What can paper-based clinical information systems tell us about the design of computerized clinical...
11
Please cite this article in press as: Miller A, et al. What can paper-based clinical information systems tell us about the design of computerized clinical information systems (CIS) in the ICU? Aust Crit Care (2010), doi:10.1016/j.aucc.2010.02.001 ARTICLE IN PRESS AUCC-89; No. of Pages 11 Australian Critical Care (2010) xxx, xxx—xxx RESEARCH REVIEW What can paper-based clinical information systems tell us about the design of computerized clinical information systems (CIS) in the ICU? A. Miller a,∗ , D. Pilcher b , N. Mercaldo a , T. Leong b , C. Scheinkestel b , J. Schildcrout a a Vanderbilt University Medical Center, Nashville, TN, United States b Intensive Care Unit, Alfred Hospital, Melbourne, Australia Received 29 July 2009; received in revised form 16 December 2009; accepted 5 February 2010 KEYWORDS Clinical information systems design; Computerized provider order entry; Clinical decision processes; Adverse events; Error Summary Background: Screen designs in computerized clinical information systems (CIS) have been modeled on their paper predecessors. However, limited understanding about how paper forms support clinical work means that we risk repeating old mistakes and creating new opportunities for error and inefficiency as illustrated by problems associated with computerized provider order entry systems. Purpose: This study was designed to elucidate principles underlying a successful ICU paper-based CIS. The research was guided by two exploratory hypotheses: (1) paper-based artefacts (charts, notes, equipment, order forms) are used differently by nurses, doctors and other healthcare professionals in different (formal and infor- mal) conversation contexts and (2) different artefacts support different decision processes that are distributed across role-based conversations. Method: All conversations undertaken at the bedsides of five patients were recorded with any supporting artefacts for five days per patient. Data was coded according to conversational role-holders, clinical decision process, conversational context and artefacts. 2133 data points were analyzed using Poisson logistic regression analyses. Results: Results show significant interactions between artefacts used during dif- ferent professional conversations in different contexts ( 2 (df=16) = 55.8, p < 0.0001). ∗ Corresponding author. Tel.: +1 615 343 1696. E-mail address: [email protected] (A. Miller). 1036-7314/ $ — see front matter © 2010 Australian College of Critical Care Nurses Ltd. Published by Elsevier Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved. doi:10.1016/j.aucc.2010.02.001
Transcript of What can paper-based clinical information systems tell us about the design of computerized clinical...
A
A
R
Wsc
ADNTCJ
a
b
R
1
d
ARTICLE IN PRESSUCC-89; No. of Pages 11
ustralian Critical Care (2010) xxx, xxx—xxx
ESEARCH REVIEW
hat can paper-based clinical informationystems tell us about the design of computerizedlinical information systems (CIS) in the ICU?
. Millera,∗,
. Pilcherb,
. Mercaldoa,. Leongb,. Scheinkestelb,. Schildcrouta
Vanderbilt University Medical Center, Nashville, TN, United StatesIntensive Care Unit, Alfred Hospital, Melbourne, Australia
eceived 29 July 2009; received in revised form 16 December 2009; accepted 5 February 2010
KEYWORDSClinical informationsystems design;Computerized providerorder entry;Clinical decisionprocesses;Adverse events;Error
SummaryBackground: Screen designs in computerized clinical information systems (CIS) havebeen modeled on their paper predecessors. However, limited understanding abouthow paper forms support clinical work means that we risk repeating old mistakesand creating new opportunities for error and inefficiency as illustrated by problemsassociated with computerized provider order entry systems.Purpose: This study was designed to elucidate principles underlying a successfulICU paper-based CIS. The research was guided by two exploratory hypotheses: (1)paper-based artefacts (charts, notes, equipment, order forms) are used differentlyby nurses, doctors and other healthcare professionals in different (formal and infor-mal) conversation contexts and (2) different artefacts support different decision
Please cite this article in press as: Miller A, et al. What can paper-based clinical information systems tellus about the design of computerized clinical information systems (CIS) in the ICU? Aust Crit Care (2010),doi:10.1016/j.aucc.2010.02.001
processes that are distributed across role-based conversations.Method: All conversations undertaken at the bedsides of five patients were recordedwith any supporting artefacts for five days per patient. Data was coded accordingto conversational role-holders, clinical decision process, conversational context andartefacts. 2133 data points were analyzed using Poisson logistic regression analyses.Results: Results show significant interactions between artefacts used during dif-ferent professional conversations in different contexts (�2
(df=16) = 55.8, p < 0.0001).
∗ Corresponding author. Tel.: +1 615 343 1696.E-mail address: [email protected] (A. Miller).
036-7314/ $ — see front matter © 2010 Australian College of Critical Care Nurses Ltd. Published by Elsevier Australia (a division of Reed International Books Australia Pty Ltd). All rights reserved.
oi:10.1016/j.aucc.2010.02.001

ARTICLE IN PRESSAUCC-89; No. of Pages 11
2 A. Miller et al.
The interaction between artefacts used during different professional conversationsfor different clinical decision processes was not statistically significant although alltwo-way interactions were statistically significant.Conclusions: Paper-based CIS have evolved to support complex interdisciplinary deci-sion processes. The translation of two design principles — support interdisciplinaryperspectives and integrate decision processes — from paper to computerized CIS mayminimize the risks associated with computerization.
e of Critical Care Nurses Ltd. Published by Elsevier Australianatio
fltpfeaarRhbbdiapobnae
ptciipfatodifiItprocesses.
© 2010 Australian Colleg(a division of Reed Inter
Introduction
Screen designs in many computerized clinicalinformation systems (CIS) have been influencedby their paper predecessors, but understandingabout how paper-based systems support clin-ical work is limited. In order to build thecase for computerization,1,2 past studies thatincluded paper charts tended to emphasize theirinadequacies while overlooking their strengths.With increased computerization, the diminishingopportunities to understand the principles under-lying paper-based systems has prompted someresearchers to undertake a more detailed study.3—5
With a more comprehensive understanding we mayminimize the risk of repeating old mistakes andavoid creating new opportunities for error and inef-ficiency. The purpose of this study was to identifyprinciples underpinning successful paper-based CISdesigns as a means for informing more effectivetechnology design. The next section shows howsome of the adverse effects of computerized medi-cation ordering and administration might have beenavoided by a deeper understanding of paper-basedmedication management.
Paper-based medication records and thenegative effects of CPOE implementation
An estimated 15—20% of hospitals in the US and insome European countries (e.g., The Netherlands)have replaced paper-based medication recordswith computerized provider order entry (CPOE)systems.4 Although benefits have accrued,5,6 thefollowing three categories of CPOE problems havebeen identified as contributing to errors with high-severity adverse outcomes.6—12
Loss of communicationRemote-user access, the ability to place or mod-
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
ify orders from different locations, is one of theproposed benefits of CPOEs. However, remote-access can reduce face-to-face conversation thatin addition to efficient information transfer and
IBds
nal Books Australia Pty Ltd). All rights reserved.
ow, promotes social connectedness, and facili-ates shared understanding about patient diseaserocesses and care plans.7,9,11,13—15 As face-to-ace conversation reduces, new inefficiencies maymerge as individuals attempt to uncover the goalsnd rationales for orders that have ‘just appeared’,nd the risk of errors increases as goals andationales are assumed and/or misunderstood.6,9,11
emote-access also reduces the visibility of role-olders such as pharmacists and the expertise theyring to care delivery processes.7,9,12 Without visi-ility, understanding about how and when to involveifferent professionals may be compromised result-ng in lack of timely advice. Remote-access canlso promote batched order entry (entering multi-le orders for different patients in one session) byften junior doctors.9,10 In this situation, orderingecomes a simple data-entry task that is discon-ected from care planning and feedback processesnd is vulnerable to transcription and other data-ntry errors.
In our study ICU, paper-based medication chartsromoted face-to-face conversation. All medica-ion charts were located at patients’ bedsides. Theare team assembled at the bedside for morn-ng rounds. During the round, orders were writtenn the context of patient assessment and carelanning discussions that integrated different pro-essional perspectives.15 Between rounds, doctorsgain came to the bedside to change medica-ion orders in response to laboratory results orther consultations.16 As others have also noted,9
octors coming to the bedside cued nurses tomminent changes and provided an opportunityor both clinicians to update their understand-ng of the patient’s situation. Thus in the studyCU, ordering was embedded within broader,eam-based decision, care planning and delivery
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
nterruptions to information and workflowerg and Toussaint3 argue that the first step in theesign of information systems should be to under-tand how information flows across different roles
ARTICLE INAUCC-89; No. of Pages 11
Paper-based clinical information systems and design of
Ftr
acplaiRaiattTacaocFcui
amolGnpirscpsabtt
sr
attafttal(RoMapi(tliii
DRmaatdteaot
pmamtwwcoonai
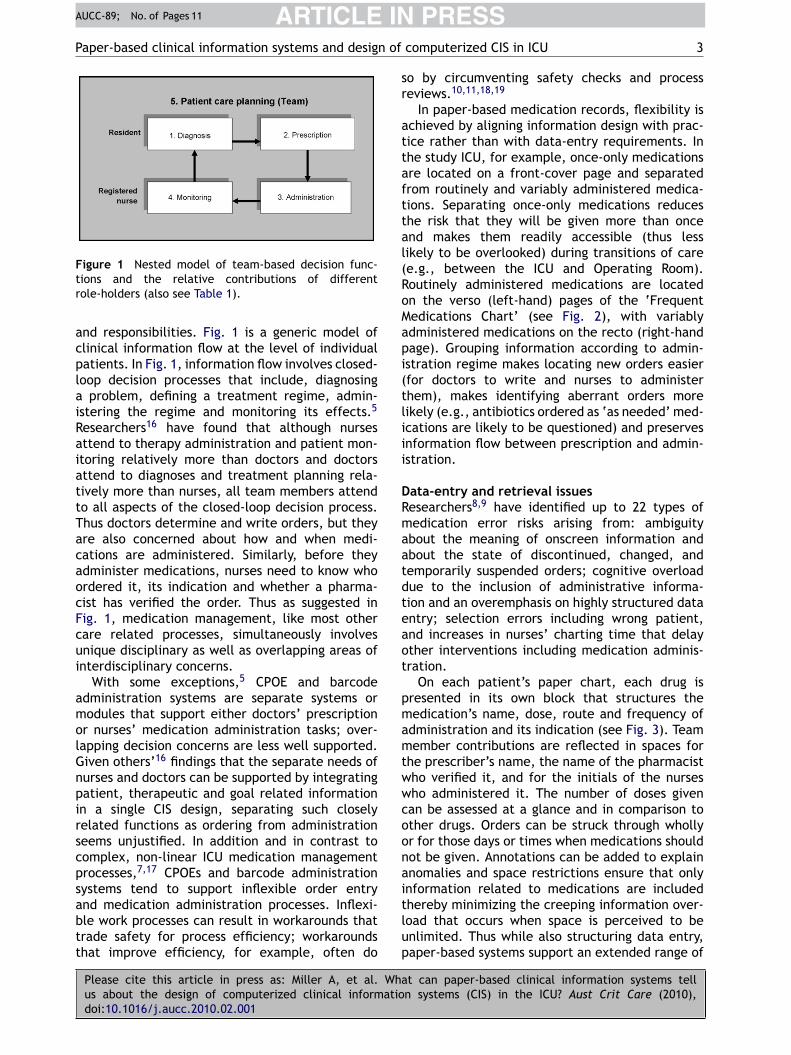
igure 1 Nested model of team-based decision func-ions and the relative contributions of differentole-holders (also see Table 1).
nd responsibilities. Fig. 1 is a generic model oflinical information flow at the level of individualatients. In Fig. 1, information flow involves closed-oop decision processes that include, diagnosing
problem, defining a treatment regime, admin-stering the regime and monitoring its effects.5
esearchers16 have found that although nursesttend to therapy administration and patient mon-toring relatively more than doctors and doctorsttend to diagnoses and treatment planning rela-ively more than nurses, all team members attendo all aspects of the closed-loop decision process.hus doctors determine and write orders, but theyre also concerned about how and when medi-ations are administered. Similarly, before theydminister medications, nurses need to know whordered it, its indication and whether a pharma-ist has verified the order. Thus as suggested inig. 1, medication management, like most otherare related processes, simultaneously involvesnique disciplinary as well as overlapping areas ofnterdisciplinary concerns.
With some exceptions,5 CPOE and barcodedministration systems are separate systems orodules that support either doctors’ prescription
r nurses’ medication administration tasks; over-apping decision concerns are less well supported.iven others’16 findings that the separate needs ofurses and doctors can be supported by integratingatient, therapeutic and goal related informationn a single CIS design, separating such closelyelated functions as ordering from administrationeems unjustified. In addition and in contrast toomplex, non-linear ICU medication managementrocesses,7,17 CPOEs and barcode administrationystems tend to support inflexible order entry
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
nd medication administration processes. Inflexi-le work processes can result in workarounds thatrade safety for process efficiency; workaroundshat improve efficiency, for example, often do
tlup
PRESScomputerized CIS in ICU 3
o by circumventing safety checks and processeviews.10,11,18,19
In paper-based medication records, flexibility ischieved by aligning information design with prac-ice rather than with data-entry requirements. Inhe study ICU, for example, once-only medicationsre located on a front-cover page and separatedrom routinely and variably administered medica-ions. Separating once-only medications reduceshe risk that they will be given more than oncend makes them readily accessible (thus lessikely to be overlooked) during transitions of caree.g., between the ICU and Operating Room).outinely administered medications are locatedn the verso (left-hand) pages of the ‘Frequentedications Chart’ (see Fig. 2), with variablydministered medications on the recto (right-handage). Grouping information according to admin-stration regime makes locating new orders easierfor doctors to write and nurses to administerhem), makes identifying aberrant orders moreikely (e.g., antibiotics ordered as ‘as needed’ med-cations are likely to be questioned) and preservesnformation flow between prescription and admin-stration.
ata-entry and retrieval issuesesearchers8,9 have identified up to 22 types ofedication error risks arising from: ambiguity
bout the meaning of onscreen information andbout the state of discontinued, changed, andemporarily suspended orders; cognitive overloadue to the inclusion of administrative informa-ion and an overemphasis on highly structured datantry; selection errors including wrong patient,nd increases in nurses’ charting time that delayther interventions including medication adminis-ration.
On each patient’s paper chart, each drug isresented in its own block that structures theedication’s name, dose, route and frequency of
dministration and its indication (see Fig. 3). Teamember contributions are reflected in spaces for
he prescriber’s name, the name of the pharmacistho verified it, and for the initials of the nursesho administered it. The number of doses givenan be assessed at a glance and in comparison tother drugs. Orders can be struck through whollyr for those days or times when medications shouldot be given. Annotations can be added to explainnomalies and space restrictions ensure that onlynformation related to medications are included
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
hereby minimizing the creeping information over-oad that occurs when space is perceived to benlimited. Thus while also structuring data entry,aper-based systems support an extended range of

Please cite this article in press as: Miller A, et al. What can paper-based clinical information systems tellus about the design of computerized clinical information systems (CIS) in the ICU? Aust Crit Care (2010),doi:10.1016/j.aucc.2010.02.001
ARTICLE IN PRESSAUCC-89; No. of Pages 11
4 A. Miller et al.
Figure 2 Frequently administered medications (see Fig. 3 for more detailed views).
Figure 3 Selected paper-based medication orders (representative, not to scale).

INA
P n of
pa
LIttmdda(mpmsfl
R
Ctuitcfceiashsgah
Hfoaswb
Hetciab‘aht
M
C
Taiaafahitpwulpm
P
FapbTwatctsp
M
M
1
2
P
ARTICLEUCC-89; No. of Pages 11
aper-based clinical information systems and desig
rescription and administration, team decision andccountability processes.
essons to be learnedn summary, paper-based medication records likehe ones in Figs. 2 and 3 are successful becausehey support interdisciplinary information flows andedication management practices in addition toata entry. The overall structure of the paper-esign supports different types of prescription anddministration criteria and care delivery contextsonce-only, routine and variably administered). Atore micro-levels, information is grouped (e.g.,rescription with administration; indications withedication name, dose, route, frequency) to pre-
erve and support information relationships andows.
esearch questions
onsistent with Berg and Toussaint’s recommenda-ion,3 the aims of this study were to examine these of artefacts in ICU decision processes by apply-ng the information flow model presented in Fig. 1o the use of artefacts during different role-holderonversations. For the purposes of this study arte-acts are defined as any tool (paper-based and/oromputerized forms, charts, equipment, notes,tc.) used by healthcare professionals to supportnformation processing and information flow. Thispproach differs from the more usual ethnographictudies of artefacts.4,5 Rather than undertake aighly contextualized analysis, we applied the deci-ion process model in Fig. 1 to provide a moreeneric characterization aimed elucidating gener-lizable principles. We used the following researchypotheses to guide our examination.
ypothesis 1 :. In the study ICU, paper-based arte-acts are used differently by nurses, doctors andther healthcare professionals in different (formalnd informal) conversation contexts. Statisticallyignificant interactions between these variablesill provide insights as to ‘how’ artefacts are used,y whom in what contexts.
ypothesis 2 :. In a paper-based ICU, differ-nt artefacts support different decision processeshat are distributed across different role-basedonversations. This hypothesis addresses the rolenteractions, artefacts and the reasons for anrtefact’s use. Statistically significant interactionsetween these variables will allow us to describe
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
why’ artefacts are important in decision contextsnd to whom and may provide some insights as toow information flows within an interdisciplinaryeam.
Tc(m
PRESScomputerized CIS in ICU 5
ethod
ontext
he study ICU was an Australian, universityffiliated metropolitan hospital admitting approx-mately 2000 patients per year and treating onverage 32 patients at once. The combined ICUnd trauma center deals with complex conditionsor, as a limited example, cardio-thoracic surgery,rtificial heart technology, transplantation, andyperbaric emergencies. In common with othernstitutions, the study hospital is undergoing aransition from a fully paper-based system to aredominantly electronic one. Although computersere introduced in 2003 to allow clinicians to lookp blood results and X-rays, at the time of data col-ection, all observations charting, medical records,rescribing, nursing care plans and handover infor-ation were paper-based.
articipants
ollowing Human Research Ethics Committeepproval, 83 doctors and nurses consented toarticipate between May and July, 2006. This num-er included all ICU doctors and 45% of nurses.he next-of-kin of five critically ill patients gaveritten consent. Three research assistants (RAs),ll psychology graduates with acute care hospi-al experience, were trained by the researcher toollect data. Training included familiarization withhe patient care-area, equipment, routines and keytaff members as well as orientation to the study’surpose and data collection procedures.
aterials
aterials setup in patients’ care-areas included:
. Three microphones, an 8-channel audio-mixingdeck to filter background noise, and a set ofheadphones. Sound was recorded onto mini-tapes in a Canon camera. No visual images werecaptured.
. A laptop computer for manually recording thedate and time, the conversation content, thespeaker’s roles (e.g., doctor, nurse, etc.) andsupporting artefacts.
rocedure
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
he researcher and RAs recorded all patient-relatedonversations and observed uses of artefactspaper-based, computerized and procedural equip-ent) continuously for five days per patient (day,

IN
S
Pcfalfw(awwstitfdpiwccral
R
Asv1(a1s
ntetotufab
ARTICLEAUCC-89; No. of Pages 11
6
night and weekend) for five patients for a total of 23days (one patient was discharged after three days).The RAs were positioned at the back of the patients’care-areas where they could see speakers andartefacts-in-use without interrupting the conver-sations. During the night-shift, the previous day’saudio-recordings were replayed and manual record-ings were corrected. RAs were quickly assimilated;there was no overt evidence that patient-relatedconversations were censored.
Data coding
The recorded conversations were divided intothematically coherent, grammatically completeconversational units (e.g., questions and answersor sentences), as distinct from speech units thatdo not require grammatical completeness.20 Con-versational units involving multiple artefacts weresubdivided so that each artefact was associatedwith the topic it supported. Once collated, the fol-lowing four variables were defined:
1. Decision process: Fig. 1 and the five decision pro-cesses (Table 1) were developed during researchfollowing this study and will be published insubsequent papers. The definition and opera-tionalization of each process is presented inTable 1. Cohen’s kappa23 for inter-coder relia-bility, calculated from three randomly selecteddays of patient data and independently codedby the researcher and a research assistant, wasgood (kappa = 0.83).
2. Roles: Conversations between different clin-ical roles included: nurse-to-nurse; doctor-to-doctor; mixed role conversations betweennurses and doctors; and conversations betweennurses or doctors and other healthcare workerssuch as pharmacists.
3. Artefacts used during clinical communicationincluded: paper-based charts (e.g., observation,fluid-balance), notes (free form text reportsand personal notes) and orders (specifically,medication charts); non-paper-based comput-erized information systems (cardiac monitors,radiology scans, laboratory results); proceduralequipment (beds, bowls, components of fluidinfusion sets, surgical instruments, ventilators);radiology equipment (echocardiograms, ultra-sound and X-ray machines); and no-artefactconversations that did not involve the use of an
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
artefact.4. Context: Whether the artefact was used dur-
ing a formal scheduled conversation (e.g., shifthandover or round) or during an informal (notformally scheduled) conversation.
(tvdu
PRESSA. Miller et al.
tatistical methods
oisson or log-linear regression models were used toharacterize the relationships among conversationeatures, (1) role, (2) context, (3) decision process,nd (4) artefact, while acknowledging or control-ing for patient differences.21 To examine evidenceor higher level (e.g., 3-way or 4-way) interactions,e conducted several of likelihood ratio Chi-square
LR�2) tests for nested models. We first constructedsaturated model that included main effects asell as 2-way, 3-way, and 4-way interactions. The 4-ay interaction was tested by comparing the LR�2
tatistic for the saturated model to the LR�2 statis-ic for the nested model that did not include thenteraction. Three-way interactions were tested inhe same manner (i.e., by comparing LR�2 statisticsor nested models). Statistical significance is evi-ence that the more complex of two nested modelsrovides a superior fit to the data. Upon identify-ng the statistically significant 3-way interactions,e calculated expected frequencies of all possibleovariate combinations and their associated 95%onfidence intervals (CIs). These quantities wereescaled to reflect counts per 100 conversations. Allnalyses were prepared using the R programminganguage.22
esults
total of 2133 entries were collected from the fivetudy patients. The data collected for each patientaried from 10 to 30% (Patient 1: 29%, 2: 29%, 3:5%, 4: 17%, 5:10%). From these 2133 entries 34%n = 798) of conversations were not supported byrtefacts, 28% were supported by charts (n = 530),6% involved equipment (n = 351) and 10% of conver-ations were supported by written orders (n = 222).
Using Poisson regression modeling, there waso statistically significant difference betweenhe fully saturated model containing all mainffects and 2-way, 3-way, and 4-way interac-ions and the simpler model that containednly the main and 2-way and 3-way interac-ions (LR�2
(df=21) = 28.2; p = 0.1345). Thus we werenable to detect a 4-way interaction between arte-act, roles, context, and decision process. Next,statistically significant interaction was observed
etween roles, conversation context and artefactLR�2 = 55.8; p-value < 0.0001). This supports
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
(df=16)he first hypothesis that different role-based con-ersations involve the use of different artefacts inifferent conversational contexts. Finally, we werenable to detect an interaction between roles,

ARTICLE IN PRESSAUCC-89; No. of Pages 11
Paper-based clinical information systems and design of computerized CIS in ICU 7
Table 1 Levels of decision processing.
Level Definition Conversational unit example
Patient care planning Conversations about the team’s objectives,goals or plans for a specific patient. Mayinclude the steps needed to achieve goalsover particular timeframes and modificationsto existing plans.
‘‘Let’s aim to extubate tomorrow.Go to CPAP now and drop thesedation right back to off over thenext 4 hours. We’ll see how shegoes over night and T-piecetomorrow at 0600. If all’s wellextubate after the round’’.
Diagnosis Conversations about a patient’s diseasestate or disease process, includingdiscussions about progress and progression,problem identification and problem solving.
‘‘He’s improved this morning, nolonger febrile, passing urine.’’‘‘The psychiatrists seem to thinkit’s a rare side-effect of thecyclosporine.’’
Prescription Highly specific directions (usually for others)to act using medication or devices (e.g.,ventilator). These directions hold the teammember legally responsible for thedirection—–they may be written or verbal.
‘‘Turn the ventilator to CPAP’’‘‘Stop the midazolam and starthaloperidol instead.’’Physician writes an order forVancomycin (observer note)Nurse checks the ordered dose.
Administration Highly specific actions associated with caredelivery processes that may be routine orspecifically prescribed.
The process of:- taking a chest X-ray;administering drugs; enactingprotocols; completing medical(CVC line insertion) or nursingprocedures
Monitoring The acquisition, comprehension and/ortransfer/transmission of information aboutpatient states, rates or plans.
‘‘His current BP is . . .’’‘‘How are we going, has his SaO2stabilized yet?’’
dvtspdaie
Hfpc
qCfist
iwfwapbcssNabtdha
ecision process and artefact (LR�2(df=59) = 41.7; p-
alue = 0.9567). Thus these data do not supporthe interaction proposed in the second hypothe-is, although the pairwise interactions: (decisionrocess and artefact—–LR�2
(df=24) = 497.7; roles andecision process—–LR�2
(df=12) = 144.6; and roles andrtefact—–LR�2
(df=18) 51.5), were all highly signif-cant (p < 0.0001). Each of the hypotheses will bexplored in greater detail in the following sections.
ypothesis 1. Paper-based artefacts are used dif-erently by nurses, doctors and other healthcarerofessionals in different (formal and informal)onversation contexts.
Fig. 4 shows the expected conversation fre-uencies (rescaled to counts per 100) and 95%Is for the significant interaction between arte-
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
acts, roles and conversational context. The rowsn Fig. 1 represent each role category, the columnshow each type of artefact, and conversation con-ext is represented using different symbols. The
Hea
They observe T-waves on thecardiac monitor
nteractions are evident by comparing the CIsithin each row and down each column. Thus,
or example, formal conversations among nursesere supported by charts more than any otherrtefact. During formal conversations charts wererimarily used among RN—RN exchanges followedy those between RN—MD. In contrast, informalonversations among nurses were associated mosttrongly with equipment (e.g., ventilators, infu-ion pumps) and unsupported verbal conversations.urse—doctor conversations have a similar profilecross conversation types, although charts supportoth formal and informal nurse—doctor conversa-ions. These two profiles differ substantially fromoctor—doctor and nurse or doctor with alliedealth professional conversations, which were notssociated with any particular artefact.
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
ypothesis 2. Different artefacts support differ-nt decision processes that are distributed acrossll role-based conversations.

ARTICLE IN PRESSAUCC-89; No. of Pages 11
8 A. Miller et al.
rtefa
simoawpa
D
T
Figure 4 Expected frequencies and 95% CIs for each aconversational contexts.
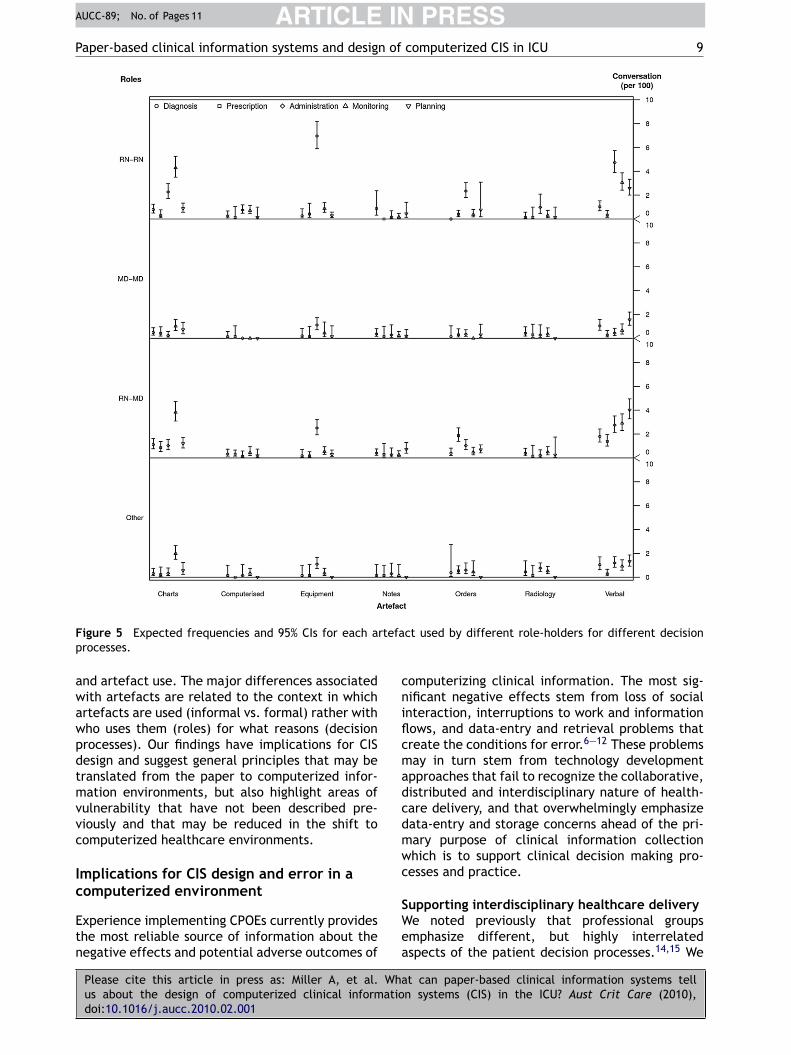
The non-significant three-way interactionbetween roles, decision processes and artefactsis clearly evident in Fig. 5. Across all roles forexample, charts (4th CI in the charts group)supported monitoring while equipment (3rd CI inthe equipment group) supported administrativeprocesses and unsupported verbal conversationswere associated with administration, monitoringand patient care planning. Thus the observeddifferences across role-based conversations wereassociated with the relative frequency of eachartefact’s use (height of the CIs) rather withfundamentally different uses of artefacts.
Fig. 5 also highlights some of the significant two-
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
way interactions. Reflecting the ‘role by decisionprocess’ interaction, conversations involving nurses(i.e., RN—RN and RN—MD) tend to involve adminis-tration, monitoring and patient care planning more
uadi
ct used by different role-holders in formal or informal
o than other role-based conversations. Represent-ng the ‘decision process by artefact’ interaction,onitoring is most closely associated with the use
f charts, administration with the use of equipmentnd patient care planning is most closely associatedith unsupported verbal exchanges. Diagnoses andrescription were largely unsupported by bedsidertefacts.
iscussion
he purpose of this study was to identify principles
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
nderpinning successful paper-based CIS designs asmeans for informing more effective computerizedesign. The results of this analysis present a highlynterdisciplinary profile of ICU decision processes
ARTICLE IN PRESSAUCC-89; No. of Pages 11
Paper-based clinical information systems and design of computerized CIS in ICU 9
F rtefap
awawpdtmvvc
Ic
Etn
cniflcmadcdmwc
igure 5 Expected frequencies and 95% CIs for each arocesses.
nd artefact use. The major differences associatedith artefacts are related to the context in whichrtefacts are used (informal vs. formal) rather withho uses them (roles) for what reasons (decisionrocesses). Our findings have implications for CISesign and suggest general principles that may beranslated from the paper to computerized infor-ation environments, but also highlight areas of
ulnerability that have not been described pre-iously and that may be reduced in the shift toomputerized healthcare environments.
mplications for CIS design and error in a
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
omputerized environment
xperience implementing CPOEs currently provideshe most reliable source of information about theegative effects and potential adverse outcomes of
SWea
ct used by different role-holders for different decision
omputerizing clinical information. The most sig-ificant negative effects stem from loss of socialnteraction, interruptions to work and informationows, and data-entry and retrieval problems thatreate the conditions for error.6—12 These problemsay in turn stem from technology development
pproaches that fail to recognize the collaborative,istributed and interdisciplinary nature of health-are delivery, and that overwhelmingly emphasizeata-entry and storage concerns ahead of the pri-ary purpose of clinical information collectionhich is to support clinical decision making pro-esses and practice.
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
upporting interdisciplinary healthcare deliverye noted previously that professional groupsmphasize different, but highly interrelatedspects of the patient decision processes.14,15 We

IN
amihri
L
TspstdarhhFnipwpsetaftttm
sbevTuit
C
Tpid
ARTICLEAUCC-89; No. of Pages 11
10
also observed that current CPOE and medicationadministration systems emphasize nurses’ or doc-tors’ data-entry tasks5,9—12; the interrelations andinterdependencies between say doctors’ ordersand nurses’ medication administration are notwell supported. In contrast, the artefacts in thestudy ICU were used by all role-holders. Thus,paper-based artefacts appear to have evolvedto support both disciplinary and interdisciplinaryperspectives (see Figs. 2 and 3) and by integratingprofessional perspectives provide a common plat-form for communication and shared understanding.In retrospect this conclusion seems obvious, butas illustrated in our introduction its importancehas clearly been overlooked in clinical informationsystems design at least with respect to CPOEs.
Using integrated tools, team members with dif-ferent professional perspectives can share, test,update, tailor and repair mutual understandingsabout the patient’s situation, about the team’sprogress against intended plans and about eachteam member’s responsibilities.13—15 Without anintegrated information system the overall commu-nication burden increases because clinicians mustactively seek out and integrate narrower disci-plinary perspectives, or else tolerate informationgaps that increase the risk of adverse events due tofaulty assumptions or misunderstandings.10,11
This study has also highlighted inadequacies,even in paper-based information systems, in thesupport of patient care planning in particular. Thereare at least two possible reasons for the lack ofartefacts supporting care planning. First, interdisci-plinary communication processes (interdisciplinaryrounds for example) are not universally acceptedas standard practice.14 Thus interdisciplinarity isarguably an emerging practice and as such theartefacts to support it are also emerging. Sec-ond, ICU patient dynamics can change rapidly. Overshort timeframes it may not be as necessary todocument team plans that are discussed duringdaily rounds and updated during informal discus-sion. However as the complexity of in-hospital carecontinues to increase as a consequence of shorterstaying sicker patients, the need for clearly definedgoals and plans that integrate information overtime and across different care delivery contextswill also increase. Computerized displays that rep-resent goals and plans, that facilitate progresstracking and that alert clinicians to deviationsfrom anticipated patient care trajectories mayassist in minimizing the incidence of breakdowns
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
in care coordination that include delayed, dupli-cated, missed or erroneous care related activities.Achieving this outcome will, however, require a fun-damental shift in systems design philosophy from
apnd
PRESSA. Miller et al.
single user-group transaction (i.e., doctor ordersedication; nurse administers medication) to an
nterdisciplinary design approach that emphasizesuman decision processes in an information envi-onment and that closes the communication andnformation flow loops represented in Fig. 1.
imitations and future research directions
his study like most research has a number ofhort-falls that limit conclusions, but which alsorovide opportunities for future research. The mostignificant limitation is that the analysis was under-aken at the level of professional group interactionsuring broad categories of conversations. Thispproach has the advantage of capturing aggregateather than individuals’ patterns of behavior, butas the disadvantage of limiting conclusions aboutow artefacts support these processes specifically.urther research is needed to better understand theature of interdisciplinary interactions with chartsn particular, including how they are used to sup-ort information flows and decision outcomes, andhat happens when these contributions are not sup-orted. Given that paper charts have evolved inpecific contexts and thus reflect the priorities andccentricities of those contexts, it will be impor-ant to examine the design of paper-based artefactscross institutions. Ideally this examination shouldocus on design invariances, those aspects of designhat are common across units. Invariances providehe broad design skeleton; differences representhose aspects of design that need to be tailored toeet the needs of different contexts.In addition, the conversations recorded in our
tudy ICU were limited to those undertaken at theedside. It is possible that some conversations,specially doctors’ diagnoses and prescription con-ersations were undertaken away from the bedside.hus physician interactions with artefacts may bender-represented. Finally, data capture was lim-ted to only one ICU, thus results may not generalizeo other ICUs or healthcare settings.
onclusions
he purpose of this study was to elucidate princi-les underlying successful paper-based CIS designsn an ICU. Thus we present the following twoesign principles as summaries of our findings
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
nd conclusions: Principle 1. Effective CISs sup-ort interdisciplinary interaction. Interdisciplinaryeeds for information should be integrated into theesign and implementation of CIS; and Principle 2.

INA
P n of
EtAte
A
TwatwSSmMMea
R
ARTICLEUCC-89; No. of Pages 11
aper-based clinical information systems and desig
ffective CIS support decision processes, informa-ion flows and practice in addition to data entry.ccurate data entry is necessary but not sufficiento the provision of high quality patient care deliv-ry.
cknowledgements
he authors acknowledge all physicians and nursesho participated in this study. The Australiannd New Zealand College of Anaesthetists fundedhis research (Grant #: 06/026). Dr. Miller’s timeas supported in part by a Vanderbilt Universitychool of Nursing fellowship. Mr. Mercaldo’s and Dr.childcrout’s time was supported by the Depart-ent of Anesthesiology at Vanderbilt Universityedical Center. Tara-Jane Clark, Janice Horslen,iles Patterson and Shannon Kennedy (VUMC) wereach involved in data collection, collation andnalysis.
eferences
1. Turley JP. A framework for the transition from nursingrecords to a nursing information system. Nurs Outlook1992;40(4):177—81.
2. Geiger G, Merrilees K, Walo R, Gordon D, Kunov H. An anal-ysis of the paper-based health record: information contentand its implications for electronic patient records. Med Info1995;8(pt1):295—8.
3. Berg M, Toussaint P. The mantra of modeling and theforgotten powers of paper: a sociotechnical view on thedevelopment of process-oriented ICT in health care. Int JMed Info 2003;69:223—34.
4. Aarts J, Koppel R. Implementation of computerizedphysician order entry in seven countries. Health Aff2009;28(2):404—14.
5. Franklin D, O’Grady K, Donyai P, Jacklin A, Barber N. Theimpact of a closed-loop electronic prescribing and adminis-tration system on prescribing errors, administration errorsand staff-time: a before and after study. Qual Saf HealthCare 2009;16:279—84.
6. Reckmann M, Westbrook J, Koh Y, Lo C, Day RO. Does com-puterized provider order entry reduce prescribing errorsfor hospital inpatients? A systematic review. JAMIA; 2009
Please cite this article in press as: Miller A, et al. Whaus about the design of computerized clinical informatiodoi:10.1016/j.aucc.2010.02.001
[PrePrint; doi:10.1197/jamia.M3050].7. Dykstra R. Computerized physician order entry and com-
munication: reciprocal impacts. In: Proceedings of theAmerican Medical informatics Association, 2002 annualsymposium. 2002. p. 230—4.
Available online at www.
PRESScomputerized CIS in ICU 11
8. Cheng CH, Goldstein MK, Geller E, Levitt RE. The effects ofCPOE on ICU workflow: an observational study. In: AmericanMedical Informatics Association 2003 symposium proceed-ings. 2003. p. 150—4.
9. Ash JS, Berg M, Coiera E. Some unintended consequencesof information technology in health care: the nature ofpatient care information system-related errors. JAMIA2004;11:104—12.
10. Koppel R, Metlay JP, Cohen A, Abaluck B, Localio AR,Kimmel SE, et al. Role of computerized physician orderentry systems in facilitating medication error. JAMA2005;293(10):1197—203.
11. Campbell EM, Sittig DF, Ash JS, Guappone KP, Dykstra R.Types of unintended consequences related to computerizedprovider order entry. JAMIA 2006;13(5):547—56.
12. Ash JS, Sittig DF, Dykstra R, Guappone K, Carpenter JD,Seshadri V. Categorizing the unintended sociotechnical con-sequences of computerized provider order entry. Int J MedInfo 2007;76S:S21—7.
13. Klein G, Feltovich PJ, Bradshaw JM, Woods DD. Commonground and coordination in joint activity. In: Rouse WB,Boff KR, editors. Organizational simulation. Hoboken, N.J.:John Wiley & Sons; 2005. p. 139—84.
14. Miller A, Scheinkestel C, Limpus A, Joseph M, KarnikA, Venkatesh B. Clinical information use by nurses andphysicians and the effects of uni- and interdisciplinaryinteraction on round and handover content in intensive careunits (ICUs). Hum Factors 2009;51(3):339—53.
15. Miller A, Scheinkestel C, Joseph M. Coordination and conti-nuity of intensive care unit (ICU) patient care. Hum Factors2009;51(3):354—67.
16. Miller A, Scheinkestel C, Steele C. The effects of clinicalinformation presentation on physicians’ and nurses’ deci-sion making in ICUs. Appl Ergon 2009;40(4):753—61.
17. Hazelhurst B, McMullen C, Gorman P, Sittig D. How the ICUfollows orders: care delivery as a complex activity system.In: American Medical Informatics Association, 2003 sympo-sium proceedings. 2003. p. 284—8.
18. Koppel R, Wetterneck T, Telles JL, Karsh BT. Work aroundsto barcode medication administration systems: their occur-rences, causes, and threats to patient safety. JAMA2008;15:408—23.
19. Walker JM, Carayon P, Leveson N, Paulus RA, Tooker J, ChinH, et al. EHR safety: the way forward to safe and effectivesystems. JAMIA 2008;15:272—7.
20. Hill CE, O’Brien KM. Helping skills: facilitating exploration,insight and action. Washington, DC: American PsychologicalAssociation; 1999.
21. Agresti A. Categorical data analysis. second edition NewYork: Wiley; 2002.
22. R Development Core Team. R: A language and environmentfor statistical computing. Vienna, Austria: R Foundation
t can paper-based clinical information systems telln systems (CIS) in the ICU? Aust Crit Care (2010),
for Statistical Computing; 2009, ISBN 3-900051-07-0, url:http://www.R-project.org (accessed 18th July 2009).
23. Cohen J. A co-efficient of agreement for nominalscales. Educational and Psychological Measurement1960;XX(1):3—46.
sciencedirect.com