Expression of ALK1 and p80 in Inflammatory Myofibroblastic Tumor and Its Mesenchymal Mimics: A Study...
8
Expression of ALK1 and p80 in Inflammatory Myofibroblastic Tumor and Its Mesenchymal Mimics: A Study of 135 Cases Melissa H. Cessna, M.D., Holly Zhou, M.D., Warren G. Sanger, Ph.D., Sherrie L. Perkins, M.D., Ph.D., Sheryl Tripp, M.T., Diane Pickering, M.S., Clark Daines, M.D., Cheryl M. Coffin, M.D. Department of Pathology, Primary Children’s Medical Center and University of Utah School of Medicine, Salt Lake City, Utah (MHC, HZ, SLP, ST, CD, CMC); and Department of Pediatrics, University of Nebraska Medical Center, Omaha, Nebraska (WGS, DP) Abnormalities of chromosome 2p23 with expres- sion of ALK1 and p80 occur in both inflammatory myofibroblastic tumor (IMT) and anaplastic large cell lymphoma. This immunohistochemical study investigates whether the ALK family of neoplasms includes fibroblastic–myofibroblastic, myogenic, and spindle cell tumors. Formalin-fixed paraffin- embedded archival tissues from 10 IMTs and 125 other soft tissue tumors were stained for ALK1 and p80 with standard immunohistochemistry. ALK1 and/or p80 reactivity was observed in a cytoplasmic pattern in IMT (4/10; 40%), malignant peripheral nerve sheath tumor (4/10; 40%), rhabdomyosar- coma (6/31; 19%), leiomyosarcoma (1/10; 10%), and malignant fibrous histiocytoma (1/11; 9%). No staining was observed in nodular fasciitis, desmoid, infantile myofibromatosis, infantile fibrosarcoma, synovial sarcoma, leiomyoma, or myofibrosarcoma. Alveolar rhabdomyosarcomas (4/16; 25%) displayed a distinctive dot-like cytoplasmic positivity. No cases displayed nuclear reactivity. Fluorescent in situ hybridization on 12 of the positive cases re- vealed a combination of abnormalities including ALK break-apart signals, nucleophosmin (NPM)/ ALK fusions, or extra copies of 2p23. This study demonstrates that in addition to IMT, abnormalities of ALK1 and p80 expression with a variety of struc- tural chromosomal changes are found in several sarcomas, especially rhabdomyosarcoma and ma- lignant peripheral nerve sheath tumor. Although immunoreactivity in non-IMTs cannot distinguish between structural abnormalities involving 2p23 or additional copies of 2p23, it supports the concept of ALK involvement in a larger group of neoplasms, some of which have other documented clonal ab- normalities. In IMT, immunohistochemistry for ALK1 and p80 is useful as an indicator of a 2p23 abnormality, but it must be interpreted in the con- text of histologic and other clinicopathologic data if used as an adjunct to differential diagnosis. KEY WORDS: ALK gene rearrangements, ALK im- munohistochemistry, Anaplastic large cell lym- phoma, Inflammatory myofibroblastic tumor. Mod Pathol 2002;15(9):931–938 Inflammatory myofibroblastic tumor (IMT), a tumor of myofibroblastic spindle cells accompanied by a lymphoplasmacytic and eosinophilic inflammatory infiltrate, and anaplastic large cell lymphoma share clonal aberrations involving the short arm of chromo- some 2 in region p21–p23 (1–5). Chromosome 2p23 is the site of the human ALK gene, which codes for anaplastic lymphoma kinase, a tyrosine kinase recep- tor and member of the insulin growth factor receptor superfamily. Antibodies to the protein product of the ALK gene detect both ALK expression associated with 2p23 rearrangements and other abnormalities in ALK deregulation. ALK rearrangements and/or ALK1 and p80 im- munoreactivity have been reported in 36 – 60% of IMTs and 8 –33% of “inflammatory pseudotumors” (3, 5, 6 –9). Fusion oncogenes have been identified in a small proportion of IMTs with ALK rearrange- ments and include TPM3-ALK and TPM4-ALK (4). In anaplastic large cell lymphoma, the clonal ab- normalities of ALK include a characteristic translo- cation t(2, 5)(p23;q35), variant translocations, and a TPM3-ALK fusion oncogene in some cases (2, 10 – 15). Various investigators have shown that ALK gene rearrangements and ALK expression are found Copyright © 2002 by The United States and Canadian Academy of Pathology, Inc. VOL. 15, NO. 9, P. 931, 2002 Printed in the U.S.A. Date of acceptance: May 20, 2002. Presented in part at the United States and Canadian Academy of Pathol- ogy, Atlanta, GA, on March 8, 2001. Address correspondence to: Cheryl M. Coffin, M.D., Department of Pa- thology, University of Utah School of Medicine, 50 North Medical Drive, Salt Lake City, UT 84132; e-mail: [email protected]; fax: 801-588-3169. DOI: 10.1097/01.MP.0000026615.04130.1F 931
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Expression of ALK1 and p80 in Inflammatory Myofibroblastic Tumor and Its Mesenchymal Mimics: A Study...

Expression of ALK1 and p80 in InflammatoryMyofibroblastic Tumor and Its Mesenchymal Mimics:A Study of 135 CasesMelissa H. Cessna, M.D., Holly Zhou, M.D., Warren G. Sanger, Ph.D., Sherrie L. Perkins, M.D., Ph.D.,Sheryl Tripp, M.T., Diane Pickering, M.S., Clark Daines, M.D., Cheryl M. Coffin, M.D.
Department of Pathology, Primary Children’s Medical Center and University of Utah School of Medicine,Salt Lake City, Utah (MHC, HZ, SLP, ST, CD, CMC); and Department of Pediatrics, University of NebraskaMedical Center, Omaha, Nebraska (WGS, DP)
Abnormalities of chromosome 2p23 with expres-sion of ALK1 and p80 occur in both inflammatorymyofibroblastic tumor (IMT) and anaplastic largecell lymphoma. This immunohistochemical studyinvestigates whether the ALK family of neoplasmsincludes fibroblastic–myofibroblastic, myogenic,and spindle cell tumors. Formalin-fixed paraffin-embedded archival tissues from 10 IMTs and 125other soft tissue tumors were stained for ALK1 andp80 with standard immunohistochemistry. ALK1and/or p80 reactivity was observed in a cytoplasmicpattern in IMT (4/10; 40%), malignant peripheralnerve sheath tumor (4/10; 40%), rhabdomyosar-coma (6/31; 19%), leiomyosarcoma (1/10; 10%), andmalignant fibrous histiocytoma (1/11; 9%). Nostaining was observed in nodular fasciitis, desmoid,infantile myofibromatosis, infantile fibrosarcoma,synovial sarcoma, leiomyoma, or myofibrosarcoma.Alveolar rhabdomyosarcomas (4/16; 25%) displayeda distinctive dot-like cytoplasmic positivity. Nocases displayed nuclear reactivity. Fluorescent insitu hybridization on 12 of the positive cases re-vealed a combination of abnormalities includingALK break-apart signals, nucleophosmin (NPM)/ALK fusions, or extra copies of 2p23. This studydemonstrates that in addition to IMT, abnormalitiesof ALK1 and p80 expression with a variety of struc-tural chromosomal changes are found in severalsarcomas, especially rhabdomyosarcoma and ma-lignant peripheral nerve sheath tumor. Althoughimmunoreactivity in non-IMTs cannot distinguish
between structural abnormalities involving 2p23 oradditional copies of 2p23, it supports the concept ofALK involvement in a larger group of neoplasms,some of which have other documented clonal ab-normalities. In IMT, immunohistochemistry forALK1 and p80 is useful as an indicator of a 2p23abnormality, but it must be interpreted in the con-text of histologic and other clinicopathologic data ifused as an adjunct to differential diagnosis.
KEY WORDS: ALK gene rearrangements, ALK im-munohistochemistry, Anaplastic large cell lym-phoma, Inflammatory myofibroblastic tumor.
Mod Pathol 2002;15(9):931–938
Inflammatory myofibroblastic tumor (IMT), a tumorof myofibroblastic spindle cells accompanied by alymphoplasmacytic and eosinophilic inflammatoryinfiltrate, and anaplastic large cell lymphoma shareclonal aberrations involving the short arm of chromo-some 2 in region p21–p23 (1–5). Chromosome 2p23 isthe site of the human ALK gene, which codes foranaplastic lymphoma kinase, a tyrosine kinase recep-tor and member of the insulin growth factor receptorsuperfamily. Antibodies to the protein product of theALK gene detect both ALK expression associated with2p23 rearrangements and other abnormalities in ALKderegulation.
ALK rearrangements and/or ALK1 and p80 im-munoreactivity have been reported in 36 – 60% ofIMTs and 8 –33% of “inflammatory pseudotumors”(3, 5, 6 –9). Fusion oncogenes have been identifiedin a small proportion of IMTs with ALK rearrange-ments and include TPM3-ALK and TPM4-ALK (4).In anaplastic large cell lymphoma, the clonal ab-normalities of ALK include a characteristic translo-cation t(2, 5)(p23;q35), variant translocations, and aTPM3-ALK fusion oncogene in some cases (2, 10 –15). Various investigators have shown that ALKgene rearrangements and ALK expression are found
Copyright © 2002 by The United States and Canadian Academy ofPathology, Inc.VOL. 15, NO. 9, P. 931, 2002 Printed in the U.S.A.Date of acceptance: May 20, 2002.Presented in part at the United States and Canadian Academy of Pathol-ogy, Atlanta, GA, on March 8, 2001.Address correspondence to: Cheryl M. Coffin, M.D., Department of Pa-thology, University of Utah School of Medicine, 50 North Medical Drive,Salt Lake City, UT 84132; e-mail: [email protected]; fax: 801-588-3169.
DOI: 10.1097/01.MP.0000026615.04130.1F
931

in cell lines of neuroblastoma, neuroectodermal tu-mors, malignant melanoma, small cell lung carci-noma, and rhabdomyosarcoma and in central ner-vous system tissue (12, 15). Thus, it appears thatstructural or functional abnormalities of the ALKgene are found in a group of mesenchymal neo-plasms including anaplastic large cell lymphoma,IMT, and possibly others.
The purpose of this study is to systematicallyinvestigate by immunohistochemical means, withselective fluorescence in situ hybridization (FISH)analysis, whether the ALK family of tumors, whosecurrent members are IMT and anaplastic large celllymphoma, also includes mesenchymal tumorswith a predominantly spindle cell phenotype andrhabdomyosarcoma.
MATERIALS AND METHODS
Case SelectionFormalin-fixed, paraffin-embedded archival tis-
sue was obtained from institutional and consulta-tion files. Cases included 10 IMTs and 125 smallround blue cell and spindle cell tumors. These in-cluded 31 rhabdomyosarcomas, 10 nodular fasciiti-des, 10 desmoid-type fibromatoses, 10 infantilemyofibromatoses, 10 infantile fibrosarcomas, 11malignant fibrous histiocytomas, 10 synovial sarco-mas, 10 malignant peripheral nerve sheath tumors,3 myofibrosarcomas, 10 leiomyomas, and 10leiomyosarcomas. The rhabdomyosarcomas in-cluded 16 alveolar and 15 embryonal (including 2anaplastic, 1 spindle cell, and 2 botyroid) types. Softtissue tumors were classified according to theWorld Health Organization Classification of SoftTissue Tumors (16), the International Classificationof Rhabdomyosarcoma (17), and published de-scriptions for myofibrosarcoma (18 –20). Clinico-pathologic and immunohistochemical findings forsome cases of IMT, rhabdomyosarcoma, and infan-tile fibrosarcoma had been previously published (1,3, 8, 21–23). Five of 10 IMTs were included in aprevious study of ALK-1 and p80 expression andchromosome 2p23 rearrangements (5), and 8 wereincluded in a separate study (8). All specimens wereoriginally diagnosed between 1976 and 2000. All ofthe inflammatory myofibroblastic tumors, rhabdo-myosarcoma, infantile myofibromatoses, infantilefibrosarcomas, and myofibrosarcomas were fromchildren and adolescents. All of the leiomyomaswere from adults. The remaining tumors occurredin both children and adults. The original surgicalpathology reports were reviewed, and the diagnoseswere confirmed by review of hematoxylin and eo-sin–stained sections and immunohistochemicalstudies. One representative block for each case wasselected for immunohistochemical staining.
Antibodies and ImmunostainingImmunohistochemical studies were performed
on 4-�m-thick formalin-fixed, paraffin-embeddedtissue sections, using a standard heat-inducedepitope retrieval method, a standard avidin– biotinperoxidase complex detection technique, and anautomated immunostainer (Ventana Medical Sys-tems, Tucson, AZ).
The monoclonal ALK1 antibody was obtainedfrom DAKO Company (Carpinteria, CA). ALK1staining was done after heat-induced epitope re-trieval in an electric pressure cooker for 3 minutes(total time in pressure cooker, 30 min) in a citratebuffer at pH 6.0. The antibody was applied at adilution of 1:25 for 32 minutes using the VentanaNexus autostainer with a basic diaminobenzidinedetection kit, endogenous peroxidase blocking, andstaining amplification kit.
The polyclonal p80NPM/ALK antibody was ob-tained from Monosan (Leiden, the Netherlands).p80 staining was done after heat-induced epitoperetrieval in an electric pressure cooker for 3 minutes(total time in pressure cooker, 30 min) in a citratebuffer at pH 6.0. The antibody was applied at adilution of 1:30 for 32 minutes using the VentanaNexus autostainer with a basic diaminobenzidinedetection kit, endogenous peroxidase blocking, andstaining amplification kit.
Appropriate positive and negative controls wereused. Reactivity was interpreted as positive or neg-ative. Positive cases were graded according to thepercentage of tumor cells with staining, with 1�representing 0 –30% positivity, 2� representing�30 –70% positivity, and 3� representing �70%positivity. Cases of positive staining were assessedas to the localization of staining to cytoplasm, nu-cleus, or both of tumor cells. Diffuse cytoplasmicstaining of nontumor cell types was not observed.
FISH Methods for Detection of t(2, 5)(p23;q35)and Other Rearrangements of 2p23 (ALK), usingALK and NPM/ALK Probes on Paraffin-Embedded Tumor Tissue
FISH procedures were performed on 4- to 5-�munstained tissue sections using an NPM/ALK two-color FISH probe specific for the t(2, 5)(p23;q35)and a two-color, break-apart ALK probe that flanksthe ALK gene region at 2p23 for detection of thealternative rearrangements involving the ALK gene.The NPM/ALK probes were obtained from Dr. SteveMorris, and the ALK break-apart probe is commer-cially available (Vysis, Downers Grove, IL). Beforethe hybridization, the slides were pretreated usingthe VP2000 automated slide processor (Vysis) usingthe program specified for paraffin slides. Briefly, theprogram included deparaffinization of the slides,followed by dehydration, 0.2 N HCL treatment for
932 Modern Pathology

15 minutes, and incubation in sodium thiocyanatefor 20 minutes at 80° C. The slides were then di-gested in protease for 15 minutes at 37° C, rinsed,and dehydrated. For FISH, three overlapping chro-mosome 5 cosmid clones (13, 15–2, and 47C12)located immediately centromeric to the NPM genelocus and an ALK P1 clone, which is homologous tothe ALK gene locus translocated in the t(2, 5), werelabeled by nick translation with Spectrum Greenand Spectrum Orange, respectively, and then puri-fied using the Bio-Spin P-30 chromatography col-umn (Bio-Rad, Hercules, CA). For each hybridiza-tion, the labeled probes were combined in equalamounts (50 ng each), lyophilized with 1 �g ofCot-1 DNA, and resuspended in LSI HybridizationBuffer (Vysis). For the cases that did not exhibit thet(2, 5), the LSI ALK (Vysis) was used according tomanufacturer’s instruction. For hybridization, 10�L of the probe mixture was placed on the pre-treated tissue section, coverslipped, and sealed. Theprobe and target DNA were co-denatured at 75° Cfor 5 minutes, followed by an overnight hybridiza-tion at 37° C using the HybRite automated FISHsystem (Vysis). After hybridization, the slides werewashed for 2 minutes in 2� SSC/0.1% NP-40 at 72°C, followed by 2 minutes in 2� SSC/0.1% NP-40 atroom temperature. The slides were counterstainedwith 4', 6-diamidino-2-phenylindole (DAPI) at aconcentration of 125 ng/mL in antifade solution.Analysis was performed on an Olympus BX51 fluo-rescence microscope equipped with appropriate fil-ters and Cytovision FISH system image capturesoftware (Applied Imaging, Santa Clara, CA). Foreach case, 100 cells were scored for the presence ofthe t(2, 5) as evidenced by juxtaposition of the red(ALK) and green (NPM) signal forming a yellow“fusion” signal. The false-positive rate for this FISHsystem, as established by University of NebraskaMedical Center Human Genetics Laboratories be-fore this study, is 0 –7%, with cutoff at 12%. For theALK break-apart probe, the cells were scored for a“separation” of the green and red signal, which isindicative of a rearrangement of the ALK gene re-gion. The false-positive rate for this test is 0 –10%,with a cutoff of 15%.
RESULTS
The immunohistochemical findings are summa-rized in Tables 1 and 2. Three of 10 IMTs, all fromchildren, showed staining for both ALK1 and p80(Fig. 1, A–C); one IMT showed expression of onlyp80. The staining pattern in all of these IMTs wasdistinctly and diffusely cytoplasmic in single well-defined cells. No cytoplasmic or nuclear staining ofnontumor cell types was observed. A fibrillary, sub-membranous, or punctate quality of the cytoplas-mic staining in these IMTs was not discernible.
Among the other mesenchymal tumors, no casesof nodular fasciitis, fibromatosis, infantile myofi-bromatosis, infantile fibrosarcoma, synovial sar-coma, myofibrosarcoma, or leiomyoma showed im-munohistochemical reactivity for either ALK1 orp80. Positivity for both ALK1 and p80 was seen infive rhabdomyosarcomas (four alveolar and oneembryonal, all from children; Fig. 2, A–C), two ma-lignant peripheral nerve sheath tumors (both fromchildren), one leiomyosarcoma (from a child), andone malignant fibrous histiocytoma (from anadult). Two additional malignant peripheral nervesheath tumors (one from an adult, one from a child)showed positivity for only p80. One other embryo-nal rhabdomyosarcoma (from a child) showed pos-itivity for only ALK1. The staining pattern in all buttwo non-IMTs was diffusely cytoplasmic. Three al-veolar rhabdomyosarcomas displayed a distinctivepunctate, dot-like pattern of cytoplasmic stainingvisible at 40 –100�. With the exception of the dot-like cytoplasmic reactivity in alveolar rhabdomyo-sarcomas, the cytoplasmic staining for ALK1 andp80 in non-IMTs was less intense than in IMTs. Thenon-IMTs with 1� positivity displayed a low per-centage of reactive cells, �10% in 6 of 10 cases. Inall of the tumors with both ALK1 and p80 staining,the same types of cells were positive with bothmarkers. Among the rhabdomyosarcomas, primi-tive round or polygonal cells and rhabdomyoblastswith eccentric nuclei and eosinophilic cytoplasmwere positive, and in general, the less differentiatedcells appeared to stain more frequently.
The FISH results for ALK1- and/or p80-positivetumors are shown in Table 3. Among the three IMTthat could be analyzed, all three had ALK rearrange-ments with the ALK break-apart probe (two classicsplits and one complex variant), and none had anNPM/ALK fusion detected. All of these IMT dis-played cytoplasm ALK1 and/or p80 reactivity.Among the six rhabdomyosarcomas that could be
TABLE 1. ALK1 and p80 Reactivity in Spindle Cell
Tumors
Diagnosis
No. Positivea/No.Tested
ALK p80
Inflammatory myofibroblastic tumor 3/10 4/10Rhabdomyosarcoma 6/31 5/31Malignant peripheral nerve sheath tumor 2/10 4/10Leiomyosarcoma 1/10 1/10Malignant fibrous histiocytoma 1/11 1/11Nodular fasciitis 0/10 0/10Desmoid fibromatosis 0/10 0/10Infantile myofibromatosis 0/10 0/10Infantile fibrosarcoma 0/10 0/10Myofibrosarcoma 0/3 0/3Leiomyoma 0/10 0/10Synovial sarcoma 0/10 0/10
a All positive cases displayed cytoplasmic reactivity without nuclearreactivity.
ALK-1, p80, and FISH in Mesenchymal Tumors (M. H. Cessna et al.) 933
analyzed, one each of embryonal and alveolar sub-types were positive for NPM/ALK and displayed dif-fuse, weak cytoplasmic ALK1 and/or p80 staining.One embryonal rhabdomyosarcoma with weak cy-toplasmic ALK1 and p80 reactivity was negative forALK rearrangements but had three copies of 2p23.Three alveolar rhabdomyosarcomas with dot-likecytoplasmic ALK1 and p80 reactivity had eitherthree to six copies of 2p23 without ALK rearrange-ments in two cases or had a complex ALK rear-rangement with the ALK break-apart probe. Onemalignant peripheral nerve sheath tumor was pos-itive for NPM/ALK by FISH and was reactive for p80.One case each of leiomyosarcoma and malignantfibrous histiocytoma had two and four copies of2p23, respectively, but lacked ALK and NPM/ALKrearrangements.
DISCUSSION
IMT is classified with intermediate neoplasms inthe current World Health Organization HistologicalTyping of Soft Tissue Tumors (16). Recent studieshave identified chromosomal abnormalities occur-ring in a proportion of pulmonary and extrapulmo-nary IMTs, lending support to the concept of IMTas a neoplasm (3–5, 9, 24 –28). These recurrent ab-normalities involve chromosome 2p21–24, are as-sociated with ALK deregulation, and are character-ized by ALK expression by immunohistochemistry(3–5). The understanding of the relationship be-tween inflammatory pseudotumor and inflamma-tory pseudotumor-like neoplasms continues toevolve, although it is clear that both reactive andneoplastic processes have histologic similarities (1,7, 29 –32).
Originally described in anaplastic large cell lym-phoma, ALK abnormalities identify a distinct sub-group of anaplastic large cell lymphomas with afavorable prognosis. Recent studies have reportedthe association of ALK expression in IMT with ayounger age at presentation (4, 5, 7). Immunohis-tochemistry for ALK expression, using both mono-clonal and polyclonal antibodies, has previouslycorrelated well with results of reverse transcriptasepolymerase chain reaction, FISH, and conventionalcytogenetics for detection of ALK abnormalities (3,
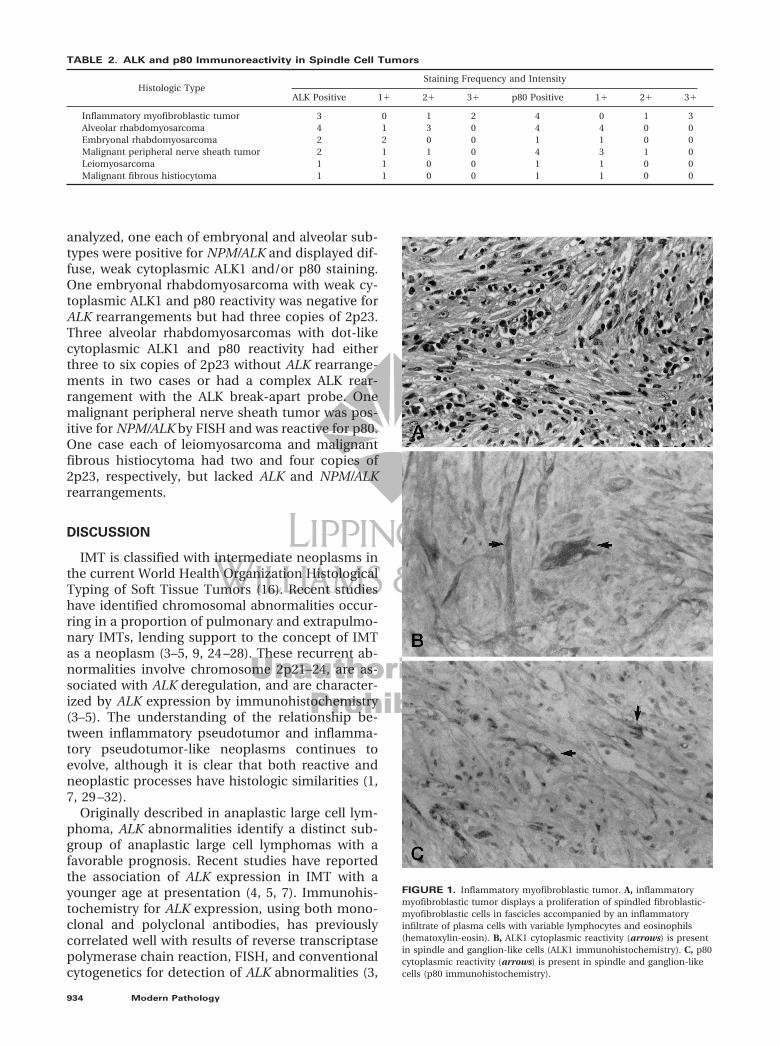
FIGURE 1. Inflammatory myofibroblastic tumor. A, inflammatorymyofibroblastic tumor displays a proliferation of spindled fibroblastic-myofibroblastic cells in fascicles accompanied by an inflammatoryinfiltrate of plasma cells with variable lymphocytes and eosinophils(hematoxylin-eosin). B, ALK1 cytoplasmic reactivity (arrows) is presentin spindle and ganglion-like cells (ALK1 immunohistochemistry). C, p80cytoplasmic reactivity (arrows) is present in spindle and ganglion-likecells (p80 immunohistochemistry).
TABLE 2. ALK and p80 Immunoreactivity in Spindle Cell Tumors
Histologic TypeStaining Frequency and Intensity
ALK Positive 1� 2� 3� p80 Positive 1� 2� 3�
Inflammatory myofibroblastic tumor 3 0 1 2 4 0 1 3Alveolar rhabdomyosarcoma 4 1 3 0 4 4 0 0Embryonal rhabdomyosarcoma 2 2 0 0 1 1 0 0Malignant peripheral nerve sheath tumor 2 1 1 0 4 3 1 0Leiomyosarcoma 1 1 0 0 1 1 0 0Malignant fibrous histiocytoma 1 1 0 0 1 1 0 0
934 Modern Pathology

5, 11, 14, 33). The similar 2p23 abnormalities in IMTand anaplastic large cell lymphoma raise the ques-tion of whether the ALK family of tumors includesother mesenchymal neoplasms, especially becauseALK tyrosine kinase gene expression has beenfound in cell lines from several tumor types (12, 15)and because neoplasms of fibroblasts and myofi-broblasts encompass a large and histologically sim-ilar group of entities. An additional question iswhether ALK immunohistochemistry is useful fordifferential diagnosis or principally for detection ofan ALK abnormality.
Previous studies have shown that ALK gene rear-rangements and/or ALK expression are found inanaplastic large cell lymphoma, IMT, and cell linesfrom neuroblastoma, neuroectodermal tumors,malignant melanoma, small cell lung carcinoma,and rhabdomyosarcoma (Table 4). Non-neoplasticcentral nervous system tissue also expresses ALK.The present study of IMT and other mesenchymalneoplasms demonstrated ALK1 and/or p80 reactiv-ity in IMTs (40%) and in rhabdomyosarcomas(19%), malignant peripheral nerve sheath tumors(40%), malignant fibrous histiocytomas (9%), andleiomyosarcomas (10%). These findings confirmthose of previous studies, which have shown ALK1immunohistochemical reactivity in 8 – 62% of IMTsand “inflammatory pseudotumors” (3, 5, 7–9, 34).The present study also confirmed the presence ofALK and/or p80 expression in rhabdomyosarco-
FIGURE 2. Alveolar rhabdomyosarcoma. A, alveolarrhabdomyosarcoma consists of small round tumor cells liningfibrovascular septa and floating in pseudoalveolar spaces (hematoxylin–eosin staining). B, ALK1 reactivity (arrows) with a distinctive dot-likecytoplasmic pattern (ALK1 immunohistochemistry). C, p80 reactivity(arrows) with a distinctive dot-like cytoplasmic pattern.
TABLE 3. FISH in ALK1/p80-Positive Mesenchymal
Tumors
Diagnosis (n)
FISH (No. of Cases)
ALK Break-ApartProbe Split
NPM/ALKFusion
Extra 2p23Copies
IMT (3) 3a 0 0ARMS (4) 1b 1 2 (3–6 copies)ERMS (2) 0 1 1 (3 copies)MPNST (2) 0 1 0LMS (1) 0 0 1 (2 copies)MFH (1) 0 0 1 (2 copies)
IMT, inflammatory myofibroblastic tumor; ARMS, alveolar rhabdo-myosarcoma; ERMS, embryonal rhabdomyosarcoma; MPNST, malignantperipheral nerve sheath tumor; LMS, leiomyosarcoma; MFH, malignantfibrous histiocytoma; NPM, nucleophosmin; FISH, fluorescence in situhybridization.
a Two IMTs had classic splits, and one had a complex variant with 1–2fusion and 2 red signals.
b One ARMS had a complex variant split signal with the ALK break-apart probe, which included three fusion and two red signals and anegative NPM/ALK signal.
TABLE 4. ALK Protein Expression by
Immunohistochemistry in Neoplastic and Normal
Tissues: Summary of 10 Series
Neoplasms PositiveNo.
Positive/TotalReference
No.
Anaplastic large celllymphoma
137/309 2, 3, 11, 13–15
Inflammatorymyofibroblastic tumor
28/68 Present study, 4, 5
Neuroblastoma 2/5 15Rhabdomyosarcoma 7/34 Present study, 12, 15Malignant peripheral nerve
sheath tumor4/10 Present study
Leiomyosarcoma 1/11 Present study, 12Malignant fibrous
histiocytoma1/10 Present study
Normal tissues reportedly positive: cerebral cortex, hypothalamus,cerebellum, basal ganglia, thalamic nuclei (12). Neoplasms reportedlynegative (present study, 2, 11–13): lymphomas other than ALCL,Hodgkin’s disease, lymphomatoid papulosis, astrocytoma, glioma, glio-blastoma, medulloblastoma, various carcinomas, germ cell tumors,Wilms’ tumor, liposarcoma, malignant rhabdoid tumor, fibrosarcoma,synovial sarcoma, carcinoid, pheochromocytoma, thymoma, melanoma,others.
ALK-1, p80, and FISH in Mesenchymal Tumors (M. H. Cessna et al.) 935
mas, especially the alveolar type, and identifiedother mesenchymal neoplasms with ALK expres-sion. Correlation of the immunohistochemical find-ings with FISH probes for ALK and NPM/ALKyielded interesting evidence of ALK rearrangementsor extra copies of 2p23 in ALK1-positive non-IMTs.All of three IMTs had either classic ALK split signalsor a complex variant fusion signal. The other nineALK1 and/or p80-reactive mesenchymal tumorsanalyzed by FISH displayed either extra copies of2p23 in five cases or ALK rearrangements, with anNPM/ALK fusion in three cases and a variant ALKfusion in one case; one case could not be analyzed.Among the alveolar rhabdomyosarcomas, there wasan association between the cytoplasmic dot-likepattern of ALK1 and p80 immunohistochemicalstaining and extra copies of 2p23. The recent studyby Cook and colleagues (8) did not demonstrateALK expression in nodular fasciitis, desmoids, orgastrointestinal stromal tumors. Lawrence and col-leagues (4) reported that ALK was not expressed innodular fasciitis, inflammatory liposarcoma, in-flammatory leiomyosarcoma, or angiomatoid ma-lignant fibrous histiocytoma.
Oncogenesis subsequent to translocations in-volving the ALK gene occurs as a result of constitu-tive expression and activation of ALK, with abnor-mal phosphorylation of cellular substrates. Basedon studies of anaplastic large cell lymphoma andIMT, a variety of genes are capable of deregulatingALK. A single fusion partner has not been found inALK-positive anaplastic large cell lymphomas;rather, a variety of fusion partners has been identi-fied, including NPM, clathrin, nonmuscular tropo-myosin (TPM3), or TRK-fused gene (TFG). Previousstudies of ALK expression in anaplastic large celllymphoma have shown recurrent characteristic lo-calization patterns for ALK protein associated withspecific ALK fusion proteins (11–13). The variantfusions give rise to different ALK immunohisto-chemical staining patterns than the typical nuclearor nuclear and cytoplasmic staining seen with thet(2, 5)(p23; q35) NPM-ALK fusion protein. The mostcommon pattern of ALK expression seen in thevariant translocations is diffuse cytoplasmic stain-ing without a significant nuclear component. TheTPM-ALK fusion genes found in IMT and anaplasticlarge cell lymphoma were associated with intense,predominantly cytoplasmic staining (4, 35). In ad-dition to identifying the TPM3-ALK and TPM4-ALKfusion genes in IMT, Lawrence and colleagues (4)identified the possibility of at least two alternativeALK fusion mechanisms in IMT, resulting in pre-dominantly cytoplasmic (3 cases) or predominantlynuclear (1 case) localization. ALK1-staining pat-terns in IMTs have recently been described as dif-fuse cytoplasmic, granular cytoplasmic, or nuclearmembranous, with the diffuse cytoplasmic pattern
occurring most frequently (8). The possibility existsthat multiple mechanisms may result in ALK dereg-ulation; for example, point mutations involving theALK gene could also cause overexpression and ab-normal trafficking of ALK between the nucleus andcytoplasm. Whether clear-cut molecular–morpho-logic correlates will emerge is a question of greatinterest.
The IMTs in our study showed a diffuse cytoplas-mic staining pattern, which was also observed inthe ALK-positive malignant peripheral nerve sheathtumors, malignant fibrous histiocytomas, andleiomyosarcomas. Three of the alveolar rhabdomy-osarcomas showed a characteristic dot-like patternof cytoplasmic staining, two of these cases had ad-ditional copies of 2p23, and one had a variant ALKfusion. This suggests that not only a specific fusiongene, but also other mechanisms can result in ALKoverexpression in neoplasms with a variety of cyto-genetic abnormalities. Alveolar rhabdomyosarcomais often associated with a recurrent translocationinvolving the FKHR gene on chromosome 13q14and the PAX3 gene at 2q35 or PAX7 gene on 1p36(36). Less is known about the cytogenetic abnor-malities in malignant peripheral nerve sheath tu-mor, malignant fibrous histiocytoma, or leiomyo-sarcoma. The data from this study suggest thatthere may be a subset of mesenchymal neoplasmsthat have in common abnormalities resulting fromALK deregulation and overexpression.
In this study, both the monoclonal antibody forALK1 and the polyclonal antibody p80 were used toevaluate ALK expression. Overall, the sensitivities ofthese antibodies was comparable, although p80 de-tected positive staining in one IMT and two malig-nant peripheral nerve sheath tumors that werenonreactive with the ALK1 antibody. Conversely,ALK1 detected ALK expression in one case of rhab-domyosarcoma that was nonreactive with the p80antibody. Overall, the ALK1 antibody staining waseasier to interpret, with a cleaner background incomparison to p80, as reported by previous inves-tigators (12, 33). As in our previous study, the im-munohistochemical expression of ALK1 and p80was strongly associated with structural or numeri-cal abnormalities of the ALK region on chromo-some 2p23 (5).
Although the ALK immunoreactivity and cytoge-netic abnormalities in rhabdomyosarcoma, malig-nant peripheral nerve sheath tumor, leiomyosar-coma, and malignant fibrous histiocytoma are asyet incompletely characterized as to numerical orstructural chromosomal abnormalities involving2p23 or as to ALK deregulation by other means, thefindings in this study support the concept of ALKinvolvement in a larger group of mesenchymal neo-plasms, some of which have other known clonalabnormalities. Immunohistochemistry for ALK1
936 Modern Pathology

and p80 is useful when positive as an indicator of2p23 rearrangement in IMT but must be inter-preted in the context of histologic and other clini-copathologic data if used as an adjunct for differ-ential diagnosis. Although the frequency of ALK1immunoreactivity in IMT ranges from 36 – 60% (5,8), ALK1 and p80 reactivity provide evidence tosupport the diagnosis of IMT, with the caveats thatthe typical histologic features are present and thatanaplastic large cell lymphoma has been excluded.When negative, careful consideration of alternativediagnoses, including nonneoplastic or inflamma-tory pseudotumors, is critical, although a signifi-cant percentage of IMTs will not exhibit ALK1 andp80 expression. Because a small proportion of var-ious sarcomas in this study demonstrated ALK1 andp80 reactivity, further investigation of the role ofALK deregulation in mesenchymal neoplasms mayyield information of potential biologic and thera-peutic significance.
Acknowledgments: The authors thank SamanthaFarr, Michelle Gonzalez, and Kristi Herrin for theirsecretarial expertise.
REFERENCES
1. Coffin CM, Watterson J, Priest JR, et al. Extrapulmonaryinflammatory myofibroblastic tumor (inflammatory pseudo-tumor). A clinicopathologic and immunohistochemicalstudy of 84 cases. Am J Surg Pathol 1995;19:859 –72.
2. Nakamura S, Shiota M, Nakagawa A, et al. Anaplastic largecell lymphoma: a distinct molecular pathologic entity: areappraisal with special reference to p80(NPM/ALK) expres-sion. Am J Surg Pathol 1997;21:1420 –32.
3. Griffin CA, Hawkins AL, Dvorak C, et al. Recurrent involve-ment of 2p23 in inflammatory myofibroblastic tumors. Can-cer Res 1999;59:2776 – 80.
4. Lawrence B, Perez-Atayde A, Hibbard MK, et al. TPM3-ALKand TPM4-ALK oncogenes in inflammatory myofibroblastictumors. Am J Pathol 2000;157:377– 84.
5. Coffin CM, Patel A, Perkins SL, et al. ALK1 and p80 expres-sion and chromosomal rearrangements involving 2p23 ininflammatory myofibroblastic tumor. Mod Pathol 2001;14:569 –76.
6. Cheuk W, Hill RW, Bacchi C, et al. Hypocellular anaplasticlarge cell lymphoma mimicking inflammatory lesions oflymph nodes. Am J Surg Pathol 2000;24:1537– 43.
7. Chan JK, Cheuk W, Shimizu M. Anaplastic lymphoma kinaseexpression in inflammatory pseudotumors. Am J Surg Pathol2001;25:761– 8.
8. Cook JR, Dehner LP, Collins M, et al. Anaplastic lymphomakinase (ALK) expression in the inflammatory myofibroblastictumor: a comparative immunohistochemical study. Am JSurg Pathol 25:1364 –71.
9. Yousem SA, Shaw H, Cieply K. Involvement of 2p23 in pul-monary inflammatory pseudotumors. Hum Pathol 2001;32:428 –33.
10. Shiota M, Fujimoto J, Takenaga M, et al. Diagnosis of t(2;5)(p23;q35)-associated Ki-1 lymphoma with immunohisto-chemistry. Blood 1994;84:3648 –52.
11. Pittaluga S, Wiodarska I, Pulford K, et al. The monoclonalantibody ALK1 identifies a distinct morphological subtype of
anaplastic large cell lymphoma associated with 2p23/ALKrearrangements. Am J Pathol 1997;151:343–51.
12. Pulford K, Lamant L, Morris SW, et al. Detection of anaplas-tic lymphoma kinase (ALK) and nucleolar protein nucleo-phosmin (NPM)-ALK proteins in normal and neoplastic cellswith the monoclonal antibody ALK1. Blood 1997;89:1394 –404.
13. Falini B, Bigerna B, Fizzotti M, et al. ALK expression definesa distinct group of T/null lymphomas (“ALK lymphomas”)with a wide morphological spectrum. Am J Pathol 1998;153:875– 86.
14. Cataldo KA, Jalal SM, Law ME, et al. Detection of t(2;5) inanaplastic large cell lymphoma: comparison of immunohis-tochemical studies, FISH, and RT-PCR in paraffin-embedded tissue. Am J Surg Pathol 1999;23:1386 –92.
15. Lamant L, Pulford K, Bischof D, et al. Expression of the ALKtyrosine kinase gene in neuroblastoma. Am J Pathol 2000;156:1711–21.
16. Weiss SW. Histologic typing of soft tissue tumors. 2nd ed.New York: Springer-Verlag, 1994.
17. Newton WA Jr, Gehan EA, Webber BL, et al. Classification ofrhabdomyosarcomas and related sarcomas. Pathologic as-pects and proposal for a new classification—an IntergroupRhabdomyosarcoma Study. Cancer 1995;76:1073– 85.
18. Eyden BB, Banerjee SS, Harris M, Mene A. A study of spindlecell sarcomas showing myofibroblastic differentiation. Ul-trastruct Pathol 1991;15:367–78.
19. Smith DM, Mahmoud HH, Jenkins JJ, Rao B, Hopkins KP,Parham DP. Myofibrosarcoma of the head and neck in chil-dren. Pediatr Pathol Lab Med 1995;15:403–18.
20. Montgomery E, Goldblum JR, Fisher C. Myofibrosarcoma: aclinicopathologic study. Am J Surg Pathol 2001;25:219 –28.
21. Coffin CM, Jaszcz W, O’Shea PA, et al. So-called congenital-infantile fibrosarcoma: does it exist and what is it? PediatrPathol 1994;14:133–50.
22. Coffin CM, Rulon J, Smith L, et al. Pathologic features ofrhabdomyosarcoma before and after treatment: a clinico-pathologic and immunohistochemical analysis. Mod Pathol1997;10:1175– 87.
23. Hussong JW, Brown M, Perkins SL, et al. Comparison of DNAploidy, histologic, and immunohistochemical findings withclinical outcome in inflammatory myofibroblastic tumors.Mod Pathol 1999;12:279 – 86.
24. Treissman SP, Gillis DA, Lee CL, et al. Omental-mesentericinflammatory pseudotumor. Cytogenetic demonstration ofgenetic changes and monoclonality in one tumor. Cancer1994;73:1433–7.
25. Hojo H, Newton WA Jr, Hamoudi AB, et al. Pseudosarcoma-tous myofibroblastic tumor of the urinary bladder in chil-dren: a study of 11 cases with review of the literature. AnIntergroup Rhabdomyosarcoma Study. Am J Surg Pathol1995;19:1224 –36.
26. Snyder CS, Dell’Aquila M, Haghighi P, et al. Clonal changesin inflammatory pseudotumor of the lung: a case report.Cancer 1995;76:1545–9.
27. Sciot R, Dal Cin P, Fletcher CD, et al. Inflammatory myofi-broblastic tumor of bone: report of two cases with evidenceof clonal chromosomal changes. Am J Surg Pathol 1997;21:1166 –72.
28. Su LD, Atayde-Perez A, Sheldon S, et al. Inflammatory myo-fibroblastic tumor: cytogenetic evidence supporting clonalorigin. Mod Pathol 1998;11:364 – 8.
29. Coffin CM, Humphrey PA, Dehner LP. Extrapulmonary in-flammatory myofibroblastic tumor: a clinical and patholog-ical survey. Semin Diagn Pathol 1998;15:85–101.
30. Dehner LP. The enigmatic inflammatory pseudotumours:the current state of our understanding, or misunderstand-ing. J Pathol 2000;192:277–9.
ALK-1, p80, and FISH in Mesenchymal Tumors (M. H. Cessna et al.) 937

31. Dehner LP, Coffin CM. Idiopathic fibrosclerotic disordersand other inflammatory pseudotumors. Semin Diagn Pathol1998;15:161–73.
32. Gomez-Roman JJ, Sanchez-Velasco P, Ocejo-Vinyals G, et al.Human herpesvirus-8 genes are expressed in pulmonaryinflammatory myofibroblastic tumor (inflammatory pseudo-tumor). Am J Surg Pathol 2001;25:624 –9.
33. Shiota M, Nakamura S, Ichinohasama R, et al. Anaplasticlarge cell lymphomas expressing the novel chimeric proteinp80NPM/ALK: a distinct clinicopathologic entity. Blood 1995;86:1954 – 60.
34. Cheuk W, Chan JK, Shek TW, et al. Inflammatorypseudotumor-like follicular dendritic cell tumor: a distinc-tive low-grade malignant intra-abdominal neoplasm withconsistent Epstein-Barr virus association. Am J Surg Pathol2001;25:721–31.
35. Lamant L, Dastugue N, Pulford K, et al. A new fusion geneTPM3-ALK in anaplastic large cell lymphoma created by a(1;2)(q25;p23) translocation. Blood 1999;93:3088 –95.
36. Barr FG, Chatten J, D’Cruz CM, et al. Molecular assays forchromosomal translocations in the diagnosis of pediatricsoft tissue sarcomas. JAMA 1995;273:553–7.
Book Review
Robboy SL, Anderson MC, Russell P: Pathologyof the Female Reproductive Tract, 929 pp,London, Churchill Livingstone, 2002($250.00).
‘When in the course of human events it becomesnecessary‘ (with an apology to Thomas Jefferson)to come up with a major new textbook of gyne-cologic pathology, the most important prerequi-site is the confluence of minds: that of a first-class publisher experienced in such matters, andthat of team of enthusiastic authors/editors will-ing to see to it that the project is completed indue time. Preferably, the putative editors shouldhave a respectable track record. In the presentcase it helped that all three editors have writtenextensively on gynecologic pathology, and it def-initely does not hurt that they have authoredchapters for books that could now be consideredas a competition of their own. For the record Ishould mention that many years ago I reviewedDr. Russell’s book on the pathology of the ova-ries, which is now in part incorporated in thepresent book; I still think that it is one of bestbooks of ovarian pathology ever written.
This voluminous book is a physically beauti-ful piece of art reflecting the know-how of boththe British publisher and the transcontinentalteam of editors and contributors. In contrast toother major textbooks of gynecologic pathology,its illustrations are almost all in color and, allother things being equal, that is an enormousadvantage—pathology is still in effect a visualdiscipline. The editors deserve compliments forassembling such a cornucopia of gross and mi-croscopic figures, and the publishers are to becongratulated for rendering them in print sobrilliantly.
The beauty of the illustrations should, how-ever, not detract one from the well-written and
masterfully edited text. By all standards it is com-prehensive, informative, and replete with usefuldata and diagnostic hints. In contrast to the ver-bosity of some other texts, this one is ratherlapidary. For my part, I find it not only moredesirable but also more admirable— concisewriting requires more effort than semiautomaticdictation of whatever comes to one’s mind. Thepresent text strikes the right balance betweenbeing comprehensive and being to the point. It isjust right for a busy pathologist swamped in hisor her daily practice with tons of surgical mate-rial. A structured and systematic approach toeach entity, applied throughout the book, willmake it also attractive to novices who may de-cide to read it cover to cover over a period ofseveral moths or even years. The tables dealingwith the differential diagnosis of closely relatedor morphologically similar entities are a featureworth mentioning, and one regrets only that thebook does not contain more of them. Tabularpresentations of immunophenotypes of varioustumors are yet another notable attraction. Thereferences are well chosen and up to date.
The review copy of this book reached me 6months after it appeared in print. One of thepossible reasons, as I learned from talking withDr. Robboy, is that the demand exceeded theinitial supply, surpassing the publisher’s expec-tations. From what I know about medical pub-lishing, I would predict that the demand willremain strong, and I predict that many morecopies of this wonderful book will be sold overthe next few years all over the world.
Ivan DamjanovUniversity of Kansas School of Medicine,Kansas City, Kansas
938 Modern Pathology