Examining Spatial Patterns of Primary Health Care Utilization ...
172
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Examining Spatial Patterns of Primary Health Care Utilization ...


Examining Spatial Patterns of Primary Health Care Utilization in Southern Honduras
A Dissertation Submitted to the Division of Research and Advanced Studies
of the University of Cincinnati in partial fulfillment of the requirements for the degree of
Doctorate of Philosophy (Ph.D.)
In the Department of Geography of the College of Arts and Sciences
2005
By Jonathan B. Baker B.A. Skidmore College, 1981
M.B.A, Widener University, 1992 M.A., West Chester University, 2002
Lin Liu, Ph.D., Chairperson

Abstract:
Examining Spatial Patterns of Primary Health Care
Utilization in Southern Honduras By Jonathan B. Baker
Chairperson: Lin Liu, Ph.D.
Primary health care utilization is poorly understood in many parts of the developing world. This
is especially true in rural places, such as Santa Lucia, Intibuca, Honduras, where there are only
three primary health care facilities servicing almost 12,000 people, where the people are poor,
and generally speaking access to care is limited. This research project focuses on trying to
understand primary health care utilization patterns in this part of southern Honduras.
Specifically, this research project examines the utilization of three health clinics operating in and
around Santa Lucia.
The delivery of health care is dependent on many factors, including the availability, cost, and
capacities of the providers; the needs, resources and decisions of the patients; and the
characteristics of the region within which the patients live. This research focuses primarily on the
patients, and tries to understand their health seeking behavior. A better understanding of
utilization can be used by health service planners to improve primary health care delivery in this
and similar locations.
The findings of this research indicate that utilization patterns can be explained, to a large extent,
by factors relating to walking [travel] time, economic status, and the combined affect of health

service type and proximity to care. These findings are consistent with findings from prior
research: Both travel time and economic status are important factors in determining primary
health care utilization. In addition, a new variable is created to examine health decision-making.
This new variable has not been considered in previous research, and is found to very significant
determinant of health facility utilization in the study area.
A modified gravity model is used to estimate the level of utilization, and is tested through the use
of log linear transformation and multi-variate regression techniques. The results here, an R-
square of .644 for a model combining three different health clinic service areas, clearly indicate
a relationship between these independent variables and utilization.


Acknowledgements I would like to gratefully acknowledge the following individuals for their contribution to my
Doctor of Philosophy degree in Geography:
Lin Liu, Ph.D., University of Cincinnati, Geography Department, for his teachings in economic
geography; his support in the analysis and preparation of my dissertation and related papers; and
his guidance through the process of completing my Ph.D. He has been my dissertation committee
chair, and I am very grateful for his contribution to this research project and the development of
a clear agenda for my future research.
Howard Stafford, Ph.D., University of Cincinnati, Geography Department, for his teachings in
Economic & Marketing Geography and support in the research, development and design of my
dissertation. In addition, I would like to thank him for his many long discussions with me on
various topics related to geography, and his support of me as a Teaching Assistant and Adjunct
Instructor.
Andrew Bazemore, M.D., University of Cincinnati, Department of Family Medicine, Institute for
Health Policy and Health Services Research, for his teachings in the area of health services, and
public health policy, and his enthusiasm and support in the development of this research project.
Furthermore, I am very grateful for his support in helping me develop a niche in International
Health research, and his contacts at Shoulder-to-Shoulder, Inc. and Hombro á Hombro, without
which this research project would not have been possible.

Nicholas Dunning, Ph.D., for his teachings in the History and Philosophy of Geography, his
expertise in fieldwork in Latin America, and his support on my dissertation committee.
Chris Carr, for his expert teachings in the area of GPS, and his assistance in data collection in
Honduras and the development of methods for this project.
Miguel Coello, for his experience and discussions related to primary health care delivery in
Santa Lucia, Intibuca, Honduras.
The following University of Cincinnati affiliates for their kind financial support of this project;
The Graduate Student Governance Association (GSGA), The Institute for Global Studies and
Affairs (IGSA), and the University Research Council (URC).
La Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente (SERNA), for
making GIS and Honduran Census data files available for use in this project.
Part of this material is based upon work supported by the National Science Foundation under
Grant No. IIS-0081434. Any opinions, findings, and conclusions or recommendations expressed
in this material are those of the author(s) and do not necessarily reflect the views of the National
Science Foundation.

- 1 -
TABLE OF CONTENTS Page List of Tables and Figures 6
List of Maps 7
Chapter One – Introduction 8
1.1 Problem Statement 9
1.2 Importance of Health Service Utilization Research 10
1.2.1 What affects utilization? 11
1.3 The Study Area 12
1.3.1 Location 12
1.3.2 History of the study area 17
1.3.3 Roads and Travel 18
1.3.4 Population 19
1.3.5 Employment 20
1.3.6 Income 21
1.3.7 Education 22
1.4 Health Services in Honduras 22
1.4.1 History on Health Services 22
1.4.2 Background on La Clinica Hombro á Hombro 23
1.4.3 Development of a rural health facility 24
1.5 Chapter Summary 25
Chapter Two – Literature Review 27
2.1 Theoretical Foundations of Prior Research 27
2.1.1 Access and Utilization to Health Care Services 27
2.1.2 Utilization 29

- 2 -
2.1.3 Utilization and Distance 30
2.1.4 Factors influencing utilization 32
2.1.5 Unit of Analysis 36
2.1.6 Theoretical Framework 37
2.2 Methods of Studying Utilization 40
2.2.1 Regression Modeling 40
2.2.2 Gravity Modeling 40
2.2.3 Comparative Descriptive Analysis 41
2.2.4 Marketing Geography and Utilization 42
2.2.5 Geographic Information Systems 43
2.2.6 Global Positioning System 45
2.3 Empirical Studies 46
2.4 Social Equity in Access to Primary Care 47
2.4.1 Access and Equity 48
2.5 Chapter Summary 49
Chapter Three – Data Acquisition 51
3.1 Acquisition of Data for the GIS 51
3.1.1 Acquisition and development of a base map 51
3.1.2 Acquisition of GPS Data in Honduras 52
3.1.3 GIS and Census Data 55
3.2 Attendance Samples 56
3.3 Qualitative Sources of Data 59
3.3.1 Key Informant Data 59
3.3.2 Key Informant Interviews 61

- 3 -
3.3.3 Informal Interviews 61
3.4 Challenges in conducting fieldwork in the developing world 61
3.5 Chapter Summary 65
Chapter Four – Descriptive Analysis 66
4.1 Unit of Analysis 66
4.2 Variables Used to Explain Utilization 66
4.2.1 Utilization Index 67
4.2.2 Distance 69
4.2.3 Walk-Time Estimate 70
4.2.4 Population Size 72
4.2.4.1 Reconciliation of Population Data 72
4.2.5 Attractiveness of Health Care Facility 76
4.2.5.1 Number of Doctors 77
4.2.5.2 Size of Health Facility 77
4.2.5.3 Operating Hours of Facility 77
4.2.6 Income 77
4.2.7 Employment Index 78
4.2.8 Economic Status 78
4.2.9 Education 79
4.2.10 Cost of Service 79
4.2.11 Road Quality 80
4.2.12 Health Choice 81
4.3 Analysis of Distance Decay 84
4.4 Comparative Analysis: Distance versus Walking-Time 85

- 4 -
4.5 Data Analysis 87
4.6 Chapter Summary 91
Chapter Five - The Predictive Model 93
5.1 Selection of the Gravity Model 93
5.2 The Model 94
5.2.1 Calculation of the Dependent Variable 97
5.3 The Four Models 98
5.4 Chapter Summary 100
Chapter Six – Results 101
6.1 Correlation Analysis 101
6.2 Results 104
6.2.1 Stepwise Regression Methodology 104
6.2.2 System Model Results 105
6.2.2.1 Visual Inspection for System Model 106
6.2.3 Magdalena Health Center Model 107
6.2.4 Santa Lucia Health Center Model 109
6.2.5 Hombro á Hombro Clinic Model 111
6.3 Comparison of the Four Models 113
6.4 Analysis and Discussion of Explanatory Variables 115
6.4.1 Walking Time 115
6.4.2 Economic Status 116
6.4.3 Choice 118
6.4.3.1 Model Improvement 120

- 5 -
6.5 Residuals Analysis 122
6.5.1 Residuals for Hombro á Hombro Model 123
6.5.2 Residuals for Overall Study Area 124
6.5.3 Residuals for Magdalena Health Center Model 126
6.5.4 Residuals for Santa Lucia Health Center Model 128
6.6 Summary of Results 129
6.7 Chapter Summary 131
Chapter Seven - Conclusions and Recommendations 133
7.1 Lessons learned in the field 135
7.2 Limitations of Fieldwork 136
7.3 Policy Implications 138
7.3.1 Accessibility Improvements 138
7.3.2 Community Assessments 139
7.3.3 Transportation Improvements 140
7.4 Future Research 140
7.5 Concluding Comments 142
Bibliography: 143
Appendix A: Bi-variate Correlations 149
Appendix B: Regression Output Table 153
Appendix C: Residuals 159
Appendix D: Key Informant Interview 162

- 6 -
List of Tables and Figures Page Figure 1.1 Average Income Comparison 21
Figure 2.1 Initial Behavioral Model 38
Figure 2.2 Hypothetical Utilization Model 39
Table 4.1 Distance Table 70
Table 4.2 Estimated Walking-Time Calculation 71
Table 4.3 Population Aggregation Worksheet 75
Table 4.4 Average Speed Calculation Matrix 81
Figure 4.1 Choice Decision Model 84
Figure 4.2 Distance Decay of Utilization 85
Table 4.5 Correlations from Distance-Time Comparison 86
Figure 4.3 Histogram of Original Data 88
Figure 4.4 Scatter Plot of Original Data 88
Figure 4.5 Histogram for ln of Utilization 89
Figure 4.6 Scatter Plot for ln Utilization and ln Walking-Time 90
Table 4.6 Kolmogorov-Smirnov Test 91
Figure 5.1 Utilization Model 96
Table 6.1 Correlation to Utilization Summary 103
Table 6.2 Stepwise Regression Coefficients – System Model 106
Table 6.3 Stepwise Regression Coefficients – Magdalena Health Center 108
Table 6.4 Stepwise Regression Coefficients – Santa Lucia Health Center 110
Table 6.5 Stepwise Regression Coefficients – Hombro á Hombro Clinic 112
Table 6.6 Comparison of Models 114

- 7 -
List of Maps Page
Map 1.1 Honduras National Map 15
Map 1.2 Honduras and Location of Study Area 16
Map 1.3 Santa Lucia Study Area – Detail 16
Map 1.4 Study Area Population Distribution 20
Map 3.1 Base Map of Study Area 56
Map 4.1 Village-Caserio Reconciliation 74
Map 4.2 Example of Population Reconciliation 76
Map 6.1 Utilization – System Model 107
Map 6.2 Utilization - Magdalena Health Center 109
Map 6.3 Utilization - Santa Lucia Health Center 111
Map 6.4 Utilization – Hombro á Hombro 113
Map 6.5 Residuals – Hombro á Hombro 121
Map 6.6 Residuals – Overall Service Area 125
Map 6.7 Residuals – Magdalena Service Area 127
Map 6.8 Residuals – Santa Lucia Service Area 129
- 8 -
CHAPTER ONE - INTRODUCTION
The following research looks at utilization of primary health care services in a rural part of
southern Honduras. Specifically, this research examines health-seeking behavior and the
associated health care decision-making process. To accomplish this goal, key variables
explaining health-seeking behavior need to be identified, and their relationship to utilization
needs to be established. In this study several key determinants of primary health care
utilization are examined and compared to actual utilization patterns. Conclusions about
health-seeking behavior are then drawn based on these relationships.
The central aim of this research, then, is to examine the spatial patterns of health care
utilization, and to suggest a model that may be used to explain health-seeking behavior. Many
places such as rural parts of Central America are poorly understood by researchers and
medical planners, and it is for this reason that significant gains in knowledge may be achieved
as a result of this study.
Such research is inherently difficult. Many sources of secondary data do not exist for many
parts of the developing world. In this research project, it was very difficult to acquire the data
needed. It was necessary to conduct extensive fieldwork in the region to collect much of the
needed information for this research project. In the end, this research combines primary data
collected in the field with data from secondary sources into a dataset that was used to examine
utilization behavior in the study area. GPS receivers were used to locate roads, trails, villages
and other geographic features in the study area; health attendance at three area clinics were
sampled; interviews of several key informants were conducted; and available secondary

- 9 -
information was gathered from sources such as the Honduran National Census. The collection
of data from these varied sources thus, enabled an opportunity to study utilization in the Santa
Lucia region of southern Honduras.
1.1 Problem Statement
The fundamental problem is to understand the spatial variation in utilization in the study area.
This problem includes the question of why certain places differ in the amount of medical care
consumed. The specific aims of this research project are threefold:
1. This study proposes that utilization can be understood by using a modified gravity model
to examine the determinants of primary health care utilization. The gravity model has not
been commonly employed in prior utilization studies.
2. This study prioritizes the factors influencing health-seeking behavior in a rural Latin
American setting. The health-seeking decision-making process is a complex process that
deserves attention, but has not been a common focus in past research. By prioritizing these
factors, health policy decisions should be more effective in improving health care
provision in this region.
3. This research tries to better understand the complex health-seeking process by creating a
variable that considers health decisions as a two-part process. It is hypothesized that a
compound variable will more accurately reflect the health-seeking decision-making
process.
The following chapter contains a description of the importance of health service research;
followed by the description of utilization; a description of the study area; a short history of the
- 10 -
study area; a section describing the development of a rural health facility and Shoulder-to-
Shoulder, Inc./La Clinica Hombro á Hombro; and concludes with a brief summary.
1.2 Importance of Health Service Utilization Research
For most people health care is initiated when they or their relatives recognize that they are
sick, but the factors that result in a patient contact with health services is very complex (Habib
and Vaughan, 1986). Variations in response to sickness and in utilization exist from person to
person and for any one person at different times (Habib and Vaughan, 1986).
Good knowledge and understanding of how people use health facilities is vital for health
resource allocation and planning (Müller et al., 1998). Studies of health services utilization
often seek to understand the frequency and trends in health service use, and the possible
mechanisms that may determine this use (Habib and Vaughan, 1986). Utilization studies,
therefore, have a wide appeal to the policy makers, managers and providers of health care,
particularly when they are able to identify areas of improvement (Habib and Vaughan, 1986).
Health planners need to understand utilization in order to improve health services. They need
to identify the important characteristics that relate to health care use and their
interrelationships, in order to make more effective health policy decisions. Understanding
utilization enables better development decisions to be made, which should result in better,
more effective primary care for the people of the region in the long run. The ultimate
justification of health services utilization studies lies in the relationship of service use to
improving the health status of the population (Habib and Vaughan, 1986).

- 11 -
Not much work has been done on health care use in developing countries since the early part
of the 1990s (Buor, 2002). During the 1960s and 70s, studies focusing on the determinants of
medical care utilization received a good deal of attention (Andersen and Newman, 1973). The
importance of this research comes from a set of social values and perceptions including: 1) a
growing consensus that all people have a right to medical care regardless of their ability to
pay; 2) the general belief that certain disadvantaged population groups are not receiving
medical care which is comparable to that available to the rest of the population; and, 3)
expectation that medical care can contribute to the general health level of the population
(Andersen and Newman, 1973).
1.2.1 What affects utilization?
The utilization of health services can be viewed as a type of individual behavior (Andersen
and Newman, 1973). According to Moore (1969), the behavioral sciences have attempted to
explain individual behavior as a function of characteristics of the individual himself,
characteristics of the environment in which he lives, and/or some interaction of these
individual and societal forces (Andersen and Newman, 1973).
Understanding health facility utilization involves trying to understand human behavior. This
is a complex and sometimes confounding process. There have been a number of key variables
used in past research to explain health care utilization. Many of these relationships have been
empirically tested, and some results are consistent, while other relationships are not. These

- 12 -
sometimes inconsistent results lead us to a conclusion that we simply do not fully understand
some relationships.
In several studies distance was discovered to be one of the most important factors relating to
health care utilization (Buor, 2002-4; Müller et al., 1998; Stock, 1983). In particular, Buor’s
2002 paper “Distance as a predominant factor in the utilization of health services in the
Kumasi metropolis, Ghana” demonstrated the critical importance of distance as it relates to
utilization of health services in the developing world.
In addition to distance, there are other factors that affect health care utilization. These include
demographic characteristics of the patients such as income level, education level, gender, and
age; geographic characteristics such as the quality of roads; and service characteristics such as
number of doctors, number of office hours, cost of service, etc. All of these factors have been
examined and many have been determined to be significant in explaining health care
utilization, as we shall see in the literature review portion of this paper. These factors are
examined in this study in an effort to better understand their effect on health-seeking behavior
in the context of a rural, developing world study area.
1.3 The Study Area
1.3.1 Location
There are 18 States (Departamentos) in Honduras. The study area is in the state of Intibucá,
which is 316,562 hectares in size. Santa Lucia is the central town in a municipality
(Municipio) with the same name. The study area is located in the southern part of the state of

- 13 -
Intibucá, within only a few miles of the El Salvador border. See Map 1.1, 1.2 and 1.3 for
spatial perspective on Honduras and the location of the study area within the country
The topography of the study area is quite mountainous with the town of Santa Lucia resting in
a narrow valley at 1,100 feet in altitude, and the nearby peak of Cerro Verde rising to 2,600
feet in altitude. The climate in the study area is semi-arid, with a weather pattern dominated
by the Pacific Ocean, yielding a rainy season from May to December and a dry season from
January to April. During recent fieldwork in the area during the January dry season,
temperatures ranged from mid 50s at night (during an unusually cold period) to mid 90s in the
afternoon.
The service area for the Hombro á Hombro health clinic was used to define the study area. A
sample of attendances from the Hombro á Hombro clinic was used to determine the study area
for this project. This sample, taken during a pilot study in December 2003, identified the
primary home locations for patients who attend the clinic.
The Hombro á Hombro clinic, a private sector (NGO) health facility, is located in the town of
Santa Lucia, the capital of the municipality of Santa Lucia. Most of the clinic’s patients come
from this municipality, though some come from the neighboring municipalities of Magdalena,
San Antonio, and Colomoncagua, and a few come from more distant locations such as El
Salvador, or Concepcion.

- 14 -
In addition to the Hombro á Hombro health clinic, two Rural Health Centers operate in the
Santa Lucia service area, one in the town of Santa Lucia, and one in the nearby town of
Magdalena. These Rural Health Centers (Centros de Salud) are operated by the Honduran
Health Ministry.
The nearest hospital is in the city of La Esperanza, the state capital, 82 kilometers to the north
of Santa Lucia, and per Rodriguez (2003), a minimum of three hours drive by fast pickup
truck. The hospital in La Esperanza is a regional hospital with limited specialty services. For
many specialty services, patients must travel to Tegucigalpa, with no certainty of being seen
in short order for their concerns. Functionally, then, the vast majority of all health care
received is performed locally in Santa Lucia (Bazemore, 2005c).

- 15 -
Map 1.1: Honduras National Map
Source CIA, 2004.

- 16 -
Santa LuciaService Area
Olancho
Yoro
Colón
Gracias a Dios
El Paraiso
Cortés
Lempira
Atlántida
Copán
Francisco Morazán
Choluteca
Comayagua
Intibucá
La Paz
Santa Bárbara
Valle
Islas de la Bahía
Honduras
Departamentos IntibucaSant Lucia
N
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente
Map 1.2 Honduras and Location of Study Area
#
#
#
#
#
##
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
Talquezal
El Barreal
El Castano
El Jicaral
La Montana
Las Aradas
Las Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
El Mosquito
La Ceibilla
Santa Lucia
Los Horcones
Los Tablones
San Francisco
Las Marias Mag
Piedra Colorada
Santa Lucia Service Area N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
# PopulationÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region by Jonathan Baker, Chris Carr, and Andrew Bazemore.
Map 1.3. Santa Lucia Study Area Detail

- 17 -
The size of the study area is at the micro scale, with an east/west width of
approximately 14.4 kilometers, by 8 kilometers north/south. The shape of the study
area is irregular, and these distances are at the greatest points. Much of the study area
fits within a 12 kilometer radius from the town of Santa Lucia, which is at its center.
The mountainous topography makes travel difficult within the service area. Per
fieldwork done in the study area, it takes on average over two hours to traverse the
study area from east to west by truck and, of course, it would take significantly longer
by foot. These measurements of the study area use a geographic information system
(GIS) to calculate the Euclidean (straight-line) distance measurements. The study area
contains the homes of over 90 percent of the patients who attend the Hombro á
Hombro clinic.
1.3.2 History of the Study Area
As we have discussed, this location is remote. As recently as the 1960s, travel from
Santa Lucia to La Esperanza required over a week using a donkey or by foot
(Rodriguez, 2003). In the 1970s, a primitive dirt road was built through the mountains
from La Esperanza to Magdalena. During the 1980s, the road was improved partly due
to the civil war in El Salvador, in an effort to assist the Honduran military with
transportation of equipment in and out of the border region (Rodriguez, 2003, 2005).
But not until 1998, with the relief efforts brought on by Hurricane Mitch, was the dirt
roadway improved as far south as Santa Lucia (Tepe, 2005).

- 18 -
1.3.3 Roads and Travel
Today, all the roads in the service area are dirt (except in the central towns like Santa
Lucia where sections are cobbled), though some are improved so that a well equipped
vehicle can sustain 25 KPH. Most of the roads, particularly in the outlying areas, are
not improved and 5-15 KPH is a common rate of travel in a well equipped truck. Map
1.4 shows the distribution of the roads in the service area and indicates road
classifications from 1-4. Roads classified from 2-4 indicate relative travel speeds
observed during recent fieldwork in the area using a GPS with 4 being the best roads
and the highest commensurate average speeds. The road classification of 1 represents
a walking path or trail which is not accessible using a vehicle. Road classifications of
1 have the lowest observed average travel speed.
Several of the villages in the study area have no road leading to them, only a walking
path. This creates a particularly large challenge with regard to accessibility, not only
for health access issues, but also for basic commercial purposes such as getting
produce to the periodic market in the town of Magdalena.
Most people in the service area only have one mode of transportation – their feet. The
results of surveys performed at the Hombro á Hombro clinic during 2003 indicate that
70% of the people coming to the clinic arrived by foot (Kurak, 2003). In addition to
walking, Kurak's surveys indicate that 28% of the patient's surveyed arrived by car or
truck, 2% by horse, and 0% by bus.

- 19 -
1.3.4 Population
According to the 2001 Honduran national census (INE, 2004), the population of the
study area is approximately 12,000 people. Census denominations are hierarchical,
with a structure similar to the U.S. census (US Census Bureau, 2005). At the top level
is the nation, then the State or Departamento. Our study area is located in the state of
Intibuca. Within each department are Municipalities (Municipio), similar to a U.S.
county. Santa Lucia and Magdalena are the two Municipalities within our study area.
Within each Municipality are the Aldeas, which vary in size, but are roughly 1-4
square kilometers in the rural locations. There are ten Aldeas in the study area. In the
context of this study, the term Aldea is used to mean a census-based areal unit, not to
be confused with the colloquial translation of the term as “village”. The word
“village” has a very specific meaning, as is defined later in this paper. The smallest
census denomination is the Caserio, similar to a neighborhood or barrio. There are
from four to 21 Caserios per Aldea, totaling 94 Caserios in the study area.
The three largest towns in the study area, Santa Lucia, Magdalena, and San Juan, have
population sizes of 917, 1054, and 990 respectively. Second tier towns are Las Lomas,
San Francisco, and San Jose, with population sizes of 754, 636, and 701 respectively.
Population distribution is depicted in Map 1.4.
Place names are frequently reused in Honduras, making demographic analysis
confusing. For example, the town of Santa Lucia is a Municipality, an Aldea, and a
Caserio. [It is important to know what level of the census hierarchy is being

- 20 -
considered for a given analysis.] The scale of this study is the Village, which is a
synthetic geographic unit made up of one or more Caserios.
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
##
#
##
#
#
#
#
#
#
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
Talquezal
El Barreal
El Castano
El Jicaral
La Montana
Las AradasLas Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
La Ceibilla
Santa Lucia
Los HorconesLos Tablones
San Francisco
Las Marias MagPiedra Colorada
Population Distribution N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
Population# 0 - 99# 100 - 217
# 218 - 431
# 432 - 754
# 755 - 1054
ÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region.
Map 1.4: Study Area Population Distribution
1.3.5 Employment
The primary occupation in the study area is agriculture, with many of the farmers
living a traditional subsistence life-style (Coello, 2003). Due to poor agricultural
conditions in the region, to supplement incomes many families have members working
as wage laborer in the major Honduran cities, or in the U.S. on a migratory basis. The
overall effect has been that few rural households exist independent of wage labor
(Stonich, 1991).

- 21 -
1.3.6 Income
Basic income for most of the employed workers in the region is approximately $6 a
day, or approximately $1,500 a year (Coello, 2003). Many people are not employed
full-time, and therefore have lower incomes. The average income per capita (GDP per
capita-purchasing power parity) was $2,600 for the nation as of 2004 (CIA, 2004), but
in our study area it is far less. The average income per capita compares with the other
Central American countries of Guatemala ($4,100), El Salvador ($4,800), and
Nicaragua ($2,300). When contrasted on a global scale, Honduras income is above the
Republic of the Congo ($700), but is far below the U.S. at $37,800 (CIA, 2004).
Figure 1.1 highlights the contrast in per capita GDP between these countries.
-5,000
10,00015,00020,00025,00030,00035,00040,000
$US
Hon
dura
s
Nic
arag
ua
Gua
tem
ala
ElSa
lvad
orC
ongo
U.S
.
Average Income (GDP/capita)
Figure 1.1 Average Income Comparisons

- 22 -
1.3.7 Education
Basic education in the study area consists of local primary schools (grades 1-6), many
in rural village locations. Junior high schools (grades 7-9) are only available in the
relatively large central towns of Santa Lucia and Magdalena. Any students continuing
their education have two options for senior high school: A liberal arts program, which
prepares students for an advanced education at the university, or a trade/technical
school for business, accounting, computers, car mechanics, etc. Many students,
particularly in the rural villages, do not continue with their education beyond the 6th
grade (Diaz, 2005).
1.4 Health Service in Honduras
1.4.1 History on health services
The Honduran health system is made up of public and private sub sectors with the public
sector consisting of the Ministry of Public Health and the Honduran Social Security Institute
(IHSS), the National Water Supply and Sewerage Service and the National Institute for the
Prevention of Alcoholism, Drug Addiction and Drug Dependence (Black et al., 2004). During
a recent study, Black et al. (2004) estimated that the coverage for the Ministry of Public
Health was 60%; Social Security covered 10-12%; and the private sector covered 10% of the
population. The Ministry of Public Health is organized into 9 health regions, and is the main
provider of health services in the public sector with 1272 health centers distributed across the
country (Black et al., 2004). Included in this number are 28 hospitals, although modern
technology and complex health care interventions are concentrated in the six national
hospitals, five of which are located in the capital (Black et al., 2004). Of the 1272 health

- 23 -
centers throughout the country, 341 are Health Centers with an attending Physician and
Dentist, and 865 are Rural Health Centers (Black et al., 2004).
The Municipio of the Santa Lucia has a limited history of continuous primary health care
delivery. The first team of medical doctors from the University of Cincinnati came to the
Santa Lucia area in 1990, prior to which there had been no consistent physician presence in
this remote region (Bazemore, 2005c). The Shoulder-to-Shoulder/Hombro á Hombro clinic
was completed in 1993. Health service in the form of nursing staff was available in the towns
of Magdalena and Santa Lucia prior to 1990. The Health Centers in Magdalena and Santa
Lucia were built around 1997 (Heck, 2005), but physician support has been intermittent for
both of these rural health centers (Coello, 2003). Therefore, it has only been quite recently
that physician care has been available to the population of the region. Prior to this, and
continuing to some extent today, there were “traditional” health providers that included
Curanderos (healers), Sabadores (massagers), Parteras (midwives), and herbalists. In most
cases, these traditional healers lack formal medical training from a University.
1.4.2 Background on La Clinica Hombro á Hombro:
Hombro á Hombro is a non-profit NGO legally registered in Honduras since 1998, but has
been operating under the sister U.S. organization Shoulder to Shoulder since 1990. It
represents a successful partnership between the University of Cincinnati, College of
Medicine, the Honduran Ministry of Health, and the Community Health Board in Santa Lucia,
Intibuca. Its mission includes providing ongoing primary health care and public health
services to residents of Santa Lucia, Honduras, and to enhance the teaching mission of the

- 24 -
College of Medicine in International Health. Over the years, the project has expanded and
now includes provision of health care, dental and nutrition services. The clinic is fully staffed,
including two full-time physicians, one full-time dentist, and two nurses. It has examination
rooms, laboratory, pharmacy, X-ray equipment and an operating room (Shoulder-to-Shoulder,
2005).
1.4.3 Development of a Rural Health Facility
When developing a rural primary health service such as the Hombro á Hombro clinic, health
planners started with an assumption of need based on the population in a specified area with
lack of primary care resources to meet this need. In the case of the Hombro á Hombro clinic,
the location was established in a central town in the region, and was partly determined by
interest and commitment from the local community. Other towns were considered, but Santa
Lucia, was selected primarily due to this combination of socio-political and need-based
considerations (Bazemore, 2005a).
In the original plan the Hombro á Hombro clinic would service an area with a roughly 12
kilometers radius around the health clinic (Heck, 2005a). Though the original plan was to
serve as primary care provider for this whole service area, due to several factors including low
levels of access, it is questionable whether significant portions of the service area are actually
able to utilize the health clinic (Bazemore, 2005b).

- 25 -
1.5 Chapter Summary
This chapter introduced the study of primary health care in Santa Lucia, Intibuca, Honduras.
This study focuses on utilization of primary care services in a poor, rural part of southern
Honduras. In order to better understand utilization patterns, this research creates a model
which can be used to predict utilization behavior in the service area. This is important for
several reasons – first, because the area is remote and poorly understood; second, because
understanding health-seeking behavior can help primary health care planners improve
services; and, third, because there are many other similar places around the world which can
benefit from the lessons learned in this research project.
This study is unique in several ways. First, it explores utilization in a new location not
previously studied. Utilization behavior has been studied in other rural developing world
locations such as Buor’s (2004) study in rural Ghana, but it has not been studied in rural parts
of Central America. Utilization behavior may vary from place to place for reasons such as
local culture, topography or political structure (to name a few). At the beginning of a research
project such as this, it is safe to say that we are not sure about how universal are the factors
that relate to utilization, and how well models will correspond to those developed in other
parts of the world.
This study differs from previous studies, which have focused on using linear models to
describe utilization behavior. This study uses a non-linear gravity model to explain utilization
behavior. It is believed that this model, which is significantly different than a linear model,
should perform better than the linear models used in past research. This is because

- 26 -
relationships such as distance to utilization may be described as non-linear (Müller, et al.,
2000), and non-linear models (such as the gravity model) are better able to predict these types
of relationships.
The next chapter will focus on a review of the research literature pertaining to health care
accessibility and utilization applied to the developing world.

- 27 -
CHAPTER TWO - LITERATURE REVIEW
This chapter reviews the previous research conducted in the field of health service geography
in the area of accessibility and utilization. Linkages are made and gaps are noted between this
project and the literature so as to identify opportunities and justification for the current
research project. The first section of this chapter summarizes the theoretical research done in
this field and explains the processes and concepts involved. The second part of this chapter
summarizes the methodological approaches used in prior studies. The final section of this
chapter reviews the empirical studies that include and examination of the data, methods, and
findings of prior research.
2.1 Theoretical Foundations of Prior Research
2.1.1 Access & Utilization to Health Care Services
Access to health care is an important part of an overall health system and has a direct impact
on the burden of disease that affects many countries in the developing world. Unfortunately,
health care, like many public services, is not equally available to all people (Joseph and
Phillips, 1984), and limited physical access to primary health care continues to be a major
impediment to achieving the goal of health care for all (Perry and Gesler, 2000).
Access to health care is concerned with the ability of a population to obtain health care
services (Black et al., 2004). It is concerned with the ability and willingness of the population
of a given area to bridge the physical gap between their home and the location of a health
facility. Access to health services is influenced by many behavioral as well as cost and
distance factors (Buor, 2002; Müller et al, 1998). Utilization of health services is increasingly

- 28 -
being viewed as a function of accessibility (Phillips, 1979; Noor et al., 2003). The distance
patients must travel in order to obtain health care service has long been recognized as a
primary determinant of the utilization of health care facilities (Stock, 1983). Health care
facilities are often geographically inaccessible to many who live in a rural area (Stock, 1983).
The distance element is particularly significant in rural parts of the developing world where
western-type health facilities are not common, and where patients are likely to make the
journey for treatment as pedestrians (Stock, 1983).
Probably the most important link or interaction in any health care delivery system is that
between consumer and provider (Meade and Earickson, 2000). An optimal distribution of
health care resources is possible only if this relationship is understood (Meade and Earickson,
2000). To improve access to health care, it is important to monitor how access varies across
both geography and subpopulations (Knickman, 1998). Assessing access across communities,
however, can be difficult (Halfon et al., 1999). Geographic information systems (GIS) can
help by combining and analyzing complex information from multiple sources and then
displaying it as maps (Phillips et al., 2000). Maps are very useful tools for investigative
research because they are visually compelling and in many cases easy to interpret. The old
adage that “a picture is worth a thousand words” relates very nicely to maps. The brain is
better able to assimilate a large amount of geographic information when it is presented in the
form of a map. Maps look at geographic data in such a way as to give features of the planet a
spatial perspective. Maps have been used for many years as a tool for examining health
concerns (Porter et al. 2004).

- 29 -
2.1.2 Utilization
Love and Lindquist (1995) define utilization as the relationship between service providers and
surrounding populations. The spatial patterns of utilization are a combination of the location
of the service used and the frequency with which each patient uses the service (Hays et al.,
1990). Accessibility often plays an important role in determining who is able or willing to use
a health service. These concepts of “accessibility” and “utilization” are inter-related. There
are two basic approaches to measuring accessibility to primary health care services: the first
involves the measurement of potential physical accessibility based upon the location of
populations relative to that of health care facilities; the second, the measuring of actual or
revealed accessibility through the analysis of utilization data (Joseph and Bantock, 1982). In
the context of this study the focus will be on the second definition based on revealed or
actualized access to primary care. The main difference between these two approaches is that
one looks at the characteristics of a place for those persons who could use a facility, and the
other one looks at the characteristics for those who already use the facility. A common point
here is that one needs to have access to a public facility in order to use (or utilize) it. A
distinction between the two approaches is that the first focuses on facility location, whereas
the second focuses on the patient, looking at health-seeking behavior.
In the context of this study utilization (the dependent variable in this study) is viewed as a
combination of clinic attendance and population for a given geographic unit. Specifically, a
utilization index is created to test the spatial variation of primary health care use. This index is
calculated by taking the attendance numbers (of a health facility) for a given geographic unit
and dividing by the population for that geographic unit. Since the spatial unit of measure is

- 30 -
the village, both the attendance numbers and the population numbers are aggregated to this
spatial unit, i.e. the village. The resulting index is an attendance number that is normalized by
population. This normalization process is performed so as to neutralize the effect of
population size on the spatial patterns of attendance.
2.1.3 Utilization and Distance
Distance from patient to health care providers, which can be called proximity, is often cited as
one of the most important factors relating to accessibility and utilization of health care
resources (Powell, 1995). Closeness to a particular doctor or facility is one of the main
reasons for using a given resource (Meade and Earickson, 2000). In developing countries
studies have shown the important role of distance in reducing the use of health facilities,
especially in rural areas (Buor, 2003). Noor et al. (2003) suggest that distance is a crucial
feature of health service use, but its application and utility to health care planning have not
been well explored. Several researchers have focused on this issue of distance as being an
important factor determining health care facility utilization (Müller, et al., 1998; Buor, 2002-
3; Noor, et al., 2003; Habib and Vaughan, 1986; Stock, 1983; Egunjobi, 1983; Joseph &
Phillips, 1984). Their results have made clear that distance is a very important factor affecting
utilization in rural areas of the developing world. Despite the importance of distance, it has
often been overlooked in a planning and decision-making context (Meade and Earickson,
2000).
The link between provider and consumer weakens with distance (Meade and Earickson,
2000). In general, the further away a health facility is from a person’s residence, the less

- 31 -
likely he/she will use it. This is a distance decay concept, where the rate of interaction varies
inversely with distance. Distance decay is derived from the gravity model, which states that
the attractional force between two objects is directly proportional to their masses and
inversely proportional to the square of the distance between them (Meade and Earickson,
2000). According to Stock (1983), distance decay models have been employed frequently in
studies of health care behavior.
Distance decay is useful in determining central place hierarchies and functional
regionalization (Meade and Earickson, 2000). In places with rapid distance decay patterns,
health services should be decentralized and locally accessible. This usually applies to low-
order services such as first aid. High-order services such as heart transplants are not as
sensitive to distance. People are willing to travel further for these [high-level] services
(Meade and Earickson, 2000). This relationship is related to the body of theory known as
Central Place Theory (see Christaller, 1966), and can help health planners develop health
delivery systems that are effective, while considering constraints such as the cost of services
provided.
In health provision research, several utilization studies have been conducted in the developing
world, focusing on the spatial distributions of patients seeking medical treatment at particular
health facilities. These studies suggest that health care facilities in developing countries are
likely to effectively serve only a small area surrounding the facility (Stock, 1983). In Nigeria,
Stock found that at a distance of 5-km from the medical facility, the per capita utilization rate
fell to one third of that of the 0-km rate. In a study in Iraq, Habib and Vaughan (1986) found

- 32 -
that after 5-km utilization rates declined to 60% of the 0-km rate. In a study in India,
Frederiksen (1964) found that the utilization rate declined by 50% for each half-mile between
the community and the facility (Buor, 2002). In a recent study in Kenya, Noor et al. (2003)
found that 60% of health facility users attended health facilities within 5-km of their home.
Buor (2002) found that most people patronize health services in metropolitan Ghana at a
distance of less than 3-km, and therefore recommends a 3-km model to study utilization.
2.1.4 Factors Influencing Utilization
The discussion from the previous section on distance and distance decay of utilization has
demonstrated its importance in health service research, but the distance issue cannot be
identified as the sole determinant. The delivery of health care is dependent on many factors,
including the capacities of the providers, the needs and capacities (socio-economic-
demographic factors) of the patients, and the characteristics of the region within which the
patients live (e.g., topography, transportation facilities and routes, settlement patterns,
government). The following discussion looks at the different variables used to explain
utilization behavior is past research.
Love and Lindquist (1995) focus on utilization, which they define as the relationship between
service providers (hospitals) and surrounding populations. This study examines actual
utilization patterns and forms conclusions about accessibility based on these patterns. Love
and Lindquist recognize that there are many factors, in addition to physical distance, that
influence the use of medical facilities. According to their study, insurance status, income,
education, occupation, age, gender, and individual preferences and perceptions all may be

- 33 -
involved in determining usage. Buor (2003) adds the factor for marital status to the studied
variables. Joseph and Phillips (1984) add social class and ethnicity as important factors
influencing utilization, but suggest they may be difficult to study given their relationship to
other studied variables such as income, occupation and education.
Income: Looking at income as an explanatory variable, Joseph and Phillips (1984) cited an
important New York study (Koos, 1954) as evidence that lower-income residents underutilize
health care services. Koos’ study suggests that lower income residents are often deterred from
seeking medical care because of cost and fear. At the same time, several studies have
suggested that lower-income residents tend to have a greater need for health care (Joseph and
Phillips, 1984). Wolfe’s (1999) research suggests a negative correlation between income and
health status. In her research, Wolfe found that from 1990 to 1995, the proportion of children
in the U.S. in very good or excellent health decreased. At the same time, this author found that
the proportion of non-poor children in very good or excellent health, increased. Wolfe's
research suggests a clear association between income and health, and that poor children are
now in worse general health than non-poor children (Wolfe, 1999). This issue of “more needy
lower income” residents underutilizing health service turned into a contentious debate in the
UK, with contradictory conclusions being made depending on the study cited (Joseph and
Phillips, 1984). The pattern of distance/utilization for low-income residents has not been
determined, and consequently offers the opportunity for further study.
Education: When looking at education as an explanatory variable, the results from Love and
Lindquist (1995), and Buor (2002), indicate there is a positive relationship between education

- 34 -
and utilization of health care facilities. It has been shown that people with higher levels of
education utilize health facilities more often than individuals with lower levels of education.
Age/Gender: Both age and gender of patients are important variables to study relating to
utilization of health care. It may be expected that as people age, and especially after
retirement, people will need health care services more for chronic and perhaps acute
conditions (Joseph and Phillips, 1984). Also, among younger age groups, utilization by
females can be increased for reasons associated with childbearing and conception. Several
studies have found that women have higher morbidity than men (Anderson and Andersen,
1972; Kohn and White 1976; Cleary et al. 1982). In spite of this higher level of morbidity,
women outlive men on average (Joseph and Phillips, 1984).
Race/Ethnicity: Joseph and Phillips (1984) suggest ethnicity may be important in
determining cultural preferences toward health care. They also suggest “diagnosis” or
“treatment” as another important variable to study. Availability of alternative sources of
medical treatment is included in this cultural preference issue. In many parts of Latin
America, people use traditional health providers known as Curanderos. They belong both
culturally and socially to the community and the local population supports their work (Perry
& Gesler, 2000).
Social Capital: Social capital may also influence utilization. This is a set of social
relationships that shape a group’s social interactions. Social capital is often connected with
places. The relative level of comfort or feeling of safety that is generated by a place or area is

- 35 -
often due to social connections, or social capital (World Bank, 2003). A person feels more
comfortable in a place he knows, or has been recommended to him/her. Family and cultural
patterns influence social capital and, hence, utilization of primary health care. Utilization of a
particular health care facility is often something that is passed on by word of mouth. In a
study of spatial attendance of health services in New Zealand, Hays et al. (1990) observed a
pattern of utilization with less spatial bounds when a family member recommended a health
service. This study concluded that people are willing to travel further to get health care if the
service has been recommended by a family member or relative.
Quality of Health Service: Received quality of health care service is an important issue in
determining health care utilization (Buor, 2002; Stock, 1983). The quality of the health
facility, the medical equipment available at the health facility, the treatment by the staff and
general relationship that the physicians have with their patients, all play an important role in
determining utilization of a health facility.
Complex Variables: As has been discussed, several variables have been used in past research
to examine utilization behavior, but human behavior is complex and not easily explained.
What determines the actual behavior may often lay in a combination of both consumer and
provider characteristics (Buor, 2003). Joseph and Poyner (1982) support this reasoning
arguing that both consumer and facility attributes interact to produce different reactions from
different persons (Buor, 2003).
- 36 -
In Fotheringham’s (1983) paper, the author suggests many types of interactions may be
considered a result of a complex two-stage decision-making process. This is a way for a
model to simultaneously consider a combination of two or more variables, and this, in turn,
may more accurately reflect the human decision-making process. This is an intuitively
appealing concept, because human decisions such as primary care utilization may be the result
of two or more sub-decisions. Consequently, this study tests this idea by using a two-stage
variable to describe health choice decisions. In past research on health service utilization, the
effect of this type of variable on a utilization model has not been examined.
2.1.5 Unit of Analysis
The study of utilization can use several different units of measure. Buor’s (2002-4) studies use
individual level survey data to examine individual patient-provider interactions. As an
alternative approach, data can be aggregated at some predefined level. Müller et al. (1998),
for example, aggregated attendance data at the household level, and further grouped data
according to age and sex of patients.
When studying utilization, some variables are best applied to individuals, while others can be
aggregated or grouped according to the needs of the study. A variable such as sex, when
aggregated at some spatial level, may not offer insight into utilization behavior because once
aggregated the numbers become close to 50/50 for men versus women for most places.
Furthermore, meaningful generalizations based on aggregated data can run into an “ecological
fallacy” problem, where making generalizations about individuals should not be made based

- 37 -
on aggregated data. Nonetheless, sometimes it is necessary in studies such as this to aggregate
data and focus on the variables and conclusions that are appropriate for the unit of analysis.
In this study a synthetic unit of measure called the “Village” is used. This is necessary
because addresses, such as those used in the U.S., do not exist in the service area. In this study
clinic attendance records are listed according to the “Village” of residence, because no
detailed house location data are available. Furthermore, the Honduran National Census does
not release individual level data, only aggregated data, at a predefined spatial scale to preserve
individual anonymity. This makes comparisons with individual level socio-demographic data
available from the census impossible, and further restricts the type of model that can be used
in the study (such as the logit model which needs individual level data). As a result this study
uses aggregated data, and works to conduct the analysis according to the constraints offered
through the use of this type of data.
2.1.6 Theoretical Framework – Utilization Models
Frameworks for the study of utilization have been developed in prior research. The initial
utilization model, the model created during the 1960s (Andersen, 1968), is shown in the figure
2.1. Andersen (1995) describes the initial utilization model as a behavioral model. This model
suggests that people’s use of health services is a function of their predisposition to use
services, factors which enable or impede use, and their need for health care (Andersen, 1995).
Some individuals have a propensity to use services more than others. This propensity toward
use can be predicted by individual characteristics which exist prior to getting sick (Andersen

- 38 -
and Newman, 1973). People with these preexisting characteristics are more likely to use
health services, because they have a greater need. These characteristics can include
demographic, social and attitudinal-belief variables (Andersen and Newman, 1973).
Figure 2.1 Initial Behavioral Model: (taken from Andersen, 1995)
Even though an individual may be predisposed to use a health service, some means must be
available for him/her to do so (Andersen and Newman, 1973). Enabling conditions make
health service resources available to the individual. These can include income, health
insurance, availability of source of care, and accessibility of the source (Andersen and
Newman, 1973). Without these enabling resources, health care utilization may not occur.
If we assume the preexistence of both predisposing and enabling factors, the individual must
still perceive the need for health service. A perception of illness is necessary for use of a
health service (Andersen and Newman, 1973). An evaluated illness is also a source of
demand for health services. The illness level represents an immediate cause of health service
use (Andersen and Newman, 1973).

- 39 -
The initial behavioral model of utilization has undergone several changes through the years.
Aday’s Utilization model (Aday and Andersen, 1974) includes a health care system
component to the model in recognition of the importance of national health policy and the
resources in the health care system (Andersen, 1995). Dutton (1986) introduced structural
barriers to the model. Andersen (1995) introduces the factor of health outcomes into the
utilization model. Trying to incorporate both behavioral and spatial factors from the previous
models, Buor (2002) creates a model that combines distance and use of health services. This
author indicates that utilization is based on provider characteristics, user characteristics, and
restrictive factors (such as distance coverage, location of facilities, and service cost) which are
a result of government policy. See figure 2.2.
Figure 2.2 Hypothetical Utilization Model (taken from Buor, 2002)
The preceding models consider many of the variables that affect utilization behavior, but do
not consider the complex nature of the human decision-making process. As Fotheringham

- 40 -
(1983) suggests, many decisions may be the result of a two-stage decision-making process.
Incorporating a two-stage decision variable into the model may be a way to improve its
explanatory as well as its predictive capacity.
2.2 Methods of Studying Utilization
2.2.1 Regression Modeling
When looking at the demand for health service, Schultz (1975) focuses on analyzing the
characteristics of the people who are serviced by a given medical facility. Schultz (1975) uses
a multi-variate regression analysis to determine the relationships between medical service
supply and several demographic demand factors. Multi-variate regression analysis, also
known as multiple regression analysis, is a statistical method for studying the relationship
between a single dependent variable and one or more independent variables (Allison, 1999). It
is unquestionably one of the most widely used statistical techniques in the social sciences
(Allison, 1999). Schultz (1975) uses this measure of correlation to help explain the factors
that relate to demand for a given health service. Bour (2002, 2003) uses a multiple regression
analysis to examine the factors that effect health facility utilization.
2.2.2 Gravity Modeling
Gravity models have been used for years to account for a wide range of interactions between
people and places. The gravity model is derived from Newton’s Law of Gravitation, and has
been used as a way of combining accessibility and availability (Guigliardo, 2004). Gravity
models have been used to represent the potential interaction between any population point and
all service points within a specific distance (Guigliardo, 2004). In past research gravity

- 41 -
models have been used in several geographic studies on access to health care (Joseph and
Bantock, 1982; Scarpaci, 1984), but no known study has used this gravity modeling approach
in a study of primary care utilization.
Müller et al’s (1998) study suggests that the distance decay pattern of patient attendances is
non-linear. This suggests that the use of a non-linear model, such as the gravity model, would
constitute a better approximation of the true relationship of these variables to utilization.
Considering that this type of model has not been used in previous utilization studies and has
been suggested to be a better fit than non-linear models, an opportunity exists to both improve
utilization modeling and at the same time add to the understanding of health care utilization.
This is a gap in the knowledge base that needs to be filled. The use of the gravity model in
utilization studies may substantially improve the predictive capacity of a utilization model and
is therefore worthy of testing in a study such as this. Furthermore, use and testing of the
gravity model represents a significant contribution to knowledge relating to utilization of
health services.
2.2.3 Comparative Descriptive Analyses
In their study on health care utilization Phillips, et al. (2000) uses both the Griffith
Commitment Index and Location Quotient Index to describe the characteristics of places
relative to usage. The Griffith Commitment Index is an analytical measure used to show the
spatial patterns of patient utilization for a given health facility. This index is calculated by
taking the total number of visits for a geographic unit, and dividing this number by the total
number of visits for the study area as a whole. This index measures the extent to which

- 42 -
patients from defined geographic areas utilize a health care facility. The results can be ranked
and mapped in a GIS, and the authors suggest including only the top 60% of clinic visits, and
designating them as primary users (Phillips, et al., 2000).
Another comparative index employed by Phillips et al. (2000) is the Location Quotient Index.
Location quotients are calculated by dividing the utilization rate for a given geographic unit
by the utilization rate for the service area as a whole, thus allowing for a focus on specific
subpopulations. A Location Quotient Index can be used to determine the proportion of the
target population that uses a health clinic for a given geographic unit. The results are
calculated and mapped in a GIS (Phillips, et al., 2000). This index can be used to evaluate
service areas and to identify underserved and over-served populations.
2.2.4 Marketing Geography and Utilization
There are strong links between marketing geography and medical facility utilization. While
markets are most often associated with the buying and selling of goods and services in a
commercial sense, markets can also be applied to activity spaces that describe general
behavior (Ricketts, 2002), and the methods used in analyzing market areas can be very helpful
in improving medical service provision in the developing world. Market area analysis has
been used in health facility utilization studies (Martin and Williams, 1992). Being able to
identify the primary and secondary trade areas reveals the spatial extent of the service area,
and shows patterns of utilization. The proximal service area method, sometimes called
“Customer Spotting” (Jones and Simmons, 1990) is a way of putting your patients on a map.
This type of Pin map is helpful in delimiting the catchment area, identifying underserved

- 43 -
areas, and identifying potential future facility locations. Thiessen polygons, spider diagrams,
and concentric circles (buffers) are other popular ways to delimit proximal service areas.
In contrast to the deterministic, destination-based, proximal service area method just
mentioned, Huff (1963) developed a probabilistic, origin-based model of trade area
delimitation. This approach is derived from the gravity model and looks at shopping behavior
of the customer, and assigns a probability of attending a given retail store based on
mathematical computation of the attraction of a store and the distance to it. This method
focuses on the perspective of each customer’s home (origin) location, and creates a
continuous probability surface. This is in contrast to the store-based perspective of the
proximal service area method mentioned in the previous paragraph.
2.2.5 Geographic Information Systems
Geographic Information Systems (GIS) are computerized systems for the storage, retrieval,
manipulation, analysis, and display of geographically referenced data. Since they can include
physical, biological, cultural, demographic, or economic information, they are valuable tools
in the natural, social, medical, and engineering sciences, as well as in business and planning
(Mark et al., 2004). GIS is a young discipline. Although cartography and mapping go back
hundreds of years, GIS began in the 1960s, and is, thus, a relatively new form of computer
science (Mark et al., 2004).
Love and Lindquist (1995) recommend the use of GIS as an aid in the analysis of medical
access issues. These authors use a GIS and its related tools as a means of efficiently capturing,
organizing, storing, and retrieving spatial data. What distinguished a GIS from other types of

- 44 -
information systems is that objects within the database are stored according to location. Thus,
hospitals and surrounding census districts [for example] can be assigned to specific locations
in the database. The GIS generates topological relationships where objects are locationally
related to one another in space, thereby enabling the researcher to conduct spatial
comparisons and other types of analytical procedures. These spatial operations and related
GIS capabilities, such as buffering and object overlay, make them ideally suited for measuring
accessibility to medical services (Love and Lindquist, 1995).
GIS has grown in popularity in public health through the past decade. Today, there are now
recurring conferences on GIS and health sponsored by organizations such as ESRI, the
American Public Health Association (APHA), the Agency for Toxic Substances and Disease
Registry (ATSDR), and others.
Geographic information systems have been helpful for understanding a variety of health care
issues such as defining hospital service areas, examining the affect of distance on access, and
disease patterns (Phillips et al., 2000). The use of GIS for the measurement of accessibility
has been popular in health care planning for several years (Parker & Campbell, 1998; Phillips
et al. 2000). A number of accessibility studies have been conducted in the developing world
utilizing GIS (Black et al. 2004; Perry & Gesler, 2000; Ayeni et al., 1987; Oppong &
Hodgson, 1994) and signify the contribution that GIS has made in health care planning and
provision research. Despite some early innovations in using GIS to understand health care
access within communities, it has remained largely underutilized (Phillips et al., 2000).

- 45 -
The World Health Organization (WHO), through both its Evidence and Information for Policy
Cluster (EIP) and the Health Analysis and Information Systems (AIS) group has been
involved in a number of initiatives to measure and analyze physical accessibility to health
care using GIS. In research related to this initiative GIS has been used in conjunction with
sophisticated software products such as AccessMod and SEGEpi to examine accessibility
across large areas, and develop location-allocation models to be used in health care planning
(Black et al., 2004). In contrast to the extensive use of GIS in accessibility studies, the use of
GIS in developing world utilization studies has been limited. This study offers an opportunity
to expand the application of GIS into the area of primary health care utilization research, and
at the same time contribute to the body of knowledge.
2.2.6 Global Positioning Systems
The Global Positioning System (GPS) refers to the series of satellites developed and launched
by the U.S. Government for navigational purposes. Used in conjunction with a GPS receiver,
these satellites can determine your exact position anywhere on the earth. GPS provides
accurate information about latitude, longitude, altitude, speed, and direction of travel
(DeLorme, 2001). The GPS can be used in field research as an easy and effective way of
collecting primary data for health care research (Bernheisel et al., 2003; Brane et al., 2004).
Furthermore, the GPS data can be easily interfaced with GIS to provide maps and other
geographic analyses.
GPS has become a common tool in health related field research. In a recent study the GPS
proved to be an effective in determining the locations of mosquitoes carrying the West Nile

- 46 -
virus (Gibbs and Emmanuel, 2005). In the developing world, GPS was used to identify the
spatial framework for an Indian village. This enabled an analysis of socio-economic,
demographic, and spatial factors related to a dengue fever outbreak in 2001 (Pratt, 2003).
GPSs have been used in other health geography studies including Tanser and Wilkinson’s
(1999) strategy for monitoring and control of tuberculosis in rural South Africa (Porter, 1999),
and in an analysis of access to primary care in Andean Bolivia (Perry and Gesler, 2000).
2.3 Empirical Studies
The impact of spatial factors on health care behavior and their implications for health care
delivery have been major themes in health service geography research (Shannon, et al., 1969;
Shannon and Defer, 1974; and Pyle, 1979). A number of studies have demonstrated the value
of geographical methodologies for health care planning purposes (Stock, 1983). In these
studies a number of different methods have been used to study accessibility and utilization.
These include a descriptive analysis of utilization (Phillips, et al, 2000); an analysis of
distance decay of utilization (Müller, et al., 1998); a population weighted average distance
analysis (ReVelle and Swain, 1970; Oppong and Hodgson, 1994), a maximal covering
analysis (Oppong and Hodgson, 1994); a regression, correlation analysis (Shultz 1975;
Gesler, 1999; Buor, 2002, 2003), negative exponential model (Stock, 1983), gravity model
(Joseph and Bantock, 1982; Scarpaci, 1984; Guagliardo, 2004), a service area analysis
(Martin and Williams, 1992); and an analysis of rural service centers using Central Place
Theory (Mallick and Routray, 2001). Geographic Information Systems (GIS) have been used
to implement several of these models and apply them to real-world case studies (Black et al.,
2004; Noor et al. 2003; Phillips et al., 2000; Perry and Gesler, 2000; Ayeni, et al., 1987;

- 47 -
Oppong and Hodgson, 1994). In these studies spatial patterns of utilization have been
mapped, modeled, and the relationship of utilization to a host of variables has been tested.
The use of health services has been widely investigated in countries and cities in the
developed world (Bailey and Phillips, 1990). Many of the significant determinants of health
care utilization have been determined and tested in developed-world locations. In the cities
and countries of the Third World, the same cannot be said with any degree of confidence
(Bailey and Phillips, 1990). Many of the factors and relationships are simply unknown. As
Hellen (1986) points out, there is no exclusively Third-World health systems research to
parallel the clear demarcation that has been drawn around ‘tropical’ medicine. For this reason,
he suggests, many of the research methods developed and refined in the Western countries
may be applied in developing countries (Bailey and Phillips, 1990).
2.4 Social Equity in Access to Primary Care
Social equity can be most simply described as “a just distribution, justly arrived at” (Harvey,
1977). Social equity can be applied to the distribution of and access to health care resources.
The idea is to have health facilities located in such a way as to be fair to the majority of the
people in a given area. Therefore, when planning a health service area, health care authorities
need to consider social equity. One can use the population weighted average distance (Church
and ReVelle, 1974) as a measure of fairness, where lower average distance locations can be
viewed, not only as more efficient, but also more equitable.

- 48 -
Noor et al. (2003) focus on the issue of equity in physical access to clinic services and use
GIS to define the population’s overall access to health care. They use regression to determine
equity of service. In this study the authors test the relationship between actual utilization and a
theoretical target level of physical accessibility (defined as percentage of population living 5-
km from nearest health facility), and conclude this is a good measure of equity (how well
actual utilization fits the theoretical target). Their results reveal a coefficient of determination
(r2) in the four tested districts between .71 and .99. The authors suggest that though there were
marked disparities in theoretical access between districts, particularly between rural and urban
areas, the predefined measures of theoretical access corresponds closely with actual usage
data. It is through the use of these and related tools that the authors believe health delivery
planning and monitoring can be conducted more equitably.
2.4.1 Access & Equity
Access has many components; geography is only one. Exploring equity and inequity in terms
of access to primary care is an important aspect that needs further study. Phillips (2000)
suggests there are two types of service areas; the “idealized” and the “actualized” service
areas. The “idealized” is what is originally planned for during the development of a health
service area; versus the “actualized” is what has actually taken place after some period of
time. These are not the same. This difference is one reason why we study issues like access to
care Bazemore (2005b).
The use of tools such as Geographic Information Systems (GIS) allows for the building of
models to test this equity issue. GIS enables us to examine how the original idealized plan is

- 49 -
working. This tool allows us to understand the delivery of varying levels of care based on
access, by allowing us to understand the distribution of access across the study area and the
identification of pockets of under-served populations (Bazemore, 2005b).
An analysis of utilization data can be used to assess the “actualized” service area, and then
compare it with the “idealized” service area. In this type of analysis health facility attendance
records are examined, and a comparison is made between “actualized” and “idealized” service
areas. For examples see Noor, et al., 2003, Phillips et al., 2000, and Bazemore et al. 2003.
2.5 Chapter Summary
In summary, this chapter reviews the prior research on the topic of access to and utilization of
health care services. Access is described as the ability of a person to overcome the physical
space that exists between his or her home location and the location of the health care provider.
It focuses on the potential for people to access a given health service. This is contrasted with
utilization, which focuses on the actual past interactions between patient and provider. These
represent people who already have used a given health service, where the focus is on the
characteristics of those interactions.
Several variables have been used in past research to explain health utilization behavior.
Variables such as distance have been well researched and the relationship to utilization is
consistently negative throughout the literature. In contrast, other variables such as income and
education provide inconsistent results. There are many other variables that could explain
health seeking behavior, but have yet to be examined adequately in health care utilization

- 50 -
studies, particularly in developing world locations. Variables such as size of facility, number
of doctors, number of operating hours, employment, type of facility, transport cost and mode
of transport all offer potential for explaining health seeking behavior and offer an opportunity
for further research. Researching these variables should offer an opportunity to better
understand the variables that help explain health seeking behavior in the developing world.
Finally, in this review several different approaches to the study of accessibility and utilization
are discussed and an opportunity for using a gravity model approach is identified. The
literature describes relationships such as distance to utilization to be non-linear. Nonetheless,
non-linear models, such as the gravity model, are not common in utilization studies.

- 51 -
CHAPTER THREE - DATA ACQUISITION
This chapter summarizes the acquisition of data used in this study. This includes a section
describing the acquisition and development of a base map; the acquisition of village and
walking routes throughout the study area via GPS receivers, and the incorporation of these
data into a GIS; the acquisition of GIS political boundary shape files and census demographic
information; and a section describing the clinic attendance samples. The second part of this
chapter looks at the qualitative data used in this study and includes a section describing the
selection of the key informants. This is followed by a discussion of the challenges in
conducting fieldwork in the developing world.
3.1 Acquisition of Data for the GIS
3.1.1 Acquisition and development of base map
In order to start a geographic analysis of this type a good base map needs to be acquired or
developed. This is a good starting point for most types of spatial analyses. Having a good base
map gives a good frame of reference for physical features in the study area relative to other
features (such as villages relative to streams).
In most parts of the developed world formatted GIS files are available from a variety of GIS
vendors, but when working in the developing world, particularly rural parts such as southern
Honduras, these GIS files are often not available. As a surrogate, this research started by
acquiring a 1:50,000 scale topographic map available from the Instituto Geografico Nacional
de Honduras [the Honduran national geographic institute] (IGN, 1984). Though this map was
originally created in 1970, topographic features do not change much over 35 years, but human

- 52 -
development features do. Nonetheless, it is the most detailed map available for this area, and
that is why it was chosen for this project. The appropriate map for the service area was
difficult to locate in the U.S., but eventually one was located at the Cornell University
Library.
This topographic map was then scanned using a large map scanner and saved in a digital
format called a TIF file. This map was later converted to a bil format that is usable in
ArcView, a common GIS software package. This process included geo-referencing nine
known points from the map and processing it with ENVI (a remote sensing software). This
processing enabled the GIS to use the known point locations as references and interpolate the
coordinates for all other places on the map. The result of this process is a GIS base map that
allows other geographic data (such as a road network) to be overlaid on top of this base map.
3.1.2 Acquisition of GPS Data in Honduras: Village locations and walking routes
The first step in the data acquisition phase involved primary collection of locations for each
village and the determination of all walking routes/trails used in the study area. The village
locations and walking routes were determined using a handheld GPS receiver. Using a local
guide to determine the location of each village, two field researchers traveled to each village
either by pick-up truck or on foot. A GPS device was used to determine the exact routes taken
and the coordinates of each village. This included all roads and pathways that the patients
used to travel from their home residence locations to the health facilities, as well as the exact
location of 31 important villages and towns in the service area. Data for each route and village
location were later downloaded into a GIS. (See Map 3.1 for more information.)

- 53 -
Many of the routes were mapped using a good four-wheel drive pickup truck. This helped
data collection to progress quickly, allowing the researchers to get to most villages in the
study area in less than two weeks. Other villages not on roads had to be mapped with GPS on
foot. During this map-building phase, local guides were used to assist in finding needed routes
and village locations.
The GPS data were added to the GIS base map so that route distance calculations and spatial
references could be made. This research used Garmin eTrex Legend and Vista GPS receivers,
which have download capabilities and accuracies generally in the 20-30 foot range. Waypoint
and route data were downloaded via DNR Garmin, a freeware program, developed by the
Minnesota Department of Natural Resources (DNR Garmin. 2004), and imported into
ArcView GIS.
The GIS village/route file requires some processing to enable it to become a fully functioning
GIS network. The first procedure involves loading the GPS file into the GIS. Garmin’s track
files (which are used to show routes traveled) are basically a “cookie crumb” trail which gives
GPS location points along the trail every few seconds. The output of this file is therefore a
large assemblage of related points. These points are added to an ArcView project view using
the “Add Event Theme” function. This point theme needs to be converted into a line theme
through one of several ArcView script extensions, such as X-Tools (DeLaune, 2001) or it can
be drawn using heads-up digitizing methods.

- 54 -
The next step in the GIS processing involves the linking of the route data and the village
waypoint data into a functioning network. This functionality is available in ArcToolbox,
which is available in ESRI’s ArcGIS 8 and 9 software packages, but not available in earlier
additions of ArcView 3.2. The first step of this process involved converting the route line
theme to a coverage using the “make shapefile into coverage” function in ArcToolbox under
conversion tools. The next step uses the “clean” function to create the topology used by the
network {Conversion Tools/Data Management Tools/Topology/Clean}. Use parameters –
Dangle length = 0; Fuzzy Tolerance = .0005 (snap distance) to insure proper connection of
dangling line segments and nodes. The final step, which creates a coverage usable by ArcGIS,
involved using ArcToolbox’s “Build” function to create the road network coverage. Be sure
to specify feature class = “line”. This last step is not necessary if ArcView is being used.
As a result of this procedure, we have a fully functioning network coverage for ArcView or
ArcGIS. ArcView’s Network Analyst is then used to calculate the shortest distance along the
road network from each village to the health clinic. {This is not to be confused with the travel
time estimation technique presented in chapter 3.} These distance measurements represent
varying levels of access in the distance decay model created for this study. This method of
measuring distance is a more accurate measure of travel impedance than simple straight-line
or Euclidean distance that has been often employed in past research such as Oppong and
Hodgson’s (1994) study on accessibility in Ghana. See map 3.1 on next page for an image of
the enhanced base map.

- 55 -
3.1.3 GIS and Census Data:
In order to understand the distribution of the population and calculate the utilization index one
needs to have population data for each village. This research uses 2001 Honduran National
Census data for population counts of each village and this information is available at their
website (INE, 2004). There are some concerns, as with any census, as to the quality and
accuracy of these data. Considering though, that this is the only officially sanctioned census, it
is assumed to be accurate. None the less, caution is recommended when using these data and
drawing conclusions based on them.
INE makes these census data available in a tabular format, but what is more valuable to a
geographic analysis such as this is when the data are associated with corresponding GIS
shapefiles. These data were made available for use in this project by the Secretaria de Estado
en los Despachos de Recursos Naturales y Ambiente [The Secretary of Nature and the
Environment] (SERNA, 2005), located in Tegucigalpa, the Honduran capital. This made geo-
demographic analysis much simpler where the GIS could be used to group and analyze
spatially referenced demographic information at detailed levels. These data were available at
the Caserio level, which is akin to the U.S. Census’ Block Group level. See Map 4.1 on next
page for a detailed view of the study area.

- 56 -
#
#
##
#
#
#
## #
#
#
# #
# #
#
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
ÊÚ
ÊÚ
ÊÚ
Basemap of Santa Lucia Study Area N
Topographic map information by Instituto Geografico Nacional (1984).Road and Village Locations by Jonathan Baker and Chris Carr
0 1000 2000 3000 4000 5000 Meters
Map 3.1: Base Map of Study Area
3.2 Attendance Samples
A systematic sample of patient attendance for each of the three health clinics in the service
area was performed during a two-week field trip to the study area in January of 2005. The
Honduran Health Ministry requires that all rural clinics keep records of the patients they are
seeing. These records, sometimes called log books, include detailed information on the
demographics (age, sex, weight, diagnosis, home location, etc.) of each patient who visits the
clinic. All three clinics in the service area keep this type of records, and samples were taken
from each clinic for the entire year of 2004. There were some challenges along the way, but

- 57 -
this process went quite well considering that the three health clinics were under no obligation
to provide this information. The following section further explains this sampling process.
For each of the three clinics home location information was extracted in a systematic method
of sampling of the clinics’ patient attendance records. This involved sampling every 10th
record from the log books for the entire year of 2004. This represents 10% of all patients seen
by the clinic over that period. This yielded patient residence locations for a sample size of 477
patients from the Hombro á Hombro clinic, 320 patients from the Santa Lucia Health Center,
and 557 patients from the Magdalena Health Center. These records represented patients
residing in 31 villages or towns. Only the patients’ home location (village) was recorded. No
names or other personal information was taken to preserve confidentiality. The information
was tallied according to the patient’s home village. The same methodology was used for all
three clinic samples.
Acquiring permission to sample the clinic’s logs turned out to be a relatively easy process.
Since this researcher is associated with the University of Cincinnati’s Medical School and
supported by the director of the Hombro á Hombro health clinic, access to Hombro á
Hombro’s log books was straight forward. The sample was performed in the clinic and took
approximately two afternoons.
A similar experience occurred with gaining access to the Santa Lucia Health Center’s records.
The long-time nurse at the Health Center, who has a good amount of influence in the
community and strong ties with the Hombro á Hombro clinic, was very helpful in providing

- 58 -
information and access to her clinic’s records. No resistance was given, and it seemed that she
understood the value of this research. This was a very positive experience and significant
amounts of other qualitative data were received during this process.
It was thought that the Magdalena clinic would be a different experience. Expectations for
trying to get a sample of the Magdalena Health Center’s records were not good from the
beginning. This clinic operates in another municipality, Magdalena. It is operated by a Cuban
social service doctor who was quite new to the area. There was some concern over the
doctor’s attitude towards American researchers coming into her clinic and asking to see their
health records. It was feared that geo-political tensions between the two respective countries
would cause a problem toward gaining access to the records. As it turned out, this was not the
case. The head clinician from the Hombro á Hombro clinic accompanied the research team to
the Magdalena clinic interview and worked as a facilitator, making the introductions and, in
general, smoothing the way for a very good, meaningful interview on the health conditions in
Magdalena. Towards the end of the meeting, the survey request was made, and access to the
records was granted.
The combined experience of these three survey experiences led to a better understanding of
the level of cooperation that exists between health facilities in this part of the world. Everyone
knows that conditions are difficult in and around Santa Lucia, and everyone tries to help if
they can with another person’s tasks. This is a very friendly, open, and constructive way to be.
When looking at the big picture, this experience was seen in sharp contrast to the overly
competitive, uncooperative way that many things happen in the US. Furthermore, by having

- 59 -
samples for all three clinics a more thorough and robust utilization model could be developed
(compared to an analysis of only a single clinic’s utilization), one that considers all of the
primary health care options available to the citizens of the study area.
3.3 Qualitative Sources of Data
3.3.1 Key Informant Data:
A significant amount of qualitative data was compiled for this study. To get these data
involved performing several interviews with key informants in the field. These were
knowledgeable individuals whose expertise on the subject matter made them appropriate for
this research questioning. Key informant data were used primarily in two areas of this
research: Firstly, to better understand many of the socio-cultural and medical aspects of the
study area and the people who live there. And secondly, the key informant interviews helped
with the interpretation of the results. These key informant interviews help to improve the
quality of the study by adding insights from knowledgeable sources in the field, and experts in
the field of international health. Descriptions of the key informants are as follows:
1. Key informant #1 was the previous head clinician at the Hombro á Hombro health
clinic in Santa Lucia, Intibuca. He is a medical doctor with over 13 years experience at
the Hombro á Hombro clinic and his knowledge of the people and the conditions in
the study area were instrumental to this research. Furthermore, his knowledge of the
Honduran health system and sources of the other geographic information made him a
very important resource for this research.
2. Key informant #2 is the current director of the Shoulder to Shoulder, Inc., Hombro á
Hombro’s American sister organization. He is a medical doctor, health policy

- 60 -
researcher, and faculty of a major university-based international health program. His
regional knowledge of medical needs, health care planning, and policy making was a
valuable resource to this research.
3. Key informant #3 was a project coordinator for PROMESA (a community
development corporation which offers community-based primary health care services
in several parts of the world) with a Masters in Social Work (MSW) and extensive
experience in health-based community assessments in Honduras.
4. Key informant #4 was the project site founder of the Hombro á Hombro health clinic,
with over 13 years experience in the Santa Lucia area. He is a medical doctor and is
the Director of the Division of Family Medicine at a major U.S. educational
institution. His background in both medical issues relating to international health, and
experience in the study area made him a very important contact.
5. Key informant #5 was the current head clinician at the Hombro á Hombro health
clinic. He is a medical doctor with over four years clinical experience in the Santa
Lucia service area. His knowledge of medical issues in the study area and contacts
throughout the community made him a very important resource.
6. Key informant #6 was the nurse practitioner at the Santa Lucia Health Center. She has
28 years experience servicing the medical needs to the people of Santa Lucia, much of
that period working without an M.D. Her knowledge of the people and the medical
situations in the service area was extensive.

- 61 -
3.3.2 Key Informant Interviews:
Most key informant interviews were handled in an informal manner with questions pertaining
to their expertise and the goals of this research prepared ahead of time. If needed an
interpreter was present to help with translation. For some applicable interviews, summary
assessment surveys were administered at the beginning of the interview so as not to bias the
responses on the surveys. In Appendix D there is a detailed question and answer interview
with the former head doctor at the Hombro á Hombro clinic, who was one of the most
important key informants interviewed during this study. This serves as a good example of the
interview method used and the types of qualitative data acquired during this process.
3.3.3 Informal Interviews:
In addition to the above key informant interviews, many informal interviews were conducted
in the process of collecting data for this research. This included a number of interviews with
school teachers; the administrative head of Hombro á Hombro and director of the school
nutrition program; a key town leader; two board members of the Hombro á Hombro clinic; a
Honduran-American Social Worker; a Peace Corps Volunteer working in the area; and two
nurses and two doctors from the two government health centers. Other interviews were
performed in the Santa Lucia community on an informal basis to help with building the
foundation of this research.
3.4 Challenges in conducting fieldwork in the developing world:
There have been a number of challenges that have confronted this researcher during the
current study. One challenge related to the acquisition of GIS political boundary files that

- 62 -
could be linked to the Honduran national census. It has taken almost two years and two trips
to Honduras to find and acquire the data for a good GIS analysis of this area. The following is
a description of the steps taken during this search.
At the beginning a thorough search of library, commercial, university and other internet-based
GIS resources (of which there are many) yielded little in the way of usable GIS files for the
study. Only country level shape files were acquired from ESRI, the publisher of ArcView.
This was in sharp contrast to the large amounts of secondary GIS information available for
most projects in a developed world location like the U.S. GIS information is easily accessible,
and its popularity so great, that it seemed surprising that no census based boundary files could
be found for Honduras, particularly considering that a good national census had been
conducted in Honduras in 2001. It was believed that the Honduran Census Institute (INE)
should have good, detailed maps to delineate the different parts of the country for the
purposes of collecting and analyzing data for the census. But where to get these GIS files?
Who to contact?
INE has a website and a good deal of census information available for researchers to
download (INE, 2004), but unfortunately none was linked to the polygon shapefiles needed to
make maps with GIS. Little progress was made contacting this Honduran agency or others
such as the Honduran Geographic Institute (IGN), directly via email, from addresses available
on several websites. Numerous emails were either not returned or were sent back as not
deliverable. It appeared that many of the links discovered during several Google searches

- 63 -
were broken or not active. This process was repeated many times over the two year period,
and resulted in a good deal of frustration.
A decisive turn in this search occurred through networking, when a key informant was
established from MERTU, the Center for Disease Control’s Central American division
located in Guatemala City. In an email this informant revealed that these GIS files existed in
Tegucigalpa, Honduras’ capital city, at the Instituto Geografico Nacional (IGN - the
Honduran national geographic institute). This instigated further failed attempts to contact
them by email, but at least this researcher was able to conclude that these files existed.
The next break in this search occurred several months later with an email to a key informant
who was a native of Tegucigalpa, and a former head clinician of the Hombro á Hombro clinic.
He suggested that there were three potential sources for these data. In addition to IGN and
INE, he suggested contacting the Secretaria de Estado en los Despachos de Recursos
Naturales y Ambiente (SERNA, 2005) [The Secretary of the Nature & the Environment] as a
potential source for these GIS files.
At this point it was concluded that the best way to locate and procure these data was going to
be during an upcoming field trip to Honduras. A group of medical personnel was going to
Santa Lucia, Honduras during January of 2005, and going through Tegucigalpa. It was
therefore determined that going to Tegucigalpa a few days early would afford the best
opportunity to find and procure these GIS data.

- 64 -
Finding addresses for these government agencies proved difficult prior to the trip to
Honduras. Upon arrival in Tegucigalpa, using a local phone book and some assistance from a
local phone operator, the addresses of these agencies were established. Also, in a valuable
phone conversation with key informant #1, the suggestion was made that the best place to
look first was SERNA. The following morning, a trip was made to SERNA’s office. This was
a very positive experience which yielded a contact with a GIS Analyst. This Analyst had the
data that was sought, but unfortunately, could not provide it without a letter of approval from
the Secretary’s office. At this point, she kindly discussed the steps needed to procure this
approval. This involved writing a proposal-type letter identifying the nature of the request,
and why this information was needed. It was explained that the request would take several
days to process. Luckily, this was done at the beginning of the trip, and upon return to
Tegucigalpa the data were provided.
Upon return to Tegucigalpa, this long search came to end when this researcher met with the
senior director of the GIS department, and was given a disk with all the data that was
requested. Upon discussion of the CD’s contents and the research plans, the director agreed to
provide additional information which linked the GIS shapefiles to the national census at the
lowest, and most detailed, spatial level. This has subsequently proven to be of great help,
since this research looks at several socio-demographic characteristics in the study area that are
available only from the national census. Furthermore, having this information at a detailed
level added to the analysis of the study area. In addition to providing a clear delineation of the
political units in the service area, this information enabled the accurate evaluation of the

- 65 -
population distribution throughout the study area. It also enabled the creation of an
employment index that could be studied in this research.
3.5 Chapter Summary
In summary, this chapter has discussed the collection of data for this study. Portions of this
chapter discussed issues relating to developing a good base map; collecting data via a GPS
and developing a GIS with these data; the acquisition of census based shape files; the
collection of qualitative data from key informants; and the challenges of conducting research
in Honduras.
Data collection is a very important part of research, particularly in a developing world
location. In contrast to developed world locations, many secondary sources of geographic and
health information are not available. This often means having to perform substantial in-
country field work. Consequently, much of the data for this study have been collected in
Honduras, and the lessons learned there were instrumental in developing this and future field
work methodologies.
The next chapter, Chapter Four, is an exploratory chapter which looks at the data and tries to
come to some preliminary conclusions based on descriptive analyses which will be used to
justify the methods and models used in this paper.

- 66 -
CHAPTER FOUR - DESCRIPTIVE ANALYSIS
This chapter is used to explore the data used in this study. This involves using descriptive
techniques to understand the variables studied, and this leads to the justification of the model
chosen for this study. This chapter starts out by giving a description of the spatial scale and a
full explanation of all of the variables used to study utilization. This is followed by an analysis
on distance decay of utilization used to describe the relationship of distance to utilization. The
final section of this chapter focuses on validating the data and focuses on determining the
normalcy of the dependent variable – the utilization index.
4.1 Unit of Analysis
The geographic unit of measure in this study is a synthesized point-based unit that will be
referred to as the “Village”. Attendance, population, utilization and other census data are
associated with the locations of these village points which were acquired with the help of
local guides and GPS receivers during fieldwork in the area. (See Maps 1.3 for the
distribution of the villages within the service area, or Map 3.1 for a more detailed topographic
map featuring these same geographic units). The population data for the village and the area
surrounding the village are estimated using a methodology described later in this chapter.
4.2 Variables Used to Explain Utilization
The next several sections detail the variables used to explain utilization behavior in the study
area. This research examines several key factors that may affect the patterns of demand for a
health facility, namely; a measure of the friction of distance from each village to each health
clinic in the service area (distance, walking time, and road quality); a measure of the

- 67 -
population size for each village; a measure of the attraction for each health care facility; a
measure of the relative level of education for each village; a measure of the level of relative
wealth for each village; a measure of employment for each village; a measure of service cost
for each health facility; a measure of road quality; and a complex measure of choice.
The selected group of variables chosen is not intended to be all inclusive. As Habib and
Vaughan (1986) point out, a decision to highlight certain variables has to be made in most
studies because utilization is the outcome of many complex interactions with numerous
factors. It is practically impossible in most studies to observe the whole process in detail and
few utilization studies can be sufficiently comprehensive to encompass all possible factors
that can play a part in this process (Bailey and Phillips, 1990). The variables chosen for this
study are described in detail in the following sections.
4.2.1 Utilization Index
The utilization index is the dependent variable in the model and is a calculated ratio which
combines attendance numbers for the three clinic samples, groups them by village, and
normalizes them by population. The result is a utilization index number for each village-to-
clinic interaction.
The numerator in the utilization index is the total number of attendances for each clinic-
village interaction and is the result of a systematic sample of attendances for the three clinics
over a year (see section 3.2). A primary hypothesis in this study is that clinic attendances are
positively related to the size of a village. Larger villages should have higher attendances, and

- 68 -
smaller villages should have lower attendances. The connection between these two variables
is intuitive and leads us to the creation of an index ratio that considers the clinic attendances
relative to the population for a given village.
The denominator of the index is the underlying population for each village. The population
for each village can be seen as a proxy for ‘need’. If we assume that all people have the same
need for health services, then the distribution of the population in the study area should equate
to the distribution of need. The utilization index, then, becomes a relative measure of the
satisfaction of the need for health service.
The use of the population variable is important because when working with an analysis such
as this, we only know the people who come to a given clinic from a given village (via the
samples). What we don’t know is who does not come to the clinic. This is a limiting factor.
One way to get around this short-coming in the analysis is to normalize the attendance data by
the population. The result is a way to compare attendance, while adjusting for the size of the
population for a given village. By normalizing the attendance data by the population we create
an index ratio where higher index numbers relate to a higher proportion of a village that is
using the clinic. Lower index numbers indicate a lower proportion of the village population
using the clinic. One minus the index ratio number, by contrast, indicates the proportion of the
population that does not use the clinic. See section 5.2.1 for a detailed description of the
calculation of the utilization index.

- 69 -
4.2.2 Distance
The following formula is used to measure two-dimensional distance. This includes only the
horizontal or flat distance between two points. GPS units were used to create a “cookie
crumb” trail network, where point locations were created at frequent intervals (determined by
the GPS every few seconds) along each trail. These GPS files were used to supply the
locational coordinates at a detailed level. X, and Y coordinates (longitude & latitude) are used
to obtain the network distances for routes throughout the study area. A UTM coordinate
system is used, with NAD-27 as the datum.
Each GPS point represents an “x”, and a “y” value. The distance formula is notated below:
( ) ( )2212
2112 yyxxd −+−= (4.1)
where,
x = the longitude coordinate (UTM Easting) of the GPS point
y = the latitude coordinate (UTM Northing) of the GPS point
for each point:
( )111 , yxP = (4.2)
( )222 , yxP = (4.3)

- 70 -
Table 4.1 Distance Table
GPS Point DistanceP1P2 d 12P3 d 23… …Pn d n-1, n
An Excel spreadsheet was used to calculate the distance of each line segment between each
set of GPS points, and combine all of the line segments into a distance matrix for each town-
to-clinic trail combination.
4.2.3 Walk-Time Estimate
Elevation changes affect the friction of distance particularly for those who walk to the clinic.
In general, it is more difficult to hike up a grade than hike on a flat terrain, and it is logical to
assume that most people will hike slower up a grade. Since this is a very mountainous terrain,
the elevation change aspect of distance is important to include in an estimate of walking time,
so there needs to be a way to adjust travel distances to incorporate elevation changes.
In this study we adjust the distances developed in the prior section by an elevation change
factor (collected from the GPS logs) in order to more accurately reflect actual walking time.
This is accomplished by using the Appalachian Mountain Club's (AMC) (Daniell and Smith.
2003) formula to estimate the hiking time from each village to each clinic. The AMC formula
indicates that it takes 30 minutes to cover one mile on flat terrain, and adds 30 minutes for
every 1,000 feet of elevation gain. Downhill stretches are treated as if they were flat, which is
30 minutes per mile. This formula is generalizable for many places and types of terrain.

- 71 -
Variations from estimates to actual time may be encountered depending on the individual’s
strength, fitness level and age. Based on preliminary research in the area, it is expected that
this formula should roughly estimate the time of travel by foot for the average person. This
methodology of estimating time of travel has been tested using a GPS to determine actual
time & distances for a few selected trail routes in the study area, and fairly estimates actual
travel time. In addition, it is believed that if inaccuracies occur, then they should occur
throughout the study area, thereby having little to no substantive impact on the study as a
whole.
This method for estimating travel time is operationalized by including a calculation in the
distance matrix spreadsheet that accounts for cumulative positive elevation changes over the
duration of each village-to-clinic trail, and adds the appropriate amount of time to the total
hiking time calculation. This should provide a very accurate identification of the elevation
change factor in the equation, and combined with the distance factor should provide a reliable
estimate of walking time from villages to clinics.
It is assumed that this method of estimating travel time is a more accurate representation of
reality for people who normally travel to the health clinic by foot (which is the majority of the
population in the service area) compared to simple distance measures. See following table for
an example of the estimated travel time calculation.

- 72 -
Table 4.2: Estimated Walking Time Calculation
Trail Network Distance Matrix for Palacio to Santa Lucia Clinic
UTM Zone
X UTM
Easting
Y UTM
Northing Z
Altitude Distance AltitudeElevation Change
Elevation Adjustment
Travel Time
Cumulative Travel Time
(meters) (meters) (meters) (meters) (feet) (minutes) (feet) (feet) (minutes) (minutes) (minutes)
16 P 347941 1537732 513 168116 P 347939 1537730 514 3.20 11 0.060 1686 5 0.15 0.21 0.21 16 P 347934 1537730 514 5.02 16 0.094 1685 -2 - 0.09 0.30 16 P 347932 1537735 505 9.81 32 0.183 1658 -27 - 0.18 0.48 16 P 347948 1537735 505 16.01 53 0.298 1656 -2 - 0.30 0.78 16 P 347967 1537744 510 21.56 71 0.402 1672 16 0.47 0.87 1.66 16 P 347976 1537749 513 10.70 35 0.199 1681 10 0.29 0.48 2.14 16 P 347981 1537758 514 10.40 34 0.194 1686 5 0.15 0.34 2.48
Distance Time
Time Adjusted Distance
4.2.4 Population Size
Population size of each village and town is an important characteristic of the study area.
These data are acquired from the 2001 Honduran Census and is applied to the denominator of
the dependent variable for the gravity model. This factor helps to determine the spatial pattern
of the population which indirectly has an influence on the location of the three clinics. All the
clinics are located in the two major towns in the service area and their large populations
therefore have a strong effect on the models. A number of problems were incurred in this
study relating to the reconciliation of clinics’ attendance records with the locations used in the
census. The following section highlights this problem and suggests a method for allocating
population numbers to the villages covered in this study.
4.2.4.1 Reconciliation of population data
A big challenge arose when trying to associate the attendance data from the clinic with
population data from the Honduran 2001 Census data. Several Caserios (the smallest
geographical unit of measure of the Honduran national census) are not accounted for with any

- 73 -
attendance numbers at the clinic. During registration at the clinic, patients are asked to
identify “the place from which they came” (this is the literal translation), and this is where the
problem arises – this is an ambiguous reference to “place”. Patients therefore, may identify
their home location as the town, village or general area that they live in. This makes it
difficult to accurately reconcile the clinic attendance data with the census data because “home
residence” could be interpreted as either a Caserio, Aldea or a Pueblo (town).
It is possible that people living in small rural places list the larger geographic unit (the Aldea),
or possibly the closest Caserio, as their home residence. It is hard to know exactly how this
“home residence” field is interpreted by the patients during admittance to the clinic,
particularly for patients residing in small rural locations. Map 4.1 offers a visual perspective
on this population reconciliation problem, where the blue dots represent places the patients’
identify as their home Villages and the red triangles represent census-based Caserios.
As a way of addressing this problem, the following methodology is used for reconciling the
attendance numbers from each clinic with the 2001 Honduran census, so that the village or
town is preserved as the unit of measure in this study, and the total population of the study
area is accounted for as accurately, and in as much spatial detail, as possible. The
methodology is as follows: A table is constructed for adding the population of each Caserio
(the smallest census unit) to the closest attending village, so that the total population for the
entire Aldea is taken into account. No assignment of Caserio population data is performed for
a Caserio located more than 1 kilometer from the nearest studied village. This helps ensure
census-based population data is representative of the proximal area of the studied village.

- 74 -
Map 4.1: Village-Caserio Reconciliation
This procedure results in a population assignment for each Caserio according to its nearest
attending Village. Also, no across border (Aldea border) population assignments are made. In
summary, this procedure is a way of allocating the population of the smaller rural
communities to the larger (geographically known) locations, which we are calling Villages for
the purpose of this study.
As an example, the Aldea of Banaderos is used to illustrate this procedure. Banaderos is an
Aldea with seven Caserios, three of which are relatively large in size and which coincide with
the “Villages” identified in samples of clinics attendance records. According to the national

- 75 -
census this Aldea has a population of 550 persons, with 118 persons not accounted for in the
Caserios which are identified with the Villages in this study (e.g. places with attendance
records from the clinics). These 118 persons are allocated to the three Caserios with
attendance records, via the nearest neighbor scheme described above. As an example, the
Caserio of El Aguila (one of the attending Caserios), which has a census population of 167,
rises by 30 to 197 persons after adding the Caserio of Las Delicias. This should more
accurately account for the small, outlying Caserios, such as Las Delicias, which is close to El
Aguila, but has no clinic attendance records. See following table and accompanying map for
more information.
Table 4.3: Population Aggregation Worksheet
Population Aggregation - Villages Plus Neighboring Caserios
Aldea NameCaserio Name (from Census)
Caserios Populations Village Name
Village Population
Banaderos El Aguila 167 El Aguila Banaderos Las Delicias 30 El Aguila 197Banaderos Banaderos 166 BanaderosBanaderos Cerro Las Tetas 20 BanaderosBanaderos La Florida 16 BanaderosBanaderos El Cohete 52 Banaderos 254Banaderos El Castano 99 El Castano 99
Aldea of Banaderos 550
Note: In the following map the geographic location of the studied villages have been
established through fieldwork in the area with a GPS and are represented by blue dots. The
locations of the census-based Caserios are the red triangles, from which the population
reassignment occurs. Additionally, the Village of El Castano is listed as being located in the
Aldea of Banaderos by the Honduran national census.

- 76 -
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
$
#
#
#
#
#
Banaderos
El Aguila
El Castano
Reyolar La Pita
Isletas
Bañaderos
El Zapote El Aguila
El Cohete
El Recod
e
La Florida
s
La Florida
Santa RitaCoyotera
a Barranca
San
Las Delicias
Los Tablones
El Guanacaste
Cerro Las Tetas
Los Tablon
resa
Portillo de
Aldea of Banaderos
0 0.5 1 1.5 Kilometers
Aldeas01
Roads11 - 22 - 33 - 4
$ Caserios# Population
Map data from the Honduras Secretaria de Estado en los Despachos de RecursosNaturales y Ambiente, and fieldwork conducted in the area.Villages are blue dots, in bold print
N
Map 4.2: Example of Population Reconciliation
4.2.5 Attractiveness of Health Care Facility: The next group of variables studied relate to
the attractiveness of a health facility. This study looks at three separate ways of measuring
attraction, namely: the size of the facility, the number of doctors, and the cost of service. Each
is measured separately, and applied to the regression model as an independent variable, in
order to determine its effect in the final model. The general hypothesis that applies to all three
measures is the more attractive health facilities have higher utilization index rates. It is

- 77 -
expected that these variables will be collinear; therefore only one will be used in the final
model. Details for each measure are as follows:
4.2.5.1 Number of Doctors: The number of full-time equivalent (FTE) doctors for
each health facility is an attraction factor tested in this study. It is hypothesized that health
facilities with a larger number of doctors would be more attractive than one with a smaller
number of doctors. Supporting information was acquired from key informants.
4.2.5.2 Size of the Health Facility: The size of all three health facilities is an
alternative measure of facility attraction tested for this study. The square footage of floor
space for each facility determines the size of each clinic, and this determines its relative
level of attraction. Jones and Simmons (1990) suggest using this method of measuring the
attraction of a facility such as a store. It is hypothesized that larger facilities have more
attraction than smaller ones. Measurements of clinic sizes were performed during
fieldwork in the area.
4.2.5.3 Operating Hours of Facility: The number of normal operating hours of a
health facility is the third measure of attraction tested in this study. It is hypothesized that
longer hours would be more attractive than shorter ones. Supporting information was
acquired from key informants.
4.2.6 Income
The levels of relative income for each village are another factor studied in this research. In
general, we know that the people of this region are poor by US standards where per capita
Gross Domestic Product (a measure of individual wealth) was $2,400 in 2004 (CIA, 2004).
Key informants estimate average income in the study area at about $1500 for those with

- 78 -
paying jobs. The literature suggests there is a significant positive relationship between income
and utilization, but a detailed examination of income levels by household or small census
units such as a Caserio was not available for this research. Secondary sources such as the
Honduran Census do not provide this information. As surrogate measures for income,
employment index and economic status variables were created to test their ability to explain
utilization behavior.
4.2.7 Employment Index
An employment index is created to examine the effect of employment on the utilization of
health services. An index value is created for each village using a composite of two 2001
Honduran Census data fields. The first field indicates the number of person’s in a Caserio that
“found work last week”, while the second field indicates the number of persons in a Caserio
that “did not find work last week”. This variable is calculated by taking the first field, and
dividing it by the summation of the two fields {a/(a+b)}. The results are an employment index
for each village, which is tested in the regression analysis.
4.2.8 Economic Status
This research uses another surrogate measure to evaluate relative income levels for each of
the villages. This involves developing a summary assessment in order to categorize the
economic status of the different villages. This summary assessment categorizes economic
conditions for each of the studied villages on a high-medium-low basis. In order to convert
the categories into a numeric format the following scheme will be used: high = 3; medium =
2; and low = 1. The five assessments are combined into an average score for each village, and

- 79 -
the natural log was applied to the result before applying this to the regression analysis. Five of
these “economic status” assessments were completed by key informants in the study area
during December of 2003.
4.2.9 Education
Education is an important variable in determining health facility utilization and is studied in
this research project. The municipality of Santa Lucia has many rural lower level schools, but
only two high-schools. This research uses 2001 Honduras national Census data to determine
percentages of a population that have attained a 6th grade education (the end of primary
education in Honduras). These data are used to determine which villages have had higher
percentages of their pupils graduate from the 6th grade. This is accomplished by taking the
number of 6th grade graduates and dividing it by the population for the village as a whole.
This higher level of educational attainment may, in turn, help explain areas of higher and
lower health facility utilization. It is a hypothesis of this study that there is a positive
relationship between the percentage of primary school graduates and clinic utilization rates.
4.2.10 Costs of Service
The cost of health service may affect utilization patterns. The cost of service variable works in
a similar way to the other previously mentioned attraction variables, only this can be thought
of more as a deterrent. It is hypothesized that higher cost private facilities, such as the
Hombro a Hombro clinic, are less attractive than cheaper public ones. This variable was
treated as a separate independent variable in the model, and the hypothesis was tested in the
regression analysis. Data were collected from key informants in the study area.

- 80 -
4.2.11 Road Quality
The quality of the road from the village to the health clinic may help determine access via
alternative means of transport. It is hypothesized that better roads lead to more truck traffic,
which leads to greater accessibility via collective pick-up trucks. If it is true that more people
are traveling by truck to the clinic, then this factor may help explain certain areas of increased
clinic utilization.
A good way of measuring the quality of the roads is through the analysis of the GPS logs, and
developing an average speed associated with each route or trail. It is logical to assume that
better roads mean higher speeds, which will be more attractive to collective truck drivers
(because they can more efficiently transport their passengers). For the purposes of this study,
a categorical ranking is created based on average speed. The following scheme is used: A zero
is given to walking trails where it was not possible to drive a truck; a one is given to average
travel velocity of 0-10 KPH; a two is given to average velocities of 11-20 KPH; and a three is
given to 21+ KPH velocities. These data are used in the gravity modeling to determine
whether there is a relationship between utilization and road quality, which has been suggested
in the literature. (See abbreviated example below.)
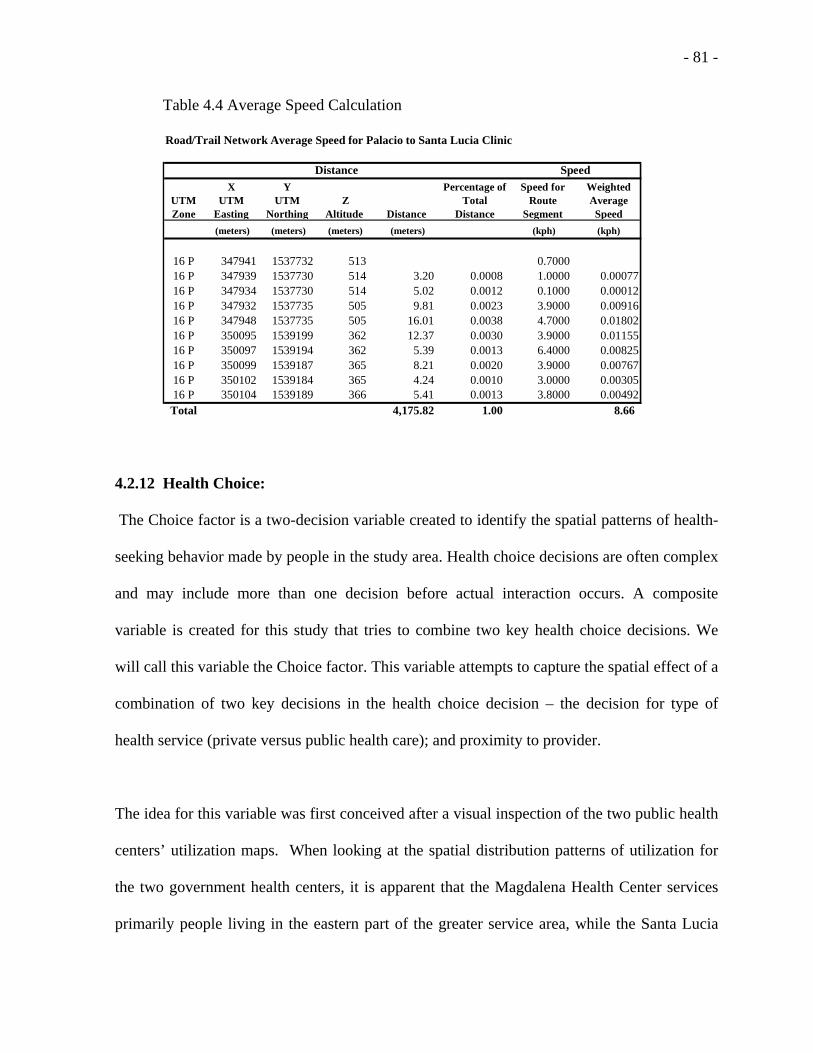
- 81 -
Table 4.4 Average Speed Calculation
Road/Trail Network Average Speed for Palacio to Santa Lucia Clinic
UTM Zone
X UTM
Easting
Y UTM
NorthingZ
Altitude Distance
Percentage of Total
Distance
Speed for Route
Segment
Weighted Average Speed
(meters) (meters) (meters) (meters) (kph) (kph)
16 P 347941 1537732 513 0.7000 16 P 347939 1537730 514 3.20 0.0008 1.0000 0.0007716 P 347934 1537730 514 5.02 0.0012 0.1000 0.0001216 P 347932 1537735 505 9.81 0.0023 3.9000 0.0091616 P 347948 1537735 505 16.01 0.0038 4.7000 0.0180216 P 350095 1539199 362 12.37 0.0030 3.9000 0.0115516 P 350097 1539194 362 5.39 0.0013 6.4000 0.0082516 P 350099 1539187 365 8.21 0.0020 3.9000 0.0076716 P 350102 1539184 365 4.24 0.0010 3.0000 0.0030516 P 350104 1539189 366 5.41 0.0013 3.8000 0.00492Total 4,175.82 1.00 8.66
SpeedDistance
4.2.12 Health Choice:
The Choice factor is a two-decision variable created to identify the spatial patterns of health-
seeking behavior made by people in the study area. Health choice decisions are often complex
and may include more than one decision before actual interaction occurs. A composite
variable is created for this study that tries to combine two key health choice decisions. We
will call this variable the Choice factor. This variable attempts to capture the spatial effect of a
combination of two key decisions in the health choice decision – the decision for type of
health service (private versus public health care); and proximity to provider.
The idea for this variable was first conceived after a visual inspection of the two public health
centers’ utilization maps. When looking at the spatial distribution patterns of utilization for
the two government health centers, it is apparent that the Magdalena Health Center services
primarily people living in the eastern part of the greater service area, while the Santa Lucia

- 82 -
Health Center primarily services people living in the western part. This creates a basic
division in the attendance patterns for public health centers, and may in part be due to the
political/administrative boundaries of the municipalities of Magdalena and Santa Lucia and
the spatial organization of the government run health centers.
The logic behind the decision-making behavior is borrowed from Fotheringham’s (1983)
paper where the author suggests many types of interactions can be considered a result of a
two-stage decision-making process. This research suggests viewing the health-seeking
behavior in the study area as a two-stage decision process involving choices. The first
decision is whether to choose a private or a public health facility, and the second is whether to
choose a health provider that is within your ‘local’ municipality, or not. The first decision
may be based on your ability to afford a private health service, or the perceived need for the
higher quality service that can be associated with a private health care service. And the second
decision assumes that you have not chosen the private health provider, and then relates to
choosing one of the government health facilities. It is believed that much of this second
decision is based on “proximity” of provider relative to the home locations of the patients, and
suggests that people have a strong bias toward patronizing the closer facility which is usually
in their local municipality.
When creating a variable to perform in the system-wide model, the first step looks at all
utilization decisions as a specific type of service choice. A value of one is assigned to all
decisions that utilize the private Hombro á Hombro clinic, and if selected no further decision
needs to be made. If the private health facility is not chosen, then a choice is made to select

- 83 -
one of the two public health centers, where a value of two is given to any village-clinic
interactions that are outside of the patient’s “home” municipality, or a value of one is given to
interactions within the “home” municipality. This distinction helps specify utilization outside
of one’s home municipality, which is an uncommon occurrence. This second decision we will
call the administrative separation factor.
In the development of this Choice factor this research made two assumptions and the results
indicate these assumptions worked to help explain health-seeking behavior (utilization). The
first of the assumptions is that the administrative separation factor is not an important factor
for the private health clinic. This assumption is investigated by mapping the residuals for the
Hombro á Hombro clinic. A visual inspection of the residuals for the private clinic supports
this assumption that there is no east/west administrative separation in the private clinic’s
utilization.
The second assumption is that this administrative separation factor is important to the public
health centers’ utilization. This is clearly indicated in the visual inspection of the public health
centers’ utilization maps showing an east/west bias in their two service areas. This
observation helps provide validation of the second assumption. More will be discussed on this
variable in the results and conclusions chapters.

- 84 -
The following figure describes the health choice decision-making process.
Figure 4.1: The Choice Decision Model:
4.3 Analysis of Distance Decay:
This paper now proceeds with an analysis that looks at the distance decay patterns in
utilization across the study area, trying to form a better understanding of the relationship
between distance and utilization. In the following analysis a graph is created to show how the
utilization index rates vary at different distances from a clinic. In this analysis the Hombro á
Hombro clinic was used as a base, and distances from this base were calculated via
ArcView’s Network Analyst functionality. Clinic attendances were then grouped by village
and aggregated at 2-km intervals. The aggregated attendance numbers were then divided by
the population for that distance interval.
The resulting graph shows a strong distance decay pattern for the utilization index. In
addition, these results suggest that the decay pattern is not linear. This is an important finding

- 85 -
because it indicates that the relationship between these variables would be best approximated
using a non-linear model such as the gravity model. The justification for using the gravity
model in this study is therefore made by looking at the figure 4.2 which describes the actual
distance decay of utilization in the study area.
Access: The Distance Decay of Utilization
0%1%2%3%4%5%6%7%8%9%
10%
1 km 3 km 5 km 7 km 9 km 11 kmDistance
Util
izat
ion
Figure 4.2 – Distance Decay of Utilization
The conclusions from this analysis of distance decay are consistent with Müller et al’s (1998)
study of the effect of distance on health attendances in Papua New Guinea, namely, that
attendance decreases substantially with distance, and the decrease is non-linear.
4.4 Comparative Analysis: Distance versus Walking-Time
The preceding argument focuses on the distance decay of utilization, and justifies the use of a
non-linear gravity model based on this analysis. Other measures of the friction of distance
may be substituted for this distance measure. This study focuses on using an alternate

- 86 -
measure, namely walking time. Given the above justification, it is important to know whether
there are substantial differences in these measures, and whether walking time can be
substituted for distance in the above analysis.
In past studies several authors have chosen to focus on the issue of distance as being the main
factor determining health care facility utilization (Stock, 1983; Joseph & Phillips, 1984;
Müller, et al., 1998; Buor, 2002). Though these measures of distance and their effect on
utilization have been documented in this research, only Buor (2002) has chosen to compare
the relationships between these two related variables.
The following correlation matrix indicates that the Ln of network distance cross-correlates
with the Ln of travel time (estimated walking time) at a .996 level. Furthermore, this
relationship is highly significant at a .000 level. It is clear from these statistics that the
variables are very similar and strongly related.
Table 4.5: Correlations from Distance-Time Comparison
Ln UtilizationLn Network
DistanceLn Travel
TimeLn Utilization Pearson Correlation 1.000 -0.440 -0.433
Sig. (p-value ) - 0.015 0.017Ln Network Distance Pearson Correlation -0.440 1.000 0.996
Sig. (p-value ) 0.015 - 0.000Ln Travel Time (Walking) Pearson Correlation -0.433 0.996 1.000
Sig. (p-value ) 0.017 0.000 -
Given the close relationship that exists between the Ln of Network Distance and the ln of
Travel Time (walking), it is logical to conclude that walking time may be substituted for

- 87 -
distance in the distance decay analysis, with little variance in the results. Furthermore, these
results infer a similar non-linear relationship between utilization and walking time.
4.5 Data Analysis
It is important to analyze the distribution of data for the dependent variable, particularly if you
are going to use it in a regression analysis. A good descriptive analysis can be accomplished
in two simple tests. The first involves creating a scatter plot of the dependent variable
(utilization) to estimated walking time, and second, a histogram of the dependent variable.
The main question we are trying to answer is whether the data are normally distributed. The
results of this analysis can then be used to determine which models are appropriate for this
analysis and which are not.
Looking at Figure 4.3, it is clear that the original data for the dependent variable (utilization
index) is not normally distributed. The lack of a “bell” shape in the histogram and the lack of
any discernable pattern in the scatter plot both confirm the original data for the dependent
variable (utilization index) is not normally distributed.

- 88 -
Figure 4.3 Histogram of Original Data
Figure 4.4: Scatter Plot of Original Data
It is a known requirement of regression modeling that the dependent variables must be
normally distributed. Therefore, in order to use multiple regression methods to test the final
model, it is important that the dependent variable have a normal distribution. So, the solution

- 89 -
is to perform a logarithmic transformation of the utilization index values in order to normalize
their distribution.
After a natural log transformation of the data, the next step is to rerun both of the previous
analytical graphs (the histogram and the scatter plot) to see if the data are now normal. When
looking at the histogram of the natural log of the utilization index, the distribution now
appears to be close to approximating a normal curve. Also, when looking at a scatter plot of
these transformed variables, a negative, relationship appears to exist between the natural log
of walking time and the natural log of utilization variables. See Figure 4.5 and 4.6 for more
information.
Figure 4.5: Histogram for ln Utilization

- 90 -
Figure 4.6: Scatter Plot for ln Utilization and ln Walking-Time
As a further test of normalcy, a one-sample Kolmogorov-Smirnov (K-S), Goodness-of-Fit
Test, is performed. The results of this test indicate a significance level of .499, which is
considered normal. {Large significance levels (p-values > .05) indicate that the observed
distribution corresponds to the theoretical [normal] distribution (SPSS, 2000)} Now a
regression analysis can be used with confidence that the distribution of the natural log of the
utilization index variable is normally distributed. See Table 4.1 for more information.

- 91 -
Table 4.6 Kolmogorov-Smirnov Test
One-Sample Kolmogorov-Smirnov Test
74-3.439461.107229
.096
.051-.096.828.499
NMeanStd. Deviation
Normal Parametersa,b
AbsolutePositiveNegative
Most ExtremeDifferences
Kolmogorov-Smirnov ZAsymp. Sig. (2-tailed)
LN_UTIL
Test distribution is Normal.a.
Calculated from data.b.
4.6 Chapter Summary
The preceding chapter explores the data used in this study, starting with several variables used
to study utilization. In addition to distance and travel (walking) time, several socio-economic-
demographic and service-based variables are considered. The development of a new
compound choice variable is discussed in some detail, and a model for this variable is
presented. This new variable is expected to improve the explanatory power of the model and
represents a substantial contribution to utilization research.
The next section of this chapter performs an analysis of distance decay of utilization and
concludes that the relationship between utilization and distance is non-linear. This observation
justifies the use of the non-linear gravity model used in this study. It is suggested that the
application of the gravity model to this area of research should result in a significant
contribution to utilization research.

- 92 -
A section of this chapter compares walking time estimates with distance as a measure of the
friction of distance. Both measures correlate highly with utilization, and it is concluded that
either measure adequately measures the distance decay effect. Thus, a justification is made
that either may be used in an analysis such as this.
The last section of this chapter looks at the dependant variable and determines through several
statistical procedures that the original data is not normally distributed and therefore
inappropriate for the planned regression analysis. This analysis is compared with a similar
analysis using naturally log transformed variables. The results indicated that the log
transformed variables adequately represent the normal distribution and therefore are
appropriate for the planned regression analysis.
This chapter justifies the use of the gravity model in this present research. The next chapter,
Chapter 5, discusses this model in more detail.

- 93 -
CHAPTER FIVE - THE PREDICTIVE MODEL
This chapter describes the model used in this study – a gravity model. The chapter is
organized as follows: The first section discusses the selection of the gravity model and why it
is used in this study. The second section describes the model and justifies the natural-log data
transformation used on the data.
5.1 Selection of the Gravity Model
When considering the type of model to use, past research has included the use of the linear
regression model (Buor, 2002-4; Shultz, 1975), the negative-exponential model (Stock, 1983),
and non-linear models such as the gravity model (Shannon et al. 1969). Müller, et al. (1998)
concludes that a relationship, such as the distance relative to utilization, is non-linear.
The conclusions drawn from the previous chapter on the analysis of the utilization data
confirm Müller et al’s (1998) conclusion, and suggest that the relationship between distance
and utilization in this study is also non-linear. The previous chapter recommends the use of
the gravity model as a better way to approximate the relationship between the studied
variables and utilization because the gravity model is a non-linear model and can account for
the curvilinear relationships, such as the distance decay of utilization described in the
previous chapter. Though the gravity model has been popular in past research relating to
accessibility to health care, no known study has used the gravity model to study primary
health care utilization. This is a new approach to studying utilization, and based on the
exploratory analyses, has the potential to yield a model that improves upon those used in past
research.

- 94 -
5.2 The Model
This research creates a complex model that tries to explain the health-seeking behavior for the
people who live in the Santa Lucia study area. This model is based on the gravity model.
The gravity model comes from Newton’s law of gravitation, which states that any two objects
in space attract one another according to a force that is proportional to the product of their
masses and inversely proportional to the square of the distance separating them (Stutz and de
Souza, 1998). Newton’s law of gravitation can be expressed as the force of attraction F, which
is equal to Mi (the mass of the first body), times Mj (the mass of the second body), divided by
the distance separating i and j (Stutz and de Souza, 1998). The basic formula of the gravity
model is as follows:
2
*
ij
ji
dMM
F = (5.1)
The gravity model has been applied to flows between two points in several areas in
geographic research, and has become popular in transportation and migration studies. A
modified form of the traditional gravity model used in this study can be expressed as follows:
)*******(17654321 αααααααβ ChoiceRQCostEconEduEmpAT
PopIY =+
=
(5.2)

- 95 -
Where
Yij = The utilization of the Hombro a Hombro clinic from village i;
Iij = Interaction from village i to clinic j. (Measured though sample of
attendances at each clinic);
Tij = Estimated walking time from village i to clinic j (measure of the friction of
distance);
Popi = The population size for each village
A1-3j = Health facility attraction measured in terms of number of doctors, number of
office hours, and size (in square footage) of facilities.
Ii = Income;
Empi = Employment (number employment as a ratio of total workforce);
Edui = Education;
Econi = Economic status (relative measure of wealth for a village);
RQij = Road Quality
Choice = A compound variable use to describe health choice decisions;
71−α = Exponent values that control their respective variables;
i = Village identifier;
j = Clinic identifier.
A symbolic representation of the model used to study the utilization of health services
in Santa Lucia, Honduras is as follows:

- 96 -
Access Factors:Travel Time (Walking)
Road Quality
Provider Characteristics:Size of Clinic
Number of DocsCost of Service
Health Choice-Type of Care:
Private vs Public
Village Characteristics:Economic Status,
Education, EmploymentHealth Status (Need)
Utilization
Health Choice-Proximity of
Health Facility
Figure 5.1 Utilization Model
This research uses a data transformation technique that converts the values for all non-linear
variables into their linear form, and tests the model using multi-variate regression analysis.
The rationale for this decision is based on four considerations. First, a multi-variate non-linear
model (such as the gravity model) should better approximate the patterns of utilization than
the standard linear model. The nature of a gravity model is different than a linear model. It is
able to accurately reflect curvilinear relationships, whereas a linear model cannot. Second, it
is impossible to assess the statistical significance of any gravity model, or variables contained
within one. Third, though a multivariate non-linear model is difficult to accurately calibrate
and interpret, the transformation of the model into its linear form should make the model

- 97 -
more operational and intuitive to interpret. Both the second and third points are necessary to
accurately calibrate the gravity model. And fourth, the preceding chapter concludes that the
dependent variable, utilization, is not normally distributed. A logarithmic transformation is
recommended to “normalize” this variable. The log-linear transformation discussed in this
section will accurately normalize the dependent variable so that it does not violate the
“normalcy” requirement of the regression model. It is believed that this preceding section has
adequately justified the log-linear transformation of all variables used in this current study.
The result is a transformed gravity model into its linear equivalent form suitable for use in a
multiple regression analysis.
With natural logarithmic transformations, the original model can be rewritten as:
ChoiceRQCostEconEduEmpATY lnlnlnlnlnlnlnlnln 7654321 αααααααβ +++++++=
(5.3)
5.2.1 Calculation of the Dependent Variable
The utilization index is the dependent variable in the gravity model and subsequent regression
analysis. The utilization index variable calculation is based on a ratio of aggregated
attendance numbers from village i to clinic j, divided by the population for village i. The
attendance numbers were taken from a systematic sample for each clinic (see the patient
samples section below for more information). The formula can be expressed as follows:
i
ijij P
IY
1+= (5.4)

- 98 -
where, Y is the utilization from village i to clinic j; I is the interaction (attendance number)
from village i to clinic j; and P is the population for village i.
Since we earlier conclude that a natural logarithmic transformation of this variable is needed,
all interaction (attendance) numbers need to be increased by one. This allows for proper
consideration of all 93 cases in the regression analysis, and keeps the regression software
(SPSS) from excluding any cases for villages with zero interactions. This is important because
zero interactions are valid cases and help to explain places with no clinic attendance. These
places need to be considered in the analysis, and not be excluded. Therefore, by adding one to
the attendance number for each case in the study we are able to keep the relative integrity of
the samples, and at the same time allow for a natural logarithmic transformation to be
performed on the utilization index for all 93 cases. The resulting utilization index can be used
to compare relative levels of utilization throughout the study area.
5.3 The Four Models:
The modified gravity model used in this study is presented in the previous section (5.2). We
can call this our system model because it encompasses all the elements needed to examine the
entire primary health care system for the Santa Lucia service area. Looking at it from the
perspective of the people who live in the service area, the system model represents all the
options available for the primary health care service. This includes one private health clinic,
and two public health centers. In this study we choose to examine all four different
configurations of our gravity model – one system model, and three individual clinic sub-
models - because they all offer a different perspective on the phenomena presented in the

- 99 -
study area. This section discusses why we need four models for this analysis, and what their
main differences are.
Why is this needed? Since the study area is composed of three individual clinic service areas,
the characteristics of the system model are derived from the characteristics of the three sub-
models. Therefore, an examination of the three individual clinic models should offer clues
about utilization behavior in the greater system-wide model. It is believed that a comparison
of the significant variables, their Betas, and their coefficients of determination, should provide
these clues.
What are the similarities/differences? The four different models all are derived from the
gravity model; all use the same formulation and the same group of explanatory variables (see
equation 5.2), and all use the same testing methodology. All four models incorporate natural
log transformations to all the variables as described and justified in the prior section (see
section 5.2).
In addition to these similarities, the individual clinic’s service areas also have several
differences. For example, the spatial distribution of the three clinics is not even. Two of the
clinics (one private, one public) are located in the large central town of Santa Lucia, while the
other public clinic is located by itself in another large town. As another example, the
topography of the study area also varies across the study area. This area is mountainous, and
as you go west of the town of Santa Lucia you encounter a large mountain. This type of
accessibility barrier is not present in the eastern portion of the study area. A third distinct

- 100 -
difference is the road quality. It is clear after conducting fieldwork in the area that the road
quality, in general, gets worse as you go south and west. These are just three of the many
differences that exist within the study area. These differences make a clear case for needing to
examine each clinic’s utilization and subsequent service area separately in order to determine
the important factors that effect utilization for each clinic.
In general, we can say that the individual clinic models, compared to the system model,
answer different sets of questions. The individual clinic models focus on the characteristics of
each individual clinic’s utilization and the differences between them, while the system model
focuses on health-seeking behavior for the entire service area and explaining these important
relationships. The first leads to the second, but different questions are asked. The latter, for
example, considers questions such as which type of health facility to attend (public versus
private choice) that aren’t pertinent when looking at an individual clinic’s model.
5.4 Chapter Summary
This chapter has provided a summary of the model used in this research project. Through the
use of the gravity model, log linear transformation, multiple regression analysis, and the
analysis of several key independent variables, a more thorough understanding of utilization
behavior is obtained for the Santa Lucia service area.
The next chapter, Chapter 6, reports on the results obtained from this model.

- 101 -
CHAPTER SIX - RESULTS This chapter summarizes the results of this research, followed by a section analyzing the
variables used to study utilization. This chapter first looks at the correlations of the variables
involved in this study. This is followed by a definition of the stepwise regression procedure
and the results of the system model and the three individual clinic models. An examination of
the performance of each model is made through the comparison of coefficients of
determination (R2), and an examination of the significance, direction, and strength of each of
the independent variables. Standardized coefficients from the regression output are examined
for similarities and differences throughout the various models studied.
6.1 Correlation Analysis
Reviewing the correlations that exist between pairs of variables, one begins to get an
understanding of the relationships that exist between each of the studied variables. In this
analysis the focus is on the ln of utilization, which is the dependent variable in the gravity and
subsequent regression models. Looking at the following summary table, these results indicate
there is a strong negative correlation between walking time and utilization. In each of the
related models this variable is indicated between the .05 and .001 significance levels. The
Choice variable also exhibits a very strong negative correlation to utilization. In every
applicable model the Choice variable is significant at the .001 level. Both of these variables
will be discussed in greater detail later in the regression analysis.

- 102 -
Other significant variables include cost of service, facility attraction measured in square
footage of clinic floor space, road quality, and educational attainment to the 6th grade level.
These variables vary in significance level but most are significant at the .05 level or better.
This analysis reveals that the facility attraction variable (determined by size of health facility),
is significant on a bi-variate basis for the system-wide model, but is later excluded from the
multiple regression models because the value of the variables becomes a constant for each of
the individual clinic models. A similar situation occurs for the cost of service variable. It is
noted that cost of service and facility attraction are cross-correlated at the .99 level. This
suggests that the two variables may be explaining the same thing, therefore only one of these
variables should be used in any final model.
This analysis indicates the economic status variable, a variable significant at the .05 level in
the final system-wide regression model, is not significant in any of the bi-variate correlations.
This research does not offer evidence on this matter, but suggests that this should be
investigated further in future research.
The road quality variable is marginally significant on a bi-variate basis for three out of the
four models, including the System-wide model, the Santa Lucia Health Center model and the
Hombro á Hombro model. The road quality is an important variable that helps to explain the
patterns of utilization for two of the three clinics, but in the context of the multi-variate
models it is not significant.

- 103 -
When visiting Santa Lucia it is apparent that collectivo truck transport is a growing mode of
transport for people of the region. The town of Santa Lucia functions as a service center for
the region with two health clinics, a high school, several markets, and a bank. Santa Lucia has
several good quality roads leading from it to several of the more remote village locations. A
number of villages to the west of Santa Lucia have a barrier to access by foot, namely Monte
Verde. Compared to the flatter eastern portions of the study area, travel by foot in the western
portion of the study area is difficult. These factors may encourage truck transportation in the
area, but primarily to places with better roads. Road quality may therefore be seen as a
surrogate for the amount of relative truck transport to a given village, and improved access
that it offers. This in turn may help to explain the spatial patterns of utilization for the region.
See the following summary table of bi-variate correlations comparing the different models, or
reference Appendix A for a complete listing of the bi-variate correlations for the entire study:
Table 6.1 Correlation to ln Utilization - Summary
VariableSystem-Wide
Model Sig.Magdalena
Health Center Sig.Santa Lucia
Health Center Sig.Hombro a
Hombro Clinic Sig.Ln Travel Time -0.550 **** -0.682 **** -0.444 ** -0.465 ***Ln Choice -0.712 **** -0.790 **** -0.700 **** -Ln Cost of Service 0.269 ***Ln Road Quality 0.181 * 0.324 * 0.393 **Ln Economic StatusLn Education 6th Gr. -0.301 *Ln Attraction (Facility Size) 0.284 **** significant at the .10 level or better; ** significant at the .05 level or better;*** significant at the .01 level or better; **** significant at the .001 level or better.

- 104 -
6.2 Results
6.2.1 Stepwise Regression Methodology
This study uses a stepwise multi-variate regression methodology available from the statistical
software package SPSS to determine the optimal mix of variables for the final regression
equation. Variables are included and excluded in the final equation according to the following
methodology: According to the SPSS documentation of the technique, at each step in the
computation, the independent variable not in the equation which has the smallest probability
of F is entered [most significant variable], if that probability is sufficiently small. Variables
already in the regression equation are removed if their probability of F becomes sufficiently
large. [The parameters for entry were set at .05, and removal at .10.] The method terminates
when no more variables are eligible for inclusion or removal (SPSS, 2000).
The stepwise regression methodology serves a second purpose. The output from the stepwise
regression gives us a ranked list of the significant variables tested in this study. This enables
us to determine the relative importance of each of the factors that influence utilization
behavior, which is one of the specific aims of this research project. This method of ranking
the predictors relative to importance was used in Buor’s (2002) study of utilization in Ghana.
The ranking of the results should help health planners determine the most important factors to
focus on when trying to improve health care provision in the region, because these are the
most important factors that effect utilization.

- 105 -
6.2.2 System Model Results
With the results of the regression analysis, we are able to summarize this relationship with the
following regression equation:
ln Y = .527 - 2.055 ln Choice -.853 ln T -.385 ln Econ
R2 = .644
Where Y equals the natural log of the utilization index, and ln Choice is the natural log of the
Choice variable, ln T equals the natural log of the estimated walking time variable, and ln
Econ equals the natural log of the economic status variable. The coefficients in the above
equation are unstandardized and the variables are ordered according to importance in the
model.
The coefficient of determination (R2) for this model is .644, and can be interpreted as meaning
that 64.4% of the variance in the ln utilization index variable is explained by the combined
variance in the ln choice, ln walking time, and ln economic status variables. This relationship
can be summarized by stating there is a statistically significant relationship between the
independent and dependent variables, and one that is moderately strong. In particular, the
variables for Choice and walking time are extremely significant. A summary of the stepwise
model development with standardized (Beta) coefficients, p-values (a measure of statistical
significance), and coefficients of determination (R2) follows:

- 106 -
Table 6.2: Stepwise Regression Coefficients - System Model
Step Variable Beta
Coefficient Sig (p-value) R2 1 Ln Choice -0.712 0.000 0.507 2 Ln Choice -0.593 0.000 0.612 Ln Time -0.346 0.000 3 Ln Choice -0.544 0.000 0.644 Ln Time -0.489 0.000 Ln Econ Status -0.222 0.006
6.2.2.1 Visual Inspection for the System Model:
This is the general system-wide model (for all three clinics) used to explain the overall health-
seeking behavior of the people in the service area. As you can see from the following map,
there are higher levels of utilization near central large towns & main roads. This is not
surprising considering access should be at its highest levels in these areas.
In contrast, points in extreme periphery exhibit low levels of utilization. Many of these
villages are south and west of Santa Lucia, over Monte Verde and along the Torola River,
which is the border with El Salvador. There are some low utilization areas in the extreme
eastern portion of the service area. These places deserve further investigation, since they may
be accessing an alternate health clinic further to the east, which is closer to them, but out of
this study area.

- 107 -
#
#
#
#
#
##
#
#
#
#
##
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
Jicaral
La Montana
Las AradasLas Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
La Ceibilla
Santa Lucia
Los Horcones
Los Tablones
San Francisco
Las Marias Mag
Utilization - Combined for All Clinics N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
Utilization# 0 - 0.047# 0.047 - 0.091
# 0.091 - 0.131
# 0.131 - 0.188
# 0.188 - 0.325
ÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region.
Map 6.1: Utilization - System Model
6.2.3 The Magdalena Health Center Model:
This is the model used to explain the overall behavior of the people attending the government
sponsored (public) Magdalena Health Center. We are able to summarize this model with the
following regression equation:
ln Y = .490 – 2.633 ln Choice -.711 ln T
R2 = .719

- 108 -
Where Y equals the natural log of the utilization index, and ln Choice is the natural log of the
Choice variable, and ln T equals the natural log of the walking time variable. The coefficients
in the equation are unstandardized.
This model has an R2 of .719, which is considered strong in explaining utilization behavior,
and is the strongest of the utilization models presented, including the system model. For this
model variables for choice, and travel time are very significant. The economic status variable,
significant in the System Model, and the Santa Lucia Health Center model, is not significant.
A summary of the stepwise model development with standardized (Beta) coefficients, p-
values (a measure of statistical significance), coefficients of determination (R2), and a map of
utilization for the Magdalena Health Center follows:
Table 6.3: Stepwise Regression Coefficients - Magdalena Health Center Model.
Step Variable Beta
Coefficient Sig (p-value) R2 1 Ln Choice -0.790 0.000 0.625 2 Ln Choice -0.596 0.000 0.719 Ln Time -0.364 0.005

- 109 -
#
#
#
#
#
##
#
#
#
#
##
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
Jicaral
La Montana
Las AradasLas Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
La Ceibilla
Santa Lucia
Los Horcones
Los Tablones
San Francisco
Las Marias Mag
Utilization - Magdalena Health Center N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
Magdalena HC# 0 - 0.002# 0.002 - 0.016
# 0.016 - 0.04
# 0.04 - 0.168
# 0.168 - 0.296
ÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region.
Map 6.2: Utilization Magdalena Health Center Model
Notice the concentration of high utilization villages in the eastern portion of the study area.
6.2.4 Santa Lucia Health Center Model:
This is the model used to explain the overall behavior of the people attending the government
sponsored Santa Lucia Health Center. We are able to summarize this model with the
following regression equation:
Y = .856 - 1.961 ln Choice - .966 ln T - .584 ln Econ
R2 = .631

- 110 -
Where Y equals the natural log of the Utilization Index, ln Choice is the natural log of the
Choice variable, ln T equals the natural log of the Walking Time variable, and ln Econ equals
the natural log of the Economic Status variable. The coefficients in the equation are
unstandardized, and the variables are ranked according to importance in the model.
This model has an R2 of .631, which is considered moderately strong in explaining utilization
behavior. The significant explanatory variables are – ln Choice, ln Walking Time, and ln
Economic Status. A summary of the stepwise model development with standardized (Beta)
coefficients, p-values (a measure of statistical significance), coefficients of determination
(R2), and a map of utilization for the Santa Lucia Health Center follows:
Table 6.4: Stepwise Regression Coefficients – Santa Lucia Health Center Model.
Step Variable Beta Coefficient Sig (p-value) R2 1 Ln Choice -0.700 0.000 0.490 2 Ln Choice -0.625 0.000 0.558 Ln Time -0.271 0.047 3 Ln Choice -0.554 0.000 0.631 Ln Time -0.512 0.004 Ln Econ Status -0.355 0.029

- 111 -
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#
#
#
#
##
#
#
#
#
#
#
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
Jicaral
La Montana
Las AradasLas Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
La Ceibilla
Santa Lucia
Los Horcones
Los Tablones
San Francisco
Las Marias Mag
Utilization - Santa Lucia Health Center N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
Santa Lucia HC# 0 - 0.004# 0.004 - 0.016
# 0.016 - 0.036
# 0.036 - 0.072
# 0.072 - 0.11
ÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region.
Map 6.3: Utilization - Santa Lucia Health Center Model
Notice the concentration of high utilization places in the western portion of the study area,
and low utilization places in the east.
6.2.5 Hombro á Hombro Clinic Model:
This is the model used to explain the behavior of the people attending the Hombro á Hombro
clinic. We are able to summarize this model with the following regression equation:
Y = -.883 - .509 ln T
R2 = .216

- 112 -
Where Y equals the natural log of the utilization index, and ln T equals the natural log of the
walking time variable. The coefficients in the equation are unstandardized.
This model has a modest R2 of .216, which is considered weak in explaining utilization
behavior, and in contrast to relatively strong results of .719 and .631 for the public health
center models. This indicates that less of the variation in utilization can be explained by
variation in the independent variables. Part of this sub-performance can be explained by lack
of the Choice variable that was significant in the other models. This variable was excluded by
the stepwise refinement procedure because there was no variation in the value of the variable
(a constant) for all the village-to-clinic interactions. In this model the only significant
explanatory variable was ln walking time. A summary of the stepwise model development
with standardized (Beta) coefficients, p-values (a measure of statistical significance), and
coefficients of determination (R2) follows:
Table 6.5: Stepwise Regression Coefficients of Independent Variables - Hombro a Hombro
Clinic.
Step Variable Beta
Coefficient Sig (p-value) R2 1 Ln Time -0.465 0.008 0.216

- 113 -
#
#
#
#
#
##
#
#
#
#
##
#
#
#
#
##
#
##
#
##
#
##
#
#
#
#ÊÚ
ÊÚ
ÊÚ
Espino
Llanitos
Palacios
San Jose
San Juan
Banaderos
El Aguila
Junquillo
Los Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
Jicaral
La Montana
Las AradasLas Marias
San Marcos
San Rafael
Santa Rita
Cordoncillo
El Leoncito
La Ceibilla
Santa Lucia
Los Horcones
Los Tablones
San Francisco
Las Marias Mag
Utilization - Hombro a Hombro Clinic N
0 2000 4000 Meters
Aldeas012
Municipios
Roads11 - 22 - 33 - 4
Hombro# 0 - 0.01# 0.01 - 0.031
# 0.031 - 0.046
# 0.046 - 0.074
# 0.074 - 0.107
ÊÚ Clinics
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region.
Map 6.4: Utilization - Hombro á Hombro Clinic.
6.3 Comparison of the Four Models
This next section compares the four models used in this study. These models all use the
gravity model as their foundation, so therefore should be similar in their mathematical
structure. The methods that were used to develop them are the same. There are some
differences too. These differences include; different spatial extents, different mixes of
significant variables, different proximal location factors, different attendance samples or

- 114 -
groups of samples to test the overall model. These all lead to different results as the preceding
sections have shown.
As an indication of the overall “fit” of a model to the actual utilization data, the coefficient of
determination, or R2, is a good statistic to use to compare different models. The R2 for the
overall system model is .644. This is similar to the R2 of .719 and .631 of the two Health
Center models. The Hombro á Hombro clinic model is somewhat lower than the others with
an R2 of .216. See table 6.5 below.
Table 6.6: Comparison of Models
Model Model Name
Number of Sig.
Factors R2
1 System Model 3 0.644
2 Magdalena Health Center 2 0.719
3 Santa Lucia Health Center 3 0.631
4 Hombro a Hombro Clinic 1 0.216
The reasons for the differences in the models’ performance, other than what has already been
specified, are a matter of speculation. The system model with its R2 of .644 could be
considered a benchmark since it represents all three samples and has three significant
variables (two of which are very significant). The wildcard factor appears to be the inclusion
(or exclusion) of the Choice variable as a determinant of level of the R2. The System Model,
the Magdalena Health Center Model and the Santa Lucia Health Center Model all indicate the
Choice factor is highly significant, and all have strong R2s. The Hombro á Hombro Clinic
- 115 -
Model does not include the Choice factor (it was excluded during the stepwise refinement
process), and subsequently its R2 is relatively weak. These results therefore lead to the
conclusion that the model estimates real world utilization better for a combined service area,
or for public health centers such as the Magdalena and Santa Lucia Health Centers. The
Hombro á Hombro Clinic’s utilization patterns appear to be more complex, and its model
needs further improvement in order to compare with the predictive capacity of the other
models.
6.4 Analysis and Discussion of Explanatory Variables:
6.4.1 Walking-Time
All models tested in this study indicate the Walking Time variable is very significant at the
.01 significance level or better, with a negative or inverse relationship to utilization. This
suggests a strong “distance-decay” effect relating to walking time. The standardized
coefficient (Beta) for walking time is -.489 for the system model, -.465 for the Hombro a
Hombro clinic model, -.512 for the Santa Lucia Health Center model, and -.364 for the
Magdalena Health Center model. These results indicate that walking-time occupies a
significant position in the utilization model.
All of the models exhibit a similar magnitude and direction in their coefficients within the
-.364 to -.512 range, with the system model being near the middle of the range at -.489. This
indicates a generally strong distance decay of utilization pattern based on walking time to the
clinics, and is consistent with other rural developing world health service research. Buor
(2004) for example found that the distance/utilization relationship in a rural part of Ghana had

- 116 -
a beta coefficient of -.504. Habib and Vaughan (1986) found that the distance/utilization
relationship in Iraq had a beta coefficient of -.300. The results of these studies may be
considered similar to the walking time decay patterns from this study since the variables for
walking time and distance are highly correlated (see Chapter 4, section 4.4, for more detail).
The Santa Lucia Health Center’s coefficient for walking time is -.512, exhibiting the sharpest
distance (time) decay pattern. This finding suggests the smallest effective service area in the
study. This is possibly due to the competition from the Hombro á Hombro clinic, located in
the same town, causing a division in the clientele base along socio-economic lines, where the
poorer members of the community attend this government health center. This conclusion is
consistent with data collected from key informants and may suggest that people who patronize
this clinic are more spatially bound, with fewer options like transportation that would allow
them to overcome the friction of distance. It seems likely that these issues stem from low
income and poverty which is endemic in the service area.
6.4.2 Economic Status:
The Economic Status variable is significant in the System-wide model and the Santa Lucia
Health Center model. Studies such as Buor (2003) have suggested a significant relationship
between income and utilization. In most prior research this relationship has been positive,
where higher incomes enable greater utilization (closes the access barrier through better
transportation, affordability of service, etc.), and lower incomes generally make access to care
difficult, if not impossible. This relates to Andersen's (1968) enabling factors, where the cost
of care, cost of transport, and other affordability issues enable or inhibit use of health services.

- 117 -
In contrast, the results of this research indicates that in the context of the model the Economic
Status variable exhibits an inverse relationship to Utilization in the study area as a whole (the
system-wide model), where it was significant at the .006 level; and at the .029 level for the
Santa Lucia Health Center, in particular. This variable was found not to be significant in the
other two models. The general conclusion drawn from the two significant tests suggests that
as economic levels decline, utilization increases...but why?
When trying to explain this relationship, this research suggests that need plays an important
role in determining utilization. There is an obvious connection between economic status and
income levels, and low income levels with poverty. It has been shown that poverty can be
associated with decreased health status. Wolfe’s (1999) economic research suggests there is a
strong [positive] correlation between poverty and poor health. Joseph and Phillips (1984)
suggest this may be related to need, where lower income residents have a greater need for
health care services. This research suggests that Joseph and Phillips' connection is valid and
that higher 'need' may be driving higher utilization in poorer parts of the study area after
considering the effect of walking time and the Choice factor.
This research suggests that the small fee associated with the two government Health Centers
service is not inhibiting utilization, otherwise the poorer members of the community would
not be utilizing the service (and there would not be this significant inverse relationship). This
evidence suggests that the service is affordable, even to the poorer members (though not
necessarily the poorest) of the service area. Furthermore, this evidence suggests that many
patients from lower economic statuses may indeed be accessing the Santa Lucia Health

- 118 -
Center’s service, in contrast to possibly a broader distribution of economic statuses for the
Hombro á Hombro clinic. Several key informants have suggested this dynamic – that the
poorer members of the community go to the government Health Centers, while the wealthier
members go to the Hombro á Hombro clinic (which is considerably more expensive).
6.4.3 Choice:
The results of this research clearly indicate that there is a very significant relationship
between the Choice factor and health facility utilization, and that health-seeking behavior is
better approximated using a two-tier decision-making approach. The implication is that the
Choice factor is the only other variable studied that compares with walking time in explaining
such a high proportion of utilization. Thus, the Choice factor, like the walking time variable,
occupies a significant position in the overall utilization model.
These results point to a strong spatial patterning in the study area associated with the two
government health centers, which appear to suggest a tendency for people who attend the
government health centers do so in the municipality in which they reside. This is not always
the case, and some people prefer to attend the health center that is the closest to, but not in,
their municipality. But this does help confirm one conclusion drawn from the economic status
section that suggests that the poor are more spatially bound due to lack of transportation
options and therefore attend the closest government health center, usually in their
municipality.

- 119 -
The results of this research do not lead to a clear conclusion as to why this variable is
significant. There are a number of theories that may suggest why health choice decisions are
linked to the home administrative unit (municipality). One theory might suggest that people
come to the main town in their municipality for various economic reasons in addition to
servicing their health care needs. This could be considered the “activity space” (Jones and
Simmons, 1990) for these individuals. Since the government health center is also located in
this large central town, then it is within their normal weekly travels or “activity space”.
Young people also could follow a similar “activity space” pattern explaining their health
choice decisions, but not necessarily for the same reasons. Many young people come to the
central towns of Santa Lucia and Magdalena for high-school. These are the only two high-
schools in the area, and travel for these individuals to these central towns becomes a common
almost daily occurrence. Once again, since the health center is located in this central town,
then it is within their “activity space”, and patronage of the local health center should be
considered the easiest place to get primary health care service.
Another related way to explain this relationship would be to suggest that the choice variable
helps explain the patterns of health-seeking behavior relating to proximity of clinic and home
residence. This could relate to Fotheringham’s (1983) “competing destinations” concept
where people choose to attend the clinic that is closest to their home residence when given the
choice of more than one service provider. This theory suggests there is a higher utility
associated with utilization of a service that is closer to the patient, than utilization of a service

- 120 -
that is further away. For the most part, with a few exceptions, the closest government health
center would be located in the central town for each municipality.
The Hombro á Hombro clinic’s patient utilization patterns do not exhibit the same
municipality-based pattern of utilization. People who attend this clinic come from all parts of
the service area regardless of the municipality from which they reside. As has been mentioned
previously, this clinic’s clientele is more socio-economically diverse and patients come from a
broad array of locations. Patients who attend this clinic (which is considerably more
expensive than the government Health Centers) may choose this provider because of the
higher quality of service associated with this private clinic. As a visual analysis of the
Hombro á Hombro clinic’s utilization shows there is no east/west spatial patterning in their
utilization. {See Hombro á Hombro clinic utilization map, Map 6.4}. This is confirmed by a
map of the residuals from the regression analysis of the Hombro á Hombro’s utilization model
that furthers this observation. See map 6.5 for more information.
6.4.3.1 Model Improvement: Does the addition of the Choice variable really improve the
model’s performance? When considering this question, a comparison of the residuals from the
model (both before and after the addition of the Choice variable) seems to be in order. An
average of the absolute value of the residuals from the regression analysis is compared for
both iterations of the model. The results indicate that the average deviation in residuals for the
model without the Choice factor is .73, compared to .57 if we include the Choice factor. This
amounts to a 21% reduction in deviation from the estimated regression line, and is a clear
indication of the model’s improvement.

- 121 -
This research has tested other measures including a modified Huff model, and simple
proximity measures to nearest health facility. Neither of these measures has been able to
capture the level of significance, and improvement in the explanatory power of the model
(indicated by the R2) that this Choice variable has. This is partly due to the compound nature
of the Choice variable. It considers a two-tier decision-making process, which more
accurately reflects the complex nature of the health-seeking decision-making process in the
context of this rural, Central American region.
ÊÚ
ÊÚ
ÊÚ#
%
#
%
#
##
#
#
%
%
#%
%
#
%
#
#
#
%
%#
#
#
%
#
#
%
%
#
#
Aguila
Espino
BarrealLeoncito
Llanitos
Tablones
Palacios
San Jose
San Juan
Banaderos Junquillo
Las Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
El Jicaral
La Montana
Las Aradas
Las Marias
Las Marias
San Marcos
San Marcos
San Rafael
Santa Rita
Cordoncillo
La Ceibilla
Santa Lucia
Los Horcones
San Francisco
El Salvador
Hombro a Hombro Clinic Residuals N
0 2000 4000 Meters
Aldeas012
Roads11 - 22 - 33 - 4
ÊÚ Clinics
Hombro a Hombro Residuals
% -2.8 - -1.4
% -1.4 - 0
# 0 - 1
# 1 - 2
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region by Jonathan Baker, Chris Carr, and Andrew Bazemore.
Map 6.5: Residuals – Hombro á Hombro Clinic

- 122 -
In summary, the Choice variable helps determine health choice decisions within the study
area. This variable considers both type of service, and proximity to provider as important
variables in the decision-making process. This composite variable is constrained so that the
decision reflects a two-tier decision-making process. This variable describes the first tier of
the health choice decision as being a-spatial (private versus public primary care service),
which is based on quality of service and other needs based considerations. After the first tier
of the decision has been made, then the decision turns to a spatial-type decision, based loosely
on proximity, through the consideration of municipality of residence.
6.5 Residuals Analysis:
The following section looks more closely at the maps of the residuals generated for this study.
Residuals are the difference between an observed value and the value predicted by the model
(SPSS, 2000). An analysis of the residuals from the estimated equation provides an
opportunity to compare the individual cases that lie the furthest from the estimated
relationship. The residual is the vertical distance an instance of the sample is away from the
calculated regression line. If the model is a close fit to the observed data then the residuals
will be small, but if it is not, then the residuals will be large. The coefficient of determination
(R2) is a measure of “goodness of fit”, and can help support an examination of the residuals
from the regression analysis.
In this research, residuals are mapped, and used to establish how well the model explains the
overall distribution of the data. In the case of the Choice variable, residuals mapping helps to

- 123 -
confirm an even distribution of residuals exists for the Hombro á Hombro clinic throughout
the study area. This is important in establishing the validity of the first assumption used in the
Choice variable, namely that there is no structural bias in the model with regard to the private,
Hombro á Hombro clinic utilization.
6.5.1 Residuals from Hombro á Hombro Model
Looking at Hombro á Hombro’s residuals map (Map 6.5) may help to identify things
occurring in the study area that are not explained well in the model. The Hombro á Hombro
utilization model has an R2 of .22 which indicates that only 22% of the deviation in utilization
is explained by the model. At the same time, this also implies that 78% of the deviation is not
accounted for in the model. Therefore, in an effort to try to explain the two greatest residuals
(largest deviations) may give some direction on how to improve the model for future research.
The two villages with the most extreme residuals (and they are quite far from the regression
line compared to the others) are Bañaderos and San Marcos, Colomoncagua. This research
suggests this error can be explained.
Bañaderos, in the extreme western periphery has a very strong positive residual, indicating a
high level of utilization relative to the model’s predicted value. This may be explained by a
new roadway servicing this once remote and isolated area. It is believed there has been a
certain amount of pent-up demand for health service in this area causing a higher than normal
level of utilization at the Hombro á Hombro clinic. After the addition of a roadway, citizens
are now able to rent a truck to transport them to the Hombro á Hombro clinic. This was
confirmed by a key informant (Suarez, 2005) at the clinic as a common way for people from

- 124 -
Bañaderos to travel the 12 plus kilometers to the Hombro á Hombro clinic. It is expected that
this utilization index rate will move towards a more normalized rate sometime in the future.
San Marcos, Colomoncagua, was a different story. This village is in the extreme eastern
periphery of the study area and has a strong negative residual, indicating a very low utilization
relative to the model’s predicted value. This research suggests that this is due to a new health
facility now operating to the east of San Marcos. This health facility is another university
sponsored health clinic (similar to Hombro á Hombro), and is closer to the people who live in
San Marcos, Colomoncagua, than any of the study area clinics. Since our study area was
originally defined in December 2003 based on attendance at the Hombro á Hombro clinic, it
is understandable that things may have changed, and people who once came from San Marcos
to attend the Hombro á Hombro clinic, no longer do so.
6.5.2 Residuals for Overall Study Area
The following section looks at a map of the residuals from the regression modeling for the
overall study area. See maps 6.6 for a visual representation of the geographical arrangement
of the regression residuals, where negative residuals [the red squares] represent areas of over-
estimation by the model, and positive residuals [the blue circles] represent areas of under-
estimation by the model. This map clearly suggests that there is an east/west bias in the
residuals for the overall service area (even after the addition of the Choice variable), that is
not accounted for by the model. One possible explanation for this is that the value of the
choice variable is assigned arbitrarily. In improving the model, future research may wish to
focus on assigning weights to the values given to the Choice variable. This, in turn, may more

- 125 -
adequately describe the east/west spatial patterns that exist in the study area, and improve the
predictive capacity of the model.
ÊÚ
ÊÚ
ÊÚ%
%
%
%
#
#%
%
%
%
%
#%
%
#
#
#
%#
%
#%
#
%
%
%
%
#
%
%
%
Aguila
Espino
BarrealLeoncito
Llanitos
Tablones
Palacios
San Jose
San Juan
Banaderos Junquillo
Las Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
El Jicaral
La Montana
Las Aradas
Las Marias
Las Marias
San Marcos
San Marcos
San Rafael
Santa Rita
Cordoncillo
La Ceibilla
Santa Lucia
Los Horcones
San Francisco
El Salvador
Overall Service Area Residuals N
0 2000 4000 Meters
Aldeas012
Roads11 - 22 - 33 - 4
ÊÚ Clinics
Total Residuals
% -2.6 - -1.25
% -1.25 - 0
# 0 - 1.25
# 1.25 - 2.6
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region by Jonathan Baker, Chris Carr, and Andrew Bazemore.
Map 6.6: Residuals – Overall Service Area
Other than the east/west patterning previously mentioned, conclusions from the residual
mapping of the overall service area are difficult to make because there is no other spatial
patterning apparent in the study area. Therefore, this map does not suggest additional
variables to study. This leaves us with a simple conclusion; the additional error in the model
could be derived from other non-spatial sources, or is random.

- 126 -
6.5.3 Residuals for Magdalena Health Center Model
The following map represents the residuals for the Magdalena Health Center. San Marcos,
Colomoncagua stands out with exceptionally low utilization relative to the predicted value
from the regression equation. Following a similar logic from the Hombro á Hombro model,
the people from San Marcos may be accessing a new clinic further to the east and outside of
this service area, thus causing their low utilization. La Ceibilla, in the southern portion of
Municipality of Magdalena, also stands out with low utilization. This may simply be
explained by relatively easy access to the town of Santa Lucia and the two clinics there. This
village has relatively high utilization for both the Hombro á Hombro clinic and the Santa
Lucia Health Center, but low utilization for the Magdalena Health Center. This would be
considered one of the exceptions, where people in this village prefer to travel to the closer
clinic, though outside of their municipality, to received primary health care.
Looking at another village with a strong negative residual, San Jose, in the western portion of
the study area, exhibits a very low utilization level relative to the Magdalena Health Center
model. When considering possible explanations, it is important to understand that San Jose is
located over seven kilometers and 2.5 hours estimated walking time from Santa Lucia, and
further from Magdalena. This friction of distance factor alone may explain this low
utilization, but it may also be more complicated than this.
When considering other factors, it is necessary to understand San Jose in the context of the
study area. Firstly, San Jose is in a different Municipio, namely San Antonio. Secondly, the
village of San Jose has its own private health clinic, but according to key informants (Coello,

- 127 -
2003) it has no resources (staff or supplies) and is normally closed. Thirdly, the town of San
Antonio has its own government health center (5.25 kilometers to the west of San Jose), so it
is likely that some of the people in San Jose are going [west] to the town of San Antonio for
their health service needs. With three alternative options for primary health care it is therefore
less likely that people will travel to Magdalena for health service.
ÊÚ
ÊÚ
ÊÚ%
%
#
%
#
##
#
%
%
%
#%
%
#
%
#
%
%
%
%%
#
#
%
#
#
#
#
#
#
Aguila
Espino
BarrealLeoncito
Llanitos
Tablones
Palacios
San Jose
San Juan
Banaderos Junquillo
Las Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
El Jicaral
La Montana
Las Aradas
Las Marias
Las Marias
San Marcos
San Marcos
San Rafael
Santa Rita
Cordoncillo
La Ceibilla
Santa Lucia
Los Horcones
San Francisco
El Salvador
Magdalena Health Center Residuals N
0 2000 4000 Meters
Aldeas012
Roads11 - 22 - 33 - 4
ÊÚ Clinics
Magdalena Residuals
% -2 - -1
% -1 - 0
# 0 - 1
# 1 - 2.2
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region by Jonathan Baker, Chris Carr, and Andrew Bazemore.
Map 6.7: Residuals – Magdalena Health Center
In contrast, Los Pozos has a utilization index level that is higher than the model predicts. This
may be explained by access from the best roadway in the area leading almost directly to the
Magdalena Health Center. It is expected that collective truck transport is both efficient and

- 128 -
cheap for people residing in this village. This village may be used as a good example of how
things might be if the transportation network is improved in the service area. See Map 6.7 of
the Magdalena Health Center residuals for more information.
6.5.4 Residuals from Santa Lucia Health Center Model
The Santa Lucia Health Center residuals map displays a pattern that can be explained with a
focus on access. The high residuals villages of Las Aradas, La Ceibilla, and San Juan, all are
relatively close to Santa Lucia and offer no major physical barrier (like a mountain) in their
pathway. Access to the Santa Lucia Health Center is relatively good for all three villages,
even if traveling by foot. The very negative residual indicated for San Francisco, on the other
hand, may be explained by the existence of two other clinics closer to this village and the
better access they provide. See Map 6.8.

- 129 -
ÊÚ
ÊÚ
ÊÚ%
%
#
%
%
#%
#
#
%
#
#%
#
%
%
%
%
%
#
%%
#
%
%
#
#
#
%
#
%
Aguila
Espino
BarrealLeoncito
Llanitos
Tablones
Palacios
San Jose
San Juan
Banaderos Junquillo
Las Lomas
Los Pozos
Magdalena
San Pablo
TalquezalEl Castano
El Jicaral
La Montana
Las Aradas
Las Marias
Las Marias
San Marcos
San Marcos
San Rafael
Santa Rita
Cordoncillo
La Ceibilla
Santa Lucia
Los Horcones
San Francisco
El Salvador
Santa Lucia Health Center Residuals N
0 2000 4000 Meters
Aldeas012
Roads11 - 22 - 33 - 4
ÊÚ Clinics
Santa Lucia HC Residuals
% -2 - -1
% -1 - 0
# 0 - 1
# 1 - 2
Map data from the Honduras Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente, and fieldwork conducted in the region by Jonathan Baker, Chris Carr, and Andrew Bazemore.
Map 6.8: Residuals – Santa Lucia Health Center
6.6 Summary of Results
From an examination of the utilization and residuals maps, we are able to conclude the
following:
• High utilization areas may be the result of good roads resulting in cheap efficient
collective truck transportation. This reduces the barrier of distance. Such may be the
case for Magdalena and Los Pozos in the system model.
• High utilization areas may be a result of new improvements in access, where before
there were none. This may be the case with the village of Bañaderos.

- 130 -
• Low utilization areas may be the result of competition from other clinics outside the
Santa Lucia service area. This may be the case with San Marcos, Colomoncagua, or
San Jose.
• There is an east/west spatial pattern in the service areas for the two public Health
Centers, one servicing the eastern municipality of Magdalena, and one servicing the
western municipalities of Santa Lucia and San Antonio.
• There is no (east/west) spatial patterning in the Hombro á Hombro clinic’s service
area.
Based on the regression analysis of the presented gravity model, this research has come to the
following general conclusions:
• There is a strong relationship between primary health care utilization and walking
time, economic status and the Choice factor. The R2 of the system-wide model is .64,
which indicates that 64% of the variance in utilization index can be explained by the
combined movement of these variables. This model may be improved with further
empirical study.
• Distance and estimated walking time are both highly related. Both variables indicate a
negative or inverse relationship with utilization, a relationship that is expected. This
inverse relationship to utilization represents a travel-time decay pattern that is
consistent with distance decay patterns from other similar developing world research
(see Buor, 2002, for comparison).
• The Choice factor is highly significant and provides an instrumental improvement in
the system-wide model’s performance. This research shows that by creating a variable

- 131 -
that combines health service choice (private versus public service) and the
municipality of residence (proximity to care) a better estimate of health-seeking
behavior results. The value of combining simple variables into a complex variable
such as this indicates the complexity of human decisions, and shows potential
direction for future research.
• The principles of the model developed in this study can be generalizable throughout
the developing world, but the parameters need to be recalibrated to reflect the unique
aspects of the new study area.
• Utilization analyses such as those performed in this study can be completed in a
relatively short period of time, given expertise in geographic field methods (including
GPS & GIS) and availability of in-country resources.
• This study yields a large amount of useful information for health service planners
working in the region.
• This model provides for a unique way of analyzing utilization in the developing world
which may be applied to other similar locations.
6.7 Chapter Summary
This chapter shows that utilization patterns can be explained to a large extent by factors
relating to walking time, economic status, and the combined affect of health service type and
proximity to care (the Choice factor). This chapter illustrates that it is difficult to have one
model that works equally well for different types of clinics. Public clinics appear to have
different factors effecting utilization patterns, compared to a private clinic.

- 132 -
In this study a modified gravity model is constructed to help explain utilization behavior in
the study area, and is tested using log transformed variables and multiple regression analysis.
Utilization patterns for the combined service area are analyzed, as are the utilization patterns
for the three individual clinics. The explanatory variables for walking time and choice were
found to be very significant in explaining utilization behavior.
The following chapter summarizes this research project and expands on the conclusions
identified in this chapter.
- 133 -
CHAPTER SEVEN: CONCLUSIONS AND RECOMMENDATIONS
This research project studies health service provision by focusing on health facility utilization
in a poor region of southern Honduras. More specifically, this study uses a combination of
spatial-interaction modeling and multiple regression techniques to develop and test a model
used to predict the spatial patterns of utilization. This study examines actual utilization
patterns from three health clinics, relates them to several socio-economic and geographic
characteristics existing in the study area, and forms conclusions about health-seeking behavior
based on those relationships.
The results of this research are consistent with other research done in the field of health
facility utilization. Utilization behavior clearly exhibits an inverse relationship to travel time.
The variable for health choice, a variable not previously studied, was found to be very
significant. Furthermore, variables for education and economic status are also found to be
significant factors explaining utilization. Since prior research provides inconsistent results
with regard to education and economic status, this research helps confirm their relationship to
utilization in a rural developing world location.
The Choice factor is a new variable not found in previous research. This is a compound
variable that considers health choices as a two-part decision process, including the selection
of service type (private versus public) and the selection of a health facility associated with
one’s home municipality. Given this variable's highly significant results, this study suggests
that health-seeking behavior is complex and is best represented by a compound variable of
this kind. This is a significant contribution to the literature not only because it helps to

- 134 -
identify spatial-interaction patterns, but also because it leads the way for future studies to
explore other combinations of variables that may further explain this complex health care
decision-making process.
This research also explores the use of a way to estimate walking travel time. In a service area
where most people walk to health services, the intuitive appeal of using walking time as an
alternative measure of the friction of distance is great. No prior research has used this method
(an established method for estimating hiking times in mountainous locations), in health
service research. Given the large amount of time committed to calculating the walking time
estimates, this research concludes that network distance, being easy and efficient to calculate
using a GIS, is the more efficient measure for future studies. Other measurements of the
friction of distance may also be considered for future research. One alternative may be to
refine the walking-time variable to a measure of "effort expended" (see Zipf, 1949) - using
calories or economic cost.
This project also contributes to the body of research through its extensive fieldwork. A great
deal of information was collected and compiled for this study through primary and secondary
sources. Techniques were developed to better assist in the collection of data in a poorly
understood place such as southern Honduras. The GPS proved to be an invaluable tool in
locating places, roads and trails in the service area, and its ability to download this collected
information for use in a GIS. Interview and sampling techniques were also developed to assist
in attaining important characteristics relating to health-seeking behavior.

- 135 -
Challenges were encountered during this study. Of particular interest was the challenge of
reconciling the clinic attendance records with the national census. A method of reconciling
the census point data with geo-referenced “Village” locations was devised using a proximal
area method of census point unit assignment. This method is flexible and offers an
opportunity to use data gathered at different scales to be aggregated to a scale that is
consistent with other sources and allows for further analysis. This is a methodological
achievement that can be used in future fieldwork applications throughout the world.
The following section describes lessons learned in the field, followed by a general discussion
on fieldwork in Honduras. This is followed by a section on policy implications geared toward
improving health services in the study area. The chapter and paper concludes with some
suggested questions for future research.
7.1 Lessons learned in the field:
The lessons learned while conducting fieldwork in Honduras were as follows:
• Organize the trip (as much as possible) in advance. Write up anticipated questions for
interviews; know you goals; research design; and what data you will need for your
research. Develop a task list and time-line. This will help ensure that your time in the
field is well spent and that you are able to get as much information as possible from a
given trip. A good research proposal should help in this regard.
• Communicate and network: talk with as many knowledgeable persons as possible to
try to understand existence, form and availability of data.

- 136 -
• The best information is not always available through internet, commercial or other
common secondary resources.
• Be patient, but persistent. Don’t give up trying to find your data.
• If all else fails, go there – it is sometimes more effective if you are in-person, rather
than a faceless name on an email.
• Above all, when conducting research in Latin America, be flexible, to accommodate
the more “relaxed” Latino way of doing things. Remember the key word for us
Gringos when in Latin America – “Tranquilo”.
In general the fieldwork experience was a very good. Without exception the Hondurans that
were encountered during the fieldwork were friendly and helpful. This researcher was
particularly impressed with the attitudes of the employees of La Clinica Hombro á Hombro,
including the doctors and staff and several key members of the Santa Lucia community, in
their willing assistance in the collection and interpretation of data needed for this research.
Furthermore, the employees of La Secretaria de Estado en los Despachos de Recursos
Naturales y Ambiente in Tegucigalpa were also very helpful in providing the very much
needed Honduran GIS/Census files.
7.2 Limitations of Fieldwork:
The limitations of the fieldwork include the following:
1. Key informant interviews – may be biased in a way based on experiences and
perceptions. Nonetheless, key informants were selected based on their knowledge of

- 137 -
the study area and expertise in the subject matter, and to reflect a balance of leadership
qualities, genders, economic strata, age, etc.
2. Economic Status variable – based on survey summary assessments. These may be
biased in some way based on perceptions of “wealthier” versus “poorer” villages. Key
informants were selected based on their comprehensive knowledge of the study area.
Basic economic data such as average household income were not available for this
study. Many families in the study area live a traditional subsistence lifestyle. In these
families there is a lack of a currency-based economy. Furthermore, there was lack of
funds to collect this type of information.
3. Census data may be inaccurate. Inaccuracy of the population counts for each village
can cause errors in the analysis. Also, the educational attainment and employment
variables were based on census data. These variables also may contain inaccurate data.
Nonetheless, the 2001 Honduran National Census is the best possible source for this
type of information because it gives detailed, unbiased demographic information.
Furthermore, the 2001 census is the most current one available for this type of
research.
4. Attendance samples do not consider repeat visits. Some chronic conditions may need
repeated visits to the clinic. The attendance samples do not consider this possibility. If
there is nonrandom distribution of frequent visitors by village, then these places can
skew the results of this analysis.
5. Utilization was not broken down by type of visit, nor chief complaint, which may
impact utilization patterns differently than the aggregate measure. Attendance samples
do not consider type and severity of illness. Chronic problems such as headaches are

- 138 -
commonly not life threatening. Other medical problems such as Dengue or Malaria
can be life threatening. Since this analysis does not consider the type or severity of
illness, it is not able to distinguish between the more important and less important
medical issues.
6. The dependant Variable (utilization) does not capture people who do not come to the
clinics, and is therefore not a direct measure of access to care. Utilization looks at the
characteristics of those who come to a health facility, whereas access looks at the
characteristics that enable or disable use of a health service. Utilization studies
consider access factors (such as distance to care) as one determinant of utilization, but
the utilization index such as the one used in this study only measures access indirectly.
The calculated utilization index ratio can infer access because it is a measure of the
relative use of the health facility (attendance divided by population). See section 4.2.1
for details on the calculation of the utilization index. This analysis is based on
utilization and does not directly measure the characteristics of those who do not come
to the clinics and is therefore a potential source of error in the study.
7.3 Policy Implications:
This section makes a few recommendations aimed at improving health care service in the
study area.
7.3.1 Accessibility Improvements:
One way to improve accessibility is to offer periodic field-clinics at auxiliary sites to be
conducted in underserved communities on a regular basis. One auxiliary site could be located

- 139 -
southwest of the main clinic (Santa Rita), another northwest (San Jose) and one southeast (Las
Lomas). The main idea here is to bring the doctors to the people, rather than to transport the
people, to the clinic. The Hombro á Hombro clinic has the infrastructure needed to get the
doctors to these auxiliary sites. These auxiliary-clinics could be acquired with little or no cost.
In the southwestern and northwestern auxiliary locations, there are already health clinics, but
no staff to run them. In the eastern auxiliary service area, an old school house or church could
be used. The treatments are often relatively simple, so no need for sophisticated equipment.
Also, the Hombro á Hombro clinic has a sufficient amount of meds to supply auxiliary site
needs.
7.3.2 Community Assessments:
This research also recommends the use of community medical assessments to evaluate high
utilization areas. If an assumption is made that high utilization places are such because of
higher than normal need, then a logical conclusion would be that there may be some medical
challenge in the village or community that needs to be addressed. An analysis similar to this
current research could be used to identify villages with abnormally high clinic utilization.
This could be combined with medical assessment expertise from visiting medical brigades. A
community assessment could then be combined with a GIS analysis to help to identify “hot
spots” which may lead to identifying situations like a contaminated water supply. Identifying
places such as these could have a large positive impact on the health status of people who live
in the area.

- 140 -
7.3.3 Transportation Improvements:
This research also recommends the investigation of improvements to the transportation
network. Significant improvements in access to care can be achieved through improvements
in the transportation network. One potential solution is targeted subsidized truck
transportation. Privately owned collective trucks are becoming more common in the Santa
Lucia service area, offering improved access to primary health care providers such as the
Hombro á Hombro clinic. A portion of the cost of this transportation could be subsidized by
the clinic and paid directly to the transportation operators. This approach could focus on those
least able to pay, such as subsistence farmers, or those living in the most remote locations.
7.4 Future Research:
The following is a list of potential research projects that can be done in Santa Lucia area or
other rural developing world locations that will help improve the understanding of health
services utilization.
The Choice variable has been shown to be effective in explaining utilization behavior in the
service area, but it can be improved. This research suggests a future project examining the
effect of weightings on the Choice variable, and the testing in other similar locations. Other
two-part choice variable may also be explored. One such combination may include questions
such as: To seek treatment or not? To use a Curandero or a clinic?
Another interesting project would be to investigate alternative variables that may help explain
utilization behavior. A variable indicating diagnosis has good potential for future research.

- 141 -
This could be used to separate chronic from acute conditions receiving attention at the
clinic(s), and might help identify variations in utilization based on medical condition. A
subsequent analysis of distance decay patterns by medical condition would provide for an
improved understanding of the friction of distance.
Another study would focus on one specific type of medical treatment such as dental treatment
at a facility such as the Hombro á Hombro clinic. The new dental facility at the Hombro á
Hombro clinic has been very successful and an investigation of utilization patterns for it
would be a very interesting enhancement to this research project.
Another very interesting project would be the investigation of improvements to the
transportation network. It is clear that improvements to the transportation network will
improve access to care issues throughout the service area, but this area is poor and
government-based transportation projects are not a probability. Nonetheless, private
transportation operators (collective truck transport) are already finding their way to the region.
As the number of these operators increase access issues should improve. An interesting future
research project would involve conducting a longitudinal study of changing utilization
patterns across the study area. A focus of this research could be on the changing patterns of
access.
An additional interesting study would examine the effect of traditional health care providers
(Curanderos) on health care utilization in the area.

- 142 -
One more suggested research project would analyze the effect of new health facilities on the
patterns of utilization in the service area. There are two new private clinics not far from Santa
Lucia. These new clinics at Santa Ana, and San Marcos de la Sierra could offer an
opportunity to further study utilization in a larger study area. This could help to support this
research project through confirmation of the models and methods used.
7.5 Concluding Comments
This research project has accomplished its goals. It has successfully developed a model for
use in primary care utilization research. Several variables, both old and new, have been
examined and tested in a micro-scale rural developing world location. This has yielded an
improved understanding of the determinants of utilization and health-seeking behavior, in
general, for the study area.

- 143 -
BIBLIOGRAPHY
Aczel, A.D. 1989. Complete Business Statistics. Boston, Irwin.
Aday, L.A. and R.M. Andersen. 1974. A Framework for the Study of Access to Medical Care. Health Services Research. 9: 208-20.
Allison, P.D. 1999. Multiple Regression. Thousand Oaks, CA, Pine Forge Press.
Andersen, R. 1968. A Behavioral Model of Families’ Use of Halth Services, Research Series No. 25. Chicago, Center for Health Administration Studies.
Andersen, R. and J. Newman. 1973. Societal and Individual Determinants of Medical Care Utilization in the United States. Milbank Memorial Fund Quarterly. 81: 95-123
Andersen, R.M. 1995. Revisiting the Behavioral Model and Access to Medical Care: Does it Matter? Journal of Health and Social Behavior. 36: 1-10.
Anderson, D. W. and R.M. Andersen. 1972. Patterns of use of health services. In H. Freeman, S. Levine and L Reeder (eds). Handbook of Medical Sociology, 2nd edition. Englewood Cliffs, New Jersey: Prentice-Hall. Cited from Joseph and Phillips (1984).
Ayeni, B., G. Rushton, and M.L. McNulty. 1987. Improving the geographical accessibility of health care in rural areas: A Nigerian case study. Social Science and Medicine. 25:1083-94.
Bailey, W. and D.R. Phillips. 1990. Spatial Patterns of Use of Health Services in the Kingston Metropolitan Area, Jamaica. Social Science and Medicine. Vol. 30 (1): 1-12.
Bazemore, A. 2005a. Interview – May 10, 2005.
Bazemore, A. 2005b. Interview – January 16, 2005.
Bazemore, A. 2005c. Interview – January 3, 2005.
Bazemore, A., R. Phillips, and T. Miyoshi. 2003. Using Geographic Information Systems to Define Healthcare Access in an Urban Community Health Center Network. ESRI International Health GIS Conference 2003, Arlington, VA. May 4-7 2003, http://gis.esri.com/library/userconf/health03/papers/pap3037.pdf
Bernheisel, C., A. Bazemore, and J. Baker. 2003. Application of GIS Technology to Disease Surveillance in a Rural Honduran Village. Poster presented at the 2003 IHMEC Conference.
Black, M., E. Steeve, P.N. Aguilar, M. Vidaurre and Z. El Morjani. 2004. Using GIS to Measure Physical Accessibility to Health Care. ESRI 2004 International Health Conference Proceedings.
Brane, S., A. Bazemore, S. Freedman, C. Kugel, L. Bishop, and J. Baker 2004. Baseline Health Assessment and Mapping of a Rural Honduran Village. 2004 IHMEC Conference Poster.
Buor, D. 2002. Distance as a predominant factor in the utilisation of health services in the Kumasi metropolis, Ghana. GeoJournal. Vol. 56: 145-157.

- 144 -
Buor, D. 2003. Analysing the primacy of distance in the utilization of health services in the Ahafo-Ano South district, Ghana. International Journal of Health Planning and Management. 18: 293-311
Buor, D. 2004. Determinants of utilisation of health services by women in rural and urban areas of Ghana. GeoJournal. 61(1): 89-102.
Christaller, W. 1966. The Central Places of Southern Germany. Translated by C.W. Baskin. Englewood Cliffs, NJ. Prentice Hall.
Church, R, and C ReVelle. 1974. The Maximal Covering Problem. Papers of the Regional Science Association. Vol 32: p. 101-18.
CIA 2004. World Factbook. Central Intelligence Agency. Downloaded from: http://www.cia.gov/cia/publications/factbook/
Cleary, P.D., D. Mechanic and J.R. Greenley. 1982. Sex differences in medical care utilization: an empirical investigation. Journal of Health and Social Behavior. 23: 106-119.
Coello, M. 2003. Interview and discussions – December 12-20, 2003
Coello, M. 2005. Interview - January 14, 2005
Cromley, E.K. and S.L. McLafferty. 2002. GIS and Public Health. New York, Guilford Press.
Daniell, G. and S. Smith. 2003. AMC White Mountain Guide, 27th edition. New Hampshire. Appalachian Mountain Club Books.
Daskin, M. 1995. Network and Discrete Location: Models, Algorithms, and Applications. New York. Wiley Interscience.
Davidson, P., R. Andersen, R. Wyn and E. Brown. 2004. A Framework for Evaluating Safety-Net and Other Community-Level Factors on Access for Low-Income Populations. Inquiry, 41(1): 21-38.
DeLaune, M. 2001. X-Tools. ArcView 3.xx Extension. Available at http://arcscripts.esri.com/
DeLourme. 2001. Pennsylvania Atlas & Gazetteer, seventh edition. DeLourme. Yarmouth, Maine.
Diaz, E. 2005. Interview – January 22, 2005.
DNR Garmin. 2004. Minnesota Department of Natural Resources, GPS software application. Downloaded from http://www.dnr.state.mn.us
Dutton, D. 1986. Financial, Organisational and Professional Factors Affecting Health Care Utilisation. Social Science and Medicine, 23 (7); 725-735.
Egunjobi, L. 1983. Factors Influencing Choice of Hospitals: A Case Study of the Northern Part of Oyo State, Nigeria. Social Science and Medicine, 17: 585-89.
Fotheringham, A.S. 1983. A new set of spatial-interaction models: the theory of Competing Destinations. Environment and Planning A. Vol. 15, 15-36.
Fredericksen H. 1964. Maintenance of malarial Eradication; Duplicated Report WHO/Mal./429, Geneva, p. 246, Table 1.

- 145 -
Gesler, W.M. 1984. Health Care in Developing Countries. Washington, DC: The Association of American Geographers.
Gesler, W.M., J.M. Jordan, A. Dragomir, G. Luta and J.G. Fryer. 1999. A Geographic Assessment of Health-Care Coverage In Two “Rural” North Carolina Communities. Southeastern Geographer. V. 39(2): 127-144.
Ghosh, A, and S. McLafferty. 1987. Developing Retail-Outlet Networks. In Location Strategies for Retail and Service Firms. Lexington, MA. Lexington Books.
Gibbs, K. and A. Emmanuel. 2004. Comprehensive GIS Application for West Nile Virus Surveillance. ESRI 2004 Health GIS Conference Proceedings.
Guagliardo, M.F. 2004. Spatial accessibility of primary care: concepts, methods, and challenges. International Journal of Health Geographics. 3:3. Available @ http://ij-healthgeographics.com/content/3/1/3
Habib, O.S. and J.P. Vaughan. 1986. The determinants of health services utilization in Southern Iraq: a household interview survey. International Journal of Epidemiology. 15: 395-403.
Halfon N., M Inkelas, H. DuPlessis, and P.W. Newacheck. 1999. Challenges in securing access to care for children. Health Affairs (Millwood), 18: 48-63.
Harvey, D. 1977. Social justice and the city. London: Edward Arnold
Hays M.S., A.R. Kearns, and W. Moran. 1990. Spatial patterns of attendance at general practitioner services. Social Science and Medicine. Vol. 31: 7. 773-781.
Heck, J. 2005a. Interview – January 21, 2005.
Heck, J. 2005b. Correspondence - March 14, 2005.
Hellen, J.A. 1986. Medical Geography and the Third World. In Medical Geography: Progress and Prospect (Edited by Pacione, M.), pp 284-332. London, Croom Helm.
Hodgart, R. L. 1978. Optimizing access to public services: A review of problems, models, and methods of locating central facilities. Progress in Human Geography. 2: 17-48.
Huff, D. L. 1963. The Probabilistic Analysis of Shopping Center Trade Areas. Land Economics. Vol. 39: 81-90.
IGN. 1984. Instituto Geografico Nacional. Tegucigalpa, Honduras, C.A.
INE. 2004. Instituto Nacional de Estadistica. Tegucigalpa, Honduras, C.A. The Honduras 2001 National Census. Downloaded from: http://www.ine-hn.org/
Jones, K. and J. Simmons. 1990. The Retail Environment. London, Routledge.
Jordan, H., P. Roderick, D. Martin, and S. Barnett. 2004. Distance, rurality and the need for care: access to health services in South West England. International Journal of Health Geographics. 3:21. September 2004. Available at: http://www.ij-healthgeographics.com/content/2/1/21
Joseph, A.E., and P. R. Bantock. 1982. Measuring Potential Physical Accessibility to General Practitioners in Rural Areas: A Method and Case Study. Social Science and Medicine. 16: 85-90.

- 146 -
Joseph, A.E. and D.R. Phillips. 1984. Accessibility & Utilization: Geographical Perspectives on Health Care Delivery. London: Harper & Row Ltd.
Joseph, A.E. and A. Poyner 1982. Interpreting patterns of public service utilisation in rural areas. Economic Geography. 58: 262-273
Knickman, J.R. 1998. A foundation executive on access measures. Health Affairs (Millwood). 17: 187-88.
Kohn, R. and K.L. White. (eds) 1976. Health Care: An International Study. Oxford: Oxford University Press.
Koos, E. 1954. The Health of Regionsville. New York: Columbia University Press. Cited from Joseph and Phillips, 1984.
Kurak, K. 2003. Unpublished health care interview surveys conducted at Shoulder-to-Shoulder health clinic during October 2003.
Love, D. and P. Lindquist. 1995. The Geographical Accessibility of Hospitals to the Aged: A Geographic Information Systems Analysis within Illinois. Health Services Research. Vol. 29: 629-51.
Mallick, R.K. and J.K. Routray. 2001. Identification and accessibility analysis of rural service centers in Kendrapara District, Orissa, India: a GIS-based application. International Journal of Applied Earth Observation and Geoinformation. 3(1): 99-105.
Mark, D.M., N. Chrisman, A.U. Frank, P.H. McHaffie, and J. Pickles. 2004. The GIS History Project. Accessed via the internet on December 20, 2004 at: http://www.geog.buffalo.edu/ncgia/gishist/bar_harbor.html
Martin, D. and H. C. W. L. Williams. 1992. Market-area analysis and accessibility to primary health-care centers. Environment and Planning A. Vol. 24 (7): 1009-19.
Meade, M.S., and R.J. Earickson. 2000. Medical Geography, 2nd edition. New York. The Guilford Press.
Moore, W.E. 1969. Social Structure and Behavior. In Lindzey, G. and E. Aronson (eds), The Handbook of Social Phychology, Vol 4, 2nd Edition. Pp. 283-322. Reading, Mass: Addison-Wesley.
Müller, I., T. Smith, S. Mellor, L. Rare, and B. Genton. 1998. The effect of distance from home on attendance at a small rural health centre in Papua New Guinea. International Journal of Epidemiology. 27: 878-884.
Neter, J., M.H. Kutner, C. J. Nachtsheim, and W. Wasserman. 1996. Applied Linear Statistical Models, 4th Edition. Chicago, Irwin.
Noor, A.M., D. Zurovac, S.I. Hay, S.A. Ochola, and R.W. Snow. 2003. Defining equity in physical access to clinical services using geographical information systems as part of malaria planning and monitoring in Kenya. Tropical Medicine and International Health. 8 (10): 917-926.
Oliver, A. and E. Mossialos. 2004. Equity of access to health care: outlining the foundations for Action. Journal of Epidemiology and Community Health. 58: 655-658.

- 147 -
Oppong J.R., Hodgson M.J. 1994. Spatial Accessibility to Health Care Facilities in Suhum District, Ghana. Professional Geographer. 46: (2): 199-209.
Parker, E.B., and J.L. Campbell. 1998. Measuring access to primary medical care: some examples of the use of geographic information systems. Health and Place. Vol. 4(2): 183-193.
Perry, B. and W. Gesler. 2000. Physical access to primary health care in Andean Bolivia. Social Science and Medicine. Vol. 50: 1177-1188.
Phillips, D.R. 1979. Spatial variations in attendance at general practitioners services. Social Science and Medicine. 13: 169-181.
Phillips, R.L., E.L. Kinman, P.G. Schnitzer, E.J. Lindbloom, and B. Ewigman. 2000. Using Geographic Information Systems to Understand Health Care Access. Archives of Family Medicine. Vol. 9: 971-978
Porter, D.E., K.A. Kirtland, M.J. Neet, J.E. Williams, and B.E. Ainsworth. 2004. Considerations for Using a Geographic Information System to Assess Environmental Supports for Physical Activity. Preventing Chronic Disease [serial online] Available from: http://www.cdc.gov/pcd/issue/2004/oct/04_0047.htm.
Porter, J.D.H. 1999. Geographical Information Systems (GIS) and the tuberculosis DOTS strategy. Tropical Medicine and International Health. Vol. 4(10): 631-633.
Powell, M. 1995. On the outside looking in: Medical geography, medical geographers and access to health care. Health and Place. Vol. 1: 41-50
Pratt, M. (editor). 2003. Down-to-Earth Approach Jumpstarts GIS for Dengue Outbreak. ArcUser. January-March, 2003. Vol. 6 (1)
Pyle, G.F. 1979. Applied Medical Geography. Wiley, New York.
ReVelle, C.S., and R.W. Swain. 1970. Central Facilities Location. Geographical Analysis. Vol. 2: 30-42.
Ricketts, T.C. 2002. Geography and Disparities in Health Care. In Guidance for the National Healthcare Disparities Report, National Academy of the Sciences.
Rodriguez, M. 2003. Interview and discussions – December 14-20, 2003.
Rodriguez, M. 2005. Interview and discussions – January 16-26, 2005.
Rushton, G. 1984. Use of location-allocation models for improving geographical accessibility of rural services in developing countries. International Regional Science Review. 9:217-40.
Scarpaci, J.L., 1984. A Methodological Note on Location-Allocation Models. American Journal of Public Health. Vol. 74 (10): 1155-1157.
Schultz, Ronald, R. 1975. A Space Potential Analysis of Physician Location. Proceedings of the Association of American Geographers. Vol. 7: 203-208.
SERNA - Secretaria de Estado en los Despachos de Recursos Naturales y Ambiente. 2005. GIS boundary shape files acquired for the 2001 Honduran National Census. Tegucigalpa.

148
Shannon G.W., R.L. Bashshur, and C.A. Metzner. 1969. The concept of distance as a factor in the accessibility and utilization of health care. Medical Care Review. Vol. 26: 143.
Shannon G.W. and G.E. Defer. 1974. Health Care Delivery: Spatial Perspectives. McGraw-Hill, New York.
Shoulder-to-Shoulder. 2005. Website accessed May 22, 2005. http://www.shouldertoshoulder.org
SPSS. 2000. Documentation accompanying release 10.1.0 of SPSS statistical analysis software. Chicago, IL.
Stock, Robert. 1983. Distance and the Utilization of Health Facilities in Rural Nigeria. Social Science Medicine. Vol. 17 (9): 563-70.
Stockburger, D.W. 2005. Multivariate Statistics: Concepts, Models, and Applications Accessed at: http://www.psychstat.smsu.edu/MultiBook/mlt06m.html 3/12/2005
Stonich, S.C. 1991. Rural Families and Income from Migration: Honduran Households in the World Economy. Journal of Latin American Studies. Vol. 23.
Stutz, F.P., and A.R. de Souza. 1998. The World Economy, third edition. Upper Saddle River, NJ, Prentice-Hall.
Suarez, M. 2005. Interview and discussions – January 16-26, 2005
Tanser F. and D. Wilkinson. 1999. Spatial implication of the tuberculosis DOTS strategy in rural South Africa: a novel application of geographic information systems and global positioning systems technologies. Tropical Medicine and International Health. 4: 634-638.
Taylor, P. 1975. Distance Decay in Spatial Interactions. Geo Abstracts Ltd. Norwich, England.
Tepe, L. 2005. Interview – March 15, 2005.
US Census Bureau. 2005. Website accessed May 20, 2005 at http://www.census.gov.
Wolfe, B. 1999. Poverty, Children’s Health, and Health Care Utilization. FRBNY - Economic Policy Review. Federal Reserve Bank of NY. September, 1999.
World Bank. 2003. Report retrieved from their website on 8.28.2003: http://www.worldbank.org/ poverty/scapital/whatsc.htm
Wyckoff, W. 1989. Central Place Theory and the Location of Services in Colorado in 1899. The Social Science Journal, 26 (4): 383-398
Zipf, G.K. 1949. Human behavior and the principle of least effort. New York, Hafner.

149
Appendix A: Bi-variate Correlations – System-wide Model
Variable Stat LN UTILLN
TIME LN_A4 LN EMPLN % EDU 6
LN ECON
LN COST LN RQ
LN CHOICE
LN_UTIL r 1 -0.55 0.284 -0.054 0.021 0.054 0.269 0.181 -0.712 (Utilization) Sig . 0.000 0.006 0.606 0.840 0.605 0.009 0.082 0.000
N 93 93 93 93 93 93 93 93 93LN_TIME r -0.55 1 -0.102 0.13 -0.252 -0.566 -0.091 -0.321 0.344
Sig 0.000 . 0.331 0.213 0.015 0 0.385 0.002 0.001N 93 93 93 93 93 93 93 93 93
LN_A4 r 0.284 -0.102 1 0 0 0 0.992 0 -0.527 (Attraction) Sig 0.006 0.331 . 1 1 1 0 1 0.000
N 93 93 93 93 93 93 93 93 93LN_EMP r -0.054 0.13 0 1 0.016 -0.059 0 -0.466 0.000
Sig 0.606 0.213 1 . 0.877 0.576 1 0 1N 93 93 93 93 93 93 93 93 93
LN % EDU 6 r 0.021 -0.252 0 0.016 1 0.123 0 0.18 0Sig 0.840 0.015 1 0.877 . 0.241 1 0.085 1N 93 93 93 93 93 93 93 93 93
LN_ECON r 0.054 -0.566 0 -0.059 0.123 1 0 0.152 0Sig 0.605 0 1 0.576 0.241 . 1 0.146 1N 93 93 93 93 93 93 93 93 93
LN_COST r 0.269 -0.091 0.992 0 0 0 1 0 -0.5Sig 0.009 0.385 0 1 1 1 . 1 0N 93 93 93 93 93 93 93 93 93
LN_Road r 0.181 -0.321 0 -0.466 0.18 0.152 0 1 0 Quality Sig 0.082 0.002 1 0 0.085 0.146 1 . 1
N 93 93 93 93 93 93 93 93 93LN CHOICE r -0.712 0.344 -0.527 0 0 0 -0.5 0 1
Sig 0.000 0.001 0 1 1 1 0 1 .N 93 93 93 93 93 93 93 93 93

150
Appendix A (continued): Bi-variate Correlations –Magdalena Health Center
Variable Stat LN UTILLN
TIME LN_A4 LN EMPLN % EDU 6
LN ECON
LN COST LN RQ
LN CHOICE
LN_UTIL1 r 1 -0.682 . -0.212 0.274 0.14 . -0.014 -0.79 (Utilization) Sig . 0 . 0.252 0.135 0.452 . 0.941 0
N 31 31 31 31 31 31 31 31 31LN_TIME r -0.682 1 . 0.28 -0.401 -0.473 . -0.163 0.535
Sig 0 . . 0.127 0.025 0.007 . 0.38 0.002N 31 31 31 31 31 31 31 31 31
LN_A4 r . . . . . . . . . (Attraction) Sig . . . . . . . . .
N 31 31 31 31 31 31 31 31 31LN_EMP r -0.212 0.28 . 1 0.016 -0.059 . -0.466 0.244
Sig 0.252 0.127 . . 0.931 0.754 . 0.008 0.187N 31 31 31 31 31 31 31 31 31
LN % EDU 6 r 0.274 -0.401 . 0.016 1 0.123 . 0.18 -0.332Sig 0.135 0.025 . 0.931 . 0.511 . 0.334 0.068N 31 31 31 31 31 31 31 31 31
LN_ECON r 0.14 -0.473 . -0.059 0.123 1 . 0.152 -0.014Sig 0.452 0.007 . 0.754 0.511 . . 0.415 0.942N 31 31 31 31 31 31 31 31 31
LN_COST r . . . . . . . . .Sig . . . . . . . . .N 31 31 31 31 31 31 31 31 31
LN_Road r -0.014 -0.163 . -0.466 0.18 0.152 . 1 0.14 Quality Sig 0.941 0.38 . 0.008 0.334 0.415 . . 0.453
N 31 31 31 31 31 31 31 31 31LN CHOICE r -0.79 0.535 . 0.244 -0.332 -0.014 . 0.14 1
Sig 0 0.002 . 0.187 0.068 0.942 . 0.453 .N 31 31 31 31 31 31 31 31 31

151
Appendix A (continued): Bi-variate Correlations – Santa Lucia Health Center
Variable Stat LN UTILLN
TIME LN_A4 LN EMPLN % EDU 6
LN ECON
LN COST LN RQ
LN CHOICE
LN_UTIL1 r 1 -0.444 . 0.14 -0.301 -0.043 . 0.324 -0.7 (Utilization) Sig . 0.012 . 0.452 0.1 0.816 . 0.076 0
N 31 31 31 31 31 31 31 31 31LN_TIME r -0.444 1 . 0.061 -0.141 -0.623 . -0.456 0.276
Sig 0.012 . . 0.743 0.451 0 . 0.01 0.132N 31 31 31 31 31 31 31 31 31
LN_A4 r . . . . . . . . . (Attraction) Sig . . . . . . . . .
N 31 31 31 31 31 31 31 31 31LN_EMP r 0.14 0.061 . 1 0.016 -0.059 . -0.466 -0.244
Sig 0.452 0.743 . . 0.931 0.754 . 0.008 0.187N 31 31 31 31 31 31 31 31 31
LN % EDU 6 r -0.301 -0.141 . 0.016 1 0.123 . 0.18 0.332Sig 0.1 0.451 . 0.931 . 0.511 . 0.334 0.068N 31 31 31 31 31 31 31 31 31
LN_ECON r -0.043 -0.623 . -0.059 0.123 1 . 0.152 0.014Sig 0.816 0 . 0.754 0.511 . . 0.415 0.942N 31 31 31 31 31 31 31 31 31
LN_COST r . . . . . . . . .Sig . . . . . . . . .N 31 31 31 31 31 31 31 31 31
LN_Road r 0.324 -0.456 . -0.466 0.18 0.152 . 1 -0.14 Quality Sig 0.076 0.01 . 0.008 0.334 0.415 . . 0.453
N 31 31 31 31 31 31 31 31 31LN CHOICE r -0.7 0.276 . -0.244 0.332 0.014 . -0.14 1
Sig 0 0.132 . 0.187 0.068 0.942 . 0.453 .N 31 31 31 31 31 31 31 31 31

152
Appendix A (continued): Bi-variate Correlations – Hombro á Hombro Clinic
Variable Stat LN UTILLN
TIME LN_A4 LN EMPLN % EDU 6
LN ECON
LN COST LN RQ
LN CHOICE
LN_UTIL1 r 1 -0.465 . -0.068 0.038 0.059 . 0.393 . (Utilization) Sig . 0.008 . 0.714 0.84 0.753 . 0.029 .
N 31 31 31 31 31 31 31 31 31LN_TIME r -0.465 1 . 0.039 -0.202 -0.634 . -0.38 .
Sig 0.008 . . 0.835 0.277 0 . 0.035 .N 31 31 31 31 31 31 31 31 31
LN_A4 r . . . . . . . . . (Attraction) Sig . . . . . . . . .
N 31 31 31 31 31 31 31 31 31LN_EMP r -0.068 0.039 . 1 0.016 -0.059 . -0.466 .
Sig 0.714 0.835 . . 0.931 0.754 . 0.008 .N 31 31 31 31 31 31 31 31 31
LN % EDU 6 r 0.038 -0.202 . 0.016 1 0.123 . 0.18 .Sig 0.84 0.277 . 0.931 . 0.511 . 0.334 .N 31 31 31 31 31 31 31 31 31
LN_ECON r 0.059 -0.634 . -0.059 0.123 1 . 0.152 .Sig 0.753 0 . 0.754 0.511 . . 0.415 .N 31 31 31 31 31 31 31 31 31
LN_COST r . . . . . . . . .Sig . . . . . . . . .N 31 31 31 31 31 31 31 31 31
LN_Road r 0.393 -0.38 . -0.466 0.18 0.152 . 1 . Quality Sig 0.029 0.035 . 0.008 0.334 0.415 . . .
N 31 31 31 31 31 31 31 31 31LN CHOICE r . . . . . . . . .
Sig . . . . . . . . .N 31 31 31 31 31 31 31 31 31

153
Appendix B: Modified Gravity Model Output Tables - System-wide model:
Model Summary
.712a .507 .501 .87609129
.783b .612 .604 .78105657
.802c .644 .632 .75285974
Model123
R R SquareAdjustedR Square
Std. Error ofthe Estimate
Predictors: (Constant), LN CHOICEa.
Predictors: (Constant), LN CHOICE, LN TIMEb.
Predictors: (Constant), LN CHOICE, LN TIME, LNECON
c.
Coefficientsa
-3.128 .111 -28.117 .000-2.689 .278 -.712 -9.672 .000
-.331 .574 -.576 .566-2.240 .264 -.593 -8.486 .000
-.604 .122 -.346 -4.949 .000.527 .632 .834 .407
-2.055 .263 -.544 -7.816 .000-.853 .147 -.489 -5.787 .000-.385 .137 -.222 -2.805 .006
(Constant)LN CHOICE(Constant)LN CHOICELN TIME(Constant)LN CHOICELN TIMELN ECON
Model1
2
3
B Std. Error
UnstandardizedCoefficients
Beta
Standardized
Coefficients
t Sig.
Dependent Variable: LN UTIL+1a.

154
Appendix B (continued): Modified Gravity Model Output Tables - System-wide model
Excluded Variablesd
-.346a -4.949 .000 -.463 .882-.126a -1.469 .145 -.153 .722-.116a -1.366 .175 -.143 .750.181a 2.533 .013 .258 1.000
-.054a -.734 .465 -.077 1.000.021a .287 .775 .030 1.000.054a .736 .464 .077 1.000
-.089b -1.153 .252 -.121 .715-.079b -1.039 .301 -.110 .743.079b 1.138 .258 .120 .883
-.009b -.139 .890 -.015 .981-.071b -1.044 .299 -.110 .928-.222b -2.805 .006 -.285 .636-.074c -.985 .327 -.104 .711-.064c -.867 .388 -.092 .738.066c .977 .331 .104 .878
-.004c -.055 .956 -.006 .980-.081c -1.230 .222 -.130 .926
LN TIMELN_A4LN_COSTLN_RQ_1LN_EMPLN_P_ED6LN ECONLN_A4LN_COSTLN_RQ_1LN_EMPLN_P_ED6LN ECONLN_A4LN_COSTLN_RQ_1LN_EMPLN_P_ED6
Model1
2
3
Beta In t Sig.Partial
Correlation Tolerance
Collinearity
Statistics
Predictors in the Model: (Constant), LN CHOICEa.
Predictors in the Model: (Constant), LN CHOICE, LN TIMEb.
Predictors in the Model: (Constant), LN CHOICE, LN TIME, LN ECONc.
Dependent Variable: LN UTIL+1d.

155
Appendix B (continued): Model Output Tables – Magdalena Clinic
Model Summary
.790a .625 .612 .92835441
.848b .719 .699 .81755448
Model12
R R SquareAdjustedR Square
Std. Error ofthe Estimate
Predictors: (Constant), LN CHOICEa.
Predictors: (Constant), LN CHOICE, LN TIMEb.
Coefficientsa
-2.629 .280 -9.393 .000-3.493 .503 -.790 -6.948 .000
.490 1.047 .468 .643-2.633 .524 -.596 -5.023 .000
-.711 .232 -.364 -3.065 .005
(Constant)LN CHOICE(Constant)LN CHOICELN TIME
Model1
2
B Std. Error
UnstandardizedCoefficients
Beta
Standardized
Coefficients
t Sig.
Dependent Variable: LN UTIL+1a.
Excluded Variablesc
-.364a -3.065 .005 -.501 .713.099a .854 .401 .159 .980
-.021a -.175 .863 -.033 .941.013a .107 .915 .020 .890.129a 1.144 .262 .211 1.000.011b .104 .918 .020 .901.038b .358 .723 .069 .909
-.085b -.761 .453 -.145 .819-.057b -.469 .643 -.090 .696
LN TIMELN_RQ_1LN_EMPLN_P_ED6LN ECONLN_RQ_1LN_EMPLN_P_ED6LN ECON
Model1
2
Beta In t Sig.Partial
Correlation Tolerance
Collinearity
Statistics
Predictors in the Model: (Constant), LN CHOICEa.
Predictors in the Model: (Constant), LN CHOICE, LN TIMEb.
Dependent Variable: LN UTIL+1c.
* The Ln A4, and Ln Cost variables were excluded because there is no variation for this model.

156
Appendix B (continued): Model Output Tables – Santa Lucia Health Center Model Summary
.700a .490 .473 .86701710
.747b .558 .527 .82135881
.794c .631 .590 .76485364
Model123
R R SquareAdjustedR Square
Std. Error ofthe Estimate
Predictors: (Constant), LN CHOICEa.
Predictors: (Constant), LN CHOICE, LN TIMEb.
Predictors: (Constant), LN CHOICE, LN TIME, LNECON
c.
Coefficientsa
-3.168 .194 -16.343 .000-2.479 .470 -.700 -5.280 .000
-.794 1.158 -.685 .499-2.213 .463 -.625 -4.782 .000
-.512 .246 -.271 -2.077 .047.856 1.295 .661 .514
-1.961 .445 -.554 -4.408 .000-.966 .303 -.512 -3.191 .004-.584 .254 -.355 -2.300 .029
(Constant)LN CHOICE(Constant)LN CHOICELN TIME(Constant)LN CHOICELN TIMELN ECON
Model1
2
3
B Std. Error
UnstandardizedCoefficients
Beta
Standardized
Coefficients
t Sig.
Dependent Variable: LN UTIL+1a.

157
Appendix B (continued): Model Output Tables – Santa Lucia Health Center
Excluded Variablesd
-.271a -2.077 .047 -.365 .924.230a 1.784 .085 .320 .980
-.032a -.232 .818 -.044 .941-.077a -.540 .594 -.101 .890-.034a -.251 .803 -.047 1.000.142b 1.007 .323 .190 .792.005b .037 .971 .007 .923
-.158b -1.154 .258 -.217 .831-.355b -2.300 .029 -.405 .575.087c .644 .525 .125 .762.017c .139 .890 .027 .921
-.176c -1.389 .177 -.263 .828
LN TIMELN_RQ_1LN_EMPLN_P_ED6LN ECONLN_RQ_1LN_EMPLN_P_ED6LN ECONLN_RQ_1LN_EMPLN_P_ED6
Model1
2
3
Beta In t Sig.Partial
Correlation Tolerance
Collinearity
Statistics
Predictors in the Model: (Constant), LN CHOICEa.
Predictors in the Model: (Constant), LN CHOICE, LN TIMEb.
Predictors in the Model: (Constant), LN CHOICE, LN TIME, LN ECONc.
Dependent Variable: LN UTIL+1d.
* The Ln A4, and Ln Cost variables were excluded because there is no variation for this model.

158
Appendix B (continued): Model Output Tables – Hombro á Hombro Clinic
Model Summary
.465a .216 .189 .72375628Model1
R R SquareAdjustedR Square
Std. Error ofthe Estimate
Predictors: (Constant), LN TIMEa.
Coefficientsa
-.883 .857 -1.030 .311-.509 .180 -.465 -2.828 .008
(Constant)LN TIME
Model1
B Std. Error
UnstandardizedCoefficients
Beta
Standardized
Coefficients
t Sig.
Dependent Variable: LN UTIL+1a.
Excluded Variablesb
.253a 1.452 .158 .265 .856-.050a -.301 .765 -.057 .998-.058a -.343 .735 -.065 .959-.394a -1.941 .062 -.344 .598
LN_RQ_1LN_EMPLN_P_ED6LN ECON
Model1
Beta In t Sig.Partial
Correlation Tolerance
Collinearity
Statistics
Predictors in the Model: (Constant), LN TIMEa.
Dependent Variable: LN UTIL+1b.
* The Ln A4, Ln Cost, and Ln CHOICE variables were excluded because there is no variation for the Hombro á Hombro clinic.
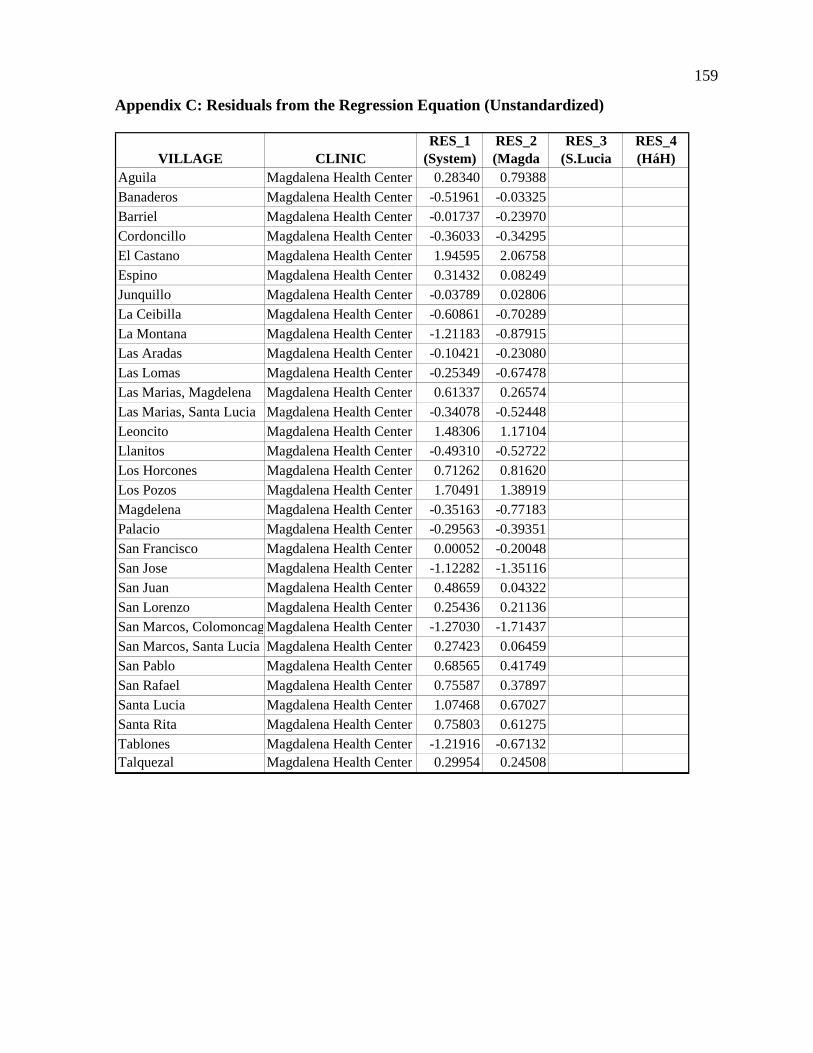
159
Appendix C: Residuals from the Regression Equation (Unstandardized)
VILLAGE CLINICRES_1
(System)RES_2 (Magda
RES_3 (S.Lucia
RES_4 (HáH)
Aguila Magdalena Health Center 0.28340 0.79388Banaderos Magdalena Health Center -0.51961 -0.03325Barriel Magdalena Health Center -0.01737 -0.23970Cordoncillo Magdalena Health Center -0.36033 -0.34295El Castano Magdalena Health Center 1.94595 2.06758Espino Magdalena Health Center 0.31432 0.08249Junquillo Magdalena Health Center -0.03789 0.02806La Ceibilla Magdalena Health Center -0.60861 -0.70289La Montana Magdalena Health Center -1.21183 -0.87915Las Aradas Magdalena Health Center -0.10421 -0.23080Las Lomas Magdalena Health Center -0.25349 -0.67478Las Marias, Magdelena Magdalena Health Center 0.61337 0.26574Las Marias, Santa Lucia Magdalena Health Center -0.34078 -0.52448Leoncito Magdalena Health Center 1.48306 1.17104Llanitos Magdalena Health Center -0.49310 -0.52722Los Horcones Magdalena Health Center 0.71262 0.81620Los Pozos Magdalena Health Center 1.70491 1.38919Magdelena Magdalena Health Center -0.35163 -0.77183Palacio Magdalena Health Center -0.29563 -0.39351San Francisco Magdalena Health Center 0.00052 -0.20048San Jose Magdalena Health Center -1.12282 -1.35116San Juan Magdalena Health Center 0.48659 0.04322San Lorenzo Magdalena Health Center 0.25436 0.21136San Marcos, Colomoncag Magdalena Health Center -1.27030 -1.71437San Marcos, Santa Lucia Magdalena Health Center 0.27423 0.06459San Pablo Magdalena Health Center 0.68565 0.41749San Rafael Magdalena Health Center 0.75587 0.37897Santa Lucia Magdalena Health Center 1.07468 0.67027Santa Rita Magdalena Health Center 0.75803 0.61275Tablones Magdalena Health Center -1.21916 -0.67132Talquezal Magdalena Health Center 0.29954 0.24508

160
Appendix C (continued): Residuals from the Regression Equation-Unstandardized
VILLAGE CLINICRES_1
(System)RES_2 (Magda
RES_3 (S.Lucia
RES_4 (HáH)
Aguila Sant Lucia Health Center 0.23457 0.05484Banaderos Sant Lucia Health Center -0.40534 -0.56862Barriel Sant Lucia Health Center -0.22985 -0.13682Cordoncillo Sant Lucia Health Center -0.43416 -0.39650El Castano Sant Lucia Health Center -0.11345 -0.08140Espino Sant Lucia Health Center -1.07901 -0.96904Junquillo Sant Lucia Health Center 0.91964 0.92574La Ceibilla Sant Lucia Health Center 1.69593 1.49860La Montana Sant Lucia Health Center -0.19352 -0.32561Las Aradas Sant Lucia Health Center 0.65128 0.70635Las Lomas Sant Lucia Health Center -0.63973 -0.55919Las Marias, Magdelena Sant Lucia Health Center 0.00868 0.05327Las Marias, Santa Lucia Sant Lucia Health Center -0.23869 -0.17108Leoncito Sant Lucia Health Center 0.80535 0.84063Llanitos Sant Lucia Health Center 0.28551 0.38464Los Horcones Sant Lucia Health Center 0.10376 -0.05737Los Pozos Sant Lucia Health Center -0.49398 -0.45205Magdelena Sant Lucia Health Center -0.52940 -0.34736Palacio Sant Lucia Health Center 0.02019 0.07815San Francisco Sant Lucia Health Center -1.80299 -1.80669San Jose Sant Lucia Health Center -0.39990 -0.20882San Juan Sant Lucia Health Center 1.18615 1.16617San Lorenzo Sant Lucia Health Center -0.63480 -0.58878San Marcos, Colomoncag Sant Lucia Health Center -0.90052 -0.80176San Marcos, Santa Lucia Sant Lucia Health Center 1.12740 1.28251San Pablo Sant Lucia Health Center 0.18509 0.34990San Rafael Sant Lucia Health Center 0.39931 0.46576Santa Lucia Sant Lucia Health Center -0.55088 -0.45176Santa Rita Sant Lucia Health Center 0.79001 0.91712Tablones Sant Lucia Health Center -0.41061 -0.62210Talquezal Sant Lucia Health Center -0.24170 -0.17873

161
Appendix C (continued): Residuals from the Regression Equation-Unstandardized
VILLAGE CLINICRES_1
(System)RES_2 (Magda
RES_3 (S.Lucia
RES_4 (HáH)
Aguila Hombro á Hombro 0.48491 0.91569Banaderos Hombro á Hombro 0.79781 1.15279Barriel Hombro á Hombro -0.49133 -0.21910Cordoncillo Hombro á Hombro -0.33807 -0.30298El Castano Hombro á Hombro 0.84810 0.81387Espino Hombro á Hombro -0.02038 0.17258Junquillo Hombro á Hombro 0.07979 0.30995La Ceibilla Hombro á Hombro 0.35619 0.74330La Montana Hombro á Hombro -1.09442 -0.59748Las Aradas Hombro á Hombro -0.48959 -0.43012Las Lomas Hombro á Hombro -1.02528 -1.20818Las Marias, Magdelena Hombro á Hombro 0.11053 0.04752Las Marias, Santa Lucia Hombro á Hombro -0.45830 -0.41243Leoncito Hombro á Hombro 0.38834 0.35720Llanitos Hombro á Hombro -0.53289 -0.67088Los Horcones Hombro á Hombro -0.32557 0.04289Los Pozos Hombro á Hombro 0.07583 0.02182Magdelena Hombro á Hombro 0.50195 0.30742Palacio Hombro á Hombro -0.42725 -0.38746San Francisco Hombro á Hombro -0.18164 -0.07642San Jose Hombro á Hombro 0.29718 0.07655San Juan Hombro á Hombro 0.28914 0.33773San Lorenzo Hombro á Hombro 0.47691 0.52306San Marcos, Colomoncag Hombro á Hombro -2.37515 -2.61787San Marcos, Santa Lucia Hombro á Hombro 0.14818 0.07250San Pablo Hombro á Hombro 0.91532 0.88259San Rafael Hombro á Hombro -0.17692 -0.31316Santa Lucia Hombro á Hombro -0.80856 -0.37572Santa Rita Hombro á Hombro 0.32965 0.18488Tablones Hombro á Hombro -0.34016 0.21717Talquezal Hombro á Hombro 0.43097 0.43228

162
Appendix D: Key Informant Interview
The following is a summary of Key Informant #1 Interview which can be used as an
example of interviews used during fieldwork for this study. The interview took place in
Santa Lucia, Honduras during December 2003, and uses a basic question and answer
format with questions prepared before the interview, and follow-up question presented
when appropriate.
Question #1: Describe the basic characteristics of the most common patients: Most
patients come from the two major nearby towns of Magdalena, and Santa Lucia (more
than 50%).
• 50% of patients are less than 5 years old, mostly female.
• 10-12 years ago most patients came from the rural villages, now mostly from two
major towns (Magdalena, & Santa Lucia). Though Magdalena has its own clinic it
does not have as good a facility (medical equipment), nor does it have as good a staff
(Doctor not always present). Consequently, many people now are choosing to travel
45 minutes by foot to come to the Santa Lucia Clinic. Good reputation of Shoulder-to-
Shoulder/Hombro a Hombro Clinic also a factor. Patients coming by car from San
Antonio also similar situation. San Antonio has clinic, but not as good a service.
Question #2: Describe the characteristics of the most serious patients: Some of the most
problematic areas are the most remote places. People coming from far away (remote)
villages, often wait too long before coming to clinic. Many go to local traditional healers,
who often give out poor advice. This delays the treatment of the patients by the clinic

163
(people think they will get better from traditional healer). Often these people come to the
clinic after the disease/medical problem gets very advanced, and sometime too late for the
clinic doctor to help (or at least help easily/quickly). If the patients came in quickly then
the Doctors would be more effective. He recommended efforts to work with local healers,
to educate them, about medical problems that should be referred to the clinic. In some
cases, this has been implemented and is working.
• This is where improving accessibility would probably help patient outcomes. If the
clinic were more accessible, then people would probably use the clinic more
frequently.
• Many patients with serious medical issues have the following characteristics: They
have a poor education (do not read); many are malnourished; come from big families
(10-12 children); and prevalence of alcoholism in the family.
Question #3: What other characteristics keep people from utilizing clinic?
• Personal biases, preferences, and misinformation:
• Hypothetical example of a prospective patient who had a friend or family
member who had a bad experience with a western doctor. This lead to a
personal bias against the western clinic.
• Patients think they need money to come to clinic. Though the clinic charges
people for the service, many people don’t have money. So they think they
cannot go to the clinic when they are sick. This is not true, and people need to
be educated to understand this.

164
• Alternative sources of health service: Traditional healers are a problem as described
above.
• Midwives are good, but only for “normal” births. Complicated births need clinic or
hospital attendance.
• Government clinic in Santa Lucia cheaper, but doesn’t always have doctor. It’s a
cheaper place to get drugs, but it doesn’t always have them. When they have drugs,
many people go there. This causes uneven flow of patients to Hombro a Hombro
clinic.
Question #4: What recommendations can be made for improving service?
• Having a doctor, nurse, and two health workers/promoters who travel out to the
villages every 2 weeks (need to be on a regular schedule). This, in effect, brings the
health care to the people. The Hombro a Hombro clinic has offered to provide
transportation and medicine, but needs funding for the salaries of the staff.
• Also discussed the possibility of having the social service doctor spend two days a
week out at the Santa Rita clinic and the San Jose clinic, both of which have a
building, but don’t have a doctor or staff. This is a good idea, but one that runs into
political problems in Tegucigalpa with the National Health Ministry.
#5: What are your thoughts on educational efforts out in the villages?
• Teach people about preventive medicine – childhood inoculations, etc.
• Brigades and traveling doctors/nurses can help with educational efforts.

165
• Health promoters in each of the villages know basic health issues. Helps refer people
to clinic if needed.
Question #6: What are the towns with local traditional healers? San Juan, Santa Lucia,
Palacios, Condoncillo, San Rafael, Junquillo, San Marcos, and Santa Rita.
Question #7: What form of transportation do most patients use to get to clinic?
• Key informant 1 and 5 collaborated on this issue and estimated that 80-85% of their
patients come to the Hombro a Hombro clinic by foot.
• When the patient is very sick, often a car/truck is hired.
Question #8: What are the most common medical problems?
• Years ago infectious diseases were the most common, but as the health of these people
improves, chronic diseases have become the most prevalent. These include: diarrhea,
upper respiratory infection (from cooking fires inside), headaches, muscle aches,
hypertension, diabetes, arthritis & pregnancy.
Question #9: What is the average number of children in a family? The average number of
children is 5.
Question #10: What is the ethnic makeup of most of the people in the service area? The
ethnic makeup of most of the people is mixed (mestizo).