
Early Pacemaker Implantation after Transcatheter Aortic Valve ...
Upload
independentCategory
view
4download
0
Functional Magnetic Resonance Imaging of Hearing-ImpairedChildren Under Sedation Before Cochlear Implantation
Ankur M. Patel, DO, Lisa D. Cahill, MA, CCC-A, Jennifer Ret, MS, Vincent Schmithorst, PhD,Daniel Choo, MD, and Scott Holland, PhDImaging Research Center, Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio.
AbstractObjective—To investigate functional magnetic resonance imaging (fMRI) in pediatric cochlearimplantation candidates with residual hearing who are under sedation for evaluation of auditoryfunction.
Design—During fMRI, subjects heard a random sequence of tones (250−4000 Hz) presented 10dB above hearing thresholds. Tones were interleaved with silence in a block-periodic fMRI designwith 30-second on-off intervals. Twenty-four axial sections (5 mm thick) covering most of the brainwere obtained every 3 seconds for a total acquisition time of 5.5 minutes.
Setting—Single tertiary academic medical institution.
Patients—Severely to profoundly hearing-impaired children (n = 10; mean age, 49.1 months).During fMRI, subjects were awake (n=2) or sedated with pentobarbital sodium if their weight was10 kg or greater (n=4) or chloral hydrate if their weight was less than 10 kg (n=4).
Main Outcome Measures—Detection of brain activation by fMRI in the primary auditory cortex(A1) in hearing-impaired patients under sedation, and correlation of A1 activation with hearing levelsmeasured after cochlear implantation.
Results—In most subjects, fMRI detected significant levels of activation in the A1 region beforecochlear implantation. The improvement in hearing threshold after cochlear implantation correlatedstrongly (linear regression coefficient, R=0.88) with the amount of activation in the A1 regiondetected by fMRI before cochlear implantation.
Conclusions—Functional MRI can be considered a means of assessing residual function in theA1 region in sedated hearing-impaired toddlers. With improvements in acquisition, processing, andsedation methods, fMRI may be translated into a prognostic indicator for outcome after cochlearimplantation in infants.
©2007 American Medical Association. All rights reserved.Correspondence: Scott Holland, PhD, Imaging Research Center, Cincinnati Children's Hospital Medical Center, 3333 Burnet Ave,Cincinnati, OH 45229−3039 ([email protected])..Author Contributions: Dr Holland had full access to all the data in the study and takes responsibility for the integrity of the data andthe accuracy of the data analysis. Study concept and design: Cahill, Choo, and Holland. Acquisition of data: Ret, Schmithorst, and Holland.Analysis and interpretation of data: Patel, Schmithorst, and Holland. Drafting of the manuscript: Patel, Cahill, and Holland. Criticalrevision of the manuscript for important intellectual content: Patel, Cahill, Ret, Schmithorst, Choo, and Holland. Statistical analysis:Schmithorst and Holland. Obtained funding: Holland. Administrative, technical, and material support: Patel, Cahill, Ret, Choo, andHolland. Study supervision: Choo and Holland.Additional Contributions: The Department of Radiology at Cincinnati Children's Hospital Medical Center performed sedationprocedures in pediatric subjects, and the Cochlear Implant Research Team identified appropriate subjects.Financial Disclosure: None reported.
NIH Public AccessAuthor ManuscriptArch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
Published in final edited form as:Arch Otolaryngol Head Neck Surg. 2007 July ; 133(7): 677–683. doi:10.1001/archotol.133.7.677.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

IT HAS BEEN ESTIMATED THAT APproximately 60 infants are born each day in the United States withsignificant hearing loss (1 to 6 infants per 1000).1-4 The effects of early hearing loss oncommunication development, as well as social and educational development, are welldocumented.5-8 A growing body of evidence now supports the benefit of early detection ofcongenital hearing loss and the concomitant implementation of early intervention strategies.9-13
Current research suggests that the development of language-relevant areas in the brain may besignificantly altered in hearing-impaired (HI) children compared with normal-hearing children.14 As with other neurocognitive systems, early language experience and biological circuitryinteract to stimulate and support mutual development of structure and function.15,16 With theadvent of universal newborn hearing screening in nearly all areas of the United States, theaverage age of diagnosis of congenital hearing impairment has now decreased to 3 to 6 months,thereby increasing the likelihood for appropriate early intervention in these infants.
Cochlear implantation is an effective way of restoring hearing in children with severe toprofound sensorineural hearing loss.17 The application of cochlear implants has extended toinclude children with pure-tone averages ranging from an 80- to 100-dB hearing level.18-20
An impetus for consideration of children with significant residual hearing for implantationarose from the sizable proportion of such children not experiencing progress with their hearingaids at the same rate as those with implants.21 Outcome studies and comparisons with hearingaid users have established that cochlear implantation can produce communication benefits,particularly improved speech understanding, even in children with significant residual hearing.19,22,23
The clinical dilemma is predicting the likelihood of substantial communication benefits fromcochlear implantation in infants and children with residual hearing. Several highly sensitivediagnostic instruments are available that reliably evaluate various aspects of peripheral hearingacuity and sensory function using nonbehavioral methods, such as the auditory brainstemresponse, otoacoustic emissions, and auditory steady-state response. However, the nature ofhigher auditory cortical processing and perception in the HI neurosystem is not wellcharacterized by the battery of instrumentation traditionally used. An objective and minimallyinvasive tool that assists in describing central auditory system function and ultimately indetermining the potential speech perception benefit from cochlear implantation is highlydesirable.
Functional magnetic resonance imaging (fMRI) has been used previously to examine brainactivation in response to auditory and language stimulation in children24 and infants.25,26
Cortical activation results in localized increases in blood flow that in turn cause a change insignal intensity in MRIs constructed using methods that are sensitive to small changes inmagnetization associated with blood oxygenation. In these MRIs, the activated andnonactivated cortices have measurably different signal intensities, and brain activation mapscan be constructed from the contrast between brain images of the activated and nonactivatedstates. This MRI method is termed blood oxygenation level–dependent (BOLD) contrast andis the technique used for fMRI.
Although sedation is typically required in pediatric populations to obtain a complete evaluation,several investigations have shown that subjects given passive auditory stimulation undervarious types of sedation have exhibited a positive BOLD signal response.27-29 Functionalneuroimaging techniques may be useful in evaluation of central auditory function in childrenwho are candidates for cochlear implantation. Specifically, fMRI may permit differentiationof brain responses corresponding to auditory detection, speech perception, and languageprocessing in normal-hearing and HI infants.30 The ability of fMRI to demonstrate neural
Patel et al. Page 2
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

representation of auditory perception may provide important information regarding variousaspects of auditory and language processing in infants and toddlers.
In the present study, we examined the relationship between preimplantation cortical activationand improvement in pure-tone audiometry thresholds after cochlear implantation in HIchildren. We hypothesized that children with severe to profound sensorineural hearing losswith residual auditory cortical activity as shown by fMRI would also have greater improvementin pure-tone auditory thresholds after cochlear implantation.
METHODSSUBJECTS
Ten HI children (median age,26 months; mean age, 49.1 months; 4 boys and 6 girls) wererecruited for this feasibility study through the Departments of Otolaryngology and Radiology,according to an institutional review board–approved protocol, and informed consent wasobtained from the parents or the guardian. The HI subjects all had at least minimal residualhearing levels, with pure-tone audiometry ranging from 75 to 115 dB, placing them in theclassification of severe to profound hearing loss. None of the subjects in this study had aconductive hearing loss, as indicated on their clinical audiograms before and after cochlearimplantation. Four patients had small internal auditory canals, as shown by preoperativecomputed tomography. To rule out a cochlear nerve aplasia, MRI studies were obtained. In 3patients, a cochlear nerve was definitively observed within the internal auditory canal. In thelast patient, interpretation of computed tomographic scans and MRI by a neuroradiologist wasequivocal for the anatomic presence of a cochlear nerve. However, physiologically, the patientdemonstrated consistent auditory responses on serial audiologic testing. Accordingly, thepresence of a (poorly) functioning cochlear nerve was assumed. Patients demonstrating noaudiologic responses and lacking definitive anatomic evidence of a cochlear nerve on high-resolution imaging studies are not considered candidates for cochlear implantation at ourinstitution.
Owing to the loudness of the MRI scanner gradients during fMRI, no auditory tone testing wasperformed during the imaging procedure. Audiological testing was performed in all subjectsas part of the standard referral pathway for cochlear implantation at our institution. Pure-toneaudiometry was performed on these subjects by a credentialed pediatric audiologist beforeimplantation using sound field audiometry. These tests were repeated after cochlearimplantation. The improvement in hearing threshold for each subject was calculated from thedifference in pure-tone average hearing thresholds before and after cochlear implantations.This difference was based on the most recent preimplantation and postimplantationaudiograms, with the most improved hearing level reported in the patient's medical chart, upto 18 months after implantation.
All sedation procedures were performed by the Department of Pediatric Radiology to obtaina clinically indicated MRI requested by the patients’ referring physician. Children weighingless than 10 kg (typical age, 0−24 months) were sedated using orally administered chloralhydrate at a dose of 75 to 100 mg/kg. Children younger than 7 years but weighing 10 kg orgreater were sedated using intravenous pentobarbital sodium (Nembutal; Baxter InternationalInc, Deerfield, Illinois) administered at a dose of 3 to 5 mg/kg. Subjects were excluded for anystandard contraindications to an MRI, such as metal implants, orthopedic pins or plates abovethe waist, and orthodontic braces.
Patel et al. Page 3
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
AUDITORY STIMULATION PARADIGMS FOR fMRIAll subjects were presented with the same block-periodic fMRI passive listening task. The taskis a frequency-modulated tone task wherein random tones ranging from 400 Hz to 1.5 kHz arepresented at 0.5- to 1.0-second intervals for 0.5 to 1.5 seconds each. Thirty-second blocks ofthese tones (the stimulus interval) are interleaved with 30-second blocks of silence (the controlinterval) to create a 5.5-minute task. The auditory input to the subjects was delivered througha calibrated magnetic resonance–compatible audio system (SS3100; Avotec Inc, Stuart,Florida), with levels set to exceed the measured audiometric hearing thresholds of each patientby approximately 10 dB.
MRI SETTINGSFollowing sedation for MRI, subjects were placed on the table in the scanner. Magneticresonance–compatible headphones (Avotec Inc) were placed over the subject's ears, and thehead was restrained within a padded head holder with additional foam pads to minimize headmotion. Prescribed clinical MRIs were completed first, and the fMRIs were added at the endof the clinical routine. Eight of 10 subjects underwent MRI on a 1.5-T scanning system withecho-speed gradients (GE Signa Horizon; General Electric Medical Systems, Milwaukee,Wisconsin); 2 subjects, on 3-T systems (Bruker Biospec 30/60 MRI system [BrukerMedizintechnik, Karlsruhe, Germany] for the nonsedated subject and a Siemens MRI system[Siemens Medical Solutions, Erlangen, Germany] for the other subject). Functional MRI wasperformed on these systems using a gradient-echo, echo planar imaging method. A time seriesof 110 echo planar imaging gradient-echo images (repetition/echo times, 3000/50milliseconds) was acquired during each fMRI paradigm at 1.5 T. At each time point, 24 axialsections (5 mm thick) were acquired, ranging from the inferior aspect of the temporal lobes tothe superior apex of the cerebrum. The other relevant fMRI settings (field of view, 22×22 cm;matrix, 64×64 pixels) were similar to those we used in a study of hemispheric dominance forlanguage in children with epilepsy using fMRI.31,32 Three-dimensional whole-brain T1-weighted inversion recovery prepped fast gradient-echo images were acquired as part of theclinical scanning protocol and were used for anatomic reference and overlay of the fMRI brainactivation maps. The same imaging settings were used on the 3-T scanners, except that theecho time was shortened to 38 milliseconds to accommodate shorter T2* at this field strength.
IMAGE RECONSTRUCTION AND POSTPROCESSINGThe 3-dimensional anatomic and fMRI data were processed using Cincinnati Children'sHospital Image Processing Software.33 This Interactive Data Language–based program (ITTCorp, Boulder, Colorado) was also used for the statistical processing of all data. Beforestatistical parameter mapping of activation from each fMRI paradigm, several preprocessingsteps were performed.
The raw echo planar imaging data was Hamming windowed before reconstruction to reducethe truncation artifacts at the edges of k-space and to reduce high-frequency noise in the images.The data were corrected for motion using a pyramid iterative coregistration algorithm.34
After collection, the fMRI data were processed using the general linear model.35 A set of cosinebasis functions was used as covariates to account for possible signal drift and aliased respiratoryand cardiac signals. The z-score maps were computed and smoothed in 3 dimensions with agaussian filter of 4-mm width. Activated pixels were detected during the tone task in a regionof interest (ROI) defined bilaterally in the auditory cortex at a threshold of P<.05 with a spatialextent threshold of 5 voxels. To create the individual activation maps displayed in Figure 1, afixed-effects analysis36 was performed to find regions of significant activation as defined inthe second sentence of this paragraph. Specificity was further improved using the clusteringmethod proposed by Xiong et al.37
Patel et al. Page 4
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The fMRI activation was parameterized by counting the number of pixels that exceeded theP<.05 threshold within an ROI defined bilaterally in the auditory cortex of each subject. TheROI was defined manually by consensus of 2 neuroimaging experts (A.M.P. and S.H.) toencompass the full extent of the primary auditory cortex (A1) located within the transversetemporal gyrus (the Heschl gyrus and Brodmann area 41), identified in each subject's anatomicimages. The A1 ROI typically spanned 3 to 5 fMRI sections (nominal section thickness, 5 mm)for the subjects and images included in this study. Within this A1 ROI, the total number ofsuprathreshold pixels was tallied and then used in the graph of Figure 2 and in the linearregression of pixel count vs improvement in hearing threshold.
RESULTSThese data are from children undergoing MRI on a 3-T MRI system (Bruker Biospec 30/60)without sedation (n=1), on a 1.5-T MRI system scanner (GE Signa Horizon) without sedation(n=2) and with sedation (n=6), and on a 3-T MRI system (Siemens Medical Solutions) withsedation (n=1). The Table shows a list of subjects, which MRI system was used, their age inmonths, and what type of sedation was administered (none, chloral hydrate, or pentobarbital),the improvement in hearing threshold (ΔHL), and the number of activated voxels identified inthe ROI.
Figure 1 depicts an activation map for a typical sedated, 2-year-old HI subject undergoing MRIon a 1.5-T MRI system. This patient was sedated with pentobarbital and had a preimplantationhearing threshold of 115 dB in both ears. The general linear model z-score map shows bothpositive and negative fMRI activation with a significance threshold of P<.05 in a single sectionthrough the A1 ROI during auditory stimulation with the tone task. Pixels labeled in yellowindicate positive BOLD activation, whereas pixels labeled in blue indicate negative BOLDactivation. The ROI covering A1 in this section is also displayed on this image. One hundredsixteen activated pixels were counted within the A1 ROI over 3 sections of the brain activationmap for this subject. Typically, the Heschl gyrus spans 3 to 4 sections (each 5 mm thick) inthese images, but only 1 of these sections is displayed in Figure 1. This image furtherdemonstrates that fMRI can indeed detect central auditory activation in children with severeto profound hearing loss. Furthermore, we observed that central auditory activation is bothpositive and negative under the influence of sedation during fMRI. This effect has beenobserved in many of the infants and toddlers in our studies, as well as in reports from otherstudies involving fMRI in infants and toddlers.25,26,29 Negative activation in fMRI correspondsto a decrease in blood oxygenation that follows increased cortical activity in a localized groupof neurons. This effect will occur if neuronal metabolism increases to meet demand but is notaccompanied by a concomitant increase in blood flow to deliver the additional oxygen requiredto support the increased cerebral metabolic rate.38
Figure 2 shows the improvement in the pure-tone audiometry hearing threshold in the 10patients before and after cochlear implantation. The differences are plotted so that the y-axisrepresents the improvement in hearing threshold after implantation (these values reflect thechange in hearing threshold from before to after implantation). The x-axis plots the number ofactivated pixels detected during the tone task in an ROI defined bilaterally in the A1 ROI,located in the transverse temporal gyrus (Heschl gyrus). When charted in this way, 2observations become apparent. First, in this limited sample of 10 subjects, fMRI effectivelydetects significant levels of A1 activation in most of the subjects, before cochlear implantation.Second, the improvement in hearing threshold after implantation correlates strongly (linearregression coefficient, R=0.88) with the amount of activation in A1 detected by fMRI beforeimplantation.
Patel et al. Page 5
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

COMMENTSevere to profoundly HI children who showed auditory cortical activation with fMRI beforecochlear implantation had statistically greater improved pure-tone audiometry thresholds afterimplantation compared with children who did not show activation. Future research is focusedon developing more stringent exclusion criteria for the HI group and on gathering a controlgroup of normal-hearing children. Nevertheless, the present results indicate that, for childrenwith residual hearing under sedation, it is possible to obtain meaningful fMRI responses toauditory stimuli that appear to be related to potential benefit from cochlear implants.
In constructing the typical activation map shown in Figure 1, we avoided the use of theTalairach reference frame and linear spatial normalization.39 Affine transformation of pediatricbrain image data to standardized dimensions defined for an adult brain is not optimal for usewith infant brain data.40,41 Distortions are particularly noticeable in the anterior temporal loberegion of the images. In earlier studies of language development in normal children, we havefound that construction of our own brain image templates for a nonlinear spatialnormalization42,43 is the best approach for spatial normalization of pediatric brain image data.44 We will consider such an approach in future studies of this young population as additionaldata accrue.
A number of factors affect the success of fMRI for detecting auditory brain stimulation,including those mentioned already as well as acoustic noise presented by the scanner itself.Consequently, we have developed a method in which auditory stimuli can be presented duringa silent interval of the MRI gradients, producing hemodynamics unrelated to sounds ofhardware (HUSH)45 Unlike previous implementations of behavior interleaved gradient fMRI,46 the HUSH method does not require long acquisition times. Non-equilibrium acquisitionsrequire modified postprocessing methods. However, the auditory activation produced by thismethod shows promise for further investigations of the developing neural substrates forauditory and language processing in HI infants and children. This technique should improvethe specificity of fMRI for evaluating candidates for cochlear implantation in the future.
It is well established that prolonged lack of auditory stimulation will result in irreversibleauditory cortical loss that is nonresponsive to cochlear implantation.47,48 Conversely, earlyimplantation (before age 18 months in cases of congenital hearing impairment) is known tofacilitate normal or near-normal speech perception/production, language, and reading skillscompared with implantation at 2 to 4 years of age.49,50 The mean age of the subject cohortreported herein was 49 months. If we exclude the two 12-year-old children, the mean age ofthe remaining 8 children was 25 months. This younger subset is more typical of the age ofimplantation in many programs at present. At our institution, we begin the cochlear implantstaging process between ages 6 and 9 months, with an average age range for implantation of12 to 18 months. It is possible that the duration of deafness in the 2 older children could accountfor some of the variability in our data. However, for both of these children, the improvementin hearing level after cochlear implantation was greater than in the children who underwentimplantation at younger ages. This trend runs counter to what might be expected from theliterature,51 suggesting that earlier implantation results in better language performance duringthe school age years. However, it is important to note that pure-tone average hearing levels asreported in the Table and Figure 2 may not be the best indicator of language performance afterimplantation. Language measures were not available on the subjects included in thispreliminary fMRI feasibility study, but one might expect that children with a longer durationof deafness might not demonstrate as great an improvement in standardized language measuresas children undergoing implantation earlier in the developmental period for language. Thisdemonstrates the critical importance of timely clinical decision making in the provision of asurgical implant and implementation of intervention for communication development.
Patel et al. Page 6
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The activation patterns observed in this cohort of children with severe to profound hearingimpairment, as shown in Figure 1, appear to replicate the typical patterns observed in normal-hearing children under sedation.52 Similar rates of positive and negative activation in A1 arefound in both groups, regardless of the form of sedation. Therefore we believe the incidenceof negative activation is not due to the sedation or the hearing impairment in this study. Rather,we hypothesize that the mixture of positive and negative activation in this cohort is aconsequence of the immature cerebrovascular system in subjects aged 1 to 3 years.
In addition, a similar pattern of A1 activation has been identified in a large cohort (n=323) ofnormal-hearing children and adolescents aged 5 to 18 years who were not sedated.53 Althoughthe activation in the sedated HI subjects in this report seems to be attenuated and to contain amixture of positive and negative activation, the similarity of the distribution of activated pixelsin the A1 ROI provides further assurance that the observed patterns correspond to the tonestimulus administered to these subjects.
A limitation of this study arises from the use of MRI systems operating at different fieldstrengths (1.5 and 3.0 T) and different forms of sedation (chloral hydrate, pentobarbital, ornone). This variability in methods might be expected to result in variability in the correlationof fMRI activation in the A1 ROI with postimplantation hearing thresholds as shown in Figure2. Unfortunately, with the limited sample size in this preliminary study, we are unable toexplore the effects of field strength on A1 activation in a statistical manner. However, despitethe built-in variability in this pilot study, the correlation between A1 activation andimprovement in hearing thresholds as shown in Figure 2 is convincing. In fact, this correlationseems to transcend the influences of sedation, field strength, duration of deafness, and otherconfounds. The robustness of this finding gives us confidence that fMRI is feasible in thiscontext and, if administered under more carefully controlled conditions, it may offer potentiallydiagnostic information.
Noninvasive assessment of the cortical response to sound input in an infant who is unable torespond reliably to behavioral auditory system assessment is important for accurate decisionmaking in the cochlear implantation staging process. Functional MRI has the potential toprovide clinicians with an advanced, objective diagnostic tool with capabilities beyondperipheral auditory system assessment. This report demonstrates the feasibility of fMRI forassessment of auditory cortical function in severe to profoundly HI infants, even with sedation.More research will be required to demonstrate the utility of fMRI or other neuroimagingmethods that highlight auditory cortical function as safe and effective approaches to predictcochlear implantation outcomes in prelingual HI infants and toddlers with residual hearing.
Funding/SupportThis study was supported in part by grants R21-DC05311 and RO1-HD38578 from the National Institutes of Health.
REFERENCES1. Kemper AR, Downs SMA. Cost-effectiveness analysis of newborn hearing screening strategies. Arch
Pediatr Adolesc Med 2000;154(5):484–488. [PubMed: 10807300]2. Cunningham M, Cox EO. Hearing assessment in infants and children: recommendations beyond
neonatal screening. Pediatrics 2003;111(2):436–440. [PubMed: 12563074]3. Bachmann KR, Arvedson JC. Early identification and intervention for children who are hearing
impaired. Pediatr Rev 1998;19(5):155–165. [PubMed: 9584525]4. Northern JL. Universal screening for infant hearing impairment [comment]. Pediatrics 1994;94(6 pt
1):955. [PubMed: 7971027]5. Moeller MP, Osberger MJ, Eccarius M. Language and learning skills of hearing-impaired students:
receptive language skills. ASHA Monogr March;1986 (23):41–53. [PubMed: 3730031]
Patel et al. Page 7
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

6. Davis JM, Elfenbein J, Schum R, Bentler RA. Effects of mild and moderate hearing impairments onlanguage, educational, and psychosocial behavior of children. J Speech Hear Disord 1986;51(1):53–62. [PubMed: 3945060]
7. Erenberg A, Lemons J, Sia C, Trunkel D, Ziring P, American Academy of Pediatrics Task Force onNewborn and Infant Hearing. Newborn and infant hearing loss: detection and intervention, 1998−1999.Pediatrics 1999;103(2):527–530. [PubMed: 9925859]
8. Joint Committee on Infant Hearing; American Academy of Audiology; American Academy ofPediatrics; American Speech-Language-Hearing Association; Directors of Speech and HearingPrograms in State Health and Welfare Agencies. Year 2000 position statement: principles andguidelines for early hearing detection and intervention programs. Pediatrics 2000;106(4):798–817.[PubMed: 11015525]
9. Kileny PR, Zwolan TA, Ashbaugh C. The influence of age at implantation on performance with acochlear implant in children. Otol Neurotol 2001;22(1):42–46. [PubMed: 11314714]
10. Knott C. Universal newborn hearing screening coming soon: “hear's” why. Neonatal Netw 2001;20(8):25–33. [PubMed: 12144101]
11. Centers for Disease Control and Prevention (CDC). Infants tested for hearing loss–United States,1999−2001. MMWR Morb Mortal Wkly Rep 2003;52(41):981–984. [PubMed: 14561955][published correction appears in MMWR Morb Mortal Wkly Rep. 2003;42(49):1210]
12. White KR. The current status of EHDI programs in the United States. Ment Retard Dev Disabil ResRev 2003;9(2):79–88. [PubMed: 12784225]
13. Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Language of early- and later-identified childrenwith hearing loss. Pediatrics 1998;102(5):1161–1171. [PubMed: 9794949]
14. Hammes DM, Novak MA, Rotz LA, Willis M, Edmondson DM, Thomas JF. Early identification andcochlear implantation: critical factors for spoken language development. Ann Otol Rhinol LaryngolSuppl May;2002 189:74–78. [PubMed: 12018355]
15. Kishon-Rabin L, Taitelbaum R, Muchnik C, Gehtler I, Kronenberg J, Hildesheimer M. Developmentof speech perception and production in children with cochlear implants. Ann Otol Rhinol LaryngolSuppl 2002;189:85–90. [PubMed: 12018357]
16. Moore DR. Auditory development and the role of experience. Br Med Bull 2002;63:171–181.[PubMed: 12324392]
17. Waltzman SB, Cohen NL. Cochlear implantation in children younger than 2 years old. Am J Otol1998;19(2):158–162. [PubMed: 9520051]
18. Eisenberg LS, Martinez AS, Sennaroglu G, Osberger MJ. Establishing new criteria in selectingchildren for a cochlear implant: performance of “platinum” hearing aid users. Ann Otol RhinolLaryngol Suppl 2000;185:30–33. [PubMed: 11140994]
19. Eisenberg LS, Kirk KI, Martinez AS, Ying EA, Miyamoto RT. Communication abilities of childrenwith aided residual hearing: comparison with cochlear implant users. Arch Otolaryngol Head NeckSurg 2004;130(5):563–569. [PubMed: 15148177]
20. Winton, L.; Hollow, R.; Dettmen, SJ. Cochlear implant speech perception selection criteria: who isa candidate now?. Paper presented at: XXVI International Congress of Audiology; Melbourne,Australia. March 17−22, 2002;
21. Skinner, MW.; Holden, LK.; Binzer, SM. Aural rehabilitation for individuals with severe andprofound hearing impairment: hearing aids, cochlear implants, counseling, and training.. In: Valente,M., editor. Strategies of Selecting and Verifying Hearing Aid Fittings. Thieme Stratton Inc; NewYork, NY: 1994. p. 267-299.
22. Dettman SJ, D'Costa WA, Dowell RC, Winton EJ, Hill KL, Williams SS. Cochlear implants forchildren with significant residual hearing. Arch Otolaryngol Head Neck Surg 2004;130(5):612–618.[PubMed: 15148185]
23. Cullen RD, Higgins C, Buss E, Clark M, Pillsbury HC III, Buchman CA. Cochlear implantation inpatients with substantial residual hearing. Laryngoscope 2004;114(12):2218–2223. [PubMed:15564849]
24. Holland SK, Plante E, Weber Byars AM, Strawsburg RH, Schmithorst VJ, Ball WS. Normal brainactivation patterns in children performing a verb generation task. Neuroimage 2001;14(4):837–843.[PubMed: 11554802]
Patel et al. Page 8
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

25. Altman NR, Bernal B. Brain activation in sedated children: auditory and visual functional MRimaging. Radiology 2001;221(1):56–63. [PubMed: 11568321]
26. Anderson AW, Marois R, Colson ER, et al. Neonatal auditory activation detected by functionalmagnetic resonance imaging. Magn Reson Imaging 2001;19(1):1–5. [PubMed: 11295339]
27. Born P, Leth H, Miranda MJ, et al. Visual activation in infants and young children studied byfunctional magnetic resonance imaging. Pediatr Res 1998;44(4):578–583. [PubMed: 9773849]
28. Born AP, Miranda MJ, Rostrup E, et al. Functional magnetic resonance imaging of the normal andabnormal visual system in early life. Neuropediatrics 2000;31(1):24–32. [PubMed: 10774992]
29. Martin E, Joeri P, Loenneker T, et al. Visual processing in infants and children studied using functionalMRI. Pediatr Res 1999;46(2):135–140. [PubMed: 10447104]
30. Holland, SK.; Choo, DI.; Ret, JK., et al. fMRI of severe to profoundly hearing impaired children priorto cochlear implantation.. Paper presented at: Ninth Symposium on Cochlear Implants in Children;Baltimore, MD. April 24, 2003;
31. Holland, SK.; Strawsburg, RH.; Weber, AM.; Dunn, RS.; Schmithorst, VJ.; Ball, WS. SymposiumNeuroradiologicum XVI; May 15−17, 1998/36th Annual Meeting of the American Society ofNeuroradiology, May 17−21, 1998; Philadelphia, Pennsylvania. Vol. 36. American Society ofNeuroradiology; Oak Brook, IL: 1998. fMRI of language distributions in pediatric epilepsy patients.;p. 83
32. Holland, SK.; Strawsburg, RS.; Weber, AM.; Dunn, RS.; Schmithorst, V.; Ball, WS. Proceedings ofthe International Society for Magnetic Resonance in Medicine 7th Scientific Meeting and Exhibition;May 22−28, 1999; Philadelphia, Pennsylvania. International Society for Magnetic Resonance inMedicine; Berkeley, CA: 1999. Differences in fMRI language activation patterns between audio andvisual presentation of the same verb generation task in pediatric epilepsy patients.. Abstract 787
33. Schmithorst, VJ.; Dardzinski, BJ. CCHIPS. [April 24, 2007].http://www.irc.cchmc.org/cchips_main.htm.
34. Thevenaz P, Ruttiman UE, Unser M. A pyramid approach to sub-pixel registration based on intensity.IEEE Trans Image Process 1998;7(1):27–41. [PubMed: 18267377]
35. Worsley KJ, Liao CH, Aston J, et al. A general statistical analysis for fMRI data. Neuroimage 2002;15(1):1–15. [PubMed: 11771969]
36. Friston KJ, Zarahn E, Josephs O, Henson RN, Dale AM. Stochastic designs in event-related fMRI.Neuroimage 1999;10(5):607–619. [PubMed: 10547338]
37. Xiong J, Gao JH, Lancaster JL, Fox PT. Clustered pixels analysis for functional MRI activation studiesof the human brain. Hum Brain Mapp 1995;3(4):287–301.
38. Buxton, RB. Introduction to Functional Magnetic Resonance Imaging: Principles and Techniques.Cambridge University Press Inc; New York, NY: 2002.
39. Talairach, J.; Tournoux, P. Co-planar Stereotaxic Atlas of the Human Brain. Thieme-Stratton Inc;New York, NY: 1988.
40. Wilke M, Schmithorst VJ, Holland SK. Assessment of spatial normalization of whole-brain magneticresonance images in children. Hum Brain Mapp 2002;17(1):48–60. [PubMed: 12203688]
41. Wilke M, Holland SK. Variability of gray and white matter during normal development: a voxel-based MRI analysis. Neuroreport 2003;14(15):1887–1890. [PubMed: 14561914]
42. Brett, M. The MNI Brain and the Talairach Atlas. Medical Research Council Cognition and BrainSciences Unit; Cambridge, England: 1999.
43. Brett M, Christoff K, Cusack R, Lancaster J. Using the Talairach atlas with the MNI template.Neuroimage 2001;13(1):85.
44. Wilke M, Schmithorst VJ, Holland SK. Normative pediatric brain data for spatial normalization andsegmentation differs from standard adult data. Magn Reson Med 2003;50(4):749–757. [PubMed:14523961]
45. Schmithorst VJ, Holland SK. Event-related fMRI technique for auditory processing withhemodynamics unrelated to acoustic gradient noise. Magn Reson Med 2004;51(2):399–402.[PubMed: 14755667]
46. Hartnick CJ, Schmithorst V, Rudolph C, Willging JP, Holland SK. Functional magnetic resonanceimaging of the pediatric swallow: imaging the cortex and the brainstem. Laryngoscope 2001;111(7):1183–1191. [PubMed: 11568539]
Patel et al. Page 9
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

47. Osberger MJ, Chute PM, Pope ML, et al. Pediatric cochlear implant candidacy issues. Am J Otol1991;12(suppl):80–88. [PubMed: 2069195]
48. Miyamoto RT, Osberger MJ, Todd SL, et al. Variables affecting implant performance in children.Laryngoscope 1994;104(9):1120–1124. [PubMed: 8072359]
49. Geers AE. Speech, language, and reading skills after early cochlear implantation. Arch OtolaryngolHead Neck Surg 2004;130(5):634–638. [PubMed: 15148189]
50. McConkey Robbins A, Koch DB, Osberger MJ, Zimmerman-Phillips S, Kishon-Rabin L. Effect ofage at cochlear implantation on auditory skill development in infants and toddlers. Arch OtolaryngolHead Neck Surg 2004;130(5):570–574. [PubMed: 15148178]
51. Miyamoto RT, Houston DM, Kirk KI, Perdew AE, Svirsky MA. Language development in deafinfants following cochlear implantation. Acta Otolaryngol 2003;123(2):241–244. [PubMed:12701749]
52. Holland, SK.; Choo, DI.; Ret, JK.; Hilbert, L.; Dunn, RS.; Schmithorst, VJ. fMRI of severe toprofoundly hearing impaired infants and toddlers under sedation.. In: Miyamoto, RT., editor.Cochlear Implants: Proceedings of the VIII International Cochlear Implant Conference; May 10−13,2004; Indianapolis, Indiana. Vol. 1273. Elsevier Science Inc; New York, NY: Nov. 2004 p. 383-386.
53. Schmithorst VJ, Holland SK, Plante E. Cognitive modules utilized for narrative comprehension inchildren: a functional magnetic resonance imaging study. Neuroimage 2006;29(1):254–266.[PubMed: 16109491]
Patel et al. Page 10
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
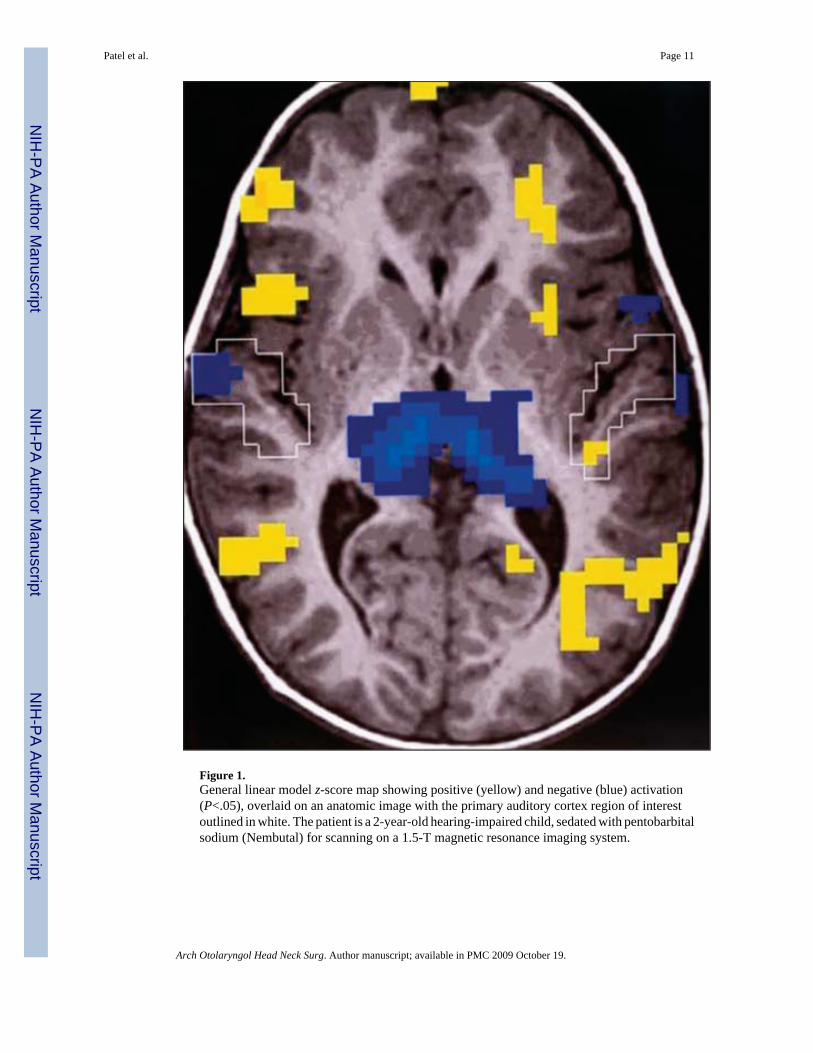
Figure 1.General linear model z-score map showing positive (yellow) and negative (blue) activation(P<.05), overlaid on an anatomic image with the primary auditory cortex region of interestoutlined in white. The patient is a 2-year-old hearing-impaired child, sedated with pentobarbitalsodium (Nembutal) for scanning on a 1.5-T magnetic resonance imaging system.
Patel et al. Page 11
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
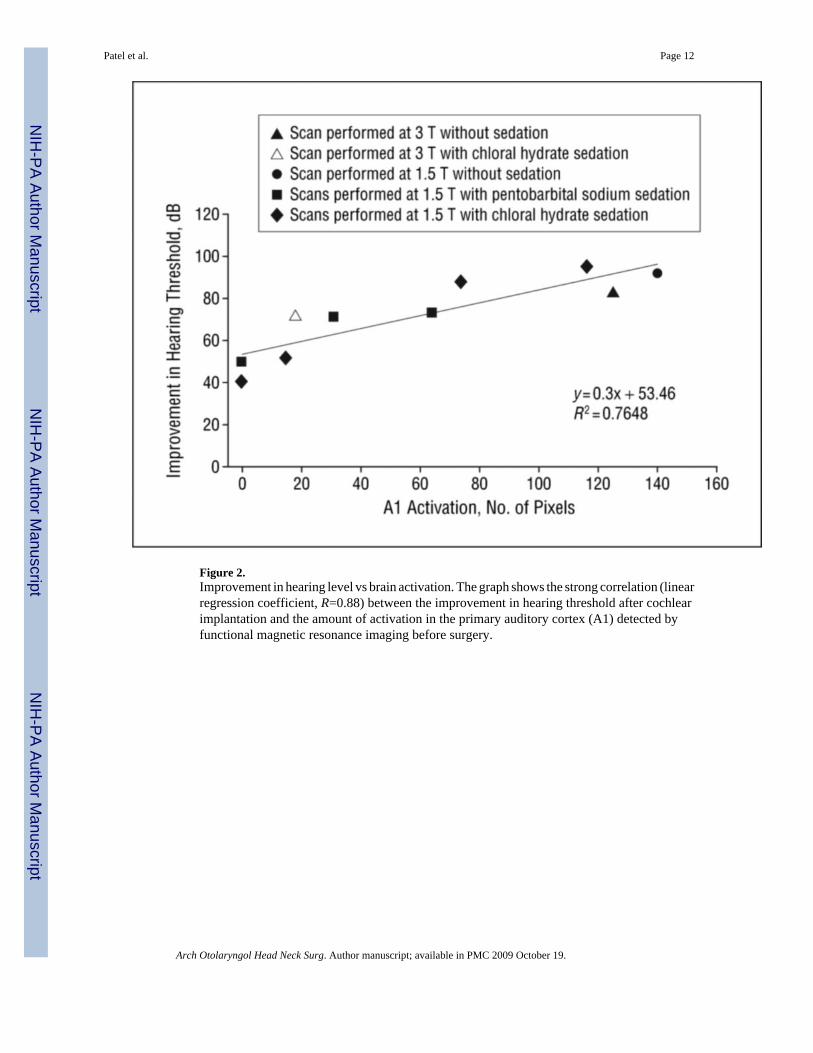
Figure 2.Improvement in hearing level vs brain activation. The graph shows the strong correlation (linearregression coefficient, R=0.88) between the improvement in hearing threshold after cochlearimplantation and the amount of activation in the primary auditory cortex (A1) detected byfunctional magnetic resonance imaging before surgery.
Patel et al. Page 12
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Patel et al. Page 13
TableSubject Age, MRI System, and Type of Sedation Used
Subject No./Age, mo MRI System (T) Sedation ΔHL, dB A1 Pixels
1/149GE (1.5)a None 92 1402/143GE (1.5)a None 82 1253/11GE (1.5)a Chloral hydrate 71 314/15GE (1.5)a Pentobarbitald 40 05/24GE (1.5)a Pentobarbitald 95 1166/33GE (1.5)a Pentobarbitald 87 747/21GE (1.5)a Chloral hydrate 50 08/20GE (1.5)a Chloral hydrate 76 649/48Siemens (3)b Chloral hydrate 72 18
10/28Bruker (3)c Pentobarbitald 52 15
Abbreviations: A1, primary auditory cortex; ΔHL, improvement in hearing threshold; MRI, magnetic resonance imaging.
aIndicates GE Signa Horizon (General Electric Medical Systems, Milwaukee, Wisconsin).
bIndicates Siemens (Siemens Medical Solutions, Erlangen, Germany).
cIndicates Bruker Biospec 30/60 (Bruker Medizintechnik, Karlsruhe, Germany).
dAdministered as pentobarbital sodium (Nembutal).
Arch Otolaryngol Head Neck Surg. Author manuscript; available in PMC 2009 October 19.
Copyright © 2022 FDOKUMEN




















