FOR MID-LEVEL MANAGERS - newconceptinfosys.net
68
SOCIAL AND BEHAVIOUR CHANGE COMMUNICATION TRAINING FOR MID-LEVEL MANAGERS Duration: Two Days
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of FOR MID-LEVEL MANAGERS - newconceptinfosys.net

SOCIAL AND BEHAVIOUR CHANGECOMMUNICATION TRAINING
FOR MID-LEVEL MANAGERSDuration: Two Days

2014
For more copies contact:Communication for Development SectionUnited Nations Children's Fund73 Lodi Estate, New Delhi, IndiaE-mail: [email protected]: www.unicef.org www.unicefiec.org www.unicef.org/india/Telephone: +91-11-24690401
SOCIAL AND BEHAVIOUR CHANGECOMMUNICATION (SBCC)TRAINING
FOR MID-LEVEL MANAGERSDuration: Two Days
3

CONTENTSDAY I Session 1 - Inauguration and Introduction 4Session 2 - Changing Paradigms in Development Communication 5Session 3 - Introduction to the ‘Tarang’ Communication Module 7Session 4 - Introduction to Communication 8Session 5 - The Behaviour Change Process 12Session 6 - Qualities of a Good Communicator 18Session 7 - Introduction to Interpersonal Communication; The
GATHER Concept20
Session 8 - ReviewandReflectionsoftheDay 22
DAY IISession 1 - RecallofDayISessions 24Session 2 - Understanding Social Inclusion and its Importance in
Social and Behaviour Change Communication24
Session 3 - Social Inclusion (Continued) 29Session 4 - How to Conduct a Group Discussion 31Session 5 - UseofaCommunityDialogueTool 34Session 6 - Understanding Teamwork 38Session 7 - Planning and Organising a Village Health and Nutrition
Day42
Session 8 - Creating a Village Health Plan and Developing a Village SBCC Plan
43
Session 9 - ValedictorySession 44
Annexures 45
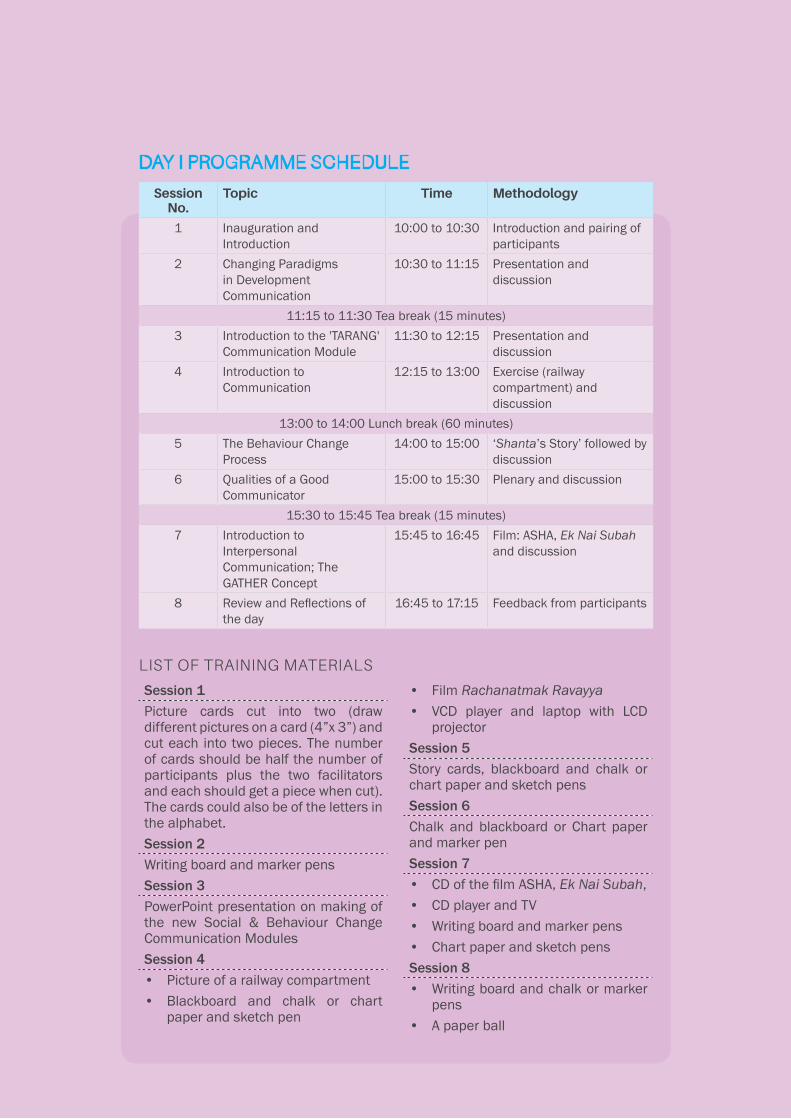
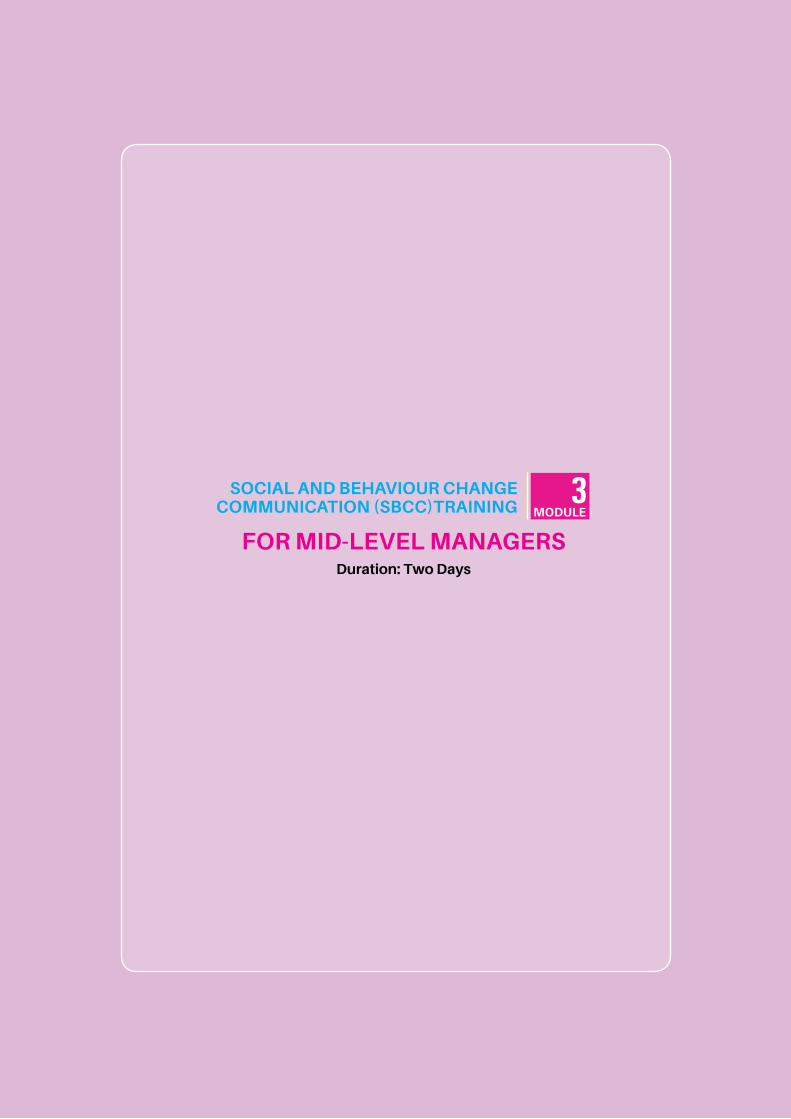
Session No.
Topic Time Methodology
1 Inauguration and Introduction
10:00 to 10:30 Introduction and pairing of participants
2 Changing Paradigms in Development Communication
10:30 to 11:15 Presentation and discussion
11:15 to 11:30 Tea break (15 minutes)3 Introduction to the 'TARANG'
Communication Module11:30 to 12:15 Presentation and
discussion4 Introduction to
Communication12:15 to 13:00 Exercise(railway
compartment) and discussion
13:00 to 14:00 Lunch break (60 minutes)5 The Behaviour Change
Process14:00 to 15:00 ‘Shanta’sStory’followedby
discussion6 Qualities of a Good
Communicator15:00 to 15:30 Plenaryanddiscussion
15:30 to 15:45 Tea break (15 minutes)7 Introduction to
Interpersonal Communication; The GATHER Concept
15:45 to 16:45 Film: ASHA, Ek Nai Subah and discussion
8 ReviewandReflectionsoftheday
16:45 to 17:15 Feedback from participants
Session 1Picture cards cut into two (draw different pictures on a card (4”x 3”) and cut each into two pieces. The number of cards should be half the number of participants plus the two facilitators and each should get a piece when cut). The cards could also be of the letters in the alphabet.Session 2Writing board and marker pensSession 3PowerPoint presentation on making of the new Social & Behaviour Change Communication ModulesSession 4• Pictureofarailwaycompartment• Blackboard and chalk or chart
paper and sketch pen
• Film Rachanatmak Ravayya• VCD player and laptop with LCD
projectorSession 5Story cards, blackboard and chalk orchart paper and sketch pensSession 6Chalk and blackboard or Chart paper and marker penSession 7• CDofthefilmASHA,Ek Nai Subah,• CDplayerandTV• Writing board and marker pens • Chart paper and sketch pensSession 8• Writing board and chalk or marker
pens • A paper ball
LIST OF TRAINING MATERIALS
DAY I PROGRAMME SCHEDULE

For Mid-Level Managers4
SESSION 1 INAUGURATION AND INTRODUCTION
SESSION OUTCOMES
At the end of the session, participants would have:
• Introducedeachother,creatingafriendlyenvironment.
MATERIALS REQUIRED
• Picture cards cut into two [draw different pictures on cards (each 4”x 3”) and cut each into two pieces. The number of cards should be half the number of participants plus the two facilitators and each should get a piece when cut]. The cards could also have the letters of the alphabet.
METHODOLOGY
Pairing using picture cards.
PROCESS
1. Oneofthefacilitatorsbeginsthesessionbysaying,“OnbehalfoftheInstitute(TrainingCentre) and facilitators’ team, Iwelcomeeachoneof you to today’ssessions on introducing the new SBCC module for field functionaries andcommunity volunteers.With communicationbecomingcentral todevelopmentprogramming, we hope that this module will be a great help to all in reaching out to families and communities to bring about social and behaviour change. We will be discussing details of the module during the course of the sessions.”
“But before that, let’s start by introducing ourselves. Some of you may beacquaintedwitheachotherandsomeofyoumaynot.Solet’strytogettoknoweach other through a simple exercise.”
2. Now put the cards cut into halves in a box the centre of the room and mix them up well. Ask each participant to come and pick a card. The two facilitators too should pickacardeach.Onceeveryonehasacard,telltheparticipants,“Eachofushasacardwithhalfapicture.Wenowhavetofindoutwhohastheotherhalfofthepicture.Pleasemovearoundandfindoutwhohastheotherhalfofthepicture.Onceyoufindthatpersonstaytogetherasapair.Start.”
3. If the total of participants and facilitators is an odd number, ask the person left outtojoinanypair;oroneofthefacilitatorsshouldnotpickacardandjoinoneof the pairs making it a triad. Once all the participants are in pairs each person should:sayhis/hername;whathe/shedoes;alsobrieflyshareoneprogrammecommunicationactivitythathe/shehasseeninthecourseofworkwhichhe/shefelt was either successful or not successful.
After each of themhas done this, whichmay take about 5minutes, ask theparticipants to sit with their partners. Now ask each one to introduce his/her partner. The facilitators also join in.
CONCLUDING THE SESSION
Concludethesessionbythankingthemforactivelyparticipatingintheexerciseandalso for sharing their experiences in programme communication. Tell the participants that we will build on the discussions in the subsequent sessions.
10:00 to 10:30 (30 minutes)

SBCC Training : Module 3 5
SESSION 2 CHANGING PARADIGMS IN DEVELOPMENT COMMUNICATION
SESSION OUTCOMES
At the end of the session, participants will be able to:
• Describe the changes that have taken place in development communication in order to bring about the desired behaviour changes.
METHODOLOGY
PowerPoint presentation and discussion
MATERIALS REQUIRED
Writing board and marker pens
PROCESS
Startthesessionbysaying,“Overthelastfewdecades,therehavebeensubtleshiftsinthewaydevelopmentcommunicatorshaveapproachedcommunicationstrategiesin influencingbehaviourchange. Ithasbeenaprocessofevolutionandtodaywehave a much more comprehensive approach to handle social and behaviour change within development programming.”
1. Ask the participants to tell how they/their department have perceivedcommunication in the past.
2. Askthemtotellthedifferencebetweenthe‘familyplanning’campaignsofthe1970s and the ‘polio campaign’ of recent times. What communication tools were used then and now?
3. Oncetheparticipantshavefinished,sumup,coveringthefollowingpoints:• In the 1950s and 1960s when development was measured using the Gross
National Product (GNP) as the indicator where capital-intensive approaches and centralised planning were the norm, it was believed that mass media would raise the aspirations of the people and bring about desired behaviour changes. A large number of radio stations and newspapers were used to disseminate messages targeting populations in the hope that this would help bringaboutchanges.Thiswasaone-wayapproach.
• Itwasthoughtthatmassmediawasimportantbecauseonlythroughthemcould the countries with limited resources hope to provide information to vast numbersbydisseminatingthemessagesattheraterequiredfordevelopment.
• It was then felt that mass communication alone would not produce the desired results, but that there was need for the dissemination of messages through opinion leaders. This brought in the initial concepts in interpersonal communication strategies where individuals within communities were inductedtospreadmessagesandinfluenceindividualsandfamilies.
• The 1970s and 1980s focused on bringing about individual behaviour change and the concept of Behaviour Change Communication (BCC) came intobeing.BCCiscloselyassociatedwithSocialMarketingStrategieswhichwere seen as a means to promote a particular behaviour or social change through communication.
10:30 to 11:15 (45 minutes)

For Mid-Level Managers6
• Almost simultaneously the concept of Information, Education andCommunication (IEC) was also evolving where the emphasis was on dissemination of messages through production and use of audio visuals and print materials.
• In all the above approaches the concept of stakeholder participation was totallymissing.Theideathatstakeholdersshouldnecessarilyparticipateinthecommunicationprocesswasbroughtoutasearlyasinthe1960swiththeworkthatwasbeingdoneinLatinAmericabyPauloFreire.Thisdidnotcatchthe attention of communication planners at that time.
• However, with human rights based programming gaining ground in the late 1990sandearly2000swhereparticipationbecameacriticalrightofeveryindividual, family or community, the concept of participatory approachesto communicationgainedprominence. Theparadigm that every individual,familyorcommunityhastheright tomake ‘informedchoices’stressedtheimportance of empowering them with the right knowledge and skills to make such choices. Communication is no more seen as a top-down approach where families and communities are targets for behaviour change. Today,development communication is considered to be a multi-stakeholder and participatoryprocesswheretheinvolvementofallstakeholdersisimportant.
• Today‘development’isseenascreatinganenvironmentinwhichpeoplecanreach their full potential and lead productive, creative lives in accordance with their needs and interests. According to the UNDP Human Development Report 2012, people are the real wealth of nations and emphasis should be on the needforexpansionoftheirchoicessothattheyleadlivesthattheyvalue.
• Intoday’sdevelopmentcontextitisimportanttounderstandthatwidesocialacceptanceabouttheneedforspecificchangehasbecomeapre-conditionforindividualbehaviourchange.Changeisofteninfluencedbyotherpeople’sexpectations,whichisinturnshapedbythecurrentsocialandculturalnorms.Therefore it is important that communication strategies address social change, creating community norms. Social and Behaviour Change Communication(SBCC) addresses both social and individual behaviour change.
4. Sum up the discussions with the following:We have seen that communication approaches have been evolving over time and todaythereisamuchmorecomprehensiveunderstandingoftheprocess.Someofthe areas that require our communication activities are given below:
CONCLUDING THE SESSION
Conclude the session with the following:• Thus, we see that a communication plan should address various stakeholders at
various levels and that the approaches at different levels could be different or a mix of different approaches, depending on the need.
To b
e re
ache
dCo
mm
unic
atio
n Ap
proa
ches
Social: Institutions and policies
Largelythrough advocacyand mass
media
Implementing agencies and functionaries
Through training and capacitybuilding
Community
Communitydialogue and mobilisation, community
media
Individuals and families
Interpersonal communication,
IEC and counselling

SBCC Training : Module 3 7
SESSION 3 INTRODUCTION TO THE ‘TARANG’ COMMUNICATION MODULE
TEA BREAK 11:15 to 11:30 (15 minutes)
SESSION OUTCOMES
At the end of the session, participants will be able to:• Describe the background against which the module has been developed, the
principles used in developing the modules and the contents of the different items.• List the items in the modules and their use at various levels.
MATERIALS REQUIRED
• Writing board with chalk/marker pens• PowerPoint presentation, LCD projector and laptop or computer
METHODOLOGY
PowerPoint presentation and discussion
PROCESS
1. Thefacilitatorbeginsthesessionbysaying:“Wewillnowhaveabriefintroductionto the new Social & Behaviour Change Communication Module that has been developed. Much work had gone in to its making including review of existing modules and materials, field visits to states and interactions with variousstakeholdersat thestate,district,blockandfield level. The facultyof varioustrainingcentreswerealsometandtheirinputstaken.Iwillnowtakeyouthrougha PowerPoint presentation that summarises how the modules were made and whattheycontain.”
2. NowstartthePowerPointpresentationandgothroughtheslidesonebyone.
3. Allow participants to raise questions during the presentation. Answer them based on the module.
CONCLUDING THE SESSION
Concludebysayingthatinthefollowingsessionswewillhaveadetailedlookatsomeoftheimportantsessionsfromthe5-DaytrainingModule.
• TheSBCCmodulesthatarebeingintroducedarelargelytoaddresscommunicationneedsatthecommunity,familyandindividuallevels.ThemodulesdealwithIPC,Counselling,IECandCommunityDialoguetools.
• We will discuss these in detail in the next few sessions.
11:30 to 12:15 (45 minutes)

For Mid-Level Managers8
SESSION 4 AN INTRODUCTION TO COMMUNICATION
SESSION OUTCOMES
At the end of the session, participants will be able to:• Describe the communication loop with the different steps therein.• Explain the need for the communicator and the receiver to be on the same
wavelength for effective communication to happen.• Give examples of why one-way communication invariably leads to distorted
messages.
MATERIALS REQUIRED
• Thepictureofarailwaycompartmentasshowninthelessonplan• Blackboard and chalk or chart paper and sketch pen• Film Rachanatmak Ravayya• VideoplayerandTVorlaptopandLCDprojector
METHODOLOGY
• The‘railwaycompartment’exercise.• Follow-up discussions.• ConcludewiththefilmRachanatmak Ravayya.
PROCESS
1. Ask for 10 Volunteers. One of the facilitators takes Volunteer #1 and leaves the traininghall.He/shegivesthevolunteerthepictureoftherailwaycompartmentandtellshim/hertostudyit(2minutestostudythepicture).
2. The facilitator informs the Volunteerthathis/hertaskwillbetoconveywhatisinthe picture to volunteer #2.
3. Once the Volunteer isreadytodescribethepicture,askhim/hertocomeintothe training room. Now the other nine Volunteers are taken out of the training hallbythesecondfacilitator.ThenVolunteer #2 from among them is called in. Ask Volunteer #1 to describe what was in the picture to Volunteer #2. Tell him/herthathe/shecanonlylistentowhatVolunteer#1issayingandcannotaskanyquestionsforclarification.OnceVolunteer #1 has completed describing the picture,askhim/hertositamongtheparticipantsandnottotalktoanyone.
4. Now call Volunteer #3 into the training hall. Ask Volunteer #2 to describe what he/she heard from Volunteer #1 to Volunteer #3. As before, Volunteer #3 cannot askanyquestions.OnceVolunteer #2 has completed, ask him/her to sit next to Volunteer#1,butnottospeakanything.
5. Repeat the process till Volunteer#6isbriefedbyVolunteer #5. Now ask Volunteer #6 to tell all the participants what he/she understood about the picture. The descriptionhe/shegiveswillbeverydifferentfromwhatisreallyinthepicture.
6. Showthepicturetoalltheparticipantssothattheyareabletoseethedistortionsthat have taken place.
12:15 to 13:00 (45 minutes)

SBCC Training : Module 3 9
7. Nowtelltheparticipantsthattheexerciseisnotyetover.CallinVolunteers7and8. Give the picture to Volunteer #7 and ask him/her to study itso that he/she can describe it to Volunteer #8. Volunteer #8 should not see the picture. Once he/she is readytodescribethepicture,takeitaway.NowaskVolunteer#7 todescribe the picture to Volunteer #8. Tell Volunteer #8 that he/she can ask questions to get clarifications. Once Volunteer #7completes describing the picture to the satisfaction of Volunteer #8, ask Volunteer #8 to describe the picture to all the participants. Once again show the picture to all participants sothattheyareabletomakeoutthedistortions.
8. Tell the participants that there is one more part to the exercise. Call in Volunteers #9and10andgivethepicturetoVolunteer#9.Askhim/hertostudythepicturesothathe/sheisabletoconveywhathe/sheseestoVolunteer#10.Oncehe/sheisready,askhim/hertodescribethepicturetoVolunteer#10andtellhim/her there are no restrictions. He/she can even show the picture and describe it. Now tell Volunteer #10 to describe the picture to the participants. Stop the exercise here; ask all participants to go back to their original seats.
9. Asktheparticipants,“Whatdidweseehere?Whatwerethedifferencesinthethree parts of the exercise? Which team/pair was able to give the best description of the picture?”Ask the following questions and note the answers:
• Howmanywomenarethere?• Howmanypersonsarethere?• Howmanychildrenarethere?• Whichlanguagehasbeenusedbytherailwaysonthecompartmentpartitions,
bypassengersontheirluggage?(Facilitatortonote:Doessomeonepointoutthateverythingiswritteninmirrorimage?)
10. Why did that team/pair succeed? Allow sufficient time for the participants toreflectandsharetheirviews.
11. The points emerging from the discussions are noted on the board.
12. Asktheparticipantswhethertheyhavehadanyexperiencewheremessagesgotdistorted.Havefivetosixparticipantssharetheirexperiences.
CONCLUDING THE SESSION
Wesawthreedifferentcommunicationstyleshere.
Case 1: The communication was one way where the listener could not ask anyquestions;he/shecouldonlylistentothevolunteer.

For Mid-Level Managers10
• Whenamessageisconveyedbyoneperson,theothershouldreceiveitwithoutdistortions. This can be ensured when the receiver gives a feedback to the sender and repeats themessageso thatclarificationscanbeprovided ifneeded.Soeffective communication should have a loop which ensures that the sender and the receiver have the same understanding.
• So when we communicate with women, families and communities it is veryimportantthatwetakefeedbackfromthemandlistentothemverycarefullytoensurethatthemessagehasbeenisunderstoodclearly.
• Ask the participants what, in their opinion, are the do's and don’ts for good, effectivecommunication.Listentosomeresponses,andthendisplaythechartbelow.
Case 2: Thelistenerwasfreetoaskquestionsandgetclarifications.Inthiscasethemessagewasbetterdeliveredcomparedtothefirstcase.
Case 3: The messenger and the listener were able to discuss the picture while looking at it. The listener fully participated in deciding what the picturedepicted.She/hewasnotjustasilentlistenerwhocouldonlyaskquestionsbutwasactivelyinvolvedindecidingwhatthepicturedepicted.Thethirdcommunicationstylegavethebestdescription.
When the message is not clear, it often gets distorted. • Some new things get added and some information goes missing. Little things
assume big proportions and big things are trivialised.• Ofthemanyfacts,onlyafewaretransmittedastheyarepassedfromoneperson
to another. • Veryoften,unusualinterpretationsaregiven,andoftenthesehavemuchtodo
with a person's mind, temperament and prejudices. • Thesecanalsoendupasrumoursorastory.Therefore, for communication to be effective there has to be a dialogue where the communicatorandlistenerareactivelyinvolvedandinteractwitheachother.
Draw the diagram as shown below on the board.
Message
Feedback
Channel
Sender Receiver

SBCC Training : Module 3 11
Part 2: VCD Rachanatmak Ravayya1. Telltheparticipantsthatyouwillbeshowingthemashortfilmtilled"Rachanatmak
Ravayya and that they should watch the film carefully and contribute to thediscussions that follow.
2. Tellthemthattheywillbeviewingthefilmintwopartsandthataftereachpartthere will be a discussion.
3. Screenthefilmandstopatthepointwhen,aftertalkingtothemother,theASHAworker takes the umbrella and walks into the village.
4. Ask the participants the following questions: What did you see here? HoweffectivelydidtheASHAworkercommunicatewiththemother?Whatwentwronginthecommunication?Askthemtorecallthecommunicationloopandreflectonwhattheysawbasedontheprinciplesofgoodcommunication.Ask“Whatcouldhave been done to improve the communication?”
5. Generateadiscussion;giveparticipantstimetoreflectandsharetheirviews.
6. List the points that emerge on the white board or on the chart paper.
7. Nowscreentherestofthefilm.
8. Attheendofthefilm,asktheparticipantsthefollowingquestions:Whatdidyouseeinthispartofthefilm?WhydidtheASHAgetapositiveresponse?WhatarethepositivefactorsASHA'swayofcommunications?
9. As the participants respond write the points on the board or chart paper.
CONCLUDING THE SESSION
Using the points listed on the board or chart paper and referring to the communication loop reiterate the reasons for communication failure as well as for effective communication.
Effective Communication
Do's
• Involveyourreceiverinthefeedback process (remember Case 2 and 3 from the exercise).
• Trytodevelopasharedexperience of communication as equal partners (remember Case 3 from the exercise).
• Act on the feedback and create opportunitiesforclarifications(remember Case 3 from the exercise).
Don’ts
• Avoidone-waycommunication(remember Case 1 from the exercise).
• Avoidlengthycommunication.In order to be effective communication should be broken into short pieces (rememberhowlengthycommunication was less effective in Case 1, and how small pieces of information coming one after another improved the communication in Case 3).

For Mid-Level Managers12
SESSION 5THE BEHAVIOUR CHANGE PROCESS
LUNCH BREAK 13:00 to 14:00 (60 minutes)
SESSION OUTCOMES
At the end of the session, participants will be able to:• List the different steps involved in the behaviour change process.• Relate personal experiences to the different steps in the behaviour change process.• Articulate the role of the communicator in each step of the behaviour change
process.• List the barriers that could occur in each stage of the behaviour change process.
MATERIALS REQUIRED
• Storycards• Black board and chalk or chart paper and sketch pens
METHODOLOGY
The session is divided into three parts:
Part I:Tellingastoryusingthestorycards.
Part II:Presentingthefirstchartdepictingthesevenstepsinbehaviourchange.
Part III: Conclusion.
PROCESS
Part I: Telling a story using the story cards
1. Usingthestorycardstonarratethefollowingstory
Ĭ Shanta’s Story
Sumitra, the ASHA of village Rampur, was concerned that a few families in the village were not bringing their babies for immunisation. So, she decided to visit their homes and explain to them the importance of immunisation and the need to get their children immunised. One of the houses she visited was that of Shanta, aladywitha6-month-oldbabywhohadneverbeenimmunised.WhenSumitra discussed the need to immunise her son, Shantasaid thather familydidnotbelieve in immunisation and that her mother-in-law and husband, Ramlal, would never allow her to immunise the child. Sumitra, in a very friendly and caringmanner, explained to ShantawhyimmunisationwasimportantthatandaskedhertoattendtheVHNDthefollowingWednesdayalongwithherbaby.Shanta promisedtodiscussthiswithherfamily.
14:00 to 15:00 (60 minutes)
SBCC Training : Module 3 13
On VHND, Sumitra noted that Shanta had not brought her babyfor immunisation and so, after the session, she took the AWW to Shanta’s house and was fortunate to meet both - Ramlal and his mother. She explained to them too the need for immunisation. After much persuasion,theyagreedtoimmunisethe child. As the ANM was still in the village theywereable toadministerthe first doses of polio andDPT aswell as BCG. Sumitrawasveryhappy.She told Shantaandherfamilythatthey should bring the baby for thesecond dose of vaccines on the next VHND the following month.
A week later, Sumitra visited Shanta’s housetofindouthowthebabywasandalsotoremindthemtobringthebabyforthe second dose. Shanta’s mother-in-law complained that the child was restless after immunisation and had fever all through the night. Sumitra explained that it was normal for some babies to get fever after immunisation and that there was no cause for concern.
On the next VHND, Shanta did not come to the PHC. Sumitra sent the AWW helper to Shanta’s house again, but she refused to come since her family was against any furtherimmunisation since the child had fever the previous time and theyhad also heard that it could cripple the child. The child, thus, missed the second dose.
For Mid-Level Managers14
Sumitra thendecidedthattheonlywayto ensure that the child got immunised was to convince Ramlal. She spoke to the Sarpanch and also to two of Ramlal’s neighbours who were his friends. Together theyhadalongdiscussionwiththefamilyinforming them that all the children in the village were being immunised and that there had been a marked reduction indiseases.Theyalsotoldthefamilythatit is the right of every child to getimmunised and that parents should not be guilty of not taking care of thehealth of the child. Both - Ramlal and
his mother were convinced and even accompanied Shanta to the PHC where the child received the second dose of vaccines. Since then the parentshavebeenverycarefulandhave ensured that the child receives all vaccinations, including against measlesandVitaminAprophylaxis.Shanta now actively advocates onthe need to get babies immunised.
2. Onceyoucompletenarratingthestory,askthefollowingquestions:• Whatdidyouthinkofthestory?DoyoufindfamilieslikeShanta’s who are
reluctanttofollowyouradvice?• How did Sumitra handle the case?Did she try to findout the reasons for
Shanta’s husband’s and mother-in-law’s opposition to immunisation? Did Shanta’sfamilyacceptheradviceandgetthechildimmunisedasadvised?
• How did Sumitra finally convince the family and win Shanta’s support in promoting health care?
• What is it that Sumitracouldhavedonebetter?(Likecounsellingthefamilyatthetimeoffirstimmunisation)
3. Allowsufficienttimefortheparticipantstoreflectandsharetheirviewsoneachof the above questions: Keep asking questions to elicit the following:
4. DuringherfirstvisittoShanta’s house, Sumitra was able to create an awareness as well as a desire in Shanta to get the child immunised. But Ramlal and her mother-in-lawinfluencedheranddissuadedherfromimmunisingthechild.
SBCC Training : Module 3 15
• OnthesecondvisitwiththeAWW,theywereabletogetRamlal, his mother and Shanta to agree to test the desiredbehaviourchangebygettingthebabyimmunisedwiththefirstdose.
• But, again, the fact that the baby had feverandalsothattheywerenotfullyconvincedaboutthecause,stoppedthefamilyfrombringingthechildforthesecond dose.
• SumitraagaininfluencedandmotivatedthefamilybybringingintheSarpanch and two of Ramlal’s friends and was successful in getting the second dose administered.
• Inthismanner,thefamilyrealisedthatitwasgoodtogetthebabyimmunisedandtofollowtheadviceoftheASHAandthereforetheycontinuedtobringthechildforimmunisationandotherservices,therebysustaining the behaviour change.
Part II: Presenting the first chart depicting the seven steps in behaviour change 14:00 to 15:00 (60 minutes)
Leading from the discussions on Shanta’sstoryinPartI,initiatediscussiononthebehaviourchangecycle.
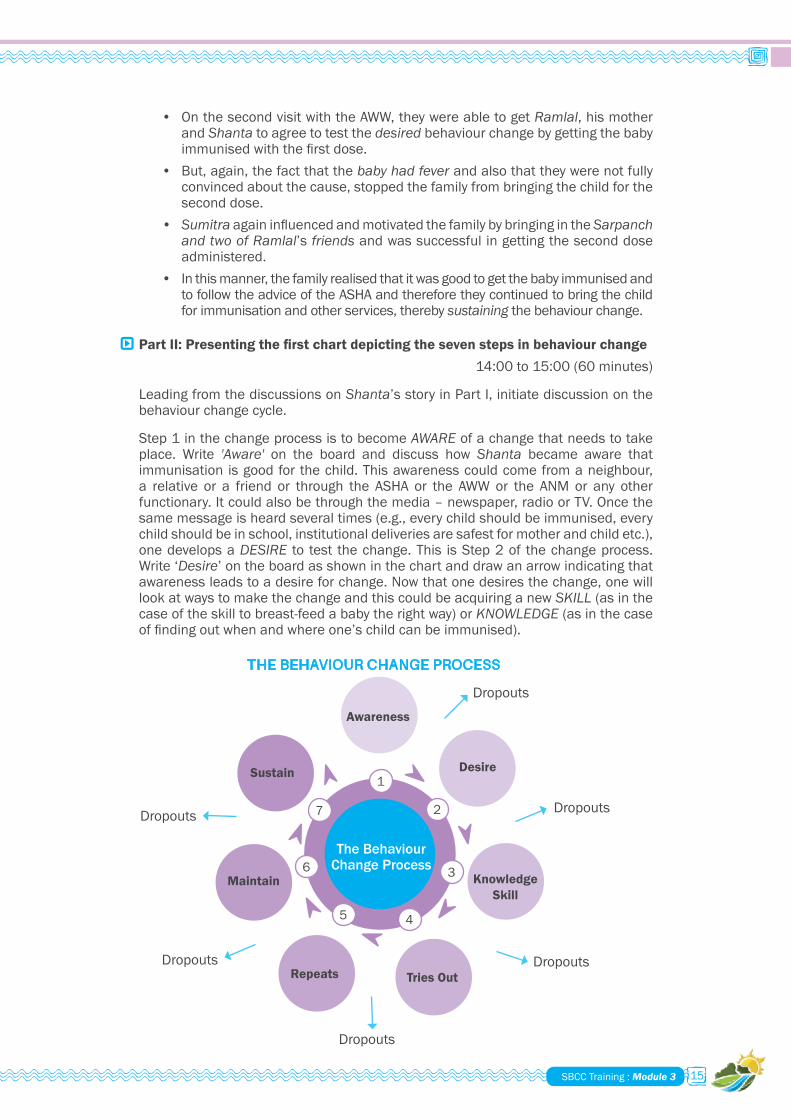
Step 1 in the change process is to become AWARE of a change that needs to take place. Write 'Aware' on the board and discuss how Shanta became aware that immunisation is good for the child. This awareness could come from a neighbour, a relative or a friend or through the ASHA or the AWW or the ANM or any otherfunctionary.Itcouldalsobethroughthemedia–newspaper,radioorTV.Oncethesamemessageisheardseveraltimes(e.g.,everychildshouldbeimmunised,everychild should be in school, institutional deliveries are safest for mother and child etc.), one develops a DESIRE to test the change. This is Step 2 of the change process. Write ‘Desire’ on the board as shown in the chart and draw an arrow indicating that awareness leads to a desire for change. Now that one desires the change, one will lookatwaystomakethechangeandthiscouldbeacquiringanewSKILL (as in the caseoftheskilltobreast-feedababytherightway)orKNOWLEDGE (as in the case offindingoutwhenandwhereone’schildcanbeimmunised).
1
2
3
45
6
7
The Behaviour Change Process
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
Awareness
Desire
Knowledge Skill
Tries OutRepeats
Maintain
Sustain
THE BEHAVIOUR CHANGE PROCESS
For Mid-Level Managers16
Therefore, Step 3 isacquiringthenecessaryskillorknowledgetomakethebehaviourchange. Write KNOWLEDGE (in Shanta’s case the knowledge was where to get the immunisationdoneforherbabyaswellasknowingthescheduleofimmunisation)or‘Skill’(asinthecaseofbeingabletobreastfeedachildtherightway)ontheboardas shown in the chart and draw an arrow to indicate that desire leads to acquiring thenecessaryknowledgeand/orskilltomakethatchange.
Now that one has acquired the knowledge and/or the skill, Step 4 will be to TRY OUT thatchange(e.g. takingthechild for immunisationfor thefirst timeorstartingtoconsumeIFAtabletsasadvisedbytheASHA).WriteTRY OUT on the board as shown in the chart and discuss this as the fourth step in the change process.
Individuals analyse the experience of trying out the change behaviour and if theassessment is negative (as in Shanta’s case), the person drops out from the process; if it ispositivethetendencyistotry itoutonceagain, inotherwordsREPEAT the action.ThisisStep5ofthecycle.WriteREPEATontheboardasshowninthediagramand discuss the same with the participants.
If the experience of Step 5 was good, one will tend to repeat the action; in other words MAINTAIN (Step 6) the behaviour and soon it becomes a SUSTAINED (Step 7) behaviour change or a habit. Write MAINTAIN and SUSTAIN on the board as in the chart with the arrows linking them and discuss these steps with the participants. The behaviourchangecycleisthuscompeted.
Mention, also, that there could be new awareness coming in and there could be a changecycleevenon thesamebehaviour following thesamecycle: forexample,switching from a ‘pinch of salt and a scoop of sugar’ to the use of ORS packets.
Inform the participants that in the actual training the participants participate in a group discussion, sharing their experiences on the behaviour change process followed by group presentations. This part is being skipped due to shortage of time. The intention here is to give glimpses of a few sessions in the module.
CONCLUDING THE SESSION
Using the diagram that was drawn in Part II of the session and the discussions, completethechartindicatingthatatanystepofthecycleonecoulddropoutfromthe behaviour change process unless there is someone motivating and ‘facilitating’ the person to make that change.
An enabling environment consists of
• Supportive relatives and neighbours.• Functionaries and volunteers and other opinion leaders through their
sustained encouragement, through counselling and dialogue and provisionofqualityservices.
• The communication media through supportive messaging.
SBCC Training : Module 3 17
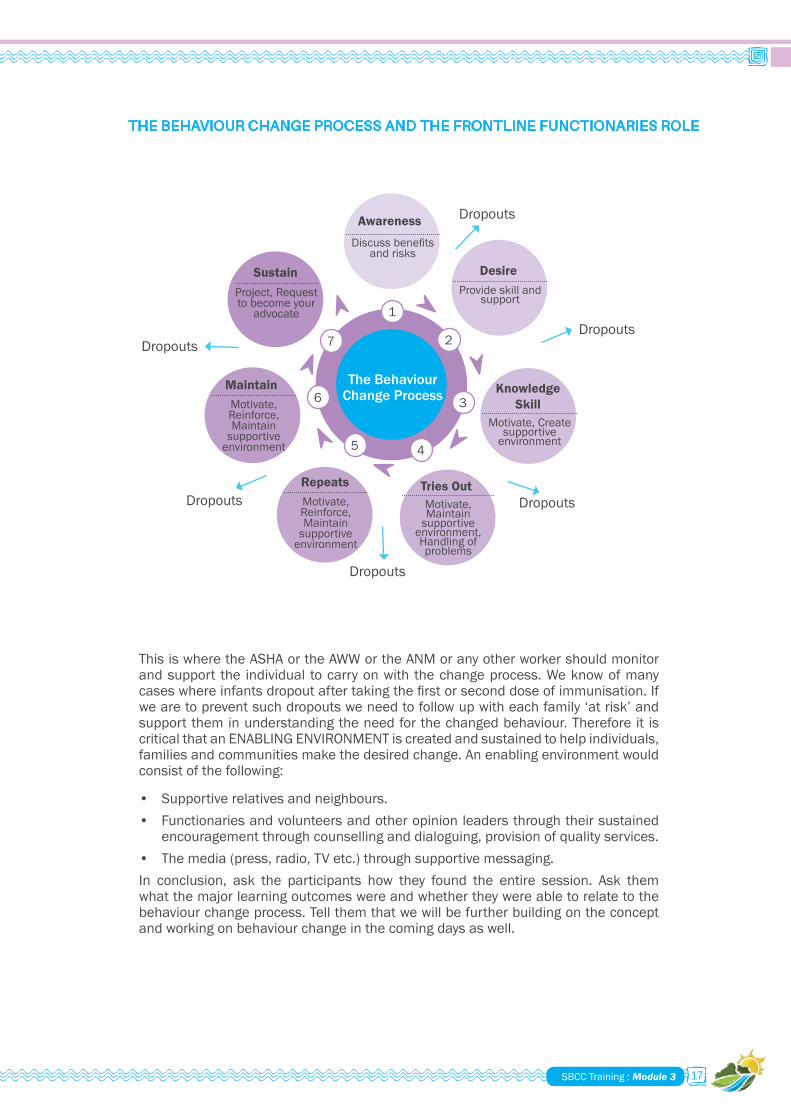
ThisiswheretheASHAortheAWWortheANMoranyotherworkershouldmonitorandsupport the individual tocarryonwith thechangeprocess.Weknowofmanycaseswhereinfantsdropoutaftertakingthefirstorseconddoseofimmunisation.Ifwearetopreventsuchdropoutsweneedtofollowupwitheachfamily‘atrisk’andsupport them in understanding the need for the changed behaviour. Therefore it is critical that an ENABLING ENVIRONMENT is created and sustained to help individuals, families and communities make the desired change. An enabling environment would consist of the following:
• Supportive relatives and neighbours.• Functionaries and volunteers and other opinion leaders through their sustained
encouragementthroughcounsellinganddialoguing,provisionofqualityservices.• The media (press, radio, TV etc.) through supportive messaging.In conclusion, ask the participants how they found the entire session. Ask themwhatthemajorlearningoutcomeswereandwhethertheywereabletorelatetothebehaviour change process. Tell them that we will be further building on the concept andworkingonbehaviourchangeinthecomingdaysaswell.
THE BEHAVIOUR CHANGE PROCESS AND THE FRONTLINE FUNCTIONARIES ROLE
1
2
3
45
6
7
The Behaviour Change Process
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
DropoutsAwareness
Desire
Knowledge Skill
Tries OutRepeats
Maintain
Sustain
Discussbenefits and risks
Project, Request tobecomeyour
advocate
Provide skill and support
Motivate, Create supportive
environment
Motivate, Reinforce, Maintain
supportive environment
Motivate, Reinforce, Maintain
supportive environment
Motivate, Maintain
supportive environment, Handling of problems
For Mid-Level Managers18
SESSION 6 QUALITIES OF A GOOD COMMUNICATOR
SESSION OUTCOME
At the end of the session, participants will be able to:
• List the knowledge skills and values/attitudes required of a good communicator.
MATERIALS REQUIRED
• Chalk and black board or chart paper and marker pen• Chart: Knowledge, Communication Skills, Values
METHODOLOGY
Lecture and discussion
PROCESS
Asktheparticipantswhatcompetencymeans.Generateadiscussion.Concludebysaying that competency is the ability of a person to carry out an activity or a task effectively, producing the desired results.
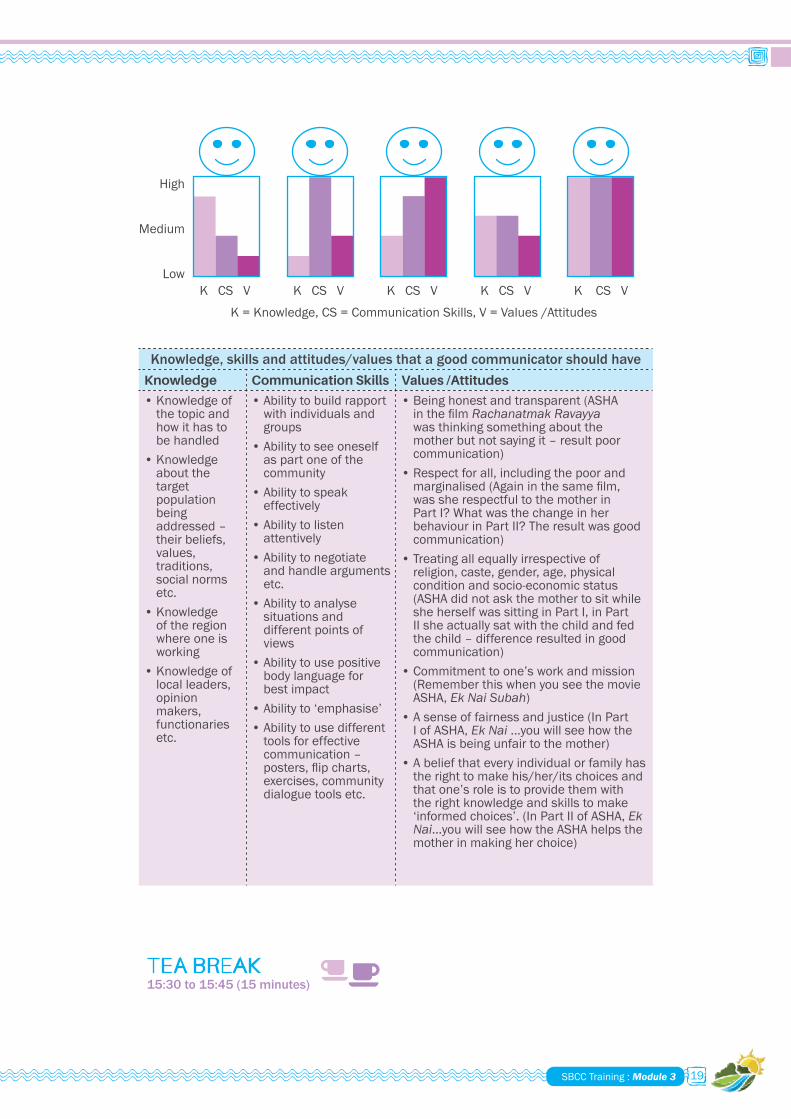
1. Thenask,“Whataretheessentialingredientsthatconstitutecompetency?”.Generateadiscussiononthis.Concludebysayingthatcompetencyconsistsofthreekeyelements:Knowledgeofthetask,skillstoperformthetaskandtheright values and attitudes that make one perform the task well. In the case of a communicator, the skills required are good communication skills. There is a chart given at the end of the session which lists knowledge, skills, values, etc. Itwillbeusefulifthischartisdisplayedinthetraininghallanddiscussed.Thiswillmakethenextstep(drawingcomparativefigures)moremeaningfulandwillimproveparticipationandthequalityofdiscussions.
2. Draw Figure 1 on the board or chart paper where the communicator has good knowledge, lower communication and much lower values and attitudes. Ask the participants what would be the performance of such a communicator. Generate a discussion on this.
3. Draw Figure 2 where the communicator’s communication skills are good, but knowledge and values are poor. What would be the performance of such a communicator?
4. Next, draw Figure 3 where the person has high values but less knowledge and communication skills. Discuss how this person would perform.
5. Draw Figure 4 where the communicator has less knowledge, low communication skills and low values. How would such a person perform?
6. Finally, draw Figure 5 where the communicator has all three aspects –knowledge, communication skills and values in equal amounts. What would be the performance of such a person?
CONCLUDING THE SESSION
From the above discussions it can be seen that a good communicator should have theknowledge,skillsandtherightvaluesandattitudestobeeffectiveinthefield.Lackofanyoneoftheabovequalitiesmakeshim/herineffective.Weneedtobemotivated and committed to bring about change within communities. Then we will findwaystoacquiretheknowledgeandskillstoperformourtasksbetter.
15:00 to 15:30 (30 minutes)
SBCC Training : Module 3 19
Knowledge, skills and attitudes/values that a good communicator should haveKnowledge Communication Skills Values /Attitudes
• Knowledge of the topic and how it has to be handled
• Knowledge about the target population being addressed–their beliefs, values, traditions, social norms etc.
• Knowledge of the region where one is working
• Knowledge of local leaders, opinion makers, functionaries etc.
• Abilitytobuildrapportwith individuals and groups
• Abilitytoseeoneselfas part one of the community
• Abilitytospeakeffectively
• Abilitytolistenattentively
• Abilitytonegotiateand handle arguments etc.
• Abilitytoanalysesituations and different points of views
• Abilitytousepositivebodylanguageforbest impact
• Abilityto‘emphasise’• Abilitytousedifferent
tools for effective communication–posters,flipcharts,exercises,communitydialogue tools etc.
• Being honest and transparent (ASHA inthefilmRachanatmak Ravayya was thinking something about the motherbutnotsayingit–resultpoorcommunication)
• Respect for all, including the poor and marginalised(Againinthesamefilm,was she respectful to the mother in Part I? What was the change in her behaviour in Part II? The result was good communication)
• Treatingallequallyirrespectiveofreligion,caste,gender,age,physicalcondition and socio-economic status (ASHA did not ask the mother to sit while she herself was sitting in Part I, in Part IIsheactuallysatwiththechildandfedthechild–differenceresultedingoodcommunication)
• Commitment to one’s work and mission (RememberthiswhenyouseethemovieASHA, Ek Nai Subah)
• A sense of fairness and justice (In Part I of ASHA, Ek Nai...youwillseehowtheASHA is being unfair to the mother)
• Abeliefthateveryindividualorfamilyhasthe right to make his/her/its choices and that one’s role is to provide them with the right knowledge and skills to make ‘informed choices’. (In Part II of ASHA, Ek Nai...youwillseehowtheASHAhelpsthemother in making her choice)
TEA BREAK15:30 to 15:45 (15 minutes)
Low K CS V
K = Knowledge, CS = Communication Skills, V = Values /Attitudes
K CS V K CS V K CS V K CS V
High
Medium

For Mid-Level Managers20
SESSION 7 INTRODUCTION TO INTERPERSONAL COMMUNICATION; THE GATHER CONCEPT
SESSION OUTCOME
At the end of the session, participants will be able to:• List what constitutes "Muskurahat" or "GATHER"anddescribe its relevance in
interpersonal communication.• Explain how effective interpersonal communication can be done.
MATERIALS REQUIRED
• ThefilmASHA, Ek Nai Subah• CDplayerandTV• Writing board, chart paper and marker pens
METHODOLOGY
Filmviewingfollowedbydiscussion.
PROCESS
• Explain the concept behind the word "Muskurahat" (eqLdqjkgV)or"GATHER"anddetail what each alphabet in the word stands for as given below:
eqLdqjkgV
eq & eqLdqjk dj vfHkoknu djsaxhAvius dk;Z{ks= esa tc vki fdlh ls Hkh feyrh gSa rc fu'p; gh izlUurk iwoZd eqLdqjkrs gq, feyrh gSaA lkFk gh lkFk] lkeus okys ds in vkSj le;kuqdwy vfHkoknu Hkh djrh gSaA
l & loky iwN dj leqnk; ls tkudkjh ysaxh fd mudh LokLF; laca/kh D;k leL;k,¡ gSa vkSj O;ogkj ifjorZu esa D;k&D;k ck/kk,¡ gSa\loky iwN dj leqnk; dh LokLF; laca/kh leL;kvksa vkSj O;ogkj ifjorZu dh ck/kkvksa dh tkudkjh ysaxhA blls leqnk; dh t+:jrksa dh tkudkjh fey ik,xh rkfd mudks vko“;drkuqlkj lgh ijke“kZ fn;k tk ldsA
dq & dq“ky LokLF; O;ogkj ds fy, mudh vko“;drkuqlkj Ik;kZIr tkudkjh nsaxhAdq“ky LokLF; O;ogkj ij ppkZ djsaxh vkSj mudh vko“;drkuqlkj ¼tksfd fiNys pj.k }kjk irk yx pqdh gaS½ tkudkjh nsaxh] [kkldj vxj vkids lkeus ubZ ekrk gks] xHkZorh L=h gks ;k fQj dksbZ fd“kksjhA dq’ky O;ogkj ij tkudkjh nsrs le; /;ku j[kuk gksxk fd bu ekrk] fd'kksjh ;k L=h dks dksbZ loky vFkok ijs'kkuh rks ugha gS\ lkFk&lkFk] ;g Hkh iwNuk gksxk fd D;k fiNys ckj nh xbZ lykg dks viukus esa dksbZ ijs'kkuh gqbZ\ vxj gqbZ rks og D;k Fkh\ vxj dksbZ u;k elyk gS rks og D;k gS\
jk & jk; cukus esa enn djsaxh( ,d ,slh jk; cukus esa] ftlls ekrk [kqn QSlys djus esa l{ke cusaAekrk ls ckr dj jk; cukus esa enn djsaxhA vxj dksbZ leL;k ugha gks rks tks ckr vPNh py jgh gS mldks vkSj lqn`<+ djsaxhA ;fn dksbZ iz'u ;k leL;k gks rks mlds fofHkUu igyqvksa ij fopkj&foe'kZ vkSj iz'u djsaxhA leL;k ls tqM+h ;fn dksbZ ubZ tkudkjh vkids ikl gS rks mlds fo"k; esa vo'; ppkZ djsaA bl tkudkjh ls gksus okys Qk;ns&uqdlku ij Hkh ppkZ djsaxhA blls ubZ ekrk] xHkZorh efgyk ;k fd'kksjh dks leL;k dk lek/kku ;k iz'u dk mŸkj <w¡<+us esa lgk;rk feysxhA bl izdkj efgyk Lo;a QSlys ysus esa l{ke cusxhA
15:45 to 16:45 (60 minutes)
SBCC Training : Module 3 21
g & gky lq/kkjus ij ppkZ djsaxh] [kkldj vxj dksbZ ijs'kkuh ;k loky gks rksAgky lq/kkjus ij ppkZ djsaxh] [kkldj vxj dksbZ ijs'kkuh ;k tfVy loky gkas rksA bl izfØ;k esa leL;k dk fuokj.k vki&vk'kk nhnh ugha djsaxh vfirq leL;k dk lek/kku <w¡<+us dh {kerk dks c<k+ok nsrs gq, enn djsaxhA lykg flQZ rc gh nsaxh tc dksbZ uqL[ks ;k lq>ko ij O;ogkj djus esa dksbZ ijs'kkuh ;k vM+pu vk jgh gksA gky lq/kjus dh ppkZ dks lekIr djus ds igys de ls de ,d ;k nks ckrksa ij lgefr cukuh pkfg,A leL;k ds lek/kku ds fØ;kUo;u ds rjhds ;k jkLrksa ij Hkh lgefr gksuh pkfg,A
V & fVdkÅ vkSj ljy laca/k dh vk'kk ds lkFk fonk ysaxhAfVdkÅ vkSj ljy laca/k dh vk'kk vkSj iqu% tYnh feyus ds okns ds lkFk fonk ysaxhA fVdkÅ laca/kksa ds fy, le;≤ ij nksckjk fey dj orZeku fLFkfr dh Hkh tkudkjh ysrh jgsaxh rkfd le; jgrs mi;qDr lq>ko fn;k tk ldsA
OR
GATHER
G–GREET the caregivers (establish rapport): It isnecessary toovercomebiasestomeetpeopleasequals.Greetingpeoplepersonallyhelpsinbuildingrapporttoagreat extent.
A–ASK caregivers (gather information): It is important to elicit the needs of the caregivers, prioritising information to make it more relevant. Asking should not be limitedtomeremedicalhistorybecauseotheraspectsofaperson’slife(lifestage,lifestyle, personality, etc.) often impact an individual’s post-counselling behaviourmorethanhis/hermedicalhistory.
T–TELL (provide information): Avoid information overload such as reciting details on all the processes at one time because there is a limit to how much information people can retain. Instead, package the information in smaller module and check for understandingafterdeliveryofeachmodule.Specificinformationorganisedlogicallyisretainedlongerandmorecompletely,especiallyiftheindividualsareencouragedto ask questions.
H–HELP the individual: This is the decision-making or problem-solving moment. The providerishelpingtheindividualsortthroughtheinformation,lifestyleandlife-stageissues to come up with various alternatives, and to consider the advantages and disadvantages of each alternative.
E –EXPLAIN to the individual: Once the individual has made a choice, the provider uses IECmaterial to help the individual remember key information. The provideralso uses IEC material to remind them of important discussion points. IEC materials reinforcekeyinformation,advantagesanddisadvantages.
R –RETURN/REFER/REALITY CHECK: Return visits or referrals should be planned. Ifnecessary,repeattheinformationgiven.
• Discuss each step in Muskurahat orGATHER indetail; clarifyanydoubts thatparticipantsmayhave.
• Once there is good understanding among participants on either of the two words, startshowingthefilmASHA, Ek Nai Subah.
• Stop the film at the point where the four questions are raised and ask theparticipants what the answers could be. Generate a discussion on the same and list all the shortcomings of the ASHA in her communication.
• Oncethisisdone,resumeshowingthefilm.Stopthefilmonceagainwhenthenext set of four questions appear. Get the participants to respond to the questions and note these points on the board or chart paper.

For Mid-Level Managers22
SESSION 8 REVIEW AND REFLECTIONS OF THE DAY
• Resumethefilmagain.Stopthefilmwhenthenextsetofquestionsappearandget the participants to respond to the questions. Link them with either Muskurahat or with ‘GATHER’ and describe how the steps that were discussed in part I of the sessionactuallyhelpedtheASHAingettingpositiveoutcomesincludingbuildingstrong relationships with the families and communities.
• Showthefinalpartofthefilmanddiscussthefilmonceagain.
CONCLUDING THE SESSION
• Onceagaindiscussthefivestepsin"Muskurahat"orthesixstepsin"GATHER"andrelatethemtowhattheysawinthefilm.
• Highlight the importance of rapport building to ensure that communication becomes effective.
• Recall the session on ‘Qualities of a Good Communicator’ and once again highlight the importance of having the right values and attitude to be an effective communicator.
SESSION OUTCOME
At the end of the session:
• Therewillbealistingofthehighlightsoftheday,thelearningsandfeedbackonthe sessions.
MATERIALS REQUIRED
• Writing board and chalk or marker pens• A paper ball
METHODOLOGY
Getting feedback and comments from participants.
PROCESS
1. Telltheparticipantsthatthisisthelastsessionofthedaywheretheycanreflectonthemajorlearningsoftheday,givetheirfeedbackonthesessionsandanyothercommentsthattheywouldliketomaketheday’ssessionsmoreeffective.Tellthemthatyouwillthrowtheballtoanyoneparticipantandhe/shewillgivehis/her comments and then throw it to the next participant for his/her comments. The comment could be in the form of a learning, an expression of what one felt duringthedayorasuggestiontomaketheday’ssessionsmoreeffective.
2. Make three columns on the board and give the headings LEARNING, FEELING andSUGGESTION.Throwtheballtoanyparticipantofyourchoiceandstarttheabove process. As the participants make their statements record them under theappropriateheading.Makesurethateachparticipantcontributesonlyonepoint. Once all the participants have contributed summarise what is written on the board.
16:45 to 17:15 (30 minutes)

SBCC Training : Module 3 23
Session No. Topic Time Methodology
1 RecallofDayIsessions 10:00 to 10:15 Discussion
2 Introduction to Social Inclusion
10:15 to 11:00 Simulation exercise and discussion
11:00 to 11:15 Tea break (15 minutes)3 Session on Social
Inclusion (continued)11:15 to 12:00 Film ‘I Am a Dalit’ and
discussion4 How to Conduct a Group
Discussion12:00 to 12:45 Use of sociogram and
discussion12:45 to 13:45 Lunch break (60 minutes)
5 UseofaCommunityDialogue Tool
13:45 to 14:45 Pulleyexerciseanddiscussion
6 Understanding Teamwork 14:45 to 15:30 Broken square exercise and discussion
15:30 to 15:45 Tea break (15 minutes)7 Planning and Organising a
VHND15.45 to 16.45 Film ASHA, Ek Din Zindagi
Ka and discussion8 Creating a Village Health
Plan and Developing a Village SBCC Plan
16.45 to 17.45 PPT presentation and discussion
9 ValedictorySession 17.45 to 18.15 Feedback from participants
Session 1No materials requiredSession 2• Six pieces of chart paper
(30 cm x 15 cm)• Markerpens(thick–preferablyof
different colours)Session 3• I am Dalit CD• Laptop and LCD or TV• DVDplayer• White board and marker pensSession 4• Chart paper and marker pensSession 5• Apulleystand• A doll
• String• A plastic bag• 12 thick VIPP cards• Blackboard and chalk or chart
paper and sketch pensSession 6• 12 pieces of the broken square.• Thekeytothebrokensquare• Black board and chalk or chart
paper and sketch pensSession 7• The film ASHA, Ek Din Zindagi Ka
(VHND)• VCD,aVCDplayerandTV• Blackboard and chalk or chart
paper and sketch pensSession 8• SBCC Plan framework (8-10) copies
LIST OF TRAINING MATERIALS:
DAY 2 PROGRAMME SCHEDULE

For Mid-Level Managers24
SESSION 1 RECALL OF DAY I SESSIONS
• Welcometheparticipantstotheseconddayoftheorientation.• Recallbrieflysessionsofday1.• Runthroughtheschedulefortheday.
SESSION 2 UNDERSTANDING SOCIAL INCLUSION AND ITS IMPORTANCE IN SOCIAL AND BEHAVIOUR CHANGE COMMUNICATION
SESSION OUTCOMES
At the end of the session, participants will be able to:• Clearly describe what "exclusion" means and understand the humiliation,
frustration, and sense of helplessness associated with it.• Sharetheir"feelings"afterhavingexperiencedtheimposedsocialrestrictionsand
getfullysensitisedtotheneedforfocussingoninclusionintheircommunicationplans.
MATERIALS REQUIRED
• Six pieces of chart paper (30 cm x 15 cm)• Markerpens(thick–preferablyofdifferentcolours)
METHODOLOGY
Simulation exercise and discussion
PROCESS
1. Divide the participants into six groups and give each group a piece of chart paper; Assign each group a role as given below:
• Group 1 members are SC/STs.• Group 2 members are WOMEN (single mothers, widows & women heading
households).• Group 3 members are DIFFERENTLY ABLED.• Group 4 members are RELIGIOUS MINORITY GROUPS.• Group 5 members are RICH/DOMINANT CASTE.• Group 6 members are HIV or LEPROSY AFFECTED PEOPLE.
Tell the participants that during the exercise, the members of each group are required to feel, think and act as people belonging to the category assigned to them and their actions should reflect the reality in society.
2. Each group is given a piece of chart paper and a marker pen to make a placard. Askthemtowriteboldlyandclearlythenameofthecategorythatisassignedtothem.
10:00 to 10:15 (15 minutes)
10:15 to 11:00 (45 minutes)

SBCC Training : Module 3 25
3. Linesaredrawn,onthefloorofthetrainingroomandallthegroupsaremadetostand at the starting point in the manner shown in the diagram below.
4. One of the facilitators reads out from a list of statements (given at the end of the session).
STARTING
LINE
GROUP 1
GROUP 2
GROUP 3
GROUP 4
GROUP 5
GROUP 6
5. Theparticipantsare requested to listencarefully toeachstatementand thendiscussamongthemselvesanddecideiftheycanfollowthe‘statements’asina real-life situation.
6. Ifanyofthegroupsfeelthattheycanperformthetaskina real-life situation theyaskamemberofthegrouptoholdtheirplacardandstepforwardsoastostandonthelineimmediatelyinfrontofthestartingpoint.
7. Conversely,ifthegroupsfeelthatitisnotpossibletoperformthetaskinareallifesituationthentheyasktheirrepresentative(holdingtheplacard)toremainwherever She/he is standing.
8. As the statements are read out, each group discusses the statement among themselves and then asks their representative to either remain where She/he is or take a step forward near the next line. This continues on until all the 10 or 12 statements are read out and acted upon.
9. The representative can keep stepping forward even after all six lines have been crossed.
10. Attheendoftheexerciseyouwouldhaveasituationwherethegroupsareindifferentpositions.TheHIV/Leprosyaffectedpeoplewouldhavemovedoneortwo steps forward, the dalits three or four and so on. The rich /dominant caste willbewayahead.

For Mid-Level Managers26
11. Once the exercise is over ask the following questions:
• Whichcategoryadvancedthemost?• Whichcategorywaslast?• What did we see here?• Howmuchdideachcategoryadvance?• Whyarethecategorieswheretheyare?• What stops people from advancing; do the categories have equal status?• Iftheansweris“no”,askwhyitisso.• Whichcategorieswerehappyandwhichwerenot?Allowthemembersofdifferentgroupstosharewhattheyfeltwhiledoingtheexercise.Didtheyfeelasenseof injustice?Tryandbringoutthefrustrations,and feelings of helplessness and sadness that some members would have felt.
Allow sufficient time for participants to reflect and share their feelings andthoughts about each of the questions. Remember we have to bring out the feelingsoftheparticipantssothattheyinternalisewhattheyarespeakingandhearing.
Ask whether this situation exists within our communities. Are people being deprived of their entitlements just because of their social and economic status, gender or health status? Allow time for the participants to share their thoughts.
CONCLUDING THE SESSION
Aswrapuptothispartofthesessionconveythefollowing:
• Therearemanyinequitiesthatstillremainwithinourcommunities• Large sections of our people remain discriminated against• TheproblemisacuteinthecaseofHIVandleprosypatients,widows,dalits
and tribals; women in general are subjected to discrimination in almost all walks of life.
GROUP 1
GROUP 2
GROUP 3
GROUP 4
GROUP 5
GROUP 6
SBCC Training : Module 3 27
• The Indian Constitution gives every individual, irrespective of the religion,caste, gender or social status She/he belongs to, equal rights. The Universal Declaration of Human Rights, the Convention on the Elimination of all Forms of Discrimination against Women (CEDAW) and the Convention on the Rights of the Child accepted all over the world recognise that everyone is bornequalandguaranteethefulfilmentofhumanrights(shortnotesonvariousconventions are given at the end of session).
• TheGovernmentofIndia,overthepastseveralyears,hasmadehumanrightscentraltodevelopmentprogramming–therighttofood,therighttolivelihood,the right to education and health care, and the right to information are all directed towardsbringingaboutequityandsocialjusticewithinourcommunities.
• ItisextremelyimportantthatanySBCCinitiativerecognisesthisbasictenetand ensures that we target those who are discriminated against and are most vulnerable. Empowering them and bringing them into the mainstream will help us to achieve our targets.
• We need to focus on inclusion in all the activities that we undertake, including home visits (select houses of the poor and marginalised), group meetings (focusonthediscriminatedandensurethattheyparticipateandsharetheirviews),servicedelivery(ensurethatthepoorandvulnerablearegivenpriorityand are covered) etc.
STATEMENTS TO BE READ OUT
How certain are you that...• Yourchildrenwillbetreatedequallyintheirschool?• Youwillreceiverationsduetoyouinthevillagerationshop?• YouwillreceivethebestofattentionwhenyougotoyourlocalPHC?• The Sarpanch, ANM, doctor, AWW, Gram Sevak etc.willvisityourhousetodiscuss
problems?• Youcanbuyamotorcycleforyoursontoattendcollege?• YoucanattendandfearlesslyparticipateinameetingbeingheldbytheANMand
AWWandthattheywilllistentoyou?• Your daughters can pursue high school studies?• You will get justice at the local Police Station?• Therewillbenoinjusticeagainstyouattheplacewhereyouwork?• Youcancelebratethenextreligiousfestivalthewayyouwant?• Youwillearnequalwagesforthesametypeofworkdonebymen?• Youwillbeableto,ifrequired,getanexpensiveoperationforamemberofyour
family?
NOTES FOR THE FACILITATORUNIVERSAL DECLARATION OF HUMAN RIGHTS (UN)
Providesequality,irrespectiveofcaste,creed,religionandregion.Allhumanbeingsareborn freeandequal indignityand rights.Theyareendowedwith reasonandconscience and should act towards one another in a spirit of brother hood.
Everyoneisentitledtoalltherightsandfreedomssetforthinthisdeclaration,withoutdistinctionofanykind,suchasrace,colour,sex,language,religion,politicalorotheropinion, national or social origin, property, birth or other status. Furthermore, nodistinction shall be made on the basis of the political, jurisdictional or international statusofthecountryorterritorytowhichapersonbelongs,whetheritbeindependent,trust,non-self-governingorunderanyotherlimitationofsovereignty.
For Mid-Level Managers28
CONVENTION ON THE ELIMINATION OF ALL FORMS OF DISCRIMINATION AGAINST WOMEN (CEDAW) The Convention on the Elimination of all Forms of Discrimination against Women (CEDAW),adopted in1979by theUNGeneralAssembly,defineswhatconstitutesdiscrimination against women and sets up an agenda for national action to end such discrimination.
TheConventiondefinesdiscriminationagainstwomenas"...anydistinction,exclusionor restriction made on the basis of sex which has the effect or purpose of impairing ornullifyingtherecognition,enjoymentorexercisebywomen, irrespectiveoftheirmarital status, on a basis of equality of men and women, of human rights andfundamentalfreedomsinthepolitical,economic,social,cultural,civiloranyotherfield."
NATIONAL COMMISSION FOR WOMEN
NCW is the apex national level organisation of India with the mandate of protecting and promoting the interests of women. Its major responsibilities include:
• Generation of legal awareness among women, thus equipping them with the knowledgeoftheirlegalrightsandwithacapacitytousetheserights.
• Assisting women in redressal of their grievances through pre-litigation services.
• FacilitatingspeedydeliveryofjusticetowomenbyorganisingParivarik Mahila Lok Adalatsindifferentpartsofthecountry.
UNITED NATIONS CONVENTION ON THE RIGHTS OF THE CHILD, 1990
Everychildhasrightswithoutdiscriminationofanykind,irrespectiveofthechild'sorhis or her parent's or legal guardian's race, colour, sex, language, religion, political orotheropinion,national,ethnicorsocialorigin,property,disability,birthorotherstatus.
The rights include protection against all forms of discrimination or punishment on the basis of the status, activities, expressed opinions or beliefs of the child's parents, legalguardiansorfamilymembers.Everychildmustberegisteredimmediatelyafterbirthandshallhavetherightfrombirthtoaname,therighttoacquireanationalityand,asfaraspossible,therighttoknowandbecaredforbyhisorherparents.
Other rights include: To diminish infant and child mortality; necessary medicalassistance and health care to all children with emphasis on the development of primaryhealthcare;tocombatdiseaseandmalnutrition;toensureappropriatepre-natalandpost-natalhealthcareformothers;toensurethatallsegmentsofsociety,in particular parents and children, are informed, have access to education and are supported in the use of basic knowledge of child health and nutrition, the advantages of breast-feeding, hygiene and environmental sanitation and the prevention ofaccidents;andtodeveloppreventivehealthcare,guidanceforparentsandfamilyplanning education and services.
TEA BREAK 11:00 to 11:15 (15 minutes)
SBCC Training : Module 3 29
SESSION 3 SOCIAL INCLUSION (CONTINUED)
SESSION OUTCOMES
At the end of the session, participants will have:• A deeper understanding of the problems of the dalit and other marginalised
communities. • Aclearerunderstandingoftheneedtofocusonexcludedsectionsofsocietyin
the Social and Behaviour Change Communication initiatives.
MATERIALS REQUIRED
• The“Iama Dalit”CD,laptopandLCDorTVandDVDplayer• Whiteboard and marker pens
METHODOLOGY
Screening of video and discussions
PROCESS
Telltheparticipants:“Wehavejustseenexclusionofgirlsandwomenjustbecausetheybelongtothefemalegender.Wearenowgoingtoseeafilmthatdepictsthepitiable condition of dalitsandthe‘oppressed’castes.Afterseeingthefilmwewilldiscuss it so that we understand the problems better.”
1. Screenthefilm
2. Attheendofthefilm,askthefollowingquestions:• Whatdidyouseeinthefilm?• Whatwerethekeyscenes?• Whatwereyourfeelingsasyouwerewatchingthefilm?• Haveyouhadsimilarpersonalexperiences?• Whicharetheothersectionsofsocietythatsufferduetoexclusion?Generateagooddiscussion.Allowsufficienttimeforparticipantstoreflectandshare their thoughts, experiences and feelings.
3. Once the discussions are over, ask the following questions:• Asdevelopmentworkers,whatmessagesdothefilmandthebottleexercise
give us?• Whatcanwedotoreachouttotheexcludedsothattheybecomepartofall
ouractivitiesandbenefitfromourservices?• List the points emerging from the discussions.
4. Now ask the following questions:• WhatarethewaysinwhichwecanmakeourSBCCstrategiesandinitiatives
more inclusive, so that we reach out to the poorest, excluded and most vulnerable?
• What changes should we bring about in our work to ensure that the excluded get included and are mainstreamed?
• List the points that emerge from the discussion and use these points to conclude the session.
11:15 to 12:00 (45 minutes)
For Mid-Level Managers30
FOR THE FACILITATOR
NOTES ON SOCIAL EXCLUSION
Social exclusion describes a process by which certain groups are systematicallydisadvantagedbecausetheyarediscriminatedagainstonthebasisoftheirethnicity,race,religion,sexualorientation,caste,descent,gender,age,disability,HIVstatus,migrantstatusorwheretheylive.Discriminationoccursinpublicinstitutions,suchasthelegalsystemoreducationandhealthservices,aswellassocialinstitutionslike the household.
Sociallyexcludedgroupssufferfromsomeorallofthesedenials.
Associalexclusionisnotonlyaboutattitudesbutisbuiltintothesocialstructure,changingattitudeswillnotnecessarilychangesocialexclusion.Thesocialstructureof a society contributes to the formation of its attitude, and the attitude in turncontributestothemaintenanceofthesocialstructure.Thereisnoeasywayoutofthishorriblyviciouscycle.
Since social exclusion is about domination, discrimination and deprivation, those who benefit from it do not want to introduce any change, while those who are discriminated against, who are supposed to be ‘inferior’, ‘incapable’, ‘less meritorious’ and ‘lower’, are not in a position to mobilise and organise to alter the existing social system. They do not want to remain in the dehumanising social order but fear that they may be subjected to repression if they resist exclusion and discrimination.
During discussions in workshops on reconstruction of the dalit identityinsixnorthernstatesbytheBiharSocial Institute, itwasfoundthatthenegativeandderogatoryperception of the dominant castes about dalits isthattheyaredirtyandfilthy,thievesandrobbers,lazy,gluttonous(pethu, khau), dishonest and ungrateful. This negates thereality.Forinstance,empiricaldatadoesnotsupporttheperceptionthatdalits aregluttons.Therealityisthatdalits,likeanyoneelse,eattosurvive.
Dalits perceptionsaboutthemselvesisthattheyarecapablebutgetnoopportunities;thattheyarehardworkingbutdonotgetthefruitsoftheirlabour;thattheyareoftenputinasituationwheretheyareforcedtoroborlie;thattheyareculturallytalentedandarenotimmoral,onthecontrarytheyaresensitiveandemotional.Somewouldargue that this perception is unrealistic, even aspirational. However, Dr. Louis argues thatacommunitythatisatthereceivingendalsohasscopeforlookingattherealityof their lives in a positive light.
Tribalsfaceapeculiardilemma.Theyhavebeenorganisingtoensuretheirrights,and protect their culture and natural resources. But whereas formerly they weretotally isolated,now theyare thevictimsofdiscrimination.Non-tribals see tribalsinaderogatorymanner,particularlytheirfoodhabitsandwaysofliving,whichareverydifferent.Thestrongemergingtribal identity,however,seesthemasthefirstinhabitantsof thiscountrywhohavecontributedmuchtotheculture,historyandheritageofIndia,thoughlittlerespectistodayshowntotheirculture,socialsystems,politicalstructuresandeconomy.
Women are the most excluded and discriminated segment of the Indian population. Patriarchy is at the coreof the structural elementdiscriminatingagainstwomen.Controlofwomen’sreproductiveabilitiesandsexualityisinmen’shands.Patriarchylimitswomen’sownershipandcontrolofpropertyandothereconomic resources,including the products of their own labour.

SBCC Training : Module 3 31
Women’smobility is constrained and their access to education and informationhindered.Overtheyears,ithasbeenrecognisedthattheexperiencesofamajorityofwomenaregroundedinbothpovertyandpatriarchy.Boththesefeedintoeachother and subject women to exclusion and exploitation.
TheMuslimcommunityisanotherexcludedgroupinIndia.TherearemoreMuslimswho live below the poverty line than any other group. They also earnmuch less(on average, Rs. 22,807 per year as against Rs. 25,653 for all others). Only 21percentofMuslimsusethepublicdistributionsystem,whichprovidessubsidisedfood grain, as compared to 33.2 percent of the general population. Enrolment of Muslim children in schools is low (61.6 percent, while it is 71.4 percent for the generalpopulation),andthedropoutrateishigher.NeitheratthepolicylevelnorinprogrammeinterventionsdoMuslimsgettheirdueshareascitizensofthiscountry.
In this environment, Dr. Louis points out, social exclusion is multiple and cumulative. For instance, a dalitortribalgirlsuffersmultipleexclusionsbybeingexcludedduetocasteandethnicreasons,andfurtherexcludedbylocationifshelivesinaruralarea where she cannot avail of facilities available to those in urban areas. If she is adifferently-abledperson,shesuffersfurtherdiscriminationbybeingdeprivedoflife-enhancing mechanisms.
Source:Extractedfromapapertitled“Socialexclusion:Challengesforcivilsocietyorganisations” (DFID)
SESSION 4 HOW TO CONDUCT A GROUP DISCUSSION
SESSION OUTCOME
At the end of the session, participants will be able to:
• Listthedo'sanddon’tsofconductingagroupdiscussionanddefinetheirroleasfacilitators of group discussions.
MATERIALS REQUIRED
• Chart paper and marker pens• Annexure: How to conduct a Group Discussion
METHODOLOGY
Group discussions and plotting discussion on a sociogram
PROCESS
1. Callsixparticipants–twowhoareveryactiveandtendtodominate,twowhoaremoderatelyactiveandtwowhoarethesilent–andaskthemtoformagroupinthe centre of the training room. Call three other participants who are active and have the other facilitator take them out of the classroom.
2. The facilitator who takes the three participants out of the classroom briefs themontheirroleas‘observers’.Tellthemthattheyhavetoobservethegroupcarefullyandthateachofthemhastocreatea‘sociogram’thatwoulddepicthow each of the group members participated in the discussion.
12:00 to 12:45 (45 minutes)

For Mid-Level Managers32
3. Give them clear instructions on how to create the sociogram. Follow the directions listed below:• Ask them to open a fresh page in their notebooks and
mark six dots that create a circle with a diameter of about 3 inches. Each dot represents one of the members who will be participating in a group discussion in the training room. The listing of the names should be in the sequence in which the group members are sitting. Now put the name of a member against each of the dots.
• When the group discussion starts, observe each member of the group. When one starts speaking observe who he/she is speaking, to and draw a straight line between the dots representing the two of them. For example, if D starts the discussion and looks at F while speaking, draw a line with an arrow from D to F as in the chart; then if F speaks looking at B draw a line with an arrow linking F and B. If C speaks next, looking at B link them both with an arrow. Keeprecordingthediscussionsbydrawinganarrowaseachmemberspeakstillattheendthereisawebdepictingthewaythediscussionswent.Incaseamemberspeakswithoutfocussingonanyoneandisspeakingtothegroupdraw an arrow from him/her to each of the others, indicating that he/she is speaking to the group. Tell the participants not to forget to mark the side chats that happen between members.
• Askthemonceagainiftheyhaveunderstoodtheirrolesclearly.Ifthereareanydoubtsclarifythem.
4. Whileonefacilitatorisbriefingthethreeobservers,theothergivesinstructionsto the six members who will be involved in the group discussion as follows:• Tellthesixparticipantsthattheywillhavetocarryonagroupdiscussionon
‘Why is Social andBehaviour Change Communication themost importantpart of our work?’Ask them to select a leader from among them to lead thediscussions.Tell themthattheywillbegiven10minutesforthegroupdiscussionandthattheycandecidehowtoconductthediscussion.
• Tell the other participants to be attentive and to assess how good the discussion was.
• Bring the three observers in and tell the group to start their discussion.• Thetwofacilitatorstooshouldobservetheparticipantscarefullyandcreate
their own sociograms of the group discussion.• Attheendof8minutes,tellthegroupthattheyhave2minutesleftandatthe
end of 10 minutes ask them to stop their discussion.• Askthesixgroupmembershowtheyfoundthegroupdiscussion,whetherall
membersparticipatedeffectively,whethertheleaderhelpedinfacilitatingthediscussion,whetheranyonedominatedetc.Askeachgroupmembertosharewhattheyfeltandhowwelloreffectivelytheycontributedtothediscussion.
• Give sufficient time for the group members to reflect and share theirexperiences.
• Then ask the rest of the participants to comment on the way the groupconducted the discussion and how effectively each member contributed.Give about 7 to 10 minutes for them to give their feedback.
• Next, ask the three observers to share their observations with the help of the sociogram.Askthefirstobservertoexplainwhatthesociogramisandwhatit depicts. In case there are gaps in his/her description, the facilitators join in and explain the sociogram in detail. The observer then explains how the discussion went using the diagram.
• Now ask the other two observers to give their observations.
A
B
C
DE
F

SBCC Training : Module 3 33
5. Next the facilitators make their own comments drawing conclusions from the sociogramspresented.Focusparticularlyonthefollowingpoints:• The role of the leader in facilitating the discussion.• The participation of individual members of the group.• Didanyonedominatethediscussionandevenpreventothersfromsharing
their views?• Wasthereanyonewhowassilentanddidnotspeakorspokeverylittle?• Was the group able to bring out relevant points on the topic given?
6. FinallythefacilitatorsgivetheirownviewsonthequalityofthegroupdiscussionandnarratethestoryoftheKingandtheKheer.
Ĭ The Story of the King and the Kheer
Therewasonceaverybenevolentkingwhoalwaysworkedforthewelfareofhispeople.Thepeoplelovedandworshippedhim.Oneday,thekingwasreflectingonhislifeandhiskingdom.Hewashappythathehadbeenamuchlovedking,always putting the welfare of his people above everything else. But he alsorealisedthatmostofhissubjectshadbecomelazyandweregettingmoreandmoredemanding.Theyhadstartedtoexpecteverythingfromthekingandthissaddenedhim.Sohedecidedtotesthispeopleandteachthemthattheytooneedtoworktoearnalivingandshouldnotbealwaysdependentonhim.
Accordingly,hemadeaplan,andtheroyalannouncers,withtheirdrums,informedthe people that the King wished to eat kheerwithhissubjects.TheyannouncedthattheKinginsistedupononecondition–eachfamilywouldhavetoprovidethemilk for the kheer while the King would provide the rice, sugar and spices.
On theappointedday, thesubjects linedup fromearlymorningwithmilkcansto give milk to the King for his kheer. A huge vessel had been placed in an open area. Each person would walk up to the vessel, climb up the ladder, pour the milk into the vessel and then climb down another ladder. This went on until the last subject had poured his milk into the vessel. The cooking of the kheer started and as promised the other ingredients came from the King. After a long wait, the kheer wasready!EveryoneincludingtheKingsatdowntoeatit.Whentheattendantsstartedserving thedelicacyand thepeople startedeating therewascompletesilence, but not for long. Soon there was a murmur which grew into a loud noise thatrosefromeverycorner,“Thisisnotkheer–thisismeetha bhaat!”
Whatreallyhappened?
7. Distributethehandouton“HowtoConductaGroupDiscussion”attachedherewith.
CONCLUDING THE SESSION
“Oursessionherewillbelikethekheer. The discussions become richer and more meaningful only when everyone contributes and shares ideas and views. It isimportant that all of us participate so that others get to know about our thoughts and feelings.”
Similarlyagroupdiscussion inthefieldgetsenrichedbyeveryone’sparticipation.Ifonlyfewpeopledominatethediscussionandsomepeoplekeepquiet,thosewhoarenotencouragedtospeakmaynotbeabletocleartheirdoubtsand/orwillnotexpress their concerns about a behaviour change. This will result into incomplete and ineffective communication.
LUNCH BREAK 12:45 to 13:45 (60 minutes)

For Mid-Level Managers34
SESSION 5 USE OF A COMMUNITY DIALOGUE TOOL
SESSION OUTCOMES
At the end of the session, participants will be able to:
• Use the outcomes of the Problem AnalysisProcess in an SBCC session using a communitydialoguetool.
• Understandtheimportanceofhavingtheparticipationofcommunitymembers,especially women, in bringing about behaviour change within families andcommunities.
MATERIALS REQUIRED
• Apulleystand• A doll• String• A plastic bag• 12 thick VIPP cards• Black board and chalk or chart paper and sketch pens.
METHODOLOGY
• Pulleyanddollexercise• Demonstration and discussions
PROCESS
1. Invite the participants to spend a few minutes discussing the low immunisation statusofchildreninoursociety.
2. Write at the centre of the board LOW IMMUNISATION STATUS OF CHILDREN and ask the participants to think of some of the main causes contributing this situation.Askthemtosharetheirthoughtsonebyone,andastheysharelistthepoints below the heading. List 10 to 12 main causes.
3. Once this is done, ask the participants the following questions: How can these problems be addressed? How could the mothers be supported to ensure full RI coverage of their children? How linkages with better earnings (like MNREGA) support full immunisation? What support can come from local governance like village health and sanitation committee for complete RI? What are the factors thatwouldhelpthem?Askthemtoreflectandsharetheirthoughtsonebyone.As they speak, list the points above ‘low immunisation status of children’ asshown in the diagram.
4. Whatweseehereisaninterplayofforcesactingin-favourofImmunisationandagainstit.ThisinterplayofoppositeforcesiscalledForceFieldAnalysis.Inorderto move the equilibrium upwards or downwards we need to alter the forces. The following exercise will show us how the forces can be altered.
(Thediagramshouldbeclearlyvisibletoall).
13:45 to 14:45 (60 minutes)

SBCC Training : Module 3 35
5. Tell the participants that they will do an exerciseusing the factors listed in the diagram and a community dialoguetool that will highlight these factors and facilitate dialogue with communities, especiallywomen.
6. Ask the participants to stand in a circle. Place the pulleystandinthecentreof the circle. Put the string through the pulleys andhang a bag on one end and a doll in a girl’s attire on the other end. The doll should be lying on thefloor.
• ANM sensitised for social intrusion.• Discussbenefitsandrisks.• Help the parents visualise child’s future.• Motivate and counsel.• Highlightimportanceandurgency.• Clear misconception.• Handle objections.• Explain in terms of changing health conditions and food habits.Th
ese
fact
ors
can
help
rais
e im
mun
isat
ion
leve
lsTh
ese
fact
ors
low
er
imm
unis
atio
n le
vels
Low immunisation status of children
• ANMdoesnot“touch“ourchildren.• No immediate threat.• Inabilityto“see”futureofthechild.• Lack of concern.• Lack of time.• Misconceptions.• Hearsayonaftereffects.
7. Tieastring(preferablyredincolour)horizontallyonefootabovethedoll,parallelto the ground. (You can also ask two participants to hold the string parallel to the ground in a straight line.)
For Mid-Level Managers36
8. Nowasktheparticipants,“Whatdoyouseehere?Whatdoesthedollrepresent?A girl?Why is she on the floor?What does the string parallel to the groundrepresent?”Generate a good discussion.
9. Concludebysayingthatthedoll(girl)isonthefloorbecausesheispoor,helpless,haspoorhealthetc.(Recallthenegativepointsfromtheanalysisdoneabove.)The string parallel to the ground represents the BPL line; the girl is below the healthline(normalbodyweight,nodisease,completeimmunisation).Whatweseenowrepresentsthepoorchildrenwithinourcommunitieswholeadadifficultlife.
10. Let’s now see how we can help this girl get out of this condition.
11. Spreadthe12thickVIPPcardsonthefloornearthedoll.Askanyoneparticipantto come forward and pick up one card. Ask him/her to write one or two words clearlyonthecardtakenfrompoint#1ofthepositivefactorsfromtheanalysisdone in the earlier part of the session. For example if point #1 is ‘ANM is sensitive towards social inclusion’, he/she should write ‘No social exclusion’ on the card.
12. Now ask him/her to explain how ‘No social exclusion’ could help improve the immunisation status for children in a minute or two. He/she then puts the card into the plastic bag hung on the string.
13. Call a second volunteer and ask him/her to pick a card and write point #2 on the card and explain how this factor will improve the immunisation status of the poor girl.
14. Call10morevolunteersfromamongtheparticipantsonebyoneandrepeattheprocesstillallthecardsonthefloorareusedandputintotheplasticbag.
15. Asthecardsareputintothebag,thegirlwillgraduallystartrisingandbythetime the seventh or eighth card is in; she will be standing and moving above the healthline.Stoptheprocesshereandask,“Whatdoweseehere?”Allowtimefortheparticipantstoreflectandgivetheiranswers.Thencontinuetheprocess.
16. Bythetimethe12th card is put in, the girl will be well above the health line.
17. Stop the exercise.
18. Now move to the second part of the exercise and discuss what happened in the firstpart.
19. Ask the participants:• Whatdidyouobserve?• Wherewasthedoll/girlatthebeginningoftheexerciseandwhy?• What happened to the doll/girl as the cards were being put in?• What position is the doll/girl in now? How did the girl come above the health
line?
20. Givesufficienttimefortheparticipantstoreflectandsharetheirthoughts.Bringout the following points:• The government is providing awide variety of services at the community
level;it isimportantthatfamiliesandcommunitiesarefullyawareoftheirentitlementsandunderstandthebenefitoftheseservicessothattheyandtheirchildrenbenefitfromtheseschemesandservices.

SBCC Training : Module 3 37
• Theseschemesandservicesareprimarilymeanttoimprovethequalityoflife,especiallythatofthepoor.
• Therearemanythingsthatcommunitiesandfamiliescoulddoontheirownthat could also improve the situation of children and women.
21. Now move on to the next part of the exercise. Remove the cards from the bag; thedollwillonceagaindropdowntothefloor.Removethestringfromthepulleysand put it on the side of the wheel. Now add cards into the plastic bag; the doll will not rise as before. Even putting all the cards will not lift the doll above the healthline.Putthestringbackonthepulleysandthedollgetsliftedagain.
22. Once this is demonstrated ask the following questions:• Didthedollgetliftedupwhenthestringwasoffthepulleys?• Whynot?
Givesufficienttimefortheparticipantstoreflectandsharetheirfeelingsandthoughts.
23. Nowsay,“Weseethatthepulleysplayavery importantrole in liftingthegirlabovethepovertyline”.Thenaskthefollowingquestions:Whatdoesthepulleyrepresent? Does it represent government schemes, the Panchayat? Does it represent functionaries like the ASHAs, AWWs, ANMs, Gram Sevaks etc., who bring communities and services together? Generate a good discussion and highlight the critical role that the functionaries play in creating awarenessamong individuals, families and communities and motivate them to avail of the services that are being provided.
CONCLUDING THE SESSION
• Asktheparticipantshowtheyfoundthesession.DidtheyfindthelinkbetweentheForceFieldAnalysisandthepulleyexercise?
• Howdidtheyfindtheuseofthepulley,dollandcardsasacommunitydialoguetool? Was it effective?
• Emphasise that it is only throughparticipationand sharing their feelings andthoughts that people internalise messages and get motivated to change.
• A sustained dialogue is essential to bring about behaviour change.
TIPS FOR THE FACILITATORS
• The length of the rope should be such that one end is 2-3 feet above the ground.• Thedollshouldbelyingonthegroundtostartwith.• The weight of six cards should be equal to the weight of the doll so that when six
cards are placed in the plastic bag, the doll and the bag are on the same level.• Do a thorough rehearsal before the actual exercise.• Initiate discussion when each card is being read and put in the bag.• Emphasisethecommunitydialoguetoolwhenwrappingupthesession.
For Mid-Level Managers38
SESSION 6 UNDERSTANDING TEAMWORK
SESSION OUTCOMES
At the end of the session, participants will get a good understanding of:• How teams should work.• What the role of each member of the team is.• Whattypeofleadershipthatwouldbringaboutthebestresults.
MATERIALS REQUIRED
• 12 pieces of the broken square• Thekey(guide)tothebrokensquare• Black board and chalk or chart paper and sketch pens
METHODOLOGY
Thebrokensquareexercisefollowedbydiscussion.
PROCESS
1. Telltheparticipants,“Oursessionnowwillbeonteamwork,whatateammeans,itscharacteristicsandtherolethatthemembersandtheleaderplay.”Askthemwhethertheybelongtoanyteam/s.Ifsomeoftheanswer“yes”,askthemwhichteamtheyaremembersofandwhotheothermembersoftheteamare.Askthemwhethertheyhaveworkedasmembersofateamandif“yes”,asktwoorthreeparticipantstosharetheirexperienceverybriefly.
2. Telltherearetwotypesofteams.Onewithinyourowndepartmentyouareapartofateamwhichcomprisesofyourcolleagues–peerlevel,juniors,andseniors.Theotherteamisoutsideyourdepartmentatthefieldlevelwhereyoucomeincontactwithpeople fromotherdepartmentsandshareacommongoal– likeANM, ASHA and AWW share a common goal of child health and development.
3. In Part A of this session, we will discuss the cross-functional teams. In Part B of this session we will discuss supportive supervision which helps in improving the intra-departmental teams’ performance.
PART A1. Nowaskforfivevolunteersandsendthemoutofthetrainingroom.Askforfive
more volunteers and send them also out of the training room.
2. Telltheotherparticipantsthatthefirstteamthatwentoutisthe‘PlanningTeam’andthesecondteamthe‘ImplementingTeam’.Showthemthesquare(key)asshown in the diagram. Also show them the 12 pieces that when put together will make the square.
3. Now leave the 12 pieces and the Guide on the table. The 12 pieces will be all mixed up and separate.
4. Address the participants inside the training room:
“You are the observers. Your task will be to observe how an individual behaves in both the planning as well as the implementing teams; also note the dynamics among the members as well as between the two teams. You will also observe different leadership styles as well as leadership transferring from one person to the other. Keep a note on each member and her/his behaviour.
14:45 to 15:30 (45 minutes)

SBCC Training : Module 3 39
At the end of the exercise you will have to share your observations with all theparticipants.
Keep your eyes and ears open; you will have a lot of fun”.
5. Call in Team #1 and tell them the following:“You are the Planning Team and you have an Implementing Team that will carry out the task of making a square under your instructions. Your task is to direct your implementing team to make a square by putting together the 12 pieces kept on the table. You will be given 5 minutes to look at the separate pieces of the square and plan how they can be put together to make a perfect square. The Guide on how the square could be made is also on the table to help you. After five minutes, the Guide will be removed.
Kindlynotethatyouarenotallowedtotouchthepieces;youcanonly lookatthem and plan as a team how the square can be made.
After5minutes,yourImplementingTeamwillbecalledinandyouwillbegivenanother5minutestoinstructandadvisethemhowtheycanmakethesquare.Again,youarenotallowedtotouchthepieceswhileinstructingyourimplementingteam. Your job is complete at the end of 5 minutes.
Your success is when your implementing team completes the square.
6. Now give the Planning Team 5 minutes to plan making the square. After 5 minutes tell them to stop and call in the Implementing Team.
7. Address the Implementing Team members:“A square has been broken into pieces. You have to put these pieces together to complete the square. You have a Planning Team that knows how this can be done and they have been given 5 minutes to give you instructions to complete the task. During these 5 minutes you are not allowed to touch the pieces. Once the Planning Team completes the instructions you will be given 10 minutes to make the square. You will not be allowed to consult any members of the Planning Team while you are making the square.
Your success in completing the square will also be the success of your planning team.
Guide to making the Square The 12 pieces that make the Square

For Mid-Level Managers40
8. AskthePlanningTeamtostartbriefingtheImplementingTeamonhowtomakethesquareusingthe12pieces.Remembertoputawaytheguide.Alsoremindthemthattheyarenotallowedtotouchthepieces.Givethem5minutestodothis.
9. At the end of 5 minutes tell the Planning Team members that their job is over and that theyshouldmoveoutleavingtheImplementingTeammemberstomakethesquare.
10. Give the Implementing Team 10 minutes to make the square. After 10 minutes ask themtostopwork.Inmostcasestheywouldnothavebeenabletocompletethetask.
11. Ask all the participants to go back to their respective seats.
12. Ask the Planning Team members the following questions:• DidyourImplementingTeamsucceedinmakingthesquare?• Areyouhappywiththeoutcome?• Whydidtheyfail?Whatwastheproblem?• WereyouabletoinstructtheImplementingTeamhowtomakethesquare?• Didyouplanwell?
Givetheteammemberssufficienttimetoreflectandrespond.
Now ask the Implementing Team members the following questions:
• Didyousucceedinaccomplishingyourtask?• Whydidyoufail?• What was the problem?• DidyourPlanningTeamgiveyoutherightinstructions?• Howwastheco-ordinationamongyourteammembers?
Givetheteammemberssufficienttimetoreflectandrespond.
13. Now ask the other participants the following questions:• WhydidtheImplementationTeamfailinitstask?• Did the Planning Team do its job well?• Whatdoyouthinkwentwrong?• Whatwerethedynamicsamongthemembersofboththeteamsandbetween
the teams?• Whoweretheleadersinthetwoteams?Whatwastheirstyleofleadership?• Were there members who were dominating? Were there members who were passive?
14. Generateagooddiscussionaroundthesequestionsandgivesufficienttimeforthe participants to respond.
15. Then ask whether the members worked as a team? What are the important characteristics of a team?
16. Bring out the following characteristics of a good team:Everygoodteamwillhave• Clear goals that all members share and aspire to achieve.• Adetailedplanwheretasksandresponsibilitiesareclearlyspeltout.• A maximum of about 15 members to be effective.• Strong bonding between members with mutual respect and appreciation. • Acodeofconductwithsomerulesandregulationsthatallmembersabideby.• Aleaderwhoisdemocraticandsensitiveandrespectedbymembers.
SBCC Training : Module 3 41
CONCLUSION PART A
Conclude thediscussionby saying, “Weareallmembersof teams– theASHA,theAWWandhelperand theANMarea team.The teamcouldbeexpandedbyincluding SHG leaders, Panchayat members, Gram Sevaks etc., depending on the tasks to be accomplished. Only when allmembers work as a teamwill weachieveresults.Everyoneshouldhavethesamegoalsandsharethesamevisionand values. Each one should play his/her role well since these roles are inter-dependent. If one member does not perform well, the team does not perform well. Thisissomethingthatallofusshouldrememberalways.
We have many challenges in the field, the greatest being creating awarenessamong families and communities and motivating them to make the right choices/decisions. Only as a team can we succeed. It is important that we strive to create a strong team at the village level consisting of the ASHA, the AWW, the helper, women and youth representatives as well as the Sarpanch and other elected representatives. Each member should have a clear understanding of the goal that needs to be achieved and the work should be delegated so that the team becomes effective and result oriented. We will see how such a team can work effectively in the next session where we will discuss the planning and organisation of the Village Health and Nutrition Day (VHND).
PART BAsk these question to the participants:
Howdoyouwantyoursupervisortobehave?Listfivegoodthingsandfivethingsthatyoudon’tlikeinyoursupervisor.Generateagooddiscussion.
Askthequestion:Whatdoyouthinkyoursubordinateswouldsayaboutyou?Doyouthinktheywillrepeatsomeofwhatyouhavesaid?Generateadiscussion.
Then display the following chart and explain the points linking it with theirobservations.
Supportive supervision is a collaborative effort between the supervisor and the healthfunctionarytohelpthehealthfunctionaryimprovehis/herperformanceandconfidence.
• The Supervisor observes the health functionary’s communication work withmothers/caregivers, and provides constructive feedback.
• TheSupervisorshouldlistentostaffandcommunity.• She/he should be able to empathise with others.• She/he should provide continuous feedback to the staff.• She/he should help each one achieve her/his targets.• She/heshouldreviewstaffperformancesperiodicallyandoffersupportformid-
course correction.
CONCLUSION PART B
Supportive Supervision is different from traditional supervision. Traditional supervision involves more aspects of inspection and control, with a focus on ensuring adherence to policies and procedures. Supportive Supervision involves jointproblem-solving to identifyareasofstrengthandaddressesanydifficulties
TEA BREAK15:30 to 15:45 (15 minutes)
For Mid-Level Managers42
SESSION OUTCOME
At the end of the session, the participants will be able to:• PlanaVillageHealthandNutritionDay(VHND),thedifferentactivitiesthatneed
to be carried out and the responsibilities of different functionaries.• Understand the need to have the Village Health and Nutrition Committee
meetings to review and plan activities for the coming months.
MATERIALS REQUIRED
• Thefilm ASHA, Ek Din Zindagi Ki (VHND)• Laptop or TV and LCD projector• Blackboard and chalk or chart paper and sketch pens
METHODOLOGY
Viewingofthefilmanddiscussions.
PROCESS
1. TelltheparticipantsthattheywillseehowagoodVHNDcanbeorganised.Askthemtowatchthefilmcarefully.
2. Familiarise yourselfwith thequestions thatare raisedduring thefilmatfixedintervalssothatyoucangeneratelivelyandusefuldiscussions.
3. Now start showing the film and stop after the first set of questions appear.Generate a discussion on the questions. Allow participants to share their thoughts. Keep the discussions to the point.
4. Oncethediscussionsareover,restartthefilm.Pauseagainwhenthenextsetofquestions appears. Generate a discussion as before.
5. Continuetheprocesstilltheendofthefilm.6. Once thediscussionon thefilm isoverask, “How isVHNDconducted inyour
villages? Do you follow what was seen in the film? What problems do youencounter?HowimportantishavingaSBCCsessiononVHND?Howdoyouplanfor it?”
7. Allowsufficienttimefortheparticipantstoreflectandrespond.
CONCLUDING THE SESSION
• ConcludebysayingtheVHNDisprobablythemostimportantdayforanyvillageanditisimportantthatweconductitinthebestwaypossible;theVillageHealth,Nutrition,WaterandSanitationCommitteeshouldberopedintosupporttheday.Frontline functionaries like the ASHA, AWW, helper, ANM etc. should work as a teamandclearlydefinetherolesasshowninthefilm.
• GettingallfamiliesandthecommunitytounderstandthatVHNDiscrucialforthehealthofchildrenandwomenisachallenge.Everychildandwomanshouldtakeadvantage of VHND.
• ItisalsoanimportantdaytoconductanSBCCsessioninaplannedwayusingagoodcommunitydialoguetool.Thesesessionsshouldbeplannedwellinadvanceandwomenshouldbeawareofthesessions.ItcouldbejointlyconductedbytheASHA, AWW and the ANM.
SESSION 7PLANNING AND ORGANISING A VILLAGE HEALTH AND NUTRITION DAY 15:45 to 16:45 (45 minutes)

SBCC Training : Module 3 43
SESSION 8CREATING A VILLAGE HEALTH PLAN AND DEVELOPING A VILLAGE SBCC PLAN
SESSION OUTCOME
At the end of the session, the participants will be able to:
• Understand the process of developing a village SBCC Plan.
MATERIALS REQUIRED
SBCC Plan templates (8-10) copies
METHODOLOGY
PowerPoint presentation and discussion.
PROCESS
1. TelltheparticipantsthattheywilllookattheprocessofcreatingavillageSBCCPlanthroughgroupwork.Whattheywillbedoingisjustanoverviewoftheprocess.Also inform them that the ASHAs, AWWs, ANMs and other functionaries who will beundergoingthe5-dayModulewillactuallydoeachstepoftheexercise.
2. FormsixgroupsandgiveonecopyofSBCCPlantemplatetoeachofthem.
3. Important: Make sure that you have read through this part of the 5-Day Module and prepare yourself for this presentation.
4. Now explain each column of the template.
5. Request the participants to make an ideal SBCC plan for their group. Give the 30 minutes to prepare this.
CONCLUDING THE SESSION
Concludebysayingthat:• A communication plan cannot be an event but a process, well planned over the
year.• One challenge is to create a supportive and enabling environment where
behaviour change is induced through social norms and the other challenge is to bring about the desired change in individuals and families.
• Communitydialogue toolsandgroupdiscussionsareeffective for creatinganenabling environment while IPC and counselling are good at the individual and familylevel.Variousaidscanbeusedtohelpincommunication.
• Social,printandelectronicmediacaneffectivelytransmitinformationandcreateawareness;thesealsoreinforcewhatisbeingdiscussedatthecommunityandfamilylevels.
• Aplanshouldlookatagoodmediamix,clearlydefineaudiencegroupsandlist
16:45 to 17:45 (60 minutes)
For Mid-Level Managers44
SESSION 9VALEDICTORY SESSION
PROCESS
• Informtheparticipantsthatday’ssessionshavecometoanendandthateachone of them is welcome to give his/her feedback and comments on the sessions as well as the SBCC module.
• List the points that emerge on the board or on a chart paper.• Conclude by saying that their support and understandingwould be critical in
rolling out such a module.
Thank all the participants for being present despite their busy schedules.
17:45 to 18:15 (30 minutes)

SBCC Training : Module 3 45
ANNEXURESANNEXURE I : Day1,Session2 – PowerPoint on Development
Paradigm and SBC Theories (given in the CD).
ANNEXURE II : Day1,Session3 – PowerPoint on TARANG SBC Communication Modules (given in the CD)
ANNEXURE III : Day1,Session4 – Thepictureofrailwaycompartment.
ANNEXURE IV : Day1,Session5 – PowerPoint of Shanta’s story (alsogiven in the CD).
ANNEXURE V : Day1,Session5 – PowerPoint of Behaviour Change Process and Roles (also given in the CD).
ANNEXURE VI : Day2,Session5 – SpecificationsforPulleyStand.
ANNEXURE VII : Day2,Session8 – SBCC Plan templates.
ANNEXURE VIII : Pre-PostFormat – SBCCTrainingforMid-levelManagers
"TELL ME, AND I WILL FORGET. SHOW ME, AND I MAY REMEMBER. INVOLVE ME, AND I WILL UNDERSTAND."
Chinese Proverb

For Mid-Level Managers46
Railwaycompartment
THE PICTURE OF A RAILWAY COMPARTMENT
ANNEXURE III Day 1 (Session 4)
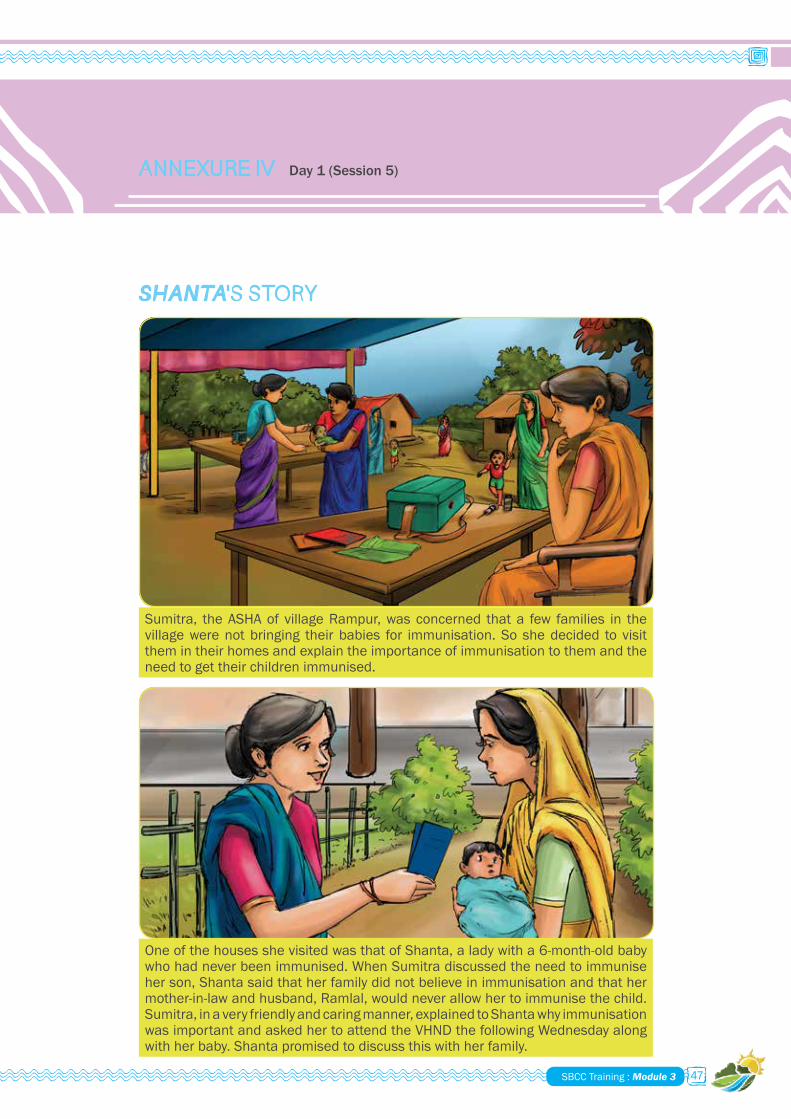
SBCC Training : Module 3 47
SHANTA 'S STORY
Sumitra, the ASHA of village Rampur, was concerned that a few families in the village were not bringing their babies for immunisation. So she decided to visit them in their homes and explain the importance of immunisation to them and the need to get their children immunised.
OneofthehousesshevisitedwasthatofShanta,aladywitha6-month-oldbabywho had never been immunised. When Sumitra discussed the need to immunise herson,Shantasaidthatherfamilydidnotbelieveinimmunisationandthathermother-in-law and husband, Ramlal, would never allow her to immunise the child. Sumitra,inaveryfriendlyandcaringmanner,explainedtoShantawhyimmunisationwasimportantandaskedhertoattendtheVHNDthefollowingWednesdayalongwithherbaby.Shantapromisedtodiscussthiswithherfamily.
ANNEXURE IV Day 1 (Session 5)
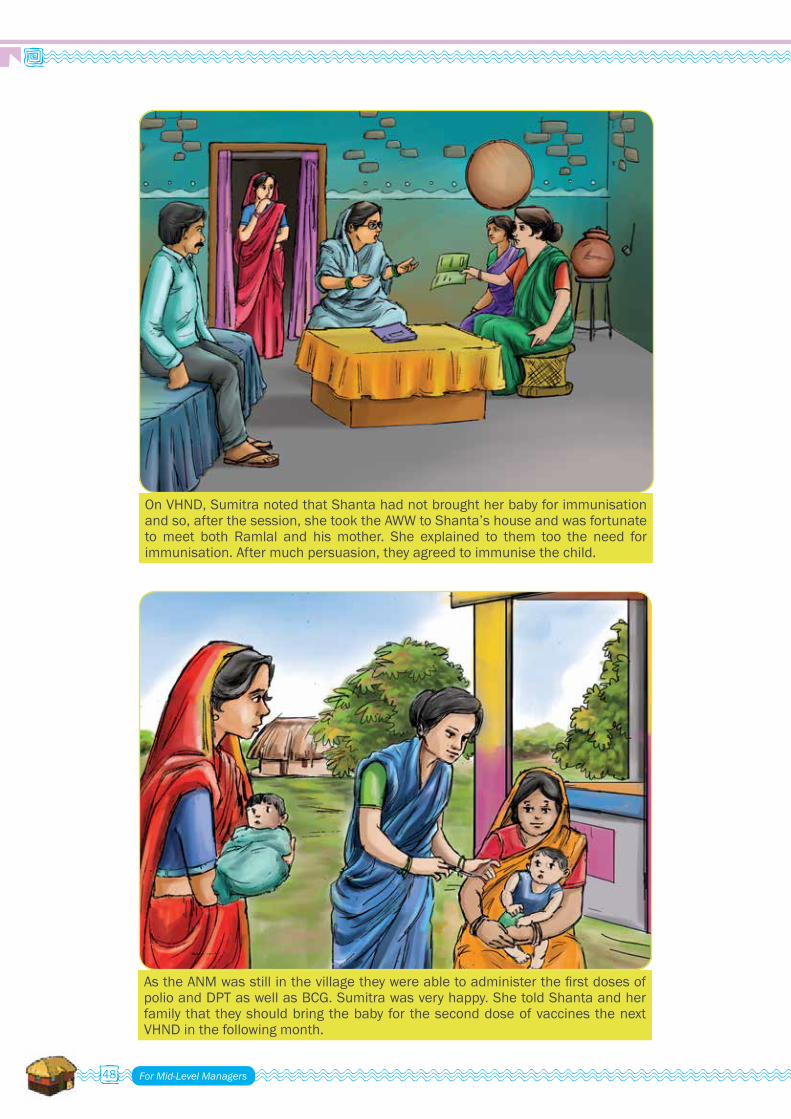
For Mid-Level Managers48
OnVHND,SumitranotedthatShantahadnotbroughtherbabyforimmunisationand so, after the session, she took the AWW to Shanta’s house and was fortunate to meet both Ramlal and his mother. She explained to them too the need for immunisation.Aftermuchpersuasion,theyagreedtoimmunisethechild.
AstheANMwasstillinthevillagetheywereabletoadministerthefirstdosesofpolioandDPTaswellasBCG.Sumitrawasveryhappy.ShetoldShantaandherfamily thattheyshouldbringthebabyfortheseconddoseofvaccinesthenextVHND in the following month.
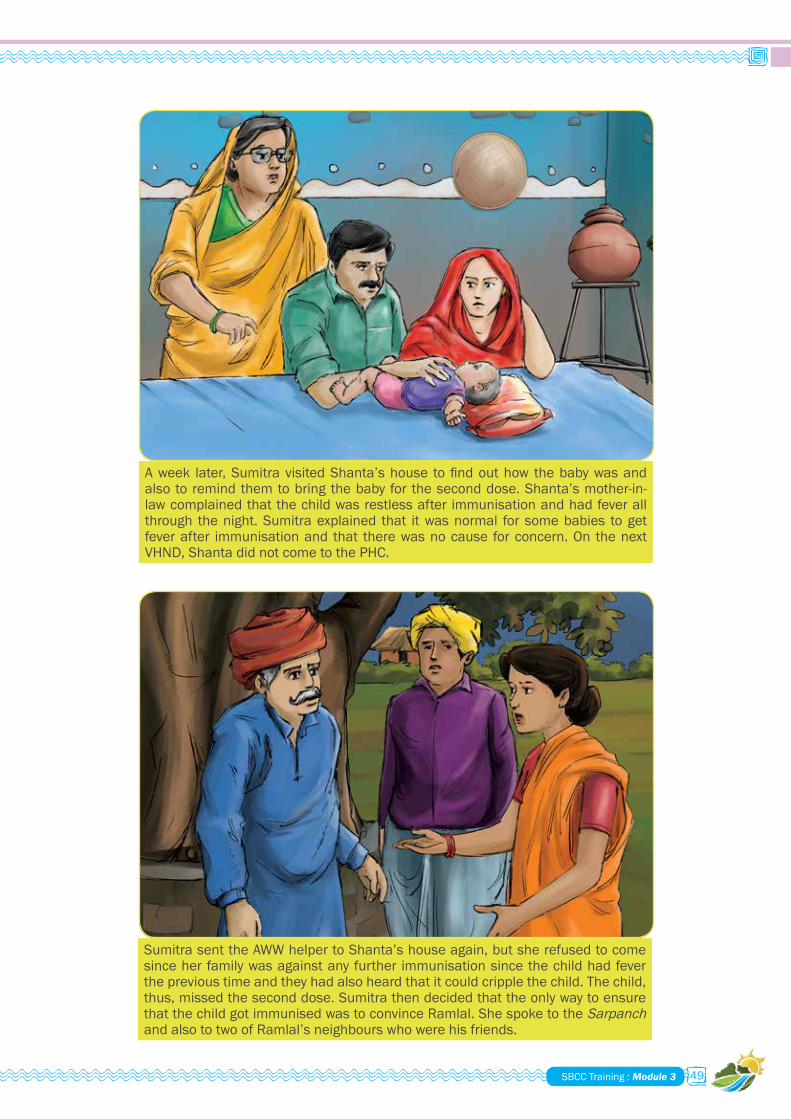
SBCC Training : Module 3 49
Aweek later,SumitravisitedShanta’shouse tofindouthow thebabywasandalsotoremindthemtobringthebabyfortheseconddose.Shanta’smother-in-law complained that the child was restless after immunisation and had fever all through the night. Sumitra explained that it was normal for some babies to get fever after immunisation and that there was no cause for concern. On the next VHND, Shanta did not come to the PHC.
Sumitra sent the AWW helper to Shanta’s house again, but she refused to come sinceherfamilywasagainstanyfurther immunisationsincethechildhadfevertheprevioustimeandtheyhadalsoheardthatitcouldcripplethechild.Thechild,thus,missedtheseconddose.Sumitrathendecidedthattheonlywaytoensurethat the child got immunised was to convince Ramlal. She spoke to the Sarpanch and also to two of Ramlal’s neighbours who were his friends.
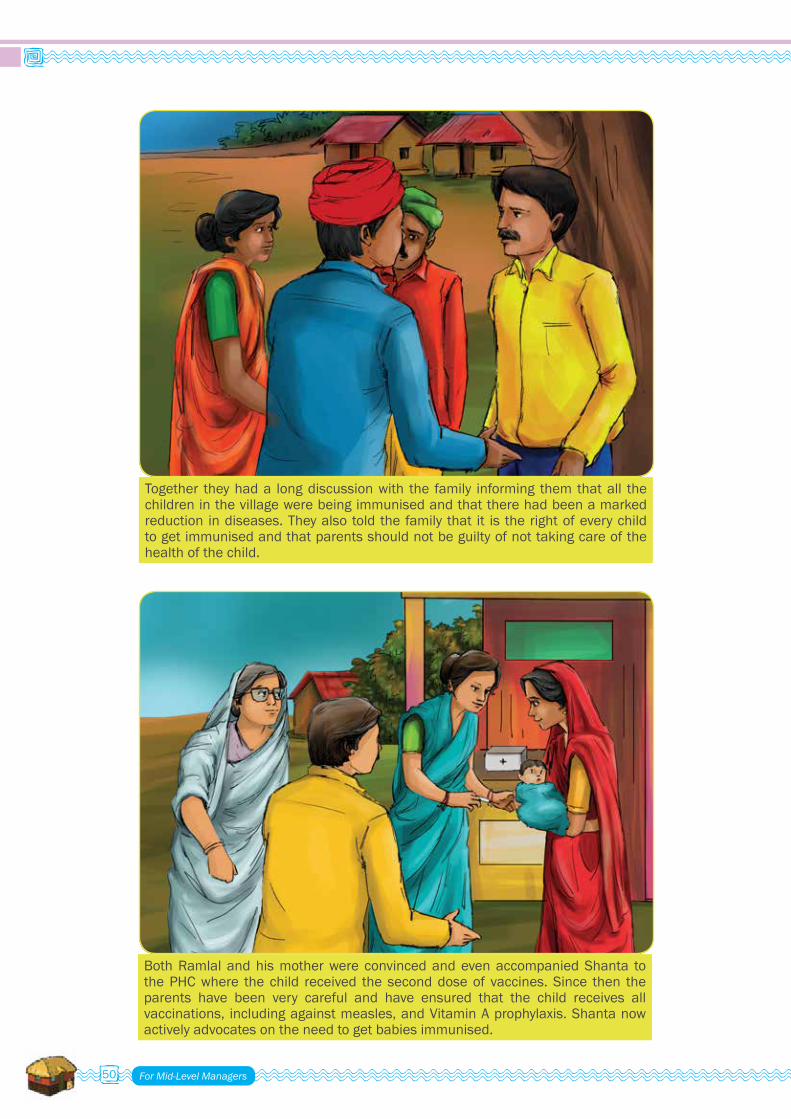
For Mid-Level Managers50
Together theyhada longdiscussionwith the family informing themthatall thechildren in the village were being immunised and that there had been a marked reduction indiseases.Theyalsotoldthefamily that it is therightofeverychildtogetimmunisedandthatparentsshouldnotbeguiltyofnottakingcareofthehealth of the child.
Both Ramlal and his mother were convinced and even accompanied Shanta to the PHC where the child received the second dose of vaccines. Since then the parents have been very careful and have ensured that the child receives allvaccinations, includingagainstmeasles,andVitaminAprophylaxis.Shantanowactivelyadvocatesontheneedtogetbabiesimmunised.

SBCC Training : Module 3 51
THE BEHAVIOUR CHANGE PROCESS
ANNEXURE V Day 1 (Session 5)
1
2
3
45
6
7
The Behaviour Change Process
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
Awareness
Desire
Knowledge Skill
Tries OutRepeats
Maintain
Sustain
An enabling environment consists of
• Supportive relatives and neighbours.• Functionaries and volunteers and other opinion leaders through their
sustained encouragement, through counselling and dialogue and provisionofqualityservices.
• The media through supportive messaging.
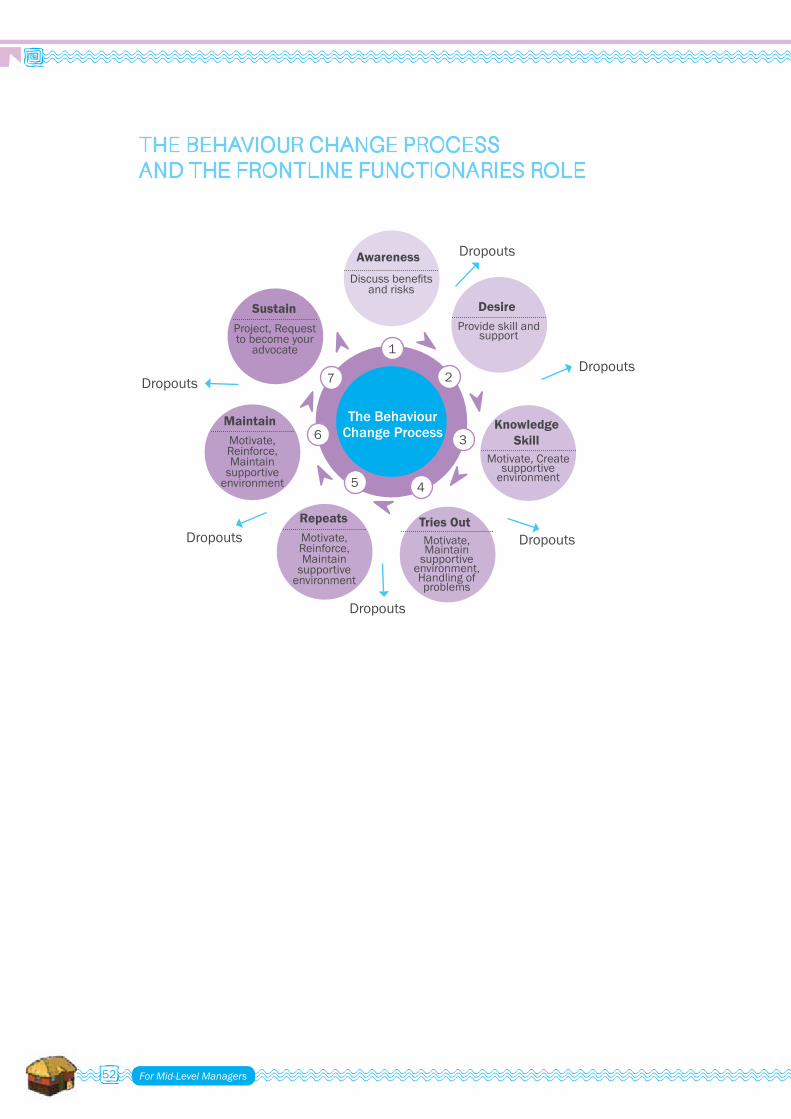
For Mid-Level Managers52
THE BEHAVIOUR CHANGE PROCESS AND THE FRONTLINE FUNCTIONARIES ROLE
1
2
3
45
6
7
The Behaviour Change Process
Dropouts
Dropouts
Dropouts
Dropouts
Dropouts
DropoutsAwareness
Desire
Knowledge Skill
Tries OutRepeats
Maintain
Sustain
Discussbenefits and risks
Project, Request tobecomeyour
advocate
Provide skill and support
Motivate, Create supportive
environment
Motivate, Reinforce, Maintain
supportive environment
Motivate, Reinforce, Maintain
supportive environment
Motivate, Maintain
supportive environment, Handling of problems

SBCC Training : Module 3 53
Dimensions: 18 inch/1.5 feet height (to be placed on the table) and14"widthwheel-to-wheel
Material: Wooden (will be polished)
ANNEXURE VI Day 2 (Session 5)
SPECIFICATIONS OF PULLEY
For Mid-Level Managers54
VILLAGE SBCC PLAN
Steps• BeginswithanalysingtheVillageHealthMaptoassessthesituation.• Reference column 2 of Village Health & Nutrition Plan template.• Develop Village Health and Nutrition Plan.• Develop Village SBCC Plan.
SBCC PLAN TEMPLATES
ANNEXURE VII Day 2 (Session 8)

SBCC Training : Module 3 55
Vill
age
SB
CC
Pla
n
Area
s of
inte
r-ve
ntio
n So
cial
& b
ehav
iour
ch
ange
list
ed
Wha
t are
the
barr
iers
or
trig
gers
to b
ehav
-io
ur c
hang
e?
Who
is to
be
addr
esse
d?
Wha
t ap-
proa
ch
shou
ld I
use?
Wha
t too
ls
or m
ater
ials
sh
ould
I us
e?
Whe
n sh
ould
I d
evel
op th
e pl
an?
Who
will
hel
p m
e?
How
sh
ould
I fo
llow
up?
How
sho
uld
I m
onito
r the
ch
ange
?
Loca
tion
of
gove
rnm
ent
serv
ice
cent
re
Wom
ensafetyshould
beco
me
a so
cial
responsibilityatthe
villa
ge le
vel.
Loca
l nor
ms
on
wom
ensafety
Villageboys,
youngmen
and
wom
en
and
villa
ge
elde
rs
Gro
up d
iscu
s-si
ons
- mixe
d gr
oups
with
ad
oles
cent
s,
men
, wom
en,
elde
rs
Open
dis
cus-
sionsandstory
telli
ng (p
ick
a storyfromthe
new
spap
er)
Orga
nise
a
spec
ial s
es-
sion
Gram
pra
d-ha
n, lo
cal r
eli-
giou
s le
ader
s
Hav
e a
mee
ting
once
in 1
5 daysfor
next
two
mon
ths
Wal
k ar
ound
the
PHC
once
in 1
5 daystoverify
the
surv
eilla
nce
grou
ps; a
sk
wom
eniftheyfeel
safe
rH
ealth
car
e se
ekin
g be
-ha
viou
r
Preg
nant
wom
en
shou
ld b
e as
king
fo
r and
ava
iling
AN
C ch
eck-
ups.
Inac
cess
ible
are
a,
delays,Lowliteracy,
old
tradi
tion,
cus
-to
ms,
dis
cour
teou
s be
havi
our o
f fro
ntlin
e fu
nctio
narie
s
Mot
hers
, hu
sban
ds,
mot
her i
n la
w
Saas
bah
u sa
mm
elan
s;
pati-
patn
i sa
mm
elan
s;
join
t hom
e vi
sit w
ith
VHSC
mem
-be
r
Orga
nise
a
grou
p m
eetin
g w
ith th
e w
omen
of
that
com
mu-
nitytoknowthe
reas
ons
for n
ot
com
ing
for A
NC.
Immediately
afterfinding
that
ther
e ar
e pr
egna
nt
wom
en in
the
community
who
hav
e no
t co
me
for A
NC
A w
oman
fro
m s
ame
grou
p w
ho h
as
com
plet
ed a
ll AN
Cs a
nd c
an
be p
roje
cted
as
a ro
le
mod
el
Every
quar
ter
Obta
in d
ata
for
ANCs
; Hom
e vi
sits
Stat
us o
f: Pr
egna
nt
wom
en &
la
ctat
ing
mot
hers
Mot
her-i
n-la
w a
nd
otherfam
ilymem
bers
supporthealthycare
prac
tices
for p
regn
ant
and
lact
atin
g m
othe
rs
and
new
born
s
Lack
of a
war
enes
s on
dan
ger s
igns
, So
cial
Nor
ms
rela
ted
toearlybathing&
cleansingofbaby&
pre-
lact
eal f
eeds
Fam
ilies
and
m
othe
r in
law
Freq
uent
ho
me
visi
tsFl
ip b
ooks
, pos
t-ers,films
Quarterly,
also
cov
er
all p
regn
ant
wom
en fr
om
thei
r reg
istra
-tio
n on
war
ds
till A
NCs
AWW
/AN
MAt
the
time
of e
ach
ANC
Hom
e vi
sits
Adol
esce
nt
girls
Wom
eninfamilyand
front
line
func
tiona
ries
expl
ain
and
disc
uss
menstrualhygiene
behaviourw
ithyoung
girls
Lack
of a
war
enes
s,
soci
al ta
boo
resu
lt-in
g in
inhi
bitio
ns to
di
scus
s w
ith /
edu-
cate
girl
s
Adol
esce
nt
girls
, mot
hers
Coun
selli
ng
sess
ions
at
scho
ol, a
nd
Anga
nwad
i ce
ntre
Gro
up m
eetin
g w
ith m
othe
rs u
s-ingdoll-pulley
Monthlymeet-
ings
Gram
pra
dhan
(if
a w
oman
) or
Pra
dhan
's w
ife
Monthly
Incr
ease
d us
e of
cle
an c
loth
/sanitarynapkins
obse
rved
thro
ugh
hom
e vi
sits
Child
ren
un-
der 6
yea
rs
RI is
reco
gnis
ed a
s a
prev
entiv
e m
easu
re;
communityrecognises
the
impo
rtan
ce o
f pre
-ve
ntiv
e be
havi
our o
ver
cura
tive
med
icin
e
Lack
of a
war
enes
s,
Trad
ition
al n
egat
ive
valu
es, I
nacc
es-
sibl
e ar
ea, n
egat
ive
attit
ude
of s
ervi
ce
providers,lowpriority
tow
ard
heal
th.
Mot
hers
, hu
sban
ds,
mot
her i
n la
w
Soci
al
dial
ogue
; use
of
relig
ious
le
ader
s
Gro
up m
eetin
g w
ith m
othe
rs u
s-ingdoll-pulley
Monthlyplans
Loca
l rel
i-gi
ous
lead
ers,
sc
hool
teac
h-er
, mot
hers
of
child
ren
with
fu
ll im
mun
isa-
tion
cove
rage
Fort
nigh
t-ly,Ongoing
verification
of 'd
ue-
lists
'
Actu
al n
umbe
r of
imm
unis
atio
ns
done;verification
with
due
list

For Mid-Level Managers56
Vill
age
SB
CC
Pla
n
Area
s of
inte
r-ve
ntio
n So
cial
& b
ehav
iour
ch
ange
list
ed
Wha
t are
the
barr
iers
or
trig
gers
to b
ehav
-io
ur c
hang
e?
Who
is to
be
addr
esse
d?
Wha
t ap-
proa
ch
shou
ld I
use?
Wha
t too
ls
or m
ater
ials
sh
ould
I us
e?
Whe
n sh
ould
I d
evel
op th
e pl
an?
Who
will
hel
p m
e?
How
sh
ould
I fo
llow
up?
How
sho
uld
I m
onito
r the
ch
ange
?
VHN
D
Crea
te d
eman
d fo
r and
pa
rtic
ipat
ion
in V
HN
D.
VHN
D is
org
anis
ed a
s a
fest
ival
like
eve
ntFa
mili
es a
nd
care
give
rsCo
nver
genc
e of
all
depa
rt-
men
ts -
espe
-ciallyHealth
and
ICD
S
Wal
l pai
ntin
gs,
child
ren
' pra
b-ha
t phe
ris'
Two
wee
ks
beforeevery
VHND/RIday
MO
I/C,
ICD
S Su
perv
isor
s,
PRI &
VH
SC
Mem
bers
, lo
cal R
MPs
, Re
ligio
us le
ad-
ers
Ongo
ing
activ
-ity,weekly
follo
w u
p w
ith d
ue
list
Num
ber o
f per
-so
ns v
isiti
ng o
n VH
ND
, inc
reas
e in
the
num
ber o
f co
unse
lling
ses
-si
ons
on a
VH
ND
Wat
er &
san
i-ta
tion
Villa
ge w
ater
and
sa
nita
tion
com
mitt
ee
(VW
SC) s
houl
d be
em
-powered;com
munity
inte
rest
in w
ater
and
safetyofw
atersources
is in
crea
sed
Wat
er is
not
see
n as
a
limite
d re
sour
ce;
Pric
e of
wat
er is
not
ac
know
ledg
ed a
s pe
ople
get
it fr
ee;
awar
enes
s on
wat
er
clea
nlin
ess
is p
oor -
w
hat l
ooks
cle
an is
pe
rcei
ved
as c
lean
All c
omm
u-nitymem
bers
-mainlypar-
ents
; VW
SC
mem
bers
Gro
up
disc
ussi
ons
on s
ourc
es
of w
ater
co
ntam
ina-
tion,
pro
per
stor
age
of
wat
er, a
nd
recyclingof
kitc
hen
wat
er
into
kitc
hen
gard
en
Community
dial
ogue
tool
doll-pulley
Quarterly
Scho
ol c
hil-
dren
; wom
enD
urin
g ho
me
visi
ts; a
t th
e vi
llage
ha
ndpu
mp
/wel
l
Hom
e vi
sits
Envi
ronm
en-
tal s
anita
tion
& h
ygie
ne
Communitytakesthe
responsibilityofmak
-in
g th
e vi
llage
OD
F
Old
prac
tices
of O
D;
Health-specially
child
ren
heal
th a
nd
wom
ensafetycanbe
trigg
ers
Men
, Wom
en,
specially
youngwom
-en
; VW
SC
mem
bers
Gro
up d
iscu
s-si
ons;
vill
age
wal
ks th
roug
h OD
site
s in
gr
oup
Wal
l pai
ntin
gs,
grou
p m
eetin
gsQu
arterlyin
cons
ulta
tion
with
Pan
-chayat
Gram
Pra
dhan
Quarterly
Hom
e vi
sits
Any
othe
r is
sue
that
the
grou
p co
mes
up
with
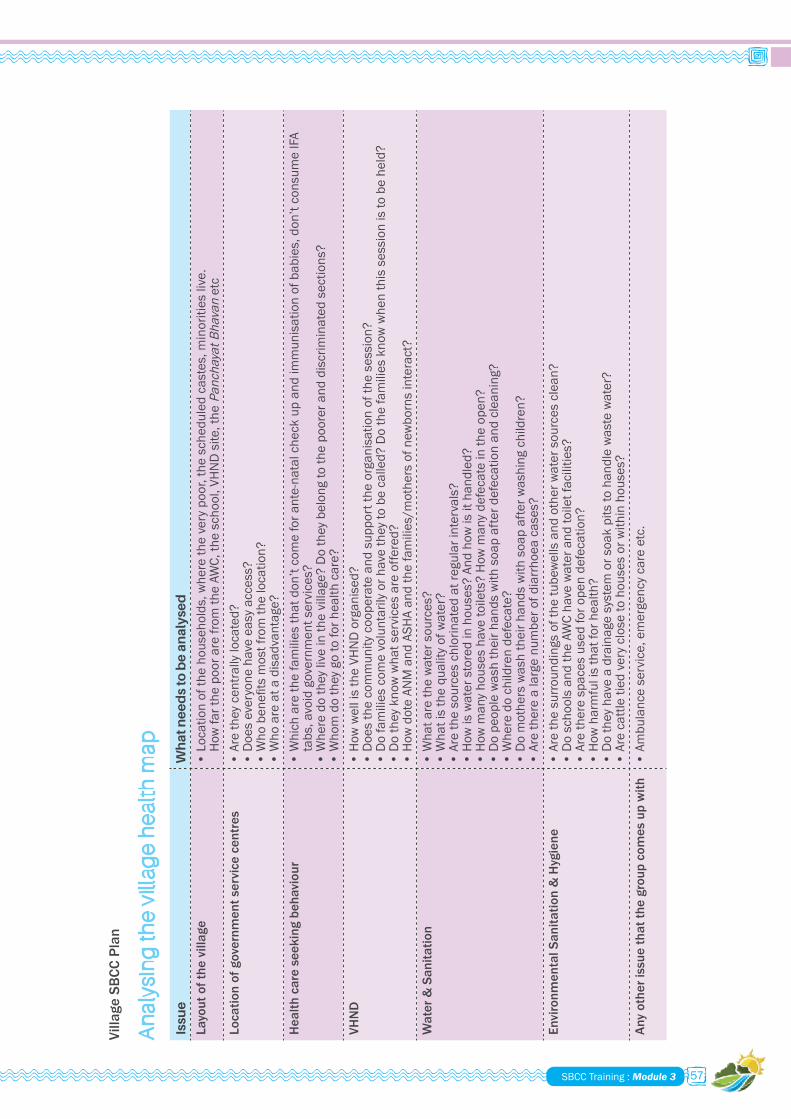
SBCC Training : Module 3 57
Issu
e
Wh
at n
ee
ds
to b
e a
nal
yse
d
Layo
ut o
f the
vill
age
• Locationofthehouseholds,wheretheverypoor,thescheduledcastes,m
inoritieslive.
How
far t
he p
oor a
re fr
om th
e AW
C, th
e sc
hool
, VH
ND
site
, the
PanchayatBhavan
etc
Loca
tion
of g
over
nmen
t ser
vice
cen
tres
•
Aretheycentrallylocated?
• Doeseveryonehaveeasyaccess?
• Whobenefitsmostfromthelocation?
• W
ho a
re a
t a d
isad
vant
age?
Hea
lth c
are
seek
ing
beha
viou
r •
Whi
ch a
re th
e fa
mili
es th
at d
on’t
com
e fo
r ant
e-na
tal c
heck
up
and
imm
unis
atio
n of
bab
ies,
don
’t co
nsum
e IF
A ta
bs, a
void
gov
ernm
ent s
ervi
ces?
•
Wheredotheyliveinthevillage?Dotheybelongtothepooreranddiscriminatedsections?
• Whomdotheygotoforhealthcare?
VHN
D
• H
ow w
ell i
s th
e VH
ND
org
anis
ed?
• Doesthecommunitycooperateandsupporttheorganisationofthesession?
• Dofamiliescom
evoluntarilyorhavetheytobecalled?Dothefamiliesknowwhenthissessionistobeheld?
• Dotheyknowwhatservicesareoffered?
• H
ow d
ote
ANM
and
ASH
A an
d th
e fa
mili
es/m
othe
rs o
f new
born
s in
tera
ct?
Wat
er &
San
itatio
n •
Wha
t are
the
wat
er s
ourc
es?
• Whatisthequalityofw
ater?
• A
re th
e so
urce
s ch
lorin
ated
at r
egul
ar in
terv
als?
•
How
is w
ater
sto
red
in h
ouse
s? A
nd h
ow is
it h
andl
ed?
• Howmanyhouseshavetoilets?Howmanydefecateintheopen?
• D
o pe
ople
was
h th
eir h
ands
with
soa
p af
ter d
efec
atio
n an
d cl
eani
ng?
• W
here
do
child
ren
defe
cate
? •
Do
mot
hers
was
h th
eir h
ands
with
soa
p af
ter w
ashi
ng c
hild
ren?
• A
re th
ere
a la
rge
num
ber o
f dia
rrho
ea c
ases
?En
viro
nmen
tal S
anita
tion
& H
ygie
ne
• A
re th
e su
rroun
ding
s of
the
tube
wel
ls a
nd o
ther
wat
er s
ourc
es c
lean
? •
Do
scho
ols
and
the
AWC
have
wat
er a
nd to
ilet f
acili
ties?
• A
re th
ere
spac
es u
sed
for o
pen
defe
catio
n?
• H
ow h
arm
ful i
s th
at fo
r hea
lth?
• Dotheyhaveadrainagesystemorsoakpitstohandlewastewater?
• Arecattletiedveryclosetohousesorwithinhouses?
Any
othe
r iss
ue th
at th
e gr
oup
com
es u
p w
ith•
Ambulanceservice,emergencycareetc.
An
alys
ing
the
vill
age
he
alth
map
Villa
ge S
BCC
Plan

For Mid-Level Managers58
Vill
age
He
alth
& N
utr
itio
n P
lan
Are
as o
f in
terv
en
tio
n
Pro
ble
ms
ide
nti
fie
d in
o
rde
r o
f pri
ori
ty
Act
ion
s re
qu
ire
d
So
cial
ch
ang
e th
at s
ho
uld
hap
pe
n w
ith
in
com
mu
nit
ies
"B
eh
avio
ur
chan
ge
that
sh
ou
ld
hap
pe
n w
ith
in fa
mili
es
(W
hat
sh
ou
ld b
e th
e d
esi
red
be
hav
iou
r ch
ang
e
that
sh
ou
ld h
app
en
at t
he
ind
ivid
ual
, fam
ily a
nd
co
mm
un
ity
leve
l so
that
exp
ect
ed
ou
tco
me
s ar
e
ach
ieve
d?)
Loca
tion
of
gove
rnm
ent
heal
th s
ervi
ce
cent
re
PHCislocatedonalonely
patchmakingitdifficult
for t
he w
omen
Sinc
e PH
C ca
n no
t be
shift
ed, t
he
surro
undi
ngs
shou
ld
be m
ade
safe
r thr
ough
su
ppor
tive
envi
ronm
ent
Wom
ensafetyshouldbecom
easocial
responsibilityatthevillagelevel.
Villageboys/youngmen/wom
en
volu
ntee
r to
form
sur
veill
ance
gro
ups
arou
nd th
e PH
C
Hea
lth c
are
seek
ing
beha
viou
r
Wom
en fr
om a
par
ticul
ar
communityarenotcom
ing
for A
NC
Expl
ore
the
caus
esW
omen
sho
uld
be w
illin
g to
talk
abo
ut th
eir
rese
rvat
ions
. Org
anis
e a
grou
p m
eetin
g w
ith
thewom
enofthatcom
munitytoknowthe
reas
ons
for n
ot c
omin
g fo
r AN
C.
Theystartcom
ingforANCsandtake
100
IFA
tabl
ets
VHN
D
Peop
le n
eed
repe
ated
re
min
ders
to c
ome
for t
he
VHN
D
VHN
D s
houl
d be
pe
rcei
ved
as a
maj
or
heal
th e
vent
Invo
lve
mul
tiple
sta
keho
lder
s - P
RI m
embe
rs,
loca
l sch
ool t
each
ers,
ICD
S/H
ealth
, NG
Os to
pu
blic
ise
the
even
t.
Fam
ilies
com
e fo
r the
VH
ND
and
di
scus
s th
eir i
ssue
s w
ith A
NM
/AW
W
Stat
us o
f:
Preg
nant
w
omen
&
lact
atin
g m
othe
rs
Wom
en d
o no
t rec
ogni
se
dang
er s
igns
just
afte
r deliveryanditprevents
seek
ing
med
ical
car
e in
tim
e
Impr
oved
HBP
NC
Mother-in-lawandotherfamilymem
bersget
invo
lved
with
chi
ld's
hea
lthMother-in-lawandotherfamily
mem
bers
reco
gnis
e da
nger
sig
ns
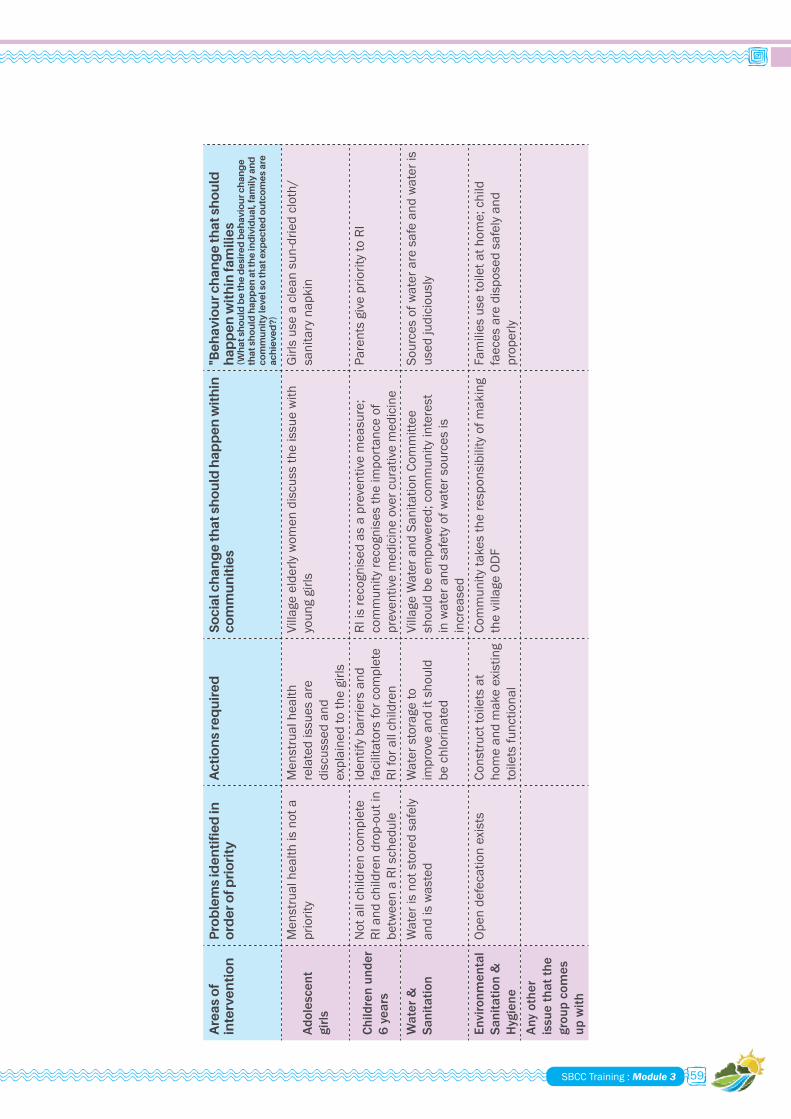
SBCC Training : Module 3 59
Are
as o
f in
terv
en
tio
n
Pro
ble
ms
ide
nti
fie
d in
o
rde
r o
f pri
ori
ty
Act
ion
s re
qu
ire
d
So
cial
ch
ang
e th
at s
ho
uld
hap
pe
n w
ith
in
com
mu
nit
ies
"B
eh
avio
ur
chan
ge
that
sh
ou
ld
hap
pe
n w
ith
in fa
mili
es
(W
hat
sh
ou
ld b
e th
e d
esi
red
be
hav
iou
r ch
ang
e
that
sh
ou
ld h
app
en
at t
he
ind
ivid
ual
, fam
ily a
nd
co
mm
un
ity
leve
l so
that
exp
ect
ed
ou
tco
me
s ar
e
ach
ieve
d?)
Adol
esce
nt
girls
Men
stru
al h
ealth
is n
ot a
priority
Men
stru
al h
ealth
re
late
d is
sues
are
di
scus
sed
and
expl
aine
d to
the
girls
Villageelderlywom
endiscusstheissuewith
younggirls
Girl
s us
e a
clea
n su
n-dr
ied
clot
h/sanitarynapkin
Child
ren
unde
r 6
year
s
Not
all
child
ren
com
plet
e RI
and
chi
ldre
n dr
op-o
ut in
be
twee
n a
RI s
ched
ule
Identifybarriersand
faci
litat
ors
for c
ompl
ete
RI fo
r all
child
ren
RI is
reco
gnis
ed a
s a
prev
entiv
e m
easu
re;
communityrecognisestheimportanceof
prev
entiv
e m
edic
ine
over
cur
ativ
e m
edic
ine
ParentsgiveprioritytoRI
Wat
er &
Sa
nita
tion
Waterisnotstoredsafely
and
is w
aste
dW
ater
sto
rage
to
impr
ove
and
it sh
ould
be
chl
orin
ated
Villa
ge W
ater
and
San
itatio
n Co
mm
ittee
shouldbeem
powered;com
munityinterest
inwaterandsafetyofwatersourcesis
incr
ease
d
Sour
ces
of w
ater
are
saf
e an
d w
ater
is
usedjudiciously
Envi
ronm
enta
l Sa
nita
tion
&
Hyg
iene
Open
def
ecat
ion
exis
tsCo
nstru
ct to
ilets
at
hom
e an
d m
ake
exis
ting
toile
ts fu
nctio
nal
Communitytakestheresponsibilityofmaking
the
villa
ge O
DF
Fam
ilies
use
toile
t at h
ome;
chi
ld
faecesaredisposedsafelyand
properly
Any
othe
r is
sue
that
the
grou
p co
mes
up
with
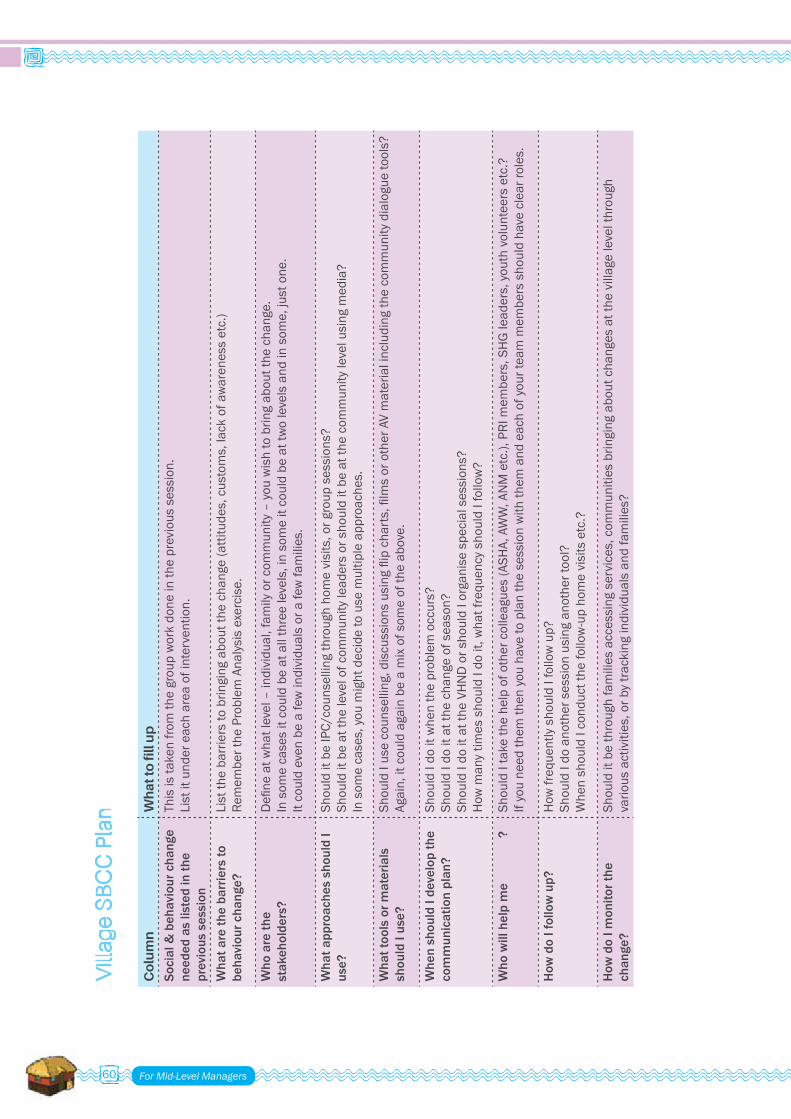
For Mid-Level Managers60
Co
lum
n
Wh
at to
fill
up
Soci
al &
beh
avio
ur c
hang
e ne
eded
as
liste
d in
the
prev
ious
ses
sion
This
is ta
ken
from
the
grou
p w
ork
done
in th
e pr
evio
us s
essi
on.
List
it u
nder
eac
h ar
ea o
f int
erve
ntio
n.
Wha
t are
the
barr
iers
to
beha
viou
r cha
nge?
List
the
barr
iers
to b
ringi
ng a
bout
the
chan
ge (a
ttitu
des,
cus
tom
s, la
ck o
f aw
aren
ess
etc.
) Remem
bertheProblem
Analysisexercise.
Who
are
the
stak
ehol
ders
? Defineatw
hatlevel–individual,fam
ilyorcom
munity–youwishtobringaboutthechange.
In s
ome
case
s it
coul
d be
at a
ll th
ree
leve
ls, i
n so
me
it co
uld
be a
t tw
o le
vels
and
in s
ome,
just
one
. It
coul
d ev
en b
e a
few
indi
vidu
als
or a
few
fam
ilies
.
Wha
t app
roac
hes
shou
ld I
use?
Shou
ld it
be
IPC/
coun
selli
ng th
roug
h ho
me
visi
ts, o
r gro
up s
essi
ons?
Shoulditbeatthelevelofcom
munityleadersorshoulditbeatthecom
munitylevelusingmedia?
Insom
ecases,youmightdecidetousemultipleapproaches.
Wha
t too
ls o
r mat
eria
ls
shou
ld I
use?
ShouldIusecounselling,discussionsusingflipcharts,filmsorotherAVmaterialincludingthecommunitydialoguetools?
Agai
n, it
cou
ld a
gain
be
a m
ix o
f som
e of
the
abov
e.
Whe
n sh
ould
I de
velo
p th
e co
mm
unic
atio
n pl
an?
Shou
ld I
do it
whe
n th
e pr
oble
m o
ccur
s?
Shou
ld I
do it
at t
he c
hang
e of
sea
son?
Sh
ould
I do
it a
t the
VH
ND
or s
houl
d I o
rgan
ise
spec
ial s
essi
ons?
Howmanytim
esshouldIdoit,whatfrequencyshouldIfollow?
Who
will
hel
p m
e ?
ShouldItakethehelpofothercolleagues(ASH
A,AWW,ANMetc.),PRImem
bers,SHGleaders,youthvolunteersetc.?
Ifyouneedthem
thenyouhavetoplanthesessionwiththem
andeachofyourteammem
bersshouldhaveclearroles.
How
do
I fol
low
up?
HowfrequentlyshouldIfollowup?
Shou
ld I
do a
noth
er s
essi
on u
sing
ano
ther
tool
? W
hen
shou
ld I
cond
uct t
he fo
llow
-up
hom
e vi
sits
etc
.?
How
do
I mon
itor t
he
chan
ge?
Shou
ld it
be
thro
ugh
fam
ilies
acc
essi
ng s
ervi
ces,
com
mun
ities
brin
ging
abo
ut c
hang
es a
t the
vill
age
leve
l thr
ough
variousactivities,orbytrackingindividualsandfamilies?
Vill
age
SB
CC
Pla
n

SBCC Training : Module 3 61
Vill
age
SB
CC
Pla
n T
em
pla
te
Are
as o
f in
terv
en
tio
n
So
cial
&
be
hav
iou
r ch
ang
e
liste
d
Wh
at
are
the
b
arri
ers
to
be
hav
iou
r ch
ang
e?
Wh
at
are
the
tr
igg
ers
to
Wh
o is
to b
e
add
ress
ed
?W
hat
ap
pro
ach
sh
ou
ld I
use
?
Wh
at
too
ls o
r m
ate
rial
s sh
ou
ld i
use
?
Wh
en
sh
ou
ld i
de
velo
p
the
pla
n?
Wh
o w
ill
he
lp m
e?
Ho
w
sho
uld
i fo
llow
up
?
Ho
w
sho
uld
i m
on
ito
r th
e
chan
ge
?
Loca
tion
of
gove
rnm
ent
heal
th s
ervi
ce
cent
re
Hea
lth c
are
seek
ing
beha
viou
r
VHN
D
Stat
us o
f:•
Pre
gnan
t w
omen
&
lact
atin
g m
othe
rs•
Ado
lesc
ent
girls
• C
hild
ren
unde
r 6 y
ears
Wat
er &
Sa
nita
tion
Envi
ronm
enta
l Sa
nita
tion
&
Hyg
iene
Any
othe
r iss
ue
that
the
grou
p co
mes
up
with

For Mid-Level Managers62
PRE-POST FORMAT –SBCC TRAINING FOR MID-LEVEL MANAGERS
THE PICTURE OF A RAILWAY COMPARTMENTANNEXURE VIII
Pre-Test Post-Test
Participant’s Name: Date:
A.Describeyourroleinfield-levelSBCCinterventionsin3-4sentences.
B. If you agree with the statements given below, please mark Y, else N
1 There is not much difference between IEC and BCC Y N2 It is not possible to change the behaviour of a person Y N3 Generallyallfamiliesinthevillageareatthesamelevelof
understanding.Y N
4 All people have equal rights, therefore there is no need to provide specialprovisionsforagrouporcommunity
Y N
5 Process of communication becomes easier with the participation of all stakeholders
Y N
6 There are seven steps in the behaviour change process Y N7 VillageHealth&SanitationCommitteescanplayanimportantrolein
creating a supportive environment for behaviour changeY N
8 BCC approaches like counselling and IPC constitute a complete and comprehensive medium for effective communication at the village level
Y N
9 Asking questions can be counter-productive in ‘Muskurahat/GATHER’ - IPC
Y N
10 Nature has divided the tasks and roles between men and women. Y N11 Convergence of various services would create confusion at a VHND Y N12 Ifapersoninterpretsamessageinawrongway,itisthatperson’s
mistakeY N
13 There is a need to run special programmes for the disadvantaged sectionsofthesociety
Y N
14 Radio and TV are media through which we can reach all people and we can change their behaviour
Y N
15 Onlyapersonwithgoodcommandonlanguagecanbeagoodcommunicator
Y N


TheCDcontainssession-wisetrainingaids–Pictures, PowerPoint Presentations, Films.

For more copies contact:Communication for Development SectionUnited Nations Children's Fund73 Lodi Estate, New Delhi, IndiaE-mail: [email protected]: www.unicef.org www.unicefiec.org www.unicef.org/india/Telephone: +91-11-24690401