. The same formatcould be used to elicit consideration ofother issues with far-reaching pos-sibilities.
After a review of the actual procedureinvolved in IVF, the students wereasked to recall the reactions of variousindividuals and groups to the an-nouncement of the first successful IVF.How did prominent scientists andtheologians react? Flow was it handledby the press? What did } Jur family,friends, or acquaintances have to sayabout it? How did you react to thenews?
Keeping these reactions to IVF inmind, the students were asked to si-lently list some of the questions thathad been raised and some of the impli-cations that had been identified. Whatlegal questions have surfaced? Howmight it affect the family? What could itmean to science?
131
Family Life
Students then shared their ideas withthe class. Each question or implicationoffered by the students was written onthe board for the entire class to see. (Anoverhead projector could be used.) Ourlist contained 26 items including ques-tions or implications such as the follow-ing.
Gives new hope to couples who havebeen childless due to tubal problems.
May help in the discovery of new con-traceptive methods.
If the child is not "normal,- who is re-sponsible?
Could reveal new information on thefirst hours and days of life.
One more step toward manipulation oflife processes.
Could increase the population.Women with tubal ligations who
changed their minds and wanted tohave a child may be able to becomepregnant.
Opens door to surrogate mothers.If several fertilized eggs die with IVF, is
this abortion?May help scientists find ways to pre-
vent sonie genetic diseases.
When all questions or implicationswere on the board, students wrote outthe three they thought carried that mostimportance in the debate over this formof reproduction. Then, they placed thenumber 3 next to the most importantquestion or implication, a 2 by the sec-ond most important, and a 1 next to thethird most important. The papers werecollected and the scores were tallied.The most commonly identified con-cerns were the question of responsibil-ity should the child be deformed, thenew hope given to couples who couldnot conceive, the ft r of manipulationof life processes, and the possibility ofthe procedure leading to new con-traceptive methods.
The followup to the exercise con-sisted of a discussion of why the ques-tions and implications that were mostoften raised by the students wereworthy of such careful thought and con-sideration.

TEACHT\IG IDEAS
Selected Impacts of Contraception
on Man and/or Society
PATRICK KIDD TOW is a graduate assis-tant in the Department of Health Educationat Southern Illinois University, Carbondale,Illinois 62901.
This teaching strategy was designedprimarily for college health surveyclasses, however, it could also beapplied to students in the senior highschool setting. This activity could followafter a unit on population growth,human sexuality, or birth control educa-tion. It involves dividing a cbss intoseparate groups to brainstorm a list ofall possible impacts from the usage ofcontraceptive methods. The topic can beexamined in view of the impact uponthe individual or society as a whole. Fif-teen minutes are usually allotted for thisportion.
After this step has been accom-plished, their next announced objectivewould be assigning symbols to each de-rived impact. These symbols (=, , or?) would represent respectively,whether they felt the concerned impact
desirable, undesirable, or questiona-lkyalue judgments must be made as agroup. There will be some items that areobviously controversial, therefore, itwould be advisable for the classroomteacher to circulate and help facilitatethe discussions when necessary. Thisportion of the activity usually involvesabout 15 minutes.
Bringing the groups back together asa class, the teacher calls upon a memberfrom each group to share the findingson the emotional impacts of contracep-tive usage. On the second round, a dif-ferent member in each group presentsthe environmental outcomes. This pro-cess continues until all six areas of con-cern are brought out for classroom dis-cussion and everyone has an opportu-nity to present their group consensus.This final part should take approxi-mately 20 minutes.
Family Life
.111
r
t /4 i e '.. . .
4'fr -e_ '
-
-
Symbol Designations+ = positive or desirable
= negative or undesirable? = questionable
Emotional Impacts1. eases fear of pregnancy out r)f a lov-
ing relationship (+)2.3.
Physical Impacts1. contraceptive devices may cause
cancer ()2.
social Impacts1. inlaws frown upon childless couple()2.3,
112
Environmental Impacts1. human race may become extinct (?)2.3.
Economic Impacts1. parents are afforded more time and
money to plan family ( +)2.3.
Religious Impacts1. considered a violation of religious be-
liefs by ministers ()2.3.
119

67 TEACHNG IDEAS
First Aid and Safety
A Working Model forSimulation Techniques
GLEN C. GILBERT is instructor of health education, Uni-versity of North Carolina at Greensboro, Greensboro,North Carolina 27412. Much of the material for this articleis from the ongoing research .by the author for his doc-toral dissertation at Ohio State University.
Instructors of emergency care are faced with the chal-lenge of educating personnel to deal with complex situa-tions that require prompt and efficient treatment. Theinstructor, largely because of time limitations, is oftenforced to rely on "one shot" coverage of the individualskills involved. Commonly such coverage is followed bya paper and pencil test in an attempt to evaluate thestudents ability to apply specific skills.
This article presents an alternative method of teachingand evaluating those skills dealt with in emergencyhealth care classes. It promotes confidence in the stu-dents' ability to employ the newly acquired skills in reallife situations, presenting a variety of situations that re-quire the application of a multiplicity of first aid skills.
The use of simulated emergency care situations is nota new idea, but this article F esents several new varia-tions on simulation design and provides a workingmodel for those persons unfamiliar with simulationtechniques.
Simulated situations can be an asset to any emergencycare program for the following reasons:
1. They provide examples of real life emergency caresituations.
2. They provide practical applk-ations of skills uw-ered in the classroom.
3. They provide practice in the analysis and evaluationof emergency situations without possible injury result-ing from judgment errors.
4. They prc, ide an alternate teaching strategy for theinstructor.
5. They provide a possible evaluation technique forinstructors.
6. They provide students with practice in performingskills under stress and thereby should increase self-confidence.
Simulations can become an integral part of an emer-gency care instructional program from the onset. Theycan be used in a variety ot ways, some ot which areoutlined below:
1. They can be used as a direct communicationstrategy by presenting the situation and the correct per-
120
formance of tirst aid procedures by the instructor or thest LI dent.
2. They can serve as an instructor-student interactionstrategy by presenting the situation and jointly (instruc-tor and class) analyzing the proper course of action andreasoning.
3. They can be a group activity with several peopleworking out a course of action and then undertaking it,This might be better in more complicated situations.
el. They can function as an independent student activ-ity by setting up an area where students come in andperform skills in varied situations.
You may wish to devise your own simulation situa-tions or ask your students to make them up for you, inwhich case each student should design one situationcomplete with symptoms and procedures. A file of suchstudent situations can be collected and made availableto students for review.
The Simulation Model: ScenarioThe student sel:Kted to perform as a first aider selects
a card, reads the number, and leaves the room.' Whilehe is out of the room the situation numbered is set up.Other students are employed as victims with symptomtags, medical alert tags, or whatever is appropriate forthe situation, placed on their person. These tags are putat the site of the simulated injury or symptom. The mate-rials which are available to the first aider are placed in thearea designated as the situation area.
The student re-enters the room upon notification andreads the card out loud to the class (he is allowed to keepit during the situation). He then examines the situation,makes a judgment based upon the symptom tags, andother information provided, and then performs theproper first aid procedures. The instructor rates the stu-dent's performance using a predesigned form.
The more realistic a situation, the better it is as alearning device. There are simulation kits available thatinclude sintulated injuries and simulated bleedingwhicn can be used, but they require a much largeramount ot time and the cost is often hiOt. The major
'Selection of situation cards should be accomplished byshuffling and the taking of the top card each time or some othermethod at the discretion of the instructor. However, it is ad-vised that a random device be employed so that students willnot feel their situation was predetermined at the will of theinstruc tor.
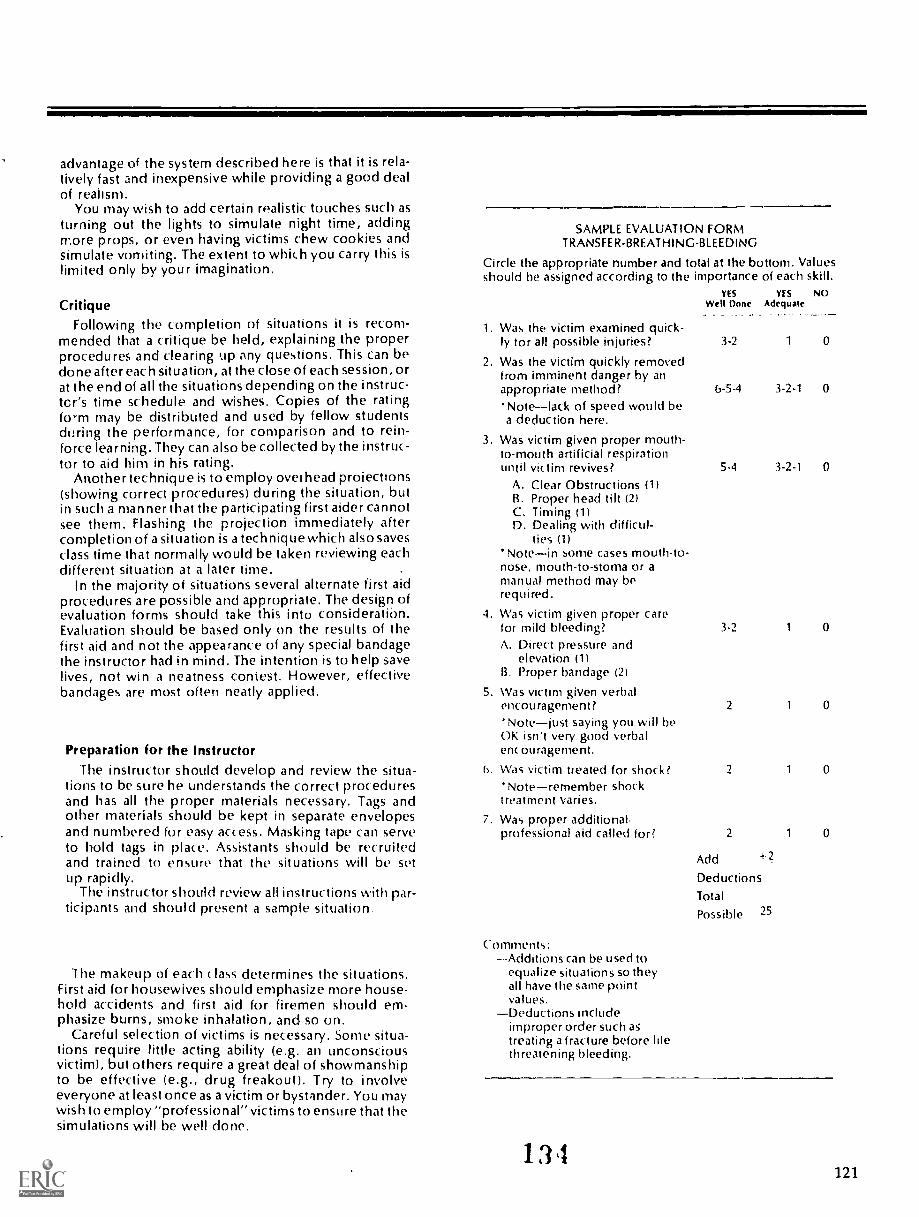
advantage of the system described here is that it is rela-tively fast and inexpensive while providing a good dealof realism.
You may wish to add certain realistic touches such asturning out the lights to simulate night time, addingmore props, or even having victims chew cookies andsimulate vomiting. The extent to which you carry this islimited only by your imagination.
CritiqueFollowing the completion of situations it is recom-
mended that a critique be held, explaining the properprocedures and clearing up any questions. This can bedone after each situation, at the close of each session, orat the end of all the situations depending on the instruc-tcr's time schedule and wishes. Copies of the ratingform may be distributed and used by fellow studentsdtrring the performance, for comparison and to rein-force learning. They can also be collected by the instruc-tor to aid him in his rating.
Another technique is to employ overhead projections(showing correct procedures) during the situation, butin such a manner that the participating first aider cannotsee them. Flashing the projection immediately aftercompletion of a situation is a technique which also savesclass time that normally would be taken reviewing eachdifferent situation at a later time.
In the majority of situations several alternate first aidprocedures are possible and appropriate. The design ofevaluation forms should take this into consideratibn.Evaluation should be based only on the results of thefirst aid and not the appearance of any special bandagethe instructor had in mind. The intention is to help savelives, not win a neatness contest. However, effectivebandages are most often neatly applied.
Preparation for the InstructorThe instructor should develop and review the situa-
tions to be sure he understands the correct proceduresand has all the proper materials necessary. Tags andother materials should be kept in separate envelopesand numbered for easy access. Masking tape can serveto hold tags in pla«. Assistants should be recruitedand trained to ensure that the situations will be setup rapidly.
The instructor should review all instructions with par-ticipants and should present a sample situation.
I he makeup of each class determines the situations.First aid for housewives should emphasize more house-hold accidents and first aid for firemen should em-phasize burns, smoke inhalation, and so on.
Careful selection of victims is necessary. Some situa-tions require little acting ability (e.g. an unconsciousvictim), but others require a great deal of showmanshipto be effective (e.g., drug freakout). Try to involveeveryone at least once as a victim or bystander. You maywish to employ "professional" victims to ensure that thesimulations will be well done.
SAMPLE EVALUATION FORMTRANSFER-BREATHING-BLEEDING
Circle the appropriate number and total at the bottom. Valuesshould be assigned according to the importance of each skill.
1. Was the victim examined quick-
YESWen Done
YESAdequate
NO
ly tor all possible injuries? 3-2 1 0
2. Was the victim quickly removedfrom imminent danger by anappropriate method? 6-5-4 3-2-1 0
Notelack of speed would bea deduction here.
3. Was victim given proper mouth-to-mouth artificial respirationuntil victim revives? 5-4 3-2-1 0
A. Clear Obstructions (1)B. Proper head tilt (2)C. Timing (1)D. Dealing with difficul-
ties (1)Notein some cases mouth-to-
nose, mouth-to-stoma or amanual method may berequired.
4. Was victim given proper carefor mild bleeding? 3-2 1 0
A. Direct pressure andelevation (1)
13. Proper bandage (2)
5. Was victim given verbalencouragement? 2 1 0
'Notejust saying you will beOK (sn't very good verbalenc ouragenlent.
1). Was victim treated for shock? 2 1 0
'Noteremember shocktreatnlent varies.
7. Was proper additional.professional aid called for? 2 1 0
Add 2
DeductionsTotal
Possible 25
Comments:--Additions can be used to
equalize situations so theyall have the same pointvalues.
Deductions includeimproper order such actreating a fracture before htethreatening bleeding.
13,4121

SAMPLE SITUATION
Situation:Your brother is playing in the garage when you hear
an explosion. There is smoke in the air and the roofappears in danger of collapsing.
Where:Your home.
Miscellaneous Information:No one else is home.
Above is the card that is given to the first aider. The informa-tion below is not seen by the first aider. It gives the directionsfor the conduct of the simulation.Position of victim:
Face down.Special Instructions for Victim:
Remain unconscious until signaled by instructor.Special Instructions for bystanders:
No bystanders present.Supplied Materials:
1. Home materials box (a box containing those first aidsupplies generally found in the home.
Tags:1. No air going in or out (1) chest2. Blue skin (1) face3. Mild bleeding (1) right forearm
PARTICIPANTS INSTRUCTIONS
1. You must treat this like a reallife situation. Nothing will beassumedyou must do all that you would in a real lifesituation. To receive credit for any procedure it must beaccomplished completely. The only exception to this isprocedures that cannot be done in the classroom such asmaking a phone call.
122
2. You may use only material provided in the testing area.3. You may not use any notes or cards other than those
provided.4. For assistance you may use only those people provided
and you musr give explicit directions for any aid theyadminister. No undirected assistance or information is tobe given by other students or victims.
5. Time will be an important factor in life threatening situa-tions. A reasonable time will be allowed for less severeinjuries, but do not waste time. (After having used a situa-tion several times an instructor will have an idea of howlong it should take to complete and may wish to set a timelimit.)
SIMULATION TAGS
Simulation tags which have symptoms written on them areconstructed for each situation and attached !oviclims by mask-ing tape. They are coded hy ulorre( :deeding, blue forbreathing difficulties and gree. I yellow for miscel-laneous symptoms.
Their size is appropriate for the symptom. This means thatsymptoms that would be obvious such as severe bleeding, havea large tag and clear fluid from the ear, are relatively small. Noattempt is made to hide tags any more than in real situations.The objective is not to trick anyone, but rather to ensure athorough examination.
Burns are listed by degrees for easy identification of properfirst aid treatment. Bleeding tags are marked mild, moderate, orsevere.
In appropriate situations medical alert tags arid cards plusmedications are supplied to further aid the first aider in diag-nosis. Medications are given in several cases to ensure under-standing of the Red Cross position on providing or giving medi-cation. Names on medications and cards should be uni-sex(i.e., Pat) so that male or female vk tims fit into all situations.
1
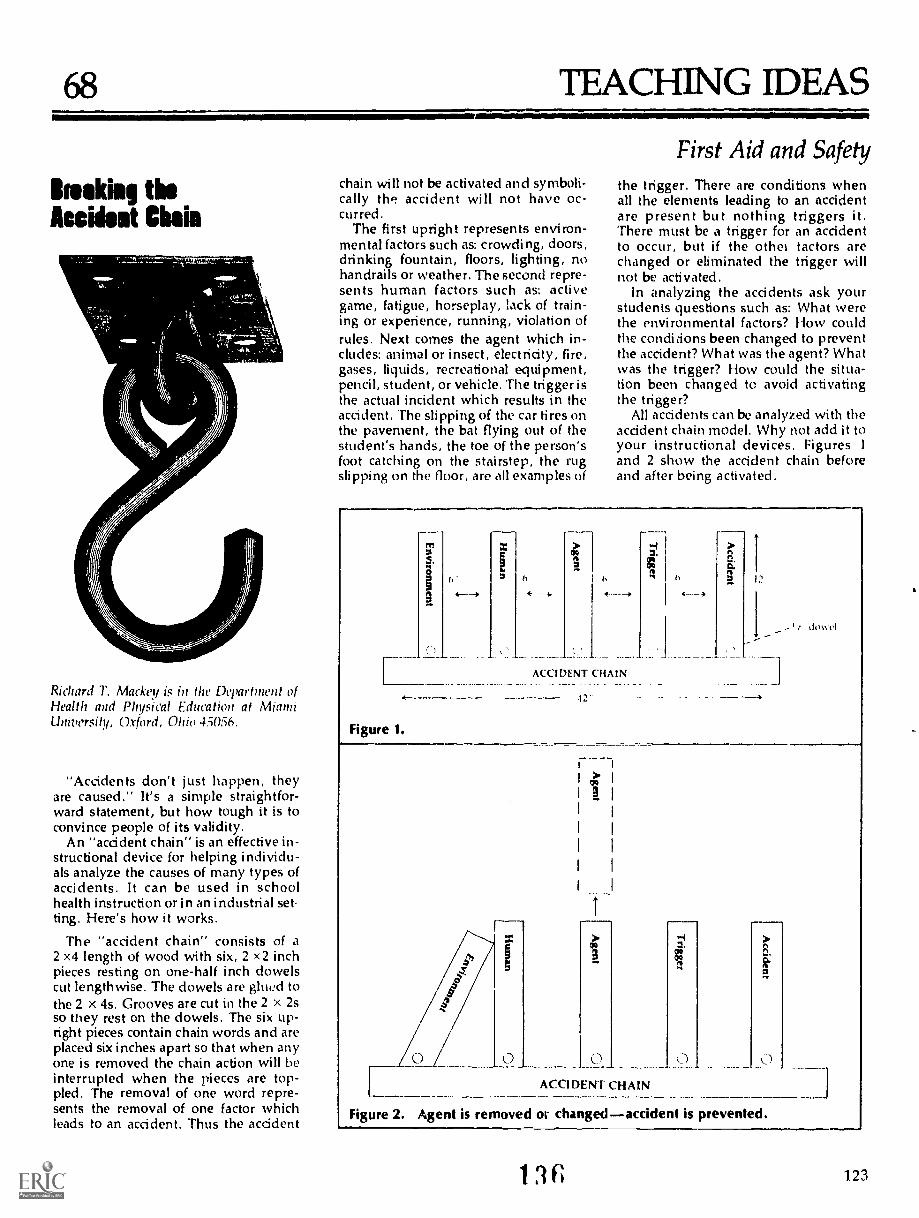
68 TEACHING IDEAS
Breaking theAccident Chain
Richard 7'. Mackey is in tlie Departnwnt ofHealth and Physical Education at MiannUniversity, Oxford, Ohio 45056.
"Accidents don't just happen, theyare caused." It's a simple straightfor-ward statement, but how tough it is toconvince people of its validity.
An "acddent chain" is an effective in-structional device for helping individu-als analyze the causes of many types ofaccidents. It can be used in schoolhealth instruction or in an industrial set.ting. Here's how it works.
The "accident chain" consists of a2 x4 length of wood with six, 2 x2 inchpieces resting on one-half inch dowelscut lengthwise. The dowels are glued tothe 2 x 4s. Grooves are cut in the 2 x 2sso they rest on the dowels. The six up-right pieces contain chain words and areplaced six inches apart so that when anyone is removed the chain action will beinterrupted when the pieces are top-pled. The removal of one word repre-sents the removal of one factor whichleads to an accident. Thus the acddent
chain will not be activated and symboli-cally tlyi accident will not have oc-curred.
The first upright represents environ-mental factors such as: crowding, doors,drinking fountain, floors, lighting, nohandrails or weather. The second repre-sents human factors such as: activegame, fatigue, horseplay, lack of train-ing or experience, running, violation ofrules. Next comes the agent which in-cludes: animal or insect, electricity, fire,gases, liquids, recreational equipment,pencil, student, or vehicle. The trigger isthe actual incident which results in theacddent. The slipping of the car tires onthe pavement, the bat flying out of thestudent's hands, the toe of the person'sfoot catching on the stairstep, the rugslipping on the floor, are all examples of
First Aid and Safetythe trigger. There are conditions whenall the elements leading to an accidentare present but nothing triggers it.There must be a trigger for an accidentto occur, but if the othel tactors arechanged or eliminated the trigger willnot be activated.
In analyzing the accidents ask yourstudents questions such as: What werethe environmental factors? How couldthe condi cions been changed to preventthe accident? What was the agent? Whatwas the trigger? How could the situa-tion been changed to avoid activatingthe tngger?
All accidents can be analyzed with theaccident chain model. Why not add it toyour instructional devices. Figures 1
and 2 show the accident chain beforeand after being activated.
yr,
s.3
of
Figure 1.
4--
1,
4-
ACCIDENT CHAIN
^
do,o.tI
0 0ACCIDENT CHAIN
Figure 2. Agent is removed or changedaccident is prevented.
1 31; 123

69 TEACHING IDEAS
CPR INNMARK KITTLESON is an instructor in theHealth Education Department atYoungstown State University, Youngstown,Ohio 44503. He is currently certified as aninstructor-trainer in CPR by the Ameritwnheart Association.
Cardiopulmonary resuscitation (CPR)has been making a lot of headlineslately. Several states have now man-dated CPR instruction to all high schoolstudents before they are allowed tograduate. Many people are turning tothe health educator to provide this CPRtraining. Through the help of theAmerican Heart Association manyhealth educators are receiving this train-ing to teach such courses. Unfortu-nately, most schools cannot provide thenecessary equipment to effectively teacha CPR course. This article discussesproblems the CPR instructor will en-counter and possible solutions to them.
ProblemsThere are several problems that
health educators face when teachingCPR in almost every learningsituationhigh school, community col-lege, university, community.
1. Size of Classlt is common tohave a great number of students en-rolled in first aid or CPR classes, whichmakes learning difficult. Many institu-tions, such as the University of Maine atFarmington, limit class size. A largegroup Ihr.its individual help and manystudents may feel neglected. Otheruniversities, such as Mankato StateUniversity, have access to paramedicstudents who are also instructors. Thisdoes alleviate the problem somewhat.
2. TimeInvariably, a few studentscannot achieve the certification becausethe manikins must be returned at a cer-tain date. If you are in a high school orcollege that does not own its own mani-kins, you muFt reserve them from in-stitutions (e.g. American Heart Associa-tion, Red Cross, hospitals, ambulancecrews) and it might take several weeksbefore they are available.
Much time is wasted during the actualclass period. Only two people can workon a manikin at a time, thus several stu-dents must sit around and lit. Tellingstudents to work with one onother in-
124
dependently on a procedure usuallydoes not work. Most students needmore structured instruction.
3. Lack of ManikinsMany schoolsand universities cannot afford mani-kins. For those who can, few have theproper number to ef:ectively ;each CPR(a 6-1 ratio is recommended by theAmerican Heart Association).
4. Areas of Certification TheAmerican Heart Association requiresthat students master four areas beforethey are certifiedobstructed airway,infant resuscitation, single and two per-son rescue. It seems almost impossiblefor one instructor to teach all those areasto a large group of students, but it canbe done. All it takes is a little imagina-tion, a little "army regimentation," anda strong voice.
5. Limitations of ManikinsAl-though the recording manikins arewell constructed, they do lack thehuman touch in several areas. It is im-portant that students work on the fol-lowing areas on a real human.
(1) The nostrils on the doll need to betough to stand the wear and tear, whichmakes them more difficult to pinch than ahuman nose.
(2) The doll's neck is more rigid dm ahuman's, so students need to practice open-ing the airway on a real human. By doing sothey find the head tilts nrich easier.
(3) Palpating the pulse is one of the mostimportant techniques. CPR done on a personwith a beating heart could result in seriousdamage. The instructor must emphasize theimportance of taking at least 10 seconds tofind the pulse. Students should practice tak-ing a pulse on a live person to know whatthat pulse feels like, where to find it, andhow hard to press.
(4) Finding the xiphold on the manikins isnot as effective. Everybody has a differentplacement for the xiphoid, thus it is impor-tant that the students have the opportunityto find xiphoids on several other humans.This is an area of concern because if thexiphoid is pressed on, it will break off andcause internal bkeding.
(5) When you are working on a human,you need to be gentle. When working with amanikin, this ,3ent1eness seems to diminishafter a few hours. The shake and shout pro-cedure, which is the first step in CPR, can bemisinterpreted as a "slugfest" with the vic-tim. Rescuers get a feeling of how hard toshake if they work on a real human. Studentslearn to gently open the airway when work-ing with a real subject. It is possible whenworking with a manikin to throw the airwayopen abruptly, which could be hazardous tothe victim.
137
First Aid and SafetyClass Management
A large class can be successfully man-aged. First concentrate on procedure;manikins are not needed. Once the pro-cedure is in student memory, learningproper compression depth and ventild-tion will come fairly quickly with prac-tice on a manikin.
The following procedure works bestfor me. Other instructors must adapt itto their needs.
Line students up in the hallway ingroups of threes. The victims lie on thefloor or on several blankets with theirheads in the same direction. One stu-dent is the observer and stands at thehead of the victim. Because of the largenumber of students it is difficult for theinstructor to observe every student. Theobserver can spot any major mistakes.The third student is the rescuer. All res-cuers should kneel on the same side ofthe victim to prevent confusion whengiving instructions; when you say righthand you mean everybody's right hand.
Start with the shake and shout andthen opening the airway. Go throughthe entire procedure until you feel thestudents have mastered the skill. Makesure students switch around to experi-ence all three roles.
There are several major areas thatneed repeated work.
1. Moving from chest to mouth and backto the chest in five seconds. This teaches thestudent Na move quickly to the mouth andget back to the chest to find proper hand po-sition. You can drill students"Find handposition, go t. mouth and ventilate; findlandmark and hand position, go to mouthand ventilate, etc." Give the students fiveseconds to ventilate before instructing themto find the landmarks. Drilling for only twominutes can give them the feel for movh.,3quickly.
2. Counting properly for efficient output.Have the student put hands in position onthe chest and without compression, count atthe right rate, then move to the head andventilate, and go back to the chest. Studentscan count together or individually. Use astop watch to see if the students are countingat the proper rate.
3. Switching with a second rescuer. Themajor problem in the two person rescue isthe switch. Locate one rescuer at the headand the second at the chest. The instructorshould do the counting and tell the rescuerswhen to switch. You can see any mixups,which there will be the first few times. Keepthis procedure going until you feel the stu-dents have mastered this procedure.
4. Finding the xiphoid. A simple drillingtechnique is to have the students find thelandmark (xiphoid), then take their hands offthe chest. Keep drilling the students by giv-ing only two seconds to find the landmarkand then having them drop their hands.

These drills allow the instructor toteach the students the basic procedurebefore they even have a chance to get onthe manikin. This will reduce needlesswork on the manikins and reduce idletime; every person is involved. The ob-server notes whether or not the rescueris doing the procedure properly, andthe victim can inform the rescuer if thehand position is incorrect. Doing thisprocedure for two hours will drill theproper procedure into the students.Students can concentrate on perfectingthe proper compression depth and ven-tilation rate when they get on the mani-kin, instead of wasting time learning theriocedure on the manikins.
Alternatives to Manikins
If you have a large class and lackenough manikins, ou can still give stu-dents a simulated compression and ven-tilation activity. Collect liquid soap bot-tles and rinse them out. Fill the bottlesabout three-quarters full with water andreseal the caps". Students should useproper hand position on the bottle andcompress. This gives a pretty good ideaof compression. Be prepared for occa-sional leaks.
For ventilation simulation, collect oldfabric softener or similar bottles andrinse them out thoroughly. Attach a
135
large balloon to the opening. With aknife, make a small slice in the middle ofthe bottle and insert the opening of asmall balloon in it. Make a larger hole(to stimulate a mouth) below the smallballoon. What you have basically is ahead and lung. Blowing into the mouthwill inflate both balloons; however, inCPR you pinch the nostrils, and thus inthis simulation you pinch the smallerballoon. This gives a pretty good idea ofhow much effort is needed to ventilate areal human. Naturally, these two simu-lations cannot match a manikin or ahuman, but they are simple, cheaptechniques to teach the general princi-ples of CPR.
1125

70 TEACHNG IDEAS
On The LevelA New TV Series for and about Teenagers
Gus T. Da lis is a consultant in health educa-tion and teaching strategies in the office of theLos Angeles County Superintendent ofSchools.
The concluding scene is the highschool yearbook office. Alice's boy-friend, Jerry enters . . .
Alice, I should have known you'd be here.Back at the scene of the crime . . . Lis-ten, do you know what's going on?
'Course I know, did you think I didn't seeGail before I left the table?
So go and deal with her, will ya?Leave me alone, ferry!But you started the whole blasted war!It's none of your business. Why don't you
just get out of here!Hey, look who's getting mad. Go shout like
that at Gail!Don't you tell me what to do! And get
something straight, I don't like to fightwith people, I can't stand up to anybodyand I'm tired of you rubbing my face intoit all of the time!
Alice is startled by the sudden openingof the &or. It's Gail . . .
hi Alice.Gail! What do you want?I wanted to talk to you . . . can I come in?
Come on . . . let me in.Alright . . . come on in . . . we have a
lot to talk about.The door closes, the screen goes black
and the credits appear. The end? Notreally. It is really a beginning. By using agroup setting and surrounding it withrelevant discussion questhns and ac-tivities, teachers can use dramatizationssuch as this one about conflict to get atsome of the gut-level issues affectingteenagers.
On The Level Series
The above scene is from a program inOn The Level, a classroom video series forfourteen-to-seventeen year olds that isbeing broadcast during the school day bymany PBS stations. This series consistsof twelve 15-minute programs, each ofwhich dramatizes a problem in the livesof this age group. Program topics in-clude: Developing self-concept, accept-ing feelings, facing conflict, thinking,
126
Mental Health
The problem here is tbat Sam doesn't want to be a baker, even though he's taken overfamily bakery for his ailing father. The scene is from On l.w Level, a new classroom videoseries for teenagers that focuses on personal and social growth.
the
;EST COPY AUILAKE 13 9
Vs4
_104-
0
.0
, d
e,
WI V. #Aige,;.7.5fAtts.
Tyrone, a would-he jazz artist, searches for his identity in "Who Am I?" a program about self-concept that is part of On the Level.
changing family relationships, alone vs.lonely, friendship, coping with stress,career aspirations, peer group member-ship, prejudice, and love.
Through program viewing along withpre- and post-viewing discussion andactivity, students are provided the op-portunity to explore the series top:cc. Itintended that this exploration willcertain personal and social groecomes for students. These outcome .clude increased:
Awareness of the interaction of emo-tional and physical health;
Skill in identifying and analyzing theinterplay between feelings and out-ward behavior;
Understanding of causes of emotionalstress and ability to cope construc-tively with such stress;
Understanding of their relations withpeers, non-parental adults, parents,and younger children.
Accompanying the video series is aLeader's/Teacher's Guide. Included inthis guide for each of the 12 videodramatizations is a program summary,background information about the pro-gram topic, student outcomes, before-and-a fter-viewing-the-program ques-tions and activities, and reproducible ac-tivity sheets. Each On The Level videoprogram has been adapted in an audioformat. Unlike the video programswhich are open-ended, each audio pro-gram gives several alternate endings.Creative use of this audio componentshould help adolescents discover thatthere are a variety of different ways todeal with a given issue. A student activ-ity book is aiao available. It serves as apersonal guide to help teenagers explorethe life issues dealt with in On The Level.The guide includes sdf quizzes, readingson the topics, and activities to encouragethinking, writing and doing. Studentscan use the guide for independent studyor for an accompaniment to the On TheLevel video or audio series.
144
Series Development
The On The Level series was producedby the Agency for Instructional Televi-sion (AIT), a nonprofit American-Canadian agency, in conjunction with aconsortium of 32 state and provincialeducation agencies. Additional fundingsupport came from the Corporation forPublic Bfoadcasting, Exxon Corporation,General Mills, the George Gund Foun-dation and Union Carbide.
The series is designed to promote thepersonal and social growth ofyoungsters fourteen-to-seventeen yearsold. The series developers e 'Me per-sonal and social growth as a process thatfosters possession of skills, information, andattributes needed to shape life events andmake constructive and maturing responses inthose events. In this context, life events arechanges in physical make-up, intellectual de-velopment, personal feelings, or changes inrelations with others or with the physicalenvironment .1
127

Planning for the series began in 1977.Using a prospectus published in 1978,A1T staff and consortium representativessharply defined the series goals in 1979.The project design team developed, inthe fall of that year, twelve program top-ics, each considered relevant to the per-sonal and social growth of high schoolage youngsters.
In order to validate the program topicsand student outcomes, secondary schoolteachers and other professionals likely touse the series were interviewed ingroups and asked to complete a take-home questionnaire. They found thetopics in personal and social growth to befamiliar and important. There was a gen-eral feeling that many of these topics arenow included in a variety of curriculumareas, that the intensity and manner inwhich they are covered varies, and thatsome topics are distinctly more difficultto teach than others. In addition, theteachers thought that the series would bean important tool for engaging teachersand students in discussions of these rel-evant issues.
From here the series was put intoproduction. Extensive evuation wasconducted with 4,000 teenagers andtheir teachers during production. Theprograms provided the catalyst forteenagers to discuss issues of importanceto them. Teenagers reacted sometimesstrongly, sometimes timidly, but almostalways with the acknowledgement thatthey were concerned about the issuesand appreciated the opportunity to talkabout them.
On the basis of student as well asteacher reactions many changes weremade in the treatment and scripts. Revi-sions included: character and plot altera-tions to make the characters and situa-tions more realistic and relevant toteenagers; and dialogue changes to en-hance the program's message and makethe programs more comprehensible.
Vehicle for Affective EducationThrough experience A1T has found
that video programming, when properlyshaped, can be useful in enhancing theaffective curriculum in schoc I settings.Such series as Ripples and InsidelOut forthe elementary school level and Self In-rorporated for the junior high level repre-sent efforts to assist teachers in dealingwith affective issues in the area of per-sonal growth and development. Withthe completion of the On The Level seriesMT has achieved a K-12 affective educa-tion program in the area of health educa-tion.
128
The programs for all these AlT seriesare particularly helpful in facilitating af-fective !earnings. That is, when properlyused they are useful in helping studentsexplore their own beliefs, opinions, andlikes and dislikes.
Effective Use of the SeriesEssentially, proper use of the On The
Level series involves (1) selection of ap-propriate questions and activities to pre-cede and follow the program, and (2) theestablishment of psychological freedomin the classroom or group setting.
The Leader's/Teacher's Guide con-tains a pool of questions and activitiesuseful in "squeezing health education af-fective juice" out of the series. For exam-ple, in using the program "Face to Face,"which centers around the conflict be-tween Alice and Gail, one of the teachersparticipating in evaluation of that pro-gram selected the following from theGuide:
Before the ProgramGet a group agreement on the defini-tion of conflict. Discuss some of thefactors that help to determine the se-verity of conflict.In small groups, make a list of the posi-tive things that can result from con-flict. The negative things.
After the ProgramAsk students to respond to the follow-ing questions: What were the conflictsin Alice's life? Did any of these con-flicts have an effect on Alice's physicaland emotional health? If so, how?Have each person write an ending tothe program's story line. (What hap-pened when Gail and Alice con-fronted each other?) Discuss the dif-ferent endings.Complete the reproducible activity"How Do You Handle Conflict?" lo-cated in the back of the guidebook(this is an instrument useful in deter-mining ways people handle conflict).Invite students to discuss the follow-ing question: How do you feel aboutfacing conflict?The most critical element in the suc-
cessful use of On The Level is the teacher.That is, what the teacher does and doesnot do as he or she interacts with teen-agers will determine the degree of suc-cess or failure in using the series. In addi-tion to utilizing relevant questions andactivities, the teacher needs to create aclassroom environment that ,:llows free,open and responsible discussion. Such apsychologically free environmentshould allow diversity without the fear
141
of recriminations from classmates or theteacher.
To establish such an environment it ishelpful for the teacher to set discussionground rules.= For example, "In our dis-cussion today let's have one personspeak at a time. Remember it's OK todisagree but don't be disagreeable whenyou do so. Also, no put downs." As thediscussion unfolds the teacher's role is tomain'ain the ground rules and to refrainfrom judging students' ideas directly orindirectly.
It was through such a teacher-established classroom environment afterviewing the program on conflict that onestudent reported that she did not feelalone. The student communicated reliefin not being "weird" because throughdiscussion she discovered she was notthe only one afraid of dealing with con-flict. Somehow there seems to be a senseof security in knowing that one's peershave similar anxieties, fears, and joys.This sense of security can come tothousands of high school students if ap-propriate affective teaching materials aswell as teaching behaviors are carefullyutilized.
Perhaps the power of the On The Level-Qries became most apparent when stu-dents responded with disappointmentand frustration at the lack of "r :al" pro-gram endings. After viewing the pro-grams students often responded withWhat happened to the rest of it? When is therest of it going to be on TV? I want to see whathappens.
Yet it was this frustration whichseemed to be a viable starting point forthe exploration of ideas and opinionsrelative to growth and development.And that is what this series is allaboutproviding a catalyst for the ex-ploration of life issues relevant to highschool students.
. _ .
'Agency for Instructional Television. Edu-cation for personal and social growth of secondaryschool st udoits. Bloomington, Indiana: Agencyfor Instructional Television, 1978.
'Agency for Instructional Television. Re-search Report 70Secondary health project: con-cepts review. Bloomington, Indiana: Agencyfor Instructional Television, 1980.
31Dalis, Gus T. and Strasser, Ben. B. Teach-ing strategies for values awareness and decisionmaking in heahh education. Thorofare, New Jer-sey: Charles B. Slack, Inc., 1977.
Anyone wishing further information aboutlocal availability of "On the Level" 'nay con-tact: AIT, Box A, Bloomington, Indiana47402, (812) 339-2203.

71 TEACHING IDEAS
Perceptions of Me
r .
,---, ,...4------.??-- 4mr,
\7
& lik
*irV4aAts0% il..
IERRO1 S. GRUN131 RG Ls coordi-nator of health education, State Uni-vers;ty of New York at Buffalo, Buf-falo, New York 14214. lie selves ascontributing editor for this SHRpaittnent, which 1,, designed to be ofparticular tiwfulnes to the class-room tea( her at all levels.
Though realizing the degree ofimmodesty of which 1 c an be ac-cused, let me risk stating that themost interesting topic to rue is me.Further, the most interesting topicto you is probably you. 1hat's noth-ing startling. We all are interestedin ourselves. Realizing this phenom-enon, educators re«mumend that!earnings m school be related to thelite experiences of the learner. It
then seems to follow that with thelearner himself the topi«)t study,the efficiency and effectiveness otthe learning process would he maxi-mized.
lhe question of the applopliate-ness of oneself as a topic tor studywithin a school setting, however. re-mains. Since one behaves on howone perc elves ieality lather than up-on reality itself, one's perceptions ofoneself will determine many healthrelated behaviors. F or example, one
possessing a positive self-conceptmight be exiwcted to walk tall (up-right) whilc one with a negativeself-concept might walk slumpedover to physically indicate "lowli-ness-; or one with a positive senseof sexual self-esteem might be out-going and pleasant, whereas onewith a negative feeling about one-self sexually might behave in a shy,withdrawn manner.
Based upon the importance ofperceptions of oneself, and, in addi-tion, how others perceive one (sincethey will behave toward othersbased upon their perceptions ofthem) activities should be devel-oped and «mducted with studentsto help them to:
1. More realistically perceivethemselves and others.
2. Explore the relationship be-tween their perceptions andhow they act.Make whatever adjustmentsthey deem necessary to be-come what they want to be.Presented in this article areexamples of such learning ac-tivities.
Sentence CompletionsUnfinished sentences which re-
quire the student to react by com-pleting them, allow for self-inquiryof a kind to which people are nota« ustigned. I xamples of such ques-tions indicate the breadth of possi-bilities and range of topics whichcan he explored With 1111,..
tional strategy.1. I often2. I seldom3. liii bored when
-4. I love to)ther children
6. I willmust
8. I am very9. I wish 1 could
10. My friends are1 I. My parents .
12. I wish13. I feel14. I'm happy when15. My body
Whereas the completion of thesesentences requires the student tothink ahcnit himself, processing theresponses in small groups allows
142
Mental Health
students to explore other childrens'perceptions of themselves. It is
hoped that surprises about certainresponses will help children bemore accepting of others and betterunderstand themselves. If the classtrusts the teacher sufficiently, thereading of the responses by theteacher might also aid the teacherto better plan instruction which per-tains to the needs of the students,
Discussion QuestionsUsing questions to stimulate
group discussions is not a recenteducational innovation, but the,types of questions suggested foruse here differ from those employedelsewhere.
1. What is the one thing thatscares you the most?
2. When are you most hurt?3. What is the very first thing
that you remember?4 What is the saddest thing
that has e er happened toyou?
5. What is the hest thing thathas eer happened to you?
6. What do you dislike mostahout school?
7 What don't you like aboutyourself?
8. What do you like most aboutyourself?What would you rather have:wealth, intelligence, or physi-cal attractiveness?
10. Who is the most intluentialperson in your life?
11. What do you wish?12. How can you he happy?13. What do you love to do the
most?14. What was the strongest feel-
ing you had last week (anger,joy, grief, etc.. , and whatcaused that feeling?
15. What is something you cantell us now that you wouldn'thae felt comfortable telling,us before?
Each group should he remindedthat there are no right or wrong an-swers to such questions md, there-fore, they should expect each per-son to respond differently. Thegroup members' role should be toask questions of the respondent\Om h will help the group to better
9.
129
understand the response, rather thanto attempt to get the group to agreeon what would be the "hest" an-swer. As a result of this exercise, itis anticipated that each student willhave a more accurate picture ofboth himself and his classmates thanprior to the exercise.
Question SociogramAn activity which can be used to
aid students to see themseh es asothers see them is the Question So-ciogram. Unlike a regular sociogramwhich asks children to lkt a num-ber of people they would like toattend a movie with, etc., the Ques-tion Sor iogram asks children toplace the name of the person inthe class most lrkek to fit the de-scription implicit in th(' question.Examples of questions whic h can beused will help to clarify this tech-nique:
1) Who most likely is
afraid of mu e?2) Who most likely cannot
resist eating a donut'Who wakes up oftenwith nightmar('s?
4) Who loves cowboymovies?
5) Who loyes romanti(movies?
6) Who most wank a lotof money'
7) Who wat( hes ,1 lot oftelevision?
8) Who most likely will bea scientist?
9) Who will he a politi-cian?
101 Who will make the bestmother or father?
1 Ii Who will never getmarried?
1)) Who will never 11,.('
drugs?11) Who is most likely to
cheat on an exam?'14) Who will Ix, the most
thoughtful lover?1S) Who will he a talking
liberal who won't doanything?
1(') Who will insist on a
small wedding'-17) Who would be the best
teacher?18) Who is apt to do anon-
ymous favcus for peo-ple?
130
19) Who will always bephysically attractive?
201 A'ho would make thebest friend?
To the left of each number, stu-dents dre requoed to place thename of one student in their groupor class. Only one name can bewritten on the blank line and eachblank line mmt have a name on it.After the responses have been made0,1(11 ( hild ( an ask eac h other c hild%VIII( ii cle riptions he most fits,thereby a«pnring others' percep-tions ot himself. To better knowoneself is the first step in improv-ing oneself.
\ fs
ir
i /yt
tA
b A aOAKS
OP% 11.0
Intimacy Questions
On«, trust has been developed ina class or group of children, ques-tions of a more intimate nature canbe explored. Best discussed in pairsto provide a close relationship,some of the following questionscan be employed hy a teacher will-ing to take risks to provide mean-ingful educational experiences:
I. What do you feel mostashamed of in your past?
2. What have you deliberatelylied about? Why?
.13
5. When do you hurt people?4. What turns you on the most?5. Do you have any health
problems? What are they?6. What are your least attrac-
tive features?7. Do you believe in God? Or-
ganired religion?8. Are your pa rents happily
married? Why? Why not?low do you feel when you
love?10. What makes you swear?11. What do \Mt think about
homosexuals?12. Do you like yourself? Why?
Why not?13, what wa,, your greatest
failure? Greatest suc c ess?
(3.
14. \Nho would citi be if you«iuld be anyone else thatyou wanted?
these questions deselop greaterbemeen two pople ssho
ore honest and trusting to beginwithmd likewise caii de elopgreater distance between two peo-ple who feel threatened by suchopenness. It is important, therefore,to employ this activity only with agroup that has matured and cantake advantage ot such an opportu-nity to mature further.

72 TEACHING IDEAS
Enhancing PositiveSelf-ConceptThrough Creativity inthe ClassroomBathara Beier is on the academic staff in tlwhealth ediwation department at thy Univer-sihi of Wisconsin, La Crosse, 54601.
I am convinced that one of the majorchallenges to teachers and other groupleaders is the creation of a self-enhancing learning environment. Somespecial people seem to do this quitenaturally out of their own authenticbeing and their commitment to others.Most of however, benefit from sug-gestions or training in allowing our cre-ative potentials to enhance a positive,humanistic environment in the class-room.
A workshop, "Creative TeachingMethods in Health," offered by theUniversity of Wisconsin La Crosse Di-vision of University Outreach, allowedthe creative process to surface in me. Asa young health director I was quite con-cerned with dispensing cognitive mate-rial to my students, but I have begun tounderstand that young people needmore than subject matter. I like tothink, now, that I teach the students,not just the subject.
Creative methods for teaching healtheducation can be written, published inbooks, and distributed nationwide, butthese ideas are only tools. Their use de-pends on you. Your use of ideas to fos-ter positive selfconcept will dependupon your own selfesteem. As JohnVasconcellos states,"Only if you are truly into your own being,possess and value yourself, feel comfortablewith and good about yourself, believe in andlive your right to be yourself-will you trulyenhance selfesteem in those young humanbeings whose selfesteem, whose lives, aretouched by you."'
Research literature is filled with re-ports indicating that cognitive learningincreases when selfconcept increases.'Following is a series of creative teach-ing methods compiled to foster a posi-tive selfconcept in students of healtheducation.Activity #1: Sharing Bags
Grade level: 10th grade
Materials needed: any size paper bagfor each student, pictures, fabric, de-corative findings, scissors, paste
Background information: In manyclasses students never have an oppor-tunity to get acquainted with theirclassmates. All of us share a need formeaningful interpersonal relationships.However, many times creating a class-room environment conducive to posi-tive interaction is awkward and dif-ficult for teachers. This activity could bea good starting point for teachers whoseek to facilitate growth in students' po-tential for interpersonal relationships.Objective: The student will have theopportunity to recognize meaningfulinformation about themselves whichcan be shared with classmates.
Procedure:1. Distribute paper bags, one to each
student.2. Instruct students to select from the
fabric, pictures, and decorations.3. Illustrate on the outside of the bag
how they think other people see them.4. On the inside of the bag, have stu-
dents illustrate how they seethemselveshow they really are.
5. Upon completion, the bags may beshared with the entire class, with asmall group or with a partner.
Follow-up questions:1. How did you feel when sharing
your creation?2. What are some of the ways you are
different from the way others see you?3. How accurately do you think you
preceive yourself?4. Do you feel good about the way
others perceive you, about the way youperceive yourself?Activity #2: tVho's Who of the WeekGrade level: 5th grade
Materials needed: background informa-tion on students in class, constructionpaper, paste.
Background information: An emergingtask in education today is to define self-esteem and to discover the process bywhich it is nurtured. The ultimate inselfesteern is found in the full posses-sion of one's total being - the intellectand the emotions and (especially) thebody in other words, in the self.
Objective: To enhance student selfcon-cept using personal data and positivereinforcement of accomplishments.
Procedu res:L Compile a "Who's Who Bulletin
Board."2. Data can be gathered about
achievements, hobbies, pets, futuregoals, family members, etc.
141
Mental Health
3. Phone calls to students' homes mayuncover information special to studentswhile promoting health education tothe parents.
4. When data is collected and writtenup, duplicate and distribute to all stu-dents in the class.
5. Pic:ures may accompany writteninformation for a pemonal touch.
6. Designate one shiclent per week tobe recognized as "Who's Who Studentof the Week."
7. Present bulletin board materials tohonored student at end of the week.
Activity #3: Who Am I?
Grade level: 3rd grade
Materials needed: 3x5 notecards, pen-cils.
Background information: Every personneeds recognition. It is expressed co-gently by the lad who says, "Mother,let's play darts. I'll throw the darts andyou say 'Wonderful.' "3
To enhance student selfconcept usingstudents' own thoughts and ideas. Togive the student recognition fromteacher and classmates.
Procedure:1. Have students write out biograph-
ical information. Include such things astalents, family happenings, hobbies,favorite places, activities, etc.
2. Collect the cards.3. On occasion, read the cards at the
beginning or end of class.4. Include a teacher description also.As health educators, promoting posi-
tive selfconcept in the classroom can bechallenging but quite rewarding. Bycreatively letting loost, involving thestudents, giving students' recognition,and by allowing the student to feel inthe classroom setting, a teacher can cre-atively enhance positive selfconcepts.As a kindergarten student put it,"When you ask me how I feel, I'm theonly one who can tell you! And I likethat!"4
'Vasconcellos, J., Chairman of the JointLegislative Committee on Educational Goalsand Evaluation, Member of the CaliforniaLegislature.
2Purkey, W. W. Self-concept and schoolachievement. Englewood Cliffs, New Jersey:Prentice-Hall, Inc., 1970.
'Baughman, M. D. Educator's handbook ofstories, quotes, and humor.
4Canfield, J., & Wells, H. C. 100 ways toenhance self-concept in the classroom. En-glewood Cliffs, New Jersey: Prentice-Hall,Inc., 1976, p. 207.
131

73 TEACHING IDEAS
Ideas from aClass in Inter-personal Relations
CAROLL KAISER teaches healtheducation at Minnetonka SeniorHigh School, Excelsior, Minnesota.Her interpersonal relations c/asses,composed of sophomores, juniors,and seniors, are the most popularof the ten health classes offeredfor credit.
Interpersonal relations stresses theimportance of self-image and self-acceptance in the development ofpersonality. Without a secure self-image and a healthy self-acceptance,a person cannot risk the emotionalinvestment necessary to relate toanother individual. With a secureself-image and healthy self-accept-ance, a person can risk the neces-sary emotional investment, and hegradually acquires a repertoire ofsuccessful behavior. Building thisrepertoire of successful behavior isa process of becoming and indi-viduation. Thus, a cyclical evolve-ment takes place: self-image andself-acceptance determine the qual-ity of interpersonal behavior; thequality of the interpersonal behaviordetermines the growth of person-ality; the growth of personalitydetermines self-image and self-ac-ceptance.
Some of the techniques I use inthe interpersonal relations classesattempt to improve self-image andself-acceptance in order to developa repertoire of successful interper-sonal behavior. One device k whatI call "Laws of the Robot." In thisexperiment I try to show studentsthat the human condition is copedwith, understandably and evenjustifiably, on a nonrational, evenemotional, basis, and that this is
not bad. In the Laws of the Robot,I pose hypothetical situations whichstudents must try to solve using apurely computerized type of logic.My direction to students is that they
132
, 4
kr'
are to consider themselves as robots.Before they are allowed to enterhuman society, they must take a testto determine whether the 'threelows" which are built into their ro-bot being are functioning properly.The laws are a functional part of thecircuitry and I further emphasizethat all circuits ore logical and can-not be altered in ,my way withoutserious damage. and that as robotsthey cannot violate the three lawseither through action or throughinoction. The laws are rigid, almostmec hanical:
robot ma\ not infurc d human orthrough inqu him ollow humoncome to horm..1 robot nitp.t obt.%
d hl111101) (.1(CW %%hew horder might conflict Mthlaw.
3 A robot impi Prole( t ik ownence lf,ng a urh prow( hon (1,1-not ( (mill( 1 with the Iasi U ,ccirndIdW
( \ I
Before the exercise is over thestudents become bogged down andalmost disfunctiondl in solving thehypothetical situations. To theirgreat frustration, logic is not enoughfor a solution because nonlogicalramifications of the problem mustbe taken into account.
Menial Health
1'
Another device I use for teachingself-awareness and self-acceptanceis what I call the -ProtoplasmicBlobs." These are o series of draw-ings or blobs faintly resemNinghumans, which elicit student inter-pretations of what the blobs arefeeling. Since it is relatively easy tocatalog gestures that people useto intensify statements, I felt thatI could use protoplasmk blobs toillustrate the subtlety of gestures,the idea being that if a studentcould perceive the-gestures in thkexperiment, Ile might more reodilyperceive them in hk everyday liv-ing. Interpreting these characters issimilar in a sense to the processpeople go through to interpret theRorschach Ink Blot Test. This par-ticular exercise k weci in conjunc-tion with a unit on body language.The exercise con.kts of 26 blobillustrations on d paper. At the bot-tom of the page are listed 26comments. The students match eachcomment with the blob character itbest expresses. For example. a stu-dent may interpret two charactersas "quarreling," and he wouldsupply a comment moq appropriatefor that depiction which might be,"please forgive me just one moretime." Students can work individu-
BEST COPY AMIABLE 145

ally or in a group where studentscompare their different interpreta-tions. Incidentally, this exercise canlead to some interesting and effec-tive role playing.
The ''Fnvironmental Box" idea isused toward the end of the unit onself-awareness as a final projec t. Itis especially effective and reward-ing for those students who are notadept verbally. The students areasked to portray or depict in visibleform a concept or feeling theypossess. They are to -remove" thisfeeling from environmental compe-tition hy "placing" it in a shoe box,fix the cover on the box-md thencut a hole in one end for the ob-server. Peering into the box and ob-serving these visual manifestationsof a student's inner life in completeisolation from an outside environ-
mental force is a most cogent ex-perience. The strength of this projectlies in the fact that the completedassignment ranges from the mostsimple illustration to the most com-plex and intricate ones, involving,in some cases. mirrors, electriclights, and small models to createillusory effects.
Since communication is an inte-gral part of interpersonal relations,I have used as an additional tech-nique a short unit on the sign lan-guage of the deaf. Often, in theverbal language we use in every-day conversation, parallel conversa-tions are conducted in w hich oneperson is not really listening to theother. Ultimately, after much paral-lel conversation, the art of reallistening is lost. Teaching studentsbasic sign language makes them
1 4 f;
aware for the firsi time of the inten-sity and the miracle of human com-munication, One is forced to lookat and study the person who is do-ing the communicating. One seesall the nuances and connotations ofwhat is said and felt. One of thehigh spots in this unit is a lecturegiven in sign language by a deaflecturer. The intensity and con-centration observed at this pointis worth a whole year of teach-ing. I might add that teach-ing this skill is not difficult or time-consuming, and the hand alphabetcan be learned in 15 or 20 minutes.Since there are hand gestures thatmake up entire words rather thanspelling out each letter in the word,I also introduce five or ten handgestures every day until each stu-dent develops quite an extensivevocabulary
133
74 TEACHING IDEAS
Role Playing as a Tool inMental Health Education
Lynn Teper is assistant professor of health educa-tion at Long Island University, Brooklyn Center,Brooklyn, New York. She was formerly an in-structor at Kingsborough Community Co /lege inBrooklyn.
Teachers of health education must transmit tostudents the concept that physical and mentalhealth are interrelated. Each is an aspect of thetotal indivki ial; each is dependent on the otherfor optimal functioning. Formerly the mentalcomponent of health was overshadowed byhealth educators !n their attempt to educate thestudent about bodily functions, but gradually,mental health has gained importance and is nowa significant aspect of many health education cur-riculums. Through units in mental health, it ishoped that students will learn to meet with someadequacy their personal, interpersonal, and socialconflicts and thus will function more completelyas young adults.
One of the tools availaL for promotinghealthy behavioral patterns is known as "socio-drama." Sociodrama is a spontaneous, impromptuexpression dramatizing intergroup relations andcollective ideologies. The students who play arole in a sociodrama do not recite from a script.A situation is presented to the class and withoutprior preparation students are chosen or volun-teer to act out the particular situation.
Man is a role player, in a sense, every day of hislife. An adolescent girl, for example, can be adaughter, a friend, a student, a member of a club,etc. Each individual is characterized by a certainrange of roles which dominates his or her behav-ior. The role player in a sociodrama is aware thathe is acting out a role, even though he may beunaware that the role, as he enacts it, revealsmany of the conflicts that confront him andothers.
The process of sociodrama unfolds as follows:
Step 1Sensitizing the groupit is important for the participants to recognize
that people perceive and interpret situations andstimuli differently. As a result of their particularinterpretation, attitudes are developed by each
134
Mental Health
individual which result in different responses.This understanding can be gained by having sev-eral students view and report on a given situation.The result will usually yield a variety of opinionsas to what took place, as when witnesses areasked to report on an accident or crime. This willreveal to some degree the lack of reliability be-tween observers due to a predisposition to selectdifferent aspects of the situation for notation. Inaddition, it will help students to see that their wayof seeing and interpreting situations is not theonly way.
Step 2The Warm Up
This step involves setting up the situation forthe sociodrama to take place. Topics for enact-ment can include conflict with the family, peergroup relationships, attitudes involved with topicsincluded in sex education or the use of narcotics.The instructor states the situation somewhat ab-stractly. Roles are described and volunteers areselected or chosen. For example: A girl is troubledby the fact that she is given little freedom fromher parents. At this point someone is chosen forthe role of the girl, another for the role of themother; father and possibly a sister or brother canenter the scene.
Step 3The Enactment
At this point, without any additional prepara-tion the role players act out what they believewould happen when the family was together.
Step 4Helping the audience observeintelligently
Much of the value of sociodrama depends onthe discussion with the class following the spon-taneous dramatization. Some of the questionscould be:
1. Do you feel that the enactment was realistic?
2. As future parents, what do you believe therole of the parent should be?
3. How do you think parents and their childrencan come to better understand one another?
147

In other situations as well as this one the prime concernshould be to discuss causes of behavior and appropri-ate ways of behaving and to encourage self-appraisal.
Step 5Replaying the situation
it is helpful for students to see how the situationlooks from different angles by switching roles. Thedaughter may become the parent or volunteers mayreplace those who have already participated. This willbring additional insights into the situation.
Step 6The Evaluation
In the evaluation it is important to emphasize thatwith positive flexible attitudes individual growth takesplace. Students need to discover for themselves thatanxiety, fears, and immobility are not inherent in anobject, event, or person, but are within themselves.The individual needs a positive attitude towardchange. To say "I'll try" means motivation for growthis present.
If real learning is to take place, problems studied inschool should deal with crucial situations in the livesof the student no matter what the subject area may be.The use of sociodrama in health education classes is
one way to implement this approach since it allowsstudents to explore some appropriate ways of dealingwith others as well as with themselves. It is a processwhereby one can look at familiar conflicts seenthrough the eyes of others. Subsequently, recognitionthat one is not alone in some of his confrontations mayresult in lessening anxiety. A three way process isestab!ished.
1. The teacher relates with the students through in-terest and involvement.
2. The students relate with one another by participa-ting, observing, and commenting on the socio-drama.
3. The students relate to the teacher by referring totht teacher for guidance and structure.
Moralizing by the teacher is curbed and condemna-tion and judgment by an adult figure are eliminated.
Involvement is a key to understanding for students.Whether the student is a role player or part of thediscussion group that evaluates the sociodrama, in-volvement is a significant outcome. Conflicts often willbe left unresolved, but hopefully the students will havewitnessed or have been a part of acting out and discus-sing a variety of ways for promoting healthy interac-tions involving the individual in his environment.
14S135
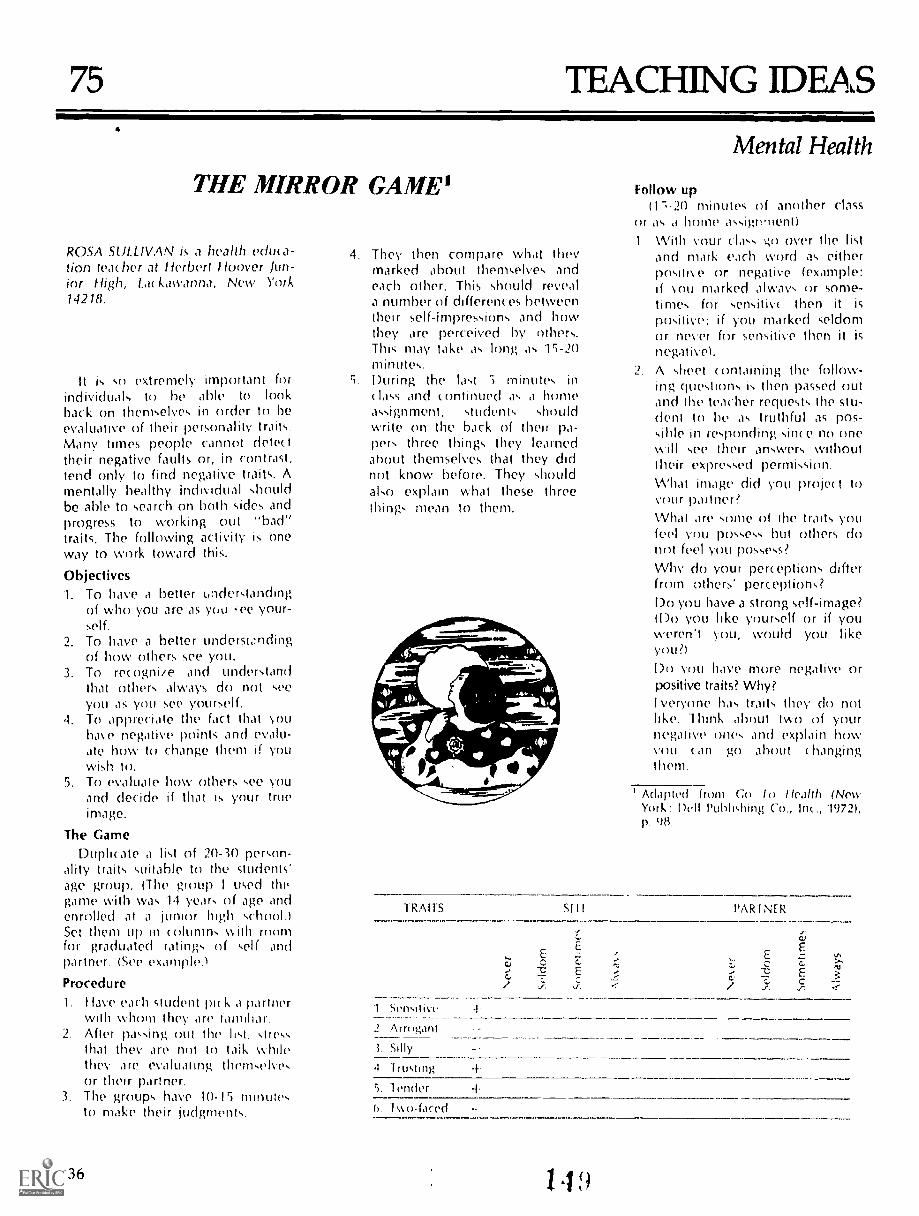
75 TEACHING IDEAS
THE MIRROR GAME'
ROSA SULLIVAN is a health educa-tion teac her at Herbert Hoover Jun-ior High, La( kawanna, New York14218.
It is so extremely important forindividuals to he able to lookback on themselves in order to beevaluative of their personality traits.Many times people cannot detecttheir negative faults or, in contrast,tend only to find negative traits. Amentally healthy individual shouldbe able to search on both sides andprogress to working out "bad"traits. The following activity is oneway to work toward this.
Objectives1. To have a better understanthng
of who you are as you ,-ee your-self.
2. To have a better underwndingof how others see you.
3. To rewgniie and understandthat others always do not seeyou as you See yourself.
4. To appreciate the fact that Youhave negative points and evalu-ate how to change them if youwkh
5. To evaluate how others see youand decide if that is your trueimage.
The GameDuplicate a list of 20-30 pep,on-
ality traits suitable to the students'age group. (The grou) I used thegame with was 14 years of age andenrolled at a junior high school.)Set them up in columns with mornfor graduated ratings of self andpartner. (See example.)
ProcedureI. !lave each student pie k 1 partner
with whom they are familiar.2. After passing out the hst, stress
that they are not to taik whilethey are evaluating themselvesor their partner.
3. The groups have 10-15 minutesto make their judgments.
136
4. They then compare what theymarked about themselves andeach other. This should reveala number of differences betweentheir self-impressions and howthey are perceived by others.This may take as long as 15-20minutes.
5. During the last S minutes in(lass and continued ,P a homeassignment, students shouldwrite on the back of their pa-pers three things they learnedabout themselves that they didnot know before. They shouldalso explain what these threethings mean to them.
TRAITS
1 Stm,atni.
2 Arrogant
AMI1
Mental Health
Follow up(I",-20 minutes of another class
or home assignment)I With Your class go over the list
and mark each word as eitherpositise or negative (example:if sou marked always or some-times for sensitive then it is
p)sitive; if you marked seldomor never for sensitive then it is
negative).2 A sheet «mtaining the follow-
ing questions Is then passed outand the teacher requests the stu-dent to he as truthful as pos-sihle in responding sin«, no onewill see their answers withouttheir expressed permission.What image did you project toyour partner?Whal ,ire ,,onle of the traits youfeel you possess but others donot feel you possess?Why do your perceptions differfrom others' perceptions?Do you have a strong self-image?(Do you like yourself or if youweren't you, would you likeyou?)
you have more negative orpositive traits? Why?Iveryone has traits they do not
Thmk about Iwo of yournegative ones and explain howvem can go about hangingthem.
I Adapted from Go lo Health (NewYork: Dell l'ubliOling Cu., nc., 1972),p. (18.
PAR1N[R
ii;
EEz VI
Cs C, >-,..
cE 31-.:.
.1. Silly
4 I rusting -f
5. 1vmier
1s,, ()Jared

76 TEACHNG IDEAS
Now to Copewith Stress inthe ClassroomCHARLES C. DAVIS is coordinator forhealth /physical education instructional pro-grams, State University College at Oswego,Oswego, New York 13126.
Learning alternative for handlingstressful situations and then giving stu-dents an experience in handling stressand developing coping ability some-thing often left out of the classroom. Aseducators we often find it difficult toplace students in situations where theycan learn practically how to handle vari-ous stressors. Much of what we say isabstract or theoretical until the student isforced to confront stress. The followingstress sheet is designed as a practical wayfor students to identify stress and thenanalyze how they cope with variousstressful situations. A deeper discussionof stress and the learning of alternativesituations to various life problems can bebetter understood. The stress sheet isadaptable for many age groups andgrade levels.
Step 1: Content
The students are tatiOt the intricatedetails of life and stress in their class. Thefollowing aspects are reviewed.1. The stress conceptwhat is stress?
discussion of Hans Selye's theory ofstress.
2. Stress as it affects our livesstress isnot inherently good or evil, it is de-pendent on the consequences of ourreactions to stressors.
3. Coping with stressGeneral Adap-tation Syndrome (GAS), the physio-logical response to stress; flight/fleeresponse or coping behavior (generalalternatives).
4. Learning ways to cope with stress--protecting the ego ideal under stress-ful situations; defense mechanisms;Maslow's hierarchy of human needs.
5. Adapting to stress--suggestions forlearning to cope with stress in a con-structive mannPr; positive and nega-tive consequences of deviations.
Step 2: Learning to Copewith Stress Constructively
Students are given a stress sheet torelate classroom theory to actual con-frontations with stressful situations. Thestudents are asked to take the followingstress sheet home and fill it out afterundergoing stress.
Stress SheetThis sheet is designed to stimulate in-
terest in and an understanding of howyou react to and cope with stress. It isalso hoped that completion of this sheetwill cause you to do some reflectivethinking on how to handle the "wearand terr of life" or stress.1. Identify: A stressful situation; the
stressor(s), internal and/or externalprimary stimulus causing the stress.
Mental Health2. Which of the following behavioral re-
sponses did you use to cope with thestress? I'lace an x next to how youresponded.
Fight Freeze FlightCompromise
Briefly describe the consequences ofyour response: it did didnot alleviate the stressful situa-tion.
3. Check any defense mechanisms thatyou used to deviate from the stressor.
avoidance regressiondeny realityfixa tionrepression sublimationprojectionother (specify)rationalization
4. Draw a line to indicate how you ex-pended energy as you pi ogressedthrough the Adaptation Syndrome.
Alarm Reaction I Stage of ResistancePrestress EnergyOutput State of Exhaustion
Time
Mit IR..
1
ThLy t
151i ZEST COPY AMMILE137

5. Sources of help. Did talking withanyone help you cope with or adaptto the stressor?no yesspecify whom
6. What deviations did you use toequalize the effect of the stress on thebody? (for example sports, reading,etc., please specify). Briefly describehow your deviations relieved thestress.
7. Did any psychologically induced paincause a physical reaction?no _____ yesspecify e g , prolonged ten-sion leads to upset stomach.
Step 3: Behavioral Outcomes
After taking home a predeterminednumber of stress sheets the studentsshould have some stress-relieving skills,such as the following.
1. Analyze some of the stressors com-mon to the experiences of students,such as competition or failure.
138
2. Understand the meaning of the termsstress, stressors, stressful situations.
3. Analyze the individual use of defensemechanisms in stressful situationsused to minimize conscious anxiety.
4. Understand that humans are affectedby and respond to stressors as totalorganisms.
5. Understand the general categories ofbehavioral responses to stress: flight,fight or compromise.
6. Understand the consequences ofconversion reactions such as psycho-logically induced pain manifestingphysical reactions when stressors arenot successfully adapted to or de-viated from.
7. Investigate how individual copingbehaviors (sports, dancing, etc.) suc-cessfully allow an individual to al-leviate stressors.
Step 4: Classroom Adaptability
1. Students can be asked to do severalstress sheets over an extended
1 5 1
period, then analyze how they copewith and adapt to stress.
2. Break students into small discussiongroups, give each group the job ofdepicting: what is stress? or what ismental health? or what is the relation-ship between stress and mentalhealth?
Give each group about 20 minutes tocome up with their pictorial descrip-tions. No words can be used in any of thethree assignments. When the allottedtime has ended, the instructor holds upthe finished product from one group andthe class responds to what they see de-picted. The same is done for the othergroups. The instructor phrases the ques-tions in a way which will extract the rela-tionship between stress and mentalhealth.
The outcome of the stress sheets exer-cise encompasses the interrelationshipof the theory of stre.-,s and how it relatesto mental health by personalizing stressthrough the stress sheets and visuallydepicting the wide interpretations ofwhat stress is.

TEACHING IDEAS
CopingWithViolence
ELAINE HALS teaches at the South ShoreHigh School in Brooklyn, New York 11236,
What can we as health educators do toreverse or at least slow down the chain ofviolence with which our students live?Our objectives should be: (1) to have stu-dents consider all life as positive, (2) toguide students in establishing construc-tive goals for the future, (3) to help stu-dents explore their values and priorities,(4) to help students explore the impact ofviolence on our society-ind (5) to assiststudents in finding nonviolent methodsof handling potentially explosive situa-tions.
These are difficult objectives to reach.How do we achieve tnem? One way is toplan for the mental health segment of the
required health course (or any other ap-propriate segment, e.g., urban problems,crime, values and goals) to include dis-cussion topics and activ.ties such as thefollowing.
Topics1. Prejudic e--its (auses and relationshipto violence2. Respect for the views of others3. Respect for the property of others4. Peer pressure; gang involvement5. Values formation (c larifi ation);priorities6. Constructive methods of problem solv-ing and dealing with stress7. Setting realistic goals for the I uture8. The impact of violence on out so( iety
Fear of involvementFear of going out aloneTendency to overreactCrimes committed in wIt-deten sePeople arming themselvesAc ceptance of violent deaths asstatistics
9. Need for feelings of self-esteemBeing recognized by others asworthwhile
10. Constructively compensating torweaknesses11. Handling emotions-learning tothink before acting12. Working towards a healthier society
How?Role of the individual
13. Value of life-own and otheisEveryone is important to someone
Activities1. Role playing
Mock court caseStudent caught cheatingRacial or ethnic role reversals
2. Values activityHave students rate the following asacceptable or unacceptable forthemselves. Discuss reasons for eachstudent's choice.a. breaking laws they don't believe inb. law enforcement agenciesc. smoking marijuanad. our governmente. cheatingf. demonstrations against the estab-lishmentg. compare students' values withthose of their parentsh. capital punishmenti. plea bargaining
3. Search for Values (PfaunvStandard,(in( innati, Ohio 1974). Read sec tion onTime, Lesson 3: "Examining PersonalGoals"4. Simoo, Sidney 13., Howe, L. W., Kir-
henbaum, Howard, Values ClarifuaHon: A Handbook of Practical Strategiestor leachers and Students (Hart Pub. Co.,New York, 1974). Play the Bomb ShelterGame (prejudice) and the I ransplantGame.
152
Mentri HealthAm I Worthwhile Task
Have eac h student talk about self fortwo minutes saying only good things.Do this activity in groups. Have thegroup members help the individualspeaking whenever necessary. Thepurpose of this activity is to help eachstudent see that he or she is worth-while.
6. Values Auction from Auction Caine byRic hard Cohen in hii graduate murse,"Health Education in the Se«-mdarySc hook," at Brooklyn College.
Give eac h student an imaginary $1,-000 to bid with, give them a valueslist, and hold an auction. If severalstudents are willing to hid the entire51,000, have each give his or her rea-son for wanting the item and thenallow the class to vote. After the auc-tion evaluate student priorities.
Items To Be Auctioned1. Invitations to all the most exciting partiesiany plac e with anyone in the whole world)every single night.2. To possess perfect health and a si rig. flex.ible, beautiful, graceful body.3. A lifetime without "hassling." No one w ill tellyou what to uo or how or when to do it.4. A dady "storm" of new ideas: originalpoems, songs, books, movies running throughyour head; visions of paintings to paint, pots tomold. buildings to design and build.5. To be the richest person in the world.6. The opportunity to direct the workings of thewhole world . . to control individuals, busi-nesses, monies, whole nations.7. No "hang-ups" whatsoever; to possessself-knowledge.8. A chance to spend a year with the greatestreligious figure of your faith-past, present. fu-ture.9. To live forever without growing old.10. The opportunity to stick up for and protectthe person or thing to which you feel thegreatest allegiance (like sticking with a friendthrough a crisis or fighting for your country,etc.).11. To have the perfect romance/or the perfec tlove relationship (s) with the person (s) of yourchoice.12. To have a computer-bank of facts and in-formation in your head; to be able to answerany questions and solve any problems whichpresent themselves to you.13. To have the strength always to do what youbelieve to be right. To be a person of integrity.14. To have the skills, know-how, and tone toreally help others and serve humanity.15. To have a real sense of what is fair and just;to deal with others as honestly and fairly aspossible.16. To be at pea«, with yourself and know thepurpose of life.17. To become a professional athlete of yourc hoice.
Health educator% will not be able toeliminate violence, but we can en«)urageour students to examine the auses aridend results of violence. We can showthem more constructive outlets for theiranger arid their frustrations-is well ashow to set and reac h positive goals for thefuture.
139
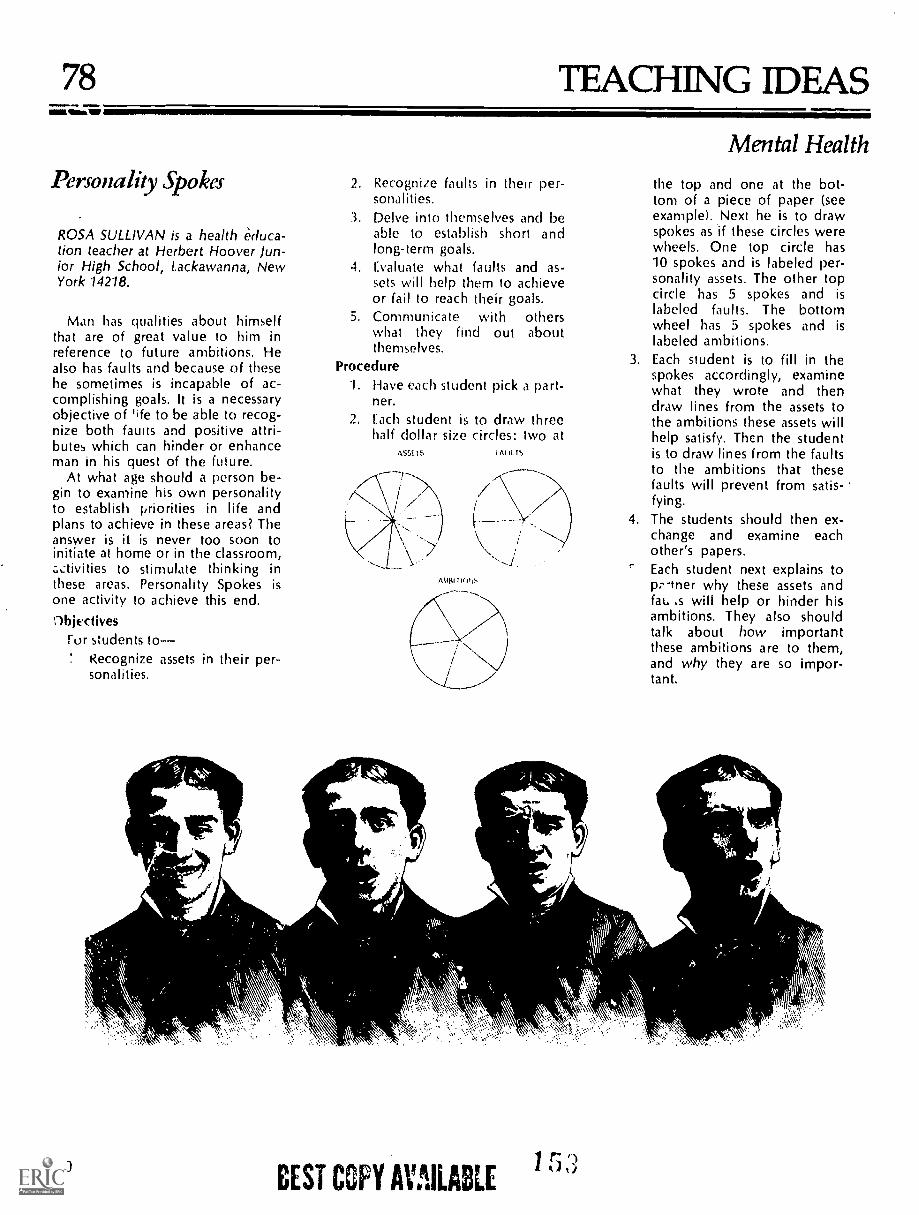
78alma
TEACHING IDEAS
Personality Spokes
ROSA SULLIVAN is a health educa-tion teacher at Herbert Hoover Jun-ior High School, Lackawanna, NewYork 14218.
Man has qualities about himselfthat are of great value to him inreference to future ambitions. Healso has faults and because of thesehe sometimes is incapable of ac-complishing goals. It is a necessaryobjective of 'ife to be able to recog-nize both faults and positive attri-butes which can hinder or enhanceman in his quest of the future.
At what age should a person be-gin to examine his own personalityto establish priorities in life andplans to achieve in these areas? Theanswer is it is never too soon toinitiate at home or in the classroom,.-.ctivities to stimulate thinking inthese areas. Personality Spokes isone activity to achieve this end.Objedives
For swdentsRecognize assets in their per-sonalities.
140
V
2. Recognize faults in their per-sonalities.
3. Delve into themselves and beable to establish short andlong-term goals.
4. Evaluate what faults and as-sets will help them to achieveor fail to reach their goals.
othersabout
5. Communicate withwhat they find outthemselves.
Procedure1. Have each student pick a part-
ner.
2. Each student is to draw threehalf dollar size circles: two at
ASSE T S f AUL 1
Mental Health
the top and one at the bot-tom of a piece of paper (seeexample). Next he is to drawspokes as if these circles werewheels. One top circle has10 spokes and is labeled per-sonality assets. The other topcircle has 5 spokes and islabeled faults. The bottomwheel has 5 spokes and islabeled ambitions.
3. Each student is to fill in thespokes accordingly, examinewhat they wrote and thendraw lines from the assets tothe ambitions these assets willhelp satisfy. Then the studentis to draw lines from the faultsto the ambitions that thesefaults will prevent from satis-fying.
4. The students should then ex-change and examine eachother's papers.Each student next explains top;--tner why these assets andfau ,s will help or hinder hisambitions. They also shouldtalk about how importantthese ambitions are to them,and why they are so impor-tant.
BEST COPY AVAILABLE
1 r:A ILI I)

79 TEACHING IDEAS
About Yourself
a
RUTH C. ENGS is assistant professor, Be-partment of Health and Safety Education,Indiana University, Bloomington, Indiana47401.
A "mentally healthy" person is oftencharacterized as having an accurate per-ception of reality, able to maintain closeinterpersonal relationships, able tocommunicate openly and honestly withothers, arid aware of personal goals, val-ues, abilities, and behavior.' Because ofthe variety of environmental stresses andour individual backgrounds, we all havedifferent problems of living. The extent towhich we learn to successfully cope withthese stresses often determines howmentally healthy we are.
One of the primary objectives of men-tal health education in the classroom is tohelp the student become aware of him-self, his communication techniques, andhis behavior as an aid in learning to copesuccessfully with life. The following warmup can help the student become ac-quainted with himself, with others, and
with the class as a whole. It can help tocreate an atmosphere for fostering opencommunication and self-knowledge lead-ing to better mental health.
These instructions should be related tothe class by the instructor:
We are now going to do some get ac-quainted exercises. We first will do a re-laxation exercise to tune in to ourselves.Then we will do several exercises to get toknow others in the class. This may be anew experience for some of you, how-ever, most people find it fun. If for somereason you find you do not wish to con-tinue, you can stop at any time. However,I'm surf you will find it enjoyable.
Relaxation (10 minutes)
1. First put your head on your desk andget comfortable in your chair or lie downon the floor and get comfortable.
2. Close your eyes, relax, and becomeaware of the sounds in the room.
3. Next, I want you to pay attention toyour breathing. Feel the air go in and out.
4. Now I want you to take a deepbreath, feel the air going in your lips,down into your lungs; feel air go out.(Repeat this two times.)
5. You should feel relaxed; in fact, it isprobably the first time you have relaxedtoday.
6. Now become aware of your feet,feel them against the floor, in your shoes.Now tighten your feet as long as you can.Now relax.
7. Become aware of your calf, (con.tinue with thighs, whole leg, shoulderand buttocks, chest, fist, neck, face,whole body).
8. You will feel relaxed; become awareof parts of your body, touching the chair(floor).
9. Now relax. And take a deep breath.
Body Trip2.The Magic GoldenBall (10 minutes)
To be used after people are in a relaxedstate.
Imagine that you see a warm goldenball in front of you.
As you watch it, it slowly begins toshrink becoming smaller and smaller.
When it is the size of a dime it movestoward you.
It gets closer and closer and finally at-taches to your forehead.
Then it turns into a magic warm goldenpaint.
It flows over your forehead, nose.Smell it, taste it.
As it flows it feels warm and glowing.When it reaches your neck the magical
paint takes on different colors and stillflr,ws over your body-----shoulders, upperarms, lower arms, fingers, chest,
1 5 4
Mental Healthstomach, genetalia, thighs, legs, feet,toes.
You are now surrounded in a warmbath of colors and feel good. I will countbackward from 10 to 1. While I am count-ing, start opening your eyes. At the countof 1 you will be wide awake and feel good.
I now want you to turn to the personnext to you and discuss what you experi-enced.
Getting Acquainted'
1. Go up to someone you do not knowbut think you might have something incommon with and would like to knowbetter. One person talks for two minuteswhile the other just listens. Then reversethe role. Now, the two of you findanother pair you do not know. Introduceyour partner to the other pair.
2. Go up to someone you think youhave nothing in common with. Sit back toback and talk. loin another pair and dis-cuss things you learned about communi-cation by sitting back to back.
3. Go up to another person you do notknow. Look each other in the eyes. Donot talk. Follow each other's handsaround as if you were looking in a mirror.Join another pair and discuss what youlearned about yourself and the other per-son by doing this.
Debriefing
1. Get back into a big circle. What didyou experience with the fantasy trip?
2. How does it feel to go up to astranger and talk ?
3. How much did you find you had incommon with the person you thoughtyou had nothing in common with ?
4. What problems did you have incommunicating back to back ?
5. What did you learn about nonverbalcommunication or about your own com-munication skills from sitting back toback ?
6. Who led in the hand mirroring?Why? What did you learn about yourselfin this exercise, about the other person?
-'Maslow, Abraham H., Toward A Psy-
chology of Being, 2nd edition, VanNostrand-Reinholt Co., Toronto, 1968.
'Adopted from Dick Price's "GestaltWorkshop," Esalen Institute, Big Sur, Cal-ifornia.
'Pfeiffer, I., and /ones, I., A Handbookof Structured Experiences for Human Re-lations Training, Vol. I-IV, University As-sociates, Iowa City, Iowa.
141

80 TEACHING IDEAS
A Lesson on Stress
JANET H. SH1RREFFS is in Depart-ment of Physiology and Health Science, BallState University, Mutwie, Indiana 47306.
A generally accepted educationalprinciple is that students learn best in anenvironment in which certain moderateto high expectations are made clear tostudents but is only minimally or mod-erately stressful. Excessive stress maybe so incapacitating that no effort on thepart of the individual can alleviate it. Itis impossible for learning to take placein an overly stressful environment inwhich the adaptive potential of studentsis exceeded. Of course, individuals dif-fer in both perceptions of stress and intheir ability to cope with stress and con-flict in their daily lives and these dif-ferences are important considerationsfor the educator in discussing stress andemotional health.
Although health educators cannotteach mental health per se, it is possibleto provide classroom experiences deal-ing with mental health and the solutionof every day problems which can helpstudents tune-in to real life situations,feel the emotions they evoke, andanalyze achons and behaviors which
142
r-""
they can use to alleviate these emotionalcrises in constructive, appropriate ways.This is the case in the following class-room technique:
Goal: (1) Learn what stress is(2) Learn what anxiety and/or angerfeels like as the result of encounteringa stressful experience(3) Learn how stress can best be han-dled in positive and constructiveways to resolve problems and reducefeelings of being "overwhelmed" byappropriate individual action.
Level: This classroom experience hasbeen used effectively at the collegelevel during a unit on mental health.The learning experience would alsobe applicable at the senior and juniorhigh school level with some modifi-cation.
Method: (1) Students should be fairlycomfortable with teacher and vice-versa.(2) Class environment should behumanistic and typically low-stressprior to the experience.(3) Teacher should have made evalu-ation requirements of the class veryspecific, including an announcementthat no unannounced quizzes wouldbe given during the semester.
155
Mental Health
Following introductory class periodsdevoted to personality developmentand enhancement of mental health, theinstructor should enter c!ass with a testor quiz which has been prepared frommaterials the students were supposed tohave lead and additional questionswhich are not from the assigned read-
Below is an example of a test ofthis type.
HES 100 Personal HealthQuiz].
Emotional Health
1. List Erikson's Eight States of Person-ality Development. (8 points)
2. In defining and describing thepsychotic personality disorders, thetext speaks of organic and functionalcauses. Describe each. (4 points)
3. Give three examples of character dis-orders. (3 points)
4. According to the text, what is anx-iety? (5 points)
Keeping very serious, announce:"You will be having a test now, pleaseremove all materials from your desks."You will notice abrupt changes in facialexpression, body movements etc., rang-ing from panic to anger which can pro-vide a basis for a discussion of bodilymanifestations of anxiety.
Pass out tests. Allow the studentsabout three minutes to look over the testand announce: "Write your feelings atthis moment on the bottom of the testpaper." A number of reactions actualstudents have reported during this ac-tivity are: complete confusion; helpless;I would like to throw my chair at you forspringing this on me; anger; completenothingness; a burst of adrenalin shotthrough my system; disgust and frustra-tion; my heart fell, anxiety, shocked,confused; feeling of total lack of control;insecure; I am feeling completely lostand kind of scared.
Announce' inmudiately after you haveasked the students to record their feel-ings on the bottom of the test page:"This is not a real test, but an experienceto get each of you to realize right nowwhat stressful situations can make youfeel like inside. (You will hear sighs ofrelief, laughter, and comments such as"I didn't think you'd do anything likethis to us, whew!")

Anxiety
Endocrine functioning as a consequence ofparasympathetic system's reactions to stress
STRESS MODEL
StressFrustration Anger Emotional Responses
Non-adrenalin Physiological ResponseAdrenalinStress
Increase in blood pressure, heart rate, sweating,dilation of pupils, etc.
Flight Fight Internalization Behavioral Adaptationwith no release
Individual differences in alleviating stress
Potentially constructive
Deal with anxiety and anger as theyoccur in small pieces.
Be assertive, honest, and real whensituations involving people createfeelings of anxiety or anger.
Select and use appropriate physicaloutlets for venting anger and anxiety(running, cycling, playing tennis, orplaying piano).
Potentially destructive
Let anger and anxiety build up by notrecognizing internal feelings and/or bynot acting on them.
Be aggressive and outwardly hostile orsubmissive when situations involvingpeople create feelings of anxiety oranger.
Attempt to hold in and repress feelingsof anger and anxiety and try to forget thesituations that caused them.
Appropriate use of defense inappropriate overuse of defensemechanisms. mechanisms.
Discussion: General questions which re-late to this experience include: What isstress? What situations are stressful toyou? How can stress resulting in angeror anxiety be handled constructivelyand destructively? What do you dowith anger when you feel it? What aresome constructive outlets for angerand anxiety? What do you think arethe dangers of repressed anger andanxiety?
Lecture: The model presented on thenext page can serve as a framework fora lecture on stress, including its emo-tional, physiological, and behavioralparameters. Health-generating reso-lution of stress should be emphasized.
Health educators cannot eliminate themany stresses their students will en-counter in their daily lives. They can,however, help students to examine thetypes of situations which evoke indi-vidual stress reactions and can discussalternative ways of coping with stress, sothat young people will be able to incor-porate health-generating behaviors intostress-provoking situations in their life-styles.
143

81 TEACHING IDEAS
NM HealthaloftSVategy
PATRICK KIDD TOW is an assistant pro-fessor in the Department of Health andPhysical Education at Old Dominion Uni-versity, Norfolk, Virginia 23508.
This teaching strategy is appropriatefor secondary school or college levelhealth classes. I have used it at the endof a mental health or drug educationunit, but it might also be applicable toany health unit which uses value clarifi-cation.
Each participant begins with a setsum of moneylet us say $25,000, andis entrusted to keep a running tally ofhow much they have spent and whatwas bought. Members of the class bidon certain aspirations, loves, or wishesin an auction. The items for auctioncould pertain to physical, emotional, so-cial, or even spiritual health.
The instructor plays the part of anauctioneer. Only he or she should knowwhat items are up for auction andshould try to keep the bids as high aspossible. Fervor and interest will growas the soaring bids become more com-petitive. The auctioneer should dealwith each item one at a time by an-nouncing and writing it on the board.After the final bid is accepted, the sell-ing price is written next to the item.
The objective of this strategy is toevoke introspection on what values theindividual cherishes. At the same time,students can see which behaviors andvalues are held in high esteem by theirpeers. The impulsive and eccentric na-ture of some participants may also be-come apparent. After completing theexercise, there will soon be an influx ofcomments and questions from the re-sults.
The following items have been auc-tioned off in a mental health class.
1. Guarantee to die a peaceful and painlessdeath when the time comes
2. Ability to prevent World War III3. Ten extra years added on to your life4. Never have to work and still be paid5. Ability to save the life of one person6. Phenomenal love for children7. Ability to play any musical instrument
desired8. Be boss and sole owner of a company9. Own the only solar-powered sports car
144
agE'
10. Travel back or forward in time andchange history
It Be considered a fantastic lover12. Be the most loved and popular politician
in the country13. Never have a sick day in your life14. Possess unrivaled intelligence or genius15. Eat as much as you want and never get
fat16. Be the author of the world's best-selling
book17. Be considered a successful financial
wizard18. Be exceptionally skilled in any sports one
desires19. Phenomenal love for animals20. Never have an enemy in the world, be
loved by all21. Die with a clean conscience, no debts,
and no sins left behind22. Guarantee to never become addicted to
any drugs23. Climb the highest mountain and survive
Mental Health
at
24. Be granted more handsomeness orbeauty
25. Reincarnation into anything or anyonedesired
Additional objectives may beachieved by modifying this auctioningstrategy. Following are some sugges-tions.
Reduce or increase the number of itemsto suit a specific health topic beingcovered.
Distribute a list of items for auction sothey may be arranged according toindividual preferences.
Allow small groups to submit publicbids as a consensus.
Permit borrowing or lending of moneyamong participants to see how manyoverextend themselves.

82 TEACHING IDEAS
People LabelingStmtegy
PATRICK K. TOW and HAL WINGARDare assistant professors in the Department ofHealth and Physical Education at OldDominion University, Norfolk, Virginia23508.
Many people are in the habit of label-ing or stereotyping other members of so-ciety. Some of these "tagged victims"may be acquaintances of those doing thelabeling. While peer group coercion hasbeen able to provide the necessary moti-vation for constructive changes in ourlives, it can also be destructive in nature.The insidious manner in which labelsand stories can spread help blow the pic-ture far out of proportion. Perhapssomeday we may come tc realize suchpractices tend to do more harm thangood.
An innocent person defamed by acirculating, malicious slander may feelthe intense social and emotional im-pacts. Public denial of such labels may beinterpreted as frantic attempts to concealguilt. There is always that tragic alterna-tive of the stigmatized acting in accor-dance with the label bestowed uponhim. On the other hand, there is also thepossibility that a label accurately depictsa person's past or present. Nevertheless,such unscrupulous denotations ex-pressed out of spite or ignorance tend todiminish the faith and trust one has inone's fcnow man.
S'agmati?.ation is only one part of thehe other is one which many of
us to on a number of occasions.:faces when listening earsievt and treat a person ac-that real or unreal stigma.tices may appear to be a
-ffo. t to prevent an individualfins the mainstream of Amen-
y Perhaps some people be--,ver actions are associated
I label warrant public de-noL, ad infinitum. The resultingsocial a..o emotional damages could beavoided f we we, e sensitized to theramifications of our persistent "pigeon-holing" behavior.
This teaching strategy is intended todraw out various prejudices, biases, and
Mental Health
CATEGORIES OF PEOPLE
Labels parent teacher
Alcoholic
Mentally
Disturbed
Homosexual
Drug
Addict
Divorcee
Total
neighbor TV star stranger Total
fears governing our lives. It will becomeobvious in discussions among highschool or college students that some con-cerns are groundless and based uponsheer ignorance. However, there will besome thoughts expressed which werebased on feelings derived from personalexperiences which might not necessarilybe refuted. Therefore, it becomes abso-lutely essential for teachers and studentsalike to pay heed to what is being said.
The teaching instrument to be used isshown as a table. The rows represent fivetypes of labels apt to be used as brandsfor certain undesirables. The columnsrepresent five categories of people thatare hypothetically given the labels. Stu-dents are directed to correlate each labelwith every category of people and assigna score to indicate the degree of tolerabil-ity they have toward these individuals.The range of scores is: 4will always beable to tolerate; 3will frequently be ableto tolerate; 2will sometimes be able totolerate; 1will seldom be able to toler-ate; 0will never be able to tolerate.
Examples of the process involvedshould be provided for the students. Forexample, a student examines thehypotb.,,fic.11 situation that one of hispardnts is an alcoholic. He may find that
.:t absolutely intolerable and assigns asc ore of zero. On the other hand, he maybe quite willing most of the time to acceptthe fact that his favorite TV star turnedout to be an alcoholic. If this is the case,the student would assign a score ofthree. In another example, a studentmay be willing to tolerate his homosex-ual teacher most of the time and scores a
1 5
three. However, he may seldom feel tol-erant enough to associate with a homo-sexual stranger and assigns a score oftwo.
A sum of totals from each row andcolumn reflect that label or category ofpeople deserving the most and least de-gree of tolerance. For example, the high-est row total found associated with di-vorcee would suggest that student ismore tolerant of divorcees than any ofthe other given labels. By the same to-ken, the highest column total, which isassociated with stranger, may indicatethat student is more tolerant of their im-proprieties than the other category ofpeople. The lowest row or column totalsmay indicate that label or category ofpeople least tolerated by the student.
Other variables besides what is givenin the table can be used in substitution.Any of the following can be added topeople categories: brother/sister, politi-cian, cousin, boy/girlfriend, or minister.Any of the following labels can be used,too: transsexual, shoplifter, murderer,marijuana smoker, hit-run driver, sui-cide attempter, child abuser, or bisexual.Of course, there are also other possiblealternatives that can be conjured up bythe teacher.
In the ensuing discussions, studentsshould begin to realize people with suchlabels used in this strategy need moreempa thy than sympathy from otherpeople. Most anyone can provide pity,but understanding is a step beyond whatthe stigmatized may expect. It is fortu-nate that changing times and people intoday's world beckon us to relent andmodify our opinions about others nowdeemed out of place in our society.
145

83 TEACHING IDEAS
Creative FoodLabels: ConsumerHealth Eduestise
HYSON
=
MOON S. CHEN, JR. is visiting assistantprofessor, Department of Health, PhysicalEducation, and Recreation, Box 4070, TexasTech University, Lubbock, Texas 79409.
Any unit or course in consumer healthshould include a section on what to ex-pect on food labels. Described in the fol-lowing outline is one way to facilitatestudent learning in food labels.
Teacher Preparation
1. Read the handout, "A Consumer'sGuide to Food Labels," by MargaretMorrison from the Tune 1977 FDAConsumer.
2. Prepare enough copies of the hand-out for distribution to each student.
3. Write the names of approximatelyfive to seven fresh fruits on strips ofpaper so that there are enough foreach class member and each fruit ismore or less equally represented.
Place these strips of paper in a bag.Students will draw these strips fortheir assignment.
Behavioral Expectations for the Student
As a result of this exercise, the studentwill be able to:
1 46
tfo.NET'A..:'.WHOLE BEAN:)4*,,..UNcoATED
TABLE/ PMa;or,..;
1. Make a food label and in doing so willbe familiar with the various compo-nents of food labeling.
2. Make judgments on the quality of var-ious food labels.
3. Experience, discuss, and categorizethe decision-making processes ofmany consumers.
Procedure
Day One
1. Introduce the topic of food labelingwith emphasis on reasons for labeling
111,1011NONIOIN
MACKEREL'S.qqqq
food, FDA requirements for foodlabels, explanations of the variouscomponents of the nutrition informa-tion label.
2. Introduce the idea of a contest to beconducted the next class day on foodlabels. Each class member draws froma paper bag a choice of a fresh fruit.These <thoices are not to be revealed toother members of the class. For thenext class assign students to read thehandout, "A Consumer's Guide toFood Labels," and make a label for thechoice they drew from the paper bagthat would conform to FDA
1 5
Nutritionguidelh,es Any information that isnot a, eilable, such as net weight, may
e es Syr: ted or made up.
3. Announce that there will be prizes(first prize and runner-up) awardedto the most original label, the mostpopular label, the most attractivelabel.
Day Two
1.
2.
3.
Have all those with the same fruitsplace their labels in one area of theclassroom. The objective is to placelabels in such a way that they will"sell" themselves. Have students puta price on their items.Once labels are in place, distributethree pieces of paper to each studentfor ballots.Instruct students to write theirchoices for the best label on their bal-lots. Students may distribute theirvoting on these ballots in any fashionthey wishall three ballots for theirchoice of best label, two ballots forone choice and one ballot for another,or one ballot for three differentchoices.
4. Invite volunteers to tally the ballots.5. After the ballots have been tallied,
announce the winning labels andaward the prizes for the best label andrunner-up. The teacher may decidewhat to do in case there are ties.
6. Prizes could be books or fruits.7. The teacher should then follow up
this exercise with a discussion on con-sumer decision-making in the mar-ketplace and ask class to share theirexperiences and their dedsion-mak-ing.
84 TEACHING IDEAS
Sensible listing
MARILYN MUDGETT is associated withthe Health Education Department, GroupHealth Cooperative. DOROTHY CULIAT ispresently evaluating the weight control pro-gram of Group Health Cooperative, 200 15thAvenue East, Seattle, Washington 98112.
Dieting is an obsession for manyAmericans. Money readily spent on faddiets, exercise devices, over-the-counterweight loss aids; miracle foods, and na-tional self-help organizations all add upto a billion dollar weight reduction in-dustry. Physical activity has been takenout of the realm of the natural and isunder the domain of big business--health spas, athletic clubs.
The search to be thin can be confusingand costly to the consumer. Studentsneed accurate, unbiased information tomake decisions about weight control andlearn how to protect their pocketbooks atthe same time. The following assign-ments are methods of educating the po-tential consumer.
1. Investigate commercial health spasand community recreational facilities.Compare cost, services offered, equip-ment available, and reputation. Investi-gate commercial dit'' qics comparingtype and length of "treatment," prom-ises made, food plan, consideration forchanging food habits, and success rate.
2. Make a study of doctors who spe-cialize in weight control. Examine pro-fessional qualifications, length of treat-ment, types of treatments (pre-packagedfoods, pills, shots, hypnosis, etc.), suc-cess rate, and possible health dangers.
3. Visit the local drugstore and make alist of the over-the-counter reducing aidsavailable or visit a library or bookstoreand note the number and titles of bookson dieting.
1 6(4)
Nutrition
4. Compile magazine and newspaperadvertisements on diets, diet aids, andslimming devices. Evaluate the reliabilityof these advertisements analyzing theuse of objective facts, pseudoscientificwords such as "cellulite" and "diuretic,"or claims to do something for nothingsuch as, "lose ugly fat while you eat thefoods you love."
'Siiadhbai;Lmi.7b.11P'a.. 4.1
5. Write to adolescent summer weightcamps and adult "fat farms" forbrochures. Figuring length of stay anddesired weight to be lost, determine howmuch each pound of weight loss wouldcost.
6. Make a survey of family and friendsto determine if they ever dieted, types ofdiets, aids, products and/or facilitiesused, success rate, and cost.
Two excellent resources for consumereducation and weight control are ThinFrom Within by Jack Osman and A Diet forLiving by Jean Mayer.
147

PART II

ForewordHealth Teaching Ideas Secondary was first published in 1983. The publication has
been very popular and has experienced a consistent demand from those interested inimproving the delivery of health education. Since 1983, the Journal of Health Educationhas cortGnued to print teaching strategies under the heading of "Teaching Ideas." Prac-tically all of these are included in the revised edition of this publication. In addition,other teaching strategies have been included that will eventually be printed in theJournal.
Although the title states "secondary," teaching strategies have been included herethat would be applicable for middle school through the college level. Users of thisvolume have the flexibility of adapting the teaching strategies to the grade level that ismost appropriate for them.
The Association for the Advancement of Health Education believes that Part IIwill add to the value of the earlier materials and make this expanded volume an excel-lent reference for all those seeking workable ideas in teaching and delivering healtheducation programs.
As editor, I wish to thank the authors for sharing their creativity and successeswith the profession. Without their willingness to make this professional contribution,the new edition could not have become a reality.
Within the covers of this book are a multitude of ideas to make health educationrelevant and exciting for the student -- and enjoyable and rewarding for the teacher. I
invite the reader to explore the innovative and successful experiences presented here.
Loren B. Bensley, Jr., EditorProfessor of Health Education
Central Michigan UniversityMount Pleasant, Michigan

Focus on Process
1G3

TEACHING IDEAS 85
The Writing Process in Health ClassVicki Steinberg and Teresa M. Fry
In Exeter Township's Health HI class,a health quarter course required forgraduation, teacher Terry Fry involvesstudents in the learning process usingvarious writing techniques. Previously,Mrs. Fry used teacher generated lec-tures, quizzes, tests, and a few learningcenters to give students a basic under-standing of human sexuality. For fouryears, Mrs. Fry used traditional meth-ods, but she was bored with the fin-ished assignments, particularly sinceshe teaches four similar classes in onequarter; therefore, a test meant 120 stu-dents turned in dull true/false or match-ing answers. Also, Mrs. Fry was con-cerned that students were not reallyinvolved in their own learning process.
Although many of the tests remainthe same, through the writing processthere is more interaction between stu-dents and between the students and theteacher. At first, Mrs. Fry tried a simpleassignment. She began hy telling theclass about her birds and the bees' talkwith her mom and her misconceptionsabout sex. Class members then wrote inclass their recollections of a similar talkwith their parents. Those students whodid not recall a talk or were sure theyhad never been involved in such a dis-cussion wrote what they will tell theirchildren. Since some of the informationis quite revealing, students who do notshare but do turn in the rough draft andeach class member receives credit forthe assignment. Using this simple writ-ing, Mrs. Fry breaks the ice, showingthat everyone has the same thoughtsand experiences. Students who havewritten in order to learn about them-selves realize how nervous both theyand their parents were.
This early success encouraged Mrs.Fry to give extra credit to students whointerview their mothers about their own
Vicki Steinberg is a teachcr in the EnglishDepartment of Exeter Township School Dis-trict in Reading, PA 19606. Teresa M. Fryis a teacher in the Physical Education!HealthDepartment of Exeter Townshi.p School Dis-trict.
births. Obviously, some students do notlive with, or even know, their birthmothers. These students have a sheet often options from which to choose, suchas to interview three different people orexpress their own views concerning sexeducation in the schools. This interviewgives the student an insight into thetimes of his birth and brings parentsand teenagers together. One boy dis-covered he had been born on the daythat Bobby Kennedy was shot and wasnamed after Kennedy, while many kidsfound their dads had been in Viet Namat the time of their births and had noteven known their baby sex. This as-signment makes students talk to theirparents pleasantly and brings themcloser for a moment or two because itgives students insight into their person-al history.
For a full week, about half waythrough the course when class membersare comfortable with each other, theFlour Baby Project begins. Here eachstudent must make a baby from a fivepound sack of flour and carry him/hereverywhere for seven days. During theweek, in order to achieve more than anaverage grade, studen:s may do twomecerent interviews about the FlourBaby Project, one to obtain the parentalview of the project and any suggestionsfor improvement and one interviewinga parent other than the student's ownconcerning being a parent. Other topicsinclude checking the finances associatedwith having a baby and writing aboutthe information.
As a culminating exercise, studentscomplete sentences such as "I learnedthat..," "I now know that..," and "Ihated that . . . At the end of the ques-tions, students may give opinions aboutthe project and how they would changethe project. After papers are turned in,the class orally reviews the ideas.
As classwork, students split up intogroups of three or four to write dia-logues about the birthing process. Afterrough drafts are completed, ,tudentsread their dialogues aloud to the class.Typical encounters mdude scenes about
the start of labor, getting to the hospitalon time, or the labor processthe phys-ical and psychological aspects of birth-ing. Students don't feel a need for agrade; they enjoy themselves and revealknowledge at the same time.
As Mrs. Fry continues to use thewriting process, she finds more uses forit. A recent addition to her course is achronological description of the steps ofthe menstrual cycle. After the lecture,studrInts write their understanding inparagraphs to clarify any mistaken con-cepts in timing and to solve problemsbefore the same question appears on atest.
Previously, each Health III classwrote research papers on various topicsfrom rape to child abuse to in vitrofertilization, but the papers were repeti-tive and copied word for word from thesource material. This problem endedwhen Mrs. Fry presented the class witha list of different ways to tackle writingthe researched material. Instead of sim-ply copying the material, students couldwrite a diary of a child abuser, a PhilDonahue interview with a surrogatemother, a dialogue between a lawyerand a rape victim, or anything similar.These options made the teacher's andthe students' jobs more enjoyable andtherefore a better learning experience.Even those students wlio wrote a tradi-tional research paper had to add a per-sonal final paragraph to humanize thetext.
The most recent writing started inclass but was finished outside class.First, the class brainstormed reasons,pro and con, for a teenager having asexual relationship. A recorder kepttrack of the ideas and the class receiveda copy the following day. Working indi-vidually, class members drafted a dis-cussion of four ideas from the list. Mrs.Fry had magazine articles available tohelp back up responses. For extra cred-it, students could have their parentsread and sign the paragraphs, againopening discussion at home throughwriting.
Because of the added written assign-
153

ments, students learn more about them-selves, other people, and their families.Tests and quizzes do not allow the closefeelings among class members or stu-dents teaching themselves to see theirfeelings.
The teacher also learns more aboutwhat members of the class know and
can adapt future work to problem spots.Through end of the quarter evaluations,she can also discover what needs to betaught di(ferently, faster or slower, or inmore detail. Fortunately, none of theextra writing is a large burden in timebecause students have found theirvoices and are interesting as well asknowledgeable.
Because the English faculty at Exeterhas been encouraging all teachers to usewriting in their classes and providingideas to make it possible in each uniquesituation, the health curriculum has be-come an exciting and enjoyable educa-tional experience for both students andteachers.
154
1 G 5

TEACHING IDEAS 86
Logo-Mania: Creative Health ArtFrank Caisbeek
The logo or trademark is a power-ful communication tool in the hands of acreative health teacher. It is useful forgetting students to examine the "human-izing" messages that health agenciesdevelop and project for themselves.Artistic symbols are used to craft alikeness or identity for the organization'smission and philosophy. These imagesare planned and developed with intentand purpose. Each is significantly dif-ferent and is a projection of the uniquequalities that an institution or agencywishes to convey about itself
The idea of a logo or trademark isvery old. Marks have been found onearly Chinese porcelain, on pottery jarsfrom ancient Greece and Rome, and ongoods from India dating back to about1300 BC (Morgan, 1986).
Set the StageStudents can be motivated to be-
come involved in logo-mania by callingtheir attention to a logo that many haveseen, but few may understand. Thecaduceus, with its two snakes entw inedin opposite directions around a wandmade of olive wood and gold, alwaysarouses their curiosity. Point out the factthat both snakes are "eyeballing" eachother and that they are surmounted bytwo wings. Students generally recog-nize that the wings are symbol ic of speed;they are sometimes affixed to a trackshoe and given as an award to the school'strack star. These wings belonged to
Frank Calsbeek is in the Health Edu-cation Divisionof Sout' westTexas StateUniversity, San Marcos, TX 78666.
Hermes, the speedy messenger of thegods in Greek mythology. The wandwas a gift from Apollo and had thepower to unite all beings divided byhate. Hermes discovered the unifyingpower of the wand when he threw itbetween two fighting snakes whopromptly wound themselves around it infriendly association. The wand also pos-sessed magical powers over dreams,waking, sleep, and even death.
Later, a single snake wrappedaround the staff came to be a symbol forAesculapi us, thc god of medicine. Todayit s the symbol of the medical profession.
Health Logos TodayHealth agencies are very sensitive
to the public 's perception of their image.Their logos take form as a symbol, setapart by unique design, with distinctivecoloring, lettering, or any combinationof these. The purpose is to give a pow-erful identity to the health agency or
1 G t;
group. Usually the logo is field-tested tosee if it accurately reflects the image thatthe organization has of itself. It mustalso mold this image in a positive way.Images can be misinterpreted,amplified,or ignored.
A healthy image will exhibit orelicit some, if not all, of the followingcharacteristics or responses: 1) strongemotional response, 2) appearance ofpower, 3) sense of experience, confi-dence, and tradition, and 4) sl ow processresulting from consistent repetition(Napoles, 1988).
Discovering a Logo's ImageFive current health logos are pro-
vided on the following page to use forreproduction as an overhead transpar-ency. They represent professional, vol-untary, and official (tax-supported)health organizations and agencies. Somemay be well known and easily recogniz-able. Others may be unfamiliar to yourclass. An identification key is given atthe end of this article.
Project these logos on a screen andhave students examine each one indi-vidually. Ask probing questions thatfocus on the following:
1. What objects do you recognize ineach logo?
2. What symbolic meaning does eachobject have?
3. To which agency/organization doesthis logo belong?
4. What do you know about the mis-sion of the agency?
5. What impression do you have aboutthe identity and image of each agency;organization?
155

pr.*4,4".
A
Creative Logo DesignHave students form six design
teams of three to five students. Ask eachteam to creatively design a logo thatprojects an image and identity for one ofthe following school-based gniups:
Team 1. A local SADD chapterTeam 2. Your cafeteria programTeam 3. The nurses' health centerTeam 4. Crossing guard programTeam 5. Custodial/janitorial serviceTeam 6. Smoking cessation group
for teensArt materials such as paper, rulers,
compasses, color markers, and otheritems should be supplied. Students maybe apprehensive at first, claiming *heyhave little or no art ability. F.L. isurethem that the thsign concept is :ntraland that perfection could be carried outlater by an art professional. What isneeded is the basic idea.
Encourage students to creativelytranslate the image and identity of eachschool service group (or others, if theyapply) into the logo design. It may benecessary to inquire from each servicegroup how it views itself and its mission.Suggest that each logo should utilizepopular colors that would make it attrac-tive for a T-shirt or coat emblem.
After all teams have completed theirdesign task, culminate the activity byhaving each group share its creationwith the other design teams. Prominentlydisplay all six logo designs and inviteschool service group members to viewthe logos and verify if their mission andidentity were accurately projected.
Logo-mania is fun. It encouragesstudents to participate in a conteinporaryart form while creating an awarenessand apprec iation for different health ser-vice groups at their school.
a.
Key to Logos
A. World Health OrganizationB. Association for the Advancement of
Health EducationC. American School Health
AssociationD. American Public Health
AssociationE. March of Dimes - Birth Defects
Foundation
Morgan, H. (1986)SymbolsofAmerica. NewYork: Viking Penguin, Inc., p. 7.
Napoles, V. (1988). Corporate identity de-sign. New York: Van Nostrand ReinholdCompany, Inc., p. 11-26.

TEACHING IDEAS 87
Overcoming Xenophobia:Learning To Accept Differences
Judith A. Baker
Health educators are often calledupon to interact with special popula-tion groups. Some of the special pop-ulations health educators serve arethe medically indigent, the homeless,the elderly, the obese, gays, the dis-abled, racial minorities, and alcohol-ics. Unfortunately, most health edu-cators and their clients have beenraised in a society which tends toview people with these characteris-tics in a negative and stereotypicalmanner (Snyder, 1986). When thesesocietal views are internalized, xeno-phobia limits the ability of healtheducators to provide quality serviceto all clients. Xenophobia is a termused here to identify the fear ofstrangers or anyone viewed as differ-ent from the norm.
The disasterous impact of xeno-phobia on the practice of health ed-ucation is apparent in the case ciinternalized ageism of elderly clients.Obstacles to early detection of breastcancer among elderly women listedby Frank-Stromborg (1986) are mythsabout older people, viewing pain asan inevitable part of aging, and at-tributing symptoms to aging ratherthan illness. Internalized ageism andits associated fatalism may lead todiminished perceptions about the se-rious consequences of developing dis-eases which might otherwise be pre-vented. And, elderly adults who haveinternalized ageist beliefs that olderpeople are clumsy, ineffectual, fear-ful, dependent, and slow (Shaie &Shaie, 1977) prevent themselves from
Judith A. Baker is an assistant pro-fessor in the Department of HealthEducation, Texas Woman's Univer-sity, Denton, TX 76204.
enjoying the opportunity to improvequality of life in later years withphysical activity.
Strategies exist to help health ed-ucators overcome negative and pro-fessionally destructive attitudestoward clients. As part of a commu-nity health education class at a mid-western university, students were en-couraged to overcome xenophobia inthemselves and others. To preparefor teaching the unit on special pop-ulations, the instructor first exam-ined her own xenophobic reactionsand participated in each of the learn-ing strategies. The only materialsnecessary were a brief xenophobicassessment questionnaire, a list of 10successful people from the specialpopulation of choice, a list of booksand movies about the special popu-lation, and a written description ofstudent assignments. Three class ses-sions were allotted for the learningunit. Each of the strategies presentedcan be adapted for use in a variety ofhealth education classes includingthose dealing with human sexuality,aging, alcohol abuse, and weight man-agement.
In the first class session, self-awareness is addressed. The first andlast names of all students enrolled inthe class are written on name tags.Students are asked to sele n one nametag other than their own and place thename tag on someone in the room towhom they believe the name be-longs. Additionally, students are askedto give a fabricated introduction basedsolely on appearances to the classabout the people they selected. Fol-lowing the introductions, class dis-cussion is generated about the ste-reotypes used during the name tagactivity. Next, students are asked torecognize how they feel about each
1Pq
of the client groups listed previouslyon a brief questionnaire. Reactions toworking closely with clients possess-ing each of the listed characteristicsare ranked by each student followingthe question: "Would you feel un-comfortable or ill-at-ease when work-ing with any of these clientsr Manyprejudice attitude questionnaires orinstruments have been developedwhich also can be used to measurexenophobic reactions (Wingard, 1981;Smith, 1973). The first session en-ables the instructor to identify one ortwo special population groups forwhich most of the students in theclass express the greatest xenopho-bic reaction.
In the second session, the instruc-tor helps students to identify all themyths commonly heard about thespecial population group of choice.Students are asked to collect factualknowledge about the characteristicor the group of people from materialsprovided in class. Misunderstand-ings and myths are corrected in classby the students.
Next, students are asked to con-sider how society oppresses peoplewith the characteristic. What labelsare commonly used to describe peo-ple with the characteristic? How doesthe label serve to perpetuate stereo-typing and oppression? Are the con-notations of the labels helpful tostrengthening the self-esteem of peo-ple with the characteristic?
Repeated and positive personal ex-posure with people who possess thecharacteristic may help to alleviatexenophobic reactions. Outside class-room assignments include the sug-gestion that students get to knowthese people socially or at least out-side a professional setting. Studentscould attend a self-help group com-
157

prised of these people. Students areprovided with a list of movies andbooks depicting the special popula-tion in a positive manner. Studentscompete by trying to identify thegreatest number of famous and suc-cessful people from the special pop-ulation.
Other ways to reduce xenophobiain addition to increased self-aware-ness, knowledge, and personal expo-sure are simulations, role plays, androle reversal. A simulation is con-ducted by having students verballyexpress their immediate reaction toeach of the following situations: ( I)you had to listen to an obese speakerin class talk about Overeaters Anon-ymous, (2) the specialist to whomyou have been referred for a medicalproblem is obese, (3) your best friendfrom childhood who came to visit isobese, (4) you discover that you areobese.
Examples of role plays and rolereversals are essay assignments about
1 58
what life would be like if 90 percentof the U.S. population were gay or ifthe student woke up tomorrow weigh-ing 50 extra pounds. In the thirdsession, dialogues based on the es-says are created and acted out bystudents in class. In addition, stu-dents report on their experiences incompleting the outside classroom as-signments.
The use of these strategies in acommunity health education class aid-ed students in comprehension of acomplex issue. Students were able togenerate their own examples of waysxenophobia acts as a barrier to thepractice of community health educa-tion.
Once students work through all thestrategies for reducing their xenopho-bia, they will be better able to workwith a greater variety of clients. Evenif they cannot identify xenophobia inthemselves, they have responsibili-ties as health educators to recognizethe problems encountered by their
clients. Clients themselves can ben-efit from experiencing these strate-gies to help overcome their internal-ized xenophobia. Quality healtheducation requires that health educa-tors engage in the professional andpersonal development necessary toovercoming xenophobia.
Frank-Stromborg. M. (1986). The role of thenurse in early detection of cancer: Popu-lations sixty-six years of age and older.Oncology Nursing Forum, 13(3), 66-74.
Schaie, L. W., & Schaie, J. P. (1977). Clinicalassessment and aging. In J. E. Birren andK. W. Schaie (eds.), Handbook of thepsychology of aging. New York: VanNostrand Reinhold.
Smith, K. (1973). The homophobic scale. In G.Weinberg, Society and the healthy homo-sexual. New York: Anchor.
Snyder, M. (1986). Self-fulfilling stereotypes.In D. Goleman and D. Heller (eds.), Thepleasures of psychology. New York: NewAmerican Library.
Wingard,J. (1981). Measures ofattitudes towardthe elderly. Experimental Aging Re-search, 6, 229-313,
TEACHING IDEAS 88
Factors Important in Teaching Confroversial IssuesAnsa Ojanlatva
A few years ago one of my assignedcourses was a required methods coursefor those intending to teach health edu-cation at the secondary school level.Most of the students in these courseswere physical education majors and asoften is the case, they were studyinghealth education as their second teach-ing field. Unfortunately, in these cir-cumstances, students often expecthealth education to be an easy field ofstudy, and therefore, by the time of theirsenior year, many still are ;ma ware of theknowledge, skills, and sensitivityneeded to teach controversial health is-sues.
Additionally, Merki' found evidencein 1976 that there is a plethora of instruc-tion about physical fitness; but life-re-lated topics such as human sexuality,mental health, and consumer issues,frequently requested by students, areoften lacking completely in the cur-riculum. This has prompted my searchfor activities which might increase stu-dent awareness of the qualifications toteach controversial issues.
I developed the following teaching/learning activity with the above statedobjective in mind. Specifically, the activ-ity concentrated on drawing out infor-mation about the following:
1. the instructor: his/her characteris-tics and professional background;
2. the subject matter: the cognitivesubstance and the continuity of it in rela-tion to other subjects;
3. the method of teaching: the plan-ning of instructional activity, the instruc-tional methods, and the possible evalua-tive procedures.
Before this session students engagedin values clarification activities and theywere aware that they would not beforced to participate. However, as futureteachers of health education, they wereencouraged to participate in the activity.In this class no one refused.
The students were told to:1. pick a topic "from the hat" (all were
Ansa Ojanlatva is in the department ofHealth Science and Human Ecology, Schoolof Natural Sciences, California State College,San Bernadino, CA 92407. Her article wasaccepted for publication in June 1980.
questions commonly asked by highschool students about sexuality), and
2. take five minutes to write down:(a) how they would answer the
question (subject matter);(b) how they would teach about it
(method of teaching);(c) what qualifications a teacher
should possess to present thematerials in an effective man-ner.
The students worked on the topicswithout discussing them with eachother. Time did not allow for all topics tobe discussed, but after the five-minuteperiod several questions were selected tobe answered:
1. What is a wet dream?2. Do women have wet dreams?3. What is masturbation?4. What is a normal penis size?5. Can the sperm supply be used up?6. What is homosexuality?The material* presented during this
session included:1. The instructor's role.
(a) knowledge required,(b) sensitivity needed for discuss-
ing the topic or issue, e.g.:(1) sensing other people,(2) feeling comfortable with
one's own sexuality.2. Subject matter.
(a) facts,(b) continuity.
3. Methods of teaching.(a) planning a program including
elements such as:(1) support from needed com-
munity groups and fromparents,
(2) personal involvement fromstudents,
(3) ddequate time for learning,feedback, and evaluation,
(4) meetings with students andtheir parents.
(b) using methods of instructionelaborating on:(1) positive vs. negative ap-
proaches,_
'The students used the following book as aresource: Read, Donald A., and Greene, Wal-ter H. Creative teaching in health. New York:MacMillan Publishing Co. Inc., 1975.
BEST COPY MAE 1 7 (4
(2) values clarification,(3) positive climate,(4) openness to any relevant
questions.(c) planning evaluative proce-
dures.The eva iation revealed that in most
cases the activity accomplished what itwas meant to accomplish. Twelve stu-dents participated in this class experi-ence, and each turned in an evaluation.Following is a synopsis of their reactionsto the questions on the evaluation sheet.1. Did you find out anything about yourselfas a teacher?
Four students indicated it was hard totalk about sex; three of them suggestedcareful preparation was essential for theoutcome; and five felt comfortable intalking about sex with the class, whoposed as high school students. The:ewas indication of not having the neededinformation to teach the subject, and ofhaving found out what to teach and whatnot to teach.
2. Did you learn anything about the re-quirements of the subject matter?
The answers ranged from "no" (twostudents) to "different things" (one stu-dent). Some of the particular require-ments were:
(a) getting your points across.(b) using teaching aids effectively.c) preparing up-to-date material.
(..1) needing more preparation thanpreviously expected.
(e) needing so much factual informa-tion, knowledge of attitudes andbehaviors, plus ability to talk andlisten.
( f) needing information from relatedsubjects such as psychology,anatomy, etc.
3. Did you learn anything about the factorsneeded to plan a controversial teaching unit?
The variety of responses makes asummary somewhat difficult. Some ofthe responses cautioned:
not to ask students to reveal per-sonal information they may notwish to reveal;to think more about how the subjectmatter may affect the student;to prepare for extreme feedback.(The responses seemed to refer to
159

possible need for counseling afterstudy of controversial issuese.g.,a student's bursting into tears dur-ing discussion of death arid dyingissues.)
Further, the answers revealed that thestudents realized the importance of thefollowing:
the need for a comfortable attitudein the teacher to make students feelcomfortable.the necessity of an organized pic-ture of the various factors in sexeducation and the particular steps toconsider.the need bor a lot of planning beforea teaching unit can be implementedthe consideration of class makeup:social background, experience.the need of the other related sub-jects in planning a unit (anatomy,psychology, sociology, human sex-uality related topics).
4. How did you feel when you had to teachthe topic?
Two students indicated they felt ner-vous because they did not know how theclass was going to react. Five studentsindicated the opposite: they felt comfort-able in talking about the issue raised.Three students indicated embarrass-ment or hesitance in the beginning. And
160
two students said they felt inadequate interms of factual knowledge.5. Any other comments?
The answers to this last question indi-cated overall feelings:
objection to an activity involvinghomosexuality."The class today was great. . . I
thought it was one of the most un-usual classes I have been to."interesting exercise (two students)."I think teaching on sexualityshould fall within the limits of theapproved curriculum if you want tokeep your job as a secondary schoolteacher."
This activity was meant to make stu-dents aware of the information, skills,and sensitivity needed to teach contro-verbial subjects. The topics were chosenbased upon issues discussed in class,which happened to be on sexuality. Inthe same manner, one might raise ques-tions about use and abuse of drugs, orany other subject for which there is noone solution.
'Merki, Donald. Personal communication,January 1980.
'Read, Donald , and Greene, Walter H.Creative teach;is, Oh. New York: MacMil-lan publish' , Inc., 1975.
I 7 1
TEACHING IDEAS 89
Teaching About Authoring Systems: InstructionalDesign Tools for Health Education
Paul D. Sarvela and Marilyn J. Karaffa
Microcomputers have become in-creasingly important as educationaltools in the health education program(Petosa & Gillespie, 1984). Adoptionof microcomputer technology has oc-curred not only for hardware sys-tems, but also for software systems.Even though there has been an in-crease in the quantity and variety ofsoftware for health education, one ofthe biggest problems facing healtheducators who try to use computer-assisted instruction (CA1) is the short-age of high quality educational soft-ware (McDermott & Belcastro. 1983;Sarvda, Ritzel, Karaffa, & Naseri,1989). Therefore, health educatorssometimes find it desirabk to devel-op CA1 to meet a specific need. Sincemany health educators do not havecomputer programming skills at thelevel neces,iary to create high qualitysoftware, riuthoring systems can serveas an ex zellent alternative. Author-ing syst.ems are software packagesthat P.re designed to create CA1through a process of mediation be-tween the author and a high-levelcomputer programming language(Whiteside & Whiteside, 1987/1988).
The purpose of this paper is topresent and describe the metheds ofa teaching technique which aims tointroduce and develop proficiency inapplying one of the authoring sys-
Paul D. Sarvela is an associate pro-fessor in the Department of HealthEducation, College of Education,Southern Illinois University at Car-bondale, Carbondale, IL 62901.Marilyn J. Karaffa is an assistantprofessor in the Department ofHealth and en.. ical Education, Col-lege of Arts and Sciences, Young-stown State University, Young-st6 1, OH 44555.
tems currently available for healtheducators, Apple SuperP1LOT. (Su-perPILOT is an authoring packagewhich enables instructors to developCA1 in an efficient and effective man-ner. Features include a comprehen-sive tutorial, an excellent set of doc-umentation materials, and foureditors: lesson text, graphics, soundeffects, and character set.) This tech-nique was designed for students en-rolled in a basic microcomputer ap-plications course at Southern IllinoisUniversity at Carbondale. With mi-nor adaptions, this approach wouldbe excellent for in-service work-shops and training programs for healtheducators wedng in a variety ofsettings (Le., schools, hospitals, com-munity agencies, and worksites).
Preparation
In private industry, computer soft-ware design and development is usu-ally dictated by a set of specifica-tions. We have. found this strategy tobe an effective way to teach designand development of health educationCA1 as well. Figure 1 shows an ex-ample of a specification that we haveprepared for use in our CA1 classes.
For e project, the instructorshould organize students into groups.It has been our experience that groupsof three or four students usually arebest. Next, documentation and pro-grams created by students (or instruc-tors) in previous sessions should bemade available to the students. Thesematerials are extremely helpful tostudents as they study the best waysto design and develop their authoringpackages.
172
Implementation and Time Frame
The lessons and activities are im-plemented in the following sequence:
(1) Introduce CAI hr).(2) Review Instructional Systems
Design (1SD) model of curric-ulum devdopment (1 hr).
(3) Discuss special curriculum de-velopment issues related to CA1(1 hr).
(4) Introduce basic SuperP1LOTcommands (1 hr).
(5) Demonstrate previously devel-oped student or instructor-generated programs (1 hr).
(6) Student review of SuperPI-LOT tutorial (3 hrs).
(7) Student design and develop-ment of CAI materials (8 hrs).
(8) Pilot testing and revision ofCA1 materials (3 hrs).
(9) Student demonstration of theirprojects to class (1 hr).
In our classes, 20 hours have beenallotted to the process of teachinghow to use the SuperP1LOT author-ing package.
Necessary Materials
The following materials are neededto implement this teaching tech-nique: one Apple 2e computer withtwo disk drives and monitor per group;one SuperP1LOT authoring systemper group; one blank disk per group;checklists for pilot testine the CA1materials (i.e., Horne & Gold, 1983);student background readings on CA1and 1SD (i.e., Bork, 1984; Sarvela &Noonan, 1988; Damarin & White,1986); and resources on tne healtheducation topic for the CAI selectedby the group (students gather thesematerials).
161
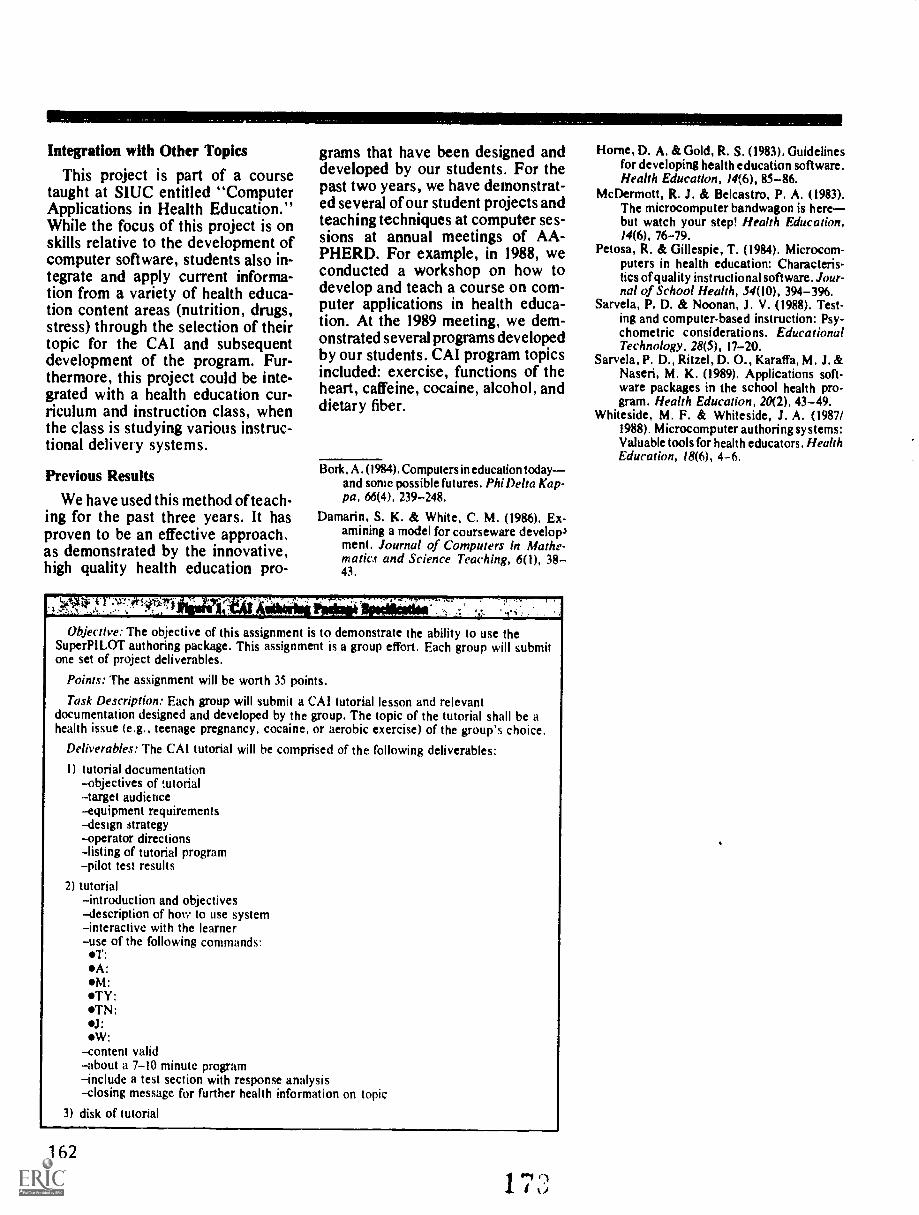
Integration with Other Topics
This project is part of a coursetaught at SIUC entitled "ComputerApplications in Health Education."While the focus of this project is onskills relative to the development ofcomputer software, students also in-tegrate and apply current informa-tion from a variety of health educa-tion content areas (nutrition, drugs,stress) through the selection of theirtopic for the CAI and subsequentdevelopment of the program. Fur-thermore, this project could be inte-grated with a health education cur-riculum and instruction class, whenthe class is studying various instruc-tional delivery systems.
Previous Results
We have used this method of teach-ing for the past three years. It hasproven to be an effective approach,as demonstrated by the innovative,high quality health education pro-
grams that have been designed anddeveloped by our students. For thepast two years, we have demonstrat-ed several of our student projects andteaching techniques at computer ses-sions at annual meetings of AA-PHERD. For example, in 1988, weconducted a workshop on how todevelop and teach a course on com-puter applications in health educa-tion. At the 1989 meeting, we dem-onstrated several programs developedby our students. CAI program topicsincluded: exercise, functions of theheart, caffeine, cocaine, alcohol, anddietary fiber.
Bork, A. (1984). Computers in education todayand some possible futures. Phi Delta Kap-pa, 66(4), 239-248.
Damarin, S. K. & White, C. M. (1986). Ex-amining a model for courseware develop.)ment. Journal of Computers in Mathe-matics and Science Teaching, 6(1), 38-43.
,)1,11 Pik*.
Objective: The objective of this assignment is to demonstrate the ability to use theSuperPILOT authoring package. This assignment is a group effort. Each group will submitone set of project deliverables.
Points: The assignment will be worth 35 points.
Task Description: Each group will submit a CAI tutorial lesson and relevantdocumentation designed and developed by the group. The topic of the tutorial shall be ahealth issue (e.g., teenage pregnancy, cocaine, or aerobic exercise) of the group's choice.
Deliverables: The CAI tutorial will he comprised of the following deliverables:
1) tutorial documentation-objectives of wtorial-target audience-equipment requirements- design strategy-operator directions- listing of tutorial program- pilot test results
2) tutorialintroduction and objectives
- description of how to use system-interactive with the learner- use of the following commands:
ST:A:SM:STY:*TN:
SW:- content valid- about a 7-10 minute program-include a test section with response analysisclosing message for further health information on topic
3) disk of tutorial
162
Horne, D. A. & Gold, R. S. (1983). Guidelinesfor developing health education soft ware.Health Education, 14(6), 85-86.
McDermott, R. J. & Belcastro, P. A. (1983).The microcomputer bandwagon is herebut watch your step! Health Education,14(6), 76-79.
Petosa, R. & Gillespie, T. (1984). Microcom-puters in health education: Characteris-tics of quality instructional software. Jour-nal of School Health, 54(10), 394-396.
Sarvela, P. D. & Noonan, J. V. (1988). Test-ing and computer-based instruction: Psy-chometric considerations. EducationalTechnology, 28(5), 17-20.
Sarvela, P. D., Ritzel, D. 0., Karaffa, M. J. &Naseri, M. K. (1989). Applications soft-ware packages in the school health pro-gram. Health Education, 20(2), 43-49.
Whiteside, M. F. & Whiteside, J. A. (1987/1988). Microcomputer authoring systems:Valuable tools for health educators. HealthEducation, 18(6), 4-6.

TEACHING IDEAS 90
TIC-TAC-TOEMary Lawler
Want to get your students interested,involved, and excited? Need somethingdifferent to motivate evetyone from thebrightest to the least gifted in yourclasses? Strike it rich with something assimple as tic-tac-toe.
In tic-tac-toe students pair up andadminister their own game by beingmaster/mistress of ceremonies, judge,and contestant at the sam Mime. Studentslove to compete and cannot be passivewhile playing this game. It's based onthe timeless game everyone knows howto play, so attention can be placed onlearning or reviewing the material athand.
First, I wrote questions and an-swers on our current unit. Questionswere then judged as easy, mediu ordifficult. Difficult questions shou. :otbe true/false, in order to eliminateguesswork. The number of questionscan be adjusted to your material or timerestraihts. Table 1 lists a sample ofquestions used in our substance abuseedition.
I began with 25 easy and mediumquestions and 6 difficult questions.Fewer difficult questions are neededbecause they earn fewer squares withinthe tic-tac-toe grid. The questions aretyped with the acceptable answers fol-lowing. For example: Chewing tobaccocauses a white patch in the mouth called
. (leukoplakia)
Mary Lawler is a teacher atGreenfield-Central High School,Greenfield, IN 46140.
One copy of each question isneeded for each two students in theclass. I used several different methodsfor preparing the necessary questions.They can be typed on colored paper,coded for the degree of difficulty. An-other way is to type all questions onwhite paper and code them for difficultyby marking the end of the sheets with theappropriate color. One copy of eachquestion is then placed in an envelope;the envelope is sealed and slit at one endto expose the color coded end of thequestions (questions can thus be selectedwithout being read). Another method isto print the questions on cardstock, ofthree different colors; these are moredurable but take more time to prepare.
The class is divided into partners tobegin the game. Once a player selects adifficulty level, their opponent reads theappropriate level question from thecardstock stack or envelope. The firstplayer answers and if correct, placestheir symbol, X or 0, in the tic-tac-toegrid. Xs or Os earned with correctresponses to easy questions can only beplaced in the four corners, mediumquestions in the mid-box, and difficultquestions in the center of the grid, asshown in Figure 1 (see next page).
Missed question3 are returned to thestack or envelope and remain in playuntil answered correctly. It is possiblethe question may recycle to be asked ofthe player who previously played it.However, it is entirely by chance andstudents are rewarded for remembering.Only the difficulty of the question is inthe control of a player, not the actualquestion selected.
Players continue taking turns untilthe game is won or a draw is declared.Players then draw a new tic-tac-toe gridand continue playing until all questionshave been answered correctly and takenout of play. Progress throughout thegame varies with ability of the students.Students in my health classes (grades 9and 10) play the entire packet in 30 to 45minutes.
Students benefit by working at aself-paced, directed activity at a difficultylevel of their own choosing. They areinvolved on task with reading, answer-ing, judging answers, and planningstrategy. The teacher's role should beonly as final judge for accuracy andfairness.
The game is easily adaptable to anysubject material and grade level. It hasbeen a fun, exciting activity that left mystudents involved, interested, and excitedover health class.
Questions andAnswersfor the
Substance Abuse Unit
Easy Questions
1.Name a drug in the narcotic cat-egory. (heroin, codeine, methadone,morphine, opium)
2. What are the narcotics used for inmedicine? (stop pain, stop a cough, stopdiarrhea)
3. What is the natural source for nar-cotics? (opium, poppy plant)
174 163

4. Where is all cocaine grown? (SouthAmerica)
5. Free-basing is a method of usingwhich drug? (cocaine)
6. Is caffeine a stitnulant? (yes)7.Can you overdose on caffeine?
(yes, but it takes a lot)8. What effect does a barbiturate have
on a person? (can calm or put you tosleep)
9.Do anti-depressants make peoplehigh? (no)
10. What group of drugs make aperson see things which aren't reallythere? (hal lucinogens)
11. --------is anythingwhich causes a change in your bodyphysically, mentally, or emotionally.(drug)
12. Stopping drug use aml gettingsick because the addiction isn't fed iscalled . (withdrawal)
13. dependenceinvolves both tolerance and withdrawal.(physical)
14. dependencemeans you think you need the drug.(psychological)
15. Name one cancer besides lungcancer caused by tobacco use. (oral,kidney, throat)
16. In 1972 cigarette ads werebanned on . (TV and radio)
17. is a diseasecaused by smoking and is both incurableand progressive. (emphysema)
18. Name three things you cannotdo while smoking, (answers will varybut may include swim, kiss, live)
19. What type of alcohol is foundin alcoholic beverages? (ethyl)
20. What is the only organ in thebody which can break down alcohol?(liver)
21. If someone had four mixeddrinks, how long would it takc to breakdown all of the alcohol in their body?(four hours)
22. Which produces a strongerbeverage: fermentation or distillation?(distillation)
23. What usually happens when theBAC level reaches 10%? (death)
24. Which happens first with al-
164
cohol use: relaxation or loss of balance?(relaxation)
25. Name the organization whichworks with teen-agers who live with analcoholic. (alateen)
Medium Questions
1.What is the disease in which fatreplace.s normal cells due to the damagedone by alcohol? (cirrhosis)
2.What is the best way to quitsmoking? (cold turkey)
3. What narcotic is often found incough medicine and pain relievers? (co-deine)
4.Name a medical use for amphet-amines. (narcolepsy or hyperactivity)
5. What is the most commonly useddrug in America? (alcohol)
6. Approximately - % of all fatalauto accidents involve alcohol. (50)
7. Which drug is the most addictive inthe world? (cocaine)
8. What is the term for needing in-creasing doses of a drug to get the sameeffect? (tolerance)
9. in tobacco makes itaddictive. (nicotine)
10. in tobacco causescancer. (tar)
11. What group is the onlyAmerican group to increase its tobaccouse? (teenage girls)
12. Which gets into your systemfaster: a smoked cigarette or chewingtobacco? (smoke)
13. Which has more tar, ammonia,carbon monoxide, and hydrogen cya-nide: mainstream or sidestream smoke?(sidestream smoke)
14. Proof is equal to --- times thcpercent of alcohol. (two)
15. is when analcoholic cannot remember. (black-outor alcohol amnesia)
16. oz. of beer has anequal amount of alcohol as ----oz. ofwine. (12:5)
17. Five ounces of has asmuch alcohol as a shot of --. (wine:hard liquor)
18. 1 1/2 oz. of whiskey has ------oz. of ethanol. (1/2)
Figure 1.
II1"

TEACHING IDEAS 9119. What is the active ingredi^nt in
marijuana? (THC or delta-9 tetrahydro-cannabinol)
20. One marijuana joint has thesame ability to cause cancer asof cigarettes. (one)
21. Name the hallucinogen whichcauses violent hallucinations and wasonce used as an anesthetic for animals.(PCP)
22. Most names for prescriptiondepressants end in . ( al)
23. When legal penalties have beendecreased for drug use or possession ithas been . (decriminalized)
24. are abused to buildmuscles and may lead to cancer andother health problems. (steroids)
25. Glue, butyl nitrate, and gasolinebelong to the group of drugs known as
. (inhalants)
Difficult Questions
1. Chewing tobacco causes a pre-cancerous white patch in the mouth called
. (leukoplakia)2. Lung cancer is % fatal. (95%)3. The lit end of a cigarette reaches
what temperature? (90) -1200 degrees
4. What would be the effect of 60milligrams of nicotine taken all at once?(death)
5. What's the difference bk tween aproblem drinker and an alcoholic? (al-coholic is addicted, problem drinker'sdrinking leads to problems but they maynot be addicted)
6. is a drug used for aver-sion therapy in treating alcoholism.(antabuse)
Picture Charades:
A Health Teaching DeviceRichard T. Mackey
Looking for a classroom activity thatyour health students will find excitingand fun-filled? Try picture charades. It'senjoyable, promotes learning effec-tively, and is particularly good in helpingstudents clarify vocabulary words youinclude in your health instruction.
The rules for pictures charades arequite simple. They are really the same asfor regular charades, but instead of act-ing out the words, participants mustdraw a picture of the word, phrase, etc.
Here are thz., rules: Divide the class intoteams of four to six members. All teamscan compete against each other at thesame time, or you can arrange otherforms of competition. The importantthing is to keep all teams actively partici-pating.
You, the teacher, can act as tlw leader,or you can appoint a student leader and
_
Richard T. Mackey is in the Department ofHealth, Physical Education and Recreation atMiami University, Oxford, Ohio.
you become an observer. The leader hasa list of four or five terms, phrases, orperhaps definitions pertaining to thehealth topics the class has been study-ing. At the start of the game, a captainfrom each team goes to the leader andgets the secret word. The captain hurriesto his or her team and draws a picture ofthe term. The captains may, in addtion todrawing the picture, sketch a dashed lineindicating the number of words or sylla-bles in the phrase or word. They mayanswer only yes or no to questions fromteammates. The team member who dis-covers the correct .m becomes the newcaptain, rushes tc e leader to verify thecorrectness of the term, and then gets anew one. The first team to identify all theterms is, of course, the winner.
You can supply the health vocabularywords or terms or invite your students todevelop a list. A list pertaining to dentalhealth, for example, could include thefollowing: fluoridation, soft bristles,unwaxed floss, bicuspid, brush and flossonce in every 24 hours, toothpaste, junkfood, and gingivitis.
If you students enjoy a challenge andyou want to add some zest to your healthclass, picture charades are for you. Afteryou see them play the game, you'll prob-ably find a way t become a participantyourself. The author did!
165

TEACHING IDEAS 92
Drawing Interpretations of HealthVicki L. Cleaver
01).9 O.061
ototA,,,sotvbot. at 1410011 gond., . I p4
HOIDE MOTIVATION SPIRITUA
PEERGROUPS SOCIAL-FRIENDS WORK
EMOTIONALHAPPY
ExERCIsE
SAO ANGRY
pEERpRESSUR`
NORM"
LIFE
SCHOOL
OEPFIE
PSYCHOLOGICAL
PHYSICAL
RESTproper hygiene
Doivoi0
7.10evs"vo
AFFECTION,SELF ESTEEM,
SECURITYPSYCHOLOGICAL
NEEDS
oo
°so
0 0 0 oe0, 0 0 oel oO 0
43 0°
0°G 0 a:ye
MISS PHYSICALLYFIT
Vicki L. Cleaver is assistant professor in theHealth, Physical Education, and RecreationDepartment, 119 Huston Huffman Center,University of Oklahoma, Norman, OK73019.
166177
Teachers often strive to effectively usea variety of teaching methods, especial-ly with large classes. A technique whichthe author has used periodically andwhich has proven successful is to havethe students draw their interpretationsof health rather than assigning an essay.
Directions for the AssignmentDivide the class into groups of four to
five students. If possible, the teachershould provide the drawing paper orposter board needed in each group. Thestudents should be advised ahead oftime to bring colored pens, pencils, ormarkers to class. Each group shoulddiscuss what health means, then dray., apicture representing their interpreta-tion. Give each group approximately 45minutes to discuss and complete thedrawing. Have each group hang theirpicture in the room. If time allows, havea representative from each group ex-plain the group's drawing.
On this page are samples of creationsby former students.
TEACHING IDEAS 93
Using Team Games to Teach HealthMark A. Croson
Roseknn Benson
Correct health information is an im-portant part of a growing student's life.However, the hea:th educator must beable to get the student's attention inorder to clarify what is fact or myth,healthy or unhealthy. A lasting impres-sion that will involve students in astimulating learning experience in theclassrom will aid retention of material.Learning by doing will result in greaterretention because learners who are re-quired to be active in the learning pro-cess must be attentive.
Purposeful activities that are basedon a student's interests include teachingstrategies involving problem solving andactive student participation, as in groupgames. Well-known team games such asvolleyball, football, and baseball arenatural vehicles to interest all students inlearning.
Three examples are described here.Student objectives could include but arenot limited to recalling or explainingkey terms, definitions, and ideas. Eachgame is appropriate for introducingmaterial with which the students arealready familiar, or revie v. ing for anexam. These games are ex !...ng activi-ties that will get everyo:ie out of his/herseat and involved in the action,
Mark A.Croson and RoseAnn Bensonare in the Department of Health. Spot tand Leisure Studies at George MasonUniversity, Fairfax, VA 22030-4444.
VERBAL`.'.13LLEYBALL
Cbissmum_shunizatianOrgaze classroom chairs into three
rows per team, facing each other.
Quail=The questions should be organized
into three levels of difficulty. Level one,the easiest questions, go to the passers.Level two, more difficult questions, goto the setters. Level three, the most dif-ficult questions, go to the spikers. Re-gardless of question difficulty, studentsmust have a set time in which to respond.Atypical time limit would be 15 seconds.
RulesThe students are organized into two
teams and a coin is flipped to determinewhich is the offensive team. The teamserving the ball is the offense and theteam receiving the ball is the defense.The individual in the offensive servingposition draws and relds a level onequestion to the passers. If they answercorrectly, the server draws and reads alevel two question to the setters. If theyanswer correctly, the server draws andreads a level three question to the spikers.If they answer correctly, the refereedraws and reads questions in the sameorder to the offensive team. The questionseries continues uru it one team misses.If the defense misses, a point is awardedto the offense. lf the offense misses, aside out Is awarded to the defense andteam members rotate:. By rotating, each
student has the opportunity to respond toquestions at all three levels of difficulty.Points can be scored only by the offen-sive team.
PenaltiesPenalties are assessed by the referee
for answering out of turn, or any inap-propriate classroom behavior. For de-fensive team penalties, a poi nt is awardedto the offensive team. For offensi v e teampenalties, side out is awarded to thedefensive team.
Three hats from which to draw eachlevel of question Pre needed.
YariatiunsThe game may be focused on indi-
viduals, small groups, or the entire teamdepending on how the teacher wants todirect who may respond to the questions.
FOOTBALLFOLLIES
QuestionsThe questions should be organized
into three levels of difficulty. Level (mequestions, the easiest, are worth 5 yards.Level two questions, more difficult, arewortn 10 yards. Level three questions,the most difficult, are worth 15 yards.Regardless of question difficulty, stu-dents must have a set time in which torespond. A typical time limit would be15 seconds.
167

RulesA diagram of a football field includ-
ing yard markeis is made on the chalk-board. The students are organized intoteams and choose the order m whichthey are to resporki to a question. A coinis flipped to determine which is theoffensive team. The offensive team stu-dent whose turn it is to answer a qaes-tion, chooses the difficulty level/yard-age. The referet, draws and reads thequestion. If the questiou is answeredcorrectly the yaids are awarded. Theoffensive team has four chances to makea first down or 10 yards. If they succeed,they continue w itn four more chances. Ifthey fail, the defensive team is awardedthe ball and has four oppertunities tomake a first down.
MaltaPenalties are assessed by the referee
for answering out of turn or for anyinappropriate classroom behavior. Thepenalty cards are shuffled and one isdrawn and assessed agairvt the guiltyteam.
Equipment and MaterialsThree football helmets are needed to
hold the three levels of questions. Awhite penalty flag is needed for thereferee to drop when a penalty is to beassessed. Penalty cards consisting of 5.10, and 15 yard losses should be madeon 5 x 8 cards. If the penalty is againstthe offensive team an additional card,"fumble," should be added. A paperfootball marked with an arrow placed onthe playing field marks direction andprogress toward a touchdown (7 points).
168
BASEBALLBOOGALOO
ChosammikganizalimThe classroom should be organized
into a diamond shape with chairs forbases and player positions.
QuestiowThe questions should be organized
into four levels of difficulty. Level onequestions, the easiest, are worth a single.Level two questions, n,ore difficult, areworth a double. Level three questions,even more difficult, are worth a triple.Level four questions, the most difficult,are worth a home run. Regardless ofquestion difficulty, students must have aset time in which to respond. A typicaltime limit would be 15 seconds.
RulaThe students are organized into two
teams and choose their batting order andfield poEition. A roster must be submittedto the umpire. A coin is flipped to de-termine which team is at bat. The offen-sive team student whose turn it is toanswer a question chooses the difficultylevel/number of bases. The umpire draws
and reads one question. The individualat bat has only one strike to correctlyanswer a question. If the question isincorrectly answered an out is assessedand the next batter is up, and so on untilthree outs. If the question is correctlyanswered the team in the field has theopportunity to throw the batter out byanswering a question of equal difficulty.Single and double questions are an-swered by the infield (as a group). Tripleand home run questions are answered bythe outfielders (as a group).
If two base runners reach basesafely, the defense may attempt to answertwo additional double questions in orderto make a double play. If they miss onequestion, the lead runner advances onebase. If they miss both questions, onerunner scores and the other advancesone base. Players advE bases as forcedby the hitters following them.
PenaltiesPenalties are assessed by the umpire
for answering out of turn or for otherinappropriate classroom behavior. If anoffensive player breaks a rule, an out isthen assessed. If a defensive playerbreaks a rule, a walk is given to theplayer at bat.

TEACHING IDEAS 94
The Concept of Health and TechniqueF ofConceptual Analysis
Joseph E. Balog
To take what there is, and use it,without waiting forever in vainfor the preconceived - to dig deepinto the actual and get somethingout of that - this doubtless is theright way to live.
-Henry James
The ancient Greeks viewedhealth as one of the greatest goods. Infact the cult of Hygeia claimed thathealth was the foremost good and "themost desirable thing" (Temkin, 1977).However, other cults cautioned againstthe glorification of health. The Stoicphilosophers did not view health as anabsolute value, but they did emphasizethe idea that health was necessary forthe practice of virtue (Temkin, 1967,1977). Regardless of where the ancientGreeks and modern day healtheducators rank the value of health, thisconcept is still at the core of theprofession's role and exist 'trice insociety. As a consequence, it is ;mpera-Live for health educators to help theirstudents and future professionals intheir understanding of what it means tobe healthy.
This is perhaps one of the mostdifficult intellectual tasks which con-fronts health educators. The reasonsfor this are many and have been dis-cussed elsewhere (Balog, 1981, 1982,1985). In general, though, studying theconcept of health remains elusive fortwo very important reasons. First, the
Joseph E. Balog is with the Departmentof Health Science, State University ofNew York, College at Brockport,Brockport, NY 14420.
concept of health is not an empiricalfact or a directly observable and objec-tive phenomenon. Rather, health is ahuman construct that is defined in ac-cordance with our cultural values, so-cial norms, and presuppositions aboutits existence. Second, the profession ofhealth education has traditionallydevoted little and formal study toanalyzing concepts in its curriculum.
The task of defining health is dif-ficult, hut the fact still remains, an un-derstanding of health is a most essentialand fundamental ingredient for being ahealth educator. Thus, healtheducators should ask of themselves,and of their students, "What doeshealth mean?" even if for no otherreason than simply that someone mayhave an answer or provide a clearer andmore insightful way of viewing health.
The following activity ispresented to help health educators infacilitating a discussion on the conceptof health while providing some basictechniques for conducting conceptualanalysis. A more detailed and thoroughdescription, which contains additionalexamples and dialogue, can be found inConceptual Questions in Health Educa-tion and Philosophical Inquiry or in EtaSigma Gamma's monograph, Ethicsand the Field of Health Education(Balog, 1982, 1985).
Conceptual Analysis Activity
The overall goal z this activity isto help students n constructing theirown view of hewn/. More specifically,the main objective of this exercise is to
1 sti
develop, record, and refine two lists ascommon features which your studentsuse h. describing why they think some-one should be considered healthy or ill.Note that including the examination onillness helps students in developingtheir views on health.
Begin this exercise by handingout a sheet of paper which asks twoquestions about a list of people. Thequestions and list may look as follows:
Conceptual Analysis Activity
Are the following people healthy?Explain.
Are the following people ill? Ex-plain.
- A person with bronchogenic car-cinoma (lung cancer).
- A person with hypertension andanginal pain.
- A student-athlete who is a topmiddle distance runner.
- An aerobic physical fitness in-structor.
- A person with dyschromaticspirochetosis (discolorization of theskin caused by a spirochete).
- A person with myopia (near-sightedness).
- A person who is a paraplegic.
As the instructor, you may wish todevelop your own list. However, if youdo use alternative examples, make surethe items on your list reflect the follow-ing ideas and techniques of conceptualanalysis.
Hand out the list and have yourstudents take it home as an assignment.The students' task is to answer the twoquestiors by writing out a brief ex-
169
planation on why they think the peopleon the list are healthy or ill. When thestudents return during the next classperiod, the instructor's main tasks are:(1) to facilitate a dialogue and (2) torecord on the board, two lists (one forhealth and one for illness) of commonterms, phrases, and/or features whichstudents use in explain;ng whether theindividuals on the handout are healthyor ill. Developing two lists and con-trasting the ingredients !or defininghealth and illness should help the classin seeing how they view these two con-
Classroom Discussion and ModelCases
Begin the discussion by using amodel case example on illness. Foryour purpose, a model case example isa person from the list who would betypically seen as being ill in our society.Choose the example of a person withhi ochogenic carcinoma.
Identify and list the common fea-tures of an illness which your studentsuse in their explanations. For example,they may offer descriptions such as anabnormal growth is present, the condi-tion can cause death, or this person'sbody is not functioning properly.
Next, select another model casesuch as the person with hypertensionand anginal pain Once again, list com-mon descriptions which the studentspresent in explaining why this person isill. Compare and merge the list by ad-ding or subtracting items which the stu-dents believe are essential criteria indetermining what is an illness.
Contrary Cases
The next step in your analysis isto use a contrary case example. A con-trary case is similar to a model case ex-cept the interest lies in inquiring intoexamples which people typicallybelieve are the opposite of an illness ordisease. The idea is to consider caseswnich people would say "Whatever anillness or disease is, this case certainlyisn't an example of it."
Choose the example of a student-athlete who is a top middle distance
1 70
runner. The objectives are (1) to com-pile a list of features which the studentsuse in describing health and (2) to com-pare and contrast this list to the abovelist on illness.
Next, use the example of theaerobic fitness instructor, and as above,compare, contrast, and merge into onelist of features which students offer intalking about health. You may find stu-dents wanting to disagree with theitems on the health list. Welcome thearguments, but also try to draw out andidentify items whien can be placed onthe list.
Counterexamples
Counterexamples are caseswhere a premise might ix true, but theconclusions are false. A person withdyschromatic spihxhetosis is a goodexample to use with this technique. Forinstance, this condition is a discoloriza-tion of the skin caused by a spirochete.Most people, including your students,would argue that this physical state isabnormal and represents an improperor unnaturat body :unctioning.However, point out that a famousmedical sociologist, David Mechanic,discovered that in a South Americantribe this condition was so common,"Indians who did not have (it) wereregarded as abnormal and were evenexcluded from marriage" (Mechanic,1968).
7 his is a good place to propose tothe class that some conditions whichmight seem abnormal, improper, andconsidered ill by some people can alsobe judged as healthy by others. Thus,this example raises the question ofwhether a person can be healthy even ifan abnormality or an improper physicalfunctioning exists. After you discussthis point, see if you need to add or sub-tract any items on your list of health andillness.
Related Cases
As the example of dyschromaticspirochetosis points out, when studentsdiscuss the concepts of health and ill-nes it isn't long before they need tostart examining related concepts like
s 1
normality, natural body designs, orproper physical functioning. Thus, thepurpose of using related cases in con-ceptual analysis is to discuss conceptswhich are similar, connected, or re-lated to the concepts of health and ill-ness.
The examples of a person withmyopia or a person who is a paraplegicare good cases for beginning thisdialogue. In both cases, students mightbe quick to agree there is present an im-proper functioning, an unnaturalfunctioning, or an abnormal function-ing, but slow tt. ::-..mclude that these in-dividuals are unhealthy. As a result,students are led to question whetherthese criteria should be on their list ofcommon feature for health or illness.
These examples also beg a discus-sion on whether a person can be physi-cally abnormal, or have an improperphysical functioning, yet at the sametime be considered healthy. Studentswill want to say, for example, "Yes aphysical limitation of improperfunctioning is present, but this does notmean these people are unhealthy." Tryto pin point the criteria they use in ar-guing and justifying their positions andadd or subtract these items to your lists.
Summary
At this point, you should haverecorded on the board two lists of com-mon features which your studentsdeveloped in describing health and ill-ness. The class, however, may still beunsure and confused about the con-cepts they have been discussing. Thus,the instructor must tie together the ac-tivity and offer a summary. In general,your summary should include the fol-lowing three points.
First, you should note that avariety of views were offered, becausehealth and illness are concepts whichindividuals define relative to their cul-tural values and presuppositions aboutthese two concepts. Second, point outthat ideas of health and illness usuallygroup into three different themes orcategories. The first theme centers onthe idea that health and illness are op-posites. The absence of one establishesthe presence of the other, i.e. health isthe absence of disease or illness. A

second theme views health and illnessin regard to how well an individualadapts, adjusts, of functions daily. Forinstance, an individual who can notcarry out his or her daily tasks would beconsidered ill. On the other hand, anindividual who functions well in lifewould be viewed as being healthy.Finally, a third popular way of viewinghealth and illness is simply by aperson's own self-assessment. In thiscase, all that really counts is how an in-dividual perceived his or her own levelof health and illness.
Next, review your list on I.ealthand determine into which category thestudent's view of health falls. Then,move on to constructing a definition ofhealth which evolves from the student'slist of health criteria.
Finally, bring the discussion fullcircle. Go back to Henry James' quoteand note that in defining health and ill-ness, there are no absolute answers.The answers people create, however,are very real and greatly influence: (1)people's attitudes toward achievinghealth; (2) which professions areresponsible for dealing with health; and(3) which patterns of dealing with
health are appropriate concerns of thehealth professions. Thus, the challengefacing students of health is to developanswers to the perplexing conceptualquestions about health and illness andargue why one is better than another.Challenge your students not to acceptpreconceived answers, but "...to digdeep into the actual and get somethingout of that - this doubtless is the rightway to live."
E alog, J. E. (1981). The concept of health andthe role of health education. Journal ofSchool Health, Sept., 461-464.
.log, J. E. (1982). The concept of health anddisease: A relativistic perspective. HealthValues: Achieving High Level We/bless, 6(5),7-13.
Ba log, J. E. (1982). Conceptual questions inhealth education and philosophical in-quiry. Journal of School Health, 52(4), 201204.
Balog, J. E., J. H. Shirreffs, R. D. Gutierre-,,& L. F. Ba log (1985). Ethics and the fieldof health education. Eta Sigma Gamma,Monograph Series, 4(1), 63-110.
Mechanic, D. (1968). Medical sociology: A se-lective view. New York: The Free Press.
Temkin, 0. (1977). The double face of Janus: Andother essays in the history of medicine. Bal-timore: The Johns Hopkins UniversityPress.
182
Temkin, 0. & L. C. Temkin, eds. (1967).Ancient medicine: Seiected papers of LudwigEdelstein. Baltimore: The Johns HopkinsUniversity Press.
171

TEACHING IDEAS 95
The Town Council Meeting: DecisionMaking Through a Large Group Role Play
James D. Brown
Health educators are often challengedto develop a strategy concerning a con-tToversial issue that includes decisionmaking, maximum participation, and abalance between information giving anddiscussion. Because the Town CouncilMeeting can be adapted to many groupsettings, many educators may enjoy anactivity that provides detailed informa-tion, dramatizations, heated debates,judgments, and fun.
DirectionsThe specific directions for this activity are:
1. Role assignments. Establish tlw councilmeeting date and assign the variousroles a few days in advance to allow fo1adequate preparation. The roles in-clude: th? mayor (1); council members(6-10); presenters for the pro side of theissue (4-6); presenters for the con sideof the issue (4-6); media representatives(1-4); and concerned citizens (3-10).Choose the role players carefully. Usu-ally it is best to use volunteers or indi-viduals known to enjoy being in front.The presenters are the key to a success-ful program because their role demandseffort and ingenuity. For example, theymay want to "plant" a few concernedcitizens. Since our local council meet-ings are televised, our role players re-cently had a wonderful time mimickingthe mannerisms of our civic leaders.
2. Information gathering. The teacher canhave most of the materials available andshould allow a few days for students togather additional resources. This couldinclude interviews with civic leadersand the members of the council, sur-veys, visiting agencies, etc. All classmembers should take part in the infor-mation gathering.
3. Choice of topic. The most apprepriatetopics are controversial issues C-at arecurrently before our state and local gov-ernments. A review of your town coun-cil's agenda may find such 0,, 1. Forexample, our class chose AI 1-nanceunder consideration by (.tuncilbanning smoking in buildingsand public transportation . i.er issues
James D. Brown is with the Department ofHealth and Physical Education, 20 Both-well, University of A4issouri, Columbia,Missouri 6'7211.
172
could be: D.WJ. legislation, drinkingage, flouridation, metal can ban, nucle-ar power, pollution controls, fire arms,seat belts, mandatory retirement for dv-ic and school employees, and manyothers.
4. Time frame and the council meeting agenda.By taking class time to give the assign-ment carefully, hold strategy meetings,complete the council meeting and de-velop some appropriate follow-up activ-ities approximately three full classmeetings can be used. The councilmeeting needs an agenda and timeschedule. A number of options can beequally effective. For example, tl:e pre-senters could have each member makea timed presentation or elect one or twomembers to role play expert testimony.Time should also be set aside to havecouncil members question the present-ers and to have the concerned citizensrespond. Once the testimony is com .pleted the members of the council voteon the issue. Prior to submitting theirnews copy to the class the followingday, the members of the media shouldinterview the participants.
5. Follow-up. During the following meet-ing have the members of the mediapresent their coverage of the proceed-ings. This could be in the form of anewspaper article or presented as aradio or TV spot. Follow the mediapresentation with a class discussion.Some of the kir-. questions for the classdiscussion might include: (1) How accu-rate were the members of the media? (2)Who changed their position on the is-sue during the council meeting andwhy? (3) What were the major pointsdeveloped on the pro and con sides ofthe issue? (4) For those who might beinterested, what activities could groupmembers take part in to support theirside of the issue at the local or statelevels?
The Teacher's RoleThe teacher's role in any controversial
issue is to guide, motivate, clarify, andhelp gather reliable sources. The teachermust remain unbiased; more specifical-ly, the teacher's role encompasses thefollowing servic?s: to help define theproblems, to evaluate student progress,
1S3
to help collect and analyze data, toguide students through the problemsolving process, to ensure decisionmaking, to develop follow-up activities,to ensure participation and to take astand on the issue, if asked, after stu-dents have expressed their decisions.
7-......
'eft
.."
-411711`;
dik- -""Ar-t-
41.

TEACHING IDEAS 96
The Health Reporter PoolDavid Wiley
Student, who are often viewed as"receptacles" in which to deposit heal th-related information, should be moreactively involved in the learning process.A primary problem with mass-prr ducet.teacher guides and curriculum manualsin health education is that they tend tofocus more on subject matter than onstudent participation. The field of healtheducation, however, presents many op-portuni ties to activel-7 involve the studentin the !catmint process. The goals ofhealth education differ from other sub-jects, such as mathematics, geography,or history, where knowledge is factualand cumulative. In health education,knowledge should be combined withefforts to influence positive health atti-tudes, effective decision-making skills,and promotion of pc sitive health be-havior.
The Health Rcporter Pool is anactivity that can combine a variety ofstudent-centered activities into a singlelesson format. The central idea of theHealth Reporter Pool activity is that astudent is er cted to role play a particularhealth-related "character." The choicesfor characters are limitless, for example,a bacterium, a carbohydrate, a drugabuser, a positive self-esteem, a gooddecision, or the human immunodefi-ciency virus (HIV). Based on class size,a number of other students are selectedto be reporters "assigned" to cover apress conference, in the presence of the
David Wiley teaches at SouthwestTexas atate University, Scn Mat cos,TX78666.
class, with each health-related charac-ter.
Several days prior to the press con-ference, the characte- and the reportersconduct research to discover facts andother health-related issues pertaining tothe character. Reporters must formulaterelevant questions such as: "What is itlike to be a bacterium?"; "What good doyou do anyone?"; or "If you are sup-posed to help humans, why do you con-stantly have to be controlled?" Theteacher can limit orexpand the types andnumberof questions based on availabilityof time and resources.
An exchange between the reporters(R) and the character (C) might go asfollows:
R I: "So tell me, what makes you, abacterium, so important?"
C: "Well, I am very important inhelping the body conduct a variety offunciions."
R2: "Would you be so kind as toelaborate on two or three of these func-tions?"
C: "First of all, I assist the intestinaltract in the digestion of food. In addition,I can help ward off certain infectiousorganisms."
R3: "PleL .e describe your relation-ship with antibiotic drugs."
C: "As you may be aware, I've ncvcrreally enjoyed being around antibiot,..cand I'll tell you why. . . ."
The Heath Reporter Pool )ft hcused with a variety of grade levels (7 -12)and diverse ability groups. In addition,this activity is structured with maximumflexibility to allow the teacher to fit it
184
into specific time frames and availabil-ity of resources. For example, the activ-ity can be used as a 10-minute introduc-tion to a new unit or as an entire classsession on a particular topic. Also, theteacher can design questions for thc par-ticipants to research or rely on the stu-dents to generate their own set of ques-tions and responses. Most importantly,no special materials are needed for thisactivity, although students should beencouraged to use appropriate props torepresent their specific character.
Advantages of using the HealthReporter Pool are numerous. MI st, itactively involves students in thc learn-ing process. Health class then becomes"something to do," rather than "some-thing to attend." Students become in-volved in researching a particular sub-ject for something besides a researchpaper or other written report. Second,topics that many students might con-sider boring (e.g., nutrition, infectiousdisease, personal health) can be madeexciting and fun. In addition, controver-sial topics (e.g., AIDS, sexuality, sub-stance abuse) can be approached froman impersonal perspective that couldserve to reduce the inherent volatility ofMP' of these issues. Third, the activity
be used with special populations.For example, classes comprised of apredominantly minority population canexamine health care issues from the per-spective of that particular group andeven carry on the interview in a lan-gcage other than English.
Fourth, the Health Reporter Poolcan be used to integrate health with othercontent areas. As an example, the prob-lem of AIDS can be examined from a
173

TEACHING IDEAS 97
sociological perspective, with the healtheducator and sociology teacher usingthe Pool to serve as an introductoryactivity in a coordinated effort to pro-vide a focus on the topic. Thus the activ-ity provides a medium to spread thehealth education curriculum across re-lated content areas within a school. Fifth,students must learn beyond rote memo-rization and advance to higher levelthinking and interaction skills. With theHealth Reporter Pool, students learn toanswer a range of questi ns focused onadvancing discussion beyond basic facts.
Finally, students have the oppor-tunity to develop public speaking skills.For many students, speaking before agroup is a very uncomfortable experi-ence. By structuring the activity care-fully, the teacher can provide studentswith the opportunity to practice speak-ing in a controlled environment. Fortho- e students who speak comfortablyin front of a group, the Pool provides anopportunity to ad lit, and have fun cre-ating an interesting interview.
The Health Reporter Pool idea hasthe potential for use in a variety of ways.Teachers have the discretion to use theactivity in a strictly controlled manneror to allow students to construct theirown interviewing activity. As this ac-tivity is used throughout the school year,the more comfortable and creative stu-dents can become in its use.
Its most important characteristic isthat it directly involves students in theprocess of learning. The Health ReporterPool provides teachers with a creativeand challenging activity in which stu-dents may develop new skills while re-fini.ig skills that already exist.
174
Health Education SupermarketMary S. Sutherland
This learning strategy is appropriatefor a secondary health education class-room or a college personal and commu-nity health course. The strategy has beenused successfully in selected health con-tent areas such as mental health, drugeducation, family health, or diseases andis applicable to any health education con-tent unit which uses value clarificationand/or decision making techniques.
The participants are grouped as animaginary family unit for a wellnessshopping trip, where they can purchaseitems to attain a more healthful lifestyle.Family members might consist of a lov-ing father and mother, each about forty-five years old. The parents are typicalhardworking individuals, both em-ployed full-time, who want the best fortheir family and desire to k Is well asbe loved. All family members are affeo.tionate. Children may display the follow-ing characteristics:
A. A single eighteen-year old son,who displays a fond for alcohol anda need to be loved.
B. A sixteen-year old daughter who isextremely popular with boys. However,her morals are suspect.
Each family unit member will thenvisit the health su:lermarket and pur-chase appropriate wellness items. Theshopping aisles may be divided as fol-lows:
Aisle oneMenti HealthAisle twoAlcoholAisle threeFamily Healtl-Aisle fourVenereal DiseaseFive items from each aisle may be pur
Mary S. Sutherland is at Florida State Uni-versity, Department of Human Services andStudies, 215 Stone Building, Tallahassee, FL32306.
chased by every family member, basedupon family health needs. Upon comple-tion of the shopping trip, each familyunit member will share reasons for his orher selected purchases and how the pur-chases will help the family improve itslevel of wellness.
Following is a sample list of availableitems in each aisle. Only the items men-tioned are to be purchased:
Aisle one items: (1) package of food,water, air; (2) package of sleep, dreams,and warmth; (3) mental illness candy; (4)shelter; (5) pill for self-love; (6) pill forparental love; (7) pill for sibling love; (8)pill for love of parents; (9) independencesyrup; (10) person's favorite music; (11)changing values mix; (12) behavior; (13)happiness; (14) emotional snacks; (15)maturity.
Aisle two items: (1) religious drink; (2)social drink; (3) machine for changingdrinking habits; (4) tape of teenagedrinking habits; (5) reality-escapingdrink; (6) excitement drink; (7) six pack ofpeer pressure drinks; (8) bottle of alcoholand driving attitudes; (9) pint of effects ofalcohol; (10) gallon of alcohol and acci-dents; (11) a heavy drinker mix; (12) pillto become an alcoholic; (13) pamphletson number of alcoholics in U.S.; (14) re-ceipt from alcoho: cost; (15) understand-ing; (16) helping hand.
Aisle three items: (1) societal pressure;(2) choice of schools; (3) communicationpackage; (4) responsibility cans; (5) cul-tural mix; (6) bag of unity; (7) can of secu-rity, (8) jar of affection; (9) pound of fam-ily pride; (10) sale on ethics.
Aisle four items: (1) bag of truth; (2)penicillin tablets; (3) appointment for thedoctors; (4) appointment to a publichealth clinic; (5) ja: of symptoms; (6)ounce of fear; (7) package of ignorance;(8) a pill for courage to tel: parents; (9)change of sex practice pill; (10) slice of itsgoing away.

TEACHING IDEAS 98
Health Education to the Third Power(Cubed?)
Susan Cross Lipnickey
They seem to be everywhere. Grand-parents have them. Parents have them.Children of all ages can bo seen withthem at school, at airports, in front ofthe television, and when they are sup-posed to be in bed sleeping. What is thisubiquitous object? Why, it is none otherthan Rubik's Cube (a trademark of IdealToy Corporation).
Rubik's Cube is a six-sided, six-col-ored manipulative object. Each side hasnine smaller squares. The object is to geteach side to contain nine squares of allone color so that there is one side whichis all orange; one which is all green; and
Susan Cross Lipnickey is an instructor inMiami University's HPER Department,Oxford, Ohio.
so forth. This manipulative puzzleworks beautifully to help explain theconcept of school health education.
There are six 'sides' to school healtheducation: for the learner there is theside of health knowledges, the side ofhealth attitudes, and the side of healthbehaviors and practices; the health 'pro-gram' also has three sides, or facets.These are the healthy school environ-ment, the health instruction which oc-curs within the school, and the schoolhealth services.
Health knowledges, in this case, referto what the student actually knows thatis the skills or information she/he hasgathered along the way: the long termbenefits of frequent aerobic exercise;how to perform CPR; the advantages of
186
wearing a seathdt; and the need forpositive ..opirg skills, to name a few.One could easily assign nine healthknowledges to each of the nine Jquareson the health knowledges side of the'cube.'
Health attitudes include how onefeels about one's own health as well ashow one feels toward the health knowl-edges she/he has gained and which arereflected in one's health practices. Doesthe student have the attitude that "itwill never happen to me" and smokecigalettes because she/he enjoys it now?
Health behaviors and practices arewhat one actually does. These practicesmay be positively or negatively influenced by the health knowledges andattitudes previously noted: brushing
1 75

and flossing one's teeth in combinationwith regular dental check-ups; drivingat a rate no greater than the speed limit;or asking for an explanation from thephysician when one doesn't understandsomething. Each health behavior exhib-ited by the student could be assigned ablock on the health behaviors/practicesside of the 'cube.'
The healthy school environment, oneof the three sides of the 'School HealthProgram' portion of Rubik's Cube iscomprised of such 'blocks' as goodlighting for the students; the opportuni-ties for peer interaction within theschool setting; and an adequate amountof time for physical exercise and eating,as well as intellectual stimulation andchallenge. The health instruction side ofthe 'School Health Education' cube hasblocks such as a field trip to a waterpurification plant; the viewing of healthfilms or discussion of current eventsrelated to health; a guest speaker froman orgarCzation such as the AmericanHeart A sociation; or the teacher deliv-ering a k lure on a current health topic.School health services, the sixth side ofour cube which is neither more nor lessimportant than the preceding five sides,is composed of such blocks as visionand scoliosis screening; the treatment ofhealth emergencies within the schoolsetting; and the administration of tuber-culin tests for faculty and staff mem-bers. There are numerous other exam-ples which could occupy the blockswhich comprise each of the six sides;the aforementioned are only a few.
School Health Education is more thanthe sum of these facets; it ie; the interre-lation of these dimensions. When one ofthese six facets of school health educa-tion is incomplete, then at least oneother dimension is affected. Just as isthe case with Rubik's Cube, there is noway to have only one of the sides in-complete. At no one time can just one ofthe dimensions be incomplete due tothe high degree of interrelatednessamong them. What we as health educa-tors must do is to realize aild appreciatethe fact that school health services arenot only tied very closely to and aredependent upon health Mstruction anda healthy school environment, but theyaffect very closely and are dependentupon the health knowledges, attitudes,and actions of the learner. It is alsoimportant for us to understand thatthere is a reciprocal relationship withthe learner affecting the program asmuch as the program affects the learner.
Going back to our Rubik's Cube ofSchool Health Education, three of the
176
sides may each consist solely of onecolor, but the side representing atti-tudes, the side representing behaviors(as affected by Tom's attitude that acci-dents only happen to others), and theside representing healthy school envi-ronment are a mixture of colors. It isquite possible then that only three, orhalf, of the sides are composed of blocksof all one color: health knowledges,nealth instruction and school healthservices.
On the other hand, positive relation-ships can exist between the learner andthe program. The following illustratesjust such a relationship with the facetsof the program affecting the learner . .
Julie is a fourth grader at Lane ElementarySchool. She, as with most fourth graders,was not an overly health conscious person.Two weeks ago, during recess, she fell andsuffered a severe laceration of her lower leftleg. The school nurse was able to stop the legfrom bleeding, take the "sting" out of thewound, and reassure her that everythingwould be okay. She explained to Julie, whilethey were waiting for her mother to come,the importance of keeping the wound cleanand giving it a clrnce to heal. The schoolnurse showed Julie how to change 'he dress-ing so she could explain it to her mother andhelp in the process. Her wound healed beau-tifully.
In this example there is primary inter-action among five of the six facets . . .
Health Knowledges: Julie learned how tochange the dressing and why it wasimporant to keep the laceration clean;Health Attitudes: we can assume she feltit was important because she followedthe directions, resulting in the completehealing of the wound; Health Behaviors:Julie followed the advice of keeping itclean and changed the dressing to aid inthe healing process; School Health Serv-ices: the school nurse was there to pro-vide emergency treatment as was need-ed; School Health Instruction: the schoolnurse not only provided information inthe form of why it was essential to keepthe wound clean, but she also taughtJulie the skill of changing a dressing.The only side of the cube not primarilyinvolved in this illustration was that ofthe healthy school environment. Theschool health services and health in-struction were responsible for influenc-ing the knowledges, attitudes and be-haviors of the learner; thus five of thesix sides of our cube became one-col-ored sides and therefore so did thesixth.
Utilizing Rubik's Cube as a conceptu-al model for the School Health Educa-tion Program allows us to incorporate
iS7
the dimensions of 'the learner' with thedimensions of 'the program.' Since nei-ther can exist without the other, it isvital for us to combine the two in onemodel and not look at 'the learner' as anentity in and of itself, or 'the program'as divorced from 'the learner.' Healthinstruction directly affects the healthknowledges of the learner--if some-thing is not taught, the learner will nothave the opportunity to learn it. If it istaught effectively, hopefully the studentwill have that knowledge to add on to astime goes on and new information islearned, as well as to draw upon whenthat particular body of knowledge pro-vides relevant information. But theknowledge of the learner can be affectedby the healthy school environment aswell: if the room is too cold or too hotthe student may be unable to concen-trate and, therefore, miss essential con-cepts; if th classroom environment isone in which the student is frightenedor intimidated by the teacher, howmuch knowledge will she/he gain?School health services, as demonstratedin the example of Julie thc fourth grad-er, also has the potential to influencethe learner's body of knowledge. Healthattitudes and practices can also be influ-enced by the programrole models ofhealth behavior, reinforcement of posi-tive health practices by the teacher, andencouragement in acquiring positivehealth behaviors not previously demon-strated by the student.
In addition, the Ftudent can influencethe three program partswhat the stu-dent knows or doesn't know mav influ-ence what is taught; the student's atti-tude may influence the rules for safetyin the school; the student's practicesmay influence the type of school healthservices required. It should also be not-ed that the three segments within 'theprogram' portion affect each other andthe same is true for the three segmentswhich comprise 'the learner' segment.The model of Rubik's Cube also affordsus the advantage of looking at each ofthe co- .ponents within the learner asmultidimensional. For example, knowl-edge is not just One item but encom-passes a myriad of pieces of informationand skills gathered from as manysources.
So, Rubik's Cube, the toy so popularamong today's children of all ages, pro-vides us with a unique approach tolooking at School Health Education as amultidisciph lary and di% 2rse entit,

TEACHING IDEAS 99
Junior High School Studentsas Facilitators of Elementary School
Health Education Carnivals
David K. Hosick and Parris R. Watts
During the early 1980s, Watts andStinson (1981) began to advocate"health education carnivals" forelementary school students. These car-nivals are similar to traditional healtheducation fairs which have beenpopular for years (Daughtrey, 1976;Lafferty, Guyton & Pratt, 1976; Mc-Kenzie, Scheer & Williams, 1981). Themost obvious similarity of the carnivalsand fairs is that they boat employ manyof the sante instructional strategies andmaterials. However, where a typicalhealth fair includes screening tests, thehealth education carnival does not.Thelatter actually is comprised of a widevariety of health education activities,incorporated into a festive, carnival-like setting; hence, the reason for itsname. Although health professionalsstill are involved in the carnivals,physicians, dentists and nurses replacetheir usual work apparel with costumesthat are more appropriately related tothe activity areas of which they are apart.
Watts and Stinson initiallydeveloped the health education car-nival concept to expose undergraduateelementary education majors to the
Parris R. Watts is an associate professorof health education at the University ofMissouri-Columbia, Columbia, MO65211. David K Hosick is the formereighth grade science and health teacherin the Phelps County Missouri SchoolDistrict. He currently is a ninth gradescience and healtn instructor at BlueSprings Junior High School, BlueSprings, MO 64015.
natural learning patterns of childrenprior to a formal student teaching ex-perience. From the beginning, objec-tives of the health education carnivalhave been the promotion of (1) per-sonal interaction between thefacilitators and children, (2) meaning-ful health education experiences forthe children, (3) cooperative involve-ment among the facilitators as theyplan and implement the activities, and(4) positive public relations within theschool and throughout the community.The authors of this article simply haveextended those expected outcomesinto a new dimension by replacing theelementary education majors withjunior high school students. In usingjunior high school students asfacilitators of an elementary schoolhealth education carnival, all four ofthe previously stated objectives wereachieved for the elementary students,
BEST COPY MAE
6-
188
their school, and the community. Invol-vement of junior high school studentsin facilitative roles enabled them to bet-ter appreciate their own health withina context of a broader based ex-perience. In addition, they were able todevelop a sense of teamwork by joiningtogether in a common cause. Also, thejunior high school students were givena great deal of responsibility for provid-ing a quality health education learningopportunity for elementary school stu-dents, and they felt much personalpride when their efforts were success-ful.
Organizing Junior High SchoolStudents as Facilitators
The carnival idea was presentedto eighth grade students of the PhelpsCounty Missouri School District as a
luoromil.:11'

part of their junior high school scienceand health education course. Videotapes of other carnivals were shownand synopses of certain journal articleswere distributed for review (Watts &Stinson, 1981; Petty & Pratt, 1982;Bays, 1986; Wolf, 1986). After studentsinformally discussed the idea amongthemselves and considered it as agroup, they decided to conduct the car-nival. It should bc noted that the healtheducation carnival was not the onlylearning activity within the course. Ahealth textbook wns utilized and tradi-tional health education class sessionswere held throughout the semester. Inpreparation for the health educationcarnival, the class was divided into fivedifferent groups. After the groups wereorganized, each was given the oppor-tunity to choose from among five healthconceptual areas included in the car-nival. Those instructional areas were(1) smoking, alcohol, and other drugs,(2) physical fitness, (3) nutrition, (4)dental health, and (5) first aid. Figure 1outlines tasks completed by studentsand by the teacher of the course duringthe nine weeks devoted to preparationfor and staging of the health educationcarnival event.
Overview of Activity Areas
Following are brief descriptionsof the five conceptual areas included inthe health education carnival.
Smoking, Alcohol, and OtherDrugs Employed a smokingmachine to demonstrate the effects ofcigarette smoke on the lungs along withthe encouragement not to smoke. Briefdescriptions of what happens within_he human body when people drink al-cohol or use other drugs. Playing of asmoking, alcohol and other drugs gamewhich included basic questions aboutthose substances, with emphasis placedon advantages of not using them. Dis-tribution of coloring books, iron-onand stick-on patches and information-al pamphlets pertaining to this activityarca.
Physical Fitness Display of amodel of the human heart and identify-ing and explaining its various anatomi-cal parts. Use of a stethoscope forstudents to listen to their heartbeats
178
and to participate in a physical activityand then listen to determine how muchfaster their hearts beat in response toexercise. Playing of a game which em-phasized the sequence of blood flowthrough the chambers of the heart andreviewed how the heart works. Dis-tribution of pamphlets and otherresource materials on blood circulationand the benefits of maintaining physi-cal fitness throughout the elementaryschool years and beyond.
Nutrition Introduction of thefour basic food groups and an explana-tion of the importance of each. Discus-sion of "junk foods" and provision ofactual substitute foods for the childrento eat selected from among the fourbasic food groups. Playing of a nutri-tion game wherein students reachedinto a sack of groceries and placed thefood item withdrawn into its properbasic food group.
Dental Health Presentation ofa skit involving the elementary studentsthemselves where they were intro-duced to dental caries and given agraham cracker to eat. Plaque revealedon their teeth and cleansed away byusing carrot and celery sticks todemonstrate how foods can help clean
the teeth. Proper brushing of the teethincluded in the skit, along with otherdental hygiene practices.
First Aid Introduction to thethree degrees of burns and ademonstration on how to properly treateach. The correct way to bandage burninjuries in order to help relieve painand prevent infection stressed. Printedresource materials dealing with burnsdistributed.
Conducting the Carnival
During the week of the healtheducation carnival, regularlyscheduled daily class periods for theeighth grade science and health courseon Tuesday, Wednesday, and Fridaywere used for the carnival. On each ofthose days, the 56-minute scheduledclass time was used to set up, conductthe carnival, and disassemble the ac-tivity areas. The first ten minutes of theclass period were used to assemble andorganize the five activity areas. Then oneach day, a different class (secondgrade on Tuesday, third grade on Wed-nesday, and fourth Grade on Friday)participated in the carnival, held in the
Figure 1. Student Task Aulgrunents and Teacher Checklist
Weeks Student Task Assignments__._.._...
1-2 Develop the activity/conceptual area, including the :ielection of a carnivaltheme and send for and/or locally secure information and resourcematerials.
3-5 Organize information received and materials secured for use in the carnivalactivity areas.
6-7 Work on banners, posters, handouts, and costuming for the activity areas.8 Complete all preparatory work and rehearse presentations to be made
within each activity area during the carnival.9 Conduct the health education carnival for the elementary school students.
Weeks leacher Checklist-
1-3 Motivate the junior high school students and offer ideas which will, in turn,generate additional ones.
4 Start to promote the carnival among the administration, faculty, and staff ofthe sc:,00l and keep students on task.
5 Secure volunteers from among school personnel to help publicize thecarnival within the elementary school and throughout the community (topromote parental and family involvement) and continue to keep thestudents progressing in their work.
6-7 Encourage carnival facilitators (students) to finalize work on their activityareas.
8 Preside over the rehearsal sessions; select student facilitators to visit theelementary school classes to promote the carnival event, and make certainthat media coverage is arranged.
Coordinate the efforts of the student facilitators during the carnival.

school gymnasium. Students in eachclass were divided into five separategroups and assigned to begin at a dif-ferent learning center. They were thenrotated through all five activity areas sothat every student was exposed to eachset of learning experiences.
All five groups of junior highschool facilitators were given sevenminutes to conduct their activity areasession. The seven minute time periodtypically consisted of one minute to in-troduce to the conceptual material, twominutes of information sharing, two tothree minutes of games or other hands-on activities for the children, and oneminute to synthesize and conclude thelearning experience. During the weeksof preparation for the carnival, thejunior high school student facilitatorswhere instructed to design the activityareas so that they would (1) be child-centered, (2) provide basic informationat the proper grade level, and (3)promote learning and fun throughoutthe experience. All three goals were ef-fectively achieved, best evidenced inthe attentive behavior and enthusiasticresponse of the elementary schoolchildren.
After all groups had rotatedthrough each station, plenty of time atthe end of the class period remained fordisassembly of activity areas and clear-ing out of the gymnasium. Witheveryone working together, there wasno need for junior high school studentsto miss any additional class time out-side the regularly assigned science andhealth class period.
Carnival Follow-Up
After the health education car-nival was over, the primary author ofthis article, who also was instructo ofthe eighth grade health class, visitedelementary school classes involved inthe experience. He found studentsstudying, completing the worksheets,and using the pamphlets and otherprinted resource materials providedfor them during the carnival. Elemen-i--y school students clearly seemed toJo more conscious of their health andexpressed considerable interest in fol-lowing good health habits they hadlearned during the carnival. Two ex-
11-
s,4,1,tifts,
14,1t vh,
x 'tk-0,1411/4 ,
,
''Kt
s:
js: r
e ,ha
tatkV
A;;riz140:i14'
11.4k.
*Icr,
arnples of the lasting impact of the car-nival on their lives were noted by thejunior high school science and healthteacher. Members of the third gradeclass confessed they had no idea thatmilk was so good for the body and theyproclaimed that they would continue todrink more of it. Members of thesccond grade class organized a "SmokeBusters" club and promised to weartheir "Don't Smoke " emblems to fur-ther demonstrate their commitment.The teacher observed that the secondgrade students remained true to theirpromise.
Additional follow-up was alsodone by teachers in each of the threeclasses involved in the health educationcarnival. During the next few classmeetings, they processed the health re-lated information and materials givento their students. Elementary schoolteachers expressed sincere apprecia-tion for the outstanding, active learningopportunity made available to theirstudents during the health educationcarnival. Teachers were surprised thatthe junior high school students couldbe so well organized, motivated, andcapable of providing such a high qualitylearning experience for their students.
i
)1114
4
What was possibly even more amazingis that we never doubted for a momentthat they could do it. Junior high schoolstudents are "naturals" as facilitators ofelementary school health educationcarnivals. Give them the chance andyou will be glad that you did!
Bays, C. T. (1986). The elementary schoolhealth fair: A process involving thewhole school in health education. Journalof School Health, 56. 292-293.
Daughtrey, G. (1976). The Norfolk publicschools health fair. Health Edacation, 7(4),36-37.
Lafferty, J., Guyton, R. & Pratt, L. E. (1976).The University of Arkansas health fair asprofessional preparation. Health Educa-tion, 7(4), 24-25.
McKenzie, J. F., Scheer, J. & Williams, I. C.(1981). The health and safety fair: Acookbook approach. Health Education,12(1), 27-29.
Petty, R. & Pratt C. (1983). Student staffedhealth fairs for older adults. Health Edu-cation, 14(2), 40-42.
Watts, P. R. & Stinson, W. J. (1981). Thehealth education carnival: Giving the oldhealth fair a face-lift. Health Education,12(6), 23-25.
Wolf, Z. R. (1986). A health fair for school-age children presented by registerednurses. journal of School Health, 56, 192--193.
179

TEACHING IDEAS 100
Thinking and WritingA Strategy for Teaching Positive Health Decision Making
Paul Villas
When an undesirable or unpleasantevent occurs, people are often remindedthat it did not have to happen. The adviceis that if a different route were taken, theunpleasant occurrence would not haveto come to fruition. A television com-mercial explains this concept perfectlyby emphasizing a particular car's brak-ing ability. The commercial promotesthe notion that vehicles do not have to becrashed to prove they are safevehiclescan be safe if you can stop them beforethey crash. The point is made that thebest way to survive an accident is neverto have one. This commercial's themebecomes the strategy for this teachingideasomething can be done before thepoint of no return is reached.
Criticism directed toward educationtoday claims that students cannot thinkcritically. Another area of concern is theinability of students to express them-selves in writing. Thinking and writingskills can both be enhanced in healtheducation courses by employing a time-line teaching activity, which allows,students the opportunity to make posi-tive health decisions at the same time.
The time-line teaching activity isdesigned with three goals in mind: pro-mote writing skills, enhance criticalthinking, and equip and direct studentstoward healthful decision making. Themain objective is to help students un-derstand the consequences of poor healthdecisions and realize that lack of aware-ness makes them select poor healthchoices. Writing and thinking skills arethe tools used to achieve the main objec-tive.
Paul Villas is with the Department ofHealth Science, New Mexico State Uni-versity, Las Cruces, NM 88003.
1 80
The Activity
The assignment begins by provid-ing each student a sheet of paper dividedinto four columns as shown in Figure 1with an explanation of the meaning ofeach area.
Micle or Event: This is the heart ofthe assignment The students are askedto select a newspaper artic le, news story,or an event they are familiar with thathad negative consequences because ofpoor health decision making. Examplessuch as suicide, vehicle accidents, teenpregnancy, anorexia nervosa, etc., couldbe used. From these articles or events,students creatively but realistically fig-ure out why poor health decisions aremade.
Trigger: Under this heading, the stu-dent speculates about what could havehappened to trigger the particular eventin the minutes, hours, or days precedingit. If the event deals with a suicide orattempted suicide, the trigger could havebeen an argument with parents or abreakup with a boyfriend/girlfriend. Ifthe event was a car accident, 'he triggermight have been driving under the influ-ence of alcohol in combination with lackof sleep.
History: This column enables thestudent to discuss situations or condi-
tions that have taken place in a person'slife that may make him/her prone tomake certain decisions. Poor self-es-teem or an inability to make any closefriends in the formative years may pro-gram a person toward a destructivelifestyle.
Post Event: The lesson or lessonslearned from the event go in this col-umn. The lesson could apply both tothose who survived or are the mainplayers in the event as well as to thosewho knew or learned about it. It. is im-portant to understand that there are con-sequences resulting from poor healthdecisions. The teaching aim is to leadstudents to resolve not to repeat theevents they are reporting on and learnthat background information leading topoor health choices can be overcome topromote positive health behaviors.
Final Note
The writing assignment could be asintensive as a teacher desires. The Ls-signment could be done on the sheet ofpaper provided, or that sheet could beused as a working paper for a moreformal writing assignment. Hopefully,by providing opportunities for studentsto figure out why poor health decisionsare made and to understand their con-sequences, they will not get themselvesin the same predicament.
History(Days, Years)
Trigger(Days, Hours,Minutes)
MolesOf Event
PostEvent
Figure 1. Time-Line Teaching Form
TEACHING IDEAS 101Nkr-sklai
Personal Health Via Community HealthLinda Olasov
A.011M11.
Traditionally, students in personalhealth classes at universities are askedto complete a variety of assignments.Among them, the most traditional of allis the term paper. Usually it is a twoway communication between the stu-dent and teacher with few others shar-ing the information. However, it is pos-sible for a teacher to offer an alternativeto the formal term paper, to offer anopportunity to the student to interact ina community health facility through asharing of information, different per-spectives, and skills.
This new partnership between stu-dents in a health education class and acommunity mental health facility hasgreat potential. It provides an opportu-nity for health students, some of whommay be in teacher education, to havecontact with exceptional people and toteach individuals with emotional/behav-ioral disturbances. It is hoped that r on-tact with these people will result inpositive attitudes for health educationstudents. And, the partnership couldbenefit the patients by infusing somestimulation through learning in an oth-erwise boring daily existence at a psy-chiatric facility.
The author, in preparation for thispaper, could find no literature dealingdirectly with the use of mental healthfacilities or hospitals as placements forstudents in personal health classes or
Linda Olasov is an assistant professor ofeducation in the Education Department,Northern Kentucky University, HighlandHeights, KY 41076.
ale
NEN
for any education students. This articlewill describe the field placement experi-ence for four students in a personalhealth class who chose to work withexceptional students in a communitymental health fadlity rather than towrite a formal term paper.
In the BeginningThe basis for this program was estab-
lished two years ago by a health educa-tor at Northern Kentucky Universitywho asked a clinical psychologist fromRol lman Psychiatric Institute in Cincin-nati, Ohio to speak to several classesabout mental health. Several groups ofstudents volunteered for a practicum atRol lman in which they helped with pa-tient recreation.
Experience with those students pro-vided incentive for the more ambitiousprogram discussed in this paper. A so-cial worker at Rol lrnan suggested anacademic program for patients, and thisbecame the basis for the placement ofstudents in a personal health class.
ObjectivesFrom the viewpoint of the university,
there were three objectives for this col-laboration: (1) provide an additionalpreservice teaching option; (2) developmore constructive attitudes through di-rect contact with emotionally disturbedpeople; and (3) provide service to thecommunity, one of the university's mis-sions.
From the perspective of the hospital,
, 1 p
this project had four primary objectives:(1) help alleviate the bored.xn and inac-tivity which many patients experiencein the hospital; (2) enhance the self-sufficiency of patients by teaching thempractical skills; (3) provide an opportu-nity for interested, qualified pathmts tobegin preparing for the General Educa-tional Development (GED) examinationwhile hcspitalized, which coltki contin-ue iollowing discharge, and, (4) edu-cate, through direct experience with acommunity mental health fariliiy, peo-ple whose chosen profession will makethem influential in the community re-gardii g attitudeF toward mentA illness.Objective three was arranged through asecond faculty member.
Information About the HospitalRollman Psychiatric Institute is a 146
bed state-funded psychiatric receivinghospital. It provides shurt-term acutecare for adults between ages 18 to 65.The mean length of stay at the time ofthis project was 29 days. The major:ty ofthe patients have psychotic episodesand have been probated. Practically allare on psychotropic medication in thehospital for symptom relief. Most pa-tients have a variety of serious behavior-al, economic, educational, and interper-sonal problems which have resultea inone or more previous hospitalizations.Iie problems are typically complex andmultidetermined. In most cases the goatof hospitalization is to return the patientto the level of functioning he or she hadin the community before hospitalizationwas required.
181

ArrangementsFour students from the personal
health class volunteered for placementat Rollman. Patients were also volun-teers and participated in the activitiesstudents offered. All students were atleast at the junior level. Except for onewho was not an education major, theothers had previous classroom expert-ence through the practicum componentof their Introduction to Educationcourse (120-135 hours).
Students were supervised both byfaculty members at the university andby hospital staff. A psychologist servedas program coordinator and liaison be-tween the two institutions and waspresent for all sessions. All studentswere required to keep and submit totheir teachers a written account of theirreactions to each session.
Of the students in the personal healthclass, four out. of 29 chose to makepresentations to patients on a hospitalward in two sessions, one week apart.The alternative was to hand in a formalterm paper. Three of these studentswere physical education majors with aminor in health education; the fourthwas a business major.
Health PresentationsThe students were able to choose any
topic related to health and to presentinformation about it. Length of the ses-sions varied in order to accommodatethe needs of the presenter and patients.Of the four students who participated,two taught individually and iwo as ateam. They scheduled their sessionswith the psychologist about two weeksin advance. One Tek before they wereto present, they submitted to their in-structor a topic, bibliographical refer-ences, a brief outline of what they in-tended to do, and how they intended todo it.
The health students piesented a totalof six programs on a ward for menduring a time when the patients wereordinarily restricted to the ward for shiftchange. Each program lasted from 30 to90 minutes. No individual or team pre-sented on consecutive weeks because ofindividual scheduling problems. Thefollowing topics listed by presenterwere offered: (1) stretching exercises,basic first aid; (2) calisthenics, bandag-ing; and (3) starting c,nversations, com-edy movie. The overlap of topics wasnot a problem due to a rapid patientturnover in the hospital, and presentersof the topic were different. There was,however, little st nse of continuity or1 82
development of topics because of sched-uling problems and each health studentpresenting two programs unrelated toeach other in content.
Student ReactionAlmost all the students expressed
some degree of anxiety or fear aboutgoing to a psychiatric facility. However,by the end of their experience, all stu-dents reacted with positive comments, osense of learning, growing, and selfworth.
The following statements from jour-nals kept by students express ther re-sponses to their experiences:
"I learned how lucky I am to hem afamily, job, and an education." "The experi-ence was one-of-a-kind." "I learned whatanother side of the world is like." "I reallyliked it, and enjoyed myself." "Thanks forthe opportunity you 'lave given me to view asituation like this. It was a first for me, and Ifeel I have learned a lot." "Mental illnessseemed spooky to me before. Since my visit toRollman's, I can see that these people justneed help, care, and understanding." "Be-ing at Rollman's gave me a real feelins of selfworth, that someone really needed me. Myspirits were lifted greatly when the patientsthanked me for coming to spend time withthem and truly wanted me to retarn."
Evaluation of the ProjectFrom the veiwpoints of both the uni-
versity and the psychiatric hospital, themajor objectives of this cooperative ven-ture were acheived. Collaboration pro-vided future teachers with an insideglimpse of a psychiatric facility. As apilot project in a novel situation, it chal-lenged their flexibility and creativity.Programs were seen as successful andworth continuing by all involved, in-cluding preservice teachers, universityfaculty, patients, and hospital staff. Theprograms given by personal health stu-dents reached many patients. The uni-versity instructor viewed the programswith Rollman as a viable method forploviding students with contact withexceptional people and for providing aunique alternative to the traditionalterm paper.
Student journals reflected a change inattitude toward institutionalized psychi-atric patients. Students generally be-came more confident in their interac-tions. All the students expressed enjoy-ment and learning as a result of theirexperience and urged continuance ofthis program as a future option for stu-dents.
A community mental health facilitycan provide a mutually beneficial expe-
1 ( f)1,J
rience both for patients who serve asstudents and for their tutors, the uni-versity students enrolled in health edu-ce tion courses. The program gives stu-dents an opportunity to practice teach-ing and gives patients an opportunity toparticipate actively, learn, broaden theirexperiences, and relieve the boredom ofinstitutional life. The real world and theivory tower can meet halfway.
Recommendations for FutureCollaborations
Several suggestions can be made tothose attempting to carry out programssuch as that described above:
(1) An individual on the hospital staffmust see the need for interaction withthe university and be committed toexpanding services to the pati.mtpopulation. There are many difficnItlogistics to work out, e.g., identifica-tion of appropriate patients, location,times, and availability of universitystudents. University personnel can-not carry out such a program withoutinhouse commitment and assistance.(2) A hospital staff member should bepresent or readily available at all ses-sions in order to alleviate studentapprehension and to handle anyemergencies.(3) Preservice teachers should haveprior classroom experiences. One par-ticipant without this prior experiencehad difficulty with his presentationand inte:action with patients. Suchstudents should only be involved ifthey could team teach with a morequalified student.(4) All students should come to thehospital the first time with someonethey know, someone who can pro-vide feedback and support. Initialteaching could be a team effort; soloteaching could follow when indicat-ed.(5) Careful coordination and schedul-ing of topics is needed for students,proviiing only two sessions of in-struction.(6) Educational activities either at theuniversity or the hospital whichmight alleviate anxiety and dissipatemyths about psychiatric patientswould be helpful. Ideally, opportuni-ties for training students in interview-ing and psychopathology, both ap-proached from a practical "how to"point of view, could be made avail-able. These subjects are quite relevantfor student volunteers both in func-tioning at the psychiatric facility andin careers as classroom teachers.
TEACHING IDEAS 102
Using College Students asSenior Peer Teachers in
Youth-to-Youth Health EducationAnthony G. Adcock
A problem often encountered in col-lege health strategy classes is how tomake the learning meaningful to stu-dents. The conscientious instructor isoften frustrated because time con-straints limit student practical experi-ence in the education process. One in-novative way to develop an effectivehands-on experience for prospectiveteachers is to have them serve as seniorpeer teachers in youth-to-youth peerteaching programs in the publicschools. Considerable evidence existsthat peer teaching programs are aneffective way of providing health educa-tion (National Institutes of Health,1980).
At Freed-Hardem.m College the firstpeer teaching model 1 developed in1981 (Adcock, Chambers, Wilson,.1981). It was prompted by local concernabout the extent o i smoking in the pub-lic schout. Several members of theschool board made an effort to ban theuse of all tobacco products on schoolproperty. One result of the publicitywas recogniticn of the need to develop aprogram which would help preventyoung people from developing thesmoking habit. It was believed that aprogram which would train high schoolstudents to teach anti-smoking contentto elementary age youth could be effec-tive in achieving this goal. Cooperationof the school board, school principals,and health teachers was assured.
ProcedureTwo outstanding students who were
willing to work with the high schoolstudents were selected from the collegestrategies class. The college studentsheld planning meetings with the districtexecutive director of the Tennessee Di-vision of the American Cancer Societywho suggested printed materials whichthe Society pi ovided. The students also
Anthony G. Adcock is an associate professorof health education at Troy State University,Troy, AL 36082
met with the high school principal andtne health teachers to discuss the youth-to-youth anti-smoking program.
The high school health teachers se-lected 15 students to participate in theprogram. The bases for their selectionwere ability to be positive non-smokingrole models and interest in the project.The high school students were in thetenth grade and were 15 or 16 years old.The sixth grade was selected as thefocus for the program because few stu-dents were already regular smok( Is, butwould soon be entering junior highschool where peer pressure to smokewould likely increase.
194
The college students conducted fourtraining sessions with the high schoolstudents. The length of the sessionsranged from 60 to 90 minutes. At thefirst session, the high school studentswere divided into five groups of threestudents each. The purpose and specificobjectives of the program were identi-fied. At the second session, specifictopics and activities were assigned toeach group. Each group was responsi-ble for one presentation of approximate-ly 45 minutes. The remaining sessionswere used to develop and refine eachpresentation.
Films and printed materials from the
183

American Cancer Society were used bythe student groups. The college stu-dents also developed materials, andseveral of the high school studems hadideas for materials which were iticorpo-rated into the presentations.
Five sixth grade classrooms of stu-dents participated in the program, con-sisting of five presentations during atwo-week period. Each group gave thesame presentation each session, only toa different classroom of sixth graders.During the presentions, senior peerteachers observed the high school stu-dents as they taught and mct with themafterwards to discuss the experienceand to offer suggestions for future ses-sions.
In 1982 all students in th.: collegehealth strategies class were required toparticipate in the youth-to-youth pro-gram. The program was organized inmuch the same way except that thecollege students were divided into fiveteams consisting of two members each.Each team worked with five high schoolstudents to develop one module in theprogram.
Since 1981, additional youth-to-youth
184
teaching modules have been developedfor drug abuse and for the prevention ofdrinking and driving. One year, theyouth-to-youth program was includedin a state grant for a community-widedrinking and driving program, and thecollege students were paid a small sti-pend for their work as senior peerteachers.
SummarySeveral benefits accrue from the use
of college students ir. a youth-to-youthteaching program. Undergraduate stu-dents who are planning to becomehealth educators gain hands-on experi-ence in program planning and in teach-ing high school students. Since the highschool students immediately applywhat they have learned, the collegestudents can see the outcomes of theirteaching in a short period of time. Inaddition, both the high school and theelementary students become enthusias-tic about the program.
Senior peer teachers returning to thecollege classroom engage in mutualproblem solving, and class meetings aretimes for sharing and helping. The col.
1 1 r1.
lege instructor serves as the resourceperson but otherwise is as much a stu-dent as everyone else in the classroom.
Experience has shown that a youth-to-youth program must be carefullyplanned to be effective. The programmust be closely supervised by the col-lege instructor, and adequate time mustbe given to preparat.on before presenta-tions. Selection of the high school stu-dents is also important to the success ofthe program. They must be good rolemodels who are self-confident enoughto present information to a group ofyounger students.
Much effort is required to successfullyconduct a youth-to-youth program us-ing college students as senior peerteachers, but the interest and excite-ment it creates are well worth the effort.---Adcock, A. G., Chambers, V., & Wilson, J.
(1981). A youth to youth smoking educa-tion program for sixth grade students.Tennessee Journal ()f Health, Physkal Educa-tion, and Recreation, 20(1), 18-19.
National Institutes of Health, (1980, June).Smoking prNrams for youth. Washington,DC: US Public Health Service, NIH 80-2156. Fil
TEACHING IDEAS 103
Judgments Required from the ResidencyCoordinator
William N. Washington
The word residency is discussed herecan be considered synonymous withfield work, internship, and field train-ing. Residency is a time when the stu-dent can practice the various processesand responsibilities of a vocation underthe supervision of a professional in thefield. Such opportunities are generallyfound in the curriculum of universityprofessional schools such as publichealth, public administration, educa-tion, medicine, social work, and certaindepartments in other universities.
The residency coordinator, an employ-ee, develops a communication link be-tween the university and the communi-ty, locates residency sites, places stu-dents in residency, counsels students inrespect to their residency experience,and in general coordinates all businessrelating to the residency program. Theresidency coordinator coordinates all
William N. Washington is an associate pro-fessor, the School of Applied Arts and Sci-ences, Department of Health Science, Sanlose State University, San lose, CA 95092
the ach 'Ries resulting from the relation-ship between the university, the stu-dent, and the agency.
Residency coordinators may be askedto perform in a specialized or generalarea. For example, within the school ofpublic health there could be several spe-cialized areas such as health education,nutrition, health services administra-tion, and population planning. In thisspecialized situatbn, a residency coor-dinator would relate only to one pro-gram, such as health education. A coor-dinator.who functions as a generalistwould relate to two or more specializedareas. A generalist may function as thecoordinato for all programs on the pro-fessional l vel.
Functior ing as a residency coordina-tor requires making many judgmentsthat effect the relationship between theuniversity, the student, and the agencyin which the student is placed. Thecoordinator's judgment could affect thereputation of the professional school
1 op
and university as reflected by the com-munity's perception of the quality of theuniversity's staff, faculty, students, andprograms. The value of the residencyexperience for the student and theaccomplishment of an agency's objec-tive by using a student are all affectedby the coordinator's judgments.
The residency program may be con-ceptualized as having at least four com-ponents: (1) preplanning and programselection, (2) residency selection andplacement, (3) residency experience,and (4) program evaluatic. Preplan-ning and program selection includethose procedures and activities neces-sary to obtain needed information fromstudents, finding potential health-relat-ed agencies willing to act as preceptors,and selecting the appropriate type ofprogram. Residency selection andplacement involve using informationpertinent to the particular experiencedesired by a student and then makingarrangements for the student to work atan appropriate facility. Field work de-scribes the actual job experience. Pro-
1 85

111=111111111O
gram evaluation analyzes all stages ofthe process relative to the successes,failures, and suggestions for improve-ment and consideration.
Judgments required from the residen-cy coordinator are discussed in terms ofthe four conceptualized componen ; ofa residency program. Preplanning andprogram selection is discussed in refer-ence to gathering information from stu-dents and making contacts with healthagencies; residency selection and place-ment is discussed in relation to informa-tion given to students about agencieswilling to act as preceptors; residency isdiscussed in relation to on-the-job expe-rience; and program evaluation is relat-ed to those judgments necessary to de-termine whether the program meets itsobjectives.
Preplanning and ProgramSelection
Information frail Students
As much rel want information as pos-sible should be obtained from the stu-dent to help the coordinator choosewhich students should have residencyexperience. In professional schools,there is a good chance that some stu-dents have already had practical careerexperience equivalent to the responsi-bilities and tasks performed by gradu-ates of the school, or equivalent to theresponsibilities and tasks a student isexpected to perform during a residencyexperience. Depending on the student'sdesire or financial status, the studentmay be working whiie attending schooland, therefore may have difficulty fit-ting in a tesidency experience. In addi-tion, the university's program may ormay not require a residency experiencefor all its students. Taking all thesesituations into account, the coordinatormust judge which students need a resi-dency.
Students who enter a professionalschool have various backgrounds andexperiences. They differ not only inwork experience, -but in academic prep-aration. Some students are interested indoing a residency soon after admissioninto the school. The coordinator mustconsider these factors and judge theappropriateness of residency for stu-dents. For example, the coordinatormay want to ensure that the studentwill perform competently in the resi-dency. To increase this potential assur-ance, the coordinator may require thestudent to complete certain acaiemiccourses and/or spend a certain time (forexample, one year) in the academic pro-1 86
gram before being considered for resi-dency.
The coordinator counsels the studentwith respect to the best type of residen-cy. This judgment could be made afterreflecting upon the background and ca-reer interest of the student. For exam-ple, if a student interested in healtheducation has had extensive communityhealth education experiences andproved competent, the coordinator mairecommend a residency experience in ahospital setting. This new settingshould concentrate on skills that needdevelopment, such as skills in adminis-tration. Working in administration mayprovide a more detailed introduction tofiscal matters, personnel, and decisionmaking relative to programs with whichthe student had no previous experience.
Contacts with Health Agencies
After the coordinator decides whichagencies to contact, and after contacth:s been made, the coordinator mustdetermine which agency is willing totake a student. The agency's willingnessgoes beyond its agreement to place astudent. hi this case, willingness infersa sincere desire to provide the studentswith learning experiences and environ-ments in which they will be acceptedand supported. In certain circum-stances, an agreement to place a studentdoes not include support and accept-ance. The coordinator must judge thewillingness of the agency, and makeplacement accordingly.
Competent Staff and Facilities
Students should be placed in agencieswith good facilities and competent staffwho have been adequately trained to dothe expected quality and quantity ofwork. The agency staff should be moreskilled than the student. Inadequate fa-cilities may mean that the studentwould be unable to observe all the pro-cesses involved in his assignment fromits beginning to completion. In suchcases. some assignments may be at-ternp4ed with insufficient input or tests,completed at another agency, or simplynot completed.
Agehcies are anxious to provideplacement for students for a variety ofreasons. Some agencies want studentsfor cheap labor, status, or to do worknone of (he agency's staff wants. ManyagencieF, however, have positive rea-sons for wanting students. The coordi-nator must judge the reasons for place-ment agreement and the appropriate-ness of the experiences in relation to theuniversity's program. The experience
must relate to program objectives. Theplacement decision should be based onwhat is best for the student, the univer-sity, and the agency.
What about the reputation of theagency? The coordinator should exam-ine statements made about and beliefsheld toward a potential preceptor andanalyze all interactions with the agencyto support or refute statements or be-liefs. The reputation of an agency isimportant because the agency's reputa-tion could be transferred to the profes-sional school due to association alone,and association with a highly respectedagency could help the community thinkhighly of the professional school. Basedon these considerations, the coordinatormust make a judgment about the impor-tance of an agency's reputation in resi-dency placement.
The coordinator should establishstandards that must be met by an agen-cy being considered for preceptorship.These standards should be of qualitythat in no way compromises the generalstandard for excellence of the entireuniversity. Of all the agencies indicatinga willingness to act as preceptors, thecoordinator should choose those thathave met or have agreed to meet therequirements.
Inform Students About Agencies
Several decisions should be made be-fore informing students about agencieswilling to act as precept9rs. The first isto det-rmine which students to recom-mend to specific agencies by taking intoconsideration the experience wanted byeakh student and the additional types ofagencies discussed by the coordinatorand the student. The coordinatorshould give the student an opportunityto interview with any agency. However,the cool dinator must also provide guid-ance to students concerning on whichagency they should concentrate theirenergies, based on interests, back-ground, and abilities. For example,some students may be interested inworking at a particular agency becauseof its prestige, rumors from other stu-dents and friends, permanent employ-ment opportunity, and/or staff composi-tion, but they may give little thought towhether the agency can provide thenecessary experience. The coordinatorshould work with the students to clarifypotential positive and negative conse-quences.
The number of students available forplacement varies from year to year andfrom semester to semester. The coordi-nator should try to have more place-

ment site opportunities than students toensure placement for all lf the coordi-nator has the philosophy that each stu-dent should have interviews with sever-al agencies and that each agency shouldbe given the opportunity to interviewseveral students for each position, thecoordinator should decide how manyinterviews each student should haveand which students should be sent forinterviews. To deal with this problem,the coordinator could contact the agen-cies, tell them how many students areavailable for interviews, and ask howmany students each agency would liketo interview. The coordinator can thencheck the files to determine which stu-dents are interested in the positionavailable at each agency. Without show-ing favoritism, the coordinator shouldinform all interested students aboutavailable positions and, using the first-come, first-served method, refer thepredetermined number of students toagencies k r interviews. The first-come,first-served rule might be relinquishedif, after se , eral interviews, the samestudents are consistently first and, as aresult, adtain an excessive number ofinterviews. An attempt should be madeto achieve a good balance in number ofinterviews.
Sometimes after several interviews,several students may be selected forplacement by more than one agency,and several may be selected by none. Astudent who has been selected by morethan one agency should not be sched-uled for additional interviews. If morethan one agency wants a particular stu-dent, this student should be asked tochoose an agency. The coordinatoi
should continue t mge interviewsfor those students o have I,ot beenselected. lf, after se A.ral unsuccessfulinterviews, a student seems discour-aged and disappointed, the coordinatorshould offer counseling, encourage-ment, and special attention by arrang-ing an interview after establishing thatthe student has an excellent opportuni-ty to be selected by that agency. Thepotential for this student to be selectedcould be increased through the absenceof competition; i.e., the coordinatorwould send only this student to theagency for an interview.
In order the selection process to oper-ate smoothly, no student should go toan agency for an interview without pri-or approval by the coordinator.
Residency ExperienceIn most cases, the residency experi-
ence is an unfamiliar situation for stu-dents. They are in a new relationshipwith the residency coordinator and theiragencies. The coordinator will need touse keen senses to judge whether astudent is having a successful residencyand should maintain constant commu-nication with the student to determinewhether the student is doing thosetasl agreed upon by the preceptor andcoordinator. All key actors will be awareof changes in the program they main-tain good communication.
The coordinator should ask the stu-dent directly whether the residency issuccessful. The answer, whether ves orno, should be followed by an explana-tion. In addition, the coordinatorshould look for both verbal and nonver-bal messages. For example, studentsmay say one thing but mean another orsay little or nothing about their experi-ence. To understand nonverbal mes-sages the coordinator should obtain ad-ditional information about the work sit-uation from the preceptor or otherpersons with whom the student works.An indepth, personal, and private dis-cussion with the student may disclosethe true success of the residency.
If a problem exists, the coordinatorshould first determine whether it relatesto tasks being performed, interactionswith the preceptor, interactions withother employees, or a combination ofthese. Then, the coordinator must solvethe problem. One possible solutionwouk. Lle counseling the student and/orthe pi :eptor. Another solution wouldbe to -ansfer the student to anotherdepartment within the same agency ortransfer the student to a new agency. Ifthe problem relates to the task, the
1 9S
coordinator could provide some techni-cal assistance or recommend assistanceresources. If the problem relates to theinteraction between the student andpreceptor, the coordinator should act asan intermediary. If neither solutionworks, the student should be trans-ferred based on the desire of the studentand/or the p-eceptor.
EvaluationTo determine the success of a pro-
gram it must be evaluated. The degreeof evaluation will depend on the evalua-tion technique's sophistication with suc-cess determined on the basis of evalua-tions from the student and preceptor.The coordinator should make a compar-ative analysis of both evaluations,whether such evaluations are open-end-ed, objective, or a combination. Thepreceptor's evaluation should be com-pared to the student's to determine thesimilarities and disparities. By compara-tive analysis the coordinator can deter-mine the validity and significance ofevaluation. For example, if both studentand preceptor are given guidelines forwriting an open-ended evaluaiion, butthe coordinator receives and this wasfollowed inappropriate and misrepre-sentative evaluations, questions wouldexist about the evaluation's validity orsignificance.
From the evaluations should comeseveral recommendations for changesand new ideas for consideration. Stu-dents may suggest (1) courses or workexperience that should act as prerequi-sites to the nesidency, (2) no futureplacement at thit agency, (3) no futureplacement under a particular supervi-sor, or (4) continuation of the past meth-od of selection and placement. The pre-ceptor may also give ideas to use infuture placement selection. The coordi-nator must decide which suggestionsshould be used in the future to help theprogram continue to evolve into a betterresidency program.
1 87

TEACHING IDEAS 104
A Community Resource Class AssignmentAnsa Ojanlatva, Ph.D.
,
z `, 4.1 "I'2.11.
"Ot
sr
41f re' -re
.or
t.t
_1-
s le
,orr ";a1",...4
Ansa Ojanlatva is coordinator of the Depart-ment of Health Science, Louisiana StateUniversity, School of HPERD, BatonRouge, LA 70803.
188
go. ..ir
9
. ,
2tOrtS_Tr
7*-
'
Arr._
Community Health Education classesmay effectively be used to introducestudents to development of tools forcommunity action. An undergraduateseminar, Health Behavior and Commu-nity Health Education, at CaliforniaState College/San Bernardino includesfrom four advisement areas: health ad-ministration and planning, environ-mental health and safety, health sciencegeneralist, and community health edu-cation. For many of them this is the firstcourse on community health education,and for some of them it is the only suchcourse in the present curriculum. Thecollege is on a quarter system whichtosome extentlimits the quantity ofwork to te accomplished at one time,and action programs to be completed bystudents will have to be reasonable. Atthe same time, the academic require-ments of these students include morehomework than normally found inmany other institutions (1 unit of 5 or 1/2of 2.5 units pei quarter), providing 1/2 to1 unit more credit per quarter. There-fore, out-of-class assignments are no'only desirable but required. The settingis outstanding for health educationprocess.
Often community activities requirethat individuals team up for action. Fewof us can alone accomplish significanttasks demanding interaction with peo-ple. This concept is brought to the class-room, and the following is an assign-ment students have to complete as par-tial fulfillment of the above statedcourse.
The assignment itself has gonethrough many transformations in differ-ent types of classes, but it appears towork best here where its purpose isclear, where the time element is appro-priate, and where the students are seri-ous enough to complete a started pro-ject. After this experience, most stu-dents move on to leldwork and mayutilize the newly acquired materials.
During the first week of class, thestudents are given a syllabus, and dicingwith it they are asked to think about atopic of major interest which eventuallycould be developed into a communityresource. Approximately half of the stu-dents do truly come up with topicswhich are realistic possibilities for a pro-ject. These alternatives are listed on theblack board during the tollowing ses-sion, the instructor adds few, and someof the students suggest additional onesas a result of brainstorming. Two dozenor more suggestions may be listed.
Once all possibilities are discussed,each student is asked to make a commit-ment and to initial one of them. Two or
more students are normally assigned toone project. The rest of the session isused to formulate conclusions of theproject ahead. This translates to defin-ing purpose, setting of goals and objec-tives, and finally division of tasks to beaccomplished.
For about five weeks the studentswork on their assignments, consultingwith the instructor when necessa-y. Areport is prepared, it is shared in class,and evaluated by the peers (Form A)and the instructor. Since these projectsare designed and completed by the stu-dents, the final outcome and formatvary from one to another. However,some cover letter information is oftenshared and includes name, address andphone number(s) of the service(s), con-tact person(s), time(s) and day(s) ofservice(s), kinds of service(s) offered,fee(s), population(s) served, type of care(primary, secondary, tertiary), andwhether the service can be reached byphysically disabled clients.
Although the project is a reasonabletask for most students, about one in 15fails to comply with the requests. Withthe process of defining roles and assign-ing tasks, most of the difficulties areworked out early. It seems that thestudents failing to complete the projecthave personal problems which seriouslyinterfere with school work.
Another difficulty seems to arisewhen business establishments are com-pared with each other. This may be dueto the competitive nature of such estab-lishments. Certain information simplywill not be available for comparisonpurposes.
Many of the students in this locationcome back to school, because they wantto do something different in their lives.Often these projects function as a modeto turn negative experiences into posi-tive ones. Sometimes the activity worksas a vehicle to learn something com-pletely different from the defined goalsand objectives of the assignment. And afew students have used the activity toeither define future fieldwork experi-ences or to provide better tools for theexisting ones. Some of the projects havebeen forwarded for use by the variouscommunity groups.
Examples of resources from the mostrecent classes include:
1. Child Abuse listing for San Bernar-dino and Riverside Counties;
2. Teenage Alcohol and Drug AbuseServices.and Resources in San Ber-nardino County and SurroundingMetropolitan Areas; (These two re-
2 (
source guides were forwarded foruse by an area school district.)
3. Veterans Resource Guide (VRG),Alcohol and Drug Abuse ProgramServices in San Bernardino Coun-ty, California, 1982; (The guidewas compiled by a veteran togeth-er with another interested studentand it is available for counselingpurposes.)
4. Counseling and Support Groupsfor Families with Terminally IllChildren;
5. ABC's/Alternative Birthing Cen-ters Resource Listing for SouthernCalifornia;
6. Guide to Ostomy Services, SanBernardino/Riverside MetropolitanArea;
7. Ulcerative Colitis: Alternatives toSurgery (including resources); and
8. Services to the Newly Blind.
4710
. 1.40004.1 .
4.vcioingov.4.1.
189

TEACHING IDEAS 105
Evaluating Health NewsMichele J. Hawkins
Proliferation ofheakh informationin the popular press is increasing atdramatic levels (Broad, 1982; Culliton,1987). Media sources that provide thishealth information also have iffolifer-ated. One needs only to pick up a news-paper or magazine to find that healthreceives heavyattention in todays press.Fluther, whlle the amount ofhealth newsgrows, the content is ever changing.What is healthy tc 'ay, may be found tobe unhealthy tomorrow. Levin (1987)states the approximate half-life of a so-called health fact is four years. Hence,formal education can no longer teachhealth facts that will remain intact duringthe course of one's life span. Levinfurther states that dianging informationregarding health leads to substantialpublic confusion about what andwho tobelieve, thus progressively diminishingeffectiveness of health messages. Com-pounding the problem is the difficultythe lay person has in understanding theinformation beingdisseminated (Yeaton,Smith, & Rogers, 1990).
In response to this proliferation ofhealth information, the public must beable to analyze the accuracy and rel-evance of information it receives. Be-ing able to analyze this information iseven more critical since the public gainsmostof its health information outside thecontext of formal education (Miller,Sliepcevich, & Vitello, 1981). There-fore, teaching skills used to analyzehealth messages critically becomes vi-tal. The following teaching exercise isdesigned to teach these skills.
Michele J. Hawkins is with the Univer-sity of Oregon, Department of Schooland Community Health, Eugene, OR97403.
"t 90
Purpose
The purpose of this educationalmethod is to teach critical thinking skillsfor analyzing health news to high schooland college students. In particular, stu-dents will be able to use criteria pro-vided to critically evaluate news stories.
Overview of the TeachingTechnique
Evaluating Health Newstakes twoclass periods (50minutes each) tocom-plete. The fffst class period consists oflecture information regarding guide-lines used to evaluate the health news.The second class period is used to allowstudents to evaluate health articles.
On day one, photocopy news sto-ries related to health (the local newspa-per is often most relevant to students).On day two, give several magazines thatcontain health news to students. (Stu-dents enjoy analyzing a wide variety ofmagazines and tabloids. I recommendincluding several that have sensationalstories, such as theEnquirer.)
The lecture covers the followingpoints: (1) Discuss importance of ana-lyzing health news today (see introduc-tion and provide relevant examples). (2)Discuss importance of understandingbasic research when evaluating healthnews. The following points maybe per-tinent:
- Health research involves testing(studies). Studies usually are done oneat a time, providing educated guesses(hypotheses) about how living beingsfunction. Since human beingsare com-plex, one experiment or study rarelyproduces complete results; therefore,
2 (1
many arperiments or studies are neededto understand phenomena under study.When studies are reported in the news,we are presented with one piece of apuzzle. Only after several studies doesa more complete picture begin toemerge.
- Research yields new knowledge,but uncovers new questions. Whenconflicting results occur, it often is be-cause the study may be slightly diferentfrom those previously conducted, witha different population (men rather thanwomen, teens rather than elderly).
- When examining health news,specific criteria should be considered.
On day twv, provide several map-zines and newspapers and have stu-dents evaluate articles in class in smallgroups. During the last 20 minutes ofclass, let students report on their find-ings.
Guidelines for EvaluatingHealth News
Credibility of the Source
Who is reporting the health infor-mation? Is it a publication known forprinting sensational stories? Or is it apublication that must check its sourcesfor accuracy? Who conducted the re-search? Was it a research group underauspices of a university or was it a pri-vate organization? Who paid for thestudy? Does the group have a "stake" inthe findings, such as a drug companyevaluating its own product?
Study Design
What type of study was done - test

tube, animals, humans? Test tube andanimal studies usually are done at thebeginning of research testingeffects ofsomething (drugs, exercise) on humans.While these studies yield important in-formation, the test done with humanbeingsyields the most information. Howmany subjects are in the study? This isimportant because many studies thatmake headlines have few people in thestudy. The larger the study, the stron-ger the findings.
What axe the characteris-tics of subjects? Arc theywomen, teens,elderly? One must be careful whengeneralizing results obtained from onegroup to another group. For instance,many studies of cholesterol involvemen and women who do not know thelevels of cholesterol that pose a threatfor women. Was there a control group?Having a control group means that onegroup did not receive the treatment(drug, exercise, diet). At the end of thestudy, the group is exantined to see howit differs from the group that receivedthe experimental procedure. If the ex-perimental group differs from the con-trol group, the change maybe attributedto the procedure.
How were subjects se-lected to be in the study? The strongeststudies use a random sampling tech-nique. A good example is using one'sschool. If you only asked students inone class questions regarding drug use,would you be able to generalize or saythat this percentage of students in the
202
school uses drugs? To be able to gener-alize about the school, everyone in theschool should have an equal chance ofbeing selected to be in the study. Draw-ing names from a hat or taking everytenth name from an alphabetical listingare examples that approximate randomselections.
Has the study been re-peated? The more times the study isrepeated with sbnilar results, the stron-ger the ftndings.
Look for qualifying wordssuch as "in animals" or "in some sub-jects." Are the results reported as factsor someone's opinions? Doesthe articleinclude what needs to be examined infuture research? What questions re-main? Does the article suggest thatpeople change their behavior becauseof these results?
Broad, W. G. (1982). Science Magazines: Thesecond wave rolls in. Science, 215, 272-273.
Culliton, B. J. (1987). Science sections in U.S.newspapers increased dramatically in thepast two years. Science, 235, p.429.
Levin, L (1987). Every silver lining has a cloud:The limits of health promotion. Socialpolicy,summer, 57-60.
Miller, A.E., Sliepcevich, E. M., & Vitello, E. M.(1981). Health-related articles in the six lead-:ng women's magazines'. Content, coverageand readership profile. Health Values, 5, 257-264.
Yeaton, W. H., Smith, D., & Rogers, K. (1990).Evaluating understanding of popular pressreports of health research. Health EducationQuarterly, 17(2), 223-234.
191

TEACHING IDEAS 106
The Classics of Epidemiology:A Critical Thinking Approach
Wesley E. Hawkins
In a recent article in the NewEngland Journal of Medicine, Fra-ser (1987) suggests that the essentialcharacteristics of a liberal arts edu-cation are "those fields that helpfree students from the limitations ofprior beliefs and experiences andthat teach important modes of think-ing so as to prepare them to ask andanswer new questions" (p. 309).Fraser further argues that epidemiol-ogy is an example of a discipline thatshould bebut rarely isincludedin a liberal arts education:
Epidemiology has features thatresemble those of the tradition-al liberal arts . . . it (epidemi-ology) emphasizes methodrather than arcane knowledgeand illustrates the approachesto problems and the kinds ofthinking that a liberal educa-tion should cultivate: the scien-tific method, analogic thinking,deductive reasoning, problem-solving within constraints, andconcern for aesthetic values.(p. 30)
Given the pedagogical promise ofepidemiology in the liberal arts, itseems appropriate to suggest teach-ing methods that allow health educa-tors to use the epidemiologic model.One such application is the ClassicStudies Inquiry Simulation using ac-tual data and simulating the actual
Wesley E. Hawkins is an assistantprofessorSchool and CommunityHealth, University of Oregon, Eu-gene, OR 97403.
1 92
11-)41. 44iy4fisi
events of classic epidemiologic stud-ies. This type of teaching strategynot only teaches specific skills inepidemiology but also captures the
excitement of reliving simulated his-torical eventsa special brand ofexcitement incurred by solving themystery of disease occurrence inpopulations .
Description of Method
Many aspects of epidemiologymay be taught through the ClassicStudies Inquiry Simulation. Thistechnique will be demonstrated forteaching major research designs andmajor rates used in epidemiology.The Classic Studies and respectiveresearch designs and rates are illus-trated in Table I.
Objectives. The epidemiologicalcontent and general process/criticalthinking objectives are: given actualdata and historical simulation ofevents for selected Classic Studies,the learner will (1) select and applythe appropriate epidemiological re-search design, (2) rply and calcu-late major epidemiological rates fortesting Piypotheses, (3) determine in-formation needed to test a hypothe-sis, (4) reorganize and synthesizedata for testing a hypothesis, and (5)draw logical inferences and appro-
Tsb1e I. amok *Wks, Reward Nips, aid LiloClassic Studies
'Toxic ShockSyndrome Study
FraminghamHeart Study
Kingston/NewburgFluoridation Study
Epidemiological Research Designs RatesCase-Control/Retrospective Odds-Ratio
Longitudinal/Prospective Relative Risk
Randomized Control Trials Relative Risk/AttributableRisk
21 3

priate conclusions after testing a hy-pothesis.
Teaching Sequence. This teachingstrategy takes three to four classperiods and involves three majorsteps: (1) A background lecture isconducted describing the major re-search designs and major rates usedin epidemiology. Two class periodsare required for this step. (2) In thenext class session, the Classic Stud-ies Inquiry Simulations (Figure 1)are presented to students in a work-sheet or computer software format.Thc simulations include historicalnarrative describing the origin,events, and purpose of the ClassicStudy and actual data presentedfrom the Classic Study with required
student tasks that meet content andinquiry objectives of the lesson. (3)The final class session requires stu-dents to present inferences drawnafter testing hypotheses based ondata from the Classic Studies. Stu-dents then are required to presentthis information in an oral presenta-tion and a class discussion format.
Conclusion
Educational techniques such asshe Class Studies Inquiry Simulationare needed for teaching criticalthinking skills. John Dewey's educa-tional philosophy of emphasizing"how to think" rather than "what tothink" seems even more relevant
given the increased demands on indi-viduals for critical thinking in ourmore complex information age.
Ast. D., & Schlesinger, E. (1956). The conclu-sion of a ten-year study of water fluori-dation. American journal of Public Health,46, 265-271.
Centers for Disease Control. (1980). Annualsummary 1980: Reported morbidity andmortality in the United States. Morbidityand Mortality Weekly Report, 1977 (26), p.293.
Dawber, T., Kannel, W., & Lye 11, L. (1963).An approach to longitudinal studies inthe community: The FraminghamStudy. Annals of the New York Academy ofSciences, 107, 593-599.
Fraser, D. (1987). Epidemiology as a liberalart. New England journal of Medicine, .316(6), 309-314.
Nowt L amok Mai Inquiry SimsClassic Study #1: Toxic Shock Syndrome Study (Centers for Disease Control, 1980)
Historical Narrative. In 1980, the Centers for Disease Control (CDC) had received reports from Wisconsin and Minnesota of women who hadcontracted a mysterious illness after the start of their menstrual period. The illness included symptoms such as confusion, aggression, and shockwith very low systolic blood pressure. Physicians diagnosed this condition as an earlier identified children's disease: Toxic Shock Syndrome(TSS).
As reports increased, the CDC began to investigate TSS. Their first report on TSS identified 55 cases, 52 of whom were women. Soonafterward CDC researchers conducted a quick telephone survey in which they contacted 52 womer who had suffered toxic shock syndrome andan equal number of their friends who had not. The women were questioned about their marital status. frequency of sexual intercourse,intercourse during menstruation, birth control practices, history of herpes or other vaginal infections, use of douches or sprays duringmenstruation, and use of tampons and sanitary napkins.
Student Simulation for TSS Study. You have been employed recently as an epidemiologist at CDC. You are asked to examine all the factorslisted above to determine if any are related to TSS. None of the variables show any relationship except for the factor "use of tampons or sanitarynapkins." Your data show that of the 52 women who had suffered Toxic Shock Syndrome, 40 had used tampons, while only 10 of the controls(friends who had not contracted Toxic Shock) had used tampons. What type of research design was conducted in the telephonesurvey? Test the hypothesis that use of tampons is related to TSS by calculating relative odds or odds ratio. Show calculationsof relative odds: For your homework assignment for the next class period, be prepared to discuss inferences you have drawnfrom testing the effect of tampon use on TSS. Be prepared to discuss how large the odds ratio will have to be to say that tampon use has an effecton TSS.
Classit Study #2: The Framinghant Heart Study (Dawber et al, 1963)Historical Narrative. In the 1940s, there had been much speculation by health officials on the causes of heart disease. In 1948 the U.S. Public
Health Service and researchers at the Harvard School of Public Health initiated a study in Framingham, Massachusetts to determine risk factorsrelated to heart disease.
Student Simulation.The year is 1948 and you have been employed recently by the U.S. Public Health Service as an epidemiologist to study riskfaaors related to heart disease. Your task is to follow subjects from Framingham for a ten-year period and obtain annual measures of serumcholesterol (the variable you are studying) and heart disease. You are asked to compute relative and attributable risk for your 10-year findingsthat found the incidence for heart disease for males ages 30-49 with serum cholesterol levels above 260 mg% as 186 per 100.000 while for maleswith cholesterol levels below 190 mg percent the incidence was 50 per 100,000. Test the hypothesis that serum cholesterol is a risk factor for heartdisease by calculating relative risk. Show catcuhtions. In addition, what type of research design did you just conduct? Foryour homework assignment, be prepared to discuss inferences you have drawn from testing the hypothesis that serum cholesterol affects heartdisease. Also be prepared to discuss the size of relative risk.
Classic Study #3: Kingston-Newburg Dental Fluorldation Study (Ast, 1956)Historical Narrative. A classic two-community (Kingston and Newburg. New York) experimental trial was the study of water fluoridation
designed by David Ast (Ast & Schlesinger, 1956), who first believed that fluoride had no effect on dental caries. Newburgh would serve as theexperimental community (water supplemented with fluoride to 1.1 and 1.2 parts per million (ppm). 'The non-supplemented .:ontrol community ofKingston would have its fluoride level unchanged at .1 ppm. The number of dental caries would be compared then to see if fluoride level had an ef-fect.
Student Simulation. You are an epidemiologist assisting David Ast in this dental fluoridation study. You examine preliminary results and findthat six to nine year-old children from the control community (Kingston) reported 23.1 decayed, missing, or filled (DMF) permanent teeth per 100erupted permanent teeth while children from the experimental community (Newburg) exhibited 10 DMF teeth per 100 permanent teeth. Test thehypothesis t.,at fluoride levels are related to tooth decay by calculating relative and attributable risk. Show calculations: . . Next,what type of research design was employed in this study? For the next class session, be prepared to discuss the inferences you have drawn fromtesting the hypothcsis that fluoride levels are linked to tooth decay. In addition, be prepared to discuss the size of relative risk.
2n4193

TEACHING IDEAS 107
Discipline: A Parenting DilenunaPatrick K. Tow and Warren L. Mc Nab
aC1:1-2.2446:7
411111PWWINE 2
-051
tcr
The philosophical continuum of pa-rental discipline ranges from "childabuse" on one extreme to "passive ac-ceptance of the child's unmanagable be-havior" on the other. Repercussion todisciplinary actions are both positive andnegative and affect both child and pa-rental health.
Attempting to apply specific discipli-nary measures to correct a child's un-acceptable behavior can often be a matterof trial and error. For each couple ex-periencing parenthood, there will hefrustration and aggravation as well aslove A nd delight.
Parents admittedly make mistakes intheir administration of discipline. Todaythe effectiveness of the traditional methodof corporal punishment is much in doubt.It is through this method that childrenquickly learn "might means right." Since
Patrick K. Tow is associate professor of HealthEducation, Department of Health, PhysicalEducation and Recreation, Old DominionUniversity, Norfolk, VA 23508. Warren L.M:Nab is associate professor of Health Ed-ucation, School of Health, Physical Educa-tion, Recreation and Dance, University ofNevada, Las Vegas, Las Vegas, NV 89154.
194
there are seldom any academic classesaddressing the problems of parenting,we are often left with past disciplinaryexperiences as our only legacy of suchskills.
The selection of behavioral manage-ment techniques by a parent dependson the child s overt behavior which isinterfering with parental rules or guide-lines.
Behavioral management is basically aset of procedures that, when appropri-ately applied, usually decrease undesir-able behavior and hopefully increasedesirable behavior. These parental pro-cedures require experience and practiceto be successful. Punishment is definedas administering an aversive conse-quence or withdrawing positive rein-forcement in order to reduce thepossibility of the recurrence of a task ordemonstration of a maladaptive behav-ior (Azrin & Holz, 1966).
Discipline is a state of order based uponrules and regulations. In its simplestterms, it is teaching people to followspecific rules.
There is a major difference betweenpunishment and discipline, however. Inpunishment, pain follows an act thatsomeone else disapproves of, and the
someone else usually provides the pain.With discipline, the pain is a natural andrealistic consequence of a person's be-havior. Unlike punishment, discipline israrely arbitrary; it asks that a child eval-uate his behavior and commit himself toa better course of action (Glasser, 1965).
Preventive behavioral management isthe best approach to parenting. Man-agement guidelines need to be estab-lished early and explained in detail, alongwith possible consequences as a resultof violating these guidelines.
The importance of parent-child com-munication is paramount in the preven-tion-behavior management continuum.Being able to discuss fully problems, po-tential crises, and the providing of pa-rental support, can perhaps reduce theprobability of future behavioral prob-lems.
Health problems pertaining to mentalhealth, sexuality, mood modifiers, nu-trition, and other related areas oftencenter around a poor self-concept or self-esteem. If potential parents realize theimportance of the development of theirchild's self-concept and facilitate open,two-way communication, disciplinetechniques will be more easily under-stood and tolerated.
The positive or negative developmentof the child depends on the parental at-titudes, values, and discipline philoso-phy which many times emulates thepositive or negative relationship they ex-perienced with their own parents.
Glasser (1965) suggests parents takethe following steps in addressing be-havioral problems:
1. Ask the child if what he/she didwas against your parental rules.
2. Ask the child to evaluate himselfas to the reason behind his/her actionsor behavior.
3. Collectively the parent(s) and childshiuld devise a plan and commitmentto do better.
4. As a parent, explain you will notaccept anything but a change in behav-ior.
5. Otherwise, specific consequencesof breaking the rules will be enforced.In following these steps, parents shouldbuild on the positive strengths of theirchildren, control emotions, and facilitatepositive communication.
The Role of Health EducationEducational methodologies which al-
low parents or prospective parents hy-pothetically to recognize potentialproblem areas, establish guidelines indisciplining children, and practice the
communication techniques which en-hance the behavioral management pro-cedure, certainly would be beneficial.Prospective parents are not prepared, nordo they realize what parental responsi-bilities encompass. Education for par-enthood segments of health educationcourses should involve a variety ofmethodologies geared toward the pre-vention, management, and communi-cation skills needed to cope with specificbehavior problems.
In professional preparation programs,health educators should provide nu-merous methodologies to students in-volving disciplinary measures. Followingis a procedure that has been successfulin providing students in health educa-tion with parental behavioral manage-ment experience.
Step 1. Identify Discipline Alternatives
Chances are that students in your classhave had first-hand experience with avariety of disciplinary measures em-ployed by their own parents. Tap intothis valuable resource at your disposal.Depend upon their past encounters tohelp shape the preliminary portion ofthe strategy by encouraging them toidentify a list of these measures.
After the brainstorming session, carryout a class tally of the number of stu-dents having experience in each of themeasures listed. This will help studentsrealize there is a commonality, thoughno absolute uniformity, in disciplinepractices among parents. It also allowsstudents the opportunity to see there aremany different and perhaps more effec-tive ways to handle disciplinary prob-lems. This list usually includes thefollowing disciplinary alternatives:
1. Corporal punishment (i.e., use ofphysical force).
2. Total loss of privileges (e.g., no TV,music, or parties).
3. Home detention (i.e, grounded athome for a period ( rime; room con-finement).
4. Fines (i.e., suspension or reducedallowance; pay a penalty).
5. p,ssignment of extra household du-ties (i.e., additional chores on top of reg-ular duties).
6. Verbal put-downs (i.e., belittle orscold).
7. Curbing of privileges (e.g., earliercurfew, restrictions).
8. Ignoring the problem (i,e., pay lit-tle or no attention to the child).No doubt there are proponents and op-ponents to one or more of these disci-plinary techniques. Part of this step
requires students to provide advantagesand disadvantages for each of the mea-sures cited.
Step 2. Examine Potential DisciplinaryProblems
After identifying specific disciplinaryalternatives, the types of problems con-fronted by new parents over the yearsshould be identified. After all, our so-ciety would like to believe its membersdesignate appropriate "punishment"tailored to the nature of the "crime"committed. Presumably the same logicwould apply to the disciplinary prob-lems created by children in a family. Thissecond step requires students to listproblems frequently encountered athome for which disciplinary measuresmay be applied. Examples of some po-tential disciplinary problems wouldprobably include:
1. Talking back or "sasing"2. Excessive TV watching3. Use of profanity4. Staying out late without checking
in5. Lying6. Shoplifting7. Fighting with peers8. Playing with matches9. Crossing streets without adult su-
pervision10. Smoking cigarettes11. Coming home drunk12. Stealing money from parents13. Crying or refusing to leave toy or
candy section of store14. Horseplay leading to property
damage15. Cheating at school16. Accepting treats from strangers17. Neglecting household chores18. Looking through pornographic
materials19. Playing hooky from school20. Running awa from home21. Eating snacks before meals22. Drunk while driving23. Crying or refusing to visit doctor's
or dentist's office24. Smoking marijuana25. Repeat traffic law offender26. Premarital pregnancy experi-
enced by daughter or caused by son27. Violation of curfew on weekday
or weekend28. Hitting the parent in anger29. Hanging around with bad com-
pany30. Failing academically at school
As one can easily surmise from this par-tial listing of disciplinary problems, someare major concerns while others do not
need redress of any kind. Yet many prtr-ents have a way of misconstruing a wideassortment of concerns as being a per-sonal matter deserving punitive action.One also sees that some concerns canbe handled differently with a young childthan with a teenager.
Step 3. Examine Specific Circumstancesand Determine a Reasonable Course ofDisciplinary Action
This step requires students in the classto be paired off in couples simulatingtwo parents.
Ask the prospective parents to ex-amine each of the situations listed anddetermine whether it truly constitutes abonafide disciplinary problem. The par-ents are then to determine the properdisciplinary action, if any, to be appliedto each of the problems listed earlier. Itmust be stressed to these pseudo-par-ents that concurrence should exist be-tween them on the final decision. Thisexercise can also be done individually tosymbolize the single parent family.
Step 4. Evaluation and Discussion of theDisciplinary Decision
The last step of this strategy involvesconvening the class to listen collectivelyto and discuss similar or different waysthese prospective parents would har,dlesuch disciplinary problems in their ownfamilies. The opportunity to discuss thereasons for variations in approaching thesame disciplinary problems should beprovided.
SummaryThe pos:tive familial relationship can
be an extremely rewarding and enjoy-able experience. The key, perhaps, isunderstanding the magnitude of the re-sponsibility of parenthood, the prepa-ration of the predictable, and coping withthe unpredictable behavioral manage-ment difficulties that one may encounteras a parent.
Even before anticipating a pregnancy,prospective parents should evaluate theneeds and goals they hope to satisfy byhaving children. Every child should bea wanted child. In having children, par-ents should feel a sense of creative ac-complishment in guiding and helping achild grow into a well-functioning adult.The parent is the most important teacherthe child will ever have. Helping theirchildren through behavior managementin developing positive physical, mental,intellectual, and social adjustments in lifecan be a wonderfully rewarding expe-
195

rience for parents. Even the best parentsmake mistakes, but with proper knowl-edge, planning, and discipline experi-ence, they can overcome many of thedifficulties of child-rearing. Good par-ents will evaluate the discipline situationand respect the child as an individual,satisfy the psychological and behavioralneeds of the child, and provide the childwith emotional security, sympathy, andunderstanding.
In the majority of school systems, par-enting and behavioral management skillsare not included in the health curricu-lum. There is a definite need for cog-nitive and effective teachings regarding
the behavioral management of children.The objective is tl provide as many rel-evant and reali: experiences as pos-sible to inform students, as potentialparents, of the responsibilities in pre-paring for parenthood.
There is a need to dispel the unreal-istic notion that as future parents theywill rear perfectly obedient children.Disciplinary measures come in manytormsheld it disdain by some andstrongly endorsed by others. Effectiveexpedmental behavioral managementtechniques encourage effective parent-child communication skills through lis-tening, critical thinking, and assertive-ness.
Health programs which include pa-rental discipline techniques can provideassistance to young people to preparefor parenthood, reduce certain predict-able health problems, and hopefully en-hance the overall health of the child andparent in the process.
Azrin, N. H., & Holz, 0. C. (1966). Punish-ment, in W. K. Honig (ed). Operant be-havior areas of research and application. NewYork: Appleton-Century-Crofts.
Glasser, W. (1965). Reality therapy. New York:Harper & Row.
UI
196
BEST CCFY AMIABLE 2( 7

TEACHING IDEAS 108
Counterbalancing Parental Concernsin Health Education
Lorraine G. DavisShirley Holder Hazlett
Across all parts of the United States,comprehensive health education pro-grams have been implemented, devel-oped, discussed, or at least considered.Because the primary purpose of schoolhealth education is to reinforce healthattitudes and practices being taught inthe home, full support from parents andcommunity members is always a goal ofhealth education coordinators and cur-riculum specialists.
Parental support is dynamic and on-going; ways of obtaining the desiredsupport should be considered. The fol-lowing statements may serve to estab-lish support for the school's role inassisting with the development or re-sponsible health attitudes and behaviorsin children.
1. The first five years of life are the mostcritical with regard to the development ofproper attitudes and behaviors.
During the early years, the family unitserves as the basic reference group fromwhich a child's attitudes and behaviorsare formed (Glover, 1978, March). Pa-rental love, warmth, and caring supportace the foundation for future decision-making (Gordon, 1981, April). Earlyconcepts become rather permanent.During these crucial development years,the public school has not yet enteredinto a position of influence.
Lorraine G. Davis is an associate professorof health in the Department of Health Edu-cation, University of Oregon, Eugene, OR97403. Shirley Holder Hazlett is project di-rector of the School Health Program, Cali-fornia State Department of Education, 721Capitol Mall, .3rd Floor, Sacramento,CA 95814.
2. Families with established regularpatterns of interactions have the highestrate of transfer of attitudes, values, andbehaviors.
Familial beliefs are transferred to chil-dren through a process of imitation ormodeling (Glover, 1978, March). As aresult of verbal and nonverbal interac-tions, the child emulates attitude andbehavior patterns of the parents (Lion-tos & Liontos, 1981, October 11). Parentswho take an active role in communicat-ing with their children are more effectivein the transferring of traits. The criticismof a child's family practices is not underscrutiny. Rather, the important of fam-ilial interaction is emphasized as theprimary determinant of character devel-opment.
3. The bond between parent and child isthe strongest of bonds; it will survivebutthe child needs freedom to explore newdirections. Parents need to provide adviceand support during this process.
Fortified with familiar guidance, thechild must interact with society. He orshe must exercise and expand the skillof responsible decision-making. Feel-ings of capability and self-worth mustbe carefully nurtured. Parents serve aprimary role (Gordon, 1981, April) in thiseffort, but support makes the processcomplete. The reinforcement of self-es-teem and personal worth provide con-sistency needed for the child's optimalmoral and social development.
4. Neither reading about it nor wishing forit gives a person a skill; skills ale acquiredthrough practice.
The child learns responsible decision-making by practicing it at home and atschool. Parents teach concepts such ashonesty, fairness, and self-respect whichare reinforced in the school setting. Thes?concepts contribute to the developmentof a lifelong skill of responsible decision-
2OR
making (Musom, 1979, February). De-cision-making must be learned, applied,and the results continuously evaluated.Health education has a goal to assist inthe provision of such skills.
5. Telling a child about something doesnot guarantee participation. Not telling achild about something does not mean helshewon't participate.
If children are to become adults whomake responsible decisions about areassuch as drug usage and sexuality, theymust be knowledgeable and informed.The less a young person knows aboutsex, the earlier he/she is likely to engagein sexual activity (Gordon, 1981, April).Adolescents informed about sexuality aremore likely to delay sexual relations(Liontos, 1981).
Knoln ledge in and of itself, void of anunderstanding of consequences of ap-;ication, is not enough. The informa-,tion combined with an examination ofshort- and long-term consequences ofbehavior is crucial in the decision-mak-ing process. Responsible decision- mak-ing is included in comprehensive healtheducation.
6. individuals who feel good aboutthemselves aren't as vulnerable forexploitation and are less likely to exploitothers (Gordon, 1981, April).
Self-esteem provides an essential mo-tivational component in responsible de-cision-making. Children who feel goodabout themselves are not as easily vic-timized as people who feel inferior.Women who have self-worth are morelikely to resist sexual advances (Kirby &Alter, 1980, November) and less likelyto promote undesirable situations. In-dividuals who are loved and know it areless likely to participate in behaviorssolely as attention-getting mechanisms.The home and school can combine ef-forts to enhance necessary feelings ofself-worth.
197

7. Parents should charge the school withexposing children to the widest range ofviews possible, for their decisions will bemade iq an increasingly complex world.Ignorance will not make decisionssimpleronly more dangerous.
Tomorrow's adults must adapt to aworld fraught with obsolescence of skillsand continuous expansion and revisionof information (Thomas, 1978, Septem-ber). Children cannot merely be armedwith nutrition facts of the '80s for thecurrent "truths" may be revised in the'90s. Parents and schools must assistchildren in learning to assess accuratelyand cope constructively with change.Basic survival skills in an ever-changingsociety include the ability to continue tomake responsible decisions in light ofnew insights.
198
8. Education is aimed at teaching peoplehow to think and decide, not what to thinkand decide.
School health education enforces pos-itive health behaviors developed early inlife. Enhancement of a capacity for re-sponsible moral reasoning rather thanthe inculcation of a specific set of valuesis the goal (Musun, 1979, February). Theabove considerations are neither rigid norexhaustive. Their purpose is to maintainan avenue of communication betweenconcerned parents and health educa-tors. An understanding of the conceptsthe statements represent may help to al-leviate some of the fears about the roleof the school in preparing people for life,particularly in tLose areas sometimesthought to be in the sole educational do-main of the home. The interchange ofideas related to these thoughts may fa-cilitate support for health education andassist families and schools in preparingchildren for the future.
2o
Glover, A. D. (1978, March). Modeling--apowerful change agent. The fourna, ofSchool Health, 48: 175-176.
Gordon, S. (1981, April). The case for a moralsex education in the schools. The icurnalof School Health, 51: 214-218.
Liontos, L. B., & Liontos, D. (1981, October11). Discussion helps ease sex educationhangups. Eugene Register-Guard.
Muson, H. (1979, February). Moral think-ingcan it be taught? Psychology Today,12: 48-68, 92.
Kirby, D., & Alter, T. (1980, November). Theexperts rate important features and out-comes of sex education programs. Thelournal of School Health, 50: 497-502.
Thomas, M. (1978, September). Back tobasicsdo we want to go? The Journal ofSchool Health, 48: 446.

TEACHING IDEAS 109
Incorporating Health Education CompetenciesInto a Content Course:
The Disease Guidebook ProjectJoanna Hayden
With competencies necessary forpractice as a health educator identi-fied (National Task Force, 1985), it isthe responsibility of those in profes-sional preparation programs to pro-vide experiences for students that willenable them to acquire these skills.Courses focusing on program plan-ning, teaching, or research methods,by their very nature, provide theseexperiences. However, even a coursesuch as human disease, which is con-tent heavy, can incorporate activitiesthat encourage acquisition of compe-tencies.
The Disease Guide Book is a projectthat incorporates health education con-petencies into a content course. Com-petencies addressed through this proj-ect include: utilization of computer-ized sources of health related infor-mation, matching an information needwith an appropriate retrieval system,accessing principle online and otherdate based health information, andappiying various processes in acquisi-tion of resource materials (NationalTask Force, 1985).
The initial step in the Disease GuideBook Project is student selection of
Joanna Hayden is with William Pater-son Colley in the Depcatment of HealthSciences, Ware, N1 07470.
disease topics. All topics to be coveredduring the semester are written onindividual pieces of paper, folded, andplaced in a bag. Each student in turnpicks a topic out of the bag. Thisprocess precludes more than one stu-dent from chosing the same topic. Italso encourages student investigationof a disease entity that may not havebeen a personal choice.
The Disease Guide Book Projectis divided into two parts, a traditionalterm paper and a guide sheet. Theterm paper includes an introductionto the disease topic or historical infor-mation, description of the populationaffected and those at risk, etiology,signs and symptoms, diagnosis, treat-ment, and prevention strategics, cur-rent research, community resources,and bibliography. Since it is difficult tolocate textbooks that contain all theinformation, this limits, to some ex-tent, use of textbooks and encouragesinvestigation into periodic literatureand various methods of data retrieval.Investigation of reference sources otherthan textbooks is encouraged furtherby requiring that references be cur-rent, no more than five years old.
To assist students in acquiringcompetencies needtrl for retrieval ofcurrent periodic literature, an intro-duction to library resources is sched-uled. This dass session is conducte i inthe library by a reference librarian. Itindudes instruction on the use of on-line databases as well as paper indexesand other health related resources.Use of indexes specific to the healthprofessions is emphasized since stu-dents tend to use the more general in-dexes.
The second part of the DiseaseGuide Book Project is a guide sheet.This is a one to two page summary ofsome of the information presented inthe term paper. The guidc sheetseventually will be compiled to formthe Disease Guide Book. The guidesheets include: defmition of the topic,population at risk, etiology, signs andsymptoms, diagnosis, treatment, riskfactors, and community resources withaddresses and telephone numbers(Figure 1). For consistency, the guidesheet is set up in the same manner byall students. It is required that stu-dents contact local, state, and nationalorganizations and agencies related totheir topic in order to request printmaterials. Obtaining materials in suf-ficient quantity for class distribution isencouraged, if materials are availableavailable free of charge.
Parts I and II of the Disease GuideBook Project are submitted togetherto the instructor for grading. Part I isgraded as a traditional term paper.Part II, the guide sheet, is correctedfor errors and omissions and returnedfor rewrite. The rewritten guide sheetand the bibliography from the termpaper tfien are returned to the in-structor. The instructor, or a studentvolunteer, compiles the guide sheetsalphabetically along with the bibliog-raphies, numbers the pages, and pre-pares a table of contents. The DiseaseGuide Book is now ready to be copiedin sufficient quantity for class distri-bution. Addition of a cover in a heav-ier gauge color paper gives a morefinished appearance. Spiral binding issuggested. 1 99

Content and length of the DiseaseGuide Book will differ each semesterbased on the number of students inthe class and topics chosen. The Dis-ease Guide Book has ranged from asfew as 28 pages covering 14 diseases toas many as 73 pages covering 35 dis-eases.
Since a substantial amount of timeis needed to correct, rewrite, compile,and copy the completed Guide Book,initial submission of materials musttake place at least six weeks prior tothe end of the semester with deadlinesstrictly adhered to. It is the instruc-tor's responsibility to correct the guidesheets quickly in order to allow suffi-cient time for rewriting and resubmis-sion. A deadline in one week for re-submission of the guide sheet is suffi-cient. If students do not meet thedeadline, their topics are omitted fromthe final Guide Book. Their grades forthe project can be reflective of this.
Although the Disease Guide Bookproject requires ongoing involvementof the instructor, student fetdback onits usefulness makes it worthwhile.Along with providing practice for dataretrieval skills, this project requiresstudents to summarize information,meet deadlines, and identify and re-quest information from communityresources. Students complete the hu-man disease course not only havinggained knowledge, but skills and auseful resource tool as well.
National Task Force on the Preparation andPractice of Health Educators. (1985). AFramework for the Development of Com-petency-Based Curricula for Entry LevelHealth Educators. New York: Author.
200
.ifeR'S MINIMDefinition/Description
Influenza is a contagious respiratory disease.
ltddence/Population at RiskThe highest incidence is seen in children between the ages of 5 to 14. Adults over 65 years ofage and those w'th chronic pulmonary and cardiac disease are more likely to be seriouslyaffected.
EtiologyInfluenza is caused by a variety of viral strains. It spreads through direct contact with infectedperson, or indicted contact through droplet infection.
Signs/SymptomsAbrupt onset of fever, muscle pains, headache, cough, chills, and weakness.
DiagnosisDiagnosis is made based on the presence of symptoms.
Treatment/PreventionBeal-est, oral hydration, and non-aspirin analgesics are used to relieve discomfort.Yearly vaccination is suggested to prevent infection in the following people:persons over 65 years of agepersons with chronic pulmonary, cardiac disease, and or metabolic diseases; children andteenagers receiving continuous aspirin therapy; residents of chronic care facilities.
Community ResourcesNational Institute of Allergy and Infectious
Diseases Office of CommunicationsBuilding 31, Roorr 7A32Bethesda, Maryland 20892(310) 496-5717
Centers for Disease Control1600 Clifton RoadAtlanta, Georgia 30329(404) 329-3311
American Lung Association--Local chapter
211

TEACHING IDEAS 110
Politics and Health
Randall R. Cottrell
During Spring term, 1988, acourse titled "Health Issues" wastaught at the University of Cincinnati:A combination of both graduate andundergraduate students enrolled inthe class which was scheduled to meetonce a week for two and one halfhours. Since it was a presidential elec-tion year and the Ohio primary wouldtake place during the term, politicsand health was one issue included inthe course. A learning activity wasdeveloped to examine presidentialcandidates' positions on a variety ofhealth issues. A description of thatlearning activity follows.
Initial objectives of the projectwere: (1) upon completion of the as-signment, students would be able toexplain each presidential candidate'sposition on selected health issues and(2) upon completion of the assign-ment, students would be able to dis-cuss how politics impact healthpolicies and decisions. Specific healthissues examined were to be selectedby students and answers were to beobtained via correspondence and/orphone conversations with eachcandidate's local or national cam-paign headquarters.
Procedures
On the first night of class, studentswere divided into groups of three andeach group was randomly assigned apresidential candidate, one who wasstill in the primary race, to research.All groups were given addresses and
Randall R. Cottrell is an associateprofessor in Health and NutritionSciences at the University of Cincin-nati, Cincinnati, OH 45221.
phone numbers for their candidate'slocal (if available) and national cam-paign headquarters. This informationhad been z7otained by the instructorprior to class from the local chapter ofThe Loague of Women Voters. Toidentify health issues on which toquestion candidates, a modifiednominal group process method wasused and involved questioning stu-dents about what they considered tobe the most important health issues oftoday. Votes were used to establishthe ten highest priority issues. Adescription of this technique can befound in the book Community HealthPlanning (Green et al., 1980).
The process of identifying issueswas in itself a valuable learning ac-tivity. Students were forced first toidentify issues, then to prioritize them.In addition they were not only lookingat issues from a health perspective,but also from a political perspective.Some of the issues identified involvedAIDS funding, abortion, family plan-ning, programs for the elderly, and ac-cess to health care.
All groups were told to obtain themost detailed information availableregarding their candidate's positionon each issue. Students were en-couraged to start this project im-mediately and to be persistent since itmight take several weeks andrepeated attempts to obtain the infor-mation. To help keep students ontask, the instructor obtained weeklyverbal progress reports on effortsgroups had made to obtain informa-tion and how successful they hadbeen. Five weeks were allotted for in-formation gathering the minimumtime period to use for this assignment.Even with the five week time frame, a
212
couple of students did not receive allthe information needed until the dayreports were due.
Student Reports and InformationProcessing
Each group was required toprepare and submit a written reportof information obtained. In addition,they were required to submit a diarydocumenting efforts to obtain infor-mation for the project. The diary wasto include copies of letters sent andresponses received and all phone con-versations documented with the nameof the person contacted, date, andtime. Further, each group was topresent orally their findings to the en-tire class. Compiling, processing, anddiscussing the information gatheredfrom oral presentations took onecomplete class period. Tht name ofeach candidate was placed across thetop of the blackboard and issues werelisted along the side. One issue was ex-amined at a time with each groupreporting their candidate's positionon that issue. It was stressed that stu-dents were not to "campaign" fortheir assigned candidate, but just toreport the facts. The class as a wholethen evaluated each candidate's posi-tion on each issue and assigned one offour rankings. A "+" was assignedwhen it was decided that thecandidate's position was favorabletoward the health issuu, a " " was as-signed if the candidate's position wasnot favorable toward the health issue,a "G" was assigned when the informa-tion available was so general that anevaluation could not be made, and a"?" was assigned when no informationcould be obtained regarding that
201

candidate's position on the healthissue in question.
Results
Overall, the anking systemrevealed many more "0" and "?"ratings than " + " or " " ratings. Ingeneral, most students were disap-pointed in the quality of the answersthey were able to obtain and theamount of effort it took to get the in-formation. Local campaign officeswere able to supply literature, butstaff members and volunteers werenot able to answer specific questions.Calling national campaign head-quarters revealed a general willing-ness to send literature, but once againlittle specific information regardinghealth issues. Two groups were told bynational campaign headquarters tosend the specific questions and theywould respond in wrking. In one caseno response was received, and in theother case the same general campaignliterature was sent a second time.
So in light of the quality of infor-mation obtained, was the learning ac-
202
tivity a failure? Absolutely not! Thisactivity got stt. dents to examine thepolitics of heakh. During the discus-sion of presidertial candidates, otherimportant issues surfaced. Studentsrealized that it is difficult to obtainspecific information necessary todetermine a candidate's position onimportant health issues. Some stu-dents questioned how we asAmericans could be informed voterswhen we cannot obtain more thangeneral platitudes from our politicalcandidates. As a class we consideredhow important politics are to healthissues, how politics can affect fundingof health programs, and how healthpriorities can be altered with a changein administrations. We also discussedhow politics plays a role in the hiringof health personnel from the federallevel on down.
Recommendations
This activity was successful in get-ting students to critique the politicalprocess, to become more informed onthe presidential candidate's positions
2 13
on a variety of issues (not necessarilyhealth issues), and to examine the roleof politics in health. The followingrecommendations are made withregard to future use of this activity:
This activity was developed foruse in a course designedprimarily for health educationmajors, but it might also be of in-terest in basic personal, com-munity, or public health classes.This activity should be tried withmature junior and senior levelhigh school students. Since theactivity has implications relatedto our political system, citizen-ship, and becoming an informedvoter, the activity could be usedas a joint health/politicalscience project.The activity should be tried withother political campaigns. Itmight be easier to obtain infor-mation from candidates in-volved in local or regional races.
Green, L. W., Kreuter, M. W., Deeds, S. G.,& Partridge, K. B. (1980). Health educationplanning: a diagnostic approach. Palo Alto,
CA: Mayfield Publishing Company.

Focus on Content
214

TEACHING IDE: iS 111
Addiction
Inoculating StudentsAgainst Using Smokeless Tobacco
Melody Powers Noland and Richard S. Riggs
According to a recent report bythe Surgeon General of the UnitedStates, use of smokeless tobacco hasincreased dramatically over the past10 years (Department of Health andHuman Services, 1986). Researchersjust now are beginning to investigateapproaches that might be most -ffec-
Melody Powers Noland and Richard S.Rigs are associate professors of healtheducation in the Health, PhysicalEducation and Recreation Departmentat the University of Kentucky, Lexi-ngton, KY 40506-0219.
,APAi,
,
,1,--' 411
tive in preventing use of smokelesstobacco. A number of approaches,however, have been shown to be effec-tive in prevention of smoking be-haviors. Effective approaches in-clude:
Emphasis on immediatephysiological effects (such as in-creased heart rate and bloodpressure) (Evans et a)., 1978)Use of peer models to deliverinterventions (Evans et a).,1978; McAlister, Perry, & Mac-coby, 1979; Hurd et al., 1980;Seffrin & Bailey, 1985)Solicitation of public commit-ment not to smoke (McAlister
2 1 5
4
JILL_
Photo: lint Kirby
et aL, 1979; Seffrin & Bailey,1985)Development of social skillsneeded to resist the temptationto begin smokirig. This has beenreferred to as "inoculation,""immunization," and "resis-tance training" (Evans, 1984).
"Inoculation" has been used insmoking and alcohol prevention(Evans et al, 1978; McAlister et a).,1979; Hurd et aL, 1980; Evans, 1984;Duryea, 1984.) This approach ex-poses young people to persuasive ar-guments or threatening messages touse alcohol or to smoke that they arelikely to encounter in the future. By
205

familiarizing students with the argu-ments before they actually hear themin life situations, students are betterable to resist use of substances such astobacco or alcohol. The name "in-oculation" comes from the concept ofinoculating individuals with "germs"(social pressure to use substances) inorder to facilitate development of"antibodies" (skills for resisting pres-sure to adopt unhealthy behaviors)(McAlister et al., 1979).
A brief explanation of conceptsinvolved in understanding the in-oculation method may be necessaryfor students. Once the framework ofthe method has been learned, applica-tion to other content areas such assexuality, consumer issues, nutrition,and other substance abuse areas ismore efficient. Since the inoculationapproach has been used effectively insmoking and alcohol use prevention,it is appealing that the same approachalso might be effective when used withsmokeless tobacco.
The subsequent teaching techni-que outlines a method which is in-tended to develop skills among juniorand senior high school youth to resistpreuure to use smokeless tobacco.This method would be introducedsubsequent to class instruction on ef-fects of smokeless and smoking tobac-co. In this method, students are learn-ing content of persuasive arguments,practicing refutations to persuasivearguments, and receiving feedback onresponses. We recommend thismethod's use as a component of amore comprehensive program that in-corporates other effective ap-proaches previously discussed (i.e.,emphasizing immediate physiologicaleffects, peer models to deliver inter-ventions, and solicitation of publiccommitments).
This method has been used suc-cessfully in a junior high school classby a peer educator that we trained.The peer educator received themethod as detailed below, reviewedthe method with us, and spent per-sonal time reviewing materials.Evaluations of the method hidicatethat it was effective in meeting thelesson's objective. The classroomteacher or a trained peer educator canteach this method in one class session.
206
Student Objective
The student will deliver effectiveverbal counterarguments to specificpeer statements that encourage use ofsmokeless tobacco.
Method
The teacher or a trained peereducator will divide the class intogroups of four or five, making surethere are a few males in each group.Groups will be instructed to select oneperson in each group whom they willtry hypothetically to talk into usingsmokeless tobacco. The person fromeach group is told what studentsremaining in the room will be doing,then asked to step outside in the hall.Small groups will brainstorm andwrite down eight to 10 comments theywould make to the student to try totalk him into using smokeless tobacco.Those students who are out in the hallwill be asked to return to the room andrejoin their groups. The groups thenwill proceed to try to talk their studentinto using smokeless tobacco.
Individuals within each groupbegin stating their persuasions for thestudent to try smokeless tobacco, thenhe or she responds to each comment.Allow this process to continue for afew minutes (approximately five to10), then stop the activity. Ask some-one from each group to read a per-suasive argument used to persuadethe student to try smokeless tobacco.The teacher or peer educator shouldwrite arguments on the board, thenask class members what they thoughtwould be a good student response inrefusing the smokeless tobacco. Stu-dents in class will not have difficultyidentifying persuasions to use thesmokeless tobacco since these will besimilar to persuasions studentsprobably have heard from others inreal life experiences. UsuaLy studentswill not have any difficulty in com-menting on persuasions to try smoke-less tobacco.
The most important part of thelesson focuses on responses to per-suasions and not on the persuasionsthemselves. The teacher/peereducator should emphasize thatcriteria for an effective response
should be (1) that the response dis-putes the accuracy of the argument'smain point or (2) whether theresponse indicates that the main pointof the argument was irrelevant to thecentral issue. These criteria should bedescribed to class members, thenclass members helped to select ordevise effective responses for variouspersuasions they have used or heardused. Write at least six or seven ofthese on the board and include boththe persuasion and a counterargu-ment that meets at least one of thecriteria identified above. If studentshave a notebook or take notes, askthem to write both the persuasive ar-gument and the effective counterar-gument in their notes.
Figure 1 shows examples of pos-sible persuasive arguments that peersmight use to convince someone to usesmokeless tobacco and suggestionsfor effective counterargumentresponses. There may be other equal-ly effective counterarguments. Ex-amples are offered as a beginningpoint for this instructional strategy.
Duryea, E. J. (1984). An application of inoc-ulation theory to preventive alcohol ed-ucation. Health Education 15(1), 4-7.
Evans, R. I. (1978). A social inoculation strat-egy to deter smoking in adolescents. InJ. D. Matarazzo, J. A. Herd, N. E. Miller& S. H. Weiss, (Eds.), Behavioral health: Ahandbook of health enhancement and diseaseprevention. New York: John Wiley, 765-774.
Evans, R. I., Rozelle, R. M., Mittelmark,M. B., Hansen, W. B., Bane, A. L. &Havis, J. (1978). Determining the onset ofsmoking in children: Knowledge of im-mediate physiological effects and copingwith peer pressure, media pressure andparent modeling. Journal of Applied SocialPsychology, 8(2), 126-135.
Hurd, P. D., Johnson, C. A., Pechacek, T.,Bast, L. P., Jacobs, D. R. & Luepker,R. V. (1980). Prevention of cigarettesmoking in seventh firade students. Jour-nal of Behavioral Medicine, 3(1), 15-28.
McAlister, A. L., Perry, C. & Maccoby, N.(1979). Adolescent smoking: Onset andprevention. Pediatrics, 63(4), 15-28.
National Institutes of Health. (1986). Thehealth consequences of using smokeless tobac-co. (DHHS Publication No. 86-2874). Be-thesda, MD: U.S. Government PrintingOffice,
Seffrin, J. R. & Bailey, W. J. (1985). Ap-proaches tc adolescents smoking cessa-tion and education. Special services in theschools, 1(3), 25-38.

It. 1
Persuasion:Response:
"It's not as bad for you as smoking."It's really hard to compare smoking with the use of smokeless tobacco. Bothproducts contain nicotine which is bad for your heart and both containcancer-causing agents. Smokeless tobacco increases your risk for mouthcancer and cigarettes increase your risk for lung cancer. If you can getcancer from both products, neither one is safe.
Persuasion: "All the guys are doing it."Response: That's not true. Only about 16 percent of males between the ages of 12 and
25 use smokeless tobacco.Persuasion: "It's coolit makes you look tough."Response: I don't see anything tough or cool looking about having that dirty stuff all
over your teeth. Tobacco has nothing to do with being cool. Anyway, if Ihave to do that to be cool, 1 would rather not be cool.
Persuasion: "All the coaches and athletes chew or dip."Response: All coaches and athletes do not chew or dip. While coaches and athletes
may use smokeless tobacco more than others, the majority of them do notuse it.
Persuasion: "It doesn't smell bad like cigarette smoke."Response: Maybe you need to smell your own breath to see how bad it smells.Persuasion: "It gives you a buzz."Response: From what I have heard, it does give you a buzz (high), but that doesn't
last very long and then you find yourself wanting another buzz, so you usemore tobacco. The result over time could be a drug dependency on tobacco.I'd rather be drug free.
Persuasion: "It helps you relax."Response: Smokeless tobacco contains nicotine which is a stimulant. Stimulants speed
up the heart rate and can increase your blood pressure. I don't call thatrelaxing.
Persuasion: "You are a chicken if you don't try it."Response: I really would be a chicken if I tried it just because you told me to. I think it
is smart not to use tobacco.Persuasion: "Plenty of people have used it for years without having any problems."Response: Not all people who use snuff or chewing tobacco have health problems, but
using smokeless tobacco increases your chances for having a number of'lealth problems such as mouth cancers and gum diseases. I'd rather notake a chance.
Persuasion: "My grandmother uses snuff. You mean you're afraid to use somethingthat doesn't bother my grandmother."
Response: Jus, ecause your grandmother uses it doesn't make it safe or right. Thatwas your grandmother's choice and not mine. I want to choose for myselfand I choose not to try smokeless tobacco.
Persuasion: "Chewing and dipping are not habit-forming like smoking cigarettes."Response: That's not true. Smokeless tabacco contains nicotine, and you can become
dependent on nicotine. Just ask people who use tobacco regularly how hardit is to for them to stop.
217 207
TEACHING IDEAS 112
AddictionThe 12 Puffs of Christmas
Warren McNab
glade Levet: 7-12
Time Frame: 30 minutes
Materials: Transparencies, overheadprojector, and a marking pen
Preparation and Implementation: Ciga-rette smoking is the largest single pre-ventable cause of illness and prematuredeath in the United States. A smoker'srisk of death is much greater because ofthe direct relationship smoking has tocoronary disease, lung cancer, emphy-sema, and chronic bronchitis.
There are many mental, social, andphysical reasons for not Rmoking. Animportant concept to emphasize to stu-dents is that they always have a c hoice asto whether to begin t a smoke (or continueto smoke).
One creative method to help youngpeople cc .nprehend and remember pre-viously identified reasons for notsmoking is to combine these reasonswith the melody of "The Twelve Days ofChristmas" song. Upon completion ofthe unit on smoking, the class is brokeninto groups of five and instructed tobrainstorm at least 12 reasons why people
Warren McNab is professor of healtheducation, School of Health, PhysicalEducation, and Recreation, Universityof Nevada, Las Vegas, NV 89154.
208
should not smoke. Students can use c lassnotes and their textbook if they cannotrecall enough mental, social, or physicalreasons for not smoking.
The groups of students are thenasked to combine these hazards/reasonswith "The Twelve Days of Christmas"melody. The first sentence should begin,"On the first day of Christmas, mycigarettes gave to me"followed byone of the reasons they identified for notsmoking "T"'^ rocedure is followed forthe 12 days..... 1its can be creative andput the reasons in any order.
The fifth reason listed should bespelled out phonetically, to indicate thispart of the song is emphasized differentlyand sung like "five golden rings" in theoriginal song. Groups can also createtheir own title for their version.
Each group then puts its list on atransparency, which is eventually pro-jected onto a screen. The class collec-tively sings the 12 reasons given in thesongs the groups have written, or certainselected songs may he sung if time isI im ited.
An alternative to this method is tohave the class brainstorm reasons not tosmoke, and a recorder writes the reasonsgiven on the board. Class members thenselect the 12 they would like to use aslyrics to "The Twelve Days of Christ-mas."
The following is an example of thiscompleted task:
215
The Twelve Puffsof Christmas
On the first day of Christmas, my
cigarettes gave to me
A whole lot of agony
2nd day - Lots of stinky clothes
3rd day - Yellow teeth and fingers
4th day - Two lungs with cancer
5th day - Leu Ko Pla Kia
6th day - Ashtray-tasting kisses
7th day - Stressful nonstop air flights
8th day - Chronic emphysema
9th day - Coughing family members
19th day - Richer thoracic surgeons
llth day - Terminal carcinoma
12th day - Mourners singing softly
This activity provides an avenue toreview material through group partici-pation that emphasizes the negative as-pects of smoking and reinforces thepositive reasons one shouid not begin tosmoke. Discussions on how to verballysay no to people offering cigarettes mayfollow this activity.

TEACHING IDEAS 113Addiction
Drive-A-TeenA Program to PreventDrinking and Driving
Susan Willey Spa lttr
Drive-A-Teen would never haveevolved had it not been for a group ofdedicated and competent high schoolstudents who welo willing to devote agreat deal of time and energy to theprogram. Many of the student volun-teers had lost close friends in alcohol-related accidents and were anxious toparticipate in a constructive way tosolve a difficult problem. Many of themwere extremely concerned about the ex-tent of the drinking behavior in theteenage community, and they werevery much aware of their impact on theyounger students. Students also ex-pressed concern about the polarizationof friendships surrounding alcohol useand the prevalent attitude that drinkingis an essential component of a goodtime. It is significant to note that thereare some students who by age 16 or 17have substantially modified their drink-ing behavior; for them, the years ofearly adolescence involved the heaviestalcohol use.
Dkive-A-Teen activities art coordinat-ed by three school faculty members whoact as program advisors: a project &rec-tor who coordinates all aspects of theprogram, a student activities coordina-tor who is responsible for developingand implementing student activities,
Susan Willey Spa lt is health coordinaior andDrive-A-Teen Project director, ChapelHillCarrboro City Schools, Chapel Hill,NC 27514.
IMO%
and a high school guidance counselorwho acts as a liaison between studentsand Drive-A-Teen staff. The faculty ad-visors have been impressed by the ma-ture views of the students, yet con-cerned by the excessive nature of someof the alcohol related experiences theydescribed. Students who all had hadexperiences related to alcohol, drinkersand nondrinkers alike, shared a concernfor their community and a strong com-mitment to finding solutions to prob-lems caused by alcohol.
Early student activities centeredaround launching the transportation
The problem of teenage drinking anddriving is only partly reflected by avail-able statistics, namely, that 60 percentof alcohol related highway fatalities areamong young people. Alcohol-relatedaccidents are responsible for serious in-jury and permanent disability. It is wellknowr that teenagers are overrepre-sented in the number of arrests madefor driving under the influence eachyear. The problem of teenage drinkingand drivirg is exacerbated by their inex-perience with both driving and drink-ing. The problem may also be measuredby the anxiety felt by pk.rents as theyworry about their teens, waiting for thatmost dreaded of all phone calls. DI ive-A-Teen grew out of a community's an-guish following a number of tragic acci-dents and represents a community's de-termination not only to end suchaccidents but to foster responsible atti-tudes toward alcohol use.
Drive-A-Teen began with a simple
1 9
question. Could accidents be preventedif teenagers had an alternative way toget home from social events that theywould trust and use? The answer to thisquestion lead to the development of theDrive-A-Teen transportation service.The service involves the use of parents,who volunteer to drive students homewhen they are stranded, usually be-cause of their own or their friends'drinking. Drive-A-Teen calls are fieldedby the local crisis telephone hotline. Thetelephone counselors help the caller toassess the situation and to consider oth-er transportation alternatives. If neces-sary, the counselor calls the Drive-A-Teen parent volunteer to relay informa-tion about the caller. The parents pickup the students and take them home.No names are ever used.
The transportation system works toprevent accidents in several ways. First,rides are offered to teens who are unsafeto drive or whose friends are unsafe tcdrive. Second, teenagers can say to eachother, "If you don't let me drive, I'mgoing to call Drive-A-Teen." Third, thevery existence of Drive-A-Teen hasraised the consciousness of the entirecommunity. Students often refrain fromdrinking before driving. Adult volun-teers have becorm more aware of theproblems involved. The message con-veyed to students is that drinking anddriving is such a serious problem thatDrive-A-Teen is willing to do almostanything to prevent it. The service thusreinforces the existing alcohol educationcurriculum.
209

Students were involved in par-ent volunteer orientation sessions, theyhelped to develop the system by whichDrive-A-Teen phone calls are fielded bythe crisiF phone service, and they spoketo their peers, personally and throughthe media. Most important, perhaps,they demonstrated by their interest andenthusiasm that the service was neededand that it would be used.
It was their efforts that provided theinitial impetus for expanding the Drive-A-Teen program to address problems ofteenage alcohol use in other ways. Theneed to keep the student body as awhole well informed about the service,coupled with the potential benefits ofinvolving students more actively in thealcohol education program, encouragedthe staff to initiate a pilot peer educationprogram. The student peer educatorsparticipated in the training programwhich involved factual informationabout alcohol, decision-making skills,clarification of values pertaining to alco-hol, elements of group facilitation, anda discussion of problem situations com-mon to teenagers. While the scope andextent of the peer education programwas limited by time and funds, it dem-onstrated the potential of peer educa-tion to augment both the transportationservice and the existing alcohol educa-tion program. The students involvedlearned to better understand and dis-cuss their own attitudes and problems210
with alcohol. The experience of leadingdiscussion groups with slightly youngerstudents gave them a greater apprecia-tion for the problems associated withalcohol, and they had the experience ofhelping to develop a new program intheir community.
The interest Drive A-Teen has gener-ated in the community has sparked anexpansion of activities into other areasrelated to alcohol use. A committee ofstudent volunteers has organized tomeet with community officials to devel-op recreation alternatives acceptable toboth teenagers and parents. Studentsalso plan to meet with representativesfrom the district attorney's office to dis-cuss the feasibility of developing sen-tencing alternatives for young peoplearrested on alcohol-related charges.
The evaluation of Drive-A-Teen willreflect the diversity of its activities. Thetransportation service provided over100 rides during its first year of opera-tion. There is no way to accurately mea-sure how many students avoided drink-ing before driving or encouraged theirfriends to avoid drinking before drivingbecause of Drive-A-Teen; 1,owever, in-formal discussions with students, par-ents, and t: achers suggest that studentsdid in fact become more responsibleregarding drinking and driving. Thestaff will continue to gather informationconcerning relevant attitudes and be-havior through the use of question-
2 ,!
naires, interviews, and informal discus-sions. Parents and students will both beincluded. Records will also be kept forevaluation purposes on all Drive-A-Teen student committee functions. Thepeer education component will be as-sessed with pre- and posttests. Thisrather formidable task will be carriedout with assistance from the HighwaySafety Research Center, University ofNorth Carolina at Chapel Hill.
Drive-A-Teen has brought togetherpeople of different ages, backgrounds,and interests to address the problem ofdrinking and driving. Drive-A-Teen be-gan in a southeastern university townwith a total population of about 50,000and a secondary student population of2,500. It seems likely, however, that thisprogram could be adapted to fit manycommunities.
Any such programs must begin withstudents and with adults whom theytrust. It is important to involve both thestudent "partiers" and the student"leaders." The need for parent volun-teers is readily apparent. Parents mustbe willing to drive at odd hours withstudents whom they may or may notknow. They must be committed to con-fidentiality, and they must be preparedfor those times when the students maybe taking advantage of the service. Analready existing telephone service isprobably necessary. The telephonecounselors must be carefully informedabout the purpose of the service, andthey must be willing to help an oftenconfused, sometimes scared youngteenager figure out if he or she reallyneeds Drive-A-Teen.
Drive-A-Teen probably would nothave been effective without an alreadyexisting alcohol education program.Students had already been exposed tothe problems surrounding alcohol use.The active support of community lead-ers is crucial. Sound and available legaladvice is essential to provide legal pa-rameters within which volunteers canfunction and to address questions asthey arise.
It is gratifying to see many teenagers,so long considered only as part of theproblem, becoming part of the solutionas well. Teenagers and adults havefound in Drive-A-Teen a forum whereideas and problems can be openly dis-cussed. The problems of drinking anddriving are not going to be solved easilyor quickly, yet Drive-A-Teen has giventhe citizens of one community the op-portunity to take joint responsibility forproblems and to work toward a solu-tion.

TEACHING IDEAS.111Elb
114
Addiction
Analyzing Cigarette SmokeDavid M. White and Linda H. Rudisill
The results of a ten year study (1975-1984) indicate a clear relationship be-tween teenagers' perceptions of theharmfulness of cigarette smoking andtheir smoking behavior. As the percentof high school students who think ciga-rette smokers harm themselves (physi-cally or in other ways) has increasedfrom 26.8 percent to 64 percent, thepercentage reporting daily use has de-creased from 26.8 percent to 18.7 per-cent (U.S.D.H.H.S., 1985). This evi-dence supports what most health edu-ca tors have believed for yearsinstruction about health risks of smok-ing is crucial, especially in the elemen-tary and middle school grades.
The following describes a lessonabout the health risks of smoking thathas proven to be interesting and effec-tive. This lesson places the student inthe unusual position of analyzing tobac-co smoke by "sampling" some of theingredients separately. It not only em-phasizes the health risks of smoking,but also encourages the student to be amore intelligent consumer by providingan experience in product analysis.
Teachers who enjoy using "props"should like this one. Though materialsrequired may present some difficulty ifthey must be transported from room toroom, they are easily assembled andcritical to the impact of the instructionalactivity. Materials needed include thefollowing: four balloons, a small glassjar of flour, a small glass of chocolatesyrup (about one cup), and a small glassjar of clear syrup, such as Karo syrup.
The following is an example of a"script" of this lesson that has beenused with junior higl- age students. Theinstructor should adjust the vocabularyfor other age groups.
David M. White is an assistant professor ofHealth Education at East Carolina Universi-ty, Greenville, NC 27858. Linda HarrillRudisill is a teacher of health and physicaleducation at Ashley Ir. High School in Gas-tonia, NC and adjunct-professor of healthmaintenance at Gardner-Webb College inBoiling Springs, NC.
Focus
How many of you have ever receivedproducts in the mail to sample, such assoap, shampoo, or toothpaste? Themakers provide a small amount for us totry and then we decide if we want topurchase the product. Suppose wecould sample one of these products bybreaking it down and trying the mainingredients, that is, by analyzing it.(Teacher may want to discuss the mean-ing of analyze). We might know muchmore about a product if we could ana-lyze it rather than simply trying a smallsample. The purpose of this lesson is tohelp you analyze a product that is usedby millions of people in the UnitedStates. Its popularity, however, hasbeen declining for several years. (Em-phasize here that it is important not tocomment on what the product is untilinstruction is complete. Have studentswrite the name of the product on a sheetof paper when they think they haveguessed correctly.)
221
Teacher InputI will not ask you to sample these
items as I describe them. When I havecompleted the discussion, you can thendecide if you want to try them. Remem-ber, if you do not want to try it, yourgrade will not be affected.
Point to balloons
The product that we are analyzing isassociated with over 500 gases and sev-eral thousand chemicals. Since I wouldhave to go to a lot of trouble to bringyou over 500 gases, I just brought two ofthem in balloons. This balloon containssome carbon monoxide. Joe, after I de-scribe the other chemicals, would youplease inhale the gas in this balloon?This gas is odorless, colorless, and, al-though this amount should not hurtyou, this gas is deadly. When you usethis product, your blood transports fiveto ten times more carbon monoxidethan normal. This is because carbonmonoxide binds to hemoglobin about240 times more strongly than oxygendoes.
Now, Joe, I know what you are think-ing. Why should only a guy try this.Sue, I would like you to choose a bal-loon and try it, too. Remember, if youuse the average amount of this productdaily, you will lose six to eight percentof your body's oxygen carrying capaci-ty.
Point to other balloons
I have put another of the gases fromthis product in these balloons. This gasis hydrogen cyanide. Hydrogen cyanide isa gas that has been used in the gaschamber. When you use the product weare analyzing the hydrogen cyanideparalyzes your cilia (teacher may needto explain the functions of the cilia here)for 20 to 30 seconds. Now, Carl, wouldyou and Judy sample this ingredient bybreathing the gas in these balloons? I'mfairly sure that the amount I have inhere will not hurt you; however, re-member that this gas paralyzes, or
2 1 1
freezes, your cilia for 20 to 30 secondseach time you use the product.
Hold up the jar of flour
In this jar I have a little arsenic.Kathy, would you sample this for uslater? I have clean spoons for both youand Tom. Arsenic is a silvery-white,tasteless, poisonous chemical used inmaking insecticides. It looks like flourand that is what it is mixed with in thisjar. Arsenic is associated with the prod-uct we are analyzing.
Hold up glass jar (about one cup) ofchocolate syrup
In this jar I have a brown stiLky sub-stance. If you use the average amount ofthe product we're analyzing, your bodywill collect about a cup of this brown,sticky substance a year. Tom, wouldyou put your finger in this jar and thenlick your finger? Susan, I know you willhelp Tom with this.
Refer students to jar of clear syrup
This substance is a poison. It can killinstantly in its pure form, but I havemixed it so that it will not kill you. Itlooks like clear syrup, so that is what itis mixed with. This poison is habit-forming. It speeds the heart rate anextra 15 to 25 beats per minute, or asmany as 10,000 extra beats a day. Also,it constricts the blood vessels and quick-ens breathing. George, would you sam-ple this for us? Remember, a one dropinjection of this substance would causedeath! Jean, you are so cooperative inclass, and I think George would feelbetter if someone else were doing this.Another thing, when you use this prod-uct, this poison reaches your brain inonly seven seconds. If it were not forthis ingredient, people would probablynot be interested in long term use of thisproduct.
Now, are you all ready to sample afew of the ingredients in this product?Before you answer, I guess I should tellyou more. (The following list of factsmay be discussed or the teacher maywant to add others and delete somefrom this list.)
If you start using this product nowand continue, you should expect to losesix and one half years of your life.
If you use it a lot, your chances ofdying between the ages of 25 and 65 areabout twice as great as for those who donot use this product.
Over 100,000 physicians have quitusing this product.
212
Before this day is over, approxi-mately 4,500 young people will havetried or started using this product. Bythe time they graduate from highschool, half the nation's teenagers willhave used this product, 18 percent on adaily basis.
About one and one half billion ofthese products are used by 54 millionAmericans for an average of about 27each day. The substances in this prod-uct are the primary cause of 360,000known deaths a year, an average of1,000 deaths a day.
Using this product is one of thelargest self-inflic ed risks a person cantake. It is responsible for more prema-ture deaths and disability than any oth-er known agent.
More people die from using thisproduct than seven times our annualdeath toll from highway accidents.
A pregnant woman who uses thisproduct may be affecting the health ofher unborn child. Comparing userswith nonusers, users have a higher per-centage of stillbirths, a greater numberof spontaneous abortions and prema-ture births, and more of the infants die afew weeks after birth. The chi:d's long-term physical and intellectual develop-ment may be adversely affected.
This product will stain your teeth,and users often have bad breath.
You might say, "Surely a person canstop using this product whenever hewants to." My reply is "not necessari-ly." Remember the habit-forming sub-s tance we mentioned. Withdrawalsymptoms for using this drug often in-clude tension, irritability, restlessness,depression, anxiety, difficulty in con-centrating, overeating, constipation, di-arrhea, insc-nnia, and an intense crav-ing for the product.
A few things that I have not men-tioned are:
If you use this product, you are1,000 percent more likely to die fromlung cancer than those who do not useit.
You are 500 percent more likely todie of chronic bronchitis and emphyse-ma if you use it.
Average users of this product are 70percent more likely to die of coronaryartery disease. They also tend to sufferfrom more respiratory infections, suchas colds, than nonusers do.
Finally, this product is so danger-ous that four rotating warning labels arerequired by law to be on the package.
If you were sent this product in themail to sample, would you be likely to
2 -
try it? If you received a box in the mailand on the outside these facts werePrinted, would you try it?
Have students name the product.End the lesson with a statement about
the importance of making wise deci-sions which influence your life in posi-tive ways. For example, the teachermight say, "You have the power toinfluence your future in vital ways. Thechoice is up to you. No one can keep youfrom smoxing, and it definitely will af-fect your entire life, however short orlong it may be. Why start and gethooked? But, if you want to smoke, goahead, it's your life, but it's the only oneyou will ever get. The only safe cigaretteis an unlit cigarette."
U.S. Dept. of Health and Human Services:Use of Licit and Illicit Drugs by America'sHigh School Students, 1975-1984 (1985).Washington, DC: U.S. GovernmentPrinting Office. U.S. Dept. of HealthHuman Services publication no. (ADM)85-1394.

TEACHING IDEAS 115
Promoting a Natural HighCatherine J. Paskert
Ever since the mid-seventies whenthe National Institute on Drug Abusereported that informational drug educa-tion programs were often ineffective indeterring youthful substance abuse,there has been a shift to more broad-based curricula. The evidence that cog-nitive approaches were sometimescounterproductive and may have influ-enced some youngsters to experimentwith drugs signaled a need for change.Trial balloons were launched to findteaching methods better suited to drugeducation. Many educators respondedby developing and trying different tech-niques, and the literature was soonflooded with ideas. None claimed to bemagic bullets, but affective approachesand especially valuing activities wereregarded as having a potential for influ-encing young people to adopt a drugfree lifestyle. Consequently, drug edu-cation programs today are mostly multi-dimensional. Important cognitive fea-tures such as basic information aboutalcohol and drugs remain, but there isan overall greater emphasis on a widevariety of affective and experientiallearning activities which aim to helpstudents develop coping skills that haveapplication to everyday living.
One of the most effective and endur-ing valuing strategies is the "Love List"or "Twenty Things That You Love ToDo" (Simon, Howe and Kirschenbaurn,1972). This learning activity, "FeelingGood," is a variation of the "Love List"and is based on the theory that peoplehave an innate need to temporarily alterconsciousness or "get high" wh:ch theywill satisfy chemically if they fail toachieve it in more natural ways, e.g.,sports, movies, music, dance, travel,art. This activity also recognizes thatdrugs are used and abused for manyreasons, but the desire to feel good orget high is what actually may be at the
Catherine I. Paskert is an associate professorin the Department of Health Professions atMontclair State College, Upper Montclair,NJ 07043.
Addiction
imorid
NIiiNV Ny 1 N N N)
3,
213
LZsi copy AMBLE 2 23

root of drug taking (Weil, 1972; Weiland Rosen, 1983).
The purpose of "Feeling Good" istwo-fold. It aims to demonstrate thatalcohol and other drugs are used andabused for a variety of reasons and thatthe very pleasures which are often at-tributed to chemical highs can beachieved naturally; that is to say,through health-promoting activities."Feeling Good" helps students arrive atthe important conclusion that the plea-sures which drug users associate withtheir chemicals of choice are also experi-enced by people engaged in legal orsocially sanctioned activities. This is anappropriate activity for students in jun-ior high school through college and alsois suited for use with educators, par-ents, and community groups concernedwith the prevention of youthful sub-stance abuse.
Description1. Ask students to list five or more of
their favorite things to do. Make itclear that this is their private listand that they will not be requiredto share its contents.
2. Instruct students to match eachactivity on their list with an adjec-tive that best describes their feel-ings during or after participating inthe activity.
3. Compile a listing of adjectives onthe chalkboard. To expedite theprocess and increase student in-volvement, ask several students tocome to the chalkboard and alter-nate taking turns recording adjec-tives when volunteered by class-mates. When all adjectives includ-ing their own have been noted onthe chalkboard, instruct recordersto sit down.
4. Ask students if any activity ontheir list of favorite things to do isillegal or socially unacceptable. Ifso, ask if they will share only theword that is paired with the illegalactivity and circle adjectives thatan, so identified.
5. Clarity at this point is especiallyimportant. The teacher might be-gin by saying, "these adjectives,with possibly a few exceptions (cir-cled words) describe how you sayyou feel when engaged in yourfavorite socially acceptable activi-ties. Think about this: do thesewords, including those circled,also describe how persons usingdrugs might possibly say theyfeel?" "Do some, most, or all ofthem apply?" "Could you elimi-
21 4
nate any of these adjectives?" :Jote:Some students will recognize thatthe pleasurable physical and psy-chological effects derived from par-ticipation in legal or socially sanc-tioned activities are not unlike thepleasure seeking effects often asso-ciated with substance abuse. Theinitial reaction of others may bethat surely none or very few of theadjectives are related to drug use.When such variations in studentresponses occur, and they oftendo, it may be partly a function ofexperience. Tessler (1980) reportsthat there are important differ-ences in the opinions of junior andsenior high school drug users andnonusers about why kids usedrugs. The nonuser groups in theTessler study identified peer pres-sure and escape as important moti-vating factors, whereas the usergroups discounted the influence ofthese and a third factorexperi-mentation. The majority of users(53.47 percent) claimed that "feel-ing good" was th principal reasonfor using drugs.
6. Continue by asking students whythey think people do drugs. Askthem to identify reasons that aretypically given to explain drug tak-ing and list the responses on thechalkboard. Among the factorsthat will likely be suggested are:peer pressure, curiosity, availabil-ity, to escape, cope, rebel, and gethigh.
7 Conclude by discussing the ideathat although people take drugsfor a variety of reasons, gettinghigh is a key factor, and for manythis may be the most critical ele-ment. At this point a case can bemade for getting turned on tosomething else 11-at is fun but,unlike drugs, is Tt iter physicallynor psychologically damaging. Or,put another way, doesn't hurt somuch and in so many ways, i.e.,shattered personal relationships,poor grades, declining health, andpossible drug charges. Most of thereported benefits of drug use canbe achieved in more accepted andnatural ways. Remind studentsthat this was illustrated by the factthat virtually all the adjectiveswhich they used to describe feel-ings associated with socially ac-cepted activities were also descrip-tive of drug taking. Doing drugs is,dernonstratably, not the only gamein town.
DiscussionThe groundwork for acceptance of
recreational drug use was set in the1960s at a time when drug taking wasfrequently a political statement. Druguse today is more casual. Among ado-lescents in particular it is often viewedin the same context as going to a movieor an athletic event, and its social ac-ceptability at parties is widespread.Moreover, the problem is both complexand deeply rooted; young people con-tinue to use and abuse drugs in unprec-edented numbers.
Educational approaches that appealto the thrill and glamour of life on anatural high, instead of scare tactics,can be effective vehicles for reachingyoung people at all levels of drug expe-rience. Most student populations in-clude some youths who are drug freeand determined to keep it that way,many who are undecided, and otherswho will use/abuse drugs no matterwhat. This learning activity can provideimportant and much needed reinforce-ment for those who are drug free as wellas those who are undecided, and couldalso be instructive to the drug users bysending the message that "feelinggood" is not an exclusive feature ofdrug taking. All young people need tobe reminded that, yes, there are alterna-tives to drinking and drugging, andthese natural high alternatives appear tobe gaining momentum. This is evi-denced by the occasional media cover-age of school community sponsoredevents such as mini-marathons whichencourage student participation withslogans that exhort, "don't get high ondrugs, get a natural high."
There is widespread agreement thatgetting turned on to themselves is thesingle most important high for youngpeople today; it is prerequisite to a drugfree lifestyle, one that is focused o.;achieving pleasure via natural ratherthan chemical means. The challenge isclear: we must convince them that "do-ing drugs" is neither the best nor theonly ticket to "feeling good."Simon, S. B., Howe, L. W. & Kirchenbaum,
H. (1972). Values clarification (a handbookfor teachers and students). New York: HartPublishing Company, Inc.
Tessler, D. J. (1980). Drugs, kids and schools.Santa Monica: Goodyear PublishingCompany, Inc.
Weil, A. (1972). l"he Natural Mmd. Boston:Houghton Mifflin.
Weil, A. & Rosen, W. (1983). Chocolate tomorphine: Understanding mind-activedrugs. Boston: Houghton Mifflin Compa-ny.

TEACHING IDEAS 116
Addiction
Alcoholics Anonymous: The Utilization ofSocial Experience in the Classroom
Robert G. Yasko
Alcohol abuse is America's numberone drug problem. Nearly 105 millionAmericans (18 years of age and older)are considered to be drinkers, i.e., theyhave had at least one drink of beveragealcohol during the past year (Carroll,1985). Among American high rchoolstudents, 93 percent have tried drink-ing, and 71 percent drink at least once amonth (Schlaadt & Shannon, 1986). It isestimated that there are 3.3 millionproblem drinkers among youth in the14-17 age range-19 percent of the 17million of this age group (Hafen & Brog,1983). Approximately 90 percent of col-lege students report drinking duringtheir academic career. Furthermore, it isconservatively estimated that there areat least 10 million alcoholics in the Unit-ed States (Johnson, 1980).
For five decades, Alcoholics Anony-mous (A.A.) has been working success-fully for men and women from everykind of background. Virtually all per-sons in our society have been exposedto alcoholism in some form or other,and it has caused us great consternationand confusion. Alcoholism affects everyaspect of society and it has been esti-mated that 36 million Americans areaffected by living with the alcoholic orby having close contact with one (Max-well, 1976). Beverage alcohol abuseleads to more problems for individuals,families, and society as a whole thanany other drug in the United States.
The Objective of Alcoholics4nonymous as a LearningExperience
St. Pierre and Miller (1986) encourageawareness as a priceless educationaltool for providing insights which triggercognition and synthesis of information.Alcohol educators should not be lured
Robert G. Yasko is an instructor in healtheducation at The Pennsylvania State Uni-versity, McKeesport Campus, McKeesport,PA 15132.
away from including awareness-raisingactivit es because of accountability ofissues.
One of the most effective learningexperiences is having students attendan "open" A.A. meeting after the factu-al knowledge of alcoholism has beenpresentedwhich must be the founda-tion of any prevention effort. This meet-ing is open to non-A.A. persons as wellas members. These meetings are themost accessible and vary in format, butusually they are of the speaker type;generally a leader and two or threespeakers who relate their storieshowit was with them, what happened, andhow it is now (Maxwell, 1984). I havefound that first-hand attendance atA.A. meetings accomplishes somethinga book can never doawareness (byseeing, hearing, and listening) of whatbecoming alcoholic is like. Thus, theobjective is not just understanding alco-holism, but awarenesswhich is an in-valuable educational experience. Fur-thermore, A.A. is one of the most effec-ti v e methods of attaining andmaintaining sobriety and this programnot only is helpful to the alcoholic, butcan also be an excellent program forpersonality development of all persons,alcoholic or nonalcoholic, drinkers ornondrinkers (Twerski, 1984).
Implementation of AlcoholicsAnonymous in the Classroom
Throughout the United States andCanada, A.A. is found in most townsand cities. A.A. can be located throughthe local telephone directory, newspa-per office, police stations, hospitals, orby contacting local priests or ministers.At the beginning of the semester, stu-dents are provided with a course sylla-bus outlining evaluation procedures.During the same class period, the A.A.project assignment is given. The assign-ment is discussed in detail. Each stu-dent will submit a written critique of hisor her experience two weeks prior to theend of the semester in order to allow
time for grading. A special case occurswhen students cannot complete theA.A. project for reasons beyond theircontrol. The instructor usually is willingto renegotiate the project with a differ-ent activity (e.g., article critique or filmreview).
The following guidelines are dis-cussed in class prior to attending A.A.:
1. Students are permitted to go insmall groups (two or three) with class-mates, friends, or relatives.
2. Students are not permitted to takeany classroom material (pencils, or pa-pers).
3. If students attend an A.A. meetingin their local community, they shouldnot be surprised to see someone therethey know.
4. The A.A. meeting is approximately60 minutes long.
5. Students may be asked by an A.A.member why they are in attendance.Their response should be: "My name is
. I am a student atand was asked to observe an 'open'A.A. meeting for a health educationclass."
6. Students also should be preparedfor a "cigarette smoke environment,"although A.A. is beginning to hold non-smoking meetings.
The instructor can add to the cogni-tive domain by asking questions thatstimulate discussion in the affective do-main. Affective instruction (which isbased on the rationale that behavior ispersonal) can assist individuals to ac-knowledge control over and responsi-bility for their own behavior. As a re-sult, attitudes about beverage alcoholare identified, discussed, modified, andconformed (Dennison et al., 1980). Theinstructor can utilize the following ques-tions to stimulate discussion in the af-fective domain when the written cri-tique is dule in class:
1. What were your thoughts beforeattending the A.A. meeting?
2. What were your thoughts duringthe A.A. meeting?
215

3. What were your thoughts whileleaving the A.A. meeting?
4. Does A.A. benefit our society?5. Explain the basic nature and opera-
tional p,ocess of A.A.6. Did you have any misconception of
what becoming alcoholic was like?7. How large was the A.A. meeting
you a ttended?8. Are there any differences between
female and male alcoholics?9. How do you now feel about drink-
ing?10. What is irresponsible and inap-
propriate beverage alcohol use?11. What characterizes responsible
and appropriate use of beverage alco-hol?
12. Would you recommend the A.A.meeting as a learning experience for afuture health class?
216
ConclusionThe author has utilized the A.A.
experience not only at the college level,but with high school teachers, coaches,nurses, as well as with adults who en-roll in a drug or alcohol awareness class.The open meetings of A.A. offer awealth of data to the interested learner.This resource has been grossly under-utilized, and valuable as learning from abook may be, it cannot compare withthe wisdom of experience. The feedbackis overwhelmingly positive, and thoughthis awareness experience is difficult toassess, the value and contribution itmakes to student growth warrants itsuse.
Carroll, C.R. (1985). Drugs in modern society.Dubuque, IA: Wm. C. Brown Publish-ers, p. 5.
ki!
.11)
I %Ir. IIIRiss.40.1114
Dennison, D., Prevet, T., & Affleck, M.(1980). Alcohol and behavior: An activatededucation approach. St. Louis: C.V. Mos-by, 77-78.
Hafen, B.Q. & Brog, M.J. (1983). Alcohol,(2nd ed.). St. Paul: West Publishing Co.p. 102.
Johnson, V. E. (198). I'll quit tomorrow: Apractical guide to alcoholism treatment. NewYork: Harper & Row Publishers, p. 1.
Maxwell, M.A. (1984). The A.A. experience: Aclose-up view for professionals. New York:McGraw-Hill Book Company, p. 9.
Maxwell, R. (1976). The booze battle. NewYork. Ballantine Books, p. 6.
Schlaadt, R.G. & Shannon, P.T. (1986).Drugs of choice: Current perspectives ondrug use (2nd ecL). Englewood Cliffs, NJ:Prentice-Hall, Inc., 146-147.
St. Pierre, R. & Miller, D.N. (1985-86). Fu-ture directions for school based alcoholeducation. Health Education, 16,(6).
Twerski, A.J. (1984). Self-discovery in recovery.Center City, MN: Hazelden EducationalMaterials.
2 J; ..7EST C MOPY A E
TEACHING IDEAS 117
"Can A Bike Run On Beer"Melvin H. Ezell, Jr .
Addiction
Each year approximately 50,000 peo-ple lose their lives on our nation's high-ways and at least 50 percent of thesedeaths involve a person under the influ-ence of alcohol (CPWT Report, 1982).Such accidents are usually attributed toa combination of physical and behavior-al impairments involving visual re-sponse and acuity, reaction time, con-centration, and overall judgment (Edlin,1982). Furthermore, as shown in Figure1, the probability of being responsiblefor ar automobile accident involving afatality increases significantly as blood-alcohol concentration increases (Per-rine, 1971).
PurposeThe purposc! of the event, "Can A
Bike Run On Beer," was to dramaticallyand objectively demonstrate the rela-tionship between blood-alcohol concen-tration and the performance of a grossmotor skill. The selected skill containedmany of the same elements involved indriving an automobile. Therefore, theparticipants and spectators were en-couraged to generalize the results whichdiscouraged driving under the influenceof alcohol,
ProcedureEight male subjects, each a moderate
to occasional drinker, were selectedfrom the Corps of Cadets of The Cita-del, The Military College of South Caro-lina, to participate in the demonstra-tion. Each subject was required to readand sign an informed consent statementwhich described the nature and pur-pose of the demonstration and indicat-ed that some risks of injury were pres-ent in the task.
The subjects were then randomly as-signed to one of two groups: Group I"The Sippers," or Group II "The Chug-gers." Each group was named for the
Melvin H. Ezell, lr. is a professor in theDepartment of Physical Education, The Cit-adel, The Military College of South Caroli-na, Charleston, SC 29409.
manner of drinking employed. The sub-jects next selected a bicycle and wereencouraged to practice riding throughthe test course. The test course itselfwas approximately two hundred yardsin length laid out on a smooth grasssurface, free of obstacles, and reason-ably safe (Figure 2).
Once subjects felt comfortable withthe task, they were required to traversethe course until each one attained base-line scores of at least ninety. Scoreswere determined by subtracting fivepoints for each error, defined as touch-ing either boundary line with the frontwheel, from an arbitrary perfect score ofone hundred.
Next, the subjects were served beer atthe rate of three ounces per fifteen-minute interval for Group I and "asrequested" for Group II. Breathalyzertests were administered by members ofthe South Carolina Highway Patrol toall subjects at thirty minute intervals.Following the breathalyzer test eachsubject was again required to completethe bicycle course as previously de-scribed.
ResultsBaseline scores established prior to
the ingestion of beer indicated that allsubjects could successfully complete thetest course at or above the selected levelof competency (ninety or above or notmore than two errors).
Subsequent scores for subjects inGroup I were all ninety or above whilescores for subjects in Group II declined
227
as a function of increasing blood alcoholconcentration. Final scores for the sub-jects in Group I were all one hundredswhile those in Group II ranged fromforty to sixty-five. Blood alcohol concen-trations for Group I remained below0.01 while subjects in Group II recordedblood alcohol concentrations of .12.16.All subjects in Group Il were, therefore,classified as legally "drunk" accordingto the laws of South Carolina.
DiscussionThe results produced through the
demonstration "Can A Bike Run OnBeer" were expected and provided thedramatic, objective illustration of therelationship between blood alcohol con-centration and the ability to perform agross motor skill. Furthermore, partici-pants and spectators readily generalizedthe results to the skill required to oper-ate a motor vehicle. The generalizationwas encouraged by the presence of po-lice officers, breathalyzer equipment,traffic accident displays, and brochures.Participants and spectators were askednumerous questions and made com-ments regarding the amount of alcoholthey typically consumed followed bydriving, swimming, and skiing.Through the demonstration, questions,and comments, it appeared to the writerand to others that a meaningful bit ofeducation was taking place. The ulti-mate results of such education are spec-ulative. However, if only c ne DUI wasaverted, the demonstration was worth-while.
RecommendationsThe following recommendations are
offered to those who might wish toconduct a similar demonstration:
Establish a meaningful philosophy forconducting such a demonstration andsecure administrative support.
Obtain assistance from local and statelaw enforcement agencies.
Publicize the event on campus andbeyond to include appropriate highschool and college groups. Notify news-paper publishers and TV stations, mak-ing certain that they are properly edu-cated regarding the nature and purpose
217

of a demonstration. This should be ac-complished through a written statementprepared by those conducting the dem-onstration.
Select an area similar to the one previ-ously described. Intramural athleticfields and football stadiums are mostappropriate if adequate spectator areasare available.
Subjects should be "drinkers" and, ofcourse, of legal age to consume alcohol-ic beverages. An informed consentstatement should be read and signed byeach subject and a witness.
Beers should be purchased by thoseconducting the demonstration an('served to the subjects in cups. Avoidassistance from beer distributors.
Bicycles should be provided in a vari-ety of sizes, all appropriate for riding ona grass surface.
Faculty and student assistance shouldbe recruited to perform the followingtasks:
Scorekeeper to record amount of beerconsumed, blood-alcohol concentra-tion, and task performance score.
"Barkeeps" (two) to serve beer to thesubjects as instructed and to reportsuch information to the scorekeeper.
Head referee to count the number oferrors and report the score to thescorekeeper.
Assistant referees (four) to throw"flags," indicating errors, and report-ing to the head referee.
Police officers (four) to operatebreathalyzers and report results to thescorekeeper, explain procedures, pro-vide displays, and literature.
Announcer to keep spectators in-formed regarding results as posted onthe scoreboard as well as to provideoccasional comments. (i.e. "reactiontime worsens by 50 percent as BACreaches 0.10")."Can A Bike Min On Beer" was co-
sponsored by The Citadel's Departmentof Physical Education and the Col-legewide Committee on Alcohol Aware-ness. The writer wishes to express ap-preciation for assistance to Dr. DebbieMiller who conducted a similar demon-stration at The College of Charleston.
Ed lin, G. & Golanty, E. (1982). Health andwellness. Boston, MA. Science Books In-ternational, p.281.
Perrine, M. W., Waller, J. A. & Harris, L. S.(1971). Alcohol and highway safety: Be-havioral and Medical Aspects. U.S. De-partment of Transportation.
Report from the Committee on Public Works andTransportation t(.. the 97th Congress, 2ndSession (1982, Sept. 23). Report No. 97-867, p.7
218
-'111F-4FAVi, .
. . ..
70
60
50
40
30
20
10
<0.01 0,03 0.05 0,07
1_ 1 1 J0.15 0.17 0.19 0.20+
Blood Alcohol Concentration, Percentage(From Perrine et al., "Alcohol and Highway Safety: Behavioral and Medical Aspects." NHTSATech. Report, DOT HS-800-599, 1971.)
rstill,'Lec.1;9-;7-4,'%1 1;s-
\*;.?" .
A Scoreboard (4' x 16')B Group I. Group II
C DisplaysD PA and BreathalyzerE Spectator Area

TEACHING IDEAS 118
Add:ction
Once Upon a Synapse: A Drug EducationSimulation in Three Acts
William M. London
In order to facilitate rational, criti-cal thinking about psychoactivedrugs as they relate to personalhealth and political controversies, in-struction about basic pharmacologi-cal principles is important. Just asinstruction about sexual physiologycan reduce "magical thinking" aboutsexual relations (e.g., pregnancy can-not result from one's first coital expe-rience), instruction about pharmacol-ogy can reduce thinking about drugsas if they were magical potions.
The main problem in teachingabout pharmacology is the complex-ity of the topic. Instructional activi-ties are needed that can make diffi-cult" pharmacological concepts asreal, relevant, interesting, and com-prehensible for students as possible.The purpose of this article is todescribe such an activity that can biconducted in college level healthscience classes and, possibly, at thesecondary level as well. The activity,"Once Upon a Synapse," can becompleted in about 45 minutes. Thebehavioral objective is to enable stu-dents to describe various mecha-nisms by which psychoactive drugshave been theorized to alter normalneuronal functioning and therebyproduce psychological effects.
At a minimum, abodt 10 studentsare needed to effectively illustratethe mechanisms. A class of 20 to 40students makes the simulation clear-er and more entertaining.
William M. London is an assistant pro-fessor in the health education programat Kent State University, Kent, OH44242.
Mate) :als
"Once Upon A Synapse" is a sim-ulation which is to be performed as athree-act play. The only instructionalmaterial needed for the actual simu-lation is a chart placed at the front ofthe room on which is listed the dra-matis personae (see Figure 1). Thechart should be large enough to bereadable by the entire class. The ri-diculous names of the characters list-ed on the chart invariably generatelaughter throughout the activitythereby making the technical natureof the topic less intimidating.
The simulation should be proceed-ed by a brief lecture on drugs and thenervous system. Recommended ma-terials for this preliminary lectureinclude overhead transparencies thatillustrate: (1) the structure of neu-rons; (2) the movement of sodiumand potassium ions across the nervecell membrane (which in the essenceof the nerve impulse); (3) the move-ment of neurotransmitter moleculesfrom presynaptic vesicles to postsyn-aptic vesicles; and (4) the reuptake ofthe neurotransmitters by the presyn-aptic neuron.
An overhead transparency thatlists various mechanisms (including
those illustrated by the simulation)by which drugs are believed to affectneuronal communication should bepresented to conclude the lesson.Such mechanisms include: (1) alter-ing membrane permeability; (2)mimicking neurotransmitters; (3)blocking neurotransmitters frombinding to receptors; (4) alteringsynthesis of neurotransmitters; (5)blocking reuptake of neurotransmit-ters; (6) altering release of neuro-transmitters; (7) altering deactiva-tion of neurotransmitters; and (8)altering storage of neurotransmit-ters in vesicles (Ray & Ksir, 1987).
Procedure
Students are seated facing thecenter of the room in a U-shapedformation with a gap of about fivefeet at the midpoint region of thecurve. The seating arrangement isused to represent two nerve cells(neurons) in the brain and the syn-apse between them. The seating ar-rangement with the initial position-ing of the characters is diagrammedin Figure 2.
Following a brief lecture on neu-rotransmission, the activity pro-ceeds in three "acts". In Act I, nor-
Ethel (or, technically, Ethyl) Alcohol a depressant drugCoco Cocaine a stimulant drugNeil Neuron a nerve cellNellie Neuren a nerve cell that receives input from Neil NeuronNorman Neurotransmitter a chemical messenger sent by Neil NeuronVic (or Vicki Vesicle) a storage bin for chemical messengers from Neil NeuronRita Receptor a receiver of chemical messages sent to Nellie Neuron
22219

mal transmission of an electricalmessage across an excitatory syn-apse is simulated. (Normal trans-mission in an inhibitory synapse canalso be simulated in a second runthrough Act I.) Act II illustrates howalcohol affects normal transmission.Act III illustrates how cocaine affectsnormal transmission.
The teacher begins by requestingvolunteers for the "lead" roles in theplay: Rita Receptor, Norman Neuro-transmitter, Ethel (or, technically,Ethyl) Alcohol, and Coco Cocaine.To help students to relate to thelock-and-key relationship betweenreceptors and neurotransmittets, itis advisable to choose a female toplay Rita and a male to play Nor-
man. (This may also generate someplayful humor!) If in the teacher'sjudgment, there is a big enoughgroup, the reality of the simulationmay be enhanced by designatingmore than one participant to playeach lead role. Each participant notassigned to a lead role is designatedas part of Neil Neuron, Nellie Neu-ron, or Vic (Vicki, if preferred) Ves-icle depending upon seating posi-tion (see Figure 2).
The teacher directs the action asfollows:Act 1: Normal Neurotransmission atan Excitatory SynapseStep 1: The nerve impuise begins withthe participant seated at the dendriticend of Neil Neuron (point A of Figure 2).
Back of Classroom
receptor site (Rita Receptor)
postsynaptic neuron(Nellie Neuron)
[ID]
nerve impulse ends
Coco Cocaine
[C]if
synapticcleft
A\ /teacher
Front of Classroom
neurotransmitter(Norman Neurotransmitter)in a vesicleVic or vicki Vesicle)
presynapdc neuron(Neil Neuron)
[A]
nerve impulse begins
Ethel Alcohol
220
The participant raises his or her armsand then places them back down. Thissignals the next participant over to do thesame and continues down the line NeilNeuron participants to point 2. The armraising and lowering procedure is likelyto be familiar to students as "the wave":a popular pastime in recent years forspectators at sporting events. Each stu-dent's arm raising and lowering repre-sents the movement of sodium and po-tassium ions across the cell membrane ateach point along the neuron.Step 2: Vic(ki) Vesicle (point B) opensup and releases Norman Neurotrans-mitter into the synapse.Step 3: Norman Neurotransmitterbinds to Rita Receptor (point C). (A hugor even a handshake will do.)Step 4: A wave begins at point C andproceeds along Nellie Neuron to point D).Step 5: Rita Receptor releases NormanNeurotransmitter.Step 6: Norman Neurotransmitter ispumped back into Vic(ki) Vesicle. (Thisprocess, known as reuptake, replenishesthe supply of neurotransmitter mole-cules). Participants are asked to be cre-ative and improvise how reuptake shouldlook.
If the teacher decides to simulatean inhibitory synapse, I recommendhaving a wave continually repeatingin Nellie Neuron that stops repeat-ing upon the binding of NormanNeurotranemitter to Rita Receptor.
The teacher can process Act I byasking the class to brainstorm how adrug that reaches the brain couldconceivably disrupt the normal neu-rotransmission process simulatedby the class. Students who haveideas on this matter should be in-structed to "become" the drug andact out the ideas that they brain-storm.
In Act Il and in Act III, the teachercan direct the class to simulate hy-pothesized actions of two common-ly abused drugs: alcohol and co-caine. The teacher may decide topass up Act II and Act III if studentsrespond well during the processingof Act I.Act II: Alcohol is ImbibedStep 1: A wave begins at point A.Step 2: Ethel Alcohol interferes with thepropagation of the wave. Ethel mightwant to hold some participants' handsdown.

Step 3: No release of Norman Neuro-transmitter. No wave begins in NellieNeuron.
Teachers can explain that manyscientists have lost confidence in thehypothesized mechanism illustratedin Act II which suggests that alcoholinterferes with membrane excitabil-ity. Many now believe that, likeother central nervous system de-pressant drugs, alcohol may mimicthe neurotransmitter, gamma-ami-nobutyric acid, which has inhibitoryeffects when it binds to its receptorsite (Ray & Ksir, 1987).
Act III: Cocaine is AdministeredStep 1: A wave begins at point A.Step 2: Vidki) Vesicle (point 8) opensup and releases Norman Neurotrans-mitter into the synapse.Step 3: Norman Neurotransmitterbinds to Rita Receptor (point C).Step 4: A wave begins at point C andproceeds along Nellie Neuron to point D.Step 5: Coco Cocaine stops Rita Recep-tor from releasing Norman Neurotrans-mitter. (Cocaine interferes with the re-uptake process).Step 6: Waves continually repeat frompoint C to point D. Students can easilyrelate this to the intensified experiencesproduced by cocaine administration.
Step 7: The teacher explains that theinterference with reuptake along withbinding of cocaine to special (unsimu-lated) receptor sites may explain thestimulation effects of cocaine. Some re-searchers also believe that the severedepression experienced by some chroniccocaine users may result from failure toreplenish the supply of neurotransmitter(Gregler & Mark, 1987).
Much more than after Act I, afterthe demonstrations of Acts II and III,students are likely to have ideas onother ways that drugs can act at theneuronal level. Thus, at this point,the teacher should repeat the brain-storming session. The teacher canthen compare the students' brain-stormed list of mechanisms with theteacher's own list on overheadtransparency (as described aboveunder "Materials"). Teachersshould ask students to imagine thepsychological effects resulting fromeach proposed mechanism of drugactivity.
It is not so important for studentsto be able to recite the names ofvarious neurotransmitters or to ex-plain the specific hypothesized ac-tions of specific drugs. Emphasis ofthe discussion should be on generalconcepts of neurotransmission anddrug actions, and how these relateto drug effects.
231
Conclusion
The actions of psychoactive drugsat the neuronal level can be a daunt-ing topic of study. "Once Upon aSynapse" makes the topic real, rel-evant, interesting, enjoyable, andcomprehensible for students by fa-cilitating group interaction.
Indeed, the simulation can beused primarily as a group energizerfor drug education programs thatemphasize social support and skillbuilding strategies.
Facilitators should be prepared foroutbursts of laughter and friendlyteasing of the student, In the leadroles. The cit ssror nvironmentwill appear chaotic ut will actuallybe carefully choreographed. Stu-dents tend to want to "get it right"and thus will tend to cooperate witha facilitator who is well-prepared.
Gregler, H.L. & Mark, H. (1987). Medicalcomplications of cocaine abuse. New En-gland Journal of Medicine, 315, 1495-4500.
Ray, 0. & Ksir, C. (1987). Drugs, Society, andHuman Behavior (4th edition). St. Louis:Times Mirror/Mosby College Publishing.
221

TEACHING IDEAS 119According to recent surveys parents
are now considering alcohol abuse aserious problem that the schools shouldaddress. This is a change from recentyears when "drug abuse" was the majorconcern. In fact, parents were often re-lieved to discover that youngsters were"only drinking" and not using othersubstances. This reawakening of popu-lar interest in the prevention of alcoholabuse provides an opportunit, for pro-gram development. So the problemfaced by health educators is not one ofgaining support for a program but,rather, one of responding in ways likelyto have an impact on the lives of stu-dents.
One does not have to visit many class-rooms to note that there seems to be agreat deal of confusion about what oughtto be included in an effective alcoholeducation program. At least four differ-ent types of programs are in use. Whilethere is generally some overlap of thedifferent types of programs, it is useful toidentify each type so that strengths andweaknesses can be noted.
One predominant type is the biologi-cal emphasis. Teachers using this ap-proach emphasize the impact of alcoholon the body. Students are acquaintedwith the properties of alcohol and how itfunctions in the body. While the knowl-edge of alcohol effects on the body is animportant aspect of any problem, it is notsufficient. First of all, the factors that in-fluence individual decision-making andthe choice to drink or not to drink are notgiven consideration. In addition, manyof these programs have a negative em-phasis. It seems to be assumed that ifstudents are made aware of all of theterrible things that alcohol does to thebody, then students will not drink.
A second type of a program in theschools tends to confuse alcohol and al-coholism education. The major thrusthere is on alcoholism and the dangers ofbecoming an alcoholic. In fact, this em-phasis has become so popular that theauthor is usually inundated in alcoholeducation courses with ques:ions aboutalcoholism and how one can tell if he orshe is an akoholic. Once again, whilesome of this information is useful, al-cohol abuse should not be confused withalcoholism. Any individual may abuse
Toni V. Savage is an associate professor in theDepartment of Curriculum and Instruction,Texas A&M University, College Station, TX77843.
222
Investigating the Social Aspectsof Alcohol Use
,I. IL\
*`& `
.00
-7-
. ,---,---
--_-----,,\ N-\% .-
# N\--:-Addiction
Tom V. Savage
alcohol at any time. In addition, this ap-proach fails to emphasize decision-mak-ing and tends to have a negative flavor.
A third approach, more common thanwe would like to admit, is the "evils ofalcohol" approach. These programs em-phasize moralizing and preaching tostudents about w:ty they should notdrink and how evil it is. Such programstend to use scare tactics that emphasizethe horrible consequences of drinking.The usual results of these classes areknowing glances passed among stu-dents, communicating that they knowbetter than fi e teacher and that theteacher is out of touch with reality. Stu-dents often assume an adversarial posi-tion of defending drinking and attemptto refute the moralistic arguments of theteacher. More than one of these types ofclasses have been brought to an embar-rassing conclusion when a student asksthe teacher, "Do you drink?".
A fourth approach may be labeled the"resource blitz." These programs featurea daily procession of resource people and
2 n
material. Police officers, reformed el-coholics, counselors from alcoholism re-habilitation programs, films, and fieldtrips are the major ingredients of thisapproach. While many of these re-sources might be worthwhile, most ofthese progiams lack focus.
And though there are elements ofthese four approaches that might be use-ful in designing an alcohol educationprogram, they all lack some critical ele-ments.
The first step in developing an alcoholeducation program involves clarificationof the goals and purposes of the pro-gram. This helps guide both the contentselected for study and the activities stu-dents will experience.
What should be the goals and pur-poses of a sound alcohol education pro-gram? Perhaps the major goal should beto help students make responsible andintelligent decisions about their drinkingbehavior. It must be recognized at thispoint that complex factors are involved

in the decision to drink. An alcohol edu-cation program must address thesecomplex factors. Learning about alcoholis only one part of this process. Studentsneed to address the sources of attitudesand behavioral expectations that influ-ence individuals to drink to the extentthat they abuse alcohol. Above all, theprogram must have a realistic focus andone that avoids adversarial relationshipsbetwe.en teacher and student.
Another component that should beaddressed in alcohol education pro-grams is that of the social context of al-cohol use. The social environment andsocial reinforcements or sant.fions have astrong impact on the attitudes and be-haviors of individuals. There are manyaspects of the social environment thatsend messages to individuals regardingappropriate drinking behaviors.
One way of beginning a study of thesocial aspects of alcohol use is to pose thefollowing questions: Why do peopledrink? What satisfactions do they getfrom drinking? How do individuals in-fluence their drinking behavior and pat-terns? What drinking behaviors and pat-terns are taught in our culture?
Several interesting projects can in-volve students in the search for answersto these types of questions. Studentsshould be allowed to gather data, statetheir findings, and analyze the impactthat social reinforcement has on their at-titudes and behavior. The role of theteacher should be one of suggestingquestions and sources of informationand prompting students to evaluate themeaning of the data.
Societal attitudes are influenced inboth obvious and subtle ways. Some ofthe more obvious means might bethrough advertisements that promotevarious forms of beverage alcohol.Other, mo..c subtle, means might befound by analyzing the content of car-toons, television programs, and movies.
Analysis of advertisements is a projectmany teachers have utilized. The firststep involves collection of advertise-ments, usually from various popularmagazines. When undertaking this proj-ect it is useful to have students identifythe magazine where the advertisementvas found. This is helpful when identify-ing the audience for which the adver-tisernent was intended. It should benoted that television commercials couldalso be included in the investigation. Asadvertisements are collected, the follow-ing questions can be posed:
1. What does the advertisementshow?
2. Why do ru think these elementswere selected for inclusion in the adver-tisement?
3. What is the message of the adver-tisement?
4. What attitudes and behaviors doesthe advertisement seem tr oe reinforc-ing?
5. What impact do advertisementshave on the attitudes and behaviors ofpeople?
6. What information is not included inthese advertisements that is important toknow?
As a follow-up, the advertisementscould be grouped, and a summary madeof the common elements and messagesthey seem to convey. For example, doesthe fact that nearly all advertisementsportray alcohol use in settings that areexciting, sexy, and fun have any impacton our views of when alcohol should beused?
A rather subtle source of informationabout alcohol use, one that is often over-looked, is the cartoon. Cartoons relatingto alcohol use are plentiful. They appearregularly in newspapers and magazines.Just the fact that cartoons with alcohol-related themes are so plentiful is a usefulbit of information to discuss. As cartoonsare collected, they could be grouped ac-cording to common themes. Cartoonscan be found illustrating nearly everyreason that could be given for drinking.The following questions could be asked:
1. What is the message of the cartoon?2. Why do you think drinking behav-
ior is portrayed as humorous?3. What reasons are given for drink-
ing in this cartoon?4. How valid are those reasons?5. Why do you think the cartoonist
chose this topic?6. What influence do jokes and car-
toons have in shaping attitudes and be-haviors of people?
A Eecond method to use with cartoonsis what is called a task card, which is away of individualizing student involve-ment. A task card might consist of a car-toon related to drinking behavior, alongwith a series of questions or tasks to becompleted by the student. For example,a cartoon might be presented that relatesto drunkenness. The following ques-tions and tasks could be included:
1. How is drunkenness portrayed inthis cartoon?
233
2. Why do many people think drunk-enness is funny?
3. Why is getting drunk the goal ofmany people when they drink?
4. Poll your classmates. How many ofthem think getting drunk is desirable?Why do they feel that way?
5. Construct a blood alcohol levelchart that shows the probable changes inbehavior associated with differentchanges in the blood alcohol level.
The project of different students andtheir task card projects should be sharedwith the class and discussed. At thispoint, it might be helpful to addresssome of the common myths surroundingalcohol use.
Another rather subtle source of infor-mation about alcohol use is the contentof television programs and movies.While some types of beverage alcoholmay not be advertised, there is a consid-erable amount of drinking behavior por-trayed during the programs.
One interesting approach is to dividethe class into the teams and have themconduct a television survey. Simple sur-vey forms can be developed and differ-ent students assigned a particular view-ing time and program. They should beasked to identify the program, thenumber of times alcohol was mentionedor used, the context of the drinking, thepurposes for which alcohol was used,the consequences of the usage, and thenumber of times any other beverage wasmentioned or used.
Students are often surprised to dis-cover that other beverages are men-tioned only rarely luring the context ofany given program It is almost as if noother beverages were available.
After a period of time, perhaps a week,the results can be tabulated and pre-sented to the class. They might pay spe-cial attention to the context of alcoholusage. How many times was it used toenhance sexuality, to relieve tension orstress, to escape an unpleasant situa-tion? Once again the students should beasked to state the types of messages thatare being sent about the use of beveragealcohol.
A sound alcohol education programmust include several components. It hasbeen the purpose of this paper to suggestways of investigating one of the compo-nents that is often overlooked, that of thesocial aspects of alcohol use. An under-standing of how these complex forcesinfluence attitudes and behaviors canhelp move students toward the goal ofresponsible decision-making.
11111
223

TEACHING IDEAS 120
Addiction
Drug Use, Misuse and Abuseas Presented in Movies
Kerry J. Redican, Barbara L. Redican and Charles R. Baffi
Movies represent a form of themass media and are an important in-strument of communication. Analysisof the effects that movies ham onpeople has produced much debateamong professionals from a variety ofdisciplines. Regar&Pss of the stand aperson takes, however, the potentialInfluence of movies on people'sknowledge, attitudes and behaviorcannot and should not be underes-timated.
Health behaviors presented inmovies often can be interpreted as"norms" to viewers. To the healtheducator, these implied "norms" maynot be the ones most conducive tohealthy lifestyles or reduction of risktaking behaviors. Examples of im-plied "norms" might be the way druguse is presented in movies. Manymovies imply that people use substan-ces to better enable them to cope orfor recreation and imply that thesereasons make it all right to use drugs.
In an effort to have studentsevaluate how movies present druguse, the following learning activity wasdeveloped. Thic activity has been usedin junior and nior high school clas-ses, as well as health educationworkshops for teachers and otherhealth profesrionals. The activity hasbeen well received by these groups.
Kerry!. Redican is an associate profes-sor of health education at VirginiaTech, Blacksburg VA 24061. BarbaraL. Redican is a registered nurse inBlacksburg VA. Charles R. Baffi is anassociate professor at Virginia Tech.
224
This learning opportunity is designedto stimulate student discussionregarding how movies present druguse. Since movies do represent an adform and since people interpretmovies in different ways, this learningopportunky should not be considered
23 ,4
to be a definitive way to analyze howdrug use is presented in movies.Structure of the LearningOpportunity
As part of a course assignment inhealth education, students can be

Directions: For the film being observed, respond to the following statements by circling one of the following choices located beside eachstatement.
sAA
SDNA
= Strongly Agree= Agree= Undecided= Disagree= Strongly Disagree= Not Applicable (drug-related scenes not in film)
Note: Information regarding scoring can be found under the Scoring and Interpretation Section.
Number of drug use scenes in the filmGenerally the scene in the film or movie:
(1) Encourages or condones the use of mood modifying substances. SA A U D SD NA(2) Does not show the negative effects of using mood modifying substances. SA A U D SD NA(3) Promotes use of mood modifying substances as a solution to boredom. SA A U D SD NA(4) Associates the use of mood modifying substances with fun or pleasure. SA A L I D SD NA(5) Encourages the use of mood modifying substances as a problem-solving
behavior. SA A U D SD NA(6) Suggests that use of mood modifying substances ia a "norm" (in other
words "everyone is doing it!"). SA A U D SD NA(7) Portrays people who abstain from using mood modifying substances as
immature, not adult, or "nerds." SA A U D SD NA(8) Shows an easy solution to the results of misus.e or abuse of mood
modifying substances. SA A U D SD NA(9) Portrays the hero or heroine as one who uses mood modifying substances. SA A U D SD NA
(10) Portrays the use of mood modifying substances as a means of enhancingperformance (intellectual, physical, spiritual, etc.). SA A U D SD NA
asked to pick out a certain film anduse the instrument in Figure 1 inevaluating how drug use is presented.
ln order to maximize the discus-sion on movies, it is best to observe thefollowing points.
Don't let students reviewmovies that are considered out-rageous in terms of their drugcontent. For example, moviessuch as Animal House orCheech and Chong filmsportray unrealistic drug-takingbehaviors.ln any given analysis, be sure tohave students determine if anyclosure was reached regardingthe negative side of drug use.For example, some films mayglorify drug use initially, but asthe movie proceeds. it is easilyseen that drug use is interferingin the person's life.
Summary
Once again, the purpose of thelearning opportunity is to stimulateclassroom discussion. Hopefully, asan end result, the student and teacherwill watch movies with a keener eyeand an insight as to how drug use isbeing presented.
Scoring and Interpretation
Step I:
Step II:
Step III:
Step IV:
Scoring: Use the following method of scoring your responses:
ISA] Strongly Agree = 5 pointsIA] Agree = 4 pointsKJ] Undecided = 3 pointsID] Disagree 2 points
(SD] Strongly Disagree = 1 pointINA] Not Applicable = 0 points
Add your points as follows:
Statement 1: Points
Statement 2: Points
Statement 3: Points
Statement 4: Points
Statement 5: Points
Statement 6: Points
Statement 7: Points
Statement 8: Points
Statement 9: Points
Statement 10: Points
Total Points: Points
After you have added up the total points, place an "X" on theappropriate point on the following line that best represents your totalpoints. Once you've placed the "X" that represents the total points,you can easily see the film's position regarding drug use.
"Anti" Drug UsePosition
10 20 40
"Pro Drug UsePosition
50
Comments regarding analysis of movie (e.g. what kind of closurewas reached?)
215225

TEACHING IDEAS 121
Learning About Alcohol Drinking Attitudes andMotivations by Examining theVocabulary of Drunkenness
William M. London Addiction
According to editors of the Dic-tionary of American Slang,"the concepthaving the most slang synonyms is drunk"(Wentworth & Flexner, 1975). The dic-tionary listed 353 of these synonyms(Levine, 1981) and 323 synonyms in itsappendix. Spears (1986) listed over 1,870synonyms, while Abel (1985) listed over1,620 slangterms defmed as intoxicated,""drunk," or various degrees of drunken-ness.
Reasons for the vastness andrichness of our vocabulary of drunken-ness are not clear (Abel, 1985). How-ever, semanticists have sulnested thathow we use language to name thingsaffects how we perceive things (Postman& Weingartner, 1969). Thus, our vo-cabulary of drunkenness reflects our cul-ture's attitudes, values, and thoughtsabout the use of alcohol (Abel, 1985).
An important role of alcoholeducators is to facilitate open discussionabout attitudes and motivations relatedto drinking and drunkenness. The pur-pose of this art icle is to describe how thatcan be accomplished by using our vo-cabulary of drunkenness to provide in-sights about alcohol in American soci-ety.
The activity is recommended aspart of alcohol education for students insecondary schools, colleges, and univer-sities. It also has been used successfullyas part of inservice training for schoolpersonnel. The activity can take from aslittle as 45 minutes to as long as 90
William M. London is an assistant profes-sor in the health education program atKent State University, Kent, 01-1 44242.
226
minutes depending upon what (if any-thing) the teacher decides to omit fromthe method described below, the dynam-ics of the group, and the size of the group.(The activity can be carried out with anyclass size.)
Method
The teacher asks each studentto draw a line down the middle of a pieceof paper. Students are given a minute tolist on the left side of the page, as manywords (including slang words) meaningsnow as they possibly can. This is fol-lowed by a brainstorming session so theteacher can write all words generated bythe students on the chalkboard. The taskis intended to confound students, andmost groups will struggle to generate 10words. The teacher must be careful notto give students too much latit.ule be-cause some especially sophisticatedgroups may come up with many morewords if allowed to use words that referto types of snow.
Students then are given a minuteta list on the right side of the page as
ards (including slang words). t.c.; drunk as they can. This, again,
awed by a brainstorming session inwnich the teacher records student re-sponses. Students tend to know enoughsynonyms to enjoy the challenge of fillingthe board with brainstormed responses.This brainstorming tends to be accom-panied by frequent outt ursts of laughterin response to many of the words, includ-ing those words typically regarded asprofane.
(To discourage students fromcalling out profane words may defeat
2;
part of the purpose of the activity by, ineffect, discouraging them from discuss-ing what the use of such words to meandrunk implies about common attitudesof Americans toward drunkenness. How-ever, at the secondary school level, theteacher may need to compromise out ofrespect for community standards.) Brain-storming continues until there are about30 seconds during which no new re-sponses are made. From a prepared listof synonyms for drunk (which can beassembled from Abel, 1985; Levine, 1981;Spears, 1981; Spears, 1986; andWentworth & Flexner, 1975) with syn-onyms having the same first letter clus-tered together, the teacher reads aloud.
In processing the activity, theteacher asks the class why it was so mucheasier to generate words for drunk thanwords for snow. After a brief discussion,the teacher explains that Eskimos have30 different words for snow, includingone for falling snow, one for "snow onthe ground," one for "drifting snow,"and one for "blowing snow." The largenumber of words reflects the impor-tance of perceiving various aspects ofnature central to Eskimo culture (Cross,1979). The teacher facilitates discussionabout what the vast number ofsynonymsfor drunk implies about attitudes towarddrunkenness in popular American cul-ture.
In groups of four to six, studentsare asked to discuss what the nature ofsynonyms for drunkenness implies aboutcommon motivations for drinking inAmerica. Students generally note thatmost of the words connote violence ordestruction (e.g., stoned, bombed) orsilliness (e.g., blotto, schnoggered), al-
though a few have more mild connota-tions (e.g., tipsy, high). The teacher re-convenes a meeting of the entire classand asks for volunteers to share whatthey concluded in their groups.
During the ensuing discussionthe teacher may wish to present relevantviewpoints of scholars for students tocritique. For example, Levine (1981)suggested that violent words are directedat what "might be thought of as ordinaryor everyday consciousness" and thus theappeal of getting drunk "is the anticipa-tion of a break with ordinary conscious-ness."
Synonyms such as "woofled"connote a degree of self-handicapping.Tucker, Vuchinich, & Sobell (1981) pro-vided experimental evidence that some-times people drink alcohol as a self-handicapping strateff. Berg las & Jones(1978, p. 406) defined a self-handicap-ping strategy as "any action or choice ofperformance setting that enhances theopportunity to externalize ( 'r excuse)failure and to internalize (reasonablyaccept credit for) success." They sug-gested that, for those who are uncertainabout their competence, to fail at a taskdue to the self-handicapping of drunken-ness normally is preferable to failurethat clearly indicates stupidity or incom-petence. Thus, self-handicapping mightbe part of the motivation for some peopleto "woofle" themselves before such chal-lenges as test-taking, proposing a firstdate, and getting up to dance at a party.
Since students are asked to dis-cuss the lesson in their small groups, theactivity can make some students noticea-bly uncomfortable (perhaps, especially,those students who tend to deny theirown alcohol abuse or those who havesignificant others who abuse alcohol).The small groups provide students anopportunity to express their feelings andto receive social support. The teachershould be available and responsive tostudents who wish to discuss furthertheir reactions to the activity. Some stu-dents may be encouraged to seek helpand the teacher must be prepared tooffer appropriate referrals.
Abel, E. L. (1985). Dictionary of alcohol useand abuse: Slang, terms, and terminolo-gy. Westport, CT: GrPenwood Press.
Berglas, S., & Jones, E. E. (1978). Drug choiceas a self-handicapping strategy in re-sponse to noncontingent success. Journalof Personality and Social Psychology, 36,405-417.
Cross, D. W. (1979). Word abuse: How thewords we use use us. New York: Coward,McCann & Geodiegan.
Levine, H. G. (1981). The vocabulary of drunk-enness. Journal of Studies on Alcohol, 42 ,1038-1051.
Postman, N., & Weingartner, C. (1969). Teach-ing as a subversive activity. New York:Dell.
Spears, R. A. (1981). Slang and euphemism.Middle Village, New York: Jonathan Dav-id Publishers.
Spears, R. A. (1986). The slang and jargon ofdrugs and drink. Metuchen, NJ: Scare-crow Press.
Tucker, J. A., Vuchinich, R. E., & Sobel!,M. B. (1981). Alcohol consumption as aself-handicapping strategy. Journal of Ab-normal Psychology, 90, 220-230.
Wentworth, H., & Flexner, S. B. (Comps. &Eds.). (1975). Dictionary of AmericanSlang, 2nd edition. New York: Crowell.
237 227

TEACHING IDEAS 122
Aging
Helping College StudentsUnderstand the Older Adult
Margaret J. Pope
Our society has seen a tremendousincrease in the number of people overthe age of 65 and in the past decade, anawareness of their problems and somepossible solutions have surfaced. Doc-tors, gerontologists, social workers,therapeutic recreators, hospital andnursing home administrators, and psy-chologists recognize the problems ofthis growing population, and manyhealth educators are aware of the gapthat exists between the older adult andthe college student.
Teaching a unit on aging in a healtheducation class at the university levelmade this author aware of the manypossibilities for older adults and college-age students to communicate. There is adefinite need for inter-generationalcommunication, and the opportunityfor mutual understanding of problemsshould be afforded the health class andthe older adult.
As an introduction to the unit, thestudents were administered a test,"Facts on AgingA Short Quiz" (Pal-more, 1977). This test contains only 25items, takes only a few minutes to com-plete, is easily scored, and gives a goodindication of misconceptions about ag-ing. The scores on this short quizshowed that the students possessed lit-tle accurate knowledge about the olderadult. Some of their misconceptionswere: The majority of old people aresenile with defective memories; old peo-ple are all alike; old people are unable tolearn anything new; physically they feelbad all the time and are totally incapableof any type of exercise; and they arementally withdrawn with little contact
Margaret I. Pope is professor, Health, Phys-ical Education and Recreation Department,Jacksonville State University, Jacksonville,AL 36265.
228
with the world outside their limitedenvironment.
The approach taken to try and allevi-ate these misconceptions was to invitefive adults from the Retired Seniors Vol-unteer Program to class. All were over65 years of age and they were still activemembers of the community.
In preparation for these visitors, theclass was divided into groups with adiscussion leader. The following broadtopics were chosen as discussions areas:(1) social life, (2) income and retirement,(3) exercise and keeping fit, (4) transpor-tation, and (5) safety and crime. Thestudents developed questions pertinentto each area. These were collected bythe discussion leader to use as points ofdiscussion with the older adults.
Following are some of the questionsthat the students asked the older adults:
What do you do for entertainment?Do you feel isolated and lonely?Do you find it hard to live on a fixed
income?Do you exercise regularly?If so, what type of exercise?Do you feel bad?Do you feel safe in your environment?Have you fallen or had a personal accident
in the last five years?Has a crime of any kind been committed
against you or your partner in the past fiveyears?
Do you ever think of death?Do you have a lot of medical bills that are
brought about by your personal health prob-lems?
What method of transportation do youuse?
Dv you feel safe using it?Would you want to live in a nursing
home?Would you want to live with your chil-
dren?What is your biggest problem in day-to-
day life?
2 3 s
On the days the older adults came,the classroom was arranged with thedesks in a circle. This allowed the olderadults to sit among the students and tofeel more relaxed and at ease. Eacholder adult was given an opportunity torelate personal information to the stu-dents, including living arrangements, ifmarried how long, the number of chil-dren, and social interests. The olderadults visited the classroom for threedays and during this time, good rapportdeveloped between them and the stu-dents. Some of the students became sointerested in the adults that theyplanned to visit them in their homes.The experience seemed to be invaluableto both generations.
At the conclusion of the class on thelast day the older adults visited, thestudents wrote individual evaluations,guided by the following questions:
Did you think this was a good learningexperience?
Did it change any of your thoughts aboutolder adults?
Would you like to see this practice contin-ued in this class?
The evaluations revealed that the stu-dents previously had a number of mis-conceptions about the older adult.Many were surprised how actively in-volved these people were in communityand social activities. Most of them hadassumed that older adults were in nurs-ing homes or health care facilities. Theywere also amazed at the amount ofmental clarity older adults possessed.This encounter seemed to change thestudents' stereotyped opinion of theolder adult as a senile member of aninstitution. They became aware that theolder adult can still be a viable andcontributing member of society.
Palmore, E. (1977) Facts on AgingA ShortQuiz. Gerontology, 17 (4).
TEACHING IDEAS 123
As Old as Trees
Yaasp
IA_
Aging
MINA. -
Glenn E. Richardson and Susan Bicknell
Ageism, a form of discriminationbased on old age, is a powerful, sociallyreinforced prejudice existing in our sod-ety. One method to combat ageism in theeducational setting is experiencing thefollowing activity, As Old as Trees.
The class is given a blank sheet ofpaper and asked to draw a symbol thatrepresents their perception of oldpeople. They are given time to completethis task, and a few are asked to sharetheir drawings and give explanations.Generally, symbols such as rockingchairs, wheelchairs, nursing homes, andcanes emerge from the participants inthis activity.
Leaving the drawings and the class-room, the group (in good weather) istaken outside near a group of trees.
Glenn E. Richardson is coordinator of AlliedHealth Studies, Department of Health andPhysical Education, Texas A&M University,College Station, TX 77843. Susan Bicknell isa Health Education Major in the Departmentof Health and Physical Education, TexasA&M University, College Station, TX77843.
Dyads are formed with one member ofthe dyad blindfolding (blindfolds areprovided by the instructor) the otherstudent. The blindfolded students areturned around two or three times to losetheir sense of direction and then in-formed by the inst:uctor that theirpartners will lead th( m to a tree within areasonable radius. Tlry are instructed toget to know the tree so that when theyreturn without a blindfold, they will beable to identify the tree. The dyads goout, each to their own tree, and the stu-dents, mostly by touch, become ac-quainted with the root systems, the tex-ture of the tree surface, the knots andbranches if within reach, and other dis-tinctive features. The student, whensatisfied that helshe knows the tree, isled back to the instructor at a centralplace, turned around two or three timesand then the blindfold is taken off.
When all have returned, the studentswho were blindfolded attempt to locatetheir trees. Generally, students are suc-cessful M this endeavor; then the othermember of the dyad is blindfolded andthe activity repeated. Following the ac-
239
tivity, discussion questions can be raisedto highlight the analogy between gettingto know a tree with its unique qualitiesand getting to know older people as in-dividuals rather than as stereotypes. Forexample:
1. For those of you who were able tofind your tree, how were you able to findit?
2. What were distinctive features witheach of your trees?
3. Did you feel environmental wearon your tree?
4. You may have identified your treewith a rough exterior, but how wouldyou judge the interior of your tree? Doyou think it still produces life-maintaining fluids to its branches andleaves? Can you tell that by looking justat the outside of the tree?
5. How can you tell that your tree isstill alive? Is there any evidence? (leaves,fruit, etc.)
6. How many seasons do you thinkyour old tree has seen? Can you imaginethe story this tree could tell if it couldrelate what it may have seen over theyears?
7. How can you relate getting to knowa tree with getting to know an older per-son?
The discussion can lead students atthis point to realize the effort to identify atree from the rough, wrinkled exterior,and how much easier it might be to iden-tify individuality in older people. Theanalogy can be drawn that as the old,rough exterior of the tree houses its lifeprocesses, so older people, though aged,still have within the throb of vitality.And sometimes we don't see the interiorwhere there is so much warmth, excite-ment, and love.
At this point a discussion of the agedas a source of wisdom, spiritual strength,comfort, and other integral sources ofliving would be treated. For a more de-tailed description of these thoughts, seethe article "Ageism: Need We Discrimi-nate." '
After the discussion the students arereturned to the class, given another pieceof paper, and asked to draw a symbol of"old age." Drawings of wine bottles,books of life, owls, trees, and oth,r sym-bols representing the concept of improv-ing with age and sources of wisdomemerge from the students. A look at theirfirst picture and a comparison with thesecond picture lead to an interesting dis-cussion of change.
'Jose, N. L., and Richardson, G. E. Ageism:need we discriminate. Journal of School Health,Vol. 50, No. 12 (September, 1980), pp. 419-421.
229

TEACHING IDEAS 124
Chronic Diseases
Digging for Healthy Hearts: A SimulatedArchaeological Dig for the Prevention of
Cardiovascular DiseaseWesley E. Hawkins
In recent years, health profession-als increasingly have targeted youngeraudiences such as high school andcollege students for education on riskfactors related to cardiovascular dis-ease. Various teaching methods havebeen implemented in providing learn-ing experiences about the preventionof cardiovascular disease. Teachingtechniques have ranged from the di-rect lecture method to more experien-tial teaching methods such as inquiryproblem solving techniques, the latterbeing the focus of the present article.
The inquiry technique emphasizesproblem solving and discovery ratherthan direct transferral of informationfrom teacher to student in the tradi-tional lecture class. As Kime,Schlaadt, and Tritsch (1977) whoadvocate the use of inquiry in healtheducation noted, "the teacher's basictask is to provide data to assist stu-dents in their search for relevant data.The teacher is a primary motivator(extrinsic) in the approach to learningas a task of discovering somethingrather than learning about it" (p. 142).More specifically, the inquiry tech-nique is a problem solving process thatfirst requires the student to gather,analyze, and categorize data for con-cept formation, and then formulategeneralizations about the data gath-
Wes Hawkins is an assistant professorin (he Department of School andCommuniry Health, University of Ore-gon, Eugene, OR 97403.
230
ered (Northwest Regional Educa-tional Laboratory, 1972).
The teaching technique describedbelow, named "Digging for HealthyHearts," uses an inquiry approach toassist young persons in examining therelationship between personal cardio-vascular disease risk and lifestylehabits. Specifically, the inquiry ap-proach that will be described in thisarticle is a simulated archaeologicaldig that depicts a hypothetical highrisk and low risk civilization for car-diovascular disease.
Purpose
The major purpose of the Diggingfor Healthy Hearts Teaching Tech-nique is to utilize an inquiry and prob-lem solving approach in educatinghigh school and college students aboutrisk factors and preventive healthbehaviors related to cardiovasculardisease.
Overview of the Teaching Technique
The Digging for Healthy Heartstechnique requires three 50 minuteclass periods for completion. The firstclass period is the simulated archaeo-logical digand requires students to usean inquiry problem solving approachexamining the relationships of per-sonal cardiovascular disease risk andlifestyle habits. Simulating an actualarchaeological dig, artifacts are bur-ied representing health behaviors of
1 U
hypothetical civilizations that wouldbe high risk and low risk for cardiovas-cular disease. For example, based onrisk factors identified in past researchon cardiovascular disease (e. g., smok-ing identified from the Framinghamstudy), artifacts such as old cigarettelighters would be buried to representthe high risk behavior of smoking. Forthe low risk civilization, artifacts suchas old cans of low fat foods (e.g., tunafish cans) would be buried.
Students are told to pretend theyare archaeologists and to start diggingfor artifacts in their assigned areas.Students are asked first to hypothesizewhich artifacts represent a low risk ora high risk civilization. During thesecond class period, student stories ofthe civilizations are presented. At thethird and final class meeting, researchfindings on risk factors related to car-diovascular disease are presented.After presentation of risk factors bythe instructor, students are asked tocompare and contrast health behav-iors of our present American civiliza-tion with their own fictional civiliza-tions derived from the archaeologicaldig.
Behavioral Objectives
(1) After visual inspection of arti-facts from the simulated archaeologi-cal dig, the student will categorizeartifacts as representative of healthbehaviors as either at-risk or preven-
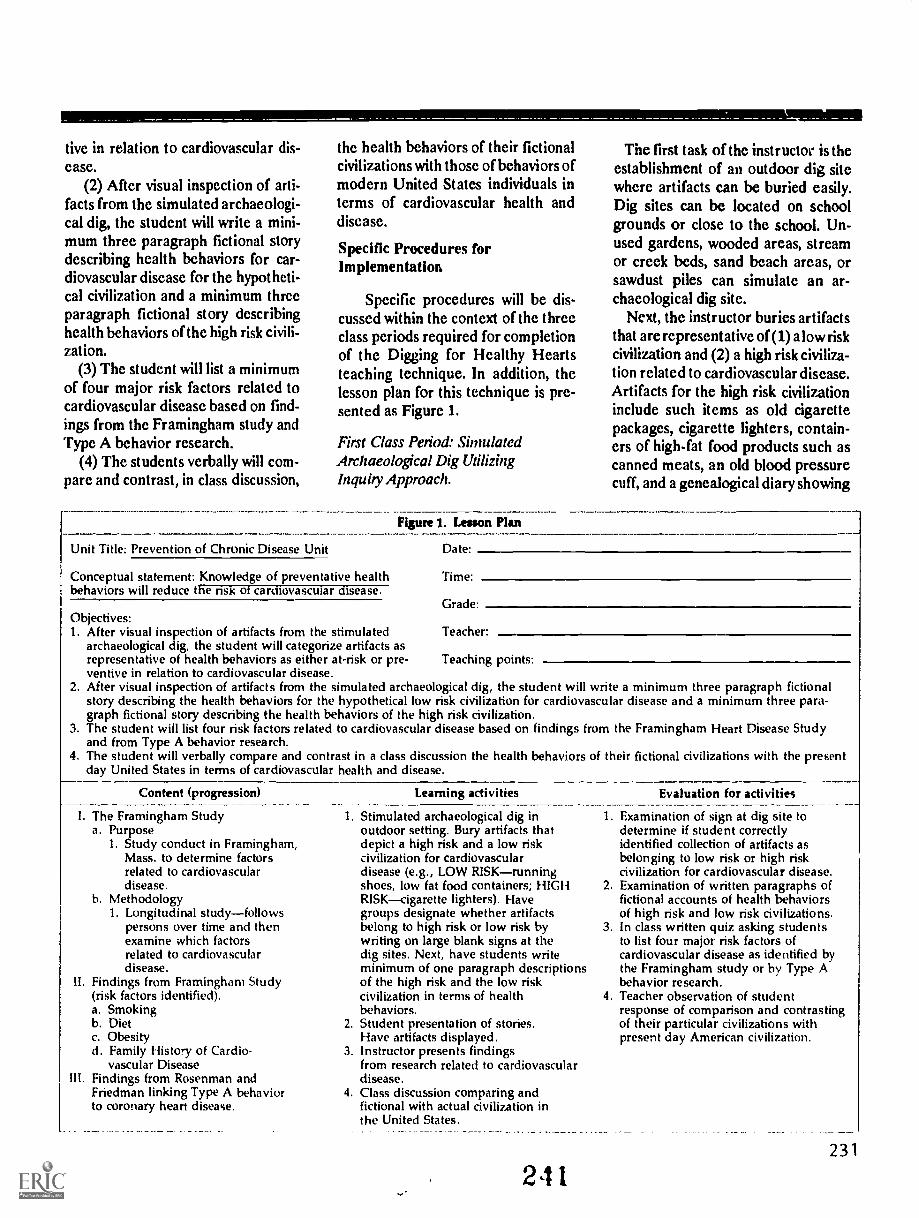
tive in relation to cardiovascular dis-ease.
(2) After visual inspection of arti-facts from the simulated archaeologi-cal dig, the student will write a mini-mum three paragraph fictional storydescribing health behaviors for car-diovascular disease for the hypotheti-cal civilization and a minimum threeparagraph fictional story describinghealth behaviors of the high risk civili-zation.
(3) Thc student will list a minimumof four major risk factors related tocardiovascular disease based on find-ings from the Framingham study andType A behavior research.
(4) The students verbally will com-pare and contrast, in class discussion,
the health behaviors of their fictionalcivilizations with those of behaviors ofmodern United States individuals interms of cardiovascular health anddisease.
Specific Procedures forImplementation
Specific procedures will be dis-cussed within the context of the threeclass periods required for completionof the Digging for Healthy Heartsteaching technique. In addition, thelesson plan for this technique is pre-sented as Figure 1.
First Class Period: SimulatedArchaeological Dig UtilizingInquiry Approach.
Figure 1. Lesson Plan
The first task of the instructor is theestablishment of an outdoor dig sitewhere artifacts can be buried easily.Dig sites can be located on schoolgrounds or close to the school. Un-used gardens, wooded areas, streamor creek beds, sand beach areas, orsawdust piles can simulate an ar-chaeological dig site.
Next, the instructor buries artifactsthat are representative of (1) a low riskcivilization and (2) a high risk civiliza-tion related to cardiovascular disease.Artifacts for the high risk civilizationinclude such items as old cigarettepackages, cigarette lighters, contain-ers of high-fat food products such ascanned meats, an old blood pressurecuff, and a genealogical diary showing
Unit Title: Prevention of Chronic Disease Unit Da te.
Conceptual statement: Knowledge of preventative health Time.behaviors will reduce the risk 01 cardiovascular disease.
GradeObjectives:I. After visual inspection of artifacts from the stimulated Teacher
archaeological dig, the student will categorize artifacts asrepresentative of health behaviors as either at-risk or pre- Teaching pointsventive in relation to cardiovascular disease.
2. After visual inspection of artifacts from the simulated archaeological dig, the student will write a minimum three paragraph fictionalstory describing the health behaviors for the hypothetical low risk civilization for cardiovascular disease and a minimum three para-graph fictional story describing the health behaviors of the high risk civilization.
3. The student will list four risk factors related to cardiovascular disease based on findings from the Framingham Heart Disease Studyand from Type A behavior research.
4. The student will verbally compare and contrast in a class discussion the health behaviors of their fictional civilizations with the presentday United States in terms of cardiovascular health and disease.
Content (progression)
I. The Framingham Studya. Purpose
1. Study conduct in Framingham,Mass. to determine factorsrelated to cardiovasculardisease.
b. Methodology1. Longitudinal studyfollows
persons over time and thenexamine which factorsrelated to cardiovasculardisease.
11. Findings from Framingham Study(risk factors identified).a. Smokingb. Dietc. Obesityd. Family History of Cardio-
vascular DiseaseIII. Findings from Rosenman and
Friedman linking Type A behaviorto coronary heart disease.
Learning activities Evaluation for activities
1. Stimulated archaeological dig inoutdoor setting. Bury artifacts thatdepict a high risk and a low riskcivilization for cardiovasculardisease (e.g., LOW RISKrunningshoes, low fat food containers; HIGHRISKcigarette lighters). Havegroups designate whether artifactsbelong to high risk or low risk bywriting on large blank signs at thedig sites. Next, have students writeminimum of one paragraph descriptionsof the high risk and the low riskcivilization in terms of healthbehaviors.
2. Student presentation of stories.Have artifacts displayed.
3. Instructor presents findingsfrom research related to cardiovasculardisease.
4. Class discussion comparing andfictional with actual civilization inthe United States.
211
1. Examination of sign at dig site todetermine if student correctlyidentified collection of artifacts asbelonging to low risk or high riskcivilization for cardiovascular disease.
2. Examination of written paragraphs offictional accounts of health behaviorsof high risk and low risk civilizations.
3. In class written quiz asking studentsto list four major risk factors ofcardiovascular disease as identified bythe Framingham study or by Type Abehavior research.
4. Teacher observation of studentresponse of comparison and contrastingof their particular civilizations withpresent day American civilization.
231

generational deaths from heart dis-ease. Traces of the low risk civilizationinclude artifacts such as exercise arti-facts (segments of racquet balls orparts of old tennis rackets), low fatfood artifacts from wooden fruit con-tainers such as apples and oranges,low fat chicken, tuna, etc. canned meatcontainers, a genealogical diary notshowing family patterns of deaths dueto cardiovascular disease, and a per-sonal date book with a stressful, heavyschedule but with planned relaxationand scheduled exercise.
High risk and low risk artifacts arekept separate when buried in differentareas at the dig site. Burying artifactsin this manner allows students tohypothesize whether artifacts repre-sent health behaviors as a high risk ora low risk civilization in relation tocardiovascular disease. To evaluatethis objective, blank signs are placed atd'fferent areas of the dig sites. Afterexaminingartifacts for their particulargroup, students are instructed to des-ignate their particular site area bywriting on the signs in large letteringeither "High Risk Civilization forCardiovascular Disease" or "LowRisk Civilization for Heart Disease."
Next, students are directed to writea minimum three paragraph fictionalstory describing the health behaviorsof a low risk and a high risk civilizationfor cardiovascular disease. Studentsare urged to make stories creative,fun, and exciting while describing thehealth behaviors of a civilization. Eachstudent is asked to complete this as-signment as homework and asked toshare the story at the follow-up sessionheld indoors the next school day. Stu-dents are asked to bring their artifactsand visually present them as they readand discuss their stories with the class.
Second Class Period: Presentation ofStudent Fictional Stories DescribingLow Risk and High Risk Civilizationsfor Cardiovascular Disease
The second class period is heldindoors in the traditional classroom
23 2
format. Students are asked to readtheir fictional stories to the class, de-scribing the particular civilizationchosen.
Third Class Period: Instructor'sPresentation of Research Findings ofRisk Factors Related to CardiovascularDisease
In the third and final class period,held inside in a traditional classroomformat, the instructor presents back-ground information on risk factorsrelated to cardiovascular disease asidentified in the Framingham, Massa-chusetts heart disease study and fromRoseman and Friedman's (1971) re-search linking Type A behavior withcoronary heart disease. After presen-tation of the risk factors is completed,the instructor, in a class discussionformat, asks students to compare andcontrast their fictional civilizationswith our present American civilizationin terms of health behaviors and car-diovascular disease.
Student ReactionHealthy Hearts
to Digging for
Various reactions from students inan introductory personal healthcourse in a large midwestern univer-sity were positive. Examples of com-ments are: "It was a fun way to learnabout heart disease, " "The dig wasfun and I learned a lot about prevent-ing heart disease," "I thought it was acrazy idea to start with, but it was funand I learned a lot, " "I liked writingthe stories about the civilizations, itwas a fun way to learn, and! think I will
2 -I 2
remember this stuff a lot better thisway."
Summary
We would do well to reconsider theimportance of inquiry as an educa-tional technique for health education.As Goodlad, Stoephasius, and Klein(1966) noted two decades agoduring aperiod of significant curriculum re-form, "Many curriculum builders seek
to organize their fields around the pri-mary structural elements of each dis-cipline: the concepts, key ideas, prin-ciples, and modes of inquiry. It is as-sumed that understanding these ele-ments (rather than merely possessingthe facts) gives the students the intel-lectual power to attack unfamiliarproblems and enables them to graspintuitively the relationship of newphenomena already experienced.Ability to think inductively becomes abuilt-in goal, and teachers are enopur-aged to let students discover meaningsfor themselves" (p. 15).
Inquiry techniques such as theDigging for Healthy Hearts teachingmethod are needed for students todiscover the meaning of what effecttheir health behaviors can have inrelationship to cardiovascular disease.
Iwould like to dedicate this article tornyfather, Eugene Hawkins, who died ofcardiovascular disease on the day thisarticle was submitted for publication.He was my teacher, my friend, and mymentor for life.
Goodlad, J., Steophasises, R., dr Klein, M.(1966). The changing school curriculum.New York: Fund for the Advancementof Education.
Kime, R., Schlaadt, R., & Tritsch, L. (1977).Health instruction: An action approach. En-glewood Cliffs, NJ: Prentice-Hall, Inc.
McCollum, J. & Davis, R. (1972). Instructor'smanual development of higher level thinkingabilities. Portland, OR: Northwest Re-gional Educational Laboratory.
Rosenman, R. & Friedman, M. (1971). Thecentral nervous system and coronaryheart disease. Hospital Practice,6(10):87-97.

TEACHING IDEAS 125Chronic Diseases
Cancer: A Mini-Documentary
From time to time, most health educa-tors get the urge to deviate from stan-dard methods of instruction and trysomething that might be out of the ordi-nary but profitable at the same time. Forthose broad topics such as cancer orheart disease, which tend to take days orweeks to cover, a mini-documentarymight bt: just the thing to use. This pro-gram is meant to be set up like 60 Minutesor 20120 but involves each student as aspecialist in his/her own field. The wholeclass can be given the opportunity to notonly produce but be the "stars" of theirown television show. The purpose of thedocumentary is to allow the studentsfreedom to select an area that intereststhem while also enabling them to be cre-ative in communicating their findings toothers. Videotaping the show enableseveryone to view the finished productand reinforces the material once again.
How the Mini-Documentary WorksEach student chooses a 3 x 5 card on a
Stephen C. Corey is group health claim ap-prover with the John Hancock Mutual LifeInsurance Company. He can be reached atP.O. Box 682, Mansfield, MA 02048.
Stephen C. Corey
particular area of cancer. On this card areseveral questions which he/she will re-search and discuss. They are also given atitle for themselves and may choose theirown name. As an example, a studentchooses cancerous tumors. His card willread:
Dr. , leading oncologistfrom Harvard.
I. What are tumors?2. What are two different types of
tumors?3. Any special tests for them?4. Any special symptoms from
them?The rest is left up to him. He must find
the correct answers and be able to reporthis findings on "TV." The following is alist which could be consulted for the re-maining cancer topics.
1. Physiology of the cancer cells2. Cancerous tumors3. Most common causes of cancer4. Cardnogens5. Warning signals of cancer6. Tests for cancer7. Treatments for cancer8. Most common cancers in women9. Cancer of the uterus
10. Breast cancer11. Most common cancers in males12. Lung cancer13. Cancer of the prostate gland14. Cancer of the testes15. Cancer of the larynx16. Oral cancer
213
17. Skin cancer18. Cancer of the esophagus19. Cancer of the stomach20. Colo-rectal cancer21. Thyroid cancer22. Hodgkin's disease23. Leukemia24. Cancer in children25. The American Cancer SocietyTwo students must be chosen to fill the
spots of commentator and interviewer.The commentator's job is to introducethe show and make some concludingstatements at the end, while the inter-viewer is responsible for accepting the 3x 5 cards from the specialists, introduc-ing them, and asking the questions. (Thestudents who have the most enthusiasmand originality seem to be best suited forthese roles.) A small "set," consistingpossibly of chairs, a table, and a lampshould be constructed so that thecamerman can focus on both of the"stars" at once. To avoid confusion andallow continuity of the show while vid-eotaping, a list should be posted so thateveryone knows when his or her inter-view is coming up. The specialist takeshis seat on the "set," gives his 3 x 5 cardto the interviewer, and when all is quiet,the cameraman gives a "ready . . ac-tion!"
As soon as the interview is finished,the next specialist comes up and getsready to go. The interviewee may alsowear a lab coat and a stethoscope to add
233

to the total effect. If each interview lastsone to two minutes, the whole show canbe completed in a single class period.
The students may be evaluated ontheir degree of research and their abilityto answer the questions correctly. With alittle enthusiasm, originality, and evenhumor, a fairly monotonous topic can bedeveloped into an exciting and refresh-ing educational tool.
Even though cancer is a prime exam-ple of the topics which could be used, themini-documentary does not need to belimited to cancer only. Therefore, topiclists for drugs and infectious diseases areincluded for future mini-documentaries.
234
Drugs
1. StimulantsInfr lious Diseases
1. Virus1 Depressants 2. Bacteria3. Hallucinogens 3. Fu ngi4. Drug abuse 4. Protozoa5. Drug misuse 5. Pathogen6. Antibiotics 6. Incubation period7. Antiseptics 7. Active immunity8. Analgesics 8. Passive immunity9. Tranquilizers 9. Diphtheria
10. Narcotics 10. Whooping cough11. Cross tolerance 11. Tetanus12. Reverse tolerance 12. Poliomyelitis13. Main effect 13. Measles14. Side effect 14. German measles15. Addiction 15. Mumps16. Withdrawal syndrome 16. Chickenpox17. Over-the-counter drugs 17. Common cold18. Medicine 18. Influenza19. Food and Drug Administration 19. Tuberculosis
(FDA) 20. Infectious mononucleosis20. Tolerance 21. Infectious hepatitis21. Synergism22. Alcohol
2 4 4

TEACHING IDEAS 126
Consumer Health
Consumer Health: Medical QuackeryCarolyn E. Cooper
An important aspect of consumerismis the evaluation of messages that areconveyed in advertisements for healthcare products or services. Only througheducated analysis can consumers decidewhich purported health care productsare quackery and which are legitimate.Since young adult consumers constitutea large target audience for advertisers, itis beneficial to teach analysis skills tostudents at the college level. Moreover,college students have indicated thatthey are interested in quackery andfraudulent health practices as a consum-er health topic (Gaines, 1984).
Therefore, a lesson plan was devel-oped to provide university students en-rolled in a lower division geileral healtheducation course with informationabout medical quackery and the oppor-tunity in small group discussims toanalyze health care advertisements. Thelesson's objective was to equip studentswith the knowledge and analytic skillsrequisite to making decisions aboutwhether or not advertisers are guilty ofquackery. The following lesson planmay be implemented either during oneor two class sessions (depending uponthe quantity of content covered) as acomponent of a larger unit on consumerhealth.
Preparation for the LessonPrior to class, photocopy advertise-
ments of suspect health care products,services, or programs. (The author se-lected advertisements from the two ma-jor newspapers in Los Angeles, the LosAngeles Times and the Herald Examiner, inaddition to the gossip tabloid, the Na-tional Enquirer. These newspapers ad-vertised such products as diet pills, sun-screens, anti-balding ointments, andvarious programs for weight reduction,acupuncture, smoking cessation, footsurgery, and impotence.) The teacher
Carolyn E. Cooper is a graduate student inthe Master of Public Health Program in theDepartment of Health Science at CaliforniaState Univergity, Northridge, CA.
should make enough copies of each adto ensure that when students are placedin groups, each group will have twoadvertisements and each group memberwill have a copy of both advertisements.Also, if possible, have different adver-tisements for each group so that no twogroups will have the same ad.
Content MaterialBefore students gather in groups to
analyze the advertisements, it may behelpful to conduct a brief lecture on thefollowing subject matter (Ensor, Means,& Henkel, 1985; Olsen, Redican, &Baffi, 1986).
I. Medical QuackeryA. Definitions
1. nostrumunproven andgenerally unscientific, se-cret "remedies" for ill-nesses
2. quackspurveyors ofmisinformation about thetreatment of disease, ill-ness or a condition
B. Common Characteristics ofQuackery1. product or service being of-
fered is a "secret" remedythat is not available from anyother source
2. sponsor claims to be battlingthe established medical pro-fession because it does notaccept his/her discovery
3. remedy or product is solddoor-to-door or by mail orderadvertisements
4. treatment is valuable for awide variety of illnesses
5. anecdotes and testimonialsare used to support claims
6. overnight success is claimed7. scare tactics are utilized8. free trial packages of medi-
cine or free first visitC. Characteristics of People Who
Are Prey to Quacks1. want instant cure for painful,
chronic, or incurable disease
245
2. want cure for ailment thatmedical practitioners havedifficulty diagnosing andtreating
3. believe they have had poorquality or unsympatheticmedical care
4. believe they cannot afford aphysician or a "high-priced"specialist
5. dissatisfied with their generalappearance and do not thinka physician will solve theproblem.
6. cannot accept the inevitableprocess of aging, i.e., bald-ness, gray hair, or wrinkles
II. Propaganda Advertising TechniquesUsed to Persuade Consumers to Buya Particular Health ProductA. Bandwagoneveryone is doing
or taking itB. Snob Appealonly the privi-
leged few use this productC. Testimonyit worked for me, so
it will work for youD. False Imageyou will be like
someone else (possibly a moviestar or athlete) if you use thisproduct
E. Rewards Appeal--free gift withproduct or upon signing up forservice
F. Humor appealuse of jokes orcatchy songs
G. Just Plain Folksordinary peo-ple use this product, just like youH. Scientific Evidencedoctorsrecommend this product
I. Non-verbal Appealextensiveuse of picturesUnderdog Appealwe're num-ber two, but we try harder
J.
Small Group DiscussionsAfter advising students of their task
to analyze these health care advertise-ments to determine if they are quack-ery, randomly assign students togroups so that each group consists offive to six students. Distribute the pho-tocopies of advertisements, discussed
235

above, to each group. (Each groupshould have two different advertise-ments to analyze.)
Distribute a 4x6 index card to eachgroup. The cards contain the followingquestions, which will be answered col-lectively by the group members.
1. What is the product, remedy, orservice being promoted?
2. Who do you believe is the intend-ed audience?
3. What type(s) of propaganda adver-tising techniques are being uti-lized?
4. What is the promised outcome?5. What characteristics does the ad
have that may make you suspi-cious of quackery?
6. Do you believe this advertisementis quackery? Why or why not?
Write the names of propaganda tech-niques, outlined in Section II of thecontent material, on the chalk board forstudents to refer to when responding to
question 3. The teacher may want tovisit each group briefly to answer ques-tions and to observe group members'interaction. Allow 20 to 30 minutes forthis exercise.
Have students select a spokespersonto present each group's answers beforethe entire class. When discussing theirgroups' advertisements, spokespersonsshould also comment on dissentingopinions, if significant. For example, itmay be interesting for the class to hearwhy three members strongly supportedthe opinion that an ad was quackerywhile three other members had the op-posite opinion.
An unexpected issue that arose whenthe author implemented this lesson wasthe origin of the advertisements. Stu-dents were curious to learn whichnewspaper co-tained which advertise-ment. The class expressed the belief thatmost of the advertisements were ob-tained from the National Enquirer, when,
in fact, the majority were selected fromthe Los Angeles Times and Herald Examin-er (perceived by the students to be con-siderably more reputable newspapersthan the Enquirer). Also, students foundit interesting that advertisements per-taining to impotence were located in thebusiness section, advertisements aboutbaldness were in t1 _ sports section, andweight loss advertisements were in thewomen's feature section.
Ensor, P.G., Means, R.K., & Henkel, B.M.(1985). Personal Health (2nd ed.). NewYork: John Wiley and Sons, 286-289.
Gaines, J. (1%4). A study of the consumerhealth interests of selected college stu-dents. Journal of School Health, 54 (11),437-438.
Olsen, L.K., Redican, K.J., & Baffi, C.R.(1986). Health Today (2nd ed.). NewYork: Macmillan Publishing Co., 554-560.
tolk.oft
041/410%1144*- e\-4340*`
0.4."$100 1000
(' e klac
0°41&-/-911°
v° 0004\S 01,1%*
SOS. *IS it404)04
236

TEACHING IDEAS 127
Environmental HealthEnvironmental Health Simulations:
Island City and ProductionGlenn E. Richardson, Alan Burns, and Janet Falcone
Often it is difficult for students toenjoy concepts associated with environ-mental health because it is difficult toapply personally. Simulation activitiesare often beneficial and make a unitmore interesting by helping studentsunderstand the complex issues associat-ed with environmental control. Thepurpose of this paper is to give twoexamples of simulation activities thatare fun, mimic or simulate environmen-tal dilemmas, and allow for active par-ticipation by many students.
Island CityThe purpose of the Island City simu-
lation is to have students understandthe environmental problems associatedwith growth and to sense some of thefrustration of city planners who dealwith the vroblems. The materials andwhat they represent in the story are asfollows:
1. Poster paper (2' x 3') is the is-
Incense represents factories.Cups, coffee filter, and water rep-
reont the water treat:nent plant./' Uncooked bearo, represent peo-
ple.!'. Ash trays are usc as incinera-
tors.6. Newspaper is solid waste.7. Coffee and tea grounds are water
pollutants.8. Tape recorded city sounds repre-
sent noise pollution.9. A non-aerosol spray or perfume
spray represents air pollution.10. Small toy cars represent the
means of transportation.
Glenn E. Richardson is chair of the Depart-ment of Health Education at the Universityof Utah, Salt Lake City, UT 84112. AlanBurns is a health and physical educationmajor in the Department of Health andPhysical Education at Texas A&M Univer-sity. Janet Falcone is in community educa-tion in the A&M Consolidated School Dis-trict, College Station, TX.
Students are divided into groups ofeight or more people (the number canvary based on the number of tasks) andeach group is given the following setup:The piece of poster paper is placed inthe middle of the group. Students areinstructed that this is their island wherethey live and cannot leave. It is theirresponsibility to keep it clean and beau-tiful. Each group is given a bag of mate-rials as described. Each student is givena bean to represent themselves on theisland and may draw a small home andselect his or her automobile. A factory(incense) where they work is also placedon the island and lighted. The watersource (cup of water), and waste dispos-al site (ash tray) are also located wherethey deem appropriate. A commercialarea of the island should be selectedwith stores, an area designated forparks, national forest, and wildlife pre-serve.
The activity begins with the followinginstructions:
I. Every 10 seconds a new bean isadded to the island, which representspopulation growth.
2. Another car is addedute.
3. Add another factoryminutes.
4. Torn paper is addedconstantly.
Each student is given athe process. The following are repre-sentative of the tasks:
1. One person maintains the cleanli-ness of the water supply.
2. One person builds new homes forevery set of three beans. Group consen-sus is necessary to determine placementor they go to a shelter which the homebuilder makes.
3. Two people help to coordinate thesubdivision and roadways connectingthe homes and factories (draw in roadswith pencil).
4. One person adds people and cars.5. Another person adds the factories.
He or she needs to get group approvalwithin 10 seconds before placing thefactories.
every min-
every two
slowly, yet
task during
2 4 7
6. One person should be responsiblefor maintaining parks and natural areason the island.
7. Someone is responsible for remov-ing and burning solid waste. (Note: Besure it is permissable to burn bits ofpaper; if not conduct the activity whereyou are permitted to do so or delete thispart of the activity.)
The instructor begins with the citysounds at very low volume and every 30seconds or so turns up the volumeslightly until it is quite loud by the endof the activity. Additionally, the instruc-tor should drop coffee or tea groundsinto the water source, causing the stu-dent responsible for the water source togo through the filtering process.
The activity continues until the chaosand confusion reach a breaking point.Discussions should revolve aroundquestions related to frustration associat-ed with controlling population growth,coordination of environmental controlservices, and cooperation among serv-ices when growth is so rapid.
Production1 he purpose of this activity is to simu-
late developing, refining, using, andrecycling of products. The student willexperience some of the frustrations as-sociated with reclaiming raw materials.
The materials necessary for this simu-lation are as follows:
1. Three 3" x 3" x 1/2" squares ofplaydough, each a different color (red,white, and blue) for each participatinggroup.
2. A clear wrap and label for eachgroup. Labels should have productssuch as car, airplane, milk carton, andbook written on them.
Divide the class into four groups (de-pending on the size of the class) andgive each group red, white, and bluesquares of playdough wrapped in clearwrap labeled as a particular product, i.e.car or airplane. There will be five stepsto this method, each step taking 5 to 7minutes.
Step / (Raw Materials to Parts): Thefirst step is for each group to take "raw
237
materials" (playdough squares) andconstruct the parts for the product indi-cated on the label. For example, if mem-bers of the group are constructing a car,then wheels, body, bumper, and lightsshould be manufactured but not assem-bled. Note: All or part of the playdoughmay be used for manufacturing partsbut any that is not used will remainbehind as waste.
Step 2 (Assembling): Moving clock-wise between groups, the students passtheir manufactured parts to the nextgroup so that every group has partsmade by a different group. The groupsare to act as assembling factories andput the product together.
Step 3 (Consumer Use): Groups thenpass their finished products clockwiseagain to the next group This is theconsumer stage The ultimate outcomeis that the product will be used andworn out. The car may get into a wreckor the milk carton smashed
Step 4 (Recycling) The products arenow passed to the next group to besalvaged and used for another purposeThe students are to take the worn out orwrecked product and make something
238
else from it, utilizing ,he same materialsand parts.
Step 5 (Restoring): he recycled prod-ucts are passed ba,lc to the originalgroups. The groups should now try torestore the product to its original rawmaterial state (three squares of red,white, and blue playdough). It will bevirtually impossible to do this becausethe colors will be mixed due to thestickiness of the playdough.
Students will be asked to smell theirhands following the activity. They willsmell the distinct smell of the play-
BEST COPY AMME 2 ,1
dough. This can represent the humanexposure as the people work with someraw materials. The students will be sointent on making their products thatthey will forget that they are being ex-posed to the "contaminants." The anal-ogy is that many times people are sointent in making money that they forgetthe health consequences of exposure totheir products.
Discussions will revolve around theissues of depletion of raw materials,factory hazards, assembly line stress,recycling, and economic issues.

TEACHING IDEAS 128
Family Life Education
Reducing Anxiety About Teaching a HumanSexuality Program
Louise Row ling
One of the problems for schools in thedevelopment of a human sexuality pro-gram is the inadequate preparation ofteachers, many of whom feel anxious,embarrassed, and h rful of questionsadolescents will ask. Preparation ofteachers of human sexuality at a preser-vice or inservice level should aim to easesome of this discomfort (McCarthy,1983).
Health educators have frequentlyused rehearsal behavior as a means ofpreparation for future events.M7Guire's (1969) concept of psychologi-cal inoculation adds to the belief thatexamining a situation, and practicingways o cope with it before it is experi-encerl ,,hould help reduce anxiety anddevelot cor ing skills. These beliefswere coi,,bined with Finn's (1981) onhow to deal with personal questionsfrom students, to develop a cognitivebehavioral technique that would enableteachers or trainee teachers to:
anticipate controversial questionsfrom adolescents relating to sexualityprepare responses that they wouldfeel comfortable verbalizinggain experience in using "the lan-guage of sex."The last aim attempted to fulfillBruess and Greenbera's (1981) criteriafo ,. sex educata-s"The teacher sex (!ducationneeds to be able to use the languageof sex easily and naturally, especial-ly in the presence of the young."
Implementation of the Activity1. Initiate a discussion focussing on
the handling of controversial is-sues in the health curriculum. Of-ten issues such as drugs and sexu-ality involve personal questions
Louise Bowling is a lecturer in the HealthEducation Department at Syu'l.ey Instituteof Education, P.O. Box 63, Camperdown2050 New South Wales, Australia.
from adolescents to the teacher.2. Present the three general ways of
responding to personal questionsproposed by Finn (1981): answerhonestly, refuse to answer, equiv-ocate or lie. Further exploration ofthese can then develop responseguidelines: ensure educational va-lue, be comfortable, be aboveboard(Finn, 1981).
3. Orient the discussion toward re-sponding to questions in humansexuality lessons. Produce a ques-tion box and ask participants towrite on a sheet of paper (anony-mously) any questions they thinkthat an adolescent may ask thatthey would feel uncomfortable orhave difficulty responding to. Thebox is collected, the questionstyped up, and a sheet of the ques-tions handed out to the partici-pants in the next session. (Thesession leader may also have add-ed some questions.) Examplescould include: "Do girls like it asmuch? Are you a virgin? Is it dan-gerous to masturbate?"
4. Participants then prepare respons-es to all the questions by discuss-ing with friends and family and/orthrough reading.
5. At a subsequent session, partici-pants are divided into smallgroups. (The session leader hasprepared question boxes, one foreach group, with the questions onindividual sheets of paper.) Eachgroup sits in a circle, one partici-pant selects a piece of paper andasks the question of the personopposite. That person responds,preferably not reading a preparedanswer, but giving the generalidea of a planned response. Thebox is passed on around the circleuntil all questions have to be askedand responded to. (The length ofthis activity wiH depend on thenumber of questions.)
249
6. Small group discussion can occurafter each question and answerand/or after the activity as a whole.Issues that may be considered are:the impact on adolescents of theresponses, how participants felt,how difficult the research was. Ageneral summary should focus onparticipants describing what theyhad gained from the exercise.
Feedback on the ActivityParticii its have stated that the activ-
ity:forced them ,o personally confrontmany issues about sexuality educa-tion;under the guise of completing anassignment, opened up topics ofdiscussion with friends and family,topics previously not broached;highlighted the need for the avail-ability of simple straightforward in-formation on sexuality for adoles-cents;made them feel more comfortable indealing with questions from adoles-cents. This was based on the beliefthat it would be harder to deal withthese questions among their "sameage" group rather than with adoles-cents in the classroom.
The author has used this process suc-cessfully a number of times at the pre-service level and believes it could beequally as effective in inservice pro-grams.
Bruess, C. & Greenberg, J. (1981). Sex educa-tion: Theory and practice. Wadsworth: Bel-mont, CA.
Finn, P. (1981). Hey, Teach! Do you drink!Journal of School Health, 51(8), 538-542.
McCarthy, W. (eu) (1983). Teaching about sex.The Australian experience. George Allen &Unwin Sydney.
McGuire, . J. (1969). The nature of atii-tude, -id attitude change. Lindzey, G.
'Irons; F. (eds). Handbook of socialp. Otology, Vol. 3, Addison Wesley:Reading, MA.
239
TEACHING IDEAS 129
Are.You Readyfor Prime Time Birth Control?
Pamela Wild and Linda Berne
Family Life Education
Grade Level: 9-12 (7-12 for high riskstudents)Time: Two class periods, 50 minuteseachMaterials: Questionnaire, paper, pen-cils, chalk board
Concepts: If a couple has sexual in-tercourse, they must perform many skillsto use birth control effectively and avoida pregnancy. It is harder for teenagers tobe effective contraceptors than for olderadults.
Teacher Background: "Why arethese kids getting pregnant when clinicsgive away free birth control?" is aquestion commonly asked by those whoare concerned with teen pregnancy.Perhaps the answer lies in the fact that ofthe annual abortions performed in theUnited States, less than a third are toteenagers. Adults, who should have theknowledge, maturity, resources, and lifeexperiences that would enable them toprevent unintended pregnancies oftendon't do much better than teens.
For adults or teens to preventpregnancies, a multitude of skills mustbe learned and used. Teenagers, however,must clear additional hurdles: denial ofimpending behavior, believing thatnothing can happen to them, failing tosee consequences of behavior, immobi-lizing fear or guilt of being "found out"or "planning it," lacking transportation
PamelaWild is with the Children andYouth Services of Chattanooga, T N.Linda Berne is professor of health edu-cation at the University of North Caro-lina, Charlotte.
240
or money, inability to express concernsor emotions about sexuality, and igno-rance of or mis:nformation about lawson confidentiality and age requirementsfor obtaining contraception.
Because life planning is so criticalto opportunity in today's world, learningthe skills to contracept and becomingmotivated to use them are major needsof teens and adults who currently are orwill be sexually active. Rather thanasking "Why do teens become preg-nant?" we should be asking "What pre-vents a teen from avoiding pregnancy?"Instruction to affect attitudes, knowl-edge, skills, and behaviors is necessaryto help youths achieve positive rela-tionships, sexual health, and maturity.
Objective: The student will identifyskills needed to be an effectivecontraceptor, determine those in whichhe/she has competence, and develop theskills that would be difficult or impos-sible to perform.
Procedure: Say "We have alreadydiscussed how it takes skills to remainabstinent when there is so much pressuretoday to be sexually active. Let's reviewsome of the skills you need to avoidunwanted sexual behavior" (see Berne& Wild, 1988). Write the skills studentssuggest on the chalkboard.
Session 1Activity 1: Say "It takesmany more skills for a person who ishaving sexual intercourse to avoid anunwanted pregnancy or STD. Divideyourselves into groups of four. Brain-storm and write down all the skills youcan think of that a person must perform
25(i
to use birth control successfully." (Theteacher should review the rules forbrainstorming.) Tell students there areabout 30 skills and challenge them tocome up with 15 or more. Give 15 min-utes for this activity and move amonggroups, prompting ideas.
Pull groups together and make amaster list of skills. Have students writethem on a sheet of paper with threecolumns to the right labeled "easy todo," "hard to do," and "impossible todo." Ask each student to make fourcopies of their sheet or make four pho-tocopies.
Homework: Say "For homework,give your 'skills survey' to four peoplenot in this class. Ask them how easy,hard, or impossible each skill would befor them to do now if they were sexuallyactive. Try to have both sexes and adultsas well as teens answer your questions.Record their age and sex, but not theirname on the sheet. We will discuss yourresults on (day due give three days)."During the interim days, teach aboutcontraception.
Seccion 2Activity 2: As studentsenter class, give each the questionnaireand have them rate their own comfort!skills and write why the skill is easy,hard, or difficult (20 minutes). Havestudents get out their homework surveysand review each skill one at a time,asking for reasons why they and otherpeople they surveyed ranked the skill asthey did. If you sense denial, play devil 'sadvocate to bring the discussion to real-ity. If you sense embarrassment, movethe discussion to "third person."

After going through the list, askstudents to identify the most difficultskilis and circle them. Have studentsbreak into groups and brainstorm sug-gestions and solutions to help a personovercome the difficulty in carrying outthe skill. Share with the class afterwardsand record ideas. Ask for "thumbs up"and "thumbs down" as to whether theythink the solutions would work.
Processing Questions:1. Can a person be sexually respon-
sible without using contraception?1 If you are too embarrassed or timid
to do these skills, are you mature enoughor in the right relationship to be havingsex? Why? Why not?
3. Whose responsibility should con-traception be? Why?
4. If two people equally share thepleasures of sex, how can the responsi-bilities be equally shared?
5. What could society do to assistsexually active teens in being bettercont.raceptors without encouraging pre-marital sex?
Closure: Ask students what theywould like to do with the new informa-tion they learned. Some possible serviceprojects are:
Write a letter or send a studentdelegation to talk about findings withthe health department, school, localnewspaper, family planning council, orlegislator.
Tour local clinics and rate theirservices as being accessible or "userfriendly" to teens.
Develop an educational pamphletor radio public service announcementdirected toward sexually active teens.
Participate in peer counselor train-ing to help learn and teach skills thatstudents have problems with.
Write a creative skit for a teenaudience and give performances. Allowthe audience to interact in a discussionof the issues.
Evaluation:I. Rate yourself:
"1" - I probably would not become
involved in a pregnancy if I were sexu-ally active.
"2" - I might become involved in apregnancy if I were sexually active.
"3" - I would become involved in apregnancy if I were sexually active.
Explain why you gave yourself therating that you did.
2. Give detailed explanations of your
strong and weak skills as well as otherpersonal strengths and weaknesses as apossible contraceptive user.
3. What could you do to improveyour birth control consumer skills?
Berne, L.A., & Wild, P.J. (1988).Teen sexualbehavior: A leader's guide to practical strat-egies with youth. Reston, VA: AAHPERD.
ARE YOU READY FOR PRIME TIME BIRTH CONTROL?
Imagine you are a sexually activeperson but are not ready for a preg-nancy. Rate your ability to do the follow-ing birth control skills:
(1) ft would be eat for me to . . .
(2) It would be had for me to . . .
(3) It would be impossible for me to . . .
1. admit to myself that I'm goingto have sexual intercourse.
2. admit to myself that I could getpregnant or impregnate my partner.
3. talk about my/my partner'spast sexual experiences to see if one orboth of us could be carrying STDs.
4. talk with partner about needingbirth control and which method is best forboth of us.
5. before having sex, decidingwith partner what we would do if a preg-nancy does occur.
6. get transportation to clinic ordoctor's office
7. go alone (or with partner) tohealth department, public clinic, or pri-vate doctor's office.
8. talk to strangers (doctor, nurse,counselor) honestly when they ask mequestions about my sex life.
9. have an internal pelvic exam,or go with my partner for a pelvic exam.
10. ask questions when I don'tunderstand the instructions.
11. read and understand the in-structions that come with birth controlmethods.
12. buy birth control methods in adrug store or out in the public eye.
13. pay for birth control methods.25
when I can not get them free at a clinic.14. store birth control in a cool,
dark, and dry place.15. practice applying and remov-
ing birth control method prior to sexualintercourse.
16. use a birth control methodcorrectly every time I have sexual inter-course.
17. use a backLp method of birthcontrol or abstain for the first four weekstaking the pill.
1 8. remember to take pill at thesame time each day, or remind partner.
19. use more than one method(pill and condom) for more protection.
20. touch my sex organs to applyand remove birth control method.
21. touch partner's sex organs tohelp apply or remove birth control method,
22. apply birth control in front ofmy partner.
23. stop myself during sexualforeplay to apply birth control methods.
24. stop sexual partner duringforeplay to apply birth control methods.
25. remember possible side ef-fects of my birth control method andknow what to do if they occur.
26. carry birth control with me, orget it before sexual foreplay begins.
27. return to clinic for regularmedical check ups.
28. remember to get more birthcontrol items before they run out.
29. continue to educate myselfand learn new information on birth con-trol methods.
45 Copyright 1990 P. Wild & L. Berne
CEST COPY AVMAKE
241
TEACHING IDEAS 130
Family Life Education
"Hey! How Did That Baby Livein That Test Tube?"
David A. Birch
Health education, like other academicareas, often relates directly to currentissues and events extensively coveredby various media. A current issue gen-erating media coverage, invitro fertiliza-tion and embryo transfer or "test tubebabies" has created curiosity amongboth adults and children.
However, even with extensive mediacoverage, not everyone understands theprocedure involved with invitro fertil-ization. Part of this confusion can betraced to the commonly used term "testtube baby." The author, in his experi-ence with junior high school students,became aware of many students whoseperception of invitro fertilization includ-ed a live baby and a test tube. Thus, tosome students, the question, "Hey!How did that baby live in that testtube?" is not as ludicrous as it mayseem.
Another contributing factor to thismisunderstanding is the tendency forboth children and adults to look at orlisten only to the headlines and not thedetails of a story. Thus if a child, or evenan adult, hears only "test tube baby," itis easy to imagine misconceptions thatcould occur.
Because it is an important currenthealth issue that could impact upon oursociety, these misunderstandings andmisconceptions can and should be dealtwith in health education classes. Thereare many areas in the health educationcurriculum which would relate directlyto invitro fertilization and embryo trans-fer. The following information andteaching ideas should assist the healtheducator in covering this topic.
BackgroundInvitro fertilization and embryo trans-
David A. Birch is with the Department ofEducational and Cultural Services, StateHouse Station 23, Augusta ME 04333.242
fer is a procedure allowing women withblocked or missing Fallopian tubes tocarry a baby in the uterus and subse-quently give birth. Prior to institution ofthis procedure, these women were con-sidered to be infertile.
Following births in England and Aus-tralia, the first American "test tubebaby" was born in January, 1982. Theterm "test tube baby" is a misnomersince the procedure involves no actualtest tu'oe.
Using r,.rtility inducing hormones tocause ovulation at a specified time, along tube with a syringe is inserted atthe time of ovulation through an inci-sion in the abdomen and used to pullfluid containing the egg cell from theovary. The egg cell is then depositedinto a petri dish which has an environ-ment similar to that inside the Fallopiantubes.
Sperm cells from the father are thendeposited into the petri dish so thatfertilization can occur. If fertilization oc-curs, the egg cell is inserted into theuterus through the vagina. If the fertil-ized egg implants itself into the wall ofthe uterus, prenatal developmentshould continue.
While this procedure offers hope tosome couples, there are objections tothis procedure. Objections focus on is-sues such as the possible discarding ofabnormal embryos, the potential risk tooffspring from the procedure, the costof the procedure, and the idea of physi-cians and scientists "playing God."
VocabularyTo understand the procedure, stu-
dents should become familiar with thefollowing vocabulary words: uterus,Fallopian tubes, ovulation, egg cell,menstrual cycle, fertilization, infertile,sperm cell, and embryo.
Classroom ActivitiesThe following activities should help
9k)
students understand cognitive aspectsrelated to invitro fertilization and em-bryo transfer:
Using a drawing, chart, or model, dem-onstrate to students the path the egg cellnormally follows through the Fallopiantube to the uterus, after ovulation.Using a drawing, chart, or model, ex-plain to students the ramifications ofblocked or missing Fallopian tubes on awoman's ability to have children.Using the same drawing, chart, or mod-el, explain to students how an egg cell isremoved from the body after ovulation,fertilized in a petri dish, and insertedinto the uterus.A:ow students to make their own au-diovisual aids and to explain and reviewthe situations listed above with theirclassmates.
Students should also be given an op-portunity to discuss related affective is-sues. A classroom discussion of the fol-lowing questions will provide this op-portunity:
Do you feel medical science has gone toofar with invitro fertilization and thatscientists are, in effect, "playing God"?Is it more appropriate for a couple that isinfertile because of blocked Fallopiantubes to opt for invitro fertilization or toadopt one of the many children a? ',blefor adoption?Should embryos that have developeddeformities before implementation bediscarded?Should private and public health insur-ance plans cover the cost of invitrofertilization and embryo transfer proce-dures?
The issue of invitro fertilization andembryo transfer or the "test tube baby"issue stimulates interest in all agegroups. Hopefully, the suggestions list-ed above will provide health educatorswith ideas for students at various levels.It is a current health issue with interestand implications for all segments of oursociety.

TEACHING IDEAS 131
Family Life Education
Actions Teach Better Than Words: Teen LifeTheater and Role Play in Sex Education
Peggy Brick
Eft
"Here comes the Teen L;fe Theater," Ishout as 12 young actors dressed inlogoed blue tee shirts run onto the stageand begin to introduce themselves. "I'mMargo and I wish my mother would tryto understand me." "I'm Leo and I wishI didn't have VD." "I'm Marni and Iwish my brother wasn't gay." "I'm Caland I wish my friends wouldn't pres-sure me to smoke." When the introduc-tions are over, the individual scenesdepicting problems of adolescent lifebegin. The audience of students, par-ents, administrators, and board of edu-cation members is confronted with 12unresolved dilemmas, such as the one
Peggy Brick, recently retired from teachingHuman Behavior, is Director of AffirmativeTeaching Associates in Englewood, New Jer-sey and sexuality educator at Planned Par-enthood of Bergen County, New Jersey.
SRt.
;he 'r '
:
f
4
called "Sex Pressure" in which Robinand Tony arrive at the front door anddiscover a note saying that Robin's par-ents won't be home until late. Tonypresses to come in, hut Robin refuses:the family has a strict rule about boys inthe house when Mom and Dad are notthere. He insists; she resists. He getsangry and leaves, taunting, "Why don'tyou grow up?" At the end of the perfor-mances, the actors remain in their roleswhile the audience questions, chal-lenges, and even joins them in tryingalternative solutions. A few weeks laterthe board of education votes unani-mously to fund this improvisational the-ater, thus adding a new dimension tothe sexuality education program at--`wight Morrow High School in Engle-wood, N.J.
After fifteen years teaching sexualityeducation, I am convinced that this ex-periencing of adolescent dilemmasthrough life-like skits presented by thetheater troupe, or in classroom role-
253
#.
play, is a powerful method of educatingfor responsible sexuality. Many sex edu-cators, busy "winning the battle" (Dick-man, 1982), developing curriculum, andfielding questions, need to be remindedthat improvisational theater may be thequintessential tool. Here the importantingredients of effective sex educationcoalesce. As students get into the act,they gain self-confidence, explore rela-tionships, critique behavior, developskills in communication and decision-making, learn to understand differentpoints of view, and dernystify sex. Inour school, the Teen Life Theater nowprovides a model that encourages role-playing activities in the regular class-rooms. In both formats students have aunique opportunity to practice con-fronting problems in their own lives.Our experience leads me to believe thatimprovisational theater should be a fun-damental part of the family life educa-tion curriculum and basic in the preparation of sex educators.
243

Although family life theaters have be-come popular in a number of youthagencies during the past ten years (Na-tional Clearinghouse for Family Plan-ning Information, 1982), few are sup-ported by a board of education as part ofthe regular school program. Ours, initi-ated by a small grant from the county'sPlanned Parenthood, has been fundedsince 1981 by a board that values thisdirect method of confronting adolescentproblems and appreciates the fact thatin our multi-ethnic community, theTheater is unusual in its ability to attractstudents from a variety of groups. It is aliving example of the intergroup cooper-ation and friendship that the board ad-vocates.
During its first two years, the troupeperformed at the state teachers' conven-tions, at institutes and workshops train-ing teachers as family life educationeducators, and at a wide variety ofschools, churches, community organi-zations, and youth groups. Within ourown district they performed in health,behavioral science, English, and biologyclasses and in a number of mini-assem-blies. Each performance is custom de-signed. During a session, following theperformance of six to twelve skits, theaudience may also get into the act.
Training the Theater TroupeTeen Life Theater is an extracurricular
activity, and 15 to 20 members trainafter school for two hours two days aweek. The members also study the is-sues they are working on through read-ing, interviews with authorities, andfilms. Each receives a copy of R. Bell'sChanging Bodies, Changing Lives (1980) asa basic resource. In addition, many ofthe actors are taking or have alreadytaken the Human Behavior coursetaught by my co-advisor and me. Thecourse and the Theater complementeach other lany ways.
At tl ling of each rehearsal,ttinte . (Spolin, 1963) defuseanx:e low n self-conscious-ness coup spirit. We start bysta- and one by one callou e. r1 a ( razy way, the groupec chnique adapted 1. Jin a
r'ivback Theater). Next, a-) the center and creates
a tion," an action usingboth voi. She moves in frontof another ,.nber who imitates her,and, as she returns to her place in thecircle, evolves her own action. The proc-ess is repeated as each invents, is imitat-ed, laughed with, encouraged.
A final warm-up might be the ma-244
chine exercise. One student begins amachine-like action with an appropriatesound. Others slowly add on, fittinginto the building machine, which finallyslows down and stops. Relaxed andenergized, students are already practic-ing acting skills: perceiving, respond-ing, imagining, creating (Siks, 1977).
During the early weeks, the directoremphasizes the most fundamental skill,concentration, as students struggle tosolve a variety of acting problems. Stu-dents must focus on each body sense,making "the object real" and trying toshare their experience with their audi-ence. They practice with half the troupe"on stage" while the other half ob-serves. As the actors learn to focus,distractions are ignored and phoninessdisappears; forgetting themselves, they"solve the problem" with increasingcredibility. By being alternately actorsand audience, students learn to evalu-ate when actions seem real and arecommunicated effectively.
Learning to ImproviseSoon the students are ready to solve
larger problems by improvising a varie-ty of scenes together. "You are on aboat. There's hardly room for all of you.It's beginning to sink. It goes under.""You are climbing a hill. It's very rocky.A strong wind comes from the summit.You reach the top and the view is beau-tiful." "You are all lifting a heavy box.You need more people. Gently now,up, up." Those observing are watchingfor concentration so complete they canfeel the cold water, the strong wind, theheaviness of the box.
Next, students experiment with be-coming different characters. The entireclass mills slowly around the room:"You are 75 and going for your dailywalk." The director gives actors time tobecome the character. Some will behealthy, striking with vigor; others willbe crippled, plodding with difficulty.E.ch time, actors create their own char-acter according to their own feelings.Later, actors will take much more timeto develop the characters in skits forperformance. For now, they are tryingto experience themselves in another'sbody, imagining how that body reacts.
Grad aally, these exercises changeself-col iscious posturers into persuasiveactors. Actors will need considerablerehearsal in creating meaningful skits,but for most of them, their acting nowwill be natural and real as comparedwith most amateurs.
They are ready to begin "playmak-ing" (Siks, 1977), developing the skits
2 c t
about adolescent life that are the es-sence of Teen Life Theater. They brain-storm all the problems they might wantto explore, select several, and divideinto small groups to plan. They work onthree areas: (1) The scene. Where andwhen is the incident occurring? What isbeyond the scene in the present? in thepast? in the future? (2) The characters.Who are they and what are their rela-tionships? (3) The Conflict. After discuss-ing these issues, they plan the basicactions and try them out.
When they feel some satisfaction, or ifthey are stuck at some point, they re-turn to the whole group to work furtherwith the director and present the germi-nating skits. Two boys are at urinals;one has a painful burning sensation,and they're off on a discussion of STDs.Three girls are in a locker room with onerefusing to smoke and suffering thejeers of her friends. A girl tells herboyfriend that she is pregnant. Parentsare upset with their son's interracialdating. A shy boy and girl struggle,merely to say "hello." A girl tries to gether alcoholic father to stop drinking.Each skit will have a fixed beginningand end, but no final resolution to theconflict. The aim of the Theater is toinvolve members of the audience in thecrisis and leave them to work out theirown solutions.
As students present rough skits, thedirector utilizes a number of techniquesto help develop the drama being impro-vised. These methods facilitate thedeeper exploration of character and sit-uation and never instruct the actor inhow to act. The director's job is to helpstudents discover the right action in theircharacter and situation in some of thefollowing ways: (1) Act out an eventthat occurred before the present scene,to help "see" what caused this situa-tion; or act out a future scene to under-stand the result of present actions. (2)Reverse roles. (3) Double: the director oranother actor stands behind the charac-ter and while shadowing the actions,occasionally speaks a thought or feelingthe character may not be expressing. (4)Coatrapuntal argument: two actors inconflict, speaking simultaneously, as-sert their own argument without re-sponding to each other. (5) Repeat thescene in pantomime. (6) Freeze thescene and ask the characters questions:"Did your mother treat you differentlybefore she remarried?" "Do you getalong better with other teachers?""Have you ever had a long-term rela-tionship with a boy?" (7) Freeze thescene and have each character assess

how the scene is "working" for them.(8) Change the pace if skit is serious,and make jt into a, comedy; if it's fast,"cool it." (9) "Physicalize" what's hap-pening: for example, a child being "tornapart" by the parents' divorce. (10)Have a character monologue with theaudience.
After eight weeks of this training,students are ready to perform beforereal audiences and to answer the chal-lenging questions that will follow. Westart off performing for classes withinthe school, but soon, we are out in thecommunity and the responses revealthe impact. Parents report they had noidea that adolescents had so many prob-lems. Teachers say the skits help themunderstand their students' attitudes to-ward school. An administrator writesthat the skits made his students awareof their own disruptive and aggressivebehaviors. A minister says it helpsmembers of his congregation realize theneed to develop a sex education pro-gram for the young people of thechurch. A professional whispers shewishes she had had the opportunity tosee such a program when she was achild being sexually abused.
Role Play in the ClasspiomThere are, of course, significant dif-
ferences between the Theater and class-room role play. Teen Life Theater is avoluntary, extracurricular activity di-rected to produce an entertaining aswell as educational performance. In theclassroom, however, I must be justifiedin taking time from other academic ac-tivities to have students play-act. Someteachers are uncomfortable with thisidea, worrying, as one wrote at a recentworkshop, that students will "goof off."And one administrator complained thathe couldn't evaluate my lesson becausethe students were role playing and hecouldn't "see me teach."
Both of these perceptions are mistak-en. Yes, students do enjoy the acting,but through it they are dealing with
roblems of real life. I find students tobe very serious about that. As for myteaching, I believe it is especially skilledand meaningful when I am facilitatingrole play. Here I am demonstrating thatthe information students are learning inmy class is not just for knowing but forusing. Role play, more than any otherin-class pedagogical technique, forcesstudents to apply learning to life. Al-though the same dilemmas can be ex-amined in writing assignments and indiscussions, the problems tend to re-main cognitive, often subject to glib and
heady solutions. But when students act,emotions and complexities surface andthe situation is experienced more fully.Acting allows students to experiencethemselves and others as whole personsin real-life contexts. With emotion-ladedmaterial such as sexuality, I find thisapproach indispensable. It is an effec-tive prelude to honest discussion, seri-ous writing, valid learning, and reten-tion.
Although seeing a Teen Life Theaterperformance reduces student fears ofacting and makes my task in the class-room easier, I still use a number ofstrategies to encourage the maximumpossible participation in role play. Iwant everyone to experience them-selves as someone else, to gain theempathy that comes from "being anoth-er." Here are three of the methods I use.
For the first, students take on a role,but do not act in front of the class.Desks are arranged in twos and, asstudents arrive, they divide into cou-ples. Each pair will negotiate contracep-
BEST COPY At" 25
_At
tive decisions in imaginary situationslisted on their assignment sheet: (1) Youare both 14 znd are considering havingintercourse for the first time. (Studentsalmost unanimously select abstinencefor this one.) (2) You are both 23, livingtogether, wanting to finish graduateschool before you get married. (3) Theman is 33 and the woman is 28; you aremarried; you do not want to have anychildren because a child would interferewith your career plans. In each case, thecouple must record their decision, notewhy they selected the method they didand what steps they would need to taketo implement their decision. After thecouples complete their work, the classdiscusses the choices: explaining, argu-ing, revising as they hear each others'reasoning.
This exercise is valuable for severalreasons. It normalizes talking 'co a part-ner about birth control. In enables stu-dents to apply their knowledge of con-traception in specific situations. It dem-onstrates that people of different ages
245
must communicate openly if they are tobe sexually responsible. Finally, itmakes clear the difference betweenmaking a decision and acting on thatdecision. This exercise is as close as Ihave come to breaking down the inhibi-tions that prevent contraceptive useamong some sexually active adoles-cents.
A second method I use to facilitatestudent comfort in role play is placingstudents first in small groups. (Oftenthey may select their own group withthe stipulation that there is at least "onemale, one female, one black, and onewhite" in each.) The group's first task isto reach agreement on what the maincharacter should do in each of five situa-tions. After the group has completedthis assignment, it chooses one to actout for the entire class. This seems to benon-threatening and almost all studentsenjoy taking part in these skits.
After each group rehearses and actsout its skit, as in the Theater, membersstay in role while the class questionsand challenges. Since others have al-ready come to their own conclusionsabout each scene, discussion is guaran-teed to be lively and meaningful.
A third method demonstrated byMartha Roper at Syracuse University in1981 involves all the students as part ofa support system for the actors on stage.For example, for a scene in which Johnis telling his mother and dad that hisgirlfriend, Jenny, is pregnant, the classwould divide into three groups: onesupporting John, one supporting hisdad, and one, his mother. Each groupwould receive a card describing its char-acter; "Jenny's mom is 44 years old, andhas two younger children: Brian, 10 andSam, 13. She has been a comrIter pro-grammer for five years and enjoys herwork but worries that she leaves hechildren alone too much. Her salary isimportant for the family, especiallysince John plans to go to college nextyear. She frequently speaks with disap-proval about teens who are sexuallypromiscuous. She has just come homefrom her aerobics class."
The card is read and the group selectsa person to play the role. The groupmakes suggestions to its character and,during the enactment of the scene, canmake recommendations in writing. Thecharacter can also leave the scene andask another member to continue theaction.
To begin, characters move to the frontand, after introducing themselves, startthe action which continues until there isa natural break. The actors are iold toreturn to their groups for coaching or246
for replacement. The scene then contin-ues until a two-minute warning signalsthe end.
Following this drama, I might do adifferent kind of processing: (1) Haveeach player share reactions about therole and feelings toward the other play-ers. (2) Have the class discuss the inter-personal dynamics that developed dur-ing the scene. (3) Discuss how the scenerelates to the students' own lives. Care-ful processing is essential to successfulrole play. The teacher's questions helpstudents understand the significance ofwhat has happened so they gain insightinto their own feelings and into humanbehavior.
Once students are accustomed to roleplay, our procedures become more in-formal. Anonymously, students submiton file cards problems they would liketo see enacted. I'll read a card, ask forvolunteers, and develop the scene onthe spot. The school year is never longenough to explore all the problems stu-dents continue to submit.
Evaluating the Effects of TeenTheater and Classroom Role Play
At a time when everyone is searchingfor hard data on the effects of sex educa-tion, the evaluations of our programs,to date, are soft: responses, both writtenand oral, from audiences and sponsor-ing organizations, taped interviewswith members of the Teen Life Theatertroupe, both as individuals and togetherin a group; hundreds of student jour-nals and essays that include discussionof theater performances and classroomrole play. There are no statistics to docu-ment significant behavior change as aresult of participation in improvisationaltheater. There are only the subjectivereports of both participants and observ-ers.
My interviews with Teen Life Theatermembers show that they believe theTheater has had a positive effect on theirlives. Many report increased feelings ofself-confidence.
Teen Life Theater also benefits itsmembers through the strong bondingthat develops between them. The The-ater nurtures friendships and gives stu-dents a positive identity.
Student responses reinforce my ownconclusions from teaching over 1,500students: improvisational theater is anessential tool for the sex educator. Itfacilitates the implementation of fourbasic goals: to provide adequate knowl-edge of human sexuality in its physical,psychological, social and moral dimen-sions; to help students clarify and ap-
256
predate their values and attitudes to-ward family and sexuality; to enhancestudent self esteem; and to increaseskills in decision-making and communi-cation. Only when students applyknowledge to life are these goals real-ized. Role play helps achieve this transi-tion. In role play, students practice theirnew leamings in life-like situations. Asthey examine relationships between ac-tors, as they defend their values in aparticular scene, as they take pride inresolving a family crisis, as they com-municate a strong belief, their knowl-edge is becoming personal and real.Through role play, sex education comesto life.
Bell, R. (1980). Changing Bodies, ChangingLives: A Book for Teens on Sex and Relation-ships. New York: Random House.
Dick :n, I. R. (1982). Winning the Battle forSex Education. New York: Sex Informa-tion and Education Council of the U.S.
National Cleannghouse for Family PlanningInformation. (August, 1982). Improvisa-tional Theatre: An Effective Outreachand Education Medium. InformationServices Bulletin.
Playback Theater, Innovative Studies.S.U.N.Y., New Paltz, New York, 12561.
Siks, G. B. (1977). Drama With Children. NewYork: Harper & Row.
Spolin, V. (1963). Improvisation for the Theater.Evanston, Illinois: Northwestern Uni-versity Press.
photo: Greg Meeker

TEACHING IDEAS 132
Family Life Education
Abortion Attitude Scale*
Linda A. Sloan
Perhaps the greatest crisis a contem-porary teenager might face is having anuntimely, unwanted pregnancy. Sincemore adolescents are sexually active andat younger ages than in past generations,the likelihood of its occurring hasreached epidemic proportions in recentyears. The pregnant teen has two majoroptions: carrying the pregnancy to termor abortion.
Abortion, although legally available inthe U.S. for almost a decade, has notceased to be a highly volatile and hotlycortested issue. Counseling the expec-tant mother on the abortion option isoften inadequate because of three majorintervening factors: (A) The counselorfrequently has personal biases about theoption; (B) It is difficult for the adoles-cent to identify her values about abor-tion; (C) Making the decision under thepressure of pregnancy may result in adifferent outcome than making a deci-sion about abortion in a noncrisis setting.
Although health educators can havelittle impact on the personal biases of thecounselor, they are in ideal positions tohelp students explore their values con-cerning abortion in nonthreatening cir-cumstances. Chances of long term nega-tive effects are reduced when one's be-haviors are compatible with one's be-liefs. Thus, helping students identify
*Health educators are reminded of the highlysensitive, controversial nature of this topic.Though there is an urgent need to help teen-agers, it is also imperative that the classroomteacher abide by district policies.
Linda A. Sloan is an assistant professor in theDepartment of Health and Physical Educa-tion, University of North Carolina at Char-lotte, Charlotte, NC 28223.
Abortion Attitude Scale
Directions: This is not a test. There are no wrong or right answers to any of the statements, sojust answer as honestly as you can. The statements ask you to tell how you feel about legalabortion (the voluntary removal of a human fetus from the mother during the first threemonths of pregnancy by a qualified medical person). Tell how you feel about each statementby circling one of the choices beside each sentence. Here is a practice statement:
SA A SlA S1D D SD Abortion should be legalized.
(SA = Strongly Agree; A = Agree; S1A = Slightly Agree.: SlD = Slightly Disagree; DDisagree; SD = Strongly Disagree)Please respond to each statement and circle only one response. No one else will see yourresponses without your permission.
SA A SlA SID D SD
5 4 3 2 1 0
5 4 3 2 1 0
; 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 I 0
5 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 1 0
5 4 3 2 1 ()
5 4 3 2 1 0
5 4 3 2 I 0
1. The supreme court should strike down legalabortions in the United States.
2. Abortion is a good way of solving an unwantedpregnancy.
3. A mother should feel obligated to bear a childshe has conceived.
4. Abortion is wrong no matter what the circum-stances are.
5. A fetus is not a person until it can live outside itsmother's body.
6. The decision to have an abortion should be thepregnant mother's.
7. Every conceived child has the right to be born.
8. A pregnant female not wanting to have achild should be encouraged to have an abortion.
9. Abortion should be considered killing a person.
10. People should not look down on those whochoose to have abortions.
11. Abortion should be an available alternative forunmarried, pregnant teenagers.
12. Persons should not have the power over the lifeor death of a fetus.
13. Unwanted children should not be brought intothe world.
14. A fetus should Ew considered a person at themoment of conception
those beliefs without the pressure of ex-tenuating circumstances may eventuallyaid them in making the best personalchoice if they ever face the situation. Theexperiences provided in the classroommay also create such dissonance as to
25 7
cause students to internalize the advan-tages of preventing pregnancy ratherthan having to cope with it once it oc-curs.
247

The health educator has little difficultylocating information on tHe history ofabortion, the medical techniques, andgroups to speak to its advantages anddisadvantages. What may be more dif-ficult to acquire is an instrument whichsomewhat objectively measures at-titudes toward abortion. To meet thisneed, the author has dc.i.c.Aoped and val-idated the following Abortion AttitudeScale for use with teenagers. The valida-tion process involved interrater agree-ment, pilot testing, reliability estimates,factor analysis to determine unidimen-sionality and hypothesis testing. Thescale was administered to populationsincluding high school and college stu-dents, active Right to Life members, andabortion service associates. The test ex-hibited a high total test estimate of relia-bility (.92) and five hypotheses weresupported on the construct validity as-sessment. Right to Life members' meanscores were 16.2 while abortion serviceassociates' scores were 55.6. All othergroups' mean scores fell in the middlerange.
248
Classroom Uses:Health teachers can use this instru-
ment in several ways:1. To generate discussion.2. For pre-post testing on abortion
unit.3. For students to administer to par-
ents and report.4. For students to administer to
friends and report.5. For students to compare results
from various groups.6. To use as a background for debate.7. To explore ranges of acceptance of
abortion (in case of rape, incest, geneticdefects, etc.).
8. To combine the scale with use ofvalues clarification techniques such as avalues continuum, popular song lyrics,etc.
r,)
Note to Teacher on Scoring:Step 1Reverse the point scale for items
1, 3, 4, 7, 9, 12, 14.Step 2Total point responses for all
items.Step 3Provide students with scoring
scale.
70-56 Strong pro abortion55-44 Moderate pro abortion43-27 Unsure26-16 Moderate pro life15-0 Strong pro life III

TEACHING IDEAS 133
Family Life Education
Marriage Yesterday and Today
Margaret J. Pope
In the Unites States today, morethan 90 percent of the population willmarry at least once. Statistics indicatethat one half or more of these mar-riages end in divorce, a rate that hasbeen rising steadily since World WarII. The median length of marriagesthat end in divorce is seven years(Nass, Libby, & Fisher, 1984). Fourout of five who divorce will remarryand many will marry more than twice.Why should so many marriages endwithin such a few years? Marriage ex-perts cannot provide one clear answer(Payne & Hahn, 1986). There is,however, a general agreement amongphysicians, sociologists, mental healthcounselors, and ministers that manyproblems that confront people inmarriage could be avoided if therewere a more realistic approach tomarriage.
People tend to marry those ofsimilar background in age, race,education, intelligence, religion,economic status, and family. One ofthe keys to a successful marriage iscommunication. Effective com-munication involves being respon-sible for working out problems as theyoccur, being a good listener, and notbeing defensive as disagreements ordifferences arise (Hamrick,Anspaugh, & Ezell, 1987). The key tohealthy disagreement is communica-tion.
While tcaching a unit on Marriageand Family Relationships in a healtheducation class at the university un-dergraduate level, I decided to initiatea different approach to th- marriage-
Margaret!. Pope is a professor of healtheducation at Jacksonville State Univer-sity, Jacksonville, AL 36265.
divorce syndrome of today's society.The objective was to discuss with fourmarried couples how they resolvetheir marriage problems. This in-volved discussion of communicationas well as other problems that arisewhen two people marry. Four coupleswere invited to visit the class on an ap-pointed day.
Two had been married over 50years and the two were college stu-dents who had married within theyear. The class was to investigate,through discussion, some of theproblems each couple had faced inadjustments to marriage. The samequestions were asked of the youngcouples and those who had been mar-ried for over 50 years. The purposewas to draw comparisons between agegroups and their approach to adjust-ment problems of marriage.
In preparation for the visit, theclass was divided into groups, eachwith a student leader. The instructorsuggested topics that could be usedfor discussion and asked the class forsuggestions. Students were told theycould not -isk questions that were per-sonal or offensive to the guests.
Broad topics chosen for discus-sion were:
Readiness for MarriageAdjustment ProblemsAgeCompatibilityEmotionalMaturityInterests
Economic and Financial SecurityFinancial GoalsOccupation of Each Partner
259
Conflict in MarriageCommunication During ConflictResolving Disagreements
Stn4cture of FqmilyChildren
Each group of studentsdeveloped questions pertinent to allbroad topics. These were previewedin class the day before the couplesvisited.
On the day of the visit, desks andchairs were arranged in a circle andapple juice was served. This allowedguests and students to socialize beforethe discussion began. The topic bothgroups of couples discussed longestwas "conflict in marriage." Student in-terest in resolving disagreements be-tween married couples was high andguests were willing to discuss theirsolutions. One of the questions to theolder couple was, "How have you heldyour marriage together for so long?"The two young couples were more in-volved with the "economic and finan-cial security" topic.
There is no formula for a success-ful marriage; however, throughpreparation, recognition of potentialproblems, and opportunity for discus-sion with married couples, studentscan become more ready for this stepin their lives. The four marriedcouples' visits to the classroomfacilitated opportunity for studentgrowth through personal interaction.
Evaluations of the process werepositive. Students indicated that thiswas a meaningful experience thatcaused them to begin to think moreseriously about marriage andproblems that might arise.
249

TEACHING IDEAS 134
Family Life Education
Teaching Abstinence to Today's TeensDee Gibbs Smalley
Again, we confront a dilemma inthe family life curriculum. Is it pos-sible to take a positive stance on absti-nence and still provide necessary in-formation to those teens who areengaging in sexual activities? If it ispossible, how do family life educatorsapproach the issue of abstinence withtheir students in a manner to accom-modate both groups - those electing toabstain and those who have chosen tobecome sexually active.
A vast majority of parents andteachers alike support abstinence as acurriculum topic. Forrest and Silver-man report that one survey revealedabout 25 percent of teachers cited ab-stinence as the most important mes-sage they have for their students.However, it, like most issues involvingsexuality, is not an easy topic to dis-cuss in a classroom filled with 30 fif-teen-year-olds. To complicate mat-ters even more, abstinence curriculaand supplemental instructional pro-grams arc lacking in quantity as wellas quality. Therefore, teachers fre-quently elect to develop their ownteaching materials. This leads teach-
Dee Gibbs Smalley is the health andphysical education curriculum devel-opment coordinator for Memphis CitySchools, Memphis, TN 38104.
250
crs to question what should be dis-cussed and how it should be presentedto students. (Alan Guttmacher Insti-tute, 1989).
In a 1986 poll, "American TeensSpeak: Sex, Myths, TV, and BirthControl," conducted by Louis Harrisand Associates, one thousand teenswere asked their opinions on a num-ber of issues. Two of the questionsincluded; (1) Why do teens not wait tohave sexual intercourse until they areolder; and (2) What reasons are mostuseful in convincing peers to iait tohave sex until they are older? (Peter-son, 1988).
Peterson reports the top four rea-sons given by teenage girls for notwanting to have sexual intercourserevolved around dangers of diseases,such as AIDS and herpes - 65 percent,and the danger of pregnancy - 62 per-cent. Fifty percent of the teens wor-ried about what their parents woulddo if they found out, and 29 percentfelt that ha-ing sex would ruin theirreputativa ',Peterson, 1988).
The 1986 Harris Poll reported thatteens felt pressure by other teenagersto go further with sex than they wanted.Since both males and females felt thispressure, those curricula materialsshould be utilized which contain ac-tivities essential to helping teens learnhow to resist this sexual pressure. It isso vitally important to empower youthto resist peer pressure. Such assertive-ness skills have lifelong value. How-ever, educators must be alert to teens'concerns where resisting peer pres-sure is involved. It is not always easy tosay "no" even after learning the skill(Peterson, 1988).
Leo reports in TIME that studiesarc surfacing which present evidence
2
that most teens are looking for anexcuse to abstain. In 1980, the teenservices program at Atlanta's GradyMemorial Hospital found that of thethousand or so girls under age 16 inthis program, many wanted to learnhow to say no without hurting any-one's feelings. The key to the theirfinal decision rests in their decision-making skills, their assertiveness, andtheir ability to communicate their valuesand feelings concerning abstinence.
In light of these critical facts, thefollowing 55 minute lesson is a sugges-tion for those teachers who lack cur-ricula materials but share the desire toteach abstinence. While the lesson isdesigned for middle school and juniorhigh school studcnts, it easily can beadapted for older students.
Instructional Objectives
The student will (1) recognize theimportance of sexual abstinence andidentify consequences of failure toabstain and (2) identify and practicetechniques of assertiveness.
Set
Begin the instruction by writingthe phrase "human sexuality" on theboard. While this is visible to students,explain that although they are sexualbeings, it is important not to act out onevery sexual feeling until they aremature enough to accept responsibili-ties for their consequences. Informstudents that the purpose of this les-son is to recognize the importance ofsexual abstinence and identify conse-quences ot failure to abstain, and toidentify and practice techniques of as-sertiveness.

Instruction
Write three headings on the boardfor all students to see. The headingsshould read: (1) Reasons FrequentlyGiven by Teens for Becoming Sexu-ally Active, (2) Reasons FrequentlyGiven by Teens for Postponing SexualActivity, and (3) Possible Consequencesof Becoming Sexually Active.
Begin with heading number 1. Al-low students to brahistorm reatonsthat teens may become sexually ac-tive. As ideas are presented, list themon the board underneath the heading.Allow sufficient time for students togenerate as many reasons as possible.Reasons may include pressure frompeers, fun or pleasure, feel grown up,love, curiosity, hold onto girl/boyfriend,lonely, rebelling against parents asseen on TV or movies, or to escapeproblems at home. Allow for interac-tion between students.
Move to heading number 2. Havestudents brainstorm reasons that teensmay postpone sexual activity. As be-fore, list them or the board whengenn.rated. Reasons may include wait-h until married, fear of pregnancy,fear of getting a sexually transmitteddisease, AIDS, afraid parents will findout may be painful, against religiousbeliefs, against value system, mightinterfere with future plans, not readyfor responsibilities of a baby, not physi-cally or emotionally ready, might ruinreputation, or simply didn't want to.Again, ,meourage discussion betweenstudents.
Finally, direct students' attentionto heading number 3. Ask students tothink of possible consequences of be-coming se;:ually active. List them un-der the heading as students generatetheir ideas. Consequences may include,but are not limited to, unwanted preg-nanry, sexually transmitted diseases,AIDS, dropping out of school becauseof pregnancy, damaged reputation, hav-ing to seek a job to svport a child,changed relationship with boy/girl-friend, parents, and friends, losing self-respect, and fc,..nng differently aboutoneself.
Ask students to compare men-tally the reasons given for becomingsexually active with possible conse-quences of becoming sexually active.Ask them to identify the list of reasonswhich would have a greater impact ontheir lives both now and in the futureand the plans, dreams, and goals theyhave set for themselves.
Explain to students that the deci-sion to become sexually active or toremain abstinent is theirs - a decisiononly they can make. Unfortunately,pressures abound in society. Pressuresfrom the media as well as peer pres-sure force many adolescents to be-come sexually active before they arephysically, emotionally, and financiallyprepared to deal with the consequences.
Inform students that many ado-lescents are not prepared to deal withthe pressure often exerted by a mem-ber of the opposite sex to becomesexually active. Therefore, being ableto say "no" assertively to a pressuresituation may be very helpful. Explainthat by knowing how to deal with thesepressures, students will have morecontrol over their lives and will be ableto make wiser decisions.
Distribute a copy of the Handout- Lines (Figure 1) to each student.Have students write their response toeach "line." After students have com-pleted the assignment, provide volun-teers with an opportunity to sharetheir response. If sufficient time re-mains, have students select the most
Continued on page 253
Fi re I. Handout-Lines
DIRECTIONS: Read each statement car:fully. Write a response to each of the following.
I. Come on! Everyone is doing it!Response:
2. If you really love me, you'll do it!Response
3. If you won't have sex with me, I won't see you again.Response:
1. Don't be afraid of what others will say.Response:
5. Having sex with me will make you a real man/womarResponse:
6. 1 promise we'll get married someday.Response:
7. Don't you want to try it to see what it's like?Response:
8. But 1 have to have it or I'll die.Response:
9. If you get pregnant, we'll get married.Response:
10. You know you want it as much as I do.Response:
11. lf you love me, prove it.Response:
12. Come on, take a drink. It will get you in the mood.Response:
2 1
251

TEACHING IDEAS 135Family Life Education
Group Discussion on Contraceptive IssuesBarbara A. Rienzo
et
The problems and consequences ofunplanned and unwanted pregnancyare ll documented in the literature.Sol, of the costs to the mother, child,and society include high infant mortal-ity rate, high rate of low birth weight orpremature babies, higher risks of hyper-tension, toxemia, and other complica-tions of pregnancy, interruption or ter-
Barbara A. Rienzo is an associate pr-iessorin the Department of Health Edu«aion,University of Florida, Gainesville, II.32611.
252
mination of education, lower job/careerpossibilities, increased rates of childabuse, and birth defects, such as mentalimpairmect and limo deformity. Mosthealth and education professionalsagree on the need for prevention ofunwanted pregnancy.
Although we do not yet have a per-fect contraceptive method many un-wanted pregnancies could be preventedthrough consistent use of an effectivecontraceptive. There are a variety ofreasons given for non-use of contracep-tives among youth. These include igno-rance, unavailability, lack of motivation,the desire to become pregnant.
The following exercise is an effectivemethod of introducing the topic of birthcontrol and facilitating discussion aboutmotivational issues surrounding the useof birth control/contraceptives by sexu-ally active young adults. It is appropri-ate for high school, college, and adultgroups.
Initially the educator has the studentstake a half-page of paper and writ"whether they are male or female at thytop. No names or distinguishing marksshould be used to preserve anonymity.The class is then instructed to listen tothe following situation. They will laterbe asked to write down their reaction.

The instructor tells the class: (The fol-lowing may be modified to fit th2 specif-ic audience)
"You have been going out with thisperson for some length of time.You really care for him or her andhave had a nice time this evening.You've been to a romantic dinnerwith candlelight and to a movie,and now you're back at your place.You are both feeling affectionateand things begin to get 'hot andheavy.' You realize that you'd real-ly like to make love with this per-son (You had not had sex with him/her before)but you don't haveany contraceptive available. Whatwould you do?"
The instructor tells the students toconsider the situation silently and towrite down on their papers as honestlyas they can what they think they woulddo in that situation. The teacher shouldbe sure to have students write downtheir answers without talking to othersto ensure that individually consideredresponses are recorded. As the studentsfinish writing (allow approximately fiveminutes), have the students fold theirsheets of paper in half. The teachershould collect the sheets personally,shuffling them as they are handed in topreserve anonymity. When all the pa-pers are collected, the instructor directsthe class to form a circle of chairs (usin,about half of the chairs) in the cent«.room. Meanwhile, the students' pap 3
should be separated into male and fe-male responses. After this is accom-plished, the teacher instructs all themales to sit in the inner circle. The classis told that this is a "fishbowl" exercisewith the following rules:
1. All the persons in the inner circleare allowed to participate in thediscussion. They are the only onespermitted to talk.
2. There should he enough chairs inthe inner circle for all members ofone sex plus one empty chair.
3. The persons in the miter circlemust remain silent. They' may onlylisten. If they wish to say some-thing, they must take the emptychair in the inner circle.
4. The persons in the inner circle willbe given the responses of the othersex by the instructor. The studentsare instructed to discuss the re-sponses in terms of by answeringthe following:
a. How do you feel about theresponse(s);
b. Do you think the response isrealistic?
c. What are the implications orconsequences of the '-sponse?
5. The instructor makes it clear ...1atthe discussion should be amongthe persons in the inner circle onlyand no personal attacks on otherpeople are permitted. (Speak in"1" statements).
The instructor may need to initiatediscussion by asking the persons in theinner circle to read the responses aloudto the group, and then use active listen-ing skills to elicit their thoughts andfeelings. The discussion time should besplit evenly between the same-sexgroups, and the instructor should allowa few minutes at the end of class time tosummarize the session. Often, addition-al time must be spent during the nextclass period to summarize the discus-sion and allow students to express theirfeelings and thoughts about the exer-cise.
The major ideas generated throughfllis exercise are:
1. Responsibility for birth control--a. Whose responsibility is it?b. How do you share the respon-
sibility?c. How do you take responsibil-
ity?d. What obligation(s) does the
male have in an unplannedpregnancy?
2. Communication--a. How do you talk about birth
control with a partner?b. When is a good time to talk
about contraception?3. Relationships
a. Does birth control responsibility vary with the type/intensityof the relationship?
4. Sex Rolesa. How do female sexuality ste-
reotype influence birth control?1. Is a girl/woman bad/loose if
she is prepared for sex?2. When a woman says "no" is
she serious? Is she taken se-riously?
b. How do male sexuality stereo-types influence birth control?1. Is a guy always out for all he
can get?2. Is it OK for a guy to say
"no"?5. Sexual behavior--
a. Is sexual intercourse the onlysatisfying end/goal of lovemak-ing?
b. Are there alternatives to sexualintercourse?
c. Is "planned" sex less excit-ing?Does sex have to bespontaneous to be good?
This exercise provides an opportunityfor students to participate actively inclass and to identify those issues whichcontribute in important ways to theirdecisions regarding contraceptive be-havior. The teacher-facilitator has theresponsibility to initiate (when neces-sary), summarize, and clarify issuesfrom each group's responses. Bothteacher and students can benefit greatlyfrom the insight achieved through talk-ing with and listening to other individ-uals.
Teaching Abstinence to Today's Teens
Continued from page 251
assertive response, the most deverresponse, and others.
Again, explain to students that thedecision to become sexually active orto remain abstinent is theirs - a deci-sion only they can make. Briefly re-view the possible consequences ofbecoming sexually active, Stress that asexual relationship can be a most grati-fying experience when a person is pre-pared physically, emotionally, and fi-nancially to deal with the consequences,
263
but it can be a terrifying experienceunder other conditions.
The Alan Guttmacher Institute. (1989). Riskand responsibility. New York: Author.
Forrest, J. D., & Silverman, J. (1989). Whatpublic school teachers teach about pre-venting pregnancy, AIDS, and sexuallytransmitted diseases. Fami6, Planning Per-spectives, 21 (2), 65-72.
Leo, J. (1986, November 24). Sex and Schools.Time, 54-63.
Peterson, L. (1988). The issue- and controversy-surrounding adolescent sexuality and ab-stinence. S1ECUS Report 17 (1), 1-8.
253
TEACHING IDEAS 136
Family Life Education
Developing and Rejuvenating RelationshipsJane W. Lammers
For some people, developing per-sonal relationships is very difficult.Equally as difficult for some is main-taining a continued interest in an oldrelationship. As Peck (1978) de-scribes, relationships go through var-ious stages, and hard work is nec-essary for relationships to flourish.
An ideal time to learn about rela-tionships and their intricacies is dur-ing the developmental period of ad-olescence, when teenagers are veryconcerned about establishing ties withtheir peers P.nd are testing their in-dependence from the immediate fam-ily (Erickson, 1982). Yet, while thenew relationships are being devel-oped, old relationships need to bemaintained and nurtured. By partic-ipating in the following activity, oneis able to experience caring for sev-eral different types of relationshipsin his life.
The activity works well with teen-agers but is applicable to anyonewho desires renewal in a relation-ship. College students, whose agesrange from 18 to elderly, have ben-efited from the experience. In healtheducation classes, the activity inte-grates well into the human sexualitysection, where a major emphasis islearning how to develop and appre-ciate a variety of relationships withfamily and friends (Educational De-velopment Center, Inc., 1983).
The overall goal of the activity is tohelp an individual experience devel-opment and nurturing of a relation-ship. Specifically, the participant willrenew a relationship with himself, aloved one, and one or more otherpeople he does not know very well.The time allotted for the activity is
lane W. Lammers is in the Departmentof Health Education at the University ofCentral Arkansas, Conway, AR 72032.254
three weeks, with one week beingdevoted to each relationship. A help-ful technique for insuring that theparticipant completes the activity isto provide an activity sheet for plan-ning and recording the results (seeTable 1 for an example of Week One).
In the first week, the participant isto renew a relationship with him-self. He is asked to analyze how wellhe has been taking care of himself bywriting down three things that hedoes to care for himself and listing inanother column three things he doesnot do. Some examples that can berecorded in the "does not do" col-umn might be general health habitsthat are recognized as beneficial forhealth: for example, exercising reg-ularly, getting adequate sleep, eat-ing well-balanced meals, managingstress, meditating, playing, and notusiag tobacco. He then chooses somespecific thing that he will do every-day for himself for one week andrecords the planned activity on aparticular day in a weekly log (eachday's activity may be the same or allor some may be different). Examplesmight include meditation for 15 min-utes, walking for 20 minutes, goingto a movie, eating breakfast, notsmoking cigarettes or chewing to-bacco, or eating more fresh fruitsand vegetables. At the end of eachday, the participant records in thedaily log what he did each day. Atthe end of the week, he writes asummary paragraph that describesthe success or failure in being goodto himself, feelings during the expe-rience, plans for the future, andgeneral comments about the activi-ty, including how he might do it ifhe tried it again.
During the second week, the par-ticipant renews a relationship with a
t; .1
loved one, either a family member ora close friend. To analyze the currentstatus of the relationship with theperson, the participant writes downthree things that he does on a reg-ular basis to nurture the relationshipand three things that he could do.Examples might include 15 minutesof uninterrupted conversation withthe other person without talkingabout himself, rubbing the person'sback, washing the person's car, send-ing a card of appreciation to the

individual for his contribution to theparticipant's life, takins the personout to eat, or keeping the person'shouse clean. For one week, the par-ticipant chooses something to doeveryday for the other person with-out telling the person he is doingthis for an assignment and recordshis planned activity in a daily log. Atthe end of each day, the participantrecords what he has done. At theend of the week, a summary para-graph is developed to describe suc-cesses, failures, feelings, and re-sponses. The participant is asked toreport what changes he might makeif he were to do the activity again.
The final week is designed for theparticipant to establish a relation-ship with someone or several otherpeople whom he does not knowvery well. Such an individual(s) might
be someone in one of his classes, hisemployer, a fellow worker, a neigh-bor, or someone he has been want-ing to meet. Each day for one week,the participant chooses somethinghe will do to enhance a new rela-tionship without letting anyone knowabout the project. '.2:ach day may bedevoted to establishing a relation-ship with the same person or adifferent person. Some examples ofways to enhance the relationshipmight be to initiate a conversation,ask someone to go to a movie orparty, offer to run an errand forsomeone, or just compliment some-one. The participant lists the plan foreach day in the daily log and then,after each day is completed, he willrecord what was done to enhance anew relationship. At the end of theweek, the participant writes a sum-
(Worksheet)
Week One: Renew a relationship with yourself.
A. Analyze how well you have been taking care of yourself. Write down three thingsthat you do or do not do on a regular basis.
Things 1 do for myself Things 1 do not do for myself
2.
3.
Choose something you will do everyday for yourself for one week. (Each day'sactivity may be different or all may be the same.) In the left hand column, write whatyou plan to do each day. In the right hand column, write what you did each day.
My daily plan
Day I
Day 2
Day 3
Day 4
Day 5
Day 6
Day 7
What I r id
C. At the end of one week, write a summary paragraph that describes your success orfailure in being good to yourself. Describe your feelings during the achvity, plans forthe future, and general analysis of the activity.
Note: Each week, the activity sheet would be modified.
265
mary paragraph reporting what hap-pened, how the participant felt aboutthe experience, how others respond-ed, and how the experiment mightbe redone.
Generally, most students willing-ly participate in the activity; but,with encouragement, those who areinitially apprehensive usually bene-fit most from the experience. Assign-ment of the activity may be all that isnecessary to encourage the studentto initiate the beginning or renewalof a desired relationship. Many stu-dents write in their reports that be-cause of the activity they began anew relationship with someone theyhad wanted but had been too afraidto meet in the past. Some have usedthe activity as an opportunity tore-establish old ties with family andfriends that previously had beensevered by a disagreement. Somestudents even become philosophi-cal. One student wrote after havingcompleted the project:
I have found the smallest of seeds sownsincerely will grow if cared for. Just likethe seeds sown, a relationship needs to benourished. A cared for relationship willgrow and produce much beneficial fruit.An ignored one will wither. Relationshipsare active and can be directly influencedby the care given them. (Anonymous,1988)
In summary, health educators canprovide opportunities for studentsto develop skills that will enhancethe quality of their lives. Caring fora relationship is an example of oneskill that can be developed. Theactivity discussed provides a practi-cal approach to learning how to carefor oneself and others. With prac-tice, individuals, whether in thehome, workplace, or community,can begin to demonstrate their con-cern for themselves and others andthus becom healthier people. In thefinal analysis, healthy relationshipsmake for healthy people.
Anonymous, (1988). Paper prepared for healtheducation general education course.
Educational Development Center, Inc. (1983).Haviv., friends. The teenage health teachingmoth r.. Department of Health and Hu-man Services (contract #200-79-0922).
Erickson, E. (1982). The life cycle completed: Areview. New York: W .W. Norton & Co.
Peck, M. S. (1978). The road less traveled. New..ork: Simon & Schuster.
255
TEACHING IDEAS 137
Family Life Education
Courtesies and Rights Within RelationshipsBethann Cinelli and Robert Nye
Courtesy, n., pl. -sies: 1. courteousbehavior 2. a polite or considerate act(Gurlanik, 1984)
Right , n.: 1. what is right, just, etc.2. a power, privilege, belonging to oneby law, nature etc. (Gurlanik, 1984)
Human relationships presentmany challenges. For many peoplethese include developing, buildingand maintaining of primary relation-ships and possible marriage. 1 hereare also many factors to a lasting loverelationship. Rosenman has iden-tified these as: self-acceptance, ap-preciation of one another, commit-ment, good communication, realisticexpectations, shared interes's and theability to face conflict effectively(Rosenman, 1979).
As part of a Love and Marriageclass, students are encouraged todevelop their own definition of love,identify desirable traits they want intheir potential mate, and then look atpartner interactions which may bedetrimental to or may enhance their
Bethann Cinelli is an assistant profes-sor of health education, West ChesterUniversity, Department of Health, WestChester, PA 19383. Robed Nye is aprofessor of health education at WestChester University.
256
r Itionship. As the course progressestiscussing helping and doing things
- each other, then to jealousy andhonesty, many students become con-fused, frustrated and angry over ex-pectations and what partners shouldand should not do for each other. Thisis most evident when discussing cour-tesies within a relationship. One cannotice quickly that students have notyet defined for themselves the dif-ferences between courtesies andrights nor what to expect or demandwithin relationships.
Crooks and Baur (1987) referto this as the "inclusion-responsefoundation." They describe this termas the "little things that count in arelationship." Often these behaviorsmay go unnoticed and, therefore, aretaken for granted. These may includeoffering to help with a chore, openingdoors, or being complimentary.Therefore the purpose of this activityis to help students distinguish be-
.. tween what they perceive to be cour-tesies within the relationship as well aswhat they perceive to be individualrights.
Activity
Instruct students to form smallgroups that are co-ed with ap-proximately four or five students. Forthe next 15 to 20 minutes, each groupwill be asked to list the most importantcourtesies (there is no mention ofrights at the; time) that they would like
Table 1. Examples of a Courtesy List from Class Discussion
Not interrupting your partner when he or she is speakingOpening doorsBeing on timeCalling your partner if you are going to be latePicking up after yourselfBeing honestShowing respect for partnerNot leaving hair ii the sinkTelling your partner there is a change in plansRemembering important dates (birthdays, anniversaries)Allowing time for friendsAllowing your wife to workFilling the gas tank when emptyWife being given money for herselfNot drinking directly out of cartons in refrigeratorNot embarrassing your partner in publicNot smoking in bedPutting toilet seat down after usePaying attention or listening when your partner is talkingBeing supportive of partner's career
266

extended to them by their partners.To record their responses, give eachgroup a large (36" X 30) sheet ofnewsprint paper and a marker. Tellstudents that they may work within theclassroom or may choose to work inthe hallway or other available rooms.
When the lists have been com-pleted, the iastructor will attach them(an example of common responsescan be found in Table 1) to wallsaround the room. Students then areasked to read over the lists while theinstructor also reviews them.However, the instructor will place acheck by the items which actually maybe considered to be individual rightsrather than courtesies. At this time, donot tell students why you are checkingany particular item. Ask the groups todiscuss each other's lists. As the ques-tions and comments trail off, ask stu-dents why they think that you havechecked certain items. If time is im-portant, after these lists have beenchecked, go right to the question of"why" these items were highlighted.
After students offer their sug-gestions, the instructor can point out
that check marks actually may indi-cate "rights" rather than "courtesies"within a relationship. These "rights"are viewed as what is just, rather thanas a courteous or considerate act. Theinst, actor should note that confusionover courtesies and rights can bedevastating to a relationship. Whatone partner may see as merely a cour-tesy, the other may believe is a rightwhich must be observed.
The follow-up discussion willthen address differences betweencourtesies and rights. Students willalso be asked a key question abouthow they feel when an expected cour-tesy is not extended to them. Oftenthey will express feelings of anger, dis-appointment or disillusionment. Itthen can be pointed out to them thatperhaps this is an indication that theyview the expected behavior as a rightrather than as a courtesy. The denialof a courtesy should not generate thedegree of anger some students ex-hibit. In different:7 g between thetwo, students r- 3cuss that thereare universal which should be
267
extended to everyone at all times, andthat there may be relationship rightswhich people define for themselveswhich may need to be identified earlyin the "getting to know each other"stage.
Conclusion
This activity is designed to offerthe students an opportunity to showhow, in actuality, (1) rights are oftenconfused with courtesies, (2) com-munication between partners is es-sential in order to define courtesiesand rights, (3) partner expectationsneed to be defined and (4) because ofvarying backgrounds, what onepartner may consider to be a courtesythe other partner may consider to bea right.
Crooks, R. & Baur, K. (1987). Our sexuality.
California: Benjamin Cummings, 226--228.
Gurlanik, D. B. (1984). Webster's new worlddictionary. New York Warner Books, 111,144.
Rosenman, M. (1979). Loving styles. Engle-wood Cliffs, NJ: Prentice 1:iall.
257

TEACHING IDEAS 138
First Aid and Safety
CPR Drilling RevisitedMark J. Kittleson
In 1980, this author published an arti-cle that discussed a possible alternativein teaching Cardiopulmonary Resuscita-tion (CPR). Entitled CPR Drilling, itsmain premise was that a great deal ofCPR instruction is spent observing an-other person performing CPR. The au-thor contended that much of this ob-serving could be reduced by more effi-cient classroom management.
Over the past several years, the ideassuggested in the 1980 article have beenrefined and researched. This article willdiscuss four specific techniques that canbe used in a CPR class to enhance thelearning of this critically needed bkill.
Bloom (1974) stated that on-task be-havior is a critical component to learn-ing any skill. Most of Bloom's research,as well as many of Bloom's followers,have only analyzed cognitive shills.Could such a theory be effective in apsychomotor skill such as CPR? Little, ifany, research has been done to supportthis concept.
Kittleson's research (1986) showedthat Bloom's time on task concept isrelevant to psycnonlotor skills. He alsowent on to shc w how Cratty's theory ofprogressive part practice can also affectCPR instruction (Cratty, 1973).
Cratty believes that in order to learn acomplex skill, one must first break theskill into several specific parts. Onlyafter mastering these specific parts canon,- put the skill together.
The skills needed to learn single res-cue CPR forms the basic of learningCPR. Once such 3kills are mastered,other techniques such as two personCPR can be taught. However, singlerescue CPR is the major technique now
Mark J. Kittleson is an assistant professor inhealth education in the Department ofHealth and Physical Education at Youngs-town State Universiti, --ungstown, OH.He is also an instructor-ti.:iner in advancedfirst aid for the American Red Cross as wellas an instrIctor-trainer in CPR for theAmerican I rt Association.
258
encouraged by the American Heart As-sociation and the American Red Cross.
A critical part of single rescue CPR isthe learning of various "parts" whichinclude: mouth-to-mouth resuscitation,proper compression rate and depth,moving quickly from the chest to givetwo ventilations, combining chest com-pressions with two ventilations, as wellas learning the steps to initiate CPR.
In Kittleson's study (1986), each ofthese skills were broken down and eachskill is practiced by an individual untilmastered. Once mastered, the individ-ual can "combine" these parts. An indi-vidual is placed in a group of three, witheach person responsible for a key com-ponent of the task. The rescuer is theperson performing the actual skill; thetimer is the individual who uses a stop-watch to detect speed; tne observer care-fully monitors the performance of therescuer. Each of the three individualsrotate a role when the rescuer completeshis/her task. Altogether, there are fourspecific tasks to complete.
This format will allow the instruc-tor(s) to spend time with those individ-uals needing special assistance. It alsosets the tone of the class that eachperson is not only responsible to learnCPR, but also is responsible to assistothers in the learning of that task.
Task One: Initiating CPRRescuer's Rost_ Imagine you have
walked into the room and you see "An-nie" lying here. Although you do notknow it at the time, Annie is in cardiacarrest. Go through the proper steps ofdetermining unresponsiveness, callingfor help, opening the airway and listen-ing for breathing, giving two fullbreaths, and checking the pulse (whilecalling for somebody to get an ambu-lance).
After you have finished taking thepulse, position yourself to performCPR. Once your hands are on the chest,you can sit back.
Timer's Role: Start the stopwatch oncethe person starts checking for unre-
2fiS
sponsiveness. Keep track of how longeach task takes. Be especially aware ofthe length of the pulse check. A roughidea for time should be as follows:
Task Seconds
Min. Max.
1. Determine Unrespon-siveness 4 8(call for help)
2. Open Airway, listenfor breathing 7 13
3. Give two full breaths 13 194. Check Pulse 17 29
(tell somebody to callan ambulance)
Observer's Role: Your job is to makecertain that the rescuer performed eachspecific criteria successfully. You are tomake certain that proper position of therescuer (as well as the victim) occur, atall times. Stop the rescuer if necessaryto point out an error.
Have each person rotate after fivecomplete performances.
Task Two: Proper VentilationThis task is to get the rescuer comfort-
able with the idea that he/she is to movequickly from the chest when giving thetwo ventilations.
Rescuer's Role: Start in chest compres-sion position. When you hear the timersay "go," leave the chest, give two fullventilations, go back to the chest posi-tion, and wait until the timer says "go"again. Make certain that you ventilateeffectively and that you pinch the nos-trils and open the airway sufficiently. . If
you get confused, or get behind in thesequence, stay on the chest until youhear the word "go" again.
Timer's Role: When the rescuer isready, say the word "go." Keep youreyes on the stopwatch. Every six sec-onds say "go" loudly to the rescuer.Keep the watch running at all times; donot stop and reset each time. For exam-ple, say "go" at start, six, twelve, eigh-teen, twenty-four seconds, etc.
Go for thirty seconds, stop, and con-tinue for another 75 seconds.
Observer's Role: Your job is to makecertain that the mannikin is resuscitatedcompletely. Make sure that the headtilt, chin lift is performed correctly, thatthe nostrils are being pinched, and thatthe rescuer's mouth completely coversthe mouth of the mannikin. Finally,make certain that the rescuer finds themannikin's xiphoid process before plac-ing hands on the mannikin's chest.
Have each person rotate roles aftercompleting one thirty second and one75 second.
Task Three: CPR CompressionsThe objective of this task is to make
certain that the rescuer is able to per-form proper chest compressions withinthe allotted time period.
Rescuer's Role: Position yourself on thechest, ready to do cardiac massage. Do15 proper chest compressions within8.5-9.0 seconds. Stop, receive yourtime, and repeat 10 times.
Timer's Role: When the rescuer startscompressing, start the stopwatch.When he/she completes the 15 compres-sions, stop the watch. Tell the rescuerhis/her time. Reset the watch, and readyyourself to time the person once again.
Observer's Role: Make absolutely cer-tain that the rescuer is compressingproperly. Also, observe whether therescuer has unnecessary movement (e.g., bobbing head).
Rotate after completion of 10 cycles.
Task Four: Combining Breathingand Compressions
This task has the objective to puttogether two of the previous tasks toform one fluid motion.
Rescuer's Role: Position yourself on themannikin's chest. At yol own discre-tion, start 15 chest compressions. Aftercompleting 15 compressions, move tothe mannikin's head and give two fullbreaths. After giving tv% o breaths, goback to the chest, and pc sition yourselfon the mannikin's chet (making sureyou find the xiphoid process). Aftergetting into this position, you may sitback.
Repeat after hearing your time eighttimes.
Timer's Role: When the rescuer startscompressions, start the watch. Whenthe rescuer completes the two breathsand returns his/her hands to the chest,stop the watch. Do not stop the watchuntil the rescuer has placed his/her
hands on the chest. Tell the rescuer thetime that this particular cycle took.
Also note how long it took for thecompressions, as well as the movementfrom chest to mouth (and back).
Observer's Role: Make certain the indi-vidual properly compresses, properlyventilates, as well as properly findshand position. The time for each cycleshould range between 13.5 to 15 sec-onds, although the time between leav-ing the chest, and returning to the chest(after breathing) should take no longerthan six seconds.
Putting It into PracticeThese progressive part practice ses-
sions should only be utilized after see-ing and practicing the general CPR se-quence. How that practice is done is upto the individual instructor. This authorpairs up each student, then directs thestudent in each CPR step (without actu-al ventilation and chest compressions).It is important that this general practiceis done before the progressive part prac-tice sessions to acquaint students withthe overview of CPR. To use the pro-gressive part practice without a generalunderstanding of CPR would not allowtotal learning to occur.
Each task, with three individuals pergroup, can be accomplished within a10-12 minute time period. Additionalgroups can be taken care of in one of thefollowing ways:
1). Placed at additional manikins topractice critical tasks such as mouth-to-mouth breathing, and chest compres-sions.
2). Placed at a non-mannikin area topractice the entire CPR sequence on amember of the group. Obviously, chestcompressions and ventilations are notpermitted. The observer also serves as atimer.
Completion of each of the tasks usual-ly provides a solid foundation of mas-tering the specific skills needed for CPR.Students also find this an acceptablemethod in that all students are involvedat all times. By observing, assisting inindividual performances, and in actualpractice, CPR skills are enhanced.
Kittleson's research (1986) analyzedthese specific tasks on effectiveness toteach single rescue CPR. The results ofhis study showed this approach to bemore efficient at teaching CPR skillswhen compared to the traditional meth-od of instruction endorsed by the Amer-ican Heart Association.
Although not statistically tested,skills involving two person CPR and
269
infant :esuscitation can also be brokendown to increase teaching effectiveness.For example, the student who practicestwo person CPR can concentrate on"CPR Switching" only, or a student canpractice ventilations on an infant. Oncethese specific skills are mastered, stu-dents can combine these skills to per-form the entire sequence.
Bloom, B.S. (1974). Time and learning. Amer-ican Psychologist, 29, 682-688.
Cratty, B.J. (1973). Teaching Motor Skills. En-glewood Cliffs, NJ: Prentice Hall, Inc.
Kittleson, Mark J. (1986). Analysis and com-parison of cardiopulmonary resuscita-tion methodology among college stu-dents. Unpublished Dissertation. TheUniversity of Akron, Akron, OH.
Kittleson, Mark J. (1980). CPR drilling, HealthEducation, 11, 22-23.
259

TEACHING IDEAS 139
First Aid and Safety
The Improvised ManikinHomemadeCPR Equipment
Mardie E. Burckes
Asta.;/
"The Improvised Manikin" is an ana-tomic dummy which the Nebraska De-partment of Health-Emergency MedicalServices designed to teach CPR in theNebraska public schools. This manikincan be made by following the simpledirections included in this article. TheNebraska Department of Health hasgiven permission to reprint the direc-tions for making the manikin, althoughthe author has made some slightchanges.
The manikin is made of the followingmaterials: pillow, styrofoam head, rub-ber bands or tape, safety pins, t-shirt,handkerchief, Laerdal chest piece andsteel chest band (optional).Directions
1. Poke hole with a pencil or cut holethrough the mouth to the hollow cen-ter core of the styrofoam head.
2. Tape or use an elastic band to hold aplastic bag to the neck. A small gar-bage bag (12" x 18") or grocery plasticbag both work well.
3. Place the plastic bag under chestpiece if one is used, otherwise placethe bag under the pillow. (The Ne-braska Department of Health uses apillow) If the bag is placed under thechest piece, the head can be tiltedback to open the airway and the chestwill rise when air is blown into themouth.
Marche E. Burckes is with the School ofHPER, University of Nebraska at Omaha,Omaha, NE 68182,
260
.hF: ?, . ,. 4 .A;4... ': 'al , 4
t° i . ' 1,0, ' u,rr.ijol.t t ^ -4U'I'd"-,crzillfZiett
X '
4. Put a shirt on the pillow and a hand-kerchief on the manikin's neck; ar-range the head, bag, and pillow asshown. Pin the bottom of the shirtsnugly near the pillow.
The manikin could cost as little as$1.00 or as much as $50.00 dependingon whether the Laerdal chest band andchest piece is used. If the chest pieceand band is not used, a clorox plasticbottle cut into a 4 inch band could beplaced over the pillow as a chest piece,but the edges should be taped or pad-ded because they could be rough.
Why use an improvised manikin?Many times schools cannot get regularCPR manikins from various agencies orcannot afford the price tag of $600 fora commercial CPR manikin. Also animprovised manikin works well in thepublic schools because it is lightweightand can be transported easily from oneclass to another.
A few safety rules should be followed
2
when using the improvised manikins.Because styrofoam is porous and diffi-cult to wash, each participant shoulduse a four inch square of wax paperwith a slit in the middle to cover themouth of the manikin when ventilating.For sanitary reasons the styrofoam headand plastic bag should be removed anddiscarded after every few classes. Theprice of this is negligiblestyrofoamhead ($1.00), plastic bag (free) and couldsave a disease outbreak in the school.
To practice with "Improvised Mani-kin," place the dummy on its back andfollow steps from the American HeartAssociation or the American Red Cross:Shake and shout, call for help, tilt thehead back to open the air passage, look,listen, feel, 4 quick breaths, pulse, callfor help, find proper hand position,cadence: 1 rescuer for an adult 15:2, 4cycles of 15:2 in one minute, repeat or 2rescuer, 5:1 following the instructedprocedures.

TEACHING IDEAS 140
Teachhig the Fourof First Aid
Mark J. Kittleson
First Aid, I now believe, can be an ex-citing and rewarding subject to teach: anopportunity to see students developskills that can be of utmost service notonly to themrelves but to others suffer-ing from illness or injury. Unfortunately,some instructors (including this author)have been guilty of terribly dry and un-rewarding courses. I believe an excitingand practicai approach to teaching firstaid, which I call "The Four C's of FirstAid," can provide the basis for an effec-tive course. Each of the four C's isequally important, for without one, theother three cannot be maximized.
4""NifNumber OneCognition
NordCognition, or the knowledge of first
aid, is an obvious essential. Withoutproper knowledge, a student could notmake appropriate choiceschoiceswhich could place the life of the victim injeopardy. Although cognition is the basisof first aid, it is not necessarily the solegoal of a first aid course, and it is not thesole responsibility of the instructor.Cognition is the prime responsibility ofthe student. If an instructor is forced tolecture on textbook material, what is thepurpose of using a text? By requiring
Mark I. Kittle:con is an instructor of HealthEducation in the HPE department at Youngs-town State University, Youngstown, OH44555. He is also certified as an Instructor-Trainer in First Aid with the American RedCross and Instructor-Trainer in CPR withthe American Heart Association.
students to read specific chapters (and tobe responsible for this information), you,as the instructor, can devote more timeto the other three C's.
To let your students realize the seri-ousness you attach to their readings,give daily quizzes on required readings.Any student who does poorly on one ortwo of these quizzes will quickly make ita point to study ahead of time.
A method this author uses to encour-age cognition (besides lecture) is toprovide all members of the first aidcourses an old first aid final. This final,develoi-ed more than five years ago,does have some outdated material, but itis an excellent tool to promote study.These tests are for students to keep.They are to put down only answers theyare sure of, and to look up the answers toquestions of which they are unsure.They are allowed to work in pairs,groups, or alone, and can use any re-source for answers or clarifications. This235-item test is used throughout thequarter; every class meeting has sometime devoted to its use. It is especiallyhandy during a quiz or major tests. Thestudents who finish their quiz early canwork on this "final" while others arefinishing. This prevents much idle time.Also, this provides an opportunity forone-on-one assistance to those studentsdesiring such help.
Number TwoConfidence
It seems rather foolhart o pxvide afirst aid course and not have studentsapply their skills. One of the main rea-sons people decide not to administer firstaid is their lack of confidence. The in-
271
structor must go out of his or her way toprovide encouragement. Although youmust be cautious and not go overboard,try to find something good in even ratherpoor results. Encouraging and promot-ing confidence is part of your job as aninstructor.
One trick found to be successful inpromoting confidence is the continualreinforcement and practice of specificskills. For example, the first day of class,and each class hereafter, the author hasa small portion of daily dass time de-voted to obstructed airway maneuversand to bandaging. By the end of thecourse, the students have mastered arather complicated procedure involvingobstructed airwayfor both consciousand unconscious victims. They are sosure of their ability to do thr procedureproperly that there is no doubt in theirminds they can come to the aid of a chok-ing victim.
The students are also proficient atbandaging--so much so that they canapply a sling, various head bandages,shoulder, chest, and hip bandages prop-erly within thirty seconds.
4"1Number ThreeCooperation
01.0,The third C also falls under the re-
sponsibility of the instructor. Since acci-dents or illness have a tendency to bringmany people together, a first aider israrely alone. He or she 1111.1e learn tocooperate and to deal with knowledge-able as well as uninformed people in thesubject of first aid.
A dassic example given by this authoris a personal account of my initial oppor-tunity to use first aid skills. As I cameupon the scene ;mmediately after an ac-cident, two men were discussing (ratherheatedly) what the proper steps shouldbe to aid an older women with a scalpinjury. While the heated discussionturned into a heated debate, I maragedto sneak in to treat the victim. Soonthereafter, the two men started hittingeach other. I am still amazed at that inci-dent. While somebody was lying on theroad bleeding profusely, two men werefightMg over proper procedure. Stu-dents must be continuously remindedthat they must learn to deal effectivelywith "know-it-alls." This author usuallyincorporates two to three simulationsduring the course, and often role-plays a"know-it-all" person (without lettingthe class realize what is happening).
261

Eventually the students develop effec-tive skills in dealing with this type ofperson.
Cooperation is also encouraged by as-signing specific tasks and grading oncooperation rather than procedure(without the students' knowledge thatcooperation is what is looked for). Givetests and have two people work on themtogether (nothing provides more realisticpressure than assigning fifty true andfalse questions and giving the studentsten minutes to answer them). Also, givecertain accident situations for which stu-dents (as a group) must list appropriatefirst aid procedures. Students realizethat not everybody interprets everythingthe same, and all have different perspec-tives regarding first aid treatment.
Number FourCreativeness
-.mod
The chances of having an ambulanceor a first aid station within easy accessafter an accident are rare. Chances areyou will be twenty miles from nowherewhen an accident occurs. Thus, it is ex-
262
.0. `,`
t
;
I/
2 7
tremely important that the instructor en-courage creative thinking. We all learn toapply slings using the triangular ban-dage, but how many people carry trian-gular bandages with them? A personmay have to use a shirt, jacket, or someother item.
The instructor needs to provide timefor the student to improvise certain firstaid equipment such as splints, ban-dages, litters, and other transporting de-vices.
Specific examples that can be utilizedare to require of students that they obtaina triangular bandage and some otherpiece of clothing. They learn their ban-dage first with the triangular bandage,and later in the course they experimentwith their extra clothing. I also encour-age them to practice applying the ban-dage (sling, forehead, scalp, etc.) onthemselves.
ConclusionMurphy's Law ("If anything can go
wrong, it will.") is a most appropriatequote to relay to your first aid class. Asinstructors of first aid, we must try toprepare students in all dimensions offirst aid. This author has found the "FourC's" of first aid an effective attempt tomeet these needs.
111
TEACHING IDEAS 141
First Aid and Safety
Mock Disaster: An Effective Lessonin Preparation for the Real Thing
Gary M. English and Cathie G. Stivers
The use of mock situations in firstaid is not new, but effective uses ofmocks are not easily found in theliterature. Through trial and error a'mock exercise has been developedthat serves as a learning tool and isevaluated easily.
This exercise takes four classperiods to complete.
First Class Introduction
As an introduction to the upcom-ing major mock, a variety of "minimock" situations are provided to en-courage students to begin thinkingabout staging a mock situation. Aseries of 3x5 cards which identifyspecific injuries, signs and/orsymptoms of victims of accident or ill-ness are distributed among classmembers. Once cards are distributed,individuals form informal groups ofthree to four members and discusstheir mock situation in terms of (1)identifying the situation, (2) listingprops that could be used to enhancethe scenario, (3) listing signs andsymptoms associated with the injury
Gary M. English is a doctoral can-didate and graduate tr -.thing assistantin the Department c; fealth "NW-don, Physical Educe m and LeisurePrograms at the University of NewMexico, Albuquerque, NM 87131.Cathie G. Myers is an assistant profe--sor in the Department at The Universityof New Mexico.
and (4) listing proper treatments forthe injury described in the mock situa-tion. The goal of this exercise is toresolve the situation by correctly Hen-tifying these four criteria.
axe the exercise is completedand class members have gained an un-derstanding of what is to be expectedof them, students are divided intoworking groups to prepare for themajor mock. Althougb is is not impor-tant that each group have an equalnumber of students, it is imperativethat there is an even number ofgroups. Once groups are formed, themajor mock forms are distributed(see Figure 1), and group planningbegins. At this time, group membersare encouraged to share phone num-bers so that members can contacteach other to arrange additionalmeetings outside class.
In concluding the first classperiod of this exercise, the instructorprovides, via overhead projector andtransparencies, an example of a com-pleted mock situation form for stu-dents to view (see Figure 1i). Whenstudents see a completed form, manyquestions are answered and muchconfusion is resolved. Finally, half thegroups are designated as victims andthe other half as rescuers, for the thirdclass period.
Second Class - Group Planning
Because of the time involved indeveloping the mock situation, theclass does not formally meet during
273
this session. Instead, students are ex-pected to gather to work with othermembers of their group in decidingwhat their group's mock will be,gathering props, and working out thelogistics needed to complete the as-signment: During this "open" classperiod, the instructor should be avail-able to clarify any questions the stu-dents may have.
Third Class - Mock Disaster, RoundOne
During this class period, groupsthat were designated as victims duringthe first class period will enact theirmock situations. Rescuers designatedat that same time will demonstratetheir first aid skills by rescuing the vic-tim group.
Fourth Class - Mock Disaster, RoundTwo
The format for this class period isidentical to that of the precedingclass. However, groups will changeroles, allowing everyone the oppor-tunity to perform as a victim and as arescuer.
Role of the Victim
The group's members selected toplay the roles of victims must fill outtheir mock forms completely. It is im-portant to stress to members of thevictim group that they are to
263

"1:4 _VV4. itA!
A ,q
Names:
Major Mock SituationVictim ReportI. Uescribe the situation you -re going 'co display:
A bus on its way to the airport has overturned. You are among the first people to arrive at the accident scene. After surveying thesituation, you find that two passengers have been anjurvd.
List the injury(s) of each individual and the signs or symptoms for those injuries. List the most severely injured individual first,followed by the next serious to the kast serious.
Victim 11. Injury: Sio,ns and symptt.ins:
Glass fragmems ill face. Bleeding around the face and head.
2. Injury: Signs and symptoms:Vehicles antenna penetrated the victim's cheek. Hieeding from the mouth, some teeth may be missing.
3. Injury: Signs and symptoms:Unsure?? Victim's pulse is weak and rapid, the skin is cold and clammy,
and the victim appears to be pale.
Victim Z1. Injury: Signs and symptoms:
Fracture of the left forearm. The arm is deformed between the wrist and the elbow.2. Injury: Signs and symptoms:
Unsure?? There is no pulse at the radial artery. However, there is extremepain when the hand is held or touched.
3. Injury: Signs and symptoms:Unsure?? The victim is complaining of pain in the area where his chest came
into contact with the seat in front of him.
II. What is the proper treatment for each victim? List treatments in the order in which they should be done. Assume that a good patientsurvey has been completed.
Victim 1Treat for shockmaintain the ABC's; keep body temperature stable; elevate the lower extremities; reassure the victim; find and treat thesource of the shock.If there are teeth missing clear the mouth and femove any broken teeth.
Remove the antenna if it is still impaled in the cheek, unless this is too difficult: then stabilize and bandage around the object. Hold agauze pad inside the cheek as well as outside. Do not leave gauze inside the mouth unless you're holding it.Do not attempt to remove any large fragments of glass. Apply a sterile dressing to wounds and bandage. Do not apply pressure towounds (doing so may cause further damage).
Transport immediately; stabilize the victim; keep the victim on his or her back.
Victim 2While performing the secondary survey it was noticed that there was extreme pain when the left hand was touched. The pain wasevident from the fingertips to the point of the suspected fracture. It was also noticed that there was no pulse at the radial artery. Anocclusion should be suspected and corrected before splinting. The rescuer must move the arm to allow circulation to be restored to thehand before splinting.
Immobilize the arm by splinting above ae.i tl.elow the suspected fracture sight. Once the arm has been immobilized, place it in a sling.Exam. le the chest area for deformities t! .e may indicate a fracture Look for the signs and symptoms of a flail chest place the victim in eilying or sitting position or wftitevi comfortable.
III. Explain why you put the victims in the order that you did.From the signs and symptoms, it was apparent that victim 1 was going into shock. To prevent the shock from progressing, it was decidedthat this person would be treated first.
Victim 2 was treated second. The problems with this indieidual became more serious as time passed. The fracterc was not a majorconcern; however, as time passed, the pain in the extremity became severe. The chest pains were attributed to the victim corning intocontact with the front seat and did not appear to be very serious.
IV. What props will you use, or how will the rescuers find the information they need to figure out what happened?Victim 1: Wire (for the antenna), broken glass around the accident sight, Chiclets (for the broken teeth).Victim 2: A short round board to portray the tracture sight; a chair to suggest the front seat.
264 27.1

demonstrate, or act out, the victimscenario whicl. they developed. Allmembers of the woup must be totallyfamilial with their own simulated in-juries and treatment for those injuries,as they will assist evaluating effec-tiveness of treatments rendered byrescuers.
To assist the rescuer, the victimmay tell the rescuer of symptoms thatcan't be seen; however, the victimshould only reveal the symptom whenthe rescuer assesses that particularbody part.
Role of the Rescuer
While victims prepare for mocksituations, rescuers should wait in ahallway or nearby classroom wherethey cannot see the victims in prepara-tion. Durhig the wait, the instructorreads the situation from the victims'major mock form. It may be neces-sary, at this time, for the instructor toremind rescuers to think carefullyabout the situation they are about toencounter. Rescuers may -,ed to bereminded especially that there may besituations in which the best thing tooffer, in terms of aid to the victim,is reassurance.
Appropriate examples include anepileptic coming out of a seizure, oran accident victim with a suspectedfracture of the thoracic vertebrae.The rescuers may choose to work as agroup or as individuals, but com-munication among rescue groupmembers is encouraged strongly. Themock is completed only when all vic-tims have been attended and theirconditions stabilized.
Evaluation
There are several ways to evav....(testudent performance during a mocksituation. To assess cognitive aspeetLof first aid, the instructor must criti-cally review each "treatment" sectionof the mock planning form. Since eachvictim identifies his/her lir ,lt.ment foreach injury, the victim is in the bestposition to assess correctr,ess of treat-ments rendered by the rr-icuer.
Because of this, victims are askedto complete an evaluation sheet as-
sessing their rescuers' performanef..),once the mock situation has con-cluded. Criteria include questionssuch as "Did the rescuer find all theinjuries without help?" "Were correcttreatments given to those injuries?""Were treatments done in correctorder of priority?" "Did rescue teammembers work well together?" Thisassessment, along with theinstructor's evaluation of how wellrescuers performed, determines agrade for the affective learning com-ponent of the mock situation.
These two compol.ents comprisethe majority of the evaluation process.A final component, then, is added tothe mock to assure that individualswithin the group contribute equally.Each individual is asked to list, cn aseparate sheet of paper, members cfhis/her group and to relate whethereach member (1) contributed morethan cther group members, (2) contributed equally to the group effort or(3) contributed less than other groupmembers.
Proven Success and Popularity
The use of the mock situation infinal weeks of a semester of college-level first aid courses has proven to besuccessful in assessing students' com-prehensive first aid knowledge andpractical skills. An added feature ofthis procedure is its popularity withstudents.
Creativity elicited by this activityadds to the excitement. In one in-stance, members of a group of NativeAmerican Indians decided they wouldadd to the confusion of the mocksituation by speaking in their nativelanguage in order to see how rescuerswould react. In another situation, avictim group displayed a spelunkingaccident and required rescuers towork in a darkened room under a longlow table. Other sit7,- tions have in-cluded skiing or can.eing accidents,motor vehicle accidents and gangfights. Possibilities are limited only bystudent imagination.
275 265
TEACHING IDEAS 142=IMMEW
First Aid and Safety
The Importance of Child Safety SeatEducationKaren D. Li ller
Injuries are the leading causeof childhood death in the United States(Baker & Waller, 1989). Total motorvehicle injuries are the leading cause adeath of children between the ages of 0to 14 in every state (Baker & Waller,1989). Based on these injury statistics, itis logical to assume that parents wouldcomply with safety seat laws by alwaysusing a child safety seat (CSS) for in-fants and toddlers. Although all 50 stateshave now enacted CSS laws, less :han 50percent of three-year-old and four-year-old children, respectively, were re-strained, 411985 (Fo&s, 1989). Research-ers have suggested that CSS expense,
Karen D. Liller is an assistant professorat the University of South Flwida Col-lege of Public Health, Tampa, FL 33612.
266
difficulties in use, confrontations withtoddlers, inaccurate beliefs and assess-ments of accident risks, and lack of rolemodels contribute to parents' reluc-tance in using CSSs.
Because many of the parentsof today's young parents did not useCSSs, this behavior has not been rein-force& Therefore, CSS education shouldbe available to parents and young adults.High school students enrolled in health,life management, parenting, and otherrelated courses also should receive thiseducation. Although most of these stu-dents are not parents, they do partici-pate in activities, such as baby- sittinginfants and toddlers, which often re-quire students to be responsible forchildren in a motor vehiue. Also, par-ents of students may not L using CSSs
27f;
with their younger children or are usingsafety seats improperly. Students canserve as role models for their family andfriends and, eventually, role models fortheir own children and future genera-tions.
CSS education should includestrategies shown effective through re-search and program implementation andevaluation. A C&S program should becomprehensive and address many rea-sons cited for low rates of compliance.An example of a two session high schoolCSS program follows. These sess:3n.sprobably will take place over three orfour class periods. However, instructorsmay shorten or lengthen the time andtailor the topics, depending on the par-ticular setting and curriculum in use.
Student Participants
Male and female studentsshould be randomly assigned to eachother to serve as a parenting unit. If thereis an unequal number of males and fe-males, two females can be paired or twomales, because there are many singleparents today who bring a friend or ac-quaintance to parenting education ses-sions. Also, if there is an unequal numberof students in the class, groups of threascan be used. Groups of "parents" shouldsit together in a large circle. Topics forteaching sessions are shown in the Ses-sion 1 and Session 2 boxes.
CSS education should be takingplace in schools and other locations suchas prenatal and postnatal classes (Ker-nish & London, 1986) and pediatricians'and obstetricians' offices. Other healthsettings such as pharmacies should have0.:S material available. Community en-

vironments such as daycares or pre-schools also should have information toshare with parents. Materials for in-structors and community settings mayinclude pamphlets, booklets, or videosavailable through local and state trans-portation safety groups, in addition tonational sponsors such as the NationalHighway Traffic Safety Admini. tration(NHTSA) or the Americau Academyof Pediatrics (AAP). This material mayneed to be revised so that it is targetedfor the audience, reflecting age, cul-tural diversity, and socioeconomic sta-tus.
Although CSS legislation hasbeen in effect for a decade, childrencontinue to be injured and killed inmotor vehicle accidents. Strict propo-nents of passive restraints such as airbass and automatic seat belts believethat passive devices are the answer tooccupant protection. However, even ifthese restraints become standard in ev-ery motor .mhicle, parents still will needto be educa!ed about CSS use withthese devices.
Individuals must be active intheir own safety. For parents and otherswho care for young children, this alsoincludes becoming active in children'ssafety.
Parenting and related classesin schools provide excellent opportuni-ties for introducing and reinforcing use
Baker, S. P., & Waller, A. E. (I 989).Childhood injury-state-by state mor-tality facts. Baltimore: The JohnsHopkins Injury Prevention Center.
Foss, R. D. (1989). Evaluation of a com-munity-wide incentive program topromote safety restraint use. Amer-ican Journal of Public Health, 79,
304-306.Kernish, R., & London, L. (1986). Strat-
egies to increase the use of childsafety seats-An assessment of cur-rent knowledge.(NHTSA Report No.DOT HS 807 116). Washington, DC:National Highway of Traffic SafetyAdministration (NTIS No. DIN H22-82-A-07197, Task 4).
of CSSs. This is a life-saving skill that hasa definite place in our clas.srooms. Thegoal of CSS education is to make asignificant impact on decline of the trag-
edy of childhood motor vehicle injuries anddeaths. With education, legislation, and im-proved CSS technology in place, schools andcommunities can help make this a reality.
Session 1
The instructor will:
I. Discuss laws, penalties, and safety features of approved infant and toddler CSSs. (Aconvertible infant/toddler seat may be used.)
2. Discuss availability of seats at a reduced cost through loaner1.-ntal communityprograms.
3. Have available various models of child safety NM, with directions and names of vehiclesin which they fit. These are available from manufacturers and loaner programs. Demon-strate proper use of an infant and toddler CSS with dolls.
4. Allow each parent to properly place a doll in both the infant and toddler scats. If timepermits, have each parent place the doll and CSS in the instructor's vehicle or otheravailable vehicles. Each student must do this properly!
5. Have each parent group discuss difficulties of using a CSS. Have them work with theirpartner/s to document questions or concerns that will be discussed at the next CSS session.
-AMIMMIIIME.111=1:!
Session 2
The instructor will:
1. Ha\ : each paup of parents read their questions and concerns to the rest of the class.The ir structor will answer the questions and conduct a brief discussion session.
2. Re view importance of using CSSs for both infants and toddlers.
3. Discuss and role-play parent/child interactions that will improve parental compliance.The instructor will need iother teacher or student to assume the role of the toddler.
4. Recruit local patentswho consistently complywith child safety seat laws to join thThese parents can be lccated through various injury or safety groups in the communityAllow these parents to respond to questions and concerns from the class.
5. Have the class view videos of parent "testimonials" on importance of using CSSs..Thisshould not be used for "shock value" but should emphasize that the health of the infantand toddler is dependent upon the parent, even when riding in a vehicle.
6. Have each class member write one or . wo paragraphs on benefits of CSS education andhow each class member will implement this behavior now (if possible) and in the future.
Complete the session by providing each class member with a certificate for successfulcompletion of the CSS education program.
277267
TEACHING IDEAS 143
HIV/AIDS
AIDS "To Tell the Truth" Gaming Activity:A Teaching Method
Jon W. Hisgen
The AIDS epidemic has created apublic outcry for effective and creativeAIDS education at all grade levels. Whathas come out is a plethora of lectures,discussion materials, and talking-headaudiovisual materials. The activity I havedeveloped asks students to look at thebillion dollar a year AIDS quackerybusiness. The students make use of thetechnique from the old television gameshow "To Tell the Truth" to discoverwho are the charlatans and who is thereliable doctor. AIDS charlatans are veryknowledgeable so some of the answerspresented by each participant are accu-rate; students must sort out the falsestatements from the correct and appro-priate re gponses.
'1">)e following are the objectives ofthis teaching method. The student will:
1. Differentiate between accurateand inaccurate AIDS information.
2. List the qualities of a healthcharlatan.
3. Analyze AIDS information scto determine the accurate medical spe-cialist.
4. Identify questionable practices.
The activity involves interviews ofthree contestants, all claiming to be areliable AIDS specialist. Only one ofthem answers all questions accurately.The other two can respond with eithercorrect or incorrect information.
Jon Hisgen is health coordinator forthe Pewaukee Public Schools, Pewaukee ,WI 53072.
268
T ree c mtestants are given a set ofanswer. a wtek before the wtivity; theyreview their narefully to learn accuratepronunciauon of all words used. Duringthe interview, a group of five panelistsask questions of any of the three con-testants, for a two-minute period. Afterthe questioning, the rest of the classdecides who the real doctor is and why.All three contestants provide some ac-curate AIDS information, but only onewill answer every question correctly. Adiscussion of each contestant's answers,beliefs, and philosophy should followthe identification of the real doctor.
The mtivity begins with the intro-duction of the three contestants. Whenasked by the announcer to "state yourname and occupation," Contestants #1,#2, and #3 all respond: "My name is Dr.(Jane, James) Bluemner and I am aspecialist working on treatments forAIDS patients."
The announcer then states: "Pondexposing genitals to the sun at
4:00 o'clock, cell injunctions thesearc some of the treatments offered forAIDS, a disease ripe for questionablecures. Dr. Bluemner has been a physi-cian specializing in the study of the HIVvirus for the past five years. The doctorhas researched retroviruses at the Centerfor Disease Control since 1985 and ispresently studying drugs that mightprevent these viruses from entering thehost nucleus. Dr. Bluemnerrecently wonthe American Meal Association re-search scholar:m:1rd. We will begin thequestioning wit!I panelist #1."
The panel sts, in turn, read the fol-lowing 21 questions, asking any of thethree contestants they chose.
"I 3
Questions
I. Why is AIDS such a great problemin our world?
2. What is your opinion about self-ueating an illness that is supposedlyuntreatable?
3. Who is at high risk for AIDS?4. What is ARC?5. Where did you get your MD degree?6. If I wanted AIDS information from
someone other than a doctor to whomshould I turn?
7. What is the most dangerous AIDStreatment on the market today?
8. What is AZT?9. Since the AIDS virus attacks the
immune system what type of AIDSproducts do you think people are likelyto sell to the unknowing AIDS patient?
10. What is the greatest problemteachers face educating about AIDS?
11. What is an AIDS guerrilla clinic?12. What is L-721 and do you think it
should be legalized?13. Do you believe in AIDS testimo-
nials?14. What can Americans do to fight
AIDS quackery?15. Why does quackery thrive so much
in our society?16. What is DNCB and why do AIDS
patients use it?17. Is DNCB legal? If so, why?13. What do you think should be done
by people in a place where they are incontact with a known AIDS patient?
19. How is AIDS transmitted?20. Huw could a person reduce his/
her risk of exposure to the AIDS virus?21. If you knew someone in your
family with AIDS what would you do?

Answers for Contestant #1
I. Acquired immune deficiency syn-drome is a worldwide concern becauseso many people are ignorant about thedisease.
2. Self-treatment plays right into thehands of the money hungry charlatan.That is what they want.
3. Men who have had anal sex withother men since 1977 and people whoshare drug paraphernalia, specificallyneedles, are examples of persons ex-hibiting high risk behaviors.
4. AIDS related complex (ARC) is apre-AIDS condition with such symptomsas severe weight loss.
5. I received my degree from LomaLinda Medical School in San Diego,California.
6. The Public Health Service and theCenter for Disease Control have someup-to-date materials.
7. An $800 treatment for pills con-taining mice immune system substancesafter being given the AIDS virus. Instantdeath!
8. A drug that has been shown to stopAIDS symptoms in some patients.
9. Most of these treatments promiseto strengthen immunity.
10. Developing guidelines for teach-ing about the disease within the valuesand concerns of every student's family.
11. A place where questionable AIDStreatments are sold or practiced.
12. It is a product made of a fat calledlecithin that was purported to hinder theAIDS virus from attacking healthy cells.I think it should be approved for experi-mental use by willing patients.
13. Only if the testimonials say thedisease is a killer.
14. Become knowledgeable of thc at-risk behaviors and the seriousness of theinfection once cont-acted.
15. People will grab at aR:). iin
when their life is at stake. The, t.hey
Lve nothing to lose.16. A chemical that diminishes the
purplish lesions of Kaposi's sarcoma, a
type of opportunistic, rare cancer thataffects AIDS patients.
17. It is a chemical used by photogra-phers in processing film.
18. Realize that if you do not engagein high-risk behaviors like anal, homo-sexual sex or sharing needles with thisperson you decrease your chance ofhaving the infected person's blood orbody fluids enter your body.
19. Mixing of blood or blood prod-ucts with an infected person's blood orbody fluids.
20. Abstinence, having only one sexpartner, and use of condoms will defi-nitely lower AIDS risks.
21. Show him/her the love and con-cern I felt for him/her before hashecontracted the disease.
Answers for Contestant n
1. There is no ultimate AIDS cure inthe foreseeable future.
2. Certain macrobiotic lifestyles likemeditation and whole grain and veg-etable diets are the only successfultreatments that can be selfftaught.
3. Anyone who gets the AIDS virusin their blood or body fluids.
4. It is a pre-AIDS condition withdiarrhea, extreme weight loss, and de-pressed immunity.
5. I received my MD degree at theUniversity of California and my nutri-tiona consultant's degree from theWholistic Health Clinic in Sacramento.
6. The HEAL group presents soundAIDS information.
7. Mail order bottles of T-cells toreplace AIDS ravaged T-cells is an ab-solutely absurd treatment.
8. A drug shown to lessen AIDSsymptoms.
9. They should buy Dr. Revici' s herbalremedy but they end up purchasing bloodserum contaminated with hepatitis Bawl AIDS. How utterly stupid!
10. Farents unwilling to allow soundhealth information for their kids.
279
11. Clinics that sell bogus healthtreatments.
12. A drug that can be made fromhealth food store ingredients. Furtherresearch needs to be done before legal-ization.
13. I support solid research like Dr.Levy's that has shown many men becamestronger after following a macrobioticlifestyle.
14. Become educated as to the stylesand techniques of the quack in our so-ciety. Be skeptical!
15. The government needs to makelaws that will scare these charlatans off.
16. A drug that has FDA approval forwarts.
17. Yes, but for warts, not AIDS.18. Let doctors try promising new
drugs with sound dietary practices onthese people without FDA intervention.
19. Sex, transfusions, and crossingplacental barriers to unborn children.
20. Develop a respon sible macrobioticlifestyle of diet, meditation, no intrave-nous drug use, and safe sex withcondoms.
21. Get him/her to macrobioticcounseling.
Answers for Contestant #3
1. Acquired immune deficiency syn-dromeis a major problem because peopleare panic stricken whenever anyone saysthe word. We need to educate!
2. I think most people cannot self-treat and must be guided by competent,trained physicians.
3. Gays, needle sharers, prostitutes,hemophiliacs, and infants of infectedmothers.
4. The beginning stages of the infec-tion.
5. The State University of New Yorkat Stony Brook with postgraduate workin the Bahamian AIDS research institute.
6. New York's HEAL group has manyeducational materials and many newtreatments.
269

7. $10,000 treatment of thymus glandextract that is available in France.
8. A quack product that claims toalleviate AIDS symptoms.
9.1 believe my life extension prod-ucts like BHT are the only effectiveAIDS treatment on the market.
10. Our teachers' lack of knowledgeof the most successful I IDS treatments.
11. ME :,es that are forced to sell soundtatments because the FDA has harassed
at into hiding.12. An effective AIDS drug that U.S.
ai;.1 Israeli rsearchers have found sue--:sful in preventing AIDS.13. If a person has been told he will
dL the,' I believe in personal accounts.4. We must realize that our medical
'em has so little to offer that alter-,les must be explored.
270
15. Because quacks are looking for aquick buck and people are al ways lookingfor a quick cure.
16. A drug that has been shown tohelp with Kaposi's sarcoma, an oppor-tunistic cancer with purple splotches.
17. Yes, it is available in clinics likemine throughout the country.
18. Show care for the AIDS patient sohe/she will feel better and live longer.
19. Anal intercourse, blood transfu-sions of infected blood, mixing of bodyfluidsharing of needles, and sex withpi t...titutes.
20. Injections of bee pollen, garlic, orblue-green algae beefs up the immunesystem.
21. Have him/her become a part ofmy life extension program.
The first contestant is the person whogave all correct responses. Contestant#2 discussed health and nutritionaltreatments that, though they were harm-less, involved claims that were loadedwith half truths and outright false state-ments; one should encourage an AIDSpatient to consume a sound, balanceddiet but not the one promoted Lymacrobiologists. Contestant #3 ex-changed many false and dangeroustreatments and iaeas with his/her pa-tients.
This approach could be used forother areas of health education. Ques-tions and answers are prepared by theteacher, but, depending on the interestand capabilities of the students, could be\vritten by the.. students themselves.

TEACHING IDEAS 144
HIVIAIDS
AIDS/HIV Teaching IdeasBarbai a Beier, J. Leslie Oganowski, Richard A. Detert, and Kenneth Becker
AIDS/HIV education is essential forthe understanding and pre' ention of thedisease. AIDS/HIV is a complex issueand thus demands a multifaceted ap-proach. The condition may be viewed asa disease issue, a decision-making issue,a sexuality issue, and a death and dyingissue.
A series of four teaching ideas arepresented as they address each of theAIDS/HIV issues. The teaching tech-niqtrs are as follows:
1. "Understanding AIDS/H1V"a disease issue
2. "Who Do You Trust?" a deci-sion-making issue
3. "A Safer Sex Continuum" a
sexuality issue4. "The Living Years" a death
and dying issue
ACTIVITY #1:"UNDERSTANDING AIDS/HIV"Obiective: After the bag demonstration,the student will be able to describe howI-HV breaks down the immune system toallow the development of AIDS.
Preparation: Prepare envelopes for eachstudent with the following shapes repre-senting parts of the blood involved i n theimmune system. Place the Illy in onlythree of the envelopes.
Barbara Beier, J. Leslie Oganowski,Richard A. Detert, and Kenneth Beckerare members of the faculty at the Uni-versity of Wisconsin-LaCrosse.
T-cells whiteblood cells
Necessary Materials:1 lunch size paper bag for each
student2 lunch size bags for teacher dem-
onstrationmarkers or crayonsprepared envelope for each student
Activity:1. Instruct the students to color or
decorate their bag to represent the skin.2. Review the steps that take place
when a germ enters the bod hv havingeach student put parts of the blood (fromtheir envelope) in the bag. The teacherdemonstrates by placing in the bag each
!ype and explaining the action; i.e.,white blood cells rust, to the place wheregerms enter and attach to the germ tomake it less dangerous to the persm.
3. Introduce the functions of the im-mune system. A healthy immune syszmiworks to destroy nearly all types ofgerms, including many bacteria and vi-ruses.
4. Writeimmun( )n the board. Havea student tell what is meant when some-one says he/she is "immune" to some-thing (protected/safe).
5. Conduct the following demonstra-tion of the activities of the immune sys-tem in fighting germs.
a. Hold two bags to represent the skinas a barrier to keep germs out. As long as
281
HIVcells
the skin remains uninjured, it holdswhat's inside the body in and keeps therest safely out.
b. Reveal a break in the skin by tear-ing part of one bag. Have students nameways a break could occur (cuts, scratc hes,burns, scrapes, br)ken bones, surgery,intravenous drugs, ear piercing, tattoos,punctures).
c. Toss some objects into the bagsrepresenting foreign bacteria, viruses,or germs. Explain that our blood con-tains white blood cells that fight germs.One kind of white blood cell (mac-rophage) moves through the blood andtissues to surround and "eat" germs.Toss some macrophage cells into thebag.
d. T-cells are another type of whiteblood cell that help fight germs. T-cellsattack and des:-..oy viruses. Add T-cellsto the. bag. Stress that some T-cells serveas "command cen ters" for the body'sbattle against germs.
e. Another kind of white blood cell iscalled a B-cell. Add the B-cells to thebag. B-cells produce chemicals calledantibodies. Explain that antibodies candestroy viruses and other germs.
f. Explain that some antibodies, evenafter destroying some germs, stay in thebody to protect in case there is anotherexposure to the same type &germ. Thaiis immunity.
271

g. Ask students "What hr pens whenthe 'command center' in a real battle isdestroyed?" Conclude that when germsattack the white blood cells (T-cells)that control the body's immune system,they can cripple the body's ability tofight off infection and diserse.
h. Ask who has an "H" in his/herenvelope. Toss the "H" into the bag.This represents an HIV condition. AIDSis caused by a virus called HIV (humanimmunodeficiency virus). HIV destroysthe "command centers" 'T-cells) of theimmune system and the body cannotfight off certain infections.
i. The person with HIV does netusually of HIV infection directlythe person with AIDS usually dies fromotherdiseases that the body can no longerfight off.
Time Frame: The bag activity itself canbe completed in a 30-40 minute classperiod. The preparatury informationcould take one class prior to the activity.Questions about symptoms of HIV,children with HIV, and feelings associ-ated with having an "H" in his/her bagcould take varying amoun.s of time.
Do discuss witN the ciasz the chancesof "having an HIV in his/her bag" andthe risks of infection. Include a discus-sion of caring for the feelings of peoplewho are infected.
ACTIVITY #2:"WHO DO YOU TRUST?"
Objective: At the completion thisactivity, students will be able to discussthe benefits and consequences of tak igrisks.
Preparation: Before students eater theroom, the teacher places objects insideeach of four large brown paper bags:(bag #1. one mouse trap that is not set;bag #2 = one small mouse trap that is set;bag #3 = one large rat trap that is set; bag#4 = one block of wood).
There is one block of wood on thecorner of the table.
272
Necessary Materials..4 large brown paper bags num-
bered I to 42 mouse traps1 large rat trap2 blocks of woodtable
Activity:I. Ask for three volunteers to come
forward who are willing to take a risk.Describe the risk as selecting one of thepaper bags. Volunteers will be asked toblindly reach to the bottom of the bagand grab whatever is in ;.t. If it is theblock of wood like the one on the cornerof the t3ble, they will receive a desig-nated amount of money.
2. Ask for three volunteers who willassist the risk takers in their adventure.Instruct these volunteers to move to theother side of the room.
3. One at a time, ask each of the threeassistants to open each of the bags andlook at the conteats. Ask them to beexpressionless as they view each of thebags. Then ask each of the assistants ifthere is a block of wood in at least one ofthe bags. Once verifie ask (one at atime) if he/she would be willing to takethe risk of reaching blindly into one ofthe bags. Some will say no; some, yes.
4. Ask each assistant to meet a risktaker and quietly whisper in his/her earwhat was seen in the bags. Then instructthe risk taker to whisper the same mes-sage to one other person in the room.Once all three have additional informa-tion about the contents, ask each of therisk takers if he/she is still willing to takethe risk. Those who say "no" can Ivseated; those who are still willing tocontinue remain standing.
5. Provide some more information tothe risk takers (and the rest of the class)by revealing the contents of bag #1.Then reveal the contents of bag #2 byunsetting the mouse trap with foldedpiece of paper. Ask again which risktakers would still be willing to blindlyreach into one of the two remainingbags.
6. Ask the assistants to provide a bitmore information to the risk takers and
252
the rest of the class by asking whether aconsequence of reaching into one of thebags could result in a) pain, b) brokenfmgers, or c) the presence of blood?Then ask again who might be willing totake the risk.
7. Teacher places remaining risktakers in the front of the room and asksthem one more time if they are willing totake the risk. If yes, mN tV bags up andask the risk takers to turn around. Bynow, most risk takers have quit!
8. Of course, the teacher stops theactivity at this point as students couldget injured if they actually reached intobag #3. The bag contents are now re-vealej.
9. Follow-up discussion:a. Ask the risk takers to tell the group
what their assistant whispered in theirear.
b. Did all the assistants see the samecontents?
c. Discuss how the risk takers thoughtthey could "beat the odds."
d. Discuss comments that encour-aged/discourage.; each from stopping orcontinuing with the activity.
e. Finally, discuss what risks each arewilling to take; which would not be saferisks; what risks are invelved with AIDS/HIV conditions.
Time Frame: This activi,y takes between20-40 minutes to complete. The timeframe may vary depending on grae?,level and the number of comments madeor points raised during the discussion.
ACTIVITY #3:"A SAFER SEX CONTINUUM"
Objective: At the completion of thisactivity the student will be able to iden-tify means of transmission of AIDS/HIV on a safer to unsafe continuum.
Prepiration: When discussing the issueof AIDS in the classroom, one way tointroduce safe and unsafe sexual prac-tices is by using the "Safer Sex Con-tinuum. This activity would be pa.t ofa larger unit on sexuality or sexually

transmitted diseases (STDs) and wouldbe utilized once the students had devel-oped a degree of comfort in discussingsexual topics.
Matedials Necrasaa:chalkboard and chalk(or newsprint and marking pens)
Activity:1. Introduce the topic by having stu-
dents consider the methods of transmis-sion of the HIV virus and sexual prac-tices. Place the continuum shown at thebottom of the page on the chalkboard.
2. At this point, ask the students to"place" a sexual activity on this con-tinuum on the appropriate position so asto indicate the "safeness" or "riskiness"of t11.3 behavior. As each behavior orsexual activity is suggested, the ele-ments inwilved in ranking that behaviorin that pos *ion should also be disc ussed.This method involves the students inanalyzing each sexual activity basedupon their knowledge of the transmis-sion of the HIV virus. It is also a methodthat could be useful in introducing sen-sitive topics such as masturbation,condom use, and anal intercourse.
3. Clarification of certain activities isa productive outcome of this activity ifstudents are allowed to engage in opendiscussion and ask questions. For in-stance, one popular misconception dis-covered with this approach was thatsome students considered a sexual mo-nogamous relationship to mean havingsex with "one person at a time.
Time Frame: This activity takes be-tween 30 and 50 minutes to completedepending upon 1) the level of knowl-edge of the students, 2) the degree ofcomfort with discussing sexual topics,and 3) the amount of discussion timeallowed.
ACTIVITY #4:"THE LIVING YEARS"
Objective: At the completion of thisactivity, the student will be able to ver-balize his/her reactions to AIDS as adeath and dying issue.
Erfrvalign: One effective way we foundto address AIDS as a death and dyingissue was to play a song that manystudents may have heard on popular hitradio stations. "The Living Years," re-corded by Mike and the Mechanics, wasplayed and students were encouraged tofollow along with the printed words.Introductory statements may include:"Think about the words and what theysay about death and dying," or, "As youlisten to the words of this song, thinkabout your thoughts on death, dying,and AIDS."
Materials Necessary:tape: "The Living Years," by Mike
and the Mechanicsprinted words to the songtape player
The Living Years
Every generationBlames the one beforeAnd all of their frustrationsCome beating in your door.
I know that I'm a prisonerTo all my father held so dearI know that I'm a hostageTo all his hopes and fearsI just wish I could have told himIn the living years.
Crumpled bits of paperFilled with imperfect thought
283
Stilted conversationsI'm afraid that's all we've got.
You say you just don't see itHe says it's perfect senseYou just can't get agreementIn this present tenseWe all talk a different languageTalking in defense.
Say it loud, say it clearYou can listen as well as you hearIt's too late when we dieTo admit we don't see eye to eye.
So we open up in quarrelBetween the present and the pastWe only sacrifice the futureIt's the bitterness that lasts.
So don't yield to the fortunesYou sometimes see as fateIt may have a new perspectiveOn a different dayAnd if you don't give up,And don't give inYou may just be OK.
Say it loud, say it clearYou can listen as well as you hearIt's too late when we dieTo admit we don't see eye to eye.
I wasn't there that morningWhen my father passed awayI did't get to tell himAll the things I had to say,I think I caught his spiritLater that same yearI'm sure I heard his echoIn my baby's new born tearsI just wish I could have told himIn the living years.
"The Living Years," Mike and the Mechan-ics (1988), Atlantic Record Corporation, 75Rockefeller Plaza, New York, NY 10019.
273
TEACHING IDEAS 145Mental and Emotional Health
Stress Manifestations Among Adolescents:Actions, Situations, and Body Responses
Chai les Regin
Grade Level: 7 - 12
Time Frame: 50 minutes
Materials: Gumby handouts, blankGumby transparency, overhead projec-tor, transparency marker. Note: any ap-propriate, genderless figure can be sub-stituted for the Gumby figure illustrated.
Background Informatin The im-pact of stress and stress related diseasesis a major concern in American society.Either the mismanagement of stress orthe use of maladaptive coping strategiesamong adolescents plays a significantrole in the major health problem areasidentified in the Surgeon General's re-port on health promotion and diseaseprevention. These problem areas includeteen pregnancy, sexually transmitteddiseases, mental illness, suicide, andhomicide.
Preparation
In the first rew classes of a stressmanagement unit, it is important to es-tablish similarities/common stresssources among students. This "we allhave stress in our lives" sensitizationallows for greater feelings of opennessand a possible reduction of the feeling of"I am the only one who has these prob-
Charles Regin is an assistant profes-sor of health eduction in the School ofI lealth, Physical Education, and Recre-ation at the University of Nevada, LasVegas, NV 89154.
274
lems." This activity is designed to ad-dress such issues. Specifically, the ob-jectives of the activity are to:
1. Describe how the stress responsecan affect a person 's physical well-being.
2. Demonstrate both similarities anddifferences in ways adolescents handle/mishandle stress.
3. Provide a supportive forum for adiscussion regarding common waysadolescents respond to stressful situa-tions.
4. Identify and describe how adoles-cents can reveal distress and eustresssources in their 'Ives.
The teacher will need enough"Gumby" handouts (sec next page) sothere is one for each student. In addition,the insuuctor will need enough Gumbyhandouts reprc heed on a second colorso that there is one for each small groupinto which the class will be divided.
Implementation
Distribute a copy of Gumby to eachstudent. Explain that the figure is arepresentation of themselves and thatthey will use it to explore how stressaffects their lives in both a positive andnegative manner.
The first step is designed to helpstudents identify how stress affects thebody. Direct the class to shade in theareas of Gumby that represent the partsof their bodies that are affected by toosuch stress. For example, some studentswill shade in the hands because. theirhands get cold when they experience toomuch stress. Other students will shade
S
in the head or stomach areas becausethey get headaches or upset stomachE Ifappropriate, this can be shown using anoverhead projector and a transparencyof Gumby.
The second step is designed to helpstudents identify current and past sourcesof stress. Tell the students that stress isboth positive (eustress) and negative(distress). The line down the middle ofthe handout separates positive and nega-tive stressors. Direct the class to fill inthe circles with terms that represent cur-rent distressful and eustressful sourcesin their lives. Examples might includemath class at school, a brother, or forolder students, their boss at work. (En-courage them to be specific rather thanwriting general terms such as school,home, or work.) Also mention that somestressors can be placed on both sides ofthe line. The horizontal line near thebottom of the handout separates currentfrom past stressors. Direct the studentsto reflect upon former stressors that theyhave "set aside" or have dealt with andlabel the circles below the line withthose past situations or people.
The third step is designed to helpstudents identify how they behave whenthey have or have had too much stress intheir lives. Direct the students to writedescriptions between the present stres-sors stating how they behave in bothnegative and positive stressful times.Positive behavior examples includesinging, exercising, or feeling happyand smil ing. Negative behavior examplesinclude yelling, picking on people, orovereating. lit the arca of past stressors,ask students to identify the behavior thathelped them deal with the stressor. Ex

amples include talking with a friend orfamily member or seeing a counselor atsc hool.
At the conclusion of this three-stepprocess, form small groups of three tofive students. Distribute the secondGumby handout and direct the studentsto fill out a composite that represents thegroup's eustress and distress situations.The teacher can conclude the activitywith these small group discussions orcan have one pei son from each groupdescribe their Gumby composite.
Variations
There is a great deal of flexibility inthis activity. Depending upon the age,readiness, and educational needs of thestudents, one, two, or all three steps canbe completed. The number of examplescan be varied at the beginning of eachstep, to help students fill in the circles orspaces between the circles.
It is also possible to use the Gumbyfigure so that the circles and spacesbetween focus on specific health educa-tion topics, such as smoking, teen preg-nancy, or AIDS. The activity can easilybe integrated into other classes that dealwith these areas. This is accomplishedby first describing a specific controver-sial situation (e.g., a teen pregnancy).The students then fill in the circles withpositive and negative behaviors (e.g.,tell parents, don't tell anyone) and thespaces in between with anticipated reac-tions by others (e.g., anger, fear, sup-port).
Note: This activity is adapted from N.L.Tubesing and D.A. Tubesing, 5truc_turedExercises in Stress Management (Duluth:Whole Person Press, 1983), pp. 21-27.
0WSNTAT
Phs-r
0 0Drawing shown smaller than it should be for actual use by students.
285

TEACHING IDEAS 146Mental and Emotional Health
An Introductory Activity for AdoiescentCommunication and Intimacy
G. Greg Wojtowicz
The purpose of this student activityis fourfold: 1) to provide students anopportunity to use intimacy as an effec-tive communication tool, 2) to familiar-ize students with the concept of "behavioral scripts," 3) to aid student transi-tions into opposite sex age groupings,and 4) to use the concept of "scripting"as a classroom management techniquein order to structure effective studentgroupings. This learning experience de-velops an awareness of individual be-havior characteristics and supports thedevelopment of communication skillsas they relate to intimacy, interpersonalbehavior, and social cognition.
Adolescence and Intimacy
The ritualistic behaviors learnedduring childhood are given practicalmeaning during adolescence. Adolescentdevelopmental issues such as autonomy,intimac y, and identity are critical as theyrelate to behavior. Schools ser to in-stitutionalize peer relationships, thusteaching the adolescent how these is-sues are linked to emotions. The adoles-cent who establishes intimate relationswith peers is challenged to socialize andcommunicate in both ideal and practicalterms. Consequently, "peers play anextremely important role n socializingadolescents into roles of adulthood"
G. Greg Wojtowicz is an assistantprofessor of health education in the De-partmel of Health Education andPhysical Education, University of Ala-bama at Birmingham, Birmingham, AL35294.
276
(Steinberg, 1985). In addition, the focusof psychosocial development shifts fromsame sex groupings to opposite sex in-teractions. This process supports theeffective translation of real values intodecision making skills and real behav-iors into problem solving techniques.This exercise in communication allowsthe student to practice intimacy skills ina controlled environment.
Behavioral Scripts
"Behioral scripts prescribestandard ways of behaving in givensettings" (Jones, Shainberg, & Byer,1985). These predetermined, uncon-scious ways of thinking and acting de-termine the who, what, why, when, andwhere of any specific behavior. Script-ing helps to integrate personality. Fail-ure to do so results in esteem fragmen-tation (Jones et al., 1985). This activityallows students to identify the variedcomponents of their scripts and givesthem an opportunity to match their scriptwith peers who have similar interests.
The technique can be adapted to fitany classroom time frame at the juniorand senior high school level. In addition ,
the activity can be effectively used tosolve problems associated with thestructuring of student groups. It requiresstudents to use those communicationskills essential to functioning as an ef-fective member of an activity group.
Objectives
This technique is designed toachieve the following four behavioralobjectives: The student will use inti-
2c E.
macy, communication skills, andknowledge of behavioral scripts in orderto:
1) identify five components of a be-havioral script,
2) identify three issues related toadolescent development,
3) list two characteristics they appre-ciate in other people, and
4) begin to appreciate the unique el-ements of other personalities.
Methods
The activity begins with a discus-sion of important issues related to ado-lescent social development, communi-cation, and behavioral scripts. Impor-tant terms such as autonomy, intimacy,and identity should be defined and dis-cussed. A numbered "behavioral script"activity sheet (Figure 1) is used to allowstudents to identify components of theirown behavioral script. Each activity sheetis identified by a number that correspondswith the numbers next to student nameson the class attendance list. Students ar..1told to put their number on their sheetand also write that number on a foamcup provided by the teacher. Studentsplace the cups on a desk or chalk tray innumerical order and then are given suf-ficient time to complete the questions ontheir activity sheet.
When they have finished, scriptsshould be posted throughout the entireroom, avoiding crowding in any onearca. Students then circulate around theroom and read each script. When theyfinish, they are instructed to c hoose threeto five scripts thai matched their inter-ests by copying the numbers found on
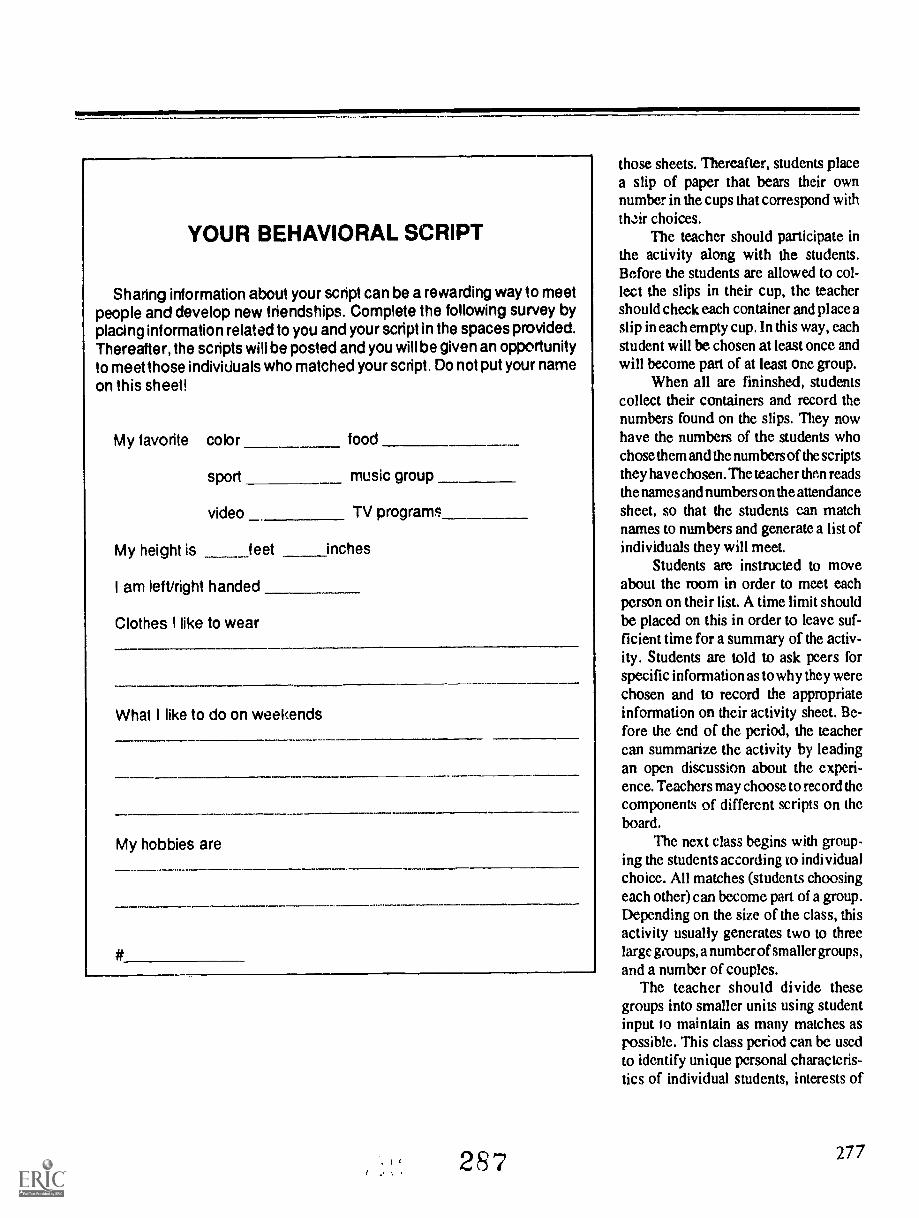
YOUR BEHAVIORAL SCRIPT
Sharing information about your script can be a rewarding way to meetpeople and develop new friendships. Complete the following survey byplacing information related to you and your script in the spaces provided.Thereafter, the scripts will be posted and you will be given an opportunityto meet those individuals who matched your script. Do not put your nameon this sheet!
My favorite color food
sport music group
video TV program
My height is feet inches
I am left/right handed
Clothes I like to wear
What I like to do on weekends
My hobbies are
#
287
those sheets. Thereafter, students placea slip of paper that bears their ownnumber in the cups that correspond withthcir choices.
The teacher should participate inthe activity along with the students.Before the students are allowed to col-lect the slips in their cup, the teachershould check each container and place aslip in each empty cup. In this way, eachstudent will be chosen at least once andwill become part of at least one group.
When all are fininshed, studentscollect their containers and record thenumbers found on the slips. They nowhave the numbers of the students whochose them and the numbers of the scriptsthey have chosen. The teacher then readsthe names and numbers on the attendancesheet, so that the students can matchnames to numbers and generate a list ofindividuals they will meet.
Students are instructed to moveabout the room in order to meet eachperson on their list. A time limit shouldbe placed on this in order to leave suf-ficient time for a summary of the activ-ity. Students are told to ask peers forspecific information as to why they werechosen and to record the appropriateinformation on their activity sheet. Be-fore the end of the period, the teachercan summarize the activity by leadingan open discussion about the experi-ence. Teachers may choose to record thecomponents of different scripts on theboard.
The next class begins with group-ing the students according to individualchoice. All matches (students choosingeach other) can become part of a group.Depending on the size of the class, thisactivity usually generates two to threelarge gioups, a number of smaller groups,and a number of couples.
The teacher should divide thesegroups into smaller units using studentinput to maintain as many matches aspossible. This class period can be usedto identify unique personal characteris-tics of individual students, interests of
277

groups, and hobbies Ihpred by the entireclass.
The groups formed can be used to:1) support development of social
skills within opposite sex groups,2) facilitate student interactions in-
volving decision making and problemsolving,
3) structure role playing activities,and
4) group students in order to developclassroom simulation games.
Groupings consisting of matchesmade by the students can improve theeffectiveness of group work by im-proving attention span, increasing mo-tivation, and augmenting student inter-actions.
Materials needed for this activityare as follows: behavioral script activitysheets, a master sheet identifying eachstudent, foam cups, small slips of paper,tape for posting the sheets, and an activ-ity content outline used to record infor-mation associat ;d with intimacy,scripting, and communication skills.
278
Conclusion
This activity provides students withthe opportunity to develop communicaLion skills essential to social cognitionand psychosocial development. Adoles-cents who experience success in class-room activities and develop effectivesocialization techniques may developpositive skills that will carry over intoadulthood In addition, teachers can usethis technique to structure effective ac-tivity groups.
This scripting methodology is suc-cessful for two reasons: 1) students aremotivated to work together because theylike one another and 2) task outcomesare easier to achieve because studentsexercise an autonomy or ownership ofthe experience after they choose mem-bers of the gioup.
This technique is most effective atthe high school level (especially grades
11 and 12) because opposite sex rela-tionships become the primary focus ofpsychosocial development. Junior high
25S
school students are more comfortableand more effective when allowed toparticipate in same sex groupings. How-ever, repeated use of this activity can aidthe transitir_%n into opposite sex group-ings. Studt'nts who lack proactive socialskills tend to somewaat 7..4rded atthe beginning of the activity. However,after they warm to the task, they tend toapproach me experience with enthusi-asm.
ReferencesFord, M. (1982). Social cognition and socialcompetence in adolescent developmentalpsychology. Developmental psychology, 18,323-340.
Jones, K.L, Shainberg, L.W., & Byer, CO.(1985). Dimensions of human sexuality.Dubuque, IA: Wm. C. Brown Publishers.College Division.
Katchaciourian, H.H. (1989). Fundamerualsof human sexuality (5th ed.). Orlando, FL:Dryden Press, Holt, Reinhart & Winston,Inc., p. 268.
Steinberg, L. (1985). Adolescence. NewYork: Alfred A. Knopf, Inc.

TEACHING IDEAS 14711111111.
Mental and Emotional Health
SHOW AND TELLDeveloping an Appreciation of Diversity
Kathryn Katzman Rolland
This two-part lesson provides a ve-hicle for high school and college levelstudents to examine the range of commonneeds and desires they share in terms ofhuman fulfillment. In addition, the ex-ercise works well as a trust-buildingexperience.
Introducfion
College students, majoring ineducation, gathered for the first class ina course that would deal with incorpo-rating materials about AIDS/HIV in theelementary and secondary school cur-riculum. Like the students in the urbancenter in which most of them willeventually teach, the class encompasseda wide range of diversity. They weremale and female, ranging in age from 20through 50, African-American, Euro-pean-American, and Latino, straight andgay, single, married, divorced and cur-and y cohabiting, returning students, one
pregnant female, single parentsandfrom a variety of economic strata.
At the first class meeting, they eyedme and each other somewhat warily.Their concern, though unspoken, waspalpable. Would they be comfortable inthis class? Would they feel out of place?Would they have anything to contribute?As educators, and particularly as healtheducators, we know these concerns well.
Kathryn Katzman Rolland is afacultymerher in the Department of Healthand Physical Education,11 timer Collegeof the City University of New York, NewYork City.
Objectives
Realizing that the class would en-compass subject matter that is contro-versial, emotional, and even frightening,I dec ided to begin with an exploration ofa more "neutral" conceptthe con-tinuum of human values. (Obviously,these are the same values that transcendand impact upon our attitudes towardAIDS and people with AIDS.) I havefound that discovering similarities fa-cilitates a more honest and sensitiveexploration of di ffet ences at a later time.My objective was to provide a forumwhere students could experience thesimilarities of their human needs in away that was at once personal and yetoffered adequate room for privacy, ifneeded.
Procedure
Because a homework assignmentis an integral part of the lesson, a pre-liminary explanation of the teacher'sexpectations is required as part of aprevious lesson.
Lesson One: As an assignment forthe following class, each student wasinstructed to "bring to class somethingthat has a special meaning for youthatmakes you feel good." The only caveatwas that living things had to be repre-sented by photographs or drawings.Realizing that I was asking students toreveal a portion of themselves to "al-most strangers," I included myself in theactivity. Students were instructed torecord their informal thoughts on the
28,
process, especially such aspects of theexercise that related to how difficult itwas to select something, v.:fat thoughtshelped them to make the final decision,and what single feelirgiemotion theirspecial "thing" elicitel. These noteswould serve as personal reference mate-rial dining the next meeting of the class.(How does it make you feel? What is itthat you respond to? Did you have adifficult time making a decision? arehelpful guidelines.) Students were in-structed not to discuss the assignmentwith any other class members until theclass met aroin.
Lesson Two: As I entered the class-room the following week, the anticipa-tion and excitement were apparent.Students were talking animatedly witheach other and their enthusiasm wasinfectious. I began the class by tellingthem that I would go first and that eachperson would go as he or she was ready.I would not call on them but everyonewas expected to participate before theend of class. In this way, they couldattend to each individual report insteadof thinking, "three more people and it'smy turn to go." A recorder kept track ofkey phrases as the discussion progressed.
Thne Frame
The class required 60 minutes for all 20students to complete their reports, but Ihave subsequently conducted the classin less time. It is important for studentsto know how long they will have todiscuss their "show and tell" when the
Continued on page 281
279

TEACHING IDEAS 148
Mental and Emotional Health
Teaching Self-AwarenessThrough Idiosyncrasies
Patrick K. Tow, Beverly Johnson and Patricia N. Smith
Pet peeves, annoying habits, oreccentricities, whatever they may becalled, are behavioral idiosyncrasieswhich everyone exhibits to some de-gree. These peculiarities develop overtime as a result of convenience, lazi-ness, or ignorance; however, most ofus are more aware of others' idiosyn-cratic behavior than of our own. Self-awareness is an elusive quality.
By itself, a behavioral idiosyncrasymight not be considered a problem ofgreat magnitude. At best, it may be aminor annoyance in an otherwise idealcharacter whose presence is appreci-ated and enjoyed. At worst, it may beconsiderer4 an extreme annoyancerequiring remediation. Whether ma-jor or minor, an annoying habit servesas a source of chronic irritation in arelationship.
Background
When people fail to recognize andput idiosyncrasies into proper per-spective, continued growth and devel-opment of interpesonal relationshipscan be stunted. The crux of a criticalinterpersonal conflict can remainunaddressed while time and attentionare consumed over minor points ofantagonism. The continual masking
Patrick K Tow is an associate professorin the Department of HPER at OldDominion University, Norfolk VA23529-0196. Beverly Johnson is Chair-person of the Department of HPER atOld Dominion University. Patricia N.Smith is an English teacher at NorviewHigh School, Norfolk, VA 23513.
280
of an underlying problem can onlycompound the gravity of a conflict andmake it more difficult to resolve. Thedegree to which someone finds certainbehaviors offensive varies accordingto one's relationship to the offendingparty. Pet peeves tr I to be exagger-ated when a person who is trusted orloved fails to line up to one's expecta-tions. Nevertheless, a tendency to-ward idealization and infatuationshould be tempered with a healthydose of reality. People are not gener-ally aware of their own idiosyncrasies,however obvious these may be to oth-ers. ;-chavioral habits may become anunconscious part of one's everydayrepertoire. Thus, overall awareness ofidiosyncrasies could bringa refreshingenlightenment to relationships.
Educational Merits of Strategy
This t.:aching strategy has realworld application that may be rootedin a lesson plan dealing with familyliving or mental health. The strategyserves as a suitable vehicle to teachself-awareness as well as an awarenessof others. It brings to a level of con-sciousness that which seldom isthought about until interpersonalconflicts surface. Even on these occa-sions, some people insist on denyingtheir part in a disharmonious relation-ship.
This lesson is not designed to sug-gest specific solutions but reveals,instead, a perspective on the trials andtribulations of relationships in gen-eral. Anyone growing up with siblingswill remember annoyances over which
2"U
family squabbles started. Marriedstudents, in particular, are able tocompose a list of chronic irritationsdisplayed by spouses. Students, whoare also parents, will certainly have alist of pet peeves about their children.In short, every stuck at will find somepersonal relevance in this lesson.
Classroom Procedure
Ideally, students should be asked tocompile anonymously a personal listof pet peeves or annoying behaviorsthey note in others, allowing studentsfreely to express personal thoughtswitl.aut fear of socia! reprisal or aviolation of persond privacy. Aftercollecting the lists, the instructorshould cite items from the lists openlyto the class. The students should pub-licly vote on each pet peeve in thefollowing manner: a raised fist withthc thumb up means that the habit isperfectly tolerable by the voter's stan-dard; a thumbs down vote reflects anintolerance for the habit. At theinstructor's discretion, a third votingoption may be crossed arms to indi-cate indecision on the part of the stu-dent.
Teachers are not obligated to makedistinctions between major or minorbehavioral problems, since the stu-dents will be value voting. This is pal:of the dilemma which they need toresolve during the voting process.
The following is a list of behavioralidiosyncrasies developed by studentsin classes on family life education andmental health:
Is inattentive during conversationsLeaves toilet seat upBites his/her fi agernailsFlirts with othersSleeps to an excessIs preoccupied with televisionDoesn't flush toiletInterrupts conversationSqueezes toothpaste tube in middleLeaves cap off the toothpaste tubeBathes or showers infrequentlyCuts fingernails or toenails in bedShows affection publiclyChanges underwear infrequentlyDrinks direcCy out of milk containerBoasts about accomplishmentsDoesn't rinse tub after useLeaves clothing or shoes lying aroundNagsDresses slovenlyTells little "white" liesCurses or swearsIs negligent about doing choresDrives with a "lead foot" on gas pedalBorrows without returning thingsBorrows without asking permissionStays out late without callingIs negligent about keeping physically
fitGossips or passes rumorsIs tardy or late frequentlySnores during sleepPicks his/her noseEats too fast or too slow
Makes major purchases withoutconsulting
Brings guests home with little or nowarning
Doesn't wash hands after using toiletWastes water or electricity
As one can see, chronic habitsfound to be irritating range from themost commonplace to the preposter-ous. The instructor may elect to gothrough this listing selectively or tohave students derive their own listsanonymously.
Conclusion
In the final analysis, what has beenaccomplished? First, students be-come more aware of their own behav-ioral idiosyncrasies and not only thoseof others. Second, they come to gripswith the fact that their actions also canbe a source of annoyance to others.Third, they are not alone in their per-ceptions of vhat constitutes irritatingbehaviors. Hoofully, some will cometo realize that minor, irritations oftenare blown out of proportion. Last, ahumorously anecdotal discussion ofpast, present, and future living experi-ences with spouses parents, friends, orsiblings is beneficial for those wantingto imp,: interpersonal relation-ships.
2 9 1
SHOW AND TELLContinued from page 279
when theassignment is presented. (Threeto five minutes is more than adequate.)Another 30 minutes was needed to ad-equat, ,ly process the information andfeelings presented. (In a high schoolclass with 30 students, we broke up intosix small groups and completed the as-signment in 38 minutes.)
Reactions
The examples that student.s selectedwere diverse and included such items asan adopted son's birth certificate, crys-tals in a leather pouch, photos of pet catsand dogs, a nephew's photograph, sev-eral stuffed animals, a credit card, twoportable cassette players, and a Bible.(Obviously, the choices will vary de-pending upon the age of the partici-pants.) What was wonderfully excitingevery time I have used this lesson wasthe ease with wtich students saw theconnections md similarities amongthemselves. For example, a "walkman"reflected the importance of music in thestudents' lives, especially as a stressmanagement technique. Pets gave un-conditional love and did nia give advice.
The common threads that studentsidentify are: security self-worth and self-esteem , accompli shment, trust, intimacy,and desiA.s. An assigned reading fromMaslow's Toward a Psycho/ogy of Be-ing (2nd ed., 1968, Van Nostrand) canbe utilized at this point. A discussion ofthese basic human needs provides anavenue for discussion of ways in whichsociety provides enabling opportunitiesas well as the kinds of barriers that exist.Students are asked to focus first onpersonal experiences and then to iden-tify the similar ways they feel societyhas helped turd hindered their develop-ment. Discussions about stereotyping,prejudice, and stigma can be an appro-priate follow-up to this lesson.
281

TEACHING IDEAS 149
Can You Name These Foods?Eileen L. Daniel
111111111M
M1111114111
440\44111,ePw""
,914%;111114110Can you name these foods by seeing
their ingredients only?1. Water, hydrogenated coconut and
palm kernel oils, sugar, corn syrup sol-ids, sodium casseinate, dextrose, poly-sorbate 60, natural and artificial flavors,sorbitan monostearate, carrageenan,guar gum and artificial color.
2. Dehydrated tomato, corn sweeten-ers, modified food starch, sugar, non-fat dry milk, salt, monosodium gluta-mate, butterfat, partially hydrogenatedcoconut oil, dehydrated onion, artificialcolor, mono and diglycerides, silicondioxide, sodium casseinate, dipotas-sium phosphate, natural and artificialflavor, citric acid, and BHA.
Eileen L. Daniel is an instructor in theDepartment of Health Science, State Univer-sity of New York, Brockport, NY 14420.
282
3. Corn syrup solids, partially hydro-genated vegetable oils, sodium cassein-ate, dipotassium phosphate, monogly-cerides, sodium tripolv-phosphate, arti-ficial flavors, beta carotene andriboflavin.
4. Sugar, dextrose, citric and malicacids, sodium citrate, natural and artifi-cial flavors, tricalcium phosphate, vita-min C, cellulose gum and artificial color.
5. Sugar, gdatin, adinic acid, sodiumcitrate, fumaric acid, artificial flavor andcolor.
Answers:1. Cool-Whip non-dairy whipped
topping2. Lipton Tomato Cup-A-Soup3. Cremora non-dairy creamer4. Tang5. Jello gelatin (any flavor)
2 0 9
Nutrition
This learning activity can be used in awide variety or ways in either a nutri-tion class or in a health education curric-ulum. Activities which are student-ori-ented are an interesting and excitingway to present a specific topic within acurriculum. A favorite activity of mine(and my students) is "can you namethese foods?" Five or more foods arelisted on an overhead projector or black-board by ingredients only. Students arethen asked to try and identify the food.Though most students fail to determinethe food by ingredients only, the activi-ty generates hvely discussion andlaughter!
Some examples of topics which can beaddressed from this activity are:
What information is on a food label?Order of ingredients indicates the
order of their predominance in the food.Additives are listed by their chemi-
cal name.Food colors :ire listed as "natural or
artificial color," not by their chemicalname.
The different forms of sugar used,i.e., dextrose, corn syrup, corn sweet-eners.
Risk versus benefit concept in usingadditives.
The changing American diet whichincorporates fabricated and conve-nience foods in increasing numbers.
Nutritional implications when wechange from foods like juices to sugar-based imitation products.
The activity can also be implementedby having the students bring in theirown ingredient lists from foods found athome or in the supermarket. Takingturns, they can display their lists andhave fellow students try to guess thefood.
Whichever way the activity is pre-sented, it has always generated muchinterest and discussion in nutrition,foods, and diet. Many students are verysurprised at exactly what goes into thefoods they eat, particularly sugars andadditives.

TEACHING IDEAS 150
Nutrition
"Digesting" Health InformationRichard A. Crosby
Ideally, health educators are in a stateof neverending search for better meth-ods. Sharing is bound to be the bestcontributor to this search.
In sharing, the author has found thisplay to be a highly motivating approachto the teaching of the digestive system."What Happened to the Apple" isgeared toward upper elementary agedstudents, but works quite well with"low achieving" junior high school stu-
ents. Audience participation allows allclass members to become involved andh Iterested.
After the narrator closes the play,stedents may want to try different roles.The play takes no more than five min-utes to perform and can easily be re-peated. Hopefully, students will memo-rize the apple's path with enthusiasm.
k
What Happened to the Apple?
Characters: Apple, Stomach, SmallIntestine, Large Intestine, Mouth andTeeth, and the entire audience
App/e: That girl just picked me up. OhNo!
Mouth and Teeth: Let's grind this appleinto small pieces so the stomach won'thave to do it. Teeth, when you're fin-ished, have the tongue move the small-er pieces back to the throat. Mouth, youturn on your hoses and wet this fooddown with saliva so that the thriatwon't complain when it swallows.
Apple: It sure is dark in here! Wheream I anyway?
Audience: You, apple, are in the stom-ach! And you look more like applesauceafter what the mouth and teeth did to
Richard A. Crosby is with the Department ofHealth Education at Central Michigan Uni-versity, Mt. Pleasant, MI 48859.
you.Apple: But how did I get here?Audience: You came down the esopha-
gus!Stomach: Oops! Looks like my rest is
over. I've got to get busy and digesmore food. It sure is rough work break-ing up carbohydrates and protein. But,at least there is no fat coming in thistime. I hate breaking up fat!
Audience: Hey, stomach, Do you likeyour job?
Stomach: Most of the time my bosstreats me pretty well, but every nowand then he delivers the wrong kind offood and I go on strike!
Apple: Whoo! Where am I going now?What's happening to me?
Audience: Don't you know apple?Your time in the stomach is up now;you have to go to the small intestine.
Small Intestine: I can't wait to absorbyou into my bloou, apple!
Apple: But what will happen to mewhen I'm in your blood?
,
29 3
Small Intestine: Your carbohydrateswill be burned for energy and yourprotein can be used for growth andrepair of the body.
Audience: Hey small intestine! Howare you going to absorb the apple?
Sma// Intestine: Well, I must admit, Itwon't be an easy task. I'll have to havehelp from my friends, Liver and Pancre-as.
Apple: There's not much of me left!But I'm st4ll here. The small intestinedidn't use all of me. I still have myroughage and some of my water.
Audience: Here comes the large intes-tine.
Large Intestine: I'm gonna be glad toget that apple in meI like roughage.I'll soak up that leftover water as well.
Narrator: The large intestine did soakup the apple's leftover water. Then thelarge intestine compacted and eliminat-ed the roughage from the body. Thebody was grateful to the apple for pro-viding so many good nutrients.
283

TEACHING IDEAS 151
6
Nutrition
Nutrition Is the Name of the GamePaula R. Zaccone
Classroom approaches that preach thedo's and don'ts of health practices havewen tlwir day. The effect of television,video and audio recording devices, andthe bombardment of advertising dictatethat educational methods aiming to cap-ture an audience must appeal as entetainment. Today it is not enough forhealth educators to appear before theirstudents with scientific facts and a sin-cere interest in their delivery. Style andprocess of delivery are as important asthe health message in determining theduration of effect.
Studies indicating why children andadults watch television (Lvl?., 1972;Robinson, 1972; Schramm, Lyle, andParker, 1961) give educators clues forplanning class activities that are enter-taining and informative. Teaching meth-ods and learning activities that are amus-ing, relate to the interests of students,and that carry a health message are morelikely to draw interest from both youngand mature students.
What follows is an approach to nutri-tion education that can be appropriatelyemployed by the health educator in avariety of educational settings. The Nu-trition Is the Name of the Game approachmay be useful to the health or physicaleducator who aims to teach that good
Paula R. Zaccone is an associate professmHealth Education at Seton Hall University,Department of Health, Physical Education,& Recreation, South Orange, NI 07079.
284
eating habits complement habits of exer-cise for the maintenance of good healthand in the prevention of disease. Thecoach whose responsibilities includeguiding athletes toward proper physicalconditioning may find that this teachingtechnique can be adapted to the specificsport interests of a particular team, e.g.,wrestling, football, basketball, baseball,track and field, hockey, etc.
Tennis, a sport which has gainedpopularity in recent times because of itsvalue for players of all ages, can aid in thedevelopment of coordination, speed,endurance, and accuracy. Introducingits techniques and terminology alongwith nutrition education further com-municates that habits of eating and exer-cise are both determinants of healthstatus.
For implementation of the tennistheme, 31 "tennis balls", 4-inch circles,need to be cut from paper or cardboard.Each ball bears a statement of nutritioninformation. In the statement, one ortwo terms are underlined that have sig-nificance for both the game of tennis andgood eating habits.
The "tennis balls" are distributea tothe students, and each in turn introducesthe statement to the class. A discussionof the statement on the ball as it appliesto the sport of tennis and to good habitsof nutrition follows.
Teachers in search of means bo inte-grate nutrition education into an alreadycrowded academic schedule may findthis approach useful. Classroomteachers and school nurses may elect to
29
n.ount the balls on a bulletin board in acalendar arrangement. For the purposeof integrating nutrition education intothe daily curriculum, each day maybegin with the disclosure of one state-ment which also bears the date.Weekend messages could be addressedon Mondays and Fridays. Brief nutritionand tennis discussions could precedeother learning activities scneduled forthe day.
The concepts that are to appear oneach of the "tennis balls" are as follows:
1. A "tennis nut" is a protein.T: Whereas "health nuts" have been
described for their tendency "to spendinordinate amounts of time maintainingand promoting their health" (Bedworth,1982), tennis nut refers to one who is fre-quently occupied by tennis play (T:Ten-nis).
N: Nutritionally speaking (N:Nutri-tion), "nuts of the edible kind aresources of protein, fats, the B vitamins,and some minerals.
2. The body is the court for the foodwe eat.
1: The tennis court is the place wherethe sport is played and the outcome isdetermined. For the doubles game, thecourt is 36 fe...et in width and 41/2 feetnarrower for the singles game.
N: The body is the place where theeffects of eating habits are determined.
I Eat within the boundaries of mod-eration.
T: The tennis court is marked by two

baselines, which are tl.v end lines of thecourt, and two sidelines.
N: Eating, too, has its limitationswhich need to be regarded for the main-tenance of good health. Excesses of eventhe most nutritious foods can becomecontributors to fat storage and the inci-dence of some diseases.
4. Eating a variety of foods is goodoffense.
1: Offense generally applies to being incontrol of the ball or having the ability toattack t le opponent. The player who isabout to serve is the offensive player.
N: Eating a variety of foods allows thebody to produce antibodies to :ounteractharmful bacteria, assures an intake of es-sential nutrients, and protects the bodyfrom acquiring toxic levels of potentiallyharmful substances.
5. Eat green and yellow vegetableswhich score for good health.
T: The accumulation of points madein the game occur as love, 15, 30, 40, andgame.
N: The accumulation of important nu-trients such as vitamins A, C, and K,iron, potassium, and fiber is provided bygreen and yellow vegetables.
6. Vegetables without salt are a com-plete set.
T: The player/s who is/are first to winsix games win(s) a set, providing there isa margin of at least two games over theopponent. A set is extended until thismargin is achieved.
N: Vegetablos derive minerals includ-ing sodium fron, the soil in which theygrow. Processing may cause moresodium to be a,A.:.led. Thus, adding moresalts to foods .ncr .ase the blood volumeand is risky to those who are susceptibleto high blood pressure. Vegetablesserved without salt as an additive arenutritionally complete.
7. Carbohydrates are body power.T: Power is the ability to provide sud-
den force to the ball.N: Carbohydrates are excellent
suppliers of suddenly needed energy forthe body. In plants, sugars and starchesare present along with vitamins andminerals, and thus provide excellentfood sources of body energy.
8. Proteins from animal and plantsources make a good match.
T: Tennis competition generally con-
eludes when one side wins two out ofthree sets.
N: Amino acids provided by bothdairy and plant sources combine to formcomplete proteins which will best servethe body's needs for proteins.
iIIII 14
"gnallilin%T..1...................fes1111111.11M011111ft
meeressuliOUNOSsmusIffilesessmesumillIfill.m...... ......--__IluilOWINIO;MININUM;;;
,
I.:312::::1_1.1:11.:::ulmiI
WI:::;;;;;;;;;;t: i1.8.11...............4.\::.. ::::::::EiriE#7..... .. .....\
,.7:li 17 , /
TtII
19. Serve fruits and vegetables for
meals and snacks.T: The method of putting the ball into
play is called a serve and is done by aplayer who stands with both feet behindthe base line and within an imaginerycontinuation of the center mark and theside line.
N: Furnishing the body with fruitsand vegetables also provides the bodywith vitamins, minerals, water, and fiberin useful combinations. Sugar derivedfrom fruits and vegetables supplies thebody with the energy needed tometabolize these nutrients. Because oftheir high nutritive density, fruits andvegetables are superior to "emptycalorie" foods as snacks.
295
10. Pace your eating or you'll suffer inthe end.
T: Pace, the rate of movement orlength of steps taken, is an importantfactor in eNecuting tennis strokes.
N: Slower rates of eating will allow forefficient mastication and processing offood for digestion, absorption, andelimination. Furthermore, a controlledeating pace allows the stomach to sendcues of satiety to the brain and the quan-ity of food eaten to be held in check.Problems related to eating too quickly(ingestion, nausea, diarrhea, and con-stipation) may be avoided by adoptingslower-paced eating habits.
11. 1. Raisins, 2. apples, 3. bananas,and 4. nuts are forehand ("four hand")foods.
T: The basic drive which includes abackswing and a follow through usingthe whole arm is known as the forehand.
N: Each of the four foods listed can beeaten by hand, requires almost no prepa-ration, and can also be convenient andnutritious as snacks.
12. Fats may be backhanded in theirappearance.
T: A backhand drive is contacting theball with the back of the hand turned inthe direction of motion.
N: Whereas fats may add flavor, theirpresence in foods often times is invisible.The moisture in cakes and pastries maybe attributable to fats which contribute tothe high caloric value of these foods. Eat-ing an excess of fatty foods has been as-sociated with the accumulation of plaqueon the walls of arteries, a condition thatis not easily identified.
13. Dieting is often the need that fol-lows an overlswing.
T: A common error in which theplayer uses too much backswing or fol-low-through frequently results in theball landing too wide or too long.
N: Binge eating, periods when eatinghabits take on an "overswing," causesthe body to store excess calories as bodyfat. Furthermore, some theorists main-tain that overeating during periods ofrapid cell division may permanently in-crease the propensity toward overfat-ness during inactivity and in adulthood.
14. Overeating is not your foot's fault.T: A foot fault is a foul committed by
the server who enters an area other thanthat behind the base line within the
285

imaginery extension of the center markand side line or who changes position bywalking or running throughout the de-livery of the service.
N: This statement suggests the needfor overeaters to take control of their owneating habits. It serves no useful purposeto blame eating binges on others. Theymay have nothing to gain or lose by theovereater's gains (i.e., "My foot causedme to overeat"). Accepting 1'esponsibil-ity for one's own eating habits and fit-ness status is a healthy approach towardcoping with disappointments.
15. "If You Drink Alcohol, Do So inModeration" (USDA, USDHHS, 1980) isa slice of good advice.
T: A slice is a short, choppy stroke inwhich the ball is hit downward withbackspin and is aimed to bounce awayfrom the opponent's reach.
N: A brief slice of nutritional advice isto avoid excessiveness in the drinking ofalcohol. For healthy, non-pregnantadults who choose to drink alcohol, therecommendation made by the NationalResearch Council (USDA, USDHHA) isto do so in moderation.
16. Let your mind, not your tummy,be the judge.
T: The official who makes the deci-sions regarding play tournaments maybe the referee, umpire. CI lines judge.
N: Sensations o; thirst and hungeralone are not accurate indicators of thebody's needs for liquids and food. Habitsof meal planning to ensure adequate in-take of all .lutrients and regular replace-ments of water lost by perspiration andexcretion are reliance on wisdom, ratherthan impulse, for good nutrition.
17. Avoid using food to bounce backfrom disappointments.
T: The term bounce back in tennis mayrefer to the ability of the ball or player torebound after a hard hit.
286
N: Those who eat in search of psYcho-logical comfort would do better to findless self-defeating methods of coping.Try exercising or becoming involved innon-food related hobbies that expendrather than store surplus calories.
18. Aim to have meat, fish, poultry, oreggs at least twice daily.
T: To aim is to direct the ball to drop ina specific spot on the court.
N: These food items share the nutri-tive values of protein, fats, niacin,thiamin, iron, and other minerals. Ef-forts should be directed toward theirconsumption at least twice daily.
19. Milk products are needed for goodform .
T: Players demonstrate good tennisform with efficient execution of tennisstrokes and strategies.
N: Milk, cheese, yogurt, even pud-dings and ice cream made from milk con-tain nutrients important for building andmaintaining strong bones and teE th.Found in milk products and specificallyresponsible for the strength of bodystructures, are vitamin D, calcium,phosphorus, and protein.
20. Rush the net, but pause throughdinner.
T: Dashing to tho front of theforecourt to play the ball as it crosses thenet or drops over is known as rushing thenet.
N: This statement points to the im-portance of controlled eating patterns.Reasonably paced ingestions of food thatallow for pleasant conversation add tothe enjoyment and longevity of the eat-ing period. Habits that encourageawareness of quantity eaten and portioncontrol enable the diner to acquire feel-ings of satiety that would escape thespeed eater.
21. No single food is perfect.T: Single play takes place when an in-
dividual player opposes one other playerin competition.
N: No one food provides the bodywith all the substances needed to carryon its physiological processes and tomaintain health. This statement invites adiscussion of the need to eat a variety offoods (#4) and the relative values offoods. While milk is considered to be ahighly nutritious food, it fails to meet thebody's needs for iron and vitamin C.Fish, often said to be "brain food," is aworthy source of protein, but lacks thecarbohydrates the brain requires for fuel.
22. Doubles of sweets can bring doublesof troubles.
T: The do-Wes gmne requires coopera-
tion and communication with a partneron a court that is wider than for singlesplay.
N: This statement addresses thehazards that are evident from eating anexcess of sugar. Tooth decay and obestityare just two of the consequences relatedto excessive sugar in the diet. Other dis-orders of the cardiovascular and diges-tive systems have been associated with asurplus of calories derived from "emptycalorie foods.
lb
1/
23. Milk is a good partner to manyfoods.
T: A tennis partner is a teammate indoubles play.
N: In addition to its vitamin and min-eral constituents (vitamin A and D, ribo-flavin, calcium, phosphorus), milk con-tains protein ideally suited for use by thebody when it combines with amino acidsfrom grains and vegetables. The aminoacids from milk and plant products aregood protein partners.
24. Sugar is the opponent of good den-tal health.
T: The player/s on the other side ofthe net during play is/are an opponent(s).
N: Sugar combines with acid in themouth to produce decay-causing bac-teria. Particularly when sugar lingers onthe teeth of children, it opposes gooddental health.
25. A well strung meal has dental flossas its follow through .
T: Tennis rackets may be strung withnylon, steel wire, or sheep gut. There issome concern that string tension that istoo tight my contribute to painful "tenniselbows, an inflammation of the pointwhere the tendons that straighten the
2.,,.r,
elbow attach. A follow through is the con-tinuation of movement after contact withthe ball is made.
N: Using dental floss after meals andbefore brushing will aid in removingcariogenic food particles and plaquefrom the teeth.
26. Eating should be neither torment,nor a tournament.
T: A tournament is a contest amongplayers to detertnine a champion.
N: Discussion about many attitudesand food-related habits that result in un-healthy eating habits may evolve. Someexamples are eatia:::: and drinking con-tests in which overindulging is encothaged, contests of rapid weight loss,using foods as rewards, and practicesthat encourage anxiety with eating suchas force feeding and eating in stressfulenvironments.
27. S is make the playing rough.T: The playing of highly skilled
players according to their ranked abilityis a practice which has been designed toensure challenge and competitionamong players.
N: Seeds and skins from various plantfoods (fruits, vegetables, nuts) as asroughage in the digestive system and aidthe body to rid itself of waste products.
28. For effective elimination, take infiber, fats, and water.
T: An elimination tournament is one inwhich the loser is disqualified fromfurther play.
N: Fiber functions to bind wasteproducts for removal from the body. Fatsand water lubricate the digestive tract sothat processing of food for digestion andexcretion is facilitated.
29. Water and sunshine make a dandydeuce.
T: Veuce in tennis refers to the scorebeing tied at 40-all.
N: The need to rep:ace body fluidslost during perious of exercise and heavyperspiration cannot be overemphasized.With higher temperatures, the body'sneed for water increases.
30. "The breakfast of champions" isdaily.
T: Champions are those who acquirethe greatest number of wins and are de-termined to be in first place at the end ofthe event.
N: Breakfast is considered to be infirst place with regard to its importancefor supplying the body with fuel and nu-trients required for each day's activities.An additional consideration is the nu-tritional fact that the breakfasts of champi-
ons need not come in a cardboard boxbearing the picture of an athlete. Instead,breakfast foods should be a combinationof those from the basic four food groups:grains, dairy, fruits and vegetables, andmeat, fish, poultry, or nuts.
31. Calories add (ad) in.T: Ad in refers to the point advantage
to the server. This follows deuce. A pointadvantage to the receiving player wouldbe called "ad-out."
N: Here, the concept of homonyms,words that sound alike but are differentin meaning, would appropriately be in-tegrated in a language arts and nutritioneducation lesson. Calories derived fromsecond servings, snacks, and rich des-serts add into the total caloric intake. Noamount of will can erase the program-ming of an ingested calorie to carry outits fuel-serving function.
32. Winning is easy to digest.T: To earn success or to achieve prog-
ress is winning for some players of ten-nis.
N: Taking responsibility for one's pat-terns of ingestion to restrict certainfoods and drinks, and putting sound nu-tritional habits into practice is winning,whether it be in the battle of the un-sightly bulge or in the fight against riskfactors.
In the process it is important to realizethat what you eat is as important aswhether you lose or gain. Harm to healthmay occur as a result of excesses of fats,salt sugar, or calories. Moreover, nutri-ent imbalances promoted by fad dietsand willfully induced starvation withhopes of achieving quick fat loss may belosing pounds without winning the ben-efits of good nutritional status.
Bedworth, A. The health educator as healthnut. Health Education, 1982, 13 (2): 27-28.
Lyle, J. Television in daily life: patterns of useoverview. In RubPnstein, E. A., Com-stock, A., & Murray, J. P. (eds.). Televi-sion and Social Behavior, Vol. 4. Washing-ton, DC: U.S. Dept. of Health, Educa-tion, & Welfare, 1972, pp. 1-32.
Robinson, J. P. Toward defining the functi(msof television. In E. A. Rubenstein, Cu. 1-stock, A., & Murray, J. P. (eds). Televisionand Social Behavior, Vol. 4. Washington,DC: U.S. Dept. of Health, Education, andWelfare, 1972, pp. 568-601.
Schramm, W., Lyle, J., & Parker, E. B. Thlevi-sion in the lives of our children. Stanford:Stanford University Press, 1961.
United S'ates Depts. of Agriculture andHealth and Human Services. Nutritionand your health: Dietary guidelines forAmericans, 1980.
297
idli:::1.111.Igilli .
0 in NI . 1111,
I . I k/A 1141 1:1 I
a:47a: .... .......INISMIIIIIIIMMI111111.1m1se................-orm
faINEPOO11111110Ensumma11111Mus1111111IONINIMa111eissoms-NNI11aii-fismou.................-1,......estsossmosiumma....1.::::::mmt-:::::,/..............-__-_......=s...:-..,,,,......----_-_..,::::::-.1:::::. ,
........,r:BEHEE-::...iir
287

TEACHING IDEAS 152
Personal Health
Sun Smart: A Peer-Led Lesson on the Effects ofTanning and Sunning on the Skin
Mary Elesha-Adams and David M. White
Many adolescents and young adultsspend a great deal of time sunning.Some university students even sched-ule classes and jobs around primesunning time. It has been our expe-rience in teaching personal healthcourses that not only do studentstypically have a number of miscon-ceptions about sun exposure and skincancer, but the information we pro-vide often has little or no influence ontheir behavior. Because almost all ofthe more than 500,000 cases of non-melanoma skin cancer developed eachyear in the United States are consid-ered to be sun-related, and recentstudies show that sun exposure is aprimary factory in the developmentof melanoma (American Cancer So-ciety, 1988), we clearly needed tofind more effective ways of deliveringhealth education. To address thisneed, we developed a peer-led lessonon the effects of tanning and sunning.By designing the course to be led bypeers, we also addressed anotherneed at the university level. Peerteaching can provide valuable, prac-tical experience for health educationmajors before their formal studentteaching or internships.
The goals of the SUN SMARTsessions are to:
1. Enable participants to make in-formed decisions regarding sunningand encourage safer sunning behav-ior, and
Mary Elesha-Adams is a health edu-cator in the Student Health Service atEast Carolina University Greenville,NC 27858-4353. David M. White is anassistant professor of health educa-tion in the Department of Health,Physical Education, Recreation, andSafety at East Carolina University,Greenville, NC 27858-4353,
2 88
2. Provide opportunities for under-graduate health education majors togain practice experience.
Development and Implementation
Sessions are coordinated by thehealth educator at the UniversityHealth Service in cooperation v. iththe Department of Health, PhysicalEducation, Recreation and Safety.The peer educators may register forthe experience as an independentstudy project and receive from one tothree semester hours of academiccredit, depending on the scope ofinvolvement.
Peer health educators are trainedin a preservice workshop. They de-velop teaching materials, role playinstructional sessions, and work ongroup facilitation skills, then are as-signed in terms to lead SUN SMARTsessions. SUN SMART sessions havebeen requested most frequently dur-ing spring semester when studentsprepare for spring vacation and sum-mer activities.
Objectives
The SUN SMART session has thefollowing objectives.
I. Students should be able to de-scribe complications caused by sun-ning including premature wrinkling,cataracts, and skin cancer.
2. Students should be able to iden-tify medications that increase the like-lihood of sensitivity to the sun, suchas birth control pills, certain antibiot-ics, antihistamines, and Accutane.
3. Students should be able to de-termine their own skin type and de-fine sun protection factor (SPF).
4. Students should be able to listtwo recommended methods to re-lieve sunburn.
5. Students should be able to iden-tify the harmful effects of tanningbeds and other indoor tanning devic-es, including skin rashes and eyeinjuries, and complications from over-exposure, such as wrinkles and skincancer.
6. Students should be able to de-scribe safer sunning techniques, suchas use of sunscreens, protective cloth-ing and sunglasses, hats and visors,and avoiding tanning between 11:00am-2:00 pm when the sun's rays arestrongest.
7. Students should be able to de-scribe self-examination proceduresfor skin cancer.
Materials and Resources
The one-hour SUN SMART ses-sions are informal, and commentsand questions are encouraged through-out the presentation. A colorful hand-out developed by the peer healtheducator is given to each participantand referred to often during the pre-sentation. The handout describes saf-er sunning tips, defines SPF, listscommon suntan preparations and theirSPF, and identifies medications thatincrease sun sensitivity. Free sun-screen and t-shirts reinforce safersunning behavior and encourage at-tendance. We also used the followingcommercially produced materials, asreinforcements:
I. "Sun Sense," a brochure de-veloped by Johnson & Johnson thatemphasizes the use of SPF and sen-sible sun protection.
2. "Skir Cancer. Early Preven-tion, Early Detection," a brochuredeveloped by the North Carolina De-partment of Human Resources thatillustrates a 10-step procedure forchecking for skin cancer.

3. "Progress Against Cancer ofthe Skin," published by the NationalInstitutes of Health, a resource forpeer health educators.
Applications
In addition to presentation at res-idence halls, peer health educatorshave provided SUN SMART demon-strations at two university health fairs.Instructors of university personalhealth and wellness courses can in-corporate SUN SMART into the ex-isting curriculum. The program canalso be presented to high school stu-dents in classes or organization andclub meetings.
Typical Misconceptions AboutSunning
We developed a pretest for useduring the SUN SMART sessionsthat focuses on high-risk groups andbehaviors, detection and treatmentof skin cancer, and perceived level of
knowledge about safer sunning. Thusfar, participants have been almostexclusively white, female, and aged18 to 23. Although almost all (98percent) knew that people with ex-cessive exposure to the sun were athigh risk for skin cancer, 17 percentdid not know that redheads andblondes were at high risk, 13 percentdid not believe that fair-skinned peo-ple were at high risk, and 12 percentdid not realize that people who sun-burn often were at high risk. Thirteenpercent of the students inaccuratelybelieved that the chances of devel-oping skin cancer were reduced eachtime the skin darkens through tan-ning. One-fourth (25 percent)did notrealize that the majority of the aver-age person's total lifetime sun expo-sure is in the first 20 years of life. Interms of screening and detection, 22percent did not think that the skinshoukl be examined at least onceyearly and 23 percent believed that it
299
is not necessary to check areas of thebody unexposed to the sun whenchecking for skin cancer.
Conclusion
The SUN SMART program hasproven to be effective in increasingknowledge and awareness of safersunning and has provided an oppor-tunity for health education majors togain valuable practical experience.Preliminary results indicate that thisteaching idea can be beneficial tostudents, faculty, and staff. An eval-uation of the effectiveness of thisapproach in changing sunning behav-ior is currently underway.
This project was funded, in part, bythe P'orth Carolina Division, Ameri-can Cancer Society, Inc.
The authors would like to thankJerri Harris for her expert editorialassistance.
American Cancer Society. (1988). Cancer factsand figures--1988. New York: Author.
289

TEACHING IDEAS 153
Personal Health
A Quick and Easy Check for Foot ProblemsDianne Boswell O'Brien
The Foot Powder TestDid you ever wonder why your pants
or skirt move slightly to the left or to theright after you have been walking? Ifyour slacks appear to be turning to theleft after you have been walking, thenyou are probably taking a longer stridewith the right foot than you are with theleft foot. One way to check to see if yourstride length is the same with both legsis to measure the distance between foot-prints. A simple powder test will tell youhow long your stride length is with eachleg.
Stride length(right leg)
(illustration 1)
To perform the test, just cover a darkfloor with a sprinkle of foot powder. Thenwalk barefooted in a straight line throughthe powder. Your footprints should beclearly visible. The powdered surfaceshould be large enough to accommodate
Dianne O'Brien is an assistant professor ofhealth education in the Department of Health,Physical Education, Recreation and Danceat P ii, State University, Murray, KY42001. In 1980, she was named the outstand-ing young professional and given the MabelLee Award by AAHPERD.
290
about three steps; for example, a right-left-right or left-right-left. This is a dis-tance of about ten feet.
Before walking onto the newly pow-dered surface, take about six natural stepsso that your normal walking cadence andpattern are established before you strikethe powdered surface.
Stride length
Once you have walked through thepowdered surface take a tape measureand measure your right stride length bymeasuring the distance from your leftbig toeprint to the heel of your right foot-print. Measure your left stride length inthe same way.
Everyone needs a footprint test
Good foot health results from intelli-gent decisions about exercise habits, footcare and shoe selection: Much can belearned from just interpreting foot-prints. The simple footprint test givenin the following paragraphs will indicatesome individualized foot care needs.
To the Teacher: This article is suitablefor students and adults who may be in ahealth or fitness class. To perform the testwith large groups, purchase a roll of butcherpaper from a restaurant supply house. Thecost will be approximately fifteen dollars.Purchase stamp pads from a book or station-ery supply shop at a cost of about five dollars.
Divide the paper into fifteen-foot sectionsand give each person a section of time paper.Have each person ink their feet with the stamppads. Perform the test as directed, but omitthe part of the test which directs the personto take several strides before 5tepping ontothe paper. When ink is used, the person willstep directly onto the paper. When checkingthe footprints, consider the first few steps asa gaining momentum. The last two stepsshould be investigated as the person's morenatural stride.
3 (4
The test assists a teacher in recognizingpotential problems of students who will beasked to participate in endurance or sportsactivities. It is especially helpful in recog-nizing problems in adult populations.
A person who has a dominate rightfoot may take a longer stride with theright kg. People who are right-handedoften have a dominate right foot.
If your right foot is dominate it mayalso be larger. You can also see size bycomparing your right and left footprints.If your right footprint is larger you shouldmake certain to try on the right shoe firstwhen fitting new shoes. If the right slikwis large enough for your right foot thonthe left shoe should also be large enoug;for your smaller left foot.
Toeing Out or Pronation
6 to 7 degreesavc rage pronation
(Illustration 2)
The average toe-out position or pron-ation is 6 to 7 degrees (See Illustra-tion 2). Toeing out increases with ageand weight increases. Toeing out de-creases as walking speed increases.(Cailliet, 1978) People who have ex-tremely pronated feet tire easily and of-ten experience leg pain.

The following exercises when done re-peatedly (15 times once a day) for sev-eral weeks will strengthen T.uscles inthe feet and legs wh;ch help to controlpronation. Recommended activities are:(1) Strengthen muscles in the calf of theleg by holding on to a chair and risingon the toes, (2) Strengthen muscles ofthe feet by picking up pencils with thetoes, (3) Strengthen feet and legs bystanding with weight on the outer bor-ders of the feet and curl toes inward andupward .
Foot StrainFoot strain may occur in the under-
exercised foot and pronated foot. Theperson who exercises infrequently andthen decides to walk a long distance orengage in a Saturday ball game is a likelycandidate for foot strain. Since 857r ofthe foot problems are caused by ill-chosen footwear, the lack of proper shoesis also a culprit in creating foot strain.Poor body mechanics and abuse throughoveruse or improperly fitting shoes cancreate excessive stress on the musclesand ligaments of the feet, thus causingchronic foot strain. Foot strain producesaching legs and feet. For brief bouts(acute) of foot strain, rest and properfoot wear are recommended. For long-term (chronic) foot strain, professionalhelp should be sought.
When foot strain persists over longperiods of time, pronation and a flat-tened transverse arch often accompanythe condition (Cailliet, 1978).
Flat FeetWhen the transverse arch (arch going
across the foot) is flattened, a footprintwill be noticably lacking the "normal"curve on the inside border of the foot(See Illustration 3).
averagearches
arches lowfeet noticeably flat
(Illustration 3)
Reading a footprint will give a personan indication of a flattened transversearch.
Some people have inherited naturallyflat feet. However, the older or heavierperson's transverse arches may be ab-normally depressed. This flattening ofthe transverse arch may cause calluseson the metatarsal heads (ball of foot).(See Illustration 4). These calluses maybe padded with commercially availablefelt pads which are designeu to relievethe pressure on the calluses.
metatarsalhead noo 0 0 00n
abnormal weight here onmetatarsal heads
(Illustration 4)
Metatarsal pads and heel pads will helprelieve the pressure on the transversearch. Metatarsal pads should be placedbehind the metatarsal heads. Strength-ening the arches of the foot, practicinggood walking mechanics and correctfootwear will help the problem. Whenthere is persistent pain, a person shouldsee a podiatrist.
Exercises for strengthening the footwere listed previously. They should beaccompanied by exercises which st:etchthe achilles tendon (Cailliet, 1978). Forexample stand about two feet away fromthe wall and lean toward the wall. Placeboth hands on the wall and lean towardthe wall keeping both feet flat on thefloor. Feel the stretch on the back of thecalf of the leg. Hold the position at least20 seconds.
Pigeon Toed WalkIn aduhs a pigeon-toed walk (Illustra-
tion 5) may be a result of improper me-chanics of the joints which are not locatedin the foot. For example, improper align-ment of the knee jcint and other mul-tiple causes will cause the feet to turninward.
(Illustration 5)
In order to adequately diagnose theproblem, assistance of professional helpis recommended. For children, earlytreatment is of utmost importance.
Distance Between FootprintsTo measure the distance between
footprints, draw an extended line fromthe edge of the big toe through the mostindented part of the arch. Do this forboth feet. Then measure the distance be-tween the lines (See Illustration 6).
big toemost indentedpart of the arch
2 to 4 inchesaverage horizontaldistance betweenfootprints
(Illustration 6)
The average horizontal distance be-tween footprints is 2 to 4 inches. Thehorizontal distance between footprintswill be influenced by width of pelvic gir-dle and overall body size. A larger frameneeds a wider base of support.
Shortened Big Toeln some footprints the great toe ap-
pears to be shorter than the second toe(Illustration 7). This condition is oftencalled Morton's toe and is usually in-
291
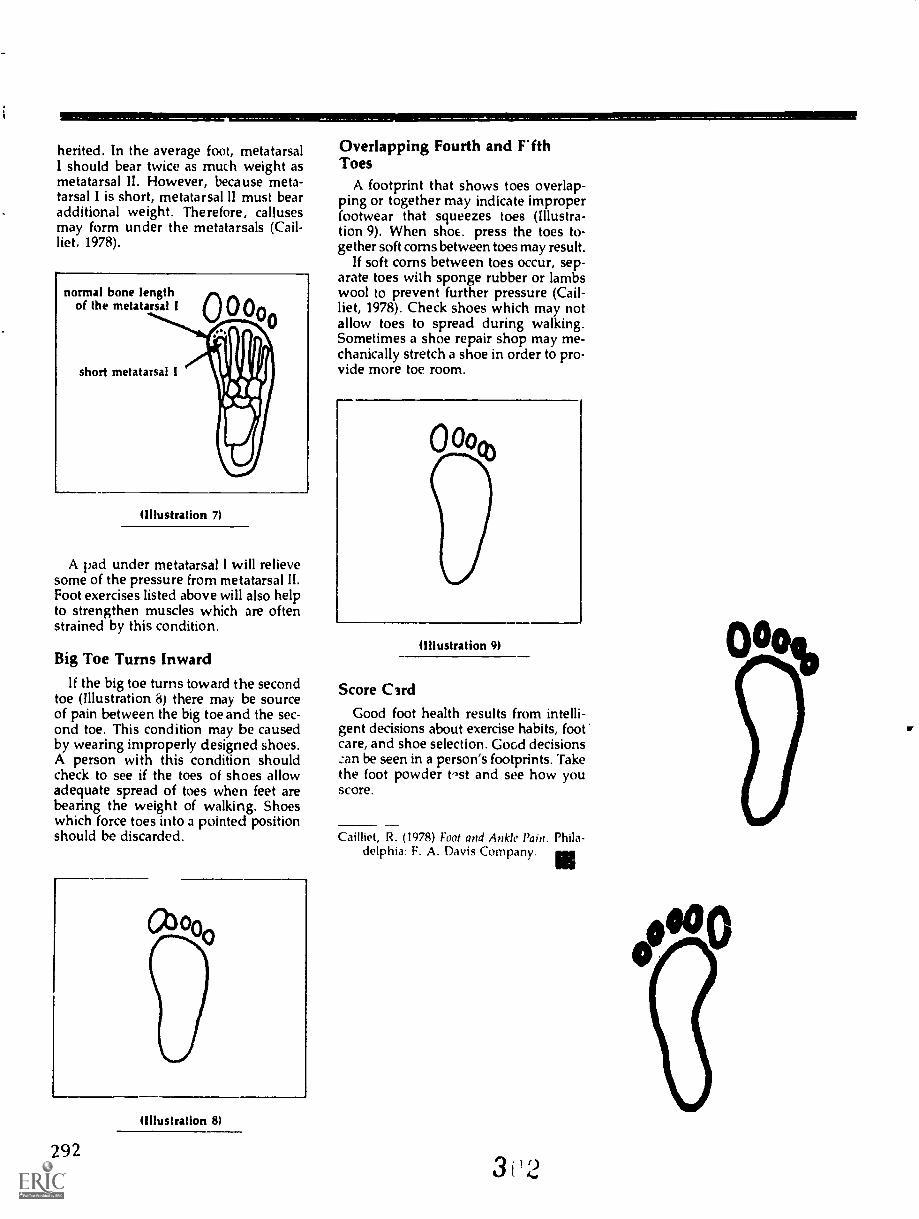
herited. In the average foot, metatarsalI should bear twice as much weight asmetatarsal II. However, because meta-tarsal I is short, metatarsal II must bearadditional weight. Therefore, callusesmay form under the metatarsals (Call-liet, 1978).
normal bone lengthof the metatarsal I
short metatarsal I
(Illustration 7)
A pad under metatarsal I will relievesome of the pressure from metatarsal II.Foot exercises listed above will also helpto strengthen muscles which are oftenstrained by this condition.
Big Toe Turns InwardIf the big toe turns toward the second
toe (Illustration 8) there may be sourceof pain between the big toe and the sec-ond toe. This condition may be causedby wearing improperly designed shoes.A person with this condition shouldcheck to see if the toes of shoes allowadequate spread of toes when feet arebearing the weight of walking. Shoeswhich force toes into a pointed positionshould be discarded.
(Illustration 8)
292
Overlapping Fourth and F'fthToes
A footprint that shows toes overlap-ping or together may indicate improperfootwear that squeezes toes (Illustra-tion 9). When shoE. press the toes to-gether soft corns between toes may result.
If soft corns between toes occur, sep-arate toes with sponge rubber or lambswool to prevent further pressure (Cail-liet, 1978). Check shoes which may notallow toes to spread during walking.Sometimes a shoe repair shop may me-chanically stretch a shoe in order to pro-vide more toe room.
00o%
(Illustration 9)
Score CirdGood foot health results from intelli-
gent decisions about exercise habits, footcare, and shoe selection. Good decisions:an be seen in a person's footprints. Takethe foot powder t-st and see how youscore.
Cailliet, R. (1978) Foot and Ankle Pain. Phila-delphia: F. A. Davis Company.
3
0000

Association for the Advancementof Health Education
1900 Assoc tion Drive, Reston, Virginia 22091(703) 476-3437
MISSION STATEMENT
The mission of the Association for the Advancement of Health Education (AAHE) isto advance health by encouraging, supporting, and assisting health professionals con-cerned with health promotion through education and other systematic strategies.
PURPOSES AND OBJECTIVES
The basic purpose of AAHE shall be to promote the advancement of health educationby providing a focal structure for the encouragement, support, and assistance of per-sons interested in concentrating their professional efforts on the improvement of healththrough the development and conduct of effective health education programs in educa-tional institutions and other community settings.
In fulfilling the above stated purposes, AAHE seeks to:
1. Provide information, resources, and services regarding health education to profes-sionals and the lay public.
2. Enhance a public awareness of the nature and purposes of health education.3. Enlist support in the development, implementation, and evaluation of health educa-
tion programs.4. Foster the development and program implementation of the philosophical basis of
health education practices.5. Promote and interpret research relating to school and community health education.6. Promulgate criteria, guidelines, and evaluation procedures for assessing the effec-
tiveness of preservice, inservice, and continuing professional education of healtheducation personnel.
7. Determine curriculum needs and assist in the development and mobilization ofresources for effective health education at all levels of education.
8. Facilitate communication between school and community personnel, and betweenprofessionals and the lay public, with respect to current health education principles,problems, and practices.
9. Provide leadership in establishing program policies criteria and evaluative proce-dures that will promote effective health education programs.
10. Inform the membership of current and pending legislation related to AAHE inter-ests and, upon request, provide professional and technical assistance in draftingpertinent legislation and related guidelines.
11. Mdintain effective liaison with Wher national health education organizations.
31'3

Health EducationTeaching Ideas:
SecondaryRevised Edition
Association for theAdvancement of Health Education
American Alliance forHealth, Physical Education,Recreation and Dance1900 Association Drive
Reston, Virginia 22091
BEST COPY AVAILABLE
30.1
ISBN 0-88314-529-4