Health promotion needs of physically disabled individuals with lower limb amputation in Rwanda
13
REHABILITATION IN PRACTICE Health promotion needs of physically disabled individuals with lower limb amputation in Rwanda SEYI L. AMOSUN 1 , EUGENE MUTIMURA 2 , & JOSE M. FRANTZ 3 1 Division of Physiotherapy, School of Health & Rehabilitation Sciences, University of Cape Town, South Africa, 2 Department of Physiotherapy, Kigali Health Institute, Kigali, Rwanda, and 3 Department of Physiotherapy, University of the Western Cape, South Africa Abstract Purpose. The objectives of the study were to identify the health-related behaviors among physically disabled individuals with lower limb amputation resident in Rwanda, the factors that influenced these behaviors, and the major issues that should be targeted in health promotion programs for physically disabled individuals with lower limb amputation. Method. A cross-sectional survey, utilizing a self-administered questionnaire, was carried out among 334 lower limb amputees who volunteered to take part in the study. In addition, a sub-sample of 15 participants was purposively selected for in-depth face-to-face interviews. Results. Many participants did not engage in physical exercises (64.7%). Others abused alcohol on daily basis (14.4%), smoked 11 – 20 cigarettes daily (13.2%), and used recreational drugs such as marijuana, opium and cocaine (9.6%). There were significant associations between the age group of the participants and participation in exercises (P = 0.001), and consuming alcohol, tobacco and recreational drugs (P = 0.001). In-depth interviews revealed factors influencing the behavior of participants. Conclusions. Participants were found to be at risk of secondary complications because of poor lifestyle choices. There is a need to develop and promote wellness-enhancing behaviors in order to enhance the health status of physically disabled individuals in Rwanda who have lower limb amputations. Keywords: Physically disabled, health promotion, health-related behaviors, Rwanda Introduction Rwanda is a mountainous, landlocked central African country. The general population profile in terms of size and geographical distribution has been profoundly distorted by the civil war between 1990 and 1995 [1]. Recently, the 2003 national census indicated a population of 8.3 million, and the adult literacy rate was 70% [2]. Due to inadequacy of healthcare facilities and lack of timely treatment intervention, both the military and civilian popula- tions remain severely physically and psychologically traumatized as a result of the war [3]. The impact of the war on youth and children had been particularly severe. The period of war resulted in a high prevalence of physical disabilities and associated secondary com- plications. Although there are no reliable statistical data on the prevalence of physical disabilities in Rwanda, the most common physical disability appears to be lower limb amputation. The Australian Medical Support Force (AS MSF) to Rwanda carried out a retrospective study of all operative surgery performed during the 1-year long deploy- ment from August 1994, and estimated the prevalence of amputations to be about 8.0% of the total 750 operations performed, the majority of which were caused by land mine blasts [1]. In addition, the annual statistical records at Central Hospital of Kigali for the period 1997 – 2000 revealed an alarming increase in number of lower limb amputation, more than 50% of which were caused by the land mines that maimed thousands of Rwandan people [4]. After the war, there was a remarkable transition from conflict management to peace and sustainable Correspondence: S. L. Amosun, Division of Physiotherapy, School of Health & Rehabilitation Sciences, Faculty of Health Sciences, University of Cape Town, Anzio Road, Observatory 7925, Republic of South Africa. Tel: 27 21 406 6205. Fax: 27 21 406 6323. E-mail: [email protected] Accepted October 2004. Disability and Rehabilitation, 2005; 27(14): 837 – 847 ISSN 0963-8288 print/ISSN 1464-5165 online # 2005 Taylor & Francis Group Ltd DOI: 10.1080/09638280400018676
Transcript of Health promotion needs of physically disabled individuals with lower limb amputation in Rwanda

REHABILITATION IN PRACTICE
Health promotion needs of physically disabled individuals with lowerlimb amputation in Rwanda
SEYI L. AMOSUN1, EUGENE MUTIMURA2, & JOSE M. FRANTZ3
1Division of Physiotherapy, School of Health & Rehabilitation Sciences, University of Cape Town, South Africa, 2Department
of Physiotherapy, Kigali Health Institute, Kigali, Rwanda, and 3Department of Physiotherapy, University of the Western
Cape, South Africa
AbstractPurpose. The objectives of the study were to identify the health-related behaviors among physically disabled individuals withlower limb amputation resident in Rwanda, the factors that influenced these behaviors, and the major issues that should betargeted in health promotion programs for physically disabled individuals with lower limb amputation.Method. A cross-sectional survey, utilizing a self-administered questionnaire, was carried out among 334 lower limbamputees who volunteered to take part in the study. In addition, a sub-sample of 15 participants was purposively selected forin-depth face-to-face interviews.Results. Many participants did not engage in physical exercises (64.7%). Others abused alcohol on daily basis (14.4%),smoked 11 – 20 cigarettes daily (13.2%), and used recreational drugs such as marijuana, opium and cocaine (9.6%). Therewere significant associations between the age group of the participants and participation in exercises (P=0.001), andconsuming alcohol, tobacco and recreational drugs (P=0.001). In-depth interviews revealed factors influencing the behaviorof participants.Conclusions. Participants were found to be at risk of secondary complications because of poor lifestyle choices. There is aneed to develop and promote wellness-enhancing behaviors in order to enhance the health status of physically disabledindividuals in Rwanda who have lower limb amputations.
Keywords: Physically disabled, health promotion, health-related behaviors, Rwanda
Introduction
Rwanda is a mountainous, landlocked central
African country. The general population profile in
terms of size and geographical distribution has been
profoundly distorted by the civil war between 1990
and 1995 [1]. Recently, the 2003 national census
indicated a population of 8.3 million, and the adult
literacy rate was 70% [2]. Due to inadequacy of
healthcare facilities and lack of timely treatment
intervention, both the military and civilian popula-
tions remain severely physically and psychologically
traumatized as a result of the war [3]. The impact of
the war on youth and children had been particularly
severe.
The period of war resulted in a high prevalence of
physical disabilities and associated secondary com-
plications. Although there are no reliable statistical
data on the prevalence of physical disabilities in
Rwanda, the most common physical disability
appears to be lower limb amputation. The Australian
Medical Support Force (AS MSF) to Rwanda
carried out a retrospective study of all operative
surgery performed during the 1-year long deploy-
ment from August 1994, and estimated the
prevalence of amputations to be about 8.0% of the
total 750 operations performed, the majority of
which were caused by land mine blasts [1]. In
addition, the annual statistical records at Central
Hospital of Kigali for the period 1997 – 2000
revealed an alarming increase in number of lower
limb amputation, more than 50% of which were
caused by the land mines that maimed thousands of
Rwandan people [4].
After the war, there was a remarkable transition
from conflict management to peace and sustainable
Correspondence: S. L. Amosun, Division of Physiotherapy, School of Health & Rehabilitation Sciences, Faculty of Health Sciences, University of Cape Town,
Anzio Road, Observatory 7925, Republic of South Africa. Tel: 27 21 406 6205. Fax: 27 21 406 6323. E-mail: [email protected]
Accepted October 2004.
Disability and Rehabilitation, 2005; 27(14): 837 – 847
ISSN 0963-8288 print/ISSN 1464-5165 online # 2005 Taylor & Francis Group Ltd
DOI: 10.1080/09638280400018676

development. The highest priority of health policy
was to enhance the quality of life of all nationals
through equity, by providing opportunities to enjoy
health and related privileges through community
participation [2]. For example, people who have had
lower limb amputation required prosthesis, along
with a substantial rehabilitation program in order to
be fully re-integrated into society [5,6]. Therefore,
part of the goal of the post-war health policy was to
promote health and wellness for people with dis-
abilities, and prevent unwarranted secondary
complications.
A number of factors are known to exacerbate the
level of physical disability. These factors included but
not limited to poverty, high level of illiteracy and
poor choice of lifestyle [2,7 – 9]. Physically disabled
individuals are often left to manage their lives with
little help [10], which often leads to frustration.
Hogan et al. [11] reported that students with physical
disabilities were more likely to engage in substance
abuse, cigarette smoking, and sedentary lifestyles
than their non-disabled fellow students. Social
isolation, low self-esteem and anxiety were also
reported among the same group of people with
physical disabilities. Other studies have advocated for
collective efforts to improve the lives of people with
physical disabilities through health-enhancing beha-
viors [12 – 14]. The strategy is to empower people
with physical disabilities to take control of their lives
by motivating them to engage in healthy lifestyle
behaviors [15 – 17]. There is the perception that
there have been few programs and little research
aimed at addressing issues of health promotion needs
among people with physical disabilities [13], parti-
cularly in African countries.
The intention of the researchers was to contribute
to the goal of promoting health and wellness for
people with physical disabilities in Rwanda, and
prevent unwarranted secondary complications. The
specific objectives of this study were therefore to
identify (i) the health-related behaviors among
physically disabled individuals with lower limb
amputation, (ii) the factors that influenced the
behaviors, and (iii) the major issues that should be
targeted by health care professionals and policy
makers in health promotion programs for physically
disabled individuals with lower limb amputation.
This is consistent with the goals of the African
Decade of Disabled People (2000 – 2009) [18] in
attempting to improve the quality of life of people
with disability in Africa.
Materials and methods
Both descriptive quantitative and qualitative analytic
designs were utilized in the study. The study was
carried out in the Republic of Rwanda with settings
at three referral hospitals and two rehabilitation
centers that are known nationally for the provision of
rehabilitation services for amputees (see Appendix I).
In addition to the subjects identified through
attendance at the above-mentioned medical facilities,
the national radio was utilized to further recruit
eligible participants. The participants were indivi-
duals aged 12 – 60 years who had either unilateral or
bilateral lower limb amputation. Inclusion criteria
included the ability to read and write, and the
cognitive ability to comprehend and complete the
questionnaire without assistance. Exclusion criteria
included severe cognitive problems and additional
disabilities such as blindness or deafness. Three
hundred and eighty-six participants volunteered to
participate in the cross-sectional survey of their own
health-related behaviors. Purposive sampling was
later used to recruit fifteen participants for face-to-
face interviews, three from each of the research
settings. Individuals who expressed willingness to be
interviewed were targeted.
Instrumentation
The instrumentation consisted of a self-administered
questionnaire based on published literature [11,14]
which were designed to identify the health-related
behaviors of participants (see Appendix II). Due to
the general low level of literacy, the wording of the
questionnaire was simplified. The questionnaire was
divided into three sections, A to C. Section A
requested for demographic characteristics such as
age, gender, marital status, employment status, level
of education, as well as disability-related character-
istics including the level of lower limb amputation.
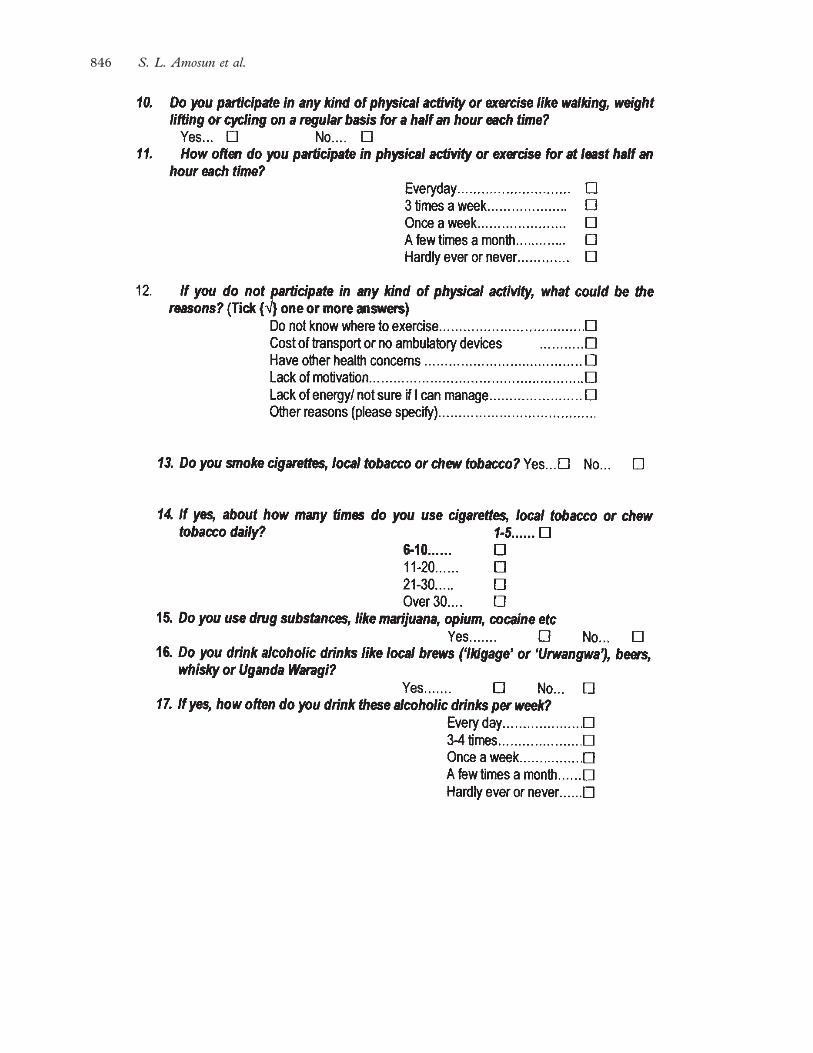
In section B, the variables assessed included
participation in physical exercises, the use of
different substances such as tobacco, recreational
drugs, and alcohol consumption. The use of tobacco
included chewing tobacco, smoking cigarettes or
smoking the local tobacco called ‘gusuguta’. The
recreational drugs included marijuana, opium, and
cocaine. Alcohol consumption included local brews,
beers, and whisky. Although there are other health-
related behaviors that influence quality of life, the
variables assessed in this study were limited to the
behaviors observed during the planning phase of the
research. Finally in section C, participants were
requested to identify programs and activities they
perceived as essential to improve their well being.
Forward and back translation was used to translate
the questionnaire from English to local Kinyarwanda
language, as the majority of the participants did not
write nor speak English.
Face-to-face interviews were used to provide in-
depth descriptions of the participants’ health-related
behaviors, and the reasons for their engagement in
838 S. L. Amosun et al.

these behaviors. The interview guide consisted of a
series of probes that endeavored to obtain an in-
depth justification of the practice of various health-
related behaviors. The interviews were directed,
purposeful conversations during which the partici-
pants’ lifestyle experiences, and the meaning
attached to those experiences were explored in detail.
Procedure
Due to the low educational background and poor
socio-economic status that characterize the majority
of the Rwandan population, many people in rural
areas do not read newspapers or watch the national
television. Therefore, for the majority of Rwandan
society, the main reliable source of information
remains the national radio. Radio announcements
and posters were therefore used to request interested
persons with lower limb amputation to participate in
the study. The prospective participants included
those who were receiving or had received rehabilita-
tion services from the five centers. The radio
announcements invited volunteers to meet with a
research team in any of the five research settings on a
given date and time. Radio announcement had
always been used as a faster and more efficient
means of communication with persons with disabil-
ities. For instance, when lower limb amputee
patients had their provisional wooden prostheses
changed to definitive polypropylene prostheses, a
large number of amputees responded to a radio
announcement.
Six newly qualified physiotherapists were recruited
and trained as field research assistants. The research
assistant in each research setting met with the
participants, explained the purpose and possible
benefits of the study to the participants, obtained
informed consent, distributed the questionnaires and
collected them after completion. At each of the
research settings, one of the authors (EM) organized
and carried out the face-to-face interviews. The
quantitative and qualitative data were analyzed
separately, but used to complement each other in
order to present a deeper understanding of the
findings of the study. The quantitative data were
analyzed descriptively using the Statistical Package
for Social Sciences (SPSS; version 10.0), and the
relationship between variables were analyzed using
the chi-square test. The common themes in the
qualitative data were also identified, using the
qualitative data to illustrate and highlight some of
the quantitative data.
Results
Out of a total of 386 participants who responded to
the radio announcements and received the question-
naires for the cross-sectional survey, 342 participants
completed the questionnaire (88.6% response rate).
However, eight of the returned questionnaires were
incomplete and therefore not eligible for data
analysis. The mean age of the participants (n=334)
was 30.4 years (SD=13.4). The socio-demographic
characteristics of the study sample, and the disability-
related characteristics of the participants are, respec-
tively, summarized in Tables I and II.
Two hundred and sixteen (64.7%) participants did
not participate in any kind of physical exercises,
while 118 (35.3%) participants participated in some
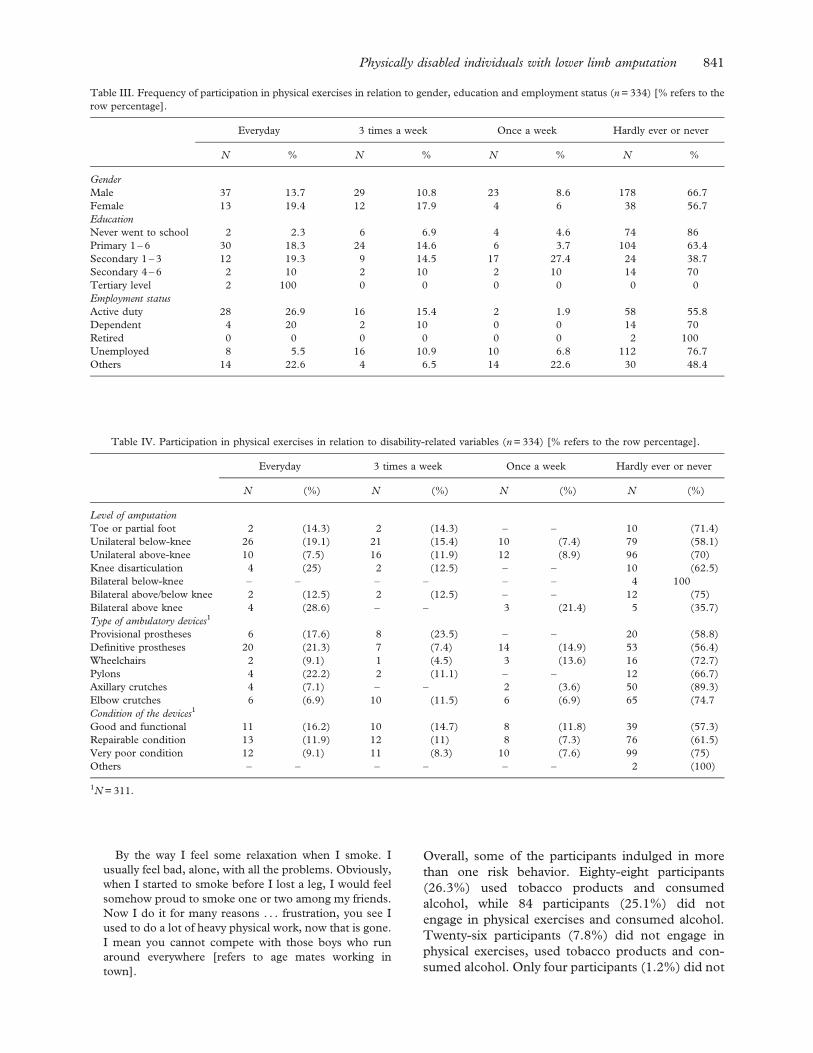
kind of physical exercises. The frequency of partici-
pation in physical exercises in relation to gender,
level of education and employment status are
summarized in Table III. Using the w2-test, there
was no significant difference in frequency of partici-
pation in physical exercises between males and
females (P=0.275), whereas the difference in fre-
quency of participation was significant for level of
education and employment status (P5 0.001 in each
case). The younger participants took part in more
physical exercise than the older participants
(P=0.001).
The frequency of participation in physical exer-
cises in relation to disability-related characteristics
are summarized in Table IV. Conclusively, the type
of ambulatory devices appeared to significantly
influence participation in physical exercises using
the w2-test (P5 0.001), but the condition of the
devices was not as significant (P5 0.05).
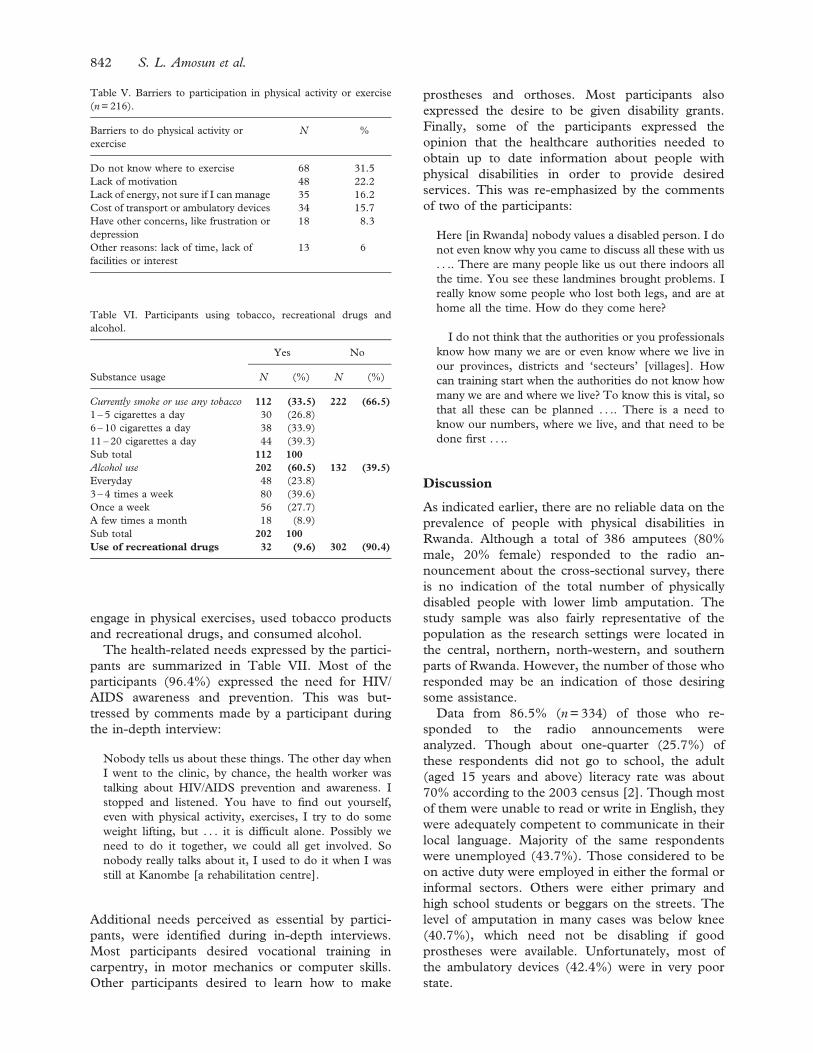
Table V gives a summary of the barriers to
participation in physical exercises among those who
hardly ever or never participated in physical exercises
(n=216). The greatest barrier to participation was
Table I. Socio-demographic characteristics of the study sample
(n=334).
Variable
measured Characteristics n %
Gender Male 267 80
Female 67 20
Marital status Single 155 46.4
Married 131 39.2
Divorced or separated 10 3.0
Widowed 38 11.4
Education Never went to school 86 25.7
Primary 1 – 6 164 49.1
Secondary 1 – 3 62 18.6
Secondary 4 – 6 20 6.0
Tertiary education 2 0.6
Employment Active duty 104 31.1
status Dependent 20 6.0
Retired 2 0.6
Unemployed 146 43.7
Others 62 18.6
Physically disabled individuals with lower limb amputation 839

lack of knowledge of where to exercise (n=68). One
of the participants in the face-to-face interview
commented:
I do not know if there are places around for us to do the
exercises. Other people [the non-disabled] do the
exercises in those places. Maybe it would be good to
do the exercises with others. I mean one would try to do
it more or less like others. I really do not know where
others like us do the exercises. It is difficult when it
comes to running up and down the stairs with those who
are well, how can one compete?
Lack of self-motivation to exercise safely was also
highlighted in the interviews:
I do not do any physical activity, not because there are
no facilities, but I have never thought about it. Where
would I start? The other time when I went to
Nyamirambo [stadium] on the day for the disabled, I
saw what the boys were doing, those boys from Gatenga
[Centre for training acrobats], I felt moved. I am sure I
can also manage those manoeuvres, but I have never
thought about those exercises. In a fact, no one has ever
encouraged me to start the exercises.
For me if I could get someone to enlighten me about
the exercises. Personally, I lack someone to motivate me,
you know. I used to do some jogging when I was young,
and felt very strong and healthy. Now I would do
something else, weight lifting . . ..
[Pauses] . . . and . . . other activities.
Table VI summarizes the frequencies at which
the participants currently used tobacco products,
hard drugs, and consumed alcoholic drinks. The
majority of smokers currently smoked 11 – 20
cigarettes daily. Over one-third of those who
consumed alcohol drank 3 – 4 times a week, and
about 10% of participants used recreational
drugs. Chi-square tests indicated a significant
association between age of the participants and
tobacco use (P=0.001) and alcohol consumption
(P=0.004). The majority of those who consumed
tobacco, alcohol and recreational drugs were in
the 21 – 30-year age group.
In-depth interviews revealed some of the reasons
why participants were using these substances. One
participant explained:
I wouldn’t like to take drugs, smoke or even drink
alcohol, but my friend, if you were in my place, you
would find yourself doing all this too. To me, life has
changed. When I lost the first leg, at least, but now
things are not easy. I feel low in society . . . [shakes head]
inferior to others, and have to accept any job. Certainly
life plans have changed, some how I try to swallow it but
. . . [stops] . . .
Another participant further explained:
Drugs, they are fine, you get self-satisfaction, get
contented with the little you have. It has many effects,
but for me, it is fine.
During in-depth interviews, it was clear that some
participants got involved in drug abuse before
amputation. However, the presence of the disability
appeared to have exacerbated the behavior. One
participant commented:
I started to take drugs nine years ago before I lost a leg.
When I lost my leg, I found myself taking more of it
[drugs]. More because when I am in low spirits, maybe
depressed, and I take it, I feel delighted and tend to
forget lots of troubles.
Additional reasons for indulging in the behaviors
expressed by two participants are given below –
I take a bit [refers to drugs] and tend not to think a
lot about my problems. I am not a professional, have
no job, yet I have to do this and that to survive, and
my family of course. I should say it is much more
difficult now to manage all this. It is very dishearten-
ing, but when I smoke, I get a settled mind. I used to
have sleep problems, now I puff one or two and go to
bed.
Table II. Disability-related characteristics of the participants
(n=334).
Variables
measured Characteristics N %
Level of Toe or partial foot 14 4.2
amputation Unilateral below-knee 136 40.7
Unilateral above-knee 134 40.1
Knee disarticulation 16 4.8
Bilateral below-knee 4 1.2
Bilateral above and below
knee
16 4.8
Bilateral above knee 14 4.2
Type of
ambulatory
device1
Provisional prostheses 34 10.9
Definitive prostheses 94 30.2
Wheelchairs 22 7.1
Pylons 18 5.9
Axillary crutches 56 18.0
Elbow crutches 87 27.9
Condition of Good and functional 68 21.9
the device1 Repairable condition 109 35.0
Very poor condition 132 42.5
Others 2 0.6
1N=311.
840 S. L. Amosun et al.
By the way I feel some relaxation when I smoke. I
usually feel bad, alone, with all the problems. Obviously,
when I started to smoke before I lost a leg, I would feel
somehow proud to smoke one or two among my friends.
Now I do it for many reasons . . . frustration, you see I
used to do a lot of heavy physical work, now that is gone.
I mean you cannot compete with those boys who run
around everywhere [refers to age mates working in
town].
Overall, some of the participants indulged in more
than one risk behavior. Eighty-eight participants
(26.3%) used tobacco products and consumed
alcohol, while 84 participants (25.1%) did not
engage in physical exercises and consumed alcohol.
Twenty-six participants (7.8%) did not engage in
physical exercises, used tobacco products and con-
sumed alcohol. Only four participants (1.2%) did not
Table III. Frequency of participation in physical exercises in relation to gender, education and employment status (n=334) [% refers to the
row percentage].
Everyday 3 times a week Once a week Hardly ever or never
N % N % N % N %
Gender
Male 37 13.7 29 10.8 23 8.6 178 66.7
Female 13 19.4 12 17.9 4 6 38 56.7
Education
Never went to school 2 2.3 6 6.9 4 4.6 74 86
Primary 1 – 6 30 18.3 24 14.6 6 3.7 104 63.4
Secondary 1 – 3 12 19.3 9 14.5 17 27.4 24 38.7
Secondary 4 – 6 2 10 2 10 2 10 14 70
Tertiary level 2 100 0 0 0 0 0 0
Employment status
Active duty 28 26.9 16 15.4 2 1.9 58 55.8
Dependent 4 20 2 10 0 0 14 70
Retired 0 0 0 0 0 0 2 100
Unemployed 8 5.5 16 10.9 10 6.8 112 76.7
Others 14 22.6 4 6.5 14 22.6 30 48.4
Table IV. Participation in physical exercises in relation to disability-related variables (n=334) [% refers to the row percentage].
Everyday 3 times a week Once a week Hardly ever or never
N (%) N (%) N (%) N (%)
Level of amputation
Toe or partial foot 2 (14.3) 2 (14.3) – – 10 (71.4)
Unilateral below-knee 26 (19.1) 21 (15.4) 10 (7.4) 79 (58.1)
Unilateral above-knee 10 (7.5) 16 (11.9) 12 (8.9) 96 (70)
Knee disarticulation 4 (25) 2 (12.5) – – 10 (62.5)
Bilateral below-knee – – – – – – 4 100
Bilateral above/below knee 2 (12.5) 2 (12.5) – – 12 (75)
Bilateral above knee 4 (28.6) – – 3 (21.4) 5 (35.7)
Type of ambulatory devices1
Provisional prostheses 6 (17.6) 8 (23.5) – – 20 (58.8)
Definitive prostheses 20 (21.3) 7 (7.4) 14 (14.9) 53 (56.4)
Wheelchairs 2 (9.1) 1 (4.5) 3 (13.6) 16 (72.7)
Pylons 4 (22.2) 2 (11.1) – – 12 (66.7)
Axillary crutches 4 (7.1) – – 2 (3.6) 50 (89.3)
Elbow crutches 6 (6.9) 10 (11.5) 6 (6.9) 65 (74.7
Condition of the devices1
Good and functional 11 (16.2) 10 (14.7) 8 (11.8) 39 (57.3)
Repairable condition 13 (11.9) 12 (11) 8 (7.3) 76 (61.5)
Very poor condition 12 (9.1) 11 (8.3) 10 (7.6) 99 (75)
Others – – – – – – 2 (100)
1N=311.
Physically disabled individuals with lower limb amputation 841
engage in physical exercises, used tobacco products
and recreational drugs, and consumed alcohol.
The health-related needs expressed by the partici-
pants are summarized in Table VII. Most of the
participants (96.4%) expressed the need for HIV/
AIDS awareness and prevention. This was but-
tressed by comments made by a participant during
the in-depth interview:
Nobody tells us about these things. The other day when
I went to the clinic, by chance, the health worker was
talking about HIV/AIDS prevention and awareness. I
stopped and listened. You have to find out yourself,
even with physical activity, exercises, I try to do some
weight lifting, but . . . it is difficult alone. Possibly we
need to do it together, we could all get involved. So
nobody really talks about it, I used to do it when I was
still at Kanombe [a rehabilitation centre].
Additional needs perceived as essential by partici-
pants, were identified during in-depth interviews.
Most participants desired vocational training in
carpentry, in motor mechanics or computer skills.
Other participants desired to learn how to make
prostheses and orthoses. Most participants also
expressed the desire to be given disability grants.
Finally, some of the participants expressed the
opinion that the healthcare authorities needed to
obtain up to date information about people with
physical disabilities in order to provide desired
services. This was re-emphasized by the comments
of two of the participants:
Here [in Rwanda] nobody values a disabled person. I do
not even know why you came to discuss all these with us
. . .. There are many people like us out there indoors all
the time. You see these landmines brought problems. I
really know some people who lost both legs, and are at
home all the time. How do they come here?
I do not think that the authorities or you professionals
know how many we are or even know where we live in
our provinces, districts and ‘secteurs’ [villages]. How
can training start when the authorities do not know how
many we are and where we live? To know this is vital, so
that all these can be planned . . .. There is a need to
know our numbers, where we live, and that need to be
done first . . ..
Discussion
As indicated earlier, there are no reliable data on the
prevalence of people with physical disabilities in
Rwanda. Although a total of 386 amputees (80%
male, 20% female) responded to the radio an-
nouncement about the cross-sectional survey, there
is no indication of the total number of physically
disabled people with lower limb amputation. The
study sample was also fairly representative of the
population as the research settings were located in
the central, northern, north-western, and southern
parts of Rwanda. However, the number of those who
responded may be an indication of those desiring
some assistance.
Data from 86.5% (n=334) of those who re-
sponded to the radio announcements were
analyzed. Though about one-quarter (25.7%) of
these respondents did not go to school, the adult
(aged 15 years and above) literacy rate was about
70% according to the 2003 census [2]. Though most
of them were unable to read or write in English, they
were adequately competent to communicate in their
local language. Majority of the same respondents
were unemployed (43.7%). Those considered to be
on active duty were employed in either the formal or
informal sectors. Others were either primary and
high school students or beggars on the streets. The
level of amputation in many cases was below knee
(40.7%), which need not be disabling if good
prostheses were available. Unfortunately, most of
the ambulatory devices (42.4%) were in very poor
state.
Table VI. Participants using tobacco, recreational drugs and
alcohol.
Yes No
Substance usage N (%) N (%)
Currently smoke or use any tobacco 112 (33.5) 222 (66.5)
1 – 5 cigarettes a day 30 (26.8)
6 – 10 cigarettes a day 38 (33.9)
11 – 20 cigarettes a day 44 (39.3)
Sub total 112 100
Alcohol use 202 (60.5) 132 (39.5)
Everyday 48 (23.8)
3 – 4 times a week 80 (39.6)
Once a week 56 (27.7)
A few times a month 18 (8.9)
Sub total 202 100
Use of recreational drugs 32 (9.6) 302 (90.4)
Table V. Barriers to participation in physical activity or exercise
(n=216).
Barriers to do physical activity or
exercise
N %
Do not know where to exercise 68 31.5
Lack of motivation 48 22.2
Lack of energy, not sure if I can manage 35 16.2
Cost of transport or ambulatory devices 34 15.7
Have other concerns, like frustration or
depression
18 8.3
Other reasons: lack of time, lack of
facilities or interest
13 6
842 S. L. Amosun et al.

The public health community in Africa has
traditionally paid little attention to the health-related
needs of people with disabilities in spite of the
growing number due to the wars and consequences
of wars. Due to various reasons, many African
countries have not managed to significantly imple-
ment programs that would help to improve the
quality of life for people with disabilities. There is
concern that disabled people are still relegated to the
margins of society as countries grapple with econom-
ic woes and civil strife. An overall sense of neglect,
despair and frustration may be perceived from the
tone of some of the comments made during the in-
depth interviews. This was captured in the com-
ments of one of the participants:
Here [in Rwanda] nobody values a disabled person . . . .
Unfortunately, there is no reliable information on the
prevailing health-related behaviors in Rwanda. How-
ever, the health-related behaviors reported in this
study among physically disabled individuals with
lower limb amputation are reflections of similar
behaviors reported among non-disabled individuals
in other African countries [18 – 21]. Unhealthy
behaviors like smoking, alcohol consumption, use
of recreational drugs, and sedentary behaviors, when
practiced for an extended period of time often lead to
a range of chronic diseases later in life. Conditions
like cardiovascular disease, diabetes and cancer
contribute to significant human and economic costs
through premature death and increased expenditure
on health. Additionally, some of the risky health-
related behaviors lead to psychological and social
problems. For example, alcohol and drug use are
often accompanied by violent behavior and family
instability [23].
Many health promotion interventions have been
developed to address health-risk behaviors among
non-disabled individuals in African countries [19 –
22]. The health promotion needs highlighted in this
study are similar to the needs of non-disabled
individuals. Increasing physical activity among this
group of people is an important public health
challenge, particularly to increase cardio respiratory
fitness. However, it seems there was no provision
made to address this and similar needs. Meeting
these needs seems to raise important management
and practice issues for healthcare services. People
with physical disabilities seem to have limited access
to mainstream health promotion services because
they are often excluded from society, either because
they are ‘segregated’ within specialist support ser-
vices in the community or because they live in
isolation with carers. Community-based health pro-
motion interventions are required to address these
issues in order to prevent the onset of secondary
disease processes or additional disability.
Conclusion and recommendations
Many of the reported health-promoting needs are
not unique to people with physical disability,
however the needs become compounded or exacer-
bated. The effects of the physical impairments
already present major challenges. Specific attention
must be paid to prevent the occurrence of secondary
disabilities, like tobacco-related diseases, which can
further drastically affect level of independence.
Proper attention to the health care needs of people
with disabilities will result in greater independence
and improved health among this population. The
following two specific recommendations are made,
in addition to the recommendations made by the
participants in this study, in order to pay better
attention to meet the health promoting needs of
lower limb amputees in Rwanda:
1. Most of the recommendations made by the
participants of this study were dependent on
what others had to do. Amputees should be
empowered to identify the type of support they
could give to each other to improve their well
being. This can be achieved through occa-
sional workshops for people with disabilities to
get together, share experiences and motivate
each other.
2. Community Health Workers (CHWs) in
Rwanda should be trained to run physical
exercise and wellness programs for people
with disabilities at community levels, in
addition to the provision of other community
based rehabilitative services.
References
1. Farrow G, Rosenfeld J, Crozier J, Wheatley P, Warfe P.
Military surgery in Rwanda. The Australian and New Zealand
J Surgery 1997;67:696 – 702.
Table VII. Perceived health-related needs of participants (n=334).
Participants’ needs Frequency %
HIV/AIDS awareness and prevention 322 96.4
Healthy lifestyle habits 318 95.2
Blood pressure control 314 94.0
Improving wellness 312 93.4
Staying physically active 308 92.2
Managing stress 302 90.4
Prevention of diabetes 300 89.8
Back care management 300 89.8
Exercise options and programs 286 85.6
Cessation of smoking 276 82.6
Weight control management 268 80.2
Physically disabled individuals with lower limb amputation 843

2. Office of the Minister of Finance and Economic Planning.
The 2003 National Census. Department of Statistics,
2004;March No. 2.
3. Geltman P, Stover E. Genocide and the plight of children in
Rwanda. J American Medical Association 1997;277:289 –
294.
4. Office of the Hospital Director. Central Hospital of Kigali
annual statistical records. Physiotherapy/Orthopaedic work-
shop department and Department of Surgery; 2000;88 – 99.
5. Dougherty PJ. Transtibial Amputees from the Vietnam War.
The J of Bone and Joint Surgery 2001;83:383 – 389.
6. World Health Organisation. Land mines – a concerted public
health response. Violence and injury prevention, Available at
http://www.who.int/violence-injury-prevention/landmine/pub-
lichealth.htm; 2000.
7. Coyle CP, Santiago MC, Shank JW, Ma GX, Boyd R.
Secondary conditions and women with physical disabilities: A
descriptive study. Archives of Physical Medicine and Rehabi-
litation 2000;81:1380 – 1387.
8. Gail KA, Nora G. Media reports on disability: A binational
comparison of types and causes of disability as reported in
major newspapers. Disability and Rehabilitation 1999;12:
420 – 431.
9. Ostir G, Carlson JE, Black SA, Rudkin L, Goodwin JS,
Markides KS. Disability in older adults 1: Prevalence, causes
and consequences. Behavioural Medicine 1999;24:147 – 157.
10. Stuifbergen AK, Rogers S. Health promotion: An essential
component of rehabilitation for persons with chronic disabling
conditions. Advances in Nursing Science 1997;19:1 – 20.
11. Hogan A, Mclellan L, Bauman A. Health promotion needs of
young people with disabilities – a population study. Disability
and Rehabilitation 2000;22:352 – 357.
12. Cooper RA, Quatrano LA, Axelson PW, Harlan W, Stineman
M, Franklin B, Krause JS, Bach J, Chambers H, Chao EYS,
Alexander M, Painter P. Research on physical activity and
health among people with disabilities: A consensus statement.
J of Rehabilitation Research and Development 1999;36:142 –
154.
13. Rimmer JH, Rubin SS, Braddock D. Barriers to exercise in
African American women with physical disabilities. Archives
of Physical Medicine and Rehabilitation 2000;81:181 – 188.
14. Stuifbergen AK, Seraphine A, Greg R. An explanatory model
of health promotion and quality of life in chronic disabling
conditions. Nursing Research 2000;49:122 – 129.
15. Breslow L. From disease prevention to health promotion.
The J of the American Medical Association 1999;281:
1030 – 1033.
16. Davis RM. Healthy People 2010:Objectives for the United
States: Impressive, but unwieldy. British Medical J
2000;320:818 – 819.
17. Kailes JI. Can disability, chronic conditions, health and
wellness coexist? The National Centre on Physical Activity
and Disability, Available at http//www.ncpad.org/, 2000.
18. African Decade of Disabled Persons (2000 – 2009). Available
at http://www.un.org/esa/socdev/enable/disafricadecade.htm
19. Peltzer K. Tobacco smoking in Black and White South
Africans. East African Medical J 2001;78:115 – 118.
20. Dundas R, Morgan M, Redfern J, Lemic-Stojcevic N, Wolfe
C. Ethnic differences in behavioural risk factors for stroke:
Implications for health promotion. Ethnic Health 2001;6:95 –
103.
21. Fisher AJ, Chalton DO. Urbanisation and adolescent risk
behaviour. South African Medical J 2001;91:243 – 249.
22. Balmer DH, Gikundi E, Billingsley MC, Kihuho FG, Kimani
M, Wang’ondu J, Njoroge H. Adolescent knowledge, values,
and coping strategies: Implications for health in sub-Saharan
Africa. J of Adolescent Health 1997;21:33 – 38.
23. World Health Organisation. The World Health Report 2002.
Reducing risks, promoting healthy life. Geneva: World Health
Organisation.
Appendix I. Research setting
The research settings included three hospitals, which
were the Central Hospital of Kigali in Kigali Ville
province, Kanombe Military Hospital in Kigali Rural
province and Ruhengeri Provincial Hospital in
Ruhengeri province. In order to make the study
representative and increase the size of the study
sample, the study was also carried out in two
rehabilitation centers considered to have a high
number of individuals with lower limb amputation.
These centers were Gatagara Centre for Physically
Handicapped Persons, and Nyagatare Military De-
mobilization Settlement.
The Central Hospital of Kigali is situated in Kigali
Ville Province in the center of Kigali, the capital city
of Rwanda. It is a teaching and national referral
hospital. It has the largest referral orthopedic work-
shop in the country to which most individuals with
lower limb amputation are referred for prosthetic
fitting and rehabilitation. Kanombe military hospital
is situated in Kigali Rural province, approximately
15 km from the center of Kigali. Kanombe military
hospital is mainly a referral hospital for the military
war casualties although it also meets the needs of the
civilian population. It has an orthopedic workshop
that provides prosthetic fitting and rehabilitation
services to a large number of lower limb amputees
nationally, mainly casualties from the national
defense force and the national police force.
Ruhengeri Hospital is found in the northwest of
the country, in Ruhengeri Province about 97 km
from Kigali. It is a provincial hospital, receiving
amputee patients referred from the northern and
north-western parts of the country for rehabilitation
and prosthetic fitting. Gatagara Centre for the
physically handicapped, named ‘Gatagara Centre des
Handicapes Physiques’, is situated in Gitarama Pro-
vince 74 km south of Kigali. The center is famous for
its quality prosthetic products, and receives a high
number of people with amputations, predominantly
from the southern and south-western parts of the
country. Nyagatare Military demobilization settle-
ment is situated in Umutara Province in Nyagatare
district, about 145 km from Kigali, to meet the
accommodation needs for many military persons
with various disabilities who were demobilized from
the national defense force.
844 S. L. Amosun et al.
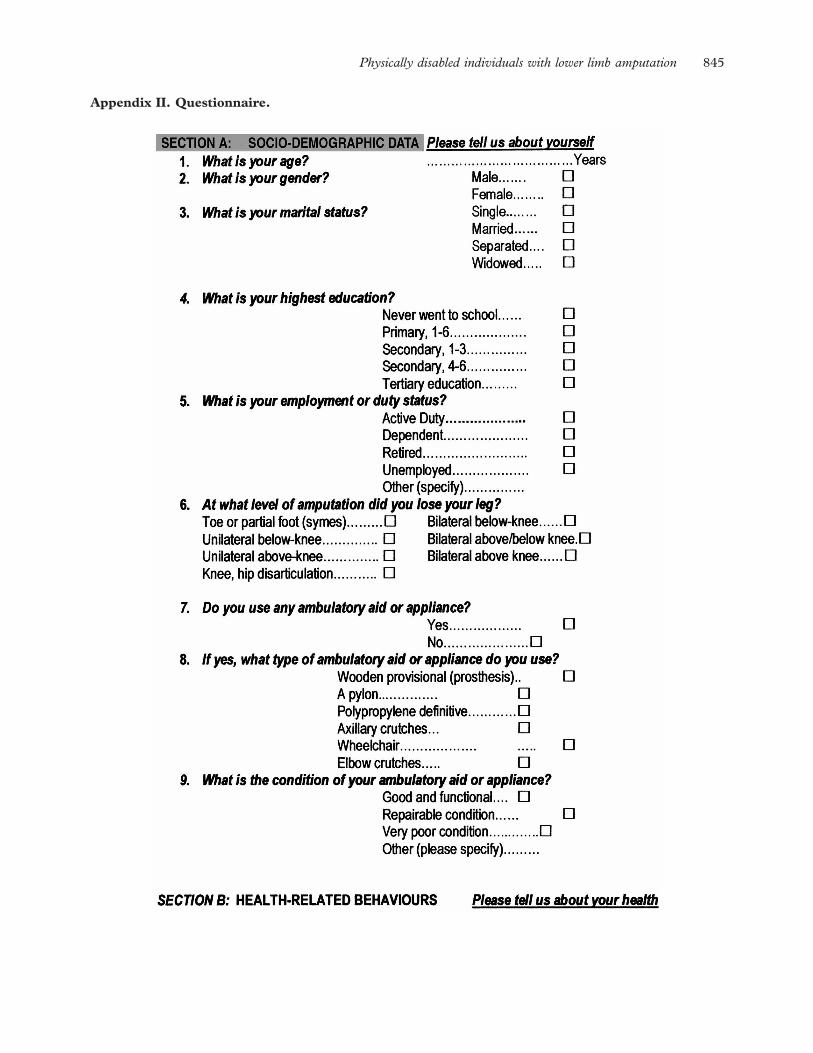
Appendix II. Questionnaire.
Physically disabled individuals with lower limb amputation 845
846 S. L. Amosun et al.
Physically disabled individuals with lower limb amputation 847