
FACTORS ASSOCIATED WITH RETENTION IN CARE ...
122
College of Medicine FACTORS ASSOCIATED WITH RETENTION IN CARE AMONG PEOPLE LIVING WITH HIV/AIDS IN UBUNGO MUNICIPALITY, TANZANIA BY SYLVIA DENIS MOSHI (MEDICAL DOCTOR- MD) A thesis submitted to the Department of Public Health and Herbal Medicine, in partial fulfillment for the degree of Master of Science in Public Health December, 2021
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of FACTORS ASSOCIATED WITH RETENTION IN CARE ...

College of Medicine
FACTORS ASSOCIATED WITH RETENTION IN CARE
AMONG PEOPLE LIVING WITH HIV/AIDS IN UBUNGO
MUNICIPALITY, TANZANIA
BY
SYLVIA DENIS MOSHI
(MEDICAL DOCTOR- MD)
A thesis submitted to the Department of Public Health and Herbal Medicine, in partial
fulfillment for the degree of Master of Science in Public Health
December, 2021

ii
Certificate of Approval
The Dissertation of Sylvia Denis Moshi is approved by the Dissertation Examination
Committee:
_______________________________________
Prof. Fanuel Lampiao
(Chairman, Post Graduate Committee)
_______________________________________
Alinane Linda Nyondo-Mipando, RNM, Ph.D.
(Supervisor)
_______________________________________
Joan Rugemalila MD, MMED
(Supervisor)
_______________________________________
Adamson S. Muula, MBBS, MPH, Ph.D.
(Head of Public Health Department)

iii
Declaration
This thesis is my original work and has not been presented for a degree award in any other
university.
Name of the Candidate: Sylvia Denis Moshi
Signature:
Date: 30th December, 2021

iv
Dedication
I dedicate this thesis to my late parents, Denis Petro Moshi and Marcellina Melkiori. My guardian
parents, Mr. & Mrs. Stewart Petro Mlang’a for their wonderful support, who made me the woman
I am today. My lovely husband for his moral support and persistent prayers.

v
Acknowledgements
I would like to firstly give thanks to the Almighty God for his wonderful mercies and blessings
upon my life throughout my studies. Indeed, the Lord God is my strength.
My sincere gratitude goes to World Bank and Inter-University Council for East Africa (IUCEA),
African Centre of Excellence in Public Health and Herbal Medicine (ACEPHEM) for the
scholarship. Without their support I wouldn’t have made it.
I would like to extend my gratitude to my supervisors: Dr. Alinane Linda Nyondo Mipando and
Dr. Joan Rugemalila for their availability, tireless support, patience and encouragement throughout
the entire period of the study.
I am greatly indebted to the management of Sinza Hospital, Mbezi Health centre and Kimara
dispensary and all the staff who gave me the opportunity and support to conduct the study in the
clinics. Special mention goes to Janeth Kweka and Juma Baraka who supported me with data
collection. Analyses of the results would not have been finally completed without the assistance
of Paul Sabuni and Dr. Severin Kabakama. Thank you for your valuable work.
Last but not least, I would like to thank my participants for voluntarily participating in the study.

vi
Abstract
Background: Globally, approximately 50% of people who have been diagnosed with HIV are
either not linked to a care provider or not retained in medical care. In sub-Saharan Africa 54% of
those who are not yet eligible for ART were lost to follow-up before becoming eligible, while 32%
of the people living with HIV who were eligible for ART were lost before initiating treatment.
Although the retention rate of HIV infected people in Tanzania has increased slowly from 39.4%
to 54.5% from 2008 to 2016, there remains some challenges in achieving optimal rates.
Methodology: A convergent mixed method design was used to determine factors associated with
retention in care among PLHIV at Ubungo municipality, Tanzania. Quantitatively, a descriptive
cross -sectional design was applied and data was collected using an interviewer-administered
questionnaire among 365 participants that were systematically selected. Quantitative data were
analyzed using SPSS software and descriptive statistics was used to summarize findings in tables,
graphs and charts. In addition, Chi square test was used to determine the factors associated with
retention in HIV care. Qualitatively, we conducted a descriptive study and drew a purposive
sample of 18 participants for In-depth Interviews and 18 health care workers for Key informant
Interviews (KII). All data were digitally recorded and then transcribed, translated, coded, analyzed
thematically. The data collection was conducted between May and July 2021.
Results: Ninety-three percent (93%) of the participants were retained in HIV/AIDS care. The
majority (81.1%) never missed their clinic appointments. The main reason for missing a clinic
appointment was forgetfulness. Eighty-seven per cent of the participants were aware of the risks
of missing appointments. However, 94.8% participants continued using the ARVs despite missing
the clinic appointment and obtained drugs from friends, relatives or another clinic. Only 1.1% of

vii
the participants were lost to follow-up. All socio- demographic charactersitics, sex, age, marital
status, education level and occupation were not associated with retention. However, sense of
wellness and good worker’s attitude were related to reported retention during the Key informant
and in-depth interviews.
Conclusion: The study reports a high rate of retention on HIV/AIDS care and treatment attributed
to awareness of alternative clinics to collect the ARVs from and the consequencies of missed-
appointment. Health care workers should strengthern counselling efforts to further minimize the
rates of missed clinic appointments of longer than six months, focusing om factors associated with
poor retention in HIV/AIDS care and treatment.

viii
Table of Contents
Certificate of Approval ................................................................................................................... ii
Declaration ..................................................................................................................................... iii
Dedication ...................................................................................................................................... iv
Acknowledgements ......................................................................................................................... v
List of Tables ............................................................................................................................... xiii
List of Figures .............................................................................................................................. xiv
Abbreviation and Acronyms ......................................................................................................... xv
Operational Definitions ............................................................................................................... xvii
Abstract .......................................................................................................................................... vi
Chapter One .................................................................................................................................... 1
1.1 Background ...................................................................................................................... 1
1.2 Problem Statement ........................................................................................................... 4
1.3 Significance for the Research Project .............................................................................. 5
1.4.1 Broad Objectives ....................................................................................................... 5
1.4.2 Specific Objectives ................................................................................................... 5
1.5 Research Questions .......................................................................................................... 5
Chapter Two: Literature Review .................................................................................................... 7
2.1 Introduction ...................................................................................................................... 7
2.2 Epidemiology of HIV/AIDS ............................................................................................ 7
2.3 Status of Retention ........................................................................................................... 8
2.4 Factors that Influence Retention in Care .......................................................................... 9

ix
2.4.1 Health System Factors .............................................................................................. 9
2.4.2 Transportation Cost and Distance to the Clinic ...................................................... 10
2.4.3 Community Based-Interventions ............................................................................ 11
2.4.4 Positive Perceptions of ART ................................................................................... 11
2.4.5 Psychosocial Factors (Stigma and Non-Disclosure) ............................................... 12
2.4.6 Faith Healing ........................................................................................................... 12
2.4.7 Use of Herbal Medicine .......................................................................................... 13
2.4.8 Family and Social Support ...................................................................................... 13
2.5 Conceptual Framework .................................................................................................. 14
Chapter Three: Research Methodolody ........................................................................................ 16
3.1 Study Design .................................................................................................................. 16
3.2 Study Site ....................................................................................................................... 16
3.3 Study Population ............................................................................................................ 18
3.4 Eligibility Criteria .......................................................................................................... 19
3.4.1 Inclusion Criteria for HIV/AIDS Participants ........................................................ 19
3.4.2 Exclusion criteria for HIV/AIDS participants ........................................................ 19
3.4.3 Inclusion Criteria for HCW’s.................................................................................. 19
3.4.4 Exclusion Criteria for HCW’s ................................................................................ 19
3.5 Study Period ................................................................................................................... 20
3.6 Sample Size .................................................................................................................... 20
3.6.1 Sample Size for Quantitative Component............................................................... 20
3.6.2 Sampling for Qualitative Component ..................................................................... 21
3.7 Sampling Procedure ....................................................................................................... 21

x
3.7.1 Quantitative Method ............................................................................................... 21
3.7.2 For Qualitative Method ........................................................................................... 22
3.7.3 Pre-Testing of Study Tools ..................................................................................... 22
3.8 Data Collection Tools..................................................................................................... 22
3.8.1 Questionnaire .......................................................................................................... 23
3.8.2 The Validity and Reliability of the Quantitative Data (Questionnaire) .................. 23
3.8.3 Key Informant Interview......................................................................................... 24
3.8.4 In-depth Interview ................................................................................................... 24
3.8.5 Credibility, Transferability, Confirmability and Dependability Of The Qualitative
Tools ................................................................................................................................. 24
3.9 Data Management .......................................................................................................... 25
3.10 Data Analysis ................................................................................................................. 25
3.10.1 Quantitative Data Analysis ..................................................................................... 25
3.10.2 Qualitative Data Analysis ........................................................................................... 26
3.11 Presentation of Results ................................................................................................... 28
3.12 Dissemination of Results ................................................................................................ 28
3.13 Ethical Consideration ..................................................................................................... 28
Chapter Four: Results ................................................................................................................... 30
4.1 Introduction .................................................................................................................... 30
4.2 Social Demographic Characteristics of the Participants ................................................ 30
4.2.1 Quantitative Interviews Participants ....................................................................... 30
4.2.2 Characteristics of Participants in the Qualitative Component ................................ 31
4.3 HIV Status Disclosure and Clinic Appointments ........................................................... 32

xi
4.4 Rentention: Ever Missed Appoiment for Six Months Or More, And ART Continuity . 37
4.4.1 Status of Retention from the Health Facilities ........................................................ 42
Chapter Five: Discussion, Conclusion and Recommendations .................................................... 44
5.1 Introduction .................................................................................................................... 44
5.2 Retention in HIV/AIDS Care and Treatment ................................................................. 44
5.3 Social Factors Associated with Retention ...................................................................... 45
5.3.1 HIV Status Disclosure............................................................................................. 45
5.3.2 Stigma and Discrimination ..................................................................................... 46
5.3.3 Traditional Healers and Faith Healing .................................................................... 47
5.4 Structural and Health System Factors Associated with Retention ................................. 47
5.5 Strengths of the Study .................................................................................................... 50
5.6 Study Limitations ........................................................................................................... 50
5.7 Conclusion ...................................................................................................................... 50
5.8 Recommendations .......................................................................................................... 51
References ..................................................................................................................................... 53
Appendices .................................................................................................................................... 64
Appendix 1: informed consent forms ........................................................................................ 64
Appendix 1.1: Informed consent form for HIV/AIDS patients in English ........................... 64
Appendix 1.2: Informed consent form for HIV/AIDS patients in Swahili .......................... 67
Appendix 1.3: Informed Consent form for In-depth Interview (IDI) for HIV/AIDS patients
in English ............................................................................................................................... 70
Appendix 1.4: Informed consent form for In-depth interview for HIV/AIDS patients in
Swahili ................................................................................................................................... 73

xii
Appendix 1.5: Informed Consent Form for Key Informant Interview (KII) in English ....... 76
Appendix 1.6: Informed consent form for Key Informant Interview in Swahili ................. 79
Appendix 2: Data Collection Tools ........................................................................................... 82
Appendix 2.1: Questionnaire in English ................................................................................ 82
Appendix 2.2: Questionnaire in Swahili ................................................................................ 87
Appendix 2.3: Topic guide for In- depth interview (IDI) for patients living with HIV/AIDS
in English ............................................................................................................................... 92
Appendix 2.4: Topic guide for In-depth Interview (IDI) for Patients living with HIV/AIDS
in Swahili ............................................................................................................................... 94
Appendix 2.5: Key Informant Interview Guide (KII) for Health Care Workers in English . 96
Appendix 2.6: Key Informant Interview Guide (KII) for Health Care Workers in Swahili . 98
Appendix 3: COMREC clearance letter .................................................................................. 100
Appendix 4: NIMR clearance letter ........................................................................................ 101
Appendix 5: Research Permit from Ubungo Municipal.......................................................... 103
Appendix 6: Gantt chart .......................................................................................................... 104
xiii
List of Tables
Table 1: Retention in care pre-determined themes for qualitative component ............................. 27
Table 2: Sociodemographic characteristics of participants in quantitative component ................ 31
Table 3: Social and demographic characteristics of KII and in-depth interviews participants .... 32
Table 4: HIV status disclosure and clinic appointments attendance ............................................. 33
Table 5: Retention, ever missed appointment for 6 months or more and access to ART ............. 39
Table 6: Association between retention to ART care and treatment ............................................ 43

xiv
List of Figures
Figure 1: Conceptual framework .................................................................................................. 15
Figure 2: (A) A Map of Tanzania showing regions, (B) Map of Dar es salaam Region showing
Municipals, and (C) Map of Ubungo Municipality showing study health facilities. ................... 18
Figure 4: Shows proportion of retention from the facilities ......................................................... 42

xv
Abbreviation and Acronyms
AIDS Acquired Immunodeficiency Syndrome
ART Antiretroviral Therapy
CBAS Community Based Adherence Support
CBHS Community Based Health Services
CBOs Community Based Organizations
CD4 Cluster of differentiation 4
CDC Centers for Disease Control and Prevention
CHW Community Health Workers
COM College of Medicine
COMREC College of Medicine Research Ethics
Committee
CTC Care and treatment Centre
HAART Highly Active Anti-retroviral Therapy
HCWs Health Care Workers
HIV Human Immunodeficiency Virus
IDI In-depth interview
IPT Isoniazid Preventive therapy
IRB Institutional Review Board
KII Key Informant Interview
LTFU Lost to follow up
MDH Management and Development for Health

xvi
MoHCDEC Ministry of Health, Community
Development, Gender, Elderly and Children
NGOs Non-Governmental Organizations
NIMR National Institute of Medical Research
PCR Polymerase Chain Reaction
PI Principal Investigator
VTC Voluntary Testing and Counselling
PLHIV People Living with Human Immunodeficiency
Virus.
RNA Ribose Nucleic Acid
SMS Short message service
MS Microsoft
SPSS Statistical Package for the Social Sciences
UKIMWI Ukosefu wa Kinga Mwilini
UNAIDS United Nations programme on HIV/AIDS
USA United States of America
SSA Sub-Saharan Africa
WHO World Health Organization

xvii
Operational Definitions
Retention in care is defined as a patient’s regular engagement with medical care at a health care
facility after initial entry into the system (1). Retention in care is defined as being alive and on
ART or being transferred out to other health facilities to continue treatment (2).
Enrollment: Entry into care after HIV diagnosis, defined as a visit with an HIV care provider
authorized to prescribe ART.
HIV cascade/continuum: sequential steps a client undergoes from HIV testing to Viral load
suppression.
Linkage: Linkage to care is the process of engaging newly diagnosed HIV-infected persons into
HIV primary care.
Visit: Contact with health care worker at a health facility.
Missed appointment: A patient is classified as having a missed appointment if they are more than
3 days, but less than or equal to 7 days, late to their expected appointment.
Lost to follow up is defined when a patient has not attended a scheduled clinic for three months
consecutively and their vital status is unknown. At the same time, two-three attempts to track those
patients have failed.
Attrition: “the number of patients who were lost to follow-up, transferred out, or died.”
Transfer out: Transfer out is initiated by the healthcare provider to the client from one ART
facility to another for continuation of HIV care.
Viral load: is the number of HIV RNA copies in a milliliter (copies/mL) of blood.
Antiretroviral therapy: is a combination of at least three anti-retroviral drugs to suppress the
HIV replication and stop the progression of HIV disease.

1
Chapter One
1.1 Background
Globally, approximately 50% of people who have been diagnosed with HIV are neither linked to
a care provider nor retained in medical care (3). In the USA less than 50% of individuals with HIV
are considered sufficiently retained in care (4). This has substantial implications for both individual
and public health outcomes. Adherence to ART as a consequence of good retention in care has
been shown to have the benefit of guaranteeing longer, healthier lives for those on treatment but
also the additional effect of limiting transmission by up to 96% and reducing the risk of maternal
to child transmission of HIV to less than 5% compared to up to 45% without treatment (5). A
study done in China found a retention rate was 58.1% among 822 PLWHIV in Changsa center
for Disease Control and prevention (6). The available literature from sub-Saharan Africa showed
that 54% of those who are not yet eligible for ART were lost to follow-up before becoming eligible,
while 32% of the people living with HIV who were eligible for ART were lost before initiating
treatment.
Tanzania has done well to control the HIV epidemic over the last decade. Scaling up access to
antiretroviral treatment (ART) has resulted in a decline of 13% in the proportion of new infections
consequently halving the number of people dying from an AIDS related illness (7). Despite that
more people living with HIV are benefitting from effective treatment, linkage to care after
diagnosis remains one of the weakest parts of Tanzania’s HIV treatment cascade. There is still a
great challenge in retaining HIV/AIDS patients in care, the retention rate has increased slowly
from 39.4% to 54.5% from 2008 to 2016 (8). A study done in Uganda, Zambia, and Tanzania in

2
2014, found that the retention rate in Tanzania after ART initiation was decreasing with increasing
years 71.0% in the first year, 62.7% in the second year, and 58.3% in the third year (9).
Both facility-based health care providers and community-based organizations (CBO) work with
clients to ensure retention in care, including limiting missed appointments and loss-to-follow-up
(LTFU) of clients. Poor retention in HIV care is a global problem affecting both developed and
developing countries. There are widespread challenges to retaining patients in care especially in
resource-limited settings (10). There is no single approach for retention that is likely to work for
everyone in all settings because retention factors vary among the clients (11). For example, many
Africans reside in rural areas where there is a lack of proximity to public health facilities and
inadequate transportation which are major impediments to accessing care (12). Although ART is
given free, factors like stigma, non-disclosure, and transport costs lead to poor retention (13).
Retention of people living with HIV/AIDS across the continuum of care is essential for optimal
health outcomes. For people living with HIV who are receiving treatment, the maintenance of
uninterrupted ART and continual monitoring are essential for sustained viral suppression, optimal
treatment outcomes, and avoidance of treatment failure and drug resistance (14). Retention in care
is necessary to ensure optimal clinical outcomes, ongoing receipt of ART, evaluate the emergence
of medication toxicities, and identification of the occurrence of treatment failure that necessitate a
switch form one ART regimen to another (15). It also provides additional benefits through
ancillary services, social support, and secondary prevention messages that help patients navigate
a lifelong and complicated infection (16).
3
At present, there is no consensus on exact definitions for retention or what constitutes ‘adequate’
retention in care (17). There is a lack of consistency which results in the inclusion of deceased
clients (18), self-transferred clients (19) as part of those that are lost to follow-up. Self-transfers
occurs when people decide to move into a new facility without informing their previous facility
staff and this is further compounded with occurrence of unregistered death due to lack of routinely
collected vital registration data in many resource-limited countries (19). Improving the
understanding of barriers to retention and establishing innovative strategies to address them are
important priorities in the implementation of research and public health (20). Tanzania emphasis
retention in care as pivotal element of adherence to antiretroviral therapy (ART) and risk reduction,
through engagement with medical care at a health care facility after initial entry into the system
(2). More formal definitions and measurements that have been utilized are required to follow up
at certain intervals to define retention in care; these definitions have typically conceptualized
retention in care based on either appointments missed or medical visits attended at regularly
defined intervals (5).
Some of the factors that affects retention in care include lack of disclosure, male sex, distance to
the clinic, travel costs, competing life activities and forgetfulness, health system factors such as
prolonged waiting time when accessing services, negative attitudes of health care works, and
stock out of drugs (21). An understanding of challenges that affect retention in HIV care is critical
as it provides information that can be used in the development of strategies that will improve
retention in care amongst HIV infected individuals. The objective of this study was to identify
factors associated with retention in care among people living with HIV/AIDS HIV in Ubungo
Municipality, Tanzania.

4
1.2 Problem Statement
Despite the implementation of strategies to optimize retention in care and adherence to ART,
clients still struggle to remain in care and adopt good behaviors as directed by their health care
providers (22). This results in increased morbidity and mortality through suboptimal viral
suppression, increased risk of drug resistance, and increased risk of HIV transmission (23). All
this leads to a higher health-care costs and a loss of or reduction in individual income, potentially
translating to lower economic productivity at individual and national level (13).
Although there is evidence on the expansion and benefits of ART to clients, some patients
discontinue with follow-up visits and treatment schedules. In other cases the reasons for
discontinuation from HIV care among people that are infected with HIV who were initially
successfully linked to care remains unknown (24). Retention of people living with HIV in care is
vital for achieving long term positive outcomes both for the individual and ART programs (24).
Retention in care remains a challenge both in developed and developing countries despite various
interventions implemented by different Non-Governmental Organizations (NGO) dealing with
HIV/AIDS. The success of PLHIV being retained in HIV/AIDS programs requires an
understanding of factors that influence retention because clients who are poorly retained in care
cause an interruption to care and this affects the client’s health and global fight of HIV/AIDS
pandemic. Given the relevance of retention in care and the gaps that are prevalent in Tanzania, this
study assessed the factors associated with retention in care among people living with HIV/AIDS
in Ubungo municipality, Tanzania.

5
1.3 Significance for the Research Project
The study has provided insights on factors associated with retention in care among PLHIV, which
is an important step in understanding and strengthening strategies that will help people living with
HIV/AIDS to be continuously engaged and retained in care. The findings from this study also
provides additional data to the National AIDS Control Program (NACP) through the Ministry of
Health, Community Development, Gender, Elderly and Children)) and Ubungo Municipal council
to improve interventions equipped to retain more PLHIV in care and other services, making them
more relevant to the needs of people living with HIV/AIDS.
1.4 Research Objectives
1.4.1 Broad Objectives
To assess factors associated with retention in care among people living with HIV/AIDS in Ubungo
municipality, Tanzania.
1.4.2 Specific Objectives
1. To determine the proportion of people retained in care among HIV positive clients
attending health centres in Ubungo Municipality for HIV/AIDS care.
2. To identify factors facilitating or limiting retention in care among people living with
HIV/AIDS in Ubungo Municipality, Tanzania.
1.5 Research Questions
1. What is the proportion of retention in care among people living with HIV/AIDS
attending health centres at Ubungo Municipality?

6
2. What are the factors facilitating or limiting retention in care among the People
Living with HIV/AIDS?
7
Chapter Two: Literature Review
2.1 Introduction
The literature review covers the epidemiology of HIV/AIDS, the status of retention in HIV/AIDS
care and the factors associated with retention in care among people living with HIV/AIDS globally,
in African setting and in Tanzania.
2.2 Epidemiology of HIV/AIDS
Globally, 37.9 million people were living with HIV at the end of 2018 (25). Although the burden
of the pandemic continues to vary considerably between countries and regions, the WHO African
region remains most severely affected, with nearly 1 in every 25 adults (3.9%) living with HIV
and accounting for more than two-thirds of the people living with HIV worldwide (26). HIV/AIDS
remains a major public health problem in sub-Saharan Africa, causing the death of millions of
adults in their prime, disrupting and impoverishing families, and turning millions of children into
orphans. Since the beginning of the epidemic, 75 million people have been infected with the HIV
and about 32 million people have died of HIV related deaths (27).
The East and Southern Africa is the region that is hit the hardest by HIV. It is home to around
6.2% of the world’s population but over half (54%) of the total number of people living with HIV
in the world (20.6 million people) are found in sub-Saharan countries of Africa (28). In 2018, there
were 800,000 new HIV infections, which is under half of the global total (24). South Africa
accounted for more than a quarter (240,000) of the region’s new infections in 2018. Seven other
countries accounted for more than 50% of new infections: Mozambique (150,000), Tanzania

8
(72,000), Uganda (53,000), Zambia (48,000), Kenya (46,000), Malawi (38,000), and Zimbabwe
(38,000) (25).
In Tanzania, 1.7 million people were living with HIV in 2019 (29). This equates to an estimated
HIV prevalence among adults of 4.8% (25) with more women infected than men (29). In the same
year, 77,000 people were newly infected with HIV, and 27,000 people died from an AIDS-related
illness (30). Among adults who initiated Antiretroviral therapy (ART), 75% are still active on
treatment after 12 months in 2019 (31). Dar es Salaam has the highest burden of HIV/AIDS with
a prevalence of 11% (27).
2.3 Status of Retention
Both in African setting and the globe, the status of retention and factors that affect retention are
almost similar. In USA, based on HIV surveillance data from 2010 through 2018, the retention in
HIV medical care among persons with diagnosed HIV has ranged from 53.6% in 2011 to 57.9%
in 2018 (32), this is far below the National HIV/AIDS Strategy 2020 goal of at least 90% retention
in HIV medical care (33). In China, a study that was done by Guoli.L. Yang on Retention in Care
and Factors Affecting It among People Living with HIV/AIDS in Changsha City, China found that
the retention rate was 58.1% (6). In African setting, retention in care is still a challenge. According
to a systematic review that was done in Sub Saharan Africa, in 2011, found that the retention rate
from ART eligibility to ART initiation was 68% (34). In Nigeria a seven year review on retention
and HIV care, found that 63% of patients were retained in care (35) as of 2015. A study done in
Uganda found the retention rate in care for 12 months was 65.7% in the year 2021 (36). In a study

9
that was done in rural Kenya found the overall retention rate among adults for one year was 94%
(37) in 2017.
2.4 Factors that Influence Retention in Care
The factors that influence retention in care include health system factors, community-based
interventions, education factors, positive perception on ART, distance to the clinic and
transportation costs, stigma and non-disclosure, faith healing, and use of herbal medicine and
family and social support.
2.4.1 Health System Factors
The health system factors that contributed to poor retention of patients in care were long waiting
times due to shortage of staff, high patient load, shortage of third-line ARV drugs, and inadequate
space in ART clinic (38). An East African study on facility-level factors influencing retention
found that, LTFU were higher in facilities without CD4 tests available on-site and with longer
Human Immunodeficiency Virus Ribonucleic Acid Polymerase Chain Reaction (HIV RNA PCR)
turnaround times, in both pre-ART and post ART respectively (39). Also, the clinic being open
more than 4 mornings per week was associated with a decreased hazard of LTFU in the ART
period (39). Increased LTFU was also observed during the pre-ART period when TB symptomatic
patients were treated within the ART program (39). Another study done in Gabon, Central Africa,
found that the main factor associated with retention to care was the initiation of ART at the first
or second clinical visit, whereas the main risk factor associated with LTFU was documented TB
(40). There was no reason highlighted for this finding. This is consistent with another study that
was done in Masaka Uganda which found that the risk of LTFU was 69% higher in patients who

10
started ART within seven days following HIV diagnosis compared to those who began ART after
seven days (41).
Clinic attendance is the key to adherence to the HIV treatment cascade and in ensuring retention
(39). Participants prefer more than one method to be reminded about their appointments and these
include appointment cards, text messages, availability of a treatment supporter, home visits (14).
Of the methods mentioned, an appointment card was the most preferred while those that didn’t
want any reminders attributed that to fear of having their status unintentionally disclosed to others
(42). Furthermore, evidence suggests that patients without a telephone set were 52% more likely
to be LTFU compared to those with a telephone set because they cannot get text messages
notifications and reminders for their clinic appointment (41).
2.4.2 Transportation Cost and Distance to the Clinic
Several studies show that distance to the clinic and transports cost is the major barrier to retention
in care in most African countries (12,38,43,44). It has been argued that in resource-limited settings
if the distance that participants have to travel to the clinic exceeds two hours the risk of non-
retention was doubled (21). Additionally in Uganda, the most common reasons for LTFU included
lack of transportation in 50% of the participants and excessive distance in 42% among the 111
participants included in the study (12). Another study done in Tanzania, Uganda, and Zambia
showed that further distance to the clinic is significantly associated with attrition (9) whereas in
India, among 106 patients who failed to return for 3 or more months, 20% cited distance and lack
of transportation as the major reasons for their non-attendance (45).

11
2.4.3 Community Based-Interventions
Interventions involving the delivery of community-based services have the strongest retention
rates. A systematic review reported that community-based adherence support (CBAS) that
consisted of home visits by Community Health Workers (CHWs) who distributed ART and
provided psychosocial and health-related support; showed significant improvements in retention
in care (46). Another systematic study that was done in Low and Middle income countries on
Community-Based Interventions to Improve and Sustain Antiretroviral Therapy Adherence,
Retention in HIV found that, the participants that were assigned to community-based ART (80.3
%) had statistically significant higher rates of treatment engagement than those in facility-based
ART (75.9 %) at the end of the follow-up period (10).
2.4.4 Positive Perceptions of ART
In a study that was done in Madagascar, found that most of the participants had a positive attitude
and perception (score ≥ 5) towards ART 75.6%, and this had a good impact on adherence to ART
services (47). Also, in a study that was done in Nigeria, it was found that a majority of the subjects
showed positive attitude towards ARV therapy, while only 23 % had poor attitude (48). They
strongly believed that ARV is efficacious in reducing viral load. On the other hand, a study that
was done in Iringa, Tanzania found that PLHIV and other participants from Iringa viewed ART
positively and considered it highly efficacious, people who were once sick and showed symptoms
of the disease upon initiation of ART their health improved and tend to seek care more and highly
retained. These participants reported that they were able to regain weight relatively quickly and
their fatigue and other symptoms diminished or disappeared (40).

12
2.4.5 Psychosocial Factors (Stigma and Non-Disclosure)
Pervasive stigma and discrimination from family members, friends, and community members have
been identified to contribute to LTFU of PLHIV on treatment (49). Individuals with poor retention
in care, due to stigma or other factors, experience difficulties in achieving a comparable CD4 cell
count, and attainment of survival benefits as compared to those who are retained in care (14).
Disclosure of an HIV-infected status remains an important factor in influencing retention in care
and non-disclosure had more negative consequences for women compared to men (50). Evidence
suggests that participants who report nondisclosure of an HIV status are twice as likely to have
poor retention in care as compared to persons who reported broad disclosure (14). Furthermore,
women experience difficulties in keeping HIV care appointments or adhering to a medication if
they conceal their HIV-positive status (51).
2.4.6 Faith Healing
Pastors who preach the gospel of faith-healing convince many patients to discontinue HIV care,
for the fact that they have been healed when they are prayed for (52). A Tanzanian study found
that many participants tend to abandon biomedical care after heard of others being cured after
pursuing healing in Miracle churches (43), furthermore, one Christian leader, stated that he
encouraged faith healing as a primary approach to treatment with repeat HIV tests to ascertain
efficacy and told congregants to seek biomedical treatment only after prayers (37). In additional,
participants in an Ethiopian study believed that holy water cures HIV, HIV is God’s punishment
and they did not think it is a virus rather it is a devil that only God can cure (53).

13
2.4.7 Use of Herbal Medicine
Some Africans believe in herbal medicines thus tend to abandon treatment in the conviction that
they are cured. The use of herbal remedies were identified as negative influences on retention in
care (38). Some traditional healers convince patients that herbal remedies can cure HIV and AIDS
since they help to boost the immunity (38). The most used traditional medicines are moringa leaves
and aloe vera juice (52). These influence the health seeking behavior of patients leading to
discontinuation of ART treatment and thus poor retention (54). A Malawian study reported that
the use of herbal medicine is reduced in urban areas compared to rural areas at 59% (55). It also
found that a larger proportion (73%) of herbal medicine users were women (55). This indicate
that despite the use of herbal medicine, women are more retained in care than men.
2.4.8 Family and Social Support
Social and family support is a strong pillar to stay in care. Family supports financially and in terms
of nutrition, ensures a balanced diet, and also provides moral support to their beloved ones, family
influence retention in care through a reminder on clinic dates, and taking of medicines (56). Lack
of family support was associated with poor retention among adolescents in a Tanzanian study (29),
while the support provided by the family has been highlighted as a necessity for a person with
HIV/AIDS because they feel supported from the family and accepted as a member of it, valid and
non-discriminated (57). Without family support, PLHIV said that their life would end and there
will be no reason and hope to fight HIV/AIDS (58). These findings were similar to another study
done in Yunnan China, which found that all of the participants were in great need of help and the
primary source of support came from their families (57). Family support included financial

14
assistance, support in the disclosure process, daily routine activities, medical assistance, or
psychological support (44).
2.5 Conceptual Framework
The conceptual framework for this study identifies factors for retention such as: health system
factors, community-based interventions, education factors, positive perception on ART, distance
to the clinic and transportation costs, stigma and non-disclosure, faith healing, and use of herbal
medicine and family and social support. The study examined the health systems, community
factors, educational, perceptions, stigma and discrimination as independent variables affecting the
retention, as dependent variable, in care among people living with HIV/AIDS in Ubungo
municipality, as presented by figure 1; the study conceptual framework.

15
Independent variables Dependent Variable
Figure 1: Conceptual framework
Source: Researcher’s Own Construct (2021)
Faith healing and use of herbal medicine
Family and social support
Health system factors
Stigma and non-disclosure
Community based interventions
Distance to the clinic and transportation
costs.
Positive perception on ART
Education factors
Retention in care

16
Chapter Three: Research Methodolody
3.1 Study Design
The study was a convergent mixed- methods cross-sectional study (59). The design was chosen
because it allowed the collection of data on several cases at a single point in time to collect a body
of quantitative and qualitative data. The qualitative component explains and complement the
quantitative approaches (60). The quantitative approach followed a health facility-based cross-
sectional study using an interviewer-administered questionnaire for participants for specific
objective 1; to determine the proportion of people retained in care among HIV positive participants
attending health centres in Ubungo Municipality for HIV/AIDS care. The qualitative approach
used a descriptive design and employed in-depth interviews with the participants, and Key
Informants Interview (KII) with HCWs, to assess the status of retention in care among
PLHIV/AIDS and to identify factors facilitating or limiting uptake of care among PLHIV/AIDS.
3.2 Study Site
The study was conducted in Ubungo municipal, one of the municipalities that constitute the city
of Dar es Salaam, Tanzania’s major business city. The municipal has a total area of 260.40km2, it
is bordered by the Kibaha District to the North, Kinondoni District to the South-East, and Kisarawe
District to the West (fig.2). The municipality is well linked by roads to other parts of the country.
Major road links are Morogoro road, Mandela Road, and Sam Nujoma Road. Administratively, it
is divided into fourteen 14 wards, which in turn are sub divided into 91 sub wards.

17
According to the 2012 population census, 845,368 people were living in Ubungo of which 409,149
were males and 436,219 females. This population grows at a rate of 5% each year and was
projected to be 1,031,349 in 2016 with 4,911 persons per square kilometers.
The municipal is estimated to have 257,837 households with an average of 4 persons per
household. The social-economic activities of people in Ubungo involve agricultural activities and
livestock keeping, small businesses, and fishing.
Ubungo municipal council is responsible for providing health services to its people in collaboration
with private sector services providers. It has a total of 68 health facilities of which 17 are
government-owned while the remaining 51 are owned by private organizations. Categorically,
Ubungo has a total of 5 hospitals, six health centers, and 57 dispensaries. All the health facilities
provide promotive, preventive, and curative care services. Currently the correct data on HIV/AIDS
prevalence and retention rate specifically for Ubungo municipality is lacking and will be
ascertained by this study.
The study was done in three health facilities in Ubungo municipality which were Sinza hospital,
Mbezi health center, and Kimara Central dispensary. These health facilities were chosen because;
firstly, the geographical distribution allowing easy accessibility to the majority of participants in
Ubungo municipality, secondly, a high population density within facilities catchment area
permitting high risk for acquiring HIV/AIDS and the third reason was health facility which
relatively serves many HVI/AIDS patients than others in Ubungo municipality

18
Figure 2: (A) A Map of Tanzania showing regions, (B) Map of Dar es salaam Region showing
Municipals, and (C) Map of Ubungo Municipality showing study health facilities
3.3 Study Population
HIV positive individuals aged 18 to 59 years receiving care at Kimara Dispensary, Mbezi Health
Centre and Sinza Hospital for more than six months since their enrollment in care.

19
3.4 Eligibility Criteria
3.4.1 Inclusion Criteria for HIV/AIDS Participants
1. HIV positive adults aged 18 to 59 years
2. Attending care and treatment clinic in Kimara Dispensary, Mbezi Health centre and
Sinza Hospital for six or more months
3. Able and willing to give consent to participate in this study.
3.4.2 Exclusion criteria for HIV/AIDS participants
1. Less than 18 years of age patients – because the researcher, wanted to study adults
so <18 years are not adults.
2. Newly enrolled in care clients (less than six months) - they will not have met
retention criteria according to Tanzania National guideline.
3.4.3 Inclusion Criteria for HCW’s
1. Doctors and nurses working in Care and Treatment center (CTC), with at least six
months’ experience working in CTC clinic.
3.4.4 Exclusion Criteria for HCW’s
1. New doctors and nurses, with less than six months- Do not have much experience
on retention.
2. Doctors and nurses who are not working in Care and Treatment center. Do not have
experience on retention.

20
3.5 Study Period
The study was conducted for 20 months. It started in April 2020 with proposal writing to December
2021 which will be the submission of the dissertation. (Appendix 8). The data collection was done
between May and July 2021.
3.6 Sample Size
3.6.1 Sample Size for Quantitative Component
The total number of study participants planned was 389 obtained using WHO formula for sample
size determination in health studies (42), however a total of 365 people living with HIV/AIDS
were interviewed.
Sample size was calculated as follows:
Sample size (n) =(𝑍2𝑃 (1−𝑃)
𝑒2 )
Sample size (n), whereas n is the desired minimum sample size, Z = Level of confidence interval
at 1.96 and e =Degree of accuracy at 0.05
P= Proportion of retention among people living with HIV/AIDS, (54.5%) taken from a study done
by Paul Mee on Changes in patterns of retention in HIV care and Antiretroviral treatment in
Tanzania between 2008 and 2016 (8).

21
The sample was divided, proportional to the number of consultations among the three health
facilities Kimara dispensary, Mbezi Health Center and Sinza Hospital.
3.6.2 Sampling for Qualitative Component
A purposive (61) sample of 18 health care providers was randomly selected as Key Informants;
drawn from the care and treatment centres; including 6 nurses, 6 doctors and 6 laboratory staff.
The 18 were further divided and translated into two for each health worker category per facility.
In the similar manner, the researcher randomly selected participants for in-depth interview; six
from each of the three-health facility, from among the participants attending the CTC services.
3.7 Sampling Procedure
3.7.1 Quantitative Method
We employed a systematic sampling approach (62). Seven working days were allocated for data
collection. The total number of HIV/AIDS consultations for seven days were 3864 (25.2%), 6762
(44.1%), and 4704 (30.7%) for Kimara, Mbezi and Sinza, respectively; equals to 15 330
consultations at the three facilities for one week. In the similar manner, the researcher divided the
sample size among the three health facilities; each facility based on the proportionate number of
HIV/AIDS consultations, the higher the consultation the higher the proportion of the sample size.
As such the sample per facility was 92 (25.2%), 161 (44.1%) and 112 (30.7%) for Kimara
dispensary, Mbezi Health Center and Sinza Hospital, respectively. To determine the daily sampling
interval, at every facility, the total number of estimated consultations for seven days was divided
by seven days, and the total sample size. Hence, every sixth HIV/AIDS client in the queue was

22
approached for consent to participate in the study those who were voluntarily willing to participate
in the study were accepted. In case the consent was denied, the next patient was chosen.
3.7.2 For Qualitative Method
At every health facility, a promotional talk was done at Care and Treatment Clinic (CTC), staff
meeting on Monday. Subsequently, randomly selected 6 health care providers and 6 clients from
each facility as KII and for in-depth interviews, respectively. The principal investigator conducted
these interviews for seven days as the research assistants did the quantitative interviews.
3.7.3 Pre-Testing of Study Tools
The questionnaire, the key informant, in-depth interviews topic guides, were pretested among 10
potential participants, 5 HCW and 5 participants, respectively. The pilot testing of these study tools
was conducted at the study in Sinza Health Centre; a center different from where the actual study
was conducted. The researcher did appropriate corrections of the study tools for questions
ambiguity and correctness. The researcher also tested the voice recording quality of the Sonny
Digital recorders.
3.8 Data Collection Tools
A topic guides for participants, key informant interview with HCW’S and in-depth interview with
participants was used (Appendix 2).

23
3.8.1 Questionnaire
Quantitative data was collected using Interviewer administered questionnaire, developed by the
investigator. Two trained research assistants and the principal investigator (Appendix 2.2),
interviewed the participant using the paper-based questionnaire in Swahili language.
3.8.2 The Validity and Reliability of the Quantitative Data (Questionnaire)
Lincoln and Guba argue that ensuring qualitative data credibility (internal validity) is one of the
most important factors in establishing trustworthiness (63). Internal validity was observed by using
standard data collection tools that was pre-tested and used during the data collection. Apart from
that data collection tools were translated into Swahili language which was used to conduct the
interviews.
The reliability of the tools was assured by using competent research assistants and pre-testing of
the tools. All research assistants were trained and get familiarized with the research objectives and
data collection tools. On each day after data collection, the principal researcher reviewed the
collected data to check for ambiguities and the necessary adjustment was made.
The researcher also ensured data dependability by keeping the detailed records that would provide
room for another researcher to conduct a similar study within the same context and replicate
results. The researcher ensured face validity by developing the questions that answered the
research objectives. In addition, to produce valid results, the content of data tools and methods
used cover all relevant parts of the subject it aims to measure.

24
3.8.3 Key Informant Interview
The key informant interview was conducted among health care workers working in CTC clinics,
using the interview guide (Appendix 2.6) on the topic related to retention in care. It involved
medical doctors, nurses and laboratory technician. Six HCW’s from each health facility was
interviewed using Swahili language. The researchers recorded the interview using the Sonny
Digital recorders.
3.8.4 In-depth Interview
The interview was conducted among HIV/AIDS adult aged 18-59 years attending clinic in the
selected health facilities (Appendix 2.4), from each health facility six participants was selected.
The interview was conducted using the interview guide on a topic related to retention in care, using
Swahili language and the recording was done.
3.8.5 Credibility, Transferability, Confirmability and Dependability Of The Qualitative
Tools
The credibility of the qualitative data collected was achieved through, persistent observations and
data collection triangulation (Key informant and In-depth interviews) and data sources (PLHIV
and health care workers). We employed member checking through reading the summary of the
findings to the participants and asked if that was a true reflection of their opinions, to ensure
accuracy (61). The researcher ensured data confirmability by documenting the procedures for
checking and rechecking the data throughout the study and by keeping the audit trail of all the
documents, that were used from the start of research to the reporting of findings (64). Data
dependability was ensured by keeping the detailed records that can be used by another researcher

25
to conduct the similar study (65). Also, the researcher described the research methods adequately
to help the future researcher do the same. Again, the researcher provided thick description of the
research content to give room for those wishes to transfer the results in a different content (63).
3.9 Data Management
All questionnaires and tapes, which were given to research assistant, were counted and signed by
the principal investigator at the back for easy identification as original copies. The research
assistant returned the questionnaires to principal investigator daily. Upon their receipt, they were
counted and checked, to ensure maximum security of data; they were stored safely in the data
storage box whose access was limited to principal investigator. Soft copy of data was stored in
principles investigator’s computer and backed-up in her flash disk. At the end of the study, all the
study materials were placed in a box secured for verification during data analysis.
3.10 Data Analysis
3.10.1 Quantitative Data Analysis
The researcher coded the responses and entered the data in the Microsoft Excel 2010 spreadsheet.
The data was exported to Statistical Package for Social Sciences (SPSS), version 20 software for
analysis. The principal researcher generated a list of queries in the data cleaning processes. In
addressing the dataset queries, the researcher and research assistants when back to the
questionnaire for missing data imputation and collecting wrong entries. Descriptive and
exploratory analysis was done to summarize data using means, median and standard deviation, and
proportions for continuous and categorical; variables, respectively. The association between
dependable variable (Retention in care) with, age, gender, education level, marital status and

26
occupation and independent variable, the chi-square test was used. A p-value of less or equals to
0.05 was considered statistically significant.
3.10.2 Qualitative Data Analysis
Data was digitally recorded, transcribed verbatim, focusing on the verbal conversation, translated
from Swahili to English. Using thematic analysis as described by Braun and Clarke (2006) (66),
both the KII and in-depth interviews were analyzed using the following steps:
The first step included familiarization with the qualitative data collected by the researchers from
Kimara Dispensary, Mbezi Health Center and Sinza Hospital. Each research assistant and the
research submitted the field notes for qualitative interviews to the principal researcher. Since the
interviews were conducted in Swahili, the principal researcher transcribed, starting with the KII
interviews for all 18 -individual recording, creating 18 different Microsoft word files. This process
was repeated for the 18 in-depth interviews.
The second step was coding process, the researcher used both inductive and deductive coding
approaches. She started deductively with a set of codes that were derived from the research
questions, but then inductively came up with new codes and iterate them as sifting through the
data. The researcher manually wrote beside the printed text the possible interesting data elements,
line by line, for all 18 KII transcribed individual notes, prior moving the 18 in-depth interviews.
After all, data have been coded and collated, the researcher aligned the codes to the pre-determined
themes (Table 1).

27
Table 1: Retention in care pre-determined themes for qualitative component
The third step involved sorting of various codes into potential themes and sub-themes by bringing
together related codes to form comprehensive themes using a table. In step four, themes were
reviewed and refined by considering both internal homogeneity and external heterogeneity to
ensure meaningful coherence of the data within themes.
The fifth step involved, defining and naming of themes, this involved identification of what each
theme is about and determining aspects of the data captured by each theme. Lastly, a concise,
coherent, logical and no repetitive descriptive report of thematic analysis was produced.
THEMES SUB - THEMES
Health system factors Good health care services
Short time to be attended
Privacy of the clinic
Community based services
Clinic date reminder
Shortage of staffs
Drug stock out
Pill count
Social factors Stigma and discrimination
Use of herbal medicine
Faith healing
Travel distance and transportation costs.
Personal factors Lack of disclosure

28
3.11 Presentation of Results
Quantitative findings were summarized in statistical tables, histograms and pie charts. Data from
qualitative component were presented and discussed as poignant quotes and or most representative
of the research findings.
3.12 Dissemination of Results
The researcher will disseminate the results of this study in writing and presentations to all health
care facilities in Ubungo Municipality. Recommendations will be made to all decision-makers and
policymakers at Ubungo municipality health facilities, Medical Officers office, and local
implementing partner Management and Development for Health (MDH) on improvements that
need to be made to improve retention in care among people living with HIV/AIDS. Also,
dissemination of results will be made to the University of Malawi College of Medicine senate, to
College of Medicine Research Ethics Committee (COMREC), and the National Institute of
Medical Research in Tanzania (NIMR). Copies will be made available at the COM library and
department of Public Health. At some point, the results from this study will be published in a peer-
reviewed open-access journal.
3.13 Ethical Consideration
The permission to conduct the study was obtained from both College of Medicine Research Ethics
Committee (COMREC), IRB number P.04/21/3294 (Appendix 5) and National Institute for
Medical Research in Tanzania (NIMR), IRB number NIMR/HQ/R.8a/Vol.IX/3615. (Appendix 6)
Permission to conduct research in health centres and hospital which are under Ubungo municipal
council was sought from the Municipal health authority (Appendix 7). In addition, written consent

29
was sought from the participants. The consent form was developed in English and translated into
Swahili language. We encouraged voluntary participation and the participants were assured that
they will not be penalized nor lose any access to medicals services that they receive should they
withdrawal from the study at any point in time. We anonymized all identifiers and identified the
participants using codes a way of safeguarding their privacy and confidentially. For an illiterate
person, the impartial witness was involved after the person had voluntarily agreed to take part in
the study.

30
Chapter Four: Results
4.1 Introduction
This chapter presents and discusses both descriptive and inferential findings from the study. In
descriptive analysis frequency tables and charts were produced to describe the study area,
characteristics of people living with HIV/AIDS, health factors and status of retention of the people
living with HIV/AIDS. The qualitative interviews results are presented as summary points after
quantitative findings with quotations from respondents drawn from the KIIs and In-depth
interviews, in italics.
4.2 Social Demographic Characteristics of the Participants
4.2.1 Quantitative Interviews Participants
In total, 365 participants responded to the questionnaire; 92 (25.4%), 161 (44.2%) and 112 (30.3%)
from Kimara dispensary, Mbezi Health Center and Sinza Hospital, respectively. Demographic data
shows that majority (32.3%) of respondents were aged 46 years and above followed by those aged
36 to 45 years (Table 2).

31
Table 2: Sociodemographic characteristics of participants in quantitative component
Variable Response Frequency Percentage
Age
Sex
13-25 39 10.7
26-35 93 25.5
36-45 115 31.5
46 and above 118 32.3
Total 365 100
Female 258 70.7
Total 365 100
Education Level No Formal Education 25 6.8
Primary 223 61.1
Secondary and above 117 32.1
Total 365 100
Occupation Employed 64 17.5
Self Employed 245 67.1
Entrepreneurship 53 14.5
Unemployed(dependent) 3 0.9
Total 365 100
Marital Status Single 140 38.4
Married 125 34.2
Divorced 21 5.8
Separated 43 11.8
Widowed 36 9.9
Total 365 100
Monthly Income Less than 10000 23 6.3
10001-50000 1 0.3
50001-100000 2 0.5
100001-200000 48 13.2
More than 200000 291 79.7
Total 365 100
4.2.2 Characteristics of Participants in the Qualitative Component
In total 18 key informants were interviewed. Equal number of doctors, nurses and laboratory
technicians were interviewed. The in-depth interviews involved 18 participants (Table 3).

32
Table 3: Social and demographic characteristics of KII and in-depth interviews participants
Key Informants Interviews
Sex
Male 8
Age (Mean, range) 32 (28-50)
Education
Tertiary level 18
Occupation
Doctors 6
Nurses 6
Lab technician 6
In-depth interviews
Gender
Male 6
Age (Mean, range) 36 (22-49)
Education
No formal education 1
Primary 8
Secondary 9
Occupation
Employed 6
Self employed 12
4.3 HIV Status Disclosure and Clinic Appointments
The majority (92.1%) of the participants interviewed had disclosed their HIV status, whereas, 7.9%
have not disclosed their HIV status (Table 4). It was reported that the majority (63.8%) of the
participants revealed that they were seeking for comfort as the main reason for disclosing their
HIV status. In addition, only 2.5% mentioned that need of financial support was reason for
disclosing their HIV status (Table 4). Furthermore, 18.9% had ever missed appointment in the past
six months.

33
Table 4: HIV status disclosure and clinic appointments attendance
Variable Response Frequency Percentage
Status of HIV disclose Yes 336 92.1
No 29 7.9
Total 365 100
Reasons for disclose HIV status Seeking for Comfort 233 63.8
Need of Financial Support 9 2.5
Any Other (my family members) 124 33.2
Total 365 100
Reasons for non-disclose of HIV
status
Stigmatized and Discriminated 348 95.3
Divorced 3 0.8
No Reason 5 1.4
Other Reasons 9 2.5
Total 365 100
Ever missed clinic appointment Yes 69 18.9
No 295 81.1
Total 365 100
Number of times missed clinic
appointments
Once 355 97.3
Twice 5 1.4
Thrice 2 0.5
More than thrice 3 0.8
Total 365 100
Awareness of health risks in
missing clinic appointments
Yes 334 91.5
No 31 8.5
Total 365 100
Counseled on the dangers of
missing appointments
Yes 319 87.4
No 46 12.6
Total 365 100
Reasons for missing clinic
appointment
Forgetfulness 337 92.3
My health has improved 8 2.2
Attend to Traditional Healers /Prayers 3 0.8
Others (use of herbal medicine) 17 4.7
Total 365 100
Also, about 33% of the participants interviewed in the study area mentioned other issues as reasons
for disclosing their HIV status apart from seeking for comfort and need of financial support. The
majority (95.3%) of the participants interviewed in the study area revealed that stigmatization and
discrimination was the main reason for not disclosing their HIV status (Table 4).
Participants in the indepth interview stated that non-disclosure occured as a measure of concealing
their status at their work places and from their marital partners. Participants further states that

34
consequently they miss their clinic appointment dates for fear of indirectly disclosing their status.
The clinic starts from Monday to Friday at 7:30A.M to 3:00 P.M. at this time I will be at
work, and therefore it makes hard for me to ask permission from my boss, as the genuine
reason for me to attend the clinic is not known (Participant 1 - IDI)
For me I am living with my husband and I have not disclosed my status to him, so whenever
he is at home and it’s my clinic day, I fail to come, unless I lie to him for other reasons
(Participant 4-IDI)
One woman mentioned that he has not disclosed her status to her husband due to fear of
separation. She depends on her husband for the living costs and so she is afraid when she
discloses her status to him, he might leave her and she will suffer as she has no other
support (Participant 2- IDI).
During the indepth interview with the participants, confidentiality and self stigimatisation were
factors that prevented one from disclosin an HIV infected status.
When I come here. I meet with people who know me, they tend to spread the news in the
community and people starts to gossip about me. So this made me to move to another clinic,
where no one knows me (Participant 3- IDI)

35
My sister in law works here as the nurse, initially I didn’t know whether she works here
until when I saw her one-day attending patients. I thank God she didn’t see me, I left the
clinic and moved to a far way clinic. If she knew I am HIV positive, she will go tell my
husband and their family will abandon me (Participant 7- IDI).
Self stigmatisation remained the main concern during the key informant interviews, a inner thought
of being descriminated due to thier HIV statuswhether implicity. Examples of this are explained
by the following statements,which make the disclosure of ones status impossible:
The patients themselves, have inner stigma, whatever you do to them accidentally, they
think it is because of their status (HCW 6- KII)
In short, this people living with HIV/AIDS, they have self-stigmatization, because even
when you mistreat them unfortunately, they think it’s because of their positive status. (HCW
10- KII)
During an indepth interview, many participants mentioned reasons for not disclosing and only
few mentioned that they had to disclose their status to family members.
We are only two in my family, so I cannot hide any thing from my sister, I had to tell her
the truth that I am HIV positive(Participant 5- IDI).

36
I disclosed my status to my family,as they have to know what’s going on with me, and also
to support me. I am not financially stable, I depend on my brother for financial support.
(Participant 4- IDI )
During quantitative interviews, the small proportion (18.9%) reported ever missed appoitment, and
when they did, the majority (97.3%) of the participants reported missing clinic appointment once,
1.4% missed clinic appointment twice while 0.8% missed clinic appointment more than thrice
(Table 4). The majority (92.3%) reported forgetfullness as the main reasons for missing clinic
appointment, while being aware of risks of missing appointment was reported by another 91.5%
of the participants (Table 4). Also, the majority (97.5%) did not access ART services during missed
appoitment period.
The main reason for me missing my clinic appointment is because, I have not disclosed my
HIV status to my husband, so whenever he is at home, and it is my clinic day I fail to come
(Participant 9- IDI).
Another participant, reported that I have not disclosed my HIV status to my Boss, so if I
am at work and it’s my clinic day, hence I fail to come. Because I cannot ask permission
every month to attend the clinic appointment as this may irritate my boss.
Other factors that were mentioned during qualitative interviews as reasons for missed appointment
were divine powers and traditional healers. The health care workers said it is very hard to counsel
them to come back, their minds tend to be washed away by these apostles

37
I know a friend of mine, who stopped using ARV’S and went to seek healing in this miracle
churches, later the situation was very bad and she ended up dying. (HCW 10)).
Some of the clients tend to attend to traditional healers and come to the hospital when the
situation is very bad. (HCW 12)
During in-depth interviews, some participants mentioned ARVs side effects such as tiredness and
weakness as a reason for stopping care and treatment. Some mentioned that they become so strong
they make you to eat a lot and the economy is not so well. Example:
Once I started using these drugs I became so weak, I can’t go to work anymore and I am
failing to do my usual activities, so I decided to stop them and continue with my herbal
drugs. (Participant 13- IDI).
On the other hand, during in-depth interview some participants mentioned that, the use of drugs
makes them feel healthy and strong. That they believe in taking drugs and they don’t wish to stop.
Since I have started using these drugs, I felt healthy and secure, drugs make me feel strong
and energetic that I don’t want to stop using them. I have never fall sick, my CD4 are good,
and currently my viral load cannot be detected (Participant 1- IDI)
4.4 Rentention: Ever Missed Appoiment for Six Months Or More, And ART
Continuity
The study shows that the majority (96.4%) of the participants ever missed follow up care and

38
treatment for less than 3 months; 1.1% for 3 – 6 months, while 2.5% for more than 6 months (Table
5). Some participants (40.8%) mentioned being reminded to take drugs during the period of lost to
follow up, 16.7% given social support, while 15.3% were reminded to attend appointments. The
majority (95.6%) of the participants mentioned that their health conditions were well during the
lost to follow up care and treatment period, 3.3?% they got sick during the lost to follow up care
and treatment, and only 1.1 % reported were always sick during the lost to follow up care and
treatment (Table 5). However, regarding access to ARVs, (94.8%) of the participants were using
ARVs when they missed clinic appointments and 5.2% were not using ARVs when missed their
clinic appointments.

39
Table 5: Retention, ever missed appointment for 6 months or more and access to ART
Factor Response Frequency Percentage
Ever missed appointment Less than 3 months 352 96.4
3 - 6 months 4 1.1
6-12 months 2 0.5
More than 12
months
7 2.0
Total 365 100
Social support during
HIV/AIDS care and treatment
Reminded to take
drugs
149 40.8
Company to the
clinic
26 7.1
Financial Support 43 11.8
Reminded to attend
appointments
56 15.3
Social Support 61 16.7
Others 30 8.2
Informed on access of other
facilities for treatment and care
Yes 306 83.8
No 59 16.2
Total 365 100
Ever sought care and treatment
services from another facility
apart from the one enrolled
Yes 65 17.8
No 300 82.2
Total 365 100
Services sought to other
facilities
Treatment 323 88.4
TB screening
Services
10 2.7
Refill 1 0.3
Others such as 31 8.6
Total 365 100
Preference of being reminded Phone Call 224 61.4
SMS 111 30.4
Home Visits/Home
Based Care 30 8.2
Total 365 100
Clients’ perception towards
health workers in clinics
Good 305 83.5
Average 45 12.3
Stigmatize Clients 7 1.9
Others
(unwillingness to
say )
8 2.3
Total 365 100

40
Of those that sought treatment during the missed appointment period, 17.8% sought care and
treatment services from other facilities apart from the one enrolled in while majority (82.2%)
never sought care and treatment services from other facilities apart from the one enrolled at.
During an Indepth interview the reasons that were mentioned for seeking care and treatment
from other facilities were being away from their usual clinic.
My work involves traveling a lot, at times it is my clinic day and I am far away from my
home. So I attend the nearby clinic to get the services. (Participants 12- IDI)
I only missed my clinic twice, by that time I was in village, I went to attend my mothers in
law funeral and I stayed for a long period (Participants 2- IDI)
Most participants, 61.4%, prefered to receive phone call as a reminder to clinic appointments,
whereas, 30.4% prefered Short Message Service (SMS) while 8.2% prefered home visit/home
based care as a reminder to clinic appointments.Regarding the participant’s perception toward
health workers, the study revealed that (83.5%) of the participants reported good attitude, 12.3%
average attitude (Table 5).
During the in-depth interviews, most of the interviewed participants mentioned that, good
customer care services from the health care workers makes them feel loved and protected.
One woman mentioned that “I come to the clinic because they don’t discriminate me, they
support me and help me in all situations just like others (Participant 6-IDI)

41
Here services are given on time, you don’t stay in queue to wait for services (Participant
17)
Other factors that were mentioned by healthcare workers were, pill count, use of community-based
health care services and putting reasonable number of clients on each clinic day to avoid
congestion.
For new clients, we tend to count their pills to correspond to the next appointment, we
don’t give extra drugs as this may cause abstinence to the clinic and hence poor retention.
(HCW 14)
Introduction of short messages has helped most clients not to miss their clinic. Before it’s their
date, clients receive a short message reminding them on their scheduled clinic.
“They get financial support from the local partner” (MDH).
“Since they have started sending messages to remind us on the clinic, I have never missed
it. At times I used to forget but for now I am happy that they remind us.” (Patient 6)
“We usually call a day before the next appointment to remind them on their clinic date,
surely this has helped to improve retention”. (Healthcare worker).
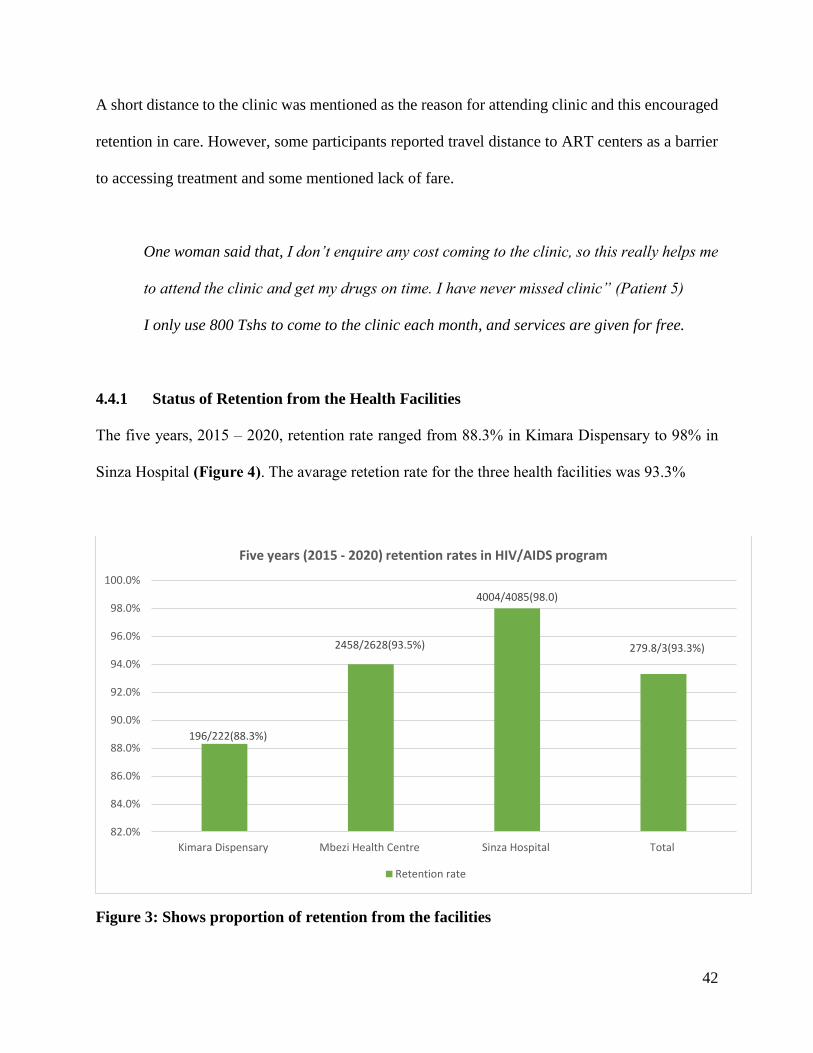
42
A short distance to the clinic was mentioned as the reason for attending clinic and this encouraged
retention in care. However, some participants reported travel distance to ART centers as a barrier
to accessing treatment and some mentioned lack of fare.
One woman said that, I don’t enquire any cost coming to the clinic, so this really helps me
to attend the clinic and get my drugs on time. I have never missed clinic” (Patient 5)
I only use 800 Tshs to come to the clinic each month, and services are given for free.
4.4.1 Status of Retention from the Health Facilities
The five years, 2015 – 2020, retention rate ranged from 88.3% in Kimara Dispensary to 98% in
Sinza Hospital (Figure 4). The avarage retetion rate for the three health facilities was 93.3%
Figure 3: Shows proportion of retention from the facilities
196/222(88.3%)
2458/2628(93.5%)
4004/4085(98.0)
279.8/3(93.3%)
82.0%
84.0%
86.0%
88.0%
90.0%
92.0%
94.0%
96.0%
98.0%
100.0%
Kimara Dispensary Mbezi Health Centre Sinza Hospital Total
Five years (2015 - 2020) retention rates in HIV/AIDS program
Retention rate

43
Table 6: Association between retention to ART care and treatment
Variable Response Retention Status Total Chi-
Square
Value
p-
value Not retained Retained
Age 13-35 3 131 134 0.004 0.951
36 and above 6 225 231
Total 9 356 365
Education
Level
No formal
education
1 38 39 0.953 0.329
Primary and
above
8 318 326
Total 9 356 365
Marital
Status
Not married 6 234 240 0.299 0.584
Married 3 122 125
Total 9 356 365
Sex Male 3 104 107 0.259 0.611
Female 6 252 258
Total 9 356 365
Occupation Employed 3 61 64 2.239 1.35
Not employed 6 295 301
Total 9 356 365
Table 6, shows that there is no significant association between retention status of clients and
charactersitics of clients namely sex, age, marital status, education level and occupation as
indicated with their p-values. All p-values are greater than 0.05. Although, more females
(252/357), a proportion of 71% were retained in care compared to 29% of male, the difference is
not statisitcally significant.

44
Chapter Five: Discussion, Conclusion and Recommendations
5.1 Introduction
The identified factors associated with retention in care were, disclosure of one’s status, reminder
messages on the next clinic appointment, good attitude of health care workers and good customer
care. The pill count method used by health care workers and putting reasonable number of clients
on each clinic day and the use of CBHS. Other mentioned reasons were short distance to the clinic
and reasonable transport cost. Mention reasons for poor retention were nondisclosure,
stigmatization and discrimination, divine powers and the use of herbal medicine.
5.2 Retention in HIV/AIDS Care and Treatment
The rate of retention among adults was above 90% UNAIDS target for 6 months after ART
initiation. This retention rate must be maintained for HIV control. Retained PLHIV are more likely
to achieve viral suppression and tend to have higher CD4 cell counts, thus prevent transmission to
the general population, improve quality of life and less likely to get opportunistic infections which
results in reduced morbidity and mortality. A nearly similar retention rate has been reported
elsewhere in Africa (67). However, the longer the time used to determine retention, the lower the
retention rates reported in Kenya and Ethiopia (9,41,53,67,68). Although the current study did not
report any significant retention rates between men and females, others have reported females being
more likely to be retained in care and treatment than men (6,7), contradicting a higher dropout in
females than males (20). The differences in the maternity care services at Antenatal Clinic (ANC)
and PMTCT programs is pivotal in providing health education to women, including HIV testing
and linkage services to improve retention in care for women. In Haiti, most women who were

45
retained in care had been diagnosed with HIV prior to pregnancy (62%) (69). The differences in
rates of retention between men and women may reflect gender differences in health-seeking
behavior. The cultural perspective makes men seek care very late, consequently late diagnosis and
presentation with advanced HIV disease and increased mortality (53,70).
Retention in care improves survival and HIV viral control, resulting in low morbidity and mortality
(68,71). If high retention is maintained, we can achieve the UN 95-95-95 goals by 2030 (72). In
programs whereby the ART services were brought closer to the populations through community
groups, retention of nearly 100% was reached (73).
5.3 Social Factors Associated with Retention
The study found out that the socio-factors that supported the high rate of retention were disclosure
of one’s status, because of seeking social and financial support. This factors are discussed below.
5.3.1 HIV Status Disclosure
Our study found that 92.1% of the study participants had disclosed their HIV status to their close
relatives and continuously received support to engage in care. A similar percentage of disclosure
was reported in Mwanza Tanzania where two hundred and fifty-two participants (93.3%) had
disclosed their HIV sero-status (74). The disclosure was very low in other studies done in African
setting, only 5% in Ethiopia (75), and remained a primary concern in Malawi during in-depth
interviews (76). In the current study, the high level of disclosure could explain the high retention
rate, as disclosure could be associated with retention (50). Similar to the current study, others have
reported reasons for disclosing one's status, such as seeking social (51,74,77) and financial support

46
(74,78). Disclosure has helped them to be reminded to take drugs and attend appointments.
According to a previous qualitative study done in Zambia by Mukumbag, participants reported
that patients do not disclose their status even to close family members, making it hard for them to
attend clinics and take drugs to keep the secret (38).
The current study reports that patients do not want to disclose their HIV status to their relatives,
their marital partners, or bosses, which has also been reported in Tanzania, Kenya, and Uganda
(51,74). Patients fear that disclosing their HIV may lead to abandonment, discrimination, and
gossip in the community (52). Separation and domestic violence were joint among marital partners,
most women depend on their partners for everything, so when they disclose their HIV status, there
is fear of separation and rejection (77). Participants reported that disclosure of HIV status to family
or friends, although initially tricky, typically resulted in more incredible social support (79).
5.3.2 Stigma and Discrimination
We found that, ninety-five per cent (95%) of participants mentioned the reasons for not disclosing
HIV/status to be stigma and discrimination. This is comparable with other studies that identified
HIV related stigmas as an essential barrier to adherence and retention in care (52), also . in Uganda
stigma was found to be a hindrance to ART access, adherence, and long-term retention in care
(36). Stigma and denial are common feelings for individuals recently diagnosed with HIV,
therefore tend to have difficulties remaining in care (41,80,81). In addition, stigma and HIV status
denial and hence poor retention to care has been shown to be associated with low immunological
status and virological suppression. Similarly, another study conducted in Kenya showed that HIV
positive patients drop out of care because they do not want to be seen in the HIV clinic and risk

47
being seen by someone they know. This stigma and discrimination could cost their social relations,
business openings, and a chance of living in harmony with people in their surroundings (82).
5.3.3 Traditional Healers and Faith Healing
Both patients and healthcare workers reported traditional and faith healing negatively affected
retention in care. Similar findings were reported as personal barriers to ART access by the focus
group discussions and in-depth interviews study conducted in Zambia (38). The use of herbal
medicinal products is very prevalent among patients taking ART; in Malawi reported 17.5% of
ART patients used herbal medicine (55)
Other patients who reported attending new churches were told that the use of anointed oil and holy
water cures HIV/AIDS, and therefore, there is no need to continue with HIV/AIDS services (53).
Patient believe in traditional healers and pastors, and so obey their instructions, so even when you
counsel the patients on the benefits of a continuum of care, their mind has already been eluded.
Participants mentioned ARV’s side effects, such as fatigue, as the reason for using of herbal
medicines, as they make patients fail to do their daily activities (52), also reported by other studies
done in Africa and elsewhere. (20,38,82)
5.4 Structural and Health System Factors Associated with Retention
This study found that 36.7% of the participants spent a bus fare of 1000 Tshs to reach the clinic
and 42.7% spent 1-2 hours to reach the clinic, and 34.5% of participants reached the clinic within
30 minutes. The 1000 Tshs bus fare is affordable to most participants, also the 30 minutes time to
2-hours spent to reach the clinic is not a barrier to retention as most participants mentioned. Lack

48
of transport money and long distance travel , which was not the case with the current study, has
been reported by similar studies (12,38). Urban settings may be at an advantage in accessibility
compared with rural areas (43). In contrast to our results, other studies conducted in Uganda and
Malawi reported lack of transport fare as a barrier to attending the ART care and treatment services
(12,76). Services designs considering the effect of transportation on retention have been
considered effective in increasing retention (21). Economic factors and time spent collecting
medications and transportation charges are among the factors related to retention.
Also, the current study reported a good health care attitude to patients, attributed to adequately
staffed clinics, contrary to what was reported elsewhere in sub-Saharan Africa such as Zambia,
where there are few health care workers to attend patients, patients get tired of waiting and go
home without being seen. (38,42). A qualitative study was done in Ethiopia also reported clinic
overcrowding and workers poor attitude affecting retention, in contrast to our study findings (82).
In recent years, multi-month prescriptions have improved retention through reduced clinic
overcrowding. However, a study that was done in Zambia in 2017 found that , because of the
second-line ART drug shortage, patients were given a one-month prescription (38).
In the current study, participants preferred phone calls reminders rather than short messages, 60%
vs 30%. Short messages reminder acceptability is very low in the current study compared with a
study done in Ethiopia, 30% versus 91% (75). A study conducted in Kenya reported that the SMS
was the effective methods in increasing ART adherence (35); mentioned by both health care
workers and patients as an effective means of retaining clients to HIV and AIDS care. Also, this
has been effective in tracing missed clients and lost to follow up back to care (83). The clients who

49
missed clinics were called after the clinic and asked about the reasons for missing the clinic. Some
mentioned forgetfulness as a reason for the missed appointment, similar to studies done in Malawi
and Kenya (76,83).
The study found that, for those clients who do not want to visit clinic for the fear of being known,
CBHS supply them with all the necessary services such as drug supply, viral load and CD4 sample
collection. These findings are similar to studies conducted in Uganda; the use of Community-based
Health Services (CBHS) played a role in maintaining clients into care through various community
services (84). In some programs, the community health workers or volunteers delivered ART at
home. In Mozambique, a demonstration project of people living with HIV used self-formed
community-based ART groups to deliver ART in the community (85). These community ART
programs made treatment readily accessible and affordable (85). A randomized controlled trial
conducted in Uganda and South Africa reported that the CHBS programs are cost-effective and
without adverse events compared to ART delivery at the clinical setup (84). Good results were
also reported elsewhere where the CBHS was implemented (86). Clients who never wanted to
come to the clinic were receiving HIV care services directly from the community. Community-
based ART programs encourage patient autonomy, build social networks, and minimize the
structural barriers, such as the cost of transport to the clinic, which in turn appear to result in better
outcomes. Community-based delivery of antiretroviral therapy for HIV, including ART initiation,
clinical and laboratory monitoring, and refills, could reduce barriers to treatment and improve viral
suppression, reducing the gap in access to care for individuals who have detectable HIV viral load,
including men who are less likely than women to be virally suppressed (86).

50
5.5 Strengths of the Study
The study used both quantitative and qualitative methods, which enabled us to explore a lot of
factors that are associated with retention in care among PLHIV beyond those that were identified
by quantitative method alone. Hence the study provided valuable insights on factors associated
with retention in care among PLHIV.
5.6 Study Limitations
Despite impressive high retention rate, the researcher failed to trace non-retained patients, which
could have prolonged the study. However, the researcher tried to reach them through phone calls
but proved to be unsuccessful. Because of the design, the self-reported missed appointment and
retention could not be correlated with attendance register records, which would have improved the
data credibility through triangulations.
5.7 Conclusion
The study reports a high rate of retention of PLHIV receiving care and treatment, this was
attributed to the awareness of the alternative clinic to collect the ARVs and the consequences of
missed-appointment. Nonetheless, over two per cent of participants have missed an appointment
for six or more months. The study has revealed the existence of stigma as demonstrated by the
significant proportion of participants who had not disclosed their HIV serostatus for fear of social
and family retribution. Still, a good proportion of participants periodically missed appointments
during the follow-up, citing forgetting the date as a significant reason. However, the continuum of
care was attained among those missing appointments due to knowledge of alternative clinics to
collect their medications.

51
The reminder of the appointment date through mobile short messages was perceived as a
significant breakthrough in minimizing missed appointments. Health workers’ attitudes,
transportation costs did not present as factors affecting retention during interviews. Similarly, other
health systems factors such as staff shortage and long waiting time was mentioned during the in-
depth and key informant interviews and factors that could contribute to reduced retention, did not
strongly come out during individual interviews.
5.8 Recommendations
Recommendations to the policymakers and health care providers:
a. Health care providers and policymakers at various levels of HIV and AIDS Care
treatment should stern the health education information about the importance of
regularly attending the CTC by the patients. The efforts could minimize the
periodically missed appointments of shorter duration hence improving adherence
to ARTs
b. Specific health educations sessions should focus on religious and traditional beliefs
that could affect the retention of services and should equally target both the clients
and the health care providers. Also health care workers should emphasis on effects
of sharing drugs as it can cause non-adherence among clients secondary to
shortages.

52
Recommendations for further research:
a. Further researches, in particular, ethnographic studies, could investigate further the
reasons for the missed appointment of longer than six months and withdrawal from
services
b. Larger and longitudinal studies, particularly cohort studies, which include more
facilities and districts in Tanzania, could demonstrate retention into HIV/AIDS care
and treatment over time rather than a cross-sectional study.

53
References
1. Roscoe C, Hachey DM. Retention in HIV care, basic HIV primary care: National HIV
curriculum. 2020.
2. Ministry of Health, Social Welfare, Gender E and C. National guidelines for the
management of HIV and AIDS. Dar Es Salaam; 2017. Report No.: 6.
3. Crawford TN. Poor retention in care one-year after viral suppression: a significant
predictor of viral rebound. AIDS Care. 2014 Nov;26(11):1393–9.
4. Centers for Disease Control and Prevention. Vital signs: HIV prevention through care and
treatment - United States. Morbidity and Mortality Weekly Report. 2011:60(47):1617-
1623.
5. Horstmann E, Brown J, Islam F, Buck J, Agins BD. Retaining HIV‐infected patients in
care: Where are we? Where do we go from here? Clin Infect Dis. 2010;50(5).
6. Yang GL, Yan J, Liu Y, Huang ZL, Long S. Retention in care and factors affecting it
among people living with HIV/AIDS in Changsha City, China. Asia Pacific J Public Heal.
2015 Mar;27(2 Suppl):86S-92S.
7. Avert. HIV and AIDS in Tanzania. [Internet]. [cited 2022 Feb 28]. Available from:
https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/tanzania
8. Mee P, Rice B, Lemsalu L, Hargreaves J, Sambu V, Harklerode R, et al. Changes in
patterns of retention in HIV care and antiretroviral treatment in Tanzania between 2008
and 2016: an analysis of routinely collected national programme data. J Glob Health.
2019;9(1):1–11.
9. Koole O, Tsui S, Wabwire-Mangen F, Kwesigabo G, Menten J, Mulenga M, et al.

54
Retention and risk factors for attrition among adults in antiretroviral treatment
programmes in Tanzania, Uganda and Zambia. Trop Med Int Heal. 2014;19(12):1397–
410.
10. Nachega BJ. Community-based interventions to improve and sustain antiretroviral therapy
adherence, retention in HIV care and clinical outcomes in low- and middle-income
countries for achieving the UNAIDS 90-90-90 targets. PMC. 2019;5:24.
11. World Health Organization. Global Health Sector Strategy on HIV 2016-2021: towards
ending AIDS. WHO: Geneva; 2016.
12. Tuller DM, Bangsberg DR, Senkungu J, Ware NC, Emenyonu N, Weiser SD.
Transportation costs impede sustained adherence and access to HAART in a clinic
population in Southwestern Uganda: a qualitative study. AIDS Behav. 2010
Aug;14(4):778–84.
13. Stricker SM, Fox KA, Baggaley R, Negussie E, de Pee S, Grede N, et al. Retention in care
and adherence to ART are critical elements of HIV care interventions. AIDS Behav. 2014
Oct 1;18(5):465–75.
14. Roscoe C, Hachey DM. Retention in HIV care: introduction and definitions. 2020.
15. Wichlinski M, Rajaram R. The Use of RONA/WACC as a proxy for investment quality. J
Econ Behav Stud. 2019;10(6A):177–85.
16. Messeri PA, Abramson DM, Aidala AA, Lee F, Lee G. The impact of ancillary HIV
services on engagement in medical care in New York City. AIDS Care. 2002
Aug;14(Suppl. 1).
17. Chi BH, Cantrell RA, Mwango A, Westfall AO, Mutale W, Limbada M, et al. An
empirical approach to defining loss to follow-up among patients enrolled in antiretroviral

55
treatment programs. Am J Epidemiol [Internet]. 2010 Apr 15 [cited 2020 Mar
30];171(8):924–31. Available from: http://www.ncbi.nlm.nih.gov/pubmed/20219765
18. Chi BH, Yiannoutsos CT, Westfall AO, Newman JE, Zhou J, Cesar C, et al. Universal
definition of loss to follow-up in HIV treatment programs: a statistical analysis of 111
facilities in Africa, Asia, and Latin America. PLoS Med [Internet]. 2011 Oct [cited 2020
Mar 30];8(10):e1001111. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/22039357
19. for Disease Control C, of HIV D, Prevention A. Understanding the HIV care continuum
[Internet]. Available from: https://www.cdc.gov/hiv/pdf/library/factsheets/
20. Makunde WH, Francis F, Mmbando BP, Kamugisha ML, Rutta AM, Mandara CI, et al.
Lost to follow up and clinical outcomes of HIV adult patients on antiretroviral therapy in
care and treatment centres in Tanga city, North-Eastern Tanzania. Tanzan J Health Res.
2012;14(4):1–10.
21. Geng EH, Nash D, Kambugu A, Zhang Y, Braitstein P, Christopoulos KA, et al. Retention
in care among HIV-infected patients in resource-limited settings: emerging insights and
new directions. Curr HIV/AIDS Rep. 2010 Nov;7(4):234–44.
22. Damulak PP, Ismail S, Manaf RA, Said SM. Interventions to improve adherence to
Antiretroviral Therapy (ART) in sub-Saharan Africa: an updated systematic review. Int J
Environ Res Public Heal. 2021;18(2477).
23. Enriquez M, McKinsey DS. Strategies to improve HIV treatment adherence in developed
countries : clinical management at the individual level. HIV/AIDS-Research Palliat Care.
2011;3:45–51.
24. UNAIDS. Joint United Nations Programme on HIV/AIDS. AIDS data 2019. UNAIDS.

56
Geneva, Switzerland; 2019.
25. UNAIDS. Joint United Nations Programme on HIV/AIDS. Global data on HIV
epidemiology and response. UNAIDS. 2021.
26. World Health Organization. HIV/AIDS overview. Geneva: WHO:-. 2019.
27. World Health Organization. HIV/AIDS fact sheet: key facts. Geneva: WHO: 2021.
28. Avert. HIV and AIDS in east and southern Africa regional overview. Avert; 2021.
29. Development R. Tanzania Human Development Report. 2000;(February).
30. National AIDS Control Programme. United Repuplic of Tanzania. Ministry of Health,
Community Development, Gender E and C. National AIDS Control Programme. National
guidelines for the management of HIV&AIDS. Dar Es Salaam; 2012. Report No.: 4.
31. Ministry of Health, Community Development, Gender E and C. Mapping HIV service
delivery strategies in Tanzania. Working Paper. Dar Es Salaam; 2017.
32. Centers for Disease Control and Prevention. Monitoring selected national HIV prevention
and care objectives by using HIV surveillance data: United States and 6 dependent areas,
2018. Vol. 25, CDC. HIV Surveillance Supplemental Report; 2020.
33. National HIV/AIDS Strategy (2022-2025) [Internet]. [cited 2021 Dec 14]. Available from:
https://www.hiv.gov/federal-response/national-hiv-aids-strategy/national-hiv-aids-
strategy-2022-2025
34. Rosen S, Fox MP. Retention in HIV care between testing and treatment in sub-Saharan
Africa: a systematic review. PLoS Med. 2011;8(7).
35. Babatunde O, Ojo OJ, Atoyebi OA, Ekpo DS, Ogundana AO, Olaniyan TO, et al. Seven
year review of retention in HIV care and treatment in federal medical centre Ido-Ekiti. Pan
Afr Med J. 2015;22:1–9.

57
36. Muwanguzi M, Lugobe HM, Ssemwanga E, Lule AP, Atwiine E, Kirabira V, et al.
Retention in HIV care and associated factors among youths aged 15–24 years in rural
southwestern Uganda. BMC Public Health. 2021;21(1):1–8.
37. Brown LB, Havliri D V, Ayieko J, Mwangwa F, Owaraganise A, Kwarisiima D, et al.
High levels of retention in care with streamlined care and universal test-and-treat in East
Africa. AIDS. 2017;30(18):2855–64.
38. Mukumbang FC, Mwale JC, Van Wyk B. Conceptualising the factors affecting retention
in care of patients on antiretroviral treatment in Kabwe District, Zambia, using the
Ecological Framework. AIDS Res Treat. 2017;2017.
39. Rachlis B, Bakoyannis G, Easterbrook P, Genberg B, Braithwaite RS, Cohen CR, et al.
Facility-level factors influencing retention of patients in HIV care in East Africa. PLoS
One. 2016 Aug 1;11(8).
40. Janssen S, Wieten RW, Stolp S, Cremers AL, Rossatanga EG, Klipstein-Grobusch K, et
al. Factors associated with retention to care in an HIV clinic in Gabon, central Africa.
PLoS One. 2015;10(10):1–14.
41. Kiwanuka J, Waila JM, Kahungu MM, Kitonsa J, Kiwanuka N, Id JK, et al. Determinants
of loss to follow-up among HIV positive patients receiving antiretroviral therapy in a test
and treat setting: a retrospective cohort study in Masaka. PLoS One. 2020;15(4).
42. Schatz E, Seeley J, Negin J, Weiss HA, Tumwekwase G, Kabunga E, et al. “for us here,
we remind ourselves”: strategies and barriers to ART access and adherence among older
Ugandans. BMC Public Health. 2019;19(1):1–13.
43. Tomori C, Kennedy CE, Brahmbhatt H, Wagman JA, Mbwambo JK, Likindikoki S, et al.
Barriers and facilitators of retention in HIV care and treatment services in Iringa,

58
Tanzania: the importance of socioeconomic and sociocultural factors. AIDS Care.
2014;26(7):907–13.
44. Ronoh, J C. Factors associated with retention in care among HIV positive adults attending
Pumwani Comprehensive Care Centre, in Nairobi County, Kenya (Masters Thesis), Jomo
Kenyatta University of Science and Technology, Kenya; 2018.
45. Joshi K, Jhanwar S, Mathur A et al. Barriers in adherence of ART (anti retroviral
treatment): an experience of ART centre of Western Rajasthan, India [abstract] Presented
at the International AIDS Conference, Mexico City, Mexico, August 3–8, 2008.
46. Murray KR, Dulli LS, Ridgeway K, Dal Santo L, De Mora DD, Olsen P, et al. Improving
retention in HIV care among adolescents and adults in low- and middle-income countries:
A systematic review of the literature. PLoS One. 2017 Sep 1;12(9).
47. Raberahona M, Lidamahasolo Z, Andriamamonjisoa J, Andriananja V, Andrianasolo RL,
Rakotoarivelo RA, et al. Knowledge, attitudes, perception and practices regarding
antiretroviral therapy among HIV-infected adults in Antananarivo, Madagascar: a cross-
sectional survey. BMC Health Serv Res. 2019;19(1):1–9.
48. Afolabi MO, Ijadunola KT, Fatusi AO, Olasode O. Knowledge of and attitude towards
antiretroviral therapy among people living with HIV/AIDS in Nigeria. TAF Prev Med
Bull. 2010;9(3):201–8.
49. UNAIDS. Joint United Nations Programme on HIV/AIDS. Stigma and discrimination
against people living with HIV remains widespread in Asia and the Pacific, report shows.
2011.
50. Umeokonkwo CD, Onoka CA, Agu PA, Ossai EN, Balogun MS, Ogbonnaya LU.
Retention in care and adherence to HIV and AIDS treatment in Anambra State Nigeria.

59
BMC Infect Dis [Internet]. 2019 Jul 22 [cited 2020 Mar 14];19(1):654. Available from:
https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-019-4293-8
51. Brown LB, Getahun M, Ayieko J, Kwarisiima D, Owaraganise A, Atukunda M, et al.
Factors predictive of successful retention in care among HIV-infected men in a universal
test-and-treat setting in Uganda and Kenya: a mixed methods analysis. PLoS One.
2019;14(1):1–16.
52. Mwale JC. Factors affecting retention in care of patients on antiretroviral treatment in the
Kabwe district, Zambia. 2016;(June):1–69.
53. Tiruneh YM, Galárraga O, Genberg B, Wilson IB. Retention in care among HIV-infected
adults in Ethiopia, 2005-2011: a mixed-methods study. PLoS One. 2016;11(6):2005–11.
54. Billong SC, Fokam J, Penda CI, Amadou S, Kob DS, Billong E, et al. Predictors of poor
retention on antiretroviral therapy as a major HIV drug resistance early warning indicator
in Cameroon : results from a nationwide systematic random sampling. BMC Infect Dis
[Internet]. 2016;1–9. Available from: http://dx.doi.org/10.1186/s12879-016-1991-3
55. Mbali H, Sithole JJK, Nyondo-Mipando AL. Prevalence and correlates of herbal medicine
use among anti-retroviral therapy (Art) clients at queen elizabeth central hospital (qech),
blantyre malawi: a cross-sectional study. Malawi Med J. 2021;33(3):153–8.
56. Adelekan B, Andrew N, Nta I, Gomwalk A, Ndembi N, Mensah C, et al. Social barriers in
accessing care by clients who returned to HIV care after transient loss to follow-up. AIDS
Res Ther [Internet]. 2019;16(1):1–7. Available from: https://doi.org/10.1186/s12981-019-
0231-5
57. Xu JF, Ming ZQ, Zhang YQ, Wang PC, Jing J, Cheng F. Family support, discrimination,
and quality of life among ART-treated HIV-infected patients: a two-year study in China.
60
Infect Dis Poverty. 2017;6(152).
58. Qypi K. The importance of family support for individuals with HIV/AIDS. Eur J Soc Sci
Stud. 2017;2(1):111–22.
59. Sandelowski M. Combining qualitative and quantitative sampling, data collection, and
analysis techniques in mixed‐method studies. Res Nurs Health. 2000;23(3):246–55.
60. Johnson RB, Christensen L. Methods of data collection in quantitative, qualitative and
mixed reserach. Educ Res Quant Qual Mix approaches [Internet]. 2017;179–206.
Available from: https://edge.sagepub.com/rbjohnson7e
61. Purposive sampling [Internet]. [cited 2021 Dec 1]. Available from: https://research-
methodology.net/sampling-in-primary-data-collection/purposive-sampling/
62. Kothari CR. Research methodology: methods and techniques. 2nd ed. New Delhi: New
Age International (P) Ltd; 2004.
63. Guba EG. Criteria for assessing naturalistic inquiries. Educ Commun Technol [Internet].
1981;29(2):75–91. Available from: http://eric.ed.gov/?id=ED297007
64. Tobin GA, Begley CM. Methodological rigour within a qualitative framework. J Adv
Nurs. 2004 Nov;48(4):388–96.
65. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis : striving to meet the
trustworthiness criteria. 2017;16:1–13.
66. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol.
2006;3(2):77–101.
67. Kiplagat J, Mwangi A, Keter A, Braitstein P, Sang E, Negin J, et al. Retention in care
among older adults living with HIV in western Kenya: a retrospective observational
cohort study. PLoS One. 2018;13(3):1–12.

61
68. Wekesa P, McLigeyo A, Owuor K, Mwangi J, Nganga E, Masamaro K. Factors associated
with 36-month loss to follow-up and mortality outcomes among HIV-infected adults on
antiretroviral therapy in Central Kenya. BMC Public Health. 2020;20(1):1–11.
69. Dionne-Odom J, Massaro C, Jogerst KM, Li Z, Deschamps MM, Destine CJ, et al.
Retention in care among HIV-infected pregnant women in Haiti with PMTCT Option B.
AIDS Res Treat. 2016;2016.
70. Mburu G, Ram M, Siu G, Bitira D, Skovdal M, Holland P. Intersectionality of HIV stigma
and masculinity in eastern Uganda: implications for involving men in HIV programmes.
BMC Public Health. 2014;14(1061).
71. Stricker SM, Fox KA, Baggaley R, Negussie E, de Pee S, Grede N, et al. Retention in
Care and Adherence to ART are Critical Elements of HIV Care Interventions. AIDS
Behav. 2014;18:465–75.
72. UNAIDS. Joint United Nations Programme on HIV/AIDS. Understanding fast-track
targets: ending the AIDS epidemic by 2030. 2015.
73. Tom Decroo; Barbara Telfer; Marc Biot; Jacob Maı¨ke´re; Sergio Dezembro; Luisa Isabel
Cumba; Carla das Dores; Kathryn Chu; Nathan Ford; Distribution of antiretroviral
treatment through self-forming groups of patients in Tete Province, Mozambique. J
Acquir Immune Defic Syndr [Internet]. 2011 Feb 1 [cited 2021 Oct 21];56(2). Available
from: https://pubmed.ncbi.nlm.nih.gov/21084990/
74. Yonah G, Fredrick F, Leyna G. HIV serostatus disclosure among people living with
HIV/AIDS in Mwanza, Tanzania. AIDS Res Ther. 2014;11(1):1–5.
75. Endebu T, Deksisa A, Dugasa W, Mulu E, Bogale T. Acceptability and feasibility of short
message service to improve ART medication adherence among people living with

62
HIV/AIDS receiving antiretroviral treatment at Adama hospital medical college, Central
Ethiopia. BMC Public Health. 2019;19(1):1–11.
76. Chirambo L, Valeta M, Banda Kamanga TM, Nyondo-Mipando AL. Factors influencing
adherence to antiretroviral treatment among adults accessing care from private health
facilities in Malawi. BMC Public Health. 2019;19(1):1–11.
77. Arrey AE, Bilsen J, Lacor P, Deschepper R. “It’s my secret”: fear of disclosure among
sub-Saharan African migrant women living with HIV/AIDS in Belgium. PLoS One.
2015;10(3):1–22.
78. Li L, Wu S, Wu Z, Sun S, Cui H, Jia M. Understanding family support for people living
with HIV/AIDS in Yunnan, China. AIDS Behav. 2006;10(5):509–17.
79. Abdallah S. Factors Associated with retention in care among patients receiving
antiretroviral therapy at Pantang Hospital, Ghana. University of Ghana; 2018.
80. Auld AF, Pelletier V, Robin EG, Shiraishi RW, Dee J, Antoine M, et al. Retention
throughout the HIV care and treatment cascade: From diagnosis to antiretroviral treatment
of adults and children living with HIV - Haiti, 1985-2015. Am J Trop Med Hyg.
2017;97(Suppl 4):57–70.
81. Ruria EC, Masaba R, Kose J, Woelk G, Mwangi E, Matu L, et al. Optimizing linkage to
care and initiation and retention on treatment of adolescents with newly diagnosed HIV
infection. Aids. 2017;31(May):S253–60.
82. Lifson AR, Demissie W, Tadesse A, Ketema K, May R, Yakob B, et al. Barriers to
retention in care as perceived by persons living with HIV in rural Ethiopia: focus group
results and recommended strategies. J Int Assoc Provid AIDS Care. 2013;12(1):32–8.
83. Lester RT, Ritvo P, Mills EJ, Kariri A, Karanja S, Chung MH, et al. Effects of a mobile
63
phone short message service on antiretroviral treatment adherence in Kenya (WelTel
Kenya1): A randomised trial. Lancet. 2010;376(9755):1838–45.
84. Barnabas R V., Szpiro AA, van Rooyen H, Asiimwe S, Pillay D, Ware NC, et al.
Community-based antiretroviral therapy versus standard clinic-based services for HIV in
South Africa and Uganda (DO ART): a randomised trial. Lancet Glob Heal.
2020;8(10):e1305–15.
85. Decroo T, Rasschaert F, Telfer B, Remartinez D, Laga M, Ford N, et al. Community-
based antiretroviral therapy programs can overcome barriers to retention of patients and
decongest health services in sub- saharan africa: a systematic review. Int Health. 2013
Sep;5(3):169–79.
86. Mukherjee JS, Barry D, Weatherford RD, Desai IK, Farmer PE. Community-based ART
programs: sustaining adherence and follow-up. Curr HIV/AIDS Rep [Internet].
2016;13(6):359–66. Available from: http://dx.doi.org/10.1007/s11904-016-0335-7
64
Appendices
Appendix 1: informed consent forms
Appendix 1.1: Informed consent form for HIV/AIDS patients in English
Study Title: Factors associated with retention in care among people living with HIV/AIDS in
Ubungo municipality, Tanzania.
Principal Investigator: Dr. Sylvia D. Moshi, a student of Master’s of Science in Public Health,
University of Malawi, College of Medicine
Research Supervisor: Dr. Linda Nyondo-Mipando and Dr. Joan Rugemalila
PI Version date: 2.0, March 24, 2021
Hello, my name is Sylvia D. Moshi and I am a student at the University of Malawi, College of
Medicine), I am conducting a study on Factors associated with retention in care among people
living with HIV/AIDS in Ubungo Municipality. I would like to seek your permission to participate
in this study, please read the consent form below.
Introduction and Purpose of the Study
This study seeks to determine proportion of people retained in care, and to asses factors associated
with retention in care among people living with HIV/AIDS in order to help find ways that would
improve retention in care among them and entire program.
Procedure
If you agree to take part in this study; Firstly, you will be asked to sign a consent form. You will
also be asked to fill in a questionnaire with the help of a trained research assistant. The interview
will not take much of your time and it will be done once. The interview will be face to face and
will also be digitally recorded. You will decide on which day and place you will be comfortable
with to have you interviewed. The study team will maintain your privacy and confidentiality at
any place that you will choose.
Secondly, we will collect some information about you such as age, tribe, religion, where you live,
and nature of your work, and also we will conduct the interview and discussions on the Factors
associated with retention in care among people living with HIV/AIDS in Ubungo municipality.

65
Risks
We do not anticipate that participation in this study will pose any physical or psychological risks
beyond what you encounter in everyday life. However, participation in this study is voluntary and
if you are uncomfortable answering a particular question, you are free to not to answer the question,
and you are free to leave the study at any time.
Benefits
The information you provide to the investigator will shed light on the factors associated with
retention in care among people living with HIV/AIDS, and the study results will assist us in
informing PLHIV, representatives of Ubungo Municipality and other stakeholders to help improve
retention among PLHIV and develop suitable strategies.
Costs and compensations:
There are no costs associated with this study. Please note that you will not receive any money for
participating in this study. You can decide not to take part in this study, and this will not affect you
in any way.
Privacy and Confidentiality:
The interviews will be conducted in a private place where no one can hear our conversation. Some
questions may be sensitive and you are encouraged not to answer, however we would like you to
answer all questions. Any information given to this study will be kept confidential. Your name
will not be used in any report coming from this study, you will be using a code. The questionnaires
and the consent form will be safely kept in a lockable cabinet accessed only by the study staff that
is the researcher, the study supervisor and COMREC. The information collected will remain
confidential. All research material will be submitted to Kamuzu University of Health Sciences
(KUHES), for official documentation purpose and they will be destroyed upon completion of the
study or when requirements are met.
Other Information
In case you have any questions you can contact the investigator Dr. Sylvia D. Moshi on +255 767
041648 or Supervisors. Dr. Joan Rugemalila on +255 784 660 517 and Dr. Linda Nyondo
Mipando on +265 999 44 12 12 and NIMR representative on +255 758 587885.
Your signature below shows that you understand the above statement and willingly agree to
participate in the study.
This consent form has been read and explained to me. I voluntarily consent to participate in this
study:
Signature: Study participant
____________________ Date: ________________________

66
OR
Thumb print………………………………. Date……………………..
Witness: Signature: …………………… Date: ……………………………
I have explained the study for the above subject and I have sought his/her understanding for
informed consent
Signature: ____________________ Date: _______________________
(Research assistant)
THANK YOU FOR YOUR TIME AND PARTICIAPTION
67
Appendix 1.2: Informed consent form for HIV/AIDS patients in Swahili
Kichwa cha utafiti: Sababu zinazohusiana na wateja wa UKIMWI kudumu kwenye huduma katika
manispaa ya Ubungo.
Mtafiti: Dk. Sylvia D. Moshi, mwanafunzi wa uzamili katika chuo kikuu cha Malawi.
Msimamizi: Dk. Linda Nyondo Mipando na Dk. Joan Rugemalila
PI TOLEO LA TAR: 2.0, Machi 24, 2021.
Habari, Mimi naitwa Sylvia Denis Moshi ni daktari na mwanafunzi wa chuo kikuuu cha Malawi,
ninafanya utafiti kuhusu sababu zinazohusiana na mteja wa UKIMWI kudumu kwenye huduma
katika manispaa ya Ubungo. Ninapenda kupata ridhaa yako ili uweze kushiriki kaatika utafiti huu.
Tafadhali soma fomu ya idhni:
Lengo na dhumuni la utafiti
Utafiti huu unalenga kutambua idadi ya wateja wanaohudhuria kikamilifu katika huduma, na pia
kujua visababishi vinavyomfanya mteja wa UKIMWI kuhudhuria au kutokuhudhuria kwenye
matibabu/huduma ili kuweza kupata suluhisho ambayo itasaidia kutatua tatizo hili kwa wateja
wote na programu zote zinazohusika na kuwasaidia wateja wa UKIMWI.
Utaratibu
Kama unakubali kushiriki katika utafiti huu, utahitajika kusaini fomu ya idhini. Pia utapewa fomu
ya maswali ya kujaza kwa msaada wa msaidizi wa utafiti. Mahojiano hayatachukua muda wako
mwingi na yatafanyika mara moja. Mahojiano haya yatakuwa uso kwa uso na pia yatarekodiwa.
Unaweza ukachagua sehemu ambayo ipo sawa kwako kufanyiwa mahojiano na muda ambao
unaoutaka wewe. Wataalamu wa utafiti watafanya mahojiano kwa usiri sana na nyaraka zote za
mahojiano zitahifadhiwa kwa usiri mkubwa mno.
Tahadhari
Hatutegemei kwamba, kwa kushiriki kwenye utafiti huu utapata tatizo lolote lile la kiafya au
kuweza kujeruhiwa. Kushiriki katika utafiti huu ni hiari kabisa na kama hutojisika kujibu baadhi
ya maswali unaruhusiwa kufanya hivyo, na pia kama unataka kujitoa katika utafiti huu uwe huru
kufanya hivyo.

68
Faida
Taarifa utakazozitoa zitapelekea kupata ujuzi juu ya visababishi vinavyomfanya mteja wa
UKIMWI kuhudhuria au kutokuhudhuria kwnye matibabu/huduma. Matokea ya huu utafiti
yatatusaidia kuweza kuwaelimisha wateja juu visababishi vinavyomfanya mteja kuhudhuria au
kutkuhudhuria, pamoja na wadau mbalimbali wanaoshiriki katika kutoa huduma kwa wateja pia
na wawakilishi wa manispaa ya Ubungo ili kuweza kutengeneza mikakati itakayosaidia kuboresha
mahudhurio.
Gharama na fidia
Hakutakuwa na malipo ya aina yoyote ile ukishiriki katika utafiti huu, jua kwamba hautapewa hela
ili kushiriki. Unaweza pia kutokushiriki katika utaafiti huu na hii haitakuathiri kwa namna yoyote
ile.
Usiri
Majadiliano yatafanyika kwa usiri mkubwa mno ambapo hakutakuwa na mtu yeyote atakayeweza
kusikia majadilaino yetu. Maelezo/taarifa yoyote ile itawekwa kwa usiri mkubwa sana. Jina lako
halitatumika katika ripoti zitakazotengenezwa. Fomu za maswali pamoja na ya ruhusa
zitahifadhiwa katika kabati inayofungwa kwa kofuli au funguo ambapo wahusika wa utafiti huu
tuu(mtafiti na tume ya utafiti ya chuo kikuu cha Malawi- COMREC) ndio wanaoweza kuzitumia.
Nyaraka zote zilizotumia kwenye utafiti huu zitakabidhiwa chuoni Malawi kwa ajili ya
kurekodiwa na zitachomwa baada ya utafiti huu kukamilika /kumalizika.
Kwa taarifa Zaidi
Ikitokea una maswali wasiliana na mtafiti Dk. Sylvia Moshi kwa namba +255 767 041648 au
wasimamizi wa utafiti Dk. Joan Rugemalila kwa namba +255 784 660 517 na Dk. Linda Nyondo
Mipando kwa namba +265 999 441212 au mwakilishi wa NIMR kwa namba: +255 758 587885
Kwa kusaini fomu hii itaonesha kwamba umesoma na kuielewa na hivyo kwa hiari yako kabisa
umeamua kushiriki kwenye utafiti huu.
Fomu hii imesmwa na kuelezewa kwangu, hivyo nimeamua kushiriki katika utafiti huu, kwa hiari
yangu.
Sahihi……………. Tarehe ……………….
(Mshiriki utafiti)
Au
Dole gumba……………………….. Tarehe …………………
Sahihi ………………………… Tarehe ……………..
(Shahidi wa mtafiti)

69
Nimetoa maelezo ya kutosha kuhusiana na huu utafiti na mteja ameridhia kushiriki katika huu
utafiti,
Sahihi………………. Tarehe………………
(Msaidizi wa utafiti)
ASANTE KWA KUSHIRIKI

70
Appendix 1.3: Informed Consent form for In-depth Interview (IDI) for HIV/AIDS patients
in English
Study Title: FACTORS ASSOCIATED WITH RETENTION IN CARE AMONG PEOPLE
LIVING WITH HIV/AIDS IN UBUNGO MUNICIPALITY, TANZANIA
Principal Investigator: Dr. Sylvia D. Moshi, Master of Science in Public Health, University of
Malawi
Research Supervisors: Dr. Linda Nyondo-Mipando and Dr. Joan Rugemalila
PI Version Date: 2.0, March 24, 2021
What you should know about this study
You are being asked to join a research study. This consent form explains the research study and
your part in the study. Please read it carefully and take as much time as you need. Please note that
your participation in this study is entirely voluntary and you may decide not to take part or to
withdraw from this study at any time. There will be no penalty if you decide to quit the study.
During the study, we will tell you if we learn any new information that might affect whether you
wish to continue to be in the study or not.
The Investigator of this study is Dr. Sylvia Denis Moshi, a student of masters of public health in
University of Malawi, College of Medicine, and my assistant is _____________. Before you
decide if you want to be a part of this study, we want you to understand the study.
The study staff will talk with you about this information. You are free to ask questions about this
study at any time. Before you decide whether to take part in this research study, you need to know
the purpose, the possible risks and benefits to you, and what will be expected of you during the
study. After the study has been fully explained to you, you can decide whether or not you want to
participate. Once you understand this study, and if you agree to take part, you will be asked to sign
this consent form or make your mark in front of someone. You will be offered a copy of this form
to keep.
Purpose of the StudyThis study seeks to determine proportion of people retained in care, and to
assess factors associated with retention in care among people living with HIV/AIDS, in order to
help find ways that would improve retention in care among them and the entire program.

71
Study Procedures
If you agree to take part in this study, you will be asked to sign a consent form or thumb print it
before the witness. About 18 participants (six from each facility) will participate in this interview.
The interview will be face to face and will also be digitally recorded. The interview will not take
much of your time and it will be done once. You will decide on which day and place you will be
comfortable with to have you interviewed. The study team will maintain your privacy and
confidentiality at any place that you will choose.
Secondly, we will collect some information about you such as age, tribe, religion, where you live,
and nature of your work, and also we will conduct the interview and discussions on the Factors
associated with retention in care among people living with HIV/AIDS in Ubungo municipality.
Risks and or discomforts
We do not anticipate major risk, some discussions may be sensitive and you are free not to answer.
However, we encourage you to answer all questions because it will help us to understand the health
care workers and client’s views on regards of the factors that are associated with retention in care
among people living with HIV/AIDS. We will make every effort to protect your privacy and
confidentiality while you are in the study and will not use your name in the study summaries.
However, in instances where you are the only one in your position others may be able to know of
your participation in the study. The discussions will take place in private.
Potential Benefits
There may be no direct benefit to you from this study. Information gained from this study may
help us understand factors that are associated with retention in care among people living with
HIV/AIDS and may inform health care workers on provision of such services in future.
Reasons why you may be withdrawn from the study without your consent.
• The study is stopped or cancelled by the Ministry of Health, community development,
gender, elderly and children (MoHCDEC), the Malawi College of Medicine Research Ethics
Committee (COMREC) and National Institute of Medical Research (NIMR).
• Staying in the study would be harmful to you.
Costs and Compensation.
There is no cost associated with this study and you will not receive payment for participation. You
are free not to participate in the study. This will not affect your job or regular health care at this
hospital.
Confidentiality
Efforts will be made to keep the questionnaires and recordings of the interviews confidential to
the extent permitted by law. However, we cannot guarantee absolute confidentiality. You will be
identified by a code. Your name will not be used in any publication of this study. The recorded
discussions will only be used for research purposes and once those requirements are met they will

72
be erased. After the interview, the consent form will be kept as per COMREC guidelines have
been met and then they will be destroyed. The interviews will use codes and not your real names.
The study records will be kept in a locked cabinet at the Kamuzu University of Health Sciences
However, your records may be reviewed by Supervisors, study staff, study monitors, department
of Public Health and College of Medicine Research Ethics Committee (COMREC).
Research Related Injury
It is unlikely that you will be injured as a result of being in this study, however if you are injured
as a result of being in this study, the study staff will give you immediate necessary treatment for
your injuries. You will not have to pay for this treatment. You will then be told where you can get
additional treatment for your injuries, if needed. There is no program for monetary compensation
or other forms of compensation for such injuries through this study. You do not give up any legal
rights by signing this consent form.
Problems or Questions
For questions about this study or a research-related injury, contact:
• Dr. Sylvia Denis. Moshi, Principal Investigator, phone number: 0767 041648/0717041648
• Dr. Joan Rugemalila research supervisor located at Muhimbili National Hospital,
department of internal medicine, phone number 0784 660 517 and
• Dr. Linda Nyondo Mipando, research Supervisor, located at the University of Malawi,
College of Medicine. Department of Health Systems and Policy, phone number, 0999 44 1212,
• And NIMR representative on +255 758 587885
If you have read the informed consent, or have had it read and explained to you, and understand
the information, and you voluntarily agree to join the study, please sign your name or make your
mark below.
____________________________ _________________________________
Participant Signature Date
______________________ ________________________
Study Staff signature Date
___________________ _________________
Witness Signature Date
-------------------------- ------------------
THANK YOU SO MUCH

73
Appendix 1.4: Informed consent form for In-depth interview for HIV/AIDS patients in
Swahili
Kichwa cha somo: Sababu zinazohusiana na wateja wa UKIMWI kudumu kwenye huduma katika
manispaa ya Ubungo
Mtafiti; Dk. Sylvia Denis Moshi, mwanafunzi wa shahada ya uzamili ya afya ya jamii katika chuo
kikuu cha afya cha Malawi
Msimamizi wa utafiti; Dk. Linda Nyondo, Mipando na Dk. Joan Rugemalila
PI TOLEO LA TAR: 2.0, Machi 24, 2021.
Unachotakiwa kufahamu kuhusu huu utafiti
Unaombwa kushiriki katika utafiti huu. Hii fomu ya idhini inaelezea kwa kina kuhusu huu utafiti
na ushiriki wako katika huu utafiti. Kwa hiyo unaombwa kutumia muda wako mwingi kuusoma
na kuuelewa. Ushiriki wako katika utafiti huu ni wa hiari kabisa na unaweza ukaamua kutoshiriki
au kujitoa wakati wowote. Hakutokuwa na utozaji wa pesa pindi utakapoamua kujitoa katika
utafiti. Wakati utaafiti unaendelea utapata fursa ya kujifunza mambo kadha wa kadha
yanayohusiana na utafiti. Utaelewa kwa undani kabisa kuhusu huu utafiti na wataalamu
wanaohusika na utafiti. Jisikie huru kabisa kuuliza maswali yoyote wakati wowote yanayohusiana
na huu utafiti. Unapaswa kujua lengo la huu utafiti na madhara au faida zitokanazo na huu utafiti
na nini cha kutegemea wakati wa utafiti. Baada ya kupata maelezo ya kutosha ndipo utakapofanya
maamuzi ya kushiriki au kutokushiriki katika utafiti. Mara ya baada ya kuelewa na kukubali
kushiriki, utaakiwa kusaini hii fomu ya idhini au kuweka alama ya dole gumba mbele ya shahidi,
na kisha utapewa nakala ya hii fomu.
Lengo la utafiti
Utafiti huu unalenga kujua kiasi/idadi ya wateja ambao wapo katika huduma na kuweza kutambua
vitu vinavyosababisha wateja wa ugonjwa wa UKIMWI kubaki au kutokubaki kwenye huduma.
Ili kuweza kutafuta njia stahiki za kuboresha na kuwafanya wateja waweze kudumu katika
huduma.
Utaratibu wa utafiti
Kama unakubali kushiriki katika utafiti huu utapaswa kusaini fomu ya idhini au kuweka alama ya
dole gumba. Jumla ya Wateja wa ugonjwa wa UKIMWI kumi na nane watashiriki katika
74
mahojiano haya, ikiwa ni washiriki sita katika kila kituo cha afya vilivyochaguliwa. Mahojiano
yatafanywa na wataalamu wa utafiti huu na yatakuwa uso kwa uso na yatarekodiwa. Mahojiano
haya hayatachukua muda mwingi na yatafanyika mara moja. pia unaweza kuchagua sehemu
ambayo utaipenda wewe kwa kufanyia mahojiano na muda ambao unautaka. Mahojiano yote
tatafanywa kwa usiri na nyaraka zitahifadhiwa kwa usiri mkubwa sana.
Tahadhari na Usumbufu
Hatutegemei kama utapata madhara yoyote, baadhi ya maswali yanaweza yakawa nyeti na jisikie
huru kabisa kutokujibu. Hata hivyo tunasisitiza uweze kujibu maswali yote maana hii itatusaidia
kuweza kupata uelewa juu ya mitazamo ya wahudumu wa afya , pamoja na wateja juu ya sababu
mbalimbali zinazowafanya wateja kudumu au kutokudumu kwenye huduma.
Faida za utafiti
Hakutakuwa na faida ya moja kwa moja zitokanazo na utafiti huu bali taarifa utakazozitoa
zitatusaidia kupata uelewa juu ya vitu vinavyosababisha wateja kudumu au kutokudumu katika
huduma, nah ii itatusaidia kuweza kujua mbinu stahiki zitakazoweza kuwadumisha wateja kwenye
huduma, pamoja na kuboresha sekya ya afya kiujumla.
Sababu zitakazopelekea kutolewa kwenye utafiti bila ya ridhaa yako ni;
I. Utafiti ukikatizwa na wizara ya afya, ustawi wa jamii, jinsia, wazee na watoto, taasisi ya
utafiti Tanzania (NIMR), tume ya utafiti Malawi (COMREC).
II. Kuendelea kubaki kwenye utafiti kutakuwa na madhara kwako.
Malipo na fidia.
Hakutakuwana malipo ya aina yoyote ile, yatokanayo na utafiti huu na unaweza kutokushiriki na
hii haita – athiri upataji wako wa huduma katika kituo.
Usiri
Jina lako halitatumika katika utafiti huu, hata hivyo utatambulika kwa namba ambayo utapewa,.
Mazungumzo yote yatafanywa kwa usiri mkubwa katika chumba ambapo hapana mtu yeyote
atakayeweza kusikia. Mazungumzo yatarekodiwa na yatatumika tuu kwenye utafiti na mara baada
ya utafiti kumalizika yataharibiwa kutokana na muelekezo wa taasisi ya masuala ya utafiti
(COMREC). Taarifa zako zitapitiwa na msimamizi wa utafiti, wataalamu wa utafiti pamoja na
idara ya afya ya jamii chuo cha afya Kamuzu, Malawi. Fomu zote za utafiti pamoja na
mazungumzo yaliyorekodiwa yatahifadhiwa katika loka/ kabati ambalo litafungwa kwa ufunguo
katika chuo cha Malawi.
Ajali zitokanazo na utafiti
Hatutegemei kuwa utapata ajali kwa kushiriki kwenye huu utafiti, hata hivyo ikitokea umeumia
kutokana na utafiti huu, wataalamu wa utafiti watakupatia matibabu yanayostahili na hutolipia
haya matibabu. Ghrama zote za matibabu zitalipwa na wataalamu wa utafiti. Hakutakuwa na
malipo au fidia yoyote kutokana na ajali.

75
Kwa mawasiliano zaidi au maulizo.
Kwa maswali kuhusu huu utafiti wasiliana na:
• Dk. Sylvia Denis Moshi, mtafiti mkuu kwa namba ya simu 0767 041648 / 0717 041648 au
kwa barua pepe; [email protected]
• Dk. Linda Nyondo Mipando, msimamizi wa utafiti chuo kikuu cha afya Malawi kwa simu
namba, +265 999 44 12 12 au kwa barua pepe; [email protected] na
• Dk. Joan Rugemalila, msimamizi wa utafiti huu pia kwa namba +255 784 660 517 au kwa
barua pepe : [email protected]
• Au mwakilishi wa NIMR kwa namba: +255 758 5878
Kama umesoma au kuelezwa na umeelewa fomu hii tafadhali weka sahihi au alama ya kidole
gumba, uweze kushiriki.
ASANTENI SANA

76
Appendix 1.5: Informed Consent Form for Key Informant Interview (KII) in English
Study Title: FACTORS ASSOCIATED WITH RETENTION IN CARE AMONG PEOPLE
LIVING WITH HIV/AIDS IN UBUNGO MUNICIPALITY, TANZANIA
Principal Investigator: Dr. Sylvia D. Moshi, a student of Master’s of Public Health, at the Kamuzu
University of Health Sciences, Malawi.
Research Supervisors: Dr. Linda Nyondo-Mipando na Dk. Joan Rugemalila
PI Version Date: Version 2.0, March 24, 2021
What you should know about this study
You are being asked to join a research study. This consent form explains the research study and
your part in the study. Please read it carefully and take as much time as you need. Please note that
your participation in this study is entirely voluntary and you may decide not to take part or to
withdraw from this study at any time. There will be no penalty if you decide to quit the study.
During the study, we will tell you if we learn any new information that might affect whether you
wish to continue to be in the study or not.
The Investigator of this study is Dr. Sylvia Denis Moshi, a student of masters of public health in
University of Malawi, College of Medicine and my assistant is _____________. Before you
decide if you want to be a part of this study, we want you to understand the study.
The study staff will talk with you about this information. You are free to ask questions about this
study at any time. Before you decide whether to take part in this research study, you need to know
the purpose, the possible risks and benefits to you, and what will be expected of you during the
study. After the study has been fully explained to you, you can decide whether or not you want to
participate. Once you understand this study, and if you agree to take part, you will be asked to sign
this consent form or make your mark in front of someone. You will be offered a copy of this form
to keep.
Purpose of the Study
This study seeks to determine proportion of people retained in care, and to asses factors associated
with retention in care among people living with HIV/AIDS, in order to help find ways that would
improve retention in care among them and the entire program.
77
Study Procedures
If you are interested to participate in this study you will need to meet some requirements. Firstly,
we will ask you to sign or thumb print this consent form before the witness. About 18 Key
Informants (6 participants from each facility) will participate in the interview. The Key informants
comprises of Doctors, nurses and lab technicians. The research staff will conduct the interviews,
it will be face to face, and it will be done once. It will also be digitally recorded.
Secondly, we will collect some information about you such as age, tribe, religion, where you live,
and nature of your work, and also we will conduct the interview and discussions on the Factors
associated with retention in care among people living with HIV/AIDS in Ubungo municipality.
Risks and or discomforts
We do not anticipate major risk, some discussions may be sensitive and you are free not to answer.
However, we encourage you to answer all questions because it will help us to understand the health
care workers and client’s views on regards of the factors that are associated with retention in care
among people living with HIV/AIDS. We will make every effort to protect your privacy and
confidentiality while you are in the study and will not use your name in the study summaries.
However, in instances where you are the only one in your position others may be able to know of
your participation in the study. The discussions will take place in private.
Potential Benefits
There may be no direct benefit to you from this study. Information gained from this study may
help us understand factors that are associated with retention in care among people living with
HIV/AIDS and may inform health care workers on provision of such services in future.
Reasons why you may be withdrawn from the study without your consent.
• The study is stopped or cancelled by the Ministry of Health, community development,
gender, elderly and children (MoHCDEC), the Malawi College of Medicine Research Ethics
Committee (COMREC) and National Institute of Medical Research (NIMR).
• Staying in the study would be harmful to you.
Costs and Compensation
There is no cost associated with this study and you will not receive payment for participation. You
are free not to participate in the study. This will not affect your job or regular health care at this
hospital.
Confidentiality
Efforts will be made to keep the questionnaires and recordings of the interviews confidential to
the extent permitted by law. However, we cannot guarantee absolute confidentiality. You will be
identified by a code. Your name will not be used in any publication of this study. The recorded
discussions will only be used for research purposes and once those requirements are met they will
be erased. After the interview, the consent form will be kept as per COMREC guidelines have

78
been met and then they will be destroyed. The interviews will use codes and not your real names.
The study records will be kept in a locked cabinet at the College of Medicine. However, your
records may be reviewed by Supervisors, study staff, study monitors, department of Public Health
and College of Medicine Research Ethics Committee (COMREC).
Research Related Injury
It is unlikely that you will be injured as a result of being in this study, however if you are injured
as a result of being in this study, the study staff will give you immediate necessary treatment for
your injuries. You will not have to pay for this treatment. You will then be told where you can get
additional treatment for your injuries, if needed. There is no program for monetary compensation
or other forms of compensation for such injuries through this study. You do not give up any legal
rights by signing this consent form.
Problems or Questions
For questions about this study or a research-related injury, contact:
• Dr. Sylvia Denis. Moshi, Principal Investigator, phone number: 0767 041648/0717041648
• Dr. Linda Nyondo Mipando, Research Supervisor, located at the University of Malawi,
Department of Health Systems and Policy, phone 0999 44 1212 and
• Dr. Joan Rugemalila, research supervisor located at Muhimbili National Hospital,
department of internal medicine, phone number 0784 660 517
• And NIMR representative on +255 758 587885
If you have read the informed consent, or have had it read and explained to you, and understand
the information, and you voluntarily agree to join the study, please sign your name or make your
mark below.
____________________________ _________________________________
Participant Signature Date
______________________________ ____________________________________
Study Staff Signature Date
______________________________ ____________________________________
Witness Signature (print) Date
THANK YOU.

79
Appendix 1.6: Informed consent form for Key Informant Interview in Swahili
Kichwa cha somo: Sababu zinazohusiana na wateja wa UKIMWI kudumu kwenye huduma katika
manispaa ya Ubungo
Mtafiti; Dk. Sylvia Denis Moshi, mwanafunzi wa shahada ya uzamili ya afya ya jamii katika chuo
kikuu cha afya Malawi.
Wasimamizi wa utafiti; Dk. Linda Nyondo, Mipando na Dr. Joan Rugemalila
PI TOLEO LA TAR: 2.0 Machi 24, 2021.
Unachotakiwa kufahamu kuhusu huu utafiti
Unaombwa kushiriki katika utafiti huu. Hii fomu ya maridhio inaelezea kwa kina kuhusu huu
utafitina ushiriki wako katika huu utafiti. Kwa hiyo unaombwa kutumia muda wako vizuri
kuusoma na kuuelewa, ushiriki wako katika utafiti huu ni wa hiari kabisa na unaweza ukaamua
kutoshiriki au kujitoa wakati wowote. Hakutokuwa na utozaji wa pesa pindi utakapoamua kujitoa
katika utafiti. Wakati utaafiti unaendelea utapata fursa ya kujifunza mambo kadha wa kadha
yanayohusiana na utafiti. Utaelewa kwa undani kabisa kuhusu huu utafiti na wataalamu
wanaohusika na utafiti. Jisikie huru kabisa kuuliza maswali yoyote wakati wowote yanayohusiana
na huu utafiti. Unapaswa kujua lengo la huu utafiti na madhara au faida zitokanazo na huu utafiti
na nini cha kutegemea wakati wa uafiti. Baada ya kupata maelezo ya kutosha ndipo utakapofanya
maamuzi ya kushiriki au kutokushiriki katika utafiti. Mara ya baada ya kuelewa na kukubali
kushiriki, utaombwa kusaini hii fomu ya maridhiano au kuweka alama ya dole gumba mbele ya
shahidi, kasha utapewa nakala yah ii fomu.
Lengo la utafiti
Utafiti huu unalenga kujua kiasi/idadi ya wateja ambao wapao katika huduma na kuweza kutambua
vitu vinavyosababisha wateja wa ugonjwa wa UKIMWI kubaki au kutokubaki kwenye huduma.
Ili kuweza kutafuta njia stahiki za kuboresha na kuwafanya wateja waweze kudumu katika
huduma.
Utaratibu wa utafiti
Wahudumu wa afya kumi na nane watashiriki katika mahojiano haya, Wataalamu hao ni
madaktari, wauguzi na wataalamu wa maabara. Mahojiano hayo yatafanywa mara moja na
wataalamu wa utafiti huu na yatakuwa uso kwa uso na pia yatarekodiwa.

80
Kama utapenda kushiriki utafiti huu utapaswa kusaini hii fomu au kuweka alama ya dole gumba
mbele ya shahidi na pia kutoa taarifa za umri wako, kabila, dini unapoishi. Tutafanya mahojiano
ya vitu vinavyosababisha wateja wa ugonjwa wa UKIMWI kubaki au kutokubaki kwenye huduma.
Tahadhari na Usumbufu
Hatutegemei kama utapata madhara yoyote, baadhi ya maswali yanaweza yakawa nyeti na jisikie
huru kabisa kutokujibu. Hata hivyo tunasisitiza uweze kujibu maswali yote maana hii itatusaidia
kuweza kupata uelewa juu ya mitazamo ya wahudumu wa afya , pamoja na wateja juu ya sababu
mbalimbali zinazowafanya wateja kudumu au kutokudumu kwenye huduma.
Faida za utafiti
Hakutakuwa na faida ya moja kwa moja zitokanazo na utafiti huu bali taarifa utakazozitoa
zitatusaidia kupata uelewa juu ya vitu vinavyosababisha wateja kudumu au kutokudumu katika
huduma, nah ii itatusaidia kuweza kujua mbinu stahiki zitakazoweza kuwadumisha wateja kwenye
huduma, pamoja na kuboresha sekya ya afya kiujumla.
Sababu zitakazopelekea kutolewa kwenye utafiti bila ya ridhaa yako ni;
III. Utafiti ukikatizwa na wizara ya afya, ustawi wa jamii, jinsia, wazee na watoto, taasisi ya
utafiti Tanzania (NIMR), tume ya utafiti Malawi (COMREC).
IV. Kuendelea kubaki kwenye utafiti kutakuwa na madhara kwako.
Malipo na fidia.
Hakutakuwana malipo ya aina yoyote ile, yatokanayo na utafiti huu na unaweza kutokushiriki nah
ii haita – athiri kazi yako.
Usiri
Jina lako halitatumika katika utafiti huu, hata hivyo utatambulika kwa namba ambayo utapewa,.
Mazungumzo yote yatafanywa kwa usiri mkubwa katika chumba ambapo hapana mtu yeyote
atakayeweza kusikia. Mazungumzo yatarekodiwa na yatatumika tuu kwenye utafiti na mara baada
ya utafiti kumalizika yataharibiwa kutokana na muelekezo wa taasisi ya masuala ya utafiti
(COMREC). Taarifa zako zitapitiwa na msimamizi wa utafiti, wataalamu wa utafiti pamoja na
idara ya afya ya jamii chuo cha Malawi. Fomu zote za utafiti pamoja na mazungumzo
yaliyorekodiwa yatahifadhiwa katika loka/ kabati ambalo litafungwa kwa ufunguo katika chuo cha
Malawi.
Ajali zitokanazo na utafiti
Hatutegemei kuwa utapata ajali kwa kushiriki kwenye huu utafiti, hata hivyo ikitokea umeumia
kutokana na utafiti huu, wataalamu wa utafiti watakupatia matibabu yanayostahili na hutolipia
haya matibabu. Ghrama zote za matibabu zitalipwa na wataalamu wa utafiti. Hakutakuwa na
malipo au fidia yoyote kutokana na ajali.
Kwa mawasiliano zaidi au maulizo.

81
Kwa maswali kuhusu huu utafiti wasiliana na:
• Dk. Sylvia Denis Moshi, mtafiti mkuu kwa namba ya simu 0767 041648 / 0717 041648 au
kwa barua pepe; [email protected]
• Dk. Linda Nyondo Mipando, msimamizi wa utafiti chuo kikuu cha afya Malawi kwa simu
namba, +265 999 44 12 12 au kwa barua pepe; [email protected]
• Dk. Joan Rugemalila, msimamizi wa utafiti huu pia kwa namba +255 784 660 517 au kwa
barua pepe: [email protected]
• Na mwakilishi wa NIMR kwa namba: +255 758 587885
Kama umesoma au kuelezwa na umeelewa fomu hii tafadhali weka sahihi au alama ya kidole
gumba, uweze kushiriki.
ASANTENI SANA

82
Appendix 2: Data Collection Tools
Appendix 2.1: Questionnaire in English
Study title: Factors associated with retention in care among PLHIV/AIDS in Ubungo
Municipality.
PI Version Date: Version 2.0, March 24, 2021
Investigators: Dr. Sylvia Denis Moshi
Research Supervisor: Dr. Linda Nyondo Mipando and Dr. Joan Rugemalila
Questionnaire No:
Client’s unique number: _______ Clinic Name: ________ Date of interview: ____
Socio demographic data
1. Gender
a) Male
b) Female
2. Age_____ Date of Birth ___________
3. Marital Status
a) Single
b) Married
c) Divorced
d) Separated
e) Widowed
4. Level of Education
a) None
b) Primary
c) Secondary
d) College/ University
5. What is your occupation?
a) Employed
b) Self-employed
c) Unemployed

83
d) Casual
6. What is your income per month? (Tshs.)
a) <10000
b) 10,000 – 50,000
c) 50,001 –100,000
d) 100,001- 200,000
e) > 200,000
f) Not willing to say
7. Have you disclosed your HIV status to anyone?
a) Yes
b) No one (Go to No. 9)
8. To whom one?
a) Spouse
b) Family members
c) Friends
9. Why did you disclose your status?
a) Seeking for comfort/support
b) Need fo financial support
c) Any other …………………………………….
10. How was their reaction
a) Positive
b) Negative
c) Unknown
11. How have you been supported seeking care?
a) Reminded to take drugs
b) Company to the clinic
c) Financial support
d) Reminded to attend my appointments
e) Social support
12. Why have you not disclosed to any one?
a) I’m afraid to be stigmatized and discriminated
b) I’m afraid to be divorced
c) I’m afraid to lose my job
d) No reason
13. Were you informed of where to go for treatment and care in case you cannot access the
facility?
a) Yes
b) No
84
14. Have you ever sought care and treatment services from another facility apart from the one
you are enrolled in?
a) Yes
b) No
15. If yes, what services were you seeking?
a) Treatment
b) Refill (ARVs/Septrin)
c) Lab tests (Viral load check)
d) Others…….
16. What is your view towards health workers in this Clinic?
a) Good
b) Average
c) They stigmatize clients
d) Others.………
17. How many hours do you take to reach to the clinic?
a) < 30 mins
b) One hour
c) Two hours
d) Three hours
e) > 3hours
18. How much do you spend for coming to the Clinic? (In Tshs)
a) None
b) 1000
c) 2000
d) 5000
e) >5000
f) Any other…………..
19. How long do you take to be attended in this Clinic?
a) < 30 Mins
b) 30 Mins
c) 1 – 2 Hours
d) 2 – 3 Hours
e) > 3 Hours
20. How do you comment on time you spend in the clinic?
a) Short
b) Average
c) Long
d) Too long
21. Do you think missing clinic appointments puts your health at risk?
a) Yes

85
b) No
22. Have you ever missed your clinic appointment for any reason?
a) Yes
b) No
23. If yes, what made you miss your clinic appointments?
a) I forgot
b) I am using herbal medicine
c) I attend to traditional healers / prayers
d) my health has improved
e) I was very sick
f) no support from friends and families
g) other reason
24. How many times have you missed your clinic appointments?
a) Once
b) Twice
c) Thrice
d) >Thrice
25. Have you been counseled on the dangers of missing your appointments, care and treatment?
a) Yes
b) No
26. For how long did you stop being followed up in care and treatment?
a) < 3 Months
b) 3 Months
c) >3 Month
d) 6 – 12 Months
e) > 12 Months
27. How was your health during this period you were lost to follow up?
a) I was well/Not sick
b) I was well initially but later got sick
c) Was always sick
d) Any other reason:……………………………..
28. Were you on ARVs when you missed your clinic appointments?
a) Yes
b) No
29. If yes, where were you accessing your ARVs?
a) I missed taking them
b) Picked at another facility
c) I borrowed from spouse/friend/relative
d) Any other reason……………………..
30. What brought you back to the clinic?

86
a) I was followed up
b) Was counseled by a friend
c) Accepted my status and decided to come back
d) I was sick
e) Any other reason:………………………
31. How do you prefer to be followed up and reminded to attend your scheduled clinic
appointments? (Tick as appropriate)
a) Phone call
b) SMS (short message service)
c) Home visit/home based care
d) Treatment buddy
e) None
Thank you for your time and participation

87
Appendix 2.2: Questionnaire in Swahili
Kichwa cha utafiti: Sababu zinazohusiana na wateja wa UKIMWI kudumu kwenye huduma
katika manispaa ya Ubungo.
PI TOLEO LA TAR: 2.0 Machi 24, 2021.
Mtafiti: Dk. Sylvia Denis Moshi, mwanafunzi wa shahada ya uzamili, katika chuo kikuu cha afya,
Malawi.
Msimamizi wa utafiti; Dk. Linda Nyondo Mipando na Dk. Joan Rugemalila
Dodoso Na…….. Namba ya mteja: --------- Jina la kliniki ………….. Tar. Ya mahojiano…
Taarifa muhimu
1. Jinsia
a) Mwanaume
b) Mwanamke
2. Umri wako
Miaka …………. Tar. Ya kuzaliwa
3. Hali ya ndoa
a) Sijaolewa/ Sijaoa
b) Nimeolewa/Nimeoa
c) Nimeachwa kwa talaka
d) Nimeachika
e) Mjane
4. Hali ya elimu
a) Sijasoma
b) Elimu ya msingi
c) Elimu ya sekondari
d) Elimu ya diploma/setifiketi
e) Elimu ya chuo kikuu
5. Kazi yako ni nini?
a) Nimeajiriwa
b) Nimejiajiri
c) Sina ajira

88
6. Kipato chako kwa mwezi ni shilingi ngapi? (Tshs.)
7. <10000
8. 10,000 – 50,000
9. 50,001 –100,000
10. 100,001- 200,000
11. > 200,000
12. Not willing to say
13. Je, umemjulisha mtu yoyote juu ya hali yako ya maambukizi?
a) Ndiyo
b) Hapana
14. Je, ni kwa nini, umetoa taarifa kuhusu hali yako ya maambukizi?
a) Kupata faraja na msaada wa kifamilia
b) Kusaidiwa kiuchumi
c) Sababu nyingine yeyote:,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,,
15. Je, umesaidiwa vipi, kupata huduma?
a) Nimekumbushwa kumeza dawa
b) Nimesindikizwa kliniki
c) Nimesaidiwa kifedha
d) Nimekumbushwa kuhudhuria kliniki
e) Sijasaidika na chochote
f) Zingine……………….
16. Ni, kwa nini hujamshirikisha mtu yoyote hali yako ya maambukizi?
a) Naogopa kunyanyapaliwa na kutengwa na jamii
b) Naogopa kuachwa na mwenza /mpenzi wangu
c) Naogopa kuachishwa kazi
d) Hakuna sababu
e) Zingine…..
17. Je, umeshawahi kushauriwa juu ya madhara ya kutokuhudhuria kliniki, kukosa huduma au
matibabu?
a) Ndiyo
b) Hapana
18. Je, umeshawahi kushauriwa mahali ambapo unaweza kupata huduma ikitokea hauwezi
kuhudhuria kwenye kituo chako?
a) Ndiyo
b) Hapana
19. Je, umeshawahi kuwaza kupata huduma kwenye kituo kingine tofauti na kituo chako cha
siku zote?
a) Ndiyo
b) Hapana
20. Kama ni ndiyo, je ni nini sababu ya kufanya hivyo?

89
a) Kupata matibabu
b) Huduma ya kituo changu hairidhishi (siyo nzuri)
c) Kuchukua dawa
d) Watoa huduma hawanijali
e) Kupata vipimo
f) Sababu nyingine…………..
21. Je, ni nini mtazamo wako kuhusu watoa huduma wa hapa kituoni?
a) Mzuri
b) Wa kawaida
c) Wananyanyapaa wateja
d) Nyingine……….
22. Je, inakuchukua masaa mangapi kufika kituoni?
a) Chini ya nusu saa
b) Nusu saa
c) Lisaa limoja hadi mawili
d) Masaa matatu
e) Zaidi ya masaa matatu
23. Je, unatumia fedha kiasi gani kuja kliniki? (Tshs)
a) Situmii fedha (natembea)
b) 1000
c) 2000
d) 5000
e) >5000
24. Je, inakuchukua muda gani kuweza kupata huduma?
a) Chini ya nusu saa
b) Nusu saa
c) Nusu saa hadi lisaa
d) Masaa mawili
e) Masaa matatu
f) Zaidi ya masaa matatu
25. Je, unauonaje muda unaoutumia kupata huduma?
a) Mfupi
b) Wa kawaida
c) Mrefu
d) Mrefu sana
26. Je, unafikiri kwamba kwa kukosa kuhudhuria klinik kunahatarisha afya yako?
a) Ndiyo
b) Hapana
27. Je, umeshawahi kukosa kuhudhuria kliniki kwa sababu yoyote ile?

90
a) Ndiyo
b) Hapana
28. Kama ndiyo, sababu ilikuwa ni nini?
a) nilisahau
b) afya yangu iliimarika hivyo nikaacha kutumia dawa
c)natumia dawa za kienyeji
d)natibiwa na waganga na maombi
e) hakuna msaada wowote pindi nikizidiwa
f) sababu nyingine yeyote
29. Je, ni mara ngapi umekosa kuhudhuria kliniki?
a) Mara moja
b) Mara mbili
c) Mara tatu
d) Zaidi ya mara tatu
30. Je, ni kwa muda gani umeacha kuja kwenye huduma?
a) Chini ya miezi mitatu
b) Ni Zaidi ya miezi mitatu
c) Miezi sita hadi kumi na mbili
d) Zaidi ya miezi kumi na mbili
31. Je, afya yako ilikuaje kwa kipindi chote ambacho ulikuwa hauhudhurii kliniki?
a) Nilikuwa sijambo/siumwi
b) Nilikuwa mzima mwanzoni, baadaye nikaanza kuumwa
c) Nilikuwa naumwa mar azote
d) Sababu nyingine
32. Je, ulikuwa unatumia dawa ulipokuwa hauhudhurii klinilk?
a) Ndiyo
b) Hapana
33. Kama ni ndiyo, je ulikuwa unapata wapi dawa?
a) Niliacha kutumia
b) Nilichukua kituo kingine
c) Nilipata kwa mwenza wangu/rafiki/ndugu
d) Sababu nyingine……………….
34. Je, ni nini kimekufanya urudi kliniki?
a) Nilifatwa kurudi kituoni
b) Nilishauriwa na rafiki yangu
c) Nimeikubali hali yangu na kuamua kurudi kwenye huduma
d) Nilikuwa naumwa
35. Je, unatamani vipi kupata huduma ya kukumbushwa kuhudhuria kliniki?
a) Kupigiwa simu
b) Kutumiwa meseji

91
c) Kutembelewa nyumbani
d) Nyingine……
Asante kwa kushiriki

92
Appendix 2.3: Topic guide for In- depth interview (IDI) for patients living with HIV/AIDS
in English
PI Version Date: 2.0, March 24, 2021
SOCIO DEMOGRAPHIC HISTORY
1. How old are you…….… years (Estimate if unsure)
2. What is your current marital status?
a) Single e) Separated
b) Married f) Divorced
c) Living with partner g) Widowed
d) Never married
3. What is your religion?
a) Roman Catholic
b) Muslim
c) (Seventh Day Adventist) SDA
d) Pentecostal
e) Anglican
f) Other (Specify) _____________
4. What is your Tribe...?
5. What is your highest level of education?
a) No schooling
b) Primary school
93
c) Secondary Education
d) Advanced Secondary Education
e) Attended College/University
6. Are you able to read?
a) Yes
b) No
7. What is your occupation?
8. Can you explain in details the factors contributing to poor retention in care among people
living with HIV/AIDS?
9. Can you explain in details the factors leading to the uptake of care among people living
with HIV/AIDS?
For question 8 and 9
Probe the factors related to:
Health systems, clinic flow, operation times and days, human resources, health
worker attitudes and skills, policies in the clinic, waiting time.
Individual factors and community factors: geographical distances, transport
cost.
10. Can you explain in detail the measures that should be done in order to improve retention
in care among people living with HIV/AIDS?
11. What are the measures that you think cannot be implemented and why?
12. What are the measures that has been implemented but still retention is poor? /Why is there
poor retention despite of the measures that has been implemented?
Probe on clinic based strategies, community based strategies and mobile strategies.
Thank you very much for your cooperation and time; you are welcome to ask questions if
any. I appreciate for sparing your time to share your views with us.

94
Appendix 2.4: Topic guide for In-depth Interview (IDI) for Patients living with HIV/AIDS
in Swahili
PI TOLEO LA TAR: 2.0 Machi 24, 2021.
TAARIFA ZA KIJAMII
1. Una umri gani? ….. (Unaweza kukadiria)
2. Je, hali yako ya kindoa ipojee?
a) Nimeolewa/ Nimeoa
b) Tunaishi wote
C) Sijaolewa/Sijaoa
d) Tumeachana
e) Tumetalakiana
f) Mjane
3. Dhehebu lako ni lini??
a) Mkatoliki
b) Muislamu
c) Mpentekoste
d) Msabato
e) Dhehebu jingine lolote: _____________
4. Kabila lako ni lipi...
5. Je elimu yako ni ipi?
a) Sijasoma
b) Shule ya msingi
c) Shule ya sekondari
d) Elimu ya chuo kikii

95
6. Je, unauwezo wa kusoma?
a) Yes
b) No
7. Je, kazi yako ni nini?
8. Je, Unaweza ukatuambia vitu/mambo gani yanayomfanya mteja wa maambukizi ya UKIMWI
kushindwa kudumu katika/kwenye huduma?
9. Je, unaweza ukatumbia vitu vinavyomfanya mteja wa maambukizi ya UKIMWI kuendelea
kubaki kwenye huduma?
Kwa swali namba 8 na 9
Peleleza vitu vinavyohusiana na:
Mfumo wa utoaji huduma, mpangilio wa kliniki, muda wa kufanya kazi na siku
za kazi, nguvu kazi wa watu/wafanyakazi, mtazamo wa wafanyakazi na
mtazamo wao pamoja na ujuzi/uzoefu sera za kliniki pamoja na muda wa
kusubiria huduma.
Sababu za mtu binafsi pamoja na za jamii: sehemu mtu anayoishi- umbali,
gharama za usafiri. n.k
10. Je, unaweza ukatuambia ni vitu gani ambavyo vinaweza kufanyika ili kuweza
kuwadumisha wateja wa maambukizi ya UKIMWI kwenye huduma?
11. Je ni vitu/mambo gani unadhani hayawezi kutekelezeka?? Na ni kwa nini?
12. Je ni vitu gani ambovyo tayari vimekwisha kufanyika lakini bado wateja hawajaweza
kubaki kwenye huduma? / Je ni kwa nini bado wateja hawabaki kwenye huduma licha ya
jitihada mbalimbali zinazofanywa na mashirika yanayofadhili hizi huduma.
Peleleza kuhusu mikakati ya kliniki, mikakati ya kijamii pamoja na kliniki za mitaani.
Mtazamo wa wahudumu kuhusu jitihada za haya mashirika.
ASANTE SANA KWA MUDA WAKO NA KWA KUWEZA KUSHIRIKI KATIKA
MAJADILIANO HAYA. KAMA UNA MASWALI YOYOTE TAFADHALI JISIKIE
HURU KUULIZA

96
Appendix 2.5: Key Informant Interview Guide (KII) for Health Care Workers in English
PI Version Date: 2.0, March 24, 2021
SOCIO DEMOGRAPHIC HISTORY
1. How old are you…….… years (Estimate if unsure)
2. What is your current marital status?
a) Never married d) Separated
b) Married e) Divorced
c) Living with partner f) Widowed
3. What is your religion?
a) Roman Catholic
b) Muslim e) Pentecostal
c) Seventh Day Adventist (SDA)
d) Anglican
f) Other (Specify) _____________
4. What is your Tribe?
5. What is your highest level of education?
a) No schooling
b) Secondary Education
c) Advanced Secondary Education
d) Attended College/University
6. Are you able to read and write?
a) Yes
b) No

97
7. What is your occupation?
8. As a medical personnel, can you explain in details the factors contributing to poor retention in
care among people living with HIV/AIDS?
9. Due to your experience, what are factors leading to the uptake of care/ retention in care among
people living with HIV/AIDS?
For question 8 and 9
Probe the factors related to:
Health systems, clinic flow, operation times and days, human resources, health
worker attitudes and skills, policies in the clinic, waiting time.
Individual factors and community factors: geographical distances, transport
cost.
Health care workers factors such as, attitude, arrogance, laziness, no caring.
10. Can you explain in detail the measures that should be done in order to improve retention
in care among people living with HIV/AIDS?
11. Due to your experience, what are the measures that you think cannot be implemented and
why?
12. What should be done in order for those factors to be implemented?
13. What are the measures that has been done but still, the retention is poor? /Why is there poor
retention despite of the measures that has been implemented?
Probe on clinic based strategies, community based strategies and mobile strategies.
THANK YOU SO MUCH

98
Appendix 2.6: Key Informant Interview Guide (KII) for Health Care Workers in Swahili
PI TOLEO LA TAR: 2.0 Machi 24, 2021.
TAARIFA ZA KIJAMII
1. Una umri gani?
2. Je, hali yako ya kindoa ipojee?
a) Sijaolewa/ Sijaoa d) Tumeachana
b) Nimeolewa/ Sijaoa e) Tumetalakiana
c) Tunaishi wote f) Mjane
3. Dhehebu lako ni lini??
a) Mkatoliki
b) Muislamu
c) Msabato
d) Mpentekoste
e) Dhehebu jingine lolote: _____________
4. Kabila lako ni lipi?
5. Je elimu yako ni ipi?
a) Sijasoma
b) Shule ya msingi
c) Shule ya sekondari
d) Elimu ya chuo kikuu
6. Je, kazi yako ni nini?
………………………………
7. Je, wewe kama muhudumu wa afya, unaweza ukatuambia ni vitu/ mambo gani yanayomfanya
mteja wa maambukizi ya UKIMWI kushindwa kudumu kwenye huduma?
8. Kwa uzoefu wako katika utoaji wa huduma kwa wateja hawa, je ni vitu gani ambavyo unaona
ndo vinawafanya wabaki kwenye huduma.

99
Kwa maswali namba 7 & 8:
Peleleza vitu vinavyohusiana na;
Mfumo wa utoaji huduma, mpangilio wa kliniki, muda wa kufanya kazi, nguvu kazi watu,
kama vile idadi ya wafanyakazi, mtazamo wa wafanyakazi pamoja na uzoefu/ujuzi, saa za
kliniki na muda wa kusuburi huduma.
Sababu za wafanyakazi kama vile ujeuri, kutokujali, uvivu, n.k
Sababu za wateja pamoja na za jamii kama vile, sehemu mtu anayotoka (umbali), gharama,
mtazamo wa jamii yake na huu ugonjwa, msaada wa familia na jamii.
9. Je unaweza ukatuambia ni vitu gani ambavyo vinaweza kufanyika ili kuweza kuwadumisha
wateja hawa kwenye huduma?
10. Kwa uzoefu wako, je unadhani ni mambo gani ambay hayawezi kutekelezeka na ni kwa nini?
11. Je, nini kifanyike ili mambo hay ohayo yaweze kutekelezeka?
12. Je ni vitu gani ambavyo tayari vimekwisha fanyika lakini bado wateja hawajaweza kubaki
kwenye huduma?
13. Je ni kwa nini bado wateja hawabaki kwenye huduma licha ya jitihada mbalimbali za mashirika
yanayofadhili hii huduma?
Peleleza kuhusu mikakati ya kliniki, mikakati ya kijamii, pamoja na kliniki za mitaani.
Mtazamo wa wahudumu kuhusu haya mashirika.
Asante Sana

100
Appendix 3: COMREC clearance letter
The chairperson of OMREC; Prof Eric Umar.

101
Appendix 4: NIMR clearance letter

102

103
Appendix 5: Research Permit from Ubungo Municipal
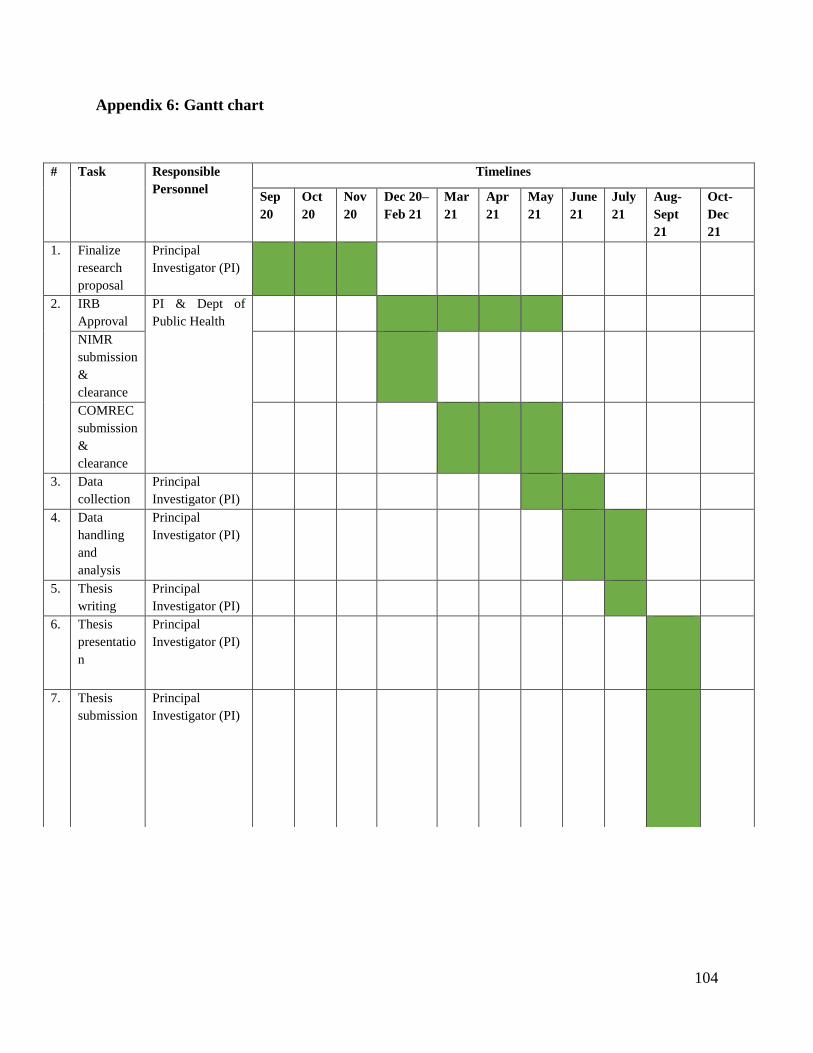
104
Appendix 6: Gantt chart
# Task Responsible
Personnel
Timelines
Sep
20
Oct
20
Nov
20
Dec 20–
Feb 21
Mar
21
Apr
21
May
21
June
21
July
21
Aug-
Sept
21
Oct-
Dec
21
1. Finalize
research
proposal
Principal
Investigator (PI)
2. IRB
Approval
PI & Dept of
Public Health
NIMR
submission
&
clearance
COMREC
submission
&
clearance
3. Data
collection
Principal
Investigator (PI)
4. Data
handling
and
analysis
Principal
Investigator (PI)
5. Thesis
writing
Principal
Investigator (PI)
6. Thesis
presentatio
n
Principal
Investigator (PI)
7. Thesis
submission
Principal
Investigator (PI)

105
8. Dissertatio
n final
submission
Principal
Investigator (PI)




















