EXPANDING the PRIVATE COMMERCIAL SECTOR'S ROLE in MEETING REPRODUCTIVE HEALTH NEEDS
80
EXPANDING the PRIVATE COMMERCIAL SECTOR’S ROLE in MEETING REPRODUCTIVE HEALTH NEEDS James E. Rosen and Shanti R. Conly POPULATION ACTION INTERNATIONAL G E T T I N G D O W N T O BUSINESS
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of EXPANDING the PRIVATE COMMERCIAL SECTOR'S ROLE in MEETING REPRODUCTIVE HEALTH NEEDS

EXPANDING the PRIVATE COMMERCIAL SECTOR’S
ROLE in MEETING REPRODUCTIVE HEALTH NEEDS
James E. Rosen and Shanti R. Conly
POPULATION ACTION INTERNATIONAL
G E TTI N
GD
OW
NT
O
BUSINESS

ABOUT POPULATION ACTION INTERNATIONAL
Population Action International (PAI) is dedicated to advancingpolicies and programs that slow population growth in order toenhance the quality of life for all people.
PAI advocates the expansion of voluntary family planning,other reproductive health services, and educational and economicopportunities for girls and women. These strategies promise toimprove the lives of individual women and their families whileslowing the world’s population growth.
To these ends, PAI seeks to increase global political and financial support for effective population policies and programsgrounded in individual rights.
PAI fosters the development of U.S. and international policyon urgent population issues through an integrated program ofpolicy research, public education and political advocacy. PAIreaches out to government leaders and opinion makers throughthe dissemination of strategic, action-oriented publications,broader efforts to inform public opinion, and coalitions with otherdevelopment, reproductive health and environmental organiza-tions.
© Population Action International, 1999
Material from this publication may be reproduced provided PopulationAction International and the authors are acknowledged as the source.
ISBN: 1-889735-05-1Library of Congress Number: 99-664885
Printed on recycled paper with organic inks.
POPULATION ACTION
INTERNATIONAL
1120 19th Street, NWSuite 550
Washington, DC 20036 USATelephone: 202-659-1833
Fax: 202-293-1795Website:
http://www.populationaction.org1999
Cover photo credits: Family: PAHO/©Carlos Gaggero Banner, left to right: Corbis Images; Photodisc; PAI/Terri Bartlett; JHU/PIP; Photodisc

James E. Rosen and Shanti R. Conly
POPULATION ACTION INTERNATIONAL
1999
BUSINESSGetting Down to
EXPANDING the PRIVATE COMMERCIAL SECTOR’S
ROLE in MEETING REPRODUCTIVE HEALTH NEEDS

Acknowledgment
We are grateful to the dozens of colleagues who so generouslygave of their time to meet with us and to share their knowledgeand expertise on the private sector. In particular we want to recog-nize the contribution of those pharmaceutical company officialswhose insights have enriched the study. For ease of reading wehave avoided use of footnotes in the text of the report, butacknowledge our heavy debt to the many experts who have writtenbefore us on this topic. For the reader’s information, a list of keysources follows the main report.
Many thanks to those colleagues outside of Population ActionInternational (PAI) who reviewed and commented on an earlierversion of the text. They include: Sigrid Anderson, Kim Beer, SteveBrooks, Michael Free, Patrick Friel, April Harding, Dana Hovig,Doug Heisler, Carl Hemmer, Barbara Janowitz, Ron Loohuys,Susan Mitchell, Steve Mobely, Maureen Norton, Richard Pollard,Steve Sinding, Isabel Stout, Bettina Tewinkel, Abdi Wardere andBill Winfrey. For providing us with their detailed analysis of Demo-graphic and Health Survey data on the commercial sector as asource of family planning our thanks to Bill Winfrey and colleaguesat the Futures Group International.
Many PAI staff helped to shape and edit the report. For excel-lent research support we thank Beverly Johnston, who preparedthe charts and tables and was a valuable sounding board at allstages of the research, writing, and publication. We also acknowl-edge the contribution of Carl Hemmer who, as consultant to PAI,drafted three of the four market profiles.
While acknowledging the invaluable contributions of our manycolleagues, the authors assume full responsibility for the opinionsexpressed in the report, as well as for any unintentional errors.

Table of Contents
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5
CHAPTER 1: Improving Reproductive Health: The Importance of the Private Sector . . . . .12
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12
The Private Sector’s Potential Contribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
The Shortfall in Public Funding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .14
The Growing Needs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
Scope of the Report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .16
CHAPTER 2: The Private For-Profit Sector’s Current Contribution to Reproductive Health Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .19
The Private Sector Role in Manufacturing and Distribution . . . . . . . . . . . . . . . . . .19
Reliance on Private Sector Sources of Reproductive Health Care . . . . . . . . . . . . . .21
CHAPTER 3: Key Factors Affecting Commercial Sector Involvement . . . . . . . . . . . . . . . . .29
Social, Economic and Demographic Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
Competition from Subsidized Products . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
The Legal and Regulatory Climate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .35
Other Factors Affecting Commercial Involvement . . . . . . . . . . . . . . . . . . . . . . . . . .39
CHAPTER 4: Strategies to Expand the Role of the Commercial Sector . . . . . . . . . . . . . . .41
Strategy #1: Target Public Programs to the Poor and Hard to Reach . . . . . . . . . . . .42
Strategy #2: Lower Legal and Regulatory Barriers . . . . . . . . . . . . . . . . . . . . . . . . . .44
Strategy #3: Initiate a Dialogue Between the Public and Private Sectors . . . . . . . . .48
Strategy #4: Create Demand for Reproductive Health Care . . . . . . . . . . . . . . . . . .49
Strategy #5: Build Commercial Markets through Sustainable Public-Private Partnerships . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .50
CHAPTER 5: Forging a New Relationship Between the Public and Private Sectors . . . . . . .55
Changing Government Attitudes about the Commercial Sector . . . . . . . . . . . . . . . .55
Increasing Donor Awareness of and Support for the Commercial Sector . . . . . . . .60
Looking to the Future . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .64
Statistical Annex . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .66
Key References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .70

BOXES: What Distinguishes the Private Sector? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .18
A Changing Climate for Local Manufacture of Contraceptives . . . . . . . . . . . . . . . .20
What is the “Right” Mix of Private and Public Roles in the Health Sector? . . . . . . .25
Crowding Out the Commercial Market in Zimbabwe . . . . . . . . . . . . . . . . . . . . . . .39
Lessons Learned from the USAID Experience . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .45
Anatomy of a Deal: Marketing Injectable Contraception in Brazil . . . . . . . . . . . . .53
Expanding Commercial Markets for Family Planning in Indonesia . . . . . . . . . . .56
Building Alliances: UNFPA’s Initiative to Expand Commercial Markets for Contraceptives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .63
FIGURES: FIGURE 1: The Growing Need for Reproductive Health Care . . . . . . . . . . . . . . . . . . .14
FIGURE 2: Projected Trends in Use of Contraception . . . . . . . . . . . . . . . . . . . . . . . . .16
FIGURE 3: Developing Countries that Manufacture Contraceptives . . . . . . . . . . . . . .20
FIGURE 4: Commercial Share of the Family Planning Market in Developing Regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .23
FIGURE 5: Change Over Time in Reliance on Commercial Sources of Contraceptives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24
FIGURE 6: Distribution of Private and Public Health Expenditures . . . . . . . . . . . . .25
FIGURE 7: Private Sources of Reproductive Health Care . . . . . . . . . . . . . . . . . . . . . .27
FIGURE 8: Worldwide Sales of Oral Contraceptives . . . . . . . . . . . . . . . . . . . . . . . . . .30
FIGURE 9: Who Benefits from Public Subsidies for Reproductive Health Care? . . . . .34
FIGURE 10: Ipas Sales of Manual Vacuum Aspiration (MVA) Instruments . . . . . . . . .37
FIGURE 11: What Targeting of Health Care Services Hopes to Achieve . . . . . . . . . . .43
FIGURE 12: Trends in Use of Injectable Contraceptives . . . . . . . . . . . . . . . . . . . . . . .46
FIGURE 13: Public-Private Partnerships in Social Marketing Initiatives . . . . . . . . . .51
FIGURE 14: Sales of Condoms through Social Marketing Programs . . . . . . . . . . . . . .58
MARKET
PROFILES: Oral Contraceptives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .30
Manual Vacuum Aspiration Instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . .36
Injectable Contraceptives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46
Condoms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .58
Table of Contents continued

EXECUTIVE SUMMARY7
Governments in developing coun-tries have an important role toplay in making reproductive
health products and services affordable forthe poor and other under-served groups.Accordingly, efforts to improve access tofamily planning and other reproductivehealth care have focused primarily on the public sector.
However, the private for-profit sector in thesecountries also has enor-mous potential to helpmeet the increasingdemand for good qual-ity reproductive healthcare. Many developingcountry households earnenough to bear all or partof their health care costs,and are willing to pay for thebetter quality and more efficientcare offered by private as compared topublic health facilities. Encouraging agreater role for the private sector canallow governments to refocus their effortson reaching the poorest and most remotecommunities.
The widening gap between stagnatingpublic funding and the rapidly increasingdemand for reproductive health carerequires that developing nations movequickly to tap the potential of the private
sector. Yet, most countries are not fullyutilizing the private sector, either as asource of additional financial resources for reproductive health or as an efficientprovider of services and commodities.
This study examines how developingcountry governments and internationaldonors can stimulate private sector
involvement in the reproductivehealth arena, with a particular
emphasis on improving theavailability of commodities
such as contraceptives,drugs for treatment ofsexually transmittedinfections (STIs), andnutritional supplements.
The report aims tohelp policymakers in
both developing anddonor countries better under-
stand the crucial role of privatebusiness in expanding access to
reproductive health care.
Many policymakers are unaware of the extent to which commercial firms arealready involved in the provision ofreproductive health care. Indeed, privatebusinesses dominate the manufacture,distribution and marketing of reproductivehealth commodities. Many consumersobtain both commodities and servicesdirectly from the private for-profit sector.
Executive Summary
Encouraging a greater role for
the private sector canallow governments to
refocus their efforts on reaching the poorest
and most remote communities.

Reliance on the commercialsector, however, varies greatlyfor different types of repro-ductive health productsand services. Con-sumers are generallymore willing to pay forcurative than for pre-ventive care. As such,they are most likely toseek out private sourcesfor delivery and abortionservices, as well as for diagno-sis and treatment of sexually trans-mitted infections. In contrast, thecommercial sector role in preventive caresuch as immunizations and nutritionalsupplementation for pregnant women isrelatively insignificant.
For family planning, reliance on thecommercial sector varies according to themethod of contraception. Almost half ofwomen using temporary methods thatrequire regular resupply of commodities—for example, oral contraceptives—obtaintheir method from a commercial source.However, the for-profit sector serves fewerthan 10 percent of women using longer-act-ing methods such as sterilization and IUDs.
The role of the commercial sectoracross countries, moreover, varies enor-mously, reflecting differences in the business environment that profoundlyinfluence a firm’s decision to invest inreproductive health care. Levels of incomeand urbanization, along with competitionfrom publicly subsidized programs, areamong the most important social and economic factors that shape the climate
for commercial activity. The sizeof the market, the demand
for reproductive healthcare and the legal andregulatory frameworkare also important.
Policymakers gener-ally have little control
over many of thesedemographic and social
factors in the short term.However, governments as well
as international donors can havesubstantial influence over the climate for
commercial involvement in reproductivehealth care over the medium and longterm. The following are specific strategiesthat can encourage the commercial sectorto expand its role.
STRATEGY #1
TARGET PUBLIC PROGRAMS TO
THE POOR AND HARD TO REACH
Governments must reorient public sectorprograms to those truly in need, so thatthey complement rather than displace commercial efforts.
There is strong evidence that subsidizedprograms serve many clients who wouldotherwise use for-profit sources. Indeed,free or highly subsidized governmenthealth programs in many countries con-tinue to help the better-off more than thepoor. Redirecting public funds to poor andhard-to-reach communities could stimulatecommercial interest in the provision ofreproductive health care, while expandingaccess to under-served groups.
8EXECUTIVE SUMMARY
Governments as well as international
donors can have substantial influenceover the climate forcommercial involve-ment in reproductive
health care.

EXECUTIVE SUMMARY9
Governments are often reluctant to target public resources for both politicaland practical reasons. Moreover, there isno simple formula guaranteed to reorientpublic programs to lower-income clients.Yet, to free up financial resources to serve these populations within budgetconstraints, governments must seek waysto shift wealthier clients to commercialsources. One solution is to concentratepublic programs in low income communi-ties and rural areas, which are least likelyto attract commercial interest.
STRATEGY #2
LOWER LEGAL AND
REGULATORY BARRIERS
Governments should change laws and regulations as needed to encourage agreater role for the private for-profit sectorin reproductive health care.
A country’s legal and regulatory frame-work deeply affects the commercial sector’sinvolvement in health. While governmentregulation is important to protect con-sumers, all too often laws and regulationsplace unnecessary limits on the for-profitsector that raise the costs or suppress salesof reproductive health products. Bans oncertain products or services, medicallyunnecessary prescription requirements,and restrictions on where and by whomproducts can be sold are among the barri-ers that most affect the for-profit sector.Other inhibiting factors include excessivedelays in product registration, tax policiesand import duties, and restrictions onbrand name advertising and promotion.
Some countries have successfullyremoved such barriers, often through theefforts of nongovernmental organizations(NGO) and international donors. In mostcountries, to move such efforts forward, it is essential to involve key actors outsidethe health sector, such as Ministry ofFinance officials and business associations.
STRATEGY #3
INITIATE A DIALOGUE BETWEEN THE
PUBLIC AND PRIVATE SECTORS
Governments and international donorsneed to better analyze the impacts of public policies on the commercial sectorand include representatives of private businesses in health care planning and decision making.
Most governments and donors lackunderstanding of the for-profit sector’scontribution to reproductive health, andare largely unaware of how their ownpolicies and programs affect the commer-cial sector’s interest in this area. Govern-ment and donor officials rarely includecommercial sector representatives in dis-cussions of population and health policyor in making major program decisions.Such lack of understanding is compoundedby a dearth of reliable information aboutmarket conditions.
To better understand how policy deci-sions affect the commercial sector, govern-ments must maintain a continuing dialoguewith private businesses. It is particularlyimportant that government actionsintended to solve public health problems

10EXECUTIVE SUMMARY
do not supplant for-profit activities that are emerging on their own. Differentdonor agencies need to agree on thetypes of assistance required in a givencountry, and coordinate their efforts sothey do not work at cross-purposes.
STRATEGY #4
CREATE DEMAND FOR
REPRODUCTIVE HEALTH CARE
Governments and donors must supportbroad public education efforts that aim toincrease demand for reproductive healthproducts and services.
In many countries, low levels ofdemand for reproductive health careinhibit the interest of commercial enter-prises. For most businesses, the costs andrisks associated with expanding marketsfor reproductive health products are pro-hibitively high. Such products typicallyaccount for a small portion of drug com-pany sales, and have limited potential togenerate substantial profits.
For these reasons, the public sectormust take the lead in funding activities tostimulate use of reproductive health careand thus encourage greater private sectorinvolvement. Many developing countrieshave successfully used national communi-cation campaigns to significantly increaseknowledge and use of family planning,HIV/AIDS and other reproductive healthservices. Governments can undertake pro-motional campaigns that broadcast mes-sages in support of broad public healthgoals, as well as the use of products andservices available through the commercialsector. To enable businesses to expandtheir own promotional campaigns, govern-
ments also need to ease restrictions onadvertising of reproductive health products.
STRATEGY #5
BUILD COMMERCIAL MARKETS
THROUGH SUSTAINABLE
PUBLIC -PRIVATE PARTNERSHIPS
Governments and donors can use a varietyof mechanisms to undertake partnershipswith the for-profit sector that share therisks of expanding commercial markets forreproductive health products.
Moving beyond their fundamentalresponsibility for creating a business cli-mate in which commercial markets canflourish, some governments and donorshave actively helped to build commercialmarkets through partnership arrangementswith private businesses. Many of theseefforts build on the social marketingapproach, in which subsidized productsare sold through commercial channels. Ina number of instances, for example, donoragencies have supported promotionalactivities in order to encourage commercialfirms to introduce new reproductive healthproducts. The commercial partnershipmodel focused initially on expanding mar-kets for contraceptives, but is increasinglybeing applied to a broader range of repro-ductive health products.
Social marketing is an important mech-anism for serving consumers unable to paythe full market price of reproductive healthproducts, while still recovering at leastpartial costs. As such, this approach meritscontinued support from governments anddonors. In many settings, governments anddonors can begin to move social marketingprograms in the direction of eventual

EXECUTIVE SUMMARY11
financial self-sufficiency. The parties to suchefforts need to work together to furtherrefine the transition from a subsidized to afully self-sustaining effort.
FORGING A NEW RELATIONSHIP
BETWEEN THE
PUBLIC AND PRIVATE SECTORS
To be successful, the strategies describedabove require a change in how govern-ments, international donors and the pri-vate commercial sector view each other. A new alliance based on openness andrecognition of the benefits of interdepen-dence must replace a legacy of mutual dis-trust and misunderstanding. Developingcountry governments and internationaldonors must assume much of the burdenfor removing the constraints to closer col-laboration and overcoming long-standingbiases and negative attitudes about the private sector.
CHANGING GOVERNMENT ATTITUDES
ABOUT THE COMMERCIAL SECTOR
In some countries where thestate has tightly controlledthe economy, many publicofficials view private sec-tor activity of any typewith suspicion. In manycountries, public healthofficials remain con-cerned that expandingthe role of the commer-cial sector in the healthsector may increase costs
and lower the quality of care. Many publicofficials also worry that plans to shift clientsfrom public to commercial sources—whichoften involve the introduction of user feesfor formerly free public services—mayreduce rather than improve access tohealth care for the poor. Meanwhile, manygovernment officials tend to overestimatethe potential interest of the commercialsector in expanding or entering the marketfor reproductive health.
As reproductive health needs mountand public funding stagnates, governmentsmust put aside their biases and activelyenlist the commercial sector’s help inachieving public health goals. Governmentsshould moreover be able to allay concernsabout the cost and quality of private careby strengthening their appropriate regula-tory role and addressing specific problemsin the private provision of health care.
INCREASING DONOR AWARENESS OF
AND SUPPORT FOR THE
COMMERCIAL SECTOR
The United States, with its largelyprivate for-profit health sys-
tem, has been a leader inpromoting models forcommercial sectorinvolvement in repro-ductive health in devel-oping countries. TheUnited Kingdom and
Germany are the onlyother bilateral donors
with a significant commit-ment to such initiatives.
A new public-privatealliance recognizing
the benefits of interdependence must
replace a legacy ofmutual distrust andmisunderstanding.

Donor agency officials in these and othercountries must also overcome biasesagainst private sector involvement. Manydonor officials, themselves civil servants,view the government role in health financ-ing and services as essential and lack anunderstanding of commercial sector inter-ests. The World Bank and United NationsPopulation Fund, the major multilateraldonors in reproductive health, generallywork through developing country governments and thus find it moredifficult to support commer-cial sector programs.
The major donoragencies in reproduc-tive health are showinga growing interest incommercial sector ini-tiatives. Still, the donorscould do much more toencourage a more positiveattitude to the private sectorby developing countries. As a firststep, donors should ensure that theircommodity support nurtures rather thanundermines healthy commercial markets.Donors should also use their influencewith governments to promote fundamentalchanges in health policy, such as reorienta-tion of government health services towardsthe poor. By promoting more efficient andequitable health systems, such actions willultimately benefit the growth of commer-cial markets. Donors can also help tobridge the information gap by supportingresearch on markets and demand forreproductive health care and sharing thisinformation with governments and thebusiness community.
LOOKING TO THE FUTURE
There is no quick and simple solution toincreasing the role of the private commer-cial sector in reproductive health care. Toachieve this end, fundamental changes areneeded in policies relating to the role andresponsibilities of governments in payingfor and providing reproductive health care.
To be effective, the strategies describedabove must also be part of a com-
prehensive approach to mak-ing the best use of scarce
public funds. This effortshould clarify public andprivate sector roles inmeeting the reproduc-tive health needs ofdifferent economic and
social groups within eachunique national context.
Fortunately, both govern-ment and businesses are begin-
ning to recognize the benefits of closercollaboration. The public sector mustbuild on these evolving attitudes andtake the actions needed to harness thecommercial sector’s full potential toimprove reproductive health and slowworld population growth.
12EXECUTIVE SUMMARY
The major donor agencies in
reproductive health areshowing a growing
interest in commercial sector initiatives.
EXECUTIVE SUMMARY13
To improve reproductive health
and slow world populationgrowth, the public sector
must take the actionsneeded to harness
the commercial sector’s full potential.
POPULATION ACTION INTERNATIONAL14
INTRODUCTION
Around the world, there is an emerging consensus that privateenterprise is the engine of economic growth and development.Market forces are widely accepted as the most dynamic and effi-cient mechanisms for meeting society’s demands for goods andservices, especially in the productive economic sectors such asagriculture and industry. Even in the social sectors, where govern-ments have traditionally played a greater role, there is growingrecognition that the private for-profit sector can help meet thepublic’s demand for education and health care.
In reproductive health, as in other areas of health care, theprivate sector’s potential importance lies in the inadequacy ofpublic funding relative to growing needs. New and innovativeapproaches involving the private sector are required to bridge this gap between stagnating financial resources and the rapidlyincreasing demand for reproductive health care.
Yet in most developing countries, the private sector is not ful-filling its potential to help meet reproductive health needs, oftenbecause governments have not created a sufficiently supportiveenvironment. Developing country governments and internationaldonor agencies do not adequately appreciate the private sector’scontribution to reproductive health. Most governments anddonors lack awareness of how their own policies and programseither encourage or deter the private sector from playing a largerrole in reproductive health.
CHAPTER 1
Improving Reproductive Health: The Importance of the Private Sector

Getting Down to Business 15
THE PRIVATE SECTOR’S POTENTIAL CONTRIBUTION
The private sector can help expand access to good qualityreproductive health care in a variety of ways.
❁ Private households represent a largely untappedsource of additional funding for reproductive health.Payments by consumers of health services and productsalready represent a major source of health care financingin both the industrialized and developing world. For repro-ductive health care too, many families are willing to pay allor part of the costs. At present, most consumer expendi-tures on health care pay for care obtained from privatesources. However, many government health systems in thedeveloping world are also introducing user fees, based onthis consumer willingness to pay.
❁ Private health facilities generally offer higher qualitycare and operate more efficiently than their publicsector counterparts. Quality is an important reason citedby consumers for seeking reproductive health care fromprivate sources; higher quality facilities are also more likelyto retain their clients. Access to private care gives consumersan alternative to often unreliable or poor quality public sec-tor health facilities, expanding consumer choices and thenumber of sources from which consumers can obtain care.The private sector’s greater efficiency also means it canpotentially serve more clients for the same cost.
❁ Expanding the role of the private sector, together withtargeting of limited public funds, can help increaseoverall access to reproductive health care. In virtuallyevery developing country, government health budgetsremain inadequate to provide good quality reproductivehealth care to the entire population, let alone keep pacewith the rapid increase in couples of childbearing age. Yetcurrently, in many countries, large numbers of relativelywell-off consumers obtain reproductive health care free orat subsidized prices from public sources, while many poorpeople have little or no access to care. By encouragingwealthier clients to use unsubsidized sources of care, gov-ernments can more easily focus their own funds on thepoorest and most remote communities.
Private house-holds represent alargely untappedsource of addi-tional funding
for reproductivehealth.

POPULATION ACTION INTERNATIONAL16
THE SHORTFALL IN PUBLIC FUNDING
Public funding for reproductive health from developing countryand donor governments remains far short of the funding needsidentified at the International Conference on Population andDevelopment (ICPD), held in Cairo in 1994. For 1996, total expen-ditures on basic reproductive health care in developing countriesare estimated at roughly $10 billion, compared to an estimated$17 billion needed by the year 2000. Developing countries providedalmost four-fifths of this amount—with governments contributingabout $7 billion and private households an estimated $1 billion.Donor governments provided $1.4 billion in grant aid, comparedto an estimated $5.7 billion needed in the year 2000.
Prospects for future increases in public funding are uncertain.While some donor countries have increased funding for popula-tion and reproductive health programs, others provide only negli-gible assistance. Many developing countries experiencingeconomic problems have cut their health budgets, including theAsian nations which account for the bulk of domestic reproductivehealth spending in the developing regions. The poorest countriesin Africa have the greatest needs but limited ability to increase theirhealth budgets. While developing and donor country governmentsneed to boost their lagging spending, alternative strategies areclearly needed to make the ICPD goals a reality.
The ICPD Programme of Action expressly acknowledges theimportance of the private sector in meeting reproductive healthgoals. The document recognizes that private as well as public
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2050
2045
2040
2035
2030
2025
2020
2015
2010
2005
2000
1995
1990
1985
1980
1975
1970
1965
1960
1955
1950
Actual Number of Women
Projected Number of Women
MIL
LIO
NS
OF
WO
ME
N A
GE
S 1
5 T
O 4
9 Y
EA
RS
Figure 1
THE GROWING NEED
for REPRODUCTIVE
HEALTH CARE
Current and Projected Numberof Women of Reproductive Agein the Developing World(UN medium projection)
Source: United Nations. World Popu-lation Prospects: The 1998 Revision.New York: UN, 1998.

Getting Down to Business 17
sector participation will be necessary to realize universal access togood quality reproductive health care by the year 2015, as part ofthe broader conference goal of improving living standards andslowing population growth. It calls for efforts to promote the roleof the private sector “in service delivery and in the production anddistribution…of high-quality reproductive health and family-plan-ning commodities and contraceptives…”
THE GROWING NEEDS
The shortfall in funding is especially acute because, while manycountries have made some progress in expanding access to repro-ductive health care, needs in this area continue to grow rapidly.
❁ The number of women of childbearing age is increasing byalmost 24 million a year. These women, together with theirmale partners, represent the key consumers of reproduc-tive health care, including family planning, prenatal careand safe delivery, and prevention and management ofHIV/AIDS and other sexually transmitted infections (STIs).
❁ More than 100 million married women in developingcountries already have an unmet need for family planning,contributing to some 36 million abortions each year. Inaddition, a growing number of couples want moderncontraception in order to achieve a smaller family size. Tomeet this growing demand, family planning programs willneed to reach an additional 250 million couples by 2015.
❁ Meanwhile, maternal death rates remain high; about600,000 women die each year in pregnancy or childbirth,including 80,000 from unsafe abortion. Yet many womenstill lack access to prenatal care and safe delivery. Unlesseconomic and health conditions and access to dietarysupplements improve, the number of women with anemiaand other nutritional deficiencies which contribute tomaternal illness and deaths could grow from 500 millionto 700 million by 2015.
❁ The AIDS epidemic is spreading rapidly; some 6 millionindividuals each year are infected with HIV. Another 300million men and women annually acquire a curable STI—a number likely to increase to over 400 million by 2015.More aggressive efforts are needed to prevent HIV andother STIs, and to diagnose and treat curable STIs.
The shortfall in funding is
especially acute becausereproductivehealth needs continue to
grow rapidly.

POPULATION ACTION INTERNATIONAL18
SCOPE OF THE REPORT
The private sector encompasses many different elements, includingboth non-profit and for-profit entities. Within the for-profit sector,the private commercial sector—i.e., private business and industry—plays a key role in the manufacture, distribution and retail sales ofreproductive health commodities. Private clinics and practitionersare engaged in the direct provision of services. In addition, privatehealth insurance schemes and employer-sponsored health pro-grams are involved in the financing of reproductive health care.
This report seeks to enhance understanding of how the pri-vate commercial sector can help expand access to reproductivehealth care, with a special focus on its role in making commodi-ties such as contraceptives, STI drugs and nutritional supple-ments more widely available. The report analyzes the scope ofthe for-profit sector’s current involvement in reproductive health,and the major factors that influence private investment in thisarea. It goes on to look more specifically at the role of privatebusiness in the supply of reproductive health commodities, andidentifies strategies developing country governments and interna-tional donors can adopt to encourage the private commercial sector to play an expanded role in this area.
0
200
400
600
800
1000
Developed Regions
Developing Regions Excluding China
China
201520051995
MIL
LIO
NS
OF
MA
RR
IED
WO
ME
N
Figure 2
PROJECTED TRENDS in USE of CONTRACEPTION1995, 2005 and 2015
Sources: United Nations. Levels and Trends of Contraceptive Use asAssessed in 1994. New York: UN, 1996;United Nations. World PopulationProspects: The 1998 Revision. New York: UN, 1998.
Getting Down to Business 19
The limited focus of this report is not to deny the private sec-tor’s other important and complementary roles, which are alsoworthy of research and analysis. It would be difficult, however, to do justice to the full range of private sector activities in a singlereport. Moreover, many of the strategies recommended in thisreport are relevant to efforts to stimulate the private provisionand financing of reproductive health care.
There are also several reasons to focus on the commercialsector, i.e. the role of private business in the supply of reproduc-tive health commodities.
❁ Commodities are the lifeblood of reproductive health programs (especially for family planning and STI treat-ment.) Depending on the type of care, they may accountfor a significant share of the costs of these activities.
❁ The private commercial sector plays an especially sig-nificant role in the supply of some reproductive healthproducts. For example, it is the leading source from which consumers obtain oral contraceptives, condomsand some other commodities.
❁ In an increasingly integrated or globalized world economy,new opportunities exist for the handful of transnationalcompanies involved in the manufacture and distribu-tion of reproductive health products to tap into marketsin the developing world.
While this report emphasizes the potential role of private business, it also acknowledges the importance of the state. Govern-ments have a crucial role to play in helping to make services afford-able for the poor and other under-served groups, and in ensuringaccess to services when private markets fail to provide adequatecare. Moreover, in many countries, there are legitimate concernsregarding the quality and cost of health care provided by the privatesector. Governments bear a responsibility to regulate the privatesector’s involvement in reproductive health—as in health caremore generally. Public funds, however, should complement ratherthan substitute for the private sector.
Public fundsshould comple-
ment ratherthan substitutefor the private
sector.

POPULATION ACTION INTERNATIONAL20
T he formulation of strategies to encouragecommercial involvement in reproductive
health care requires an understanding of thedifferences between the private sector and thenongovernmental and public sectors. A keydistinction is the character of ownership andthe motivations of owners:
❁ Private businesses are owned by indi-viduals or share holders and exist toearn a profit that is distributed amongthe owners.
❁ Nongovernmental organizations ornon-profits are also private, but definetheir mission in terms of achievingsome social or public health goalrather than securing profits.
❁ Public sector organizations such ashealth ministries are instruments ofthe state established to achieve thepolitical and social objectives of thegovernment, usually including goalsfor improving public health.
Each sector, while distinct in ownershipand motivation, may draw upon both publicand private funds. Commercial suppliers,manufacturers, and distributors sell to otherprivate firms or to governments and interna-tional donor agencies. Nongovernmental orga-nizations have traditionally received fundingfrom public sources (donor and developingcountry governments) and charitable contribu-
tions, but often rely on payments from clients to atleast partially cover costs. Government programs,customarily funded from general tax revenues andinternational grants and loans, are increasinglyseeking to recover at least some of their coststhrough user fees.
The lines between the sectors—never com-pletely clear as shown by the examples above—are blurring even further:
❁ Nongovernmental organizations areincreasingly becoming “social enterprises”earning profits which they plow back intoactivities to support their social goals,rather than distributing them to ownersor shareholders like a commercial firm. A number of national family planningassociations in Latin America now operatein this mold.
❁ Physicians and other health workers inprivate practice often see themselves aspromoting public health goals as well asoperating as for-profit businesses.
❁ Joint government-private ownership, particularly of manufacturing facilities forreproductive health products, is anotherarrangement which cuts across defini-tional lines.
❁ Finally, there is a growing trend for commercial firms to assume managementof publicly owned facilities in order topromote more efficient operation.
WHAT DISTINGUISHES THE PRIVATE SECTOR?

Getting Down to Business 21
R eproductive health care is a multibillion dollar worldwideindustry, with sales of contraceptives alone generatingsome $3 billion in revenues each year. The private com-
mercial sector is deeply involved at all points along the chain ofsupply that links the producers of reproductive health productsand services to consumers.
THE PRIVATE SECTOR ROLE IN
MANUFACTURING AND DISTRIBUTION
The manufacture of commodities such as contraceptives, drugs fortreatment of sexually transmitted infections, iron supplements andthe medical supplies used in reproductive health programs is over-whelmingly an activity involving private for-profit firms. Productionof contraceptives in particular is dominated by a relatively smallnumber of large transnational companies. China, India and someother developing countries still operate state-owned productionfacilities, many of which were built with financing from interna-tional donors (see box on page 20), but even these are increas-ingly being run as profit-oriented businesses.
Private, commercial firms have a similarly important role in thedistribution and marketing of reproductive health commodities.Large, multinational drug and medical supply firms either use theirown distribution and marketing channels or contract with indepen-dent commercial agents to distribute and sell their products. Inthe past, many public sector programs have purchased commodi-ties directly from manufacturers or wholesalers and used their owndistribution systems to deliver these commodities to clinics andhospitals. Governments are, however, increasingly turning to com-mercial firms or nonprofit organizations to handle distribution ofcommodities, again in the interests of greater efficiency.
CHAPTER 2
Production ofcontraceptivesis dominated
by a relativelysmall number
of largetransnational
companies.
The Private For-Profit Sector’s Current Contribution to Reproductive Health Care
POPULATION ACTION INTERNATIONAL22
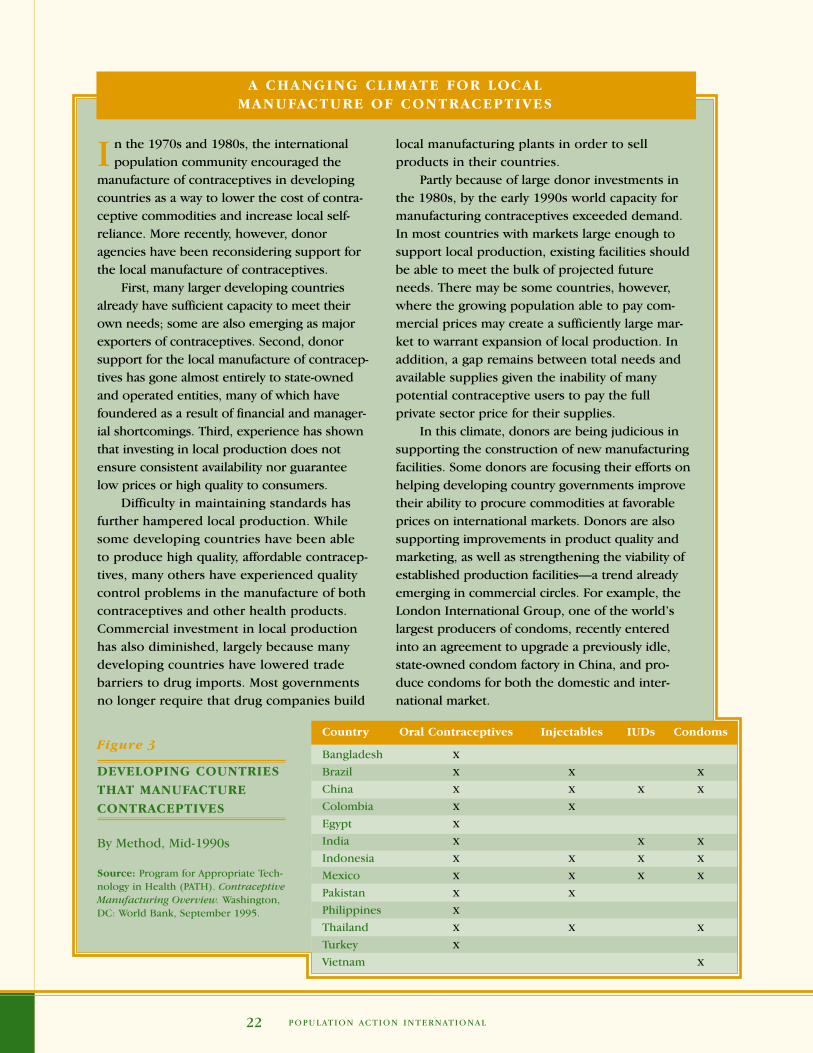
I n the 1970s and 1980s, the internationalpopulation community encouraged the
manufacture of contraceptives in developingcountries as a way to lower the cost of contra-ceptive commodities and increase local self-reliance. More recently, however, donoragencies have been reconsidering support forthe local manufacture of contraceptives.
First, many larger developing countriesalready have sufficient capacity to meet theirown needs; some are also emerging as majorexporters of contraceptives. Second, donorsupport for the local manufacture of contracep-tives has gone almost entirely to state-ownedand operated entities, many of which havefoundered as a result of financial and manager-ial shortcomings. Third, experience has shownthat investing in local production does notensure consistent availability nor guaranteelow prices or high quality to consumers.
Difficulty in maintaining standards hasfurther hampered local production. Whilesome developing countries have been ableto produce high quality, affordable contracep-tives, many others have experienced qualitycontrol problems in the manufacture of bothcontraceptives and other health products.Commercial investment in local productionhas also diminished, largely because manydeveloping countries have lowered tradebarriers to drug imports. Most governmentsno longer require that drug companies build
local manufacturing plants in order to sell products in their countries.
Partly because of large donor investments inthe 1980s, by the early 1990s world capacity formanufacturing contraceptives exceeded demand.In most countries with markets large enough tosupport local production, existing facilities shouldbe able to meet the bulk of projected futureneeds. There may be some countries, however,where the growing population able to pay com-mercial prices may create a sufficiently large mar-ket to warrant expansion of local production. Inaddition, a gap remains between total needs andavailable supplies given the inability of manypotential contraceptive users to pay the full private sector price for their supplies.
In this climate, donors are being judicious insupporting the construction of new manufacturingfacilities. Some donors are focusing their efforts onhelping developing country governments improvetheir ability to procure commodities at favorableprices on international markets. Donors are alsosupporting improvements in product quality andmarketing, as well as strengthening the viability ofestablished production facilities—a trend alreadyemerging in commercial circles. For example, theLondon International Group, one of the world’slargest producers of condoms, recently enteredinto an agreement to upgrade a previously idle,state-owned condom factory in China, and pro-duce condoms for both the domestic and inter-national market.
Figure 3
DEVELOPING COUNTRIES
THAT MANUFACTURE
CONTRACEPTIVES
By Method, Mid-1990s
Source: Program for Appropriate Tech-nology in Health (PATH). ContraceptiveManufacturing Overview. Washington,DC: World Bank, September 1995.
Country Oral Contraceptives Injectables IUDs Condoms
Bangladesh X
Brazil X X X
China X X X X
Colombia X X
Egypt X
India X X X
Indonesia X X X X
Mexico X X X X
Pakistan X X
Philippines X
Thailand X X X
Turkey X
Vietnam X
A CHANGING CLIMATE FOR LOCAL MANUFACTURE OF CONTRACEPTIVES

Getting Down to Business 23
RELIANCE ON PRIVATE SECTOR SOURCES OF
REPRODUCTIVE HEALTH CARE
In the small towns and cities of virtually every developing country,consumers who can afford to pay have the option of seekingreproductive health care from clinics, pharmacies and retail storesthat operate for profit. People “shop around” for reproductivehealth care as they do for other goods, deciding to use public,NGO or for-profit sources after taking into account factors such asprice, quality, travel costs and waiting time.
Surveys and other studies suggest that many people look to theprivate sector for reproductive health care. However, the qualityand completeness of information on the private sector varies widely.Although national surveys in many developing countries typicallyreport detailed information on where women obtain family plan-ning, definitions of the private sector are not consistent acrosscountries or between one survey and the next for the same country.Unfortunately, for other reproductive health care, the informationavailable on the degree of reliance on public and private sources ismuch sparser and even poorer in quality. Such data draw mainly onsmall-scale and anecdotal studies, which cannot be used to makecross-country comparisons or analyze trends worldwide.
It is also often difficult to make a distinction between purelyfor-profit sources of care and those that operate with some degreeof public subsidy. In many countries, for example, a substantialproportion of contraceptives purchased through private pharma-cies are subsidized through social marketing programs.
Many individuals also use private sources for some types ofhealth care while choosing public sources for others. For example,women commonly use private prenatal care, then deliver their childin a public hospital. Similarly, in Indonesia, almost 40 percent ofwomen obtaining oral contraceptives from the public sector chooseprivate, commercial sources for at least some other maternity andchild health care.
Reliance on the Private Sector for Family Planning
For the developing world as a whole, 12 percent of all family plan-ning users, or roughly 50 million women, obtain contraceptionfrom commercial sources. However, an extremely small percentageof users rely on commercial sources in the two largest developingcountries—under 1 percent in China and just 13 percent in India.Outside of China and India, fully one-third of women in the devel-oping world rely on commercial sources for family planning.
Many peoplelook to the
private sectorfor reproductive
health care.

POPULATION ACTION INTERNATIONAL24
There is striking variation in the commercial sector share,ranging from under 5 percent in countries such as China, Kazakstanand Rwanda, to over 50 percent in Bolivia, the Dominican Repub-lic, Egypt and Paraguay. The proportion of women using for-profitsources of family planning tends to be higher in Latin America andthe Caribbean (46 percent) and the Middle East and North Africa(44 percent) than in sub-Saharan Africa (27 percent) and Asia (26percent, excluding China and India).
Consumers rely much more heavily on commercial sourcesfor temporary than for longer-acting family planning methods.Almost half of couples using condoms and oral and injectablecontraceptives obtain their supplies from the profit-oriented sector.(Roughly one in six of these users, however, purchases contracep-tives at below-market prices through social marketing programs.)By contrast, for-profit facilities serve fewer than 10 percent ofclients using sterilization or IUDs.
These averages mask enormous variance among countries andwithin regions. In Latin America, for example, only 22 percent ofwomen obtain oral contraceptives from private for-profit sources inHaiti, compared to 94 percent in Colombia. The commercial sectorshare of the condom market in sub-Saharan Africa similarly rangesfrom 9 percent in Rwanda to almost 100 percent in the Sudan.
Even in countries where the commercial share is high, substan-tial room for future growth of the market may exist. In Nigeria, thecommercial sector share is 40 percent. Yet, with just 4 percent ofwomen using modern contraception, the potential for expansionof the overall market is large. Similarly, in the Sudan, while virtu-ally all condoms are purchased from commercial sources, less than1 percent of couples use condoms as a family planning method.
Comparisons across countries show no evidence of any rela-tionship between reliance on commercial sources of family plan-ning and overall levels of contraceptive use. Within countries,however, the commercial share of the market for contraceptivesappears to be increasing. In 16 of 26 countries for which data ontrends over time are available, overall commercial market share hasrisen over time. In Ghana, for example, as use of modern contra-ception rose from 5 to 10 percent between 1988 and 1993, thecommercial share doubled from 24 to 48 percent. In Indonesia,too, the commercial sector share rose from 12 percent in 1987 to40 percent in 1997, along with overall family planning use. It isnoteworthy that in a number of these countries, governments anddonors made explicit efforts to increase the for-profit sector’s role.
Elsewhere, the commercial share of the market has fallen overtime—sometimes sharply, as in Egypt, where the commercial sharedropped from 71 percent to 51 percent between 1988 and 1995.Still, the absolute number of women served by for-profit sourceshas not decreased in any country; any decline in market share for
Consumers relymore heavily
on commercialsources for
temporary thanfor longer-actingfamily planning
methods.

Getting Down to Business 25
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
A L L M O D E R N M E T H O D S
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
O R A L C O N T R AC E P T I V E S
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
I U D s
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
I N J E C TA B L E C O N T R AC E P T I V E S
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
F E M A L E S T E R I L I Z AT I O N
0 10 20 30 40 50 60 70 80 90Latin America and the Caribbean
Asia Excluding China and IndiaAsia
Middle East and North AfricaSub-Saharan Africa
Developing World Excluding China and IndiaDeveloping World
C O N D O M S
Figure 4
COMMERCIAL SHARE ofthe FAMILY PLANNING
MARKET in DEVELOPING
REGIONS
Percent of Women Using aModern Contraceptive WhoObtain Their Method from aCommercial Source
Sources: The Futures Group Interna-tional; UN Population Division; vari-ous Demographic and Health Surveys. For a detailed description of sourcesand methodology, see note for the Statistical Annex.

POPULATION ACTION INTERNATIONAL26
the commercial sector has been offset by a combination of therapid increase in the number of women of childbearing age andthe growing demand for family planning.
Globally, however, the size of the market for contraceptives, atabout $3 billion in sales a year, is small compared to an estimated$300 billion in total annual pharmaceutical sales worldwide. More-over, oral contraceptives account for fully two-thirds of the revenuesgenerated by worldwide contraceptive sales—with 90 percent ofrevenues from oral contraceptive sales coming from developedcountries. The markets—and potential for profits—for other con-traceptive methods remain relatively small; condoms, for example,generate only about $150 million in annual worldwide sales bymanufacturers. Still, prospects are good for future growth indeveloping country markets for condoms and hormonal methodssuch as pills and injectables.
Figure 5
CHANGE OVER TIME
in RELIANCE on COMMERCIAL SOURCES
of CONTRACEPTIVES
Percent of Women Using aModern Contraceptive WhoObtain Their Method from aCommercial Source, Mid-1980sto Mid-1990s, Various Countries
Sources: Demographic and Health Sur-veys; The Futures Group International.
0
10
20
30
40
50
60
70
80
Peru
Guatem
ala
Domin
ican R
epubl
ic
Colom
bia
Brazil
Bolivia
Turk
ey
Phili
ppines
Moro
cco
Jord
an
Indones
iaEgy
pt
Bangla
desh
Zimba
bwe
Zambi
a
Uganda
Togo
Tanza
nia
Seneg
al
Niger
Mad
agas
car
Mali
Mala
wi
Kenya
Ghana
Camer
oon
CO
MM
ER
CIA
L S
EC
TO
R M
AR
KE
T S
HA
RE
S U B - S A H A R A N A F R I C A A S I A A N D N E A R E A S TL AT I N A M E R I C A A N D
T H E C A R I B B E A N
Third Survey
Second Survey
First Survey

Getting Down to Business 27
E conomic theory justifies some degree ofgovernment involvement in financing and
providing the reproductive health servicesoutlined in the Cairo Programme of Action,especially where these services benefit thelarger society as well as the individuals whouse them. The state also has a role in ensuringthat the poor, who could not otherwise affordcare at market prices, can obtain essentialreproductive health information, products andservices. However, determining the optimalpublic-private mix in addressing health careneeds is a complex task.
For the developing world as a whole, private households account for roughly half of all health spending; however, this propor-tion varies considerably across countries. Theprivate share is smallest—about 30 percent—in the former socialist economies, and ranges
between 40 and60 percent inmost other devel-oping countries.In India, privatehouseholds
account for 78 percent of total health spending. The wide variation of health systems across
countries and the unique conditions that shapethem have led many observers to conclude thatthere is no single, best combination of public andprivate roles. As a recent World Bank health policydocument states, “neither sector is effective byitself—each needs the other. Both too much andtoo little involvement by either sector are oftenassociated with problems.” The U.S. Agency forInternational Development (USAID) takes a similarcountry specific approach in its efforts to helpdeveloping countries improve their health systems.
Nevertheless, as the role of the state in thefinancing and provision of social services under-goes a reappraisal, many observers now questionthe dominance of governments in health care.Developing countries with the most success inachieving health goals have encouraged a greaterprivate role in the actual provision of care, whilefocusing government efforts on providing healthinformation, setting policy, improving regulationsto ensure the quality of health care and servingthe truly needy.
0 10 20 30 40 50 60 70 80 90 100
Publicly FinancedPrivately Financed
Eastern Europe and Central Asia
High Income Countries
Sub-Saharan Africa
East Asia and the Pacific
Middle East and North Africa
Latin America and the Caribbean
South Asia
P E R C E N T O F T O TA L H E A LT H S P E N D I N G
Figure 6
DISTRIBUTION of PRIVATE and PUBLIC
HEALTH EXPENDITURES
Developing Regions and HighIncome Countries, Circa 1994
Source: George Schieber and Akiko Maeda.“A Curmudgeon’s Guide to FinancingHealth Care in Developing Countries.” In Innovations in Health Care Financing. Proceedings of a World Bank Conference. Washington,DC, 10-11 March 1997, ed. George Schieber. Washington, DC: World Bank, 1997: 1-40.
WHAT IS THE “RIGHT ” MIX OF PRIVATE AND PUBLICROLES IN THE HEALTH SECTOR?

POPULATION ACTION INTERNATIONAL28
Sources of Other Reproductive Health Care
Reliance on private for-profit sources varies greatly for other typesof reproductive health care.
❁ The vast majority of women choose private sources ofhealth care for prenatal care and delivery. Some 60 per-cent of births in developing countries still take place athome, where most women receive care from trained pri-vate midwives or traditional birth attendants. Only a smallgroup of women give birth in for-profit clinics or hospitals.For prenatal care, the proportion of women seeking privatecare varies. In Morocco, half of all women see a privatehealth worker for prenatal care; in Peru, the Philippines,and Tunisia, one-quarter of women seeking care use privatesources for prenatal services.
❁ Few pregnant mothers and infants receive tetanus andother routine immunizations from commercial sources;most use government facilities for these preventive ser-vices. Little information is available about where pregnantwomen obtain nutritional supplements such as ironfolate tablets, but available studies suggest the commercialsector role is small.
❁ The private for-profit sector plays a large role in the diag-nosis and treatment of sexually transmitted infections.Typically, men who experience symptoms of an STI eithertreat themselves, or seek care from a traditional healthpractitioner, pharmacist, or private physician. In a study in Cameroon, 60 percent of men first obtained treatmentfrom the commercial sector, and the vast majority pur-chased remedies from pharmacies and other for-profitsources. Women with reproductive tract infections arethought to be less likely than men to seek private care,because they are more accustomed to using public clinicsfor other reproductive health care and often have lessaccess to the funds needed for private treatment.
The vast majority of
women chooseprivate sources
for prenatal careand delivery.

Getting Down to Business 29
STUDY SAMPLE FINDINGS
STI TREATMENT
Cameroon 189 young men with an 61% of men obtain initial treatment for
Crabbe et al. (1996) STI in two large towns STI-related symptoms from the private sector
Ghana 764 clients of an STI/AIDS 75% of clients self-medicate with one or more
Adu-Sarkodie (1997) clinic in a small city antimicrobial drugs before seeking clinical care
United States National survey of 3,432 men 49% of respondents with an STI receive
Brackbill et al. (1999) and women ages 18 to 59 treatment from a private doctor
South Africa 4,781 STI patients over a 35% of clients seek treatment
Wilkinson et al. (1998) 5-month period in one from private doctors
largely rural health district
Kenya 380 STI patients at Roughly one-third of patients obtain initial
Moses et al. (1994) eight public clinics treatment elsewhere; 63% of those patients
received care from the private sector
MATERNAL HEALTH AND NUTRITION
Philippines National survey of 15,029 23% of women use private facilities
East-West Center (1996) women ages 15 to 49 for their first prenatal visit
Bolivia, Guatemala, Botswana, National surveys of women In four of five countries, less than 20% of
Sudan and Uganda ages 15 to 49 women use the private sector for tetanus
Berman and Rose (1996) toxoid vaccination
Morocco and Tunisia National surveys of women 48% of women in Morocco and 25% of women
Berman and Rose (1996) ages 15 to 49 in Tunisia use the private sector for prenatal care
Malawi 210 pregnant women in 10% of pregnant women purchase iron
Williams et al. (1997) villages and tea estate tablets from commercial sources
compounds in one district
ABORTION AND POSTABORTION CARE
Nigeria 119 women receiving treatment 60% of patients had the initial procedure
Konje and Obisesan (1991) for abortion complications in a performed at a private hospital or clinic
large public hospital
Figure 7
PRIVATE SOURCES
of REPRODUCTIVE
HEALTH CARE
Findings from Recent Studies
See Key Reference list for full citations.

POPULATION ACTION INTERNATIONAL30
❁ The degree to which women use private for-profit abortioncare depends largely on the legal status of abortion in acountry. Where severe restrictions exist, the majority ofwomen will either induce an abortion alone or seek outclandestine private providers. In Nigeria, where abortion is legal only to save a woman’s life, 60 percent of womenwho sought treatment at a public hospital for complica-tions from unsafe abortion had the initial procedure at aprivate hospital or clinic. Where abortion is permitted forbroad social and economic reasons, women appear morelikely to use public sector services. For example, after theSouth African parliament legalized early abortion in 1997,public hospitals reported a surge in the number of womenseeking the procedure. Many women, however, still preferprivate care out of concern for quality and confidentiality.
❁ For-profit providers play a less central role in postabortioncare. Where the majority of abortions are clandestine,poorer women are most likely to suffer complicationsfrom unsafe abortion, yet are least able to pay for expen-sive private treatment. In addition, private, clandestineabortion providers typically do not offer family planning—a key element of postabortion care.
These disparities in reliance on the private commercial sectorreflect differences in the willingness of consumers to pay for spe-cific types of health care, in particular their greater willingness topay for curative than for preventive care. But they also reflect dif-ferences across countries in the social and economic factors whichshape the general business environment and influence the com-mercial sector’s decision to invest in reproductive health care.
The private for-profit sector
plays a largerole in the
diagnosis and treatment of
sexually transmittedinfections.

Getting Down to Business 31
F or any business, the decision to make an investment iscomplex and reflects a combination of factors. In repro-ductive health, too, a number of factors account for vary-
ing levels of commercial sector involvement across countries. A better understanding of the conditions that facilitate suchinvestments is crucial to formulating effective strategies toexpand the commercial sector role.
SOCIAL, ECONOMIC AND DEMOGRAPHIC FACTORS
Population size and density, current demand, income levels andavailability of basic infrastructure are important elements of thegeneral business environment that affect commercial decisions toenter or expand markets. Most of these conditions remain outsidethe short-term influence of policymakers; together, however, theyhave a profound effect on the volume of sales and profits compa-nies can generate and on the cost of their business operations.
Population size is key to commercial interest. To remainviable, businesses at all points along the supply chain must have apotential market large enough to generate sufficient revenues tocover their costs. Developing countries with larger populationsthus tend to attract more interest from commercial firms. Of theten countries where the commercial sector share of the familyplanning market is greatest, six (Colombia, Turkey, Egypt, Mexico,Brazil and Indonesia) have populations of more than 40 million.
Population density is also important to profitability, and is onereason why pharmacies and private medical practitioners tend to beconcentrated in urban areas. Commercial distribution networks fordrugs and medical supplies typically do not reach regions with alow population density. It is often not economical for sales repre-sentatives of pharmaceutical companies to visit remote or sparselypopulated areas, since expected sales volume is not high enoughto cover the costs of promotion and distribution. In Pakistan, forexample, one drug company limits its sales representatives to visit-ing towns with 5 or more doctors, owing to cost considerations.
CHAPTER 3
Key Factors Affecting Commercial Sector Involvement
Developingcountries withlarger, moreurbanized
populationstend to attractmore interestfrom commer-
cial firms.

32MARKET PROFILE
IMPROVING THE PRODUCTCurrently technology makes a variety ofimprovements in oral contraceptives feasible.However, profits are too small and the poten-tial liabilities from lawsuits in developed countries are too large to stimulate the industry to develop and launch new forms of oral contraceptives.
MANUFACTURINGA few large multinational drug companiesdominate the manufacture of oral contracep-tives. Wyeth-Ayerst and Ortho in the UnitedStates, Schering in Germany, and the Dutchfirm Organon account for 80 percent of prod-uct sales worldwide. For Schering and Organon,roughly a quarter of their overall revenuesderive from the sale of oral contraceptives.For Wyeth-Ayerst, by contrast, sales of theircontraceptive products make up less than 10percent of overall product sales.
The need for exacting quality control andhighly skilled workers limits production of oralcontraceptives to settings in relatively devel-oped countries. Plants can operate profitablyonly when geared to mass production, and
MARKET SIZEOral contraceptives are one of the most popu-lar methods for women seeking temporaryprotection against pregnancy. In the develop-ing world, the nearly 50 million users of oralcontraceptives account for 13 percent of thosewomen practicing modern family planning.Worldwide sales of oral contraceptives yieldover $2 billion annually, about 80 percent ofrevenues from the sale of family planningproducts worldwide. Manufacturers earn 90percent of these revenues in industrializedcountries, where just one-third of users reside.
THE PRODUCTPills combining the hormones estrogen andprogestin are the most widely used productson the market; a second, less common formu-lation are progestin only pills, intendedprimarily for breastfeeding women. Over thelast three decades, manufacturers have reducedthe amount of hormones contained in the oralpill to diminish the undesirable side effects ofhigher dosages. Packaged in 21 and 28 day blis-ter packs, pill cycles sometimes include severalgradations of dosage over a woman’s cycle.
MARKET PROFILE
Oral Contraceptives
Figure 8
WORLDWIDE SALES ofORAL CONTRACEPTIVES
Percent Share by Company, 1992
Source: Polly Harrison and Allan Rosenfield, eds. Contraceptive Researchand Development: Looking to theFuture. Washington, DC: NationalAcademy Press, 1996.
9%A L L O T H E R S
3%PA R K E - DAV I S
3%SYNTEX4%
S E A R L E
12%O R GA N O N
18%SCHERING AG
22%O RT H O
29%W Y E T H
T O TA L S A L E S : $ U S 2 . 1 B I L L I O N

MARKET PROFILE33
require dependable supplies of critical rawmaterials. Manufacturing facilities are primarilylocated in the United States, Germany, Canada,the Netherlands, the United Kingdom andHungary, but also operate in roughly a dozendeveloping countries. Plants in China are state-owned, India and Egypt host a mix of publicand privately-owned producers, and elsewhereproduction is in the hands of private firms.
CONSUMER SOURCES OF SUPPLYIn the developing world, three out of fivewomen who use oral contraceptives obtaintheir supplies free or at nominal charges frompublic sector institutions such as ministries ofhealth and social security systems, or from non-profit family planning associations. Pharmaciesand other retail outlets supply some 20 millioncustomers; of these, 4 million purchase theproduct at below-market prices through socialmarketing initiatives in 33 developing countries.
DONOR ROLESInternational donors play a vital role in financ-ing the use of oral contraceptives in developingcountries. Donors provide about 300 millioncycles of pills annually, or enough to supplyroughly three-quarters of all women who obtainthe method from public or non-profit sources.Donor support will continue to be crucial to
make supplies available to poorwomen and to fund research toimprove the product.
OPPORTUNITIES FOR MARKET GROWTHAlmost all growth in the use of oralcontraceptives will likely come fromthe developing world, where thenumber of younger women—themain users of the method—areincreasing rapidly. The growingpopularity of injectable hormonalcontraception may, however, dampenfuture market growth, and the poten-tial for expansion of commercialmarkets is uneven across regions.The likelihood for market growth is lower in Latin America and theCaribbean, where levels of contra-ceptive use and commercial sectorinvolvement are already high. InAsia and Africa, by contrast, prospectsare good for market expansion. Thetrend towards fewer restrictions onbrand-name advertising of prescrip-tion drugs holds particular promisefor efforts to boost commercial salesof the method.
Ma
rket
Pro
file

POPULATION ACTION INTERNATIONAL34
Research confirms that highly urbanized countries are more likelyto have a strong commercial family planning presence.
Current Demand (also referred to as actual market size)greatly influences commercial sector involvement. “If the marketsare already there,” notes one observer, “commercial companieswill pursue opportunities.” Companies generally find it morecost-effective to compete for existing consumers than to invest in expanding the market by wooing public sector or new clients.Moreover, businesses often view expanding markets for reproduc-tive health products as expensive and risky. For example, thepotential market for iron pills is huge—effectively, all women ofreproductive age—and current use of these supplements is low in most countries. Yet few commercial producers are willing togamble that advertising and other promotional activities will payoff in increased sales of their product.
A further disincentive for investing in market expansion is thatreproductive health products typically account for only a smallportion of drug company sales and profits. Sales representativesare under pressure to visit several pharmacies or physicians eachday and to promote as many as 30 different items. They have littleincentive to spend much time on items such as contraceptives,which often do not generate a large volume of sales or high profitmargins. Moreover, firms generally focus promotional efforts onnew products with greater profit potential; many contraceptivebrands have been on the market for several years.
Income levels are a key factor affecting the willingness of for-profit firms to enter a new market or to invest in market expan-sion. Contraceptive manufacturers earn just 20 percent of theirrevenues from sales in developing countries, even though two-thirds of the world’s contraceptive users live in the developingworld. “In many poorer countries,” observes one pharmaceuticalcompany executive, “people just don’t have the wherewithal topay market prices for reproductive health products.”
Not surprisingly, the commercial sector share of the familyplanning market tends to be greater in countries and regions with higher per capita incomes. Latin America, for example, has a highly developed commercial sector, because most countries in the region have substantial middle and upper class groups withadequate purchasing power. By contrast, commercial sector involve-ment is low in sub-Saharan Africa, where consumer buying poweris much more limited.
Nonetheless, other factors such as a large and viable middle classcan create a favorable climate for business even where most peopleare relatively poor. For example, although average purchasing powerin India is low, the middle class is large enough to attract significantinvestments from international pharmaceutical companies.
The commercialsector share of the family
planning markettends to begreater in
countries andregions withhigher per
capita incomes.

Getting Down to Business 35
The degree to which a basic economic and commercialinfrastructure has been established is also a key considerationfor businesses interested in operating in a country. Well-function-ing transport and communications systems, and reliable bankingand credit facilities, are particularly important to fostering a posi-tive business climate. Inadequate infrastructure can eliminate alarge share of the potential market for a product by placing con-sumers beyond the easy reach of distribution networks, andincreasing costs to the point where maintaining a businessbecomes unprofitable.
COMPETITION FROM SUBSIDIZED PRODUCTS
The presence of large public sector programs that provide low-costor free reproductive health care without regard to the ability ofclients to pay can strongly inhibit the development of commercialmarkets. By pricing products and services below levels at whichthe commercial sector can operate profitably, subsidized programstake away clients who would otherwise use for-profit sources.
The business community is particularly critical of publicly-funded efforts that undermine established commercial markets. Arepresentative of a multinational drug company notes the loss ofmarket share in Nigeria that occurred, in his view, when the publicsector began to distribute free contraceptives supplied by interna-tional donors. “We often want to make an investment in a country,only to find that public sector strategies run counter to commercialsector business strategies,” says this official. Faced with the uncer-tainty of government and donor actions, firms frequently opt not togamble on new markets. They will often undertake partnershipswith the public sector only with assurances that the country will notlater be flooded with free commodities from international donors.
Analyses confirm that subsidized programs have an inhibitingeffect on for-profit activity. A study of family planning market sharein 45 countries shows an association between strong governmentprograms and a small commercial presence. In Peru, the govern-ment’s decision to greatly strengthen the public sector programand provide free services is thought to have precipitated a sharpdrop in the commercial share of the family planning market.
Governments may decide that the benefits of public subsidiesfor reproductive health care outweigh any inhibiting effects oncommercial sector involvement. In making these decisions, how-ever, policymakers need to explicitly take into consideration thepotential impacts on the private sector.
Still, in some countries, subsidized programs have not inhib-ited for-profit efforts. In Turkey, a strong public sector programco-exists with a healthy commercial market, in part because the
Faced with theuncertainty of
government and donor
actions, firmsfrequently optnot to gamble
on new markets.

POPULATION ACTION INTERNATIONAL36
large population allows businesses to attract customers in num-bers sufficient to maintain profits. Moreover, while untargetedpublic programs may hamper commercial efforts, the absence ofstrong government programs is itself no guarantee of commercialinterest. There are many countries with weak public sector healthsystems, particularly in sub-Saharan Africa, where the commercialsector has failed to aggressively invest in reproductive healthcare—usually because other necessary conditions for such invest-ment have not been met.
Another form of competition from subsidized or low priceproducts occurs when corrupt government officials redirect com-modities meant for distribution through subsidized channels forcommercial sale for their own financial gain. Drug company exec-utives cite such “leakage” as a serious challenge to establishingviable commercial markets. In Thailand, for example, the diversionof oral contraceptives from the public sector program in nearbyBangladesh to the market in Thailand has reportedly hurt commer-cial sales. In smaller markets, even relatively low levels of productleakage can reduce profitability to the point where commercialsales are no longer viable.
Figure 9
WHO BENEFITS from PUBLIC SUBSIDIES
for REPRODUCTIVE
HEALTH CARE?
Findings from Recent Studies
See Key Reference list for full citations.
STUDY SAMPLE FINDINGS
Vietnam Survey of 1,890 households The richest 20% of the population receives Behrman and Knowles in seven provinces 28.4% of family planning subsidies; the (1998) poorest 20% receives just 15.2% of subsidies
El Salvador National survey of 65% of women using subsidized hospital Farrell et al. 9,000 households birthing care are from high and middle-(1994) income households
Indonesia National survey of 54% of high-income households and 80% Winfrey and Heaton 12,631 households of low-income households obtain family (1996) planning services from subsidized sources
Peru National survey of 28,951 20% of women obtaining family planning Futures Group women ages 15 to 49 services from the public sector can fully (1997) pay for such services
Côte d’Ivoire Survey of 2,171 individuals 60% of people viewing a publicly-funded Shapiro and Meekers in a large city and two televised AIDS prevention program are (1999) small towns from middle and upper income groups;
70% of respondents purchasing the subsidized brand of social marketing condoms are from middle and upperincome groups
Getting Down to Business 37
Leakage is difficult to detect, and there is a need to furtherstudy the extent of the problem. One executive estimates that afifth of donated contraceptives in some countries are diverted tocommercial channels. Donors can help reduce leakage by strength-ening training in commodity management for staff in public sectorprograms, and by holding recipient governments accountablewhen donated commodities are diverted to the black market.
THE LEGAL AND REGULATORY CLIMATE
The laws and regulations that set the framework for a country’seconomic activity and govern the provision of health care have aprofound effect on commercial involvement in the health sector.Both the public and commercial sectors recognize that regulationis needed to protect consumers from unscrupulous or harmfulpractices. Nevertheless, laws and regulations often unnecessarilylimit the provision of family planning and reproductive health careon a profit-making basis.
Regulations affecting the delivery of reproductive healthcare can increase supplier costs and suppress sales of reproductivehealth products. Those having the largest impact on the commer-cial sector include:
❁ bans on reproductive health products or services, includingpolicies restricting the availability of all or some contracep-tives in some former French colonies of sub-Saharan Africaand laws in many countries that restrict abortion;
❁ medically unnecessary prescription requirements for hormonal contraception and for drugs used in the treat-ment of sexually transmitted infections;
❁ limitations on where contraceptives can be sold;
❁ medically unnecessary requirements regarding the types of health workers who can provide various products andservices; and
❁ excessive delays in product registration, licensing and certification.
Illustrations of these types of constraints are the limitationsmany countries place on the ability of nurses and midwives to set up private practices and on their authority to prescribe theantibiotics that are used in STI treatment.
Regulation,although needed
to protect consumers,
often unneces-sarily limits the
provision ofreproductivehealth care.

38MARKET PROFILE
MARKET SIZEAbout 700,000 women yearly undergo manualvacuum aspiration (MVA) for abortion and treat-ment of postabortion complications, roughly 5percent of all such procedures performed bytrained health workers in the developing world.A small but rapidly number of abortions in theUnited States—some 100,000 annually—areperformed with MVA. Worldwide revenues fromthe sale of MVA instruments are tiny—roughly$1 million a year, of which sales to developingcountries account for 85 percent.
THE PRODUCTMVA was introduced 25 years ago as a safer,simpler, and more cost-effective alternative totraditional methods of uterine evacuation inearly pregnancy. The technique has particularapplication in poor countries for treating com-plications from unsafe abortion. The MVA tech-nology consists of a large syringe attached to along, thin plastic tube inserted into the uterus.The syringe generates a vacuum using a spe-cially designed locking mechanism which, whenactivated, empties the contents of the uterusthrough the tube. MVA operates in the sameway as the electric pump that is the standardtechnology in the United States and Europe.MVA instruments are generally sold in kitswhich include a syringe along with half adozen of the tubes, called cannulae. Withproper maintenance, the better-quality syringesare routinely used more than 50 times.
IMPROVING THE PRODUCTBecause of the controversy over abortion andlow profit potential, interest from donor countrygovernments and commercial manufacturers inimproving MVA technologies is very limited. As aresult, the product today has changed little fromearly models. One possible area for improve-ment would be making the syringe from anewer plastic that is more easily sterilized.
MANUFACTURINGThe world’s largest manufacturer of MVA instru-ments is the U.S. nonprofit organization Ipas,which in 1997 sold 45,000 syringes and 200,000cannulae. Currently, only one other U.S. firmmakes a syringe for MVA. However, the firmdoes little to market them globally. Manufactur-ers in India and Vietnam produce lower-qualityinstruments. Ipas has helped to set up manu-facture of its instruments in a few developingcountries, notably India. Markets in all but thelargest countries, however, are too small to justify local production.
CONSUMER SOURCES OF SUPPLYMost MVA instruments are marketed directly tophysicians. Ipas sells roughly half of its produc-tion to the commercial sector, including aboutone-third to commercial distributors in over 20developing countries and one-fifth to individualdoctors. Particularly strong commercial marketsfor MVA instruments have emerged in Nigeriaand Turkey, in large part due to the willingnessof a few key local individuals to develop thefor-profit market. NGOs, donor agencies anddeveloping country governments account forthe rest of MVA purchases.
MARKET PROFILE
Manual Vacuum Aspiration Instruments

MARKET PROFILE39
DONOR ROLESInternational donors currently purchase abouthalf the supply of MVA instruments. Privatefoundations have been particularly important inthe dissemination of MVA technology, given thereticence of official aid agencies to associatethemselves with abortion-related activities. Inthe wake of the 1994 International Conferenceon Population and Development and its stresson improving postabortion care, some donorcountries have begun to fund training in MVAand purchase of instruments, especially fortreatment of abortion complications. AlthoughUSAID supports research and training inpostabortion care, its current policy prohibitsthe agency from purchasing MVA instruments,even if only for treating abortion complications.
Donors will continue to play a key role insupporting efforts to educate developing coun-try policymakers and the general public on theprevalence and health impact of unsafe abor-tion. More open discussion of abortion will helpcreate a more favorable climate for availabilityand use of techniques such as MVA.
OPPORTUNITIES FOR MARKET GROWTHThe prospects for rapid growth in sales of MVAinstruments are good, but revenues will con-tinue to be relatively small. Projections putannual sales of the technology at just $3 millionwithin 5 years. At these levels, MVA technologywould be used for about 3.5 million abortionsannually. The increasing availability of safe and
effective abortion drugs could signifi-cantly reduce the need for MVA andother surgical abortion techniques.Most of the growth in market forMVA is likely to occur in developingcountries; the United States is one ofthe few countries in the developedworld where there is potential forgrowth in MVA sales.
The key to expanding commer-cial sales of the instruments is theestablishment of reliable and sustain-able local channels of distribution.This step requires official action toapprove and license the product andcoordination among governmentsand the donors and technical assis-tance agencies working to improveabortion and postabortion care. Gov-ernment recognition of MVA makesit far easier to set up these channels.Introducing MVA into public sectorprograms is thus crucial for the even-tual emergence of a commercial mar-ket for MVA instruments, sinceofficial acceptance of the technologylegitimizes the practice for the privatesector. Another important strategy toestablishing commercial distributionis to emphasize the multiple uses ofMVA—for example, its use for collect-ing uterine cells for diagnosis of can-cer and other diseases.
Figure 10
IPAS SALES of MANUAL
VACUUM ASPIRATION
(MVA) INSTRUMENTS
Percent Share By Purchaser, 1997
Source: Ipas.27%
M U LT I L AT E R A L A N DB I L AT E R A L D O N O R S
20%P R I VAT E
I N D I V I D UA L S
20%INTERNATIONAL
NGOS
33%C O M M E R C I A L D I S T R I B U T O R S
T O TA L S A L E S : $ U S 1 . 0 M I L L I O N
Ma
rket
Pro
file

POPULATION ACTION INTERNATIONAL40
Tax policies and import duties can raise costs to producers,wholesalers, and retailers, and thus cut profits. Although intendedto help governments improve budget shortfalls and spur economicgrowth, the following types of policies can work against efforts toachieve public health objectives.
❁ Sales taxes on reproductive health products and services, as high as 20 percent in some countries, impose costs oncommercial suppliers that are passed on to the consumer.
❁ In many countries, imports destined for commercial marketsare heavily taxed, while donated goods are usually importedfree of charge, putting commercial firms at a further disad-vantage in competing with subsidized programs.
❁ In countries such as the Philippines, commercial importsof contraceptives are exempt from import duties, but theprocess to obtain the exemption is often cumbersome,time-consuming and costly.
❁ Obtaining import licenses and securing the foreign exchangeneeded to buy imported drugs is a major problem in placessuch as Russia, which is privatizing the formerly state-rundrug distribution and retailing network.
Restrictions on brand advertising and promotion also discourage commercial interest. Until recently, most countriesprohibited consumer advertising of specific brands of contracep-tives and other reproductive health products. Although restrictionson brand-name advertising are diminishing, they still remain inmany countries. Government regulations in the Philippines, forexample, prohibit the advertisement of all prescription drugs—including oral and injectable contraceptives. Jamaica allowsbrand-specific advertising of condoms, but still prohibits such promotion for hormonal contraceptives.
Meanwhile, commercial firms are reluctant to place genericadvertisements to stimulate use of these products because suchadvertising may also benefit their competitors. Most firms alsoperceive this type of generic promotion to be the responsibility of the public sector.
Price controls and threats to intellectual property rightsare two additional concerns for businesses. In Egypt, Jordan andelsewhere, government controls on the price of oral contracep-tives—intended to make products more affordable—have discour-aged commercial sector interest. In South Africa, a major U.S.-basedpharmaceutical company suspended plans to set up productionfacilities over concerns that weak patent protections would makeit unprofitable to manufacture products in the country.
Restrictions onbrand nameadvertising
and promotiondiscourage commercial
interest.
Getting Down to Business 41
A positive legal and regulatory climate, while necessary forcommercial viability of a product, is not by itself a guarantee ofprofitability. “Policy isn’t everything, it’s only a part of the picture,”says a U.S. foreign aid official familiar with efforts to increase theinvolvement of the commercial sector in providing reproductivehealth care. The impact of regulatory constraints varies tremen-dously. In some countries, excessive regulation is an importantconstraint on commercial activity. Yet, elsewhere, a favorable legaland regulatory climate has not been matched by a vibrant commer-cial response, often because demand for reproductive health careand purchasing power are too low.
OTHER FACTORS AFFECTING
COMMERCIAL INVOLVEMENT
The political environment for the provision of reproductivehealth care often has an important influence on business deci-sions. Firms work hard to maintain good relations with govern-ment officials and to project a positive public image. Companiesoften shy away from involvement in abortion and family planningto avoid embroilment in religious or ethical conflicts—and thepotential harm to their business interests.
The risks of such controversies can be considerable. When thepharmaceutical company Pharmacia & Upjohn introduced itsinjectable contraceptive Depo-Provera onto the commercial marketin the Philippines, the Catholic church organized a boycott of thecompany’s entire line of products. As a result of the controversy,
I n Zimbabwe, a strong government programhas slowed development of a commercial
market for contraceptives. With a highly liter-ate population of 11 million, a relatively highannual per capita income for the region ofabout $600, and among the highest levels ofcontraceptive use in the region, Zimbabwewould seem ripe for commercial interest. Yet,just one in ten oral contraceptive users obtainssupplies from for-profit sources.
The government’s family planning pro-gram has been very successful in expandingaccess to family planning in Zimbabwe. How-
ever, the decision to distribute contraceptives free,regardless of ability to pay, has driven out virtuallyall commercial players. Even though the govern-ment has initiated efforts to wean higher-incomeusers from highly subsidized public sector services,the dominance of the state-run program continuesto discourage the involvement of the commercialsector. Pill manufacturers who do not already haveproducts on the local market have shown limitedinterest in establishing commercial operations inZimbabwe, in part reflecting concern that con-sumers will not pay commercial prices for prod-ucts they have been receiving free.
CROWDING OUT THE COMMERCIAL MARKET IN ZIMBABWE

POPULATION ACTION INTERNATIONAL42
many pharmacies refused to sell Depo-Provera, and the firm scaledback its promotional activities. Fearing a similar public reaction,other companies selling hormonal contraceptives abandoned theirplans to more aggressively promote such products.
Corruption is a major problem for commercial firms operatingin developing countries, one which can significantly raise the costof doing business and cut into profitability. U.S. companies, facingsanctions for bribery under existing U.S. law, often complain theyare at a disadvantage compared to foreign competitors who arenot held to the same ethical standards.
Finally, knowledge about market conditions in the develop-ing world is frequently limited. Government policymakers typicallyknow little about the commercial sector and may unintentionallyinhibit the growth of commercial markets, thus hampering theachievement of public health goals. Businesses themselves operatewithout full information, and their analysis of markets can beflawed. Distributors and sales representatives often do not usepublicly available survey information regarding current and poten-tial demand for reproductive health care. Moreover, data on com-mercial sales for many developing countries are incomplete andunreliable, and marketing of products commonly proceeds on atrial and error basis.
STRATEGY #1:
Looking across countries, the factors that appear to have themost influence on the commercial sector’s interest in reproductivehealth include levels of income and urbanization, along withperceived competition from publicly subsidized programs. Yet, as some of the examples cited above suggest, the situation differsgreatly from country to country; other factors may be of equal orgreater importance for any particular country or product.
Many of the factors influencing commercial sector involvementare beyond the immediate control of developing country govern-ments. There is little potential to change population size and density over the short term; similarly, raising income levels andimproving basic economic infrastructure—though appropriateareas of government action—are typically long-term undertakings.
Yet, governments as well as international donors can have substantial influence over a number of factors in the short andmedium term. These include the scope of publicly funded pro-grams, together with policies regarding subsidization of productsand services; the legal and regulatory framework; and the level ofdemand for reproductive health care. The following section dis-cusses how governments and donors can influence these factorsto encourage the commercial sector to play a greater role.
Governmentsand interna-tional donors
can influence anumber of the
factors thatdetermine thecommercial
sector’s interestin reproductive
health.
Getting Down to Business 43
CHAPTER 4
I n all developing countries, governments and internationaldonor agencies can utilize a variety of strategies to explicitlyencourage the commercial sector to expand its role in repro-
ductive health care. To be effective, such strategies need to be partof a comprehensive approach to clarifying public and private sec-tor roles in serving the reproductive health needs of different eco-nomic and social groups, and making the best use of scarce publicfunds. Governments and donors need to define these roles in thecontext of each country’s specific situation, based on fundamentalconditions such as market size, demand for reproductive healthcare, and the ability of consumers to pay for such care.
In reality, the poorest and least developed countries will needto provide significant subsidies for reproductive health care for theforeseeable future. These subsidies may be provided through pub-lic sector and NGO programs and approaches such as social mar-keting that make low-cost products and services available throughcommercial channels. Wealthier developing countries have a lesserneed for subsidies, and governments in these countries shouldencourage the commercial sector to play a larger role.
In any particular country, the mix of strategies, and the extentof reliance on the public and private sectors respectively, will vary.But in general, the primary responsibility of governments is to laythe groundwork for a viable commercial market and create a posi-tive business climate for the provision of reproductive health care.Some governments and donors have gone further, however, andtaken a more active role in helping to build commercial marketsthrough various partnership arrangements with private businesses.
Specific strategies that governments and donors can undertaketo encourage the commercial sector to expand its role include:
❁ reorienting public sector programs to those truly in need, so that they complement rather than displace commercial efforts;
❁ changing laws and regulations necessary to encourage agreater role for the private for-profit sector in reproductivehealth care;
In any particular
country, the mix of strategies
to expand the commercial
sector role will vary.
Strategies to Expand the Role of the Commercial Sector
POPULATION ACTION INTERNATIONAL44
❁ analyzing the impacts of public policies on the commercialsector and including representatives of private businessesin health care planning and decision making;
❁ supporting broad public education activities aimed atincreasing demand for reproductive health products andservices; and
❁ undertaking public-private partnerships aimed at sharingthe risks of expanding commercial markets for reproduc-tive health products.
STRATEGY #1
TARGET PUBLIC PROGRAMS TO THE
POOR AND HARD TO REACH
Perhaps the single most important step that governments can taketo stimulate commercial interest in the provision of reproductivehealth care is to redirect public funds towards serving the poorand hard-to-reach. To increase access to reproductive health care,governments must become far more discriminating in targetingtheir programs to those truly in need. Despite official rhetoric, freeor highly subsidized government health programs in many coun-tries continue to help the better-off more than the poor.
The state has a critical role in extending reproductive healthcare to those unable to afford market prices and to remote orsparsely-populated areas where it is unprofitable for commercialfirms to operate. But to free up financial resources to serve thesepopulations within existing budget constraints, governments needto shift wealthier clients to commercial sources.
There is enormous potential for this strategy to reduce thefinancial burdens on the public sector. Based on a conservative esti-mate that just one-fifth of public sector family planning clients inthe developing world could pay the full cost of care, shifting theseconsumers to commercial sources would reduce the number ofclients served by the public sector by roughly 75 million worldwide.
Unfortunately, most governments and donors have failed torecognize the potential of targeting to achieve public health goals.“Getting the government and donors to recognize that the statecannot do it all is the hardest step,” notes one observer. Many gov-ernments continue to offer free reproductive health care, regardlessof ability to pay, because they believe the benefits to society out-weigh the costs. Government health officials also tend to focus onthe volume of publicly provided care rather than the total coverageof health services provided by all sectors. Donors, for their part,have tended to focus on the level of products and services provided,rather than the income levels of those served.
Governmentsmust redirect
their programsto serving thepoor and hard
to reach.
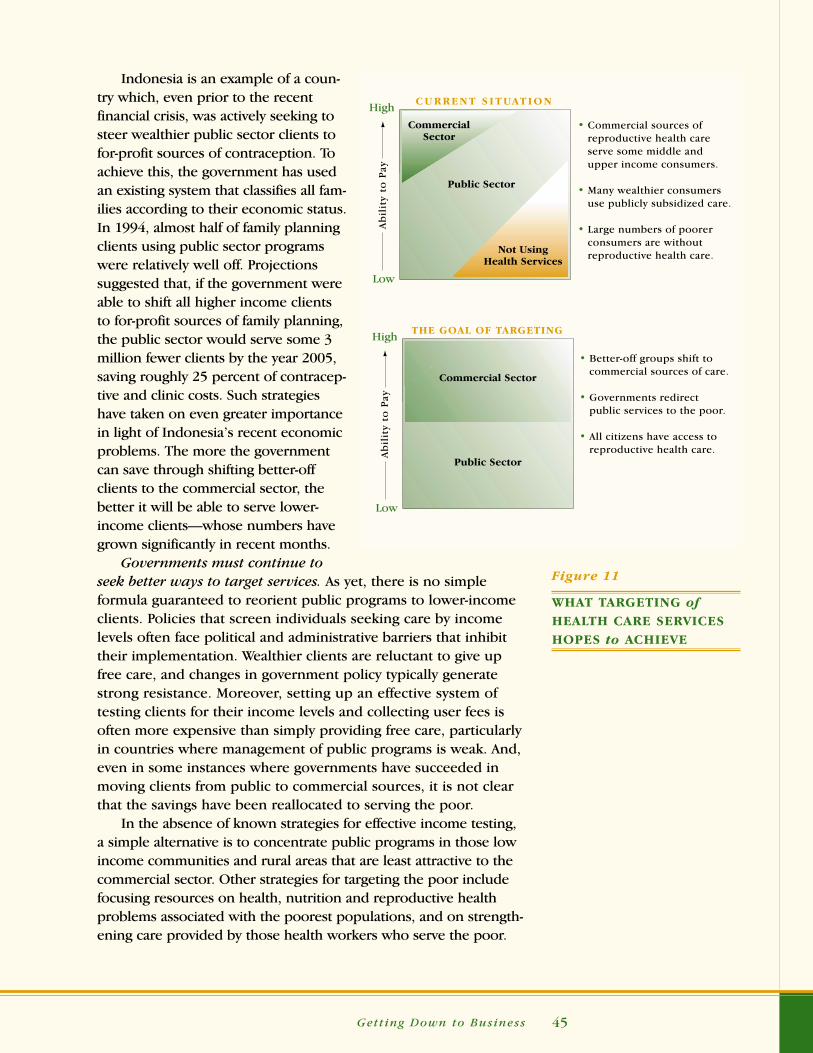
Getting Down to Business 45
Indonesia is an example of a coun-try which, even prior to the recentfinancial crisis, was actively seeking tosteer wealthier public sector clients tofor-profit sources of contraception. Toachieve this, the government has usedan existing system that classifies all fam-ilies according to their economic status.In 1994, almost half of family planningclients using public sector programswere relatively well off. Projectionssuggested that, if the government wereable to shift all higher income clientsto for-profit sources of family planning,the public sector would serve some 3million fewer clients by the year 2005,saving roughly 25 percent of contracep-tive and clinic costs. Such strategieshave taken on even greater importancein light of Indonesia’s recent economicproblems. The more the governmentcan save through shifting better-offclients to the commercial sector, thebetter it will be able to serve lower-income clients—whose numbers havegrown significantly in recent months.
Governments must continue toseek better ways to target services. As yet, there is no simple formula guaranteed to reorient public programs to lower-incomeclients. Policies that screen individuals seeking care by incomelevels often face political and administrative barriers that inhibittheir implementation. Wealthier clients are reluctant to give upfree care, and changes in government policy typically generatestrong resistance. Moreover, setting up an effective system oftesting clients for their income levels and collecting user fees isoften more expensive than simply providing free care, particularlyin countries where management of public programs is weak. And,even in some instances where governments have succeeded inmoving clients from public to commercial sources, it is not clearthat the savings have been reallocated to serving the poor.
In the absence of known strategies for effective income testing,a simple alternative is to concentrate public programs in those lowincome communities and rural areas that are least attractive to thecommercial sector. Other strategies for targeting the poor includefocusing resources on health, nutrition and reproductive healthproblems associated with the poorest populations, and on strength-ening care provided by those health workers who serve the poor.
Figure 11
WHAT TARGETING ofHEALTH CARE SERVICES
HOPES to ACHIEVE
High
Low
Commercial Sector
Public Sector
THE GOAL OF TARGETING
• Better-off groups shift to commercial sources of care.
• Governments redirect public services to the poor.
• All citizens have access to reproductive health care.A
bil
ity
to P
ay
High
Low
CommercialSector
Public Sector
Not UsingHealth Services
Ab
ilit
y to
Pay
C U R R E N T S I T UAT I O N
• Commercial sources of reproductive health care serve some middle and upper income consumers.
• Many wealthier consumers use publicly subsidized care.
• Large numbers of poorer consumers are without reproductive health care.

POPULATION ACTION INTERNATIONAL46
STRATEGY #2
LOWER LEGAL AND REGULATORY BARRIERS
Governments should limit legal and regulatory barriers thatdiscourage the use of for-profit sources of reproductive healthcare. Efforts in a number of countries have succeeded in reduc-ing such barriers.
❁ In Egypt in 1993, population program advocates were successful in convincing regulatory authorities to legalizethe sale of the injectable contraceptive Depo-Provera incommercial pharmacies. Government regulations, however,still allow only physicians to administer injections.
❁ In Brazil, condom companies joined with AIDS activists to convince the government to reduce tariffs on the rawmaterials used in condom production, arguing that lower-ing tariffs would promote public health goals.
❁ In Zimbabwe, population organizations successfully lob-bied for the elimination of import duties on condoms and forreductions of 5 to 10 percent in tariffs on other contraceptives.
Particularly in addressing tax and import policies, it is vital thatthe dialogue involve not only health officials but also other keystakeholders, for example Ministry of Finance officials and businessgroups. It should also be recognized that such efforts are likely tomeet with some resistance. For example, in the Philippines, healthofficials proposed exempting oral contraceptives from an acrossthe board import tariff on drugs. Analyses indicated that, at lowercommercial prices, a large number of public sector clients wouldshift to purchasing pills from pharmacies. This in turn would havereduced the burden on government health facilities and generatedsavings that more than offset the loss in revenues from eliminatingthe tariff on oral contraceptives. Still, government revenue depart-ment officials opposed the change.
Governmentsshould limit
legal and regulatory
barriers thatdiscourage theuse of for-profit
reproductivehealth care.

Getting Down to Business 47
Governments also need to ease restrictions on advertising ofreproductive health products. Many Latin American countries arefollowing the lead of the United States in loosening restrictions onadvertising of brand name drugs, and there is slow progresstowards reducing these barriers in other regions. Governmentsand donor technical assistance agencies should encourage compa-nies to view increased freedom to advertise as a cost-effective wayto expand their markets. Nevertheless, for many drug companieswhich until recently relied almost exclusively on a marketing strat-egy aimed at medical personnel, the switch to advertising directlyto consumers requires a major shift in marketing approach.
T wo decades of USAID-supported efforts toexpand the commercial sector’s involvement
in the marketing of reproductive health productshave yielded the following lessons.
❁ Building partnerships with commercialfirms requires that international donoragencies acknowledge the profit motiveand use a business-like approach in theirdealings with the commercial sector.
❁ Donor agencies do not have to offer largeamounts of direct financing or subsidiesto the commercial sector to create suc-cessful partnerships in the health sector.Private for-profit manufacturers, distribu-tors and retailers will invest their ownfunds in a partnership if there is a viablebusiness opportunity.
❁ Distribution of free or heavily subsidizedproducts discourages the commercial sec-tor from entering or expanding markets.
❁ Demand creation, through modern marketing and advertising techniques, is an important requirement for com-mercial sector success.
❁ To be effective, partnerships with the com-mercial sector must address policy and traderelated issues such as brand registration,import licensing and trademark protection.
❁ Activities that integrate family planningwith other health services which are profitable and in demand stand the bestchance of financial success and commer-cial sector response.
❁ Segmenting the market and tailoring messages to the desired audiences isessential to the effectiveness of social marketing efforts.
❁ Donors can help establish markets foraffordable products by supporting innova-tive advertising and promotion and thentransferring the program to a local com-mercial or NGO partner.
❁ Rather than competing for clients, the private for-profit and non-profit sectorsshould work together to achieve commongoals. For example, commercial distributorscan form successful partnerships with NGOsto sell products in rural areas where com-mercial distribution networks do not reach.
LESSONS LEARNED FROM THE USAID EXPERIENCE
Adapted from USAID, Commercial and Private Sector Strategies Results Package, 1998.
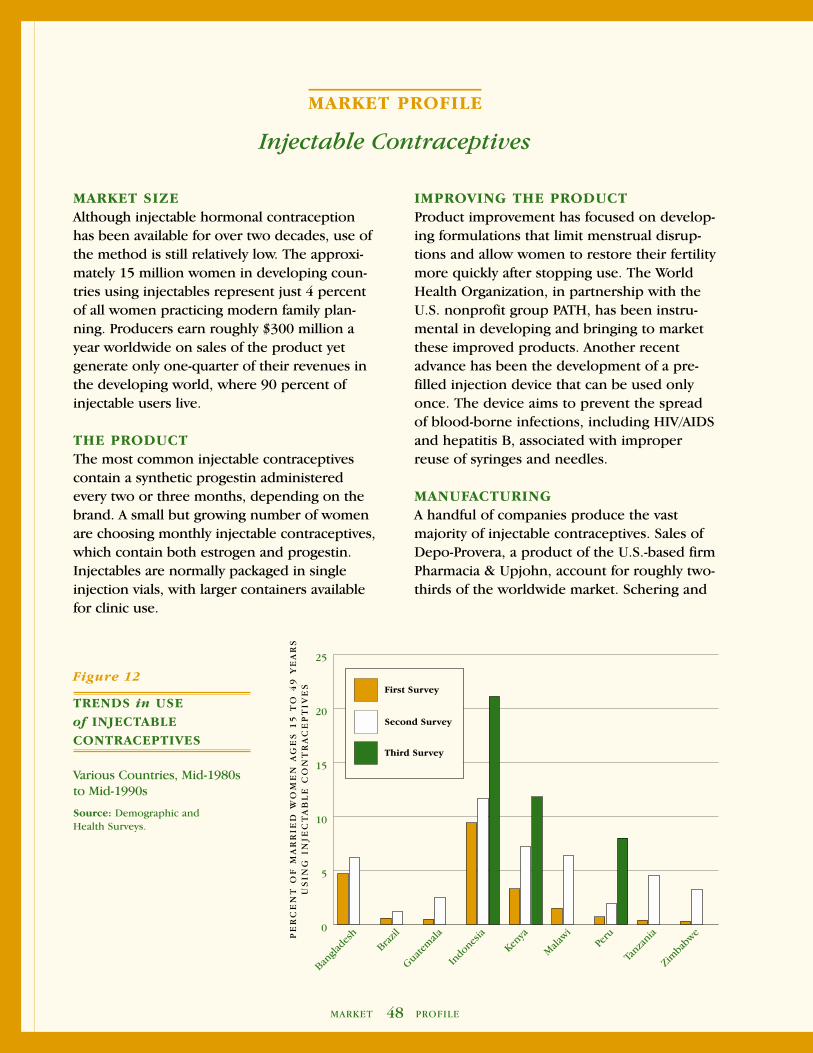
48MARKET PROFILE
IMPROVING THE PRODUCTProduct improvement has focused on develop-ing formulations that limit menstrual disrup-tions and allow women to restore their fertilitymore quickly after stopping use. The WorldHealth Organization, in partnership with theU.S. nonprofit group PATH, has been instru-mental in developing and bringing to marketthese improved products. Another recentadvance has been the development of a pre-filled injection device that can be used onlyonce. The device aims to prevent the spreadof blood-borne infections, including HIV/AIDSand hepatitis B, associated with improperreuse of syringes and needles.
MANUFACTURINGA handful of companies produce the vastmajority of injectable contraceptives. Sales ofDepo-Provera, a product of the U.S.-based firmPharmacia & Upjohn, account for roughly two-thirds of the worldwide market. Schering and
MARKET SIZEAlthough injectable hormonal contraceptionhas been available for over two decades, use ofthe method is still relatively low. The approxi-mately 15 million women in developing coun-tries using injectables represent just 4 percentof all women practicing modern family plan-ning. Producers earn roughly $300 million ayear worldwide on sales of the product yetgenerate only one-quarter of their revenues inthe developing world, where 90 percent ofinjectable users live.
THE PRODUCTThe most common injectable contraceptivescontain a synthetic progestin administeredevery two or three months, depending on thebrand. A small but growing number of womenare choosing monthly injectable contraceptives,which contain both estrogen and progestin.Injectables are normally packaged in singleinjection vials, with larger containers availablefor clinic use.
MARKET PROFILE
Injectable Contraceptives
Figure 12
TRENDS in USE
of INJECTABLE
CONTRACEPTIVES
Various Countries, Mid-1980s to Mid-1990s
Source: Demographic and Health Surveys.
0
5
10
15
20
25
Zimba
bwe
Tanza
niaPe
ru
Mala
wi
Kenya
Indones
ia
Guatem
ala
Brazil
Bangla
desh
Third Survey
Second Survey
First Survey
PE
RC
EN
T O
F M
AR
RIE
D W
OM
EN
AG
ES
15
TO
49
YE
AR
SU
SIN
G I
NJE
CT
AB
LE
CO
NT
RA
CE
PT
IVE
S

MARKET PROFILE49
Organon make other popular brands. Manu-facturing facilities are located in the UnitedStates, Belgium, Germany, Mexico and Indo-nesia. A monthly injectable, Cyclofem, is pro-duced by two private firms in Indonesia andone in Mexico.
CONSUMER SOURCES OF SUPPLYAbout one-half of women using injectables indeveloping countries obtain the method fromcommercial sources such as pharmacies andprivate physicians; this proportion is muchlower in sub-Saharan Africa and higher incountries of Latin America and the Caribbean.About 1.4 million couples in 22 countries nowobtain injectables at subsidized prices throughsocial marketing programs. The largest sucheffort is in Indonesia, where over a millioncouples buy the socially marketed product.
DONOR ROLESDonor support has been crucial to makinginjectable contraception available in develop-ing regions. International aid agencies provideabout 24 million doses annually, enough toserve almost half the women using themethod. The donors have also encouragedindustry to pursue research aimed at improv-ing existing injectable formulations.
OPPORTUNITIES FOR MARKET GROWTHUse of injectable contraception, although stilllow, is projected to grow faster than for anyother method of family planning. Recent surveysconfirm a surge in the popularity of injectablesin many countries, including in the UnitedStates. Almost half of the recent rise in modernmethod use in Africa can be attributed to thegrowing acceptance of injectable contraception.
Women switching from oral con-traceptives and other, less effectivemethods of temporary family plan-ning account for a significant part ofthe recent increase in injectable use.Many women prefer the injectionbecause it frees them from remem-bering to take a pill every day, andallows them to keep their contracep-tive use confidential.
Prospects for expanding com-mercial markets are somewhatmixed. Large untapped pools ofpotential users remain in placessuch as India, which only recentlyapproved commercial sales of themethod, and where the governmentprogram still does not offer injecta-bles as an option. In India and else-where, however, regulatory barriersremain an important constraint torapid commercial market growth.The need to assure high quality carethrough careful training of healthworkers in proper counseling anddelivery of services will further slowcommercial growth.
In most countries, injectables arealso more expensive than oral con-traceptives because of the additionalcost of administering the injection.Moreover, companies marketinginjectables have generally set priceshigh and aimed their promotionalefforts at a relatively small group ofwealthy women. The higher cost willlikely remain a barrier for manywomen wishing to use the method.
Ma
rket
Pro
file

POPULATION ACTION INTERNATIONAL50
STRATEGY #3
INITIATE A DIALOGUE BETWEEN THE
PUBLIC AND PRIVATE SECTORS
Governments and donor agencies need a better awareness ofhow their actions affect the commercial sector. A public sector thatunderstands the impact of its actions on private business is bettersituated to encourage an expanded role for the for-profit sector, aswell as to achieve national goals for improving reproductive health.
Government must consult private businesses in major deci-sions relating to the role of the commercial sector. It is rare forcommercial sector representatives to be invited to participate inpopulation or health policy discussions, or to be consulted byeither donors or government decisionmakers. In formulatingnational strategies, policymakers often assign a role and specificgoals for the commercial sector, and are then disappointed whencommercial firms do not act according to the plan. “There has tobe open communication between the government, donors andthe business community in a particular market,” notes one donorofficial, adding, “Coordination of timing and objectives of thevarious players is important.”
It is crucial for the different donor agencies in a country toreach consensus on the types of assistance required in that countryand to coordinate their efforts. Yet, donors often work at cross-pur-poses: one donor may have financial self-sufficiency of reproduc-tive health programs and building commercial markets as primaryobjectives, while for another donor the urgent need to achievepublic health goals may override cost considerations. In Honduras,for example, one aid agency is supporting the transformation of asubsidized social marketing effort into a fully self-sufficient com-mercial venture. Meanwhile, another donor is planning to fundfree distribution of condoms on a major scale, a move likely toundermine efforts to expand commercial markets.
Governments must also ensure that in their eagerness to solvepublic health problems they do not crowd out for-profit activitiesthat are emerging on their own. Public officials may underestimatethe degree to which the commercial sector is already active inproviding reproductive health services to consumers, especially in areas such as the treatment of sexually transmitted infections,where a strong motivation to seek curative care exists.
There has to be open
communicationbetween the government,donors and the businesscommunity.

Getting Down to Business 51
STRATEGY #4
CREATE DEMAND FOR REPRODUCTIVE HEALTH CARE
Governments and donors can encourage private sector involve-ment by supporting broad public education aimed at stimulatinguse of reproductive health care. Only the public sector can affordto engage in broad-based demand creation activities; although thecommercial sector as a whole may benefit from such campaigns,no single company can justify these types of investments.
In many developing countries, national level communicationcampaigns have significantly increased knowledge about familyplanning, HIV/AIDS and other reproductive health services, andare linked to greater use of reproductive health care. Such activitiespromote the general benefits of reproductive health care and helpto legitimize the use of reproductive health products and services.They also provide information to the public on how productswork, to whom they are most beneficial, and where consumerscan go to obtain both products and services.
The most effective of these broad-based efforts combine a vari-ety of approaches that communicate to a range of audiences, forexample, mass media campaigns for the general public, workshopsfor policy makers and health workers, education and informationin communities for families and community leaders, education andinformation for couples at health clinics, and outreach on sexualhealth and family planning to youth. Governmental financial andpolitical support is crucial to the success of such campaigns,because of the high cost of promotion and because of the sensitiv-ity of sexual and reproductive health issues in many countries andthe resulting potential for political controversy. In many countries,effective publicly-sponsored media campaigns have significantlycontributed to the success of reproductive health programs.
A number of countries have undertaken promotional cam-paigns that broadcast messages in support of broad public healthgoals as well as specific products and services available through thecommercial sector. Several countries have sponsored marketing ofcommercially-available reproductive health services and productsunder a common logo, including the Blue Circle and Gold Circlecampaigns in Indonesia, Couples Choice in Philippines, Green Starin Pakistan, and Red Apple in Uzbekistan. In Pakistan in less thantwo years, a thousand female private practice physicians joined theGreen Star program, which provides participants with training infamily planning and contraceptive commodities for sale to clients.
Only the public sectorcan afford to
engage inbroad-based
demand creationactivities.
POPULATION ACTION INTERNATIONAL52
STRATEGY #5
BUILD COMMERCIAL MARKETS THROUGH
SUSTAINABLE PUBLIC -PRIVATE PARTNERSHIPS
Governments and donors can utilize a variety of mechanisms toshare the risks of establishing and expanding markets with com-mercial partners. Social marketing—the promotion and sale ofsubsidized products through commercial channels—is the mostcommon approach to actively building commercial markets forreproductive health products. Social marketing programs currentlyoperate in some 60 countries, providing family planning servicesto about 10 million couples, in addition to a variety of otherhealth products.
Governments and donors should continue to support socialmarketing as an important strategy for serving lower and lower-middle income consumers. Social marketing programs accustomconsumers to paying something towards the cost of a product and,by using existing commercial distribution networks, often reachpopulations that the public sector does not serve.
Where market conditions are ripe, governments and donorscan begin to move social marketing programs in the direction ofeventual financial self-sufficiency. Partnership arrangements withthe commercial sector can play a key role in promoting this goal.Under such arrangements in a number of countries, for-profit dis-tributors of reproductive health products have reached formalagreements with governments and international donor agencies tomaintain prices at levels affordable to the middle and lower-middleclass consumers most likely to switch from subsidized public sec-tor programs. In return, governments and donors have shared thecosts of an expanded marketing effort. The goal of these initiativeshas been to encourage commercial partners to sustain large-scalemarketing of affordable products after the withdrawal of donorand public sector funding.
The U.S. Agency for International Development has been apioneer in this area, developing such partnerships in almost 20countries, most of which already have viable commercial marketsor significant potential for market expansion. USAID plans toexpand reliance on this strategy under a recently-initiated programaimed at promoting commercial sector involvement. The UnitedNations Population Fund (UNFPA) is also exploring such partner-ships in its first major effort to promote the expansion of commer-cial markets for contraceptives.
Partnershiparrangementswith the com-mercial sector
can move socialmarketing pro-grams toward
financial self-sufficiency.

Getting Down to Business 53
Figure 13
PUBLIC-PRIVATE PART-
NERSHIPS in SOCIAL
MARKETING INITIATIVES
Examples from the SOMARC IIIProject, 1993 to 1998
Source: The Futures Group International.
Country Contraceptive Methods Commercial Partner
MIDDLE EAST, NORTH AFRICA AND EUROPE
Egypt IUDs FEI Products, Inc.
Injectables Pharmacia & Upjohn
Turkey Oral Contraceptives Organon
Schering A.G.
Wyeth
Injectables Pharmacia & Upjohn
Ukraine Oral Contraceptives Gedeon Richter
Organon
Schering A.G.
ASIA
India Oral Contraceptives Wyeth
Indonesia Condoms London International Group
Oral Contraceptives Schering A.G.
Injectables Pharmacia & Upjohn
Kazakstan Oral Contraceptives Gedeon Richter
Organon
Schering A.G.
Injectables Pharmacia & Upjohn
LATIN AMERICA AND THE CARIBBEAN
Jamaica Oral Contraceptives Gedeon Richter
Schering A.G.
IUDs FEI Products, Inc.
Injectables Pharmacia & Upjohn
Mexico Oral Contraceptives Schering A.G.
Peru Condoms CSI
Oral Contraceptives Schering A.G.
Wyeth
IUDs FEI Products, Inc.
Injectables Pharmacia & Upjohn
POPULATION ACTION INTERNATIONAL54
Experience with the commercial partnership model to datehas primarily been with contraceptives.
❁ In the Dominican Republic, the German pharmaceuticalmanufacturer Schering agreed to cut the price of its oralcontraceptive brand in half, in exchange for advertising paidfor by the USAID-funded social marketing organization.
❁ In Brazil, Pharmacia & Upjohn initially sought to marketits injectable contraceptive Depo-Provera to wealthy cus-tomers at a high price. In exchange for marketing supportfrom USAID, the company agreed to cut its price in halfand promote the product to less well-off consumers (seebox on page 51).
These partnership arrangements are also gradually beingutilized to expand markets for a broader range of reproductivehealth products. In Indonesia, government interest in reducingreliance on free distribution of iron folate tablets spurred an agree-ment between USAID, local pharmaceutical companies and theassociation of private midwives to boost commercial sales of ironsupplements to pregnant women. Manufacturers agreed to reducethe price to wholesalers and consumers in exchange for USAIDfunding for promotional activities.
“The key to negotiating the agreement was telling each partyhow they will benefit,” notes the official who helped broker thedeal. The success of the program has spurred drug companies todo their own promotion of iron supplements in anticipation oflarge increases in product sales. “Amazingly,” notes one interna-tional expert on maternal nutrition, “these types of efforts to tapinto the commercial sector and people’s willingness to pay havenot received much attention, especially given how little these programs actually cost.”
Public-private sector partnerships have also been undertaken toimprove treatment of common sexually transmitted infections, butthese have had only limited success to date. Pilot programs to sellprepackaged kits containing drugs in Cameroon, Uganda and thePhilippines have encountered opposition from public health authori-ties who view the initiative as encouraging self-medication. Despitethese problems, given the willingness of many consumers—espe-cially men—to pay the full private sector price for such treatment,continued efforts are needed to explore effective ways to treat suchinfections through commercially-marketed products.
Continued efforts are needed
to explore effective ways
to treat sexually transmitted
infections throughcommercially
marketed products.

Getting Down to Business 55
T he recent experience in marketing thethree-month injectable Depo-Provera in
Brazil illustrates both the potential of partner-ships between governments, donors, and thecommercial sector as well as the limitations ofsuch a strategy.
In 1997, the government of Brazilapproved the commercial sale of Depo-Provera. USAID had an interest in making theproduct available to a wide range of con-sumers in Brazil, and asked the Futures GroupInternational (a U.S. technical assistanceagency) to approach Pharmacia & Upjohn inBrazil (the local importer and distributor ofthe product) about introducing Depo-Proverathrough a social marketing program.
During preliminary discussions, theFutures Group discovered that the distributorplanned to market the injectable to a relativelysmall group of high-income Brazilian women.The distributor’s own calculations showed that,taking the traditional marketing approach ofpromoting Depo-Provera to physicians, it couldsell about 70,000 doses at $20 per injection.
The Futures Group, using informationfrom a recent demographic and health surveyin Brazil, showed company officials that an
alternative, mass-marketing strategy could greatlyincrease the volume of sales and increase profits.After extensive negotiations—and despite con-cerns over negative reactions from the CatholicChurch and conservative members of the medicalestablishment—Pharmacia & Upjohn agreed totry the new strategy and cut its price by half.Meanwhile, USAID offered to spend $1 million tosupport the launch of the product and associatedpromotional expenses.
Early sales of Depo-Provera appeared promis-ing, running at almost double initial projections.After a year, however, Pharmacia & Upjohn pulledout of the partnership, claiming that revenue levelswere not sufficient to continue the effort. Thecompany has abandoned the direct-to-consumerapproach and raised the price of the product.Observers point to contractual limitations as amajor reason for the collapse of the deal. Becausethe agreement with Pharmacia & Upjohn camenear the end of its own contract with USAID, theFutures Group was unable to negotiate more thana one-year deal with the company. USAID remainsconvinced, however, of the viability of its initialstrategy, and has begun negotiations with anothermanufacturer of injectables to undertake a similarmarketing campaign.
Adapted from Patricia Allman, Marketing Social Marketing to Commercial Partners: What’s in it for Them? 1998.
ANATOMY OF A DEAL: MARKETING INJECTABLE CONTRACEPTION IN BRAZIL

POPULATION ACTION INTERNATIONAL56
To date, there has been little rigorous evaluation of theseefforts to transform subsidized programs into fully commercialventures, and of the impact of social marketing programs on theexpansion of commercial markets. Qualitative analyses suggestthat the movement from subsidized social marketing to fully sus-tainable programs is a slow and not always successful process.
“We need to work more on bridging mechanisms to makethese efforts more effective,” notes one executive whose companyhas partnered with international donors in a number of countries.Specific mechanisms for achieving this transition require moreattention during initial discussions with manufacturers and distrib-utors. In particular, pricing and willingness to pay studies areneeded to help determine the long-term commercial viability ofsuch efforts.
International donors and the technical assistance agenciesthey support have played a key role in brokering agreements withcommercial firms and in educating the business community aboutsuccessful and innovative alliances. Governments need to expandtheir involvement beyond the role of mere guarantors of theseagreements, to more actively negotiate and offer their own finan-cial and technical resources as part of these agreements.
Internationaldonors and
the technicalassistance
agencies theysupport haveplayed a key
role in brokeringagreements
with commer-cial firms.

Getting Down to Business 57
T he public-private partnerships described in the precedingsection require a new relationship among governments,international donors and the private commercial sector. In
too many countries, the relationship between governments and pri-vate business has been adversarial and marked by mutual mistrust.In many instances, governments and donors need to overcomelong-standing biases and negative attitudes about the private sectorthat remain a constraint to closer collaboration. Public officials needto recognize the benefits of working with the private sector andbuild a relationship based on greater openness and trust.
CHANGING GOVERNMENT ATTITUDES ABOUT
THE COMMERCIAL SECTOR
In many developing countries, government officials still harborviews about the business community that inhibit the commercialsector from reaching its full potential as a provider of reproductivehealth care. Countries with a tradition of state control over theeconomy—including China, Vietnam, and Russia and the newlyindependent states—are among the most resistant to expandingcommercial sector involvement. The government of Vietnam, forexample, has been reluctant to relinquish its dominance as aprovider of health services and take on a greater role in regulatingthe private health sector. In Egypt, following years of state controlover the economy, government distrust of the for-profit sectorremains among the most significant constraints to commercial sec-tor involvement in family planning. By contrast, countries whichhave long relied on a market economy, for example Indonesia andthe Philippines, are more open to commercial sector involvement.
One reason public officials are sometimes wary about expand-ing the role of the commercial sector is a concern that such anemphasis may increase costs and lower the quality of health care.Some studies have shown that profit-oriented, private practitionersmay be more likely to provide inappropriate or unnecessary treat-ment, or to cut costs in ways that reduce the quality of services.
CHAPTER 5
Forging a New Relationship Between the Public and Private Sectors
Public officials need to recognize the benefits of working
with the private sector.

POPULATION ACTION INTERNATIONAL58
Over the last decade, the commercial sector’s role as a source of family plan-
ning products and services in Indonesia hasexpanded enormously. Much of this increasecan be traced to government efforts that havehelped to create a favorable climate for commercial activity.
Although the public sector dominatedprovision of family planning products and ser-vices in the first two decades of the nationalpopulation program, government policieswere already helping to lay the groundworkfor commercial expansion. The national familyplanning program linked a large and effectivenetwork of services with a strong effort toinform and educate couples on contraception.Family planning use increased from under 10percent of married women when the nationalprogram was established in the late 1960s toalmost 60 percent by 1997. The governmentfocus on rural areas—where the commercialsector has relatively little interest in providingcare—reduced competition with commercialsector providers whose natural clientele werebetter-off, urban consumers.
Spurred initially by an economic downturnthat reduced public funding, beginning in themid-1980s the government has taken variousactions to accelerate the development of com-mercial markets for family planning, including:
❁ legal and regulatory reform of thepharmaceutical industry to increasecommercial interest in investing in theexpansion of local markets for contra-ceptive commodities;
❁ a sustained, nationwide, government-sponsored advertising campaign topromote private family planning ser-vices and products under a common“Blue Circle” logo;
❁ training in family planning for midwives—who in Indonesia are free to establish private practice, and are authorized to provide all contraceptive methods with the exception of sterilization;
❁ heavy promotion of the concept that bet-ter-off clients should shoulder some or allof their family planning costs, coupledmore recently with efforts to implementincome tests to ensure that publicly-fundedservices serve primarily the poor; and
❁ support for private health insurance thatincludes coverage for family planning.
These changes spurred an impressiveresponse by the for-profit sector. For example, the seven-fold increase between 1989 and 1994in sales of oral contraceptives marketed under theBlue Circle logo convinced a major pharmaceuti-cal company to open a new local factory for oralcontraceptives. Together with strong economicgrowth that increased consumer buying power,the efforts described above helped raise the for-profit sector’s share of the family planning marketfrom 12 to 40 percent between 1987 and 1997—an extraordinarily rapid increase.
Whether this trend will continue in the wakeof Indonesia’s recent financial crisis is uncertain.Although many consumers are still willing to payfor contraceptives, there is some evidence that thecombination of falling incomes and rising privatehealth care costs has forced many consumers toswitch to lower-cost public services. The govern-ment family planning program, meanwhile, isintensifying efforts to target its resources towardsserving the poor.
EXPANDING COMMERCIAL MARKETS FOR FAMILY PLANNING IN INDONESIA

Getting Down to Business 59
Of particular concern is the adequacy of information provided toclients who purchase reproductive health commodities at pharma-cies or other commercial outlets. For users of hormonal contracep-tion, lack of adequate information on who should use theseproducts, how to use them and potentially serious side-effects canresult in physical harm. Similar problems may be associated withconsumers who purchase drugs for treatment of sexually transmit-ted infections through pharmacies without prior consultation witha trained health worker. Many social marketing programs haveattempted to address this problem through training of pharmacyworkers and others who sell reproductive health products, butthese efforts have had only partial success.
Many public officials also worry that the drive to shift clientsfrom public to commercial sources may reduce the access thatpoor people have to health care. In many countries where the gov-ernment has instituted user fees for health services, utilization ofpublic services has fallen; children and the poor are often the hard-est hit by such price increases. Many health officials also perceivethe commercial sector as reluctant to provide services with astrong public health component that often benefit the poor most,including immunization, prevention of sexually transmitted infec-tions, and provision of health information.
At the same time that many government officials are wary ofgreater commercial sector involvement, they also tend to haveunrealistic expectations regarding the potential interest of the com-mercial sector in expanding or entering markets. “In general,”notes an official at a large U.S. contraceptive manufacturing firm,“the commercial and public sectors have dramatically differentviews of what can be considered viable markets.” In some coun-tries, government and donor officials have unrealistically expectedthe commercial sector to “take over” all or partial responsibility forreproductive health care after a donor has decided to withdrawassistance from a country.
Priorities for Governments: While many of the concernsexpressed above are legitimate, governments could do muchmore to recognize and facilitate the potential contribution of private businesses.
❁ In an era of escalating needs and stagnant funding, all governments need to look to the commercial sector for help in achieving public health goals. Even in countriessuch as China and Vietnam where the state has traditionallydominated health provision, private sector health servicesare growing rapidly—not as a result of a clear policy butrather to fill in the gaps in government services. The spreadof the market economy worldwide has reinforced this trend.
Governmentscould do
much more to facilitate the potential contribution
of private businesses.

60MARKET PROFILE
IMPROVING THE PRODUCTCondom manufacturers frequently introduceincremental changes in design to improve ormaintain product appeal. Enhancements focuson increasing resistance to tearing, changing thetexture, and adding spermicidal lubrication. Anew condom made of a thin, durable plasticrepresents an important alternative for userswho are allergic to latex. Plastic condoms arealso less vulnerable to light and high tempera-tures, and can be used with oil-based lubricants.Within the developing world, however, mostconsumers will likely continue to prefer thelatex condom as it costs significantly less thanthe plastic variety.
With the exception of limited donor supportfor development of the plastic condom, there islittle funding outside of industry for productimprovements. Donor requirements to meetmore stringent international standards have,however, spurred significant enhancements inthe quality of condoms.
MARKET SIZECondoms have long been used for both protec-tion against unwanted pregnancy and diseaseprevention. About 30 million couples in thedeveloping world use condoms for family plan-ning—roughly one-quarter of those using a tem-porary, modern method of family planning.Another 50 million men use condoms primarilywith sex workers and other casual sexual con-tacts to avoid contracting a sexually transmittedinfection. Sales of the roughly 5.5 billion con-doms used each year in developing countriesgenerate only about $150 million in revenuesfor manufacturers.
THE PRODUCT Nearly all of the condoms currently sold aremade of latex and are packaged singly or instrips of 3 to 5 pieces. Condom colors, shapesand textures vary according to the brand.
MARKET PROFILE
Condoms
Figure 14
SALES of CONDOMS
THROUGH SOCIAL
MARKETING PROGRAMS
1991 to 1997
Source: DKT International. Contra-ceptive Social Marketing Statistics, 7 vols. Washington, DC: DKT Inter-national, 1992-1998.
0
200
400
600
800
1000
1997199619951994199319921991
MIL
LIO
NS
OF
CO
ND
OM
S

MARKET PROFILE61
MANUFACTURINGRelatively few companies account for the bulkof worldwide condom supply. These include theLondon International Group (United Kingdom),Ansell (United States), Dongkuk (Korea), Seo-hung (Korea), Fuji (Japan), and Hindustan Latex(India). The economics of latex condom manu-facturing requires mass production for the dip-ping process, exacting quality control, and easyaccess to high quality latex supplies and tomarkets that can absorb large quantities of out-put. Manufacturing occurs principally in theUnited States, India, China, Korea, Thailandand Malaysia. Condom packaging operationscan be located in a broader range of placesbecause they require less stringent technicalspecifications and smaller quantities. One firmin Mexico imports bulk condoms from Germanyand packages them locally. Companies in anumber of other developing countries importcondoms in generic packages, then place theproduct in boxes under a local brand name.
CONSUMER SOURCES OF SUPPLYSlightly under half of all couples in developingcountries using condoms to plan their familiessecure their supplies from a commercialsource—typically private pharmacies and smallstores. Government sources are most commonin countries of the Middle East and North Africaregion while pharmacies supply the bulk of con-dom users in Latin America. Social marketingprograms in 50 countries—most of themfocused on HIV/AIDS prevention—sell almostone billion condoms a year at subsidized prices.More than half this total, however, is sold in justthree South Asian countries—India, Bangladeshand Pakistan—primarily for family planning.
DONOR ROLESSupport from international donors has beencritical to the growing popularity of condomsin the developing world. From 1995 to 1997,donors provided about 1.4 billion condomsannually for both family planning and STI prevention programs.
OPPORTUNITIES FOR MARKET GROWTHVirtually all recent growth in con-dom use has occurred in poorercountries, in large part spurred byaggressive programs to prevent thespread of HIV/AIDS. The growth incondom sales is flat in most of thedeveloped world, where, outside ofJapan, condoms are not widely used.
Although other methods of fam-ily planning offer temporary protec-tion against unwanted pregnancy,the condom is unique among contra-ceptives in its ability to also protectthe user against sexually transmittedinfections. The recently introducedfemale condom now gives womenan important option to providethemselves with similar protection.However, its high cost relative to themale condom limits its use in devel-oping countries beyond suppliesprovided by international donors.
Many experts believe there is stillhuge potential for growth in the con-dom market for prevention ofHIV/AIDS and other sexually transmit-ted infections, especially among ado-lescents. Sales of socially marketedcondoms increased 70 percentbetween 1992 and 1997. Neverthe-less, important barriers remain togrowth in commercial markets forcondoms. Low purchasing power ofthe groups most in need of condomsfor disease prevention is among themost significant barriers. TheHIV/AIDS epidemic is particularlydevastating in the poorest countries,including many countries in sub-Saharan Africa, and in Asian countriessuch as India and China. Continuedpublic subsidies for wealthier con-sumers also inhibit commercial market expansion.
Ma
rket
Pro
file
POPULATION ACTION INTERNATIONAL62
❁ Governments should balance justifiable concerns aboutthe cost and quality of private sector health care with thepotential for better achieving public health goals throughgreater commercial sector involvement. As noted earlier,governments have a important role in regulating the pri-vate sector role in reproductive health care—and in healthcare more generally. In particular, there is a need for pub-lic sector regulation of the variable quality of private for-profit health care. Yet, over-regulation often unnecessarilyinhibits the commercial sector’s efficient functioning.Moreover, specific strategies can be developed to addresssuch problems as the inadequate information given toclients purchasing products from pharmacies. For exam-ple, pharmacy staff should receive more and better train-ing, and manufacturers and distributors can utilizealternative means of getting information to clients, forexample through improved package inserts.
❁ While governments need to be more open to the privatesector, they also need to recognize when underlying socialand economic conditions are not ripe for commercialexpansion. Failure to be realistic about the commercialsector’s ability to reach markets profitably can lead to seri-ous miscalculations about the ability of for-profit actors toachieve goals set by national reproductive health programs.For example, family planning officials in Indonesia—acountry where overall commercial involvement in familyplanning has increased dramatically in recent decades—assumed 20 years ago that the commercial sector wouldoffer family planning in remote areas. Yet, the lack of prof-itable opportunities in sparsely-populated regions of thecountry has generated little interest on the part of commer-cial firms in marketing their products in these areas.
INCREASING DONOR AWARENESS OF
AND SUPPORT FOR THE COMMERCIAL SECTOR
Interest on the part of international donor agencies in expandingthe role of the commercial sector has been growing over the pasttwo decades, a trend that has accelerated as the financial con-straints on donors and governments have become more acute.Still, initiatives to expand commercial sector involvement mustalso overcome resistance on the part of some donor agencies.
Donor agency views on commercial sector initiatives varywidely, in part reflecting philosophical and societal differencesamong donor nations. The United States, with its largely private
Governmentscan develop
specific strategies toaddress the
variable qualityof private for-profit
health care.
Getting Down to Business 63
for-profit health system, has been the foremost proponent ofmarket solutions to reproductive health problems in developingcountries. In virtually all other industrialized countries, most peo-ple obtain health care from publicly-funded or publicly-providedprograms. Notes one U.S. observer, “Many other countries don’tblink an eye when thinking about a strong public role for healthcare, in the same way that we in the United States assume thateducation is a state responsibility.”
A further obstacle to increasing the role of the commercialsector in reproductive health is that the culture of donor assistanceis for the most part unsympathetic to the commercial sector.Donor agency staff working in the reproductive health arena aregovernment officials themselves; many see a strong governmentpresence in health financing and services as essential to achievingpublic health goals, and are reluctant to divert limited funds tocommercial sector initiatives.
“Donors are to a certain extent committed to and aware of theneed to involve commercial partners,” says an official at one U.S.technical assistance agency, “but they lack good information onboth the motivations and potential of the for-profit sector.” Thislack of understanding reinforces existing biases against commercialsector initiatives while nurturing mistaken beliefs regarding whatthe commercial sector can realistically achieve. Notes one observer,“A lot of the donors think commercial sector involvement is aquick answer to the problem of financing government programs.”
The United States has been a leader in promoting models forprivate sector involvement. In the early 1980s, during the Reaganadministration, which placed a high value on free economic mar-kets, USAID began allocating significant financial and technicalresources to such initiatives. After almost two decades of both suc-cesses and failures in this area, the agency has built up significantexpertise in designing and implementing innovative and flexibleprograms that promote public-private partnerships.
Because of its long experience with such approaches, USAIDhas fairly realistic expectations of the role the commercial sectorcan play. Yet, there is still considerable debate within the agencyover the level of resources and effort that should be devoted toinitiatives to increase commercial sector involvement. Many USAIDpopulation and health staff, moreover, lack a good understandingof commercial sector issues.
The United Kingdom and Germany are the only bilateraldonors besides the United States that have made a significantcommitment to commercial sector initiatives in reproductivehealth, almost exclusively through social marketing efforts. Aidpolicies of both donors favor a highly subsidized approach tosuch efforts. In keeping with its strong mandate to serve the poor,the British aid program requires that the social marketing programs
The UnitedStates has been
a leader inpromotingmodels for
private sectorinvolvement.

POPULATION ACTION INTERNATIONAL64
it funds focus on low-income consumers. Neither the British northe German population assistance program has shown much inter-est in the types of public-private partnerships pioneered by USAID.Even in Pakistan, where the British are partnering with a localcommercial contraceptive distributor, aid officials do not expectthe program to become financially self-sufficient in the long run.
Multilateral donors generally work through developingcountry governments and thus find it more difficult to channeltechnical and financial resources to commercial sector programs.A current initiative by the United Nations Population Fund tobroker partnerships among donors, governments, and commer-cial manufacturers of oral contraceptives marks an important firststep for the agency (see box on page 61). The World Bank loansmoney to the public sector and thus is even more restricted in itsability to develop commercial sector initiatives. A positive recentstep by the World Bank is the push for the Bank’s private invest-ment arm, the International Finance Corporation (IFC), toincrease its lending for commercial health activities. The IFC hasestablished a specialized unit in one of its regional departmentsto develop investments in health care, an area in which the IFChad previously shown little interest.
Priorities for International Donors: The preceding discus-sion illustrates the variable and relatively limited interest in andability of donors to directly support commercial initiatives. Never-theless, donor agencies can take a number of steps to promote amore positive overall stance towards the role of the private sectorin reproductive health care.
❁ At a minimum, aid agencies should avoid supportingactivities that undermine healthy commercial markets.Especially in their commodity assistance and in their sup-port for social marketing, donors need to convince busi-ness interests that they respect commercial markets andwill not act in ways that undercut profits. Striking the rightbalance between nurturing commercial markets and achiev-ing critical public health goals is often difficult, however.This is particularly true in the case of efforts to increasecommercial sales of condoms on the one hand and expandfree distribution on the other, in light of the urgent needto prevent the spread of the devastating AIDS epidemic.
❁ Donors are uniquely situated to influence governmentpolicy and promote an environment that facilitates therole of the commercial sector. Donor agencies can play anespecially important role in their policy discussions withgovernments in urging the reorientation of publicly sup-ported health care to the needy and the removal of
Aid agenciesshould avoid
supportingactivities that
underminehealthy commer-
cial markets.

Getting Down to Business 65
In 1997, the United Nations Population Fund(UNFPA) for the first time initiated a highly
visible push for greater involvement of thecommercial sector. The program, carried outunder UNFPA’s Global Initiative on Contracep-tive Requirements and Logistics ManagementNeeds, aims to expand commercial markets forfamily planning products and promote public-private partnerships to reduce contraceptivecosts. Sponsors of the effort include the Rocke-feller and Packard Foundations and the U.K.’sDepartment for International Development.
Through dialogue between governments,donors and commercial firms, UNFPA hopesto convince companies to lower prices andexpand markets in exchange for commitmentsby governments to improve the tax and regu-latory climate for commercial activity. Donoragencies would contribute to such dealsthrough support for advertising and othermarketing costs.
UNFPA is focusing first on oral contracep-tives, because of their importance as a methodof family planning and because oral pillsaccount for almost four-fifths of the cost of allcontraceptive commodities. Moreover, thereare relatively few manufacturers of oral contra-ceptives worldwide, and many are accustomed
to working with the public sector on similarinitiatives supported by USAID.
A novel aspect of the initiative is that for thefirst time representatives of international donoragencies, developing country governments andthe commercial sector are sitting around the sametable discussing strategies to expand commercialmarkets. An initial meeting in July 1997 broughttogether bilateral and multilateral donor agenciesincluding the World Bank, health and finance offi-cials from developing countries, and the majorproducers of oral contraceptives.
UNFPA has followed up with specific efforts toassess interest among government officials andcommercial sector representatives in Egypt, Ghana,India, Indonesia, South Africa and Thailand. A meet-ing in November 1998 brought together the mainpartners from those countries where the greatestpotential exists for negotiating such agreements.
Some experts point out that UNFPA is spend-ing little of its own money on the initiative—andthat commercial sector programs have until nowreceived limited interest within the Fund, and lackbroad support and understanding within UNFPA.Most observers, however, agree that UNFPA isbreaking new ground and moving in a positivedirection by taking on a greater role in expandingcommercial markets.
BUILDING ALLIANCES: UNFPA’S INITIATIVE TO EXPAND COMMERCIAL MARKETS FOR CONTRACEPTIVES

POPULATION ACTION INTERNATIONAL66
unnecessary legal and regulatory barriers to commercialsector involvement. The World Bank, in particular, hasenormous influence on developing country policies; it isalready taking the lead, in concert with other donors, tohelp developing countries establish more efficient andequitable health systems. Such reforms are key to redirect-ing public funds from curative to preventive health careand to encouraging better-off populations to seek carefrom private sources—changes that will in the long termbenefit the growth of commercial markets. The donors arealso more likely to have an impact if they coordinateefforts to influence policy and speak with one voice.
❁ Donors can serve both government and business interestsby gathering and sharing information on markets and thedemand for reproductive health care. For example, thecountry-level demographic and health surveys sponsoredby donors could routinely include questions on prices paidfor reproductive health products and the ability of con-sumers to pay for such products. Such surveys should alsowork towards adoption of standard definitions of socioeco-nomic status to allow cross-country comparison and analy-ses of reproductive health markets.
LOOKING TO THE FUTURE
Current trends favor an expansion of the private commercialsector’s role in reproductive health care.
First, the attitudes of public sector officials towards the privatesector in general are changing. Today, both developing and donorcountry governments increasingly recognize that the private sectorcomplements their efforts, and are working to foster its growth.There is unprecedented acceptance that the private sector is ofparamount importance to overall economic development.
The long-standing reluctance of many large transnational cor-porations to invest in developing country markets is also fading.With the globalization of the world economy, these companies—including the major producers of reproductive health commodi-ties—now recognize the huge potential market represented by the80 percent of the world’s population who live in the developingworld. There is a new appreciation that expanding into emergingmarkets is key to maximizing long-term profits. In the past decade,private capital flows from industrialized to developing countrieshave risen, especially to middle-income countries and those withlarge populations, even as official development aid has declined.
Donors canwork with
governments topromote an
environmentthat facilitates
the role of the commercial
sector.

Getting Down to Business 67
Finally, transnational companies in the reproductive healthfield appear more open to the idea of partnerships with the publicsector. Several such companies have gained experience in recentyears with donor–sponsored initiatives to increase commercial sec-tor involvement. Moreover, the relatively small number of compa-nies involved in the manufacture and distribution of reproductivehealth products worldwide facilitates the replication of such part-nerships across countries. The fact that several major internationaldonors are also large clients of these companies is a further factorfacilitating closer public-private partnerships.
As these trends converge, there is a new appreciation of thebenefits of closer collaboration and a greater willingness to worktogether on the part of both government and businesses. Suchchanges in attitude are the first step towards enabling the privatecommercial sector to assume a more vibrant and dynamic role inmeeting reproductive health needs. The challenge now is for gov-ernments and international donors to build on their emergingawareness of the private sector’s potential contribution to repro-ductive health. The public sector needs to move vigorously aheadwith the policy changes and actions needed to make the commer-cial sector a full partner in the international effort to improvereproductive health and slow world population growth.
There is a newappreciation
of the benefitsof closer collab-oration on the
part of bothgovernment
and business.

POPULATION ACTION INTERNATIONAL68
DATA SOURCES AND METHODOLOGY
Data Sources: Information for the 60 countries included in theStatistical Annex comes primarily from the Demographic andHealth Surveys (DHS), nationally representative studies carriedout periodically in many developing countries. Figures for 22 ofthe 60 countries are drawn from an unpublished analysis of theDHS data performed by the Futures Group International. For anadditional 35 countries, commercial sector market share is basedon calculations from published DHS country reports. For 3 coun-tries—China, India, and Thailand—the Annex draws on non-DHSsources: the 1992 National Fertility and Family Planning Survey,China; the India National Family Health Survey 1992-93; and theThailand National Contraceptive Prevalence Survey 1996. For allcountries, data from the most recent survey is used.
Definitions of Commercial Sector: Although they lack astandard definition for the commercial sector, the DHS surveys docollect fairly detailed information on sources of contraception. Thefollowing categories are included in the calculation of commercialmarket share used in the Annex: private hospitals, private clinics,private doctors and midwives, pharmacies, and markets or shops.While these groupings are not completely consistent across coun-tries, they do provide a good approximation of the commercialsector presence. For countries where the DHS does not clearly distinguish between private commercial and private nonprofitsources, the commercial share has been estimated after consulta-tion with international and in-country experts.
Methodology to Calculate Regional Averages: Regionalaverages are weighted by the number of married women ages 15to 49 using modern contraception. The weighted average foreach region is calculated by summing the total number of womenobtaining methods from commercial sources and dividing thisfigure by the total number of women using modern contraception.Although these averages are based only on the countries with survey information, almost 90 percent of women of reproductiveage using modern contraception in the developing world reside in these 60 countries.
Statistical Annex
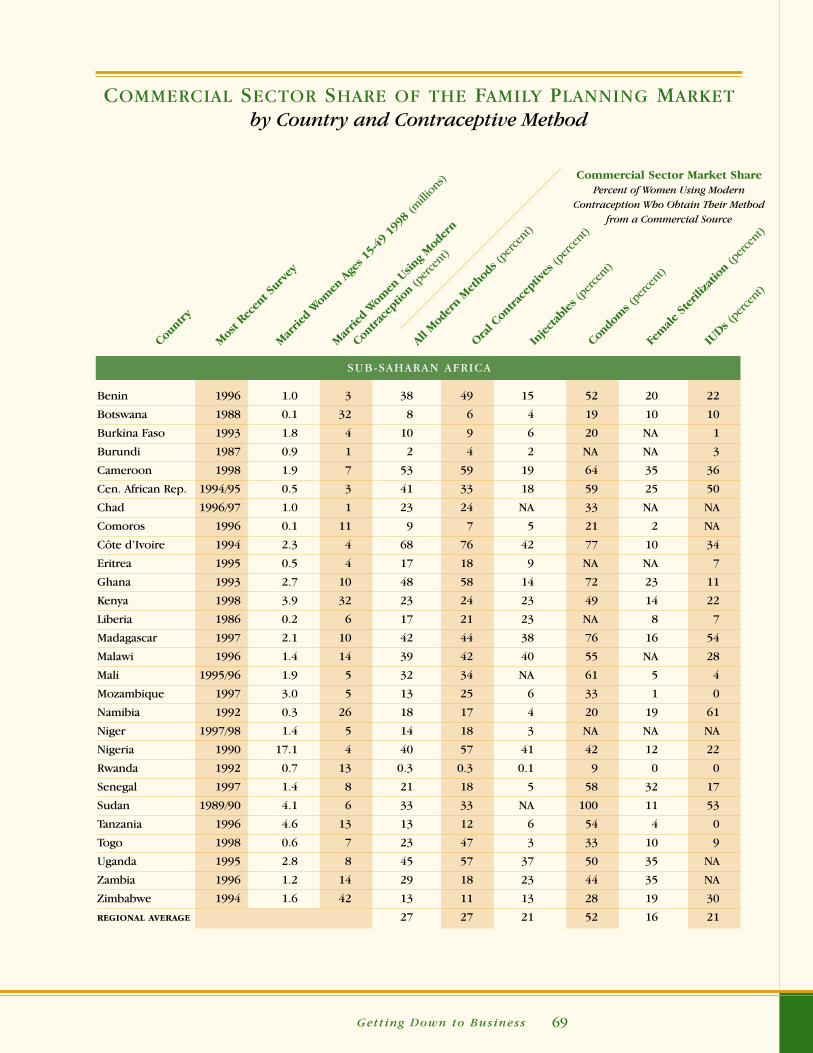
Getting Down to Business 69
Count
ry
Mos
t Rec
ent S
urve
y
Mar
ried
Wom
en A
ges 1
5-49
199
8 (m
illion
s)
Mar
ried
Wom
en U
sing
Mod
ern
Contra
cept
ion
(per
cent
)
All M
oder
n M
etho
ds (p
erce
nt)
Oral C
ontra
cept
ives
(per
cent
)
Inject
ables (
perce
nt)
Condo
ms (
perce
nt)
Fem
ale St
erili
zatio
n (p
erce
nt)
IUDs (
perce
nt)
COMMERCIAL SECTOR SHARE OF THE FAMILY PLANNING MARKETby Country and Contraceptive Method
Commercial Sector Market SharePercent of Women Using Modern
Contraception Who Obtain Their Method from a Commercial Source
SUB-SAHARAN AFRICA
Benin 1996 1.0 3 38 49 15 52 20 22
Botswana 1988 0.1 32 8 6 4 19 10 10
Burkina Faso 1993 1.8 4 10 9 6 20 NA 1
Burundi 1987 0.9 1 2 4 2 NA NA 3
Cameroon 1998 1.9 7 53 59 19 64 35 36
Cen. African Rep. 1994/95 0.5 3 41 33 18 59 25 50
Chad 1996/97 1.0 1 23 24 NA 33 NA NA
Comoros 1996 0.1 11 9 7 5 21 2 NA
Côte d’Ivoire 1994 2.3 4 68 76 42 77 10 34
Eritrea 1995 0.5 4 17 18 9 NA NA 7
Ghana 1993 2.7 10 48 58 14 72 23 11
Kenya 1998 3.9 32 23 24 23 49 14 22
Liberia 1986 0.2 6 17 21 23 NA 8 7
Madagascar 1997 2.1 10 42 44 38 76 16 54
Malawi 1996 1.4 14 39 42 40 55 NA 28
Mali 1995/96 1.9 5 32 34 NA 61 5 4
Mozambique 1997 3.0 5 13 25 6 33 1 0
Namibia 1992 0.3 26 18 17 4 20 19 61
Niger 1997/98 1.4 5 14 18 3 NA NA NA
Nigeria 1990 17.1 4 40 57 41 42 12 22
Rwanda 1992 0.7 13 0.3 0.3 0.1 9 0 0
Senegal 1997 1.4 8 21 18 5 58 32 17
Sudan 1989/90 4.1 6 33 33 NA 100 11 53
Tanzania 1996 4.6 13 13 12 6 54 4 0
Togo 1998 0.6 7 23 47 3 33 10 9
Uganda 1995 2.8 8 45 57 37 50 35 NA
Zambia 1996 1.2 14 29 18 23 44 35 NA
Zimbabwe 1994 1.6 42 13 11 13 28 19 30
REGIONAL AVERAGE 27 27 21 52 16 21
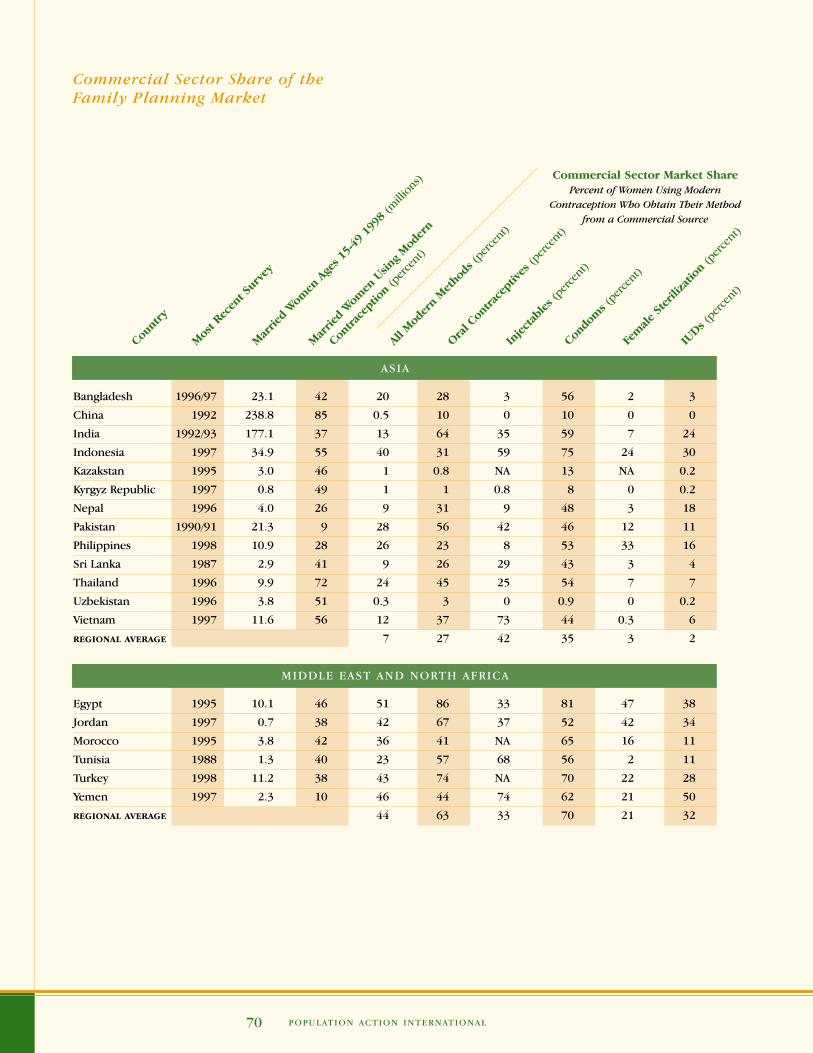
POPULATION ACTION INTERNATIONAL70
ASIA
Bangladesh 1996/97 23.1 42 20 28 3 56 2 3
China 1992 238.8 85 0.5 10 0 10 0 0
India 1992/93 177.1 37 13 64 35 59 7 24
Indonesia 1997 34.9 55 40 31 59 75 24 30
Kazakstan 1995 3.0 46 1 0.8 NA 13 NA 0.2
Kyrgyz Republic 1997 0.8 49 1 1 0.8 8 0 0.2
Nepal 1996 4.0 26 9 31 9 48 3 18
Pakistan 1990/91 21.3 9 28 56 42 46 12 11
Philippines 1998 10.9 28 26 23 8 53 33 16
Sri Lanka 1987 2.9 41 9 26 29 43 3 4
Thailand 1996 9.9 72 24 45 25 54 7 7
Uzbekistan 1996 3.8 51 0.3 3 0 0.9 0 0.2
Vietnam 1997 11.6 56 12 37 73 44 0.3 6
REGIONAL AVERAGE 7 27 42 35 3 2
MIDDLE EAST AND NORTH AFRICA
Egypt 1995 10.1 46 51 86 33 81 47 38
Jordan 1997 0.7 38 42 67 37 52 42 34
Morocco 1995 3.8 42 36 41 NA 65 16 11
Tunisia 1988 1.3 40 23 57 68 56 2 11
Turkey 1998 11.2 38 43 74 NA 70 22 28
Yemen 1997 2.3 10 46 44 74 62 21 50
REGIONAL AVERAGE 44 63 33 70 21 32
Count
ry
Mos
t Rec
ent S
urve
y
Mar
ried
Wom
en A
ges 1
5-49
199
8 (m
illion
s)
Mar
ried
Wom
en U
sing
Mod
ern
Contra
cept
ion
(per
cent
)
All M
oder
n M
etho
ds (p
erce
nt)
Oral C
ontra
cept
ives
(per
cent
)
Inject
ables (
perce
nt)
Condo
ms (
perce
nt)
Fem
ale St
erili
zatio
n (p
erce
nt)
IUDs (
perce
nt)
Commercial Sector Market SharePercent of Women Using Modern
Contraception Who Obtain Their Method from a Commercial Source
Commercial Sector Share of theFamily Planning Market

Getting Down to Business 71
Sources: Demographic and Health Surveys; The Futures Group International;United Nations Population Division
LATIN AMERICA AND THE CARIBBEAN
Bolivia 1998 1.1 25 50 78 72 78 28 41
Brazil 1996 26.8 70 54 90 94 76 27 48
Colombia 1995 5.6 59 43 94 97 95 12 20
Dominican Rep. 1996 1.1 59 50 66 47 72 46 28
Ecuador 1987 1.9 36 36 38 85 48 32 34
El Salvador 1985 0.9 44 10 32 69 68 3 7
Guatemala 1995 1.4 27 29 30 36 72 22 27
Haiti 1994/95 1.1 13 22 22 7 67 4 27
Mexico 1987 14.6 45 36 66 84 54 21 19
Nicaragua 1998 0.7 57 16 34 32 41 6 9
Paraguay 1990 0.7 35 66 75 87 87 40 49
Peru 1996 3.4 41 25 33 11 69 17 14
Trinidad and
Tobago 1987 0.2 44 46 61 61 57 12 24
REGIONAL AVERAGE 46 81 68 74 24 23
Count
ry
Mos
t Rec
ent S
urve
y
Mar
ried
Wom
en A
ges 1
5-49
199
8 (m
illion
s)
Mar
ried
Wom
en U
sing
Mod
ern
Contra
cept
ion
(per
cent
)
All M
oder
n M
etho
ds (p
erce
nt)
Oral C
ontra
cept
ives
(per
cent
)
Inject
ables (
perce
nt)
Condo
ms (
perce
nt)
Fem
ale St
erili
zatio
n (p
erce
nt)
IUDs (
perce
nt)
Commercial Sector Market SharePercent of Women Using Modern
Contraception Who Obtain Their Method from a Commercial Source
Commercial Sector Share of theFamily Planning Market

POPULATION ACTION INTERNATIONAL72
Adu-Sarkodie, Y.A. “Antimicrobial Self-Medication in PatientsAttending a Sexually Transmitted Diseases Clinic.” InternationalJournal of STD & AIDS, no.8 (1997).
AIDSCAP. “HIV/AIDS Prevention: Mobilizing the Private Sector.”AIDSCaptions 2, no. 1 (March 1995).
Allman, Patricia. “Marketing Social Marketing to Commercial Partners: What’s in It for Them?” Paper presented at the 1998Innovations in Social Marketing Conference, Washington, DC,June 1998.
Becker, Stan et al. “The Determinants of Use of Maternal and ChildHealth Services in Metro Cebu, the Philippines.” Health Transi-tion Review 3, no. 1 (1993): 77-89.
Bennett, Sara et al. “Carrot and Stick: State Mechanisms to Influ-ence Private Provider Behavior.” Health Policy and Planning 9,no. 1 (1994):1-13.
Berman, Peter and Laura Rose. “The Role of Private Providers inMaternal and Child Health and Family Planning Services inDeveloping Countries.” Health Policy and Planning 11, no. 2(1996): 142-155.
Cakir, H. Volkan and Jeffrey J. Sine. Segmentation in Turkey’s Family Planning Market. The POLICY Project. Washington, DC:The Futures Group International, July 1997.
Castro Leal et al. “Public Social Spending in Africa: Do the PoorBenefit?” World Bank Poverty Council. Washington, DC: WorldBank, December 1997. Unpublished.
Centre for Operations Research and Training. Situation Analysisof Medical Termination of Pregnancy (MTP) Services in UttarPradesh. Baroda, India: Centre for Operations Research andTraining, August 1997.
Conly, Shanti and Shyami de Silva. Paying Their Fair Share? DonorCountries and International Population Assistance. Washing-ton, DC: Population Action International, 1998.
Key References

Getting Down to Business 73
Crabbe, F. et al. “Why Do Men with Urethritis in Cameroon Preferto Seek Care in the Informal Health Sector?” GenitourinaryMedicine 72 (1996).
Cross, Harry E. Policy Issues in Expanding Private Sector FamilyPlanning. Options for Population Policy Project (The OPTIONSProject). Policy Paper Series, no. 3. Washington, DC: The FuturesGroup International, 1993.
Desai, Jaikishan. “The Private Sector in Family Planning Services:Demand and Supply Issues.” Washington, DC: The FuturesGroup International, 1997. Unpublished.
East-West Center, Program on Population. “Who Uses ReproductiveHealth Services in the Philippines (and Who Doesn’t)?” Asia-Pacific Population and Policy, no. 37 (April 1996).
Family Health International. “Evaluating Family Planning Costs.”Network 18, no. 2 (Winter 1998).
Feeley, Frank. Practical Pointers for Conducting Commercial SectorFamily Planning Regulatory Assessments. Arlington, Virginia:The PROFIT Project, 1997.
Foreit, Karen G. Private Sector Approaches to Effective FamilyPlanning. Population and Human Resources Department. PolicyResearch Working Papers, WPS 940. Washington, DC: WorldBank, 1992.
The Futures Group International. Family Planning CommercialSector Initiatives in Peru: A Feasibility Study. Washington, DC:The Futures Group International, 1997.
Gertler, Paul and Jeffrey S. Hammer. “Strategies for Pricing PubliclyProvided Health Services.” In Innovations in Health CareFinancing: Proceedings of a World Bank Conference, March 10-11, 1997, ed. George J. Schieber. Washington, DC: WorldBank, 1997: 127-154.
Griffin, Charles C. The Private Sector and Health Care Policy inDeveloping Countries. Discussion Paper, no. 4. Washington, DC:International Finance Corporation, 1989.
Handyside, Alan et al. Evaluation of the Social Marketing forChange (SOMARC III) Project. Poptech Report, no. 95-053-039.Arlington, Virginia: Population Technical Assistance Project, 1996.
Hanson, Kara, Lilani Kumaranayaki, and Ian Thomas. SupplyingSubsidised Contraceptives: Economic Rationale and Pro-gramme Issues for Promoting Sustainability. Health and Popu-lation Division, United Kingdom Department for InternationalDevelopment. London: Options Consultancy Services Limited,August 1998.

POPULATION ACTION INTERNATIONAL74
Harrison, Polly F. and Allan Rosenfield. Contraceptive Researchand Development: Looking to the Future. Washington, DC:National Academy Press, 1996.
Hopstock, Paul, Ann Sherpick, and Carla Briceno. Providers andConsumers of Commercial Family Planning Services in Devel-oping Countries. Arlington, Virginia: The Profit Project, 1997.
Janowitz, Barbara and John H. Bratt. “What Do We Really Knowabout the Impact of Price Changes on Contraceptive Use.”International Family Planning Perspectives 22, no. 1 (March1996): 38-40.
Janowitz, Barbara, Diana Measham, and Caroline West. Issues inthe Finance of Family Planning Services in Sub-Saharan Africa.Research Triangle Park, North Carolina: Family Health Interna-tional, 1999.
Kean, Linda Griffin. Summary Proceedings: Invitational Meetingof Experts on Opportunities for Commercial Sector Involvementin Developing Country Family Planning Services. Arlington,Virginia: The PROFIT Project, October 1996.
Kenney, Genevieve. Assessing Legal and Regulatory Reform inFamily Planning: Manual on Legal and Regulatory Reform.Options for Population Policy Project (The OPTIONS Project).Policy Paper Series, no.1. Washington, DC: The Futures GroupInternational, 1993.
Kimball, Ann Marie and Myo Thant. “A Role for Businesses in HIVPrevention in Asia.” The Lancet 347 (June 15, 1996):1670-1672.
Kincaid, Mary et al. The Transition to the Commercial Sector:What Happens to Socially Marketed Products after Graduatingfrom USAID Support? Somarc III Project Special Study, no.1.Washington, DC: The Futures Group International, April 1997.
Lamptey, Peter. “Expanding the Partnership—The Private Sector’sRole in HIV/AIDS Prevention.” AIDSCaptions 3, no. 2 (July 1996).
Lande, Robert E. and Judith S. Geller. “Paying for Family Planning.”Population Reports, J-39 (November 1991).
Lewis, Maureen and Genevieve Kenney. The Private Sector andFamily Planning in Developing Countries: Its Role, Achievementsand Potential. Population and Human Resources DepartmentWorking Paper. Washington, DC: World Bank, 1988.
Mitchell, Susan. Conducting a Private Sector Family PlanningCountry Assessment. Arlington, Virginia: The PROFIT Project,September 1997.

Getting Down to Business 75
Musgrove, Philip. Public and Private Roles in Health. World BankDiscussion Paper, no. 339. Washington, DC: World Bank, 1997.
Opportunities for Micronutrient Interventions (The OMNI Project).Knowledge, Attitudes, and Practices of Pregnant WomenRegarding, the Problem of Anemia, its Consequences, andTreatment. Qualitative Research in 6 Districts of Bolivia. La Paz, Bolivia: The OMNI Project, June 1997.
Private Initiative for Primary Healthcare Project (Initiatives). Initia-tives Private Sector Toolkit: A Step by Step Guide for Workingwith the Private Health Sector. Arlington, Virginia: John SnowResearch & Training Institute, 1997.
Private Initiative for Primary Healthcare Project (Initiatives).Lessons Learned in the Initiatives Project, 1992-1997. MeetingReport. Arlington, Virginia: John Snow Research & TrainingInstitute, June 1997.
The POLICY Project, Planning and Finance Group. “Value forMoney in Reproductive Health: Issues and Options for Govern-ments and Donors.” Washington, DC: The Futures Group Inter-national, December 3, 1998. Draft.
Program for Appropriate Technology in Health (PATH). Funda-mental Issues Affecting the Feasibility of Local ContraceptiveProduction. Washington, DC: World Bank, September 1995.
______. Contraceptive Manufacturing Overview. Washington, DC:World Bank, September 1995.
Psacharopoulos, George and Nguyen Xuan Nguyen. The Role ofthe Government and the Private Sector in Fighting Poverty.World Bank Technical Paper, no. 346. Washington, DC: WorldBank, 1997.
Ravenholt, Betty Butler and Madiha Said. Analysis of the Legaland Regulatory Environment for Family Planning in Egypt: An Update. The POLICY Project. Washington, DC: The FuturesGroup International, November 1997.
Ravenholt, Betty. “From Deal to Delivery: Partnerships with theCommercial Sector.” Paper presented at the SOMARC LessonsLearned from Social Marketing Conference, Washington, DC,September 22, 1998.
Ravenholt, Betty. Potential for Increased Involvement of the Commercial Sector in Family Planning Service Delivery in the Philippines: Assessment and Initial Strategies. The POLICYProject. Washington, DC: The Futures Group International, July 1996.
POPULATION ACTION INTERNATIONAL76
Schieber, George and Akiko Maeda. “A Curmudgeon’s Guide toFinancing Health Care in Developing Countries.” In Innovationsin Health Care Financing: Proceedings of a World Bank Confer-ence, March10-11, 1997, ed. George Schieber. Washington, DC:World Bank, 1997: 1-40.
Stanback, John. Perspectives on Local Manufacture of Contracep-tives in Developing Countries. Arlington, Virginia: The PROFITProject, 1997.
UNFPA. Consultative Meeting on Expanding Commercial Marketfor Oral Contraceptives in Developing Countries. TechnicalReport, no 41. New York: UNFPA, 1997.
______. Local Production of Contraceptives. Evaluation Report, no. 10. New York: UNFPA, 1995.
United Kingdom Overseas Development Administration. Sexualand Reproductive Health Social Marketing Projects: A Summaryof Experiences from Activities Supported by UK/ODA. London:United Kingdom Overseas Development Administration, March 1997.
Van der Gaag, Jacques. Private and Public Initiatives. WorkingTogether for Health and Education. Washington, DC: The WorldBank, 1995.
Williams, Linda et al. “Reducing Iron Deficiency and Anaemia inWomen of Reproductive Age in Thyolo District, Malawi. Reportof a Baseline Survey.” Arlington, Virginia: The MotherCare Pro-ject, March 1997. Unpublished.
Winfrey, William et al. The Commercial Sector in Family Planning.The POLICY Project Working Paper, no. 4. Washington, DC: TheFutures Group International, 1999. Forthcoming.
Winfrey, William and Laura Heaton. Market Segmentation Analysisof the Indonesian Family Planning Market: Consumer, Providerand Product Market Segments and Public Sector ProcurementCosts of Family Planning under Different Scenarios of PrivateSector Participation. Options for Population Policy Project (TheOPTIONSII Project). Washington, DC: The Futures Group Inter-national, April 1996.
World Bank. Confronting AIDS: Public Priorities in a Global Epidemic. New York: Oxford University Press, 1997.
______. Financing Health Services in Developing Countries. An Agenda for Reform. Washington, DC: World Bank, 1987
______. Sector Strategy: Health, Nutrition, and Population. Washington, DC: World Bank, 1997.

Getting Down to Business 77

COLOPHON
Getting Down to Business: Expanding the Private CommercialSector’s Role in Meeting Reproductive Health Needs was composedin ITC Garamond and produced on a Macintosh G3 in QuarkXpress.It was printed on Mega Dull 80# cover and text.

William H. Draper, Jr.National and Honorary Chair1965-1974
OFFICERS
National ChairpersonConstance Spahn
National Co-ChairsWilliam H. Draper, IIIRobin Chandler DukeVictoria P. SantJoseph D. Tydings
TreasurerScott M. Spangler
SecretaryPhyllis Tilson Piotrow
PresidentAmy Coen
DIRECTORS
Vincent AnkuVicki-Ann E. AsseveroAnthony C. BeilensonPouru P. BhiwandiAnne K. BingamanNorman E. BorlaugSharon L. CampMarion M. Dawson CarrWilliam Clark, Jr.A.W. ClausenPhilander P. Claxton, Jr.Barber B. ConableHenry H. FowlerBill GreenKaval GulhatiJulia J. HendersonLawrence R. KeganC. Payne LucasEdwin M. MartinRobert S. McNamaraWendy B. MorganYolonda RichardsonAllan RosenfieldFred T. SaiIsabel V. SawhillElmer Boyd StaatsTimothy L. TowellJoseph C. WheelerWilliam D. Zabel
Director of Publications: Judith HindsDesigned by: Chadick and KimballPrinted by: Colorcraft of Virginia

POPULATION ACTION INTERNATIONAL
1120 19TH STREET, NW, SUITE 550
WASHINGTON, DC 20036 USA