
Frequency of elevated Hepatocellular Carcinoma (HCC) biomarkers in patients with advanced hepatitis...
10
CLINICAL ADVANCES IN LIVER, PANCREAS, AND BILIARY TRACT Des--Carboxy Prothrombin and -Fetoprotein as Biomarkers for the Early Detection of Hepatocellular Carcinoma ANNA S. LOK,* RICHARD K. STERLING, ‡ JAMES E. EVERHART, § ELIZABETH C. WRIGHT, § JOHN C. HOEFS, ¶ ADRIAN M. DI BISCEGLIE, # TIMOTHY R. MORGAN, ¶, ** HAE–YOUNG KIM, ‡‡ WILLIAM M. LEE, §§ HERBERT L. BONKOVSKY, ,¶¶ JULES L. DIENSTAG, ## and the HALT-C Trial Group *Division of Gastroenterology, University of Michigan Medical Center, Ann Arbor, Michigan; ‡ Hepatology Section, Virginia Commonwealth University Medical Center, Richmond, Virginia; § Division of Digestive Diseases and Nutrition, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Department of Health and Human Services, Bethesda, Maryland, ¶ Division of Gastroenterology, University of California-Irvine, Irvine, California; # Division of Gastroenterology and Hepatology, Saint Louis University School of Medicine, St. Louis, Missouri; **Gastroenterology Service, VA Long Beach Healthcare System, Long Beach, California; ‡‡ New England Research Institutes, Watertown, Massachusetts; §§ Division of Digestive and Liver Diseases, University of Texas Southwestern Medical Center, Dallas, Texas; Department of Medicine and ¶¶ Department of Molecular and Structural Biology and The Liver-Biliary-Pancreatic Center, University of Connecticut Health Center, Farmington, Connecticut; and ## Gastrointestinal Unit (Medical Services), Massachusetts General Hospital and the Department of Medicine, Harvard Medical School, Boston, Massachusetts See related articles, Miura H on page xxiv, Miyahara K et al on page e17, and Singal AK et al on page 192 in CGH. BACKGROUND & AIMS: The outcome of patients with hepatocellular carcinoma (HCC) remains poor because of late diagnosis. The aim of this study was to compare the accuracy of -fetoprotein (AFP) and des--carboxy pro- thrombin (DCP) in the early diagnosis of HCC. METH- ODS: Among 1031 patients randomized in the Hepatitis C Antiviral Long-term Treatment Against Cirrhosis (HALT-C) Trial, a nested case-control study of 39 HCC cases (24 early stage) and 77 matched controls was conducted to compare the performance of AFP and DCP. Testing was performed on sera from 12 months prior (month 12) to the time of HCC diagnosis (month 0). RESULTS: The sensitivity and specificity of DCP at month 0 was 74% and 86%, respec- tively, at a cutoff of 40 mAU/mL and 43% and 100%, respectively, at a cutoff of 150 mAU/mL. The sensitivity and specificity of AFP at month 0 was 61% and 81% at a cutoff of 20 ng/mL and 22% and 100% at a cutoff of 200 ng/mL. At month 12, the sensitivity and specificity at the low cutoff was 43% and 94%, respectively, for DCP and 47% and 75%, respectively, for AFP. Combining both markers in- creased the sensitivity to 91% at month 0 and 73% at month 12, but the specificity decreased to 74% and 71%, respec- tively. Diagnosis of early HCC was triggered by surveillance ultrasound in 14, doubling of AFP in 5, and combination of tests in 5 patients. CONCLUSIONS: Biomarkers are needed to complement ultrasound in the detection of early HCC, but neither DCP nor AFP is optimal. View this article’s video abstract at www.gastrojournal.org H epatocellular carcinoma (HCC) is the sixth most common malignancy and the third most com- mon cause of cancer-related death worldwide. 1 The incidence of HCC in the United States is increasing and is largely attributed to hepatitis C. 2 Whereas the survival of patients with most malignancies has im- proved over the last decade, 5-year survival of patients with HCC has remained less than 10%. 3 The poor outcome of patients with HCC is related to the late detection, with more than two thirds of patients diag- nosed at advanced stages of disease. 4 Cirrhosis of any cause and chronic infection with hepatitis B virus (HBV) or hepatitis C virus (HCV) are the most com- mon risk factors for HCC. 5 Thus, surveillance of pop- ulations at-risk may detect tumors at an early stage when curative interventions can be implemented. Sev- eral studies reported a benefit of HCC surveillance on survival, 6,7 and guidelines from professional organiza- tions recommend HCC surveillance for at-risk popula- tions. 5,8 A major problem with HCC surveillance is the lack of reliable biomarkers. -Fetoprotein (AFP) is the most widely used biomarker for HCC surveillance; however, not all HCCs secrete AFP. Furthermore, AFP may be elevated in patients with chronic liver disease in the absence of HCC. The low sensitivity and specificity of Abbreviations used in this paper: AFP, -fetoprotein; AUROC, area under receiver operating characteristic curve; CT, computed tomogra- phy; DCP, des--carboxy prothrombin; HALT-C, Hepatitis C Antiviral Long-term Treatment Against Cirrhosis; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; MRI, magnetic resonance imaging. © 2010 by the AGA Institute 0016-5085/10/$36.00 doi:10.1053/j.gastro.2009.10.031 CLINICAL ADVANCES IN LIVER, PANCREAS, AND BILIARY TRACT GASTROENTEROLOGY 2010;138:493–502
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Frequency of elevated Hepatocellular Carcinoma (HCC) biomarkers in patients with advanced hepatitis...

CA
DE
AAH
*RDGLMCM
BhlatOATstoHstrsoAc7c1tutne
V
LIN
ICA
LA
DV
AN
CES
LIV
ER,PA
NCREA
S,N
DBIL
IARY
TRA
CT
GASTROENTEROLOGY 2010;138:493–502
LINICAL ADVANCES IN LIVER, PANCREAS,ND BILIARY TRACT
es-�-Carboxy Prothrombin and �-Fetoprotein as Biomarkers for thearly Detection of Hepatocellular Carcinoma
NNA S. LOK,* RICHARD K. STERLING,‡ JAMES E. EVERHART,§ ELIZABETH C. WRIGHT,§ JOHN C. HOEFS,¶
DRIAN M. DI BISCEGLIE,# TIMOTHY R. MORGAN,¶,** HAE–YOUNG KIM,‡‡ WILLIAM M. LEE,§§
ERBERT L. BONKOVSKY,� �,¶¶ JULES L. DIENSTAG,## and the HALT-C Trial Group
Division of Gastroenterology, University of Michigan Medical Center, Ann Arbor, Michigan; ‡Hepatology Section, Virginia Commonwealth University Medical Center,ichmond, Virginia; §Division of Digestive Diseases and Nutrition, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health,epartment of Health and Human Services, Bethesda, Maryland, ¶Division of Gastroenterology, University of California-Irvine, Irvine, California; #Division ofastroenterology and Hepatology, Saint Louis University School of Medicine, St. Louis, Missouri; **Gastroenterology Service, VA Long Beach Healthcare System,ong Beach, California; ‡‡New England Research Institutes, Watertown, Massachusetts; §§Division of Digestive and Liver Diseases, University of Texas Southwesternedical Center, Dallas, Texas; � �Department of Medicine and ¶¶Department of Molecular and Structural Biology and The Liver-Biliary-Pancreatic Center, University of
##
onnecticut Health Center, Farmington, Connecticut; and Gastrointestinal Unit (Medical Services), Massachusetts General Hospital and the Department ofedicine, Harvard Medical School, Boston, MassachusettsHmiaspwodnc(muwestt
ownea
upLH
C IN A
See related articles, Miura H on page xxiv,Miyahara K et al on page e17, and Singal AKet al on page 192 in CGH.
ACKGROUND & AIMS: The outcome of patients withepatocellular carcinoma (HCC) remains poor because of
ate diagnosis. The aim of this study was to compare theccuracy of �-fetoprotein (AFP) and des-�-carboxy pro-hrombin (DCP) in the early diagnosis of HCC. METH-
DS: Among 1031 patients randomized in the Hepatitis Cntiviral Long-term Treatment Against Cirrhosis (HALT-C)rial, a nested case-control study of 39 HCC cases (24 early
tage) and 77 matched controls was conducted to comparehe performance of AFP and DCP. Testing was performedn sera from 12 months prior (month �12) to the time ofCC diagnosis (month 0). RESULTS: The sensitivity and
pecificity of DCP at month 0 was 74% and 86%, respec-ively, at a cutoff of 40 mAU/mL and 43% and 100%,espectively, at a cutoff of 150 mAU/mL. The sensitivity andpecificity of AFP at month 0 was 61% and 81% at a cutofff 20 ng/mL and 22% and 100% at a cutoff of 200 ng/mL.t month �12, the sensitivity and specificity at the lowutoff was 43% and 94%, respectively, for DCP and 47% and5%, respectively, for AFP. Combining both markers in-reased the sensitivity to 91% at month 0 and 73% at month2, but the specificity decreased to 74% and 71%, respec-ively. Diagnosis of early HCC was triggered by surveillanceltrasound in 14, doubling of AFP in 5, and combination ofests in 5 patients. CONCLUSIONS: Biomarkers areeeded to complement ultrasound in the detection ofarly HCC, but neither DCP nor AFP is optimal.
iew this article’s video abstract at www.gastrojournal.org
epatocellular carcinoma (HCC) is the sixth mostcommon malignancy and the third most com-
on cause of cancer-related death worldwide.1 Thencidence of HCC in the United States is increasingnd is largely attributed to hepatitis C.2 Whereas theurvival of patients with most malignancies has im-roved over the last decade, 5-year survival of patientsith HCC has remained less than 10%.3 The poorutcome of patients with HCC is related to the lateetection, with more than two thirds of patients diag-osed at advanced stages of disease.4 Cirrhosis of anyause and chronic infection with hepatitis B virusHBV) or hepatitis C virus (HCV) are the most com-
on risk factors for HCC.5 Thus, surveillance of pop-lations at-risk may detect tumors at an early stagehen curative interventions can be implemented. Sev-
ral studies reported a benefit of HCC surveillance onurvival,6,7 and guidelines from professional organiza-ions recommend HCC surveillance for at-risk popula-ions.5,8
A major problem with HCC surveillance is the lackf reliable biomarkers. �-Fetoprotein (AFP) is the mostidely used biomarker for HCC surveillance; however,ot all HCCs secrete AFP. Furthermore, AFP may belevated in patients with chronic liver disease in thebsence of HCC. The low sensitivity and specificity of
Abbreviations used in this paper: AFP, �-fetoprotein; AUROC, areander receiver operating characteristic curve; CT, computed tomogra-hy; DCP, des-�-carboxy prothrombin; HALT-C, Hepatitis C Antiviralong-term Treatment Against Cirrhosis; HCC, hepatocellular carcinoma;CV, hepatitis C virus; MRI, magnetic resonance imaging.
© 2010 by the AGA Institute0016-5085/10/$36.00
doi:10.1053/j.gastro.2009.10.031

AaGaHdob
wDgppidbWl
fHaubiamboTpostrnoomrwipFfai(odDpwu
sarmnhsht
oeserttCUrmtf
pHmiahoi(lactmwtdrrddtfincd
CLIN
ICA
LA
DV
AN
CES
INLIV
ER,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
494 LOK ET AL GASTROENTEROLOGY Vol. 138, No. 2
FP in detecting early HCC led the American Associ-tion for the Study of Liver Diseases (AASLD) Practiceuidelines Committee to recommend that ultrasound
lone (without AFP) be used for HCC surveillance.5
owever, the interpretation of ultrasound is operatorependent and can be difficult in persons who arebese or have underlying cirrhosis. Therefore, reliableiomarkers to complement ultrasound are needed.Des-�-carboxy prothrombin (DCP) has been used
idely in Japan for HCC diagnosis and surveillance.9 –16
CP is an abnormal prothrombin molecule that isenerated as a result of an acquired defect in theosttranslational carboxylation of the prothrombinrecursor in malignant cells; this prothrombin defect
n malignant cells is similar to the deficit in vitamin Keficiency and has been called prothrombin inducedy vitamin K absence.17,18 Experience with DCP inestern countries, particularly the United States, is
imited.To date, most studies on HCC biomarkers have
ocused on the accuracy of these markers at the time ofCC diagnosis. Few studies have included cohorts of
t-risk persons followed prospectively to determine thetility of these markers in detecting early stage HCC,efore clinical manifestations.19 Of note, some studies
ncluded patients with early stage liver disease, who aret low risk of HCC, and, in most studies, the perfor-ance of the biomarkers was assessed by focusing on
aseline values rather than on serial determinationsver time.13,20 –26 The Hepatitis C Antiviral Long-termreatment Against Cirrhosis (HALT-C) Trial enrolledatients with chronic hepatitis C and bridging fibrosisr cirrhosis who failed to respond or to achieve austained virologic response (SVR) to combinationherapy with pegylated interferon (peginterferon) andibavirin. These patients were randomized to mainte-ance therapy with peginterferon alfa-2a 90 �g/weekr to no treatment for 3.5 years.27,28 One of the goalsf the HALT-C Trial was to identify and validate serumarkers for the surveillance of HCC. In an earlier
eport on 1145 patients enrolled in the lead-in phase,e observed that baseline AFP levels were �20 ng/mL
n 16.6% of patients and were significantly higher inatients with cirrhosis, in women, and black patients.29
urthermore, AFP levels decreased during peginter-eron and ribavirin treatment. The aims of the currentnalysis were to (1) compare the impact of demograph-cs and liver histology on baseline AFP and DCP values,2) compare the effect of maintenance peginterferonn changes in AFP and DCP values during the ran-omized study, (3) determine the accuracy of AFP andCP in the detection of HCC during a 12-montheriod before HCC diagnosis, and (4) determinehether an increase in AFP or a suspicious nodule on
ltrasound occurred earlier in the HCC cases. oPatients and MethodsHALT-C Trial Design, HCC Definition,and SurveillanceThe design of the HALT-C Trial has been de-
cribed previously.27,28 All patients were required to haven ultrasound, computed tomography (CT), or magneticesonance imaging (MRI) with no evidence of hepatic
ass lesions suspicious for HCC and a serum AFP �200g/mL prior to enrollment (except for 3 patients whoad AFP values of 206, 212, and 315 ng/mL). Liver biopsypecimens were reviewed in conference by a panel of 12epatic pathologists, who used the Ishak scoring systemo stage fibrosis (0 – 6).30
Patients were seen every 3 months during the 3.5 yearsf the randomized trial. Blood samples were collected atach visit for subsequent research testing including as-ays for HCC biomarkers. AFP levels at enrollment andvery 3 months were tested at the local clinical laborato-ies. DCP levels at enrollment and during follow-up wereested on all patients with an enzyme immunoassay (pro-hrombin induced by vitamin K absence [PIVKA II]; Eisaiompany, Tokyo, Japan) in a central laboratory at theniversity of Michigan. Ultrasound examinations were
epeated 6 months after enrollment and again every 12onths. Patients with an elevated or rising AFP and
hose with new lesions on ultrasound were evaluatedurther by CT or MRI.
Two definitions of HCC were adopted as describedreviously, 1 for “definite” HCC and 1 for “presumed”CC.31 Definite HCC was defined by histologic confir-ation or a new mass lesion on imaging with AFP levels
ncreasing to �1000 ng/mL. Presumed HCC was defineds a new mass lesion on ultrasound in the absence ofistology and AFP �1000 ng/mL in conjunction with 1f the following characteristics: (1) 2 liver imaging stud-
es showing a mass lesion with characteristics of HCCarterial enhancement � wash out), (2) progressively en-arging lesion on ultrasound leading to death, or (3) 1dditional imaging study showing a mass lesion withharacteristics of HCC that either increased in size overime or was accompanied by AFP level �200 ng/mL and
ore than tripling of baseline value. All cases of HCCere adjudicated by an outcomes review panel to ascer-
ain that they met predefined diagnostic criteria and toetermine the date when these criteria were first met. Theadiology reports of all HCC cases were retrospectivelyeviewed by the HCC working group to determine theate when the last imaging showed no hepatic lesion, theate when imaging first revealed a suspicious nodule, andhe tumor stage at diagnosis. Early stage HCC was de-ned as a single tumor nodule �3 cm in diameter witho evidence of vascular invasion or metastasis. For eachase, the HCC working group also determined whether aoubling in AFP or a lesion detected on ultrasound
ccurred earlier. A doubling of AFP instead of an abso-
l3bgA
tdFlrimolmHfTcTafi
hcaH
CCvuaectbatsr
iwTif1Ffi
tAscioaaemtl
a(cmswC4iHnHw
wfi(3Smtv1w�st�w3n
CLI
NIC
AL
AD
VA
NCES
INLI
VER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
February 2010 BIOMARKERS FOR EARLY DETECTION OF HCC 495
ute cutoff value was chosen because all patients had-month AFP monitoring; because 19% of patients hadaseline AFP values exceeding 20 ng/mL; and becauseender, race, cirrhosis, and interferon therapy can affectFP values.
Nested Case-Control StudyA nested case-control study was used to compare
he accuracy of AFP and DCP in the detection of HCCuring a 12-month period before the diagnosis of HCC.or this study, all 39 HCC cases (33 definite [32 histo-
ogically confirmed] and 6 presumed) diagnosed betweenandomization and 3.8 years after randomization werencluded. For each case, 2 controls without HCC—
atched for treatment assignment, presence of cirrhosisn baseline biopsy, and length of follow-up—were se-
ected. Blood samples at the time of HCC diagnosis andonths �3, �6, �9, and �12 before the diagnosis ofCC from HCC cases and at corresponding time points
rom the matched controls were tested for AFP and DCP.ime 0 for the controls corresponded to the study visitlosest to the time of HCC diagnosis in the matched case.o ensure that the controls did not have subclinical HCCt time 0, only patients who had more than 12 monthsollow-up beyond time 0 with no evidence of HCC werencluded in the matching process.
One control was subsequently excluded because ofigh DCP values related to coumadin use, leaving 77ontrols. DCP values were not available to investigatorsnd, therefore, played no prospective role in diagnosis ofCC in contrast to AFP and ultrasound.
Statistical AnalysesStatistical analyses were performed at the Data
oordinating Center with SAS release 9.1 (SAS Institute,ary, NC). Because of the wide range in AFP and DCPalues, log10 AFP and log10 DCP were used for all analysesnless specified otherwise. Comparisons of baseline AFPnd DCP values according to fibrosis strata, gender, race/thnicity, and age were performed with t test and Wil-oxon rank sum test. The effect of maintenance pegin-erferon treatment on AFP and DCP values was analyzedy comparing changes in these values between year 3.5fter randomization and time of randomization in the 2reatment groups. For this analysis, control patients whoubsequently developed HCC (beyond year 3.8) and thoseeceiving coumadin were excluded.
For the nested case-control study, baseline character-stics of HCC cases and matched controls were comparedith conditional logistic regression for matched pairs.he selected controls were also compared to the remain-
ng non-HCC patients with either a �2 or a t test. Trendsor both AFP and DCP values during specific times in the2 months before the diagnosis of HCC were compared.or patients with missing DCP values because of insuf-
cient stored samples, the mean values before and after ghe missing values (�3 months) were used. Changes inFP and DCP over the 12 months prior to HCC diagno-
is were compared with mixed linear models. For analysesomparing the accuracy of AFP and DCP in differentiat-ng HCC cases from controls, area under the receiverperator characteristic curve (AUROC) was calculated,nd only patients with available values for both markerst the same time point were included. Controls werexcluded if data were not available for their case. Un-atched logistic regression was used to calculate sensi-
ivity, specificity, and ROC curves. A 2-sided significanceevel of 5% was used for all analyses.
ResultsBaseline AFP and DCP Values of AllRandomized PatientsOf the 1050 patients randomized, baseline AFP
nd/or DCP values were not available in 19. Thus, 103198.2%) patients were included in this analysis. Baselineharacteristics of these patients (39 HCC cases, 77atched controls, and 915 other non-HCC patients) are
hown in Table 1. The mean age of these 1031 patientsas 50 years, 29% were women, and 18% were black.irrhosis was present on baseline biopsy specimens in1% of patients. Half (49%) of the patients were random-
zed to maintenance peginterferon. The results of theALT-C Trial showed that low-dose peginterferon hado effect on outcomes including the development ofCC28,31; therefore, patients in the 2 treatment groupsere combined for this analysis.
Impact of Demographics and Liver Histologyon Baseline AFP and DCP ValuesBoth AFP (P � .0001) and DCP (P � .0001) values
ere significantly higher in patients with cirrhosis (Ishakbrosis score, 5 or 6) than in those with bridging fibrosis
Ishak score, 3 or 4). Mean � SD AFP values were 23.6 �6.4 and 13.3 � 22.7 ng/mL (P � .0001), whereas mean �D DCP values were 48.8 � 114.7 and 35.2 � 85.3AU/mL (P � .0001) for patients with cirrhosis and for
hose with bridging fibrosis, respectively. Whereas AFPalues were higher in women than in men (19.6 � 29.7 vs6.7 � 29.5 ng/mL, respectively, P � .0004), DCP valuesere higher in men than in women (44.5 � 115.9 vs 31.825.8 mAU/mL, respectively, P � .002). AFP values were
ignificantly higher in black patients than in white pa-ients (23.1 � 29.4 vs 15.6 � 28.7 ng/mL, respectively, P
.0001), whereas DCP values were significantly higher inhite patients than in black patients (43.9 � 114.6 vs0.2 � 21.9 mAU/mL, respectively, P � .0005). Age hado effect on baseline AFP or DCP values.
Impact of Peginterferon on AFP and DCPValues in Patients With No HCCDuring the randomized phase, mean DCP values
radually increased among both treated and untreated
pitimecptvii1d
a
(ngva
aof2ba�m
T
ND
M
V
L
H
CEM
MNa
b .
CLIN
ICA
LA
DV
AN
CES
INLIV
ER,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
496 LOK ET AL GASTROENTEROLOGY Vol. 138, No. 2
atients but to a similar degree. The mean DCP valuesncreased from 36.6 mAU/mL at the time of randomiza-ion to 53.1 mAU/mL at the end of the 3.5-year random-zed study in the treated patients and from 35.4 to 50.8
AU/mL in the untreated patients (P � .65 for differ-nces of means at the end of the randomized study). Inontrast, mean AFP values remained lower among theatients randomized to receive peginterferon, althoughhe changes in both groups were minor. The mean AFPalues decreased from 17.1 ng/mL at the time of random-zation to 15.7 ng/mL at the end of the randomized studyn the treated patients but increased from 17.1 ng/mL to9.0 ng/mL in the untreated patients (P � .046 forifferences of means at the end of the randomized study).
Case-Control Study on the Accuracy of AFPand DCP in the Diagnosis of HCCThe baseline characteristics of the 39 HCC cases
able 1. Baseline Characteristics of HCC Cases and Controls
HCC cases
o. of patients 39emographicsAge, y 51.9 � 5.6Sex, % female 18Race/ethnicity, %
Non-Hispanic white 62Hispanic 5Black 28Others 5
etabolic factorsBMI (kg/m2) 27.8 � 4.3Diabetes, % 18
iral factorsHCV genotype 1, % 90HCV RNA, log10 IU/mL 6.37 � 0.54
aboratory resultsHemoglobin, g/dL 14.8 � 1.6WBCa � 1000/mm3 4.9 � 1.4Plateletb � 1000/mm3 123 � 51
104 (58–288)Albumin, g/dLa 3.7 � 0.4AST, U/L 123 � 80ALT, U/L 141 � 116Alkaline phosphatase, U/La 131 � 62
119 (50–341)Total bilirubin, mg/dL 0.9 � 0.4INRb 1.08 � 0.08
CC markersAFP, ng/mL 30.7 � 36.9Log10 AFP, ng/mLa 1.25 � 0.44DCP, mAU/mL 55.8 � 54.9Log10 DCP, mAU/mLb 1.6 � 0.34
irrhosis on biopsy, % 56sophageal varices, %b 53aintenance IFN, % 49
edian and range apply to rows for platelet and alkaline phosphatasOTE. Data provided are percentages or means � SD. Median (rangP � .05 for comparisons between HCC cases and matched controlsP � .01 for comparisons between HCC cases and matched controls
nd 77 controls are shown in Table 1. Twenty-four m
61.5%) HCC cases had early tumors at the time of diag-osis. The cases and controls were well matched for age,ender, and race/ethnicity. HCC cases had more ad-anced liver disease and higher baseline DCP (P � .002)nd AFP values than the controls (P � .02).
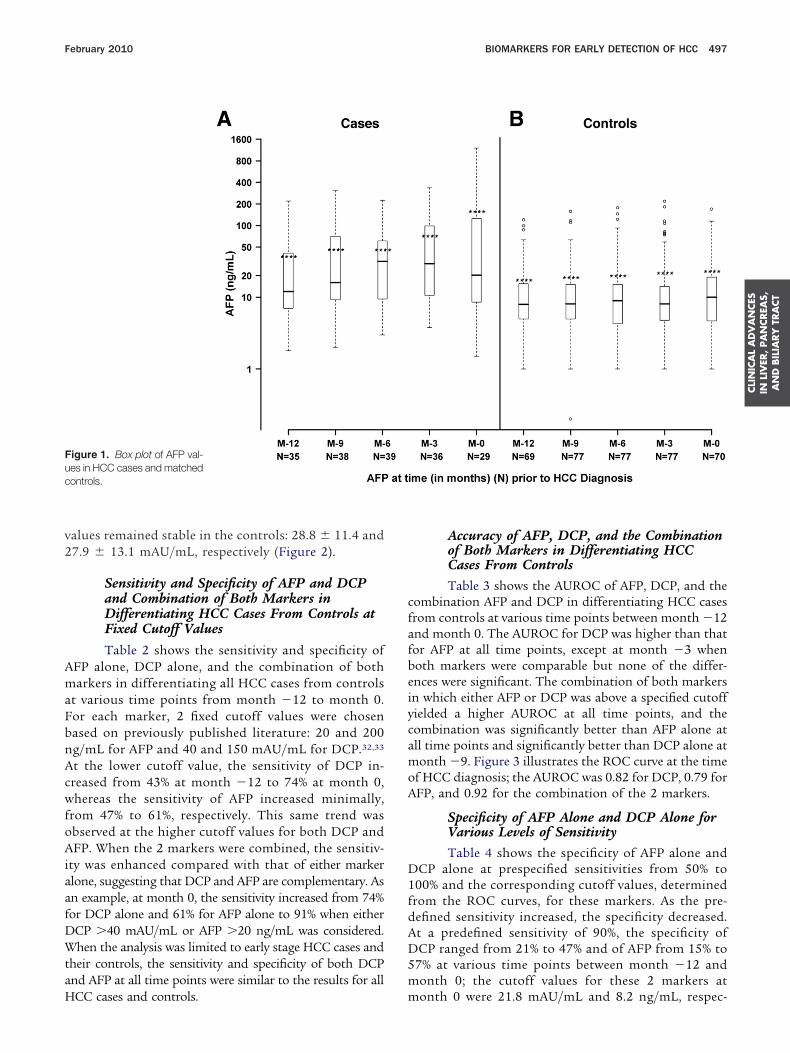
Changes in AFP and DCP Values BetweenMonth �12 and Month 0
Figure 1 displays AFP values in the HCC casesnd controls at months �12, �9, �6, �3, and 0 (timef HCC diagnosis). Mean � SD AFP values increasedrom 37.0 � 51.3 ng/mL at month �12 to 157.6 �96.6 ng/mL at month 0 in the HCC cases (P � .0001)ut remained unchanged in the controls: 17.4 � 25.8nd 23.0 � 34.2 ng/mL, respectively. Similarly, mean
SD DCP values increased from 79.1 � 172.5AU/mL at month �12 to 413.4 � 597.7 mAU/mL at
Matched controls Other non-HCC patients
77 915
51.6 � 8.3 50.0 � 7.125 30
60 736 8
32 161 2
29.4 � 4.7 30.0 � 5.638 23
96 936.44 � 0.6 6.44 � 0.52
14.8 � 1.4 15.0 � 1.45.8 � 1.9 5.8 � 1.9
155 � 54 167 � 67148 (51–331) 162 (39–426)
3.8 � 0.4 3.9 � 0.498 � 68 85 � 56
113 � 74 105 � 76106 � 49 98 � 4492 (48–308) 89 (20–478)0.8 � 0.4 0.8 � 0.4
1.02 � 0.08 1.04 � 0.12
20.4 � 33.3 16.7 � 28.81.02 � 0.47 0.97 � 0.4227.9 � 13.0 41.3 � 103.91.40 � 0.19 1.47 � 0.26
57 3924 2549 49
provided for variables that are not normally distributed.
e.e) is.onth 0 (P � .0001) in the HCC cases, whereas DCP
v2
AmaFbnAcwfoAiaafDWtaH
cfafbeiycamoA
D1fdAD5m
Fuc
CLI
NIC
AL
AD
VA
NCES
INLI
VER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
February 2010 BIOMARKERS FOR EARLY DETECTION OF HCC 497
alues remained stable in the controls: 28.8 � 11.4 and7.9 � 13.1 mAU/mL, respectively (Figure 2).
Sensitivity and Specificity of AFP and DCPand Combination of Both Markers inDifferentiating HCC Cases From Controls atFixed Cutoff Values
Table 2 shows the sensitivity and specificity ofFP alone, DCP alone, and the combination of botharkers in differentiating all HCC cases from controls
t various time points from month �12 to month 0.or each marker, 2 fixed cutoff values were chosenased on previously published literature: 20 and 200g/mL for AFP and 40 and 150 mAU/mL for DCP.32,33
t the lower cutoff value, the sensitivity of DCP in-reased from 43% at month �12 to 74% at month 0,hereas the sensitivity of AFP increased minimally,
rom 47% to 61%, respectively. This same trend wasbserved at the higher cutoff values for both DCP andFP. When the 2 markers were combined, the sensitiv-
ty was enhanced compared with that of either markerlone, suggesting that DCP and AFP are complementary. Asn example, at month 0, the sensitivity increased from 74%or DCP alone and 61% for AFP alone to 91% when eitherCP �40 mAU/mL or AFP �20 ng/mL was considered.hen the analysis was limited to early stage HCC cases and
heir controls, the sensitivity and specificity of both DCPnd AFP at all time points were similar to the results for all
igure 1. Box plot of AFP val-es in HCC cases and matchedontrols.
CC cases and controls. m
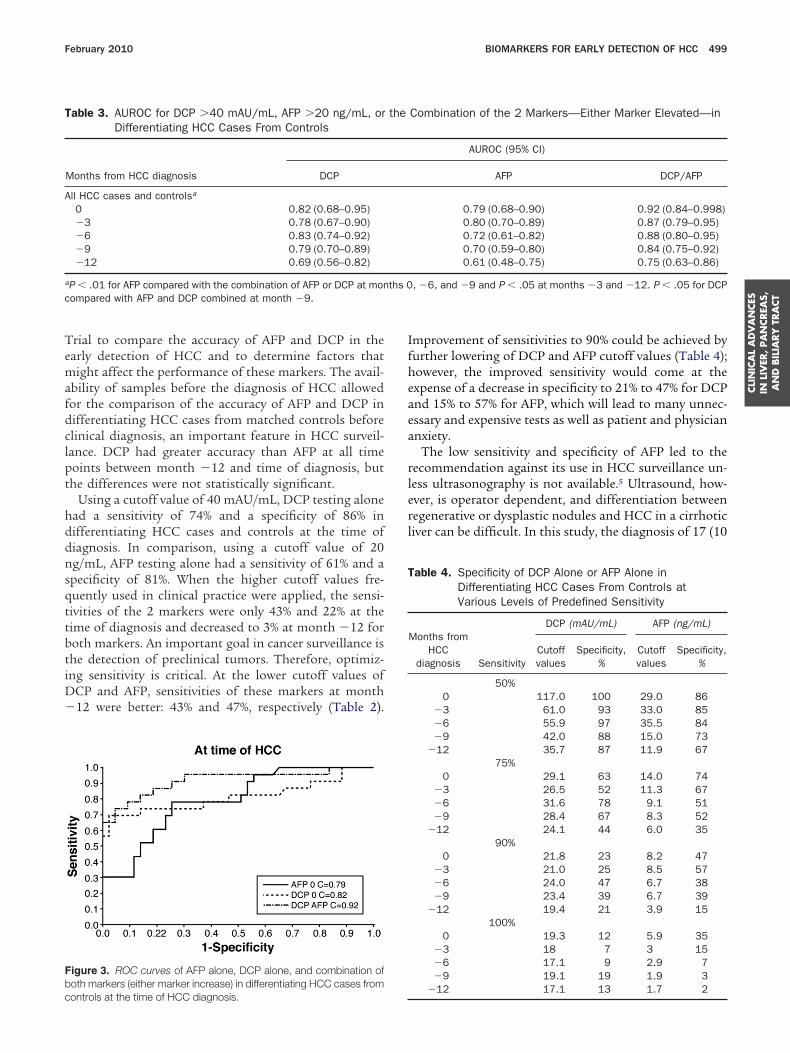
Accuracy of AFP, DCP, and the Combinationof Both Markers in Differentiating HCCCases From ControlsTable 3 shows the AUROC of AFP, DCP, and the
ombination AFP and DCP in differentiating HCC casesrom controls at various time points between month �12nd month 0. The AUROC for DCP was higher than thator AFP at all time points, except at month �3 whenoth markers were comparable but none of the differ-nces were significant. The combination of both markersn which either AFP or DCP was above a specified cutoffielded a higher AUROC at all time points, and theombination was significantly better than AFP alone atll time points and significantly better than DCP alone atonth �9. Figure 3 illustrates the ROC curve at the time
f HCC diagnosis; the AUROC was 0.82 for DCP, 0.79 forFP, and 0.92 for the combination of the 2 markers.
Specificity of AFP Alone and DCP Alone forVarious Levels of SensitivityTable 4 shows the specificity of AFP alone and
CP alone at prespecified sensitivities from 50% to00% and the corresponding cutoff values, determinedrom the ROC curves, for these markers. As the pre-efined sensitivity increased, the specificity decreased.t a predefined sensitivity of 90%, the specificity ofCP ranged from 21% to 47% and of AFP from 15% to
7% at various time points between month �12 andonth 0; the cutoff values for these 2 markers at
onth 0 were 21.8 mAU/mL and 8.2 ng/mL, respec-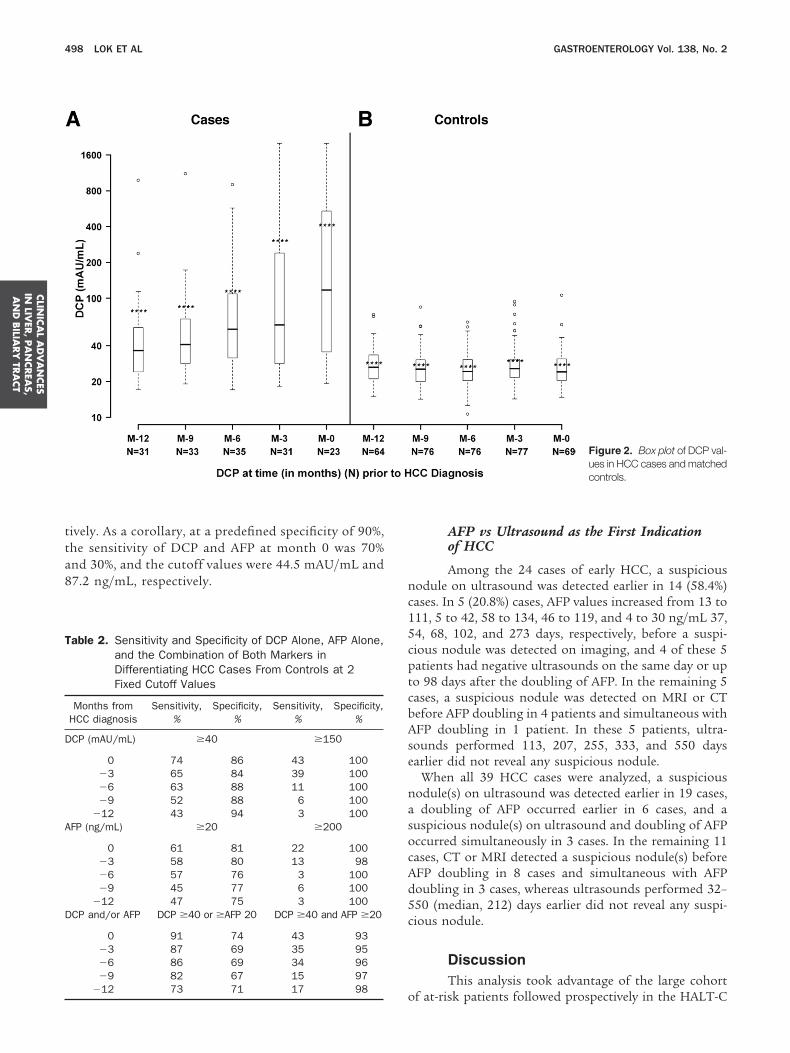
tta8 n
c15cptcbAse
nasocAd5c
T
D
A
D
CLIN
ICA
LA
DV
AN
CES
INLIV
ER,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
498 LOK ET AL GASTROENTEROLOGY Vol. 138, No. 2
ively. As a corollary, at a predefined specificity of 90%,he sensitivity of DCP and AFP at month 0 was 70%nd 30%, and the cutoff values were 44.5 mAU/mL and7.2 ng/mL, respectively.
able 2. Sensitivity and Specificity of DCP Alone, AFP Alone,and the Combination of Both Markers inDifferentiating HCC Cases From Controls at 2Fixed Cutoff Values
Months fromHCC diagnosis
Sensitivity,%
Specificity,%
Sensitivity,%
Specificity,%
CP (mAU/mL) �40 �150
0 74 86 43 100�3 65 84 39 100�6 63 88 11 100�9 52 88 6 100
�12 43 94 3 100FP (ng/mL) �20 �200
0 61 81 22 100�3 58 80 13 98�6 57 76 3 100�9 45 77 6 100
�12 47 75 3 100CP and/or AFP DCP �40 or �AFP 20 DCP �40 and AFP �20
0 91 74 43 93�3 87 69 35 95�6 86 69 34 96�9 82 67 15 97
o�12 73 71 17 98
AFP vs Ultrasound as the First Indicationof HCC
Among the 24 cases of early HCC, a suspiciousodule on ultrasound was detected earlier in 14 (58.4%)ases. In 5 (20.8%) cases, AFP values increased from 13 to11, 5 to 42, 58 to 134, 46 to 119, and 4 to 30 ng/mL 37,4, 68, 102, and 273 days, respectively, before a suspi-ious nodule was detected on imaging, and 4 of these 5atients had negative ultrasounds on the same day or upo 98 days after the doubling of AFP. In the remaining 5ases, a suspicious nodule was detected on MRI or CTefore AFP doubling in 4 patients and simultaneous withFP doubling in 1 patient. In these 5 patients, ultra-
ounds performed 113, 207, 255, 333, and 550 daysarlier did not reveal any suspicious nodule.
When all 39 HCC cases were analyzed, a suspiciousodule(s) on ultrasound was detected earlier in 19 cases,doubling of AFP occurred earlier in 6 cases, and a
uspicious nodule(s) on ultrasound and doubling of AFPccurred simultaneously in 3 cases. In the remaining 11ases, CT or MRI detected a suspicious nodule(s) beforeFP doubling in 8 cases and simultaneous with AFPoubling in 3 cases, whereas ultrasounds performed 32–50 (median, 212) days earlier did not reveal any suspi-ious nodule.
DiscussionThis analysis took advantage of the large cohort
Figure 2. Box plot of DCP val-ues in HCC cases and matchedcontrols.
f at-risk patients followed prospectively in the HALT-C
Temafdclpt
hddnsqttbtiD�
Ifheaea
rlerl
Fbc
T
A
a
c
T
CLI
NIC
AL
AD
VA
NCES
INLI
VER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
February 2010 BIOMARKERS FOR EARLY DETECTION OF HCC 499
rial to compare the accuracy of AFP and DCP in thearly detection of HCC and to determine factors thatight affect the performance of these markers. The avail-
bility of samples before the diagnosis of HCC allowedor the comparison of the accuracy of AFP and DCP inifferentiating HCC cases from matched controls beforelinical diagnosis, an important feature in HCC surveil-ance. DCP had greater accuracy than AFP at all timeoints between month �12 and time of diagnosis, buthe differences were not statistically significant.
Using a cutoff value of 40 mAU/mL, DCP testing alonead a sensitivity of 74% and a specificity of 86% inifferentiating HCC cases and controls at the time ofiagnosis. In comparison, using a cutoff value of 20g/mL, AFP testing alone had a sensitivity of 61% and apecificity of 81%. When the higher cutoff values fre-uently used in clinical practice were applied, the sensi-ivities of the 2 markers were only 43% and 22% at theime of diagnosis and decreased to 3% at month �12 foroth markers. An important goal in cancer surveillance ishe detection of preclinical tumors. Therefore, optimiz-ng sensitivity is critical. At the lower cutoff values of
CP and AFP, sensitivities of these markers at month12 were better: 43% and 47%, respectively (Table 2).
igure 3. ROC curves of AFP alone, DCP alone, and combination ofoth markers (either marker increase) in differentiating HCC cases from
able 3. AUROC for DCP �40 mAU/mL, AFP �20 ng/mL, orDifferentiating HCC Cases From Controls
Months from HCC diagnosis DCP
ll HCC cases and controlsa
0 0.82 (0.68–0.95)�3 0.78 (0.67–0.90)�6 0.83 (0.74–0.92)�9 0.79 (0.70–0.89)�12 0.69 (0.56–0.82)
P � .01 for AFP compared with the combination of AFP or DCP at monompared with AFP and DCP combined at month �9.
ontrols at the time of HCC diagnosis.
mprovement of sensitivities to 90% could be achieved byurther lowering of DCP and AFP cutoff values (Table 4);owever, the improved sensitivity would come at thexpense of a decrease in specificity to 21% to 47% for DCPnd 15% to 57% for AFP, which will lead to many unnec-ssary and expensive tests as well as patient and physiciannxiety.
The low sensitivity and specificity of AFP led to theecommendation against its use in HCC surveillance un-ess ultrasonography is not available.5 Ultrasound, how-ver, is operator dependent, and differentiation betweenegenerative or dysplastic nodules and HCC in a cirrhoticiver can be difficult. In this study, the diagnosis of 17 (10
Combination of the 2 Markers—Either Marker Elevated—in
AUROC (95% CI)
AFP DCP/AFP
0.79 (0.68–0.90) 0.92 (0.84–0.998)0.80 (0.70–0.89) 0.87 (0.79–0.95)0.72 (0.61–0.82) 0.88 (0.80–0.95)0.70 (0.59–0.80) 0.84 (0.75–0.92)0.61 (0.48–0.75) 0.75 (0.63–0.86)
, �6, and �9 and P � .05 at months �3 and �12. P � .05 for DCP
able 4. Specificity of DCP Alone or AFP Alone inDifferentiating HCC Cases From Controls atVarious Levels of Predefined Sensitivity
Months fromHCC
diagnosis Sensitivity
DCP (mAU/mL) AFP (ng/mL)
Cutoffvalues
Specificity,%
Cutoffvalues
Specificity,%
50%0 117.0 100 29.0 86
�3 61.0 93 33.0 85�6 55.9 97 35.5 84�9 42.0 88 15.0 73
�12 35.7 87 11.9 6775%
0 29.1 63 14.0 74�3 26.5 52 11.3 67�6 31.6 78 9.1 51�9 28.4 67 8.3 52
�12 24.1 44 6.0 3590%
0 21.8 23 8.2 47�3 21.0 25 8.5 57�6 24.0 47 6.7 38�9 23.4 39 6.7 39
�12 19.4 21 3.9 15100%
0 19.3 12 5.9 35�3 18 7 3 15�6 17.1 9 2.9 7�9 19.1 19 1.9 3
the
ths 0
�12 17.1 13 1.7 2

oaMctkswurmpNinnA
DdmA1cD
busraltbittohtrAApDcfiaaiobrDct
rctaitt
deamcfaswawe
nwatwtooDf
wamawordwsusstcigH
tonA
CLIN
ICA
LA
DV
AN
CES
INLIV
ER,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
500 LOK ET AL GASTROENTEROLOGY Vol. 138, No. 2
f 24 early HCC) of 39 HCC cases was first triggered byn increase in AFP and/or suspicious nodule on CT orRI. Although the HALT-C HCC surveillance protocol
alled for annual rather than every 6 months ultrasound,his is consistent with the AASLD guidelines.5 We ac-nowledge that some patients did not adhere to theurveillance protocol, but 8 patients had ultrasoundsithin 6 months of HCC diagnosis, and 6 patients hadltrasounds within 12 months of diagnosis that did noteveal any suspicious nodule. Admittedly, tumor nodules
ay have been present on ultrasounds in some of theseatients and were missed by inexperienced radiologists.evertheless, these results reflect the real world experience
n which ultrasounds are frequently performed in commu-ity hospitals and not at academic liver centers. Therefore,ew biomarkers with better sensitivity and specificity thanFP to complement ultrasound are needed.Several case-control studies have shown sensitivities ofCP of 28% to 89% and specificities of 87% to 96% in theiagnosis of HCC.10 –12,33,34 In some studies, DCP wasore sensitive than AFP,12,33,34 whereas, in other studies,FP was more sensitive.10,11 A recent Japanese study of377 HCC patients and 355 non-HCC controls withhronic hepatitis or cirrhosis showed that the accuracy ofCP was inferior to AFP, particularly for small tumors.15
Various factors may influence the performance of HCCiomarkers, including patient demographics, cause ofnderlying liver disease, presence of cirrhosis, tumortage, and tumor biology.35–38 Thus, Nguyen et al haveeported that AFP was less sensitive in diagnosing HCCmong African American patients with hepatitis C-re-ated cirrhosis compared with non-African American pa-ients.38 In an earlier report of the HALT-C Trial data,aseline AFP values were noted to be significantly higher
n patients with cirrhosis, in women, and in black pa-ients.29 Increased AFP values in patients with cirrhosis vshose with earlier stage liver disease had been reported inther studies and attributed to increased liver injury andepatocyte turnover. This is supported by the observa-ion of a decline in AFP values during peginterferon andibavirin treatment and a correlation between decrease inFP and decrease in ALT values during treatment.29
nalysis of the baseline DCP and AFP values of 1031atients included in the current analysis showed thatCP values were also significantly higher in patients with
irrhosis but lower in women and in black patients. Thending that patient demographics influenced both DCPnd AFP values but in opposite directions was surprisingnd merits further investigation. This observation mightmpact the accuracy of these biomarkers in the detectionf HCC and underscores the importance of recall policiesased on changes in biomarker values from baselineather than absolute cutoff values in HCC surveillance.ata from the randomized phase of the HALT-C Trial
onfirmed that AFP values decreased during interferon
reatment. The effect, however, was minimal and possibly Helated to the use of a lower dose of peginterferon. Inontrast, DCP values were not affected by interferonreatment. The performance of cancer biomarkers maylso be influenced by tumor stage; 24 of the 39 HCC casesn this analysis had early stage tumors. It is reassuringhat the accuracy of DCP and AFP in detecting early stageumors was similar to that of all tumors.
Neither DCP alone nor AFP alone was optimal in theetection of HCC, but the combination of both markersnhanced the sensitivity, indicating that these 2 markersre complementary. At a DCP cutoff value of �40AU/mL or AFP value of �20 ng/mL, sensitivity in-
reased from 61% and 74% for each marker alone to 91%or both markers combined at month 0 and from 43%nd 47% to 73% at month �12. Several other studies alsohowed that DCP and AFP are complementary,14,16,39
hich is consistent with the fact that production of DCPnd AFP in HCC occurs through different pathways andith our finding that gender and race had opposite
ffects on these 2 markers.This study has several strengths including a homoge-
ous underlying cause for liver disease in all patients,ell-matched cases and controls, prospective follow-up oft least 12 months to rule out undiagnosed HCC amonghe controls, and predefined criteria for diagnosis of HCCith further review of each case by a panel of investiga-
ors. A unique aspect of our analysis was the availabilityf samples dating back 12 months before the diagnosisf HCC, allowing the assessment of the performance ofCP and AFP in differentiating preclinical HCC cases
rom controls.The most important limitations in the current analysis
ere the small number of HCC cases and the incompletevailability of samples at all of the time points fromonth �12 to month 0. Also, because study sites were
ware of AFP but not DCP results, a confounding biasas introduced that may have influenced investigators torder additional testing based on AFP but not DCPesults and, hence, the accuracy of AFP vs DCP for HCCiagnosis. Furthermore, only 61.5% of patients presentedith early stage HCC. Noncompliance with the HCC
urveillance protocol and variations in interpretation ofltrasound may have contributed to the delay in diagno-is in some cases, but there is a clear need for bettercreening strategies. The differential effects of interferonreatment on AFP and DCP values may have confoundedomparisons of the accuracy of these 2 markers, but thempact is likely to be small. Finally, our results cannot beeneralized to patients with liver disease not caused byCV or to patients who are not white or black.In conclusion, this case-control study demonstrated
hat DCP was not superior to AFP in the early detectionf HCC in patients with advanced hepatitis C and thateither AFP alone, DCP alone, nor the combination ofFP and DCP was sufficiently accurate to be used for
CC surveillance. The sensitivity of these markers was
mltcaiiauttaHetcet
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
CLI
NIC
AL
AD
VA
NCES
INLI
VER
,PA
NCREA
S,A
ND
BIL
IARY
TRA
CT
February 2010 BIOMARKERS FOR EARLY DETECTION OF HCC 501
aximal at the time of HCC diagnosis and considerablyower at earlier time points. Nevertheless, increasing AFPriggered the evaluation that led to the diagnosis of someases of early HCC. This study demonstrated that DCPnd AFP are complementary; therefore, prospective stud-es should be conducted to determine whether combin-ng both markers will improve the detection of early HCCnd to establish the optimal cutoff values that should besed for patient recall and further testing. In addition,he influence of patient demographics and interferonreatment on DCP and AFP values should be confirmednd their impact on the performance of these markers inCC surveillance determined. Until better serum mark-
rs are available, ultrasonography remains the preferredool for HCC surveillance, but reliable biomarkers toomplement ultrasound may improve the detection ofarly HCC in clinical practice, in which setting interpre-ation of ultrasound is variable.
References
1. Kamangar F, Dores GM, Anderson WF. Patterns of cancer inci-dence, mortality, and prevalence across five continents: definingpriorities to reduce cancer disparities in different geographicregions of the world. J Clin Oncol 2006;24:2137–2150.
2. El-Serag HB. Hepatocellular carcinoma: recent trends in theUnited States. Gastroenterology 2004;127:S27–S34.
3. Everhart JE. Primary liver cancer. In: Everhart JE, ed. Burden ofdigestive diseases in the United States. Department of Healthand Human Services, Public Health Service, National Institutes ofHealth, National Institute of Diabetes and Digestive and KidneyDiseases. Washington, DC: US Government Printing Office,2008; NIH Publication No. 09-6443 2008:49–52.
4. Stravitz RT, Heuman DM, Chand N, et al. Surveillance for hepa-tocellular carcinoma in patients with cirrhosis improves outcome.Am J Med 2008;121:119–126.
5. Bruix J, Sherman M. Management of hepatocellular carcinoma.Hepatology 2005;42:1208–1236.
6. Zhang BH, Yang BH, Tang ZY. Randomized controlled trial ofscreening for hepatocellular carcinoma. J Cancer Res Clin Oncol2004;130:417–422.
7. McMahon BJ, Bulkow L, Harpster A, et al. Screening for hepato-cellular carcinoma in Alaska natives infected with chronic hepa-titis B: a 16-year population-based study. Hepatology 2000;32:842–846.
8. Bruix J, Sherman M, Llovet JM, et al. Clinical management ofhepatocellular carcinoma. Conclusions of the Barcelona-2000EASL conference. European Association for the Study of the Liver.J Hepatol 2001;35:421–430.
9. Makuuchi M, Kokudo N, Arii S, et al. Development of evidence-based clinical guidelines for the diagnosis and treatment of hep-atocellular carcinoma in Japan. Hepatol Res 2008;38:37–51.
0. Aoyagi Y, Oguro M, Yanagi M, et al. Clinical significance ofsimultaneous determinations of �-fetoprotein and des-�-carboxyprothrombin in monitoring recurrence in patients with hepatocel-lular carcinoma. Cancer 1996;77:1781–6.
1. Nomura F, Ishijima M, Kuwa K, et al. Serum des-�-carboxy pro-thrombin levels determined by a new generation of sensitiveimmunoassays in patients with small-sized hepatocellular carci-noma. Am J Gastroenterol 1999;94:650–654.
2. Mita Y, Aoyagi Y, Yanagi M, et al. The usefulness of determiningdes-�-carboxy prothrombin by sensitive enzyme immunoassay inthe early diagnosis of patients with hepatocellular carcinoma.
Cancer 1998;82:1643–1648.3. Ishii M, Gama H, Chida N, et al. Simultaneous measurements ofserum �-fetoprotein and protein induced by vitamin K absence fordetecting hepatocellular carcinoma. South Tohoku District StudyGroup. Am J Gastroenterol 2000;95:1036–1040.
4. Hamamura K, Shiratori Y, Shiina S, et al. Unique clinical charac-teristics of patients with hepatocellular carcinoma who presentwith high plasma des-�-carboxy prothrombin and low serum �-fe-toprotein. Cancer 2000;88:1557–1564.
5. Nakamura S, Nouso K, Sakaguchi K, et al. Sensitivity and spec-ificity of des-�-carboxy prothrombin for diagnosis of patients withhepatocellular carcinomas varies according to tumor size. Am JGastroenterol 2006;101:2038–2043.
6. Okuda H, Obata H, Nakanishi T, et al. Production of abnormalprothrombin (des-�-carboxy prothrombin) by hepatocellular carci-noma. A clinical and experimental study. J Hepatol 1987;4:357–363.
7. Liebman HA, Furie BC, Tong MJ, et al. Des-�-carboxy (abnormal)prothrombin as a serum marker of primary hepatocellular carci-noma. N Engl J Med 1984;310:1427–1431.
8. Stenflo J, Fernlund P, Egan W, et al. Vitamin K dependent modi-fications of glutamic acid residues in prothrombin. Proc Natl AcadSci U S A 1974;71:2730–2733.
9. Marrero JA. Screening tests for hepatocellular carcinoma. ClinLiver Dis 2005;9:235–251.
0. Ikoma J, Kaito M, Ishihara T, et al. Early diagnosis of hepatocel-lular carcinoma using a sensitive assay for serum des-�-carboxyprothrombin: a prospective study. Hepatogastroenterology 2002;49:235–238.
1. Pateron D, Ganne N, Trinchet JC, et al. Prospective study ofscreening for hepatocellular carcinoma in Caucasian patientswith cirrhosis. J Hepatol 1994;20:65–71.
2. Oka H, Tamori A, Kuroki T, et al. Prospective study of �-fetopro-tein in cirrhotic patients monitored for development of hepatocel-lular carcinoma. Hepatology 1994;19:61–66.
3. Bolondi L, Sofia S, Siringo S, et al. Surveillance programme ofcirrhotic patients for early diagnosis and treatment of hepatocel-lular carcinoma: a cost-effectiveness analysis. Gut 2001;48:251–259.
4. Tong MJ, Blatt LM, Kao VW. Surveillance for hepatocellular car-cinoma in patients with chronic viral hepatitis in the UnitedStates of America. J Gastroenterol Hepatol 2001;16:553–559.
5. Chalasani N, Horlander JC Sr, Said A, et al. Screening for hepa-tocellular carcinoma in patients with advanced cirrhosis. Am JGastroenterol 1999;94:2988–2993.
6. Izuno K, Fujiyama S, Yamasaki K, et al. Early detection of hepa-tocellular carcinoma associated with cirrhosis by combined as-say of des-�-carboxy prothrombin and �-fetoprotein: a prospec-tive study. Hepatogastroenterology 1995;42:387–393.
7. Lee WM, Dienstag JL, Lindsay KL, et al. Evolution of the HALT-CTrial: pegylated interferon as maintenance therapy for chronichepatitis C in previous interferon nonresponders. Control ClinTrials 2004;25:472–492.
8. Di Bisceglie AM, Shiffman ML, Everson GT, et al. Prolongedtherapy of advanced chronic hepatitis C with low-dose peginter-feron. N Engl J Med 2008;359:2429–2441.
9. Di Bisceglie AM, Sterling RK, Chung RT, et al. Serum �-fetopro-tein levels in patients with advanced hepatitis C: results from theHALT-C Trial. J Hepatol 2005;43:434–441.
0. Ishak K, Baptista A, Bianchi L, et al. Histological grading andstaging of chronic hepatitis. J Hepatol 1995;22:696–699.
1. Lok AS, Seeff LB, Morgan TR, et al. Incidence of hepatocellularcarcinoma and associated risk factors in hepatitis C-related ad-vanced liver disease. Gastroenterology 2009;136:138–148.
2. Gupta S, Bent S, Kohlwes J. Test characteristics of �-fetoproteinfor detecting hepatocellular carcinoma in patients with hepatitisC. A systematic review and critical analysis. Ann Intern Med
2003;139:46–50.
3
3
3
3
3
3
3
R
GTa
A
N
N
ioi
(M
M
NE
2CAG
NGC
gM
(RSSM
9G
NMFR
(SH
aGR
DB
DA
DL
G
ML
nf
C
arobcWrLa
F
DAtGCNCAoa
CLIN
ICA
LA
DV
AN
CES
INLIV
ER,PA
NCREA
S,A
ND
BILIA
RY
TRA
CT
502 LOK ET AL GASTROENTEROLOGY Vol. 138, No. 2
3. Marrero JA, Su GL, Wei W, et al. Des-� carboxyprothrombin candifferentiate hepatocellular carcinoma from nonmalignant chronicliver disease in American patients. Hepatology 2003;37:1114–1121.
4. Lamerz R, Runge M, Stieber P, et al. Use of serum PIVKA-II (DCP)determination for differentiation between benign and malignantliver diseases. Anticancer Res 1999;19:2489–2493.
5. Toyoda H, Kumada T, Osaki Y, et al. Staging hepatocellularcarcinoma by a novel scoring system (BALAD score) based onserum markers. Clin Gastroenterol Hepatol 2006;4:1528–1536.
6. Volk ML, Hernandez JC, Su GL, et al. Risk factors for hepatocel-lular carcinoma may impair the performance of biomarkers: acomparison of AFP, DCP, and AFP-L3. Cancer Biomark 2007;3:79–87.
7. Yano Y, Yamashita F, Kuwaki K, et al. Clinical features of hepa-titis C virus-related hepatocellular carcinoma and their associa-tion with �-fetoprotein and protein induced by vitamin K absenceor antagonist-II. Liver Int 2006;26:789–795.
8. Nguyen MH, Garcia RT, Simpson PW, et al. Racial differences ineffectiveness of �-fetoprotein for diagnosis of hepatocellular car-cinoma in hepatitis C virus cirrhosis. Hepatology 2002;36:410–417.
9. Beale G, Chattopadhyay D, Gray J, et al. AFP, PIVKAII, GP3,SCCA-1 and follisatin as surveillance biomarkers for hepatocel-lular cancer in non-alcoholic and alcoholic fatty liver disease.BMC Cancer 2008;8:200.
Received July 23, 2009. Accepted October 13, 2009.
eprint requestsAddress requests for reprints to: Anna S. Lok, MD, Division of
astroenterology, University of Michigan Health System, 3912aubman Center, SPC 5362, Ann Arbor, MI 48109. e-mail:[email protected]; fax: 734-936-7024.
cknowledgmentsThis is publication No. 45 from the HALT-C Trial Group.The HALT-C Trial is registered with clinicaltrials.gov (No.
CT00006164).H.L.B.’s current address is Carolinas Medical Center, Charlotte,
orth Carolina.
In addition to the authors of this manuscript, the followingndividuals were instrumental in the planning, conduct, and/or caref patients enrolled in this study at each of the participating
nstitutions as follows:
University of Massachusetts Medical Center, Worcester, MA:contract N01-DK-9-2326) Gyongyi Szabo, MD; Barbara F. Banner,D; Maureen Cormier, RN; Donna Giansiracusa, RN.University of Connecticut Health Center, Farmington, CT: (grant01RR-06192) Gloria Borders, RN; Michelle Kelley, RN, ANP.Saint Louis University School of Medicine, St Louis, MO: (contract
01-DK-9-2324) Bruce Bacon, MD; Brent Neuschwander–Tetri, MD;lizabeth M. Brunt, MD; Debra King, RN.Massachusetts General Hospital, Boston, MA: (contract N01-DK-9-
319, grant M01RR-01066, grant 1 UL1 RR025758-01, Harvardlinical and Translational Science Center) Raymond T. Chung, MD;ndrea E. Reid, MD; Atul K. Bhan, MD; Wallis A. Molchen; Cara C.ooch.University of Colorado School of Medicine, Denver, CO: (contract
01-DK-9-2327, grant M01RR-00051, grant 1 UL1 RR 025780-01)regory T. Everson, MD; S. Russell Nash, MD; Jennifer DeSanto, RN;arol McKinley, RN.University of California-Irvine, Irvine, CA: (contract N01-DK-9-2320,
rant M01RR-00827) John R. Craig, MD; M. Mazen Jamal, MD,
PH; Muhammad Sheikh, MD; Choon Park, RN. tUniversity of Texas Southwestern Medical Center, Dallas, TX:contract N01-DK-9-2321, grant M01RR-00633, grant 1 UL1R024982-01, North and Central Texas Clinical and Translationalcience Initiative) Thomas E. Rogers, MD; Peter F. Malet, MD; Janelhelton; Nicole Crowder, LVN; Rivka Elbein, RN, BSN; Nancy Liston,PH.University of Southern California, Los Angeles, CA: (Contract N01-DK-
-2325, grant M01RR-00043) Karen L. Lindsay, MD, MMM; Suganthaovindarajan, MD; Carol B. Jones, RN; Susan L. Milstein, RN.University of Michigan Medical Center, Ann Arbor, MI: (contract
01-DK-9-2323, grant M01RR-00042, grant 1 UL1 RR024986,ichigan Center for Clinical and Health Research) Robert J.
ontana, MD; Joel K. Greenson, MD; Grace L. Su, MD; Pamela A.ichtmyer, LPN, CCRC; R. Tess Bonham, BS; Mita Ghosh, BS.Virginia Commonwealth University Health System, Richmond, VA:
contract N01-DK-9-2322, grant M01RR-00065) Mitchell L.hiffman, MD; Melissa J. Contos, MD; A. Scott Mills, MD; Charlotteofmann, RN; Paula Smith, RN.Liver Diseases Branch, National Institute of Diabetes and Digestive
nd Kidney Diseases, National Institutes of Health, Bethesda, MD: Marc. Ghany, MD; T. Jake Liang, MD; David Kleiner, MD, PhD; Yoon Park,N; Elenita Rivera, RN; Vanessa Haynes–Williams, RN.National Institute of Diabetes and Digestive and Kidney Diseases,
ivision of Digestive Diseases and Nutrition, Bethesda, MD: Leonard. Seeff, MD; Patricia R. Robuck, PhD; Jay H. Hoofnagle, MD.University of Washington, Seattle, WA: (contract N01-DK-9-2318)
avid R. Gretch, MD, PhD; Chihiro Morishima, MD; Minjun Chungpodaca, BS, ASCP; Rohit Shankar, BC, ASCP; Natalia Antonov, MEd.New England Research Institutes, Watertown, MA: (contract N01-
K-9-2328) Kristin K. Snow, MSc, ScD; Anne M. Stoddard, ScD;inda Massey; Teresa M. Curto, MSW, MPH.Armed Forces Institute of Pathology, Washington, DC: Zachary D.
oodman, MD.Data and Safety Monitoring Board Members: (chair) Gary L. Davis,D; Guadalupe Garcia-Tsao, MD; Michael Kutner, PhD; Stanley M.
emon, MD; Robert P. Perrillo, MD.
The content is solely the responsibility of the authors and doesot necessarily represent the official views of the National Centeror Research Resources or the National Institutes of Health.
onflicts of interestThe authors disclose the following:Financial relationships of the authors with Hoffmann-La Roche, Inc.,
re as follows: A.S. Lok is a consultant; R.K. Sterling is a consultant,eceives research support, and is on the speaker’s bureau; J.C. Hoefs isn the speaker’s bureau; T.R. Morgan is a consultant, on the speaker’sureau, and receives research support; A.M. Di Bisceglie is aonsultant, on the speaker’s bureau, and receives research support;.M. Lee receives research support; and H.L. Bonkovsky receives
esearch support. Financial relationships of the authors with Eisai Co,td, are as follows: A.S. Lok receives research support. The remaininguthors disclose no conflicts.
undingSupported by the National Institute of Diabetes & Digestive & Kidney
iseases (contract numbers are listed below); the National Institute ofllergy and Infectious Diseases (NIAID); the National Cancer Institute;
he National Center for Minority Health and Health Disparities; byeneral Clinical Research Center and Clinical and Translational Scienceenter grants from the National Center for Research Resources andational Institutes of Health (grant numbers are listed below); by Eisaio, Ltd, through a Materials Cooperative Research and Developmentgreement (M-CRADA) with the National Institutes of Health for testingf des-�-carboxy prothrombin; and by Hoffmann–La Roche, Inc, throughCooperative Research and Development Agreement (CRADA) with
he National Institutes of Health.




















