Expression of TAG-72 In Ovarian Cancer and Its Correlation With Tumor Stage and Patient Prognosis
11
Expression of TAG-72 in ovarian cancer and its correlation with tumor stage and patient prognosis Moorthy P. Ponnusamy a,1 , Ganesh Venkatraman a,1 , Ajay P. Singh a , Subhash C. Chauhan a , Sonny L. Johansson b , Maneesh Jain a , Lynnette Smith c , John S. Davis a,d,e , Steven W. Remmenga d , Surinder K. Batra a,b,f, * a Department of Biochemistry and Molecular Biology, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA b Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA c Department of Preventive and Societal Medicine, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA d Department of Obstetrics and Gynecology, University of Nebraska Medical Center, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA e Omaha VA Medical Center, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA f Eppley Institute for Research in Cancer and Allied Diseases, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA Received 24 October 2006; received in revised form 21 November 2006; accepted 22 November 2006 Abstract Tumor associated glycoprotein-72 (TAG-72), a pancarcinoma antigen, was initially identified in cancer tissues by its immunoreactivity to a monoclonal antibody B72.3. In this study, we have analyzed the expression and localization profiles of TAG-72 in ovarian cancer tissue samples of different stages and histological subtypes by immunohistochemistry using a second generation high affinity monoclonal antibody CC49. We have also studied the expression of TAG-72 in ovarian can- cer cell lines by confocal microscopy and immunoblot analyses. A correlation between TAG-72 expression and localization with patients’ prognosis was also analyzed using Kaplan–Meier analysis. Eighty eight percent of the ovarian cancer tissue samples (n = 43) showed immunoreactivity with CC49 antibody. The expression of TAG-72 in advanced stage cancer tis- sues (mean composite score = 3.7) was significantly higher (p = 0.035) compared to the early stage tumors (mean composite score = 2.3). However, no significant correlation of TAG-72 was observed with histological tumor types. A marginal cor- relation of TAG-72 staining with patients’ survival was observed. Interestingly, the membrane localization of TAG-72 in tumors was significantly (p = 0.0082) associated to the poor clinical outcome, while cytoplasmic staining was correlated sig- nificantly to a better prognosis (p = 0.0051). Immunoblot analysis demonstrated the expression of TAG-72 in three ovarian cancer cell lines (OVCAR3, SB247 and COV362.4). In conclusion, the tumor-specific expression of TAG-72 and its asso- ciation with disease stage indicate its potential as a marker for effective disease management and targeted cancer therapy. Ó 2006 Elsevier Ireland Ltd. All rights reserved. Keywords: TAG-72; Ovarian cancer; Diagnosis; Prognosis; Therapy 0304-3835/$ - see front matter Ó 2006 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.canlet.2006.11.025 * Corresponding author. Tel.: +1 402 559 5455; fax: +1 402 559 6650. E-mail address: [email protected] (S.K. Batra). 1 Both these authors have equally contributed to this manuscript. Cancer Letters 251 (2007) 247–257 www.elsevier.com/locate/canlet
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Expression of TAG-72 In Ovarian Cancer and Its Correlation With Tumor Stage and Patient Prognosis

Cancer Letters 251 (2007) 247–257
www.elsevier.com/locate/canlet
Expression of TAG-72 in ovarian cancer and its correlationwith tumor stage and patient prognosis
Moorthy P. Ponnusamy a,1, Ganesh Venkatraman a,1, Ajay P. Singh a,Subhash C. Chauhan a, Sonny L. Johansson b, Maneesh Jain a, Lynnette Smith c,
John S. Davis a,d,e, Steven W. Remmenga d, Surinder K. Batra a,b,f,*
a Department of Biochemistry and Molecular Biology, University of Nebraska Medical Center, Omaha, NE 68198-5870, USAb Department of Pathology and Microbiology, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA
c Department of Preventive and Societal Medicine, University of Nebraska Medical Center, Omaha, NE 68198-5870, USAd Department of Obstetrics and Gynecology, University of Nebraska Medical Center, University of Nebraska Medical Center,
Omaha, NE 68198-5870, USAe Omaha VA Medical Center, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA
f Eppley Institute for Research in Cancer and Allied Diseases, University of Nebraska Medical Center, Omaha, NE 68198-5870, USA
Received 24 October 2006; received in revised form 21 November 2006; accepted 22 November 2006
Abstract
Tumor associated glycoprotein-72 (TAG-72), a pancarcinoma antigen, was initially identified in cancer tissues by itsimmunoreactivity to a monoclonal antibody B72.3. In this study, we have analyzed the expression and localization profilesof TAG-72 in ovarian cancer tissue samples of different stages and histological subtypes by immunohistochemistry using asecond generation high affinity monoclonal antibody CC49. We have also studied the expression of TAG-72 in ovarian can-cer cell lines by confocal microscopy and immunoblot analyses. A correlation between TAG-72 expression and localizationwith patients’ prognosis was also analyzed using Kaplan–Meier analysis. Eighty eight percent of the ovarian cancer tissuesamples (n = 43) showed immunoreactivity with CC49 antibody. The expression of TAG-72 in advanced stage cancer tis-sues (mean composite score = 3.7) was significantly higher (p = 0.035) compared to the early stage tumors (mean compositescore = 2.3). However, no significant correlation of TAG-72 was observed with histological tumor types. A marginal cor-relation of TAG-72 staining with patients’ survival was observed. Interestingly, the membrane localization of TAG-72 intumors was significantly (p = 0.0082) associated to the poor clinical outcome, while cytoplasmic staining was correlated sig-nificantly to a better prognosis (p = 0.0051). Immunoblot analysis demonstrated the expression of TAG-72 in three ovariancancer cell lines (OVCAR3, SB247 and COV362.4). In conclusion, the tumor-specific expression of TAG-72 and its asso-ciation with disease stage indicate its potential as a marker for effective disease management and targeted cancer therapy.� 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: TAG-72; Ovarian cancer; Diagnosis; Prognosis; Therapy
0304-3835/$ - see front matter � 2006 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.canlet.2006.11.025
* Corresponding author. Tel.: +1 402 559 5455; fax: +1 402 559 6650.E-mail address: [email protected] (S.K. Batra).
1 Both these authors have equally contributed to this manuscript.
248 M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257
1. Introduction
According to the American Cancer Society, ovar-ian cancer is the most lethal gynecological malignancyand the fourth leading cause of cancer-related deathsin women in the United States. Approximately 20,180new cases will be diagnosed and 15,310 women willdie due to ovarian cancer in the year 2006 [1]. No con-siderable improvement has been reported in the sur-vival of ovarian cancer patients in the past 30 yearsand the five-year survival still remains to be only35% after diagnosis. Epithelial ovarian cancer(EOC), the most common type among all forms ofthe ovarian cancers, is highly malignant and is fre-quently associated with widespread intra-peritonealmetastasis and ascites [2,3]. The survival of ovariancancer patients can be improved significantly if treat-ed at an early stage, however, presently, only 23% ofthe cases are detected at stage I due to lack of earlydiagnostic markers [4,5].
The current diagnostic methods have shown lim-itations in early detection of ovarian cancer and themajority (>70%) of the cases are diagnosed only atadvanced stages (III and IV) when cancer hasalready spread into the peritoneal cavity [4,6–9].The CA125 serum assay is one of the most utilizedtumor marker tests for the detection of epithelialcancers of the ovary [4,10]. The specificity of CA125 assay, however, is limited due to its elevationin benign conditions such as endometriosis, pelvicinflammatory disease and pregnancy [6,7,10–12].Similarly, other methods, such as the trans-vaginalsonogram, and pelvic palpation being used for thedetection of ovarian cancer have limitations due tothe lack of specificity. The proteins that are specifi-cally present and/or overexpressed in cancer tissuesmay be utilized as disease markers and therapeutictargets. TAG-72 is a high molecular weight tumorassociated glycoprotein, which is known to be over-expressed in various carcinomas including ovariancancer [13]. In previous studies, it has been clearlydemonstrated that TAG-72 is not expressed in nor-mal adult tissues except secretary endometrial tissues[14]. Thus, the tumor tissue restricted expression ofTAG-72 makes it an ideal candidate for cancerimmunodiagnosis and targeted immunotherapy.Several antibodies reactive to TAG-72 have beengenerated thus far. B72.3, a TAG-72 reactive mono-clonal antibody, generated by immunization of micewith a membrane enriched fraction of human breastcarcinoma cells [15–17] has been utilized to analyzeTAG-72 expression in different types of cancers
[18]. In other studies, a second generation monoclo-nal antibody CC49, showing higher affinity and sev-eral times more specificity to detect TAG-72compared to the B72.3 antibody, has been used tocheck the expression and to treat the metastatic car-cinoma by radioimmunotherapy [19–22]. CC49monoclonal antibody recognizes the sialyl-Tn andsialyl-T [23,24], the two carbohydrate epitopespresent on mucin like glycoproteins. Since multiplecopies of these epitopes can be present on a singleglycoproteins, the CC49 antibody may provide ahigher sensitivity. The preclinical use of CC49 andits engineered single chain Fv (scFv) forms have beendemonstrated in targeted radioimmunotherapy withexcellent pharmacokinetics and biodistribution[25–28].
In the present study, we have analyzed theexpression of TAG-72 in ovarian cancer cell linesand tissues using CC49 monoclonal antibody. Theoverall objective was to study the correlation of itsexpression and localization profiles with tumorstage (early versus advanced), histological subtype(serous, clear cell, mucinous and endometrioid)and patient’s prognosis.
2. Materials and methods
2.1. Tissue specimen and cell lines
Forty-three ovarian cancer and 3 normal ovarian tis-sue samples (paraffin-embedded) were used in this study.Samples were obtained after approval of the protocol bythe Institutional Review Board (IRB) at the University ofNebraska Medical Center, Omaha, NE. Four micronthick paraffin sections were cut and stained with hema-toxylin and eosin for pathological evaluation. The histo-logical type and pathological stage were assessed by asurgical pathologist (S.L.J.) according to the guidelinesof World Health Organization (WHO) and Americanjoint committee on cancer (AJCC), respectively. In addi-tion, ten ovarian cancer cell lines [SKOV3, OVCAR3COV362.4, COV664, COV434, PA1, SB247, KGNA2780 and A2780 CISR (Cisplatin resistant)] were alsostudied. All the cell lines were grown in ATCC specifiedculture media.
2.2. Immunohistochemistry
Four micron (4 lm) thick sections from paraffinembedded blocks were prepared by tissue microtomyand were mounted on the slides. Sections were deparaffi-nized using EZ-DeWaxTM (Bio Genex, San Ramon, CA)and then rehydrated with graded alcohols. Heat-inducedantigen retrieval was performed in citrate buffer (pH

M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257 249
6.0) by heating slides in a microwave oven at 700 W for15 min. Sections were then processed for the immunohis-tochemistry as described previously [29,30]. In brief, thetissue sections were washed three times with phosphatebuffer saline (PBS) and incubated with Vectastain normalhorse serum (Vector ABC kit, Vector Laboratories, Bur-lingame, CA) for 30 min at room temperature to blocknon-specific binding. Endogenous peroxidase activitywas quenched by incubating sections in 3% H2O2 inPBS for 20 min. Sections were then incubated with anti-TAG72 mouse monoclonal antibody (CC49) for 60 minat room temperature and washed with PBS-T containing0.05% Tween 20 (3 · 5 min) before incubating with horseradish peroxidase-labeled secondary antibody (VectorLaboratories) for 30 min. Slides were washed again(3 · 5 min) with PBS-T before incubating with the ABCsolution (Vector Laboratories). The reaction color wasdeveloped by incubating sections with 3,3 0-diaminobenzi-dine reagent (DAB) (Vector Laboratories) as per manu-facturer’s instructions. The slides were washed withwater, counter-stained with hematoxylin, dehydratedand mounted with Vectamount permanent mountingmedia (Vector Laboratories).
2.3. Assessment of immunoperoxidase staining
All slides were observed under Nikon E400 LightMicroscope and representative photographs were taken.The intensity and percent immunoreactivity of the CC49MAb was scored. Staining intensity was graded on a 0–3 scale (0 for no staining, + for weak immunoreactivity;++ for moderate immunoreactivity; and +++ for strongimmunoreactivity). The percentage of cells that showedpositive immunoreactivity within the tissue section wasscored as follows: 1 for 0–25%; 2 for 26–50%; 3 for 51–75%; and 4 for 76–100%. The values of the staining inten-sity and the percent immunoreactive cells were multipliedto obtain a composite score ranging from 0 to 12.
2.4. Confocal immunofluorescence microscopy
Ovarian cancer cells were processed for confocalmicroscopy as described previously [29,30]. Briefly, cellswere grown at 37 �C for 24 h on sterile glass cover slips,washed with Hanks buffer containing 0.1 M HEPES andfixed in ice-cold methanol at �20 �C for 2 min. To preventnon-specific binding, cells were blocked with 10% goatserum in phosphate buffered saline containing 0.05%Tween 20 (PBS-T) for 30 min, followed by incubationwith anti-TAG-72 monoclonal antibody (CC49) dilutedin PBS (1:200) for 60 min at room temperature. Cells werewashed 4 · 5 min with PBS-T and then incubated withFITC-conjugated goat anti-mouse secondary antibodies(1:400) for 30 min. Cells were washed (5 · 5 min) andmounted on glass slides in anti-fade Vectashield mountingmedium (Vector Laboratories).
2.5. Western blot analysis
Ovarian cancer cell lines were processed for proteinextraction and Western blotting by both SDS–agaroseand acrylamide gel electrophoresis, as previously described[29,30]. Briefly, the cells were lysed in RIPA buffer(100 mM Tris, 5 mM EDTA, 5% NP40; pH 8.0) containingprotease inhibitors (1 mM phenyl-methyl sulfonyl fluoride,1 lg/ml aprotinin, 1 lg/ml leupeptin) and kept at 4 �C for30 min. Cell lysates were passed through one freeze thawcycle to disrupt the cell membranes, centrifuged at14,000 rpm for 30 min at 4 �C and supernatants were col-lected. The lysates were heat denatured in reducing SDSsample buffer, resolved on either10% SDS–polyacrylamideor 2% SDS–agarose gel by electrophoresis and subsequentlytransferred on to PVDF membranes. The membranes wereblocked in 5% nonfat dry milk in PBS for 2 h and incubatedwith anti-TAG-72 MAb (CC49) (1:5000) or anti-b-actinmonoclonal antibody (1:5000) for 2 h at room tempera-ture. The membranes were washed (6 · 10 min) in PBSTat room temperature, incubated with horseradish peroxi-dase-conjugated goat anti-mouse secondary antibodies(1:2000) (Amersham Biosciences) for 1 h at room tempera-ture and washed 5 · 10 min with PBST. The signal wasdetected with ECL Chemiluminescence Kit (AmershamBiosciences, Buckinghamshire, UK).
2.6. Statistical analysis
Mean composite scores were compared between stagegroups and tumor types with t-tests and analysis of vari-ance, respectively. Stage and tumor types were examinedfor associations with TAG-72 staining using Fisher’sexact test. Various TAG-72 group combinations wereexamined. Overall survival times were calculated asmonths from diagnosis to death from any cause or dateof last follow-up. Patients alive at last follow-up weretreated as censored. Survival distributions were estimatedusing the Kaplan–Meier method and the log-rank test wasused to compare distributions between TAG-72 stainingscore categories, composite score, stage, and tumor type.p-values less than 0.05 were considered to be statisticallysignificant.
3. Results
3.1. TAG-72 is overexpressed in ovarian tumors and
correlated with tumor stage
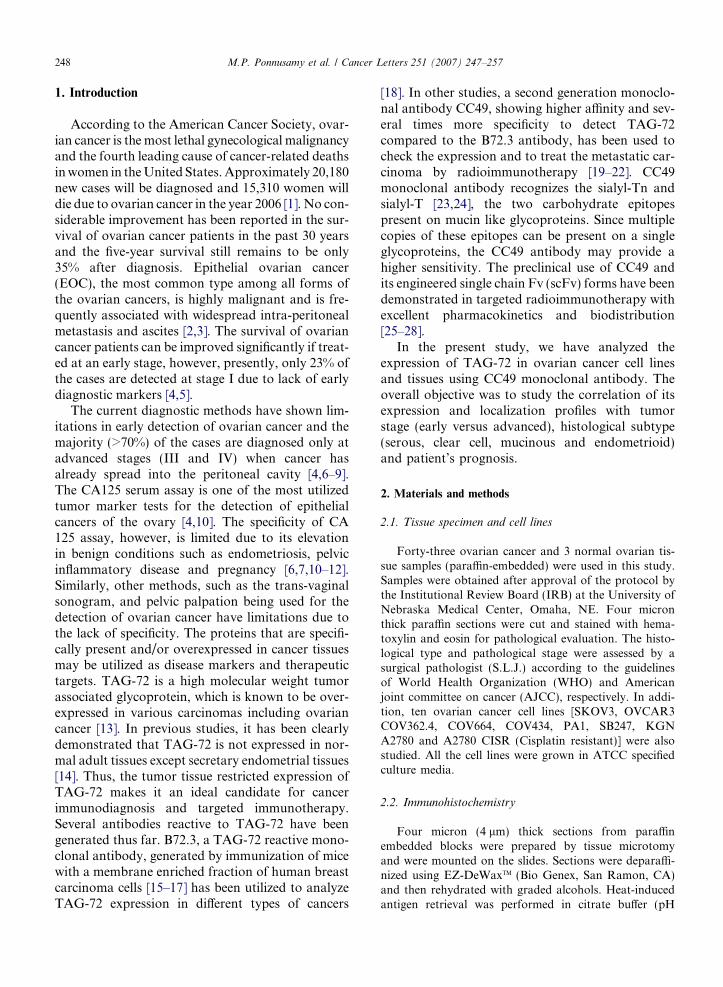
Immunoperoxidase staining of TAG-72 using a secondgeneration monoclonal antibody, CC49, showed positiveimmunoreactivity in 88% of the ovarian cancer samples,while normal ovary samples (n = 3) failed to show anyimmunoreactivity. A representative pattern of TAG-72expression in different histological tumor types (serous,clear cell, endometrioid and mucinous) and in the normal
250 M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257
ovary is shown in Fig. 1. In order to evaluate the correla-tion of the TAG-72 overexpression with cancer stage,tumor samples were grouped into early (stages I and II,n = 10) and advanced (stages III and IV, n = 33) stages.Among 10 early stage samples, 90% of the samplesshowed immunoreactivity for CC49 with weak (n = 2)and moderate (n = 7) staining and a mean compositescore of 2.3. In advance stage tumor samples, 84.8%expressed TAG-72. Among this group, CC49 immuno-staining was weak (n = 3), moderate (n = 21) and strong(n = 4), with a mean composite score of 3.7 (Table 1). Sta-tistical analysis revealed that the mean composite score of
Fig. 1. TAG-72 expression in different histological types of ovarian caembedded ovarian cancer and normal ovary tissue sections were procantibody (1:250). Expression of TAG-72 is shown in (a) serous (b) clearand one of the mucinous ovarian tumor samples failed to show a detect400·.
TAG-72 immunostaining was significantly higher(p = 0.035) in advanced stage ovarian tumors comparedto the early stage samples. However, no significant corre-lation was observed among different histological tumortypes (Table 1).
3.2. Association of TAG-72 localization with ovarian cancer
stage and histological types
We next examined if there existed a correlation betweenTAG-72 localization (cytoplasmic/membrane-bound/lu-minal) and tumor stage or histological subtypes of
ncer and normal ovary tissue samples. Formalin-fixed, paraffin-essed for immunohistochemical analysis using CC49 monoclonalcell; (c) endometroid; (d) mucinous ovarian tumors. Normal ovaryable level of TAG-72 expression (e and f). Original magnification,
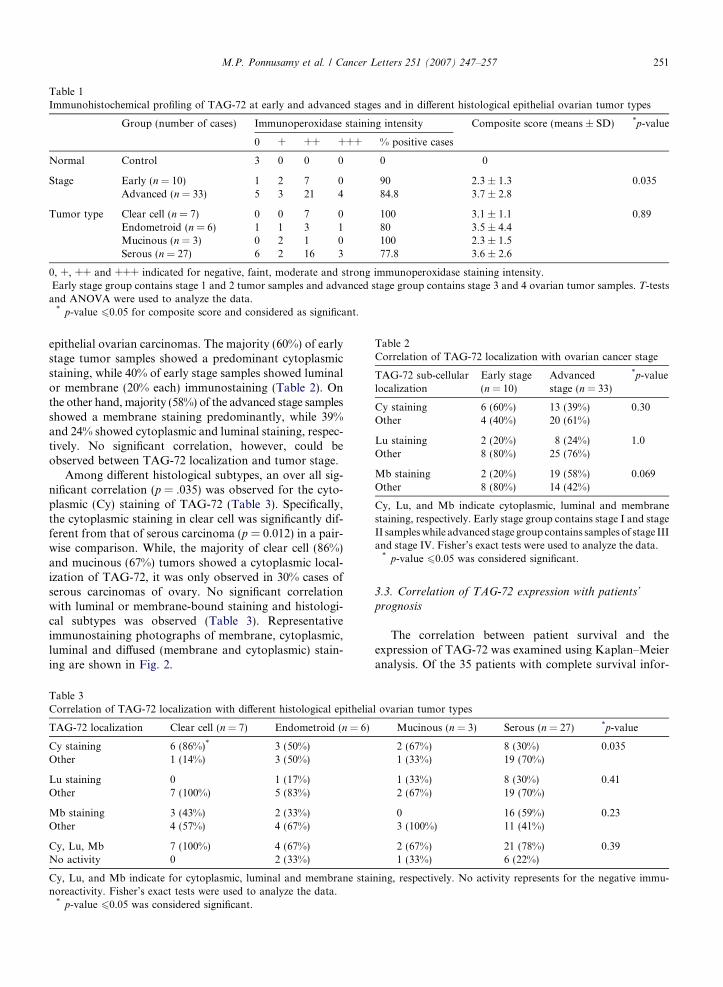
Table 2Correlation of TAG-72 localization with ovarian cancer stage
TAG-72 sub-cellularlocalization
Early stage(n = 10)
Advancedstage (n = 33)
*p-value
Cy staining 6 (60%) 13 (39%) 0.30Other 4 (40%) 20 (61%)
Lu staining 2 (20%) 8 (24%) 1.0Other 8 (80%) 25 (76%)
Mb staining 2 (20%) 19 (58%) 0.069Other 8 (80%) 14 (42%)
Cy, Lu, and Mb indicate cytoplasmic, luminal and membranestaining, respectively. Early stage group contains stage I and stageII samples while advanced stage group contains samples of stage IIIand stage IV. Fisher’s exact tests were used to analyze the data.
* p-value 60.05 was considered significant.
Table 1Immunohistochemical profiling of TAG-72 at early and advanced stages and in different histological epithelial ovarian tumor types
Group (number of cases) Immunoperoxidase staining intensity Composite score (means ± SD) *p-value
0 + ++ +++ % positive cases
Normal Control 3 0 0 0 0 0
Stage Early (n = 10) 1 2 7 0 90 2.3 ± 1.3 0.035Advanced (n = 33) 5 3 21 4 84.8 3.7 ± 2.8
Tumor type Clear cell (n = 7) 0 0 7 0 100 3.1 ± 1.1 0.89Endometroid (n = 6) 1 1 3 1 80 3.5 ± 4.4Mucinous (n = 3) 0 2 1 0 100 2.3 ± 1.5Serous (n = 27) 6 2 16 3 77.8 3.6 ± 2.6
0, +, ++ and +++ indicated for negative, faint, moderate and strong immunoperoxidase staining intensity.Early stage group contains stage 1 and 2 tumor samples and advanced stage group contains stage 3 and 4 ovarian tumor samples. T-tests
and ANOVA were used to analyze the data.* p-value 60.05 for composite score and considered as significant.
M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257 251
epithelial ovarian carcinomas. The majority (60%) of earlystage tumor samples showed a predominant cytoplasmicstaining, while 40% of early stage samples showed luminalor membrane (20% each) immunostaining (Table 2). Onthe other hand, majority (58%) of the advanced stage samplesshowed a membrane staining predominantly, while 39%and 24% showed cytoplasmic and luminal staining, respec-tively. No significant correlation, however, could beobserved between TAG-72 localization and tumor stage.
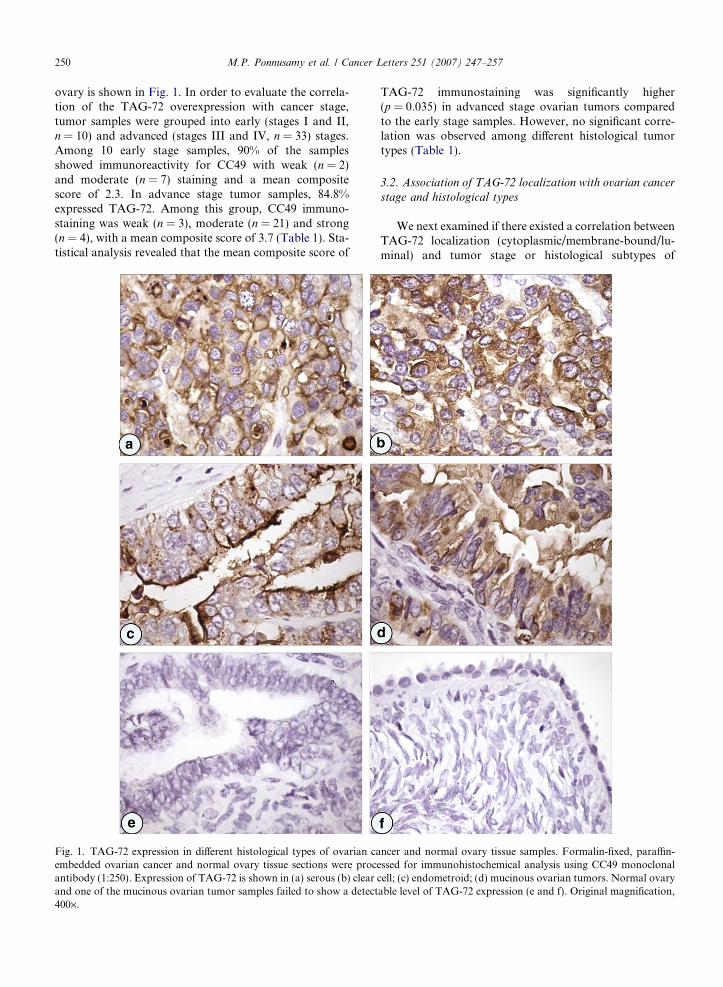
Among different histological subtypes, an over all sig-nificant correlation (p = .035) was observed for the cyto-plasmic (Cy) staining of TAG-72 (Table 3). Specifically,the cytoplasmic staining in clear cell was significantly dif-ferent from that of serous carcinoma (p = 0.012) in a pair-wise comparison. While, the majority of clear cell (86%)and mucinous (67%) tumors showed a cytoplasmic local-ization of TAG-72, it was only observed in 30% cases ofserous carcinomas of ovary. No significant correlationwith luminal or membrane-bound staining and histologi-cal subtypes was observed (Table 3). Representativeimmunostaining photographs of membrane, cytoplasmic,luminal and diffused (membrane and cytoplasmic) stain-ing are shown in Fig. 2.
Table 3Correlation of TAG-72 localization with different histological epithelia
TAG-72 localization Clear cell (n = 7) Endometroid (n = 6)
Cy staining 6 (86%)* 3 (50%)Other 1 (14%) 3 (50%)
Lu staining 0 1 (17%)Other 7 (100%) 5 (83%)
Mb staining 3 (43%) 2 (33%)Other 4 (57%) 4 (67%)
Cy, Lu, Mb 7 (100%) 4 (67%)No activity 0 2 (33%)
Cy, Lu, and Mb indicate for cytoplasmic, luminal and membrane stainoreactivity. Fisher’s exact tests were used to analyze the data.
* p-value 60.05 was considered significant.
3.3. Correlation of TAG-72 expression with patients’
prognosis
The correlation between patient survival and theexpression of TAG-72 was examined using Kaplan–Meieranalysis. Of the 35 patients with complete survival infor-
l ovarian tumor types
Mucinous (n = 3) Serous (n = 27) *p-value
2 (67%) 8 (30%) 0.0351 (33%) 19 (70%)
1 (33%) 8 (30%) 0.412 (67%) 19 (70%)
0 16 (59%) 0.233 (100%) 11 (41%)
2 (67%) 21 (78%) 0.391 (33%) 6 (22%)
ning, respectively. No activity represents for the negative immu-
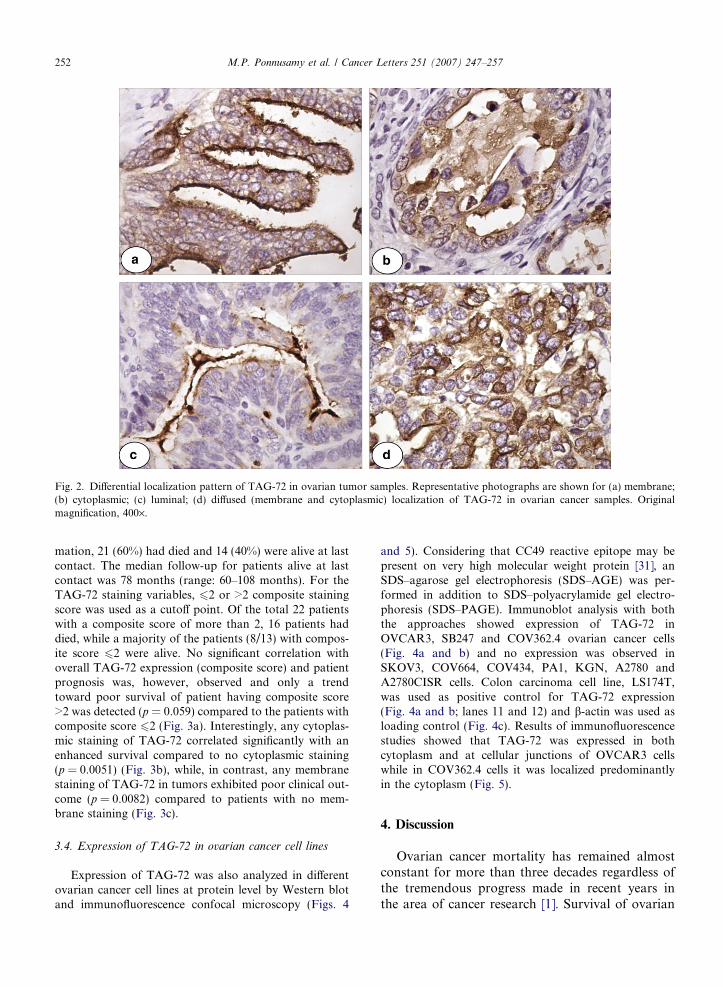
Fig. 2. Differential localization pattern of TAG-72 in ovarian tumor samples. Representative photographs are shown for (a) membrane;(b) cytoplasmic; (c) luminal; (d) diffused (membrane and cytoplasmic) localization of TAG-72 in ovarian cancer samples. Originalmagnification, 400·.
252 M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257
mation, 21 (60%) had died and 14 (40%) were alive at lastcontact. The median follow-up for patients alive at lastcontact was 78 months (range: 60–108 months). For theTAG-72 staining variables, 62 or >2 composite stainingscore was used as a cutoff point. Of the total 22 patientswith a composite score of more than 2, 16 patients haddied, while a majority of the patients (8/13) with compos-ite score 62 were alive. No significant correlation withoverall TAG-72 expression (composite score) and patientprognosis was, however, observed and only a trendtoward poor survival of patient having composite score>2 was detected (p = 0.059) compared to the patients withcomposite score 62 (Fig. 3a). Interestingly, any cytoplas-mic staining of TAG-72 correlated significantly with anenhanced survival compared to no cytoplasmic staining(p = 0.0051) (Fig. 3b), while, in contrast, any membranestaining of TAG-72 in tumors exhibited poor clinical out-come (p = 0.0082) compared to patients with no mem-brane staining (Fig. 3c).
3.4. Expression of TAG-72 in ovarian cancer cell lines
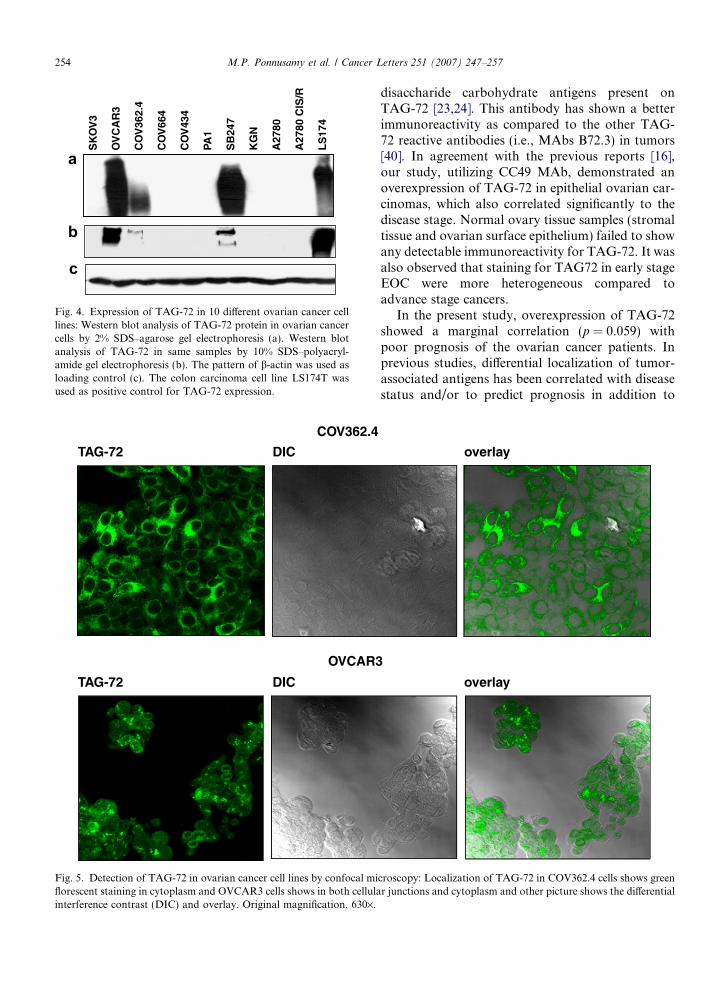
Expression of TAG-72 was also analyzed in differentovarian cancer cell lines at protein level by Western blotand immunofluorescence confocal microscopy (Figs. 4
and 5). Considering that CC49 reactive epitope may bepresent on very high molecular weight protein [31], anSDS–agarose gel electrophoresis (SDS–AGE) was per-formed in addition to SDS–polyacrylamide gel electro-phoresis (SDS–PAGE). Immunoblot analysis with boththe approaches showed expression of TAG-72 inOVCAR3, SB247 and COV362.4 ovarian cancer cells(Fig. 4a and b) and no expression was observed inSKOV3, COV664, COV434, PA1, KGN, A2780 andA2780CISR cells. Colon carcinoma cell line, LS174T,was used as positive control for TAG-72 expression(Fig. 4a and b; lanes 11 and 12) and b-actin was used asloading control (Fig. 4c). Results of immunofluorescencestudies showed that TAG-72 was expressed in bothcytoplasm and at cellular junctions of OVCAR3 cellswhile in COV362.4 cells it was localized predominantlyin the cytoplasm (Fig. 5).
4. Discussion
Ovarian cancer mortality has remained almostconstant for more than three decades regardless ofthe tremendous progress made in recent years inthe area of cancer research [1]. Survival of ovarian

c
a
> 2 6 16 22
Composite score CNSR FAIL TOTAL
<=2 8 5 13.
Test: p=0.059
0.00.10.20.30.40.50.60.70.80.91.0
Months
Pro
port
ion
Pro
port
ion
|
| |
1.00.90.80.70.60.50.40.30.20.10.0
1200 12 24 36 48 60 72 84 96 108
Mb CNSR FAIL TOTAL MEDIAN
Any Mb 4 17 21 36Other 10 4 14 .
Months
Test: p=0.0082
||
||||
1.00.90.80.70.60.50.40.30.20.10.0
120Months
0 12 24 36 48 60 72 84 96 1081200 12 24 36 48 60 72 84 96 108
b
Cy CNSR FAIL TOTAL MEDIAN
Any Cy 11 6 17 .Other 3 15 18 36
Pro
port
ion
Test: p=0.0051
Fig. 3. Kaplan–Meier analysis for the correlation of TAG-72 expression (a) overall survival by composite score; (b) overall survival bycytoplasmic staining; (c) overall survival by membrane staining. A marginal significant correlation (p = 0.059) was observed betweenTAG-72 expression and poor patient survival. A significant correlation between membrane sub-cellular localization of TAG-72(p = 0.0051) was observed in ovarian cancer patients. CNSR, patient censored (alive); FAIL, patients dead; TOTAL, total number of casesand composite score values of immunostaining indicated as P2 and >2(A).
M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257 253
cancer patients can be improved considerably if newmethods of early diagnosis and therapy are devel-oped [5,8]. In the present study, we examined theexpression and localization profiles of TAG-72 inovarian tumor samples and studied its associationwith tumor stage, histological subtype and patients’prognosis. Our study demonstrated an overexpres-sion of TAG-72 in epithelial ovarian carcinoma thatcorrelated significantly (p = 0.035) with tumorstage, but not with histological subtype (Table 1).Nonetheless, an over all significant correlation ofcytoplasmic staining (p = 0.035) with histologicalsubtypes was observed (Table 3) with clear cell Cystaining showing significant difference from serousCy staining in a pair-wise comparison (p = 0.012).Furthermore, patients with any cytoplasmic stain-ing exhibited a better survival, while any membranestaining correlated with poor prognosis. However,
overall TAG-72 expression did not show significantlinkage with patient’s prognosis.
In earlier studies, TAG-72 expression has beenexploited for selective gene delivery [32], radioimmu-notherapy [33] and radioimaging [34,35]. TAG-72expression in epithelial ovarian carcinomas has alsobeen analyzed in previous studies [13,36,37]. Thesestudies either utilized a lower affinity antibodyB72.3 [13,37] or a second generation, higher affinitymonoclonal antibody CC49 [16]. All these studieshave demonstrated an overexpression of TAG-72in majority of malignant epithelial cells comparedto normal or benign lesions. Due to the high specific-ity and strong immunoreactivity to target antigen,CC49 antibody has entered in clinical trials for theimaging and treatment of various carcinomas [20–22,33,38,39]. CC49 monoclonal antibody recognizesthe sialyl-Tn and sialyl-T epitopes, which are
d
COV362.4
OVCAR3
TAG-72 DIC
TAG-72 DIC
Fig. 5. Detection of TAG-72 in ovarian cancer cell lines by confocal miflorescent staining in cytoplasm and OVCAR3 cells shows in both cellulainterference contrast (DIC) and overlay. Original magnification, 630·.
SK
OV
3
OV
CA
R3
CO
V36
2.4
CO
V66
4
CO
V43
4
PA1
SB
247
KG
N
A27
80
A27
80 C
IS/R
LS
174
a
b
c
Fig. 4. Expression of TAG-72 in 10 different ovarian cancer celllines: Western blot analysis of TAG-72 protein in ovarian cancercells by 2% SDS–agarose gel electrophoresis (a). Western blotanalysis of TAG-72 in same samples by 10% SDS–polyacryl-amide gel electrophoresis (b). The pattern of b-actin was used asloading control (c). The colon carcinoma cell line LS174T wasused as positive control for TAG-72 expression.
254 M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257
disaccharide carbohydrate antigens present onTAG-72 [23,24]. This antibody has shown a betterimmunoreactivity as compared to the other TAG-72 reactive antibodies (i.e., MAbs B72.3) in tumors[40]. In agreement with the previous reports [16],our study, utilizing CC49 MAb, demonstrated anoverexpression of TAG-72 in epithelial ovarian car-cinomas, which also correlated significantly to thedisease stage. Normal ovary tissue samples (stromaltissue and ovarian surface epithelium) failed to showany detectable immunoreactivity for TAG-72. It wasalso observed that staining for TAG72 in early stageEOC were more heterogeneous compared toadvance stage cancers.
In the present study, overexpression of TAG-72showed a marginal correlation (p = 0.059) withpoor prognosis of the ovarian cancer patients. Inprevious studies, differential localization of tumor-associated antigens has been correlated with diseasestatus and/or to predict prognosis in addition to
overlay
overlay
croscopy: Localization of TAG-72 in COV362.4 cells shows greenr junctions and cytoplasm and other picture shows the differential

M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257 255
their aberrant expression [41–43]. In a study byShigeto et al, localization of EGFR in the cytoplasmcorrelated with poor prognosis in pancreatic adeno-carcinoma patients [43]. Similarly, cytoplasmiclocalization of p27kip1, a cyclin-dependent kinaseinhibitor that regulates cellular progression fromG1 to S phase, is independently associated with poorsurvival in late stage ovarian carcinomas irrespec-tive of tumor histotype [42]. In a retrospective studyof breast carcinomas, the cytoplasmic expression oftransmembrane mucin MUC1 has been correlatedwith poor prognosis [41]. The analysis of theTAG-72 localization in the present study exhibitedfour patterns of TAG-72 localization [cytoplasmic,membrane bound, luminal and diffused (both mem-brane and cytoplasmic)]. Interestingly, the mem-brane staining of TAG-72 correlated significantlywith the poor patient survival (p = 0.0082), whilethe cytoplasmic staining indicated better prognosisof patients compared to all others. Furthermore,the cytoplasmic localization of TAG-72 correlatedwith the clear-cell shows significant difference whencompared with serous CY staining (p = 0.012) how-ever, it did not correlate with tumor stage. This wasconsistent with the previous study [36] that alsofound no significant difference in the membraneand cytoplasmic expression of TAG-72 in the pri-mary and metastatic lesions.
We have also studied the TAG-72 expression byimmunoblot analysis in established ovarian cancercell lines. Among the 10 cell lines examined, onlythree cell lines (OVCAR3, SB247 and COV362.4)showed TAG-72 expression. Furthermore, immuno-fluorescence study demonstrated TAG-72 localiza-tion both in the cytoplasm and at cellularjunctions in OVCAR3 cells, while it was presentonly in the cytoplasm of COV362.4 cells. The resultsfrom this study substantiate the importance ofTAG-72 as a valid target for diagnosis and therapyof EOC. Monoclonal antibody CC49 has alreadybeen exploited for radioimmunotherapy of EOC.Besides we have generated and characterized scFvsto CC49 that have extensively been evaluated in pre-clinical studies for tumor targeting [25,26].
In conclusion, our immunohistochemical dataclearly indicate that TAG-72 is an overexpressedglycoprotein that can find multiple uses as atarget for ovarian cancer diagnosis and diseasemanagement. Furthermore, the TAG-72 express-ing cell line identified in this study can beuseful for studying targeted therapy in animalmodel.
Acknowledgements
This work was supported by a grant fromDepartment of Defense OC040592 and the OlsonCenter for Women’s Health. We thank Mr. ErikMoore for excellent technical support and Ms. KristiL. W. Berger for editing the manuscript. We alsothank the Director of the Tissue Bank at UNMC,Dr Julia Bridge, for providing tissue samples. TheNCI Cancer Center Grant (P30 CA36727) toUNMC and CHTN Western Division, Case Wes-tern Reserve University, Cleveland, Ohio, is greatlyacknowledged for providing the additional tissuesfor this study. The Mab CC49 was a gift from Dr.David Colcher and is greatly acknowledged. Theovarian cell lines COV362.4 and COV644 were ob-tained from Dr. C.E. van der Minne, Leiden Uni-versity Medical Center, Leiden, The Netherlands.
References
[1] A. Jemal, R. Siegel, E. Ward, T. Murray, J. Xu, C. Smigal,M.J. Thun, Cancer statistics, 2006, CA Cancer J. Clin. 56(2006) 106–130.
[2] N. Auersperg, M.I. Edelson, S.C. Mok, S.W. Johnson, T.C.Hamilton, The biology of ovarian cancer, Semin. Oncol. 25(1998) 281–304.
[3] N. Auersperg, A.S. Wong, K.C. Choi, S.K. Kang, P.C.Leung, Ovarian surface epithelium: biology, endocrinology,and pathology, Endocr. Rev. 22 (2001) 255–288.
[4] F. exander-Sefre, U. Menon, I.J. Jacobs, Ovarian cancerscreening, Hosp. Med. 63 (2002) 210–213.
[5] R.F. Ozols, Update on the management of ovarian cancer,Cancer J. 8 (Suppl) (2002) S22–S30.
[6] R.C. Bast Jr., Status of tumor markers in ovarian cancerscreening, J. Clin. Oncol. 21 (2003) 200–205.
[7] I.J. Jacobs, U. Menon, Progress and challenges in screeningfor early detection of ovarian cancer, Mol. Cell Proteomics 3(2004) 355–366.
[8] U. Menon, I.J. Jacobs, Recent developments in ovarian cancerscreening, Curr. Opin. Obstet. Gynecol. 12 (2000) 39–42.
[9] U. Menon, I. Jacobs, Screening for ovarian cancer, BestPract. Res. Clin. Obstet. Gynaecol. 16 (2002) 469–482.
[10] H.A. Fritsche, R.C. Bast, CA 125 in ovarian cancer:advances and controversy, Clin. Chem. 44 (1998)1379–1380.
[11] R.C. Bast Jr., F.J. Xu, Y.H. Yu, S. Barnhill, Z. Zhang, G.B.Mills, CA 125: the past and the future, Int. J. Biol. Markers13 (1998) 179–187.
[12] I.J. Jacobs, D.H. Oram, R.C. Bast Jr., Strategies forimproving the specificity of screening for ovarian cancerwith tumor-associated antigens CA 125, CA 15-3, and TAG72.3, Obstet. Gynecol. 80 (1992) 396–399.
[13] A. Thor, N. Ohuchi, C.A. Szpak, W.W. Johnston, J. Schlom,Distribution of oncofetal antigen tumor-associated glyco-protein-72 defined by monoclonal antibody B72.3, CancerRes. 46 (1986) 3118–3124.
256 M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257
[14] A. Thor, M.J. Viglione, R. Muraro, N. Ohuchi, J. Schlom,F. Gorstein, Monoclonal antibody B72.3 reactivity withhuman endometrium: a study of normal and malignanttissues, Int. J. Gynecol. Pathol. 6 (1987) 235–247.
[15] D. Colcher, P.H. Hand, M. Nuti, J. Schlom, A spectrum ofmonoclonal antibodies reactive with human mammarytumor cells, Proc. Natl. Acad. Sci. USA 78 (1981)3199–3203.
[16] D. Colcher, M.F. Minelli, M. Roselli, R. Muraro, D.Simpson-Milenic, J. Schlom, Radioimmunolocalization ofhuman carcinoma xenografts with B72.3 second generationmonoclonal antibodies, Cancer Res. 48 (1988) 4597–4603.
[17] D.M. Colcher, D.E. Milenic, J. Schlom, Generation andcharacterization of monoclonal antibody B72.3. Experimen-tal and preclinical studies, Target. Diagn.Ther. 6 (1992)23–44.
[18] W.W. Johnston, C.A. Szpak, S.C. Lottich, A. Thor, J.Schlom, Use of a monoclonal antibody (B72.3) as a novelimmunohistochemical adjunct for the diagnosis of carcino-mas in fine needle aspiration biopsy specimens, Hum. Pathol.17 (1986) 501–513.
[19] S.K. Batra, M. Jain, U.A. Wittel, S.C. Chauhan, D. Colcher,Pharmacokinetics and biodistribution of genetically engi-neered antibodies, Curr. Opin. Biotechnol. 13 (2002)603–608.
[20] R.F. Meredith, A.J. Bueschen, M.B. Khazaeli, W.E. Plott,W.E. Grizzle, R.H. Wheeler, J. Schlom, C.D. Russell, T. Liu,A.F. LoBuglio, Treatment of metastatic prostate carcinomawith radiolabeled antibody CC49, J. Nucl. Med. 35 (1994)1017–1022.
[21] R.F. Meredith, E.E. Partridge, R.D. Alvarez, M.B. Khaza-eli, G. Plott, C.D. Russell, R.H. Wheeler, T. Liu, W.E.Grizzle, J. Schlom, A.F. LoBuglio, Intraperitoneal radioim-munotherapy of ovarian cancer with lutetium-177-CC49, J.Nucl. Med. 37 (1996) 1491–1496.
[22] F. Robert, E.M. Busby, A.F. LoBuglio, Chemotherapytolerance after radioimmunotherapy with 90Y-CC49 mono-clonal antibody in patients with advanced non-small cell lungcancer: clinical effects and hematologic toxicity, CancerBiother. Radiopharm. 18 (2003) 317–325.
[23] F.G. Hanisch, G. Uhlenbruck, H. Egge, J. Peter-Katalinic, AB72.3 second-generation-monoclonal antibody (CC49)defines the mucin-carried carbohydrate epitope Gal beta(1-3) [NeuAc alpha(2-6)]GalNAc, Biol. Chem. Hoppe Seyler370 (1989) 21–26.
[24] H.S. Silverman, M. Sutton-Smith, K. McDermott, P. Heal,S.H. Leir, H.R. Morris, M.A. Hollingsworth, A. Dell, A.Harris, The contribution of tandem repeat number to the O-glycosylation of mucins, Glycobiology 13 (2003) 265–277.
[25] S.C. Chauhan, M. Jain, E.D. Moore, U.A. Wittel, J. Li, P.R.Gwilt, D. Colcher, S.K. Batra, Pharmacokinetics andbiodistribution of 177Lu-labeled multivalent single-chainFv construct of the pancarcinoma monoclonal antibodyCC49, Eur. J. Nucl. Med. Mol. Imaging 32 (2005) 264–273.
[26] A. Goel, D. Colcher, J. Baranowska-Kortylewicz, S. Augus-tine, B.J. Booth, G. Pavlinkova, S.K. Batra, Geneticallyengineered tetravalent single-chain Fv of the pancarcinomamonoclonal antibody CC49: improved biodistribution andpotential for therapeutic application, Cancer Res. 60 (2000)6964–6971.
[27] S.V. Kashmiri, L. Shu, E.A. Padlan, D.E. Milenic, J.Schlom, P.H. Hand, Generation, characterization, and
in vivo studies of humanized anticarcinoma antibodyCC49, Hybridoma 14 (1995) 461–473.
[28] S.M. Larson, A.M. El-Shirbiny, C.R. Divgi, G. Sgouros,R.D. Finn, J. Tschmelitsch, A. Picon, M. Whitlow, J.Schlom, J. Zhang, A.M. Cohen, Single chain antigen bindingprotein (sFv CC49): first human studies in colorectalcarcinoma metastatic to liver, Cancer 80 (1997) 2458–2468.
[29] N. Moniaux, G.C. Varshney, S.C. Chauhan, M.C. Copin,M. Jain, U.A. Wittel, M. Andrianifahanana, J.P. Aubert,S.K. Batra, Generation and characterization of anti-MUC4monoclonal antibodies reactive with normal and cancer cellsin humans, J. Histochem. Cytochem. 52 (2004) 253–261.
[30] A.P. Singh, N. Moniaux, S.C. Chauhan, J.L. Meza, S.K.Batra, Inhibition of MUC4 expression suppresses pancreatictumor cell growth and metastasis, Cancer Res. 64 (2004)622–630.
[31] X. Filella, S. Friese, H.J. Roth, S. Nussbaum, B. Wehnl,Technical performance of the Elecsys CA 72-4 test–develop-ment and field study, Anticancer Res. 20 (2000) 5229–5232.
[32] F.J. Kelly, C.R. Miller, D.J. Buchsbaum, J. Gomez-Navar-ro, M.N. Barnes, R.D. Alvarez, D.T. Curiel, Selectivity ofTAG-72-targeted adenovirus gene transfer to primary ovar-ian carcinoma cells versus autologous mesothelial cellsin vitro, Clin. Cancer Res. 6 (2000) 4323–4333.
[33] R.D. Alvarez, W.K. Huh, M.B. Khazaeli, R.F. Meredith,E.E. Partridge, L.C. Kilgore, W.E. Grizzle, S. Shen, J.M.Austin, M.N. Barnes, D. Carey, J. Schlom, A.F. LoBuglio,A Phase I study of combined modality (90)Yttrium-CC49intraperitoneal radioimmunotherapy for ovarian cancer,Clin. Cancer Res. 8 (2002) 2806–2811.
[34] J. Bell, C. Mojzisik, G. Hinkle Jr., H. Derman, J. Schlom, E.Martin, Intraoperative radioimmunodetection of ovariancancer using monoclonal antibody B72.3 and a portablegamma-detecting probe, Obstet. Gynecol. 76 (1990) 607–611.
[35] D.G. McIntosh, D. Colcher, T. Seemayer, M.L. Smith, Theintraoperative detection of ovarian adenocarcinoma usingradiolabeled CC49 monoclonal antibody and a hand-heldgamma-detecting probe, Cancer Biother. Radiopharm. 12(1997) 287–294.
[36] D.C. Chhieng, C. Rodriguez-Burford, L.I. Talley, H. Sviglin,C.R. Stockard, M.J. Kleinberg, M.N. Barnes, E.E. Partridge,M.B. Khazaeli, W.E. Grizzle, Expression of CEA, Tag-72, andLewis-Y antigen in primary and metastatic lesions of ovariancarcinoma, Hum. Pathol. 34 (2003) 1016–1021.
[37] A. Thor, F. Gorstein, N. Ohuchi, C.A. Szpak, W.W.Johnston, J. Schlom, Tumor-associated glycoprotein(TAG-72) in ovarian carcinomas defined by monoclonalantibody B72.3, J. Natl. Cancer Inst. 76 (1986) 995–1006.
[38] R.D. Alvarez, E.E. Partridge, M.B. Khazaeli, G. Plott, M.Austin, L. Kilgore, C.D. Russell, T. Liu, W.E. Grizzle, J.Schlom, A.F. LoBuglio, R.F. Meredith, Intraperitonealradioimmunotherapy of ovarian cancer with 177Lu-CC49:a phase I/II study, Gynecol. Oncol. 65 (1997) 94–101.
[39] R.F. Meredith, M.B. Khazaeli, W.E. Plott, W.E. Grizzle, T.Liu, J. Schlom, C.D. Russell, R.H. Wheeler, A.F. LoBuglio,Phase II study of dual 131I-labeled monoclonal antibodytherapy with interferon in patients with metastatic colorectalcancer, Clin. Cancer Res. 2 (1996) 1811–1818.
[40] R. Muraro, M. Kuroki, D. Wunderlich, D.J. Poole, D.Colcher, A. Thor, J.W. Greiner, J.F. Simpson, A. Molinolo,P. Noguchi, Generation and characterization of B72.3second generation monoclonal antibodies reactive with the

M.P. Ponnusamy et al. / Cancer Letters 251 (2007) 247–257 257
tumor-associated glycoprotein 72 antigen, Cancer Res. 48(1988) 4588–4596.
[41] M.A. McGuckin, M.D. Walsh, B.G. Hohn, B.G. Ward,R.G. Wright, Prognostic significance of MUC1 epithelialmucin expression in breast cancer, Hum. Pathol. 26 (1995)432–439.
[42] D.G. Rosen, G. Yang, K.Q. Cai, R.C. Bast Jr., D.M.Gershenson, E.G. Silva, J. Liu, Subcellular localization of
p27kip1 expression predicts poor prognosis in humanovarian cancer, Clin. Cancer Res. 11 (2005) 632–637.
[43] S. Ueda, S. Ogata, H. Tsuda, N. Kawarabayashi, M.Kimura, Y. Sugiura, S. Tamai, O. Matsubara, K. Hatsuse,H. Mochizuki, The correlation between cytoplasmic overex-pression of epidermal growth factor receptor and tumoraggressiveness: poor prognosis in patients with pancreaticductal adenocarcinoma, Pancreas 29 (2004) e1–e8.