
Ecdysone agonist inducible transcription in transgenic tobacco plants

1
Title: GnRH agonist during luteal phase for women undergoing assisted reproductive techniques:
systematic review and meta-analysis of randomized controlled trials
Short title: GnRH agonist during luteal phase support
Authors: Wellington P Martins, Rui A Ferriani, Paula A Navarro, Carolina O Nastri
Affiliation: Department of Obstetrics and Gynecology, Ribeirao Preto Medical School, University of Sao
Paulo (DGO-FMRP-USP), Ribeirao Preto, Brazil
Correspondence: Wellington P Martins. Address: Av. Bandeirantes, 3900 – 8 andar - HCRP - Campus
Universitario; City: Ribeirao Preto; State: Sao Paulo; Country: Brazil; Postal code: 14048-900. Phone:
+55(16)3602-2583; Fax: +55(16)3633-0946; E-mail: [email protected].

2
Abstract
Objective: To identify, appraise and summarize the available evidence regarding the effectiveness and
safety of adding GnRH agonist during luteal phase for women undergoing assisted reproductive techniques.
Methods: In this systematic review and meta-analysis, we searched for randomized controlled trials
(RCTs) comparing the addition of GnRH agonist during luteal phase compared with standard luteal phase
support. We searched seven electronic databases and hand-searched the reference list of included studies
and related reviews. Our primary outcome was live birth or ongoing pregnancy per randomized woman. Our
secondary outcomes were clinical pregnancy per randomized woman; miscarriage per clinical pregnancy;
adverse perinatal outcome; and congenital malformations.
Results: The evidence from 10 studies examining 3,056 women showed a relative risk (RR) for Live Birth
or Ongoing Pregnancy = 1.26; 95% CI = 1.04-1.53; I² = 58%. Sensitivity analysis excluding the studies that did
not report live birth and those at high risk of bias resulted in one study examining 181 women with a RR =
1.07; 95% CI = 0.73-1.58. Subgroup analysis separating the studies by single/multiple doses of GnRH agonists
or by ovarian stimulation with GnRH agonist/antagonist was not able to explain the observed heterogeneity.
The quality of the evidence was deemed to be very low: it was downgraded because of the limitation of the
included studies, imprecision, inconsistency across the studies’ results, and suspicion of publication bias.
None of the included studies reported adverse perinatal outcomes or congenital malformations.
Conclusion: There is evidence that adding GnRH agonist during luteal phase improves ongoing pregnancy.
However, this evidence is of very low quality and there is no evidence about adverse perinatal outcomes and
congenital malformations. We therefore believe that including this intervention on clinical practice would be
still premature.
Keywords: Luteal phase support; Infertility; Subfertility; IVF; ICSI; Assisted Reproduction.
3
Introduction
Assisted reproductive techniques (ART) frequently involve controlled ovarian stimulation (COS) aiming
the development of multiple follicles and, ultimately, the formation of multiple embryos to improve efficacy
of the treatment. The recruitment of multiple follicles boosts the estradiol production, and abnormally high
levels of estrogen are observed during COS. After aspiration of these follicles, multiple corpora lutea are
formed, which keeps on the abnormally high production of steroids 1, 2. In a natural pregnancy, LH is
continuously produced after the ovulation surge and only decreases when human chorionic gonadotropin
(hCG) from the growing throphoblast takes over. Conversely, in ART cycles, the high steroid levels exert a
negative feedback in the pituitary gland prematurely inhibiting the production of LH 2. The consequence is
the shortening of the luteal phase, a situation called premature luteolysis 1.
To overcome this issue, a pharmacological support during the luteal phase is used to improve pregnancy
rates. Many combinations of estradiol, progesterone, and hCG are frequently used to enhance directly or
indirectly the low progesterone level 3. More recently, gonadotropin-releasing hormone (GnRH) agonist was
introduced for luteal phase support 4, 5. The first hypothesis is that the GnRH agonist could extend LH
production throughout the luteal phase thus preventing the occurrence of premature luteolysis and
consequently improving pregnancy rates 1. Nonetheless, it was observed that a single GnRH agonist dose by
the time of implantation could improve pregnancy rate in recipients after artificial endometrial preparation
with GnRH down regulation followed by estrogen and progesterone 5. The increase in pregnancy rate in
recipients without corpus luteum lead to the hypothesis of a direct effect of the agonist on the early embryo
2, 5; although a direct effect on the endometrium cannot be ruled out. Evidence from in vitro studies suggest
that GnRH agonist acts directly on the preimplantation embryos as its receptor is extensively expressed in
human morula and blastocyst embryos 6. Porcine and murine preimplantation embryo development is
enhanced when embryos are incubated with GnRH agonists and diminished when incubated with antagonist
7, 8.

4
Because of the potential embryonic/fetal effects, adverse perinatal outcomes and congenital
malformations are important safety outcomes, and they have been scarcely reported. Although the lack of
information regarding the fetal safety of GnRH agonist use in early pregnancy and an apparent inconsistency
among the clinical studies’ results, three previous systematic reviews concluded that there was a benefit
from the intervention 1, 9, 10. This intervention has been subject of intensive study and new data are emerging
pointing out the need of a comprehensive and judicious systematic review of the literature 11. The objective
of the present systematic review and meta-analysis is to identify, appraise and summarize the evidence from
randomized controlled trials examining and weighing the efficacy and safety of using GnRH agonist during
the luteal phase.

5
Material and Methods
Protocol registration
The protocol of this review was registered on the International prospective register of systematic reviews
(PROSPERO): CRD42014014895.
Eligibility criteria
Study design: Parallel group and cross-over randomized controlled trials (RCTs) were considered eligible. If
a cross-over trial is included, only data from the first treatment of each participant would be considered for
analysis. We didn’t include pseudo-randomized studies or studies that randomized embryos or oocytes.
Participants: Women undergoing ART; studies examining women undergoing IUI or timed-intercourse were
not included. Interventions: Addition of GnRH agonist during luteal phase compared with standard luteal
phase support and no other relevant difference between intervention and control group.
Information sources and search strategy
We searched for published studies in the following electronic databases: Cochrane Central Register of
Controlled Trials (CENTRAL), PubMed, and Scopus. We searched for study protocols on the following
databases: Current Controlled Trials (www.controlled-trials.com), ClinicalTrials.gov
(http://clinicaltrials.gov/ct2/search), and the World Health Organization International Clinical Trials Registry
Platform search portal (http://apps.who.int/trialsearch/Default.aspx). We searched for conference abstracts
on Web of Science. Additionally we hand-searched the reference list of included studies and related reviews.
The following terms were used, adjusting for each database as necessary: ((in vitro fertilization) OR (IVF)
OR (intracytoplasmic sperm) OR (ICSI) OR (embryo) OR (blastocyst)) AND ((Agonist) OR (Buserelin) OR
(Goserelin) OR (Leuprolide) OR (Nafarelin) OR (Triptorelin)) AND (luteal) AND (random* OR trial). We did not
impose any publication date or language limits for the searches.
Study selection

6
Titles and abstracts were reviewed independently by two review authors (CON and WPM) checking for
duplicates and using the pre-established criteria for inclusion. These authors retrieved the full-text
manuscripts of trials considered to be potentially eligible for inclusion and independently evaluated eligibility
of these trials. Disagreements were solved by consensus. We corresponded with study investigators as
required, to clarify study eligibility. There was no limitation on language, publication date or publication
status.
Data collection process
We extracted data from included trials using a data extraction form designed and pilot-tested by the
authors. In the cases we identified a study with multiple records (e.g. publication, abstract, protocol
registration), we used the main trial report as reference and additional details could be supplemented from
secondary sources. We corresponded with study investigators in order to solve any query, as required. Data
were extracted independently in a standardized manner by two authors (CON and WPM); disagreements
were solved by consensus.
Data items
Study characteristics: authors; country; institution; funding sources; conflicts of interest; informed
consent; ethical approval; study design; period of enrollment; eligibility criteria; number of participants in
each group at each stage; age and BMI (mean ± SD) of participants; number of oocytes retrieved; number of
embryos transferred per woman; and implantation rate.
Primary outcomes: Live birth / ongoing pregnancy per randomized woman (birth of twins/triplets will be
counted as a single live birth). We preferentially used data for live birth; however, when live birth was not
reported, we used data for ongoing pregnancy (intrauterine live fetus with a gestational age ≥ 12 weeks) as a
surrogate for live birth, since the difference between ongoing pregnancy and live birth is frequently not large,
as less than 1% of the pregnancies will result in a stillbirth 12, 13.
Secondary outcomes: Clinical pregnancy per randomized woman (ultrasonographic visualization of one or
more gestational sacs or definitive clinical signs of pregnancy); miscarriage per clinical pregnancy (single fetal

7
demise in twins or triplet pregnancies will not be counted as a miscarriage); adverse perinatal outcome
(gestational diabetes, pregnancy-induced hypertension, pre-eclampsia, large or small for gestational age,
preterm birth, acidosis, intensive care unit admission, and pre- and perinatal mortality); and congenital
malformations.
Dealing with missing data: When miscarriage was not reported but authors reported clinical pregnancy
and ongoing pregnancy, the number of miscarriages was considered as being equal to the difference
between the number of clinical pregnancies and ongoing pregnancies.
Risk of bias in individual studies
Two authors (CON and WPM) independently assessed the risk of selection bias; performance bias;
detection bias; attrition bias; reporting bias; and other potential sources of bias (e.g. difference in the
number of embryos transferred, age of participants, co-interventions, early stopping). We did not consider
that blinding is likely to influence the risk of performance and detection bias for the review outcomes.
Disagreements were solved by consensus. To judge the risk of bias, we followed The Cochrane
Collaboration's criteria for judging risk of bias 14: the studies were classified as being of 'low', 'high' or
'unclear' risk of bias.
Summary measures
The effects of the intervention were summarized as risk ratio (RR) and the precision of the estimates were
evaluated by the 95% CI. We considered the clinical relevance of all comparisons taking into account the
precision of the estimates; we determined the number needed to treat for an additional beneficial outcome
(NNTB) or an additional harmful outcome (NNTH) when a significant difference was observed.
Synthesis of results
All results were combined for meta-analysis using Review Manager 5.3 (Copenhagen: The Nordic
Cochrane Centre, The Cochrane Collaboration, 2014). Heterogeneity was assessed subjectively and by the I²
statistic. An increase in the risk of a particular outcome, which may be beneficial (e.g. live birth) or

8
detrimental (e.g. miscarriage), was displayed graphically in the meta-analyses to the right of the center line
and a decrease in the risk of an outcome to the left of the center line.
Risk of bias across studies
In view of the difficulty of detecting and correcting for publication bias and other reporting biases, the
authors tried to minimize their potential impact by ensuring a comprehensive search for eligible studies and
by being alert for duplication of data. A funnel plot was planned to be used only if ten or more studies were
included to explore the possibility of small study effects (a tendency for estimates of the intervention effect
to be more beneficial in smaller studies). However, it was not employed since only 7 studies were included.
Additional analyses
We performed sensitivity analysis to verify whether the conclusions would be different if eligibility was
restricted to studies at low risk of bias and if data for ongoing pregnancy was not pooled with live birth.
In order to examine the observed heterogeneity, we performed two subgroup analyses separating the
studies by:
- Single vs. Multiple doses of GnRH agonist;
- Agonist vs. Antagonist protocol.
Overall quality of the body of evidence
A table was generated to summarize the review findings. The quality of evidence for the main outcomes
was evaluated using the following the Grading of Recommendations Assessment, Development and
Evaluation (GRADE) Working Group recommendation 15: we considered the limitations of included studies,
inconsistency of effect, imprecision, indirectness, and risk of publication bias.
The quality of the evidence (and its interpretation) was judged as follow: High quality = Further research is
very unlikely to change our confidence in the estimate of effect; Moderate quality = Further research is likely
to have an important impact on our confidence in the estimate of effect and may change the estimate; Low
quality = Further research is very likely to have an important impact on our confidence in the estimate of

9
effect and is likely to change the estimate; Very low quality = We are very uncertain about the estimate. The
judgments about evidence quality were justified, documented and incorporated into the reporting of results
for each outcome.

10
Results
Study selection
The electronic search was last run in Mar-22-2015 and a total of 882 records were retrieved: CENTRAL =
189; PubMed = 216; Scopus = 406; Web of Science = 23; ClinicalTrials.gov = 48; Current Controlled-trials = 0;
WHO ICTRP = 0. One additional record was retrieved through manual search of reference lists of potentially
eligible studies and related reviews. Therefore 883 records were assessed for eligibility; we removed 860
records on the basis of title and abstract: there were 334 duplicates and 526 records clearly did not meet the
eligibility criteria. We further examined 23 records for eligibility:
- 10 studies (from 12 records) were included in this review: 2 studies with 2 records each 16-18 and more 8
studies with one record each 11, 19-25.
- 5 studies (from 5 records) are awaiting classification: there are 4 ongoing studies 26-29 and 1 study with
unknown status 30.
- 6 studies (from 7 records) were excluded: 3 studies (from 3 records) were not randomized or were
pseudo-randomized 4, 5, 31; 1 study (from 1 record) examined only women undergoing IUI 32; 1 study (from 2
records) was excluded because the triggering was performed with GnRHa in the intervention group and with
hCG in the control group 33, 34; 1 study (from1 record) was terminated without results 35.
The study flow diagram is presented in Figure 1.
Study characteristics and participants
The characteristics of the 10 studies including eligibility criteria are reported in Table 1.
Outcomes
- 8/10 studies reported either live birth or ongoing pregnancy: 3 studies reported live birth 16, 20, 24; and 5
studies reported ongoing pregnancy 11, 17, 19, 22, 23;
- 10/10 studies reported clinical pregnancy;
- Data for miscarriage were retrieved from 8/10 studies: 3 studies reported miscarriage 19, 20, 23 and in the

11
other 5 studies we determined the number of miscarriages as being equal to the difference between clinical
pregnancy and ongoing pregnancy or live birth 11, 16, 17, 22, 24.
- No study reported adverse perinatal outcomes or congenital malformations.
Risk of bias within studies
- 5/10 studies 16, 19, 23, 24 were considered to be at unclear risk of selection bias because although they used
computer generated randomization, there were no details regarding allocation concealment. The other 5/10
studies were considered to be at low risk of selection bias. Blinding was not considered to be relevant for the
reproductive outcomes evaluated.
- 3/10 studies 20, 23, 24 were considered to be at high risk of attrition bias: one study recruited 234 women,
but analyzed only 120 without providing reasons 20; one study lost follow up of 9.8% of the participants in
the intervention group and of 2.4% in the control group 24; one lost follow up of 16% in one of the study
arms and of 5% of the control group 23; the other 6/9 studies were considered to be at low risk of attrition
bias.
- 10/10 studies were considered to be at low risk of performance, detection, reporting, and other source
of bias.
- 1/10 studies 11 was judged to be at unclear risk of other bias, as women in the control group had slightly
higher age and body mass index.
Results of individual studies
The results of individual studies are presented in Figures 2-4.
Synthesis of results
Live birth / ongoing pregnancy (Supplemental Figure 1): The evidence from 8 studies examining 2,776
women showed a RR = 1.26; 95% CI = 1.04-1.53; I² = 58%. Sensitivity analysis excluding the studies not
reporting live birth and those at high risk of bias resulted in one study examining 181 women with a RR =
1.07; 95% CI = 0.73-1.58. Subgroup analysis separating the studies by single or multiple doses of GnRH

12
agonists was not able to explain the observed heterogeneity (Supplemental Figure 2). In the same way,
subgroup analysis separating the studies by agonist and antagonist cycles was not able to explain the
observed heterogeneity (Figure 2); however, all the studies that did not observe any benefit of using GnRH
agonist during luteal phase were those using an agonist protocol for controlled ovarian stimulation; while
the two studies examining this intervention in GnRH antagonist protocol observed more ongoing
pregnancies in the intervention group (Figure 2).
Clinical pregnancy (Figure 3): The evidence from 10 studies examining 3,056 women showed a RR = 1.28;
95% CI = 1.08-1.52; I² = 61%. Sensitivity analysis excluding the studies at high risk of bias resulted in 7 studies
examining 2,503 women with a RR = 1.15; and 95% CI = 0.98-1.34; I² = 49%.
Miscarriage (Figure 4): The evidence from 8 studies examining 1,077 clinical pregnancies showed a RR =
0.82; 95% CI = 0.60-1.10; I² = 26%. Sensitivity analysis excluding the studies at high risk of bias resulted in 5
studies examining 892 clinical pregnancies with a RR = 0.92; and 95% CI = 0.72-1.19; I² = 0%.
Risk of bias across studies
Small study effect was suspected because the studies suggesting benefit of the intervention were the
most imprecise while the most precise studies suggested no effect; and also, there is no imprecise study
pointing to “harm” (Supplemental Figure 3). The funnel plot analysis for the only outcome reported by all 10
studies – clinical pregnancy – showed a clear asymmetry, highly suggestive of publication bias.
Additional analysis
Sensitivity analysis and subgroup analyses were reported along with the synthesis of the results.

13
Discussion
Summary of the evidence
In despite of the relatively large number of studies and participants included, we are still very uncertain
about the estimate of the effect and its precision (Table 2). The results of the individual studies are
inconsistent, which translates both into substantial heterogeneity and into a large confidence interval. We
also suspected that the dissemination of research findings could have been influenced by the nature and
direction of results. The included studies partially answered the review question, as no data regarding fetal
safety was identified.
Quality of the evidence
The quality of the evidence for Live birth/Ongoing Pregnancy and Clinical Pregnancy was downgraded for
four reasons. Firstly, the RCTs included in the present review presented serious limitations and only two
from the ten included studies were deemed at low risk of bias in every domain. Only one study reporting
Live Birth was considered to be at low risk of bias, and the estimate of this single study suggests no effect
against a benefit of the intervention when considering data from all studies. The estimate for Clinical
Pregnancy considering only the studies not at high risk of bias suggests no effect against a benefit of the
intervention when considering data from all studies. Secondly, the quality was downgraded in one level
because of imprecision: although there is a relatively large number of participants and events, the 95% CI of
the relative risk and of the NNTB are wide (Table 2), not being sufficiently precise to ascertain whether the
benefit would be clinically irrelevant or large. The third reason for downgrading was the unexplainable
inconsistency across studies: some precise studies had observed no effect whether other had observed a
benefit of the intervention. Lastly, the quality was downgraded because of a strong suspicion of publication
bias.
The quality of the evidence for Miscarriage was downgraded one level because of limitations of the
studies included in this review. It was also downgraded two levels because of serious imprecision: the
14
number of events was low (less than 100 per group) and the 95% CI of the relative risk (0.56-1.14) is very
wide, not being sufficiently precise to ascertain whether there is a large benefit or a small harm.
Agreements and disagreements with other studies
We found three other reviews on this subject published a few years ago 1, 9, 10. Overall, we adopted more
strict eligibility criteria allowing the inclusion of only truly randomized studies in which the studied groups
differed only in the use of GnRh agonist in the luteal phase; in order to obtain a meaningful conclusion.
Evidence in this field is emerging quickly, and the four new RCTs we found and included in this update are
responsible for 40.6% of the weight in the estimates and for the inclusion of 1,251 women.
And still, evidence regarding its safety is scarce. Although GnRH agonist for luteal support does not seem
to affect the risk of miscarriage, no study reported the occurrence of congenital malformations. Although
there are some reports of lack of effect on pregnancy outcomes when GnRH agonist was inadvertent
administrated during early pregnancy 34, the use during pregnancy is contra-indicated by the manufacturer
laboratory (Suprecur®, Sanofi-Aventis, Frankfurt, Germany).
The evidence available at the present does not allow us to ascertain which would be the most likely
mechanism of action of GnRH during the luteal phase. When observing the subgroup analysis in Figure 2, we
have that, in spite of a marginally significant benefit in the subgroup ‘Antagonist protocol’, this subgroup is
not different from the subgroup ‘Agonist protocol’; P = 0.20. However, only two small studies used
antagonist protocol for COS. Considering that the premature luteolysis could be an important issue to
overcome; cycles in which the pituitary function is blocked with GnRH antagonists would be more likely to
benefit from GnRH agonist in the luteal phase than those cycles in which the pituitary function is blocked by
GnRH agonist.
Nevertheless, the hypothesis of a direct effect of GnRH agonist on the embryo is supported by in vitro 6-8
and clinical findings 5. Evidence compiled in this meta-analysis does not allow us to either corroborate or
undermine such hypothesis; which brings about the need of evaluating safety outcomes before using the
intervention in clinical practice.

15
Conclusions
There is very low quality evidence that adding GnRH agonist during luteal phase improves ongoing and
clinical pregnancy, particularly in antagonist cycles. Nevertheless, there is no evidence about its safety,
considering both adverse perinatal outcomes and congenital malformations. Given the biological rationale,
future studies could focus in stablishing the effect of the intervention in cycles using antagonist protocols for
COS. We therefore believe that including this intervention in clinical practice without more studies would be
premature. This review should be updated in the near future as there are a few ongoing studies examining
this intervention.

16
Authors’ role:
WPM: Study conception and design; Data acquisition and analysis; Interpretation of the results; Drafting
the manuscript; Final approval; Agreement to be accountable for all aspects of the work in ensuring that
questions related to the accuracy or integrity of any part of the work are appropriately investigated and
resolved.
PAN: Interpretation of the results; Revising the manuscript critically for important intellectual content;
Final approval; Agreement to be accountable for all aspects of the work in ensuring that questions related to
the accuracy or integrity of any part of the work are appropriately investigated and resolved.
RAF: Interpretation of the results; Revising the manuscript critically for important intellectual content;
Final approval; Agreement to be accountable for all aspects of the work in ensuring that questions related to
the accuracy or integrity of any part of the work are appropriately investigated and resolved.
CON: Data acquisition and analysis; Interpretation of the results; Revising the manuscript critically for
important intellectual content; Final approval; Agreement to be accountable for all aspects of the work in
ensuring that questions related to the accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Acknowledgements: We would like to thank Dr Abha Majumdar and Dr Abdelhamid Benmachiche who
have kindly provided additional information regarding their studies.
Funding: Medical School of Ribeirao Preto, University of Sao Paulo (FMRP-USP), Brazil; The National
Council for Scientific and Technological Development (CNPq), Brazil; Foundation to Support Education,
Research and Care, University Hospital, Medical School of Ribeirao Preto, University of Sao Paulo (FAEPA),
Brazil. The funders had no role in study design, data collection and analysis, decision to publish, or
preparation of the manuscript.
Conflict of interests: None declared.

17
References
1. van der Linden M, Buckingham K, Farquhar C, Kremer JA, Metwally M. Luteal phase support for
assisted reproduction cycles. Cochrane Database Syst Rev 2011; CD009154.
2. Fatemi HM. The luteal phase after 3 decades of IVF: what do we know? Reprod Biomed Online 2009;
19 Suppl 4: 4331.
3. Gizzo S, Andrisani A, Esposito F, Noventa M, Di Gangi S, Angioni S, Litta P, Gangemi M, Nardelli GB.
Which luteal phase support is better for each IVF stimulation protocol to achieve the highest pregnancy
rate? A superiority randomized clinical trial. Gynecol Endocrinol 2014; 1-7.
4. Fujii S, Sato S, Fukui A, Kimura H, Kasai G, Saito Y. Continuous administration of gonadotrophin-
releasing hormone agonist during the luteal phase in IVF. Hum Reprod 2001; 16: 1671-1675.
5. Tesarik J, Hazout A, Mendoza C. Enhancement of embryo developmental potential by a single
administration of GnRH agonist at the time of implantation. Hum Reprod 2004; 19: 1176-1180.
6. Casan EM, Raga F, Polan ML. GnRH mRNA and protein expression in human preimplantation
embryos. Mol Hum Reprod 1999; 5: 234-239.
7. Nam DH, Lee SH, Kim HS, Lee GS, Jeong YW, Kim S, Kim JH, Kang SK, Lee BC, Hwang WS. The role of
gonadotropin-releasing hormone (GnRH) and its receptor in development of porcine preimplantation
embryos derived from in vitro fertilization. Theriogenology 2005; 63: 190-201.
8. Raga F, Casan EM, Kruessel J, Wen Y, Bonilla-Musoles F, Polan ML. The role of gonadotropin-
releasing hormone in murine preimplantation embryonic development. Endocrinology 1999; 140: 3705-
3712.
9. Kyrou D, Kolibianakis EM, Fatemi HM, Tarlatzi TB, Devroey P, Tarlatzis BC. Increased live birth rates
with GnRH agonist addition for luteal support in ICSI/IVF cycles: a systematic review and meta-analysis. Hum
Reprod Update 2011; 17: 734-740.
10. Oliveira JB, Baruffi R, Petersen CG, Mauri AL, Cavagna M, Franco JG, Jr. Administration of single-dose
GnRH agonist in the luteal phase in ICSI cycles: a meta-analysis. Reprod Biol Endocrinol 2010; 8: 107.

18
11. Aboulghar MA, Marie H, Amin YM, Aboulghar MM, Nasr A, Serour GI, Mansour RT. GnRH agonist
plus vaginal progesterone for luteal phase support in ICSI cycles: a randomized study. Reprod Biomed Online
2015; 30: 52-56.
12. Gordon A, Raynes-Greenow C, McGeechan K, Morris J, Jeffery H. Risk factors for antepartum
stillbirth and the influence of maternal age in New South Wales Australia: a population based study. BMC
Pregnancy Childbirth 2013; 13: 12.
13. Reddy UM, Laughon SK, Sun L, Troendle J, Willinger M, Zhang J. Prepregnancy risk factors for
antepartum stillbirth in the United States. Obstet Gynecol 2010; 116: 1119-1126.
14. Higgins J, Green S. (editors). Cochrane Handbook for Systematic Reviews of Interventions Version
5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-
handbook.org.
15. Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, Norris S, Falck-Ytter Y, Glasziou P, DeBeer H,
Jaeschke R, Rind D, Meerpohl J, Dahm P, Schunemann HJ. GRADE guidelines: 1. Introduction-GRADE
evidence profiles and summary of findings tables. Journal of clinical epidemiology 2011; 64: 383-394.
16. Isikoglu M, Ozgur K, Oehninger S. Extension of GnRH agonist through the luteal phase to improve the
outcome of intracytoplasmic sperm injection. J Reprod Med 2007; 52: 639-644.
17. Ata B, Yakin K, Balaban B, Urman B. GnRH agonist protocol administration in the luteal phase in ICSI-
ET cycles stimulated with the long GnRH agonist protocol: a randomized, controlled double blind study. Hum
Reprod 2008; 23: 668-673.
18. Ozgur K, Isikoglu M, Seleker M. Continuation of gonadotropin releasing hormone agonist during the
luteal phase in in vitro fertilization patients: is it beneficial? Fertility and Sterility 2002; 78: S53.
19. Inamdar DB, Majumdar A. Evaluation of the impact of gonadotropin-releasing hormone agonist as an
adjuvant in luteal-phase support on IVF outcome. J Hum Reprod Sci 2012; 5: 279-284.
20. Qublan H, Amarin Z, Al-Qudah M, Diab F, Nawasreh M, Malkawi S, Balawneh M. Luteal phase
support with GnRH-a improves implantation and pregnancy rates in IVF cycles with endometrium of <or=7
mm on day of egg retrieval. Hum Fertil 2008; 11: 43-47.

19
21. Razieh DF, Maryam AR, Nasim T. Beneficial effect of luteal-phase gonadotropin-releasing hormone
agonist administration on implantation rate after intracytoplasmic sperm injection. Taiwan J Obstet Gynecol
2009; 48: 245-248.
22. Tesarik J, Hazout A, Mendoza-Tesarik R, Mendoza N, Mendoza C. Beneficial effect of luteal-phase
GnRH agonist administration on embryo implantation after ICSI in both GnRH agonist- and antagonist-
treated ovarian stimulation cycles. Hum Reprod 2006; 21: 2572-2579.
23. Yildiz GA, Sukur YE, Ates C, Aytac R. The addition of gonadotrophin releasing hormone agonist to
routine luteal phase support in intracytoplasmic sperm injection and embryo transfer cycles: a randomized
clinical trial. Eur J Obstet Gynecol Reprod Biol 2014; 182C: 66-70.
24. Isik AZ, Caglar GS, Sozen E, Akarsu C, Tuncay G, Ozbicer T, Vicdan K. Single-dose GnRH agonist
administration in the luteal phase of GnRH antagonist cycles: a prospective randomized study. Reprod
Biomed Online 2009; 19: 472-477.
25. Zafardoust S, Jeddi-Tehrani M, Akhondi MM, Sadeghi MR, Kamali K, Mokhtar S, Badehnoosh B,
Arjmand-Teymouri F, Fatemi F, Mohammadzadeh A. Effect of administration of single dose GnRH agonist in
luteal phase on outcome of ICSI-ET cycles in women with previous history of IVF/ICSI failure: A randomized
controlled trial. J Reprod Infertil 2015; 16: 116-120.
26. Benmachiche A, Boularak A. Luteal Supplementation With GnRH-agonist After GnRH-agonist
Triggering in Combination With Low Dose HCG in IVF. ClinicalTrials.gov 2014; NCT02053779.
27. QFS. GnRH Agonist and Progesterone Versus Progesterone Only for Luteal Phase Support in
Antagonist Cycles (GALA). ClinicalTrials.gov 2014; NCT02262416.
28. Cengaver N. The Effect of GnRH Agonist Administered in the Luteal Phase on ART Cycle Outcomes.
ClinicalTrials.gov 2014; NCT02114645.
29. Brigante CMM, Mignini Renzini M, Dal Canto M, Coticchio G, Comi R, Fadini R. Efficacy of luteal
phase support with GnRH agonists: a preliminary comparative study. Fertility and Sterility 2013; 100: S299.
30. Tsafrir A, Margalioth E. Luteal-Phase GnRH Agonist Administration in Frozen-Thawed IVF Embryo
Transfer Cycles. ClinicalTrials.gov 2007; NCT00542126.

20
31. AboHamila F, Maged A, AboulFoutouh I. Progesterone supplementation is just enough for luteal
phase support in ICSI cycles. KAJOG 2011; 2: 14-19.
32. Bellver J, Labarta E, Bosch E, Melo MA, Vidal C, Remohi J, Pellicer A. GnRH agonist administration at
the time of implantation does not improve pregnancy outcome in intrauterine insemination cycles: a
randomized controlled trial. Fertil Steril 2010; 94: 1065-1071.
33. Loumaye E, Pirard C, Donnez J. GnRH agonist as a novel luteal support: Results of a pilot study. Hum
Reprod 2004; 19: i4.
34. Pirard C, Donnez J, Loumaye E. GnRH agonist as luteal phase support in assisted reproduction
technique cycles: results of a pilot study. Hum Reprod 2006; 21: 1894-1900.
35. Ata B, Urman B. Single Dose Gonadotropin-releasing Hormone (GnRH) Agonist Administration in the
Luteal Phase of GnRH Antagonist Stimulated ICSI-ET Cycles. ClinicalTrials.gov 2009; NCT01007851.
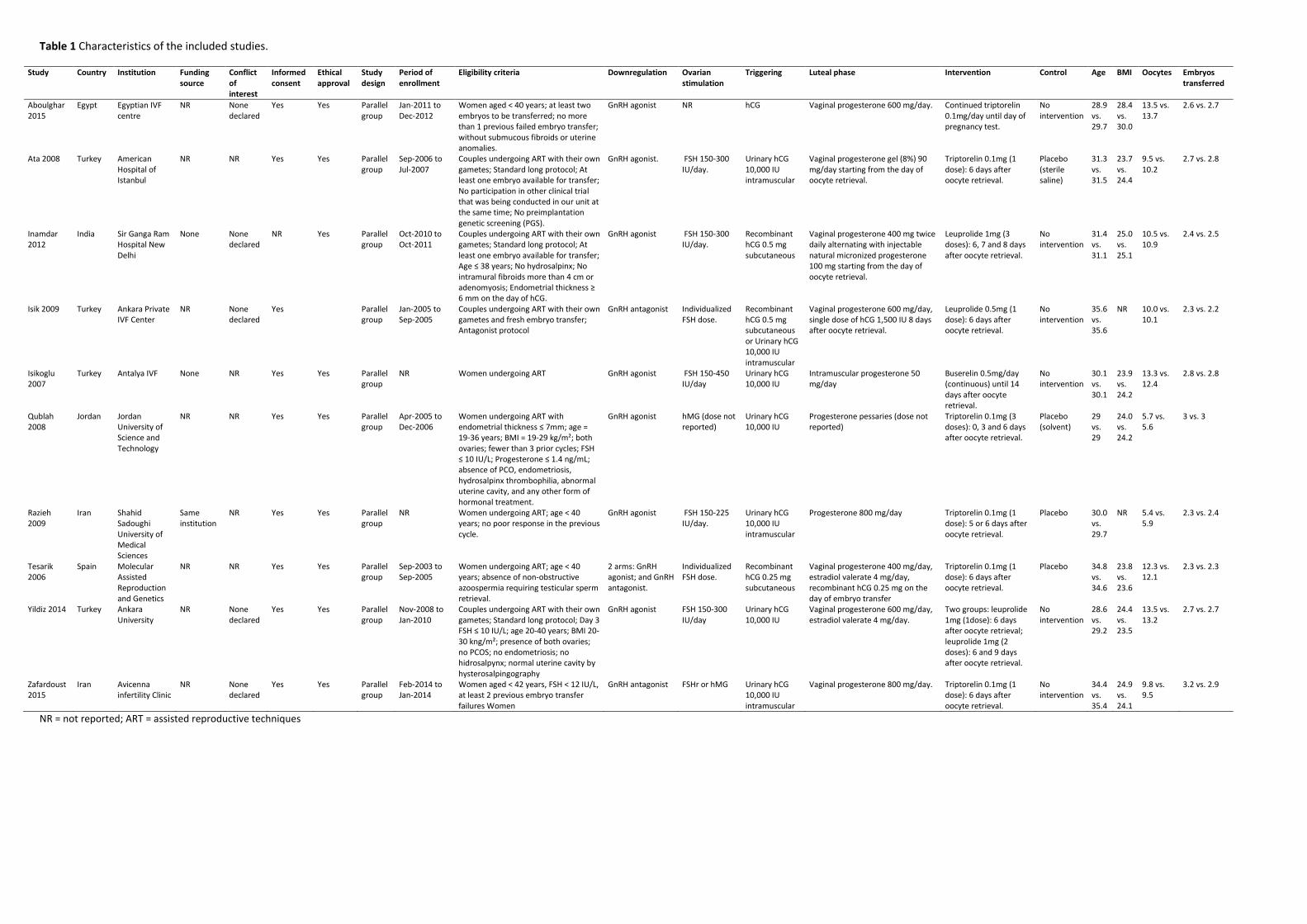
Table 1 Characteristics of the included studies.
Study Country Institution Funding source
Conflict of interest
Informed consent
Ethical approval
Study design
Period of enrollment
Eligibility criteria Downregulation Ovarian stimulation
Triggering Luteal phase Intervention Control Age BMI Oocytes Embryos transferred
Aboulghar 2015
Egypt Egyptian IVF centre
NR None declared
Yes Yes Parallel group
Jan-2011 to Dec-2012
Women aged < 40 years; at least two embryos to be transferred; no more than 1 previous failed embryo transfer; without submucous fibroids or uterine anomalies.
GnRH agonist NR hCG Vaginal progesterone 600 mg/day. Continued triptorelin 0.1mg/day until day of pregnancy test.
No intervention
28.9 vs. 29.7
28.4 vs. 30.0
13.5 vs. 13.7
2.6 vs. 2.7
Ata 2008 Turkey American Hospital of Istanbul
NR NR Yes Yes Parallel group
Sep-2006 to Jul-2007
Couples undergoing ART with their own gametes; Standard long protocol; At least one embryo available for transfer; No participation in other clinical trial that was being conducted in our unit at the same time; No preimplantation genetic screening (PGS).
GnRH agonist. FSH 150-300 IU/day.
Urinary hCG 10,000 IU intramuscular
Vaginal progesterone gel (8%) 90 mg/day starting from the day of oocyte retrieval.
Triptorelin 0.1mg (1 dose): 6 days after oocyte retrieval.
Placebo (sterile saline)
31.3 vs. 31.5
23.7 vs. 24.4
9.5 vs. 10.2
2.7 vs. 2.8
Inamdar 2012
India Sir Ganga Ram Hospital New Delhi
None None declared
NR Yes Parallel group
Oct-2010 to Oct-2011
Couples undergoing ART with their own gametes; Standard long protocol; At least one embryo available for transfer; Age ≤ 38 years; No hydrosalpinx; No intramural fibroids more than 4 cm or adenomyosis; Endometrial thickness ≥ 6 mm on the day of hCG.
GnRH agonist FSH 150-300 IU/day.
Recombinant hCG 0.5 mg subcutaneous
Vaginal progesterone 400 mg twice daily alternating with injectable natural micronized progesterone 100 mg starting from the day of oocyte retrieval.
Leuprolide 1mg (3 doses): 6, 7 and 8 days after oocyte retrieval.
No intervention
31.4 vs. 31.1
25.0 vs. 25.1
10.5 vs. 10.9
2.4 vs. 2.5
Isik 2009 Turkey Ankara Private IVF Center
NR None declared
Yes Parallel group
Jan-2005 to Sep-2005
Couples undergoing ART with their own gametes and fresh embryo transfer; Antagonist protocol
GnRH antagonist Individualized FSH dose.
Recombinant hCG 0.5 mg subcutaneous or Urinary hCG 10,000 IU intramuscular
Vaginal progesterone 600 mg/day, single dose of hCG 1,500 IU 8 days after oocyte retrieval.
Leuprolide 0.5mg (1 dose): 6 days after oocyte retrieval.
No intervention
35.6 vs. 35.6
NR 10.0 vs. 10.1
2.3 vs. 2.2
Isikoglu 2007
Turkey Antalya IVF None NR Yes Yes Parallel group
NR Women undergoing ART GnRH agonist FSH 150-450 IU/day
Urinary hCG 10,000 IU
Intramuscular progesterone 50 mg/day
Buserelin 0.5mg/day (continuous) until 14 days after oocyte retrieval.
No intervention
30.1 vs. 30.1
23.9 vs. 24.2
13.3 vs. 12.4
2.8 vs. 2.8
Qublah 2008
Jordan Jordan University of Science and Technology
NR NR Yes Yes Parallel group
Apr-2005 to Dec-2006
Women undergoing ART with endometrial thickness ≤ 7mm; age = 19-36 years; BMI = 19-29 kg/m²; both ovaries; fewer than 3 prior cycles; FSH ≤ 10 IU/L; Progesterone ≤ 1.4 ng/mL; absence of PCO, endometriosis, hydrosalpinx thrombophilia, abnormal uterine cavity, and any other form of hormonal treatment.
GnRH agonist hMG (dose not reported)
Urinary hCG 10,000 IU
Progesterone pessaries (dose not reported)
Triptorelin 0.1mg (3 doses): 0, 3 and 6 days after oocyte retrieval.
Placebo (solvent)
29 vs. 29
24.0 vs. 24.2
5.7 vs. 5.6
3 vs. 3
Razieh 2009
Iran Shahid Sadoughi University of Medical Sciences
Same institution
NR Yes Yes Parallel group
NR Women undergoing ART; age < 40 years; no poor response in the previous cycle.
GnRH agonist FSH 150-225 IU/day.
Urinary hCG 10,000 IU intramuscular
Progesterone 800 mg/day Triptorelin 0.1mg (1 dose): 5 or 6 days after oocyte retrieval.
Placebo 30.0 vs. 29.7
NR 5.4 vs. 5.9
2.3 vs. 2.4
Tesarik 2006
Spain Molecular Assisted Reproduction and Genetics
NR NR Yes Yes Parallel group
Sep-2003 to Sep-2005
Women undergoing ART; age < 40 years; absence of non-obstructive azoospermia requiring testicular sperm retrieval.
2 arms: GnRH agonist; and GnRH antagonist.
Individualized FSH dose.
Recombinant hCG 0.25 mg subcutaneous
Vaginal progesterone 400 mg/day, estradiol valerate 4 mg/day, recombinant hCG 0.25 mg on the day of embryo transfer
Triptorelin 0.1mg (1 dose): 6 days after oocyte retrieval.
Placebo 34.8 vs. 34.6
23.8 vs. 23.6
12.3 vs. 12.1
2.3 vs. 2.3
Yildiz 2014 Turkey Ankara University
NR None declared
Yes Yes Parallel group
Nov-2008 to Jan-2010
Couples undergoing ART with their own gametes; Standard long protocol; Day 3 FSH ≤ 10 IU/L; age 20-40 years; BMI 20-30 kng/m²; presence of both ovaries; no PCOS; no endometriosis; no hidrosalpynx; normal uterine cavity by hysterosalpingography
GnRH agonist FSH 150-300 IU/day
Urinary hCG 10,000 IU
Vaginal progesterone 600 mg/day, estradiol valerate 4 mg/day.
Two groups: leuprolide 1mg (1dose): 6 days after oocyte retrieval; leuprolide 1mg (2 doses): 6 and 9 days after oocyte retrieval.
No intervention
28.6 vs. 29.2
24.4 vs. 23.5
13.5 vs. 13.2
2.7 vs. 2.7
Zafardoust 2015
Iran Avicenna infertility Clinic
NR None declared
Yes Yes Parallel group
Feb-2014 to Jan-2014
Women aged < 42 years, FSH < 12 IU/L, at least 2 previous embryo transfer failures Women
GnRH antagonist FSHr or hMG Urinary hCG 10,000 IU intramuscular
Vaginal progesterone 800 mg/day. Triptorelin 0.1mg (1 dose): 6 days after oocyte retrieval.
No intervention
34.4 vs. 35.4
24.9 vs. 24.1
9.8 vs. 9.5
3.2 vs. 2.9
NR = not reported; ART = assisted reproductive techniques

Table 2 Summary of findings table.
Absolute chance/risk (95% CI) a NNTB (95% CI) RR (95% CI) N participants / studies Interpretation Quality of evidence
Standard LPS GnRH agonist
Live birth / Ongoing Pregnancy 27.8% 35.0% (28.9-42.5%) 14 (7-90) 1.26 [1.04, 1.53] 2,776 /8 Benefit Very Low*
Clinical pregnancy 33.1% 42.4% (35.8-50.3%) 11 (6-38) 1.28 (1.08-1.52) 3,056 / 10 Benefit Very Low*
Miscarriage per clinical pregnancy 21.8% 17.9% (13.1-24.0%) - 0.82 (0.60-1.10) 1,077 /8 No evidence of
effect Low**
Adverse perinatal outcomes No evidence from RCTs
Congenital malformations No evidence from RCTs
CI = confidence interval; LPS = luteal phase support; NNTB = number needed to treat for an additional beneficial outcome or to reduce and adverse outcome; RR = relative risk. a = The absolute risk in the Standard LPS was determined as the average risk in these groups; the absolute risk in the GnRH agonist group and its 95% CI was determined using the RR and its 95% CI. b = The NNTB for miscarriage was determined for the number of women initially treated. * = Downgraded because of low quality of the included studies, serious inconsistency among studies, serious imprecision of the estimates, and high suspicion of publication bias. ** = Downgraded because of very serious imprecision.

Figure 1 Flowchart of study selection.

Figure 2 Forest plot for live birth / ongoing pregnancy: subgroup analysis separating the studies by Agonist vs. Antagonist
protocol.

Figure 3 Forest plot for clinical pregnancy.

Figure 4 Forest plot for miscarriage.

Supplemental Figure 1 Forest plot for Live Birth / Ongoing Pregnancy.

Supplemental Figure 2 Forest plot for Live Birth / Ongoing Pregnancy: subgroup analysis separating the studies by
Single vs. Multiple doses of GnRH agonist.

Supplemental Figure 3 Funnel plot for Clinical Pregnancy.
Copyright © 2022 FDOKUMEN




















