Factors associated with variability in length of sick leave because of acute low back pain in Chile
6
Clinical Study Factors associated with variability in length of sick leave because of acute low back pain in Chile Claudio Diaz-Ledezma, MD a,b , Julio Urrutia, MD c, * , Jose Romeo, DSc d , Alfonso Chelen, MD b , Leonardo Gonza ´lez-Wilhelm, MD, MSc b , Cristian Lavarello, MD b a Department of Orthopaedic Surgery, Mutual de Seguridad C.Ch.C., Clinica Alemana, Universidad del Desarrollo, Av. Manquehue 1410, Santiago, Chile b COMPIN Metropolitano, SEREMI de Salud Metropolitano, Moneda 1040, Santiago, Chile c Department of Orthopaedic Surgery, Pontificia Universidad Catolica de Chile, Marcoleta 352, Santiago, Chile d Departamento de Matema´ticas, Universidad de Santiago de Chile, Alameda 3363, Santiago, Chile Received 8 May 2009; revised 4 August 2009; accepted 16 September 2009 Abstract BACKGROUND CONTEXT: Acute low back pain (LBP) is a frequent cause of physician visits and sick leave. Patients with longer sick leave account for most costs associated with LBP. Most research on risk factors for prolonged sick leave because of LBP has been done in Anglo-Saxon or Northern European populations with occupational LBP. Few studies have been conducted in less affluent Latin countries. PURPOSE: To investigate the prevalence of acute LBP as a cause of sick leave and the variables associated with longer work absence (WA) because of acute LBP in Chile. STUDY DESIGN: A retrospective study of nonoccupational sick leave certificates issued in a 1-year period by the Chilean Public Health System. PATIENT SAMPLE: Ten thousand cases with nonoccupational sick leave certificates issued with the diagnosis of acute LBP. OUTCOME MEASURES: Prevalence of acute LBP as a cause of sick leave, days of WA, and subsidy payment. METHODS: A review of sick leave certificates from patients with different diagnoses was done to determine the prevalence of acute LBP as a cause of sick leave. We investigated whether age, gen- der, history of at least one episode of sick leave in the previous year because of acute LBP or because of other diagnoses, stipendiary subsidy paid (converted to US $), work activity, occupation, and the specialty of the attending physician influenced the length of sick leave. RESULTS: Acute LBP represented 5.4% of cases causing sick leave. Patients with acute LBP who had significantly longer sick leave than the rest of the population were patients with an episode of WA because of LBP in the previous year (14% longer sick leave than patients without that history), manual workers (35% longer than nonmanual workers), and patients seen by orthopedic surgeons (43% longer than patients seen by other medical specialists). Nonpregnant women and men had similar durations of sick leave because of acute LBP. CONCLUSIONS: Physicians who treat patients with LBP should be aware of these variables as- sociated with longer sick leave because of acute LBP, which represents a significant burden to any society and is an important epidemiologic problem. Ó 2009 Elsevier Inc. All rights reserved. Keywords: Low back pain; Sick leave; Prevalence; Cost of Illness; Absenteeism Introduction Low back pain (LBP) is a prevalent public health prob- lem. Acute LBP is one of the most frequent causes of physician visits [1,2] and is associated with an important socioeconomic burden [3–5]. During recent years, the eco- nomic costs associated with LBP have grown, mainly FDA device/drug status: not applicable. Author disclosures: JU (consulting, Simpirica Spine). * Corresponding author. Department of Orthopaedic Surgery, Pontifi- cia Universidad Catolica de Chile, Marcoleta 352, Santiago, Chile. Tel.: (56) 2-2070101; fax: (56) 2-2067148. E-mail address: [email protected] (J. Urrutia) 1529-9430/09/$ – see front matter Ó 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.spinee.2009.09.004 The Spine Journal - (2009) - ARTICLE IN PRESS
-
Upload
independent -
Category
Documents
-
view
6 -
download
0
Transcript of Factors associated with variability in length of sick leave because of acute low back pain in Chile

ARTICLE IN PRESS
The Spine Journal - (2009) -
Clinical Study
Factors associated with variability in length of sick leave becauseof acute low back pain in Chile
Claudio Diaz-Ledezma, MDa,b, Julio Urrutia, MDc,*, Jose Romeo, DScd, Alfonso Chelen, MDb,Leonardo Gonzalez-Wilhelm, MD, MScb, Cristian Lavarello, MDb
aDepartment of Orthopaedic Surgery, Mutual de Seguridad C.Ch.C., Clinica Alemana, Universidad del Desarrollo, Av. Manquehue 1410, Santiago, ChilebCOMPIN Metropolitano, SEREMI de Salud Metropolitano, Moneda 1040, Santiago, Chile
cDepartment of Orthopaedic Surgery, Pontificia Universidad Catolica de Chile, Marcoleta 352, Santiago, ChiledDepartamento de Matematicas, Universidad de Santiago de Chile, Alameda 3363, Santiago, Chile
Received 8 May 2009; revised 4 August 2009; accepted 16 September 2009
Abstract BACKGROUND CONTEXT: Acute low bac
FDA device/drug
Author disclosure
1529-9430/09/$ – see
doi:10.1016/j.spinee.2
k pain (LBP) is a frequent cause of physician visitsand sick leave. Patients with longer sick leave account for most costs associated with LBP. Mostresearch on risk factors for prolonged sick leave because of LBP has been done in Anglo-Saxonor Northern European populations with occupational LBP. Few studies have been conducted in lessaffluent Latin countries.PURPOSE: To investigate the prevalence of acute LBP as a cause of sick leave and the variablesassociated with longer work absence (WA) because of acute LBP in Chile.STUDY DESIGN: A retrospective study of nonoccupational sick leave certificates issued in a1-year period by the Chilean Public Health System.PATIENT SAMPLE: Ten thousand cases with nonoccupational sick leave certificates issued withthe diagnosis of acute LBP.OUTCOME MEASURES: Prevalence of acute LBP as a cause of sick leave, days of WA, andsubsidy payment.METHODS: A review of sick leave certificates from patients with different diagnoses was done todetermine the prevalence of acute LBP as a cause of sick leave. We investigated whether age, gen-der, history of at least one episode of sick leave in the previous year because of acute LBP orbecause of other diagnoses, stipendiary subsidy paid (converted to US $), work activity, occupation,and the specialty of the attending physician influenced the length of sick leave.RESULTS: Acute LBP represented 5.4% of cases causing sick leave. Patients with acute LBP whohad significantly longer sick leave than the rest of the population were patients with an episode ofWA because of LBP in the previous year (14% longer sick leave than patients without that history),manual workers (35% longer than nonmanual workers), and patients seen by orthopedic surgeons(43% longer than patients seen by other medical specialists). Nonpregnant women and men hadsimilar durations of sick leave because of acute LBP.CONCLUSIONS: Physicians who treat patients with LBP should be aware of these variables as-sociated with longer sick leave because of acute LBP, which represents a significant burden to anysociety and is an important epidemiologic problem. � 2009 Elsevier Inc. All rights reserved.
Keywords: Low back pain; Sick leave; Prevalence; Cost of Illness; Absenteeism
Introduction
Low back pain (LBP) is a prevalent public health prob-lem. Acute LBP is one of the most frequent causes of
status: not applicable.
s: JU (consulting, Simpirica Spine).
front matter � 2009 Elsevier Inc. All rights reserved.
009.09.004
physician visits [1,2] and is associated with an importantsocioeconomic burden [3–5]. During recent years, the eco-nomic costs associated with LBP have grown, mainly
* Corresponding author. Department of Orthopaedic Surgery, Pontifi-
cia Universidad Catolica de Chile, Marcoleta 352, Santiago, Chile. Tel.:
(56) 2-2070101; fax: (56) 2-2067148.
E-mail address: [email protected] (J. Urrutia)

2 C. Diaz-Ledezma et al. / The Spine Journal - (2009) -
ARTICLE IN PRESS
because of an increase in sickness and workers’ compensa-tion claims [6].
An important part of the burden associated with acuteLBP is sick leave [7–9] in spite of the recommendation thatpatients who suffer from acute LBP should stay active andcontinue normal activities, including work if possible[10–12]. A Dutch study reported that 20% of patients withLBP report absences from work [13].
Most patients with acute LBP can return to work aftera short time, and the cases requiring longer sick leaveaccount for most costs associated with LBP [14]. Prognos-tic factors for LBP disability have been reported by severalstudies [9,15,16]. Among the predictive factors that influ-ence longer sick leave are psychosocial determinants (eg,attitudes, beliefs, mood state, anxiety, depression, socialdysfunction, job satisfaction) [17,18], severity of disability[9,16,17], duration of pain before sick leave [16], gender[9], physically demanding work [18,19], age [9,15,18,19],and amount of compensation received [9,20]. Most of thesestudies have been performed in Anglo-Saxon or NorthernEuropean populations [1–8,13], and mainly patients withwork-related LBP have been studied. However, legal, cul-tural, and sociodemographic differences may affect LBP-related disability [21,22] and physicians’ determination ofthe need for sick leave in these patients. Few studies havebeen performed in Hispanic countries to predict chronicdisability related to acute LBP [23], and only one studyhas been conducted in a Latin American country, in a pop-ulation of work-related LBP [24].
The aims of our study were to determine the prevalenceof acute LBP as a cause of non–work-related sick leave ina middle- and low-income population of workers in Chile,to describe the sociodemographic characteristics of thosepatients, and to determine the factors associated with moreprolonged sick leave. In addition, we estimated the annualexpenditures associated with subsidy payments to Chileanpatients with acute LBP.
Table 1
Work activities and occupations of patients with sick leave certificates
because of acute low back pain
Work activities/occupation %
Work activities
Commercial 13.0
Construction 13.8
Finances 5.0
Manufacturing 9.0
Public services 13.6
Transportation 10.9
Nonspecified 30.8
Others (minery, agriculture, and others) 3.9
Total 100
Occupation
Administrative 13.0
Manual worker 51.1
Professional 5.2
Salesperson 5.0
Technician 6.1
Others 19.6
Total 100
Materials and methods
In Chile, patients with non–work-related diseases takingsick leave receive an official sick leave certificate. The sickleave certificates of patients affiliated with the PublicHealth System must be evaluated by the Commission ofPreventive Medicine and Disability (COMPIN) forapproval or rejection. If COMPIN resolves to accept theprescription of sick leave, the worker has the right to takesick leave and receive subsidy payments. It must be noted,however, that the first 3 days of sick leave are not paid forby insurance unless rest is prescribed for 11 days or longer;for example, if a patient takes sick leave for 5 days, hereceives payment for 2 days.
The Chilean Public Health System (ChPHS) recorded785,064 sick leave certificates because of non–work-relateddiseases in a population of 4,433,165 beneficiaries in 2005
[25]. These certificates were mainly for unique members;however, some of them may represent multiple claims fromthe same individual.
To obtain our sample, we randomly chose 10,000 sickleave certificates from patients with diagnoses of variousnon–work-related diseases, prescribed between October2006 and October 2007. The inclusion criterion was a diag-nosis of acute LBP (including diagnosis of LBP and lum-bago), which was defined as an episode that had lastedfor less than 4 weeks [26] and was preceded and followedby at least 1 day at work, as proposed by de Vet et al. [27].Exclusion criteria were diagnoses of work-related LBP(which in Chilean legislation is defined as an episode thatstarts related to a specific work event), pregnancy-relatedLBP [28], sciatica, and patients with a previous history ofcontinuous sick leave secondary to LBP longer than 4weeks in the previous year (not preceded and followed byat least 1 day at work) to study only patients with acuteLBP.
To identify the factors associated with variability inlength of sick leave in patients with acute LBP, we studiedwhether age, gender, history of a precedent sick leave cer-tificate because of acute LBP or for other diagnoses in theprevious year, amount of stipend paid (converted to US $),and the medical specialty of the attending physician whoindicated the work absence (WA) were related to the lengthof sick leave prescribed. We also studied the different workactivities and occupations of the population studied (Table1) and their relation to the period of WA.
We calculated the expenditures associated with subsidypayments considering the total number of sick leave certif-icates in the study period, the prevalence of acute LBPamong them, and the mean amount paid in subsidy for eachpatient with acute LBP.
3C. Diaz-Ledezma et al. / The Spine Journal - (2009) -
ARTICLE IN PRESS
To obtain a representative sample size, using a margin oferror of 5%, a confidence level of 95%, and a response dis-tribution of 50%, the minimal sample size estimated was384 patients with acute LBP. The statistical analyses wereperformed using STATA 10.0 (StataCorp LP, College Sta-tion, TX, USA).
To perform a multivariable analysis, a zero-truncatedPoisson regression model was used for all observed covari-ates (age, gender, history of a precedent sick leave certifi-cate because of acute LBP or for other diagnoses in theprevious year, stipendiary subsidy paid, work activity,occupation, and the medical specialty of the attending phy-sician who indicated the WA) to examine how they affectedthe target outcome (days of WA). All statistical compari-sons were tested at the a50.05 level of significance.
Results
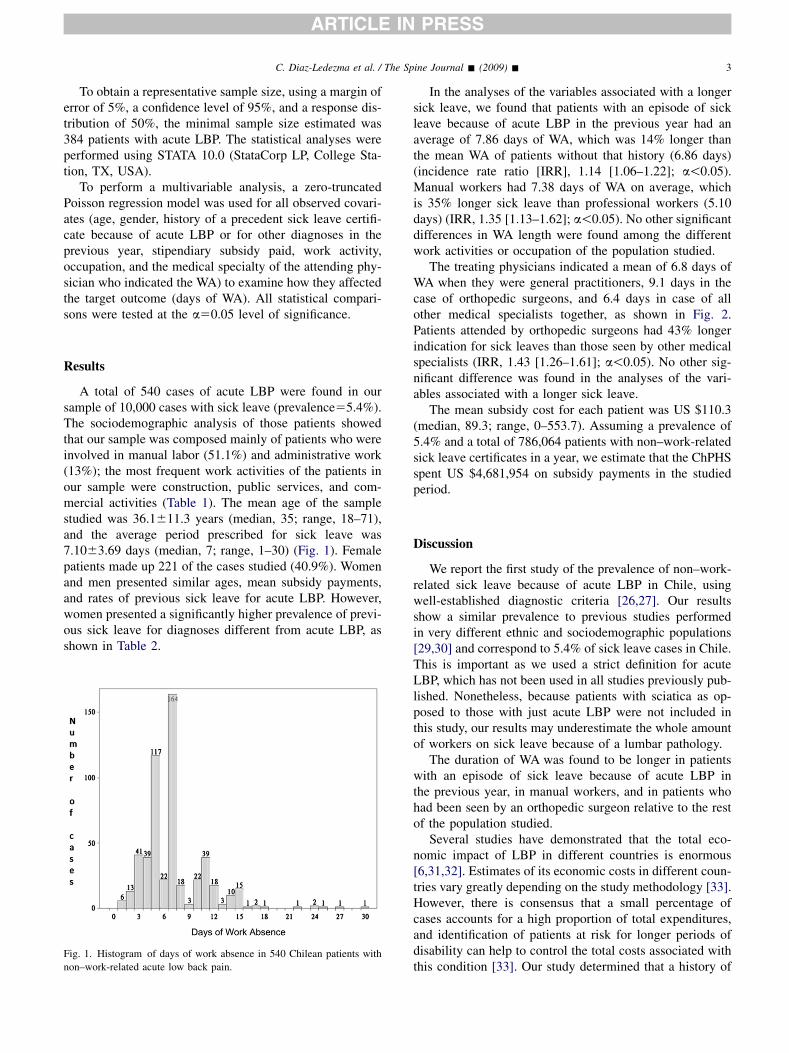
A total of 540 cases of acute LBP were found in oursample of 10,000 cases with sick leave (prevalence55.4%).The sociodemographic analysis of those patients showedthat our sample was composed mainly of patients who wereinvolved in manual labor (51.1%) and administrative work(13%); the most frequent work activities of the patients inour sample were construction, public services, and com-mercial activities (Table 1). The mean age of the samplestudied was 36.1611.3 years (median, 35; range, 18–71),and the average period prescribed for sick leave was7.1063.69 days (median, 7; range, 1–30) (Fig. 1). Femalepatients made up 221 of the cases studied (40.9%). Womenand men presented similar ages, mean subsidy payments,and rates of previous sick leave for acute LBP. However,women presented a significantly higher prevalence of previ-ous sick leave for diagnoses different from acute LBP, asshown in Table 2.
Fig. 1. Histogram of days of work absence in 540 Chilean patients with
non–work-related acute low back pain.
In the analyses of the variables associated with a longersick leave, we found that patients with an episode of sickleave because of acute LBP in the previous year had anaverage of 7.86 days of WA, which was 14% longer thanthe mean WA of patients without that history (6.86 days)(incidence rate ratio [IRR], 1.14 [1.06–1.22]; a!0.05).Manual workers had 7.38 days of WA on average, whichis 35% longer sick leave than professional workers (5.10days) (IRR, 1.35 [1.13–1.62]; a!0.05). No other significantdifferences in WA length were found among the differentwork activities or occupation of the population studied.
The treating physicians indicated a mean of 6.8 days ofWA when they were general practitioners, 9.1 days in thecase of orthopedic surgeons, and 6.4 days in case of allother medical specialists together, as shown in Fig. 2.Patients attended by orthopedic surgeons had 43% longerindication for sick leaves than those seen by other medicalspecialists (IRR, 1.43 [1.26–1.61]; a!0.05). No other sig-nificant difference was found in the analyses of the vari-ables associated with a longer sick leave.
The mean subsidy cost for each patient was US $110.3(median, 89.3; range, 0–553.7). Assuming a prevalence of5.4% and a total of 786,064 patients with non–work-relatedsick leave certificates in a year, we estimate that the ChPHSspent US $4,681,954 on subsidy payments in the studiedperiod.
Discussion
We report the first study of the prevalence of non–work-related sick leave because of acute LBP in Chile, usingwell-established diagnostic criteria [26,27]. Our resultsshow a similar prevalence to previous studies performedin very different ethnic and sociodemographic populations[29,30] and correspond to 5.4% of sick leave cases in Chile.This is important as we used a strict definition for acuteLBP, which has not been used in all studies previously pub-lished. Nonetheless, because patients with sciatica as op-posed to those with just acute LBP were not included inthis study, our results may underestimate the whole amountof workers on sick leave because of a lumbar pathology.
The duration of WA was found to be longer in patientswith an episode of sick leave because of acute LBP inthe previous year, in manual workers, and in patients whohad been seen by an orthopedic surgeon relative to the restof the population studied.
Several studies have demonstrated that the total eco-nomic impact of LBP in different countries is enormous[6,31,32]. Estimates of its economic costs in different coun-tries vary greatly depending on the study methodology [33].However, there is consensus that a small percentage ofcases accounts for a high proportion of total expenditures,and identification of patients at risk for longer periods ofdisability can help to control the total costs associated withthis condition [33]. Our study determined that a history of

Table 2
Studied variables in patients with sick leave secondary to acute LBP
Patients All Men Women p Value
Number of cases (%) 540 319 (59.1) 221 (40.9)
Age, y (mean6SD) 36.1611.1 36.2611.3 35.8610.8 .6
Days of WA (mean6SD) 7.163.8 6.863.0 7.364.0 .1
Subsidy payment in US $ (mean6SD) 110.3693.6 112.1696.2 107.7689.6 .5
Previous WA because of LBP, n (%) 129 (23) 70 (21) 59 (26) .2
Previous WA because of other causes, n (%) 210 (61) 102 (31) 108 (48) !.01
LBP, low back pain; SD, standard deviation; WA, work absence.
4 C. Diaz-Ledezma et al. / The Spine Journal - (2009) -
ARTICLE IN PRESS
an episode of sick leave because of LBP in the previousyear is associated with longer WA. There is controversialevidence on the use of history of LBP as a prognostic factorfor duration of sick leave: Wasiak et al. [34] have found thata history of LBP is a risk factor for WA; however, in a sys-tematic review of the literature, Steenstra et al. [9] foundthat a history of LBP is not predictive of the duration ofsick leave. Our study specifically evaluated the presenceof a previous episode of WA because of acute LBP in theprior year, not just the history of LBP, which may explainour results. Future prospective studies should help to clarifythis epidemiologic situation.
Heavy load work has been previously described as a pre-dictor of longer duration of sick leave [9,16–18]. The cur-rent study found that manual workers (considered as thosewho perform heavy work) were prescribed longer sickleave periods than nonmanual workers. Our study specifi-cally differentiated work activity and occupation, as thesame work activity can be shared by patients with very dif-ferent occupations (eg, industry can be a work activity fora manager or for a manual worker). Kinkade [35] advisedstaying active but avoiding heavy lifting, bending, twisting,and prolonged sitting for patients with LBP, as early returnto productive activity has shown to decrease disability.
Fig. 2. Days of prescribed sick leave because of acute low back pain
grouped by medical specialty of attending physician.
However, as modification of work duties is not always pos-sible for manual workers, this may explain their longer WA.
It has been reported that people of working age consti-tute a large proportion of physician visits for back symp-toms, and up to 60% of patients with back pain aretreated by primary care physicians [36]; our study is com-posed of a comparable population. In our study, patientsseen by orthopedic surgeons received an indication of lon-ger periods of sick leave than those seen by other physi-cians. Previous data show that specialists usuallyprescribe longer durations of WA than general physicians[8]. The patients seen by orthopedic surgeons may repre-sent a subpopulation of more severe cases, which might ex-plain that finding, as COMPIN does not make a differenceto authorize different sick leave duration depending on thespecialty of the physician who indicates the WA.
Our study could not evaluate the severity of LBP or dis-ability, which are variables that have been found to be asso-ciated with the length of WA [8,16]. In addition, we did notevaluate psychosocial factors, which have been associatedwith prolonged disability in cases of LBP [15,17,18,37,38].
The current study did not find that age and gender wererisk factors for prolonged sick leave. However, our studyexcluded pregnant patients. Previous data showing thatthe proportion of WAs related to LBP does not differ be-tween nonpregnant women and men [26] were confirmedby our study.
The amount of compensation received is also considereda risk factor for longer sick leave because of LBP [9,20].From our data, we cannot evaluate the effect of the Chileanregulation that warrants full subsidy payment only if sickleave is prescribed for 11 days or longer as a factor thatmay explain prescription of longer WA.
Finally, we also tried to determine the costs associatedwith subsidy payments for acute LBP in the ChPHS. Wedid not try to estimate the expenditures associated with directhealth-care [4] or indirect costs, such as work absenteeismand loss of productivity, which are usually significantly high-er [5,6]. We did not intend to estimate all the expenditures as-sociated with subsidy payment related to LBP either, as ourstudy specifically excluded patients with chronic LBP, whichusually accounts for most back pain costs.
However, as our study included patients from the publichealth insurance system, which covers 70% of the Chileanpopulation [39], the group studied is representative of

5C. Diaz-Ledezma et al. / The Spine Journal - (2009) -
ARTICLE IN PRESS
a significant proportion of the Chilean population. Notably,this population of middle- and low-income workersobtained a mean subsidy payment for WA because of acuteLBP equivalent to 38% of the minimal obligatory monthlystipend in Chile. This is a significant amount consideringthat the mean sick leave duration was 7.10 days, and the sti-pend paid covered only some days of disability in manycases.
Conclusions
In a Chilean population of patients with acute non–work-related LBP, those who had an episode of WAbecause of LBP in the previous year, manual workers,and patients treated by orthopedic surgeons presented lon-ger sick leave durations than the rest of the population.Nonpregnant women and men had similar durations of sickleave because of acute LBP. The results from this study ina Chilean population are similar to those found in Anglo-Saxon and Northern European populations. All physicianswho treat patients with LBP should be aware of these riskfactors, as sick leave associated with LBP is a significantburden to any society and an important epidemiologicproblem.
References
[1] Hart LG, Deyo RA, Cherkin DC. Physician office visits for low back
pain. Frequency, clinical evaluation, and treatment patterns from
a U.S. national survey. Spine 1995;20:11–9.
[2] Deyo RA, Mirza SK, Martin BI. Back pain prevalence and visit rates:
estimates from U.S. national surveys, 2002. Spine 2006;31:2724–7.
[3] Luo X, Pietrobon R, Sun SX, et al. Estimates and patterns of direct
health care expenditures among individuals with back pain in the
United States. Spine 2004;29:79–86.
[4] Ekman M, Johnell O, Lidgren L. The economic cost of low back pain
in Sweden in 2001. Acta Orthop 2005;76:275–84.
[5] Maniadakis N, Gray A. The economic burden of back pain in the UK.
Pain 2000;84:95–103.
[6] Tubach F, Leclerc A, Landre MF, et al. Risk factors for sick leave due
to low back pain: a prospective study. J Occup Environ Med 2002;44:
451–8.
[7] Carey TS, Evans AT, Hadler NM, et al. Acute severe low back pain:
a population based survey of prevalence and care-seeking. Spine
1996;21:339–44.
[8] Steenstra IA, Koopman FS, Knol DL, et al. Prognostic factors for
duration of sick leave due to low-back pain in Dutch health care pro-
fessionals. J Occup Rehabil 2005;15:591–605.
[9] Steenstra IA, Verbeek JH, Heymans MW, et al. Prognostic factors for
duration of sick leave in patients sick listed with acute low back pain:
a systematic review of the literature. Occup Environ Med 2005;62:
851–60. [review].
[10] Hagen KB, Jamtvedt G, Hilde G, et al. The updated cochrane review
of bed rest for low back pain and sciatica. Spine 2005;30:542–6.
[11] Koes BW, van Tulder MW, Ostelo R, et al. Clinical guidelines for the
management of low back pain in primary care: an international com-
parison. Spine 2001;26:2504–13.
[12] Van Tulder M, Becker A, Bekkering T, et al. for the COST B13
Working Group on Guidelines for the Management of Acute Low
Back Pain in Primary Care. Chapter 3. European guidelines for the
management of acute nonspecific low back pain in primary care.
Eur Spine J 2006;15(Suppl 2):169–91.
[13] Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands:
prevalences, consequences and risk groups, the DMC(3)-study. Pain
2003;102:167–78.
[14] Pengel LH, Herbert RD, Maher CG, et al. Acute low back pain: sys-
tematic review of its prognosis. BMJ 2003;327:323.
[15] IJzelenberg W, Burdorf A. Risk factors for musculoskeletal symptoms
and ensuing health care use and sick leave. Spine 2005;30:1550–6.
[16] Du Bois M, Szpalski M, Donceel P. Patients at risk for long-term sick
leave because of low back pain. Spine J 2009;9:350–9.
[17] Pincus T, Vlaeyen JW, Kendall NA, et al. Cognitive-behavioral ther-
apy and psychosocial factors in low back pain: directions for the
future. Spine 2002;27:E133–8.
[18] Fransen M, Woodward M, Norton R, et al. Risk factors associated
with the transition from acute to chronic occupational back pain.
Spine 2002;27:92–8.
[19] Dasinger LK, Krause N, Deegan LJ, et al. Physical workplace factors
and return to work after compensated low back injury: a disability
phase-specific analysis. J Occup Environ Med 2000;42:323–33.
[20] Gatchel RJ, Polatin PB, Mayer TG. The dominant role of psychoso-
cial risk factors in the development of chronic low back pain disabil-
ity. Spine 1995;20:2702–9.
[21] Kovacs FM, Muriel A, Abriaira V, et al. Spanish Back Pain Research
Network. The influence of fear avoidance beliefs on disability and
quality of life is sparse in Spanish low back pain patients. Spine
2005;30:E676–82.
[22] Kovacs F, Abraira V, Muriel A, et al. Prognostic factors for neurore-
flexotherapy in the treatment of subacute and chronic neck and back
pain: a study of predictors of clinical outcome in routine practice of
the Spanish National Health Service. Spine 2007;32:1621–8.
[23] Kovacs FM, Abraira V, Zamora J, et al. The transition from acute to sub
acute and chronic low back pain: a study based on determinants of qual-
ity of life and prediction of chronic disability. Spine 2005;30:1786–92.
[24] Soriano ER, Zingoni C, Lucco F, Catoggio LJ. Consultations for
work related low back pain in Argentina. J Rheumatol 2002;29:
1029–33.
[25] Superintendencia de Salud de Chile. Available at: http://www.super
salud.cl/documentacion/569/articles-2522_recurso_1.pdf. Accessed
October 27, 2005.
[26] Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of low
back pain: a joint clinical practice guideline from the American Col-
lege of Physicians and the American Pain Society. Ann Intern Med
2007;147:478–91.
[27] de Vet HC, Heymans MW, Dunn KM, et al. Episodes of low back
pain: a proposal for uniform definitions to be used in research. Spine
2002;27:2409–16.
[28] Sydsjo A, Alexanderson K, Dastserri M, et al. Gender differences in
sick leave related to back pain diagnoses: influence of pregnancy.
Spine 2003;28:385–9.
[29] Ghaffari M, Alipour A, Jensen I, et al. Low back pain among Iranian
industrial workers. Occup Med (Lond) 2006;56:455–60.
[30] Vingard E, Mortimer M, Wiktorin C, et al. Musculoskeletal Inter-
vention Center-Norrtalje Study Group. Seeking care for low back
pain in the general population: a two-year follow-up study: results
from the MUSIC-Norrtalje Study. Spine 2002;27:2159–65.
[31] Ekman M, Jonhagen S, Hunsche E, et al. Burden of illness of chronic
low back pain in Sweden: a cross-sectional, retrospective study in pri-
mary care setting. Spine 2005;30:1777–85.
[32] Walker BF, Muller R, Grant WD. Low back pain in Australian adults:
the economic burden. Asia Pac J Public Health 2003;15:79–87.
[33] Dagenais S, Caro J, Haldeman S. A systematic review of low back
pain cost of illness studies in the United States and internationally.
Spine J 2008;8:8–20.
[34] Wasiak R, Verma S, Pransky G, et al. Risk factors for recurrent epi-
sodes of care and work disability: case of low back pain. J Occup
Environ Med 2004;46:68–76.
6 C. Diaz-Ledezma et al. / The Spine Journal - (2009) -
ARTICLE IN PRESS
[35] Kinkade S. Evaluation and treatment of acute low back pain. Am
Fam Physician 2007;75:1181–8. 1190–1192.
[36] Cypress BK. Characteristics of physician visits for back symptoms:
a national perspective. Am J Public Health 1983;73:389–95.
[37] Buer N, Linton SJ. Fear-avoidance beliefs and catastrophizing: occur-
rence and risk factor in back pain and ADL in the general population.
Pain 2002;99:485–91.
[38] Carragee EJ, Alamin TF, Miller JL, et al. Discographic, MRI and psy-
chosocial determinants of low back pain disability and remission:
a prospective study in subjects with benign persistent back pain.
Spine J 2005;5:24–35.
[39] Fondo Nacional de Salud de Chile FONASA. Available at: https://fon.
fonasa.cl/prontus_fonasa/site/artic/20070112/asocfile/01_demografia_
pagina_web__15_09_2008_ja.xls. Accessed January 9, 2009.