Healthcare Education Handbook - Kansas Hospital Association
109
Kansas Healthcare Education Council Healthcare Education Handbook Published by the Kansas Healthcare Education Council
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Healthcare Education Handbook - Kansas Hospital Association
Kansas Healthcare Education Council
Healthcare
Education
Handbook
Published by the Kansas Healthcare Education Council
Kansas Healthcare Education Council
Table of Contents
I. Overview of the Educator’s Role in a Kansas Hospital
II. Organization of the Hospital Education Department
III. Requirements
A. State licensure and certification requirements
B. General education recommendations for Kansas hospital staff members:
C. Regulatory Training
D. Life Safety Classes
E. Record-Keeping Requirements
F. Additional Course Curriculum Utilized by Hospitals
IV. Developing the Hospital Educational Program
A. Annual Planning
B. Educational Evaluation
V. Competency Management
A. Elements of Performance
B. Verification Cycle
C. Standards & Ideas
VI. KSBN Continuing Education Requirements
A. Interactive CNE Offerings
B. Independent Study Program
C. Interactive Video (ITV)
D. Computer Assisted Instruction
VII. Policies & Procedures for Long-term Continuing Education Providers
A. Needs Assessment
B. Program Evaluation
C. Evaluation Criteria, Narrative Description
VIII. The Nursing Education Program
IX. Providing Continuing Education
A. Continuing Education Definitions
B. ANCC Certification
C. Preparing a Course
- Objectives, Curriculum Design, Stages of Learning,
- Cognitive, Affective, & Psychomotor Domain
X. Bibliography & Recommended Journals
XI. Appendix
A Seating
B. Digital Native Learner
C. Notes & Articles
Kansas Healthcare Education Council
Page 3
Acknowledgement
It is with grateful appreciation to the members of KaHEC that this handbook has been compiled. Kansas
Association of Nursing Continuing Education Providers, now incorporated with the Kansas Healthcare
Education Council (KaHEC), was for many years an excellent organizational resource for healthcare educators
within the State of Kansas. Their contribution to this handbook with specific information regarding continuing
education is greatly appreciated. The KaHEC Board of Directors has chosen to provide this resource to assist
not only those providers of nursing continuing education, but also for those responsible for organizing
healthcare education across departmental lines within the Kansas hospital setting.
Introduction
It is the philosophy of KaHEC that education beyond basic preparation for one’s role in a hospital setting, is
the individual responsibility of every nurse, doctor, healthcare professional and/or staff member. Therefore, it
is the goal of this handbook to assist the hospital educator in the development and sustainment of a hospital
educational program that will not only meet individual requirements, but will exceed the standards set forth by
regulatory and professional governing entities.
Specific emphasis is given in this handbook for hospitals which provide continuing nursing education (CNE).
Continuing nursing education is one means of maintaining competency and enhancing skills for hospital
nurses and contributes to the personal and professional growth of the nurse. Many, if not all, of the principles
set forth for establishing a successful nursing education program are applicable to an entire hospital education
program and so the hospital educator, even if not a provider of clinical education, is encouraged to reference
this section of the KaHEC Healthcare Education Handbook.
For the Kansas hospital educator, some of the first steps in entering this role can be challenging if not
overwhelming. Identifying one’s specific duties and the organizational structure are key to a successful tenure.
It would seem that in many hospital settings, the educational needs are frequently exceeding the educator’s
ability to answer the demands. There’s always more to be taught, more to be assessed, more to be filed, etc.
For the educator, the goal of establishing work / life balance, yet meeting the existing demands while
strategizing for the future, requires careful organization and a watchful eye to not place unreasonable
expectations on oneself or on staff assisting with these responsibilities.
It is our hope and desire that this reference tool will be a source of encouragement and assistance to the Kansas
hospital educator. Please note that this is not a complete work, but a fluid document, always under revision as
regulations change and new opportunities are presented.

Kansas Healthcare Education Council
The Journey...
“I’m impressed,” stated the KDHE
State Surveyor, “it’s not often that I
find an education department that is so
thorough in meeting educational
requirements.” Melinda, Education
Coordinator at KaHEC Regional, was
pleased at the surveyor’s comments;
but, immediately reflected on the ardu-
ous journey that had led to this valued
compliment as well as all those that
had enabled the successes she now
enjoyed…
Three years before...
“Can I help you?” the Admissions
clerk asked the nervous Melinda
Havercamp RN who stood before her.
“Yes, could you let Jane Campbell,
DON know that I’m here or point out
her office to me please?” “Ms Camp-
bell is somewhere on the nursing unit.
If you turn right after leaving this
area, you can ask the nurses where she
might be working.” Melinda headed
in the general direction indicated and
eventually happened upon the DON
who was working with the Nursing
Supervisor. “Oh Melinda, I’m glad
you’re finally here!” The senior nurse
was apparently very excited over see-
ing her newest recruit and quickly
introduced her to the staff in the imme-
diate area, as the new Education Co-
ordinator. After being escorted to
her new desk area, introduced to
countless individuals, provided with a
computer, passwords, a badge, and
given a quick tour of the facility,
Melinda settled down to organize her-
self. Momentarily Melinda was dumb-
founded as she feared that all her edu-
cation had not prepared her for this
moment…Where do I start? What has
been done? What is needed?
The Educator’s Role in a
Kansas Hospital
Simply put, the Kansas hospital
employee charged with the oversight
of the education department, is
responsible to ensure that all
regulatory, organizational, and professional educational
requirements are met for all staff within the hospital. Depending on
the licensure of the facility and the regulatory agencies governing
compliance, educational requirements may differ slightly from one
organization to another.
⇒ The education coordinator is to be familiar with educational
requirements and oversee / ensure compliance.
⇒ The education coordinator is crucial in providing a well-
organized program that meets on-going staff educational
requirements, competency management, annual evaluations,
record-keeping and organizational development.
⇒ Typically, the education coordinator will develop, with the
assistance of other hospital department directors, an over-all
annual education calendar.
⇒ The education coordinator will ensure that needed classes are
organized and meet all necessary requirements for continuing
education hours.
⇒ The education coordinator will ensure that Kansas State Board of
Education requirements are met if the hospital is certified as a
Long-Term Provider of continuing education.
Helpful Hint: Restraint education should be provided
on a periodic basis after initial orientation education.
The Joint Commission permits organizations to deter-
mine the time frame for ongoing education, but it is im-
plied that it should occur no less than every three
years.
I’m hir
ed...no
w
what?
??
Page 4
Kansas Healthcare Education Council
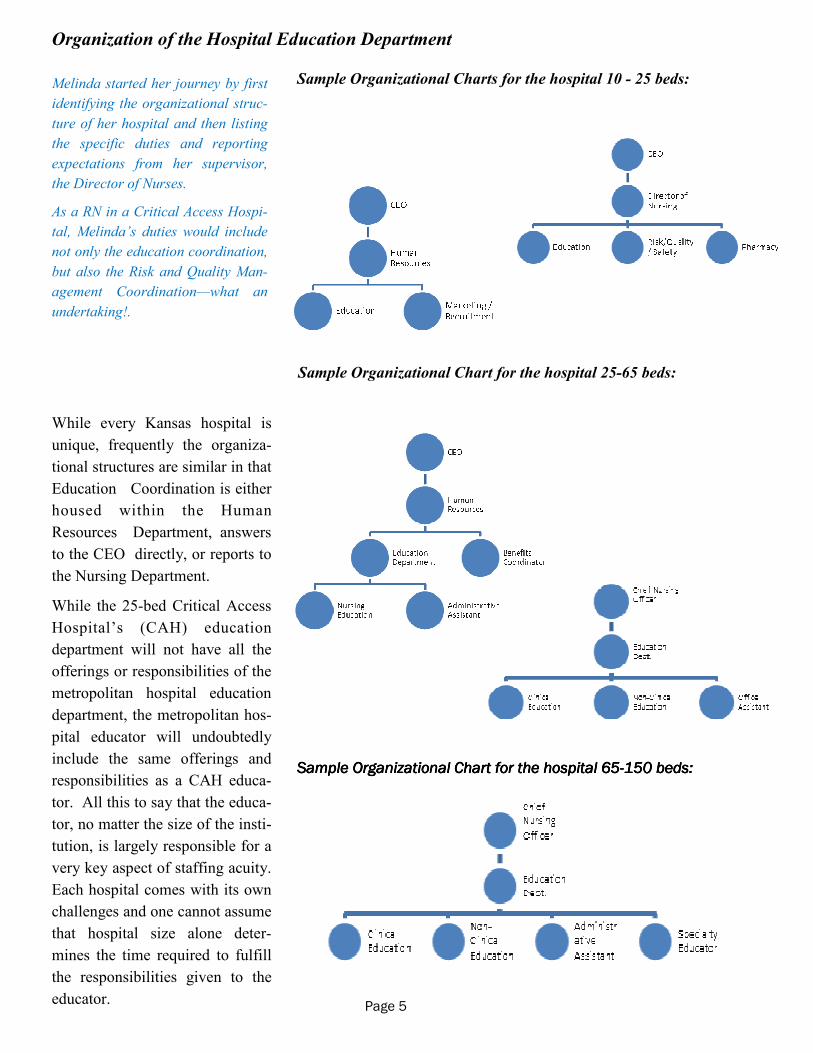
Sample Organizational Charts for the hospital 10 - 25 beds:
Sample Organizational Chart for the hospital 25-65 beds:
Sample Organizational Chart for the hospital 65Sample Organizational Chart for the hospital 65Sample Organizational Chart for the hospital 65Sample Organizational Chart for the hospital 65----150 beds:150 beds:150 beds:150 beds:
While every Kansas hospital is
unique, frequently the organiza-
tional structures are similar in that
Education Coordination is either
housed within the Human
Resources Department, answers
to the CEO directly, or reports to
the Nursing Department.
While the 25-bed Critical Access
Hospital’s (CAH) education
department will not have all the
offerings or responsibilities of the
metropolitan hospital education
department, the metropolitan hos-
pital educator will undoubtedly
include the same offerings and
responsibilities as a CAH educa-
tor. All this to say that the educa-
tor, no matter the size of the insti-
tution, is largely responsible for a
very key aspect of staffing acuity.
Each hospital comes with its own
challenges and one cannot assume
that hospital size alone deter-
mines the time required to fulfill
the responsibilities given to the
educator.
Melinda started her journey by first
identifying the organizational struc-
ture of her hospital and then listing
the specific duties and reporting
expectations from her supervisor,
the Director of Nurses.
As a RN in a Critical Access Hospi-
tal, Melinda’s duties would include
not only the education coordination,
but also the Risk and Quality Man-
agement Coordination—what an
undertaking!.
Page 5
Organization of the Hospital Education Department
Kansas Healthcare Education Council
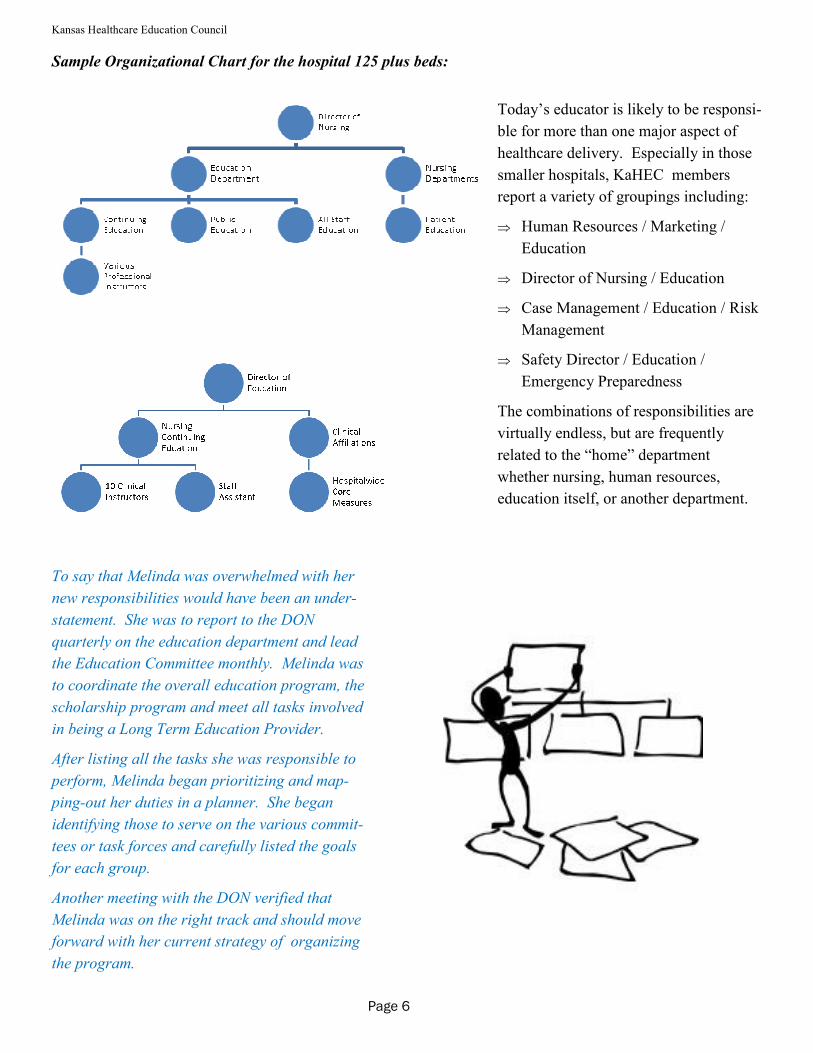
Sample Organizational Chart for the hospital 125 plus beds:
Today’s educator is likely to be responsi-
ble for more than one major aspect of
healthcare delivery. Especially in those
smaller hospitals, KaHEC members
report a variety of groupings including:
⇒ Human Resources / Marketing /
Education
⇒ Director of Nursing / Education
⇒ Case Management / Education / Risk
Management
⇒ Safety Director / Education /
Emergency Preparedness
The combinations of responsibilities are
virtually endless, but are frequently
related to the “home” department
whether nursing, human resources,
education itself, or another department.
To say that Melinda was overwhelmed with her
new responsibilities would have been an under-
statement. She was to report to the DON
quarterly on the education department and lead
the Education Committee monthly. Melinda was
to coordinate the overall education program, the
scholarship program and meet all tasks involved
in being a Long Term Education Provider.
After listing all the tasks she was responsible to
perform, Melinda began prioritizing and map-
ping-out her duties in a planner. She began
identifying those to serve on the various commit-
tees or task forces and carefully listed the goals
for each group.
Another meeting with the DON verified that
Melinda was on the right track and should move
forward with her current strategy of organizing
the program.
Page 6

Kansas Healthcare Education Council
For the hospital educator there are at least five distinct aspects of
education that must be addressed:
A. Safety
B. Compliance and Organizational-related Curriculum
C. Competency Programs & Assessments
D. Continuing Educational Requirements for Staff
E. Record-keeping
F. CME and /or CNE qualifications and requirements
Education recommended for the education coordinator /
director is largely contingent on the responsibilities dele-
gated. For many years, the focus on hospital education was
almost solely on the nursing department; therefore, many if
not most hospital educators in Kansas have a degree as a
Registered Nurse or higher clinical education. For those hos-
pitals that are providers of Continuing Nursing Education,
some hospitals require a Master’s Degree or an Advanced
Practice Registered Nurse for the education coordinator.
With increasing costs and with nursing staff shortages, the
education coordinator may not have a clinical degree, but
rather an alternate professional degree with a proclivity or
interest to adult education as well as the needed organiza-
tional skills. Close coordination with the nursing department
can enable an education coordinator to successfully organize,
but not lead, a nursing continuing education without actually
holding a nursing degree. For those hospital educators who
are not responsible to provide clinical instruction, a bachelor
or master’s degree in education is most advantageous with
experience or emphasis in adult learning methodologies. Ad-
ditionally, because of the nature of the education coordina-
tor’s job, proficiency in project management is extremely as-
sistive.
With her goals firmly identified for each
of her major areas of responsibility, and
committee tasks and task members iden-
tified, Melinda now turned her attention
to ensuring that one of her foremost du-
ties was well underway - curriculum.
In the past, the hospital had not had a
well-defined process for identifying the
“mandatory” courses to be presented to
both clinical and non-clinical personnel.
Melinda wanted to change this hap-
hazard approach and implement a con-
sistent procedure for annual education
course selection.
She began by researching what courses
were required by the hospital’s regula-
tory agency, CMS. Then she added
those courses that department directors
indicated were also required. Finally,
after consulting with the best practices
of other hospitals, she added a few
classes that supported the mission of the
hospital and would be assistive in im-
proving identified problem areas.
Helpful Hint: It is important for hospitals to make a decision as to the frequency of education that
will be provided to staff on the various topics. There are only a few topics that regulatory agencies
require annually. For some, MDRO, central line–associated bloodstream infections (CLABSI), sur-
gical site infections (SSI), and waived testing is mandatory. Education and training on the use of re-
straint, and MDRO, CLABSI, and SSI are sometimes also provided at the time of hire.
Page 7
Kansas Healthcare Education Council
Requirements Profession: Continuing Education Requirements: Doctors (MD or DO) 50 CME hours every year Physician Assistants 100 CME hours every two years Advanced Practice Registered Nurses 30 credits every 2 years* Registered Nurses 30 credits every 2 years Licensed Practical Nurses 30 CEUs every 2 years Physical Therapists 40 CEUs each 2 year licensing period Physical Therapy Assistants 20 CEUs each 2 year licensing period Occupational Therapists 40 CEU’s every 2 years (odd numbered years) Speech Therapists 20 CEU’s every 2 years Medical Laboratory Technicians No CEU requirements Psychologist 50 hours every 2 years Radiography (August 15-September 30 annually) 12 CEUs Nuclear Medicine 12 CEUs Radiation Therapy 12 CEUs Respiratory Therapists 12 CEUs annually Registered Dietitian 75 hours every 5 years Licensed Dietitian 15 hours every 2 years Social Workers 40 hours every 2 years
General education recommendations for many Kansas hospital staff members:
Regulatory Training:
Infection Control Reporting Abuse and Neglect Care for Specific Populations Restraint and Seclusion Rights & Responsibilities Ethical Considerations Compliance Program Patients' Rights Risk Management
Life Safety Classes:
All Hazards Awareness Disaster Preparedness Hospital Incident Command System Electrical Safety Fall Prevention Course Fire Safety Hand Hygiene Hazard Communication Infection Prevention and Control for Non-Clinical Staff Medical Radiation Safety Missing or Abducted Child Moving, Lifting and Repetitive Motion Slips, Trips and Falls HIPAA
Human Resource Topics:
Sexual Harassment
Page 8
Kansas Healthcare Education Council
Additional Course Curriculum Utilized by Hospitals: Leadership-enhancing coursework:
KHA Leadership Academy (offered in the summer months) Franklin-Covey Courses: 7 Habits of Highly Effective People, 7 Habits of Highly Effective
Managers, Project Management, 4 Disciplines of Execution
Communication Skill Enhancements:
Crucial Conversations, Crucial Confrontations, Influencer by Vital Smarts
Interpersonal Skill Development / Teamwork:
Customer Service: Disney Customer Service The Florence Philosophy Studer Group Courses / Books
Conflict Management
Health / Nutrition / Wellness
Personality Identification
Colors Personality Course DISC System
Personagenics Meyers-Briggs Inventory
HFAP Standards for Annual Education:
• Infection control including blood borne pathogens and airborne pathogens • Quality Assessment / Performance Improvement (QAPI) • Life Safety • Equipment / device safety as needed • Hazardous waste and materials safety • Information Management including confidentiality, computer access, and medical records confidentiality • Patient Rights • In addition, education is required on the prevention, identification, and reporting of suspected abuse
(including sexual assault) and neglect to each healthcare worker, regardless of discipline.
Record Keeping:
Helpful Hint: Develop a pattern
of offering the same courses
regularly (during the same time
periods each year) so that staff
can expect to re-certify without
having their certifications lapse.
Page 9
- The KHA Record & Retention Guide 2011 suggests that a Personnel File (which often includes competencies,
education, in-services, etc.) be kept for each employee for, “Not less than 7 years after termination of employ-
ment.” CFR 1602-14 requires retention for one year after termination or until final disposition of any charge
or action. Kansas law requires retention five years after termination. See KAR 50-2-2. We recommend the
longer period to provide for retention beyond the statute of limitations on a written employment contract,
which is five years.
- Records regarding continuing medical courses offered in the hospital are to be kept permanently.
Kansas Healthcare Education Council
Developing the Hospital Educational Program Whether assuming responsibility for an established hospital education program or providing initial
education program organization, the educator will need to address the following in the total
educational program:
A. Evaluations & Annual Assessments Annually the educator will need to identify the foreseeable required and desired needs of hospital
personnel within each department. Based on established goals of the hospital governance addi-tional classes / topics may also need to be included in the curriculum plan. This type of assessment is frequently done through a Hospital-wide Educational Assessment given to managers. The fol-lowing is a sample annual assessment. (See Appendix for Samples)
B. Classes based on infrequency of a procedure or Nursing Competency Assessment Results C. Orientation / On-Boarding D. Core Curriculum Requirements E. Hospital-specific classes frequently included
F. Annual Hospital-wide Education Program examples: On-line Educational Programs CareLearning HealthStream Swank Healthcare Live Educational Programs In-house Directed Contract Taught Pre-Packaged Programs
Combination Programs Competency Management
Hospital-wide Competency Program Management Unit / Department specific Competency Program Management
G. Resources for education documentation and certificates LMS (Learning Management Systems) providers, e.g. ACE Ware H. Departmental continuing education program I. Documentation Required: Policies & Procedures Manual CAH Review and Signature Requirement Other licensure requirements: Proof of education required for hospital certification JACHO licensed HVAP licensed CMS licensed KDHE Proof of education for employees, transcripts J. Competency Management K. Competency Record-keeping Helpful Hint: An effective education and training program should
be divided into thirds. One-third is for didactic training, one-third is
for direct observation, and one-third is for simulation.
Page 10
Kansas Healthcare Education Council
Standard Education Courses
AFM&A Advanced Fetal Monitoring and Assessment
BLS Basic Life Support, two year certification, clinical and non-clinical courses available, pre-requisite requirement for ACLS
ENPC Emergency Nursing Pediatric Course, five-year certification for nurses only
PALS Pediatric Advanced Life Support, two year certification for nurses, PA’s, APRN’s, MD’s or DO’s.
ACLS Advanced Cardiac Life Support, two year certification for nurses, PA’s, APRN’s, MD’s or DO’s. Pre-requisite for ATLS course.
ATLS Advanced Trauma Life Support, four year certification for medical providers only (PA’s, APRN’s, MD’s and DO’s).
IFMC Intermediate Fetal Monitoring Course
NRP Neonatal Resuscitation Program, every two years.
ONS Chemo Chemotherapy & Biotherapy Course, RN’s only and renewed every two years RTTDC Rural Trauma Team Development Course, designed to help the emergency room response team (radiology, laboratory services, respiratory services, emergency room provider, EMS staff, etc. to work collaboratively for the welfare of the patient).
Stable Neonatal education program to focus exclusively on the post-resuscitation/pre-transport stabilization care of sick infants. Four year certification.
TNCC Trauma Nursing Core Course, four year certification for RN’s and APRN’s.
With her mandatory curriculum identified for the year, Melinda now divided up the coursework. She discov-
ered early on in the process of identifying curriculum that she had several areas to consider and so divided-up
the curriculum into Clinical and Non-Clinical curriculum and further identified curriculum for general orien-
tation, 90-Day orientation, competency improvement, and annual mandatory in-services. By noting the
months that BLS, ACLS, ENPC, etc. were typically offered, she was able to identify map-out her curriculum
for the entire year. She placed her findings into a chart so as to streamline the process for ensuing years. At
the same time she revamped the survey she had provided to department directors so that it would accurately
reflect the information she had just gathered from them.
Helpful Hint: Pre-Establish Names / Titles of Courses and be consistent in recording courses for easy retrieval i.e.: (Date) ACLS or Advanced Cardiac Life Support, (Date)
Page 11
Kansas Healthcare Education Council
It had been a rough couple of weeks for Melinda, but at last she felt like
she was starting to get the Education Department organized to her liking.
One big aspect of this department was, of course, curriculum identifica-
tion. Now that that task was done, Melinda needed to identify exactly what
mediums were going to be used to present the curriculum. Certainly she
could not teach every course! How would she track it all and what about
scheduling!
After researching several companies that provide online education pro-
grams for hospitals, Melinda settled-on a company that would provide all
the identified mandatory classes, allow for private courses to be added,
and had all the tracking and reporting capabilities the hospital needed.
The online educational program would serve as the backbone to provide
the KaHEC Regional Hospital mandatory education curriculum.
Competency Management
Competency Management can be organized in a variety of ways, but should always be closely tied with a
hospital’s quality improvement program. In deciding what skills need to be included in an annual competency
assessment, topics / skills should be based on the following: high risk/low frequency, identified skill gap,
regulatory compliance, new equipment or policy /procedure. In some Kansas hospitals, the following clinical
procedures are to have a competency assessment performed annually:
• Multi-Drug Resistant Organisms (MDRO)*
• Central Line–Associated Bloodstream Infections (CLABSI)*
• Surgical Site Infections*
• Use of Restraint
*Competency is to also frequently given at time of hire.
Various methods for competency assessment include:
1. Competency Assessment Day(s) - These are typically mandatory sessions in which various stations are
established that allow for return demonstration after a brief tutorial or
explanation of the procedure is provided.
2. Live monthly or bi-monthly educational session that include a competency
assessment.
3. Assigned on-line classes or printed education sessions with return demon-
stration or other form of competency assessment provided that verifies the
skill required.
4. Packets given to staff with required completion dates.
(See samples from St. Jude Children’s Research Hospital in Appendix)
Page 12
Kansas Healthcare Education Council
Melinda and the Director of Nursing
discussed at length the best strategy
for managing competency assess-
ment of the clinical staff. After con-
firming the list of competencies that
needed verification, it was decided
to develop packets of education that
included:
• Bladder Scanner /
• Chest tube insertion / drainage
• Stryker Beds
• BIPAP
• Crashcart / Defibrillator / EKG
• PICC / Portacaths / IV / Veno-
scope
• Multi-Drug Resistant Organisms
• Central Line–Associated Blood-
stream Infections (CLABSI)
• Surgical Site Infections
• Bariatric Transfer-slide
• Glucometer
• Dysrhythmia Test
• KCI Wound VAC
• Body Mechanics
• HazMat Protocol Skills
The assigned packets had not only a
summary of the policy and / or
needed skill, but also an identified
means of competency assessment
that would be completed by a speci-
fied date and returned to Melinda.
In reviewing the plan, Melinda made
sure that variety was included in the
assessments and that each objective
was attainable. Furthermore, she
created specific guidelines for
returning the packets to ensure time-
liness.
Elements of Performance*
1. The hospital defines the competencies it requires of its staff who
provide patient care, treatment, or services.
2. The hospital uses assessment methods to determine the individual’s
competence in the skills being assessed. NOTE: Methods may in-
clude test taking, return demonstration, or the use of simulation.
3. An individual with the educational background, experience, or
knowledge related to the skills being reviewed assesses competence.
NOTE: When a suitable individual cannot be found to assess staff
competence, the hospital can utilize an outside individual for this
task. Alternatively, the hospital may consult the competency guide-
lines from an appropriate professional organization to make its as-
sessment.
4. Staff competence is initially assessed and documented as part of ori-
entation.
5. Staff competence is assessed and documented once every three
years, or more frequently as required by hospital policy or in accor-
dance with law and regulation.
6. The hospital takes action when a staff member’s competence does
not meet expectations.
Principles to Follow Regarding Competency:
• Competency assessment should assess, on an ongoing basis, that you
have the right staff abilities to carry out your current organizational
goals and objectives.
• Competency assessment is an ongoing process:
- Basic: at time of hiring, licensure, registration, certification,
interview questions, previous experience.
- Initial: the knowledge, technical / clinical, interpersonal,
critical thinking skills and abilities required at
completion of orientation and before practicing
independently.
- Ongoing: build on the already established knowledge, skills,
and abilities. Reflect the new, changing, high risk, and
problematic aspects of the job as it evolves over time.
• The annual competency assessment process is not comprehensive
like the competency validation that occurs during orientation. Once
the employee has demonstrated that he or she has knowledge and the
ability to perform the position’s assigned responsibilities, tasks, and
skills, competency is established.*
*Provided by Dr. Samuel L. Maceri, MPA, DNSc, RN, NEA-BC,
Director, Education & Support St. Jude Children’s Research Hospital.
Kansas Healthcare Education Council
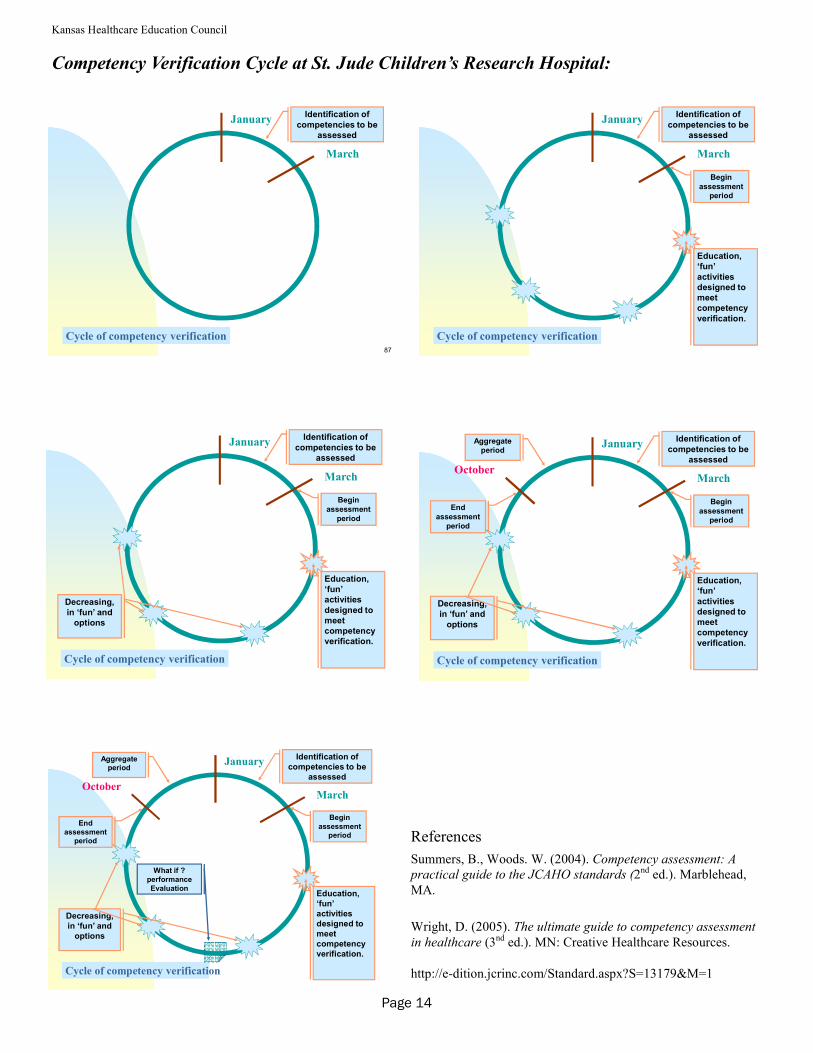
Competency Verification Cycle at St. Jude Children’s Research Hospital:
Cycle of competency verification
January
March
Identification of
competencies to be
assessed
87
89Cycle of competency verification
January
March
Identification of
competencies to be
assessed
Begin
assessment
period
Education,
‘fun’
activities
designed to
meet
competency
verification.
90Cycle of competency verification
January
March
Identification of
competencies to be
assessed
Begin
assessment
period
Education,
‘fun’
activities
designed to
meet
competency
verification.
Decreasing,
in ‘fun’ and
options
92Cycle of competency verification
January
March
Identification of
competencies to be
assessed
Begin
assessment
period
Education,
‘fun’
activities
designed to
meet
competency
verification.
Decreasing,
in ‘fun’ and
options
End
assessment
period
Aggregate
period
October
93Cycle of competency verification
January
March
Identification of
competencies to be
assessed
Begin
assessment
period
Education,
‘fun’
activities
designed to
meet
competency
verification.
Decreasing,
in ‘fun’ and
options
End
assessment
period
Aggregate
period
What if ?
performance
Evaluation
October
References
Summers, B., Woods. W. (2004). Competency assessment: A
practical guide to the JCAHO standards (2nd ed.). Marblehead,
MA.
Wright, D. (2005). The ultimate guide to competency assessment
in healthcare (3nd ed.). MN: Creative Healthcare Resources.
http://e-dition.jcrinc.com/Standard.aspx?S=13179&M=1
Page 14
Kansas Healthcare Education Council
- Blood transfusions and IV medications are administered by personnel who are trained and working within their scope of practice.
- Restraint competency is required as part of orientation and subsequently on a periodic basis consistent with
hospital policy including:
a. Techniques to identify staff and patient behaviors, events, and environmental factors that may trigger
circumstances that require the use of a restraint of seclusion
b. The use of nonphysical intervention skills
c. Choosing the least restrictive intervention based on an individualized assessment of the patient’s medi-
cal , or behavioral status or condition.
d. The safe application and use of all types of restraint or seclusion used in the hospital, including training
in how to recognize and respond to sights of physical and psychological distress (for example, positional or
asphyxia)
e. Clinical identification of specific behavioral changes that indicate the restraint or seclusion is no longer
necessary
f. Monitoring the physical and psychological well-being of the patient who is restrained or secluded, in-
cluding but not limited to respiratory and circulatory status, skin integrity, vital signs, and any special require-
ments specified by hospital policy associated with the 1-hour fact-to-face evaluation
g. The use of first aid techniques and certification in the use of cardiopulmonary resuscitation including
required periodic recertification.
Healthcare Facilities Accreditation Program (HFAP) Competency Standards
HFAP standards state, “Staff is competent in knowledge, skills, and ability to perform their responsibilities as
appropriate. An objective process for assessing and evaluating the competence of all employees is performed
at defined intervals. Competency is an on- going process. The facility will define the skills to be assessed
annually and those skills to be assessed at defined intervals.”
Competency Day Theme Ideas
· Have a Titanic theme with boarding passes for check-off lists and navigational maps for various stations.
· One of our KaHEC educators recently tried a County Fair theme with cotton candy, apples and stations each having a
county fair flare.
· St. John Medical Center in Tulsa, OK used a Survivor theme. If a nurse completed a competency, he or she could earn
immunity. They even used Survivor-themed music.
· You might try a “Tune-up” theme. Use a car’s trouble-shooting maintenance list and check the “monitors,” “oil level,”
etc. in the various parts of the “Service Station.”
· “Tuning-up your Instruments” might work if you’d like to use a music theme for your competency day. Make sure the
right “notes” are played in Meditech or whatever documentation program you need to review.
· Don’t forget about a game day theme whether it’s a football team and you’re arranging competencies in “huddles” or a
game show theme with teams and choices such as Jeopardy.
Page 15
Kansas Healthcare Education Council
Kansas Trauma Level Designation & Educational Requirements
A component in the development of a trauma care system is the designation of definitive trauma care facilities.
The system is a network of definitive care facilities that provides a range of care for all injured patients. In
most trauma systems a combination of designated trauma centers will coexist with other acute facility stan-
dards. The standards are established by the American College of Surgeons Committee on Trauma (ACS-
COT). This committee is the oldest standing committee of the college, established in 1922.
The classification of levels is not significant of the level of medical, but as a ranking of resource depth. The
commitment to quality care must be the same regardless of resources. All levels must participate in state and
regional trauma system planning, development, and operation within a region. Examples are:
Participation in state and regional trauma advisory committees
Leadership in state and regional medical audit committees
Regular collaboration with Regional Committees on Trauma, EMS, or other agencies to promote develop-
ment of state and regional systems
Participation in media and legislative education to promote and develop trauma systems
Participation in state and regional trauma needs assessment or injury surveillance
Participation in the development of a state or regional trauma plan or state trauma registry
Provision of technical assistance and education to regional hospitals and providers for the purposes of im-
proving system performance
A physician should be designated as the emergency department director. Physicians providing care are recom-
mended to be Advanced Trauma Life Support® (ATLS®) trained. Physicians providing emergency coverage
need to meet three categories: board certification, clinical involvement, and education. ATLS® certification
is for four years.
Trauma registry data must be collected and analyzed by every trauma center. The data must be reviewed by
the trauma director and trauma manager and reported to the appropriate committees within the facility. The
data must be submitted to the National Trauma Data Bank® (NTDB®) quarterly to be analyzed at a national
level.
Performance Improvement plus Patient Safety (PIPS) is a vital component of trauma care. Trauma care should
be efficacious, safe, and cost-effective. A major objective of PIPS is to reduce inappropriate variation in care
and to improve patient safety.
Level I
The Level I facility is a regional resource trauma center that provides tertiary care central to the trauma care
system. The facility must have the capability of providing leadership and total care for every aspect of injury,
from prevention to rehabilitation. The Level I center must have adequate depth of personnel and resources
serving as a lead hospital for the trauma system. Because of the large amount of resources for personnel and
Page 16
Kansas Healthcare Education Council
facility, resources required for patient care, education, and research, most Level I trauma centers are university
-based teaching hospitals. A Level I trauma center must admit at least 1,200 trauma patients yearly or have
240 admissions with an Injury Severity Score (ISS) of more than 15 for the trauma panel surgeons or general
surgeons on call.
Must have 24-hour in-house availability of the attending surgeon with a maximum acceptable response time of
15 minutes tracked from patient arrival. The trauma surgeon must be dedicated to the trauma center when on
duty and have a published backup call schedule. A board certified neurosurgeon must be promptly available at
all times for trauma service.
Level II
A Level II trauma center provides trauma care in two distinct environments. The first is a population-dense
area where the Level II center may supplement the clinical activity and expertise of a Level I institution. The
second Level II environment serves as the lead trauma facility for a geographic area with a Level I is not geo-
graphically close.
The trauma director must have responsibility for determining each general surgeon’s ability to participate, be
present in the emergency department for major resuscitations, be present at operative procedures and actively
involved in the critical care of all seriously injured patients. 24-hour in-house availability with a maximum
acceptable response time of 15 minutes tracked from patient arrival. The trauma surgeon must be dedicated to
the trauma center while on duty with a published backup call schedule. A board certified neurosurgeon must
be promptly available at all times to the trauma service.
Level III
The Level III trauma center should have the capability to initially manage the majority of injured patients and
have transfer agreements with a Level I or II trauma center for patients who exceed the available resources.
The Level III trauma center must have continuous general surgical coverage. Trauma panel surgeons must re-
spond promptly to activations; remain knowledgeable in trauma care principles, and participate in performance
review activities. The Level III trauma center expects that the surgeon will be in the emergency department on
patient arrival with a maximum acceptable response time of 30 minutes tracked from patient arrival.
Level III trauma centers may frequently treat patients who may ultimately require transfer to a higher level of
care. Well-defined transfer plans are essential. Injury prevention and control, outreach activities to the local
community, and education programs for nurses, physicians, and allied health care workers involved with
trauma are functions of the Level III trauma center. A board certified neurosurgeon may or may not be avail-
able and if not transfer agreements must be in place.
Level IV
A Level IV trauma center is located in a rural area and usually supplements care within a larger trauma system.
Level IV facility provides initial evaluation and assessment of injured patients, but most patients will require
transfer to a higher level of trauma care. A Level IV facility must have 24-hour emergency coverage by a
Page 17
Kansas Healthcare Education Council
physician, specialty coverage may or may not be available, but a well-organized resuscitation team is impor-
tant and well-defined transfer plans are essential.
Clinical Services
Anesthesia services must be available 24-hours a day and in-house for Level I and Level II trauma centers.
Anesthesiologists for Level I and Level II centers must be board-certified in anesthesiology. In Level III hos-
pital anesthesiologists or CRNAs must be promptly available.
An operating room must be readily available and staffed for a Level I trauma center. For Level II and III cen-
ters an adequately staffed and readily available operating room must be available in a timely manner.
Radiology services must be prompt available or by tele-radiology. Conventional radiography and computed
tomography (CT) must be available to all trauma centers 24-hours per day.
Laboratory services must be prompt and available 24-hours per day.
Physician Assistant (PA) and Advanced Registered Nurse Practitioner (APRN) can take ATLS® to be a mem-
ber of the trauma team.
Educational Opportunities for Nursing staff
A requirement for trauma education is a necessity for trauma team personnel. Opportunities for training are
Advanced Burn Life Support ©(ABLS©) 4 year certification
Trauma Nurse Core Course (TNCC) 4 year certification
All information for guidance in trauma level criteria can be obtained through the Kansas Trauma Program.
Additional can be obtained through the American College of Surgeons (American College of Surgeons [ACS],
2006). Note: An updated ACS manual is in the process of being updated.
Reference
American College of Surgeons. (2006). Resources for optimal care of the injured patient 2006 (2 ed.). Chicago, IL: American College of Surgeons.
Page 18

Kansas Healthcare Education Council
Notes
Page 19
Kansas Healthcare Education Council
Page 20
Kansas State Board of Nursing (KSBN)
Mission
The mission of the Board of Nursing is to assure the citizens of Kansas of safe and competent practice by
nurses and mental health technicians.
Continuing Education
The Kansas State Board of Nursing recognizes nurses as adult learners with continuing education needs as
professionals and licensees. To facilitate the learning needs of licensees, KSBN has established the following
options for acquisition of CNE:
Long-Term CNE Providers - persons, organizations, or institutions approved by the Board to
implement multiple offerings for CNE credit towards RN, LPN, and LMHT re-licensure.
Single-Program Providers - persons, organizations, or institutions approved by the Board for a two
-year period to implement a single topic CNE offering.
Individual Offering Approval (IOA) - a means of facilitating continuing nursing education credit for
learning experiences that are not approved by a recognized nursing organization. The individual
licensee must submit an individual offering approval form and required documentation to provide
written justification of how the learning experience will enhance their practice of nursing.
College Course Credit - satisfactory completion of an academic course taken as a part of a nursing
degree completion program will be accepted by KSBN for re-licensure. Other college courses should
be submitted using the Individual Offering Approval process. One hour of college credit = 15 hours of
CNE.
Other Approved Offerings - Continuing education offerings approved by a national nursing
organization (ANCC, NLN, etc.) or any state board of nursing are accepted by the KSBN for re-
licensure in Kansas.
Meetings
The Continuing Education Committee of the Kansas State Board of Nursing consists of Governor appointed
members, staff, and CNE providers. The committee meets five times per year in conjunction with the KSBN
meetings and reviews providership applications, renewal applications, annual reports, and CNE rules and
regulations. The meetings are open to all interested persons.
More Information
To obtain a copy of the Kansas Nurse Practice Act, the CNE Rules and Regulations or other information about
the CNE functions of the Kansas State Board of Nursing, contact the Nursing Practice Specialist - CNE at the
KSBN at 785-296-5062, or visit the KSBN Website at www.ksbn.org.
Kansas Healthcare Education Council
Page 21
Developing an Interactive CNE Offering
The following information has been developed to offer the reader the experience of many nursing continuing
education coordinators that have been working within the guidelines and regulations of a mandatory system. It
is hoped that the information will provide answers to many questions on how to plan, implement, and evaluate
nursing continuing education offerings.
I. Assessment
Assess Learner’s Needs - Formal and Informal
A. Prior to conducting a needs assessment you should
1. Determine a needs assessment framework/model.
2. Determine the source(s) of the needs assessment data - individual,
organizational, society.
B. Steps in the needs assessment
1. Determine the purpose.
2. Define the scope of the assessment.
3. Assess resources and constraints for conducting the assessment.
4. Elicit support.
5. Select appropriate methods - existing instruments vs. designing your own.
6. Collect the data using the appropriate methodology - questionnaires,
interviews, mail surveys, observations, etc.
7. Analyze data.
8. Prioritize needs.
9. Plan the offerings based on the needs assessment.
C. Suggested approaches to needs assessment
1. Ask questions of perspective participants, employers, nurse
colleagues, and consumers. (i.e. focus groups)
2. Include a needs assessment question on each offering evaluation.
3. Review current literature and research findings.
4. Conduct a formal needs assessment utilizing a questionnaire/survey tool (refer to the
literature for suggestions on questionnaire development).
5. Consult an advisory committee or colleagues/peers.
Kansas Healthcare Education Council
Page 22
See Needs Assessment section for more information.
D. Selecting an Advisory Committee
1. Determine purpose and function.
2. Determine appropriate membership based upon purpose and function (i.e. - educators, learners, consumers, clinical experts).
3. Limit membership to a manageable number.
4. If necessary, form subcommittees.
E. Assess Resources - people and material for conducting an offering
1. Operating budget.
2. Faculty.
3. Hardware.
4. Supplies.
5. Facilities. II. Planning
A. Prior to planning a nursing continuing education offering, select a method to organize and document the process. Dolphin, Holtzclau, 1983, pp. 159-160.
1. PERT—The Program (or Project) Evaluation and Review Technique, commonly abbreviated PERT, is a statistical tool, used in project management, that is designed to analyze and represent the tasks involved in completing a given project.
2. Calendar flow chart.
B. Steps in the planning process
1. Identify the topic area and target audience.
2. Establish a planning committee based upon specific expertise determined by the topic or purpose of the offering. Be sure to involve someone with a background in education and someone that represents the target audience. The size of the planning committee should be congruent with the size and tasks of the offering itself.
3. Clarify the goals of the offering.
Helpful Hint: Several Online Options are available free for use
collecting your needs assessment data. These instruments will also
compile the data for you as well. See below for some available
options or search for free online survey options.
http://www.surveymonkey.com/
http://kwiksurveys.com/
http://www.zoomerang.com/
Kansas Healthcare Education Council
Page 23
4. Determine format of the offering (e.g. one day, two day, concurrent sessions, practice session, demonstration, etc). Keep in mind principles of adult learning.
5. Establish a time and location for the offering:
a. Be aware of various factors that may contribute to timing (e.g. other offerings that
may affect participation, preference of target audience, potential for inclement
weather, etc.).
b. Secure a location early in the planning especially if seeking hotel accommodations.
c. Determine criteria for selection of offering site (e.g. location, meals, sleeping rooms,
comfort, breakout rooms, etc.).
6. Select a title for the offering. The title should reflect the content of the offering.
7. Develop measurable objectives or learning outcomes.
a. Objectives must be stated in terms of behaviors that will assure that the broad goals
have been met.
b. The number of objectives depends upon the complexity of the offering goal.
8. Develop offering content based upon the goal and objectives. Be certain that the
objectives and content can be accomplished in the designated time frame. Be specific
about the time the presentations begin and end.
9. Collaborate with speaker to determine the most appropriate teaching/learning strategies. Be
sure they are appropriate to the content, objectives and time frame.
10. Establish a prospective agenda with designated times for break and meals.
11. Calculate the number of contact hours according to formula approved by Kansas State
Board of Nursing. (50 min=1 CNE)
12. Identify speakers for the selected content:
a. Use established criteria for selection of speakers (e.g. credentials, expertise, ability
to present, style and manner of presence, availability, reputation, etc.).
b. Establish who will contact the potential speaker.
c. Coordinate objectives and content with the speaker.
d. Establish honoraria (if appropriate) and other expenses.
e. Request a current vita from the speaker.
f. Discuss teaching/learning strategies with the speaker.
g. Send a letter of confirmation to the speaker outlining details of the offering. Request
specific objectives, content outline, handout materials, and bibliography for course
notebooks or as handout materials for participants. Also ask about audiovisual needs. If
an honorarium is involved, a formal contract may be beneficial. This contract can
Kansas Healthcare Education Council
Page 24
specify the sponsoring organization’s responsibilities as well as the expectations of the
speaker.
h. Establish a time for receipt of above material.
i. Follow up phone calls or letters should be done as necessary.
13. Determine how you want to evaluate the offering. (Kirkpatrick, 1994)
• Level I: Reaction: participant satisfaction
• Level II: Learning: to what extend did the participants increase knowledge, improve skills and/or change behavior?
• Level III: Behavior: To what extent do they apply the information?
• Level IV: Results: What final results occurred? (quality, cost etc.)
C. Budget
1. Prepare an estimated budget for the specific program or offering.
2. There are many factors considered in identifying costs of a single
offering. Samples of budget reports are included in this section.
3. Be sure to consider direct (honoraria, refreshments, film rental, etc.) as well as indirect costs (services, facilities, record-keeping, etc.).
D. Marketing
1. Determine target audience (e.g. RN, LPN, LMHT, and geographic area).
2. Determine most appropriate means to reach the target audience:
a. Journal advertisements (some professional journals have free advertisements for continuing education, others require a fee to advertise) most require 3 - 4 months lead-time.
b. Kansas State Board of Nursing Newsletter, Kansas Nurse, American Nurse, Council Newsletters.
c. Newspapers, radio, television, flyers.
d. Convention booths.
e. Direct mailing to the individual or institution. Direct mail is the preferred method for
best results but sometimes difficult to obtain or maintain mailing lists. Use your own mailing list or purchase lists from specific agencies or associations (e.g. ANA, Councils, journals, etc.).
3. If mailing third class (least expensive), mail at least 6-10 weeks prior to date of offering. a. You must plan ahead to be sure brochure is ready to mail on time.
Kansas Healthcare Education Council
Page 25
4. Send additional brochures to planning committee and speakers to help market the
offering.
5. Send brochures to selected agencies, organizations, or individuals who can help market
the offering for you.
6. Be creative with your marketing techniques.
7. Evaluate your marketing techniques.
E. Brochure
1. Brochures and promotional materials are the mainstay of continuing education. They should communicate the message clearly.
2. The following are suggestions and considerations to include on the brochure: a. Sponsorship. b. Title. c. Dates, times, and locations. d. Advisory board/planning committee. e. Testimonials. f. Speakers. g. Purpose. h. Objectives. i. Target audience. j. Schedule and content. k. Fees and what they include. l. Contact hours and accreditation statement. (See the KSBN regulations for their
approved statement which must appear on each brochure). m. Registration forms. n. Phone number and name for additional information. o. Cancellation/refund policy. p. Accommodations (if necessary). q. Parking. r. Tax deduction information.
F. Co-sponsorship
1. If co-sponsoring a program decide who is responsible for the following:
a. Administration of the budget. b. Determination of objectives and content. c. Selection of faculty/presenters. d. Awarding of contact hours. e. Record keeping for offering. f. Evaluation.
2. Obtain a signed letter of agreement addressing above responsibilities.
III. Implementation
A. Know the plan and review the plan with all involved in assisting with the implementation.
Kansas Healthcare Education Council
Page 26
B. Maintain Records 1. Records are kept for each offering and include the following:
a. Title. b. Name and title of person administratively responsible for implementing the offering. c. Names and title of planning committee. d. Name, title and vita for each faculty/presenter. e. Starting and ending dates. f. Name and address of facility where offering was held. g. Objectives, content, time frame, teaching methods, and method used to evaluate
the offering. h. Description of target audience. i. Method used to determine need for the offering.
j. Names and license numbers of participants and number of contact hours awarded
to each.
k. Number of contact hours awarded for offering. L. Summary of participant's evaluations. m. A copy of co-sponsorship agreement, if applicable.
2. Develop a system for storage of records, which allows for retrieval of essential information. 3. Keep records for at least five years. 4. Maintain confidentiality of record keeping system.
C. Day of the Program
1. Be sure that all speakers are in town. 2. Registration
a. Arrange for registration table. b. Be sure you have enough assistance to keep flow of registrants moving. c. Provide registration table staff with packets of materials, name tags, and sign-in
sheets.
3. Conference Room(s)
a. Be sure microphones are on and ready to use.
b. Be sure required audiovisual equipment is:
1. Present
2. Working and focused properly.
3. Extra bulbs for all audiovisual equipment are present and someone is there to change them.
c. Be sure seating arrangements are as planned. 1. Leave space between chairs for arms of participants. 2. Walking space between rows of chairs. 3. Keep chairs away from exit doors to:
a. Enable easy entrance and exit. b. Avoid disruption of participants due to noise in hall.
D. Greeter
1. Be available to greet participants. 2. Be available at registration table to assist registration staff.
Helpful Hint: All of these records
can be stored electronically. Your
signed rosters can be scanned and
filed.
Kansas Healthcare Education Council
Page 27
3. Be available to handle emergencies.
E. Begin program 1. Begin program on time. (A MUST) 2. Greet assembled group. 3. Extend welcome. 4. Introductory remarks.
a. Be sure each participant has a copy of:
• Course outline
• Each handout
• References
• Evaluation tools (Encourage to complete)
• Brochure of future programs if appropriate
b. Announce.
• Location of water fountains, bathrooms
• Time of breaks and where
• Time of lunch and location if provided
• Time afternoon session begins if applicable
5. Introduce speaker.
a. The vita will provide pertinent information. The introduction should be short and should serve to provide both the credentials of the speaker and something interesting about the speaker.
b. Lead the applause as speaker approaches podium. c. Assist speaker with microphone. Move from speaker area
as unobtrusively as possible.
6. Conference management. a. Maintain physical comfort of the room. Adjust air-conditioner, fans, etc. b. Be available to answer questions. c. Obtain additional materials as necessary. d. Socialize with participants during breaks and lunch to gain feedback and
presentation reaction. e. Arrange lunch for speaker. f. Adjust lighting when audiovisuals are being used for maximum viewing.
g. Deliver messages to participants. (Usually a note and confine to emergencies). h. Be available to make announcements as break time. i. Be available to call participants back to seats following breaks, lunch, etc. j. Arrange or follow-up closure - include:
1. Brief appreciation comments to speaker. 2. Request for evaluations. 3. Identify where certificates of attendance may be obtained.
4. Wish them a safe trip home.
Kansas Healthcare Education Council
Page 28
k. Be available to socialize with participants or speaker or both as offering
concludes.
l. Assist speaker in collecting materials and departing.
m. Post offering follow-up:
1. Return audiovisual equipment and other teaching aids to appropriate
area.
2. Compile evaluation data and prepare a report. 3. Draft notes of appreciation to:
• Speaker(s)
• Staff who have been helpful
• Co-sponsors
• Planning Committee 4. When all bills are in, finalize the budget.
IV. Evaluation
A. Evaluating Educational Offerings 1. Each educational offering should be evaluated at its conclusion. 2. Ample literature is available on designing and using effective evaluation tools. 3. The following evaluation components should be included on your evaluation tool:
a. Learner’s achievement of offering objectives. b. Teaching effectiveness of each individual faculty member/presenter. c. Relevance of content to goals and learner’s needs. d. Appropriateness of physical facilities. e. Achievement of personal objectives by participants.
4. Use the results of your evaluations for planning future offerings.
Many hospitals develop some type of computer-based training modules. Although this
method is probably the simplest to provide, not all education and training should be
conducted in this manner.
Kansas Healthcare Education Council
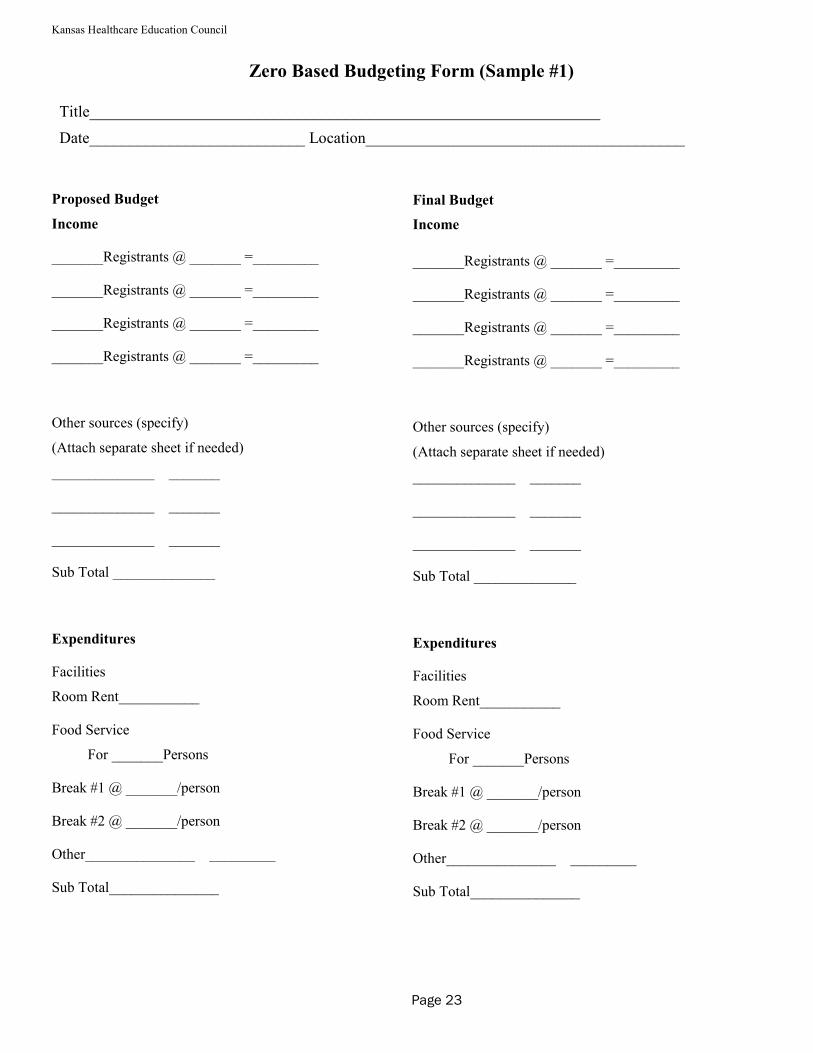
Proposed Budget
Income
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
Other sources (specify)
(Attach separate sheet if needed)
______________ _______
______________ _______
______________ _______
Sub Total ______________
Expenditures
Facilities
Room Rent___________
Food Service
For _______Persons
Break #1 @ _______/person
Break #2 @ _______/person
Other_______________ _________
Sub Total_______________
Zero Based Budgeting Form (Sample #1)
Title________________________________________________________________
Date___________________________ Location________________________________________
Final Budget
Income
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
_______Registrants @ _______ =_________
Other sources (specify)
(Attach separate sheet if needed)
______________ _______
______________ _______
______________ _______
Sub Total ______________
Expenditures
Facilities
Room Rent___________
Food Service
For _______Persons
Break #1 @ _______/person
Break #2 @ _______/person
Other_______________ _________
Sub Total_______________
Page 23

Kansas Healthcare Education Council
Income & Expenditures (Sample #2)Income & Expenditures (Sample #2)Income & Expenditures (Sample #2)Income & Expenditures (Sample #2)
WORKSHOP/SEMINAR________________________________________________
DATE___________________________LOCATION__________________________
ATTENDANCE: Employees _____________ Other _____________ Total Income _____________
TOTAL INCOME: ____________
TOTAL EXPENDITURES: ____________
NumberNumberNumberNumber
CostCostCostCost
TotalTotalTotalTotal
INCOMEINCOMEINCOMEINCOME
Tuition/Fees
Other
EXPENDITURESEXPENDITURESEXPENDITURESEXPENDITURES
Brochure:Brochure:Brochure:Brochure:
Printing
Xeroxing
Other
Mailing cost:Mailing cost:Mailing cost:Mailing cost:
Supplies:Supplies:Supplies:Supplies:
Handouts
AV Equipment
Other
Speaker:Speaker:Speaker:Speaker:
Honorarium/Fee
Mileage/Car Rental
Plane Fare
Hotel/Meals
Refreshments:Refreshments:Refreshments:Refreshments:
Meals
Breaks
Other Expenses:Other Expenses:Other Expenses:Other Expenses:
Room Rent
Other
Kansas Healthcare Education Council
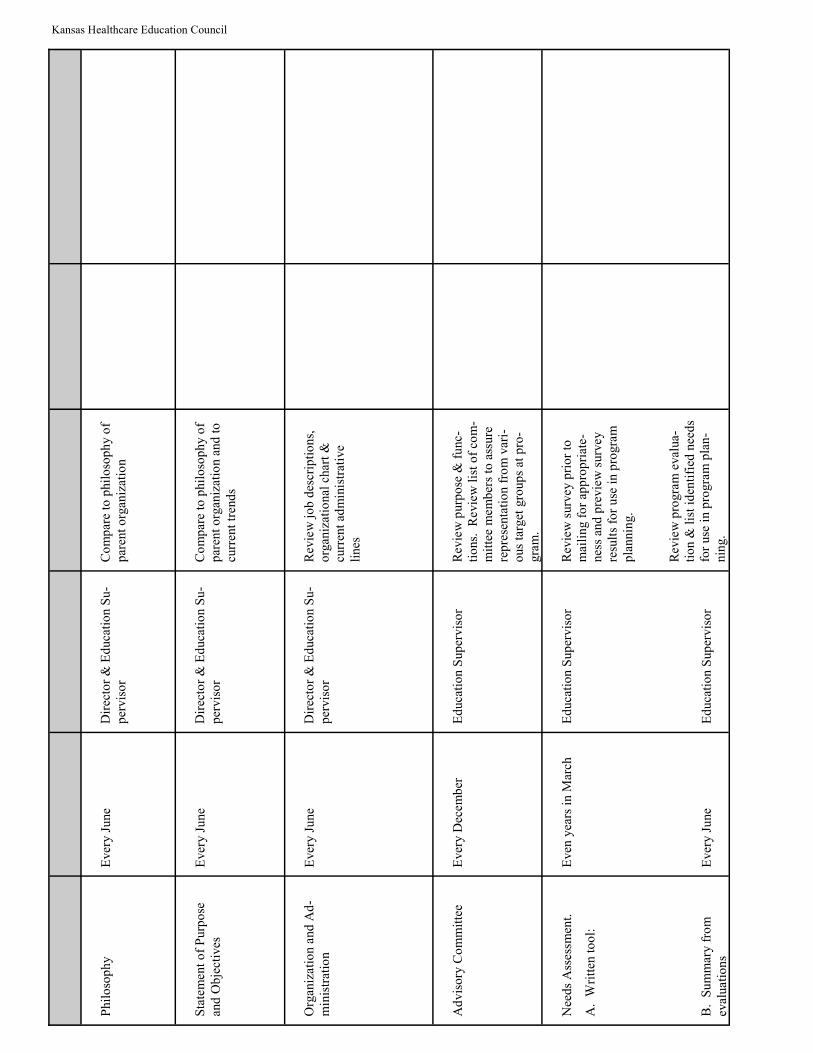
Phil
oso
ph
y
Ever
y J
une
Dir
ecto
r &
Ed
uca
tio
n S
u-
per
vis
or
Co
mp
are
to p
hil
oso
ph
y o
f
par
ent
org
aniz
atio
n
Sta
tem
ent
of
Purp
ose
and
Ob
ject
ives
Ever
y J
une
Dir
ecto
r &
Ed
uca
tio
n S
u-
per
vis
or
Co
mp
are
to p
hil
oso
ph
y o
f p
aren
t o
rgan
izat
ion a
nd
to
curr
ent
tren
ds
Org
aniz
atio
n a
nd
Ad
-
min
istr
atio
n
Ever
y J
une
Dir
ecto
r &
Ed
uca
tio
n S
u-
per
vis
or
Rev
iew
jo
b d
escr
ipti
ons,
o
rgan
izat
ional
char
t &
cu
rren
t ad
min
istr
ativ
e
lines
Ad
vis
ory
Co
mm
itte
e
Ever
y D
ecem
ber
Ed
uca
tio
n S
up
ervis
or
Rev
iew
purp
ose
& f
unc-
tio
ns.
R
evie
w l
ist
of
com
-m
itte
e m
emb
ers
to a
ssure
re
pre
senta
tio
n f
rom
var
i-o
us
targ
et g
roup
s at
pro
-
gra
m.
Nee
ds
Ass
essm
ent.
A.
Wri
tten
to
ol:
B.
Su
mm
ary f
rom
eval
uat
ion
s
Even
yea
rs i
n M
arch
Ever
y J
une
Ed
uca
tio
n S
up
ervis
or
Ed
uca
tio
n S
up
ervis
or
Rev
iew
surv
ey p
rio
r to
m
aili
ng f
or
app
rop
riat
e-
nes
s an
d p
revie
w s
urv
ey
resu
lts
for
use
in p
rogra
m
pla
nnin
g.
Rev
iew
pro
gra
m e
val
ua-
tio
n &
lis
t id
enti
fied
nee
ds
for
use
in p
rogra
m p
lan
-
nin
g.
Kansas Healthcare Education Council
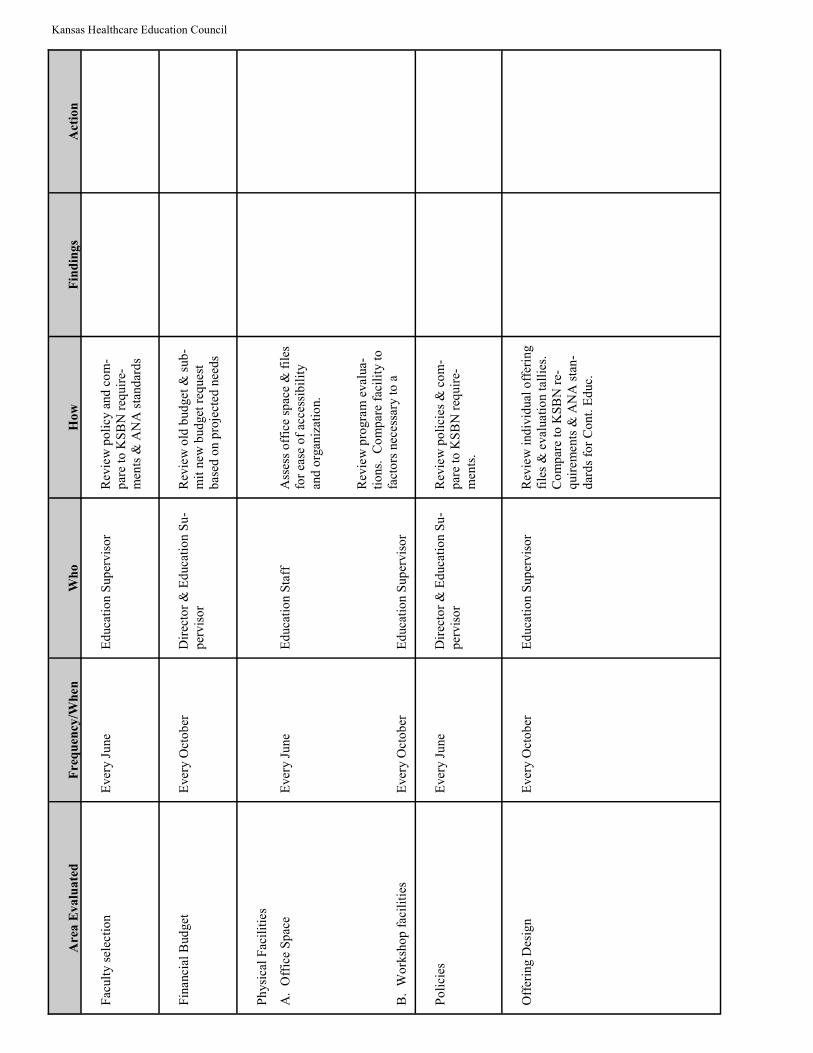
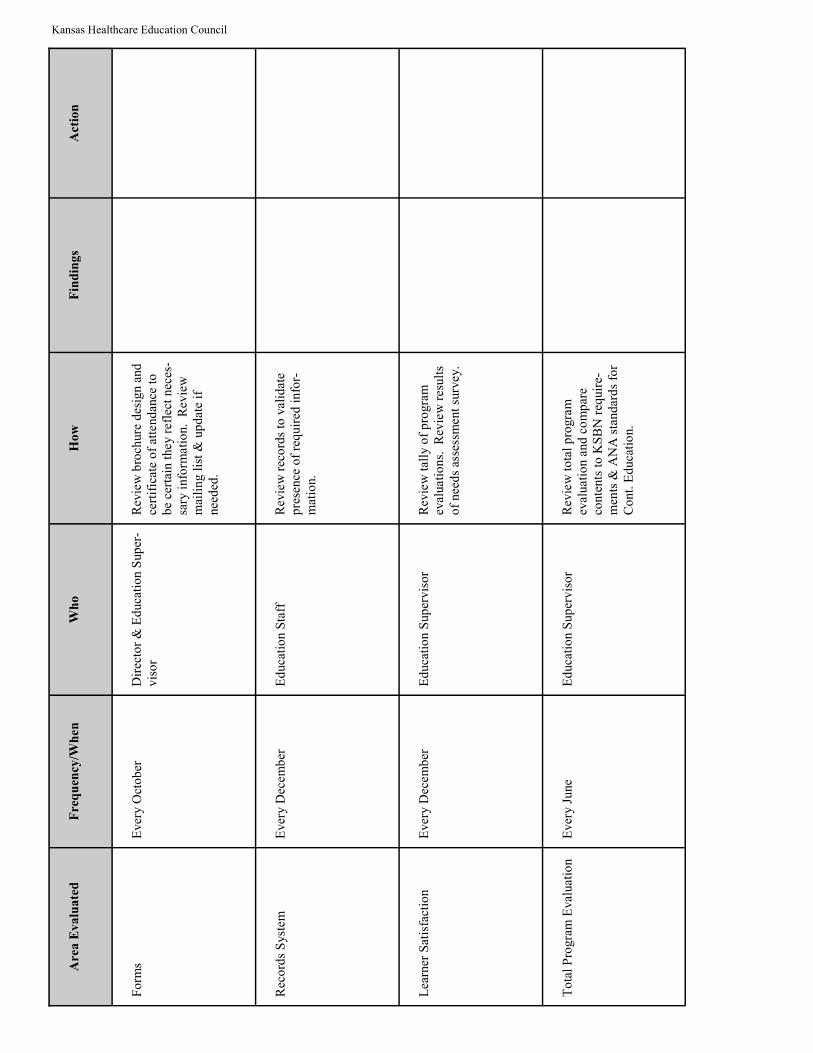
Area Evaluated
Frequency/When
Who
How
Findings
Action
Fac
ult
y s
elec
tio
n
Ever
y J
une
Ed
uca
tio
n S
up
ervis
or
Rev
iew
po
licy
and
co
m-
par
e to
KS
BN
req
uir
e-m
ents
& A
NA
sta
nd
ard
s
Fin
anci
al B
ud
get
Ever
y O
cto
ber
Dir
ecto
r &
Ed
uca
tio
n S
u-
per
vis
or
Rev
iew
old
bud
get
& s
ub
-m
it n
ew b
ud
get
req
ues
t b
ased
on p
roje
cted
nee
ds
Ph
ysi
cal
Fac
ilit
ies
A.
Off
ice
Sp
ace
B.
Wo
rksh
op
fac
ilit
ies
Ever
y J
une
Ever
y O
cto
ber
Ed
uca
tio
n S
taff
Ed
uca
tio
n S
up
ervis
or
Ass
ess
off
ice
spac
e &
fil
es
for
ease
of
acce
ssib
ilit
y
and
org
aniz
atio
n.
Rev
iew
pro
gra
m e
val
ua-
tio
ns.
C
om
par
e fa
cili
ty t
o
fact
ors
nec
essa
ry t
o a
Po
lici
es
Ever
y J
une
Dir
ecto
r &
Ed
uca
tio
n S
u-
per
vis
or
Rev
iew
po
lici
es &
co
m-
par
e to
KS
BN
req
uir
e-
men
ts.
Off
erin
g D
esig
n
Ever
y O
cto
ber
Ed
uca
tio
n S
up
ervis
or
Rev
iew
ind
ivid
ual
off
erin
g
file
s &
eval
uat
ion t
alli
es.
C
om
par
e to
KS
BN
re-
quir
emen
ts &
AN
A s
tan
-
dar
ds
for
Co
nt.
Ed
uc.
Kansas Healthcare Education Council
Area Evaluated
Frequency/When
Who
How
Findings
Action
Fo
rms
Ever
y O
cto
ber
Dir
ecto
r &
Ed
uca
tio
n S
up
er-
vis
or
Rev
iew
bro
chure
des
ign a
nd
ce
rtif
icat
e o
f at
tend
ance
to
b
e ce
rtai
n t
hey
ref
lect
nec
es-
sary
info
rmat
ion.
Rev
iew
m
aili
ng l
ist
& u
pd
ate
if
nee
ded
.
Rec
ord
s S
yst
em
Ever
y D
ecem
ber
Ed
uca
tio
n S
taff
Rev
iew
rec
ord
s to
val
idat
e p
rese
nce
of
req
uir
ed i
nfo
r-
mat
ion.
Lea
rner
Sat
isfa
ctio
n
Ever
y D
ecem
ber
Ed
uca
tio
n S
up
ervis
or
Rev
iew
tal
ly o
f p
rogra
m
eval
uat
ion
s.
Rev
iew
res
ult
s
of
nee
ds
asse
ssm
ent
surv
ey.
To
tal
Pro
gra
m E
val
uat
ion
Ever
y J
une
Ed
uca
tio
n S
up
ervis
or
Rev
iew
to
tal
pro
gra
m
eval
uat
ion a
nd
co
mp
are
conte
nts
to
KS
BN
req
uir
e-m
ents
& A
NA
sta
nd
ard
s fo
r
Co
nt.
Ed
uca
tio
n.
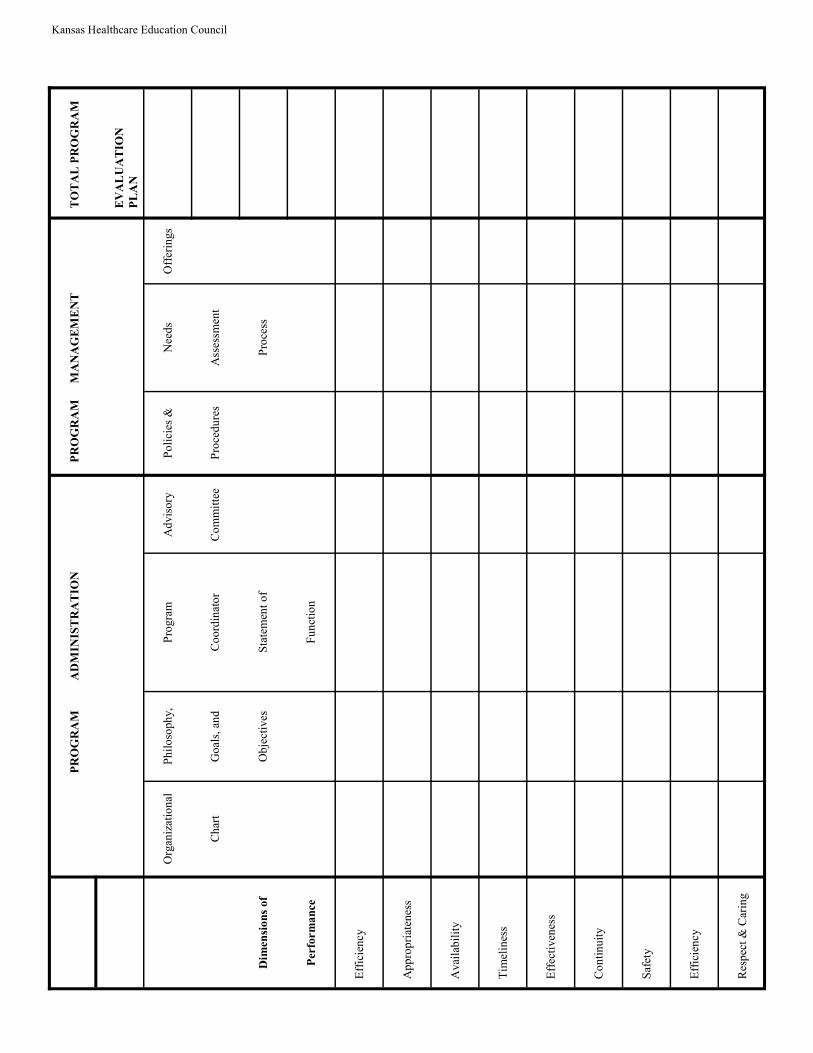
Kansas Healthcare Education Council
PROGRAM
ADMINISTRATION
PROGRAM
MANAGEMENT
TOTAL PROGRAM
EVALUATION
PLAN
Org
aniz
atio
nal
Ph
ilo
soph
y,
Pro
gra
m
Ad
vis
ory
Po
lici
es &
Nee
ds
Off
erin
gs
Ch
art
Go
als,
an
d
Co
ord
inat
or
Co
mm
itte
e
Pro
ced
ure
s
Ass
essm
ent
Dimensions of
Ob
ject
ives
Sta
tem
ent
of
Pro
cess
Performance
Fu
nct
ion
Eff
icie
ncy
Ap
pro
pri
aten
ess
Avai
lab
ilit
y
Tim
elin
ess
Eff
ecti
ven
ess
Co
nti
nu
ity
Saf
ety
Eff
icie
ncy
Res
pec
t &
Car
ing
Kansas Healthcare Education Council
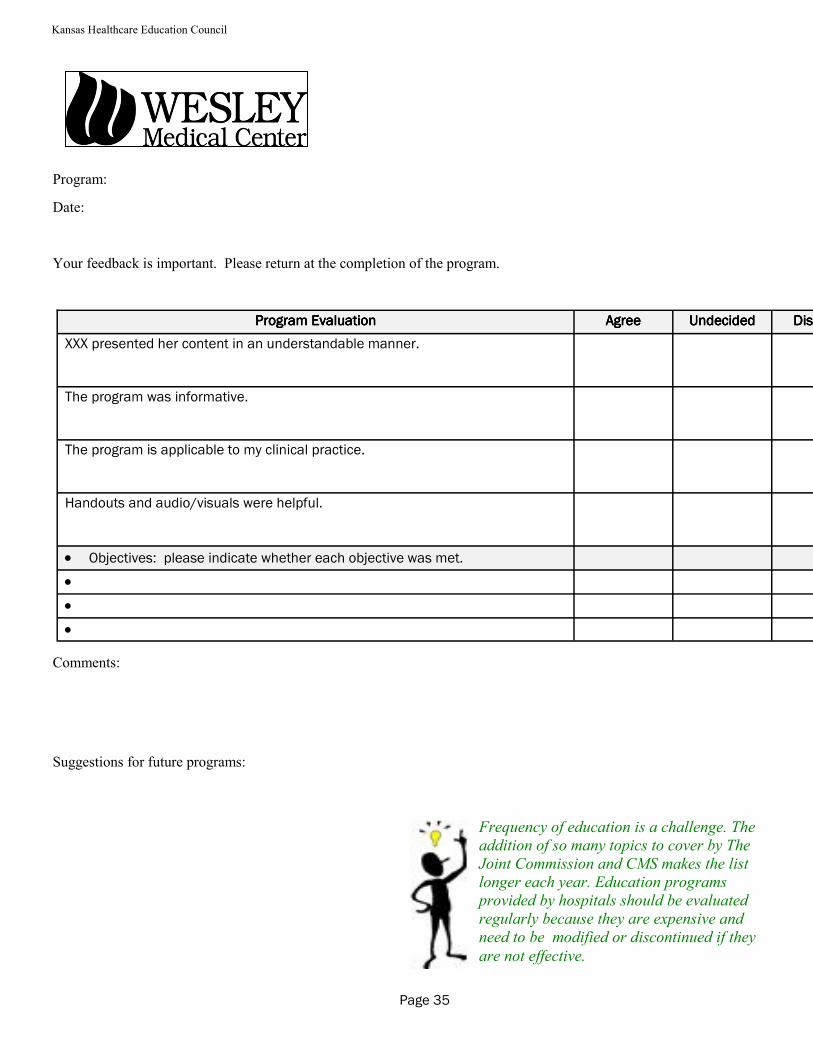
Program:
Date:
Your feedback is important. Please return at the completion of the program.
Comments:
Suggestions for future programs:
Program EvaluationProgram EvaluationProgram EvaluationProgram Evaluation AgreeAgreeAgreeAgree UndecidedUndecidedUndecidedUndecided DisagreeDisagreeDisagreeDisagree
XXX presented her content in an understandable manner.
The program was informative.
The program is applicable to my clinical practice.
Handouts and audio/visuals were helpful.
• Objectives: please indicate whether each objective was met.
•
•
•
Frequency of education is a challenge. The
addition of so many topics to cover by The
Joint Commission and CMS makes the list
longer each year. Education programs
provided by hospitals should be evaluated
regularly because they are expensive and
need to be modified or discontinued if they
are not effective.
Page 35
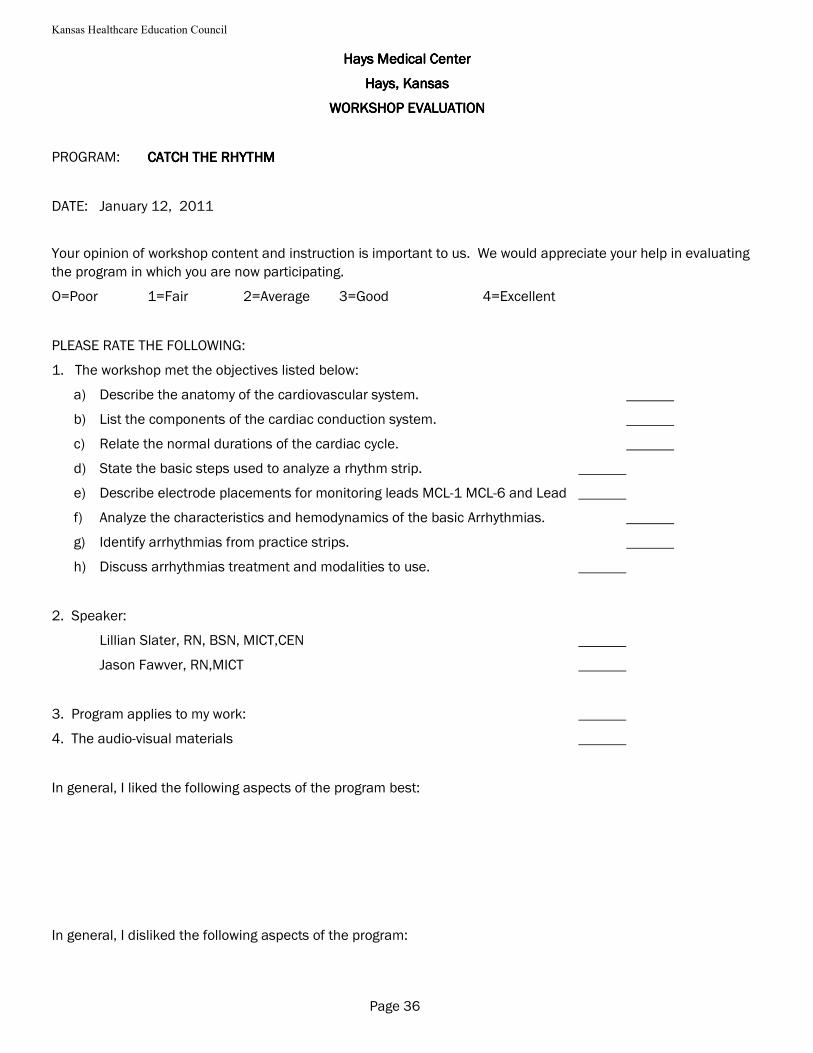
Kansas Healthcare Education Council
Hays Medical CenterHays Medical CenterHays Medical CenterHays Medical Center
Hays, KansasHays, KansasHays, KansasHays, Kansas
WORKSHOP EVALUATIONWORKSHOP EVALUATIONWORKSHOP EVALUATIONWORKSHOP EVALUATION
PROGRAM: CATCH THE RHYTHMCATCH THE RHYTHMCATCH THE RHYTHMCATCH THE RHYTHM
DATE: January 12, 2011
Your opinion of workshop content and instruction is important to us. We would appreciate your help in evaluating
the program in which you are now participating.
O=Poor 1=Fair 2=Average 3=Good 4=Excellent
PLEASE RATE THE FOLLOWING:
1. The workshop met the objectives listed below:
a) Describe the anatomy of the cardiovascular system.
b) List the components of the cardiac conduction system.
c) Relate the normal durations of the cardiac cycle.
d) State the basic steps used to analyze a rhythm strip.
e) Describe electrode placements for monitoring leads MCL-1 MCL-6 and Lead
f) Analyze the characteristics and hemodynamics of the basic Arrhythmias.
g) Identify arrhythmias from practice strips.
h) Discuss arrhythmias treatment and modalities to use.
2. Speaker:
Lillian Slater, RN, BSN, MICT,CEN
Jason Fawver, RN,MICT
3. Program applies to my work:
4. The audio-visual materials
In general, I liked the following aspects of the program best:
In general, I disliked the following aspects of the program:
Page 36
Kansas Healthcare Education Council
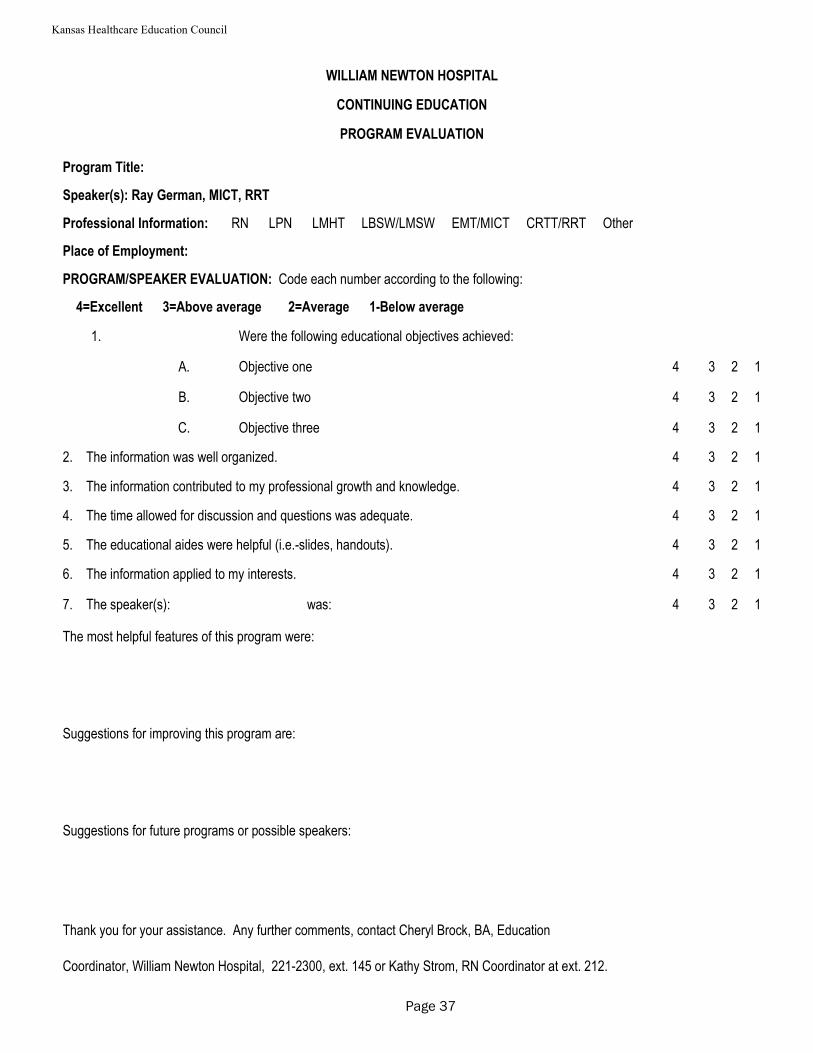
WILLIAM NEWTON HOSPITAL
CONTINUING EDUCATION
PROGRAM EVALUATION
Program Title:
Speaker(s): Ray German, MICT, RRT
Professional Information: RN LPN LMHT LBSW/LMSW EMT/MICT CRTT/RRT Other
Place of Employment:
PROGRAM/SPEAKER EVALUATION: Code each number according to the following:
4=Excellent 3=Above average 2=Average 1-Below average
1. Were the following educational objectives achieved:
A. Objective one 4 3 2 1
B. Objective two 4 3 2 1
C. Objective three 4 3 2 1
2. The information was well organized. 4 3 2 1
3. The information contributed to my professional growth and knowledge. 4 3 2 1
4. The time allowed for discussion and questions was adequate. 4 3 2 1
5. The educational aides were helpful (i.e.-slides, handouts). 4 3 2 1
6. The information applied to my interests. 4 3 2 1
7. The speaker(s): was: 4 3 2 1
The most helpful features of this program were:
Suggestions for improving this program are:
Suggestions for future programs or possible speakers:
Thank you for your assistance. Any further comments, contact Cheryl Brock, BA, Education
Coordinator, William Newton Hospital, 221-2300, ext. 145 or Kathy Strom, RN Coordinator at ext. 212.
Page 37
Kansas Healthcare Education Council
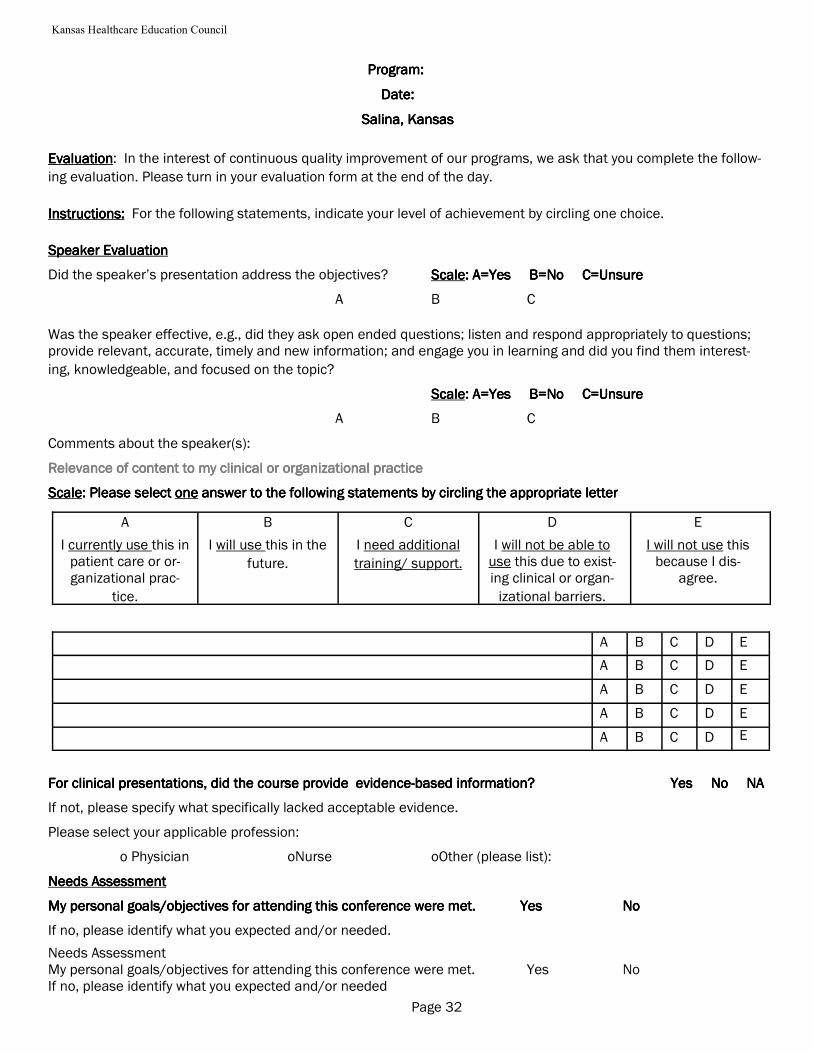
Program: Program: Program: Program:
Date: Date: Date: Date:
Salina, KansasSalina, KansasSalina, KansasSalina, Kansas
EvaluationEvaluationEvaluationEvaluation: In the interest of continuous quality improvement of our programs, we ask that you complete the follow-
ing evaluation. Please turn in your evaluation form at the end of the day.
Instructions:Instructions:Instructions:Instructions: For the following statements, indicate your level of achievement by circling one choice.
Speaker EvaluationSpeaker EvaluationSpeaker EvaluationSpeaker Evaluation
Did the speaker’s presentation address the objectives? ScaleScaleScaleScale: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure
A B C
Was the speaker effective, e.g., did they ask open ended questions; listen and respond appropriately to questions; provide relevant, accurate, timely and new information; and engage you in learning and did you find them interest-
ing, knowledgeable, and focused on the topic?
ScaleScaleScaleScale: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure: A=Yes B=No C=Unsure
A B C
Comments about the speaker(s):
Relevance of content to my clinical or organizational practice Relevance of content to my clinical or organizational practice Relevance of content to my clinical or organizational practice Relevance of content to my clinical or organizational practice
ScaleScaleScaleScale: Please select : Please select : Please select : Please select oneoneoneone answer to the following statements by circling the appropriate letteranswer to the following statements by circling the appropriate letteranswer to the following statements by circling the appropriate letteranswer to the following statements by circling the appropriate letter
For clinical presentations, did the course provide evidenceFor clinical presentations, did the course provide evidenceFor clinical presentations, did the course provide evidenceFor clinical presentations, did the course provide evidence----based information? based information? based information? based information? Yes No NAYes No NAYes No NAYes No NA
If not, please specify what specifically lacked acceptable evidence.
Please select your applicable profession:
o Physician oNurse oOther (please list):
Needs Assessment Needs Assessment Needs Assessment Needs Assessment
My personal goals/objectives for attending this conference were met.My personal goals/objectives for attending this conference were met.My personal goals/objectives for attending this conference were met.My personal goals/objectives for attending this conference were met. YesYesYesYes NoNoNoNo
If no, please identify what you expected and/or needed.
Needs Assessment My personal goals/objectives for attending this conference were met. Yes No If no, please identify what you expected and/or needed
A
I currently use this in patient care or or-ganizational prac-
tice.
B
I will use this in the
future.
C
I need additional
training/ support.
D
I will not be able to use this due to exist-ing clinical or organ-
izational barriers.
E
I will not use this because I dis-
agree.
A B C D E
A B C D E
A B C D E
A B C D E
A B C D E
Page 32
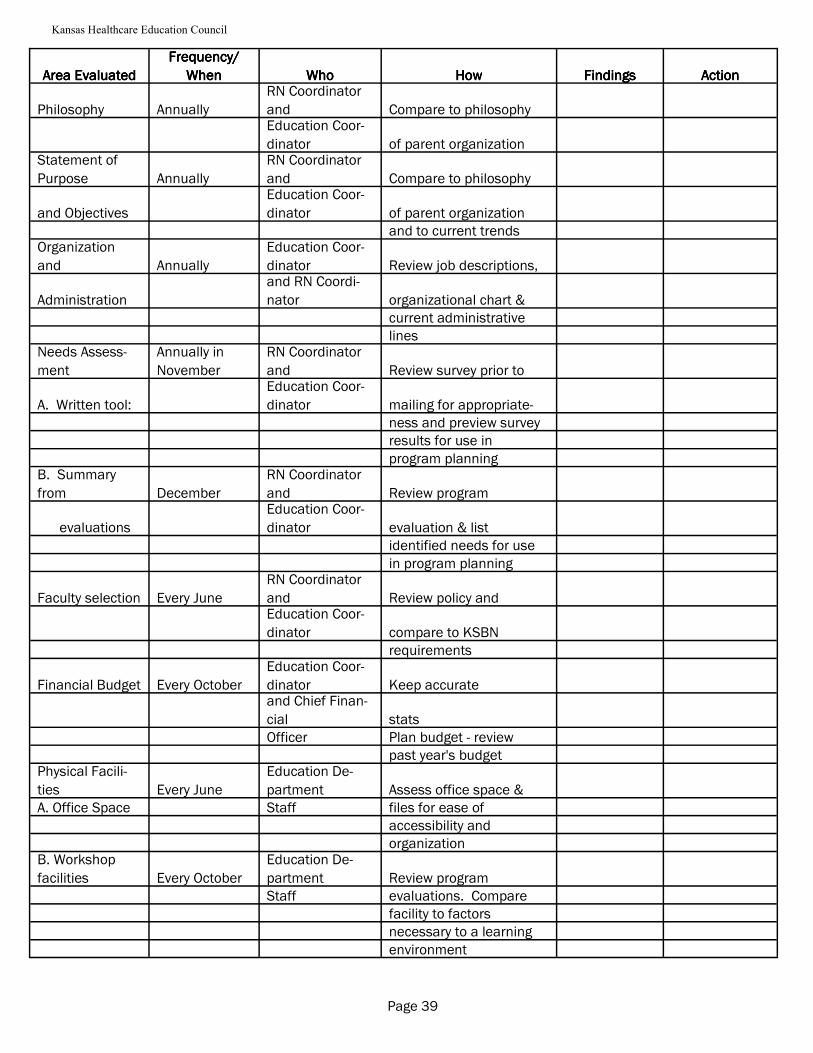
Kansas Healthcare Education Council
Area EvaluatedArea EvaluatedArea EvaluatedArea Evaluated
Frequency/Frequency/Frequency/Frequency/
WhenWhenWhenWhen WhoWhoWhoWho HowHowHowHow FindingsFindingsFindingsFindings ActionActionActionAction
Philosophy Annually
RN Coordinator
and Compare to philosophy
Education Coor-
dinator of parent organization Statement of
Purpose Annually
RN Coordinator
and Compare to philosophy
and Objectives
Education Coor-
dinator of parent organization
and to current trends Organization
and Annually
Education Coor-
dinator Review job descriptions,
Administration
and RN Coordi-
nator organizational chart &
current administrative
lines Needs Assess-
ment
Annually in
November
RN Coordinator
and Review survey prior to
A. Written tool:
Education Coor-
dinator mailing for appropriate-
ness and preview survey
results for use in
program planning B. Summary
from December
RN Coordinator
and Review program
evaluations
Education Coor-
dinator evaluation & list
identified needs for use
in program planning
Faculty selection Every June
RN Coordinator
and Review policy and
Education Coor-
dinator compare to KSBN
requirements
Financial Budget Every October
Education Coor-
dinator Keep accurate
and Chief Finan-
cial stats
Officer Plan budget - review
past year's budget Physical Facili-
ties Every June
Education De-
partment Assess office space &
A. Office Space Staff files for ease of
accessibility and
organization B. Workshop
facilities Every October
Education De-
partment Review program
Staff evaluations. Compare
facility to factors
necessary to a learning
environment
Page 39
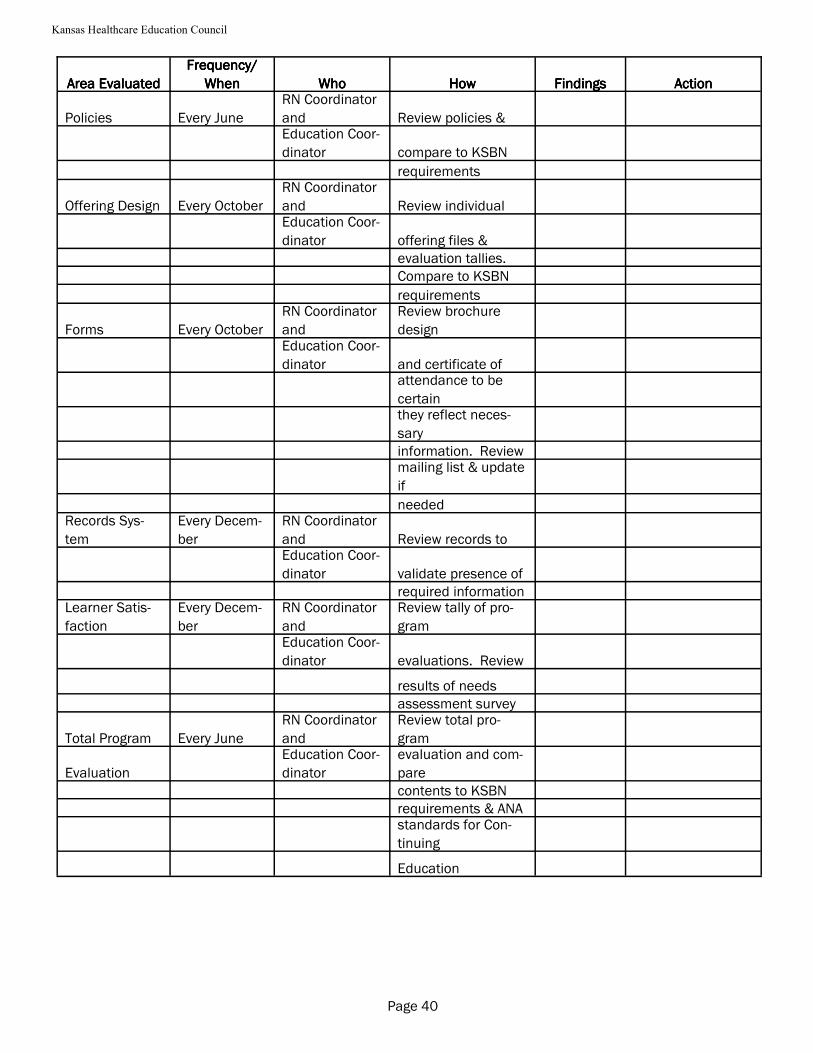
Kansas Healthcare Education Council
Policies Every June
RN Coordinator
and Review policies &
Education Coor-
dinator compare to KSBN
requirements
Offering Design Every October
RN Coordinator
and Review individual
Education Coor-
dinator offering files &
evaluation tallies.
Compare to KSBN
requirements
Forms Every October
RN Coordinator
and
Review brochure
design
Education Coor-
dinator and certificate of
attendance to be
certain
they reflect neces-
sary
information. Review
mailing list & update
if
needed Records Sys-
tem
Every Decem-
ber
RN Coordinator
and Review records to
Education Coor-
dinator validate presence of
required information Learner Satis-
faction
Every Decem-
ber
RN Coordinator
and
Review tally of pro-
gram
Education Coor-
dinator evaluations. Review
results of needs
assessment survey
Total Program Every June
RN Coordinator
and
Review total pro-
gram
Evaluation
Education Coor-
dinator
evaluation and com-
pare
contents to KSBN
requirements & ANA
standards for Con-
tinuing
Education
Area EvaluatedArea EvaluatedArea EvaluatedArea Evaluated
Frequency/Frequency/Frequency/Frequency/
WhenWhenWhenWhen WhoWhoWhoWho HowHowHowHow FindingsFindingsFindingsFindings ActionActionActionAction
Page 40
Kansas Healthcare Education Council
Kansas Association of Nursing Continuing Education Providers
Independent Study (Self-study Programs)
Number of Hours Permitted
The Kansas State Board of Nursing currently permits registered nurses, licensed practical nurses and licensed
mental health technicians to earn 30 contact hours/renewal period via independent study. Contact hours
earned via independent study must be designated independent study on the certificate.
Rationale for Offering Independent Study
1. Provides a means of offering individualized instruction to meet specific learning needs, i.e. care of the
cardiac patient.
2. Provides a means of verifying attainment of knowledge and/or level of competence.
3. Provides an alternative for individuals whose schedules do not permit attendance at seminars or other
scheduled offerings.
4. Provides a service for individuals who are facing license renewal deadlines.
Challenges to Offering Independent Study
1. Independent study is labor intensive---each registration, test and certificate is handled individually.
2. It is sometimes difficult to obtain independent study programs. Unless you develop your own (this as-
sumes expertise in a specific area and time to do it), it is often difficult to find programs at a cost you
can afford.
3. Independent study programs require updating just like any other offering. This may require additional
resources, either human or financial.
4. The number of hours assigned to a specific independent study program must be verified. Pilot the in-
dependent study program on a number of nurses (usually three to five). Ask the pilot group to record
the time it takes to complete the entire study. Take an average of the time submitted by the pilot group.
As you obtain participant evaluations and feedback, use this information to verify the hours or change
them if necessary.
Page 41
Kansas Healthcare Education Council
Where to Obtain Independent Study Programs
1. Purchase from the author for resale
(Author retains the copyright to the program.)
Advantages
A. You can provide programs with only a small investment in inventory.
B. You buy a finished product. It will be up-to-date or you need not buy it again.
Disadvantages
A. Most authors will expect you to actively market the independent study; may require that you enter
into a contractual agreement with the author defining specific expectations.
2. Author develops a specific independent study for you
(You/your institution owns the copyright to the program.)
Advantages
A. In the long run, this is usually the most cost- effective way to offer programs. You can generate
revenue through volume over time.
Disadvantages
A. Program development usually takes a good bit of time. You may need to have several conferences
with the author to define content, check on progress and evaluate the final product.
B. Beginning costs can be expensive---depending on who you find to write the independent study,
sometimes as much as $1000-$1500/independent study.
C. Since you own the independent, you will be responsible for updating it periodically. This is usually
an additional cost.
Designing Independent Study Materials
When designing educational activities that are intended for self-instruction, follow the same basic format used
for designing interactive offerings. The following guidelines will help in designing self-learning programs.
1. Conduct a Needs Analysis
Follow the same procedure for determining learning needs as for other educational programs.
2. Develop Objectives
The same steps should be followed for developing learning objectives as with other offerings. In most
cases, independent study is best suited for cognitive learning. Psychomotor skills are not usually
Page 42
Kansas Healthcare Education Council
learned effectively via independent study. It is possible to combine independent study materials with
in-class demonstrations and hands-on practice.
3. Develop Independent Study Materials
Guidelines to keep in mind when designing self-learning materials include:
· Develop an outline, based on the objectives
· Use as few words as possible to get the point across.
· Use examples to illustrate major points.
· If possible, use visuals such as pictures, graphs, and charts.
· Include a bibliography.
4. Evaluate the Program
Provide a written evaluation to obtain participant feedback. This can be very helpful in designing fu-
ture self-learning modules. Feedback regarding both the content and the completion process is useful.
Documenting Completion of Independent Study
You will need some criteria for determining satisfactory completion of the offering. This is usually done by
means of a test.
Some authors want to grade the test themselves, write feedback for the participant, etc. In this situation, the
test is returned to the author and the author notifies you that the participant has satisfactorily completed the
independent study. You then send the certificate to the participant. This can be a very involved process and
one that takes clear guidelines for implementation.
It is much easier to develop a short answer test and grade it in-house. This can be done by support staff. This
also facilitates being able to process the independent study in a timely manner for the participant.
Interactive Video (ITV)
Continuing education provided via ITV is totally interactive and can be given contact hour credit just like any
other offering. During the presentation, a participant at any site has the opportunity to interact with the pre-
senter, and the presenter with the participant. The main advantage to using ITV is that it reaches a lot of peo-
ple with little travel time. A continuing education offering provided by ITV is planned like any other offering.
The speaker must be comfortable with the ITV format.
One of these two basic formats for setting up the offering can be followed:
I. Host site invites other sites to participate
The host site is responsible for making technical arrangements at each invited site, sends
out offering announcements, maintains the offering files, collects fees from all
participants, and is responsible for all costs. The host site is also responsible for
sending handouts, evaluations, and sign in rosters to each remote site. At the
Page 43
Kansas Healthcare Education Council
conclusion of the offering, the remote sites sends all receipts, rosters, and evaluations
to the host site. The host site is then responsible for issuing continuing education certificates.
II. Remote site asks to join the host site
The remote site is responsible for making technical arrangements to join the program,
secures from the host site all information to maintain their CNE files, and accepts
responsibility for all costs at the remote site. The remote site also maintains their own
rosters, evaluations, and issues their own continuing education certificates. The speaker
honorarium is usually shared by each site.
Computer Assisted Instruction (CAI)
CAI may be provided for continuing nursing education and is considered to be interactive, therefore all thirty
(30) contact hours for relicensure can be obtained through this modality.
There are numerous companies with computer programs appropriate for CNE. Many of the programs already
have continuing education approval through various nursing organizations such as ANA, AJN, AACN, or a
KSBN provider can approve these through their providership.
The cost of each program may vary from $250 to $800.
Determining Contact Hours
To determine how many contact hours to award to the program, several nurses should complete the program
and record the length of time it took for each nurse to complete the activities. The number of hours to award to
the program would be an average of those times.
Verification of Completion
Most programs do have a post test included with a predetermined passing score needed for successful comple-
tion. Some of the programs allow the test results to be printed and some do not. For those that do not allow
the results to be printed, an educator must be contracted to come and verify the results once the nurse has com-
pleted the program.
Advantages
* Allows the nurse to complete all thirty (30) contact hours at their own pace and at times convenient for
their own personal schedules plus choose topics of personal interest.
Disadvantages
* Users may not be familiar with computers, thus requiring someone to be available to assist with using the
computer.
* A contact person must always be available during business hours for questions and technical problems.
* Nurses waiting until the last minute to obtain CNE for relicensure may not be able to receive the certifi-
cate the day they complete the program since verification of successful completion must be obtained.
Page 44
Kansas Healthcare Education Council
Policies and Procedures
I. Required for Long Term Providers of CNE (KAR 60-9-105, 60-5-107)
A. Registration
1. Roster
Example: The attendance roster will be identical to the KSBN sample roster and will be type
written. The roster shall identify the provider’s name, address, phone number, provider
number, the course title, the CNE. The list of names will be alphabetized and will include the
license numbers of the participants.
2. Sign in process
Example: Participants must sign in at the beginning of each offering with their name exactly
as it appears on their nursing license. The sign in process is monitored by registration staff.
Each registrant is asked to verify personal information on the roster. Sign in sheets are col-
lected within fifteen (15) minutes of the start of the offering. At no time are sign in sheets left
unattended in a public place.
B. Attendance
1. Late arrival/early departure
Example: An offering shall consist of a minimum of 30 minutes (0.6 hours). Fractions of
hours over 30 minutes may be given with the approval of the Education Supervisor based on
0.1 contact hours for every 5 minutes of presentation time. Participants can be no more than
15 minutes late to a continuing education offering and must attend the entire offering to
receive contact hour credit. Exception: participants must attend the entire time for offerings
of one contact hour or less. The coordinator has the right/responsibility to deny or reduce
credit hours awarded if the participant arrives late or leaves prior to the completion of the
offering.
2. Partial Credit
Example: Partial credit may be granted with the approval of the coordinator for participants
arriving late or leaving early due to emergency situations. Partial credit may also be awarded
in the event a program-in-progress must be canceled suddenly due to unexpected circum-
stances (i.e. blizzard) or for attendance during one day of a two day offering.
C. Certificates
Example: Certificates of attendance will be awarded to participants after completion of a
continuing education offering. The certificate will contain:
* provider’s name, address, and provider number
* title of the course
* date(s) of attendance
* number of CNE contact hours awarded
Page 45
Kansas Healthcare Education Council
* signature of the individual responsible for CNE
* name, address, and license number of the participant
* type of credit awarded if applicable (instructor, independent study)
D. Offering Announcement
Example: Offering announcements for continuing education will include the following
information:
* title of course offering
* date(s), time(s), and location
* purpose and offering objectives
* agenda
* speaker(s) and credentials
* target audience
* non-discrimination policy statement
* ADA policy statement
* fees
* cancellation/refund policy
* contact hours awarded
* the provider statement and provider number (as per KSBN guidelines)
* provider’s name, number, and address
* sponsorship information
E. Instructor Selection Criteria
Example: Instructors are selected on the basis of their comprehensive knowledge and experi-
ence relevant to the program content, their ability to relate to adult learners, and their commit-
ment to excellence in presentation style. For non-nurse presenters, degree and/or experience
in an allied field is required (education, psychology, social work, nursing home administra-
tion, business, law, etc.) Non-nurse presenters must show evidence of tailoring their
presentations to nursing issues and health-care settings.
F. Records
1. Location of Files
Example: All continuing nursing education files are maintained in a secure manner in the
CNE Department.
2. System of Record Keeping
Page 46
Kansas Healthcare Education Council
Helpful Hint: When a new employee
joins your staff, make sure you document
all the information you might need in the
future including address, phone number,
license number, current certifications, etc.
The information is helpful for Human
Resources and Education.
Example: Records are kept in folders and filed in chronological order by offering date.
Records for the current and past two years are kept in a locked file cabinet.
3. Contents of CNE Files
4. Example: Each individual continuing education offering folder will
contain the following:
* offering announcement
* curriculum vitae for speaker(s)
* evaluations with summaries
* sign in rosters
* attendance roster
* handouts
* bibliography
* agenda
* objectives
* budget information
* correspondence
4. Security Measures Example: Records are kept in a secured manner (locked filing cabinet or
on computer) with only the coordinator and designated others having access to the files.
II. Policies (The following policies and procedures are not only helpful to have in place but may also be re-
quired to KSBN for providership).
A. Restrictions H. Laboratory time ratio in offerings
B. Cancellation I. Contract Services
C. Auditing J. Co-sponsorship
D. Fees* K. Outreach Program
E. Refunds* L. Independent home study courses
F. Insufficient funds and check policy* M. Instructor Credit
G. Audiovisual/audio taping N. Educational Setting
Page 47
*See appendix for sample policy and procedure.
Kansas Healthcare Education Council
Needs Assessment
The assessment of learning needs is the first step in designing an effective learning experience. Using multiple
sources for identifying needs gives more accurate information about needs than does one source. It is also im-
portant to consider the response rate from the method selected. A smaller response rate would require greater
consensus to indicate a need.
Needs Assessment Methods
1. Advisory Groups - A group not to exceed 8-9 people who attend to share ideas in their area of practice
2. Brainstorming - A representative group who are willing to generate ideas without criticism or praise for
their clinical area.
3. Checklists - Readily available data such as orientation checklists which can indicate learning needs.
4. Delphi Technique - A specific strategy to obtain consensus. Questionnaires are sent to a targeted group,
responses are summarized, and a new version of the questionnaire is sent to the same responders for ad-
ditional response.
5. Interviews - An opportunity to share in-depth views, expand on areas of particular concern, and provide
examples to clarify points.
6. Literature Analysis - Keeping current with the literature in various areas of nursing is important to ana-
lyze trends and project learning needs for future programs.
7. Nominal Group Process - A method designed to create consensus through individual ranking of items
and a pooling of scores.
8. Observations - Direct observation of work performance can illicit learning needs.
9. Questionnaires - Most common type of needs assessment. These surveys
focus only on the respondent’s opinion as opposed to their actual knowledge or skill.
10. Rating Scales - A Likert scale commonly has response ranges from 1 to 5,
with 1 representing most or least and 5 representing the other extreme.
11. Records and Report Analysis - Careful analysis of data reports such as quality assurance reports often
reflect institutional need.
12. Services and Institutional Changes - Changes in the existing services of and institution provide indica-
tors for learning needs.
13. Telephone Surveys - Telephone surveys tend to illicit more accurate responses than face-to-face inter-
views.
Page 48
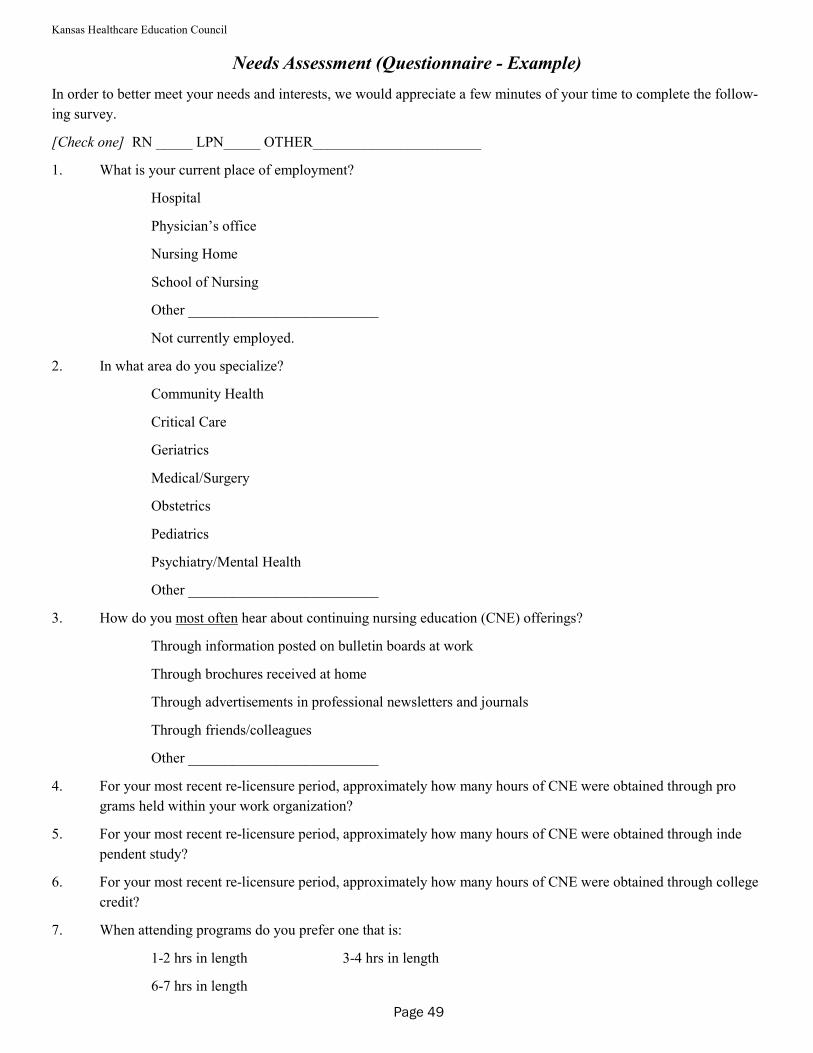
Kansas Healthcare Education Council
Needs Assessment (Questionnaire - Example)
In order to better meet your needs and interests, we would appreciate a few minutes of your time to complete the follow-
ing survey.
[Check one] RN _____ LPN_____ OTHER_______________________
1. What is your current place of employment?
Hospital
Physician’s office
Nursing Home
School of Nursing
Other __________________________
Not currently employed.
2. In what area do you specialize?
Community Health
Critical Care
Geriatrics
Medical/Surgery
Obstetrics
Pediatrics
Psychiatry/Mental Health
Other __________________________
3. How do you most often hear about continuing nursing education (CNE) offerings?
Through information posted on bulletin boards at work
Through brochures received at home
Through advertisements in professional newsletters and journals
Through friends/colleagues
Other __________________________
4. For your most recent re-licensure period, approximately how many hours of CNE were obtained through pro
grams held within your work organization?
5. For your most recent re-licensure period, approximately how many hours of CNE were obtained through inde
pendent study?
6. For your most recent re-licensure period, approximately how many hours of CNE were obtained through college
credit?
7. When attending programs do you prefer one that is:
1-2 hrs in length 3-4 hrs in length
6-7 hrs in length
Page 49
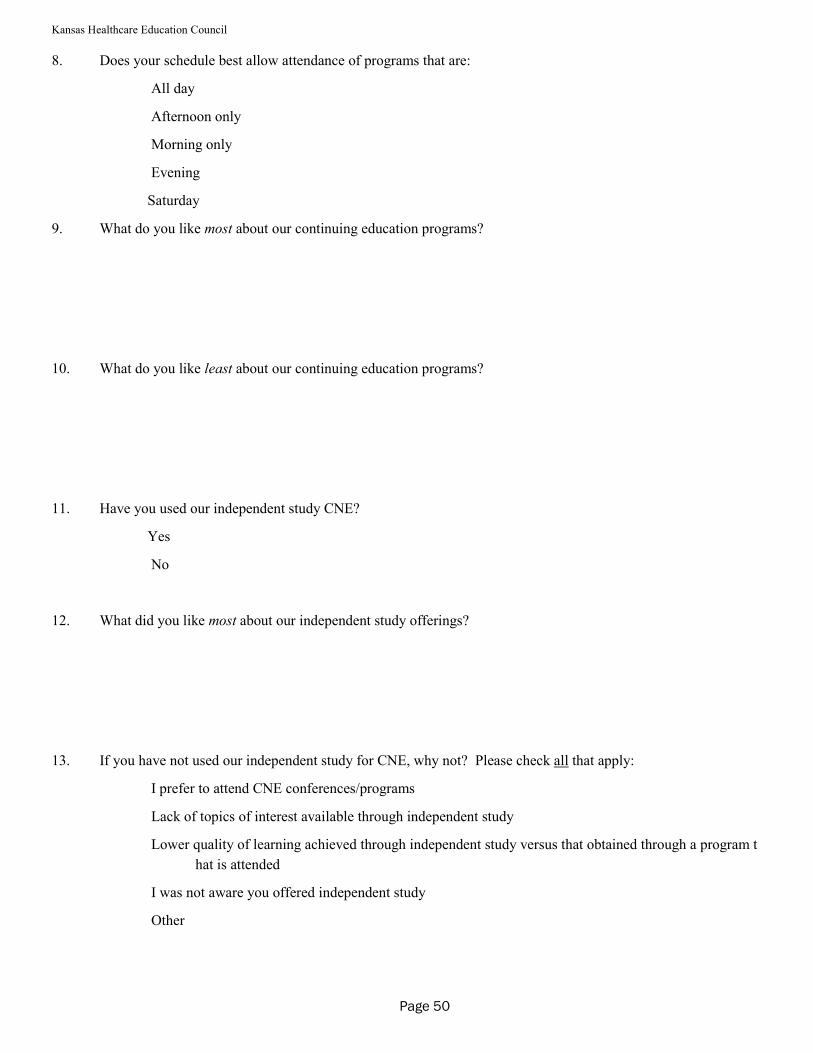
Kansas Healthcare Education Council
8. Does your schedule best allow attendance of programs that are:
All day
Afternoon only
Morning only
Evening
Saturday
9. What do you like most about our continuing education programs?
10. What do you like least about our continuing education programs?
11. Have you used our independent study CNE?
Yes
No
12. What did you like most about our independent study offerings?
13. If you have not used our independent study for CNE, why not? Please check all that apply:
I prefer to attend CNE conferences/programs
Lack of topics of interest available through independent study
Lower quality of learning achieved through independent study versus that obtained through a program t
hat is attended
I was not aware you offered independent study
Other
Page 50
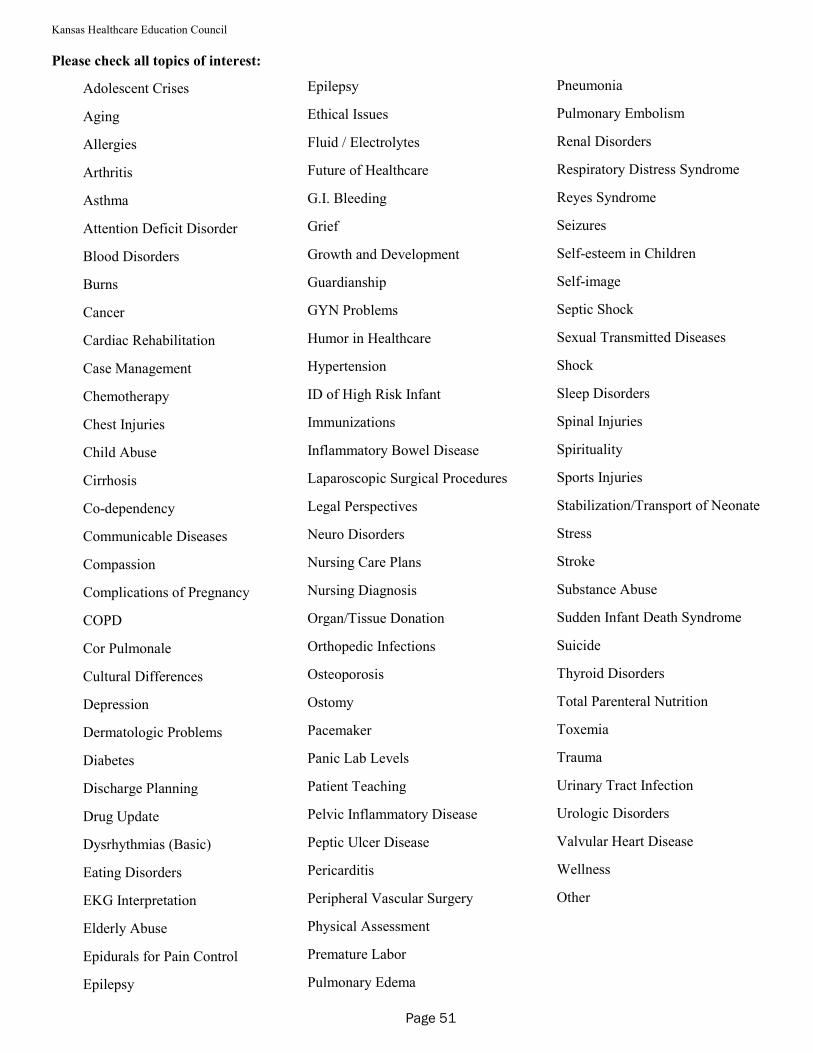
Kansas Healthcare Education Council
Please check all topics of interest:
Adolescent Crises
Aging
Allergies
Arthritis
Asthma
Attention Deficit Disorder
Blood Disorders
Burns
Cancer
Cardiac Rehabilitation
Case Management
Chemotherapy
Chest Injuries
Child Abuse
Cirrhosis
Co-dependency
Communicable Diseases
Compassion
Complications of Pregnancy
COPD
Cor Pulmonale
Cultural Differences
Depression
Dermatologic Problems
Diabetes
Discharge Planning
Drug Update
Dysrhythmias (Basic)
Eating Disorders
EKG Interpretation
Elderly Abuse
Epidurals for Pain Control
Epilepsy
Epilepsy
Ethical Issues
Fluid / Electrolytes
Future of Healthcare
G.I. Bleeding
Grief
Growth and Development
Guardianship
GYN Problems
Humor in Healthcare
Hypertension
ID of High Risk Infant
Immunizations
Inflammatory Bowel Disease
Laparoscopic Surgical Procedures
Legal Perspectives
Neuro Disorders
Nursing Care Plans
Nursing Diagnosis
Organ/Tissue Donation
Orthopedic Infections
Osteoporosis
Ostomy
Pacemaker
Panic Lab Levels
Patient Teaching
Pelvic Inflammatory Disease
Peptic Ulcer Disease
Pericarditis
Peripheral Vascular Surgery
Physical Assessment
Premature Labor
Pulmonary Edema
Pneumonia
Pulmonary Embolism
Renal Disorders
Respiratory Distress Syndrome
Reyes Syndrome
Seizures
Self-esteem in Children
Self-image
Septic Shock
Sexual Transmitted Diseases
Shock
Sleep Disorders
Spinal Injuries
Spirituality
Sports Injuries
Stabilization/Transport of Neonate
Stress
Stroke
Substance Abuse
Sudden Infant Death Syndrome
Suicide
Thyroid Disorders
Total Parenteral Nutrition
Toxemia
Trauma
Urinary Tract Infection
Urologic Disorders
Valvular Heart Disease
Wellness
Other
Page 51
Kansas Healthcare Education Council
Total Program Evaluation
The total program evaluation plan should provide a systematic process for collecting and analyzing the data
needed to determine if the providership is doing the right thing and doing the right thing well. The plan identi-
fies and describes all components of the plan used to evaluate the overall performance of the CNE provider-
ship.
What is to be Evaluated
The total program evaluation plan must evaluate the entire program:
* Program Administration
Organizational chart
Philosophy, goals, and objectives
Program coordinator job description
Advisory Committee
*Program Management
Policies and procedures
Needs assessment process
Offerings
*Total Program Evaluation Plan
Evaluate the plan itself - the ability of the plan to measure overall performance (i.e. effectiveness, appropri-
ateness, efficiency, etc.) of the CNE providership.
This is not an evaluation of individual educational offerings.
When is the evaluation done
The total program evaluation is done at least annually and is reported in the annual report to the KSBN.
How is the evaluation done
The plan may be presented as a narrative, as a chart, as a matrix, or in any format appropriate for the provider-
ship.
Page 52
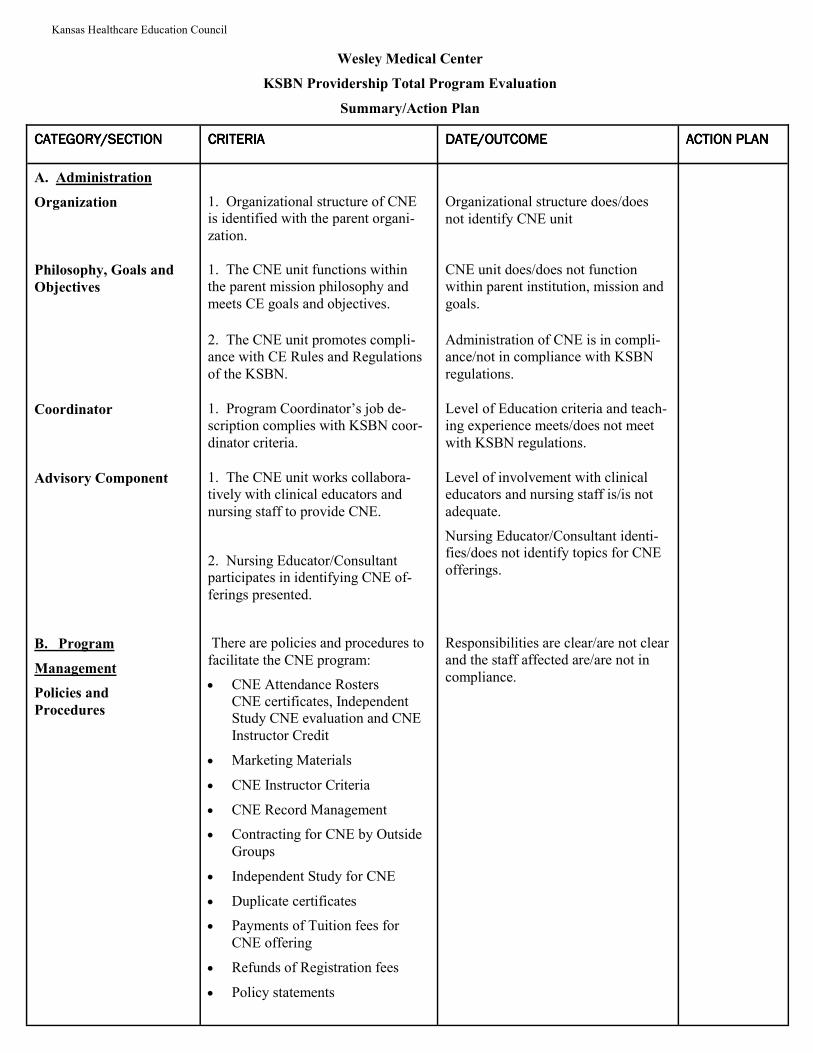
Kansas Healthcare Education Council
Wesley Medical Center
KSBN Providership Total Program Evaluation
Summary/Action Plan
CATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTION CRITERIACRITERIACRITERIACRITERIA DATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOME ACTION PLANACTION PLANACTION PLANACTION PLAN
A. Administration
Organization
1. Organizational structure of CNE is identified with the parent organi-
zation.
Organizational structure does/does
not identify CNE unit
Philosophy, Goals and
Objectives
1. The CNE unit functions within the parent mission philosophy and
meets CE goals and objectives.
CNE unit does/does not function within parent institution, mission and
goals.
2. The CNE unit promotes compli-ance with CE Rules and Regulations
of the KSBN.
Administration of CNE is in compli-ance/not in compliance with KSBN
regulations.
Coordinator
1. Program Coordinator’s job de-scription complies with KSBN coor-
dinator criteria.
Level of Education criteria and teach-ing experience meets/does not meet
with KSBN regulations.
Advisory Component 1. The CNE unit works collabora-tively with clinical educators and
nursing staff to provide CNE.
2. Nursing Educator/Consultant participates in identifying CNE of-
ferings presented.
Level of involvement with clinical educators and nursing staff is/is not
adequate.
Nursing Educator/Consultant identi-fies/does not identify topics for CNE
offerings.
B. Program
Management
Policies and
Procedures
There are policies and procedures to
facilitate the CNE program:
• CNE Attendance Rosters CNE certificates, Independent Study CNE evaluation and CNE
Instructor Credit
• Marketing Materials
• CNE Instructor Criteria
• CNE Record Management
• Contracting for CNE by Outside
Groups
• Independent Study for CNE
• Duplicate certificates
• Payments of Tuition fees for
CNE offering
• Refunds of Registration fees
• Policy statements
Responsibilities are clear/are not clear and the staff affected are/are not in
compliance.
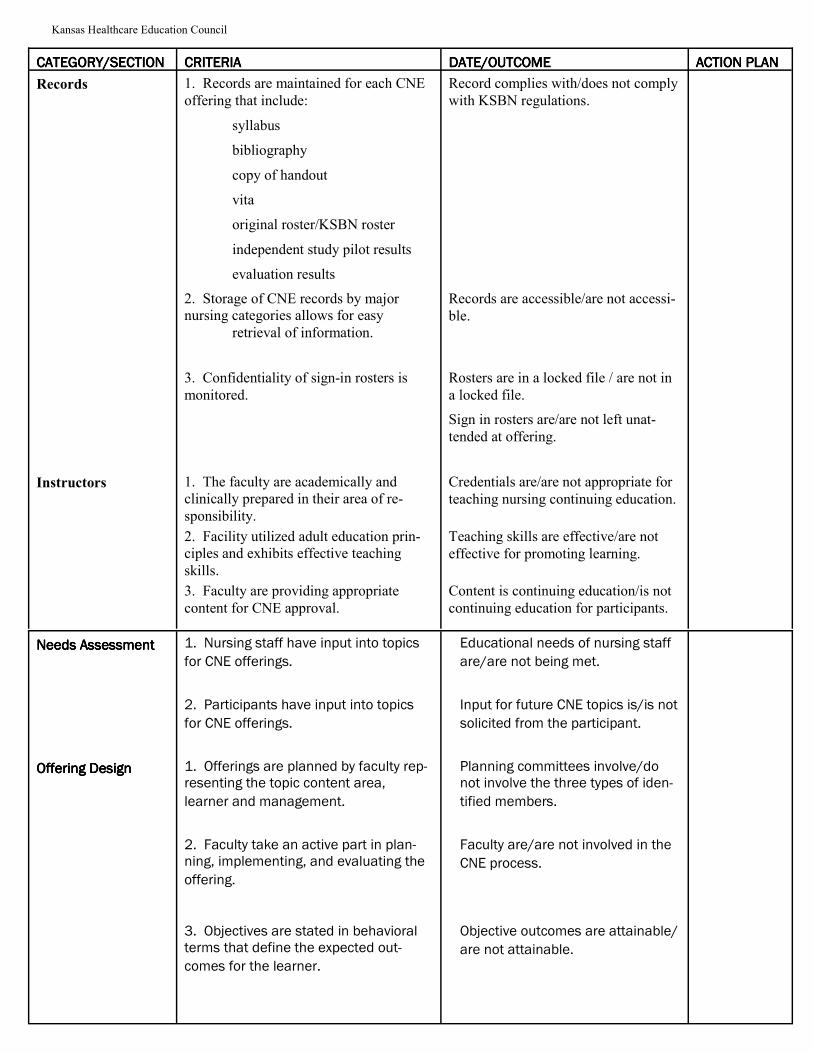
Kansas Healthcare Education Council
CATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTION CRITERIACRITERIACRITERIACRITERIA DATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOME ACTION PLANACTION PLANACTION PLANACTION PLAN
Records
1. Records are maintained for each CNE
offering that include:
syllabus
bibliography
copy of handout
vita
original roster/KSBN roster
independent study pilot results
evaluation results
2. Storage of CNE records by major nursing categories allows for easy
retrieval of information.
Record complies with/does not comply
with KSBN regulations.
Records are accessible/are not accessi-
ble.
3. Confidentiality of sign-in rosters is
monitored.
Rosters are in a locked file / are not in
a locked file.
Sign in rosters are/are not left unat-
tended at offering.
Instructors
1. The faculty are academically and clinically prepared in their area of re-
sponsibility.
Credentials are/are not appropriate for
teaching nursing continuing education.
2. Facility utilized adult education prin-ciples and exhibits effective teaching
skills.
Teaching skills are effective/are not
effective for promoting learning.
3. Faculty are providing appropriate
content for CNE approval.
Content is continuing education/is not
continuing education for participants.
Needs AssessmentNeeds AssessmentNeeds AssessmentNeeds Assessment 1. Nursing staff have input into topics
for CNE offerings.
Educational needs of nursing staff
are/are not being met.
2. Participants have input into topics
for CNE offerings.
Input for future CNE topics is/is not
solicited from the participant.
Offering DesignOffering DesignOffering DesignOffering Design
1. Offerings are planned by faculty rep-resenting the topic content area,
learner and management.
Planning committees involve/do not involve the three types of iden-
tified members.
2. Faculty take an active part in plan-ning, implementing, and evaluating the
offering.
Faculty are/are not involved in the
CNE process.
3. Objectives are stated in behavioral terms that define the expected out-
comes for the learner.
Objective outcomes are attainable/
are not attainable.
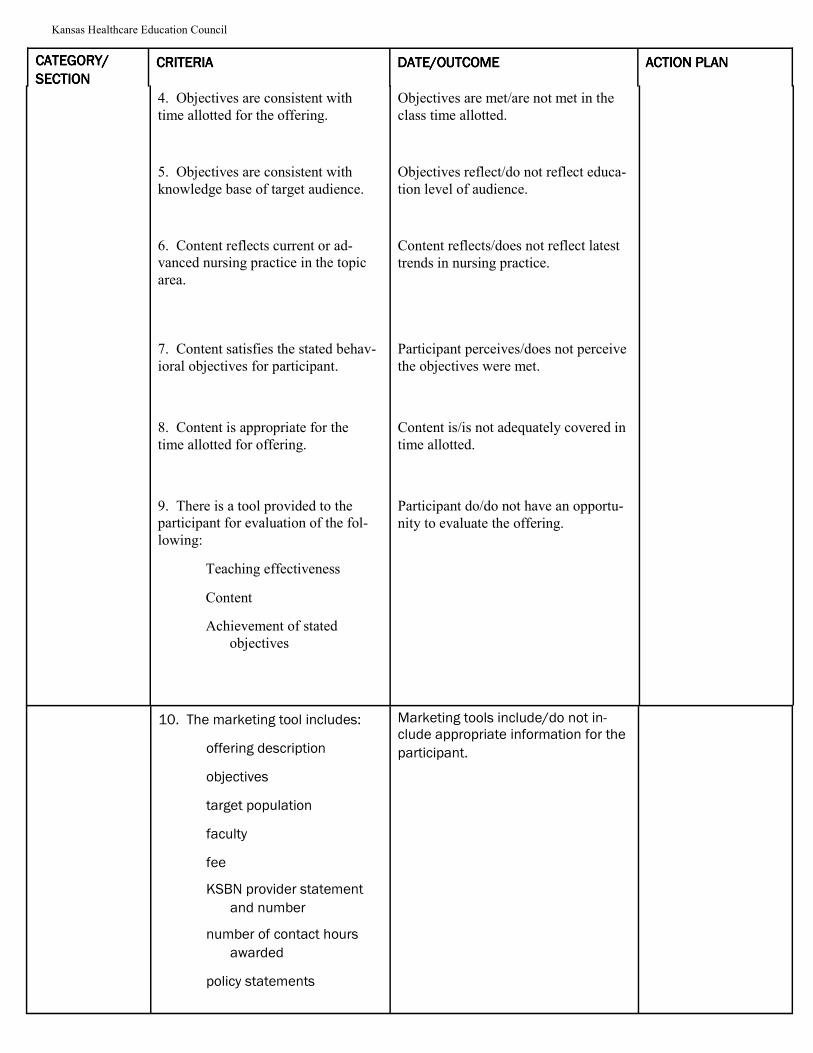
Kansas Healthcare Education Council
CATEGORY/CATEGORY/CATEGORY/CATEGORY/
SECTIONSECTIONSECTIONSECTION CRITERIACRITERIACRITERIACRITERIA DATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOME ACTION PLANACTION PLANACTION PLANACTION PLAN
4. Objectives are consistent with
time allotted for the offering.
Objectives are met/are not met in the
class time allotted.
5. Objectives are consistent with
knowledge base of target audience.
Objectives reflect/do not reflect educa-
tion level of audience.
6. Content reflects current or ad-vanced nursing practice in the topic
area.
Content reflects/does not reflect latest
trends in nursing practice.
7. Content satisfies the stated behav-
ioral objectives for participant.
Participant perceives/does not perceive
the objectives were met.
8. Content is appropriate for the
time allotted for offering.
Content is/is not adequately covered in
time allotted.
9. There is a tool provided to the participant for evaluation of the fol-
lowing:
Teaching effectiveness
Content
Achievement of stated
objectives
Participant do/do not have an opportu-
nity to evaluate the offering.
10. The marketing tool includes:
offering description
objectives
target population
faculty
fee
KSBN provider statement
and number
number of contact hours
awarded
policy statements
Marketing tools include/do not in-clude appropriate information for the
participant.
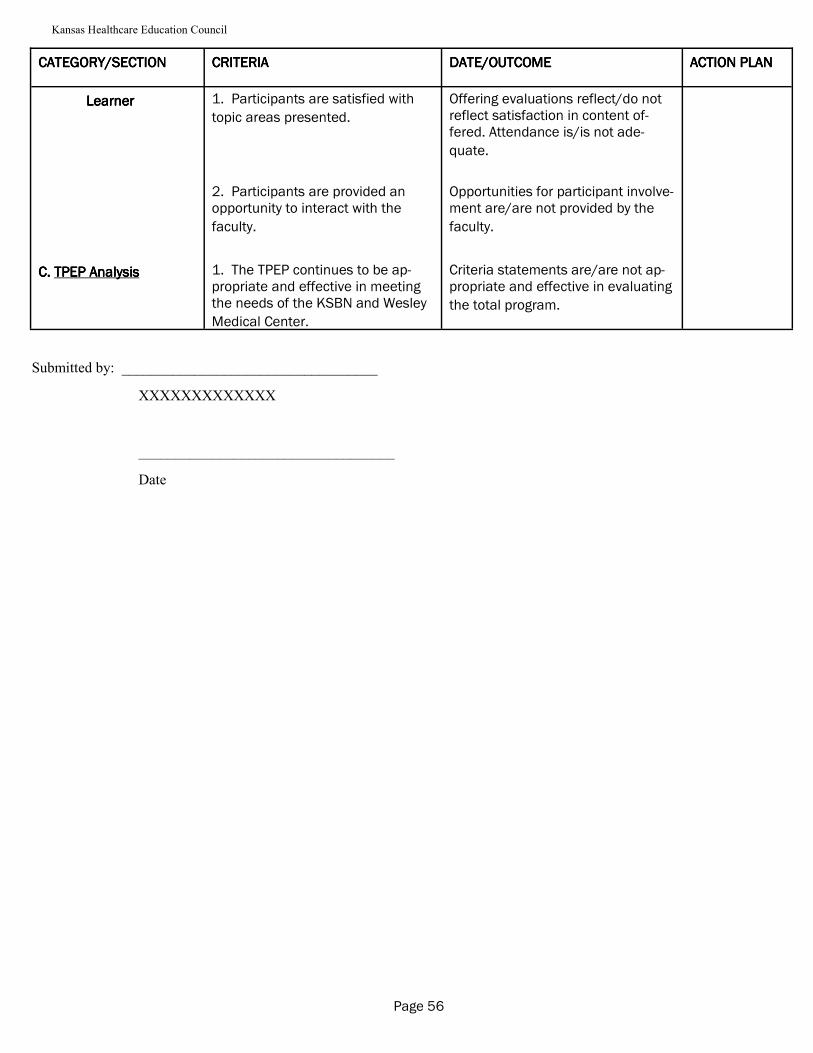
Kansas Healthcare Education Council
CATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTIONCATEGORY/SECTION CRITERIACRITERIACRITERIACRITERIA DATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOMEDATE/OUTCOME ACTION PLANACTION PLANACTION PLANACTION PLAN
LearnerLearnerLearnerLearner 1. Participants are satisfied with
topic areas presented.
Offering evaluations reflect/do not reflect satisfaction in content of-fered. Attendance is/is not ade-
quate.
2. Participants are provided an opportunity to interact with the
faculty.
Opportunities for participant involve-ment are/are not provided by the
faculty.
C. C. C. C. TPEP AnalysisTPEP AnalysisTPEP AnalysisTPEP Analysis 1. The TPEP continues to be ap-propriate and effective in meeting the needs of the KSBN and Wesley
Medical Center.
Criteria statements are/are not ap-propriate and effective in evaluating
the total program.
Submitted by: ___________________________________
XXXXXXXXXXXXX
___________________________________
Date
Page 56
Kansas Healthcare Education Council
PROGRAM EVALUATION
Dwight D. Eisenhower VA Medical Center
Continuing Nursing Education Provider Program
This Total Program Evaluation Plan was adapted from the Dimensions of Performance as described by the
Joint Commission on the Accreditation of Health Care Organizations. The plan is designed to answer the
questions:
Are we doing the right thing?
Efficacy
Appropriateness
Are we doing the right thing well?
Availability
Timeliness
Effectiveness
Continuity
Safety
Efficiency
Respect and Caring
During the first year of using this plan, review the program administration, program management, and total
program evaluation using a 1-5 scale to determine the degree of efficacy, appropriateness, availability, timeli-
ness, effectiveness, continuity, safety, efficiency, and respect and caring (5=no room for improvement,
4=exceeding standard, 3=meeting standard, 2=less than acceptable, 1= not acceptable, 0=not being done at
all).
In subsequent year, review the program administration, program management, and total program evaluation
using a “Rating of Change Scale” such as: +5=very much better, +4=much better, +3=moderately better, +2=a
little better, +1=almost the same, hardly any better at all, 0=no change, -1=almost the same, hardly any worse,
-2=a little worse, -3=moderately worse, -4=much worse, -5=very much worse.
Page 57
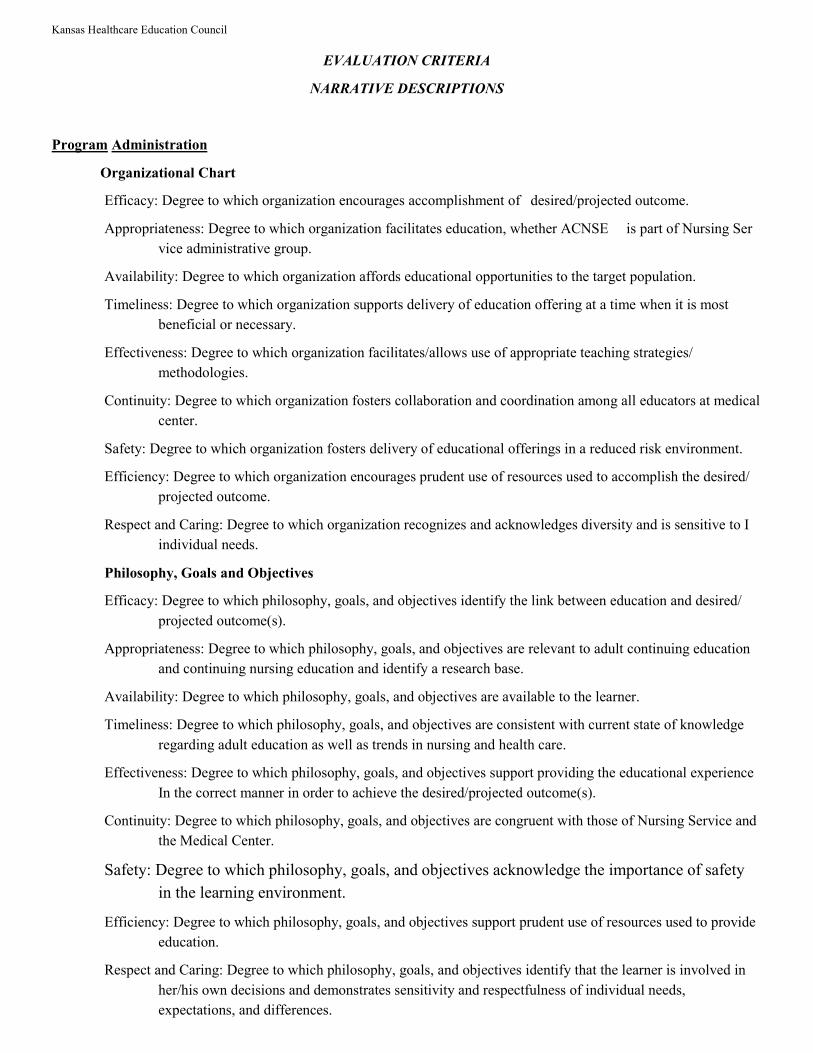
Kansas Healthcare Education Council
EVALUATION CRITERIA
NARRATIVE DESCRIPTIONS
Program Administration
Organizational Chart
Efficacy: Degree to which organization encourages accomplishment of desired/projected outcome.
Appropriateness: Degree to which organization facilitates education, whether ACNSE is part of Nursing Ser
vice administrative group.
Availability: Degree to which organization affords educational opportunities to the target population.
Timeliness: Degree to which organization supports delivery of education offering at a time when it is most
beneficial or necessary.
Effectiveness: Degree to which organization facilitates/allows use of appropriate teaching strategies/
methodologies.
Continuity: Degree to which organization fosters collaboration and coordination among all educators at medical
center.
Safety: Degree to which organization fosters delivery of educational offerings in a reduced risk environment.
Efficiency: Degree to which organization encourages prudent use of resources used to accomplish the desired/
projected outcome.
Respect and Caring: Degree to which organization recognizes and acknowledges diversity and is sensitive to I
individual needs.
Philosophy, Goals and Objectives
Efficacy: Degree to which philosophy, goals, and objectives identify the link between education and desired/
projected outcome(s).
Appropriateness: Degree to which philosophy, goals, and objectives are relevant to adult continuing education
and continuing nursing education and identify a research base.
Availability: Degree to which philosophy, goals, and objectives are available to the learner.
Timeliness: Degree to which philosophy, goals, and objectives are consistent with current state of knowledge
regarding adult education as well as trends in nursing and health care.
Effectiveness: Degree to which philosophy, goals, and objectives support providing the educational experience
In the correct manner in order to achieve the desired/projected outcome(s).
Continuity: Degree to which philosophy, goals, and objectives are congruent with those of Nursing Service and
the Medical Center.
Safety: Degree to which philosophy, goals, and objectives acknowledge the importance of safety
in the learning environment.
Efficiency: Degree to which philosophy, goals, and objectives support prudent use of resources used to provide
education.
Respect and Caring: Degree to which philosophy, goals, and objectives identify that the learner is involved in
her/his own decisions and demonstrates sensitivity and respectfulness of individual needs,
expectations, and differences.
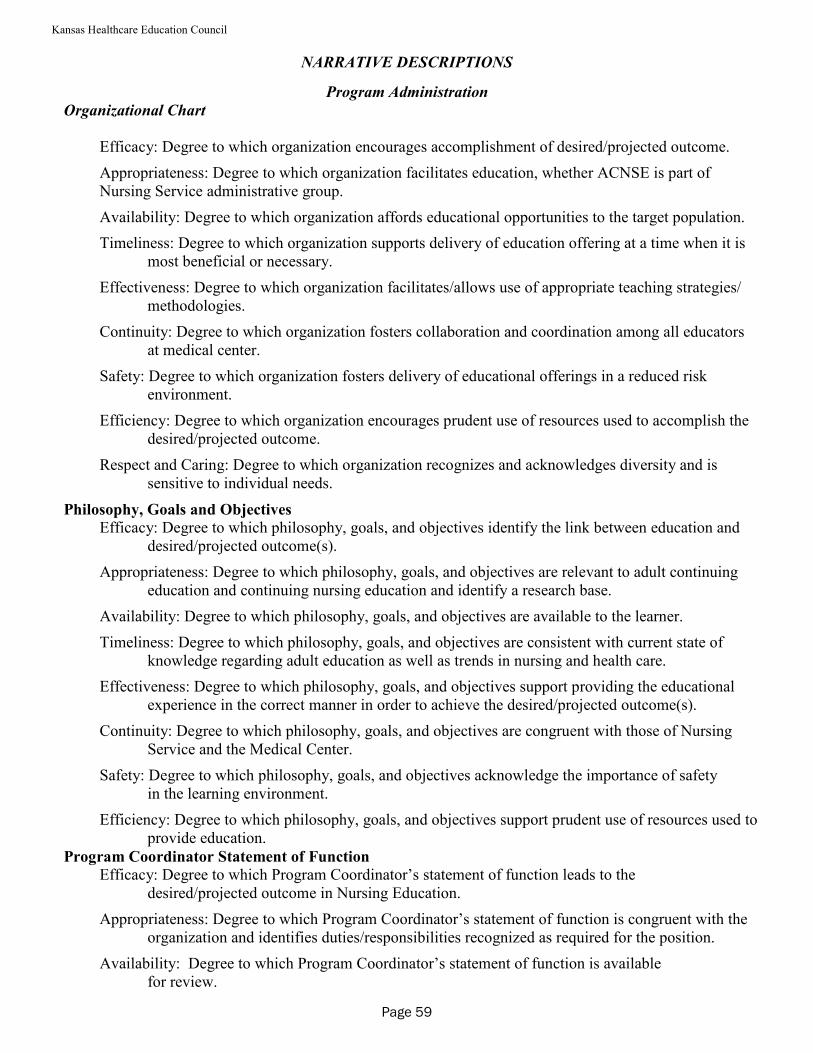
Kansas Healthcare Education Council
NARRATIVE DESCRIPTIONS
Program Administration
Organizational Chart
Efficacy: Degree to which organization encourages accomplishment of desired/projected outcome.
Appropriateness: Degree to which organization facilitates education, whether ACNSE is part of Nursing Service administrative group.
Availability: Degree to which organization affords educational opportunities to the target population.
Timeliness: Degree to which organization supports delivery of education offering at a time when it is most beneficial or necessary.
Effectiveness: Degree to which organization facilitates/allows use of appropriate teaching strategies/ methodologies.
Continuity: Degree to which organization fosters collaboration and coordination among all educators at medical center.
Safety: Degree to which organization fosters delivery of educational offerings in a reduced risk environment.
Efficiency: Degree to which organization encourages prudent use of resources used to accomplish the desired/projected outcome.
Respect and Caring: Degree to which organization recognizes and acknowledges diversity and is sensitive to individual needs.
Philosophy, Goals and Objectives
Efficacy: Degree to which philosophy, goals, and objectives identify the link between education and desired/projected outcome(s).
Appropriateness: Degree to which philosophy, goals, and objectives are relevant to adult continuing education and continuing nursing education and identify a research base.
Availability: Degree to which philosophy, goals, and objectives are available to the learner.
Timeliness: Degree to which philosophy, goals, and objectives are consistent with current state of knowledge regarding adult education as well as trends in nursing and health care.
Effectiveness: Degree to which philosophy, goals, and objectives support providing the educational experience in the correct manner in order to achieve the desired/projected outcome(s).
Continuity: Degree to which philosophy, goals, and objectives are congruent with those of Nursing Service and the Medical Center.
Safety: Degree to which philosophy, goals, and objectives acknowledge the importance of safety in the learning environment.
Efficiency: Degree to which philosophy, goals, and objectives support prudent use of resources used to provide education.
Program Coordinator Statement of Function
Efficacy: Degree to which Program Coordinator’s statement of function leads to the desired/projected outcome in Nursing Education.
Appropriateness: Degree to which Program Coordinator’s statement of function is congruent with the organization and identifies duties/responsibilities recognized as required for the position.
Availability: Degree to which Program Coordinator’s statement of function is available for review.
Page 59
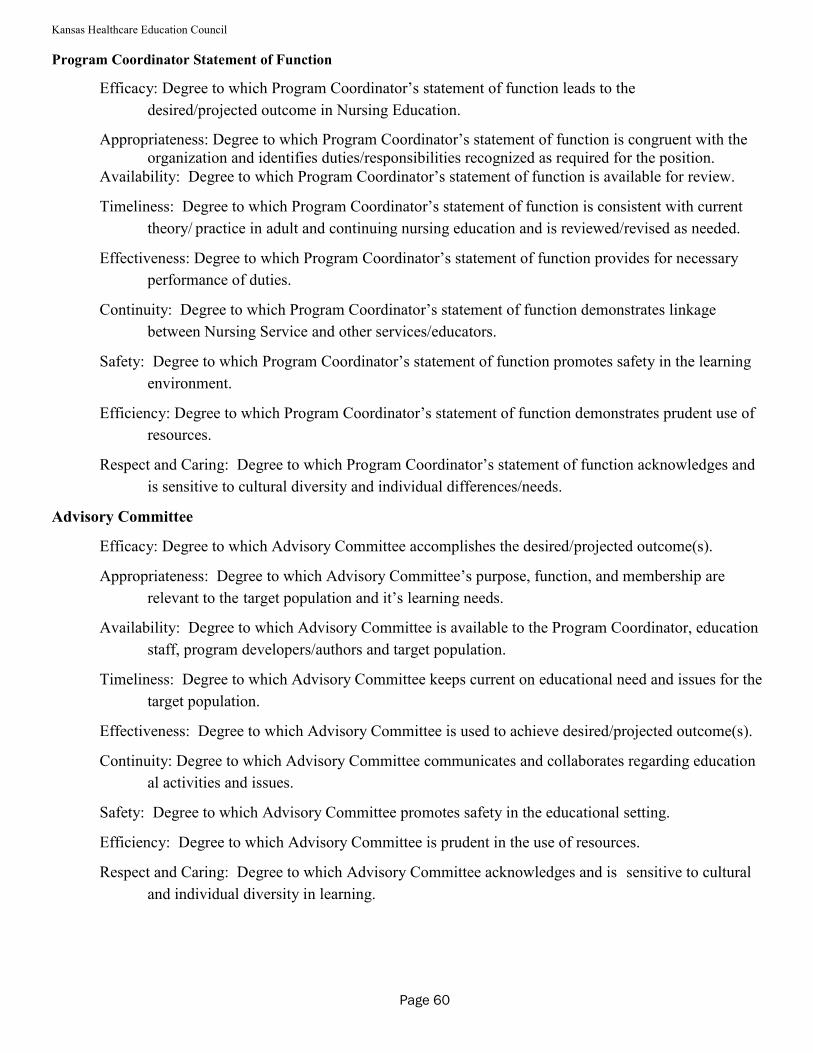
Kansas Healthcare Education Council
Program Coordinator Statement of Function
Efficacy: Degree to which Program Coordinator’s statement of function leads to the
desired/projected outcome in Nursing Education.
Appropriateness: Degree to which Program Coordinator’s statement of function is congruent with the organization and identifies duties/responsibilities recognized as required for the position.
Availability: Degree to which Program Coordinator’s statement of function is available for review.
Timeliness: Degree to which Program Coordinator’s statement of function is consistent with current
theory/ practice in adult and continuing nursing education and is reviewed/revised as needed.
Effectiveness: Degree to which Program Coordinator’s statement of function provides for necessary
performance of duties.
Continuity: Degree to which Program Coordinator’s statement of function demonstrates linkage
between Nursing Service and other services/educators.
Safety: Degree to which Program Coordinator’s statement of function promotes safety in the learning
environment.
Efficiency: Degree to which Program Coordinator’s statement of function demonstrates prudent use of
resources.
Respect and Caring: Degree to which Program Coordinator’s statement of function acknowledges and
is sensitive to cultural diversity and individual differences/needs.
Advisory Committee
Efficacy: Degree to which Advisory Committee accomplishes the desired/projected outcome(s).
Appropriateness: Degree to which Advisory Committee’s purpose, function, and membership are
relevant to the target population and it’s learning needs.
Availability: Degree to which Advisory Committee is available to the Program Coordinator, education
staff, program developers/authors and target population.
Timeliness: Degree to which Advisory Committee keeps current on educational need and issues for the
target population.
Effectiveness: Degree to which Advisory Committee is used to achieve desired/projected outcome(s).
Continuity: Degree to which Advisory Committee communicates and collaborates regarding education
al activities and issues.
Safety: Degree to which Advisory Committee promotes safety in the educational setting.
Efficiency: Degree to which Advisory Committee is prudent in the use of resources.
Respect and Caring: Degree to which Advisory Committee acknowledges and is sensitive to cultural
and individual diversity in learning.
Page 60
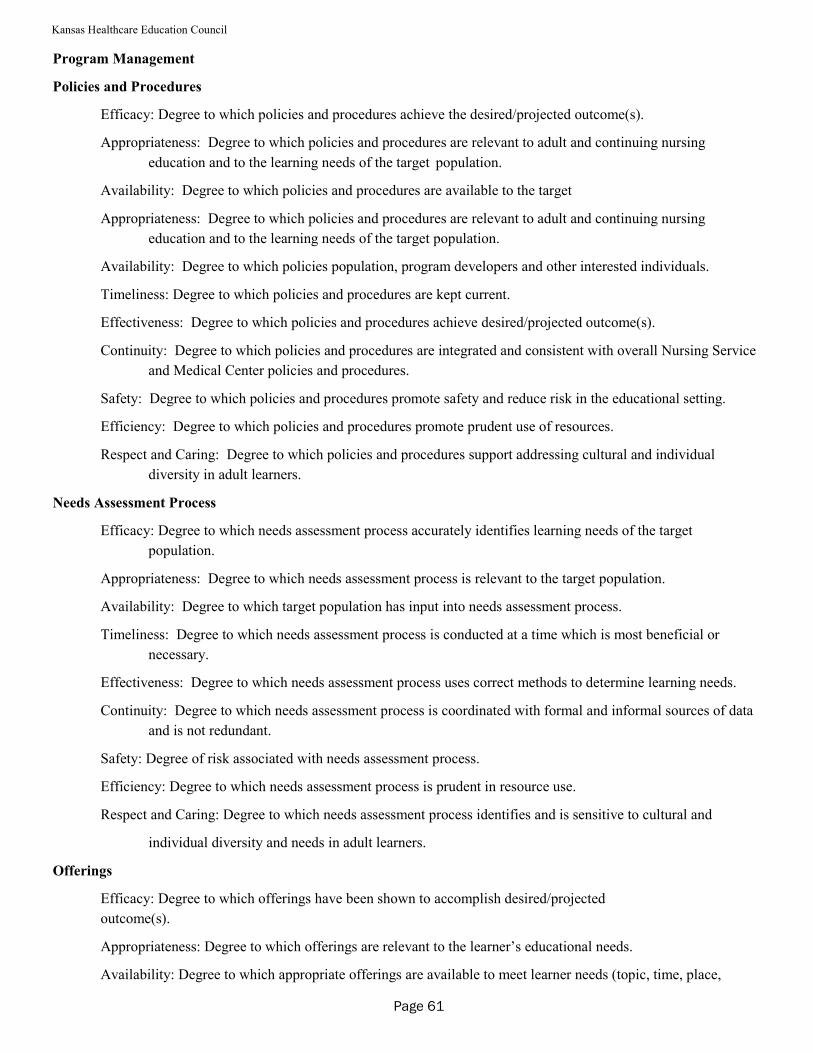
Kansas Healthcare Education Council
Program Management
Policies and Procedures
Efficacy: Degree to which policies and procedures achieve the desired/projected outcome(s).
Appropriateness: Degree to which policies and procedures are relevant to adult and continuing nursing
education and to the learning needs of the target population.
Availability: Degree to which policies and procedures are available to the target
Appropriateness: Degree to which policies and procedures are relevant to adult and continuing nursing
education and to the learning needs of the target population.
Availability: Degree to which policies population, program developers and other interested individuals.
Timeliness: Degree to which policies and procedures are kept current.
Effectiveness: Degree to which policies and procedures achieve desired/projected outcome(s).
Continuity: Degree to which policies and procedures are integrated and consistent with overall Nursing Service
and Medical Center policies and procedures.
Safety: Degree to which policies and procedures promote safety and reduce risk in the educational setting.
Efficiency: Degree to which policies and procedures promote prudent use of resources.
Respect and Caring: Degree to which policies and procedures support addressing cultural and individual
diversity in adult learners.
Needs Assessment Process
Efficacy: Degree to which needs assessment process accurately identifies learning needs of the target
population.
Appropriateness: Degree to which needs assessment process is relevant to the target population.
Availability: Degree to which target population has input into needs assessment process.
Timeliness: Degree to which needs assessment process is conducted at a time which is most beneficial or
necessary.
Effectiveness: Degree to which needs assessment process uses correct methods to determine learning needs.
Continuity: Degree to which needs assessment process is coordinated with formal and informal sources of data
and is not redundant.
Safety: Degree of risk associated with needs assessment process.
Efficiency: Degree to which needs assessment process is prudent in resource use.
Respect and Caring: Degree to which needs assessment process identifies and is sensitive to cultural and
individual diversity and needs in adult learners.
Offerings
Efficacy: Degree to which offerings have been shown to accomplish desired/projected
outcome(s).
Appropriateness: Degree to which offerings are relevant to the learner’s educational needs.
Availability: Degree to which appropriate offerings are available to meet learner needs (topic, time, place,
Page 61
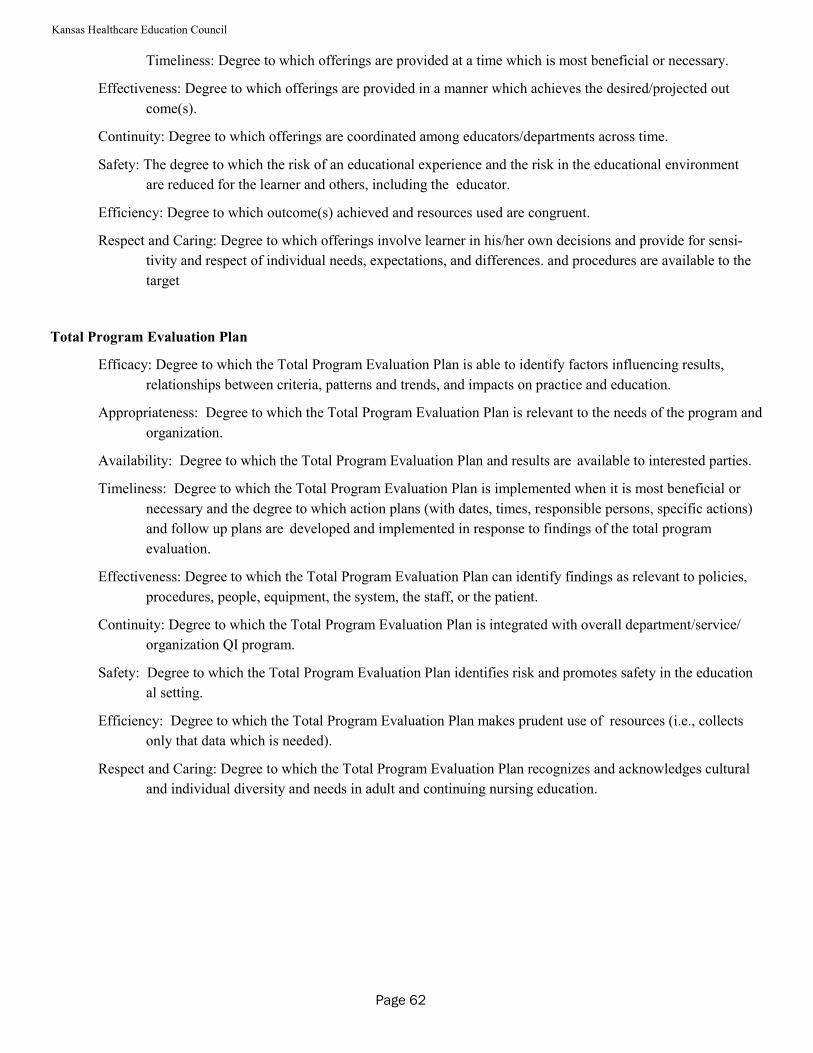
Kansas Healthcare Education Council
Timeliness: Degree to which offerings are provided at a time which is most beneficial or necessary.
Effectiveness: Degree to which offerings are provided in a manner which achieves the desired/projected out
come(s).
Continuity: Degree to which offerings are coordinated among educators/departments across time.
Safety: The degree to which the risk of an educational experience and the risk in the educational environment
are reduced for the learner and others, including the educator.
Efficiency: Degree to which outcome(s) achieved and resources used are congruent.
Respect and Caring: Degree to which offerings involve learner in his/her own decisions and provide for sensi-
tivity and respect of individual needs, expectations, and differences. and procedures are available to the
target
Total Program Evaluation Plan
Efficacy: Degree to which the Total Program Evaluation Plan is able to identify factors influencing results,
relationships between criteria, patterns and trends, and impacts on practice and education.
Appropriateness: Degree to which the Total Program Evaluation Plan is relevant to the needs of the program and
organization.
Availability: Degree to which the Total Program Evaluation Plan and results are available to interested parties.
Timeliness: Degree to which the Total Program Evaluation Plan is implemented when it is most beneficial or
necessary and the degree to which action plans (with dates, times, responsible persons, specific actions)
and follow up plans are developed and implemented in response to findings of the total program
evaluation.
Effectiveness: Degree to which the Total Program Evaluation Plan can identify findings as relevant to policies,
procedures, people, equipment, the system, the staff, or the patient.
Continuity: Degree to which the Total Program Evaluation Plan is integrated with overall department/service/
organization QI program.
Safety: Degree to which the Total Program Evaluation Plan identifies risk and promotes safety in the education
al setting.
Efficiency: Degree to which the Total Program Evaluation Plan makes prudent use of resources (i.e., collects
only that data which is needed).
Respect and Caring: Degree to which the Total Program Evaluation Plan recognizes and acknowledges cultural
and individual diversity and needs in adult and continuing nursing education.
Page 62
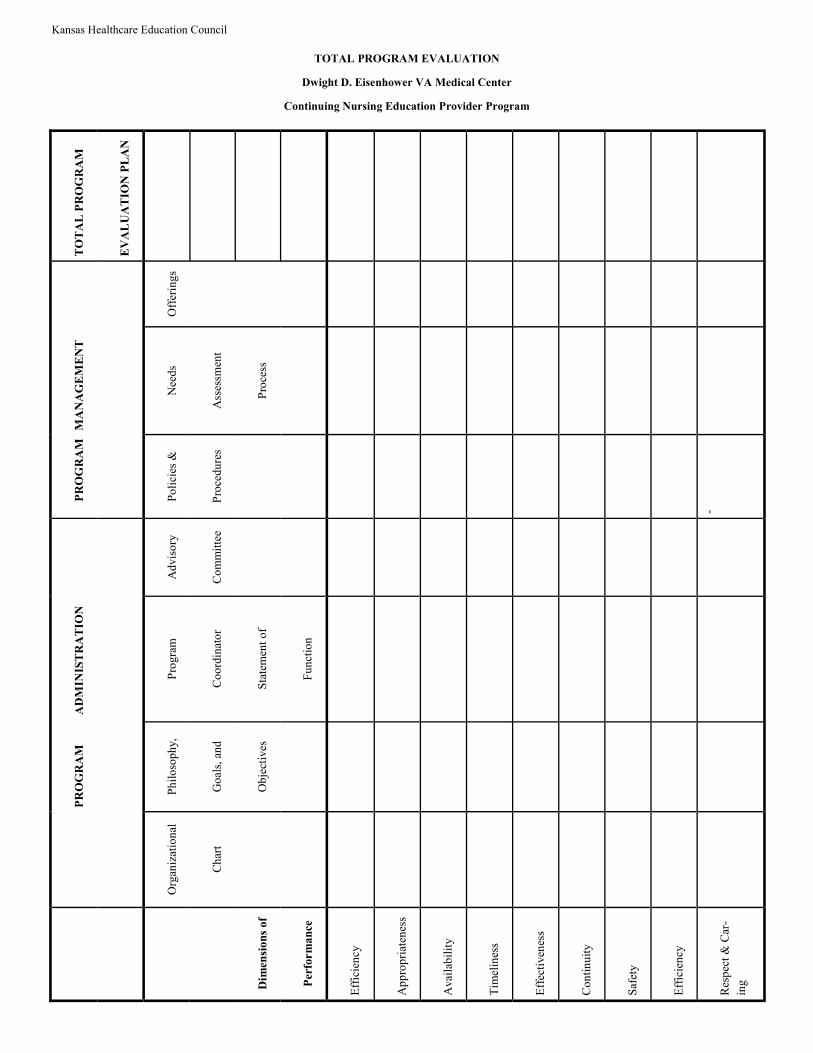
Kansas Healthcare Education Council
TOTAL PROGRAM EVALUATION
Dwight D. Eisenhower VA Medical Center
Continuing Nursing Education Provider Program
PROGRAM
ADMINISTRATION
PROGRAM
MANAGEMENT
TOTAL PROGRAM
EVALUATION PLAN
Org
aniz
atio
nal
Ph
ilo
soph
y,
Pro
gra
m
Ad
vis
ory
Po
lici
es &
Nee
ds
Off
erin
gs
Ch
art
Go
als,
an
d
Co
ord
inat
or
Co
mm
itte
e
Pro
ced
ure
s
Ass
essm
ent
Dimensions of
Ob
ject
ives
Sta
tem
ent
of
Pro
cess
Performance
Fu
nct
ion
Eff
icie
ncy
Ap
pro
pri
aten
ess
Avai
lab
ilit
y
Tim
elin
ess
Eff
ecti
ven
ess
Co
nti
nu
ity
Saf
ety
Eff
icie
ncy
Res
pec
t &
Car
-
ing
-
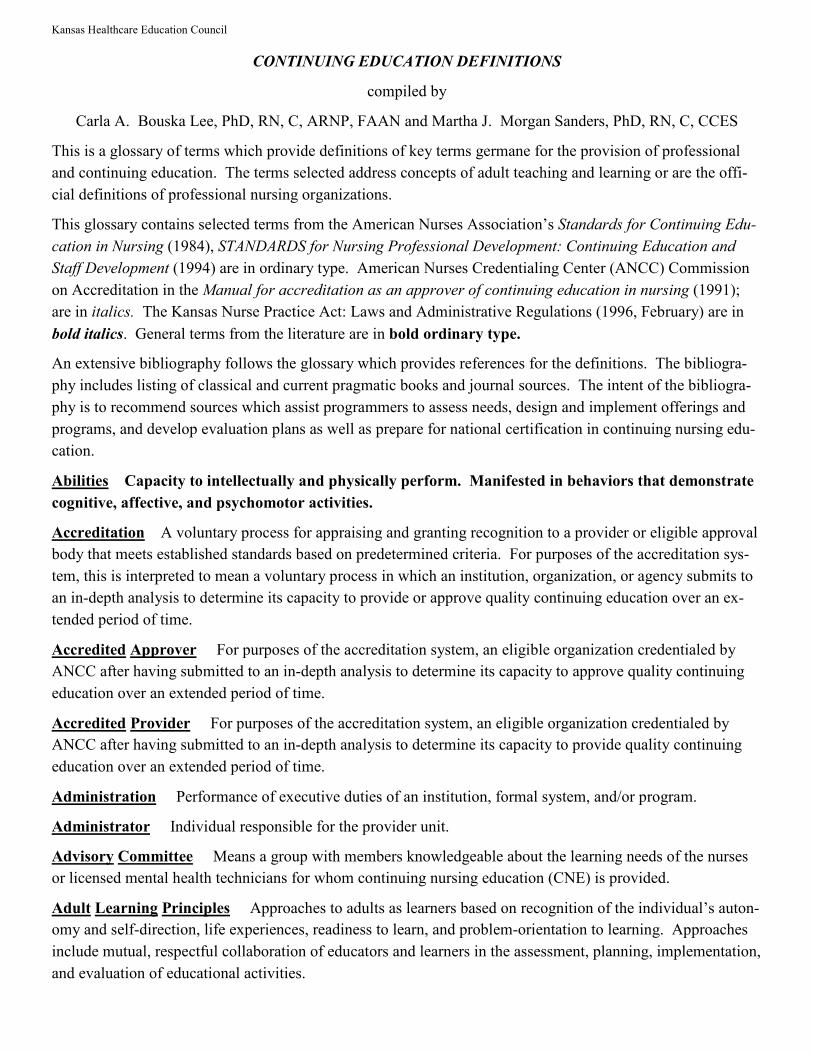
Kansas Healthcare Education Council
CONTINUING EDUCATION DEFINITIONS
compiled by
Carla A. Bouska Lee, PhD, RN, C, ARNP, FAAN and Martha J. Morgan Sanders, PhD, RN, C, CCES
This is a glossary of terms which provide definitions of key terms germane for the provision of professional
and continuing education. The terms selected address concepts of adult teaching and learning or are the offi-
cial definitions of professional nursing organizations.
This glossary contains selected terms from the American Nurses Association’s Standards for Continuing Edu-
cation in Nursing (1984), STANDARDS for Nursing Professional Development: Continuing Education and
Staff Development (1994) are in ordinary type. American Nurses Credentialing Center (ANCC) Commission
on Accreditation in the Manual for accreditation as an approver of continuing education in nursing (1991);
are in italics. The Kansas Nurse Practice Act: Laws and Administrative Regulations (1996, February) are in
bold italics. General terms from the literature are in bold ordinary type.
An extensive bibliography follows the glossary which provides references for the definitions. The bibliogra-
phy includes listing of classical and current pragmatic books and journal sources. The intent of the bibliogra-
phy is to recommend sources which assist programmers to assess needs, design and implement offerings and
programs, and develop evaluation plans as well as prepare for national certification in continuing nursing edu-
cation.
Abilities Capacity to intellectually and physically perform. Manifested in behaviors that demonstrate
cognitive, affective, and psychomotor activities.
Accreditation A voluntary process for appraising and granting recognition to a provider or eligible approval
body that meets established standards based on predetermined criteria. For purposes of the accreditation sys-
tem, this is interpreted to mean a voluntary process in which an institution, organization, or agency submits to
an in-depth analysis to determine its capacity to provide or approve quality continuing education over an ex-
tended period of time.
Accredited Approver For purposes of the accreditation system, an eligible organization credentialed by
ANCC after having submitted to an in-depth analysis to determine its capacity to approve quality continuing
education over an extended period of time.
Accredited Provider For purposes of the accreditation system, an eligible organization credentialed by
ANCC after having submitted to an in-depth analysis to determine its capacity to provide quality continuing
education over an extended period of time.
Administration Performance of executive duties of an institution, formal system, and/or program.
Administrator Individual responsible for the provider unit.
Advisory Committee Means a group with members knowledgeable about the learning needs of the nurses
or licensed mental health technicians for whom continuing nursing education (CNE) is provided.
Adult Learning Principles Approaches to adults as learners based on recognition of the individual’s auton-
omy and self-direction, life experiences, readiness to learn, and problem-orientation to learning. Approaches
include mutual, respectful collaboration of educators and learners in the assessment, planning, implementation,
and evaluation of educational activities.
Kansas Healthcare Education Council
Agency Relation in which one person, the agent, acts on behalf of another with the authority of the latter.
See regulatory agency.
Andragogy The art and science of helping adults learn; discipline of knowledge and technology related to
adult learning.
Approval (Continuing Education) A voluntary process for appraising and granting recognition of a provider or
a program that meets established standards based on predetermined criteria. For purposes of the accreditation
system, a decision made by an accredited approver that the criteria for approval of continuing education have
been met. Means the act of determining that a course offering meets applicable standards based on review of
either the total program or the individual offering.
Approval Unit For purposes of the accreditation system, the administrative body responsible for coordinat-
ing all aspects of the continuing education approval process.
Approved Provider Means a person, organization, or institution approved by the board, that is responsible
for the development, administration and evaluation of the CNE program or offering.
Association An organization of persons having a common interest; also called a society.
Behavioral Objectives Intended outcome of instruction stated as a specific behavior of the learner that can
be measured by performance. Means the intended outcome of instruction stated as measurable learner
behaviors.
Certificate A document which is proof of completion of contact hours.
Certification The state of being certified, usually granted by regulatory or professional organizations.
Clinical Hours Learning experiences for the attainment of clinical skills. One contact hour equals three clini-
cal hours.
College Course Means a course taken through a college which enhances an individual’s professional devel-
opment. It shall include: (a) a course successfully completed within the renewal period that is part of a pro-
gram leading to a nursing degree; or (b) a course with a demonstrated relationship to the practice of nursing. It
shall not include any incomplete, audited or failed course. One college credit hour equals 15 contact hours.
Colloquium Usually an academic meeting at which specialists present addresses on a topic or related topics
followed by answers to questions related to the topics presented.
Competent Qualified or capable.
Computer-Based Instruction Means a learning application that provides computer control to solve an in-
structional problem or to facilitate an instructional opportunity. Because the learner actively participates in
reciprocal dialogue with the communication system, Computer-based instruction shall e considered interactive
learning for CNE.
Concept A class of a number of objectives, events, things, and/or behaviors that differ in appearance.
Conference A meeting of several persons or a representative assembly to discuss matters of common con-
cern.
Page 65
Kansas Healthcare Education Council
Consultation Provision of professional or expert advise.
Contact Hour A unit of measurement that describes 50 minutes of an approved, organized learning experi-
ence. For purposes of the accreditation system, contact hours also may be awarded for offerings organized as
independent study. Means 50 minutes of participation in a learning experience organized by an approved pro-
vider.
Content Subject matter of, or definitive information about an educational activity which relates to the be-
havioral objectives.
Continuing Education Those learning activities intended to build upon the educational and experiential
bases of the professional nurse for the enhancement of practice, education, administration, research, or theory
development to the end of improving the health of the public. (see Continuing Nursing Education)
Continuing Education Unit (CEU) Ten contact hours of participation in an organized continuing experi-
ence that meets the criteria published by the National Council on the Continuing Education Unit, including re-
sponsible sponsorship, capable direction, and qualified instruction.
Continuing Nursing Education (CNE) Means an organized systematic, and evaluative educational experi-
ence beyond the basic preparation which is designed to increase knowledge, improve skills and develop atti-
tudes that enhance nursing and improve health care to the public. CNE does not include in-service education,
on-the-job training, job orientation or education designed for the general public. (see Continuing Education)
Coordinator Person who acts to seek harmonious functioning of all parts of a system for effective results.
Co-provide For purposes of the accreditation system, the process for planning, developing and implement-
ing an educational activity by two or more providers.
Co-sponsor See co-provide.
Criteria Indicators by which standards may be measured and evaluated.
Curriculum Planned program of study usually sponsored by formal institution.
Curriculum vitae For purposes of the accreditation system, a succinct resume which specifies education
and professional qualifications.
Deferral For purposes of the accreditation system, a decision made to delay action on an application.
Denial For purposes of the accreditation system, a decision made by the appropriate body to disapprove the
application.
Director Individual responsible for bringing together and managing elements needed for a continuing edu-
cation provider unit or program; coordinator.
Distance Education Education occurring without the direct, 1:1 relationship, on-site, physical proximity
with the teacher, i.e., spatial separation. (see Education)
Education Any formal act or experience that has a formative effect on the mind, character, or physical abil-
ity of an individual; process by which society, through its schools, deliberately transmits its accumulated
knowledge, values, and skills.
Educational Activity A planned, organized effort aimed at accomplishing educational objectives.
Kansas Healthcare Education Council
Educational Design A plan for instruction consisting of a minimum of a documented assessment of learn-
ing needs, behavioral objectives, content outline, teaching methods, learning experiences, resource utilization
plan, and evaluation strategies.
Educational Objective A statement of a learner-oriented outcome of an educational activity.
Educational Staff People planning the educational design.
Educator A nurse whose practice is nursing continuing education or staff development.
Endorsed CNE Provider An individual, organization, or institution accredited as a provider of CNE by an
organization or body whose function is to grant CNE approval; and reviewed by the board and determined to
have met board CNE provider standards and requirements.
Evaluation A systematic process by which a judgment is made about the quality of consequences, out-
comes, effects, or merit of a provider unity or educational activities. For purposes of the accreditation system,
evaluation is a systematic assessment of administration, program and learning outcomes.
Goal Broadly stated objective. For purposes of the accreditation system, this is further defined as a state-
ment of broad direction or general intent.
Guidelines For purposes of the accreditation system, statements for direction in implementing criteria and
policies.
Health Care Consumer Individuals, groups, or communities who are participants in the health care deliv-
ery system.
Independent Study For purposes of the accreditation system, a self-paced learning activity developed for
individual use which may be institutionally offered (provider-directed) or self-prescribed (self-directed).
Means CNE designed for individual study and monitored by an approved Kansas provider or meeting the re-
quirements of K.A.R. 60-9-107, including research, professional papers and other authorship.
Individual Offering Approval (IOA) The act of determining that an offering not previously approved for
CNE meets applicable standards.
In-service Education Activities intended to assist the professional nurse to acquire, maintain, and/or in-
crease the level of competence in fulfilling his/her assigned responsibilities specific to the expectations of the
employer.
On-The-Job Training Means planned learning activities in the work setting designed to assist the individ-
ual in fulfilling job responsibilities. Inservice education and on-the-job training, including institution-specific
resuscitation courses, are not CNE.
Institute A brief intensive course of instruction on selected topics related to a specific field, e.g., urban stud-
ies.
Instruction The action, practice, or profession of teaching; teaching learning process.
Instructor One who instructs or teaches b providing authoritative information or advice.
Instructor Credit Contact hours awarded by an approved provider, or if the offering is not by an approved
provider by the board, to the individual who prepared and presents the CNE. A 50 minute presentation equals
two contact hours of instructor credit. The minimum presentation length is 50 minutes.
Page 67
Kansas Healthcare Education Council
Interdisciplinary Continuing Education Planned, organized learning experiences designed for a target
audience of members of two or more separate but interrelated professions.
Learning The progressive process of acquisition of knowledge, skills, and attitudes which result in a change
of behavior in the learner.
Learning Needs Assessment A process of determining deficits in knowledge, skills or attitudes identified as
necessary and capable of being achieved through learning experiences. (see Needs Assessment)
Lecture One-way discourse given before a group for instructional purposes.
Lesson Plan Smallest organized part of the curriculum, a schedule, or outline to serve as guide for instruc-
tion.
Liability An obligation to do or refrain from doing something; a duty which eventually must be performed.
Licensee One to whom a license is granted.
Licensure A right granted which gives the holder permission to perform actions that could not be legally
done without such permission; to exercise a certain privilege; to carry on a particular business; or to pursue a
certain occupation.
Monitor For purposes of the accreditation system, a periodic assessment to determine continuing compli-
ance with the criteria.
Need Discrepancy between what is desired and what exists.
Needs Assessment Process by which a discrepancy between what is desired and what exists is identified.
Nursing Professional Development Lifelong process of active participation in learning activities to en-
hance professional practice.
Objective See behavioral objective
Offering For purposes of the accreditation system, an offering is a single educational activity that may be
presented once or repeated. A single CNE learning experience designed to enhance knowledge, skills and atti-
tudes related to nursing. An offering shall consist of at least one contact hour.
Orientation The means by which new staff are introduced to the philosophy, goals, policies, procedures,
role expectations, physical facilities, and special services in a specific work setting. Orientation is provided at
a time of employment and at other times when changes in roles and responsibilities of occur in a specific work
setting. Means formal or informal instruction designed to acquaint new employees with the institution and the
position. Orientation is not CNE.
Outcome Assessment Measurement and evaluation of intended result or end of a plan of study, learning
program, or other components of a program.
Panel Presentation Presentation in which a small group discusses a topic or issue without making prepared
speeches and either with or without active participation by the audience.
Partial Credit Means the actual number of contact hours awarded by an approved provider when an indi-
vidual attends only part of a CNE offering.
Page 68
Kansas Healthcare Education Council
Pedagogy The art and science of teaching children; literally interpreted as the art and science of teaching
and educating.
Philosophy A statement of beliefs.
Planning Committee For purposes of the accreditation system, a group of knowledgeable persons, includ-
ing, potential participants or representatives of target audience, brought together for the purposes of planning
an educational activity.
Program A planned, organized effort directed toward accomplishing educational objectives; in continuing
education, an individual offering or group of offerings; in nursing education, a planned, organized effort lead-
ing to an academic degree. For purposes of the accreditation system, a program is a series of offerings/
educational sessions with a common theme and common overall goals. Attendees may be allowed to choose
among several individual/concurrent educational sessions. An example of a program might be a conference or
course (with multiple sessions). Means an organized effort to achieve overall continuing education goals.
Provider An individual, institution, organization, or agency responsible for the development, implementa-
tion, evaluation, financing, record keeping, and staff development activities.
Provider Unit The administrative body responsible for coordinating all aspects of the nursing continuing
education activities.
Purpose A statement describing why and for whom an educational program has been designed.
Quality Assurance An internal process to ensure the excellence of continuing education activities. The
process includes measurement of the degree to which intents or goals are met, and the introduction of changes
based on information supplied by the measurement with the view toward improvement of the total continuing
education effort.
Registration The act of making a list, catalogue, schedule, or register which has the purpose and effect
of giving notice and preventing fraud and deception.
Regulations Rules or other directives issued by administrative agencies that must have specific au-
thorization to issue directives and upon such authorization must usually follow prescribed conditions,
such as prior notification of the proposed action in a public record and an invitation for public com-
ment.
Page 69
Kansas Healthcare Education Council
Regulatory Agency A government body responsible for control and supervision of a particular activity or
area of public interest.
Refresher Course A course of study providing review of basic preparation and current developments in
nursing practice a refresher course may be used for CNE.
Resources Individuals, materials, space, and funds needed to implement an educational program.
Revoke For purposes of the accreditation system, to rescind approved/accredited status.
Satisfactory Completion Acceptable performance.
Schedule A timetable indicating the time and sequence of organization in the learning experiences; se-
quence structure for learning may be vertical or horizontal.
Seminar Organized guided discussion with focus on the discovery of new relationships by participating in-
dividuals.
Sponsor See Provider
Staff Development Those learning activities which facilitate the nurse’s job-related performance A process
consisting of orientation, inservice education, and continuing education for the purpose of promoting the de-
velopment of personnel within any employment setting, consistent with the goals and responsibilities of the
employer. Orientation, inservice education and continuing nursing education for the purpose of promoting the
development of personnel within the employment setting.
Standard A norm that expresses an agreed-upon level of excellence that has been developed to character-
ize, to lead to criteria for measurement, and to provide guidance in achieving excellence in education.
Symposium (a) Different phases of a broad topic are presented in speeches or lecture without interruption.
Each member presents a different approach to a selected phase of a broad topic.
Target Audience Group for which a learning experience has been designed.
Teaching Methods An orderly process of instruction an evaluation of results. Methods include both formal
and informal processes, e.g., lecture and spontaneous discussion, respectively.
Teleconference An interactive telecommunication offering of CNE.
Total Program Evaluation A systematic process by which a provider analyzes outcomes of the overall con-
tinuing nursing education providership in order to make subsequent decisions.
Workshop A brief, intensive educational program for a small group of people that emphasizes participation
in problem solving.
Page 70
Kansas Healthcare Education Council
Certification From the American Nurses Credentialing Center
for Nursing Continuing Education /Staff Development
Certification is the process by which ANCC Boards on Certification validate, based upon predetermined stan-
dards, an individual registered nurse’s qualifications, knowledge and practice in a defined functional or clinical
area of nursing.
The American Nurses Association, Inc. established the ANA Certification Program in 1973 to provide tangible
recognition of professional achievement in a defined functional or clinical area of nursing.
Certification is reserved for those nurses who have met requirements for clinical or functional practice in a
specialized field, pursued education beyond basic nursing preparation and received the endorsement of their
peers. After meeting these criteria, nurses take certification examinations based on nationally recognized stan-
dards of nursing practice to demonstrate their special knowledge and skills which surpass those required for
licensure.
ELIGIBILITY REQUIREMENTS
1. Currently hold an active RN license in the United States or its territories;
AND
2. Hold a baccalaureate or higher degree in nursing;
AND
3. Have practiced as an actively licensed registered nurse in nursing continuing education and/or staff devel-
opment for a minimum of 4,000 hours during the past 5 years. This requirement may be met if your pri-
mary responsibilities are teaching, managing or consulting in nursing continuing education/staff develop-
ment for the stated number of hours.
AND
4. Currently practice as an actively licensed registered nurse in nursing continuing education and/or staff de-
velopment an average of 20 hours or more per week. This requirement may be met if your primary respon-
sibilities are teaching, managing or consulting in nursing continuing education/staff development for the
stated number of hours.
AND
5. Have 20 contact hours of continuing education and/or its equivalent in academic credits, applicable to nurs-
ing continuing education and staff development within the past 2 years; documentation of continuing edu-
cation and/or academic credit must be submitted.
EXAMINATION TOPICS
1. Foundations of practice
2. Educational process
3. Management of offerings and programs
4. Roles
Page 71
Kansas Healthcare Education Council
Tests are given in June and October.
Your credential designation after successful completion of the exam will be RN, C.
The certification is valid for 5 years. After completing stipulated practice requirements, you may choose to re-
certify by examination or by obtaining appropriate contact hours of continuing education.
To obtain a certification catalog, application forms, or additional information contact:
American Nurses Credentialing Center
600 Maryland Ave., SW Suite 100 West
Washington, DC 20024-2571
(800) 284-CERT
FAX: (202)651-7004
www.nursecredentialing.org
Information obtained from the 1996 Certification Catalog from ANCC
Page 72
4http://karws.gso.uri.edu/JFK/Critical_thinking/MSNBC_show/012000.jpg
Kansas Healthcare Education Council
Preparing a Continuing Education Course
Many times staff will ask can something be offered for continuing education credit. The criteria for credit is based in part on the definition of the course’s purpose. First, define whether the course is continuing education or in-service
education or staff development.
According to the Kansas nurse practice act, continuing education is defined as: "Learning experiences intended to build on education and experiential basis of the registered professional and licensed practical nurse for enhance-
ment of: Practice, Education, Research & Theory Development to the end of improving the health of the public."
In-service Education is considered to be activities intended to assist the profession nurse to acquire, maintain and/or increase the level of competence in fulfilling his/her assigned responsibilities specific to the expectations of the employer. And On-the-Job-Training means planned learning activities in the work setting designed to assist the individual in fulfilling job responsibilities. In-service education and On-the-Job-Training, including institution
specific resuscitation courses are not continuing nursing education.
Staff Development means orientation, in-service education, and continuing nursing education for the purpose of promoting the development of personnel within the employment setting. Potential instructors should contact the CE person in the Department of Organizational Development to discuss the course. In the discussion the follow-
ing topics will be addressed:
- Title that reflects the content
- Measurable objectives or learning outcomes
- Copy of outline, handouts and bibliography. (Note references should be not be older than 3-5 years)
- Curriculum Vitae for each instructor
- A list of participants should be sent in advance to the Department of Organizational Development so a roster and
certificates can be made.
- Other factors to consider, when to schedule, room scheduling, who is responsible for getting the brochure/flyer
out, target audience, cost, refreshments, who will make the handouts, etc.
Writing Objectives
A measurable or behavioral objective is one, in which a certain behavior on the part of the learner is met.
That is at the end of the program the participant will be able to do something he/she could not do or do as well before
the program.
Objectives are usually stated like this:
- At the completion of the program the learner will be able to:
- Identify three areas of the body of high risk for decubitus ulcer
- Describe three methods of increasing circulation to pressures areas
- Demonstrate the application of op-site for protection of a pressure area.
Parts of an objective include:
- Situation - the stimulus situation, the given or the circumstances under which the behavior will be observed
- At the completion of this program
- Learned capability - refers to the type of learning outcome the demonstrated behavior represents, strictly de-
fined by certain verbs for each level of intellectual skill
- Object - the content of the learner's performance
- Action verb - how the performance will be completed. (See attached list)
- Tools, constraints, and conditions - the special tools, needed the constraints to or the actual condition under
which the performance will be observed.
Kansas Healthcare Education Council
The following phrases are too broad to be measurable, so the learner cannot demonstrate a change in knowledge,
behavior, skill or attitude.
At the completion of this program the learner will:
Learn more about decubitus care
Enhance the understanding of circulation
Appreciate the significance of stasis to decubiti
Measurable objectives might read as follows:
At the completion of this class the learner will be able to:
Describe how to stage a decubitus ulcer.
Identify factors that predispose a patient to developing a decubitus ulcer.
Describe appropriate nursing interventions for a decubitus ulcer.
Sometimes the objective has to do with affective or attitudinal change rather than a behavior change. An example of
this might be:
At the end of this program the learner will be able to:
Express a personal opinion about euthanasia with children based on facts presented in this program.
Describe one's feeling as about a Living Will based on discussion in this program.
Page 74
Advanced Practice Registered Nurse Continuing Education Requirements:
According to the Kansas Nurse Practice Act Statutes & Administrative Regulations, KSA 65-1117
“Continuing nursing education means learning experiences intended to build upon the educational and experi-
ential bases of the registered professional and licensed practical nurse for the enhancement of practice, educa-
tion, administration, research or theory development to the end of improving the health of the public.” There-
fore with regard to providing continuing education credit for APRNs, the following is the application of this
regulation as presented by William L. Anderson, JD,RN, Education Specialist: Long-Term Providers of Con-
tinuing Education credit can assign APRN continuing education credit on the course certificate and bro-
chures / announcements for programs deemed appropriate to meet the definition of, “enhancement of prac-
tice.” Typically, those programs pre-approved for Continuing Medical Education (CME) for doctors qualify
for this definition. Additionally, full or partial credit is currently being offered for ACLS, PALS, ENPC, etc.
when the content is deemed appropriate for the advanced practice role. Note: An APRN who practices as a
midwife will likely need a different genre of advanced curriculum than the APRN who specializes in cancer
treatment. If the Long Term Provider is unsure of unable to determine the level of credit to be assigned, the
provider involved can complete the paperwork required for an independent study along with course objec-
tives, etc. and submit the paperwork to KSBN for assigned credit. Providers of continuing education credit
are to be careful to track and document the credit provided.

Kansas Healthcare Education Council
Use objectives to:
• Establish measurable development objectives
• Write outcomes
• Define objective measures.
• Plan CNE
• Demonstrate results – change in staff performance
• Justify and validate ratings of learner performance
• Monitor individual development during orientation
Pick List • Pin-points • Discriminates between • Selects among (chooses) • Derives • Abstracts from • Filters (through) (out) • Connects (physically or graphically) • Writes • Codes • Tests • Shares • Presents
• Applies rules to / toward (procedure / build) • Negotiates • Judges when to • Evaluates (quality of) • Generates • Diagrams • Lists • Collects (data / facts) • Searches for • Validates • Plays role of • Assign • Cross-matches
Behavioral Objective Defined
An objective is a clear and unambiguous description of expectations for learners: it includes three components:
learner behavior conditions of performance, and performance criteria.
Three Parts of a Behavioral Objective
Learner Behavior – skill or knowledge to be gained and the action or skill the learner is able TO DO.
Knowledge. Remembering information Comprehension. Explaining the meaning of information. Application. Using abstractions in concrete situations. Analysis. Breaking down a whole into component parts. Synthesis. Putting parts together to form a new and integrated whole Evaluation. Making judgments about the merits of ideas, materials, or phenomena
Conditions of Performance – under what circumstances or context will the behavior be performed?
Performance Criteria – how well is the behavior to be done; compared to what standard?
Page 75
Objectives Continued:
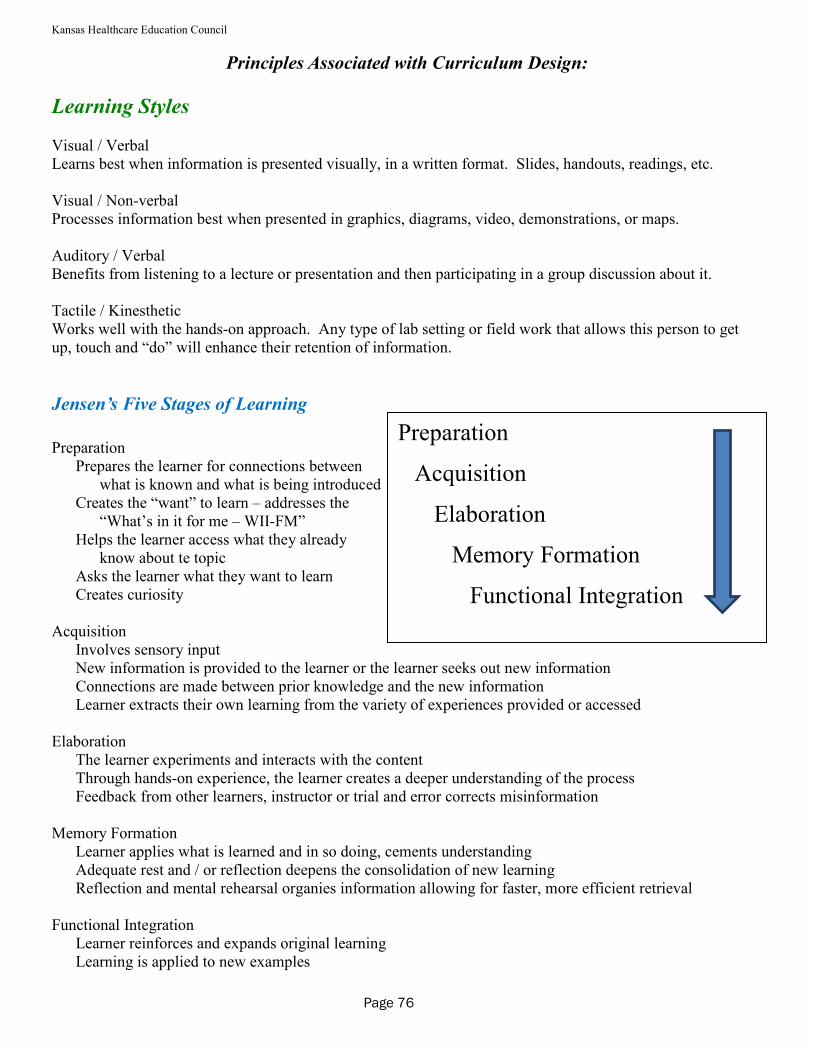
Kansas Healthcare Education Council
Page 76
Learning Styles Visual / Verbal Learns best when information is presented visually, in a written format. Slides, handouts, readings, etc. Visual / Non-verbal Processes information best when presented in graphics, diagrams, video, demonstrations, or maps. Auditory / Verbal Benefits from listening to a lecture or presentation and then participating in a group discussion about it. Tactile / Kinesthetic Works well with the hands-on approach. Any type of lab setting or field work that allows this person to get up, touch and “do” will enhance their retention of information.
Jensen’s Five Stages of Learning
Preparation
Prepares the learner for connections between what is known and what is being introduced
Creates the “want” to learn – addresses the “What’s in it for me – WII-FM”
Helps the learner access what they already know about te topic
Asks the learner what they want to learn Creates curiosity
Acquisition
Involves sensory input New information is provided to the learner or the learner seeks out new information Connections are made between prior knowledge and the new information Learner extracts their own learning from the variety of experiences provided or accessed
Elaboration
The learner experiments and interacts with the content Through hands-on experience, the learner creates a deeper understanding of the process Feedback from other learners, instructor or trial and error corrects misinformation
Memory Formation
Learner applies what is learned and in so doing, cements understanding Adequate rest and / or reflection deepens the consolidation of new learning Reflection and mental rehearsal organies information allowing for faster, more efficient retrieval
Functional Integration
Learner reinforces and expands original learning Learning is applied to new examples
Preparation
Acquisition
Elaboration
Memory Formation
Functional Integration
Principles Associated with Curriculum Design:
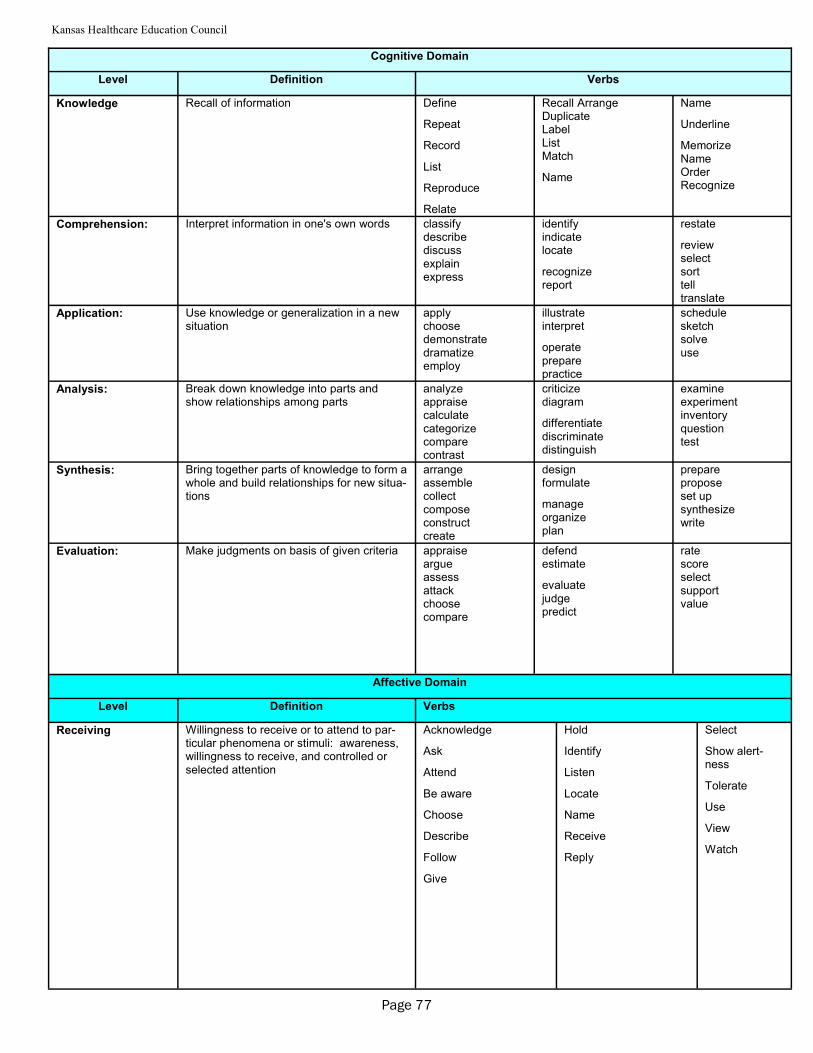
Kansas Healthcare Education Council
Cognitive Domain
Level Definition Verbs
Knowledge Recall of information Define
Repeat
Record
List
Reproduce
Relate
Recall Arrange Duplicate Label List Match
Name
Name
Underline
Memorize Name Order Recognize
Comprehension: Interpret information in one's own words classify describe discuss explain express
identify indicate locate
recognize report
restate
review select sort tell translate
Application: Use knowledge or generalization in a new situation
apply choose demonstrate dramatize employ
illustrate interpret
operate prepare practice
schedule sketch solve use
Analysis: Break down knowledge into parts and show relationships among parts
analyze appraise calculate categorize compare contrast
criticize diagram
differentiate discriminate distinguish
examine experiment inventory question test
Synthesis: Bring together parts of knowledge to form a whole and build relationships for new situa-tions
arrange assemble collect compose construct create
design formulate
manage organize plan
prepare propose set up synthesize write
Evaluation: Make judgments on basis of given criteria appraise argue assess attack choose compare
defend estimate
evaluate judge predict
rate score select support value
Affective Domain
Level Definition Verbs
Receiving Willingness to receive or to attend to par-ticular phenomena or stimuli: awareness, willingness to receive, and controlled or selected attention
Acknowledge
Ask
Attend
Be aware
Choose
Describe
Follow
Give
Hold
Identify
Listen
Locate
Name
Receive
Reply
Select
Show alert-ness
Tolerate
Use
View
Watch
Page 77
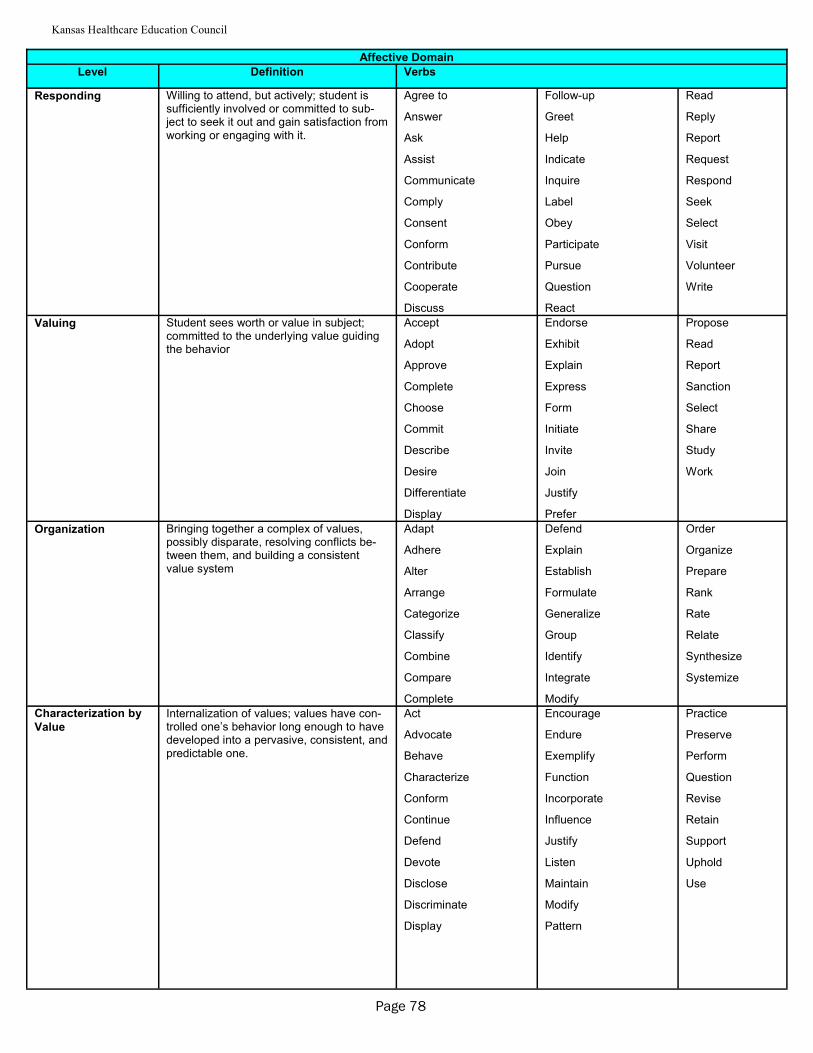
Kansas Healthcare Education Council
Affective Domain
Level Definition Verbs
Responding Willing to attend, but actively; student is sufficiently involved or committed to sub-ject to seek it out and gain satisfaction from working or engaging with it.
Agree to
Answer
Ask
Assist
Communicate
Comply
Consent
Conform
Contribute
Cooperate
Discuss
Follow-up
Greet
Help
Indicate
Inquire
Label
Obey
Participate
Pursue
Question
React
Read
Reply
Report
Request
Respond
Seek
Select
Visit
Volunteer
Write
Valuing Student sees worth or value in subject; committed to the underlying value guiding the behavior
Accept
Adopt
Approve
Complete
Choose
Commit
Describe
Desire
Differentiate
Display
Endorse
Exhibit
Explain
Express
Form
Initiate
Invite
Join
Justify
Prefer
Propose
Read
Report
Sanction
Select
Share
Study
Work
Organization Bringing together a complex of values, possibly disparate, resolving conflicts be-tween them, and building a consistent value system
Adapt
Adhere
Alter
Arrange
Categorize
Classify
Combine
Compare
Complete
Defend
Explain
Establish
Formulate
Generalize
Group
Identify
Integrate
Modify
Order
Organize
Prepare
Rank
Rate
Relate
Synthesize
Systemize
Characterization by
Value
Internalization of values; values have con-trolled one’s behavior long enough to have developed into a pervasive, consistent, and predictable one.
Act
Advocate
Behave
Characterize
Conform
Continue
Defend
Devote
Disclose
Discriminate
Display
Encourage
Endure
Exemplify
Function
Incorporate
Influence
Justify
Listen
Maintain
Modify
Pattern
Practice
Preserve
Perform
Question
Revise
Retain
Support
Uphold
Use
Page 78
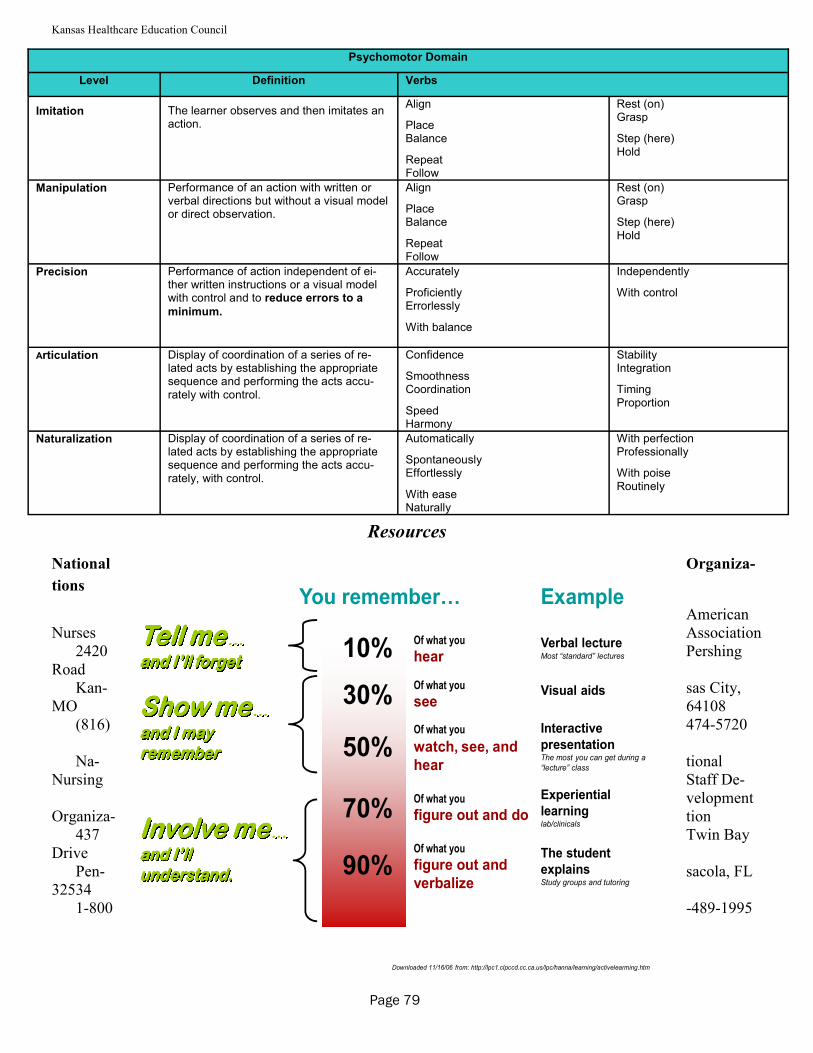
Kansas Healthcare Education Council
Resources
National Organiza-
tions
American Nurses Association
2420 Pershing Road
Kan- sas City, MO 64108
(816) 474-5720 Na- tional
Nursing Staff De-velopment
Organiza- tion 437 Twin Bay
Drive Pen- sacola, FL
32534 1-800 -489-1995
Psychomotor Domain
Level Definition Verbs
Imitation
The learner observes and then imitates an action.
Align
Place Balance
Repeat Follow
Rest (on) Grasp
Step (here) Hold
Manipulation Performance of an action with written or verbal directions but without a visual model or direct observation.
Align
Place Balance
Repeat Follow
Rest (on) Grasp
Step (here) Hold
Precision Performance of action independent of ei-ther written instructions or a visual model with control and to reduce errors to a
minimum.
Accurately
Proficiently Errorlessly
With balance
Independently
With control
Articulation Display of coordination of a series of re-lated acts by establishing the appropriate sequence and performing the acts accu-rately with control.
Confidence
Smoothness Coordination
Speed Harmony
Stability Integration
Timing Proportion
Naturalization Display of coordination of a series of re-lated acts by establishing the appropriate sequence and performing the acts accu-rately, with control.
Automatically
Spontaneously Effortlessly
With ease Naturally
With perfection Professionally
With poise Routinely
Page 79
17
You remember/
The student
explainsStudy groups and tutoring
Of what you
figure out and
verbalize90%
Experiential
learninglab/clinicals
Of what you
figure out and do70%
Interactive
presentationThe most you can get during a
“lecture” class
Of what you
watch, see, and
hear50%
Visual aidsOf what you
see30%
Verbal lectureMost “standard” lectures
Of what you
hear
Example
Tell meTell meTell meTell me…………
and I’ll forgetand I’ll forgetand I’ll forgetand I’ll forget
Show meShow meShow meShow me…………
and I may and I may and I may and I may rememberrememberrememberremember
Involve meInvolve meInvolve meInvolve me…………
and I’ll and I’ll and I’ll and I’ll understand.understand.understand.understand.
10%
Downloaded 11/16/06 from: http://lpc1.clpccd.cc.ca.us/lpc/hanna/learning/activelearming.htm
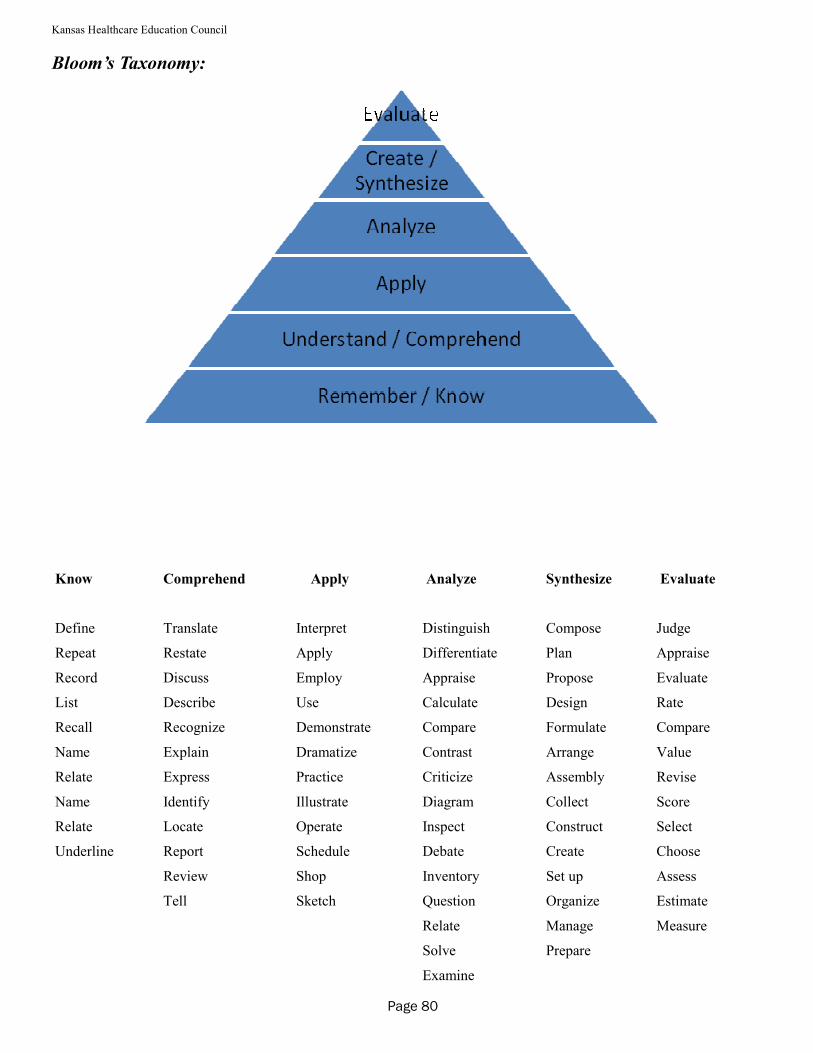
Kansas Healthcare Education Council
Know
Define
Repeat
Record
List
Recall
Name
Relate
Name
Relate
Underline
Comprehend
Translate
Restate
Discuss
Describe
Recognize
Explain
Express
Identify
Locate
Report
Review
Tell
Apply
Interpret
Apply
Employ
Use
Demonstrate
Dramatize
Practice
Illustrate
Operate
Schedule
Shop
Sketch
Analyze
Distinguish
Differentiate
Appraise
Calculate
Compare
Contrast
Criticize
Diagram
Inspect
Debate
Inventory
Question
Relate
Solve
Examine
Synthesize
Compose
Plan
Propose
Design
Formulate
Arrange
Assembly
Collect
Construct
Create
Set up
Organize
Manage
Prepare
Evaluate
Judge
Appraise
Evaluate
Rate
Compare
Value
Revise
Score
Select
Choose
Assess
Estimate
Measure
Page 80
Bloom’s Taxonomy:
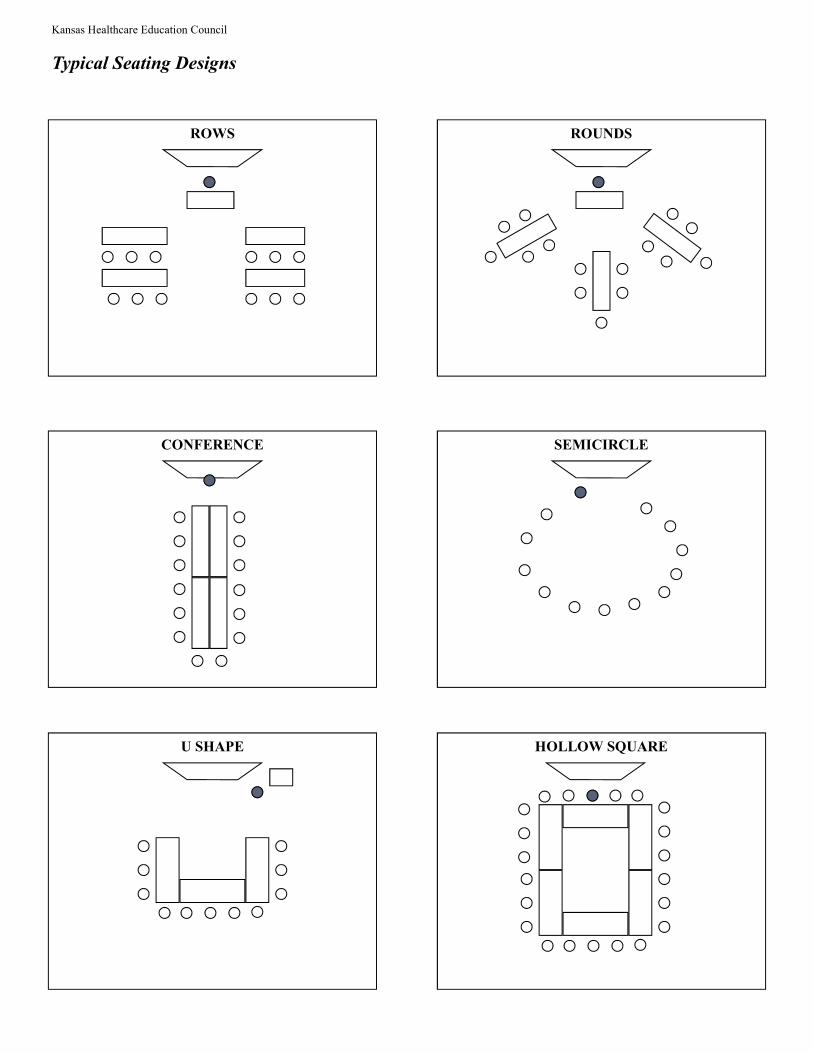
Kansas Healthcare Education Council
Typical Seating Designs
ROWS ROUNDS
SEMICIRCLE CONFERENCE
U SHAPE HOLLOW SQUARE
Kansas Healthcare Education Council
Digital Native Learner M. Paula Daoust, PhD (Blue Cross & Blue Shield of Kansas Institute) presented the following information re-
gard teaching the “Digital Native” Learner for the Spring KaHEC Conference April 26, 2013.
Definition of a Digital Native:
Someone who grew up using digital technology; computers, video games, smart phones, internet, mp3’s, social media (i.e., Facebook, chat, texting, Twitter), etc.
Someone who has never known a world without digital technology. The Digital Learner is characterized as using “Butterfly” brain activity:
rapid access skim and leave programmed for speed and interactivity hyper-text minds (leap around cognitive structures) parallel NOT sequential (linear) thinking multi-tasking (parallel processing)
The Digital Learner is accustomed to:
twitch speed multi-tasking random-access graphics-first active interaction being connected fun & fantasy quick payoff
Learning Strengths of the Digital Native:
accustomed to group work comfortable with active learning multi-tasking technology experts short-term goal and achievement oriented learn from failure – trial and error motivated by money and earning potential prefer games to “serious” work graphics awareness long attention span for active learning events random access
pattern detection in chaos scientific thinking collateral learning decision-making prioritizing creativity problem-solving risk-taking inductive thinking tactical thinking literacy
Learning Challenges of the Digital Native Impatient with “long” documents Expects instant gratification Require more structure and mentoring Limited vision – difficulty seeing the “big” picture Abstract reasoning
Planning Not sequential or linear thinkers Short attention-span for “old” learning strategies Recognition Development of mental models for new constructs Critical thinking

Kansas Healthcare Education Council

Kansas Healthcare Education Council
Page 84
BIBLIOGRAPHY
* priority references
# classic or foundational resources
^ certification review
Books & Journal Articles
Abruzzesle, R.S. (1992). Nursing staff development: strategies for success. St. Louis: Mosby.
* American Nurses Association. (1995). Scope and standards for nurse administrators. Washington,
DC: American Nurses Publishing.
*^ American Nurses Association. (1994). Standards for continuing education and staff development.
Washington, DC: American Nurses Publishing.
ANCC Commission on Accreditation. (1995). Manual for accreditation as an approver of continuing edu-
cation in nursing. Washington, DC: Author.
* Angelo, T.A., & Cross, K.P. (1993). Classroom assessment techniques: A handbook for college teach-
ers. San Francisco: Jossey-Bass.
*^ Bard, R., Bell, C.R., Stephen, L., & Webster, L. (1987). The trainer=s professional development
handbook. San Francisco: Jossey-Bass.
# Bloom, B. (1956). Taxonomy of education objectives: The classification of educational goals. New
York: McKay.
# Boyle, P.G. (1981) Planning better programs. New York: McGraw-Hill.
Brookfield, S.D. (1990). The skillful teacher. San Francisco: Jossey-Bass.
^ Brookfield, S.D. (1988). Developing critical thinkers: Challenging adults to explore alternative ways
of thinking and acting. San Francisco: Jossey-Bass.
Kansas Healthcare Education Council
* Bryson, J.M. (1989). Strategic planning for public and nonprofit organization: A guide to strengthen-
ing and sustaining organizational achievement. San Francisco: Jossey-Bass.
*^ Caffarella, R.S. (1994). Planning programs for adult learners: A practical guide for trainers and staff
developers. San Francisco: Jossey-Bass.
Carter, J., & Powell, D. (1992). Teacher leaders and staff developers. Journal of Staff Development, 13
(1), 8-12.
*^ Cervero, R.M. (1988). Effective continuing education for professionals. San Francisco: Jossey-Bass
Cervero, R.M., & Assaretto, J.F. (1990). Visions for the future of continuing professional education. Ath-
ens, GA: University of Georgia, Georgia Center for Continuing Education.
Cervero, R.M., & Wilson, A.L. (1994). Planning responsibility for adult education: A guide to negotiating
power and interests. San Francisco: Jossey-Bass
# Cooper, S., & Heenan, C. (1980). Preparing, designing, leading workshops: A humanistic approach.
New York: Van Nostrand Reinhold.
Covey, S.R. (1991). Principle-centered leadership. New York: Simon & Schuster.
Craddock, E. (1993). Developing the facilitator role in the clinical area. Nursing Education Today, 13,
217-234.
Cranton P. (1994). Understanding and promoting transformative learning: a guide for educators of adults.
San Francisco: Jossey-Bass
*^ Cranton, P. (1989). Planning instruction for adults. Toronto: Wall & Thompson.
* Daloz, L.A. (1986). Effective teaching and mentoring. San Francisco: Jossey-Bass
* Davis, B.G. (1993). Tools for teaching. San Francisco: Jossey-Bass
Page 85
Kansas Healthcare Education Council
Del Bueno, D.J., & Freund, C.M. (1986). Politics and policy in nursing administration: A case book.
Ownings Mills, ND: Rynd Communication.
* De Toryay, R., & Thompson, M.A. (1987). Strategies for teaching nursing (3rd ed.). Albany, NY:
Delmar
* Draves, W.A. (1995). Energizing the learning environment. Manhattan, KS: learning Resources Net-
work (LERN).
^ Draves, W.A. (1984). How to teach adults. Manhattan, KS: Learning Resources Network (LERN).
Duning, B.S., Van Kekerix, M.J., & Zaborowski, L.M. (1993). Reaching learners through telecommuni-
cations. San Francisco: Jossey-Bass
Farquharson, A. (1995). Teaching in practice: How professionals can work effectively with clients, pa-
tients, and colleagues. San Francisco: Jossey-Bass
Fox, V.J., Rothrock, J.D., & Skelton, M. (1992). The mentoring relationship. American Operating Nurse
Journal, 56(5), 858-867.
*^ Galbraith, M.W. (Ed.). (1990). Adult learning methods: A guide to effective instruction. Malabar,
FL: Krieger.
Galbraith, M.W. (Ed.). 1990). Education through community organizations. New Directions for Adult
and continuing Education, 47. San Francisco: Jossey-Bass
*^ Gilley, J.W., & Eggland, S.A. (1989). Principles of human resource development. Reading, MA: Ad-
dison-Wesley.
Good, C. (1959). Dictionary of education. New York: McGraw-Hill.
Grifis, S.H. (1991). Law dictionary. New York: Barron=s Educational Series.
Page 86
Kansas Healthcare Education Council
* Gronlund, N.E., & Linn, R.L. (1990). Measurement and evaluation in teaching (6th ed.). New York:
Macmillan.
^ Hardy, M.E$., & Conway, M.E. (1988). Role theory; perspectives for health professionals. Norwalk,
CT: Appleton & Lange.
Harris, J. (1989). Successful cosponsorships in continuing education. Manhattan, KS Learning Resources
Network (LERN).
Heimlich, J.E., & Norland, E. (1994). Developing teaching style in adult education. San Francisco:
Jossey-Bass
Hiemstra, R. (Ed.). (1991). Creating environments for effective adult learning. New Directions for Adult
and continuing Education, 50. San Francisco: Jossey-Bass
*^ Hiemstra, R., & Sisco, B. (1990). Individualizing instruction: Making learning personal, empowering,
and successful. San Francisco: Jossey-Bass
Kahler, A.A., Morgan, B., Holes, G.E., & Bundy, C.E. (1985). Methods in adult education. Danville, IL:
Interstate Printers & Publishers.
Kelly, K.J. (1992). Nursing staff development: Current competence, future focus. Philadelphia: Lippin-
cott.
Kirkpatrick, DL (1994), Evaluating training programs: The Four levels. San Francisco:Berrett-Koehler
Publishers
Knowles, M.S. (1986). Using learning contracts: practical approaches to individualizing and structuring
instruction. San Francisco: Jossey-Bass
*^ Knowles, M.S. (1980). The modern practice of adult education. Chicago: Follett.
Lee, C.A.B. (1984). Philosophy of language development: Toward refinement of professionalism. Wich-
ita, KS: Wichita State University (research project: education glossary.).
Page 87
Kansas Healthcare Education Council
Lee, C.A.B. (1986). Mentoring as facilitator of developmental process. Kansas Nurse, 61(2), 1-3.
Lee, C.A.B. (1986). Writing as a form of professional development and creative expression. Kansas
Nurse, 61(4), 1-3.
LeFevre, R.A. (1995). Critical thinking in nursing: a practical approach. Philadelphia: W.B. Saunders.
London, M. (1988). Change agents: New roles and innovation strategies for human resource profession-
als. San Francisco: Jossey-Bass
Lorenzi, N.M., & Riley, R.T. (1995). Organizational aspects of health informatics: Managing technologi-
cal change. New York: Springer-Verlag.
# Madaus, G.F., Scriven, M., & Stufflebeam, D.L. (1983). Evaluation models: Viewpoints on educa-
tional and human services evaluation. Boston: Kluwer-Nijhoff.
# Mager, R.F. (1984). Preparing instructional objectives (2nd ed.). Belmont, CA: David S. Lake.
^ Matkin, G.W. (1985). Effective budgeting in continuing education: A comprehensive guide to im-
proving program planning and organizational performance. San Francisco: Jossey-Bass
* Merriam, S.B. (1993). An update on adult learning theory. New Directions for Adult and Continuing
Education, 57. San Francisco: Jossey-Bass
Merriam, S.B., & Caffarella, R.S. (1991). Learning in adulthood. San Francisco: Jossey-Bass
Mesirow, J. (1991). Transformative dimensions of adult learning. San Francisco: Jossey-Bass.
* Meyers, C. (1988). Teaching students to think critically. San Francisco: Jossey-Bass
National University Continuing Education Association. (1987). Challenges for continuing higher educa-
tion leadership: Corporate/campus collaboration. Washington, DC: Author.
Page 88
Kansas Healthcare Education Council
Oleske, D.M. (Ed.). (1995). Epidemiology and the delivery of health care services: Methods and applica-
tions. New York: Plenum Press.
PEW Health Professions Commission. (1995). Health professions education and managed care: Chal-
lenges and necessary responses. Washington, DC: Author.
* Piskurich, G.M. (Ed.). (1993). Handbook of instructional technology. New York: McGraw-Hill.
Popham, J.W. (1969). Instructional objectives. Chicago: Rand McNally.
Sparks, D. (1992). Becoming an authentic consultant: an interview with Peter Block. Journal of Staff De-
velopment, 13(3), 12-15.
* Spritzer-Lehmann, R. (1994). Nursing management desk reference: concepts, skills, & strategies.
Philadelphia: Saunders.
* State of Kansas. (1987). Kansas statutes administration [K.S.A. 65-4921 through 65-4930]. Topeka,
KS: Author.
* State of Kansas. (1996, February). Kansas nurse practice act [K.S.A. 65-1113 through 65-1137;
K.A.R. 60-1-102 through 60-16-105]. Topeka, KS: Kansas State Board of Nursing.
* Straka, D., & O=Malley, J. (1994). A professional development model: Rewarding excellence in nurs-
ing practice. Seminars for Nurse Managers, 2(3), 167-174.
Strother, G.B., & Klus, J.P. (1982). Administration of continuing education. Belmont, CA: Wadsworth.
* Sullivan, E.J., & Decker, P.J. (1992). Instructors resource manual for effective management in nursing
(3rd ed.). Redwood City, Ca: Addison-Wesley.
* Sullivan, E.J., & decker, P.J. (1992). Effective management in nursing (3rd ed.). Redwood City, CA:
Addison-Wesley.
Page 89
Kansas Healthcare Education Council
# Tyler, R.W. (1949). Basic Principles of curriculum and instruction. Chicago: University of Chicago
Press.
Verduin, .R., & Clark, T.A. (1991). Distance education: The foundations of effective practice. San Fran-
cisco: Jossey-Bass
Webster=s ninth new collegiate dictionary. (1991). Springfield, MA: Merriam-Webster.
* Wholey, J.W., Hatry, H.P., & Newcomer, K.E. (Eds.) (1994). Handbook of practical program evalua-
tion. San Francisco: Jossey-Bass.
Wlodkowski, R.J. (1993). Enhancing adult motivation to learn: A guide to improving instruction and in-
creasing learner achievement. San Francisco: Jossey-Bass.
Page 90
Additional Resources National Organizations American Nurses Association 2420 Pershing Road Kansas City, MO 64108 (816) 474-5720 National Nursing Staff Development Organization 437 Twin Bay Drive Pensacola, FL 32534 1-800-489-1995 State Organizations Kansas Healthcare Education Council c/o Kansas Hospital Association P.O. Box 2308 Topeka, KS 66601-2308 (785) 233-7436 Kansas State Board of Nursing Landon State Office Building 900 SW Jackson Suite 551S Topeka, KS 66612-1256 (785) 296-5062 www.ksbn.org
Kansas State Nurses Association 700 SW Jackson Suite 601 Topeka, KS 66603 (785) 233-8638
Kansas Healthcare Education Council
Journals Suggested for Regular Reading
A practitioner in continuing education may find the following journals directed to continuing education and
staff development helpful.
Adult and Continuing Education Today. Manhattan, KS: Learning Resources Network [LERN].
Adult Education Quarterly: A Journal of Research and Theory. (ISSN 0741-7136) Washington, DC:
American Association for Adult and Continuing Education [AAACE].
Adult Learning. (ISSN 1045-1595) Washington, DC: American Association for Education [AAACE].
Continuing Higher Education Review: The Journal of the National University Continuing Education Asso-
ciation. Columbus, OH: Ohio State University, Office of Continuing Education.
Human Resource Development Quarterly. (ISSN 1044-8004) San Francisco: Jossey-Bass (sponsored
by the American Society for Training and Development [ASTD]).
Journal of Continuing Education in Nursing. (ISSN 0022-0125) Thorofare, NJ: Slack.
Journal of Continuing Education in the Health Professions. New York: Alliance of Continuing Medical
Education, Taylor & Francis.
Journal of Nursing Staff Development. Philadelphia: Lippincott.
New Directions for Adult and Continuing Education. (ISSN 0195-2242) San Francisco: Jossey-Bass.
Nurse Educator. (ISSN 0363-3624) Philadelphia: Lippincott.
T.H.E. Journal (Technological Horizons in Education). (ISSN 0192-592x) Tustin, CA: T.H.E. Journal.
Page 91
Kansas Healthcare Education Council
Page 92
REGISTRATION / FEES FOR
CONTINUING EDUCATION OFFERINGS
Sample
Pre-registration is required for most continuing education offerings and will be so stated on the offering an-nouncement. The registration fee must accompany the pre-registration form (see fees below). All information on the pre-registration form should be as it appears on the participant’s license. Participants may assume con-firmation of registration unless notified. Waiting List In the case of over-registrations, a waiting list will be started and the individual notified. If cancellations oc-cur, the first person on the waiting list will be taken. If unable to contact the individual within a reasonable pe-riod, the next person will be contacted. Walk-ins Walk-ins are accepted at continuing education offerings if seating is available (see fees below). Children / Non-registered Persons Participants attending continuing education offerings have paid for a learning experience. Due to limited seat-ing and because children can be distracting to others, children and non-registered persons will not be allowed at continuing education offerings. Calculation of Fees Continuing education offerings will be provided on a break-even basis. Income will be matched as closely as possible with expenses. Expenses may include: 1. faculty honorarium and expenses (mileage, meals, accommodations, etc.); 2. facility rent - if off hospital premises; 3. printing; 4. mailing; 5. materials (xeroxing, tape rental, etc); 6. refreshments; 7. education supervisor’s time; Tuition will be calculated by adding the projected costs of the above items and dividing by the estimated num-ber of paying attendees. A written agreement will be sent to all course speakers for their signature and returned for our records. The agreement will specify approved expenses for the speaker. Registration Fees Pre-registered non Newman Regional Health (NRH) participants including physicians - full fees with the ex-ception of the program speakers. Retired employees (20 years or more employment at NRH), current NRH board members and spouses, and active auxiliary members and volunteer chaplains - half price tuition.
(1 of 2)
Kansas Healthcare Education Council
Page 93
Sample
Walk-in non-NRH participants - full fees plus $5.00 additional charge.
NRH employees and ESU Newman Division of Nursing employees - no charge in most cases. The Education
Dept. reserves the right to set a discounted fee for employees at offerings in which expenses are projected to
be high.
PRN NRH employees - may attend at NRH employee rate if they have worked within 30 days prior to a
scheduled offering (inservice days will not count toward working time).
NRH employees on leave of absence or FMLA - may attend at NRH employee rate for 6 months. After 6
months, the employee will be expected to pay the stated non-NRH registration fee. This includes employees
on medical leave, educational leave, workers compensation, etc.
ESU Newman Division of Nursing students - will follow the same policies as NRH employees if seating is
available. Certificates will be issued only upon request and no contact hours will be provided unless a specific
request is made.
Students from other nursing educational institutions - if seating is available, a flat fee of $5.00 per student
will be charged to cover refreshments, xeroxing, etc. These individuals must be full-time students in an ac-
credited school of nursing to qualify for this rate. Certificates will be issued only upon request but no contact
hours will be provided.
Insufficient Fund Checks
If it is known prior to the program that a check did not clear the bank, the CNE certificate will be held until
the participant pays for the course in cash. Any checks which do not clear the bank following the program
will be referred to the NRH Fiscal Services Dept. to attempt to collect payment for the program.
Cancellations/Refunds
If pre-registered for a program and unable to attend, the registration fee will be refunded if the NRH Educa-
tion Department is notified at least 24 hours prior to the offering. There is a $5.00 charge for processing can-
cellations.
If an offering must be canceled due to inclement weather, speaker illness, etc., NRH will notify all partici-
pants as soon as possible. A full refund of tuition fees will be made.
(2 of 2)
Kansas Healthcare Education Council
Page 94
Sample
INDEPENDENT STUDY
CONTINUING EDUCATION
Newman Regional Health offers several courses for independent study for employees only. The Education Su-
pervisor will review these courses to verify the appropriateness for continuing education credit.
The number of contact hours awarded will be based on the time required to complete the offering using pilot
testers (See Awarding Contact Hours Policy).
Participants must schedule a time to complete the independent study offerings.
Following completion of the independent study course and successful completion of the post test or return
demonstration, the participant will complete a course evaluation and sign the attendance roster. A certificate of
attendance will be awarded to the participant indicating “Independent Study” credit. The post test, sign-in ros-
ter, and participant evaluation will be maintained in a secure manner in the Education Department for a period
of two years.

Kansas Healthcare Education Council
Notes
Page 95

Kansas Healthcare Education Council
11-2013 Edition
Teaching Nursing’s Next
Generation
Judith W. Herrman, PhD, RN, ANEF Professor
School of Nursing University of Delaware
April 16, 2014
2/14/2014
1
Teaching Nursing’s Next Generation
Judith W. Herrman, PhD, RN, ANEF
Professor
School of Nursing University of Delaware
Objectives • Discuss generational differences that impact
the teaching-learning process.
• Identify the barriers to creative teaching in a variety of learning environments.
• Describe creative teaching strategies for use with diverse learners and in a variety of settings.
• Analyze the integration of creative teaching strategies into personal practice.
Why are you here?
• What is the most challenging part of education?
• What makes you feel best about teaching?
• What makes you feel frustrated in teaching?
• Why did you pick education as a career?
Today’s 2.9 million nurses?
• Age—average 46.8 (highest ever); 41%>50; 9% <30 years
• Mean salary $57, 785
• Age at graduation – BSN 26.3; AD/Dip 31.8
• Gender – 6% male
• Race – 12.6 self-identified as minority
Who are today’s nurses?
• Career trajectory: 83% employed; 37% MS or doctorate; More full time than ever before
• Educational level
– 25% diploma
– 42% ADN
– 32% BSN
• 56% in hospitals; 14% ambulatory; 30% other
• Focus on our similarities and our differences!
Today’s nurses • Are a varied, unique, and diverse group-Changing
demographics—diverse individuals, diverse ideas of behavior
• Changing views on of leadership
• Changing attention spans—expectations
• Lack of confidence in social institutions
• Less prepared for the rigors of academics and the workplace
• Less cognizant of the “chain of command”
• More complex lives—greater levels of stress, working, other obligations, and are frequently “overwhelmed”
2/14/2014
2
When were they Young?
•Technology
•Rewards systems
•Work ethic
• Learning Styles
•Teaching Methods
• Attentive, respectful, and passive • Like lecture and traditional methods • Motivated to learn and work • Build on previous wisdom • Respect the “wiseness” of others • Learn best when respected for
current knowledge and life experiences
• Follow orders • Less comfortable with interactive
methods or group work
Veterans—1922-1945
• Students and parents of students • Demanding and accepting • High standards for teaching and
learning • May or may not accept technology • Responsibility of learning is on the
quality of the teaching—like traditional teaching
• Motivated if topic is relevant and useful • Wish to be respected for experiences • Learn best by “doing”—do well with
experiential teaching strategies
Boomers 1946-1964 • Respond to creativity in teaching and
learning
• Technology and innovation=Challenge
• Enjoy to learn—learning needs to be enjoyable
• Education as a step to a goal
• Balance of work and play
Generation Xers—1965-1980
• Learn at a rapid pace
• Comfortable with innovation
• Expect learning to have a creative side
• Advocate for their own learning needs
• Live at “one with technology”— digital natives versus digital immigrants
• Embrace group work
Generation Why—1981-1990 The millennials—1990-present • Risk-takers
• Highly motivated to learn “their way.”
• Need content to be made relevant to “their reality.”
• Technology is a way to express creativity
• Varied levels of readiness for academics
• Pluralist learning— learning to accept “gray areas” and the “iffy” parts of nursing.
2/14/2014
3
Why Creative Teaching • How can we enhance learning?
• Create learning experiences which are fun, relevant, memorable, and focusing?
• Construct these experiences to meet the needs of diverse generations and individuals?
• We can use Creative Teaching Strategies!
• Barriers to Creative Teaching!
• Making Creative Teaching work in your setting!
Strategies to build a thinking and learning community: Ice Breakers
• Many group exercises may be considered
“icebreakers.”
• Why are you here?
Common and Different Already did this!!!!
• Talk to your neighbor to the left of you
• Find four things that you have in common
• Find four things that you have which are
different
• Adapting this strategy for many
needs, content, or classes—
culture, experiences, and more
Ice Breaker Example: Which shape best describes you as a nurse?
• Organized, structured, rigid, task oriented, concrete, no ideas…all do
• People lovers, caring, nurturing, harmony
• Period of transition, confused, don’t know what to choose
• Leaders, make decisions, works well with squares, in charge, delegate
• Creative, relaxed, idea people, little work/results
Team-building...
Setting priorities icebreaker
• Give each student three index cards
• Have them write the three most important things in their life, one on each card
• Ask them to give up one card….then another…
• Uses: Setting priorities, poverty, aging, others?
Scavenger Hunt
• Look for things • Use things • Of important areas • Case study Scavenger Hunt • Meet the people • Enlist the unit’s/agency’s/etc. support
• Computer scavenger hunt • Make it brief and fun • Takes a while…. use over and over again
2/14/2014
4
The same information
• Give two groups two different sets of information…
• Gives another perspective..
• How does it impact or thoughts and behaviors?
• How does that impact our nursing care?
• Relate to clinical situations
• Reinforce empathy, not knowing the whole story, etc.
Grand Rounds
• Confidentiality • Build on and improve the
medical model • Enlist the patient’s AND
family’s permission/assistance • Ask client’s their perceptions of
priorities
Equipment Review
• Make sure learners have
ability to see and feel each
piece of equipment
• Include a review of the equipment
frequently used in this clinical
environment
• Enlist the help of agency
staff and equipment reps
Stories…. • Using lay literature
– All I really need to know I learned in kindergarten
• Business and newspaper columns
• Comics • Nursing Moments • War Stories • Children’s books • Clinical Anecdotes • Put it in Perspective...
Strategies to build priority setting skills:
Pause for Priority Setting After teaching, discussing
a topic, or demonstrating in lab, ask students:
–“What’s the Big deal?”
–“What’s the point?”
–“First nursing priority?”
–“First nursing action?”
– “Why is this so important?”
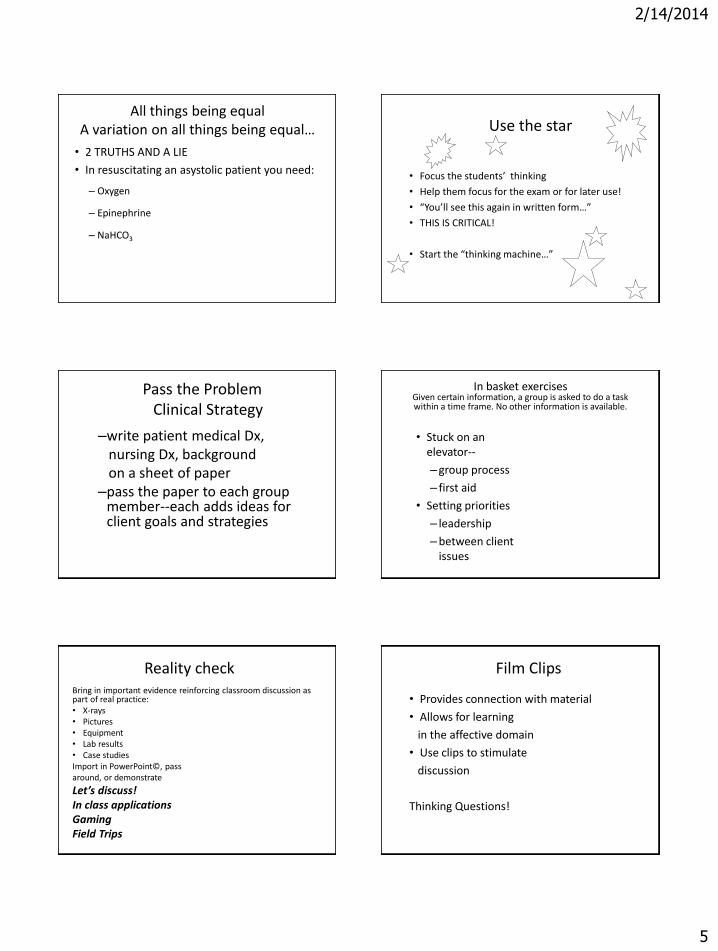
2/14/2014
5
All things being equal A variation on all things being equal…
• 2 TRUTHS AND A LIE
• In resuscitating an asystolic patient you need:
– Oxygen
– Epinephrine
– NaHCO3
Use the star
• Focus the students’ thinking
• Help them focus for the exam or for later use!
• “You’ll see this again in written form…”
• THIS IS CRITICAL!
• Start the “thinking machine…”
Pass the Problem Clinical Strategy
–write patient medical Dx, nursing Dx, background on a sheet of paper –pass the paper to each group
member--each adds ideas for client goals and strategies
In basket exercises Given certain information, a group is asked to do a task within a time frame. No other information is available.
• Stuck on an elevator--
–group process
– first aid
• Setting priorities
– leadership
–between client issues
Reality check Bring in important evidence reinforcing classroom discussion as part of real practice: • X-rays • Pictures • Equipment • Lab results • Case studies Import in PowerPoint©, pass around, or demonstrate
Let’s discuss! In class applications Gaming Field Trips
Film Clips
• Provides connection with material
• Allows for learning
in the affective domain
• Use clips to stimulate
discussion
Thinking Questions!
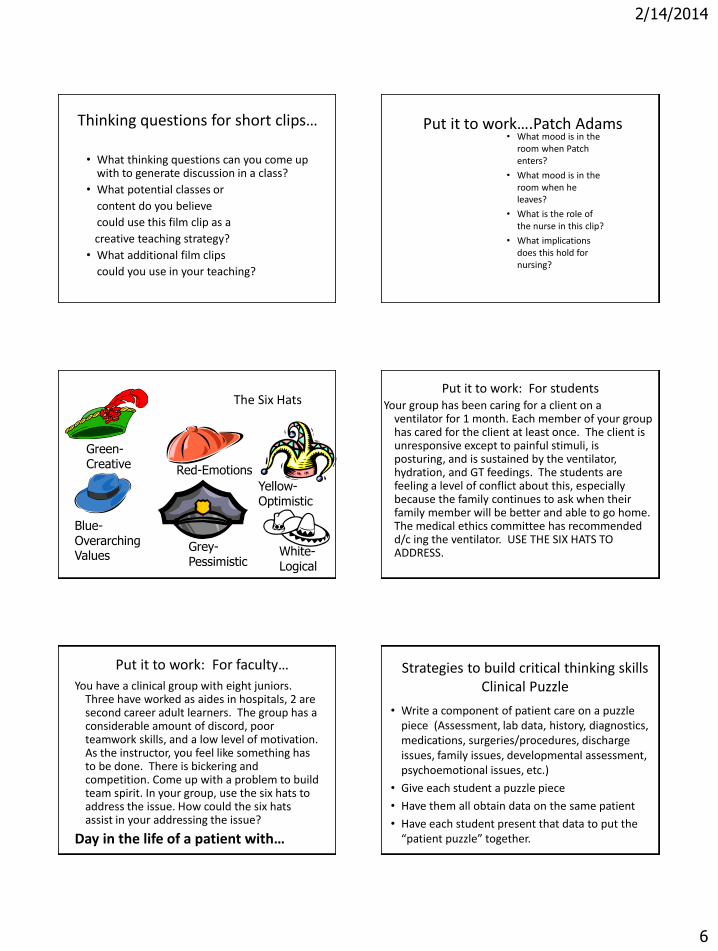
2/14/2014
6
Thinking questions for short clips…
• What thinking questions can you come up with to generate discussion in a class?
• What potential classes or
content do you believe
could use this film clip as a
creative teaching strategy?
• What additional film clips
could you use in your teaching?
Put it to work….Patch Adams • What mood is in the
room when Patch enters?
• What mood is in the room when he leaves?
• What is the role of the nurse in this clip?
• What implications does this hold for nursing?
The Six Hats
Green-Creative
Grey-Pessimistic
Red-Emotions
Yellow- Optimistic
Blue- Overarching Values White-
Logical
Put it to work: For students Your group has been caring for a client on a
ventilator for 1 month. Each member of your group has cared for the client at least once. The client is unresponsive except to painful stimuli, is posturing, and is sustained by the ventilator, hydration, and GT feedings. The students are feeling a level of conflict about this, especially because the family continues to ask when their family member will be better and able to go home. The medical ethics committee has recommended d/c ing the ventilator. USE THE SIX HATS TO ADDRESS.
Put it to work: For faculty…
You have a clinical group with eight juniors. Three have worked as aides in hospitals, 2 are second career adult learners. The group has a considerable amount of discord, poor teamwork skills, and a low level of motivation. As the instructor, you feel like something has to be done. There is bickering and competition. Come up with a problem to build team spirit. In your group, use the six hats to address the issue. How could the six hats assist in your addressing the issue?
Day in the life of a patient with…
Strategies to build critical thinking skills Clinical Puzzle
• Write a component of patient care on a puzzle piece (Assessment, lab data, history, diagnostics, medications, surgeries/procedures, discharge issues, family issues, developmental assessment, psychoemotional issues, etc.)
• Give each student a puzzle piece
• Have them all obtain data on the same patient
• Have each student present that data to put the “patient puzzle” together.
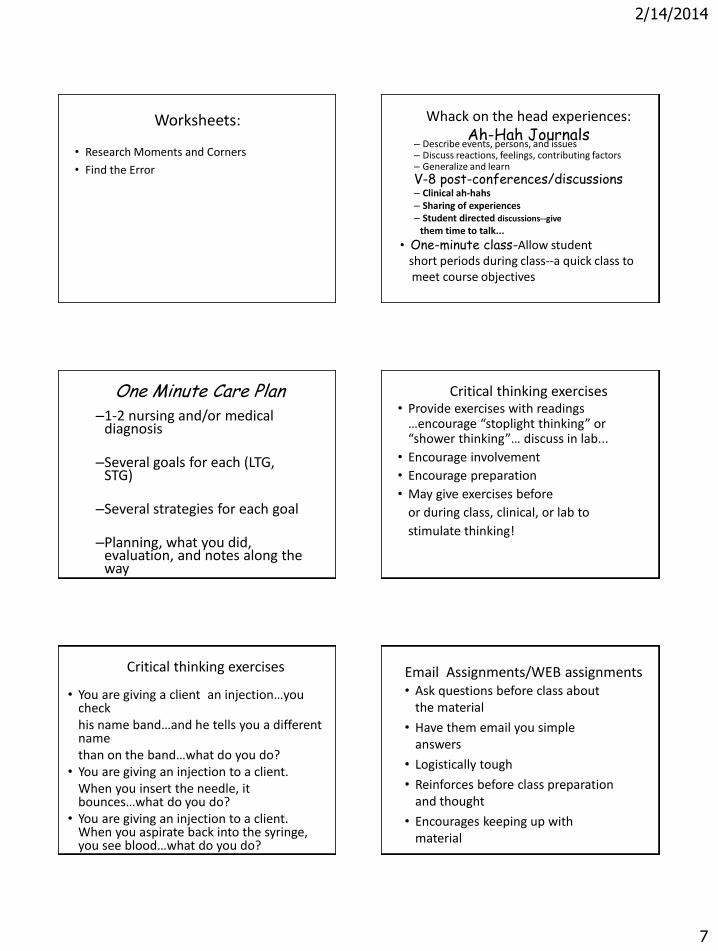
2/14/2014
7
Worksheets:
• Research Moments and Corners
• Find the Error
Whack on the head experiences: Ah-Hah Journals
– Describe events, persons, and issues – Discuss reactions, feelings, contributing factors – Generalize and learn
V-8 post-conferences/discussions – Clinical ah-hahs – Sharing of experiences – Student directed discussions--give
them time to talk...
• One-minute class-Allow student short periods during class--a quick class to meet course objectives
One Minute Care Plan –1-2 nursing and/or medical
diagnosis –Several goals for each (LTG,
STG) –Several strategies for each goal
–Planning, what you did,
evaluation, and notes along the way
–Discuss in pre/post-conference or in group discussion
Critical thinking exercises • Provide exercises with readings
…encourage “stoplight thinking” or “shower thinking”… discuss in lab...
• Encourage involvement
• Encourage preparation
• May give exercises before
or during class, clinical, or lab to
stimulate thinking!
Critical thinking exercises
• You are giving a client an injection…you check
his name band…and he tells you a different name
than on the band…what do you do? • You are giving an injection to a client. When you insert the needle, it
bounces…what do you do? • You are giving an injection to a client.
When you aspirate back into the syringe, you see blood…what do you do?
Email Assignments/WEB assignments • Ask questions before class about
the material
• Have them email you simple answers
• Logistically tough
• Reinforces before class preparation and thought
• Encourages keeping up with material
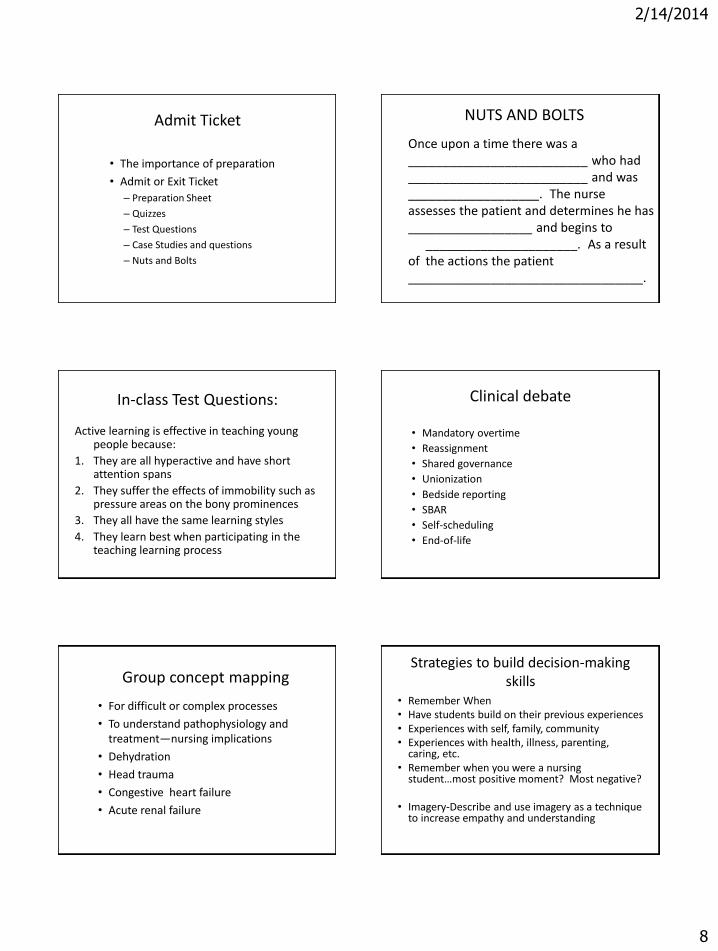
2/14/2014
8
Admit Ticket
• The importance of preparation
• Admit or Exit Ticket
– Preparation Sheet
– Quizzes
– Test Questions
– Case Studies and questions
– Nuts and Bolts
NUTS AND BOLTS
Once upon a time there was a __________________________ who had __________________________ and was ___________________. The nurse assesses the patient and determines he has __________________ and begins to ______________________. As a result of the actions the patient __________________________________.
In-class Test Questions:
Active learning is effective in teaching young people because:
1. They are all hyperactive and have short attention spans
2. They suffer the effects of immobility such as pressure areas on the bony prominences
3. They all have the same learning styles
4. They learn best when participating in the teaching learning process
Clinical debate
• Mandatory overtime
• Reassignment
• Shared governance
• Unionization
• Bedside reporting
• SBAR
• Self-scheduling
• End-of-life
Group concept mapping
• For difficult or complex processes
• To understand pathophysiology and treatment—nursing implications
• Dehydration
• Head trauma
• Congestive heart failure
• Acute renal failure
Strategies to build decision-making skills
• Remember When • Have students build on their previous experiences • Experiences with self, family, community • Experiences with health, illness, parenting,
caring, etc. • Remember when you were a nursing
student…most positive moment? Most negative?
• Imagery-Describe and use imagery as a technique to increase empathy and understanding
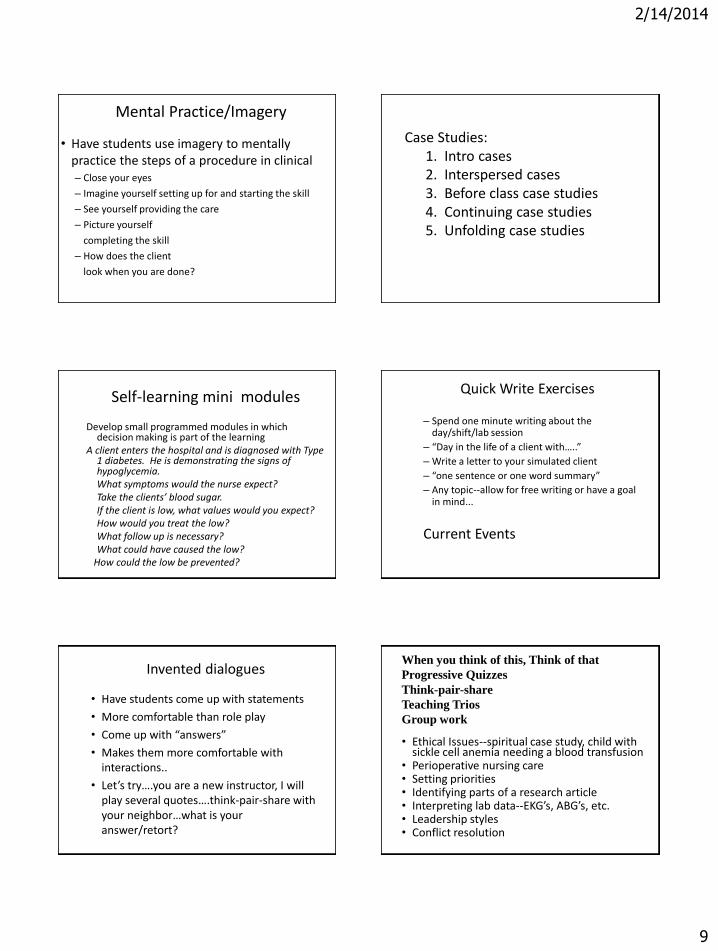
2/14/2014
9
Mental Practice/Imagery
• Have students use imagery to mentally practice the steps of a procedure in clinical – Close your eyes
– Imagine yourself setting up for and starting the skill
– See yourself providing the care
– Picture yourself
completing the skill
– How does the client
look when you are done?
Case Studies: 1. Intro cases 2. Interspersed cases 3. Before class case studies 4. Continuing case studies 5. Unfolding case studies
Self-learning mini modules
Develop small programmed modules in which decision making is part of the learning
A client enters the hospital and is diagnosed with Type 1 diabetes. He is demonstrating the signs of hypoglycemia.
What symptoms would the nurse expect? Take the clients’ blood sugar. If the client is low, what values would you expect? How would you treat the low? What follow up is necessary? What could have caused the low? How could the low be prevented?
Quick Write Exercises
– Spend one minute writing about the day/shift/lab session
– “Day in the life of a client with…..”
– Write a letter to your simulated client
– “one sentence or one word summary”
– Any topic--allow for free writing or have a goal in mind...
Current Events
Invented dialogues
• Have students come up with statements
• More comfortable than role play
• Come up with “answers”
• Makes them more comfortable with interactions..
• Let’s try….you are a new instructor, I will play several quotes….think-pair-share with your neighbor…what is your answer/retort?
• Ethical Issues--spiritual case study, child with sickle cell anemia needing a blood transfusion
• Perioperative nursing care • Setting priorities • Identifying parts of a research article • Interpreting lab data--EKG’s, ABG’s, etc. • Leadership styles • Conflict resolution
When you think of this, Think of that
Progressive Quizzes
Think-pair-share
Teaching Trios
Group work
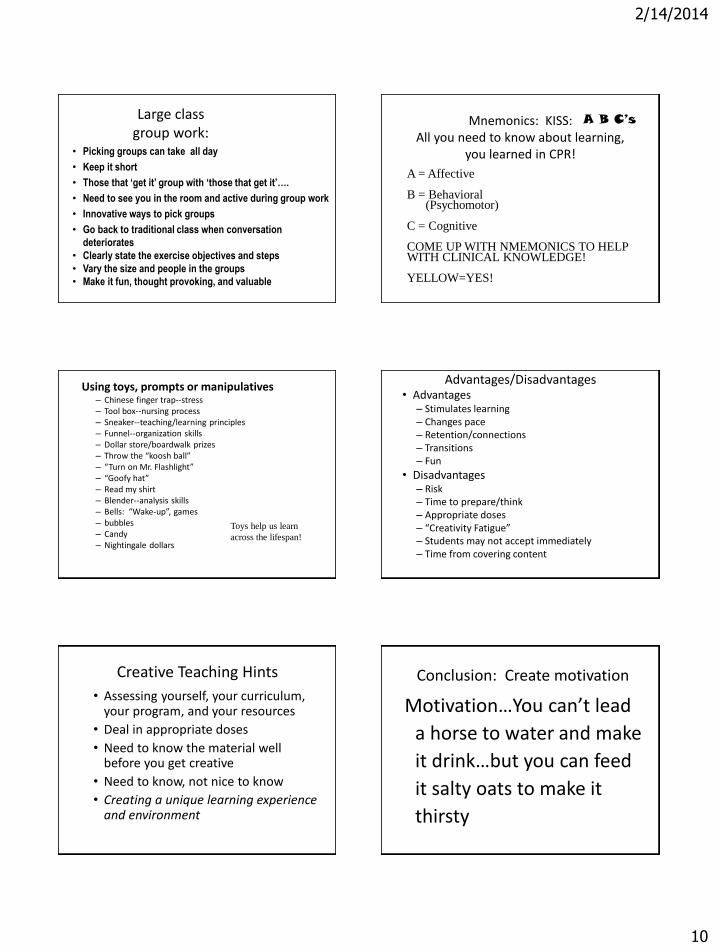
2/14/2014
10
Large class group work:
• Picking groups can take all day
• Keep it short
• Those that ‘get it’ group with ‘those that get it’….
• Need to see you in the room and active during group work
• Innovative ways to pick groups
• Go back to traditional class when conversation
deteriorates
• Clearly state the exercise objectives and steps
• Vary the size and people in the groups
• Make it fun, thought provoking, and valuable
Mnemonics: KISS: All you need to know about learning,
you learned in CPR!
A = Affective B = Behavioral (Psychomotor) C = Cognitive COME UP WITH NMEMONICS TO HELP WITH CLINICAL KNOWLEDGE! YELLOW=YES!
A B C’s
Using toys, prompts or manipulatives – Chinese finger trap--stress – Tool box--nursing process – Sneaker--teaching/learning principles – Funnel--organization skills – Dollar store/boardwalk prizes – Throw the “koosh ball” – “Turn on Mr. Flashlight” – “Goofy hat” – Read my shirt – Blender--analysis skills – Bells: “Wake-up”, games – bubbles – Candy – Nightingale dollars
Toys help us learn
across the lifespan!
Advantages/Disadvantages • Advantages
– Stimulates learning – Changes pace – Retention/connections – Transitions – Fun
• Disadvantages – Risk – Time to prepare/think – Appropriate doses – “Creativity Fatigue” – Students may not accept immediately – Time from covering content
Creative Teaching Hints
• Assessing yourself, your curriculum, your program, and your resources
• Deal in appropriate doses
• Need to know the material well before you get creative
• Need to know, not nice to know
• Creating a unique learning experience and environment
Conclusion: Create motivation
Motivation…You can’t lead
a horse to water and make
it drink…but you can feed
it salty oats to make it
thirsty
1
JudithW.Herrman,PhD,[email protected]
References
Benner,P.(2009).Educatingnurses:Acallforradicaltransformation.NewYork:
JosseyBass.Billings,D.,&Halstead,J.(2013).Teachinginnursing:Aguideforfaculty.
Philadelphia:Saunders.Bradshaw,M.,&Lowenstein,A.(2013).Innovativeteachingstrategiesinnursingand
therelatedhealthprofessions.NewYork:JonesandBartlett.DeYoung,S.(2008).TeachingStrategiesforNurseEducators.UpperSaddleRiver,
NJ:PrenticeHall.Glendon,K.&Ulrich,D.L.(1997).Unfoldingcases:Anexperientiallearningmodel.
NurseEducator,22(4),15‐18.Glendon,K.,&Ulrich,D.L.(2000).Unfoldingcases:Experiencingtherealitiesof
clinicalnursingpractice.UpperSaddleRiver,NJ:PrenticeHall.Herrman,J.W.(2011).Keepingtheirattention:Innovativestrategiesfornursing
education.JournalofContinuingEducationinNursing,42(10),449‐456.Herrman,J.(2008).Creativeteachingstrategiesforthenurseeducator.Philadelphia:
FADavis.Herrman,J.(2006).Usingfilmclipstoenhancenursingeducation.NurseEducator,
31(6).Herrman,J.(2002).The60‐secondnurseeducator:Creativestrategiestoinspire
learning.NursingEducationPerspectives,23(5),222‐227.Herrman,J.,Saunders,A.,&Selekman,J.(1998).Beyondhospitalwalls:Educating
pediatricnursesforthenextmillennium.PediatricNursing,24,96‐99.Penn,B.(2008).Masteringtheteachingrole:Aguidefornurseeducators.
Philadelphia,PA:F.A.Davis.Ulrich,D.L.&Glendon,K.J.(2005).Interactivegrouplearning:Strategiesfornurse
educators.NewYork:Springer..
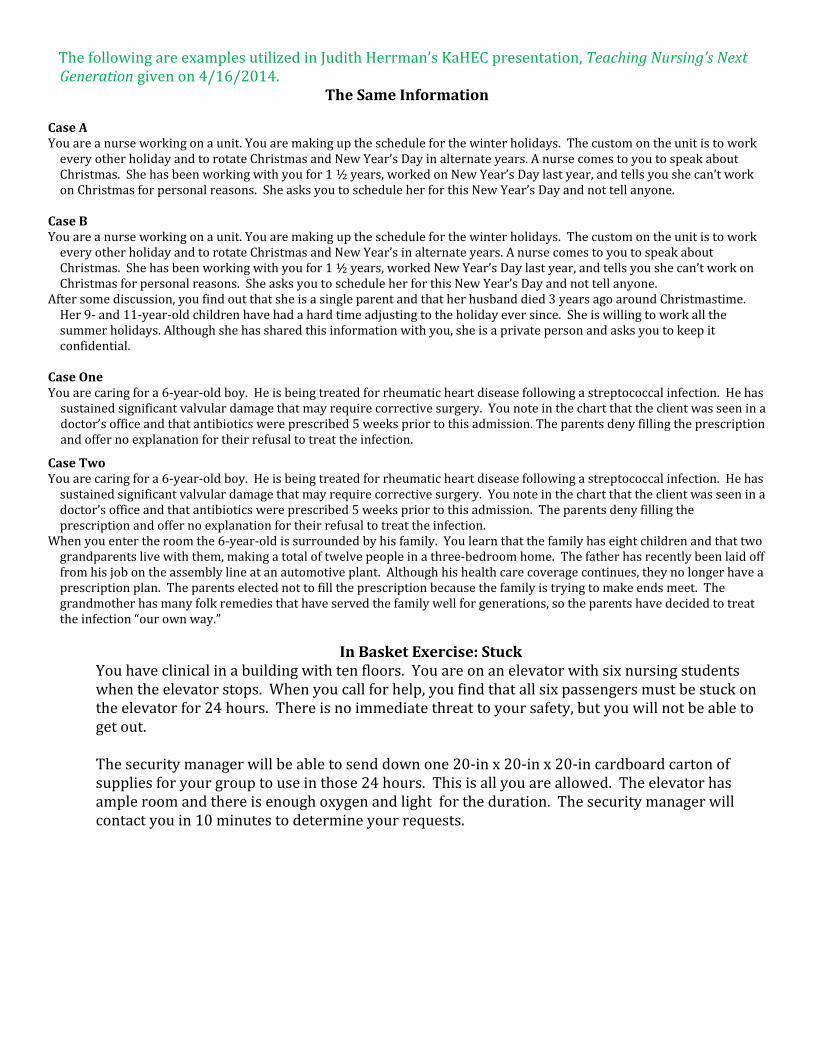
ThefollowingareexamplesutilizedinJudithHerrman’sKaHECpresentation,TeachingNursing’sNextGenerationgivenon4/16/2014.
TheSameInformationCaseAYouareanurseworkingonaunit.Youaremakingupthescheduleforthewinterholidays.ThecustomontheunitistoworkeveryotherholidayandtorotateChristmasandNewYear’sDayinalternateyears.AnursecomestoyoutospeakaboutChristmas.Shehasbeenworkingwithyoufor1½years,workedonNewYear’sDaylastyear,andtellsyoushecan’tworkonChristmasforpersonalreasons.SheasksyoutoscheduleherforthisNewYear’sDayandnottellanyone.
CaseBYouareanurseworkingonaunit.Youaremakingupthescheduleforthewinterholidays.ThecustomontheunitistoworkeveryotherholidayandtorotateChristmasandNewYear’sinalternateyears.AnursecomestoyoutospeakaboutChristmas.Shehasbeenworkingwithyoufor1½years,workedNewYear’sDaylastyear,andtellsyoushecan’tworkonChristmasforpersonalreasons.SheasksyoutoscheduleherforthisNewYear’sDayandnottellanyone.
Aftersomediscussion,youfindoutthatsheisasingleparentandthatherhusbanddied3yearsagoaroundChristmastime.Her9‐and11‐year‐oldchildrenhavehadahardtimeadjustingtotheholidayeversince.Sheiswillingtoworkallthesummerholidays.Althoughshehassharedthisinformationwithyou,sheisaprivatepersonandasksyoutokeepitconfidential.
CaseOneYouarecaringfora6‐year‐oldboy.Heisbeingtreatedforrheumaticheartdiseasefollowingastreptococcalinfection.Hehassustainedsignificantvalvulardamagethatmayrequirecorrectivesurgery.Younoteinthechartthattheclientwasseeninadoctor’sofficeandthatantibioticswereprescribed5weekspriortothisadmission.Theparentsdenyfillingtheprescriptionandoffernoexplanationfortheirrefusaltotreattheinfection.
CaseTwoYouarecaringfora6‐year‐oldboy.Heisbeingtreatedforrheumaticheartdiseasefollowingastreptococcalinfection.Hehassustainedsignificantvalvulardamagethatmayrequirecorrectivesurgery.Younoteinthechartthattheclientwasseeninadoctor’sofficeandthatantibioticswereprescribed5weekspriortothisadmission.Theparentsdenyfillingtheprescriptionandoffernoexplanationfortheirrefusaltotreattheinfection.
Whenyouentertheroomthe6‐year‐oldissurroundedbyhisfamily.Youlearnthatthefamilyhaseightchildrenandthattwograndparentslivewiththem,makingatotaloftwelvepeopleinathree‐bedroomhome.Thefatherhasrecentlybeenlaidofffromhisjobontheassemblylineatanautomotiveplant.Althoughhishealthcarecoveragecontinues,theynolongerhaveaprescriptionplan.Theparentselectednottofilltheprescriptionbecausethefamilyistryingtomakeendsmeet.Thegrandmotherhasmanyfolkremediesthathaveservedthefamilywellforgenerations,sotheparentshavedecidedtotreattheinfection“ourownway.”
InBasketExercise:Stuck
Youhaveclinicalinabuildingwithtenfloors.Youareonanelevatorwithsixnursingstudentswhentheelevatorstops.Whenyoucallforhelp,youfindthatallsixpassengersmustbestuckontheelevatorfor24hours.Thereisnoimmediatethreattoyoursafety,butyouwillnotbeabletogetout. Thesecuritymanagerwillbeabletosenddownone20‐inx20‐inx20‐incardboardcartonofsuppliesforyourgrouptouseinthose24hours.Thisisallyouareallowed.Theelevatorhasampleroomandthereisenoughoxygenandlightfortheduration.Thesecuritymanagerwillcontactyouin10minutestodetermineyourrequests.