
Heart Weight Affects Spontaneous Defibrillation But Not Ventricular Fibrillation Threshold
8
Reprinted with permission from PACING AND CLINICAL ELECTROPHYSIOLOGY, Volume 17, No. 12, December 1994 Copyright O 1994 by Futura Publishing Company, Inc., Armonk, NY 105040418 Heart Weight Affects Spontaneous Defibrillation But Not Ventricular Fibrillation Threshold ESTELA RUIZ and MAX E. '\IALENTINUZZI From the Laboratorio de Bioingenieria, Facultad de Ciencias Exactas y Tecnologfa (FACET), Universidad Nacional de Tucumtin (UNT), and the Institute Superior de Investigaciones Biol6gicas (INSIBIO), Consejo Nacional de Investigaciones Cientificas y TBcnicas (CONICET- UNT), Tucumfin, Argentina RUIZ, E., ma.: Heart Weight Affects SpontaneousDefibrillation But Not Ventricular Fibrillation Thresh- old. Among the factors involved in the induction, generalization, and reversion of cardiac fibrillation, the amount of tissue is a determinant factor. One question is whether an increase in myocardial mass would or would not require the same electrical threshold. Accordingly, one objective was to determine if ventricular weight [VW) has any effect on the fibrillation thresholds (FTs). A second objective was to find a possible relationship between spontaneous defibrillation [SPDE)and heart weight. FifLy mongrel dogs of both sexes were used, of which 26 were 2- to 10-week-old puppies. The rest were adult animals of undetermined age. Fibrillation was induced with two types of stimuli directly applied to the heart. The stimuli were a train of rectangular pulses [TP)not synchronized with the ECG, and single pulses [SP) synchronized with and delayed from the R wave. TP type was used in one group with paddle electrodes; and the TP and SP types were used in a second group with hook electrodes. For both types, stimulation started at a low current and was increased untilfibrillation was triggered. Once defibrillated, either sponta- neously or by electrical shock, the procedure was repeated. Correlation coeficients between FT and VW were low [< 0.4), and scaling of the thresholds to VW resulted in hyperbolic relationship,for all cases, thus suggesting independence of the two parameters. SPDE fell sharply with weight. For values higher than 12 grams it was essentially nonexistent. VW does not have any effect on the FT but it dramatically influences the capacity of the myocardium to revert the arrhythmia by itself. (PACE 1994; 17[Pt. I]: 2255-2262) fibrillation threshold, spontaneous defibrillation, mass, weight Introduction Supported by Consejo Nacional de Investigaciones Cientfficas y TBcnicas (CONICET, PID 3134-700-88) and by Consejo de Among the factors involved in the induction, Investigaciones de la Universidad Nacional de Tucumk generalization, and reversion of cardiac fibrilla- (CIUNT, Program NO. 57). tion, the arnomt of tissue (either atrial or ventricu- This paper is part of EstelaRuiz' doctoral dissertation, "Vulner- lar) is a determinant factor. As early as 1887, Mac- abilidad del coraz6n de mamffero a la fibrilacibn:la masa car- ~ i l l i - I implicitly to the importance of diaca como variable fibrilatoria" (Mammalian heart vulnerabil- ity to fibrillation: cardiac mass as fibrillatory variable), carried the myocardial mass in the maintenance of fibrilla- out at the Laboratorio de Bioingenieria under the direction of tion. One of the traditional theories to explain this M.E. Valentinuzzi, and submitted to the Facultad de Ciencias phenomenon (circus motion or reentry Naturales, Universidad Nacional de Tucumh, Tucumk, Ar- gentina, December 1991. theory) considers the necessity of a minimal Address for reprints: Max E. Valentinuzzi. Bioingenieria, C.C. route-obviously related to a minimal size, in turn 28, Suc. 2, (4000).Tucuman, Argentina. Fax: 54-81-24-2174. related to weight-for the depolarizing fkont to Received January 11,1994; revision March 30,1994; accepted reach fhe already recovered initial point, to restart ~pril 12.1994. the circuit.' In 1944, Martinez3 demonstrated ex- PACE, Vol. 17 December 1994, Part I
-
Upload
unt-argentina -
Category
Documents
-
view
3 -
download
0
Transcript of Heart Weight Affects Spontaneous Defibrillation But Not Ventricular Fibrillation Threshold

Reprinted with permission from PACING AND CLINICAL ELECTROPHYSIOLOGY, Volume 17, No. 12, December 1994 Copyright O 1994 by Futura Publishing Company, Inc., Armonk, NY 105040418
Heart Weight Affects Spontaneous Defibrillation But Not Ventricular Fibrillation Threshold
ESTELA RUIZ and MAX E. '\IALENTINUZZI From the Laboratorio de Bioingenieria, Facultad de Ciencias Exactas y Tecnologfa (FACET), Universidad Nacional de Tucumtin (UNT), and the Institute Superior de Investigaciones Biol6gicas (INSIBIO), Consejo Nacional de Investigaciones Cientificas y TBcnicas (CONICET- UNT), Tucumfin, Argentina
RUIZ, E., ma.: Heart Weight Affects Spontaneous Defibrillation But Not Ventricular Fibrillation Thresh- old. Among the factors involved in the induction, generalization, and reversion of cardiac fibrillation, the amount of tissue is a determinant factor. One question is whether an increase in myocardial mass would or would not require the same electrical threshold. Accordingly, one objective was to determine i f ventricular weight [VW) has any effect on the fibrillation thresholds (FTs). A second objective was to find a possible relationship between spontaneous defibrillation [SPDE) and heart weight. FifLy mongrel dogs of both sexes were used, of which 26 were 2- to 10-week-old puppies. The rest were adult animals of undetermined age. Fibrillation was induced with two types of stimuli directly applied to the heart. The stimuli were a train of rectangular pulses [TP) not synchronized with the ECG, and single pulses [SP) synchronized with and delayed from the R wave. TP type was used in one group with paddle electrodes; and the TP and SP types were used in a second group with hook electrodes. For both types, stimulation started at a low current and was increased untilfibrillation was triggered. Once defibrillated, either sponta- neously or by electrical shock, the procedure was repeated. Correlation coeficients between FT and VW were low [< 0.4), and scaling of the thresholds to V W resulted in hyperbolic relationship, for all cases, thus suggesting independence of the two parameters. SPDE fell sharply with weight. For values higher than 12 grams it was essentially nonexistent. VW does not have any effect on the FT but it dramatically influences the capacity of the myocardium to revert the arrhythmia by itself. (PACE 1994; 17[Pt. I]: 2255-2262)
fibrillation threshold, spontaneous defibrillation, mass, weight
Introduction Supported by Consejo Nacional de Investigaciones Cientfficas y TBcnicas (CONICET, PID 3134-700-88) and by Consejo de Among the factors involved in the induction, Investigaciones de la Universidad Nacional de Tucumk generalization, and reversion of cardiac fibrilla- (CIUNT, Program NO. 57). tion, the arnomt of tissue (either atrial or ventricu- This paper is part of EstelaRuiz' doctoral dissertation, "Vulner- lar) is a determinant factor. As early as 1887, Mac- abilidad del coraz6n de mamffero a la fibrilacibn: la masa car- ~ i l l i - I implicitly to the importance of diaca como variable fibrilatoria" (Mammalian heart vulnerabil- ity to fibrillation: cardiac mass as fibrillatory variable), carried the myocardial mass in the maintenance of fibrilla- out at the Laboratorio de Bioingenieria under the direction of tion. One of the traditional theories to explain this M.E. Valentinuzzi, and submitted to the Facultad de Ciencias phenomenon (circus motion or reentry Naturales, Universidad Nacional de Tucumh, Tucumk, Ar- gentina, December 1991. theory) considers the necessity of a minimal Address for reprints: Max E. Valentinuzzi. Bioingenieria, C.C. route-obviously related to a minimal size, in turn 28, Suc. 2, (4000). Tucuman, Argentina. Fax: 54-81-24-2174. related to weight-for the depolarizing fkont to Received January 11,1994; revision March 30,1994; accepted reach fhe already recovered initial point, to restart ~ p r i l 12.1994. the circuit.' In 1944, Martinez3 demonstrated ex-
PACE, Vol. 17 December 1994, Part I

RUIZ, ET AL.
perimentally that the capacity of a piece of myo- cardium to fibrillate increases with the size of the sample. Moe and Abildskov? defined fibrillation as the coexisting state of many disorderly wavelet fronts. If the number is large enough, as in a large heart, the probability is low for all the elements to be in phase (e.g., all in the refractory state or all recovered). If, instead, the number of wavelets is small, the probability for them to get in phase and resume the sinus rhythm becomes higher. The lat- ter case would be called a spontaneous defibrilla- tion (SPDE). Several authors showed that size has a definite influence on the maintenance and spon- taneous reversion of the ~ h y t h m i a , ~ - ~ while oth- ers tried to quantitate the minimum size of myo- cardial mass needed to induce fibrillation.'
If the concept of minimal mass to sustain fi- brillation is accepted and the minimum stimulat- ing amplitude to induce the arrhythmia is mea- sured, one may ask whether an increase in myocar- dial mass would require the same electrical threshold. Thus, the objective was to determine if ventricular weight (VW) has any effect on the ventricular fibrillation thresholds (VFTs). A sec- ond objective was to find a possible relationship between SPDE and heart weight.
Materials and Methods Preliminary Protocol
A total of 50 mongrel dogs of both sexes were used, 26 of which were 2- to 10-week-old puppies. Animals were provided by the "Instituto AntirrAb- ico de la Provincia de Tucumh" and the guide- lines of the American Physiological Society were followed. The rest were adult animals of undeter- mined age. They were anesthetized with morphine clorohydrate (15 mg/kg, sc) and sodium pentobar- bital(10 mg/kg, IV). In the case of puppies, pento.
barbital was initially injected subcutaneously until the desired level of anesthesia was reached. An artery was exposed for the measurement of blood pressure (with a Statham transducer) and to remove blood samples. A vein was used for the administration of physiological solution, anesthe- sia, and sodium bicarbonate, when needed. Medial thoracotomy along the sternum was the route of access to the heart. ECG and arterial pressure were continuously monitored (Gould 6800 recorder, Cleveland, OH, USA) while rectal temperature (measured with a mercury thermometer), pH, p02, and pCOz (model 161, Corning Gas Analyzer, Corning, NY, USA) were periodically tested (at 45- min intervals). An electric blanket maintained body temperature while infusion of sodium bicar- bonate and/or adjustment of the respirator (rate and depth) kept the acid-base equilibrium within the 7.35-7.45 pH range.
Electrodes and Fibrillating Stimuli
Animals were randomly divided into two groups. For group GA, a pair of paddles (664 mm2, similar to those used in transventricular defibrilla- tion) were applied to both sides of the heart. On the other hand, for group GB, a pair of stainless steel hooks were inserted on the medial anterior right ventricular surface area. The effective contact area per electrode was 11 mm2.
Two types of electrical stimuli were applied: (1) a train of rectangular pulses (TP) of 1-second duration, 50 Hz, with 2-msec pulse width, not syn- chronized with the ECG; and (2) a single 5-msec rectangular pulse (SP) synchronized and delayed with respect to the R wave. Stimulation of the TP type was used for group GA and both TP and SP types for group GB. Table I summarizes the total number of animals, groups, weights, electrodes, and stimuli.
Table I.
Summary of Groups GA and GB
No. of Animals BW (range) VW (range) Electrode Type Stimulus Type
G A 17 0.75-1 1 .OO Kg 4.8-84.5 g Spoon TP GB 33 0.70-14.00 Ka 4.2-102.0 a Hook TP & SP
Out of the total 33 animals in GB, only 31 were tested with SP and 28 with TP for the reasons explained in the text. BW = body weight; SP = synchronized single pulse; TP = nonsynchronized train of pulses; VW = ventricular weight.
December 1994, Part I PACE, Vol. 17

HEART WEIGHT
Electrical Fibrillation Threshold Measurement
For either stimulus type, stimulation started with a low current amplitude and was increased until fibrillation was triggered. Once defibrillated, either spontaneously or by electrical shock, the procedure was repeated following an up-down al- g ~ r i t h m . ~ ~ ' ~ For group GB, the initial stimulus was chosen at random to avoid any possible bias. Ran- domization has been used and recommended by others.1° Adult animals were defibrillated imme- diately after fibrillation, whereas in the case of the puppies a 30-second waiting period elapsed to allow for possible spontaneous normalization. If normalization did not occur, an electrical dis- charge was then applied. Each animal underwent between 10 to 12 fibrillation episodes and, in gen- eral, the same number or slightly more defibrilla- tion episodes. The number of the latter episodes must be kept low to minimize heart damage. Its ideal level is attained when the number of defi- brillations is equal to the number of fibrillations. After electrical reversal, a recovery period of at least 5 minutes was permitted before another se- quence was initiated. Return to a normal ECG was usually the criterion for recovery along wltn nor- mal acid-base balance. In other words, most of the time a longer waiting interval was allowed. The defibrillator was equipment designed and built in the laboratory.'*
The threshold for each animal was obtained from the threshold band concept,'' i.e., for each animal the applied current attempting fibrillation was plotted as a function of time. A band B is de- fined between the maximum value that did not trigger fibrillation and the minimum value that did produce fibrillation. The mid-range value of this band was taken as the VFT for that particular ani- mal. The width of the band could well be consid- ered as an estimator of intra-animal repeatability. Another way is to collect all the values within the band and calculate the average with its SD. The coefficient of variation obtained would measure repeatability within a single animal. Numerical data collected from dogs, sloths, and cats, yielded that the mid-range value does not differ signifi- cantly from the average value within the band.13 This "fibrillation band" contains values that may or may not trigger the phenomenon with a 50% probability of success. Thus, this definition would take account of the random variations intrinsic in
VFT (mA)
Figure 1. Ventricular fibrillation thresholds (VFTs) in mA as a function of ventricular weight (VW), for group GA using paddle electrodes (P) and train of pulses (TP). The right side: avemge value (AVG) = 14.1 mA, with standard deviation (SD) = 4.3 mA.
the threshold concept. Group GA had 17 such val- ues (one per animal) and, thus, the average I, to esti- mate the constant fibrillation threshold (FT) was calculated over such a set. Group GB had instead, respectively, 31 and 28 values per stimulus type, out of a total of 33 animals (Table I, Figs. 1-3).
V F T (mA)
Figure 2. Ventricular fibrillation thresholds (VFTs) in mA as a function of ventricular weight (VW), for group GB using hook electrodes (H) and synchronized single pulses (SP). The right side: average value (AVG) = 1 6.8 mA, with standard deviation (SD) = 7.4 mA.
PACE, Vol. 17 December 1994, Part I 2257

RUIZ, ET AL.
VFT (mA)
Figure 3. Ventricular fibrillation thresholds (VFTs) in mA as a function of ventricular weight (VW), for group GB using hook electrodes (H) and synchronized single pulses (SP). The right side: average value (AVG) = 0.91 mA, with standard deviation (SD) = 0.44 mA.
Based on previous s t~d ies , '~* '~ . '~ the average overall expected reproducibility of the three stim- ulating methods, estimated by the coefficient of variation, would be 26.8% +_ 13.9. While for TP applied with paddles the average overall repro- ducibilty was 28.0% and 25.2%, for TP applied with hooks, and SP applied with hooks it was 44.4% and 38.9%, re~pectively.'~.'~
When the experiment ended, the full heart was excised, cutting off the arterial and venous "tails." It was then weighed and the two atria were removed, and then the ventricles were weighed by themselves.
Results
Figure 4, panel A illustrates a typical fibrilla- tion episode, induced in this case by a TP, and its spontaneous reversal about 20 seconds later (Fig. 4, panel B). Figure 5, panel B shows an electrical defibrillation after the induction shown in Figure 5, panel A. The postdefibrillatory record of Figure 5, panel B is bradycardic with blocks, as opposed to the somewhat better morphology of the former spontaneous case.
Figure 1 displays the VFT (mA) obtained from group GA (17 dogs), stimulated with TP applied via paddles, as a function of VW. Figures 2 and 3 show similar results for group GB (33 dogs), using
hook electrodes, for SP and TP applied to 31 and 28 animals, respectively. Most of the animals of group GB were tested with both types of stimuli, however, the actual numbers (31 and 28) were somewhat lower because, for reasons of stability of the preparations, it was not possible to test all of them with both stimuli. As expected, the SP values are at least one order of magnitude higher, or more, than the values found for TP, for the same type of electrodes and location.
For the experiments reported in Figures 1-3, the coefficients of variations were, respectively, 30.6%, 43.9%, and 48.4%; the latter two were higher than the maximum limit predicted by the expected (26.8% + 13.9% = 40.7%) (see Materi- als and Methods) but, nontheless, still comparable with values reported in the literat~re,'~.'~.'~ espe- cially if the comparison is made with the same method. These values lie within what can be ex- pected from any biological variable in general. In fact, some authors have reported coefficients of variations as high as 60%.15 The measurement of VFT seems to be characterized by a large disper- sion.
Simple visual inspection does not anticipate any relationship between VET and VW because no particular trend is apparent, although the three graphs might offer the impression of a slight de- crease from left to right, that is, in the direction of growing VW. However, Pearson product-moment correlation coefficients (calculated with STAT- PAK [ver. 2.1, Northwest Analytical, Inc., Port- land, OR, USA]) were extremely low, 0.391 for GA, 0.273 for GB (TP), and 0.251 for GB (SP), which, at a 0.01 significance level, either by the traditional Fisher's table16 or by application of the t-test," yielded values not large enough to reject the as- sumption that there is no trend relating the two variables (the null hypothesis of r = 0 is accepted), thus, confirming the first suggestion. When a curve fitting program (to linear, second-degree polynom- ial, logarithmic, and exponential functions) was applied to the experimental data of the three fig- ures, all four yielded correlation values < 0.4, which discouraged the existence of any type of in- fluence of weight on the FT.
Figure 6 shows the percent of SPDE of each animal (groups GA and GB pooled together) as a function of VW. It sharply decreases as the latter increases, showing a neat zero cut at about 12 grams.
2258 December 1-994, Part I PACE, Vol. 17

HEART WEIGHT
SU mrn Hg
-
Figure 4. Triggering of a fibrillation episode by a train of Figure 5. Triggering of a fibrillation episode by a train of pulses (TP) with the typical drop to zero arterial pressure pulses (TP) with its typical drop to zero arterial pressure (AP) shown in panel A, and spontaneous defibrillation (AP) shown in panel A, and defibrillation by a discharge (SPDE) shown in panel B. The surface ECG shows the (D) shown in the panel B. Fiffy seconds have elapsed R wave in the left upper corner being replaced by the between the onset and end of fibrillation. Observe the fibrillatory F waves affer the TP. Calibrations are shown A-V block and obvious S-Tsegment elevation along with on the figure. a poorer blood pressure recovery, due to blocks, as com-
pared to the spontaneous phenomenon of Figure 4, panel B.
Discussion Since the VFT value depends weatlv on the electrode size and location,-and on the" type of
Cardiac electrical stimulation is frequently sti,lus,~s two types of each were chosen for a used in experimental physiology and in clinical location so that if threshold weight cardiology as a method to study the effects of anti- changed results were not masked by the above- arrh~thmic drugs or the responses in a given Pa- mentioned technological parameters. thology, to find the adequate stimulation levels if Coefficients of correlation were always ex- a pacemaker is to be implanted or, as in our case, tremely low (usually < 0.4) when FTs were statisti- to quantitate vulnerability to fibrillation in ventri- cally analyzed against VW. Curve fitting did not cles of different sizes. lead to any standard shape or trend either.
PACE, Vol. 17 December 1994, Part I 2259
RUIZ, ET AL.
SPDE (%)
20 Critical mass?
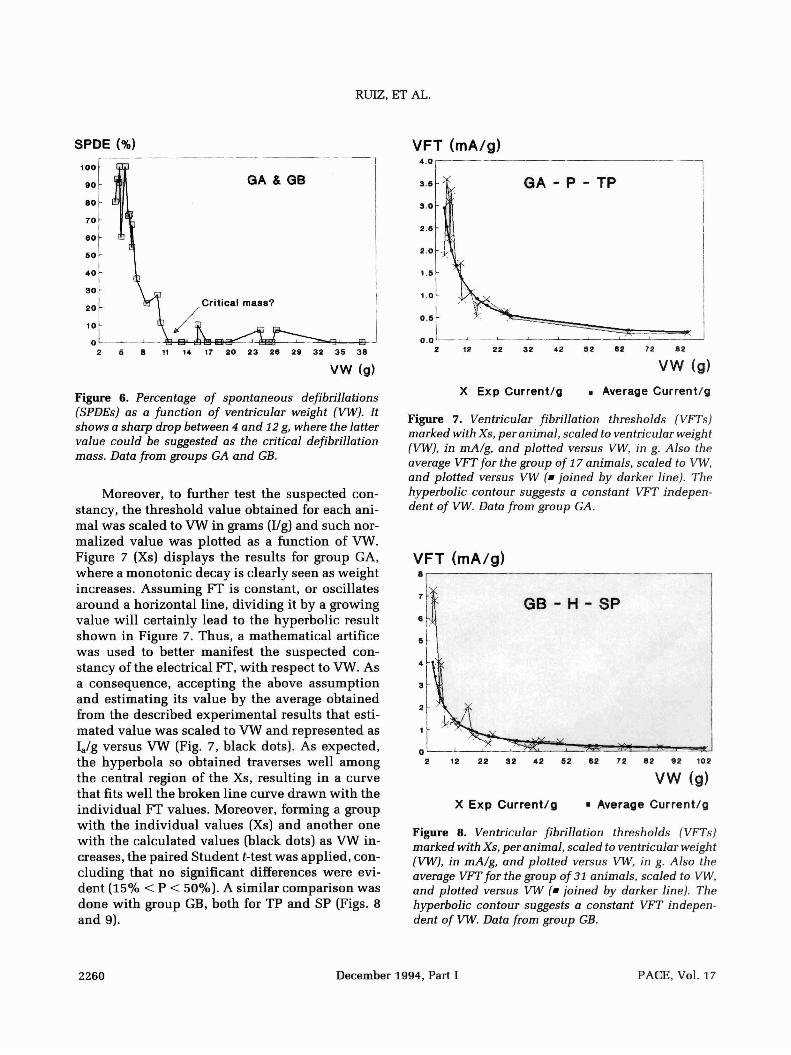
Figure 6. Percentage of spontaneous defibrillations (SPDEs) as a function of ventricular weight (VW). It shows a sharp drop between 4 and 12 g, where the latter value could be suggested as the critical defibrillation mass. Data from groups GA and GB.
Moreover, to further test the suspected con- stancy, the threshold value obtained for each ani- mal was scaled to VW in grams (Ilg) and such nor- malized value was plotted as a function of VW. Figure 7 (Xs) displays the results for group GA, where a monotonic decay is clearly seen as weight increases. Assuming FT is constant, or oscillates around a horizontal line, dividing it by a growing value will certainly lead to the hyperbolic result shown in Figure 7. Thus, a mathematical artifice was used to better manifest the suspected con- stancy of the electrical FT, with respect to VW. As a consequence, accepting the above assumption and estimating its value by the average obtained from the described experimental results that esti- mated value was scaled to VW and represented as I,/g versus VW (Fig. 7, black dots). As expected, the hyperbola so obtained traverses well among the central region of the Xs, resulting in a curve that fits well the broken line curve drawn with the individual FT values. Moreover, forming a group with the individual values (Xs) and another one with the calculated values (black dots) as VW in- creases, the paired Student t-test was applied, con- cluding that no significant differences were evi- dent (15% < P < 50%). A similar comparison was done with group GB, both for TP and SP (Figs. 8 and 9).
VFT (mA/g) - -1
X Exp Current/g . Average Current/g
Figure 7. Ventricular fibrillation thresholds (VFTs) marked with Xs, per animal, scaled to ventricular weight (VW), in mA/g, and plotted versus VW, in g. Also the average VFT for the group of 17 animals, scaled to VW, and plotted versus VW (=joined by darker line). The hyperbolic contour suggests a constant VFT indepen- dent of VW. Data from group GA.
VFT (mA/g) 8, 1
X Exp Current/g . Average Current/g
Figure 8. Ventricular fibrillation thresholds (VFTs) marked with Xs, per animal, scaled to ventricular weight (VW), in mA/g, and plotted versus VW, in g. Also the avemge VFT for the group of 31 animals, scaled to VW, and plotted versus VW (= joined by darker line). The hyperbolic contour suggests a constant VFT indepen- dent of VW. Data from group GB.
2260 December 1994, Part I PACE, Vol. 17

HEART WEIGHT
VFT (mA/g) 0.301 ?r: 1
X Exp Current/g r Average Current/g
Figure 9. Ventricular fibrillation thresholds (VFTs), marked with Xs, per animal, scaled to ventricular weight (VW), in mA/g, and plotted versus VW, in g. Also the average VFT for the group of 28 animals, scaled to VW, and plotted versus VW (r joined by darker line). The hyperbolic contour suggests a constant VFT indepen- dent of VW. Data from group GB.
Our results cannot be compared directly with others because no data have been found relating VFT with ventricular size. Rosen et a1.18 measured VFT in the isolated right and left ventricles of rats obtaining the same value, in spite of the difference in size. The same article describes how a preload maneuver (increasing the end-diastolic volume) produces a decrease in the VFT, especially in larger ventricles. They concluded that ventricular mass and wall stress would favor the development of arrhythmias. Stretch seems to affect VFT much more than even size. In observing their values one can see that without stretch,the average VFT in small ventricles (73 mg) was exactly equal to the value obtained in the large ones (122 mg). Thus, these data would support the contention reached herein. Sohail et al.I9 found that ventricular dilata- tion consistently decreased VFT-although this fact is not related to size, which is this article's main concern-however, an interesting result is the marked difference in VFT between the right and left ventricular values, the latter always being, with or without stretch, much lower than the for- mer (5.55 mA vs 13.28 mA, on the average, using
TP). Such difference might be explained by the shorter refractory period of the left ventricle (as reported by these authors) and to differences in vascularization and innervation. We rule out any size related effect. In fact, it may seem unrealistic to treat both ventricles as separate structures in a global phenomenon such as fibrillation. Recently, Stramba-Badiale et a1.20 reported that removal of either vagal or right cardiac sympathetic activity increases susceptibility to ventricular fibrillation during the first weeks of life. They used single stimuli and their VFT are similar to those reported here. Thus, developmental abnormalities would favor cardiac electrical instabilities that, in turn, may lead to arrhythmias. Size, with its strong in- fluence on spontaneous reversal, may prevent greater incidences of ventricular fibrillation epi- sodes in infants. No good data, clinical nor labora- tory, have been found to support this statement.
The ability to defibrillate spontaneously (i.e., stopping the uncoordinated activity and resuming the normal rhythm without external intervention), decreased dramatically as ventricular size in- creased, as expected, in agreement with observa- tions made by othem5-' However, the data pre- sented here are more complete because they cover a wider range (VW from 4.2-102 g, or a ratio > 24) for the same animal species. Attention should be called to the 30-second waiting period imposed in these experiments to protect the myocardium. Longer times led to quick diaphragmatic and body movements probably related to hypoxia. The pos- sibility cannot be ruled out of a SPDE after that interval, as reported by Szabuniewicz et a1.6 Thus, the values herein given should only be considered as an approximate estimation. It is thus concluded that VW is the predominant variable in the ability to defibrillate spontaneously. Fibrillation time and weight did not seem to reflect any relationship either. Figure 6 shows a sharp drop to zero proba- bility, essentially, for a VW of about 1 2 grams (dis- regarding the few cases with very low probability around 16 and 25-33 g). The possible existence of a maximal mass for SPDE is thus suggested, con- ceptually similar to the minimal mass to sustain fibrillation, but not necessarily numerically coin- cident. More experimental observations are re- quired to better validate this concept.
Kralios et a1." reported that the vulnerability
PACE, Vol. 17 December 1994, Part I 2261

RUIZ. ET AL.
of the neonatal dog heart to electrical induction of ventricular fibrillation decreases progressively during early age, and that SPDE decreases precipi- tously between the second and fourth week of age. These authors, however, did not take into account the possible role of VW.
up the phenomenon (by the application of the threshold stimulating level), the generalization mechanisms take care of the rest, therefore leading the myocardium into the arrhythmia. On the other hand, VW dramatically affects the possibility of self-recovery of the myocardium.
Conclusion
VW does not have any effect on the electrical FT. Probably, once the critical minimal mass starts
References
MacWilliam JA. Fibrillar contraction of the heart. J Physiol 1887; 8:296-310. Garrey WE. The nature of fibrillary contraction of the heart: Its relation to tissue mass and form. Am J Physiol 1914; 33:397-414. Martinez C. La masa miochdica media fibrilable e influencias que la modifican (in Spanish): The average myocardial fibrillable mass and influences that modify it. Medicina 1944; 4:109-132. Moe GK, Abildskov JA. Atrial fibrillation as a self- sustained arrhythmia independent of focal dis- charge. Am Heart J 1959; 58:59-70. Oliveira LH, Peres da Costa C, Huggins SE. Cardiac mass, blood temperature and ventricular fibrilla- tion, a study of comparative physiology of the three-toed sloth and domestic cat. Comp Biochem Physiol 1980; 67A:483-490. Szabuniewicz M, McCrady JD, Clark DR, et al. Ven- tricular fibrillation and spontaneous recovery in the dog. Southwest Vet 1968; 21. Szabuniewicz M, Hoff HE, McCrady JD. Sponta- neous ventricular defibrillation in the armadillo. Cardiovasc Res Center Bull 1970; 8:135-147. West TC, Landa JF. Minimal mass required for in- duction of a sustained arrhythmia in isolated atrial segments. Am J Physiol 1962; 202:232-236. Armayor MR, Savino GV, Valentinuzzi ME, et al. Ventricular defibrillation thresholds with capaci- tor discharge. Med Biol Eng Comput 1979; 17: 435-442. Cha YM, Peters BB, Birgersdotter-Green U, et al. A reappraisal of ventricular fibrillation threshold testing. Am J Physiol1993; 264(Heart Circ Physiol 33):H1005-H1010. Savino GV, Clavin OE, Guill6n SG, et al. Defibrila- dor cardiac0 capacitivo controlado a tiristor. Rev Mex Ing Biomed 1979; 2:20-24. Valentinuzzi ME, Ruiz E, Peres da Costa C. Ventric- ular fibrillation thresholds in the three-toed sloth
Acknowledgments: The technical assistance of Rafael Fi- gueroa, Hugo Griffasi, Julio Rodriguez, and Ricardo Medina Cisterna is duly recognized. Laboratorios Verardo (Buenos Aires) supplied, h e of charge, the morphine salt.
(Bradypus tridactylus). Acta Physiol Pharmacol Latinoam 1984; 34:313-322. Ruiz E. Vulnerabilidad del coraz6n de mamifero a la fibrilaci6n: La masa cardiaca como variable fibrilatoria. Doctoral Dissertation (in Spanish): Mammalian heart vulnerability to fibrillation: Car- diac mass as fibrillatory variable. Laboratorio de Bioingenieria, Universidad Nacional deTucumh, 1991. Ruiz E, Russo JA, Savino GV, et al. Ventricular fi- brillation threshold in the dog determined with defibrillating paddles. Med Biol Eng Comput 1985; 23:281-284. Ruiz E, Arredondo ME, Valentinuzzi ME, et al. Ventricular fibrillation threshold: Influence of type of electrical stimulus. J Clin Eng 1987; 12: 233-237. Cantatore de Frank NM. Manual de Estadistica Aplicada (in Spanish). Buenos Aires, Argentina, Editorial Hemisferio Sur, S.A. 1980-83. Glantz SA. Primer of Biostatistics. Second edition. New York, McGraw-Hill, 1987. Rosen S, Lahorra M, Cohen M, et al. Ventricular fibrillation thresholds are influenced by left ven- tricular stretch and mass in absence of ischaemia. Cardiovasc Res 1991; 25:458-462. Sohail J, Williams GR, Mann DE, et al. Effect of acute ventricular dilatation on fibrillation thresh- olds in the isolated rabbit heart. Am J Physiol1992; 263(Heart Circ Physiol 32):H1306-H1310. Strarnba-Badiale M, Lazzarotti M, Schwartz PJ. De- velopment of cardiac innervation, ventricular fi- brillation, and sudden infant death syndrome. Am J Physiol 1992; 263(Heart Circ Physiol 32):H1514- H1522. Kralios FA, Millar CK, Kralios AC. Developmental changes of ventricular fibrillation threshold and spontaneous defibrillation in young dogs. J Dev Physiol 1992; 17:163-167.
December 1994, Part I




















