
Frontline 88 for web
40
NEWS — EDUCATION — BEHAVIOUR— BURNOUT SPECIAL EDUCATION Volume 88 • Autumn 2012 F RONTLINE THE IRISH VOICE FOR INTELLECTUAL DISABILITY
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Frontline 88 for web

NEWS — EDUCATION — BEHAVIOUR— BURNOUT
SPECIALEDUCATION
Volume 88 • Autumn 2012
F R O N T L I N ETHE I R I SH VO ICE FOR INTELLECTUAL D I SAB I L I TY

2 frontline Autumn 2012
Volume 88 • Autumn 2012
CONTENTS
09 Introduction to the Special Educationissue of Frontline by Minister for Education& Skills Ruairí Quinn, TD.
10 Mainstream inclusion—Challenges,opportunities and the need for equityDamian White reflects on the impact on children of thecutbacks on SNAs in our primary schools.
12 A progression opportunity for individuals with intellectualdisabilities: A look at the LIFE (Leading Into Further Education)ProgrammeKathleen Deasy and Sinead Murphy.
14 Personal perspectives on educationKatherine O’Leary and her daughter Julie share their perspectives on educationin Ireland for those with intellectual disabilities.
16 Influencing service improvement and change througheducationDeirdre Corby of DCU explains how a new module draws teams of individualstogether to work on projects specifically focused on improving and changingservices for people with intellectual disability
18 Supporting LÁMH users at schoolMary Cullen explains the LÁMH sign language system in Irish schools. REGULARS
03 Editorial
04 News Update—Government publishes Report ofthe Value for Money and PolicyReview of Disability Services—National Carers’ Strategyrecognises value of carers—Success for deaf student inLeaving Cert!—Rehab Group to fund JoanneO’Riordan documentary—Frontline is going live ...—Another First for WilliamLoughnane—Protest reverses budget cuts toPAs—MENCAP calls for closure ofinstitutions in the UK—Minister Burton says there is nochange to disability allowancecriteria—National Disability StrategyImplementation Plan—Disability organisations call foraction on school leavers
F R O N T L I N E
26
FEATURE: EDUCATION
MAIN ARTICLES07 Interview: Interview with
Paddy Connolly CEO ofInclusion Ireland
10 Inclusion: The Rosary GardenPaul Henry describes a garden built aspart of the Eucharistic Congress.
22 Person-centred planning:Person-centred active supportin IrelandJulie Beadle-Brown and Judy Ryanexplain what person-centred activesupport is all about for people withdisabilities.
24 Burnout: Staff coping andburnout in intellectualdisability servicesSile Murphy and Claude Wattersprovide an overview of measures toprevent staff burnout, and potentialinterventions for staff withinintellectual disability services who areexperiencing burnout.
26 Angelman Syndrome:Promising therapeutic avenuesfor Angelman SyndromeBernard Dan explains the symptomsof Angelman Syndrome and explorespossible therapies.
28 Change: A nationalprogramme of change inchildren’s disability servicesCaroline Canton makes the argumentfor a national programme of changein children’s disability services.
30 Change: Lost opportunitiesfor people with intellectualdisability in institutional caresettingsDonal Fitzsimons explains how theintroduction of person-centred plans(PCPs) into disability services inrecent times brought with it anassumption that the PCP was robustenough to safeguard against thedeleterious effects of life incongregate settings.
33 Pain: The problem of chronicpain in people with anintellectual disabilityBrian Maguire reports on the highincidence of people with ID livingwith chronic pain.
18
06
34 Behaviour: Fun with foodKaren Mings examines behaviouralproblems for children with autismrelating to food and suggests funand rewarding methods to resolvethese issues.
36 Nursing network: Developingsupport for intellectualdisability practice: NursingNetwork In DisabilitiesIreland (NNIDI)Owen Doody and Therese Danahertrace the formation of NursingNetwork in Disabilities Ireland.
38 Reading: The Star book club

3
EditorStephen Kealy
Editorial BoardOwen DoodyMitchel FlemingColin GriffithsSiobhán KaneMichael McKeonKathy O’GradyMary de PaorNiamh PowerJean SpainMichael TeehanAngelina Veiga
Published byFrontline Magazine Ltd.
Design and ProductionNiamh Power, Print Design Services
Printed byOpus Print
ISSN 0791–1270Published Quarterly
Supported byThe People inNeed Trust
Frontline Magazine Ltd. is a ‘not forprofit’ organisation, formed solely topublish the magazine Frontline.Copyright resides with the individualauthors, but permission to reproduceany article must be obtained in writingfrom Frontline.
Views expressed in Frontline are thoseof the authors themselves and notnecessarily those of the editor oreditorial board. Letters to the editor are welcomed.Name and address should be provided;they will be published unless otherwiserequested. Articles may be submitted for possiblepublication in Frontline. Guidelines forauthors are available from the editor.Items on meetings, conferences etc.should be submitted well in advance ofevents, to meet the magazinepublication schedule.
Frontline editorial address for letters,articles and other items for inclusion:Frontline Magazine Ltd.Unit C2, The SteelworksFoley Street, Dublin 1E-mail: [email protected]: www.frontline-ireland.netSubscriptions: [email protected]. Chy No: 18745
LEARNING
GUBU-Grotesque, unbelievable, bizarre and unprecedented.Who would have thought that a government would allowitself again to be in such a position—and yet that is exactlywhat happened. If a decision was made, for example, on the
basis of gender, to reduce the earnings of women, there would be, and rightly so, atsunami of outrage from every corner of the country. Well maybe not from everyone—some Neanderthal decision-maker may be lurking in the long grass operating theprinciples of GUBU.
How else could you possibly explain a decision to cut support to people withdisabilities to have full and meaningful lives in the community, while at the same timepublicly acknowledging the achievements of all our paralympic athletes. Suchachievements are hard-won and supported by many, particularly family, friends, paidcarers and, of course, personal assistants. Are some decision makers, because of theirabilities, just simply incapable of ‘walking in the shoes’ of people with disabilities? Do theylack the empathy to appreciate the effort it takes to do something small withoutassistance—to move a hand or a finger or to change the position of one’s body.
This issue of Frontline has an educational theme. Yet again, decisions are made that dolittle to continue active and personal support for people with disabilities in the educationalsystem—decisions that may even be harbingers of worst things to come. Is there anunderstanding of how difficult it is for a child with an intellectual disability in amainstream class to track an extended explanation in the classroom if there is notsomeone available to mediate that experience? Is there an understanding of the need tominimise confusion so that a person with an intellectual disability can learn at his or herown developmental level? Is there an appreciation of the need to constantly review theteaching approach vis a vis evidence-based research? We know IT can enhance thelearning experiences of all children, but particularly children with disabilities. Is thisunderstanding reflected in classrooms and in teacher training colleges? Is there aninvestment in educational research that will bridge classroom practice with internationalunderstandings?
Relationship is an essential component of progress and achievement. The medal-winning paralympians, without exception, linked their success to the close relationshipsestablished between carers, their parents, brothers and sisters, extended family, personalassistants, friends and many other people in their lives. This understanding was reiteratedby all who gave interviews about the joy of their participation and all of them, includingthose who did not gain medals, were winners. The educational supports for people withdisabilities have to foster and support effort, no matter how small and, yes, it does requirecontinuing investment.
Thankfully, that GUBU decision has since been partially reversed — but will similiarsuch decisions continue to be made at the expense of disabled and vulnerable peoplebecause they are seen as soft options?
* * * * * * * * * * * *
Issue 87 saw the re-publication of an article by Owen Doody, Maria Bailey and RosemaryLyons, ‘Primary care for persons with intellectual disabilities: Issues for practice. The articlewas re-published to focus attention once again on the health and well-being of peoplewith intellectual disabilities living in the community, a meaningful living optionsignificantly under threat, given the group think of the HSE and government on reducing,even possibly irreversibly eroding, essential supports which have been so hard won.
Stephen Kealy
Contributors to this issue:
Julie Beadle-BrownCaroline CantonDeirdre CorbyMary CullenBernard DanTherese DanaherKathleen Deasy
C RED I T S
frontline Autumn 2012
F R O M T H E E D I T O R
Owen DoodyDonal FitzsimonsPaul HenryBrian MaguireKaren MingsSile MurphySinead Murphy
Katherine O’LearyJulie O’LearyMinister Ruairí QuinnJudy RyanClaude WattersDamian White
Cover: Angus Mac Lellan,who graduated from theSeasamh /WIT Certificatein Leadership & AdvocacyCourse in 2009, picturedhere with his Mum.

4 frontline Autumn 2012
N E W S U P D AT E
An Taoiseach Enda Kenny and Tánaiste Eamon Gilmore attended the launch on 19 July 2012 of the National Carers’Strategy. The Strategy says that the value and contribution of carers should be recognised and it sets out a series of goals,including the need to recognise the needs of carers through the provision of income supports. It also identifies the need forother supports for carers, including information, training that will empower them and help them to manage their physicaland mental health needs. Speaking at the launch, Minister of State at the Department of Health Kathleen Lynch said shehopes carers will be ‘recognised, supported and empowered’ as a result of the newly-published National Carers’ Strategy,while Mr Kenny said it was time for Ireland to formally acknowledge and to care for carers. The Cabinet sub-committee onsocial policy, which is chaired by Mr Kenny, will monitor the progress of the strategy, which was published by the Departmentof Health and is available at http://www.dohc.ie/publications/national_carers_strategy.html.
National Carers’ Strategy recognises value of carers
Speaking at the launch in July of the Report of theValue for Money and Policy Review of the Disability ServicesProgramme, Minister of State Kathleen Lynch TD saidgovernment is committed to the vision of people with adisability being supported to achieve ‘full inclusion andself-determination through access to the individualisedpersonal social supports and services needed to live afully included life in the community’. The Report saysthe following vision statement should be the guidingprinciple on a ‘revitalised and re-orientated DisabilityServices Programme’:
To contribute to the realisation of a society where peoplewith disabilities are supported to participate to their fullpotential in economic and social life and have access toa range of quality personal social supports and servicesto enhance their quality of life and well-being.
The Report highlights serious deficiencies in theplanning, monitoring and delivery of services to peoplewith a disability. It also states that major issues
Government publishes Report of the Value forMoney and Policy Review of Disability Services
identified in the 2005 review of disability services by theComptroller and Auditor General have not been actedon, including the lack of ‘performance data’ ondisability services, and that standards for services havenot been introduced.
Responding to the Report, Inclusion Ireland CEOPaddy Connolly said a major barrier to implementingthe recommendations of this report is the limitedcapacity to deliver, at HSE level: ‘The report highlightsthat the National Disability Unit of the HSE which haslead responsibility for planning, monitoring andevaluation of the disability programme has no authorityover resource allocation matters or operational servicedelivery. It will be critical that the restructuring of theHSE incorporates a sufficiently resourced andempowered disability unit.’ He also said Minister Lynchmust outline how people with a disability and theirfamilies will be consulted about the implementation ofthe Review.
SUCCESS FOR DEAF STUDENT IN LEAVING CERT!The Irish Times recently reported on the achievement of Killian McDonnell fromKilsallaghan, Co. Meath. Killian is deaf and has Down Syndrome, and his mother Teresabelieves he is the first deaf student with this condition to have passed the Leaving Cert.‘According to every inquiry we made… this is a first,’ she said.Killian completed his studies in Ashbourne Community School through Irish SignLanguage (ISL). In an interview earlier this year with the Fingal Independent Killian said ‘Ilove school. The students and teachers are great. The students in my class have learnedsome ISL.’
Killian received support in the classroom from ISL language support worker, CiaraClarke, who translated the curriculum from English to ISL and assisted Killian’scommunication with teachers and pupils. Killian said ‘Ciara is brilliant, I reallyappreciate all her hard work, I could not be at school without her support.’ Remarkably,Killian started learning ISL only five years ago.
Killian now plans to complete a two–year intensive literacy course and hopes totravel and work in different countries in the future. He is interested in drama and hasbeen an active member of the Dublin Theatre of the Deaf.
Killian’s achievement underlines the finding in the recent NCSE report on theeducation of deaf children which recognised that deaf children can achieve the sameeducational success as their hearing peers with the right support. DeafHear believesKillian’s determination to succeed can inspire other deaf students into the future.
DeafHear congratulates Killian on his great achievement and wishes him everysuccess in his future studies.
Reprinted from DeafHear.ie

5frontline Autumn 2012
N E W S U P D AT E
No Limbs, No Limits, the film that is to examine theextraordinary life of 16 year old Cork-born Joanne O’Riordanmade a significant step towards becoming a reality this week,when the Rehab Group announced it is to provide €25,000towards the making of the film.
The Rehab Group has pledged the funding along withprofessional support to filmmaker and Joanne’s olderbrother, Steven O’Riordan. Joanne is one of only sevenpeople in the world with an extremely rare physicalcondition called Total Amelia, which means she was bornwithout all four limbs.
Speaking about the decision to support the film, AngelaKerins, Rehab Group CEO said, “Steven and Joanne’s film isa momentous opportunity to share the incredible story of ayoung determined girl and her family. It is a chance to showpeople how those with disabilities can and do, overcomechallenges, what are at times enormous challenges.
“At Rehab we strongly believe in encouraging peoplewith disabilities to share their stories. It’s a hugely importantpart of demonstrating how people with disabilities can leadvery full lives and also improves wider public understandingof disability. Rehab’s motto is ‘Investing in People, ChangingPerspectives’ and we hope that through Rehab’s support
REHAB GROUP TO FUND JOANNE O’RIORDAN DOCUMENTARYJoanne’s story will help to change the perspectives of allthose who see the film.”
Welcoming the funding, the film’s director StevenO’Riordan said, “I’m thrilled that the Rehab Group haverowed in to support this film. Joanne’s story is not onlyinteresting one, but it’s also an important one too. Thanks toRehab’s generous support, this story can now be told.”
The film will focus on Joanne’s life at home, school, workand follow her as she travels to the UN to deliver a landmarkaddress. It will also feature interviews with key members ofher family and the experts that have helped her during the16 years.
The Rehab Group is urging other organisations withavailable funds to support the project so as to ensure thisimportant story is told.
The Rehab Group has a history of encouraging theparticipation of people with disabilities in the arts, includingtheatre, the visual arts and film and previously supported themaking of Academy Award winning My Left Foot, which toldthe story of quadriplegic author Christy Brown. The RehabGroup has also provided training enabling people withdisabilities to learn the skills they need to develop careers inthe dynamic arts and media sector.
Frontline is going live...Frontline is currently revamping its website sothat it is more accessible for our readers.Kwame, our volunteer Website Developer isdoing tremendous work changing our existingwebsite. Please bear with us as we try to get itright. Soon you will be able to see back issues,read the current issue, search back issue articles,subscribe and renew your yearly subscription onthe website. Keep an eye on your inbox foryour new password and instructions on how tochange it so you can continue to access Frontlinein a digital format but in an easier manner. Ournew web address is http://www.frontline-ireland.com. Check us out on facebook too!
IRISH INSTITUTE OF PSYCHOANALYTIC PSYCHOTHERAPY107, Baggot Street Lower, Dublin 2.
ROOMS AVAILABLE TO RENT
There are meeting/training/reading/consultation rooms available at:Irish Institute of Psychoanalytic Psychotherapy,
107, Baggot Street Lower, Dublin 2
from September 2012.
Expressions of interest/enquiries to be sent to:Theresa Merrigan at:
Email: [email protected] Tel: 087-4120758

6 frontline Autumn 2012
N E W S U P D AT E
A Special Olympics gold medallist has become the first person in thecountry with Down Syndrome to pass his driving test.
William Loughnane (26), from Clooney-Quin, Co Clare, got rid of hisL plates after recently passing the theory and driving test.
His latest achievement has been hailed by Pat Clarke, the president ofDown Syndrome Ireland.
Mr Clarke said that, to the best of his knowledge, William was the firstperson in Ireland with Down Syndrome to hold a full driving licence. ‘Forpeople with Down Syndrome it shows that if they persevere they will getto where they want to get to,’ he added.
William, who works in a Centra shop in Ennis, won two gold medals,three silver and two bronze for gymnastics at the 2003 Special Olympicgames in Dublin. Four years later, he claimed six gold and one bronzemedal in China.
His father Liam helped him with the principles of driving. ‘I showedhim the ropes. He only started in November,’ Liam said.
ANOTHER FIRST FOR WILLIAM LOUGHNANE
Proposed cuts to Personal Assistant (PA) budgets werereversed following a protest by the Leaders Alliance ofdisability activists, on 4 September. The protest was heldoutside Government Buildings and coincided with the firstCabinet meeting after the summer recess. A core group ofthe protesters stayed at Government Buildings overnightand were joined by a group led by the Centres forIndependent Living, for another protest on 5 September.Leaders Alliance spokesperson John Roche said the protestaimed to highlight the ‘disgraceful, retrograde andinhumane cuts’ to frontline services. On 31August, the HSEhad announced a €130million cost reduction plan thatincluded a €10million cut to Personal Assistant hours, and a€1.7million cut from Home Care Packages. Cuts tohomecare packages were not reversed at the time ofwriting.
Inclusion Ireland warned that although the PA cuts willno longer go ahead, €10 million will still be taken from thedisability budget and people with disabilities and theirfamilies will bear the brunt of this cut. The Department ofHealth statement announcing the reversal of the decision tocut the PA budget said ‘the Minister has told the HSE todistribute adjustments across the sector with a focus oncutting administration, training and travel costs, and bettercash management by agencies involved.’
Inclusion Ireland CEO Paddy Connolly said ‘both thisgovernment and the previous government have been sayingfor several years that greater efficiencies are needed in thedisability sector and there must be cuts to administration,travel and training in the first instance. Does thegovernment believe there is scope for a further €10 millionto be taken in these types of costs from the disability sector?If so, why did Minister Reilly and Disability Minister KathleenLynch not seek these savings prior to targeting PersonalAssistants?’
Although the Leaders Alliance called off their protest,they said they would resume the protest if the HSE DirectorGeneral Tony O’Brien did not agree to meet them within thenext 14 days. They said they cannot trust the government’sword when it comes to supporting people with disabilities.
Protest reverses budget cuts to PAs
FRONTLINE is looking forenthusiastic and motivatedindividuals willing to join theeditorial board.
Board members attend aneditorial meeting 4 to 6 times ayear).
The first position calls for anindividual who can contribute
to the production of the magazine by writing orsourcing articles (and/or book, conference or seminarreviews) and promoting the magazine to new audiences.
The second position calls for an individual withwebsite experience who will take on the very importantrole of updating the website, on line subscriptions andarranging for any other technical duties that are associatedwith the role.
An understanding of and familiarity with IntellectualDisability is desirable. Both roles include mentoringsupport from an existing board member. Commitmentrequested for a minimum of 1 year. Contact Angelina formore information on 085 818 4343.
MAGAZINE:F R O N T L I N EVolunteer Editoral Board member
2 positions available
The Open Training College have two new links:
The facebook link is:www.facebook.com/theopentrainingcollege
The twitter link is: www.twitter.com/myotc
Open Training College. Tel: (01) 2988544www.opentrainingcollege.com
OPEN TRAINING COLLEGE LINKS

7frontline Autumn 2012
N E W S U P D AT E
DISABILITY ORGANISATIONS CALL FORACTION ON SCHOOL LEAVERS
A number of disability organisations, including InclusionIreland, the National Parents and Siblings Alliance and IrishAutism Action, in addition to local organisations from theMidwest, came together to demand action for school leaverswithout post-school placements in July.
A number of months ago, the HSE identified approximately660 young adults with an intellectual disability and/or autismleaving school, who need further support from disabilityservices. In July, 153 of these young adults had no furthereducation, training, or day service placement confirmed forSeptember. In mid-August, 98 school leavers were still withoutplaces, according to Paddy Connolly, CEO of Inclusion Ireland,who said: ‘Minister Lynch must take responsibility for thissituation. Government cannot say they were not forewarned—this situation has repeated itself annually since 2008, yet youngadults with disabilities and their families are again facing asummer of uncertainty and stress as they wait to be toldwhether a service will materialise in September. Clearly, thisshows disjointed leadership.’
‘Government, through the HSE, try to place young adults indisability services with no input from the person with a disabilityon their own ambitions or preferences for the future. They areinstead told where they are going and what they are doing.There seems to be no forward planning in government on thisissue. Young adults with disabilities are not permitted to build afuture; instead they are slotted into whatever box is available.’
Tony Murray, PRO of the National Parents and SiblingsAlliance, said: ‘Even those who do secure some form ofplacement in September may not receive the service that bestsupports their needs. For example, many will get a three-dayservice, when a five-day service would better support them.When people are being squeezed into any available placements,then questions must also be raised about the quality of service.’
As well as those leaving school, at the time of writing, afurther 54 adults leaving post-school training are still looking forfurther support from disability services. In July, this number wasat 73.
Speaking on RTÉ’s This Week programme on 22 July,Minister Kathleen Lynch said additional funding was not madeavailable to service providers this year for school leavers, butthat ‘service providers, not all of them, but the majority ofthem, have stepped up to the plate and really beenextraordinarily generous and done incredible things.’
Inclusion Ireland says ‘further education, training and dayservice options must be available, and planning must start nowfor what will happen in 2013 and after that, so as we’re not leftin this situation again next year. Government must ensureeveryone who needs a service receives it and future planningmust take place that includes the voice of the person with adisability.’
The organisations who called for action on this issue were:Inclusion Ireland, National Parents and Siblings Alliance, IrishAutism Action, Parents and Friends Daughters of CharityServices Lisnagry Limerick, North Tipperary Autism SupportGroup, South Tipperary Autism Support Group, Áras Folláin,Nenagh, Co. Tipperary, Lámh Cúnamh, Ennis, Co. Clare, PavingThe Way parents, Clifden, Co Galway, Clare Federation forPeople with Special Needs, Ennis Voices for Autism, Co. Clare,Clare Crusaders, Co. Clare and ConnectAbilities, Co. Clare.
National Disability StrategyImplementation Plan
MINISTER BURTON SAYS THERE ISNO CHANGE TO DISABILITY
ALLOWANCE CRITERIAMinister for Social Protection Joan Burton has said nochanges have been made to the qualification criteria forreceipt of the Disability Allowance. Speaking in August,Minister Burton was responding to reports that the refusalrate for initial applications for Disability Allowance hasrisen from 54% in 2010 to 61% in the first quarter of2012. Between January and April 2012, the Department ofSocial Protection turned down 4823 applications.
Cuts announced in the Budget in recent years meanthat people on Disability Allowance are down €847.60 ayear since 2008. An €8 weekly cut to Disability Allowancewas announced in Budget 2012. This is on top of an€8.30 cut in 2009, amounting to €16.30 a week in justtwo years (from €204.30 in 2008 to the current rate of€188 a week).
A spokesperson for Minister Burton said the criteriahad not been changed and that the scheme is notbudget-capped.
The UK organisations Mencap and the ChallengingBehaviour Foundation are campaigning to end poor careand abuse at large, institutional-style services for peoplewith a learning disability. They recently launched a newcampaign report called ‘Out of sight’. It tells the storiesof James, Chrissy, Joe, Emmanuel and Victoria, whoexperienced neglect and abuse in institutions. The reportcomes one year on from the BBC Panorama programme,which exposed shocking abuse of people with anintellectual disability at Winterbourne View, anassessment and treatment unit near Bristol.
In response to that broadcast, the Care QualityCommission carried out inspections of 145 assessmentand treatment units and care homes for people withdisabilities. Their report showed that half of all serviceswere not meeting essential standards around care andwelfare and protecting people from abuse. Mencap andthe Challenging Behaviour Foundation are calling for thephased closure of large, institutional-style services forpeople with a learning disability, and their replacementby appropriate local services. More information isavailable at www.mencap.org.uk/outofsight.
MENCAP calls for closure ofinstitutions in the UK
The government has begun to draft a NationalDisability Strategy Implementation Plan. The followinggoals are the basis for commitments in the Plan and formonitoring its implementation:
— Equal citizens— Independence and choice— Participation— Maximised potential.
Under each goal a number of specific objectives are set,and performance indicators are to be identified for eachaction. The Plan is expected to be completed in theautumn.

8 frontline Autumn 2012
I N T E R V I E W
Taking over as CEO of Inclusion Ireland has occurred at atime of cost constraints affecting most voluntaryorganizations. What impact will this have for definingpriorities?There have been cutbacks across the voluntary sector, and thefocus of Inclusion Ireland is the impact of these cuts on peoplewith an intellectual disability and their families. While this hashad an adverse impact on many areas, the challenge forInclusion Ireland is not just what cuts are happening atpresent, but also what the future vision is for people with anintellectual disability and how we can work to achieve that,despite ongoing funding restraints. In many ways the cutsaffecting people at present amplify the need for InclusionIreland as a central voice to advocate for the rights of peoplewith an intellectual disability and their families.Unfortunately, the language of cuts and austerity is the firstthing to trip off the lips of policy makers, but the rights ofpeople with disabilities and their families are not diminishedby a recession. It is important that Inclusion Ireland, inpartnership with others (particularly people with disabilitiesand their families), remains focused on the goal of achievingthe supports that people with disabilities need to live the lifethey choose with equal opportunities to all others.
There are many voluntary disability organisations in thecountry. Why is Inclusion Ireland different?I am not aware of any other organisation that has a fifty yearhistory of advocating for the rights of people with anintellectual disability and their families. Inclusion Ireland,more than any other organization, has led out publicly oncritical issues such as modern capacity law and independentinspection of disability services. But it is not our differencethat is important, rather the belief system of theorganization—one that puts the rights of people with adisability and their families at the centre of everything it does.Inclusion Ireland is only relevant as long as families andpeople with an intellectual disability feel it is representingthem, that they have its support and that they are not isolatedin trying to secure the supports they need, whether forthemselves as people with an intellectual disability or asparents and siblings advocating for their family members.
What are the challenges for retaining an involved,inclusive membership, given Inclusion’s broad remit?Inclusion Ireland’s central vision is that of people with anintellectual disability living and participating in thecommunity with equal rights as citizens, to live the life of theirchoice to their fullest potential. While this vision provides auniting force under which our membership stands, it is truethat we cannot, nor should we, try to represent the broad
spectrum of interests in the disability arena. There are peopleand groups, and I’m thinking of parents and family members,self-advocates, adults with an intellectual disability not alignedto self-advocacy groups etc, who do not enjoy the resources,access to policy makers and level of influence that others enjoy.If Inclusion Ireland is to be relevant, to offer something unique,to achieve real change and improvement in the lives of peoplewith a disability—and, remember, that is what it is ultimatelyabout—then these are the people Inclusion Ireland has to have atthe centre of its work and to be most vociferous in supportingand representing.
What are the challenges for achieving active nationalmember participation to achieve the aims and objectives ofInclusion Ireland?There is enormous drive, commitment, passion and abilityamongst people with intellectual disabilities and their familymembers; there is palpable anger at the daily struggles peoplehave to undertake to achieve the basic supports they need andhave a right to. I see enormous potential for Inclusion Ireland topartner with people to harness that energy and, to bring us backto your first question, to ensure not only that there are notfurther cuts but, more importantly, to insist and ensure thatpeople with an intellectual disability and parents are at thecentre of the planned change programme—not just representedon various committees in a token fashion, but resourced to be atthe table as drivers of policy and service changes. Specifically, anearly priority for me is to ensure that Inclusion Ireland is aresource, in terms of information and coordination, to parentsand parent groups. To this end, I have in recent weeks convenedmeetings with a number of parents in Galway and Dublin, andwill in the comings weeks be holding similar meetings in Corkand the Northwest, to better understand how we can do morefor parents. Central to this is the method of communicationwith parents. Of equal importance is how Inclusion Irelandworks with people with an intellectual disability to ensure theircollective voice is heard and, while we are involved in initiatingthe emergence of a National Self-Advocacy Network, we are alsoanxious to promote the emergence of self-advocacy groupsaround the country.
The absence of national standards open to scrutiny inintellectual disability services has been a concern forInclusion Ireland for a very long time, but especially in thelast decade. How can Inclusion Ireland contribute to theimplementation of national standards?Inclusion Ireland will continue to advocate for standards untilthe Minister for Health announces the date for theirimplementation, which we understand will be mid-2013. But thestandards are only one element of a robust system of checks and
INTERVIEW WITHPADDY CONNOLLYCEO of Inclusion Ireland

9frontline Autumn 2012
The Editorial Board of Frontline invites contributionsfor forthcoming issues, the themes of which are:
Issue 89 (December 2012)—Celebrating Disability
Issue 90 (March 2013)—Advocating for People with Disabilities
Issue 91 (June 2013)—Forensic challenges for people withDisabilities
Issue 92 (September 2013)—Supported Employment for people withDisabilities
Issue 93 (December 2013)—Older People with Disabilities
What is of particular interest to the readership is a focuson people’s abilities and achievements. Gallery pictures
provide a wonderful picture of people and theirachievements—do not hesitate to forward editorial andpictorial stories. There are so many achievements to
celebrate, and lessons to be learned. It is important to getthat message disseminated far and wide. Please help
Frontline to do this by your articles and good news stories.
F R O N T L I N E
balances in the provision of a rights-based person-centrednational disability services. Other critical elements includemoving away from exchequer funding being delivered inblock grants to service providers towards individualisedfunding, the availability of a menu of supports whichprovide real choice (not just a reconfiguration of what’salready on offer), and a broad spectrum of advocacyprovision which includes the present provision ofrepresentative advocacy, but also state-wide self-advocacygroups and more. Also critical to a robust and safe disabilityprogramme is that citizens are at the centre of planning andevaluating that system. We have a long way to go toensuring parents and people with an intellectual disabilityare viewed as genuine partners and placed at the centre ofthe change programme. So to answer: yes, we will continueto push for a robust inspection programme, but we only seethat as a small, albeit important, element of a wider changeagenda.
How will your previous employment achievementsinform your role as CEO of Inclusion Ireland?I have been involved in community organising for overtwenty years and certain themes are ever-present; one of thestrongest of these is the lack of genuine consultationbetween statutory agencies and citizens. Another is howgood Ireland is at producing policy documents, but howpoor we are at implementing them. I hope to bring what Ihave learnt about getting people together to act collectivelyto achieve real change. To work for change requires ananalysis of what needs to change, and an understanding ofhow society and the way it distributes resources sustainsinequality. I had a meeting recently with a group of parentswith children with a disability—some had adult childrenothers younger children—what was most disturbing aboutthis meeting was how the younger parents were goingthrough the same battles for supports and services as theparents who had being advocating for two or more decades.While it is true to say that the government significantlyincreased the amount invested in disability services duringthe past decade, it is also true that they failed abysmally toreform how services were delivered; they failed (andcontinue to fail) to put the citizen at the centre. I have beeninvolved in a number of campaigns that sought to ensurethat communities and individuals were consulted as equalsin the design and implementation of policy programmesand this will be important to Inclusion Ireland goingforward.
Increasingly, the number of parents with an intellectualfisability are the subject of childcare proceedings. HasInclusion a role to support parents with a disability asparents?Unfortunately, there are occasions when children will beremoved to the care of state for their own welfare andprotection. This is the case for children of all parents.However, as international studies have found, parents withan intellectual disability are up to 50 times more likely tohave their children removed to state care than other parents.Going to court can be extremely daunting and intimidating.Access to an independent advocate has been shown toremove many of the barriers faced by parents withintellectual disability. Inclusion Ireland has providedspecialist advocacy support to parents with an intellectual
disability to enable them to defend themselves in court. Thenumber of requests for this support has increased significantlyin recent years.
It is also our experience that parents with an intellectualdisability have received inadequate support in their parentingbefore proceedings are initiated. Inclusion Ireland hasadvocated for the introduction of policies and programmesthat will support parents with an intellectual disability in theirparenting role.
In a broader context, Inclusion Ireland continues toadvocate for the ratification of the UN Convention on theRights of Persons with Disabilities. The Convention reaffirmsthe right of people with a disability in all matters relating tomarriage, family, parenthood and relationships, on an equalbasis with others. It says that governments should provideappropriate assistance to people with a disability in theperformance of their child rearing responsibilities.
Would you like to share with readers three priorities forInclusion Ireland over the next two years?— To promote the right of people with an intellectual
disability to advocate for themselves by building a nationalnetwork of self-advocacy groups around Ireland and bysupporting the emergence of an independent nationalnetwork of self-advocates.
— To work in partnership with parents and parentgroups/associations to build a unified, cohesive and strongparents’ voice at national level.
— To campaign for the full implementation of the NationalDisability Strategy and against further cuts in disabilityexpenditure.

10 frontline Autumn 2012
I N C L U S I O N
THE ROSARY GARDEN
It is August 15th and we have justcancelled a family trip to theHorseshow at the RDS, as the rain
teems down and the nation battensdown for a storm. We are obviously notas hardy as the loosely-namedInternational Eucharistic CongressInclusion Team who faced a ‘week ofwet’ to construct the ‘Rosary Garden’and ‘Wheat Stand’ at the RDS twomonths ago in preparation for thethousands of national andinternational visitors to IEC-2012.
The team was made up of peoplefrom across the country who chose tomake a real contribution to thisinternational occasion. People were
more interested in having real roles—demonstrating what they do in theirwork and the roles they can play in thecommunity. This was far moreimportant to people than just turningup as part of the event. The organisersof the IEC 2012 were keen on the ideaof a garden as a quiet place for peopleto relax and rest during Congress and toenjoy our Irish summer! The gardenconcept was open to competition. Withsome sponsorship from the IrishFarmers Association and The IrishFarmers Journal, our proposal, designand location at the Poor ClareMonastery on Simmonscourt Road wasaccepted.
Amid a week of rain from 5-9June, the garden came into being. Myabiding memory is of the persistentgood humour amid the pressure thatalways accompanies such a project,and the welcome, warmth andcomfort food continually supplied bythe Poor Clares to keep our spirits up.Parkside Nurseries in Waterford grewand supplied the plants. CintraNurseries led the landscaping, alongwith Burton Hall, Clean Sweep, DoveHouse and Moore Abbey. During theCongress, people linked to servicesacross the country assisted daily inmanaging the garden and welcomingvisitors. Friday had a specialemphasis, with the workshop‘Including People at the Margins’being presented by the SunflowerFarm group from Roscommon andBrother Donatus Forkan (PriorGeneral of the Hospitaller Order of StJohn of God) who came from Rome tocontribute. Over 300 people fromIreland and abroad attended theworkshop.
On reflection, it was worth askingthe original question—how couldpeople contribute and build newrelationships through the Congress.Participants’ comments reflected this:‘It is something we should build on anddo again’; Being part of a big occasionwas great and being in the home ofLeinster Rugby was the best part (atLeinster’s RDS Grounds); I’d love totalk more about our work in Cintra onlocal radio’ ‘The nuns (Poor Clares) wereso kind and asked us to stay in touch’.
A plaque will be mounted tocommemorate the Rosary Garden andthose who prepared and provided it.Some of the organisations we got toknow are continuing to be in contactwith us since the project: Agri Aware,Blooms, Spred, Leinster Rugby, TidyTowns – Entente Florale, ACT, IFA /Macra, Social Farming Across Borders(SoFAB). We plan to keep in touchwith whatever grows from here,through a newssheet ‘Become whatwe have received’ and gettingtogether socially and practically incommunity and parish roles. FL
Paul Henry
‘It was a really nice piece of work to be part of, nice to see other people enjoy it.’(Team Member from Burton Hall)

11frontline Autumn 2012
Although we are now operating in a time of severeeconomic difficulty, I want to assure you that bothmyself and my colleagues in government arecommitted to prioritising funding for specialeducational needs (SEN) services. Approximately15% of the entire budget of the Department ofEducation and Skills—some €1.3 billion—will bespent in support of children with special educationalneeds this year. Despite our current financial challenges, SEN
funding has not been reduced and the overallnumbers of Special Needs Assistants and Resource
Teachers in the school system has been maintained. Such commitment has been crucial to the provision of inclusive education. This government
will continue to prioritise special education provision to ensure that all children with SENcontinue to receive an education appropriate to their needs.One of the things which we can be proudest of in our education system over recent decades
is the extent to which the education of children with special needs has been incorporated intothe mainstream education system. The majority of children with special needs are noweducated in their local mainstream schools, within their community, along with their friendsand neighbours.The advantages of this policy of inclusion are twofold. Children with special educational
needs benefit from being educated in their local schools, and their teachers and classmateshave the opportunity to acquire a greater level of awareness and knowledge of diversity anddifferent abilities. Ultimately this has a wider societal benefit. Some students still require specialist interventions in a special school or class. The
Department of Education & Skills (DES), in conjunction with the National Council for SpecialEducation, makes provision for special classes and schools to cater for children who haveparticular significant needs. These classes have lower pupil teacher ratios, so that moreindividual attention can be given. Special classes are established in mainstream schools, to provide for as much inclusion as
possible. This school year, 91 new special classes opened, bringing the total number of specialclasses in mainstream schools across thecountry to 640. DES also provides for a range of
special schools for children with the mostcomplex needs requiring specialistinterventions. In this way, there areprovisions available to cater for the fullrange of SEN. We will continue with this policy of
inclusive education, while also trying toimprove special educational services,taking into account best internationalpractices and research.I wish to assure parents that whatever
your child’s level of special need, there isa place for your child in our educationsystem and supports which can beprovided, and this will continue.
Introduction to the Special Education issue of Frontlineby Minister for Education & Skills Ruairí Quinn T.D.
12 frontline Autumn 2012
E D U C AT I O N
MAINSTREAM INCLUSION—Challenges, opportunities
and the need for equity
Iwas sitting in my noisy old Opel at ared traffic light in Castleknock,revving to prevent an embarrassing
cut-out in the stylish suburb where Iworked as a young teacher. Glancingsideways I spotted Philip, a wheelchair-bound student on the pavement,smiling in his usual cheeky way. Henodded towards the school ahead,while making hand gestures as if hewas a young Marlon Brando about toeasy ride his Harley Davison across thedesert. I responded in kind and, pullingdown my imaginary goggles, revvedagain. Philip, thrilled with thechallenge, catapulted his chair forwardwith a quick gear shift, encouraging meto ‘eat his dust’ as I awaited the lightchange. Moments later I was tootingthe horn and passing him by as hemade his steady way. My ‘ hare’ wasagain overtaken by his ‘tortoise’ at thenext traffic lights and by the time Idrove into the school car park, Philipwas waving at me from the front door. Ialmost had to queue to ‘high five’ him,such was his popularity amongclassmates.
Children argued over whose turn itwas to help Philip with the daily choreshe found difficult. Many wanted him astheir ‘best friend.’ He was a regularbirthday party attendee, and parentsenjoyed the thought that their childrenhad such empathy for their friendwhose mobility was so restricted.
Our little race took place more than20 years ago. Much has changed, andchanged again, for pupils and teacherslike Philip and me in the interim.Special Needs Assistants, once as scarceas TDs at a junior ministers Dáilpresentation, increased and multipliedin numbers until one-in-three adults inschools were so employed. KathySynnott and other campaigners onbehalf of children with special needsraised awareness of issues and gainedrights through the courts and the ballotbox. Applications for SNA and resourceteaching support were almost assuredof approval once the criteria were met.
I can recall one class in a local schoolfrom around the millennium where amainstream class teacher competed forspace with 6 SNAs in a classroom, eachassigned to an individual child. Someschools had more SNAs than teacherson staff.
Before the Celtic Tiger cametumbling down the tree, all educationpartners realised that change wasnecessary. The Department ofEducation and Science (as it then was)sought to limit SNAs to a maximum ofone per classroom. As the shock of thebanking collapse took hold, the sametree was attacked from the bottom forits’ low hanging fruit—the recent andrapidly expanded number of SNAs. Alimit of 10,365 employees wasimposed on the service. Whether anapplicant child would be grantedsupport was dependent on that figurenot being breached. SNAs were nowshared between pupils, not always inthe same class. Many were grantedreduced hours.
My young friend Philip, I’m sure,has gone on to have a happy andproductive life, though I regrettablycan’t confirm it as I too moved on soonafter that. Children I have sinceencountered with similar disabilitieshave, by and large, enjoyed similardegrees of popularity. By coincidence,as I write, RTÉ News is carrying thestory of Killian MacDonnell’sachievement in overcoming the jointdisabilities of profound deafness andDown Syndrome to pass his AppliedLeaving Certificate. His achievement iscelebrated by everyone associated withhim, including extraordinary SNAs andteachers and his peers who regard himso highly.
As popular as a child with obviousphysical disabilities may be with peers,the opposite frequently applies tochildren with ADHD, ASD, ODD orAspergers Syndrome. These are thechildren who are suffering most fromreduced SNA numbers and the 15%decrease in allocated resource hours.When children with non-physicaldisabilities have SNA support, it isusually applied in a way that helpsdisguise the intended beneficiary,particularly in junior classes. Often,children in the class are completelyunaware that the extra adult is assignedto anyone in particular, such is thesubtlety and professionalism the twocolleagues bring to their work.
The criteria for granting SNAsupport now effectively limit the serviceto those with extreme physicaldisability or those adjudged by aclinical psychologist to be a danger tothemselves or others. Critically, thisleaves many children with a non-physical disability outside the loop.Their condition may involve a lack ofsocial skills, an unwillingness to share
Damian White reflects on the impact onchildren of the cutbacks on SNAs in ourprimary schools.
An old teacher once advisedme that a child whose onlytalent is hammering nails
should have the opportunityto do so in school. With thisin mind, I have always foundit important to find out,through talking to and
observing the child, what theyenjoy and what they have atalent for, before giving themall possible opportunities to
display their ability.

13frontline Autumn 2012
or cooperate with others, a propensityfor over-reacting to the least stimuli,positive or negative, or a lack ofconcentration in class. This can leadto increased need for correction by theteacher and frustration for thechildren themselves. Where a childwith ADHD over-reacts on a regularbasis and upsets or strikes anotherchild, figuring out if there is bullyinginvolved and which child is thevictim can be a complex issue for theteacher. Is the child who strikes outwhen ‘his buttons are pushed’—abully? If the same childrencontinuously provoke and are lashedout against, where lies the greatestfault? In such cases, it is notuncommon to have both sets ofparents at the principal’s door,screaming ‘bully’ at the other party.
A child who loses their tempereasily through no fault of their ownand acts inappropriately towardsanother child quickly becomesunpopular with peers, if there is noobvious physical reason to suggestthat they are in any way different.After a number of such incidents,peers become openly hostile towardssuch a child, accentuating theproblem. Parents ask for their child tobe moved away from the child theyconsider disruptive, adding furtherissues for the teacher. Many of these
issues could be countered by having anSNA available. However, access to SNAsupport for such children may now beno more than 15 hours per week,leaving them over 13 hours to fend forthemselves.
So, how do you integrate childrenwith special needs into mainstreamschooling, especially in these tighttimes? Schools with ASD units take agradual approach, introducingintegration for subjects such as visualarts, religion (where appropriate) andPE, with academic subjects coming laterin the process. Schools with sensory andcooking facilities sometimes bring inthe mainstream classes to use thefacilities along with their autistic peers.Many schools use a ‘Buddy System’ tofoster integration during playtime.School plays and concerts also offerchances to integrate children withspecial needs. An old teacher onceadvised me that a child whose onlytalent is hammering nails should havethe opportunity to do so in school.With this in mind, I have always foundit important to find out, throughtalking to and observing the child, whatthey enjoy and what they have a talentfor, before giving them all possibleopportunities to display their ability.
In every primary school, academicsubjects are but one spoke in the wheelof a day’s proceedings. Children can
learn valuable lessons fromorganising the library, attendinggreen schools meetings, or updatingthe school’s website or blog. Gettingthe PE equipment ready for a lesson,rearranging displays, gardening,attending the bird feeders or settingout the GP room for eveningfunctions all contain nuggets ofinclusive learning and the potentialfor self-esteem enhancement.Children with their own vegetable oregg enterprises can design anddisplay advertisements on anassigned school noticeboard, or onthe schools website. Differentiationbased on each child’s needs andabilities means homework is given inproportion to the child’s ability tocomplete the task.
Cuts in access to resourceteaching and SNAs, as well ascrippling reductions in DEISprovision, mean that schools arefighting a rearguard action tomaintain a quality of service forpupils with special needs. The SpecialEducation Support Service (SESS) is ofhuge importance to schools, as theyprovide an excellent advice, trainingand back-up to teachers, principalsand SNAs. Any cut in this servicewould be a real disaster for childrenwith special needs and thoseproviding for them.
Daily, schools seek to provideequality of educational opportunityto each and every child. Maintainingthis as our ideal keeps us focussed onthe job at hand. However, the cuts inservice have had a serious effect onequity in the system. Only arestoration of services and areprioritisation by the DES can ensurethat the child with a non-physicaldisability can enjoy and benefit fromtheir school experience as much asmy friend Philip. FL
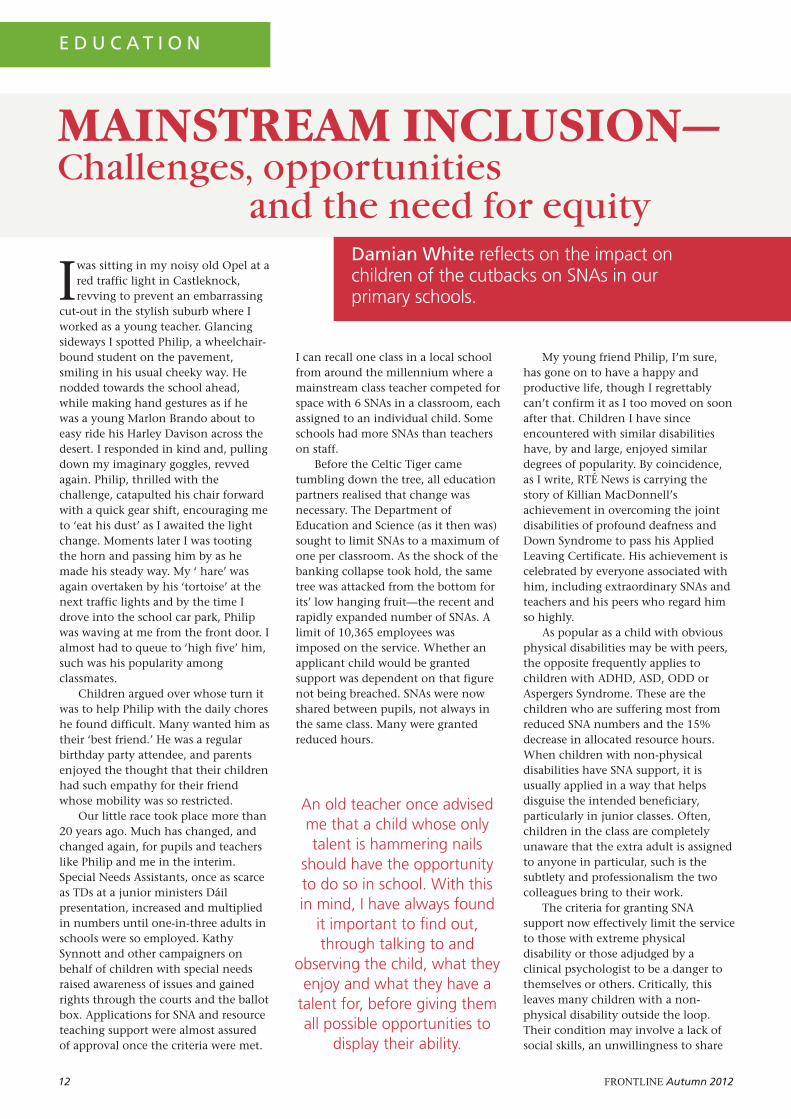
Above: 11-year-old Rebecca Walsh who is blind and has learning disabilities being helped by herfull time special needs assistant (SNA), Judith O'Malley at St Anthony's Special School in Castlebar,Co. Mayo. Rebecca will no longer have a full-time special needs assistant (SNA) as a result of 4SNAs out of 13 in the entire school being cut following a review. Photograph by Keith Heneghan, phocus.ie.
Damian White is Principal of ScoilShinchill, Killeigh, Tullamore, Co. Offalysince 1994. In 1999 he was a foundermember of The Irish Primary Principals’Network (IPPN) and has been a memberof their national executive ever since.He is editor of IPPNs magazineLeadership + where he also contributesa regular column. Damian is married toMarguerite, who is also a schoolprincipal. They have 3 children.

14 frontline Autumn 2012
E D U C AT I O N
IntroductionRights-based statutes such as theDisability Act (2005), the Education forPersons with Special Needs Act (2004)and the Qualifications (Education andTraining) Act (1999) have influencededucational provision in Ireland. Parallelto legislation, beneficial policydocuments, including the EUMemorandum on Lifelong Learning (2000)and the Learning for Life, White Paper onAdult Education (2000), as well as theBack to Education Initiative (BTEI),endeavour to promote further educationoptions for individuals. Yet, there arelimited tertiary education opportunitiesavailable for young adults withintellectual disabilities in Ireland.
Currently midway through its thirdcycle (2011-2013), The LIFE (Leadinginto Further Education) Programmeprovides access to further education foryoung individuals with intellectualdisabilities. This programme wasdeveloped in response to an identifiedgap in provision for learners withintellectual disabilities leavingmainstream second-level school. It is atwo year BTEI programme for adults 18-25 with mild to moderate intellectualdisabilities and/or with AutisticSpectrum Disorder, with the aim ofassisting the transition from mainstreamsecond-level education into furthereducation and training. The pilot
programme was launched in September2007, as a partnership venture betweenthe Health Service Executive (HSE), DúnLaoghaire VEC and Carmona Services.Subsequently, STEP joined thepartnership for the following programmecycle (2009-2011) and have continuedon the current programme cycle whichbegan in September of 2011 to runthrough to June 2013. Additionally,other service providers (Sunbeam HouseServices and Enable Ireland) have joinedthis partnership approach bycontributing to programme content.
The LIFE ProgrammePotential participants between 18-25years of age are referred to the LIFEprogramme by local services and schools.Participants are expected to be able totravel independently, and to participateand work collaboratively in a groupsetting. Subsequently, referrals gothrough an interview process to ensurethat the programme is appropriate to theneeds of the potential learners. The LIFEprogramme comprises two parts: theCore Skills programme and theComplementary Programme.
Dún Laoghaire VEC run the CoreSkills programme in a mainstreamenvironment in a variety of locationsaround Dún Laoghaire, Co. Dublin.Classes take place three days a week atDLVEC Educational Support Services inMulgrave Street, Dún Laoghaire Collegeof Further Education and the Institute ofArt, Design and Technology. Participantshave an opportunity to achieve a FETACLevel 3 Certificate in General Learning.The curriculum consists of core skillsubjects such as communications,personal effectiveness, mathematics andcomputer literacy. Elective subjectsinclude drama, intercultural awareness,health-related fitness and self-advocacy.Tutors use innovative teaching
techniques and creative assessmentmethodologies in order to give thelearners the best opportunities todemonstrate and evidence their learningas required by FETAC. It is important tonote that in instances where learners didnot meet the assessment criteria in agiven module, tutors were able to adaptthe programme to meet individualneeds, thus enabling learners to improvetheir competencies in key areas, even ifaccreditation was not possible. Thus thefocus shifts to the individual level andaccommodates the needs of learners, firstand foremost.
Along with the three days of FETACclasses, the Complementary Programmeoffers additional classes. Historically,Carmona Services and STEP wereresponsible for the organisation anddelivery of the complementaryprogramme, because a large majority ofparticipants were referred from theirservices. Recent focus has shifted toclasses being offered by a variety ofservice providers in an effort to shareexpertise and resources. In contrast tothe FETAC Core Skills element, theComplementary Programme aims at amore holistic approach to learning andfocuses on social and life skills. This isreflected in such classes as the friendshipprogramme, healthy eating, cooking,student representation, work skills,literacy, newsletter, current affairs andconflict resolution. As an example of thefocus on participation in the community,one of the programmes, Streetwise, isdelivered jointly by Carmona Servicesand the Garda Siochána. It offers anawareness of safety and protection in theneighbourhood. Additionally, one of themost positive outcomes to date on theComplementary Programme is theparticipation by the learners on Ireland’sNational Award Challenge, the GaisceBronze President’s Award.
A progression opportunity forindividuals with intellectual disabilities:
A look at the LIFE(Leading Into FurtherEducation) Programme

15frontline Autumn 2012
Participants and outcomesSeven participants took part in the firstprogramme cycle in 2007-2009. Threeof the seven achieved full Level 3Certificates in General Learning withthe remaining achieving a number ofminor awards. After completion of theLIFE programme, four of theparticipants went into paid supportedemployment, with the remaining threeparticipating in further educationaloptions. In the 2009-2011 programmecycle, eighteen learners completed theprogramme. Approximately half of theparticipants received Level 3Certificates in General Learning, eventhough they did not complete all therequired modules. Although, they didnot complete the coursework for Level3 mathematics, some of the learnershad previously completed this moduleprior to participating on the LIFEprogramme, thus, highlighting theflexibility of the FETAC framework.Participants who did not complete afull award, achieved minor awards orcomponent certificates containingsomewhere between five to sevenmodules. The following are theprogression routes for the participantson the second cycle: one learnerworking on the Leaving Cert Applied,nine learners attempting furthereducational opportunities, and eighton work experience or supported paidemployment. In 2011, seventeenparticipants enrolled on the third cycleof the programme, and they anticipateprogression outcomes equalling thosein previous cycles.
ConclusionAs a mainstream option for individualswith intellectual disabilities, thelearners have remained for the mostpart segregated within a mainstreamsetting. In essence, The LIFEprogramme could be defined by Zafft,Hart & Zimbrich (2003) as aSubstantially Separate Post SecondaryEducation Model for young adultswith disabilities; thus students attendclasses with other students withdisabilities within a mainstreamenvironment. Although the LIFEprogramme remains segregated, itsbenefits lie in the flexibility of theFETAC curriculum that fostersprogression opportunities for furthermainstream qualifications, which isaptly described by the name LeadingInto Further Education. FETAC classes onthe LIFE programme are adapted or
modified, but assessment is based onstandardised ‘specific learningobjectives’ (SLO). SLOs are the samefor anyone who takes part in thespecific FETAC module. Thusrequirements for achievement in aFETAC Level 3 module on the LIFEprogramme are equal to the sameFETAC Level 3 class in any further-education setting. This allows greaterscope for progression, opening routesto other services within thecommunity (beyond the disabilityarea). Therefore, learners who havecompleted the LIFE programme mayattempt higher FETAC levels and movetowards further educationopportunities in other mainstreamsettings.
In addition to the academicachievement, the complementary partof the programme fosters theformation of individual values andattitudes. The learners gain self-assurance, autonomy and learn how todemonstrate self-advocacy through aneducational setting. The experiencesand personal growth of the learnerswho have previously participated onthe overall programme have beenextremely constructive. All thelearners have demonstrated improvedsocial skills and have exhibited agreater level of independence, self-confidence and personal effectiveness.In adulthood, the opportunities totake part in lifelong learning arecritical to self-purpose and ‘personalwell being’ (Stodden & Whelley, 2004,p.6).
‘Transition from childhood toadulthood is a defining moment ineach person’s life, albeit celebrateddiversely across cultures. Young adultswith intellectual disabilities especiallyrely on support to negotiate thisdevelopmental stage’ (May, 2000, citedin Hogg & Langa, 2005, p.29). Thecore of this programme was thedevelopment of a model wherebylearners with intellectual disabilitieswould be aided and encouragedthrough this transition. Likewise, themerits of this innovativelearner/person-centred programmewere acknowledged when theyreceived (in 2009) an AONTAS StarAward in the Nationwide Category.
Most importantly, the sense ofhaving had and enjoyed the ‘collegeexperience’ is expressed by many whohave completed their two years withinthe programme.
Previous learners have commented:‘Everything has changed for me since Icame to college. I am more independentand confident.’ ‘I have learned about exercise, health,being safe, to respect people and how tobe calm and patient.’ FL
Kathleen Deasy and Sinead Murphy
ReferencesCommission of the European
Communities 2000. Commission StaffWorking Paper. The EU Memorandumon Lifelong Learning. SEC (2000)1832.
Department of Education and Science2000. Learning for life, white paper onadult education, Dublin: TheStationery Office.
Education for Persons with SpecialEducational Needs Act, 2004retrieved 3rd August 2012 fromhttp://www.irishstatutebook.ie/pdf/2004/en.act.2004.0030.pdf
Hogg, J. and Langa, A. 2005. Assessingadults with intellectual disability – Aservice provider’s guide. Edinburgh:Wiley-Blackwell.
Stodden, R. and Whelley, T. 2004.Postsecondary education and personswith intellectual disabilities: Anintroduction. Education and Trainingin Developmental Disabilities, 39, 6-15.
The Disability Act (2005) retrieved 3rdAugust 2012 fromhttp://www.oireachtas.ie/documents/bills28/acts/2005/a1405.pdf
Qualifications (Education and Training)Act (1999) retrieved 3rd August 2012fromhttp://www.oireachtas.ie/documents/bills28/acts/1999/a2699.pdf
Zafft, C., Hart, D. and Zimbrich, K. 2004.College career connection: A study ofyouth with intellectual disabilitiesand the impact of postsecondaryeducation. Education and Training inDevelopmental Disabilities, 39, 45-53.
Kathleen Deasy is the LIFE ProgrammeCoordinator for Dún Laoghaire VEC.Sinead Murphy was part of the LIFEProgramme Steering Group responsiblefor the development of the LIFEprogramme. A copy of the LIFE PilotProgramme Report (2012) may beaccessed at www.dlvec.ie. For furtherinformation or questions regarding theprogramme, contact Kathleen Deasy [email protected].

16 frontline Autumn 2012
KATHERINE’SPERSPECTIVEStarting school is the first step intoformal education. Progression to postprimary school can be challenging.Leaving school is exciting because it isthe time when you get to chose thepath of learning for yourself. Your ticketis the CAO form. Your destinationcould be university, an institute oftechnology or any number of colleges.Your family and friends wish you well.You might be moving away from home.This is the stuff of normal life andregular families. So what happens ifthere is somebody who needs extra helpor falls into the bracket that is definedas having ‘special needs’? Then the pathis utterly different.
Drawing from my own experienceas the mother of Diarmuid, who is ayoung man with an intellectualdisability (ID); I am convinced that ourIrish system has many positives, butalso many gaps. Some people with IDhave a very good service, while othersmay have none at all. Standardisationacross the system is a difficulty. Thepolicy is to move towards inclusiveeducation and I believe education isinclusive when students with specialneeds are educated in their local schoolin age-appropriate classrooms alongsidetheir non-disabled peers, with thenecessary supports to enableparticipation while also meeting theirindividual needs. While I’m passionateabout this view I remain concernedabout what might happen to peoplewith severe ID, hence I do not envisagethe phasing out of the special schoolsystem.
There will be difficulties inimplementing inclusive educationacross the Irish education system. Atpresent our class sizes are too big andthis means that more special needs
assistants (SNAs) are needed, to avoidpupils with ID becoming isolated. Tobe successful inclusive educationrequires the relationships between allstake holders to be on the one voice.This process will not proceed withouttensions.
The value of a diagnosis or a label,while we may not like it, doesguarantee a certain level of service. Forthis reason assessments need to bedone quickly. At primary level thereare two choices for the child withspecial educational needs (SEN): to goto a special school or to go to the localnational school. This is a very personalchoice for parents. The parents makethe choice in the best interest of theirchild and in consideration of theirown circumstances. Many pupils needthe support of a special needs assistant(SNA) in order to be able to cope inmainstream school.
We chose the option of specialschool for Diarmuid. There were anumber of things that influenced ourdecision. Diarmuid had medical issuesand we felt that he would be safer in aspecial school where his needs wereunderstood. He had difficulty withspeech so we thought he might receivebetter speech therapy in a specialschool. We’d been told that the gapbetween mainstream pupils and thosewith special needs widens as the pupilsget older. From my experience as ateacher I have found this to be true.Hence, many pupils with (SEN) revertto the special school system whileothers struggle through the postprimary system with little support.Surely this is not equitable or fair?
It is seriously challenging forpeople with an intellectual disability tofind suitable options after leavingschool. Generally there is only oneavenue and that is attending a localdisability service. Over the years,
provision of places has been sporadicand there seems to be no plan forpeople with an intellectual disabilityafter the age of eighteen. This issimply not acceptable and clientsshould not be pawns in disputesbetween the HSE and disabilityservices throughout the country.Putting more clients into disabilityservices that are already under pressureis not sustainable. Society has movedon from merely offering care to peoplewith ID. They need individuallytailored programmes, individualeducation plans (IEPs) up to schoolleaving age and person-centred plans(PCPs) after that. Education is key tosuccess, but it must be worthwhilelearning, such as programmes towardsindependent living, personal care, theworking environment and definingtheir own futures.
The challenge for administrators inIreland will be to get the numbersright. The various departmentsinvolved must then put funding inplace to provide places for the peopleleaving school. All people, with orwithout disabilities, are entitled to aneducation. There are manystakeholders involved: teachers,teacher training colleges, the NationalCouncil for Special Education, thewider Department of Education andSkills, the voluntary disabilityagencies, the curriculum developmentagencies—along with parents andpupils. It is difficult to get all agenciescooperating when resources are tight.Nevertheless we must educate peoplewith SEN so that they can live betterlives, reach their potential andcontribute to society.
Being educated in the same schoolas one’s siblings without having totravel long distances and going on tocollege seem to be straightforwardambitions, yet they are still not a
PERSONALPERSPECTIVES ON EDUCATION
E D U C AT I O N
Katherine O’Leary and her daughter Julie sharetheir perspectives on education in Ireland for those with intellectual disabilities.

17frontline Autumn 2012
reality for everyone. As a parent andteacher I find it hard to have therequired patience, but as someone whois sometimes involved in shapingpolicy I know that things are changing.
It is important that the DisabilityStrategy and Education for Persons withSpecial Educational Needs Act (EPSEN2004) are put in place to allowmovement towards fully inclusiveschools, to enable all pupils to have anopportunity to learn together. I lookforward to a time when there is a placeon the CAO form for disability services.The vehicle for accreditation is therethrough FETAC. We just need to putthe programmes in place.
There are good people in oursystem. I encounter them every day.People with SEN can and will be betterserved in the future, but it requires allthe stakeholders to work together.
JULIE’S PERSPECTIVEEducation is a human right, which putsit as a high priority in the eyes of Irishsociety, and if I am honest I am verylucky that achieving in this sphere isheld in such high regard because it iswhere I excelled and got anopportunity to show my true colours. Ihave a physical disability, cerebralpalsy, which very obviously impacts onmy mobility. When people meet mefirst, before I open my mouth, theyoften assume that there is no brainoperating behind the scene, and it isvery frustrating. My greatest weapon incombating this misconception is myeducation.
I attended mainstream education allthe way up. I was lucky, I just neededthe playing field to be levelled a littlebit. I availed of extra time for examsand a scribe. At third level I also hadsupport with transport and educationalassistants. All these little thingsculminated in me achieving a degree inapplied psychology from UCC and anMA in journalism from NUI Galway. Iam extremely proud of the letters I cannow put after my name. They affirmmy ability and diminish my disability.With every step in education I take, mydisability has less and less of an impactbecause my achievements cannot bedisputed. It is an incredible feeling andI want everyone to experience it.
For people with an intellectualdisability, it is not quite asstraightforward to achieve effectiveinclusion. Due to the fact that people
with an intellectual disability rely onservice providers to avail of educationand because the emphasis is oneducating people to the age of 18,many people do not and cannotbenefit from further education. Furthereducation is the part that allows us totruly flourish and to define ourindividuality and it should be availablein some shape or form to allindividuals in Ireland, withoutexception.
Some people may be reading thisand thinking it is all a pipedream, butif we reach for the moon we mightland on the stars. Lifelong learning is afocus in all of our further educationinstitutions, so it should also betailored and offered to people withspecial needs of all kinds. I am notsaying that people with an intellectualdisability should fit into theconventional system we have. I feel thesystem should be flexible to fit allkinds of abilities.
My brother Diarmuid has DownSyndrome and he wants nothing morethan to go to college. I want the verysame for him, and we as a family won’trest until he gets it. He is an achieverand wants to be the same as me andmy other brothers Philip and Colm. Heshould be afforded that opportunity.Unfortunately, in Cork where we livethere are not enough doors to knockon yet!
A concrete example of realinclusion working on the ground is theGoing to College Project in NUIGalway. The pilot project which beganin 2011 is enabling eight students withintellectual disabilities to study at theuniversity in the undergraduateprogramme of their choice. Studentsare registered full-time students and arefully included in undergraduatelectures, tutorials, labs and group work,with opportunities to volunteer and doa work placement. I have met all eightstudents and they are all thriving totheir potential. It’s a great example of auniversity/community partnership, allworking together to achieve socialchange. There is a great buzz about thisproject and it will undoubtedly gofrom strength to strength into thefuture.
Like most further educationinitiatives, the Going to College Projectis dependent on funding, and due tothe tough economic climate, it getsharder and harder to secure the money,but people have great ingenuity and a
sense of innovation and most of the timewhere there is a will, there is a way. Itsaddens me when funding is a thing thatholds real progress back!
I am so proud of NUI Galway for allthe hard work they have put into thispioneering project. There are otherprojects and programmes around thecountry, but they group people withintellectual disabilities rather thanintegrating them with the wider studentbody and tailoring programmes andsupport to individual needs. Realinclusion means everyone together. I amaware that some people need moresupport than others; in terms of howinclusion works it is not a one-size-fits-all outfit. It takes hard work, thought,reflection and perseverance by so manypeople, not least the learners themselves.
Achievement in my eyes is a relativeconcept. The most importantcomponent is potential. If an individualis reaching their potential, that is allanyone can ask for, but we mustcontinue to ensure that everyone has theopportunity to explore their potentialand find an outlet to achieve it!
I will remain steadfast in mypipedream, only because I know in myheart that it will become reality. When Iwas in school, there was nobody in myclasses with an intellectual disability. Inschools around the country there is realinclusion happening and now mybrother studies with a student with anintellectual disability in his degree inArts and Human Rights in NUI Galway.
I know particularly for parents andsiblings of those with intellectualdisabilities it can be hard to keep thefaith if the person you love does not geta place and seems to be left behind, but Ipromise with all my heart there aremany of us working to ensure that thiswill change. We are making it happenone step at a time, we have come a longway and have further to go, so pleasehang in there with us! FL
Katherine O’Leary and Julie O’Leary.
Katherine O’Leary is married to Tim whois a dairy farmer. They have four adultchildren, Julie, Diarmuid, Philip and Colm.Diarmuid is 24 and has Down Syndrome.Katherine is a director of Inclusion Irelandand Cope Foundation. She teaches homeeconomics in Our Lady of Good CounselSpecial School and is a columnist with theIrish Farmers Journal.

18 frontline Autumn 2012
People with intellectual disability are beginning to findopportunities opening up in post-Secondary and third-level education. Some institutions have been offering
courses for a number of years, with specifically designedprogrammes being the most common. More recently moremainstream options are being developed which encourage allstudents to study together with awards achieved at differentlevels.
A module is a unit of education that allows itsparticipants to explore one important area of life. In themodule being explained in this article, we look at how threeordinary stakeholders of an intellectual disability service canbring about service change. Students who have attended thismodule in Dublin City University have reported feelingempowered to bring about changes and improvements intheir services. The ability of this module to build capacity inindividuals and services is supported by the evidence frominformal and formal feedback of students and serviceproviders and reflects the policies that are currently drivingnational and international practice changes. This modulegives a voice to people with intellectual disability, family andordinary staff members as they achieve personal and teamgoals. Based on early evaluations and feedback, it seems fairto say that this module can make real practical changes to thelives of people with intellectual disabilities who attend theservices that have been involved in this project.
This module brings together teams of three people towork on a service improvement or change project. Teamsconsist of a staff member, a person with intellectual disabilityand a family member (not connected to the person with ID).There is equality among the team members, encouragingthem to develop a collaborative attitude throughout theproject. Called ‘Improving Service with CooperativeLearning’, the module teaches the students how to worktogether as a team and research options to complete a projectthat will make things better in their service. A minimum offour teams of three people undertake the module eachacademic year.
TeamBecause the service is held in common by all participants inthe team, they all have a stake in improving or changingthings for the better. While teams apply together to DublinCity University to take the module, all students must makeindividual applications which are considered by the academicteam. All students are registered with the university, haveaccess to all facilities and receive a student card valid for oneacademic year. Informal learning (learning gained through
the experience of life) is equally valued as formal education.One person put it in her own words, saying: ‘do you meanbecause I have lived in residential care for twenty years I knowas much about this service as the staff?’
InfluencesA significant influence to the development and maintenanceof this module has been the commitment and support of asteering group which involves service providers, familymembers and representatives of advocacy organisations suchas Inclusion Ireland and the National Parents and SiblingsAlliance. When a service undertakes to nominate a team, thisis just the beginning for them—they provide funding, andmuch more. This includes providing a mentor from theservice who will facilitate the team to progress their project. Inpractical teams, this involves a senior member of staff givingtheir time as well as ensuring the team is provided with theresources required.
The University provides a focus for the educational aspect,while national policy will underpin much of the direction theprojects take. Policies that focus on access to mainstream andinvolving people in decisions about their services arehighlighted, and students are encouraged to consider these.
EducationThe module uses a cooperative model of education, includingpractical recommendations made by the students themselves.This cooperative approach requires that students workcollaboratively and simultaneously with each other, yet thereis an understanding and provision made for individual
E D U C AT I O N
INFLUENCING SERVICEIMPROVEMENT AND CHANGETHROUGH EDUCATIONDeirdre Corby of DCU explains how a new module draws teams ofindividuals together to work on projects specifically focused on improvingand changing services for people with intellectual disability
KEY ELEMENTS OF IMPROVING SERVICE WITHCOOPERATIVE LEARNING

19frontline Autumn 2012
students’ preferences and abilities. Classes all take place in theSchool of Nursing and Human Sciences in Dublin CityUniversity, where students attend one day a month duringone academic year, from October to May. Three universitylecturers facilitate the module, each taking responsibility foraspects of educational input and support for teams. Eachteam is allocated a lecturer who provides the team academicsupport, in addition to the practical support provided by theservice-based mentor. Team teaching is the main classroommethod employed—an approach that encourages students toparticipate in all activities.
Individual and team progress reports are essentialelements of each university day and students are offeredopportunities to present their ongoing work. Problem-solvingwithin and between the teams is invaluable, providing aunique opportunity for all students to investigate what ispositive within other services.
One student, Breda, gives her views andfeedbackAs a parent of a child with an intellectual disability, I waspart of the team from Kildare services who attended thismodule. Our team began by picking a unit of 48 peoplewithin our services, in which to base ourproject. We askedpeople and discovered that they would like more choices,moremeaningful activities and more communityparticipation. We then used a questionnaire to see the level ofinterest in expanding an existing community farming schemeand in the introduction of weaving. The result was thatapproximately 50% were interested in participating in socialfarming and a similar percentage in learning how to weave.
The team then decided on a two-fold plan for theproject—to expand the social farming scheme and tointroduce a weaving programme to the unit. We felt thatgiving these additional choices would address some of theissues raised. After a lot of hard work, many meetings, visitsto other service providers, farms and wool suppliers, theproject was up and running.
Four people took part in an expanded social farmingscheme over a six week period. it is hoped to further expandthe scheme to include more people. With regard to theweaving, a table loom and peg loom have been installed inthe unit, staff members have been trained in weaving skillsand lots of people are weaving successfully. Donations oflooms and training of staff by another service provider, thefinancing of wool by the director of services in KildareServices and the provision of wool by a well-known weavingcompany have all helped our efforts with the weavingproject. We hope that the projects we started will continueinto the future.
Our team found this course very educational andinformative. The areas covered by the lectures included thedifferent services available in the area of intellectualdisability, social inclusion, project management, leadership,teamwork, various reports published regarding intellectualdisability and future proposals in this area. Guest speakersalso told of their experiences in arriving at satisfactoryarrangements for day and residential services for their familymember. A lecturer was assigned to each team and wasavailable to assist the team whenever necessary. Thisincluded, in our case, visiting and assisting our team at theservice headquarters and visiting the farm and weavingservice involved in our project.
Our team feels that the trialogue of a person with anintellectual disability, a staff member and a parent workingtogether to achieve a goal can be a successful way of gettingresults. We feel that the success of our project as a result of thecourse at Dublin City University has brought about animprovement in the service we are involved with and has thusenhanced somewhat the quality of life of some individualswith intellectual disability. (Breda Pierse)
LegacyThe overall vision of this project is to create a ‘legacy effect’ ofbenefit, not only for the students but the organisations orservices they represent. A sense of achievement and doingsomething practical and useful is reflected in studentdiscussions at the end of the module. The universityexperience too has been very much enjoyed. While studentsidentified that there was significant, and perhaps unexpected,work in progressing their project, the fact that the projects aretheir own ideas put into practice has resulted in students notwanting to leave. They speak about how they can continue towork together after the module, and friendships are begunand maintained. The ripple effect is felt with individuals, andalso within services as staff, in particular, report feeling astronger commitment and feel this module has helped themto understand what people with intellectual disability needand want from their service.
Conclusion Past student feedback is really valued and influencesimprovements on how the next module is run. Anyoneinterested in applying for the programme, or withqueriesabout it, should contact Deirdre Corby, at DCU (tel: 017008524; email [email protected]. Those who havecompleted the module and service providers who havesupported teams to attend are also happy to be contacted. FL
Deirdre Corby, Therese Danaher and Richard Jackson, Lecturers,DCU. Breda Pierse, student, DCU.
Deirdre Corby is a lecturer in the Schoolof Nursing and Human Sciences, DublinCity University and the modulecoordinator for the module "ImprovingService with Cooperative Learning". Shehas a nursing background in services forpeople with intellectual disability and hasbeen working in nurse education for overten years. She is currently undertaking aPhD programme examining the
experiences of people with intellectual disability in postsecondary and third level education in the Republic of Ireland.
While students identified that there wassignificant, and perhaps unexpected, work inprogressing their project, the fact that theprojects are their own ideas put into practicehas resulted in students not wanting to leave.

20 frontline Autumn 2012
The first day of school is anexciting and important event in achild’s (and family’s!) life. For
children who use a mode ofcommunication other than speech,along with the preparation of booksand uniform will be the need to helpprepare the school to support the newpupil’s communication system.
Augmentative or alternativecommunication (AAC)Everybody communicates in their ownway. For some, this might mean usinga mode of augmentative or alternativecommunication (AAC): ‘a set of toolsand strategies that an individual uses tosolve everyday communicative challenges’(ISAAC). AAC supports include signs,communication books andcommunication devices. Having accessto a method of communication enablesthe child to interact, express theirwants and needs and buildrelationships. AAC supports can be‘high-tech’ or ‘low-tech’. PictureExchange Communication System(PECS), speech output devices and someApps are aided forms of AAC. Lámhmanual signs are unaided, i.e. usingLámh signs doesn’t involve anythingother than the person’s hands andbody.
For someone who has experienceddifficulties with communication, AACsupport can make a vital difference.Using a form of AAC can mean havingthe opportunity to experience moreaspects of life, i.e. ‘participation,achievement, independence, inclusion andfun’ (Locke).
Lámh signsThe AAC system that some childrenand adults use is the Lámh manual signsystem. Lámh manual signs (or key wordsigns) have been developed for use bychildren and adults with intellectualdisability and communication needs inIreland. Manual signs can supportcommunication in the following ways:Signs, being visual, can be easier toremember than what is heard.Signs emphasise small differences inspoken words, for example between‘sleep’ and ‘sweet’ or ‘dog’ and ‘doll’.This helps the child to pay attention tothese differences and so understandbetter what is happening in theclassroom.
Signs can be easier to imitate. Theseattempts give an opportunity to matchthe spoken word to the sign and so toachieve better understanding of theword and possible practice saying it.Early attempts at words are oftenunclear. If the person uses a sign aswell, communication partners caninterpret correctly and give a positiveexperience of communication so thechild is more likely to try again.A tactile, as well as a visual way ofremembering the word, i.e. you can‘feel’ yourself making the sign.Using signs takes the focus off speech.The child who is not under pressure totalk may be more likely to establishspoken language skills at their ownpace.
There are 500 Lámh signs, used tosign key words in a sentence. Speech isalways used with Lámh signs. SomeLámh users may use sign for a period of
time and then may drop the signswhen their speech develops, or theymay use Lámh throughout their lives.Lámh is based on Irish Sign Language(ISL) and on natural gesture.
Lámh users may use a larger orsmaller number of signs. They may usea number of signs themselves andcomprehend those signs along withother signs. Lámh signs may be usedalong with sounds, words and othermodes of communication.
Lámh at schoolThe child who uses Lámh will havebeen supported by a team that hasincluded a speech and languagetherapist. They will already have acommunication programme or plan inplace which will provide usefulguidance to those now supportingthem in school. Families will beexperienced in using the child’scommunication system, and will play akey role in providing initial andongoing information to SNAs, teachersand others.
In the classroom, if those aroundthe Lámh user can become familiarwith Lámh signs and use some signsthemselves, the child will have theopportunity to participate in schoollife from the start. Along with schoolstaff members, peers are alsocommunication partners and can besupported to learn about theirclassmate’s communication system.They are often enthusiastic signers, aswell as being interested in learningabout Lámh. The role of thecommunication partner is important:
SUPPORTINGLÁMH USERSAT SCHOOL
Mary Cullen explains theLÁMH sign languagesystem in Irish schools.
E D U C AT I O N

frontline Autumn 2012 21
‘Communication is a cooperativeundertaking and the successful use ofaugmentative and alternativecommunication (AAC) systems is asdependent on the communicationpartner as it is on the user.’ (Murphyet al)
Sign users are more likely to use signwith someone they have seen signing.The most effective way to use signs is toinclude them in day-to-day activitiesand routines. This is a signingenvironment, where sign is part ofeveryday life. This is more effectivethan setting aside specific ‘Lámh time’,which can lead to having signs onlybeing used during this set time by alimited number of people. Using Lámhin context also ensures that the signsbeing used are relevant and will supportthe child’s communication:1. Use signs in natural contexts, e.g. at
circle time or when givinginstructions to the class.
2. Offer opportunities for makingchoices, to encourage sign use, e.g.red crayon or blue one.
3. Try structured opportunities for signpractice within routines, e.g.‘forgetting’ to give the child theirbook so that they need to ask for it.
4. Introduce topics of conversationthat will be of interest to the child.e.g. talk about their pet (based onBeukelman & Mirenda)
Where those creating the signingenvironment at school can accesssupport and training, a signingenvironment can be put in place. Oneof the tools that can be used in theclassroom is the Lámh-a-Song DVD,which includes well-known songs foryoung children such as Old MacDonaldand The Wheels on the Bus, performed
using Lámh signs. These songs are usuallyused in classrooms with gestures andactions to accompany the words, so it iseasy to ‘swap’ Lámh signs for thosegestures and actions.
Lámh training If a child is a Lámh user, families willknow which of the 500 Lámh signs theirchild is using and can introduce some ofthose signs to those in the school.Families may have already attended theLámh Family Course run by the child’sspeech and language therapist or serviceprovider. SNAs and teachers may beshown some signs from the child’sspeech and language therapist or supportteam.
In addition to information specific tothe Lámh user, a Lámh course such as theModule-One Lámh Course, is where signscan be learned and sign materials aredistributed. An average of 1,400 staffmembers from various disciplines attendLámh staff training each year (based ontraining delivered in the past four years,see www.lamh.org). Lámh trainingfocuses on communication, the signingenvironment and encouraging sign use,
as well as the mechanics of signing.Teachers attend Lámh training organisedby local service providers where thechild receives their supports such asspeech and language therapy, or by theSpecial Education Support Service (SESS)www.sess.ie . SNAs and other supportstaff attend training organised by serviceproviders, family support organisationsor other groups. FL
Mary Cullen, Lámh Project Manager (with contribution from Eleanor Stanton,Lámh Tutor)
For more information about Lámh seewww.lamh.org or contact Mary Cullen,Lámh Project Manager, Lámh DevelopmentOffice, Innovation Centre, Carlow I.T.,Kilkenny Rd, Carlow 059-9139657.
References:Beukelman, D. and Mirenda, P. 2005
Augmentative and alternativecommunication: Supporting childrenand adults with complexcommunication needs. Baltimore MD,Paul H. Brookes.
ISAAC, International Society forAugmentative and AlternativeCommunication website, www.isaac-online.org
Locke, P.A. 2000 Quality education forstudents: It’s easier than you think(Centre on Disabilities: Technologyand Persons with DisabilitiesConference 2000) California StateUniversity.
Murphy, J., Marková, I., Collins, S.,McCall, F. and Moodie, E. 1995 Therole of the communication partner inaugmentative and alternativecommunication (AAC), InternationalJournal of Language & CommunicationDisorders 30 (S1), pp. 603-7 (Firstpublished online: 8 Apr 2011)

22 frontline Autumn 2012
Person-centred active support is the key to increasingengagement in meaningful activities and relationships which,is itself, is key to achieving a good quality of liflife. It is very
difficult to grow in independence and experience social inclusion orchoice and control if you never a range of experiences.
In person-centred active support, staff:— See every moment as potential—every activity, task or
interaction at home, at work or in the community is anopportunity for the person being supported to be involved, evenif not for long or if they can only do a small part of the activity.
— Use a ‘little and often’ approach, working at the pace of theindividual and keeping tasks and support simple,
— Provide just the right amount of help and support for eachindividual in each activity, and
— Maximise choice and control for the person they support.
There are two fundamental components to making sure activesupport is implemented. Organisations need to ensure that staffboth have the skills to use person-centred active support and aremotivated to work in this way. In terms of ensuring staff have theskills to do person-centred active support, training is the key andresearch has shown that both classroom-based training and hands-on training are essential.
The Nurse and Midwifery Planning and Development unit(NMPD, Tullamore) recently provided funding support for 11individuals from intellectual disability services in the Midlandsregion to train as trainers in person-centred active support. Theparticipants work in a range of services, including residentialsettings and day services. The first day of the training involved anintroduction to person-centred active support, using worksheets,videos and anecdotes to illustrate the essential components of thesystem. Day Two combined hands-on training with the opportunityfor trainers to observe and think about the feedback they would
PERSON-CENTREDACTIVESUPPORT INIRELANDPerson-centred active support is a way of
supporting people with disabilities which
puts the person at the centre of their own
lives and focuses on enabling and
empowering people to experience a range
of activities both new and familiar, in a wide
range of different contexts, with just enough
help and support so that people grow in
independence, have real choices and control
over their lives and become a valued
member of their community. Julie Beadle-
Brown and Judy Ryan explain.
Hill
cres
t, U
K

23frontline Autumn 2012
give. A number of service user volunteers came to the venueand were supported by the trainers to engage in a range ofactivities, including making their lunch, baking, cleaning etc.Although they had never been to the venue and many ofthem hadn’t met the person supporting them before, theysuccessfully participated and appeared to enjoy themselves.Day Three of the training focused on training and practiceleadership and also allowed participants to discuss some of theissues they thought they might meet curing their training. Keyissues included anticipated resistance from some staff, atendency to care for people and do things for them (ratherthan enabling them to be as independent as possible), theperception that they wouldn’t have time to do active supportbecause they of too much paperwork, lack of opportunitybecause of the size of their service setting, and a lockedkitchen and lack of funding for adapting the environment tomake it accessible. These are similar issues to those raised intraining sessions with staff in almost every organisation acrossthe world.
As noted above, training is only one element ofimplementing person-centred active support within anyorganisation. It is also necessary to identify what motivatesstaff to work the way they do. There are a number of elementsof motivation, all of which have to be considered:— The personal attitudes of staff— The values of management and how these are perceived by
staff—do staff believe that managers think that the quality
of life of the people supported and whether they enablepeople using person-centred active support is the mostimportant element of their work? Is this apparent in allaspects of the organisation?
— The consequences of doing or not doing active support forstaff; do those who are good at enabling people receiverecognition and are those disciplined who do not (even afteradditional training and support)?
If organisations do not pay attention to the motivational contextand the informal culture of the services, it is unlikely thattraining will be as effective as it could be, or perhaps not effectiveat all. However, if both the motivational context and training arein place, then the positive impact on the quality of life of thepeople supported can be extensive. FL
Further readingMansell, J. and Beadle-Brown, J. 2012 Active support: Enabling and
empowering people with intellectual disabilities. London: JessicaKingsley Publishers.
Ashman, B., Ockenden, J., Beadle-Brown, J. and Mansell, J. 2010Person-centred active support: A handbook. Brighton, UK:Pavilion Publishing.
Beadle-Brown, J., Hutchinson, A. and Whelton, B. 2008 A betterlife: The implementation and effect of person-centred activesupport in the Avenues Trust, Tizard Learning Disability Review13 (4), 15-24.
P E R S O N - C E N T R E DP L A N N I N G

24 frontline Autumn 2012
people to distance themselves bothcognitively and emotionally from theirwork. It is the most extensively reportedand researched aspect of burnout.Emotional exhaustion generallyprecipitates the two other documenteddimensions of burnout—depersonalisation and reduced personalachievement. As such, it is useful forservices to monitor and recognise theearliest signs of emotional exhaustion inorder to intervene to prevent burnout.
Depersonalisation represents theinterpersonal dimension of burnout. Itis self-protective initially—an attempt byindividuals to cope with work stress bydistancing themselves from others. Itmanifests itself in a callous or uncaringresponse that often includes a loss ofidealism. This distancing isaccomplished by developing a cynical orindifferent attitude. Depersonalisationdevelops in reaction to emotionalexhaustion.
Reduced personal accomplishmentdenotes the self-evaluation dimension ofburnout. It is characterised by feelings ofreduced productivity and competence.This lowered sense of self-efficacy hasbeen associated with depression and aninability to cope with the demands ofthe job (Maslach and Goldberg 2001).
The Conservation of Resourcesmodel (Hobfall and Shirom 2000)provides a means for understanding the
The main features of burnout arean overwhelming exhaustion,feelings of cynicism, frustration,
anger, failure and ineffectiveness.Burnout negatively affects bothpersonal and social functioning. It isassociated with absenteeism, intentionto leave the job and actual employeeturnover. Burnout results in reducedemployee satisfaction and reducedquality of care for service users. Rose,Jones, and Fletcher (1998) reported thatstaff exhibiting higher levels of stresshave been observed to undertake fewerpositive interactions with service users.
Measuring and monitoring staffburnoutThe predominant measure of burnoutin research and clinical diagnosis is theMaslach Burnout Inventory HumanServices Survey (MBI-HSS; Maslach andJackson 1981.) This measure assessesburnout through three dimensions:emotional exhaustion,depersonalisation and reduced personalaccomplishment.
Emotional exhaustion representsthe basic stress dimension of burnout.Features associated with this dimensionare emotional over-extension, negativeaffect, lack of energy and a perceptionthat one’s emotional resources havebeen depleted. Exhaustion is not justan experience or emotion; it may lead
process through which burnoutoccurs. This theory posits thatindividuals endeavour to obtain, retainand protect things they value (termed‘resources’). These include materialresources such as money, personalresources such as self-esteem,condition resources such as socialsupport, and status and energyresources such as credit, knowledge.Stress arises from actual or potentialloss of resources. Resources are linked,thus loss of one resource leads tofurther loss. A loss of confidence inmanaging stressful situations at workmay impact on self-esteem, which mayimpact on reputation or perceivedstatus as an employee. This cycle isreferred to as a loss cycle and it helpsto explain the links between the threedimensions of burnout posited byMaslach. The opposite also holds—anincrease in resources leads to a gaincycle; mastery of a task at work leadsto increase in self esteem, feelings ofaccomplishment and status as a valuedemployee. This theory suggests thatservices should be actively working topromote resource gain to prevent theprocess of burnout.
Maslach advocated examiningburnout in the person-organisationcontext. Maslach identifies six areaswhere a person-job mismatch canbecome apparent:
STAFF COPING AND BURNOUT ININTELLECTUAL DISABILITY SERVICES
Burnout can be described as a prolongedresponse to chronic interpersonal and emotionalstressors in the work environment. Staff burnoutis considered an occupational hazard in people-oriented professions and it is commonlyreported amongst frontline staff working inintellectual disability services. In this article SileMurphy and Claude Watters provide anoverview of measures to prevent staff burnout,and potential interventions for staff withinintellectual disability services who areexperiencing burnout. The role of staffattributions within the context of challengingbehaviour will be examined.
B U R N O U T

25frontline Autumn 2012
Howard, Rose and Levenson (2009)compared groups of staff who worked ina direct supportive capacity in medium-secure units and community settingswith adults with intellectual disabilities.All staff in the medium-secure settingreceived training in managingaggressive behaviours, as opposed toonly eight staff in the communitysetting. Although staff in the medium-secure setting were exposed toconsiderably more incidents ofchallenging behaviour, they reportedlower levels of fear and higher levels ofself-efficacy than community staff. Asimilar finding from Chung and Corbett(1998) was that staff working withpeople with intellectual disabilitiesreported lack of training as a cause ofstress.
Other forms of training such asemotion-focused interventions havealso demonstrated some beneficialresults. There is some evidence reportedfor the efficacy of interventions basedon cognitive behaviour therapy (CBT),acceptance and commitment therapy(ACT) and mindfulness approaches toenhance staff coping responses andpreventing burnout. CBT is a problem-focused coping strategy that addressesdysfunctional emotions, behaviours andcognitions through goal-orientated,systematic processes. Problem-focusedstrategies identify and alleviate thestressors giving rise to the strain. CBTattempts to teach people to bettercontrol their thoughts and feelings.Gardner et al. (2005) found that CBTand a behavioural coping model wereshown to be effective in reducing workrelated stress.
Acceptance and commitmenttherapy (ACT) is an emotion-focusedcoping strategy that targets undesirablethoughts and emotions aroused by workstressors. It encourages people to live inaccordance with their values and tocontact the present moment withopenness and acceptance. ACT attemptsto teach people to notice and acceptunpleasant or difficult thoughts andfeelings without trying to change them.
Noone and Hastings (2010) reportedsome positive findings through theirPACT (Promotion of Acceptance inCarers and Teachers) workshop. Theone-and-a-half day PACT workshop isbased on the core principles ofacceptance and commitment therapy.Thirty-four staff were provided withinformation on stress and well-beingbefore and after their PACT workshops.
1) Work overload—the most obvious, iswhere job demands surpass humancapabilities
2) Lack of control—employees do nothave scope to innovate, customise orimprove. This results in lowering ofself-efficacy or not feelingresponsible for outcomes in work
3) Insufficient rewards—deficiencies ofeither external (salary) or internal(sense of accomplishment) on thejob
4) Breakdown of community—peoplegetting isolated in work, orunresolved conflict with otherpeople in employment
5) Absence of fairness—inequity in payor work load or promotions handledinappropriately 6) Value conflict—people feeling constrained to dothings they feel are unethical or thatgo against their own set of values.
The most frequently reported workstressor among disability support staff ischallenging behaviour among serviceusers (Jenkins et al. 1997, Hastings2002). Emerson et al. (1987) definedchallenging behaviour as ‘culturallyabnormal behaviour of such intensity,frequency or duration that the physicalsafety of the person or others is placedin serious jeopardy, or behaviour whichis likely to seriously limit or deny accessto the use of ordinary communityfacilities’. Although challengingbehaviour is a known work stressor, therelationship between challengingbehaviour and burnout is unclear. Somestudies indicate a relationship (e.g. Millsand Rose 2011), and some find norelationship (e.g. Mutkins, Brown andThorsteinsson 2011). There is someresearch that suggests that it is not thelevel of the challenging behaviourwhich impacts on staff stress, but theway that such behaviour is viewed bystaff (Phillips and Rose 2012).
Dilworth, Philips, Rose and Factors(2011) reported that staff consideredphysically aggressive behaviours asbeing more under the control of theindividual than self-injurious behaviour;thus physically aggressive behaviourswere associated with more negativeemotions experienced by staff.
These results point to a role for stafftraining with regard to challengingbehaviour. Psycho-education regardingthe function of the behaviour mayimpact on staff attributions and mayhelp reduce negative emotionsexperienced by staff.
A control group of six staff alsocompleted the measures over a six-weekperiod. Two-thirds of participants hadimproved well-being scores, asmeasured by the General HealthQuestionnaire (GHQ-12). Staffperceptions of work stressors (measuredby the Staff Stressor Questionnaire(SSQ)) did not lower significantly overthe same time period. These resultssuggest that the ACT strategies did nothave a direct impact on levels of workstress, but rather that they influencedthe manner in which individuals copedwith this stress.
Singh and colleagues havedeveloped a mindfulness skills-trainingprogramme for staff, incorporating theuse of meditation exercises. Mindfulnessapproaches involve a non-judgementalawareness of the present moment(Kabat-Zinn 2003). Benefits reportedinclude a reduction in use of physicalrestraints and medications (Singh et al.2009), levels of aggression (Singh etal.2006) and increased levels ofhappiness among service users withprofound multiple disabilities (Singh etal. 2004).
This brief review has discussed therisk of staff burnout amongst frontlineworkers who provide supports toindividuals with intellectual disabilities,particularly amongst staff supportingindividuals with challenging behaviour.We have described ways of measuringand preventing staff burnout byproviding positive work environmentswith cognisance taken of the person-jobmatch. Finally, we have presented thefindings of promising research on theprovision of staff training and supportusing mindfulness, cognitivebehavioural therapy and acceptanceand commitment therapy principlesthat may offer means of improving staffwell-being and the quality of carereceived by service users. FL
Sile Murphy is a psychologist in clinicaltraining with the National University ofIreland, Galway. Sile completed herintellectual disability placement with theMuiriosa Foundation at Moore Abbey in2012.
Claude Watters studied psychology inTrinity College Dublin and graduated in2011. Claude has been working in avoluntary capacity with the clinicalpsychology team at the MuiriosaFoundation, Moore Abbey since 2011.

26 frontline Autumn 2012
Angelman Syndrome is a rare genetic condition that bearsthe name of the British paediatrician who described threechildren who presented with characteristic features in the
1960s. Affected individuals show developmental delay, intellectualdisability, have (practically) no spoken words and an exuberant,contagiously happy temperament, smiling nearly all the time andlaughing a lot, tending to stick out their tongue, and loving to playwith water with wanton enjoyment. They may also have epilepsy,as well as various problems with coordinating their movements,and their EEG (brainwave recording) often shows recognisablepatterns. Angelman Syndrome is due to lack of expression of agene called UBE3A in brain cells. Although the condition is geneticin origin, it usually occurs in unrelated individuals rather, than inseveral members of a family. The UBE3A gene was known beforescientists suspected its implication in Angelman Syndrome. A fewof its functions have been described, but more remain to bediscovered. It is not well understood how the genetic defect leadsto abnormalities in brain maturation, control of movements,organisation of intelligence, problems of speech or of sleep,epilepsy and the peculiar behaviour. Current hypotheses relate tovarious processes underlying the way brain cells communicatewith each other.
The medical genetics of Angelman Syndrome is particularlycomplex. In all our cells, we have two copies of the UBE3A gene:one is passed on to us from our mother and the other one fromour father. In brain cells, the UBE3A gene is normally expressedonly from the copy inherited from the mother, while the copyfrom the father remains (virtually) silent. This is because just nextto UBE3A, there is a control centre which acts as a DO NOT READ!signal. On the maternal chromosome, this control centre isdeactivated (by a chemical process called methylation). As a result,the DO NOT READ! signal is not produced and UBE3A can beeffectively expressed.
A N G E L M A NS Y N D R O M E
PROMISINGTHERAPEUTIC AVENUESFOR ANGELMANSYNDROME
Left: Cartoon illustrating the molecular classes that underlie AngelmanSyndrome. ((c) Christyan Fox 2012). Chromosome 15 inherited from themother is represented by a woman, the one inherited from the father bya man. One Way sign indicates expression of UBE3A allele. Dead End signindicates allele inactivation. Roadworks sign indicates gene deletion ormutation. Right turn sign indicates activation of silent allele. (1) In thetypical situation, the chromosome 15 inherited from the mother carriesan epigenetic signal enabling UBE3A gene expression whereas thepaternal allele is inactive. (2) In case of deletion or mutation of thematernal copy, this cannot be expressed while the paternal allele isinactive as in the typical situation. (3) In case of imprinting defect, bothalleles are inactive. (5) Promoting the expression of the paternal allelemight be a promising therapeutic avenue.
Bernard Dan explains the symptoms of AngelmanSyndrome and explores possible therapies.

27frontline Autumn 2012
Different mechanisms may prevent normal expression ofthe UBE3A gene and thus cause Angelman Syndrome, asillustrated in the cartoon by Christyan Fox, who is the father ofa boy with Angelman Syndrome. There may be a deletion or amutation of the maternal copy of UBE3A. More rarely, theproblem is the absence of the imprinting that marks thechromosome inherited from the mother, as such. This is called‘imprinting defect’: the methylation pattern that should blockthe DO NOT READ! signal of the control centre is not there, sothe UBE3A gene cannot be read. Or the whole chromosomethat should be inherited from the mother is absent and theindividual has two copies of this chromosome from the father,both with silenced UBE3A: this is referred to as paternal‘uniparental disomy’. All these mechanisms prevent expressionof the UBE3A gene, either because the gene itself is abnormal(deletion or mutation), or because it cannot be read becausethere is no methylation inactivating the DO NOT READ! signal(imprinting defect or uniparental disomy). Thus, they all resultin Angelman Syndrome, but the severity of the manifestationsmay vary according to the underlying mechanism. Forexample, intellectual disability, speech problems and epilepsytend to be less severe in individuals with imprinting defect oruniparental disomy, than in those with a deletion of amutation.
Seeing these variations in severity according to the geneticmechanism, some scientists have thought that there mayactually be a very weak expression of the intact copy of theUBE3A gene, despite the presence of the silencing DO NOTREAD! signal.
Thanks to genetic engineering approaches, labs can‘produce’ mice with the genetic defect and study selectedaspects of their functioning, hoping that it is representativeenough of that of humans with Angelman Syndrome. In fact,mice tolerate the genetic abnormality much better thanpeople, and it is not easy (if at all possible) to tell thegenetically modified mice from the normal ones with thenaked eye. These mouse models of Angelman Syndrome havehelped us understand fine neurological abnormalities, usingmouse-adapted tests for problem-solving, for movementcoordination and recordings of various parts of the brain. Theyhave also allowed much progress in the understanding ofinteraction between genes and the effect of the gene defect atmany microscopic levels. A number of teams worldwide(including our own) are involved in various aspects of thisresearch. In the last few years, there have been more and moreencouraging results. Recently, the team led by Ed Weeberfound improvements in the electrical functioning of the brainand in motor performance of a mouse model, followingadministration of a specific antibiotic. These results still needto be confirmed and it is currently not clear how the drugworks. Still, a study is currently being carried out in humanswith Angelman Syndrome.
Since 2000, several teams of researchers have attempted tofind ways to promote the expression of the copy of UBE3Awhich is intact, but non-functional because of this silencingsignal without much success until a recent breakthrough. Ateam led by Ben Philpot and Marky Zylka tested more than2000 drugs in mice in order to see if some of them couldactivate the paternal copy of UBE3A. They found that selectedanticancer drugs and, in particular, one called topotecan, canunsilence this copy of the gene in the mice they studied bydisrupting the DO NOT READ! signal. In human medicalpractice, topotecan is used for its toxicity, in order to kill cancer
cells. This may have great implications for developing newstrategies of pharmacological management of AngelmanSyndrome, alhough a lot of questions need to be answeredbefore we know if and how these early results in animalexperiments can impact individuals with AngelmanSyndrome. This process, which has brought about greatsuccesses in many fields, is typical of medical science: withdue respect for ethics, and in the patients’ best interest, it mustfollow a sound, stepwise road. And results obtained inAngelman Syndrome may prove useful for a wide range ofneurodevelopmental genetic disorders.
Current understanding which founds developmentalmedicine and much of child neurology emphasises theimportance of maturational factors, experience-driven brainplasticity and the notion of critical periods that occursequentially in a hierarchical order in embryonic, fetal andearly postnatal life. Plasticity can imply windows ofopportunity for optimising developmental trajectories asaimed for in ‘early intervention’ programmes, but it isconstrained by these critical periods to a large extent.Therefore, there is currently no indication thatneurodevelopmental genetic disorders might be cured byrestoring normal gene expression, replacing or otherwiseinterfering with gene product, or bypassing the mutationaltogether, as we do not know (yet) how we could allowunconstrained brain plasticity to take place. The perspectivemight change when we gain better understanding of the rolethe concerned genes on brain development and function.
The diagnosis of Angelman Syndrome is often made late inthe history of brain development: at the earliest in infants andin most individuals in older children. It must also be borne inmind that it wouldn’t be correct to interpret as a cure theimprovement or even normalisation of selected, specificaspects of the neurological functioning of animal models ofAngelman Syndrome. Nevertheless, results from animalstudies are likely to lead to the development of treatments thataim to improve how individuals with Angelman Syndromeuse their own potential. Meanwhile, efforts into improvingmanagement need to rest very largely on improvingphysiological or adaptive functioning, with a view tosymptomatic relief and on individually-tailored habilitationprogrammes aimed at optimising development, quality of lifeand participation. Validated guidelines for clinicalmanagement of individuals with Angelman Syndrome,developed by an international, multidisciplinary groups(including the mum of young man with AngelmanSyndrome), are available from the Dyscerne website(http://www.dyscerne.org/dysc/digitalAssets/0/263_Angelman_Guidelines.pdf ). FL
Bernard Dan is the head of the Department ofNeurology at the Children’s Hospital inBrussels, Belgium, and Professor ofNeurophysiology and DevelopmentalNeurology at the Université Libre de Bruxelles.He has been involved in clinical and basicresearch on Angelman Syndrome, published atextbook on this condition (Mac Keith Press2008), but he also wrote an award-winningnovel, Le livre de Joseph (Aube 2001).

28 frontline Autumn 2012
If your child has a disability, being ableto get services and supports shouldn’tdepend on where you live or the nature
of your child’s needs.Disability services for children have a
long history in Ireland and manyorganisations provide excellent support forchildren and their families. They have ahigh level of expertise and family-centredinterdisciplinary teams, with nearlyeverything provided in one location. Thisis unlike the fractured way services aredelivered in some other countries, whichcan involve families travelling to manydifferent centres to get the services theirchild needs.
However, because services in Irelandhave developed independently and maylook after only one specific group ofchildren who have a particular disability,there is wide variation in the servicesavailable in different parts of the countryand for different categories of disability.For instance, there may be a service forchildren with an intellectual disability inyour locality, but none for children with aphysical disability or with autism. As aconsequence, some children and theirfamilies have little or no access to services.
We need a more equitable andconsistent way to provide services forchildren with disabilities and must work
together to achieve the greatest benefitpossible within our resources.
A national programme is changingthe way services are provided across thecountry. It is based on therecommendations of the Report of theNational Reference Group onMultidisciplinary Services for Childrenaged 5-18 Years (available on the HSEwebsite (http://www.hse.ie/eng/services/Publications/services/Disability/DisabilityServices)).
The organisation of services in thefutureMany children with delays indevelopment will be able to have theirneeds met by their local Primary Careservices (public health nurse, communityspeech and language therapy, familydoctor, community physiotherapy etc).Early intervention and school-agedisability teams in each Network areawill provide a more specialised service forthose children who require it (a Healthand Social Care Network is an area with apopulation of approximately 50,000).
As the Primary Care and Networkteams will be looking after children witha wide range of difficulties, they need tobe supported by specialist services infields requiring a high level of expertise.
Examples of these areas are high-techassistive technology and programmes formanaging challenging behaviour. Thespecialist services will be involved inconsultation on individual children andtraining, as well as providing directintervention with children whenneeded.
How will this be different? Instead ofhaving separate services in an area forchildren with learning disability orphysical disability or autism, all childrenwho need a team disability service willhave access to their local earlyintervention or school age team. Thismeans that health professionals andparents, instead of trying to find theirway through a maze of services, willknow where a child should be referred.Importantly our aim is that no familywill be left without a service.
How is the programme beingorganised? A National Co-ordinatingGroup, with representatives of disabilityorganisations, parents, the HSE, and theDepartments of Health and Education, isleading, monitoring and guiding theprogramme. There are regional leads andlocal leads for the programme across thecountry (see panel for names of RegionalLeads if you want to find out about yourlocal area and how to get involved).
C H A N G ECaroline Canton makes theargument for a nationalprogramme of change inchildren’s disability services.
A NATIONAL PROGRAMME OF CHANGEIN CHILDREN’S DISABILITY SERVICES

29frontline Autumn 2012
Local Implementation GroupsIn local areas (based usually on LocalHealth Office boundaries though not inall cases) the local leads have broughttogether representatives from services andparents, to see how current services canbe reorganised to achieve this improvedstructure. This includes finding out whatis currently available for children withdisabilities, planning how best to usethese resources and making surethroughout that there is goodconsultation and communication.Because there will be guidance anddirection from the national level of theproject, local areas will have support andassistance and there will be a consistentapproach throughout the country.
Other InitiativesAs this is a national programme ofchange in the way children’s disabilityservices are delivered, it is offering usopportunities to look more widely atgeneral issues in the way we supportchildren with disabilities and theirfamilies. The National CoordinatingGroup has formed national workinggroups to look at specific areas. Membersof the working groups include parents,representatives of the professional bodiesand others bringing specific expertise.They also are consulting widely to drawon as much real experience as possible.
Health and EducationHealth services, schools and parents needto develop closer working relationships sothat, together, they can ensure thatchildren with disabilities make the mostof their education. Parents deserve issuesconcerning the development of theirchildren to be addressed in a holistic
manner and not as two separate ‘health’and ‘education’ components. The sectorsare separately organised and their task isto make sure that parents can’t see thejoin! Representatives of education areinvolved in this programme at all levelsand this is seen as an invaluableopportunity to advance a co-ordinatedapproach.
Learning from experienceHealth services in some areas, such as inthe mid-west, north-east and west of thecountry, had already come together a fewyears ago and changed to provide unifiedservices. While in each case they say thatthe change took effort, commitment andpersistence and that more still needs to bedone, they have found it has resulted in amuch improved way of providingaccessible comprehensive services whichaddress the needs of all children withdisabilities. Here are some of thecomments from parents with childrenattending the Limerick Early InterventionService where there are now teams whoeach provide services for all childrenwithin a Network area:
‘My child has benefited enormously fromthe services he has received from the EarlyIntervention Centre, which includedPhysiotherapy, Early Intervention andSpeech and Language therapy.’‘It’s great that a team is available andknows your situation before any session sothat you don’t spend more timeexplaining everything again.’‘Everything happened very quickly andthat was a relief.’
Comment from staff of Meath Children’sDisability Services which is for all childrenof school age who require a team serviceregardless of their disability:
‘Moving from having a specialist caseload(e.g. only working with children withautism) to a more mixed one was not asdifficult as we thought it would be, andstaff retention has actually improvedmarkedly because working with childrenwho have varied needs is less stressful andmore rewarding.’
These experiences of staff and parents willbe of great assistance to others as theyplan what needs to be done and how togo about it in their own local area.
What stage has the programmereached?Because of the way services havedeveloped, each part of the country iscoming from varying situations and
therefore at differing stages. The localimplementation groups have been giventhe objective under the HSE NationalService Plan 2012 of agreeing this yeartheir plan for change. This will includean agreement on the principles servicesshould work to, and governancestructures, policies and procedures forservices. Each group is currently workingto this end.
It is expected that the wholeprogramme will take a couple of years tocomplete. It is very important that it iscarefully planned and implemented withfull consultation and information for allconcerned. Limited resources are ofcourse an issue and it may take a longtime to achieve a comprehensive servicestructure throughout the country.However if we have the vision of wherewe want to be and get the structuresright, we can build on firm foundations.
The vision for when theprogramme is completed� One clear pathway to services for all
children with disabilities according toneed.
� Effective teams working inpartnership with parents.
� Resources used to the greatest benefitfor all children and families.
� Health and education workingtogether to support children toachieve their potential. FL
www.hseland.ie (This is the HSE’s Learningand Development website which is open forall to enrol, not just HSE staff. There is awealth of information and written materialof interest on this site, including theProgressing Disability Services for Children &Young People programme. When you haveenrolled go to Practice and DevelopmentHubs, then click on the Change Hub. On thetop line you will see ReconfigurationResources, click on that and open ProgressingChildren’s Disability Services. You will findthe key documents such as the Report of theReference Group on MultidisciplinaryServices for Children and guidelines as theyare issued, plus an extensive library ofexisting service documents and relevantarticles.
REGIONAL LEADS FOR THEPROGRAMME
South: (Kerry, Cork, Waterford, Wexford,Carlow, Kilkenny, South Tipperary) Aisling Lenihan: [email protected]
West: (Donegal, Sligo, Leitrim, WestCavan, Roscommon, Mayo, Galway,Clare, Limerick).
North: (Tipperary) Gerard Tully: [email protected]
Dublin Mid Leinster: (Dublin south ofthe Liffey, Wicklow, Kildare, Laois, Offaly,Longford, Westmeath) Bernie Nyhan: [email protected]
Dublin North East: (Dublin north of theLiffey, Meath, Louth, Cavan, Monaghan)Anne Melly: [email protected]
Caroline Cantan is a social worker byprofession and is Clinical Co-ordinator ofEnable Ireland Children’s Services inTallaght in Dublin. She is NationalProgramme Co-ordinator for theProgressing Disability Services forChildren & Young People programme.

30 frontline Autumn 2012
Lost opportunities for people with intellectualdisability in institutional care settings
The institutionalisation of people with intellectual disability in Irelandduring the twentieth century was at the time considered a helpfulresponse that would improve the lives of people with intellectualdisability and their families. Institutions provided a regime of care thatmet basic biological needs in a secluded, self-sufficient environmentthat perpetuated itself. For the individual with intellectual disability therewere many missed opportunities for self-determination and communityparticipation. Donal Fitzsimons explains how the introduction ofperson-centred plans (PCPs) into disability services in recent timesbrought with it an assumption that the PCP was robust enough tosafeguard against the deleterious effects of life in congregate settings.
Arecent study, ‘A case studyanalysis of person-centred planningfor people with intellectual
disabilities following their transfer frominstitutional care’, examined the lives often individuals with intellectualdisability who were removed from theirfamilies, taken into institutional careand later transferred to live in houses inthe community. The researchconsidered the perspective from threesources: the person with intellectualdisability, their family member andtheir key worker. For many of theseindividuals the priority was that theywere removed from family homes andcared for in hospital settings where theywere nourished and medicated. Theywere subjected to the austere andconforming regimes of institutionalcare. Opportunities for learning wererestricted to what could be taught inspecial segregated settings, oftenwithout application to their everydaylife. This study found that there weremany missed opportunities for theperson with intellectual disability tolearn the life skills necessary to have anindependent life of their own making(see Table 1).
Armed with this knowledge, it isimportant that when we considereducation for people with intellectualdisability it is essential to also create aculture of learning experiences thatpromotes their dignity, while at thesame time preparing them for lifeindependence.
Case studyThe following excerpts from a detailedcase study of Teresa (pseudonym),illustrate how vulnerable people’s lives are:
Teresa was born prematurely in themid-1960s and weighed less than threepounds. This low birth weight placed herat risk of developmental delay. She livedwith her father and mother in their smallhome situated on the outskirts of a rural
village. Teresa’s case notes indicate thather parents had 12 children. When shewas three years of age she was placed ina large children’s ward, of the localpsychiatric hospital. She was placedthere because, according to her mother,she was ‘completely unmanageable athome’. When Teresa was six years ofage, she was moved to a specialresidential and education centre under
C H A N G E
TABLE 1: THE LEGACY OF INSTITUTIONAL CARE AND PRACTICESAND LOST OPPORTUNITIES FOR EDUCATION
Person with intellectual disability— Alienation from family, mainstream education & community life – antithesis of
normalisation.— A loss of personhood & control of their lives.— Relinquished to patient status.— Acquiescence.— Loss of confidence and self esteem.— Restricted to the menu of special services.— At the mercy of staff that are paid to be with them.
Family members of the person with intellectual disability— No control in their family member being taken into care. — Years later it is assumed that they can re-engage in the person’s life. This leads
to confusion, anxiety and fear.— The concern that if they display any confidence that they will be expected to
engage in direct care.— Afraid to complain or really say what they think.— Deference to staff.
Key worker for the person with intellectual disability— Attitude of ownership to people in state care.— Institutional practices persist in community houses.— Institutional hierarchy of conflicting roles.

31frontline Autumn 2012
the care of an order of nuns. She wasreported as doing ‘reasonably well’ inspecial school, acquiring very basicacademic skills. During this period from1971 to 1983 she did not have thebenefit of normal family life.
When Teresa graduated from ‘specialschool’ it was envisaged that she wouldattend a residential rehabilitationprogramme. However, this did nottranspire due to her unwillingness to goto yet another residential facility. Teresareturned to live at home with herfamily. Teresa reported that she was veryhappy during this stage of her life. It isnoted that she displayed someadjustment difficulties at home whichtook the form of temper tantrums andacting out aggressively towards others.As a result of these behaviours, Teresa’sparents sought an out-of-homeplacement for her. Teresa was admittedto a large residential centre for peoplewith intellectual disabilities in 1985.Shortly after her admission to thecentre, her mother passed away. Someten years later her father died, thusmaking it increasingly unlikely thatTeresa would ever return home. Her lifebecame inextricably bound to theformal intellectual disability serviceprovision.
In the large residential centre whereTeresa resided there were manyinstitutional practices, such asdormitory style accommodation, centralmeal preparation and central laundry.Residents were expected to conform.There were set unit meal times, wakingtimes, bed times, shared leisureactivities such as viewing the sametelevision programme, going for walksand communal personal hygienepractices. Teresa, while in the largeresidential centre, made threeallegations of an abusive nature. Whenreflecting on her past life she remarked:
‘I have lived in three institutions and Ididn’t like any of them, you would haveto share dormitories and I didn’t likethe food, you didn’t get out much andthere was nothing to do other than domessages for the staff.’
After about a year living in thisresidential centre, Teresa was removedto a group home in the area. Teresamoved with women that she had beenresiding with in the large residentialcentre. Because of the move Teresa nowhad her own bedroom, participated inmeal preparation, and her lifestyle wasmore conventional. She was also given a
day placement in the occupationaltherapy unit in the psychiatric hospitalwhere she had resided as a child,working in supported employment inthe laundry. Initially Teresa got on wellin her community residence, but wasfrequently returned to the largeresidential centre in response to ‘badbehaviour’.
Teresa currently resides in acommunity residence, approximatelyfour miles on the outskirts of a largetown. She attends a day service in thistown on four days per week and anactivation unit in another part of thetown for the fifth day. Teresa reportsthat she is now happy in this house andalso with her day service. During herday programme Teresa reported that sheengages in many activities such as arttherapy, reflexology, communityinclusion including going for coffee,shopping, using local amenities such asthe swimming pool, church or cinema.
Teresa stated that she has feelings ofnot being listened to, of her voice nothaving power, views of others beingtaken as fact whilst her views arediscredited in her eyes. When one asksTeresa ‘how are you, Teresa?’ she willreply ‘the staff say I’m very good’ or forinstance it is noted that she is in goodform, she is likely to reply ‘the tabletsare working’ or ‘I went to the doctorand he told me the tablets are working’.This study found that a commonfeature of institutionalisation was thatthe person with intellectual disabilityrelinquishes control and responsibilityfor their own lives and has an over-reliance on medical and nursingopinions.
When Teresa is treated unfairly in apunitive manner she is more likely toengage in acting-out behaviours and thather reputation as ‘difficult’ is fulfilled.Teresa, like many people with intellectualdisability, is often seen as being in a stateof ‘eternal childhood’ and is treated withstrategies reminiscent of the past wherechildren were punished when they wereperceived as being ‘bold’. Moreenlightened protocols around positivebehaviour supports can be found inTeresa’s care plan so that she can besupported to have a more self-determined lifestyle rather than withinthe more restrictive and punitivebehaviour management strategies of thepast. Teresa does not see herself as beingtrustworthy or having ordinaryentitlements such as a key to her ownfront door. She states ‘I might lose it.’Her leisure pursuits are restricted to‘special’ events. These include attendingthe local Special Olympics and themonthly parents and friends disco forpeople with intellectual disability.
When asked if she participated inbuying groceries for the house she stated‘Well, we shop online using the internetfor groceries.’ When probed about herparticipation in this activity she stated‘no I can’t use a computer. I am not thatgood at it. I think the staff do it. Thefood is delivered to the house. It is agreat service.’ When Teresa was asked ifshe participated in preparing andcooking meals in the house she replied:
‘The care assistants do that. We don’t gonear it because we are not allowed gonear the cooker, we’re not let. I wouldhelp to serve out the dinner but I am notallowed near the cooker.’

32 frontline Autumn 2012
When Teresa was asked whether sheparticipated in doing her own laundry,she replied:
‘Well if I was shown how to use it and ifI got it started, I wouldn’t mind learning.I do help by clearing up the table,emptying the dishwasher, bring theclothes off the line, sweep the floor andset the table, things like that.’
Teresa attributes her current level ofhappiness to the successful role ofmedication and to her care plan. Shestates ‘the key worker says the care plan isworking’ and ‘the doctor says themedication is doing its job.’ Teresa spokeof herself in an objective way, forexample, stating ‘takes me’ and‘handover’ about herself. She continuallyspoke of herself in the third person. Shereferred to her peers as ‘clients’ and statesthat when she goes on holiday ‘anotherclient goes with me.’ When planningseasonal breaks she describes herself asbeing at the mercy of her sisters to ‘take’her home. She describes her brothers ashaving ‘no interest in my life.’
Teresa also commented that while sheis currently happy in her house, she doesfeel insecure. She attributes this to beingmoved many times withoutconsultation—even in the recent past sheleft her community residence onemorning to be brought by the staff to adifferent house. This was done tofacilitate another service user who wasterminally ill. She said:
‘Well, I had to move to another house thereason being was that another residentwas sick. You see they needed a singleroom for him and I had to give him myroom. I didn’t mind, but sure what couldI do. I had no choice.’
Teresa described being moved without herknowledge as ‘very upsetting’; however,Teresa made the comment that she is now‘very happy with her life.’
Teresa’s sister perceived Teresa as nowhaving a ‘wonderful life’. She emphasisedthe importance of ‘dignity and respect forpeople with intellectual disability’. Shestated that Teresa ‘does not like being
spoken down to and that this causes herto get stressed’. She alluded to anothercommunity placement where Teresa wasunhappy. She was moved there withouther knowing to free up a room. Thiscaused great distress in her life and shebelieved that her sister was ‘heading for abreakdown. She was on anti-depressantsand was suicidal. I live in fear that theywill do that to her again.’
Teresa’s sister points out that Teresa’slifestyle is not very person-centred in thatTeresa lacks any real choice in her dailyactivities. She had some reservations withregard to Teresa’s level of activity. Shedoesn’t think that she should be toldwhat to do. She stated that Teresa is ‘toldto do art, but if she is not in the mood todo art, it doesn’t matter, she still has to doit.’ She remarked that in the past, beingsent back to the large residential centrewhen Teresa became difficult, was ‘notvery professional.’ She articulated again,however, a sense of reservation about‘saying too much’ because of anunderlying fear that following anycriticism ‘I would be told to take her out’,implying that she would have theresponsibility for Teresa’s care if she wascritical of the quality of her currentservice provision.
ConclusionIn summary, this study confirms theimperative of learning from theinstitutional legacy of the past and themodel of care that exists today. Ithighlights the importance of looking ateach person with intellectual disabilityindividually. If Teresa had been given thesupports that she required to learn in herown home in her own locality, perhapsher life skills would have developed whereshe would have been a contributingmember of her community. It isimportant to view education as a lifelongopportunity to learn, rather than beingrestricted to a classroom setting. Mansellet al. (2009), in their work on person-centred active supports, illustrate theimportance of every moment as anopportunity to learn. By ‘doing’ withpeople and giving them the active
supports they require, people withintellectual disability are enabled to becapable of full community participation.
If society has the courage to learnfrom people like Teresa, it would equipvarious stakeholders such as policymakers, government departments, serviceproviders and families with theunderstanding that institutional practicesclearly have limitations that continue tothe present day. The desired future iswhere people with intellectual disabilitywill be seen as individuals, with allstakeholders having a sharedunderstanding and vision in the capacityof the person with intellectual disabilityto lead full and active lives in an inclusivesociety that is not defined by, orsegregated by, their disability. In keepingwith the spirit of New directions (2012)and Time to move on from congregatedsettings (2011), the imperative is to look atindividuals with intellectual disability‘one person at a time’, in order to turn‘lost opportunities’ into occasions forlifelong learning. FL
ReferencesFitzsimons, D. 2012 A case study analysis
of person-ventred-planning for peoplewith intellectual disabilities followingtheir transfer from institutional care.Unpublished PhD thesis. TrinityCollege Dublin.
Health Service Executive 2012 Newdirections: Review of HSE day servicesand implementation plan 2012-2016.Dublin.
Health Service Executive 2011 Time tomove on from congregated settings: Astrategy for community inclusion.Dublin.
Mansell, J, Beadle Brown, J., Ashman, B.and Ockendon, J. 2009 Person-centredactive support. Brighton, UK: PavilionPublishing.
It is important to view education as a lifelong opportunity tolearn, rather than being restricted to a classroom setting ... By ‘doing’ with people and giving them the active supportsthey require, people with intellectual disability are enabled tobe capable of full community participation.
C H A N G E
Donal Fitzsimons qualified as an RNID in1992. He graduated with a BA (hons) inhealthcare management from AthloneInstitute of Technology in 2003 andgraduated with an MBA from CoventryUniversity. Donal has submitted his PhDthesis to Trinity College Dublin entitled‘An evaluation of Person-Centred-Planning for people with intellectualdisabilities following their transfer frominstitutional care’. He has held clinical andmanagerial positions in Ireland andabroad. He is currently employed by theHSE and holds the position of Manager ofDisability Services with responsibility forLongford, Westmeath, Laois and Offaly.

33frontline Autumn 2012
Everyone experiences pain at sometime or another—a headache, a soreback or a sprained muscle are normal
experiences—but in most cases, the painsettles and disappears in hours or days, oroccasionally after a few weeks. However,some people experience pain that is alwayspresent. Chronic pain is defined as painthat lasts for at least three months and isthere all the time or almost all the time.While many people are born with physicalconditions or disabilities that cause pain,others may develop pain at any stage oftheir lives, from childhood to old age. Thismay be as a result of an accident or injury,the effects of the body aging (the joints canbecome painful as we age), or pain maydevelop spontaneously—in the absence of aspecific injury to the body. In some cases,chronic pain can last for years and evendecades or can be present for the entirety ofa person’s life.
Chronic pain poses a major healthburden, with an estimated 19% ofEuropeans affected. A recent study carriedout at the Centre for Pain Research atNational University of Ireland, Galway,found that almost one-third of peoplesurveyed had chronic pain. The PRIMEStudy (Prevalence, Impact and Cost ofChronic Non-Cancer Pain in Ireland) alsoestimated that pain costs around €4bn peryear, when medical treatments, hospitalvisits, medication, loss of employment andsocial welfare payments are taken intoaccount. Clearly, chronic pain is a verysignificant health problem in Ireland, as itis throughout the rest of the world.
There has, however, existed a long-standing belief that people with anintellectual disability may be insensitive topain, or at least that they have a higherthreshold for pain than the generalpopulation. Consequently, people with anintellectual disability have usually beenexcluded from the study of chronic pain.The idea that people with an intellectualdisability are incapable of either painsensation or expression has been recognisedas unfounded, resulting in an increasedinterest in the extent of pain problems
among this group and in the challengesindividuals with an intellectual disabilityexperience in expressing their pain. It isnow recognised that the experience of painfor people with an intellectual disability isno different from that of the generalpopulation, although pain might beexpressed differently in people who cannotcommunicate verbally or whose vocabularyfor describing pain is not as well developedas it is for others.
In order to understand the extent ofthe problem of chronic pain in people withan intellectual disability, researchers at NUIGalway have conducted two studies ofchronic pain by asking caregivers (family orpaid care staff) to describe whether theperson they care for may have chronicpain. These studies were published in TheJournal of Intellectual Disability (McGuire,Daly and Smyth 2009), based on a surveyof around 150 people. A second largerstudy was published in the medical journalPain (Walsh, Morrison and McGuire 2011),after a survey of 2000 carers, of whom 750replied. Overall, the studies found thataround 15% of people with an intellectualdisability were reported by their carers tohave chronic pain. The researchers notedthat this was considerably less than the33% identified in the general population inthe PRIME study. They concluded thatchronic pain in people with an intellectualdisability may be ‘under-recognised andunder-treated’. Those reported to havechronic pain had symptoms for an averageof 6.3 years. More females were reported toexperience chronic pain than males,although age, communication ability andlevel of intellectual disability were not anydifferent in those with and without pain.However, the presence of pain was morelikely in people with cerebral palsy,physical disability and reports ofchallenging behaviour. A sizeable portionof those with chronic pain also experiencedlimitations in daily living; over 78% ofcarers reported that the service user hadbecome upset or distressed by pain. Over80% were receiving some form oftreatment for their pain, with most seeing a
family doctor, rather than a specialist,and using over-the-counter pain killers asthe primary form of pain treatment.Hardly any of those with pain wereattending a specialist pain clinic or takingprescribed medications. The resultsoverall indicated that chronic pain is asignificant problem for people with anintellectual disability, with a proportionof service users living with daily pain formany years and experiencing limitationsin daily functioning, emotional well-being and quality of life.
In the general population, newapproaches to pain management aredeveloping. As well as using medicationand physical therapies to manage pain,most treatment centres now offerpsychological approaches to painmanagement, which can be veryeffective. However, hardly any of thepeople in the surveys were seeing apsychologist for help with painmanagement. A clinical psychologist inNUI Galway, Sharon McManus, did herresearch thesis on the use of a successfulpsychological treatment for chronic paincalled cognitive therapy. The researchersfound that the treatment was of somehelp to people with an intellectualdisability in teaching pain managementcoping skills. The results of the study willbe published soon in The Journal ofIntellectual Disability Research. Theapproaches used have been developedinto a book called Feeling better publishedby Pavilion Press in the UK. The book iswritten for carers of people with anintellectual disability and providespractical advice and strategies for helpingpeople with an intellectual disability whohave chronic pain.
The researchers at NUI Galway arecarrying out more studies in this area.They have started a study to see if youngwomen with menstrual pain can behelped to develop pain managementstrategies and they also plan to ask peoplewith an intellectual disability themselvesabout their own experience of pain in astudy later this year. FL
THE PROBLEM OF CHRONICPAIN IN PEOPLE WITH ANINTELLECTUAL DISABILITYBrian Maguire reports on the high incidence of peoplewith ID living with chronic pain.

34 frontline Autumn 2012
— Mealtime routine—small groups withfamiliar peers sitting at table as ameans to model behaviour, inclusionand sociability. Eating at table (familyall together) is actively encouraged.Consideration to seating comfort andheight to maximise vision and accessto the food. ‘Own place’ for sense ofsecurity and routine is also addressed.
— Consideration to the child’s likes anddislikes in terms of favourite colour,themed cutlery and crockery areimportant.
— Small portion size on plate todiscourage over-eating, over filling ofmouth and for visual acceptability
— Engagement of the child in groceryshopping and healthy food choices,with the aim to create anticipationand enjoyment of meals.
— Making gradual food changes, e.g.gradually thickening, changingtexture, and increasing variety.
— Awareness of the child’s hunger cuesand not insisting on a ‘clean plate’approach. Even babies who turnaway from the breast/bottle sendsignals that they are full.
FUNWITHFOOD
The goal of the committee was to promotea positive and enjoyable healthy eatingexperience for those with foodbehavioural issues. Emphasis was placedon supporting each child’s individualneeds by developing tailored eating plans
General intervention strategiesThe committee kept in mind recognisedbest-practice intervention strategies,which included:— Oral play activities known to have
potential in developing oral processingand oral awareness in a non-threatening manner. Activitiesinvolved sessions on blowing bubbles,blowing out cheeks, blowing musicalinstruments, funny facial expressionswith emphasis on mouth gesturing,cheek and chin massage, kissingnoises.
— Creation of a positive, calm andrelaxed atmosphere
— Contingent positive reinforcement(preferred foods contingent onconsumption of refused foods).
Non-edible rewards, e.g. a favouriteactivity/toy and praise.
Many children with autism havebehavioural issues relating tofood, diet and healthy eating.
These include: — Self-restricted diet— Avoidance of unfamiliar foods— Food preference according to visual
appearance (colour, shape)— Difficulty with sensory processing
(avoidance of particulartastes/textures)
— Difficulty with oral motor control
Particular eating patterns— fear of contamination (foods
touching on plate)— crumbling food before putting in
mouth— hand/ fingers in mouth while
chewing— overfilling mouth.
With these considerations in mind, a‘Fun with Food Committee’ wasestablished with representatives fromvarious disciplines—nursing, social care,school staff, speech and languagetherapy, play therapy and the head chef.
Karen Mings examinesbehavioural problems forchildren with autism relatingto food and suggests funand rewarding methods toresolve these issues.
B E H A V I O U R

35frontline Autumn 2012
— Provide opportunity for food playand exploration using the handsoutside of mealtimes.
— Make scrapbook/poster—‘foods I likeand foods I would like to try’
— Social stories and visual cues.
St Paul’s therapeutic interventioninvolves:— A positive fun approach with
individual eating plan— A team and parent partnership
approach with clear channels ofcommunication (communicationbook, food diaries)
— Intervention strategies planned,implemented, monitored andprogress evaluated monthly.
Case History 1—JohnJohn is a six-year-old boy who exhibitsselectivity and rigidity in food choices,avoiding new and unfamiliar foods anddisplaying a preference for foodsaccording to colour and texture. Hechooses to eat dry crunchy food itemsover that of ‘wet’ sloppy foods. He is avery active boy and can maintain focusfor a very short period of time. Sitting atthe table for any length of time presentsa challenge to him.
Intervention strategies� Sensory sessions—floor-time food
exploration where the child wasencouraged to handle, play with andtaste ‘wet’ food textures, e.g. ricepudding, custard, yogurt, bakedbeans, mashed banana, meltedchocolate, gravy with mashedpotatoes/vegetables.
� Floor-time sessions to introduce newfoods (taste or texture) outside ofmealtimes. Small pieces of the newfood were used and randomly placed,encouraging the child to self-selectthe new food.
� Over time the new foods wereintroduced as part of the meal with asmall amount mixed in with afavourite food. Exposure to one newfood or food texture needed tohappen at least twelve times, in orderto achieve familiarity andacceptance. Reward and praise wereessential for each step in touching ortasting.
� At mealtimes, one designated personsupported the child. A therapeutic‘weighted vest’ helped to ground andsteady him and improved correctsitting position at the table. Atherapy lumpy ‘slip-proof’ cushion
was useful to discourage deliberatesliding to the floor. PECS, as visualcues, helped focus on eating anddrinking and also encouraged him torequest and make food choices.
While tasting and accepting ‘new’ foodsis slow, John is making good progresseating more sloppy wet food textures. Henow sits at the table with two peers andremains seated for longer periods.Mealtimes are calm, with the child keptfully engaged using PECS to indicatefood choices. When finished, Johnbrings his plate to the sink, establishingclosure to his mealtime.
Case History 2. JaneJane is a five-year-old girl who exhibitssensory difficulties around food texture.She prefers her dinner almost pureedand is hesitant to chew and swallowmore solid food items. She crumblesfood on her plate or against her mouth,using her fingers. Jane doesn’t recognisewhen her mouth is full and tends tooverfill it, with a risk of choking.
Intervention strategies� Auto-motor preparation, which
involvew gentle pressure andmassage of her cheeks, mouth andchin, overseen by an occupationaltherapist
� ‘Dry’ and ‘messy’ play sessions.Initially Jane was allowed to weargloves. Over time the glove fingerswere cut off, and ultimatelyremoved.
� Floor-time food ‘texture’ explorationsessions were outside of mealtimes.
� ‘Chewellery’—involving differentchew material/textures on a key ring
� At mealtimes one designated personundertook hand-over-handassistance initially, with the use ofthe fork/spoon. Praise for appropriateeating proved very effective ‘Nicechewing!’
� Jane was encouraged to keep herhands away from her face, whichdiscouraged her putting her fingersin her mouth or crumbling food.Food consistency towards firmer,solid foods was increased, e.g. 20%lumpy/solid and 80% mashed, then30% lumpy food, etc. Smallmanageable portions were put onher plate and guidance was given asto the appropriate amount of foodon the (small) spoon or fork, whichavoided spillage and over filling ofher mouth. The use of PECS at the
table provided opportunities tocommunicate and slow down eating.
� Praise was given when the food waseaten and closure was established forJane when she removed herbib/apron and brought her plate tothe sink. She was rewarded with afavourite activity/treat afterwards, tohelp reinforce the desired behaviour.
Jane has progressed with the level oftexture tolerated, which has beenaugmented by allowing her to mash alittle of the food herself, using a fork.Overall progress is reported with Jane nolonger overfilling or putting her fingersin or around her mouth to crumble thefood.
The ‘Fun with Food Committee’ isdedicated to supporting and workingalongside parents in understanding andovercoming the fears and challengesexperienced by their child relating tofood and eating. The committeecontinues to develop and embrace newstrategies in supporting the needs of thechild. FL
Recommended books:McCurtin, A. 2007 The fun with food
programme, Victoria, Australia:Speechmark.
Winstock, A. 2005, Eating and drinkingdifficulties in children. Victoria,Australia, Speechmark.
Karen Mingsgraduated from UCDin 1984 with anhonours degree inEnglish & History andHigher Diploma in
Education. She has worked in St Paul’sService for children with Autism since1986 in the role of Houseparent /Childcare Leader. Ms Mings has muchexperience working as part of a multi-disciplinary team in St Paul’s Serviceincluding Residential & Respite care, StPaul’s Special School, Community Houseliving & Early Intervention therapeuticservice. Working in partnership withparents she has developed andimplemented individual interventionprogrammes to maximise potential inthe areas of socialisation, daily livingskills, communication & independencefor service users ranging in age from 4–18 years old.

36 frontline Autumn 2012
In the 1980s, nurse tutors working inwhat were known at the time asschools of nursing attached to eight
services, formed the ‘Nurse TeachersGroup’. However, given thedevelopment in nurse education andtraining and the move to third-leveleducation in 2002, the group needed to
Development of Nursing andMidwifery, after a successful applicationfor funding was made by the steeringgroup.
The workshop took place at AllHallows’ College, Dublin, on 8December 2009, with activities entitled(1) Design a Person and (2) Describeyour Person. The first activity involvedsmall groups thinking about humanbeings, their hopes, dreams, fears andfantasies and the reality of living with adisability. Arts and crafts materials wereused to illustrate their vision. Theactivity enabled the participants to‘design’ an intellectual disability nursewho would be fit for purpose for thenext fifty years. The second activityrequired participants to concentrate onbuilding ‘the best nurse to get the bestresults for [the] person’. The aspectsidentified as important for this futurenurse were: person-centredness, arights-based approach, qualitystandards, multi- and inter-disciplinarycollaboration and social inclusion. Oneof the produts of the day can be seen inPicture 1, where the group designed anddescribed the person.
Evaluation forms were distributed toall participants and a total of 28 werereturned on the day. The participantswere asked in five questions to rate theirlevel of happiness, and the very positiveresponses are shown in Figure 1.
consider its future. In 2007 it wasdecided that the group shouldcontinue, but with a new shape andfocus. This new focus opened the doorfor representation from not only theeducation institutes, but also frompractice areas and intellectual disabilityservices. The result is the formation ofthe Nursing Network in IntellectualDisability Ireland (NNIDI). The networkwas developed by a steering group,comprising representatives from thethird-level sector, service providers,practice development teams andprofessional development units. Theoverall aim and objectives of NNIDIinclude promoting an intellectualdisability network in Ireland andfacilitating events that would supportnetworking in intellectual disabilitynursing in ireland. As 2009 saw the50th anniversary of the establishment ofintellectual disability nursing inIreland, the group decided to mark theoccasion by running a uniquecelebratory event, Intellectual DisabilityNursing – Towards the Future. This was ahalf-day workshop for people with anintellectual disability (service users),nurses, nursing students and carers. Itwas facilitated by Helen Laverty, anurse teacher/health lecturer workingin the University of Nottingham. Theevent was supported by the NationalCouncil for the Professional
DEVELOPING SUPPORT FORINTELLECTUAL DISABILITY PRACTICE:Nursing Network In Disabilities Ireland (NNIDI)
Owen Doody and Therese Danaher trace the formation ofNursing Network in Disabilities Ireland.
Picture 1

37frontline Autumn 2012
Also in 2010, the steering group ofNNIDI worked to expand itsmembership with key personnel inservices and education across thecountry. This resulted in thirteensteering group members who meet in2011 with a view to consolidating theaims and objectives of NNIDI andidentifying ways of achieving them.The following was agreed:
Aim: To promote and support networkingin the field of intellectual disability inIreland.
Objectives:— To promote an intellectual
disability nurses network inIreland.
— To develop local/regional networksin order to build capacity fornetworking.
— To support the nursing network inintellectual disability, Irelandthrough organising or faciliatingoccasional events.
— To contribute to national forumsand circulate webpage links topromote awareness of bothnational and strategic policydocuments relevant to intellectualdisability.
— To review this initiative in 2013.
Terms of references— To actively promote the
engagement of persons with theNNIDI (online and through
Overall the event went well andparticipants reported a high level ofsatisfaction with the event in theevaluation forms. As a spin off of the2009 Intellectual Disability Nursing –Towards the Future workshop,information was gathered and thefeedback forms were used to develop aposter (Picture 2) which was presentedat the National Network of LearningDisability Nurses’ National NetworkConference, 2010 (Reasonable Adjustmentto Care: From Rhetoric to Reality), whichwas held at the University of York.
services and professionalorganisations).
— To develop a ‘resource bank’ ofinformation pertinent to issuesconcerning intellectual disabilitypeople in Ireland (e.g. policydocuments, website list, care issuesetc).
— To identify a link/lead person onspecific subject areas (e.g. epilepsy,mental health, ageing, health needsetc).
— To organise or facilitate an eventthat promotes issues relevant topersons with intellectual disabilityor their carers.
— To produce an annual report of theNNIDI activities (available on webor distributed).
It is envisaged that networking will be acornerstone of future activities anddevelopment for intellectual disabilitynurses and it is this belief that has beenthe motivation for this initiative. Themembers of the NNIDI welcome you tospread the word of our existence,recommend us to a colleague and linkin with our service as often as possible.Through networking we can link withpeople of similar interest and makecontact with those with whom we maylearn or gain support. For furtherinformation, please [email protected] or log onto the group’swebsite http://www.nnidi.com. Wewould also like to draw attention to ourNNIDI Conference on Wednesday 26September 2012 in Dr. Steeven’sHopsital Dublin. This event will bringpeople from professional, academic andpolitical arenas together to discuss thevision for intellectual disability nursingin Ireland now and into the future. FL
Owen Doody, Lecturerin IntellectualDisability Nursing,Department of Nursingand Midwifery,University of [email protected]
Therese Danaher,Lecturer in IntellectualDisability Nursing,School of Nursing andHuman Sciences,Dublin City [email protected]
Figure 1: Quantitative Responses
Picture 2
N U R S I N GN E T W O R K

38 frontline Autumn 2012
R E A D I N G
THE STAR BOOK CLUB
suitable venue was somewhat time-consuming as our chosen venueneeded to be on board with our idea,wheelchair friendly and quiet enoughfor us to hear each other readingaloud. We found all of these traits inStarbucks in Blanchardstown, wherethe staff’s enthusiasm and kindnessmade our book club even moreenjoyable. (We would like to say ahuge thank you to them.)
Although we arrived prepared eachweek, we came across obstacles such asthe attendance of book club membersand the time commitment requiredfrom both staff and service users.Other difficulties included preparationof materials for the meetings becauseof limited access to the internet,printing and laminating services.
The books we chose were all fromthe Open Door Series (New IslandBooks) a collection written by wellknown authors for adults with literacydifficulties. These books work well, asthere are plenty of topics to choosefrom, and they are generally eight toten chapters long, allowing us tocomplete a book per term. These bookswere easily adapted for our serviceusers who had lower literacy levelsthan others; this included usingpictures and objects as supports, aswell as identifying and defining keywords and storylines. The bookschosen also provided scope foractivities during our book club, such asidentifying the bridges of Dublin fromBullet and the Ark (Sheridan 2008), and
There are many challenges atpresent to be faced working inhealth care in Ireland, in
particular the barriers that both staffand service users face with currentcutbacks and limited resourceprovisions. In the face of thesechallenges it is important to becreative and innovative in order toprovide services that best meet theneeds of those service users that wework with and, in turn, maximisetheir potential. With this in mind,the Book Club in St Vincent’s Centrewas founded just over a year ago andwas a result of several disciplinescoming together in shared expertise.
The idea first came from ourlibrarian, Grace Hillis, andcommunity nurse, Jane O’Connell,after they discovered a book entitledThe next chapter book club (Fish andRabidoux 2009) which detailed aninclusive and dynamic model forcreating a book club to suit peoplewith intellectual disabilities. Theattraction of The Next Chapter BookClub was that there was a particularemphasis on communityparticipation and involvement, anidea we felt echoed the sentiments ofthe HSE report New directions (HSE2012), which called for a ‘blurring ofboundaries between “special” and“mainstream” services’. By creating acommunity-based book club for ourservice users we would be able to takea ‘mainstream’ idea and combine itwith the goals of our service users.Essentially, the creation of a bookclub would be multifaceted; not onlywould we be addressing personalobjectives such as literacy, but therewould be opportunities to focus oncommunication, interaction andsocial involvement. Essentially, thebook club gave both service users andstaff the opportunity to engage in anexciting and interesting venture thatwe hoped would positively impactthe quality of service being provided,as well as the quality of life of theservice users.
Through a group effort frommembers of the multidisciplinaryteam, staff and service users, our StarBook Club was formed! Finding a
a bus tour around Dublin city followingOld money, new money (Sheridan 2000).
On reflecting after the first bookclub, feedback was overwhelminglypositive, viewing it a worthwhileventure for service users and staff alike.This resulted in the formation of asecond book club for service usersliving in a different community area, aswell as the continuation of the firstbook club. From our experiences of thefirst book club, we were then able toprovide training to other staff membersso that they could also run book clubsindependently. Although theorganisation and running required a lotof time and effort from service usersand staff, we felt the gains in socialinteractions and literacy definitelyjustified the work involved. We wouldhighly recommend others to followsuit! (and we would welcome anycomments or queries.) FL
Rachel Gorman & Olive Gormley Speechand Language Therapy Department’Daughters of Charity, [email protected]@docservice.ie
ReferencesHealth Service Executive. (2012). New
Directions Review of HSE Day Servicesand Implementation Plan 2012 –2016. Dublin. HSE
Fish, T & Rabidoux, P. (2009). NextChapter Book Club. Bethesda.Woodbine House Inc.
Sheridan, P. (2000). Old Money, NewMoney. Dublin. New Island
Sheridan, P. (2008). Bullet and the Ark.Dublin. New Island.

39frontline Autumn 2012
This seminar will consider some of the key issues in working with children, adolescents and adults with intellectual disabilities who have sexually harmful behaviours or sexually offend.
This seminar will focus on:
Safeguarding
Speakers:
Disability Psychotherapy Ireland with the Institute of Psychotherapy and Disability
and Respond announce
‘Forensic Disabilities’
45.00€

To subscribe, please emailFrontline [email protected] fill in the form across andsend to:
Unit C2The SteelworksFoley StreetDublin 1
Frontline has been published since1989 and deals with issues of interestto frontline workers, those with alearning disability and their families.
ANNUAL SUBSCRIPTION RATES (2012)
Individuals: €26.00
Parents Associations and Schools: €50.00
Organisations (service units) and Libraries: €95.00* * Organisations will receive two copies of each issue plus back-issue access online
Additional magazine copies available at these annual rates: 1: €20.00 2: €40.00 3: €50.00 5: €80.00 10: €140.00
Payment DetailsCheque Postal Order/Draft
Order Form
Name:
Address:
Tel:
Email:
Please provide email address
Renewal New Subscription
�
Bank Transfer (EFT)Pay directly to Frontline Magazine Ltd:AIB, 52 Upper Baggot Street, Dublin 4A/c no: 19596030Bank sort code 93-10-63
F R O N T L I N ESubscribe to
F R O N T L I N E




















