
LGBT Health Care in Health Settings
32
L.G.B.T. HEALTH: WITHOUT EQUALITY, THERE IS NO QUALITY Presented by: Josh Hyatt DHSc, MHL, CPHRM
-
Upload
hms-harvard -
Category
Documents
-
view
6 -
download
0
Transcript of LGBT Health Care in Health Settings
L.G.B.T. HEALTH:WITHOUT EQUALITY,
THERE IS NO QUALITY Presented by:Josh Hyatt DHSc, MHL, CPHRM

SPEAKER
Dr. Josh Hyatt, DHSc, MHL, CPHRMSenior Risk Management SpecialistMajor Medical Professional Liability Insurance Carrier.Adjunct Professor: Health Law, Medical Ethics, Health Leadership, Health Communication and Education.
2
DISCLAIMERS Discussions of sexuality and gender can be controversial in nature
There is no intent to change the participants core values or moral convictions
The focus of this presentation is to start a dialogue with health care providers on the health care disparities and barriers to care that the LGBT community faces everyday

OBJECTIVESFollowing this session participants should be able to: Identify and evaluate some health disparities in the LGBT community and their impact on public health overall.
Analytically evaluate the legal and ethical risks that health care institutions face related to LGBT health care issues.
Develop plans that work towards reducing health disparities in the LGBT community and improve overall quality of care.
LGBT TERMS
LGBT
Ally
Sexual Orientation Gender
Identity
Trans
Coming Out
Cisgender
What other terms can you think of that you want to
discuss?
SELF-AWARENESS What are your personal attitudes towards LGBT issues? What has shaped them? Is sexual orientation a biological determinate? Is gender a biological determinate? Does it really matter?
6
WORDS
A. GaydarB. Queen C. DykeD. Sexual PreferenceE. FaggotF. Butch / FemmeG. Breeder
H. Fag Hag / Fag StagI. TrannyJ. TransvestiteK. Drag Queen/KingL. QueerM. FruitN. Nancy Boy
Identify the word(s) you have negative associations with:
Words have power.

EXERCISE EXERCISE: Write 5 words or phrases that you associate with LGBT individuals
Write 5 words or phrases that you associate with LGBT rights
Write 5 words or phrases that you associate with LGBT health care
9
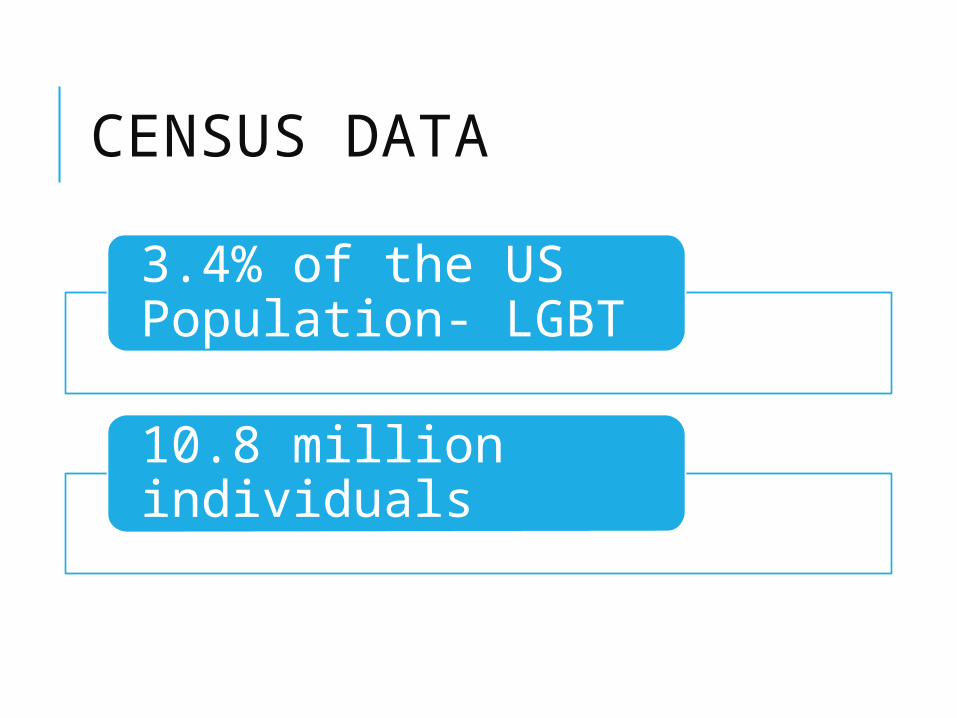
CENSUS DATA
3.4% of the US Population- LGBT
10.8 million individuals
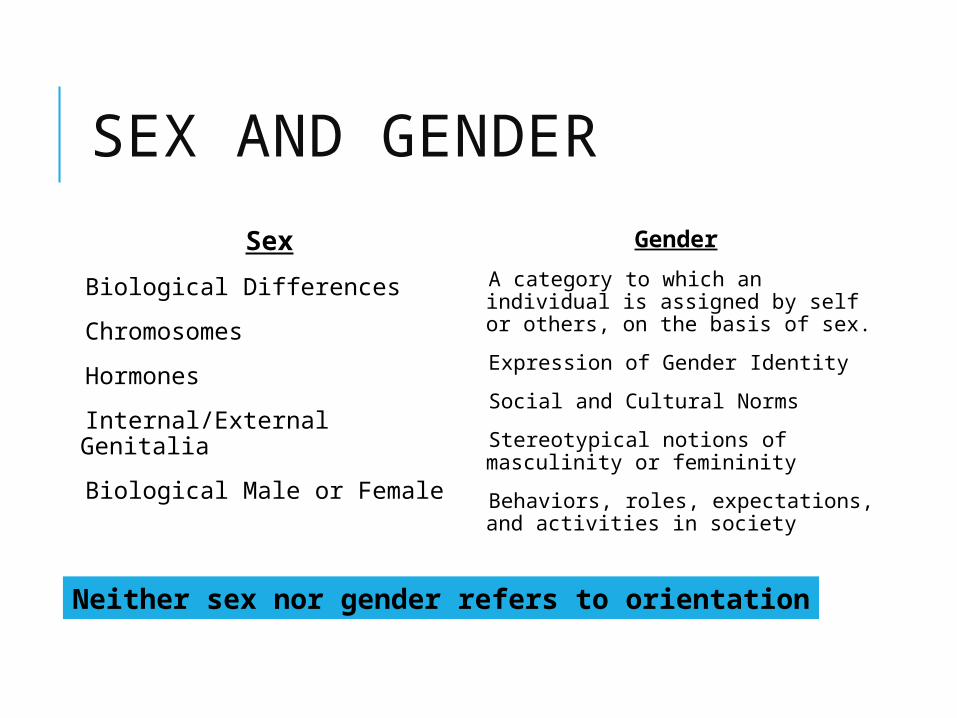
SEX AND GENDERSex
Biological Differences Chromosomes Hormones Internal/External Genitalia Biological Male or Female
Gender A category to which an individual is assigned by self or others, on the basis of sex. Expression of Gender Identity Social and Cultural Norms Stereotypical notions of masculinity or femininity Behaviors, roles, expectations, and activities in society
Neither sex nor gender refers to orientation

DISCRIMINATION FACING THE LGBT COMMUNITY Homophobia
Transphobia
Reparative Therapy
Religious and Social Ostracism
Victimization, Bullying, and Abuse
HEALTH DISPARITIES IN THE LGBT COMMUNITY HIV/AIDS
Cancer Mental Health Smoking Eating Disorders/Obesity Poverty Access to Care Violence (Bullying, Community, Family, Domestic)
LGBT DISPARITIES The primary cause(s) of health disparities in the LGBT community include:
A.Perceived and actual discrimination B.Social stigmatizationC.Unfair marketing of productsD.Lack of positive role-models in the
mediaE.Patchwork of state laws

HEALTHY PEOPLE 2020The reasons for this goal included:Health disparities linked to social stigma and discrimination
Impact of non-acceptance of sexual orientation or gender identification on adolescents and young adults
Lack of health insurance coverage for same-sex Increased rates of psychiatric and substance abusePrevalence of attempted and actual suicide Increased amount of violence and bullying experienced by the community
HETERONORMATIVITY A belief that:
Favors opposite-sex relationships
Encourages distinct gender roles
16

HETERONORMATIVITY Institutional Systems:
Rules/Policies: Visitation Rights Forms/Documents Website Information Training That Ignores LGBT Health Issues
17
QUESTIONS What institutional heteronormality practices can you identify in your facility? How many of you have cultural competency programs in your facility? How many of you include LGBT in that training? How many market to the LGBT community or have specific programs?
18

MICRO-MESSAGING Subtle messages that devalue, discourage, or impugn others
Double-blind Effect: Lack of options result in a sense of penalty, censure, or deprivation
19

MICRO-MESSAGING Examples: Eye contact Tone of voice Body language Hetero-normal terms on forms Gender pronoun issues
20
QUESTIONS What are some micro-messaging you see in your home? What are some micro-messaging you see in the general population? What are some micro-messaging you see in your workplace?
21
MINORITY STRESS MODELSexual minority health disparities are linked to stressors induced by a hostile and homophobic culture, which results in the
Harassment, Maltreatment Discrimination Victimization
SELF-IDENTITY AND COMING OUT Self-identity Coming Out
Outing
Acceptance or denial of an individual’s sexual orientation can be a defining
aspect of their life as it can directly influence the risk of negative, self-
destructive behaviors.
COMING OUT- PROVIDER’S ROLE Provider-patient relationship
Positive, non-judgmental experience will often lead to a more positive self-image
Confidentiality laws are inconsistent in federal and state laws

BARRIERS TO CARE
Perception that LGBT couples are less committed
Fear of social rejection and isolation
Lack of understanding of LGBT issues
Fear of disclosure
Stigmatization
BARRIERS TO CAREContributing Factors: Lack of awareness and LGBT training in medical and nursing school, Presumption of a heterosexual orientation by care givers, Discomfort when asking about or discussing sexual orientation, and Lack of LGBT presence in health care settings and leadership roles
BARRIERS TO TRAINING Cultural and Institutional bias Fear of Backlash Lack of Qualified Speakers Addressing Micro-messages Very Difficult to Change Culture
27
RISK MANAGEMENT ISSUES IN LGBT CARE Access to Care Marriage/Civil Union/ Domestic Partnership End-Of-Life Decision Making Visitation Rights Spousal Insurance Rights
RECOMMENDATIONS- COMMUNICATION Don’t conflate sex and gender in the trans community or overemphasize sexual orientation in the LGB community.
Procedural changes (forms, posters, etc.)
Scripts to structure patient encounters
Language on marketing and websites
Identify services that could be controversial
Integrated and open culture

RECOMMENDATIONS- EDUCATIONAL
Establish LGBT cultural competency programs
Narratives should focus on characteristics, not behaviors. Focus on the ethical care and services
Micro-messaging
Avoid “victim” and “oppressor” dynamics
Avoid the “Black and White” discussion of sexual orientation and gender identity
RECOMMENDATIONS- INDIVIDUAL Identify moral distress components
Identify own biases, attitudes, and assumptions
Differentiate between “couch” issues and “institutional” issues
Identify when personal judgments may be creating micro-messaging