Handovers From the OR to the ICU
19
Handovers From the OR to the ICU Alberto S. Bonifacio, BSN, MHA* Durham Veterans Affairs Medical Center Durham, North Carolina Noa Segall, PhDw Duke University Medical Center Durham, North Carolina Atilio Barbeito, MD, MPHwzz Durham Veterans Affairs Medical Center Durham, North Carolina Jeffrey Taekman, MDw Duke University Medical Center Durham, North Carolina Rebecca Schroeder, MD, MMCiwzz Durham Veterans Affairs Medical Center Durham, North Carolina Jonathan B. Mark, MDwzz Durham Veterans Affairs Medical Center, Durham, North Carolina The case was long and difficult—a redo sternotomy and coronary artery bypass grafting procedure on a fragile 82-year-old patient. While you are pushing the bed down the hallway, you move cautiously toward the intensive care unit (ICU) because the patient is hemodynamically unstable and receiving high doses of inotropes and intra-aortic balloon pump support. Upon rounding a corner, equipment temporarily being stored in the hallway forces you to swerve forcefully disconnecting the helium tubing from the balloon pump. Alarms chiming, you quickly make it to your assigned ICU bed space to find the receiving ICU nurse absent. She left the bedside to look for a missing pressure cable. You handover the bag-mask system to the respiratory therapist, and she asks whether you had any problems with intubation or ventilation. You want to tell her that intubation was difficult, but you notice that the arterial pressure is very low. “Please don’t disconnect the a-line yet,” you ask the INTERNATIONAL ANESTHESIOLOGY CLINICS Volume 51, Number 1, 43–61 r 2013, Lippincott Williams & Wilkins www.anesthesiaclinics.com | 43 FROM THE *PATIENT SAFETY CENTER OF INQUIRY ; zDEPARTMENT OF ANESTHESIOLOGY AND wDEPARTMENT OF ANESTHESIOLOGY REPRINTS:JONATHAN B. MARK, MD, DEPARTMENT OF ANESTHESIOLOGY ,DURHAM VETERANS AFFAIRS MEDICAL CENTER, 508 FULTON STREET DURHAM, NC 27705. E-MAIL: JONATHAN.MARK@DUKE.EDU
Transcript of Handovers From the OR to the ICU
Handovers From the OR to the ICU
Alberto S. Bonifacio, BSN, MHA*Durham Veterans Affairs Medical CenterDurham, North Carolina
Noa Segall, PhDwDuke University Medical CenterDurham, North Carolina
Atilio Barbeito, MD, MPHwzzDurham Veterans Affairs Medical CenterDurham, North Carolina
Jeffrey Taekman, MDwDuke University Medical CenterDurham, North Carolina
Rebecca Schroeder, MD, MMCiwzzDurham Veterans Affairs Medical CenterDurham, North Carolina
Jonathan B. Mark, MDwzzDurham Veterans Affairs Medical Center,Durham, North Carolina
The case was long and difficult—a redo sternotomy and coronaryartery bypass grafting procedure on a fragile 82-year-old patient. Whileyou are pushing the bed down the hallway, you move cautiously towardthe intensive care unit (ICU) because the patient is hemodynamicallyunstable and receiving high doses of inotropes and intra-aortic balloonpump support. Upon rounding a corner, equipment temporarily beingstored in the hallway forces you to swerve forcefully disconnecting thehelium tubing from the balloon pump. Alarms chiming, you quicklymake it to your assigned ICU bed space to find the receiving ICU nurseabsent. She left the bedside to look for a missing pressure cable. Youhandover the bag-mask system to the respiratory therapist, and she askswhether you had any problems with intubation or ventilation. You wantto tell her that intubation was difficult, but you notice that the arterialpressure is very low. “Please don’t disconnect the a-line yet,” you ask the
INTERNATIONAL ANESTHESIOLOGY CLINICSVolume 51, Number 1, 43–61r 2013, Lippincott Williams & Wilkins
www.anesthesiaclinics.com | 43
FROM THE *PATIENT SAFETY CENTER OF INQUIRY ; zDEPARTMENT OF ANESTHESIOLOGY AND wDEPARTMENT OF
ANESTHESIOLOGY
REPRINTS: JONATHAN B. MARK, MD, DEPARTMENT OF ANESTHESIOLOGY, DURHAM VETERANS AFFAIRS MEDICAL
CENTER, 508 FULTON STREET DURHAM, NC 27705. E-MAIL: [email protected]
resident as you push 5 mcg of intravenous epinephrine and administer afluid bolus. Meanwhile, the surgeon is talking to the ICU attending inthe hallway and giving details of the procedure. You would love to hear,but the TV is on (looks like it may rain tomorrow).
With the balloon pump working and vital signs recovering, yougather your paperwork and deliver your report to the patient’s primaryICU nurse: “He is on 0.07 mcg/kg/min of epinephrine. His EF was lowto start with. We gave him 2000 mL of crystalloid. Last ACT was 106.”The nurse takes notes on the back of her insulin sheet.
Twenty minutes later, you walk out, carrying the monitor and theoxygen tank. “That was a tough case,” the surgeon comments as heaccompanies you out the door. At the desk, the ICU resident, now alone,is trying to figure out why the patient needs to be ventricularly paced,but gets interrupted by the nurse who asks “Is he really supposed to beon 15 units per hour of insulin?”
’ Introduction
The problems caused by ineffective patient handovers are wellknown and common—we have all experienced them. In today’sincreasingly complex and integrated health care system, the safetyof our patients depends upon the seamless transitions of care betweenclinical care teams, treatment areas, and support systems. Patient hand-overs, defined as the transfer of information, professional responsibility,and accountability between individuals and teams,1 are the processesthat span the gaps between critical junctures and ensure that continuityof care is maintained. [The terms handover and handoff are usedinterchangeably in the medical literature to describe the transitions inpatient care as defined above. We prefer the term handover (and use itin this chapter) because we feel it conveys a clearer sense of teamworkand continued commitment to the seamless care of the patient.] Thesetransfers of care, however, have been shown to be fraught with technicaland communication errors2–4 that have been linked to adverse eventsand patient harm.2,5–8 For example, handover failures account for halfof the sentinel events rooted in “communication failures” as reported bythe Joint Commission9 and also for 20% of all malpractice claims in theUnited States.10
In response to these and a growing number of similar findings, newresident workload restrictions,11 and increased regulatory demand toimprove health care performance and outcomes, interest in patienthandovers has grown significantly. The Joint Commission, for example,now requires health care providers to “implement a standardizedapproach to handover communications including an opportunity to askand respond to questions” (National Patient Safety Goal 02.05.01).11
44 ’ Bonifacio et al
www.anesthesiaclinics.com
The Accreditation Council for Graduate Medical Education, recognizingthe impact of resident work hour mandates,12 requires residencyprograms to design clinical assignments to minimize the number of caretransitions, ensure and monitor structured handover processes, andensure that trainees are competent in communicating with teammembers during handover.13 Despite these robust efforts to improvethe safety of handovers, they remain high-risk, error-prone, andvulnerable points in the continuum of care.
’ Types of Handovers
A clear distinction is beginning to emerge between distinct types ofintrafacility handovers. The first is a handover that is usually performedat the end of a shift when a provider who is caring for several patientstransfers information about each patient to his or her replacement.Commonly called “sign-out,” or “within-unit,”14 this handover endswith a formal or informal transfer of responsibility for the care of thesepatients. This type of handover usually occurs between 2 clinicians ofsimilar disciplines such as house officers on a medicine ward, nurses inan intensive care unit (ICU), or between 2 consultant physicians whocross-cover each other at different times during the week.
The second type of handover is the transfer of a patient from 1location in the hospital to another with a different team assuming carefor that patient. These “between-unit” handovers not only involvea transfer of information and responsibility, but also a physical transferof the patient. Most transfers that require a change in level of care(eg, ICU to step-down or emergency to ward, etc.) involve “between-unit” handovers.
’ The Operating Room (OR) to ICU Handover
A variant of the “between-unit handover” is the transfer ofpostoperative patients from the OR to a postoperative care area suchas the ICU handover or postanesthesia care unit. Unlike the otherbetween-unit handovers, this handover involves some unique qualitiessuch as a delivering team comprised of 2 services (anesthesia andsurgery) instead of 1, the need to communicate details about a recentand significant event (the surgical procedure), and the commonpresence of invasive monitoring, tubes and drains, etc.
Although more complex than within-unit or shift handovers,postoperative handovers have received relatively little attention. Fewerthan 25 articles have been published since 1999 that focus specifically onOR to ICU patient handovers.15 Of these, the few that tested specificinterventions have limited generalizability owing to small sample sizes, afocus on 1 population type (pediatric cardiac surgery), and absence of
Handovers From the OR to the ICU ’ 45
www.anesthesiaclinics.com
outcome data.2,4,16–18 This chapter will describe current knowledgeabout OR to ICU handovers, provide strategies to improve handoversafety and reliability, and offer guidance on implementing change andsustaining improvements in care.
’ Characteristics of the OR to ICU Handover
The OR to ICU handover is dynamic and complex. In this process,an OR team is charged with transporting a patient and supportequipment while simultaneously monitoring and performing anyneeded therapeutic tasks such as manual ventilation. Upon arriving inthe ICU, the OR team joins a separate ICU team to transfer monitoringand support equipment to local systems while important informationabout the patient’s status and plan of care is transmitted. The process isfurther complicated as delivering team members with correspondinglydifferent perspectives on the course of the surgery must transmitinformation to a second team that is often simultaneously stabilizing,assessing, and initiating care plans for the patient. Furthermore, thisprocess is often informal, unstructured, and nonstandardized19 and, as aresult, inconsistent and highly variable.
As such, it is evident how handovers give rise to so many proceduraland communication errors. In the next sections, we will describe the3 crucial components of OR to ICU handovers: (1) the physical transferof the patient; (2) the transfer of information; and (3) the transferof responsibility and care.
Physical Transfer
Acutely ill or physically compromised patients recovering from high-risk procedures may experience rapid, life-threatening complications atany time during the transfer process. Movement of the patient from theOR table to a hospital bed may cause physiological disturbances relatedto positional changes and shifts in blood volume leading to cardiopul-monary instability. In transit, the patient is especially vulnerable asessential emergency resources such as suction, defibrillators, and criticalpersonnel, may be unavailable.
Physically moving the patient also raises the risk for displacement ordislodgement of critical lines and tubes. A complex surgical patient may beconnected to >2 dozen tubes, lines, drains, and monitoring cables thateasily tangle and disconnect. Free-rolling equipment transported with thepatient such as intravenous poles or circulation assist devices are oftendifficult to maneuver and add to the task saturation for transport teams.Separation of these cumbersome pieces from the bed because of insufficientpersonnel, crowded hallways, elevators, and poor coordination of the bedmovement are common sources of technical and attention errors.
46 ’ Bonifacio et al
www.anesthesiaclinics.com

Patient transport also presents an opportunity for significant periodsduring which the patient may be inadequately monitored. Postoperativecare transitions routinely require a minimum of 2 interruptions inmonitoring: (1) a transfer from the fixed OR to a mobile transportsystem; and (2) a transfer from the mobile to the fixed ICU monitoringsystem. Poor preparation of equipment (missing cables or dysfunctionalcomponents), accidental disconnections, and delayed transfer becauseof tangled cables may prolong unmonitored periods. Inattention of thetransport team, or distraction related to multitasking, may likewise leadto poor patient monitoring.
Information Transfer
Because of the condition of the postsurgical patient, the quantity andcomplexity of information exchange may be great. Not only is this dataset extensive and significant, but the transfer occurs between 2 highlyspecialized teams that work in functionally disparate environments.Members of the delivering team may prioritize and share informationbased upon their clinical roles and make inaccurate assumptions aboutwhat the members of the receiving team need or wish to hear.15 Forexample, an anesthesiologist may focus on the “anesthesia data set” (eg,airway difficulties, intake and output, etc.) because it is the informationwith which he or she is most familiar and considers most important. Theresult is often a lengthy but incomplete transfer of disorganizedinformation from which the receiving team must extract those pointsin which they are most interested. Differences in communicationstyle, hierarchical constraints, and a lack of structure further confoundthe process and contribute to communication failures.20 Chang andcolleagues reported that although deliverers of a handover thoughttheir report contained “the most important piece of information,”receivers disagreed 60% of the time.21 Another descriptive studyreported that anesthesiologists failed to transfer all of the essentialinformation in 67% of OR to postanesthesia care unit handovers.Interestingly, the study also noted that information related to anesthesia(eg, intraoperative analgesia) was reported most often while surgery-related information (eg, course of surgery) was reported least often.22
Another barrier to effective communication is the absence of keyteam members from the handover. For example, if the surgeon is notpresent, the anesthesia provider may be left to communicate all of theintraoperative information, thereby increasing the likelihood of infor-mation omissions or inaccuracies related to surgical details and planof care.19 Furthermore, critical team members may be functionallyexcluded from the report even if physically present such as whena surgeon and anesthesiologist speak privately with the ICU physician,whereas the ICU nurse is busy performing clinical tasks. Although
Handovers From the OR to the ICU ’ 47
www.anesthesiaclinics.com

present, the nurse becomes effectively excluded from the exchange ofinformation. This may also occur if the report delivered is inaudiblebecause of soft speech or a noisy environment. Regardless of reason,exclusion from the report may lead to data omission, duplication, orinaccuracy as team members are unable to cross-check and verify patientinformation.
Another common error and handover failure mode is inattentioncaused by the concurrent performance of tasks while attempting toreceive information. For example, a nurse attempting to calibrate aninvasive blood pressure transducer while simultaneously receivingreport may have difficulty comprehending and retaining the informa-tion delivered. Furthermore, errors may also occur with the physicaltask (calibrating the blood pressure transducer) as the nurse switchesattention between the 2 tasks. The nurse must then cognitivelyreassemble abstracted bits of information or later request the informa-tion from a team member who received it (yet another handover andopportunity for miscommunication).
The distraction-rich environment of an ICU is yet another barrierto effective handovers. Concentration and attention from both thedeliverers and receivers of critical information are essential for asuccessful exchange; however, they are often surrounded by auditoryand visual distractions such as alarming monitors, intercom announce-ments, and sometimes even patient televisions. Also common arecognitive disruptions caused by staff interrupting the informationexchange to discuss issues unrelated to the handover.23 Finally, timepressure related to OR scheduling or shift changes may causeunnecessary abbreviation or even deferral of the handover altogether.These factors combine to place handovers at high risk for communi-cation failure, adverse events, and patient harm.
Transfer of Responsibility
The formal transfer of responsibility for the patient is most often thefinal step in the handover occurring after the information is delivered.Like the physical and information transfer, the transfer of authority andresponsibility is usually informal rather than explicitly articulated.24 Thispresents yet another opportunity for patient harm because of uncertaintyabout patient care goals, who is ultimately responsible for the care of thepatient, and to whom questions or instructions should be directed.
’ A Practical Guide to Improving PostoperativeHandovers
Although variable in quality and lacking in strong evidence, thebody of literature offering insight and recommendations for OR to ICU
48 ’ Bonifacio et al
www.anesthesiaclinics.com

handovers is growing and improving. In a recent literature review,Segall and colleagues identified 24 articles that offered recommenda-tions for improving handovers. Fourteen of these supported theirinterventions with some level of evidence with 4 describing intervention-based studies. In addition to recommendations for physical andinformation transfer, many authors emphasized the importance ofeffective teamwork skills during handovers.15 Incorporating theseconcepts into the design of handovers has the potential for improvinghandover safety and reliability by addressing many of the modes offailure mentioned earlier.
Handover Teamwork and Structure
Five strategies to improve OR to ICU handovers have been broadlyrecommended in the recent literature.15 Each recommendation will bediscussed in further detail in the following sections.! Standardize the process.! Complete urgent clinical tasks before the information transfer.! Allow only patient-specific discussions during verbal handovers.! Require that all relevant team members be present.! Provide training in team skills and communication.
Standardizing the process is important as it will provide all handoverparticipants with a broad understanding and clear expectations as tohow the process should work. In other words, it is a plan that getseveryone on the “same page.” Defining roles and responsibilities willenable the concurrent completion of numerous tasks while ensuringthat important items are not forgotten. As team members becomecomfortable with the “routine,” the cognitive demand on workingmemory will decrease resulting in an improved understanding andretention of information. Codifying the standard into a formal protocolwill further enhance efforts by improving compliance thereby reducingvariability in the process. As teams become more familiar and adept atexecuting a standardized process such as the one we describe, the abilityof individuals to cross-monitor each other, anticipate each other’sactions, and detect potential process failures improves.
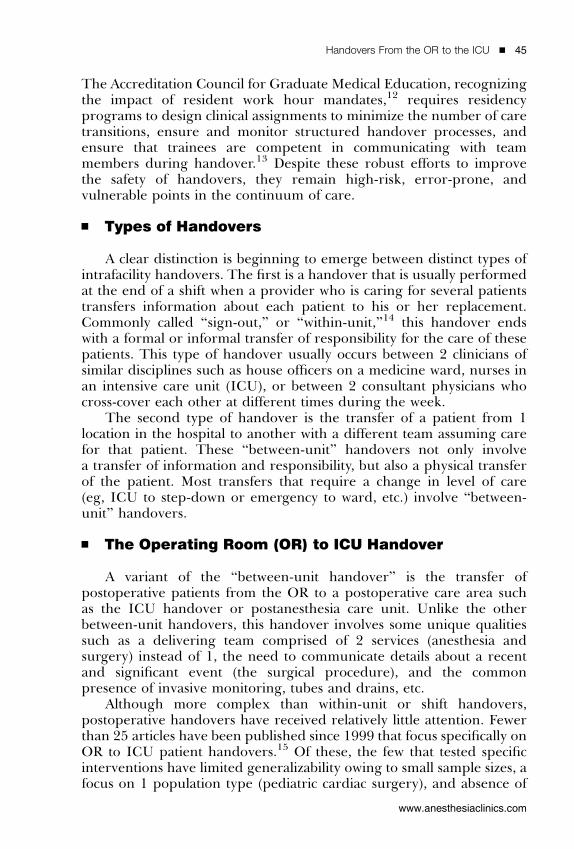
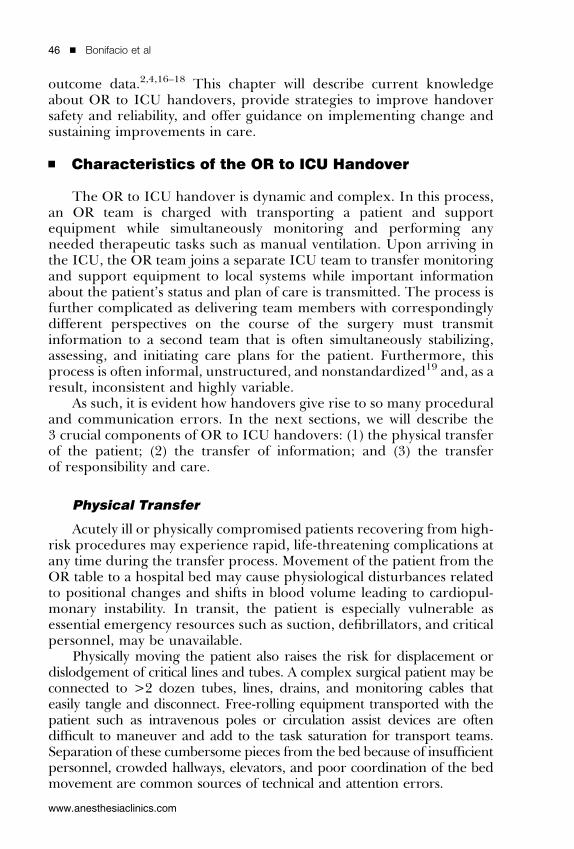
The matrix depicted in Figure 1 is an example of a standardizedprocess for the transfer of the patient upon arrival to the ICU. It is readlike a musical score, with roles on the y-axis and time/events on the x-axis. Figures 2, 3 are sample diagrams of staff positions and suggestionsfor task allocation for receiving surgical patients in the ICU.
Establishing a scalable and flexible yet standardized protocol for theOR to ICU handover will enhance the situational awareness (SA) of allteam members. Endsley25 has formally defined SA as “the perception ofthe elements in the environment within a volume of time and space, the
Handovers From the OR to the ICU ’ 49
www.anesthesiaclinics.com
comprehension of their meaning and the projection of their status inthe near future.” This definition breaks the concept of SA into 3 distinctlevels: (1) level 1—perception of the environment; (2) level2—comprehension of the meaning of this information; and (3) level3—projection of events or actions in the future based on the perceptionand comprehension. With a good sense of SA, team members are highly“in tune” with what is occurring around them, enabling them toperceive what is happening, anticipate what may occur, and create a planof how to react. SA can be enhanced by using effective teamcommunication strategies. For example, asking team members to “callout” vital signs as they appear on the ICU monitor display or otherpieces of information (eg, identification of an unexpected hemorrhageor a change in infusion rates during handover) will get all members onthe same page without disrupting the performance of their individualtasks.
Designating a handover leader may also be helpful. The handoverleader will facilitate smooth execution of the process by initiating andconcluding the handover and determining when to deviate from the
Figure 1. Standardized process for handover at bedside. The handover roles are identified onthe y-axis while the time course of events is depicted on the x-axis. Time 0 indicates the arrival ofpatient to the intensive care unit (ICU). BP indicates blood pressure; CRNA, certified registerednurse anesthetist; CVP, central venous pressure; ECG, electrocardiogram; ETT, endotracheal tube;MD, medical doctor; NGT, nasogastric tube; NIBP, noninvasive blood pressure; OR, operatingroom; PAP, pulmonary arterial pressure; RN, registered nurse; SPO2, pulse oximeter oxygensaturation; TDCO, thermodilution cardiac output.
50 ’ Bonifacio et al
www.anesthesiaclinics.com
routine (eg, in cases with unexpected patient deterioration or criticalequipment failure). The handover leader will also be charged withmediating interpersonal conflicts and setting the tone for effectiveteamwork and cooperation.
Other teamwork skills that may enhance the process include theestablishment and enforcement of communication ground rules. Theseinclude allowing only 1 person to speak at a time, ensuring the receivingteam is ready to receive report before information delivery, and estab-lishing a common language or method to address conflict. A variety ofvalidated programs offer teamwork strategies such as Team STEPPS(Team STEPPS: Team Strategies and Tools to Enhance Performance andPatient Safety) CUS (I am Concerned, I am Uncomfortable, Stop)26; orCrew Resource Management’s 3W’s (What I see, What I I’m concernedabout, What I want).27
Physical Transfer
At times it seems that Murphy’s Law, “if anything can go wrong, itwill,” is the only constant in the transport of critically ill patients, especiallywhen furthest away from help. Strategies should be implemented to
Figure 2. Initial team positions and tasks upon patient arrival in the intensive care unit (ICU).Upon arrival to the ICU, the handover teams first establish monitoring and complete critical tasksbefore transferring information. Personnel not directly involved in the initial transfer of monitor andequipment are asked to remain away from the bedside (behind the “hot line”) until needed. RNindicates registered nurse; RT, receiving team.
Handovers From the OR to the ICU ’ 51
www.anesthesiaclinics.com
prevent mishaps and mitigate their effects when they occur. Theseinclude meticulous preparation of equipment, nurturing a proactivemindset, and developing contingency plans. The Guidelines for the Inter-and Intra-hospital Transport of Critical Ill Patients published by the Societyof Critical Care Medicine describes good strategies relevant to OR toICU handovers.28
Equipment issues are common during patient handovers.29 Beforetransport, it is important to ensure that necessary equipment is in goodworking order (ie, functional monitor, batteries for infusion pumps,intravenous pole wheels, full oxygen cylinders, functional bag-valve maskventilation devices, etc.). Depending on the distance to be traveled andavailability of code carts along the way, it may be advisable to travel with atransport kit with basic resuscitation and airway equipment and drugs.
During the physical transfer of the patient, handover team membersmust anticipate and be prepared to manage life-threatening post-operative complications. Some handover models, for example, prohibitthe disassembly of OR monitor and ventilation systems (eg, ORventilator circuit) until the patient is determined to be safe for transport.
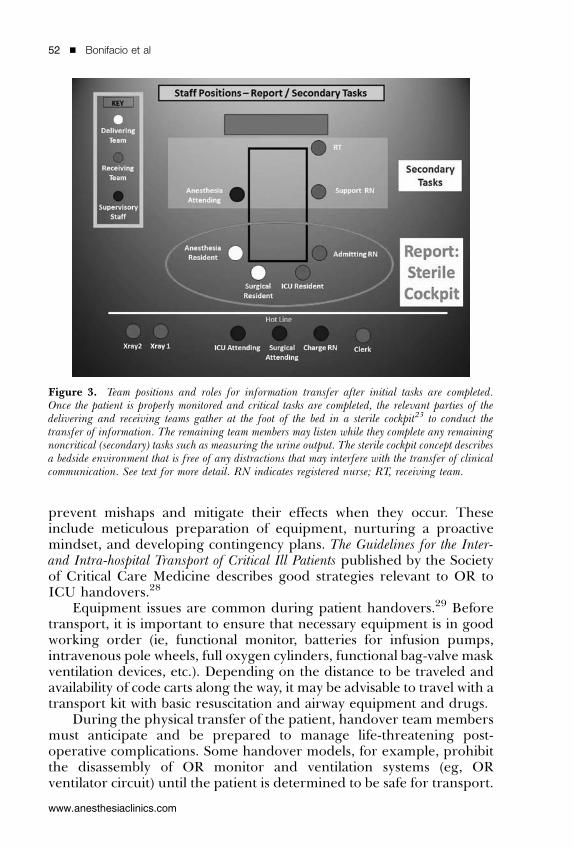
Figure 3. Team positions and roles for information transfer after initial tasks are completed.Once the patient is properly monitored and critical tasks are completed, the relevant parties of thedelivering and receiving teams gather at the foot of the bed in a sterile cockpit23 to conduct thetransfer of information. The remaining team members may listen while they complete any remainingnoncritical (secondary) tasks such as measuring the urine output. The sterile cockpit concept describesa bedside environment that is free of any distractions that may interfere with the transfer of clinicalcommunication. See text for more detail. RN indicates registered nurse; RT, receiving team.
52 ’ Bonifacio et al
www.anesthesiaclinics.com

It is also helpful to familiarize transport teams with the location of codecarts, alternate treatment areas, and means of summoning help in case itis needed. Sending a person in advance to reserve an elevator or clearthe hallway of equipment or people is often helpful as well.
Information Transfer
Information communicated by the delivering team must enable thereceiving team to perform 3 vital tasks: (1) prepare the staff, environment,and other resources for patient arrival; (2) provide immediate medicalcare upon patient arrival; and (3) provide care consistent with the overallcare plan upon assuming responsibility. The appropriate type and amountof information should be communicated clearly, accurately, and efficiently.
The flow of information should begin as soon as the surgeryschedule is published or the decision is made to admit a patient to theunit. Providing the ICU with a list of expected patients allows unitmanagers to plan for bed and staffing needs. Before the patient’s arrivalto the ICU, a patient-specific report will help the ICU prepare for thepatient’s arrival. This “preliminary” report, communicated verbally,electronically, or in writing, should contain sufficient information toallow the receiving team to develop a clinical picture of the patient,appropriately prepare space and equipment (eg, ventilators, isolation,etc.), and manage staff and workload. A number of health informationsystems now provide real-time electronic anesthesia records that enablethe ICU staff to monitor the patient’s clinical status during surgery.Although not formally evaluated in the OR to ICU handover literature,this mode of communication has the potential to offer the ICU teama very detailed view of the patient’s condition during surgery.
Figure 4 is an example of a manually completed worksheet intendedto prepare the ICU for patient arrival. This preliminary report wasdesigned for the OR circulating nurse and anesthesia provider tocomplete at a convenient time during the case (usually 45 to 60 minbefore patient transfer). ICU and OR staff collaboratively developed theform for the specific purpose of preparing the ICU physical environ-ment and staff expectations for patient arrival. It is not intended toprovide detailed clinical information or to duplicate data that will behanded over after patient arrival. The form makes use of colors,borders, spacing, and visual depictions to enhance usability andcomprehension. Phone calls are then made by OR personnel nearsurgical wound closure and just before patient transport to update thereceiving team of any significant changes or special instructions.
A detailed verbal report should be provided to the receiving teamafter arrival to the ICU. This bedside report should adequately describethe patient’s current status, outline a plan of care, and inform thereceiving team of any special considerations. A list of handover
Handovers From the OR to the ICU ’ 53
www.anesthesiaclinics.com

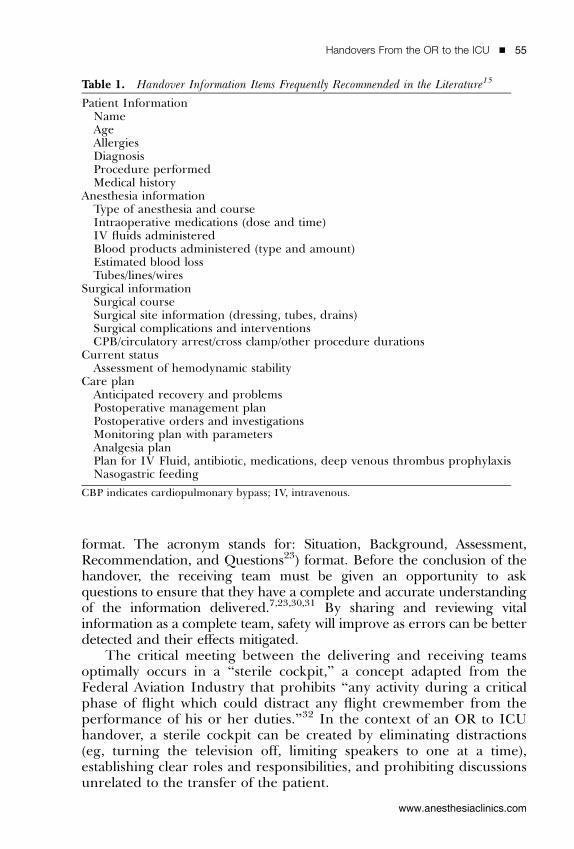
information items frequently cited in the literature can be found inthe Table 1. Although most have intrinsic face validity, it may proveimpractical or even detrimental to include them all. Instead, a minimumdata set should be created that will satisfy the informational needs of thedelivering OR and receiving ICU teams.
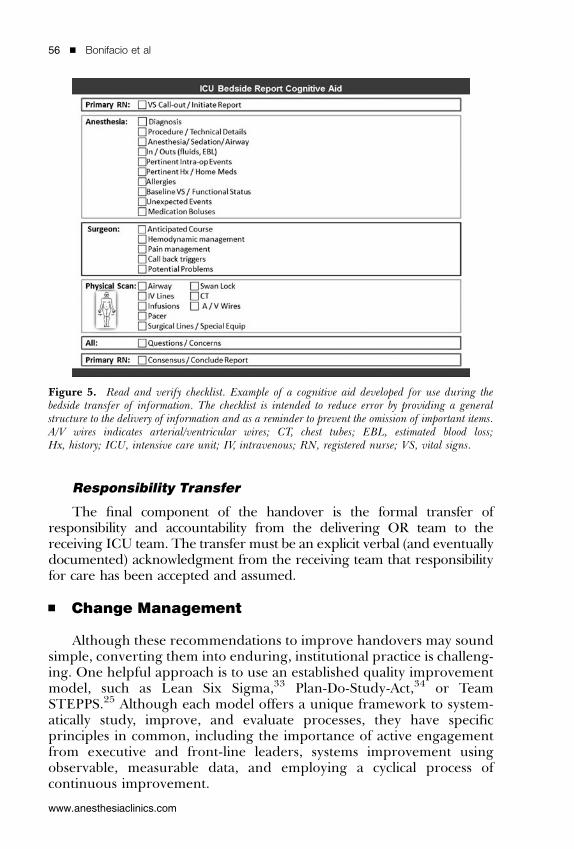
A single, face-to-face, interactive discussion at the patient’s bedsidethat involves all relevant team members is a powerful strategy toimprove handovers. Participation from all team members enables cross-checking and validation of information transferred and creates anopportunity to rapidly perform a joint physical scan of the patient toverify the location and condition of lines, tubes, drains, incisions, andany active therapy being delivered such as vasoactive drug infusions.“Read and verify” checklists may be used as quick memory aidsto provide logical structure to the report and ensure that all importantitems have been addressed. Figure 5 is an example of such a checklistorganized in a modified SBARQ (SBARQ is an acronym for a techniqueused to communicate information in a standardized and easily understood
Figure 4. Preliminary report. Example of a hand-written report intended to prepare the ICU stafffor patient arrival. The report is to be completed by the anesthesiology provider and circulator at aconvenient time during the case. It is not intended to provide detailed clinical information or toduplicate data that will be handed over after patient arrival. Anes indicates anesthesiology provider;DOB, date of birth; ETA, estimated time of arrival; Gtts, infusions; HEP, hepatitis; HIV, humanimmunodeficiency virus; ICU, intensive care unit; IV, Intravenous Line; MRSA, methicillin-resistant Staphylococcusaureus; NTG, nitroglycerin; OR, operating room; OGT/NGT, orogastrictube/nasogastric tube; PMHX, past medical history; Pt, patient; RN, registered nurse; SSN, patientor social security number; VRE, vancomycin-resistant enterococcus.
54 ’ Bonifacio et al
www.anesthesiaclinics.com
format. The acronym stands for: Situation, Background, Assessment,Recommendation, and Questions23) format. Before the conclusion of thehandover, the receiving team must be given an opportunity to askquestions to ensure that they have a complete and accurate understandingof the information delivered.7,23,30,31 By sharing and reviewing vitalinformation as a complete team, safety will improve as errors can be betterdetected and their effects mitigated.
The critical meeting between the delivering and receiving teamsoptimally occurs in a “sterile cockpit,” a concept adapted from theFederal Aviation Industry that prohibits “any activity during a criticalphase of flight which could distract any flight crewmember from theperformance of his or her duties.”32 In the context of an OR to ICUhandover, a sterile cockpit can be created by eliminating distractions(eg, turning the television off, limiting speakers to one at a time),establishing clear roles and responsibilities, and prohibiting discussionsunrelated to the transfer of the patient.
Table 1. Handover Information Items Frequently Recommended in the Literature15
Patient InformationNameAgeAllergiesDiagnosisProcedure performedMedical history
Anesthesia informationType of anesthesia and courseIntraoperative medications (dose and time)IV fluids administeredBlood products administered (type and amount)Estimated blood lossTubes/lines/wires
Surgical informationSurgical courseSurgical site information (dressing, tubes, drains)Surgical complications and interventionsCPB/circulatory arrest/cross clamp/other procedure durations
Current statusAssessment of hemodynamic stability
Care planAnticipated recovery and problemsPostoperative management planPostoperative orders and investigationsMonitoring plan with parametersAnalgesia planPlan for IV Fluid, antibiotic, medications, deep venous thrombus prophylaxisNasogastric feeding
CBP indicates cardiopulmonary bypass; IV, intravenous.
Handovers From the OR to the ICU ’ 55
www.anesthesiaclinics.com
Responsibility Transfer
The final component of the handover is the formal transfer ofresponsibility and accountability from the delivering OR team to thereceiving ICU team. The transfer must be an explicit verbal (and eventuallydocumented) acknowledgment from the receiving team that responsibilityfor care has been accepted and assumed.
’ Change Management
Although these recommendations to improve handovers may soundsimple, converting them into enduring, institutional practice is challeng-ing. One helpful approach is to use an established quality improvementmodel, such as Lean Six Sigma,33 Plan-Do-Study-Act,34 or TeamSTEPPS.25 Although each model offers a unique framework to system-atically study, improve, and evaluate processes, they have specificprinciples in common, including the importance of active engagementfrom executive and front-line leaders, systems improvement usingobservable, measurable data, and employing a cyclical process ofcontinuous improvement.
Figure 5. Read and verify checklist. Example of a cognitive aid developed for use during thebedside transfer of information. The checklist is intended to reduce error by providing a generalstructure to the delivery of information and as a reminder to prevent the omission of important items.A/V wires indicates arterial/ventricular wires; CT, chest tubes; EBL, estimated blood loss;Hx, history; ICU, intensive care unit; IV, intravenous; RN, registered nurse; VS, vital signs.
56 ’ Bonifacio et al
www.anesthesiaclinics.com

Before beginning a project to improve patient handovers, it will beimportant to gain the support and active engagement of leaders andother key stakeholders. Explicit support in writing, and ideally activeinvolvement, from formal leaders at all levels gives the project legitimacyand establishes expectations from subordinate leaders. Their supportwill be essential to overcoming barriers to change. Getting early supportfrom front-line workers who possess influence over resources and staffwill also increase the likelihood of effective change.
At the heart of any quality improvement framework lies a systematiccycle of continuous improvement where processes are methodicallyexamined, modified based on facts learned, and then reexamined todetermine if the desired outcomes were achieved. By first studying aprocess, an accurate assessment of existing practices can be made,increasing the likelihood that new strategies address root, and notproximal causes of errors. The type and amount of data collected willdepend on the scope of the project and the resources available.
An objective and detailed description of current handovers canbe achieved by direct field observations. Using an observation check-list, 1 or 2 trained observers can collect data that can be compiled tocreate process maps or other visual depictions of the current handoversystem. A deeper understanding may be gained by combining this“snapshot” with contextual data collected from those involved in thehandover. Through interviews, surveys, and focus groups, investigatorscan draw upon the experiences, perspectives, and ideas of handoverteam members to gain deeper insight into the process and developsolutions that may better meet the needs of its end users. By addingcontext to what is observed, investigators will be better able to recognizepatterns in handovers, identify subtle or rare events not capturedbecause of a small sample size, and decipher differences betweenperceptions and reality. Consequently, the sense of ownership and buy-in fostered through staff participation will play importantly duringimplementation.
Before implementation, process modeling, or simulating the newhandover process in a controlled environment, can facilitate thedetection of faults in the design. Including stakeholders in this effortwill promote a sense of ownership and generate support for theproposed changes. Once the new process is sufficiently refined throughiterative testing in simulation, piloting on live patients can be conducted.
Implementation
Many would agree that strategy development is easy when com-pared with implementation and sustainment. The only published studyknown that examined the sustainability of a postoperative handoverintervention reported that only partial compliance with strategies to
Handovers From the OR to the ICU ’ 57
www.anesthesiaclinics.com
improve information transfer and limit interruptions was achieved3 years after implementation.35
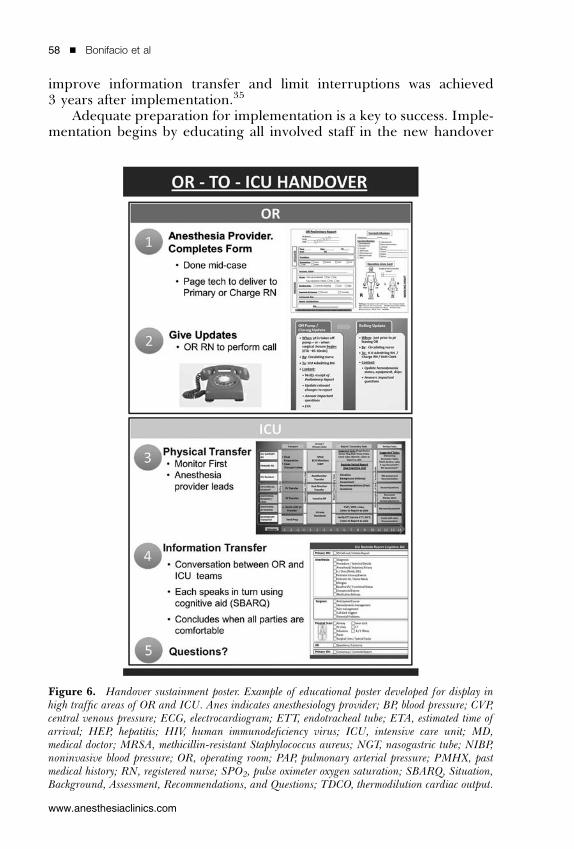
Adequate preparation for implementation is a key to success. Imple-mentation begins by educating all involved staff in the new handover
Figure 6. Handover sustainment poster. Example of educational poster developed for display inhigh traffic areas of OR and ICU. Anes indicates anesthesiology provider; BP, blood pressure; CVP,central venous pressure; ECG, electrocardiogram; ETT, endotracheal tube; ETA, estimated time ofarrival; HEP, hepatitis; HIV, human immunodeficiency virus; ICU, intensive care unit; MD,medical doctor; MRSA, methicillin-resistant Staphylococcus aureus; NGT, nasogastric tube; NIBP,noninvasive blood pressure; OR, operating room; PAP, pulmonary arterial pressure; PMHX, pastmedical history; RN, registered nurse; SPO2, pulse oximeter oxygen saturation; SBARQ, Situation,Background, Assessment, Recommendations, and Questions; TDCO, thermodilution cardiac output.
58 ’ Bonifacio et al
www.anesthesiaclinics.com

strategies. Informative emails, flyers, posters, newsletter articles, andbrief presentations during OR and ICU staff meetings are usefulmethods of publicizing the new process. Easy-to-understand checklistsand protocols serve to explain the redesigned handover process and tofacilitate the transition (Fig. 6). These materials should be widelyavailable in break rooms, nursing stations, education classrooms, andother common areas. Introductions by formal leaders, informal supportby front-line champions, and a genuine demonstration of enthusiasm byprocess owners will help in generating excitement and buy-in.
Training must be schedule-friendly, impactful, and fun. In healthcare, simulation is an effective educational strategy36 and is increasinglyassociated with improved patient care.37 However, some forms ofsimulation such as high-fidelity mannequin-based simulation, can beprohibitively expensive. Recent evidence has shown that other, lesscostly forms of simulation can be equally effective in the learning processand in the transfer of skills to patient care.38 Alternative forms ofsimulation such as games-based learning offer several advantages overmannequin-based simulation, including scalability, standardization,distributability, accessibility, convenience, and built-in assessment.39
Multimodal training platforms, which blend these and other learningsolutions such as active coaching, may maximize efficacy and efficiency.Current handover training initiatives such as 3Di Teams developed atDuke University employ this concept by first allowing learners to masterconcepts in games-based learning before moving to high-fidelitysimulation to begin interprofessional learning and to focus on nuancesof care.
Implementation of the new handover process, or “Go live” day,should be a celebrated event. It is important to immerse the target unitswith resources to facilitate the transition, address unplanned issues thatmay arise, and support the staff. The active endorsement or even merepresence of both formal and informal leaders will demonstrate theircommitment to improvement and convey the project’s importance.Active coaching in the new handover by process owners or frontlineleaders is key to success.
This level of support can be scaled down as the process gainstraction. Codifying the new handover into policy will establish it as aclear expectation. Once the handover is being performed regularly,versions of the instruments used to initially examine the process can bereapplied to compare results. Further refinements can then be madeusing these data.
The authors have no conflicts of interest to disclose .
Handovers From the OR to the ICU ’ 59
www.anesthesiaclinics.com

’ References
1. Jeffcott SA, Evans SM, Cameron PA, et al. Improving measurement in clinicalhandover. Qual Saf Health Care. 2009;18:272–276.
2. Mistry K, Landrigan C, Goldmann D, et al. Communication error during post-operative patient hand off in the pediatric intensive care unit. Crit Care Med.2005;33:A12.
3. Nagpal K, Abboudi M, Fischler L, et al. Evaluation of postoperative handover using atool to assess information transfer and teamwork. Ann Surg. 2011;253:831–837.
4. Catchpole KR, de Leval MR, McEwan A, et al. Patient handover from surgery tointensive care: using formula 1 pit-stop and aviation models to improve safety andquality. Paediatr Anaesth. 2007;17:470–478.
5. de Leval MR, Carthey JC, Wright DJ, et al. Human factors and cardiac surgery:a multicenter study. J Thorac Cardiovasc Surg. 2000;119:661–672.
6. Arora V, Johnson J, Lovinger D, et al. Communication failures in patient sign-out andsuggestions for improvement: a critical incident analysis. Qual Saf Health Care.2005;14:401–407.
7. Mazzocco K, Petitti DB, Fong KT, et al. Surgical team behaviors and patient outcomes.Am J Surg. 2009;197:678–685.
8. Kitch B, Cooper J, Zapol W, et al. Handoffs causing patient harm: a survey of medicaland surgical house staff. Jt Comm J Qual Patient Saf. 2008;34:563–570.
9. Improving America’s Hospitals: The Joint Commission Annual Report on Quality andSafety, 2007. Available at: http://www.jointcommission.org/assets/1/6/2007_Annual_Report.pdf. Accessed June 22, 2012.
10. Singh H, Thomas EJ, Petersen LA, et al. Medical errors involving trainees: a study ofclosed malpractice claims from 5 insurers. Arch Intern Med. 2007;167:2030–2036.
11. The Joint Commission Announces the 2009 Patient Safety Goals [The JointCommission Perspectives], 2008. Available at: http://www.jcrinc.com/common/PDFs/fpdfs/pubs/pdfs/JCReqs/JCP-07-08-S1.pdf. Accessed July 19, 2012.
12. ACGME Duty Hours Standards Fact Sheet. Available at: http://www.acgme.org/acWebsite/newsRoom/newsRm_dutyHours.asp. Accessed June 22, 2012.
13. Common Program Requirements. 2011. Available at: http://www.acgme.org/acwebsite/home/Common_Program_Requirements_07012011.pdf. Accessed June22, 2012.
14. Hilligross B, Cohen MD. The unappreciated challenges of between-unit handoffs:negotiating and coordinating across boundaries. Ann Int Med; 2012. Available at:http://www.sciencedirect.com/science/article/pii/S0196064412003769. Accessed June22, 2012.
15. Segall N, Bonifacio AS, Schroeder RA, et al. Can we make postoperative patienthandovers safer? A systematic review of the literature. Anesth Analg. 2012;115:102–115.
16. Craig R, Moxey L, Young D, et al. Strengthening handover communication inpediatric cardiac intensive care. Paediatr Anaesth. 2012;22:393–399.
17. Joy BF, Elliott E, Hardy C, et al. Standardized multidisciplinary protocol improveshandover of cardiac surgery patients to the intensive care unit. Pediatr Crit Care Med.2011;12:304–308.
18. Zavalkoff SR, Razack SI, Lavoie J, et al. Handover after pediatric heart surgery: asimple tool improves information exchange. Pediatr Crit Care Med. 2011;12:309–313.
19. Smith AF, Pope C, Goodwin D, et al. Interprofessional handover and patient safety inanaesthesia: observational study of handovers in the recovery room. Br J Anaesth.2008;101:332–337.
20. Chang V, Arora V, Lev-Ari S, et al. Interns overestimate the effectiveness of theirhandoff communication. Pediatrics. 2010;125:491–496.
60 ’ Bonifacio et al
www.anesthesiaclinics.com

21. Leonard M, Graham S, Bonacum D. The human factor: the critical importance ofeffective teamwork and communication in providing safe care. Qual Saf Health Care.2004;13:i85–i90.
22. Anwari JS. Quality of handover to the postanaesthesia care unit nurse. Anaesthesia.2002;57:488–493.
23. Mistry K, Jaggers J, Lodge A, et al. Using six sigmas methodology to improvehandoff communication in high-risk patients. In: Henriksen K, Battles JB, Keyes,MA, et al, eds. Advances in Patient Safety: New Directions and Alternative Approaches.Rockville, MD: Agency for Healthcare Research and Quality 2008.
24. Smith AF, Mishra K. Interaction between anaesthetists, their patients, and theanaesthesia team. Br J Anaesth. 2010;105:60–68.
25. Endsley MR. Design and evaluation for situation awareness enhancement, Proceedings of theHuman Factors Society 32nd Annual Meeting. Santa Monica, CA: Human Factors Society;1988:97–101.
26. Pocket Guide Team STEPPS. Available at: http://www.ahrq.gov/teamsteppstools/instructor/essentials/pocketguide.htm#sbar. Accessed June 22, 2012.
27. Sculli G. Clinical Crew Resource Management Workshop, Learning Session Module.2012;19.
28. Warren J, Fromm R, Orr R, et al. Guidelines for in the inter- and intrahospitaltransport of critically ill patients. Crit Care Med. 2004;32:256–262.
29. Beckmann U, Gillies DM, Berenholtz SM, et al. Incidents relating to the intra-hospital transfer of critically ill patients: an analysis of the reports submitted to theAustralian Incident Monitoring Study in Intensive Care. Inten Care Med. 2004;30:1579–1585.
30. Amato-Vealey E, Barba M, Vealey R. Hand-off communication: a requisite forperioperative patient safety. AORN J. 2008;88:763–774.
31. Manser T, Foster S, Gisin S, et al. Assessing the quality of patient handoffs at caretransitions. Qual Saf Health Care. 2010;19:e44, 1-5.
32. Electronic Code of Federal Regulations. Available at: http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?c = ecfr&sid = 9d09dce07297bd83dafe799d9cd823d4&rgn = div8&view =text&node = 14:3.0.1.1.7.20.3.8&idno = 14. Accessed June 22, 2012.
33. Carrigan M, Kujawa D. Six sigma in health care management and strategy. HealthCare Manag. 2006;25:133–141.
34. Science of Improvement: How to Improve. Available at: http://www.ihi.org/knowl-edge/Pages/HowtoImprove/ScienceofImprovementHowtoImprove.aspx. AccessedJuly 19, 2012.
35. Chen JG, Wright MC, Smith PB, et al. Adaptation of a postoperative handoffcommunication process for children with heart disease: a quantitative study. Am J MedQual. 2011;26:380–386.
36. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for healthprofessions education: a systematic review and meta-analysis. JAMA. 2011;306:978–988.
37. McGaghie WC, Draycott TJ, Dunn WF, et al. Evaluating the impact of simulation ontranslational patient outcomes. Simul Healthc. 2011;6:S42–S47.
38. Norman G, Dore K, Grierson L. The minimal relationship between simulationfidelity and transfer of learning. Med Educ. 2012;46:636–647.
39. Taekman JM, Shelley K. Virtual environments in healthcare: immersion, disruption,and flow. Int Anesthesiol Clin. 2010;48:101–121.
Handovers From the OR to the ICU ’ 61
www.anesthesiaclinics.com