FULL - Journal of Canine Development & Research
135
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of FULL - Journal of Canine Development & Research

126
Journal of Canine Development & Research 2013
JOURNAL OF CANINE DEVELOPMENT & RESEARCH
PROFESSOR (DR.) ANIL AHUJADEPARTMENT OF CLINICAL VETERINARY MEDICINE
COLLEGE OF VETERINARY AND ANIMAL SCIENCE, RAJUVAS BIKANER- 334 001 (RAJASTHAN) INDIA
Phone : 0151- 2544243 (O), 2543726 (R)Mobile : 09414230453
E-mail : [email protected] : www.jcdrindia.com
EXECUTIVE EDITORS
PROF (Dr.) D.K. BIHANIDept. of Cil. Vety. Medicine
PROF (Dr.) G.N. PUROHITDept. of Gyne. & Obst.
ASSISTANT EDITORS
Dr. DEEPIKA DHURIADept. of Cil. Vety. Medicine
Dr. ANIL LANGERDept. of Cil. Vety. Medicine
COVER DESIGNAASHISH AHUJA
E D I T O RADVISORY CUM
EDITORIAL BOARDArora, P. K.(Faridabad)
Ashok Kumar(Hisar)
Gahlot, A. K.(Bikaner)
Gupta, S. K.(Jammu)
Kachwaha, R. N.(Bikaner)
Kapoor, P. K.(Hisar)
Pathak, K. M. L.(Delhi)
Purohit, S.K.(Jodhpur)
Sharma, S.N.(Bikaner)
Tanwar, R.K.(Bikaner)
Varshney, J. P.(Surat)
CANINE PUBLISHING HOUSEPUSHAP BHAWAN, B-48, SADUL GANJ
BIKANER - 334 003 (RAJASTHAN)INDIA
Web
Pencil
Web
Pencil

127
Journal of Canine Development & Research 2013
Publication of articles and other correspondence may be made to:
Professor (Dr.) Anil AhujaB.V.Sc. & A.H., M.V.Sc., Ph.D., FISACP
Editor, Journal of Canine Development & ResearchProfessor & Head, Department of Clinical Veterinary Medicine
College of Veterinary & Animal Science, RAJUVAS, Bikaner - 334 001 (Rajasthan) INDIA
Phone : 0151-2544243 (O)0151-2543726 (R)
Mobile : 09414230453
E-mail : [email protected]
Website : www.jcdrindia.com
Laser type set at Pooja Computers & Printers, Bikaner Tel. No. 9928645198
Journal of Canine Development & Research ANNUAL SUBSCRIPTION (one issue)
For InstitutionsRs. 1200.00 or US$ 110 or £ 65 or DM 130 or Euro 90
For Vets & OthersRs. 500.00 or US$ 50 or £ 30 or DM 60 or Euro 50
Send a demand draft in favour of “Canine Publishing House” payableat ICICI, JNV Colony, Bikaner through registered mail to CaninePublishing House, B-48, Sadul Ganj, Bikaner - 334 003 (Rajasthan).
Web
Pencil
130
Journal of Canine Development & Research 2013
CONTENTSS. No. Title and Autors’s Name Page No.
EditorialCanine Research
1. Disseminated Intravascular Coagulation (DIC) in Canine - 1-8Old Disease with New HopeArabinda Adak, Rajesh Eswarappa and S. K. Mukhopadhayay
2. Update on History, Etio-Pathogenesis and Clinical signs of 9-15Leptospirosis in DogsAnkita Sharma, Anil Ahuja , Sunil Tamoli,Mukesh Srivastava, J.P. Kachhawa,Mamta Daga and Khushbu Kannojia
3. Advanced Diagnosis in Canine Scabies 17-23Anil Langer, Altaf Hussain and S.K. Gupta
4. A Study on Electrocardiographic Values of 25-29Arrhythmic DogsPriyanka, Anil Ahuja, J.P. Varshney, A.P.Singh and Deepika Dhuria
5. Pathogenecity Trials of Escherichia Coli 31-36from Pyometric BitchesVarun Bassessar, Yamini Verma and Madhu Swamy
6. Effect of Therapeutic Management on Electrocardiographic 37-45Parameters in Dialated Cardiomyopathy Affected DogsVelhankar, R.D. and D.V. Keskar
7. Hemato-Biochemical Alterations in Canine Pyometra 47-51Varun Bassessar, Yamini Verma and Madhu Swamy
8. Vertebral Heart Score in Saint Bernard Breed of Dogs 53-55Anil Ahuja, Mamta Daga, Ankita Sharma, Jitender Bargujar, D.K.Bihani,Pradeep Abusuria, Mahender Tanwar and Anil Langer
9. Prevalence of Canine Corona Virus in Dogs 56-58Shanaz Bashir, Altaf Hussain and Anil Langer
10. Therapeutic Management of Demodicosis in Dogs 59-62Ramakant and Mukesh Srivastava
11. Therapeutic Management of Snake Bite in Dogs 63-65D.K. Bihani, D.K Saini, B.L.Sharma, S. Kumar and M. L. Sain
12. Flea Allergy Dermatitis and its Therapeutic 66-68Management in DogsJ.P. Kachhawa, Anil Ahuja, A.P. Singh, D.K. Bihani, Sanjhali Soren,Deepika Dhuria, Ankita Sharma, and Mamta Daga
13. Successful Management of Canine Pyometra 69-71Kuldip Dwivedi
14 Renal Failure in Dog 72-74M.L. Sain, D. K. Bihani, Mukesh Srivastava, R. K. Khinchi and N. K. Singh
15. Management of Ascites in a Dog 75-77A.K. Srivastava and B. Syed
16. Sertoli Cell Tumour in a Dog and its Surgical Management 78-80Arabinda Adak, Vinay Chaturvedi, V. K. Tripathi and S. K. Mukhopadhayay
Web
Pencil
131
Journal of Canine Development & Research 2013
17. Use of Decolorized Iodine in Alopecia of Canine 81-82Bhanu K Khajuria, Anisha Tiwari and S.K. Gupta
18. Diaphyseal Oblique Fracture of Femur and It’s 83-87Surgical Management in a DogJayakrushna Das, Sidhartha Sankar Behera,Manas Ranjan Senapati and Monalisa Behera
19. Successful Management of Dystocia in a Bitch 88-89Kuldip Dwivedi
20. Surgical Management of Vaginal leiomyoma of Canine 90-92Rai Somil and Chandrapuria V.P
21. Vaginal Fibroma and Urinary Incontinence in a Bitch 93-96Sidhartha Sankar Behera, Jayakrushna Das,Monalisa Behera and Manas Ranjan Senapati
22. Canine Transmissible Venereal Tumor of a Dog and 97-101its Surgical ManagementJayakrushna Das, Sidhartha Sankar Behera, Manas Ranjan Senapati, MonalisaBehera, Snehasis Pradhan, Manas Ranjan Praharaj and Prasanta Kumar Nanda
Canine Practice23. Update on Use of Medicated Shampoo in Companion 102-111
Animal DermatologyMukesh Srivastava, Anil Ahuja, S. Kachhawaha, J.P Kachhawa,Ankita Sharma, M. Daga, N.K.Singh and Khusbu Kannojia
24. Advancement in Dental Care in Canines : An Overview 112-116J.P. Kachhawa, Anil Ahuja, A. P. Singh, D.K.Bihani,Deepika Dhuria,
Jitender Bargujar and Anil Langar
25. The Neapolitan Mastiff- A Breed Review 117-118R.N.Kachwaha1, Basant Bais and G. Choudhary
Feline Research and Practice
226. Bronchial Asthma in a Cat 119-123A.K. Srivastava and B. Syed
27. The Bengal Cat - A Breed Review 124-125S.K.Vyas, Anil Ahuja, Anil Langer and Deepika Dhuria
Author Index, Subject Index and Guidelines for Contributors
DISCLAIMERThe views, claims, suggestions and/or commitments in the articles are the sole and
total responsibility of the author(s). JCDR’s editors need not necssarily agree/disagree tothese and will not be responsible for any liability/loss/injury/damage arising out of these
Web
Pencil
139
Journal of Canine Development & Research 2013
Dear Reader,In the era of canine growth in India I am presenting the 9th Volume of JCDR.I am
cheer up to observe that most of the canine clinics of the metros are equipped withadvance diagnostic modalities and the clinicians gained the lot of professional skills.Present issue of JCDR contain review on Disseminated Intravascular Coagulopathy,
Leptospirosis in dogs and advances in diagnosis of Scabies. Canine research sectionincludes a electrocardiographic (ECG) studies of Arrhythmic dogs, therapeuticmanagement of Dialated Cardiomyopathy in dogs, and put on record vertebral heart
score of Saint Bernard dogs. Therapeutic management of demodicosis, flea allergydermatitis in dogs are useful guidelines for canine practitioners. Prevalence of caninecorona virus is an important report. Use of decolorized iodine in alopecia is a
interested trail. Pathogenecity trails of Escherichia coli from pyometric bitches,hemato-biochemical and management of pyometra are quite informative. Caninesurgeon enhance their professional competence going through articles on surgical
management of sertoli cell tumour of dog, vaginal leiomyoma, fibroma and venerealtumor in bitches. The canine practice section contains very sensitive topic of caninedermatology- use of medicated shampoo, dental care in canines and tips of most
loveable giant breed Neapolitan Mastiff.Feline research and practice section is represent bronchial asthma in a cat and abreed review of Bengal cat.
As usual JCDR would welcome contributors to the Journal.
ANIL AHUJA
From the Desk of Editor ..........
Web
Pencil


1
Journal of Canine Development & Research 2013
REVIEW ARTICLE
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
DISSEMINATED INTRAVASCULAR COAGULATION (DIC) IN CANINE - OLDDISEASE WITH NEW HOPE*Arabinda Adak1, Rajesh Eswarappa2 and S. K. Mukhopadhayay3
Department of ToxicologyJai Research Foundation, Vapi – 396 195( Gujarat)
1Associate Scientist II, Dept. of Pathology, Vanta Bioscience, K2, 11 Cross street, SIPCOT Industrial Estate,Gummidipoondi, Tamilnadu - 601201 2 Test Facility Director, Vanta Bioscience, Gummidipoondi, Tamilnadu3 Professor and Head, Dept. of Pathology, West Bengal University of Animal and Fishery Sciences, Belgachia,Kolkata 700 037*Corresponding author e-mail - [email protected]
A B S T R A C T
Disseminated intravascular coagulation (DIC) is a serious, oftenfatal, life-threatening condition in humans and animals. It is acomplication of a wide spectrum of disorders including sepsis,neoplasms, infectious diseases and various inflammatoryconditions. The key event in the pathogenesis of DIC is systemicactivation of coagulation cascade leading to thrombosis. It isgenerally diagnosed based on the presence of an underlyingdisease that causes DIC combined with various laboratory teststhat suggest problems in the coagulation system. Despite thegloomy prediction, animals with DIC can survive, if the underlyingcause is a treatable illness and the coagulation abnormalities aretreated appropriately and promptly. As DIC is associated withorgan failure and often a fatal condition, prognosis variesdepending on the underlying disorder, the extent of theintravascular thrombosis (clotting) and the response of the dogto the therapy.
Key words :CanineDiagnosisDisseminated intravascular-coagulationEtiologyPathophysiologyPrognosis
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
Disseminated intravascular coagulation alsoknown as “DIC” or “Dysfibrinogen
syndrome”, is a complex syndrome of disordersand deregulation of the coagulation. It is thecontinuum in clinico-pathological severity, whichis characterized by diffuse intra vascular
thrombosis causing haemostatic defect due toreduction in clotting factors and platelets as a resultof their utilization in thrombotic process (Wada,2004; Coliman et al., 1979). Although the firstclinical observation on DIC were reported in 19
th
century, the condition of widespread and
Vol (9) 1-8

2
Journal of Canine Development & Research 2013
disordered coagulation has probably affected theanimals for as long as trauma and infections havebeset them and now-a-days, it has become anemerging problem in many breeds and strains ofcanines and thereby a headache to the cliniciansas this condition can occur in dogs of any age,breed or sex. When compared to humans, it isless common in dogs, judging by the lack of clinicalreports. To some extent, this may be due toshortage in documentation attributable to limitedapplication of suitable diagnostic tests in emergencypatients. It’s importance is supported by two keyobservations. Firstly, the presence of DICincreases the risk of mortality beyond thatassociated with primary disease (Levi, 2009).Secondly, the removal of it’s underlying cause doesnot necessarily alleviate the process in all cases .As these disorders develop slowly and the affectedanimal dies unknowingly, the acronym has beentruely synonymous with “Death Is Coming” (DIC).There is paucity of information on this disease inIndian literature. This is an updated overview ofDIC and how its onset may indicate the turningpoint from which an adaptive response becomesmaladaptive and potentially ominous to the host.This article could be helpful for the veterinarians indaily contacts with patients and hopefully couldshift this problem from laboratories to veterinaryclinics.
Etiological factors
Disseminated intravascular coagulation is never aprimary disease per se, but a serious and oftenlife- threatening complication of a variety ofdiseases (Grindem et al., 1991). Sepsis and thesystemic inflammatory response syndrome (SIRS)are the most common causes in humans and dogs(Hackner, 2007). The various diseases andconditions associated with DIC in canines are asfollows:1.Neoplasia: It includes gastric cancer (Takeda
et al., 2014; Takashima et al., 2010; Rhee et al.,2010), rectal cancer (Higashiyama et al., 2011),hemangioma, hemangiosarcoma (Legendre andKrehbiel, 1977), mammary carcinoma (Jaillardonet al., 2012; Maruyama et al., 2004), metastaticthyroid carcinoma, prostatic adenocarcinoma,lymphoma, cholangiocarcinoma.2.Infectious disorders: It includes sepsis,bacterial endocarditis, leptospirosis, InfectiousCanine Hepatitis, babesiosis, dirofilariasis,angiostrongylosis (Kruse et al., 2013; Ramseyet al., 1996), lung worm infection (Schmitz andMoritz, 2009) and leishmaniasis (Honse et al.,2013; Font et al., 1994)3.Inflammatory conditions: It includessuppurative dermat itis, suppurativebronchopneumonia, acute hepatic necrosis,chronic active hepatitis, pancreatitis andhemorrhagic gastroenteritis.4.Miscellaneous: Shock, heatstroke, venomoussnakebite, cirrhosis (Ho et al., 1998),aflatoxicosis, Immune-mediated hemolytic anemia(Carr et al., 2002), cold agglutinin disease,nephrotic syndrome (Ritt et al., 1997), gastricdilatation- volvulus (Uhrikova et al., 2011;Monnet, 2003), congestive heart failure, valvularfibrosis, diaphragmatic hernia, perioperativecomplications, embryonic mycetoma, renalamyloidosis, pulmonary thromoembolism, hepaticlipidosis and renal amyloidosis.
Pathophysiology
The pathogenesis of DIC is complex and centerson the enhanced generation of thrombin in vivo.The contributing components include increasedtissue factor expression, suboptimal function ofnatural anticoagulant systems, dysregulation offibrinolysis and increased anionic phospholipidavailability (Levi et al., 2009). However, the keyevent in DIC is systematic activation of coagulationto an extent, which cannot be contained by thebody anticoagulant mechanisms (Vlastin et al.,

3
Journal of Canine Development & Research 2013
2004). It includes the following mechanisms:● Activation of the coagulation cascade leads tofibrin formation from fibrinogen by the action ofthrombin deposition in the microvasculature i.e.thrombosis (Kitchens, 2009). Thrombus formationresults in ischemia and end organ damage.● This activation of coagulation results inconsumption and depletion of coagulation factors,including procoagulant factors (especially thosethat are non-enzymatic factors fibrinogen, factorV and factor VIII) and anticoagulant factors suchas AT-III (Slappendel, 1988).● Platelets activated by the thrombin generatedfrom coagulation, become trapped by fibrindeposited in the microvasulature and participatein formation of intravascular thrombi. This leadsto thrombocytopenia followed by bleeding(Brooks et al., 2009). Red cells are also damagedby fibrin in the microvasculature leading toformation of schistocytes.● Plasmin, the active enzyme of fibrinolysis, isgenerated by tissue plasminogen activator and itdegrades fibrin clots as well as circulating fibrinogenthereby elevating the concentration of fibrindegradation products (FDPs).● There has been a recent challenge however tothe basic assumptions and interpretations of thepathophysiology of DIC. A study of sepsis andDIC in animal models has shown that a highly-expressed receptor on the surface of hepatocytes,termed the Ashwell-Morell receptor, is responsiblefor thrombocytopenia in bacteremia and sepsis dueto streptococcal pneumoniae (SPN) and possiblyother pathogens. The thrombocytopenia observedin SPN sepsis was not due to increasedconsumption of coagulation factors such asplatelets, but instead was the result of thisreceptor’s activity enabling hepatocytes to ingestand rapidly clear platelets from circulation. Byremoving pro-thrombotic components before theyparticipate in the coagulopathy of DIC, theAshwell-Morell receptor lessens the severity of
DIC, reducing thrombosis and tissue necrosis andpromoting survival. The hemorrhage observed inDIC and among some tissues lacking this receptormay thereby be secondary to increased thrombosiswith loss of the mechanical vascular barrier.
Clinical findings
Owing to the dynamic and progressive nature ofDIC, clinical signs vary considerably and rangefrom no signs, to signs of organ failure associatedwith microvascular thrombosis and culminating inovert signs of bleeding (Hackner, 2007). Signsassociated with DIC depend on the individual dog,the length of time they have been ill and theunderlying condition (Vlastin et al., 2004).Clinically this disorder is divided into two forms:a) Acute (fulminant) form and b) chronic (subclinical) form.a) Acute form-It is a hemorrhagic disordercharacterized by multiple petechiae, ecchymoseson skin, mucosal bleeding, visceral hemorrhages,oozing from surgical, traumatic and venipuncturesites, deep tissue hematomas, acral cyanosis andgangrene etc. It is usually seen after true acutetrauma or as secondary to the primary disease.Acute DIC is often fatal with multiorgan failure andcirculatory collapse. Acute DIC is more commonlyobserved in dogs and is rare in cats (Choi, 2005).b) Chronic form-It is more subtle, usually doesn’thave spontaneous bleeding and characterized bysuperficial venous thrombosis, signs of deep venousor arterial thrombosis, and serial thromboticepisodes (Brooks, 2000). It is the most commonform seen in dogs with concomitant malignancy orchronic disorders.
Diagnosis
Disseminated intravascular coagulation is usuallydifficult to diagnose as it can be triggered by manyunrelated diseases and the clinical manifestationsare variable and so there is quasi-consensus aboutthe definitive diagnosis (Stokol, 2012). There is

4
Journal of Canine Development & Research 2013
not a single test that diagnoses DIC (Maxson,2000). Disseminated intravascular coagulation isgenerally diagnosed based on the presence of anunderlying disease that causes DIC combined withlaboratory tests that suggest problems in thecoagulation (clotting) system (Levi and Thachil,2009). Diagnosis is based on following criteria:Complete medical history and thorough physicalexamination to find out clinical findings and thepresence of underlying diseases known to beassociated with DIC. Special attention should bepaid to any evidence of bruising or bleeding.Complete blood count (CBC) including Packedcell volume (PCV) can discover anemia (too fewoxygen-carrying red blood cells), abnormal plateletnumbers (too few or too many blood clotting cells)and abnormal white blood cell counts (too few ortoo many infection-fighting cells). The plateletcount is usually decreased in DIC (DeLoughery,2009).Clotting tests such as an activated clotting time(ACT), prothrombin time (PT) and activated partialthromboplastin time (APTT) are used to determineif anemia and/or bleeding are due to the inabilityof the animal to clot its blood (Ho et al., 1998;Kaneko and Wada, 2011; Bateman et al., 1999;Uhrikova et al., 2013). These values are greatlyprolonged in the hemorrhagic phase of DIC. Thevalues can be short in the early phases. As the dogis being treated, it is recommended to repeat theseblood tests to confirm that they normalize.Serum fibrinogen concentration and fibrindegradation products (FDPs) are tests used toidentify the presence of breakdown products offibrin (called fibrin degradation products -FDPs)can serve as an important clue to the presence ofDIC (Brooks, 2000; Uhrikova et al., 2013). Theyare elevated with DIC.The International Society on Thrombosis andHemostasis (ISTH) recommends a diagnosticscoring algorithm for patients with DIC (Toh andHoots, 2007). If the patient has underlying disease
known to be associated with DIC, then routinehemostatic tests are performed. Test results areassigned a score of 0 to 3 based on the extent ofabnormality, and cumulative scores of 5 or greaterare considered compatible with overt DIC. Giventhe dynamic nature of DIC, recommendations areto repeat the algorithm daily in at-risk patients. Aprospective evaluation of this scoring system inICU patients revealed high sensitivity andspecificity and a strong correlation between anincreasing DIC score and mortality. A similarscoring system has been developed and evaluatedin dogs with DIC-associated conditions (Wiinberget al., 2010; Mischke, 2010). This model, whichestablishes a score based on PT, aPTT, fibrinogenand D-dimers (Machida et al., 2010), was shownto have a good sensitivity and specificity, withpositive and negative predictive values of approx.80%. However, Studies have been performed totry to establish the cut-off levels for D-dimermeasurements that define a ‘moderate’ or ‘strong’increase because this is required in order to usethe scoring system (mentioned above). As issuesremain regarding the accuracy of high D-dimerestimations with current assay systems and workis ongoing for standardising reagents for thispurpose, precise definitions of D-dimer cut-offlevels are not meaningful at the current time. As aresult, D-dimer assay results need to be interpretedbased on the clinician’s experience andconsideration of the clinical circumstances andother available laboratory investigations (Levi etal., 2009).
In summary, hemogram and serum chemistry indogs with DIC will reveal hypofibrinogenemia,increased FDPs (more than 1:10) and D-dimersconcentrations (Stokol et al., 2000), prolongedaPTT, decreased antithrombin III concentration(50-80%), hemolytic anemia, thrombocytopenia(20-80,000/ml), increased schistocytes, left shiftneutrophilia, rarely neutropenia, hyperbilirubinemia,

5
Journal of Canine Development & Research 2013
hyperphosphatemia, increased liver enzymes,decreased total CO
2 (metabolic acidosis) and
possibly panhypoprotenemia (severe bleeding).Additional tests may be recommended on case-by-case basis. They may be recommended tohelp evaluate or determine the underlying causefor DIC (Stokol, 2012). These tests include:· Serum biochemical profile to determine potentialunderlying causes of DIC.· Analysis of the urine to check abnormalities thatbe contributing to this problem. It consists ofhemoglobinurea, bilirubinurea, occasionalproteinurea and cylindruria (urine sample shouldnot be obtained via cystocentesis).Abdominal Radiograph (X-ray) may be done torule out changes in size of organs like the liver orkidneys or to look for evidence of abdominaltumors. Kidney disease, intestinal disease, diseaseof the adrenal gland or certain abdominal tumorsmay be present as an underlying cause for DIC(Kaneko and Wada, 2011).
Treatment
Despite the lack of a standardized protocol forclinical management, aggressive medical andnursing care can play a prominent role in the clinicaloutcome of the patient with DIC (Maxson, 2000).Patients with DIC will require initial in-hospitalstabilization. Treatment is primarily directed at theunderlying disease. In-hospital therapy includesintensive care and frequent evaluation of bleedingand blood clotting parameters (Levi et al., 2009).The goal is to treat the underlying condition whiletrying to control hemorrhage that results from DIC.While treatment of DIC needs to be individualized,the following principles are helpful:1)Diagnose and remove or treat the underlyingcause of the DIC (Levi et al., 2009).2) Supportive care: Aggressive fluid therapy withcrystalloids or plasma extenders (dextran) is anessential component of case management tomaintain good tissue perfusion to dilute activated
clotting and fibrinolytic factors and to flush outmicrothrombi and to maintain precapillary andarteriole patency to increase blood flow to hypoxicareas (Feldman et al., 2000). Corticosteroids canbe used for the establishment of perfusion.3) Prevent secondary complications by maintainingoxygen mask, cage oxygen or nasopharyngealcatheter, by checking secondary bacterialinfections and by correcting acidosis and cardiacarrhythmias.4) Prevent intravascular coagulation by theadministration of heparin, aspirin, blood or bloodproducts (Mohamed and Seif, 2010). Low-molecular weight heparin may have been moreappropriate choice in view of some reports, thathigh molecular fractions of standard heparin havea platelet proaggregating effect (Mischke andJacobs, 2001).Heparin dose ranges: mini, low, intermediate andhigh doses 5-10, 100-200 , 300-500 and/750-1000 U/kg bwt sc or iv tid, respectively.Therapy: Add the initial mini-dose heparin to theblood/plasma prior to transfusion and wait for 30minutes at room temperature. Use the intermediateor high dose heparin if marked azotemia, isosthenicurine, increased liver enzymes, dyspnea orhypoxemia supervene. If overheparinizationoccurs, use protamine sulfate slow iv infusion (1mg / 100 U of the last dose of heparin given) as50% of the calculated dose one hour after heparinand 25% given two hours after heparin. Onceclinical and cinicopathological features haveimproved, taper the heparin dose gradually over3 to 4 days.Aspirin dosages: aspirin is not an effectivetreatment in most of the dogs with acute DIC, butcan be used to manage chronic cases or to preventrecurrences @ 5 –10 mg / kg bwt po bid.Plasma that has been frozen soon after collection(fresh frozen plasma) may be administered toprovide clotting factors in cases of DIC after thedog has been treated with heparin to prevent

6
Journal of Canine Development & Research 2013
ongoing coagulation. Sometimes heparin is mixedin with the fresh frozen plasma (Levi et al., 2009).Blood transfusions may be recommended for dogswith anemia or blood loss.
Prognosis
Prognosis varies depending on the underlyingdisorder, the extent of the intravascular thrombosis(clotting) and the response of the dog to the therapyas because DIC is associated with organ failureand it is often fatal condition. However, withappropriate care, patients with DIC can have afavorable outcome. The prognosis for the dogswith DIC, regardless of cause, is often grim: DICis associated with substantial mortality in humansand in animals. Mortality rates of 50-77% arereported in dogs and 93% in cats (Hackner,2007). DIC with sepsis has a significantly higherrate of death than DIC associated with trauma.Thus, dogs with DIC = grave prognosis unless theinitial cause is eliminated quickly and appropriatetherapy is initiated as soon as possible.
ReferencesBateman, S.W., Mathews, K.A., Abrams-Ogg, A.C.,
Lumsden, .JH., Johnstone, I.B. and Hillers,T.K.(1999). Evaluation of point-of-care tests fordiagnosis of disseminated intravascular coagu-lation in dogs admitted to an intensive care unit.J Am Vet Med Assoc., 215(6):805-810.
Brooks, M. (2000). Coagulopathies and thrombosis. In:Textbook of Veterinary Internal Medicine, 5th
Ed. W.B.Saunders, Philadelphia: 1829-1841Brooks, M.B., Catalfamo, L.J., Brown, A., Ivanova and
Lovaglio, J. (2009). A hereditary bleeding disor-der of dogs caused by a lack of plateletprocoagulant activity. Blood. 99(7): 2434-2441.
Carr, A.P., 2002 Panciera, D.L. and Kidd, L. (2002). Prog-nostic factor for mortality and thromoembolismin canine immune- mediated hemolytic anemia-a retrospective study of 72 dogs. J.Vet. Inter.Med., 16 (5): 501-503.
Choi, Y. (2005). Disseminated Intravascular Coagulation(DIC), Winter Newsletter., Indiana Animal Dis-
ease Diagnostic Model. Purdue University.Coliman, R.W., Robboy, S.J. and Minna, J.D. (1979). Dis-
seminated Intravascular Coagulation - an ap-proach. Am J. Med., 52: 679-689.
DeLoughery, T.G. (2009). Thrombocytopenia and otherhot topics. Am J Clin Oncol., 32(4), S13-S17.
Feldman, B.F., Kirby, R. and Caldin, M. (2000). Recogni-tion and treatment of Disseminated Intravas-cular Coagulation. In Bonagura J. Ed. Kirk’sCurrent Veterinary Therapy XIII. Philadelphia,WB Saunders: 190-194.
Font, A., Gines, C, Closa, J.M. and Mascort, J. (1994).Visceral leishmaniasis and disseminated intra-vascular coagulation in a dog. J Am Vet MedAssoc., 204 (7):1043-1044.
Grindem, C.D., Breitschwerdt, E.B., Corbett, W.T. andJans, H.E.(1991). Epidemiological survey ofthrombocytopaenia in dogs- a report on 987cases. Vet Clin Pathol, 20:38-43.
Hackner, S. G. (2007). Disseminated Intravascular Co-agulation- An update for the clinician. News-letter. Cornell University. Pp. 1-5.
Higashiyama, A., Kudo, M. and Nagasako, T. (2011).Successful chemotherapy of carcinomatosis ofthe bone marrow with disseminated intravas-cular coagulation from a rectal carcinoma foundby eosinophilia. Nihon Shokakibyo GakkaiZasshi, 108: 1244-1251.
Ho, C.H., Hou, M. C., Lin, H. C., Lee, S.D. and Liu, S. M.(1998). Can advanced haemostatic parametersdetect disseminated intravascular coagulationmore accurately in patients with cirrhosis of liver.Zhonghua Yi Xue Za Zhi., 61(6): 332-338.
Honse, C.O., Figueiredo, F.B., De Alencar, N.X., Madeira,Mde F., Gremião, I.D. and Schubach, T.M.(2013). Disseminated intravascular coagulationin a dog naturally infected by LeishmaniaChagasi from Rio de Janeiro - Brazil. Vet Res.,9:43.
Jaillardon, L., Barthélemy, A., Goy-Thollot, I., Pouzot-Nevoret, C. and Fournel-Fleury, C. (2012). Mam-mary gland carcinoma in a dog with peripheralblood and bone marrow involvement associ-ated with disseminated intravascular coagula-tion. Vet Clin Pathol., 41(2):261-265.
Kaneko, T. and Wada, H. (2011). Diagnostic criteria andlaboratory tests for disseminated intravascular
7
Journal of Canine Development & Research 2013
coagulation. J Clin Exp Hematop., 51(2), 67-76.Kitchens, C.S. (2009). Thrombocytopenia and thrombo-
sis in disseminated intravascular coagulation(DIC). Hematology Am Soc Hematol., 4, 240-246.
Kruse, B.D., Hartmann, K., Groth, A., Schulz, B. andWehner, A.(2013). Disseminated intravascularcoagulopathy in a dog with Angiostrongylusvasorum infection. Tierarztl Prax Ausg KKleintiere Heimtiere. 41(6):401-407.
Legendre, A.M. and Krehbiel, J.D. (1977). Disseminatedintravascular coagulation in a dog with he-mothorax and hemangiosarcoma. J Am Vet MedAssoc. 171(10):1070-1071.
Levi, M., Toh C.H., Thachil, J. and Watson, H.G. (2009).Guidelines for the diagnosis and managementof disseminated intravascular coagulation. Brit-ish Committee for Standards in Haematology.Br J Haematol. 145(1):24-33.
Machida, T, Kokubu, H, Matsuda, K, Miyoshi, K, Uchida,E (2010). Clinical use of D-dimer measurementfor the diagnosis of disseminated intravascularcoagulation in dogs. J. Vet. Med. Sci., 72: 1301–1306.
Maruyama, H., Miura, T., Sakai, M., Koie, H., Yamaya, Y.,Shibuya, H., Sato, T., Watari, T., Takeuchi, A.,Tokuriki, M. and Hasegawa, A. (2004). The inci-dence of disseminated intravascular coagula-tion in dogs with malignant tumor. J Vet MedSci., 66 (5):573-575.
Maxson, J.H. (2000). Management of disseminated intra-vascular coagulation. Crit Care Nurs Clin NorthAm.,12(3):341-52.
Mischke, R. and Jacobs, C. (2001). The monitoring ofheparin administration by screening tests inexperimental dogs. Res Vet Sci., 70 (2): 101-108.
Mischke, R. (2010). Disseminated intravascular coagula-tion in dogs: are scoring systems of value? Sep.,185(3): 243-244.
Mohamed, A. and Seif, G. (2010). Disseminated Intra-vascular Coagulation in Obstertrics, Pregnancyand Gynaecology: Criteria for Diagnosis andManagement. Ain Shams Journal of Anesthe-siology. 3 (2): 94-108.
Monnet, E. (2003). Gastric dilatation-volvulus syndromein dogs. Vet. Clinics of North America: SmallAnim Practice. 33: 987–1005.
Ramsey, I.K., Littlewood, J.D., Dunn, J.K. andHerrtage, M.E. (1996). Role of chronic dissemi-nated intravascular coagulation in a case ofcanine angiostrongylosis. Vet Rec. 138(15):360-3.
Rhee, J., Han, S.W., Oh, D.Y., Im, S.A., Kim, T.Y. and Bang,Y.J. (2010). Clinicopathologic features and clini-cal outcomes of gastric cancer that initially pre-sents with disseminated intravascular coagu-lation: a retrospective study. J GastroenterolHepatol, 25: 1537-1542.
Ritt, M. G.,1997 Rogers, K.S. and Thomas, J.S. (1997).Nephrotic syndrome resulting in thromboem-bolic disease and disseminated intravascularcoagulation in dog. J. Anim Hosp Assoc., 33(5):385-391.
Schmitz, S. and Moritz, A. (2009). Chronic disseminatedintravascular coagulopathy in a dog with lungworm infection. Schweiz ArchTierheilkd.,151(6):281-286.
Slappendel, R.J. (1988). Disseminated intravascular co-agulation. Vet Clin North Am Small Anim Pract.,18(1):169-84.
Stokol, T., Brooks, M.B., Erb, H.N. and Maudlin, G.E.(2000). D-dimer concentration substrate inhealthy and dogs with disseminated intravas-cular coagulation. Am. J. Vet. Res. 61(4): 393-398.
Stokol, T. (2012). Laboratory diagnosis of disseminatedintravascular coagulation in dogs and cats: thepast, the present and the future. Vet Clin NorthAm Small Anim Pract., 42(1):189-202.
Takeda, H., Nishikawa, H., Tsumura, T., Sekikawa, A.,Maruo, T., Okabe, Y., Kimura, T., Wakasa, T.and Osaki, Y. (2014). Prominenthypereosinophilia with disseminated intravas-cular coagulation as an unusual presentationof advanced gastr ic cancer. InternMed.53(6):563-569.
Takashima, A., Shirao, K. and Hirashima, Y. (2010). Se-quential chemotherapy with methotrexate and5-fluorouracil for chemotherapy-naïve ad-vanced gastric cancer with disseminated intra-vascular coagulationat initial diagnosis. J Can-cer Res Clin Oncol. 136: 243-248.
Toh C.H. and Hoots W.K. (2007). The scoring system ofthe Scientific and Standardisation Committee

8
Journal of Canine Development & Research 2013
on Disseminated Intravascular Coagulation ofthe International Society on Thrombosis andHaemostasis: a 5-year overview. J. of Throm-bosis and Hemostasis, 5, 604–606.
Uhrikova, I., Rehakova, K., Rauserova-Lexuamlova, L.and Doubek, J. (2011). Initial HMGB1 values indogs with gastric dilatation and volvulus - apilot study. Vet. Clin. Pathol., 40: 587-589.
Uhrikova, I., Machackova, K., Rauserova-Lexmaulova,L. , Rehakova, K. and Doubek, J. (2013). Dis-seminated intravascular coagulation in dogswith gastric dilatation-volvulus syndrome.Veterinarni Medicina, 58 (11): 587–590.
Vlastin, M., Rauser, P., Fichtel, T. and Novonty, J. (2004).Disseminated Intravascular Coagulation of thedogs, Acta Vet Brno.73: 497-505.
Wada, H (2004): Disseminated intravascular coagulation.Clinical Chemistry Acta., 344, 13-21.
Wiinberg, B., Jensen, A..L, Johansson, P.I., Kjelgaard-Hansen, M., Rozanski, E., Tranholm, M. andKristensen, A.T. (2010). Development of a modelbased scoring system for diagnosis of caninedisseminated intravascular coagulation withindependent assessment of sensitivity andspecificity. Vet J. 185(3): 292-298.

9
Journal of Canine Development & Research 2013
REVIEW ARTICLEUPDATE ON HISTORY, ETIO-PATHOGENESIS AND CLINICAL SIGNS OFLEPTOSPIROSIS IN DOGS*Ankita Sharma1, Anil Ahuja2 , Sunil Tamoli1,Mukesh Srivastava3 , J.P. Kachhawa4, Mamta Daga1 and KhushbuKannojia5
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege Of Veterinary and Animal Science, RAJUVAS, Bikaner -334 001 (Rajasthan)
1,5P.G.Scholar 2Professor and Head 3Ph.D Scholar 4Teaching Associate 5Deptt. Of ABG*Corresponding author e-mail - [email protected]
A B S T R A C T
Leptospirosis is a bacterial disease affecting several mammalianspecies, including human beings with reservoies in companionanimals, livestock and wild animals. In dogs, it is spread mainlyby rodents that act as a maintenance host for severalLeptospiraserovars. Until recently, the most common signsobserved in affected dogs consisted of icterus and haemorrhagicdiathesis, but today the most prevalent clinical signs are attributedto acute renal failure. The current literature gives a peer reviewof leptospirosis in dogs. This review considers the history,epidemiological feature, pathogenesis and clinical signs of thisemerging zoonotic disease.
Key words :ELISALeptospirosisMonoclonal antibodiesRice Field DiseaseSeven day feverWeils disease
A R T I C L E H I S T O R Y
Received : November 28, 2013Revised : December 12, 2013Accepted : December 22, 2013
Canine leptospirosis is a bacterial zoonosis withworldwide distribution (Ghneim et al., 2007)
causing renal and hepat ic dysfunction,coagulopathies and other abnormalities (Arent etal., 2012; Miller et al., 2011; Andre-Fontaine,2006) with a case fatality rate of 10–20% in dogs(Harkin et al., 1996). It is caused by infection withthe motile spirochetal bacterium of the genus,Leptospira (Bharti et al., 2003) more commonlyin countries with a warm, humid climate that allowthe bacteria to thrive (Sykes et al., 2011). Almostevery known species of rodent, mammal ormarsupial or even humans can be a reservoir or
incidental host for Leptospira (Picardeau, 2013).The incubation period is approximately seven daysbut it depends on dose, strain and host (Sykes etal., 2011). Out of 250 serovars, six to eight arethought pathogenic for the dog (Adin and Cowgill,2000 and Levett, 2001), which include serovarsbratislava, canicola, icterohaemorrhagiae,grippotyphosa and pomona. Each serovar has aprimary or definitive host that maintains theorganism and contributes to its dissemination inthe environment. Although all mammals may besusceptible to infection, clinical signs are expectedto be most severe with non–host-adapted
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 9-15

10
Journal of Canine Development & Research 2013
serovars, whereas the definitive host is typicallyinfected at a young age and is thought to mostcommonly exhibit minimal clinical disease(Goldstein et al., 2006). In the United States,leptospirosis in dogs has reported to be associatedwith Leptospira interrogans serovars canicolaand icterohaemorrhagiae (Adin and Cowgill,2000). During the past 10 years, however, therehas been an increase in the number of dogs withleptospirosis from which clinicians have isolatedor detected serologic evidence to support theinvolvement of L. Kirschneri serovargrippotyphosa, L interrogans serovar bratislava,and L. Interrogans serovar pamona (Wardet al., 2002). In Germany, the predominantserovars seem to be grippotyphosa, saxkoebing,icterohaemorrhagiea, canicola, and Bratislava,while in Italy major identified serovars includesbratislava and grippotyphosa (Scanziani et al.,2002 and Geisen et al., 2007).
History
The history of Leptospira dates back to nineteenthcentury and disease was described under a varietyof names such as griesinger bilious typhoid, biliousor hepatic fever, hepatic typhoid, icteric typhoid,catarrhal icterus, and febrile icterus (Terpstra,2006). In 1886, Adolf Weil, Professor of Medicineat Heidelberg whose name has been given to thedisease in humans, first described this disease butthe distinction between leptospirosis, yellow fever,and other diseases with icterus was not clear(Edward and Hodder , 1990). In 1914, RyoKichei Inada and his colleagues in Kyushu, Japan,observed the spiralorganisms in the liver of a guineapig inoculated with blood taken from four Japaneseminors presumed to have Weil’s disease. Theynamed the organisms Spirochaitaicterohaemorrhagiae (Inada et al., 1916), and in1917, Hideyo Noguchi renamed the genus asLeptospira (Noguchi, 1928). In the next 15 yearsmany of the important serovarieties prevalent
throughout the world and their host sources werediscovered (Kmely and Dikken, 1993). Before1960, L interrogans serovaricterohaemorrhagiae and canicola were believedresponsible for most clinical cases of canineleptospirosis as acute or subacute hepatic and renalfailure, characterized by acute hemorrhagicdiathesis, icterus, or uremia (Brown et al., 1996).The detailed structure of Leptospira was studiedunder electron microscope during the 1960 and1970 (Noguchi, 1928). In 1972, leptospirosisresearchers developed a preoccupation withserological classification, based only on absorptionand cross-agglutination of antisera. By 1980,enzyme-linked immunosorbant assay (ELISA)methods were developed to analyze non-agglutinating as well as agglutinating antigens andapplied with monoclonal antibodies to identifyepitopes involved in the immunity and useful forclassification. The current system of geneticclassification was adopted in 1994 (Edward andHodder , 1990). In the last 15 years, developmentshave included lipopolysaccharide derivation of theantigens involved in the immunity, and moleculartechniques like polymerase chain reaction (PCR)has been developed for identification and geneticspeciation (Adler et al., 1980). Recently multilocussequence typing method has been used forgenotyping of Leptospira (Ahmed et al., 2006).Leptospirosis is known to be endemic in India sincethe early 20th century (Chowdry, 1903; Woolley,1911, 1913; De Castro, 1922; Barker, 1926).Most outbreaks of leptospirosis in India arereported from the coastal regions of the states ofGujarat, Maharashtra, West Bengal, Orissa,Kerala, Tamil Nadu, Karnataka and the AndamanIslands. Highest rates occur during October toNovember which coincides with the monsoonseason in these parts. Significant outbreaks havebeen observed in Orissa (Faine, 1994; Sehgal etal., 2001), Mumbai and the Andaman archipelago(Sehgal et al., 1995; Singh et al., 1999).

11
Journal of Canine Development & Research 2013
Etiology
Leptospira is a Gram-negative, aerobic bacteriumthat belongs to the order Spirochaetales, familyLeptospiracae and genus Leptospira (Zuerner,2010). The bacterium has a helical appearancewith a hook on each end and is as thin as a sewingthread (0,1 x 6-20 ìm) (Holt, 1978), and motilethrough two periplasmic flagella (Levett, 2001).The bacterium has an inner membrane and an outermembrane containing lipopolysaccharides (Holt,1978). The genus was formerly divided into twospecies L. interrogans, comprising all pathogenicstrains, and L. biflexa containing the saprophyticstrains isolated from the environment. Thesespecies were further divided into serogroups,serovarieties, and strains, based on shared antigens.Over 60 serovarieties of L. biflexa and more than250 serovarieties of L. interrogans have beenrecognized (Coleman, 2006 ). Leptospira bacteriaprefer a moist, warm environment, with an optimalgrowth temperature of 28-30°C. They can surviveup to 180 days in wet soil and for many months insurface water (McDonough, 2013).
Epidemiology
According to the occupational groups involved andthe nature of the disease presentations, differentnames of disease have been used, e.g. Seven-Day Fever found commonly in Japan, CaneCutter’s Disease in Australia, Rice FieldLeptospirosis in Indonesia and Fort Bragg Feverin the US, Weil’s Disease in many countries,including India and other South-East AsianCountries, China, continental Europe and England.It occurs in tropical, subtropical and temperatezones (Sehgal, 1995), but remains a grosslyneglected disease and is under-recognizedclinically because of the difficulty of diagnosis andthe wide variety of clinical manifestations(Hartskeerl, 2006). Boqvist et al. (2012) andAdin and Cowgill (2000) reported positivecorrelation between rainfall and seropositivity for
leptospirosis in pigs.The dog serves as the reservoir host only for thepathogenic L. interrogans serovar canicola. Thereservoir hosts for the other serovars includecommon rodents, skunks, raccoons, farm animals,and deer, which can carry and excrete the bacteriain their urine for extended periods (Baldwin andAtkins, 1987). The reservoir hosts suffer from achronic infection with Leptospira in their kidneys,as the leptospires colonize the surface of renalproximal tubular epithelial cells (Adler andMoctezuma, 2010; Picardeau, 2013). To becomea reservoir host depends on many factors, such asurine pH in the host, environment and possibilitiesof coming into contact with the bacterium. If twoanimals of a potential reservoir species are infectedone of them can become a reservoir host whilethe other does not (Sophie, 2013). Each serovaris adapted to one or more mammals as a primaryor definitive or reservoir host. Adapted reservoirhosts are thought to harbour persistent infectionwithout signs of disease and can shed organismsin their urine for months to years after infection asbacteria are maintained in the renal tubules ofreservoir hosts and excreted in the urine. The othertype of mammalian host is the incidental host thatbecomes infected with a specific serovar that isnot adapted to living chronically in this species ofmammal. Incidental hosts tend to develop clinicaldisease and either clears the organisms or die, theyrarely develop a chronic carrier state (Goldstein,2006).The most frequent sources of infection are urine,kidneys, surface water, mud and soil (Forbes etal., 2012; Ngbede et al., 2012; Picardeau, 2013).Leptospires are presumed to enter via smallabrasions or other breaches of the surfaceintegument. They may also enter directly into thebloodstream or lymphatic system via theconjunctiva, the genital tract in some animals, thenasopharyngeal mucosa, possibly through acribriform plate, the lungs following inhalation of

12
Journal of Canine Development & Research 2013
aerosols, or through an invasion of the placentafrom the mother to the foetus at any stage ofpregnancy in mammals. Drinking or inhalation ofcontaminated water following can also causedisease (Faine , 1994). The organism survives onlytransiently in undiluted acidic urine (pH 5.0 to 5.5)as neutral to basic pH is favourable for its survival.Dilute or non-concentrated urine provides asuitable habitat. Freezing markedly decreasessurvival of the organism outside the host, likelycontributing to a seasonal pattern of infection incolder climates. Ambient temperatures between0°C and 25°C favour survival of the organism.Therefore, rainfall, temperature, and pHrequirements may explain the apparent increasedincidence of canine leptospirosis in late summerand early fall, in the southern, semitropical belt ofthe United States, and in similar climatic regionsworldwide. Seasonality in many parts of thecountry is associated with rainfall (Goldstein et al.,2006 and Ward et al., 2002).Incubation period may be as short as a few days,the organisms replicating rapidly within the bloodas early as 1 day after infection before invadingtissues (Saravanan et al., 1999). The incubationperiod in experimental studies has been 7 days,but varies depending on the infecting dose, strain,and host immune response. Shorter incubationperiods can occur with large inoculate, and longerincubation periods may occur after low-grade,chronic infections of the renal tubules orhepatocytes, with clinical illness not being detecteduntil sometime after renal or hepatic injury ( Sykeset al., 2011; Forbes et al., 2012 and Langstonand Heuter, 2003). After penetration intosusceptible host, leptospires begin to multiply asearly as 1 day after entering the blood vascularspace (Geisen et al., 2007). This initiates aleptospiremic phase, which lasts a few daysinvolving rapid replication of the bacteria andendothelial damage. After this phase, invasion of avariety of end organs, including the kidneys, liver,
spleen, central nervous system, eyes, and genitaltract can occur. Leptospires damage organs byreplicating and inducing cytokine production andinflammatory cell invasion. Host susceptibility andthe virulence of the organism will determine theextent of damage to internal organs (Midwinter etal., 1994).The initial replication mainly damagesthe endothelial cells and only later the kidneys andliver. Leptospires enter the cerebrospinal fluid(CSF) in the early septicaemic phase of the illness,but there is little evidence of inflammatory responsein the CSF (Wesley et al., 1995)Failure of integrity of the cell membrane ofendothelial cells lining of the small blood vessels inall parts of the body are due to the action of theglycoprotein toxin of Leptospira (Farr, 1995),which causes haemorrhage. The extent of damageto internal organs varies seems to depend on thevirulence of the organism, including serovar andstrain, the inoculum, and host susceptibility(Scanziani et al., 2002), also, an organ can beseverely affected even though the animal recoversclinically (Greene et al., 2006).After the leptospiremic phase, the following organsare typically targeted by the bacteria:Kidneys: Ischemia from damage to blood vesselsin renal cortex leads to renal tubular necrosisparticularly of proximal convoluted tubules. Theresulting anatomical damage causes renal failurethat can be fatal (Visith and Kearkiat, 2005).Interstitial nephritis may be a chronic manifestationof acute disease in dogs (Goldstein , 2010).Liver: Liver cell necrosis caused by ischemia andthe destruction of hepatic architecture leads to thecharacteristic jaundice, failure of blood clottingmechanisms (Farr, 1995).This was thought acommon occurrence in serovaricterohaemorrhagiae (Brown et al., 1996).Endothelium: Tissue edema and disseminatedintravascular coagulation may occur within the firstfew days of infection as a result an acute endothelialinjury (Greene et al., 2006).

13
Journal of Canine Development & Research 2013
Lung: Lung changes includes pulmonaryhaemorrhage, most likely due to endothelialdamage and vasculitis (Scanziani et al., 2002).Secondary immune-mediated disease(polyarthritis, haemolytic anemia etc.) has also beensuspected (Friedland et al., 1991).Additional body systems may also be damagedduring the acute phase of infection like benignmeningitis is produced when leptospires invade thecentral nervous system, uveitis may occur innaturally occurring and experimentally inducedcanine leptospirosis in addition to abortion andinfertility resulting from transplacental transmissionof leptospires (Friedland et al. 1991). Previousexposure either naturally or vaccinal to the sameserovar is likely to provide some degree ofimmunity although the duration of immunity afternatural infection and the degree of cross protectionbetween serovars are unknown in dogs. A recentstudy comparing different commercially availablevaccines showed only a mild serologic responseto a series of two vaccinations but good immunitywhen challenged 1 year after the second vaccine(Klaasen et al., 2003).
Clinical Signs
Leptospirosis may present as peracute, acute,subacute, or chronic disease and clinical signsdepend on the serovar, the individual’s immuneresponse, and how quickly treatment is instituted.Large breed, male, outdoor, middle-aged dogs areaffected most commonly. (Langston et al., 2003)but young animals often get a more severe formof leptospirosis compared to adults (Greene et al.,2006). Per acute leptospiral infections can causedeath with few clinical signs, while acute infectionsare often associated with pyrexia, shivering, andmuscle tenderness; vomiting, dehydration, andshock, coagulopathies like hematemesis,hematochezia, melena, epistaxis, and petechiation.Terminally ill dogs become depressed andhypothermic; hepatic and renal failure is not
typically present. Subacute infections are thoughtto be the most commonly recognized form ofleptospirosis, which is manifested with pyrexia,anorexia, vomiting, dehydration, polydipsia,lethargy fever diarrhoea and apathy (Lappin,2010). Myalgia and paraspinal hyperesthesia mayresult from muscular, meningeal, or renalinflammation. Mucous membranes appearinjected, and petechiation and ecchymoses arepresent. Conjunctivitis, rhinitis, and tonsillitis areusually accompanied by cough and dyspnea.Acute renal failure develops in 83-100% dogs(Adin and Cowgill, 2000) and is associated withpolyuria/polydipsia, which may progress to oliguriaor anuria. Gastrointestinal signs tend to more severeand persistent in dogs with leptospirosis comparedwith other causes of acute renal failure. Intestinalintussusceptions have occurred in dogs withgastrointestinal involvement and respiratory signsmay occur in a small number of dogs withleptospirosis (3 -20% ) (Rentko et al., 1992 andBirnbaum et al., 1998). Pulmonary hemorrhage,edema, acute respiratory distress syndrome, andinterstitial pneumonitis have been observed tooccur (Harkin and Gartrell,1996 ; Birnbaum etal., 1998).Liver failure is usually less severe thanrenal failure, although was a prominent part ofhistorical leptospirosis. Ventricular tachyarrhythmiaand eventual myocardial damage can occur in dogswhere the heart is involved (Greene et al., 2006).The mildest forms evolve to fever, anorexia,vomiting, dehydration and apathy and the chronicform may be unapparent, culminating in chronicrenal insufficiency (Santim et al., 2006).Additionally, healthy dogs in kennels, multi-doghouseholds, neighbourhoods, or other areas whereinfection has been documented should be screenedand monitored for signs of leptospirosis. In otheranimals such as cattle, pigs and horses abortion iscommon but this is rarely the case with dogs(Picardeau, 2013).
14
Journal of Canine Development & Research 2013
ReferencesAdin, C.A.; Cowgill, L.D. (2000) Treatment and outcome
of dogs with leptospirosis: 36 cases (1990-1998).J. Am. Vet. Med. Assoc. 216: 371-5.
Adler, B.; Murphy, A.M.; Locarnini, S.A.; Faine, S. (1980)Detection of specific anti-leptospiral immuno-globulins M and G in human serum by solid-phase enzyme-linked immunosorbent assay. JClin. Microbiol. 11:452-7.
Adler, B. and Moctezuma, A.P. (2010) Leptospira andLeptospirosis. Veterinary Microbiology. 140:287-296.
Ahmed, N.; Devi, S.M.; Valverde, M.L. et al. (2006)Multilocus sequence typing method for identi-fication and genotypic classification of patho-genic Leptospira species. Ann. Clin. Microbiol.Antimicrob. 5: 28.
Andre-Fontaine, G. (2006) Canine Leptospirosis-Do wehave a problem? Vet. Microbiol. 117:19–24.
Arent, Z.J.; Andrews, S.; Adamama-Moraitou, K.;Gilmore, C.; Pardali, D. and Ellis, W.A. (2012)Emergence of novel Leptospiraserovars: a needfor adjusting vaccination policies for dogs. Epi-demiology and Infection. 24: 1-6.
Baldwin, C.J.; Atkins, C.E. (1987) Leptospirosis in dogs.Compendium on Continuing Education for thePracticing Veterinarian. 9:499–507.
Barker, F.A. (1926) Leptospirosis: With special referenceto the existence ofspirochaetosisicterohaemorrhagica, or Weil’sdisease in the Andaman Islands. Indian Medi-cal Gazette. 61: 479–488.
Bharti A.R., Nally J.E. and Ricaldi JN.(2003). Leptospiro-sis: a zoonotic disease of globalimportance.Lancet Infect Dis.3(12):757-71.
Birnbaum, N.; Barr, S.C.; Center, S.A. et al. (1998) Natu-rally acquired leptospirosis in 36 dogs: sero-logical and clinicopathological features. J. SmallAnim. Pract. 39:231-236.
Boqvist, S.; Eliasson-Sellin, L.; Bergström, K. andMagnusson, U. (2012) The association betweenrainfall and seropositivity to Leptospira in out-door reared pigs. The Veterinary Journal. 1: 135-139.
Brown, C.A.; Roberts, A.W.; Miller, M.A. et al. (1996)Leptospira interroganssero var grippotyphosa
infection in dogs. J. Am. Vet. Med. Assoc. 209:1265–7.Chowdry, A.K. (1903) Jaundice at Port Blair, Andaman
Islands. Indian Medical Gazette. 38: 409–412.Coleman, T.J. (2006) Leptospira. In: Greenwood D, Slack
RCB, Peutherer JF, eds. Medical Microbiology.16th ed. London: Churchill Livingstone,Elsevier. 352-7.
De Castro, A.B. (1922) Toxic Jaundice of unknown ori-gin. Indian Medical Gazette. 57: 292.
Edward, A. and Hodder, S. (1990) Leptospirosis. In: TopleyWW, Wilson GS, Parker MT, Collier LH, eds.Topley& Wilson’s Principles of Bacteriology,Virology and Immunity. Vol. 3. 8th ed. London:Hodder Arnold. 619.
Faine, S. (1994) Leptospira and Leptospirosis. CRC Press,Boca Raton, Florida USA.
Farr, R.W. (1995) Leptospirosis. Clin Infect Dis. 21: 16.Forbes, A.E.; Zochowski, W.J.; Dubrey, S.W. and
Sivaprakasam, V. (2012) Leptospirosis andWeil’s disease in the UK. Quarterly Journal ofMedicine. 105:1151–1162.
Friedland, J.S. and Warrell, D.A. (1991) The Jarisch-Herxheimer reaction in leptospirosis: possiblepathogenesis and review. Rev. Infect. Dis.13:207–10.
Geisen, V.; Stengel, C.; Brem, S. et al. (2007) Canineleptospirosis infections—clinical signs andoutcome with different suspectedLeptospiraserogroups (42 cases). J. Small Anim.Pract. 48(6):324–8.
Ghneim, G.S.; Viers, J.H.; Chomel, B.B.; Kass, P.H.;Descollonges, D.A.; Johnson, M.L. (2007) Useof a case-control study and geographic infor-mation systems to determine environmental anddemographic risk factors for canine leptospiro-sis. Vet. Res. 38: 37–50.
Goldstein, R.E.; Lin, R.C.; Langston, C.E. et al. (2006)Influence of infecting serogroup on clinical fea-tures of leptospirosis in dogs. J. Vet. Intern.Med. 20(3):489–94.
Greene, C.E., Sykes, J.E., Moore, G.E., Goldstein, R.E. &Schultz, R.D. (2006) Chapter 42: Leptospirosis.In Greene, C.E. (editor) Infectious Diseases ofthe dog and cat. 4. ed. St Louis, SaundersElsevier. 431-447.
Harkin, K.R. and Gartrell, C.L. (1996) Canine leptospiro-sis in New Jersey and Michigan: 17 cases (1990-1995). J. Am. Anim.Hosp.Assoc. 32:495-501.
Hartskeerl RA. (2006)Leptospirosis: current status andfuture trends. Ind. J Med Microbiol . 24:309.
Holt, S.C. (1978) Anatomy and Chemistry of Spirochetes.Microbiological reviews. 42(1):114-160.
Inada, R.; Ido, Y.; Hoki, R.; Kaneko, R.; Ito, H. (1916) Theetiology mode of infection and specific therapyof Weil’s disease. J. Exp. Med. 23:377-402.
15
Journal of Canine Development & Research 2013
Klaasen, H.L.; Molkenboer, M.J.; Vrijenhoek, M.P. et al.(2003) Duration of immunity in dogs vaccinatedagainst leptospirosis with a bivalent inactivatedvaccine. Vet. Microbiol. 95(1-2):121–32.
Kmely, E. and Dikken, H. (1993) Classification of the spe-cific Leptospirainterrogans and the history ofits serovars. Groningen: University PressGroningen.
Langston, C.E. and Heuter, K.J. (2003) Leptospirosis. Are-emerging zoonotic disease. Vet. Clin. NorthAm. Small Anim. Pract. 33: 791-807.
Lappin, M. (2010) Doençasriquetsianaspolissistêmicas.In: NELSON, R. W.; COUTO, C. G.Medicinainterna de pequenosanimais. 4ed., Riode Janeiro: Elsevier ,pp. 1322-1335.
Levett, P.N.(2001) Leptospirosis. Clin. Microbiol. Rev.14: 296-326.
McDonough, P.L. (2013) Leptospirosis in Dogs – Cur-rent Status. [online] (2001-07-19). Available from:h t t p : / / w w w. i v i s . o r g / a d v a n c e s /infect_dis_carmichael/mcdonough/ivis.pdf[2013-01-02]
Midwinter, A.; Vinh, T.; Faine, S. et al. (1994) Character-ization of an antigenic oligosaccharide fromLeptospirainterrogansserovar Pomona and itsrole in immunity. In: Infect Immun. 62: 5477-5482.
Miller, M.D., Annis, K.M., Lappin, M.R. &Lunn, K.F.(2011) Variability in Results of the MicroscopicAgglutination Test in Dogs with Clinical Lep-tospirosis and Dogs Vaccinated against Lep-tospirosis. J. Vet. Int.Med.25 : 426-432.
Ngbede, E.O., Radi, M.A., Kwanashie, C.N., Okolocha,E.C., Gugong, V.T. and Hambolu, S.E. (2012)Serological prevalence of leptospirosis in cattleslaughtered in the Zango abattoir in Zaria,Kaduna State, Nigeria. VeterinariaItaliana. 48 (2):179-184.
Noguchi, H. (1928) The spirochaetes. In: Jordan EO, FalkIS, eds. Newer knowledge of bacteriology andimmunology. Chicago: University of ChicagoPress. 452-97.
Picardeau, M. (2013) Diagnosis and epidemiology of lep-tospirosis [online] (2013-01-18). Available from:Médecineet Maladies Infectieuses, http://dx.doi.org/10.1016/j.medmal.2012.11.005 [2013-01-28]
Rentko, V.T.; Clark, N.; Ross, L.A. et al. (1992) Canineleptospirosis. A retrospective study of 17 cases.J. Vet. Intern. Med. 6:235-44.
Santim, K.; Blacence, A.; Nadvorny, A.; Wolffnbuttel,S.; Cardoso, M. R. I.;Schimidt, V. (2006) Pesquisa
de aglutininas anti-leptospiraemcães comsuspeitaclínica de leptospirose.ClínicaVeterinária, São Paulo, 6( 60): 48-52.
Saravanan, R.; Rajendra, P.; Garajan, S.P. (1999) Clinical,bacteriologic and histopathologic studies oninduced leptospirosis in stray dog pups. In-dian J. Pathol. Microbiol. 42:463–469.
Scanziani, E.; Origgi, F.; Giusti, A.M. et al. (2002) Sero-logical survey of leptospiral infection in ken-nelled dogs in Italy. J. Small Anim. Pract. 43:154–7.
Sehgal, S.C.; Murhekar, M.V. and Sugunan, A.P. (1995)Outbreak of Leptospirosis with pulmonary in-volvement in North Andaman. Indian Journalof Medical Research. 102: 9-12.
Singh, S.S.; Vijayachari, P.; Sinha, A.; Sugunan, A. P.;Rashid, M. A and Sehgal SC (1999). Clinico-epidemiological study of hospitalized casessevere leptospirosis. Indian Journal of MedicalResearch, 109: 94–99.
Sophie, Hedberg. Leptospirosis in dogs in Lima, PeruDescription of changes in serology, hematol-ogy, blood chemistry and urinalysis before andafter one month of treatment. Uppsala 2013.
Sykes, J.E.; Hartmann, K.; Lunn, K.F.; Moore, G.E.;Stoddard, R.A. and Goldstein, R.E. (2011) 2010ACVIM Small Animal Consensus Statement onLeptospirosis: Diagnosis, Epidemiology, Treat-ment, and Prevention. Journal of Veterinary In-ternal Medicine. 25: 1-13.
Terpstra, W.J.(2006) Historical perspectives in leptospiro-sis. Indian J. Med. Microbiol. 24: 316-20.
Visith S.and Kearkiat P. (2005)Nephropathy in leptospiro-sis. J Postgrad Med. 51:184-8.
Ward MP, Glickman L.T. and Guptill L.E. (2002). Preva-lence of and risk factors for leptospirosis amongdogs in the United States and Canada: 677 cases(1970-1998). J Am Vet Med Assoc 2002;220:53-8.
Wesley, Farr R. (1995) Leptospirosis. Clin Infect Dis. 21:1-8.
Woolley, J.M. (1913) Malaria in Andamans. Indian Medi-cal Gazette. 48: 266–267.
Woolley, J.M. (1911) Malaria in Andamans. Indian Medi-cal Gazette. 46: 409–411.
Zuerner, R. L. (2010) Genus Leptospira. In Krieg, N.R.,Staley, J. T., Brown, D. R., Hedlund, B., Paster,B. J., Ward, N., Ludwig, W. & Whitman, W. B.(editors) Bergey’s Manual of Systematic Bac-teriology. 2. ed. New York, NY, USA, Springer-Verlag, Vol 4. 232-242.
16
Journal of Canine Development & Research 2013

17
Journal of Canine Development & Research 2013
REVIEW ARTICLEADVANCED DIAGNOSIS IN CANINE SCABIES*Anil Langer1, Altaf Hussain2 and S.K. Gupta3
Department of Veterinary MedicineArawali Veterinary College, Bajor, Sikar-332 001 (Rajasthan)
1&2Assistant Professor 2Dept. of AGB 3Dean ,Faculty of Vety. Sci. & A. H, SKUAST, R.S.Pura, Jammu (J & K).*Corresponding author e-mail : [email protected]
A B S T R A C T
Scabies is a contagious disease of humans and other mammals,caused by the mite Sarcoptes scabiei, a burrowing mite.Generally canine scabies is diagnosed via clinical signs andmicroscopic examination of skin scrapings from the lesions.Presently diagnosis of canine scabies is reviewed and advancediagnostic tests are enlightened.They are pinnal-pedal reflex,dermatoscopy, antigen detection , PCR diagnostic, Intradermalskin test, histologic examination, antibody detection -Serologicalexamination, S. scabiei gene discovery, immunodiagnostic assayusing recombinant S. scabiei allergens and therapeutic diagnosis.
Key words :DermatoscopyGene discoveryImmunodiagnosisPinnal-pedal reflexSarcoptic scabiei
A R T I C L E H I S T O R Y
Received : February 18, 2013Revised : April 14, 2013Accepted : April 24, 2013
Canine scabies is a nonseasonal, intenselypruritic, transmissible infestation of the skin
of dogs caused due to development andreproduction of burrowing mite Sarcoptes scabieivar. canis (Muller et al., 1989; Tahsin and Kerem2013). It is clinically characterized by erythematouspapular eruptions involving ventral aspects of thechest, abdomen, pinnae, elbows and hocks(Pachauri, 1999). It represents 2-4% ofdermatology cases and is one of the major causesof marked pruritus in dogs (Carlotti, 2004). Thesynonyms of canine scabies are canine sarcopticmange and canine sarcoptic acariasis (Newburyand Moriello, 2006; Bochkov, 2010; OIE, 2013).
Diagnosis
Diagnosis is via clinical signs and microscopicexamination of skin scrapings (Soulsby, 1982;OIE, 2013), but experience has shown that thesensitivity of these traditional tests is less than 50per cent (Walton and Currie, 2007). Detectingvisible lesions can be difficult, as they are oftenobscured by eczema or impetigo or are atypical.Detection of burrows with India ink was advocatedmore than 20 years ago (Woodley and Saurat,1981), but the test is often impractical and is notroutinely used. Presumptive diagnosis can be madeon the basis of a typical history of pruritus, whichworsens at night, the distribution of the
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 17-23

18
Journal of Canine Development & Research 2013
inflammatory papules, and a history of contact withother scabies cases (McCarthy et al., 2004).Diagnosis of canine scabies is made from thehistory, physical examination and by the findingsof mites or eggs in multiple deep skin scrapingstaken wherever possible from non-traumatizedlesions at predilection sites. A characteristic, butnot pathognomonic, sign of pinnal-pedal reflex canalso be elicited as a diagnostic method (Pachauri,1999). Histologic and serological exam also helpin diagnosis. In this review we discribe thediagnostic modalities for the diagnosis of caninescabies.
1. History
History of dog coming in contact with a pruriticdog, or roaming outdoors, or becoming pruriticafter being boarded, or after visit to a veterinaryclinic may indicate possible contact with scabiesinfested dog or fomites (Pachauri, 1999).
2. Physical examination
Upon physical examination, presence oferythematous papular eruptions or papulo-crustouslesion at predilection sites or all over the bodyshould be suspected for scabies (Pachauri, 1999).
3. Pinnal-pedal reflex
In addition to the lesions and topography describedabove, the pinnal-pedal reflex should be lookedfor (Carlotti, 2004; Darzi et al., 2007). When theear margin (with or without visible lesions) isrubbed, particularly at the site where the pinna isfolded, this triggers an attempt to scratch by thedog’s hind leg. This zone may give a “sandy” feelingwhen palpated. In the French literature it is called“Henry’s zone” after the name of a parasitologistwho noticed in the 1920s both its infestation ofmites and its sensitivity to stimulation. The pinnal-pedal reflex is only suggestive and not specific; itoccurs in about 80 per cent of scabies cases butalso in about 20 per cent of other pruriticdermatoses (Carlotti, 2004). It can also be
observed in dogs with seborrheic ear disease fromother causes (Krantz and Walter, 2009; Hay,2009; Bochkov and Mironov, 2011).
4. Microscopic examination of skin scrapings
Definitive diagnosis is based on the identificationof mites, eggs, egg-shell fragments, or mite fecalpellets from skin scrapings (e.g., from scabieticpapules or from under the fingernails) or by thedetection of the mite at the end of its burrow(Walton and Currie, 2007; Bochkov and Mironov,2011). Sarcoptic mites are difficult to find, andtherefore multiple deep scrapings are indicated.In about one-half of the cases, no mites will befound (Orkin and Maibach, 1978), but if theclinical features are suggestive, presumptivediagnosis of canine scabies can be made (Mulleret al., 1989). When scrapings are positive, thenumber of visualized mites remains low (1 or 2).In very rare cases, called Norwegian scabies, highnumbers of mites can be found in thick crusts.(Bochkov,2010)
5. Dermatoscopy
Epiluminescence microscopy and high-resolutionvideodermatoscopy are noninvasive techniquesthat allow detailed inspection of the patients skin,from the surface to the superficial papillary dermis(Argenziano et al., 1997; Haas and Sterry, 2001;Micali et al., 2004). Diagnosis is by observationsof the “jet-with-contrail” pattern in the skinrepresenting a mite and its burrow. Due todifficulties obtaining skin scrapings from somepatients, e.g., infants, and the lack of sensitivity ofclassical methods, dermatoscopy might beinformative (Haas and Sterry, 2001), but studiesperformed on large cohorts are lacking (Micali etal., 2004; Chosidow, 2006) and limited due tohigh cost of the equipment (Andrews et al., 2009).
6. Antigen detection and PCR diagnostics
The key weakness of a scabies PCR diagnostic isthat, as with microscopy diagnosis, it relies on the

19
Journal of Canine Development & Research 2013
physical presence of a mite or mite part in thesample. Therefore, it is unlikely to become a viabletest for widespread use, due to the generally lowmite burden and, thus, low sensitivity (OIE, 2013).PCR followed by enzyme-linked immunosorbentassay detection of the PCR product has beensuggested to be a sensitive technique fordiagnosing patients with atypical scabies (Bezoldet al., 2001). However, the method described islabor-intensive and time-consuming (Walton andCurrie, 2007).
7. Intradermal skin test
The intradermal skin test method is not feasible touse with whole-mite extract due to the inability toculture sufficient quantities of S. scabiei.Furthermore, whole-mite extracts obtained fromanimal models contain a heterogenous mixture ofhost and parasite antigens, including house dustmite cross-reactive epitopes, and vary incomposition, potency, and purity. Patients withscabies often present to clinicians with ageneralized pruritus of unknown cause. Purified,well-characterized recombinant scabies miteallergens with standardized protein contents couldpotentially be utilized in the future for scabies skintest assays for clinically difficult-to-diagnose casesand for immunotherapy (Walton and Currie, 2007;OIE, 2013).
8. Histologic examination
A skin biopsy may confirm the diagnosis of scabiesif a mite or parts of it can be identified. However,in most cases, the histological appearance is thatof nonspecific, delayed hypersensitivity withsuperficial and deep perivascular inflammatorymononuclear cell infiltrates with numerouseosinophils, papillary edema, and epidermalspongiosis (Falk and Eide, 1981; Bochkov, 2010).Cutaneous histopathology is rarely diagnosticbecause it is exceptional to visualize a mite in askin biopsy. Generally, skin biopsies show a non-
specific superficial peri-vascular hyperplasticdermatitis. Lymphocytes, histiocytes andeosinophils predominate, suggesting a cutaneoushypersensitivity reaction. The number ofeosinophils is higher in chronic lesions. Sometimes,foyers of eosinophilic necrosis in the superficialepidermis may suggest the trail of the burrowingmite but this sign is not pathognomonic and is seenperhaps only in about 50 per cent of the cases.Marked epidermal hyperplasia is controversial asa suggestive sign (Carlotti, 2004; Bochkov, 2010).
9. Antibody detection (Serologicalexamination)
Studies document that scabies mite infestationcauses the production of measurable antibodies ininfested host species (Arlian et al., 2004; Falkand Bolle, 1980). Furthermore, host IgG has beendemonstrated in the anterior midgut and esophagusof fresh mites (Rapp et al., 2006; Willis et al.,2006). Enzyme- linked immunosorbent assayshave been developed for the detection ofantibodies to S. scabiei in pigs and dogs (Bornsteinet al., 1996; Bornstein and Wallgren, 1997;Hollanders et al., 1997). These assays rely onwhole-mite antigen preparations derived from S.scabiei var. suis and the itch-mite of the red fox,S. scabiei var. vulpes, and therefore havelimitations in availability and specificity. A studylooking at cross-reacting IgG antibodies to the foxmite antigen in human scabies reported a sensitivityof only 48 per cent, in comparison with 80 percent in pig scabies and 84 per cent in dog scabies(Haas et al., 2005). This is not surprising, asstudies using molecular markers suggest that S.scabiei organisms from humans and animals aregenetically distinct and that interbreeding or cross-infection appears to be extremely rare (Walton etal., 1999; Walton et al., 2004). Seroconversioncan take up to 5 weeks after inoculation and 1 to3 weeks after the first symptoms, so testing shouldnot be done at a too early stage. Sera of dogs

20
Journal of Canine Development & Research 2013
infested with other parasites (Cheyletiella yasguri,Demodex canis, Otodectes cynotis,Linognathus setosus), dogs affected with fleaallergy dermatitis, or atopic dogs that are sensitisedto Dermatophagoides farinae and D.pteronyssinus give a negative reaction to this test.In contrast dogs with scabies can show positivereactions to these house dust mites, both in vivo(skin-tests) and in vitro (IgE and IgG assays). Thisclearly indicates that false positive reaction tohouse dust mites extracts may lead to diagnosticerrors in dogs affected with scabies (Carlotti, 2004;Bochkov, 2010; OIE, 2013).Cross-reactivity between scabies miteinfestations and house dust mite allergyInvestigations have demonstrated that patientssensitive to house dust mites but with no history ofscabies have circulating IgE antibodies thatrecognize antigens in S. scabiei var. canis extract(Arlian et al., 1991). Furthermore, Western blotand radioallergosorbent assays have demonstratedthat individuals with scabies showed strong IgEbinding to house dust mite extract (Falk and Bolle,1980). The specific cross-reactive moleculesremain unidentified but may represent somepolysaccharide-related IgE cross-reactivity(Malandain, 2005). Scabies mites and house dustmites are phylogenetically related arthropods, andit is not surprising that they or their excretions orsecretions have homologous allergens. However,it is unknown how many of these will be cross-reactive or what the clinical significance of any suchcross-reactivity is. For example, studies on cross-reactivity between the group 5 allergens of housedust mites Dermatophagoides pteronyssinus andBlomia tropicalis (Der p 5 and Blo t 5) have beenundertaken, and although they have 43 per centamino acid identity, they have been found not tobe cross-reactive (Kuo et al., 2003).
10. S. scabiei gene discovery
A major limitation in biomedical research on
scabies has been the difficulty of obtaining mites insufficient numbers, due to the generally low parasiteburden and the lack of an in-vitro culture system.To overcome this, cDNA libraries have now beenconstructed from S. scabiei var. hominis and S.scabiei var. vulpes (Fischer et al., 2003a; Fischeret al., 2003b; Ljunggren et al., 2003), and largeexpressed sequence tag databases containing bothpartial and complete DNA sequences of S. scabieigenes have been established. From thesedatabases, scabies mite homologues to most ofthe known house dust mite allergens have now beenidentified, as well as many other relevant molecules(Dougall et al., 2005.; Fischer et al., 2003a; Holtet al., 2003; Holt et al., 2004; Mattsson et al.,2001; Pettersson et al., 2005). Recombinantantigens promise a continuous, reproduciblequantity of allergenic proteins in a purified formsuitable for use in in-vitro assays (Hicks andElston, 2009; Bochkov, 2010; OIE, 2013).
11. Immunodiagnostic assay usingrecombinant S. scabiei allergens
Recently, a number of scabies mite homologuesto house dust mite allergens have been cloned,expressed, and affinity purified. These includemature forms of both active and inactivehomologues of the cysteine protease group 1allergens (Holt et al., 2004), mature forms ofactive and inactive homologues of the serineprotease group 3 allergens (Holt et al., 2003), amu class and a delta class glutathione S-transferasegroup 8 allergen (Dougall et al., 2005; Petterssonet al., 2005), and a homologue to the C terminusof an apolipoprotein group 14 allergen (Harumalet al., 2003; Bochkov, 2010; OIE, 2013).Immunohistochemical staining of sections of humanskin which was highly infested with S. scabiei mitesshowed that anti-group 8 and anti-group 14antibodies (generated in mice and rabbits,respectively) localized to the internal organs of thescabies mites and the cuticle, with minor staining

21
Journal of Canine Development & Research 2013
in the digestive system (Harumal et al., 2003).Moreover, the group 1 and group 3 scabies miteallergens have now been expressed in Pichiapastoris, with considerable evidence that they arein native conformation and that they are localizedto the digestive system of the mite (Willis et al.,2006). Studies are now under way to evaluate thediagnostic potential of the identified proteins bycharacterizing specific human and animal humoraland cellular immune responses. Serologicalfeatures that are diagnostically important are theinterval between exposure to infection and antibodyresponse and the nature of the antibodies that makeup the response.
12. Response to therapy (Therapeuticdiagnosis)
One of the best diagnostic aids is the promptresponse to therapy. Diagnosis of a disease basedon the patient’s response to specific therapy isanother approach utilized to diagnose sarcopticmange. In case chronically pruritic dog that havethe classical signs of scabies does not yield mitesor eggs on repeated microscopic examinations ofskin scrapings, the dog should be treated forsarcoptic mange. If the dog has a positive responseto therapy, one can make a presumptive diagnosisof scabies (Tahsin and Kerem, 2013; Bochkov,2010; OIE, 2013; Sudhakara and Nalini, 2013).A good response to systemic glucorticoid therapyoccurs in about 40 per cent of the cases andconsequently does not allow the exclusion ofscabies. However, a good response maysometimes be difficult to interpret because otherparasitic diseases can also respond to acaricides/insecticides (cheyletiellosis, oto-acariasis,trombiculosis, pediculosis, flea allergy dermatitis)(Carlotti, 2004).
13. Other diagnostic techniques
Other laboratory aids are of less significance, buta few patients will have mites in the feces. A
hemogram may reveal eosinophilia and/ornonregenerative anemia (Muller et al., 1989).Aujla et al. (2000) reported leucocytosis andneutrophilia in scabies as haematologicalalterations. In one haematological study significant(P<0.05) neutrophilia and leucocytosis in dogsinfested with sarcoptic mange was reported bySarma et al. (2005).
Future Prospects
1) Since confirmatory diagnosis of canine scabiesis difficult, there is need to look for more reliablediagnostic techniques.2) Using an appropriate recombinant antigen, thedevelopment of an S. scabiei immunodiagnosticassay is a real possibility. Its development willenable the selective treatment of affectedindividuals and animals, reducing the requirementfor mass treatment and the associated costs. Thisshould decrease the potential for escalating miteresistance and provide another means ofcontrolling scabies in highly affected areas. Thereis little evidence that simple mass treatment iseffective in the long term. Molecular studies aimedat improved diagnosis and better therapeuticoptions will significantly contribute to reductionsin the high prevalence of scabies observedcurrently in resource-poor communities.3) Even though there are effective chemicalcompounds available to treat canine scabies, someserious side-effects are associated with their use.Therefore, there is a need to look for drugs ofherbal origin which are devoid of deleterious effectsof drugs in use presently.
ReferencesAndrews, R.M.; McCarthy, J.; Carapetis, J.R. and Currie,
B.J. (2009). “Skin disorders, including pyoderma, scabies, and tinea infections”.Pediatr.Clin. North Am. 56 (6): 1421–40.
Argenziano, G.; Fabbrocini, G. and Delfino, M. (1997).Epiluminescence microscopy. Arch. Dermatol.133: 751–753.
Arlian, L.G.; Morgan, M.S.; Estes, S.A.; Walton, S.F.;

22
Journal of Canine Development & Research 2013
Kemp, D.J. and Currie, B.J. (2004). CirculatingIgE in patients with ordinary and crusted sca-bies. J. Med. Entomol. 41: 74–77.
Arlian, L.G.; Vyszenski-Moher, D.L.; Ahmed, S.G. andEstes, S.A. (1991). Cross-antigenicity betweenthe scabies mite, Sarcoptes scabiei, and thehouse dust mite, Dermatophagoidespteronyssinus. J. Investig. Dermatol. 96: 349–354.
Aujla, R.S.; Singla, L.D.; Juyal, P.D. and Gupta, P.P. (2000).Prevalence and pathology of mange-mite infes-tations in dogs. J. Vet. Parasitol. 14 (1): 45-49.
Bezold, G.; Lange, M.; Schiener, R.; Palmedo, G.; Sander,C.A.; Kerscher, M. and Peter, R.U. (2001). Hid-den scabies: Diagnosis by polymerase chainreaction. Br. J. Dermatol. 144: 614–618.
Bochkov A.V. (2010). A review of mammal-associatedPsoroptidia (Acariformes: Astigmata). Acarina,18: 99–260.
Bochkov A.V. and Mironov S.V. (2011). Phylogeny andsystematics of mammal-associated psorptidianmites (Acariformes: Astigmata: Psoroptidia)derived from external morphology. Invert. Syst.25: 22–59.
Bornstein, S. and Wallgren, P. (1997). Serodiagnosis ofsarcoptic mange in pigs. Vet. Rec. 141: 8–12.
Bornstein, S.; Thebo, P. and Zakrisson, G. (1996). Evalu-ation of an enzyme linked immunosorbant as-say (ELISA) for the serological diagnosis ofcanine sarcoptic mange. Vet. Dermatol. 7 (1):21–28.
Carlotti, D. N. (2004). Canine scabies: An update. In: 29thWorld Congress of the World Small Animal Vet-erinary Association. October 6-9, Rhodes,Greece.
Chosidow, O. (2006). Scabies. N. Engl. J. Med. 354: 1718–1727.
Darzi, M.M.; Mir, M.S.; Shahardar, R.A.; and Pandit, B.A.(2007). Clinicopathologal, histochemical andtherapeutic studies on concurrent sarcoptic andnotoedric acariasis in rabbit (oryctolagus cu-niculus). Vet. Arhiv. 77: 167-75.
Dougall, A.; Holt, D.C.; Fischer, K.; Currie, B.J.; Kemp,D.J. and Walton, S.F. (2005). Identification andcharacterization of Sarcoptes scabiei andDermatophagoides pteronyssinus glutathionetransferases: Implication as a major potentialallergen in crusted scabies. Am. J. Trop. Med.Hyg. 73: 977–984.
Falk, E.S. and Eide, T. J. (1981). Histologic and clinicalfindings in human scabies. Int. J. Dermatol. 20:
600–605. Fischer, Ka.; Holt, D. C.; Harumal, P.;Currie, B.J.; Walton, S.F. and Kemp, D.J. (2003).Generation and characterization of cDNA clonesfrom Sarcoptes scabiei var. hominis for an ex-pressed sequence tag library: Identification ofhomologues of house dust mite allergens. Am.J. Trop. Med. Hyg. 68: 61–64.
Falk, E.S., and Bolle, R. (1980). In vitro demonstration ofspecific immunological hypersensitivity to sca-bies mite. Br. J. Dermatol. 103: 367–373.
Fischer, Kb., Holt, D.C.; Wilson, P.; Davis, J.; Hewitt, V.;Johnson, M.; McGrath, A.; Currie, B.J.; Walton,S. F. and Kemp, D.J. (2003). Normalization of acDNA library cloned in lZAP by a long PCRand cDNA reassociation procedure. Bio Tech-niques. 34: 250–254.
Haas, N. and Sterry, W. (2001). The use of ELM to moni-tor the success of antiscabietic treatment.Epiluminescence light microscopy. Arch.Dermatol. 137: 1656–1657.
Haas, N.; Wagemann, B.; Hermes, B.; Henz, B.M.; Heile,C. and Schein, E. (2005). Crossreacting IgG an-tibodies against fox mite antigens in humanscabies. Arch. Dermatol. Res. 296: 327–331.
Harumal, P.; Morgan, M.S.; Walton, S.F.; Holt, D.C.; Rode,J.; Arlian, L.G.; Currie, B.J. and Kemp, D.J. (2003).Identification of a homologue of a house dustmite allergen in a cDNA library from Sarcoptesscabiei var. hominis and evaluation of its vac-cine potential in a rabbit/S. scabiei var. canismodel. Am. J. Trop. Med. Hyg. 68: 54–60.
Hay, R.J. (2009). “Scabies and pyodermas—diagnosisand treatment”. Dermatol Ther. 22 (6): 466–74.
Hicks, M.I. and Elston, D.M. (2009).“Scabies”. Dermatologic therapy 22 (4): 279–92.
Hollanders, W.; Vercruysse, J.; Raes, S. and Bornstein,S. (1997). Evaluation of an enzyme-linkedimmunosorbent assay (ELISA) for the serologi-cal diagnosis of sarcoptic mange in swine. Vet.Parasitol. 69: 117–123.
Holt, D.C.; Fischer, K.; Allen, G.E.; Wilson, D.; Wilson,P.; Slade, R.; Currie, B.J.; Walton, S.F. and Kemp,D.J. (2003). Mechanisms for a novel immuneevasion strategy in the scabies mite Sarcoptesscabiei: A multigene family of inactivated serineproteases. J. Investig. Dermatol. 121: 1419–1424.
Holt, D.C.; Fischer, K.; Pizzutto, S.J.; Currie, B.J.; Walton,S.F. and Kemp, D.J. (2004). A multigene familyof inactivated cysteine proteases in Sarcoptesscabiei. J. Investig. Dermatol. 123: 240–241.

23
Journal of Canine Development & Research 2013
Krantz G.W. and Walter D.E. (2009). A Manual of Acarol-ogy, 3rd Edition. Texas Tech University Press,Lubbock, Texas, USA.
Kuo, I.C.; Cheong, N.; Trakultivakorn, M.; Lee, B.W. andChua, K.Y. (2003). An extensive study of hu-man IgE cross-reactivity of Blo t 5 and Der p 5.J. Allergy Clin. Immunol. 111: 603–609.
Ljunggren, E.L.; Nilsson, D. and Mattsson, J.G. (2003).Expressed sequence tag analysis of Sarcoptesscabiei. Parasitology. 127: 139–145.
Malandain, H. (2005). IgE-reactive carbohydrate epitopes-classification, cross-reactivity, and clinical im-pact. Allerg. Immunol. (Paris) 37: 122–128.
Mattsson, J.G.; Ljunggren, E.L. and Bergstrom, K. (2001).Paramyosin from the parasitic mite Sarcoptesscabiei: cDNA cloning and heterologous ex-pression. Parasitology. 122: 555–562.
McCarthy, J.S.; Kemp, D.J.; Walton, S.F. and Currie, B.J.(2004). Scabies: more than just an irritation.Postgrad. Med. J. 80: 382–387.
Micali, G.; Lacarrubba, F. and Tedeschi, A. (2004).Videodermatoscopy enhances the ability tomonitor efficacy of scabies treatment and al-lows optimal timing of drug application. J. Eur.Acad. Dermatol. Venereol. 18: 153–154.
Muller, G.H.; Kirk, R.W. and Scott, D.W. (1989). Parasiticskin diseases. In: Small Animal Dermatology.4th edn. W. B. Saunders Company Ltd., Phila-delphia. p. 396-404.
Newbury, S. and Moriello, K.A. (2006). Skin diseases ofanimals in shelters: triage strategy and treat-ment recommendations for common diseases.In Campbell, KL (ed.) The Veterinary Clinics ofNorth America Small Animal Practice: Up-dates in Dermatology. W.B. Saunders Co. Phila-delphia, p. 78.
OIE Terrestrial Manual (2013). Mange. NB: Versionadopted by the World Assembly of Delegates.Chapter 2.9.8.
Orkin, M. and Maibach, H. I. (1978). Scabies in children.Symposium on Pediatric Dermatology. Pediatr.Clin. North Am. 25: 371-386.
Pachauri, S.P. (1999). Sarcoptic mange. In: Canine Pre-ventive Medicine . Nilay Publications,Pantnagar. p. 633-637.
Pettersson, E.U.; Ljunggren, E.L.; Morrison, D.A. andMattsson, J.G. (2005). Functional analysis and
localisation of a delta-class glutathione S-trans-ferase from Sarcoptes scabiei. Int. J. Parasitol.35: 39–48.
Rapp, C.M.; Morgan, M.S. and Arlian, L.G. (2006). Pres-ence of host immunoglobulin in the gut of Sar-coptes scabiei (Acari: Sarcoptidae). J. Med.Entomol. 43: 539–542.
Sarma, K.; Borthakur, S.K. and Kalita, G. (2005). Incidenceof mange mite infestation in dogs - a report. J.Vet. Parasitol. 19 (2): 147-148.
Soulsby, E.J.L. (1982). Helminth, arthropods and proto-zoa of domesticated animals, 7th Ed. Baillieretindall, London, p. 482-86.
Sudhakara, B. and Nalini, K.K. (2013). Canine scabies-its therapeutic management and Zoonotic im-portance. Polivet 14 (2): 292-294.
Tahsin, B.D. and Kerem U. (2013). Comparable ef? cacyof topical eprinomectin and permethrin for treat-ment of sarcoptic mange in dogs. VeterinarskiArhiv. 83 (4): 393-402.
Walton, S.; Choy, J.L.; Bonson, A.; Valle, A.; McBroom,J.; Taplin, D.; Arlian, L.; Mathews, J.; Currie, B.and Kemp, D. (1999). Genetically distinct dog-derived and human-derived Sarcoptes scabieiin scabies-endemic communities in northernAustralia. Am. J. Trop. Med. Hyg. 61: 542–547.
Walton, S.F. and Currie, B.J. (2007). Problems in diagnos-ing scabies, a global disease in human and ani-mal populations. Clin. Microbiol. Rev. 20 (2):268–279.
Walton, S.F. and Currie, B.J. (2007). ”Problems in Diag-nosing Scabies, a Global Disease in Human andAnimal Populations”. Clinical MicrobiologyReviews 20 (2): 268–79.
Walton, S.F.; Dougall, A.; Pizzutto, S.; Holt, D.C.; Taplin,D.; Arlian, L.G.; Morgan, M.; Currie, B.J. andKemp., D.J. (2004). Genetic epidemiology ofSarcoptes scabiei (Acari: Sarcoptidae) in north-ern Australia. Int. J. Parasitol. 34: 839–849.
Willis, C.; Fischer, K.; Walton, S.F.; Currie, B.J. and Kemp,D.J. (2006). Scabies mite inactivated serine pro-tease paralogues are present both internally inthe mite gut and externally in feces. Am. J. Trop.Med. Hyg. 75: 683–687.
Woodley, D., and Saurat, J.H. (1981). The Burrow InkTest and the scabies mite. J. Am. Acad.Dermatol. 4: 715–722.
24
Journal of Canine Development & Research 2013
With Best Compliments From :
Suman Sales CorporationDealers in
Surgical, Scientific & Laboratory Requiste,Chemicals, Glassware & Equipment
Add. : B-6-61, Sudarshna Nagar, BikanerTel. : 9929181564, 9667176904
S CS

25
Journal of Canine Development & Research 2013
RESEARCH ARTICLEA STUDY ON ELECTROCARDIOGRAPHIC VALUES OF ARRHYTHMIC DOGSPriyanka1, *Anil Ahuja2, J.P. Varshney3 , A.P.Singh4 and Deepika Dhuria1
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege of Veterinary and Animal Science, RAJUVAS, Bikaner-334 001 (Rajasthan).
1Veterinary Officer 2Professor and Head 3Sr.Consultant,Nandni Hospital, Surat 4 Professor*Crresponding author e-mail : [email protected]
A B S T R A C T
In the present study electrocardiographic values of 96 arrhythmicdogs were measured. The arrhythmic dogs were presented witha wide variety of clinical signs such as weakness, depression,exercise intolerance, lethargy, refractory appetite, syncope,dullness, easy exertion, and posterior weakness. Forteen typesof arrhythma were observed in the study. Sinus tachycardia waselectrocardiographically characterized by increased heart rate192.2 ± 4.97 where as sinus arrhythmia showed variation in R-R interval = 10%. Bradycardia was reflected by heart rate = 60beats per minute. P wave of different amplitude and configurationwith a constant P-R interval were characteristic feature ofwandering pacemaker. Atrial tachycardia was characterized byrepeated premature complexes and rapid atrial heart rate. Incase of Atrial premature complexes heart rate was normal withirregular rhythm owing to premature P’ wave. (‘f’ wave) in placeof P wave, Ventricular tachycardia had repeated VPC. Sinusblock were characterized by long pauses (more than twice R-Rinterval) and regularly irregular rhythm, 1st
degree AV block by
increased P-R interval (0.15 sec.) and 2nd
degree heart block byprogressively increase in P-R interval. P wave was absent witoutP-R interval in dogs with silent atrium.
Key words :Arrhythmic dogsBradycardiaElectrocardiographic valuesSinus tachycardia
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
C ardiac arrhythmias are defined asdisturbances in rhythm and/or rate of heart,
abnormalities of impulse formation and conduction(Miller and Tilley, 1995). Electrocardiography(ECG) is an examination method that graphicallyshows electric actions of the heart, recorded over
a given period from the body surface of an animal.Today, Electrocardiography is the most precisemethod in diagnosing arrhythmias.Present studyreport the various arrhythmias on the basis ofECG.
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 25-29
26
Journal of Canine Development & Research 2013
Materials and methods
Present work was carried out at College ofVeterinary and Animal Science, Bikaner andPanjarapole Prerit Nandini Veterinary Hospital,Surat from December 2011 to March 2012.Electrocardiographic tracing were recorded oncardiart 108T-MK-VI, a single channel, 12 leadelectrocardiographs (BPL India Ltd.) machine andMagic R machine (Maestros Company).All animals had been positioned in right lateralrecumbancy with standard ECG leads on the limbin agreement with Tilly’s recommendation. Paperspeed of 25 mm/sec. and 1 cm = 1mv amplitudewere selected. Four to five beats were recordedon each lead and a longer rhythm strip was run onlead II. The amplitude of the complexes anddifferent intervals were measured as per guidelinegiven by Tilley (1985). In the present studyelectrocardiographic values of 96 arrhythmic dogswere measured. The arrhythmic dogs werepresented with a wide variety of clinical signs suchas weakness, depression, exercise intolerance,lethargy, refractory appetite, syncope, dullness,easy exertion, and posterior weakness.
Results and discussion
On the basis of ECG observations of P-QRS-Tof complexes and their intervals, heart rate andrhythm in arrhythmic dogs with forteen types ofarrhythmia in presented in the table 1.As per table 1 the mean value of P (0.04 ± 0 sec.,0.23 ± 0.013 mv), P-R interval (0.089± 0.002sec.), QRS complex (0.04± 0 sec.), ST segment(0.053 ± 0.002 sec), T wave (0.064± 0.003 sec,0.29 ± 0.003 mv), R-R interval (0.33± 0.009 sec),were within normal range in dogs with sinustachycardia. However, heart rate was = 160 forlarge breeds and = 180 for toy breeds with a meanof 192.2± 4.97 beats per minutes as suggestedby other workers (Tilley, 1985; Varshney andTiwarri, 2002 a, b). It may be physiologicassociated with exercise, stress, anxiousness, pain
or may be Drug-induced due to atropine orglycopyrrolate, methylxanthines (theophylline),excessive thyroid supplementation, catecholamines(epinephrine, dobutamine) or may be Pathologicdue to fever, shock, hyperthyroidism, anemia,hypoxia, and congestive heart failure.The values of all components P (0.04± 0 sec.,0.18±0.019 mv), P-R interval (0.101±0.006 sec),QRS complex (0.04 ± 0 sec), T wave (0.07±0.006 sec, 0.24± 0.031 mv) were also within rangelimit in dogs with sinus arrhythmia except R-Rinterval that showed variation = 10% agreeingwith the observation of Muir et al. (1975).In bradycardiac dogs, all the ECG measurementsP (0.04 ±0 sec., 0.125 ± 0.025mv), P-R interval(0.11 ±0.01sec), QRS complex (0.04 ±0.005sec.), ST segment (0.12 ±0 sec.), T wave (0.05±0.01 sec., 0.1 ±0 mv) R-R interval (0.88 ±0.08sec.) were normal except that heart rate was =60 beats per minute similarly also observed byVarshney and Dey (2000). It may be physiologicaleg. during sleep, the heart rate of many dogs dropsto 30 to 40 bpm. Calm animals or athletic animalsat rest may have a physiologic sinus bradycardia.It may be Drug-induced due to anesthetics andsedatives, digoxin, calcium channel blockers, betablockers or pathologic due to hypothermia,hypothyroidism, sick sinus syndrome (SSS).In present study wandering pacemakerelectrocardiographs characterized by differentconfiguration and amplitude of ‘P’ wave. The meanvalues of QRS duration; ST segment; T waveduration and amplitude; R-R interval and heart ratewere 0.04 ± 0 sec., 0.076 ± 0.013 sec., 0.076±0.013 sec., 0.32 ± 0.058 mv, 0.52 ± 0.036 sec.and 120 ± 6.32 beats/min, respectively. Similar topresent results Changkija (2007) also reportedthat electrocardiographic profile in dogs withwandering pacemaker, is characterizes by P waveof different amplitude and configuration and aconstant P-R interval. Tilley (1985) ascribed toshifting of pacemaker within SA node or between

27
Journal of Canine Development & Research 2013
SA node and AV junction.In atrial tachycardia mean value of P waveamplitude and duration; PR interval; QRS duration;ST segment; T wave duration and amplitude; R-Rinterval and ventricular heart rate were 0.04 ±0sec., 0.23 ± 0.088 mv, 0.086 ± 0.006 sec., 0.04± 0 sec., 0.046 ± 0.0066sec., 0.046 ± 0.006sec.,0.23 ± 0.088mv, 0.41 ± 0.013 sec., 150 ± 5.77beats/min .Atrial tachycardia characterizes by rapidheart rate with more APC. The configuration of P’wave was a little different than that of P wave.Rest electrocardiographic indices were withinnormal range. It appears that atrial tachycardia maybe due to an enhanced automaticity of an ectopicfocus or re- entry (Josephson and Kastor, 1977).Atrial fibrillation characterizes by fine oscillation/or ‘f’ wave. QRS duration; ST segment; T waveduration and amplitude; R-R interval andventricular heart rate were 0.04 ± 0 sec., 0.052±0.008 sec., 0.4 ±0.071 sec., 0.456 ±0.045 mv,and 132 ± 7.348 beats/min, respectively.Thisfinding is an agreement with observation ofChangkija (2007) and Varshney et al. (2011a).Causes of atrial fibrillation includes Structural heartdisease eg. advanced degenerative valve disease,dilated cardiomyopathy, atrial neoplasia, congenitalheart disease.Electrocardiographs of atrialpremature complexes were characterized byadditional P’ waves occasionally. Mean value Pwave amplitude and duration; PR interval; QRSduration; ST segment; T wave duration andamplitude; R-R interval and heart rate were 0.04±0sec., 0.17 ± 0.067 mv, 0.11 ± 0.0067 sec., 0.04± 0 sec., 0.08 ± 0 sec., 0.05 ± 0.006 sec., 0.2 ±0.057 mv, 0.54 ± 0.059 sec., 110 ± 11.55 beats/min, respectively . Similar to present study Guytonand Hall (2004) also reported APC with shortenedP-R interval, indicating that the ectopic origin ofthe beat is in the atrium near the AV node. GenerallyCauses of APC includes any disease associatedwith atrial enlargement, such as degenerative valvedisease, congenital heart disease, or
cardiomyopathy. Other causes include hypoxia,atrial neoplasia, and chronic obstructive pulmonarydisease.AV junctional escape rhythm characterizes by anegative ‘P’ wave that replaces the regular P wave.Mean value P wave amplitude and duration; PRinterval; QRS duration; ST segment; T waveduration and amplitude; R-R interval and heart ratewere negative 0.04 sec., 0.1 mv, 0.04 sec, 0.08sec., 0.06 sec., 0.5 mv, 0.64 sec., 110 beats/min,respectively .Similarly Kumar et al. (2011) alsoreported AV junctional escape rhythm withnegative P wave disrupting the normal P waverhythm. Heart rate, QRS complex and T wavewere normal but the rhythm was irregular due tothe premature P’ waves.Presently in Ventricular premature complex Meanvalues of P wave amplitude and duration; PRinterval; QRS duration; ST segment; T waveduration and amplitude; R-R interval and heart ratewere 0.04 sec., 0.2 mv, .0.04 sec., 0.04 sec., 0.08sec., 0.06 sec., 0.6 mv, 0.48 sec., 140 beats/min,respectively and at one place QRS complex wasbizarre unassociated with regular P wave. The Rwave of premature complex was merged with thepreceding T wave (R over T phenomena). Thesefindings are in agreement with the observation ofVarshney et al. (2011b) and kumar et al. (2011).The R over T phenomenon also reported in fourdogs by Duerr et al. (2007). VPCs arise from anectopic focus or foci within the ventricularmyocardium. Depolarisation therefore occurs inan abnormal direction through the myocardium andthe impulse conducts from cell to cell (not withinthe conduction tissue).In Ventricular tachycardia mean values of P waveamplitude and duration; PR interval; QRS duration;ST segment; T wave duration and amplitude; R-Rinterval and heart rate were 0.04 sec., 0.3 mv,0.08 sec, 0.04 sec., 0.04 sec., 0.18 sec., 0.4 mv,0.52 sec. and 108 beats/min, respectively.Electrocardiograph characterizes by presence of
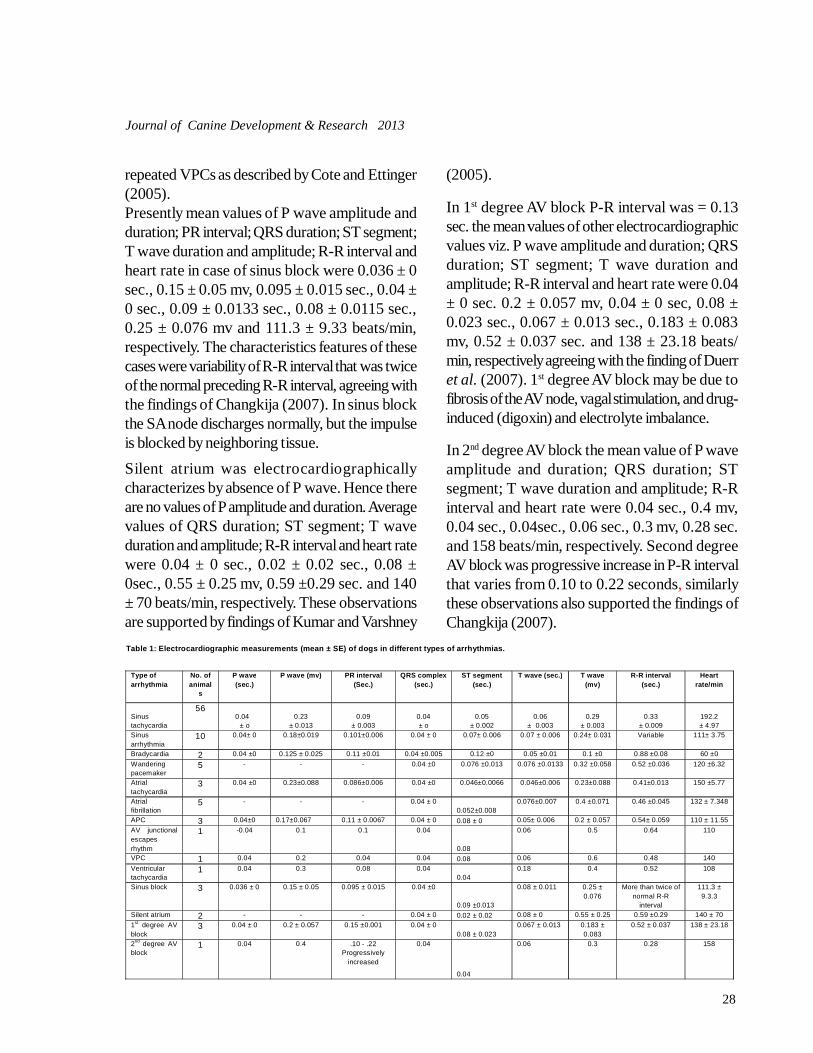
28
Journal of Canine Development & Research 2013
repeated VPCs as described by Cote and Ettinger(2005).Presently mean values of P wave amplitude andduration; PR interval; QRS duration; ST segment;T wave duration and amplitude; R-R interval andheart rate in case of sinus block were 0.036 ± 0sec., 0.15 ± 0.05 mv, 0.095 ± 0.015 sec., 0.04 ±0 sec., 0.09 ± 0.0133 sec., 0.08 ± 0.0115 sec.,0.25 ± 0.076 mv and 111.3 ± 9.33 beats/min,respectively. The characteristics features of thesecases were variability of R-R interval that was twiceof the normal preceding R-R interval, agreeing withthe findings of Changkija (2007). In sinus blockthe SA node discharges normally, but the impulseis blocked by neighboring tissue.Silent atrium was electrocardiographicallycharacterizes by absence of P wave. Hence thereare no values of P amplitude and duration. Averagevalues of QRS duration; ST segment; T waveduration and amplitude; R-R interval and heart ratewere 0.04 ± 0 sec., 0.02 ± 0.02 sec., 0.08 ±0sec., 0.55 ± 0.25 mv, 0.59 ±0.29 sec. and 140± 70 beats/min, respectively. These observationsare supported by findings of Kumar and Varshney
(2005).
In 1st degree AV block P-R interval was = 0.13sec. the mean values of other electrocardiographicvalues viz. P wave amplitude and duration; QRSduration; ST segment; T wave duration andamplitude; R-R interval and heart rate were 0.04± 0 sec. 0.2 ± 0.057 mv, 0.04 ± 0 sec, 0.08 ±0.023 sec., 0.067 ± 0.013 sec., 0.183 ± 0.083mv, 0.52 ± 0.037 sec. and 138 ± 23.18 beats/min, respectively agreeing with the finding of Duerret al. (2007). 1st degree AV block may be due tofibrosis of the AV node, vagal stimulation, and drug-induced (digoxin) and electrolyte imbalance.
In 2nd degree AV block the mean value of P waveamplitude and duration; QRS duration; STsegment; T wave duration and amplitude; R-Rinterval and heart rate were 0.04 sec., 0.4 mv,0.04 sec., 0.04sec., 0.06 sec., 0.3 mv, 0.28 sec.and 158 beats/min, respectively. Second degreeAV block was progressive increase in P-R intervalthat varies from 0.10 to 0.22 seconds, similarlythese observations also supported the findings ofChangkija (2007).
Table 1: Electrocardiographic measurements (mean ± SE) of dogs in different types of arrhythmias.
Type of arrhythmia
No. of animal
s
P wave (sec.)
P wave (mv) PR interval (Sec.)
QRS complex (sec.)
ST segment (sec.)
T wave (sec.) T wave (mv)
R-R interval (sec.)
Heart rate/min
Sinus tachycardia
56 0.04
± o 0.23
± 0.013 0.09
± 0.003 0.04 ± o
0.05 ± 0.002
0.06 ± 0.003
0.29 ± 0.003
0.33 ± 0.009
192.2 ± 4.97
Sinus arrhythmia
10 0.04± 0 0.18±0.019 0.101±0.006 0.04 ± 0 0.07± 0.006 0.07 ± 0.006 0.24± 0.031 Variable 111± 3.75
Bradycardia 2 0.04 ±0 0.125 ± 0.025 0.11 ±0.01 0.04 ±0.005 0.12 ±0 0.05 ±0.01 0.1 ±0 0.88 ±0.08 60 ±0 Wandering pacemaker
5 - - - 0.04 ±0 0.076 ±0.013 0.076 ±0.0133 0.32 ±0.058 0.52 ±0.036 120 ±6.32
Atrial tachycardia
3 0.04 ±0 0.23±0.088 0.086±0.006 0.04 ±0 0.046±0.0066 0.046±0.006 0.23±0.088 0.41±0.013 150 ±5.77
Atrial fibrillation
5 - - - 0.04 ± 0 0.052±0.008
0.076±0.007 0.4 ±0.071 0.46 ±0.045 132 ± 7.348
APC 3 0.04±0 0.17±0.067 0.11 ± 0.0067 0.04 ± 0 0.08 ± 0 0.05± 0.006 0.2 ± 0.057 0.54± 0.059 110 ± 11.55 AV junctional escapes rhythm
1 -0.04 0.1 0.1 0.04
0.08
0.06 0.5 0.64 110
VPC 1 0.04 0.2 0.04 0.04 0.08 0.06 0.6 0.48 140 Ventricular tachycardia
1 0.04 0.3 0.08 0.04 0.04
0.18 0.4 0.52 108
Sinus block 3 0.036 ± 0 0.15 ± 0.05 0.095 ± 0.015 0.04 ±0
0.09 ±0.013
0.08 ± 0.011 0.25 ± 0.076
More than twice of normal R-R
interval
111.3 ± 9.3.3
Silent atrium 2 - - - 0.04 ± 0 0.02 ± 0.02 0.08 ± 0 0.55 ± 0.25 0.59 ±0.29 140 ± 70 1st degree AV block
3 0.04 ± 0 0.2 ± 0.057 0.15 ±0.001 0.04 ± 0 0.08 ± 0.023
0.067 ± 0.013 0.183 ± 0.083
0.52 ± 0.037 138 ± 23.18
2nd degree AV block
1 0.04 0.4 .10 - .22 Progressively
increased
0.04
0.04
0.06 0.3 0.28 158

29
Journal of Canine Development & Research 2013
ReferencesChangkija, B. (2007). Electrocardiographic studies in
dogs with references to management ofcardiac tachyarrhythmias by alternate days.Indian Veter inary Research Insti tude,Izatnagar. M.V.Sc Thesis.
Cote, E., Ettinger, S. J. (2005). Electrocardiography andcardiac arrhy- thmias. In: Ettinger, S.J., Feldman E. C., ed. Textbook of veter- inaryinternal medicine, 6th edn. St Louis: Saunders,p 1040-1076.
Duerr, F. M., Carr, A. P., Duke T., Shmon, C. L., Monnet,E. (2007): Prevalence of perioperativearrhythmia in 50 young healthy dogs. .Cana.Vet. J., 48(2):162-177.
Guyton, A. C. and Hall, J. E. (2004). Textbook ofMedical Physiology.11th edn. Philadelphia, S.W. Saunders Company, p 106.
Josephson, M. E. , Kastor, J . A. (1977). Supraventricular tachycardia: mechanismsand management. Ann. Intern. Med., 87:346–358.
Kumar, A., Varshney J. P. (2005). Atrial stand still in aGerman Shepherd dog. Clinical article. Indianvet. Med. J., 29:225-226.
Kumar, K. S., Tirumale Rao, D. S., and Snigari, N. A.(2011). Electrocardiographic diagnosis ofcardiac diseases in dogs. A study of two year(2007-2009). Intas Polyvet, 12:254-260.
Miller, M. S. and Tilley, L. P. (1995). Treatment of
cardiac ar rhythmia and conductiondisturbances. In Miller and Tilley: manual ofcanine and feline cardiology, 2nd edn. W. B.Saunders co., p 371-411.
Muir, W. W., Werner, L. L. and Hamlin, R. L. (1975).Antiarrhythmic effects of diazepam duringcoronary artery oclusion in dogs. Am. J. Vet.Res., 36:1203-1206.
Tilley, L. P. (1985). Essentials of canine and falineelectrocardiography interpretation andtr eatmen t. 2 nd edn . Lea and Febiger,Philadelphia, p 320.
Varshney, J. P. Tiwari, P. (2002a). Electrocardiographicand cl in ic-biochemical fea tures oft rypanosomosis in dogs wi th natura linfection of Trypanosoma Evansi. J. Can.Dev. Res., 2:51-54.
Varshney, J. P. Tiwari, P. (2002b). Electrocardiographicchanges in canine parvoviral infection. J. Can.Dev. Res., 2:23-27.
Varshney, J. P., Deshmukh, V. V. and Chouchary, P. S.(2011 a). Atrial fibrillation/atrial flutteres indogs and it’s management. Intas Polivet,12:271-273.
Varshney, J. P., Deshmukh, V. V. and Choudhary, P. S.(2011 b). Congestive heart failure in dogs. Aprospective study. Intas Polyvet, 12:261-267.
Varshney, J. P. and S. Dey (2000). Sinus brady-arrhythmia in dog and its treatment. IndianJ. Vet. Med., 20(2):105-106.
30
Journal of Canine Development & Research 2013
JOURNAL OF CANINEDEVELOPMENT AND RESEARCH
SUBSCRIPTION FORM
The annual subscription (one issue) rates are as under:
For Institutions Rs. 1200.00 or US$ 110 or £ 65 or DM 130 or Euro 90For Vets & Others Rs. 500.00 or US$ 50 or £ 30 or DM 60 or Euro 50
VOLUME 1, 2, 3, 4, 5, 6 ,7 & 8 ARE ALSO AVAILABLE
Please enroll me as a subscriber and send me the issue of Journalof Canine Development & Research. I am enclosing herewitha Demand Draft No. ....................Dated .............Amount............towards the annual subscription for the volume ...............................,in favour of the CANINE PUBLISHING HOUSE, BIKNAER.
NAME ................................................................................... PROFESSION ................................................................................... ADDRESS ...................................................................................
...................................................................................
Filled subscription form should be mailed by Regd. Post to:
CANINE PUBLISHING HOUSEPUSHAP BHAWAN, B-48, SADUL GANJ
BIKANER- 334 003 (RAJ.)
31
Journal of Canine Development & Research 2013
RESEARCH ARTICLE
Journal of Canine Development & ResearchISSN : 0973-3272 Accessible at : www.jcdrindia.com
PATHOGENECITY TRIALS OF ESCHERICHIA COLI FROM PYOMETRICBITCHES*Varun Bassessar1, Yamini Verma2 and Madhu Swamy3
Department of Veterinary PathologyCollege of Veterinary Science and Animal Husbandry, N D V S U, Jabalpur-482 001 (MP)
1 Ph.D. Scholar2 Associate Professor 3 Professor and Head*Corresponding author e-mail : [email protected]
A B S T R A C T
The aim of the present work was to establish the pathogenecity ofEscherichia coli (E coli), the predominant isolate obtained frompyometric female dogs. The study was carried out on White Albinorats of either sex weighing 80-150 g. Albino rats were divided intotwo groups as control and experimental with 10 animals in eachgroup. The control group was given Standard feed and water and0.3ml. of PBS (intra-peritoneum) while the experimental groupwas given Standard feed and water and inoculums’ of E.coli (0.3ml. adjusted to 1 × 10
9 CFU/ml). The experimental rats were
sacrificed on day 7 and day 14. Hemato-biochemical studies alongwith the detailed histo-pathological examination were performedat the time of sacrifice. Smear prepared from the perianal swabsof rats inoculated with E. coli revealed the presence of gramnegative rods after 4
th day of inoculation. The haematological
parameters showed no significant variation from the control groupat both the intervals. The values of ALT, AST and ALP wereincreased in experimental animals at both 7
th and 14
th day. The
carcass of all the animals inoculated with E. coli were septicaemicand the liver, kidney and intestine showed marked microscopicchanges. The E. coli isolates from uterine exudate of caninepyometra is pathogenic and can infect other species as evidencedby pathogenecity trials conducted in rats.
Key words :CaninePathogenecity trialPyometraRats
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
Pyometra is the accumulation of purulentmaterial within the uterine lumen. It is of
particular importance to the veterinary practitioner,since early recognition, diagnosis and appropriateintervention is required to avoid fatal consequences(Varun et al.,2011;Nagar et al.,2008,Velhankar
et al.,2008) . It is classically a disease of thediestrual animals and can be classified as opencervix or closed cervix, with latter being a medicalemergency requiring rapid intervention to preventsubsequent sepsis and potential patient death(Smith, 2006). Closed cervix pyometra is
Vol (9) 31-36

32
Journal of Canine Development & Research 2013
particularly dangerous because septicemia andtoxemia may develop rapidly and if left untreatedcan result in patient death.
Past investigations of the bacteriaassociated with canine pyometra have been few.However, it has been well established that the mostcommon infecting agent is Escherichia coli, whichis isolated in 59% to 96% of pyometra cases(Tsumura et al., 2003). Certain serotypes of E.coli, such as 02, 04, 06, 075, 10, 11 and 032, 12appear to be isolated more commonly than otherserotypes from dogs with pyometra (Tsumura etal., 2003). Like other
gram-negative bacteria, the
E. coli cell wall has endotoxins. Endotoxemia isbelieved
to be responsible for many of the clinical
signs associated with pyometra. If rupture of the
infected uterus occurs, bacterial peritonitis and/or
sepsis may result, with a guarded to poor prognosis.
Occasionally, other agents (e.g., Klebsiella spp.,Streptococci spp., Staphylococci spp. andPseudomonas spp.) have also been isolated fromthe uterus of an infected animals (Fransson et al.,1997; Dhaliwal et al., 1999 ; Coggan et al.,2008).
Materials and methods
The work was conducted in Departmentof Veterinary Pathology, College of VeterinaryScience and Animal Husbandry, NDVSU,Jabalpur, Madhya Pradesh. The study was carriedout on White Albino rats of either sex weighing80-150 g. The animals were acclimatized for 7days prior to use. The animals were maintained ina 12/12 hours light/dark cycle with good hygieniccondition and were kept on a standard diet withwater ad libitum following the CPCSEA norms.For the pathogeneicity trails White Albino ratswere divided into two groups as shown in table 1.Escherichia coli isolated from the vaginaldischarge of the pyometric animals was taken forthe preparation of the inoculums. The test organismwas grown overnight on tryptic soy broth (TSB)at 37
0C. To test the purity of culture, direct smear
was prepared from the broth culture, stained withGram’s staining method and examinedmicroscopically. Young broth culture of eachisolate was subjected to 3000 rpm centrifugationat low temperature for 20 minutes. The cell pelletsof each group were suspended in PBS to a
Group No. of animals Treatment Sacrifice Collection of material
Control 10 Standard feed & water + 0.3ml. of PBS (intraperitonally, i.p.)
First Sacrifice on 7 th day (5 animals)
Second sacrifice on 14th day (5 animals)
i. Perianal swab collected on 3rd day.
ii. Blood collected for haemato-biochemical studies at the time of sacrifice.
iii. Lung, liver, kidney and intestine collected for gross and histopathological studies.
Experimental Group
10 Standard feed & water + Inoculum of E.coli (0.3 ml. adjusted to 1 × 109 CFU/ml (i.p.)
First Sacrifice on 7 th day (5 animals)
Second sacrifice on 14th day (5 animals)
(Same as above)
Table 1: Pathogenecity trials of Escherichia coli in rats
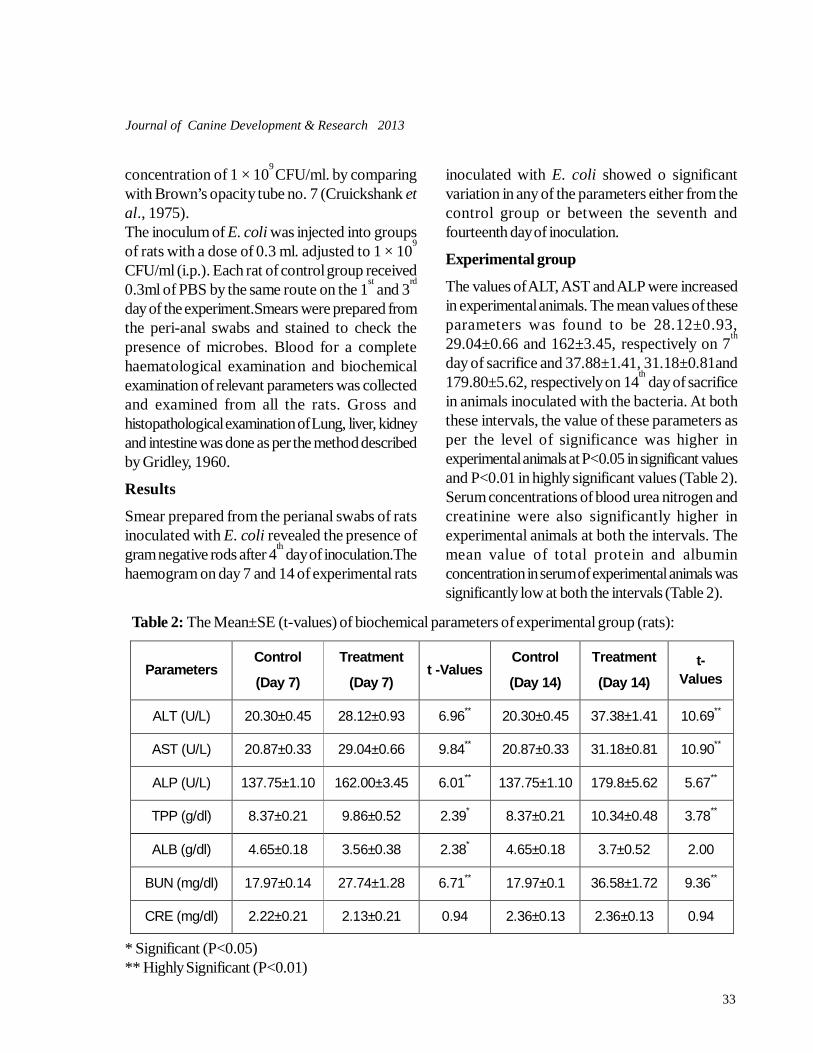
33
Journal of Canine Development & Research 2013
Parameters Control
(Day 7)
Treatment
(Day 7) t -Values
Control
(Day 14)
Treatment
(Day 14) t-
Values
ALT (U/L) 20.30±0.45 28.12±0.93 6.96** 20.30±0.45 37.38±1.41 10.69**
AST (U/L) 20.87±0.33 29.04±0.66 9.84** 20.87±0.33 31.18±0.81 10.90**
ALP (U/L) 137.75±1.10 162.00±3.45 6.01** 137.75±1.10 179.8±5.62 5.67**
TPP (g/dl) 8.37±0.21 9.86±0.52 2.39* 8.37±0.21 10.34±0.48 3.78**
ALB (g/dl) 4.65±0.18 3.56±0.38 2.38* 4.65±0.18 3.7±0.52 2.00
BUN (mg/dl) 17.97±0.14 27.74±1.28 6.71** 17.97±0.1 36.58±1.72 9.36**
CRE (mg/dl) 2.22±0.21 2.13±0.21 0.94 2.36±0.13 2.36±0.13 0.94
* Significant (P<0.05)** Highly Significant (P<0.01)
concentration of 1 × 109 CFU/ml. by comparing
with Brown’s opacity tube no. 7 (Cruickshank etal., 1975).The inoculum of E. coli was injected into groupsof rats with a dose of 0.3 ml. adjusted to 1 × 10
9
CFU/ml (i.p.). Each rat of control group received0.3ml of PBS by the same route on the 1
st and 3
rd
day of the experiment.Smears were prepared fromthe peri-anal swabs and stained to check thepresence of microbes. Blood for a completehaematological examination and biochemicalexamination of relevant parameters was collectedand examined from all the rats. Gross andhistopathological examination of Lung, liver, kidneyand intestine was done as per the method describedby Gridley, 1960.
Results
Smear prepared from the perianal swabs of ratsinoculated with E. coli revealed the presence ofgram negative rods after 4
th day of inoculation.The
haemogram on day 7 and 14 of experimental rats
inoculated with E. coli showed o significantvariation in any of the parameters either from thecontrol group or between the seventh andfourteenth day of inoculation.
Experimental group
The values of ALT, AST and ALP were increasedin experimental animals. The mean values of theseparameters was found to be 28.12±0.93,29.04±0.66 and 162±3.45, respectively on 7
th
day of sacrifice and 37.88±1.41, 31.18±0.81and179.80±5.62, respectively on 14
th day of sacrifice
in animals inoculated with the bacteria. At boththese intervals, the value of these parameters asper the level of significance was higher inexperimental animals at P<0.05 in significant valuesand P<0.01 in highly significant values (Table 2).Serum concentrations of blood urea nitrogen andcreatinine were also significantly higher inexperimental animals at both the intervals. Themean value of total protein and albuminconcentration in serum of experimental animals wassignificantly low at both the intervals (Table 2).
Table 2: The Mean±SE (t-values) of biochemical parameters of experimental group (rats):
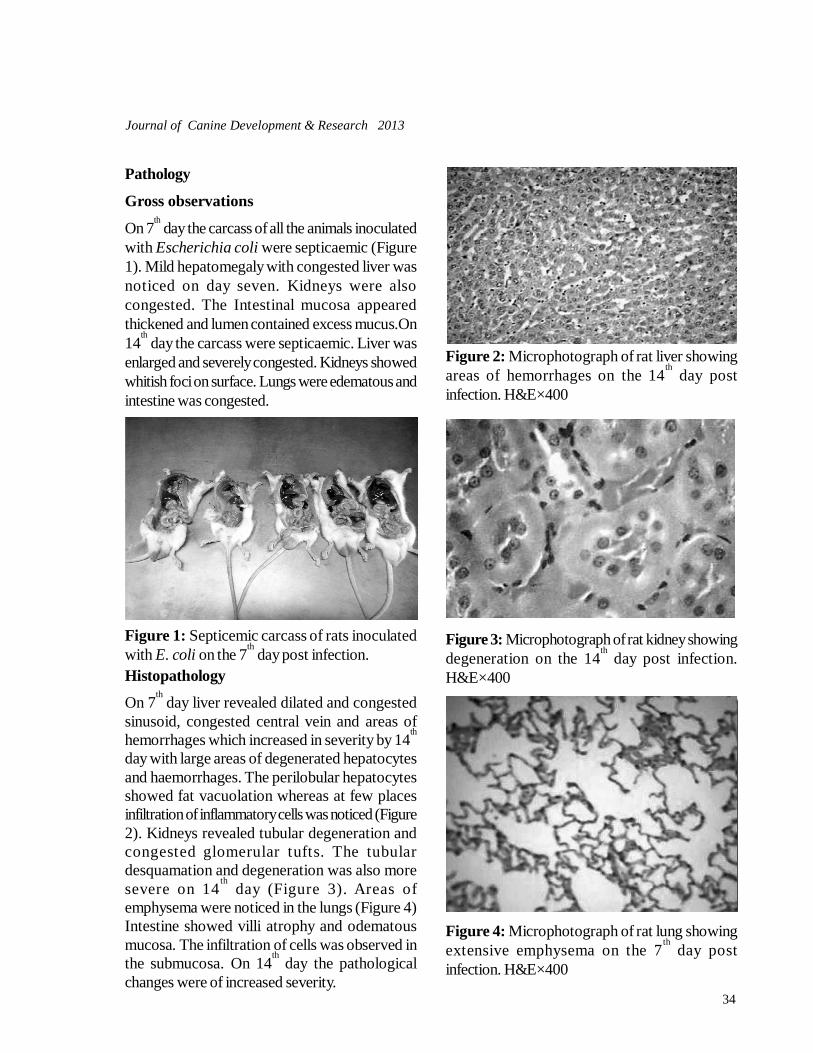
34
Journal of Canine Development & Research 2013
Figure 1: Septicemic carcass of rats inoculatedwith E. coli on the 7
th day post infection.
Pathology
Gross observations
On 7th day the carcass of all the animals inoculated
with Escherichia coli were septicaemic (Figure1). Mild hepatomegaly with congested liver wasnoticed on day seven. Kidneys were alsocongested. The Intestinal mucosa appearedthickened and lumen contained excess mucus.On14
th day the carcass were septicaemic. Liver was
enlarged and severely congested. Kidneys showedwhitish foci on surface. Lungs were edematous andintestine was congested.
Histopathology
On 7th day liver revealed dilated and congested
sinusoid, congested central vein and areas ofhemorrhages which increased in severity by 14
th
day with large areas of degenerated hepatocytesand haemorrhages. The perilobular hepatocytesshowed fat vacuolation whereas at few placesinfiltration of inflammatory cells was noticed (Figure2). Kidneys revealed tubular degeneration andcongested glomerular tufts. The tubulardesquamation and degeneration was also moresevere on 14
th day (Figure 3). Areas of
emphysema were noticed in the lungs (Figure 4)Intestine showed villi atrophy and odematousmucosa. The infiltration of cells was observed inthe submucosa. On 14
th day the pathological
changes were of increased severity.
Figure 2: Microphotograph of rat liver showingareas of hemorrhages on the 14
th day post
infection. H&E×400
Figure 3: Microphotograph of rat kidney showingdegeneration on the 14
th day post infection.
H&E×400
Figure 4: Microphotograph of rat lung showingextensive emphysema on the 7
th day post
infection. H&E×400

35
Journal of Canine Development & Research 2013
Discussion
Pathogenecity trial of the predominant bacterium(E. coli) isolated from uterine exudates wasconducted in albino rats. The biochemicalabnormalities reflected liver and kidneydegenerative changes. Microscopic examinationof the tissues also revealed moderate liver, kidney,and lung and intestinal lesions in the infectedanimals. The changes were more severe in the laterinterval of experimental studies.Gupta and Srivastava (2012) conducted work onthe experimental rats which were fed cow urineand challenged with E. coli infection.Pathomorphological examination of rats succumbedto infection revealed changes of acute non-suppurative hepatitis characterized by paracental/centrilobular necrosis with infiltration of neutrophilsand macrophages, thickening of alveolar septa dueto congestion of blood vessels with peribronchiallymphoid cuffing, congestion of myocardial bloodvessels and at places separation of myofibres withdegeneration of myocardium; slightly swollen, darkbrown kidneys showing congested cortimedullaryjunction with increased cellularity and vacuolizationof glomerular loops along with tubular degenerationand thickened intestinal walls with congestion alongwith the presence of catarrhal to haemorrhagicexudates. Acute non suppurative hepatitis,thickening of alveolar septa with peribronchial andperivascular lymphoid cuffing and hyperplasia ofbronchial epithelium and findings of lesions ofcatarrhal to haemorrhagic enteritis were alsoobserved by other workers in spontaneous andexperimental E. coli infection in kids by Azmi andJha (1994) and Sharma (2000); in lambs by Men-Shikova and Baltaev (1995) and in calves by Singhand Singh (1983).It must be considered that dogs are animals thatare living in close proximity to man for thousandsof years and have an important role in thetransmission of E. coli to other animals and to man.As pyometra is considered one of the main
diseases in the female dogs, its pathologyrepresents a potential risk to public health becauseof the fact that the vaginal secretion can be a sourceof infection to man.
ReferencesAzmi, S. and G.J. Jha (1994). Pathology of induced E. coli
infection in kids. Indian J. Vet. Pathol., 18(1):47-49.
Coggan, J.A., P.A. Melville, D.E. Olivera, C.M. Faustino,M. Moreno, and A.M. Benites (2008). Micro-biological and histopathological aspect of ca-nine pyometra. Brazilian Journal of Microbi-ology. 39: 477-483.
Cruickshank, R., J.P. Dugie, B.P. Marimon and R.H.A.Swain (1975). Medical Microbiology, 12th edn,Publ. Churchill Livingstone, New York. pp. 202-203.
Dhaliwal, G.K., C.W. England, and D.E. Noakes (1999).Oestrogen and progesterone receptors in theuterine wall of bitches with cystic endometrialhyperplasia/pyometra. Vet. Rec., 145(16): 455–457.
Fransson, B., A.S. Lagerstedt, and P. Jonsson (1997).Bacteriological findings, blood chemistry pro-file and plasma endotoxin levels in bitches withpyometra or other uterine disease. J. Vet. Med.A. Physiol. Pathol. Clin. Med., 44(7): 417-426.
Gridley, M. F. (1960). Manual of histological & specialstaining techniques. Publ., McGraw-hill BookCompany, Inc.New York. 202 p.
Gupta, A. and A.K. Srivastava (2012). Effect of cow urineagainst experimental E. coli infection in rats: Ahistopathological study. Indian J. Vet. Pathol.,36(1): 107-109.
Men-Shikova, Z.N. and S.P. Baltaev (1995). Study of theultrastructure of epithelial cells of the small in-testine mucosa of gnotobiotic lambs with ex-perimental E.coli infection. Sbornik-Nauchnykh- Tvudor Moskovskaya-Veterinarnaya- Akademiya., 79(1): 110-114.
Nagar D.,Purohit G.N.and Mehta J.S(2008).Prevalence ofreproductive conditions in bitches. J.CanineDev.Res.7:7-10.
Pramod Kumar, G.N. Purohit, J.S. Mehta, Amit Kumar,Vikash Choudhary, Chandra Shekher andKamlesh Jeengar. (2010) Clinical fundings andtherapy of pyometra in bitches. J Canine Dev.Res. 6: 79-82.
Sharma, V.K. (2000). E. coli induced diarrhea in neonatal

36
Journal of Canine Development & Research 2013
kids-A clinicopathological and pathomorpho-logical study. M.V.Sc. thesis submitted to theC.S.A. University of Ag. And Tech. Kanpur,(U.P.).
Singh, G.K. and N.P. Singh (1983). Clinicopathologicalstudy of experimental calf scour induced by E.coli strain (0:129). Indian J. Vet. Pathol., 7: 31-34.
Smith, F.O. (2006). Canine pyometra. Theriogenology.66: 610 - 612.
Tsumura, H., E. Hiyama, T. Kodama, T. Sueda and T.Yokoyama, (2003). Relevance of antimicrobial
agent-induced endotoxin release from in vitrocultured Escherichia coli and in vivo experi-mental infection with gram-negative bacilli. Int.J. Antimicrob. Agents., 21: 463-470.
Varun Bassessar, Yamini Verma and MadhuSwamy(2011). Canine Pyometra: An Update onEtio-Pathogenesis. J.Canine Dev.Res.7:1-7
Velhankar R.D., Dighe D.G., Gaikwad, R.V. and KeskarD.V.( 2008 ) Multifocal paroxysmal ventriculartachycardia subsequent to pyometra in bitches.J.Canine Dev.Res.5:13-15.

37
Journal of Canine Development & Research 2013
RESEARCH ARTICLEEFFECT OF THERAPEUTIC MANAGEMENT ON ELECTROCARDIOGRAPHICPARAMETERS IN DIALATED CARDIOMYOPATHY AFFECTED DOGS*Velhankar, R.D.1 and D.V. Keskar 2
Department of Clinical Medicine, Ethics and JurisprudenceBombay Veterinary College, Parel, Mumbai – 400 012 (Maharashtra)
1 Assistant Professor, 2 Professor and Head Part of the Thesis submitted to Maharashtra Animal and FisherySciences University, Nagpur, for the award of degree of Doctor of Philosophy.*Corresponding author e-mail : [email protected]
A B S T R A C T
Electro cardio graphy (ECG) was recorded in 23 dialatedcardiomyopathy (DCM) affected dogs and 11 apparently healthydogs. The DCM affected dogs were suggested a treatmentprotocol for a period of 30 days. Due to severity of disease, 12dogs died (Died group of dogs) and 11 dogs survived and reportedfor post therapeutic evaluation after 30 days (After treatmentGroup).Out of these 23 DCM affected dogs, Five dogs sufferedatrial fibrillation (21.74%). ECG in DCM affected dogs showeda significant increase (P 0.05) in heart rate, P wave width, Pwave amplitude, QRS width and amplitude. The dogs in DCMgroup showed electrocardiographic evidence of left atrialenlargement and left ventricular enlargement. The heart rate indied group of dogs was higher (NS) by 21.57%, on percentilebasis, than the Survived group of dogs. Therapeutic managementfor a period of 30 days, prolonged the PR interval and QT interval,on percentile basis, by 18.18 % and 1.91% with the consequentialreduction in heart rate by 9.54%.
Key words :Atrial fibrillationDigoxinDialated cardiomyopathyElectrocardiogram
A R T I C L E H I S T O R Y
Received : November 28, 2013Revised : December 12, 2013Accepted : December 22, 2013
Electrocardiogram (ECG) is a quick, costeffective, field utility, portable and fairly reliable
diagnostic tool for the diagnosis of DilatedCardiomyopathy (DCM) in dogs. ECG is agraphical representation of magnitude or patternof electrical flux / activity produced in an orderlyand repetitive manner or cyclical fashion, during
each cardiac cycle, due to contraction andrelaxation of atria and ventricles.The electrical activity produced duringdepolarization or repolarization of a cardiacmuscle fibre, due to ionic shift across the cellmembrane, is directly proportional to its length andthickness (Bolton,1975). Therefore, this is the
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 37-45

38
Journal of Canine Development & Research 2013
reason why the lengthen or hypertrophied cardiacmuscle fibres in the dilated or hypertrophied heartproduce the current of greater magnitude,reflecting on the electrocardiogram in the form ofcomplexes of greater width (wider) and greaterheight (amplitude).Fox et al. (1988), DeFransesco (2001), Dukes-McEwan et al. (2003), Israel (2003) and Tilleyet al.(2008) have reported electrocardiographicalterations in DCM affected dogs. They alsoreported tachyrrthmias and atrial fibrillation as beingthe most common rhythmabnormality. Oyama et al. (2007) recommendedto encourage screening of dogs for dilatedcardiomyopathy used for breeding belonging topredisposed breeds and involve the use of a Holtermonitor (a 24 hour ambulatory ECG) to monitorfor arrhythmias, as they are often present beforesignificant changes in the myocardial contractility.Therefore, authors suggested use of combinationof ECG and echocardiography for diagnosis ofoccult cardiomyopathy.Present study measured, recorded and compareddifferent electrocardiographic parameters like Pwave (width and amplitude) , PR interval, QRScomplexes (width and amplitude), QT interval, STsegment, T wave and Mean Electrical axis , priorto and 30 days after the therapy - both in DCMaffected dogs and in apparently healthy dogs usingthe method as described by Tilley (1992).
Materials and methods
This study was conducted at Chandrika ChimanlalDoshi Cardiovascular Unit for animals –established at the Department of Medicine,Bombay Veterinary College, Parel and TeachingVeterinary Clinical Complex (TVCC), Parel. Thedogs, without any age, breed or sex prejudice,presented at TVCC for various ailments, werescreened and those with the history and complaintof weakness, lethargy, respiratory distress,exercise intolerance, coughing and or cyanosis
were selected. Their body weights were recordedon Libra weighing scale while body condition score(on 1-5 scale) was determined as per Ettinger andFeldman (2005) and body surface area wascalculated as per Withrow and MacEwen (1995).These dogs were then subjected to thoroughclinical examination as per, Fox et al. (1988),Ettinger and Feldman (2005) and Tilley et al.(2008). It comprised of careful cardiac auscultationfor its rate, rhythm while murmurs were graded asper Ettinger and Suter (1970). Auscultation oflungs yielded severity of congestion and bronchialsounds. Pulse was noted for its rate, regularity,amplitude and deficit- if any. Systolic bloodpressure was recorded with the help of “Vet Dop”by Doppler method and Arterial oxygen saturationof haemoglobin (SpO
2) was recorded by using a
finger tip pulse oximeter. Dorso-ventral and lateralthoracic radiographs of these dogs were taken andcardiac index was calculated as per Hamlin (1968)using DV view, while lateral view was used tocalculate vertebral heart size as per Buchanan andBucheler (1995). Electrocardiogram of these dogswas recorded as per the method recommendedby Tilley (1992) and lead II @ 50 mm / sec speedwas used for measuring and calculating the variousparameters. The dogs showing radiographic andelectrocardiographic evidence of cardiomegaly –were further subjected to echocardio-graphicexamination for confirmation of cardiacenlargement as per the method described by Foxet al. (1988), Nyland and Mattoon (1995) andTilley et al. (2008).During the period of study, adapting to the abovementioned protocol and using these diagnosticmodalities, 23 dogs were detected and confirmedto suffer from DCM and constituted “DCMgroup”. These DCM (dilated cardiomyopathy)cases were prescribed a therapy based on therecommendations by Tilley and Smith Jr., 2000and Atkins (2004, 2005, 2007a, 2007b and2007c). It comprised a positive inotropic agent

39
Journal of Canine Development & Research 2013
digoxin @ 0.01 mg/kg bwt. bid, Enalapril @ 0.5mg/kg bwt. od, Furosemide @ 2-4 mg/ kg bwt.bid, orally/im/iv, depending on severity ofpulmonary congestion/ pulmonary oedema alongwith Spironolactone, an aldosterone antagonist @2 mg/ kg bwt orally bid (0.5-2.5 mg/kg bwt ) anda neutraceutical - l- carnitine was administered inall the dogs of DCM group @ 50 mg/Kg BID.(Sarita Devi and Jani, 2009)]. These treatmentcases were followed up at the OPD, TVCC, Pareland requested to report for re-evaluation after aperiod of one month (30 days) by subjecting tothe same tests to assess the treatment response interms of clinical recovery and cardiac performance.However, due to severity of disease, out of 23DCM cases, 12 cases died within a month (Diedgroup of dogs) and only 11 dogs survived(Survived group of dogs). These 11 dogsreported after a period of one month for re-evaluation and underwent same set of testsdescribed earlier. This group of 11 survived dogsafter post therapeutic assessment formed the“After treatment group”.
The “Healthy Control Group”- herein afterreferred to as “Control Group”- comprisedanother 11 apparently healthy dogs of any age,breed or sex – without any complaint of weakness,lethargy, exercise intolerance, respiratory distressor coughing – with their owners’ voluntaryparticipation in this study, were selected andunderwent all these tests referred to at above andserved as Healthy Control Group.
Results and discussion
The range of body weight, body surface area andbody condition score in control group of dogs was12-50kg, 0.53-1.37 m
2 and 2-4 (1-5 scale) with
their corresponding (Mean± SE) as 28.78 ± 2.73kg, 0.94 ± 0.06 m
2 and 3.45 ± 0.21 (1-5 scale)
while the range of body weight, body surface areaand body condition score in DCM group of dogs
were 7-45 kg, 0.37-1.26 m2 and 1-4 (1-5 scale)
with their corresponding (Mean ± SE) as 27.74 ±2.44 kg, 0.90± 0.06 m
2 and 2.83 ± 0.21 (1- 5
scale) respectively. All these three parametersbetween control group and DCM group did notdiffer significantly (P = 0.05).
Electrocardiograms were taken in the dogsbelonging to control and DCM group and theirinterpretation was recorded. In the control group, the rhythm of heart in all the dogs was sinusarrhythmia (slight variation in R-R interval) and asper Tilley (1992), this sinus arrhythmia is a normalfeature of canine heart. The heart rate averaged at114.64 ± 5.26 (mean ± SE) bpm (Table 1). Theaverage width and amplitude of P wave in controlgroup with its corresponding mean ± SE as0.04±0.0 seconds and 0.17 ±0.01 mV while themean PR interval observed with its average (mean± SE) at 0.11±0.00 seconds. The mean width andamplitude of QRS complexes averaged (mean ±SE) as 0.05±0.0 seconds and 1.05±0.11 mVrespectively. The QT interval in this groupmeasured (mean ± SE) 0.22±0.01 seconds. STsegment, in control group dogs did not show anyabnormal deviation (depression /elevation) fromthe base line. T wave in majority of cases wasnegative and normal in configuration (neither tall /peaked or shifting polarity nor biphasic). Meanelectrical axis averaged (mean ± SE) 73.64
0 ±
4.270. The values of the various ECG parameters
in control group viz heart rate, rhythm, P wave,PR interval, QRS complex, ST segment, QTinterval and mean electrical axis – were within thenormal physiological range recommended by Tilley(1992), Fox et al.(1988) and Tilley et al.(2008).Therefore, the electrocardiograms recorded in thedogs of control group were within normal limitsand did not show any electrocardiographicevidence of dilated cardiomyopathy or arrhythmia.At the same time, ECG’s were also recorded inall the 23 dogs in DCM group and their resultswere as under:

40
Journal of Canine Development & Research 2013
Table1: Range and Mean ± SE of Electrocardiographic Parameters in Control and DCM groupsusing Student “t” Test
The rhythm of 5 dogs in the DCM group was atrialfibrillation while other 18 dogs had sinus arrhythmiaas their cardiac rhythm. These electrocardiographicobservations in the present study corroborate withthe findings of DeFransesco (2001), Dukes-McEwan et al. (2003) – who described atrialfibrillation as most common arrhythmia in dogs withDCM. In the present study out of 5 dogs in DCMgroup suffering from atrial fibrillation, 3 were largebreed and other 2 were weighing above 22 Kg.All these dogs suffered from dilatedcardiomyopathy. These observations are inconsonance with Israel (2003) and Tidholm andJonsson (1996) who opined that presence of atrialfibrillation was a probable sign of presence ofdilated cardiomyopathy in large breed dogs.Meurs (2005) described atrial fibrillation as oneof the characteristic arrhythmia associated withdilated cardiomyopathy and it was present in 5cases out of 23 (21.74 %) in this group. The
average heart rate (mean ± SE) recorded in DCMgroup was 143.22 ± 8.35 bpm and it wassignificantly higher (P = 0.05) than in the controlgroup (Table 1). This observation is in agreementwith the findings of Gelzer et al.(2004), whoobserved excessive heart rates in dogs with DCMand attributed it to atrial fibrillation and thatexacerbated the signs CHF. ECG was very muchuseful as a cost effective diagnostic tool in thisproject and helped to identify the cases of rhythmdisturbances and dilated cardiomyopathy. Similarviews were expressed by DeFransesco (2001).The mean width and amplitude of P waves in dogsof DCM group, with their corresponding averages(mean ± SE), was 0.06 ± 0.00 seconds and 0.23± 0.02 mV respectively. The PR interval (alsodescribed as PQ interval) averaged 0.11±0.01seconds (mean ± SE). While comparing theseobservations with control group, it was evidentthat P waves in DCM group were significantly
Sr. No
Parameters Unit Range Control Group
Mean±SE Control Group
Range DCM
Group
Mean±SE DCM
Group
“t” Calcu-lated
D.F.
1 Heart rate bpm 84-150 114.64± 5.26
78-225 143.22± 8.35 2.286*
32
2 P wave (width) sec 0.04-0.04 0.04± 0.00
0.05-0.07 0.06± 0.00 10.677*
32
3 P wave (Amplitude) mV 0.1-0.2 0.17± 0.01
0.15-0.4 0.23± 0.02 2.413*
32
4 PR interval sec 0.09-0.13 0.11± 0.00
0.08-0.17 0.11 ± 0.01 0.219 NS
32
5 QRS complex (width)
sec 0.04-0.05 0.05± 0.00
0.04-0.08 0.06 ± 0.00 5.210*
32
6 QRS complex (Amplitude)
mV 0.6-1.6 1.05± 0.11
1.3-3.8 1.71 ± 0.17 2.639*
32
7 QT interval sec 0.18-0.24 0.22± 0.01
0.16-0.25 0.20 ± 0.01 1.304 NS
32
8 Mean Electrical Axis degree 60-90 73.64± 4.27
60-90 82.83 ± 2.47 1.987 NS
32
“t 32
” Critical/Table value at 5% = 2.037 * Significant at P = 0.05, NS –non significant (P =0.05) Sec - Seconds,

41
Journal of Canine Development & Research 2013
wider and taller (P = 0.05) than in control group(Table 1). However after comparing the data ofDCM group with the standard range recommendedby Tilley (1992), it showed wide P waves- whichimplied enlargement of left atrium. That means allthe dogs in the DCM group had enlarged left atrium.The PR interval in control and DCM groupmeasured (mean ± SE) as 0.11 ± 0.00 and 0.11 ±0.01 seconds. Thus, PR interval in both the groupswas within normal recommended limits and didnot differ significantly (P = 0.05) (Table 1). QRScomplexes in the dogs of DCM group had theiraverage (mean ± SE) for width and amplitude as0.06 ± 0.00 seconds and 1.71 ± 0.17 mV,respectively. Comparing the data between controland DCM group, it clearly demonstrated asignificant increase (P = 0.05) in width andamplitude of QRS complexes (Table 1). Thesevalues were also higher than the standardprescribed values by Tilley (1992). The increasedwidth of QRS complexes, their increasedamplitude, slurring of T wave – implied leftventricular enlargement. The QT interval in controlgroup and DCM group had their respectiveaverages (mean ± SE) as 0.22 ± 0.01 and 0.20 ±0.01 seconds. QT interval in both the groups didnot differ significantly (P = 0.05) (Table 1). Theaverage (mean ± SE) value of Mean Electrical Axis(MEA) in control group and DCM group were73.64
0±4.27
0 and 82.83
0 ± 2.47
0 respectively.
Mean Electrical Axis in both the groups did notdiffer significantly (P = 0.05) (Table 1). ST slurring/ coving was observed in 17/23 cases in DCMgroup while it was not evident in any case of controlgroup. According to Tilley (1992), ST slurringindicated left ventricular enlargement. Thus, thesedogs in DCM group had electrocardiographicevidence of left ventricular enlargement. T wavesin most of the dogs in DCM group were wider ordeeper than control group of dogs. The main causesof alteration in amplitude and width of T waves,according to Tilley (1992), generally indicated
either myocardial hypoxia or electrolyte imbalance.The serum electrolytes (particularly K
+) in the
DCM group of dogs were within normal limits andthus the probable cause of these wider T waveswas myocardial hypoxia secondary to dilatedcardiomyopathy. Collectively, the dogs of DCMgroup had wide P waves and wide QRScomplexes indicating that these dogs had left atrialand or left ventricular enlargement. Theseobservations are in agreement with those of Foxet al. (1988), Tilley (1992) and Bonagura (2001)who observed typical abnormalities with cardiacenlargement in dogs as wide or tall P waves / QRScomplexes and ST wave slurring. Present studydemonstrated and recorded all of thesecharacteristics reported by these authors. Hence,it was concluded that all the dogs included in theDCM group had electrocardiographic evidenceof left atrial and left ventricular enlargement.Comparison of ECG measurements insurvived group and died group of DCMaffected dogs : The mean heart rate at the timeof recording ECG in survived group of dogsmeasured (mean ± SE) 128.73 ± 12.03 bpm.While in died group of dogs, it averaged as156.28± 10.67 bpm. In all, five dogs suffered fromatrial fibrillation and all of them belonged to diedgroup of dogs. There was a non significant increase(P = 0.05)“t
10” Table value at 5% level = 2.228 , sec -
seconds * Significant at P = 0.05, NS –nonsignificant (P = 0.05)
This reduction in heart rate could beattributed to the therapeutic effect of digoxin andis in agreement with the views expressed by Foxet al. (1988), who reported that digitalisglycosides helped slowing of AV nodal conductionand prolonged the AV nodal refractory period. Thecomparable homologous data was not availablefor comparison in the referred literature.The mean PR interval in the Survived group of
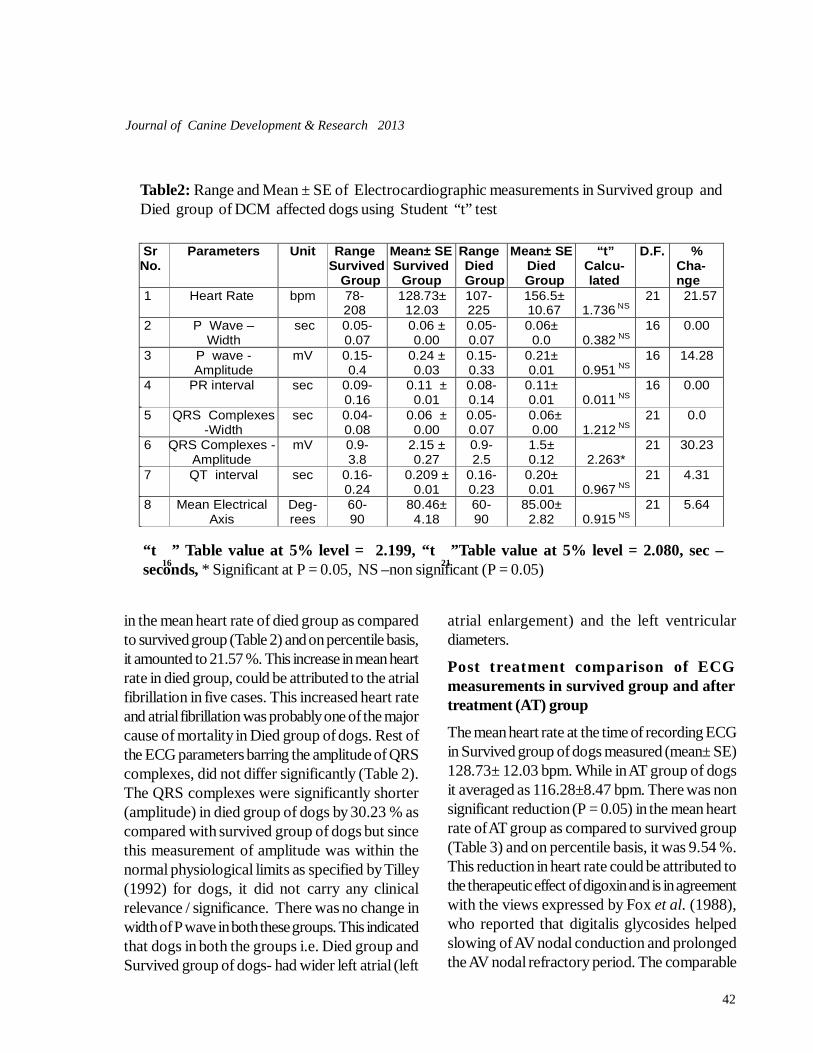
42
Journal of Canine Development & Research 2013
Table2: Range and Mean ± SE of Electrocardiographic measurements in Survived group andDied group of DCM affected dogs using Student “t” test
in the mean heart rate of died group as comparedto survived group (Table 2) and on percentile basis,it amounted to 21.57 %. This increase in mean heartrate in died group, could be attributed to the atrialfibrillation in five cases. This increased heart rateand atrial fibrillation was probably one of the majorcause of mortality in Died group of dogs. Rest ofthe ECG parameters barring the amplitude of QRScomplexes, did not differ significantly (Table 2).The QRS complexes were significantly shorter(amplitude) in died group of dogs by 30.23 % ascompared with survived group of dogs but sincethis measurement of amplitude was within thenormal physiological limits as specified by Tilley(1992) for dogs, it did not carry any clinicalrelevance / significance. There was no change inwidth of P wave in both these groups. This indicatedthat dogs in both the groups i.e. Died group andSurvived group of dogs- had wider left atrial (left
atrial enlargement) and the left ventriculardiameters.
Post treatment comparison of ECGmeasurements in survived group and aftertreatment (AT) group
The mean heart rate at the time of recording ECGin Survived group of dogs measured (mean± SE)128.73± 12.03 bpm. While in AT group of dogsit averaged as 116.28±8.47 bpm. There was nonsignificant reduction (P = 0.05) in the mean heartrate of AT group as compared to survived group(Table 3) and on percentile basis, it was 9.54 %.This reduction in heart rate could be attributed tothe therapeutic effect of digoxin and is in agreementwith the views expressed by Fox et al. (1988),who reported that digitalis glycosides helpedslowing of AV nodal conduction and prolongedthe AV nodal refractory period. The comparable
“t 16
” Table value at 5% level = 2.199, “t 21
”Table value at 5% level = 2.080, sec –seconds, * Significant at P = 0.05, NS –non significant (P = 0.05)
Sr No.
Parameters Unit Range Survived
Group
Mean± SE Survived
Group
Range Died Group
Mean± SE Died Group
“t” Calcu-lated
D.F.
% Cha- nge
1 Heart Rate bpm 78- 208
128.73± 12.03
107- 225
156.5± 10.67 1.736 NS
21 21.57
2 P Wave – Width
sec 0.05-0.07
0.06 ± 0.00
0.05-0.07
0.06± 0.0 0.382 NS
16 0.00
3 P wave - Amplitude
mV 0.15- 0.4
0.24 ± 0.03
0.15- 0.33
0.21± 0.01 0.951 NS
16 14.28
4 PR interval sec 0.09-0.16
0.11 ± 0.01
0.08-0.14
0.11± 0.01 0.011 NS
16 0.00
5 QRS Complexes -Width
sec 0.04-0.08
0.06 ± 0.00
0.05-0.07
0.06± 0.00 1.212 NS
21 0.0
6 QRS Complexes - Amplitude
mV 0.9- 3.8
2.15 ± 0.27
0.9- 2.5
1.5± 0.12 2.263*
21 30.23
7 QT interval sec 0.16-0.24
0.209 ± 0.01
0.16-0.23
0.20± 0.01
0.967 NS
21 4.31
8 Mean Electrical Axis
Deg-rees
60- 90
80.46± 4.18
60- 90
85.00± 2.82 0.915 NS
21 5.64
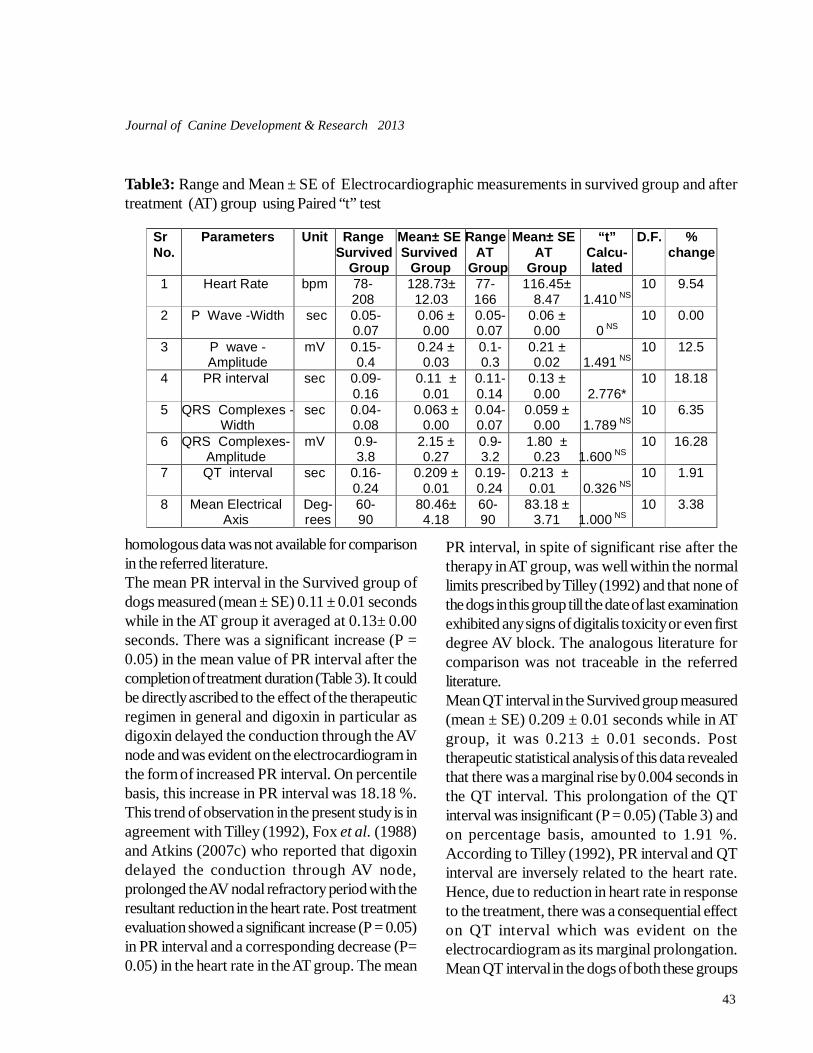
43
Journal of Canine Development & Research 2013
Sr No.
Parameters Unit Range Survived
Group
Mean± SE Survived
Group
Range AT
Group
Mean± SE AT
Group
“t” Calcu- lated
D.F. % change
1 Heart Rate bpm 78- 208
128.73± 12.03
77- 166
116.45± 8.47 1.410 NS
10 9.54
2 P Wave -Width sec
0.05- 0.07
0.06 ± 0.00
0.05-0.07
0.06 ± 0.00 0 NS
10 0.00
3 P wave - Amplitude
mV 0.15- 0.4
0.24 ± 0.03
0.1- 0.3
0.21 ± 0.02 1.491 NS
10 12.5
4 PR interval sec 0.09- 0.16
0.11 ± 0.01
0.11-0.14
0.13 ± 0.00 2.776*
10 18.18
5 QRS Complexes -Width
sec 0.04- 0.08
0.063 ± 0.00
0.04-0.07
0.059 ± 0.00 1.789 NS
10 6.35
6 QRS Complexes-Amplitude
mV 0.9- 3.8
2.15 ± 0.27
0.9- 3.2
1.80 ± 0.23 1.600 NS
10 16.28
7 QT interval sec 0.16- 0.24
0.209 ± 0.01
0.19-0.24
0.213 ± 0.01
0.326 NS
10 1.91
8 Mean Electrical Axis
Deg-rees
60- 90
80.46± 4.18
60- 90
83.18 ± 3.71 1.000 NS
10 3.38
Table3: Range and Mean ± SE of Electrocardiographic measurements in survived group and aftertreatment (AT) group using Paired “t” test
homologous data was not available for comparisonin the referred literature.The mean PR interval in the Survived group ofdogs measured (mean ± SE) 0.11 ± 0.01 secondswhile in the AT group it averaged at 0.13± 0.00seconds. There was a significant increase (P =0.05) in the mean value of PR interval after thecompletion of treatment duration (Table 3). It couldbe directly ascribed to the effect of the therapeuticregimen in general and digoxin in particular asdigoxin delayed the conduction through the AVnode and was evident on the electrocardiogram inthe form of increased PR interval. On percentilebasis, this increase in PR interval was 18.18 %.This trend of observation in the present study is inagreement with Tilley (1992), Fox et al. (1988)and Atkins (2007c) who reported that digoxindelayed the conduction through AV node,prolonged the AV nodal refractory period with theresultant reduction in the heart rate. Post treatmentevaluation showed a significant increase (P = 0.05)in PR interval and a corresponding decrease (P=0.05) in the heart rate in the AT group. The mean
PR interval, in spite of significant rise after thetherapy in AT group, was well within the normallimits prescribed by Tilley (1992) and that none ofthe dogs in this group till the date of last examinationexhibited any signs of digitalis toxicity or even firstdegree AV block. The analogous literature forcomparison was not traceable in the referredliterature.Mean QT interval in the Survived group measured(mean ± SE) 0.209 ± 0.01 seconds while in ATgroup, it was 0.213 ± 0.01 seconds. Posttherapeutic statistical analysis of this data revealedthat there was a marginal rise by 0.004 seconds inthe QT interval. This prolongation of the QTinterval was insignificant (P = 0.05) (Table 3) andon percentage basis, amounted to 1.91 %.According to Tilley (1992), PR interval and QTinterval are inversely related to the heart rate.Hence, due to reduction in heart rate in responseto the treatment, there was a consequential effecton QT interval which was evident on theelectrocardiogram as its marginal prolongation.Mean QT interval in the dogs of both these groups

44
Journal of Canine Development & Research 2013
were within the normal physiological limitspublished by Tilley (1992). Hence this QTprolongation also improved the cardiac output.Similar type of observations by other workers onthis topic, for comparison, was unavailable in thereferred literature.Therapeutic regimen for 30 days, as expected too,did not bring about any significant alteration / change- beyond the physiological limits as specified byTilley (1992), in the other ECG parameters like Pwave (width and amplitude), QRS complexes(width and amplitude), mean electrical axis – whencompared in these two groups (Table 3).Analogous observations by other workers on thistopic, for comparison, were unavailable in thereferred literature.
ReferencesAtkins,C.E. (2004). Therapeutic advances in the man-
agement of heart diseases: An overview. A Dis-trict of Columbia Academy of Veteriary Medi-cine, Lecture notes , Pp -1-18
Atkins , C. E. (2005). Canine Heart failure – Current Con-cepts : Strengths and weaknesses. Proceedingof the North Am. Vet. Conference Jan. 8th -12th ,Orlando, Florida. Reprinted in the IVIS websitewith the permission of the NAVC. http://www.ivis.org
Atkins, C. E. (2007a) Angiotensin Converting-EnzymeInhibitors and the Kidney.32th WSAVA Con-gress, Sydney, Australia , August 19th – 23rd .
Atkins, C. E. (2007b) An approach to asymptomatic ac-quired heart disease in dogs. Proceedings ofthe WSAVA Congress, Sydney, Australia.
Atkins, C. E. (2007c) Therapeutic Advances in the man-agement of heart diseases. An Overview. Pro-ceedings of the WSAVA Congress, Sydney,Australia.
Bolton, G. R. (1975) In “Hand Book of Canine Electrocar-diography”. WB Saunders Company,Philadelphia,USA. Pp 112, 113.
Bonagura, J. (2001) Cardiomyopathy. 26th World SmallAnimal Association World Congress –Vancouver.
Buchanan,J.W. and J. Bucheler, (1995) Vertebral scalesystem to measure canine heart size inradiographs.J.Am.Vet Med.Assoc 206 : 194-199.
DeFransesco, T. (2001) Advanced discussions in the di-agnosis of heart failure. In a publication on“Advances in the management of cardiac pa-tients” Sponsored / Published by Waltham andMerial ,USA. Pp : 3 – 11
Dukes-McEwan J., M. Borgarelli, A. Tidholm, A. C.Vollmar and J. Häggström (2003) ProposedGuidelines for the Diagnosis of Canine Idio-pathic Dilated Cardiomyopathy. J. Vet. Cardiol-ogy 5 : 2
Ettinger, S. J. and P. F. Suter (1970) Canine Cardiology,W. B. Saunders Company , PA, USA. Pp 14, 29,65.
Ettinger, S. J. and E. C. Feldman (2005) Textbook of Vet-erinary Internal Medicine (Diseases of Dog andCat), 6th edn. W.B Saunders Publications, Phila-delphia.
Fox P. R., D. Sisson and N. S. Moise (1988) In “Text Bookof Canine and Feline Myocardial diseases ofDogs” WB Saunders Company,PA. USA..Pp230,356-378,.
Gelzer A. R. M., M. S. Kraus N. S. and Moise (2004)Assessment of antiarrhythmic drug efficacy tocontrol heart rate in dogs with atrial fibrillationusing 24-hour ambulatory electrocardiographic(Holter) recordings. abstract 14th ECVIM-CACongress, reprinted J. Vet. Int. Med.. 18 (5) :779.
Hamlin, R. L. (1968) Analysis of the cardiac silhouette indorsoventral radiographs from dogs with heartdiseases. J.Am.Vet.Med.Assoc. 153(11):1446-1452.
Israël, N. V. (2003) Idiopathic dilated cardiomyopathy inthe dog: diagnostic approach. UK VET : 8 : 1 –5.
Meurs, K. M. (2005) Canine Dilated Cardiomyopathy –Insights In to Diagnosis and Management. Pro-ceeding of the. North Am. Vet. Conf. Jan. 8th –12th , 2005, Orlando, Florida.
Nyland, J. S. and T. G. Mattoon (1995, copy right 2000)Small Animal Diagnostic Ultrasound, 2nd Edi-tion, Saunders, Philadelphia, PA, 19106. Pp 354-379, 380, 393-397, 406.
Oyama, M.A.; D. Sisson and P.F.Solter (2007) Prospec-tive screening for occult cardiomyo-pathy indogs by measurement of plasma atrial natriureticpeptide, B-type natriuretic peptide,
and cardiac troponin-I concentrations. AJVR, Vol 68, No.1, January 2007, Pp. 42-47.
Sarita Devi R. G. and A. Jani (2009) Review on NutritionalManagement of Cardiac Disorders in Canines.

45
Journal of Canine Development & Research 2013
Vet. World 12 (2) : 482 – 485.Tidholm, A and L. Jonsson (1996) Dilated cardiomyopa-
thy in Newfoundland: A study of 37 cases (1983-1994). J. Am. Hosp. Assoc. 32 : 465.
Tilley, L. P. (1992) Essentials of canine and feline Electro-cardiography (Interpretation and treatment).Edition, Lea and Febiger (Philadelphia and Lon-don). Pp : 146 and 147.
Tilley, L. P. and F. W. K. Smith Jr. (2000) Cardiomyopathy– Dilated – Dogs 5 minutes Veterinary Consult(Canine and Feline). 2nd Edition, Lippincott
Williams and Wilkins, 351 West Camden Street,Baltimore, Maryland USA. Pp. : 476,522 –523.
Tilley, L. P., F. W. K. Smith (Jr), M. A. Oyama and M. M.Sleeper (2008) Manual of Canine and FelineCardiology. 4th Edition, ISBN: 978-1-4160-2398-2 Saunders (Elsevier) Saint Louis , Missouri.USA. Pp.: 52, 90,91, 115,139 – 149, 180, 277, 296and 297.
Withrow, S. J. and E. G. MacEwen (1995) Small AnimalClinical Oncology, 2nd edn. WB Saunders Com-pany, Philadelphia, PA, USA.
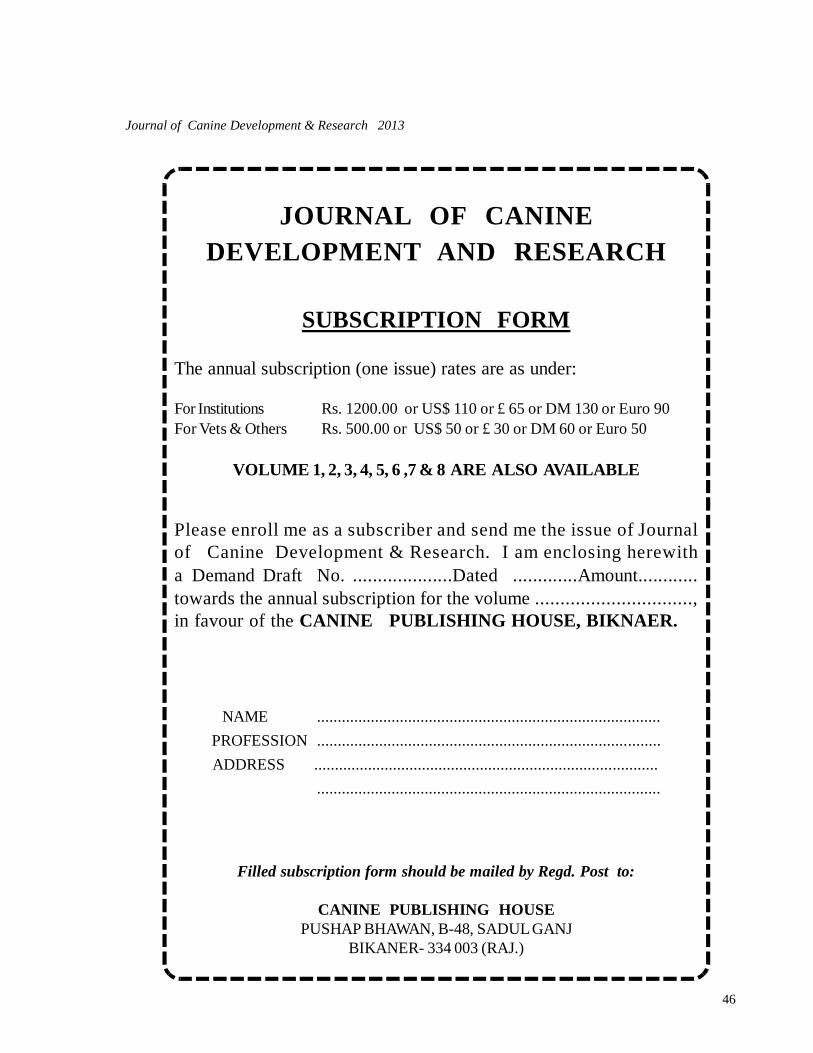
46
Journal of Canine Development & Research 2013
JOURNAL OF CANINEDEVELOPMENT AND RESEARCH
SUBSCRIPTION FORM
The annual subscription (one issue) rates are as under:
For Institutions Rs. 1200.00 or US$ 110 or £ 65 or DM 130 or Euro 90For Vets & Others Rs. 500.00 or US$ 50 or £ 30 or DM 60 or Euro 50
VOLUME 1, 2, 3, 4, 5, 6 ,7 & 8 ARE ALSO AVAILABLE
Please enroll me as a subscriber and send me the issue of Journalof Canine Development & Research. I am enclosing herewitha Demand Draft No. ....................Dated .............Amount............towards the annual subscription for the volume ...............................,in favour of the CANINE PUBLISHING HOUSE, BIKNAER.
NAME ................................................................................... PROFESSION ................................................................................... ADDRESS ...................................................................................
...................................................................................
Filled subscription form should be mailed by Regd. Post to:
CANINE PUBLISHING HOUSEPUSHAP BHAWAN, B-48, SADUL GANJ
BIKANER- 334 003 (RAJ.)

47
Journal of Canine Development & Research 2013
RESEARCH ARTICLEHEMATO-BIOCHEMICAL ALTERATIONS IN CANINE PYOMETRA*Varun Bassessar1; Yamini Verma2 and Madhu Swamy3
Department of Veterinary PathologyCollege of Veterinary Science and Animal Husbandry,NDVSU , Jabalpur-482 001 (M.P.)
1Ph. D Scholar 2Associate Professor 3Professor and Head*Corresponding author e-mail : [email protected]
A B S T R A C T
A study was conducted to investigate the hemato-biochemicalalterations in 20 pyometric dogs. Pyometra was found in animalsbetween age group of 3-10 years; however, the maximum casesof pyometra were noticed at 4 years of age. The results ofhaematological studies comprising haemoglobin estimation (HG,g/dl), total erythrocyte count (TEC, millions/µl), Packed cellvolume (PCV, %), Mean corpuscular haemoglobin (MCH,picogram), Mean corpuscular haemoglobin concentration(MCHC, g/dl), Total leukocyte count (TLC, thousands/µl) anddifferential leukocyte count (DLC) revealed marked anaemia,leukocytosis, neutrophilia and elevated number of band cells.However, there were significant elevation of serum ALT, AST,ALP, bilirubin and BUN but decrease in protein and albuminconcentration was observed.
Key words :CanineCanine pyometraHemato-biochemical
A R T I C L E H I S T O R Y
Received : April 28, 2013Revised : July 12, 2013Accepted : July 22, 2013
Canine pyometra is a clinical syndrome thataffects adult intact bitches, causing a variety
of clinical and pathological signs of genital andsystemic disease (Sahoo et al., 2005). It is ofparticular importance to the veterinary practitioner,since early recognition, diagnosis and appropriateintervention is required to avoid fatalconsequences.
Materials and methods
The work was conducted in Department ofVeterinary Pathology and Teaching VeterinaryClinical Service Complex (TVCSC), College of
Veterinary Science and Animal Husbandry, NanajiDeshmukh Veterinary Science University, Jabalpur,Madhya Pradesh. Twenty female dogs above 3years of age suspected for pyometra, registeredat TVCSC, during the study period of 8 months(Jan - Aug 09) were included in the study. Inaddition, six clinically healthy dogs undergoingelective ovariohysterectomy were taken as control.Blood for a complete haematological examinationand biochemical examination of relevantparameters was collected from all the pyometraaffected bitches. In addition to this, blood sampleswere also obtained from 5 clinically healthy bitches
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 47-51

48
Journal of Canine Development & Research 2013
undergoing elective ovariohysterectomy to serveas control. A complete blood count was done usingthe automated blood analyzer (Abacus). Inaddition, blood smears were prepared, stainedand were examined for differential leukocyte countand presence of band cells. The analysis of alaninetransferase (ALT) and aspartate transferase (AST)alkaline phosphatase (ALP) total protein (TP),albumin (ALB), creatinine (CRE), blood ureanitrogen (BUN) was done on blood ChemistrySemi Auto Analyzer (CHEM-5 PLUS).
Results and discussion
Pyometra was found in animals between age groupof 3-10 years, however, the maximum cases ofpyometra were noticed at 4 years. Chastain et al.(1999) opined that nulliparous bitches and bitchesof more than 4 years of age seem to bepredisposed to pyometra. In a study conductedby Fakuda (2001) in a colony of Beagles, 15.2%of the bitches more than 4 yrs. of age were affected,whereas the mean age was 9.4±0.4 years at thetime of clinical signs. In a group of 192 bitchestreated medically for pyometra, the mean agereported was 2.4 years by Feldman and Nelson(2004). Thus, our observations coincide with thoseof earlier workers.
Breed wise incidence was recorded as highest inPomeranians (10), followed by German Shepherd(8) , Labrador (1) and Daschound (1). Earlier,Smith (2006) reported that Rottweiler, SaintBernard, Chow Chow, Golden Retriever,Miniature Schnauzer, Irish terrier, Airedale Terrier,Cavelier King, Charles Spaniel, Rough Collie andBernese Mountain dogs to be predisposed topyometra. Egenvalt et al. (2001) claimed thatbreeds with a low risk of pyometra includeDrevers, German Shepard, Daschunds andSwedish Hounds. The sample size in the presentinvestigations is too low to draw any suchconclusions.The results of haematological studies comprisinghaemoglobin estimation (HG, g/dl), totalerythrocyte count (TEC, millions/µl), Packed cellvolume (PCV, %), Mean corpuscular haemoglobin(MCH, picogram), Mean corpuscularhaemoglobin concentration (MCHC, g/dl), Totalleukocyte count (TLC, thousands/µl) anddifferential leukocyte count (DLC) revealedmarked anaemia, leukocytosis, neutrophilia andmore numbers of band cells in the peripheral bloodsmear (Table-1 and Figure -1).
Figure 1: Blood smear from pyometric dog showing band cells. Leishman’s stain × 1000.
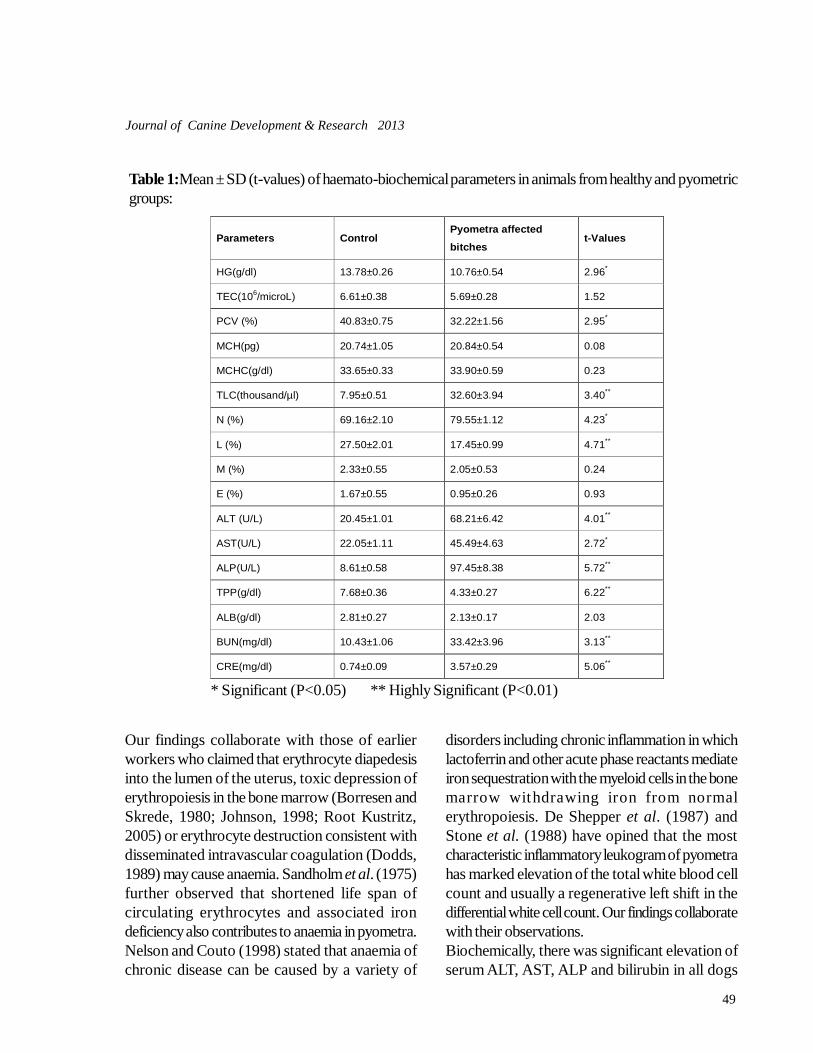
49
Journal of Canine Development & Research 2013
Our findings collaborate with those of earlierworkers who claimed that erythrocyte diapedesisinto the lumen of the uterus, toxic depression oferythropoiesis in the bone marrow (Borresen andSkrede, 1980; Johnson, 1998; Root Kustritz,2005) or erythrocyte destruction consistent withdisseminated intravascular coagulation (Dodds,1989) may cause anaemia. Sandholm et al. (1975)further observed that shortened life span ofcirculating erythrocytes and associated irondeficiency also contributes to anaemia in pyometra.Nelson and Couto (1998) stated that anaemia ofchronic disease can be caused by a variety of
disorders including chronic inflammation in whichlactoferrin and other acute phase reactants mediateiron sequestration with the myeloid cells in the bonemarrow withdrawing iron from normalerythropoiesis. De Shepper et al. (1987) andStone et al. (1988) have opined that the mostcharacteristic inflammatory leukogram of pyometrahas marked elevation of the total white blood cellcount and usually a regenerative left shift in thedifferential white cell count. Our findings collaboratewith their observations.Biochemically, there was significant elevation ofserum ALT, AST, ALP and bilirubin in all dogs
Parameters Control Pyometra affected
bitches t-Values
HG(g/dl) 13.78±0.26 10.76±0.54 2.96*
TEC(106/microL) 6.61±0.38 5.69±0.28 1.52
PCV (%) 40.83±0.75 32.22±1.56 2.95*
MCH(pg) 20.74±1.05 20.84±0.54 0.08
MCHC(g/dl) 33.65±0.33 33.90±0.59 0.23
TLC(thousand/µl) 7.95±0.51 32.60±3.94 3.40**
N (%) 69.16±2.10 79.55±1.12 4.23*
L (%) 27.50±2.01 17.45±0.99 4.71**
M (%) 2.33±0.55 2.05±0.53 0.24
E (%) 1.67±0.55 0.95±0.26 0.93
ALT (U/L) 20.45±1.01 68.21±6.42 4.01**
AST(U/L) 22.05±1.11 45.49±4.63 2.72*
ALP(U/L) 8.61±0.58 97.45±8.38 5.72**
TPP(g/dl) 7.68±0.36 4.33±0.27 6.22**
ALB(g/dl) 2.81±0.27 2.13±0.17 2.03
BUN(mg/dl) 10.43±1.06 33.42±3.96 3.13**
CRE(mg/dl) 0.74±0.09 3.57±0.29 5.06**
Table 1:Mean ± SD (t-values) of haemato-biochemical parameters in animals from healthy and pyometricgroups:
* Significant (P<0.05) ** Highly Significant (P<0.01)

50
Journal of Canine Development & Research 2013
with pyometra. Hepatocellular damage caused bysepticaemia and hepatic circulation and cellularhypoxia in dehydrated bitches and intrahepaticcholestasis could be attributed as the cause forrise in these parameters. Similar findings have beenreported by earlier workers (Borresen andSkrede, 1980; Wheaton et al., 1989; Ravishankaret al., 2004; Nath et al., 2009 and Sahoo et al.,2012). Fransson et al. (1997) reported a highserum level of ALP during haemato-biochemicalstudies of pyometra dogs similar to our findings.Sodikoff et al. (1995) have stated that majorcauses of increased serum ALP activity in dogsare cholestatic liver disease and excessiveexogenous corticosteroids.A constant finding in all the cases with pyometrawas a decrease in protein and albuminconcentration in serum. These again increased andwere comparable to normal values after treatmentor ovariohystertectomy of animals. Borresen andSkrede (1980) have opined that plasma proteinchanges in pyometra dogs are the result of acutephase reactions. Fantoni et al. (1999) have statedthat sepsis and endotoxemia cause increasedvascular permeability and contribute to loss ofprotein. Earlier, Ravishankar et al. (2004) havereported a hypoalbuminemia andhyperglobulinemia in cases of pyometra with totalplasma protein concentration remaining unchanged.However, in our studies we observed a decreasein total plasma protein and albumin in all dogs withpyometra which may be attributed to theirdehydrated status.Increased blood urea nitrogen levels in animalssuffering from pyometra were observed whichdecreased after treatment and as condition of theanimal improved. Similar to present findingsJayathangaraj et al. (1994); Ravishankar et al.(2004) and Sahoo et al. (2012) recordedincreased BUN levels in dogs with pyometra.However, Renton et al. (1993) and Troxel et al.(2002) recorded normal BUN levels in the cases
of pyometra. Increased BUN level can have pre-renal, renal or post-renal causes. Sodikoff (1995)has stressed that urinalysis with determination ofspecific gravity and evaluation of sediment can beused to differentiate pre-renal azotemia fromazotemia of renal origin. Isothenuria (specificgravity <1.010±0.002) suggests a renal causewhile a higher urine specific gravity suggests pre-renal or post renal cause. A rise in serum creatininevalue was recorded in all cases of pyometra whichis in agreement with the findings of Stone et al.(1988) and Ravishankar et al. (2004). Theworkers have postulated that elevated serum ureanitrogen and creatinine levels might be due toorganic tissue destruction observed in pyometra.Thus, all the dogs with pyometra showed significantabnormalities in blood indicative of liver or kidneydysfunction associated with pyometra.
ReferencesBorressen, B. and Skrede, S. (1980). Pyometra in the dog-
a pathophysiological investigation V. the pres-ence of intrahepatic cholestasis and an “acutephase reaction”. Nord. Vet. Med., 32(9): 378-386.
Chastain, C.B., Panciera, D. and Waters, C. (1999). Asso-ciations between age, parity, hormonal therapyand breed, and pyometra in Finnish dogs. SmallAnim. Endocrinol., 9: 8.
De Schepper, J., Stock, J.V. and Capiau, E. (1987). Anaemiaand leucocytosis in one hundred and twelvedogs with pyometra. J. Small Anim. Pract.,28(2): 137-145.
Doods, W.J. (1989). Haemostasis. In: J.J. Kaneko (ed.)Clinical Biochemistry of Domestic Animals. 4th
edn., Publ., Academic Press, San Diego, pp. 274-315.
Egenvalt, A., Hagman, R., Bonnet, B., Hedhammar, A.,Olsson, P. and Lagerstedt, A.S. (2001). Breedrisk of pyometra in insured dogs in Sweden. J.Vet. Intl. Med., 15: 530–538.
Fakuda, S. (2001). Incidence of pyometra in colony- raisedBeagle dogs. Exp. Anim., 50: 325-328.
Fantoni, D.T., Junior, J.O.A., Futema, F., Cortopassi, S.R.,Miglati, E.R., Faustino, M. and De Oliveira, C.M.(1999). Intravenous abministration of hypertonicsodium chloride solution with dextran or iso-

51
Journal of Canine Development & Research 2013
tonic sodium chloride solution for treatment ofseptic shock secondary to pyometra in dogs. J.Am. Vet. Med. Assoc., 215(9): 1283-1287.
Feldman, E.C. and Nelson, R.W. (2004). Cystic endome-trial hyperplasia/pyometra complex. In: KerseyR, editor, Canine and Feline endocrinology andreproduction. W.B. Saunders Co., pp 852- 867.
Fransson, B., Lagerstedt, A.S. and Jonsson, P. (1997).Bacteriological findings, blood chemistry pro-file and plasma endotoxin levels in bitches withpyometra or other uterine disease. J. Vet. Med.A. Physiol. Pathol. Clin. Med., 44(7): 417-426.
Jayathangaraj, M.G., Prathaban, S., Ayyappan, S. andDhanapalan, P. (1994). Unusual case of pyome-tra in a bitch: A case review. Vet. J. 71: 496-498.
Johnson, C.A. (1998). Cystic endometrial hyperplasia andpyometra, In: R.W. Nelson and C.G. Couto (ed.)Small Animal Internal Medicine. 2nd edn., Publ.,Mosby, St. Louis, pp 870-873.
Nath, K., Tiwari, S.K., Sharda, R., Garg, S. and kalim, M.O.(2009). Pyometra induced biochemical changesin bitches. Indian Vet. J., 86: 853-855.
Nelson, R.W. and Couto, I.T. (1998). Pyometra. Vet. Clin.N. Am., 16: 561-576.
Ravishankar, N., Manoharmurli, B., Balchandran, C.,Sumitra, M., Manikandan, P. andPuvanakrishnan, R. (2004). Haemato-biochemi-cal alterations and pathological changes in ca-nine pyometra. Indian J. Vet. Pathol., 28(1): 14-17.
Renton, J.P., Boyd, J.S. and Harvey, M.J.A. (1993). Ob-servations on the treatment and diagnosis ofopen pyometra in the bitch. J. Repord. Fertil.Suppl., 47: 465-469.
Root-Kustritz, M.V. (2005). Cystic endometrial hyperpla-sia and pyometra. In: S.G. Ettinger and E.C.Feldman (ed.) Textbook of Veterinary InternalMedicine. 6th edn., Pubu., Elsevier Saunders,St. Louis, pp 1676-1680.
Sahoo, M., Panda, S.K., Sahoo, N.R., Mohapatra, H.K.and Nath, I. (2005). A clinico-pathological in-vestigation on canine pyometra. Indian J. Vet.Pathol., 29(2): 54.
Sandhlom, M., Vasenius, H. and Kivisto, A.K. (1975).Pathogenesis of canine pyometra. J. Amer. Vet.Med. Assoc., 167: 1006-1010.
Smith, F.O. (2006). Canine pyometra. Theriogenology.66: 610 - 612.
Sodikoff, C.H. (1995). Laboratory Profiles of Small Ani-mal Diseases: A guide to Laboratory Diagno-sis. 2nd edn. Publ., Mosby-year Book, pp 435.
Stone, E.A., Littman, M.P., Robertson, J.L. and Bovee,K.C. (1988). Renal dysfunction with pyometra.J. Vet. Med. Ass., 193: 457-64.
Stone, E.A., Littman, M.P., Robertson, J.L. and Bovee,K.C. (1988). Renal dysfunction with pyometra.J. Vet. Med. Ass., 193: 457-64.
Troxel, M.T., Cornetta, A.M., Pastor, K.F., Hartzband, L.E.and Besancon, M.F. (2002). Severe hematome-tra in a dog with cystic endometrial hyperpla-sia/pyometra complex. J.Am. Anim. Hosp.Assoc., 38: 85-89.
Wheaton, L.G., Johnson, A.L., Parkar, A.J. and Kneller,S.K. (1989). Results and complications of sur-gical treatment of pyometra: A review of 80cases. J. Am. Anim. Hosp. Assoc., 25: 563-568.
52
Journal of Canine Development & Research 2013
JOURNAL OF CANINEDEVELOPMENT AND RESEARCH
SUBSCRIPTION FORM
The annual subscription (one issue) rates are as under:
For Institutions Rs. 1200.00 or US$ 110 or £ 65 or DM 130 or Euro 90For Vets & Others Rs. 500.00 or US$ 50 or £ 30 or DM 60 or Euro 50
VOLUME 1, 2, 3, 4, 5, 6 ,7 & 8 ARE ALSO AVAILABLE
Please enroll me as a subscriber and send me the issue of Journalof Canine Development & Research. I am enclosing herewitha Demand Draft No. ....................Dated .............Amount............towards the annual subscription for the volume ...............................,in favour of the CANINE PUBLISHING HOUSE, BIKNAER.
NAME ................................................................................... PROFESSION ................................................................................... ADDRESS ...................................................................................
...................................................................................
Filled subscription form should be mailed by Regd. Post to:
CANINE PUBLISHING HOUSEPUSHAP BHAWAN, B-48, SADUL GANJ
BIKANER- 334 003 (RAJ.)

53
Journal of Canine Development & Research 2013
RESEARCH ARTICLE
Journal of Canine Development & ResearchISSN : 0973-3272 Accessible at : www.jcdrindia.com
VERTEBRAL HEART SCORE IN SAINT BERNARD BREED OF DOGS*Anil Ahuja1, Mamta Daga2, Ankita Sharma2, Jitender Bargujar3, D.K.Bihani4, Pradeep Abusuria3, Mahender Tanwar5
and Anil Langer3
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege Of Veterinary and Animal Science, RAJUVAS, Bikaner -334 001 (Rajasthan)
1Professor and Head 2PG Scholar 3Teaching Associate 4Professor 5Ph.D Scholar,Deptt. of S & R*Corresponding author E-mail – [email protected]
A B S T R A C T
Key words :Saint BernardThoracic radiographyVertebral heart score
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
Radiographic interpretation for heart can bedone by number of ways such as gross
examination or by using different measurementslike cardiothoracic ratio, relationship with inter-costal spaces or vertebral heart score (Mudasiret al., 2013). Earlier cardiothoracic ratio and aspecification of 2.5 to 3.5 inter-costal spaces (witha deep and wide thorax, respectively) had beenintroduced for dogs using lateral radiographicviews, but variations in the axis of the heart and itssilhoutte, thoracic conformation, respiratory phase,rib superimposition and imprecise measurementpoints (Gulanber et al., 2005) were majorlimitations in its use. These techniques have beensupplemented by vertebral heart score system, inwhich the heart length and width on the thoracicradiograph is compared with the vertebral length.
Gulanber et al.(2005) also suggested that vertebralheart score may be useful in assessing the changein size of the heart in a patient over time as there isgood correlation between the growth of differentvisceral organs and vertebral body length.Knowledge of inter-breed variation in the thoracicconformation and selection of proper referencevalue may further enhance the value of vertebralheart score technique in diagnosis of cardiacenlargement in dogs, evaluate clinical response totherapy or progression of disease (Root and Bahr,2002). Lamb et al. (2001) suggested the use ofbreed-specific VHS values to get high specificityin diagnosis of cardiomegaly. Keeping in view theimportance of breed specific VHS, present studywas palnned to standardize the VHS in SaintBernard breed of dog.
Present communication describes the vertebral heart score(VHS) in Saint Bernard breed of dogs in healthy state, as goodrelations are known to exist between vertebrae length and heartsize. Cardiac measurements are more useful when the normalrange is breed and sex specific and relatively narrow. Resultshowed a VHS of 10.70 ± 0.18 vertebrae with distribution rangeof 9.24 to 11.80 vertebrae in this breed. The longitudinal axiswas 6.11± 0.13, while short axis was 4.61± 0.13 vertebrae.
Vol (9) 53-55

54
Journal of Canine Development & Research 2013
Materials and methods
Six healthy Saint Bernard dogs, irrespective of sexwith mean age of 2.6 years were selected afterclinical (physical examination and auscultation) andlaboratory evaluation (haemato-biochemical andurinalysis). Left lateral thoracic radiographs weretaken during inspiration as suggested by Gulanberet al. (2005) in least stress condition without useof any anesthetic agents (Srivastava et al., 2011).The long axis B of the heart, reflecting the combinedsize of the left atrium and left ventricle wasmeasured from the ventral border of the left mainstem bronchus to the cardiac apex. The short axisA was measured at the widest point of the cardiacimage on a line perpendicular to the long axis atthe level of the caudal vena cava (Buchanan andBucheler, 1995). Measurements were recordedin centimeters for statistical analyses. Long andshort axis measurements were compared to thevertebrae starting at the cranial edge of T4 tocaudally and result expressed in units of vertebrallengths was obtained for each axis (fig-1). Themeasurements of the long and short axes wererecorded in terms of the numbers of vertebraecovered and the two numbers were then addedtogether to give the value of the VHS and data areexpressed as mean ± SE.
Results and discussion
The vertebral heart score in clinically healthy SaintBernard dogs was 10.70 ± 0.18 vertebrae withdistribution range of 9.24 to 11.80 vertebrae. Thelongitudinal axis was 6.11± 0.13, while short axiswas 4.61± 0.13 vertebrae. The recognition ofinterbreed variations of cardiac dimensions has ledto the development of breed-specific ranges forechocardiography in dogs (Nakayama et al.,2001), in the same direction Lamb et al. (2001)published breed-specific VHS ranges for somepopular breeds of dogs like Doberman, Labradorretriever and Boxer etc. In present study the rangeof VHS for Saint Bernard dog is 10.70 ± 0.18
vertebrae, which is found closer to Labradorretriever having VHS score of 10.8 ± 0.6 vertebrae(Lamb et al., 2001), but was slightly above thanVHS in initial study of Buchanan and Bucheler(1995), who reported the mean VHS of 9.7 ±0.5 vertebrae. Distribution of VHS range was 9.24to 11.80 vertebrae; this finding was in agreementwith Buchanan and Bucheler (1995), who reporteda wide clinical range of 8.5 to 10.5 vertebraeirrespective of breed. More researches in thisdirection are required as cardiac measurementsare likely to be useful only when the normal rangeis relatively narrow (Lamb et al., 2000). Sleeperand Buchanan (2001) recommended that sexshould be taken into account when evaluating thepossibility of cardiomegaly on the basis of theVHS. Vertebral heart score values for heart sizecan be affected by several factors like individualvariations in the actual heart size, vertebral lengthbetween breeds of dog need to be considered, aswell as the presence of narrowed disc spaces.Hansson et al. (2005) have suggested thepossibility of inter individual variation inmeasurement. Gulanber et al. (2005) suggestedone positional fault as a cause of wronginterpretation of VHS, they suggested that inlateral radiography if X-ray beams and thorax arenot exactly vertical on each other, VHS will bechanged and this fact should be taken intoconsideration while interpretating radiograph. Inthe present study the radiographs were taken andevaluated in the standard position to rectify thepositional variation in VHS. Besides shape andsize of heart, thoracic radiography can be used toget the status regarding pulmonary circulation andamount of pulmonary edema (Richard et al.,2007). Other method of VHS measurementintroduced the VHS unit (length of body and discusof T4) with the aim to express the heart size bycomparing it with the length of one specificvertebra, which simplifies the calculations verymuch (Spasojevic et al., 2007). For practical

55
Journal of Canine Development & Research 2013
reasons the T4 vertebra may be used as a reference unit, as this vertebra is the cranial reference point forVHS measurements.
Fig-1. Showing measurement of long axis B and short axis A of heart adding the number of vertebralbodies for the long and short axis to generate a VHS.
ReferencesBuchanan, J.W. and Bucheler, J. (1995). Vertebral scale
system to measure canine heart size in radio-graphs. J. Am. Vet. Med. Assoc., 206: 194-199.
Gulanber, E.G. and Ramazan, G. (2005). Vertebral ScaleSystem to Measure Heart Size in Thoracic Ra-diographs of Turkish Shepherd (Kangal) Dogs.Turk J Vet Anim Sci. 2005; 29723-726.
Hansson, K., Haggstrom, J., Kvart, C. and Lord, P. (2005).Interobserver variability of vertebral heart sizemeasurements in dogs with normal and enlargedhearts. Vet. Radiol.Ultrasound. 46: 122-30.
Lamb CR, Wikeley H, Boswood A, Pfeiffer DU (2001).Use of breed-specific ranges for the vertebralheart scale as an aid to the radiographic diag-nosis of cardiac disease in dogs. Vet Rec.148(23):707-711.
Lamb, C.R., Tyler, M., Boswood, A., Skelly, B. J. and Cain, M. (2000) Assessment of the value of thevertebral heart scale in the radiographic diag-nosis of cardiac disease in dogs. VeterinaryRecord. 146:687-690
Mudasir Bashir Gugjoo, Mozammel Hoque, AbhishekChander Saxena, Malik Mohammed ShamsuzZama, Amarpal (2013) Scale System to MeasureHeart Size in Dogs in Thoracic Radiographs .Advances in Animal and Veterinary Sciences. 1(1): 1 – 4.
Nakayama, H., Nakayama, T. and Hamlin, R.L.(2001).Correlation of cardiac enlargement as assessedby vertebral heart size and echocardiographicand electrocardiographic findings in dogs withevolving cardiomegaly due to rapid ventricularpacing. J. Vet. Intern. Med. 15: 217–221.
Richard, Woolley., Paul, Smith. and Elizabeth Munro.(2007). Effects of Treatment Type on VertebralHeart Size in dogs with Myxomatous MitralValve Disease. Intern J Appl Res Vet Med. 5 (1):43-48
Root, C.R. and Bahr, R.J. (2002). The heart and great ves-sels in Textbook of diagnostic veterinary radi-ology, Thrall DE (ed) 4 edition, W.B. SaundersCompany, Philadelphia. pp: 402-419.
Sleeper, M.M. and Buchanan, J.W. (2001).Vertebral scalesystem to measure heart size in growing pup-pies. J. Am. Vet. Med. Assoc. 219: 57-59.
Spasojevic, K, L., Krstic N. and Trailovic, RD (2007).Comparison of Three Methods of MeasuringVertebral Heart Size in German Shepherd Dogs.Acta Veterinaria (Beograd), 57, 2-3,133-141.
Srivastava, M., Srivastava, A and Sharma, B. (2011).Management of Congestive Heart Failure in Dogwith Pimobendan. Veterinary Practitioner 12 (2):190-191.

56
Journal of Canine Development & Research 2013
RESEARCH ARTICLEPREVALENCE OF CANINE CORONA VIRUS IN DOGS*Shanaz Bashir1 , Altaf Hussain2and Anil Langer3
Department of Epidemiology and Veterinary Preventive MedicineCollege of Veterinary Science, DUVASU , Mathura- 281001(U.P.)
1,2,3Assistant Professor 2Dept. of AGB 3 Department of Veterinary Medicine2,3 Arawali Veterinary College, Bajor, Sikar-332 001 (Rajasthan)*Corresponding author e-mail : [email protected]
A B S T R A C T
This study was carried out to access the prevalence of CanineCoronavirus (CCV) in dogs suffering from diarrhea in somedistricts of Uttar Pradesh, India. Forty five fecal samples werecollected from diarrheic dogs below 1 year age between March2011 to June 2011. Prevalence of CCV in these dogs was foundto be 10.64%. The test was carried out with a commercial CCVAg test kit. This study presents a report on the prevalence ofCCV in parts of UP and suggests that CCV can be a cause ofviral diarrhea in dogs in this area.
Key words :Canine coronavirusDiarrheaImmunochromatography
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : May 12, 2013Accepted : June 22, 2013
Canine Corona virus (CCV) has the potentialto spread rapidly between dogs owing to its
high contagious nature. Infected dogs shed thevirus in their feces for 2 weeks or even longer.There is no age or breed predisposition. CCVdiarrhea can lead to severe dehydration and death(Appel et al., 1980; Miller et al., 1980). Thediarrhea may be hemorrhagic or non-hemorrhagicand the affected animals recover spontaneouslywithin a week. If more severe, the infection canprove fatal within a few days after infection(Evermann et al., 2005; Hoskins et al., 1998).There is rapid spread of infection among the dogpopulation apart from CCV being a secondaryinvader; there is need of rapid diagnosis of CCV
infection (Squires, 2003; Decaro et al., 2004).Diagnosis of CCV infection on the basis of clinicalfindings is not definitive. There are a number oflaboratory methods for the detection of CCV likeELISA, PCR, monoclonal antibodies, etc.However, these tests are time consuming andexpensive and difficult to perform under fieldconditions. A rapid method which can be appliedunder field conditions is theImmunochromatography Assay. Commercialimmunochromatography kits (CCV Ag Test) havehigh specificity and sensitivity of 98% and 100%,respectively (Soma et al., 2001; Pratelli, 2002).Present study was based on the detection of CCVantigens using Immunochromatography (IC).
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 56-58
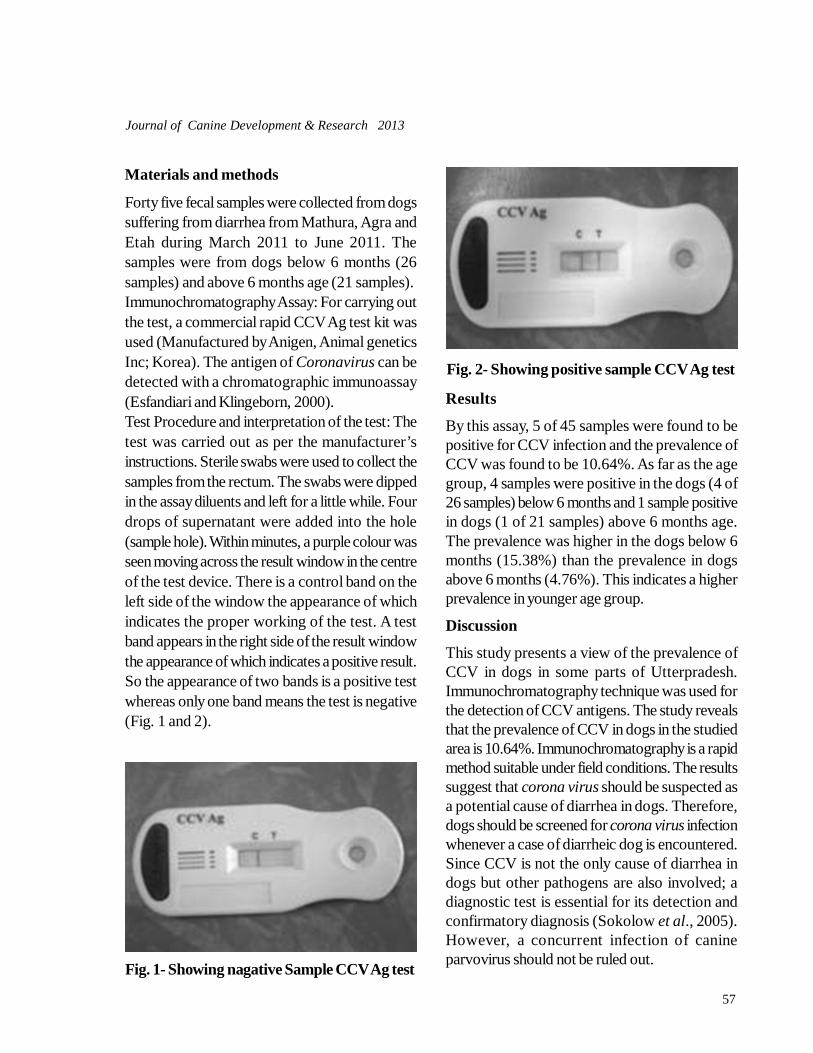
57
Journal of Canine Development & Research 2013
Materials and methods
Forty five fecal samples were collected from dogssuffering from diarrhea from Mathura, Agra andEtah during March 2011 to June 2011. Thesamples were from dogs below 6 months (26samples) and above 6 months age (21 samples).Immunochromatography Assay: For carrying outthe test, a commercial rapid CCV Ag test kit wasused (Manufactured by Anigen, Animal geneticsInc; Korea). The antigen of Coronavirus can bedetected with a chromatographic immunoassay(Esfandiari and Klingeborn, 2000).Test Procedure and interpretation of the test: Thetest was carried out as per the manufacturer’sinstructions. Sterile swabs were used to collect thesamples from the rectum. The swabs were dippedin the assay diluents and left for a little while. Fourdrops of supernatant were added into the hole(sample hole). Within minutes, a purple colour wasseen moving across the result window in the centreof the test device. There is a control band on theleft side of the window the appearance of whichindicates the proper working of the test. A testband appears in the right side of the result windowthe appearance of which indicates a positive result.So the appearance of two bands is a positive testwhereas only one band means the test is negative(Fig. 1 and 2).
Fig. 1- Showing nagative Sample CCV Ag test
Fig. 2- Showing positive sample CCV Ag test
Results
By this assay, 5 of 45 samples were found to bepositive for CCV infection and the prevalence ofCCV was found to be 10.64%. As far as the agegroup, 4 samples were positive in the dogs (4 of26 samples) below 6 months and 1 sample positivein dogs (1 of 21 samples) above 6 months age.The prevalence was higher in the dogs below 6months (15.38%) than the prevalence in dogsabove 6 months (4.76%). This indicates a higherprevalence in younger age group.
Discussion
This study presents a view of the prevalence ofCCV in dogs in some parts of Utterpradesh.Immunochromatography technique was used forthe detection of CCV antigens. The study revealsthat the prevalence of CCV in dogs in the studiedarea is 10.64%. Immunochromatography is a rapidmethod suitable under field conditions. The resultssuggest that corona virus should be suspected asa potential cause of diarrhea in dogs. Therefore,dogs should be screened for corona virus infectionwhenever a case of diarrheic dog is encountered.Since CCV is not the only cause of diarrhea indogs but other pathogens are also involved; adiagnostic test is essential for its detection andconfirmatory diagnosis (Sokolow et al., 2005).However, a concurrent infection of canineparvovirus should not be ruled out.

58
Journal of Canine Development & Research 2013
CCV spreads rapidly among dogs and theknowledge of its prevalence and detection isessential to isolate the affected dogs. CCV alsoremains in the environment for a significant period(Hoskins, 1998).In Italy, antibodies against CCV were detectedusing ELISA and nearly 73.5% of the serumsamples were found positive (Pratelli et al., 2002).In Australia, a study carried out for many yearsshowed that 40.8% sera of kenelled dogs werepositive for CCV antibodies (Naylor et al., 2001).14% fecal samples of dogs were found positivefor CCV infection in Chennai (Sareendranath etal., 1992).Diarrhea, weight loss and severe dehydration maylead to death (Appel, 1987). Young puppies areaffected more (Hoskins, 1998). Present study alsosuggests an increased prevalence in young dogsbelow 6 months age. Regular vaccinations shouldbe carried out against Coronavirus for being apotential cause of diarrhea in dogs.
ReferencesAppel, M. J. (1987) Canine Coronavirus in viral infec-
tions of carnivores. InM. J. Appel, Ed., ElsevierScience Publishers, Amsterdam, The Nether-lands. 115-122.
Decaro, N., Camero, M., Greco, G., Zizzo, N., Tinelli, A.,Campolo, M., Pratelli, A. and Buonavoglia, C.(2004) Canine distemper and related diseases:report of a severe outbreak in a kennel. NewMicrobiol. 27: 177-181.
Esfandiari, J., Klingeborn, B. (2002) A comparative studyof a new rapid and one- step test for the detec-tion of parvovirus in feces from dogs, cats andmink. J Vet Med 47: 145-153.
Evermann, J.F., Abbott, J.R., Han, S. (2005) CanineCoronavirus-associated puppy mortality with-out evidence of concurrent canine parvovirusinfection. J Vet Diagn Invest. 17; 610-614.
Hoskins, D.J. (1998) Canine Viral enteritis. In: InfectiousDiseases of the Dogs and Cats. Greene, C.E.(Ed), 2nd Ed., W.B. Saunders Co., Philadelphia,pp. 45-49.
Naylor, M.J., Monckton, R.P., Lehrbach, P.R. and Deane,E. M. (2001) Canine Coronavirus in Austra-lian dogs. Aust Vet J. 79: 116-119.
Pratelli, A., Elia, G., Martella V. (2002) Prevalence of Ca-nine Coronavirus antibodies by an enzyme-linked immunosorbent assay in dogs in thesouth of Italy. J Virol Meth. 102: 67-71.
Pratelli, A., Tinelli, A., Decaro, N., Camero, M., Elia, G.,Gentile, A. and Buonavoglia, C. (2002) PCR as-say for the detection and identification of atypi-cal Canine Coronavirus in dogs. J Virol Meth-ods. 106: 209-213.
Sareendranath, M. R. (1992) Vet Bull. 6: 12.Sokolow. S.H., Rand, C., Marks, S.L., Drazenovich, N.L.,
Kather, E.J., Foley J.E. (2005) Epidemiologicevaluation of diarrhea in dogs in an animal shel-ter. Am J Vet Res. 66: 1018 1024.
Soma, T., Hara, M., Ishii, H., Yamamoto, S. (2001) Anti-body testing against Canine Coronavirusimmunoperoxidase plaque staining. Vet ResCommun. 25: 327-336.
Squires, R. A. (2003) An update on aspects of viral gas-trointestinal diseases of dogs and cats. N Z Vet.J. 51: 252-261.

59
Journal of Canine Development & Research 2013
RESEARCH ARTICLETHERAPEUTIC MANAGEMENT OF DEMODICOSIS IN DOGSRamakant1 and *Mukesh Srivastava1
Department of Veterinary Clinical Medicine, Ethics and JurisprudenceCollege of Veterinary Science and Animal Husbandry, DUVASU, Mathura-281 001 (U.P.)
1 Assistant Professor*Corresponding author e-mail:[email protected]
A B S T R A C T
Demodicosis was diagnosed and treated in 20 dogs irrespectiveof age, sex and breed. Screening was done on basis ofmicroscopic examination of skin scrapping and dermatologicalclinical examination. The infected dogs were treated withcombined therapy of ivermectin, topically application of amitrazalong with supportive therapy for secondary bacterial infectionand imuunomodulation. Out of 20 cases, 16 cases responded totherapy in 4 weeks of treatment.
Key words :AmitrazDemodicosisDogIvermectin.
A R T I C L E H I S T O R Y
Received : October 22, 2012Revised : November 16, 2012Accepted : November 26, 2012
Canine demodicosis is a common, noncontagious, inflammatory parasitic
dermatosis characterized by excessiveproliferation of the commensal mite Demodexcanis within hair follicles and sebaceous gland. Themost common species, Demodex canis is aresident in their hair follicles, and sebaceous glandsof skin and is part of normal fauna (Henpf andHat, 1988) and are transmitted from the bitch tothe pups during the first few days of life (Greveand Gaafar, 1966). Demodicosis is classified aslocalized and generalized according to extent ofthe disease. Localized demodicosis mostcommonly occurs in young dogs of less than oneyear of age and as a mild and benign self-limitingdisease with spontaneous remission in mostpatients (Mueller, 2004). The disease is considered
to be generalized when a dog has five or morelocalized lesions, when an entire body region (e.g.,facial area) is involved, or where the completeinvolvement of two or more feet occurs (Scott etal., 1995). Demodicosis is commonly reported inassociation with defect in the integrity of immunesystem particularly an inherited specific T celldeficiency (Fontaine, 2008). Success rate ofAmitraz rinse increases with the concentration andfrequency of the rinse. The approved concentrationis 0.025% every other week, but treatmentprotocols that involve either washing alternatehalves of the dog daily or weekly treatment withamitraz in concentrations of 1.25% have beenreported (Hugnet et al., 2001). Ivermectin as aweekly injection has not been associated with goodsuccess rates (Mueller, 2012), also it may be used
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 59-62

60
Journal of Canine Development & Research 2013
in conjunction with amitraz therapy (Srivastava etal., 2012). Present study reports the therapeuticmanagement of demodicosis in dogs with combinedtherapy of Ivermectin and Amitraz..
Materials and methods
Study was conducted on clinical cases presentedin Teaching Veterinary Clinical Complex,DUVASU, Mathura. A total of 48 clinical casesof dermatitis were screened irrespective of theirage, sex and breeds, which have reported to havehistory of itching, shedding of hairs, various degreeof alopecia, hyper-pigmentation of skin andrepulsive odour. Observations were done forclassical signs of demodicosis like focal alopecia,periocular alopecia erythema, and scalingappearing on the distal limbs and the face,comedones, follicular papules and pustules alongwith crusting and ulceration (Fig1, 2 and 3).Multiple skin scrapings were collected from differentlesions of the body specialy from periphery of thelesions with the help of liquid paraffin smearedscalpel until blood oozed out from lesions. Thescraped materials examined microscopically fordetection of mites using standard techniques(Soulsby, 1982). Skin scrapping examinationshowed demodicosis in 20 dogs (Fig-4). Theinfected dogs were treated with combined therapyof Ivermectin @ 0.2mg/kg. b.wt. sc at weeklyinterval for 4 weeks, Chlorphenramine maleate @0.4 mg/ kg. b.wt. im, Lincomycin @20mg/kg.b.wt. im for 7 to 10 days, Immuno- modulatorSyrup Immunol (Marketed by Himalaya Drug Co.,Bangalore) @ 5ml bid po for 3 weeks along withtopical application of solution of Amitraz 12.5%@ 4ml/liter of water, twice in a week for a month.
Results and discussion
Out of forty eight clinical cases of dermatitis in dogsshowing classical lesion of demodicosis, , twentycases (41.66%) were found positive for Demodexcanis based on skin scrapping examination (Fig.5
& 6). Out of 20 cases, 16 cases respondeed wellfor combination therapy of Ivermectin and Amitraz,which was similar to Srivastava et al. (2012), whosuggested to use this combined therapry in amitrazresistant cases of demodicosis. Ivermectin is amacrolide that can acts against arthropods, whichselectively binds to glutamate gated and gamma-amino butyric acids (GABA) gated chloridechannels in mite’s nervous system, resulting in cellhyper polarizations, mite parasites and finally death,but due to its untoward reaction, this drug iscontraindicated in Coolies and English Sheep dogs.The drugs have to be given under supervisions forside effects like ataxia, mydriasis, tremors, stupor,salivation bradycardia and respiratory arrest (Tater,2008). Amitraz inhibit enzyme monoamine oxidasethat inhibits metabolism neurotransmitter causesparalysis and death of ectoparasites (Sandhu andRampal, 2006) by increasing nervous activity oftarget ectoparasites. Combination therapy ofIvermectin and Amitraz was used to havesynergistic effects against mites, although failureof treatment has been attributed to insecticideresistance or incorrect application (James et al.,1993; Keys et al., 1993). Immuno-modulator wasused in the present study consideringimmunological suppression due to endoparasitismor malnutrition in young dogs and corticosteroidstherapy, endocrine disease, neoplasia andchemotherapy in older dogs are consideredpredisposing factors for demodicosis (Muller etal., 2012). Chlorphenramine maleate is an H-1receptor antagonist, inhibits the release of histaminethat reduces the itching and inflammations (Sandhuand Rampal, 2006).
Acknowledgement
The Authors are highly thankful to the Dean,College of Veterinary and Animal Sciences,DUVASU, Mathura for providing necessaryfacilities to carry out this clinical work.
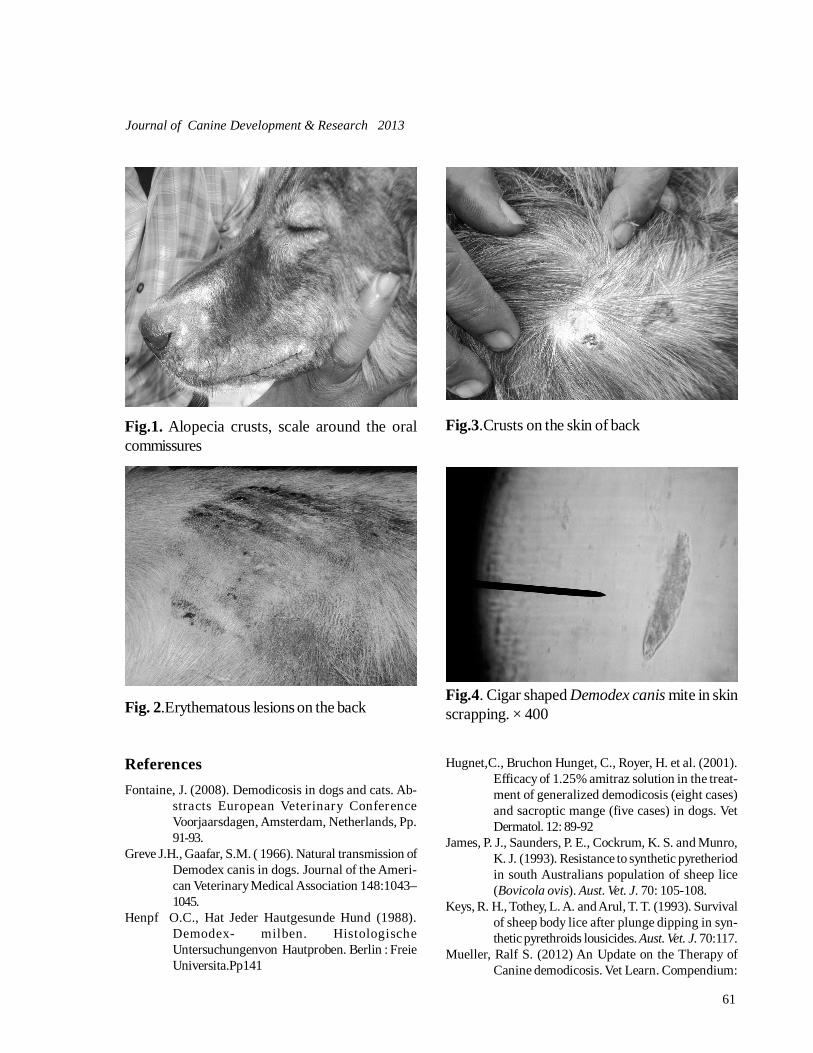
61
Journal of Canine Development & Research 2013
Fig.1. Alopecia crusts, scale around the oralcommissures
Fig. 2.Erythematous lesions on the back
Fig.3.Crusts on the skin of back
Fig.4. Cigar shaped Demodex canis mite in skinscrapping. × 400
ReferencesFontaine, J. (2008). Demodicosis in dogs and cats. Ab-
stracts European Veterinary ConferenceVoorjaarsdagen, Amsterdam, Netherlands, Pp.91-93.
Greve J.H., Gaafar, S.M. ( 1966). Natural transmission ofDemodex canis in dogs. Journal of the Ameri-can Veterinary Medical Association 148:1043–1045.
Henpf O.C., Hat Jeder Hautgesunde Hund (1988).Demodex- milben. HistologischeUntersuchungenvon Hautproben. Berlin : FreieUniversita.Pp141
Hugnet,C., Bruchon Hunget, C., Royer, H. et al. (2001).Efficacy of 1.25% amitraz solution in the treat-ment of generalized demodicosis (eight cases)and sacroptic mange (five cases) in dogs. VetDermatol. 12: 89-92
James, P. J., Saunders, P. E., Cockrum, K. S. and Munro,K. J. (1993). Resistance to synthetic pyretheriodin south Australians population of sheep lice(Bovicola ovis). Aust. Vet. J. 70: 105-108.
Keys, R. H., Tothey, L. A. and Arul, T. T. (1993). Survivalof sheep body lice after plunge dipping in syn-thetic pyrethroids lousicides. Aust. Vet. J. 70:117.
Mueller, Ralf S. (2012) An Update on the Therapy ofCanine demodicosis. Vet Learn. Compendium:

62
Journal of Canine Development & Research 2013
Continuing Education for Veterinarians. E1-4.Muller, R. S., Bensignor, E., Ferrer, L., Holm, B., Lamarie,
S., Paradis, M. and Shipstone M. A. (2012).Treatment of Demodicosis in dogs: 2011 Clini-cal Practice guidelines Vet. Dermatol 23: 86.
Muller, R.S. (2004). Treatment protocols for demodicosis:an evidence-based review. Vet Dermatol..15(2):75-89.
Nutting, W. B. and Desch, C. E. (1978). Demodex canisre-description and re-evaluation, Cornell Vet.68:139-149.
Sandhu, H. S. and Rampal, S. (2006). Essentials of Veteri-nary Pharmacology and Therapeutics, 1st Edn.Publ., Kalyani Publishers., Ludhiana, Pp. 398,454, 1250-1253.
Scott, D. W.,. Miller, W. H. and Griffin, C. E. (1995).In.Muller and Kirk’s Small Animal Dermatology.Parasitic skin diseases. 5th ed., W. B. Saunders,Philadelphia. Pp. 417-432.
Soulsby EJL. (1982) Helminths, Arthropods and Proto-zoa of Domesticated Animals. 7th edn., BailliereTindall., London. Pp. 35-740.
Srivastava, M., Srivastava A and B. Sharma. (2012). Man-agement of Amitraz resistant cases of CanineDemodecosis by Ivermectin. Ind. Vet. Journal.89(6):81-82
Tater, K. C. (2008).Canine and feline demodicosis. DVMMagazine, Veterinary Medicine. cited at veteri-nary medicine.dvm360.com /vetmed /article /article Detail .jsp id =535123 &sk=&pageID=6

63
Journal of Canine Development & Research 2013
RESEARCH ARTICLETHERAPEUTIC MANAGEMENT OF SNAKE BITE IN DOGS*D.K. Bihani1, D.K Saini2, B.L.Sharma3, S. Kumar3 and M. L. Sain3
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege of Veterinary & Animal Science, RAJUVAS, Bikaner – 334 001(Rajasthan)
1Professor 2MVSc.Scholar 3Veterinary Officer,A.H.Dept., Rajasthan Govt.*Corresponding author e-mail :[email protected]
A B S T R A C T
Present communication describes the successful managementof snake bite in two dogs. Prominent signs were vomiting,twitching of muscles, salivation, abnormal gait, panting and dilatedpupil. Dogs were treated with reconstituted polyvalent anti snakevenom, dexamethasone, botropase, amoxirum forte along withtetanus toxoid. Appreciable improvement was observed in 5 hrsof therapy but complete recovery was recorded in five days.
Key words :DogPolyvalent anti snake venomSnake bite
A R T I C L E H I S T O R Y
Received : March 10, 2013Revised : June 2, 2013Accepted : June 22, 2013
Snake bites and insect stings are mostcommonly encountered biotoxins (Mount,
1989). Most of the cases of snake bite have beenreported in dogs and horses (Garg, 2002), butcat is usually not attacked due to its greatercaution and superior agility while hunting (Shukla,2009). Snake bite with envenomation should betreated as an emergency. Rapid examination andinitiation of proper treatment is essential (Vijay,et al., 2001) as delayed and inadequate treatmentmay lead to untoward consequences (Ananda etal., 2009). Based on the system affected, snakevenoms may be classified as hemotoxic andneurotoxic depending on (Gregory and John,2002). Present communication describessuccessful therapeutic management of snake bitein two dogs.
Case history, clinical and biochemicalexamination
One male and one female Alsatian dog agedbetween two to two and half years were presentedto canine outdoor of TVCC, CVAS, Bikaner withthe complaint of frothy salivation, dull anddepressed demeanor, ataxic gait, vomiting,twitching of muscles, salivation, abnormal gait,panting and dilated pupil. History revealed snakebite as a common problem in that location.Physical examination showed cyanotic swollenareas with fang marks on tip of nose and left forepaw. Based on the history and physical examinationof the dogs, the cases were suspected forsnakebite, but species of the snake was notidentified by the owner. Vital parameters like rectaltemperature, pulse and respiratory rate of male
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 63-65

64
Journal of Canine Development & Research 2013
dog were 37oC, 45/ min and 19/min while in female
dog the parameters, were 37.4oC, 47/ min and
20/ min,respectively. Additionally furtherexamination of both the cases revealed presenceof cold extremities and decreased body reflexes.The blood samples from both the dogs werecollected with and without ethylene-diamine-tetra-acetic acid for hematological parameters andbiochemical parameters - serum alanineaminotransferase, aspartae amino trasferase andcreatinine estimation. The hematologicalparameters revealed decreased hemoglobinconcentration (12.6 g/dl, 13.2 g/dl) and packedcell volume (35%, 40%) in male and femaleAlsatian, respectively. The biochemical valuesshowed elevated levels of alanine aminotransferase(80 IU/dl, 90 IU/dl), aspartate amino trasferase(29.5 IU/dl and 30.8 IU/dl) and creatinine (2.2mg/dl, 1.96 mg/ dl) in male and female Alsatian,respectively.
Therapy and discussion
The animal was kept in a calm and quiet place andit was made to lie on lateral recumbency with itshead little below the level of the rest of the bodyso as to minimize the circulatory spread of thevenom. The fang mark area of the skin wasthoroughly washed with 5% potassiumpermanganate solution (Suchitra et al., 2010).These dog were treated with polyvalent anti snakevenom 10 ml slow iv in NSS 500 ml,dexamethasone 1mg/kg bwt. im, botropase 1mlim and amoxirum forte 300 mg im b.i.d. on firstday along with tetanus toxoid 3000 IU. After 5hrs the dogs were active, normal and there wasno relapse of the signs were observed.Dexamethasone, botropase and amoxirum fortewere repeated in the above mentioned doses andschedule for two more days. The antibiotic therapywas continued for 5 days to both the dogs withcomplete recovery in one week. The alterationsin the hematological parameters might be due to
damage to the blood cells by snake venom. Theincreased values of alanine aminotransferase andcreatinine may be due to the hepatotoxic andnephrotoxic effect of snake venom (O’Shea,2005). Polyvalent snake anti-venom was preferredin the present case as it provides protection againstthe venom of four (common cobra, common krait,saw scaled viper and russell’s viper) species ofthe snakes. The use of steroids in snake bites isstill debated; while some say they have nospecific role, their administration reduceinflammatory process. Additionally, sometimeslyophilized polyvalent anti-snake venom may causeanaphylactic reactions (Sai et al, 2008) toovercome the untoward effect to antivenom,dexamethasone injection was given to the dogs.However, in the present study corticosteroid waspreferred over antihistamines as in certain times itpotentiates the toxic action of the snake venom.The use the corticosteroid prior to the polyvalentsnake anti-venom also inhibits serum sickness(Shukla, 2009). The use of tetanus toxoidprovides protection against the tetanus spore thatmight have entered animal body from contaminatedsnake mouth (Shukla, 2009).The other components of snake venoms areglycoproteins, lipids, and biogenic amines, suchas histamine, serotonin and neurotransmitters(catecholamines and acetylcholine) (Klaassen,2008). Passing of blood in the urine observed inAlsatian dog can be hypothesized to thehaematotoxic effect of snake venom which mayinterfere with many components of the haemostaticsystem (Wolff, 2006). Moreover, the toxins suchas the haemorrhagins cause spontaneous bleedingin the gingival sulci, nose, skin and gastrointestinal.However, such bleeding tendencies were notnoticed in either of the two cases except hematuriain Alsatian dog. Clinical signs such as frothysalivation, dullness muscular weakness withabnormal gait observed in the present study canbe attributed to the enzymatic and non enzymatic

65
Journal of Canine Development & Research 2013
compounds in the snake venom. According toKlaassen (2008), hyalurinadase cleaves internalglycoside bonds in certain acid muco-polysaccharides resulting decreased viscosity ofconnective tissues allowing other fractions of venomto penetrate the tissues. The cyanotic edemaobserved at the site of bite may be attributed toenzyme hyaluronidase which acts as a spreadingfactor.
References
Ananda, K. J., Mohan, K., Ansar Kamran and R. Sharada(2009). Snake bite in dogs and its successfultreatment. Veterinary World. 2(2): 66-67
Garg, S. K. (2002). In Zootoxins. Veterinary Toxiciology,CBS publishers and Distributers 1st Edn NewDelhi.
Gregory Juckett., and John G. Hancox. Venomous Snake-bites in the United States: Management Reviewand Update . American Family Physician. 65 (7): 1367-1374.
Klaassen, C.D. (2008). Properties and Toxicities of ani-mal Venoms. In:Toxicology . 7th Edn, McGraw-Hill, New Delhi. pp 1093-1098.
Mount, M. E. (1989): Toxicology, S.J. Ettinger (ed.), Intext book of Veterinary Internal Medicine, Vol.1, 3rd Edn., W.B. Saunders Co., Philadelphia,London. pp. 72.
O’Shea, M. (2005). Venomous Snakes of the World.Princeton: Princeton University Press.
Sai Butcha Rao, M., Satish Kumar and Thirumala Rao,D.S. (2008): Intas Polivet., 9(1), 16.
Shukla, P .C. (2009): Snake bite in animals and itstreatment. Pashudhan, 35(2): 2-4..
Suchitra, B. R., M. C. Anilkumar and G. P. Kalmath.( 2010)Clinical Management of Snake bite in a dog.Veterinary World. 3(5):234.
Vijay Kumar, G., et al. (2001). Snake envenomation in adog- A case report. Indian Vet. Journal, 78:1148-1149.
Wolff, F. A. D. (2006). Natural Toxins. In: Clarke’s Analy-sis of Drugs and Poison. Pharmaceutical press,London, Electronic Version.
66
Journal of Canine Development & Research 2013
RESEARCH ARTICLEFLEA ALLERGY DERMATITIS AND ITS THERAPEUTICMANAGEMENT IN DOGS*J.P. Kachhawa1, Anil Ahuja2, A.P. Singh3, D.K. Bihani3, Sanjhali Soren1, Dipika Dhuria4, Ankita Sharma5, and Mamta Daga5
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege of Veterinary and Animal Science, RAJUVAS ,Bikaner -334 001 (Rajasthan)
1Teaching Associate 2Professor & Head 3Professor 4 Instructor 5M. V. Sc. Scholar*Corresponding author e-mail :[email protected]
A B S T R A C T
Flea allergy dermatitis is a hypersensitivity reaction to componentsof fleas, especially allergens in flea saliva. Twelve cases werepresented in Canine Outdoor of TVCC of College of Veterinaryand Animal Science, Bikaner with history of itching, alopeciaand redness on body. The clinical examination revealed pruritus,crusts, hyperpigmentation, papules, lichenification, hypotrichia,pustules, hyperkeratosis and diagnosed as Flea allergy dermatitisby wet paper flea test. All the dogs were treated with fipronil,predenisolone, marbofloxacin, and syrup containing Omega 3and Omega 6 fatty acids. All the dogs were recovered 21 daysafter commencement of treatment.
Key words :DermatitisFipronilFlea
A R T I C L E H I S T O R Y
Received : Novmber 28, 2013Revised : December 16, 2013Accepted : December 31, 2013
Flea allergy dermatitis (FAD) is an immunologicdisease of dogs caused by Ctenocephalides
canis. The host has hypersensitive reaction to fleasaliva which contains a variety of histamine-likecompounds, enzymes, polypeptides, and aminoacids that span a wide range of sizes from 40 to66 KDa (Halliwell et al., 1987). This results insevere pruritus, hair loss, crusty lesions and rashalong the upper back, tail region and down theback and inside of the hind legs (Ahuja et al.,2001; Dryden, and Broce, 2002). Flea allergydermatitis is the most common dermatologicdisease of dogs around the world (Halliwell et al.,1987; Blagburn, and Dryden, 2009). Fleas from
other mammals or birds that have been capturedor hunted by dogs may form transient associationswith dogs (Dryden, 1993). The ectoparasites ofpet animals have the potential to develop resistanceso new and effective treatments are important(Coles and Dryden, 2014).
Case history and clinical examination
Twelve dogs presented to Canine Outdoor ofTeaching Veterinary Clinical Complex of Collegeof Veterinary and Animal Science, Bikaner fromAugust to October 2013 were induded in thisstudy. All the dogs had history of itching, rednesson were included in this study back and around
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 66-68
67
Journal of Canine Development & Research 2013
the tail, presence of fleas over the body and dogsgroom and biting themselves excessively. Clinicalexamination revealed erythema, alopecia,seborrhoea, crusts, hyperpigmentation, papules,excoriations, lichenification, hypotrichia, epidermal,bullae, pustules, hyperkeratosis in all dogs. Threedogs had tail-head puritus extending to the lumbo-sacral area while nine dogs had pruritus on ventralabdomen, caudal and medial thighs. The diseasewas diagnosed on the basis of thorough history,clinical examination and identification of fleas andflea dirt detection by wet paper flea test. A wetpaper placed under or near the dog, hair coatbrushed with finger and debris collected on thepaper. The flea faeces give rise to blood stainedstreaks on the paper which were readly visible(Chandler et al., 1979).
Therapy and results
All the dogs suffering from FAD were treated withadulticide phenylpyrazoles compound, fipronil0.5% shampoo (Zerotick, Cure & Care BiotecPvt. Ltd. Delhi) on weekly interval along withsupportive treatment with predenisolone @ 1.0mg/kg b.wt, po for five days, marbofloxacine @2.5mg/kg bwt po for seven days and syrupcontaining Omega-3 and Omega-6 fatty acids(Glossycoat, Venkey’s India Ltd. Pune) for threeweeks. After three weeks all the dogs were freeform fleas and got rid from pruritus and otherclinical signs observed when they were presentedfor the treatment except alopecia whichdisappeared gradually.
Discussion
Most flea species differ from many otherectoparasites by their lack of host specificity andby the fact that most of their life cycle is spent offthe host in the environment (Kwochka and Bevier,1987). Treatment requires appropriate knowledgeof the flea life cycle and flea related biology, andunderstanding of the mode of action of the relevant
flea control products (Cadiergues, 2009).The present cases were observed during themonths August to October of 2013. Optimumenvironmental conditions for flea propagation andsurvival include temperatures between 20 and30°C with a relative humidity greater than 70%(Rust and Dryden, 1997; Lance et al., 2005). Theclinical signs alopecia, seborrhoea, crusts,hyperpigmentation, papules, excoriations,lichenification, hypotrichia, epidermal, collaretes,bullae, pustules, hyperkeratosis were similar to thatobserved previously by Koutinas et al. (1995) andKotnik (2007). Type I immediate hypersensitivity,type IV delayed hypersensitivity, and cutaneousbasophil hypersensitivity to salivary antigen areconsidered as immunologic participants in fleaallergy dermatitis (Gross & Halliwell, 1985). A latephase IgE-mediated reaction also may contributeto the pathogenesis.Fipronil binds to two different glutamate-gatedchloride channels of neurons in the central nervoussystem, sharing a common binding site withcyclodienes (Zhao et al., 2003; Zhao et al.,2004). Fipronil reduced flea counts by 98%(Medleau et al., 2003), and 97.3%, (Rohdich etal., 2014) in dogs suffering from FAD. Systemicuse of prednisolone, 1 to 2mg/kg po bd, to stopthe pruritus associated with FAD. Fatty acid aresupplements containing omega-3 fatty acids helpfulin controlling concurrent atopy, alleviating dry skin,and modulating the production of inflammatorymediators (Craig, 2006). An appropriate systemicantibiotic was administered for treatment ofsecondary pyoderma due to bacterial invasion forat least 5 to 7days (Kotnik, 2007).The prognosis of FAD is good if strict flea controlis practiced. Despite the availability of safe,effective compounds, treating FAD remains achallenge. An integrated approach to treatmentshould be adopted, involving all the players in theflea life cycle the FAD patient, all in-contact pets,and the environment (Cadiergues, 2009).

68
Journal of Canine Development & Research 2013
Acknowledgement
The authors are thankful for Dean, CVAS, Bikanerfor providing necessary facilities to present researchwork.
ReferencesAhuja, A., Bihani, D.K., and Mali, M.M. (2001). Flea al-
lergy dermatitis: summer eczema. J. CanineDev.Res.1: 78-79.
Blagburn, B.L. and Dryden, M.W. (2009). Biology, treat-ment, and control of flea and tick infestations.Vet Clin Small Anim., 39:1173-1200.
Cadiergues, M.C. (2009). Flea control in flea allergic dogsand cats. EJCAP, 19 (3): 261-267.
Chandler, E.A., Evans, J.M., Sington, W.B., Startup, F.G.,Sutton, J.B., and Taverner, W.O., (1979). In: Ca-nine medicine and therapeutics, Blackwell sci-entific publication Oxford, London. Pp. 200-1.
Coles,T.B. and Dryden, M.W. (2014). Insecticide/acari-cide resistance in fleas and ticks infesting dogsand cats. Parasit Vectors, 7:8.
Craig E. G. (2006). Saunders manual of small animal prac-tice, third Edn. Saunders Elsevier St. Louis,Missouri. Pp. 68-69.
Dryden, M.W. (1993). Biology of fleas of dogs and cats.Comp. Cont. Educ. Pract. Vet. 15: 569-579
Dryden, M.W. and Broce, A.B. (2002). Integrated fleacontrol: Flea control for the 21st century.Compend Contin Educ Pract Vet., 24 (Supp11):36-9.
Gross, T.L. & Halliwell, R.E.W. (1985) Lesions of experi-mental flea bite hypersensitivity in the dog. VetPathol 22, 78–81.
Halliwell, R.E., Preston, J.F., Nesbitt, J.G. (1987). Aspectsof the immunopathogenesis of flea allergy der-matitis in dogs. Vet Immunol Immunopathol.17: 483–494.
Kotnik, T. (2007). Retrospective study of presumably al-lergic dogs examined over a one year period atthe Veterinary Faculty, University of Ljubljana,Slovenia. Vet. Arhiv 77: 453-462.
Koutinas A.F., Papazahariadou, M. G., Rallis, T. S., Tzivara,N. H., Himonas, C. A. (1995). Flea species fromdogs and cats in northern Greece: environmen-tal and clinical implications. Veterinary Parasi-tology 58: 109-115
Kwochka, K.W. and Bevier, D.E. (1987). Flea dermatitis.In: G.H. Nesbitt (Editor), Contemporary Issuesin Small Animal Practice, Vol. 8—Dermatology.Churchill Livingstone, New York, Pp. 21 -55.
Lance, A.D., Todd, N.J, Joy, E.M., Lindsey, S. S. (2005).Fleas parasitizing domestic dogs in Georgia,USA: Species composition and seasonal abun-dance. Veterinary Parasitology 130: 157–162.
Medleau, L., Clekis, T, McArthur, T.R., Alva, R., Barrick,R.A., Jeannin, P. (2003) Evaluation of fipronilspot-on in the treatment of flea allergic dermati-tis in dogs. J Small Anim Pract. 44(2): 71-75.
Rohdich, N., Roepke, R.K.A. and Zschiesche, E. (2014).A randomized, blinded, controlled and multi-centered field study comparing the efficacy andsafety of Bravecto™ (fluralaner) against Front-line™ (fipronil) in flea- and tick infested dogs.Parasites & Vectors, 7:83.
Rust, M.K., and Dryden, M.W. (1997). The biology, ecol-ogy, and management of the cat flea. AnnualReview of Entomology, 42: 451-473.
Zhao, X., Salgado, V.L., Yeh, J.Z., Narahashi, T. (2003).Differential actions of fipronil and dieldrin in-secticides on GABA-gated chloride channelsin cockroach neurons. J Pharmacol Exp Ther.306(3): 914- 924.
Zhao, X., Yeh, J.Z., Salgado, V.L., Narahashi, T. (2004).Fipronil is a potent open channel blocker ofglutamate-activated chloride channels in cock-roach neurons. J Pharmacol Exp Ther. 310(1):192- 201.

69
Journal of Canine Development & Research 2013
RESEARCH ARTICLESUCCESSFUL MANAGEMENT OF CANINE PYOMETRA*Kuldip Dwivedi 1
Department of Obstetrics & GynecologyCollege of Veterinary Science & Animal Husbandry, DUVASU, Mathura -281 001 (U.P.)
1Assistant Professor*Corresponding author e-mail : [email protected]
A B S T R A C T
Present case report describes failure of medical management inpyometra in 6 year old Labrador bitch. Major clinicalmanifestations were anorexia, vomiting, fever, distendedabdomen, lethargies and depression. Per vaginal examinationshowed a scanty amount of yellow brown pus, whileultrasonographic examination showed some hypoechoic honeycomb like pouches in uterus which confirmed pyometra. Thebitch underwent ovario-hysterctomy with uneventful recovery.
Key words :BitchOvario-hysterectomyPyometra
A R T I C L E H I S T O R Y
Received : March 12, 2013Revised : June 02, 2013Accepted : June 22, 2013
Infection and pus in uterus is a serious and lifethreatening condition of older age bitches but
can occur at any age, whether bred or not. Theincidence of pyometra in dogs is approximately24% before 10 years of age (Hagman et al.,2004).Nagar et al.(2008) reported 31.7% whilePramod et al.(2011) reported 12.12% prevalenceof pyometra among reproductive conditions inbitches. In approximately 90% of cases,Escherichia coli is a main causal agent (Susi etal., 2006). This bacterium produces endotoxins(that are capable of initiating the cytokine cascadeand the release of many inflammatory mediators.E. coli is thought to be the cause of the local andsystemic inflammatory reactions associated withpyometra. Because of long luteal phase of estrouscycle and predominance of progesterone, animmunosuppressive hormone, reduces the entry
of white blood cells in uterus and causes thickeningof wall of uterus and thus reduces its ability toconstrict and evacuate the accumulated fluid andpathogens, which consequently can lead tosecondary infection.Sonographic diagnosis ofpyometra is easy when large volumes of fluid/pusare present in the uterus(Qureshi etal.,2002;Pramod et al.,2010).
History and clinical examination
A 6 year old Labrador bitch was presented toTVCC, College of Veterinary Science & AnimalHusbandry, Mathura with a history of anorexia andvomiting. History revealed beginning of problemtwo months ago after previous estrus. Ownerconsulted two three times local vets and diagnosedas trans-vaginal tumor and treated accordingly.Consequently animal got no relief even after
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 69-71

70
Journal of Canine Development & Research 2013
treatment of 3 weeks. On clinical examinationinitially fever was recorded which subsequently fellto normal. Animal was lethargic, depressed, fattywith a distended abdomen. Per vaginal examinationshowed a scanty amount of yellow brown pus,while ultrasonographic examination showed somehypoechoic honey comb like pouches in uteruswhich confirmed pyometra. Blood hemoglobinwas 7.4 gm% while leukocyte count was 68000/cmm.
Treatment and discussion
Treatment for trans-vaginal tumor was discontinuedand medical Treatment for pyometra was initiatedwith Tab. Cabergoline @ 50 µg for 4 days andCloprostenol (vetmate)@ 25 µg im on fouralternate days. After some time animal restoredappetite and stopped vomiting and became normal,but as the treatment was discontinued previoussymptoms became evident and finally ovario-hysterctomy was done aseptically as discribedpreviously (Smith,2006) with uneventful recovery(Fig.1 and 2).During the early luteal phase, the increasedprogesterone concentration suppresses cellular
immunity (Sugiura et al., 2004). E. coli is themost prevalent organism that causes pyometra inthe dog and cat (Coggan et al., 2008; Bassessaret al., 2011) and is normally present in the urineand feces of affected bitches (Tsumagari et al.,2005). Estradiol causes cervical dilation duringestrous, and therefore allows bacteria that are partof the normal flora of the vagina (especially E.coli and Streptococcus spp.) to ascend into theuterus. The combination of reduced local immunityand favorable uterine conditions for thesepathogens allow for bacterial colonization andproliferation. Recently, it was reported thatinoculation of E. coli into the uterus on days 11 to20 and 20 to 30 after the luteinizing hormone peakcaused canine pyometra, because at that time theuterus is most susceptible to infection (Smith,2006). The cases of canine pyometra arepresented late for treatment as the symptomsbecome evident at later stages of disease. Medicaltreatment is not reliable as chances of relapse arehigher therefore (Nelson et al.,1982; Pretzer,2008), ovario-hysterectomy is only reliable andsafe treatment for canine pyometra (Pramod etal.,2010).
Fig. 1 Uterine horn filled with pus

71
Journal of Canine Development & Research 2013
Fig.2.An exteriorized uterus during an ovariohysterectomy for pyometra.
ReferencesBassessar Varun, Yamini Verma and Madhu Swamy
(2011) Canine Pyometra : an update on etio-pathogenesis J. Canine Dev. Res. 7:1-7.
Biswas D., Das S., Das B. C., Saifuddin A. K. Md. (2012).Pyometra in a German Shepherd Dog. J Vet Adv,2(1) 34-38.
Barton C (1992). Diseases of the Uterus - Cystic Endome-trial Hyperplasia/Pyometra Complex. In: Hand-book of Small Animal Practice, Morgan, R.V.(Ed). 2nd Edition. New York: ChurchillLivingstone, Pp: 655-658.
Coggan, J.A., Melville, P.A., de-Oliveira, C.M Faustino,M., Moreno, A.M and Benites NR (2008). Mi-crobiological and Histopathological Aspects ofCanine pyometra. Brazilian J. Microb, 39, 477-783.
Hagman, R. (2004). New Aspects of Canine Pyometra.Studies on epidemiology and pathogenesis.PhD. Thesis, The Swedish University of Agri-cultural Sciences, Uppsala, Sweden.
Nagar,D; Purohit, G.N. and Mehat, J.S. (2008) Prevalenceof reproductive conditions in bitches. J. CanineDev. Res. 5: 7-10.
Nelson, R.W., Feldman, E.C., Stabenfeldt GH. (1982).Treatment of canine pyometra and endometri-tis with prostaglandin F2 alpha. J Am Vet MedAssoc, 181, 899-903.
Pretzer, S.D.(2008). Clinical presentation of canine pyo-metra and mucometra: a review.Theriogenology,70: 359-363.
Pramod Kumar, G.N.Purojit, Yogesh Barolia, Sumit Yadav
and Jatinder Bargujar (2010). Clinical findingsand therapy of pyometra in bitches J. CanineDev. Res. 6: 79-82.
Pramod Kumar, G.N.Purojit, J,S.Mehta, Amit Kumar, VikasChoudhary, Chander Shekhar, and KamleshJeengar (2011). Prevalence of reproductive dis-orders in bitches. J. Canine Dev. Res. 7:29-35.
S.M.Qureshi, T.K.Gahlot, P. Bishnoi, Suresh Jhirwal andG.N.Purohit,(2002).Sonographic diagnosis ofpyometra in bitches J. Canine Dev. Res. 2: 61-62.
Roberts S. J. (1982) Uterine Inertia. In: Veterinary Obstet-rics & Genital Diseases. 2nd ed. CBS publish-ers and distributors. Pp. 231.
Smith, F.O (2006). Canine pyometra. Theriogenology, 66:610– 612.
Susi, A., Iris, R., Madeleine, H. (2006). Canine Pyometra:New Approaches to an Old Disease. In: Proc31st World Small Animal Veterinary Conference,Czech Republic.
Sugiura, K., Nishikawa, M., Ishiguro, K., Tajima, T., Inaba,M., Torii, R., Hatoya, S., Wijewardana, V.,Kumagai, D., Tamada, H., Sawada, T., Ikehara,S. and Inaba, T (2004). Effect of ovarian hor-mones on periodical changes in immune resis-tance associated with estrous cycle in thebeagle bitch. Immunobiology, 209: 619–27.
Tsumagari, S., Ishinazaka, T., Kamata, H., Ohba, S., Tanaka,S., Ishii, M., Memon, M.A (2005). Induction ofcanine pyometra by inoculation of Escherichiacoli into the uterus and its relationship to re-productive features. Anim. Reprod. Sci., 87: 301–308
72
Journal of Canine Development & Research 2013
RESEARCH ARTICLERENAL FAILURE IN DOG*M.L. Sain1, D. K. Bihani2, Mukesh Srivastava3, R. K. Khinchi4 and N. K. Singh4
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege of Veterinary and Animal Science, RAJUVAS, Bikaner- 334 001 (Rajasthan)
1Veterinary Officer,A.H.Dept., Rajasthan Govt. 2Professor 3Ph.D. scholar 4MVSc.Scholar*Corresponding author e-mail : [email protected]
A B S T R A C T
Present case report describes renal failure in an 8 year oldDoberman male dog, which was diagnosed thorough history,clinical examination and serum biochemistry. Dog was treatedwith furesimide and continuous infusion dopamine along withother supportive and fluid therapy but dog does not respond forthe treatment possibly due to presentation in end stage of chronickidney disease.
Key words :DogDopamineRenal failure
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
The kidneys are responsible for maintaininghomeostasis in the body, failure leads to
derangements of fluid, electrolyte, and acid-basebalance (Cathy, 2008). Incidence of renal diseaseincreases with age due to progressive loss ofnephron mass in every mammalian species, excepthorses (Grauer, 1992). Bilateral renal calcinosis isalso responcible for renal faliure (Bishnoi etal.,2004). Renal failure is a common clinicalproblem occurring in 2-5% of dogs (Lora-Michiels et al., 2001) and third leading cause ofdeath in canines. Robertson (2001) reported thatby the age of 5 years, nearly 60% of dogs showrenal lesions and decrements in renal function whichapproaches 90% by ten years. Renal dysfunctionis routinely identified by elevations in blood ureanitrogen (BUN) and serum creatinine, but azotemiais usually not present until an animal has lost
approximately 75% of its total renal function (Ross,1995). Loop diuretics, such as furosemide, canincrease urine flow without increasing GFR(McClellan et al., 2006). Despite the increase inurine output, loop diuretics do not improveoutcome, which suggests that patients that respondhave less severe renal failure, resulting in a betteroutcome for recovery in dependent of drug therapy(DeVriese et al., 2003). Dopamine infusionincreases renal blood flow in a dose-dependentmanner the dose range varies between species(Christopher et al., 1999). In dogs low-dosedopamine results in an increase in glomerularfiltration rate (GFR) (Lee, 1993). Present casereport describes the management of renal failurein a dog with furesimide and continuous infusiondopamine along with supportive therapy.
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 72-74

73
Journal of Canine Development & Research 2013
Case history and clinical observations
A 8 year old Doberman male dog (24 kg bodyweight) presented to the Outdoor of ClinicalMedicine, TVCC, of the College of Veterinary andAnimal Science, Bikaner, with the complaint ofpersistent vomiting since one week, andunresponsiveness to common antiemetics and othersupportive therapy. Clinical examination showedpaleness of mucous membrane, dehydration ofmore than 8% (based on skin tenting time 10second and capillary refill time of 4 second),oliguria and melena. All the vital parameters werealmost within normal range except tachypnoea (70/min) to panting and tachycardia (120/min). Noabnormality was detected on lung auscultation andabdominal palpation. Considering the history,animal data and clinical examination tentativediagnosis was made for renal failure, which wasconfirmed by kidney function test including BUNand serum creatnine and routine urinalysis.
Diagnosis
Kidney function showed higher degree of azotemiaand creatinemia (BUN-450 mg/dl and serumcreatnine 8.4mg/dl), which confirmed the renalfailure. Hematology showed normocyticnormochromic anemia (Hb- 8.0 gm %, PCV- 28% , MCV- 60 fl) and leucocytosis along withneutrophilia. Urinalysis was nonspecific except highspecific gravity of urine (1.035). Based on the resultof blood and urine examination the case wasconfirmed for renal failure.
Treatment and discussion
Treatment was initiated with 5% DNS 500 ml overhydration of the dog with equal amount of RingerLactate and Normal Saline (total 500 ml) in 24hrs along with Ampicillin @ 5 mg/kg bwt iv,Sucralfate @ 1 gm / day po, Iron Sucrose @200mg iv, Pentaperazole @ 1mg/ kg bwt, iv,Furesimide 4 mg/kg , iv bds and Decadurabolin25 mg im biweekly (Ahuja et al., 2010). The
above treatment was continued for 2 days, whichwas followed by Dopamine @ 2 µgm/kg/min ascontinuous infusion for 10 hrs daily for 7 days andfuresimide. The dog was further evaluated byclinical examination and kidney function test. after7 days, which showed clinical improvement in theform of subsidence of melena and regaining ofappetite but kidney function test were almost thesame (BUN- 300 mg/dl and Serum creatnine- 7.8mg/dl). Critically ill patients with acute renal failure(ARF) carry a higher risk specially in increasedage, and oliguria (Brivet et al., 1996). ARF inthe acutely ill patient may result from vascular,glomerular, interstitial, or obstructive injury,ischaemic tubular injury is the final commonpathway in the majority of cases (Duke, 1999).Dopamine is an endogenous diuretic andcatecholamine that is active and adrenergic anddopaminergic receptors. As a low-dose infusion(e.g. 1 - 5 µg/kg/min) it has been advocated fordecades as a promising renoprotective agent(Goldberg, 1972). Its inotropic effects mayimprove cardiac output and renal perfusionpressure and its intra-renal dopaminergic-1receptor agonist properties reduce renal vascularresistance, proximal tubular Na+ reabsorbtion(Duke and Bersten, 1992) and improve medullaryoxygenation in the presence of selective medullaryvasoconstriction (Fink et al., 1985). A number ofischaemic and nephrotoxic models of ARFsupport dopamine as a renoprotective agent(Duke and Bersten, 1992) but renal vasodilatationdoes not necessarily occur in the compromisedkidney and its diuretic action increases urine outputbut not creatinine clearance (Bersten and Rutten,1995). Use of furesemide in renal failure was basedon evidence of renal vasodilator properties inanimal models, the potential to flush ‘blocked’tubules, clinical reports of improved outcome, andevidence of lower mortality in patients withpolyuric ARF (Honda and Hishida, 1993). Butpresent case have failed to demonstrate any

74
Journal of Canine Development & Research 2013
ReferencesAhuja, Anil., Gahlot, T.K., Parashar, M.C. and
R.K.Dedar.(2010). Chronic renal failure in a dogdue to renal calcinosis – a case report. J.CanineDev. Res. 6: 83-85.
Bersten AD, Rutten AJ. (1995). Renovascular interactionof epinephrine, dopamine and intraperitonealsepsis. Crit Care Med. 23:537-544.
Bishnoi .P; Ahuja, A; Gahlot, T.K;Jhirwal S.K andRajpurohit G(2004) Bilateral renal calculi in adog. J.Canine Dev. Res. 4: 25-28.
Brivet FG, Kleinknecht DJ, Loirat P, Landais PJ. (1996).Acute renal failure in intensive care units—causes, outcome, and prognostic factors ofhospital mortality; a prospective, multicenterstudy. French Study Group on Acute RenalFailure. Crit Care Med. 24:192-198.
Cathy Langston (2008). Managing Fluid and ElectrolyteDisorders in Renal Failure. Vet Clin Small Anim.38: 677–697.
Christopher J Burton and Charles R V Tomson. (1999).Can the use of low-dose dopamine for treat-ment of acute renal failure be justified? PostgradMed J. 75: 269-274
DeVriese AS. (2003). Prevention and treatment of acuterenal failure in sepsis .J Am Soc Nephrol.14:792–805.
Duke G. J. (1999). Renal Protective Agents: A ReviewCritical Care and Resuscitation. 1: 265-275
Duke GJ and Bersten AD. (1992). Dopamine and renal
outcome benefit of combined therapy of furesimideand dopamine, suggested reason is presentationof case in end stage of disease, It is concludedthat management of renal failure is most successfulif initiated early (Grauer and Lane, 1995).
salvage in the critically ill patient. Anaesth In-tensive Care. 20: 277-302.
Fink MP, Nelson R, Roethel R. (1985). Low-dose dopam-ine preserves renal blood flow in endotoxinshocked dogs treated with ibuprofen. J SurgRes. 38:582-591.
Goldberg LI. (1972). Cardiovascular and renal actionsof dopamine: potential clinical applications.Pharmacol Review. 24:1-29.
Grauer, G. (1992). “Glomerulonephritis.” Seminars in Vet-erinary Medicine and Surgery (Small Animal)7(3): 187-97.
Grauer, G.F. and I.F. Lane. (1995). Acute Renal Failure InText book of Veterinary Internal Medicine,Ettinger, S.J. and E.C.Feldman (Eds.). WBSaunders Co., Philadelphia, PA USA., Pp: 851-855.
Honda N, Hishida A. (1993) Pathophysiology of experi-mental nonoliguric renal failure. Kidney Int.43:513-521.
Lee MR. (1993). Dopamine and the kidney: ten years on.Clin Sci.84:357–75.
Lora-Michiels, M., Anzola, K.G. and Solano, M. (2001).Quantitative and qualitative scintigraphic mea-surement of renal function in dogs exposed totoxic doses of Gentamicin. Vet. Radiol. Ultra-sound. 42 (6): 553-561.
McClellan JM, Goldstein RE, Erb H.N. (2006). Effects ofadministration of ?uids and diuretics on Glom-erular ?ltration rate,renal blood flow, and urineoutput in healthy awake cats.AmJVet Res.67:715–22.
Robertson, J. (2001). The kidney in the aging dog.Pathobiology of the Aging Dog. (Blacksburg,Iowa State University Press.
Ross, L.A. (1995). Assessment of renal function in thedog and cat. (In: RW, Kirk. (Ed.) Current Veteri-nary Therapy IX. W.B. Saunders, Philadelphia.

75
Journal of Canine Development & Research 2013
CLINICAL ARTICLEMANAGEMENT OF ASCITES IN A DOG*A.K. Srivastava1 and B. Syed1
Faculty of Veterinary Medicine, Jigjiga University, Jigjiga, Ethiopia.
1 Professor* Corresponding author e-mail :[email protected]
A B S T R A C T
Hepatic origin ascites was diagnosed and treated in a 6 yearmale boxer dog, prominent signs were distended abdomen,difficulty in breathing, frequent vomition, hollow flanks withprominent spines. Radiography showed ground glass like densityof the abdomen, while hemato-biochemical showed anemia andhepatic dysfunction. Treatment was done with diuretics,antibiotics, fructodex, recovery was recorded in six days oftreatment.
Key words :AscitesBoxer DogHepatic Dysfunction
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
Ascites is caused by the leakage of fluid intothe abdomen from blood vessels, lymphatics,
internal organs or abdominal masses (Press et al.,1982). Common causes of ascites includenephrotic syndrome (Runa et al., 2013), cirrhosis(progressive damage and scarring) of the liver(Srivastva and Syed, 2012), right-sided congestiveheart failure, hypoproteinemia ,ruptured bladder,peritonitis and abdominal cancer. Sunil et al.(2003)reported that 85% of cases of ascites in dogs aredue to liver disorders and 15 % due to kidneydysfunction. They further reported dullness,depression and anorexia with pendulous abdomenand on tactile percussions fluid sounds as majorclinical manifestations. Abdominal radiographs,ultrasonography as recommended by Anne- LaureEtiene et al. (2013), evaluation of the ascitic fluidled to a diagnosis of chyloabdomen. Presently acase of ascites is reported.
Case history and clinical examination
A male Boxer dog of about 6yrs age presented tothe Faculty of Veterinary Medicine, Jijgjiga withprogressive lethargy and a severely distendedabdomen, difficulty in breathing, frequent vomition,hollow flanks with prominent spines. Conjunctivalmucous membrane was pale and temperature waswithin normal range, changes in urinary and bowelhabits, sudden weakness. Tactile percussion ofabdominal cavity revealed fluid thrills. Ascitic fluidwas transudate as it was negative to Revaltareaction, faecal of dog was negative for parasiticinfection and helminthic ova and urine sample didnot reveal presence of sugar, albumin acetone, bilesalts or bile pigments. Hematology revealeddecrease in the red cells, while biochemical profileshowed elevations in ALT, AST and ALKPenzymes. Decreases in BUN, albumin, cholesteroland blood glucose indicated decreased liver
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 75-77

76
Journal of Canine Development & Research 2013
functional capability. Abdominal X-ray showedsignificant ascites due to which the abdominalstructures were obscured by the nature of the fluid.On ultrasonography, fluid in the abdomenenhanced the images, providing for greater detail,which allowed evaluation of the liver, kidneys,spleen and pancreas.
Treatment and discussion
About 1.0 lit ascitic fluid was aspirated asepticallyemploying therapeutic abdominocentesis, as therewas a large amount of fluid in the abdomencompressing the diaphragm and leading to difficultyin breathing. A needle was inserted into theabdominal wall and fluid drained to relieve thepressure, making breathing easier and the dog wascomfortable but all the fluid was not removed,however, because losing too much fluid from thebody might lead to shifts in fluid homeostasis andshock. Diuretics (Furosemide) - Lasix @ 4 mg/kg bwt was administered to increase fluidexcretion, ampicillin 500 mg i/m to fight infectionsfor 6 consecutive days. Fluid balance wasmaintained with Fructodex 200 ml i/v daily.Additionally Betnelan 1.0 mg tab orally, daily for5 days and liver tonic 2.5 ml i/m on alternate daysfor 10 days were also supplemented. The dog whenexamined after a week, showed markedimprovement as there was absence of oedema ofindependent parts and vomition and had normalappetite. After 20 days, the animal developed slightoedema of in dependent parts and dullness. So itwas treated with the same drugs for one weekagain which resulted in improvement. Animalrecovered completely after a week.Combination of portal hypertension and moderatehypoalbuminemia often produces ascites in dogswith liver dysfunction (Jan, 2009). Because of thehigh reserve capacity of the liver, hypoalbuminemiaoccurs only when liver function is chronically andseverely impaired such as chronic hepatitis/cirrhosisand severe forms of portal vein hypoplasia
(Szatmari and Rothuizen, 2006). However, evenin the most severe cases, the synthesis of albuminis only moderately reduced and reduced osmoticpressure may be the only cause of edema/asciteswhen albumin concentrations reduce to a criticallevel. Therefore portal hypertension must bepresent in liver diseases in order to cause ascites,also, liver diseases causing portal hypertension giverise to different liver dysfunctions, such as reducedprotein and albumin production. In dogs withsevere cholestasis, associated with high systemicplasma levels of different bile acids have beenshown to inhibit the activity of 11 b-hydroxysteroiddehydrogenase (OHSD), which prevent cortisolfrom binding to the aldosterone receptor (Fossumet al., 1986). Cortisol is present in about tenfoldexcess to aldosterone, and has the same affinityfor the aldosterone receptor. On binding, cortisolactivates the intracellular aldosterone pathways andthen acts as aldosterone. OHSD converts cortisolinto cortisone, which does not bind to the receptor(Stauffer et al., 2002). Inhibition of the enzymeby bile acids may cause unexpectedhyperaldosteronism, exerted by cortisol, andcondition may lead to ascites, hydrothorax, oredema, which is refractory to most diuretics butresponds well to spironolactone, an aldosteronereceptor antagonist. The cause of ascites formationis reflected in the type of ascitic fluid (Gerritzen etal., 2006) With pre and posthepatic causes thereis a high portal blood pressure and congestion ofthe splanchnic vascular bed, therefore abdominalfree fluid then contains lymph, plasma, anderythrocytes. The fluid is more or less turbid andpink-colored. If the cause is intrahepatic, there isonly moderate portal hypertension andhypoalbuminemia and increased hepatic andsplanchnic lymph production, which exceeds thecapacity of the lymphatic system, causing a clear,nonhemorrhagic, colorless transudate (or yellowishin cases of icterus). The diagnosis of the underlyingcause of ascites starts by examining a few milliliters

77
Journal of Canine Development & Research 2013
of ascitic fluid. If cardiac failure can be excludedwith physical examination, pink- colored fluidindicates either portal vein or thoracic vena cavaobstruction. Clear colorless transudate indicatesan intrahepatic disease requiring liver biopsy forfinal diagnosis. Clear colorless transudate may alsooccur in nonhepatic diseases associated with severealbumin loss (nephrotic syndrome and protein-losing enteropathy). Pink colored fluid may be seenwith some abdominal tumors, although this is rare.The ascitic fluid may contain a large amount ofalbumin due to diffusion of this low molecularweight protein out of the circulation. Completeremoval of the abdominal fluid in animals with portalhypertension is useless (the cause remains and theascites recurs quickly) and undesirable. The ascitescan be treated more effectively by a low-sodiumdiet and potassium sparing diuretics (Pradhan etal., 2008).
ReferencesAnne- Laura Etiene, Romian Cavrenne, Kris Gommeran,
Geraldine Bolen and Valeria Busoni (2013). Cis-terna Chyli in eight dogs and four cats. Veteri-nary Radiology and Ultrasound,54(4): 398-402.
Fossum, T.W., Jacobs, R.M., Birchard, S.J. (1986). Evalu-ation of cholesterol and triglyceride concentra-tions in differentiating chylous and nonchylouspleural effusions in dogs and cats. J Am VetMed Assoc., 188(1):49–51.
Gerritzen-.Bruing MJ, van den Ingh TS, Rothuizen J.(2006). Diagnostic value of fasting plasma am-monia and bile acid concentrations in identifi-
cation of portosystemic shunting in dogs. J VetIntern Med.20:13-9.
Jan Rothuizen. (2009). Important Clinical SyndromesAssociated with Liver Disease. Vet CIin SmallAnim.39: 419-437.
Pradhan, M.S., Dakshinkar, N.P., Waghaye, U.G. andBodkhe, A.M. (2008). Successful treatment ofAscites of hepatic origin in Dog. VeterinaryWorld, 1(1):23.
Press, O.W., Press, N.O., Kaufman, S.D. (1982).Evalua-tion and management of chylous ascites. AnnIntern Med. 96(3):358–364.
Runa Rortveit, Anna Vigdis Eggertsdottir, RagnarThomassen, Forde Lingas and John HegsetJansen (2013). A clinical study of canine col-lagen type III glomerulopathy. BMC VeterinaryResearch.9: 218.
Srivastva, A.K. and Syed, B. (2012). Management ofAscites in Cats. Ind J Canine Prac, 4(2): 86-87.
Stauffer AT, Rochat MK and Dick B.( 2002) Chenode-oxycholic acid and deoxycholic acid inhibit 11beta-’hydroxysteroid dehydrogenase type 2and cause cortisol- induced transcriptional ac-tivation of the mineralocorticoid receptor. J BiolChem.277:26286-92.
Sunil Kumar, Anil Ahuja, D.K. Bihani and A.K. Gahlot(2003). Studies on canine ascites J. Canine Dev.Res. 3: 9-17.
Szatmari V, Rothuizen J. ( 2006) Ultrasonographic identi-fication and characterization of congenitalportosystemic shunts and portal hypertensivedisorders in dogs and cats. In: WSAVA LiverStandardization Group, editor. WSAVA stan-dards for clinical and histological diagnosis ofcanine and feline liver diseases. Edinburgh(UK): Churchill Livingstone.Pp. 1540.
78
Journal of Canine Development & Research 2013
CLINICAL ARTICLESERTOLI CELL TUMOUR IN A DOG AND ITS SURGICALMANAGEMENT*Arabinda Adak1, Vinay Chaturvedi2, V. K. Tripathi3 and S. K. Mukhopadhayay4
Department of PathologyBombay Veterinary College, Parel, Mumbai - 400 012 (Maharashtra)
1,2,3M.V.Sc. Scholar 2Dept. of Surgery 3 Dept. of Medicine 4Professor & Head, Dept of Pathology, WBUAFS, Kolkata.*Corresponding author e-mail : Arabinda.Adak @vantabio.com
A B S T R A C T
A five year old Doberman dog was presented to BombayVeterinary College Hospital with a complaint of swelling at thescrotal region and improper gait for last three months. The lefttesticle was enlarged with hard consistency while thecorresponding right testicle was small, flabby and atrophied.Orchiectomy was performed to remove both the testicles undergeneral anaesthesia. Histopathological examination confirmedthe tumour mass as sertoli cell tumour. The dog made anuneventful recovery post surgical excision of the tumour mass.
Key words :IntrascrotalOrchiectomySertoli cell tumour
A R T I C L E H I S T O R Y
Received : February 20, 2013Revised : June 04, 2013Accepted : June 22, 2013
Sertoli cell tumor (sustentacular cell tumour) isa form of testicular tumor and is usually linked
with undescended testicles or cryptorchidism(Saegusa et al., 2011 and Quartuccio et al.,2012). It is fairly common in dogs and rare in catsand horses (Moulton, 1978). Although relativelyrare, testicular tumour is the most common solidorgan malignancy in young men and remains aleading cause of cancer death in this population(Ye and Ulbright, 2012). It is reported that up to14 per cent sertoli cell tumors in dogs are malignantand metastasize to surrounding lymph nodes in thebody and other organs (Peters and Vom, 1996).The average age of affected dogs is eight to nineyears and there is no breed predilection. Thepresent paper deals with a case of intrascrotalsertoli cell tumour in a five year old Doberman
dog and it’s successful surgical treatment.
Case history and clinical examination
A five year old Doberman dog was presented toBombay Veterinary College Hospital with acomplaint of swelling at the scrotal region andimproper gait for the last three months. Clinicalexamination revealed that the left testicle wasenlarged with hard consistency while thecorresponding right testicle was small, flabby, andatrophied (Fig. 1). There was typical bilateralalopecia, especially on the ventral aspect of theabdomen. The dog was otherwise healthy withnormal appetite and physiological parameters werealso normal. Considering it to be a case of testiculartumour, it was decided to perform radical surgery.
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 78-80

79
Journal of Canine Development & Research 2013
Surgical treatment
The animal was premedicated with triflupromazine@1 mg/kg bwt iv and atropine sulfate (0.65 mg)sc . After 15 minutes, general anaesthesia wasinduced by thiopentone sodium @7.5 mg/kg bwtiv and maintained with the same according to thecondition. After preparing the site for asepticsurgery, an elliptical incision was given around thebase of the scrotum and it was separated from thesubcutaneous tissue by blunt dissection. Afterhemostasis, both the testicles were removed andthe incision was closed in routine manner. Thetumour mass was preserved in 10% neutralbuffered formalin for histopathological examination.Post operatively, lactated Ringer’s solution 500ml iv, meloxicum 0.2 mg/kg bwt sc andstreptopenicillin 10,000 IU/ kg bwt im were givenfor 7 days. Skin wound was dressed withnitrofurazone ointment for 10 days.
Results and discussion
In the present case, symptoms of feminization wereabsent as it usually occurs in extrascrotal sertolicell tumour in cryptorchid dogs (Damodaran etal., 1974 ; Quartuccio et al., 2012).Grossly, the external surface of the growth wassmooth and the tumour was enclosed by aglistening white capsule that was well vascularized.The tumour was bulging out on cut section andwas irregularly lobulated (Fig.2). The tumour was
7cm x5cm x4.5cm in size and weighed 67 gmswhereas this tumour (confirmed as sertoli celltumour) generally grows to measure about 5 cmin greatest diameter, about 1 cm smaller thanseminoma and several cms larger than interstitialcell tumour (Cotchin, 1960).Histopathological examination revealed tubules ofmultilayered neoplastic cells separated by thickcollagenous connective tissue septa. The neoplasticcells were arranged with their long axisperpendicular to the basement membrane of thetubules. In some areas, the neoplastic cells spilledout of the tubules into the stoma, forming into solidinfiltrating cords or broad sheets. There were nocharacteristic features of malignancy. Based onabove gross and histopathological changes, thecase was confirmed as sertoli cell tumour. Thegross and microscopic findings were in agreementwith previous reports (Moulton, 1978, Jones etal., 1997 ; Mikuz, 2002). In the present case, thedog was completely recovered on removal of thetumour mass and there was no complication seeneven after six months. Thus surgical excision oftestes or orchiectomy seemed to be an effectivetreatment for sertoli cell tumour as reported byearlier workers (Dhaliwal et. al., 1999).
Acknowledgements
The authors are thankful to the Dean, BombayVeterinary College for providing the necessary facilities.
Fig. 1: Dog showing enlargement of the lefttesticle and atrophy of right testicle
Fig. 2: Transverse section of tumour massshowing irregular lobulation

80
Journal of Canine Development & Research 2013
ReferencesCotchin, E. (1960). Tumours of farm animals: A survey of
tumours examined at the Royal Veterinary Col-lege, London, during 1950-60. Vet. Rec. 72: 816-823.
Damodaran, S.G., Ramachandra, P.V. and Parthasarathy,K.R. (1974). Testicular neoplasms in canines.Cheiron. 3: 107-111.
Dhaliwal R.S., Kitchell B.E., Knight B.L. and SchmidtB.R. (1999). Treatment of aggressive testiculartumors in four dogs. J Am Anim Hosp Assoc.,35(4):311-318.
Jones, T.C., Hunt, R.D. and King, W.W. (1997). Veteri-nary Pathology, 6th edn. Williams & Wilkins, AWaverly company, Baltimore, Maryland, U.S.A,pp 1210-1211.
Mikuz G. (2002). WHO classification of testicular tumors.Verh Dtsch Ges Pathol., 86:67-75.
Moulton, J.E. (1978). Tumours in Domestic Animals. 2nd
edn. University of California Press, Berkeleyand Los Angeles, pp 309-312.
Peters M.A. and Van Sluijs F.J. (1996). Testicular tumorsin dogs: a literature review. TijdschrDiergeneeskd.121(2):36-38.
Quartuccio M., Marino G., Garufi G., Cristarella S. andZanghì A.(2012). Sertoli cell tumors associatedwith feminizing syndrome and spermatic cordtorsion in two cryptorchid dogs. J Vet Sci.,13(2):207-209.
Saegusa Y., Hayashi H., Taniai E., Imaoka M., Ohishi T.,Wang L., Mitsumori K. and Shibutani M. (2011).Spermatocytic seminoma with neuroectodermaldifferentiation and sertoli cell tumor in a dog.Vet. Pathology. 48(5):1024-1028.
Ye H. and Ulbright T.M. (2012). Difficult differential di-agnoses in testicular pathology. Arch PatholLab Med., 136(4):435-446.
81
Journal of Canine Development & Research 2013
CLINICAL ARTICLEUSE OF DECOLORIZED IODINE IN ALOPECIA OF CANINE*Bhanu K Khajuria1, Anisha Tiwari2 and S.K. Gupta3
Department of Veterinary Medicine, Faculty of Veterinary Science & Animal Husbandry, SKUAST, R.S.Pura,Jammu -180 009(J & K).
2 Department of Veterinary Parasitology, College of Veterinary Science, GADVASU, Ludhiana.3Dean
* Corresponding auther e-mail : [email protected]
A B S T R A C T
Therapeutic studies of four cases of alopecia in dogs in group I(2 dogs) with decolorized Iodine and group II (2 dogs) withomega 3 and 6 fatty acids, orally is reported and found afterencreasing results in dogs of group I.Key words :
AlopeciaDecolorized IodineErythemaVascularity
A R T I C L E H I S T O R Y
Received : March 07, 2013Revised : July 10, 2013Accepted : August 22, 2013
Alopecia is defined as a complete or partiallack of hair in areas where hair normally are
present. It is quite common in dogs as either aprimary problem or as a secondary result of anotherunderlying condition. There are distinct differencesbetween cases of alopecia in which grown hairfibers are lost, those in which stumps of hair fibersremain, and those in which the hair root itself isshed from the hair follicle (Merck Manuals, 2008).Hair comes from follicles which may be in theanagen phase (period of active growth) or telogenphase (resting period). Normally, this process isnicely balanced so that the animal is covered inhair all of the time. Very rarely, animals can endup with excessive amounts of hair, however, whenthis process goes wrong, they end up with alopeciawhich means loss of hair in any amount up to
complete baldness. It may be partial, in which thehair density is merely reduced, or total, in whichthe area of affected skin is devoid of hair (Peter,2005). Iodine is a common aid for skin conditions,such as acne, as well as hair loss. (Edward ,2011).Presently therapeutic studies of four cases ofalopecia in dogs is reported.
History,clinical examination and therapy
Four cases of alopecia (Two Labradors of agebetween 1.5 to 2 years, one pug of age 8 monthsand 1 German Shepard (GSD ) of age 1 year)were presented to the local pet clinic of Jammu.Alopecia due to unknown reason was found to bethe cause in all the cases. These dogs are devidedin the group I and II. In group I (one Labradorand one GSD) Decolorized iodine was applied
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 81-82

82
Journal of Canine Development & Research 2013
for two week on the alopecic area once daily.Active ingredients of decolorized iodine: Alcohol(45%), Ammonium and, Potassium Iodides (6.7 -7.1%), Inactive Ingredient: Purified water.In group II
(one Labrador and one pug) both the
dogs were treated with omega 3 and 6 fatty acids-Omege 3 (1 Part) + Omega 6 (10 Parts)-each10 ml cantains total 6600 mg and given @ 0.5ml/kg bwt per day orally for one month along withthe regular brushing.
Results and discussion.
In group I due to irritation caused by the iodinethere was erythema, on the area where there wasno hairs which occurred due to the increasedvascularity of the area. After one week there wasgrowth of small hairs on hairless area. Moreoverthere was drastic reduction in the hair fall. After 3weeks there was complete hair growth on the baldarea and hair fall reduced by 90%.In group II, there was no change in the alopeciearea and continuous hair fall even after one monthof treatment.The prognosis for recovery from alopecia is goodin most cases, if the underlying cause of hair loss isidentified and treated. If the skin has suffered
extensive scarring, hair regrowth will be morelimited. Topical iodine may benefit people withalopecia by causing a mild irritating reaction thatstimulates hair growthd. Barb (2011) reported thatdecolorized iodine successfully used for the face,take a q-tip and dab the dermatitis. According toThappa et al.(2001) topical iodine is successfullyused for patients with alopecia as a first line oftreatment, however, more aggressive treatmentsincluding corticosteroid injections may beprescribed if topical irritants don’t work.
ReferenceBarb (2011) Many Uses of Iodine. https://
www.facebook.com/note.php. note_id=10150149964445242 .Published on March 7.
Edward Group (2011) Uses of Iodine and Other Tips,Research, and Resources. http://www.globalhealingcenter.com/natural-health/uses-for-iodine .Published on March 16.
Peter Hill. (2005) Clinical approach to alopecia in dogs -will the hair grow back? In proceeding of theNorth American Veterinary Conference,Orlando, Florida. Pp- 263-268.
Merck Manual (2008) The Merck Veterinary Manual.Edited by Siegmund and McLean. Merck & Co.,Rahway, N.J., U.S.A..onlinelibrary.wiley.com/doi/10.1111/j.1751-0813.1962...x/abstract
Thappa DM et al.(2001) Alopecia Areata. Ind. J. Derma-tology, Venereology, and Leprology; 67:127-129.
83
Journal of Canine Development & Research 2013
CLINICAL ARTICLEDIAPHYSEAL OBLIQUE FRACTURE OF FEMUR AND IT’SSURGICAL MANAGEMENT IN A DOG*Jayakrushna Das1, Sidhartha Sankar Behera2, Manas Ranjan Senapati3 and Monalisa Behera4
Department of Veterinary Surgery and RadiologyCollege of Veterinary Science and Animal Husbandry, OUAT. Bhubaneswar-751 003 (Odisha)
1Assistant Professor 2,3,4PhD Scholar 3Dept. of Vety. Biochemistry 4 Dept. of Vety. Pathology*Corresponding author e-mail : [email protected] and [email protected]
A B S T R A C T
A 7 years old female Spitz dog was presented with history oflameness along with non-weight bearing on left hind limb causedafter jumping from a height since a week. Lateral radiograph byC-arm of left femur revealed complete, oblique fracture. Undergeneral anaesthesia using atropine sulphate, xylazine andketamine open reduction and internal fixation with intramedullarySteinman pinning and circlage wiring were done. Theimmobilization was further strengthened by application of Thomassplint. Post-operatively antibiotic, analgesic and regular dressingof the wound was carried out. On 35
th post-operative day the
immobilizers were removed and the dog recovered well.
Key words :Femoral fractureInternal, External Immobilization
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
F racture of long bone is a commonlyencountered orthopaedic problem in canine
practice. Among the prevalence of fracture ofvarious bones of pelvic limb the incidence washighest in femur followed by tibia and fibula (Simonet al., 2010). Femur is the most commonlyfractured bones accounting to 45% of long bonefractures in small animals. Of these 28% occur indistal physeal/epiphyseal region and majority ofwhich are Salter-Harris type I or II fractures(Harasen, 2003a,b). High velocity injuries are themost common type of trauma that causes femoralfractures in veterinary patients (Fossum, 1997).Most of the injuries result from automobile
accidents, but gunshot injuries and blunt traumaare also common. Although metaphyseal anddiaphyseal fractures are more common in maturedogs, proximal or distal physeal fractures are morecommon in puppies. Most femur fractures areobserved as closed fractures because of heavyoverlying muscle while some open fractures mayoccur because of penetrating injury such as agunshot wound (Singh and Saha, 2012).
Case history and clinical observations
A female Spitz dog weighing14 kg and 7 yearsold was presented with history of non-weightbearing and lameness of left hind limb after jumping
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 83-87
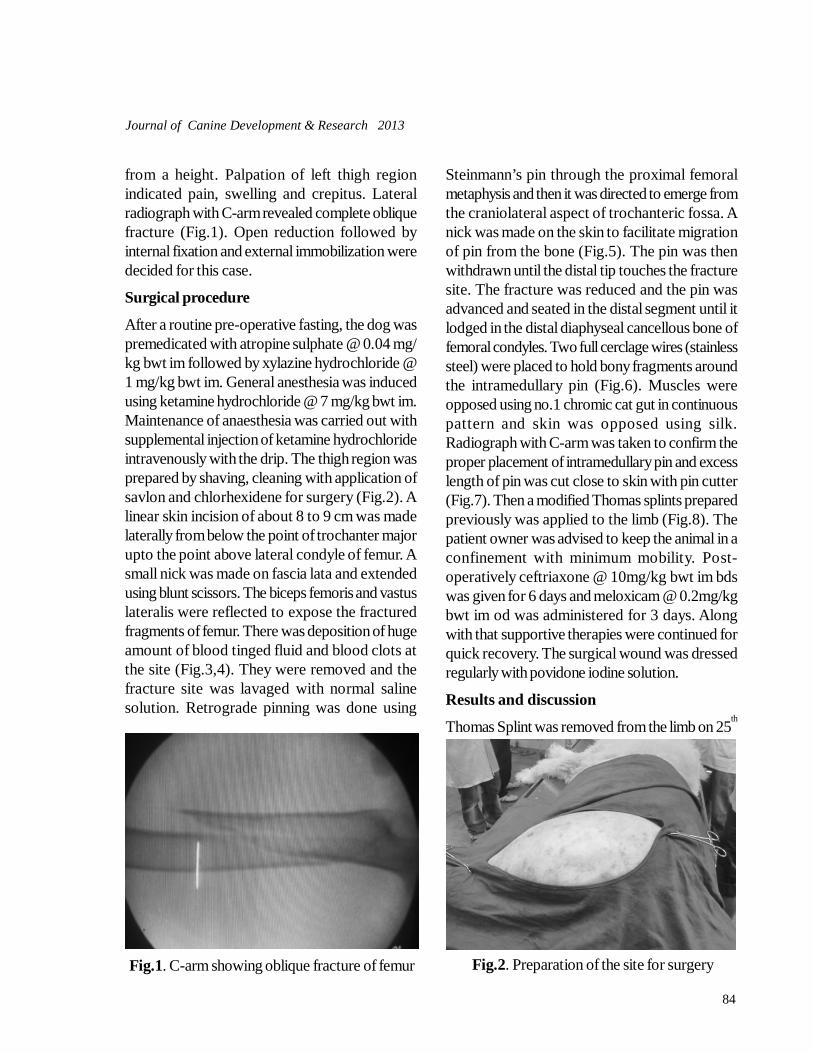
84
Journal of Canine Development & Research 2013
from a height. Palpation of left thigh regionindicated pain, swelling and crepitus. Lateralradiograph with C-arm revealed complete obliquefracture (Fig.1). Open reduction followed byinternal fixation and external immobilization weredecided for this case.
Surgical procedure
After a routine pre-operative fasting, the dog waspremedicated with atropine sulphate @ 0.04 mg/kg bwt im followed by xylazine hydrochloride @1 mg/kg bwt im. General anesthesia was inducedusing ketamine hydrochloride @ 7 mg/kg bwt im.Maintenance of anaesthesia was carried out withsupplemental injection of ketamine hydrochlorideintravenously with the drip. The thigh region wasprepared by shaving, cleaning with application ofsavlon and chlorhexidene for surgery (Fig.2). Alinear skin incision of about 8 to 9 cm was madelaterally from below the point of trochanter majorupto the point above lateral condyle of femur. Asmall nick was made on fascia lata and extendedusing blunt scissors. The biceps femoris and vastuslateralis were reflected to expose the fracturedfragments of femur. There was deposition of hugeamount of blood tinged fluid and blood clots atthe site (Fig.3,4). They were removed and thefracture site was lavaged with normal salinesolution. Retrograde pinning was done using
Steinmann’s pin through the proximal femoralmetaphysis and then it was directed to emerge fromthe craniolateral aspect of trochanteric fossa. Anick was made on the skin to facilitate migrationof pin from the bone (Fig.5). The pin was thenwithdrawn until the distal tip touches the fracturesite. The fracture was reduced and the pin wasadvanced and seated in the distal segment until itlodged in the distal diaphyseal cancellous bone offemoral condyles. Two full cerclage wires (stainlesssteel) were placed to hold bony fragments aroundthe intramedullary pin (Fig.6). Muscles wereopposed using no.1 chromic cat gut in continuouspattern and skin was opposed using silk.Radiograph with C-arm was taken to confirm theproper placement of intramedullary pin and excesslength of pin was cut close to skin with pin cutter(Fig.7). Then a modified Thomas splints preparedpreviously was applied to the limb (Fig.8). Thepatient owner was advised to keep the animal in aconfinement with minimum mobility. Post-operatively ceftriaxone @ 10mg/kg bwt im bdswas given for 6 days and meloxicam @ 0.2mg/kgbwt im od was administered for 3 days. Alongwith that supportive therapies were continued forquick recovery. The surgical wound was dressedregularly with povidone iodine solution.
Results and discussion
Thomas Splint was removed from the limb on 25th
Fig.1. C-arm showing oblique fracture of femur Fig.2. Preparation of the site for surgery
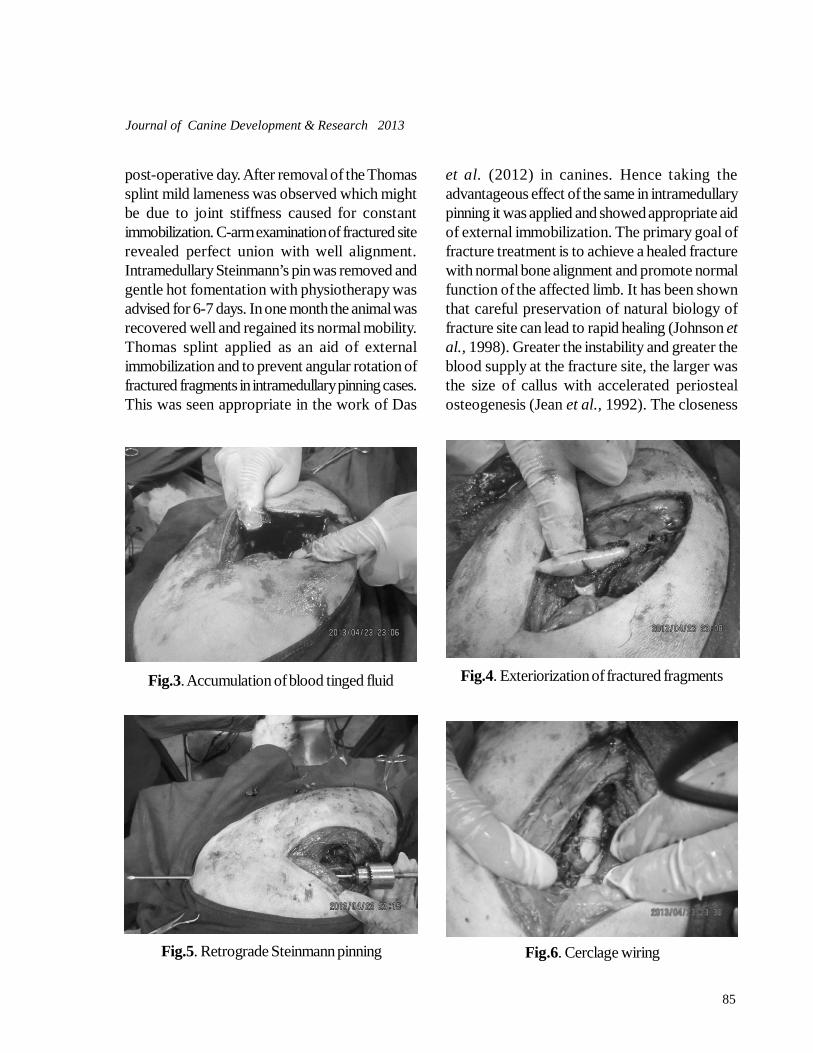
85
Journal of Canine Development & Research 2013
post-operative day. After removal of the Thomassplint mild lameness was observed which mightbe due to joint stiffness caused for constantimmobilization. C-arm examination of fractured siterevealed perfect union with well alignment.Intramedullary Steinmann’s pin was removed andgentle hot fomentation with physiotherapy wasadvised for 6-7 days. In one month the animal wasrecovered well and regained its normal mobility.Thomas splint applied as an aid of externalimmobilization and to prevent angular rotation offractured fragments in intramedullary pinning cases.This was seen appropriate in the work of Das
et al. (2012) in canines. Hence taking theadvantageous effect of the same in intramedullarypinning it was applied and showed appropriate aidof external immobilization. The primary goal offracture treatment is to achieve a healed fracturewith normal bone alignment and promote normalfunction of the affected limb. It has been shownthat careful preservation of natural biology offracture site can lead to rapid healing (Johnson etal., 1998). Greater the instability and greater theblood supply at the fracture site, the larger wasthe size of callus with accelerated periostealosteogenesis (Jean et al., 1992). The closeness
Fig.3. Accumulation of blood tinged fluid Fig.4. Exteriorization of fractured fragments
Fig.5. Retrograde Steinmann pinning Fig.6. Cerclage wiring
86
Journal of Canine Development & Research 2013
of the abdominal wall to proximal femur and thebulky surrounding musculature, limits the use ofcoaptation and external skeletal fixation for femoralfractures (Tiwari et al., 2012). The intramedullarypinning with cerclage wiring are the commonesttreatment for diaphyseal femur fracture in dogs(Rani et al., 2007). In the present case owing toits spiral diaphysial fracture both intrmedullarypinning and circlase wiring using stainless steelsuture wiring was done for proper fracturealignment.McLaughlin (1999) reported that stack pinningusing two Steinmann pins placed in the medullarycavity of femur provided stability in fracturedfragments and cerclage wires used to stabiliseoblique fractures provided stability byinterfragmentary compression in dogs. Rani et al.(2007) stated that double intramedullary pinningwith cerclage wiring was an excellent techniquefor femoral diaphyseal oblique fracture in dogs.The stated method provided alignment androtational stability by their tight fit at the fracturesite. Orthopedic wire hemicerclage or full cerclagewires provide interfragmentary compressionbetween oblique, spiral or comminuted fracturefragments. The use of hemicerclage or full cerclagewires alone without an intramedullary device iscontraindicated and provides fixation failure
(Newton and Nunamaker, 1985). Here the casewas managed effectively by use of singleintramedullary pin of matching diameter withmedullary cavity along with cerclage wiring withoutany complications except mild joint stiffness. Theimmobilization was further strengthened byapplication of Thomas splint which was also helpfulin providing rotational rigidity. Post-surgicalcomplications with femoral fracture repair includeimplant loosening, fatigue or outright failure as aresult of excessive stress on the implant andsubsequent bone resorption. Most of thesecomplications are frequently encountered in largeand active patients as it has a negative mechanicaleffect on fracture healing. Other causes of implantfailure in cases of comminution includedevascularized bone fragments and small fracturegap caused by unsuccessful reduction andstabilization (Fossum et al., 1997). However, inthe present case no such complications wereobserved. From the present study it was seen thatthe intramedullary pin along with cerclage wiresand Thomas splint application were relatively easierto implant than other forms of fixation which yieldgood result. Hence it can be effectively used forimmobilization of femoral diaphyseal obliquefracture in dogs.
Fig.7. C-arm after immobilization Fig.8. Application of Thomas splint

87
Journal of Canine Development & Research 2013
References
Das, J., Behera, S.S. and Hembram, A. (2012). Intramedul-lary pinning and modified Thomas splint appli-cation for the management of bilateral fractureof femure and tibia in a pup. Intas Polivet. 13:426-828.
Fossum, T.W. (1997). Femoral Diaphyseal Fracture. In:Small Animal Surgery. Don Ladig (ed.) Mosby,Inc. A Harcourt Health Science Company. St.Louis, Missouri, Pp: 853-863.
Harasen, G. (2003a). Common long bone fractures in smallanimal practice- part 1. Can Vet J 44: 333-34.
Harasen, G. (2003b). Common long bone fractures in smallanimal practice- part 2. Can Vet J 44: 503-04.
Jean, G., DeBowes, R.M., Hull, B.L. and Constable, P.D.(1992). Intramedullary pinning of femoral dia-physeal fractures in neonatal calves: 12 cases(1980-1990). J. Am. Vet. Med. Assoc. 200: 1372-76.
Johnson, A.L., Smith, C.W. and Schaeffer, D.J. (1998).Fragment reconstruction and bone plate fixa-tion compared with bridging plate fixation fortreating highly comminuted femoral fractures
in dogs: 35 cases (1987-1997). J. Amer. Vet. Med.Assoc. 213: 1157-61.
McLaughlin, R. (1999). Internal fixation. Vet. Cl. North.Am. Sm. Anim. Pract. 29: 1097-1115.
Newton, C.D. and Nunamaker D.M. (1985). Fracture ofthe Femur. In: Textbook of Small Animal Or-thopedics” J.B. Lippincott Company.
Rani, R.U., Kathiresan, D. and Vairavasamy, K. (2007).Fracture pattern of femur in canines and theirsurgical management. Indian Vet. J. 84: 1310-12.
Simon, Shiju M., Ganesh, R., Ayyappan, S., Rao, G. D.,Suresh Kumar, R., Kundave, V. R. and Das, B. C.(2010). Incidences of pelvic limb fractures indogs: A survey of 478 cases. Vet. World. 3:120-21.
Singh, D.K. and Saha, M.K. (2012). Intramedullary Pin-ning and use of Cerclage Wires for the Man-agement of Diaphyseal Comminuted FemoralFracture in a Dog. Intas Polivet. 13 (II): 420-421.
Tiwari, S.K., Kashyap, D.K. and Sharda, R. (2012). Femo-ral Fracture and its Surgical Management us-ing Intramedullary Pinning in a Dog. IntasPolivet.13 (II): 422-423

88
Journal of Canine Development & Research 2013
CLINICAL ARTICLESUCCESSFUL MANAGEMENT OF DYSTOCIA IN A BITCH*Kuldip Dwivedi 1
Department of Obstetrics & GynaecologyCollege of Veterinary Science & Animal Husbandry, DUVASU, Mathura -281 001 (U.P.)
Assistant Professor*Corresponding author e-mail: [email protected]
A B S T R A C T
A 4 year old Labrador bitch was brought with a hanging pupfrom vulva and history of delivery of three dead pups since last24 hrs. The successful obstetrical management with the help ofoxytocin, 5% DNS, valethemate bromide, calcium gluconate,ceftriaxon and meloxicum was done.Key words :
BitchDystociaUterine inertia
A R T I C L E H I S T O R Y
Received : Jan 28, 2013Revised : June 12 ,2013Accepted : June 22, 2013
The incidence of dystocia in the bitch variesfrom 5-7% (Purohit and Gaur, 2004).
Secondary uterine inertia occurs after the bitch hasbeen in labour for some time. One or more puppiesmay have been born but then contractions stopbefore all puppies have been delivered (Purohitand Gaur, 2004). This condition is more commonin older bitches and can be due to exhaustedmuscles in the uterus or to glucose or calciumdeficiencies (Purohit and Sharma, 2004; Nagaret al., 2008). Calcium is the most importantelectrolyte regulating myometrial contractions.Commonly used protocols for medical treatmentinclude oxytocin administration, which can berepeated after 30 minutes if successful. If theoxytocin injection does not result in the birth of apup within 30 minutes, intravenous calciumgluconate may be administered, especially in
hypocalcemic bitches. The calcium infusion mayalso be followed by another oxytocin injection.(Johnston et al., 2001; Purohit and Sharma,2004). To determine the appropriate therapy, thecause of dystocia (obstructive vs nonobstructive)must be determined and the condition of the animalassessed. A thorough history regarding breedingdates, previous parturitions, pelvic trauma, etc. isdesirable (Barber, 2003).
Case history
A 4 year old Labrador bitch was brought toT.V.C.C. ,College of Veterinary Science & AnimalHusbandry Mathura with a hanging pup in vulvaand history of whelping process since last threedays. Three dead pups were delivered and no pupwas came out since last 24 hrs. but one was hangingfrom vulva .
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol (9) 88-89
89
Journal of Canine Development & Research 2013
Obstetrical management and discussion
Bitch was restrained properly and cleaned withpotassium per magnate solution in perinial region .Proper lubrication of hanging fetus and birth canalwith the help of disposable syringe were done andthe hanging fetus was removed by oblique tractionafter securing the forelimbs . The bitch was thenallowed for a slow walk and a Gentle massage ondog’s abdominal area with light pressure and slowup-down movements. The bitch was givenoxytocin 5 IU in 100ml of 5% DNS and epidocin(Valethemate bromide) 2 ml im to initiate theuterine contractions and cervical dialation,respectively followed by 5ml of calciumgluconate10 % iv. On vaginal examination anotherpup was in approach of finger tips. Massage onbitch’s nipples was given and a smooth digitalstimulus was provided. This will release thehormone oxytocin, which can bring oncontractions. Hind limbs and pelvis were felt Awhelping forceps was introduced and pup wasgrasped with the forceps and was taken out withgentle manoeuvre. The bitch was treated withantibiotic i.e. Ceftriaxon 250 mg im bds andmeloxicum 5 mg im for a period of 3 days with anuneventful recovery.
Presently secondary uterine inertia in bitchresulted because of lodging of featus in the birthcanal and delivery of three dead pups since last
24 hrs. The bitch responded with oxytocin , 5%DNS, epidocin, calcium gluconate similar toprevious reports (Johnston et al., 2001; Purohitand Sharma, 2004; Vellanki, 2010). Similar to ourreport epidocin was successfully used for cervicaldialation in women ( Vellanki, 2010).The use ofantibiotic ceftriaxon to control the bacterialinfection and antiinflamatory meloxicum evidencedencouraging results in this case.
ReferencesBarber JA. (2003) Parturition and Dystocia. In: Root Kustritz
MV, ed. Small animal theriogenology, St. Louis:Elsevier,pp.241-281.
Johnston SD, Root Kustritz MV, Olson PNS(2001). CanineParturition—Eutocia and Dystocia, In: Canineand feline theriogenology, Philadelphia: WBSaunders Co, pp.105-128.
Nagar,D; Purohit, G.N. and Mehat, J.S. (2008) Prevalence ofreproductive conditions in bitches. J. Canine Dev.Res. 5: 7-10.
Purohit G.N. and Gaur M. (2004) Dystocia in the bitch andqueen: A review J. Canine Dev. Res. 4:90-100.
Purohit, G.N. and Sharma, A (2004) Dystocia in bitches dueto uterine inertia. J. Canine Dev. Res. 4: 22-24.
Roberts S. J. (1982). Uterine Inertia. In: Veterinary Obstet-rics & Genital Diseases. 2nd ed. CBS publishersand distributors. pp. 231.
Romagnoli S., de Souza F. F. , Rota A., Vannozzi I. (2004) Pro-longed interval between parturition of normal livepups in a bitch. Journal of Small Animal Prac-tice 45 (5), 249–253.
Vellanki S. V. (2010). Comparision of Buscopan and epidosinon cervical dialation in labour. Global J. Med. Res.10(2): 18-21.Fig.1. Photograph showing hanging pup from vulva.
Fig.2. Dead pup taken out from vulva.
90
Journal of Canine Development & Research 2013
CLINICAL ARTICLESURGICAL MANAGEMENT OF VAGINAL LEIOMYOMA OF CANINERai Somil1 and *Chandrapuria V.P2
Department of Surgery and RadiologyCollege of Veterinary Science and A.H.,NDVSU, Jabalpur (M.P.)
1PhD Scholar, 2Professor & Head* Corresponding author e-mail : [email protected]
A B S T R A C T
Six female dogs were presented with the acute signs ofconstipation, dysuria and swelled vulva. Clinical examinationrevealed multiple, smooth, encapsulated leiomyomas of varioussizes in the vaginal wall. These leiomyomas were surgicallymanaged successfully and all the dogs recovered uneventfully.Key words :
EpisiotomyLeiomyoma
A R T I C L E H I S T O R Y
Received : August 20, 2013Revised : October 15, 2013Accepted : November 22, 2013
Neoplasia of the canine female genital systemis rare (Soderberg, 1986) and occurs mainly
in old animals (Dorn and Prister, 1987; Purohit etal., 2004; Singh et al., 2014). Early detection isdifficult as in most cases, coexistent chronicdiseases mask the initial signs of neoplasia(Morrison, 1989; Kitchell, 1993). The maintumors involved are leiomyoma and fibroma(Purohit et al., 2004) which may develop inextraluminal mode and therefore, affect thefunction of neighboring organs (Grooters, 1998,Weissman et al., 2013 and McDonald et al.,2011). Surgical excision is the first therapeuticchoice if mass is localized (Salomon et al., 2004,Karagiannis et al., 2011 and Shammi et al.,2010). The survival time and duration of remissionshow unfavorable data in old animals (Holmes,1992). The present report of vaginal leiomyomain six female dogs describes unusual growth led to
successful recovery following surgical excision.Materials and methodsAll the female dogs were presented with the acutesigns of constipation, dysuria and swelled vulva.Clinical examination revealed multiple, smooth,encapsulated tumors of various sizes in the vaginalwall which compressed the rectum posing physicalhindrance to defecate or even urinate. Their breedand age is presented in table 1.
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Case No. Breed Age 1. Pomeranian 11.5 years 2. Labrador 9.5 years 3. Pomeranian 9 years 4. Boxer 12.5 years 5. Pomeranian 14 years 6. ND 13 years
Table 1. Age and breed of dogs with vaginalleiomyoma
Vol (9) 90-92
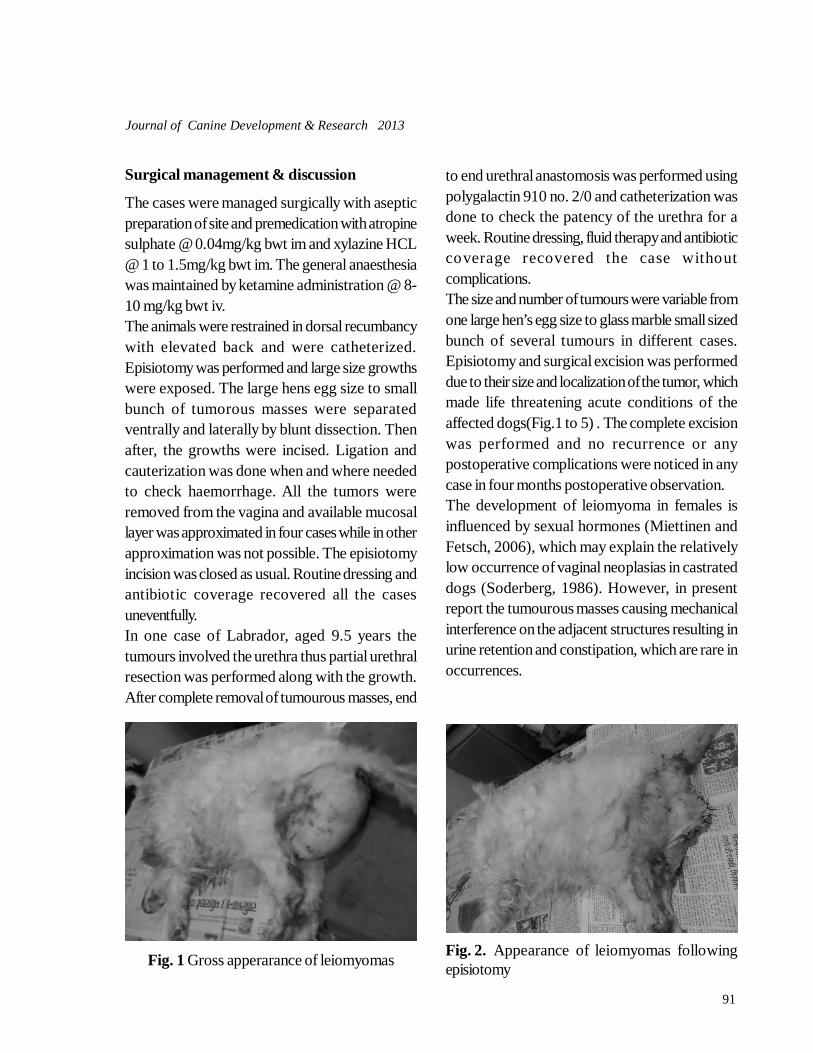
91
Journal of Canine Development & Research 2013
Surgical management & discussion
The cases were managed surgically with asepticpreparation of site and premedication with atropinesulphate @ 0.04mg/kg bwt im and xylazine HCL@ 1 to 1.5mg/kg bwt im. The general anaesthesiawas maintained by ketamine administration @ 8-10 mg/kg bwt iv.The animals were restrained in dorsal recumbancywith elevated back and were catheterized.Episiotomy was performed and large size growthswere exposed. The large hens egg size to smallbunch of tumorous masses were separatedventrally and laterally by blunt dissection. Thenafter, the growths were incised. Ligation andcauterization was done when and where neededto check haemorrhage. All the tumors wereremoved from the vagina and available mucosallayer was approximated in four cases while in otherapproximation was not possible. The episiotomyincision was closed as usual. Routine dressing andantibiotic coverage recovered all the casesuneventfully.In one case of Labrador, aged 9.5 years thetumours involved the urethra thus partial urethralresection was performed along with the growth.After complete removal of tumourous masses, end
to end urethral anastomosis was performed usingpolygalactin 910 no. 2/0 and catheterization wasdone to check the patency of the urethra for aweek. Routine dressing, fluid therapy and antibioticcoverage recovered the case withoutcomplications.The size and number of tumours were variable fromone large hen’s egg size to glass marble small sizedbunch of several tumours in different cases.Episiotomy and surgical excision was performeddue to their size and localization of the tumor, whichmade life threatening acute conditions of theaffected dogs(Fig.1 to 5) . The complete excisionwas performed and no recurrence or anypostoperative complications were noticed in anycase in four months postoperative observation.The development of leiomyoma in females isinfluenced by sexual hormones (Miettinen andFetsch, 2006), which may explain the relativelylow occurrence of vaginal neoplasias in castrateddogs (Soderberg, 1986). However, in presentreport the tumourous masses causing mechanicalinterference on the adjacent structures resulting inurine retention and constipation, which are rare inoccurrences.
Fig. 2. Appearance of leiomyomas followingepisiotomyFig. 1 Gross apperarance of leiomyomas
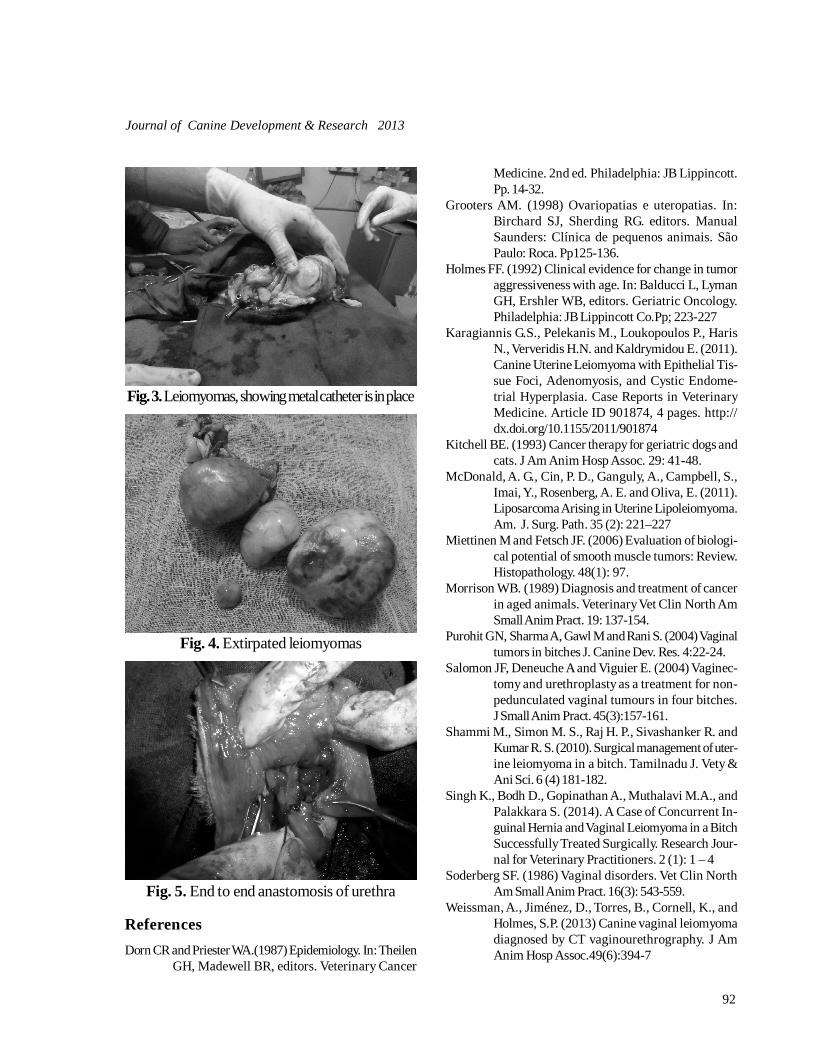
92
Journal of Canine Development & Research 2013
Fig. 3. Leiomyomas, showing metal catheter is in place
Fig. 4. Extirpated leiomyomas
Fig. 5. End to end anastomosis of urethra
ReferencesDorn CR and Priester WA.(1987) Epidemiology. In: Theilen
GH, Madewell BR, editors. Veterinary Cancer
Medicine. 2nd ed. Philadelphia: JB Lippincott.Pp. 14-32.
Grooters AM. (1998) Ovariopatias e uteropatias. In:Birchard SJ, Sherding RG. editors. ManualSaunders: Clínica de pequenos animais. SãoPaulo: Roca. Pp125-136.
Holmes FF. (1992) Clinical evidence for change in tumoraggressiveness with age. In: Balducci L, LymanGH, Ershler WB, editors. Geriatric Oncology.Philadelphia: JB Lippincott Co.Pp; 223-227
Karagiannis G.S., Pelekanis M., Loukopoulos P., HarisN., Ververidis H.N. and Kaldrymidou E. (2011).Canine Uterine Leiomyoma with Epithelial Tis-sue Foci, Adenomyosis, and Cystic Endome-trial Hyperplasia. Case Reports in VeterinaryMedicine. Article ID 901874, 4 pages. http://dx.doi.org/10.1155/2011/901874
Kitchell BE. (1993) Cancer therapy for geriatric dogs andcats. J Am Anim Hosp Assoc. 29: 41-48.
McDonald, A. G., Cin, P. D., Ganguly, A., Campbell, S.,Imai, Y., Rosenberg, A. E. and Oliva, E. (2011).Liposarcoma Arising in Uterine Lipoleiomyoma.Am. J. Surg. Path. 35 (2): 221–227
Miettinen M and Fetsch JF. (2006) Evaluation of biologi-cal potential of smooth muscle tumors: Review.Histopathology. 48(1): 97.
Morrison WB. (1989) Diagnosis and treatment of cancerin aged animals. Veterinary Vet Clin North AmSmall Anim Pract. 19: 137-154.
Purohit GN, Sharma A, Gawl M and Rani S. (2004) Vaginaltumors in bitches J. Canine Dev. Res. 4:22-24.
Salomon JF, Deneuche A and Viguier E. (2004) Vaginec-tomy and urethroplasty as a treatment for non-pedunculated vaginal tumours in four bitches.J Small Anim Pract. 45(3):157-161.
Shammi M., Simon M. S., Raj H. P., Sivashanker R. andKumar R. S. (2010). Surgical management of uter-ine leiomyoma in a bitch. Tamilnadu J. Vety &Ani Sci. 6 (4) 181-182.
Singh K., Bodh D., Gopinathan A., Muthalavi M.A., andPalakkara S. (2014). A Case of Concurrent In-guinal Hernia and Vaginal Leiomyoma in a BitchSuccessfully Treated Surgically. Research Jour-nal for Veterinary Practitioners. 2 (1): 1 – 4
Soderberg SF. (1986) Vaginal disorders. Vet Clin NorthAm Small Anim Pract. 16(3): 543-559.
Weissman, A., Jiménez, D., Torres, B., Cornell, K., andHolmes, S.P. (2013) Canine vaginal leiomyomadiagnosed by CT vaginourethrography. J AmAnim Hosp Assoc.49(6):394-7
93
Journal of Canine Development & Research 2013
CLINICAL ARTICLEVAGINAL FIBROMA AND URINARY INCONTINENCE IN A BITCH*Sidhartha Sankar Behera1, Jayakrushna Das2, Monalisa Behera3 and Manas Ranjan Senapati4
Department of Veterinary Surgery and Radiology College of Vety. Sci. and A. H., O U A T, Bhubaneswar-751 003 (Odisha)
1,3,4PhD Scholar 2 Assistant Professor 3Dept. of Vety. Pathology, 4Dept. of Vety. Biochemistry* Corresponding author e-mail : [email protected]
A B S T R A C T
One 10 year old nulliparous Spitz dog was presented withcomplain of vulval bleeding and licking the site along withtenesmus, haematuria, dysuria, urinary incontinence and faecaltenesmus. On physical examination, bulging of the perineum wasnoticed. Vaginal examination showed a smooth surface tumourmass attached to vaginal wall. Under general anaesthesia usingatropine sulphate, xylazine hydrochloride and ketaminehydrochloride episiotomy was conducted and the tumour masswas excised. Post-operatively antibiotics and analgesics wereadministered. On 10
th post-operative day sutures were removed
and the dog recovered well.
Key words :DogUrinary incontinenceVaginal fibroma
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
The most common types of tumours found inthe genital tract of bitches are benign, smooth
muscle tumours of the vagina and vulva (Rollonet al., 2008). Benign mesenchymal tumours suchas leiomyoma, fibroma or fibroleiomyoma are mostcommon and may affect uterus, cervix or vagina(Atlee et al., 1991; Moe and Lium, 1997; Purohitet al., 2004). Vulvar and vaginal tumours accountfor 2.4%-3.0% of canine neoplasms (Brodey andRoszel, 1967). Entire, aged dogs (mean age 10–11 years), particularly nulliparous animals are atrisk of benign mesenchymal tumours, where aslipoma affects slightly younger bitches (James and
McGavin, 2012). Extraluminal tumours present asslow growing perineal masses whereas intraluminalforms may present as polyps protruding throughthe vulval lips especially when the animal strainsor is in estrus. There is an association betweenbenign smooth muscle tumours and estrogenproduction in the dog. Such tumours rarely occurin spayed animals unless they have receivedestrogen therapy for some reason (Kenanny et al.,2013). Regarding treatment option in addition tosurgical excision of the mass, ovario-hysterectomywas suggested as this would prevent the recurrenceof benign tumours (Sahay et al., 1985).
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol(9) 93-96

94
Journal of Canine Development & Research 2013
Case history and observations
One 10 year old nulliparous Spitz dog waspresented with complain of vulval bleeding andlicking, tenesmus, haematuria, dysuria, urinaryincontinence and faecal tenesmus. The dog hadregular oestrus cycles and had not received anyprevious hormonal treatment. On physicalexamination, bulging of the perineum was noticed.Vaginal examination showed a tumour like massattached to vaginal wall. Tumour mass was firmwith a smooth surface on palpation occupying itslumen. Lateral radiograph of thorax and abdomenrevealed no metastatic lesion. Tentatively it wasdiagnosed as a case of vaginal tumour and surgicalcorrection was advised.
Treatment
The animal was fasted for twelve hours prior tosurgery and water was withheld for eight hoursprior to surgery. General anaesthesia was inducedwith combination of atropine sulphate @ 0.04mg/kg bwt, xylazine hydrochloride @ 1mg/kg bwt andKetamine hydrochloride @ 5 mg/kg bwt im.During operation maintenance of anaesthesia wasdone with ketamine hydrochloride iv. The dog waspositioned in lateral recumbency. The perineal skinwas shaved and prepared for surgery. Aftercatheterization of urethra, an episiotomy incisionwas made from the level of the caudodorsal aspectof the horizontal vaginal canal to the dorsalcommissure of the vulval cleft. With the help ofscissors subcutaneous muscle and mucosal layerwas incised and then the tumour mass wasexposed. It was attached to the posterior boarderof vagina and was exposed by blunt dissection.The mass was found to be smooth, oval and hardin consistency(Fig.1) after complete separationfrom the surrounding tissue. It was hold by pullingoutwardly and transfixation knot was placed closeto the base using chromic catgut no-1. One curvedhaemostatic forceps was applied at the base ofmass to provide excellent homeostasis and to
prevent bleeding. Then the tumour mass wasexcised carefully above the knot and sent forhistopathological examination. The episiotomy wasclosed by standard manner. Post-operativelyceftriaxone @ 10 mg/kg bwt im for 5 days andmeloxicam @ 0.2mg/kg bwt im for 3 days weregiven. On 10
th post-operative day sutures were
removed.
Results and discussion
After surgery there was normal defecation,urination and no discharge was noticed. Thissuggested that the tumour mass had createdobstruction and the discharge might be due toscratching and licking by the animal. Tumours offemale genital system in bitch occur most frequentlyin the vagina and vulva and rarely in the uterus orovary. Vaginal and vulval tumours are usually benignand carry a good prognosis (Joanna and Jane,2001). Those are variably referred as leiomyomas,fibroleiomyomas, fibromas and polyps, dependingon the amount of connective tissue present (Klein,2001; MacLachlan and Kennedy, 2002). Theydo not interfere with fertility but may interfere withbreeding and parturition and associated withdystocia. Benign vulvar or vaginal tumours developin older and sexually intact females with a meanage range of 10-12 years (Morrison, 2002). Thesetumours may develop in extraluminal mode andtherefore affect the function of neighbouring organs(Grooters, 1998). Here the tumour mass had alsocreated obstruction to rectum and urinary passage.Histopathological examination of the tissue showedinterlacing bundles of fibrous connective tissue withspindle shaped nuclei, suggestive of fibroma(Fig.2). Since most vaginal and vulvar tumours arebenign type hence, surgical resection combinedwith ovariohysterectomy carries a good prognosis(Kenanny et al., 2013). Salomon et al. (2004)also stated that surgical excision is the firsttherapeutic choice when total ablation is possibleand can be associated to castration (Thacher and
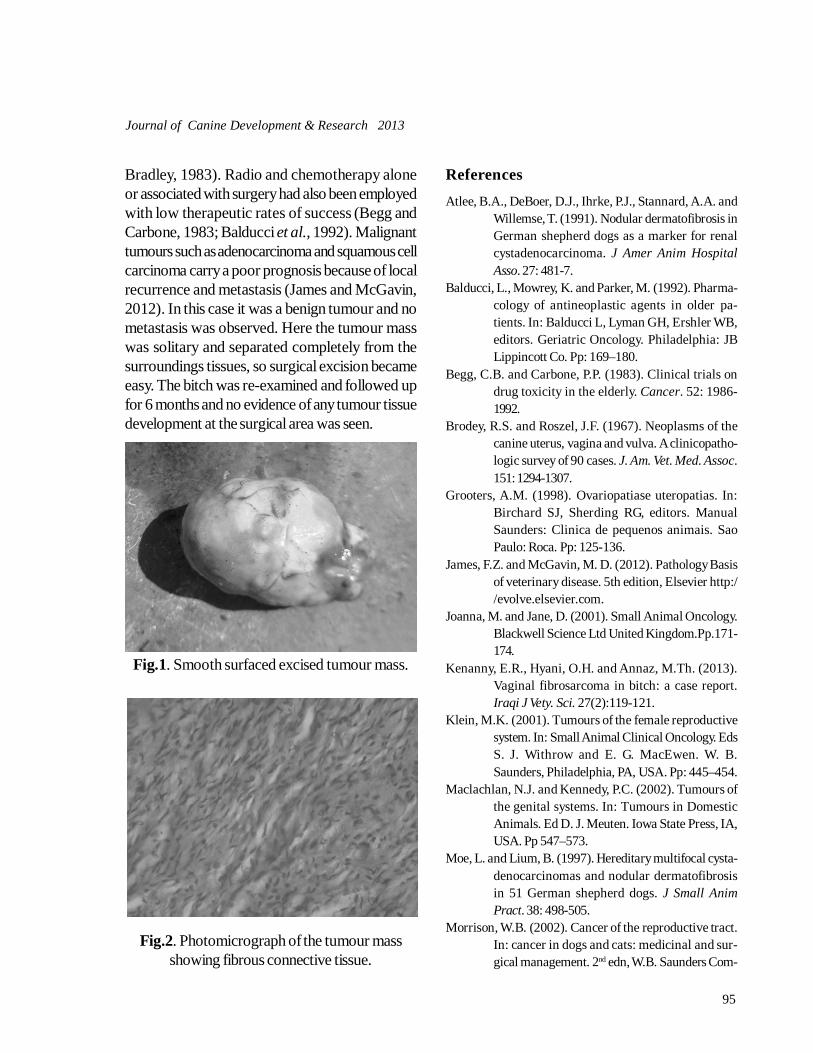
95
Journal of Canine Development & Research 2013
Bradley, 1983). Radio and chemotherapy aloneor associated with surgery had also been employedwith low therapeutic rates of success (Begg andCarbone, 1983; Balducci et al., 1992). Malignanttumours such as adenocarcinoma and squamous cellcarcinoma carry a poor prognosis because of localrecurrence and metastasis (James and McGavin,2012). In this case it was a benign tumour and nometastasis was observed. Here the tumour masswas solitary and separated completely from thesurroundings tissues, so surgical excision becameeasy. The bitch was re-examined and followed upfor 6 months and no evidence of any tumour tissuedevelopment at the surgical area was seen.
Fig.1. Smooth surfaced excised tumour mass.
Fig.2. Photomicrograph of the tumour massshowing fibrous connective tissue.
ReferencesAtlee, B.A., DeBoer, D.J., Ihrke, P.J., Stannard, A.A. and
Willemse, T. (1991). Nodular dermatofibrosis inGerman shepherd dogs as a marker for renalcystadenocarcinoma. J Amer Anim HospitalAsso. 27: 481-7.
Balducci, L., Mowrey, K. and Parker, M. (1992). Pharma-cology of antineoplastic agents in older pa-tients. In: Balducci L, Lyman GH, Ershler WB,editors. Geriatric Oncology. Philadelphia: JBLippincott Co. Pp: 169–180.
Begg, C.B. and Carbone, P.P. (1983). Clinical trials ondrug toxicity in the elderly. Cancer. 52: 1986-1992.
Brodey, R.S. and Roszel, J.F. (1967). Neoplasms of thecanine uterus, vagina and vulva. A clinicopatho-logic survey of 90 cases. J. Am. Vet. Med. Assoc.151: 1294-1307.
Grooters, A.M. (1998). Ovariopatiase uteropatias. In:Birchard SJ, Sherding RG, editors. ManualSaunders: Clinica de pequenos animais. SaoPaulo: Roca. Pp: 125-136.
James, F.Z. and McGavin, M. D. (2012). Pathology Basisof veterinary disease. 5th edition, Elsevier http://evolve.elsevier.com.
Joanna, M. and Jane, D. (2001). Small Animal Oncology.Blackwell Science Ltd United Kingdom.Pp.171-174.
Kenanny, E.R., Hyani, O.H. and Annaz, M.Th. (2013).Vaginal fibrosarcoma in bitch: a case report.Iraqi J Vety. Sci. 27(2):119-121.
Klein, M.K. (2001). Tumours of the female reproductivesystem. In: Small Animal Clinical Oncology. EdsS. J. Withrow and E. G. MacEwen. W. B.Saunders, Philadelphia, PA, USA. Pp: 445–454.
Maclachlan, N.J. and Kennedy, P.C. (2002). Tumours ofthe genital systems. In: Tumours in DomesticAnimals. Ed D. J. Meuten. Iowa State Press, IA,USA. Pp 547–573.
Moe, L. and Lium, B. (1997). Hereditary multifocal cysta-denocarcinomas and nodular dermatofibrosisin 51 German shepherd dogs. J Small AnimPract. 38: 498-505.
Morrison, W.B. (2002). Cancer of the reproductive tract.In: cancer in dogs and cats: medicinal and sur-gical management. 2nd edn, W.B. Saunders Com-

96
Journal of Canine Development & Research 2013
pany, Philadelphia.Pp: 555-564.Purohit G.N., Sharma A, Gaur M. and Rani S. (2004)
Vagenal tamors in bitches. J. Canine Dev. Res.4:22-24.
Rollon, E., Millan, Y. and Martin, J. and Mulas, D. (2008).Effects of aglepristone, a progesterone recep-tor antagonist, in a dog with a vaginal fibroma.J Small Anim Pract. 49: 41–43.
Sahay, P.N., Dass, L.L., Khan, A.A. and Singh, K.K. (1985).Urinary incontinence in a bitch caused by vagi-nal fibroma. Vet. Rec. 116: 76-77.
Salomon, J.F., Deneuche, A. and Viguier, E. (2004). Vagi-nectomy and urethroplasty as a treatment fornon-pedunculated vaginal tumours in fourbitches. J Small Anim Pract. 45(3):157-161.
Thacher, C. and Bradley, R.L. (1983). Vulvar and vaginaltumours in the dog: a retrospective study. J AmVet Med Assoc. 183(6): 690-692.

97
Journal of Canine Development & Research 2013
CLINICAL ARTICLECANINE TRANSMISSIBLE VENEREAL TUMOR OF A DOG AND ITSSURGICAL MANAGEMENTJayakrushna Das1*, Sidhartha Sankar Behera2, Manas Ranjan Senapati3, Monalisa Behera4, Snehasis Pradhan5,Manas Ranjan Praharaj5 and Prasanta Kumar Nanda5
Department of Veterinary Surgery and RadiologyCollege of Vety. Sci. and A.H., OUAT, Bhubaneswar-751 003(Odisha)
1Assistant Professor 2.3,4 PhD Scholar 3Dept.of Vety. Biochemistry 4Dept. of Vety Pathology 5 UG Students*Corresponding author e.mail: [email protected] & [email protected]
A B S T R A C T
One two year old male mongrel dog weighing 12 kg body weightwas presented with the complain of severely ulcerated andproliferated growths on and around the scrotum. History, clinicaland cytological examination of the mass revealed as case ofcanine transmissible venereal tumour. Under general anaesthesiathe tumour mass was excised and the area was cauterized withsilver nitrate sticks. For complete removal of the remnant tumourmass and to avoid recurrence chemotherapy with vincristinesulphate @ 0.025 mg/kg bwt iv was advised with 10% dextrosesolution after a week and then at 15 days interval for two times.After 12
th day the skin suture was removed. The dog recovered
well without any recurrence.
Key words :DogSurgeryTransmissible venereal tumour
A R T I C L E H I S T O R Y
Received : April 23, 2013Revised : July 18, 2013Accepted : August 22, 2013
Transmissible venereal tumour (TVT) is anaturally occurring, coitally transmitted
neoplasm of the dog that usually affects the externalgenitalia (Nak et al., 2005; Purohit, 2008).Transmissible venereal tumour is seen most oftenin young, free roaming and sexually active dogs(Feldman and Nelson, 1987; Das and Das, 2000;Purohit et al., 2004). This affects the externalgenitalia and is transmitted from animal to animalthrough sexual contacts but may also occurs bydog bites, sniffs or licks the tumour affected areas(Bloom, 1954; Das et al., 1989; Purohit, 2008;
Khan et al., 2009). In the male dog, the tumour isusually located on the caudal part of penis fromcrura to bulbus glandis or the area of glans penisand occasionally on the prepuce (Purohit, 2008).TVT may also develop at extra genital sites, evenwhen there are no genital lesions, such as skin,nasal cavity or mouth. The ultimate goal oftreatment of tumour is complete cure, which maybe achieved by surgical excision, radiotherapy,immunotherapy and chemotherapy (Misirlioglu etal., 1999; Das and Das, 2000; Purohit, 2008).Recurrence following surgical excision is common
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol(9) 97-101

98
Journal of Canine Development & Research 2013
and was recorded in 12–68% of cases (Das andDas, 2000).
Case history and observations
One two year old male mongrel dog weighing 12kg body weight was presented with the complainof severely ulcerated and proliferated growths onand around the scrotum (Fig. 1). Before one monthit started as a small ulcer and afterwards itproliferated rapidly. Though the dog was kept bythe owner, but was allowed to mix with other straydogs. So it was suspected for TVT. Cytologicalexamination of the ulcerated mass was done whichconfirmed it a case of canine transmissible venerealtumour (CTVT). As the tumour mass was verymuch extensive, it was decided for surgicalcorrection followed by chemotherapy.
Treatment and results
On the day of presentation dressing of the ulceratedmass was done and the dog was kept underantibiotic coverage. The owner was advised topresent the animal on next day after keeping 12hour fasting. General anaesthesia was induced usingatropine sulphate @ 0.04 mg/kg bwt im, xylazinehydrochloride @ 1 mg/kg bwt im and ketaminehydrochloride @ 5 mg/kg bwt im. A nasogastricfeeding tube was introduced into the urethralorifice to keep the patency of urethra. With helpof allis forceps and scissors the tumour mass wascarefully dissected (Fig.2). Tumour mass wasexcised completely and sent for histopathologicalstudy (Fig.3). Both testicles were damaged byinvasion of the tumour mass. So ablation of thetotal scrotal sac was done. After complete excisionof the tumour mass the affected area wascauterized with silver nitrate sticks andsimultaneously neutralised with isotonic salinesolutions. Adrenaline was sprayed to controlcapillary bleeding and terramycine topical wasinstilled at the site. Fixing of the nasogastric feedingtube was done to the wall of the prepuce.
Subcutaneous tissue was apposed by using 2-0chromic catgut in continuous manner. Appositionof skin wound was done in interrupted mannerusing nylon (Fig.4). The dog was treated withceftriaxone @ 10 mg/ kg bwt im for 7 days andmeloxicam @ 0.3 mg/kg bwt im with multivitamin2 ml im. for 3 days. Since it was severely affectedwith CTVT and to avoid recurrence, vincristinesulphate @ 0.025 mg/kg bwt iv was advised with10% dextrose solution after a week and then at15 days interval for two times. After 12
th day the
skin suture was removed. The dog recovered wellwith normal micturation.
Discussion
The dog was not castrated and was also allowedto mix with other dogs. Hence probably it mighthave acquired the infection while mating with theinfected dogs. Venereal tumours are most commonduring the period of maximum sexual activity indogs and the animals are particularly at highest riskwhen females exhibit the signs of oestrus. Dogs ofany breed, age or sex are susceptible (Kimeto andMugera, 1974; Betamuzi, 1992). The continuousdischarge from the external genitalia, soiling thefloor, carpet and even clothes, is a great nuisancefor the owner. The bloody discharges may beconfused with oestrus, urethritis or cystitis and inthe male, with prostatitis (Das and Das, 2000).Here there was also bleeding while dragging themass on the ground. The ignorance of the studowners and lack of stringent legislation formonitoring the sexual health of dogs are the maincauses of the widespread distribution of this diseasethroughout the country. Diagnosis is based on theenvironmental history as well as clinical andcytological findings (Purohit, 2008). Biopsy forhistological examination is the most reliable methodfor diagnosis, but cytology is usually diagnostic. Inthis case we diagnosed initially by cytologicalexamination. Further after surgical excisionhistopathological examination of the tissue sample

99
Journal of Canine Development & Research 2013
revealed round, oval and polyhedral cells havingfine granular acidophilic cytoplasm in it. The largehyperchromatic nucleus and fine connective tissuestroma was suggestive of venereal granuloma(Fig.5).Metastasis is reported to occur in less than 5% ofthe cases. Metastasis of TVT to the skin, regionallymph nodes, tonsils, eyes, brain, pituitary, nose,tongue, lips, mammary region and thoracic andabdominal viscera has been reported (Feldmanand Nelson, 1987; Das and Das, 2000; Nak etal., 2004). Here no such metastasis was noticed.Several treatment models have been tried forcomplete cure of the disease, but the treatmentsthat have proved to be most effective for TVT arechemotherapy or radiotherapy (Rogers, 1997).Chemotherapy of TVT has been attempted usingcyclophosphamide, methotrexate,cyclophosphamide and prednisone, vinblastinewith cyclophosphamide or methotrexate, andvincristine and doxorubicin (Rogers, 1997; Dasand Das, 2000; Nak, 2001). However, amongthe different chemotherapeutic agents, single agenttherapy with vincristine at the rate of 0.025 mg/kgbwt iv at weekly intervals of two to five treatmentshas been found to be most effective, safe andconvenient (Calvert et al., 1982; Amber et al.,1990; Singh et al., 1996). In the present case weadopted both surgical and three doses ofchemotherapy of vincristine sulphate and gotsuccess. The toxicities of greatest concern aftervincristine treatment are gastrointestinal upset,myelosuppression and local tissue injury due todrug extravasation (Rogers, 1997). Neutropenia,eosinopenia, lymphocytosis, monocytosis andsignificant decreases in Hb, total erythrocyte andtotal leucocyte values can be observed duringvincristine treatment (Dinesh et al., 1993; Nak,2001). Here no such untoward effect wasobserved. Recurrence was minimal whencastration or ovario-hysterectomy was practisedalong with chemotherapy (Pandey et al., 1989).
An autogenous vaccine supplemented withlevamisol may also be used to prevent recurrenceof tumour following surgical excision (Pandey et
Fig.1. Ulcerated tumour mass on and aroundthe scrotal area
Fig.2. Complete excision of the tumour mass
Fig.3. Excised tumour mass

100
Journal of Canine Development & Research 2013
Fig.4. Skin apposition after surgery
Fig.5. Photomicrograph of excised tumourtissue (H & E X 400)
al., 1977, 1989; Panchbhai et al., 1990). We didnot observe any recurrences in a follow-up periodof up to 9 months. Here total ablation of the scrotumand chemotherapy after surgery might be thereason for non-recurrence.
ReferencesAmber, E.I., Henderson, R.A., Adeyanju, J.B. and Gyang,
E.O. (1990). Single-drug chemotheraphy of ca-nine transmissible venereal tumour with cyclo-phosphamide, methotrexate or vincristine. J. Vet.Intern. Med. 4: 144-147.
Betamuzi, E.K. (1992). Risk factors associated with ca-nine TVT in Tanzania. Prev. Vet. Med., 13: 13-17.
Bloom, F. (1954). Pathology of dog and cat. Americanveterinary publication Eastern Illinois. Pp. 275.
Calvert, C.A., Leifer, C.E. and MacEwen, E.G. (1982). Vin-cristine for treatment of transmissible venerealtumours in the dog. J. Am. Vet. Med. Assoc.181: 163-164.
Das, A.K., Das, U., Das, D.K. and Sengupta, J. (1989).Metastasis of canine transmissible of venerealsarcoma in a dog. Ind. Vet. J. 10 (1): 74-75.
Das, U. and Das, A.K.(2000). Review of canine transmis-sible venereal sarcoma. Veterinary ResearchCommunications, 24 (8): 545-556.
Dinesh, N.M., Ranganath, B.N., Jayadevappa, S.M. andSrinivas, C.L. (1993). Effect of vincristine sul-phate on canine transmissible venerealtumours-haematological and biochemical stud-ies. Indian Vet. J. 70: 741-744.
Feldman, E.C. and Nelson, R.W. (1987). Canine and Fe-line Endocrinology and Reproduction. W.B.Saunders Company, Philadelphia, PA, Pp. 475-477.
Khan, L.A., Khante, G.S., Raut, B.M., Bodkhe, A.M.,Chavan, M.S., Pagrut, N.S. and Bobde, S.P.(2009). Incidence of Venereal Granuloma andits Medicinal treatment in stray dogs of Nagpurcity. Veterinary World. 2(1): 13-14.
Kimeto, B. and Mugera, G.M. (1974). Transmissible ve-nereal tumour of dog in Kenya. Bulletin of Ani-mal Health and Production, 22: 327-329.
Misirlioglu, D., Seyrek-Intas, K., Kahraman, M.M.,Ozbilgin, S., Ozyigit, M.O., Cangul, I.T., Sevimli,A. and Buyukcoban, M. (1999). A study aboutthe effects of paramunity activator BaypamunN on the prophylaxis and treatment of caninetransmissible venereal tumor (CTVT): macro-scopical findings. Kafkas Univ. Vet. Fak. Derg.5: 1-8.
Nak, D. (2001). Transmissible venereal tumor in bitch.Y.Y.U. Sagl. Bil. Derg. 7: 152-155.
Nak, D., Misirlioglu, D., Nak, Y., Seyrek-Intas, K. andTek, H.B. (2004). Transmissible venereal tumorwith mammary gland metastase in a bitch. Vet.Bilimleri Derg. 20: 99-102.
Nak, D., Nak, Y., Cangul, I.T. and Tuna, B. (2005). A Clinico-pathological Study on the Effect of Vincristineon Transmissible Venereal Tumour in Dogs. J.Vet. Med. A. 52: 366–370
Panchbhai, V.S., Karpe, A.G., Kulkarni, G.B. and Kulkarni,S.K. (1990). Use of autogenous vaccine in trans-missible canine venereal tumour. Ind. Vet. J., 67:983-984.
Pandey, S.K., Chandpuria, V.P., Bhargava, M.K. andTiwari, S.K. (1989). Incidence, treatment, ap-

101
Journal of Canine Development & Research 2013
proach and metastasis of canine transmissiblevenereal sarcoma. Ind. J.Anim. Sci., 59: 510-513.
Pandey, S.K., Dhawedkar, R.G. and Patel, M.R. (1977).Canine transmissible venereal sarcoma. Clini-cal trial with autogenous formalized vaccine.Ind. Vet. J. 54: 852-853.
Purohit G.N. (2008) Canine transmissible tumor: A reviewThe Intesnet J Vet Med. 6:1-19.
Purohit G.N., Sharma A, Gaur M. and Rani S. (2004)
Vagenal tumors in bitches J. Canine Dev. Res.4:22-24
Rogers, K.S. (1997). Transmissible Venereal Tumor. Compcontin Educ Prac Vet., 19(9): 1036-1045.
Singh, J., Rana, J.S., Sood, N., Pangawkar, G.R. and Gupta,P.P. (1996). Clinico-pathological studies on theeffect of different antineoplastic chemotherapyregimens on transmissible venereal tumours indogs. Vet. Res. Commun. 20: 71-81

102
Journal of Canine Development & Research 2013
GENERAL ARTICLEUPDATE ON USE OF MEDICATED SHAMPOO IN COMPANIONANIMAL DERMATOLOGY*Mukesh Srivastava1, Anil Ahuja2, S. Kachhawaha1, J.P Kachhawa3, Ankita Sharma3, M. Daga3, N.K.Singh3 andKhusbu Kannojia4
Department of Clinical Veterinary Medicine, Ethics & JurisprudenceCollege of Veterinary and Animal Science, RAJUVAS, Bikaner-334 001 (Rajasthan)
1 Ph.D. Scholar 2 Profesor & Head 3,4 PG Scholar, 4 Dept.of AGB*Corresponding author e-mail:[email protected]
A B S T R A C T
Utility of shampoo therapy in canine dermatological disorders,basic difference in human and canine skin, functions of shampoo,frequency, method and contact time, pre-shampooing preparationof dog, various type of shampoo for different need of dog andfunction of active ingredients of shampoo is described.Key words :
Dermatological disorderDogsShampoo therapy
A R T I C L E H I S T O R Y
Received : March 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
In spite of tremendous progress in caninedermatology, there is still a certain amount of
art as well as science in devising the optimumtopical therapy (Halliwell, 1991); additionallyincreasing use of shampoo has sparked theemergence of several medicated shampoos. Skindiseases have two major concerns i.e. microbialproliferation and inflammation. Microbialproliferation can be checked with antibiotics orantiseptics, while inflammation is often controlledwith systemic glucocorticoids. Long term use ofsystemic steroid therapy may affect the way theimmune system can deal with microbial challengeand the issue of antibiotic resistances anddisturbance of cutaneous microflora is an increasingconcern. New therapeutic options, that do notdepend on antibiotics is shampoo therapy. This
form of therapy is very useful for owners as theycan do it without the need of any special equipmentat home. Traditional shampoo formulations arecomposed of surfactants (cleansing agents, foamingagents and conditioners) as well as thickeners,softeners, sequestering agents, preservatives,fragrance and sometimes opacifiers and colouringadditives with various therapeutic agents.Surfactants are amphiphilic molecules, i.e.molecules with a dual affinity, both for water andoil. Surfactants are composed of a hydrophilic partand a lipophilic part, they have propensity forabsorption on various interfaces (oil/water, air/water), modifying the properties of the interface(decreasing the interface tension and stabilizationof the interface). In water, surfactants form micellestructures allowing surfactant to emulsify, render
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol(9) 102-111

103
Journal of Canine Development & Research 2013
soluble and disperse oils, dirt and debris.Surfactants can be classified into 4 groups,according to their ionic nature: anionic, cationic,non-ionic, and amphoteric surfactants. Petshampoos are formulated combinations ofsurfactants combining superior cleansingproperties, a perfect local tolerance, a physiologicalpH adapted to the canine skin and easiness ofrinsing. The efficacy of shampoos on skin hydrationcan be evaluated by using different techniquesincluding transepidermal water loss measurement,corneocyte counts, measurement of corneal layerthickness, stripping, chemical analysis of lipid film,water content measurement, surface biopsies andcorneometry (Groux and Bensignor, 2000). Outof these most reliable one is corneometry. To getbenefited from shampoo therapy, it is important toknow the types of shampoo available their activeingredients, and their judicious use.
Basic difference in dog and human skin
The human epidermis is 10 to 15 layers thick andnormally has a 28-day transit time from the basalcell to the cornified cell, whereas canine skin variesfrom 3 to 5 cell layers, with turnover timesdecreased by more than one week, as comparedwith humans. Beside this, canine skin has a nearlyneutral pH of 7.5, while human skin has an acidicpH of 5.5. This means that even mild babyshampoo is far too acidic and can harm dog’s skin.Bathing with a shampoo formulated for the pH ofhuman skin may decrease the surface pH of a pet’sskin and potentially result in irritation, drying,scaling, and changes in superficial bacteria. Onlyshampoos formulated for veterinary use should beused on animals.
Functions of shampoo- various functions ofshampoo are as-1- Shampoo therapy have mechanical cleansingeffect that removes detrimental material (scales,crusts, debris, exudates) or organisms (invading
pathogens) and rancid smelly fats (Carlotti, 2006)from the skin surface and cleaning out of pores toallow the flow of normal skin oils from the hairfollicles. It also reduces doggie smell which is dueto rancidification of fatty acids on the skin and inthe coat.2- This form of therapy leads to direct access oftherapeutic agent to diseased tissue without priordilution, to produce immediate action whichreduces the need for systemic therapy as it act insynergy with systemic treatments, helping to reducethe dose or frequency of the latter, or providing aquicker or stronger response. With this therapythere is reduced systemic absorption and fewersystemic adverse reactions (De Jaham, 2003).3- The combination of dog hair and man madefibers, like carpet, furniture, and even dog bedsencourage the build-up of static electricity. Thiscan attract high concentrations of commonallergens such as dust mites onto the skin.Shampoo therapy reduces allergen and bacterialpopulation by washing off trapped pollens on theskin (Christa and Ariane, 2007).4- Rehydration of the skin helps to close the gapsin the skin to maintain a barrier that prevents entryof foreign material into the skin. Water in itself isan excellent skin hydrator, but if not left on longenough, evaporation and drying of the surfacelayers of the skin may result. Too long a contacttime will result in the dishpan hands syndrome,whereby the skin becomes macerated.5- Medically supervised therapeutic bathing helpsthe skin recover from many diseases. Acts insynergy with systemic treatments, helping to reducethe dose or frequency of the latter, or providing aquicker or stronger response. (De Jaham, 2003).6- Shampoo therapy is unique in improving skinand coat aspect, resulting in increased ownersatisfaction.7- This form of therapy often permits the use oflower potency products (Cathy, 1998).8- On the long term, topical therapy is often helpful

104
Journal of Canine Development & Research 2013
to prevent relapses and control chronic skindiseases.
Frequency, method and contact time forshampoo
The frequency depends on the presence of skindisease as well as the shampoo being used andthe owner’s willingness. Owner compliance isimportant as this form of therapy is very timeconsuming. Procedure involves first application forcleaning purpose followed by rinse, then secondapplication for treatment, which should be at leastfor 5 minutes, better if 10 minutes followed by finalthorough rinse (Carlotti, 2006). Commonly,shampooing may be required two to three times aweek until adequate control of scale, grease, andodor is achieved. Thereafter, a maintenancefrequency of once weekly or once monthly maybe used or it may be reduced gradually to longestinterval over which treatment is still effective (usually1 to 2 weeks). In severe cases it is necessary towash the dog every second day or even daily untilremission is achieved, after that when the diseaseis in remission, it can be reduced to weekly orfortnightly. This length of contact time variesbetween 5 and 15 minutes according to choice ofproduct, concentration, type of base, and the skincondition. This contact time allows hydration ofthe skin and provides sufficient time for penetrationand action of the shampoo ingredients. Water, itselfis a good hydrating agent, but if not left on longenough may results in evaporation and drying ofthe surface of the skin. Long contact time will resultin the dishpan hands syndrome, where macerationof skin occurs. After shampooing the skin shouldthen be rinsed thoroughly with warm water for atleast 5 minutes, to prevent irritation and to enablethe skin to become adequately hydrated.Conventional dose of shampoo is 2 ml shampooper kilogram bodyweight (Loflath et al., 2007).
Pre-shampooing preparations
This includes placing cotton balls in the ear canals
and using a lubricant in the eyes. Any shampoothat has been retained within the eye can be quicklyremoved with lubricant flushing the eyes at thecompletion of the bath. In long haired dogs it mightbe useful to clip the dog to ensure good penetrationof the active ingredients to the skin surface (Christaand Ariane, 2007). If a costly medicated shampoois needed, it may be helpful to bathe first with aninexpensive product, such as a flea shampoo,dishwashing liquid or grooming shampoo to removegrease, debris and dirt. As a result, the medicatedshampoo will have a better contact with the skin(Sonja, 2011)
Various agents in medicated shampoo
Medicated shampoos should be chosen for eachdog and each case individually based on the coatcondition, effect required and efficacy ofingredients. Sometimes therapeutic agent needs tobe changed following the development of side-effects, rebound effects or change in clinicalpresentation (e.g. transition from greasy seborrheato dry seborrhea).Care should be taken while selecting a shampoo,especially if the dog’s skin is irritated, dry orotherwise abnormal or unusual, as few conditionsmay aggravate through the use of incorrectshampoo (Srivastava and Bhagwat, 2009).1-Keratomodulating agents : Keratomodulatingagents which leads to restoration of normalkeratinocyte multiplication and keratinisationproducing cytostatic effect on basal cells, therebyreducing their rate of division these agents areknown as keratoplastic agent Keratomodulatingagents which cause elimination of excess corneallayer production, either by increasingdesquamation or by reducing intercellular cohesionare known as keratolytic agents. Some of theseagents also work as antiseborrhoeic agents, whichact at the level of the sebaceous gland and its duct(Carlotti and Bensignor, 2002). Many parasiticdiseases (e g scabies, cheyletiellosis) and flea allergy

105
Journal of Canine Development & Research 2013
dermatitis can cause a keratoseborrhoeic disorderand the affected animals will benefit fromapplication of keratomodulating shampoos(Halliwell, 1991).2-Antiseborrhoeic agents : Antiseborrhoeicagents inhibit or reduce sebum production by thesebaceous glands, and helps in clearing of theducts. Seborrhea is the excess scale formation thatresults from abnormal cell migration, increased celldivision in the stratum basale, biochemicalanomalies in keratin production, and aberrationsin intercellular lipid production. Antiseborrheicshampoos are used primarily for eliminating surfacescale by causing cell damage and ballooning,resulting in softening and shedding of the stratumcorneum (keratolysis), and decreasing cellturnover rate by growth inhibitory effects on basalcells (keratoplasty). Important agents in thiscategory are sulfur, salicylic acid, coal tar, seleniumsulfide, ammonium lactate, phytosphingosine andbenzoyl peroxide. Zinc gluconate hasantiseborrhoeic properties by down regulatingsebum production. Vitamin B6 (pyridoxine) alsoplays a role in sebum secretion and there is asynergistic effect, of unknown mechanism, withzinc. There are two morphologic forms ofseborrhea, which may be seen in combination onthe same animal (Sonja, 2011).Seborrhea sicca : Animals are usually presentedwith a dry skin; focal or diffuse scaling (white orgrayish, usually non-adherent scales). Thesefindings imply a decreased sebum productionalthough much of the dryness may be due toepidermal dehydration.Seborrhea oleosa: Patients present with thick,tenacious, yellowish, oily accumulations, which areodiferous. This implies excessive sebumproduction. The coat often appears to be dullbecause of abnormal light refraction.3- Antibacterial agents :Antibacterial shampooscontain ingredients like benzoyl peroxide,chlorhexidine, ethyl lactate, povidone-iodine,
hexetidine or piroctone olamine. Benzoyl peroxide,organic iodine compounds, chlorhexidine andtriclosan are able to kill Staphylococcus intermediuson the skin (Kwochka and Kowalski, 1991).These agents reduce the cutaneous bacterialpopulation, remove tissue debris, allowing directcontact of the active ingredient with the organismand promoting drainage (Scott et al., 2001).4- Antipruritic agents : Cool water bathdecreases pruritus by soothing the skin and washingaway inflammatory mediators and potentialallergens. Controlled studies on efficacy ofantipruritic shampoos are lacking (Scott et al.,2001). Antipruritic shampoos are consideredgenerally as adjunctive treatments as they are rarelyaffective as the sole therapy (Halliwell, 1991).Topical antipruritic therapy is gaining increasinginterest as adjunctive therapy to control itching. Itis believed that itching results from noxious agentsand allergens being absorbed through the skin.5- Antiparasitic agents : Common indicationsof these agents include scabies, cheyletiellosis,otodectic mange, tick infestation, trombiculosis andpediculosis. Antiparasitic shampoos mostlycontains organochlorines, natural pyrethrins orsynthetic pyrethroids which is not considered verygood antiparasitic rinses and dips (Scott et al.,2001) as they are rinsed and cannot act during asufficient time (Curtis, 1998). Also there is usuallylittle or no residual action once the shampoo isrinsed off and treated animal is immediatelyvulnerable to reinfestation by host-seeking fleas.These shampoos have limited application in thelong-term management of flea infestation (Carlottiand Jacobs, 2000). Permethrin shampoo havingratio of 60:40 (trans:cis) in 1% concentration maybe successfully used for management(Yolande,2005). Shampoo containing deltamethrin(0.07%) has been shown to maintain more than90 % antifeeding effect during the hour followingchallenge for one week (Franc,and Cadiergues,1999).

106
Journal of Canine Development & Research 2013
6- Antifungal agents - Mostly antimycoticshampoos are used as adjunctive therapy fordermatophytosis and Malassezia dermatitis. Theylimit contagiosity in case of dermatophytosis butare not effective when used without systemictherapy (DeBoer and Moriello, 1995). Howeverimmediate and residual in vivo antifungal effect wasreported with a shampoo containing piroctoneolamine against Malassezia pachydermatis(Bourdeau et al., 1999). Non antifungalshampoos or shampoos with insufficient antifungalproperties can disseminate spores (Moriello andDeBoer, 1995). However, keratomodulatingshampoos are used before antifungal topicaltherapy when there is a keratoseborrhoeic disorderand they are then beneficial in removing infectedscales and crusts. Miconazole shampoo isconsidered to be as effective as lime sulfur andenilconazole in treating dermatophytosis (Morielloand DeBoer, 1995). Cases that are complicatedby concurrent Malassezia are treated with acombination containing miconazole (2%) andchlrohexidine (2 to 4%) or combination ofchlorhexidine (2%) and ketoconazole (1%) as likerinses of lime sulfur and enilconazole. (Bond etal., 1995).
Ingredients of medicated shampoo and theirfunction
a- Salicylic acid : It is a keratolytic agent becauseof its desquamating property via direct effect onintercellular cement. It also causes reduction in skinpH which leads to an increase in the waterabsorption by keratin consequently improvedhydratation of skin. Salicylic acid actssynergistically with sulphur and its efficacy varieswith concentration.Attributes of salicylic acid include keratoplastic,keratolytic, antipruritic, astringent, andbaceriostatic activity. The keratolytic activity ofsalicylic acid is produced by decreasing surfacepH, resulting in increased hydration of keratin and
thus swelling of cells in the stratum corneum.Salicylic acid also solubilizes the natural bindingmaterial between cells, promoting the shedding ofattached surface cells.b- Sulphur : It is keratolytic agent as it formshydrogen sulphide in the corneal layer and havesynergistic effect with salicylic acid. This synergismappears optimal when both substances areincorporated into the shampoo in equalconcentrations (Leyden, 1987). It is alsokeratoplastic because it interacts with epidermalcysteine to form cystine, an important componentof the corneal layer (Scott et al., 2001). It is aclassic antiseborrhoeic agent but because of itsdrying effect may trigger a rebound effect. Theefficacy of the sulfur relies on its direct interactionwith the skin, therefore sulfur is often formulatedas a colloid to increase its surface area forenhanced contact with the skin. Other property ofsulfur includes antifungal, antibacterial, andantiparasitic (mites and lice but not fleas) (Randall,2005) as a result of hydrogen sulfide andpentathionic acid formation from the combinationof sulfur with cystine. Sulfur has also beendemonstrated to decrease itching and is extremelysafe, even on newborn animals. When added inequal proportions, sulfur and salicylic acid improvethe overall effect of antiseborrheic shampoos. Theconditions for which sulfur/salicylic acidcombinations are prescribed include primarykeratinization abnormalities causing a dry scalingdermatosis or conditions secondary to bacterialpyoderma, parasitic infections, allergy, autoimmunedisorders, environmental influences, and metabolicimbalances such as hypothyroidism.c- Coal tar : Tar is a complex mixture of aromatichydrocarbons, with many constituents (more than10,000). It is hard to determine which isresponsible for therapeutic effects. It is akeratoplastic agent, reduces nuclear synthesis inthe epidermal basal layers (Kwochka, 1993),besides antiseptic and antipruritic agent.. Smell and

107
Journal of Canine Development & Research 2013
consistency of commercial preparations sometimesmake it difficult to use, although deodorizedveterinary preparations are now available. Side-effects like skin drying, discolouration of pale coatsand irritation) have been reported with highconcentrations (over 3 %). Quite often, tarshampoos are combined with sulfur and salicylicacid, which allows for a decreased concentrationof tar to provide the desired keratolytic activity.Treatments should be discontinued or followed bya conditioning rinse if drying or irritation occurs.The staining properties of tar shampoos prohibittheir use in white-coated show dogs.Characteristics of tars include antimitotic,keratolytic, antipruritic, degreasing, and anti-inflammatory activity. The antimitotic effects of tarsare a result of suppression of epidermal growthand DNA synthesis of the stratum basale. Theprimary clinical application of tar shampoos is inthe treatment of dogs with very oily skin. The higherthe concentration of tar, the better its effects, buthigh concentrations increase susceptibility tocontact allergies, excessive drying, or skin irritation.Concentrations greater than 4% refined tar havebeen shown to be irritating.d- Selenium disulphide : It is keratolytic andkeratoplastic (impaired disulphide bridge formationin keratin), antiseborrheic and a potent degreaserbut has limited usage because of its staining, drying,and irritating effects, especially to the mucousmembranes and the scrotum. Disadvantage isrebound increase in scaling. With the availabilityof less irritating degreasing products, seleniumtends to be used as a last resort for thoseseborrhoeic dogs that do not respond to otherproducts.e- Ammonium lactate : It is effective in removingexcessive scale by virtue of its keratoplastic activity(Jennings, 1998). It seems to stimulate the livingepidermis, correcting defects in keratinocytemultiplication and maturation, so useful inseborrhoeic disorders. This facilitates terminal
keratinocyte differentiation, leading to more normaldesquamation (Lavker, 1992). Ammonium lactatehas moisturizing properties (Vilaplana, 1992).Clinical studies in human indicate that ammoniumlactate is well-tolerated, even used over prolongedperiods (Klaus, 1990).f- Benzoyl peroxide : It is metabolized in the skinto benzoic acid and much of its microbiocidalactivity probably derives from the lowered skinpH (Halliwell, 1991). This disrupts microbial cellmembranes (Burkhart et al., 2000). It is anoxidizing agent, which releases nascent oxygen intothe skin and produces a series of chemical reactionsresulting in permeability changes and rupture ofbacterial membranes (Guaguère, 1996). Inaddition to being antibacterial, keratolytic anddegreasing, it is antiseborrhoeic causing sebumhydrolysis and reducing sebaceous gland activity.Campbell (1994) reported that 3% benzoylperoxide shampoos increase transepidermal waterloss and decrease skin surface lipid concentrationand corneocyte counts. It exerts a follicular flushingaction (Scott et al., 2001) which is very usefulwhen treating comedone disorders, follicularhyperkeratosis (Guaguere, 1996) anddemodecosis. It is generally used in concentrationsof 2 to 3 %, which are well tolerated but inconcentrations above 5% side-effects likeirritations, erythematosus rash ad pain n have beenreported (Guaguere, 1996). Benzoyl peroxide hasdrying and bleaching effect and should thereforenot be used in dry seborrhea and owners shouldbe warned about the bleaching effect so, emollientsare indicated after using this product. It is reportedthat 61 % of dogs responded well to a 2.5 %benzoyl peroxide shampoo, without concurrenttherapy in folliculitis. While in cases of superficialpyoderma, 70 % of responded well to a 2.5 %benzoyl peroxide shampoo (Ascher et al., 1990).Benzoyl peroxide is considered the most effectivefor Staph. intermedius in comparison to otherantimicrobials. Benzoyl peroxide has excellent
108
Journal of Canine Development & Research 2013
keratolytic activity and its residual antibacterialspectrum of 48 hours makes benzoyl peroxide oneof the most active antibacterial agents. Animals withsensitive skin may develop excessive drying orirritation; however, this can be relieved byalternating treatments with a milder product or byusing emollients. Benzoyl peroxides generally donot lather well. Loeffler et al. (2011) reportedequally efficacy of 3 per cent chlorhexidinegluconate and 2.5 per cent benzoyl peroxideshampoo was as sole antibacterial treatment indogs with superficial pyoderma.g- Essential fatty acids/ Moisturizers : In everyskin disorders, particularly in dry seborrhoea, thereis need for increasing the humidity of the animal’sskin. It has been demonstrated that skinhydratation is less in dogs with scaling disorderthan in normal dogs (Cadiot et al., 2000). Localapplication of essential fatty acids has also beenproposed to soften and rehydrate the skin, andreduce trans-cutaneous water loss (Carlotti andJacobs, 2000). Moisturizers include suchcategories as emollients and humectants. Emollientsare vegetable and animal oil products that protectand soften the skin by filling in the spaces betweenthe dry skin flakes, thus smoothing roughenedsurfaces of the stratum corneum and principallycomposed of fatty acid polyesters, vegetable oils,mineral oils and lanolin. Lipid emollients, containinglanolin alcohols, liquid paraffin or mineral oils arenow rarely used. Non-lipid emollients haverehydrating and softening properties. They reducesmell and improve coat appearance without thegreasing effect. The high molecular weight of theiractive ingredients and their hygroscopic naturemake them effective surface protecting agents.Examples include lactic acid, glycerin, propyleneglycol, urea and chitosanide. Active agents canbe combined with moisturisers: colloidal oatmealextracts and aloe vera for antipruritic activity, andcoal tar for keratolytic and keratoplastic activity.Humectants rehydrate the skin without using oils
as they act by pulling moisture to the skin from thepet’s own body fluids. The active ingredients inthis category include lactic acid, urea, carboxylicacid, glycerin, and propylene glycol. Humectants,on the other hand, can be used daily to aid inalleviating dry, scaly conditions. Various veterinaryshampoos have incorporated essential fatty acidsfor their softening and moisturizing properties. Onestudy has demonstrated that in seborrhoeic dogs,abnormal transepidermal water loss could becorrected by applying linoleic acid (Campbell andKirkwood,1993). Some shampoos containmoisturizers: glycerin, lactic acid and fatty acidpolyesters. Moisturizers can be stored inmultilamellar structures for prolonged release(spherulites), or mono/oligolamellar bodies(liposomes) to ensure hydration level. Tretter andMueller, (2010) recorded decreasedtransepidermal water loss and pruritus In atopicdogs by application of essential oils andunsaturated fatty acids once weekly for 8 weeks.Chlrohexidine : It is a synthetic biguanideantiseptic, very effective against most bacteria(Gram + and-ve), fungi, and yeasts except somePseudomonas and Serratia strains. It isbactericidal by action on cytoplasmic membranewhich causes leak of intracellular componentsleading to rapid killing of microbes with a 36-hourresidual activity. Concentrations vary in shampoosfrom 0.5 to 4% (diacetate or digluconate),however, 3- 4% formulation has been quiteimpressive in clinical cases (Ferrandis, 2003).Chlrohexidine also shows a good residual antibioticeffect due to its remanence (Kwochka andKowalski, 1991). Chlrohexidine is less irritatingthan benzoyl peroxide and is therefore preferablein dogs with sensitive and dry skin. Three percentchlorhexidine and 2.5 per cent benzoyl peroxideshampoo with frequency of twice weekly wasfound similarly effective in canine bacterialovergrowth syndrome (Viaud et al., 2012).Schilling and Mueller (2012) reported that

109
Journal of Canine Development & Research 2013
medicated shampoo cotaining chlorhexidine,lactoferrin, piroctone olamine, chitosan andessential fatty acids is effective in mild to moderateallergic pruritus without secondary skin infectionswith frequency of twice weekly for four weeks,but there was no statistically significant differencein the canine atopic dermatitis extent and severityindex.h- Povidone iodine : It is a iodophore whichslowly releases iodine to tissues (Scott et al.,2001). The titratable iodine is usually of the orderof 0.2 to 0.4 per cent. It is bactericidal and acts ina few seconds at 0.005 % (Curtis, 1998)). It hasalso a prophylactic effect due to its remanence(Kwochka and Kowalski, 1991). It is relativelydrying which can be compensated by emollientsin shampoos. It can be irritant and staining(Guaguère, 1996). Iodine preparations havedecreased in popularity as a result of their unwantedproperties and the development of more efficientproducts. Iodine has good activity against bacteria,viruses, and fungi, especially when combined withpyrrolidone nitrogen. Residual effects last only 6to 8 hours. Side effects include irritation, staining,and contact hypersensitivity.i- Ethyl lactate : Ethyl lactate is hydrolyzed toethanol and lactic acid, which lowers the skin pH.Its mode of action is therefore similar to benzoylperoxide (De Jaham, 2003). It is used inconcentration of 10 %, which is rarely followedby undesirable side effects (irritation, erythema,pruritus) (Guaguère, 1996). In a comparativestudy to benzoyl peroxide, 90 % of dogs withsuperficial pyoderma responded well to a 10 %ethyl lactate shampoo (Ascher et al., 1990). In arecent study comparing two groups of 10 dogswith superficial pyoderma, it was shown thatutilization of a 10 % ethyl lactate shampoo twiceweekly reduces the length of systemic antibioticneeded in canine superficial pyoderma (De Jaham,2003).j- Corticosteroids : Corticosteroid can also be
used in shampoo form as antipruritic agent, 1%hydrocortisone and 0.01% fluocinolone acetonide;a fluorinated corticosteroid can be used for thispurpose with oatmeal base. Topical application offluorinated corticosteroid can be associated withsystemic absorption and adrenal suppression.There is minimal residual activity noted withcorticosteroid shampoo.k- Oatmeal : Up to 8% colloidal oatmeal is asafe and effective antipruritic agent either alone orcan be combined with diphenhydramine even forchronic use. Oatmeal is formulated as a colloid,which provides a large surface area. The noxiousagents and allergens are absorbed by the oatmealand subsequently washed away, eliminating thesource of irritation and inflammation. Theseproducts are extremely safe, but tend to provideshort term relief (24-48 hours) of mild pruritus,also it has no antibacterial or antifungal properties(Randall, 2005). Topical anesthetics and anti-inflammatory agents anesthetic like 1% pramoxinehydrochloride (Scott, 2000), omega-6 fatty acids,0.01% fluocinolone acetonide has antipruritic effectbut without side effects like cutaneous sensitivityand methemoglobinouria as with lidocaine andbenzocaine. Sulfur Lyme dip is a very effectivenonsteroidal antipruritic agent can be applied asrinse and allowed to dry on the animal providingresidual effect. In addition to antipruritic effect, itis also antiparasitic and antifungal. Linoleic acidand L- rhamnose has been shown to improvecutaneous barrier function in the dogs. L-rhamnose also decreases the inflammatorymediators, that are involved in the pathogenesis ofatopic dermatitis.l- Imidazoles : It act by interfering with cell wallformation in fungal and yeast organisms, whichincreases cellular permeability, thus suppressingmetabolic function and inhibiting growth. There hasalso been evidence that ketoconazole exerts aninhibitory effect on keratinocytes in culture.It is obvious that shampoos play a major role in

110
Journal of Canine Development & Research 2013
veterinary medicine. It is also becoming increasinglydifficult to remain abreast of all the availableinformation and products. By understanding theprinciples of the various categories of shampoos,one can select an appropriate medicated shampoo(Bloom, 2007). Clinical improvement is the maincriterion in evaluating the efficacy of a shampoo.The efficacy of shampoos on skin hydration, thesurface lipid fi lm and stratum corneum, which isof great importance in keratoseborrhoeicdisorders, can be evaluated objectively using avariety of techniques, including transepidermalwater loss (TEWL) measurement and many others,but they have been deemed to be not reproducibleand thus useless. Prolonging the action of activeingredients has been made possible: liposomesprolong the moisturizing effect and Spherulitesincrease bioavailability of therapeutic agents andpromote immediate and residual moisturisingproperties (reinforced by chitosanide). Also,microemulsions enhance bio-availability of activeingredients, which readily diffuse, and they alsohave an effective cleansing effect.
References Ascher, F., Maynard, L., Laurent, J. and Goubet, B. (1990).
Controlled trial of ethyl lactate and benzoylperoxide shampoos in the management of ca-nine surface pyoderma and superficial pyo-derma. In : Advances in Veterinary Dermatol-ogy Volume 1, Eds Von Tscharner C, HalliwellREW, Baillière Tindall, London, Pp.375-382.
Bloom, P.B. (2007) How to Choose the Right Shampoo.in: NAVC Proceedings. North American Veteri-nary Conference (Eds). Publisher: NAVC(www.tnavc.org). Internet Publisher: Interna-tional Veterinary Information Service, Ithaca NY(available at .ivis.org)
Bond, R., Rose, J.F., Ellis, J.W. and Lloyd, D.H. (1995).Comparison of two shampoos for treatment ofMalassezia pachydermatis-associated sebor-rhoeic dermatitis in basset hounds. J Small AnimPract. 36: 99-104.
Bourdeau, P., Blumstein, P., Ibish, C., Gardey, L., Jasmin,P. and Gatto, H, (1999). Antifungal activity of apiroctone shampoo against Malassezia popu-
lations after single treatment in the dog. In Pro-ceedings 16 Annual Congress of the EuropeanSociety of Veterinary Dermatology and Euro-pean College of Veterinary Dermatology,Helsinki, Pp.155.
Burkhart, C. N., Specht, K. and Neckers, D. (2000). Syn-ergistic activity of benzoyl peroxide and eryth-romycin. Skin Pharmacol Appl Skin Physiol 13:292-296.
Cadiot, C., Ibisch, C., Bourdeau, P. and Gatto, H. (2000).In vitro assay for detection of caninekeratinocyte activation : preliminary results forpharmacological tests of activation/regulation.Vet Dermatol, 11 (1): 58.
Campbell, K.J. (1994). Effects of four antiseborrheic sham-poos on transepidermal water losses, hydratationof the stratum corneum, skin surface lipid con-centration, skin surface pH and corneocyte countin dogs. In: Proceedings of the tenth annualmeeting of the American Academy of VeterinaryDermatology and American College of VeterinaryDermatology, Charleston. Pp.85.
Campbell K.J., Kirkwood A.R. (1993) Effects of topicaloils on TEWL in dogs with seborrhea sicca. In: Adv. Vet. Derm. II, Eds Ihrke PJ, Mason IS,White SD, Pergamon Press,Oxford.Pp-157-162.
Carlotti, D.N. (2006). Optimizing topical therapy in thedog. In: Proceedings 31st WSAVA Congress,Prague, Czech Republic.
Carlotti, D.N. and Bensignor, E. (2002) Management ofkeratosseborrhoeic disorders. Eur J Comp AnimPract. 12: 123-133.
Carlotti, D.N. and Jacobs, D.E. (2000). Therapy, controland prevention of flea allergy dermatitis in dogsand cats. Vet Dermatol, 11: 83-98.
Cathy Curtis.( 1998). Use and abuse of topical dermato-logical therapy in dogs and cats Part 1. Sham-poo therapy In Practice ;20:244-251.
Christa, Horvath. and Ariane, Neuber (2007). Manage-ment of canine pyoderma.UK Vet. 12(1): 1-7
Curtis, C.F (1998). Use and abuse of topical dermatologi-cal therapy in dogs and cats. Part 1- shampootherapy. In Practice, 244-251.
De Jaham C, (2003). Effects of an ethyl lactate shampooin conjunction with a systemic antibiotic in thetreatment of canine superficial bacterial pyo-derma in an open-label, nonplacebo controlledstudy.Veterinary Therapeutics, 4 (1): 94-100
De Jaham, C. (2003). Effects of an ethyl lactate shampooin conjunction with a systemic antibiotic in thetreatment of canine superficial bacterial pyo-
111
Journal of Canine Development & Research 2013
derma in an open-label, non-placebo-controlledstudy. Vet Ther 4: 94- 100.
De Jaham, C. (2003). Effects of an ethyl lactate shampooin conjunction with a systemic antibiotic in thetreatment of canine superficial bacterial pyo-derma in an open-label, non-placebo controlledstudy. Veterinary Therapeutics, 4 (1): 94-100.
DeBoer, D.J and Moriello, K.A. (1995). Inability of twotopical treatments to influence the course ofexperimentally induced dermatophytosis incats. J Am Vet Med Assoc, 207: 52-57.
Ferrandis, A. (2003). Formulating a chlrorhexidine basedshampoo: a galenic challenge. In: Proceedingsof Virbac European Symposium, Skin Biologyand Innovations in Dermatology, Pp.21-26.
Franc, M. and Cadiergues, MC. (1999). Activity of adeltamethrin shampoo against Ctenocephalidesfelis and Rhipicephalus sanguineus in dogs.Vet Parasitol.. 81(4):341-6.
Groux, D. and Bensignor E (2000). Skin characteristicsmeasured by trans-epidermal water loss,corneometry and sebometry are not valuabletools to evaluate the effects of topical treat-ments in dogs. Vet Dermatol, 11(1): 60
Guaguere, E. (1996). Topical treatment of canine and fe-line pyoderma. Vet Dermatol. 7: 145-151.
Halliwell, Rew. (1991). Rational use of shampoos in veteri-nary dermatology. J Small Anim Pract 32 : 401-407.
Jennings, M..B. (1998). Comparison of salicylic acid andurea versus ammonium lactate for the treatmentof foot xerosis. A randomized, double-blind clini-cal study. J Am Podiatr Med Assoc 88: 332-336.
Klaus, M.V. (1990). Evaluation of ammonium lactate inthe treatment of seborrheic keratoses. J AmAcad Dermatol. 22: 199-203.
Kwochka, K.W. (1993). Symptomatic Topical Therapy ofScaling Disorders. In: Current Veterinary Der-matology (Griffin CE, Kwochka KW, MacDonald JM, Edrs) Mosby Year Book, St Louis,Pp.191-202.
Kwochka, K.W. and Kowalski, J. J. (1991). Prophylacticefficacy of four antibacterial shampoos againstStaphylococcus intermedius in dogs. Am J VetRes 52: 115-158.
Lavker, R.M. (1992). Effects of topical ammonium lactateon cutaneous atrophy from a potent topical cor-ticosteroid. J Am Acad Dermatol. 26: 535-544.
Leyden, J.J. (1987). Effects of sulfur and salicylic acid in ashampoo base in the treatment of dandruff: adouble-blind study using corneocyte counts andclinical grading. Acta Derm Venereol. 39: 557.
Loeffler, A., M. A. Cobb., R. Bond (2011). Comparison ofa chlorhexidine and a benzoyl peroxide sham-poo as sole treatment in canine superficial pyo-derma. Veterinary Record. 169:249
Loflath, A., Von, Voigts-Rhetz. A., Jaeger, K., Schmid, M.,Kuechenhoff, H. and Mueller, R.S. (2007). Theefficacy of a commercial shampoo andwhirlpooling in the treatment of canine pruritus- a double-blinded, randomized, placebo-con-trolled study. Vet Dermatol.18(6): 427-31.
Moriello, K.A. and DeBoer, D.J. (1995). Feline dermato-phytosis. Recent advances and recommenda-tions for therapy. Vet Clin. North Am Small AnimPract 25 : 901-921.
Randall, C. Thomas. (2005) Canine Atopic Dermatitis: Oldand New Therapies. In Proceeding of the NAVCNorth American Veterinary Conference, Or-lando, Florida. Pp.285-288
Schilling, J. and R. S. Mueller. (2012). Double-blinded,placebo-controlled study to evaluate an anti-pruritic shampoo for dogs with allergic pruri-tus. Veterinary Record.171:97
Scott, D.W., Miller, W.H. and Griffin, C.E. (2001). Mullerand Kirk’s Small Animal Dermatology, 6th edn,WB Saunders Company, Philadelphia.
Scott, W. (2000). A clinical study of the efficacy of twocommercial veterinary pramoxine cream rinsesin the management of pruritus in atopic dogs.Canine Pract 25 : 15-18
Sonja, Zabel. (2011). Shampoo use in Veterinary Medi-cine. In Proceedings of the 36th World SmallAnimal Veterinary Congress , Jeju, Korea.Pp.290-296
Srivastava, P.C. and Bhagwat, V.G (2009). Evaluation ofERINA Plus as a coat conditioner in canines.Veterinary World. 1 (12): 361-362
Tretter,S . and Mueller, R.S. (2010). The influence of topi-cal unsaturated fatty acids and essential oilson normal and atopic dogs- a pilot study. VetDerm. 21: 311-328
Viaud, S., L. Maynard and A. Sanquer (2012). Compari-son of two shampoos as sole treatment for ca-nine bacterial overgrowth syndrome. VeterinaryRecord: 170:675
Vilaplana, J. (1992). Clinical and non-invasive evaluationof 12% ammonium lactate emulsion for the treat-ment of dry skin in atopic and non-atopic sub-jects. Acta Derm Venereol 72 : 28-33
Yolande, M. B. (2005). Parasitic infections. In The Veteri-nary Formulary, 6th edn. British Veterinary As-sociation. Pp.214
112
Journal of Canine Development & Research 2013
GENERAL ARTICLEADVANCEMENT IN DENTAL CARE IN CANINES : AN OVERVIEW*J.P. Kachhawa1, Anil Ahuja2 ,A. P. Singh3, D.K.Bihani3 , Deepika Dhuria
4, Jitender Bargujar1 and Anil Langar1
Department of Clinical Veterinary Medicine, Ethics and JurisprudenceCollege Of Veterinary and Animal Science, RAJUVAS, Bikaner-334 001 (Rajasthan)
1Teaching Associate 2Professor & Head 3Professor 4Veterinary Officer*Corresponding author e-mail : [email protected]
A B S T R A C T
Dental care is necessary to provide optimum health and qualityof life. most of the time, they results from multi-factorial infection,with predominant signs of halitosis, ptyalism, dysphagia, behavioralterations, altered gingival colour, gingival bleeding, tooth mobility,periodontal and periapical abscesses. Present paper reviewedthe clinical manifestations, method of oral examination, treatmentoptions including scaling, root planning, polishing, client educationand home care.
Key words :Client educationGingivitisHalitosisPeriodontal disease
A R T I C L E H I S T O R Y
Received : December 22, 2013Revised : January 10, 2014Accepted : January 20, 2014
Periodontal disease (PD) is one of the mostcommon infectious diseases affecting adult
dogs and cats of any age, with up to 80% of animalsof all breeds affected (Harvey, 1998) and Riggioet al., 2011). It often begins with halitosis (oralmalodor) as the first detectable sign (Culhamand Rawlings, 1998). Periodontitis is irreversibleand affect’s the deeper tissues backing the teeth,permanently damaging the surrounding bone andperiodontal ligament and resulting in increasedperiodontal pocket depth and tooth loss. Thisdisease progresses through stages, including plaqueaccumulation, calculus or tartar accumulation,inflammation of the gingiva, periodontal pocketformation, alveolar bone resorption, tooth mobility,and tooth loss (Shipp and Fahrenkrug, 1992).Dental plaque covers mineralized calculus
deposits, composed primarily of calcium phosphatebetween and within remnants of formerly viablemicroorganisms (White, 1997). Periodontaldisease has been described as a multi-factorialinfection (Lindhe et al., 1973). The etiology ofcanine periodontal disease is poorly studied,although gram-negative anaerobic bacteria havebeen associated in the disease (Hennet andHarvey, 1992 and Boyce et al., 1995). Incontrast to periodontitis, gingivitis is completelyreversible and is known by the characteristic signsof halitosis, bleeding, inflammation, redness andswelling of the gingivae. Diseases of the oralcavity, if left untreated, are often painful and cancontribute to other local or systemic diseases(Holmstrom, et al., 2005). Veterinary dentistry isone of the fastest growing areas of veterinary
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol(9) 112-116

113
Journal of Canine Development & Research 2013
medicine today (Holmstrom et al., 2013). Someof the newer innovations in the field will help tokeep pets in better dental health (Baxter, 2013).This paper is an attempt to review the clinicalmanifestations, method of oral examination,treatment options including scaling, root planning,polishing, client education and home care.
Clinical manifestations
Periodontal disease is not a single disease, butrather a group of diseases with similar patterns andsymptoms affecting the periodontium (Kinane etal., 2005). The most obvious clinical signs includehalitosis, ptyalism, dysphagia, behavior alterations,altered gingival colour, gingival bleeding, toothmobility, periodontal and periapical abscesses,nasal discharge, sneezing, osteomyelitis, contactulcers, intranasal dental migration, and oronasaland oroantral fistulas (Kesel, 2000). A diagnosisof periodontal disease relies on interpreting clinicalsigns, full-mouth examination (including periodontalprobing), and intraoral radiographic exams (Klein,2008).
History, oral examination and imaging
The history must include, home care, diet, accessto treats and chews, chewing habits, current andprevious dental care and procedures, previousdiseases, allergies, and medications currentlyadministered (Holmstrom, et al., 2013). In asmall-breed dog without home care, periodontaldisease can start as early as 9 months of age but inlarge breed dogs it start some years later (Goldenet al., 1982; Holmstrom, et al., 2005).Evaluate the head and oral cavity visually and bypalpation. Areas like lymph nodes, nose, lips,mucous membrane, vestibule, palatal and lingualsurface of the mouth, dorsal and ventral aspect oftongue, tonsils and salivary ducts should beevaluated (Holmstrom, et al., 2005). Dentalradiography is a diagnostic tool for diagnosis,which permits the evaluation of alveolar bone loss,
abscesses, fractures, retained root tips, malformedteeth, resorptive root lesions and otherabnormalities that cannot be seen with the nakedeye. Intraoral radiography has been proven todetect important pathology in 27.8% of dogs and41.7% of cats without showing any clinicalabnormality. Specific or localized radiographs areessential for accurate evaluation and diagnosiswhen oral pathology is found (Holmstrong et al.,2004).
Treatment
Traditional treatment for dental disease hasincluded dental chews, rinses, brushing, antibiotics,anti-inflammatories, and dental cleanings. Thetreatment consists of superficial debridement,careful mechanical oral hygiene, rinsing withchlorhexidine and daily re-evaluation (Herrera etal., 2014). A traditional saying has always been“It is good to chew, it is better to rinse, and it isbest to brush.” Following methods are suggestedfor proper dental care and prevention and controlof periodontal diseases-1. The careful plaque and calculus removal fromthe tooth crown, gingival sulcus and root surfacesis essential for the prevention and control ofperiodontal diseases (Kamath and Nayak, 2014).Plaque removal can be accomplished by acombination of home care procedures that includemechanical and chemical plaque reductiontechniques (e.g. tooth brushing with dentifrices,topical application of chemical plaque retardantssuch as 0.12–0.2% chlorhexidine gluconate),dietary manipulation (special diet and chew toys)and regular professional periodontal therapy(Niemiec, 2008). Dental chew reduces in plaque,calculus accumulation and oral malodor significantlywhile improving gingival indices (Quest, 2013).2. Antimicrobials used to suppress subgingivalplaque accumulation should be effective againstgram-positive aerobes, as well as gram-negativeanaerobes, which are the initiators of gingival

114
Journal of Canine Development & Research 2013
inflammation and destruction (Harvey and Emily1993; Harvey, 1995; Marcello et al., 2011).Clindamycin hydrochloride @ 11 mg/kg/bwt/daypo has been used in conjunction with dentalprocedures because it is active againststaphylococcal, anaerobic (gram-positive andgram-negative), and polymicrobial dentalinfections (Dow and Jones,1998; Zetner et al.,2002). Its wide spectrum of activity (Zurenkoand Gorbach,1992) , excellent tissue and bonepenetration (Novak, 1992), and efficacy inpurulent environments (Ehrenfeld, 1992) makesit well-suited for this condition. A topical 2%clindamycin hydrochloride gel has mucoadhesiveproperties and also may function as a physicalbarrier to the introduction of bacteria (Johnston etal., 2011). Bowersock et al. (2000) reported highefficacy of clindamycine and chlorhexidine acetateagainst bacteremia before and after dental scalingin dogs with periodontitis.Amoxicillin/clavulanate and metronidazole seem tobe particularly effective antimicrobials. These maybe used for a week before periodontal surgeryand 7–10 days postoperatively as intermittenttherapy in selected patients (impaired host defencesor failure of conventional root debridement)(Lobprise, 2007 and Niemiec, 2008). Locallydelivered antimicrobials (perioceutics), such asdoxycycline gel, can be applied to teeth that havebeen cleaned and polished (Niemiec, 2008).Systemic use of doxycycline @ 2 mg/kg/bwt/daypo appeared to be an appropriate antimicrobialregimen for dogs with periodontitis (Kim et al.,2013). Dog studies revealed that periocline andthe gel containing 5% (w/w) tinidazole, couldsignificantly decrease symptoms of periodontitis(Qin et al., 2012).3. Use well-monitored inhalation anesthesia withcuffed intubation when performing dental cleanings.These techniques increase safety, reduce stress,decrease the chances of adverse sequelae (e.g.,inhalation pneumonia), and they are essential for
thorough and efficient evaluation and treatment(Holmstrom et al., 2005). With progressiveperiodontal disease, advanced periodontal surgerybecame the only option. To treat patients with deeppockets and bone loss, mucogingival surgery (flapexposure) and open curettage are required(Niemiec, 2008). New therapies have started withthe aim of inducing periodontal regeneration andinclude: soft tissue grafts, bone replacement grafts,root biomodifications, enamel matrix derivatives,use of bioactive products such as bonemorphogenic protein, guided tissue regeneration,and their combinations (Greenwell, 2001).Currently final modality for periodontal disease istooth extraction (Niemiec, 2008).
Scaling, root planning and polishing
Non-surgical periodontal therapy is always the firstline treatment and involves scaling (a combinationof hand scaling, mechanical scaling, polishing andsulcular lavage) and closed root debridement undergeneral anaesthesia. Non-surgical handinstruments, scalers and curettes are used forperiodontal therapy and the most access tosubgingival calculus (Kamath and Nayak, 2014).Scaling may be done both supragingivally andsubgingivally with a piezoelectric ultrasonic scaler.Ultrasonic instruments oscillate at very high speeds,causing micro vibrations that aid in calculus andsubgingival plaque removal (Kamath and Nayak,2014). Arabaci et al. (2007) found that thepiezoelectric system was more efficient in calculusremoval compared to hand instrumentation.Presently, numerous types of lasers have been usedfor calculus removal (Braun et al., 2003).
Client education and home care
Regular home care for disease control is vital inaddition to professional removal of plaque that isgenerally very effective in controlling mostinflammatory periodontal diseases (Drisko, 2001).The home care plan includes the frequency,duration, and methods of rinsing and brushing;

115
Journal of Canine Development & Research 2013
applying sealant and the use of special food anddental chews. At the time of discharge of patient,potential complications like bleeding, coughing,dehiscence infection, halitosis, vomiting and painshould be discussed with owner (Hennet andHarvey, 1992). Provide antibiotic and othermedication for inflammation and pain only asindicated (Hennet, 1995).Evaluate pets with gingivitis at least every 6 monthsand those with periodontitis at least every 3 to 6months. Advanced periodontal diseases requiremonthly examinations until the disease is controlled.Pets can live longer, healthier lives if oral healthcare is managed and maintained (Verstraete et al.,1998).Start a dental care routine as early as possible indog’s life so he get used to the feeling of having histeeth brushed and inspected. Puppies have 28deciduous teeth that typically fall out by about sixmonths of age. By this time, dog should be gettinghis teeth brushed regularly. Never brush dog’s teethwith human toothpaste as it can make your dogsick, use special enzymatic toothpaste madeespecially for dogs (Holmstrom et al., 2013).Plaque begins to turn into tartar or calculus within24-48 hours, so daily brushing is recommended.Brushing of dog teeth should be considered aroundthe same time of owner so it will be easier toremember. If there are some difficulties to brushdog’s teeth use oral rinses and dental treats madeespecially for dogs (Beckman, 2012). Avoid realbones as they may not only lead to gastrointestinalupset, they may also cause tooth fractures.
ReferencesArabaci, T., Cicek, Y., Canakci, C.F., (2007). Sonic and
ultrasonic scalers in periodontal treatment: areview. Int. J. Dent. Hyg. 5: 2–12.
Baxter, C. (2013). Veterinary dentistry: a clinician’s view-point. Dent Update. 40 (5):386-8, 390.
Beckman, B.W. (2012). Patient management for periodon-tal therapy. In: Niemiec BA, ed. Veterinary peri-odontology. Ames (IA): Wiley-Blackwell;:305–12.
Bowersock, T.L., Wu, C.C., Inskeep, G.A., Chester, S.T.(2000). Prevention of bacteremia in dogs un-dergoing dental scaling by prior administrationof oral clindamycin or chlorhexidine oral rinse.J Vet Dent. 17(1):11-6.
Boyce, E.N., Ching, R.J.W., Logan, E.I., Hunt, J.H.,Maseman, D.C., Gaeddert, K.L., King, C.T., Reid,E.E. andHefferren, J.J., (1995). Occurrence ofgram-negative black-pigmented anaerobes insubgingival plaque during the development ofcanine periodontal disease. Clinical InfectiousDiseases. 20 (2)S :317–319.
Braun, A., Krause, F., Nolden, R., Frentzen, M. (2003).Subjective intensity of pain during the treat-ment of periodontal lesions with the Vector‘-system. J. Periodontal. Res. 38: 135–140.
Culham, N. and Rawlings, J.M. (1998). Oral malodor andits relevance to periodontal disease in the dog.J Vet Dent. 15:165–168.
Dow, S.W., and Jones, R.L. (1988). Anaerobic infections,part II: Diagnosis and treatment. CompendContin Educ Pract Vet.9: 827–838.
Drisko, C.H. (2001). Nonsurgical periodontal therapy.Periodontol 2000.; 25:77-88.
Ehrenfeld, M. (1992). Clindamycin in the treatment ofdental infections. In: Zambrano D, ed.Clindamycin in the Treatment of Human Infec-tions. Kalamazoo: The Upjohn Co,; Chp 11: 1–24.
Golden, A.L., Stoller, N. and Harvey, C.E., (1982). A sur-vey of oral and dental diseases in dogsanesthesized at a veterinary hospital. Journalof the American Animal Hospital Association,18: 891–899.
Greenwell, H. (2001). Committee on Research, Scienceand Therapy, American Academy of Periodon-tology. Position paper: Guidelines for periodon-tal therapy Journal of Periodontology, 72, Pp.1624–1628
Harvey, C.E. (1998). Periodontal disease in dogs. Etio-pathogenesis, prevalence, and signi?cance.Veterinary Clinics of North America: SmallAnim.Pract. 28:1111–1128.
Harvey, C.E. and Emily, P.P. (1993). Periodontal disease.In: Harvey, C.E., Emily, P.P. (Eds.), Small AnimalDentistry. Mosby, St. Louis, USA, Pp. 89–144.
Harvey, C.E., Thornsberry,C., and Miller, B.R. (1995)Subgingival bacteria-Comparison of culture re-sults in dogs and cats with gingivitis. J Vet Dent,12:147–150.
Hennet, P. (1995). Periodental disease and oral microbi-
116
Journal of Canine Development & Research 2013
ology. In: crossley DA, Penman, eds. Annualof Small animal dentistry. 2nd ed. Shgurington,England: British small Veterinary Assoc. Pp. 105-113.
Hennet, P.R. and Harvey, C.E. (1992). Natural develop-ment of periodontal disease in the dog: a re-view of clinical, anatomical and histological fea-tures. Journal of Veterinary Dentistry. 9 (3) :13–19.
Herrera, D., Alonso, B., de Arriba, L., Santa Cruz, I.,Serrano, C., Sanz, M. (2014). Acute periodontallesions. Periodontol 2000. 65(1):149-77.
Holmstrom, S. E., Bellows, J., Colmery, B., Conway, M.L., Knutson, K., Vitoux, J. (2005). AAHA DentalCare Guidelines for Dogs and Cats. J Am AnimHosp Assoc, 41: 1-7.
Holmstrom, S.E., Bellows, J., Juriga, S., Knutson, K.,Niemiec, B.A., Perrone, J. (2013). AAHA dentalcare guidelines for dogs and cats. J Am AnimHosp Assoc. 49(2):75-82.
Holmstrong, S.E., Frost-Fitch, P. and Eisner, E.R. (2004).Veterinary Dental Technique for the small Ani-mal Practitioner. 3rd ed. Philadelphia: WBSaunders.
Johnston, T,P., Mondal, P., Pal, D., MacGee, S.,Stromberg, A.J., Alur, H. (2011).Canine peri-odontal disease control using a clindamycinhydrochloride gel. J Vet Dent. 28(4):224-9.
Kamath, D.G. and Nayak, S.U. (2014). Detection, removaland prevention of calculus: Literature Review.The Saudi Dental Journal 26:7–13.
Kesel, M.L. (2000). Periodontal disease M.L. Kesel (Ed.),Veterinary Dentistry for the Small Animal Tech-nician (First Ed.), Ames, Iowa State UniversityPress, USA, Pp. 67–80.
Kim, S.E., Kim, S., Jeong, M., Lee, Y., Ahn, J.T., Park,Y.W., Ahn, J.S., Lee, E., Ryu, D.Y., Seo, K. (2013).Experimental determination of asubantimicrobial dosage of doxycycline hyclatefor treatment of periodontitis in Beagles. Am JVet Res. 74(1):130-5.
Kinane, D.F., Shiba, H. and Hart, T.C. (2005). The geneticbasis of periodontitis Periodontology, 39 : 91–117.
Klein, T. (2008). Predisposing factors and gross exami-nation findings in periodontal disease ClinicalTechniques in Small Animal Practice, 15 : 189–196
Lindhe, J., Hamp, S.-E., and Loe, H. (1973). Experimentalperiodontitis in the beagle dog. Journal of Peri-odontal Research 8: 1–10.
Lobprise, H.B. (2007). Periodontal disease: PeriodontitisH.B. Lobprise (Ed.), Blackwell’s Five MinuteVeterinary Consult Clinical Companion SmallAnimal Dentistry (First Ed.), Ames, Iowa StateUniversity Press, USA, Pp. 172–180
Marcello P. Riggio, Alan Lennon, David J. Taylor, andDavid Bennett (2011). Molecular identi?cationof bacteria associated with canine periodontalDisease.Veterinary Microbiology, 150: 394–400
Niemiec, B.A. (2008). Periodontal therapy Topics in Com-panion Animal Medicine, 23 : 81–90.
Novak, E. (1992). Clindamycin: Clinical pharmacology.In: Zambrano D, ed. Clindamycin in the Treat-ment of Human Infections. Kalamazoo: TheUpjohn Co, Chp 2: 1–14.
Qin, Y., Yuan, M., Li, L., Li, W. and Xue, J. (2012), Formu-lation and evaluation of in situ forming PLAimplant containing tinidazole for the treatmentof periodontitis. J. Biomed. Mater.Res.,100(8):2197-2202.
Quest, B.W. (2013). Oral health benefits of a daily dentalchew in dogs. J Vet Dent. 30(2):84-87.
Shipp, A.D., Fahrenkrug, P. (1992). Periodontics. In:Shipp AD, Fahrenkrug P, eds. Practitioners’guide to veterinary dentistry. Glendale: GriffinPrinting Company, Pp.47–49.
Verstraete, F.J., Kass, P.H., Terpak, C.H. (1998). Diagnos-tic value of full-mouth radiography in cats. AmJ Vet Res;59(6):692–695.
White, D.J. (1997). Dental calculus: recent insights intooccurrence, formation, prevention, removal andoral health effects of supragingival and sub-gingival deposits. Eur J Oral Sci. 105 (5):508-522.
Zetner, K. and Thiemann G. (1993). The antimicrobial ef-fectiveness of clindamycin in diseases of theoral cavity. J Vet Dent; 10:6–9.
Zetner, K., Pum, G., Rausch, W.D., Rausch-Fan, X.H.,Hung, S.T. (2002). Effect of clindamycin hydro-chloride on gingival crevicular fluid and immunemediators in beagles. Vet Ther. 3(2):177-188.
Zurenko, G.E. and Gorbach, S.L. (1992). Clindamycin: Anti-microbial activity. In: Zambrano D, ed.Clindamycin in the Treatment of Human Infec-tions. Kalamazoo: The Upjohn Co,; Chp 1: 1–22.

119
Journal of Canine Development & Research 2013
CLINICAL ARTICLEBRONCHIAL ASTHMA IN A CAT*A.K. Srivastava1 and B. Syed1
Faculty of Veterinary Medicine, Jigjiga University, Jigjiga, Ethiopia.
1 Professor*Crresponding author email : [email protected]
A B S T R A C T
A 4 years old female Siamese cat presented to the Faculty ofVeterinary Medicine, Jijgjiga for several episodes of wheezing,coughing and respiratory distress. Complete blood count revealedonly the increased numbers of circulating eosinophils. Thoracicradiography recorded increased bronchial and interstitial patternswith alveolar densities.The cat recovered completely with oxygentherapy; bronchodilator -inhaled terbutaline long-actingtheophylline; corticosteroid- prednisolone; inhaled fluticasoneand marbofloxacin with in 15 days.
Key words :Bronchial asthmaBronchodilatorsCorticosteroid therapyDyspnea, donutsInhalation therapyTracheo-bronchial treeTachypneaTramlines
A R T I C L E H I S T O R Y
Received : April 28, 2013Revised : June 12, 2013Accepted : June 22, 2013
F eline bronchial asthma is a commonrespiratory condition caused by altered
immunosenstivity of the respiratory tract to inhaledallergens. This hyper responsiveness causes variousstructural and chemical changes in thetracheobronchial tree, including adrenergic-cholinergic imbalance and abnormal mucousproduction. All of these modifications may manifestas commonly recognized clinical signs. Obstructiveand allergic lung diseases affect many cats and aresometimes called asthma, bronchitis, or bronchialasthma. Unfortunately, these diseases are not easilyclassified and probably represent a variety of lungdisorders. Asthma may be defined as an
obstructive, reversible disease that affects thelower respiratory tract. It is characterized bybronchial hyper-reaction that causes a reductionin the bronchial diameter and an excessive mucoussecretion which results in a variety of signs,including coughing, wheezing and respiratorydistress. It is a rare condition in the animal kingdomthat has only been described with thesecharacteristics in the feline and human species(Padrid, 2010).First recognized in 1906 (Hill, 1906), asthma isone of the most common lung diseases in cats withconsiderable morbidity and eventual mortality. Thisrespiratory condition has been given various names:
Journal of Canine Development & ResearchISSN : 0973-3272 website : www.jcdrindia.com
Vol(9) 119-123

120
Journal of Canine Development & Research 2013
lower airway feline disease, allergic feline asthma,allergic acute bronchitis, immune- mediated lowerrespiratory tract disease and feline bronchialdisease. In any case, it must be clear that felineasthma is caused by an exaggerated immunereaction towards an inhaled allergen that generatesspecific chemical and structural changes in thetracheo-bronchial tree. Clinically, feline asthma isevidenced by the relatively variable presence ofcoughing, wheezing, exercise intolerance andrespiratory distress that can settle spontaneouslyor in response to medical treatment (Padrid, 2010;Bay and Johnson, 2005; Byers and Dhupa, 2005).The incidence of feline asthma is probably under-estimated but it is thought to affect 1% of thepopulation. It is the most frequent cause ofcoughing in cats. Although it affects cats of anyage, it is more common in young and middle-agedcats. The Siamese breed may be over-representedwith a prevalence that can be up to 5%. Thissuggests that there is a genetic predispositionsimilar to the human situation (Padrid, 2010;Thébault, 2004).Approximately only 20% of cats with feline asthmahave peripheral eosinophillia. This is not a veryspecific finding because there are other conditionsthat can demonstrate this (e.g. lung parasites,gastrointestinal parasites, heart worms,ectoparasites) (Bay and Johnson, 2005; Cohn,2007). Cats with asthma may show a stressleucogram, but this is also not specific. Bloodchemistry seldom provides relevant informationregarding lung disease, yet there are certain teststhat can help eliminate some potential conditionsfrom the differential diagnosis. It is worthconsidering a serum test for Toxoplasma gondii,and in areas where Dirofilaria immitis is endemic,it is recommended to perform serum tests fordetection of antigen and heart worm antibody incats with respiratory signs (Bay and Johnson,2005; Byers and Dhupa, 2005). In endemic areas,these lung parasites should be excluded by
proper fecal testing, including flotation with orwithout centrifugation techniques (to detectParagonimus and Capillaria eggs) andBaermann sedimentation (to detect larvae ofAeluro- strongylus) (Padrid, 2010; Bay andJohnson, 2005; Byers and Dhupa, 2005).When a cat has respiratory symptoms that arethought to indicate asthma, a therapeutic trial canbe carried out by the administration ofbronchodilators. Coughing and wheezing in catswith asthma normally disappear 10 minutes afteradministering bronchodilators (terbutaline 0.01 mg/kg bwt iv, im or sc; albuterol 100 ìg inhaled. Mostasthmatic cats respond to treatment in 5-7 dayswith a high-dose corticosteroid therapy and, if noevident improvement is shown, the diagnosis forfeline asthma should be re- viewed (Padrid, 2010;Bay and Johnson, 2005). The treatment for asthmaas a disease must be focused on the control ofinflammation in order to preventbronchoconstriction. Inhalation therapy isconsidered a key solution for human asthmamanagement and now a days it is widelyrecommended to treat feline asthma (Cohn, 2009;Cohn et al., 2008; Powell, 2007; Reinero et al.,2009). Alternative therapies that may be beneficialto manage feline asthma are available, but moreinvestigation is required in order to prove theirefficacy.
Case report
A four years old female Siamese cat was referredto the Faculty of Veterinary Medicine, Jijgjiga withsymptoms of wheezing, coughing and respiratorydistress with a crouched position with the neckextending during these coughing episodes.Occasionally, sneezing and vomiting or retchingwere noted.On physical examination: inspiratory andexpiratory loud airway sounds was auscultated.Duration of expiration was much longer thaninspiration. An end-expiratory grunt was heard as

121
Journal of Canine Development & Research 2013
well as abrupt cessation of airflow near endexpiration. Expiratory wheezes were also commonfindings on physical exam. The cat was having acombination of expiratory wheezes, inspiratorycrackles and loud respiratory sounds.Occasionally, lung sounds were quiet because ofsevere air trapping within the lungs.Carefulauscultation of the heart to differentiate cardiacdisease from respiratory conditions was done.Complete blood count, blood chemistry, fecalexamination and urinalysis were performed whichrevealed only the increased numbers of circulatingeosinophils. Thoracic radiography (chest X-ray)was done (Figure 1 and 2).Findings recorded wereincreased bronchial and interstitial patterns withalveolar densities. Peribronchial infiltrate was there,which is described as ‘donuts’ on the ventrodorsalview and ‘tramlines’ on the lateral view. There washyperlucent lung areas and flattening and caudaldisplacement of the diaphragm. There were airtrapping and hyperinflation. Atelectasis of the rightmiddle lung lobe and mediastinal shift to the righthave also been noted. Heartworm test; Felineleukemia and feline immunodeficiency virus testswere conducted which were found negative.The cat was administered following therapy:Oxygen therapy; Bronchodilator -Inhaledterbutaline - 0.325-0.625 mg/cat po tid; Long-acting theophylline -25 mg/kg bwt po at night;Corticosteroid- Prednisolone -1 mg/kg bwt pobid for 5 days, then od for 5 days and every 48hours for 5 days; Inhaled fluticasone -110-220µg bid. These medications work to alleviateinflamed airways and halt excess mucusproduction. To check secondary bacterialinfections, specially the Mycoplasma; prophylacticantibiotics -Marbofloxacin@ 2.75mg/kg bwt pood was given for 10 days.The pet owner was advised using a minimally dustycat litter; Avoiding aerosols and/or carpet cleaningproducts; Eliminating exposure to cigarette or cigarsmoke; Minimizing exposure to wool blankets and/
or carpeting; Keeping the environment comfortablycool; Minimizing stress and using a HEPA filter inthe home.
Results and discussion
The cat recovered completely with in 15 days.When the airway of the cat is sensitive to certainstimuli, exposure to these agents leads to narrowingof the airways. The inciting agents are usually directirritants to the airways or things that provoke anallergic response in the respiratory tract. Regardlessof the cause, the end-result is the same: musclespasms in the bronchi (breathing tubes),inflammation, buildup of mucus, and accumulationof cellular material. In addition, the inability to clearthe bronchi of this material leaves the cat susceptibleto secondary infections. Blocked airways mayhave air trapped distally which reduces thoraciccompressibility; as noted above this may causethe thorax to become barrel-shaped; same hasbeen reported by many reserchers (Padrid, 2010;Bay and Johnson, 2005; Cohn, 2007; Thébault,2004).Blood tests revealed peripheral eosinophillia. Stoolexamination was done to eliminate the cause; asAelurostrongylus abstrusus, Paragonimuskellicotti or Capillaria aerophila infections cancause coughing and respiratory harshness in cats.The classic radiographic pattern of this cat withasthma tends to show swelling of the bronchialwalls, generally described as “donuts” and “railwaylines” (Figure 1 and 2). In addition there wasevidence of increased radiolucency of the lungsand flattening and caudal displacement of thediaphragm, recognized when observing thediaphragmatic pillars around the lumbar vertebraearea L1-L2. The radiographs of the cat alsorevealed an increased density of the right middlelung lobe and a central displacement towards theright. This sign is related to the presence ofatelectasis in the lung lobe as a result of accumulationof mucus in the bronchi. Even though atelectasis
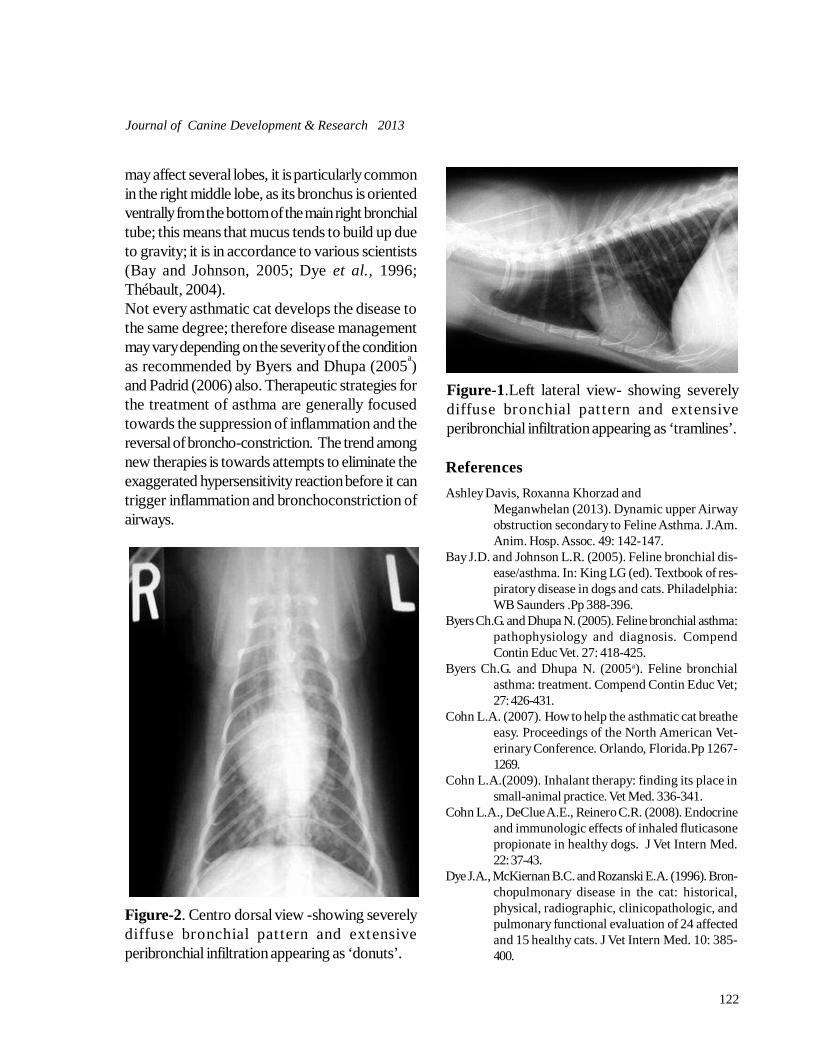
122
Journal of Canine Development & Research 2013
may affect several lobes, it is particularly commonin the right middle lobe, as its bronchus is orientedventrally from the bottom of the main right bronchialtube; this means that mucus tends to build up dueto gravity; it is in accordance to various scientists(Bay and Johnson, 2005; Dye et al., 1996;Thébault, 2004).Not every asthmatic cat develops the disease tothe same degree; therefore disease managementmay vary depending on the severity of the conditionas recommended by Byers and Dhupa (2005
a)
and Padrid (2006) also. Therapeutic strategies forthe treatment of asthma are generally focusedtowards the suppression of inflammation and thereversal of broncho-constriction. The trend amongnew therapies is towards attempts to eliminate theexaggerated hypersensitivity reaction before it cantrigger inflammation and bronchoconstriction ofairways.
Figure-1.Left lateral view- showing severelydiffuse bronchial pat tern and extensiveperibronchial infiltration appearing as ‘tramlines’.
Figure-2. Centro dorsal view -showing severelydiffuse bronchial pat tern and extensiveperibronchial infiltration appearing as ‘donuts’.
ReferencesAshley Davis, Roxanna Khorzad and
Meganwhelan (2013). Dynamic upper Airwayobstruction secondary to Feline Asthma. J.Am.Anim. Hosp. Assoc. 49: 142-147.
Bay J.D. and Johnson L.R. (2005). Feline bronchial dis-ease/asthma. In: King LG (ed). Textbook of res-piratory disease in dogs and cats. Philadelphia:WB Saunders .Pp 388-396.
Byers Ch.G. and Dhupa N. (2005). Feline bronchial asthma:pathophysiology and diagnosis. CompendContin Educ Vet. 27: 418-425.
Byers Ch.G. and Dhupa N. (2005a). Feline bronchialasthma: treatment. Compend Contin Educ Vet;27: 426-431.
Cohn L.A. (2007). How to help the asthmatic cat breatheeasy. Proceedings of the North American Vet-erinary Conference. Orlando, Florida.Pp 1267-1269.
Cohn L.A.(2009). Inhalant therapy: finding its place insmall-animal practice. Vet Med. 336-341.
Cohn L.A., DeClue A.E., Reinero C.R. (2008). Endocrineand immunologic effects of inhaled fluticasonepropionate in healthy dogs. J Vet Intern Med.22: 37-43.
Dye J.A., McKiernan B.C. and Rozanski E.A. (1996). Bron-chopulmonary disease in the cat: historical,physical, radiographic, clinicopathologic, andpulmonary functional evaluation of 24 affectedand 15 healthy cats. J Vet Intern Med. 10: 385-400.

123
Journal of Canine Development & Research 2013
Hill J.W. (1906) In: Jenkins WR ed: The diseases of thecats. Diseases of the respiratory organs.. NewYork.Pp 11-22.
Padrid P.A.(2006). Use of inhaled medications to treatrespiratory diseases in dogs and cats. J AmAnim Hosp Assoc. 42:165-169.
Padrid P. (2010). Asthma. In: August JR (ed). Consulta-tions in feline internal medicine. Philadelphia:WB Saunders.Pp 447-458.
Powell L.L. (2007). Inhalation therapy. Proceedings ofthe North American Veterinary Conference. Or-lando, Florida.Pp 220-221.
Reinero C.R., Delgado C. and Spinka C. (2009). Enanti-omer-specific effects of albuterol on airway in-flammation in healthy and asthmatic cats. IntArch Allergy Immunol. 150: 43-50.
Thébault A. (2004). Affections respiratoires chez le chat:diagnostic et traitement de l’asthme du chat.Point Vét. 248: 26-30.
132
Journal of Canine Development & Research 2013
Author’s IndexAdak, A. 1,78Eswarappa, R. 1Mukhopadhayay, S.K. 1,78Sharma, A. 9, 53, 66, 102Ahuja, A. 9, 25, 53, 66,
102, 112, 124Tamoli, S. 9 Srivastava, M. 9, 59, 66, 72,102Kachhawa, J. 9, 66, 102, 112Daga, M. 9, 53, 66, 102Kannojia, K. 9, 102Langer, A. 17, 53, 56, 112, 124Hussain, A. 17 ,56Gupta, S.K. 17, 81Priyanka 25Varshney, J.P. 25Singh, A.P. 25, 66, 112Bassessar, V. 31,47Verma, Y. 31,47Swamy, M. 31,47Velhankar, R.D. 37Keskar, D.V. 37Bargujar, J. 53, 112Bihani, D.K. 53, 63, 66, 72, 112Abusuria, P. 53Tanwar, M. 53Bashir S. 56Ramakant 59Saini, D.K. 63
Sharma, B.L. 63Kumar, S. 63Soren, S. 66Dhuria, D. 25, 66, 112,124Dwivedi, K. 69, 88Sain, M.L. 63,72Khinchi, R.K. 72Singh, N.K. 72 Srivastava, A.K. 75, 119Syed, B. 75, 119Chaturvedi, V. 78Tripathi, V.K. 78Khajuria, B.K. 81Tiwari, A. 81Das, J. 83, 93, 97Behera, S. S. 83, 93, 97Senapati, M.R. 83, 93, 97Behera, M. 83, 93, 97Chandrapuria, V.P. 90Somil, R. 90Pradhan, S. 97Praharaj, M.R. 97Nanda, P.K. 97Kachhawaha, S. 102Singh, N.K. 102Kachhawaha, R.N. 117Bais, B. 117Choudhary, G. 117Vyas, S.K. 124
133
Journal of Canine Development & Research 2013
SUBJECT - INDEXDisseminated intravascular 1Leptospirosis 9Dermatoscopy 17Gene discovery 17Arrhythmic dogs 25Electrocardiographic values 25Pyometra 31Atrial fibrillation 37Digoxin 37Thoracic radiography 53Vertebral heart score 53Corona virus 56Immunochromatography 56Amitraz 59Demodicosis 59Polyvalent anti snake venom 63Snake bite 63Fipronil 66Ovario-hysterectomy 69Dopamine 72Ascites 75Orchiectomy 78Decolorized iodine 81Femoral fracture 83Dystocia 88Episiotomy 90Vaginal fibroma 93Shampoo therapy 102Gingivitis 112Police Dog 117Bronchial asthma 119
Bronchodialator 119Bengal cat 124Chlorhexidine 113 Fibrinolysis 03Thrombocytopenia 3Plasma Extenders 5Heparin 5Aspirin 5Protamine sulphate 5Fresh frozen plasma 5Dilated cardiomyopathy 38Enalapril 39Spirolactone 39Immuno-modulator 60Omega 3& 6Fatty acids 67Renal failure 72Sucralfate 73 Decadurabolin 73Fructodex 76C-Arm 84,86Thomas splint 85,86Steinmann’s pin 85Benzoyl peroxide 107Selenium disulphide 107Oatmeal 109Halitosis 112Tooth Scaling 114Donuts 121Tramlines 121
128
Journal of Canine Development & Research 2013
The Journal of Canine Development &Research (JCDR) is published every year
by the Canine Publishing House, Bikaner. JCDRcovers review/ research articles, general articles,clinical case reports, thesis abstract and tit bitsregarding canines & felines.
Submission of Manuscript: The manuscripts areaccepted on the basis of scientific importance andsuitability for publication on the understanding thatthey have not been published, submitted or acceptedfor publication wholly or partly, in any languageelse where. The copyright of papers, accepted forpublication, will belong to the Canine PublishingHouse, Bikaner. It is necessary that allauthors of the article should be annualsubscriber of the JCDR(@Rs.500/-)Further, the processing charges @ Rs. 400/- per article shall be charged,however theminimum charges will be Rs1500/-. Thecharges of 10 sets of reprint are optionalas per number of pages.
The manuscripts should be mailed throughregistered post to DR. ANIL AHUJA, Editor,JCDR, Department of Clinical Veterinary Medicine,College of Veterinary and Animal Science,Bikaner-334 001 (Rajasthan) INDIA or CaninePublishing House, Pushap Bhawan, B-48, SadulGanj, Bikaner-334 003 (Rajasthan) INDIA.
The manuscripts should be type written, on one sideof the paper ( A 4 size) with 4 cm margins anddouble spacing throughout, except in the abstracts,footnotes and references which should be in singlespacing. It should be sent in duplicate. Each pageof the manuscript should be numbered on the topright hand side corner, including the title page,references, tables, etc. All the pages should containrunning title of the paper and surname ofauthor(s) at the top. A copy of the manuscript willbe required on a floppy 1.44 MB in Page Maker6.5 or in MS Word Office, Windows. Manuscriptmay be sent through E-Mail : [email protected]
The manuscripts should be organised in thefollowing order in general:
1. Title: Papers should be headed with full title,the initials and surname(s) of the author(s) andaddress of the institution where the work wascarried out. A shortened version of the title shouldalso be supplied for running headlines. the serialtitles are not acceptable, so each paper should havean individual title.
2. Abstract: This shoud not exceed 250 wordsand should outline briefly the purpose of the study,important findings and conclusions.
3. Key words: Provide three to six key words.
4. Introduction: This part should state briefly thenature and purpose of the work together with theimportant findings of previous workers.
5. Materials and Methods: The author(s) shoulddescribe materials, methods, apparatus,experimental procedure and statistical methods indetail to allow other workers to reproduce theresults. Sub-heading may be used in this part.
6. Results: The clinical/experimental data shouldbe presented clearly and concisely.
7. Discussion: This should focus the interpretationof clinical/experimental findings. References in thispart should be cited as follows ....... as observedby Kalra et al. (1994) or in parentheses ........ werefound (Kohli et al., 1994, Pathak and Arora, 1995).
8. Acknowledgement(s): This should be short.Grants and technical help provided should beacknowledged.
9. References: All publications cited in the textshould be presented in the form of a list ofreferences arranged alphabetically according toauthors’ surnames. Don’t give serial numbers. Usethe usual system for arranging the reference. Thevolume number and page number of the journalsand those of the text citations should be essentiallymentioned.
GUIDELINES FOR CONTRIBUTORS

129
Journal of Canine Development & Research 2013
Roman numerals. Each table should have a briefand self-explanatory title. Duplication of data in thetable and text should be avoided.
11. Figures: Only good quality, unfolded andunmounted glossy prints of half-tone illustrationsand clear line drawings in India ink are acceptable.The number of figure, the author’s name, top andbottom of the figure should be indicated lightly onthe back side specially in the case of photographsby soft pencil. Figures should be numberedsequentially by Arabic numbers. Each illustrationshould have a caption. The captions to all figuresshould be typed on a separate sheet of manuscript.All the figures should be referred to in the text andtheir approximate place be indicated on the margin.A statement of the magnification of illustrationsshould be given wherever applicable. The author(s)are required to bear the cost of reproducton of theillustrations. Coloured illustrations are alsoaccepted. The processing charge of each black& white and coloured photograph shall be Rs.50/- and 500/, respectively.
12.Clinical Articles
Clinical case reports of interesting and rare natureare published under this heading. The article sentfor publication under this head, should not contain
more than three typed pages including referencesand illustrations and should be marked ‘ClinicalArticle’ at the right upper corner of the first pageof manuscript. An abstract of the case is notnecessary. The manuscript should contain historyand important clinical observations of the case,tentative diagnosis and its confirmation, line oftreatment used and fate of the case. At least, itshould have a biref discussion on the line oftreatment and conclusion. All these can be givenin separate paragraphs sequentially and sub-heading are not required.
The acknowledgement, if necessary may be givenbut it should be as short as possible. The referencesshould be given as per the format for the researcharticles.
Reprints: The leading author of an accepted articlewill be supplied reprints on request and advancepayment at the rate as under:
No. of pages Cost per 10 sets1-2 Rs. 200.003-4 Rs. 400.005-6 Rs. 600.007-10 Rs. 800.00