Gender Preference and Birthspacing in Matlab, Bangladesh
18
Demography, Vol. 30, No.3, August 1993 Gender Preference and Birth Spacing in Matlab, Bangladesh* Mizanur Rahman International Centre for Diarrhoeal Disease Research GPO Box 128 Dhaka 1000 Bangladesh Julie DaVanzo RAND 1700 Main Street Santa Monica California 90407-2138 Gender preference, particularly son preference, is believed to sustain high fertility in many Asian countries, but previous research shows unclear effects. We examine and compare gender-preference effects on fertility in two otherwise comparable populations in Bangladesh that differ markedly in their access to and use of contraception. We expect, and find, stronger effects of gender preference in the population that has more access to contraception and higher levels of contraceptive use. Thus gender preference may emerge as a significant barrier to further national family planning efforts in Bangladesh. We find that if a woman has at least one daughter, the risk of a subsequent birth is related negatively to the number of sons. Women with no daughters also experience a higher risk of having a subsequent birth; this finding suggests that there is also some preference for daughters. Son preference is strong in both the early and later stages of family formation, but women also want to have at least one daughter after having several sons. Parents both in traditional societies (both historical and contemporary) and in highly modern societies typically have some preferences, from a mild to an extreme degree, about the gender composition of their children. Gender preference is due to a complex interplay of • This paper is based on part of Mizanur Rahman's PhD dissertation, submitted to the Johns Hopkins University. Additional research was conducted while he was a postdoctoral fellow at RAND, and was supported by a grant to RAND from the William and Flora Hewlett Foundation. Julie DaVanzo's participation was supported by Grant POI-HD28372 from the National Institute for Child Health and Development (NICHO) to RAND. The data used in this study were collected and processed by the International Centre for Diarrhoeal Disease Research, Bangladesh (lCDDR,B). Donor agencies of ICDDR,B, including those who supported this study, are the aid agencies of the governments of Australia, Bangladesh, Belgium, Canada, Denmark, France, Japan, the Netherlands, Norway, Saudi Arabia, Sweden, Switzerland, the United Kingdom, and the United States; international organizations, including the United Nations Development Programme, the United Nations Fund for Population Activities. the United Nations Children's Fund, and the World Health Organization; and private foundations. including the Ford Foundation. the Rockefeller Foundation, and the Sasakawa Foundation. We would like to sincerely thank W. Henry Mosley and Stan Becker for their suggestions and comments during the early stage of the analysis, and Gary Bjork, Jacob Klerman, Jack Molyneaux. and Omar Rahman for their suggestions at a later stage. We acknowledge the support of Michael Strong in this research. An earlier version of the paper was presented at the annual meeting of the Population Association of America, held in Washington, DC, March 21-23, 1991. Copyright II:> 1993 Population Association of America 315
Transcript of Gender Preference and Birthspacing in Matlab, Bangladesh

Demography, Vol. 30, No.3, August 1993
Gender Preference and Birth Spacing inMatlab, Bangladesh*
Mizanur RahmanInternational Centre for Diarrhoeal Disease ResearchGPO Box 128Dhaka 1000Bangladesh
Julie DaVanzoRAND1700 Main StreetSanta Monica California 90407-2138
Gender preference, particularly son preference, is believed to sustain high fertility inmany Asian countries, but previous research shows unclear effects. We examine andcompare gender-preference effects on fertility in two otherwise comparablepopulations in Bangladesh that differ markedly in their access to and use ofcontraception. We expect, and find, stronger effects of gender preference in thepopulation that has more access to contraception and higher levels of contraceptiveuse. Thus gender preference may emerge as a significant barrier to further nationalfamily planning efforts in Bangladesh. We find that if a woman has at least onedaughter, the risk of a subsequent birth is related negatively to the number of sons.Women with no daughters also experience a higher risk of having a subsequent birth;this finding suggests that there is also some preference for daughters. Son preferenceis strong in both the early and later stages of family formation, but women also wantto have at least one daughter after having several sons.
Parents both in traditional societies (both historical and contemporary) and in highlymodern societies typically have some preferences, from a mild to an extreme degree, aboutthe gender composition of their children. Gender preference is due to a complex interplay of
• This paper is based on part of Mizanur Rahman's PhD dissertation, submitted to the Johns HopkinsUniversity. Additional research was conducted while he was a postdoctoral fellow at RAND, and was supported bya grant to RAND from the William and Flora Hewlett Foundation. Julie DaVanzo's participation was supported byGrant POI-HD28372 from the National Institute for Child Health and Development (NICHO) to RAND. The dataused in this study were collected and processed by the International Centre for Diarrhoeal Disease Research,Bangladesh (lCDDR,B). Donor agencies of ICDDR,B, including those who supported this study, are the aidagencies of the governments of Australia, Bangladesh, Belgium, Canada, Denmark, France, Japan, theNetherlands, Norway, Saudi Arabia, Sweden, Switzerland, the United Kingdom, and the United States;international organizations, including the United Nations Development Programme, the United Nations Fund forPopulation Activities. the United Nations Children's Fund, and the World Health Organization; and privatefoundations. including the Ford Foundation. the Rockefeller Foundation, and the Sasakawa Foundation. We wouldlike to sincerely thank W. Henry Mosley and Stan Becker for their suggestions and comments during the earlystage of the analysis, and Gary Bjork, Jacob Klerman, Jack Molyneaux. and Omar Rahman for their suggestionsat a later stage. We acknowledge the support of Michael Strong in this research. An earlier version of the paper waspresented at the annual meeting of the Population Association of America, held in Washington, DC, March 21-23,1991.
Copyright II:> 1993 Population Association of America
315
316 Demography, Vol. 30, No.3, August 1993
economic, social (including cultural and religious), and psychological factors. In many lessdeveloped countries of Asia, where women are economically and socially dependent onmen, sons generally are preferred over daughters. These preferences are reflected quiteclearly in fertility attitudes, but conflicting results are observed regarding the effects of thesepreferences on actual fertility.
In this paper we analyze the fertility implications of gender preference in a traditionalsociety that has a relatively high level of contraceptive prevalence. Because parents arebetter able to realize their intention of having a preferred composition of children whencontraception is readily available, we hypothesize that the effect of gender preference onfertility will be stronger with greater availability and use of contraception, and thus, thatgender preference will sustain relatively high fertility in situations where otherwise it mightdecrease further. We pursue this issue by examining the patterns of birth spacing in"treatment" and "comparison" areas of Matlab, Bangladesh. The contraceptive prevalencerate in the treatment area had risen to more than 60% by 1992 because of a carefullydesigned family planning program, whereas the rate in the comparison area has remained atabout 25-30% (Koenig et al. 1991). In this study we have the unique opportunity tocompare the effects of gender preference on fertility in two populations with the samegeneral social and economic setting and at the same period of time but with remarkabledifferences in their access to and use of contraception. We use prospective data, over aperiod of five years, from the Matlab population register, a demographic archive of knownaccuracy and completeness which has existed for more than 25 years. We also investigatethe possibility that parents may have some preference for daughters in addition to apreference for sons, and we examine how the effects of gender preference vary over thereproductive life cycle.
In the following sections of this paper we review the literature on gender preferenceand its effect on fertility and on the proximate determinants of fertility; present ourhypotheses; describe our study area, data, and methods; present the major findings of thestudy; and conclude with a summary of the features, findings, and implications of thisresearch.
GENDER PREFERENCE AND FERTILITY BEHAVIOR: AREVIEW OF THE LITERATURE
In a global comparison, Williamson (1976) constructed attitudinal scales measuringson preference which are based on the information collected in various surveys on thedesired gender composition of children. She categorized most of the countries in Asia ashaving strong to very strong son preference. Cleland, Verrall, and Vaessen (1983) alsoanalyzed attitudinal data for a cross-national comparison of son preference and reachedsimilar conclusions. Findings from studies based on stated preferences in a number ofcountries corroborate the cross-national studies (Ahmed 1981; Bairagi and Langsten 1986;Coombs and Sun 1978; Karki 1988; Khan and Sirageldin 1977).
A number of studies have been carried out since the 1960s to examine the effect of thegender composition of surviving children (GCSC) on fertility, as measured by the number ofchildren ever born (CEB), parity progression ratios (PPR), probability of subsequent birth,birth intervals, or contraceptive prevalence. The results vary widely from strong effects tono effects.
Marked effects of son preference on fertility have been observed in Korea and Taiwan,where stated preferences for sons are strong. The PPR and the probability of subsequentbirth were related negatively and significantly to the number of sons (Coombs 1979;
Gender Preference and Birth Spacing in Matlab, Bangladesh 317
Coombs and Sun 1978; Park 1978, 1983), and contraceptive use was related positively tothe number of sons (Arnold 1985; Coombs and Sun 1978). In Malaysia, no significant effectof son preference was observed on fertility among Malays, but Chinese tended to continuechildbearing until they had a son (Leung 1988).
In south and west Asia, where stated son preference is strong to very strong, noconsistent associations between the number of sons and fertility have been observed.Repetto (1972) noted a positive association between the number of sons and fertility: that is,families that lacked sons or had a high proportion of daughters tended to have fewerchildren. These results were not consistent with the expectation that subsequent fertilitywould be lower among the mothers with a high proportion of sons than among those with ahigher proportion of daughters (i.e., the expectation that those who had more sons wouldstop childbearing sooner). Studies in India and Pakistan in the 1960-1970 period provide noclear evidence that son preference significantly affects fertility (De Tray 1984; Mukherji1977), though one later study finds a strong negative association between the number ofsons and fertility in India (Das 1987). Cleland, Verrall, and Vaessen (1983) found no effectof son preference on subsequent fertility in Bangladesh, Jordan, or Syria, but found mild tomoderately negative effects in Nepal and Pakistan in the 1950s, 1960s, and 1970s. Arnold(1987) examined data on 27 countries in the late 1960s, 1970s, and early 1980s, andconcluded that in most cases, the gender composition of children has only a weak effect onfertility and contraceptive use.
In Bangladesh, a weak effect of son preference on contraceptive use was observed inthe 1970s, when contraceptive prevalence was low (Amin and Mariam 1987; Bairagi andLangsten 1986). The probability of a subsequent birth was related to GCSC in Matlab,Bangladesh in the early 1980s, but the impact was not substantial: it was estimated thatfertility would be reduced by only 4-8% if gender preference were removed (ChowdhuryandBairagi 1991). In a similar period in Matlab, however, Rahman et al. (1992) observeda profound effect of GCSC preference on the acceptance and continuation of contraception.
These conflicting results have led several authors to propose various hypotheses.Cleland et al. (1983) and De Tray (1984) argued that one may not observe a relationshipbetween GCSC and fertility, despite strong statements of son preference, because couplesdo not necessarily translate their intentions into actual fertility behavior. Both Repetto(1972) and McClelland (1979) hypothesized that son preference may lead to a positiverelationship between the number of sons and fertility for economic and psychologicalreasons: because sons are a source of economic gain to the family, while daughters are afinancial burden, couples with a high proportion of sons may feel themselves under lesspressure to limit family size than couples with a high proportion of daughters. Consequentlythe former may continue childbearing but the latter may limit their fertility. Couples with ahigh proportion of daughters may have a strong desire for sons, but they may feel that thedisadvantages associated with having another daughter outweigh the perceived benefits ofhaving a son. These couples also may think that the probability of having a daughter ishigher for them than for others. Therefore, they may not be willing to risk having anotherchild for fear that they will have a girl and will be worse off than they are with their currentnumber of children. In this case (on the basis of the assumption that families consider riskin their fertility decisions), fertility may vary directly, not inversely, with the number ofsons.
The inconsistency in the fmdings on the effects of GCSC on fertility in previous studiesalso may be due to methodological problems, including the use of less than ideal analyticalmethods, inappropriate dependent variables, and inaccurate data.!
As the above literature review suggests, gender-preference research has givenoverwhelming attention to son preference and has tended to overlook the possibility thatsome parents also may prefer for daughters. Parents, particularly mothers, may have some
318 Demography, Vol. 30, No.3, August 1993
preferences for daughters for economic and other reasons. In rural Asian societies,housework (cooking, cleaning, fetching water and firewood, caring for the children and theold, washing clothes, and serving food to family members) and family farming (cropprocessing, tending domestic animals, and raising poultry, all done around the home) areregarded as "women's work." A daughter helps the mother greatly in these tasks (while ason works outside the home), beginning in childhood and continuing until her marriage,when she leaves her parents' home. In addition, daughters are more likely than sons (anddaughters-in-law) to provide emotional support to the mother in different stages of life.
We find some indications from data on family size and composition (Ahmed 1981) andon fertility (Chowdhury and Bairagi 1991) in Bangladesh and some other south Asiancountries (Nag 1991) that women would like to have one daughter after several sons. In arecent cross-national study, Arnold (1991) found that preference for equal numbers of sonsand of daughters is quite common in 27 countries that participated in the Demographic andHealth Surveys. These studies, however, made no particular effort to examine the strengthand the more specific pattern of daughter preference.
GENDER PREFERENCE AND THE PROXIMATEDETERMINANTS OF FERTILITY
If the gender composition of surviving children (GCSC) affects decisions regardingsubsequent fertility, it does so through one or more "proximate determinants" or"intermediate fertility variables." These are contraceptive use, marital pattern (divorce andpolygamy), coital frequency and voluntary abstinence, induced abortion, and breastfeeding. Among these variables, contraceptive use is likely to be influenced most stronglyby gender preference to have a potential impact on fertility because it is the key variable fordeliberate control of fertility. Use of contraception, in Coale's (1973) terminology, must bewithin the "calculus of conscious choice." When preferences regarding GCSC are strongand when contraceptive use is widespread, couples may want to achieve a desired number ofsons (and daughters) before they use contraception to limit the size of their family. Evidencefrom many countries suggests that contraceptive practice is influenced strongly by genderpreference (see, for example, Arnold 1985 for Korea; Coombs and Sun 1978 for Taiwan;Gadalla, McCarthy, and Campbell 1985 for Egypt; and Rahman et al. 1992 forBangladesh). As noted in the literature review above, son preference has been observed tohave strong effects on fertility in areas and periods with relatively high contraceptive use,but little or no effect of GCSC on fertility has been found when and where contraceptive usewas relatively low.
Divorce and polygamy may result from the pressure of an unfavorable GCSC (Merrill1989). Coital frequency and voluntary sexual abstinence were found to be related to GCSCin an in-depth study of 20 women in a village in northern India; three women whose firstchild was a son tried to delay having a subsequent birth through sexual abstinence so thatthey would be able to pay more attention to their son (Khan et al. 1989). Induced abortionis another proximate determinant that may be influenced by GCSC, though we know of nostudies that have investigated this possibility. Duration of breast-feeding also may be relatedto a child's gender; in Bangladesh. for example. boys are given supplements earlier thangirls (Brown et al. 1982; Huffman et al. 1987). Effects through polygamy. divorce, andbreast-feeding could lead to a positive association between fertility and the number orproportion of sons, but the gender preference effects of these determinants are likely to berelatively small and they may be offset to some extent by effects through other proximatedeterminants (e.g .• coital frequency and abstinence). Thus the impact of gender preference
Gender Preference and Birth Spacing in Matlab, Bangladesh 319
on fertility is expected to be small among populations without widespread access tocontraception, but such impact is expected to increase (other things being equal) as theavailability of contraception increases.
HYPOTHESES
We hypothesize that mothers in Matlab have a strong preference about the gendercomposition of their surviving children; in particular, they want several surviving sons andat least one surviving daughter. Mothers perceive that sons will strengthen the economic andsocial status of the family and the relative maternal position; thus they want to have sons inthe early stage of family formation so that the sons will enter the labor force before thefather grows old or dies. Those women who fail to have a surviving son during the earlystage of family formation will continue childbearing to have at least one son. Further, afterbearing several sons, mothers also want to have at least one daughter because daughters arevalued for the support they can provide to mothers in household activities and on otheroccasions.
Because of these preferences, parents will stop or delay childbearing if they haveachieved the preferred number and gender composition of children, but otherwise willcontinue having children. The fertility implications will fit the following pattern: for a givennumber of surviving children, the probability of having a subsequent birth will be I)associated negatively with the number of surviving sons and 2) higher among women whohave no son or no daughter than among women who have children of both sexes. We expectthat the first relationship is more likely than the second to be observed in an early stage offamily formation.
We expect that the above-mentioned preferences will be realized more fully in apopulation that has ready access to contraceptive technology because couples in such apopulation are more able to achieve their fertility choices. Thus the basic premise of thispaper is that gender preference will have a greater influence on fertility where contraceptionis readily available and widely used; we expect to see little or no effect of gender preferenceon fertility in a population that does not use contraception. In particular we expect that in theformer setting, parents will stop or delay childbearing if they have achieved the preferredGCSC, but otherwise will continue having children.
We test these hypotheses by comparing "treatment" and "comparison" areas inMatlab, Bangladesh. We expect that effects of gender composition on fertility will bestronger in the treatment area, where contraception is much more widely available andwhere contraceptive use is substantially higher, than in the comparison area. Within thetreatment area, we expect that gender composition will have stronger effects among theusers than among the nonusers of contraception, though we recognize that the use ofcontraception itself may be a behavioral response to gender preference; indeed, this has beenfound in Matlab (Rahman 1990; Rahman et al. 1992). We also examine whether the effectsof gender preference differ between families in the early stage of family formation and thosein a more advanced stage; we do so by allowing the effects of the GCSC to differ with thenumber of surviving children.
SETTING, DATA, AND METHODSThe Study Area
Matlab is a rural, riverine subdistrict located about 35 miles south of Dhaka, the capitalof Bangladesh. The area is isolated and relatively inaccessible because of lack of
320 Demography, Vol. 30, No.3, August 1993
transportation, except river transportation. Subsistence rice agriculture and fishing dominatethe economy. Social institutions are predominantly traditional (e.g., women are secludedfrom economic and social activities), despite the steady increase in modernizing influencesof commercial contact with urban areas.
Matlab is well known for its "Demographic Surveillance System" (DSS), a populationlaboratory that has been operated in the locality since 1966 by the International Centre forDiarrhoeal Disease Research, Bangladesh (ICDDR,B). The DSS has been used since 1977to examine questions about the demographic effectiveness of family planning services.Demographic dynamics are monitored in the "treatment" and the "comparison" areas, andprovide comprehensive data on the impact of health and family planning services in Matlab.Each area has a population of approximately 100,000.
In the treatment area, family planning services have been provided intensively since1977 through house-to-house delivery of contraceptive devices and information by trainedvillage women. The service program has been associated with marked increases in the useof contraception and with correspondingly pronounced declines in fertility (Phillips et al.1982, 1988).2 In 1977 the total fertility rate (TFR) was over 6.5 in both areas. By 1990 theperiod TFR had fallen to a little below 4.0 in the treatment area. In contrast, it was slightlyover 5.0 in the comparison area, where family planning and health services are provided bythe government program.
The Data
The DSS records vital events in both areas of Matlab. A service statistics system, the"Record Keeping System" (RKS), maintains information on dynamics of contraceptive useonly in the treatment area; hence we cannot distinguish between users and nonusers ofcontraception in the comparison area. The dates of contraceptive acceptance, discontinuation, and changing of methods are available from the RKS; these dates can be linked to DSSdata on births, deaths, migrations, and changes in marital status. Information onsocioeconomic conditions, household environment, and other background characteristics arecompiled in periodic house-to-house censuses in the DSS area. The last such census wasundertaken in mid-1982. Each individual in the DSS area has a unique and permanentidentification number, which permits cross-referencing and linking of information overtime.
The sample for this study consists of the 7,510 mothers who had a singleton live birth(known here as the "index" birth or child) in the Matlab DSS area during the 1982 calendaryear. Thus the sample would exclude those who already have completed their families; suchwomen might be disproportionately those who have achieved their desired GCSc. Alongitudinal record has been created for each mother to include DSS information (migration,death, and subsequent birth) for five years after the index birth. The record also containsbackground information on maternal education, religion, and preceding births and childdeaths to the mother in the five years before the index child's birth.
Among the 7,510 mothers, 3,435 came from the treatment area. For the mothers in thisarea, we obtained additional information by linking the RKS data files, which include thedates of acceptance and discontinuation of contraception, as well as of changing methods, inthe five-year follow-up period. Of the 3,435 records in the treatment area, 3,145 could belinked successfully for both DSS and RKS information. About 8% of the records wereunmatched for the information on contraceptive dynamics; they are excluded from thisanalysis. The birth-spacing behavior of unmatched individuals did not differ significantlyfrom that of the individuals included in the analysis; hence selection bias, arising from theinability to match some records to the RKS, is unlikely.
Gender Preference and Birth Spacing in Matlab, Bangladesh
The Analysis
321
Subsequent live birth within 59 months (and related conception within 50 months) ofthe birth of the index child is the event of interest as the dependent variable. We disregardadditional live births (if any) after the first subsequent birth in the 6O-month follow-upperiod. Out-migration (n=448) and death (n= 101) of the women before subsequentconception are censoring events.
Methods of analysis. Both bivariate and multivariate analyses are employed. In thebivariate analyses, we consider the simple probability of a live birth's occurring in the fiveyears following the birth of the index child and how this probability differs by GCSC foreach number of the surviving children; the timing of the birth is not considered. Incalculating the probability, we assumed that the censoring events were distributed linearlyover time. We also conducted descriptive analyses of the timing of giving birth by GCSCover postpartum time, but do not present these results here because they do not differmarkedly from the multivariate results discussed below.3
Using the probability distributions by GCSC and a method proposed by Arnold (1985),we also examine the extent to which fertility would be reduced if no gender preferenceexisted in the population. The method compares the expected number of births with theobserved births; the former are estimated by applying the probabilities in the most favorablegender composition groups. We assume that for a given number of children, the gendercomposition group with the lowest probability of a subsequent birth is the most favorablecomposition with respect to gender preference. 4
In the multivariate analysis, we use hazards regression models (Cox 1972) to model therisk of subsequent conception leading to live birth.> We estimated waiting time toconception by subtracting nine months from the interval between live births. In an effort tospecify the hazards model correctly, we performed several diagnostic tests, primarily tolearn whether any covariate had a nonproportional (time-dependent) effect (Lawless 1982).On the basis of these tests, we found that the effect of the variable "children ever born" onsubsequent conception becomes non-proportional after 33 months following the birth of theindex child. In particular, the log-minus-log curve of the proportion giving birth for womenwith four or more children was parallel to the other curve up to 33 months and becamenearly flat after that point (Rahman 1990). Therefore, we use generalized hazards modelsfor the analysis; estimation is based on discrete-time hazards models (Allison 1982). Weused a three-monthly interval of time to reduce computing cost. The censored cases areretained in the risk set of analysis until time of the woman's death or migration.
Measures of gender composition. The principal explanatory variable of interest is thegender composition of surviving children, including the index child. In the bivariateanalysis we compare the proportions with a subsequent birth across various numbers ofsurviving sons for a given number of surviving children. In determining the number ofsurviving children, we consider survival status of the index child before subsequentconception. The number of surviving children, however, was not adjusted for the mortalityof the older children after 1982. Because the median previous birth interval is greater than36 months, most of the previous children who had survived until the birth of the index childhad passed the age of highest mortality risk by the time the index child was born. Mortalityafter that age should not substantially alter the gender composition of surviving children.
The multivariate analysis focuses on larger families (four or more children) andincludes three variables to capture the hypothesized nonlinear effects of gender composition.The first variable is the number of surviving sons. Second, we include a dichotomousvariable "no surviving son." This variable takes the value of 1 if the woman has nosurviving son, and the value of 0 otherwise, to allow for an additional effect of there beingno sons. Third, to capture the effect of daughter preference, a dichotomous variable "no
322 Demography, Vol. 30, No.3, August 1993
surviving daughter" takes the value of I if there is no surviving daughter in the family, andthe value of 0 otherwise. These variables are entered in the models along with the variable"children ever bom."6
In using these variables to represent the effects of gender preference, we assume thatthe parents' decision to have a subsequent child is based on the overall number and gendercomposition of children in the family. In preliminary analyses we also investigated theextent to which subsequent fertility is influenced by the gender of the index child. The indexchild's gender, however, had significant predictive power only when the overallcomposition of the children was not considered; thus, it is not included in the analysespresented here.
Other variables considered. The net effect of gender composition is evaluated inmodels that include other variables known to affect birth spacing. These other variables aremother's age, survival status of the index child, mother's educational attainment, religion ofthe household, and area (treatment or comparison). Survival status of the index child isentered in the hazards model as a time-varying covariate." The variable "index child died"takes the value of 0 if the index child was still alive at the end of the time interval underconsideration, and the value of 1 if the index child had died during that interval or earlier.Religion and area are treated as dichotomous variables: Hindus and Muslims are coded as 1and 0 respectively; the treatment area is given a value of 1, while the comparison area isgiven a value of O.
To test the hypothesis that gender-preference effects increase with the availability anduse of contraception, we include in the models the interactions of the gender compositionvariables and the dichotomous indicator for the treatment area. We have also includedinteractions to examine whether gender-preference effects vary by the experience of childdeath, mother's education, and religion. For instance, the death of a son may lead to morerapid replacement than the death of a daughter. Furthermore. gender preference may bedifferent for the uneducated than for the educated, as well as for different religious groups.Uneducated mothers, for example, may be more traditional and hence may have strongergender preferences than educated mothers.
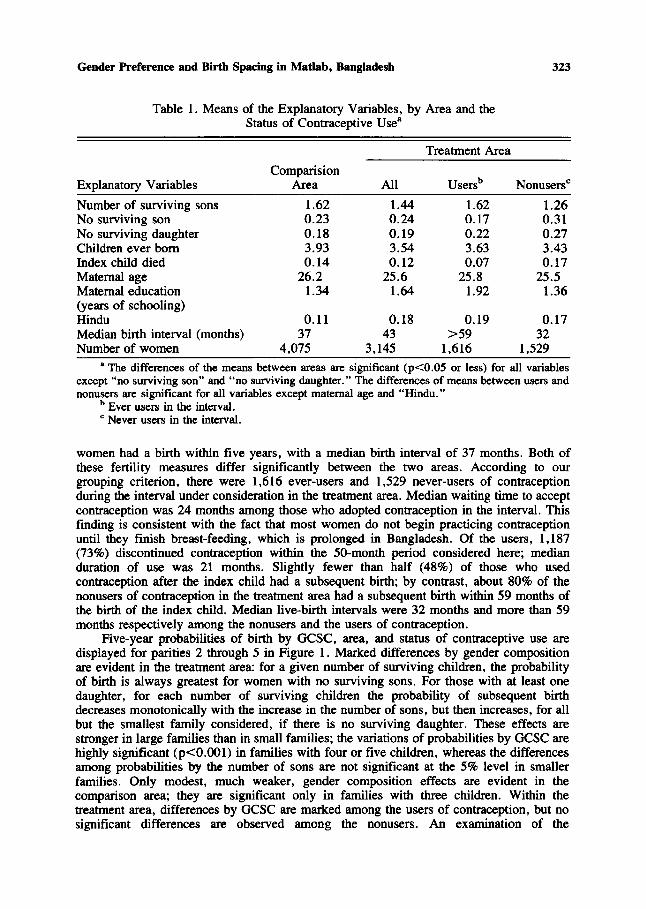
Table 1 displays means of explanatory variables by area and by status of contraceptiveuse.! Because contraceptive use is higher in the treatment area than in the comparison area,the average number of children ever born (and thus the average number of surviving sons)is lower in the treatment area. Within the treatment area, the average number of survivingsons is significantly higher among users than among nonusers of contraception. The numberof children ever born is also higher, but not to the same degree. The proportions of womenwith no surviving son or no surviving daughter are significantly lower among the users thanamong the nonusers of contraception in the treatment area; this finding suggests thatcontraceptive use in the treatment area is influenced by whether the parents have children ofboth genders. Indeed, this situation was found in an analysis of contraceptive use in Matlab(Rahman et al. 1992). Women in the treatment area have significantly better socioeconomicconditions, measured by maternal education, than women in the comparison area. There aremore Hindus in the treatment area than in the comparison area. These differences in the twopopulations' background characteristics existed when the villages were grouped intotreatment and comparison areas (Chowdhury and Phillips 1985).
RESULTSBivariate Analysis
In the treatment area, 63% of the 3,145 women had a subsequent live birth within fiveyears, with a median birth interval of 43 months. In the comparison area, 66% of the 4,075
Gender Preference and Birth Spacing in Matlab, Bangladesh
Table 1. Means of the Explanatory Variables, by Area and theStatus of Contraceptive Use"
323
Treatment Area
ComparisionExplanatory Variables Area All Usersb Nonusers"
Number of surviving sons 1.62 1.44 1.62 1.26No surviving son 0.23 0.24 0.17 0.31No surviving daughter 0.18 0.19 0.22 0.27Children ever born 3.93 3.54 3.63 3.43Index child died 0.14 0.12 0.07 0.17Maternal age 26.2 25.6 25.8 25.5Maternal education 1.34 1.64 1.92 1.36(years of schooling)Hindu 0.11 0.18 0.19 0.17Median birth interval (months) 37 43 >59 32Number of women 4,075 3,145 1,616 1,529
a The differences of the means between areas are significant (p<O.05 or less) for all variablesexcept "no surviving son" and "no surviving daughter." The differences of means between users andnonusers are significant for all variables except maternal age and "Hindu."
b Ever users in the interval.c Never users in the interval.
women had a birth within five years, with a median birth interval of 37 months. Both ofthese fertility measures differ significantly between the two areas. According to ourgrouping criterion, there were 1,616 ever-users and 1,529 never-users of contraceptionduring the interval under consideration in the treatment area. Median waiting time to acceptcontraception was 24 months among those who adopted contraception in the interval. Thisfinding is consistent with the fact that most women do not begin practicing contraceptionuntil they finish breast-feeding, which is prolonged in Bangladesh. Of the users, 1,187(73%) discontinued contraception within the 50-month period considered here; medianduration of use was 21 months. Slightly fewer than half (48%) of those who usedcontraception after the index child had a subsequent birth; by contrast, about 80% of thenonusers of contraception in the treatment area had a subsequent birth within 59 months ofthe birth of the index child. Median live-birth intervals were 32 months and more than 59months respectively among the nonusers and the users of contraception.
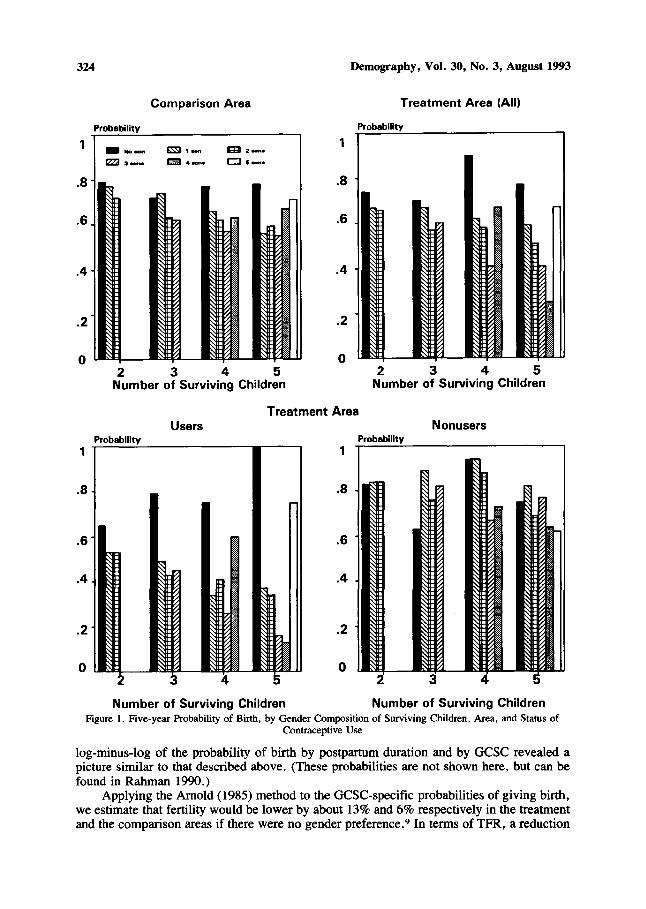
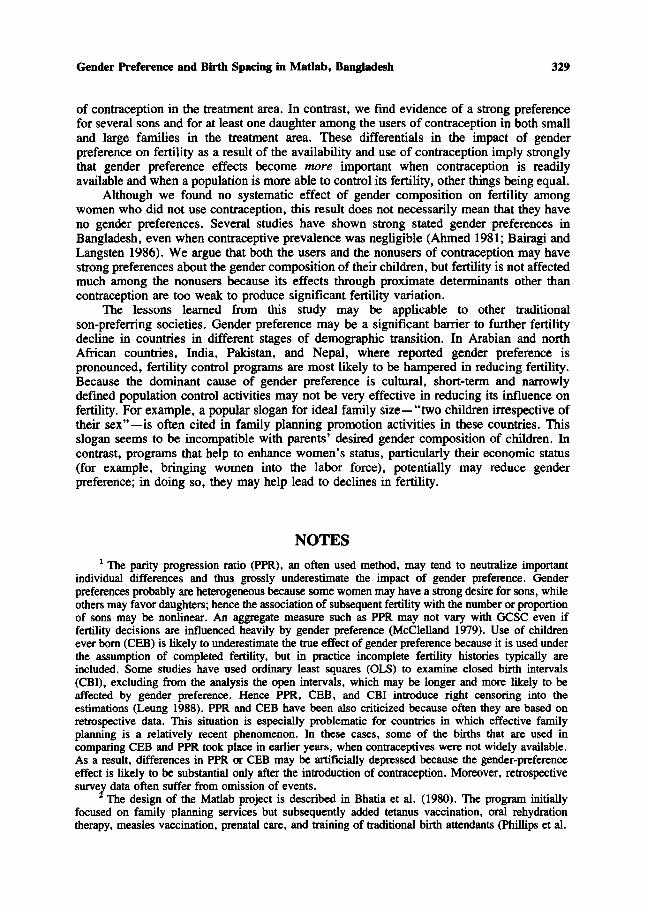
Five-year probabilities of birth by GCSC, area, and status of contraceptive use aredisplayed for parities 2 through 5 in Figure 1. Marked differences by gender compositionare evident in the treatment area: for a given number of surviving children, the probabilityof birth is always greatest for women with no surviving sons. For those with at least onedaughter, for each number of surviving children the probability of subsequent birthdecreases monotonically with the increase in the number of sons, but then increases, for allbut the smallest family considered, if there is no surviving daughter. These effects arestronger in large families than in small families; the variations of probabilities by GCSC arehighly significant (p<O.OOl) in families with four or five children, whereas the differencesamong probabilities by the number of sons are not significant at the 5% level in smallerfamilies. Only modest, much weaker, gender composition effects are evident in thecomparison area; they are significant only in families with three children. Within thetreatment area, differences by GCSC are marked among the users of contraception, but nosignificant differences are observed among the nonusers. An examination of the
324
Comparison Area
Probability
Demography, Vol. 30, No.3, August 1993
Treatment Area (All)
Probability
1_No_rzzJ 3 ....
m 2 .....
CJ leon.
1
.8
.6
.4
.2
o2 3 4 5
Number of Surviving Children
.8
.6
.4
.2
o2 345
Number of Surviving Children
UsersTreatment Area
Nonusers
1
.8
.6
.4
.2
o
Probability Probability1
.8
.6
.4
.2
o2 3 4 5
Number of Surviving Children Number of Surviving ChildrenFigure 1. Five-year Probability of Birth, by Gender Composition of Surviving Children, Area, and Status of
Contraceptive Use
log-minus-Iog of the probability of birth by postpartum duration and by GCSC revealed apicture similar to that described above, (These probabilities are not shown here, but can befound in Rahman 1990,)
Applying the Arnold (1985) method to the GCSC-specific probabilities of giving birth,we estimate that fertility would be lower by about 13% and 6% respectively in the treatmentand the comparison areas if there were no gender preference." In terms of TFR, a reduction
Gender Preference and Birth Spacing in Matlab, Bangladesh 325
of 0.59 birth could occur in the treatment area and 0.34 birth in the comparison area; in1982-1986 the average TFRs in these areas were 4.5 and 6.0 respectively. These estimates,however, are likely to be the lower bound: Bairagi (1987) showed that this methodunderestimates the true effect because of possible parity-specific heterogeneity ofpreferences.
Multivariate Analysis
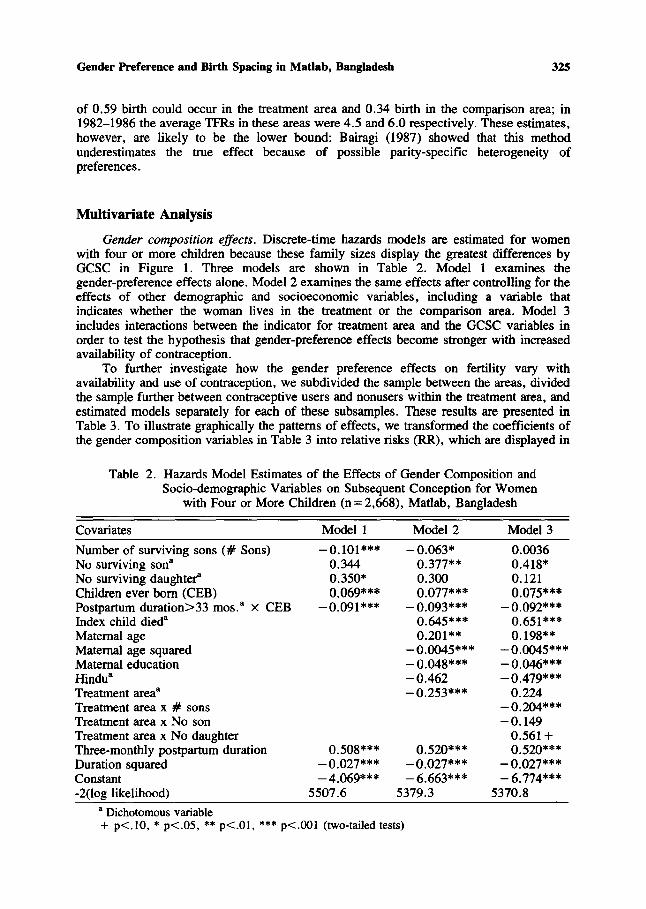
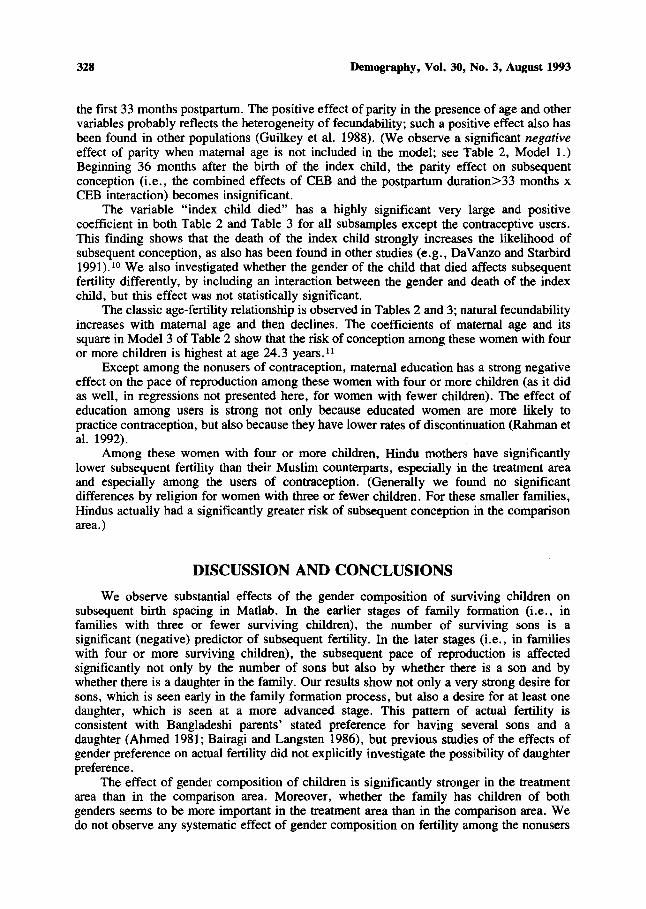
Gender composition effects. Discrete-time hazards models are estimated for womenwith four or more children because these family sizes display the greatest differences byGCSC in Figure 1. Three models are shown in Table 2. Model I examines thegender-preference effects alone. Model 2 examines the same effects after controlling for theeffects of other demographic and socioeconomic variables, including a variable thatindicates whether the woman lives in the treatment or the comparison area. Model 3includes interactions between the indicator for treatment area and the GCSC variables inorder to test the hypothesis that gender-preference effects become stronger with increasedavailability of contraception.
To further investigate how the gender preference effects on fertility vary withavailability and use of contraception, we subdivided the sample between the areas, dividedthe sample further between contraceptive users and nonusers within the treatment area, andestimated models separately for each of these subsamples. These results are presented inTable 3. To illustrate graphically the patterns of effects, we transformed the coefficients ofthe gender composition variables in Table 3 into relative risks (RR), which are displayed in
Table 2. Hazards Model Estimates of the Effects of Gender Composition andSocio-demographic Variables on Subsequent Conception for Women
with Four or More Children (n = 2,668), Matlab, Bangladesh
Covariates
Number of surviving sons (# Sons)No surviving son"No surviving daughter"Children ever born (CEB)Postpartum duration>33 mos." x CEBIndex child died"Maternal ageMaternal age squaredMaternal educationHindua
Treatment area"Treatment area x # sonsTreatment area x No sonTreatment area x No daughterThree-monthly postpartum durationDuration squaredConstant-2(log likelihood)
Modell
-0.101***0.3440.350*0.069***
-0.091 ***
0.508***-0.027***-4.069***
5507.6
Model 2
-0.063*0.377**0.3000.077***
-0.093***0.645***0.201**
-0.0045***-0.048***-0.462-0.253***
0.520***-0.027***-6.663***
5379.3
Model 3
0.00360.418*0.1210.075***
-0.092***0.651 ***0.198**
-0.0045***-0.046***-0.479***
0.224-0.204***-0.149
0.561 +0.520***
-0.027***-6.774***
5370.8
a Dichotomous variable+ p<.lO. * p<.05. ** p<.OI. *** p<.OOI (two-tailed tests)
326 Demography, Vol. 30, No.3, August 1993
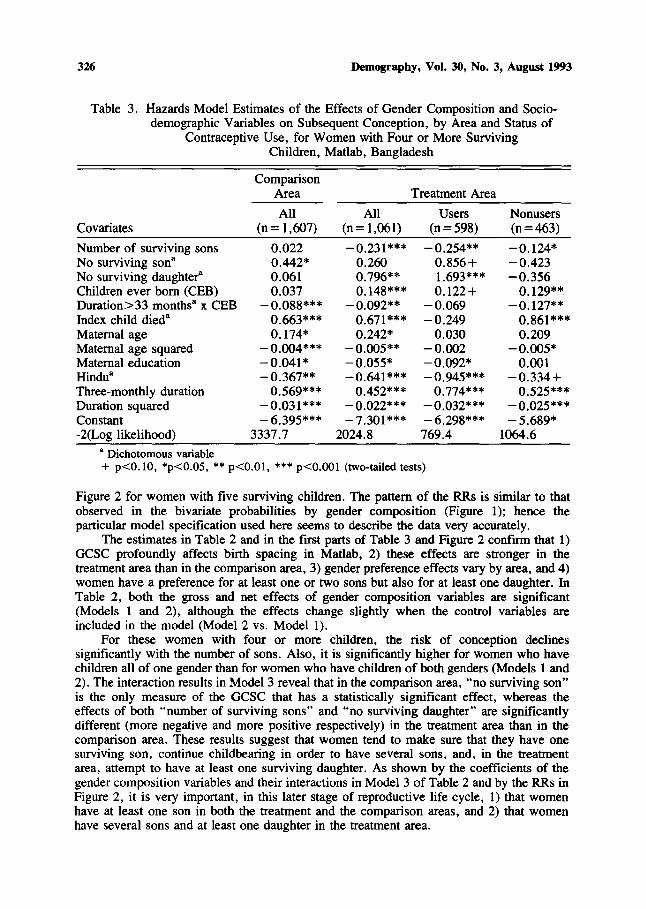
Table 3. Hazards Model Estimates of the Effects of Gender Composition and Sociodemographic Variables on Subsequent Conception, by Area and Status of
Contraceptive Use, for Women with Four or More SurvivingChildren, Matlab, Bangladesh
Covariates
Number of surviving sonsNo surviving son"No surviving daughter"Children ever born (CEB)Duration>33 months" x CEBIndex child died"Maternal ageMaternal age squaredMaternal educationHindu"Three-monthly durationDuration squaredConstant-2(Log likelihood)
ComparisonArea
All(n= 1,607)
0.0220.442*0.0610.037
-0.088***0.663***0.174*
-0.004***-0.041*-0.367**
0.569***-0.031***-6.395***
3337.7
All(n= 1,061)
-0.231***0.2600.796**0.148***
-0.092**0.671***0.242*
-0.005**-0.055*-0.641 ***
0.452***-0.022***-7.301***
2024.8
Treatment Area
Users(n =598)
-0.254**0.856+1.693***0.122+
-0.069-0.249
0.030-0.002-0.092*-0.945***
0.774***-0.032***-6.298***769.4
Nonusers(n =463)
-0.124*-0.423-0.356
0.129**-0.127**
0.861***0.209
-0.005*0.001
-0.334+0.525***
-0.025***-5.689*
1064.6
• Dichotomous variable+ p<O.lO, *p<O.05, ** p<O.OI, *** p<O.OOI (two-tailed tests)
Figure 2 for women with five surviving children. The pattern of the RRs is similar to thatobserved in the bivariate probabilities by gender composition (Figure 1); hence theparticular model specification used here seems to describe the data very accurately.
The estimates in Table 2 and in the first parts of Table 3 and Figure 2 confirm that 1)GCSC profoundly affects birth spacing in Matlab, 2) these effects are stronger in thetreatment area than in the comparison area, 3) gender preference effects vary by area, and 4)women have a preference for at least one or two sons but also for at least one daughter. InTable 2, both the gross and net effects of gender composition variables are significant(Models 1 and 2), although the effects change slightly when the control variables areincluded in the model (Model 2 vs. Modell).
For these women with four or more children, the risk of conception declinessignificantly with the number of sons. Also, it is significantly higher for women who havechildren all of one gender than for women who have children of both genders (Models 1 and2). The interaction results in Model 3 reveal that in the comparison area, "no surviving son"is the only measure of the GCSC that has a statistically significant effect, whereas theeffects of both "number of surviving sons" and "no surviving daughter" are significantlydifferent (more negative and more positive respectively) in the treatment area than in thecomparison area. These results suggest that women tend to make sure that they have onesurviving son, continue childbearing in order to have several sons, and, in the treatmentarea, attempt to have at least one surviving daughter. As shown by the coefficients of thegender composition variables and their interactions in Model 3 of Table 2 and by the RRs inFigure 2, it is very important, in this later stage of reproductive life cycle, 1) that womenhave at least one son in both the treatment and the comparison areas, and 2) that womenhave several sons and at least one daughter in the treatment area.
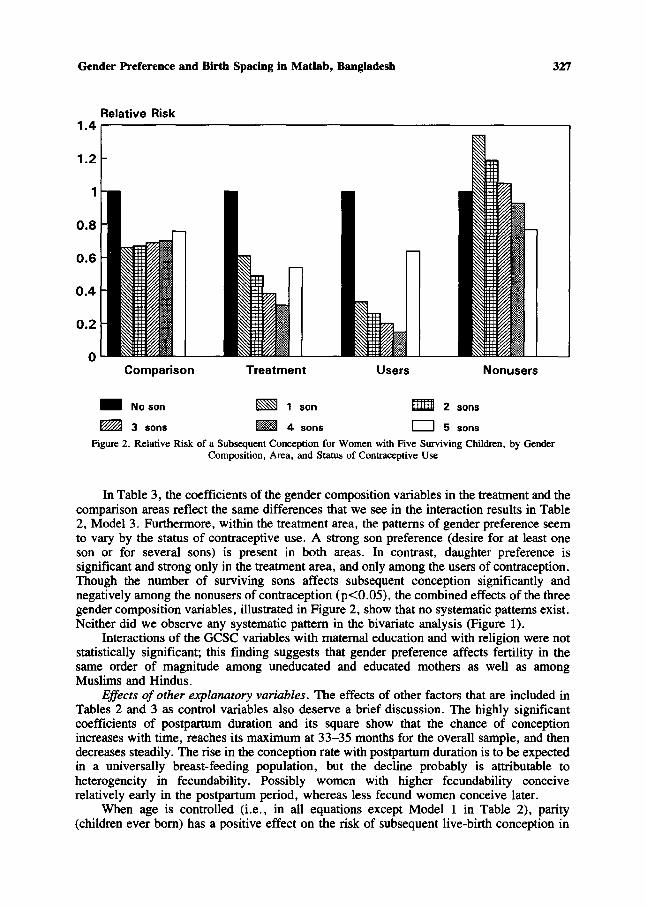
Gender Preference and Birth Spacing in Matlab, Bangladesh 327
Relative Risk1.4.-----------------------------.,
1.2
1
0.8
0.6
0.4
0.2
oComparison
No son
3 sons
Treatment
1 son
4 sons
Users
mm 2
D 5
sons
sons
Nonusers
Figure 2. Relative Risk of a Subsequent Conception for Women with Five Surviving Children, by GenderComposition, Area, and Status of Contraceptive Use
In Table 3, the coefficients of the gender composition variables in the treatment and thecomparison areas reflect the same differences that we see in the interaction results in Table2, Model 3. Furthermore, within the treatment area, the patterns of gender preference seemto vary by the status of contraceptive use. A strong son preference (desire for at least oneson or for several sons) is present in both areas. In contrast, daughter preference issignificant and strong only in the treatment area, and only among the users of contraception.Though the number of surviving sons affects subsequent conception significantly andnegatively among the nonusers of contraception (p<O.05), the combined effects of the threegender composition variables, illustrated in Figure 2, show that no systematic patterns exist.Neither did we observe any systematic pattern in the bivariate analysis (Figure 1).
Interactions of the GCSC variables with maternal education and with religion were notstatistically significant; this finding suggests that gender preference affects fertility in thesame order of magnitude among uneducated and educated mothers as well as amongMuslims and Hindus.
Effects of other explanatory variables. The effects of other factors that are included inTables 2 and 3 as control variables also deserve a brief discussion. The highly significantcoefficients of postpartum duration and its square show that the chance of conceptionincreases with time, reaches its maximum at 33-35 months for the overall sample, and thendecreases steadily. The rise in the conception rate with postpartum duration is to be expectedin a universally breast-feeding population, but the decline probably is attributable toheterogeneity in fecundability. Possibly women with higher fecundability conceiverelatively early in the postpartum period, whereas less fecund women conceive later.
When age is controlled (i.e., in all equations except Model I in Table 2), parity(children ever born) has a positive effect on the risk of subsequent live-birth conception in
328 Demography, Vol. 30, No.3, August 1993
the first 33 months postpartum. The positive effect of parity in the presence of age and othervariables probably reflects the heterogeneity of fecundability; such a positive effect also hasbeen found in other populations (Guilkey et al. 1988). (We observe a significant negativeeffect of parity when maternal age is not included in the model; see Table 2, Modell.)Beginning 36 months after the birth of the index child, the parity effect on subsequentconception (i.e., the combined effects of CEB and the postpartum duration>33 months xCEB interaction) becomes insignificant.
The variable "index child died" has a highly significant very large and positivecoefficient in both Table 2 and Table 3 for all subsamples except the contraceptive users.This finding shows that the death of the index child strongly increases the likelihood ofsubsequent conception, as also has been found in other studies (e.g., DaVanzo and Starbird1991).10 We also investigated whether the gender of the child that died affects subsequentfertility differently, by including an interaction between the gender and death of the indexchild, but this effect was not statistically significant.
The classic age-fertility relationship is observed in Tables 2 and 3; natural fecundabilityincreases with maternal age and then declines. The coefficients of maternal age and itssquare in Model 3 of Table 2 show that the risk of conception among these women with fouror more children is highest at age 24.3 years. 11
Except among the nonusers of contraception, maternal education has a strong negativeeffect on the pace of reproduction among these women with four or more children (as it didas well, in regressions not presented here, for women with fewer children). The effect ofeducation among users is strong not only because educated women are more likely topractice contraception, but also because they have lower rates of discontinuation (Rahman etal. 1992).
Among these women with four or more children, Hindu mothers have significantlylower subsequent fertility than their Muslim counterparts, especially in the treatment areaand especially among the users of contraception. (Generally we found no significantdifferences by religion for women with three or fewer children. For these smaller families,Hindus actually had a significantly greater risk of subsequent conception in the comparisonarea.)
DISCUSSION AND CONCLUSIONS
We observe substantial effects of the gender composition of surviving children onsubsequent birth spacing in Matlab. In the earlier stages of family formation (i.e., infamilies with three or fewer surviving children), the number of surviving sons is asignificant (negative) predictor of subsequent fertility. In the later stages (i.e., in familieswith four or more surviving children), the subsequent pace of reproduction is affectedsignificantly not only by the number of sons but also by whether there is a son and bywhether there is a daughter in the family. Our results show not only a very strong desire forsons, which is seen early in the family formation process, but also a desire for at least onedaughter, which is seen at a more advanced stage. This pattern of actual fertility isconsistent with Bangladeshi parents' stated preference for having several sons and adaughter (Ahmed 1981; Bairagi and Langsten 1986), but previous studies of the effects ofgender preference on actual fertility did not explicitly investigate the possibility of daughterpreference.
The effect of gender composition of children is significantly stronger in the treatmentarea than in the comparison area. Moreover, whether the family has children of bothgenders seems to be more important in the treatment area than in the comparison area. Wedo not observe any systematic effect of gender composition on fertility among the nonusers
Gender Preference and Birth Spacing in Matlab, Bangladesh 329
of contraception in the treatment area. In contrast, we find evidence of a strong preferencefor several sons and for at least one daughter among the users of contraception in both smalland large families in the treatment area. These differentials in the impact of genderpreference on fertility as a result of the availability and use of contraception imply stronglythat gender preference effects become more important when contraception is readilyavailable and when a population is more able to control its fertility, other things being equal.
Although we found no systematic effect of gender composition on fertility amongwomen who did not use contraception, this result does not necessarily mean that they haveno gender preferences. Several studies have shown strong stated gender preferences inBangladesh, even when contraceptive prevalence was negligible (Ahmed 1981; Bairagi andLangsten 1986). We argue that both the users and the nonusers of contraception may havestrong preferences about the gender composition of their children, but fertility is not affectedmuch among the nonusers because its effects through proximate determinants other thancontraception are too weak: to produce significant fertility variation.
The lessons learned from this study may be applicable to other traditionalson-preferring societies. Gender preference may be a significant barrier to further fertilitydecline in countries in different stages of demographic transition. In Arabian and northAfrican countries, India, Pakistan, and Nepal, where reported gender preference ispronounced, fertility control programs are most likely to be hampered in reducing fertility.Because the dominant cause of gender preference is cultural, short-term and narrowlydefined population control activities may not be very effective in reducing its influence onfertility. For example, a popular slogan for ideal family size- "two children irrespective oftheir sex" -is often cited in family planning promotion activities in these countries. Thisslogan seems to be incompatible with parents' desired gender composition of children. Incontrast, programs that help to enhance women's status, particularly their economic status(for example, bringing women into the labor force), potentially may reduce genderpreference; in doing so, they may help lead to declines in fertility.
NOTES
1 The parity progression ratio (PPR), an often used method, may tend to neutralize importantindividual differences and thus grossly underestimate the impact of gender preference. Genderpreferences probably are heterogeneous because some women may have a strong desire for sons, whileothers may favor daughters; hence the association of subsequent fertility with the number or proportionof sons may be nonlinear. An aggregate measure such as PPR may not vary with GCSC even iffertility decisions are influenced heavily by gender preference (McClelland 1979). Use of childrenever born (CEB) is likely to underestimate the true effect of gender preference because it is used underthe assumption of completed fertility, but in practice incomplete fertility histories typically areincluded. Some studies have used ordinary least squares (OLS) to examine closed birth intervals(CBI), excluding from the analysis the open intervals, which may be longer and more likely to beaffected by gender preference. Hence PPR, CEB, and CBI introduce right censoring into theestimations (Leung 1988). PPR and CEB have been also criticized because often they are based onretrospective data. This situation is especially problematic for countries in which effective familyplanning is a relatively recent phenomenon. In these cases, some of the births that are used incomparing CEB and PPR took place in earlier years, when contraceptives were not widely available.As a result, differences in PPR or CEB may be artificially depressed because the gender-preferenceeffect is likely to be substantial only after the introduction of contraception. Moreover, retrospectivesurvel data often suffer from omission of events.
The design of the Matlab project is described in Bhatia et al. (1980). The program initiallyfocused on family planning services but subsequently added tetanus vaccination, oral rehydrationtherapy, measles vaccination, prenatal care, and training of traditional birth attendants (Phillips et al.
330 Demography, Vol. 30, No.3, August 1993
1984). Among the 1,626 contraceptive users in the treatment area, the methods used are injectables(43%), IUDs (29%), oral pills (13%), sterilizations (6%), and others (9%).
3 In order to consider the timing of births, we calculated maximum-likelihood estimates of theprobability of not giving birth (S(t», using the product-limit, or Kaplan-Meier (1958), method. Theprobabilities of giving birth were examined in graphic form after a log-minus-log transformation[log{-log(l-S(t»}], which helped to linearize the curves and to reveal nonproportional effects (Lawless1982). These results are not presented here, but can be found in Rahman (1990).
4 Among the mothers with four surviving children, for example, if the probability of having asubsequent birth is lowest among those who have three sons and one daughter, we assume that thesemothers are the most satisfied with their GCsc.
5 We consider conception rather than birth for two reasons. First, this approach reducescomputation cost in the discrete-time hazards models (the length of the interval is reduced by 9months). Second, the variables under consideration mostly affect whether a conception occurs. Forexample, death of the index child after the subsequent conception but before that next birth would notaffect that conception. Although DSS collects information on miscarriages and stillbirths, we restrictthe analysis to conceptions that resulted in live births, for the following reasons: 1) The completenessof coverage, particularly of early fetal wastage, is likely to be unsatisfactory, and 2) duration ofgestation is not always available.
6 In preliminary analyses we also estimated separate regressions for each number of survivingchildren and included dummy variables for all possible gender compositions but one. The results werevery similar to the more parsimonious specification used here, but had less statistical power becausesamples were smaller.
7 Note, however, that early infant death occurs more frequently after a short previous birthinterval (National Research Council 1989); thus the women who lost their index children before thesubsequent conception may belong to a selective group of women with higher risk of short intervals.There are strong biological and behavioral reasons, however, why a child's death can cause a shorterinterval (e.g., DaVanzo and Starbird 1991).
8 In the multivariate analysis, we use a time-varying scheme to group women into users andnonusers of contraception. We started with all women in the treatment area who were nonusers ofcontraception at the birth of the index child. At the beginning of each ordinal month since that point,we ask "Has the woman accepted contraception?" If the answer is "yes," the woman enters the groupof users of contraception and remains there throughout the period of 50 months, whether or not shelater discontinues use. A woman remains in the group of nonusers if the answer continues to be "no."For this classification, we only consider contraceptive behavior after the birth of the index child; theuse of contraception before the birth of the index child is not considered. For the means in Table 1 westratify women into those who ever used contraception in the interval following the birth of the indexchild and those who never used contraception in that interval.
9 This (Arnold) analysis uses the total sample (all parities). Employing a similar methodology,Chowdhury and Bairagi (1991) found that fertility would be reduced by 8% and 4% respectively in thetreatment and comparison areas. The difference between our estimates and theirs is probably related todiferences in methodology and the period of study. We examine data from 1982 through 1987,whereas their study used data only up to 1985; contraceptive use increased greatly in 1986 and 1987and, as we have seen here, gender preference effects are likely to increase with increases incontraceptive use. Moreover, Chowdhury and Bairagi probably underestimated the gendercomposition effects further by not considering the mortality of the youngest child during the period ofexposure to the subsequent conception.
10 These results suggest that women who have four or more children and are practicingcontraception do not, on average, discontinue contraceptive use when a child dies. (The positive andsignificant effect for nonusers probably occurs because the child's death truncates breast-feeding. Theaverage duration postpartum is shorter for the nonusers; hence they are more likely to bebreast-feeding when the child dies. Also the contraceptive effect of breast-feeding is stronger earlier inthe postpartum period.) By contrast, in analyses not presented here, we found a positive andsignificant effect of the index child's death on the likelihood of subsequent conception forcontraceptive users with three or fewer children. In fact, that effect was nearly twice as large as the(also significant) effect estimated for non-users with three or fewer children.
11 According to the coefficients in Model 3 of Table 2, the maximum risk of conception occurs
Gender Preference and Birth Spacing in Matlab, Bangladesh 331
among the women who were age 22.0 at the birth of the index child. On average, these women are24.3 years old at the time of their subsequent conception because median time to subsequentconception is 39 months for this sample.
REFERENCES
Ahmed, Nilufer R. 1981. "Family Size and Sex Preferences among Women in Rural Bangladesh."Studies in Family Planning 12:100-9.
Allison, Paul. 1982. "Discrete-Time Methods for the Analysis of Event Histories." pp. 61-98 inSociological Methodology 1982, edited by S. Linhardt. San Francisco: Jossey-Bass.
Amin, Ruhu1 and A. G. Mariam. 1987. "Son Preference in Bangladesh: An Emerging Barrier toFertility Regulation." Journal ofBiosocial Science 19:221-28.
Arnold, Fred. 1985. "Measuring the Effect of Sex Preference on Fertility: The Case of Korea."Demography 22:280-88.
__. 1987. "The Effect of Sex Preference on Fertility and Family Planning: Empirical Evidence."Population Bulletin of the United Nations 23/24-1987:44-55.
___. 1991. "Sex Preference for Children and Its Demographic and Health Implications." Pp.249-73 in Proceedings of the Demographic and Health Surveys World Conference, Vol. 1.Columbia, MD: IRDlMacro International, Inc.
Bairagi, Radheshyam. 1987. "A Comment on Fred Arnold's "Measuring the Effect of Sex Preferenceon Fertility'." Demography 24:137-38.
Bairagi, Radheshyam and Ray L. Langsten. 1986. "Sex Preference for Children and Its Implicationsfor Fertility in Rural Bangladesh." Studies in Family Planning 17:302-07.
Bhatia, Shushum, W. Henry Mosley, Abu S. G. Faruque, and Jotsnamoy Chakraborty. 1980. "TheMatlab Family Planning-Health Services Project." Studies in Family Planning 11:202-12.
Brown, Kenneth H., Robert E. Black, Stan Becker, Shamsun Nahar, and J. Sawyer. 1982."Consumption of Foods and Nutrients by Weanlings in Rural Bangladesh." American Journal ofClinical Nutrition 36:878-89.
Chowdhury, Aminul I. and James F. Phillips. 1985. "Socio-economic Status Differentials amongCurrently Married Women of Reproductive Age: FP Services Project, 1974 Matlab Census."Journal of Family Welfare 31:3-11.
Chowdhury, Mridul K. and Radheshyam Bairagi. 1991. "Son Preference and Fertility inBangladesh." Population and Development Review 16:749-57.
Cleland, John, Jane Verrall, and Martin Vaessen. 1983. "Preferences for the Sex of Children andTheir Influence on Reproductive Behavior." World Fertility Survey Comparative Studies:Cross-National Summaries No. 27. Voorburg: International Statistical Institute.
Coale, Ansley J. 1973. "The Demographic Transition." pp. 53-72 in International PopulationConference 1973, Vol. 1. Liege: International Union for the Scientific Study of Population.
Coombs, Lo1ogeneC. 1979. "Prospective Fertility and Underlying Preferences: A Longitudinal Studyin Taiwan." Population Studies 33:447-55.
Coombs, Lologene C. and Te-Hsiung Sun. 1978. "Family Composition Preferences in a DevelopingCulture: The Case of Taiwan." Population Studies 32:43-64.
Cox, D.R. 1972. "Regression Models and Life Tables." Journal of the Royal Statistical SocietyB34:187-202.
Das, Narayan. 1987. "Sex Preference and Fertility Behavior: A Study of Recent Indian Data."Demography 24:517-30.
DaVanzo, Julie and Ellen H. Starbird. 1991. "Correlates of Short Interbirth Intervals in PeninsularMalaysia: Their Pathways of Influence through Breastfeeding and Contraceptive Use." Studies inFamily Planning 22:241-54.
De Tray, Dennis. 1984. "Son Preference in Pakistan: An Analysis of Intentions versus Behavior."Research in Population Economics 5:185-200.
Gadalla, Saad, James McCarthy, and Oona Campbell. 1985. "How the Number of Sons InfluencesContraceptive Use in Menoufia Governorate, Egypt." Studies in Family Planning 16:164-69.
Guilkey, David K., Ronald R. Rindfuss, Barry M. Popkin, John S. Akin, and Vincent Paqueo. 1988.
332 Demography, Vol. 30, No.3, August 1993
"Child Spacing in the Philippines: The Effect of Current Characteristics and RuralDevelopment." Population Studies 42:259-73.
Huffman, Sandra L., Kathleen Ford, Hubert A. Allen, and P. Streble 1987. "Nutrition and Fertility inBangladesh: Breastfeeding and Post Pactum Amenorrhoea." Population Studies 41:447~2.
Kaplan, E. and P. Meier. 1958. "Non-Parametric Estimation from Incomplete Observation." Journalof the American Statistical Association 53:457-81.
Karki, Yagya B. 1988. "Sex Preference and the Value of Sons and Daughters in Nepal." Studies inFamily Planning 19:169-78.
Khan, M. Ali and Ismail Sirageldin. 1977. "Son Preference and Demand for Additional Children inPakistan." Demography 14:481-96.
Khan, M. E., R. Anker, S. K. G. Dastidar, and S. Bairathi. 1989. "Inequalities between Men andWomen in Nutrition and Family Welfare Services: An In-Depth Enquiry in an Indian Village."pp. 175-99 in Selected Readings in the Cultural, Social, and Behavioral Determinants ofHealth,edited by J. C. Caldwell and G. Santow. Canberra: Highland Press.
Koenig, Michael A., Ubaidur Rob, Mehrab A. Khan, Jotsnamoy Chakraborty, Gillian H. C. Foo, andVincent Fauveau. 1991. Contraceptive Use in Matlab, Bangladesh in 1990: Levels, Trends, andExplanations. MCH-FP Extension Project Working Paper 65. Dhaka: International Centre forDiarrhoeal Disease Research, Bangladesh.
Lawless, J.F. 1982. Statistical Models and Methods for Life Time Data. New York: Wiley.Leung, Siu F. 1988. "On the Test of Sex Preference." Journal of Population Economics 1:95-114.McClelland, Gary H. 1979. "Determining the Impact of Sex Preferences on Fertility: A Consideration
of Parity Progression Ratio, Dominance, and Stopping Rule Measures." Demography16:377-88.
Merrill, Deborah. 1989. "Children's Gender and Marital Dissolution: Evidence from DevelopingCountries." Paper presented at the annual meetings of the Population Association of America,Baltimore.
Mukherji, S. 1977. "Desire for Children and Observed Fertility." Journal of Family Welfare24:16-22.
Nag. Moni. 1991. "Sex Preference in Bangladesh, India, and Pakistan, and Its Effect on Fertility."Working Paper 27. New York: Population Council.
National Research Council. 1989. Contraception and Reproduction: Health Consequences for Womenand Children in the Developing World. Washington, DC: National Academy Press.
Park, Chai Bin. 1978. "The Fourth Korean Child: The Effect of Son Preference on SubsequentFertility." Journal of Biosocial Science 10:95-106.
___. 1983. "Preference for Sons, Family Size, and Sex Ratio: An Empirical Study in Korea."Demography 20:333-52.
Phillips, James F., Ruth Simmons, Jotsnamoy Chakraborty, and Aminul I. Chowdhury. 1984."Integrating Health Services into an MCH-FP Program: Lessons from Matlab, Bangladesh."Studies in Family Planning 14:153~1.
Phillips, James F., Ruth Simmons, Michael A. Koenig, and Jotsnamoy Chakraborty. 1988."Determinants of Reproductive Change in a Traditional Society: Evidence from Matlab,Bangladesh." Studies in Family Planning 19:313-34.
Phillips, James F., Wayne Stinson, Shushum Bhatia, and Jotsnamoy Chakraborty. 1982. "TheDemographic Impact of the Family Planning Health Services Project in Matlab, Bangladesh."Studies in Family Planning 15:62-73.
Rahman, Mizanur. 1990. "Gender Preference, Fertility Behavior, and Excess Female Child Mortalityin Matlab, Bangladesh." Doctoral dissertation, The Johns Hopkins University.
Rahman, Mizanur, Jalaluddin Akbar, James F. Phillips, and Stan Becker. 1992. "Sex Composition ofChildren and Contraceptive Use in Matlab, Bangladesh." Studies in Family Planning 23:229-42.
Repetto, Robert. 1972. "Son Preference and Fertility Behavior in Developing Countries." Studies inFamily Planning 3:7~.
Williamson, Nancy E. 1976. Sons or Daughters: A Cross Cultural Survey of Parental Preferences.Beverly Hills: Sage.