Finding the self: A behavioral measure and its clinical implications
14
Psychotherapy Volume 38/Summer 2001/Number 2 FINDING THE SELF: A BEHAVIORAL MEASURE AND ITS CLINICAL IMPLICATIONS JONATHAN W. KANTER CHAUNCEY R. PARKER ROBERT J. KOHLENBERG University of Washington We present a clinical model of the development of self . The model focuses on the early learning responsible for linguistic self-referents such as "I" and "me." This model offers an account for why some patients, such as those with borderline personality disorder (BPD), feel that they "do not know who they are" or that their sense of self is controlled by other people, while other patients have a sense of a secure, stable self that is not prey to the whims of others. We administered a new self-report instrument, the Experiencing of Self Scale, which measures the degree to which other people influence the experience of self, along with the Self- Esteem Scale and the Dissociative Experiences Scale to 284 undergraduate students and 14 BPD patients. We found that the degree to which other people influence the experience of self depended on the nature and closeness of the people involved, that those in our BPD sample suffered from excessive influence of other people over the experience of self relative to the undergraduates, and that the degree of influence correlated Correspondence regarding this article should be addressed to Robert J. Kohlenberg, Department of Psychology, Box 351635, University of Washington, Seattle, WA 98195-1635. E-mail: [email protected] predictably with high dissociation and low self-esteem. Implications for conceptualizing BPD and narcissistic personality disorder are discussed, and clinical applications are suggested. For clinicians, perhaps no concept is more fa- miliar than that of the self. Consider the following verbatim comments by a patient we will call Beatrice: Beatrice: It's so damn hard to be real, to be me. Therapist: If you aren't you, who are you? Beatrice: I'm whoever someone else wants me to be. I don't even know when I'm being myself. Beatrice's comments highlight some difficult clinical issues. How can a clinician help Beatrice find her "real" self? What exactly is this self to which Beatrice refers? Can it be precisely defined and specified in a clinically-useful manner? Bea- trice's self seemingly possesses incongruous attri- butes that lead us into a quagmire when we try to describe it. First, it changes with other people's wants. However, Beatrice also implied that there is a quality of her self that is more "real" than is that which changes with other people's wants. This self is unchanging and not controlled by others. On the other hand, it is difficult for Bea- trice to be this self, and she does not even know when she is being it. Thus, Beatrice's self is a complicated structure with qualities that change with other people's wants but also has other quali- ties that are unchanging and not controlled by others. Further, as Beatrice describes it, these other unchanging qualities are more foreign to her but are held in higher esteem as more real. In an attempt to make sense of this phenomena, a multitude of theories of the self have been pre- sented that provide a rationale for what the self 198
-
Upload
washington -
Category
Documents
-
view
1 -
download
0
Transcript of Finding the self: A behavioral measure and its clinical implications
Psychotherapy Volume 38/Summer 2001/Number 2
FINDING THE SELF: A BEHAVIORAL MEASURE AND ITSCLINICAL IMPLICATIONS
JONATHAN W. KANTERCHAUNCEY R. PARKER
ROBERT J. KOHLENBERGUniversity of Washington
We present a clinical model of thedevelopment of self . The model focuseson the early learning responsible forlinguistic self-referents such as "I" and"me." This model offers an account forwhy some patients, such as those withborderline personality disorder (BPD),feel that they "do not know who they are"or that their sense of self is controlled byother people, while other patients havea sense of a secure, stable self that is notprey to the whims of others. Weadministered a new self-reportinstrument, the Experiencing of SelfScale, which measures the degree towhich other people influence theexperience of self, along with the Self-Esteem Scale and the DissociativeExperiences Scale to 284 undergraduatestudents and 14 BPD patients. We foundthat the degree to which other peopleinfluence the experience of self dependedon the nature and closeness of the peopleinvolved, that those in our BPD samplesuffered from excessive influence of otherpeople over the experience of self relativeto the undergraduates, and that thedegree of influence correlated
Correspondence regarding this article should be addressedto Robert J. Kohlenberg, Department of Psychology, Box351635, University of Washington, Seattle, WA 98195-1635.E-mail: [email protected]
predictably with high dissociation andlow self-esteem. Implications forconceptualizing BPD and narcissisticpersonality disorder are discussed, andclinical applications are suggested.
For clinicians, perhaps no concept is more fa-miliar than that of the self. Consider the followingverbatim comments by a patient we will callBeatrice:
Beatrice: It's so damn hard to be real, to be me.Therapist: If you aren't you, who are you?Beatrice: I'm whoever someone else wants me to be. I don'teven know when I'm being myself.
Beatrice's comments highlight some difficultclinical issues. How can a clinician help Beatricefind her "real" self? What exactly is this self towhich Beatrice refers? Can it be precisely definedand specified in a clinically-useful manner? Bea-trice's self seemingly possesses incongruous attri-butes that lead us into a quagmire when we tryto describe it. First, it changes with other people'swants. However, Beatrice also implied that thereis a quality of her self that is more "real" than isthat which changes with other people's wants.This self is unchanging and not controlled byothers. On the other hand, it is difficult for Bea-trice to be this self, and she does not even knowwhen she is being it. Thus, Beatrice's self is acomplicated structure with qualities that changewith other people's wants but also has other quali-ties that are unchanging and not controlled byothers. Further, as Beatrice describes it, theseother unchanging qualities are more foreign toher but are held in higher esteem as more real.
In an attempt to make sense of this phenomena,a multitude of theories of the self have been pre-sented that provide a rationale for what the self
198
Finding the Self
is, how it develops and how this developmentcan go awry and contribute to psychopathology.Some, like Kohut's (1971, 1977) psychodynamicself psychology and Bandura's (1977) social-cognitive construct of self-efficacy, have been ac-cepted for many years by adherents to these par-ticular theoretical approaches (see Baker andBaker, 1987, for an overview of Kohut's system,and Markus and Wurf, 1987, for a review ofcognitive theories of the self). However, manydo not find any one theory adequate, as evidencedby the abundance of new theories of the self oraspects of the self that continually are generated.For example, a scan of the table of contents of arecent review of psychoanalytic theories of theself (Socor, 1997) reveals theories on the inten-tional self, representational self, interpersonalself, ascendant self, totalitarian self, phenomenalself, good-enough self, basic self, personal self,contained self, unthought self, allusional self, andcertain self, as well as Kohut's theory of self.Clinical cognitive researchers also have proposedalternatives to Banduras's self construct and re-lated them to clinical problems, including depres-sion (e.g., Segal & Vella, 1990), anxiety andphobias (e.g., Hope, Rapee, Heimberg, & Dom-beck, 1990; Williams, 1995), eating disorders(e.g., Vitousek & Ewald, 1993), and depressionin children (e.g., Hammen & Goodman-Brown,1990). A recent chapter (Robins, Norem, &Cheek, 1999) reviewing social and personalityapproaches to the self documented at least 37different self-concept theories.
It seems that there is a problem here. Perhapsresearchers are developing theories that cliniciansdo not find externally valid or clinically useful,or clinicians are developing theories which re-searchers do not find internally valid or otherwisereject on empirical grounds. For whatever reason,there seems to be no consensus and a great dealof confusion, and the production of new theoriescontinues at an alarming rate. The proliferationof approaches has led two major self researchersto ask, in the titles of their articles, "Will the realself or selves please stand up?" (Lewis, 1992)and "Is anyone in charge?" (Greenwald, 1982).
The difficulty could be due to the "homuncu-lus" problem, the logical fallacy of explainingperception and behavior by positing a directive"person within the person" that in turn guidesperception and behavior (Smith, 1993; Westin,1999, p. 400). In this case, the logical fallacy isthat positing some form of a "self to explain a
person's experience of self is not an explanationat all in that it does not account for what, in turn,directs the self. A proposed self could never befound adequate as a theory because an additionalexplanation is always necessary.
Because a behavioral approach1 markedly dif-fers from other approaches in its treatment ofproposed mental entities, it offers a new vantagepoint that might clarify the confusion. The depar-ture, and potential solution, of behaviorists is theview that mental entities—such as the self—sim-ply do not exist. It immediately must be clarifiedthat behaviorists do not deny mental experience;they only eschew treating that experience as anentity or homunculus. For example, while behav-iorists argue that cognitive structures or schemasdo not exist, they are very interested in the experi-ence and process of thinking and in thoughts(when viewed as the products of thinking). Simi-larly, behaviorists do not deny the experience ofself; they do object to viewing the self as anythingother than an experience of the individual. Froma behavioral view, the confusing profusion of selfconstructs is understandable given the inherentimpossibility of accounting for the experience ofself with a hypothetical construct; this approachalways leaves the door open for proposals of addi-tional, alternative constructs.
A behavioral model of the self, therefore, at-tempts to account for the experience of self andhow it develops without offering a mental entityor hypothetical construct as an explanation. Atleast three lines of behavioral research and theo-retical investigation into the experience of selfrecently have begun (Dymond & Barnes, 1994,1995,1996,1997; Hayes, 1984,1995a; Kohlenb-erg & Tsai, 1991, 1995), all evolving from thework of B. F. Skinner (e.g., 1945, 1953, 1957,1974). Together, they form a body of work thatcaptures the full, complex experience of self, pro-vides a complete developmental model, and es-tablishes a framework to guide future research.
In this article, we will describe Kohlenberg andTsai's behavioral theory of the experience of self.The theory is intended for clinicians who may or
1 There are several different behavioral approaches. In thisarticle, we refer specifically to radical, or Skinnerian behav-iorism. Others refer to this approach as contextualism, behav-ior analysis, at functional analysis, and each label conveysdifferent meanings and emphases to those in these fields.These differences will not be addressed in this article.
199
J. W. Kanter, C. R. Parker & R. J. Kohlenberg
may not be familiar with a behavioral approach.Subsequently, we will present data from a prelim-inary investigation in support of this theory. Weconclude by comparing this approach to severalsimilar approaches, discuss the clinical advan-tages of a behavioral approach, and present sev-eral clinical implications.
A Behavioral Approach to the Experience ofSelf
Although this might be surprising to manyreaders, many behaviorists consider the experi-ence of self to be an important area of study(Hayes & Wilson, 1993; Kohlenberg & Tsai,1991; Moore, 1980; Skinner, 1945, 1953, 1974).Many nonbehaviorists believe that Skinner deniedthe existence of private experiences such as theexperience of self; in fact Skinner sought to ex-plain private experiences of all types, includingthe experience of self, thinking, feeling, loving,and so on. The Skinnerian view differs from mostother schools of thought in psychology in whatconstitutes an adequate explanation for a privateexperience. Skinner viewed private experiencesas private behaviors, which could be accountedfor with the same learning and change processesas could public behaviors. Skinner did not denythe existence of private experiences, rather heobjected to substituting a mental entity for thatexperience. For example, Skinner did not objectto the notion of unconscious processes. In fact,Skinner (1974) wrote, "It is often said, particu-larly by psychoanalysts, that behaviorism cannotdeal with the unconscious. The fact is that, tobegin with, it deals with nothing else (p. 153)."Skinner did object to notions that reify uncon-scious processes into "an unconscious" that thenis offered as a cause of behavior. (Although Skin-ner [1945, 1953] clearly articulated this position50 years ago, the debate on his position lamenta-bly continues. See Dougher, 1993; Alford, Rich-ards, & Hanych, 1995; and Hayes, 1995a forrecent examples.)
According to Skinner one must accomplish twoaims to fully account for a behavior. First, onemust specify the context in which the behavioroccurs and distinguish this context from those inwhich the behavior does not occur. Skinnertermed the salient features of this context discrim-inative stimuli. Second, one must describe thehistorical factors that account for why a particularbehavior is more likely to occur in a particularcontext. Skinner termed this process the re-
inforcement history. The specific discriminativestimuli for a behavior, the behavior itself, andhistorical reinforcers for the behavior comprisethe three terms in the three-term contingency.
Skinner (1974) briefly outlined a behavioralaccount of the experience of the self that formsthe basis for Kohlenberg and Tsai's (1991, 1995)more recent conceptualization. Because the expe-rience of self is necessarily private and unavaila-ble to all but the person having the experience,Skinner operationalized the experience of self asknowing one's self, specifically as the behaviorof verbally discriminating one's own behavior(Skinner, 1974, pp. 34-35). In other words,Skinner attempted to account for what linguistsrefer to as self-referential speech. The view thatself-referents and the self are two sides of thesame coin is essentially consistent with views ex-pressed in linguistic literature on the developmentof self-referents. Denzin (1972) and Fraiberg(1977), for example, proposed that pronouns andproper names develop along with the child's con-cept of self and that identity confusion is concomi-tant with difficulties in language development.Own-name use (e.g., referring to one's self asJonathan) has been viewed as an emergence of theself (Denzin, 1972). Waterman and Shatz (1982)state that their subjects were "aware of their indi-viduality" (p. 153) when they began to use per-sonal pronouns.
Skinner (1974) began with the premise that theexperience of self is of social origin. According toSkinner, developing children learn to provide self-referents because the social community asks ques-tions (provides discriminative stimuli), such as,"What did you do yesterday?" and "How do youfeel right now?" and reinforce2 self-referent re-sponses accordingly. Others ask these questions be-cause self-referents are useful for understandinghow a person thinks or feels and for predictingwhat that person might do. Although initially self-referents are public, the private experience of self
2 Another common misconception is that reinforcement in-volves presenting a reward such as giving a child food forspeaking or tokens for smiling. This would be referred to asarbitrary, or contrived, reinforcement. Instead, we are speak-ing of natural reinforcement, which in this case refers tonatural responses of caregivers, such as smiling, showingexcitement, complying with a request, or otherwise re-sponding accordingly to the child's correct self-referentialspeech.
200
Finding the Self
emerges as a consequence of this history as onelearns to self-reference silently and privately. Thisprivate behavior is useful to the person himself orherself, for managing, controlling, or giving rea-sons for his or her own behavior. Situations thatrequire managing, controlling, or giving reasons forone's own behavior serve as discriminative stimulifor experiencing one's self, which is reinforced by ahistory of successful responding in these situations.
Kohlenberg and Tsai (1991, 1995), startingwith Skinner's premises, argued that the experi-ence of self can be accounted for by identifyingand describing the terms of the three-term contin-gency, the behavior itself (the second term) beinga developing child's use of the self-referent "I."To illustrate, accounting for a person's experienceof heat involves identifying and describing thecontext in which a person says, "I am hot" (e.g.,high temperature, high humidity, lots of cloth-ing). A complete account would also identify anddescribe historical factors (e.g., growing up inAlaska or Hawaii, growing up with parents whoresponded to or ignored a shivering child) thatexplain individual differences in responding tocontextual factors with "I am hot." For the experi-ence of self, the analysis of the self-referent "I"was viewed as a prototype for the analysis ofother verbal responses that function similarly to"I," such as "me," "baby," "Davie," or "Dottie"(own name), and even "you" (when used by ayoung child to refer to oneself).
For example, suppose a child just learning totalk states, "I am hungry." In actuality, the childmight say something like "eat" or "food now"but, functionally, these statements correspond tothe generic "I am hungry," so this term is usedto simplify the analysis. At first, this statementmight or might not correspond with the internal,private state of hunger. It is the caregiver's jobto discern the true state of affairs and respondappropriately. How does a caregiver know that achild is hungry? The caregiver cannot contact theprivate experience of the child to verify the accu-racy of the statement; the caregiver can only lookto public cues. The experience of hunger doeshave some reliable public correlates to which acaregiver can look, such as the length of timesince the child's last meal, how quickly and rav-enously the child eats if the caregiver gives herfood, and if the child looks tired or acts cranky.A caregiver might accurately determine that thechild is, indeed, hungry and respond, "Oh, youare hungry? Let's give you something to eat,"
then giving the child something to eat. Behavior-ally, this caregiver response reinforces the childfor correctly contacting and responding to the pri-vate experience of hunger, making it more likelythat the child will respond, "I am hungry" whenin contact with this experience in the future. Inbehavioral terms, given this ideal history, overtime the private experience of hunger comes tocontrol the response, "I am hungry."
Unfortunately, some caregivers might not no-tice these public correlates, but might rely onother events and circumstances, such as the timeof day, that do not correlate as reliably with theprivate experience. A caregiver might respond,"No, you're not hungry; it is only four o'clock."The child is not reinforced for contacting the pri-vate experience that might otherwise come to con-trol "I am hungry," and the likelihood that thechild will correctly contact the private experiencein the future has been weakened, or at least hasnot been strengthened. This kind of contingencymakes it more likely that "I am hungry" becomespublicly controlled by, namely, the clock.
Other environments offer other kinds of contin-gencies. For example, Linehan (Heard & Linehan,1993; Linehan, 1993) described the invalidating en-vironments integral to the development of border-line personality disorder (BPD). Linehan suggestedthat individuals with BPD were raised in emotion-ally invalidating environments, in which caregiversinconsistently reinforce, negate, or punish the indi-vidual's experiences and descriptions of his or herown affect or events not observed or agreed to bythe caregiver.3 In these environments, caregiversmight respond, for example, "No, you're not hun-gry. I'll tell you when you're hungry." This typeof caregiver might only feed the child when thecaregiver is hungry, not assessing for hunger in thechild at other times. This kind of contingency makesit more likely that "I am hungry" specifically be-comes controlled by the caregiver. If this kind ofcontingency is pervasive, private experiences willnot gain much control for this child.
3 Although this article focuses on the role of the invalidatingenvironment in the development of problems with the self forpatients with BPD, it is important to note that Linehan'sbiosocial theory proposes a transaction between biologicallybased emotional vulnerabilities or deficits in emotion regula-tion systems and an emotionally invalidating environment,and research exists in support of biologically based deficitsas well (e.g., Cowdry, Pickar, & Davies, 1985).
201
J. W. Kanter, C. R. Parker & R. J. Kohlenberg
Kohlenberg and Tsai did not suggest that learn-ing "I am hungry" is a singular event. Like windand rain wearing down a rock, it is a gradual,cumulative process. The examples are purpose-fully simplified and stereotyped to clarify the roleof the fundamental behavioral processes that maybe involved, and may not precisely correspondto how a child learns "I am hungry" in the naturalenvironment. In real life, learning is likely tobe haphazard and inconsistent. "I am hungry"is probably acquired through multiple processes,including learning and other processes less rele-vant to this analysis (e.g., learning of meaningthrough definition).
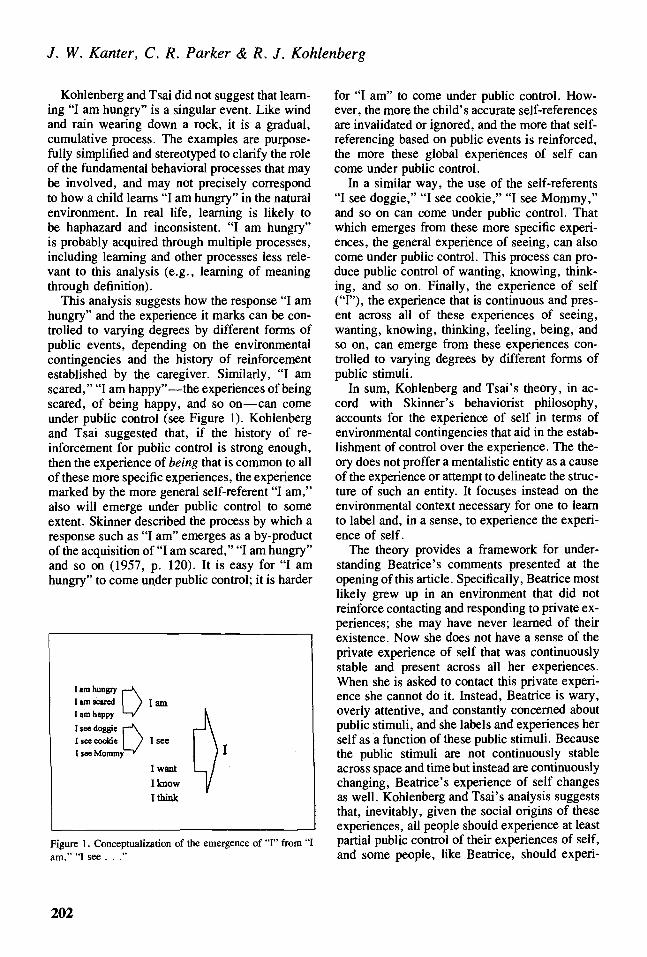
This analysis suggests how the response "I amhungry" and the experience it marks can be con-trolled to varying degrees by different forms ofpublic events, depending on the environmentalcontingencies and the history of reinforcementestablished by the caregiver. Similarly, "I amscared," "I am happy"—the experiences of beingscared, of being happy, and so on—can comeunder public control (see Figure 1). Kohlenbergand Tsai suggested that, if the history of re-inforcement for public control is strong enough,then the experience of being that is common to allof these more specific experiences, the experiencemarked by the more general self-referent "I am,"also will emerge under public control to someextent. Skinner described the process by which aresponse such as "I am" emerges as a by-productof the acquisition of "I am scared," "I am hungry"and so on (1957, p. 120). It is easy for "I amhungry" to come under public control; it is harder
D lamI am hungrylam scaredI am happy
I see doggie r~\I see cookie ) I seeI see Mommy '
I wantI knowI think
Figure 1. Conceptualization of the emergence of "I" from "Iam," "I see . . ."
for "I am" to come under public control. How-ever, the more the child's accurate self-referencesare invalidated or ignored, and the more that self-referencing based on public events is reinforced,the more these global experiences of self cancome under public control.
In a similar way, the use of the self-referents"I see doggie," "I see cookie," "I see Mommy,"and so on can come under public control. Thatwhich emerges from these more specific experi-ences, the general experience of seeing, can alsocome under public control. This process can pro-duce public control of wanting, knowing, think-ing, and so on. Finally, the experience of self("I"), the experience that is continuous and pres-ent across all of these experiences of seeing,wanting, knowing, thinking, feeling, being, andso on, can emerge from these experiences con-trolled to varying degrees by different forms ofpublic stimuli.
In sum, Kohlenberg and Tsai's theory, in ac-cord with Skinner's behaviorist philosophy,accounts for the experience of self in terms ofenvironmental contingencies that aid in the estab-lishment of control over the experience. The the-ory does not proffer a mentalistic entity as a causeof the experience or attempt to delineate the struc-ture of such an entity. It focuses instead on theenvironmental context necessary for one to learnto label and, in a sense, to experience the experi-ence of self.
The theory provides a framework for under-standing Beatrice's comments presented at theopening of this article. Specifically, Beatrice mostlikely grew up in an environment that did notreinforce contacting and responding to private ex-periences; she may have never learned of theirexistence. Now she does not have a sense of theprivate experience of self that was continuouslystable and present across all her experiences.When she is asked to contact this private experi-ence she cannot do it. Instead, Beatrice is wary,overly attentive, and constantly concerned aboutpublic stimuli, and she labels and experiences herself as a function of these public stimuli. Becausethe public stimuli are not continuously stableacross space and time but instead are continuouslychanging, Beatrice's experience of self changesas well. Kohlenberg and Tsai's analysis suggeststhat, inevitably, given the social origins of theseexperiences, all people should experience at leastpartial public control of their experiences of self,and some people, like Beatrice, should experi-
202
Finding the Self
ence considerable public control. The degree ofpublic control should be predictable from one'spresent context and one's reinforcement history,which includes cultural factors.
In this study, a measure of public control overthe experience of self was developed, the Experi-ence of Self Scale (BOSS). Three predictions con-cerning the criterion and construct validity of theBOSS were evaluated.
Prediction 1: Salient Public Stimuli Influence theExperience of Self
One technique for demonstrating that a particu-lar stimulus influences a particular behavior isto vary the salience of the stimulus and show acorresponding variation in behavior. Accordingto this account, the self emerges under variousdegrees of public stimulus control. If the experi-ence of self can be influenced by public stimuli,varying the salience of a particular public stimulusshould produce variations in its influence on theexperience of self. The more salient the publicstimulus, the more influence it should exert.
Prediction 2: Self-Esteem and DissociationRelate to Public Control of the Experience of Self
From a behavioral perspective, the term self-esteem may refer to a set of behaviors that involvedescribing and experiencing oneself in positiveterms, acting confidently and assertively in novelsituations, and so on. A large literature existssupporting the connection between invalidating,dysfunctional, or otherwise problematic child-hood environments and measures of low self-esteem. For example, Miller, Landry, Smith, andSwank (1997) reported that a mother's child-centered perspective mediated the relationship be-tween child-rearing history and child self-esteem.Post and Robinson (1998) showed that beingraised in alcoholic environments related to lowerself-esteem. Similarly, Guglielmo, Polak, andSullivan (1985) argued that familial environmentsin which the parent prefers alternative pleasuresto involvement with the child are linked to lowself-esteem. According to the present analysis,these invalidating environments should produceexperiences of self under greater public control.Therefore, a measure of self-esteem should relateto a measure of public control of the self: Thelower the self-esteem, the higher the public con-trol.
Similarly, the relationship between extreme in-validating environments and dissociation is well
established (e.g., Putnam, 1985). In addition,dissociation, by definition, involves losing con-tact with one's experience of self. Therefore, ameasure of dissociation should relate to a measureof public control of the self: The greater the disso-ciation, the greater the public control.
Prediction 3: A Clinical Sample Diagnosed withBorderline Personality Disorder (BPD) WillReport Greater Public Control over theExperience of Self than Will an UndergraduateCollege Sample
Problems of the self are particularly prevalentin BPD. One of the defining diagnostic criteriafor BPD is, "Identity disturbance: markedly andpersistently unstable self-image or sense of self"(Diagnostic and Statistical Manual of MentalDisorders-4th ed. [DSM-IV]; American Psychiat-ric Association, 1994, p. 654). Heard and Li-nehan (1993) explain that most theoretical formu-lations of BPD posit dysregulations in theindividual's self or sense of self as explanationsfor the behavioral problems associated with BPD.Kohlenberg and Tsai's analysis provides an ac-count for why problems of the self are prevalentin BPD. This account is consistent with Linehan's(1993) description of the emotionally invalidatingenvironments in which BPD individuals wereraised. In these environments, caregivers disre-gard, negate, punish, or otherwise invalidate thedeveloping child's needs and emotional experi-ences. Kohlenberg and Tsai's analysis suggeststhat these environments provide the conditionsnecessary for the establishment of an unusuallystrong degree of public control over the experi-ence of self. Given an extremely invalidating en-vironment, an individual's experience of selfmight be impaired, limited, or completely lackingin the absence of a significant relationship. There-fore, subjects with BPD should show greater pub-lic control over the experience of self than shouldan undergraduate sample.
Method
Measures
The Experiencing of Self Scale (EOSS; Parker,Beitz, & Kohlenberg, 1996). The EOSS is a self-report measure of public control over the experi-ence of self. The experience of self, as markedby verbal self-referents, was referenced by agroup of statements beginning with "My feelings. . . ," "My wants . . . ," "My opinions . . . ,"
203
J. W. Kanter, C. R. Parker &R. J. Kohlenberg
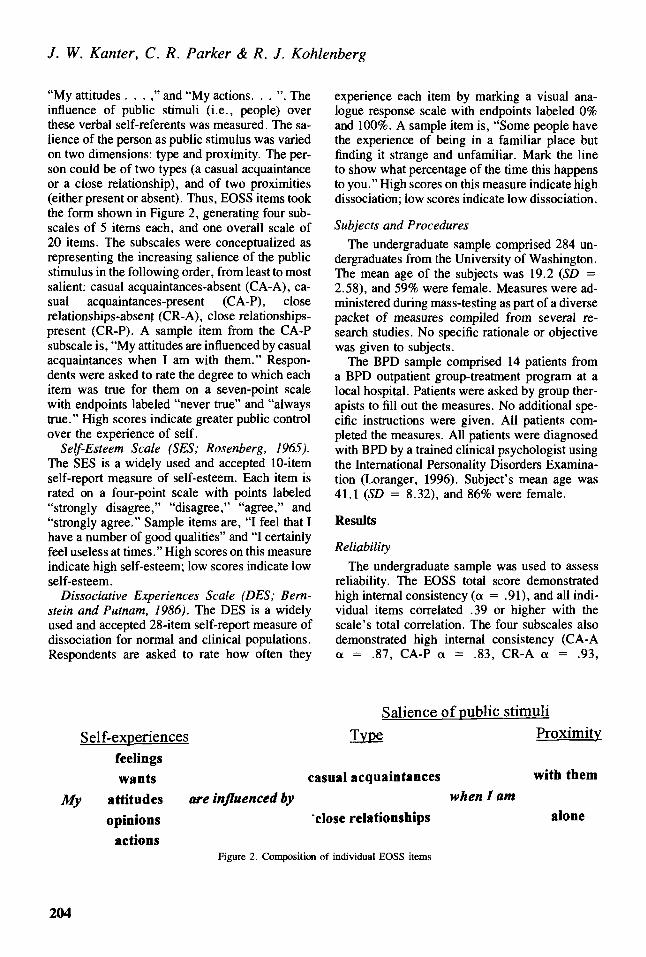
"My attitudes . . . ," and "My actions. . . ". Theinfluence of public stimuli (i.e., people) overthese verbal self-referents was measured. The sa-lience of the person as public stimulus was variedon two dimensions: type and proximity. The per-son could be of two types (a casual acquaintanceor a close relationship), and of two proximities(either present or absent). Thus, BOSS items tookthe form shown in Figure 2, generating four sub-scales of 5 items each, and one overall scale of20 items. The subscales were conceptualized asrepresenting the increasing salience of the publicstimulus in the following order, from least to mostsalient: casual acquaintances-absent (CA-A), ca-sual acquaintances-present (CA-P), closerelationships-absent (CR-A), close relationships-present (CR-P). A sample item from the CA-Psubscale is, "My attitudes are influenced by casualacquaintances when I am with them." Respon-dents were asked to rate the degree to which eachitem was true for them on a seven-point scalewith endpoints labeled "never true" and "alwaystrue." High scores indicate greater public controlover the experience of self.
Self-Esteem Scale (SES; Rosenberg, 1965).The SES is a widely used and accepted 10-itemself-report measure of self-esteem. Each item israted on a four-point scale with points labeled"strongly disagree," "disagree," "agree," and"strongly agree." Sample items are, "I feel that Ihave a number of good qualities" and "I certainlyfeel useless at times." High scores on this measureindicate high self-esteem; low scores indicate lowself-esteem.
Dissociative Experiences Scale (DES; Bern-stein and Putnam, 1986). The DES is a widelyused and accepted 28-item self-report measure ofdissociation for normal and clinical populations.Respondents are asked to rate how often they
experience each item by marking a visual ana-logue response scale with endpoints labeled 0%and 100%. A sample item is, "Some people havethe experience of being in a familiar place butfinding it strange and unfamiliar. Mark the lineto show what percentage of the time this happensto you." High scores on this measure indicate highdissociation; low scores indicate low dissociation.
Subjects and ProceduresThe undergraduate sample comprised 284 un-
dergraduates from the University of Washington.The mean age of the subjects was 19.2 (SD -2.58), and 59% were female. Measures were ad-ministered during mass-testing as part of a diversepacket of measures compiled from several re-search studies. No specific rationale or objectivewas given to subjects.
The BPD sample comprised 14 patients froma BPD outpatient group-treatment program at alocal hospital. Patients were asked by group ther-apists to fill out the measures. No additional spe-cific instructions were given. All patients com-pleted the measures. All patients were diagnosedwith BPD by a trained clinical psychologist usingthe International Personality Disorders Examina-tion (Loranger, 1996). Subject's mean age was41.1 (SD = 8.32), and 86% were female.
Results
ReliabilityThe undergraduate sample was used to assess
reliability. The BOSS total score demonstratedhigh internal consistency (a = .91), and all indi-vidual items correlated .39 or higher with thescale's total correlation. The four subscales alsodemonstrated high internal consistency (CA-Aa = .87, CA-P a = .83, CR-A a = .93,
Salience of public stimuli
Self-experiences Type Proximityfeelingswants casual acquaintances with them
My attitudes are influenced by when I amopinions "close relationships alone
actionsFigure 2. Composition of individual BOSS items
204
Finding the Self
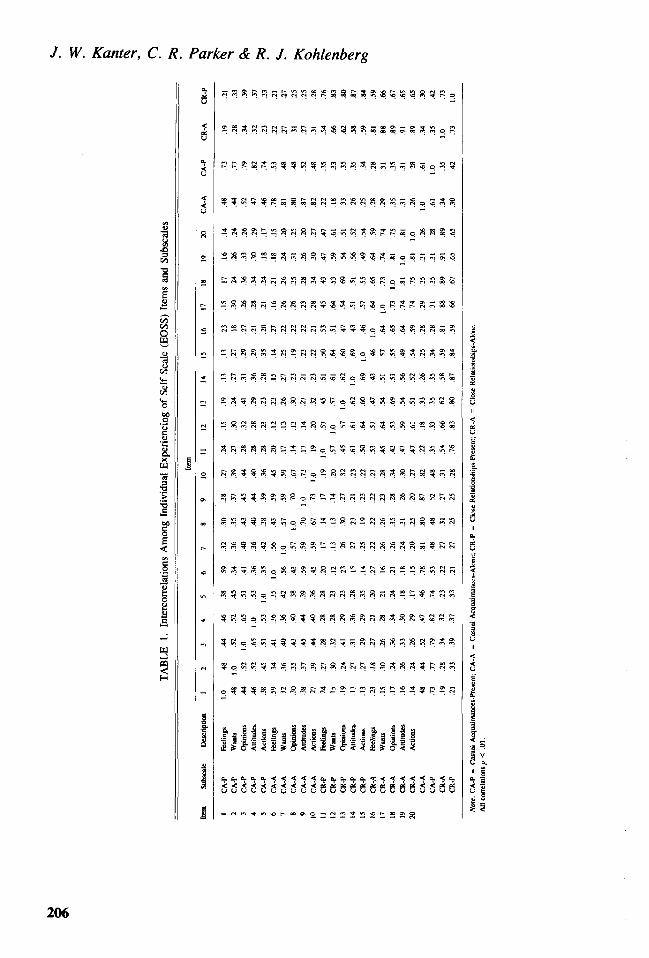
CR-P a = .88). Table 1 presents the intercorrela-tions among individual BOSS items and thefour subscales.
To empirically assess the four subscales, a con-firmatory factor analysis (CFA) was conducted us-ing the covariance matrix. A confirmatory ratherthan exploratory analysis was conducted to test theempirical fit of theoretically derived subscales ratherthan deriving atheoretical subscales empirically(Kline, 1998, p. 191). Maximum likelihood estima-tion was used with listwise deletion of missing data.The results for this CFA indicated that the foursubscales provide a good fit to the data, \2(164) =459.43, p < .0001, Comparative Fit Index = .92,Non-Normed Fit Index = .90, Normed Fit Index =.88, Root Mean Square Error of Approximation =.08. Table 2 presents the factor loadings of individ-ual BOSS items on their respective subscales.
Prediction 1: Salient Public Stimuli Influence theExperience of Self
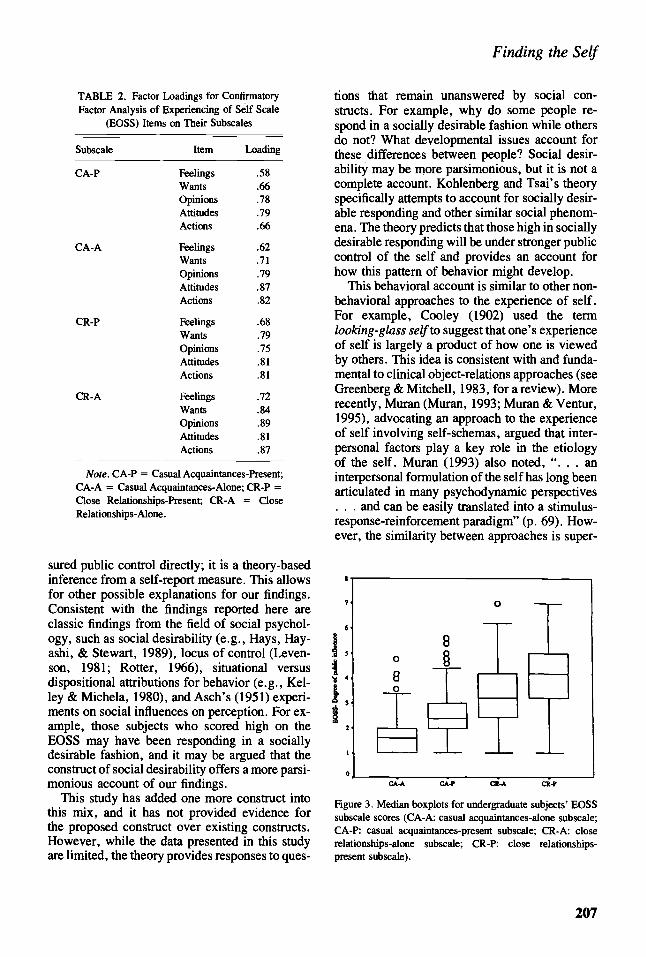
The undergraduate sample was used to test pre-diction 1. Figure 3 shows median boxplots forundergraduate subjects' BOSS subscale scores.As predicted, subjects were significantly moreinfluenced by the public stimuli as the salienceof the public stimuli increased (within-subjectsF[3, 936] = 518, p < .001). Present close rela-tionships exerted the most public control (CR-P,M = 4.10.SD = 1.16), followed by absent closerelationships (CR-A, M = 3.39, SD = 1.29),present casual acquaintances (CA-P, M = 2.52,SD — 0.87), and absent casual acquaintances(CA-A, M = 1.72, SD = 0.75).
Prediction 2: Self-Esteem and DissociationRelate to the Experience of Self
The undergraduate sample was also used to testPrediction 2. Table 3 presents means, standarddeviations, and ranges of BOSS, DBS, and SESscores for the undergraduate sample. BOSSscores correlated significantly with the SES (r =- .26, p < .001) and with the DBS (r = .34,
p < .001) in the predicted directions. As BOSSscores increased, DES scores increased and SESscores decreased.
Prediction 3: A Clinical Sample Diagnosed withBorderline Personality Disorder (BPD) Will ShowGreater Public Control over the Experience of Selfthan Will an Undergraduate College Sample
Table 3 also shows the BPD patients' scoreson the BOSS, DES, and SES. Because the under-
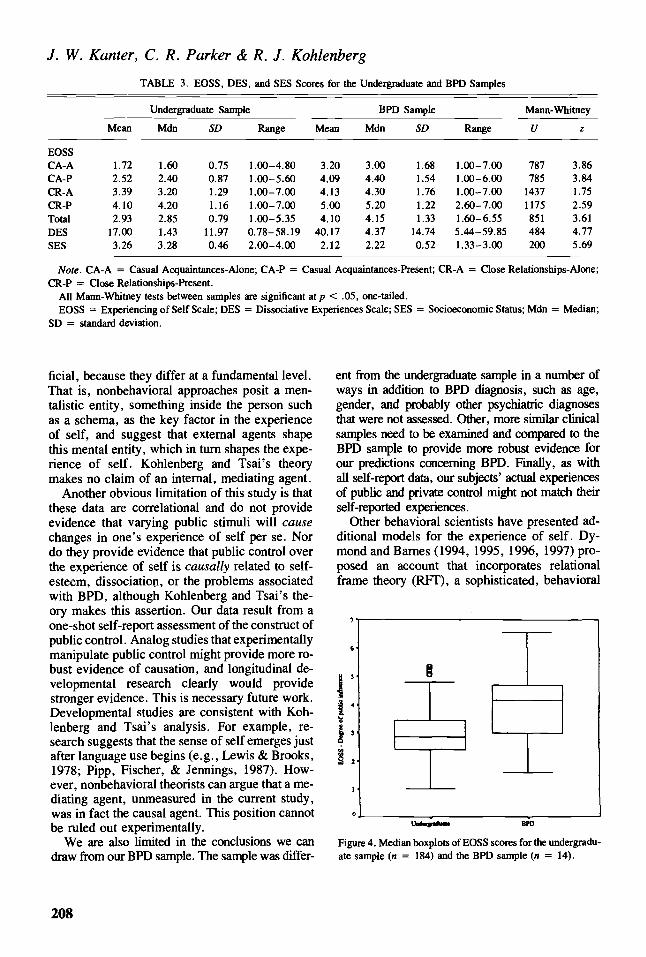
graduate sample and the BPD sample were nota-bly different in size and variance of scores, Mann-Whitney tests were used to test for differencesbetween these groups. The BPD sample scoredsignificantly higher than did the undergraduatesample on all BOSS subscales and on the DES andsignificantly lower on the SES. Figure 4 presentsboxplots of overall BOSS scores for both groups.
Because the BPD sample consisted of only 14patients, we also looked at their individual scoresto help determine if the result on overall BOSSscores is clinically meaningful. Only 2 of the14 BPD patients scored below the undergraduatemean of 2.93. Eight BPD patients (57%) scoredover one standard deviation above the undergrad-uate mean, and six (43%) scored over two stan-dard deviations above the undergraduate mean.In fact, 2 of the 14 BPD patients scored higherthan any of the 284 undergraduates.
DiscussionThe BOSS produced several predicted results.
As predicted, the degree of public stimuli's influ-ence over the experience of self varied with theirsalience. In particular, subjects reported that closerelationships were more influential over the expe-rience of self than were casual acquaintances, andstimuli were more influential when present thanabsent. Although this finding has a good deal offace validity—we expect a present, close rela-tionship to be more influential than an absent,casual acquaintance—it is important to note that,to our knowledge, Kohlenberg and Tsai's theoryis the only theory of the development of the expe-rience of self to explicitly account for it.
Also as predicted, in an undergraduate sample,the degree of public control over the experienceof self covaried with self-esteem and dissociation.In addition, a clinical sample diagnosed with BPDshowed greater public control over the experienceof self than did the undergraduate sample. Thelatter finding is particularly striking given thesmall size and large variance of the BPD sample,which limited the statistical power of this compar-ison. The strong public control over the experi-ence of self for the BPD sample relative to theundergraduates was predictable, given the preva-lence of problems of the self in this population,and is in accord with Linehan's (1993) notion ofthe invalidating environment.
This study has a number of limitations thatrestrict the confidence with which we can drawconclusions. Most importantly, we have not mea-
205
J. W. Kanter, C. R. Parker & R. J. Kohlenberg
son
I
oor- - — O
S M (*} — (Q 2 S M ® 3
I 5 S S !? !
i 111 i 11J11r f l l lSf III
s a
206
Finding the Self
TABLE 2. Factor Loadings for ConfirmatoryFactor Analysis of Experiencing of Self Scale
(BOSS) Items on Their Subscales
Subscale
CA-P
CA-A
CR-P
CR-A
Item
FeelingsWantsOpinionsAttitudesActions
FeelingsWantsOpinionsAttitudesActions
FeelingsWantsOpinionsAttitudesActions
FeelingsWantsOpinionsAttitudesActions
Loading
.58
.66
.78
.79
.66
.62
.71
.79
.87
.82
.68
.79
.75
.81
.81
.72
.84
.89
.81
.87
Note. CA-P = Casual Acquaintances-Present;CA-A = Casual Acquaintances-Alone; CR-P =Close Relationships-Present; CR-A = CloseRelationships-Alone.
sured public control directly; it is a theory-basedinference from a self-report measure. This allowsfor other possible explanations for our findings.Consistent with the findings reported here areclassic findings from the field of social psychol-ogy, such as social desirability (e.g., Hays, Hay-ashi, & Stewart, 1989), locus of control (Leven-son, 1981; Rotter, 1966), situational versusdispositional attributions for behavior (e.g., Kel-ley & Michela, 1980), and Asch's (1951) experi-ments on social influences on perception. For ex-ample, those subjects who scored high on theBOSS may have been responding in a sociallydesirable fashion, and it may be argued that theconstruct of social desirability offers a more parsi-monious account of our findings.
This study has added one more construct intothis mix, and it has not provided evidence forthe proposed construct over existing constructs.However, while the data presented in this studyare limited, the theory provides responses to ques-
tions that remain unanswered by social con-structs. For example, why do some people re-spond in a socially desirable fashion while othersdo not? What developmental issues account forthese differences between people? Social desir-ability may be more parsimonious, but it is not acomplete account. Kohlenberg and Tsai's theoryspecifically attempts to account for socially desir-able responding and other similar social phenom-ena. The theory predicts that those high in sociallydesirable responding will be under stronger publiccontrol of the self and provides an account forhow this pattern of behavior might develop.
This behavioral account is similar to other non-behavioral approaches to the experience of self.For example, Cooley (1902) used the termlooking-glass self to suggest that one's experienceof self is largely a product of how one is viewedby others. This idea is consistent with and funda-mental to clinical object-relations approaches (seeGreenberg & Mitchell, 1983, for a review). Morerecently, Muran (Muran, 1993; Muran & Ventur,1995), advocating an approach to the experienceof self involving self-schemas, argued that inter-personal factors play a key role in the etiologyof the self. Muran (1993) also noted, " . . . aninterpersonal formulation of the self has long beenarticulated in many psychodynamic perspectives. . . and can be easily translated into a stimulus-response-reinforcement paradigm" (p. 69). How-ever, the similarity between approaches is super-
i.
Figure 3. Median boxplots for undergraduate subjects' BOSSsubscale scores (CA-A: casual acquaintances-alone subscale;CA-P: casual acquaintances-present subscale; CR-A: closerelationships-alone subscale; CR-P: close relationships-present subscale).
207
J. W. Kanter, C. R. Parker & R. J. Kohlenberg
TABLE 3. EOSS, DBS, and SES Scores for the Undergraduate and BPD Samples
Undergraduate Sample BPD Sample
Mean Mdn SD Range Mean Mdn SD Range
Mann-Whitney
U z
EOSSCA-ACA-PCR-ACR-PTotalDESSES
1.722.523.394.102.93
17.003.26
1.602.403.204.202.851.433.28
00110
110
758729167997 (46 :
.00-4.80
.00-5.60
.00-7.00
.00-7.00
.00-5.35J.78-58.192.00-4.00
3.204.094.135.004.10
40.172.12
3.004.404.305.204.154.372.22
1.681.541.761.221.33
14.740.52
1.00-7.001.00-6.001.00-7.002.60-7.001.60-6.555.44-59.851.33-3.00
787785
14371175851484200
3.863.841.752.593.614.775.69
Note. CA-A = Casual Acquaintances-Alone; CA-P = Casual Acquaintances-Present; CR-A = Close Relationships-Alone;CR-P = Close Relationships-Present.
All Mann-Whitney tests between samples are significant at/> < .05, one-tailed.EOSS = Experiencing of Self Scale; DES = Dissociative Experiences Scale; SES = Socioeconomic Status; Mdn = Median;
SD = standard deviation.
ficial, because they differ at a fundamental level.That is, nonbehavioral approaches posit a men-talistic entity, something inside the person suchas a schema, as the key factor in the experienceof self, and suggest that external agents shapethis mental entity, which in turn shapes the expe-rience of self. Kohlenberg and Tsai's theorymakes no claim of an internal, mediating agent.
Another obvious limitation of this study is thatthese data are correlational and do not provideevidence that varying public stimuli will causechanges in one's experience of self per se. Nordo they provide evidence that public control overthe experience of self is causally related to self-esteem, dissociation, or the problems associatedwith BPD, although Kohlenberg and Tsai's the-ory makes this assertion. Our data result from aone-shot self-report assessment of the construct ofpublic control. Analog studies that experimentallymanipulate public control might provide more ro-bust evidence of causation, and longitudinal de-velopmental research clearly would providestronger evidence. This is necessary future work.Developmental studies are consistent with Koh-lenberg and Tsai's analysis. For example, re-search suggests that the sense of self emerges justafter language use begins (e.g., Lewis & Brooks,1978; Pipp, Fischer, & Jennings, 1987). How-ever, nonbehavioral theorists can argue that a me-diating agent, unmeasured in the current study,was in fact the causal agent. This position cannotbe ruled out experimentally.
We are also limited in the conclusions we candraw from our BPD sample. The sample was differ-
ent from the undergraduate sample in a number ofways in addition to BPD diagnosis, such as age,gender, and probably other psychiatric diagnosesthat were not assessed. Other, more similar clinicalsamples need to be examined and compared to theBPD sample to provide more robust evidence forour predictions concerning BPD. Finally, as withall self-report data, our subjects' actual experiencesof public and private control might not match theirself-reported experiences.
Other behavioral scientists have presented ad-ditional models for the experience of self. Dy-mond and Barnes (1994, 1995, 1996, 1997) pro-posed an account that incorporates relationalframe theory (RFT), a sophisticated, behavioral
Figure 4. Median boxplots of EOSS scores for the undergradu-ate sample (n = 184) and the BPD sample (n = 14).
208
Finding the Self
approach to language (e.g., Barnes, 1994; Hayes,1994; Hayes & Barnes, 1997; Hayes & Wilson,1993). A full exposition of RFT is beyond thescope of this article. Briefly, the springboard forRFT is that Skinner's (1957) analysis of lan-guage, which relied heavily on the three-termcontingency, was incomplete. RFT characterizeslanguage and cognition as derived, multidirec-tional and complex systems of stimulus relations,in which three-term contingencies play a part(also see Anderson, Hawkins, & Scotti, 1997;Hayes, 1991). RFT proposes that much of humanlanguage and cognition can be characterized byarbitrarily applicable relational framing, whichaccounts for how developing children so quicklylearn language with limited direct training (seeHayes, 1991, for a full analysis). Dymond andBarnes accumulated support for their model ofself-awareness with a series of analog studies(1994, 1995, 1996, 1997). Specifically, theydemonstrated that a complex history involvingrelational framing and specific contingencies canproduce new self-referents that were not directlytrained. They suggested mat this experimentalprocedure provides a useful analog for the naturaldevelopment of self-awareness.
Hayes (1984, 1995a), also using RFT, pre-sented a theoretical analysis that described threeclinically relevant senses of self: self as conceptu-alized content, self as verbal process, and self ascontext. The self as conceptualized content refersto the defining beliefs and categorizations thatpeople have and make about themselves, such as"I am who I am" or "I am bad." The self as verbalprocess refers to people's self-reports about feel-ings, emotions, and other behaviors, such as "Iam angry." The self as context refers to people'sexperience of self as a particular perspective orpoint of view that is consistent and predictable.In other words, the self as context is that which isexperienced from behind one's eyes, the contextfrom which the other senses of self are experi-enced. Although Hayes presented these conceptsas theoretically rather than empirically derived,he provided a thorough rationale and suggestedclinical applications, such as are found in accep-tance and commitment therapy (Hayes, Strosahl,& Wilson, 1999; Hayes & Wilson, 1994).
A behavioral account of the experience of selfis particularly useful given recent behavioral for-ays into the field of adult outpatient psychother-apy. Nelson-Gray, Gaynor, and Korotitsch (1997)noted a growing interest in new behavioral treat-
ments for adult outpatient psychotherapy such asfunctional analytic psychotherapy (Kohlenberg &Tsai, 1991) and acceptance and commitment ther-apy (Hayes, Strosahl, & Wilson, 1999; Hayes &Wilson, 1994). These treatments target difficult-to-treat patients and patients with problems that tradi-tionally have been defined as personality disorders,for whom problems of the self are ubiquitous. Theyalso aim to be applicable for the general adult outpa-tient psychotherapy population, not just for specificdisorders and specific settings as has been the casefor traditional behavioral treatments.
This approach to the experience of self can beclinically useful for characterizing patients whoexhibit problems of the self. These patients canrange from those with less severe problems, suchas difficulty knowing what they want and feel,extreme sensitivity to the opinions of others, dif-ficulty being spontaneous or creative, and narcis-sistic personality disorder, to more severe prob-lems, such as borderline personality disorder ordissociative identity disorder (Kohlenberg &Tsai, 1991; see also Phelps, 2000, for an accountof dissociative identity disorder). All of theseproblems can be seen as variants of public controlover the experience of self. For example, thisapproach suggests that those with narcissistic per-sonality disorder grew up under typical conditionsfor the establishment of public control over theexperience of self, but also were reinforced inlimited or superficial ways for being charming,demanding, beautiful (usually in females), orpowerful (usually in males). A person with sucha background lacks private control over "I," andthus has difficulty differentiating someone else'sneeds from his or her own. This person has unduereliance on other people (e.g., through praise andadmiration, gifts) for a sense of self, and knowshow to control and manipulate others (e.g.,through charm or power) to make relationshipsmore tolerable.
This approach suggests that the experience ofself has its origins in the environment and there-fore can be environmentally influenced, facilitat-ing the use of a wide range of therapeutic inter-ventions to ameliorate excessive public control.For patients with excessive public control, theircaregivers originally shaped responding to publicrather than private stimuli. Therapists likewisecan shape responding to private stimuli for thesepatients. For example, a patient with excessivepublic control might have difficulty contributingto setting a psychotherapy agenda, relying on the
209
J. W. Kanter, C. R. Parker & R. J. Kohlenberg
therapist's wishes rather than his or her privatewants or desires. This account suggests a gradualprocess of shaping this patient first to contact,then to respond according to his or her privatewants or desires rather than to the therapist's.
For example, even the technique of free associ-ation can be used by behavioral clinicians, not touncover hidden meanings or to make use of thecontent produced, but as an opportunity to shaperesponding to private rather than public stimuli.Consider the instruction, 'Tell me all the thoughts,feelings, and images that enter your mind; do notcensor anything; report everything that comes up,even if it seems trivial, unimportant, or embar-rassing." This technique can be used to minimizethe influence of external cues from the clinicianand facilitate the patient's direct response to privatestimuli with, "I feel this" or "I see this image."Free association tasks can be varied in their structureto suit the patient's level of public control and grad-ually shape private control. Initial tasks might in-clude sentence completion and word association.Then, as the patient achieves success with thesetasks, tasks involving mental imagery and self-ob-servation of private responses can be introduced.
In summary, it is the intention of this article tosensitize clinicians to the degree of public controlover the experience of self in their clients and tostimulate the use of techniques that aid in theestablishment of private control. While the datapresented in this article are limited and prelimi-nary, it is recognized that all empirical data on "theself" necessarily are limited by the impossibility ofdirect contact with it. However, the theory pre-sented herein can account for this limited data aswell as for the wealth of data generated by alternatetheories of the self and other similar constructs. Wehope that this article will stimulate interest in abehavioral approach to the experience of self andthat clinicians will consider the utility of a behav-ioral approach to other difficult clinical issues thattraditionally have been defined as nonbehavioral.
ReferencesALFORD, B. A., RICHARDS, C. A., & HANYCH, J. M. (1995).
The causal status of private events. The Behavior Therapist,18, 57-58.
American Psychiatric Association. (1994). Diagnostic andstatistical manual of mental disorders (4th ed.). Washing-ton, DC: Author.
ANDERSON, C. M., HAWKINS, R. P., & Scorn, J. R. (1997).Private events in behavior analysis: Conceptual basis andclinical relevance. Behavior Therapy, 28, 157-179.
ASCH, S. E. (1951). Effects of group pressure upon the modi-fication and distortion of judgment. In H. Guetzkow (Ed.),
Groups, leadership, and men (pp. 177—190). Pittsburgh:Carnegie.
BAKER, H. S., & BAKER, M. N. (1987). Heinz Kohut's SelfPsychology: An overview. American Journal of Psychiatry,144, 1-9.
BANDURA, A. (1977). Self-efficacy: Toward a unifying theoryof behavior change. Psychological Review, 84, 191-215.
BARNES, D. (1994). Stimulus equivalence and relational frametheory. The Psychological Record, 44,91-124.
BERNSTEIN, E. M., & PUTNAM, F. W. (1986). Development,reliability, and validity of a dissociation scale. The Journalof Nervous and Mental Disease, 174(12), 727-735.
COOLEY, C. H. (1902). Human nature and the social order.New York: Charles Scribner's Sons.
COWDRY, R. W., PICKAR, D., & DAVIES, R. (1985). Symp-toms and EEC findings in the borderline syndrome. Interna-tional Journal of Psychiatry in Medicine, 15, 201-211.
DENZIN, N. (1972). The genesis of self in early childhood.Sociological Quarterly, 13, 271-314.
DOUGHER, M. J. (1993). On the advantages and implicationsof a radical behavioral treatment of private events. TheBehavior Therapist, 16, 204-206.
DYMOND, S., & BARNES, D. (1994). A transfer of self-discrimination response functions through equivalence rela-tions. Journal of the Experimental Analysis of Behavior,62, 251-267.
DYMOND, S., & BARNES, D. (1995). A transfer of self-discrimination response functions in accordance with thearbitrarily applicable relations of sameness, more-than, andless-than. Journal of the Experimental Analysis of Behav-ior, 64, 163- 184.
DYMOND, S., & BARNES, D. (1996). A transfer of self-discrimination response functions in accordance with thearbitrarily applicable relations of sameness and opposition.The Psychological Record, 46, 271-300.
DYMOND, S., & BARNES, D. (1997). Behavior-analytic ap-proaches to self-awareness. The Psychological Record,47, 181-200.
FRAIBERG, S. (1977). Insights from the blind. Comparative stud-ies of blind and sighted infants. New York: Basic Books.
GREENBERG, J. R., & MITCHELL, S. A. (1983). Object rela-tions in psychoanalytic theory. Cambridge, MA: HarvardUniversity Press.
GREENWALD, A. G. (1982). Is Anyone in Charge? Person-alysis versus the principle of personal unity. In J. Suls(Eds.), Psychological perspectives on the self (pp. 151-181). Hillsdale, NJ: Lawrence Erlbaum.
GUGLIELMO, R., POLAK, R., & SULLIVAN, A. P. (1985). De-velopment of self esteem as a function of familial reception.Journal of Drug Education, 15(3), 277-284.
HAMMEN, C., & GOODMAN-BROWN, T. (1990). Self-schemasand vulnerability to specific life stress in children at riskfor depression. Cognitive Therapy and Research, 14(2),215-227.
HAYES, S. C. (1984). Making sense of spirituality. Behavior-ism, 12, 99-110.
HAYES, S. C. (1991). A relational control theory of stimulusequivalence. In L. J. Hayes & P. N. Chase (Eds.), Dia-logues on verbal behavior (pp. 19-40). Reno, NV: Con-text Press.
HAYES, S. C. (1994). Relational frame theory: A functionalapproach to verbal events. In S. C. Hayes, L. J. Hayes,M. Sato, & K. Ono (Eds.), Behavior analysis of languageand cognition (pp. 9-30). Reno, NV: Context Press.
210
Finding the Self
HAYES, S. C. (1995a). Knowing selves. The Behavior Thera-pist, 18(5), 94-96.
HAYES, S. C., & BARNES, D. (1997). Analyzing derived stim-ulus relations requires more than the concept of stimulusclass. Journal of the Experimental Analysis of Behavior,68(2), 235-244.
HAYES, S. C., STROSAHL, K. D., & WILSON, K. G. (1999).Acceptance and commitment therapy: An experiential ap-proach to behavior changes. New York: Guilford.
HAYES, S. C., & WILSON, K. G. (1993). Some applied impli-cations of a contemporary behavior-analytic account of ver-bal events. The Behavior Analyst, 16, 283-301.
HAYES, S. C., & WILSON, K. G. (1994). Acceptance andcommitment therapy: Altering the verbal support for experi-ential avoidance. The Behavior Analyst, 17, 289-303.
HAYS, R. D., HAYASHI, T., & STEWART, A. L. (1989). Afive-item measure of socially desirable response set. Educa-tional and Psychological Measurement, 49, 629-636.
HEARD, H., & LINEHAN, M. (1993). Problems of self andborderline personality disorder: A dialectical behavioralanalysis. In Z. Segal & S. Blatt (Eds.), The self in emotionaldistress (pp. 301-333). New York: Guilford.
HOPE, D. A., RAPEE, R. M., HEIMBERG, R. G., & DOMBECK,M. J. (1990). Representation of the self in social phobia:Vulnerability to social threat. Cognitive Therapy and Re-search, 14(2), 177-189.
KELLEY, H. H., & MICHELA, J. L. (1980). Attribution theoryand research. Annual Review of Psychology, 31, 457-501.
KLINE, R. B. (1998). Principles and practice of structuralequation modeling. New York: Guilford.
KOHLENBERG, R. J., & TSAI, M. (1991). Functional analyticpsychotherapy: Creating intense and curative therapeuticrelationships. New York: Plenum.
KOHLENBERG, R. J., & TSAI, M. (1995). I speak, therefore Iam: A behavioral approach to understanding problems ofthe self. The Behavior Therapist, 18, 113-124.
KOHUT, H. (1971). The analysis of the self. New York: Inter-national Universities Press.
KOHUT, H. (1977). The restoration of the self. New York:International Universities Press.
LEVENSON, H. (1981). Differentiating among internality,powerful others, and chance. In H. Lefcourt (Ed.), Re-search with the locus of control construct, Vol. 1, assess-ment methods (pp. 15-63). New York: Academic Press.
LEWIS, M. (1992). Will the real self or selves please standup? Psychological Inquiry, 3(2), 123-124.
LEWIS, M., & BROOKS, J. (1978). Self-knowledge and emo-tional development. In M. Lewis & L. A. Rosenblum(Eds.), The development of affect (pp. 205-226). NewYork: Plenum.
LINEHAN, M. M. (1993). Cognitive behavioral treatment ofborderline personality disorder. New York: Guilford.
LORANGER , A. (1996). Manual for the International Personal-ity Disorders Examination. White Plains, NY: New YorkHospital-Cornell Medical Center.
MARKUS, H., & WURF, E. (1987). The dynamic self-concept:A social psychological perspective. Annual Review of Psy-chology, 38, 299-337.
MILLER, L. C. L., LANDRY, S. H., SMITH, K. E., & SWANK,P. R. (1997). The role of child-centered perspectives in amodel of parenting. Journal of Experimental Child Psychol-ogy, 66(3), 341-361.
MOORE, J. (1980). On behaviorism and private events. ThePsychological Record, 30, 459-475.
MURAN, J. C. (1993). The self in cognitive-behavioral re-search: An interpersonal perspective. The Behavior Thera-pist, /6(3), 69-73.
MURAN, J. C., & VENTUR, E. D. (1995). The operant self.The Behavior Therapist, 18(5), 91-94.
NELSON-GRAY, R., GAYNOR, S. T., & KOROTTTSCH, W. J.(1997). Behavior therapy: Distinct but acculturated. Behav-ior Therapy, 28, 563-572.
PARKER, C. R., BEITZ, K., & KOHLENBERG, R. J. (1996,May). The Experience of Self Scale (EOSS): A measure ofprivate and public stimulus control of the experience ofself. Poster presented at the annual meeting of the Associa-tion for Behavior Analysis, Orlando, FL.
PHELPS, B. J. (2000). Dissociative identity disorder: The rele-vance of behavior analysis. The Psychological Record,50, 235-249.
PIPP, S., FISCHER, K. W., & JENNINGS, S. (1987). Acquisitionof self- and mother knowledge in infancy. DevelopmentalPsychology, 2J, 86-96.
POST, P., & ROBINSON, B. E. (1998). School-age children ofalcoholics and nonalcoholics: Their anxiety, self-esteem,and locus of control. Professional School Counseling,1(5), 36-40.
PUTNAM, F. W. (1985). Dissociation as a response to extremetrauma. In R. P. Kluft (Ed.), The childhood antecedentsof multiple personality (pp. 65-97). Washington, DC:American Psychiatric Press.
ROBINS, R. W., NOREM, J. K., & CHEEK, J. M. (1999).Naturalizing the self. In L. A. Pervin & O. P. John (Eds.),Handbook of personality: Theory and research (pp. 443-477). New York: Guilford.
ROSENBERG, M. (1965). Society and the adolescent self-image. Princeton, NJ: Princeton University Press.
ROTTER, J. B. (1966). Generalized expectancies for internalversus external control of reinforcement. PsychologicalMonographs, 80.
SEGAL, Z. V., & VELLA, D. D. (1990). Self-schema in majordepression: Replication and extension of a priming method-ology. Cognitive Therapy and Research, 14(2), 161 — 176.
SKINNER, B. F. (1945). The operational analysis of psycholog-ical terms. Psychological Review, 52, 270-277.
SKINNER, B. F. (1953). Science and human behavior. NewYork: Macmillan.
SKINNER, B. F. (1957). Verbal behavior. New York:Appleton-Century-Crofts.
SKINNER, B. F. (1974). About behaviorism. New York:Knopf.
SMITH, R. E. (1993). Psychology. St. Paul, MN: West.SOCOR, B. J. (1997). Conceiving the self: Presence and ab-
sence in psychoanalytic theory. Madison, CT: InternationalUniversities Press.
VITOUSEK, K. B., & EWALD, L. S. (1993). Self-representationin eating disorders: A cognitive perspective. In Z. Segal &S. Blatt (Eds.), The self in emotional distress (pp.221-266). New York: Guilford.
WATERMAN, P., & SHATZ, M. (1982). The acquisition of per-sonal pronouns and proper names by an identical twin pair.Journal of Speech and Hearing Disorders, 25, 149-154.
WESTIN, D. (1999). Mind, brain, and culture. New York:John Wiley.
WILLIAMS, S. L. (1995). The concept of self is necessaryin the scientific study of phobia. The Behavior Therapist,18(3), 52-55.
211