
Middleware für Ubiquitäre Systeme: Ein Modellgetriebener ...
Upload
khangminh22Category
view
6download
0
SCCD : N.G.
AFRICAN DEVELOPMENT FUND GUI/PSHH/2000/01Language: EnglishOriginal: French
APPRAISAL REPORT
THE HEALTH SYSTEM STRENGTHENING(HEALTH III)
REPUBLIC OF GUINEA
COUNTRY DEPARTMENT OCDWWEST REGION MAY 2000

TABLE OF CONTENTS
Page
PROJECT BRIEF, CURRENCIES AND MEASURES, LIST OF TABLES,LIST OF ANNEXES, ACRONYMS AND ABBREVIATIONS, BASIC DATA,PROJECT SUMMARY, PROJECT MATRIX (i-xi)
1. ORIGINE AND HISTORY OF THE PROJECT ............................................................... 1
2. THE SECTOR.................................................................................................................... 1
2.1 The Health Situation....................................................................................................... 12.2. Government's Policy and Programme of Action of the Sector....................................... 22.3. Institutional Framework and Organisation of the Sector................................................ 22.4. Human Resources of the sector ...................................................................................... 32.5. Financing of the Health Sector ....................................................................................... 42.6. Other Donor Interventions in the sector ......................................................................... 42.7. Health Sector Constraints ............................................................................................... 5
3. THE PROJECT AREA ...................................................................................................... 6
3.1 Building of the System's Capacities ............................................................................... 63.2 Support to Safe Motherhood Programmes/STDs/AIDS and Malaria Control ............... 73.3 District Health Care ....................................................................................................... 8
4. THE PROJECT .................................................................................................................. 8
4.1 Design and Rationale...................................................................................................... 84.2 The Project Area and Beneficiaries ................................................................................ 94.3 Strategic Setting of the Project ..................................................................................... 104.4 Project Objectives......................................................................................................... 104.5 Project Description ....................................................................................................... 104.6 Environmental Impact .................................................................................................. 164.7 Project Costs................................................................................................................. 164.8 Sources of Finance and Schedule of Expenditure ........................................................ 19
5. PROJECT IMPLEMENTATION..................................................................................... 20
5.1 Executing Agency......................................................................................................... 205.2 Institutional Arrangements ........................................................................................... 215.3 Supervision and Implementation Schedule .................................................................. 235.4 Procurement of Goods, Works and Services................................................................ 245.5 Disbursements .............................................................................................................. 275.6 Monitoring and Evaluation........................................................................................... 275.7 Accounting and Audit................................................................................................... 285.8 Aid Coordination.......................................................................................................... 28

TABLE OF CONTENTS (cont'd)
6. SUSTAINABILITY AND PROJECT RISKS.................................................................. 29
6.1 Recurrent Costs ............................................................................................................ 296.2 Sustainability of the Project.......................................................................................... 296.3 Critical Risks and Mitigation Measures ....................................................................... 30
7 ACHIEVEMENTS OF THE PROJECT .......................................................................... 30
7.1 Economic Impact.......................................................................................................... 307.2 Social Impact ................................................................................................................ 31
8. CONCLUSION AND RECOMMENDATIONS ............................................................. 31
8.1 Conclusion.................................................................................................................... 318.2 Recommendations and Conditionalities....................................................................... 32
This report was prepared following the mission to Guinea in May 2000 conducted by Mrs. B. Ba(Health Expert and Head of mission) and a Consultant Architect. Dr. R. Wanji, Health Expert,helped in finalising the report. Questions on this report should be addressed to R. CRESSMAN,Division Manager, OCDW.5 (Extendion 4112) and Mr. E. G. TAYLOR-LEWIS, Director OCDW(Extension 4152).

(i)AFRICAN DEVELOPMENT FUND
01 B.P. 1387 ABIDJAN 01Tel :20 20-44-44 : Fax :20 21-77-53
PROJECT BRIEFDate : May 2000
The information given hereunder is intended to provide some guidance to prospectivesuppliers, contractors and consultants and other persons interested in the procurement ofgoods and services for projects approved by the Boards of Directors of the Bank Group. Moredetailed information may be obtained form the executing agency of the borrower.
1. COUNTRY AND TITLE OF PROJECT: Guinea : Health System Strengthening(HSSP) Health Project III
2. LOCATION : Conakry and its suburbs and MiddleGuinea
3. BORROWER : Republic of Guinea
4. EXECUTING AGENCY : Project Coordination Unit within theMinistry of Health in Conakry c/o theSecretary General Fax 224 41 46 86
5. PROJECT DESCRIPTION:
The project’s sectoral objective is to help upgrade the state of health of Guineanpopulations in general, and in particular, mother and child health. In this regard, activitiespertaining to this project are geared towards the following specific objectives: an improvedaccess to health services in the suburbs of Conakry, in Tougué, Gaoual, and Koundara; (ii)higher quality of health care and services in general, and especially in the project area.
The project will be executed over a period of five years, and comprises the fourfollowing components: (i) building of the system’s capacities; (ii) support to safe pregnancyprogrammes, control of STDs/AIDS and malaria; (iii) improved health cover in MiddleGuinea and in Conakry; (iv) project management
6. TOTAL COSTi) In foreign exchange : UA 6.56 millionii) In local currency cost : UA 1.33 millioniii) Total cost : UA 7.89 million
7. BANK GROUP FINANCING
ADF : UA 6.50 millionTAF : UA 0.60 million
8. OTHER SOURCE OF FINANCEThe Guinean Government : UA 0.79 million
9. DATE OF APPROVALOF ADF LOAN AND TAF GRANT : September 2000

(ii)
10. ESTIMATED DATE OF START-UPAND DURATION : As from March 2001; 5 years
11. PROCUREMENT OF GOODS AND SERVICES
Civil Works: International competitive bidding except for the rehabilitation of theoperating blocks to be undertaken under UNICEF responsibility.
Goods
International shopping for the procurement of teaching and administrativefurnishings;
Local shopping for the procurement of equipment for the Project Coordination Unit(PCU) and the main directorates of the Ministry of Health;
Direct negotiation with UNPRA (United Nations Procurement Agency) for theprocurement of the remaining equipment (e.g. equipment for health centres in chargeof malaria control);
Limited international competitive bidding (including UNPRA) for the supply ofmedicines to the Central Pharmacy of Guinea (CPG);
Direct negotiation with the CPG for the supply of medicines to health facilities ;
Services
Short-list: All technical assistance services required for implementing the project’sactivities (architectural studies and supervision, management, accounting, studies,training, audit) will be procured on the basis of a short-list except for WHO services(overseas training) and UNICEF services (reduction of maternal mortality andprocurement of equipment) which will be procured through direct negotiations.
Direct negotiations with health personnel and training institutions for the conduct oflocal training programmes;
Call for candidates for the recruitment of NGOs in charge of extension activities forimpregnated mosquito nets, IEC outreach activities, surveys and training in AIDScontrol and;
Shortlist: for the selection of consultants in charge of providing specialised instructionin teaching methods and mutual aid services.

(iii)
CURRENCY EQUIVALENTS(May 2000)
UA 1 = GNF 1 649.89 USD 1 = GNF 1 250.665GNF 1 = UA 0.0006061 UA 1 = USD 1.31921
UNITS AND MEASURES
Metric System
FISCAL YEAR
1st January – 31st December
LIST OF TABLESPage
2.1 Evolution of State and MOH budgets 42.2 Interventions of major donors 54.1 Cost of project by component 174.2 Cost of project by category of expenditure 174.3 Cost of project by source of finance 184.4 Cost of project by category of expenditure and source of finance 184.5 Schedule of expenditure by component 194.6 Schedule of expenditure by category of expenditure 204.7 Schedule of expenditure by source of finance 205.1 Schedule of project implementation 235.2 Provisions for the procurement of goods, works and services 24
LIST OF ANNEXESNo of pages
1 Administrative map of Guinea 12 Organisation chart of the PCU 13 Estimated schedule of project implementation 14 List of goods and services 15 Table of contents of project implementation manual 1

(iv)
ACRONYMS AND ABBREVIATIONS
AIDS Acquired Immune Deficiency SyndromeAS Aide santé (Health Auxiliary)ATS Agent technique de santé (Technical Health Agent)AV Accoucheuses villageoises (Village Matrons)BI Bamako InitiativeCFC Chloro-fluo Carbonés (Chloro-fluoro carbon)CFG Central Pharmacy of GuineaCHD Community Health DirectorateCOGES Comité de gestion (Management Committee)CPC Consultation primaire curative (Curative Primary Consultation)CPN Consultation prénatale (Prenatal Consultation)CTC Comité technique de coordination (Technical Coordinating Committee)DH District HospitalDIEM Division de l’Infrastructure, de l’Equipement et de la Maintenance
(Division for Infrastructure, Equipment and Maintenance)DNLP Direction Nationale de la Pharmacie et des Laboratoires
(National Directorate for Pharmacy and Laboratories)DNEHS Direction nationale des établissements hospitaliers et de soins
(National Directorate in Charge of Hospitals)DNSP Direction nationale de la santé publique (National Public Health Directorate)DPS Direction préfectorale de la santé (District Health Directorate)ED Essential DrugsEDS Enquête démographique de santé (Population Health Survey)EPV Enlarged Programme of VaccinationGNF Guinean FrancHBTS InhabitantsHC Health CentreIEC Information, Education, CommunicationMEG Médicaments Essentiels Génériques (Essential Drugs)MMR Maternal Mortality RateMOH Ministry of HealthNH National HospitalPASSIP Projet d’Appui au Système de Santé de l’Intérieur du Pays
(Support Project to Health Systems in the Interior of the country)PCU Project Coordinating UnitPHC Primary Health CarePMA Paquet minimum d’activités (Minimum Health Package)PNDS Plan national de développement sanitaire (National Health Development Plan)PRISCO Projet de réhabilitation des infrastructures sanitaires de Conakry
(Conakry Infrastructures Rehabilitation Project)PSN Projet-Santé-Nutrition (Health and Nutrition Project)RBM Roll Back MalariaRH Regional HospitalRHC Rural Health CentreRHI Regional Health InspectorateRTHC Regional Technical Health Committee

(v)
ACRONYMS AND ABBREVIATIONS (cont’d)
SNISG Système national d’information sanitaire et de gestion(National Health Information and Management System)
SSEI Service de la statistique, des études et de l’information(Statistics, Studies and Information Services)
SP Safe PregnancySTDs Sexually Transmitted DiseasesUHC Urban Health CentreUNICEF United Nations Children FundUNPRA United Nations Procurement AgencyWHO World Health Organisation
(vi)
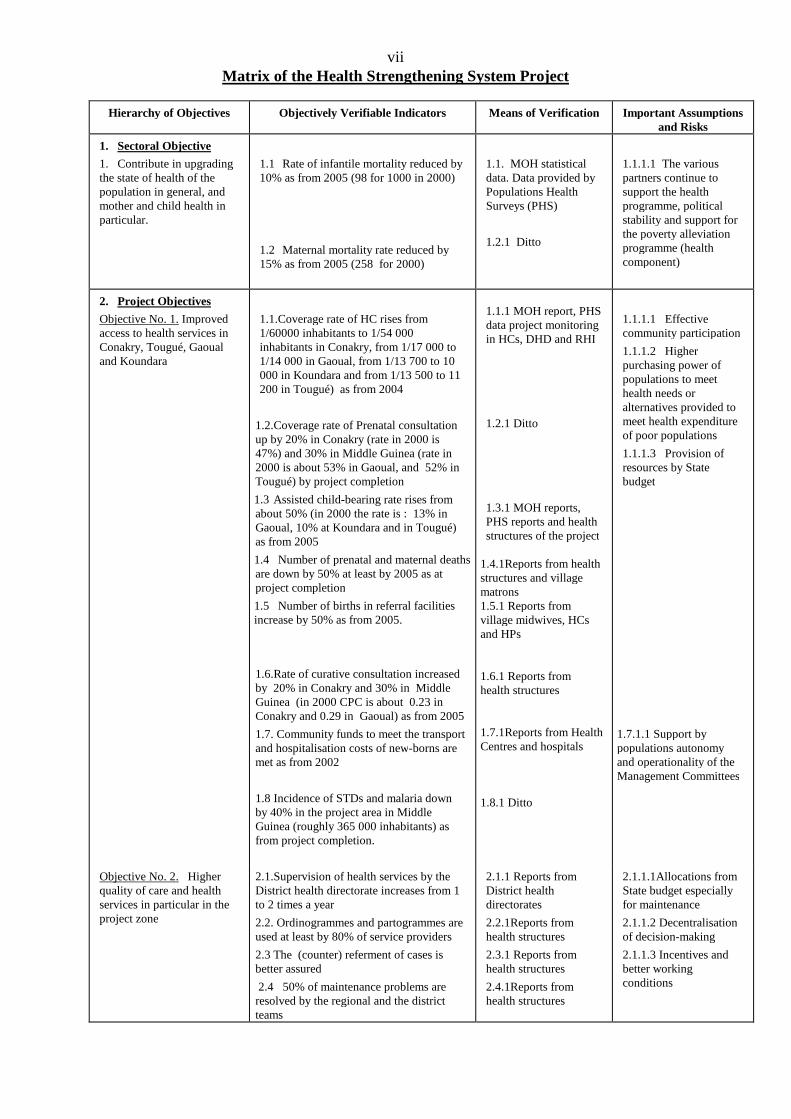
viiMatrix of the Health Strengthening System Project
Hierarchy of Objectives Objectively Verifiable Indicators Means of Verification Important Assumptionsand Risks
1. Sectoral Objective
1. Contribute in upgradingthe state of health of thepopulation in general, andmother and child health inparticular.
1.1 Rate of infantile mortality reduced by10% as from 2005 (98 for 1000 in 2000)
1.2 Maternal mortality rate reduced by15% as from 2005 (258 for 2000)
1.1. MOH statisticaldata. Data provided byPopulations HealthSurveys (PHS)
1.2.1 Ditto
1.1.1.1 The variouspartners continue tosupport the healthprogramme, politicalstability and support forthe poverty alleviationprogramme (healthcomponent)
2. Project Objectives
Objective No. 1. Improvedaccess to health services inConakry, Tougué, Gaoualand Koundara
1.1.Coverage rate of HC rises from1/60000 inhabitants to 1/54 000inhabitants in Conakry, from 1/17 000 to1/14 000 in Gaoual, from 1/13 700 to 10000 in Koundara and from 1/13 500 to 11200 in Tougué) as from 2004
1.2.Coverage rate of Prenatal consultationup by 20% in Conakry (rate in 2000 is47%) and 30% in Middle Guinea (rate in2000 is about 53% in Gaoual, and 52% inTougué) by project completion
1.3 Assisted child-bearing rate rises fromabout 50% (in 2000 the rate is : 13% inGaoual, 10% at Koundara and in Tougué)as from 2005
1.4 Number of prenatal and maternal deathsare down by 50% at least by 2005 as atproject completion
1.5 Number of births in referral facilitiesincrease by 50% as from 2005.
1.6.Rate of curative consultation increasedby 20% in Conakry and 30% in MiddleGuinea (in 2000 CPC is about 0.23 inConakry and 0.29 in Gaoual) as from 2005
1.7. Community funds to meet the transportand hospitalisation costs of new-borns aremet as from 2002
1.8 Incidence of STDs and malaria downby 40% in the project area in MiddleGuinea (roughly 365 000 inhabitants) asfrom project completion.
1.1.1 MOH report, PHSdata project monitoringin HCs, DHD and RHI
1.2.1 Ditto
1.3.1 MOH reports,PHS reports and healthstructures of the project
1.4.1Reports from healthstructures and villagematrons1.5.1 Reports fromvillage midwives, HCsand HPs
1.6.1 Reports fromhealth structures
1.7.1Reports from HealthCentres and hospitals
1.8.1 Ditto
1.1.1.1 Effectivecommunity participation
1.1.1.2 Higherpurchasing power ofpopulations to meethealth needs oralternatives provided tomeet health expenditureof poor populations
1.1.1.3 Provision ofresources by Statebudget
1.7.1.1 Support bypopulations autonomyand operationality of theManagement Committees
Objective No. 2. Higherquality of care and healthservices in particular in theproject zone
2.1.Supervision of health services by theDistrict health directorate increases from 1to 2 times a year
2.2. Ordinogrammes and partogrammes areused at least by 80% of service providers
2.3 The (counter) referment of cases isbetter assured
2.4 50% of maintenance problems areresolved by the regional and the districtteams
2.1.1 Reports fromDistrict healthdirectorates
2.2.1Reports fromhealth structures
2.3.1 Reports fromhealth structures
2.4.1Reports fromhealth structures
2.1.1.1Allocations fromState budget especiallyfor maintenance
2.1.1.2 Decentralisationof decision-making
2.1.1.3 Incentives andbetter workingconditions

vii
Hierarchy of Objectives Objectively Verifiable Indicators Means of Verification Important Assumptionsand Risks
3. Outcome
Outcome of Objective 1
1. Provision of improvedservices:
2. District health structuresare operational
3. The mutual aid facility isoperational andefficient
Outcome of Objective 2
1. Skills and know-how oftechnical staffstrengthened
2. Higher quality of servicesprovided by personnel
1.1.1. 7 Health Centres set up, 3gynecological and obstretical blocks andmaternity of National Hospitalsrehabilitated and equipped, 23 existingRHCs equipped and 1 HC rehabilitated andequipped and all these structures areoperational.
1.1.2. The ratio of health/populationpersonnel is higher.
1.2.1 Activities pertaining to safepregnancy, STDs/AIDS and malariacontrol are carried out
1.2.2 The referment and counter-referment system is operational in thevarious districts.
1.3.1 Populations participate in theirown health care by setting up villagehealth funds
1.3.2 Information/Educationprogrammes for 365 000 persons
1.3.3 Percentage of recurrent costs metby village communities
2.1.1 Technical agents (250) providedwith training in planning, maintenancemanagement, health economy, communityfinance, operational research.
2.1.2 760 village agents are trained
2.2.1 Higher number of consultations
2.2.2 The number of cases referred tothe different health structures on theincrease (Village, H.P., H.C)
2.2.3 The number of maternal deathsdecrease
1.1.1.1 Supervisionreports and minutes ofreception
1.1.2.1 Reports fromhealth structures
1.2.1.1 Project reports
1.2.2.1Reports fromhealth structures
1.3.1.1 Reports fromhealth structures andvillage health funds
1.3.2.1 Supervisionreports
1.3.3.1 Reports fromhealth structures
2.1.1.1 Project reports
2.1.2.1 Project report
2.1.2.1 Reports fromhealth structures
2.2.2.1 Ditto
2.2.3.1 Reports fromhealth structures
1.1.1.1.1 Smoothimplementation of workswithin the deadline
1.1.2.1.1 Structures areprovided with therequisite personnel
1.2.1.1.1 Provision ofcounterpart funds
1.2.1.2 Provision ofhuman resources
1.3.1.1 Community fundsfor meeting the transportcosts and hospitalisationof new borns areavailable.

vii4. Activities
Activities to attain objectiveNo. 1
1. Setting up of projectcoordination unit
2. Procurement ofequipment and supplyof works, goods andservices to the variousdirectorates of theMOH
3. Construction andrehabilitation of healthinfrastructure andaccommodation
4. Procurement of vehicles,ambulances, motorbikesand medical equipment
5. Procurement of genericdrugs and products forimpregnated mosquitonets.
Activities to attain objectiveNo. 2
1. Training of MOH cadresin management,planning, maintenanceand laboratorytechniques etc.
2. Allocation of operatingbudget, procurement ofcomputer hardware andprovision of technicalassistance.
3. Training in healtheconomics
4. Study tours.
5. Training of medical andpara-medical experts.
6. Training of midwives(760 village matrons)
Budget allocation
(in UA million)
Cat. of Expenses F.E. L.C Total
A. Studies & Superv. 0.15 - 0.17B. Const./Rehab. 1.61 0.20 1.81C. Furniture 0.22 0.02 0.24D. Equip./Material 1.58 - 1.58E. Drugs 0.37 - 0.37F. Tech. Assistance 0.71 - 0.71G. Training 0.64 0.32 0.96H. Oper. Costs 0.26 0.60 0.86I. Audit 0.08 - 0.08
Cost of base total 5.62 1.14 6.76Contingencies 0.32 0.08 0.40Price Escal. 0.62 0.11 0.73
Tot. cost of Project 6.56 1.33 7.89
Financing Plan
(in UA million)
SOURCES F.E. L.C. Total
ADF 5.96 0.54 6.50TAF 0.60 - 0.60Government - 0.79 0.79
Total 6.56 1.33 7.89
1.Minutes andevaluation of bids
3 Minutes ofreception
4 Ditto
4., 5, 6 Ditto
Ditto
1. Invitation to tenderaccording to scheduleand programme
2. Compliance withprocedures andcontracts forprocurement ofgoods and services
3. Timely approval bythe Bank
4. Timely submission ofdisbursementrequests according toschedule
1. Invitation to tenderaccording to scheduleand programme
2. Compliance withprocedures andcontracts forprocurement forgoods and services
3. Timely approval bythe Bank
4 Timely submission ofdisbursement requests

(x)
ANALYTICAL SUMMARY
1. PROJECT GENESIS
In order to address the difficulties and constraints encountered in the health sector, theGovernment of Guinea reviewed its health policy and contacted various donors including theBank Group to which a request was addressed in August 1999. This project is in keeping withthe health policy of the Government and the Bank and consolidates the achievements of pasthealth projects financed by the Bank Group. The project is pursuant to the request made bythe Government and was prepared and evaluated respectively in March 1999 and May 2000.Furthermore, the project is in line with the objectives of the government’s poverty alleviationprogramme being elaborated and with the priorities of the Bank strategy document for 1999-2001.
2. BANK GROUP LOAN AND GRANT
The ADF loan and TAF grant amounting respectively to UA 6.5 million and UA 0.6million will be used to finance 100% of foreign exchange costs. The contribution of the loanand the grant in local currency financing for only 7% of total project cost.
3. PROJECT OBJECTIVE
The project’s sectoral objective is to help improve the state of health of the Guineanpopulation in general and in particular, mother and child health. In this regard, activitiespertaining to this project are geared towards the following specific objectives: i) improvedaccess to health services in the suburbs of Conakry, in Tougué, Gaoual, and Koundara; (ii)higher quality of health care and services in general, and especially in the project area.
4. PROJECT ACHIEVEMENTS
To attain the set objectives, the project comprises four components: (i) strengtheningof the health system capacities; (ii) support to maternal health programmes, control ofSTDs/AIDS and malaria; (iii) improved sanitary coverage in Middle Guinea and in Conakry;(iv) project management. At the end of the implementation period of five years, the outcomecould be summarised as follows: the construction of a training centre and rehabilitation of asecond one, an upgraded sanitary coverage of poor regions in Conakry and in Middle Guineaby the construction and equipping of 8 health centres, the equipping of 23 existing rural healthcentres and the rehabilitation of a district hospital, the improved health of at least 600,000women in Conakry and in Middle Guinea; the training of around 900 agents (maintenance,planning, emergency midwifery, mutual aid service etc.): training of 760 village midwives,sensitisation campaigns, information and communication of more than 365,000 persons invarious fields, the development of village mutual-aid systems for an improved mother andchild health and provision of essential medicines.

(xi)
5. PROJECT COSTS
The total cost of the project exclusive of tax and customs duties is about UA 7.89million including UA 6.56 million in foreign exchange and UA 1.33 million in local currency.
6. SOURCES OF FINANCE
The project will be jointly financed by an ADF loan, a TAF grant and contributionfrom the Government. ADF contribution will take care of local currency costs (UA 0.54million) and accounts for 6.8% of the total cost (UA 7.89 million). The Government’scontribution (UA 0.79 million) accounting for 10% of the project’s total cost will partiallyfinance local currency expenditures, particularly in the “construction and rehabilitation”category (UA 0.17 million) and “operating costs” (UA 0.62 million). ADF contribution willbe used to finance all categories of the project.
7. PROJECT IMPLEMETNATION
Coordination of the project’s activities is the responsibility of a Project CoordinatingUnit (PCU) comprising a coordinator, a civil engineer, a procurement specialist, an accountingfirm, technical assistance and support staff. All middle-grade staff will be seconded fromgovernment. The PCU will be assisted by a steering committee and the already existingcommittees. The project’s activities will be implemented by the MOH and any other partnerinvolved in the project’s management (WHO, UNICEF, NGOs, Village Committees etc.)under the responsibility of the PCU. The project will be implemented in five (5) years.
8. CONCLUSIONS AND RECOMMENDATIONS
The project is in line with the Government’s health policy and aims at improving thestate of health of Guineans in general and the most deprived populations (women andchildren) in the periurban areas of Conakry and in three of the poorest districts in MiddleGuinea in particular. The project will help to increase economic and geographical access toprimary care. The project’s achievement will contribute in improving the state of health ofGuinean populations in general and mother and child health in particular.
In view of the foregoing, it is recommended that a loan not exceeding UA 6.5 millionplus a TAF grant of UA 0.6 million be granted to the Government of Guinea. The loan willbe subject to the general conditions of the Bank and the special conditions as specified in theloan agreement.

1. ORIGIN AND HISTORY OF THE PROJECT
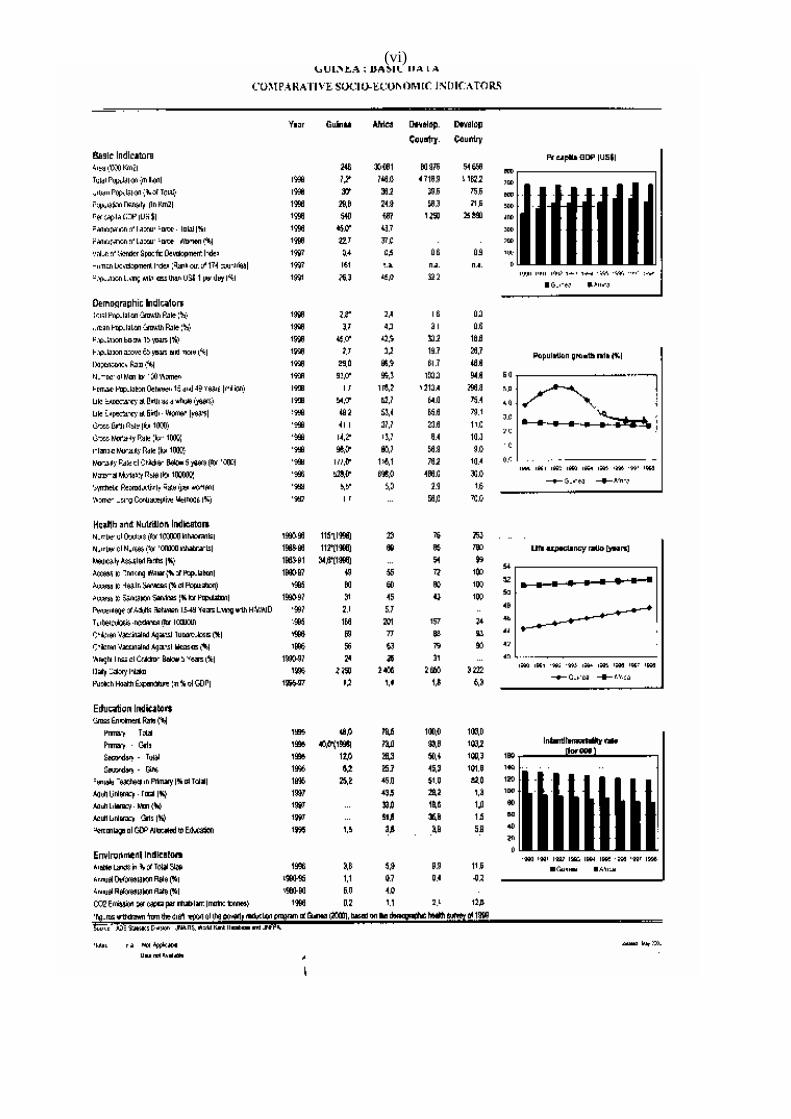
1.1 Guinea has a population of about 7.2 million inhabitants of which 45% are below 15years and 70% live in rural areas, and growing at an annual rate of 2.8% at the national leveland 6% in Conakry, the capital. This rate is higher in the suburbs of Conakry. The urbansprawl in Conakry which accounts for about 1.1 million people (one fifth of total population) isexplained by the existence of a migratory influx due to rural exodus and the rising numbers ofrefugees. Around 40% of Guinean population live below the breadline fixed at 300 USD.Girls’ and boys enrolment in primary schools stand at 40% and 68% respectively. Only 49% ofthe population have access to drinking water. Life expectancy at birth countrywide, is roughly54 years, with a gross mortality rate of 14.2 for a thousand. With regard to health, maternal,infantile and infant/juvenile mortality rates are high and are respectively about 528 for 100,000live-births, 98 for a thousand and 177 for one thousand births. Health coverage is poor inConakry, in the suburbs and in Middle Guinea.
1.2 The Government has just elaborated its health policy based on primary health care whichserves as an intervention framework for the various health development partners, including theBank Group. In September 1998, the Government initiated the identification of the priorityareas of this project which fits into the national health policy. Furthermore, the project is in linewith the Bank strategy in Guinea as defined in its Country Strategy Paper, aiming inter alia, atupgrading basic health infrastructure and living conditions of Guinean populations. In responseto the Government’s request, two preparation and evaluation missions visited Guinea in order tohelp prepare the project. The project’s design and execution will take account of achievementsand lessons drawn from past health projects. This project equally embraces the new povertyalleviation strategy in Guinea, which is being finalised.
1.3 The Bank has already financed two health projects, namely, the Conakry infrastructuresrehabilitation project (PRISCO) approved in 1987 and the pharmaceutical rehabilitation sectorproject approved in 1989. The PRISCO project helped to rehabilitate and equip sevenhealth/maternity centres, two polyclinics in Conakry and provided institutional support to theMinistry of Health. The second project helped in strengthening and enhancing the publicpharmaceutical sector through the enforcement of pharmaceutical regulations, revival of theCentral Pharmacy of Guinea, the training of chemists and setting up of four regionalpharmaceutical depots. All structures rehabilitated and built thanks to these two projects are ingood working order. However, due to the economic situation these projects’ implementationwas greatly delayed. The projects’ activities have been completed and lessons drawn in theirimplementation based on PCR missions conducted at the end of 1999 call for improvementswith respect to the following points: (i) a good definition of institutional anchorage to ensureefficient implementation; (ii) the full time secondment of a coordinator during the period ofimplementation and; (iii) close collaboration between the Ministries of the Economy andFinance, Planning and Health.
2. THE SECTOR
2.1 The Health Situation
The health situation has remarkably improved between 1992 and 1999 according to theinterim report (May 2000) on poverty alleviation in Guinea. Indeed, during this period,infantile as well as infant and juvenile mortality rates fell from 153 and 229 for 1000 to 98 and177 for 1000. During the same period, the maternal mortality rate went down from 666 to 528for 100,000 live births. The epidemiological profile is characterised by the predominance of

2
infectious and parasitical diseases. Malaria accounts for 33% of morbidity cases. In 1998, thenumber of cumulated AIDS cases was around 5,307 (of which 78% of young people aged 20 to30 years) corresponding to a rise of 29.9% compared to 1997. The prevalence rate ofHIV/AIDS rate was about 2% in 1999 in the age group between 15-45 years.
2.2. Government’s Policy and Programme of Action of the Sector
With the support of health development partners, the national health policy based onprimary health care was reviewed during the National Health Forum, held in Conakry in May1997. This policy seeks to ensure equal access to health care for the Guinean populations, offerservices of quality to the populations in general and in particular to the mother and child whilstcontinuing to provide care services. To attain these objectives, the strategies drawn by the Statelay emphasis on the decentralisation of the health system, the strengthening of sanitary coverand managerial capacity as well as a more efficient integrated disease control. Reforms in thehealth sector have helped to improve the health system by implementing primary health careprogrammes, setting up a National Health Information System (NHIS), restructuring nationalhospitals, and improving human, material and financial resources. A health map has beenprepared and adopted, so that today, consultations are held between the central level, thedecentralised administrative authorities and the populations for the setting up of healthinfrastructure.
2.3. Institutional Framework and Organisation of the Sector
2.3.1 Administratively and technically the Guinean health system is divided into three levels.The central level is composed of the Ministers cabinet and General Secretariat, having under itsauthority: (i) the three national directorates, namely, Public Health, Hospitals, the Pharmacy andLaboratories, (ii) support service, i.e. the Administrative and Finance Directorate, Statistics,Engineering and Information Department and the Strategic Training Unit. At the regional level,there are eight (8) Regional Health Inspectorates (RHIs) and the district (38 DHD) is in chargeof supervising urban and rural health centres; as well as implementing the different healthprogrammes. An organisation chart of the MOH is included in the project’s executionhandbook. On the technical level, care providing services follow the same pattern, at the top ofthe pyramid are the National Hospitals (2 NH) in the middle, the Regional Hospitals (4 RH) andat the bottom, the district hospitals (33) the Health Centres (366) and health posts (305).
Private Sector
2.3.2 The private sector in Guinea is gradually developing. In fact, curative private concernsrun about 265 polyclinics and medical cabinets that are generally located in urban areas.Furthermore, various private enterprises provide health structures for their staff, the largest ofwhich are the Fria and Kamsar hospitals. The medical laboratories, drugstores and wholesalesupplies of pharmaceutical products complete this private set-up. There is an evident revival ofthe private sector as some health personnel seek to do business in this sector.
NGOs and Religious Bodies
2.3.3 With regard to private non-profit making institutions, certain primary health care centresare run by religious bodies throughout the country. There are around twenty national andinternational NGOs active in the health sector of which nine are active in the fight againstSTDs. In general, NGOs are present in only a few regions and intervene in specific areas.Within the framework of the project, NGOs will be involved in IEC activities, in training and

3
surveys on AIDS control and the popularizing of impregnated mosquito nets. NGOs involvedin AIDS control in Guinea conduct IEC programmes for the intention of commercial sexworkers, truckers, the military, fishermen and dockers. Furthermore, they provide informationon income generating activities to people infected by AIDS, conduct training programmes inIEC and provide treatment for people infected by AIDS etc.
Traditional Medicine
2.3.4 Traditional medicine holds right of place in the Guinean health system. A policy ontraditional medicine has been laid down and seeks to valorise beneficial and meaningfulpractices against harmful diseases, and this, within the framework of the Primary Health Careprogramme. In this way traditional healers are identified and listed in the two natural regions,lower Guinea and the forest region. This effort of identification will be pursued in the otherregions for a better knowledge of this curative care system and to encourage closercollaboration with public health structures. Besides, some people consult “faith healers” fortheir health problems.
Drug Supply
2.3.5 Public health structures and some private structures are provided in medicines andpharmaceutical products through the EPV/PHC Programme/essential medicines and at theCentral Pharmacy of Guinea (CPG) instituted as a public concern (public establishment ofindustrial and commercial vocation). The medicines are then sold to patients through the costrecovery system as recommended by the Bamako Initiative, and so facilitates the replenishmentof stocks.
2.3.6 On the whole, the institutional framework and the sector’s organisation are runningsmoothly and likened to those of many African countries. However, there are a fewshortcomings with respect to the performance of the different structures. In fact the centraldirectorates still lack the required human and financial resources to effectively implement thenational health policy or provide regular support to decentralised services. Anyway, thedecentralisation of activities at the regional and district levels does not always go hand in handwith the requisite resources and operating budgets are still low. The rate of use and quality ofservices are poor.
2.4. Human Resources of the sector
Health activities as a whole are the responsibility of 6556 health agents, (910 doctors,368 midwives, 1236 health auxiliaries, 2764 technical health agents and 202 pharmacists), withthe administrative personnel completing this array of technicians. At the national level, thepopulation ratios for doctors, midwives, health auxiliaries technical health agents arerespectively around 1/8 000 inhabitants, 1/20 000 inhabitants, 1/5 800 inhabitants and 1/2 600inhabitants. In comparison with WHO standards, the number of doctors is acceptable (1 doctorfor 10 000) as well as that of nursing staff, i.e. health auxiliaries and technical health agents(WHO standards: 1 nurse for 5000 inhabitants). These figures however conceal the shortage oftrained staff and the unequal distribution of human resources countrywide. In fact, Conakry(15% of the population) accounts for around 48% of doctors, and 50% of midwives and nurses.With regard to training, the country has 1 faculty of medicine, 1 Pharmacy and Odonto-stomatology department for the preliminary training of medical personnel (doctors, dentists,pharmacists) 1 National School of Health in Kindia providing training for paramedicalpersonnel (nurses, midwives, technicians) as well as the secondary health schools, in Labé,

4
Kankan in N’zérékoré. Aware of the acute shortage in health personnel, Guinea adopted apermanent training master plan respectively in 1995 and in 1998 with the view to rationalisinghealth staff training and use. Furthermore, a health master plan for Conakry is being prepared.
2.5 Financing of the Health Sector
The financing of the sector is provided by the State, the donor community and theprivate sector (private profit and non-profit ventures and the populations). An analysis ofpublic financing of the sector show a steady rise in health sector allocations in State budget(excluding from public debt) between 1990 and 1997 (from 6 to 8% over the period). From1998 to 2000 operating expenditure exclusive of salaries (32% of health budget) are essentiallyfinanced by the National Development Budget (NDB); external financing and households (bymeans of a costs recovery system set up in Guinea since 1988) provide the rest. The tablebelow is a summary of the evolution of the operating budget, exclusive of salaries and thecapital health budget from 1998 to 2000 compared to global State budget.
Table 2.1Evolution of MOH Budget and State Budget
(in GNF billion)
Description1998
(realised)1999
(realised)2000
(estimate)
MOH Budget (NDB)- Investments-Operating expenditure exclusive of salaries
19.562.29
17.27
13.100.80
12.30
28.133.37
24.76
Total State Budget (NDB)- Investments- Operating expenditure exclusive of salaries
249.9041.40
208.50
284.2648.90
235.36
368.1966.04
302.15
% (MOH/State) Investments% (MOH/State) Operating expenditure exclusive of salaries% (MOH/State) Total exclusive of salaries
5.538.287.82
1.635.224.60
5.108.197.64
2.6 Other Donor Interventions
Donors finance only a little part of the operating budget. For instance, the EuropeanUnion provides counterpart funds for the health sector and from 1998 to 2000, the operatingbudget rose from 1.5 billion GNF to 3.54 billion GNF. Capital expenditure is mainly providedthrough external resources. From 1998 to 2000, external capital financing in the sector rosefrom 28.64 billion GNF to 59.31 billion, corresponding to 92% and 94% respectively ofinvestments in the sector. Table 2.2 summarises the interventions of major donors in the sector.

5
Table 2.2Interventions of Major Donors
Donors Period Scope, area of intervention and locality Amountin GNFbillion
UNICEF 1997-2001 Nationwide - maternal and infantile health-STDs/AIDS-Nutrition-support to districts-support at national level
12.59
World Bank 1996-2002 Nationwide – 1 health and nutrition project and 1 generichealth project including STD/AIDS
55.02
European Union 1999-2002 Nationwide – hospitals administration and management ofoperating budget of MOH and health administration – safeblood transfusion-support to health system-urban health
40.20
GTZ 1995-2001 Guékédou, Kissidigou-Diguiraye-Dabola-Siguiri-support todistricts, technical assistance
50.42
CAID 1996-2001 Conakry-Boké-Kamsar-Fria-Boffa-Dubréka-STDs/AIDScontrol-epidemiological surveillance
3.44
WHO 1996-2001 Nationwide – health policy–vaccination –training-STDs/AIDS-malaria-reproductive health institutional support.
9.13
UNFPA 1995-1999 Nationwide – reproductive health-institutional support 2.48French Cooperation 1997-2001 Rehabilitation of hospitals in Mamou-Kindia-Gaoual-Conakry-
Technical assistance to MOH-Training5.00
ADB 1987-1999 Maternal and child health-strengthening of pharmaceuticalsector
29.86
USAID 1997-2002 Nationwide but particularly Higher Guinea and Forest regions-Conakry-STDs/AIDS-reproductive health
37.78
TOTAL 205.10
2.7 Health Sector Constraints
2.7.1 In spite of the Government’s efforts to address the above-mentioned health situation,constraints in the sector’s improvement and development persist, maternal and infantilemortality rates are still high, malaria is the leading cause of morbidity and mortality and theAIDS epidemic is spreading faster and faster. These constraints are due to the poor cover anduse of health services, a shortage of trained personnel, inadequate financial resources andproblems concerning the system’s management and maintenance.
Institutional Constraints
2.7.2 The inadequate health cover is more acute in Conakry and its environs. The capital andthe pockets of poverty in Middle Guinea lack the basic health infrastructure. The drug supplydepots are often out of stock and cannot meet the demands of health structures. Besides,decentralisation and devolution of duties are not often accompanied by the allocation ofadequate financial resources to Regional inspectorates and district directorates. This constitutesan impediment in the implementation of health programmes and the right supervision of healthactivities.
Human Resources Constraints
2.7.3 The training of health personnel, particularly that of midwives has for the past yearsbeen neglected. Training of personnel in medical and para-medical specialisation is notprovided locally, which is a serious handicap that must be addressed. In fact, there areshortcomings in the fields of managerial training and in public health. The unequal distributionof personnel between health establishments in the capital and those in the interior constitutes animportant snag in the system. Furthermore, there are critical, weaknesses as regards the

6
capacity of these services to coordinate the Ministry’s administrative and managerial activitiesand provide the necessary technical support to the decentralised structures of the MOH at thecentral level.
Constraints regarding financial resources, management and maintenance of the system
2.7.4 The State’s budgetary allocation to the health sector is inadequate (around 5% in 1999,well below the 10% recommended by the WHO). This leads to failings in the management ofthe system both at the central level and the periphery. Although decentralised at the periphery,the statistical services still lack the required resources to collect, manage, analyse and use datanecessary for planning and decision-making. The division in charge of maintenance needs to beprovided with the necessary human and financial resources to implement the national policy onmaintenance adopted since 1999. The strengthening of the costs recovery system in nationalhealth infrastructure should offset some operational difficulties.
3. THE PROJECT AREA
The project will focus on the system’s capacity building, support to safe pregnancyprogrammes, STDs/AIDS, the fight against malaria, and provision of basic health care at thedistrict level (prefectures or communes).
3.1 Building of the System’s Capacities
3.1.1 An upgraded quality of services and the good performance of the health system dependon several factors of which the availability of qualified personnel, the existence of a goodsystem of maintenance, an efficient health planning and information system, the availablenessof effective generic drugs and the appropriate financing of the health system, including popularparticipation (cost recovery, mutual-aid system etc.). In this way, one of the project thrusts willbe to strengthen continuous training activities in keeping with the objectives of the PermanentTraining Master-Plan adopted in 1998 by the Government.
3.1.2 The system of maintenance of built up property and MOH equipment leaves much to bedesired. In fact, the poor system of maintenance can be explained by the absence of qualifiedmaintenance staff and the appropriate working tools; the use of below-standard equipment inhospitals and administrative structures, the encumbrance of unreliable biomedical equipmentprovided as grants; an inadequate budget allocated to maintenance and the lack of a culture ofmaintenance. Due to the lack of preventive maintenance, health buildings are amortised in 10years instead of 25 years (according to the findings of a study recently conducted in May 2000by the KFW on the health region in Conakry). In the past five years the budget earmarked formaintenance accounted for only 0.6% of the health budget. Likewise, in the health structures,the maintenance budget is equally low when compared to the procurement cost of 8% forequipment and logistics and 1% for buildings. In order to address the current problems ofmaintenance in the health sector, the Government elaborated a policy on maintenance in 1999the overall objective of which is to set up mechanisms that would help to ensure the smooth andsustainable running of these structures.

7
3.1.3 At the Ministry of Health, the planning departments of the National Health Informationand Management System and Research are under the Department of Statistics, Engineering andInformation. The principal duty of the planning bureau is to help the MOH in its planningactivities (elaboration of the national health development plan, priority programmes, and annualplans of action in the various services both at the central level and in the periphery). Theplanning bureau manned by one person (without any logistics) cannot accomplish its duties.The support provided by the central administration to the decentralised planning processremains inadequate. Besides, data generated by the information system and results ofoperational research are not always used for the purposes of planning and decision-making.
3.1.4 Todate, the drug steck-out of stocks still remains a problem. A recent study on thesupply and distribution systems of essential drugs in Guinea, conducted by the Ministry ofHealth in July 1999, highlighted the difficulties encountered by the supply outlets (the CPG andthe EPV/PHC Unit) namely: exhaustion of stocks and management problems. In order to makethe CPC more efficient, certain recommendations concerning administrative and financialmanagement as well as increasing the stocks of medicines were formulated. A meeting ofdonors will be organised by the MOH to search for the financing required to implement theserecommendations.
3.2 Support to Safe Motherhood Programmes/ STD/AIDS and Malaria Control
Safe Motherhood
3.2.1 With a maternal mortality rate of 528 for 100,000 live births in 1999 according to theMOH and 880 for 100,000 according to the United Nations, the Government of Guinea accordshigh priority to actions fostering safe pregnancy. The Government had drawn, since 1992 anational safe pregnancy programme with the support of several donors. Pilot actions had beenundertaken in the various regions of the country and contribute in bringing down these rates.From 1992 to 1999, sustained efforts had helped to obtain certain improvements with thereduction of the MMR from 666 to 528 for 100,000 births. Nonetheless, this rate still remainshigh. The general objective of the health policy is to reduce mortality by 40% by 2010, andduring the same period, reduce in particular, infantile mortality from 87.5 for 1000 to 70 for1000 and maternal mortality from 520 for 100,000 live births to 350 for 100,000.
STDs/HIV/AIDS
3.2.2 Considering that HIV/AIDS is a problem of development, the Government of Guinea issince 1998, in the process of implementing its AIDS control programme, the major objectivesof which are to reduce the propagation of HIV infection, to provide treatment for persons livingwith HIV and reduce the socio-economic impact of HIV/AIDS. The rate of incidence of STDsamong young people over 15 years old is around 18.1 for 1000 (in 1999) and the prevalence rateof HIV/AIDS is about 2% in the age group between 15-45 years. Data on the prevalence ofHIV/AIDS are not reliable and information on epidemiological surveillance system is scanty.The prevalence rate is certainly higher in urban areas, due to a high number of refugees, thepresence of mining and dams sites and the crossroads of different towns. Under the AIDScontrol programme, the Government will focus on reducing the spread of AIDS, treatment forinfected persons and the reduction of the socio-economic impact of HIV/AIDS.

8
Malaria
3.2.3 Malaria is endemic in Guinea, it is the first cause for consultation in health facilities (30-40%) and the major cause of death in hospitals. It was only in1992 that the Governmentupdated a national malaria control programme and adopted a related policy in 1993. Theprogramme aims at the proper management of malaria cases, prophylactic treatment forpregnant women and the promotion of individual protection by the use of impregnatedmosquito nets. With the financial backing of development partners, several activities have beenundertaken, but coverage in the districts and communes is low and the health centres are notalways provided with anti-malaria drugs and accessories required to check cases of malaria.For 2000, the MOH whilst subscribing to the Roll Back Malaria initiative has envisaged toreduce by 50% the overall incidence of malaria, that of acute malaria by 39%, and deaths bychronic cases of malaria in the health establishments by 25%.
3.3 District Health Care
The operational structures of basic health are inadequate countrywide. This shortcomingis particularly acute in Middle Guinea and the suburbs of Conakry with a high level of urbansprawl. Middle Guinea has been identified as one of the poorest natural regions in the countrywith about 51% of the population considered poor (annual income below 300 USD). Theincidence of poverty is lower in Lower Guinea (42%) , the Forest Regions (33%) and Conakry(7%). The health indicators in Middle Guinea are weak. The maternal mortality index is about754 for 100,000 live births compared to the national average of 528. The medical coverage rateof births is low in the region (10% in Tougué whereas the national average is roughly 25%).Only 18% of deliveries in Middle Guinea are assisted by a doctor or a midwife, whereas thispercentage is around 35% at the national level, 33% in Lower Guinea, 21% in Upper Guineaand 37% in the Forest Regions.
4. THE PROECT
4.1 Design and Rationale
4.1.1 The project meets the concerns of the government as regards the putting in place of alarge-scale poverty alleviation programme in general, and more importantly a health sectordevelopment programme. The project was prepared and evaluated with the close collaborationof beneficiary populations, development partners, namely, the World Bank, UNDP, UNICEF,UNFPA, WHO, European Union, French (AFD), German (GTZ and KFW) and Canadian(CAID), American and Japanese Cooperation; community association leaders and civil society.During the preparation and evaluation missions, the project sites visited were used as aframework of discussion with health personnel, health development partners in Guinea and thepopulations through the health committees. Subjects for discussions were centered on theirperception of the health problems in their respective regions. The project in line with the newBank Group health policy is in keeping with the priority areas of the Guinean government andseeks to improve the system’s efficiency. Therefore, all the parties concerned by the projectparticipated in its formulation during the course of discussions held in the different placesvisited, in conversations at different levels and with representatives of the online ministriesinvolved first and foremost in these activities.
4.1.2 The PHC strategy will help ensure a more tactful treatment of the main health problemsof the populations. This efficiency will be obtained through the increased supply of basictreatment, especially in the capital and deprived regions, the financing of activities that

9
contribute in reducing maternal and infantile mortality, STDs/AIDS and malaria control,through the rehabilitation and equipping of basic health infrastructure, and also with a betterperformance of care-providers at the different echelons of the health pyramid and supervision ofactivities. This project completes and strengthens other donor interventions in the periphery ofConakry and in Middle Guinea. The lessons drawn from the 2 completed health projects willbe taken into account, especially, the strengthening of the implementation unit, the involvementof the technical directorates of the Ministry and beneficiaries in project implementation andmanagement, the decentralisation of centres of authority and a better coordination with theMinistry of the Economy and Finance.
4.2 The Project Area and Beneficiaries
Project Areas
4.2.1 The areas concerned by the project are the outskirts of Conakry as well as the districts ofTougué, Gaoual and Koundara in Middle Guinea. The choice of these regions is justifiedbecause the number of basic health infrastructure is inadequate, especially in the suburbs ofConakry where urban sprawl is highest due to rural exodus and the influx of refugees from thesub-region. Furthermore, Middle Guinea is one of the two poorest regions with a poverty rateof 51% (40% at the national level). Again, this region has the highest rate of maternal mortality(754 maternal deaths for 100,000 live births, whereas the national average stands at 528 for100,000 live births). The district of Gaoual has only 8 rural health centers (RHC) i.e. one RHCfor 17,625 inhabitants whereas the norm is 1 health centre for 7,000 inhabitants. In 1999, theeffective coverage of this district in pre-natal consultation was about 53% and curative primaryconsultation (CPC) about 29%. Besides, the coverage rate of deliveries is about 13%. Itequally disposes of about a dozen health posts and a district hospital. The district of Koundarahas 7 RHCs, i.e. one RHC for 13,712 inhabitants, about a dozen health posts and a very oldregional hospital. The district of Tougué with a total population of 124,136 inhabitants, has 9RHCs, i.e. one RHC for 12,792 inhabitants, 9 operating health posts and one regional hospital.
4.2.2 Today Conakry is extending further and farer from the existing health centres. The townhas 18 HCs, 3 communal medical centres and 2 national hospitals. The communes of Matoto(4 centres for 400,603 inhabitants) and Ratoma (6 centres for 325,379 inhabitants) seeminglyreceive less coverage, although they are the most populated areas of the capital. The coverageratios as defined in the national health map correspond to 1 health centre for 10 to 20,000inhabitants in urban areas. With such a low coverage, Conakry has on average 1 HC forroughly 60,000 inhabitants. This situation calls for corrective measures.
Project Beneficiaries
4.2.3 The population of Conakry and its environs (1.1 million inhabitants) and that of MiddleGuinea (2.2 million inhabitants) benefit most from the project and account for 45% of thecountry’s total population. More importantly, training activities, support to the system ofmaintenance and to regional inspectorates are more beneficial to Middle Guinea as a whole.However, the strengthening of health cover concerns, other than Conakry, the districts ofGaoual (145,028 inhabitants), Tougué (124,136 inhabitants) and Koundara (95,988 inhabitants).The reduction of maternal mortality, STDs/AIDS control and the fight against malaria are asmany activities undertaken in these districts. The target populations are essentially mothers andchildren under five years that would have a ready need for the health services.

10
4.3 Strategic Setting of the Project
4.3.1 The project’s strategy is in keeping with the challenges and priority areas found in thenational health policy paper, in the Government’s poverty alleviation policy on one hand andthe Bank Group’s Country Strategy Paper (CSP) for Guinea for 1999-2001 on the other. Thestrategy and project activities complement those of other donors and tend to improve the healthof the populations and sustain the achievements of the sector. The project will draw from theexperience and expertise of UN organisations, i.e. WHO and UNICEF, as they have acomparative advantage in areas such as the management of training programmes, activitiesrelated to safe pregnancy and the procurement of medical equipment. The project willcontribute in addressing problems that impede the smooth development of an efficient healthsystem aimed at improving the state of health of the Guinean population in general and moreimportantly that of the most deprived. Thus, the project’s areas of intervention are as follows:(i) the strengthening of the system’s capacities (ii) support to national and infantile healthprogrammes, STDs/AIDS control and the fight against malaria and (iii) the strengthening ofdistrict health care.
4.3.2 Indeed, the project’s strategy lays down activities effectively contributing to upgrade thehealth of the populations. Thus, in addition to curative health activities, the project will focuson preventive activities especially IEC with respect to safe pregnancy, STDs/AIDS control andthe fight against malaria. Again, the training programmes to be financed will help to upgradethe quality of personnel that will provide proper services to the populations. The financing ofmaintenance activities will contribute in implementing the Government’s policy in this regardand help to upgrade the durability of buildings and equipment. Assistance provided to theplanning and information system will make possible a more effective support to decentralisedhealth systems especially in terms of elaborating regional and district health plans andimplementation of the national health development plan.
4.4 Project Objectives
The project’s sectoral objective is to help upgrade the state of health of the Guineanpopulations and in particular that of the mother and the child. The specific objectives of theproject are as follows (i) 'improve access to health services in Conakry, Tougué, Gaoual, theKoundara ; (ii) upgrade health care quality and health services in general and particularly in theproject area.
4.5 Project Description
4.5.1 To attain the set objectives the project comprises four components: i) strengthening ofthe system’s capacities; ii) support to priority programmes such as safe pregnancy, STDs/AIDScontrol and the fight against malaria, (iii) improve health cover in Middle Guinea and inConakry; and (iv) project management. At the end of the implementation period of five years,the realisations and activities expected in the project area are as follows:
I. Strengthening of the system’s capacities
- 1 continuous training centre rehabilitated and equipped in Maférinyah;- 1 newly constructed and equipped training centre in Donka;- 3 MOH directorates provided with logistics and offices;- the National Quality Control Laboratory equipped;- 2 health cadres trained in health economics;

11
- 1 curative guide elaborated, reproduced in 2000 copies and distributed;- 8 agents from the Maférinyah centre trained;- 240 agents trained in various fields (maintenance, planning etc.) ;
II. Support to safe motherhood STDs/AIDS control and the fight against malaria
- 3 operating blocks in gynaecology/obstetrics and maternity rehabilitated and equipped;- 3 blood transfusion laboratories equipped;- 3 ambulances acquired and equipped with a radio-communication system;- 29 RHCs (including 23 and 6 new ones) equipped with technical equipment, motor
bikes, radios and solar modules;- 760 agents trained and equipped with delivery kits;- a mutual aid fund for support to obstretical referment is put in place by the local
communities in each rural sub district;- 365,000 people familiarised in IEC techniques on safe pregnancy and 3 information and
sensitisation workshops (75 agents) conducted- 2 skill-based workshops (1 national 126 participants and 1 in Middle Guinea/170
participants) on the use of partogrammes;- 30 agents trained in treating sick children;- the STDs/HIV/AIDS survey system strengthened;- 10 trainers trained to conduct surveys on STDs/AIDS;- 30 agents trained to conduct surveys on STDs/AIDS- IEC techniques for the prevention of HIV/AIDS;- 150 health agents and community agents are trained in the popularisation of insecticide
treated mosquito nets, 3 agents receive training in entomology, 30 receive training intreating acute cases of malaria, 9 agents are trained in insecticide treating techniques and30 laboratory technicians receive further training;
- 50 units of insecticide-treated mosquito nets are installed, insecticide-treating equipmentand anti-malaria drugs procured;
- 3 surveillance sites to test the efficiency of chloroquine are set up.
III. Improvement of health coverage in Middle Guinea and Conakry
- 2 Urban health centres and 5 regional health centres built and 1 rehabilitated, equippedand supplied with drugs ;
- 5 houses for heads of the health centres built and 1 rehabilitated;- 2 regional hospitals and 9 district hospitals provided with maintenance equipment;- 3 motor-bikes and 3 computer kits for 3 regional hospitals, 9 motorbikes procured for 9
district hospitals.
4.5.2 The project will finance activities the realisation of which will concern the ninefollowing categories of expenditure: A. Architectural studies and supervision; B.Construction/Rehabilitation; C. Furniture; D. Equipment; E. Medicines; F. TechnicalAssistance; G. Training; H. Operating Costs; I. Audit. The list of detailed project costs ispresented in annex 4 in the execution handbook. The detailed activities of the project bycomponent are described below:
Component I: Strengthening of the system’s capacities
4.5.3 Within the framework of this component, the project will contribute in upgrading theskills of health personnel through the strengthening and installation of training centres in
12
Maferinya and Donka and the training of health administration cadres in different fields such asmaintenance, planning, research methodology, financing and health economy. Furthermore,technical assistance equipment, logistics and essential medicines will be provided to thedifferent technical services in order to enhance their respective performances.
4.5.4 The project will provide financing for studies, the supervision of rehabilitation andextension works of the Donka training centre (346 m2) lodged in the University TeachingHospital in Donka. An engineering firm will be responsible for civil engineering studies andsupervision under the control of the civil engineer of the PCU and the division forinfrastructure, equipment and maintenance. The schedule of architectural works is reproducedas an annex in the project implementation document.
4.5.5 The project will provide financing for the extension of the permanent training centre inMaférinyah (491 m2) through the construction of a documentation centre, the setting up ofadditional teaching infrastructure as well as the construction of more residence halls forstudents, increasing the Centre’s intake from 16 to 32 students including four houses for thetrainers. The project will also finance the construction of a meeting room, three offices and amulti-purpose room. Concerning the training centre in the Donka hospital, the project willfinance the construction of a new building including two classrooms of 25 places each, adocumentation centre for 20 places, two demonstration rooms, a staff room for 10 places, twooffices, one secretariat, an enclosure, and system roads.
4.5.6 The project will provide the required office and household furniture for the Maférinyaand Donka training centres, it will also provide equipment for the training centres as well as thedifferent technical services of the MOH, both training centres will be equipped with computerhardware, a photocopier and necessary documentation. The Maférinya centre will be providedwith a solar energy kit and one 4 x 4 vehicle, and the strategic training unit will receive twocomputers, documentation and one 4 x 4 vehicle. The project will provide support to thedivision of infrastructure, equipment and maintenance by procuring a double cabin 4 x 4 vehiclefor the supervision of project sites and the regional machinery and maintenance centres. Theplanning section of the MOH will be equipped with two computers and one 4 x 4 vehicle. Theproject will support the National Health Information and Management System by the provisionof a computer, a photocopier, and a binding machine. Forty four agents in charge of healthstatistics at the district level will be equipped with motorbikes to allow them to collect andanalyse health data. The Central Pharmacy of Guinea will be supplied with about a dozencomputers.
4.5.7 In order to improve the availability of medicines, the project will provide the CentralPharmacy with a stock of drugs as well as additional equipment and reagents from the NationalQuality Control Laboratory. The replenishment of the medical stocks of the Central Pharmacywill be subject to the Government’s implementing of recommendations made during theevaluation of the medicines supply system conducted by the MOH in July 1999. Therecommendations concern, inter alia, the merger of the Central Pharmacy with the EssentialDrugs Unit, the restructuring of the Central Pharmacy, the promotion of generic drugs, thereplenishment of stocks, budgetary support, rehabilitation of computer hardware, technical

13
assistance in pharmacy and marketing. The stock of drugs to be provided to the CentralPharmacy will be sold to health structures and replenished through the turn-over realised by thefirm.
4.5.8 With regard to training activities, the project will back-up training programmes for thefollowing agents: 2 cadres in health economy for a six-month overseas training course; 8agents from the Maférinyah Training Centre in local teaching methods, 6 bio-medical engineersin planning and maintenance management and further training overseas in bio-medicaltechnology for 5 months; 15 promoters of mutual aid health associations for 15 days locally; 30mutual aid health leaders for 7 days locally; 6 agents in community financing for 4 monthsabroad; 60 persons in research methodology for 35 days in Labé and in Guékédou; 13 agents inepidemiology, 12 for 4 months and 1 for 2 years in Bamako; 3 agents (12 months) for overseastraining in planning; 55 agents for 15 days locally in district administration; 1 agent in healthsociology for two years abroad.
4.5.9 Concerning technical assistance, the project will finance the services of a consultant (6pers/months) to conduct a study on the putting in place of a trust fund that will guarantee theaccess of firms importing medicines to foreign exchange. It has also been envisaged to financetechnical assistance services (6 persons/months) for the carrying out of training in teachingmethods for 8 agents at the Maférinya centre. Technical assistance (8 persons/months) will beprovided for the running and management of training programmes at the higher training centrein Donka. Furthermore, the project will finance consultant services (0.5 person/month) for thetraining of mutual aid health promoters and leaders and consultant services (2 persons/months)to elaborate and disseminate a curative guide for the rational prescription of medicines. Theguide will contain health care prescription alternatives for the sick depending on local currentpathologies, economic factors or the costs of treatment. The planning division will receive theservices of a consultant (1 person/month) for the preparation of a workshop on theadministration of districts. The project will sign an agreement with the WHO for themanagement of overseas training. It will also meet the costs of supervision, and themaintenance of vehicles and equipment for the activities of this component.
Component II: Support to safe motherhood programmes/STDs/AIDS control and thefight against malaria
4.5.10 Under this component the project will finance, support activities to safe pregnancyprogrammes, AIDS and malaria control in the health districts. Concerning the safe pregnancyprogrammes, the project will finance social mobilisation activities and IEC techniques with theview to sensitising the populations, setting up a mutual-aid association as well as aninformation system. The project will equally provide training for staff and village agents,through UNICEF and delivery kits for village agents. It will finance the rehabilitation andequipment in gynecology and obstretical and maternity blocks and provide additionalequipment for existing health centres and the laboratories of district hospitals. With regard tomalaria control activities, the project will finance IEC programmes and training, theprocurement of equipment, products, impregnation units and medicines. As far as theSTDs/AIDS control is concerned, the project will lay emphasis on surveys, IEC activities,training and procurement of medicines for treating sexually-transmitted diseases.
4.5.11 Concerning support to the safe pregnancy programme, the project will finance therenovation of the gynecology and obstretic operating blocks and the maternity wards of thedistrict hospitals in Gaoual and Tougué. The blocks and maternities will be equipped as well asthe three laboratories in the district hospitals of Gaoual, Tougué and Koundara. These three

14
hospitals will also be provided with three ambulances and three 4 x 4 vehicles. The 23 ruralhealth centres existing in the three districts as well as 6 new ones to be set up the project will besupplied with 29 motorbikes, technical equipment, a radio-communication system and solarmodules. Seven hundred and sixty delivery kits will be distributed to the village agents. Theproject will finance UNICEF technical assistance services for the procurement ofgynaecological and obstretic equipment for the implementing and coordination of activitieslinked to reproductive health. It will meet consultancy costs for a period of 3.5 persons-monthsfor the training of health staff in IEC techniques and the use of partogrammes.
4.5.12 With regard to malaria control, the project will focus on the financing of the resourcesrequired for the treatment of nets, the popularisation of their use and the training of healthpersonnel and community agents in providing treatment for acute cases of malaria. In this way,the project will finance the installation of about 50 insecticide-treating units in Gaoual, Touguéand Koundara, the procurement of 75 impregnation kits and 10,000 litres of insecticide, theconfection of management tools, 100,000 impregnation cards and 50 registers. Each districtwill manage its stock of material, which, in turn will be transferred to impregnation units underthe responsibility of the health personnel and the management committees that will apply thetariff as fixed by the cost recovery policy. The project’s activities in malaria controlcomplement those of other donors, such as the WHO, UNICEF, Japanese Cooperation thatsupply the centres with bednets.
4.5.13 The project will provide local training for 50 health agents and 100 district communityagents for 5 days in the popularisation techniques and use of impregnated bed-nets, andtreatment for acute cases of malaria. In addition, about 30 laboratory technicians will receivefurther training for 5 days. The project will meet the costs of training relating to the printing ofmodules and payment of subsistence allowances. As to involving beneficiaries andstakeholders in the project’s implementation, 50 health agents, 100 community agents andvarious population groups, especially women’s groupings, will receive training sessions in theextension and use of impregnated bednets. The health agents will attend local skill-basedseminars on the treatment of acute cases of malaria, impregnation techniques as well aslaboratory techniques. Three health agents will undergo training in medical entomology.
4.5.14 Concerning AIDS control, about ten trainers will be trained, who in turn, will providetraining to about thirty health agents to conduct probable STDs/AIDS incidence surveys (IP6and IP7) that will be carried out under the project. The project will finance the procurement ofsundry supplies made up of teaching aids, audio-visual support for education, talk shows,audio, radio and television programmes on STDs/AIDS control for the general public, schoolsand colleges. More importantly, the project will finance IEC activities and training for thefollowing groups: (i) deprived women in the periurban areas of Conakry and the urban areas ofKoundara, Gaoual and Tougué; (ii) journalists; (iii) young people in the project’s rural areas;(iv) health personnel of communities in the project areas. IEC activities, surveys and trainingprogrammes will be undertaken by international and national NGOs through competitivebidding.
4.5.15 For a large-scale dissemination of information on the AIDS epidemic, journalists (press,radio and television) will attend training sessions on IEC techniques during the course ofproject implementation. AIDS control activities in the environs of Conakry and the urban areasof Koundara, Gaoual and Tougué, are geared towards the female population comprisingcommercial sex workers, widows and young girls. With the backing of NGOs specialised inAIDS control, IEC messages will be transmitted by “peer educators”, i.e. influent women andwomen’s associations. Proferred advice will help to increase women’s awareness of the

15
dangers of unprotected sex and means of protection, the need to carry out tests, information onavailable treatment, treatment for people infected by the virus and advice on income generatingactivities to women who want to abandon the commercial sex trade. In the rural areas of theproject, IEC activities in the fight against STDs/AIDS for school children, dropouts and non-enrolled children as well as children orphaned by AIDS will be financed. In addition,Community health personnel will be provided with the adequate training enabling them toprovide better care for persons infected by sexually transmitted diseases and proffer informedadvice to AIDS patients and their families.
Component III: Upgrading of the health coverage in Middle Guinea and Conakry
4.5.16 Under this component, the project will finance the construction and equipping of eighthealth centres in the suburbs of Conakry and in Middle Guinea as well as the rehabilitation andequipping of the maternity and administrative wing of the district hospital in Koundara. Thesehealth centres will be supplied with the furniture and medicines needed for their smoothrunning. The project will equally meet the costs of engineering and supervision for theconstruction of 6 health centres and the rehabilitation of the Koundara hospital in MiddleGuinea. The project will strengthen the health cover of the periphery of Conakry through theconstruction of two health centres (336 m2 for one urban health centre), one at Simbaya Gare(commune of Ratoma) and the other at Yimbaya school (commune of Matoto). Theconstruction plans will be based on already existing architectural plans.
4.5.17 In Middle Guinea, the project will finance the reinforcement of health structures in thefollowing sub-districts: (i) in Gaoual, the construction and equipping of two rural health centresincluding accommodation in Wedoubourg and Kakoni; (ii) in Koundara, the reconstruction ofthe RHC in Guigan plus accommodation, the rehabilitation of the RHC in Youkounkoum andaccommodation for the head of centre; (iii) in Tougué, additional hospital equipment, theconstruction of RHCs (including accommodation for the head of centre) in Fello Koundoua andKoura Tongo. The average built in area for an RHC is about 197 m2 and 110 m2. for housing.In addition to all these structures, the project will also finance the sinking of boreholes and theinstallation of incinerators. The maternity and administrative block of the regional hospital inKoundara (432 m2) will be rebuilt by the project. In order to render the health systemoperational, the project will finance supervision strengthening activities and provide logisticsupport for the functioning of Regional Health Inspectorates (RHIs), District HealthDirectorates (DHDs) and health centres.
Component IV: Project Management
4.5.18 Under the component, the project will use the former premises of the PharmaceuticalSector Rehabilitation Project funded by the Bank. Its execution has been completed.Nonetheless, the project will meet the costs of office furniture and equip the PCU with therequired logistics, in particular, two vehicles, one motorbike, three computers, one telecopierand a photocopying machine. Technical assistance services, (18 persons/months) will beprovided in project management, training and civil engineering. Furthermore, it will finance therecruitment of an accounting firm for the setting up of an accounting system and keeping ofaccounts throughout the project’s duration as well as an audit firm for the auditing of the annual

16
accounts. Again, the project will pay salaries to the Project Coordinator, a civil engineer and aProcurement specialist, all three will be civil servants. The project will also pay salaries to thesupport staff and meet the operating costs of the PCU.
4.6 Environmental Impact
4.6.1 The project is a category II environmental project. The project’s impact on theenvironment will be limited since the setting up of civil engineering structures will be few. Allthe same, technical steps will be taken to avoid erosion, gullying, rain-water stagnation orflooding. Construction and rehabilitation works carried out under the project will comply withthe required hygiene and sanitation standards, depending on the geographical features of thesites. It is further envisaged to include an esthetic façade to new constructions (tree-planting,site development and anti-erosion measures). Training provided to health personnel willinclude an “environment” component to enable these agents monitor environmental aspects.The aerosols to be incorporated in the malaria control equipment will be devoid of Chloro-fluo-carbon. Finally each new centre will be equipped with an incinerator for the disposal of solidwaste.
4.6.2 Environmental measures will be integrated in the bidding documents, the appreciationcriteria of which will include the arrangements envisaged by the bidders for the eventualcarrying out of impact studies. Environmental monitoring will be directly ensured by healthpersonnel working within the structures that will be set up by the project. In view of preservinga healthier environment, the Government has adopted an environment code and instituted aNational Council for the Environment. On the legislative plane, the country has enacted theapplication instruments for the environment code.
4.7 Project Costs
4.7.1 The project’s costs exclusive of tax and customs duties are estimated at UA 7.89million. ADF and TAF contributions stand respectively at UA 6.5 million and UA 0.6 millionand Government’s participation amounting to UA 0.79 million. A provision for contingenciesis included in the different categories of expenditure (10% for civil engineering and 5% forother categories of expenditure except for medicines, a lump sum has been earmarked forprocurement) as well as an annual provision for price escalation estimated at 4% for localcurrency spending and 3.5% for foreign exchange spending. Local currency inflation is basedon the macro-economic framework projections which take account of the importance of inputsrelating to the evolution of energy requirements that add up to a considerable sum in local costs.Foreign exchange inflation take account of the eventuality of construction works being executedby international firms outside the OCDE countries. Cost were estimated during the appraisalmission on the basis of information obtained from the Ministry of Finance and the differentstakeholders in the health and construction sectors including the World Bank. Tables 4.1 and4.2 are a summary of the project’s costs by component and by category of expenditure.

17
Table 4.1Project Cost by Component
<–––––– GNF million –––––> <–– UA million –> % %
COMPONENT F.E. L.C. Total F.E. L.C. Total F.E. Tot.
1. Reinforcement of the system’scapacities
2 462.68 683.45 3 146.13 1.49 0.41 1.90 78 24
2. Support to safe-pregnancyprogrammes STDs/AIDS/Malaria
1 762.09 589.15 2 351.24 1.07 0.36 1.43 75 18
3. Improvement of health cover inMiddle Guinea and Conakry
3 924.03 349.65 4 273.67 2.39 0.21 2.60 92 33
4. Project Management 1 104.63 249.75 1 354.38 0.67 0.16 0.83 82 11
Total Base Cost 9 253.42 1 872.00 11 125.42 5.62 1.14 6.76 83 86
Contingencies 580.69 109.18 689.88 0.32 0.08 0.40 84 5
Price Escalation 1 022.39 186.82 1 209.21 0.62 0.11 0.73 85 9
Total Project Cost 10 856.50 2 168.01 13 024.51 6.56 1.33 7.89 83 100
Table 4.2Cost of Project by Category of Expenditure
<––––––– CFAF millions ––––––
><––– UA million –––> % %
Categories of expenditure F.E. L.C. Total F.E. L.C. Total F.E. Tot.
A. Studies and supervision 247.35 - 247.35 0.15 - 0.15 100 2
B. Construction/Rehabilit. 2 656.82 311.69 2 968.51 1.61 0.20 1.81 89 23
C. Furniture 361.37 40.15 401.52 0.22 0.02 0.24 90 3
D. Equipment 2 610.15 - 2 610.15 1.58 - 1.58 100 20
E. Medicines 611.88 - 611.88 0.37 - 0.37 100 5
F. Technical Assistance 1 162.47 - 1 162.47 0.71 - 0.71 100 9
G. Training 1 053.28 528.22 1 581.50 0.64 0.32 0.96 67 12
H. Operating Charges 425.11 991.94 1 417.05 0.26 0.60 0.86 30 11
I. Audit 125.00 - 125.00 0.08 - 0.08 100 1
Total Base Cost 9 253.42 1 872.00 11 125.42 5.62 1.14 6.76 83 86
Contingencies 580.69 109.18 689.88 0.32 0.08 0.40 84 5
Price Escalation 1 022.39 186.82 1 209.21 0.62 0.11 0.73 85 9
Total Project Cost 10 856.50 2 168.01 13 024.51 6.56 1.33 7.89 83% 100%
4.7.2 The project will be jointly financed by the ADF, the TAF and the Government asmentioned in tables 4.3. and 4.4 below:

18
Table 4.3Sources of Finance
(in UA million)
SOURCES F.E. L.C. TOTAL %
ADF 5.96 0.54 6.50 82
TAF 0.60 - 0.60 8
Government - 0.79 0.79 10
TOTAL 6.56 1.33 7.89 100
Percentage 83.1% 16.9% 100.0%
Table 4.4Cost of Project by Category of Expenditure and Source of Finance
CATEGORY <––––– ADF –––––> <––––– TAF –––––> Govt. <––––– Total –––––> %
OF EXPEND. F.E. L.C. Tot. F.E. L.C. Tot. L.C.. F.E. L.C. Tot. Tot.
A. Studies andsupervision
0.17 - 0.17 - - - - 0.17 - 0.17 2
B. Construc./Reha. 1.96 0.08 2.04 - - - 0.17 1.96 0.25 2.21 28
C. Furniture 0.26 0.02 0.28 - - - - 0.26 0.02 0.28 4
D. Equipment 1.83 - 1.83 - - - - 1.83 - 1.83 23
E. Medicines 0.39 - 0.39 - - - - 0.39 - 0.39 5
F. Technical Assist. 0.83 - 0.83 - - 0.83 - 0.83 11
G. Training 0.14 0.38 0.52 0.60 - - - 0.74 0.38 1.12 14
H. Operating Costs 0.29 0.06 0.35 - - - 0.62 0.29 0.68 0.97 12
I. Audit 0.09 - 0.09 - - - 0.09 - 0.09 1
Total 5.96 0.54 6.50 0.60 - 0.60 0.79 6.56 1.33 7.89 100
% du Total 76 7 82 8 0 8 10 83 17 100
4.7.3 The ADF and TAF contributions in the amount of UA 6.5 million and 0.6 millionrespectively i.e. a total of UA 7.10 million accounts for 90% of the project's total cost and 100%of foreign exchange costs (UA 6.56 million). Their local currency contribution accounts for 7%of the project’s total cost. The Government’s participation accounts for 10% of ADF financingand 10% of TAF financing, accounting for 10% of the project’s total cost and corresponding toUA 0.79 million. The ADF loan will serve to finance all categories of expenditure whilst theTAF grant will help to finance training for the building of the health system’s capacities. TheGovernment’s contribution will meet 59% of the total cost in local currency and will beallocated to category B (Construction/Rehabilitation) and H (Operating Costs) expenditure.

19
4.7.4 ADF participation in local currency costs is justified by the following reasons:
i) In general, the ADF does not finance local currency expenditure, nevertheless, inthis project and in keeping with the poverty reduction objectives, 7% of ADFresources will be allocated in local currency ;
ii) These expenditure are justified by the type of goods and services to be procured,which essentially concern local manpower, local aggregates for construction:components that will contribute in poverty reduction.
iii) It should be noted that Guinea has pursued the re-organisation of its expenditurepattern for the benefit of priority social sectors (basic social infrastructure)during the course of its successive public expenditure reviews. In this regard, itstill benefits from external budgetary support assistance. ADF contribution inlocal currency will prevent the country from sliding further into more debt with anon-concessional loan because of budgetary discipline and commitment to donordirectives under the structural adjustment programme.
4.8 Sources of Finance and Schedule of Expenditure
The project will be implemented over a period of 5 years according to the list of goodsand services detailed in annex 5 and the schedules of expenditure by component, categories ofexpenditure and sources of finance presented in the tables below:
Table 4.5Schedule of Expenditure by Component
COMPONENT 2001 2002 2003 2004 2005 Total %
1. Capacity building of the health system - 1.12 0.76 0.22 0.08 2.18 28
2. Support to maternityprogrammes/STDs/AIDS/Malaria
0.020.94 0.37
0.220.09
1.6421
3. Improving the health cover of MiddleGuinea and Conakry
0.021.20 1.18
0.710.01
3.1240
4. Support to project implementation 0.22 0.18 0.18 0.19 0.18 0.95 12
Total Project Cost 0.26 3.44 2.49 1.34 0.36 7.89 100
% of total 3 44 32 17 5 100

20
Table 4.6Schedule of Expenditure by Category of Expenditure
(UA million)
CATEGORY OF EXPENDITURE 2001 2002 2003 2004 2005 Total %
A. Studies and Supervision 0.02 0.12 0.03 - - 0.17 2
B. Construction/Rehab. - 0.84 1.07 0.30 - 2.21 28
C. Furniture - 0.10 0.02 0.16 - 0.28 4
D. Equipment 0.07 1.09 0.41 0.26 - 1.83 23
E. Medicines 0.01 0.32 0.06 - - 0.39 5
F. Technical Assistance 0.10 0.26 0.21 0.15 0.11 0.83 11
G. Training 0.01 0.54 0.38 0.19 - 1.12 14
H. Operating Costs 0.04 0.15 0.29 0.26 0.23 0.97 12
I. Audit 0.01 0.02 0.02 0.02 0.02 0.09 1
Total Project Cost 0.26 3.44 2.49 1.34 0.36 7.89 100
% of Total 3 44 32 17 5 100 100
Table 4.7Schedule of Expenditure by Sources of Finance
(UA million)
SOURCES OFFINANCE
2001 2002 2003 2004 2005 Total %
ADF 0.22 2.99 2.02 1.04 0.21 6,50 82
FAT 0.01 0.29 0.20 0.10 - 0,60 8
Government 0.03 0.16 0.27 0.20 0.15 0,79 10
Total Project Cost 0.26 3.44 2.49 1.34 0.36 7,89 100
5. PROJECT IMPLEMENTATION
5.1 Executing Agency
5.1.1 The project’s implementation will be entrusted to the future Project Coordinating Unit(PCU), its organisation chart is reproduced in annex 2 of the report. The premises of a formerhealth project financed by the ADF will be used, with the State meeting most of the localcurrency costs of the PCU, especially, the payment of salaries of staff on secondment. ThePCU will be answerable to the Secretary General of the Ministry of Health and will be providedwith the appropriate human material and financial resources to accomplish its mission. It willbe manned throughout the project’s implementation by a National Coordinator, a civil engineerversed in the procurement of furniture and equipment, a procurement specialist, an accountingfirm and support staff. Given that the two former coordinators of health projects financed bythe ADF have been transferred to other functions, a new coordinator will be recruited. TheCoordinator will be a civil servant with, on one hand, a good knowledge in the managing of theGuinean health system, and on the other, a professional experience of at least five (5) years.Furthermore, the Coordinator should master the rules and procedures of the Bank Group, or theWorld Bank with regard to project management. The curriculum vitae of civil servantsearmarked by the PCU should be submitted for Bank’s approval prior to secondment.

21
5.1.2 The PCU based in Conakry will be in charge of management and coordination of theproject’s activities. It will be responsible for financial and administrative management and willprepare in collaboration with the concerned technical services and partners, the project’sprogramme of activities. It will submit, after cross-checking, all requests for payment and willsee to the timely disbursement of ADF, TAF and Government funds. It will regularly submit,quarterly progress reports and the annual audit reports to the Bank. It will coordinate theprocurement of all goods, services and works of the project, according to the Bank’s rules andprocedures. It will be strengthened by technical assistance, 6 persons/months a year for 3 years,in project management and training. It will also be assisted by a Technical CoordinatingCommittee and the group of directorates comprising all the technical directorates of the MOHthat will meet regularly to examine, among other things, the implementation of all healthprojects. The technical directorates of the Ministry of Health as well as regional and districthealth services will directly carry out the activities of the project that concern them. The PCUwill be assisted by the UN institutions that have a comparative advantage in the execution ofcertain components of the project, namely WHO for overseas training, UNICEF forimplementation and coordination of safe pregnancy activities and procurement of equipment.
5.2 Institutional Arrangements
5.2.1 The central level comprises the group of Directors and the Technical CoordinationCommittee (TCC), both under the chairmanship of the Secretary General responsible for thecoordinating and monitoring of central services, projects and programmes, including the projectunder consideration. The TCC meets regularly and is made up of the Directors of the centralservices of the MOH, health programmes managers, representatives from the Ministries of LandAdministration, Finance, Budget and representatives of health developments partners. Aregular coordination of the project’s activities will be ensured by a sub committee emanatingfrom these structures and will be composed of the technical Directorates directly involved in theimplementation of the project’s activities (NPHD, DSEI, NDP, CPG, NDHs) a representativefrom the Ministry of the Economy, Finance and Planning, a representative of UNICEF andWHO and a representative of NGOs active in AIDS control. This committee will meetperiodically to monitor the execution of activities and propose solutions to problemsencountered in project management. The administrative costs to be paid to UNICEF and WHOwill be negotiated at the signing of the protocols and will remain within the limits of thepercentages used by UN agencies in the execution of similar projects. UNICEF and WHO willelaborate individually a detailed budget which will be submitted to the Bank for approval.
5.2.2 The implementation of the first component namely, the building of the system’scapacities will be the responsibility of the central directorates. In this regard, the Division ofInfrastructure, Equipment and Maintenance (DIEM) within the National Directorate ofHospitals (NDH) will play a crucial role in the procurement and monitoring of civil engineeringworks and equipment. In fact, the DIEM will assist the engineering firm to be recruited in theengineering and monitoring of civil engineering works. It will also be involved in theelaboration of bidding documents for civil engineering, furniture and equipment. The NationalDirectorate of Health will actively participate in the preparing of a protocol with WHO for themanagement of overseas training courses. The strategic training unit and the MaférinyaTraining Centre will assist the project in the selection of experts for further training as well asin the planning and organisation of training. The National Directorate of Planning and the CPGwill help the MOH in preparing the bidding documents for the procurement of medicines for theCPG, additional equipment for the national control laboratory as well as the monitoring of thestudy on the trust fund for the procurement of imported medicines. The department of statistics,

22
engineering and information will monitor the implementation of activities geared towards thestrengthening of the planning division and the national information and management system.
5.2.3 Concerning the implementation of the second component at the central level, theNational Directorate of Health will assist the PCU in the planning and implementing ofactivities concerning support to safe pregnancy programmes, STDs/AIDS control and the fightagainst malaria. It will actively participate in the preparing of the protocol of agreement withUNICEF. As to the implementing of the activities of the third component, the DIEM will playa fundamental role in the preparation of tender documents, the monitoring of the constructionwork of health structures as well as the procurement, installation and maintenance ofequipment. The central directorates involved in project implementation will be represented inthe committee that will meet periodically to examine the management and coordination of theproject’s activities.
5.2.4 At the regional level, the regional technical health committee (RTHC) will meetregularly to ensure the monitoring and coordination of activities developed by the differenthealth structures in the region. The managers of the regional Inspectorate, the district directorsof health, hospital directors, the managers of regional branches, the representatives ofprofessional associations, NGOs and donors will participate in these meetings. The regionalhealth inspectorates in Boké and Labé will be responsible for the projects activities at theregional level. The district technical health committee (DTHC) will meet regularly and withsame membership as the above-mentioned committees, but at the district level. The districthealth agents and personnel of health structures in Conakry, Tougué, Gaoual and Koundara,health committees and NGOs will be in charge of the implementation and monitoring of projectactivities with the backing of the PCU, UNICEF and WHO.
5.2.5 The WHO will assist the MOH in the organisation and management of overseas trainingcourses. More importantly, according to a protocol agreement to be signed with theGovernment and approved by the Bank, WHO will assist the project in the preparation of a planand a training plan, will contact the specialised training institutions, will evaluate, with theMOH, the costs of training activities on the basis of information obtained and from the projectdocument and will sit at the selection committee for candidates (at the MOH). Again, WHOwill be responsible for travel arrangements of students, the payment of their allowances andtraining costs with the funds disbursed by the Bank.
5.2.6 UNICEF will be responsible for the procurement of equipment with the United NationsProcurement Agency and the implementation and monitoring of activities relating to the safepregnancy programme. It will prepare, in concert with the MOH and the PCU, the protocolagreement incorporating the terms of reference and financial estimates of the activities to beimplemented, drawing from UNICEF experience in the reduction of maternal mortality in thedistrict of Dabola. UNICEF will carry out social mobilisation activities, IEC and advocacy infavour of the female populations with the view to familiarising them with the problems ofmother and child health as well as the putting into place community funds for the provision ofcare and treatment of women during pregnancy, the training of village agents and healthpersonnel involved in the programme’s execution.

23
5.2.7 UNICEF will be in charge not only of the procurement of equipment for newlyconstructed health structures but also for the rehabilitation of the operating blocks andmaternities in Tougué and Gaoual and their equipping; the procurement by the UN ProcurementAgency of laboratory equipment and blood-transfusion apparatus for the three district hospitalsof Tougué, Gaoual and Koundara, the equipping of 23 existing centres of these three districtsincluding a radio-communication system and 760 delivery kits, the provision of logistics forsupervision and referment (3 4 x 4 vehicles and 3 ambulances for 3 hospitals). UNICEF willsubmit quarterly progress reports, requests for disbursement and the supporting documents tothe PCV. UNICEF has the required expertise to supervise and coordinate the activities that willbe undertaken by health personnel, consultants, NGOs and the population.
5.3 Supervision and Implementation Schedule
The programme will be implemented over a period of five years as per the planmentioned in annex 3 and summarised below:
Table 5.1Project Implementation Schedule
Programme of Activities
Activities Dates In Charge
I. Approval publication
Approval loan signing and publication Sept – November 2000 ADF/Govt
Loan effectiveness March 2001 MOH/ADF
II. Project implementation
Recruitment of PCU personnel and launching January-April 2001 MOH/ADF/PCU
Procurement of equipment and vehicles March- May 2001 PCU/Suppliers
Supervisions missions (3 sup. every other year) andannual audit
Nov. 2001-Dec.2005 MOH/PCU/ADF
Mid term review September 2003 MOH/PCU/ADF
III. Capacity building of the system
Studies and preparation of bidding documents for civilengineering
January-June 2001 DIEM/PCU/ADF/Bureau
Selection of firm and civil engineering works July 2001- Jan. 2002 Firms
Procurement and installation of furniture and equipment January 2002-Dec.2002
PCU/DIEM
Planning and organisation of overseas training April 2001-Dec. 2004 PCU/MOH/WHO
Procurement of medicines for the Central Pharmacy ofGuinea
January 2002-Oct.2002
PCU/MOH/CPG/ADF
Conduct of study from trust fund for medicines andapproval
June-August 2001 PCU/NDP/Admin./FIN/MOH/CPG
IV. Support to safe pregnancy STDs/AIDS control and malaria
Preparation of Protocol Agreement with UNICEF andapproval
March –July 2001 PCU/UNICEF/MOH
Selection of firms and rehabilitation of maternityblocks/hospitals
August 2001-Nov.2002
PCU/DIEM/UNICEF
Procurement of equipment for maternity blocks for the 3Hospitals and equipment for 29 RHCs
July-December 2002 UNICEF/DIEM/PCU/DP/DHD
Safe pregnancy activities, STDs/AIDS and malariacontrol
July 2001-December2005
UNICEF/NGO/HealthPersonnel/HealthCommittee/POPCarriers
V. Improving the health cover of Middle Guinea and Conakry
Confirmation of construction sites September 2000 PCU/MOH
Preparation of bidding documents for civil engineering February-May 2001 PCU/Bureau/DIEM
Preparation of civil engineering contracts May-June 2001 DIEM/Bureau/PCU
Construction and equipping of HCs/equipment ofDHD/NHIMS decentralised/machinery for hospitals
January 2002 toJanuary 2004
Firms./UNICEF/DIEM

24
5.4 Procurement of Goods, Works and Services
5.4.1 The procurement of goods, works and services concerning the categories of expenditurefinanced by the project will be done according to ADF rules and procedures by using the Bank’sstandard bidding documents. The list of goods and services detailed in annex 4 is summarisedin table 5.2 below:
Table 5.2Arrangements concerning the procurement of goods and services (in UA million)
Categories of expenditure I.B L.S. OthersShort List Fin.
Govt. Total
1. Civil engineering works
1.1 Construction/Reh. 2 Training centres1.2 Rehab. of 2 Blocks/maternity and hosp
0.21 [0.20]0.06 [0.04]a
0.010.02
0.210.06
[0.20][0.04]
1.3 Construct /reconst. of 8 HC & Rehab.1 HP 1.94 [1.80] 0.14 1.94 [1.80]
Sub-total Civil engineering works - 2.21 [2.04]
2. Goods
2.1. Furniture for 2 Training Centres 0.01 [0.01]b 0.01 [0.01]2.2 Furniture for HCs and 1 Hosp.(Koundara)
0.27 [0.27]a 0.27 [0.27]
2.3 Equipt. Training Centres. MOHDirectorates
0.44 [0.44] 0.44 [0.44]
2.4. Equip maternity blocks/support toprogrammes
0.64 [0.64]a 0.64 [0.64]
2.5. Equip. HCs + machinery and maintenance 0.69 [0.69]a 0.69 [0.69]
2.6. Equipment PCU 0.06 [0.06] 0.06 [0.06]
2.7 Medicines CPG 0.32 [0.32]c 0.32 [0.32]
2.8 Medicines for HCs + Malaria + STDs 0.07 [0.07]d 0.07 [0.07]
Sub-total Goods 2.50 [2.50]
3. Training/IEC/Social Mobilisation
3.1. Overseas training and study trips 0.57 [0.57]e 0.57 [0.57]3.2 Training/IEC/Soc. Mob. (Prog. UNICEF) 0.17 [0.17]a - 0.17 [0.17]3.3 Training/surveys/IEC/STDs/AIDS controlpopularisation insecticide treated bed nets
0.17 [0.17]f 0.17 [0.17]
3.4 local training/surveys 0.17 [0.17]g 0.04 [0.04] 0.21 [0.21]
Sub-total - Training 1.12 [1.12]
4. Consultancy Services -
4.1. Studies and Supervision 0.17 [0.17] 0.17 [0.17]4.2 Technical Assistance 0.06 [0.06]h 0.78 [0.78] 0.84 [0.84]
4.3 Audit 0.09 [0.09] 0.09 [0.09]
Sub-total Consultancy Services 1.10 [1.10]
5. Miscellaneous -
5.1. Operating Costs 0.97 [0.35]i 0.62 0.97 [0.35]
Total 2.15 [2.00] 0.50 [0.50] 4.17 [3.53] 1.08 [1.08] 0.79 7.89 [7.10]
a : Protocol UNICEF/UNPRAb : International shoppingc: Restricted international competitive biddingd : For procurement on the basis of direct negotiations with the CPGe : Overseas training under WHO as intermediary with training institutionsf : Call for candidates on the basis of TORg :Other training programmes and activities to be undertaken either by local staff or by NGOs through direct negotiationsh: Management costs paid to WHO and UNICEFi : Operating costs and goods and services for the PCU and health structures involved in project execution

25
5.4.2 Architectural studies and supervision (UA 017 million); The services of engineeringfirms required for the conduct of architectural studies, the preparing of bidding documents forcivil engineering and the follow-up of works will be procured on the basis of a short list inaccordance with Bank rules of procedure.
5.4.3 Construction and rehabilitation (UA 2.21 million);
- International competitive bidding for construction works and rehabilitation of Health Centresin Conakry and Middle Guinea, for the maternity block and administrative building of thedistrict hospital of Koundara and the centres for further training (UA 2.15 million) ;
- Direct negotiation with UNICEF for the rehabilitation of the operating blocks in Tougué,Gaoual and Koundara and the maternity blocks in Gaoual and Tougué (UA 0.06 million) to beimplemented under the safe pregnancy programme.
5.4.4 Furniture (UA 0.28 million)
- International shopping for the procurement of furniture for the teaching and administrativesections of the Maférinya and Donka training centres (because of their specificity) and thehealth structures.
- Direct negotiation with UNPRA for the procurement of medical furniture (included in medicalequipment) for the HCs in Conakry and Middle Guinea and the Koundara hospital.
5.4.5 Equipment (UA 1.83 million)
- Local competitive bidding for the procurement of equipment (photocopiers, and computers)and vehicles for the training centres and central directorates (UA 0.44 million) and equipmentfor the PCU (UA 0.06 million). These suppliers have local representations that providemaintenance services. The local procurement of this equipment is justified because localsupplies are available and procurement at short notice to enable the PCU and central services tofunction smoothly and effectively.
- Direction negotiation with UNPRA for equipment (UA 0.64 million) of the maternity blocksin Tougué and Gaoual including ambulances and radio-communications systems as well asmalaria-control equipment (insecticide-treated bed nets, impregnation kits) and for theprocurement of medical equipment for the HCs, vehicles for the district health directorates andmaintenance machinery (UA 0.69 million).
5.4.6 Medicines (UA 0.39 million)
- Limited international competition for the procurement of medicines to replenish stocks ofmedicines to be supplied to the Central Pharmacy of Guinea (UA 0.32 million). UNPRA willbe consulted for this bidding.
- Direct negotiation with the Central Pharmacy of Guinea for the procurement of the initialstock of medicines for the health centres and additional medicines for the malaria and STDscontrol programmes (UA 0.07 million).

26
5.4.7 Technical assistance (UA 0.84 million); Technical assistance services required for theimplementing of project activities (project management, training, accounts etc.) will beprocured on the basis of a short list except for WHO and UNICEF services (UA 0.06 million) tobe procured through direct negotiation.
5.4.8 Audit (UA 0.09 million); the services of an audit firm throughout the project’s durationwill be procured on the basis of a short list.
5.4.9 Training (UA 1.12 million)
- Direct negotiation with the WHO (specialised training institution) for the management ofoverseas training and study tours (UA 0.57 million;
- Direct negotiation with health personnel, and training institutions that will conduct themajority of training programmes (UA 0.21 million); health personnel trainers will not be paidhonoraria but subsistence allowances varying between GNF 25,000 and GNF 35,000 (UA 15-UA 20) and the duration of training courses will not exceed 15 days;
- Applications for recruitment of an NGO in charge of implementing IEC techniques, trainingand AIDS control surveys (UA 0.10 million) as well as the popularisation of insecticide-treatedbed nets (UA 0.07 million);
- Short list for the carrying out of more specialised local training programmes particularly inmutual-aid associations, teaching methods and planning (UA 0.04 million); these contractsamount to 27,810,000 GNF (about UA 17,000). The subsistence allowances for trainers varybetween 25,000 GNF and 35,000 GNF;
- Direct Negotiation with UNICEF for the training of village health social mobilisation agentsand the training of personnel in emergency obstetrics.
5.4.10 Functioning (UA 0.97 million) ; goods and services will be procured through localshopping. The functioning component comprises travelling costs and allowances directly paidto service providers.
5.4.11 The local rules and regulations on procurement of the Republic of Guinea have beenexamined and found acceptable. The Project Coordinating Unit will be in charge of all contractawards for goods, services and training. In addition to the cadres that will be seconded to thePCU, technical assistance will be provided for about 6 man/months a year for 3 years, aconsultancy firm will be recruited to provide the requisite support to the PCU especially inproject management and training.
Information note on the procurement of goods and services
5.4.12 The information note on the procurement of goods and services will be discussed andadopted during the course of negotiations and will be published in the “Business Development”journal as soon as the loan is approved by the Bank’s Board of Directors.

27
Evaluation procedures
5.4.13 The following documents will be submitted for the Bank’s consideration prior topublication:
i) Special information note on the procurement of goods and services,ii) Bidding documents and invitation to consultants,iii) Bidding documents for civil engineering works,iv) Evaluation reports of bids containing recommendation on contract awards,v) Draft contracts in case the contract model included in the bidding documents have
been modified.
5.5 Disbursements
Given that the rate of disbursement in an indicator of a project’s performance andmanagement, the necessary steps will be taken to ensure the availability and transparent use ofresources for the project. The PCU will be responsible for cross-checking suppliers’ servicesagainst the specifications and will prepare requests for disbursement before submission to theADB. The amount for disbursement should not be below UA 20,000 for TAF and ADFpayments, except for requests concerning technical assistance and training. Two special anddistinct accounts will be opened, one to receive ADF and TAF resources for projectmanagement and the other, the counterpart fund. The first disbursement will be effected asfrom loan effectiveness and following the satisfactory fulfilment of conditions precedent to firstdisbursement. The account opened to receive ADF resources will be replenished after thespending of at lest 50% of the preceding operating funds, as soon as the supporting documentsare approved by the ADB.
5.6 Monitoring and Evaluation
Progress Reports
5.6.1 The various directorates involved in the project as well as UNICEF and WHO willsubmit to the PCU, quarterly and annual reports on the progress of their activities within theframework of the project. The PCU, with the assistance of an audit firm will prepare the annualaudit reports of the project’s accounts. The Project Coordinating Unit will compile the reportsfor submission to the Bank. On the project’s completion, the Government and the Bank willeach prepare a project completion report.
Supervision
5.6.2 The Project Coordinating Unit will be responsible for the project’s implementation andensure its permanent supervision. A project launch workshop will be organised with theparticipation of the Bank’s experts, as from the project’s start-up. Furthermore, the Bank willconduct periodical supervision missions (three supervision missions every other year) with theactive participation of all stakeholders involved in the project’s implementation. Copies ofthese supervision mission reports will be submitted to the authorities for action.

28
Mid-term Review
5.6.3 A tripartite mid-term review (ADF, Government and technical partners) will beundertaken after 30 months of project implementation. The purpose of the review will be tomeasure the progress made in the project’s implementation as compared to set objectives anddefine the corrective measures that may eventually be required. The review will concern all theparties involved in the project’s implementation including the representatives of beneficiaries.
Monitoring and evaluation
5.6.4 The PCU will put in place a mechanism for the monitoring and evaluation of theproject’s indicators (included in the logical framework) and the project’s realisations that willbe cross-checked during the supervision missions and the mid-term review. On the basis ofinformation contained in the project matrix it will prepare, a performance chart of simpleindicators, in close collaboration with the statistics services of the MOH and other technicaldirectorates involved in the project’s implementation, for a regular monitoring of the project’sperformances. Besides, the monitoring mechanism set up will take into account the othermonitoring mechanisms used by other health development partners for a more effectivecoordination.
5.7 Accounting and Audit
The project’s accounts will be kept by the PCU with the help of an accounting firmspecially recruited to this end. The accounts will be audited annually by an independent firm ofinternational repute. The audit reports should be prepared immediately after each fiscal yearand submitted to the Bank 6 months following the end of each fiscal year.
5.8 Aid Coordination
5.8.1 Since Guinea is a member of the consultative group, the last meeting was held in June1998. Coordination is developed through formal and informal sectoral meetings. Donorcontributions are often in keeping with areas of priority, defined on one hand by the EnhancedStructural Adjustment Facility (ESAF) 1997-99, by the Structural Adjustment Credit III (SAC)of the IDA, and on the other, by the sectoral development policy letters punctuated by sectoralround tables.
5.8.2 The donors active in the health sector meet periodically and the Government holdsannual meetings with the health development partners. During the project’s design, thepreparation and evaluation missions held discussions with the health development partners,namely, the World Bank, UNDP, UNICEF, UNFPA, WHO, European Union, French, German,Canadian, American and Japanese Cooperation agencies. All these institutions have showntheir appreciation for the participatory approach adopted by the Bank and have expressed to themission their desire to institute effective collaboration. During the course of its implementationthe project will draw from the experiences of the other development partners, for instance, thatof Canadian Cooperation (CAID) in the field of communication and that of UNICEF in thereduction of maternal mortality. In Conakry itself, project implementation will, morespecifically, be undertaken in collaboration with German Cooperation (KfW) and the EuropeanUnion . The KFW is in the process of elaborating a health master-plan for Conakry, but hasstill to define its areas of intervention. The EU will pursue its support to the health directoratein Conakry and the various community health directorates.

29
5.8.3 In Middle Guinea, the World Bank is currently running two projects, the HealthNutrition Project (HNP) and the Population Health Reproduction Project to be completedrespectively end 2000 and end 2002. The HNP has financed the construction of the districthealth directorate and contributed in the financing of the operating costs of the regional healthand the district health inspectorates. Regarding the Population Health Reproduction Project(GPHP), its interventions will be re-centered on STDs/AIDS control activities and willcomplement the Bank’s intervention. With respect to safe pregnancy, the MOH had with thebacking of the GPHP initiated women’s groupings with the view to setting up mutual villagefunds, with the project completing these efforts. With its project (PASSIP) about to belaunched, the European Union could help in the health development of this region.
6. SUSTAINABILITY AND PROJECT RISKS
6.1 Recurrent Costs
The project essentially seeks to consolidate and rehabilitate existing infrastructure andservices. Thus the recurrent costs generated by the project will be limited and will be injectedmainly in the construction of the new HCs in Conakry and in Middle Guinea, as well as theputting in place and extension of training and further training centres for health personnel. Thetotal amount of recurrent costs over five years is about 366 million GNF (UA 0.22 million) i.e.around 73.4 million GNF per annum (UA 0.04 million). These recurrent costs will includetravel costs and supervision of health personnel, and a few functioning costs (fuel, supplies etc.)and maintenance costs. The recurrent costs generated by the project account for 0.26% of theoperating budget allocated to the MOH (28.3 billion GNF in 2000) and accounts for 0.01% ofthe State operating budget (505.8 billion GNF in 2000). All the health structures to be set upunder the project will be located in Conakry and in Middle Guinea and they will institute asystem of cost recovery that will generate additional income to the budget allocated by theState. These resources will help to meet recurrent costs. In 1998 the income generated by thecost recovery system amounted to 3.4 billion GNF obtained from the health centres and around2 billion GNF from hospitals. The most dynamic and organised health centres succeed infinancing the recruitment of support staff (maintenance personnel) and even purchase their ownmotorbikes. To this should be added the resources mobilised by private concerns for the healthof their workers and their families.
6.2 Sustainability of the Project
The project has not built a lot of new infrastructure and the majority of structuressupported by the project already exist and the activities fit perfectly into the work programmesof health personnel. The project will invest considerable resources in training, and in this waywill contribute in improving personnel skills whose work will have a positive impact on thequality of service provided and on the population’s health. The training of trainers in severalfields of activity will help to provide training on the cascade principle for other groups of healthpersonnel. On the project’s completion, these activities will be pursued and the project’simpact will in this way be sustained. The engineers and bio-medical assistants trained inmaintenance techniques will help in maintaining the bio-medical equipment of the Ministry ofHealth. The health structures built, rehabilitated and equipped will serve the populationsseveral years after the project’s completion and contribute in improving their state of health.Furthermore, the cost recovery system put in place makes it possible to generate financialresources to ensure the smooth functioning of health structures, except for salaries whichremain at the charge of the State. Community participation in decision-making in the

30
management of health services will facilitate ownership of the project’s realisations by thepopulations and ensure the sustainability of the services.
6.3 Critical Risks and Mitigation Measures
6.3.1 The project’s implementation is based on the following assumptions:
6.3.2 Household purchasing power does not decease in the next few years so much so thattheir participation is effective (and/or alternatives are put in place for meeting the health costsof deprived populations) and that the cost recovery of health services and medicine is pursuedin order to sustain the actions of priority health programmes. The Government is in process ofimplementing its poverty reduction policy, the outcome of which will contribute in increasingthe income of populations. Furthermore, the application of the essential medicines policyfacilitates the populations financial accessibility to medicines.
6.3.3 The budget allocations of the Ministry of Health have been increased in order to supportsocial sectors in the fight against poverty. In keeping with the priorities expressed by thepopulations during the consultations for the preparation of the strategy of assistance to Guineain 1997/98 the Government gave high priority to health and thus allocated considerableresources to the sector. From 1999 to 2000 the budget allocated to the MOH exclusive ofsalaries increased from 5% to 8% and attaining 10% as recommended by WHO. Besides, theGovernment will provide the estimated counterpart fund within the framework of the project.
6.3.4 Generic medicines are available; the Government has adopted a generic medicinespolicy and has set up two structures (the EVP/PHC unit and the CFG) responsible for supplyingthe EDs. The cost recovery of medicines is in effect in all the structures. The Government hasthe backing of various donors, of which the Bank, in its drive to implement its medicines policyand reduce to the minimum the frequent shortages.
6.3.5 Decision-making has effectively been decentralised and the out-reach services have beenprovided with the required resources to accomplish their mission. The pursual ofdecentralisation in the health systems management should be put into effect by the provision ofthe financial resources for the periphery. With the increase in budget allocations mentioned inparagraph 6.3.3, this risk will be lessened in that the budgets for regional inspectorates anddepartmental health directorates will augment. Besides, with its new poverty alleviationprogramme, the Government will provide stronger support to decentralised services.
6.3.6 The necessary personnel have effectively been transferred to the new structures builtunder the project. This risk will be lessened since it is among the preliminary conditions thatGovernment will have to fulfill before start up of the project.
7 ACHIEVEMENTS OF THE PROJECT
7.1 Economic Impact
7.1.1 The project has a considerable economic impact as illustrated by its components andactivities. Indeed, by saving lives and reducing the morbidity status of Guineans, the projectwill increase the productivity of individuals, and beyond, their contribution to the country’seconomy. The capacity building of health personnel will contribute in upgrading personnelboth in quality and in quantity, which personnel will improve upon services offered to thepopulations in general and to the deprived classes in particular. The project's support to

31
maintenance will help in the durableness of buildings and equipment, resulting in aconsiderable gain of resources which otherwise would have gone to waste for lack of preventiveand curative maintenance. The project will invest in peripheral health more effective thantertiary health and in essential generic medicines which have a higher impact than molecules.Community participation will increase ownership by the populations of the project’s activitiesand its economic impact.
7.1.2 The economic impact of the reduction of maternal and infantile mortality, ofSTDs/AIDS control and of the fight against malaria leaves no shadow of doubt. The findings ofthe Heads of State Summit on Malaria in Nigeria in April 2000, state that the annual loss ineconomic growth due to malaria (in endemic countries like Guinea) is roughly 1.3% per annum.This means that in 15 years, the Gross Domestic Product (GDP) of Guinea will decrease by20% of what it should have been without malaria. AIDS is no longer a health problem, but aneconomic problem. The improved health of deprived populations contributes in reducingpoverty at this level.
7.2 Social Impact
7.2.1 The Government’s goal with regard to poverty is to facilitate access of the mostdeprived to basic social services. Populations in the suburbs of Conakry and in Middle Guineahalf of whom are considered poor, will be the main beneficiaries of the project. The incidencerate of poverty in Middle Guinea is about 51%. The project will contribute to reducing povertyin the country and open up access to primary health care, especially in the poorest parts of thecountry. Again, by helping to upgrade health the project will help in enhancing the productivityof the populations and increase children’s enrolment who will spend less time at home becauseof their state of morbidity.
7.2.2 The project will have a remarkable impact on women by helping to reduce maternalmortality. The project will facilitate the access of health services to women and to children thatmake up the most vulnerable groups of society. The rehabilitation of health structures and theprovision of surgical services and training in midwifery will help to provide better care forwomen in the age of reproduction. In addition, the setting up of a radio-communication systemwithin the health structures and the procurement of an ambulance will facilitate the evacuationof women in labour to referral health structures. Around 600,000 women will benefit from theproject’s impact.
7.2.3 Investments in the construction, rehabilitation and equipping of health structures willenable the system to offer better health services. By providing its contribution to public healthtraining institutions and medical and para-medical specialisations, the project will help inenhancing the performance of the Guinean health system. Training activities will be a crucialfactor in motivating health personnel. The second factor of motivation is the improvedconditions of work provided by the project. Health agents, will, in this way devote themselvesto the service of the populations and so provide them with better treatment. The strengtheningof the district health system as envisaged by the project will provide the Government of Guineawith the best means to ensure effective health care for its populations, especially those living inthe project’s areas of intervention.8. CONCLUSIONS AND RECOMMENDATIONS
8.1 Conclusions

32
The project is in keeping with the national health policy and aims at improving the stateof health of Guineans in general, and more importantly that of the most deprived groups(women and children) in the periurban areas of Conakry and the poorest districts in MiddleGuinea. The project will focus on the development of basic health treatment with the view toincreasing the populations economic and geographical accessibility to this type of care. Theproject’s outcome will contribute in improving the health cover in Conakry and in MiddleGuinea by the opening of eight health centres and the rehabilitation of the district hospital,helping thus in upgrading the health of at least 600,000 women.
8.2 Recommendations and Conditionalities
In view of the foregoing it is recommended that a loan not exceeding UA 6.5 million,and a TAF grant in the amount of UA 0.6 million be granted to the Government of Guinea. Theloan will be subject to the general conditions of the Bank and to the following specificconditionalities:
A) Conditions precedent to the effectiveness of the loan agreement
The loan’s effectiveness is subject to the fulfilment by the Borrower of the conditionsprovided in section 5.01 of the General Conditions.
B) Conditions precedent to first disbursement
The ADF shall proceed with the first disbursement of the loan proceeds only if the Borrower,not withstanding the entry into force of this Agreement, shall have met the Fund’s satisfactionthe following conditions:
i) show proof of the establishment of the Project Coordination Unit (PCU) withinthe Ministry of Health and of the secondment of the required civil servants (aproject coordinator, a civil engineer, a procurement specialist) to work full timeon the project and ensure its smooth running. The qualifications and experiencesof the civil servants retained should be acceptable to the ADF (paragraph 5.1.1)
ii) show proof of the transfer of the former premises occupied by thePharmaceutical Sector Strengthening Project to the Project Coordination Unitproject placed under the authority of the Ministry of Health or of itsrepresentative (paragraph 4.5.19);
iii) show proof of the allocation of the land necessary for the construction of atraining centre and the new health infrastructure in Conakry, Tougué, Gaoualand Koundara (paragraphs 4.5.5 and 4.5.18);
iv) show proof of the opening of two accounts; (i) one account in the Central Bankof the Republic of Guinea for the annual deposit of the counterpart funds (ii)another in a commercial bank where the ADF and TAF resources will be paid(paragraph 5.5);
v) show proof of the setting up of a sub-committee comprising the technicaldirectorates directly involved in the implementing of the project’s activities(National Health Directorate, Department of Statistics, Engineering andInformation, DNP, CPG, National Directorate of Hospitals), a representative ofthe Ministry of the Economy, Finance and Planning, a representative from

33
UNICEF and from the WHO, a representative of NGOs, participating in the fightagainst STDs and AIDS (paragraph 5.2.1) ;
C) Other conditions
i) communicate to the Fund, latest six months after loan effectiveness, thenominative list of personnel that will be seconded to the training centre inConakry (paragraph 6.3.6);
ii) communicate to the Fund, three months prior to completion of the constructionworks of each health structure, the list of personnel for secondment to ensuretheir smooth functioning (paragraph 6.3.6);
iii) submit to the Fund, latest six months following loan effectiveness, the protocolof agreement with the WHO including a detailed training plan of overseastraining specifying the choice of institutions, candidates, training programmesand costs (paragraph 4.5.9);
iv) implement, latest by June 2002, the recommendations of the study on the supplysystems and distribution of essential medicines in Guinea (July 1999), and this,prior to the submission of the bidding documents on the procurement ofmedicines destined to replenish the stock of medicines to be provided to the CPG(paragraph 4.5.7).
v) communicate to the Fund, a copy of the protocol agreement signed with UNICEFregarding maternal mortality (including the local training of midwives) inGaoual, Koundara and Tougué (paragraph 5.2.6).

Republic of Guinea ANNEX 1HSSP/Health III MAP LOCATING PROJECT SITES
This map has been drawn exclusively for the use of the readers of the report to which it is attached. The names used and the borders shown do not imply on
the part of the Bank Group and its members any judgement concerning the legal status of a territory or any approval of acceptance of these borders.

ANNEX 2Page 1 of 1
Republic of GuineaHealth System Strengthening Project (Health III)
_
Organisation Chart of the Project Coordination Unit
Secretary General of MOH
Steering Committee
Strategic Training Unit
I
NDHs
I
Office of Secretary General
I
DNPL
I
Statistics Engineering and Inform.
I
Representative Unicef
I
Representative WHO
I
Representative NGO
I
NDH
I
CPG
Project Coordination
Coordinator
I
Secretary
I
Driver/Messenger
Accounting
Firm
Financial Administration
I
Accounts
Monitoring and Evaulation
Unit
Procurement of Furn (DIEM)
I
Procurement Specialist
I
Logistics (DIEM)
Technical Assistance
Project Management and
Monitoring
Project
Partners
WHO
NGO
Unicef/UNPRA


Republic of Guinea ANNEX 4HSSP Project/Health III Page 1/1
List of goods and services by category of expenditure(in UA million)
Sources of finance ______ ADF ______ Covt. ______ TAF ______ ______ Total ______ %
Category of expenditure F.E.. L.C. Tot. F.E.. L.C. L.C. Tot. F.E.. L.C. Tot. Tot.
A. ARCHIT.STUDIES, SUP. BC 0.15 - 0.15 - - - - 0.15 - 0.15 0.02
Cont. 0.01 - 0.01 - - - - 0.01 - 0.01
P.E. 0.01 - 0.01 - - - - 0.01 - 0.01
T.C. 0.17 - 0.17 - - - - 0.17 - 0.17
B. CONSTRUC. REHAB. BC 1.61 0.06 1.67 0.14 - - - 1.61 0.20 1.81 0.27
Cont. 0.16 0.01 0.17 0.01 - - - 0.16 0.02 0.18
P.E. 0.19 0.01 0.20 0.02 - - - 0.19 0.03 0.22
T.C. 1.96 0.08 2.04 0.17 - - - 1.96 0.25 2.21
C. FURNITURE BC 0.22 0.02 0.24 - - - - 0.22 0.02 0.24 0.04
Cont. 0.01 - 0.01 - - - - 0.01 - 0.01
P.E. 0.03 - 0.03 - - - - 0.03 - 0.03
T.C. 0.26 0.02 0.28 - - - - 0.26 0.02 0.28
D. EQUIPMENT BC 1.58 - 1.58 - - - - 1.58 - 1.58 0.23
Cont. 0.08 - 0.08 - - - - 0.08 - 0.08
P.E. 0.17 - 0.17 - - - - 0.17 - 0.17
T.C. 1.83 - 1.83 - - - - 1.83 - 1.83
E. MEDICINES BC 0.37 - 0.37 - - - - 0.37 - 0.37 0.05
Cont. - - - - - - - - - -
P.E. 0.02 - 0.02 - - - - 0.02 - 0.02
T.C. 0.39 - 0.39 - - - - 0.39 - 0.39
F. TECH. ASSISTANCE BC 0.71 - 0.71 - - - - 0.71 - 0.71 0.11
Cont. 0.03 - 0.03 - - - - 0.03 - 0.03
P.E. 0.09 - 0.09 - - - - 0.09 - 0.09
T.C. 0.83 - 0.83 - - - - 0.83 - 0.83
G. TRAINING BC 0.12 0.32 0.44 - 0.52 - 0.52 0.64 0.32 0.96 0.14
Cont. - 0.02 0.02 - 0.03 - 0.03 0.03 0.02 0.05
P.E. 0.02 0.04 0.06 - 0.05 - 0.05 0.07 0.04 0.11
T.C. 0.14 0.38 0.52 - 0.60 - 0.60 0.74 0.38 1.12
H. OPERATING COSTS BC 0.26 0.06 0.32 0.54 - - - 0.26 0.60 0.86 0.13
Cont. - - - 0.04 - - - - 0.04 0.04
P.E. 0.03 0.00 0.03 0.04 - - - 0.03 0.04 0.07
T.C. 0.29 0.06 0.35 0.62 - - - 0.29 0.68 0.97
I. AUDIT BC 0,08 - 0,08 - - - - 0.08 - 0.08 0.01
Cont. - - - - - - - - - -
P.E. 0,01 - 0,01 - - - - 0.01 - 0.01
T.C. 0,09 - 0,09 - - - - 0.09 - 0.09
Total BC 5.10 0.46 5.56 0.68 0.52 - 0.52 5.62 1.14 6.76 1.00
Cont. 0.29 0.03 0.32 0.05 0.03 - 0.03 0.32 0.08 0.40
P.E. 0.57 0.05 0.62 0.06 0.05 - 0.05 0.62 0.11 0.73
T.C. 5.96 0.54 6.50 0.79 0.60 - 0.60 6.56 1.33 7.89
BC: Base CostCont.: ContingenciesP.E.: Price EscalationT.C.: Total Cost

ANNEX 5Page 1 of 1
Republic of Guinea
HSSP/Health III
CONTENTS OF IMPLEMENTATION MANUAL
Chapter 1 Presentation of Project
Chapter 2 Institutional Framework
Chapter 3 Elaboration procedure of plans of operation
Chapter 4 Procedures for procurement of goods and services
Chapter 5 Financial procedures
Chapter 6 Monitoring and accounting procedures
Chapter 7 Monitoring operations
Annexes
Annex 1 Detailed implementation schedule of project monitoring and evaluationAnnex 2 TOR of experts (personnel of PCU and Technical assistance)Annex 3 TOR of execution partners (WHO and UNICEF)Annex 4 Detailed CostsAnnex 5 Invitation to tenders, standard bidding documentsAnnex 6 Bidding documents – procurement for suppliesAnnex 7 Bidding documents – procurement for worksAnnex 8 Architectural worksAnnex 9 Supervision Plan
Copyright © 2022 FDOKUMEN




















