
Inference for Ecological Dynamical Systems: A Case Study of Two Endemic Diseases
Upload
dibrugarhuniversityCategory
view
2download
0
Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1 9
Introduction
M alaria continues to be a major health problem particularly for India and is spread over 35 states and union territories.
The hilly regions of Northeast India are endemic for malaria. The eight states in this region record about 0.07-0.1 million (Plasmodium falciparum) malaria cases annually accounting for 12% of total reported cases in India.[1] Assam itself accounts for 31.94% of the total reported P. falciparum cases from Northeastern region. The problem is compounded by P falciparum resistance. In India, resistance of P. falciparum to chloroquine (CQ), the cheapest and the most widely used drug was first reported
in the year 1973 from Karbi-Anglong district and during 1974 in Nagaon district of Assam state.[2-5] India introduced sulphadoxine-pyrimethamine (SP) combination in 1982 as a second line of treatment.[2] The antifolate drug pyrimethamine acts on the P. falciparum dihydrofolate reductase (Pfdhfr) enzyme and therefore inhibits the folate biosynthesis pathway of the parasite.[6,7] Sulfonamides act on parasite enzyme P. falciparum dihydropteroate synthetase (Pfdhps) which is responsible for folate metabolism.[8,9] Resistance is mediated by certain point mutations in Pfdhfr and Pfdhps which reduce its capacity to bind to this drug, resulting in the emergence of resistant parasite strains.[6,10,11] P. falciparum dhfr mutations N51I, C59R, S108N, and I164L and dhps mutations S436A,A437G, K540E, A581G, and A613S/T give rise to sulfadoxine and pyrimethamine resistance (SPR).[10] These mutations occur in a stepwise manner and the parasite bearing a higher number of dhfr-dhps mutations shows a higher level of SPR.[12,13] Resistance to SP has been reported in many countries.[14-18] Few studies have evaluated the prevalence of mutations in Pfdhfr and Pfdhps genes associated with SPR among the P. falciparum field isolates in Assam. However, the information is limited. Hence the present study was undertaken.
ABSTRACTBackground: The emergence of antimalarial drug resistance malaria parasite is widespread in North eastern region of India. During January 2012-December 2013, we conducted active surveillance for detection of antifolate resistance-associated genetic polymorphisms in Plasmodium falciparum malaria parasite from different malaria endemic areas of Assam. Materials and Methods: A total of 281 field samples were collected from suspected malaria patients of which 106 malaria P. falciparum positive cases were detected in microscopic slide examination. A nested PCR was done for amplification of a 648 bp portion of the dhfr gene and 710 bp portion of the dhps gene. Results: Mutation analysis revealed existence of three different haplotypes of the P. falciparum dhfr gene of which ANRNI was highly prevalent (90%). Triple mutant haplotypes AIRNI (N51I + C59R + S108N) of the dhfr gene associated with pyrimethamine resistance were prevalent in Chirang district of Assam. Whereas, dhps mutation study revealed that triple mutant haplotype AGEAA (S436A + A437G + K540E) associated with Sulphadoxine resistance was found among 26% of P. falciparum field isolates. However, P. falciparum dhfr-dhps two locus mutation analysis showed that there were a total of nine dhfr-dhps genotypes. Conclusion: It was noticed that 93.62% (88/94) isolates had mutations in the sequences of both enzymes, which is an indication of prevalence of high grade of Sulphadoxine — pyrimethamine resistance in P. falciparum malaria parasites in Assam.
KEY WORDS: Antifolate, Assam, dhfr-dhps, haplotypes, P. falciparum, sulphadoxine-pyrimethamine
Genetic polymorphisms associated with sulphadoxine-pyrimethamine drug resistance among Plasmodium falciparum field isolates in malaria endemic areas of AssamSharma J, Dutta P, Khan SA, Soni M, Dey D, Mahanta J
Division of Entomology and Filariasis, Regional Medical Research Centre (ICMR), NER, Dibrugarh, Assam, India
Address for correspondence: Dr. Prafulla Dutta, E-mail: [email protected]
Access this article onlineQuick Response Code: Website:
www.jpgmonline.com
DOI:
10.4103/0022-3859.147019
PubMed ID:
25511211
Received : 26-01-2014Review completed : 21-03-2014Accepted : 13-08-2014
Original Article

Sharma J, et al.: Antifolate resistance malaria parasites in Assam
10 Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1
Figure 1: Amplification of 648 bp portion of the dhfr gene and 710 bp portion of the dhps gene
Materials and Methods
EthicsThe study protocol was approved by the Ethics committee of the Regional malaria research center, Indian Council of Medical Research and written, informed consent was taken from all participants or their guardians. Assent was taken from children over the age of 7 years.
Study periodThe study was carried out during period from January 2012 to December 2013 through household visits as well as samples collected from patients with fever who were attending malaria clinics/Primary Health Centre (PHC) in malaria endemic areas of Assam.
Study areaAssam state (89° 42′ E to 96° E longitude and 24° 8′ N to 28° 2′ N latitude) which included Tinsukia, Sonitpur, Sivasagar, NC Hills, Lakhimpur, Karbi Anglong, Jorhat, Golaghat, Dibrugarh and Chirang districts.
Selection criteriaPatients with microscopic confirmed P. falciparum mono infection were eligible for enrolment irrespective of age, sex and disease severity. The patients who took antibiotics were excluded from the study. Clinical history was recorded for each subject. A brief epidemiological and demographical history was also collected from each participant using a structured questionnaire.
Patients and samplesTwo milliliter intravenous samples were collected from 281 individuals (aged from range 1.6 to 70 years) with fever/suspected with malaria infection/asymptomatic patients having history of malaria. Among 281 collected samples, 218 patients showed symptoms of malaria and the remaining 63 individuals were asymptomatic.
Microscopic examinationThick and thin blood smears were prepared for all blood samples and stained with 10% Giemsa stain and examined under light microscopy. Samples were considered negative when no parasite was detected after examining 100X microscopic fields. Further Polymerase chain reaction was done in microscopic positive malaria P. falciparum samples for authentication. Number of parasites/µl of blood (thick/thin film) was calculated by number of observed asexual parasites � total WBC/RBC count per µl against 200 WBC in 100 microscopic fields/total nos. of RBC screened in 25 microscopic fields.
Detection of malaria parasite by PCRDNA extraction was done from 200 µl of whole blood samples using the QIAamp DNA Mini spin columns kit (Millipore Corporation). The extracted DNA was thereafter amplified by the PCR using a set of primers as described by Snounou et al. 1996.[19] The amplified product was detected by electrophoresis on 1.5% agarose gel containing ethidium bromide and visualized on an ultraviolet transillumination.
The Gel photographs were taken and specific amplified bands at 205 bp were observed.
Amplification of dhfr and dhps genesA nested PCR method was used in all samples. 5 µl of purified DNA were added to a final reaction volume of 50 µl to amplify a 648 base pair (bp) portion of the dhfr gene [Figure 1] by using specific set of primers.[20] Similarly, a 710 bp portion of the dhps gene [Figure 1] was amplified by the use of specific primers.[20] All the amplification was performed in a Thermal cycler (Gene Amp®PCR System 9700 and Veriti, Applied Biosystems, Foster City, CA, USA). The amplified products were visualized by electrophoresis under UV transillumination. The amplified products were further purified with the QIAquick PCR purification kit (QIAGEN) before sequencing and sequenced commercially (Macrogen Inc. Seoul, Korea through Anshul Biotechnologies, Hyderabad, India). Sequencing was performed on an automated sequencer using standard protocols.
Statistical analysisThe Statistical Package for Social Science (SPSS) version 16 was used. Continuous data were expressed as mean and standard deviation. Categorical data were expressed as percentages. The sequencing products were further edited in Bio-edit software. Single nucleotide polymorphisms of the concerned genes were detected through bioinformatics software DnaSP version v. 5.10.01.
Results
DemographicsA total of 281 blood samples (age range 1.6-70 years) were collected for microscopic examination, of which 37.72% (106/281) samples were positive for P. falciparum. Two of the 281 samples were positive for P. vivax and 2.49% (7/281) had mixed infection (P. falciparum + P. vivax). All the age groups and both the sexes were found affected with malarial infection. The largest numbers of P. falciparum cases were reported from Karbi Anglong district of Assam with a high proportion of infectivity [Tables 1 and 2]. A+ and B+ blood groups were more susceptible to malaria P. falciparum infection. It was seen that 38/63 (60.32%) of the total

Sharma J, et al.: Antifolate resistance malaria parasites in Assam
Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1 11
Table 1: District wise suspected/confirmed malaria P. falciparum (Pf)-positive cases in AssamDistrict Nos. of suspected
malaria casesNos. of malaria
Pf-positive cases
Tinsukia 35 11
Sonitpur 7 0
Sivasagar 33 11
NC Hills 15 13
Lakhimpur 25 11
Karbi Anglong 29 26
Jorhat 30 9
Golaghat 8 7
Dibrugarh 86 7
Chirang 13 11
Total 281 106
Table 2: Demographic characteristics among suspected/confirmed malaria P. falciparum (Pf)-positive cases in AssamAge groups (in year) Nos. of suspected
malaria casesNos. of malaria
Pf-positive cases
1 to 10 53 33
11 to 20 67 17
21 to 30 63 28
31 to 40 49 14
41 to 50 30 8
51 above 19 6
Male 156 54
Female 125 52
Total 281 106
Table 3: Locality wise circulation of dhfr genotypes of P. falciparum isolates in Assam linked with pyrimethamine resistanceDistricts P. falciparum dhfr genotype (Nos. of isolates)
ANCSI (wild type) ANRNI AIRNI
Karbi Anglong (n=25) 2 23 —
NC Hills (n=13) 1 12 —
Chirang (n=9) — 7 2
Golaghat (n=7) 1 6 —
Dibrugarh (n=7) 1 6 —
Sivasagar (n=11) 1 10 —
Tinsukia (n=11) 1 10 —
Lakhimpur (n=8) 0 8 —
Jorhat (n=9) 1 8 —
Total 08 90 2
asymptomatic cases were P. falciparum positive whereas 68/218 (31.19%) of the symptomatic cases showed malarial P. falciparum infectivity. The mean parasite count was 4.35% (3.206; range 0.2% -15%).
Mutation analysis and haplotype diversityA total of 106 (one hundred and six) P. falciparum-infected blood samples were studied for mutation analysis of P. falciparum dhfr and P. falciparum dhps genotypes among the isolates in different malaria endemic areas of Assam. Analysis was finally possible for 100 (one hundred) amplified products independently for both the genes. The Pfdhfr gene analysis revealed the existence of three haplotypes: Two associated with drug-resistance profile (ANRNI and AIRNI) and the ANCSI associated with SP sensitivity [Table 3]. Haplotype ANRNI is a double mutant (C59R+S108N) which has moderate levels of resistance to pyrimethamine while haplotype AIRNI is a triple mutant (N51I+C59R+S108N) having a higher level of resistance. The wild-type ANCSI was present in only 8% (8/100) of the isolates, whereas double-mutation ANRNI haplotype was prevalent in 90% (90/100) of analyzed samples and the triple mutant AIRNI was the least common and was recorded in only 2% (2/100) of P. falciparum isolates. The prevalence of C59R and S108N mutation in the dhfr sequence among the isolates is indicative of the key point mutation. Any other mutation should be associated with them linked with treatment failure. Mutation analysis at nucleotide level showed that at nucleotide position 152, A-T mutation (N51I), at nucleotide position 175,T-C (C59R) and at nucleotide position 323,G-A mutation (S108N) leads to the occurrence of ANRNI and AIRNI haplotype.
The analysis of dhps mutation study revealed the presence of 7 haplotypes of which 6 were associated with drug-resistance profile (FAKAA, AGKAA, SGKGA, SGKAA, AGEAA and FGKAA) and the wild-type SAKAA haplotype [Table 4]. It was seen that the P. falciparum dhps haplotype FAKAA having a single mutation was found among 26%, wild-type haplotype in 7% isolates. Three different types of double mutant haplotypes were observed in the P. falciparum field isolates. Double-mutant haplotype AGKAA (S436A+A437G) was observed among 23%, SGKGA (A437G+A581G) among 8% and FGKAA (S436F+A437G) among 4% (4/100) isolates. The triple-mutant haplotype AGEAA (S436A+A437G+K540E) was seen among 26% isolates. At the nucleotide level it was seen that in nucleotide position 1306, T-G mutations (S436A), at 1307 position, C-T (S436F) mutation and at nucleotide site 1310, C-G (A437G) were associated with the occurrence of haplotype FAKAA, AGKAA, SGKAA and FGKAA. Likewise, at nucleotide location 1618, A-G (K540E) and mutation from C-G at nucleotide position 1742 (A581G) were accountable for the occurrence of other haplotypes of the Pfdhps gene associated with alternate level of sulphadoxine resistance.
The P. falciparum dhfr-dhps two loci mutation analysis showed that there were a total of nine dhfr-dhps two loci genotypes present among the isolates [Table 5]. Triple mutant haplotypes for both (AIRNI-AGEAA) dhfr-dhps genes were observed only in Chirang district of Assam. ANRNI-FAKAA was found
predominantly in Karbi Anglong, NC Hills, Chirang and Sivasagar district. ANRNI-AGKAA and ANRNI-AGEAA were the next common dhfr-dhps haplotypes. Only 5/94 (5.32%) of the total isolates had wild-type sequence for both enzymes while the rest 89/94 (94.68%) had mutations in either one gene or both genes (single to quadruple). It was seen that
Sharma J, et al.: Antifolate resistance malaria parasites in Assam
12 Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1
Table 5: Distribution of P. falciparum dhfr and dhps two locus genotype in the isolates of AssamP. falciparum dhfr and dhps two locus genotype among the isolates of AssamTwo locus genotype
Chirang (n = 9)
Dibrugarh (n = 7)
Golaghat (n = 7)
Jorhat (n = 9)
Lakhimpur (n = 8)
N.C Hills (n = 11)
Sivasagar (n = 11)
Tinsukia (n = 11)
Karbi Anglong (n = 21)
ANCSI-SAKAA — 1 1 1 — — 1 1 —
ANRNI- SAKAA — — — — — — — — 1
ANRNI-FAKAA 2 — — — — 8 4 — 11
ANRNI-AGKAA — 2 2 2 2 1 6 4 4
ANRNI-SGKGA — — — — — 2 — — 5
ANRNI-SGKAA 4 — — 2 — — — — —
ANRNI-AGEAA — 4 4 2 6 — — 6 —
ANRNI-FGKAA 1 — — 2 — — — — —
AIRNI -AGEAA 2 — — — — — — — —
9 7 7 9 8 11 11 11 21
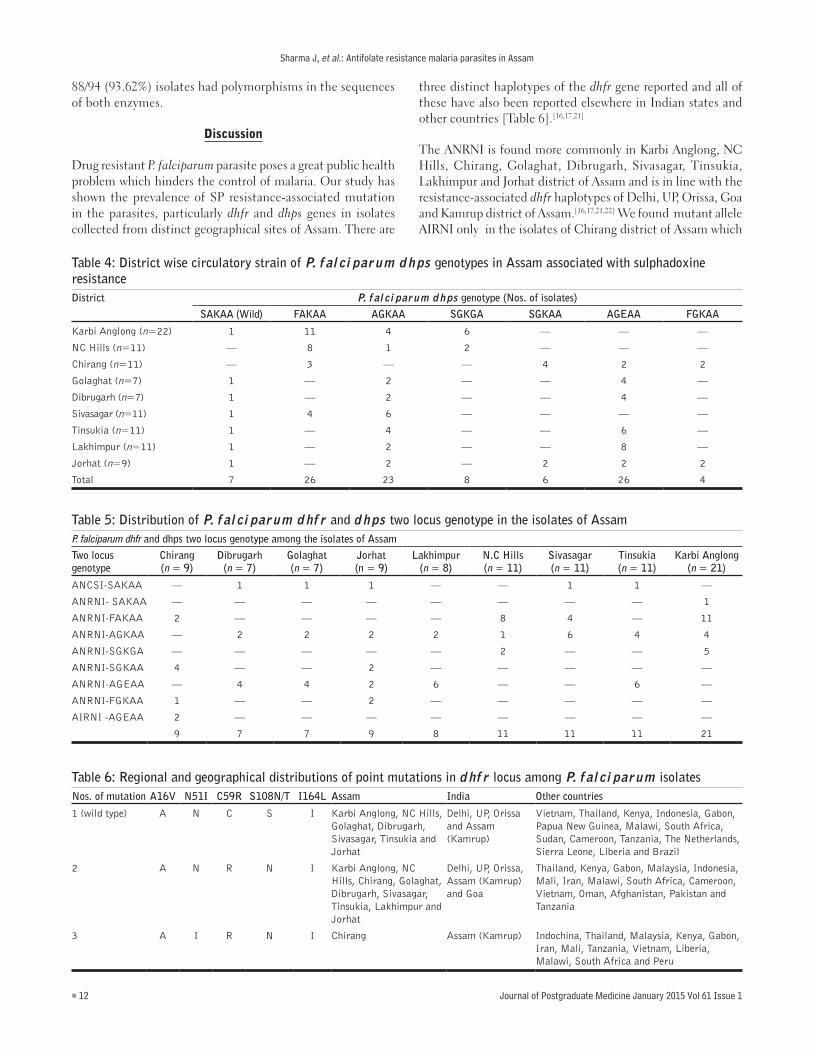
Table 6: Regional and geographical distributions of point mutations in dhfr locus among P. falciparum isolatesNos. of mutation A16V N51I C59R S108N/T I164L Assam India Other countries
1 (wild type) A N C S I Karbi Anglong, NC Hills, Golaghat, Dibrugarh, Sivasagar, Tinsukia and Jorhat
Delhi, UP, Orissa and Assam (Kamrup)
Vietnam, Thailand, Kenya, Indonesia, Gabon, Papua New Guinea, Malawi, South Africa, Sudan, Cameroon, Tanzania, The Netherlands, Sierra Leone, Liberia and Brazil
2 A N R N I Karbi Anglong, NC Hills, Chirang, Golaghat, Dibrugarh, Sivasagar, Tinsukia, Lakhimpur and Jorhat
Delhi, UP, Orissa, Assam (Kamrup) and Goa
Thailand, Kenya, Gabon, Malaysia, Indonesia, Mali, Iran, Malawi, South Africa, Cameroon, Vietnam, Oman, Afghanistan, Pakistan and Tanzania
3 A I R N I Chirang Assam (Kamrup) Indochina, Thailand, Malaysia, Kenya, Gabon, Iran, Mali, Tanzania, Vietnam, Liberia, Malawi, South Africa and Peru
Table 4: District wise circulatory strain of P. falciparum dhps genotypes in Assam associated with sulphadoxine resistance District P. falciparum dhps genotype (Nos. of isolates)
SAKAA (Wild) FAKAA AGKAA SGKGA SGKAA AGEAA FGKAA
Karbi Anglong (n=22) 1 11 4 6 — — —
NC Hills (n=11) — 8 1 2 — — —
Chirang (n=11) — 3 — — 4 2 2
Golaghat (n=7) 1 — 2 — — 4 —
Dibrugarh (n=7) 1 — 2 — — 4 —
Sivasagar (n=11) 1 4 6 — — — —
Tinsukia (n=11) 1 — 4 — — 6 —
Lakhimpur (n=11) 1 — 2 — — 8 —
Jorhat (n=9) 1 — 2 — 2 2 2
Total 7 26 23 8 6 26 4
88/94 (93.62%) isolates had polymorphisms in the sequences of both enzymes.
Discussion
Drug resistant P. falciparum parasite poses a great public health problem which hinders the control of malaria. Our study has shown the prevalence of SP resistance-associated mutation in the parasites, particularly dhfr and dhps genes in isolates collected from distinct geographical sites of Assam. There are
three distinct haplotypes of the dhfr gene reported and all of these have also been reported elsewhere in Indian states and other countries [Table 6].[16,17,21]
The ANRNI is found more commonly in Karbi Anglong, NC Hills, Chirang, Golaghat, Dibrugarh, Sivasagar, Tinsukia, Lakhimpur and Jorhat district of Assam and is in line with the resistance-associated dhfr haplotypes of Delhi, UP, Orissa, Goa and Kamrup district of Assam.[16,17,21,22] We found mutant allele AIRNI only in the isolates of Chirang district of Assam which

Sharma J, et al.: Antifolate resistance malaria parasites in Assam
Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1 13
Table 7: Regional and geographical distributions of point mutations in dhps locus among P. falciparum isolatesNos. of mutation S436 F/A A437/G K 540E A 581G A 613 Assam India Other countries
1 (wild type) S A K A A Karbi Anglong, Golaghat, Dibrugarh, Sivasagar, Tinsukia, Lakhimpur and Jorhat
Delhi, UP, Orissa, Assam (Kamrup)and Goa
Vietnam, Thailand, Afghanistan, Oman, Yemen, Sudan, Tanzania, Gambia, Papua New Guinea, Brazil, Pakistan Kenya, Indonesia, Gabon, Malaysia, Iran, Malawi and South Africa
2 F A K A A Karbi Anglong, NC Hills, Chirang and Sivasagar
Delhi, UP, Orissa, Assam (Kamrup)and Goa
Kenya
3 A G K A A Karbi Anglong, NC Hills, Chirang, Dibrugarh, Sivasagar, Tinsukia, Lakhimpur and Jorhat
Assam (Kamrup) Thailand, Vietnam and Gabon
4 S G K G A Karbi Anglong and NC Hills Assam (Kamrup) Malaysia, Vietnam, Kenya, Tanzania, Thailand, Male and Venezuela
5 S G K A A Chirang and Jorhat Delhi, UP, Orissa, Assam (Kamrup) and Goa
Kenya, Mali, Tanzania, Brazil, Liberia, South Africa, Sudan, Venezuela, Indonesia, Malaysia, Gabon and Iran
6 A G E A A Chirang, Dibrugarh, Tinsukia, Lakhimpur, Golaghat and Jorhat
Orissa and Assam (Kamrup)
Thailand
7 F G K A A Chirang and Jorhat Not found Indonesia, Malaysia, Thailand and Kenya
is similar to the P.falciparum dhfr alleles reported earlier from Kamrup district.[16,17,21,22] The high prevalence of Pfdhfr 59R+ S108N mutation in our study indicates decreased susceptibility to pyrimethamine in different localities of Assam. Only 2% isolates in our study had the triple resistance-associated haplotype.
Pfdhps mutation analysis revealed predominance of triple mutant Pfdhps AGEAA (26%) haplotypes in Assam which also indicates a high grade of sulphadoxine resistance. To our knowledge, 6/7 genotypes reported here are also present in other parts of India [Table 7]. On the other hand several of the dhfr-dhps (AICNL, AIRTI, SGEAS, AGEGA, FGEGA) genotypes reported from other countries like Peru, Gabon, Thailand were not seen among our isolates.[16,17,21] A novel dhps haplotype (FGKAA) was seen from Chirang and Jorhat district of Assam which has not been reported earlier from Indian P. falciparum field isolates but is reported from other countries [Table 7].
P. falciparum dhfr and dhps two loci genotype among the field isolates of Chirang district of Assam showed that two patients had infections with triple Pfdhfr + triple Pfdhps mutant haplotypes which is known to be associated with high grade of SPR. Double mutant Pfdhr + Pfdhps was found only in 1.06% (1/94) of the field isolates, whereas triple Pfdhr + Pfdhps was found in 32.98% (31/94) and quadruple mutant Pfdhr + Pfdhps haplotype was detected among 60.64% (57/94) of P. falciparum field isolates in different malaria endemic areas of Assam. Rates of mutation differed from district to district. The presence of multiple mutations in the genes for both enzymes is an indication that resistance has reached an alarming level. These findings indicate that a high grade of SPR is seen in Assam and that the drug may not be a good choice to combine with artesunate. A recent study conducted by Sharma J et al. in 2014 revealed point mutations in PfATPase6 gene among the
isolates of Arunachal Pradesh, but without clinical correlation.[23] Artemisinin combination (ACT (AS+SP) combination is being implemented by the Government of India in 67 districts of the North Eastern States. The high rate of SPR-associated mutations is a cause for concern and should be taken into account during policy planning. Regular molecular surveillance is required in the field for better management of malaria control through optimal use antimalarial drugs.
References
1. Available from: http://www.nvbdcp.gov.in/mp-assam.html. AES/JE cases and deaths in the country since 2008 [Last accessed on 2014 Jan 17].
2. Misra SP. In-vivo resistance to chloroquine and sulpha pyrimethamine combination in P. falciparum in India. Proc Natl Acad Sci India 1996;66:123-8.
3. Sharma VP. Current scenario of malaria in India. Parassitologia 1999;41:349-53.
4. Sharma YD, Biswas S, Pillai CR, Ansari MA, Adak T, Devi CU. High prevalence of chloroquine resistant Plasmodium falciparum infection in Rajasthan epidemic. Acta Trop 1996;62:135-41.
5. Vinayak S, Biswas S, Dev V, Kumar A, Ansari MA, Sharma YD. Prevalence of the K76T mutation in the pfcrt gene of Plasmodium falciparum among chloroquine responders in India. Acta Trop 2003;87:287-93.
6. Gregson A, Plowe CV. Mechanisms of resistance of malaria parasites to antifolates. Pharmacol Rev 2005; 57:117-45.
7. Yuvaniyama J, Chitnumsub P, Kamchonwongpaisan S, Vanichtanankul J, Sirawaraporn W, Taylor P, et al. Insights into antifolate resistance from malarial DHFR-TS structures. Nat Struct Biol 2003;10:357-65.
8. Bzik DJ, Li WB, Horii T, Inselburg J. Molecular cloning and sequence analysis of the Plasmodium falciparum dihydrofolate reductase-thymidylate synthase gene. Proc Natl Acad Sci U S A 1987; 84:8360-4.
9. Triglia T, Cowman AF. Primary structure and expression of the dihydropteroate synthetase gene of Plasmodium falciparum. Proc Natl Acad Sci U S A 1994;91:7149-53.
10. Cowman AF, Morry MJ, Biggs BA, Cross GA, Foote SJ. Amino acid changes linked to pyrimethamine resistance in the dihydrofolate reductase-thymidylate synthase gene of Plasmodium falciparum. Proc Natl Acad Sci U S A 1988;85:9109-13.
11. Peterson DS, Walliker D, Wellems TE. Evidence that a point mutation

Sharma J, et al.: Antifolate resistance malaria parasites in Assam
14 Journal of Postgraduate Medicine January 2015 Vol 61 Issue 1
in dihydrofolate reductase-thymidylate synthase confers resistance to pyrimethamine in falciparum malaria. Proc Natl Acad Sci U S A 1988;85:9114-8.
12. Kublin JG, Witzig RS, Shankar AH, Zurita JQ, Gilman RH, Guarda JA, et al. Molecular assays for surveillance of antifolate-resistant malaria. Lancet 1998;351:1629-30.
13. Wang P, Lee CS, Bayoumi R, Djimde A, Doumbo O, Swedberg G, et al. Resistance to antifolates in Plasmodium falciparum monitored by sequence analysis of dihydropteroate synthetase and dihydrofolate reductase alleles in a larger number of field samples of diverse origin. Mol Biochem Parasitol 1997;89:161-77.
14. Gama BE, de Oliveira NK, Zalis MG, de Souza JM, Santos F, Daniel-Rebeiro CT, et al. Chloroquine and sulphadoxine-pyrimethamine sensitivity of Plasmodium falciparum parasites in a Brazilian endemic area. Malar J 2009;8:156.
15. Pearce RJ, Drakeley C, Chandramohan D, Mosha F, Roper C. Molecular determination of point mutation haplotypes in the dihydrofolate reductase and dihydropteorate synthase of Plasmodium falciparum in three districts of northern Tanzania. Antimicrob Agents Chemother 2003;47:1347-54.
16. Ahmed A, Bararia D, Vinayak S, Yameen M, Biswas S, Dev V, et al. Plasmodium falciparum isolates in India exhibit a progressive increase in mutations associated with sulphadoxine-pyrimethamine resistance. Antimicrob Agents Chemother 2004;48:879-89.
17. Ahmed A, Das MK, Dev V, Saifi MA, Wajihullah, Sharma YD. Quadruple mutation in dihydrofolate reductase of Plasmodium falciparum isolates from Car Nicobar Island, India. Antimicrob Agents Chemother 2006;50:1546-9.
18. Jambou R, Legrand E, Niang M, Khim N, Lim P, Volney B, et al. Resistance of Plasmodium falciparum field isolates to in-vitro
artemether and point mutations of the SERCA-type PfATPase6. Lancet 2005; 366:1960-3.
19. Snounou G, Viriyakosol S, Zhu XP, Jarra W, Pinheiro L, do Rosario VE, et al. High sensitivity of detection of human malaria parasites by the use of nested polymerase chain reaction. Mol Biochem Parasitol 1993;61:315-20.
20. Jelinek T, Rønn AM, Lemnge MM, Curtis J, Mhina J, Duraisingh MT, et al. Polymorphisms in the dihydrofolate reductase (DHFR) and dihydropteroate synthetase (DHPS) genes of Plasmodium falciparum and in vivo resistance to sulphadoxine/pyrimethamine in isolates from Tanzania. Trop Med Int Health 1998;3:605-9.
21. Ahmed A, Lumb V, Das MK, Dev V, Wajihullah, Sharma YD, Prevalence of mutations associated with higher levels of sulphadoxine-pyrimethamine resistance in Plasmodium falciparum isolates from Car Nicobar Island and Assam, India. Antimicrob Agents Chemother 2006;50:3934-8.
22. Ghanchi NK, Ursing J, Beg MA, Veiga MI, Jafri S, Mårtensson A. Prevalence of resistance associated polymorphisms in Plasmodium falciparum field isolates from Southern Pakistan. Maler J 2011;10:18.
23. Sharma J, Dutta P, Khan SA, Soni M, Mahanta J. Detection of point mutation in Plasmodium falciparum ATPase6 gene associated with artemisinin resistance from Assam and Arunachal Pradesh. J Vector Borne Dis 2014;51.
How to cite this article: Sharma J, Dutta P, Khan SA, Soni M, Dey D, Mahanta J. Genetic polymorphisms associated with sulphadoxine-pyrimethamine drug resistance among Plasmodium falciparum field isolates in malaria endemic areas of Assam. J Postgrad Med 2015;61:9-14.
Source of Support: Nil, Conflict of Interest: None declared.
Announcement
Android AppA free application to browse and search the journal’s content is now available for Android based mobiles and devices. The application provides “Table of Contents” of the latest issues, which are stored on the device for future offline browsing. Internet connection is required to access the back issues and search facility. The application is compatible with all the versions of Android. The application can be downloaded from https://market.android.com/details?id=comm.app.medknow. For suggestions and comments do write back to us.
Copyright © 2022 FDOKUMEN




















