
Inhibition of differentiation in myoblasts deprived of the interferon-related protein PC4

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CLINICAL RESEARCHHeart failure/cardiomyopathy
Four-year follow-up of treatment withintramyocardial skeletal myoblasts injectionin patients with ischaemic cardiomyopathyCaroline E. Veltman1, Osama I.I. Soliman1, Marcel L. Geleijnse1, Wim B. Vletter1,Pieter C. Smits1, Folkert J. ten Cate1, Luc J. Jordaens1, Aggie H.H.M. Balk1,Patrick W. Serruys1, Eric Boersma1, Ron T. van Domburg1, andWim J. van der Giessen1,2*
1Department of Cardiology, Erasmus University Medical Centre, Thoraxcentre, Room Ba 587, Erasmus MC, Gravendijkwal 230, PO Box 2040, 3015 CE Rotterdam, TheNetherlands; and 2Interuniversity Cardiology Institute of the Netherlands, ICIN-KNAW, Utrecht, The Netherlands
Received 31 October 2007; revised 22 March 2008; accepted 4 April 2008; online publish-ahead-of-print 25 April 2008
Aims Studies reporting improved left ventricular (LV) function of percutaneous skeletal myoblast (SkM) injection in patientswith ischaemic cardiomyopathy had follow-up not exceeding 12 months, and did not include a control group. Ourgroup has reported evidence for myoblast efficacy in the first five out of the 14 treated patients. The objective of thepresent evaluation was to assess if these effects were sustained at long-term follow-up. We compared function ofpatients treated with SkM 4 years earlier with a matched control group. Secondary endpoints included mortality,NYHA class, N-terminal pro-B-natriuretic peptide levels, incidence of arrhythmias, and quality of life.
Methodsand results
Fourteen patients with ischaemic cardiomyopathy who underwent SkM injection were compared with 28 non-ran-domized control patients matched for age, sex, location, and extent of myocardial infarction. Contrast echocardio-graphy and tissue Doppler imaging (TDI) was performed to compare global and regional LV function. At 4-yearfollow-up, three patients (21%) had died in the treated group and 11 patients (39%) in the control group(P ¼ 0.8). In the survivors, LV ejection fraction (EF) was 35+10% and 37+9% in the SkM group and 36+8%and 36+6% in the controls at baseline and 4 years follow-up, respectively (P ¼ 0.96 between groups at follow-up). TDI-derived systolic velocity in the injected sites was 5.4+1.8 cm/s in the SkM group when compared with5.1+1.6 cm/s in corresponding sites in the control group (P ¼ 0.47). None of the secondary endpoints showed adifference between the groups. However, in the patients fitted with an internal cardioverter defibrillator, morearrhythmias leading to interventions occurred in the treated group than in the control group, 87% and 13%, respect-ively (P ¼ 0.015).
Conclusion Percutaneous intramyocardial SkM injection in ischaemic cardiomyopathy has no sustained positive effect on restingglobal or regional LV function, respectively, at 4-year follow-up. Moreover, the procedure may induce a higher risk ofdeveloping serious arrhythmias, but larger patient series are required before more precise characterization of thesafety and efficacy profile of the procedure is possible.
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Heart failure † Stem cells † Follow-up studies † Echocardiography † LV function
IntroductionAdult myocardium is incapable of effective, spontaneous regener-ation after ischaemic injury causing the injured area to develop
into fibrous, non-contractile scar tissue. Therefore, heart failure(HF) following myocardial infarction (MI) can be viewed as adisease of cellular deficiency. The remaining healthy muscle mustcompensate for the loss in left ventricular (LV) function by
* Corresponding author. Tel: þ31 10 703 52 45, Fax: þ31 10 703 43 20, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2008. For permissions please email: [email protected].
European Heart Journal (2008) 29, 1386–1396doi:10.1093/eurheartj/ehn171
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

means of compensatory hypertrophy and dilatation of the LV. Thedirect injection of autologous stem cells into the myocardial infarctarea has been proposed to prevent deterioration of LV functionand the post-infarct remodelling process. In pre-clinical studies,implantation of either skeletal myoblast cells (SkM) or bonemarrow stem cells (BMC) suggested replacement of non-functioning myocardial scar with functioning muscle and improve-ment in myocardial performance.1 –3 Preliminary data in humansubjects receiving SkM as adjunct to coronary artery bypass graft-ing (CABG) indicate that cell implantation also improves LV func-tion.4 Phase I trials showed that autologous SkM transplantation forthe treatment of post-infarction HF was feasible.5,6 Our group hasreported enhancement of LV systolic function in the first fivepatients receiving SkM as a stand-alone procedure by percuta-neous approach after a follow-up of 3 months, which was sustainedup to 6 months.7 In addition, by using the more sensitive techniqueof pressure–volume loops, we could demonstrate a significantincrease in several indices of systolic function up to 12 monthsof follow-up.8 Both the surgical and the percutaneous studywere, however, small phase two trials without a control group.The objective of the present evaluation was to assess if earliereffects of myoblast injections were sustained at long-termfollow-up. In the present study, we compared the treated patientswith a matched control group with respect to global and regionalLV function as measured by contrast echocardiography includingtissue Doppler imaging (TDI) after an average follow-up of 4years. We also assessed the long-term safety of percutaneousinjection of SkM by its effects on arrhythmias.
Methods
Study populationSymptomatic patients with chronic ischaemic cardiomyopathybecause of a previous MI involving the anterior, inferior, or lateralwall were included in the study. In total, 15 patients were treatedwith autologous SkMs in the period 2001–03. One patient refusedinformed consent leaving 14 patients for long-term follow-up (myo-blast group). For each treated patient, we selected two controlsmatched using the following method: we performed a search forappropriate patients during the period 2001–03 in our patient data-base using the following search terms: MI and echocardiography.From the resulting 200 patients, we matched two per each treatedpatient, using the following matching criteria: age (range 5 years);sex, time since occurrence of the MI (range 5 years); LV ejectionfraction (LVEF) (range 8%); location of the MI. Eligibility for inclusionfor the treatment arm was based on: (i) age between 40 and 80 yearsold; (ii) LVEF between 20 and 45%; (iii) presence of a prior Q-waveMI and a large area of akinesia of the LV, confirmed by either LVangiography or echocardiography; (iv) New York Heart Association(NYHA) symptom class II or III. The main exclusion criteria were:(i) MI within 90 days before start of follow-up; (ii) HF secondaryto valvular disease; (iii) severe non-cardiac illness that might affectsurvival or interfere with the interpretation of the study results.The median follow-up time was 48 [interquartile range (IQR)37–58 months)] months in both groups. The study was approvedby the Medical Ethics Committee of Erasmus MC. Patients gavewritten informed consent.
Cell therapy procedureThe SkMs were obtained via a biopsy of the patient quadriceps muscleunder local anaesthesia. A median of 11 g (range 8.1–13.3 g) of musclebiopsy was excised through a 10 cm long surgical incision. The trans-port conditions were monitored using a programmable temperaturemonitor (Sensitech, Beverly, MA, USA). Upon receipt at the culturingfacility, biopsies were processed according to Bioheart Inc, MyoCellTM
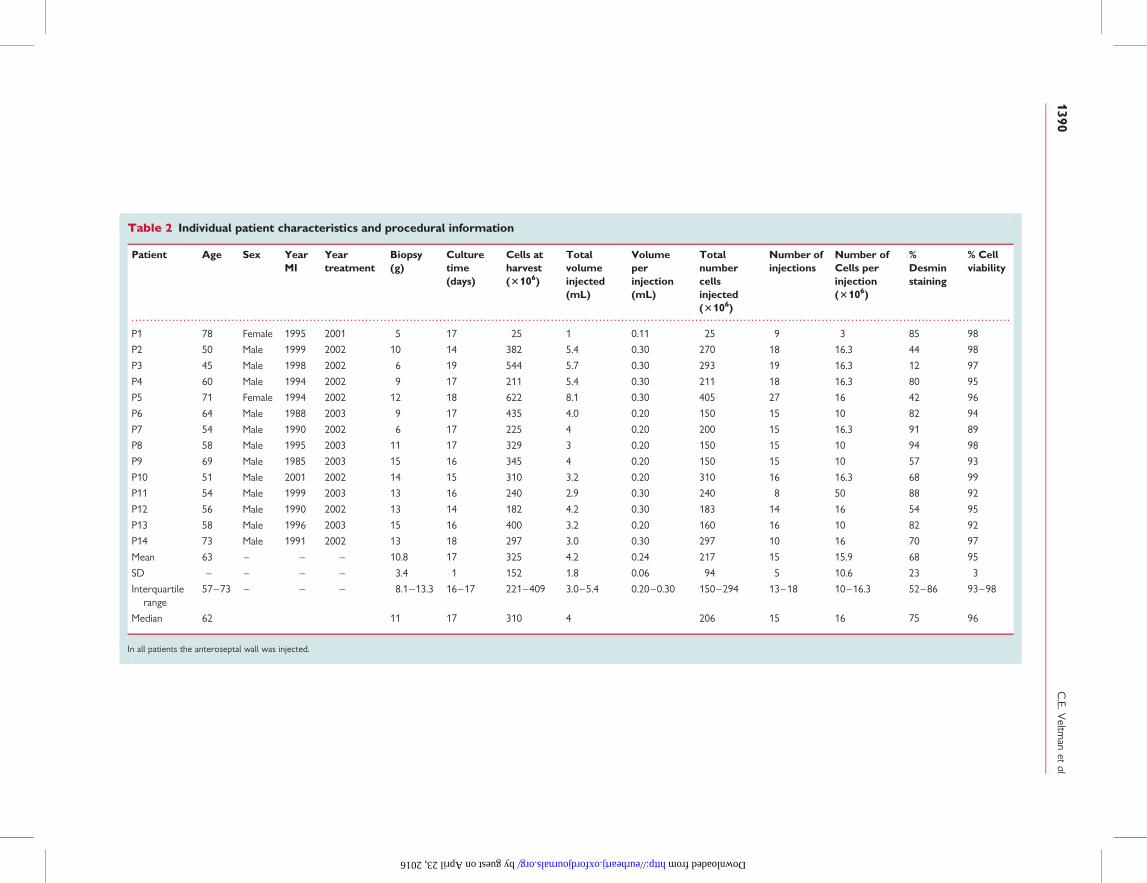
protocols as described earlier.7 The cell re-injection procedure wasperformed in the cardiac catheterization laboratory after a cultureperiod of approximately 17 days, which resulted in a mean of 325million harvested cells. Transendocardial injections were made usinga needle injection catheter as described before.7 The injections weremade within the scar region with a known wall thickness of morethan 5 mm as assessed by echocardiography. Treated patients receivedeight to 27 injections of 0.11–0.30 mL, containing three to 50 millioncells per injection. A median of 206 (IQR 150–294) million totalnumber of cells was injected in the anteroseptal wall in all patients.The cells had a mean desmin staining of 68+ 23% and a viability of95+3%. Procedural complications did not occur.
Study endpointsThe primary endpoints were changes in global and regional LV functionover time within both groups and the difference in LV functionbetween the myoblast and the control group at 4 years. The assess-ment of LV function included LV end-diastolic diameter (LV-EDD),LV end-diastolic volume (LV-EDV), LVEF, myocardial performanceindex (Tei index), and TDI-derived regional peak systolic velocity.
Secondary endpoints were cardiac mortality, arrhythmias, change inNYHA class, the six-minute walking distance, hospitalization for eitherangina, arrhythmias, or HF, N-terminal pro-B-natriuretic peptide(NT-pro-BNP) levels, and finally health-related quality of life measuredwith the Short-Form Health Survey-36 (SF-36) questionnaire. Theoccurrence of arrhythmias was measured during the follow-upperiod by the internal cardioverter defibrillator (ICD) in all patients.We also measured the frequency and severity of arrhythmias deter-mined by 24 h-Holter monitoring in all patients at the end of thefollow-up period. The SF-36 questionnaire was divided into eight sub-scales: Physical Functioning, Role Physical Functioning, Mental Health,Vitality, Bodily Pain, and General Health.9 Scores on the subscaleswere linearly converted to a score between 0 and 100, with ahigher score representing a better functioning.
The endpoints NYHA class, LV-EDD, LV-EDV, and LVEF wereassessed at baseline as well as at follow-up in the treated and thecontrol patients. The arrhythmias measured by ICD were assessedduring the 4-year follow-up period. All other secondary endpointswere measured only at the end of follow-up.
EchocardiographyAt baseline and at 4-year follow-up two-dimensional echocardiographywas performed including contrast LV opacification, while at follow-upalso TDI assessment was done. All patients were examined using aniE33 7500-ultrasound system (Philips, Best, The Netherlands) with aS3 transducer according to the recommendations of the AmericanSociety of Echocardiography.10,11 LV-EDD and LV end-systolic diam-eter (LV-ESD) were measured. LV-EDV, LV end-systolic volume(LV-ESV), and LVEF (by modified bi-plane Simpson rule) were calcu-lated from the apical four-chamber and two-chamber views.12 Toimprove the reproducibility of two-dimensional echocardiographicassessment of LVEF, LV opacification using a commercially availablecontrast agent (SonoVue, Bracco, Geneva, Switzerland) was done.
Percutaneous myoblast therapy: long-term follow-up 1387
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

A bolus of 0.5 mL SonoVue was administered via iv route withadditional boluses of 0.25 mL when needed.
Tissue Doppler imagingTDI was applied by placing the sample volume at both sides of themitral annulus in the apical four-, two-, and three-chamber views.13
Gain and filter settings were adjusted as needed to eliminate back-ground noises and to allow for a clear tissue signal. Pulsed-wave TDIvelocities were recorded end-expiratory at a sweep speed of100 mm/s and measured using electronic callipers with the worksta-tion EnConcert (Philips, Best, The Netherlands). From the six mitralannular velocity profiles, the systolic wave (Sm) and the early diastolicwave (E0) were measured. The mitral annular E/E0 ratio was calculatedfrom the postero-septal and antero-lateral mitral annulus, as previouslydescribed.14 –16 For each patient, the average of at least three measure-ments was calculated. The myocardial performance index, defined asisovolumic contraction time plus isovolumic relaxation time dividedby ejection time was calculated from the postero-septal and antero-lateral mitral annulus TDI velocity profile, as previously described.16,17
Internal cardioverter defibrillatorinterrogationDuring the 4-year follow-up, arrhythmias assessed by interrogation ofthe ICDs and defined as sustained ventricular fibrillation or poly-morphic ventricular tachycardia (VT) and sustained monomorphicVT at a rate .120 b.p.m., were measured in the 17 patients fittedwith an ICD (nine treated patients and eight control patients). Theoutcome measurement was intervention by the ICD. An interventionwas defined as anti-tachycardia pacing or shocks for all causes. Anintervention can either be appropriate or inappropriate. An appropri-ate therapy means intervention for ventricular arrhythmias by the ICD.An example of inappropriate intervention is a shock delivered by ICDbecause of atrial tachycardia. An independent expert electrophysiolo-gist blinded to the treatment group reviewed all ICD data.
Statistical analysesKolmogorov–Smirnov test to evaluate normality was used for all vari-ables in the analysis. Differences between patients and controls wereanalysed using the unpaired Student’s t-test or Mann–Whitney Utest as appropriate. Continuous variables are presented as mean+SD or as median (IQR) when normal or skewed distribution, respect-ively. Categorical data presented as frequencies were compared usingthe x2 test or Fisher’s exact test depending on the distribution. Pre-selected baseline characteristics were: age, sex, time since prior MI,localization of the first MI, occurrence of multiple MI’s, treatmentwith CABG of PCI, implantation of ICD, LV function, NYHA class, car-diovascular risk factors like multi-vessel disease, hypertension,hypercholesterolaemia, diabetes mellitus, smoking, family history andbody mass index, and comorbidities like cerebrovascular accidentand chronic obstructive pulmonary disease. All tests were two-sidedand P , 0.05 was considered statistically significant. All statisticswere performed using the SPSS 13.0 software package (SPSS Inc,Chicago, IL, USA).
ResultsA total of 42 patients were enrolled in the study: 14 patientstreated with myoblasts and 28 matched controls. Baseline charac-teristics are summarized in Table 1. The median age was 62 (IQR57–73) years. The median time after MI was 8 (IQR 3–12)
years in the myoblast group and 8 (4–12) years in the controlgroup. In all treated patients, the location of the infarct area wasthe LV anterior wall caused by their first MI or if they had multipleMI’s in their second or third MI. There was no difference in cardiachistory between the two groups in all pre-selected baseline charac-teristics, except for implantation of ICD (P ¼ 0.065). ICD implan-tation was performed per protocol because of safety issues in themyoblast group after the fifth patient was treated with SkM duringthe trial. Both the myoblast-treated patients and the controlpatients were on stable medication regimen (aspirin, angiotension-converting enzyme inhibitors, b-blockers, diuretics, and statins)during the follow-up period. Procedural characteristics of theSkM group are summarized in Table 2.
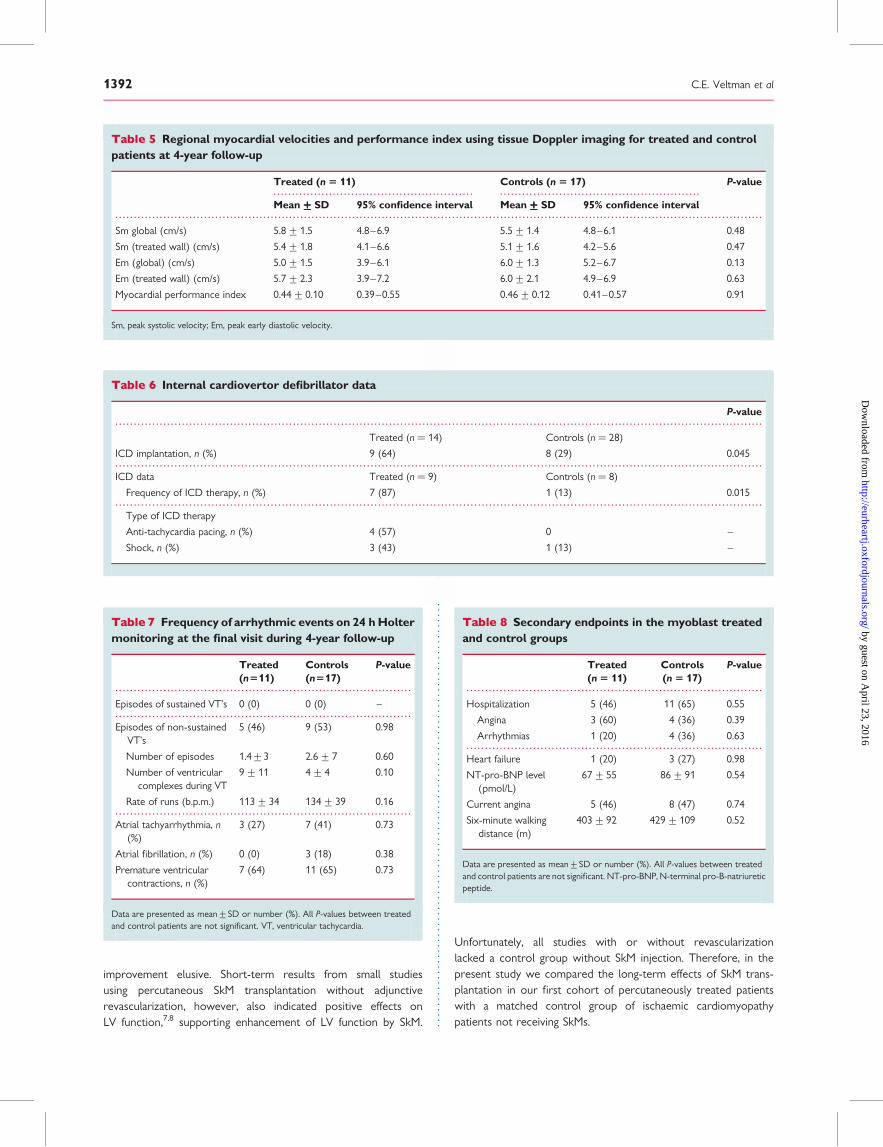
Primary endpointsLeft ventricular geometry and functionAfter 4-year follow-up, the myoblast group contained 11 patientsand the control group had 17 patients. Twenty-eight patientsunderwent contrast echocardiography at follow-up. LV-EDD,LV-ESD, LV-EDVI, and LV-ESVI showed no difference betweenthe two groups at baseline. Likewise, LVEF was similar betweenthe SkM-treated patients and the controls, 32+9% vs. 36+ 8%,respectively, P ¼ 0.29 (Table 3). Comparing baseline with follow-updata in only survivors of both groups also showed no difference.The LVEF as well as the LV-EDD, LV-ESD, LV-EDVI, and LV-ESVIwere similar between the treated and control group (Table 4). Indi-vidual data show that both in the treated as well as in the controlgroup, changes in LVEF over time varied between the individualpatients within one group. When comparing the mean baselineLVEF with the mean LVEF within one group, there is no changein LVEF over time (Figure 1). The myocardial performance indexand regional TDI-derived peak systolic velocities were not differentbetween the SkMs treated patients and the control patients. Alsothe mean systolic mitral annular velocity of the injected wall (theantero-septal wall) was similar in treated patients (5.4+1.8 cm/s)compared with control patients (5.1+ 1.6 cm/s, P ¼ 0.47). Also,early diastolic velocity was similar in the injected walls of themyoblast-treated and control groups (Table 5).
Secondary endpointsCardiac mortalityAt 4-years follow-up, 14 patients from the total study population(30%) had died, three patients (21%) in the myoblast groupand 11 patients (39%) in the control group (P ¼ 0.8). The firstmyoblast-treated patient died 9 days after procedure because ofan arrhythmic event. This patient belonged to the early phase ofthe trial and did not have an ICD. A second myoblast-treatedpatient died of cardiogenic shock following an electrical storm 1month after the procedure, despite the presence of an ICD.Because severe non-lethal arrhythmias also occurred in oneother patient shortly after the procedure in the first cohort ofpatients (non-ICD cohort) the later treated patients were allfitted with an ICD before the cell injection procedure. Anothertreated patient died of HF after 43 months. In the control group,seven patients died because of HF (64% of total death in controlgroup), one (9%) patient died because of ventricular fibrillation,and three (27%) patients died from non-cardiac causes.
C.E. Veltman et al1388
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

ArrhythmiasWe compared the nine treated with the eight control patientsfitted with an ICD at follow-up. In the treated group, seven outof nine patients (87%) had received an intervention, comparedwith one out of eight patients (13%) in the control group (P ¼0.015) (Table 6).
At the end of the follow-up, Holter monitoring was performedin all survivors. The mean time of Holter monitoring was 21 h.Episodes of non-sustained VT’s were recorded in five patients(46%) in the myoblast-treated group and nine (53%) in thecontrol group (P ¼ 0.7). The ventricular rate of the VT’s in thepatients of the myoblast group was slow (111–130 b.p.m.) witha mean length of nine ventricular complexes. In the controlgroup, fast VT’s (156–191 b.p.m.) with a mean length of four ven-tricular complexes were found in five patients. Episodes of sus-tained ventricular arrhythmias were not observed in eithergroup (Table 7).
Physical health statusNo difference was found between the myoblast patients and thecontrols in hospitalization, including the reasons of re-admissions,NT-pro-BNP levels, and presence of angina during ordinary activityand performance during six-minute walk exercise test (Table 8).The NYHA class improved in the treated group (3.0+ 0.5 to2.6+ 0.7). In this group, 36% of the patients improved in functionalclass. The other 64% of the patients remained in the same class.None of the patients worsened in functional class. In the controlgroup, 18% of the patients improved in functional class, but 36%of the patients worsened in functional class. The remaining 46%stayed in the same NYHA functional class. There was no statisti-cally significant difference between the groups (Figure 2).
Quality-of-life questionnaireIn all eight subscales of the SF-36 questionnaire, the scores weresimilar between the groups (Figure 3).
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Baseline characteristics
Characteristics Treated (n 5 14) Control (n 5 28) P-value
Demographics
Age (years) 62 (57–73) 62 (57–67) 0.58
Female sex 2 (14) 4 (14) –
Cardiac history
Time since prior myocardial infarction (years) 8 (3–12) 8 (4–12) 0.59
Multiple myocardial infarction 7 (50) 9 (32) 0.43
Previous coronary artery bypass grafting 2 (14) 12 (43) 0.12
Previous percutaneous coronary intervention 12 (86) 22 (79) 0.90
Internal cardioverter defibrillator 9 (64)* 8 (29) 0.065
Localization first myocardial infarction
Anterior 12 (86) 21 (75) 0.67
Inferior 1 (7) 6 (21) 0.48
Posterior 1 (7) 1 (4) 0.74
New York Heart Association functional class 3.0+0.5 2.8+0.8 0.40
II 2 (14) 9 (32) 0.38
III 12 (86) 19 (68) 0.38
Major risk factors
Multi-vessel disease 5 (36) 9 (32) 0.93
Hypertension 6 (43) 13 (46) 0.88
Hypercholesterolaemia 6 (43) 15 (54) 0.73
Diabetes mellitus 5 (36) 10 (36) –
Current smoking 6 (43) 12 (43) –
Positive family history 6 (43) 7 (25) 0.40
Body mass index (kg/m2) 25+4 23+5 0.20
Co-morbidities
Cerebrovascular accident 3 (21) 3 (11) 0.69
Chronic obstructive pulmonary diseases 2 (14) 1 (4) 0.59
Data are presented as median (interquartile range), mean+SD, or number (%).*P ¼ 0.045 for treated vs. control patients. All other P-values between treated and control patients are not significant.
Percutaneous myoblast therapy: long-term follow-up 1389
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Individual patient characteristics and procedural information
Patient Age Sex YearMI
Yeartreatment
Biopsy(g)
Culturetime(days)
Cells atharvest(3106)
Totalvolumeinjected(mL)
Volumeperinjection(mL)
Totalnumbercellsinjected(3106)
Number ofinjections
Number ofCells perinjection(3106)
%Desminstaining
% Cellviability
P1 78 Female 1995 2001 5 17 25 1 0.11 25 9 3 85 98
P2 50 Male 1999 2002 10 14 382 5.4 0.30 270 18 16.3 44 98
P3 45 Male 1998 2002 6 19 544 5.7 0.30 293 19 16.3 12 97
P4 60 Male 1994 2002 9 17 211 5.4 0.30 211 18 16.3 80 95
P5 71 Female 1994 2002 12 18 622 8.1 0.30 405 27 16 42 96
P6 64 Male 1988 2003 9 17 435 4.0 0.20 150 15 10 82 94
P7 54 Male 1990 2002 6 17 225 4 0.20 200 15 16.3 91 89
P8 58 Male 1995 2003 11 17 329 3 0.20 150 15 10 94 98
P9 69 Male 1985 2003 15 16 345 4 0.20 150 15 10 57 93
P10 51 Male 2001 2002 14 15 310 3.2 0.20 310 16 16.3 68 99
P11 54 Male 1999 2003 13 16 240 2.9 0.30 240 8 50 88 92
P12 56 Male 1990 2002 13 14 182 4.2 0.30 183 14 16 54 95
P13 58 Male 1996 2003 15 16 400 3.2 0.20 160 16 10 82 92
P14 73 Male 1991 2002 13 18 297 3.0 0.30 297 10 16 70 97
Mean 63 – – – 10.8 17 325 4.2 0.24 217 15 15.9 68 95
SD – – – – 3.4 1 152 1.8 0.06 94 5 10.6 23 3
Interquartilerange
57–73 – – – 8.1–13.3 16–17 221–409 3.0–5.4 0.20–0.30 150–294 13–18 10–16.3 52–86 93–98
Median 62 11 17 310 4 206 15 16 75 96
In all patients the anteroseptal wall was injected.
C.E.V
eltman
etal
1390
by guest on April 23, 2016 http://eurheartj.oxfordjournals.org/ Downloaded from

DiscussionIn pre-clinical studies, implantation of SkM suggested replacementof non-functioning myocardial scar with functioning muscle andimprovement in myocardial performance.1,3,18,19 Data in humans
receiving SkM as adjunct to CABG indicate that cell implantationindeed may lead to improvement of LV function both on short-term,20 as well as after 4 years.6,21,22 It is obvious, however, thatconcomitant myocardial revascularization makes a separateappreciation of the role of cell transplantation in LV function
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 3 Left ventricle structure and ejection fraction on echocardiography at baseline
Treated (n 5 14) Controls (n 5 28) P-value
Mean+++++SD 95% CI Mean+++++SD 95% CI
LV-EDD (mm) 61+7 57–66 64+4 61–68 0.29
LV-ESD (mm) 48+7 46–56 52+5 48–57 0.62
LV-EDVI (mL/m2) 106+42 84–127 92+29 81–104 0.21
LV-ESVI (mL/m2) 72+32 54–91 60+27 50–71 0.21
LVEF (%) 32+9 27–38 36+8 32–39 0.29
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 4 Changes in left ventricle structure and ejection fraction on echocardiography
Treated(n 5 11)Baseline
95% CI Treated(n 5 11)
Follow-up
95% CI P-valuewithin
treated
Controls(n 5 17)Baseline
95% CI Controls(n 5 17)
Follow-up
95% CI P-valuewithin
controls
P-valuebetweengroups atFollow-up
LV-EDD (mm) 62+8 57–67 62+8 57–67 0.85 64+4 61–66 62+8 58–66 0.60 0.97
LV-ESD (mm) 47+7 44–56 54+8 48–59 0.37 52+5 48–55 52+9 48–57 0.29 0.74
LV-EDVI (mL/m2) 106+42 76–137 107+38 80–137 0.97 94+29 79–109 109+35 92–128 0.05 0.89
LV-ESVI (mL/m2) 72+31 44–99 70+30 48–91 0.79 62+26 48–75 71+29 56–86 0.13 0.93
LVEF (%) 35+10 28–41 37+9 30–42 0.75 36+8 32–40 38+6 32–40 0.95 0.96
Baseline vs. 4-year follow-up of patients that survived the follow-up period. Only survivors. Data are presented as mean+SD and 95% CI. All P-values between groups and forfollow-up vs. baseline are not significant. EDD, end-diastolic diameter; EDVI, end-diastolic volume indexed to body surface area; ESVI, end-systolic volume indexed to body surfacearea; EF, ejection fraction; LV, left ventricular.
Figure 1 Individual data of changes in left ventricular ejection fraction from baseline to 4-year follow-up in the treated group of skeletal myo-blast cells (left) and the control group (right). The mean data and standard deviation are represented in blue.
Percutaneous myoblast therapy: long-term follow-up 1391
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
improvement elusive. Short-term results from small studiesusing percutaneous SkM transplantation without adjunctiverevascularization, however, also indicated positive effects onLV function,7,8 supporting enhancement of LV function by SkM.
Unfortunately, all studies with or without revascularizationlacked a control group without SkM injection. Therefore, in thepresent study we compared the long-term effects of SkM trans-plantation in our first cohort of percutaneously treated patientswith a matched control group of ischaemic cardiomyopathypatients not receiving SkMs.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 7 Frequency of arrhythmic events on 24 h Holtermonitoring at the final visit during 4-year follow-up
Treated(n511)
Controls(n517)
P-value
Episodes of sustained VT’s 0 (0) 0 (0) –
Episodes of non-sustainedVT’s
5 (46) 9 (53) 0.98
Number of episodes 1.4+3 2.6+7 0.60
Number of ventricularcomplexes during VT
9+11 4+4 0.10
Rate of runs (b.p.m.) 113+34 134+39 0.16
Atrial tachyarrhythmia, n(%)
3 (27) 7 (41) 0.73
Atrial fibrillation, n (%) 0 (0) 3 (18) 0.38
Premature ventricularcontractions, n (%)
7 (64) 11 (65) 0.73
Data are presented as mean+SD or number (%). All P-values between treatedand control patients are not significant. VT, ventricular tachycardia.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 5 Regional myocardial velocities and performance index using tissue Doppler imaging for treated and controlpatients at 4-year follow-up
Treated (n 5 11) Controls (n 5 17) P-value
Mean+++++SD 95% confidence interval Mean+++++SD 95% confidence interval
Sm global (cm/s) 5.8+1.5 4.8–6.9 5.5+1.4 4.8–6.1 0.48
Sm (treated wall) (cm/s) 5.4+1.8 4.1–6.6 5.1+1.6 4.2–5.6 0.47
Em (global) (cm/s) 5.0+1.5 3.9–6.1 6.0+1.3 5.2–6.7 0.13
Em (treated wall) (cm/s) 5.7+2.3 3.9–7.2 6.0+2.1 4.9–6.9 0.63
Myocardial performance index 0.44+0.10 0.39–0.55 0.46+0.12 0.41–0.57 0.91
Sm, peak systolic velocity; Em, peak early diastolic velocity.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 6 Internal cardiovertor defibrillator data
P-value
Treated (n ¼ 14) Controls (n ¼ 28)
ICD implantation, n (%) 9 (64) 8 (29) 0.045
ICD data Treated (n ¼ 9) Controls (n ¼ 8)
Frequency of ICD therapy, n (%) 7 (87) 1 (13) 0.015
Type of ICD therapy
Anti-tachycardia pacing, n (%) 4 (57) 0 –
Shock, n (%) 3 (43) 1 (13) –
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 8 Secondary endpoints in the myoblast treatedand control groups
Treated(n 5 11)
Controls(n 5 17)
P-value
Hospitalization 5 (46) 11 (65) 0.55
Angina 3 (60) 4 (36) 0.39
Arrhythmias 1 (20) 4 (36) 0.63
Heart failure 1 (20) 3 (27) 0.98
NT-pro-BNP level(pmol/L)
67+55 86+91 0.54
Current angina 5 (46) 8 (47) 0.74
Six-minute walkingdistance (m)
403+92 429+109 0.52
Data are presented as mean+SD or number (%). All P-values between treatedand control patients are not significant. NT-pro-BNP, N-terminal pro-B-natriureticpeptide.
C.E. Veltman et al1392
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

Primary endpointIn this 4-year follow-up study, we sought to evaluate the long-termsafety and efficacy of the percutaneous endocardial transplantationof autologous skeletal myoblasts in chronic ischaemic HF patients.The results of the present study indicate that transplantation ofautologous SkMs in patients with depressed LV function becauseof a prior MI does not improve LV function compared with age-,sex-, and LV function matched controls at 4-year follow-up. LVinternal diameters and volumes as well as LVEF did not changeover time and were similar between the treated and control
groups. In this context, it is of interest that most non-controlled,initial studies insinuated that untreated patients with ischaemicHF would show a decline in LV function. The present study indi-cates that the survivors in such a patient group remains remarkablystable over time, which is most likely because of improved medicaltherapy. These results are in agreement with results of the MAGICtrial where at 6-month follow-up both treated and placebo groupshad comparable changes in global and regional LV function.23 Theyalso emphasized a decrease in LV volume in the high-dose myo-blast group, where in the present study only a trend towards adecrease in LV-EDVI was found. We support their conclusionthat more study should be directed to the anti-remodelling poten-tial of cell therapy. The use of contrast-enhanced echo like in thepresent study, which improves the reproducibility should be con-sidered in such trials.24.
Secondary endpointsThe short-term frequency of severe VT’s has been emphasizedsince the first clinical study with SkMs,4 but the long-term risk ofarrhythmias after treatment with myoblasts was thus farunknown. In the present study, albeit small sample, we observeda difference in the patients fitted with an ICD, i.e. more interven-tions occurred in the SkM group than in the control group.
This indicates that the concerns around arrhythmias and myo-blast therapy may still be valid. However, during 24 h-Holter moni-toring at the end of follow-up, a significant amount of ventriculararrhythmias was found in both groups. Almost half of the patientsin the treated group as well as in the control group experiencedepisodes of non-sustained VT’s.
The higher frequency of arrhythmias in the treated group inthe present study was seen also very early in treated group in
Figure 2 New York Heart Association functional class frombaseline to 4-year follow-up in the skeletal myoblast cellstreated vs. control patients.
Figure 3 Quality-of-life Short-Form Health Survey-36 questionnaire subscale scores in the skeletal myoblast cells treated vs. control patients.BP, bodily pain; GH, general health; MH, mental health; PF, physical functioning; REF, role emotional functioning; RPF, role physical functioning;SF, social functioning; VI, vitality.
Percutaneous myoblast therapy: long-term follow-up 1393
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

the MAGIC trial. However, at 6-month follow-up, thefrequency of arrhythmias was similar in the treated and placebogroups.23 Importantly, we have a 4-year follow-up period in thepresent study where most of the ICD events took place after6 months.
Consistent with the primary endpoints, in this study a differencein exercise capacity, hospitalization, NT-pro-BNP levels, andhealth-related quality of life was not shown. There was a trendtowards improvement of NYHA functional class over time in thetreated group (P ¼ 0.08), while the NYHA functional classremained the same over time in the control group. This suggeststhat the SkM-treated patients performed better and had a betterclinical presentation than the patients in the control group.However, it is well recognized that in open studies evaluating inva-sive procedures, a substantial role for the placebo effect may beexpected.25 In addition, results from the quality-of-life question-naire did not point to the same direction.
Unresolved issuesAlmost all small, phase I clinical trials showed improvement in LVfunction after SkM injection, but the results from larger, andmore important randomized controlled trials treating patientswith SkM injection are still pending. In the MAGIC trial (Myo-blast Autologous Grafting in Ischemic Cardiomyopathy trial),patients were randomized into three groups (n ¼ 97 total)receiving 400 � 106 or 800 � 106 SkMs, or medium only. Themajor adverse cardiac events did not show any differencebetween the groups at 30 days as well as at 6 months. Likewise,myoblast injection did not improve either global or regional LVfunction at 6-month follow-up in the treated patients over thatin the placebo group. Of note, the incidence of ventriculararrhythmias was also similar between the groups.23 Theseresults indicate that the number of cells injected might not bethe most decisive factor for success, as the neutral results inthe MAGIC trial were observed with four times the numberof cells as in the present study. A more important variablemay be the studied population, because in trials conducted inthe acute phase of MI more, albeit modest, positive resultswere obtained.26 – 30 Alternatively, the phenotype of the injectedcells might be essential to obtain better functional improve-ments, as cells allowed to differentiate into a preferred lineagein vitro before re-injection may provide better results as shownin a pre-clinical study.31
Study limitationsThe efficacy assessment could be underpowered in this study bythe small sample of myoblast-treated population. Lack of statisticalsignificance is in this respect no conclusive evidence for lack ofeffect. However, our group has reported evidence for myoblastefficacy in five out of the 14 treated patients, which are describedin this study, at 12 months follow-up.7 The objective of the presentevaluation was to assess if these effects were sustained atlong-term.
The trial was neither randomized nor blinded. However, thematching between the two groups was performed as fair as poss-ible. The control group was matched for age, sex, and time sinceprior MI and localization of the infarction area, and LVEF.
Because we did not match on ICD presence, we should be cau-tious in the interpretation of the difference in arrhythmia in bothgroups. The patients in the treated group were fitted with ICDper protocol, where the control patients were fitted with ICDfor clinical indications. As expected, we observed considerable(average 30%) mortality in our study population over a period of4 years, but the baseline LVEF data of those patients who dieddid not differ from the survivors. Still this does not exclude a selec-tion bias introduced by loss of patients with a worse LVEF, becausethe patients who died might have been the patients with the mostprogressive decrease in clinical performance over time. This couldhave been resolved by, for instance, interim analysis every 6months during the follow-up period. However, this was notincluded in the original study design.
ConclusionsThis study shows that intramyocardial SkM injection in chronicischaemic HF patients has no sustained positive effect on restingglobal and regional LV function when compared with matched con-trols over a 4-year follow-up period. In addition, the ICD read-outsduring the course of follow-up, but not the 24 h arrhythmia moni-toring at 4 years, indicate a potential higher risk of developing ven-tricular arrhythmias.
Conflict of interest: none declared.
References1. Atkins BZ, Hueman MT, Meuchel JM, Cottman MJ, Hutcheson KA,
Taylor DA. Myogenic cell transplantation improves in vivo regionalperformance in infarcted rabbit myocardium. J Heart Lung Trans-plant 1999;18:1173–1180.
2. Orlic D, Kajstura J, Chimenti S, Jakoniuk I, Anderson SM, Li B,Pickel J, McKay R, Nadal-Ginard B, Bodine DM, Leri A,Anversa P. Bone marrow cells regenerate infarcted myocardium.Nature 2001;410:701–705.
3. Taylor DA, Atkins BZ, Hungspreugs P, Jones TR, Reedy MC,Hutcheson KA, Glower DD, Kraus WE. Regenerating functionalmyocardium: improved performance after skeletal myoblast trans-plantation. Nat Med 1998;4:929–933.
4. Menasche P, Hagege AA, Vilquin JT, Desnos M, Abergel E,Pouzet B, Bel A, Sarateanu S, Scorsin M, Schwartz K, Bruneval P,Benbunan M, Marolleau JP, Duboc D. Autologous skeletal myo-blast transplantation for severe postinfarction left ventricular dys-function. J Am Coll Cardiol 2003;41:1078–1083.
5. Siminiak T, Kalawski R, Fiszer D, Jerzykowska O, Rzezniczak J,Rozwadowska N, Kurpisz M. Autologous skeletal myoblast trans-plantation for the treatment of postinfarction myocardial injury:phase I clinical study with 12 months of follow-up. Am Heart J2004;148:531–537.
6. Dib N, Michler RE, Pagani FD, Wright S, Kereiakes DJ, Lengerich R,Binkley P, Buchele D, Anand I, Swingen C, Di Carli MF, Thomas JD,Jaber WA, Opie SR, Campbell A, McCarthy P, Yeager M,Dilsizian V, Griffith BP, Korn R, Kreuger SK, Ghazoul M,MacLellan WR, Fonarow G, Eisen HJ, Dinsmore J, Diethrich E.Safety and feasibility of autologous myoblast transplantation inpatients with ischemic cardiomyopathy: four-year follow-up. Circu-lation 2005;112:1748–1755.
C.E. Veltman et al1394
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from

7. Smits PC, van Geuns RJ, Poldermans D, Bountioukos M,Onderwater EE, Lee CH, Maat AP, Serruys PW. Catheter-basedintramyocardial injection of autologous skeletal myoblasts as aprimary treatment of ischemic heart failure: clinical experiencewith six-month follow-up. J Am Coll Cardiol 2003;42:2063–2069.
8. Steendijk P, Smits PC, Valgimigli M, van der Giessen WJ,Onderwater EE, Serruys PW. Intramyocardial injection of skeletalmyoblasts: long-term follow-up with pressure-volume loops. NatClin Pract Cardiovasc Med 2006;3(Suppl. 1):S94–S100.
9. Aaronson NK, Muller M, Cohen PD, Essink-Bot ML, Fekkes M,Sanderman R, Sprangers MA, te Velde A, Verrips E. Translation,validation, and norming of the Dutch language version of theSF-36 Health Survey in community and chronic disease popu-lations. J Clin Epidemiol 1998;51:1055–1068.
10. Cheitlin MD, Alpert JS, Armstrong WF, Aurigemma GP, Beller GA,Bierman FZ, Davidson TW, Davis JL, Douglas PS, Gillam LD,Lewis RP, Pearlman AS, Philbrick JT, Shah PM, Williams RG,Ritchie JL, Eagle KA, Gardner TJ, Garson A, Gibbons RJ,O’Rourke RA, Ryan TJ. ACC/AHA guidelines for the clinical appli-cation of echocardiography: executive summary. A report of theAmerican College of Cardiology/American Heart AssociationTask Force on practice guidelines (Committee on Clinical Appli-cation of Echocardiography). Developed in collaboration withthe American Society of Echocardiography. J Am Coll Cardiol1997;29:862–879.
11. Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA.Recommendations for quantification of Doppler echocardiogra-phy: a report from the Doppler Quantification Task Force ofthe Nomenclature and Standards Committee of the AmericanSociety of Echocardiography. J Am Soc Echocardiogr 2002;15:167–184.
12. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E,Pellikka PA, Picard MH, Roman MJ, Seward J, Shanewise JS,Solomon SD, Spencer KT, Sutton MS, Stewart WJ. Recommen-dations for chamber quantification: a report from the AmericanSociety of Echocardiography’s Guidelines and Standards Commit-tee and the Chamber Quantification Writing Group, developed inconjunction with the European Association of Echocardiography, abranch of the European Society of Cardiology. J Am Soc Echocar-diogr 2005;18:1440–1463.
13. Waggoner AD, Bierig SM. Tissue Doppler imaging: a useful echo-cardiographic method for the cardiac sonographer to assess systo-lic and diastolic ventricular function. J Am Soc Echocardiogr 2001;14:1143–1152.
14. Diwan A, McCulloch M, Lawrie GM, Reardon MJ, Nagueh SF.Doppler estimation of left ventricular filling pressures in patientswith mitral valve disease. Circulation 2005;111:3281–3289.
15. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA,Quinones MA. Doppler tissue imaging: a noninvasive techniquefor evaluation of left ventricular relaxation and estimation offilling pressures. J Am Coll Cardiol 1997;30:1527–1533.
16. Soliman OI, Theuns DA, ten Cate FJ, Anwar AM, Nemes A,Vletter WB, Jordaens LJ, Geleijnse ML. Baseline predictors ofcardiac events after cardiac resynchronization therapy in patientswith heart failure secondary to ischemic or nonischemic etiology.Am J Cardiol 2007;100:464–469.
17. Tei C, Ling LH, Hodge DO, Bailey KR, Oh JK, Rodeheffer RJ,Tajik AJ, Seward JB. New index of combined systolic and diastolicmyocardial performance: a simple and reproducible measure ofcardiac function—a study in normals and dilated cardiomyopathy.J Cardiol 1995;26:357–366.
18. Laflamme MA, Murry CE. Regenerating the heart. Nat Biotechnol2005;23:845–856.
19. Murry CE, Wiseman RW, Schwartz SM, Hauschka SD. Skeletalmyoblast transplantation for repair of myocardial necrosis. J ClinInvest 1996;98:2512–2523.
20. Hagege AA, Carrion C, Menasche P, Vilquin JT, Duboc D,Marolleau JP, Desnos M, Bruneval P. Viability and differentiationof autologous skeletal myoblast grafts in ischaemic cardiomyopa-thy. Lancet 2003;361:491–492.
21. Hagege AA, Marolleau JP, Vilquin JT, Alheritiere A, Peyrard S,Duboc D, Abergel E, Messas E, Mousseaux E, Schwartz K,Desnos M, Menasche P. Skeletal myoblast transplantation inischemic heart failure: long-term follow-up of the first phase Icohort of patients. Circulation 2006;114(Suppl. 1):I108–I113.
22. Pagani FD, DerSimonian H, Zawadzka A, Wetzel K, Edge AS,Jacoby DB, Dinsmore JH, Wright S, Aretz TH, Eisen HJ,Aaronson KD. Autologous skeletal myoblasts transplanted toischemia-damaged myocardium in humans. Histological analysisof cell survival and differentiation. J Am Coll Cardiol 2003;41:879–888.
23. Menasche P, Alfieri O, Janssens S, McKenna W, Reichenspurner H,Trinquart L, Vilquin JT, Marolleau JP, Seymour B, Larghero J, Lake S,Chatellier G, Solomon S, Desnos M, Hagege AA. The MyoblastAutologous Grafting in Ischemic Cardiomyopathy (MAGIC) trial:first randomized placebo-controlled study of myoblast transplan-tation. Circulation 2008;117:1189–1200.
24. Galema TW, Geleijnse ML, Yap SC, van Domburg RT, Biagini E,Vletter WB, Ten Cate FJ. Assessment of left ventricular ejectionfraction after myocardial infarction using contrast echocardiogra-phy. Eur J Echocardiogr 2007.
25. Leon MB, Kornowski R, Downey WE, Weisz G, Baim DS,Bonow RO, Hendel RC, Cohen DJ, Gervino E, Laham R,Lembo NJ, Moses JW, Kuntz RE. A blinded, randomized, placebo-controlled trial of percutaneous laser myocardial revascularizationto improve angina symptoms in patients with severe coronarydisease. J Am Coll Cardiol 2005;46:1812–1819.
26. Assmus B, Honold J, Schachinger V, Britten MB, Fischer-Rasokat U,Lehmann R, Teupe C, Pistorius K, Martin H, Abolmaali ND,Tonn T, Dimmeler S, Zeiher AM. Transcoronary transplantationof progenitor cells after myocardial infarction. N Engl J Med2006;355:1222–1232.
27. Janssens S, Dubois C, Bogaert J, Theunissen K, Deroose C,Desmet W, Kalantzi M, Herbots L, Sinnaeve P, Dens J,Maertens J, Rademakers F, Dymarkowski S, Gheysens O, VanCleemput J, Bormans G, Nuyts J, Belmans A, Mortelmans L,Boogaerts M, Van de Werf F. Autologous bone marrow-derivedstem-cell transfer in patients with ST-segment elevation myocar-dial infarction: double-blind, randomised controlled trial. Lancet2006;367:113–121.
28. Kang HJ, Lee HY, Na SH, Chang SA, Park KW, Kim HK, Kim SY,Chang HJ, Lee W, Kang WJ, Koo BK, Kim YJ, Lee DS,Sohn DW, Han KS, Oh BH, Park YB, Kim HS. Differential effectof intracoronary infusion of mobilized peripheral blood stemcells by granulocyte colony-stimulating factor on left ventricularfunction and remodeling in patients with acute myocardial infarc-tion versus old myocardial infarction: the MAGIC Cell-3-DES ran-domized, controlled trial. Circulation 2006;114(Suppl. 1):I145–I151.
29. Lunde K, Solheim S, Aakhus S, Arnesen H, Abdelnoor M,Egeland T, Endresen K, Ilebekk A, Mangschau A, Fjeld JG,Smith HJ, Taraldsrud E, Grogaard HK, Bjornerheim R, Brekke M,Muller C, Hopp E, Ragnarsson A, Brinchmann JE, Forfang K.
Percutaneous myoblast therapy: long-term follow-up 1395
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
Intracoronary injection of mononuclear bone marrow cells inacute myocardial infarction. N Engl J Med 2006;355:1199–1209.
30. Schachinger V, Erbs S, Elsasser A, Haberbosch W, Hambrecht R,Holschermann H, Yu J, Corti R, Mathey DG, Hamm CW,Suselbeck T, Assmus B, Tonn T, Dimmeler S, Zeiher AM. Intracor-onary bone marrow-derived progenitor cells in acute myocardialinfarction. N Engl J Med 2006;355:1210–1221.
31. Bartunek J, Croissant JD, Wijns W, Gofflot S, de Lavareille A,Vanderheyden M, Kaluzhny Y, Mazouz N, Willemsen P,Penicka M, Mathieu M, Homsy C, De Bruyne B, McEntee K,Lee IW, Heyndrickx GR. Pretreatment of adult bone marrowmesenchymal stem cells with cardiomyogenic growth factors andrepair of the chronically infarcted myocardium. Am J PhysiolHeart Circ Physiol 2007;292:H1095–H1104.
CLINICAL VIGNETTE. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
doi:10.1093/eurheartj/ehm579Online publish-ahead-of-print 22 December 2007
Haemoptysis and complete atrioventricular blockPatrizio Pascale1*, John O. Prior2, Pierre-Nicolas Carron3, Etienne Pruvot1, and Olivier Muller1
1Service of Cardiology, Centre Hospitalier Universitaire Vaudois (CHUV), – BH7, Av. Bugnon 11, Lausanne 1011, Switzerland; 2Nuclear Medicine Department, CentreHospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland; and 3Emergency Department, Centre Hospitalier Universitaire Vaudois (CHUV), Lausanne, Switzerland
* Corresponding author. Tel: þ41213140069, Fax: þ41213140055, Email: [email protected]
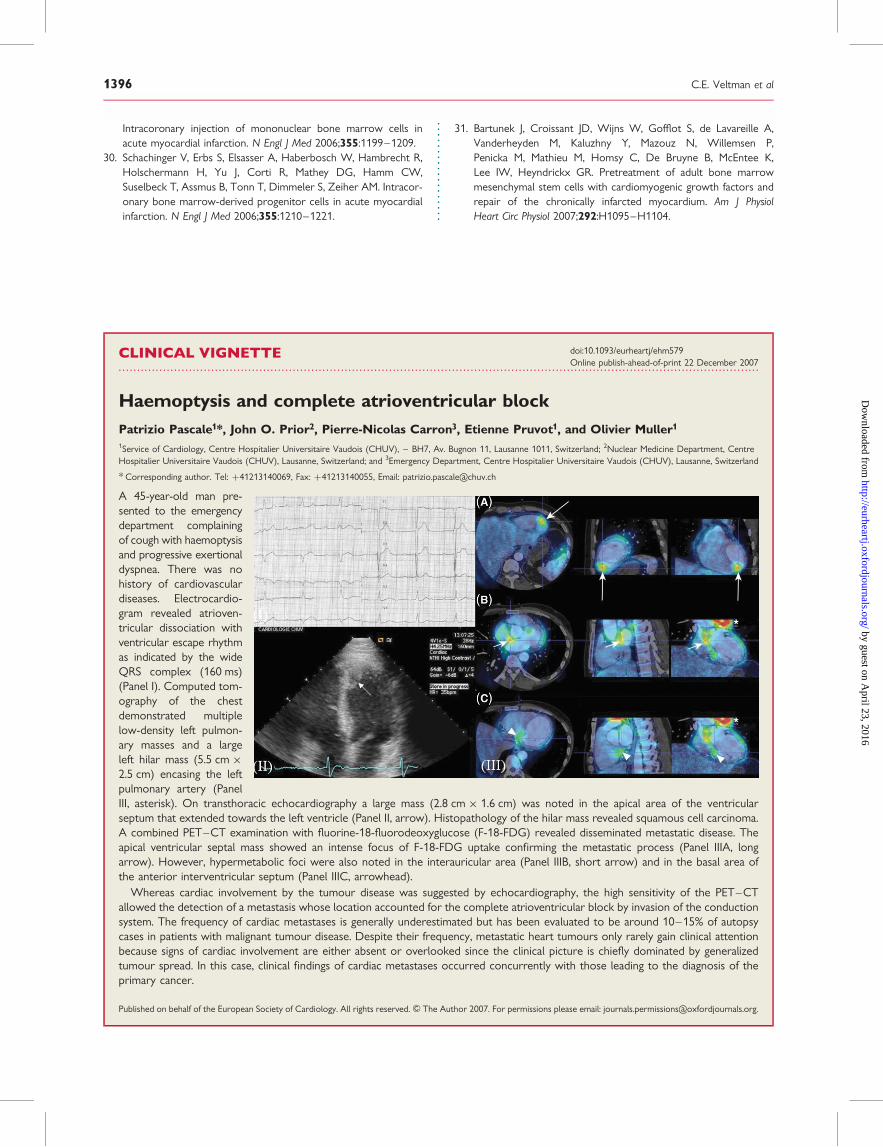
A 45-year-old man pre-sented to the emergencydepartment complainingof cough with haemoptysisand progressive exertionaldyspnea. There was nohistory of cardiovasculardiseases. Electrocardio-gram revealed atrioven-tricular dissociation withventricular escape rhythmas indicated by the wideQRS complex (160 ms)(Panel I). Computed tom-ography of the chestdemonstrated multiplelow-density left pulmon-ary masses and a largeleft hilar mass (5.5 cm �2.5 cm) encasing the leftpulmonary artery (PanelIII, asterisk). On transthoracic echocardiography a large mass (2.8 cm � 1.6 cm) was noted in the apical area of the ventricularseptum that extended towards the left ventricle (Panel II, arrow). Histopathology of the hilar mass revealed squamous cell carcinoma.A combined PET–CT examination with fluorine-18-fluorodeoxyglucose (F-18-FDG) revealed disseminated metastatic disease. Theapical ventricular septal mass showed an intense focus of F-18-FDG uptake confirming the metastatic process (Panel IIIA, longarrow). However, hypermetabolic foci were also noted in the interauricular area (Panel IIIB, short arrow) and in the basal area ofthe anterior interventricular septum (Panel IIIC, arrowhead).
Whereas cardiac involvement by the tumour disease was suggested by echocardiography, the high sensitivity of the PET–CTallowed the detection of a metastasis whose location accounted for the complete atrioventricular block by invasion of the conductionsystem. The frequency of cardiac metastases is generally underestimated but has been evaluated to be around 10–15% of autopsycases in patients with malignant tumour disease. Despite their frequency, metastatic heart tumours only rarely gain clinical attentionbecause signs of cardiac involvement are either absent or overlooked since the clinical picture is chiefly dominated by generalizedtumour spread. In this case, clinical findings of cardiac metastases occurred concurrently with those leading to the diagnosis of theprimary cancer.
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2007. For permissions please email: [email protected].
C.E. Veltman et al1396
by guest on April 23, 2016
http://eurheartj.oxfordjournals.org/D
ownloaded from
Copyright © 2022 FDOKUMEN




















