
FDG PET-CT in the Management of Primary Breast Lymphoma
7
ORIGINAL ARTICLE FDG PET-CT in the Management of Primary Breast Lymphoma Amburanjan Santra, MD, Rakesh Kumar, MD, Ramamohan Reddy, MD, Dhanapathi Halanaik, MD, Rajender Kumar, MD, Chandra Sekhar Bal, MD, and Arun Malhotra, MD, PhD Materials and Methods: Primary breast lymphoma (PBL) is a rare disease and its management differs from other breast cancers. The purpose of this study is to evaluate the role of FDG PET-CT in the management of PBL. We carried out 16 PET-CT scans and reviewed the literature. A total of 16 FDG PET-CT scans were done in 8 female patients with PBL with a median age of 49 years (range: 27– 68). Of the 16 PET-CT scans, 1 scan was done for primary diagnosis and staging (1 patient), 2 for staging (2 patients), 7 for evaluation of treatment response (6 patients), and 6 for detecting recurrence (4 patients). PET-CT image interpretation and analysis were performed qualitatively (visually) and semiquantitatively using stan- dardized uptake value (SUV). Absence of uptake in the postchemotherapy follow-up PET-CT scan was considered as a complete response, and a fall of more than 50% of baseline SUV was considered as a significant response. Results: One patient was successfully diagnosed to have PBL and staged using PET-CT. Two patients were correctly staged with the help of FDG PET-CT. Complete response was noted in all 6 patients (3 had a positive baseline scan and showed complete resolution of FDG uptake, the other 3 who did not have baseline PET-CT and lesions were detected on CT, and also showed complete resolution). Of the 4 patients evaluated for recurrence, 1 patient was positive and 3 patients were negative for recurrence in follow-up PET-CT scans done after 18, 22, and 24 months, respectively. Conclusion: FDG PET-CT has a definitive role in every step of management (diagnosis, staging, treatment response evaluation, and detection of recur- rence) in patients with primary breast lymphoma. Key Words: FDG PET-CT, primary breast lymphoma, NHL, diffuse large B-cell lymphoma (Clin Nucl Med 2009;34: 000 – 000) P rimary breast lymphoma (PBL) is a rare disease, which com- prises 0.04% to 0.53% of all primary malignant tumors of the breast. It affects less than 1% of patients with non-Hodgkin lym- phoma (NHL), and accounts for 1.7% to 2.2% of extranodal lym- phomas. 1–3 Most breast lymphomas are of diffuse B-cell type NHL. 4–5 Incidence of primary and secondary lymphomas in breasts is almost equal. 4 Though rare, bilateral breast involvement has also been reported. 5 The clinical presentation and radiologic features of this condition do not differ from those of breast cancer. Despite the clinical and radiographic similarities between the 2 tumor types, their treatments differ radically. A recent study reported that mas- tectomy offered no benefit in the treatment of PBL, and treatment that included chemotherapy or radiation therapy or both, provided benefits with regard to both survival and recurrence rates. 6 Hence, it is important to accurately distinguish lymphomas from other breast malignancies to appropriately triage patients for treatment. It is very important when choosing a therapeutic strategy for PBL, to accu- rately evaluate the spread and stage of the disease. Screening with conventional mammography along with physical examination is a sensitive method for the early detection of breast lesions. However, conventional screen-film mammog- raphy has limited sensitivity for detection of breast lesions in breasts with dense fibroglandular tissue. 7 Ultrasonography (USG) can differentiate solid lesions from cystic lesions, but it still cannot exclude breast cancer or lymphoma. Magnetic resonance imaging (MRI) is highly sensitive, but it is less specific for the diagnosis of breast cancer. The usefulness of flurodeoxyglucose positron emission to- mography (FDG-PET), including PET-CT, for the staging, treatment monitoring, and restaging of lymphoma has already been proven. 7 FDG-PET has documented its role in the evaluation of breast cancer as well. However, there are only few reports in the literature regarding the role of FDG-PET in the management of PBL. 8 –12 In the present study, we report a series of 8 cases of PBL in which 16 scans of FDG PET-CT were done and used successfully for initial diagnosis, staging, evaluation of treatment response, and restaging. In addition, we reviewed the literature for evaluating the role of PET imaging in the management of PBL. MATERIALS AND METHODS Patients A total of 7400 patients underwent FDG PET-CT scans from September 2005 to April 2007 in our PET-CT center. Of these, 8 patients were found to have PBL and were included in this study. Five patients had left-sided breast lesions, while 3 had the disease in the right breast. All patients were female with a median age of 49 years (range: 27– 68 years). All patients were referred for a PET/CT scan for various indications. Characteristics of all patients and indications of the PET-CT scan are enumerated in Table 1. A total 16 PET-CT scans were performed in these 8 patients. All patients were histopathologically confirmed by biopsy or FNAC either be- fore or immediately after first PET-CT scans. All patients were with NHL, 7 had diffuse large B-cell type lymphoma (DLBCL), and 1 had mixed phenotypic in nature (phenotypic markers are positive for both T and B cells). PET-CT Imaging All 8 patients underwent whole-body PET-CT scans. Patients were asked to report after 4 hours of fasting on the morning of the PET-CT scan. None of them was diabetic. All of them were asked to rest in a quiet room after an intravenous injection of 10 mCi (370 MBq) of flurodeoxyglucose (FDG). A whole-body PET-CT scan was acquired on a Biograph scanner (Siemens, Germany) 60 min- utes after FDG injection. After the acquisition, data were transferred to a workstation for processing and interpretation. After reconstruc- tion, the images were displayed in axial, sagittal, and coronal planes. The image interpretation and analysis was performed qualitatively (visually) and semiquantitatively using standardized uptake value (SUV). A fall of more than 50% of the baseline SUV in postche- motherapy follow-up, PET-CT scan was considered as a significant response. Complete resolution of the breast lesion in posttreatment Received for publication December 17, 2008; revision accepted July 8, 2009. From the Department of Nuclear Medicine, All India Institute of Medical Sciences, New Delhi, India. Reprints: Rakesh Kumar, MD, Department of Nuclear Medicine, All India Institute of Medical Sciences, E-81, Ansari Nagar (East), AIIMS Campus, New Delhi 110029, India. E-mail: [email protected]. Copyright © 2009 by Lippincott Williams & Wilkins ISSN: 0363-9762/09/3412-0001 balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S1 10/1/09 8:51 Art: RLU201195 Clinical Nuclear Medicine • Volume 34, Number 12, December 2009 www.nuclearmed.com | 1 AQ:3 T1
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of FDG PET-CT in the Management of Primary Breast Lymphoma

ORIGINAL ARTICLE
FDG PET-CT in the Management of Primary Breast LymphomaAmburanjan Santra, MD, Rakesh Kumar, MD, Ramamohan Reddy, MD, Dhanapathi Halanaik, MD,
Rajender Kumar, MD, Chandra Sekhar Bal, MD, and Arun Malhotra, MD, PhD
Materials and Methods: Primary breast lymphoma (PBL) is a rare diseaseand its management differs from other breast cancers. The purpose of thisstudy is to evaluate the role of FDG PET-CT in the management of PBL. Wecarried out 16 PET-CT scans and reviewed the literature.
A total of 16 FDG PET-CT scans were done in 8 female patients withPBL with a median age of 49 years (range: 27–68). Of the 16 PET-CT scans,1 scan was done for primary diagnosis and staging (1 patient), 2 for staging(2 patients), 7 for evaluation of treatment response (6 patients), and 6 fordetecting recurrence (4 patients). PET-CT image interpretation and analysiswere performed qualitatively (visually) and semiquantitatively using stan-dardized uptake value (SUV). Absence of uptake in the postchemotherapyfollow-up PET-CT scan was considered as a complete response, and a fall ofmore than 50% of baseline SUV was considered as a significant response.Results: One patient was successfully diagnosed to have PBL and stagedusing PET-CT. Two patients were correctly staged with the help of FDGPET-CT. Complete response was noted in all 6 patients (3 had a positivebaseline scan and showed complete resolution of FDG uptake, the other 3who did not have baseline PET-CT and lesions were detected on CT, andalso showed complete resolution). Of the 4 patients evaluated for recurrence,1 patient was positive and 3 patients were negative for recurrence infollow-up PET-CT scans done after 18, 22, and 24 months, respectively.Conclusion: FDG PET-CT has a definitive role in every step of management(diagnosis, staging, treatment response evaluation, and detection of recur-rence) in patients with primary breast lymphoma.
Key Words: FDG PET-CT, primary breast lymphoma, NHL, diffuse largeB-cell lymphoma
(Clin Nucl Med 2009;34: 000–000)
Primary breast lymphoma (PBL) is a rare disease, which com-prises 0.04% to 0.53% of all primary malignant tumors of the
breast. It affects less than 1% of patients with non-Hodgkin lym-phoma (NHL), and accounts for 1.7% to 2.2% of extranodal lym-phomas.1–3 Most breast lymphomas are of diffuse B-cell typeNHL.4–5 Incidence of primary and secondary lymphomas in breastsis almost equal.4 Though rare, bilateral breast involvement has alsobeen reported.5 The clinical presentation and radiologic features ofthis condition do not differ from those of breast cancer. Despite theclinical and radiographic similarities between the 2 tumor types,their treatments differ radically. A recent study reported that mas-tectomy offered no benefit in the treatment of PBL, and treatmentthat included chemotherapy or radiation therapy or both, providedbenefits with regard to both survival and recurrence rates.6 Hence, itis important to accurately distinguish lymphomas from other breastmalignancies to appropriately triage patients for treatment. It is very
important when choosing a therapeutic strategy for PBL, to accu-rately evaluate the spread and stage of the disease.
Screening with conventional mammography along withphysical examination is a sensitive method for the early detectionof breast lesions. However, conventional screen-film mammog-raphy has limited sensitivity for detection of breast lesions inbreasts with dense fibroglandular tissue.7 Ultrasonography (USG)can differentiate solid lesions from cystic lesions, but it stillcannot exclude breast cancer or lymphoma. Magnetic resonanceimaging (MRI) is highly sensitive, but it is less specific for thediagnosis of breast cancer.
The usefulness of flurodeoxyglucose positron emission to-mography (FDG-PET), including PET-CT, for the staging, treatmentmonitoring, and restaging of lymphoma has already been proven.7
FDG-PET has documented its role in the evaluation of breast canceras well. However, there are only few reports in the literatureregarding the role of FDG-PET in the management of PBL.8–12 Inthe present study, we report a series of 8 cases of PBL in which 16scans of FDG PET-CT were done and used successfully for initialdiagnosis, staging, evaluation of treatment response, and restaging.In addition, we reviewed the literature for evaluating the role of PETimaging in the management of PBL.
MATERIALS AND METHODS
PatientsA total of 7400 patients underwent FDG PET-CT scans from
September 2005 to April 2007 in our PET-CT center. Of these, 8patients were found to have PBL and were included in this study.Five patients had left-sided breast lesions, while 3 had the disease inthe right breast. All patients were female with a median age of 49years (range: 27–68 years). All patients were referred for a PET/CTscan for various indications. Characteristics of all patients andindications of the PET-CT scan are enumerated in Table 1. A total16 PET-CT scans were performed in these 8 patients. All patientswere histopathologically confirmed by biopsy or FNAC either be-fore or immediately after first PET-CT scans. All patients were withNHL, 7 had diffuse large B-cell type lymphoma (DLBCL), and 1had mixed phenotypic in nature (phenotypic markers are positive forboth T and B cells).
PET-CT ImagingAll 8 patients underwent whole-body PET-CT scans. Patients
were asked to report after 4 hours of fasting on the morning of thePET-CT scan. None of them was diabetic. All of them were askedto rest in a quiet room after an intravenous injection of 10 mCi (370MBq) of flurodeoxyglucose (FDG). A whole-body PET-CT scanwas acquired on a Biograph scanner (Siemens, Germany) 60 min-utes after FDG injection. After the acquisition, data were transferredto a workstation for processing and interpretation. After reconstruc-tion, the images were displayed in axial, sagittal, and coronal planes.The image interpretation and analysis was performed qualitatively(visually) and semiquantitatively using standardized uptake value(SUV). A fall of more than 50% of the baseline SUV in postche-motherapy follow-up, PET-CT scan was considered as a significantresponse. Complete resolution of the breast lesion in posttreatment
Received for publication December 17, 2008; revision accepted July 8, 2009.From the Department of Nuclear Medicine, All India Institute of Medical
Sciences, New Delhi, India.Reprints: Rakesh Kumar, MD, Department of Nuclear Medicine, All India
Institute of Medical Sciences, E-81, Ansari Nagar (East), AIIMS Campus,New Delhi 110029, India. E-mail: [email protected].
Copyright © 2009 by Lippincott Williams & WilkinsISSN: 0363-9762/09/3412-0001
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Clinical Nuclear Medicine • Volume 34, Number 12, December 2009 www.nuclearmed.com | 1
AQ:3
T1
PET-CT scan when compared with pretreatment scan was consid-ered as complete response.
RESULTSA total of 16 FDG PET-CT scans were performed in 8
patients. PET-CT scan was done for different indications in differentpatients. PET-CT findings of all patients are shown in Table 1.
DiagnosisOne of the 8 patients (patient 4) was successfully diagnosed
to have a PBL in her left breast. This patient had a clinically palpablemass in the left breast but conventional imaging modalities, mam-mography, and ultrasonography failed to demonstrate the lesion.PET-CT detected a well-defined mass with central necrosis in the
left breast showing intense FDG uptake in the margin of the tumor.Fine needle aspiration cytology (FNAC) was taken from the area ofincreased uptake, which demonstrated DLBCL.
Initial StagingThree patients were staged with the help of FDG PET-CT.
Two of them (patients 1 and 2) came directly for staging after aconfirmed diagnosis of PBL (Fig. 1). Another patient (patient 4)presented with a breast mass and was diagnosed by PET-CT, thesame scan being used for initial staging. The PET-CT scan waspositive in all PBLs. Patient 1 had intense homogenous uptake in thelarge 9 cm mass in the left breast involving the overlying skin. Inaddition, involvement of ipsilateral intramammary and axillarylymph nodes (LNs) was observed. She was treated with chemother-
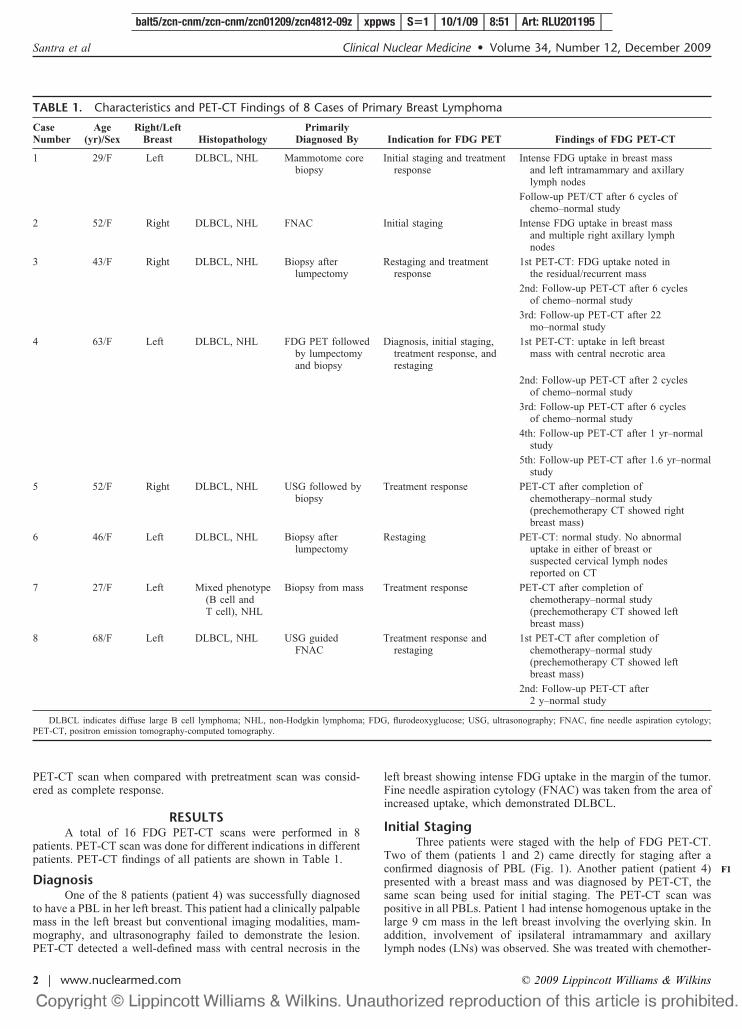
TABLE 1. Characteristics and PET-CT Findings of 8 Cases of Primary Breast Lymphoma
CaseNumber
Age(yr)/Sex
Right/LeftBreast Histopathology
PrimarilyDiagnosed By Indication for FDG PET Findings of FDG PET-CT
1 29/F Left DLBCL, NHL Mammotome corebiopsy
Initial staging and treatmentresponse
Intense FDG uptake in breast massand left intramammary and axillarylymph nodes
Follow-up PET/CT after 6 cycles ofchemo–normal study
2 52/F Right DLBCL, NHL FNAC Initial staging Intense FDG uptake in breast massand multiple right axillary lymphnodes
3 43/F Right DLBCL, NHL Biopsy afterlumpectomy
Restaging and treatmentresponse
1st PET-CT: FDG uptake noted inthe residual/recurrent mass
2nd: Follow-up PET-CT after 6 cyclesof chemo–normal study
3rd: Follow-up PET-CT after 22mo–normal study
4 63/F Left DLBCL, NHL FDG PET followedby lumpectomyand biopsy
Diagnosis, initial staging,treatment response, andrestaging
1st PET-CT: uptake in left breastmass with central necrotic area
2nd: Follow-up PET-CT after 2 cyclesof chemo–normal study
3rd: Follow-up PET-CT after 6 cyclesof chemo–normal study
4th: Follow-up PET-CT after 1 yr–normalstudy
5th: Follow-up PET-CT after 1.6 yr–normalstudy
5 52/F Right DLBCL, NHL USG followed bybiopsy
Treatment response PET-CT after completion ofchemotherapy–normal study(prechemotherapy CT showed rightbreast mass)
6 46/F Left DLBCL, NHL Biopsy afterlumpectomy
Restaging PET-CT: normal study. No abnormaluptake in either of breast orsuspected cervical lymph nodesreported on CT
7 27/F Left Mixed phenotype(B cell andT cell), NHL
Biopsy from mass Treatment response PET-CT after completion ofchemotherapy–normal study(prechemotherapy CT showed leftbreast mass)
8 68/F Left DLBCL, NHL USG guidedFNAC
Treatment response andrestaging
1st PET-CT after completion ofchemotherapy–normal study(prechemotherapy CT showed leftbreast mass)
2nd: Follow-up PET-CT after2 y–normal study
DLBCL indicates diffuse large B cell lymphoma; NHL, non-Hodgkin lymphoma; FDG, flurodeoxyglucose; USG, ultrasonography; FNAC, fine needle aspiration cytology;PET-CT, positron emission tomography-computed tomography.
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Santra et al Clinical Nuclear Medicine • Volume 34, Number 12, December 2009
2 | www.nuclearmed.com © 2009 Lippincott Williams & Wilkins
F1

FIGURE 1. Axial sections of CT (A), PET (B), PET-CT (C) showing a primary lesion in the left breast with intense homogenous fluro-deoxyglucose (FDG) uptake (upper row). Axial sections of CT, PET, and PET-CT showing an ipsilateral axillary lymph node with FDGuptake (lower row). Maximum intensity projection (MIP) whole-body PET image (D) shows a primary breast lesion with ipsilateralaxillary lymph node involvement.
FIGURE 2. Pretreatment axial sections of CT, PET, PET-CT, and MIP images (upper row) showing the primary lesion in the leftbreast with intense FDG uptake. Two mediastinal lymph nodes showing FDG PET in pretreatment MIP were inflammatory. Post-treatment (2 cycles) axial sections of CT, PET, PET-CT, and MIP images (middle row) showing resolution of a primary lesion in theleft breast. Posttreatment (6 cycles) axial sections of CT, PET, PET-CT, and MIP images (lower row) showing normal FDG uptake inthe left breast and the rest of the body.
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Clinical Nuclear Medicine • Volume 34, Number 12, December 2009 Management of Primary Breast Lymphoma
© 2009 Lippincott Williams & Wilkins www.nuclearmed.com | 3
apy. Patient 2 had intense FDG uptake in the right breast mass andin multiple right axillary lymph nodes. In patient 4, PET-CT dem-onstrated intense FDG uptake in the left breast with a centralhypometabolic area. No other lesion was noted in the rest of thebody. She was treated with lumpectomy and chemotherapy.
Treatment Response EvaluationA total of 6 patients underwent PET-CT scans for evaluation
of treatment response. Three had baseline FDG PET-CT scans. Onepatient (patient 4) underwent serial PET/CT scans at baseline after 2cycles and after completion of chemotherapy (Fig. 2). Two patients(patients 1 and 3) had PET/CT at baseline and after 6 cycles. Completeresponse to treatment was noted in scans after 2 cycles (patient 4) andafter completion of chemotherapy in all these cases. Three patients(patients 5, 7, and 8) had no baseline pretreatment PET-CT, and wereevaluated using conventional imaging modalities. They were advisedto have PET-CT soon after completion of chemotherapy to evaluatethe response. All the 3 cases had a normal study with resolution ofprechemotherapy lesions seen on CT.
RestagingFour patients (patients 3, 4, 6, and 8) were evaluated for
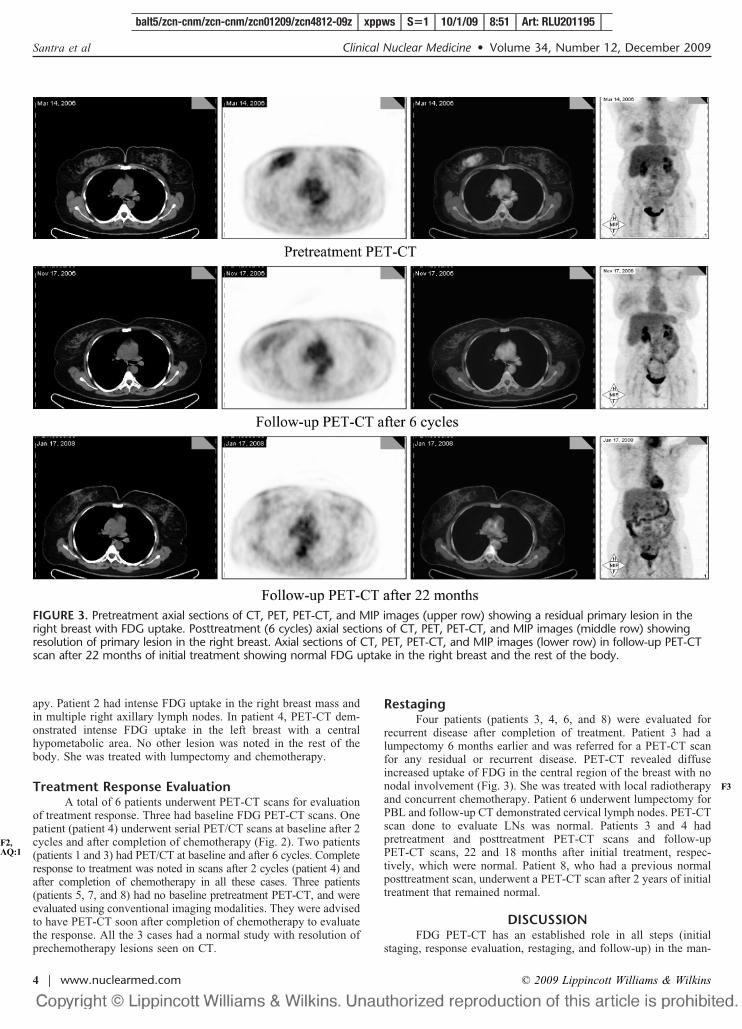
recurrent disease after completion of treatment. Patient 3 had alumpectomy 6 months earlier and was referred for a PET-CT scanfor any residual or recurrent disease. PET-CT revealed diffuseincreased uptake of FDG in the central region of the breast with nonodal involvement (Fig. 3). She was treated with local radiotherapyand concurrent chemotherapy. Patient 6 underwent lumpectomy forPBL and follow-up CT demonstrated cervical lymph nodes. PET-CTscan done to evaluate LNs was normal. Patients 3 and 4 hadpretreatment and posttreatment PET-CT scans and follow-upPET-CT scans, 22 and 18 months after initial treatment, respec-tively, which were normal. Patient 8, who had a previous normalposttreatment scan, underwent a PET-CT scan after 2 years of initialtreatment that remained normal.
DISCUSSIONFDG PET-CT has an established role in all steps (initial
staging, response evaluation, restaging, and follow-up) in the man-
FIGURE 3. Pretreatment axial sections of CT, PET, PET-CT, and MIP images (upper row) showing a residual primary lesion in theright breast with FDG uptake. Posttreatment (6 cycles) axial sections of CT, PET, PET-CT, and MIP images (middle row) showingresolution of primary lesion in the right breast. Axial sections of CT, PET, PET-CT, and MIP images (lower row) in follow-up PET-CTscan after 22 months of initial treatment showing normal FDG uptake in the right breast and the rest of the body.
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Santra et al Clinical Nuclear Medicine • Volume 34, Number 12, December 2009
4 | www.nuclearmed.com © 2009 Lippincott Williams & Wilkins
F2,AQ:1
F3
agement of high-grade NHL and Hodgkin disease.7 There arereasonably enough data in the literature about the effectiveness ofFDG PET-CT in different extranodal lymphomas of rare sites suchas pituitary, sinonasal region, testis, adrenal, bone, ocular region,and thyroid.13–19 In the present study, we tried to find out how anFDG PET-CT scan helps in the management of PBL, a rare extran-odal lymphoma. PBL is a rare but crucial disease from the manage-ment perspective. PBL is defined as the absence of concurrentwidespread lymphoma (with the exception of ipsilateral axillarynodes) and no previous diagnosis of extramammary lymphoma.3
Giardini et al reported an incidence of 0.1% in more than 25,000primary malignant tumors of the breast treated over a 30-yearperiod.20 Vignot et al, reported that NHL of the breast represented0.04% to 0.05% of malignant lesions of the mammary gland in asingle institution.21 Most breast lymphomas are of the DLBCL type.There are only a few reports about the role of an FDG-PET scan forthe management of PBL.8–12 A brief review of these cases has beentabulated in Table 2. In the case reports by Kumar et al, Nihashi etal, and Jung et al, conventional modalities used for detection ofbreast cancer failed to detect the breast tumors. Recently, Yang et alretrospectively analyzed the findings of various imaging techniquesused in 27 patients with breast lymphoma, where 10 patientsunderwent FDG PET scanning. Of the 10 patients, 6 had PBL. Theauthors in this study mentioned that mammography and USGfindings are inconsistent, whereas all 6 patients had diffuse homog-enous FDG uptake on PET scan. Moreover, whole-body PET/CThas the advantage of detecting the other sites of involvement. Yanget al have also carried out follow-up PET studies in all patients afterapproximately 8 to 12 weeks of initiation of chemotherapy and PETdemonstrated complete response in all patients.
We analyzed the data of 18 cases of PBL, 10 cases alreadypublished and 8 cases reported in this study, where FDG-PET wasused for management. All the 18 patients were women. The medianage was 50.5 years, and age range varied from 27 to 76 years. Ofthese, 16 patients had unilateral while 2 patients had bilateral breastinvolvement. Therefore, a total of 20 breasts had disease involve-ment and the ratio of right to left breasts was 9:11. Of the 20 breastlesions, 16 had DLBCL NHL, 2 had Burkitt lymphoma, and oneeach had mixed phenotype (B-cell and T-cell) and follicular NHL.
The histopathological diagnosis was made by biopsy in 15 and byFNAC in 5 breasts. The common indications for PET/PET-CT wereinitial staging followed by evaluation of treatment response andrestaging. For initial staging, PET was positive in all 16 lesions of 14patients, leading to a sensitivity of 100% for detection of PBL. PETdemonstrated diffuse homogenous uptake in the lymphomatousbreast mass in 14 of 16 breast lesions, while 2 had a doughnut-likeappearance, with FDG uptake in the margins and a central hypo-metabolic area. All except 2 patients had disease in one breast alone.One patient had left intramammary and axillary lymph nodes alongwith PBL and the other had multiple right axillary nodes in additionto the primary. PET was used for evaluation of treatment responsein 12 patients, and showed complete resolution of the disease aftercompletion of chemotherapy in all patients. Among these completeresponders, 3 patients had follow-up PET-CT scans 18, 22, and 24months after completion of initial treatment. These scans were foundto have a normal study. Therefore, PET-CT had good prognosticvalues in PBL, similar to what have been described for nodallymphoma. PET was also found to play an important role inrestaging of PBL after completion of treatment. Though numbers arelimited, PET demonstrated high negative and positive predictivevalues in restaging of patients with PBL.
One of the limitations of this study is the small number ofpatients. We are aware that a definite conclusion regarding the roleof FDG PET in the management of PBL can only be drawn from astudy recruiting a large number of patients. However, it is verydifficult to conduct such a study at a single center due to the lowincidence of PBL. But after reviewing the literature and with ourown experience, we feel that PET/PET-CT plays an important rolein the management of PBL. These findings are similar to thosealready established regarding the role of PET/PET-CT in patientswith high-grade nodal and extranodal NHL. In conclusion, based onthe review of already published data and our own data, PET/PET-CThas a definitive role in the initial staging, treatment response eval-uation, and restaging in patients with primary breast lymphoma.
REFERENCES1. Misra A, Kapur BML, Rath GK. Primary breast lymphoma. J Surg Oncol.
1991;47:265–270.
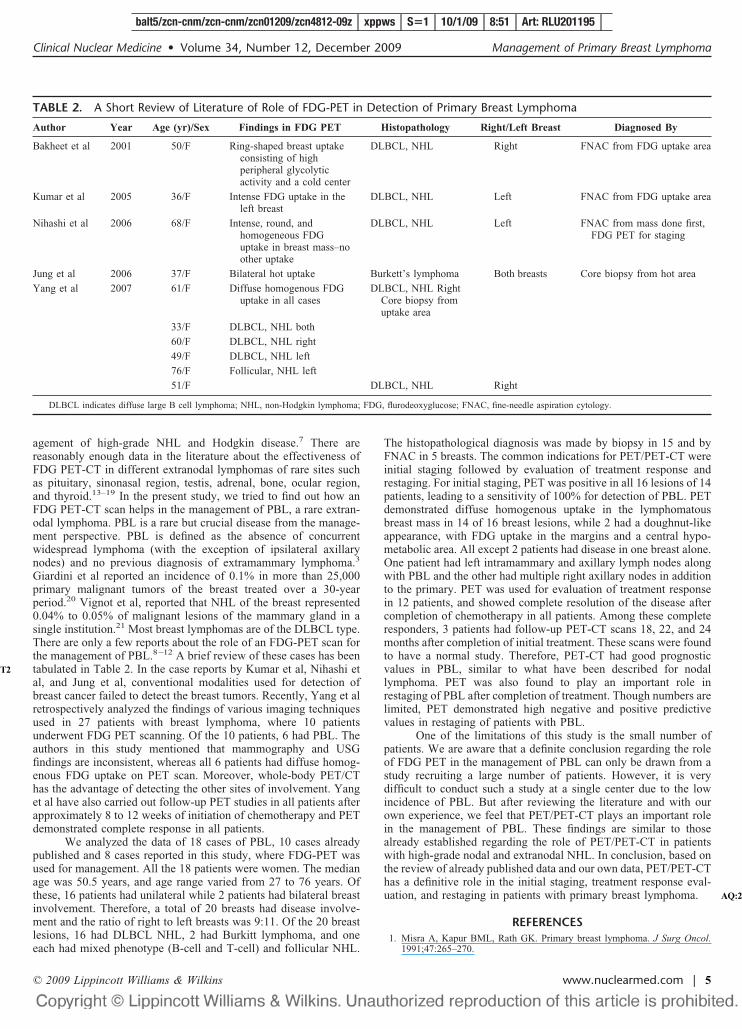
TABLE 2. A Short Review of Literature of Role of FDG-PET in Detection of Primary Breast Lymphoma
Author Year Age (yr)/Sex Findings in FDG PET Histopathology Right/Left Breast Diagnosed By
Bakheet et al 2001 50/F Ring-shaped breast uptakeconsisting of highperipheral glycolyticactivity and a cold center
DLBCL, NHL Right FNAC from FDG uptake area
Kumar et al 2005 36/F Intense FDG uptake in theleft breast
DLBCL, NHL Left FNAC from FDG uptake area
Nihashi et al 2006 68/F Intense, round, andhomogeneous FDGuptake in breast mass–noother uptake
DLBCL, NHL Left FNAC from mass done first,FDG PET for staging
Jung et al 2006 37/F Bilateral hot uptake Burkett’s lymphoma Both breasts Core biopsy from hot area
Yang et al 2007 61/F Diffuse homogenous FDGuptake in all cases
DLBCL, NHL RightCore biopsy fromuptake area
33/F DLBCL, NHL both
60/F DLBCL, NHL right
49/F DLBCL, NHL left
76/F Follicular, NHL left
51/F DLBCL, NHL Right
DLBCL indicates diffuse large B cell lymphoma; NHL, non-Hodgkin lymphoma; FDG, flurodeoxyglucose; FNAC, fine-needle aspiration cytology.
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Clinical Nuclear Medicine • Volume 34, Number 12, December 2009 Management of Primary Breast Lymphoma
© 2009 Lippincott Williams & Wilkins www.nuclearmed.com | 5
T2
AQ:2

2. Mason HS, Johari V, March DE, et al. Primary breast lymphoma: radiologicand pathologic findings. Breast J. 2005;11:495–496.
3. Wiseman C, Liao KT. Primary lymphoma of the breast. Cancer. 1972;29:1705–1712.
4. Topalovski M, Crisan D, Mattson JC. Lymphoma of the breast: a clinico-pathologic study of primary and secondary cases. Arch Pathol Lab Med.1999;123:1208–1218.
5. Shapiro M, Mansur. Bilateral primary breast lymphoma. Am J Clin Oncol.2001;24:85–86.
6. Jennings WC, Baker RS, Murray SS, et al. Primary breast lymphoma: the roleof mastectomy and the importance of lymph node status. Ann Surg. 2007;245:784–789.
7. Kumar R, Maillard I, Scuster JS, et al. Utility of flourudeoxyglucose-PETimaging in the management of patients with Hodgkin’s and non-Hodgkin’slymphoma. Radiol Clin North Am. 2004;42:1083–1100.
8. Nihashi T, Hayasaka K, Itou T, et al. Findings of fluorine-18-FDG PET inextranodal origin lymphoma–in three cases of diffuse large B cell typelymphoma. Ann Nucl Med. 2006;20:689–693.
9. Kumar R, Xiu Y, Dhurairaj T, et al. F-18 FDG positron emission tomographyin non-Hodgkin lymphoma of the breast. Clin Nucl Med. 2005;30:246–248.
10. Bakheet SM, Bakheet R, Ezzat A, et al. F-18 FDG positron emissiontomography in primary breast non-Hodgkin’s lymphoma. Clin Nucl Med.2001;26:299–301.
11. Jung HK, Kim E, Yun M, et al. Bilateral breast involvement in Burkitt’slymphoma detected only by FDG-PET. Clin Imaging. 2006;30:57–59.
12. Yang WT, Lane DL, Le-Petross HT, et al. Breast lymphoma: imagingfindings of 32 tumors in 27 patients. Breast Imaging. 2007;245:692–702.
13. Soussan M, Wartski M, Ezra J, et al. Non-Hodgkin lymphoma localization inthe pituitary gland: diagnosed by FDG-PET/CT. Clin Nucl Med. 2008;33:111–112.
14. Scalcione LR, Katz DS, Santoro MS, et al. Primary testicular lymphomainvolving the spermatic cord and gonadal vein. Clin Nucl Med. 2009;34:222–223.
15. Batlle JC, Zhuang H, Potenta S, et al. Hodgkin disease in the sinonasal regiondetected by FDG PET. Clin Nucl Med. 2004;29:449.
16. Lin EC. FDG PET/CT for assessing therapy response in primary thyroidlymphoma. Clin Nucl Med. 2007;32:152–153.
17. Chamroonrat W, Houseni M, Bing Z, et al. Non-Hodgkin’s lymphoma of thebone can mimic osteomyelitis on FDG PET. Clin Nucl Med. 2007;32:252–254.
18. Kumar R, Xiu Y, Mavi A, et al. FDG-PET imaging in primary bilateraladrenal lymphoma: a case report and review of the literature. Clin Nucl Med.2005;30:222–230.
19. Gayed I, Eskandari MF, McLaughlin P, et al. Value of positron emissiontomography in staging ocular adnexal lymphomas and evaluating their re-sponse to therapy. Ophthalmic Surg Lasers Imaging. 2007;38:319–325.
20. Giardini R, Piccolo C, Rilke F. Primary non-Hodgkin’s lymphomas of thefemale breast. Cancer. 1992;69:725–735.
21. Vignot S, Ledoussal V, Nodiot P, et al. Non-Hodgkin’s lymphoma of thebreast: a report of 19 cases and a review of the literature. Clin Lymphoma.2005;6:37–42.
balt5/zcn-cnm/zcn-cnm/zcn01209/zcn4812-09z xppws S�1 10/1/09 8:51 Art: RLU201195
Santra et al Clinical Nuclear Medicine • Volume 34, Number 12, December 2009
6 | www.nuclearmed.com © 2009 Lippincott Williams & Wilkins

JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 1 OUTPUT: Thu Oct 1 08:51:59 2009/balt5/zcn�cnm/zcn�cnm/zcn01209/zcn4812�09z
AQ3—Please confirm whether the details inserted (by the copyeditor) in the corresponding addressare correct.
AQ1—Please confirm whether the change made conveys the intended meaning.
AQ2—Please note that references 13–21 have been renumbered per journal style. Please check theaccuracy of the corresponding citations in the text.
AUTHOR QUERIES
AUTHOR PLEASE ANSWER ALL QUERIES 1




















