HEALTH - ETDA
267
The Pennsylvania State University The Graduate School College of Earth and Mineral Sciences RESPONSIBILITY FOR EXPOSURE: HEALTH GOVERNANCE OF RESPIRABLE CRYSTALLINE SILICA IN THE HYDRAULIC FRACTURING INDUSTRY A Dissertation in Geography by Arielle Leah Hesse 2018 Arielle Leah Hesse Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy May 2018
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of HEALTH - ETDA
The Pennsylvania State University
The Graduate School
College of Earth and Mineral Sciences
RESPONSIBILITY FOR EXPOSURE: HEALTH GOVERNANCE OF
RESPIRABLE CRYSTALLINE SILICA IN THE HYDRAULIC FRACTURING
INDUSTRY
A Dissertation in
Geography
by
Arielle Leah Hesse
2018 Arielle Leah Hesse
Submitted in Partial Fulfillment
of the Requirements
for the Degree of
Doctor of Philosophy
May 2018
ii
The dissertation of Arielle L. Hesse was reviewed and approved* by the following:
Melissa Wright
Professor Geography and Women’s, Gender and Sexuality Studies
Dissertation Co-Advisor
Chair of Committee
Brian King
Associate Professor of Geography
Dissertation Co-Advisor
Lorraine Dowler
Associate Professor Geography and Women’s, Gender and Sexuality Studies
Kai Schafft
Associate Professor of Education and Rural Sociology
Cynthia Brewer
Professor of Geography
Head of the Department of Geography
*Signatures are on file in the Graduate School

iii
Abstract
Since the late 2000s, the controversial application of hydraulic fracturing has been used to
extract unconventional oil and gas from shale rock in the U.S. During the fracturing
process, workers can be exposed to concerning levels of respirable crystalline silica, a
human carcinogen. These developments occur within an existing and evolving regulatory
framework in the U.S. for dealing with occupational safety and health.
This dissertation examines the state’s governance mechanisms to address workers’
exposures to respirable crystalline silica, a human carcinogen, during hydraulic fracturing
for oil and gas extraction in the US. I show how the state’s regulatory mechanisms embody
dueling responsibilities to workers and industry and undermine workers’ rights to a
healthful workplace through the ways that regulations are confounded by discursive and
material expressions of the spatial and temporal properties of the industry. By drawing on
analytical tools provided by feminist theories of responsibility, the dissertation rethinks the
ways health geographers have engaged with the concept to offer new ways of thinking
about how the state constitutes and responds to health risk. By examining the rulemaking
process, inspection procedures and workers’ compensation, the dissertation offers
empirical and theoretical interventions to unpack the state’s interests in human health,
illustrating how the rationalities and techniques used to govern human health are
representative of multiple conflicting commitments and encode problematic assumptions
about responsibility, space, and time, that belie efforts to protect workers.

iv
Table of Contents
List of Figures ................................................................................................................... vi
List of Tables ................................................................................................................... vii
List of Abbreviations ..................................................................................................... viii
Acknowledgements ........................................................................................................... x
1. Chapter 1: Introduction ........................................................................................... 1 The Case Examples .................................................................................................................... 4 Why responsibility?.................................................................................................................... 6 OSH Governance in the US ....................................................................................................... 8 OSH and Oil and Gas............................................................................................................... 13 Hydraulic Fracturing ............................................................................................................... 14 Health Geography and Responsibility: Theoretical Framework ........................................ 18
Health Governance................................................................................................................. 20 Health Justice ......................................................................................................................... 22 Responsibility, Care, and the Neoliberal State ...................................................................... 23
Methods ..................................................................................................................................... 40 Participant Observation and Interviews ................................................................................. 41 Textual Sources and Analysis ................................................................................................ 46
Dissertation Outline ................................................................................................................. 48
2. Chapter 2: Rulemaking: Is OSHA’s Principal Responsibility to Protect
Industry or the Workers? .............................................................................................. 51 Rethinking the State’s Interest in Health: Responsibility as Negotiated ............................ 53 Permissible Exposure Limits: Regulating Risk, Silica, Industry and Workers ................. 56 Silica Hazards in Hydraulic Fracturing ................................................................................. 61
The dose makes the poison? RCS as an unknown risk in hydraulic fracturing ..................... 65 Negotiating Health Risks: for whom? .................................................................................... 68
Is Silicosis Even a Problem? Absolution from Responsibility .............................................. 70 The Health of Industry: The Cost of Movement and Materials ............................................. 81 Infeasible Engineering Controls ............................................................................................ 90 Workers’ Responsibility: Respirators are the Only Option ................................................... 93
OSH Act and Rulemaking: Regulating Risk, Negotiating Responsibilities ...................... 100 Negotiating Risks: OSHA Responds ................................................................................... 103
Conclusions ............................................................................................................................. 106
3. Chapter 3: Enforcement: Spatial and Temporal Practices Absolve
Responsibility as Liability ............................................................................................ 109 Responsibility as Liability, the Subcontracted Workplace, and Health Exposures......... 111 Fragmented Oversight: Institutional Context of OSHA Enforcement ............................. 116 Responsibility-as-liability: Inspections ................................................................................. 120
Subcontracting and Flexible Work in the Oilfield ............................................................... 122 Avoiding Blame: Barriers to Inspections ............................................................................. 129 “Geography Detectives”: Finding Well Sites in a Landscape of Fixed Resources ............. 134 Avoiding Categorization: Fissuring, Subcontracting and NAICS Codes ............................ 137

v
Hierarchy of Controls: Engineering Controls and Respiratory Protection .......................... 141 Institutional capacities ........................................................................................................... 151
Fines and Blameworthiness ................................................................................................. 153 Authority to Inspect: Emphasis Programs ........................................................................... 155
Conclusions ............................................................................................................................. 156
4. Chapter 4: Workers’ Compensation: Finding Fault in ‘Fault-less’
Responsibility ................................................................................................................ 159 Practices of Responsibility, Liability, and Blame: .............................................................. 161 From Common Law to Employer Liability to Workmen’s Compensation ...................... 164 Who is liable? .......................................................................................................................... 167 What is compensable? Occupational Disease ...................................................................... 172 Rating the Impact of Workplaces on Bodies ....................................................................... 178 Spatiality of Temporal Limits ............................................................................................... 179
Defining “Dusty Diseases”: “The Hitch,” and Silicosis Compensation .............................. 185 Workers’ Compensation in the Oilfield: Texas and Pennsylvania ...................................... 192
Workers’ Responsibility through Other Parts of the State ................................................ 195 Conclusion ............................................................................................................................... 199
5. Chapter 5: Conclusion: Mapping New Geographies of Responsibility in
Occupational Health ..................................................................................................... 203 New Directions: Health Geographies of Occupational Health and Responsibility .......... 207
An Interest in Health?: Rethinking the State’s Responsibility for Occupational Health ..... 208 Health for whom or for what?: Rethinking Health Responsibility as Multiple through
Rulemaking, Inspections, and Workers’ Compensation ...................................................... 210 Future Theoretical Engagements: Mapping Responsibility in OSH ................................. 217 Future Policy Considerations for OSH: Shifting approaches to responsibility ............... 223 Conclusion ............................................................................................................................... 228
Works Cited ................................................................................................................... 231
Workers’ Compensation Statutes ................................................................................ 251

vi
List of Figures
Figure 1.1: Marcellus Shale Coalition Promotion (Marcellus Shale Coalition, 2017a). .................. 1 Figure 1.2: Marcellus Shale Coalition Promotion (Marcellus Shale Coalition, 2017b). .................. 2 Figure 1.3: Shale Basins, (U.S. Energy Information Administration, 2015) ................................. 14 Figure 1.4: Diagram of Hydraulic Fracturing Operations, (OSHA 802188, 2011, p. 165) ............ 14 Figure 2.1: Silica Regulations Timeline ......................................................................................... 61 Figure 2.2: Mountain Mover, Points of filling (OSHA 802188, 2011, p. 308) .............................. 62 Figure 2.3: Mountain Mover and Plume of Dust (OSHA 802188, 2011, p. 184) .......................... 63 Figure 2.4: Crow’s Nest (OSHA & NIOSH, 2012) ........................................................................ 63 Figure 2.5: Dr. Borak's Presentation, March 19, 2014 ................................................................... 71 Figure 2.6: CDC Mortality Data (Johnson, Freedman, & Chajet, 2014, p. 7) ............................... 72 Figure 2.7: API testimony at the RCS Informal Hearings, April 4, 2014 (A. Hesse). ................... 83 Figure 2.8: Energy Nation Poster ................................................................................................... 84 Figure 2.9: PA Jobs Rally (A. Hesse) ............................................................................................. 84 Figure 2.10: Universal Well Services Presentation (Ross, 2010) ................................................... 88 Figure 2.11: PowerPoint Slide from API’s presentation (Exhibit 148) .......................................... 92 Figure 3.1: Hierarchy of Controls (CDC, 2016) ........................................................................... 141 Figure 3.2: Ted inspecting Joe’s Face (Lawhorn-Cryden, 2015) ................................................. 149 Figure 3.3: Joe noting his beard growth (Lawhorn-Cryden, 2015) .............................................. 149 Figure 4.1: Time Limitations for Occupational Illnesses, Notices ............................................... 181 Figure 4.2: Occupational Disease Claims, Since Knowledge of Disease or Disability ............... 183 Figure 4.3: Occupational Disease Claims: Time Limitations Since Last Hazardous Exposure ... 184 Figure 4.5: Joe Breathing through a coffee stirrer (Lawhorn-Cryden, 2015) ............................... 188 Figure 4.6: Silicosis and Pneumoconiosis Claims: Time Limitations Since Last Hazardous
Exposure ............................................................................................................................... 189 Figure 4.7: Silicosis and Pneumoconiosis Claims: Time Limitations Since Knowledge of
Disease/Disability ................................................................................................................. 190 Figure 5.1: Previous OSHA Website ............................................................................................ 204 Figure 5.2: OSHA logo for silica hazards .................................................................................... 205

vii
List of Tables
Table 2.1: Statutes, Court Cases, and Executive Orders in OSHA Rulemaking .......................... 102 Table 4.1: Examples of occupational disease definitions. ............................................................ 177 Table 4.2: Top Oil and Gas States, Sept. 2017 (U.S. EIA, 2017) ................................................ 182 Table 4.3: Definitions of Silicosis for Silicosis Claims ................................................................ 190

viii
List of Abbreviations
ACC American Chemistry Council
ACGIH American Conference of Governmental Industrial Hygienists
ADA Americans with Disabilities Act
AFL-CIO American Federation of Labor and Congress of Industrial Organization
API American Petroleum Institute
AXPC American Exploration and Production Council
CDC Center for Disease Control
Chamber The U.S. Chamber of Commerce
COBRA Consolidated Omnibus Reconciliation Act
CSHO Compliance Safety and Health Officer
DPM Diesel Particulate Matter
E&P Exploration and Production
EPA Environmental Protection Agency
ERG Eastern Research Group
FMLA Family Medical Leave Act
FOIA Freedom of Information Act
HoC Hierarchy of Controls
IARC International Agency for Research on Cancer
ILO International Labor Organization
IPAA Independent Petroleum Association of America
IRB Institutional Review Board
NAICS North American Industry Classification System
NETL National Energy Technology Laboratory
NIOSH National Institutes of Occupational Safety and Health
NPRM Notice of Proposed Rulemaking
OEL Occupational Exposure Limit
OSH Occupational Safety and Health
OSHA Occupational Safety and Health Administration
PATHS Pennsylvania Training for Health and Safety
PEL Permissible Exposure Limit
PPE Personal Protective Equipment
RCS Respirable Crystalline Silica
REL Recommended Exposure Limit
SIMOPS Simultaneous Operations
SSDI Social Security Disability Insurance
STEPS Service, Transmission, Exploration, and Production Safety Network
SVEP Severe Violator Enforcement Program
TLV Threshold Limit Value
TWA Time Weighted Average
ix
USDOL United States Department of Labor
WHD Wage and Hour Division
WHO World Health Organization

x
Acknowledgements
This research received support from a National Science Foundation (NSF) Doctoral
Dissertation Improvement Grant (DDRI #1434222). The conclusions in this dissertation
do not necessarily reflect the views of the NSF. This research also received Enrichment
Funds and PLACE Lab funds from the Department of Geography at Penn State. The
conclusions in this dissertation do not necessarily reflect the views of the department.
This dissertation would not have been possible without the help and support of many
colleagues within the Departments of Geography, Women, Gender and Sexuality Studies,
and Agricultural Economics, Sociology, and Education at Penn State, and great friends in
State College and elsewhere. Special thanks to the members of Team Accountable, the
Nature Society Working Group, and the Energy Reading Group, who read drafts of
proposals and discussed this project with me over many years. Jase Bernhardt, Jenna
Christian, Dana Cuomo, Carolyn Fish, Russ Hedberg, Nicole Laliberté, Vanessa Massaro,
Aparna Parikh, Nari Senanayake, and Jamie Shinn, all deserve mention for the help and
support they have provided over the years in the ways of conversations, long runs, editorial
guidance, and continued motivation. Jennifer Titanski-Hooper deserves special mention
for the continued help, support, and guidance that she and her family, Mike and Gwen,
have provided me over many years of friendship.
My work with Jennifer Baka, Kathy Brasier, Kirby Calvert, Tim Kelsey, Leland Glenna,
Shannon Monnat, and Kai Schafft have shaped how I have come to understand the
changing landscapes surrounding unconventional and gas development. Working with
these individuals has been greatly influential. Thanks to my committee including Lorraine
Dowler and Kai Schafft for their helpful comments and feedback, and of course to my
advisors, Brian King and Melissa Wright, who have offered comments and guiding
direction through many drafts of proposals and dissertation chapters over the years.
Thanks to my family, Paula Hesse and Dena Bunis for their unwavering support, Libby,
whose sat by my side through every revision, and Brian Hesse, whose memory will always
inspire me with his curiosity and love of learning. Finally, I owe the most thanks to Sam
Stehle, who has been the greatest support system throughout this project.
1
1. Chapter 1: Introduction
Since the late 2000s, regions of the U.S. with significant growth in unconventional
oil and gas have undergone what some call an “energy renaissance.” Unconventional fuels
have been advertised as the path to “Renewal. Prosperity.” reviving the figure of the U.S.’s
industrial past, the hard-working, white American man from post-industrial decline (Figure
1.1). Assertions buttressed by inflated job estimates and optimistic forecasts about the
longevity of the industry, unconventional extraction purports to offer “Good Jobs. Good
Pay. An investment in your family’s future and the future of America” (Figure 1.2). Most
investments, however, have risks. With so much attention paid to the number of jobs that
industry creates, far less has been spoken of their quality, even as this oilfield1 work entails
the potential for significant bodily harm (Witter et al. 2014). In this investment, risk lies in
potential short and long-term consequences to one’s health despite assurances by the state
that workers have the right to a safe and healthful workplace in the US. A central concern
of this dissertation is how governance mechanisms that regulate workplace responsibilities
for health risk simultaneously reifying this dichotomous narrative.
Figure 1.1: Marcellus Shale Coalition Promotion (Marcellus Shale Coalition, 2017a).
This dissertation examines how existing governance mechanisms for occupational
health distribute responsibility for health risk to particular actors and how they intersect
with the spatio-temporal characteristics of the hydraulic fracturing industry’s operations to
shape responsibility for health risk. Shale fuel extraction and the process of hydraulic
1 Oilfield or oil patch are catch-all terms for upstream oil and gas development. This spatial terminology
(“field,” “patch”) is often not particular to any one region of extractive activity.
2
fracturing has spatial and temporal features that materially challenge existing mechanisms
to regulate the industry and manifest in narratives that contrast worker responsibility for
health risk with industry’s vitality. Efforts to regulate airborne exposures such as silica, a
well-known occupational hazard, illustrate these processes. This is due to the challenges of
measuring silica exposures within the extractive process, the long latency of many of
silica’s human health impacts, the flexibility of extractive activities, and the assumptions
that underlie the regulatory mechanisms themselves.
Figure 1.2: Marcellus Shale Coalition Promotion (Marcellus Shale Coalition, 2017b).
The existing regulatory frameworks for occupational safety and health (OSH) in
the U.S. diffuse responsibility for OSH among the state, industry, and workers in ways that
call for examination by geographers. Federal OSH regulations stipulate that the state ensure
that employers are responsible for providing workers with access to a “safe and healthful”
working environment in which workers make decisions about working ‘safely.’ After
workers get sick, state workers’ compensation laws promise workers faultless access to
funds and medical care. In both instances, workers are seen to be ‘distanced’ from
responsibility, while state and industry are allocated duties to protect them. While
progressive by some measures, this shift does not displace the state’s commitments to
liberal values, and in the state’s failures, problematically reinforces them. Moreover, in the
3
context of hydraulic fracturing and similar industries, the flexibility of the industry’s spatial
and temporal patterns challenges how the state distributes responsibility. In so far as the
state’s efforts are insufficient, workers are ultimately left to protect themselves. This
dissertation examines this regulatory environment in the context of the occupational health
risks in the oil and gas industry by focusing on the state’s mechanisms that respond to the
human health risk from occupational exposures to silica during hydraulic fracturing.
By probing how regulatory mechanisms define who is responsible for OSH
exposure, this study calls on health geographers to reexamine relationships among
institutions and individuals that influence human health. I argue that health geographers
have much to contribute to the study of human health in relation to resource extraction and
its risks by connecting feminist political philosophy on responsibility (i.e. Young, 2008)
with critical geographies of health governance. This entails not only studying ways
individuals are made responsible for risk but also questioning how institutions
conceptualize and operationalize responsibility such that regulatory mechanisms can be
rethought to address structural processes. Such a framework provides tools for
understanding how the state’s interest in protecting worker health, is both confounded by,
but also acquiescent to the spatialities and temporalities of extractive practices. The state’s
interest in worker health capitulates concern and consideration for industry health and
focuses on responsibility as liability such that the state decontextualizes the broader
structural processes that produce unsafe health exposures, limiting the utility of its own
regulatory and enforcement efforts. The complexity of the state’s governance mechanisms
ultimately leaves workers individually responsible for health risk from work. Three case
examples illustrate these processes.
4
The Case Examples
State and federal frameworks that ostensibly ‘distance’ workers from responsibility
for OSH partially stem from a long-standing recognition within public health that many
workers lack control over working conditions, that workplace cultures and employer
demands lead employees to make ‘unsafe’ decisions even when faced with ‘safer’
alternatives, and that employers should be responsible for providing a workplace with
minimal risk based on state-sanctioned standards. Before substantial federal involvement
in OSH in 1970, for a century state-level factory legislation and workers’ compensation
interceded in the relationship between workers and employers to diminish OSH
responsibilities historically placed onto workers (Noble, 1986; Asher 1991; Rogers, 2009).
The frameworks that have sought to alter the structural context of workplace risk
warrant skepticism. While by some measures workplaces have become safer and more
healthful, workers continue to be knowingly exposed to risks and bear the long-term bodily
consequences. Issues of capture, lack of institutional capacity, and lagging regulations
provide some answers as to why governance mechanisms have been insufficient, yet they
do not go far enough to critique the ideals behind the frameworks themselves, namely how
efforts to shift responsibility through regulation continue to rely on problematic notions of
the concept that do not fundamentally alter social relations. Feminist critiques of theories
of responsibility (Walker, 2008; Young, 2008) offer the concept newly theorized as
practiced, negotiated, and political, and provides the dissertation a lens to examine how
governance mechanisms reproduce structures of health responsibility.
Rulemaking and Responsibility as a Negotiated Duty to Protect: In this chapter, I
examine the state’s negotiations of its multiple responsibilities in the context of
occupational health. Workers’ rights to a safe and healthful workplace embody not only
5
the state’s responsibilities to protect workers but also employers. Drawing on
conceptualizations of responsibility as negotiated and practiced (Walker, 2008), I examine
participatory venues that the state produces when it writes new regulations (rulemaking),
spaces where it openly negotiates its conflicting responsibilities. I show how public
comment processes perpetuate discourses about responsibility for health risk through the
context of the oilfield. No organized representation of workers within upstream oil and gas
means that the dominant narrative perpetuated is that of trade lobbyists and industry
members who employ arguments to absolve themselves of responsibility and reify a
paradigm in which workers are responsible for health risk.
Inspections and Responsibility as Liability: I examine the state’s efforts to enforce
regulations through a conceptualization of responsibility as liability, whereby employers
are found responsible for health hazards in the workplace. Using Young’s critique of
responsibility as liability (2008), I show how inspections encode a conceptualization of
responsibility that constrains OSHA’s ability to react dynamically and structurally to OSH
concerns, including occupational exposures to silica and the Occupational Safety and
Health (OSHA)’s capacity to enforce its own regulations. Moreover, the rationalities and
techniques of inspections reinforce premises that workplaces are private spaces that require
special justification for state interference. Thus, spatial and temporal dynamics of this
flexible industry can impinge on OSHA’s efforts to inspect oil and gas workplaces and
illustrate reasons why conceptualizations of responsibility need to address structural
patterns of work and geographic contexts, rather than only discrete exposures.
Workers’ Compensation and No-Fault Responsibility: This chapter examines
workers’ compensation’s way of regulating responsibility ‘without fault.’ Drawing again

6
on Young’s critique of liability, I show how this attempt to redefine responsibility for
workplace injury and disease nonetheless continues to rely upon fault-finding frameworks.
By concentrating on spatial and temporal requirements for occupational disease, I illustrate
how the state’s ways of ‘finding occupational’ belie common patterns of hydraulic
fracturing work and common disease progression, making workers responsible for seeking
recompense through other social insurances. These laws foster uneven and inequitable
health relationships through exclusionary applications of time and space.
Why responsibility?
As it is used today, ‘responsibility’ is an interestingly ambiguous or multi-
layered term. In one sense, someone who is responsible for an event can be
said to be the author of that event. This is the original sense of ‘responsible’,
which links it with causality or agency. Another meaning of responsibility
is where we speak of someone being responsible if he or she acts in an
ethical or accountable manner. Responsibility also however means
obligation, or liability, and this is the most interesting sense to counterpose
with risk (Giddens, 1999, p. 8, my emphasis).
Responsibility is a multifaceted idea. Sometimes it is used as a synonym for
obligation or duty… Understood as an ethical concept, responsibility is
often used in the sense of something that is accountable or attributable, and
hence worthy of praise or blame (Eshleman 2009). Yet the term is also a
political term. Its meaning derives from the notions of “response” and
“responsible,” made into a more abstract noun by adding the suffix “-ity.”
In making something that is relational into something more abstract, the
etymological origin of responsibility already points to some of its key
elements: it is by nature relational, existing in the relationships among
people rather than in individuals themselves. Further, by being a response,
responsibility is dynamic rather than fixed, an abstraction about something
concrete. (Tronto, 2013, p. 50, my emphasis).
Responsibility is about relationships. It defines who should be accountable to
another and under what circumstances. Yet, questions abound: Is responsibility blame
(backward-looking), guilt (backward-looking), or obligation (forward-looking)? Is it moral
or political? Is it a concept unique to individuals or can it be collective or shared? What is
the role of agency in responsibility and can someone or something be responsible absent a
7
causal relationship? While responsibility can be a backward-looking relationship (Julia is
responsible for the harm she caused Dustin), it can also have a forward-looking meaning
(Julia is responsible for helping Dustin because of their familial relationship). Face-to-face
interactions often define relationships of responsibility, yet as feminist scholars have
shown, these connections can extend over distances and need not have direct causal
connections (Massey, 2004; Lawson, 2007; Young, 2008).
Young conceptualizes responsibility at two inter-related levels (2008): the
interactional (Julia is responsible to Dustin because of their familial relationship) and the
structural (Julia is responsible to the systems of environmental injustice in Appalachia
through her carbon-based lifestyle). Identifying the moral responsibility of individuals has
traditionally entailed causation, knowledge, and choice (Noorman, 2012, in Zwitter, 2014)
requirements further embedded and given power by liability within the U.S. legal system.
While most theories of responsibility focus on individuals, the extent to which they
manifest for groups or collectives engenders questions of intent, culpability, and agency.
Thus, the nature of shared and collective responsibility, and if either or both can apply to
corporations (for example, in the work of Peter French) or states, and to what effect, is
debated. Occupational health regulation provides an example from which to explore these
questions, not only because of the kinds of actors it enrolls, the state, workers, and industry,
but also because it aims at least in principle to be ‘humanitarian’ in some of its effects.
Occupational health is fundamentally a concept about the responsibility for risk and
uncertainty of what happens to individuals at work. It is not a state of the body; rather it is
a combination of institutional structures, socio-economic processes, and individual actions
that respond to the potential for poor health outcomes resulting from bodies laboring in
8
workplaces. The way institutions respond to this ‘problem’ reflect specific ways of thinking
about the body, risk, and the role of the state in social and economic life. OSH frameworks
stress that workers be given a context in which to make OSH decisions, acting as
autonomous, rational individuals. Thus, the right to occupational health, as prescribed in
U.S. law, is actually the right to a healthy workplace, the right to a space with limited health
risk where it is possible to make ‘healthy’ choices.
Occupational health captures debates about individualism, freedom, and agency.
Do workers take on risk knowingly and thus bear its health consequences? Alternatively,
are employers responsible for the health impediments that arise from activities from which
they profit? What if employers do not know the risks? What, if any, is the state’s
responsibility to diminish the bodily impacts of economic activities or to intercede in the
relationship between workers and employers? For more than a century, the state has
weighed in on these questions, requiring employers to abide by regulations and laws that
make employers responsible for providing a safe and healthful workplace and liable for
some ill-health outcomes. However, as this dissertation discusses, such a distribution of
responsibility has not been fully realized. As is common under a neoliberal state,
responsibility for risk is shifted to the individual. This shift is further justified by workers’
relationships to care including actions and feelings to protect and insulate their coworkers,
the nation, and their employers from harm. In some cases, this works to valorize and reward
risky work, and normalize workers’ risk and vulnerability to long term disease. Thus, what
would seem like a relatively straightforward distribution of responsibility is not.
OSH Governance in the US
Responsibilities within OSH frameworks have origins in 17th and 18th century
9
western moral and political philosophy2, and incorporate notions about the role of the state,
free will, and agency of the Second Industrial Revolution and Progressive Era. In the late-
19th and early-20th centuries, laws, programs, and social norms reflected shifting ideas
about the state’s responsibilities for its social body, which increasingly included forms of
social insurance and state assistance (O’Malley, 2004; Dean, 2009). Workplace hazards
arose as a problem to be managed at a moment when increasingly the state took
responsibility for its working citizenry and the health of its population, efforts seen as “part
of a broader project to ‘preserve the race’ in the face of urbanization and mass production”
(Markowitz & Rosner, 2002, p. 13; see also Sellers, 1997; Rogers, 2009)3.
New scientific groups, industry organizations, and unions established roles and
responsibilities for the state, industry, scientists, and workers to resolve problems of illness
and injury that resulted from work (Rosner & Markowitz, 1987; Rogers 2009). Emergent
scientific fields, such as industrial hygiene and toxicology, sought to shape the
identification, measurement, and elimination of hazardous workplace exposures (Sellers,
1997; Markowitz & Rosner, 2002; Murphy, 2006)4. Such research contributed to what
would become OSH: new organizations, rules, regulations, and norms to guide employers
and individuals to perform work in ‘safe’ ways under the auspices of being good for the
2 John Locke’s enduring ideas about the limited role of the state and the exercise of a rational actor’s
natural rights underpin contemporary economic theories that frame OSH debates about appropriate
governance mechanisms (Nobel, 1986; Dorman, 1996; Holmes, 2013; Horton, 2016). These ideas now
function under neoliberal processes where the neoliberal subject is an autonomous actor who takes on
responsibilities for risk once considered an issue of collective responsibility (England, 2010, p. 137). 3 This was contemporaneous to a shift in thinking about disease as having roots in social causes rather
than bacterial ones (Nash, 2006). While many public health practitioners focused on controlling
infection under germ theory or the bacteriological consensus, social reformers began identifying social
determinants of health. Markowitz and Rosner (2002) show how insurance agents embraced this social
reform analysis, and rather than public health officials helped recognize silicosis’s relationship to
workplace exposure rather than diseases like tuberculosis. 4 The depoliticized and clinical practice of industrial hygiene and toxicology gave these new sciences
increased influence throughout the 20th century (Sellers, 1997; Murphy, 2006).
10
population and the economy. OSH simultaneously encapsulates the state’s commitment to
its human population and private enterprise. Accordingly, the state has governed OSH
through coordination with non-state institutions to various ends, be that the protection and
management of society, the reduction of costs and minimization of liability, or individuals’
bodily integrity, well-being, and self-actualization (O’Malley, 2004; Dean, 2009).
Strategies to govern OSH in the U.S. developed predominantly at the state-level5.
The shift from common-law doctrines to employer liability and the establishment of
workers’ compensation and factory legislation specified state interference in the
relationship between employees and employers (McCaffrey, 1986), most notably by
changing the responsibility for risk (Bale, 1987; Sellers, 1997; O’Malley, 2004).
Throughout the 20th century, labor and public health movements successfully garnered
regulatory attention for certain OSH issues. However, industry science and industry’s
technological capacities strongly shaped these regulations efforts (Markowitz & Rosner,
1995). Many regulatory mechanisms in place today stem from industry’s influence in the
interwar period and immediately following WWII, including efforts to establish and
enforce exposure limits and the inclusion of occupational disease within workers’
compensation. I return to these later in the dissertation to analyze how these mechanisms
express visions of responsibility that frustrate the state’s own goals.
The states managed OSH until a decade of political pressure and activism in the
1960s from labor and lobbying from some industry groups resulted in federal regulation
5 However, some developments on the federal level regarding the definition of risk would shape the
context for later federal regulation of risk (Vogel, 2008). A shift from a more protective per se standard
to de minimus risk standard in 1958 that reflected the commonly accepted dose-response relationship,
“inscribed into law the notion that chemical risks were a function not of the hazard itself, but dependent
upon the exposure” (Vogel, 2008, p. 669).
11
(Donnelly, 1982; Asher 1991; Vike, 2007)6. The 1970 OSH Act that created OSHA
declared that workers had the federal right to a safe and healthful workplace. This was one
of the final programs implemented in this period and reflected ideas about the state’s role
in providing specific populations with protections (Harmon, 1995; Young, 2008). OSHA,
under the U.S. Department of Labor (USDOL), was given authority to set and enforce
workplace standards. Both industry and labor received concessions in the final law: labor
was allowed to participate in workplace inspections and standard setting, and industry
maintained the fragmentation of OSH oversight in ‘state-plan’ systems and the continued
delivery of workers’ compensation through the states.
The degree to which the state should adopt a paternalistic role through its laws or
enable workers to act as rational actors and choose risky work has been long-debated and
has influenced regulatory efforts (see Viscusi, 1983; Noble, 1986; Dorman, 1996; Sellers,
1997). Yet, these develops that drew directly from activism in the 1960s reflected a tact
towards social problems whereby certain social groups were afforded federal protections,
rights, and direct aid, including workers (Harmon, 1995; Young, 2008). For some, this
expressed a welcome benevolence of the state (Harmon, 1995). However, notions of
personal responsibility that denied structural determinants swiftly rebuked it (Young,
2008), emboldened by neoliberal risk narratives. These ideas shape dominant framings of
public health in the U.S. today, including OSH. They have further justified the approaches
taken by OSHA over the last four decades in the ways that it conceives of and addresses
6 There is some disagreement over the OSH Act’s origins. In the 1950s and 1960s, OSH reforms were
not the primary concern of many labor groups (Noble, 1986; Vike, 2007). Donnelly (1982) finds that
the activism by workers targeted at their union leaders shifted organized labor’s focus towards
advocating for what would become the OSH Act. While Donnelly (1982) is skeptical that activism on
the part of environmentalists influenced OSH Act debates, others give more credit to the broader activist
communities of the period in advancing OSH issues at the federal level (Nobel, 1986; Asher, 1991).
12
workplace risk, particularly as pertains to its regulations, enforcement, and expansion of
voluntary programs.
Since its inception, OSHA’s role has been subject to prevailing political ideologies
about the role of government in regulating health and environmental risk. The 1970’s
skepticism of big government stirred deregulatory and government accountability
movements that influenced the funding dedicated in federal budgets for the establishment
and enforcement of occupational health rules (Noble, 1986). OSHA, under the Reagan
administration, deepened these trends through deregulation and the implementation of
significant barriers to regulatory efforts (Noble, 1986; Wahl & Gunkel, 1999; Markowitz
& Rosner, 2002; Vike, 2007) which have had a lasting legacy on ways that OSHA
negotiates its responsibilities (Vogel, 2012). Many neoliberal policies and programs have
persisted and even expanded under Presidents H. Bush, Clinton, W. Bush, Obama, and
Trump, although their contours have varied across political affiliations7. Still, as discussed
in Chapters 2 and 3, important consistencies over the last four decades in OSHA’s activities
include increasingly burdensome requirements for rulemaking, which simultaneously
magnify the state’s responsibilities to prove health risk and weaken the state’s regulatory
authority, and the persistence and expansion of voluntary compliance programs.
The OSH Act also created the National Institutes of Occupational Safety and Health
(NIOSH). NIOSH operates under the Center for Disease Control (CDC) and has no
7 Democratic administrations tend to focus on enforcement more than Republican ones, which often
expand partnerships with industry. The Trump administration is expected to review several Obama-era
enforcement policies, like the use of the Severe Violator Program, and has expanded alliances with
industry lobbies, including the American Chemistry Council. Tone and inflection can change too.
OSHA under Trump republished its website on silica, switching from a more embodied description of
silicosis of the Obama-era to a disembodied, clinical account of the disease; see chapter 5. Trump’s
OSHA has also stopped reporting worker deaths on its website and has reduced the number of press
releases on egregious health and safety violations by employers.
13
enforcement authority but provides research, guidance, and recommendations on
workplace hazards. One area of research has been upstream oil and gas, with a focus on
hydraulic fracturing. Given the industry’s proprietary nature, NIOSH’s work is some of the
only published original research on OSH and hydraulic fracturing, enabled by
collaborations with industry partners. I discuss its contributions to this knowledge in
Chapter 2.
OSH and Oil and Gas
In the early 2000s, testing of combined technologies, horizontal and hydraulic
fracturing, into shale rock to extract unconventional oil and gas, proved successful (Rabe
& Borick, 2013) widening the extent of and opening new regions for oilfield activities
across the U.S. (McGraw, 2012; Wilber, 2012; Gold, 2014). Until these technologies were
combined, the industry had been unable to commercially extract oil and gas from shale
sources8. Unlike conventional oil and gas that pool within reservoirs, unconventional shale
fuels are trapped within source rock. Freeing the hydrocarbons requires the creation of
small fissures, or cracks, in the rock (NETL, 2013; U.S. EIA, 2016).
8 If it is successful or economical is debatable given investigations by the Securities and Exchange
Commission and others over the industry’s financing (Hargreaves, 2011; U.S. Securities and Exchange
Commission, 2014; Cusick, 2013; Resnick-Ault and Schneyer, 2016).

14
Figure 1.3: Shale Basins, (U.S. Energy Information Administration, 2015)
These deposits of decayed organic material date to the Devonian and Mississippian
geologic ages and contain varying quantities of oil, gas, and other light hydrocarbons
(Ground Water Protection Council and ALL Consulting, 2009). Shale plays9 in the U.S.
have opened in many US states (U.S. EIA, 2016) (Figure 1.3), although the development
and production of these plays have fluctuated with energy prices and estimated reserves.
Hydraulic Fracturing
Figure 1.4: Diagram of Hydraulic Fracturing Operations, (OSHA 802188, 2011, p. 165)
Hydraulic fracturing (Figure 1.4) is just one component of the multi-stage industrial
process used in upstream development of unconventional shale fuels. To first drill the well,
workers guide the drill bit vertically several thousand feet and then horizontally for several
9 A ‘play’ is an area of extraction, often named for the oil and gas bearing geologic formation.
15
thousand feet along the rock formation (NETL, 2013; Schlumberger Oilfield Glossary,
2016b), and then case the well with layers of steel and cement (API, 2009). The well drilled,
a new crew conducts the completion, when hydraulic fracturing occurs.
Well servicing companies, including firms such as Halliburton, Baker Hughes, or
Trican, employ specialized teams to pump a combination of millions of gallons of water,
thousands of tons of sand, and a mixture of chemicals into the well at high pressures to
further open the perforations made in the shale by small explosives (NETL, 2013). Sand
seeps into the fissures, holding them open to allow hydrocarbons to flow. Perforation and
injection of drilling fluids occurs in short stages over several days or weeks. A proportion
of the water, sand, and chemicals pumped into the well typically returns to the surface,
known as flowback (NETL, 2013; Esswein et al., 2014); then the well moves into the
production phase (Schlumberger Oilfield Glossary, 2016a). Shale wells typically
experience high initial production rates that taper off; companies may re-fracture wells later
to increase flow rates (Jacobs, 2014). One well pad can host multiple wells due to the
vertical and horizontal orientations of wellbores. Different stages of the production process
can be ongoing at a well site, requiring the coordination of available labor and
infrastructure and completions teams may use ‘zipperfracs’ (Halliburton, 2012b) or
‘simufracs’ to frack more than one well at a time.
This dissertation examines who is responsible for risk with a focus on workers’
exposure to a carcinogen, silica, that comprises 99% of the sand used in hydraulic
fracturing (OSHA & NIOSH, 2012) and is often higher mesh10. Silica causes several
10 Sand size selection depends on its application and can vary based on mesh size roundedness and
resistance; this contributes to the dust produced. There are alternatives to sand, including ceramic
proppants and resin coated sand but are often costlier.
16
debilitating and fatal diseases, including silicosis. The geography of the hydraulic
fracturing worksite, its work practices, and the spatialities and temporalities of the industry,
influence how silica becomes an occupational health hazard. Chapter 2 discuss these issues.
Pennsylvania and Texas
I conducted much of my research in Pennsylvania, with additional activities and
events in Texas. The different regional histories of these states with the oil and gas industry
and experiences with long-term respiratory diseases are instructive. While Pennsylvania
lays claim to the first oil well drilled in 1859, regions of Texas extensively developed oil
throughout the 19th and 20th centuries. Markers of its long relationship with oil fill the
Texan landscape, pump jacks and derricks, often rusted, litter parts of west and south
Texas. Huge refineries along the coast solidify the centrality of the full production chain to
the state. Indeed, in downtown Houston, many major energy companies have international
headquarters. Similarly, health concerns from the industry have flowed through Texas.
Incidents linking sandblasting for cleaning oil tanks in Texas resulted in silicosis crises in
the 1970s, 1980s, and 1990s (Rosner & Markowitz, 2000). Following World War II, the
oilfields in the Gulf Coast increased operations, leading workers to be exposed while
cleaning oil storage tanks using silica as an abrasive. Silica exposures during oil tank
cleaning would resurface in the 1970s during the OPEC crisis and its intensification of
industrial activities (Rosner & Markowitz, 2000). Explosions and chemical leaks from
refineries have engendered decades-long environmental justice struggles between local
communities and the adjacent refineries on which some communities also rely (Lerner,
2010). Texas has experienced an expansion of its oil and gas industry due to development
in the Barnett, Eagle Ford, and Haynesville Shales, but this growth has been within a well-
established oil industry with well-documented health issues.

17
Pennsylvania’s gas industry is largely the product of the recent shift towards large-
scale industrialization that facilitates unconventional shale gas extraction in the Marcellus
Shale. However, its history with industrial disease is significant. Instances of “coal miners’
consumption,” identified by physicians in the mid-nineteenth century in Pennsylvania,
swelled in the latter half of the century as new industrial tools increased the rate of dust
production and exposures. Industrial insurance agents, who clustered these diseases to
specific industries, would help identify these exposures as silicosis (Sellers, 1997; Rosner
& Markowitz, 2006). In northeastern and southwestern Pennsylvania, anthracite and
bituminous coal’s history, and black lung, a deadly lung disease caused by exposures to
coal dust, are part of the regional identity11. Changing political economies of coal led
workers to be exposed to silica through the late 20th century. As miners in the east dug
deeper and through silica-rich layers of rock to access new sources of coal, they were also
exposed to silica and later developed respiratory diseases (Rosner & Markowitz, 2000).
Despite regulations to control the disease and the industry’s shift away from underground
mining and towards mechanization and strip mining, black lung continues to be prevalent
among older miners but young Appalachian surface miners (Laney, et al., 2012; Blackley,
et al., 2016). Hydraulic fracturing in Pennsylvania has developed with its own regional
characteristics in the northeast and southwest parts of the state. Industrial lung diseases
have been endemic to these areas and provide a poignant setting as exposures to respiratory
11 Several oilfield workers that I spoke with talked about their experiences with the coal industry, as
miners themselves or as the sons of miners. One had recently lost his father to the disease. Another
worker had acquired a lung disease from a previous job and had moved to safety work in the oilfield
because it was less strenuous. For both, lung disease was considered a part of the jobs men like
themselves do, interweaving a sense of self with health risk.
18
hazards resurface through unconventional oil and gas extraction12.
Health Geography and Responsibility: Theoretical Framework
Although the workforce is central to arguments that justify the industry, scholars
have insufficiently examined the frameworks that regulate the health risks from those jobs.
Social science scholarship on unconventional fuels and health has largely excluded workers
(for exceptions see Filteau, 2014, 2015a, 2015b; Brundage, 2011; Brundage et al., 2011;
Jacquet, 2011; Witter et al., 2014). Instead, public and academic attention in the U.S. has
primarily focused on environmental and public health risks of extractive activities,
surveying, for example, the often-underdeveloped state-led regulatory framework to
protect air and water resources and limited federal oversight of oil and gas activities
(McKenzie et al., 2012; Adgate, Goldstein, & McKenzie, 2014; Warner & Shapiro, 2013;
Andrews & McCarthy, 2014; Jacquet, 2014; Rabe, 2014; Casey et al., 2016; Rasmussen et
al., 2016; Wiseman, 2016; Zirogiannis et al., 2016). Theories of environmental justice draw
attention to distributive and procedural injustice wrought through unconventional fuels
(Willow, 2014; Kennedy, Schafft, & Howard, 2017), yet more analysis is needed to
translate these concerns to occupational health. OSH frameworks afford opportunities to
examine the emergence of the hydraulic fracturing industry within existing social and
political contexts and its relationships to human health.
Health geography has been largely silent on the relationships between health and
unconventional fuel development and has been slow to examine health and OSH
regulation. However, cognate literatures that many health geographers utilize have long
12 Silicosis was also identified in this period in the nail cutting industry in Wheeling, West Virginia,
over the southwest border with Pennsylvania, and southeastern border with Ohio (Sellers, 1997).
Wheeling has become a hub of shale oil and gas activity as a crossroads of major interstates.
19
illustrated how workers bear the embodied consequences of industrial labor. The historical
roots and gendered and racialized dynamics of this burden have been well-documented
within public health (Messing, 1998), labor history (Derickson, 1998, 2013a, 2013b;
Rosner & Markowitz, 2003, 2006), medical anthropology (Holmes, 2013; Horton, 2016;
Little, P., 2017), feminist geography (Wright, 2006), and history of science (Sellers, 1997;
Murphy, 2006; Nash, 2006). Health geography centers on ways that space and time operate
as material and discursive processes to shape health risk, and thus should more significantly
engage in occupational settings wherein particularly the modes of production use time and
space to shape productivity in ways that impact (and often disregard) human health. This
study illustrates this opportunity through occupational health regulation and responsibility.
Specifically, it shows how spatial and temporal patterns of industry and occupational
exposures intersect with responsibility defined and enacted by the state, and how at this
intersection, the state’s governance mechanisms function to shift responsibility onto
individual workers through its insufficiencies, ignorances, and failures.
Thus, here I focus on the dissertation’s scholarly setting within health geography.
Health geographers have long considered that health is a social construction and material
state of the body (Kearns & Moon, 2002; Jackson & Neely, 2015), that relationships
between places and health exist, and that their study can reveal significant trends and
patterns (Kearns & Moon, 2002). For many, health is a conceptual tool to examine how
political, economic, social, cultural, and environmental processes transpire across space
and time, and reproduce imaginaries about people and places (Craddock, 1995, 2000;
Biehler, 2009; Brown, 2009; Carter, 2012). Others engaged more closely with spatial
analysis and spatial epidemiology illustrate how patterns of exposure, poverty, and access

20
to care influence health outcomes, often to understand if health is about the place itself or
the people living there (Guthman & Mansfield 2013; Rosenberg, 2013; Foley & Kavanagh,
2014). I explore two dimensions of this subfield, health governance and health justice,
before arguing that health geography re-conceive responsibility in its approach to the
relationship between institutions and individuals when considering human health.
Health Governance
Governance, the processes that produce, maintain, and order socio-spatial
relationships between individuals and institutions, provides language useful to consider the
vast apparatuses that direct conduct in space and time. Geographers have illustrated the
power relations encoded in spatial practices of laws, regulations, and policies surrounding
the promotion of healthy places and healthy bodies (Brown, 2009; Evans & Colls, 2009;
Guthman, 2011; Mansfield, 2012b). Foucauldian analyses of power have been instructive
here, as they illustrate how norms of behavior, self-regulation, techniques of measurement
and observation, and direct intervention coalesce to govern individuals and populations;
Foucault’s notion of biopolitics – or the politics of life – and biopower – the effect of
disciplinary power on the body – has driven much of this scholarship (Parr, 2004; Brown
& Bell, 2008; Brown, 2009; Brown & Knopp, 2010; Mansfield 2012b, 2012c). Health
governance literature often centers on the production of health subjects through
authoritative ways of ‘seeing,’ often starting from, but also exceeding, the state.
Conceptually, governmentality and/or biopower are part of systems of power in which
health discourses, health metrics, government analyses, and public health programs encode
forms of self-discipline including self-monitoring, pertaining to public health (Brown,
2009; Rose, 2009; Brown & Knopp, 2010; Mansfield, 2012a, 2012b; Carter, 2015). Some
use these insights to critique neoliberal configurations of power, thereby showing the

21
relationship between capitalism and personal understandings of health. Guthman (2011)
argues that obesity has been presented as an ‘epidemic,’ thus creating a public health
imaginary ameliorated through prescribed ways of being and eating. For Guthman, the
body becomes a spatial fix for capitalism.
Morality as a means of health-subject formation also frames this scholarship.
‘Moral panic’ that accompanies certain sexual practices, cleanliness, body size, etc. works
to justify state action, shape individual bodily practices, and reifies existing power relations
that deem some bodies ‘ill,’ ‘in need of correction,’ or ‘deviant’ (Brown 2009; Guthman
2011). Exploring the production of health knowledge has revealed mechanisms underlying
the making of ‘ill’ bodies regarding chronic illness, lifestyle, and risk (Brown & Duncan,
2002; Parr, 2002; Keil and Ali, 2007; Guthman, 2011). Others have turned to
‘responsibilitization’ and individual responsibility, focusing on the responsibility of
individuals, how they are made to be responsible and internalize messages of responsibility
and risk, and how this relates to neoliberal forms of power (Kearns & Collins, 2010;
Mansfield, 2012a; 2012b; Little, 2017).
These studies illustrate how the state identifies and seeks to manage a health
‘problem,’ often framing solutions through prevailing narratives of science, public health,
and morality. OSH illustrates how these narratives are constrained further within the OSH
context through the ways the state regulates responsibility, through liability, and enacts its
multiple responsibilities that fall under the ‘problem’ of occupational health. These
governance mechanisms buttress personal responsibility narratives for OSH of the
industry, but moreover, reinforce liberal values surrounding the rational subject and the
extent of the authority of the state particularly when intervening in private industry. Under
22
the rubric of OSH, the state has sought multiple ends, be that the management and
protection of populations, the reduction of costs and minimization of liability, or concern
for future bodily integrity, well-being, and self-actualization. Here, I understand the state
as an entity produced through the enactment of its authority through laws, policies and
regulations, and its role in the coordination of conduct through multiple forms of power. I
draw upon Foucauldian analyses of power, and strategies and modes of power employed
by the state (Rose & Miller, 2008; Dean, 2009), and thus remain consistent with ways that
health geographers have theorized the state and governance.
Health Justice
A related approach to examining health has been described as ‘health justice’
although what is meant by ‘justice’ is often only loosely articulated (Rosenberg, 2013).
Although methodologically split, much of this scholarship reveals patterns and
relationships that result in unequal distributions of health risk and exposure and is often
closely aligned with environmental justice scholarship (Pearce et al., 2010; Rosenberg,
2013). It gives attention to who bears health burdens, and where, and prompts a focus on
the body and place. This literature has shown how socio-economic issues such as income
inequality, proximity to industrial activities and transportation, access to care and
medicine, and food availability influence health outcomes (Pearce et al., 2010; Saha et al.,
2011; Foley & Kavanagh, 2014; Collins et al., 2015). Research crossing environmental and
health justice has utilized these findings to show how structural processes influence
discrete instances of environmental injustice (Tschakert & Singha, 2007; Hanchette, 2008),
shifting away from causal narratives required in law and public health (Pulido, 2000;
Masuda & Crabtree, 2010). It explores health policy questions about who has access to and
who benefits from given health regimes (Brown & Baker, 2012; Sparke & Anguelov,
23
2012). It often tackles neoliberalism in two related senses: by examining deregulatory
efforts that began in the 1970s and 1980s whereby the state was weakened in line with
neoliberal ideologies, and by exploring how the state has become characterized by
economizing logics whereby neoliberal values and governance have been reoriented
around risk, uncertainty, and biopolitical power (Rose, 1996; O’Malley, 2004; Rabinow &
Rose, 2006). Geographers have sought to consider health by ‘unpacking’ the environment
and its relationship to health and justice (King, 2009; Jackson & Neely, 2015) and has paid
attention to the body as a dynamic socio-nature itself (Guthman & Mansfield, 2013). This
addressed frameworks wherein the environment has been theorized statically.
Many health justice studies continue to focus on issues of proximity and
distribution; a critique also leveled at environmental justice literature (Walker, 2009;
Holifield, 2012). More analysis at the intersection of health and justice needs to examine
how health is structural, relational, and forged through process and participation. Indeed,
some have recently illustrated how the language of capabilities has been influential in
environmental justice literature (Edwards, Reid, & Hunter, 2015). There are parallels here
to Ruger’s (2010) and Venkatapuram’s work on health justice (2011). Both draw upon
Amartya Sen to offer a context for thinking about this “capability to be healthy,” health as
not merely a bodily state, or in Ruger’s terms, the “health capability paradigm.” The case
examples in this dissertation help illustrate how the right to a space in which one can make
healthy decisions may not be sufficient to address the justice questions that the capabilities
approach seeks to mend. Focusing on how the state enacts its authority in OSH articulates
the procedures and processes that these emphases miss.
Responsibility, Care, and the Neoliberal State
Critical approaches to responsibility and care have shaped scholarship in geography
24
over more than two decades (Smith, 1997; Proctor, 1998; Massey, 2004; Popke, 2006;
Lawson, 2007; Popke, 2007; Sparke, 2007; Carmalt & Faubion, 2010; McEwan &
Goodman, 2010; Milligan & Power, 2010; Barnett et al., 2011; Noxolo, Raghuram, &
Madge, 2012; Olson, 2017). Feminist contributions have rebuked notions that relationships
of care or responsibility emerge solely through proximity but rather have re-theorized
responsibility and care as extending to ‘distant others’ (Noxolo, Raghuram, & Madge,
2012; Massey, 2004; Lawson, 2007). I argue that this focus on the individual needs to be
considered within patterns of responsibility at the institutional level, focusing on
institutional mechanisms which purport to shift responsibility onto larger entities to
diminish ‘individual responsibility.’
This feminist scholarship on responsibility has helped geographers to explore
neoliberal processes and the contraction of the welfare state through aforementioned
“responsibilization” whereby the state increasingly encodes individuals with responsibility
for services formerly the purview of the state (Brown & Baker, 2012; Staeheli, 2013; Bell,
Hollows, & Jones, 2015; Glasgow & Schrecker, 2016), including the management of risk
(Bickerstaff, Simmons & Pidgeon, 2008; Mansfield, 2012a, 2012b).
Feminist care ethics has had a different impact particularly in health geography,
opening new empirical examinations of practices of care and self-care, and spaces of care
and care-scapes (Brown, 2003; Parr 2003; Greenhough, 2010; Milligan & Wiles, 2010;
Milligan, 2014). Care has also offered normative values from which to approach health-
related research (Parr 2003; Carmault & Faubion, 2010). Still, care and responsibility have
often had a synergistic history within their applications, particularly when care has been
used to examine the distribution of labor and social reproduction, and the kinds of caring

25
responsibilities left to women in the ‘private’ space of the home (Domosh, 1998).
Feminist theories of responsibility and care critique ‘traditional’ understandings of
morality and justice by attending to lived experience and relationality in the shaping of
moral and social life and knowledge (Gilligan, 1982; Noddings, 1984; Tronto, 1993;
Grasswick, 2003; Noddings, 2002; Held, 2006; Walker, 2008; Young, 2008; Tronto, 2013).
While definitions of care and responsibility are multiple, most theorists illustrate how both
are not only moral feelings but also political practice (Walker, 2008; Young, 2008; Tronto,
2013) that transcend place, space, and time (Massey, 2004; Held 2006; Lawson, 2006;
Young 2008), and thus have utility for geographic analyses of power.
Early feminist care ethics challenged models of morality and justice that were built
around particularly masculinist ideals (Gilligan, 1982; Noddings, 1984). Care offers a
distinct ethical value that highlights the relationality of moral life, illustrating uneven
relationships and inequalities through care (Kittay, 1999; Held, 2006), and the
interdependency of individuals (Kittay, 1999). This has increasingly shown care to be a
relationship of dependency that is more complex and multi-directional than ‘care-er’ and
‘cared for’ (Held, 2006; Milligan & Wiles, 2010). Indeed, care is both a lens on social
processes and an ethical standpoint. For geographers,
care is more than simply a social relation with moral or ethical dimensions;
it can also be the basis for an alternative ethical standpoint, with
implications for how we view traditional notions of citizenship and politics
(Popke, 2006, p. 506).
Still, what this means has been rethought through theoretical debates that have questioned
if care is complimentary, additive, or replacement for ‘traditional’ values of morality and
justice, if care and justice can co-exist, and the primacy of care (Held, 2006; Tronto, 2013).
Theories of responsibility have sought to understand how it is both a process of

26
‘taking’ and ‘assigning,’ (Fiore, 2003). ‘Taking’ indicates its relationship to agency, while
‘assigning’ denotes responsibility’s top-down qualities. As such, it can be traced and
mapped in the ways it is taken up and refused to understand the contours of social and
political practice (Fiore, 2003; Grasswick 2003; Walker 2008; Noxolo, Raghuram, &
Madge, 2012). Like feminist ethics of care, its use within feminist scholarship has
reoriented commitments of moral philosophy to values that are more relational, specific,
and adaptive to diverse social processes (Fiore 2003). Rooted in critiques of idealized
versions of morality (Walker, 2008), responsibility has also offered a new commitment and
analytic for the production of knowledge (Grasswick 2003; Code, 2006; Walker, 2008). As
will shortly be discussed, feminist theorizations of responsibility have further offered
challenges to virtue theory and luck egalitarianism (Hughes, 2003; Young, 2008),
discourses of personal responsibility (Fiore, 2003; Young, 2008) often underpinning
neoliberal policy (Jaggar, 2003; Tronto 2013) and utilitarian and distributive approaches
to justice (Young, 1990; 2008).
While many offer these concepts to advance ways of evaluating social life, their
use has not been without criticism, caution, and complication (Held, 2006; Noxolo,
Raghuram, & Madge, 2012; Hankivsky, 2014; Murphy 2015). In its early iterations, critics
of care ethics suggested its focus renormalized women as being the ones who ‘naturally’
do care work (Held, 2006). Post-colonial scholars have cautioned that state-led calls for
responsibility can be acts of absolution that obscure the ways its espousers are imbricated
within unjust processes of global inequality (Noxolo, Raghuram, & Madge, 2012).
Responsible relations create and are created by problematic and contradictory power
relations, where actions coded as ‘responsible’ are often violent, transcend boundaries, and

27
justify states of exception (Noxolo, Raghuram, & Madge, 2012; see also Sparke, 2007).
These critiques often use the concepts more analytically to examine power, for example,
in the health and scientific discourses (Faria, 2008; Mansfield, 2012a; 2012b), feminist
health activism (Murphy, 2015), shifts from the welfare state and neoliberal state (England,
2010),, and the sequestration of care to the private realm and work and justice to the public
realm (Boyer, 2003; Held, 2006; Popke, 2006). For Murphy, critical evaluations of ‘care’
for example, do not deny a ‘politics of care’ but rather illustrate how care itself is not inured
from the social structures to which it responds.
This vexation of care is important because there is an ongoing temptation
within feminist scholarship to view positive affect and care as a route to
emancipated science and alternative knowledge-making without critically
examining the ways positive feelings, sympathy, and other forms of
attachment can work with and through the grain of hegemonic structures,
rather than against them. (Murphy, 2015, p. 719).
Care has remained a significant dimension of feminist ethics (although feminist ethics
should not be equated with care ethics) and has become a way to shift thinking about the
actions and feelings of individuals and institutions. These two dimensions that have been
significant for geographers’ work, particularly in its theorization of a relational subject that
challenges the rational individual that underpins so much of moral philosophy (Popke,
2006, p. 506). Across both concerns of care and responsibility, the extent to which
institutions can and should adopt these concepts or be theorized as ‘taking’ or ‘being
assigned’ them are significant. As Held (2006) rightly points out, the social risks for not
thinking about care beyond the space of the interpersonal (or the family, as it is often
assumed) are high, and thus the reasons for seeing care in social institutions are great.
To the extent that we are economically interdependent, we need and want
public policies and arrangements that will enable us to provide care to those
we care about (who need not be limited to our immediate ‘‘loved ones’’)
and that will enable us to receive care when we need it… If a contractual
28
model is applied directly to situations of economic interdependence, it treats
the economically powerless and the economically powerful as if they were
equally autonomous, obscuring the conditions conducive to exploitation
and deprivation (Held, 2006, p. 81).
Indeed, thinking through the lens care is transformative (Popke, 2006, p. 506, citing Brown,
2003; Staeheli, 2003). Claims that the institutions should incorporate ‘care’ into its policies
or broaden its ‘responsibilities’ can extend to the ways we see institutions as caring and
responsible. Such ascriptions, however, raise two related issues.
First, we can trace the role of the state through its position on care and responsibility
and understand how its internal logics perpetually facilitate exploitation, domination, and
paradoxically a shifting of responsibility and a lack of care, even when its ‘assigning’ to
the state is meant to do the opposite. Second, in theorizing institutions or collectives as
being caring and responsible, we risk imparting them with moral agency, or moral standing.
The results of this concern can be seen through Peter French’s work on corporate
responsibility, where he argues for seeing corporations as ‘moral persons’ (1979) or seeing
the “actions of corporations” as “redescriptions of the actions of humans”(1992, p. 100,
see also French, 1984). While French makes compelling arguments about seeing
corporations, responsible for, particularly given the long-term challenges posed by
ascribing responsibilities for environmental damage in both a legal and moral sense (see
Chapter 9, Responsibility Matters (1992), for a brief discussion of the Exxon Valdez Spill),
seeing corporations as moral agents with moral and legal standing is not without
consequences. The relationship of French’s argument to corporate personhood is
concerning. Brown (2015) extensively discusses the dangers of this move by examining
Citizen’s United, wherein corporations take on liberal rights through processes she relates

29
to the insipid extension of neoliberalism into all aspects of democratic life13.
Responsibility in this dissertation plays a larger role than care, the reasons for which
I elaborate on below. Theories of responsibility provide a lens to engage with whom and
what is valued in society by examining the underlying power relationships embedded in
who is ‘ideally’ responsible and who ultimately is responsible. Health geographers can use
the concept as an organizing framework to consider the relationships that flow from
governance mechanisms that are multi-scalar, forward- and backward-looking, and
negotiated in everyday practice. To that end, I reconsider how the state negotiates is own
responsibilities and distributes responsibilities amongst actors when it comes to issues of
health risk and particularly occupational health risk.
I ground my analysis most strongly in Iris Marion Young’s notion of responsibility,
extensively detailed in Responsibility for Justice (2008), but also discussed in other works
(1990, p. 151; 2003; 2006). However, it would be incorrect to suggest that Young is the
only one who makes the critiques I discuss or that responsibility provides a replacement
for care. Indeed, Held’s thinking on the relationship of care and justice and discussion of
personal responsibility and virtue ethics (2006) offer some similar analyses. Tronto’s
“caring responsibilities” (2013) also offers useful ways of considering the analysis in this
dissertation, a contribution that itself draws upon components of Young and Walker’s
theories of responsibility.
However, Young’s analysis is compelling for this project in three ways. First, her
critique of liability offers a useful tool to see the limits of causation and intentionality
13 While we have seen within health geography and geography more generally, an effort to expand
agency and ethical consideration to non-human actors, the normative dimensions of these extensions
need to be carefully considered.
30
within structurally produced injustice under a diminished welfare and/or neoliberal state,
as is pertinent to the context of OSH in the US. Second, Young’s critique of ‘personal
responsibility narratives’ and a move away from ‘intent,’ ‘actions,’ or ‘character’ of the
agent, such as those found in virtue theory, are useful for considering OSH policy. This is
because questions of ‘assumed risk’ and ‘adequate compensation’ often diminish, explain,
and justify workers’ exposures to hazardous substances, and issues of ‘distance’ and ‘lack
of knowledge’ produced through subcontracting and other flexible mechanisms work to
absolve companies of responsibility. Third, by thinking through responsibility as forward-
looking through structural processes, Young directs more attention to contributions and
positions within social structures, an effort to move away from debates about the moral
character of individuals that helps my own interests in distancing from debates concerning
if workers are well enough compensated or ‘know’ the risks, as both discourses operate to
absolve others of their complacency within the structural processes that expose workers to
risk. Further, such an argument is compelling given my interest in thinking about
institutions as ‘responsible’ for injustice, but also my hesitancy in offering institutions
moral and political standing and, moreover, feeling, even as this concern is not fully
satisfied by this theorization.
Responsibility for Justice
Iris Marion Young’s posthumously published work, Responsibility for Justice,
develops the social connection model as a framework for forward-looking responsibility
that addresses structural injustice and critiques of models of responsibility rooted in
liability. Young theorizes responsibility in the context of structural injustice, explaining
structure in a way that can be used to consider the processes, institutions, and individuals
that produce OSH. Drawing on Rawls’ declaration, Young herself asserts that the “subject

31
of justice is structure” (2008, p. 44). Structures are a means of looking at society through a
series of processes and flows (2008, p. 70) involving the “accumulated outcomes of the
actions of the masses of individuals enacting their projects, often uncoordinated with many
others” (2008, p. 63). For Young, these results may themselves be anathema to the original
intent of the actors, a key consideration given the ostensible goal of OSH, to protect
workers’ health14.
Young articulates her theory of structural injustices through the Social Connection
Model by identifying injustices as processes through which groups or categories of
individuals are led to systematic risk of disadvantage and dispossession. For Young, the
challenge is to draw together moral and political philosophy such that responsibility can be
rethought in forward-looking ways to address structural problems. “To [Young]
responsibility is political, because it is collective, involves public discourse, and aims at
changing the social structure” (Neuhaüser, 2014, p. 242). Young’s model stems from a
concern that most theories of responsibility focus on individual instances of blame or fault,
do not address structural injustices, and obfuscate how normalized behaviors reproduce
them (Young, 2008); blameworthiness encoded in many of our existing frameworks for
responsibility insufficiently addresses structural roots of injustice. As she explains, “the
purposes of social practices of finding guilty, blaming, finding fault, holding strictly liable
are to focus on particular agents in order to sanction or demand compliance from them
alone” (2008, p. 105).15 She critiques responsibilities that focus narrowly on fault or blame,
14 The modest successes or outright failures of OSH structures to adequately protect workers over the
last century suggest that the concept may be more a euphemism that insulates employers and the state
from actually protecting workers. Still, many involved in OSH believe their actions make workplaces
safer, even if working within a flawed system. 15 While blame, fault, guilt and liability have different meanings and implications, Young often uses
these terms in combination when critiquing about responsibility as a causal relationship.
32
revealing how individual units of disparate parts of a system are responsible for
remediating injustice even if they are not directly culpable. For Young, “when injustice is
structural, there is no clear culprit to blame and therefore no agent clearly liable for
rectification” (Young 2008, 95). Young seeks to distance the social connection model from
questions of guilt and liability. However, as will be discussed shortly, liability has some
utility within an OSH context.
Other elements of Young’s analysis entail critique and re-readings of theories of
responsibility in public policy, virtue theory and luck egalitarianism, and Arendt’s writings
on responsibility. Virtue theory’s focus on moral character as a source of ill-standing, harm,
or, in her examples, poverty, offers nearly no contextualization of individuals within social
structures, and moreover centers on the moral character of individuals rather than the
broader systems and peoples that contribute to and reproduce injustice (Young, 2008). For
Young, virtue ethics strips people of their context, absolves others in their relationship to
injustice and fixates on consideration of morality, choices, and behaviors of individuals.
Even as Dworkin’s theory of luck endorses the idea of a welfare state as it tries to make
sense of ill-circumstances that result from arbitrary conditions and personal choice, for
Young, it “focuses largely on attributes of persons and ignores or rejects a theoretical place
for bringing social structures into view” (2008, p. 30). These critiques are useful in thinking
about OSH rules and regulations that seek to regulate behavior of actors to minimize risk,
and where behavior and ‘assumed risk’ underpin ideas that ‘workers know’ the risks they
assume and hence take responsibility for them. Focusing on behaviors and knowledge miss
the broader processes that place workers in exposure’s way in the first place. Thus, I take
Young’s critiques of responsibility as an entry point to understanding how OSH operates,
33
what it reproduces, and how it can be rethought through a more expansive
conceptualization of responsibility.
Young’s model is useful to examine OSH because of its treatment of time and
structure. It approaches issues of justice through a temporal framework; it is mostly
forward-looking, and thus forces us to engage with who bears responsibility for the
outcome of a hazard, but moreover, who should be responsible for changing the structure
that produces OSH risk. She finds that all those who contribute to unjust systems, even
those most unjustly impacted, have relationships of responsibility to change them, although
these responsibilities are not equal (Young, 2008, p. 97). This is helpful as many OSH
discourses focus on workers who ‘choose’ risky work or structures that make ‘safe choices’
impossible. In denying these binaries, she theorizes responsibility as collective and
forward-looking for structural change. While skeptical of liability as a means to influence
structural change, Young does not deny the utility of liability as a form of responsibility,
particularly when considering discrete harms done by corporations. Her proposal to rethink
responsibility provides alternative and active ways of thinking about health and health risk.
Geographers have embraced elements of this approach to rethink global
connections and the responsibilities to others they engender. As Barnett et al. (2011) write,
“taking responsibility…is theorized in terms of how distributed actions join actors together,
feeding into wider networks of cooperation that reach out and influence events elsewhere”
(p. 9). Young differentiates responsibility through power, privilege, and the ability to act
and has aligns with feminist geographers’ efforts to conceptualize global-local connections
through responsibility (Massey, 2004; Lawson, 2007). Further, her model conceptualizes
actors as unevenly imbricated in unjust structures and processes.

34
Neuhaüser (2014) extends the Social Connection Model by addressing what he sees
as its insufficient specification of the role of corporate actors, and hasty dismissal of fault
and blame. For Neuhaüser, Young does not answer if corporate actors are enrolled in the
social connection model as passive background agents, or, if “... corporate actors are
actually responsible agents themselves who can take over a part of the forward-looking
responsibility to overcome structural injustice” (Neuhaüser, 2014, p. 241). In considering
the implications of corporations or industries as being moral units or political actors,
Neuhaüser integrates more extensively both forward- and backward-looking responsibility
where these agents are held accountable for the acts they cause, but where they also have
a responsibility to change structures from which they profit that are unjust.
Neuhaüser links moral, legal and political responsibility through his efforts to
rectify ‘backward-looking’ responsibility with Young’s approach, adopting the stance of
Peter French and others that imbues corporations with agency, and allows their status as a
“moral agent.” As Pasternak describes, this means,
As moral agents, groups are morally responsible for their actions (in the
sense of backward-looking attributions of blame and praise). And as moral
agents groups can be task-responsible (in the sense of forward-looking
duties and obligations) (Pasternak, 2014, p.222).16
Neuhaüser aims to rectify inconsistencies within Young’s approach, namely surrounding a
normative theory of justice, its dealings with collective and shared responsibility, and her
16 Pasternak shows how theories of corporate responsibility, or the ‘corporate agency thesis,’ fail to
distinguish between moral and task responsibility. Pasternak is concerned by slippage as philosophers
deal with the heterogeneity of groups; this particularly occurs when blame is ascribed to a group but not
its individual members. She uses the example of corporate task responsibility to illustrate these
concerns, as it is often those members who end up enacting the forward-looking obligations and provoke
questions surrounding “industry” is framed in opposition to “workers.” Young’s approach to
responsibility for justice, such that it inclusive everyone, while maintaining an emphasis on the
distributed and necessarily unequal ways that responsibility is allocated, provide a useful counterpoint
to issues Pasternak raises. This is further supplemented by Neuhaüser’s emphasis on using guilt and
liability as mechanisms through which to address the “fair distribution of responsibility.”
35
dismissal for blameworthiness within her theory of responsibility. Notably, rather than
dismiss the utility of blame, it is “sufficient to prove that profit was made from the injustice
to further inquire whether there is a culpable involvement associated with this profit”
(Neuhaüser, 2014, p. 245). Thus, Neuhaüser uses the idea of culpability for an injustice,
broadly understood, as a mechanism by which to distribute forward-looking responsibility.
How the state views its own responsibilities and ascribes responsibilities reflects
and reproduces liberal and neoliberal notions of rational actors, personal responsibility, and
the state’s authority to intervene in private industry, that have underpinned the state’s
approaches to responsibility for OSH risk. While the dissertation draws on these insights
to understand responsibility as political, it acknowledges that practically, utilizing the idea
of industry or corporate actors as being political or moral units has additional conceptual
implications and raises theoretical tensions. Seeing industry as a political and responsible
actor has complex ramifications when considering ‘whose health’ matters when the state’s
responsibilities to workers and employers are not clear, as considered in Chapter 2. Many
of these concerns about viewing corporations as having individuals’ rights are well
articulated in raised by Brown (2015), as previously mentioned. However, seeing industry
as a unit with responsibility and agency has utility when considering its responsibility
towards structural dynamics that produce exposures to health risk, as discussed in Chapter
3, when considering a more expansive notion of responsibility for structural processes.
Mapping Responsibilities and Caring Responsibilities
Walker’s Moral Understandings draws attention to practices of responsibility.
Finding ideal constructions of responsibility insufficient, she emphasizes how
responsibility is practiced in the everyday, how responsibilities are multiple, and thus how
they are negotiated through systems of power and privilege. Responsibility reflects power

36
relations in that it is defined, assigned, and assumed through political processes, which do
not work in isolation. This work underscores that responsibilities are not singular, but
multiple, and illustrates the significance of considering not only how responsibility is
distributed in a theoretical sense, but how it is enacted. Her ideas emphasize what can be
learned from charting how responsibility unfolds through occupational health governance,
particularly about who and what is valued in society. This mirrors with Young’s concern
for responsibility’s definition, and responsibility’s relationship to the perpetuation of social
exclusions and injustices. Like care theorists, for Walker many everyday responsibilities
emerge out of relationships of dependency, opening up questions of vulnerability and
responsibility through differing forms of connection.
…social arrangements create of exacerbate vulnerabilities, which
vulnerabilities (some of them unnecessary) then entail responsibilities. But
as I have argued, delineating and delegating responsibilities is itself a large
in fundamental part of anything we might call a social arrangement,
practice, or system. The scheme of distributing responsibilities itself is a
determinant not only of particular responsibilities but of particular
vulnerabilities as well. Responsibility assignments render some people
vulnerable to particular others in particular ways for certain
things…(Walker 2008, p. 96, my emphasis).
Discourses surrounding work, working relationships, and OSH in the oilfield rely upon and
exchange between responsibility and vulnerability. Workers are responsible for their
coworkers, producing energy for the nation; workers sometimes must choose between
doing work quickly or doing work safely. Sometimes being responsible also means being
vulnerable, thus in some contexts, this comes as a form of personal sacrifice.
Walker’s ideas about “mapping responsibility” (2008, p. 86) have been widely
influential, shaping how scholars consider tracing social relationships to understand
systems of power, and more specifically in showing relationships between morality and
politics, even if she herself does not make that claim (Tronto, 2013). It is particularly useful
37
here, for thinking also about the relationship between responsibilities towards and social
vulnerabilities produced through social practices.
While the dissertation largely focuses on responsibility, Tronto’s work on ‘caring
responsibilities’ (2013) provides ways of thinking about multiple relations of care that are
significant for OSH. Drawing on Young’s analysis of structural injustice and Walker’s
account of an ethics of responsibility most strongly, Tronto explains how thinking about
‘caring responsibilities’ offers a different lens into democratic life. Privileging caring (for
Tronto, responsibility is a kind of care) offers a way to think about the decisions and
distributions of care.
Some forms of responsibility can appear to be contractual, but for an ethic
of care, one needs always to go beyond simple agreements to look more
closely at the power allocation in exchanges about responsibility. One needs
to focus also upon relationships among people, and not simply upon isolated
individuals, in making decisions about care (Tronto, 2013, p. 55).
This relational approach to viewing responsibilities requires thinking beyond distributions
of responsibility determined by rules and regulations, and considering the relationships
produced through caring relations, be that care for one’s fellow workers, one’s employer,
or one’s nation. These relationships of care underpin many of the discourses of OSH that
valorize certain kinds of risk, vulnerability, and ultimately sacrifice, examples of which are
discussed in the dissertation. Moreover, care-at-work can function to reinforce narratives
of personal responsibility.
Tronto (2013) also draws attention to irresponsibility, focusing on “epistemological
ignorance” (pp. 58-59) as a means to shift responsibility through ignorance of broader
structural conditions. Importantly, she draws attention to Pettit’s (2007) work on the Exxon
Valdez Spill, and the ways the multinational energy company utilized an “institutional
structure that deliberately diffuses and obscures lines of authority” (Tronto, 2013, p.60).

38
This is a key way that the neoliberal state has operated with respect to risk.
Risk, responsibility, and the Neoliberal State
The state has taken multiple approaches to civil society and the economy; through
liberal, welfare, and neoliberal processes the state has employed different rationalities and
techniques to govern risk, responsibility, and care (Rose, 1996; O’Malley, 2012; Tronto,
2013). The interference of the state in economic activities in the early 20th century, relied
upon core liberal ideas of a rational actor, but also incorporated new ideas about the role
of the state in mediating risks from economic activities. At various points in mid-century,
these ideas coalesced around policies and regulations to offer the populations and specific
groups protections from the state. These welfare programs, however, were strongly
rebuked, reformed, and replaced by neoliberal logics and programs. Particularly in the
latter half of the 20th century, responsibilities and caring activities that had been adopted
by the state were increasingly (re)placed on individuals under neoliberal processes and a
focus on self-governance (Jaggar, 2003; Silvey, 2009; England, 2010; Laliberté, 2015).
“The ideal neoliberal subject is the self-governing, autonomous market player” (England,
2010, p. 137). Further, the neoliberal subject bears the responsibility for social problems.
Discourses of citizenship, formerly configured around collective
responsibility, ameliorating social risk and social entitlements, have shifted
towards the neoliberal values of possessive individualism, consumerism,
and individual responsibility. In this neoliberalized frame, social problems
are recast as failures of the individual rather than the result of structural
inequalities, and the ‘good citizen’ is an atomized. (England, 2010, 136-
137).
For feminist scholars, examining the relationship between state powers, neoliberal
policies, and everyday life, has significant political contours. State power is not rooted only
at the institutional scale but can be seen in and through differently scaled social practices
(England, 2010, p. 134). This reveals ways that the state’s distribution of care and

39
responsibility are gendered, not only in divisions of public/private, but in the ways that
work/care are valued (Tronto, 2013).
In the 1990s, shifts surrounding welfare reform and welfare to work, continued to
reify distinctions of work and social reproduction relying on gendered stereotypes (Boyer,
2003), by tethering state support to ‘work’ that the state sanctioned. While much of these
discussions have focused on the ways that ‘care’ and ‘work ethic’ represent the
normalization of economic life, and public and private (Tronto, 2013), significantly
particular forms of care underpin the structures and discourses on which OSH relies, and
moreover, OSH discourses of personal responsibility depend.
These shifts in thinking about responsibility, care, and risk, paralleled a shift in how
to approach risk in the US. This is particularly evident when tracing the relationships
between the state, society, and the economy under OSH, and particularly when focusing
on the institution of OSHA. OSHA was one of the last enacted social protection programs
that emerged from social movements of the 1960s; while many neoliberal responses had
been to diminish the state’s role through deregulation, this has not been the only tool, nor
the most significant one to OSHA, Rather, through the implementation of extensive
regulation, paperwork, and requirements, OSHA’s ability to regulate has been diminished
through practical concerns (see Chapter 2). These changes have paralleled developments
in who is responsible for proving risk (Vogel, 2012) and the state’s relationship to the
precautionary principle, wherein as the state increasingly has been burdened with proving
economic activities cause harm (Vogel, 2012). The diminished capacity of the state is an
additional important dimension. Not only is OSHA underfunded and understaffed (see
Chapter 3), it is uniquely less powerful than other regulatory agencies in the strength of its

40
regulations and its ability to leverage fines (see Chapter 3). Thus, under neoliberalism, risk
and responsibility for risk, shifts onto individuals through diverse practices, of which many
are on display through this dissertation’s discussion of OSHA policy and workers’
compensation statutes. Thus here, the dissertation uses the lens of the neoliberal state to
contribute to diverse theorizations the “use of individualisation of responsibility for risk as
a management strategy by the state and other institutions” (Bickerstaff, Pigeon, &
Simmons, 2008, p.1315).
I return to these frameworks for thinking about health and its relationships to risk,
responsibility, care, and governance throughout the dissertation. Notably from this
discussion, these theorists provide ways of thinking about responsibility as a practiced,
negotiated, multiple, and inherently political concept that defines relationships between
differently scaled actors, and is tethered to neoliberal processes of the state. A focus on
responsibility for occupational health offers health geographers an opportunity to consider
not only distributional concerns of health and risk (who is exposed/unhealthy and where)
but requires examining the contexts, processes, and procedures that shape structures of
occupational health at multiple scales.
Methods
I conducted this research between October 2013 and August 2017, with the most
intense periods of data collection occurring between October 2013 and May 2015, and
employed participant observation, interviews and textual analysis. Drawing inspiration
from feminist sociologists and anthropologists (Marcus, 1995; Smith, 2005, 2006), I sought
to track the processes responsible for defining, enforcing, and perpetuating responsibility
for OSH in the oilfield. A reflexive approach further recognizes the power relationships
embedded in research but also draws attention to how the researcher is integral to the

41
knowledge produced. Positionality changes through different spaces and interactions, and
shapes the questions asked, the information gathered, and how the research impacts others.
My methods allowed me to trace social relations that shape occupational health as
it materializes through regulatory interventions situated in historical and material contexts.
My research took place in a variety of sites and changed as I engaged it, particularly as I
had not foreseen how difficult it would be to access the industry. Mulvaney (2014)
describes using multi-sited methods to overcome barriers of secretive industries that thwart
attempts to study them and was useful in tracing OSH in the oil and gas industry17. As
forms of access which I was counting on—to workers, regulators, industry members, and
well sites––infrequently materialized, I reshaped my research strategies around data that
was available. OSH is not a particular place but unfolds across space and through multiple
domains. Thus, the data presented here reflect different physical and digital sites.
Participant Observation and Interviews
To understand the dynamics of the industry, and specifically OSH, I engaged in
participant observation at industry events and conferences, in communities experiencing
development, and at government hearings. This occurred in two phases, while I was based
out of Williamsport, Pennsylvania, for ten months in 2013 and 2014, and while based in
State College, Pennsylvania, from summer 2014 until August 2017. In both periods, I made
frequent trips to other parts of the region and neighboring states, and to Washington, D.C.,
17 The industry, at times secretive and wary of researchers, is hard to access, thus despite nearly eight
dozen emails and telephone calls to various companies and trade organizations, I did not gain formal
access to it. I received few responses from direct outreach. Two companies referred me the Marcellus
Shale Coalition, which I repeatedly contacted with no response. Another directed me to a local branch
of a national safety organization that would not allow me to attend its meetings. A few OSH equipment
companies responded but ignored interview requests. Even gatekeepers at Penn State’s Marcellus Shale
Center for Outreach and Research unsuccessfully connected me with regional companies.
42
and Texas. I also conducted preliminary research in 2012 and the summer of 2013, taking
health and safety courses and visiting well sites in August 2013.
In October 2013, I moved to Williamsport, a hub of shale development in north-
central Pennsylvania. The industry was posited as a boon for both the region and the nation
because of its potential to secure energy supplies and jobs for the U.S. in a declining area.
I was in Williamsport during a ‘boom’ period, however, the landscape has changed in
recent years. The pace and scale of shale gas introduced a form of industrialization that is
spatially mobile and temporary, subject to quick changes in markets and investor
confidence. From Williamsport, I traveled to family-friendly18 employment and trade fairs
for the industry including Pennsylvania Energy Days at Lycoming County Fair Grounds
near Williamsport and the Energy Jobs Rally in Harrisburg, the state capitol, I took classes
at a local training center, and involved myself in parts of the community, including running
in a 5K race sponsored by Inflection Energy. I hung out at local bars, striking up
conversations with workers and industry executives and surveyed development in
northcentral and northeastern Pennsylvania. I also noted differences in the northeastern
part of the state to the southwestern, spending hours driving around rural parts of the state,
stopping in at local restaurants and stores that catered to the industry.
When I began the project, a near-finished Ph.D. student had warned me of the
difficulties of studying oilfield workers, on which his own research centered. I learned that
I also had limited access to this population because of who I am and what people assumed
18 These events often showcased themes stereotypical of white, working class, and rural Pennsylvania.
Events drew upon iconography of American nationalism in posters and logos; camo print adorned
giveaways, and connections often were made to farming. These differed from events I heard about which
hired groups such as “Off-site Entertainment,” a company formerly based in Williamsport that provided
scantily clad, white young women to barbeques, fairs, and restaurant events.
43
about me. I quickly discovered at trade shows, industry events, and even within my
institution, that individuals were concerned with what side I was on with regards to
hydraulic fracturing; conversations often were mediated by the extent to which I could
demonstrate ‘sympathetic neutrality’ towards shale oil and gas extraction. At times, I was
asked pointedly if I was a fracktivist and in one instance, someone who knew me outside
of research asked if I had “switched sides.” The organizers of the regional oil and gas safety
organization STEPS PA, which holds meetings every few months in State College, would
not tell me where meetings were held given their concerns about potential fractivism.
Due to the hours most workers keep, bars where one of the few places I could access
workers to interview them about their perception of silica risks but meant many of
interactions were fueled by alcohol and limited my ability to obtain consent. As I engaged
in these conversations, some nights finding people to talk to, others less successful, I found
this method of data gathering unable to achieve what I intended. Still, these conversations
added to my understanding of how some workers viewed OSH issues (as one worker
explained, OSHA was impinging on this “last man’s man- man’s” job). In other spaces, I
met individuals who knew of those who had entered into the industry, but in all but one
instance, was not able to obtain an interview. Workers often sign non-disclosure
agreements with their employers, and in these encounters, I was not able to garner the
requisite trust. Still, these experiences shape my understandings of OSH and the industry.
From State College, I redoubled my efforts to focus on OSH events. This took me
to several conferences focused on shale fuels and OSH. These conferences paralleled ways
that OSH, the responsibilities of employers, workers, and the state were being discussed in
training material and industry conferences. I engaged in conversations with individuals

44
from NIOSH, OSHA, and USDOL, which helped facilitate interviews. I draw on these
participatory experiences of OSH that enabled conversations with diverse groups involved
in OSH and the oilfield in my empirical chapters.
I also researched in eastern and southern Texas during three trips (Dec. 2014, May
2015, and Dec. 2016). One trip was dedicated to driving around the Eagleford Shale and
interviewing OSHA officials at local offices. I drove to well pads around towns such as
College Station, Beeville, Victoria, Karnes, Bryan, and Edna, by way of mostly back roads
as I searched for well-pads I could see from permit data or on the iPhone app RigData (a
source discussed in Chapter 3). I stayed San Antonio and Austin where OSHA offices were
located and conducted interviews19. In 2014 and 2016, I also attended the University of
Texas Arlington’s OSHA Oil and Gas Conference in Houston, Texas. These conferences
brought together health and safety professionals, human resource representatives, and
OSHA and NIOSH officials for two-days. Boasting large exhibitions and plenary speeches,
the conferences attracted hundreds of attendees and offered a unique opportunity to listen
to and participate in conversations about OSH in the oilfield, with a focus on OSHA
programs and NIOSH research. Both conferences had sessions, discussions, and vendors
devoted to silica, sources of information that I draw on in the empirical chapters.
A key component of my participant observation was the interviews I was able to
have with over 175 individuals at conferences and trade expos. Expos provided a unique
way to access OSH, as they provided access to individuals with the express purpose of
19 Although the industry is highly mobile, there are differences in the ways that workers are viewed, the
makeup of the workforce, and the relationship between seeing workers as insider and outsider,
something I did not experience to the same extent during my trips to Texas as I did in Pennsylvania. Oil
was in the fabric of the environment, even if new extractive activities had increased the number of
people and pace of development in the landscape. On several occasions, members of the industry
expressed to me how it was easier to work in Texas because the resistance to the industry was far less
45
talking to people interested in their work. I spoke to representatives from large operators,
safety associations, completions companies, safety equipment providers, government
agencies including OSHA, NIOSH, and the Bureau of Labor Statistics, and academic
institutions and their extension services. Individuals would speak at length about their
company’s product, and I became conversant in drug testing, behavior-based safety
programs, mini-bag house dust collection systems, respirator types and filters, and drone
technology. Through these experiences, I developed a more complex understanding of
OSH narratives as these interviews forced me to both learn and apply the language of OSH
to have meaningful discussions that went beyond silica exposure.
My fieldwork also coincided with the publication of a proposed new rule for silica
in September 2013, the first in 40 years, and the public hearings that OSHA held to discuss
its proposal in March and April 2014. I attended these hearings in Washington, D.C., at the
Department of Labor in the Frances Perkins Building, which afforded me a unique
opportunity to observe how OSHA negotiated responsibility in a public context and focus
on the days in which testimony focused on the hydraulic fracturing industry. Many of the
issues discussed at these hearings overlapped with what I was observing in my other
research activities and thus directly drew together the relationship between industry’s
approach to OSH and the regulatory environment, described in Chapter 2.
Finally, I draw on semi-structured interviews with eighteen government
representatives, including OSHA and NIOSH, and open-ended interviews with four health
and safety instructors. These occurred in government offices, academic contexts, and over
the phone. Particularly in instances where issues or inspections were being litigated,
government officials were guarded and/or only spoke on background. I asked questions
46
regarding the key occupation health concerns on wellsites, including silica concerns,
challenges to inspecting oil and gas well sites, tools and techniques used to inspect and
regulate oil and gas industry members, challenges of inspecting silica, developing silica
regulations for the oil and gas industry, and efforts to create a research portfolio
surrounding oil and gas health and safety concerns20. As per my IRB, my interviews were
conducted on the premise of confidentiality, and therefore I did not collect identifying
information from my participants. This was primarily due to the nature of the industry, the
high level of secrecy and anxiety that shrouds it, as well as the threat of litigation for
government officials. I also engaged in informational requests where I asked direct
questions regarding technical interpretations of law or research over email with state
workers’ compensation offices, state departments of labor, OSHA, and NIOSH.
Textual Sources and Analysis
In addition to these interviews and participant observation, I turned to multiple
textual sources for data. I classify these into three subtypes: laws and regulations,
government records, and OSH materials. Discourse and textual analysis enable the
researcher to analyze not only what is said, the knowledge that is conveyed between author
and audience through visual and textual media, but also the power relationships that are
being produced and maintained through that relationship (Rose, 2007) and can be a useful
tool for analysis of policy and government documents given the rules that govern their
20 The industry’s contentiousness was reflected in how some OSHA offices viewed my requests for
information. As I saw in an inspection record, OSHA is aware of fracktism and fractivists, discussing
one woman in internal email. Many OSHA offices never returned my requests for interviews, either in
2014, 2015, or 2017, by phone or letters, which I describe in Chapter 3. Some offices were skeptical of
me, unsure as to why a geographer would care about multi-employer policies and exposure monitoring.
One OSHA officer berated me on the phone for using the term ‘hydraulic fracturing’ in a letter, a sign
that I was potentially a ‘fracktivist;’ the office never returned requests to be interviewed.
47
production through the state’s authority (Hewitt, 2009). Axial coding helped make sense
of the complexity of documents I examined. It is an iterative process in which the
researcher produces categories of data which allow for the aggregation and disaggregation
of data around key themes (Wicks, 2010), and is useful for working with diverse data types.
I acquired textual data through OSH courses I attended at job fairs, information sent
to me by research participants, Internet searches, and my participation in Webinars. Course
information covers my participation in the courses21 at several training centers, and
includes materials from the class I help co-teach on confined space and rescue, where I
acted not only as an ‘expert,’ but also in charge of implementing discourses of safety. On
more than one occasion, workers in these courses sought me out to talk further or because
they wanted to provide me additional health and safety resources via email. Per IRB
requirements, I was not to use these courses as recruitment sites but my observations during
these classes were informative in understanding competing discourses of workplace safety.
Additional textual material included industry publications, advertisements, and best
practice guides; health and safety materials developed by OSHA, including “Hazard
Alerts” for the oil and gas industry, the minutes and notes from meetings from the STEPS
Network, and NIOSH and STEPS safety videos available online. Finally, I attended
webinars from safety organizations that focused on the oil and gas industry or silica and
analyzed the slides from those presentations, and other materials made available. I also
acquired from government websites, including regulations.gov that stores public comments
and evidence submitted on rulemaking and copies of public hearings’ transcripts,
21 These include: PEC SafeLand, Fall Protection, Confined Space, Confined Space Rescue, Oil and Gas
for Health and Safety Professionals, Shell Blue Book, Oil and Gas Industry: General Course; Worker
Right-to-Know; Safety is a Personal Decision, OSHA Record Keeping, PATHS: Workplace Violence
Safety, New OSHA Regulations on Record Keeping; Respirable Crystalline Silica.

48
USDOL’s Data Reporting Website that provides metadata on inspections, and Freedom of
Information Act Requests that provided detailed records of inspections. I reviewed
documents from the Government Accountability Office (GAO) that have evaluated
OSHA’s activities since its inception, but which has its own administrative history and
viewpoint on federal activities (McCaffrey, 1982)22. I watched live streams of a
Congressional hearing and speeches about the silica rulemaking and virtually attended
several webinars on the final silica rule. I examined laws, regulations, and proposed
rulemakings, including drafts and the final version of the silica rule and workers’
compensation statutes for each of the 50 states, accessed through LexisNexis Legal and
directly from state administrative codes on official state government websites.
As with any data source, the information these provide is partial and limited. These
data come from diverse organizations and authors; thus, in my analysis, I have made efforts
to critically engage with the texts, not merely as a source of information, but as a
representation of relationships between actors involved in OSH. Not only is the information
mediated by the epistemology and goals of the authors and curators and their intended
audiences, but my reading of these texts is also infused by my own perspective.
Dissertation Outline
These data, my analysis of secondary sources on the history of OSH in the U.S. and
the oil and gas industry, and my theoretical interests suffuse the empirical chapters of the
dissertation. These chapters explore how different notions of responsibility shape the
governance of occupational health risk in the U.S. oilfield. Chapter 2 examines how OSHA
negotiates its responsibilities to protect workers and the economy. Administrative
22 For McCaffrey (1982), the GAO is the “Institutionalized Critic of Lagging Regulatory Action.”

49
rulemaking, how OSHA develops standards to ensure the right to a safe and healthful
workplace, requires the state balance responsibilities to mitigate risk to workers and to
industry. Administrative rulemaking places workers’ bodies in opposition to the vitality of
the hydraulic fracturing industry. This enables the industry to utilize its flexibility as a
discourse to posit that it is unknowable and ungovernable in order to challenge existing
scientific evidence and analysis as uncertain, and to insist that workers are best at
protecting themselves from RCS. Thus, the industry shifts responsibility away from itself
and onto workers and offers arguments that position the state’s interest in industry health,
as paramount in the consideration of how to best protect human worker health. Rulemaking
requirements provide industry opportunities to recycle narratives that distance themselves
from accountability for unsafe work practices and obligations to mitigate risk. I draw
parallels between the hydraulic fracturing industry’s discourses during rulemaking and its
discourse of worker responsibility for OSH.
Chapter 3 examines how the state enacts its ideal distribution of responsibility
through a responsibility-as-blame paradigm. Enforcement mechanisms are techniques
OSHA uses to regulate employers who regulate employees. I argue that workers’
responsibility to manage health risk emerges from an institutional structure that focuses on
employers’ responsibilities. In essence, OSHA lacks sufficient tools to regulate industrial
structure. The chapter shows how the flexibility of the industry has material consequences
for the techniques OSHA uses to gather knowledge about hydraulic fracturing and regulate
silica at well sites. OSHA’s inability to capture the flexibility of hydraulic fracturing allows
the industry to avoid oversight, but also it supports its argument, as seen in Chapter 2, that
due to its spatial and temporal flexibilities, hydraulic fracturing is unknowable and thus

50
ungovernable. These oversights are material expressions of the discourse industry utilizes
to dissolve OSH responsibility to workers, as examined in Chapter 2, that emphatically
argues workers’ use of respirators is protective for workers.
Chapter 4 examines how the state determines who is responsible for mitigating the
effects of silicosis after a worker gets ill, in a context in which responsibility is declared to
be no-fault. The chapter argues that the State fails to ‘see’ many ill workers because they
have not been exposed to RCS or gotten ill from RCS in the right way, leading workers to
be responsible for managing an occupationally-acquired disease on their own. In
negotiating the conflicts between ill workers’ and exposing employers, the State struck the
compensation bargain where workers gave up their rights to sue employers in exchange for
no-fault insurance for the harms faced at work. Yet, these laws foster uneven and
inequitable health-relationships as they use exclusionary applications of time and space to
define ‘compensability’ that belie silicosis disease progression and common patterns of
work in hydraulic fracturing, and other flexible industries.
The concluding chapter provides a summary of these chapters and identifies areas
for future theoretical and empirical work. I now turn to the first empirical chapter on
rulemaking.
51
2. Chapter 2: Rulemaking: Is OSHA’s Principal Responsibility to
Protect Industry or the Workers?
[T]he process by which TLVs and, ultimately, standards have been set,
whether for asbestos, silica, or other dangerous substances, has been part of
a compromise between the health of workers and the economic health of
industry (Rosner & Markowitz, 2006, p. 253).
Around 9:30 a.m., on March 17, 2014, Administrative Law Judge Purcell convened
informal public hearings23 in Washington D.C., on OSHA’s proposed permissible exposure
limit (PEL)24 for respirable crystalline silica (RCS). I arrived at the USDOL’s Francis
Perkins Building early, having taken the Red Line to Judiciary Square, jostling on the D.C.
Metro with others going to work in the heart of the federal government. Once inside, I
presented identification and passed through a metal detector into an atrium where signs
pointed me to the Caesar Chavez Auditorium. I settled into a cushioned seat in the back,
observing clusters forming in the aisles. In a room occupied predominantly by white,
middle-aged men, to my eye, groups were differentiated by the details of their clothing: the
fit of their suits, the material on their shoes, the gel in their hair, and the size of their watches
and cufflinks25. Superficial differences, however, signified ones of great substance. Over
three weeks, these lawyers, lobbyists, scientists, and labor advocates engaged in debates
over the state’s responsibility for protecting industries vis-à-vis its responsibility to protect
23 This is a technical term. However, a judge presided over the proceedings and participants were
required to submit a Notice of Intent to Appear in order to speak and ask questions. 24 Other terms for limits include Threshold Limit Values (TLVs), Occupational Exposure Limits
(OELs), and Recommended Exposure Limits (RELs). These terms are political and social artifacts
(Murphy, 2006), and vary in what they represent. Associated with different organizations, some have
the force of law while others are recommendations. 25 I was not the only one note of how clothes reflect power dynamics. A former solicitor for OSHA
speaking to OSHA’s attorneys, women: “I have one piece of advice. I don’t know Ms. Robinson from
the Solicitor’s Office, but one advice to solicitors. Always wear a better suit than the industry attorneys,
and make sure it’s American made/unionmade. I’m wearing a suit that’s American made/union
made….Now, I don’t know whether women – there are any women’s suits that are available that are
American made/union made, but there are men’s –Hickey Freeman, and this is Tallia Uomo” (OSHA,
2014, April 3, 3784-5).

52
the workers employed in them. Notably limited were voices from workers exposed to silica.
Workers’ testimonies were concentrated to a few days and experiences from a few
industries, and not hydraulic fracturing. Instead, participants debated mortality statistics,
exposure thresholds, and the costs of engineering controls.
These hearings would distill decades-old debates over occupational exposure limits
to RCS. As part of administrative rulemaking, specifically the procedures agencies follow
in gathering evidence when exercising regulatory authority, the hearings exposed
negotiations pertaining to how the state realizes workers’ “right to a safe and healthful
workplace” as promised in the OSH Act. OSHA rulemaking starts from the premise that
the state is responsible for ensuring this right by regulating employers’ practices to reduce
workplace risks. However, there is a disconnect between this premise and its practice.
In this chapter, I argue that the governance of health risk is shaped by unresolved
questions about toward whom OSHA has the greater responsibility, to industry or to
workers. Rulemaking, or the process of writing regulations, places these tensions on full
display. The tensions produced are complicated not only by the opposing interests of
industry and workers but also by OSHA’s complicity in failing to definitively support one
or the other, despite its mandate. In negotiating the question of whether it is most
responsible to workers or to industry, the state offers regulated parties opportunities to
comment on the rulemaking and to present evidence through public hearings and written
public comment periods. However, one of the effects of offering these participatory
opportunities is that industry representatives utilize the rules of rulemaking to perpetuate
discourses that place industry’s health and vitality above that of workers, and where
workers are primarily responsible for mitigating the health risks to which they are subject
53
within the industry. Such an analysis allows us to consider how negotiations of
responsibility fit into broader narratives of health risk. These narratives of health risk
illustrate how entangled within the state’s interest in ‘worker health’ is a concern for
‘industry health.’ These processes develop from a long history in which the state has
responded industrial capitalism’s impacts on human bodies. Occupational health, then, is
a microcosm of the state’s tenacious responsibilities to its public citizenry and its private
industries. I use the hydraulic fracturing industry’s participation in rulemaking for silica to
illustrate this.
During the hearing, industry groups, such as the U.S. Chamber of Commerce (the
Chamber), the American Chemistry Council Respirable Crystalline Silica Panel (ACC),
and the American Petroleum Institute (API), downplayed industry’s accountability for
unsafe work practices and minimized industry’s obligations to mitigate risk. Employing
the requirements that OSHA uses to weigh its own responsibilities, industry challenged
scientific evidence, deployed its spatial and temporal flexibility as a strategic discourse to
posit the industry as unknowable and ungovernable, and insisted that workers are best at
protecting themselves from RCS. In denying industry’s responsibility for the health of its
workers, industry representatives shift this responsibility to individual workers. Examining
the discourses that surrounded efforts to update the state’s RCS standard reveals the
tensions that underlie state’s interest and definition of worker health. Namely, the state has
not resolved if it is more responsible to workers health or to private industry. The chapter
shows how the state’s requirements insufficiently resolve its responsibilities to workers
and to industry and give industry’s discourses a public venue through rulemaking.
Rethinking the State’s Interest in Health: Responsibility as Negotiated
This chapter builds upon health geography’s engagement with health governance

54
by offering responsibility as an organizing analytic to consider the negotiations that shape
health risk. This reframes how health geography has engaged with state and institutional
processes by focusing on the state’s negotiation of its multiple commitments when
governing health risk. As discussed in Chapter 1, health geographers have shown how
health emerges through the state’s rationalities and techniques of power that encode and
reproduce ideas about space and bodies, including how bodies internalize self-disciplining
logics surrounding health that facilitate the governance of populations. This focus on the
production of individual health behaviors pairs with scholarship that emphasizes the
problematic ways that health is reified at the site of the individual body, and that instead
contributes readings of disease and illness which center on structural processes and their
historical and spatial contexts (Holmes, 2013; Horton, 2016; King, 2017).
However, the complexity of how the state views ‘occupational health,’ which has
unique rationalities that separate it from public health, has been relatively understudied in
health geography. While critical of how the state and its public health agencies incorporate
problematic notions about bodies or are swayed by external influences, I illustrate how the
state’s interest in human health is constituted by its conflicting commitments to private
industry and the population. Worker health sits at the intersection of these two concerns,
and thus is constituted by a consideration of both. This analysis shows how the way the
state regulates health risk reflects its competing commitments. The state has many interests,
with which one is rarely imbued with absolute significance. For occupational health risk in
the U.S., these responsibilities are openly written into the ways the state defines and
55
regulates human health risk26. This chapter provides an example of how the state’s
competing commitments to workers and industry unfold through the rulemaking process.
OSHA’s rulemaking process uniquely requires public hearings27 as it adjudicates what
constitutes significant health risks for workers and for industry, fostering spaces where
health knowledge—namely whose health matters most—is contested. This offers industry
an opportunity to infuse elements of the ways that it sees OSH concerns into regulatory
spaces, and posits itself as unknowable and ungovernable, leveraging the uncertainty
regarding its spatial configurations as a discursive tool to shape narratives of responsibility
for health risks from silica. Here, I focus on how the state’s requirements for defining
human health risk enable narratives in which industry is imbued with human qualities, its
own ‘health,’ which needs to be protected, and which is contrasted with human health.
These requirements, discussed at the end of the chapter have magnified over several
decades, requiring more analysis and consideration of risk’ to human health and industry’s
health. These requirements diminish the state’s ability to write new regulations for
occupational health risk by drawing out the regulatory process, while at the same time
reifying long standing discourses and tensions of OSH.
As introduced in Chapter 1, I draw insights from theorists skeptical of the ways
responsibility operates within neoliberal democracies, showing how responsibilities are
produced through the discourses and practices of governance, and how they reproduce a
false dichotomy between freedom and personal responsibility, and structural determinism
26 While I focus on occupational health, regulations encode similar concerns and requirements for
environmental health. There are differences, however. While EPA frequently uses cost-benefit analysis,
OSHA evaluates “costs and benefits,” with slightly different evaluative requirements. 27 The OSH Act stipulates public hearings as a requirement of rulemaking, a requirement unique to the
agency although other agencies may use them under certain circumstances.
56
(Young, 2008) and draw attention to “rationalist” conceptions of responsible government
action that surface under market capitalism and the bureaucratic state (Harmon, 1995).
Such theories illustrate how the organization and distribution of responsibility among
actors, and the resolution of conflicts between them, reveal something about who and what
is valued in society (Walker, 2007, p. 11; Young, 2008). Thus, I trace the implications of
responsibilities to protect that emerge through administrative rulemaking at OSHA.
Permissible Exposure Limits: Regulating Risk, Silica, Industry and Workers
The state makes employers accountable for the health risks that workers face when
they have been exposed to silica above the level permitted by federal regulations. To this
end, OSHA establishes Permissible Exposure Limits (PELs) to define what constitutes a
“safe workplace.” An exposure limit constitutes an assessment of risk (Ziem & Castleman,
2000), and it operates as a state-sanctioned level of acceptable risk. Such limits are
commonly understood to be objective assessments that ensure a very low risk to workers’
health and function as a key “solution” to the hazardous respiratory conditions that
characterize many industrial workplaces. Through workplace inspections, the state
enforces exposure limits by levying fines and remediation requirements when workplaces
are found to be exposing workers above this state-sanctioned level of healthfulness.
In the first half of the 20th century, exposure limits gained legitimacy through the
state, industry, and public health institutions that endorsed them (Rosner & Markowitz,
2006). Yet, instead of reflecting the scientific evidence and ensuring the highest possible
protection for the workers, limits and thresholds have often reflected the financial interests
and technological capabilities of industry rather than the health of the workers. Once a limit
is established, the question as to who is responsible for ensuring that workers are not
exposed to a substance above a given level, employers or workers, has been a subject of
57
continuous debate.
Finding a solution to problems caused by silica and silicosis became a regulatory
concern of several U.S. states in the 1920s and 1930s (Rosner & Markowitz, 2006).
Sickened mine and foundry workers drew attention to silica through litigation, and states
began to legislate occupational disease, sometimes at the behest of employers who sought
to limit their mounting liability (Bale, 1987; Rosner & Markowitz, 2006).
Tragedy drew further scrutiny. In the 1931, during the construction of a tunnel for
a hydroelectric dam in Gauley Bridge, West Virginia, employers knowingly exposed
workers to high levels of silica without providing any protective equipment. In this
instance, which became known as the Hawks Nest Disaster hundreds and perhaps
thousands of workers, many of whom were African American men, developed acute
silicosis. Hundreds died within a matter of months or a few years of exposure (Cherniack,
1986). By the mid-1930s, silicosis had become “the king of occupational diseases” (Rosner
& Markowitz, 2006, p. 75).
In response, industry engaged in a concerted effort to pivot the public’s attention
away from silicosis. Rather than aiming to eradicate the disease, industry groups aimed for
“the virtual elimination of silicosis from popular discourse” (Markowitz & Rosner, 1995,
p. 254). This ‘solution’ to silicosis would absolve industry from further collective
responsibility for changing industrial practices in favor of workers. Towards this goal, the
Air Hygiene Association, an industry-academia collaboration with the Mellon Institute in
Pittsburgh, Pennsylvania, steered silicosis studies and debate. In 1936, it participated in the
USDOL’s National Silicosis Conference, which endorsed an industry standard for silica
without acknowledging the health risks associated with it (Markowitz & Rosner, 1995, p.

58
255)28. The standard limit was not binding, and debates continued in industry organizations
such as the American Council of Government Industrial Hygienists (ACGIH), unions, and
state legislatures about appropriate, often voluntary, exposure limits to silica (Rosner &
Markowitz, 2000). In the ensuing decades, the public increasingly accepted the limit
established at the National Silicosis Conference as a measure of safety that “successfully”
addressed silicosis despite persistent concerns from public health scientists and officials
(Markowitz & Rosner, 1995)29. A 1955 U.S. Bureau of Mines report, for example,
expressed concern that although many believed workers were adequately protected from
silicosis, uncertainties remained; these warnings would not change the conclusion by many
that silicosis was a disease of the past (Markowitz & Rosner, 1995, p. 258).
The federal government became responsible for setting PELs in the 1970s
following the OSH Act. The Act charged OSHA with responsibility for identifying
hazardous substances and regulating them on a hazard-by-hazard basis, with one exception:
Congress allowed OSHA to utilize ACGIH and trade organization standards from the
1950s and 1960s in setting its initial PELs (Kerwin & Furlong, 2010), which had been
strongly shaped by industry (Markowitz & Rosner, 1995; Rappaport, 1993; Ziem &
28 Rosner and Markowitz (1995) bluntly describe its influence here: “These committees were dominated
by Air Hygiene Foundation members and other experts who developed a consensus that would define
the silicosis issue in the coming years and even decades. The agenda being developed was ostensibly a
product of objective scientific and technical discussions. But the discussions were framed by the very
real social crisis facing industry and the solutions were constrained by the economic decisions of
individual firms. Workers were to be protected through engineering methods that did not disrupt
existing technologies or the continued use of sand in blasting. A consensus developed that
technologically feasible engineering and medical standards could be developed to prevent silicosis from
shortening a person’s work” (pp. 40-41, my emphasis). 29 Who these regulations were meant to protect was of some debate (Rosner & Markowitz, 2006). Like
debates on exposure limits, concern was over if regulations should protect ‘average’ workers, able-
bodied white men, or other categories of workers. In the case of lead exposure, this led to the removal
of ‘abnormal’ or fragile women’s bodies from particular environments and was emblematic of the
“sexism of industrial hygiene” (Markowitz & Rosner, 2002, p. 125, see also Murphy, 2006). Similarly,
the science used to define OSH problems and solutions has myopically focused on men (Messing, 1998).
59
Castleman, 2000). Based on these “‘start-up’ standards,” OSHA avoided what would have
been a time-consuming process of rulemaking for each of the 425 air contaminant standards
it implemented (OSHA, 2016, p. 16294)30. In 1971, OSHA established a PEL for RCS of
approximately 100 μg/m3—a level that was taken from the ACGIH 1968 recommendations
(OSHA, 2016, p. 16294)31. Already problematic, these PELs were then enforced by an
agency that would see its authority diminished throughout the as increasing regulatory
burdens, institutional pressures, and the influence on scientific knowledge from industry
diminished OSHA’s authority described in the OSH Act.
Three years later, in 1974, NIOSH determined that OSHA’s PEL for silica was
insufficiently protective. Cases of silicosis from Gulf Coast states had prompted NIOSH to
investigate silica exposure in the oil and gas and maritime industries (Rosner & Markowitz,
2000). In 1974, NIOSH issued a report that endorsed a recommended exposure limit (REL)
of 50 μg/m3 for a 10-hour time-weighted average and proposed that silica be banned as an
abrasive blasting agent (Rosner & Markowitz, 2000). Strong industry opposition coalesced
around the Silica Safety Association’s resistance to the implementation of a lower PEL.
The Association argued that respirators provided sufficient protection and that the NIOSH
REL would put the industry in jeopardy by imposing intolerably high costs (Markowitz &
Rosner, 1995). The association’s efforts were successful: several decades passed before
OSHA acted on NIOSH’s 1974 recommendations, during which these arguments
30 To circumvent this process, in 1989, the agency attempted to revise 376 PELs. However, the 11th
Circuit found that OSHA had not demonstrated either the need for the new PELs or their feasibility
(OSHA, 2016, p. 16294). Subsequently, OSHA has not tried to revise PELs en-masse. 31 In 1971, OSHA set a PEL for quartz allowing general industry to follow one of two formulas: particle
count or mass (OSHA, 2016, p. 16294). This PEL did not mandate training or medical surveillance.
Under the new 2016 rule, PELs are not established by a formula: all industries have the same limit, and
requirements now include medical evaluations and monitoring for workers regularly exposed to the
“action level” of 25 μg/m3 (OSHA, 2016).
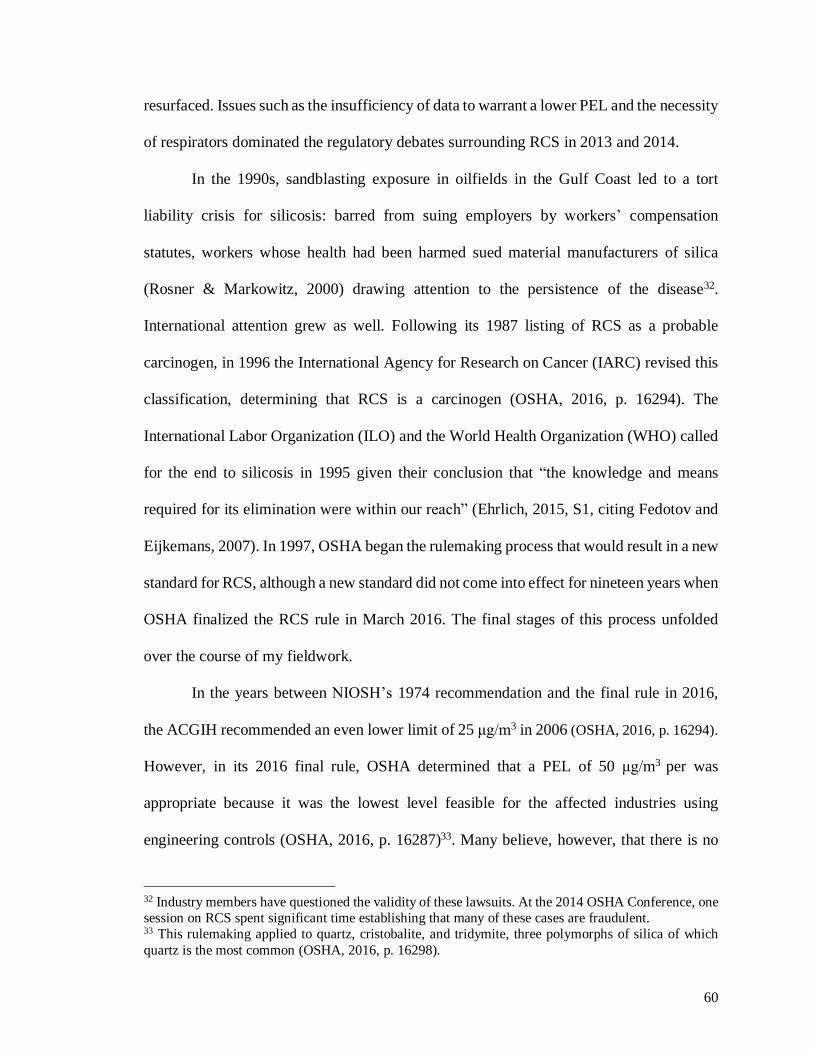
60
resurfaced. Issues such as the insufficiency of data to warrant a lower PEL and the necessity
of respirators dominated the regulatory debates surrounding RCS in 2013 and 2014.
In the 1990s, sandblasting exposure in oilfields in the Gulf Coast led to a tort
liability crisis for silicosis: barred from suing employers by workers’ compensation
statutes, workers whose health had been harmed sued material manufacturers of silica
(Rosner & Markowitz, 2000) drawing attention to the persistence of the disease32.
International attention grew as well. Following its 1987 listing of RCS as a probable
carcinogen, in 1996 the International Agency for Research on Cancer (IARC) revised this
classification, determining that RCS is a carcinogen (OSHA, 2016, p. 16294). The
International Labor Organization (ILO) and the World Health Organization (WHO) called
for the end to silicosis in 1995 given their conclusion that “the knowledge and means
required for its elimination were within our reach” (Ehrlich, 2015, S1, citing Fedotov and
Eijkemans, 2007). In 1997, OSHA began the rulemaking process that would result in a new
standard for RCS, although a new standard did not come into effect for nineteen years when
OSHA finalized the RCS rule in March 2016. The final stages of this process unfolded
over the course of my fieldwork.
In the years between NIOSH’s 1974 recommendation and the final rule in 2016,
the ACGIH recommended an even lower limit of 25 μg/m3 in 2006 (OSHA, 2016, p. 16294).
However, in its 2016 final rule, OSHA determined that a PEL of 50 μg/m3 per was
appropriate because it was the lowest level feasible for the affected industries using
engineering controls (OSHA, 2016, p. 16287)33. Many believe, however, that there is no
32 Industry members have questioned the validity of these lawsuits. At the 2014 OSHA Conference, one
session on RCS spent significant time establishing that many of these cases are fraudulent. 33 This rulemaking applied to quartz, cristobalite, and tridymite, three polymorphs of silica of which
quartz is the most common (OSHA, 2016, p. 16298).
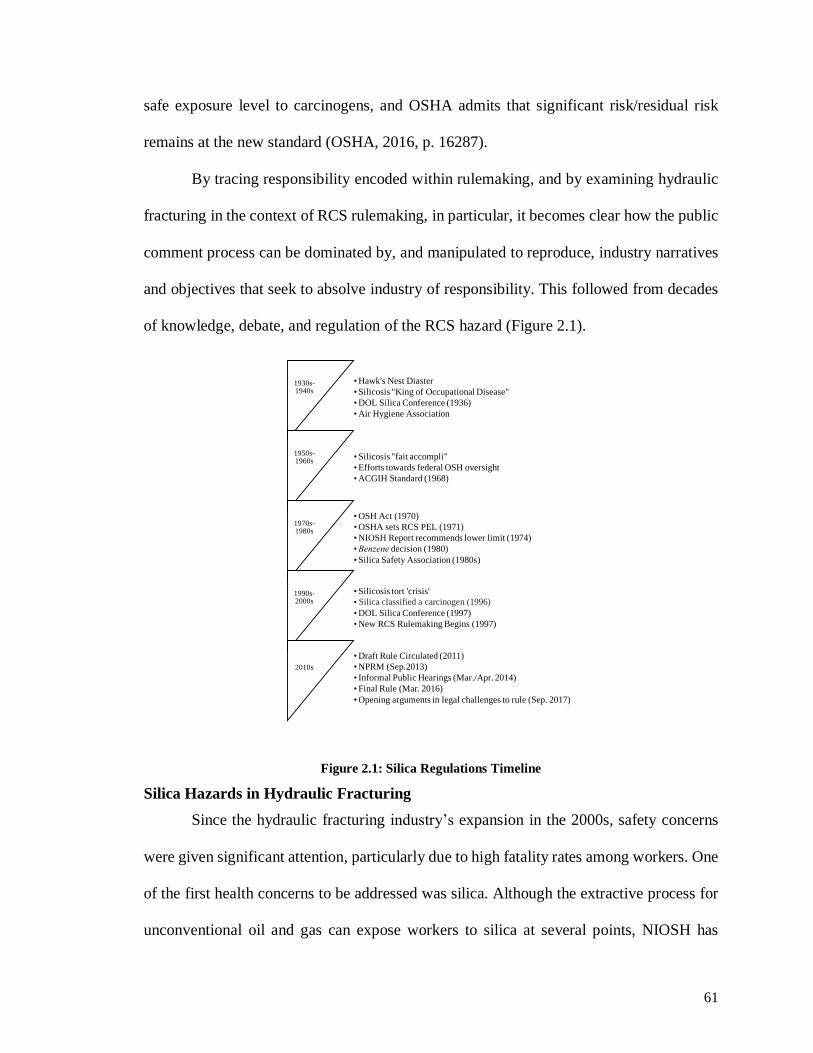
61
safe exposure level to carcinogens, and OSHA admits that significant risk/residual risk
remains at the new standard (OSHA, 2016, p. 16287).
By tracing responsibility encoded within rulemaking, and by examining hydraulic
fracturing in the context of RCS rulemaking, in particular, it becomes clear how the public
comment process can be dominated by, and manipulated to reproduce, industry narratives
and objectives that seek to absolve industry of responsibility. This followed from decades
of knowledge, debate, and regulation of the RCS hazard (Figure 2.1).
Figure 2.1: Silica Regulations Timeline
Silica Hazards in Hydraulic Fracturing
Since the hydraulic fracturing industry’s expansion in the 2000s, safety concerns
were given significant attention, particularly due to high fatality rates among workers. One
of the first health concerns to be addressed was silica. Although the extractive process for
unconventional oil and gas can expose workers to silica at several points, NIOSH has
1930s-1940s
•Hawk's Nest Diaster
•Silicosis "King of Occupational Disease"
•DOL Silica Conference (1936)
•Air Hygiene Association
1950s-1960s
•Silicosis "fait accompli"
•Efforts towards federal OSH oversight
•ACGIH Standard (1968)
1970s-1980s
•OSH Act (1970)
•OSHA sets RCS PEL (1971)
•NIOSH Report recommends lower limit (1974)
•Benzene decision (1980)
•Silica Safety Association (1980s)
1990s-2000s
•Silicosis tort 'crisis'
•Silica a definitely classified a carcinogen (1996)
•DOL Silica Conference (1997)
•New RCS Rulemaking Begins (1997)
2010s
•Draft Rule Circulated (2011)
•NPRM (Sep.2013)
• Informal Public Hearings (Mar./Apr. 2014)
•Final Rule (Mar. 2016)
•Opening arguments in legal challenges to rule (Sep. 2017)
Silica classified a carcinogen (1996)

62
recorded dangerous exposures during hydraulic fracturing, including levels that exceed
exposure limits and protective values of commonly used respirators (Esswein et al.,
2013)34. Significant exposures occur during the material handling of sand as it is mixed
into the hydraulic fracturing fluid when a stage is being pumped. Sand trucks deliver sand
onsite and pneumatically transfer sand to the sand mover, also known as a mountain mover
(Halliburton, 2012a) or sand chief (Franklin Well Services, Inc., 2016) (Figure 2.2).
Figure 2.2: Mountain Mover, Points of filling (OSHA 802188, 2011, p. 308)
In this process of off-loading, compressed air moves sand through fill ports that are on the
sides of the sand mover (Esswein et al., 2013) and can generate a visible ‘dust cloud’ that
enshrouds well sites (Figure 2.3). OSHA describes this process:
Sand is forced in from the trailer and into the Mountain Mover bin. At the
top of the bin, air escapes through a filter the shape of a large pillow. A
particulate plume is visible during bin filling. The plume rises into the air
high above the entire fracing operation. (OSHA Inspection 802188, 2011,
p. 163).
34 A variety of sampling equipment can measure airborne dust. Esswein et al. (2013) used personal
sampling pumps with sampling cassettess to capture Personal Breathing Zones (PBZ). The accuracy of
different equipment were debated at length during the informal hearings for the new rule. In general,
these samplers draw in air to collect a sample, which, when analyzed in a lab, can indicate what
proportion of the airbone dust is silica.
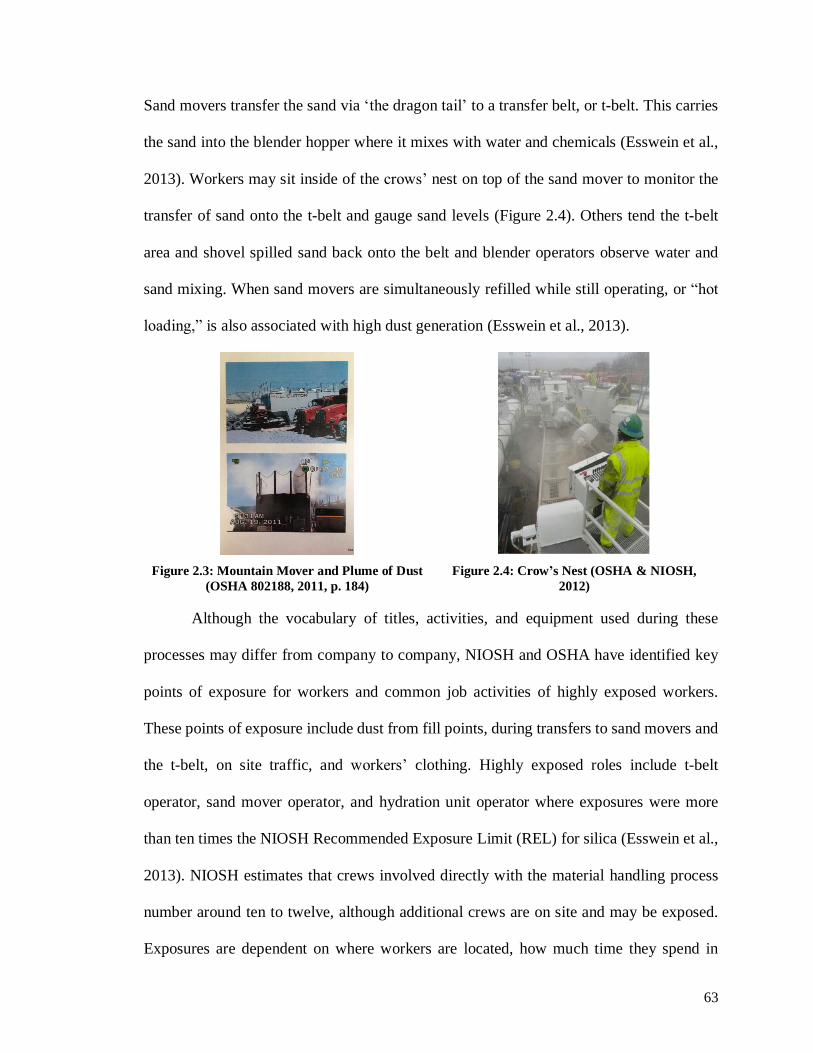
63
Sand movers transfer the sand via ‘the dragon tail’ to a transfer belt, or t-belt. This carries
the sand into the blender hopper where it mixes with water and chemicals (Esswein et al.,
2013). Workers may sit inside of the crows’ nest on top of the sand mover to monitor the
transfer of sand onto the t-belt and gauge sand levels (Figure 2.4). Others tend the t-belt
area and shovel spilled sand back onto the belt and blender operators observe water and
sand mixing. When sand movers are simultaneously refilled while still operating, or “hot
loading,” is also associated with high dust generation (Esswein et al., 2013).
Figure 2.3: Mountain Mover and Plume of Dust
(OSHA 802188, 2011, p. 184)
Figure 2.4: Crow’s Nest (OSHA & NIOSH,
2012)
Although the vocabulary of titles, activities, and equipment used during these
processes may differ from company to company, NIOSH and OSHA have identified key
points of exposure for workers and common job activities of highly exposed workers.
These points of exposure include dust from fill points, during transfers to sand movers and
the t-belt, on site traffic, and workers’ clothing. Highly exposed roles include t-belt
operator, sand mover operator, and hydration unit operator where exposures were more
than ten times the NIOSH Recommended Exposure Limit (REL) for silica (Esswein et al.,
2013). NIOSH estimates that crews involved directly with the material handling process
number around ten to twelve, although additional crews are on site and may be exposed.
Exposures are dependent on where workers are located, how much time they spend in
64
enclosed areas with air filtration, the weather and the wind, and the configuration of the
equipment (Esswein et al. 2013). Thus, the geography of the worksite can influence the
exposures workers experience, which workers experience them, and their magnitude.
Respirable crystalline silica (RCS)35,36 is a known carcinogen associated with lung
cancer, renal disease, autoimmune disease, and the fibrotic lung disease silicosis (Leung,
Tak Sun Yu, & Chen, 2012). Silicosis is a progressive disease caused almost exclusively
by occupational exposures to RCS. When RCS particles enter the lower respiratory system,
the particle inflames the lung, but an individual cannot expel the particle (OEHHA, 2005).
The body responds by producing fibrotic scar tissue, creating scarring or nodules, and
increasingly loses its ability to respire (CDC, 2002, 2010; Leung, Tak Sun Yu, & Chen,
2012). Silicosis has three primary forms: acute, accelerated, and simple chronic, depending
on the duration and magnitude of exposures, latency it takes the disease to develop, and
the kind of scarring produced (CDC, 2010; Leung, Tak Sun Yu, & Chen, 2012). Silicosis
is irreversible, is associated with several comorbidities and often leads to death. Known,
nearly exclusively, as an occupational disease37, it afflicts mostly white males according to
recorded silicosis mortality in the U.S (Mazurek et al., 2015). Its relationship to ‘life-style’
activities such as smoking contributes to debates about who is responsible for the disease;
nonetheless it is one of the oldest identified occupational diseases that has already afflicted
workers in areas conducting hydraulic fracturing.
35 The respirable fraction of dust that is considered an occupational hazard is 10 or less microns in
diameter. While I refer to both RCS and silica, it is the respirable size that is considered hazardous. 36 In addition to hydraulic fracturing, workers are exposed to RCS in sandblasting operations (used as
an abrasive cleaning agent, for example, during oil tank cleaning), manufacturing, construction, foundry
work, coal mining, homebuilding, bricklaying, and quarrying, among others (CDC, 2002). 37 Silicosis can be an environmental hazard (Markowitz & Rosner, 2002). Hydraulic fracturing has
increased mining for silica sand in the mid-western U.S., raising concerns for the sand mining
communities, as well as places through which sand is transported by rail.
65
The oilfield has long been a risky place to work38 of which RCS is only one of
several occupational health hazards. Other hazards are present at worksites constantly
while others are temporally bounded to certain work activities and environments. For
example, while volatile organic compounds off-gas from equipment and infrastructure,
multiple fatalities from hydrocarbon exposures during tank gauging have been documented
by NIOSH (Harrison et al., 2016). NIOSH has also found high levels of benzene, a
carcinogen, in the urine of workers involved in flowback operations (Esswein et al., 2014).
Low oxygen environments, and ‘sweet gas’ or hydrogen sulfide, a fatal fume that occurs
naturally in many regions, are also potential hazards and responsible for workers’ deaths.
Still, silica is one of the occupational health concerns that has garnered significant concern
from industry and government. The timing of their concern, however, is important to the
arguments made during the rulemaking process.
The dose makes the poison? RCS as an unknown risk in hydraulic fracturing
The dose makes the poison. This adage represents the traditional view of the
relationship between exposure to a hazardous substance and the illness resulting from that
exposure39. This assessment may go some way toward explaining OSHA’s admitted
prolonged lack of awareness of the RCS risks posed by hydraulic fracturing. It was not
until a study on RCS exposure was published by NIOSH that overexposure to RCS in
hydraulic fracturing attracted OSHA’s attention40. Indeed, one OSHA official explained to
me that the inclusion of the industry was a last-minute addendum to make sure that
38 I focus on onshore, upstream oil and gas, emphasizing hydraulic fracturing and exposures to silica. 39 Guthman and Mansfield (2013) and Vogel (2008) illustrate how this principle has been challenged
by new fields of environmental epigenetics and endocrine disruptors. Vogel illustrates how these ideas
were encoded within regulatory law and shape how the state regulates risk. 40 In 2012, OSHA and NIOSH published a hazard alert on RCS in hydraulic fracturing (OSHA &
NIOSH, 2012).
66
hydraulic fracturing was in the final rule, a sentiment echoed by OSHA officials giving
presentations at OSH conferences, and a narrative that supported industry’s own position
that it also did not know of the silica hazard. While silica sand was knowingly being used
in the industry, that the magnitude of the exposures was potentially dangerous to its
workers was seemingly unknown.
Representatives of the oil and gas industry have claimed that the risks posed by
RCS in hydraulic fracturing were not known until the late 2000s, even though silica sand
used in abrasive blasting in the oilfield had been at the center of the tort crisis just a few
years before. At keynote presentations that I attended at both the 2014 and 2016 UT
Arlington bi-annual OSHA Oil and Gas Safety and Health Conference, industry
representatives applauded themselves for taking quick action to address the risks posed by
silica once RCS had been identified as a problem. In sessions devoted to silica, industry
leaders espoused similar sentiments and credited the National Safety Transmission
Exploration and Production Safety (STEPS) group in conjunction with NIOSH and OSHA
representatives with enabling this action. This served to suggest that industry had taken
responsibility for their workers’ health, and as will be developed throughout the chapter,
worked as part of a broader strategy to suggest that OSHA did not need to further regulate
the industry, and absolved industry of responsibility for further action, particularly that
mandated by OSHA.
Illustrating these successes in identifying the silica problem, STEPS, NIOSH, and
OSHA formed a strategic alliance during the 2014 conference and renewed it two years
later in 2016. When I asked members of STEPs, OSHA, and NIOSH about the partnership,
many replied that it would further formalize existing efforts to organize research and

67
outreach. Several OSHA Area offices I interviewed indicated that their regional alliances
were important ways that OSH information was shared amongst industry, public health,
and regulatory stakeholders. Members of STEPS, often employees of oil and gas
companies, have also contributed to NIOSH’s National Occupational Research Agenda
(NORA) for Oil and Gas, which has helped to prioritize research into silica. STEPS also
organized the Respirable Silica Focus Group, through which industry, OSHA, and NIOSH
shared information regarding RCS exposure when this became recognized as a problem.
Meeting presentations, the minutes of which are made available on their national website,
spanned respirator use to engineering control technology. Despite this prominence, STEPS
did not give testimony at the hearings, although several of its members presented at the
hearings on behalf of their companies or primary organizations.
Industry’s narrative is that it was not aware of the magnitude of the silica problem
in hydraulic fracturing, but that once apprised of the risks it has taken responsibility and
moved to quickly address the problem. Despite this activity around silica, industry groups
continued to take the position that RCS exposure did not warrant a lower PEL, nor should
respirators be stopped as a compliance method. The belief was that industry, working
internally, had addressed the problem.
Industry representatives, however, were not alone in being slow to act. OSHA did
not address the relationship between RCS and hydraulic fracturing in rulemaking until an
advanced stage in the rulemaking process. Hydraulic fracturing was first substantively
included in the Preliminary Economic Analysis for the Notice of Proposed Rulemaking
(NPRM) in 2013. It was included in Appendix A of this document which comprises eighty
pages on NPRM’s impact on hydraulic fracturing. The impact described therein was based
68
on research conducted principally by OSHA’s contractor, the Eastern Research Group
(ERG). However, this research was not conducted until many other processes for
rulemaking had been completed, including Small Business review panels, a principal
contention for industry representatives. Thus, its late inclusion set the tone for the
rulemaking debates which I observed in 2014, which already were primed to be adversarial.
Negotiating Health Risks: for whom?
The debates I observed at OSHA’s hearings entailed strategic interpretations of
OSHA’s responsibilities offered with the purpose of advancing certain interests (industry’s
health) at the expense of others (workers’ health). According to the first narrative offered
by industry representatives, it was not necessary for OSHA to take steps to further protect
the workers. The reason: current rates of silicosis mortality did not obligate the industry to
meet a lower PEL because mortality rates were decreasing and could not be attributed to
current industrial practices. During the time that I spent in the Caesar Chavez Auditorium
during the public hearings, I heard industry-affiliated speakers offer the same arguments
with tedious repetition and an intense focus on the technical aspects of the regulation. When
the hydraulic fracturing industry was discussed, its content spilled outside the regulatory
environment and drew parallels to the trainings, conferences, and events I was attending
for OSH, and the promotional literature circulated by oil and gas industry groups. Many
arguments were rooted in ways that industry generally, and the oil and gas industry
specifically, framed OSH concerns, with a focus on safety over health, the immediate and
discrete, over the long-term and unseen, consequences, all with an eye towards establishing
the uniqueness and unpredictability of the industry.
Each day when I attended the hearings, I sat down in the center back row of seats.
Union representatives and members of other workers’ organizations, who comprised the
69
most demographically diverse group at the hearings, invariably sat to my left. Industry,
represented predominantly by white men, gathered in several groups to my right. Members
of the groups infrequently mixed, and with a few exceptions, provided rough boundaries
for the arguments that would be presented. Three tables were positioned across the flag-
accented stage, the outer two draped in blue cloth were embellished with the USDOL crest.
A rotating panel of scientists and OSHA representatives sat at the table stage left. Those
giving testimony sat stage right. One of two older white men, the presiding administrative
law judges, occupied the center table, from which they periodically intervened in tense
interrogations, reminded commenters to introduce themselves for the transcript, and kept
the hearings on schedule. I focus here on industry, in part, because so few members of labor
organizations gave specific voice to oil and gas concerns, and these came mostly by way
of question and answer. Labor unions, although charged with representing their own
membership, would at times include questions about hydraulic fracturing. Yet throughout
the hearings, it was industry that dominated the narrative, not only about the hydraulic
fracturing industry, but also by setting the discourse around a few key themes including
“significant risk.” Repeating these arguments across dozens of industry groups, by sheer
numbers and provocativeness of argument, at times, industry established its voice as the
one to be rejected41.
Before these parties gathered in Washington, D.C., for the informal hearings in
March and April 2014, the process of debating OSHA’s rule had been underway via written
41 This is not to say that unions were unheard. To the contrary, OSHA in its final rule spends significant
time on labor concerns and criticisms. However, many of the issues raised by industry had to be
addressed by labor. It was industry’s narrative on the rulemaking that framed much of the testimony,
particularly surrounding issues of hydraulic fracturing.

70
comments submitted to OSHA between September 2013 and February 201442. Following
the hearings, OSHA received post-hearing comments until August 2014. In total, OSHA
received 1,786 submissions (2,068 comments), including over 980 attachments, mostly
letters and reports provided by the industries affected by the rule43. The rulemaking docket
also includes 2,458 supporting documents, principally transcripts and exhibits from the
hearings, scientific studies, and exposure assessments, all of which were subject to review
and response before OSHA issued its final rule in March 2016. A total of 137 documents
presented to OSHA included some analysis of hydraulic fracturing. In addition to
reviewing these documents, I also examined documents from major trade organizations to
identify the relevance of the oil and gas industry arguments to other industries.
Is Silicosis Even a Problem? Absolution from Responsibility
Industry groups contested the proposed rule by forwarding their own narratives
about responsibility, arguing on the one hand that there was no significant risk they were
responsible for mitigating, and on the other, that OSHA was ignoring their responsibilities
towards industry’s needs. First, industry representatives sought to demonstrate that workers
were not at significant risk when exposed at the 100 µg/m3 PEL. Thus, according to
industry, a stronger PEL was not warranted. Using CDC data to dispute OSHA’s
interpretation of risk, industry distanced current industrial practices from incidences of
42 Regulations.gov retains information pertinent to rulemaking from most federal agencies and hosts the
comments submitted to federal agencies during the notice and comment period. 43 Policy scholars have tried to rationalize these activities. In Yackee’s view, comments “provide a new
source of information and expertise to the bureaucracy” and “the bureaucracy can reduce future court
challenges by responding to the concerns expressed within comments” (2005, p. 106). This is in keeping
with what one OSHA official told me about the utility of public hearings. Adopted rules also set a
precedent for future rulemaking. In RCS rulemaking, some commentators were concerned about the
impact of OSHA’s PEL on MSHA’s approach to updating RCS limits.
71
disease and argued that the 100 µg/m3 PEL was sufficient to protect workers44.
On the third day of the hearings, shortly after 9:30 a.m. on March 19th, 2014, the
Chamber’s counsel, Henry Chajet, took the stage. His ostentatious demeanor commanded
the auditorium, as it would throughout the hearings, as he introduced four scientists who
would defend the Chamber’s opposition to the proposed rule. OSHA had determined that
a reduced PEL for 50µg/m3 was necessary to address human health risks from RCS. The
Chamber disagreed. Speaking on its behalf, Dr. Jonathan Borak of Yale’s Medical School
offered an argument in which he opposed OSHA’s determination of significant risk.
Projecting the core of his message on a sloppily italicized PowerPoint slide, he challenged
OSHA’s conclusions as lacking “direct evidence” (Figure 2.5) an argument he grounded
in an analysis of CDC silicosis mortality data.
Figure 2.5: Dr. Borak's Presentation, March 19, 2014
Borak spoke confidently and assertively to deny OSHA’s position that a stronger
PEL was necessary. Using the CDC data, Borak concluded that too few people were dying
of silicosis to warrant a stronger standard. He emphasized that the number of people dying
from this disease had been in decline since 1968, using a chart that would be so repeatedly
presented, it inspired sighs and groans from the part of the room occupied by labor activists
(Figure 2.6), and which Borak would himself refer to as “that familiar CDC chart.”
44 I examine narratives offered by oil and gas trade groups such as the API and lobbies that analyzed
hydraulic fracturing such as the Chamber and the ACC. “Industry” refers to these speakers.

72
Figure 2.6: CDC Mortality Data (Johnson, Freedman, & Chajet, 2014, p. 7)
On this basis, Borak argued that the current PEL was sufficiently protective:
The implications of the latency and the survival durations are fairly
straightforward, going back to that familiar CDC chart. If you consider that
a mean latency of 30 years, and a mean survival of 20 years—and I
understand that that’s a simplification, but for the moment, if you assume
it, then the fact is that virtually all cases reported as a mortality were first
exposed in a period that preceded the adoption of the PEL and the enactment
of the OSHA Act [sic]. […] And it suggests that the data have only limited
probative value with respect to whether this speaks to the permissible
exposure limit and its adequacy in protecting workers. (OSHA, 2014,
March 19, pp. 280-281).
Interpreting the CDC data alongside claims that the mean latency of silicosis is 30 years
(the far end of most estimates), and that individuals live with silicosis for 20 years, his
argument attributes diseases seen in the CDC data to industrial practices that predated the
implementation of the 100 μg/m3 PEL. Thus, Borak absolved recent industrial practices of
any accountability for instances of the disease. Borak all but explicitly stated that the 20
years a person survives with silicosis and the deteriorating health of those suffering from
the disease during this period did not constitute a significant measure of risk—a sentiment
he would return to during the question and answer period. Industry sought to use temporal
distance to absolve itself from responsibility for silicosis deaths seen in the data but also
towards utilizing further controls for silica exposures. In essence, Borak manipulated time

73
to suggest that what was currently being done was sufficient.
Borak’s testimony reflected what the Chamber argued in its written comments, that
the decline in silicosis mortality indicated that OSHA had misinterpreted the CDC’s data,
which the Chamber labeled as “Trustworthy” (Figure 2.6). In the Chamber’s stated view,
OSHA’s analysis was flawed: its evidence of significant risk was based on “speculative
statistical analysis and modeling,” and its conclusions were in direct conflict with the CDC
data (Johnson, Freedman, & Chajet, 2014, p. 8). The Chamber dismissed OSHA’s claim
that the CDC data undercounted silicosis deaths45, arguing that discrepancies of this kind
did not diminish the industry’s broader message that silicosis had declined under the
current PEL. “There is no contradicting the reality of the clear and welcome steep trend
toward eliminating silica-related mortality” (Johnson, Freedman, & Chajet, 2014, p. 8).
API and Independent Petroleum Association of America (IPAA) made this point
repeatedly in written and oral comments. They argued that Borak had drawn the “rational”
conclusion that the current PEL had solved silicosis in the U.S., and distanced recent
industrial practices from responsibility for mortality associated with the disease
represented in the CDC data (API & IPAA, 2014, p. 9). In short, OSHA’s proposal for a
stronger PEL was based on an incomplete and erroneous interpretation of the available data
and for this reason was unwarranted and irrational.
This argument about the reliability of government data regarding mortality took a
turn from its earlier iterations in the 1970s (Rosner & Markowitz, 1995). In response to the
NIOSH 1974 report, industry challenged the sufficiency of NIOSH silicosis data that
endorsed a lower limit (Rosner & Markowitz, 1995, p. 257). In contrast, here, CDC data
45 There is no national registry for silicosis morbidity or mortality. The CDC’s estimates reflect causes
of death listed on death certificates.

74
were championed as demonstrating the protectiveness of the 100 μg/m3 PEL and that
current industrial practices were not generally responsible for putting workers in danger.
For industry’s argument, the CDC data served to illustrate that industry was already
meeting its responsibilities to protect workers. Essentially, industry argued that new
regulations were unnecessary because its own correct interpretation of the data demonstrate
how they were already being responsible towards protecting workers.
Not all of the CDC data were beyond criticism. Despite the industry’s praise for
NIOSH at OSH conferences including during plenaries and sessions devoted to NIOSH
research on the industry, trade organizations challenged the representativeness of NIOSH’s
study showing workers were subject to a high level of RCS exposure at hydraulic fracturing
sites. Industry representatives argued that sampling was “inadequate to determine
representative exposure profiles” (API & IPAA, 2014, p. 3). According to Halliburton:
Absent evidence that the six sites were randomly selected or were
representative of U.S. hydraulic fracturing sites in general, the exposure
profiles used by OSHA cannot be properly extrapolated to all workers in
the hydraulic fracturing industry. (de Bernardo, 2014, p. 8).
The unrepresentativeness of NIOSH’s exposure monitoring underscored industry’s
contention, discussed shortly, that worksites are all different, but also that overexposure
might not be as significant as indicated by the NIOSH data. Industry members offered this
critique strongly during the process of rulemaking. Yet, when pressed in regard to sharing
direct measurements of exposure that could show ways that the NIOSH data were incorrect,
an expert for the Chamber offered a disgruntled and far from informative reply: he could
not directly confirm the representativeness of the NIOSH data because he was bound by
confidentiality, but that he did not see a “marked difference” between the data he was
familiar with and the NIOSH work, and thus that the NIOSH data were “not completely

75
erroneous.” He painfully acknowledged that NIOSH research might be indicative of a
problem in the oilfield, reflected in this exchange:
DR. COBLE: And then have you ever seen any exposure monitoring data
from hydraulic fracking sites, other than the data in the OSHA—in the
NIOSH report that OSHA is utilizing? Is there any additional data that
you’re aware of that we could use for—to enhance our analysis?
DR. KNUTSON: Yes, I have.
DR. COBLE: Would you be able to submit some of that for —
DR. KNUTSON: I’ve got confidentiality agreements, so I can’t answer that.
Just roughly speaking, I did not see a marked difference.
DR. COBLE: So that the NIOSH data may be fairly representative, in your
mind, of an uncontrolled situation at a fracking site?
DR. KNUTSON: Well, it’s not completely erroneous. It —
DR. COBLE: Yes, okay.
DR. KNUTSON: Obviously, the problem with many monitoring data that
occurs in hydraulic fracturing is that there’s no two sites that are the same.
You’ve got the situation where the number of hoppers that you’ve got, the
conveyors, the type of sand, the size of the sand, the length of the
campaigns, all of these things change. (OSHA, 2014, March 19, pp. 499-
500).
In reiterating the possible unrepresentativeness of NIOSH’s findings, Knutson’s final
point, that well sites are all different, is an issue I return to in the next section.
Industry recycled the mid-20th century sentiment that silicosis is sufficiently
controlled by the established limit within the framework of rulemaking requirements.
When the oil and gas industry gave testimony during the closing days of the hearings,
Kenny Jordan, executive director of the Association of Energy Service Companies, echoed
this point, figuratively wagging a finger at OSHA, a tone and attitude many industry
members expressed:
MR. JORDAN: [I]t might be useful to remind OSHA also that fatalities in
silicosis ha[ve] fallen dramatically. In OSHA’s own preliminary reports,
fatalities attributed to silicosis have fallen from 1,156 deaths in 1968 to 161
in 2005. It is our belief that the current standard is very effective and such
a conclusion can be supported by the substantial decrease in fatalities.
76
(OSHA, 2014, April 4, p. 4060).
Jordan stated that fewer deaths meant that a “very effective” PEL had resolved questions
about the extent to which workers needed to be protected from contracting silicosis. By
implication what matters is how many people die, not the consequences of living with a
respiratory disease, and that there is an acceptable level of deaths. Additionally, comments
from the API mirrored language from the Chamber to argue that the downward sloping
trend in silica-related deaths suggested that there was no need for a lower PEL:
OSHA’s conclusion contrasts sharply with the actual data demonstrating
[…] that silicosis mortality has been reduced by approximately 90% since
1968 […] there is no contradicting the reality of the clear trend towards the
goal of elimination of silica related mortality in the United States. (Johnson,
Freedman, & Chajet, 2014, p. 7).
Just as mid-20th century industry groups had argued that silicosis was solved, these
statements emphasize a fait-accompli sentiment: silicosis deaths have declined, and the
PEL is an “effective” solution. Thus the “goal” has been achieved. Although people were
still contracting silicosis, the situation did not warrant regulatory action to reduce exposure:
This is not to say that silicosis has disappeared in the American workplace.
There is no denying that cases of silicosis continue to occur in the United
States. […] But the fact that cases of silicosis continue to be found does not
indicate that the current general industry PEL of 100 μg/m3 is insufficiently
protective or that reducing the PEL to 50 μg/m3 is necessary to eliminate a
significant risk of silicosis among American workers. (ACC, 2014, p. 5).
Such arguments rested on an interpretation of risk measured by mortality—more precisely,
an acceptable level of mortality—thereby absolving industry of the responsibility for
mitigating exposure. Borak presented this position when he responded to a question
regarding whether silicosis was the only risk posed by RCS worth considering. Here again,
the tensions between the parties participating in the hearings were on display:
DR. GOLDSMITH: I’m here as a representative of George Washington
University in Georgetown, but I’m not paid by anyone.
77
I have just an observation and a question for the panel. Back behind you all
is this graph of CDC decline in silicosis mortality, and I would tend to
suggest that there is certainly a reason for something positive to be said
about this.
[…] But my question is, is this the right thing to be looking at? Shouldn’t
we be looking at all of the silica-related disease, not just silicosis? […]
DR. BORAK: Let me take a first cut. I agree with Dr. Goldsmith. I think
that the slide you are seeing is a tribute to an important public health
success. Whether it’s complete or not is a separate issue. It reflects a
substantial decrease in deaths related to a preventable cause. Whether those
exposures occurred before or after OSHA should not diminish the
magnitude of the success. (OSHA, 2014, March 19, pp. 348-349).
Signaling his discomfort with Borak’s academic-industry affiliations, Goldsmith pressed
Borak to acknowledge RCS-related disease beyond silicosis. Borak began with the
rhetorical move of stating his agreement with Goldsmith, but only with the latter’s
concession that some progress has been made, not with the question Goldsmith presented.
Instead, Borak pivoted to the narrative he wanted to construct from the data, reiterating that
“this has been a wonderful success. So that’s my contribution to answering your question”
(OSHA, 2014, p. 351). Undeterred, in an effort to redirect Borak, Goldsmith followed up:
DR. GOLDSMITH: And don’t you also think that we should be looking at
a broader set of disease than simply looking at silicosis mortality?
DR. BORAK: Ah, yes, I think we are looking [at] a wide array of disease.
This happens to be a clearly documented and dramatic statement regarding
one of those most important disease[s], one of which is a signature disease.
I think that the question is not that—I, certainly, as a physician, do not
regard any of these diseases as unimportant, either to people or to the public
health. My concern had to do with whether 100 ppm PEL was or wasn’t
protective, and whether there were data, okay. But I certainly would not tell
you that these other disease[s] are unimportant. That would be a terrible
thing for me to say. (OSHA, 2014, March 19, p. 351).
At this point, Judge Solomon abruptly ended this line of questioning for time. Although
coming much closer to Goldsmith’s position, Borak did not fully concede Goldsmith’s
argument. While agreeing that other RCS-diseases exist and should be given consideration,
78
he reemphasized his point that the current PEL is already protective based largely on his
analysis of mortality data.
This admission is significant, as later in the day, a consultant for the ACC46 offered
testimony that challenged the relationship between silica and silicosis. During this
testimony, the auditorium was markedly less full, and those that were left audibly disagreed
with many of his provocative claims about the futility of not only the well-established
relationship between silica and silicosis but also the reliability of scientific methods. Still,
such arguments that dispute accepted scientific facts serve to shift discursive spaces.
Michaels (2008) and Oreskes & Conway (2011) both chart how these efforts are
accomplished by industry through regulatory and governance spaces through campaigns of
“doubt.” This kind of uncertainty-as-discourse parallels how the industry sought to
represent its own physical movements, layouts, and patterns, discussed in the next section.
A few days later, Chajet brought up the exchange between Goldsmith and Borak
with more verbose language to reframe Goldsmith’s line of questioning in reference to the
“marvelous achievement” of the decline in deaths from silicosis.
MR. CHAJET: But we also believe that the current performance of
American industry is the most incredible success story in occupational
health in the last 100 years. And if you look at these CDC numbers, you can
look at them all day long, and they show nothing but incredible achievement
of trend, the discussion that took place the other day by David Goldsmith
and one of our witnesses exemplify. David Goldsmith, Dr. Goldsmith was
one of the first people that ever talked to me about silica disease 30 years
ago or more, and this achievement is a marvelous achievement. It is the best
set of data we have, and you can try to change that data all you want, but it
is the Center for Disease Control data. And if you run analysis of this, no
matter how you analyze it, it’s a steeply, steeply declining trend and a
tremendous success story that needs to be and will be continued. (OSHA,
2014, March 21, pp. 1130-1131).
46 This consultant, Anthony “Tony” Cox now heads the EPA’s Clean Air Advisory Committee for the
Trump Administration.
79
While industry dominated many parts of the hearings and established the narrative
by which all others were forced to react, they were not the only voices visible. Many peer
reviewers, OSHA representatives, and labor advocates aggressively challenged these
arguments absolving industry from accountability for silicosis deaths. The hearings did not
focus entirely on the content of the proposed rule. Instead, they also reflected broader
power negotiations between the constituents. Many at the hearings clearly knew each other
from years and even decades of debate and indicated their familiarity with one another
during the question and answer sessions. Individuals uncomfortably shifted in their seats,
and their sighs signaled their frustration when industry, labor, or OSHA advanced specific
arguments. Chajet, Peg Seminario of the AFL-CIO, and others regularly posed questions
to illicit narrow points regarding their respective organizations’ positions on the rule and
on the nature and limits of OSHA’s authority. The question and answer periods following
testimony could become tense, at times moving far away from the topic of RCS exposure.
When the debate turned to Borak’s understanding of the scientific method, for example,
like many discussions, this focus not only intensified combativeness of the two sides but
also challenged the participants’ expertise as much as their arguments.
Even with these voices challenging industry, oilfield workers were unrepresented.
A few labor advocates brought up hydraulic fracturing, but there were no specific voices
that advocated on their behalf. Particularly powerful testimony was offered by sickened
and exposed foundry workers and construction workers47. The requirements of rulemaking
that give individuals and industry members the opportunity to participate placed many in
47 Some of this testimony that focused on the experience of living with silicosis would later appear on
OSHA’s website on silica and the new rule. This and similar text would be removed when the website
was updated around the time of the first implementation date for the new standard in October 2017.

80
the room on the defensive, defending against the industry narrative that distanced
themselves from responsibility for silicosis by focusing its concern on the visible, tangible,
and quantifiable outcome of silica exposure, i.e., deaths from silicosis. As the ‘dose makes
the poison’ suggests, it is not just that workers are exposed, but how much, and that they
ultimately die from the consequences of these exposures.
The visible and immediate in OSH often engenders more concern than what is less
immediate and clearly recognizable as an occupational hazard. As former USDOL assistant
secretary Michaels (the head of OSHA) said of the hydraulic fracturing industry in an
interview with E&E News, “No one says ‘keep working’ when somebody’s lost a body
part” (Soraghan, 2017). Long-term issues, where ill health harms take years to develop, are
less examined, a sentiment echoed by NIOSH in interviews, informal conversations, and
conference presentations. In the training materials from the courses I have taken, safety is
the dominant topic. In one 4-day, 40-hour course, one 3-hour unit was devoted to health
concerns including silica. In another 8-hour course, two pages were dedicated health issues,
whereas the remaining 60 pages covered safety. Industry is often most concerned with what
happens during a working day and issues that can be easily attributed to what happens at a
worksite.
This translates to slogans and best practices that emphasize reducing incidents.
Some firms stress “Zero Incidents,” whereas others underscore low recordable injury rates.
Contracts with servicing companies are awarded based on, among other things, injury rates,
which serve as a signal for liability and insurance costs. Many contractors are required to
provide documentation of their injury rates and the OSH programs they have developed
through the reporting systems such as ISNetworld. Trade shows I attended featured table

81
after table of exhibitors offering OSH services to manage risk, either by running or writing
safety programs or doing training with workers. In listening to many company pitches, I
noticed that most relied on strategies specifically designed to gain buy-in from workers
through behavior modification, including safety-incentive programs and surveillance
strategies. Behaviorally-based safety shifts the burden of governing risk away from
industry to the individual. Still, more than one vendor at the 2014 Safety Conference spoke
disparagingly of OSHA’s dismissal of behavior-based safety, under the direction of then
Assistant Secretary Michaels, due to the ways those practices make workers responsible
for mitigating risk.
“Incident” or “event” does not capture the harm caused by RCS exposure because
it is unlikely to produce recordable incidents that industry and OSHA measure and track.
If a worker does develop a silica-related illness, this will occur away from the oilfield,
years after repeated exposure. It can be difficult to show causality between silica-related
disease and exposure. The impact of RCS is largely “unseen” through the industry’s OSH
lens. Given that the most visible, quantifiable, and stark consequence of RCS exposure is
a dead silicotic, it is fitting that the industry’s narrative focuses on a reduced risk of silicosis
mortality. For the industry, the only “significant risk” is death. This viewpoint provided
the background against which industry argued that OSHA’s rule risked industry’s vitality
while generating no gains for workers.
The Health of Industry: The Cost of Movement and Materials
MR. JORDAN: Yeah. Frack sites are such a wide variety of animals,
depending on how many phases you’re pumping (OSHA, 2014, April 4, p.
4079).
MR. D’ANGELO: […] the limitations on employee exposures are both
special and temporal. (OSHA, 2014, April 4, p. 4081).

82
Feasibility tests of the proposed rule that are mandated for OSHA rulemaking
enabled the industry to compare its own vitality to that of its workers and to create a
narrative in which respirators are the most feasible compliance option, thereby shifting
industry’s responsibility onto the workers. Here, industry made the case that its health is
threatened by OSHA’s efforts to regulate RCS exposure, not just by mandating a new limit,
but by telling the industry how it must mitigate RCS exposure. In Appendix A of the
NPRM, OSHA had provided multiple suggestions for industry to reduce exposure through
engineering controls that change the equipment and machinery and diminish the need to
require workers to wear personal protective equipment (PPE)48.
During the final week of the hearings, members of the oil and gas industry’s major
trade groups took to the stage at OSHA’s informal public hearings. API counsel, Wayne
D’Angelo49 (Figure 2.7), a young-looking white man, read prepared testimony on the
“Industry’s Commitment to Workforce Safety”:
MR. D’ANGELO: While hydraulic fracturing is not a new technology, its
use in conjunction with technologies such as horizontal drilling is more
recent. Without question, the intersection of these technologies has changed
the way the world looks at energy and has delivered tremendous benefits to
the U.S. economy. (OSHA, 2014, April 4, p. 4025).
D’Angelo and others championed the significant shifts in the U.S. and world energy
economy triggered by hydraulic fracturing.
48 OSHA writes in Appendix A: “if the control technologies that have been used in other industries can
be successfully transferred to the hydraulic fracturing setting, the compliance costs would equal less
than one percent of average revenues and less than five percent of average profits for recent years for
the hydraulic fracturing sector as a whole and for small entities” (OSHA, 2013, p. A-67). While OSHA
estimated the costs of these modifications to be modest, API staunchly refuted its economic analysis,
claiming in most categories that OSHA had underestimated or failed to estimate the costs of the
regulation (API & IPAA, 2014). 49 D’Angelo is no longer counsel for API, and is partner at Kelley Drye, a practice that specializes in
energy law.

83
Figure 2.7: API testimony at the RCS Informal Hearings, April 4, 2014 (A. Hesse).
He continued:
MR. D’ANGELO: Not only has hydraulic fracturing helped make the
United States the world’s top hydrocarbon producer, this helped create
high-paying jobs, a renaissance of domestic manufacturing and historic
lows in our nation’s trade deficit. At the same time, the increased use of
natural gas has helped reduce America’s greenhouse gas emissions to levels
previously considered unattainable. (OSHA, 2014, April 4, pp. 4025-4026).
Citing “the unquestionable importance” (OSHA, 2014, April 4, p. 4026) of hydraulic
fracturing to the economic and environmental goals of the U.S., D’Angelo argued that
OSHA’s rulemaking has far-reaching consequences50. By implication, D’Angelo claimed
that a threat to the industry is a threat to the US.
50 Murphy (2017) describes the emergence of the ‘economy’ imbued with affect of weighty significance
in the mid-20th century. Mitchell (2006) too describes significance imbued through the making of the
‘economy’ in the early 20th century as an object of governance. Both signal the heftiness granted
arguments about the ‘economy.’ API’s claims have historical precedent. For example, Standard Oil used
the significance of the oil and gas industry to the nation’s economy and development to justify the
necessity of lead additives in gasoline in the 1920s in the U.S. (Markowitz & Rosner, 2002).

84
Figure 2.8: Energy Nation Poster
Figure 2.9: PA Jobs Rally (A. Hesse)
This well-oiled argument, rehashed through advocacy programs such as Energy Nation
(Figure 2.8) and United Shale Advocates (Figure 2.9), organized by API and the Marcellus
Shale Coalition, respectively, advocates “responsible regulation” in television commercials
and letter-writing campaigns, as well as in tradeshows, and industry demonstrations I have
attended, where the tension between too-tough regulation and the industry’s ability to self-
regulate is frequently on the display. This responsibility is to industry first such that
regulations do not harm the economic engine to which these narratives attribute revitalized
domestic energy production and stronger national security (Figure 2.9). For his part,
another industry representative, Jordan proclaimed that the industry had precipitated
“unprecedented economic growth” and would soon render the U.S. independent of other
countries for its energy (OSHA, 2014, p. 4058).
D’Angelo’s testimony established what was at stake in regulating the industry
before turning to more specific arguments about the RCS rule. He began by arguing that
OSHA’s economic and technological feasibility analysis mischaracterized the industry’s
spatial and temporal configurations, which, he argued, do not follow predictable patterns:
MR. D’ANGELO: From both an economic and technological perspective,
most of OSHA’s errors derive from the fact that OSHA viewed the
hydraulic fracturing industry as just another industry subject to the proposed
rule. But the hydraulic fracturing industry is not the same as other industries.

85
The hydraulic fracturing industry works in uncontrolled and widely
differing outdoor environments that change weekly, if not more frequently.
And no two workplaces or equipment configurations are ever the same. If
you have been to one hydraulic fracturing site, you’ve been to one hydraulic
fracturing site. (OSHA, 2014, April 4, p. 4029, my emphasis).
Just as the Chamber, the ACC, and API discredited OSHA’s interpretation of significant
risk, D’Angelo condemned OSHA’s feasibility analyses, stressing the agency’s inability to
gather knowledge given the variable nature of the conditions under which the industry
operates. By API’s account, every hydraulic fracturing worksite is different, making it
impossible to accurately analyze the rule’s economic feasibility. As Jordan put it, “So what
are the costs of the proposed rule? The answer is that OSHA has no idea. In fact, nobody
does” (OSHA, 2014, p. 4052).
Yet, both API and IPAA had argued in comments jointly submitted several months
earlier that the rule would undoubtedly prove too costly. They stated that the proposed rule
“would likely exceed $366,000,000” and that it “threatens the existence of all small
hydraulic fracturing businesses, and therefore, the competitive structure of the entire
hydraulic fracturing industry” (API & IPAA, 2014, p. 78). The flexible subcontracted
configuration of the industry was seen to be endangered by the rule, placing the entire
industry at risk. Although it is common for industry groups to argue that the cost of
regulation is ruinous, for the hydraulic fracturing industry this argument was made through
spatial and temporal arguments about the uniqueness of the industry making the costs of
the rule prohibitive and the use of engineering controls infeasible, hence making reliance
on respirators essential. This argument is a way of shifting responsibility onto individual
workers. Here, it is not so much willful ignorance of the broader processes that cause
workers to be exposed, but that other control mechanisms are infeasible and would be too
costly for the industry. This discursive shifting of responsibility is produced through
86
consideration of considering industry’s vitality.
In challenging OSHA’s contention that hydraulic fracturing could use engineering
controls, industry groups stressed the variability and unique nature of the industry’s spatial
and temporal patterns. Not only are employers “constantly moving their employees and
equipment from well site to well site in a particular area” (API & IPAA, 2014, p. 80), they
move “personnel and equipment into other active regions of the U.S.” (API & IPAA, 2014,
p. 80). API pressed that OSHA had failed to consider how hydraulic fracturing was
different from other industries:
In the hydraulic fracturing industry, employers are constantly moving their
employees and equipment from well site to well site in a particular area to
conduct well stimulation work, including relocating personnel and
equipment into other active regions of the U.S. Each well may have
different footprints and surface limitations that require unique
configurations of equipment. The size and complexity of the stimulation
work may require use of different combinations of equipment and/or
proppant. Employee schedules in the hydraulic fracturing industry are such
that specific employees may not be paired with specific equipment or tasks.
(API & IPAA, 2014, p. 80).
API’s “may” statements suggest that the configurations of equipment and materials and
volumes of proppant were not conducive to generalization. This suggests a way that
uncertainty is produced; the question is not just the science is uncertain (Michaels, 2008;
Oreskes & Conway, 2011), or that the exposures are imperceptible (Murphy 2006) or
immeasurable, but rather that the industry’s day-to-day operations that rely on spatially
variable practices confound the federal regulation of its practices51. This effort to refute
OSHA’s analysis by asserting its own unpredictability extended into post-hearing
51 Industry has opposed most federal regulation of hydraulic fracturing in favor of state-level regulations
arguing that the states can adapt to the unique practices of the industry within particular states. The
structure of OSH regulations between federal OSHA and state-plans makes this state-level strategy
impossible. Instead the argument here focuses on no-regulation due to the industry’s spatial variability.

87
comments in which API argued that the kind of soil encountered in hydraulic fracturing
could have a material effect on a company’s operations:
Factors like whether the well pad is situated on indigenous soils, caliche or
sand, limestone, granite or sandstone (the quartz content of which varies
widely) can also affect the situation. These factors are outside the control of
the oil service companies but can greatly impact exposures. (API, 2014, p.
4).
API suggested that service companies should not be responsible for mitigating exposure
with engineering controls given the extreme differences in the conditions in which
exposure can occur, framing these factors, including climate, soil content, and regulatory
environments (API, 2014, p. 4) as being out of their control. The irony of this rhetoric of
the responsibility of industry is that at times it relied on the structural constraints of
industry, the location of oil and the subcontracted nature, to absolve itself of responsibility.
Structural constraints are the very narrative that advocates of personal responsibility of
dismiss, as for Young, “the rhetoric of personal responsibility encourages an isolated,
atomistic way of thinking about individuals” (Young, 2008, p.23)52. Indeed, although
industry contended, as detailed in the next section, that workers should bear responsibility
for their health and industry’s health by wearing of respirators, industry’s argument about
its own responsibility to protect workers is synonymous with an irony that Young
highlights. “People who participate in social processes frequently deny the suggestion that
we bear responsibility in relation to them on the grounds that we confront forces that give
us no choice but to act as we do”(Young, 2008, p. 154).
52 For Young, the tendency of the rhetoric of responsibility to focus on either the structural constraints
or personal responsibility is one of its key failings. She details how influential social policy thinkers of
the mid-century recoiled to the so called ‘determinist sociological’ tendency vehemently ascribed
injustices to social structure, rather than individuals poor choices. For Young, their instance on personal
responsibility narratives builds from an argumentative position based in a false dichotomy of either
agency or structure, and one in which does not account for the background conditions of society to
themselves be inherently unjust (2008, p.3-27).

88
Even ERG’s supporting evidence to Appendix A of the Proposed Rulemaking, the
evidence used by OSHA’s contractor, included a presentation from Universal Well
Services, annotated with the words “Very Unique” to describe its layout (Figure 2.10).
Such a phrase imperfectly reinforces the uniqueness of the industry, giving no evidence to
indicate what is unique about it. Even as the idea implies a norm from which Universal’s
configuration diverges, this configuration looks like those I have seen on a well site,
projected in conference presentations, drawn for me by an OSHA official, and diagramed
in reports. Still, in one of my Freedom of Information Act Requests, images of the well site
were redacted, as the company claimed its layout was a trade secret.
Figure 2.10: Universal Well Services Presentation (Ross, 2010)
Industry invested serious concern with regards to the complications posed by the
movement of materials and goods. It was not only that materials moved rapidly between
sites operating under dynamic conditions but that this took place across state boundaries
and regulatory environments. According to industry, these circumstances compounded the
cost of its proposed rule. At the hearings, Steve Crookshank, an economist with API, stated
that OSHA had failed to consider how these costs would be felt at each site, magnifying
the proposed rule’s costs, and illustrating OSHA’s mistaken analysis of the industry:
MR. CROOKSHANK: Consider transportation, assembly, and dismantling
89
costs. OSHA assumes that, just like in the static workplace found in general
industry, the hydraulic fracturing industry need only bolt on its emission
controls once and will incur no further costs despite constantly moving
equipment on a per job basis. The reality is that control equipment would
need to be transported separately, and will need to be assembled and
dismantled at each different hydraulic fracturing site. These are not one-
time costs. These are costs incurred on every job site. (OSHA, 2014, April
4, p. 4055).
In Crookshank’s account, it would be necessary to transport equipment to and from
worksites, and that each worksite would incur costs in setting up control measures. In
Knutson’s view, these costs would be compounded because each site is unique in light of
the variability of its configurations and kinds of sand-moving equipment:
Each site is nearly unique and the number and type of the material handling
equipment varies from one site to another. Consequently, any control
system needs to be modular (or dedicated to a single piece of equipment)
and flexible. Moreover, when the equipment is moved to a new site, the
equipment does not move as a unit but could be split up and sent to several
different sites or to storage until needed for another project. (Knutson, 2014,
p. 7, my emphasis).
Together, these issues made engineering control costs prohibitive. According to this
perspective, OSHA had failed to meet its responsibility toward industry in terms of
implementing only regulations that were economically feasible such that regulations did
not place the industry at risk.
The materials and their movement repeatedly roused more concern from the
industry than did the people working on them. The workers were all but invisible in the
discussion of feasibility. As evidence of this, API and IPAA recognized the abrasive
properties of the sand on their equipment:
Sand is extremely abrasive. As such, it can damage equipment and
significantly shorten the useful life of equipment used in environments with
large amounts of sand. (API & IPAA, 2014, p. 70).
Without acknowledging what sand does to the human body, industry showed significant

90
concern for what it does to its equipment. However, concern for how exposure to sand
might adversely affect employees’ lungs was overlooked.
Industry was resistant to considering engineering controls that would reduce
exposure, arguing that the cost of lowering the PEL through engineering controls would
threaten the industry because of the industry’s flexibility. The industry should be free from
using engineering control measures to protect workers because of its competitive structure,
in essence, its own vitality, was threatened. This argument would form the foundation of
industry’s position that due to technological limitations neither the 100 μg/m3 nor the 50
μg/m3 standards could be met without the use of respirators.
Infeasible Engineering Controls
In its proposed rule, OSHA had recommended that hydraulic fracturing firms use
engineering controls from sand control systems used in other industries. Reacting to this
technological feasibility analysis, industry objected to what they characterized as OSHA’s
reliance on control measures from what they described as less evolved industries. The
purpose was to distance industry from responsibility for providing engineering controls
and to support the conclusion that respirators were the only option, such that the
responsibility for protecting the health of the workers was shifted almost entirely to the
workers themselves.
In one example, OSHA had used dust containment efforts at a site in India as a
basis for comparison and for offering regulatory suggestions. Industry representatives,
however, rebutted OSHA’s suggestions in the very clearest terms, stating that “the
comparison of the Indian stone crushing operation to hydraulic fracturing is, at best,
tenuous” (Knutson, 2014, p. 3), “purely coincidental” (Knutson, 2014, p. 17) and
“impermissibly relies on reasoning by analogy that engineering controls studied at two
91
vastly different and primitive industrial sites, in India and Iran, will be effective in the U.S.
fracking industry” (Johnson, Freedman, & Chajet, 2014, p. 22). Scolding OSHA for its
attempt to apply control measures from “primitive” sites to the more high-tech environment
of hydraulic fracturing, the Chamber argued that the two industries were wildly dissimilar
such that neither India nor Iran should be looked to for evidence of feasibility in relation
to regulating hydraulic fracturing. During the hearings, Knutson drew a visual contrast
between the Indian stone-crushing operation and hydraulic fracturing:
DR. KNUTSON: They have a beautiful picture in the report that really
explains what’s going on. They have a woman with a basket of rocks on her
head walking up to the crusher, another woman standing at the crusher with
a basket of rocks waiting to dump it into the crusher, and another woman
walking out of what appears to be a tunnel—appears, because there’s so
much dust in the air you can’t see what’s going on, that would have been
directly under the crusher, again with a basket on her head full of crystalline
silica. (OSHA, 2014, March 19, p. 456).
Offering a picture of an extremely primitive and feminine workplace, as an exotic other,
Knutson dramatically argued that these industrial practices cannot show hydraulic
fracturing anything about dust control. Finally, he wondered, “How this can be related to
hydraulic fracturing that is mechanically moving 20 sacks per minute through a carefully
controlled system, I’m at a loss” (pp. 456-458). Thus, he brought his account of OSHA’s
foolishness in relating these operations to the predominantly male and mechanized
hydraulic fracturing operations in the U.S. to an end.
A few days later, Chamber’s council, Chajet was more direct during his testimony,
arguing that “primitive sites” could not be compared to the “mechanized mechanical
system” characteristic of hydraulic fracturing. His bewilderment implied that such a
comparison was actually an affront to the rulemaking process:
MR. CHAJET: Let me just see if I have this slide to show you what Dr.
Gerhard Knutson was talking about. This is the worksite that OSHA used

92
to compare to the American hydraulic fracking industry to determine
potentially feasible engineering controls. And another worksite with similar
conditions.
This is not acceptable in rulemaking in the United States to draw feasibility
conclusions from these types of conditions. We just don’t look at primitive
worksites and say it’s feasible from their use of a control to our use of a
mechanized mechanical system. It doesn’t work. (OSHA, 2014, March 21,
pp. 1133-1134).
Two weeks later at the hearings, the API made this juxtaposition directly with a side-by-
side visual to complement D’Angelo’s remarks about the dissimilarity between the Indian
example and the “complex modern hydraulic fracturing site” (Figure 2.11):
Mr. D’ANGELO: The photo I have up on my slide is a picture of the rock
crushing equipment that was studied in the Indian study and a complex
modern hydraulic fracturing site. Not only is the equipment dissimilar, the
exposures are dissimilar, the employee interactions with the emissions are
far different. […] How is such a conclusion supportable? (OSHA, 2014,
April 4, p. 4037).
Figure 2.11: PowerPoint Slide from API’s presentation (Exhibit 148)
It was not just that these comparisons were preposterous to industry representatives.
For them, OSHA’s rushed and insufficient analysis posed a significant risk to industry.
Returning to the language of fear and threat, Halliburton wrote that he “fears that the entire
industry will face significant compliance problems and costs imposed by the Rule” (de
93
Bernardo, 2014, p. 3)53. Many expressed alarm that the outcomes of OSHA’s flawed
science and analysis would be disastrous. In expressing this concern, the American
Exploration and Production Council (AXPC) weighed workers’ lives against the interests
of industry on the basis of feasibility as follows:
Compelling industry to install infeasible and ineffective controls at great
cost will do little to protect workers but will inflict significant economic
harm on the E&P industry and domestic oil and gas production. It is because
of the compliance impossibility posed by OSHA’s proposed rule—and the
intensely flawed and careless analysis purporting to justify the rule—that
AXPC submits these comments, which fully endorse API/IPAA’s
comments and incorporate them by reference, in strong opposition to the
proposed rule. (Thompson, 2011, p. 2)54.
According to industry, the variability of its work processes hindered systematic knowledge
to recommend feasible engineering controls. The requirements of OSHA’s rulemaking
justified the argument that OSHA’s stipulated engineering controls would be disastrously
costly due to the flexibility of hydraulic fracturing practices and the variability of the
conditions in which it takes place. These threats to industry would do little for workers
given that OSHA’s “significant risk” determination was unsubstantiated due to a
decreasing mortality rate for silicosis.
Workers’ Responsibility: Respirators are the Only Option
In addition to suggesting engineering controls, OSHA’s proposed rule disallowed
respirators as a means of compliance with the PEL. Industry fiercely opposed this
provision. Just as flexibility made engineering controls infeasible, industry’s flexibility
became a device to shift responsibility from the industry to the workers. Industry
representatives were steadfast in their view that compliance was feasible only through the
53 Mark de Bernardo representing Halliburton, is at Jackson Lewis, a law firm specializing in workplace
law. At the time, Chajet was also at Jackson Lewis but is now at Husch Blackwell. 54 E&P refers to “exploration and production.”
94
use of respirators. For example, the Marcellus Shale Coalition offered the following
argument:
The mobile and transient nature of hydraulic fracturing operations has a
significant impact on the technologies and processes that can successfully
be employed to protect workers from Respirable Crystalline Silica (RCS).
A primary mechanism of protecting workers from exposure to RCS at
hydraulic fracturing sites is the use of respirators. […] OSHA has
incorrectly assumed that control sand practices deployed at stationary
factory environments would be applicable to mobile and transient hydraulic
fracturing operations. Such an approach is not supported by data and is
therefore arbitrary and entirely inappropriate. (Spigelmyer, 2014, p. 2)55.
Given the special choreography of actors at a hydraulic fracturing site, which
industry suggested OSHA did not adequately appreciate, industry representatives argued
that respirators constitute the most effective way of protecting workers from exposure to
RCS. When pressed about this topic at the hearings, the D’Angelo affirmed that respirators
were necessary to meet even the current PEL. As silicosis has already been “solved,” the
D’Angelo questioned why current practices should be changed at all:
MR. O’CONNOR: This is Dave O’Connor. Do I understand correctly that
the panel members view not only the proposed PEL of 50 μg/m3
as
infeasible in hydraulic fracturing operations, but also the current PEL of
approximately 100 μg/m3?
MR. D’ANGELO: This is Wayne D’Angelo. We believe it’s infeasible to
meet—in many cases infeasible to meet the current PEL without use of
respirators, yes.
MR. O’CONNOR: Mr. Jordan, do you hold that view as well?
MR. JORDAN: I say given that the history and as we’ve seen the cases of
silicosis decrease, I haven’t seen the most recent numbers, that the current
level of 100 has been bringing that down for a number of years. So our
argument is why change it when what’s in place seems to be getting us to a
point—no death is acceptable, but at least getting us a point as we lower. So
our preference would obviously be to leave it where it is.
MR. O’CONNOR: Yes. But do you believe that engineering and work
practice controls can currently achieve a level of 100 μg/m3
of air in
55 David Spigelmyer is president of the Marcellus Shale Coalition.

95
hydraulic fracturing operations?
MR. JORDAN: From what we have seen so far from an engineering control
standpoint, no, not without the use of respirators. (OSHA, 2014, April 4, pp.
4121-4122).
Industry representatives, therefore, directly argued that compliance with OSHA’s
regulations can only be achieved through workers using PPE—i.e., respirators—which
shifts responsibility for taking steps to mitigate health risks from the industry to its workers.
Even as industry stressed the challenges its spatial and temporal flexibility poses to
protecting workers with engineering controls, it celebrated itself for developing tools to
address the variability, mobility, and high turnover of its labor force56. During his
testimony, Jordan made special note of the course, Safeland, a collaboration involving
several companies to orient workers to well-site hazards. The course, the very name of
which speaks to the preeminence of safety over health, awards workers a card that they can
use to move between employers, thereby enabling the industry to avoid retraining its
workforce. Although he lauded the industry for taking this step, it is a technique long used
in general industry and construction for OSHA awareness training. In his explanation of
the program, Jordan revisited the idea that the industry has only recently become aware of
the risks associated with silica and applauded it for including a section on silica in the
course. In this account, industry is credited with taking steps to protect the workers for no
other reason than alerting them to the hazard. As described in Chapter 1, however claims
of being and acting responsible, however warrant scrutiny, as they can be used to shift
responsibility, and overshadow or obscure harmful and irresponsible activities (Noxolo,
56 Industry groups seldom mentioned workers (this was left largely to unions, public citizens, and worker
representatives). However, when describing how turnover impacts the industry in response to a question,
Jordan discussed turnover of “blue collar” “kids coming out of high school” who would either change
companies for “a quarter more an hour,” or “he” would find out that “this isn’t the business for them,”
after experiencing the lifestyle of hydraulic fracturing (OSHA, 2014, April 4, 4116).

96
Raghuram, & Madge, 2012; Tronto, 2013).
When Jordan mentioned that silica was included in the course, I made a note to go
back to my course materials. I had taken the SafeLand course at a regional training center
in Pennsylvania a few months earlier but recalled that silica had received only a very brief
mention. In fact, upon looking again at the course materials, I found that silica was barely
mentioned at all. Unlike chemical hazards, such as benzene and lead, each of which
received a bolded title in the course text and also appeared in the table of contents, silica
was mentioned only under the subheading of Physical Hazards, without any special
designation in the text. From the SafeLand course book:
There are many types of dusts that can cause health problems if proper
precautions are not taken. Silica dust, paint dust, including lead particles,
high air pressure and high noise levels all pose hazardous threats to those
working near sandblasting.
Hydraulic fracturing sand contains 99% silica. Transporting, moving and
refilling silica sand into and through sand movers, along transfer belts and
into blender hoppers can release dusts containing silica into the air. Workers
can be exposed if they breathe the dust into their lungs. Breathing silica can
cause an irreversible but preventable disease called silicosis. (PEC/Premier
Safety Management, 2012, pp. Module 2, page 14).
Nowhere is it explained that what silicosis does to the body is not only irreversible, but
carcinogenic and fatal. Nor are any protective techniques even mentioned. It would be up
to individual instructors to elaborate these points. However, although some instructors I
worked with and interviewed took the health risks associated with silica very seriously,
others considered dust to be just a normalized part of the job.
Narratives about the inability to use engineering controls and the necessity of
97
respirators persist even as companies develop engineering controls for the industry57,
including John Oren of SandBox Logistics who presented testimony at the hearing.
SandBox Logistics presented their technique for sand delivery that avoids the use of the t-
belt to reduce exposures, and which they believed to be a commercially viable, feasible
technology for controlling silica exposure during the handling of materials that include this
substance in their composition. In a sparsely occupied auditorium, Oren challenged the
narrative to which most in the industry were committed. Indeed, during the question and
answer period, D’Angelo pressed Oren’s optimistic outlook regarding Sandbox’s costs,
implicitly suggesting that the mechanism was not as economical as advertised.
Another equipment manufacturer, HalenHardy58, also presented testimony.
Developed in central Pennsylvania, HalenHardy’s MASHH Mobile Air Shower blows
sand off workers’ uniforms before they take off their respirators—a solution only
applicable when workers wear respirators to protect themselves from RCS because they
are exposed in the first instance. Still, the shower had won the Technology Showcase
Award the previous year at the Shale Insight Conference, was a finalist for the
Environmental, Health and Safety Innovation Award at the Oil and Gas Awards in 2013,
and would go on to win the Technology Development of the Year Award in 2013
(HalenHardy, 2017). Yet, even as industry groups rewarded this solution that fit its
paradigm regarding how to solve the RCS problem, their representative, Donny Beaver,
admitted that hydraulic fracturing’s adoption of their technology had been “slower” than
57 At the 2014 OSHA Oil and Gas Conference that December, I attended a roundtable where others
developing control systems presented compliance options. In 2016, many on the panel returned, this
time to discuss if, and how well, their measures reduced exposures at or below the new PEL. 58 I requested an interview with HalenHardy following the hearings, my request was ignored after
several email exchanges.

98
desired and that they had expanded into the construction industry (OSHA, 2014, p. 3918).
The insistence on compliance through respirators was also represented in an
awareness video developed by members of the industry. In 2016, the STEPS organization
released a training video on the hazards of RCS exposure. A safety manager, Ted, training
“the new guy” Joe on silica hazards, made statements including: “We watch out for each
other,” and “Everyone’s gonna be watchin’ ya’ to make sure you have this mask on.” Most
significantly however, Ted tells Joe that his company will “make sure you know where the
hazards are and how to protect yourself” (Lawhorn-Cryden, 2015, my emphasis). While
the video recounts engineering controls for silica, it places significant emphasis on the use
of respirators as a means of compliance and even mentions “air showers for employees to
clean them off” as an appropriate engineering control (Lawhorn-Cryden, 2015). The group
applauded for addressing issues relating to RCS explicitly makes workers responsible for
protecting themselves.
After OSHA had finalized the silica rule, industry maintained that respirators were
needed despite OSHA’s instance that they could not be used to meet the PEL long-term.
The month after the final rule was announced in 2016, Chajet gave testimony to the House
of Representative’s Subcommittee on Workplace Protections. He argued against OSHA’s
prohibition of respirators as a final means of compliance and was adamant that respirators
were protective, stating, “I do not even call them respirators, they are mini-environments”
(U.S. House of Representatives: Subcommittee on Workforce Protections, 2016, p. 74).
However, respirators transfer responsibility for safety and health to an individual
worker, who must be properly fitted for a respirator, must wear it correctly (in some
instances it is necessary for the worker to be clean shaven), and must don a respirator every
99
time s/he faces a silica hazard. If they are to remain protected, workers cannot remove their
respirators, whether to speak through communication equipment or to get a deeper breath
of air. NIOSH reported clean-shaveness as a troubling issue repeatedly seen on worksites,
one that calls into question the seal between a worker’s face and the respirator, and hence
the device’s effectiveness (NIOSH 2010, 2011a, 2011b). These are significant reasons that
underscore PPE’s place at the bottom of the hierarchy of controls, discussed in Chapter 3.
PPE requires that equipment be available, that proper training and fitting for the equipment
be provided, and that workers use the equipment properly.
Thus, shifting of responsibility to the individual through respirators ultimately
serves industry, leaving risk and risk outcomes a function of proper worker use of PPE.
Harmon, a political theorist working in public administration and writing about
responsibilities within bureaucracies, notes:
The conservative variant [of agency] over-asserts the individual by
depicting him or her as the exclusive object of blameworthiness for
irresponsible behavior. This allows collectivities to maintain an official
posture of innocence of complicity in creating these conditions in which
such behavior may be rational in a perverse but nonetheless real sense.
(Harmon, 1995, p. 129).
By insisting that the principal responsibility for mitigating health risks falls to workers by
offering respirators as the primary means of protection, industry reinforces the idea that
workers must function as agents, who, for themselves and for their families, make rational
choices in their own self-interest to mitigate health risks. A failure to wear respirators
would simply become the responsibility of workers, rather than of industry. This is a
hallmark of risk and responsibility under neoliberalism; here, even as the state professes to
seek control measures that diminish individual responsibilities, its activities to not
undermine these logics. Indeed, the state’s own requirements for rulemaking provides

100
venues in which discourses surrounding individual responsibilities and industry’s
absolution of responsibility can be reproduced. This reproduces moral agents whose
voluntary actions enact their responsibility—a problematic assumption, as these moral
agents are seen as having the freedom to exercise their agency to protect themselves from
health risks.
OSH Act and Rulemaking: Regulating Risk, Negotiating Responsibilities
The public hearings and comments submitted are a reflection of the OSH Acts
mandate, its interpretation through the courts, and the rules and requirements of rulemaking
stipulated by federal statute and executive orders. The authority granted OSHA in the OSH
Act to set PELs was the result of years of intense negotiations in Congress over the state’s
responsibility to industry and to workers. The OSH Act did not resolve these negotiations,
and its ambiguities have been subject to judicial review. The court’s interpretation of
Congress’s intention during the writing of the Act has had a profound impact on how
OSHA now attempts to fulfill its mandate through rulemaking (Michaels, 2008; Kerwin &
Furlong, 2010; Vogel, 2012), how it negotiates its responsibilities, and how it charts
relationships among workers, industry, and the state.
A key reason so much of the hearings focused on establishing risk is due to the
1980 decision in Industrial Union Department, AFL-CIO v the American Petroleum
Institute, where the Supreme Court found that OSHA must demonstrate the existence of
“significant risk” in setting a standard. Citing the legislative debates over the OSH Act, the
Court reasoned that Congress intended the right to a safe and healthful workplace to be a
qualified right. Within reason, the state could meet its responsibility to protect workers
even when risk existed in the workplace:
But “safe” is not the equivalent of “risk-free.” A workplace can hardly be
101
considered “unsafe” unless it threatens workers with a significant harm.
Therefore, before the Secretary can promulgate any permanent health or
safety standard, he must make a threshold finding that the place of
employment is unsafe in the sense that significant risks are present and can
be eliminated or lessened by a change in practices. (Industrial Union
Department v. American Petroleum Institute, 1980).
The ruling had several implications. OSHA must show that a workplace is not safe; safe
does not mean “risk-free,” but rather free of “significant harm,” and that a new PEL would
be protective against “significant risk.” Insofar as OSHA can determine that a certain level
of exposure is unsafe and that a new PEL would be protective, OSHA can establish
standards to enact the right to a safe and healthful workplace59. This presumption places
workers at a disadvantage to industry by stating that a workplace is deemed to be safe
unless shown to be otherwise. Extrapolated to health, the issue is not the healthfulness of a
workplace, but rather the determination of its unhealthfulness, by the identification of the
presence of significant risk. Decisions in American Textile Manufacturers Institute v
Donovan (1980) and U.S. Steelworkers of America v Marshall (1981) further identified
that in rulemaking OSHA is required to use feasibility tests (GAO, 2011). These now
strongly shape OSHA rulemaking.
Since the 1980s, the U.S. has increasingly regulated environmental and
occupational risk through risk assessment, economic impact studies, and evaluations of the
technological capabilities of affected industries, buttressed by judicial interpretations of
statutes (Vogel, 2012). While often neoliberal policy is associated with less government,
not more (England, 2010), in this instance, more layers of bureaucratic requirements that
59 Under 29 U.S.C. § 654, 5(a)1, the General Duty Clause, OSHA can cite workplaces for exposing
workers to a known but unregulated hazard. However, exactly what constitutes a hazard is subject to
how the General Duty Clause is interpreted, which may differ from one administration to the next and
by different federal courts when its use is under appeal.

102
account for industry’s needs produces a context in which less regulation is actually
achieved. Strides toward “accountability” and “regulatory flexibility” have been codified
as administrative requirements for rulemaking through executive orders and legislative
action (Vogel, 2012), and have often been associated with neoliberal policies and the
“capture” of governance and democratic rights by economizing logics (Brown, 2015). This
is particularly important to consider in public comment during rulemaking, where industry
and workers are can participate and make claims on the state.
Table 2.1: Statutes, Court Cases, and Executive Orders in OSHA Rulemaking
Act/Order/Ruling Date Purpose
Administrative Procedure
Act 1946 General rulemaking procedures, including rules on publishing
notices of proposed rulemaking, public participation
Regulatory Flexibility Act 1980 Requires regulatory flexibility analysis; inclusion of small
entities in rulemaking
Industrial Union
Department, AFL-CIO v.
API
1980 Supreme Court decision that requires only significant risks be
regulated; requires risk-assessments; “Benzene”
American Textile Mfrs.
Inst., Inc. v. Donovan 1981 No cost-benefit analysis in OSHA rulemaking; “Cotton Dust”;
feasibility analysis required
U.S. Steelworkers of
America v. Marshall 1981 Establishes feasibility as technical and economic
Executive Order 12866 1993 “Regulatory Planning and Review”; requires OIRA/OMB review
of proposed and final rulemaking; submissions of draft regulation
Small Business
Regulatory Enforcement
Fairness Act
1996 Provides small businesses enhanced participation and leverage;
requires consideration of small business needs, includes CRA
Congressional Review
Act (CRA) 1996 Within 60-legislative days after publication of a standard,
Congress can overturn regulation, with presidential signature
The issue is therefore not just workers’ health. OSHA considers “what is possible
technologically, operationally, and financially” (Kerwin & Furlong, 2010, p. 58) for
impacted industries. “Rulemaking gives precise form to the benefits we enjoy under a wide
range of statutes. In the process, it fixes the actual costs we incur in meeting the ambitious
objectives of our many public programs” (Kerwin & Furlong, 2010, p. 2). Thus, OSHA
103
must meet three tests in negotiating its responsibilities: First, OSHA must establish that the
rule addresses significant risk to worker health. Second, OSHA must show the economic
feasibility of effected industries to be compliant. Finally, OSHA must demonstrate the
technological feasibility of effected industries to be compliant. OSHA gathers, analyzes,
and reports data around these objectives, including during hearings and public comment
periods. Other requirements structure the rulemaking process, expand oversight of
rulemaking to other agencies and branches of government, and include the voices of
regulated parties, namely those of industry groups (Table 2.1). OSHA had to respond to
opinions forwarded by participants, which it did in its final rule. In its responses, both in
the final rule, and also during the hearings, the requirements of rulemaking have limited
the ways that OSHA weighed its competing responsibilities.
Negotiating Risks: OSHA Responds
OSHA’s final rule responded to many arguments made during the hearings and in
the submitted comments about risk and feasibility. In its final analyses, OSHA asserted its
authority to consider mortality and morbidity when assessing risk and that its ability to
regulate risk for workers is “not a mathematical straitjacket” (OSHA, 2016, p. 16290). Yet,
when public health presenters argued that OSHA needed to more fully incorporate quality
of life concerns, OSHA pressed them for a way to quantify those issues, reflecting the
usefulness of such figures to regulators and OSHA’s efforts to negotiate its responsibilities:
MS. ROBINSON: You specifically note the ability to work, engage in
family and community life and otherwise be productive members of society,
as problems that people afflicted with silica-related diseases have.
And I’m wondering if you have any other information that you will be able
to submit to the record, maybe in post-hearing comments, so it would help
OSHA to sort of quantify these issues. (OSHA, 2014, April 1, p. 3764, my
emphasis).
104
Even if OSHA does not quantify all the risks, and as one official explained to me, has to
engage in some forms of qualitative analysis, its authority is not limitless. In its final rule,
OSHA stated that it does not have the power “to establish a utopia free from any hazards”
(116 Cong. Rec. 37614 (1970), Leg. Hist. 480–482) in OSHA, 2016, p. 16290). Instead,
OSHA can mandate that risks be eliminated as long as it is feasible for all affected
industries. Rulemaking requires OSHA to negotiate the “health” of two different bodies;
OSHA reiterated that its principal responsibility is to protect the workers—but only in so
far as regulations are feasible (OSHA, 2016, p. 16289). Significant risk may persist, as is
the case for RCS:
The Agency considers the level of risk remaining at the new PEL to be
significant. However, based on the evidence evaluated during the
rulemaking process, OSHA has determined a PEL of 50 mg/m3 is
appropriate because it is the lowest level feasible for all affected industries.
(OSHA, 2016, p. 16287)
In contrast to the many pages spent on significant risk, OSHA’s reaction to the hydraulic
fracturing industry’s argument that its flexibility is not conducive to generalization was
limited, but it did strongly contest their knowledge claims:
Due to an unusually rich data set, and the great similarity of different
fracturing operations, both with respect to the equipment used and the
current levels of control, OSHA was able to estimate which controls are
necessary to go from an uncontrolled situation to the preceding PEL and
which are necessary to get from the preceding PEL to the new PEL in the
hydraulic fracturing industry. (OSHA, 2016, pp. Footnote 28, 16472, my
emphasis).
In a separate addendum, OSHA offered other reasons why its data set on which it based its
rulemaking was representative, using some of the industry’s own concessions to contest
their broader narrative:
However, they provided no explanation why geological basin would affect
the exposure levels. API acknowledged that it does not have data to indicate
that the topography differences of basins affect exposures (Document ID
105
3589, Tr. 4126). Additionally, Chamber of Commerce witness Dr. Knutson
testified that he has seen industry exposure monitoring data from hydraulic
fracturing sites other than the data in the record, and that he did not see a
marked difference between this industry data and the data in OSHA’s
exposure profile (Document ID 3576, Tr. 500). Dr. Knutson testified that
he was unable to submit this industry data to the record due to
confidentiality agreements (Document ID 3576, Tr. 500).
Though dismissive of the flexibility argument, OSHA accepted that engineering controls
might not be fully commercially available and delayed hydraulic fracturing’s requirements
to meet the PEL with engineering controls for five years, or until June 2021. This allows
industry to meet the new PEL using respirators until that time. According to one OSHA
official, a key issue was that while from their evidence OSHA recognized that the
industry’s dust control technologies needed more time to become economically viable, they
did not provide evidence that these technologies were not going to work.
Even as OSHA interpreted significant risk and feasibility in ways more protective
of workers, how OSHA weighed its responsibilities provides industry with a discursive
space through which to reproduce narratives that reinterpret OSHA’s obligations and to
absolve itself of accountability for health risks and shift responsibility to the workers. The
central question remains as to whom these regulations are responsible. Furthermore, even
though the final rule has been enacted, industry’s narratives about OSH risk can prove
influential as the rule remains subject to challenges from outside and within the new
administration.
The final rule was published on March 25, 2016, with the first implementation dates
for the construction industry beginning September 24, 201760. Unlike other rules that were
60 Full enforcement for the construction industry began October 23th, 2017. In the intervening month
OSHA indicated that it would be accommodating to employers making ‘good faith efforts’ to be
compliant with the rule. September 23th, 2017 was a delayed start date from the original date of June
23th, 2017. OSHA indicated that it wanted to provide additional time for companies to meet compliance,
106
subject to the Congressional Review Act and were repealed when the new administration
and Congress took office, the silica rule has gone into effect, although the ultimate fate of
the rule is still unknown. During his confirmation hearings, now Secretary Acosta’s to
would not confirm if the silica rule would be reviewed under President Trump’s Executive
Order 13771 that directs agencies to review rules and reduce regulatory burdens by
repealing two rules for every new one and in a cost-neutral way. Significantly, at least in
the short term, the agency is defending the legal challenges to the rule. Immediately after
the rule was published, ten lawsuits were filed by both industry and labor organizations,
and oral arguments were heard in September 2017 at the District Court of Appeals in
Washington, D.C. These oral arguments recycled many of the same arguments documented
in this chapter. How the courts ultimately rule, in what is could be long legal challenge will
have significant implications for the ways OSHA views feasibility and significant risk in
the future as its rulemaking efforts continue to negotiate the agency’s responsibilities to
industry and to workers. On December 22, 2017, the three-judge Appellate panel including
Merrick Garland, Karen Henderson, and David Tatel, upheld the rule, including on the
basis of significant risk. The Chamber and its industry collation has not announced if it
plans to appeal the decision. Barring these potential appeals, while industry’s narrative of
significant risk was given a platform, it did not sway the final outcome. However,
industry’s narrative of its spatial and temporal flexibility did gain the industry time to
continue using respirators as a means of compliance.
Conclusions
Rulemaking is a venue in which, under the auspices of guaranteeing workers the
and its own compliance assistance information had been only recently been made available. In the years
that I have watched OSHA, delayed enforcement dates are not uncommon.
107
right to a safe and healthful workplace, OSHA formally negotiates its responsibilities to
workers and to industry, due to the requirements established by the state, but also the
history of vested interest groups. Rulemaking establishes the state with dueling obligations
to protect industry and workers, which it attempts to rectify “rationally” through three tests
of significant risk and feasibility. The evidentiary basis on which OSHA is to balance these
responsibilities opens rulemaking to comment from regulated and affected parties.
Tracing the negotiation of responsibility through this participatory mechanism
illustrates how certain ways of conceptualizing OSH are reproduced. In this instance,
industry uses this space to interpret data and circumstances to distance itself from
accountability to the state and transfer responsibility for acting on health risks to workers.
It should now be clear that the neoliberal economic world view, which
posits individual responsibility as the only meaningful level upon which to
understand responsibility, functions as one of these irresponsibility
machines. (Tronto, 2013, p. 61).
What Tronto makes clear is the varied ways that not only individual responsibility is
reinforced by the discourses and institutional processes within neoliberal institutions, but
moreover, how individual responsibility serves to absolve other actors of their compliancy
within unjust systems.
Although rulemaking embodies the state’s paternalistic responsibilities in terms of
protecting the economy and working people, its rules and requirements facilitate the
perpetuation of long-standing narratives about responsibility for workers’ health. Industry
perpetuates narratives that value workers through their deaths and advances “feasibility”
arguments wherein due to its flexible configurations, it can only fulfill those obligations to
protect workers’ health by shifting that responsibility onto workers. Rulemaking is not
divorced from broader processes of the state, industry and society. As Mitchell writes, these
108
processes are reciprocal.
The power to regulate and control is not simply a capacity stored within the
state, from where it extends out into society. The apparent boundary of the
state does not mark the limit of the processes of regulation. It is itself a
product of those processes. (Mitchell, 2006, p. 175).
The arguments that circulate and perpetuate through rulemaking are historical vestiges, but
also reflections of current power dynamics that shape the relationships between workers,
the state, and industry. The decisions the state makes about regulating health are complex,
political negotiations that weigh competing truths about not only science and knowledge
but about which bodies’ health –workers’ or industry’s– matter most.
Rulemaking makes plain the ways that the state’s interest in health risk is a tenuous
negotiation. By tracing the negotiation of the states’ responsibilities, OSH rights are shown
not to be absolute but rather to embody a concern for both the fleshy, bodily health of
workers, and the immaterial discursive vitality of industry. The ambiguities of the state’s
negotiations reveal some of the consequences of locating responsibility within a non-
human agent, whose health can be threatened and evaluated against a living body.

109
3. Chapter 3: Enforcement: Spatial and Temporal Practices Absolve
Responsibility as Liability
When I drove around parts of rural Pennsylvania, West Virginia, and Ohio, in areas
beset with oil and gas development from hydraulic fracturing between 2013 and 2015,
activity was everywhere and nowhere. Equipment facilities and man camps lined highways
and state roads. Twin axles and crew cab trucks whizzed by on country lanes. Pipeline
right-of-ways cut through thick forest. Yet, the nexus of this activity, the well pad, was
often obscured by the landscape. Forest and hills made it difficult to spot wells from the
road. There were clues about its locations: posted signs and newly bonded roads,
sometimes caravans of industry vehicles marking a path to the site. In my efforts to observe
industry activity—what one friend called a “safari”—I utilized state-permitting data and
GPS coordinates, and downloaded phone apps with rig locations; even with these tools, I
still drove around for hours searching for well sites. In some cases, members of a nearby
community told me where to find well sites. Other times, I trusted that twenty or thirty
minutes on a single lane road up a hill or down a dirt path would eventually lead me to a
well, but often decided not to trespass on roads marked private, even when that seemed the
only way to get to the well. Frequently even when I did find a well site, there was no one
around, and nothing was happening. In south-central Texas where the oil and gas industry
is ubiquitous, rigs were prominent in its flat landscapes. Yet, even with visual cues, it was
not always possible to find the path to get to the well site. Wells were often at the end of
circuitous dirt roads that acted as dividing lines between farmland. I took roads unmarked
on maps to drive towards a rig, but there too I found inactive sites.
The temporality and the rurality of many landscapes of hydraulic fracturing matter
for the state’s role in enforcing its notions of responsibility for OSH. These aspects

110
challenge how the state ascribes blame for hazardous and unhealthy workplaces–
inspections–and signal the need to think creatively about the ways responsibility for
healthy workplaces is imagined and administered.
This chapter examines how the state enacts its ideal distribution of responsibility.
In this schematic, OSHA regulates employers who regulate employees
(OSHA→Industry→Worker) to understand the implications of a responsibility paradigm
within health governance. This chapter argues that OSHA enforcement utilizes a
responsibility-as-liability61 paradigm that constrains its efforts to protect a worker’s right
to a safe and healthful workplace. This approach pursues causal connections to ascribe an
outcome to an action and actor. As Young writes, “…to identify some factor or agent for a
condition means to absolve others. But such a monocausal conception is implausible”
(Young, 2008, p. 18).62 It prescribes a remediation but fails to contextualize disease risk
within broader processes and ultimately reproduces limitations on the state’s authority to
interfere in private workplaces.
I illustrate how responsibility-as-liability focuses on the enforcement of regulations
in which individual companies are held responsible for creating unhealthful working
conditions captured by a snapshot of exposures at a particular place and time. The chapter
shows how this model is confounded by the flexibility of the hydraulic fracturing industry
and the contexts in which this flexibility unfolds. The hydraulic fracturing industry operates
61 Here I am using liability to mean ways of finding an employer legally responsible for a discrete
instance of failing to meet the state’s standards for workplace conditions. 62 Young (2008) is motivated to address ways that individuals and institutions “distance ourselves from
responsibility” (p. 169) for structural injustice. Thus, her primary focus is on civil society and non-state
actors. Young is concerned by the tendency to look to governments for the provision of social needs
and the pursuit of social justice, despite the state’s failings across multiple contexts, and the successes
of private interests in arguing against a strong state. “So what is missing from the “It’s not my job–it’s
the government’s job” position is the recognition that the state’s power to promote justice depends to a
significant extent on the active support of its citizens in that endeavor” (Young, 2008, p. 169).
111
with spatial and temporal flexibility utilizing a subcontracted structure. This has material
consequences for the techniques OSHA uses to regulate hydraulic fracturing and silica
exposures. OSHA lacks the enforcement tools and the means of collecting information
necessary to match industry’s structure and spatial and temporal patterns. OSHA’s focus
on blameworthy events denies the broader structures under which OSH problems emerge
and are intensified, and through which industry is able to avoid oversight. The chapter
shows how this notion of responsibility limits OSHA’s conceptualization of OSH
problems, making it unable to account for the structural dynamics that shape unhealthful
workplaces and that confound enforcement techniques. Tracing the practices of enforcing
responsibility through inspections reveals how inspections techniques and rationalities
reinforce limitations on the state’s authority to regulate private workplaces. By diagnosing
practices as healthful or unhealthful, OSHA’s enforcement logics overlook modalities of
responsibility outside the responsibility-as-blame paradigm that could provide alternative
methods for achieving OSHA’s mandate. Other theorizations of responsibility can
approach OSH regulation as forward-looking by focusing on the structural conditions that
support and maintain unsafe working conditions and that challenge oversight.
Responsibility as Liability, the Subcontracted Workplace, and Health Exposures
The modern workplace has been profoundly transformed. Employment is
no longer the clear relationship between a well-defined employer and a
worker. The basic terms of employment—hiring, evaluation, pay,
supervision, training, coordination—are now the result of multiple
organizations. Responsibility for conditions has become blurred (Weil,
2014, p. 7, my emphasis).
This chapter shows how the context and structure of hydraulic fracturing work blur,
in a blame-worthy sense, responsibility for health risk. The model of OSH responsibility
offered by OSHA is noteworthy, as it focuses on providing a context in which workers
112
should be able to act healthfully but does not guarantee them a bodily state. This means
that OSHA does not assure that workers are free of illness or a certain level of bodily
integrity. Rather, it means that workers should be provided a workplace the state deems
unlikely to negatively impact the body because of its conditions. For Young (2008),
theories of responsibility that focus blame insufficiently addresses structural roots of
injustice and obfuscate how normalized behaviors reproduce those injustices.
A blame language can be inappropriate and unproductive in the context of
issues of structural injustice because it tends to divide people….This
oversimplifies the causes of injustice and renders most people
comparatively unable to help remedy the problem (Young, 2008, p. 116).
As she explains further “the purposes of social practices of finding guilty, blaming,
finding fault, holding strictly liable are to focus on particular agents in order to sanction or
demand compliance from them alone” (2008, p. 105). OSHA’s enforcement in the oilfield
is an exercise in ‘finding blame,’ where individual companies are held responsible for
discrete hazardous conditions. OSHA’s standards enforce “a normal set of background
conditions that we consider morally acceptable if not ideal” (Young, 2008, p. 107) that
ostensibly provide workers access to a “safe and healthful workplace.” Young considers
forward-looking relationships and those that address structural injustice, finding these
liability-rooted ways of ascribing responsibility inadequate. For Young, blame, fault, and
liability, are not synonymous with her theorization of responsibility.
The chapter shows practical reasons why a focus on a blame-worthy event, one in
which liability can be identified, rooted in OSHA’s inspections is insufficient to address
the hazards of hydraulic fracturing workplaces. Most significantly, the logistics of locating
a well site and arriving during an exposure confound enforcement efforts. Structural
conditions of hydraulic fracturing produce environments where unsafe, and hazardous
113
working conditions flourish, specifically through just-in-time practices and “fissured” or
subcontracted workplaces that segregate workers based on tasks. These structures bifurcate
industry actors, making contractors (and the workers they employ), beholden to the needs
and desires of overseeing operators.
To underscore the unjust processes produced and maintained by subcontracting, the
chapter draws on others who have written about its how it facilitates contexts in which
industry can avoid oversight. Subcontracting has been a specific strategy in industries to
reduce and distance overseeing employers from responsibility, a strategy of reorganizing
labor well noted by geographers over the last several decades (Harvey, 1989). As Collins
(2003) writes, “subcontracting introduced new layers of social relations between workers
and owners and altered the legal relationship between employees and the firm” (p.61).
Subcontracting blurs who is responsible in the workplace. These altered structures
confound the states’ responsibilities to regulate employers and ‘protect’ workplaces under
the auspices of OSH (Weil, 2014).
Charting the utility of these flexible work arrangements in producing advantages to
employers while increasing the precariousness for workers, Coe (2012) agrees with Wills’
conviction that subcontracting is “paradigmatic” (2009, see also Wills et al., 2009), writing,
Wills (2009) convincingly diagnoses subcontracting as the central
mechanism involved, which both brings workers into downward
competition with each other and can make it hard to discern the ultimate
employer of precarious workers. (Coe, 2012, p. 275, my emphasis).
It is not just workers who are in downward competition but also firms. For Weil (2014),
flexibility is a fundamental component of the “fissuring” of workplaces, the stratification
of firms, and the increased vulnerability of workers. For him, the larger concern is where
flexibility allows actors “to skirt the social costs resulting from that flexibility” (p. 288).
114
“Fissured” represents a cleavage of activities wherein “it has become far less expensive to
contract with other organizations–or create new organizational forms–to undertake
activities that are part of producing goods or providing services” (Weil, 2014, p. 44), a key
insight into the organization of the oilfield. Additionally, for Benner, flexibility has two
key senses relevant to considering OSH: flexible work and flexible employment (2002).
Flexible work “refers to the actual tasks performed by workers in the process of economic
activity, while “employment” refers to the contractual relationship (both explicit and
implicit) that shapes labor control and compensation” (Benner, 2002, p. 15). OSHA
regulation mostly focuses on the regulation of work, yet flexible employment shapes when
and where its standards apply and is what OSHA lacks the authority to regulate.
This chapter uses these insights to show how the flexibility of location and
organizational structure can exacerbate health governance oversights by exploiting the
geographies of resources that locate work in remote and difficult to find locations. It
suggests that health geographers not only can consider how the relations of work influence
health risk, but also how the state’s efforts to regulate health are confounded by these
structures of flexibility. Insofar as social costs stem from flexibility, and that flexibility
allows firms to allude oversight, OSH regulatory intervention should be reframed to
regulate flexible structures of work63, rather than discretely as an action-actor-consequence
paradigm of responsibility currently employed by OSHA. Walker’s (2008) attention the
practices of responsibility rather than their ideal state, puts a finer point on this emphasis.
As it connects to the way the state finds blameworthy events in workplaces, and
63 Young (2008) relies on a loose meaning of structure as a constellation of institutions, actors, and
processes, and oscillates between using the terms structure and structural processes. ‘Flexibility’ here
considers the ‘structure’ and ‘structural processes’ that contribute to unhealthful working conditions,
and which corporations and state actors may be seen to be responsible in perpetuating.
115
thus finds liability in particular employers, this chapter draws upon health geography’s
emphasis on the ways that ‘objective’ and ‘scientific’ thinking give legitimacy to and shape
how relationships between health, disease, and places are identified. Sampling done by
industrial hygienists utilize tools of rendering exposures ‘perceptible’ that signal the
‘realness’ of workplace risk (Murphy, 2006)64, but also are subject to epistemological and
material constraints like weather, wind, and being at the worksite during an exposure. As
Murphy writes,
Chemical exposures were, and are, notoriously difficult to prove. They are
composed of molecules invisible to the unaided eye (if not the nose) and are
usually only investigated well after the initial moment of their presence
(Murphy, 2006, p. 83).
The concerns recognizing context and structural processes in the production of human
health risk are also informative here. Horton, for example, charts the role farm organization
plays in farmworker heat death, and questions how this is related to broader labor and
immigration policies (Horton, 2016). Here, I build on such analyses by considering how
the subcontracted organization of the oilfield intersects with the underlying assumptions
that guide how the state seeks to protect workplaces from silica hazards. I critique the
techniques of identifying exposure as a way to ascribe blame onto industry by illustrating
how this method absolves industry from responsibility for producing hazardous conditions
in its failures and insufficiencies. I further place these processes within dominant narratives
of the oilfield and of OSH that not only reinforce the idea of individual responsibility, but
64 Murphy explains this further how “exposures are contentious events. They involve litigation, blame,
neglect, and suffering” and how the way we conceive or exposures are rooted in epistemologies that
have been developed in producing science such “chemical exposure and their health effects as uncertain,
that is, as events that one cannot do something about” (2006, 10). While significant, this chapter does
not delve into the campaigns of uncertainty that enshroud sampling, litigation of OSHA findings, or
epistemologies of OSHA investigators trained in industrial hygiene.
116
incentivize particular types of care and belonging that can serve to justify workers’
exposures to risk. Varied forms of caring valorized by narratives in the oilfield as workers
supporting the nation or their employer can clash with other forms of caring within OSH
objectives such as caring for one’s coworkers and returning home to one’s family and
friends. I make these arguments by drawing on interviews with OSHA65, participant
observation at oil and gas industry conference and trade events, my trips driving around
parts of the Utica, Marcellus and Eagle Ford Shales (PA, OH, WV, and TX), and textual
analysis of inspection case files66.
Fragmented Oversight: Institutional Context of OSHA Enforcement
In the late 19th and early 20th centuries, emerging liberal rationalities displaced a
classical view of the relationship between the state, the market, and society, at times
embracing moralistic and paternalistic roles for the state, including intervening in the
relationship between employers and employees (Rogers, 2009). Yet, surrounding these
debates were key tensions regarding the degree to which employers, rather than employees,
bore responsibility for these circumstances. Some championed regulations rooted in the
“producer pays principle” which held employers accountable for the hazards and harms of
workplaces. Others saw workers as individuals who rationally chose employment
65 I contacted OSHA offices in Pennsylvania, Texas, and Oklahoma in 2014 and 2015, focusing on
offices that had conducted silica inspections. Broadening my analysis in 2017, I began calling offices
in areas with high hydraulic fracturing with more general questions. After hearing several times that
OSHA does not do interviews because it is an “enforcement agency,” one office suggested that I send
in a formal request. I sent letters to 23 area offices that had reported inspections under a category used
for hydraulic fracturing and followed up with calls. This category captures more than just hydraulic
fracturing. Thus, three offices responded that they did do hydraulic fracturing inspections. Of those
remaining, I spoke with officials in 12 offices, sometimes with more than one person. These interviews
covered general issues on oil and gas inspections and hydraulic fracturing activities specifically. 66 Case files document inspection activities, and communication, fines, and abatement activities. These
include inspector narratives, checklists, and worksheets inspectors have jotted and sketched and
sampling reports. They also contain correspondence between OSHA and employers, including emails,
exposure data, remediation plans, and employer health and safety manuals.
117
opportunities where dangerous work would be rewarded and incentivized through pay
(Dorman, 1996, p. 32).
As the state weighed in on these concerns, it approached OSH issues in primarily
three ways: legal liability, worker compensation, and factory legislation (Noble, 1986).
Legal liability gave workers the ability to sue their employers for injury and illness. The
burden of proof was high and required proven willfulness on the part of employers (Bale,
1987; Sellers, 1997). As discussed in Chapter 4, the workers’ compensation bargain in the
early 20th century provided workers with no-fault insurance for the injuries they faced at
work but prohibited workers from accessing tort law in all but a few circumstances. Factory
legislation, an idea imported from Germany and England (Noble, 1986; Rogers, 2009),
involved the setting and enforcement of standards through investigations beginning in the
mid-nineteenth century. Its precedent would underpin “command-and-control regulation”
that enables the State to require employers to meet standards, and how (Noble, 1986, p.
30). This strategy engenders notions of blame.
Turn-of-the-century reformers advocated for regulatory interventions to influence
the organization of work on the shop floor such that workers could make rational decisions
for themselves (Noble, 1986, p. 19; Dorman, 2006, p. 37). Through factory legislation, no
longer were employees solely responsible for uncertain outcomes. Employers now had
obligations to meet standards, could be blamed for producing the hazard and the hazardous
outcome, and possessed responsibilities to remediate the danger. Over the next several
decades, the states primarily developed workplace standards and led workplace safety
efforts (Asher, 1991). Federal involvement was limited. The USDOL gained Cabinet-level
status in 1913 (MacLaury, 2016 (1988)) and its initial efforts focused on protections for
118
workers, particularly federal employees. By the 1930s, USDOL had broadened its purview
to aspects of private workplaces, again particularly for wages, overtime, and oversight of
federal contractors (Asher, 1991), but most OSH regulations remained at the state-level
until the 1970s (Noble, 1986).
In the 1960s, labor activists found traction in Johnson’s Great Society which sought
to concentrate social regulation at the federal level (Noble, 1986; Asher, 1991). Late in the
Johnson Administration and at the beginning of the Nixon Administration, OSH concerns
were drafted as legislation in what would become the OSH Act of 1970 (Noble, 1986). The
Act proved to be a multidimensional compromise between labor and business interests in
its final form (Vike, 2007). Labor gains were significant in the legislation. The Act placed
OSHA within the USDOL—much to the chagrin of industry—where it held powers to
establish and enforce OSH standards. The Act also allowed for workers’ involvement in
standard setting and workplace inspections. Nonetheless, industry also had some victories.
The resulting regulatory apparatus for OSH governance was fragmented; the compromise
had limited OSHA’s powers by diffusing oversight of compliance, research, and standard-
setting among OSHA, state-plan programs, NIOSH and the Occupational Safety and
Health Review Commission (Vike, 2007, p. 573)67. OSHA also did not take over OSH
activities from the Bureau of Mines. In 1977, the Mine Safety and Health Act created the
Mine Safety and Health Administration (MSHA)68. MSHA and OSHA oversee most
67 Other federal and state agencies overlap with OSH issues including protections for workers
for overtime, minimum wages, and break-time. Under USDOL, the Wage and Hour Division (WHD)
enforces the Fair Labor Standards Act and its provisions for worker classification and compensation.
The Employment and Training Administration funds the development of apprenticeship and safety
awareness programs and funded ShaleNET, a consortium of northeastern colleges and universities,
$19.9 million to develop training for shale workers (ShaleNET, 2016). 68 This replaced the Mining Enforcement and Safety Administration established in 1973 that had
succeeded the Bureau of Mines first established in 1910 (MSHA, n.d.).
119
private workplaces but enforce their own health and safety standards. For example,
OSHA’s new PEL for RCS applies to hydraulic fracturing. The workers who mine the
silica sand used in hydraulic fracturing, however, are covered by MSHA’s more permissive
standard. Although a new MSHA standard was proposed under Obama based on OSHA’s
new standard. It is unclear if will be pursued under the Trump Administration. Conversely,
MSHA has a standard for Diesel Particulate Matter (DPM) in underground mining. While
DPM is a concern during hydraulic fracturing when site configurations concentrate
emissions from frac pumps, OSHA does not have a PEL for DPM, as I learned from NIOSH
presenters at an industry OSH conference.
Today, OSHA enforcement and compliance falls to ninety area offices divided
among ten regions. As has been reported by the GAO and was marked in my interviews,
individual area and regional offices retain different operating cultures and may implement
geographically focused programs, even if the standards they enforce are the same. Within
the ten regions, twenty-eight states have implemented State Plans which must include
standards as stringent or more stringent than federal regulations69. However, state-plan
enforcement varies widely (GAO, 2013, p. 4) and has repeatedly garnered scrutiny and
calls for more federal oversight and standardization (GAO, 1982, 1988, 1993).
Federal OSHA offices cover some of the most intense areas of hydraulic fracturing
for unconventional fuels including Pennsylvania, Texas, and North Dakota. Still, of the
3,521 inspections conducted for Support Services in the Oil and Gas Industry between 2006
and 2016, State Plan inspections accounted for 21% (746) of inspections. The most were
69 Of these twenty-eight state plan states, six cover state and local government workers. The remaining
twenty-two (twenty-one states and Puerto Rico) cover private and public workplaces.

120
conducted in New Mexico (282) and Wyoming (196)70. States and localities (i.e.,
townships, cities, and municipalities) can levy regulations pertinent to OSH, and RCS
specifically, as seen in California, New Jersey and several cities (CPWR, 2016)71. Both a
practical and theoretical concern, Blomley and Baken (1992) and Blomley (1990), question
at what scale the state should regulate worker safety concerns, with a particular focus on
the role of local and community regulations of OSH issues. Given the stagnation of many
federal OSH reforms in the last several decades, OSH activists and labor scholars
increasingly have looked to state and local regulation to achieve better OSH oversight.
OSHA has few governance mechanisms that account for industries that do not
follow the vertical, factory models around which many early regulations were built. RCS
poses additional challenges as exposures are fleeting and impacted by weather conditions
and well locations are often remote. OSHA faces significant hurdles to implementing new
techniques to account for these issues. How hydraulic fracturing’s flexibilities complicate
efforts to investigate exposures to silica illustrate this.
Responsibility-as-liability: Inspections
OSHA penalties are a critical enforcement strategy meant to deter
employers from violating safety and health standards. (GAO, 2004).
Inspections encode a logic that makes employers responsible for hazards and
hazardous outcomes in workplaces. OSHA regulates employers who regulate employees.
This distribution of oversight seeks to temper workers’ responsibility to maintain safe
working practices and instead focuses on the context produced by an employer that can be
70 Wyoming has developed oil and gas industry-specific OSH regulations. 71 Canadian provinces impose OELs for most substances. For silica, these OELs range from
0.025mg/m3 for example in Alberta to .1 mg/m3 for example in Ontario (Government of Alberta, 2009;
Ontario Ministry of Labor, 2015).

121
hazardous: the workplace. This engenders responsibility-as-liability enforced through
inspections, fines, and abatement requirements where employers are found responsible for
the condition of their workplaces. For Young,
The point of locating guilt or leveling blame is precisely to single out: to
say that this person, or these people, by virtue of what they have done, bear
direct moral and often legal responsibility for the wrong or a crime, whereas
others do not because their actions have not done the deeds. The practice of
blaming or finding guilty requires singling out some from others, and
applying some sanction against them or requiring compensation from them.
(Young, 2008, pp. 76-77).
Through its enforcement efforts, OSHA finds a company responsible for exposing a worker
to risk and also levies of fines. First, OSHA has to get on site to document the blame-
worthy event for which it can find employers liable for failing to meet the state’s standards.
How the state can get on site is mediated by complex rules, procedures and processes with
serve to limit the state’s authority to regulate private workplaces.
Whether an inspection is the result of a complaint, referral, or programmed, a
Compliance Safety and Health Officer (CSHO) conducts an inspection, and in the case of
health or RCS inspections, is often a certified industrial hygienist. Protocols identified in
the Field Operations Manual (FOM), among many other directives and guidance, detail
how CSHOs should enact OSHA’s authority. A typical inspection begins after a CSHO
arrives and gains entry to a facility. Once onsite, the CSHO conducts an opening
conference, informing employers of the inspection and their rights, and requesting
documentation and records. A CSHO then performs a walk around, interviews employees,
and collects samples, notes, photographs, and video of the worksite. The inspection ends
in a closing conference during which the CSHO and the employer discuss violations,
employer rights and responsibilities, and potential hazard remedies. It warrants emphasis
that these inspections do not keep pace with hydraulic fracturing activities. The code most
122
likely to capture hydraulic fracturing contractors in the U.S. between 2007 and 2016 (3228)
accounted for 3.1% of the total rig count in that period (103,259)72. These are significant
considerations given that inspections are a primary means by which OSHA implements its
model for responsibility.
Subcontracting and Flexible Work in the Oilfield
The flexibility of the industry can hamper OSHA inspections. In the oilfield,
subcontracting produces a workplace theater where multiple teams work among each other
completing tasks with chemicals, electrical sources, large machinery, and equipment under
high pressures. Subcontracting was on view during a well site visit I took with Penn State’s
Marcellus Center for Outreach and Research. After driving along back roads through
forests and farmland deep into northeastern Pennsylvania, we arrived at a well site at the
start of a frac stage73. Piling out of a fifteen-passenger van, we donned fire-retardant suits,
shoe covers, hearing and eye protection, and hard hats, before being introduced to our
guide, a representative of the site’s operator, Southwest Energy. A large white man likely
in his thirties, he asked us to be cautious with our photography; one of the servicing
companies completing the frac did not want their name to be visible in any pictures. As he
showed us around the site, we walked across the well pad liner, avoiding pipes and stepping
over hoses at least a foot in diameter. In the bright sun of a late summer morning, it was
loud and hot. The area vibrated, and the noise grew louder as the engines supplying
72 U.S. EIA data for rig counts from 2006 to Nov. 2016. Given three codes that may capture oil and gas
activities, (213112 (inspection count: 3228), 213111 (inspection count: 2392), and 211111(inspection
count: 1095) this rises to 6715, or 6.5% of all rigs. However, these figures overestimate well sites
inspected as they capture more activities than just those at a well. 73 Frac is standard short-hand for hydraulic fracture; the lack of the ‘k’ in this spelling is in keeping with
industry practices. Frack is commonly used by fracktivists, or opponents of the industrial practice.
However, it is used on industry-supporting merchandise where Frack replaces its obscene counterpart
in slogans.
123
horsepower to the frac ramped up. Workers from different contractors moved around us.
One, his full-piece respirator reflecting the sunlight, wore long gloves extending up his
arms to protect him from the acids he was handling. Others dragged hoses. Some wielded
wrenches three feet long. We climbed a ladder to the top of a sand king so we could take
in a full view of the site; the scene highlighted groupings of workers each engaged in their
tasks. Back on the ground, the representative explained how he did not employ many of
the workers we saw involved in tasks. Rather, we were observing subcontracting at work.
In the oilfield’s subcontracted structure, an operator employs multiple
subcontractors to engage in task-specific activities for short periods, and for many basins,
in remote locations. Sometimes referred to as a kind of “organized chaos,” this situation is
called SIMOPS (Simultaneous Operations) and can impact the health and safety of
operations negatively. As Weil explains:
A second characteristic of the fissured workplace in subcontracted
organizations is coordination problems: the more tasks are divided among
different business entities, the harder it becomes to coordinate them. The
private incentives pushing toward fissuring the workplace thereby create
social problems and costs in the form of increased safety and health risks
and, at worst, deaths at the workplace (Weil, 2014, p. 100).
Subcontracting is neither a new phenomenon nor unique to oil and gas. In this iteration, it
exploits advances in speed, technology, industrialization, and labor specialization. It
influences industry’s competitive structure, benefits from hazy employment relationships,
and ultimately reduces costs by maximizing the movement of people and equipment.
Subcontracting impacts which workers are exposed to silica, the circumstances
under which employers expose workers to silica, and if and how OSHA can hold employers
blame-worthy for exposures. Employees most likely to be exposed to silica work for
subcontractors who specialize in hydraulic fracturing completions. These can be large
124
firms like Halliburton, Keane, or Baker-Hughes, or smaller contractors. Sand teams may
work at one site over the course of a day or may move between several sites, potentially
incurring exposures at each location. These servicing companies compete for contracts
from operators. Contracts may be awarded based on a subcontractor’s record of safety and
contractor rating systems and safety programs, dynamics that incentivize less reporting of
injury and illness, in addition to their regional availability and cost of services. This system
distances operators from its risks and social costs, by design. Operators benefit from a
system where they can set high safety standards, but often ignore patterns where
subcontractors, and their employees cut corners to meet production demands, including the
speed with which they complete tasks, and through cultures of under-reporting. In fact, in
the STEPS video introduced in chapter 2, Safety Manager Ted, hurries his own safety
training, saying to new guy Joe, “Well, it sounds like they’re starting to pump [a stage]
now, so we better get through this so you can get to work” (Lawhorn-Cryden, 2015). Even
in a safety video produced by a safety organization, the need to get to work and quickly is
so normalized that it takes precedence over the need to explain health and safety hazards
of the workplace.
This structure and the discourses surrounding OSH reinforce a system wherein
there are disincentives for hydraulic fracturing workers to follow OSH procedures, despite
the “commitment to safety” proffered by industry leaders. Health and safety courses,
workshops and conferences, encourage workers and safety managers to think of themselves
as part of their employer’s team, enrolling them in this structure. OSH training materials
and at OSH conferences emphasize particular forms of sanctioned care and emotion often
rooted in an idea that workers have families they want to get home to. These sanctioned
125
forms of care incentivized OSH practices by portraying workers as striving to get home
safely to their families and helping to keep coworkers and brothers safe, but also while
producing energy for the nation. Repeatedly, workers are asked not to just consider their
own risk, but to keep in mind those at home, and one’s family on the oilfield.
During the 2014 OSHA Oil and Gas Conference, one oil and gas executive’s
plenary talk discussed safety as an emotion; he and other leaders tearfully described
wrenching experiences of telling wives and mothers that their men were not coming home
after fatal accidents. The concept of “making safety personal” was a repeated mantra, the
idea that in order to help workers be safe, they had to care about what it would mean for
their own loved ones. In emphasizing a particular kind of sanctioned paternalistic emotion
to take care of one’s family and friends, and one’s employer, these narratives underscore
that workers need to look out for themselves so as to not put employers in these emotionally
compromising positions. Tensions surrounding how hazards should be managed, if they
should be managed, and by whom, run through these OSH discourses. OSH narratives are
inconsistent. Industry’s position that they are responsible for certain OSH concerns
contrasts with narratives about workers’ responsibilities to their employer and family, and
risk-taking to match demands of work.
Normalized and valorized risk shapes the responsibility narratives in the oil and gas
industry that respond to these hazards and are significant to modalities of OSH that focus
on behavior-based safety, mantras of ‘zero-incidents,’ or efforts to ‘get home safe.’ Here,
OSH works to institutionalize care at work. Significantly, caring at work facilitates shifting
responsibility to the individual worker. At the OSHA conference in 2014, “making safety
personal” was a repeated mantra, the idea that in order to help workers be safe, workers

126
had to understand how the things they cared about would also be at risk if they performed
work unsafely.
Hope is not a method. I say again, hope is not a method. By that I mean,
hoping to eliminate workplace fatalities is not a method for achieving that
noble vision. The elimination of death as an indirect consequence of our
efforts to explore for and produce the energy resources needed to fuel a
global economy requires multiple strategies. I firmly believe that one such
strategy that we must pursue to eliminate workplace deaths is by making
safety personal for every man, woman, and child in our workplace family.
(Warren Huber, 2014 OSHA Oil and Gas Conference, my emphasis).
To make safety personal frames workers’ care for their families and other co-workers as
an emotion endorsed by the industry and warranted by the risks workers face in the oilfield.
Workers’ emotion could help keep them safe. This acceptable form of care in the
workplace, while possibly a pragmatic strategy, also connects safety to personal
responsibility. First, being responsible becomes a function of caring in the right way, and
second, a lack of care could lead to irresponsible, unsafe behavior. Notably, this executive
also takes this opportunity in his speech to also distance the industry itself from direct
culpability for fatalities in the industry.
In the context where risk is normalized74, the industry has utilized OSH approaches
from other high hazard industries, including the military and has explicitly looked to hire
ex-military personnel. The relationships between oilfield OSH and the military are quite
explicit. The basic oilfield awareness training includes a unit on counterterrorism, OSH
conferences feature military speakers, and workshops draw on military protocols as ways
to manage OSH. Former members of the armed forces were often asked to stand up during
74 OSH has often grappled with questions of who needs protection and how much. Sellers (1997) uses
coal mining songs to illustrate the persistent imaginary of industrial workers as a white man who does
not need protection. That most OSH laws reflect risks in ‘high hazard industries’ also further illustrates
how OSH has reflected only certain kinds of laboring bodies (Murphy, 2006).
127
conference plenaries; applause would erupt as many men rose from their seats for
acknowledgment. Former military members I interacted with during my research often
referred back to their service in Iraq or Afghanistan as being higher risk than oilfield work
and that they had faced death repeatedly.
The military is a sector in which employment is often idealized through its
relationship to sacrifice and where the risks of work are noble. Comparisons between the
oil and gas industry and the military are more pernicious given the discourses that surround
the industry, both those in support and those against. In addition to often being described
as an industry that fuels the nation, as exemplified by the quote in the previous paragraph,
pro-industry events draw directly on symbolism within US nationalism (see Figures 2.8
and 2.9). Films such as Frack Nation and the Marcellus Shale Coalition’s Truthland (a
response to the anti-fracking film Gasland) make impassioned arguments about the ways
oil and gas development secures the nation and helps protect a particular white, agrarian
way of life. Imagery and rhetoric of US nationalism are used to indicate the weightiness
and significance of oil and gas development and to justify the risks workers face and
workers’ potential sacrifice. The language of sacrifice is itself a part of the rhetoric of
surrounding unconventional oil and gas development75. Dr. Terry Engelder, then a Penn
State professor in geosciences (now emeritus), made a highly controversial comment in
2010 when he described about areas developing Marcellus Shale resources in 2010 with
75 This vocabulary has become a significant dimension of anti-fracking imaginary in Pennsylvania as
well. For example, James Guignard, an English professor at Mansfield University in Northeastern,
Pennsylvania, entitled his narrative of being a cyclist, community member, and teacher in the midst of
boom, Pedaling the Sacrifice Zone: Writing, Teaching, and Living above the Marcellus Shale
(2015).The idea of a sacrifice zone is not unique to this context, but instead often refers to areas that
have been environmentally degraded due to industrial and extractive activities (Fox, 1999; Lerner, 2010;
Shade, 2015).
128
this language. It is not just risk that is normalized, but also sacrifice.
Hydraulic fracturing landscapes contain markers of these discourses. When I
started researching the oil and gas industry in the early 2010s in the Marcellus Shale region
of the northeastern U.S., I stumbled upon a recently opened safety supply store in
southwestern Pennsylvania that catered to the industry. I went inside, curious about why
workers needed to buy their own equipment if, as I had thought, employers were
responsible for providing protective equipment to their workforce. Mannequins, outfitted
in fire retardant suits and goggles, posed amidst displays of safety gloves, hard hats,
harnesses, and respirators. The clerk told me that often companies do not provide quality
equipment or enough equipment to workers; they may wear through boots, for example,
faster than they are replaced. I would later learn that some companies have used better
safety gear, like heated jackets, as a reward, but also that other workers, classified as
independent contractors, supply this equipment themselves76.
The store also captured narratives of workers I was encountering in my fieldwork.
I returned to the store several times, intrigued by the way its merchandise distilled much
of what I heard at health and safety conferences and courses, and how it commodified
individual responsibility for health through a very public expression of how governance
mechanisms for OSH lay the responsibility for health risk on workers. Indeed, as many
OSH narratives emphasize the need to get home safe at the end of the day, and to stay safe
to protect ones’ family and friends, this store also had oilfield themed children’s toys,
clothing for oilfield wives and other merchandise77. Within these contexts, OSHA enforces
76 Most of the safety equipment in the store catered to men. On a return visit, I noticed the store was
carrying women’s sizes for some safety gear, including pink fire-retardant suits. 77 The ‘family man’ is part of multiple representations of workers, as explored in Filteau’s work (2015a,
2015b). He finds multiple masculinities shape perceptions of ‘insider’/ ‘outsider,’ local, and belonging,
129
its regulations surrounding what it deems appropriate workplace conditions.
A key incentive of subcontracting is to make the ascription of responsibility more
complicated, and distance operators from the social costs of their operations. Thus, these
subcontracted working environments challenge tools that OSHA has to enforce its
regulations; some problems stem from the extent of OSHA’s authority, while others
emerge from the geography of the industry, the topography of the area, and the factors that
make measuring silica exposures through the inspection process particularly challenging.
Avoiding Blame: Barriers to Inspections
Inspections are an effort to ascribe blame to an employer when an OSH hazard is
found. While OSHA has the authority to investigate exposures, rights and courtesies
afforded employers dampen its efforts. The state lacks extensive authority to intervene in
private workplaces and can only do so under certain conditions. The state’s authority to
regulate influences where and when the state can operate, and by extension shapes the
spaces as being workplaces in which certain regulations do and do not matter. OSHA’s
arrival at a worksite does not cause a work stoppage. Instead, limitations on OSHA’s
authority mean that employers can delay inspections with certain tactics. This can mean
that the concerning exposures have dissipated before OSHA can capture measurements.
For example, an employer can insist on legal representation and that the company conduct
side-by-side sampling. As one example, a CSHO describes an investigation of RCS
exposures at a well site at the Castroglavanni Farm Pad in Pennsylvania. A company
attorney for Baker Hughes delayed OSHA’s investigation by three hours while the CSHO
waited for a representative to arrive:
themes reflected in the store merchandise. Moreover, in the merchandise, representations of oilfield
masculinities were also suffused with sexualized and racialized notions of workers.
130
On this inspection, sampling was delayed for the first 3 hours that hydraulic
fracturing was taking place due to the company’s attorney not allowing
sampling until a representative from the company arrived. The
concentration of silica for the short time sampled was 0.126mg/m3. The
concentration was almost at the calculated PEL of 0.137 (OSHA Inspection
943011, p. 51).
The inspection began at 7:45 a.m. In the inspection diary, the CSHO notes phone calls at
8:26 a.m. with the company attorney who wanted side-by-side sampling, but no one arrives
until after 11 a.m. (OSHA Inspection 943011, p. 107). Other parts of the inspection diary
record that the CSHO contacted the Area Director for guidance, per FOM directives, and
was instructed to wait for the company representative (OSHA Inspection 943011, p. 107).
Delayed by several hours, the sampling, once conducted, showed exposures just below the
PEL. Still, the CSHO documented how the employer limited the inspection and potential
unhealthful exposure to silica and illustrated how easily confounded the tools of inspecting
workplaces – exposure sampling – can be.
Employers can refuse entry and require that the CSHO return with a warrant
(OSHA, 2011). Employers may also procrastinate when producing documents reviewed
during the opening conference. One OSHA inspector discussed such tactics at length,
indicating they can be significant as silica exposures may change based on weather
conditions like rain and prevailing winds. As noted in one closing conference: “Discussed
that it was raining on day of the inspection. Lower level found” (OSHA, 2013, p. 104).
NIOSH has indicated the significance of weather and wind in exposures in its informational
material it has presented to industry members at conferences, where prevailing winds can
greatly impact the magnitude of exposures, and bear consideration when looking at the
layout of the worksite and where controlled access areas should be located. Yet, for OSHA,
weather can also mean the difference between ascribing blame or not. Thus, where a site
131
is located and how the wellsite is laid out in its configuration, and the environmental
conditions produces spaces as in compliance or not and shape the state’s ability to enforce
regulations in workplaces in important ways.
While these delays may not be wholly unique to the oilfield, other impediments to
inspections occur due to the remote location of many well sites and just-in-time practices
that coordinate the presence of infrastructure and people onsite only during their discrete
tasks. OSHA lacks the ability to regulate these spatial and temporal practices, and adapts
to, or is ultimately confounded, by them. Records that indicate that inspections may fail to
take place because CSHOs arrive to find no activity at the well site exemplify this. In this
example, when the CSHO arrived on site in response to a complaint in Tunkhannock,
Pennsylvania, the CSHO found no activity at the Baker Hughes site.
5-23-2014. CSHO onsite for inspection. Process not active. No hydraulic
fracturing activities (water trucks/sand trucks/ per crane/sand movers)
observed at site. No Inspection. (OSHA Inspection 978294, p. 001)
The phrase “process not active” recorded in the inspection diary and inspection metadata,
reflects the “hurry up and wait” nature of the hydraulic fracturing industry. Unproductive
time is costly; operators may direct resources to worksites when labor and equipment
become available. This can lead to unpredictable and hurried work. Moreover, wells may
be drilled several months before the commencement of hydraulic fracturing. According to
several OSHA officials, there are many unknowns about the actual schedule of activities.
Wells may be drilled, but not hydraulically fractured for a period. As OSHA officials who
used permitting data discussed with me, even if OSHA uses permits to identify and locate
wells, start dates can be misleading as they may not reflect the actual work schedule. As
one CSHO noted in an inspection diary of the workplace, “Never know when going to be
busy” (OSHA Inspection 981830, 2014, p. 148). Indeed, in my surveys of areas
132
experiencing shale development, it was not uncommon to find a well pad with little to no
infrastructure or to find a well pad stalled at some stage in development.
This temporal concern is a significant confounding issue facing many OSHA area
offices. Finding well sites doing hydraulic fracturing—not in some other stage of
development—was repeatedly mentioned. At some offices, using the coordinates of the
well site and other tools, they can find well sites, but it is “finding the activity” that is
illusive. It is not uncommon for an inspection to fail to go ahead as planned because the
process is discovered not to be active when the CSHO arrives. In this example, the site was
already finished with its activities, requiring the CSHO to open up a new inspection to visit
other sites.
11/9/12. opened follow up, learned the Parachute location was completed -
> process not active -> learned of new locations -> opened Program Planned
inspection. (OSHA, 2014).
While missing the activity is a concern for silica, it also applies to many other health and
safety concerns in the oilfield that emerge during particular worksite activities. As this
example, shows, OSHA does have some discretion to investigate worksites and adapt its
tools to the spatial and temporal logics of worksites. Finding no activity does not
necessarily preclude an investigation. In some instances, CSHOs may return if the well site
will be active later, but as several OSHA officials described, this is based on the
circumstances of the worksite.
04-26-2013. CSHO onsite for inspection. Employer not actively performing
hydraulic fracturing. Conducted opening/walkaround. Sampling to be
scheduled.
05-03-13. CSHO onsite for exp monitoring for silica. (OSHA, 2013).
In this example, the CSHO, finding no active hydraulic fracturing activities, returned a
week later to do exposure monitoring when the CSHO knew the site would be active. And,

133
even though the employer knew that an inspection was imminent, the CSHO still found
overexposures from the monitoring conducted in the return visit.
These workarounds are not applicable in all situations. As mentioned previously,
hydraulic fracturing is completed in stages, meaning infrastructure comes and goes with
relative frequency depending on the stage at hand. Activities can occur one day and stop
the next. Decisions about whether or not to schedule a follow-up inspection depend on the
circumstances of the worksite and are at the discretion of the area office.
There are spatial problems as well. The distribution of worksites can inhibit the
CSHO from implementing parts of an inspection. These factors may impact an opening
conference and walk around, or delay monitoring and sampling. A report from an
inspection conducted out of the San Antonio Office in Texas illustrates the difficulty
produced by the spatial distribution of worksites.
The walk-around did not occur because the drivers and sand pusher work
12 hour shifts in numerous areas within a 150 mile radius of Pleasanton.
Once coordination for an active frack sand delivery was established it was
led by Mr. Livingston on Feb 13, 2013, in attendance at the Frack site was
the local safety manager, Mr. Phil Baxter, the corporates Safety Manager,
Mr. David Serach. On the EOG site was the senior safety specialist, Mr.
Josh Onderek, CSP. Personal Air Sampling was conducted for the delivery
drivers, however drivers could be anywhere within 150 miles of the main
office for the second delivery or picking up sand from Victoria, Texas or
making another delivery of a load of sand to another frack site. (OSHA
Inspection 679378, 2013, p. 17).
When the CSHO first goes out to inspect, they learn that employees could be anywhere in
a 150-mile radius, complicating the CSHO’s efforts to monitor workers hauling and
handling sand. Still, the CSHO coordinates with the employer to inspect on a day when the
employer will be working for EOG, a large operator, and finds overexposures to the PEL.
While the workers wore respirators, the employer had provided them with insufficiently
protective N95 dust masks (OSHA Inspection 679378, 2013).

134
“Geography Detectives”: Finding Well Sites in a Landscape of Fixed Resources
It is not just finding the activity but finding the well site first that proves challenging
in some areas. As one OSHA official put it, CSHOs become “geography detectives” when
trying to find well sites in remote locations. This does not mean that a CSHO does not
eventually locate the site, but it can take a lot of time. This is true in parts of Pennsylvania
where much of development occurs in rural, often wooded areas in rolling hills and
mountains. The landscape makes it difficult to see well sites from the road, and newly
paved access roads, not always marked on maps, can make wayfinding more difficult. One
official in the northeast suggested that it was different finding well sites there than “in the
flatlands” where you can see “the dust clouds” from well site activity. As I described at the
beginning of the chapter, it was easier for me to spot wells in the flat land because towering
infrastructure was visible at a distance. Although officials reported being able to see
activity in flatter land, they also reported that it could be difficult to access the site, given
long distances, and sparse roads that lead to activity.
Another OSHA official in the northeast, indicated their luck in asking for directions
to well sites in rural areas learning to, “turn at this rock” to get to the site in question when
describing how hard it can be to find locations without reliable GPS or directions. In my
experience, finding the roads to travel to get to the well site could still be difficult, and
often the easiest way to find a well site, even with GPS locations, was to follow large
trucks, a technique echoed by one OSHA official.
When OSHA is determining if an employer is responsible for a hazard at a well
site, it matters if time is spent looking for the worksite itself. In one example from an
inspection report, the CSHO investigates a referral filed to the OSHA Area Office in
Wilkes-Barre, Pennsylvania, at 3:45 p.m. the previous day. Arriving in a sparsely populated
135
area of Bradford County in the morning, the CSHO looks for a well pad where visible dust
clouds had recorded on the YouTube video forwarded to the office. The CSHO notes
observations of other well sites, “questioning local citizens,” and referencing RigData,
described momentarily. When the CSHO finally locates and arrives at the Talisman well,
it is 12:15 p.m. and hydraulic fracturing had been completed for over four hours.
After briefly gathering information from company representatives, the CSHO logs an exit
time of 12:30 p.m. The state’s authority to regulate mediated through its ability to find well
site active, is shaped by the flexible conditions of the industry.
This outcome was predicted in an email exchange between the Area Office Director
in Wilkes-Barre and the Regional Office in Philadelphia at the time of the complaint:
“Please keep in mind that the fracking operations I would expect have been completed
since the video was taken a week ago” (OSHA Inspection 685459, 2012, p. 16). In fact,
the inspector was only late by several hours. The spatial and temporal characteristics of the
industry, ranging from where it is located to its industrial practices can elude OSHA’s
efforts. Even if the well site is quickly located, as one inspector described to me, it can be
a difficult to get to the site while the exposure is occurring, because hydraulic fracturing
takes place in stages when teams of subcontractors can come on site to complete discrete
tasks. The intersection of the organization of the industry, the location of the work, and the
techniques of finding blame for health risk work together in many ways to confound OSHA
efforts to govern health risk.
OSHA does not gather systematic data about where wells are being drilled or about
when they are doing hydraulic fracturing. From my conversations with different area
offices and review of inspections from different regions, the use of available data, be it
136
permit data from the State or RigData, varies. RigData is an industry service that provides
data about the location of oil and gas activities. I learned from OSHA officials that RigData
can be purchased by regional offices for area offices. Region 3 uses this service, which
includes Pennsylvania and West Virginia, and is purchased by the Regional Office in
Philadelphia. At the time of my conversations with Region 5 offices, which includes Ohio,
they did not.
OSHA does not have a central reporting system for employers to inform OSHA
about its activities. Thus, there is no central location that OSHA can query about the oil
and gas industry to implement an inspection when the specific site is unknown. This
contrasts from construction, where OSHA has a database that aims to maintain geographic
information of worksites (OSHA, 2011, pp. 2-10). When I asked on official why no efforts
had been made to create a reporting system, they explained that OSHA is limited in how it
can target locations for inspections and that changes to the current standards were
impractical. Were OSHA to require a specific industry to report where they were operating,
they would have to go through a rulemaking process, with regulations subject to the
Paperwork Reduction Act, something that has limited what OSHA has considered
requiring for reporting.
Available information about well activity from the state can vary state-to-state.
Many states, like Pennsylvania, report spud data, or the dates wells are drilled, but this does
not provide additional information about other stages of development which may be weeks
or months later. Arkansas, by contrast, provides detailed geographic information on a
weekly basis on well activity from permits to completions that CSHOs can use to find well
sites in certain stages of activity. The Texas Railroad Commission also has more specific

137
information, although not publically available, and in some instances, may work with
OSHA to use these data for inspections. However, this is dependent not only on the staffing
and resources of an individual area office but also the institutional capacities of the
commission. Other states do not make this information available, a situation that frustrates
some OSHA officials with whom I spoke. While proxy databases exist regarding wells that
have been drilled and rig locations that might serve to identify hydraulic fracturing
worksites produced by the oil and gas industry (RigData), area offices do not coordinate to
share the types of tools other area offices are using. A mechanism to locate well sites would
be helpful even if it would still be reactive to the structural conditions emerging from the
flexibility of the industry and the geography of the shale basins that challenge enforcement.
However, exposures are not just the product of one worksite’s condition but are situated
within the broader context of the industry’s practices, many of which belie OSHA’s
oversight efforts.
Avoiding Categorization: Fissuring, Subcontracting and NAICS Codes
The specialization of hydraulic fracturing—supported by and maintained by
subcontracting—is not reflected in the classification systems used to categorize inspections
and employers. Under the North American Industrial Classification System (NAICS) no
code exclusively represents hydraulic fracturing activities78. Most silica-related hydraulic
fracturing activities fall under NAICS 213112, Support Services for Oil and Gas. Hydraulic
fracturing, however, only accounts for a small portion of these activities and silica-related
activities may be under several other codes (ERG, 2013). There is no standard specific to
78 Efforts to work around these limitations include the Fatalities in the Oil and Gas Industry (FOG)
project organized by NIOSH. Although it uses NAICS codes (211, 213111, 213112), FOG examines
fatality deemed to be related to Upstream Oil and Gas regardless of its NAICS classification by
combining data sources from OSHA, BLS data and news media (NIOSH, 2015).
138
the oil and gas industry. OSHA’s General Industry Standards (29 CFR 1910) pertain in
most contexts, including those most likely to include silica overexposures, but
Construction Standards (29 CFR 1926) also apply when workers are involved in well pad
and road construction. Upstream oil and gas is also exempt from certain requirements, such
as process safety management79, some provisions of lock-out-tag-out (a process for de-
energizing equipment and electricity sources), and benzene standards.
The structure of the industry has been particularly advantageous for evading the
tools used to categorize employers for the purposes of subjecting employers to
requirements and programs. Were oil and gas industry’s injury rate higher, and less reliant
on many small-sized firms, it would be subject to more stringent reporting requirements
(King, 2016). Employers are required to report injury or illness that meet certain
“recordable” thresholds of harm; however, the way OSHA has traditionally captured the
prevalence of injury and illness has been unable to account for the industry.
Although oil and gas industry’s fatality rates far exceed the national average, its
injury rates were below average until implementation of OSHA’s new programs to tighten
gaps in the data it collects. In 2015, new rules required the report of any hospitalizations
and particular accidents, such as the loss of an eye or an amputation. These reports of
serious injuries showed that subcontractors for the oil and gas industry had some of the
highest rates of severe injuries of any industry in 2015 (Lee, 2016). These required reports
also suggest that there is a strong culture of non-reporting of less-severe injuries. Strong
incentives may have kept injury counts low and produced a pattern of under-reporting
injuries on OSHA 300 logs, documents used for injury recordkeeping (King, 2016). Firm
79 This is a management program for the handling and management of high hazard materials.
139
size can also stipulate the reach of these reporting requirements. Small-sized employers are
not subject to many of these reporting rules unless high injury rates place their industry
under special scrutiny (King, 2016). Still, the industry was recently listed under OSHA’s
severe violator program (Galassi, 2015)80.
At health and safety conferences, I saw an emphasis subtly placed on
underreporting. Low injury rates make subcontractors appear more competitive for bids
with operators. Discussions at national conferences and at conferences for OSH in
Pennsylvania that I attended regularly covered how to keep injuries or illnesses from
becoming “recordable" incidents under the auspices that it would be wasteful to over-treat
a worker. Employers do not record all injuries or illness. By avoiding thresholds such as
treatment beyond first aid or prescription strength medicine, a workers’ illness or injury
could be treated without triggering a recordable event81.
OSHA regulations also only apply to certain employment relationships. OSHA
regulations do not apply to all workers, but only to those who work for an employer in a
capacity in which the employer can be held responsible. OSHA thus is concerned with the
nature of the relationship between companies and workers. In hydraulic fracturing,
subcontracting dominates this relationship. Operators employ drilling, completion, and
service companies, who may, in turn, employ subcontractors, who may also subcontract
work to other subcontractors or independent contractors. The ‘responsibility’ of these
80 The nominee for OSHA is expected to review, and possibly curtail the use of the severe violator
program. Now applied to the oil and gas industry, a severe violator enforcement case means that
employers may be subject to different provisions when settling cases with OSHA, required follow-up
inspections, a designation on OSHA’s website, among others (OSHA, 2013). Workplaces found to have
multiple willful, repeated or failure to abate violations during a non-fatality investigation will be
classified as a severe violator enforcement case (Galassi, 2015). 81 Employees of firms of ten or fewer employees may be exempt under certain conditions. For example,
if an employers’ DART Rate, or the number of Days Away, Restricted or Transferred, falls below the
national average, their worksite may be exempted from certain kinds of inspections (OSHA, 2016).
140
operators to the activities undertaken by subcontractors is not always clear.
While some employers may use temporary employment agencies, individual
workers may classify as independent contractors who are exempt from most employment
and labor laws, including OSH regulations. Independent contractors are designated as
individuals who control their own work, a designation that has repeatedly been misapplied
in the oilfield. The WHD of the USDOL has investigated hydraulic fracturing for violations
of The Fair Labor Standards Act due to such misclassifications; in several cases in
Pennsylvania and Texas, companies have been required to pay back wages (Fehling, 2014;
Vorys, 2014; WHD, 2015a, 2015b; U.S. DOL 2016).
Even if workers are appropriately classified as employees, subcontracting can
produce a race to the bottom. As Weil has described, “[t]he more layers between the
primary corporation and its many subcontractors, the more likely there will be wage, and
other labor violations as businesses seek to lower labor costs and maximize profit margins”
(as quoted in WHD, 2015a). Many major operators require subcontractors document OSH
programs and comply with the operator’s own OSH rules. However, subcontractors can
purchase the documentation of health and safety programs they provide to operators with
little customization to a subcontractors’ specific practices. Small contractors may also cut
safety corners because they lack the resources to implement controls depending on the
operator. Small contractors form the foundation of firms operating in hydraulic fracturing,
a situation in which larger operators benefit.
At the 2016 OSHA Oil and Gas Conference in Houston, outgoing Assistant
Secretary Michaels cited these concerns produced by subcontracting, highlighting how
workers employed by small contractors are the most vulnerable in subcontracting structure.
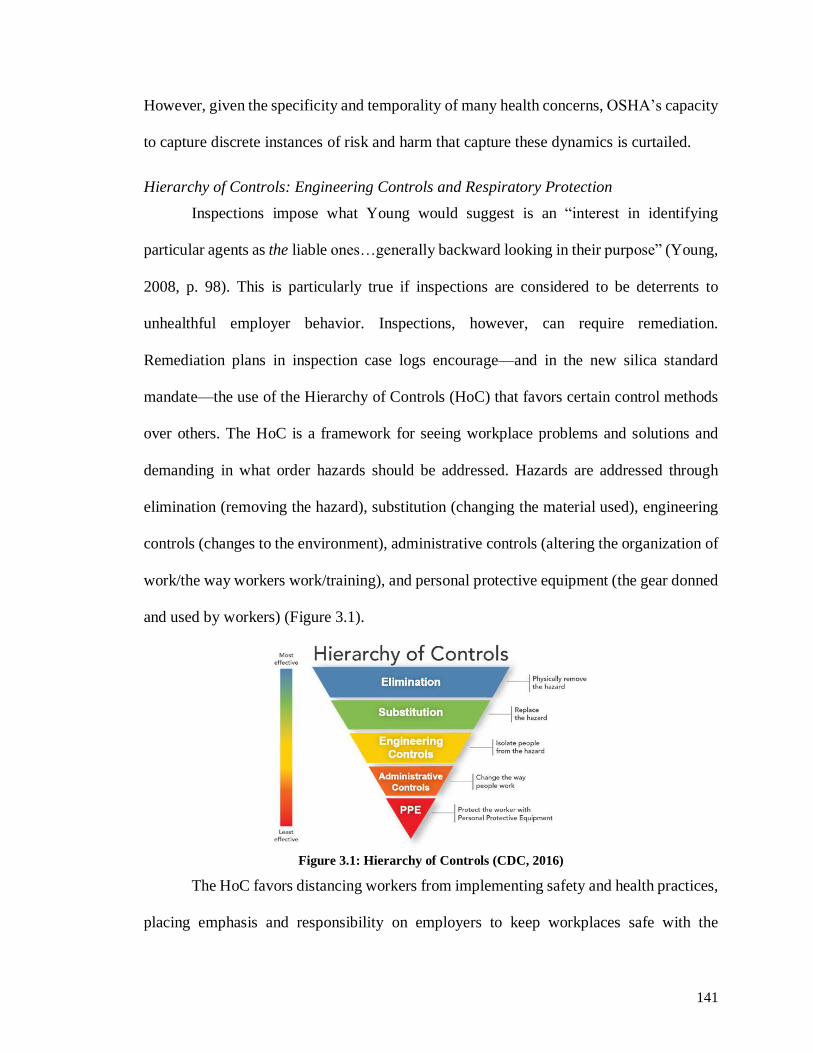
141
However, given the specificity and temporality of many health concerns, OSHA’s capacity
to capture discrete instances of risk and harm that capture these dynamics is curtailed.
Hierarchy of Controls: Engineering Controls and Respiratory Protection
Inspections impose what Young would suggest is an “interest in identifying
particular agents as the liable ones…generally backward looking in their purpose” (Young,
2008, p. 98). This is particularly true if inspections are considered to be deterrents to
unhealthful employer behavior. Inspections, however, can require remediation.
Remediation plans in inspection case logs encourage—and in the new silica standard
mandate—the use of the Hierarchy of Controls (HoC) that favors certain control methods
over others. The HoC is a framework for seeing workplace problems and solutions and
demanding in what order hazards should be addressed. Hazards are addressed through
elimination (removing the hazard), substitution (changing the material used), engineering
controls (changes to the environment), administrative controls (altering the organization of
work/the way workers work/training), and personal protective equipment (the gear donned
and used by workers) (Figure 3.1).
Figure 3.1: Hierarchy of Controls (CDC, 2016)
The HoC favors distancing workers from implementing safety and health practices,
placing emphasis and responsibility on employers to keep workplaces safe with the
142
assistance of expert knowledge and technology. Significantly, the HoC contrasts to how
Horton (2016) has described responsibility for heat illness and OSH. For Horton,
A growing literature in the occupational health sciences employs this focus
on individual decision making in its attempts to reduce heat illness among
farmworkers. Emphasizing the need for “health education and health
promotion,” the literature tends to portray heat illness as the result of poor
knowledge and faulty choices (Horton, 2016, p. 4).
The HoC complicates, although it does not invalidate, this reading of OSH responsibility82.
The HoC relies on a distrust of worker’s decision making such that they cannot be trusted
to act rationally in an OSH sense. Employers are required to implement controls first before
PPE is used by employees. When placed within the context of OSHA’s regulatory structure
the HoC illustrates how responsibility to control risk is produced through a hierarchy that
requires employers act first. Health and education messages in the oilfield often utilize
elements behaviorally based safety, but other parts of OSH, and particularly those endorsed
by OSHA, at least in theory, subscribe to the HoC’s hierarchical model of responsibility.
When a contractor has been required to abate RCS overexposures, OSHA has
emphasized engineering controls83. However, employers may argue the structure of the
industry poses challenges, suggesting that the way OSHA requires abatement may not be
fairly distributed amongst actors given the broader structure of the industry. In this
example, the representative from Chalk Mountain, the cited employer, argues that the
structure of the industry, where a subcontractor rents the equipment it uses from another
82 For example, administrative controls, a high tier on the HoC, includes employer requirements as well
as training, which often place workers are responsible for health. 83 OSHA has also required remediation plans that are extensive for overexposures for RCS such as
occurred following an inspection of Halliburton in Grand Junction, Colorado (OSHA Inspection 98326,
2014). The 300-page inspection file includes months of exposures evaluation, remediation reports,
updated exposure monitoring of remediation, and plans. These remediation documents identify points
of exposure to RCS and tools and techniques for remediation, which Halliburton then implemented.
These documents represent OSHA’s authority to dictate changes to the labor process to reduce
exposures, even as the employer may have flexibility in how it responds.

143
provider to complete a job, prevents compliance efforts.
Employer does not agree with citation 1 item 4, saying that it would be
unfair to implement engineering controls on equipment that does not belong
to his company. The movers belong to the drilling company (EOG resources
on this site), but may be rented to the drilling companies. Mr. Livingston
stated [Exempted]. CSHO explained that an employer would receive an
engineering citation for silica because the personal monitoring results were
above the PEL. CSHO informed that employers are responsible for keeping
employee exposures below the PEL. (OSHA Inspection 842583, 2013).
In this case, who is responsible for abatement? For OSHA, this is relatively
straightforward: the controlling employer. However, the company may be renting the
equipment to keep costs low such that they are awarded the contract in the first place. The
contextual factors for a company’s activities are not considered. For OSHA’s purposes, the
equipment is unsafe, and it is the responsibility of the employer to remediate. Despite the
employer’s arguments regarding the infeasibility of implementing controls, the CSHO, in
this case, cited the employer.
Lack of new equipment may also be used to suggest reasons for the absence of
engineering controls.
23. Employer Knowledge: On 04/04/2013, the employer [Exempted] Site
Safety Leader) state(sic) that he knew that employees at the site were
exposed to silica dust. [Exempted] state that he assumed employees at the
site were overexposed but had not seen any monitoring data. [Exempted]
state that engineering controls were not utilized to reduce employee
exposure to silica. [Exempted] state he was informed that Halliburton’s new
sand movers, Sand Castles, produced less dust. [Exempted] stated that the
Halliburton did not have enough Sand Castles for all crews so Mountain
Movers were still used at this site. [Exempted] state that employees working
within the vicinity of the Mountain Movers were required to wear
respiratory protection (OSHA Inspection 98326, 2014, p. 39).
The CSHO documents here what the employer knew of the hazard, showing that the safety
leader for Halliburton knew that there was more protective equipment in his organization
144
and that he was aware that employees were likely exposed84. Given the number of
worksites Halliburton was working on at the time, the organization lacked the resources to
provide more protective movers to all worksites. Rather than slow the work, Halliburton
supplied employees with respirators. The citation here is not for the organization of work,
but for the discrete exposure. Would it be prudent for the industry to slow down work so
that only safe equipment was being used? This, unfortunately, contradicts the “hurry up
and wait,” “get the job done” culture I observed within OSH spaces that normalized and
incentivized the standards associated with the industry’s structure. At one OSH conference
in a session focused on silica, attendees praised new technologies that sped up the hydraulic
fracturing process further. Holmes raises what is jeopardized through by considering risk,
responsibility, and blame through individualizing notions without accounting for context:
When risk and blame are individualized, the solutions imagined and
interventions planned focus on changing the behavior of the individual.
However, attempting to intervene on individual behavior in such contexts
draws attention away from the structural forces producing mortal danger
and death in the first place. (Holmes, 2013, p. 26).
While Homes focuses on individualization through bodies, the HoC reproduces these
processes at the employer level by focusing on controlling discrete hazards. OSH
discourses, by contrast, “make safety personal.”
The difficulties posed by the structure of the industry are not unknown to OSHA.
Returning to his remarks to the 2016 OSHA Oil and Gas Safety and Health Conference,
outgoing OSHA’s Assistant Secretary Michaels stressed that the subcontracted, complex
structure of the oil and gas industry was particularly concerning because of the challenges
it poses to health and safety. These challenges include the use of smaller subcontractors
84 Employer knowledge of hazardous conditions is one of the criteria OSHA uses to determine “serious”
violation types (OSHA, 2015, pp. 4-13).
145
who do not have the means or knowledge to implement OSH programs sufficiently, and
who work for small profit margins and are encouraged to work at high speeds due to the
demands of the industry.
OSHA can enforce the Multiemployer Policy to cite operators under certain
circumstances if OSHA designates an operator a “controlling employer” (OSHA, 1999).
While it has not consistently been implemented across administrations, OSHA expanded
its use according to Michaels, which he indicated at several industry conference speeches.
In the Multiemployer Policy, OSHA has a reactionary tool to address the challenges posed
by subcontracting. However, it is not consistently applied to inspections at oil and gas and
hydraulic fracturing site. Of areas offices I spoke with, this policy neither seemed to be
widely in use, nor in use at all in the hydraulic fracturing industry; the policy was more a
concern for construction. The multi-employer policy does also not dictate changing
industry’s structure. Indeed, to be cited, an employer must be considered “controlling,”
meaning the mechanism still focuses on causal relationships, leaving the broader structure
and forces that help produce health risk unregulated. OSHA endorses a responsibility
rooted in blame where an employer is blamed for unhealthful exposure.
The emphasis on exposure necessarily entails attention to bodies. Thus, I turn to
examples where OSHA does focus on bodies through its enforcement. OSHA signals its
preference in the HoC to remove workers from the decision-making process as much as
possible, limiting worker responsibility for implementing health and safety controls and in
fact the new silica standard allows for only a few exceptions for respirators as a means of
control. OSHA seeks to remove workers from hazards and only in the last instance, through
personal protective equipment (PPE). Absent engineering or administrative controls,
146
controlling exposure falls to an individual worker’s proper use of PPE.
OSHA has strong reasons for wanting workers to be protected from exposures
without the use of respirators. As first mentioned in Chapter 2, respirators can be
improperly used; they are hot and uncomfortable, facial hair impedes their seal, workers
are not adequately trained and fit-tested, and sometimes employees find they prevent their
other job-related tasks. Some workers may remove the respirator mid-shift, allowing sand
to accumulate on the inside of the respirator, only to don respirator again later in the shift.
At the time of the inspection, the employee (a) worked as a sand counter for
6 months and performed hydraulic fracturing operations for 12hrs/d – 2
weeks/month. The employee (a) worked on top of the sand movers
(mountain Movers) and visually checked inside the thief hatches (access
ports) to ensure an accurate count of proppant (silica sand) inside each
chamber. The employee (a) was required to wear respiratory protection and
wore a N95 dusk mask. The employee (a) did not properly don his 2-strap
N95 respirator and only utilized one strap. The employee (a) allowed the
lower strap to hang loose so that he could raise the respirator to effectively
use his headset communication radio. Improper use of the respirator
increased the employee (a)/s exposure to respirable crystalline silica.
(OSHA Inspection 98326, 2014, p. 38).
This employee, required to visually assess the volumes of proppant in a sand mover, was
seen to improperly wear his respirator while working. Leaving one strap of his respirator
that would secure the mask unhooked, this broke the seal between the face and the mask,
diminishing the respirator’s effectiveness. According to the CSHO’s notes, he did this to
speak on the radio. Significantly, the employer was cited for the infraction, not the
employee. Even though OSHA did not fine the employee, the inspection log reports that
the employee had a history of not following rules and that the company would discipline
him for not following respiratory protection protocol. While this follows the “proper”
distribution of OSH responsibility following OSHA’s logics, these forms of blame do not
address underlying concerns about why the work is structured such that the employee
147
needed to speak through a communicator while being exposed to silica. OSHA does not
place blame on employees officially (it does not fine employees), but that does not mean
that its efforts at enforcement deal with the underlying concerns about workplace
environments that stipulate that employers are blame-worthy and responsible, nor are
immune to the broader discourses that focus on blaming workers for their behavior.
OSHA does not completely absolve workers of responsibility, but it does not
impose punitive measures such it directly controls workers’ bodies or behaviors.
Section 5(b) of the Act states: “Each employee shall comply with
occupational safety and health standards and all rules, regulations, and
orders issued pursuant to the Act which are applicable to his own actions
and conduct.” The Act does not provide for the issuance of citations or the
proposal of penalties against employees. Employers are responsible for
employee compliance with the standards. (OSHA, 2011, pp. 3-10, my
emphasis).
Employers are directed to ensure their employees follow OSH rules. Workers are given an
assurance of an environment, not a bodily state, that is facilitated by the employer and
ensured by OSHA. Employee compliance is the responsibility of employers. OSHA
regulates workers through proxy; thus, OSHA can also regulate how employers monitor
their employees’ bodies through citations for incomplete fit testing of respirators.
Employers must ensure their employees have learned how to properly wear, seal, and test
respirators before their use, and that employees are physically capable of wearing one.
Employees were required to wear half-face elastomeric respirators (3M)
and had not been fit tested on an annual basis. Both Employees, sand
operator and blender operator, work within zones that Baker Hughes has
established as requiring respirators due to dust exposures. Employees have
been overexposed to silica during the hydraulic fracturing operations
according to Baker Hughes results on other sites. OSHA inspections have
documented overexposures to silica at two inspections where sampling was
performed. (OSHA Inspection 943011, 2013, p. 51).
As the CSHO documents, Baker Hughes knew of the hazards posed by RCS exposure but
148
failed to ensure that their employees could safely wear respirators, per OSHA requirements
that safe use of respirators includes annual fit testing by the employer.
Medical evaluations to clear employees for respirator use is only one concern.
OSHA is also concerned with employer’s monitoring of employee’s facial hair.
23. Employer Knowledge: . . . The Safety Superintendent issued half face
APRs to employees at the site. The Safety Superintendent state that
employees had been provided respiratory training, fit tests, and medical
evaluations . . . Both employees had facial hair that could impede the APR
seal. The Safety Superintendent allowed the employees to continue to work
without shaving. (OSHA Inspection 98326, 2014).
In contrast to a previous example, the language of this inspection focuses on the actions of
the Safety Superintendent, not the employees. The issue, as framed in the inspection case
file, is that the superintendent allowed employees to continue with work without shaving,
not that the employees did not shave. Here the CSHO reflects the ways OSHA’s mandate
focuses on regulating employees’ bodies by regulating their employers. This means
employers are responsible for surveilling and disciplining workers through the policing of
facial hair85.
Employers’ respiratory protection programs may dictate acceptable facial hair
growth, styles, or grooming are conveyed through worker training and documented in
respiratory protection programs. The training video produced in Texas by the STEPS
Network on RCS hazards ends with the safety manager, Ted, offering the new employee,
Joe, a disposable razor and shaving cream to remove his stubble before going to work.
85 OSHA’s concerns about facial hair are echoed by observations in NIOSH reports. Notes from
NIOSH’s field visits speculate that the facial hair they saw on workers might interfere with the
protective values of the respirators. “[S]ince many of the workers had facial hair (beards, goatees and
sideburns) that came into contact with the sealing surface of a respiratory, the degree of respiratory
protection for the workers is unknown” (NIOSH, Redacted, p. 4). These observations suggest that
employers are not enforcing shaving policies, nor are employees self-regulating.

149
Leaning over to look more closely at Joe’s face (Figure 3.2 and Figure 3.3), Ted says,
Well here’s a good example of a company rule for ya. When’s the last time
you shaved amigo? You know that respirator’s not going to seal with that
stubble on your face. (Lawhorn-Cryden, 2015).
Figure 3.2: Ted inspecting Joe’s Face (Lawhorn-Cryden, 2015)
Figure 3.3: Joe noting his beard growth (Lawhorn-Cryden, 2015)
When this exchange between Joe and Ted was produced in 2015, STEPS knew that OSHA
wanted workers to be protected from silica using engineering controls. Yet, it reinforced
the narrative that silica hazards should be controlled by respirators and not engineering
controls seen in Chapter 2. To do so, safety manager Ted employs the casual language of
friendship used in occupational health discourse to soften his own surveillance of Joe and
his grooming practices. Yet the language is not so neutral, as in attempting to disrupt the
hierarchy of work, his patronizing tone reinforces it. Further, not only does the focus on
facial hair reify the gendered dynamics of the industry, that being safe and healthful
150
requires particular kinds of enacting masculinity, the methods Ted uses to convey of his
paternalism (at the behest of his employer) . Particular bodies (Joe’s) are deemed irrational,
and in need of protection, yet a discourse which simultaneously demands that these same
‘irrational’ bodies take responsibility for their own health. The ‘rational’ calculus accepts
individual responsibility for health risk to fulfill other responsibilities to employers and
family. As Joe states, “Ok, Ted, I really appreciate the info, and I’m sure my family does
too. Now I understand why it’s so important to follow company policy” (Lawhorn-Cryden,
2015). Joe accepts in this exchange that he would be at fault where he not to shave and then
subsequently become ill. Drawing upon workers’ emotional desires to go home to their
families, OSH training reinforces workers’ responsibility for safe work.
This is perhaps even more concerning given that safety manager Ted offers this
practical advice under the auspices of helping keep Joe safe. This may indeed be Ted’s
intention. Many safety managers I spoke with at conferences cared about their workers and
did not want them to get hurt or sick. Yet, they also found themselves in a bind. They
offered workers advice that they thought the workers would likely not take for reasons of
workplace culture, pride, or other norms and pressures, but also found themselves trying
to insulate their employers from harm as well. Here, Ted reinforces the personal
responsibility narrative that absolves employers of their role in producing health hazards.
Thus, when implemented and enforced, training and programs enable employers to regulate
their employee’s bodies through their own narratives of responsibility for health risk86.
86 OSHA can fine employers for failing to provide workers with information about hazards they face.
This assumes that with information from labels and symbols or access to information from Material
Safety Data Sheets, employees can make more informed decisions to protect themselves and comply
with employer rules, again reinforcing the idea that workers just need the information to behave
‘rationally’ regarding OSH.

151
In many ways, a worker’s long-term health relies on the proper use of control
methods, be they engineering controls or respirators, and the proper grooming, fitting, and
training they require. In these examples, OSHA’s regulation of OSH hinges on its ability
to observe discrete infractions, its ability to find companies responsible for placing bodies
at risk at a particular place and time. The distribution of responsibility under OSHA centers
on the employer citations, fines, and abatement and are tethered to a narrow conception of
responsibility, that is unable to consider other factors, particularly structural factors, that
shape and even produce health and safety risks. Be the focus of an inspection on the
employers’ behavior or the employers’ control of an employee’s behavior, the focus is on
a discrete blameworthy event.
Institutional capacities
Federal OSHA’s institutional capacities also figure into the oversight of OSH and
OSHA’s efforts to enforce standards and warrant discussion here. OSHA’s budget is
subject to Congressional approval and has been nearly flat for three years (OSHA, n.d.)87.
Today, between state and federal offices, 2,200 inspectors oversee 8 million work sites and
130 million workers, translating to one compliance officer per 59,000 workers (OSHA,
n.d.). While this varies from office to office, one area office in the mid-west reported that
they do not have the staffing levels to do inspections unless a complaint is filed. The lack
of institutional capacity is a long-standing concern of GAO reports and has prompted
efforts to target high-hazard industries, triage inspections, and create compliance through
voluntarist measures (GAO, 1978). The effectiveness of inspections and enforcement have
87 OSHA has consistently had low ratios of inspectors to workers, and a 1978 report estimated that
OSHA and individual states had inspected less than 1% of workplaces (GAO, 1978). A 1990 report
stated that OSHA had around 800 inspectors for 3.6 million workplaces, covering 55 million workers
(GAO, 1990).

152
been recently called into question, particularly due to the low levels of fines (GAO, 2013).
Since OSHA’s inception, scholars have debated how fragmentation and a lack of
institutional capacity have been maintained and to whose benefit. For some, this system
controls capitalism to capital’s benefit, but never enough to threaten accumulation
(McCaffrey, 1982, p. xvii; Noble, 1986). For others, OSHA regulations reflect the success
of internal or external interests, either as a “balance among private interest groups” or as a
reflection of the agency’s internal politics (McCaffrey, 1982, p. xvii). Rather than see these
as opposed, moments of OSHA’s history can be read across these theoretical positions
(McCaffrey, 1982). OSHA’s evolution over the last forty-seven years has not been
unidirectional. For example, the Carter Administration took a more activist approach to
enforcement than had Nixon’s or Ford’s (Noble, 1986). Yet OSHA still was limited by
concerns over inflation and the impact of regulation on business (McCaffrey, 1982). Under
Reagan, deregulatory efforts saw the diminishment of OSHA’s enforcement authority
(Vike, 2007) and requirements to further incorporate industry and economic concerns
persist (Noble, 1986; Michaels, 2008). These demands for government accountability and
corporate-interest paralleled a resurgence in the “acceptable risk” narrative of Adam Smith,
updated in Viscusi’s “Risk by Choice” (1983) that buttressed laissez-faire approach to OSH
(Dorman, 2006, p. 37) and a focus on individual responsibility of rational workers for
workplace risk. Voluntary programs and employer assistance for small businesses have
developed through the 1990s, 2000s, and 2010s under different administrations.
From an enforcement perspective, executive leadership has influenced the
interpretation and implementation of programs and standards such as the general duty
clause and the multi-employer citation policy (McCaffrey, 1982; Shapiro & Rabinowitz,
153
1997; Headrick, Serra, & Twombly, 2008). While the power of the executive in this agency
matters greatly, approaches—be they enforcement or voluntary compliance focused—have
not been mutually exclusive. Obama’s OSHA implemented programs to target hazardous
employers and increase fines even as it simultaneously increased partnerships with
industries exemplified by voluntarist terms like “cooperation” and “education” (Noble,
1986). These undertakings aim to improve OSHA-employer relationships for better OSH
outcomes on a voluntary basis and are in many ways a practical response to OSHA
institutional constraints concerning the oil and gas industry. OSHA’s partnerships do not
address these structural issues.
OSHA consultation offices also assist mid- and small-sized companies’ regulations
(OSHA, 2011, pp. 2-1) and some programs confer benefits to employers, including
exemptions from programmed inspections and reductions in fines (OSHA, 2011). OSHA
also distributes information to employers about emerging concerns and participates in
industry conferences, strategic partnerships, and alliances. As discussed in Chapter 2,
OSHA joined with NIOSH and National STEPS to facilitate shared communication,
research, and organizing, including “Safety Stand-Downs” (OSHA, 2016; OSHA Region
VI, 2015). OSHA uses these mechanisms to incentivize, rather than demand, compliance.
These programs remain focused on fixing discrete problems—be it silica, road safety, tank
gauging fatalities, or fall hazards—even as these voluntary measures suggest that industry
members take responsibility. OSHA’s key deterrence strategy is penalties, a form of blame
levied in fines and violations resulting from inspections. This way of conceptualizing
responsibility confirms that there is an individual unit to which blame can be ascribed.
Fines and Blameworthiness
OSHA operates endorses individual employers as moral and political units who can
154
be held responsible for creating hazardous and unhealthful working conditions. When
doing so, it can levy fines on employers. Fines are the monetary value the State places on
the hazards and risks workers face. The first time since 1990, OSHA increased its fines to
match inflation, under the Bipartisan Budget Act of 2015. Serious violations now receive
penalties over $12,000 (Smith, 2016) up from $7,000, and willful and repeat violations are
just over $125,000, increased from $70,000. However, OSHA frequently reduces fines
significantly, even for fatalities (McCluskey et al., 2016). OSHA may negotiate fines with
violating employers, reducing for good faith measures, the size of the company and its
history, or if an employer immediately remediates; in 2012, OSHA reduced fines if
employers abate violations directly, accounting for $1.28 million in 2012 (McCluskey et
al. 2016).
Many inspections I reviewed utilized the Expedited Informal Settlement process.
Informal settlements were implemented by OSHA in 1980, and as its name implies, such
settlements are seen to shorten the process of hazard correction and abatement.
Justifications for these tools include the reduction of litigation costs to OSHA and small
businesses (GAO, 1984, pp. i-ii). Thus, OSHA offers incentives to hasten abatement, even
if it means that symbols of a company’s blameworthiness—citations and fines—are
reduced.
These fines, expedited or not, are extremely low. In 2015, the Department of Justice
began the Worker Endangerment Initiative to investigate OSH crimes under environmental
statutes, which have higher, more severe penalties (DOJ, 2016). Concerns over the severity
of civil penalties arise amidst weak and rarely enforced criminal penalties which are
misdemeanors (Committee on Health, Education, Labor and Pensions, 2008). Still, fines

155
and criminal prosecution emphasize finding individuals blameworthy of hazardous
conditions and outcomes. These enforcement techniques do not address concerns about the
structure of the industry under which these hazards are produced, and moreover, under
which who is responsible is blurred88.
Authority to Inspect: Emphasis Programs
OSHA triages its inspections for most concerns when OSHA receives a complaint
or referral. Its staffing levels shape which spaces remained closed from state scrutiny, and
which become open. For silica, most reports trigger an onsite inspection because silica has
been under National and Regional Emphasis Programs, programs that prioritize OSH
concerns by triggering onsite investigations to complaints, directing focus on certain
exposing industries, increasing outreach to affected industries, among other strategies89.
Still, inspections for silica lagged far behind the number of well sites.
OSHA offices that enforce these programs report variations in their level of
authority to inspect well sites. Some offices in Region VI and Region VII, which include
Texas, Kansas and Arkansas, reported to me the authority to inspect if a well site is seen
from the road, while other offices also reported that these well sites had to be located in
randomly generated regions for the inspection to occur in a legal way. Other offices in
Region VI, and in Region III, which includes Pennsylvania, indicated that they did not
inspect well sites in this way, either because they lacked the staff to perform such
inspections, or because they did not have the authority. They had to be careful not to target
88 Obama’s USDOL sought to clarify ambiguities regarding employer-employee relationships,
including who is a ‘controlling employer;’ the Trump Administration removed this clarifying guidance
for these relationships in June 2017. 89 These programs may explain why at an OSH conference in 2014 participants spoke disparagingly of
the “YouTube Lady,” a woman in Northern Pennsylvania, who they described as sending videos of
silica at well sites to OSHA to try to trigger onsite investigations.
156
one worksite unfairly. Several OSHA officials explained to me that this caution reflects
how offices interpret the directives in regional emphasis programs for oil and gas but also
is influenced by how regional federal courts have interpreted OSHA’s enforcement
authority and if an inspection would stand up to being challenged. These differences are
significant and shape the context in which OSHA enforces its standards for silica within
the context of the industry’s subcontracted structure.
Conclusions
John Howard, the director NIOSH, has written that non-standard work
arrangements, which can include subcontracting, warrant the OSH community’s attention.
While nonstandard work arrangements may offer expanded economic
opportunities for businesses, mounting evidence shows that these novel
ways of working pose occupational health and safety risks for some
workers. What kinds of risks, how much risk, and the number of workers
who bear the risks from nonstandard work arrangements are not entirely
clear. (Howard, 2017, p, 7).
But when describing how these should be addressed, he relies on a paradigm of OSH that
focuses on discrete instances of risk, and that is mirrored in OSHA enforcement strategies
for finding blame and liability. His article offers that OSH professionals should be
identifying “interventions to mitigate or eliminate those risks” (Howard, 2017, p. 7) from
non-standard work arrangements, rather than offering that these work arrangements be the
subject of reform themselves. Here, like in enforcement efforts, by focusing on the unique
encounters that unfold at work—the discrete risks—discourses in OSH limit the ways that
responsibility can be envisioned.
Responsibility-as-liability has practical and theoretical limitations when applied to
OSHA’s ability to ensure workers the right to a safe and healthful workplace. This
approach engendered by OSHA inspections pursues causal connections to ascribe an

157
exposure to an employer through citations and fines, as well as demanding a remediation
of the hazard, often to make workplaces safer in the future. While OSHA is self-limited by
its rules and regulations, the flexibility of work and employment of the hydraulic fracturing
industry exploits regulatory oversights. OSHA lacks the enforcement tools and means of
collecting information necessary to match industry’s flexibility. This reveals OSHA’s
limited capacity to regulate responsibility stemming from structures and processes that
produce unhealthful working conditions.
OSHA’s form of health governance, with its focus on blame-worthy events and
their legal implications, is confounded by the spatial and temporal properties of the industry
and represents a focus on responsibility that fails to consider the complexity of the context
in which exposure occurs. OSHA’s focus on blameworthy events and the work belies the
broader structures under which OSH problems emerge and are intensified, and through
which industry more easily avoids oversight. Space and time are confounding factors in
health governance.
Young argues that “the social connection model of responsibility says that
individuals bear responsibility for structural injustice because they contribute by their
actions to the processes that produce unjust outcomes” (2008, p.105). Indeed, Young and
Neuhaüser illustrate the importance of understanding how individuals, events, and
ultimately injustices are not isolated, but rather imbricated within complex structures. It
follows then, that responsibility be considered not solely to the “exposing” employer, but
more broadly to the collective responsibility of those imbricated in those structures
OSHA enforcement ignores other modalities of responsibility outside the
responsibility-as-blame paradigm that could provide alternative methods for achieving

158
OSHA’s mandate. Flexibility either through work or employment creates firms who are
less accountable yet profit from unsafe working practices. Efforts to create a responsibility
to reorganize should not be equally distributed. “The acceptance of responsibility for
structural injustice is often costly for agents, and this leads to the question of who should
bear the weight of responsibility and the costs coming with it” (Neuhaüser, 2014), but
rather should be conceptualized through the power relations that produce bifurcated actors
within the oilfield’s subcontracted structure.
This chapter has considered how the structures of work and their relationship to
exposures shape the state’s efforts to enforce its model of responsibility for health risk
through inspections. As industry actors are unable to be held accountable—they are
absolved—through both the discourses of OSH and the material practices of finding blame.
The chapter demonstrates how tracing responsibility and critiquing its formations under a
liability model rooted in discrete exposures, misses the broader contexts in which OSH risk
emerge, and work to absolve industry of responsibility for health risk, and towards
remediation.
159
4. Chapter 4: Workers’ Compensation: Finding Fault in ‘Fault-less’
Responsibility
Insurance, we all know, transfers risk. Yet, what we usually think of as a
transfer of risk is also a transfer of responsibility. (Baker, 2002).
As a form of social insurance, workers’ compensation fundamentally deals with
questions of risk and responsibility. Workers’ compensation distributes risk for
occupational hazards and determines who is responsible for providing for injuries or
illnesses incurred through work. Its intentions purport to be both moral and economic,
aiming to restore life after harm and to return the smooth movement of populations and
economy. Unlike other OSH mechanisms, workers’ compensation does not focus on
demonstrable blame as an instrument to assign responsibility. Under the compensation
bargain, employees give up rights to sue employers in exchange for no-fault insurance for
the dangers faced at work. Yet, workers’ compensation compensates workers who have
been exposed or fallen ill in an “appropriate” way, making workers bear the burden of the
spatio-temporalities of their industry should they become ill otherwise.
This chapter illustrates the practicalities inherent to this model of responsibility
where workers’ compensation eligibility is determined not only by a body’s physical
attributes (the state of illness, and its severity), but also its spatiotemporal attributes (where
and when a worker have labored and lived, and in what time they have gotten ill) while no-
fault in nature. Employers may be liable, but workers bear the responsibility to not only
make a claim but also become sick in the right way. The chapter argues that standards that
accompany this “fault-less” insurance neglect the flexibility of a workers’ employment and
also characteristics of long-term lung diseases. Here, then, the distinction between blame,
fault, and liability becomes significant. The responsibility to act—to make a claim on the
160
state– falls to the employee, even when an employer is liable. Yet, when the spatio-
temporal characteristics of an employee’s disease or work history absolves the employer
and the state of liability, by default, the state blames for employee for their condition,
leading the employee to be responsible for finding means of remediation.90As discussed in
chapter 1, the neoliberal state shifts responsibility and care onto individuals; here this
occurs in two ways. First workers are responsible for showing that their illness is
occupational under exclusionary definitions of workers’ compensation that have encoded
within its rules since its inception. Second, faced with the lack of access to this ‘exclusive
remedy’ workers must turn to their families and other social insurances provided by the
state, themselves often insufficient, to find assistance for their illness.
While fault is, in theory, not the preeminent concern under workers’ compensation,
fault still lingers, having been replaced by concern for what is defined as “occupational.”
As a matter of health governance, this illustrates how responsibility for health is produced
by the exclusions facilitated by governance structures, flexible employment, spatial
variability, and persistent underlying assumptions about the relationship between
employers and employees. These patterns of health responsibility have specific
manifestations within the oilfield due to the spatiotemporal practices of the industry. As I
demonstrate in this chapter, silicosis requirements, in particular, illustrate these processes.
The practices of this industry are not singularly unique and are found across a variety of
different industries. Thus, the confluence of workers’ compensation schemes and the
hydraulic fracturing industry’s flexibility have implications for other sectors, and more
90 As will be seen at the end of this chapter, there are some complexities to this construction.
Pennsylvania has allowed workers to pursue torts of employers in some cases where workers’ diseases
manifest outside of the statute of limitations for diseases. This provides a different mechanism by which
employers could be found responsible, albeit to different evidentiary standards.
161
generally can contribute a shifted lens and new context for the ways that health geographers
to approach the definition of ‘disease’, and the ways that caring responsibilities for health
emerge out of institutional processes.
Practices of Responsibility, Liability, and Blame:
This “geography of responsibility” opens the way for critical assessments
of how, and upon whom, responsibilities fall, and how the topography of a
particular social life regulates the flow of shared understandings about who
is going to be expected to see to and account for situations, outcomes, or
tasks. (Walker, 2008, 86).
This chapter takes as its central starting point the idea that responsibility is
practiced. It is not enough to know that workers’ compensation shifts the burden of risk
through “fault-less” liability; instead, this shift necessitates charting who can act, and under
what circumstances; it requires examining the processes of providing workers with access
to these fault-less compensatory funds. Walker’s focus on responsibility is significant in
that she does not limit the analysis only to “purely” moral norms but situates them within
a “social world” (p. 217). Building from Young’s critique of responsibility through liability
and blame, this chapter explores how the mechanisms used to assign liability can
themselves be unjust.
Under what I call the liability model of responsibility, I include all such
practices of assigning responsibility under the law an in moral judgment
that seek to identify liable parties for the purposes of sanctioning, punishing
or exacting compensation or redress. (Young, 2008, p.98)
In the case of workers’ compensation, the state seeks to shape norms by establishing
guidelines for whom and what are compensable under certain contexts. Workers’
compensation illustrates how governance of health and responsibility specifically is
refashioned under the term occupational. The state’s ways of ‘finding occupational’ belie
common patterns of hydraulic fracturing work and common disease progression, making
162
workers responsible for seeking recompense through other social insurances. These laws
foster uneven and inequitable health-relationships through exclusionary applications of
time and space.
The analysis builds upon work in health geography and cognate fields that examine
the political-economic processes that shape discourses of health and disease. Specifically,
these scholars illustrate how scientific and medical narratives about the causes of disease
are reproduced and co-constitutive of particular social, political, economic, and ecological
processes. Recent efforts have further argued that such examinations be placed within a
historical context, a particular concern for those examining political ecologies of health
(King 2009; Jackson & Neely, 2015), but also those who trace the governance processes
surrounding health (Craddock, 2000; Brown, 2009). Narratives of where disease comes
from, and how it can be measured and identified shape what has become occupational
health (Murphy 2006; Nash 2006), and strongly influence the ways that diseases are viewed
under workers’ compensation, particularly surrounding the biomedical model of disease
(Barnetson, 2010). For Barnetson, the relationship between workers compensation and the
biomedical model emerges within the Canadian system due to strict requirements of
causality that see disease rooted within one discrete event. While there are similar
requirements in the U.S., I focus here on ways the workers’ compensation system also
reflects and embodies the state’s the competing responsibilities, namely cost internalization
and humanitarian remediation through its definition of disease in problematic ways. I
connect these legal definitions, which encode particular spatial and temporal assumptions
about disease, with the hydraulic fracturing industry’s flexible labor practices, to show how
workers’ compensation requirement intersect with hydraulic fracturing industry’s spatio-
163
temporality flexibility to render it anew as an exclusionary social insurance.
This analysis builds on health geographers’ attention to movement in the production
of health. As Guthman and Mansfield write, movement conceptually charts new ways of
thinking about health and health risk through time and space:
Yet, just as chemicals move in and out of bodies, they move in and out of
particular spaces. People are mobile as well; those exposed elsewhere may
reveal diseases not from those spaces, while those in those spaces might not
be manifesting the disease (2013, p. 498).
Stasis, then, should not be an assumption of the governance mechanisms that seek to
address health risk. Wherein both bodies and workplaces are mobile over time, it is neither
just the body or the disease risk that move, it is both.
Responsibility as it is encoded in workers’ compensation, makes workers
responsible for the movement within their industry. Thus, the chapter contributes to
understanding how health risk is produced through not just the distribution, of the disease,
by state’s procedures for recognizing it. Here, I draw upon geographers’ history of
examining how laws and policies engender particular spatial practices to produce
inclusions and exclusions around race, class, sexuality, and gender (Craddock, 2000;
Biehler, 2009; Brown, 2009; Carter, 2012). This chapter’s focus is not so much on health
outcomes, but rather on examining the procedures used by the state to ‘recognize’ or ‘see’
diseased bodies. I examine space and time as mechanisms of exclusion when considering
who is responsible for the consequences of health risk for occupational disease, a process
that varies from state to state. Raising concerns regarding health justice and the availability
of access to this social insurance, workers’ compensation requirements can push workers
to seek compensation from other social insurance programs, or, in a few states, seek
recompense through the courts, further intensifying these uneven geographies.
164
This chapter analyzes workers’ compensation statutes in all fifty states and
Washington, D.C. Although it focuses on hydraulic fracturing activities, examining all
states is necessary when considering that workers do not tend to stay in oilfield work for
significant periods. Additionally, the chapter draws on interviews with health and safety
instructors, participant observation at workers’ compensation and occupational safety and
health conferences, and textual analysis of worker safety and health materials.
From Common Law to Employer Liability to Workmen’s Compensation
We usually conceive the process that brought about the harm as a discrete,
bounded even that breaks away from the ongoing normal flow. Punishment,
redress, or compensation aims to restore normality, or to “make whole,” in
relation to the baseline circumstance. (Young, 2008, p. 107).
In the U.S., workers’ compensation addressed concerns over litigation between
employers and employees that had arisen in the late-19th century (Rogers, 2009). Workers
sued in state courts for compensation of wages or payment of medical expenses due to
workplace injuries (Bale, 1987) and disease in a small number of cases (Bale, 1988). The
courts interpreted common law under a doctrine of “due care” which considered the free
market a fair distributor of industrialization’s impacts, and under which “laborers bore the
risk of accidents resulting from the usual work hazards, while employers assumed the
burden of those resulting from their failure to exercise proper care” (Rogers, 2009, p. 16).
The courts required that workers show negligence or willfulness by the employer, a high
burden of proof for the employee (Bale, 1987). Workers had responsibility for the hazards
they faced at work, having voluntarily and rationally entered a working relationship.
While “employer liability” asserted that “the employer was held negligent if he
violated the common-law duty of providing a reasonably safe place to work” (Bale, 1987,
p. 36; see also Sellers, 1997), employers could utilize three defenses to refute an
165
employee’s claims of harm. The “fellow servant rule” barred recoveries if a fellow
employee caused the injury. “Contributory negligence” denied compensation to injured
workers found to have in any way been at fault, and under “assumption of risk” workers
assumed the known risks of their workplace because of employment (Bale, 1987, p. 36).
Fault was a central concern in this ascription of responsibility. Workers had to show
that the employer was willfully and negligently at fault and that neither they nor another
employee contributed to the injury or illness. While many cases were dismissed or found
in favor of the employer, in some cases, large sums were awarded amounting to what Bale
has called “a compensation crisis for capital” (Bale, 1987, pp. 36-37) and what others
contend was a “crisis of uncompensated injuries and deaths” (Torrey, 2010). As juries
awarded large sums, insurance companies responded by raising coverage rates (Bale, 1987,
p. 48). The insurance industry flourished under these emerging industrial conditions. They
began collecting data, finding patterns between industrial conditions, diseases, illnesses,
and death (Bale, 1988; Sellers, 1997; Rosner & Markowitz, 2006). Under welfare capitalist
initiatives, many employers instituted workers’ insurance and benefits programs, at times
using punitive and coercive measures to ensure uptake (Asher, 1987). In other cases,
workers could purchase workers’ insurance or life insurance, although costs were often
associated with the perceived risk of the industry (Bale, 1987; O’Malley, 2004).
The idea that the free-market would deal with the consequences of workplace
hazards fell out of favor as new ideas about the role the state could take to provide the
welfare of its citizenry acknowledged the problems, economic and humanitarian, that
emerged as many workers failed to gain adequate compensation through the courts or
insurance. Social reformers sought to reshape litigious relationships (Rogers, 2009), efforts
166
that first materialized in a federal workers’ compensation program for civil servants in
1908 and then through state-based workmen’s compensation programs over the next
decade, establishing the system still in place today (Rogers, 2009; Szymendera, 2017). It
is worth noting that the history of corporate insurance, medical surveillance by companies,
and other policies in the early 20th century also influenced these developments concerning
workers’ compensation for injury and disease as companies saw these efforts as good
business also (Sellers, 1997).
The legislative success of the compensation laws had only become possible
as many corporate officials had come to agree with judges and legislators
that the unlimited bodily damage allowed in the nineteenth-century
workplace was morally wrong and even economically wasteful in the
extreme. Yet increasingly owners and managers had become convinced that
more careful tending of their employees’ health could bring tangible profits.
(Sellers, 1997, p. 107).
Workers’ compensation required that employees “agreed” to the compensation
bargain as a consequence of their employment (Rosner & Markowitz, 2006; Rogers,
2009)91. Indeed, it is implied within most employment arrangements and thus enables the
state imposes its model of responsibility on employers and workers. The state took
responsibility for mediating the relationship between workers and employers—
conceptualizing responsibility through no-fault insurance—where irrespective of fault or
blame, employers, their insurance companies, and the state held responsibility for
providing compensation for injury. Benefits were diminished from what might be awarded
in a lawsuit, but workers no longer had to prove that employers had been neglectful or
willful in enabling unsafe working conditions in court. The bargain permitted an employee
91 If employers held insurance, at first voluntarily, they were protected from litigation. Policymakers
worried that mandatory workers’ compensation would violate employers’ rights to due process until the
U.S. Supreme Court held that it did not in 1917 (Duncan, 2003). After workers’ compensation became
compulsory in most states, workers ostensibly agreed to this bargain by nature of their employment.
167
to seek recompense if they met certain requirements. Reformers expected workers’
compensation would incentivize employers to maintain safe working conditions such that
their insurance costs would not rise due to injury (Rogers, 2009). These hopes were not
actualized over the last century, raising questions about for whom these systems provide
and protect.
No workers’ compensation program in the U.S. is identical to any other states’
program, and no federal standard or oversight directs state programs (USDOL, 2016).
Workers’ compensation, with a few exceptions, has stayed the responsibility of individual
states92, leading its implementation to be geographically uneven, and moreover, its
recompense insufficient (Grabell & Berkes, 2015; OSHA, 2015; USDOL, 2016). At least
thirty-three states have diminished benefits available through workers’ compensation and
made eligibility requirements more demanding since 2003; wide disparities exist in
the payment and care across states (Grabell & Berkes, 2015) and efforts to eliminate
fraudulent claims and reduce program costs have produced stifling requirements for
workers, including complex medical evaluation requirements that often benefit employers
rather than employees.
Who is liable?
Since its introduction, workers’ compensation has only applied to certain workers.
Workers’ compensation might better be called employee compensation as these benefits
are only available to employees who are harmed under certain conditions. Workers’
compensation laws exclude independent contractors, and evaluative measures can be used
to determine if a worker was engaged in activities as an employee at the time that they
92 In the 1980s and 1990s, federal compensatory schemes developed for black lung victims from coal
mines and for irradiated workers exposed in U.S. National Laboratories (Michaels, 2008).
168
encountered the hazard. In Pennsylvania, this includes if the worker was furthering the
interests of the employer93. Indeed, much of workers’ compensation seeks to distance
employers from being ‘unjustly’ held liable for a workers’ injuries or illness for which they
did not directly contribute, even if that belies the structural processes in which they operate.
This is an anathema for Young:
Where there are structural injustices finding that some people are guilty of
perpetrating specific wrongful actions does not absolve others who actions
contribute to the outcomes from bearing responsibility in a different way.
(2008, p. 106).
The upstream oil and gas industry uses subcontracted labor and independent
contractors; both challenge efforts to determine the “responsible” employer. In the case of
independent contractors, there is no “responsible” employer; these workers are exempt
from workers’ compensation. However, subcontracting, a central component to oil and gas
operations discussed in Chapter 3, can complicate who is the responsible employer as both
the subcontractor and the operator seeking to distance themselves from the costs of health
and safety by not holding workers’ compensation insurance94. Ohio has developed clear
statute to capture this, as it describes under the section of its workers’ compensation
website devoted to oil and gas:
Many employers believe they can shield themselves from workers’
compensation liability by using subcontractor relationships rather than
hiring employees. This is only true if and when all involved contractors
comply with Ohio workers’ compensation requirements.
Ohio law – Ohio Revised Code 4123.01 – states that the liability of a non-
complying subcontractor is transferred to the general contractor. Therefore,
the best way for the general contractor to avoid such liability is to ensure
each of its subcontractors has valid Ohio workers’ compensation coverage.
93 Bathroom breaks, smoking breaks, and meals are covered as part of the natural course of work. 94 This was and has been a central strategy of corporations to ‘distance’ themselves from the medical
and health costs of their operations, very deliberately detailed in the coal industry’s example of the
“Massey Doctrine” (Weil, 2014).
169
(Ohio Bureau of Workers’ Compensation, 2017).
In Ohio, the subcontractor must also hold insurance, or the liability moves on to the general
contractor (or operator, in the case of oil and gas). The employer or their insurance
company holds financial responsibility for paying for the claim for benefits, lost wages,
and medical expenses. These chains of liability are straightforward in most cases of
accidents and injuries; the employer liable is the employer where the injury, a discrete
event, occurred.
Determining who is responsible can be more complicated for diseases of long
latency, where temporal issues then come into play. States often stipulate that the employer
responsible be the one where the last hazardous exposure occurred. A state may require
this exposure to have occurred over some period, such as for sixty-days, twelve months, or
two years, but only apply in the case of certain diseases, and under certain conditions. For
example, in Pennsylvania,
The employer liable for compensation . . . shall be the employer in whose
employment the employee was last exposed for a period of not less than one
year to the hazard of the occupational disease claimed. In the event the
employee did not work in an exposure at least one year for any employer
during the three hundred week period prior to disability or death, the
employer liable for the compensation shall be that employer giving the
longest period of employment in which the employee was exposed to the
hazards of the disease claimed (77 P. S. § 1514).
The question of liability is highly specific to the context of an individual’s employment.
Similarly, in Colorado,
In the case of silicosis, asbestosis, or anthracosis, the only employer and
insurance carrier liable shall be the last employer in whose employment the
employee was last exposed to harmful quantities of silicon dioxide (SiO2)
dust, asbestos dust, or coal dust on each of at least sixty days or more and
the insurance carrier, if any, on the risk when the employee was last so
exposed under such employer.
While the state provides the framework by which employers can be held accountable, it

170
simultaneously stipulates the requirements that employees and their ailments must meet.
These efforts to compensate disease help fulfill workers’ compensation’s both moral and
economic goals by limiting liability and reducing compensable claims.
First, workers’ compensation provides for ill workers, and second, it insulates
employers from undue OSH costs. Thus, much focus within these programs and statutes
centers on making workers’ compensation less costly, more efficient, and more insulated
from fraudulent claims. This perspective on providing benefits in a way that is both
economical and beneficial to the employer, and through the development of an insurance
agency itself, mirrors OSH and workers’ compensation values as well as their perspectives
on employees and employers. At health and safety conferences for the oil and gas industry,
sessions returned to questions of workers’ compensation issues where it was assumed that
many workers were filing false reports to get extra money and time off. Many people were
concerned with mitigating workers’ compensation fraud, assuming workers would file
fraudulent claims for non-work-related injuries and illness. It was not just about keeping
workers safe, but about reducing the costs from workers’ compensation claims, particularly
when workers did not, in the eyes of the employer, warrant compensation. The boundary
of the working day, for example, if something happened while a worker was in a parking
lot, or driving to work, were commonly debated issues as health and safety professionals
and HR reps tried to determine the spatial and temporal extents of their liability.
This sentiment colored sessions at the Pennsylvania Department of Labor and
Industry Annual Workers’ Compensation Conference in 2016 held for human resource
officers, adjusters and lawyers. Its sessions often focused on disgruntled employees,
managing a company’s liability, and preventing employees who try to take advantage of

171
employers who “show humanity” through good faith efforts. For example, sessions
included #socialdetection –Deep Internet Mining covering techniques to detect fraudulent
claims through social media, As the Claim Turns, a two-part series on extensive (and
potentially drama-filled) claims process, and Employment Law Interaction with Workers’
Compensation: A Case Study which used examples to illustrate when other federal
programs like ADA, FMLA, and COBRA applied, sometimes in exclusion of workers’
compensation. In this Employment Law session, discussion centered around cases where
employees were trying to get more money out of employers than the employers felt their
employees were owed, a skepticism that spilled into discussions on ways to reduce claims
and costs. Across these conferences and milieu, whether a worker’s ailment was
compensable, whether they were a compensable employee, whether they engaged in
furthering the interests of the employer during a “natural” workday, and to what extent
medical evidence substantiated that the worker was ill in the first place was of issue. These
forms of investigation focus squarely on the harmed individual, and not the context of
work; they seek to root out workers’ compensation cases where the employee is actually
responsible, to absolve the employer of liability.
Reducing fraudulent claims from workers is only one consideration to secure the
economic health of this insurance mechanism. West Virginia’s website reads:
The West Virginia workers’ compensation market is thriving! There are
over 260 carriers offering workers’ compensation insurance to West
Virginia employers. Currently, there are over 200 carriers writing policies
in our state. Since the workers’ compensation legislative changes went into
effect in 2006, the aggregate loss costs have decreased over 72%. (West
Virginia Office of the Insurance Commissioner, 2017).
Some states provide insurance discounts to employers who take part in safety classes and/or
organize safety committees (groups of employees who collaborate around safety issues).

172
These programs are meant to make workplaces safer at the outset such that there are fewer
workers’ compensation claims. In Pennsylvania, many safety classes are available in online
webinar formats. Offered by Pennsylvania Training for Health and Safety (PATHS),
PATHS classes I have taken included and promoted behavior-based safety techniques.
These included course materials that seek to promote behavior change through, for
example, the “Ten Commandments of Safety and Health” where the blame for accidents is
found in worker behavior, even if liability lies with the employer. Such programs reinforce
ideas about workers’ responsibility for health even as statute technically holds employers
responsible. While compensable employee comes with added layers of assumptions about
a workers’ responsibility for health, this is only the first consideration. There are significant
requirements for what ailments are compensable that place the burden of showing
‘occupational’ on the worker. These burdens are not only rooted in the status of the body-
as diseased-but in where, how, and for how long a body labored.
What is compensable? Occupational Disease
The first workers’ compensation programs provided compensation for some,
but not all, occupational injuries by establishing what counted as ‘occupational’ to limit
compensable injury (Rogers, 2009). Of issue was if and how it could be shown that an
injury was incurred during work. Industry recognized that no-fault insurance could be
advantageous for occupational diseases as well and lobbied for its inclusion in workers’
compensation when occupational disease litigation drew concern in the 1920s and 1930s
(Rosner & Markowitz, 2006). These competing interests, encoded in occupational disease
litigation from its earliest iterations, has convoluted what compensation is meant to achieve
and what is ‘fair compensation.’ Indeed, the idea of ‘fair compensation,’ and for whom (the
employer or the employee) has often swayed towards employers.
173
Labor historians have charted how silicosis was a linchpin in the development of
many worker protections in the 1930s including the scheduling of occupational diseases in
workers’ compensation statutes. Silicosis, once known as the ‘king of occupational
diseases’ (Rosner & Markowitz, 2006) in the 1930s instigated and hastened many states’
inclusion of occupational diseases under workers’ compensation statutes (Rogers, 2009).
Concerns regarding silicosis and occupational diseases stemmed from exposures in the
mines and foundries (Rosner & Markowitz, 2006; Rogers, 2009). Mounting litigation and
the deaths that resulted from the Hawk’s Nest disaster made clear including occupational
disease under workers’ compensation advantageous to both labor and industry groups,
although these groups approaches and demands differed widely (Rogers, 2009),
particularly following litigation the disaster’s cases (Sellers, 1997). In the ensuing decade,
labor lobbied for “blanket” coverage of occupational disease, while industry campaigned
for restrictive inclusion, where it even supported these efforts, opining the potential for its
inclusion to be “ruinous,” and many states ultimately opted to implement “compromises”
(Rogers, 2009, p.163).
Although occupational injuries had been covered by many states, the introduction
of occupational disease challenged these systems that had developed around primarily
acute injuries where causation was clear. By contrast, silicosis, and other occupational
diseases that result from often repeat exposures over periods of time were more challenging
under this framework. Strikingly, many state statutes sought to contain the costs of
occupational diseases’ inclusion by limiting who was able to file for these funds. These
limitations included the degree to which a person was disabled, and when they were last
exposed. How the states handled instituting these limitations has had lasting legacies; here,
174
of note have been the persistent way that space and time have been used to limit bodies’
accesses to the compensation bargain.
Some states sought to cover silicosis and other ‘dusty lung diseases’ first, and then
incorporated other occupational diseases at a later date (Rogers, 2009). Other states focused
on incorporating occupational diseases more broadly, sometimes under “Occupational
Disease Acts” or by expanding the definition of ‘injury’ to include occupational disease
(Larson, 1973). “Viewed nationally, then, the Depression-era silicosis crisis expanded state
compensation of disease coverage but left gaps and limitations” (Rogers, 2009, p. 164). It
also produced an uneven patchwork of limitations for both occupational disease and
silicosis. “The key operative concepts affecting the various silicosis limitations vary so
much from state to state that no overall generalizations about their definition are possible”
(Larson, 1973). These legislative histories left lasting legacies on present-day statutes.
Even as the 1970s saw modest efforts to update occupational disease laws (Larson 1973;
Kutchins, 1981) most efforts maintained the limiting spirit of their original intent.
Workers’ compensation programs relieved workers of the burden of showing
employer fault in workplace ailments and instead established a burden of proof: that an
ailment is occupationally acquired. To insulate employers from liability for the disease to
which their workplace may not have directly contributed, workers’ compensation excludes
bodies that are unable to meet the thresholds the State establishes for what is occupational.
Thus, the definition of “occupational disease” constrains what can be compensated and are
significant (see Table 4.1 for examples).
Some states define occupational diseases within their definition for injury, offering
that the term “injury” includes disease, even as many injuries occur immediately after

175
exposure to a hazard or accident, and diseases may take years to develop. With injuries, its
relationship to a particular hazard at a specific point and time, the cause and effect linkages,
are clear. Many occupationally acquired diseases take years of repeat exposures to develop
and lack that same direct cause-effect relationship. Other states have specific statutes for
occupational disease, but in either case, the attachment of the term “occupational” to the
disease or injury signals that liability lays with someone other than the afflicted worker if
the ailment is work-related.
The workplace conditions must be shown to be at fault. In other words, work must
be the space in which a workers’ body encountered a distinct risk that could have caused
the harm. In Oklahoma,
“Occupational disease,” as used in this act, unless the context otherwise
requires, means any disease that results in disability or death and arises out
of and in the course of the occupation or employment of the employee or
naturally follows or unavoidably results from an injury as that term is
defined in this act. A causal connection between the occupation or
employment and the occupational disease shall be established by a
preponderance of the evidence (OK §85A-65-D-1., my emphasis).
The workplace (and by virtue the employer) must be shown to be at fault by a
preponderance of evidence. The burden of proof has not changed that drastically;
employers may not have to be negligent, but they do have to be at fault.
Definitions of occupational disease further limit what is deemed “compensable.” In
Ohio:
(F) “Occupational disease” means a disease contracted in the course of
employment, which by its causes and the characteristics of its manifestation
or the condition of the employment results in a hazard which distinguishes
the employment in character from employment generally, and the
employment creates a risk of contracting the disease in greater degree and
in a different manner from the public in general. (OH § 4123.01, my
emphasis).
Here, not only is the requirement that the disease is occupational, it must be shown
176
to arise from employment in a way that is beyond the risk faced by the general public.
While the state is cautious to make employers liable for something which their activities
did not directly contribute, such a standard simplifies the relationship between disease,
exposure, and outcome. The requirements of workers’ compensation statutes, focused on
the discrete exposures measured in laboratories that were used to attribute exposure to
disease provided more ways of limiting compensation. As Murphy writes,
Enshrined in investigation protocols, juridical precedents, and workers’
compensation rules, the use of such technologies and the formulation of
specific causality became necessary to prove the very existence of
occupational illness (Murphy, 2006, p. 59, my emphasis).
Statutes may omit diseases of “ordinary life” or those that cannot be shown to be
“occupational” in origin. Definitions of occupational disease may enumerate exhaustive
exclusions, or list the only diseases the state deems compensable. Sometimes they do both.
In the case of silicosis, it is widely considered to be a disease only occupationally-acquired.
However, silica exposure is also carcinogenic, can cause renal disease and autoimmune
disorders, but it is difficult to show that these ailments have occupational origins, and
instead can be attributed to multiple sources, including “lifestyle choices.” Compensability
may also be limited by temporal and geographic characteristics of the disease and of work,
detailed in later sections.
Thus, in sum, states define injury under disease, applying logics first founded on
often discrete injurious events onto ailments that may arise out of repetitive exposures.
Many states also preclude diseases of ordinary life or any disease that may have been
equally impacted by exposures faced outside of work. Mental illness is generally excluded.
Moreover, although one of the original intentions of workers’ compensation was to shift
the burden of proof off of the employee, many states require, in the case of occupational

177
disease, that a causal connection is demonstrated by a “preponderance of evidence.” Put
most directly by Wyoming, “The employee has a greater burden of proof in proving
compensability of “injuries which occur over a substantial period of time” (Wyo. Stat. §
27-14-603(a)).
Table 4.1: Examples of occupational disease definitions.
State Code Key points
Alaska AS §23.30.395 (24) “injury” means accidental injury or death arising out
of and in the course of employment, and an occupational disease or
infection that arises naturally out of the employment or that naturally or
unavoidably results from an accidental injury; “injury” includes breakage
or damage to eyeglasses, hearing aids, dentures, or any prosthetic devices
that function as part of the body and further includes an injury caused by
the wilful act of a third person directed against an employee because of
the employment
Injury is inclusive
of disease
Arkansas AR 11-9-601. Compensation generally. (e) (1) (A) “Occupational
disease,” as used in this chapter, unless the context otherwise requires,
means any disease that results in disability or death and arises out of and
in the course of the occupation or employment of the employee or
naturally follows or unavoidably results from an injury as that term is
defined in this chapter. (B) However, a causal connection between the occupation or employment and the occupational disease must be
established by a preponderance of the evidence. (2) No compensation
shall be payable for any contagious or infectious disease unless
contracted in the course of employment in or immediate connection with
a hospital or sanitorium in which persons suffering from that disease are
cared for or treated. (3) No compensation shall be payable for any
ordinary disease of life to which the general public is exposed.
Causal connection
from a
“preponderance of
evidence”
No compensation for “ordinary
disease of life”
Iowa IA §85A.8: An occupational disease must be incidental to the character
of the business, and a direct causal connection with the employment must
be shown. A disease from a hazard where the employee was equally
exposed outside the employment is not compensable.
Casual connection
Cannot be “equally
exposed” outside
work
Montana MT39-73-104 Eligibility requirements for benefits. (23) (a)
“Occupational disease” means harm, damage, or death arising out of or
contracted in the course and scope of employment caused by events
occurring on more than a single day or work shift. (b) The term does not
include a physical or mental condition arising from emotional or mental
stress or from a nonphysical stimulus or activity.
Must have a
relationship to
working day
Excludes mental
illness
178
Nevada NV § 617.430(2). An occupational disease shall be deemed to arise out
of and in the course of the employment if: (a) there is a direct causal
connection between the conditions under which the work is performed
and the occupational disease, (b) it can be seen to have followed as a
natural incident of the work as a result of the exposure occasioned by the
nature of the employment, (c) it can be fairly traced to the employment
as the proximate cause, and (d) it does not come from a hazard to which
workmen would have been equally exposed outside of the employment.
Causal relationship
Cannot be “equally
exposed” outside
work
South
Carolina SC § 42-11-10. “Occupational disease” defined. (A) “Occupational
disease” means a disease arising out of and in the course of employment
that is due to hazards in excess of those ordinarily incident to
employment and is peculiar to the occupation in which the employee is
engaged. A disease is considered an occupational disease only if caused
by a hazard recognized as peculiar to a particular trade, process,
occupation, or employment as a direct result of continuous exposure to
the normal working conditions of that particular trade, process,
occupation, or employment. In a claim for an occupational disease, the
employee shall establish that the occupational disease arose directly and
naturally from exposure in this State to the hazards peculiar to the
particular employment by a preponderance of the evidence.
Relationship
between hazard in
employment and
disease shown
through
“preponderance of
the evidence”
Rating the Impact of Workplaces on Bodies
Having a disease is not often significant enough to warrant compensation.
Compensation often requires demonstrable harm and the loss of one’s ability to work.
When occupational diseases were included under workers’ compensation, industry pressed
for their inclusion based on if the worker was disabled, how severely, and to what extent it
had impeded their ability to work (Rosner & Markowitz, 2006). Occupational diseases
were included in workers’ compensation statutes in a “negative” way, as efforts were
“primarily aimed at limiting coverage for diseases” (Kutchins, 1981, p. 217).
Today, workers’ bodies may be classified as suffering from “temporary partial
disability,” “permanent partial disability,” “temporary total disability,” or “permanent total
disability.” Restrictions persist in what are considered “impairment-based,” “loss-of-
earnings-capacity,” “wage-loss,” or “bifurcated” workers’ compensation systems where
eligibility for compensation is assessed by a body’s inability to work, wage diminishment,
the degree of impairment, and the expected duration of disease (National Academy of
179
Social Insurance, 2010). Benefits may be diminished commensurate with the degree of
disability and the degree to which other, non-work-related ailments influence a condition.
In these cases, the knowledge of a medical provider can limit or expand access to benefits.
For example, doctors’ opinions determine if, and if so, by how much, an ill worker’s
occupational affliction is compounded by a pre-existing condition such as asthma. For
occupational disease lifestyle choices such as smoking can be used by doctors to reduce or
invalidate claims altogether (Hopkins, 2015). A claim, therefore, is subject to certain
assumptions about how workers should also be caring for their bodies “responsibly,” and
seeks to limit anything for which an employer cannot be “blamed.” The use of the term
“occupational” merely shifts the language of blame.
Finally, to obtain “expert” knowledge often, employers require workers to use
employer-approved or insurance-approved medical providers to demonstrate that the
ailment is occupational. Doctors do not always provide objective analysis as has been
documented within the coal industry and the denial of hundreds of claims of black lung
disease (Hamby, 2014). Although some states allow workers to get second opinions, and/or
use a doctor of their own choosing, this varies by state. Claims may be litigated; in
Pennsylvania, it is up to a Workers’ Compensation Judge to evaluate the scientific evidence
to follow. There are other requirements for gaining eligibility that produce exclusions and
inclusions from spatial and temporal limits for disease manifestation, exposure, and work.
Spatiality of Temporal Limits
The workers’ compensation system requires a worker and their ailment fulfill
eligibility requirements under certain spatial and geographic logics that have developed
over different legislative histories. Each state’s statute has changed over the last century
with laws, exclusions, provisions, addenda, and case law that are dense and confusing.
180
Some retain incredibly vague requirements, while others provide tediously detailed
definitions and procedures for occupational disease claim. The complexity of how these
systems work produces a system that insufficiently meets the needs of ill workers. While
in theory, workers’ compensation serves as a mechanism by which the State seeks to
mediate the relationship between workers and employers and fulfill four key
responsibilities — humanitarianism, cost internalization, promotion of safety, and
vocational rehabilitation (Torrey, 2010), some states statutes preclude flexible employment
and moreover ignore common disease progression, including silicosis. Forms of ignorance,
willful or otherwise, are related to mechanisms of irresponsibility, a process Tronto
connects to Mills’ concept of ‘epistemological ignorance’ (Tronto, 2013). Ignorance, in its
various forms, is powerful too shaping knowledge, social processes that respond to risk
(for a collection of papers on this, see Proctor & Schiebinger, 2008). Here, by ignoring the
ways that disease progress, occupational disease statutes shift responsibility back onto
workers.
Workers must report the injury to begin the compensation process when injured or
ill due to a workplace hazard, accident, or exposure. These guidelines stipulate the behavior
of the ill worker. These behavioral requirements, not just the definitions of disease
themselves, produce inclusions and exclusions for those whose illness conforms to these
norms, and those that fall outside the purview of the state. Claims and notices are the first
steps in being recognized by an employer and by the State as another class of worker, an
ill employee, and to claim the benefits afforded by the compensation bargain. These
processes are a form of claims-making on the state to be recognized. Yet, the provision of
a service is not enough and is often mediated through complex procedures and forms of
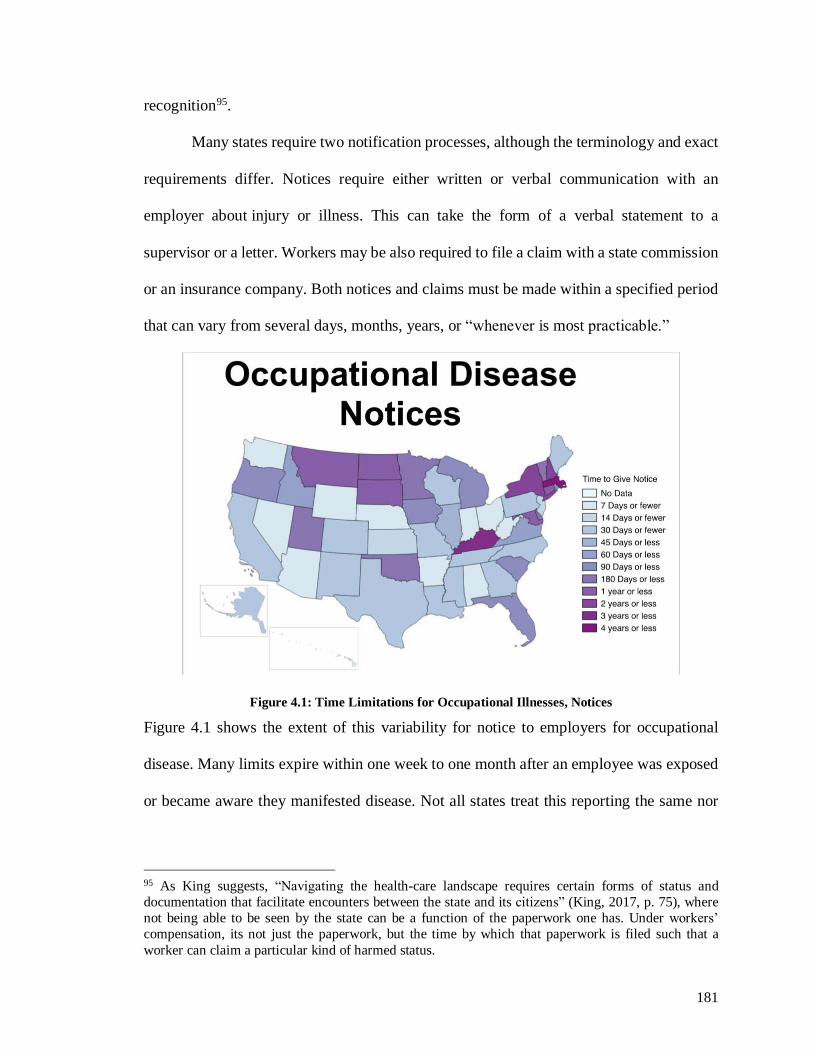
181
recognition95.
Many states require two notification processes, although the terminology and exact
requirements differ. Notices require either written or verbal communication with an
employer about injury or illness. This can take the form of a verbal statement to a
supervisor or a letter. Workers may be also required to file a claim with a state commission
or an insurance company. Both notices and claims must be made within a specified period
that can vary from several days, months, years, or “whenever is most practicable.”
Figure 4.1: Time Limitations for Occupational Illnesses, Notices
Figure 4.1 shows the extent of this variability for notice to employers for occupational
disease. Many limits expire within one week to one month after an employee was exposed
or became aware they manifested disease. Not all states treat this reporting the same nor
95 As King suggests, “Navigating the health-care landscape requires certain forms of status and
documentation that facilitate encounters between the state and its citizens” (King, 2017, p. 75), where
not being able to be seen by the state can be a function of the paperwork one has. Under workers’
compensation, its not just the paperwork, but the time by which that paperwork is filed such that a
worker can claim a particular kind of harmed status.

182
do they standardize when these “clocks” begin. However, within top oil and gas producing
states (Table 4.2) almost all notice requirements occur within one month (Pennsylvania,
Colorado, Texas), some as short as one week (Wyoming, West Virginia, Ohio). Failure to
give notice does not always disqualify a worker from compensation, but again, this depends
on the state and the type of claim.
Table 4.2: Top Oil and Gas States, Sept. 2017 (U.S. EIA, 2017)
State Oil (thousand
barrels/day)
Natural Gas (million
cubic feet/day)
Alaska 482 (3) 8,512 (3)
Colorado 397 4,667
Louisiana 133 6,325
North Dakota 1,081 (2) 1,933
Ohio 53 5,334
Oklahoma 469 7,009
Pennsylvania 18 14,808 (2)
Texas 3,574 (1) 21,560 (1)
West Virginia 26 4,585
Wyoming 215 4,722
Variability among states extends to occupational disease claims. Many states
stipulate that claims be filed within a period after a worker has become aware of their
disease, should have known of the disease, or since the disease manifests (Figure 4.2).
Often only a few years in length, these are more permissive requirements. Forty states
require claims following the employee’s knowledge, the average time being two years.
While adjacent states are often similar, in areas with hydraulic fracturing activities (e.g.,
Pennsylvania, West Virginia, Texas, Ohio, Colorado, North Dakota, and Oklahoma) these
requirements can range from within one year to within five.
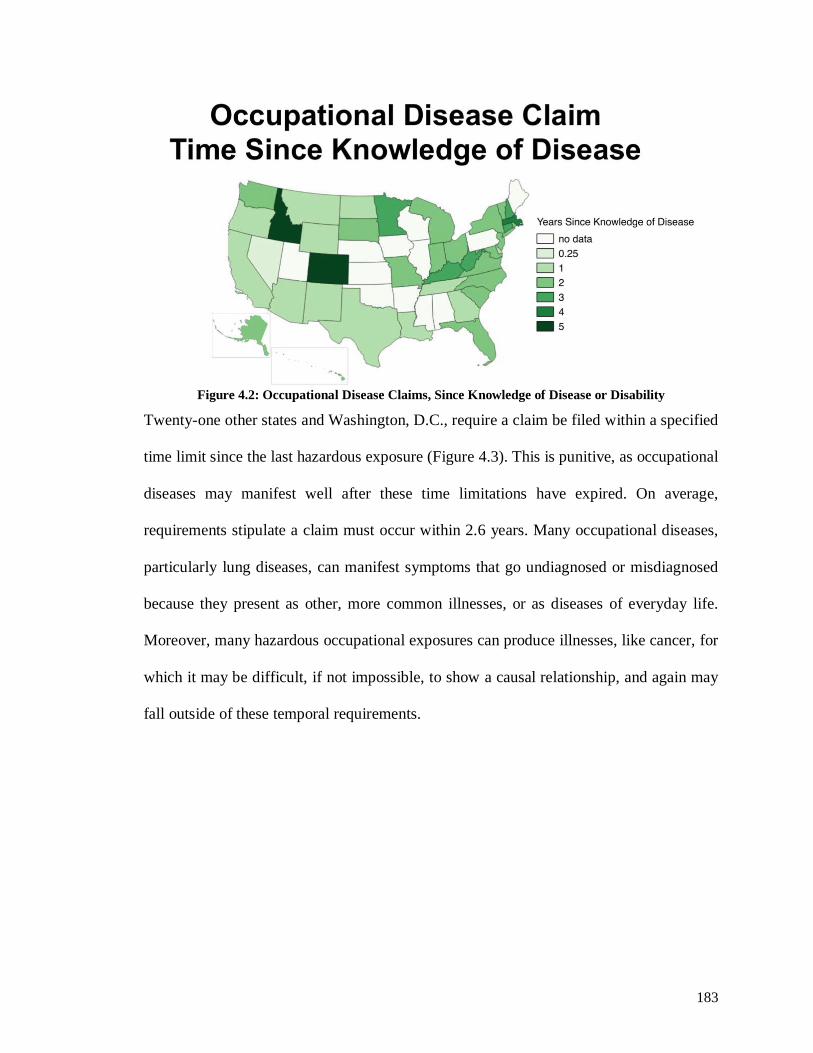
183
Figure 4.2: Occupational Disease Claims, Since Knowledge of Disease or Disability
Twenty-one other states and Washington, D.C., require a claim be filed within a specified
time limit since the last hazardous exposure (Figure 4.3). This is punitive, as occupational
diseases may manifest well after these time limitations have expired. On average,
requirements stipulate a claim must occur within 2.6 years. Many occupational diseases,
particularly lung diseases, can manifest symptoms that go undiagnosed or misdiagnosed
because they present as other, more common illnesses, or as diseases of everyday life.
Moreover, many hazardous occupational exposures can produce illnesses, like cancer, for
which it may be difficult, if not impossible, to show a causal relationship, and again may
fall outside of these temporal requirements.
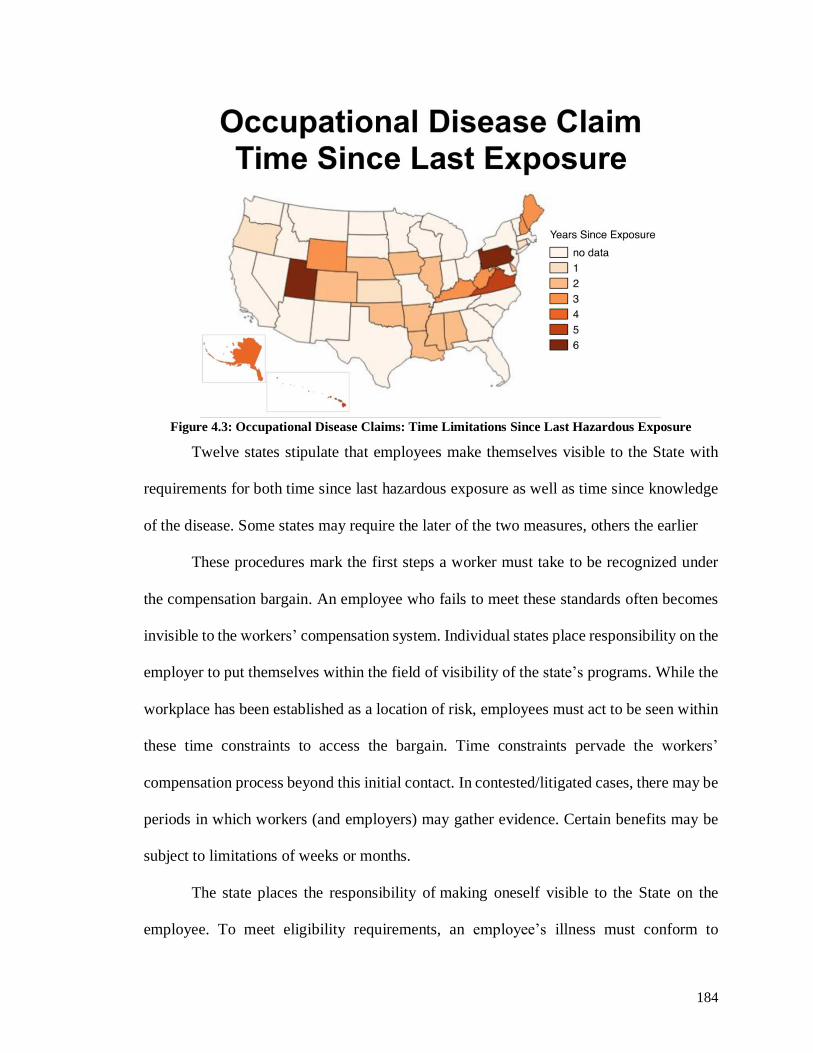
184
Figure 4.3: Occupational Disease Claims: Time Limitations Since Last Hazardous Exposure
Twelve states stipulate that employees make themselves visible to the State with
requirements for both time since last hazardous exposure as well as time since knowledge
of the disease. Some states may require the later of the two measures, others the earlier
These procedures mark the first steps a worker must take to be recognized under
the compensation bargain. An employee who fails to meet these standards often becomes
invisible to the workers’ compensation system. Individual states place responsibility on the
employer to put themselves within the field of visibility of the state’s programs. While the
workplace has been established as a location of risk, employees must act to be seen within
these time constraints to access the bargain. Time constraints pervade the workers’
compensation process beyond this initial contact. In contested/litigated cases, there may be
periods in which workers (and employers) may gather evidence. Certain benefits may be
subject to limitations of weeks or months.
The state places the responsibility of making oneself visible to the State on the
employee. To meet eligibility requirements, an employee’s illness must conform to
185
geographic and temporal parameters established by the state that limits what can be
compensated. Moreover, some states specifically articulate requirements for the silicosis,
“dusty diseases” and other pneumoconioses in both their requirements for claims and their
definitions of the disease.
Defining “Dusty Diseases”: “The Hitch,” and Silicosis Compensation
Workers’ compensation in many states precludes a worker from filing
compensation because their disease manifests outside of the time limitations set by the
state. However, this may also occur due to the flexibility of their employment. The ways
many states compensate long-latency diseases like silicosis does not conform to temporary
and transient employment. Many workers’ compensation statutes fail to accommodate the
structure of many industries, including workers involved in hydraulic fracturing activities
in the oil and gas industry.
Examining the “hitch” shows how the dynamics of industry and illness confound
the workers’ compensation requirements. A work schedule in the oilfield is known as a
“hitch.” Rotations vary across companies, but they are periods of intense work followed
by a break period of several days, weeks, or months. Workers may work twelve to sixteen-
hour days, two weeks on, two weeks off, three weeks on, one week off, or even six months
on, six months off, depending on where they work and for whom they work. Although
workers often stay in a general region during a hitch, workers can cross state borders
multiple times, working in layered or adjacent shale plays. The industry experiences high
turnover; individuals move in and out of oilfield work and between companies to avoid
layoffs or to secure better pay and better “hitches” (“better” geographic locations or on-off
schedules). Many oilfield workers may also come from other high-hazard industries, such
as mining, construction, defense services, and agriculture which may have exposed them
186
to health hazards over the years, including respirable crystalline silica. Many of the workers
I encountered at bars, and industry events had come from other dusty trades like coal or
construction.
When I drove around an area experiencing significant oil and gas development from
hydraulic fracturing—even in states where the industry has been long developed—trucks
from out of state or out of the country were noteworthy in small towns. During my time in
northeastern Pennsylvania, I became something of a license plate expert; at a distance, I
could identify the simplicity of a Texas license plate, the italicized lettering of tags from
Alberta, or iconic statute to the left side of plates from Oklahoma. While these tags often
are used to symbolize how oil and gas jobs, in some areas “not going to locals” or signal a
new wave of development and leases, they are also a key marker of the mobility of the
workers themselves. When eligibility requirements for compensation require certain
configurations of work, namely spatial fixity over a period of time, these patterns of work
are exclusionary to the governance structures that make employers liable for workplace
diseases like silicosis.
Hydraulic fracturing workers face hazards from exposure to silica most
significantly during hydraulic fracturing, particularly workers engaged in the material
handling of sand used in hydraulic fracturing, although lower-level exposures can occur
during other parts of the extractive process. During interviews with two health and safety
instructors, the instructors stressed how oil and gas was a great job, but that it was a dusty
one. Dust was just seen to be part of the job. The normalization of risk mirrors the
normalization of chronic pain and other ailments. In conversations at trade shows, drug test
companies and safety trainers would discuss with me the challenges of prescription drug
187
abuse to manage chronic pain. At long-term stay hotels, I found leaflets for chiropractors
and pain management clinics were posted alongside takeout menus for wings and local
sports bars. It is expected that work in this industry takes a heavy toll on the worker’s body.
Discursively, work takes on outsized importance because of the risk. Exposure to risk is a
key component to the ways workers are represented in both trade publications and health
and safety conferences. Even as the narrative is “we work safely” by implementing controls
on the hazards faced, the original, risky context is valorized; for example, workers are
lauded at conferences for the work they do, because it is dangerous, as they produce oil
and gas for the nation; often these claims are made by comparing oil and gas work and
safety procedures to those undertaken by the military and NASA. Here, examining how
discourses of risk help shape workers’ responsibilities underscores the relationship
between responsibility and vulnerability (Walker, 2008), where the long-term health
consequences of work are just a component of what it means to be a good and responsible
worker.
It follows then that the assumption of risk shapes the implicit and explicit ways that
workers are represented as being responsible for their own health. In the STEPs Safety
Video, new guy Joe suggests that wearing a respirator is going to be uncomfortable in the
heat of Texas. His new manager, Ted responds by emphasizing upon Joe how he will need
to consider in his day-to-day discomfort in wearing a respirator alongside the long-term
consequences of not wearing the mask. (Figure 4.5):
Joe: It’s pretty hot out here, Ted. This dusk mask–its just going to make it
worse.
Ted: Here, Joe. Take one of these straws. Try breathing through that. Now
breathe through it a little bit. Imagine walking around having to breathe
through that. The disease caused by silica, silicosis, is just like breathing
through that straw
188
Joe: Wow. That’s tough. (Lawhorn-Cryden, 2015).
Figure 4.4: Joe Breathing through a coffee stirrer (Lawhorn-Cryden, 2015)
Implicitly, Joe is being told that he needs to consider his life years from now if he does not
correctly and consistently wear the respirator. He takes on responsibility for mediating the
exposures his employer exposes him too, being asked to compromise short-term, but
meaningful discomforts in the face of potential long-term impacts. He moreover may lack
access to the benefits of the workers’ compensation bargain.
The spatial and temporal dynamics of the hitch would preclude many workers from
claiming for silicosis. As was discussed earlier, workers must file claims within a certain
amount of time and some states, although not all, have time requirements for silicosis,
dusty lung diseases, and other pneumoconioses. Like with general occupational disease
claims, these differ from state to state and are stipulated based on when a disease manifests,
the time since the last injurious exposure, or the later/earlier of the two dates. Figure 4.6
shows states that limit silicosis claims based on time since last hazardous exposure,
including several are states with extensive hydraulic fracturing activity such as West
Virginia and Oklahoma. In these states, the time requirements would preclude an employee
from filing a silicosis claim in the case of chronic silicosis, and in most cases accelerated
silicosis. In West Virginia and Oklahoma, these exclusions begin just three years after the
last hazardous exposure.

189
Figure 4.5: Silicosis and Pneumoconiosis Claims: Time Limitations Since Last Hazardous Exposure
The clock for other states’ requirements for silicosis claims begins at the time an
employee knew of the disease or at the time the disease manifested. This standard based
on knowledge of the disease or its manifestation is more permissive (Figure 4.7). Again,
several states heavily engaged in hydraulic fracturing activities have these limitations,
including Colorado and Oklahoma. If a worker gets an accurate diagnosis of silicosis
within the time requirements can be an issue. Because silicosis presents like several other
lung diseases, it often is not diagnosed until its later stages or after death, if at all. Several
states, including Oklahoma, West Virginia, and New Mexico, also stipulate temporal
requirements for time since last exposure and time since knowledge of the disease. In the
case of Oklahoma, an individual has one year to claim following knowledge, of the disease,
but within three years since the last exposure.
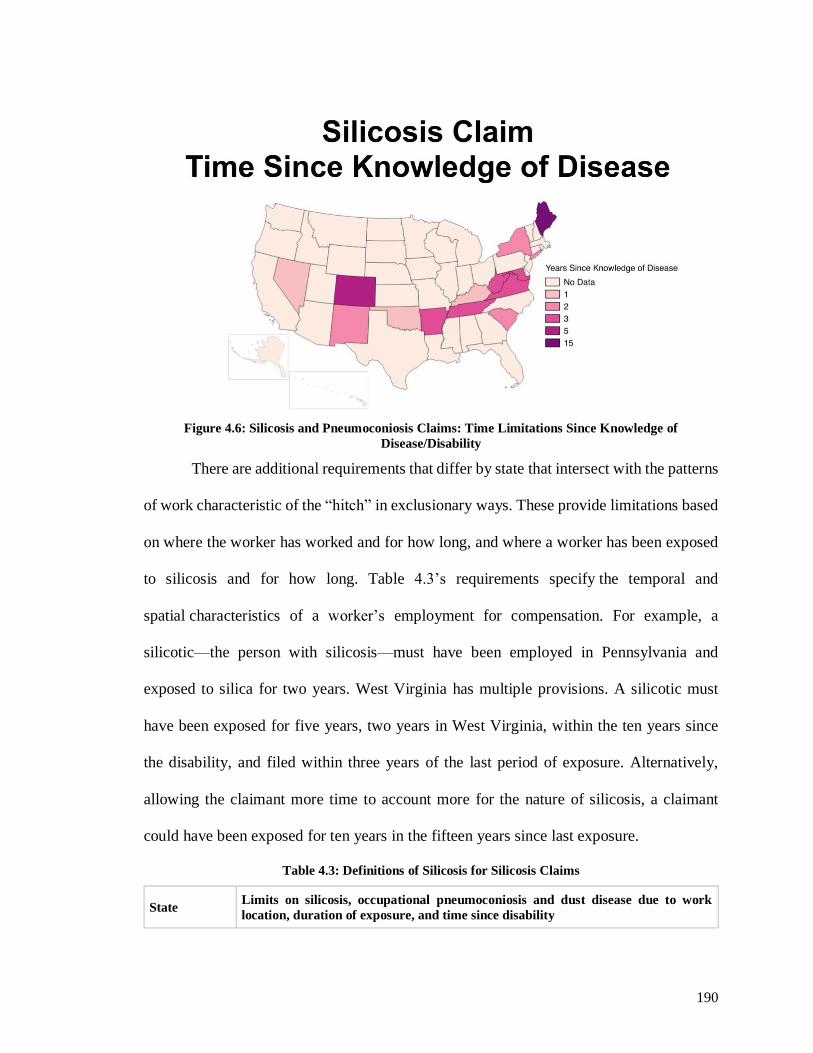
190
Figure 4.6: Silicosis and Pneumoconiosis Claims: Time Limitations Since Knowledge of
Disease/Disability
There are additional requirements that differ by state that intersect with the patterns
of work characteristic of the “hitch” in exclusionary ways. These provide limitations based
on where the worker has worked and for how long, and where a worker has been exposed
to silicosis and for how long. Table 4.3’s requirements specify the temporal and
spatial characteristics of a worker’s employment for compensation. For example, a
silicotic—the person with silicosis—must have been employed in Pennsylvania and
exposed to silica for two years. West Virginia has multiple provisions. A silicotic must
have been exposed for five years, two years in West Virginia, within the ten years since
the disability, and filed within three years of the last period of exposure. Alternatively,
allowing the claimant more time to account more for the nature of silicosis, a claimant
could have been exposed for ten years in the fifteen years since last exposure.
Table 4.3: Definitions of Silicosis for Silicosis Claims
State Limits on silicosis, occupational pneumoconiosis and dust disease due to work
location, duration of exposure, and time since disability

191
Alabama In the 5 years prior to injury, must have experienced 12 months exposures in each of the
12 months; the employee has 2 years from last exposure to file claim
Arkansas In 10 years prior to disablement, must have been exposed for 5 years, 2 of which must
have been in Arkansas; the disablement must occur within 3 years of last exposure
Idaho In 10 years prior to disablement, must have been exposed for 5 years, the last 2 of which
must have been in Idaho
Iowa In 10 years prior to the disability, must have been exposed for 5 years, 2 of which must
have been in Iowa
Kansas In 10 years prior to disability, must have been exposed for 5 years, 2 of which must have
been in Kansas; must manifest with 3 years
Kentucky Continuously exposed for 2 years in Kentucky
Maine In 15 years prior to disablement, must have been exposed for 2 years
Montana Must have inhabited Montana for previous 10 years
Nevada Must have been exposed to harmful amounts of silicon dioxide while employed in Nevada
for 1 year
New Mexico In 10 years prior to disability, must have been exposed during 1250 work shifts in New
Mexico; disablement must occur within 2 years of employment with whom claim is filed
Oklahoma In 10 years prior to disability, must have been exposed for 5 years, 2 of which must have
been in Oklahoma
Pennsylvania In 10 years prior to disability, must have 2 years aggregated exposure while employed in
Pennsylvania; must manifest with 300 weeks
South Dakota Must have been exposed for 2 years in South Dakota
West Virginia
In 10 years prior to disability, must have been exposed continuously for 5 years, 2 of
which must have been in West Virginia; Or 10 years exposure in 15 years since last
exposure; Claim must be filed within 3 years of last period of exposure of 60 days or
more, or within 3 years since diagnosis
These spatial and temporal parameters determine the compensability of disease. Many of
these requirements make workers exposed to silica in the hydraulic fracturing industry who
may develop lung diseases into the future ineligible for workers’ compensation due to the
nature of the disease and due to the characteristics of their work. They would be burdened
with the responsibility for occupational acquired disease by the nature of states’ exclusions.
Oilfield workers engaged in hydraulic fracturing work may be employed in one
state over a period of years, but only for a short duration as workers move from site to site
and traverse state boundaries to complete jobs. Workers may also shift employers over the
192
course of several months and find themselves employed in different states. Workers who
are exposed to silica in hydraulic fracturing operations, at its highest levels during material
handling, and at lower levels from well-site activities and construction, may not be captured
by this law once they begin to be symptomatic because of their employment history. Their
disease may not manifest in time to claim for benefits. Indeed, a key impetus for these
exclusions was to reduce and insulate costs, even from their earliest introduction into
workers’ compensation statutes in the 1930s. As these legacies have persisted to the
present, they continue to include these cost-limiting restrictions.
Workers’ Compensation in the Oilfield: Texas and Pennsylvania
There are several models for compensation represented across areas of extensive
hydraulic fracturing; these models have additional implications for occupational disease
and silicosis claims, and what it means for responsibility. For example, Texas uses an “opt-
out” strategy to workers’ compensation. As the name implies, this system allows employers
to opt-out of the compensation bargain. Texas’ system is more than a century old and
allows employers write their own compensation insurance and/or be subject to litigation.
Opt-out programs frequently have fewer benefits, shorter time claims periods, and have
little or no state or independent oversight. Employees do not have the option to opt-in or
out, employers do. Opt-out indicates a movement away from the intentions of the workers’
compensation bargain. Such measures favor employers, allow programs to be written to
the needs of individual employers, and shifts the injury and illness burden back to workers.
It is submitted that opt-out legislation is an overreaching pro-business
measure which, under the veil of innovative reform, will unconscionably
shifts costs of work injuries and deaths from employers to injured workers
and others. And a troubling part of this machination is the denial to injured
workers of access to the workers’ compensation adjudication system, or
some true equivalent, so that in case of dispute due process can be afforded
(Torrey, 2015, p. 9).

193
Employees may not have leverage in negotiating, mediating, or litigating
settlements as “non-subscriber” employers may require employees to sign arbitrations
agreements as a precondition of their employment (Torrey, 2015); some have indicated
that employers and their insurers are granted expansive discretion in changing the benefits
structure. Several southern states have tried to adopt this model recently, through a new
movement spearheaded by the Association of Responsible Alternatives to Workers’
Compensation built on Texas’s law (Grabell & Berkes, 2015; Torrey, 2015). However,
opt-out was recently setback when Oklahoma declared its program unconstitutional by the
state supreme court. The USDOL also began investigating Texas’s opt-out plans under the
Obama administration (Berkes, 2016).
In Texas, when workers’ compensation does apply, the Workers’ Compensation
Division within the Texas Department of Insurance does not have special provisions for
silicosis. Rather occupational diseases are only compensable if an employee gives notice
to an employer within 30 days after knowledge that the injury is work-related and files a
claim within one year. These requirements do not reflect the disease latency of chronic
silicosis.
Pennsylvania does not follow the “opt-out” model but may be setting a precedent
for other states through its case law regarding diseases of long latency. The Department of
Labor and Industry oversees the Commonwealth’s Bureau of Workers’ Compensation
which administers the Pennsylvania Workers’ Compensation Act and Occupational
Disease Act covering many of workers’ ailments, including occupational diseases, with
specific provisions for silicosis. Employers in Pennsylvania must hold workers’
compensation insurance, the state’s insurance fund, or be self-insured.
194
Workers’ silicosis claims must meet criteria codified by the Pennsylvania
Occupational Disease Act. Workers seeking compensation for disability or death from
several lung diseases, specifically, silicosis, anthraco-silicosis, coal worker’s
pneumoconiosis, or asbestosis must have been employed and exposed in Pennsylvania for
at least a combined two years in the ten years before the disability began and workers must
file for occupational diseases within 300 weeks (77 Pa. Stat. § 412). The parameters for
exposure to silica while employed in Pennsylvania and the window in which the disease
must have caused disability precludes many silicotics. For hydraulic fracturing, this may
prove even more challenging as they may not be employed in Pennsylvania for two years,
nor will they develop the disease in time to claim for benefits.
However, in 2013, the Pennsylvania Supreme Court ruled in Tooey v. AK Steel
Corporation that if occupational disease, in this case, asbestosis, manifests outside of the
prescribed temporal limits established under workers’ compensation then the immunity
from liability provided by the Workers’ Compensation Act does not apply, and a worker
can pursue civil cases against their employers. This decision included scrutiny of the
purpose of the Workers’ Compensation Act, and it’s stated “remedial” and “humanitarian”
goals.
[W]hen reviewing issues concerning the Act, we are mindful that the Act is
remedial in nature and its purpose is to benefit the workers of this
Commonwealth. Thus, the Act is to be liberally construed to effectuate its
humanitarian objectives, and borderline interpretations are to be construed
in the injured party’s favor. (Tooey v. AK Steel Corporation, 2013 p. 9).
The ruling focuses on the grammar within the Act that blurs its applicability to occupational
diseases that fall outside of the specific requirements. Drawing from the humanitarian spirit
of the law to restore injured workers, the Court unbound workers from the exclusive
remedy by finding they were not precluded from seeking damages. The court concluded
195
that because the State’s limitations exclude a worker from being “seen” by the workers’
compensation bargain, the bargain does not apply, thereby allowing them to seek
recompense through the courts. It has yet to be determined if and how this ruling will
impact Pennsylvania and other states. However, it points to the other mechanisms that
workers can seek for relief, such as torts and other forms of social insurance. Significantly
with respect to other social insurance, the court’s efforts to be humanitarian, caring, or
careful, in the application of the exclusive remedy of workers’ compensation, shifts the
burdens to other parts of the state that themselves insufficiently provide workers relief for
their occupationally acquired disease.
Workers’ Responsibility through Other Parts of the State
The apparent growth of the contingent workforce challenges existing
structures of data collection, legal responsibility and liability, and future
planning for social safety net programs. (Foley, et al. 2014, 773).
Although the workers’ compensation system reflects the responsibilities and
obligations of the state to take responsibility for its working society, the State has
intervened through other mechanisms for the good of society.
The welfare corporate society embodies at least three important principles
largely absent from earlier, more laissez-faire liberal capitalism: (1) the
principle that economic activity should be socially or collectively regulated
for the purposes of maximizing the collective welfare; (2) the principle that
citizens have a right to have some basic needs met by society and that where
private mechanisms fail the state has an obligation to institute policies
directed at meeting those needs; and (3) the principle of formal equality and
impersonal procedures, in contrast to more arbitrary and personalized forms
of authority and more coercive forms of inducing cooperation. (Young,
1990, p. 67).
Social insurance, at the state and federal level, has, in theory, affirmed the State’s
obligations to regulate economic activities in the interest of society and to ensure that
individuals have access to basic needs. Such efforts shift towards bureaucratic structures
196
wherein hierarchies, rules, and procedures are utilized to provide fair distributions and
outcomes. This has engendered multiple forms of social insurance that seek to capture
different kinds of harms and needs that the state must meet. While Young speaks highly of
the development of the welfare state, rooted in the idea of insurance-based compensation,
she also indicates its logical shortcomings and highlights, how disadvantaged peoples,
To a large extent, though not entirely, they are conditioned by
institutionalized rules and social practices that put people in differential
positions of power in relation to others, give some people higher status than
others, or afford them a wide range of options for their actions compared to
others (Young, 2008, p.39).
Indeed, while workers’ compensation provides one way to examine the ways that bodies
are measured in relation to one another, their worthiness of being compensated, this occurs
across all welfare programs. Inclusions and exclusions are made through a vast array of
social programs that determine the types of bodies that deserve state support or
intervention.
Through the compensation bargain, the state purposely limits workers’ ability to be
seen by other parts of the state. “[I]n practical terms, the workers’ compensation system
represents an enforced social compact.12 In trade for statutory coverage, workers are barred
from pursuing actions at law” (Kutchins, 1981, p. 213). The bargain limits what workers
can receive in return for their injuries. “To be barred from bringing an action for intentional
employer wrong-doing is a significant loss for workers” (Kutchins, 1981, pp. 214).
There are few options left to workers seeking monetary compensation or
recognition by the State for the harms they incurred through work. Workers can seek tort
litigation. These commonly must be brought against material manufacturers, who have, in
response to increased silicosis tort litigation in the 1990s and early 2000s leveraged several
of their own defenses (Cook, 2005). Although the recent ruling in Pennsylvania under
197
Tooey v. AK Steele may change how workers pursue silicosis claims in some places, more
commonly, workers turn to other parts of the state to seek relief from lost wages, medical
expenses, and the wear and tear of disease on daily life when they are excluded from the
purview of workers’ compensation.
A harmed worker may seek remediation through different social services if they
meet the eligibility requirements for those programs.
Other social benefit systems—including Social Security retirement benefits,
Social Security Disability Insurance (SSDI), Medicare, and, most recently,
health care provided under the Affordable Care Act—have expanded our
social safety net, while the workers’ compensation safety net has been
shrinking. There is growing evidence that costs of workplace-related
disability are being transferred to other benefit programs, placing additional
strains on these programs at a time when they are already under
considerable stress (Utterback et. al, 2016, pp. 5-6).
The USDOL found that cost shifting is particularly pernicious in high hazard industries,
where employers pay relatively little for the large costs their injuries place on individuals.
Findings of cost shifting, and the burdens families bear when workers’ compensation is
insufficient or unattainable concur with recent journalistic investigations of workers’
compensation that have additionally found unethical outcomes in the ways that these
programs provide compensation (Hopkins, 2015; Grabell & Berkes, 2015). Workers do not
receive adequate funds for their injuries and are forced to find recognition from other parts
of the state or self-fund the costs of work’s harms to the body. This requires workers find
ways to make their illness “visible” to different social services depending on the nature of
the issue. Moreover, access to such funds has been the basis for the diminishment of second
injury funds which were developed after World War II and would have captured those
workers in less “traditional” work structures where diseases were the product of current
work and previous experience (USDOL, 2016, pp. 18-19).

198
The programs to which costs are shifted are commonly grounded in different ideas
about how the state should intervene in “life.” This results in different benefit structures
and eligibility requirements. For example, Social Security Disability insurance is meant to
provide “partial income replacement to workers with significant work histories who
experience a severe disability that makes them unable to perform not only their past job
but any job in the national economy.” Workers’ compensation, by contrast, is for wages
and medical care specifically for to work-related ailments (USDOL, 2016, p. 30). Perhaps
more pernicious is that cost shifting moves costs to both individuals and families, but also
a social safety net program is largely paid for by contributions from payroll.
It is important to note that workers’ compensation costs are largely paid by
employers, with experience-rating to encourage employers to ensure
workplace safety. SSDI, on the other hand, is funded largely by payroll
contributions from nearly all workers and employers; contributions from the
current workers and employers – along with interest on the program’s
reserves and a small amount of revenue from income taxes on benefits –
fund the benefits of the current beneficiaries. (USDOL, 2016, p. 31).
Even as costs shift to other government programs, compensation and care of workers often
falls to individual workers and their families (Leigh & Marcin, 2012; Buffie & Baker,
2015; Hopkins, 2015). This cost-shifting is also a movement in the responsibilities for care
to the families of ill workers and workers themselves. As described in chapter 1, care and
responsibility help illustrate the relationality and networks through which social life
unfolds that cut across different levels of analysis. Here, it is not just that responsibility for
care is shifted to individuals but also that the shift occurs through the failure of the social
welfare system to adequately incorporate care and responsibility in its programs.
Workers’ compensation is a complex and bifurcated mechanism by which the State
sees injured workers, but it is not the only part of the state that measures, monitors, and
manages. The state sees through many programs using requirements that produce
199
inclusions and exclusions based on the underlying rationale for the program, or the
requirements established to show harm through a lawsuit. In each instance, the state
evaluates individual claims on the State, even as it seeks to manage its population. Taken
as a whole, the system—rather than restoring bodies, populations, and economies—
provides insufficient compensation to workers while simultaneously reproducing
mechanisms by which employers can shift the cost, burdens and harm their economic
activities produce. A key concern for health geographers, many of these insufficiencies
stem from the use of space and time to exclude.
Conclusion
At the same time, we can see that care is badly needed in the public domain.
Welfare programs are an intrinsic part of what contemporary states with the
resources to do so provide, and no feminist should fail to acknowledge the
social responsibilities they reflect, however poorly… Almost all feminists
recognize that there should be much more social and public concern for
providing care than there now is in the United States, although it should be
provided in appropriate and empowering ways very different from those in
place. There should be greatly increased public concern for child care,
education, and health care, infused with the values of care. (Held, 2006, p.
69)
Insofar as workers’ compensation aims to produce a social insurance that provides
for injured and ill workers, the mechanisms by which it seeks to achieve those aims, and
the contradictions internal to those efforts, need further examination. Here, not only are the
workers’ compensation programs insufficient, they internalized exclusionary logics and
requirements that undermine the humanitarian dimensions of workers’ compensation’s
stated goals. This chapter has tried to understand how through its efforts to be both
humanitarian and cost-limiting, the state has sought to shift responsibility and care for
workplace illness to workers, their families, and other parts of the state.
By examining how the state defines ‘occupational’ it is possible to see how first
200
particular ideas about bodies and configurations of workplaces, and second ideas about the
state’s responsibilities to minimize costs and provide humanitarian relief to workers, come
together under workers’ compensation statutes. The Occupational Safety and Health
Administration (OSHA) estimates that 2.5 million workers in the United States are
annually exposed to silica, and according to OSHA’s own analysis 30% of general industry
measurements exceed the older, more permissive PEL, and “19% exceeded it by 3 times
or greater” (OSHA, 2013). No national occupational disease registry exists to capture how
many individuals die of silicosis annually, and while its own analysis of death certificates
indicates that silicosis is declining, the CDC reports significant limitations in using these
data. Moreover, there are limitations when using workers’ compensation data due to
underreporting, lack of standardization, and the complexity introduced by contingent,
subcontracted, or non-traditional arrangements of labor (Foley, et al., 2014). Thus, there is
little definitive information to help illustrate the distributive impacts of silica exposures.
However, it is possible to illustrate how the procedures of filing a claim not only
contribute to this lack of data, but also themselves create injustices where certain kinds of
bodies are unable to make claims on the state. The governance of responsibility for health
is a spatiotemporal process, wrought by confusing, exclusive requirements, that further
silos long latency health concerns, reinforcing the adage “out of sight, out of mind”
discussed in Chapter 2. The workers’ compensation system reflects the responsibilities and
obligations of the State to take responsibility for its society and its economy. This involves
direct intervention by the State in the activities of employers, but also, workers.
Under workers’ compensation, the state affirmed that private economic activity
should be regulated for society’s benefit and that the state had the authority to intervene in
201
this capacity. How this has occurred has varied widely from state to state and body to body.
Through workers’ compensation, the State purports to protects workers by providing the
framework by which, in most cases, an employer or their insurance company is made to
pay for a harmed employee. However, such paternalistic responsibilities conflict, as was
the case in Chapter 2. Workers’ compensation programs also encode the State’s obligations
to employers: to protect them from unnecessary claims and costly litigation. It does so by
producing exclusions based on space and time. The state alleges that it is possible to know
what is best and fair for workers and employers, yet the state does not meet its obligations
to provide for, protect, and reintegrate those who have been excluded by way of illness.
How the state defines workers ailments as occupational and hence compensable is
illustrated through the spatial and temporal restrictions the state imposes. Not only are
benefits often insufficient, but they also exclude portions of society based on the eligibility
requirements used to “see” workers and their ailments that do not account for the
manifestation of diseases, nor the geographic and temporal patterns of work and
employment that workers in high hazard industries, like hydraulic fracturing, may face.
While employers might be liable under certain conditions, the responsibility to act fall to
workers to show that their ailment is occupational. Moreover, workers bear the
responsibility for the way their disease progresses and the spatial and temporal patterns of
their industry, depending on the state(s) they have worked in and for how long; in some
instances, this burden removes employers’ liability, and shifts responsibility onto workers
to find remediation through other parts of the state.
The techniques make certain bodies visible and others not, often in ways that belie
the progression of occupational diseases and the dynamics of the labor process. Through
202
the definition of occupational and specifications of diseases, programs have used
spatiotemporal parameters to limit compensable injuries and diseases, and individual
bodies. While fault is not the preeminent concern for compensability under workers’
compensation, the question of blame still lingers regarding whether a ‘workplace’ can be
seen to be at fault and if an employee can show that a disease is ‘occupational’ according
to the standards for that threshold set by the state. These limits make invisible workers in
industries that rely on itinerant labor, temporary workers, impermanent or mobile
worksites, and other labor practices where workers frequently move, change employers, or
are intermittently employed and exposed.
Taken as a whole, workers’ compensation, rather than restoring the flourishing of
bodies, populations, and economies, provides insufficient compensation to workers at the
same time it reproduces mechanisms by which employers can cost shift the burdens harms
from their economic activities produce. Indeed, workers’ compensation programs present
a form of social insurance that transfers risk back on to workers and on to other parts of
welfare state through other social insurances. As a matter of health governance, this
illustrates how responsibility for health is shaped by the exclusions produced by
governance structures, flexible employment, and spatial variability.
203
5. Chapter 5: Conclusion: Mapping New Geographies of
Responsibility in Occupational Health
As first described in Chapter 1, responsibility is about relationships, defining
accountability, expectations, and caring activities among institutions, groups, and
individuals for past circumstances and future possibilities. In OSH, many of these
responsibilities emerge through the laws and regulations defined and enacted by the state.
Chapters 2, 3, and 4 have examined different regulatory mechanisms through which this
occurs, including rulemaking, inspections, and workers’ compensation. However,
responsibilities for OSH can be contextualized and implied by the state in subtler ways.
Such methods are reflected in recent changes to OSHA’s website for silica. In October
2017, OSHA updated its website on silica, coinciding with the first implementation dates
of its new silica rule. The old version of the website had used quotes, some from the
informal hearings during the silica rulemaking, that registered the embodied consequences
of silica exposure for working bodies (Figure 5.1):
“Take a straw about the diameter of a dime and try to draw air through that
straw. And as time progresses, shrink the diameter of the straw. And then
put a bag over your head, because you slowly suffocate.” Lanny Wade,
safety and health consultant
“We are people, just like anyone else, and we deserve to have good health
just like anybody else.” Jonas Mendoza, Construction Worker.

204
Figure 5.1: Previous OSHA Website96
OSHA’s website had given voice to those who bore silica’s consequences, workers and
their families, not the most well-funded or the loudest. It had acknowledged the humanity
embedded within OSHA regulations, illustrating that there was something more behind the
highly technical and clinical language that comprises much of what constitutes its rules.
OSHA’s old silica website reflected its responsibility to protect workers.
The updated webpage substituted this narrative with one more accommodating of
OSHA’s responsibilities towards industry. The tacit ways silica impacts bodies and lives
are gone. The new website replaces this text with disembodied descriptions. It now states
that crystalline silica is abundant and that the respirable kind is smaller than the sand seen
at the beach or playground. More than once, the website stresses how small these particles
are. Now absent are statements such as “OSHA’s Final Rule to Protect Workers…” and
“Rule requires engineering controls to keep workers from breathing silica dust,” assertions
96 This image was generated using http://web.archive.org, a non-profit organization that records digital
traces on the internet.

205
and provisions many industry lobbyists contested during the rulemaking process. Other
information has been moved elsewhere and stripped of its old packaging. Once prominent
text that reported that the rule would result in 600 lives saved, prevent 900 new cases of
silicosis, and have $7.7 billion in net annual benefits is buried deep within a FAQs page. It
is not that basic facts are now absent, but how the information is conveyed and prioritized.
The website’s changed language, new look, and logo (Figure 5.2) is an indication
of a different attitude towards OSH; one that looks far more sanitized and clinical, more
cooperative with industry’s positions. This is perhaps best exemplified by what OSHA
intimates about responsibility in its silica logo. It reads: “Control Silica Dust. Breathe
Easier.” The grammar suggests that those who breathe are also those who control dust; the
responsibility to protect falls to the worker doing the breathing. These frameworks are
consequential. While such a change does not immediately signal a change in laws and
regulations, it sets a different stage for their enactment, a different tone for the ways rules
and regulations will be weighed, and a shifted context through which OSH problems will
be identified and approached.
Figure 5.2: OSHA logo for silica hazards
OSH continues to be a contested concept about the responsibility for risk and
uncertainty of what happens to individuals at work. It summons debates about
individualism, freedom, and agency and to whom or to what the state is more responsible,
206
industry or workers. Even as the state assures workers a right to a safe and healthful
workplace, the framework it uses to do so—that employers provide employees access to
safe workplaces—is not straightforward or fully realized, as is discussed in the empirical
chapters of the dissertation.
Health geographers have a long-standing concern regarding how individual
responsibilities for health and health risk are produced. It is not just that individuals are
made responsible for health risk; responsibilities persist and are reproduced at the
institutional level. This dissertation traced responsibilities, showing how, in particular, the
state’s concern for worker health is not absolute but emerges through the state’s
negotiations of responsibilities to different entities. It reexamined the relationships between
structural processes and bodies that shape human health. In OSH, the state has taken on
responsibilities to primarily two groups–workers and industry–whose interests do not
necessarily or often overlap. Occupational health provided this dissertation with a rich
context to trace responsibilities, as OSHA’s regulations ostensibly seek to rebalance
responsibilities for health risk but are also confounded by structural processes of work and
employment as exemplified by the hydraulic fracturing industry and its exposures to silica.
These institutional responsibilities have a complex relationship to the discourses of
responsibility associated with workers. The state’s efforts to distribute responsibilities are
entangled with, contradicted by, and reinforce discourses within OSH that stipulate
workers’ personal responsibilities often incentivized through sanctioned forms of caring.
Workers’ relationships to care valorize and reward the risks of oilfield work and
vulnerability to long-term disease. Workers are trained to protect and insulate their
coworkers from risk, ‘get home safe,’ but also produce energy for their nation and their

207
employers. Despite laws and regulations to the contrary, OSH discourses shift
responsibility for health risk to individuals. Not only does this occur through institutional
processes, procedures, and their insufficiencies, it is reinforced though relationships to care
in OSH training and discourse. Here, in the absence of a realized state framework for OSH,
the oilfield paradoxically valorizes and rewards risky work at the same time it incentivizes
workers to be safe by caring for fellow workers and their families.
In the remainder of this chapter, I suggest new engagements for health geography
that stem from this research, review the findings of the empirical chapters, and offer future
directions for the dissertation regarding theory and policy.
New Directions: Health Geographies of Occupational Health and Responsibility
This dissertation illustrated the value of using occupational health as a lens to
understand the historically contingent web of structures, processes, and social norms
reproduced at the institutional and individual level that shape human health. Although both
qualitative and quantitative analyses within health geography have grappled with the
influence of place on bodies and bodies on place, its central focus has not often been on
occupational health. Occupational health provides an opportunity to think about the
relationships between human health and place, as it, by its nature, asserts a relationship
between them: it is health as produced by and through relationships between working
bodies and their workplaces. Occupational health offers a way to think through key
normative tensions surrounding what health and health risk mean, who is responsible for
health and health risk, and who has a right to health. The dissertation demonstrated that
health geographers have rich empirical opportunities to continue to conceptualize and
theorize health in new institutional contexts and through different OSH concerns.
Occupational health is not just about bodies and their workplaces but is mediated
208
through institutional rules and regulations. It is a constellation of institutional structures,
socio-economic processes, and individual actions that seek to mitigate the risk and
uncertainty of the bodily outcomes of individuals at work. In the U.S., occupational health
is posited as a right to a particular workplace, the right to a context in which to make
‘healthy’ decisions. Such a framework, as shown through this dissertation, has significant
limitations as it continues to focus on individualized actions rooted in notions of rational
actors/workers, and embodies a concern for the health of industry as well.
Thus, occupational health is a constructed concept that expresses the relationships
between bodies and laboring in particular places, sustained through rules and regulations
that not only regulate individual bodies but also regulate industry and the state itself. The
responsibilities of the state are multiple, negotiated, and often contradictory. How these
institutional responsibilities are conceptualized and unfold through time have an impact on
human health and exposure to health risk. As discussed in Chapter 1, the concept of
responsibility has helped geographers to explore neoliberal processes particularly around
the management of risk (Bickerstaff, Simmons & Pidgeon, 2008; Mansfield, 2012a,
2012b). While these often focus on the production of individual responsibilities produced
through policies, discourse, and social norms, it is equally important to consider how
responsibilities are defined, shifted, and contested institutionally. Each of the empirical
chapters seeks to map the relationships that define and are defined by multiple institutional
responsibilities. Thus, this dissertation called on health geographers to think about the
nuances of the state and its interests in protecting human health by tracing relationships of
responsibility.
An Interest in Health?: Rethinking the State’s Responsibility for Occupational Health
Health geographers have opened the ‘black box’ of the body and have sought to
209
complicate the environment and render it active in academic conceptions of health
(Guthman & Mansfield, 2013). From intersectional approaches to political ecologies of
health to a simultaneous emphasis on socio-natures of the environment and the body, health
geography has become a dynamic field that explores the complex relationship between
health and place despite persistent friction surrounding its methodological divisions and
theoretical pluralism. New foci on the liveliness of viruses and bacteria and their co-
dependencies on the body, and examinations of the environment that insist on its dynamism
within human and non-human health, have reshaped the scales and relations geographers
explore to more complex and more ephemeral processes (Guthman & Mansfield, 2013;
King & Crews, 2013; Jackson & Neely, 2015).
Health geographers have more domains through which to unpack the state’s
interests in human health, and how it is constituted through spatial practices and
assumptions, particularly by examining occupational health. Health geographers focus on
how health emerges through rationalities and techniques of power that encode self-
disciplining logics to facilitate the governance of populations. These produce a politics of
the body in how individuals should care for one another, and also how an individual should
be responsible towards and care for itself (Mansfield, 2012a, 2012b; Murphy, 2015). While
the actions of the state are problematized for reproducing homophobia, racism, and sexism,
rarely are the underlying commitments of the state seen as being competing, multiple, or
incompatible. Similar issues could be directed towards efforts within health geography to
understand the ways that the neoliberal state shifts responsibilities for care through logics
of self-care, and thus reinforces individual responsibility for health risk. Concerns for the
infusion of neoliberal thinking into health programs and policies do not go far enough to

210
examine the commitments of the state to ‘industry’s’ health as well.
Chapter 2 and Chapter 4 considered how the ‘problem’ of workers’ health sits at
the intersection of the state’s competing commitments to its citizenry and their well-being,
but also the development of a flourishing economy. This dissertation took seriously the
idea that the state’s interest in human health is itself a product of complex institutional
processes that distribute, negotiate, and reify particular paradigms of responsibility. This is
important as health geographers engage in discussions surrounding the ‘right to health,’
within human rights frameworks (Carmalt & Faubion, 2010), wherein the focus turns to “a
broadly conceived set of elements required for humans to be as healthy as possible”
(Carmalt & Faubion, 2010, p. 298) but where the other interests the state has, which may
well compete with its interest in health, are under-examined. In summary, occupational
health offers health geographers empirical opportunities to richly engage and deepen many
of its theoretical interests in ways that have normative implications for how we
conceptualize human health.
Health for whom or for what?: Rethinking Health Responsibility as Multiple through
Rulemaking, Inspections, and Workers’ Compensation
In rethinking responsibility, I suggested not only a shift in focus from the individual
to the institutional, but I also emphasized a more complicated idea of what the concept
means as it manifests within institutional regulations and practices for health. This means
seeing responsibility of and for health and health risk as forward- and backward-looking,
and as mediated through discrete events and structural processes. Each chapter of the
dissertation took a distinct approach to thinking about responsibility by unpacking a
mechanism the state uses to regulate responsibility for OSH in the oilfield. In each case, it
is not just that the state distributes responsibilities, but how it distributes responsibilities

211
for health risk and to what effect. I use a summary of the chapters of the dissertation to
identify future contributions of this framework for health geography.
Chapter 2 examined how responsibility is negotiated in participatory spaces of
rulemaking. The chapter found that not only is the state responsible towards the health of
both workers and industry but that its mechanism for writing new regulations and
negotiating its own responsibilities reproduce problematic ways of conceptualizing OSH.
Using the example of recent silica rulemaking, this chapter reframed how health geography
has engaged with the state by showing that the ways it regulates health risk reflect its
competing commitments. The governance of health risk is shaped by unresolved questions
about to whom OSHA has the greater responsibility, industry or workers.
In regulating occupational health, OSHA considers not only the health of workers
but also that of industry. The rules and regulations of rulemaking reflect how the neoliberal
state has reoriented relationships to risk and responsibility. The state has dueling
obligations to protect industry and workers, which it mediates through three tests of
significant risk and feasibility. OSHA bears the burden of meeting these tests, and OSHA’s
success or failure in doing so is the basis on which regulated and affected parties can contest
proposed regulations. These tests include concern for industry’s ability to implement new
regulations without threatening industry’s vitality in addition to concerns for human health.
Rulemaking allows for the personification of industry as a moral entity and as an entity
that has ‘health,’ an allowance which has consequences. In the arena of rulemaking,
industry is able to reproduce a narrative in which its own health is protected by individual
workers’ use of respirators, a narrative in keeping with broader trends within OSH in the
oilfield. Regulations would have shifted the burden of protection from workers themselves
212
on to individual companies. Industry further utilized this platform of rulemaking to deny
its own responsibility for producing silicosis deaths and to suggest that its own vitality
precluded it from implementing measures to protect workers health.
The chapter also showed how health risk responsibilities are produced through the
discourses and practices of governance which reify and rely upon “rationalist” notions of
government action and individual bodies. Such a focus laid bare the ways that the
organization and practice of responsibility among actors demonstrates who and what is
valued (Walker, 2008). Under the premise of guaranteeing workers the right to a safe and
healthful workplace, rulemaking is the venue in which OSHA negotiates its responsibilities
to workers and to industry that have developed through a long history of vested interest
groups. In summary, Chapter 2 showed that the state’s interest in human health manifests
as complex, political negotiations that weigh competing truths about to which health,
workers’ or industry’s, it is most responsible. In so doing, it also showed the complexities
of seeing industry as able to make claims on the state for the protection of its own vitality,
offering new ways for health geographers to trace responsibilities for health risk.
Chapter 3 showed how conceptualizing industry as a unit capable of ‘responsibility’
has utility, however, when examining the enforcement of OSHA standards. OSHA
requirements utilize a model where OSHA is responsible for assuring that employers
provide a safe and healthful workplace. OSHA focuses on employers’ provisions of
contexts in which workers should be able to act healthfully. This does not guarantee
workers a healthful bodily state. OSHA finds employers responsible and liable for creating
unhealthful workplaces when OSHA discovers an employer has failed to meet OSHA’s
standards for what constitutes a safe and healthful workplace.
213
Chapter 3 examined how responsibility-as-liability enacted through OSHA’s
enforcement of regulations holds individual companies responsible for creating unhealthful
working conditions measured by exposures at a certain place and time. This approach
requires a discrete overexposure to silica to ascribe a punitive outcome (an OSHA citation)
to an employer. The state’s conceptualization of responsibility, however, fails to
contextualize the emergence of health risk through structural patterns of work and
employment. It relies upon finding responsibility for risk in individualistic and isolated
instances, rather than by more broadly considering structural processes that themselves
confound OSHA’s enforcement policies. This is further problematic as OSH discourses
absolve industry of responsibility by locating responsibility within individual workers,
particularly by valorizing forms of care, that not only reinforce, but in some instances are
contradictory to, OSH goals. Thus, OSHA’s logics of enforcement overlook existing tools
that could help diminish oversights posed by subcontracting and fail to contextualize the
contexts in which OSH risk emerges.
The oilfield’s organization and operating locations provide the industry means to
absolve itself of responsibility for health risk because blame cannot be found. Specifically,
Chapter 3 drew upon interviews, participant observation, and analysis of OSHA inspection
records to illustrate barriers to inspections in the oilfield. These included not being able to
find well sites given their remote location, not being able to find hydraulic fracturing sites
while they were operating given the short duration of silica exposing activities, and the
complex factors that shape exposures including weather and equipment layouts. Thus,
Chapter 3 illustrated what health geographers could gain from exploring occupational
health more extensively, demonstrating how the subcontracted organization of the oilfield

214
intersects with the underlying assumptions that guide how the state seeks to protect
workplaces from silica hazards. Structural conditions of hydraulic fracturing enable
hazardous working conditions and allow industry members to allude oversight by
distancing overseeing companies from the actual exposure, or by merely making it difficult
for the state to measure exposure. Young’s Social Connection Model (2008) reframed these
issues by providing language and critique to see industry as responsible towards structural
processes from which it profits.
By drawing on Young’s critique, Chapter 3 showed how OSHA’s model is
confounded by the flexibility of the hydraulic fracturing industry and the contexts in which
this flexibility unfolds. An organization of work that by design shifts responsibilities away
from larger companies, subcontracting has material consequences for the techniques used
to govern human health, including those that regulate hydraulic fracturing and silica
exposures. Indeed, inspections techniques and rationalities work to limit the state’s
authority to govern occupational health in part because of the limited ways OSHA
conceptualizes responsibility. In summary, Chapter 3 showed how OSHA’s framework for
workplace responsibility is insufficient as it leaves OSHA subject to the structural
dynamics that not only shape unhealthful workplace conditions but that also confound its
own enforcement efforts. This underscored the need within health geography to examine
the relationship between the geography of industry and the governance of health risk.
Finally, Chapter 4 explored the problematic ways that responsibility is enforced
through narratives of liability and blame by considering responsibility-without-fault in
workers’ compensation in the US. This chapter examined how the requirements for
workers’ compensation of occupational disease, and how these intersected with the

215
spatiality of oilfield work. Ostensibly this social insurance shifts concerns about who
caused the disease off of workers by not requiring workers show who was at fault. Workers’
compensation nevertheless has developed such that workers bear this burden in multiple
ways. Specifically, using the hydraulic fracturing industry and silicosis as examples, the
chapter examined how responsibility for occupational disease is produced by the
exclusions encoded within workers’ compensation statutes, flexible employment and work,
and persistent underlying assumptions about the relationship between employers and
employees.
Workers’ compensation statutes burden workers with the responsibility for the way
their diseases progress and the spatial and temporal patterns of their industry. The state
paradoxically re-inscribes responsibility on individual workers through requirements that
“see” workers and their ailments under particular requirements. These often exclude the
latency of many diseases and are ignorant to the spatial patterns of work and employment
of many high hazard industries, including hydraulic fracturing. In some instances, where
worker’s compensation relief is inaccessible due to these restrictions, workers must find
remediation through other parts of the state and from their social networks. Such patterns
take on specific contours in the oilfield due to the spatiotemporal practices of the industry
but also are illustrative of concerns regarding workers’ compensation that apply to other
highly mobile industries.
Significantly, the definition of what constitutes a compensable illness uses time and
space as exclusionary measures for workers’ access to compensation. Employers may be
liable, but workers bear the responsibility to become sick in the right way. Workers’
compensation relies upon exclusions to this social insurance that belie the latency of many

216
occupational diseases and patterns of flexible employment. This functions to shift
responsibility (and care work) onto workers and their families. The chapter showed the
significance of tracing the procedural requirements embedded within practices of OSH
responsibilities by the state. Even when the state seeks to assign responsibility without a
notion of fault, it continues to rely on definitions of causality that place responsibility back
onto workers.
The state uses a framework for responsibility that enrolls the state’s obligations to
employers: to protect them from unnecessary claims and costly litigation. Thus, due to the
state’s interests in not only being humanitarian, but also cost-reducing for industry, the
workers’ compensation system reproduces a form of fault-finding by another name —
occupational. Chapter 4 illustrated how finding an ailment ‘occupational’ means that
workers’ compensation eligibility is determined by a body’s physical and spatiotemporal
attributes such that ‘blame’ and ‘fault’ are re-inscribed in the system. The chapter showed
how the state’s responsibilities to minimize costs and offer workers humanitarian relief for
workplace illness manifest in the definitions of ‘occupational’ within these statutes.
In summary, Chapter 4 illustrated how, instead of achieving its stated goals
(restoring bodies, populations, and economies), workers’ compensation transfers risk and
operates as a mechanism that shifts the burdens of harms from economic activities back
onto workers. Importantly, this chapter used the example of silicosis claims and the
hydraulic fracturing industry to illustrate how health governance and responsibility for
health emerge through exclusions produced by governance structures, flexible
employment, and disease latency. While health geographers have shown the ways that
prevailing paradigms within the health and medical sciences shape institutional definitions

217
of health, this chapter reveals how laws and regulations encode different concerns in their
framing of health through a focus on responsibility.
Together, these chapters illustrated how individuals and institutions are connected
through complex relationships of responsibility, often that center around protecting
‘health’– industry’s and workers’– from risk. Tracing multiple notions of responsibility
revealed how workers and OSH are connected to one another, through time and space, and
by policies and regulations that dictate relationships of responsibility This approach
highlighted how the state ideally structures responsibility for and towards health risk and
the processes the state uses to enact that distribution of responsibility. It showed how the
state’s efforts to ostensibly redistribute responsibility reproduce the individualistic notions
of responsibility that circulate through OSH, contributing to our understanding of the
processes that shape health governance, but also that influence health justice.
These insights helped ground the ways this dissertation unraveled the complexity
of health governance and its consequences. Health governance in this context flows from
ways that the state’s interest in worker health concedes concern and consideration for
industry health. The way the state defines responsibility decontextualizes the broader
structural processes that produce unsafe health exposures. This works to limit the state’s
own regulatory and enforcement efforts and reinforce longstanding discourses about
responsibility for occupational health risk. This system, through diverse channels,
inconsistencies, oversights, and powerful narratives, works to leave workers individually
responsible for occupational health risk.
Future Theoretical Engagements: Mapping Responsibility in OSH
While the dissertation examined the ways that tracing a reimagined responsibility
provides a new analytic lens for health geography, future engagements of this research
218
could expand upon several themes in greater detail that would provide important synergies
with other parts of the discipline and the social sciences more broadly. For example, the
concept of uncertainty offers other directions for the study of OSH and responsibilities for
and towards health risk. Uncertainties abound in the OSH context, be they material (the
ability to measure an exposure (See Murphy, 2006)) or discursive (narratives of
unknowability in rulemaking (See Michaels, 2008)). Uncertainty underpins OSH in the
oilfield, as OSH policies and procedures seek to insulate workers and employers from the
unknown consequences of work be they physical, financial, clinical, or otherwise. This
would contribute to the growing interests within health geography surrounding the
production and circulation of uncertainty, particularly that research which seeks to
“account for why this uncertainty exists and how it is claimed, produced and reconstructed
by different interest groups across time and space” (Senanayake & King, 2017, p. 6).
A key component of this literature to date has focused on uncertainty– real,
‘manufactured,’ or intrinsic to science. The uncertainty of scientific knowledge, how it is
produced, managed, circulated, and given authority through particular populations, social
practices and culture, the state’s activities, and the scientific enterprise itself such that it
produces power relations and impacts social and science policy (Murphy 2006; Wagner &
Steinzor, 2006; Michaels, 2008; Zinn, 2008). This emphasis on how science claims are
produced to sustain and maintain particular power relationships and achieve particular
political ends could be used to more fully conceptualize ways that material and discursive
forms of uncertainty emerge in OSH in the oilfield. While uncertainty figures into the
‘science’ of regulatory activities, it has other dimensions. For example, Hall has recently
written on the relationship between temporary employment and the uncertain outcomes of

219
injury reporting in influencing how workers deal with their injuries (Hall, 2016). Others
have written on the multiplicity of uncertainties and ‘unknowns’ and the ability of states to
capture or control them (O’Malley, 2004). The empirical contributions of this dissertation
could contribute a new dimension from which to examine OSH and uncertainty through a
particularly geographic lens by focusing on the multiple dimensions of the ‘uncertainty’ of
hydraulic fracturing’s flexible operations and how it influences the regulation of risk.
Another future direction of this dissertation would be a more thorough undertaking
of the relationship between OSH, the imaginaries of workers encoded with OSH policies
and regulations, and its relationship to regulating health risk through engagement with
feminist and critical scholarship. In many instances OSH has historically utilized an
imaginary of the ‘average’ white male body, a rational actor not in need of protection,
excluding bodies that are seen as more fragile and irrational through the ways they are
racialized or gendered (Sellers, 1997; Messing, 1998; Markowitz & Rosner, 2002; Murphy,
2006). Yet, simultaneously this white male body is rendered disposable; in the case of the
oilfield, for the ways ‘his’ labor reproduces the ‘nation’ and its geopolitical and
geoeconomic goals. Here, feminist health geography could provide useful insights to
understanding the relationships between health, gendered and racialized identities, and
OSH activities that much of the empirical discussion of OSH in the oilfield could also
contribute to. Men’s experiences of health are mediated through multiple negotiated
masculinities (Courtenay, 2000; Courtenay & Keeling, 2000; Thien & Del Casion, 2012),
and is a negotiation that may be influenced by the organization of a company’s safety
structure (Filteau, 2014). As health narratives often reify dominant narratives of individual
responsibility, so too do health narratives reinforce and privilege masculine, white,

220
heterosexuality especially in science and policy surrounding health (Del Casino, 2007;
Brown, 2009; Sothern & Dyck, 2009; Brown & Knopp, 2010; Mansfield, 2012c).
OSH requires particular ideas of the self, of work, and of the population, as it relies
upon the multiple, and often contradictory strategies of self-monitoring, regulation and
direct intervention to shape workplace culture, space, and behavior. These processes are
significant to understanding the context of OSH for extractive industries which have
historically centered around and symbolized certain kinds of masculinity (Scott, 2010).
Future directions from this dissertation could connect how these ideas of the laboring self
and health are connected to and reproduced by the ways that the state regulates OSH
concerns. As OSH has often focused on the white, heterosexual man, its structures have
also produced and excluded those populations it views as marginal. Feminist geography
provides a lens into the reproduction of sexist and racialized power relations and provides
a framework for critically examining the role the state has in governing workers’ bodies
further. Thus, by drawing on the OSH imaginary of a worker, as mediated through
regulatory spaces, future research could more fully trace the justice implications at the
intersection of health, identity, and policy through a particularly feminist and geographic
lens. This would provide ways of further developing this dissertation’s engagement with
not only responsibility but also care. Questions of the relationship between care, gendered
processes, and gendered identities have been central to the theorizing of care and the
relationship of care and responsibility to feminist ethics and justice (Tronto, 1993; Held,
2006; Tronto, 2013).
The reduction of care to the private realm reserved for women, as something
below politics, has been challenged by feminist geographers inspired
particularly by the work of feminist political theorists who posit care as the
key to social accountability and responsible citizenship (see, for example,
221
Tronto, 1993). (McEwan & Goodman, 2010, p. 104).
For Tronto (2013), the relationship between hegemonic masculinities and discourses of
‘tough guys’ not caring is significant a dimension to the reproduction of many of these
processes. With more attention to the ways the oil and gas industry, through OSH in
particular, requires care-at-work, and sanctions particular forms of care, the dissertation
could contribute a different lens on the ways that care both is used to reinforce, but also
undermine public/private distinctions and gendered social relations.
Much of this dissertation focused on the ways that the state has reoriented its
responsibilities to working individuals such that it achieves its aims to protect the economy
and its public. Still, the dissertation has not examined how individuals and populations
internalize the state’s logics in ways that are self-regulating and self-disciplining. This
could be a future direction for the research presented in this dissertation. Such a focus
would necessarily entail far greater attention to biopolitical forms of power within OSH
and could engage with feminist geographers who have sought to understand the
relationship between power/knowledge and the reproduction of oppressive institutions,
particularly patriarchy and capitalism, through prevailing forms of governance (Pykett,
2012). This research seeks to understand the politics of everyday life and have drawn upon
theorizations of biopower and discipline to understand how through direct rule, and self-
regulation, institutions, particularly the state and the family, coordinate social control
(Mills, 2011; Staeheli, 2013; Smith, 2016). As mentioned in the introduction, much of the
focus in health geography on responsibility has been looking at issues of
responsibilitization, particularly as individuals internalize logics about self-care and self-
management. Thus, the ideas about the self, and how much workers internalize them, are
key lingering questions. Such questions may also pose challenges to Young’s social

222
connection model that need to be further considered.
With respect to the state, feminist geographers have also emphasized how the state
produces gendered, racialized and sexed bodies through state programs, policies, and law
(MacLeavy, 2007). The law acts to produce certain truths about bodies that produce and
maintain power relations and is also the mechanism by which it wields fear and shapes
understandings of the self. Critical and feminist scholarship could be further explored in
this dissertation through more engagement with the notion of public and private that has
driven much critical and feminist scholarship over the last three decades. As previously
mentioned, one dimension of this is the ways that care and responsibility work to reinforce
particular ideas about bodies in space. While health geographers have at times implicitly
and explicitly examined issues of public and private with regards to women’s health (Dyck
et al., 2001; Parr, 2004) and public health programs (Biehler, 2009), a more substantial
focus would help illustrate the reproduction of central liberal tensions that emerge through
governmental and biopolitical power over bodies and health. In particular, feminist
theorists and geographers, including Iris Marion Young, have focused on the ways that
public-private divisions restrict different groups from full participation in social life or as
citizens. For women, this is often rooted in notions of the home, and the maintenance of
patriarchal power. These scholars have shown how despite its rhetorical use as an
impermeable boundary, public and private are blurred in practice, where it suits particular
needs, particularly as it has allowed the state to reinstate its own patriarchal roles and
responsibilities.
Another approach to furthering the engagements of this dissertation would be to
more fully theorize the ways that the state’s rules and regulations self-regulate its own

223
authority to reinforce notions of public and private. This is particularly evident in the ways
OSHA enforces regulations for OSH. Much like Cuomo has shown how domestic violence
response seeks to root out ‘bad’ male heads of household while re-articulating and re-
asserting the privacy of the home and the public/private divide (Cuomo, 2015), much could
be further explored about the ways inspections, for example seek to expose ‘bad’ industry
actors, while maintaining workplaces as a space relatively free of direct state oversight.
Such avenues would provide new ways of thinking about what health governance protects
and reproduces through the logics that inform its activities.
Indeed, such critical geographic and feminist analysis has provided clear examples
of the ways that law is mutually constitutive of space, both public and private, inclusionary
and exclusionary (Blomley and Bakken, 1992; Brickell & Cuomo, 2017). State logics and
laws thus mediate public and private, and individuals and industry, and binds workers and
employers to certain OSH responsibilities and conditions of employment. These are
particularly significant insofar as laws not only create and reproduce space and time, but
also embody particular assumptions about space and time, as has been seen in the examples
in this dissertation. Exploring the relationships between the co-constitution of law and
space can be further enhanced by studies of occupational health.
In summary, there are many theoretical opportunities for this research to expand
and to consider further. Deeper engagements with uncertainty, gender and identity,
biopolitics, and the production of public and private through conceptualizations of caring
responsibilities in OSH and the state’s laws and regulations could provide more insights
not only for geographers but also policymakers.
Future Policy Considerations for OSH: Shifting approaches to responsibility
This dissertation challenged the techniques and rationalities that underpin how the

224
state approaches securing workers’ a right to a safe and healthful workplace. It highlighted
the problematic ways that OSH is framed by the state and reinforced through its procedures.
It also underscored practical concerns and considerations that policymakers could use to
help guide future decisions such that workers’ health receives the attention and weighting
that the ‘right to a safe and healthful workplace’ suggests.
First, Chapter 2 illustrated the ways that the state has not yet fully decided to whom
the state is more responsible, workers or industry. OSHA is burdened with showing ill
harm to workers from certain chemicals and no (or manageable) harm to industry. Practices
are deemed safe until shown otherwise. This approach to risk, one that displaces a
precautionary approach through, in particular, many Supreme Court interpretations (See
Chapter 2, also Vogel, 2012), automatically places industry in the privileged position.
Industry can expose workers until their practices are shown to be to be harmful to workers
and can use contestations over knowledge and scientific legitimacy to slow if not impede
regulatory change (Michaels, 2008). Policymakers can propose and implement policies and
future legislation that work to shift, if not reverse the approach within the US to
environmental and human health risks that has been reactionary rather than precautionary
(for some comparisons and suggestions, see Vogel (2012)’s discussion of the EU’s shifting
approach to regulation).
As shown in Chapter 2, rulemaking further reifies this permissive approach by
forcing OSHA to meet feasibility tests of its new rules. Changing requirements to make
industry members identify ways of being complaint with OSH regulations would be one
small step towards shifting these burdens. More significant change could include requiring
industry to show that the products and practices used have, or can be made to have, minimal
225
risk. While such small change would itself be difficult given the political realities of the
federal government, they are goals to work towards for policymakers interested in
reweighing the state’s obligations.
Another approach stemming from the findings in Chapter 2 would be to utilize state
and local regulatory frameworks to change laws surrounding silica and other hazardous
substances. States with state-plan OSHA could implement and enforce stronger limits to
exposures to substances known to be hazardous; many localities also can regulate activities
in workplaces and could, for example, outlaw practices that expose workers to certain risks.
This is already a practice being pursued by many labor groups, but one that could be
expanded to include concerning activities in industries that are not formally represented by
organized labor.
Chapter 3 highlighted problems with the ways that the state enforces its regulations.
Laws and regulations can be strict, but lack consequence if they are not enforced. Chapter
3 elaborated on different ways that the hydraulic fracturing industry is able to allude
OSHA’s oversight, including the ways the flexibility and location of the industry impede
inspection efforts. Some of the most practical considerations from this chapter include
developing a database of where and when industrial practices are ongoing so that inspectors
have a better chance of finding worksites and monitoring the hazardous exposures of
concern. With respect to hydraulic fracturing, some states already require this kind of
reporting about oil and gas work practices. The construction industry also maintains a
database of this nature through a state university. OSHA could rely upon one of its many
training centers, or its voluntary partnerships with universities and industry to help
maintain these types of records and provide a centralized database that inspectors could

226
query.
Further, OSHA could more fully enforce its multi-employer policy, introduced in
Chapter 3, and expand its definition of a controlling employer, or the employers deemed
responsible for the conditions of work. This would allow OSHA to issue citations to more
industry members within the subcontracted structure responsible for producing hazardous
working conditions. The immediate employer would not be the only one cited for an
individual hazardous exposure. Instead, OSHA could trace responsibility back to the
overseeing contractors and operators. These recommendations would not undermine the
current system of subcontracting but would provide ways of closing some of the gaps in
oversight that emerge through the ways OSHA’s definition of responsibility for OSH risk
is enforced.
Chapter 4 detailed insufficiencies and exclusions central to the ways the state
navigates its humanitarian and cost limiting goals for workplace illness. These exclusions
should be removed to reflect the nature of occupational disease and the spatial mobility
and other realities of many industries. These changes to statute would need to be
accomplished on a state by state basis or through the implementation of a federal workers’
compensation system.
Moreover, the burden of proof in workers’ compensation still often rests with the
employee. Further changes could involve requiring employers or their insurance
companies to show that workers had not been exposed to hazardous substances that caused
the illness; employers are required to keep safety data sheets on all hazardous substances
in the workplace as well as implement programs to remediate concerning substances.
Employers thus could provide the data to show that workers were not exposed. Omissions
227
in data would require great forms of deceit to disprove a workers’ claim, were the
concerning substance present. This would also shift the reporting responsibilities,
somewhat, off of workers and on to the industries who benefited from their labor. Still,
these changes would not fundamentally reverse or fix the underlying and uneven
insufficiencies within the workers’ compensation system, of which more funding, complete
overhauls, if not an entirely new system, is likely required.
Finally, OSH training and materials themselves could be carefully reframed with
respect to silica and other hazards. Many models in the oilfield seek to reinforce and re-
inscribe workers as the most, and best, way to mitigate OSH concerns. Narratives that place
workers at the center of identifying and mitigating health risks, particularly from
substances that they do not have to be exposed to in the first place (there are alternatives to
silica, including ceramics and coated silica), underscore institutional processes that cause
workers to bear the burden of health risk. This is not to say that workers should not be
trained in how to keep themselves out of harm’s way. Workers should be made aware of
the risks of work and given tools to manage many of them. It would be hard to argue that
workers should not be taught how to avoid slips in wet circumstances, how to de-energize
power supplies, or how to use wetting methods when cleaning environments to reduce dust.
However, not all hazards need a worker to mitigate them. Many can be addressed through
engineering controls, substitutions, and administrative controls and workers should be
made aware of these control technologies, so, when at all feasible, workers have the
knowledge to request different solutions to hazards.
Behavioral models that place the burden on workers to mitigate and ‘take
responsibility’ for their health can also reinforce notions that workers’ exposures to the risk

228
were their fault in the first place. This ultimately shifts responsibility away from the
employers for whom, in many cases, these risks were produced as a consequence of their
industrial efforts. While training should offer methods for workers to keep themselves safe,
these should not reproduce the notion that workers themselves are responsible for the
hazards and their health consequences, nor should they reinforce discourses which valorize
and incentivize risk-taking.
In the same way, official discourses from OSHA could be reframed. OSHA could
use its language and role in producing knowledge about workplace safety and health to
better underscore different relationships of responsibility. As the introduction to this
chapter indicates, how OSH problems are framed shapes implicit messages about who is
responsible for OSH risk. OSHA could utilize understandings of OSH risk that make more
central its own commitments to worker health.
In summary, the analysis and findings of Chapters 2, 3, and 4 offer ways of thinking
about regulatory mechanisms through responsibility that can inform directions to take OSH
policy in the future. Although the suggestions above work within the existing frameworks
for OSH in the US, they do seek to change the tenor of the state’s approach towards
responsibility for OSH. This includes seeing responsibility more expansively so as to
include the subcontracted nature of many OSH risks, and moreover, shifting the burden of
who must show risk onto the industries and employers who produce them.
Conclusion
So think real hard, Joe, before you take that respirator off. Make sure you’re
in a safe area. We do our part here to try to make sure we provide a safe
work environment, but you gotta do your part too. (Lawhorn-Cryden, 2015).
Responsibilities for OSH emerge through complex frameworks that are set and
enacted by the state, but which are also shaped and furthered through industry’s narratives.
229
As manager Ted from the STEPS Silica Training Video explains to Joe in vocabulary that
echoes the state’s regulatory language, responsibilities lie with many parties. However, the
final, most immediate responsibility falls to workers even when that regulatory framework
distributes responsibility elsewhere. This occurs through complex negotiations of
responsibilities, not only of workers deciding whether or not to wear a respirator, but also
in the negotiations of responsibilities by the state. OSH both exceeds and is directed by
how the state views its responsibilities and implements those it imposes onto others.
Regulatory frameworks for OSH in the U.S. diffuse responsibility in problematic
ways. This dissertation used the context of the occupational exposures to silica in hydraulic
fracturing to call on health geographers to reexamine relationships among institutions and
individuals that influence human health. The dissertation has argued that tracing
responsibilities as they manifest at the institutional level can provide a new lens to examine
the governance of health risk. Responsibilities can be multiple but also distributed amongst
actors in ways that bear examination as they reproduce structures in which workers are
exposed to, and made responsible for, workplace hazards. For Young,
Part of the difficulty of seeing structures, moreover, is that we do not
experience particular institutions, particular material facts or particular rules
as themselves the source of constraint: the constraint occurs through the
joint action of individuals within institutions and given physical conditions
as they affect our possibilities. (Young, 2008, p.55).
By focusing on occupational health, health geographers have an opportunity to
conceptualize these processes through laws and regulations that stipulate a relationship
between workplaces and human health. These insights provide health geographers not only
new empirical and theoretical directions, but also tools to engage in and contribute to policy
discussions regarding how the state seeks to protect and provide for human health.
Responsibility for OSH unfolds through complex negotiations, frameworks,

230
discourses, and practices. The state’s interest in OSH is mediated through, often competing,
responsibilities to other entities. Thus, the provision and protection of the right to a safe
and healthful workplace is not simple or fully realized. As exemplified by the changes to
OSHA’s website, in the U.S., the underlying conceptions used by the state to articulate its
commitments to working people are ever more significant as the new administration seeks
to rebalance its responsibilities to workers and employers in both blunt and subtle ways.

231
Works Cited
ACC (American Chemistry Council). (2014, August 18). Post-Hearing Brief of the
American Chemistry Council Crystalline Silica Panel. OSHA-2010-0034-4209,
ACC.
Adgate, J. L., Goldstein, B. D., & McKenzie, L. M. (2014). Potential Public Health
Hazards, Exposures and Health Effects from Unconventional Natural Gas
Development. Environmental Science and Technology, 48 (15), 8307-8320.
Andrews, E., & McCarthy, J. (2014). Scale, shale, and the state: political ecologies and
legal geographies of shale gas development in Pennsylvania. Journal of
Environmental Studies and Science, 4(1), 7-16.
API (American Petroleum Institute). (2009). Hydraulic Fracturing Operations – Well
Construction and Integrity. API.
———. (2014). Post-Hearing Comments from the American Petroleum Institute (78 Fed
Reg. 56274 (Sept. 12, 2013)). OSHA-2010-0034. API.
API (American Petroleum Institute) & IPAA (Independent Petroleum Association of
America). (2014). Comments of the American Petroleum Institute (“API”) and the
Independent Petroleum Association of America (“IPAA”) in Response to the
Occupational Safety & Health Administration (“OSHA”) Proposed Rule entitled
“Occupational Exposure to Respirable Crystalline Silica” (78 Fed. Reg. 56274
(Sept. 12, 2013)). OSHA-2010-0034- 2301, API & IPAA.
Asher, R. (1987). The Limits of Big Business Paternalism: Relief for Injured Workers in
the Years before Workmen’s Compensation. In D. Rosner, & G. E. Markowitz,
Dying for Work: Workers’ Safety and Health in Twentieth-Century America (pp.
19-33). Bloomington, Indiana: Indiana University Press.
———. (1991). Organized Labor and the Origins of the Occupational Safety and Health
Act. New Solutions, 24(3), 279-301.
Bale, A. (1987). America’s First Compensation Crisis: Conflict over the Value and
Meaning of Workplace Injuries under the Employers’ Liability System. In D.
Rosner, & G. E. Markowitz, Dying for Work: Workers’ Safety and Health in
Twentieth-Century America (pp. 34-52). Bloomington, Indiana: Indiana
University Press.
———. (1988). Assuming the Risks: Occupational Disease in the Years Before Workers’
Compensation. American Journal of Industrial Medicine, 13, 499-514.
Barnetson, B. (2010). The Political Economy of Workplace Injury in Canada. Athabasca
University Press.
Barnett, C., Cloke, P., Clarke, N., & Malpass, A. (2011). Globalizing Responsibility: The
Political Rationalities of Ethical Consumption. West Sussex, United Kingdom:
Wiley-Blackwell.
Bell, D., Hollows, J., & Jones, S. (2017). Campaigning culinary documentaries and the
responsibilization of food crises. Geoforum, 84, 179-187.
Benner, C. (2002). Work in the New Economy: Flexible Labor Markets in Silicon Valley.
Malden, Massachusetts: Blackwell Publishing.

232
Berkes, H. (2016, March 25). Labor Secretary Calls Workers’ Comp Opt-Out Plans
‘Pathway to Poverty’. National Public Radio. Retrieved October 7, 2017
http://www.npr.org/sections/thetwo-way/2016/03/25/471849458/labor-secretary-
calls-workers-comp-opt-out-plans-a-pathway-to-poverty
Bickerstaff, K., Simmons, P., & Pidgeon, N. (2008). Constructing responsibilities for
risk: negotiating citizen-state relations. Environment and Planning A, 40, 1312-
1320.
Biehler, D. D. (2009). Permeable homes: A historical political ecology of insects and
pesticides in U.S. public housing. Geoforum, 40(6), 1014-1023.
Blackley, D., Crum, J., Haldin, C., Storey, E., & Laney, A. S. (2016, December 16).
Resurgence of Progressive Massive Fibrosis in Coal Miners — Eastern Kentucky,
2016. Morbidity and Mortality Weekly Report, 65(49), 1385-1389.
Blomley, N. K. (1990). Federalism, Place, and the Regulation of Worker Safety.
Economic Geography, 66(1), 22-46.
Blomley, N. K., & Baken, J. C. (1992). Spacing Out: Towards a Critical Geography of
Law. Osgoode Hall Law Journal, 30(3), 622-690.
Boyer, K. (2003). At work, At Home? New Geographies of Work and Care-giving under
Welfare Reform in the US. Space and Polity, 1, 75-86.
Brickell, K. and Cuomo. D. (2017). Feminist Geolegality. Progress in Human
Geography, First Published October 23, 2017.
Brown, B., and Baker, S. (2012). Responsible citizens: Individuals, health and policy
under neoliberalism. London, United Kingdom: Anthem Press.
Brown, M. (2003). Hospice and the spatial paradoxes of terminal care. Environment and
Planning A, 35, 833-851.
———. (2009). 2008 Urban Geography Plenary Lecture-Public Health as Urban Politics,
Urban Geography: Venereal Biopower in Seattle, 1943-1983. Urban Geography,
30(1), 1-29.
Brown, M., & Knopp, L. (2010). Between anatamo- and bio-politics: geographies of
sexual health in wartime Seattle. Political geography, 29(7), 392-403.
Brown, T., & Bell, M. (2008). Imperial or postcolonial governance? Dissecting the
genealogy of a global public health strategy. Social Science and Medicine, 67(10),
1571-1579.
Brown, T., & Duncan, D. (2002). Placing geographies of public health. Area, 34(4), 361-
369.
Brown, W. (2015). Undoing the Demos: Neoliberalism’s Stealth Revolution. Cambridge,
Massachusetts: MIT Press.
Brundage, T. (2011). A Study Examining the Value of Pre-employment Training
Conducted by the Marcellus Shale Education and Training Center in Response to
the Needs of the Gas and Oil Industry. University Park, Pennsylvania: The
Pennsylvania State University.
http://irtd.ed.psu.edu:5000/pdfnew/FinalDissertationSubmittedtoDLPon9711.pdf
233
Brundage, T., Kelsey, T., Lobdell, J., Michael, L., Jacquet, J,. Ladlee, J., Lorson, J., and
Murphy, T. (2011). Pennsylvania Statewide Marcellus Shale Workforce Needs
Assessment. Marcellus Shale Education & Training Center.
Buffie, N., & Baker, D. (2015). Rising Disability Payments: Are Cuts to Workers’
Compensation Part of the Story? Center for Economic and Policy Research.
Carmalt, J.C. & Faubion, T. (2010). Normative approaches to critical health geography.
Progress in Human Geography, 34(3), 292-308.
Carter, E. (2012). Enemy in the Blood: Malaria, Environment, and Development in
Argentina. Tuscaloosa, Alabama: University of Alabama Press.
———. (2015). Making the Blue Zones: Neoliberalism and nudges in public health
promotion. Social Science and Medicine, 133, 374-382.
Casey, J., Savitz, D. A., Ramsmussen, S. G., Ogburn, E., Pollak, J., Mercer, D. G., &
Schwartz, B. S. (2016). Unconventional natural gas development and birth
outcomes in Pennsylvania, USA. Epidemiology, 27(2), 163-172.
CDC (Center for Disease Control). (2002). Health Effects of Occupational Exposure to
Respirable Crystalline Silica. CDC, Department of Health and Human Services.
Cincinnati, Ohio.
———. (2016). Hierarchy of Controls. CDC, Department of Health and Human Services.
Retrieved November 28, 2017
https://www.cdc.gov/niosh/topics/hierarchy/images/hierarchycontrols.jpg
Cherniack, M. (1986). The Hawk’s Nest Incident: America’s Worst Industrial Disaster.
New Haven, Connecticut: Yale University Press.
Coe, N. (2012). Geographies of production III: Making space for labour. Progress in
Human Geography. 37(2), 271-284.
Collins, J. (2009). Gender, Labor, and Power in the Global Apparel Industry. Chicago,
Illinois: University of Chicago Press
Collins, T., Gineski, S., Chakraborty, J., Montgomery, M., & Hernandez, M. (2015).
Downscaling Environmental Justice Analysis: Determinants of Household-Level
Hazardous Air Pollutant Exposure in Greater Houston. Annals of the Association
of American Geographers, 105(4), 684-703.
Cook, J. (2005). The Availability of Intermediary-Based “Arguments” in Texas Silicosis
Litigation. St. B. Tex. Environmental Law Journal, 35, 169-191.
Courtenay, W. H. (2000). Constructions of masculinity and their influence on men's well
being: a theory of gender and health. Social science and Medicine, 50(10), pp.
1385-1401.
Courtenay, W. H. & Keeling, R. P. (2000). Men, Gender, and Health: Toward an
Interdisciplinary Approach. Journal of the American College Health, 48(6), 243-
246.
Craddock, S. (1995). Sewers and scapegoats: Spatial metaphors of smallpox in nineteenth
century San Francisco. Social Science and Medicine, 41(7), 957-968.
———. (2000). Disease, social identity, and risk: rethinking the geography of AIDS.
Transactions of the Institute of British Geographers, 25(2), 153-168.
234
Cuomo. D., (2015). Policing Citizenship: The State Response to Intimate Partner
Violence in Center County, Pennsylvania. (Unpublished Doctoral Dissertation).
The Pennsylvania State University. University Park, Pennsylvania.
Cusick, M. (2013, March 1). SEC Investigating Outgoing Chesapeake Energy CEO
Aubrey McClendon. StateImpact Pennsylvania. Retrieved June 29, 2016
Dean, M. (2009). Governmentality: Power and Rule in Modern Society. London: Sage.
de Bernardo, M. A. (2014). Halliburton Energy Services, Inc. Comments to NPRM on
Occupational Exposure to Crystalline Silica (Docket No. OSHA 2010-0034).
OSHA Docket 2010-0034-2302, Halliburton.
Del Casino Jr., V. J., 2007. Flaccid theory and the geographies of sexual health in the age
of Viagra. Health and Place, 13(4), pp. 904-911.
Derickson, A. (1998). Black Lung: Anatomy of a Public Health Disaster. Ithaca, New
York: Cornell University Press.
———. (2013a). Dangerously Sleepy. Philadelphia, Pennsylvania: University of
Pennsylvania Press.
———. (2013b). “Nuisance Dust”: Unprotective Limits for Exposure to Coal Mine Dust
in the United States, 1934–1969. American Journal of Public Health, 103(2), 238-
249.
Domosh, M. (1998). Geography and Gender: home, again? Progress in Human
Geography, 22(2), 276-282.
Donnelly, P. (1982). The Origins of the Occupational Safety and Health Act of 1970.
Social Problems, 30(1), 12-25.
Dorman, P. (1996). Markets and Morality: Economics, Dangerous Work, and the Value
of Human Life. Cambridge, United Kingdom: Cambridge University Press.
———. (2006). Regulating Risk at Work: Is Expert Paternalism the Answer to Worker
Irrationality? In V. Morgensen, Worker Safety Under Siege: Labor, Capital and
the Politics of Workplace Safety in a Deregulated World. Armonk, New York:
M.E. Sharpe.
Duncan, G. (2003). Workers’ compensation and the governance of pain. Economy and
Society, 32(3), 449-477.
Dyck. I., Davis Lewis, N., & McClafferty, S.2001. Geographies of Women’s Health,
Routledge.
Edwards, G. A., Reid, L., & Hunter, C. (2015). Environmental justice, capabilities, and
the theorization of well-being. Progress in Human Geography, 40(6), 754-769.
Ehrlich, R. (2015). History and Medicine — the Case of Silicosis. American Journal of
Industrial Medicine, 58, S1-S2.
England, K. (2010). Home, Work and the Shifting Geographies of Care. Ethics, Place
and the Environment, 13(2), 131-150.
ERG (Eastern Research Group). (2013). Hydraulic Fracturing and Worker Exposure to
Silica. Submitted to Office of Regulatory Analysis Occupational Safety and
Health Administration, U.S. Department of Labor.
235
Esswein, E. J., Breitenstein, M., Snawder, J., Kiefer, M., & Sieber, W. K. (2013).
Occupational Exposures to Respirable Crystalline Silica During Hydraulic
Fracturing. Journal of Occupational and Environmental Hygiene, 10(7), 347-356.
Esswein, E., Snawder, J., King, B., Breitenstein, M., Alexander-Scott, M., & Kiefer, M.
(2014). Evaluation of Some Potential Chemical Exposure Risks During Flowback
Operations in Unconventional Oil and Gas Extraction: Preliminary Results.
Journal of Occupational and Environmental Hygiene, 11(10), D174-D184.
Evan, B. & Colls, R. (2009). Measuring Fatness, Governing Bodies: The Spatialities of
the Body Mass Index (BMI) in Anti-Obesity Politics. Antipode, 41(5),1051-1083.
Falzon, M. A. (2009). Multi-sited ethnography: theory, praxis and locality in
contemporary research. London, United Kingdom: Routledge.
Faria, C. (2008). Privileging prevention, gendering responsibility: an analysis of the
Ghanaian campaign against HIV/AIDS. Social & Cultural Geography, 9(1), 41-
73.
Fedotov, I. A., Eijkemans, G. J. M. (2007). The ILO/WHO global programme for the
elimination of silicosis (GPES). World Health Organisation GOHNET
Newsletter, 12, 1–4.
Fehling, D. (2014, June 24). Feds Target Oil and Gas Industry for Underpaying Workers.
NPR StateImpact Texas. Retrieved July 2, 2016
https://stateimpact.npr.org/texas/2014/06/24/feds-target-oil-gas-industry-for-
underpaying-workers/
Filteau, M. (2014). Who Are Those Guys? Constructing the Oilfield’s New Dominant
Masculinity. Men and Masculinities, 17(4), 396-416.
———. (2015a). A Localized Masculine Crisis: Local Men’s Subordination within the
Marcellus Shale Region’s Masculine Structure. Rural Sociology, 80 (4), 431–455
———. (2015b). Go Back to Texas, Gas Bastards! How a Newcomer Population of
Itinerant Energy Workers Manage Dirty Work Stigma in The Marcellus Shale
Region. Society and Natural Resources, 28(11), 1153-1167.
Fiore, R.L. (2003). Recognition, Responsibility, and Rights: An Introduction. In, Fiore,
R.N. & Nelson, H.L. Recognition, Responsibility, and Rights. Oxford, United
Kingdom: Rowman & Littlefield.
Foley, M., Ruser, J., Shor, G., Shuford, H., & Synatur, E. (2014). Contingent Workers:
Workers’ Compensation Analysis Strategies and Limitations. Journal of
Industrial Medicine, 57 , 764-775
Foley, R., & Kavanagh, A. (2014). Health and spatial justice. In G. Kearns, D. Meredith,
& J. Morrissey, Spatial Justice and the Irish Crisis. Royal Irish Academy.
Fox, J. (1999). Mountaintop Removal in West Virginia: An Environmental Sacrifice
Zone. Organization and Environment 12(2), 163–183.
Franklin Well Services, Inc. (2016). Fracturing Equipment. Franklin Well Services.
Retrieved June 28, 2016 http://www.franklinwell.com/equipment/fracturing.php
French, P.A. (1979). The Corporation as a moral person. American Philosophical
Quarterly, 16(3), 207-215.

236
———. (1984). Collective and Corporate Responsibility. New York, New York
Columbia University Press.
———. (1992). Responsibility Matters. Kansas: University Press of Kansas.
Galassi, T. (2015). Inclusion of Upstream Oil and Gas Hazards to the High-Emphasis
Hazards in the Severe Violator Enforcement Program (SVEP). Memorandum,
OSHA, U.S. Department of Labor.
GAO (United States Government Accountability Office). (1978a). Sporadic Workplace
Weak for Lethal and Other Serious Health Hazards. Washington, D.C.: GAO.
———. (1978b). Workplace Inspection Program Weak in Detecting and Abating Serious
Hazards. Washington, D.C.: GAO.
———. (1982). Letter to Secretary Donova: Improvements Needed in Monitoring State
Plans for Occupational Safety and Health. Washington, D.C.: GAO.
———. (1984). Informal Settlement of OSHA Citations: Comments On The Legal Basis
And Other Selected Issues. Washington, D.C.: GAO.
———. (1988). OSHA’s Monitoring and Evaluation of State Programs. Washington,
D.C.: GAO.
———. (1990). Options for Improving Safety and Health in the Workplace. Washington,
D.C.: GAO.
———. (1993). Changes Needed in the Combined Federal-State Approach. Washington,
D.C.: GAO.
———. (2004). OSHA’s Oversight of Its Civil Penalty Determination and Violation
Abatement Processes Has Limitations. Washington, D.C.: GAO.
———. (2011). Procedural and Analytical Requirements at OSHA and Other Agencies.
GAO.
———. (2013). OSHA Can Better Respond to State-Run Programs Facing Challenges.
GAO.
Giddens, A. (1999). Risk and Responsibility. The Modern Law Review, 62(1), 1-10.
Gilligan, C. (1982). In a Different Voice. Cambridge, Massachussetts: Harvard University
Press.
Glasgow, S. & Schrecker, T. (2016). The double burden of neoliberalism?
Noncommunicable disease policies and the global political economy of risk.
Health & Place, 39, 204-211.
Gochfeld, M. (2005). Chronologic History of Occupational Medicine. Journal of
Occupational & Environmental Medicine, 47(2), 96-114.
Gold, R. (2014). The Boom: How Fracking Ignited the American Energy Revolution and
Changed the World. New York, New York: Simon and Schuster.
Grabell, M., & Berkes, H. (2015, March 4). The Demolition of Workers’ Comp.
ProPublica. Retrieved July 13, 2016 https://www.propublica.org/article/the-
demolition-of-workers-compensation
Grasswick, H.E. (2003). Impurities of Epistemic Responsibility: Developing a Practice-
Oriented Epistemology. In, Fiore, R.N. & Nelson, H.L. Recognition,
Responsibility, and Rights. Oxford, United Kingdom: Rowman & Littlefield.
237
Greenhough, B. (2010). Citizenship, care, and companionship: Approaching geographies
of health and bioscience. Progress in Human Geography, 35(2), 153-171.
Ground Water Protection Council and ALL Consulting. (2009). Modern Shale Gas
Development in the United States: A Primer. U.S. Department of Energy Office
of Fossil Energy and National Energy Technology Laboratory.
Guignard, J. (2015). Pedaling the Sacrifice Zone: Teaching, Writing, and Living above
the Marcellus Shale. Wardlaw.
Guthman, J. (2011). Weighing In: Obesity, Food Justice, and the Limits of Capitalism.
Berkeley, California: University of California Press.
Guthman, J., & Mansfield, B. (2012). The implications of environmental epigenetics A
new direction for geographic inquiry on health, space, and nature-society
relations. Progress in Human Geography, 37(4), 486-504.
HalenHardy. (2017). Awards. HalenHardy. Retrieved May 7, 2017
https://www.halenhardy.com/history-awards/
Hall, A. (2016). Trust, uncertainty and reporting hazards and injuries. Healht, Risk &
Society, 18 (7-8), 427-448.
Halliburton. (2012a). Model FSR-2500 Mountain Mover® Proppant Storage/Conveyor.
Retrieved June 28, 2016
http://www.halliburton.com/public/pe/contents/Data_Sheets/web/H/H09429.pdf
———. (2012b). PEMEX increased production and improved completion time with
“zipper frac” technique.
http://www.halliburton.com/public/cps/contents/Case_Histories/web/H09754%20
Pemex%20Zipper%20Frac%20CS.pdf
Hamby, C. (2014, July 22). Black lung claims by 1,100 coal miners may have been
wrongly denied. The Center for Public Integrity. Retrieved October 6, 2017,
https://www.publicintegrity.org/2014/07/22/15131/black-lung-claims-1100-coal-
miners-may-have-been-wrongly-denied
Hanchette, C. (2008). The political ecology of lead poisoning in eastern North Carolina.
Health & Place, 14(2), 209-216.
Hankivsky, O. (2014). Rethinking Care Ethics: On the Promise and Potential of an
Intersectional Analysis. American Political Science Review, 108(2), 252-264.
Hargreaves, S. (2011, August 3). A warning for shale gas investors. CNN Money.
Retrieved June 29, 2016.
http://money.cnn.com/2011/08/03/news/companies/shale-gas-sec/index.htm
Harmon, M. (1995). Responsibility as Paradox: A Critique of Rational Discourse on
Government. Thousand Oaks, California: Sage Publishing.
Harrison, R. J., Retzer, K., Kosnett, M. J., Hodgson, M., Jordan, T., Ridl, S., & Kiefer,
M. (2016, January 15). Sudden Deaths Among Oil and Gas Extraction Workers
Resulting from Oxygen Deficiency and Inhalation of Hydrocarbon Gases and
Vapors — United States, January 2010–March 2015. Morbidity and Mortality
Weekly Report, 65(1), 6-9.
Harvey, D. (1989). A Condition of Post-Modernity. Cambridge, Massachusetts:
Blackwell.
238
Headrick, B., Serra, G., & Twombly, J. (2008). Enforcement and Oversight Using
Congressional Oversight to Shape OSHA Bureaucratic Behavior. Journal of
Public Administration Research and Theory, 18, 33-55.
Held, V. (2006). The Ethics of Care: Personal, Political, and Global. New York, New
York: Oxford University Press.
Hewitt, S. (2009). Discourse Analysis and Public Policy Research. Centre for Rural
Economy, Newcastle University. Centre for Rural Economy Discussion Paper
Series No. 24.
Holifield, R. (2012). Environmental Justice as Recognition and Participation in Risk
Assessment: Negotiating and Translating Health Risk at a Superfund Site in
Indian Country. Annals of the Association of American Geographers, 102(3), 591-
613.
Holmes, S. (2013). Fresh Fruit, Broken Bodies: Migrant Farmworkers in the United
States. Berkley, California: University of California Press.
Horton, S. B. (2016). They Leave Their Kidneys in the Fields: Illness, Injury, and
Illegality among U.S. Farmworkers. Berkley, California: University of California
Press.
Hopkins, J. S. (2015, November 4). Disease victims often shut out of workers’ comp
system. The Center for Public Integrity. Retrieved July 13, 2016
https://www.publicintegrity.org/2015/11/04/18816/disease-victims-often-shut-
out-workers-comp-system
Howard, J. (2017). Nonstandard Work Arrangements and Worker Health and Safety.
American Journal of Industrial Medicine, 60, 1-10.
Hughes, C.L. (2003). Integrity and Vulnerability. In, Fiore, R.N. & Nelson, H.L.
Recognition, Responsibility, and Rights. Oxford, United Kingdom: Rowman &
Littlefield.
Industrial Union Department v. American Petroleum Institute. 448 U.S. 607. Supreme
Court of the United States. (1980).
Jackson, P., & Neely, A. H. (2015). Triangulating health Toward a practice of a political
ecology of health. Progress in Human Geography, 39(1), 47-64.
Jacobs, T. (2014, May 19). Renewing Mature Shale Wells Through Refracturing. Society
of Petroleum Engineers. Retrieved July 2, 2016,
http://www.spe.org/news/article/renewing-mature-shale-wells-through-
refracturing
Jacquet, J. (2011). Workforce Development Challenges in the Natural Gas Industry.
Cornell University City and Regional Planning.
———. (2014). Review of Risks to Communities for Shale Energy Development.
Environment Science and Technology, 48(15), 8321-8333.
Jaggar, A. M. (2003). Women and Neoliberal Globalization: Debt Burdens Undermine
Women’s Health in the Global South. In, Fiore, R.N. & Nelson, H.L. Recognition,
Responsibility, and Rights. Oxford, United Kingdom: Rowman & Littlefield.
Johnson, R. K., Freedman, M., & Chajet, H. (2014). U.S. Chamber of Commerce
Comments on Occupational Safety and Health Administration Proposed Rule on

239
Occupational Exposure to Respirable Crystalline Silica Docket No. OSHA-2010-
0034-4233, The U.S. Chamber of Commerce.
Kearns, R., & Collins, D. (2010). Health Geography. In T. Brown, S. McLafferty, & G.
Moon, A Companion to Health and Medical Geography. Malden, Massachusetts:
Blackwell.
Kearns, R., & Moon, G. (2002). From Medical to Health Geography: Novelty, Place and
Theory After a Decade of Change. Progress in Human Geography, 26(5), 605-
625.
Keil, R. & Ali, H. (2007). Governing the Sick City: Urban Governance in the Age of
Emerging Infectious Disease. Antipode, 39 (5), 846-873.
Kennedy, A., Schafft, K., & Howard, T. (2017). Taking away David’s sling:
Environmental justice and land-use conflict in extractive resource development
The International Journal of Justice and Sustainability, 22(8), 952-968.
Kerwin, C. M., & Furlong, S. R. (2010). Rulemaking: How Government Agencies Write
Law and Make Policy. Washington, D.C.: CQ Press.
King, B. (2009). Political ecologies of health. Progress in Human Geography, 34(1), 38-
55.
———. (2017). States of Disease. Oakland, California: University of California Press.
King, B., & Crews, K. A. (2013). Ecologies and Politics of Health. Routledge.
King, P. (2016, May 17). Oil and gas slips through cracks of new OSHA rule. Energy
Wire. Retrieved December 3, 2017 http://www.eenews.net/stories/1060037351
Kittay, E.F. (1999). Love’s Labor: Essays on Women, Equality and Dependency. New
York, New York: Routledge Press.
Knutson, G. (2014). Comments of the Gerhard Knutson of Knutson Ventilation, on
behalf of in Response to the Occupational Safety & Health Administration
(“OSHA”) Proposed Rule entitled “Occupational Exposure to Respirable
Crystalline Silica” (78 Fed. Reg. 56274 (Sept. 12, 2013). OSHA-2010-0034-2264.
Kutchins, A. (1981). The Most Exclusive Remedy Is No Remedy at All: Workers’
Compensation Coverage for Occupational Diseases. Labor Law Journal, 32(4)
212-228.
Laliberté, N. (2015). Geographies of Human Rights: Mapping Responsibility. Geography
Compass, 9(2), 57-67.
Laney, S. A., Wolfe, A.L, Petsonk, E.L, &Haldin, C. (2012, June 15). Pneumoconiosis
and Advanced Occupational Lung Disease Among Surface Coal Miners — 16
States, 2010–2011. Morbidity and Mortality Weekly Report, 61(23), 431-434.
Larson, A. (1974). Occupational Diseases under Workmen’s Compensation Laws.
University of Richmond Law Review, 9, 86-114
Lawhorn-Cryden, E. (Producer). (2015). The Respirable Crystalline Silica Video for On
Shore E&P [Motion Picture].
Lawson, V. (2007). Geographies of Care and Responsibility. Annals of the Association of
American Geographers, 97(1), 1-11.

240
Leigh, J. P., & Marcin, J. P. (2012). Workers’ Compensation Benefits and Shifting Costs
for Occupational Injury and Illness. Journal of Occupational & Environmental
Medicine, 54(4), 445-450.
Lerner, S. (2010). Sacrifice Zones. Cambridge, Massachusetts: MIT Press.
Leung, C. C., Tak Sun Yu, I., & Chen, W. (2012). Silicosis. Lancet, 379, 2008-2018.
Little, J. (2017). Running, health and the disciplining of women’s bodies: The influence
of technology and nature. Health & Place. 46, 322-327.
Little, P. (2017). Corporate Mortality Files and Late Industrial Necropolitics. Medical
Anthropology Quarterly, doi: 10.1111/maq.12417
MacLaury, J. (2016 (1988)). History of the Department of Labor, 1913-1988. U.S.
Department of Labor. Chapter 1: Start-up of the Department and World War I
1913-1921. U.S. DOL. Retrieved June 16, 2016
https://www.dol.gov/general/aboutdol/history/hs75menu
MacLeavy, J.,(2007). Engendering New Labour's Workfarist Regime: Exploring the
intersection of welfare state restructuring and labour market policies in the UK.
Gender, Place and Culture, 14(6), pp. 721-743.
Mansfield, B. (2012a). Environmental Health as Biosecurity: “Seafood Choices,” Risk,
and the Pregnant Woman as Threshold. Annals of the Association of American
Geographers, 102(5), 969-976.
———. (2012b). Gendered biopolitics of public health: regulation and discipline
in seafood consumption advisories. Environment and Planning D: Society and
Space, 30 (4), 588-602.
———. (2012c). Race and the new epigenetic biopolitics of environmental health.
BioSocieties, 7, 352-372.
Marcellus Shale Coalition. (2017a). Job Portal. Retrieved October 5, 2017,
http://marcelluscoalition.org/wp-content/uploads/2012/02/job_banner.jpg
———. (2017b). Employment resources. Retrieved October 5, 2017,
http://marcelluscoalition.org/wp-content/uploads/2012/02/job_resources.jpg
Marcus, G. E. (1995). Ethnography In/Of The World System: The Emergence of Multi-
Sited Ethnography. Annual Review of Anthropology, 25, 95-117.
Markowitz, G., & Rosner, D. (1995). The limits of thresholds: silica and the politics of
science, 1935 to 1990. American journal of public health, 85(2), 253.
———. 2002. Deceit and Denial: The Deadly Politics of Industrial Pollution. Berkley,
California: University of California Press.
Massey, D. (2004). Geographies of responsibility. Geografiska Annaler, 86B (1), 5-18.
Masuda, J., & Crabtree, A. (2010). Environmental justice in the therapeutic inner city.
Health & Place. 16, 656-665.
Mazurek, J.M., Schleiff, P.L., Wood, J.M., Hendricks, S.A., & Weston, A. (2015, June
19). Notes from the Field: Update: Silicosis Mortality — United States, 1999–
2013. Morbidity and Mortality Weekly Report, 64 (23),653-654.
McCaffrey, D. (1982). OSHA and the Politics of Health Regulation. New York, New
York: Plenum Press.
241
McCluskey, M. T., McGarity, T., Shapiro, S., & Tracy, K. (2016). OSHA’s Discount on
Danger OSHA Should Revise Its Informal Settlement Policies to Maximize the
Deterrent Value of Citations. Center for Progressive Reform.
McEwan, C. & Goodman, M.K. (2010). Place Geography and the Ethics of Care:
Introductory Remarks on the Geographies of Ethics, Responsibility and Care.
Ethics, Place and Environment, 13(2), 103-112.
McGraw, S. (2012). The End of Country: Dispatches from the Frack Zone. New York,
New York: Random House.
McKenzie, L., Witter, R. Z., Newman, L. S., & Adgate, J. L. (2012). Human health risk
assessment of air emissions from development of unconventional natural gas
resources. Science of the Total Environment, 424, 79-87.
Messing, K. (1998). One-Eyed Science: Occupational Health and Women Workers.
Philadelphia, Pennsylvania: Temple University Press.
Michaels, D. (2008). Doubt is Their Product: How Industry’s Assault on Science
Threatens Your Health. New York, New York: Oxford University Press.
Miewald, C. E., & McCann, E. J. (2004). Gender struggle, scale, and the production of
place in the Appalachian coalfields. Environment and Planning A, 36, 1045-1064.
Mills, S. (2011). Scouting for girls? Gender and the Scout Movement in Britain. Gender,
Place & Culture, 18(4), pp. 537-556.
Milligan, C., & Power, A. (2010). The Changing Geography of Care. In T. Brown, S.
McLafferty, & G. Moon, A Companion to Health and Medical Geography. West
Sussex, United Kingdom: Blackwell Publishing.
Milligan, C. & Wiles, J. (2010). Landscapes of care. Progress in Human Geography,
34(6), 736-754.
Mitchell, T. (2006). Society, Economy, and the State Effect. In, Sharma, A. & Gupta, A.
The Anthropology of the State. Malden, Massachusetts: Blackwell Publishing.
MSHA. (n.d.). History of Mine Safety and Health Legislation. MSHA. Retrieved June
16, 2016 http://arlweb.msha.gov/MSHAINFO/MSHAINF2.HTM
Mulvaney, D. (2014). Are green jobs just jobs? Cadmium narratives in the life cycle of
Photovoltaics. Geoforum, 54, 178-186.
Murphy, M. (2006). Sick Building Syndrome and the Problem of Uncertainty:
Environmental Politics, Technoscience, and Women Workers. Durham, North
Carolina: Duke University Press.
———. (2015). Unsettling care: Troubling transnational itineraries of care in feminist
health practices. Social Studies of Science, 45 (5), 717-737.
———. (2017). The Economization of Life. Durham, North Carolina: Duke University
Press.
National Academy of Social Insurance. (2010). Workers’ Compensation: Benefits,
Coverage, and Costs.
NETL(National Energy Technology Laboratory). (2013). Modern Shale Gas
Development in the United States: An Update. Strategic Center for Natural Gas
and Oil, U.S. Department of Energy.
242
Neuhaüser, C. (2014). Structural Injustice and the Distribution of Forward-Looking
Responsibility. In, P. A. French, & H. K. Wettstein, Eds. Forward Looking
Collective Responsibility Midwest Studies in Philosophy, XXXVIII, pp. 232-251.
NIOSH (National Institutes of Occupational Safety and Health). 2010. NIOSH Report on
Hydraulic Fracturing Site 1, 2010. OSHA 2010-0034-1541 NIOSH, CDC, U.S.
Department of Health and Human Services.
———. 2011a. NIOSH Report on Hydraulic Fracturing Site 2, 2011. OSHA-2010-0034-
1542, NIOSH, CDC, U.S. Department of Health and Human Services.
———. 2011b. NIOSH Report on Hydraulic Fracturing Site 6, 2011. OSHA-2010-0034-
1546, NIOSH, CDC, U.S. Department of Health and Human Services.
———. (2015, March 15). Fatalities in the Oil and Gas Extraction Industry (FOG).
NIOSH. Retrieved July 2, 2016 http://www.cdc.gov/niosh/topics/fog/about.html
Noble, C. (1986). Liberalism at Work: The rise and Fall of OSHA. Philadelphia,
Pennsylvania: Temple University Press.
Noddings, N. (1984). Caring, a Feminine Approach to Ethics & Moral Education.
Berkley, California: University of California Press.
———. (2002). Starting at Home: Caring and Social Policy. Berkley, California:
University of California Press.
Noxolo, P, Raghuram, P, &Madge, C. (2012). Unsettling responsibility: postcolonial
interventions. Transactions of the Instituted of British Geographers, 40(1), 55-65.
Olson, E. (2017.) Geography and ethics III: Whither the next moral turn? Progress in
Human Geography, https://doi.org/10.1177/0309132517732174
Ontario Ministry of Labor. (2015). Current Occupational Exposure Limits for Ontario
Workplaces Required under Regulation 833. Retrieved June 16, 2016
https://www.labour.gov.on.ca/english/hs/pubs/oel_table.php
OSHA (Occupational Safety and Health Administration) & NIOSH (National Institutes
of Occupational Safety and Health). (2012). Hazard Alert: Worker Exposure to
Silica during Hydraulic Fracturing. OSHA & NIOSH.
OSHA (Occupational Safety and Health Administration). (1999). Multi-Employer
Citation Policy. OSHA Instruction, OSHA, U.S. Department of Labor.
———. (2008). National Emphasis Program – Crystalline Silica. OSHA Instruction,
OSHA, U.S. Department of Labor.
———. (2011). Field Operations Manual (FOM). OSHA, U.S. Department of Labor.
———. (2012). The OSHA Rulemaking Process. (Directorate of Standards and
Guidance). OSHA, U.S. Department of Labor. Retrieved July 6, 2016
https://www.osha.gov/OSHA_FlowChart.pdf
———. (2013). Notice of Proposed Rulemaking: Occupational Exposure to Respirable
Crystalline Silica. Federal Register: 2013-20997, Docket # OSHA-2010-0034-
1721.
———. (2014, March 18). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3579.
243
———. (2014, March 19). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3576.
———. (2014, March 20). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3576.
———. (2014, March 21). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3578.
———. (2014, March 24). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3580.
———. (2014, April 1). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3586.
———. (2014, April 3). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3588.
———. (2014, April 4). Informal Public Hearings for the Proposed Rule on
Occupational Exposure to Respirable Crystalline Silica. Washington, D.C.:
OSHA, U.S. Department of Labor. Docket # OSHA-2010-0034-3589.
———. (2013). Severe Violator Enforcement Program: White Paper. OSHA, U.S.
Department of Labor.
———. (2016). 29 CFR 1910 1915 and 1926 Occupational Exposure to Respirable
Crystalline Silica; Final Rule, Part II. U.S. Department of Labor. Federal Register.
———. (2016). Enforcement Exemptions and Limitations under the Appropriations Act.
OSHA, U.S. Department of Labor.
https://osha.gov/pls/oshaweb/owadisp.show_document?p_table=DIRECTIVES&
p_id=1519
———. (2016). OSHA Fact Sheet: OSHA Inspections. OSHA, U.S. Department of
Labor.
———. (2016, July 1). Association of Energy Service Companies (AESC) Provides Well
Servicing Rig Orientation for OSHA Staff. OSHA, U.S. Department of Labor.
Retrieved June 2, 2016
https://www.osha.gov/dcsp/success_stories/alliances/regional/reg6_success_storie
s.html#aesc_servicing_rig
———. (2016, December 1). OSHA QuickTakes. OSHA QuickTakes, 15(26). OSHA,
U.S. Department of Labor.
———. (2017, Jan 13). OSHA Penalties. OSHA, U.S. Department of Labor. Retrieved
July 2, 2017 https://www.osha.gov/penalties/
———. (2017). Silica E-Tool.
———. (n.d.). Commonly Used Statistics. OSHA, U.S. Department of Labor. Retrieved
June 16, 2016 https://www.osha.gov/oshstats/commonstats.html
244
OSHA Inspection 679378. (2013). Inspection Case File 679378, Valley Vessel
Fabricators, Inc. OSHA, U.S. Department of Labor.
OSHA Inspection 685459. (2012). Inspection Case File 685459, Trican Well Service.
OSHA, U.S. Department of Labor.
OSHA Inspection 802188. (2011). Inspection Case File 802188, Halliburton Energy
Services. OSHA, U.S. Department of Labor.
OSHA Inspection 842583. (2013). Inspection Case File 842583, Chalk Mountain. OSHA,
U.S. Department of Labor.
OSHA Inspection 899235. (2014). Inspection Case File 899235, Halliburton Energy
Services. OSHA, U.S. Department of Labor.
OSHA Inspection 902898. (2013). Inspection Case File 902898, Baker Hughes. OSHA,
U.S. Department of Labor.
OSHA Inspection 981830. (2014). Inspection Case File 981830, Tranz, Inc. OSHA, U.S.
Department of Labor.
OSHA Inspection 922385. (2014). Inspection Case File 922385, Nabors. OSHA, U.S.
Department of Labor.
OSHA Inspection 943011. (2013). Inspection Case File 943011, Baker Hughes. OSHA,
U.S. Department of Labor.
OSHA Inspection 978294. (2014). Inspection Case File 978294, Baker-Hughes. OSHA,
U.S. Department of Labor.
OSHA Inspection 98326. (2014). Inspection Case File 98326, Halliburton Energy
Services. OSHA, U.S. Department of Labor.
OSHA Region VI. (2015). Step Up For Safety in the Upstream Oil and Gas Industry.
OSHA Region VI. Retrieved July 2, 2016 http://www.oshastanddown.org/
OEHHA (Office of Environmental Health Hazard Assessment). (2005). Chronic Toxicity
Summary: Silica (Crystalline, Respirable). State of California.
O’Malley, P. (2004). Risk, Uncertainty and Government. London, United Kingdom: The
GlassHouse Press.
Oreskes, N., & Conway, E. M. (2011). Merchants of Doubt: How a Handful of Scientists
Obscured the Truth on Issues from Tobacco Smoke to Global Warming. New
York, New York: Bloomsburg Publishing.
Parr, H. (2002). New body-geographies: the embodied spaces of health. Environment and
Planning D: Society and Space, 20 (2), 74-94.
———. (2003). Medical geography: care and caring. Progress in Human Geography,
27(2), 212-221.
———. (2004). Medical geography: critical medical and health geography? Progress in
Human Geography, 28(2), 246-257.
Pearce, J., Richardson, E., Mitchell, R., & Shortt, N. (2010). Environmental justice and
health: the implications of the socio-spatial distribution of multiple environmental
deprivation for health inequalities in the United Kingdom. Transactions of the
Institute of British Geographers, 35(4), 522-539.

245
PEC/Premier Safety Management. (2012). Basic Orientation Student Workbook.
Mandeville, LA: PEC Premier Safety Management, Inc.
Pettit, P. (2002). Responsibility, Inc. Ethics, 117(1), 171-201.
Popke, J. (2006). Geography and ethics: everyday meditations through care and
consumption. Progress in Human Geography, 30 (4), 504-512.
———. (2007). Geography and ethics: spaces of cosmopolitan responsibility. Progress
in Human Geography, 31(4), 509-518.
Proctor, R. & Schiebinger, L. (2008). Agnotology: The making & unmaking of ignorance.
Stanford, California: Stanford University Press.
Pulido, L. (2000). Rethinking Environmental Racism: White Privilege and Urban
Development in California. Annals of the Association of American Geographers,
90 (1), 12-40.
Pykett, J. (2012). The New Maternal State: The Gendered Politics of Governing through
Behaviour Change. Antipode, 44(1), pp. 217-238.
Rabe, B. (2014). Shale Play Politics: The Intergovernmental Odyssey of American Shale
Governance. Environment Science and Technology, 48(15), 8369-8375.
Rabe, B. G., & Borick, C. (2013). Conventional Politics for Unconventional Drilling?
Lessons from Pennsylvania’s Early Move into Fracking Policy Development.
Review of Policy Research, 30(3), 321-340.
Rabinow, P., & Rose, N. (2006). Biopower Today. Biosocieties, 1(2), 195-217.
Rappaport, S. (1993). Threshold limit values, permissible exposure limits, and feasibility:
The bases for exposure limits in the United States. American Journal of Industrial
Medicine, 23(5), 683-694.
Rasmussen, S., Ogburn, E., McCormack, M., Casey, J., Bandeen-Roche, K., Dione, M.
G., & Schwartz, B. (2016). Association Between Unconventional Natural Gas
Development in the Marcellus Shale and Asthma Exacerbations. JAMA Internal
Medicine, 176(9), 1334-1343.
Resnick-Ault, J., & Schneyer, J. (2016, June 27). Texas ‘Frack Master’ bilked investors
out of millions, SEC says. Reuters. Retrieved June 29, 2016
http://www.reuters.com/article/us-breitling-energy-fraud-idUSKCN0ZD0BL
Rogers, D. (2009). Making Capitalism Safe: Work Safety and Health Regulation in
America, 1880-1940. Urbana, Illinois: University of Illinois Press.
Rose, N. (1996). Governing “advanced” liberal democracies. In A. Barry, T. Osborne, &
N. Rose, Foucault and Political Reason (pp. 37-64). London, United Kingdom:
University of Chicago Press.
Rose, N. & Miller, P. (2008). Governing the Present: Administering Economic, Social
and Personal Life. Polity.
Rose, G. (2007). Visual Methodologies: An Introduction to the Interpretation of Visual
Materials. London, United Kingdom: Sage.
Rosenberg, M. (2013). Health geography I: Social justice, idealist theory, health and
health care. Progress in Human Geography, 38(3), 466-475.
Rosner, D., & Markowitz, G. (1987). Research of Advocacy: Federal Occupational
Safety and Health Policies during the New Deal. In D. Rosner, & G. E.

246
Markowitz, Dying for Work: Workers’ Safety and Health in Twentieth-century
America (pp. 83-102). Bloomington: Indiana University Press.
———. (1995). Workers, Industry, and the Control of Information: Silicosis and the Air
Hygiene Foundation. Journal of Public Health Policy, 16(1), 29-58.
———. (2000). From Dust to Dust: The Birth and Re-Birth of National Concern About
Silicosis. In S. Kroll-Smith, P. M. Brown, & V. Gunther, Illness and the
Environment: A Reader in Contested Medicine. New York City, New York: New
York University Press.
———. (2006). Deadly Dust: Silicosis and the On-going Struggle to Protect Workers’
Health (2nd ed.). Ann Arbor, Michigan: University of Michigan Press.
Ross, D. (2010). Overview of Hydraulic Fracturing. Universal Well Services. OSHA-
2010-0034-1606.
Ruger, J.P. (2010). Health Capability: Conceptualization and Operationalization.
American Journal of Public Health, 100(1), 41-49.
Schlumberger Oilfield Glossary. (2016a). Production. Schlumberger. Retrieved July 13,
2016 http://www.glossary.oilfield.slb.com/Terms/p/production.aspx
———. (2016b). Horizontal Drilling. Schlumberger. Retrieved July 13, 2016
http://www.glossary.oilfield.slb.com/Terms/h/horizontal_drilling.aspx
Scott, R. R. (2010). Removing Mountains: Extracting Nature and Identity in the
Appalachian Coalfields. Minneapolis: University of Minnesota Press.
Sellers, C. (1997). Hazards of the Job: From Industrial Disease to Environmental Health
Science. Chapel Hill, North Carolina: The University of North Carolina Press.
Senanayake, N. & King, B. (2017). Health-environment futures: Complexity, uncertainty,
and bodies. Progress in Human Geography, DOI: 10.1177/0309132517743322
Shade, L. (2015). Sustainable development or sacrifice zone? Politics below the surface
in post-neoliberal Ecuador. The Extractive Industries and Society 2(4), 775–784.
ShaleNET. (2016). About. Retrieved December 3, 2016 http://www.shalenet.org/about
Shapiro, S. A., & Rabinowitz, R. S. (1997). Punishment versus cooperation in regulatory
enforcement: a case study of OSHA. Administrative Law Review, 49(713), 713-
762.
Silvey, R. (2009). Development and geography: anxious times, anemic geographies, and
migration. Progress in Human Geography, 33(4), 507-515.
Scott, R. R. (2010). Removing Mountains: Extracting Nature and Identity in the
Appalachian Coalfields. Minneapolis: University of Minnesota Press.
Sothern, M. & Dyck, I. (2009). “… a Penis Is Not Needed in Order to Pee”: Sex and
Gender in Health Geography. In Brown, T., McLafferty, S., Moon, G., A
companion to health and medical geography. Blackwell.
Smith, D.M. (1997). Geography and ethics: a moral turn? Progress in Human
Geography, 21(4), 583-590.
Smith, D. (2005). Institutional Ethnography: A Sociology for People. Lanham, Maryland:
Alta Mira Press.
———. (2006). Institutional Ethnography as Practice. Rowman & Littlefield.

247
Smith, C. E. (2016). Caring practices: the connection between logics of state and
domestic violence in Cairo, Egypt. Gender Place and Culture, 23(9), pp. 1227-
1239.
Smith, S. (2016, June 30). Discount on Danger: Is OSHA Giving Too Many Discounts to
Employers that Injure or Kill Workers?. Environmental Health and Safety Today.
Retrieved July 1, 2016 http://ehstoday.com/osha/discount-danger-osha-giving-
too-many-discounts-employers-injure-or-kill-workers
Sparke, M. and Anguelov, D. (2012). H1N1, globalization, and the epidemiology of
inequality. Health & Place, 18 (4), 726-736.
Soraghan, M. (2017, May 2). Oil and gas industry leads in severe injuries. E&E News.
Retrieved May 6, 2017 https://www.eenews.net/stories/1060053892/print
Sothern, M. & Dyck, I. (2009). “… a Penis Is Not Needed in Order to Pee”: Sex and
Gender in Health Geography. In Brown, T., McLafferty, S., Moon, G., A
companion to health and medical geography. Blackwell.
Sparke, M. (2007). Geopolitical Fears, Geoeconomic Hopes, and the Responsibilities of
Geography. Annals of the Association of American Geographers, 92(2), 338-349.
Spigelmyer, D. (2014). Re: Comments on Proposed Rule entitled “Occupational
Exposure to Respirable Crystalline Silica” (78 Fed. Reg. 56274 (Sept. 12, 2013)).
Marcellus Shale Coalition. OSHA-2010-0034-2311.
Staeheli, L. (2003). Women and the work of community. Environment and Planning A,
35, 815-831.
———. (2013). Whose Responsibility Is It? Obligation, Citizenship and Social Welfare.
Antipode, 45(3), 521-540
Superior Silica Sand, 2016. Frac Sand Grades: Proppant Market Differentiation.
Retreived June 27, 2016 http://sssand.com/frac-sand-grades/
Szymendera, S.D. (2017, April 20). Workers’ Compensation: Overview and Issues. CRS
Report R44580. Washington. D.C.: Congressional Research Service.
Talisman Energy. (2014). Talisman Energy Inc. U.S. Safety Handbook
Thien, D. & Del Casino, V. J. (2012). (Un)Healthy Men, Masculinities, and the
Geographies of Health. Annals of the Association of American Geographers,
102(5), 1146-1156.
Torrey, D.B. (2010-2011). The Commonwealth Court of Pennsylvania and the Workers’
Compensation Act: Background and Jurisprudence, Judge Alexander F. Barbieri
and Selected Precedents. Widener Law Journal. 20, 87.
———. (2015, November 20). The Opt-Out of Workers’ Compensation Legislation in
the South States. MCLE New England.
Tronto, J. (1993). Moral Boundaries: A Political Argument for an Ethic of Care. New
York, New York: Routledge.
———. 2013. Caring Democracy: Markets, Equality, and Justice. New York, New
York: New York University Press.
Tschakert, P., & Singha, K. (2007). Contaminated identities: Mercury and
marginalization in Ghana’s artisanal mining sector. Geoforum, 38, 1304-1321.
248
U.S. DOJ (U.S. Department of Justice). (2016). The Worker Endangerment Initiative.
U.S. DOJ. Retrieved December 3, 2017 https://www.justice.gov/enrd/worker-
endangerment/about
U.S. DOL (U.S. Department of Labor). (2016b). Misclassification of Employees as
Independent Contractors Quick Links. U.S. DOL Retrieved July 2, 2016
https://www.dol.gov/whd/workers/misclassification/
U.S. EIA (U.S. Energy Information Administration). (2015). Lower 48 states shale plays
EIA. Retrieved June 29, 2016 http://www.eia.gov/oil_gas/rpd/shale_gas.pdf
———. (2016, June 16). Shale in the United States. EIA. Retrieved June 29, 2016
http://www.eia.gov/energy_in_brief/article/shale_in_the_united_states.cfm
———.(2017, November 30). Crude Oil and Natural Gas Production. Retrieved
December 4, 2017. https://www.eia.gov/petroleum/production/#ng-tab
U.S. House of Representatives: Subcommittee on Workforce Protections. (2016, April
19). Reviewing Recent Changes to OSHA’s Silica Standards. Serial No. 114-46.
Washington, D.C.: U.S. Government Publishing Office.
U.S. Securities and Exchange Commission. (2014, August 15). SEC Announces Charges
in Houston-Based Scheme Touting Technology to End Fracking. Retrieved June
29, 2016
http://www.sec.gov/News/PressRelease/Detail/PressRelease/1370542654953
U.S. Senate Committee on Health, Education, Labor and Pensions. (2008). Discounting
Death: OSHA’s Failure To Punish Safety Violations That Kill Workers. United
States Senate.
Utterback, D. F., Meyers, A. R., & Wurzelbacher, S. J. (2016). Workers’ Compensation
Insurance: A Primer for Public Health. National Institute for Occupational Safety
and Health, CDC, Department of Health and Human Services. Government.
Venkatapuram, S. (2011). Health Justice: An Argument from the Capabilities Approach.
Malden, Massachusetts: Polity.
Vike, J. (2007). The Bureaucracy as a Battleground: Contentious Politics Surrounding
OSHA 1980-2004. Politics and Policy, 35(3), 507-607.
Viscusi, W. (1983). Risk By Choice: Regulating Health and Safety in the Workplace.
Cambridge, Massachusetts: Harvard University Press.
Vogel, S. (2008) From ‘the Dose Makes the Poison’ to ‘the Timing Makes the Poison’:
Conceptualizing Risk in the Synthetic Age. Environmental History 13: 667-673.
Vogel, D. (2012). The Politics of Precaution: Regulating Health, Safety, and
Environmental Risks in Europe and the United States. Princeton, New Jersey:
Princeton University Press.
Vorys. (2014, December 14). Oil and Gas Alert: Pros and Cons: Use of Independent
Contractors in the Oil and Gas Industry. Retrieved July 2, 2016
http://www.vorys.com/publications-1367.html
WHD (Wage and Hour Division). (2015a, March 30). News Release: U.S. Department of
Labor finds oil and gas industry workers in New Mexico, West Texas underpaid
by more than $1.3M. Retrieved July 19, 2016
https://www.dol.gov/opa/media/press/whd/WHD20150501.htm

249
———. (2015b, September 22). News Release: Halliburton pays nearly $18.3 million in
overtime owed to more than 1,000 employees nationwide after U.S. Labor
Department investigation. Retrieved July 19, 2016
https://www.dol.gov/opa/media/press/whd/WHD20151647.htm
Wagner, W. & Steinzor, R., 2006. Introduction: Principled Science. In, Wagner, W. &
Steinzor, R.. Rescuing Science from Politics: Regulation and the Distortion of
Scientific Research. Cambridge: Cambridge University Press.
Wahl, A. M., & Gunkel, S. E. (1999). Due Process, Resource Mobilization, and the
Occupational Safety and Health Administration, 1971–1996: The Politics of
Social Regulation in Historical Perspective. Social Problems, 46(1), 591-616.
Walker, G. (2009). Beyond Distribution and Proximity: Exploring the Multiple
Spatialities of Environmental Justice. Antipode, 41(4), 614-636.
Walker, M. U. (2008). Moral Understandings: A Feminist Study in Ethics. Oxford,
United Kingdom: Oxford University Press.
Warner, B., & Shapiro, J. (2013). Fractured, Fragmented Federalism: A Study in
Fracking Regulatory Policy. Publis: The Journal of Federalism, 43(3), 474-496.
Weil, D. (2014). The Fissured Workplace: Why Work Became So Bad for So Many and
What Can Be Done to Improve It. Cambridge, Massachusetts: Harvard University
Press.
West Virginia Office of the Insurance Commissioner. (2017). Latest News. Retreived
December 4, 2017 http://www.wvinsurance.gov/WorkersCompensation.aspx
Wicks, D. (2010). Coding: Axial Coding. In A. J. Mills, & G. Durepos, Encyclopedia of
Case Study Research. Thousand Oaks, California: Sage Publications.
Wilber, T. (2012). Under the Surface: Fracking, Fortunes, and the Fate of the Marcellus
Shale. Ithaca, New York: Cornell University Press.
Willow, A. J. (2014). The new politics of environmental degradation: Un/expected
landscapes of disempowerment and vulnerability. Journal of Political Ecology.
21(1), 237-257.
Wills, J. (2009), Subcontracted employment and its challenge to labor. Labor Studies
Journal. 34, 441–460.
Wiseman, H. (2014). The Capacity of State to Govern Shale Gas Development Risks.
Environmental Science and Technology, 48, 8376-8387.
Witter, R., Tenney, L., Clark, S., & Newman, L. S. (2014). Occupational Exposures in
the Oil and Gas Extraction Industry: State of the Science and Research
Recommendations. American Journal of Industrial Medicine, 57, 847-856.
Wright, M. (2013). Disposable Women and Other Myths of Global Capitalism. New
York, New York: Routledge.
Young, I. M. (1990). Justice and the Politics of Difference. Princeton, New Jersey:
Princeton University Press.
———. (2003). From guilt to solidarity; sweatshops and political responsibility. Dissent,
Spring, 29-44.
———. (2006). Responsibility and Global Justice: A Social Connection Model. Social
Philosophy and Policy, 23(1), 102-130.

250
———. (2008). Responsibility for Justice. Oxford, United Kingdom: Oxford University
Press.
Ziem, G., & Castleman, B. (2000). Threshold Limit Values: Historical Perspectives and
Current Practice. In Kroll-Smith, S., Gunter,V. J., & Brown, P. M., Illness and the
Environment: A Reader in Contested Medicine. New York, New York: New York
University Press.
Zinn, J. O. (2008). Introduction: the Contribution of Sociology to the Discourse on Risk
and Uncertainty. In: Zinn, J.O. Social Theories of Risk and Uncertainty: An
Introduction. Malden, Massachusetts: Blackwell Publishing.
Zirogiannis, N., Alcorn, J., Rupp, J., Carley, S., & Graham, J. D. (2016). State regulation
of unconventional gas development in the U.S.: An empirical evaluation. Energy
Research and Social Science, 11, 142-154.
Zwitter, A. (2014). Big Data Ethics. Big Data & Society, July-December 1-6.

251
Workers’ Compensation Statutes
*accessed via LexisNexis Legal
Ala. Code § 25-5- 110 Definitions, Occupational pneumoconiosis
Ala. Code § 25-5- 117 Workers’ Compensation, Limitation Period for Claims or Actions
For Compensation.
Alaska Stat. § 23.30.105 Time for Filing Claims.
Alaska Stat. § 23.30.395 Definitions.
Alaska Stat. §23.30.100(a)(d) Workers’ Compensation Act, Time for Filing Claims
Ariz. Rev. Stat. § 23-901.01 Workers’ Compensation, Occupational Disease; Proximate
Causation; Definitions.
Ariz. Rev. Stat. § 23-901.02 Liability of Last Employer.
Ariz. Rev. Stat. § 23-908 (E) Workers’ Compensation, Liability of Last Employer;
Exception.
Ariz. Rev. Stat. § 23-1061 Payment of Compensation
Ark. Code Ann. § 11-9-601 Compensation Generally
Ark. Code Ann. § 11-9-602 Workers' Compensation, Occupational Disease,
Compensation for Silicosis or Asbestosis.
Ark. Code Ann. § § 11-9-702(a)(2). Compensation Claims—Filing.
Cal. LAB. Code § 5500.5 Workers’ Compensation and Insurance, Compensation
Proceedings, Applications and Answers.
Col. Rev. Stat. §8-40-201 Definitions.
Col. Rev. Stat. § 8-41-206 Workers’ Compensation Act, Disability Beginning Five Years
After Injury.
Col. Rev. Stat. § 8-41-304 Workers’ Compensation Act, Last Employer Liable -
Exception.
Col. Rev. Stat §8-43-103 Workers’ Compensation Act, Notice of Injury - Time Limit.
Col. Rev. Stat § 8-43-103 Notice of Injury Time Limit.
Conn. Gen. Stat. § Sec. 31-275 Workers’ Compensation Act Definitions.
Conn. Gen. Stat. 31-294 Workers’ Compensation Act, Notice of Claim for
Compensation. Notice Contesting Liability. Exception for Dependents of Certain
Deceased Employees.
Del. Code Tit.19 § 2301 General Provisions.
Del. Code Tit.19 § 2342 Determination and Payment of Benefits.
Del. Code Tit.19 § 2361 Limitation Periods for Claims.
DC Code § 32-1501 Definitions.
DC Code § 32-1510. Occupational disease.
DC Code § 32-1514.Workers’ Compensation, Limitation Periods for Claims.
Fla. Stat. § 440.15 Workers’ Compensation Occupational Diseases.
Fla. Stat. § 440.19 Workers’ Compensation, Time Bars To Filing Petitions For Benefits.
252
Ga. Code. Ann. § 34-9-281. Workers’ Compensation, Compensation for Occupational
Disease, Prerequisites to Compensation for Occupational Disease.
Haw. Rev. Stat. § 386-82 Hawai‘i Workers’ Compensation Law Claim for
Compensation; Limitation of Time.
Idaho Code Ann. § 72-438 Workers’ Compensation and Related Laws, Occupational
Diseases.
Idaho Code Ann. § § 72-102 Workers’ Compensation and Related Laws Definitions
Idaho Code Ann. § 72-443 Workers’ Compensation and Related Laws, Period of
Exposure in Silicosis Cases.
Idaho Code Ann. § 72-445 Workers’ Compensation and Related Laws Compensation for
Total Disability or Death from Complicated Silicosis.
Idaho Code Ann. §72-448 Workers’ Compensation and Related Laws Notice and
Limitations.
820 Ill. Comp. State § 310/1 Workers’ Occupational Disease Act Citation of
Act; definitions; presumption of exposure; parties liable; limitations.
Ind. Code Ann. § 22-3-7-9 Worker's Occupational Diseases Compensation Definitions;
applicability of chapter; exemptions
Ind. Code § 22-3-7-10 Worker's Occupational Diseases Compensation Definitions,
Occupational Disease.
Ind. Code § 22-3-7-32. Worker's Occupational Diseases Compensation Notices
Ind. Code Ann. § 22-3-7-33 Worker's Occupational Diseases Compensation Exposure;
presumptions; joint employee.
Iowa Code §85A.8 Occupational Disease, Defined.
Iowa Code § 85A.12 Occupational Disease Compensation. Disablement or death
following exposure — limitations.
Iowa Code 85A.13 Occupational Disease. Provisions relating to pneumoconiosis.
Iowa Code §85A.18 Occupational Disease, Notice of Disability.
Kan. Stat. Ann. § 44-5a01. Occupational diseases. Occupational diseases; treated as
injuries by accident under workmen's compensation act; defined; limitations of
liability; aggravations.
Kan. Stat. Ann. §44-5a09. Occupational diseases. Silicosis defined.
Kan. Stat. Ann. §44-5a10. Occupational diseases. Disability or death from silicosis;
compensation rights.
Kan. Stat. Ann. § 44-5a13. Occupational diseases. Compensation for death from silicosis
complicated with other disease; how paid.
Ky. Rev. Stat. § 342.001. Workers’ Compensation Act. Definitions.
Ky. Rev. Stat. Ann. §342.316.4. Workers’ Compensation Act. Liability of employer and
previous employers for occupational disease -- Claims procedure -- Time
limitations on claims -- Determination of liable employer -- Effect of concluded
coal workers' pneumoconiosis claim -- Applicability of consensus procedure.
La. Rev. Stat. § 23:1031.1. Labor and Workers’ Compensation. Occupational disease.

253
Me. Stat. tit.39-A 885 Pt A § 603. Occupational Disease Defined.
Me. Stat. tit.39-A 885 Pt A § 609. Occupational Disease Law. Compensation Limits.
Silicosis.
Me. Stat. tit.39-A 885 Pt A § 613. Occupational Disease Law Silicosis
Md. Lab & Emp Code § 9-101(2016) (b) Workers’ Compensation. Definitions.
Md. Lab & Emp Code § 9-705. Workers’ Compensation. Notice to employer --
Occupational disease
Md. Lab & Emp Code § 9-711. Workers’ Compensation. Claim application -
Disablement or death from occupational disease.
Mass. Gen Laws ch. 152 § 26 Workers’ Compensation. Definitions.
Mass. Gen. Laws ch. 152 § 41 Workers’ Compensation. Notice of proceedings for
compensation; limitation of actions.
Mass. Gen. Laws ch. 152 § 44. Workers’ Compensation. Notices.
Mich. Comp. Laws § 418.441 Workers’ Disability Compensation Act Claim for
occupational disease and death resulting from occupational disease; requirements;
commencement; time limit.
Minn. Stat. §176.151 Workers’ Compensation. Time Limitations.
Minn. Stat. §176.021 Workers’ Compensation. Occupational Disease
Miss. Code Ann. § 71-3-3 Workers’ Compensation Definitions
Miss. Code § 71-3-7. Workers’ Compensation General Provisions. Liability for payment
of compensation.
Miss. Code § 71-3-35. Workers’ Compensation General Provisions. Limitation.
Mo. Rev. Stat. § 287.020. Workers' Compensation Law Definitions
Mo. Rev. Stat. § 287.063.1. Workers' Compensation Law. Occupational diseases,
presumption of exposure--last employer liable--statute of limitations, starts
running, when.
Mo. Rev. Stat. § 287.020. Workers' Compensation Law Definitions
Mo. Rev. Stat.§ 287.420. Written notice of injury to be given to employer--exceptions
Mo. Rev. Stat. § 287.420.1. Workers’ Compensation Law. Written notice of injury to be
given to employer--exceptions.
Mo. Rev. Stat. § 287.430.1. Workers’ Compensation Law. Limitation as to action,
exception.
Mont. Code. Ann § 39-71-601. Workers’ Compensation. Statute of limitation on
presentment of claim -- waiver.
Mont. Code Ann. § 39-71-407. Workers’ Compensation. Liability of Employers.
Mont. Code Ann. § 39-71-407(13). Workers’ Compensation.
Mont. Code Ann. § 39-71-407(10). Workers’ Compensation.
Mont. Code Ann. § 39-71-713. Workers’ Compensation. Diminution of Compensation.
Mont. Code. Ann §39-71-715. Workers’ Compensation. Benefits for pneumoconiosis --
definition.

254
Neb. Rev. Stat. § 48-137 Labor. Compensation claims; actions; statute of limitations;
exceptions.
Nev. Rev. Stat. § 617.344. Occupational Diseases. Claim for compensation:
Requirements for diseased employee, dependent or representative to file claim
Nev. Rev. Stat. § 617.010. Occupational Diseases
Nev. Rev. Stat. §617.140. Occupational Diseases “Silicosis” defined.
Nev. Rev. Stat. § 617.342. Occupational Diseases. Notice of Occupational Disease.
Nev. Rev. Stat. § 617.344. Claim for compensation: Requirements for diseased
employee, dependent or representative to file claim; form.
Nev. Rev. Stat. § 617.450. Occupational Diseases. Specific occupational diseases;
schedule.
Nev. Rev. Stat. § 617.460. Occupational Diseases. Silicosis and diseases related to
asbestos as occupational diseases; compensation and claims.
Nev. Rev. Stat. §617.470. Occupational Diseases Occupational diseases of respiratory
tract resulting from exposure to dusts.
N.H. Rev. Stat. Ann. § 281-A:16. Definitions
N.H. Rev. Stat. Ann. § 281-A:19. Workers’ Compensation. Notice of Injury.
N. J. Rev. Stat. § 34:15-34. Workers’ Compensation. Time for claiming compensation for
occupational disease.
N. J. Rev. Stat. § 34:15-31. “Compensable occupational disease” defined
N.M. Stat. Ann. 52-3-10. Employer liability for compensation; conditions when no
payment to be made.
N.M. Stat. Ann. §52-3-11. Last employer liable; exception.
N.M. Stat. Ann. §52-3-16. Claim to be filed for occupational disease benefits; effect of
failure to give required notice or to file claim within allowed time.
N.M. Stat. Ann. §52-3-32, Occupational diseases; proximate causation.
N.M. Stat. Ann. §52-3-33. Occupational diseases; definition.
N.M. Stat. Ann. §52-3-42. Limitation on filing of claims; rights barred unless timely
filed.
12 N.Y. CCR ch. V. § 2. Workers’ Compensation. Occupational disease.
12 N.Y. CCR ch. V. § 28. Workers’ Compensation. Limitation of right to compensation
12 N.Y. CCR ch. V. § 45. Workers’ Compensation. Notice to employers
N.C. Gen. Stat. § 97-58. Workers’ Compensation Act. Time limit for filing claims.
N.C. Gen. Stat. § 97-24. Right to compensation barred after two years; destruction of
records.
N.C. Gen. Stat.§ 97-22. Notice of accident to employer.
N.C. Gen. Stat. §97-58. Time for Filing Claims.
N.C. Gen. Stat. § 97-53. Occupational diseases enumerated; when due to exposure to
chemicals.
N.D. Cent. Code § 65.05.01 Claims and Compensation. Claims for benefits - When and
where filed.
N.D. Cent. Code, § 65-01-02. Compensable injury.
255
N.D.Cent..Cod § 65-05-01. Silicosis.
Ohio Rev. Code § 4123.01 Workers’ Compensation. Definitions.
Ohio Rev. Code § 4123.28 Workers’ Compensation. Record of injuries and occupational
diseases; reports.
Ohio Rev. Code. § 4123.68 Workers’ Compensation. Schedule of compensable
occupational diseases.
Ohio Rev. Code. § 4123.85 Workers’ Compensation. Claims for compensation or
benefits in cases of occupational diseases.
85A Okl. St§ 65. Occupational Disease.
85A Okl. St § 66. Asbestosis--Silicosis--Definition--Limitation on Compensation
85A Okl. St § 69. Statute of Limitations--Initial Claim--Claim for Additional
Compensation--Failure to File—Exception.
Or. Rev. Stat. § 656.802 Occupational Disease Law. Occupational disease.
Or. Rev. Stat. § 656.807 Occupational Disease Law. Time for filing of claims for
occupational disease.
77 Pa. Stat. § 27.1. Occupational diseases; definitions.
77 Pa. Stat. § 412. Workers’ Compensation Act Liability and Compensation
Compensation for silicosis, anthraco-silicosis, coal worker's pneumoconiosis, or
asbestosis.
77 Pa. Stat. § 602. Claims for Compensation.
R.I. Gen. Laws § 28-34-1. Workers’ Compensation. Definitions.
R.I. Gen. Laws § 28-34-2 Workers' Compensation – Occupational Diseases.
Occupational diseases listed – Treatment as compensable injury.
R.I. Gen. Laws § 28-34-4 Workers' Compensation – Occupational Diseases Relationship
of disease to employment – Time of bringing suit.
R.I. Gen. Laws § 28-34-9. Workers' Compensation. Notice to employer of claim.
R.I. Gen. Laws §28-35-57. Workers' Compensation. Limitations of claims.
S.C. Code § 42-11-10. Workers' Compensation. “Occupational disease” defined.
S.C. Code § 42-11-20. Workers' Compensation. “Disablement” and “disability” defined.
S.C. Code § 42-15-40. Workers' Compensation. Time for filing claim; filing by registered
mail.
S.C. Code § 42-11-60. Workers' Compensation. Requirements for compensation for
pulmonary diseases.
S.C. Code § 42-11-70. Workers' Compensation. Time in which disease must have been
contracted.
S.D. Codified Law § 62-8-1. Definition of terms.
S.D. Codified Law § 62-8-4. Right to compensation -- Applicability of workers'
compensation law.
S.D. Codified Law § 62-8-11. Occupational Disease Disability. Filing time to qualify for
disability or death compensation.

256
S.D. Codified Law § 62-8-14. Occupational Disease Disability Silicosis cases--Period of
exposure.
Tenn. Code Ann § 50-6-301. Workers’ Compensation Law. Occupational diseases
defined.
Tenn. Code Ann § 50-6-302. Retroactivity -- Coal worker’s pneumoconiosis, effect of
federal law.
Tenn. Code Ann § 50-6-303. Compensation and benefits.
Tenn. Code Ann § 50-6-305. Workers’ Compensation Law. Notice of contraction of
disease and claim for compensation.
Tenn. Code Ann § 50-6-306. Workers’ Compensation Law. Statute of limitations
Tex. LAB Code § 409.001. Workers’ Compensation Act; Notice of Injury to Employer.
Claim for Compensation. Occupational disease.
Utah LAB Code §34A-3-103. Occupational Disease Act.
Utah LAB Code §34A-3-109. Utah Occupational Disease Act. Limitations -- Rights
barred if not filed within limits -- Burden of proof.
Vt. Stat. Ann. tit. 21, § 601. Definitions.
Vt. Stat. Ann. tit.3 § 656. Notice of injury and claim for compensation.
Vt. Stat. Ann. tit.3 §1700. Vermont Workers’ Compensation and Occupational Disease
Rules. Statute of limitations.
Vt. Stat. Ann. tit.3 §1800. Vermont Workers’ Compensation and Occupational Disease
Rules. Occupational disease claims.
Va. Code Ann. §65.2-405. Workers’ Compensation. Notice to be given.
Va. Code Ann § 65.2-400. Workers’ Compensation. Occupational disease defined.
Va. Code Ann. §65.2-405. Workers’ Compensation. Notice to be given.
Va. Code Ann § 65.2-406. Workers’ Compensation. Limitation upon claim; diseases
covered by limitation.
Rev Wash. Code § 51.08.140. Occupational disease.
Rev Wash. Code § 51.28.055. Industrial Insurance. Time limitation for filing claim for
occupational disease—Notice—Hearing loss claims—Rules.
W. Va. Code § 23-4-1. Workers’ Compensation. To whom compensation fund disbursed;
occupational pneumoconiosis and other occupational diseases included in “injury”
and “personal injury”; definition of occupational pneumoconiosis and other
occupational diseases; rebuttable presumption for cardiovascular injury and
disease or pulmonary disease for firefighters.
W. Va. Code § 23-4-15. Workers’ Compensation. Application for benefits.
Wis. Stat. §102.12. Workers’ Compensation. Notice of injury, exception.
Wis. Stat. §§102.17. Workers’ Compensation. Statute of Limitations.
Wyo. Stat. §27-14-503. Workers’ Compensation. Statute of Limitations.
VITA
Arielle Leah Hesse
EDUCATION
2018 Ph.D. Geography, The Pennsylvania State University, University Park, PA
Minor: Women’s Studies
2011 M.Sc Geographical Sciences: Society and Space, University of Bristol, UK
2010 B.A. The Pennsylvania State University, University Park, PA
Major, Geography, with Honors, French and Francophone Studies, Jewish
Studies, Minor: English
RELATED PUBLICATIONS AND REPORTS
2017 Hesse, A. Governance at the intersection of health and energy, in Handbook on
Geographies of Energy, eds. B. Solomon and K. Calvert. Edward Elgar.
2016 Hesse, A., Kelsey, T., Pohlman, M. Economic Changes in Pennsylvania
within the Context of Marcellus Shale Development. Marcellus Shale Impacts
Study Wave 2. Center for Rural Pennsylvania.
2016 Brasier, K. Chandler, R. Glenna, L., Hesse, A., Kelsey, T., Monnat, S.,
Perchinski, J., Schafft, K., and Suchyta, M. 2016. Marcellus Shale Impacts Study
Wave 2: Chronicling Social and Economic Change in Southwest Pennsylvania.
Final Report to the Center for Rural PA
2016 Monnat, S. M., Ely, D., Suchyta, M., Chandler, R.F., and Hesse, A. 2016. Health
Insurance Coverage, Health Care Utilization, and Health Outcomes within the
Context of Marcellus Shale Development. The Marcellus Shale Impacts Study,
Wave 2. Center for Rural PA.
2016 Hesse, A. Baka, J., and Calvert, K. 2016. Enclosure and Exclusion within
Emerging Forms of Energy Resource Extraction: Shale Fuels and Biofuels, in
Palgrave Handbook of the International Political Economy of Energy, eds. T. Van
de Graaf and B. Sovacool.
2011 Andrews, E. and Hesse, A. 2011. Draft Technical Report prepared for the US
National Climate Assessment Case Study: Marcellus Shale: Impacts and
Intersections with Climate Change. Prepared for Climate Change in the Northeast.
SELECTED RESEARCH GRANTS & AWARDS
2014 National Science Foundation Doctoral Dissertation Improvement Grant
2012 Honorable Mention, National Science Foundation Graduate Research Fellowship
2011 Anne C. Wilson Graduate Student Award, Penn State
2010 John W. White Graduate Fellowship: Penn State Faculty Senate
RELATED RESEARCH
Research Asst, Penn State; Evidence in US Hydraulic Fracturing Rulemaking
Research Asst, Penn State; Impact of Model Policy: Analysis of State Fluid Disclosure
Laws for Hydraulic Fracturing
Research Asst, Penn State; The Marcellus Shale Impacts Study: Chronicling Social and
Economic Change in Southwest PA