FUTURE DIRECTIONS IN THE DRUG & BIOPHARMACEUTIC DEVELOPMENT AND NEUROPSYCHOPHARMACOLOGICAL...
44
Eric John Nordstrom Eric John Nordstrom Department(s) of Pharmacology Department(s) of Pharmacology and Neuroscience and Neuroscience Medical School and Medical School and College of Biological Sciences College of Biological Sciences University of Minnesota University of Minnesota Hennepin Faculty Associates Hennepin Faculty Associates Hennepin County Medical Center Hennepin County Medical Center Transgene Transgenic Effect FUTURE DIRECTIONS IN THE FUTURE DIRECTIONS IN THE DRUG & BIOPHARMACEUTIC DEVELOPMENT AND DRUG & BIOPHARMACEUTIC DEVELOPMENT AND NEUROPSYCHOPHARMACOLOGICAL NEUROPSYCHOPHARMACOLOGICAL TREATMENT OF TOURETTE’S SYNDROME TREATMENT OF TOURETTE’S SYNDROME AND RELATED DISORDERS AND RELATED DISORDERS . . New Drug Behavio r
-
Upload
spanalumni -
Category
Documents
-
view
0 -
download
0
Transcript of FUTURE DIRECTIONS IN THE DRUG & BIOPHARMACEUTIC DEVELOPMENT AND NEUROPSYCHOPHARMACOLOGICAL...
Eric John NordstromEric John NordstromDepartment(s) of Pharmacology Department(s) of Pharmacology and Neuroscienceand NeuroscienceMedical School and Medical School and College of Biological Sciences College of Biological Sciences University of MinnesotaUniversity of Minnesota
Hennepin Faculty AssociatesHennepin Faculty AssociatesHennepin County Medical CenterHennepin County Medical Center
Transgene
TransgenicEffect
FUTURE DIRECTIONS IN THE FUTURE DIRECTIONS IN THE DRUG & BIOPHARMACEUTIC DEVELOPMENT AND DRUG & BIOPHARMACEUTIC DEVELOPMENT AND
NEUROPSYCHOPHARMACOLOGICALNEUROPSYCHOPHARMACOLOGICALTREATMENT OF TOURETTE’S SYNDROME TREATMENT OF TOURETTE’S SYNDROME
AND RELATED DISORDERSAND RELATED DISORDERS. .
NewDrug
Behavior
DESCRIPTIONAL CONDITIONS… ECHOS FROM THE PAST
Sir,…my mind is liable to be excited by trifling and unsubstantial causes; disposed to cleave to unpleasant usages, to dwell on dreadful consequences from really trifling circumstances, to be appalled with vain apprehensions, and to cherish disgusts and disagreeable associations; indeed, to labor under a fixidity of ideas which causes my misery.
How Sir, can this dreadful state of mind be cured? Can I be made to possess less feeling, and more resolution to resist moral influences on the mind; to bear vexatious or distressing incidents; and to break away this association, this fixidity of ideas?
Ben Rush 1812…

CENTRAL OBJECTIVES UNDERLYING THE FOLOWING STUDIES…• Generate a mouse model that phenotypically mimics or emulates primary symptoms of these disorders.
• Identify the neural pathways and neurochemistry contributing to TS-OCD-ADHD-TTM.
• Research pharmacological compounds that not only may partially and/or completely eliminate symptoms exhibited in mouse model, but minimize the presence of side effects.
BEHAVIORAL CHARACTERISTICS or ESSENTIAL SYMPTOMS OF OCD,
TS, AND TTMTS (Tourette’s Syndrome)TS (Tourette’s Syndrome)• multiple motor and/or vocal tics (i.e., explosive utterances)
• urge-driven complex or complicated movements
• Aggravated by anxiety, stress, boredom, etc.• occurs many times a day…and in bouts• onset before age 18…typically detected around age 7
• Often secondary to TS and ADHD

VARIOUS TYPES OF TICS
. Graph taken from Advances in Neurology 35: Gillies dela Tourette Syndrome by Friedhaff and Chase, 1982.

BEHAVIORAL CHARACTERISTICS or ESSENTIAL SYMPTOMS OF OCD,
TS, AND TTM
OCD (obsessive-compulsive disorder)OCD (obsessive-compulsive disorder)• thematic obsessions (i.e., fearing uncertainty)
• senseless and perseverant rituals or compulsions
• …as a means to “neutralize” fear-provoking obsession and eliminate anxiety
• A cyclical engagement performed for prolonged periods of times
• Greatly interferes with daily activities • Often secondary to TS and ADHD

OCD Patients Behaviorally Persevere and/or Repeat•Must feel “just right”Must feel “just right”
•Cannot halt activityCannot halt activity
OCD vs. Normal Bathroom Ritualclothes mirror Q-tip
blow-dry towel floss toilet
hair style brush teeth wash hands
shower
302520151050 35 40
time (minutes)
NormalOCD

BEHAVIORAL CHARACTERISTICS or ESSENTIAL SYMPTOMS OF OCD,
TS, AND TTM
TTM (trichotillomania disorder)TTM (trichotillomania disorder)• Recurrent bouts of hair pulling--resulting in noticeable hair loss
• Mounting sense of tension prior to pulling hair
• Gratification and/or relief during hairpulling
• …however, typically patient is embarrassed and upset by these actions
• Minor player in the TS-OCD-ADHD-TTM behavioral spetrum

TRICHOTILLOMANIA…IMAGE DEPICTING CHRONICALLY PLUCKED AND PULLED
HAIR

NUMEROUS CONTRIBUTING FACTORS...NUMEROUS OUTCOMES
GENETICS and AUTOIMMUNE…many developments amassing greater issues of casual complexitiesGENETIC FACTORSGENETIC FACTORS• Autosomal Dominant inheritance…considerable phenotypic variability (even among monozygotic twin pairs)
• Many proposed gene candidates (e.g., CNTNAP2, chromosomal aberrations, etc.). However, genetic abnormalities are isolated cases, and/or involved in many other phenotypic anomalies (mental retardation, etc.)
AUTOIMMUNEAUTOIMMUNE• PANDAS (“Pediatric Autoimmune Psychiatric Disorders After Streptococcal Infection”).Possible mechanism: Inflammation or damage in the striatum, the target of CNS forebrain excitatory inputs.

NEURAL CIRCUITY ANDNEUROTRANSMITTERS UNDERLYING
THESE SPECTRUM DISORDERS
FRONTAL CORTEXFRONTAL CORTEX• Orbital Frontal Cortex (OFC)• Somatosensory Cortex (sensorimotor and association areas)
• ThalamusBASAL GANGLIABASAL GANGLIA• Striatum (Caudate and Putamen)• Substantia NigraLIMBIC SYSTEMLIMBIC SYSTEM• Amygdala

BEHAVIORAL SEQUENCE
SNc
DIRI-DIR
GLUTAMATERGIC PROJECTION
D2 D1
MODULATING DOPAMINE
CORTEX OFC, SS, PFC
NEURAL CIRCUITY ANDNEURAL CIRCUITY ANDNEUROTRANSMITTERS NEUROTRANSMITTERS UNDERLYING THESE UNDERLYING THESE SPECTRUM DISORDERS…SPECTRUM DISORDERS…Cortico-striato-thalamo-cortical loop overview
NEOSTRIATUM
AMYGDALA INPUT
GLOBUS PALLIDUS
THALAMUS

IMPLICATED NEUROTRANSMITTERS… THE “DOPAMINE HYPOTHESIS” OF TS
• Earliest pharmacological treatments for TS involved potent D2 receptor antagonists (typical neuroleptics) such as Haloperidol, Pimozide, etc., which suggested abnormalities in DA transmission.
• Treatment was effective in both juveniles and adults alike.
• Typically, these treatment regiments were often difficult to manage or maintain based upon numerous and frequently unfavorable side effects (e.g., tardive dyskinesia, sedation, cognitive dulling, etc.)
• To this day these typical neuroleptics (e.g., Haloperidol) remain the most commonly used treatment for ticcing behaviors.
• Dopaminergic drugs can produce “stereotypies” which may be behaviorally similar to compulsions.

BEHAVIORAL SEQUENCE
SNc
DIRI-DIR
GLUTAMATERGIC PROJECTION
D1
DA
CORTEXNEURAL CIRCUITY ANDNEURAL CIRCUITY ANDNEUROTRANSMITTERS NEUROTRANSMITTERS UNDERLYING THESE SPECTRUM UNDERLYING THESE SPECTRUM DISODERS…DISODERS…
D2D2D2
• ABNORMAL DA LEVELS UNDERLYING SYMPTOMOLOGY?
• KNOWN AS THE “DOPAMINE HYPOTHESIS”
• DATA FOUND NOT TO BE CONCLUSIVE
IMPLICATED NEUROTRANSMITTERS… NORADRENERGIC (NA)
NEUROTRANSMISSION AND TS
• Reduced NA metabolite levels have been shown in some TS patients—suggesting noradrenergic deficit
• Presynaptic NA neurotransmission is thought to influence cortical and limbic Glu neurotransmission
• Alpha adrenergic receptor agonist clonidine has been effective in treating TS patients
SEROTONIN (5HT) AND GLUTAMATE INVOLVEMENT IN TS
• SSRI’S (e.g., Prozac) and 5-HT antagonists (e.g., Ritanserin and Ketanserin) have been used to treat TS-OCD-TTM, albeit with inconclusive responses.
• Cortical glutamatergic-releasing neurons co-express 5HT receptors that can be blocked by 5HT antagonists resulting perhaps, in less GLU output.
• …more specifically, atypical antipsychotics have much greater efficacy and fewer side effects during treatment of TS, and in some cases TTM.
• Some studies have shown the 5HT metabolites levels are lower in OCD-TTM patients suggesting abnormalities in 5HT tranmission.

SEROTONIN (5HT) AND GLUTAMATE INVOLVEMENT IN TS
• Neurosurgery such as Leucotomy (severs glutamtatergic projections between cortex and striatum) has been shown to reduce TS and OCD behaviors in patients.
• Cortical, Limbic and Striatal regions or efferent targets are hyperactive (showing increased metabolism) in TS and OCD patients
In summary, both dopamine and serotonin transmission is indeed involved in these disorders—however, hyperexcitation of glutamatergic projecting cortical neurons appears to be the primary underlying cause
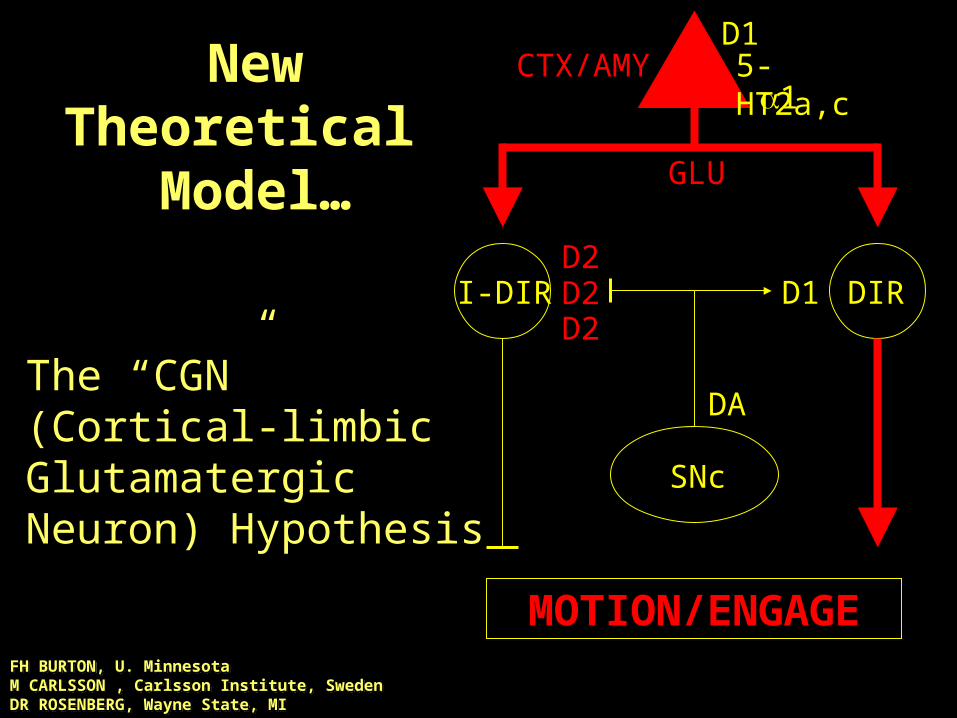
MOTION/ENGAGE
SNc
DIRI-DIR
GLU
D1
DA
CTX/AMYNew Theoretical
Model…
The “CGN”(Cortical-limbic Glutamatergic Neuron) Hypothesis
D2D2
D2
D15-HT2a,c1
FH BURTON, U. MinnesotaM CARLSSON , Carlsson Institute, SwedenDR ROSENBERG, Wayne State, MI
Behavioral Circuit Testing & Drug Development and Screen
Begin by transgenic mouse modeling…
• Hyperactivating the candidate cortical-limbic glutamatergic (CGN) neuron subtypes in these regions of the CNS
• Then determine whether the transgenic mouse expresses any phenotypic behavioral characteristics that compliment the symptoms found in human TS-OCD-TTM.
STRUCTURAL VIEW OF D1CT-7 TRANSGENE
D1 promoterD1 5' UT
D1 116bp intronSV40 SD/SA
CT ORFSV40 polyadenylation site
1 kb
EE S
mRNAprotein
N N
Human D1 dopamine receptor promoter-cholera toxin fusion transgene.
cholera toxin (CT) is used to cause the G-protein cycle to remain in a “locked state” thereby increasing cAMP and neuronal activity and/or neurotransmitter release in D1 receptor expressing neurons
…in other words, these neuronal subsets are identified as being “neuropotientiated” within their respective cns departments
CT causes D1+ neurons to be hyperexcitableD1CT-7 lineage has D1+ expression that cortical-limbic restricted

Cholera Toxin (CT)…Mechanism of Action
…Because of the effect on adenylate cyclase, cholera toxin and its purified A subunit are frequently used for the study of signal transduction mechanisms.
blocksGTPase of blocksGTPase of alpha subunitalpha subunit

D1CT-7 Transgene-Induced Neuron Subset Hyper-
responsiveness
Layers II-III of piriform and somatosensory/insular cortex – these
neurons are thought to excite orbitofrontal and corticostriatal
glutamate outputCampbell et al., J. Neurosci. 19, 5044-5063 (1999).
CT ISH D1 IHC
CPu CPuII-III II-III

Campbell et al., J. Neurosci. 19, 5044-5063 (1999).
D1CT-7 Transgene-Induced Neuron Subset Hyper-
responsiveness
Intercalated nucleus of the amygdala – these neurons are thought to increase excitatory glutamatergic output from the amygdala

The Prominent Phenotypic or Behavioral Abnormalities expressed in D1CT-7 MICE
• Perseverant or repetitive episodes-analogous to compulsive engagements found within human obsessive-compulsive cycle
• Twitching or tic-like behavior-analogous to motor tics found in human ts
• Abnormal frequency and duration of groom episodes, resulting in loss of hair and/or skin abrasions
…and their response to treatment?
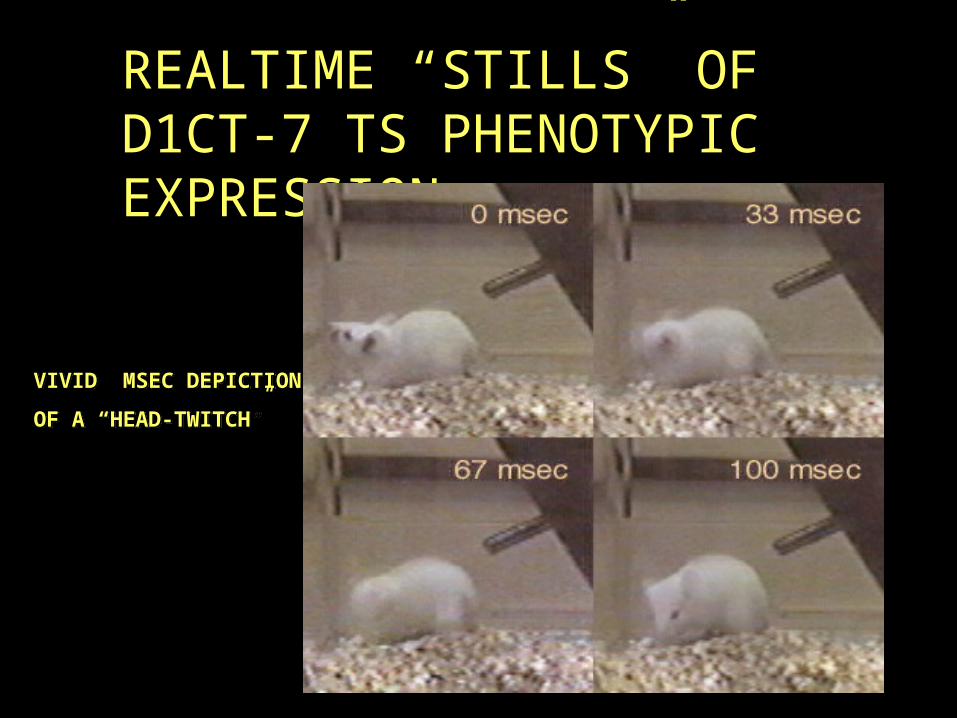
REALTIME “STILLS” OF D1CT-7 TS PHENOTYPIC EXPRESSION
VIVID MSEC DEPICTION OF A “HEAD-TWITCH”
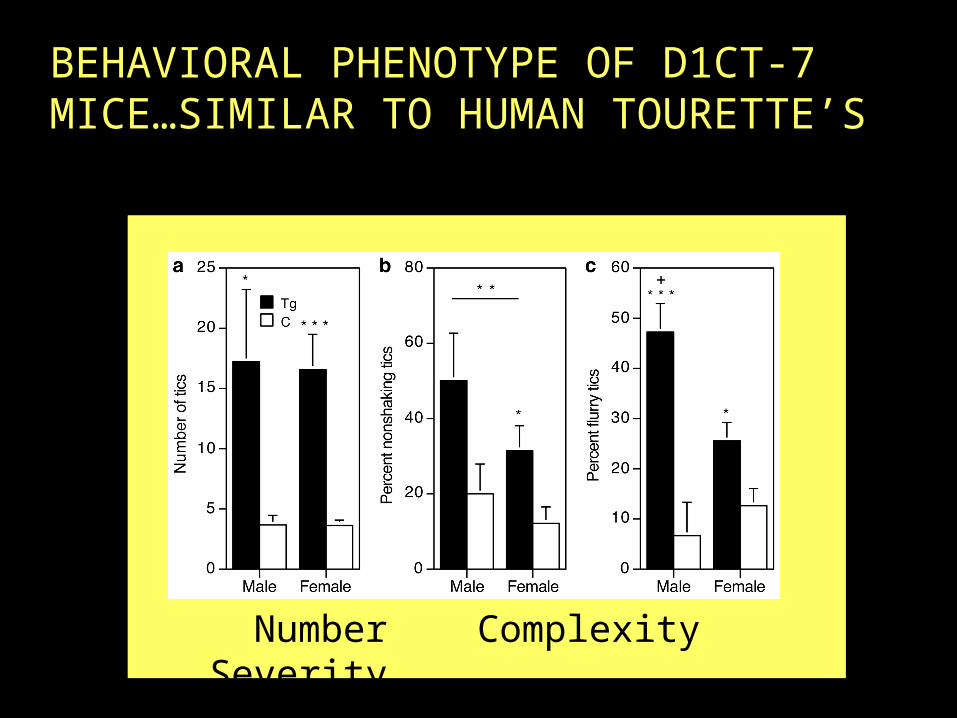
BEHAVIORAL PHENOTYPE OF D1CT-7 MICE…SIMILAR TO HUMAN TOURETTE’S
Number Complexity Severity
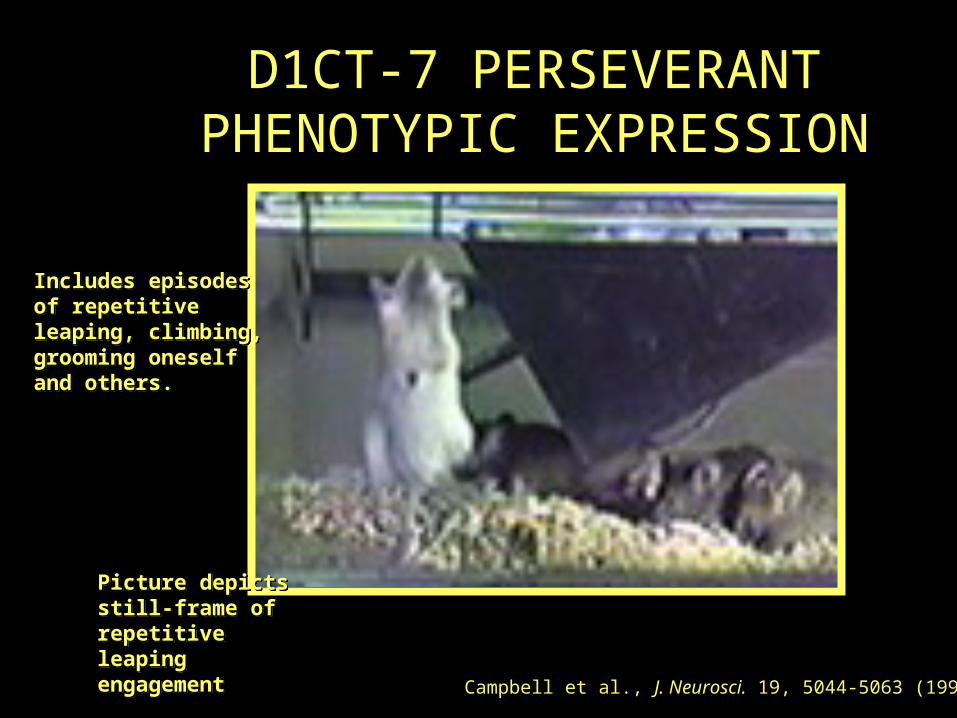
D1CT-7 PERSEVERANT PHENOTYPIC EXPRESSION
Campbell et al., J. Neurosci. 19, 5044-5063 (1999).
Includes episodes of repetitive leaping, climbing, grooming oneself and others.
Picture depicts still-frame of repetitive leaping engagement

BEHAVIORAL WAVEFORM ANALYSIS OF D1CT-7 MICE VS. HUMAN OCD
OCD vs. Normal Bathroom Ritualclothes mirror Q-tip
blow-dry towel floss toilet
hair style brush teeth wash hands
shower
302520151050 35 40
time (minutes)
NormalOCD
0
1
2
3
4
5
6
7
8
9
10
11
12
13
0
250
500
750
1000
Behavior
0
1
2
3
4
5
6
7
8
9
10
11
12
13
0
250
500
750
1000
Time (seconds)
BehaviorCONTROL TRANSGENIC
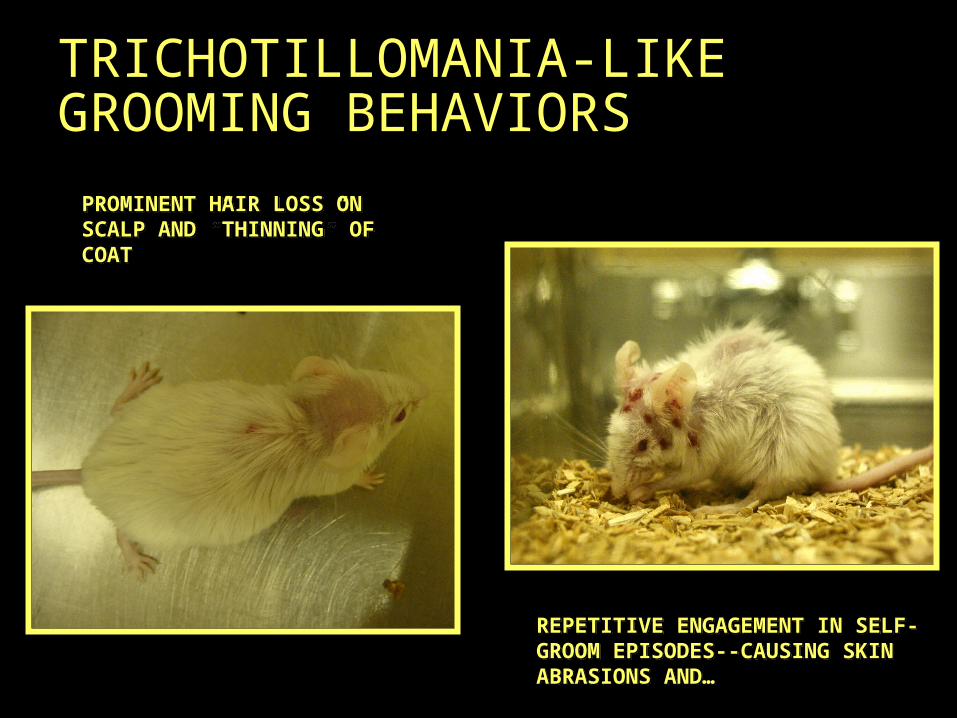
TRICHOTILLOMANIA-LIKE GROOMING BEHAVIORS
REPETITIVE ENGAGEMENT IN SELF-GROOM EPISODES--CAUSING SKIN ABRASIONS AND…
PROMINENT HAIR LOSS ON SCALP AND ”THINNING” OF COAT
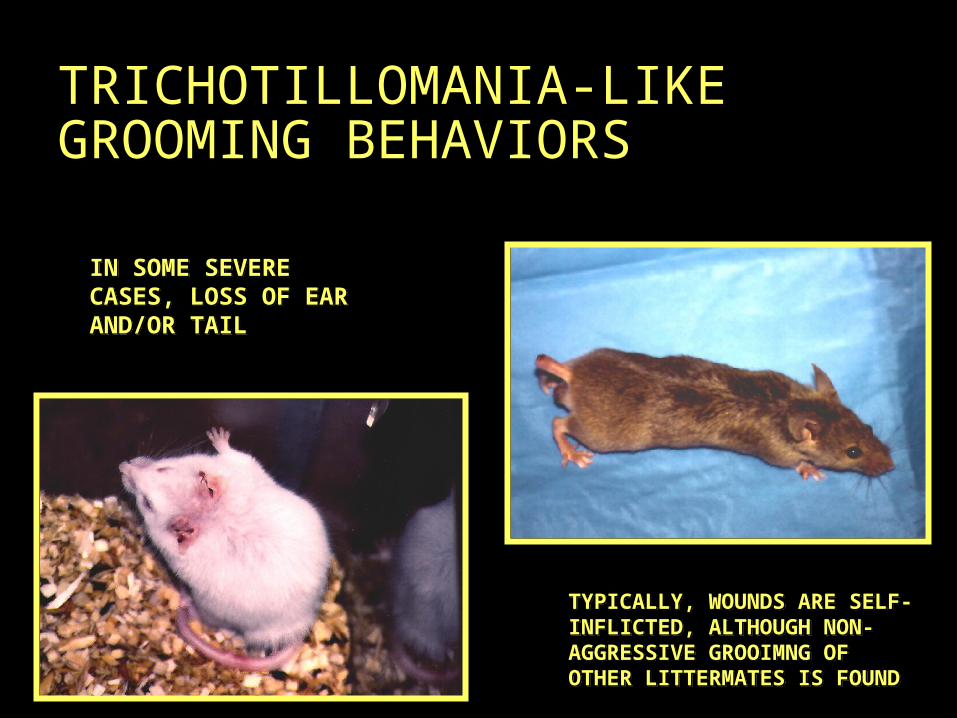
TRICHOTILLOMANIA-LIKE GROOMING BEHAVIORS
IN SOME SEVERE CASES, LOSS OF EAR AND/OR TAIL
TYPICALLY, WOUNDS ARE SELF-INFLICTED, ALTHOUGH NON-AGGRESSIVE GROOIMNG OF OTHER LITTERMATES IS FOUND
Behavioral Pharmacological Investigation
Finding the “therapeutic window”
1) Determine whether the drugs “normalize” behavioral abnormalities within the context of a minimization of side-effects
Indirect evidence to strengthen “CGN MODEL”1) Design drug experiments around the probable
receptor targets thought to be contributing factors within the CGN model
and…
Developing a Pharmacological Compound
Screening Assay• Individualistic
differences in developmental, biological, and environmental factors will continue to reinforce further research into the elucidation of undiscovered pharmacological targets…as a consequence more compounds will need to be developed and/or tested to treat any and all of these disorders
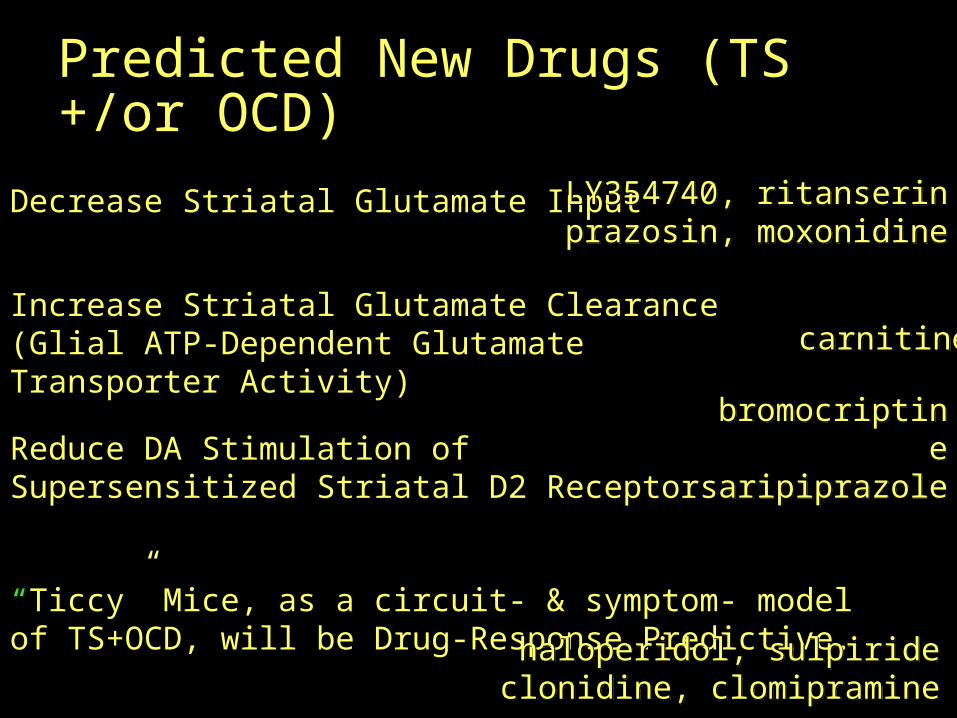
Predicted New Drugs (TS +/or OCD)
Decrease Striatal Glutamate Input
Increase Striatal Glutamate Clearance (Glial ATP-Dependent Glutamate Transporter Activity)
“Ticcy” Mice, as a circuit- & symptom- model of TS+OCD, will be Drug-Response Predictive.
Reduce DA Stimulation of Supersensitized Striatal D2 Receptors
LY354740, ritanserinprazosin, moxonidine
bromocriptine
aripiprazole
carnitine
haloperidol, sulpirideclonidine, clomipramine

MOTION/ENGAGE
SNc
DIRI-DIR
GLU
D1DA
CTX/AMY Current Drugs
Antagonists ofD2 receptors (haldol)5-HT re-uptake (clomipramine)
Agonists of2 receptors (clonidine)presynaptic D2 receptors (bromocriptine)
D2D2
D2
clonidineclomipramine
D2
haldol
bromocriptine
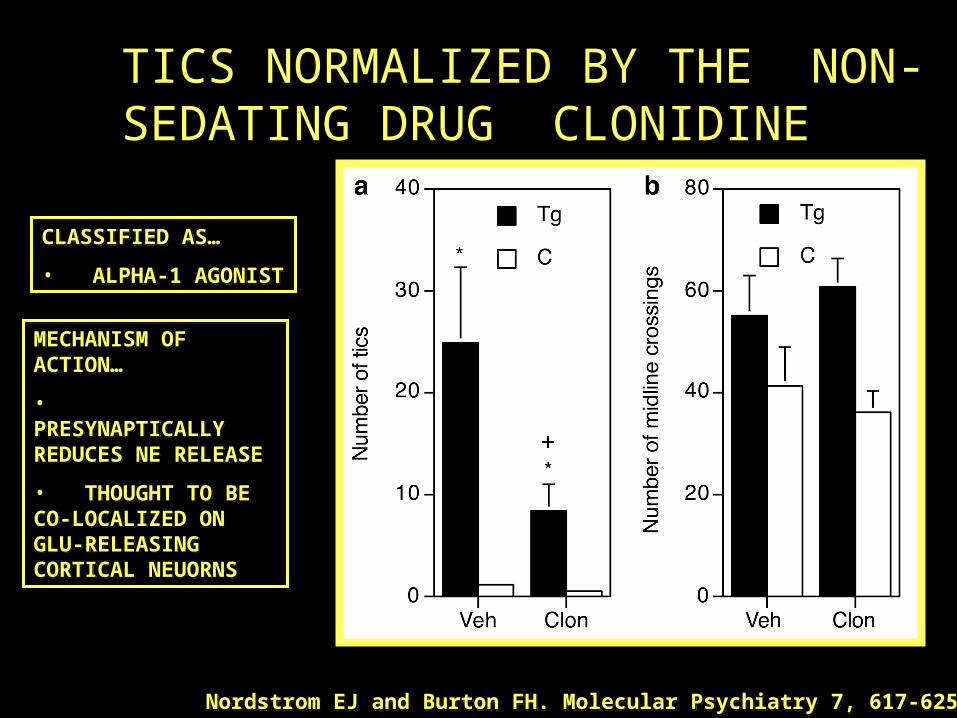
TICS NORMALIZED BY THE NON-SEDATING DRUG CLONIDINE
CLASSIFIED AS…• ALPHA-1 AGONIST
MECHANISM OF ACTION…• PRESYNAPTICALLY REDUCES NE RELEASE• THOUGHT TO BE CO-LOCALIZED ON GLU-RELEASING CORTICAL NEUORNS
Nordstrom EJ and Burton FH. Molecular Psychiatry 7, 617-625 (2002)
0
10
20
30
40
50
Number of Tics
Saline 1.0 mg/kg RIT
Drug
ControlTransgenic
++
**
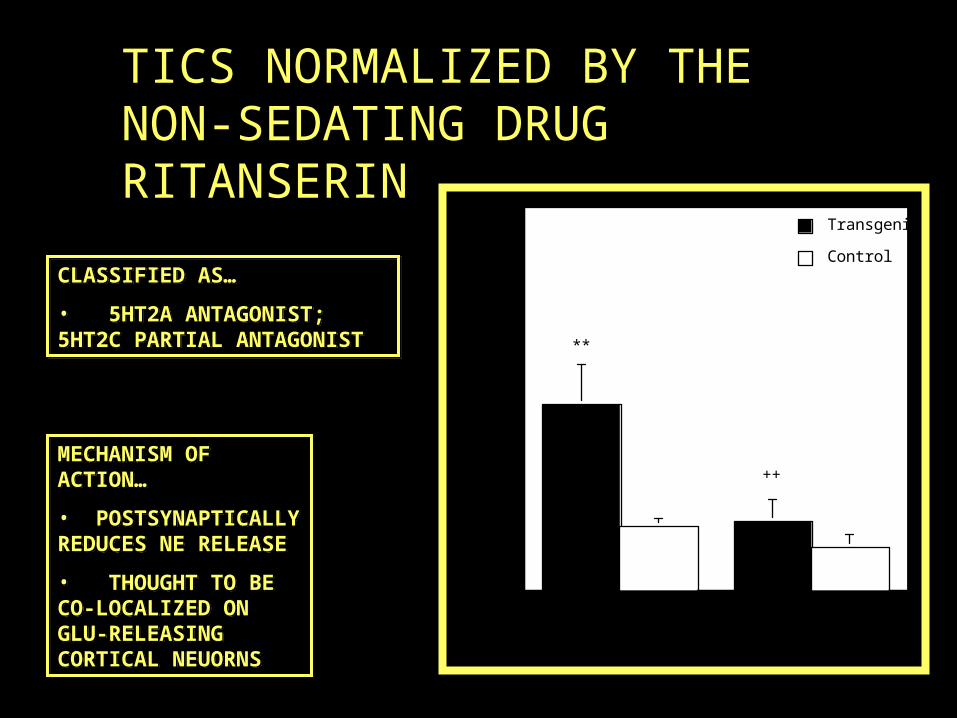
TICS NORMALIZED BY THE NON-SEDATING DRUG RITANSERIN
CLASSIFIED AS…• 5HT2A ANTAGONIST; 5HT2C PARTIAL ANTAGONIST
MECHANISM OF ACTION…• POSTSYNAPTICALLY REDUCES NE RELEASE• THOUGHT TO BE CO-LOCALIZED ON GLU-RELEASING CORTICAL NEUORNS
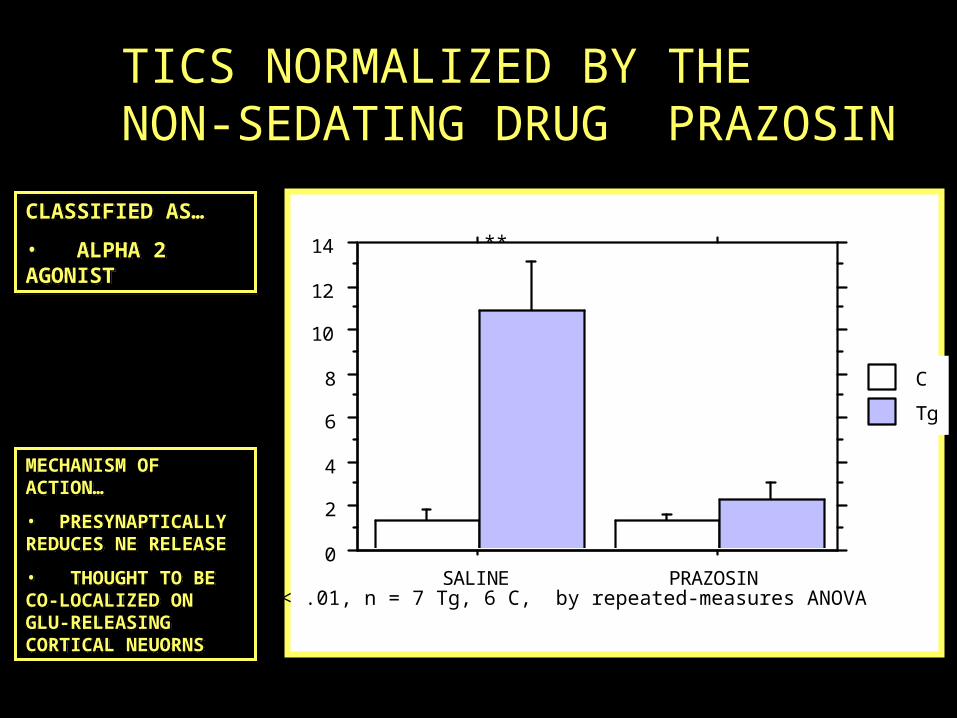
0
2
4
6
8
10
12
14
Cell Mean
SALINE PRAZOSINCell
TgC
Interaction Bar Plot for Dose Effect: Category for Dose * GENOTYPE Error Bars: ± 1 Standard Error(s)
Numb
er o
f Ti
cs
** p < .01, n = 7 Tg, 6 C, by repeated-measures ANOVA
**
TICS NORMALIZED BY THE NON-SEDATING DRUG PRAZOSIN
CLASSIFIED AS…• ALPHA 2 AGONIST
MECHANISM OF ACTION…• PRESYNAPTICALLY REDUCES NE RELEASE• THOUGHT TO BE CO-LOCALIZED ON GLU-RELEASING CORTICAL NEUORNS
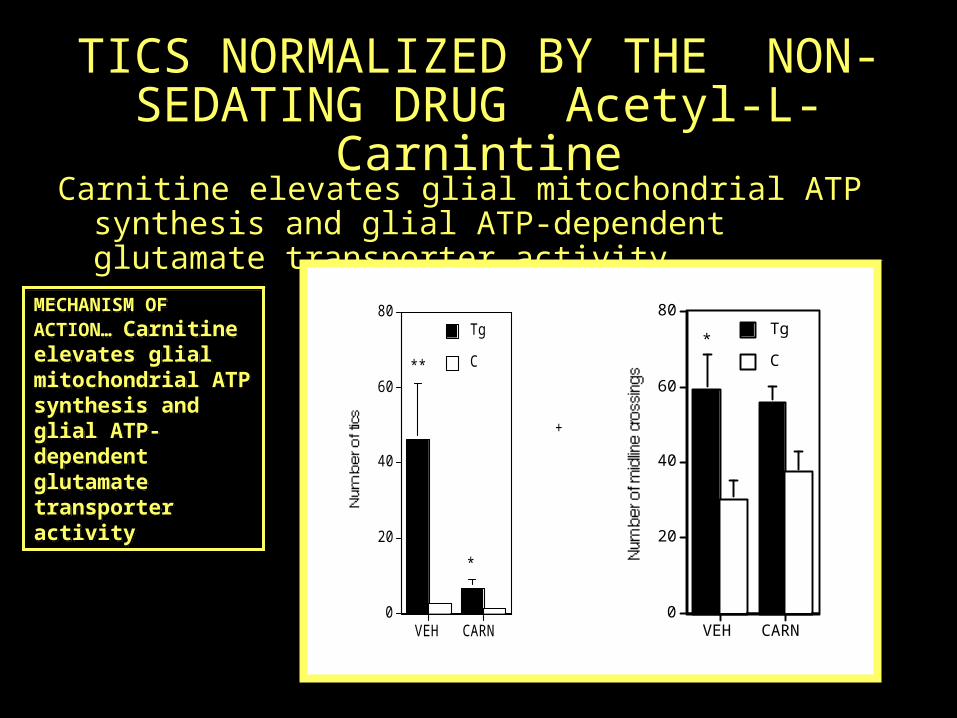
TICS NORMALIZED BY THE NON-SEDATING DRUG Acetyl-L-
CarnintineCarnitine elevates glial mitochondrial ATP synthesis and glial ATP-dependent glutamate transporter activity
0
20
40
60
80
VEH CARN
CTg
+
***
0
20
40
60
80
VEH CARN
CTg
+
*
**
MECHANISM OF ACTION… Carnitine elevates glial mitochondrial ATP synthesis and glial ATP-dependent glutamate transporter activity
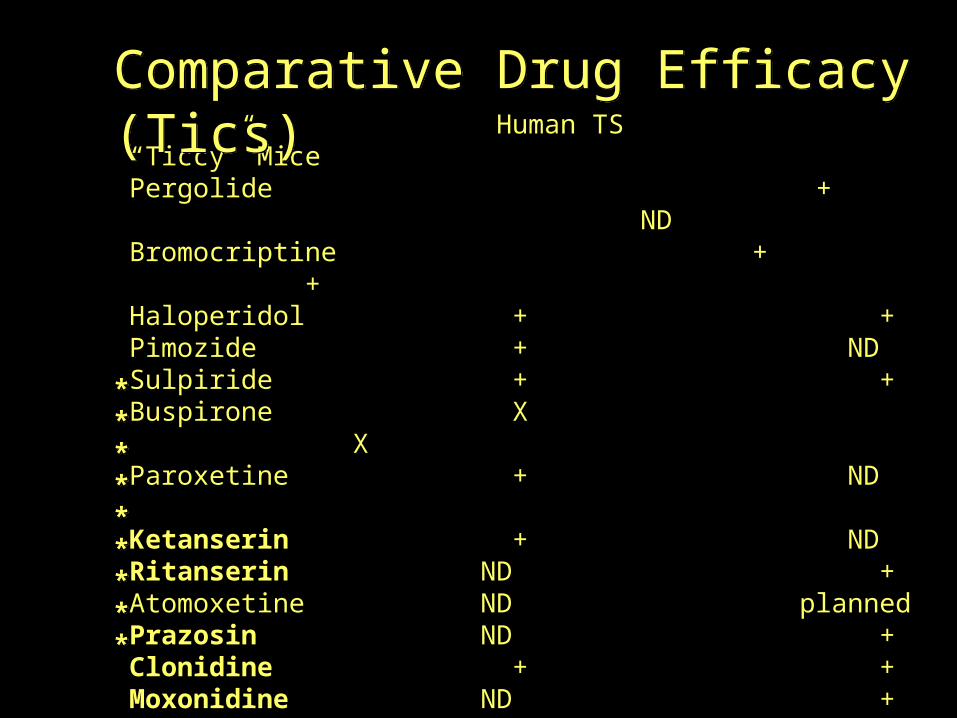
Human TS “Ticcy” MicePergolide + NDBromocriptine +
+Haloperidol + +Pimozide + NDSulpiride + +Buspirone X XParoxetine + ND Ketanserin + NDRitanserin ND +Atomoxetine ND plannedPrazosin ND +Clonidine + + Moxonidine ND +Mecamylamine - -Delta-9-THC + plannedCarnitine ND +
* drugs initially predicted by us or others to work in human TS
Comparative Drug Efficacy (Tics)
*********
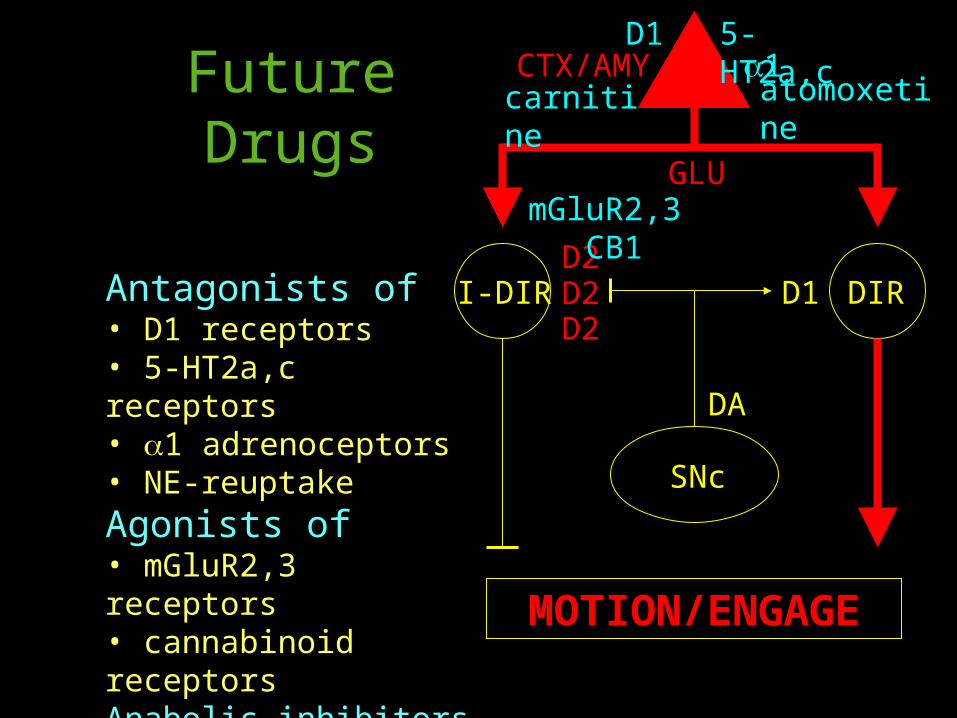
MOTION/ENGAGE
SNc
DIRI-DIR
GLU
D1
DA
CTX/AMYFuture Drugs
Antagonists of• D1 receptors• 5-HT2a,c receptors• 1 adrenoceptors• NE-reuptakeAgonists of• mGluR2,3 receptors• cannabinoid receptorsAnabolic inhibitors of• glutamate synthesis
D2D2
D2
D1 5-HT2a,c1
mGluR2,3 CB1
carnitine
atomoxetine
FUTURE DIRECTIONS
Screen “Ticcy” mice with predicted TS+OCD drugs and develop as orphan disease TS, TTM drugs
Compare “Ticcy” mice’s CNS biochemical and neurotransmitter changes to other animal models of TS, OCD and TTM, as well as psychosis.
Contrast “Ticcy” (D1CT) mice’s CNS biochemical and neurotransmitter changes to predicted opposite (antipodal) changes in D1KO-based and other animal models of classical ADHD
• Inducing hyperexcitability in cortical & limbic neurons that trigger glutamate output to the striatum mimics the symptoms, compensatory striatal changes & drug responses of human TS+OCD
• TS+OCD from either genetic neuron hyperexcitability (Cntnap2 gene loss) or PANDAS (striatal inflammation) may be due to abnormally high striatal glutamate levels
• Drugs that either decrease striatal glutamate input, increase striatal glutamate clearance, or antagonize glutamate-supersensitized receptors may prove to be useful new therapeutics for TS, OCD and related disorders
CONCLUDING REMARKS

U PHARMACOLOGY Frank H. BurtonMike McGrath, Katie C. Bittner, Anthony J. Travanty, Clinton R. Parks III, Josh Jackson, and Nathan Jorgenson
U CHEMISTRY Michael T. Bowser and Kylie B. O’Brien
ACKNOWLEDGEMENTS
…the D1CT-7 Mouse Colony