Examining the nature of interprofessional education in primary care settings: a review of the...
59
Examining the nature of interprofessional education in primary care settings: a review of the literature Scott Reeves Joanne Goldman University of Toronto
Transcript of Examining the nature of interprofessional education in primary care settings: a review of the...

Examining the nature of interprofessional education in
primary care settings: a review of the literature
Scott Reeves
Joanne Goldman
University of Toronto

2
Contents Boxes................................................................................................................................ 4 Tables............................................................................................................................... 4 Executive summary .......................................................................................................... 5 Acknowledgements .......................................................................................................... 7 Introduction....................................................................................................................... 8
This review in context ................................................................................................... 8 Report overview ............................................................................................................ 8
Section 1: Review Methodology ..................................................................................... 10
1.1. Aim and objectives............................................................................................... 10 1.2. Definitions ............................................................................................................ 10 1.3. Search strategies ................................................................................................. 10 1.4. Excluded initiatives .............................................................................................. 12
Section 2: Interprofessional education: an overview ...................................................... 13
2.1. Background issues............................................................................................... 13 2.1.1. The emergence of interprofessional education ............................................. 13 2.1.2. Terms and terminology.................................................................................. 14 2.1.3. Interaction...................................................................................................... 15
2.2. Learning issues.................................................................................................... 16 2.2.1. The timing of interprofessional education...................................................... 16 2.2.2. Theories and concepts .................................................................................. 17 2.2.3. The role of competencies .............................................................................. 20
2.3. Facilitation issues................................................................................................. 21 2.3.1. Facilitator attributes ....................................................................................... 21 2.3.3. Facilitator preparation.................................................................................... 22
2.4. Organisational issues........................................................................................... 22 2.4.1. Commitment .................................................................................................. 22 2.4.2. Logistics ........................................................................................................ 23 2.4.3. Presage, process, product ............................................................................ 24
Section 3: Interprofessional education in primary care................................................... 25
3.1. The interprofessional initiatives............................................................................ 25 3.2. Evaluating the initiatives ...................................................................................... 31
3.2.1. Evaluation design .......................................................................................... 31 3.2.2. Data collection and analysis.......................................................................... 32 3.2.3. Limitations ..................................................................................................... 34
3.3. Reported outcomes.............................................................................................. 35 3.3.1. Learner reactions .......................................................................................... 36 3.3.2. Changes in attitudes/perceptions .................................................................. 37 3.3.3. Acquisition of knowledge/skills ...................................................................... 37 3.3.4. Changes in behaviour ................................................................................... 37 3.3.5. Changes in organizational practice ............................................................... 38

3
3.3.6. Improvements to care.................................................................................... 38 Section 4: Conclusions and implications ........................................................................ 40
4.1. Conclusions...................................................................................................... 40 4.2. Recommendations ........................................................................................... 41
References ..................................................................................................................... 42 Appendices..................................................................................................................... 58
Appendix 1: Broad search strategy............................................................................. 58 Appendix 2: Focused search strategy......................................................................... 59

4
Boxes Box 1: A policy advocating interprofessional collaboration........................................... 13 Box 2: Multiple interactive learning methods ................................................................ 15 Box 3: An e-based interprofessional education initiative .............................................. 16 Box 4: A post-licensure initiative for primary care teams.............................................. 26 Box 5: An initiative aimed at improving patient care..................................................... 28 Box 6: An interprofessional education initiative led by higher education...................... 29 Box 7: Use of a quality improvement theory................................................................. 30 Box 8: Use of problem-based learning theory within interprofessional education ........ 31 Box 9: An example of a controlled before-and-after design in interprofessional education ........................................................................................................... 32 Box 10: A longitudinal evaluation ................................................................................... 32 Box 11: An example of a qualitative evaluation.............................................................. 34 Box 12: An initiative reporting changes to attitudes and knowledge .............................. 36 Box 13: An initiative reporting changes in knowledge/skills ........................................... 37 Box 14: An initiative reporting improvements to patient/client care ................................ 38 Tables Table 1: Interactive learning methods .......................................................................... 15 Table 2: Development of the attitudes, skills and knowledge....................................... 17 Table 3: Inhibitors for interprofessional education (Pirrie et al. 1998) .......................... 23 Table 4: Geographic location........................................................................................ 25 Table 5: Stage .............................................................................................................. 25 Table 6: Duration .......................................................................................................... 26 Table 7: Qualification.................................................................................................... 27 Table 8: Aim of the interprofessional education ........................................................... 27 Table 9: Participants..................................................................................................... 28 Table 10: Institutional leadership.................................................................................... 29 Table 11: Methods of learning ........................................................................................ 30 Table 12: Underpinning theory ....................................................................................... 30 Table 13: Evaluation Design........................................................................................... 31 Table 14: Data collection ................................................................................................ 32 Table 15: Data analysis .................................................................................................. 32 Table 16: Methodological limitations .............................................................................. 34 Table 17: Outcome typology modified by Barr et al. (2000) .......................................... 35 Table 18: Reported outcomes ........................................................................................ 35

5
Executive summary Interprofessional education is being increasingly recognized and supported for its potential in improving collaboration between the various health and social care professions. A series of literature reviews on interprofessional education have been recently undertaken in order to increase our understanding of the existing knowledge in this area, and directions for future research and practice (e.g. Zwarenstein et al. 2001, Freeth et al. 2002, Barr et al. 2005). This report builds upon these other reviews, but provides a unique perspective in its focus on interprofessional education undertaken in primary care settings. Objectives and methods This review addresses the following two key objectives: To provide an overview of key concepts, issues and principles related to
interprofessional education. To provide a description of the nature of interprofessional education initiatives which
have been undertaken within a primary health care context. To address these main objectives, two separate but overlapping search strategies were employed. These search strategies involved the identification of relevant interprofessional education initiatives from previous systematic reviews, a comprehensive search of Medline, CINAHL, ERIC, ASSIA, ABI, and Embase, as well as hand searches of health and social care journals and a search of the Internet. Findings The information gathered from the first search strategy, provides insight into critical issues to be considered in the development and implementation of an IPE initiative. Drawing upon this literature, interprofessional education has been defined as “occasions when two or more professions (or students) learn from and about each other to improve collaboration and the quality of care”. The review describes critical issues that need to be addressed in the planning of such initiatives, including: interactive learning methods, the timing of interprofessional education, theories of adult education, the role of competencies, facilitation issues, and organizational issues. The general overview provides contextual information to understand the results and implications of the research studies on interprofessional education in primary care. The second search strategy resulted in the identification of 154 initiatives that met the definitions for both ‘interprofessional education’ and ‘primary care’ set out in this review. The following highlights the nature and outcomes of these studies: The majority of the studies (57%) were undertaken in the United States; only nine
were based in Canada. The majority (63%) were post-licensure initiatives, including six of the Canadian subset, lasted for more than seven days, aimed to improve the quality of care delivered to patients/clients, and were led by clinical service-based institutions. Pre-licensure initiatives generally aimed to improve interprofessional collaboration and were organized by higher education institutions. Initiatives
6
included a range of professionals, but nurses and physicians were the two largest participant groups.
The seminar or workshop discussion interactive method was the most commonly employed interactive learning method, but initiatives often employed two or more interactive methods; only a small number of initiatives employed an explicit use of theory to inform the initiative.
The weak post-intervention design was the most commonly used evaluation design; 36% of interventions used quasi-experimental or experimental designs, 14% of initiatives used a longitudinal design. Most initiatives used multiple methods of data collection; the questionnaire was the most frequently used tool. A significant number of initiatives did not adequately describe the evaluation or data collection and analysis approach.
The outcomes were classified according to an outcome typology modified for interprofessional education (Barr et al. 2000), which includes: reaction, modification of attitudes/perceptions, acquisition of knowledge/skills, behavioural change, change in organizational practice, and benefits to patients/clients. The bulk of initiatives tend to report positive outcomes connected to their use of interprofessional education.
The findings in this report are interspersed with vignettes from interprofessional education initiatives that will provide the reader with a better understanding of the types of initiatives that have been undertaken, the results obtained, and the need for further comprehensive evaluation. Conclusions The findings of this review resonate with those of previous reviews. The generally positive results show that interprofessional education can improve interprofessional collaboration and potentially lead to improved and health and social care. On the other hand, these initiatives have significant theoretical and methodological limitations, as noted in other reviews, which precludes a comprehensive understanding of the most effective strategies for interprofessional education. Recommendations In order to move towards this goal of increasing our knowledge of how to best plan and implement interprofessional education to achieve desired outcomes, the following two recommendations emerge from this report: Further rigorous and comprehensive (i.e. multi-method) research is necessary to
increase our understanding of the nature and impact related to interprofessional education. Further longitudinal research is needed to better understand the long-term impact of this type of educational activity within primary care.
Increased use of theoretical work, drawn from the adult learning literature, is needed when planning interprofessional education.

7
Acknowledgements This review was funded by the Ontario Ministry for Health and Long Term Care, as part of a larger commissioned project located within the Primary Health Care Transition Fund aimed at Actively Building Capacity in Collaborative Research. We would like to thank Laure Perrier, Knowledge Translation Program at the University of Toronto for all her advice and support with our numerous searches of the literature for this review.

8
Introduction This literature review on interprofessional education in primary care forms part of a wider collaborative project undertaken by colleagues based at the University of Toronto, University of Ottawa, University of Western Ontario, Queen’s University and McMaster University, which was funded by the Ontario Ministry for Health and Long Term Care under their Primary Health Care Transition Fund. As has been repeatedly emphasized by policymakers, researchers, and educators, changes to primary health care models must be accompanied by changes to the educational system (e.g. Pringle 2000, Romanow, 2002). The move towards multidisciplinary team-based practice requires that health and social care professionals involved in these practices participate in interprofessional education that provides them with the knowledge and skills to effectively practice together. However, it is imperative that such a relatively new form of education is informed by research that provides evidence relating the most appropriate learning and teaching approaches to maximise its strengths for developing attitudes, skills and knowledge for effective interprofessional practice. In meeting this aim, the report identifies a number of key factors that need to be considered in the planning and implementation of interprofessional education within a primary health context. This review in context Given the growing interest in the potential use and impact of interprofessional education in this country and abroad, a number of reviews in this subject area have been completed. Some of the earliest literature reviews were undertaken a decade ago (Barr & Shaw 1995, Barr & Waterton 1996) and provided some useful descriptions of early interprofessional education initiatives in the United Kingdom. This work was followed by reviews of the evidence base for interprofessional education across clinical settings (Zwarenstein et al. 2001, 2005, Barr et al. 2000, 2005, Freeth et al. 2002). In addition, reviewers examined the impact of interprofessional education in specific clinical settings such as mental health (Reeves 2001) and assessed the evidence in relation to pre-licensure learners (Cooper et al. 2001). More recently, researchers have begun examining the range of factors that facilitate and inhibit the use of interprofessional education (Oandasan & Reeves 2005a&b). It is important to emphasize that this review of interprofessional education builds upon this preceding work and the findings published in these reviews. More specifically, as will be described in the methodology section, it draws upon a number of the techniques and some of the data from a small number of these previous reviews. However, this review is unique in the respect that it is focused on interprofessional education that has been undertaken within primary care settings. Report overview This report is structured in four main sections. The first presents the methods employed to search and collate the literature on interprofessional education. The second section

9
The third section presents a more focused examination of the evaluative literature on interprofessional education related to primary care settings. The final section offers conclusions and recommendations for the development of interprofessional education within primary care.

10
Section 1: Review Methodology This section of the report offers a brief description of the aims and objectives of this review, and definitions and methods employed to search and identify suitable material. 1.1. Aim and objectives The aim of this review was to search and identify published and unpublished documents containing descriptions, discussions and/or evaluations of interprofessional education initiatives undertaken within primary care context. Linked to this overarching aim were the following objectives 1. To provide an overview of key concepts, issues and principles related to
interprofessional education. 2. To provide a description of the nature of interprofessional education initiatives which
have been undertaken within a primary health care context. For the purposes of this report, an ‘initiative’ is regarded as an interprofessional education curriculum, course, module or program that has been evaluated and provides a description of its outcomes. 1.2. Definitions The following two definitions were employed for the literature review. Interprofessional education was defined as:
Occasions when members (or students) of two or more professions associated with health or social care engage in learning with, from and about each other.
After discussion the follow definition of ‘primary care’ was agreed upon:
A patient's first point of contact with a doctor or other health care team member (e.g. nurse, pharmacist). Primary care includes but is not limited to: disease management and prevention, disease cure, rehabilitation, palliative care and health promotion.
The use of these definitions provided clear parameters in the search for relevant literature. In effect, these definitions acted as the two inclusion criteria for this review. 1.3. Search strategies In order to address both research objectives presented above, the review employed two separate but overlapping search strategies: a ‘broad’ strategy and a ‘focused’ strategy. 1.3.1. Broad search strategy To address the first objective, a broad interprofessional education search strategy was developed (see Appendix 1). This search involved a three-step process.

11
Firstly, a strategy designed for searching an electronic database was developed. This strategy, a modification of previous approaches used in related review work (Freeth et al.. 2002, Oandasan & Reeves 2005a&b), was aimed at ensuring that a broad spread of the interprofessional education literature (e.g. discussion, opinion and policy papers) would be identified. The search strategy was used in the following six electronic databases: Medline (medicine) CINAHL (nursing and allied health professionals) ERIC (education) ASSIA (social sciences) ABI (organisational) Embase (health and social care) These databases were selected to ensure representation of a wide range of relevant sources. All databases were searched from 1990 to 2005.1 Secondly, hand searches of health and social care journals that published interprofessional initiatives (e.g. Journal of Interprofessional Care, Medical Education, International Journal of Rehabilitation and Therapy, Academic Medicine, Social Work Education, Learning in Health and Social Care) were also undertaken to identify any relevant papers missed by the electronic database searches. Finally, a search of the Internet was undertaken using key terms from the search strategy to locate books, policy documents and the grey (unpublished) literature. As result of these searches, over 500 papers, documents and books on interprofessional education were identified and deemed as potentially relevant information for the review, i.e. each met the definition for interprofessional education as outlined above. Information from these sources has been selectively included in this review to highlight key concepts and issues linked to interprofessional education. This background information helps to position the findings focussing on interprofessional education in the primary care setting and the conclusions and recommendations for the development of interprofessional education within this context. 1.3.2. Focused search strategy To address the second objective, a more focused search strategy was developed to identify key sources containing interprofessional education initiatives undertaken in primary care settings. This search involved a four-stage process. Firstly, the material from previous reviews, in which two of the authors had been involved (Freeth et al. 2002, Oandasan & Reeves 2005a&b), were searched for interprofessional education initiatives that met the agreed definitions. 1 Experience of the literature gathered from previous review work (Barr et al. 2000, Reeves 2001, Oandasan & Reeves 2005a) indicated that there is little of interest related to interprofessional education published before 1990.

12
Secondly, the broader search strategy was modified to search for interprofessional education initiatives undertaken in primary care settings (see Appendix 2). The six databases outlined above (Medline, CINAHL, ERIC, ASSIA, ABI and Embase) were again employed for the focused search. Given that the previous reviews, noted in stage one, had searched for interprofessional education initiatives from the late 1960s to 1998 across these different databases, and the relevant articles would have been identified, this search concentrated on the years from 1999 to 2005.2 Thirdly, the results from the hand searches of health and social care journals and the Internet searches were re-scrutinised to identify any relevant material. As a result of these efforts, 154 initiatives were identified as falling within the more restrictive parameters of meeting definitions for both ‘interprofessional education’ and ‘primary care’ outlined above. 1.4. Excluded initiatives A number of initiatives were excluded as they failed to meet one or both elements of the definition criteria. For example, although a number of initiatives were interprofessional in nature, upon closer inspection, they were not educationally-oriented (e.g. Bateman et al. 2003, Dieleman et al. 2004). A small number of initiatives were excluded because despite having some mention of interprofessional education activity, frequently within a CQI project, the actual description of the education was so poor that it was not clear what education was actually delivered (e.g. Valk et al. 2004). In addition, a few papers were excluded, as although there was interprofessional teaching about collaboration, there was only one professional group involved in the learning (e.g. Keough et al. 2002), thus failing to meet the required definition of “learning with, from and about each other”.
2 Inevitably, a small number of duplicate interprofessional education initiatives were found from the first and second stage searches, which were all removed from the review.

13
Section 2: Interprofessional education: an overview This second section of the report presents selected findings from the broad search to provide an insight into the key issues related to interprofessional education. The section is divided into four parts: background issues that describe this type of educational activity; learning related issues; facilitation related issues; and organizational issues that can affect the implementation of interprofessional education. 2.1. Background issues The following offers an insight into why interprofessional education emerged in health and social care, before it considers the language of interprofessional education and the need for interactive methods. 2.1.1. The emergence of interprofessional education Effective collaboration between the various health and social care professions has long been regarded as an essential ingredient for delivering high quality patient care (e.g. Barker 1964, Shaw 1970, Kindig 1975, Evers 1981, Gregson et al.. 1991, Firth-Cozens 1998, Rafferty et al.. 2001, Penthybridge 2004). A growing body of research evidence is demonstrating that effective collaboration can reduce staff absenteeism (Lies & Sunderland 2001), create a more satisfying work environment (McGrath 1991), and improve the quality of care delivered to patients (Feiger & Schmitt 1979, Schmitt 2001, Litaker et al.. 2003), and patient outcomes (Zwarenstein et al. 2004). The international health and social care policy literature have regularly re-emphasized the value of collaboration (e.g. World Health Organisation 1976, 1988, Department of Health 2000, 2001, 2002), and in Canada, there have been numerous federal, provincial, and institutional initiatives to promote and facilitate multidisciplinary team-based care. Box 1 provides an example.
Under the Ontario primary care reform agenda, Family Health Teams are being formed to bring together different health care providers to coordinate the highest quality of care (Ontario Ministry of Health and Long Term Care, 2006) and The Royal College of Physicians and Surgeons of Canada has identified the “Physician as Collaborator” as a core competency for students completing residency programs (The Royal College of Physicians and Surgeons of Canada, 2000).
Box 1: A policy advocating interprofessional collaboration
While particular instances of effective collaboration between health care professions have been identified and/or studied, and the ideal of effective collaboration is espoused, interprofessional interactions continue to be problematic. For example, interprofessional relationships are often undermined by boundary infringements, a lack of understanding of one another’s roles and poorly co-ordinated teamwork (e.g. Hughes 1988, Walby et al.. 1994, Allen 1997, Skjørshammer 2001, Pethybridge 2004).

14
In an effort to improve interprofessional practice, policy documents advocate the use of interprofessional education (e.g. Department of Health 1989, 1997, 2000, 2001, 2002, Committee of Vice Chancellors and Principals 1997, O’Neil & Pew Health Professions Commission 1993, College of Occupational Therapists 2000, General Medical Council 2001, Nursing and Midwifery Council 2002, World Health Organisation 1976, 1988, Romanow 2002, Health Canada 2003).3 The collective view of these policies and the wider literature (e.g. Szasz 1969, MacDougall & Elahi 1974, Jones 1986, Barr 1994, Larson 1999) is that because professionals are trained separately from one another they are not equipped with the attitudes, skills or knowledge to work effectively together to deliver patient care. The World Health Organisation (1988:16-17) states:
"[Interprofessional education] develops the ability of students to share knowledge and skills collaboratively and thereby provide individuals and the community with more efficient health care ".
In response to this emphasis on interprofessional education, there has been a steady growth of such initiatives within health and social care systems, most notably in the United Kingdom, Canada, United States, continental Europe and Australia (Goble 1994, Tope 1996, Graham & Wealthall 1999, Ross & Southgate 2000, Barr 2002, Oandasan et al. 2004). These widespread and diverse activities have been reported in both pre-licensure (e.g. Parsell et al.. 1998, Scott et al.. 2005) and post licensure education (e.g. O'Boyle et al.. 1995, Jones & Salmon 2001, McKeown et al.. 2005). Interprofessional education has been reported in university-based courses (e.g. Gill & Ling 1995, Hind et al.. 2003) and also based in clinical practice (e.g. Falconer et al.. 1993, Elliot et al.. 2002). It can form a part of a continuous quality improvement (CQI) or total quality management (TQM) initiative (e.g. Hunter & Love 1996, Cleghorn & Baker 2000). Interprofessional education can occur in primary health care (Gentry et al.. 2001) and acute settings (e.g. Harmon et al.. 1998, Elliot et al.. 2002) and involve a range of different health and social care professions, such as doctors, nurses, occupational therapists, audiologists and pharmacists (e.g. Arlton 1986, DePoy et al.. 1997). The evolving literature, which draws upon empirical studies, adult learning theories and professional experience, provides an insight into the key issues and principles related to the use of interprofessional education. The remainder of this section presents some of these issues and principles to provide the reader with a firmer grasp of how they affect the development and implementation of interprofessional education. 2.1.2. Terms and terminology The literature continues to employ a variety of phrases, such as ‘shared learning’, ‘multiprofessional education’ and ‘interdisciplinary education’ to describe interprofessional education. As a result, Pirrie (1999:122) has argued that this term can now be considered a “fuzzy concept.” To help clarify this confusion, CAIPE (1997) 3 More detailed discussion of these policies and their implications for interprofessional education can be found in both Pittilo & Ross (1998) and Forman & Nyatanga (1999).

15
developed the definition of interprofessional education which has a focus on interaction between participants from different professional groups and aims to develop the attitudes, knowledge, skills and behaviour required for effective collaboration. This definition has now been adopted by a number of authors in the field (e.g. Barr 1996, 2002, Hammick 1998). For Harden (1998), if the goal of interprofessional education is to teach collaborative practice, then the content must be on interdisciplinary knowledge, skills and attitudes. He maintains that one must not confuse teaching medical content foci (or any other profession specific content) with the primary goals of collaborative practice. For example, health professional students may be brought together to study about HIV management, but unless they are learning ‘how to work together’ in the management of HIV they will be learning in parallel. This is a classic example of multi-professional learning, which has a role in health professional education, but where there is no interaction between participants. 2.1.3. Interaction In offering a more comprehensive insight into the interactive nature of interprofessional education, Barr (2002) outlines a range of different types of interactive learning methods used in interprofessional education (see Table 1).
Learning method Examples Exchange-based seminar-based discussions Observation-based joint visits to patients/clients Problem-focused problem-based learning Simulation-based simulating clinical practice Practice-based interprofessional clinical placements
Table 1: Interactive learning methods
In relation to the literature, one discovers that these five learning activities are regularly employed within interprofessional education initiatives. For example, Freeth et al.. (1999) report the use of exchange-based learning in an interprofessional seminar focused on discussing how general practitioners (family doctors), practice nurses, district nurses and pharmacists can enhance their joint work in the care of patients with Alzheimer’s disease. To maximize opportunities for interaction, several learning activities are typically employed within interprofessional education initiatives (see Box 2).
Mires et al.. (1999) describe a short interprofessional course for 141 medical and 35 midwifery students. The course aimed to improve students’ attitudes towards each other’s professional group and their knowledge of working together. The course consisted of a number of different interactive learning methods including three PBL sessions, a two-hour clinical skills session and a two-hour seminar. The authors found that students reported improvements in their attitudes towards each other’s profession and increases in their knowledge of working together.
Box 2: Multiple interactive learning methods

16
In addition, electronic learning (e-learning) methods, such as electronic bulletin boards and video conferencing, are increasingly being used within interprofessional education (e.g. Farrell 2005). See Box 3 for an example of an e-based initiative.
Cornish et al. (2004) describe an initiative for health professionals working separately in remote rural locations across Canada who undertook a short interprofessional course that employed video-conferencing technology. The course allowed 34 physicians, nurses and social workers to participate in presentations and discussions on issues linked to patient care. Although participants found the use of video-conferencing technology helpful for enhancing interprofessional cohesion the reliability of the equipment was, at times, problematic. Nevertheless, following a number of technical refinements, it is hoped that this program can be expanded to incorporate other health and social care practitioners located in rural settings in the country.
Box 3: An e-based interprofessional education initiative The use of e-learning allows students based in separate geographical locations to interact electronically (in either a synchronous or asynchronous fashion) while they learn together. Often, interprofessional education initiatives that employ e-learning methods also use traditional learning methods, such as seminar discussions, to create a ‘blended learning’ approach (e.g. Richardson & Cooper 2003). 2.2. Learning issues This section presents the relevant literature relating to the key learning issues and concepts that underpin interprofessional education. The section offers an insight into the debate around when to implement interprofessional education, learning theories and concepts pertinent to interprofessional education, and the role of competencies in shaping the planning of interprofessional education. 2.2.1. The timing of interprofessional education There is currently some debate on identifying the most 'effective' time to deliver interprofessional education. For some authors, pre-qualifying interprofessional education is more effective as it can help diminish the negative effects of professional socialization, such as hostile stereotyping (e.g. Tope 1996, Horder 1996, Graham & Wealthall 1999). Pryce & Reeves (1997) found that first year medical, nursing and dental students had already developed a range of deeply embedded stereotypical notions of one another’s professional groups as they started on an interprofessional course. In contrast, other authors (e.g. Dombeck 1997, Pirrie et al.. 1998) maintain that post-qualifying interprofessional education is more effective, as participants have a firmer understanding of their own professional identity and role. For Dombeck (1997:15), learning to collaborate with other professional groups can be difficult when “one is unsure of one’s professional identity". Post-licensure practitioners may regard the

17
introduction of interprofessional education initiatives in clinical practice settings with suspicion (Falconer et al.., 1993), which is unsurprising since interprofessional education is generally introduced into these environments to change and enhance present practice. The implication that current practices are not adequate may result in resistance to interprofessional education. A further viewpoint in this debate advocates that interprofessional education should form a part of all practitioners’ on-going professional development, starting in their pre-qualification programmes and continuing throughout their careers. This will ensure that early learning is built upon:
"Interprofessional experience and learning could and should be consciously and deliberately built into education opportunities available to practitioners as they move along […] further and higher education and to professional training, practice and continuing professional development" (Mathias & Thompson 1997:103).
Reeves & Summerfield Mann (2003) have outlined particular attitudes, knowledge and skills required for effective collaboration that may be most appropriately developed through interprofessional education at each of the pre-licensure and post-licensure stages (see Table 2).
Pre-licensure Post-licensure Attitudes -Appreciate interprofessional collaboration -Accept other professional’s views/ideas
Attitudes -Willingness to exchange viewpoints and information
Knowledge -Understand roles of other professions
Knowledge -Understand how professional roles interrelate with others
Skills -Communicate with learners from other professions
Skills -Collaborate and negotiate with other professions -Work collaboratively with professionals
Table 2: Development of the attitudes, skills and knowledge As evidence for the most effective time to deliver interprofessional education remains elusive (e.g. Hall & Weaver 2001), this debate continues. 2.2.2. Theories and concepts Although there is little explicit use of adult learning theory within the interprofessional education literature, it is possible to identify its implicit use in a number of publications. Classic theories of adult education often used in interprofessional education are Knowles' (1980) theory of adult learning, Schön's (1987) theory of reflection, Barrows &

18
Tamblin's (1980) theory of problem based learning (PBL) and Kolb's (1984) theory of experiential learning. In addition, the use of teamwork models (Gilbert et al.., 2000) and theories of group behaviour (Carpenter et al. 2003) have contributed to the successful development of interprofessional education initiatives. From this use of learning theory arise a number of important concepts that need to be understood when using an interprofessional education approach. Key learning concepts to emerge from the literature are: relevance, status, balance, size and stability, and informality. Each concept is considered in turn. 2.2.2.1. Relevance Providing relevant learning experiences is a key element of Knowles’ (1980) theory of adult learning. Consequently, it is not surprising that learners’ reactions to interprofessional education are more favourable when they see a direct relevance between their educational experiences and current or future practices (e.g. Parsell & Bligh, 1998; Pirrie et al.., 1998). Hence, many interprofessional education initiatives employ learning approaches that are based in, or have a substantial part of the course based in, clinical practice (e.g. Reeves & Freeth 2002). Where interprofessional education occurs at the pre-licensure level within higher education institutions, one often finds that these courses incorporate some form of clinical input, whether it is a clinical placement, (Kipp & Pimlott, 2003; Wahlström & Sandén, 1998), the use of a simulated clinical environment (Freeth & Nicol, 1998) or meeting service users to talk about their health needs (Reeves, 2000). 2.2.2.2. Status Studies have shown that students sometimes felt that interprofessional learning was not as important as their profession-specific learning experiences (e.g. Dienst & Byl, 1981; Fallsberg & Wijma, 1999), and there was student resistance to collaborative activities when interprofessional education did not meet their learning needs, specifically in terms of developing their profession-specific competencies (Fallsberg & Hammar 2000, Reeves & Freeth 2002). As interprofessional education initiatives aim to improve collaborative practice for the future, students could perceive these aims as too remote for them, given their focus on learning profession specific skills and knowledge. Eliciting public support from professional leaders (Funnell et al.., 1992) and recruiting high quality tutors to deliver the education (Loxley, 1997) have been suggested as ways to improve the status of interprofessional education. An elective (voluntary) interprofessional education initiative, can give the message that this type of learning is low status, thus reducing the learner’s commitment. However, it is also argued that learner choice can ensure that those participants will be more committed and interested in their interprofessional learning experiences (e.g. Lary et al.., 1997, Reeves & Summerfield Mann 2003). In addition, if interprofessional education experiences are not assessed in a way that gives equal weight to other uni-professional courses, their status is again questioned (e.g. Reeves, 2000). As practitioners usually undertake interprofessional education on a voluntary basis, there can be little incentive

19
for them to participate, other than professional development and/or a sense of altruism related to improving patient/client care. 2.2.2.3. Balance For interactive learning and interprofessional interaction to take place, there is a need to attain and maintain a ‘balance’ within learning groups (e.g. Funnell et al. 1992, Gill & Ling 1995). For these authors, an equal mix of professionals in the group is a crucial element in achieving group balance; if the group make-up is skewed too heavily in favour of one profession, it will inhibit interaction, as the larger professional group can dominate (Pryce & Reeves 1997). In post-licensure educational initiatives, it may be difficult to group balance since there is a disproportionate number of health professionals working together in a team in the clinical practice setting. For example, on the hospital ward there may be more nurses and physicians compared to pharmacists and social workers.
2.2.2.4. Size and stability For effective learning to occur, Gill & Ling (1995) recommend that a learning group should consist of around eight to ten members. Where groups are over ten members, problems related to poorer quality interactions can be encountered (e.g. Hughes & Lucas, 1997). Looking more widely at the literature, one can see that interprofessional education initiatives generally report group sizes of between five and ten learners (e.g. DePoy et al. 1997), and on occasions, dyads of learners have worked together (Nash & Hoy, 1993; Green et al.., 1996). Fiscal restraints, of course, may cause difficulties in creating such small group learning formats (e.g. Miller et al.., 1999).
Interaction is enhanced if learners work together within a stable group, with little ‘turnover’ in terms of established members leaving and new ones joining the group (Loxley, 1980; Forbes & Fitzsimons 1993). According to the literature, this issue can be especially difficult to achieve for post-licensure interprofessional education activities. For example, when an interprofessional education course is conducted over a number of weeks, workloads may deter practitioners from attending, and hence group stability is disrupted (e.g. Hart & Fletcher 1999, Freeth et al. 2000). For learners undertaking full-time pre-licensure education, effective timetabling across professional courses is the key to creating group stability. 2.2.2.5. Informality Like uni-professional health education, most interprofessional education occurs in a formal setting (classroom, practice placement, etc). However, as Freeth et al. (2005) point out, one should not overlook the informal learning that can occur within interprofessional education. In pre-licensure interprofessional education, this interaction may have an impact on changing professional students’ socialization processes (Erkel et al.., 1995; Salvatori & Berry, 2003). Pryce & Reeves (1997) found that medical, nursing and dental students continued to discuss aspects of their learning whilst socializing together after their formal learning was completed. Time in the local cafeteria or time together car-pooling can be useful settings for sharing informal experiences among pre-licensure students (Casto, 1994; LaSala et al.., 1997). It may be important

20
to set aside time in the structured learning environment in order to create informal learning opportunities. 2.2.3. The role of competencies The issue of what should be taught within interprofessional education initiatives is increasingly being informed by the literature detailing a range of desirable collaborative competencies (e.g. Barr 1998, Hornby & Atkins 2000). Arguably, the production of collaborative competencies by health educational accreditation bodies is important as they drive the development of interprofessional education. For example, The College of Family Physicians of Canada’s recent report on Family Practice Networks (College of Family Physicians of Canada 2000) sees the need for the development of collaborative competences to ensure good interprofessional team relations and patient care. This initiative can be seen as building upon similar efforts, such as The Royal College of Physicians and Surgeons of Canada’s statements that students should demonstrate competency in carrying out the role of the “Physician as Collaborator” before they complete their residency programs (Royal College of Physicians and Surgeons of Canada, 2000). To be competent as a “collaborator” a physician should be able to:
“Effectively consult with other physicians and health care professionals in partnership with the patient and care providers. [The specialist] recognizes the roles and expertise of the other individuals involved and explicitly integrates the opinions of the patient and caregivers into management plans” (Royal College of Physicians and Surgeons of Canada, 2000:6).
The move towards competency-based interprofessional education is underway. Its shape will be determined by the context and the educational leaders who bring forth the competencies they want their students to adopt into practice. How these competencies are taught depends upon a number of factors embedded within the context of learning for health professional education programs. It is through careful consideration of all of these factors that the best pedagogical approach to teaching interprofessional education can be developed. For the post-licensure stage, the literature contains descriptions of the types of competencies that may be required of health professionals to work collaboratively. For example, in their work with physicians and nurse practitioners, Way et al.. (2001), identified seven essential elements for successful collaborative practice: co-operation, assertiveness, responsibility/accountability, autonomy, communication, co-ordination, mutual trust and respect. Barr (1998) also provides an outline of key interprofessional education competencies highlighting specific knowledge, skills and attitudes, including: knowledge of each other’s roles, a willingness to work together, trust and mutual respect. A later review of the teamwork literature, (D’Amour et al. 2004) also indicated that effective collaborative practice is contingent on team members who demonstrate such competencies.

21
2.3. Facilitation issues This section presents the relevant literature on the key facilitation issues and concepts related to interprofessional education. The section initially offers an outline of the range of facilitator attributes required by faculty, the teaching strategies they might employ with an interprofessional group of learners and the types of preparation they might undertake before commencing this type of work. 2.3.1. Facilitator attributes The role of the interprofessional facilitator is regarded as pivotal in the interprofessional education literature (e.g. Barr, 1994; Parsell & Bligh, 1998; Cleghorn & Baker, 2000). As well as having a good knowledge of group learning theories (see Jaques 1998) facilitators need practical skills, experience and confidence to meet the differing demands of an interprofessional group. As Barr (1996:244) argues:
"[The interprofessional facilitator needs to be] attuned to the dynamics of interprofessional learning, skilled in optimizing learning opportunities, valuing the distinctive experience and expertise which each of the participating professions brings."
Holland (2002:221) outlines the range of skills required for an effective interprofessional education facilitator: knowledge of the professions, understanding of the current practice issues faced by professionals, knowledge of interprofessional learning programme, and expertise and experience of interprofessional collaboration. Without this range of knowledge and skills, facilitation of interprofessional groups has been found to be inconsistent between participating professionals (Freeth & Nicol 1998, Reeves 2000). 2.3.2 Facilitation strategies It is argued that facilitators need to focus on facets of facilitation that involve both team formation and team maintenance in order to positively affect interaction between learners, and thus maximize the opportunities for enhancing their knowledge and skills for collaboration (e.g. Headrick et al.., 1998; Parsell & Bligh, 1998). Facilitators must be prepared to encounter interprofessional friction between learners when they are working together (Hammick 1998). It is felt that problems can arise between learners particularly over ‘sensitive’ areas such as a misunderstanding over professional roles. Offering more autonomy to groups during their learning can help to optimize good interaction between learners versus interaction between learners and the facilitator. This allows for the development of self-directed learning opportunities, particularly if the group has a mature system of facilitating their own discussions (Thomas, 1995). This method of facilitation works particularly well for post-licensure practitioners (e.g. Howkins & Allison, 1997). However, the literature offers little in the way of empirical accounts of the effectiveness of these facilitator approaches, consequently there is a need for research into which facilitation methods work best. In addition, there is a need for facilitators to create a non-threatening environment. This follows Knowles’ (1980) view that a key requirement for effective adult learning is the

22
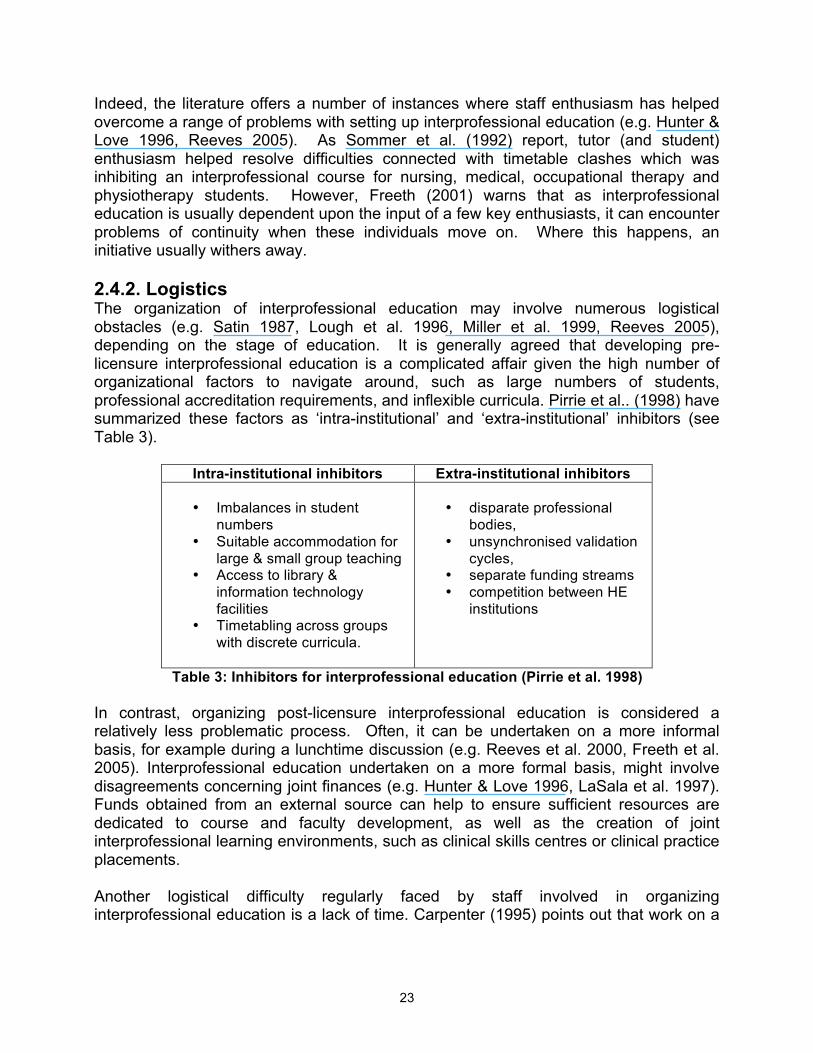
creation of a non-threatening learning environment in which learners felt psychologically safe. Given the history of social and economic inequalities that exist between the members of different health and social care professions, this principle is the cornerstone of the development of any interprofessional education course (Freeth et al. 2005). 2.3.3. Facilitator preparation In considering the type of preparation for facilitators, the interprofessional education literature again falls short. Although a number of authors stress the need for good interprofessional facilitation, little is offered in terms of suggestions which could actually inform potential facilitators. Much of the literature, although sparse, states that facilitators should have knowledge and experience of facilitating small groups and working in an interprofessional fashion (e.g. Funnell, 1995; Lary et al.., 1997). Some authors also state that it is important that facilitators understand issues of power and hierarchy which are connected to the everyday practice of the health care teams (Thomas, 1995; Miller et al.., 1999). Therefore it seems that good preparation is central to the success of an interprofessional initiative but it is not yet known what type of preparation is needed and whether preparation indeed improves interprofessional education success. 2.4. Organisational issues This section presents the relevant literature on the key organizational issues and concepts connected to interprofessional education. The section initially discusses the need for organizational commitment to ensure that this type of educational activity can be developed and delivered in an effective manner. It also outlines the range of logistical issues that need attention to operationalize an interprofessional education initiative. Finally, the section considers how a presage, process and product model might help the organization of interprofessional education. 2.4.1. Commitment It is generally agreed that institutional commitment, particularly from senior management, is a key component in the development of interprofessional education (e.g. Pirrie et al. 1998). As Casto (1994a&b) argues, senior management commitment from all participating organizations ensures that funding, staff and physical resources (e.g. classrooms) are all made available. The literature also acknowledges the need to obtain commitment from the course planners (Lough et al. 1996, Lary et al. 1997). This factor is considered particularly important, given the number of reports in which disinterested or sceptical staff have inhibited the development of this form of education (e.g. Mathias & Thompson 1997, Graham & Wealthall 1999). To overcome such scepticism, it is recommended that staff who are committed to interprofessional education should be recruited to undertake this work (e.g. Sommer et al. 1992, Lough et al. 1996) since they will be prepared to devote their time, energy and enthusiasm to overcoming the various educational, professional and logistical difficulties associated with this activity.
23
Indeed, the literature offers a number of instances where staff enthusiasm has helped overcome a range of problems with setting up interprofessional education (e.g. Hunter & Love 1996, Reeves 2005). As Sommer et al. (1992) report, tutor (and student) enthusiasm helped resolve difficulties connected with timetable clashes which was inhibiting an interprofessional course for nursing, medical, occupational therapy and physiotherapy students. However, Freeth (2001) warns that as interprofessional education is usually dependent upon the input of a few key enthusiasts, it can encounter problems of continuity when these individuals move on. Where this happens, an initiative usually withers away. 2.4.2. Logistics The organization of interprofessional education may involve numerous logistical obstacles (e.g. Satin 1987, Lough et al. 1996, Miller et al. 1999, Reeves 2005), depending on the stage of education. It is generally agreed that developing pre-licensure interprofessional education is a complicated affair given the high number of organizational factors to navigate around, such as large numbers of students, professional accreditation requirements, and inflexible curricula. Pirrie et al.. (1998) have summarized these factors as ‘intra-institutional’ and ‘extra-institutional’ inhibitors (see Table 3).
Intra-institutional inhibitors Extra-institutional inhibitors
• Imbalances in student numbers
• Suitable accommodation for large & small group teaching
• Access to library & information technology facilities
• Timetabling across groups with discrete curricula.
• disparate professional
bodies, • unsynchronised validation
cycles, • separate funding streams • competition between HE
institutions
Table 3: Inhibitors for interprofessional education (Pirrie et al. 1998) In contrast, organizing post-licensure interprofessional education is considered a relatively less problematic process. Often, it can be undertaken on a more informal basis, for example during a lunchtime discussion (e.g. Reeves et al. 2000, Freeth et al. 2005). Interprofessional education undertaken on a more formal basis, might involve disagreements concerning joint finances (e.g. Hunter & Love 1996, LaSala et al. 1997). Funds obtained from an external source can help to ensure sufficient resources are dedicated to course and faculty development, as well as the creation of joint interprofessional learning environments, such as clinical skills centres or clinical practice placements. Another logistical difficulty regularly faced by staff involved in organizing interprofessional education is a lack of time. Carpenter (1995) points out that work on a

24
collaborative project is usually undertaken on top of a normal workload therefore attending joint planning meetings can be difficult. 2.4.3. Presage, process, product Recently, Freeth & Reeves (2004) have outlined how the organization of interprofessional education might be supported by use of the 3P (presage-process-product) model. Biggs (1993) devised the 3P model as a conceptual approach to how learning and teaching opportunities might be planned and implemented. Within this model, ‘presage factors’ are regarded as the socio-political context for education and the characteristics of the individuals who participate in learning and teaching. ‘Process factors’ are regarded as the approaches to learning and teaching that are employed in an educational experience and ‘product factors’ are seen as the learning outcomes. Applying the 3P model to interprofessional education, Freeth & Reeves (2004) discuss how this type of education has been shaped by a number of presage factors such as government policies and negative professional stereotypes held by both teachers and learners, the various facilitation approaches and types of assessment that can be employed (process factors), as well as the various learning outcomes that can be achieved to promote collaboration (product factors).

25
Section 3: Interprofessional education in primary care As noted above, 154 primary care interprofessional education initiatives (i.e. courses, modules, programs that had been evaluated) qualified for inclusion in this part of the review. While this part of the report presents material gathered from a search of international initiatives, where useful, it will concentrate on the small subset of Canadian initiatives. 3.1. The interprofessional initiatives This section presents an insight into the general nature of the interprofessional education reported in the 154 primary care initiatives included in the review. 3.1.1. Geography The bulk of primary care interprofessional education initiatives (87 studies, 57%) were undertaken in the United States (see Table 4).
Country Frequency Untied States 87 (57%) United Kingdom 42 (27%) Australia 11 (8%) Canada 9 (6%) Finland 2 (1%) Malta 1 (>1%) Turkey 1 (>1%) United Arab Emirates 1 (>1%)
Table 4: Geographic location In contrast, only nine initiatives were located from Canada (Jones & Dunn 1974, van der Horst et al. 1995, Mann et al. 1996, Hartrick 2000, Cornish et al. 2003, Korabek 2004, Crutcher et al. 2004, Farris et al. 2004, Barker & Oandasan 2005). 3.1.2. Stage Table 5 shows that the bulk of primary care interprofessional education initiatives took place after licensure (98 initiatives, 63%). In the Canadian subset, five initiatives were delivered to post-licensure participants (e.g. Mann et al. 1996, Hartrick 2000, Cornish et al. 2003, Korabek 2004, Farris et al. 2004), three were delivered to pre-licensure students (Jones & Dunn 1974, van der Horst et al. 1995, Crutcher et al. 2004) and one was delivered to both pre- and post licensure participants (Barker & Oandasan 2005).
Stage Frequency Post-licensure 98 (63%) Pre-licensure 42 (27%) Mixed 14 (10%)
Table 5: Stage

26
Box 4 provides an example of a post-licensure interprofessional education initiative for two primary care teams based in the UK.
Long (1996) provided an insight into the effects of delivering a three-day interprofessional residential course for members of two primary care teams consisting of general practitioners, practice nurses, practice managers, district nurses and health visitors based in the UK. The aim of the course was to provide an opportunity for team building and to provide a catalyst for enhancing collaboration. It was decided that the course should be offered to both teams on a residential basis to ensure that members could focus on their interprofessional learning without the distraction of work pressures. Time away from work was negotiated with colleagues who deferred their attendance to another time. Interviews with the course participants revealed that they valued the course for providing them with time to understand each other’s professional role and responsibilities. It was also felt that the course allowed them to start communicating in a more systematic manner.
Box 4: A post-licensure initiative for primary care teams As discussed in Section 2.4.2, the relative ease of establishing interprofessional education initiatives at the post-licensure level, where staff do not have to navigate their way through numerous logistical difficulties, means that this disparity between pre and post-licensure is inevitable. However, it is possible that this unevenness may eventually diminish, as in a number of countries such as the UK (Department of Health 2001), government policy is promoting pre-licensure interprofessional education. 3.1.3. Duration Table 6 indicates that most primary care interprofessional education initiatives (77 initiatives, 50%) involved more than seven days of participant interaction.
Duration Frequency Over 7 days 77 (50%) 2-7 days 46 (29%) Under 1 day 16 (11%) Unclear 15 (10%)
Table 6: Duration In these cases, contact was generally spread over several months, often when participants were involved in a series of interprofessional sessions related to the implementation of a continuous quality improvement (CQI) or a total quality management (TQM) initiative (e.g. Ketola et al. 2000, Rubenstien et al. 2002). 3.1.4. Qualification Most of the interprofessional education initiatives based in primary care (90 initiatives, 58%) offered no form of academic award or educational credit to participants (see Table 7).

27
Type of qualification Frequency
None 90 (58%) Unclear 26 (17%) Higher education award/accreditation 24 (15%) Continuing education credit 14 (10%)
Table 7: Qualification None of the Canadian initiatives offered any form of award or credit. In a relatively large number of initiatives (26 initiatives, 17%), insufficient information was provided to determine if any award was offered to participants. Where a credit or award was provided, this tended to be in the form a Master’s degree (Lacey 1998), an award given as part of a pre-licensure course (Horak et al.. 1998), continuing professional credits (Mayall et al. 2004) or a certificate of attendance (Rutter & Hagart 1990). 3.1.5. Aim Table 8 indicates that the aim of most primary care interprofessional education initiatives was to improve interprofessional collaboration (70 initiatives, 45%).
Interprofessional education aim Frequency Improving interprofessional collaboration 70 (45%) Improving the quality of care delivered to patients/clients
51 (33%)
Improving interprofessional collaboration and improving the quality of care delivered to patients/clients
33 (22%)
Table 8: Aim of the interprofessional education In general, initiatives which aimed at improving interprofessional collaboration were delivered to pre-licensure participants (30 initiatives, 19 %) (e.g. van der Horst et al. 1995, Crutcher et al. 2004). In contrast, the bulk of initiatives which aimed at improving the quality of care delivered to patients/clients (51 initiatives, 33%) (e.g. Hartrick 2000, Korabek 2004) were delivered to post-licensure participants. Box 5 offers an example of an interprofessional education initiative designed to improve the care received by patients with depression.
Thompson et al. (2000) undertook an RCT to evaluate the impact on patient care of implementing a practice guideline for the treatment of depression. Fifty-nine general practices were recruited into the study. Practices were randomised to the intervention group (made up from 29 pairs of general practitioners and practice nurses) who received interprofessional sessions on the guideline, or to the control group (made up from 30 pairs) who did not receive these sessions until completion of the study. To assess the impact of the new guideline, questionnaires were distributed before and after the delivery of the interprofessional sessions. Depression scale scores of patients treated by the practitioners in both groups were also collected, as well as data on practitioners’ ability to recognise depression. It was found that the new guideline
28
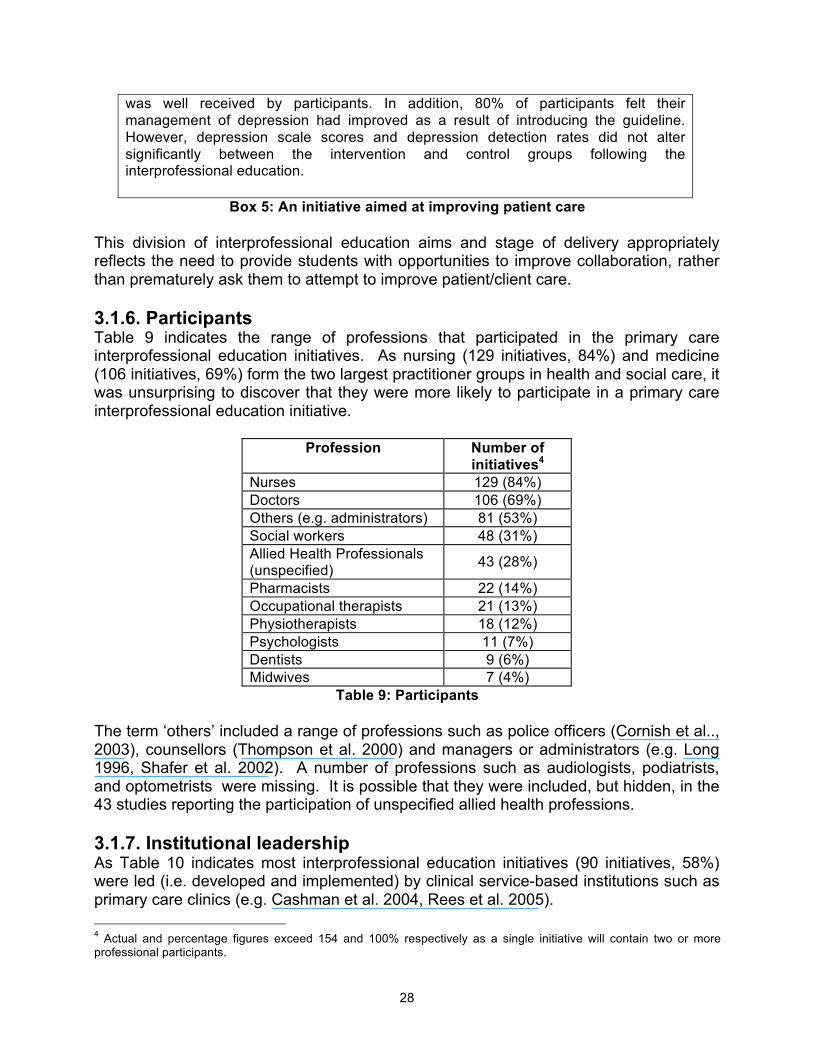
was well received by participants. In addition, 80% of participants felt their management of depression had improved as a result of introducing the guideline. However, depression scale scores and depression detection rates did not alter significantly between the intervention and control groups following the interprofessional education.
Box 5: An initiative aimed at improving patient care This division of interprofessional education aims and stage of delivery appropriately reflects the need to provide students with opportunities to improve collaboration, rather than prematurely ask them to attempt to improve patient/client care. 3.1.6. Participants Table 9 indicates the range of professions that participated in the primary care interprofessional education initiatives. As nursing (129 initiatives, 84%) and medicine (106 initiatives, 69%) form the two largest practitioner groups in health and social care, it was unsurprising to discover that they were more likely to participate in a primary care interprofessional education initiative.
Profession Number of initiatives4
Nurses 129 (84%) Doctors 106 (69%) Others (e.g. administrators) 81 (53%) Social workers 48 (31%) Allied Health Professionals (unspecified) 43 (28%)
Pharmacists 22 (14%) Occupational therapists 21 (13%) Physiotherapists 18 (12%) Psychologists 11 (7%) Dentists 9 (6%) Midwives 7 (4%)
Table 9: Participants The term ‘others’ included a range of professions such as police officers (Cornish et al.., 2003), counsellors (Thompson et al. 2000) and managers or administrators (e.g. Long 1996, Shafer et al. 2002). A number of professions such as audiologists, podiatrists, and optometrists were missing. It is possible that they were included, but hidden, in the 43 studies reporting the participation of unspecified allied health professions. 3.1.7. Institutional leadership As Table 10 indicates most interprofessional education initiatives (90 initiatives, 58%) were led (i.e. developed and implemented) by clinical service-based institutions such as primary care clinics (e.g. Cashman et al. 2004, Rees et al. 2005). 4 Actual and percentage figures exceed 154 and 100% respectively as a single initiative will contain two or more professional participants.

29
Lead institution Frequency
Service 90 (58%) Higher education 46 (30%) Joint 18 (12%)
Table 10: Institutional leadership Nevertheless, a third of initiatives (46 initiatives, 30%) were led by higher education institutions. This group of initiatives were usually delivered to pre-licensure students in the form of practice placements (e.g. Hayward et al. 1996, Reeves 2000). Box 6 provides an example of such an initiative.
van der Horst et al. (1995) described an interprofessional primary care placement for pre-qualification students from a number of professional groups including medicine, nursing, occupational therapy, physiotherapy and social work based in Canada. The aim of the placement was to enhance student understanding of interprofessional teamwork and improve their knowledge of the needs of users of community health services. Working in small interprofessional teams, students undertook a range of learning activities, such as observations of community interprofessional health teams, interviews with local community experts, interviews with the users of community health services, to gather information on teamwork and community-related issues. Students also attended seminars where their information is shared and discussed with their tutors and peers. Data gathered at the end of the placement revealed that the students enjoyed their interprofessional experiences. In addition, students felt that their knowledge of interprofessional and community issues was improved as a result of their participation in the placement.
Box 6: An interprofessional education initiative led by higher education 3.1.8. Learning methods Section 2.1.3, outlined Barr’s (2002) typology of interactive learning methods as a useful way of categorizing the range of learning activities employed in interprofessional education initiatives. Using a slightly modified version of this typology,5 Table 11 indicates that exchange-based learning (i.e. seminar or workshop discussions) was the most commonly employed method (97 initiatives, 63%). The ‘guideline development’ learning method (33 initiatives, 21%) describes initiatives which employed interprofessional education to introduce new clinical approaches or guidelines to enhance patient/client care (e.g. Bluespruce et al. 2001, Rubenstein et al. 2002). As noted in Section 2.1.3, in general interprofessional education initiatives often employ two or more interactive learning methods. This was the case for the 154 initiatives that qualified for inclusion in the review. Of these, it was found that 37 initiatives (24%) employed two methods, 29 (19%) initiatives employed three methods, 16 initiatives (10%) employed four methods and 3 initiatives (2%) employed five methods.
5 Barr’s (2002) typology has been expanded to include three additional learning methods that emerged from this review: received learning (shared lectures), guideline development (learning together to implement an improvement in the delivery of care) and e-learning (interactive electronic methods that assisted communication).

30
Learning method Frequency6
Exchange 97 (63%) Received7 64 (42%) Practice 39 (25%) Problem-focused 34 (22%) Guideline development 33 (21%) Observation 18 (12%) Simulation 13 (8%) e-learning 1 (>1%)
Table 11: Methods of learning Of the initiative that employed two interactive learning methods, a popular combination (21 initiatives, 14%) was to combine exchange-based learning with received (didactic) learning, such as lectures (e.g. Berman et al. 2000, Mayall et al. 2004). 3.1.9. Underpinning theory Table 12 indicates that there was little explicit use of theory across the 154 primary care interprofessional education initiatives. In total, only 24 initiatives (15%) employed an explicit theory drawn either from the adult learning or quality improvement literature.
Theory Frequency Adult learning (implicitly employed) 104 (68%) Quality improvement (implicitly employed) 26 (17%) Quality improvement (explicitly employed) 13 (8%) Adult learning (explicitly employed) 11 (7%)
Table 12: Underpinning theory In relation to the 13 (8%) initiatives that explicitly drew upon learning organization theory, these tended to use principles of TQM or CQI, in particular the Plan-Do-Study-Act approach (e.g. Shafer et al. 2002). (See Box 7).
Cox et al. (1999) present findings a continuous quality improvement project they established in a seven partner general practice based in the UK. The aim of the project was to improve the service delivered to patients by reducing time wasted by reception staff. Following a Plan-Do-Study-Act approach to quality improvement, an interprofessional team consisting of a general practitioner, four receptionists and the practice manager was set up to study current work practice and initiate improvements to service delivery. Once this phase was completed, suggested improvements were disseminated and implemented by staff. Audit data collected over a six-month period following these changes revealed that general practitioners and receptions were working more effective together, with a reduction of both time wastage and patient complaints.
Box 7: Use of a quality improvement theory 6 Totals exceed 154 (100%) due to the use of multiple learning methods within a single initiative. 7 As ‘received’ learning is a non-interactive learning method, its use within the initiatives was always in combination with an interactive method, usually an exchange-based method.

31
Of the 11 initiatives (7%) that explicitly drew upon theoretical perspectives from adult learning, Knowles’ theory of adult learning, Kolb’s theory of experiential learning and/or Schön’s theory of reflection (Lia-Hoagberg et al.. 1997, Barker & Oandasan 2005) were used. Only two of the Canadian initiatives used an explicit underpinning theory: Mann et al. (1996) who employed Barrow & Tamblyn’s (1980) problem-based learning (PBL) theory (see Box 8), while Barker & Oandasan (2005) employed a combination of PBL theory and Knowles’ (1980) adult learning theory in their interprofessional initiative.
Drawing upon Barrow & Tamblyn’s theory of PBL, Mann et al. (1996) describe an interprofessional course to improve understanding of health promotion issues for 35 doctors, nurses, dieticians, pharmacists and social workers based in Canada. Working in small interprofessional groups, participants were encouraged to discuss four problem-based cases linked to various aspects of health promotion and agree upon ‘solutions’ to the problems contained in each case. An evaluation of the course indicated that participants enjoyed their interprofessional experiences and acquired a better understanding of each other’s roles. Box 8: Use of Problem-based learning theory within interprofessional education
3.2. Evaluating the initiatives This section offers an outline of the approaches to evaluation employed within the 154 initiatives included in the review. Specifically, it reports on the evaluation designs employed, how data were gathered and analysed, and also on the nature of methodological limitations. 3.2.1. Evaluation design Table 13 outlines the range of evaluation designs employed across the 154 primary care interprofessional education initiatives. The post-intervention design was the most commonly used, with 49 initiatives (32%) employing this approach (e.g. Revel & Yussuf 2003, Larivaara & Taanila 2004). This design is generally considered weak, as the collection of data following the intervention (the delivery of the interprofessional education) means that it is difficult to tell if any change that has occurred is attributable to the intervention or not. The popularity of this design, however, may be determined by resource (time and money) constraints.
Research Design Frequency Post-intervention 49 (32%) Before-and-after 35 (23%) Longitudinal 21 (14%) Unclear 15 (10%) Case study 11 (7%) Controlled before-and-after 8 (5%) Randomised control trial 8 (5%) Before-during-and-after 5 (3%) Action research 2 (1%)
Table 13: Evaluation Design

32
Just over a third of the initiatives (56 initiatives, 36%) used quasi-experimental or experimental designs – before-and-after studies, before-during-and-after studies; controlled before-and-after studies (CBAs) and randomized controlled trials (RCTs) (e.g. Rees et al. 2005, Crutcher et al. 2004). In general, this type of evaluation design is more robust as the collection of baseline data, the inclusion of control groups and/or the use of randomization mean that they can more effectively detect change related to an intervention such as interprofessional education. Box 9 provides an example of the use of an experimental (CBA) design within interprofessional education.
Rutter & Hagart (1990) describe the development and evaluation of an interprofessional diploma in alcohol counselling and consultation based in the UK. Participants included nurses, social workers, a probation officer, an occupational therapist and a general practitioner. The course was delivered in one-two week full-time blocks over a period of one year. To assess the impact of this course on participants, a controlled before-and-after research design was adopted with the collection of questionnaire, interview and observational data. Findings revealed that participants enjoyed the course and reported that their knowledge of issues around interprofessional collaboration within the field of alcohol counselling improved. However, it was found that their attitudes and the quality of their interactions over the duration of the course remained largely unaltered. Data from the ‘controlled’ participants also remained unchanged.
Box 9: An example of a controlled before-and-after design in interprofessional education It was encouraging to identify 21 of the initiatives (14%) that used a longitudinal design (e.g. Korabek et al.. 2004), as this type of design provides valuable accounts of the longer-term effects of interprofessional education (usually over weeks or months) on participants’ collaborative practice and the quality of care. Box 10 provides an example of an initiative that incorporated a longitudinal design in their evaluation work.
Foy et al. (2002) describe an interprofessional education program for members of 21 primary care teams based in the UK. Participants initially attended three interprofessional critical appraisal workshops that aimed to enhance their skills in assessing research that could inform their clinical practice. During the workshops the teams also identified a clinical topic relating to their own practice and formulated a question that required further evidence to answer. They then searched the evidence and critically appraised the literature. The teams then drew up action plans and targets based on their research findings. The overall aim of this part of their training was to use the evidence they had collected to change an aspect of their professional or organizational practice. During the six months following the workshops, each team met with a facilitator to review progress on their action plan and to resolve any problems that they encountered. Participants reported team communication and service delivery improvements. For example, the evidence that one team found indicated a need to reduce antibiotic prescribing for children. A collaborative effort

33
between the doctors and health visitors to do so resulted in an evidence-based policy on prescribing and the production of a practice leaflet explaining the new policy to clients.
Box 10: A longitudinal evaluation However, It was concerning to discover that 15 initiatives (10%) did not provide sufficient information to identify which research design was employed. 3.2.2. Data collection and analysis Most initiatives tended to collect multiple forms of data (e.g. questionnaires, audit data, interviews and observations) in their evaluations (see Table 14). Combining methods helps ensure that an evaluation can provide a more detailed and plausible account of interprofessional education. Of the initiatives that employed two or more methods of data collection, the most popular were the combined use of questionnaires and interviews (Larivaara & Taanila 2004, Taylor et al. 2001).
Data Gathered Frequency Multiple methods8 61 (39%) Questionnaire 49 (32%) Unclear 21 (14%) Clinical audit 14 (9%) Interview 9 (6%)
Table 14: Data collection
Questionnaires (49 initiatives, 32%) were the most common sole method of data collection (Underwood et al.. 2002, Cashman et al.. 2004). The relative ease and low expense of gathering this type of data may account for their popularity. However, the questionnaires used in these initiatives were, in general, pilot tools and therefore not validated. Consequently, these restricted the rigor of these studies. It was also disappointing to discover that 21 of the initiatives (14%) contained such poor descriptions of their approaches to gathering data that it was problematic to identify specific method(s) of data collection. In relation to the approach take with data analysis, as displayed in Table 15, most of the initiatives adopted a quantitative approach (71 initiatives, 46%).
Approach to data analysis
Frequency
Quantitative 71 (46%) Unclear 44 (29%) Mixed 26 (17%) Qualitative 13 (8%)
Table 15: Data analysis
8 These include methods such as questionnaires, interviews and/or observations.

34
The lack of qualitative work is somewhat concerning, as helpful in-depth accounts of participants’ experiences of interprofessional education are neglected. Box 11 provides an example of a rare qualitative initiative.
Barker & Oandasan (2005) describe a family medicine teaching site which developed an educational initiative to expose trainees to interprofessional care processes and learning with a number of different health care practitioners. A formative evaluation was undertaken using qualitative interviews with family medicine residents. A semi-structured guide was developed that explored knowledge, skills and attitudes related to interprofessional care, and shared experiences of the interprofessional collaboration processes. Following data analysis, it was found that residents' perspectives on their collaborative learning revolved around four key themes: changes to understanding and practice of interprofessional care; personal impact of interprofessional collaboration; learning about other health professionals; tension and challenges of interprofessional learning and working. It was also reported that while the residents enjoyed this educational experience, they felt that faculty supervisors did provide some ‘mixed messages’ in relation to the value of collaborating with other health professionals.
Box 11: An example of a qualitative evaluation It was again disappointing to discover that a number of initiatives (44 initiatives, 14%) contained such poor descriptions of their approaches to data analysis that it was difficult to attribute an analytical approach. 3.2.3. Limitations An overwhelming 109 initiatives (71%) did not discuss the methodological limitations contained in their evaluation work (see Table 16). Although word restrictions in journals may partially account for lack of attention to methodological weaknesses, the failure to address this aspect of an evaluation limits the overall credibility of these initiatives.
Methodological limitations Frequency Not discussed/addressed 109 (71%) Multiple biases (e.g. performance, detection, selection) 24 (16%)
Performance 10 (6%) Detection 10 (6%) Selection 1 (>1%)
Table 16: Methodological limitations Mayall et al. (2004) provide a useful example of an initiative that did offer an account of the multiple methodological limitations associated with their work. In their paper, which described an evaluation of a short interprofessional education course to primary care practitioners, Mayall et al. (2000) discussed: the limitations associated with a small sample size, the lack of collection of follow-up data and their inability to exactly match pre/post questionnaire data due to the need for respondent confidentiality.

35
3.3. Reported outcomes In attempting to collate and understand the significance of the various types of outcomes related to interprofessional education, Barr et al. (2000) expanded Kirkpatrick’s classic educational outcomes typology from four to six outcomes to incorporate changes in patient care (see Table 17).
Level Description of outcome
1. Reaction Learners’ views on the learning experience and its interprofessional nature.
2a. Modification of attitudes / perceptions
Changes in reciprocal attitudes or perceptions between participant groups. Changes in perception or attitude towards the value and/or use of team approaches to caring for a specific client group.
2b. Acquisition of knowledge / skills
Including knowledge and skills linked to interprofessional collaboration.
3. Behavioural change Identifies individuals’ transfer of interprofessional learning to their practice setting and changed professional practice.
4a. Change in organisational practice
Wider changes in the organisation and delivery of care.
4b. Benefits to patients / clients
Improvements in health or well being of patients / clients.
Table 17: Outcome typology modified by Barr et al. (2000) This typology has now been incorporated in a number of other interprofessional education reviews (e.g. Reeves 2001, Freeth et al. 2002, Barr et al. 2005). In general, its use is regarded as helpful in beginning to classify, in a systematic manner, the varied outcomes that flow from interprofessional education. By employing this typology, Table 18 reveals that the bulk of initiatives tend to report positive outcomes connected to their use of interprofessional education.
Level Positive Mixed Neutral Negative 1. Reactions 89 (58%) 8 (5%) - - 2a. Attitudes/Perceptions 35 (23%) 4 (3%) 2 (1%) - 2b. Knowledge/Skills 71 (46%) 3 (2%) - - 3. Behaviour 32 (21%) 3 (2%) 2 (1%) - 4a.Organisational practice 45 (29%) 6 (4%) 2 (1%) - 4b. Patient benefit 17 (11%) 4 (3%) 1 (>1%) -
Table 18: Reported outcomes9
9 Totals exceed 154 (100%) due to the use of multiple reporting of outcomes within a single initiative.

36
In general, it was found that those initiatives which reported changes to attitudes (level 2a) also reported changes in knowledge/skills (level 2b). Box 12 provides an example of such an initiative.
Crutcher et al. (2004) describe an interprofessional education program in diabetes care based in Canada. Objectives included knowledge increase in type 2 diabetes care and examining the effect of uni-professional versus interprofessional small groups on learning outcomes. A total of 61 baccalaureate nursing students, four pharmacy students and 56 family practice residents participated in a half-day program. Participants were randomly assigned to multi- versus uni-professional groups. A questionnaire assessing knowledge, attitudes and perceived role responsibilities was anonymously completed in a pre-test/post-test manner. The program was delivered in two sessions that combined larger and small group activities. Participants and educators showed interest in multi-professional education. While no change in knowledge was found, moderate changes in attitudes (with a lessening of attitudinal differences) and significant changes in perceptions of role (from uni-professional responsibility to shared responsibilities) were noted. Nurses in uni-professional groups demonstrated the greatest attitudinal and role perception changes. The contribution of the patient as teacher was prominent. Further exploration and rigorous analysis of the utility of MPE in diverse settings is warranted.
Box 12: An initiative reporting changes to attitudes and knowledge In addition, initiatives that reported change to organizational practice (level 4a) also reported improvements to patient/client care (level 4b) (e.g. Farris et al. 2004, Korabek et al. 2004). This section goes on to describe the nature of the different outcomes reported in the 154 initiatives to provide a more informed understanding of the impacts of interprofessional education. 3.3.1. Learner reactions Ninety-seven initiatives (63%) reported some form of change in participants’ reactions to their interprofessional education experience. In general, these initiatives assessed reaction in terms of: Learner satisfaction (Partis 2001, Revel & Yussuf 2003) Valuing or enjoying the interprofessional experience (Underwood et al. 2002) Boxes 4, 6 and 8 provide examples of interprofessional education initiatives that have reported changes at this level. It could be argued that reporting reaction type outcomes does not provide a very useful indicator of the effects of interprofessional education, especially when compared with changes that improve patient/client care. Nevertheless, one could also argue that learner reactions provide a basis for change in other areas, like attitudes, knowledge and behaviour, as without a positive reaction to interprofessional education, it is unlikely that these other outcomes will be met.

37
3.3.2. Changes in attitudes/perceptions Forty-one initiatives (27%) assessed changes in attitudes or perceptions towards another profession or interprofessional collaboration. Typically, this type of outcome was measured in terms of changes of attitudes/perceptions: To other professional groups (Reeves 2000) About collaboration/teamwork (Hartrick 2000, Leeper et al. 2001) In addition to the reporting of positive outcomes, 4 initiatives (3%) reported mixed (positives and neutral) outcomes and 2 initiatives (1%) report neutral outcomes. Box 11 provides an example of an initiative which reports changes in attitudes and/or perceptions. 3.3.3. Acquisition of knowledge/skills Seventy-one initiatives (46%) reported changes in collaborative knowledge or skills (level 2b). Reported changes in knowledge or skills included: Enhanced understanding of roles and responsibilities of other health and social care
professionals (e.g. Rutter & Hagart 1990, Mann et al. 1996) Improved knowledge of the nature of interprofessional teamwork (e.g. van der Horst
1995, Barker & Oandasan 2005) Box 13 provides an example of an interprofessional education initiative that reported changes at this level.
Bluespruce et al.. (2001) describe an interprofessional course that aimed to improve health and social care practitioners’ attitudes towards and understanding of human immunodeficiency virus (HIV). Forty-nine health and social care staff from two primary care clinics based in a large managed care organization in the US took part in the program. Participants included doctors, nurses and social workers. Participants were initially offered four interprofessional sessions in which they undertook team discussions, role-plays and patient case stories. To help reinforce the learning from the sessions, participants were offered written materials (e.g. HIV risk management protocols), ‘on-the-job’ team support, and two further interactive sessions. The authors measured the following outcomes: changes in participants’ attitudes towards HIV, and knowledge and skills of the management of the virus. It was found that participants reported significant improvements in terms of their knowledge and skills of working together with HIV-positive patients.
Box 13: An initiative reporting changes in knowledge/skills 3.3.4. Changes in behaviour Initiatives that reported behaviour change (37 initiatives, 24%) tended to focus on descriptions of interprofessional co-operation and communication, or development of closer links between professions (e.g. Hartrick 2000, Revel & Yussuf 2003, Rees et al.

38
2005). See Boxes 4 and 7 for examples of interprofessional education initiatives that report a change in interprofessional behaviour. In addition to the reporting of positive outcomes, 3 initiatives (2%) reported mixed (positives and neutral) outcomes and 2 initiatives (1%) report neutral outcomes at this particular level. However, it was found that the conceptualization and operationalization of this particular outcome was, in general, problematic as initiatives provided only anecdotal reports rather than robustly measured outcomes. 3.3.5. Changes in organizational practice ??? reported changes in organisational practice. Studies reporting outcomes at this level tended to include qualified practitioners who worked on initiatives aimed at improving the quality of patient/client care. Measures used to report changes in organizational practice included: Inter-organizational working patterns (Bond 1999, Farris 2004); Documentation of patient records (Hearnshaw et al. 2001, Macfarlane et al. 2005) In addition to the reporting of positive outcomes, six initiatives (4%) reported mixed (positive and neutral) outcomes and two initiatives (1%) reported neutral outcomes at this level. Box 10 provides an example of an initiative that reported a change at this level. 3.3.6. Improvements to care Twenty-two initiatives (15%) reported changes to patient/client care (Level 4b). This group of initiatives focused on reporting change centred around: Clinical outcomes such as medication adherence (Farris et al. 2004), detection rates
(Thompson et al. 2000) Patient/client satisfaction (e.g. Korabek et al. 2004) Box 14 provides an example of an interprofessional education initiative reporting at level 4b.
Jackson & Bircher (2002) describe the use of a learning organization approach that provided the foundation for an interprofessional initiative which aimed to enhance the delivery of care to the patients of a general practice in the UK. A large patient list combined with the poor organization of the practice led the primary care team to seek external assistance to ensure the practice could more effectively meet the needs of its patients. An external facilitator was located who worked with team members individually and collectively to identify their current challenges and to develop an implementation plan to resolve them. Findings from an evaluation of this initiative found that a number of benefits to patient care were realized as a result of this initiative. These include: more targeted health promotion advice to patients; a reduction of blood pressure for patients with chronic heart disease; higher proportion

39
of older patients receiving the influenza vaccine; and reduced waiting times for prescribed drugs
Box 14: An initiative reporting improvements to patient/client care While initiatives which reported change at this level provided some useful insights into the effects of interprofessional education for patients/client, collection of satisfaction data was problematic. This was because patient satisfaction data tended to be based upon unvalidated questionnaires.

40
Section 4: Conclusions and implications This final section of the review present key conclusions and implications based on the findings from the general interprofessional education literature and the 154 primary care interprofessional education initiatives that qualified for inclusion in this work. 4.1. Conclusions This review of interprofessional education in primary care provides a synopsis of the initiatives that have been undertaken, the nature of their evaluations, and the results obtained. The following section provides an overview of the results, and positions them in relation to the broader literature on interprofessional education. The majority of initiatives included in this review were based in the United States,
were post-licensure, and offered no form of academic award or educational credit. About half of the initiatives took place over a period of more than 7 days, often in the context of CQI or TQM work.
Generally, initiatives involving pre-licensure participants were led by higher
educational institutions, and aimed to improve interprofessional collaboration; initiatives that involved post-licensure participants tended to occur within primary care team clinic contexts, and aimed to improve quality of care delivered to patients/clients.
Nurses and physicians were the two largest professional participant groups, which
reflects their proportional representation in the health and social care field, but a range of other health and social care professionals were also involved.
There was little explicit use of educational theory to underpin initiatives; those that
did, used TQM or CQI, or elements of adult or experiential learning or reflection. Seminar or workshop discussions were the most commonly used interactive learning
method employed. The range of outcomes evaluated included: reactions to intervention, changes in
attitudes/perceptions, acquisition of knowledge and skills, changes in behaviour, and improvements to care. As previously noted, all of these outcomes are valuable goals and worthy of evaluation, as positive reactions and changes in attitudes/perceptions lay the groundwork to changes in behaviour and professional practice. Thus, according to these results, interprofessional education can have a positive impact at various levels, and ultimately lead to improved health and social care.
These initiatives do, however, share the same theoretical and methodological
limitations noted in previous reviews (Barr et al. 2000, Reeves 2001, Freeth et al. 2002). There is little explicit usage of theory to underpin the bulk of interprofessional education initiatives, and thus theoretical issues discussed in Section 2, such as relevance, status, balance, and size and stability are not formally addressed in the initiatives. In addition, there is little acknowledgement of the range of factors that

41
affect interprofessional education initiatives, such as the stage when the education is offered to learners, the role of competencies, and/or teaching issues.
While all initiatives required an element of interaction to qualify for inclusion in this
review, in accordance with the interprofessional education definition (see Section 1.2), there was a limited discussion of the nature of interaction, which precludes our understanding about the effectiveness of the interactive learning strategies that were employed.
From a methodological perspective, about a third of the studies utilized the limiting
post-intervention design, and many results were based on the use of questionnaires, which have limited ability to capture robust information and a comprehensive understanding of the outcomes. In addition, measures of behaviour changes were poorly conceptualized and operationalized, often consisting of simple self-reported accounts; measurements of improvements were also problematic.
4.2. Recommendations This review provides some insight into important initial strides in the field of interprofessional education in primary care, but underscores the need for more systematic approaches to the planning and evaluation of interprofessional education to increase our understanding of the most effective means of conducting this type of education. Therefore the following recommendations are offered: Further rigorous and comprehensive (i.e. multi-method) research is necessary to
increase our understanding of the nature (i.e. interactive learning processes) and impact (I.e. learning outcomes) related to interprofessional education. Wherever possible, future evaluations should include a longitudinal element in their work to begin to understand the long-term impact of this type of educational activity within primary care.
A better use of theoretical work, drawn from the adult learning literature, is needed
when planning an interprofessional education to help to securely underpin this type of activity. Freeth & Reeves (2004) revised 3P model of teaching and learning may also be a useful framework to employ during the planning phase of an interprofessional education initiative.
It is anticipated that the incorporation of both the suggested recommendations for planning and research related to interprofessional education should help to build an effective, comprehensive strategy to encourage students, health professionals, administrators and policymakers to buy-into, and/or to continue to support this type of educational activity in future years.

42
References Alderson P, Farsides B & Williams C (2002) Examining ethics in practice: health service professionals' evaluations of in-hospital ethics seminars. Nursing Ethics; 9:508-521.
Allen D (1997) The nursing-medical boundary: a negotiated order? Sociology of Health and Illness; 19:498-520.
Arlton D (1986) A paying health promotion clinic: combining client services and student learning. Journal of Allied Health; 15:3-10.
Atwal A (2002) Getting the evidence into practice: the challenges and successes of action research. British Journal of Occupational Therapy; 65:335-341.
Bailey D (2002) Training together – part 2: an exploration of the evaluation of a shared learning programme on dual diagnosis for specialist drugs workers and approved social workers (ASWs). Social Work Education; 21:685-699.
Baker R, Sorrie R, Reddish S & Hearnshaw H (1995) The facilitation of multiprofessional clinical audit in primary health care teams-from audit to quality assurance. Journal of Interprofessional Care; 9:237-244.
Barber G, Borders K, Holland B & Roberts K. (1997) Life Span Forum: an interdisciplinary training experience. Gerontology & Geriatrics Education; 18:47-59.
Barker J (1964) Team work in the service of the mentally ill. Nursing Mirror; 199:285-287.
Barker KK & Oandasan I (2005) Interprofessional care review with medical residents: lessons learned, tensions aired--a pilot study. Journal of Interprofessional Care; 19:207-214.
Barr H (1998) Competent to collaborate: towards a competency-based model for interprofessional education. Journal of Interprofessional Care; 12:181-188.
Barr H (1994) Perspectives on Shared Learning. CAIPE, London.
Barr H (1996) Ends and means in interprofessional education: towards a typology. Education for Health; 9:341-352.
Barr H (2002) Interprofessional Education: Today, Yesterday and Tomorrow. Learning and Support Network: Centre for Health Sciences and Practice, London.
Barr H, Koppel I, Reeves S, Hammick M, Freeth D (2005) Effective Interprofessional Education: Assumption, Argument and Evidence. Blackwell, London.

43
Barr H & Shaw I (1995) Shared Learning: Selected Examples from the Literature. CAIPE, London.
Barr H & Waterton S (1996) Interprofessional Education in Health and Social Care in the United Kingdom: A report of a CAIPE survey. CAIPE, London.
Barr H, Freeth D, Hammick M, Koppel I & Reeves S (2000) Evaluations of Interprofessional Education: A United Kingdom Review for Health and Social Care. BERA/CAIPE, London.
Barrows H & Tamblin R (1980) Problem Based Learning. New York: Springer Publications.
Bateman H, Bailey P & McLellan H (2003) Of rocks and safe channels: learning to navigate as an interprofessional team. Journal of Interprofessional Care; 17:141-150.
Berman S, Miller AC, Rosen C & Bicchieri S (2000) Assessment training and team functioning for treating children with disabilities. Archives of Physical Medicine & Rehabilitation; 81:628-633.
Biggs J (1993) From theory to practice: a cognitive systems approach. Higher Education Research and Development; 12:73-85.
Bluespruce J, Dodge W, Grothaus L, Wheeler K, Rebolledo V, Carey J, McAfee, T & Thompson R (2001) HIV prevention in primary care: impact of a clinical intervention", AIDS Patient Care and Studies; 15:243-253.
Bond M (1999) Placing poverty on the agenda of a primary health care team: an evaluation of an action research project. Health and Social Care in the Community; 7:9-16.
Brown S (2000) Outcomes analysis of a pain management project for two rural hospitals. Journal of Nursing Care Quality; 14:28-34.
Carpenter J (1995) Interprofessional education for medical and nursing students: evaluation of a programme. Medical Education; 29:265-272.
Carpenter J, Barnes D & Dickinson C (2003a) Making a Modern Mental Health Care Force: Evaluation of the Birmingham University Interprofessional Training Programme in Community Mental Health 1998-2002. Internal Research Report. University of Durham, Durham. Carpenter J & Hewstone M (1996) Shared learning for doctors and social workers. British Journal of Social Work; 26:239-57.

44
Cashman S, Reidy P, Cody K, Lemay C (2004) Developing and measuring progress toward collaborative, integrated, interdisciplinary health care teams. Journal of Interprofessional Care; 18:183-196.
Casto M (1994a) Education for interprofessional practice. In: M Casto & M Julia (eds). Interprofessional Care and Collaborative Practice. Brooks/Cole, Belmont.
Casto M (1994b) Interprofessional work in the USA. In: A Leathard (ed). Going Interprofessional: Working Together in Health and Welfare. Routledge, London.
CAIPE (Centre for the Advancement of Interprofessional Education) (1997) Interprofessional education: a definition. CAIPE, London.
Cleghorn G & Baker G (2000) What faculty need to learn about improvement and how to teach it to others. Journal of Interprofessional Care; 14:147-59.
College of Occupational Therapists (2000) Code of Ethics and Professional Conduct for Occupational Therapists. College of Occupational Therapists, London.
College of Family Physicians of Canada (2000) Primary Care and Family Medicine in Canada: A Prescription for Renewal. College of Family Physicians of Canada, Ontario. Committee of Vice Chancellors and Principals (1997) Survey of Interprofessional Education and Training. Health Professionals Committee. CVCP, London.
Cooper H, Carlisle C, Gibbs T & Watkins C (2001) Developing an evidence base for interdisciplinary learning: a systematic review. Journal of Advanced Nursing; 2:228-237.
Cornish P, Church E, Callanan T, Bethune C, Robbins C & Miller R (2003) Rural interdisciplinary mental health team building via satellite: a demonstration project. Telemedicine Journal & E-Health; 9:63-71.
Cox S, Wilcock P & Young J (1999) Improving the repeat prescribing process in a busy general practice. A study using continuous quality improvement methodology. Quality in Health Care; 8:119-125.
Crutcher R, Then K, Edwards A, Taylor K & Norton P (2004) Multi-professional education in diabetes. Medical Teacher; 26:435-43.
Dalton JA, Carlson J, Blau W, Lindley C, Greer, SM & Youngblood R (2001) Documentation of pain assessment and treatment: how are we doing? Pain Management Nursing; 2:54-64.
D'Amour D, Beaulieau MD, San Martin Rodriguez L & Ferrada-Videla M. (2004) Key Elements of Collaborative Practive & Frameworks: Conceptual Basis for Interdisciplinary Practice. In: Oandasan I, D'Amour D, Zwarenstein M, Barker K, Purden M, Beaulieau MD, Reeves S, Nasmith L, Bosco C, Ginsburg L, & Tregunno D. Interdisciplinary

45
Education for Collaborative, Patient-Centred Practice: Research & Findings Report. Ottawa, Health Canada.
Department of Health (1989) Caring for People: Community Care in the Next Decade and Beyond. HMSO, London.
Department of Health (1997) The New NHS. Modern. Dependable. DoH, London.
Department of Health (2000) A Health Service of all the Talents: Developing the NHS Workforce. DoH, London.
Department of Health (2001) Working Together – Learning Together: A Framework for Lifelong learning for the NHS. DoH, London.
Department of Health (2002) Learning from Bristol: The DH Response to the Report of the Public Inquiry into Children’s Health Surgery at the Bristol Royal Infirmary 1984-1995. DoH, London.
DePoy E, Wood C & Miller M (1997) Educating allied health professionals: an interdisciplinary effort. Journal of Allied Health; 26:127-32.
Dieleman S, Farris K, Feeny D, Johnson J, Tsuyuki R, Brilliant S (2004) Primary health care teams: team members' perceptions of the collaborative process. Journal of Interprofessional Care; 18:75-78,
Dienst E & Byl N (1981) Evaluation of an educational program in health care teams. Journal of Community Health; 6:282-298.
Dombeck M (1997) Professional personhood: training, territoriality and tolerance. Journal of Interprofessional Care; 11: 9-21.
Elliott R, Woodward M & Oborne C (2002) Antithrombotic prescribing in atrial fibrillation: application of a prescribing indicator and multidisciplinary feedback to improve prescribing. Age and Ageing; 31:391-396.
Erkel E, Nivens A & Kennedy D (1995) Intensive immersion of nursing students in rural interdisciplinary care. Journal of Nursing Education; 34:359-365.
Evers H (1981) Multidisciplinary teams in geriatric wards: myth or reality? Journal of Advanced Nursing; 6:205-214.
Falconer J, Roth E, Sutin J, Strasser D & Chang R (1993) The critical path method in stroke rehabilitation: lessons from an experiment in cost containment and outcome improvement. Quarterly Review Bulletin; 19:8-16.

46
Fallsberg M & Wijma K (1999) Student attitudes towards the goals of an interprofessional Training Ward. Medical Teacher; 6:576-581.
Fallsberg M & Hammar M (2000) Strategies and focus at an integrated, interprofessional Training Ward. Journal of Interprofessional Care; 14:337-350.
Farrell M (2005) Enabling interprofessional education: the potential of e-learning. In: C Carlisle, H Cooper & D Mercer (eds). Interprofessional Education: an Agenda for Healthcare Professionals. Quay Books, Salisbury.
Farrell M, Schmitt M & Heinemann G (2001) Informal roles and the stages of team development. Journal of Interprofessional Care; 15:281-295.
Farris KB, Côté I, Feeny D, Johnson JA, Tsuyuki RT, Brilliant S & Dieleman S (2004) Canadian Family Physician; 50 :998-1003.
Feiger S & Schmitt M (1979) Collegiality in interdisciplinary health teams: its measurements and its effects. Social Science and Medicine; 13:217-229.
Firth-Cozens J (1998) Celebrating teamwork. Quality in Health Care; 7(Suppl):S3-S7.
Forbes E & Fitzsimons V (1993) Education: the key for holistic interdisciplinary collaboration. Holistic Nurse Practice; 7:1-10.
Freeth D (2001) Sustaining interprofessional collaboration. Journal of Interprofessional Care; 15:37-46.
Freeth D & Nicol M (1998) Learning clinical skills: an interprofessional approach. Nurse Education Today; 18:455-61.
Freeth D, Meyer J, Reeves S & Spilsbury K (1999) Linking interprofessional education to user benefit: of drops in the ocean and stalactites. Advancing Clinical Nursing; 3:127-135.
Freeth D, Nicol M, Reeves S, Wood D. (2000) Clinical governance: an interprofessional approach. Journal of Interprofessional Care; 14:292-3.
Freeth D, Hammick M, Koppel I, Reeves S & Barr H (2002) A Critical Review of Evaluations of Interprofessional Education. Learning and Support Network: Centre for Health Sciences and Practice. London.
Freeth D & Reeves S (2004) Learning to work together: using presage, process, product (3P) model to highlight decisions and possibilities. Journal of Interprofessional Care; 18:43-56.

47
Freeth D, Hammick M, Reeves S, Koppel I & Barr H (2005) Effective Interprofessional Education: Development, Delivery and Evaluation. London: Blackwell Science
Funnell P (1995) Exploring the value of interprofessional shared learning. In: K Soothill, L Mackay & C Webb (eds). Interprofessional Relations in Health Care. Edward Arnold, London.
Funnell P, Gill J & Ling J (1992) Competence through interprofessional shared learning. In: P Pace (ed). Developing and measuring competence (Aspects of Education and Training Technology XXV). Kogan Page, London.
Gazarian M, Henry RL, Wales SR, Micallef BE, Rood EM, O'Meara MW & Numa AH (2001) Evaluating the effectiveness of evidence-based guidelines for the use of spacer devices in children with acute asthma. Medical Journal of Australia; 174:394-397.
General Medical Council (2001) Good Medical Practice. General Medical Council, London.
Gentry M, Iceton J & Milne D (2001) Managing challenging behaviour in the community: methods and results of interactive staff training. Health & Social Care in the Community; 9:143-150.
Gibbon B, Watkins C, Barer D, Waters K, Davies S, Lightbody L & Leathley M (2002) Can staff attitudes to team working in stroke care be improved? Journal of Advanced Nursing; 40:105-111.
Gilbert J, Camp R, Cole C, Bruce C, Fielding D & Stanton S (2000) Preparing students for interprofessional teamwork in health care. Journal of Interprofessional Care; 14:223-235.
Gill J & Ling J (1995) Interprofessional shared learning: a curriculum for collaboration. In: K Soothill, L Mackay & C Webb (eds). Interprofessional Relations in Health Care. Edward Arnold, London.
Graham J & Wealthall S (1999) Interdisciplinary education for the health professions: taking the risk for community gain. Focus on Health Professional Education; 1:49-69.
Green R, Cavell G & Jackson S (1996) Interprofessional clinical education of medical and pharmacy students. Medical Education; 30:129-133.
Gregson B, Cartlidge A & Bond J (1991) Interprofessional collaboration in primary health care organisations. Royal College of General Practitioners, London.

48
Hammick M (1998) Interprofessional education: concept, theory and application. Journal of Interprofessional Care; 12:323-32.
Harden R (1998) AMEE Guide No. 12: Multiprofessional education: Part 1 – effective multiprofessional education: a three-dimensional perspective. Medical Teacher; 20:402-408.
Harmon R, Sheehy L & Davis D (1998) The utility of external performance measurement tools in program evaluation. Rehabilitation Nursing; 23:8-11.
Hart E & Fletcher J (1999) Learning how to change: a selective analysis of literature and experience of how teams learn and organisations change. Journal of Interprofessional Care; 13:53-63.
Hartrick G (2000) Developing health-promoting practice with families: one pedagogical experience. Journal of Advanced Nursing; 31:27-34.
Hayward K, Powell L & McRoberts J (1996) Changes in student perceptions of interdisciplinary practice in the rural setting. Journal of Allied Health; 25:315-27.
Headrick L, Wilcock P & Batalden P (1998) Interprofessional working and continuing medical education. British Medical Journal; 316:771-74.
Health Canada (2003) First Ministers’ Accord on Health Care Renewal. Health Canada, Toronto.
Hearnshaw H, Hopkins J, Wild A, MacKinnon M, Gadsby R & Dale J (2001) Mandatory, multidisciplinary education in diabetes care. Can it meet the needs of primary care organisations? Practical Diabetes International; 18:274-280.
Heckman M, Ajdari S, Esquivel M, Chernof B, Tamm N, Landowski L & Guterman J (1998) Quality improvement principles in practice: the reduction of umbilical cord blood errors in the labor and delivery suite. Journal of Nursing Care Quality; 12:47-54.
Hind M, Norman I, Cooper S, Gill E, Hilton R, Judd P & Newby S (2003) Interprofessional perceptions of health care students. Journal of Interprofessional Care; 17:21-34.
Holland K (2002) Inter-professional education and practice: the role of the teacher/facilitator. Nurse Education in Practice; 2:221-222.
Horak B, O'Leary K & Carlson L (1998) Preparing health care professionals for quality improvement: the George Washington University/George Mason University experience. Quality Management Health Care; 6:21-30.

49
Horbar JD, Rogowski J, Plsek PE, Delmore P, Edwards WH, Hocker J, Kantak AD, Lewallen P, Lewis W, Lewit E, McCarroll CJ, Mujsce D, Payne NR, Shiono P, Soll RF, Leahy K & Carpenter JH (2001) Collaborative quality improvement for neonatal intensive care. NIC/Q Project Investigators of the Vermont Oxford Network. Pediatrics; 107:14-22.
Horder J (1996) The Centre for the Advancement of Interprofessional Education. Education for Health; 9:397-400.
Hornby S & Atkins J (2000) Collaborative Care: Interprofessional, Interagency and Interpersonal. (2nd Edition). Oxford, Blackwell.
Howkins E & Allison A (1997) Shared learning for primary health care teams: a success story. Nurse Education Today; 17:225-231.
Hughes D (1988) When nurse knows best: some aspects of nurse/doctor interaction in a casualty department. Sociology of Health and Illness; 16:184-202.
Hughes L & Lucas J (1997) An evaluation of problem based learning in the multiprofessional education curriculum for the health professions. Journal of Interprofessional Care; 11:77-88.
Hunter M & Love C (1996) Total quality management and the reduction of inpatient violence and cost in a forensic psychiatric hospital. Psychiatric Services; 47:751-754.
Jaques D (1998) Learning in Groups (2nd ed). Kogan Page, London.
Jones R (1986) Working Together, Learning Together. Royal College of General Practitioners, London.
Jones P & Dunn E (1974) Education for the health team: a pilot project. International Journal of Nursing Studies ; 11:61-69. Jones M & Salmon D (2001) The practitioner as policy analyst: a study of student reflections of an interprofessional course in higher education. Journal of Interprofessional Care; 15:67-77.
Keough M, Field T & Gurwitz J (2002) A model of community-based interdisciplinary team training in the care of the frail elderly. Academic Medicine; 77:936.
Ketola E, Sipila R, Makela M & Klockars M (2000) Quality improvement programme for cardiovascular disease risk factor recording in primary care. Quality in Health Care; 9:175-180.
Kindig D (1975) Interdisciplinary education for primary health care team delivery. Journal of Medical Education; 50:97-110.

50
Kipp J & Pimlott J (2003) Meeting the challenges of an interprofessional clinical placement program. Paper presented at The 5th Alberta Meeting on Medical Education, Jasper, Alberta.
Knowles M (1980) The Modern Practice of Adult Education - From Pedagogy to Androgogy (revised). Chicago: Follett Publishing Co.
Kolb D (1984) Experiential Learning. Englewood Cliffs, New Jersey: Prentice-Hall.
Korabek B, Slauenwhite C, Rosenau P & Ross L (2004) Innovations in seniors’ care : Home care/physician partnership. Nursing Leadership; 17:65-78.
Lacey P (1998) Interdisciplinary training for staff working with people with profound and multiple learning disabilities. Journal of Interprofessional Care; 12:43-52.
Larivaara P & Taanila A (2004) Towards interprofessional family oriented teamwork in primary services: the evaluation of an education programme. Journal of Interprofessional Care; 18:153-164.
Larson E (1999) The impact of physician-nurse interaction on patient care. Holistic Nursing Practice; 13:38-46.
Lary M, Lavigne S, Muma S, Jones S & Hoeft H (1997) Breaking down barriers: multidisciplinary education model. Journal of Allied Health; 26:63-69.
LaSala K, Hopper S, Rissmeyer D & Shipe D (1997) Rural health care & interdisciplinary education. Nursing and Health Care Perspectives; 18:292-298.
Leeper J, Hullett S & Want L (2001) Rural Alabama Health Professional Training Consortium : six-year evaluation results. Family & Community Health; 24 :18-26.
Lia-Hoagberg B, Nelson P & Chase R (1997) An interdisciplinary health team training program for school staff in Minnesota. Journal of School Health; 67:94-97.
Lies V & Sunderland K (2001) Organisational Change. A Review for Health Care Managers, Professionals and Researchers. London School of Hygiene and Tropical Medicine, London.
Litaker D, Mion L, Planavsky L, Kippes C, Mehta N & Frolkis J (2003) Physician-nurse practitioner teams in chronic disease management: the impact on costs, clinical effectiveness and patients’ perception of care. Journal of Interprofessional Care; 17:223-238.
Long S (1996) Primary health care team workshop: team members' perspectives. Journal of Advanced Nursing; 23:935-41.

51
Lough M, Schmidt K & Swain G (1996) An interdisciplinary educational model for professions students in a family practice center. Nurse Educator; 21:27-31.
Loxley A (1980) A study of a multi-disciplinary in-service in the interests of health care. Social Work Service; 9:35-43.
Loxley A (1997) Collaboration in Health and Welfare: Working with Difference. Jessica Kingsley, London.
MacDougall M & Elahi V (1974) A multidisciplinary learning experience. Journal of Medical Education; 49:752-755.
Macfarlane F, Greenhalgh T, Schofield T & Desombre T (2004) RCGP Quality Team Development programme : an illuminative evaluation. Quality & Safety in Health Care; 13:356-362.
Mann K, Viscount P, Cogdon A, Davidson K, Langille D & Maccara M (1996) Multidisciplinary learning in continuing professional education: the Heart Health Nova Scotia experience. Journal of Continuing Education in the Health Professions; 16:50-60.
Mathias P & Thompson T (1997) Preparation for interprofessional work: trends in education, training and the structure of qualification in the United Kingdom. In: J Øvretveit, P Mathias & T Thompson (eds). Interprofessional Working for Health and Social Care. Macmillan, Basingstoke.
Mayall E, Oathamshaw S, Lovell K & Pusey H (2004) Development and piloting of a multidisciplinary training course for detecting and managing depression in the older person. Journal of Psychiatric and Mental Health Nursing; 11:165-171.
McGrath M (1991) Multidisciplinary Teamwork. Avebury, Aldershot.
McKeown M, Blundell P, Lord J & Haigh C (2005) Organic training and development: working with mental health teams directly in the workplace. In: C Carlisle, H Cooper & D Mercer (eds). Interprofessional Education: an Agenda for Healthcare Professionals. Quay Books, Salisbury.
Miller C, Ross N, & Freeman M (1999) Shared Learning and Clinical Teamwork: New Directions in Multiprofessional Practice. London: ENB.
Milne DL, Keegan D, Westerman C, & Dudley M (2000) Systematic process and outcome evaluation of brief staff training in psychosocial interventions for severe mental illness. Journal of Behavior Therapy and Experimental Psychiatry; 2:87-101.
Mires G, Williams F, Harden R, Howie P, McCarey M & Robertson A (1999) Multiprofessional education in undergraduate curricula can work. Medical Teacher; 21:281-285.

52
Mires G, Williams F, Harden R & Howie P (2001) The benefits of a multiprofessional education programme can be sustained. Medical Teacher; 23:300-304.
Mohr C, Phillips A, Curran J, & Rymill A (2002) Interagency training in dual disability. Australasian Psychiatry; 10:356-364.
Morey JC, Simon R, Jay GD, Wears RL, Salisbury M, Dukes KA & Berns SD (2002) Error reduction and performance improvement in the emergency department through formal teamwork training: evaluation results of the MedTeams project. Health Services Research; 37:1553-1581.
Nash A & Hoy A (1993) Terminal care in the community – an evaluation of residential workshops for general practitioner/district nurse teams. Palliative Medicine; 7:5-17.
Nursing and Midwifery Council (2002) Code of Professional Conduct. Nursing and Midwifery Council, London. Oandasan I & Reeves S (2005a) Key elements for interprofessional education. Part 1: the learner, the educator and the learning context. Journal of Interprofessional Care; 19(Suppl 1):21-38. Oandasan I & Reeves S (2005b) Key elements of interprofessional education. Part 2: factors and processes and outcomes. Journal of Interprofessional Care; 19(Suppl 1):39-48. Oandasan I, D'Amour D, Zwarenstein M, Barker K, Purden M, Beaulieau MD, Reeves S, Nasmith L, Bosco C, Ginsburg L & Tregunno D (2004) Interdisciplinary Education for Collaborative, Patient-Centred Practice: Research & Findings Report. Ottawa, ON: Health Canada. O'Boyle M, Paniagua F, Wassef A & Holzer C (1995), Training health professionals in the recognition and treatment of depression. Psychiatric Services; 46:616-618. O’Neil E & Pew Health Professions Commission (1993) Recreating Health Professional Practice for a New Century. Pew Health, San Francisco.
Ontario Ministry of Health and Long Term Care (2006) Family Health Teams http://www.health.gov.on.ca/transformation/fht/fht_mn.html (accessed on 25 January 2006).
Overdyk FJ, Harvey SC, Fishman RL & Shippey F (1998) Successful strategies for improving operating room efficiency at academic institutions. Anesthesia & Analgesia; 86:896-906.
Parsell G & Bligh J (1998) Educational principles underpinning successful shared learning. Medical Teacher; 20:522-29.
Parsell G, Spalding R & Bligh J (1998) Shared Goals, shared learning: evaluation of a multiprofessional course for undergraduate students. Medical Education; 32:304-11.

53
Partis M (2001) A multidisciplinary education project in primary care. British Journal of Community Nursing; 6:68-73.
Pethybridge J (2004) How team working influences discharge planning from hospital: a study of four multi-disciplinary teams in an acute hospital in England. Journal of Interprofessional Care; 18:29-41.
Pilon C, Leathley M, London R, McLean S, Phang P, Priestley R, Rosenberg F, Singer J, Anis A & Dodek P (1997) Practice guideline for arterial blood gas measurement in the intensive care unit decreases numbers and increases appropriateness of tests. Critical Care Medicine; 25:1308-1313.
Pirrie A (1999) Rocky mountains and tired Indians: on territories and tribes. Reflections on multidisciplinary education in the health professions. British Education Research Journal; 25:113-126.
Pirrie A, Wilson V, Harden R & Elsegood J (1998) AMEE Guide No. 12: Multiprofessional education part 2 – promoting cohesive practice in health care. Medical Teacher; 20:409-416.
Price J, Ekleberry A, Grover A, Melendy S, Baddam K, McMahon J, Villalba M, Johnson M & Zervos MJ (1999) Evaluation of clinical practice guidelines on outcome of infection in patients in the surgical intensive care unit.[comment]. Critical Care Medicine; 27:2118-2124.
Pryce A & Reeves S (1997) An Evaluation of the Effectiveness of Multidisciplinary Education for Medical, Dental and Nursing students: a Case Study. Internal Research Report. City University, London.
Rafferty A, Ball J & Aiken H (2001) Are teamwork and professional autonomy compatible, and do they result in improved hospital care? Quality in Health Care; 10(Suppl):S32-S37.
Rees G, Edmunds S & Huby G (2005) Evaluation and development of integrated teams: The use of Significant Event Analysis. Journal of Interprofessional Care; 19:125-136.
Reeves S (2000) Community-based interprofessional education for medical, nursing and dental students. Health and Social Care in the Community; 8:269-276.
Reeves S (2001) A review of the effects of interprofessional education on staff involved in the care of adults with mental health problems. Journal of Psychiatric and Mental Health Nursing; 8:533-542.
Reeves S, Freeth D, Nicol M & Wood D (2000) A joint learning venture between new nurses and junior doctors. Nursing Times; 96(38):39-40.

54
Reeves S & Freeth D (2002) The London Training Ward: an innovative interprofessional learning initiative. Journal of Interprofessional Care; 16:41-52.
Reeves S & Summerfield Mann L (2003) Key issues in developing and delivering interprofessional education. International Journal of Therapy and Rehabilitation; 10:310-313.
Reeves S. (2005) Developing and delivering practice-based interprofessional education: successes and challenges. Unpublished PhD Thesis. City University, London.
Revel T & Yussuf H (2003) Taking primary care continuing professional education to rural areas: lessons from the United Arab Emirates. The Australian Journal of Rural Health; 11:271-276.
Richardson B & Cooper N (2003) Developing a virtual interdisciplinary research community in higher education. Journal of Interprofessional Care; 17:173-182.
Roberts C, Howe A, Winterburn S & Fox N (2000) Not as easy as it sounds: a qualitative study of a shared learning project between medical and nursing undergraduate students. Medical Teacher; 22:386-387.
Romanow R (2002) Building on Values: The Future of Health Care in Canada. Final Report of the Commission of the Future of Health Care in Canada, November 2002.
Ross F & Southgate L (2000) Learning together in medical and nursing training: aspirations and activity. Medical Education; 34:739-743.
Royal College of Physicians and Surgeons of Canada. (2000). Can MEDS 2000 project: Skills for the new millenium: report of the societal needs working group. Ottawa, ON.: The Royal College of Physicians and Surgeons of Canada
Rubenstein L, Parker L, Meredith L, Altschuler A, dePillis E, Hernandez J & Gordon N (2002) Understanding team-based quality improvement for depression in primary care. Health Services Research; 37:1009-1029.
Rutter D & Hagart J (1990) Alcohol training in south-east England: a survey and evaluation. Alcohol & Alcoholism; 25:699-709.
Salvatori P & Berry S (2003) Implementing Interprofessional Education in Ontario: A Pilot Study. Paper presented at the 5th Alberta Medical Education Conference, Jasper, Alberta, Canada.
Satin D (1987) The difficulties of interdisciplinary education: lessons from three failures and a success. Educational Gerontology; 13:53-69.
55
Schmitt M (2001) Collaboration improves the quality of care: methodological challenges and evidence from US health care research. Journal of Interprofessional Care; 15:47-66.
Schön D (1987) Educating the Reflective Practitioner. Jossey-Bass, San Francisco.
Schreiber MA, Holcomb JB, Conaway CW, Campbell KD, Wall M & Mattox KL (2002) Military trauma training performed in a civilian trauma center. Journal of Surgical Research; 104:8-14.
Scott S, Harrison A, Baker T & Wills J (2005) Interdisciplinary community partnership for health professional students. Journal of Allied Health; 34:31-35.
Shafer M, Tebb K, Pantell R, Wibbelsman C, Neuhaus J, Tipton A, Kunin S, Ko T, Schweppe D & Bergman D (2002) Effect of a clinical practice improvement intervention on Chlamydial screening among adolescent girls. JAMA; 288:2846-2852.
Shaw M (1970) Communication Processes. Penguin, London.
Skjørshammer M (2001) Co-operation and conflict in a hospital: interprofessional differences in perception and management of conflicts. Journal of Interprofessional Care; 15:7-18.
Sommer S, Silagy C & Rose A (1992) The teaching of multidisciplinary care. Medical Journal of Australia; 157:31-37.
Szasz G (1969) Interprofessional education in the health sciences. Millbank Memorial Fund Quarterly; 47:449-475.
Taylor J, Blue I & Misan G (2001) Approach to sustainable primary health care service delivery for rural and remote South Australia. Australian Journal of Rural Health; 9:304-310.
Thomas M (1995) Learning to be a better team player: initiatives in continuing education in primary care. In: K Soothill, L Mackay & C Webb (eds). Interprofessional Relations in Health Care. Edward Arnold, London.
Thompson C, Kinmonth A, Stevens L, Peveler R, Stevens A, Ostler K, Pickering R, Baker N, Henson A, Preece J, Cooper D & Campbell M (2000) Effects of a clinical-practice guideline and practice-based education on detection and outcome of depression in primary care: Hampshire Depression Project randomised controlled trial, Lancet; 355:185-191.
Tope R (1996) Integrated Interdisciplinary Learning Between Health and Social Care Professions: A Feasibility Study. Avebury, Aldershot.

56
Treadwell MJ, Franck LS & Vichinsky E (2002) Using quality improvement strategies to enhance pediatric pain assessment. International Journal for Quality in Health Care; 14:39-47.
Underwood M, O’Meara S, Harvey E & The UK BEAM Trial Team (2002) The acceptability to primary care staff of a multidisciplinary training package on acute back pain guidelines. Family Practice; 19:511-515.
Valk G, Renders C, Kriegsman D, Newton K, Twisk J, van Eijk J, van der Wal G & Wagner E (2004) Quality of care for patients with type 2 diabetes mellitus in the Netherlands and the United States: a comparison of two quality improvement programs. Health Services Research; 39:709-725.
Van der Horst M, Turpie I & Nelson W (1995) St Joseph's Community Centre model of community-based interdisciplinary health care team education. Health and Social Care in the Community; 3:33-42.
van Staa A, Visser A & van der Z (2000) Caring for caregivers: experiences and evaluation of interventions for a palliative care team. Patient Education & Counseling; 41:93-105.
Wahlström O & Sandén I (1998) Multiprofessional Training Ward at Linköping University: early experience. Education for Health; 11:225-31.
Walby S, Greenwell J, Mackay L & Soothill K (1994) Medicine and Nursing: Professions in a Changing Health Service. Sage, London.
Walsh P, Garbs C, Goodwin M & Wolff E (1995) An impact evaluation of a VA geriatric team development program. Gerontology and Geriatrics Education; 15:19-35.
Way D, Jones L & Baskerville N (2001) Improving the effectiveness of primary health care through nurse practitioner / family physician structured collaborative practice. University of Ottawa, Ottawa. World Health Organisation (1976) Continuing Education of Health Personnel. WHO Regional Office for Europe, Copenhagen.
World Health Organisation (1988) Learning together to Work Together. WHO, Geneva.
Zwarenstein M, Reeves S, Barr H, Hammick M, Koppel I & Atkins J (2001) Interprofessional Education: Effects on Professional Practice and Health Care Outcomes. (Cochrane Review). The Cochrane Library, Issue 3, (Oxford, Update Software).
Zwarenstein M, Reeves S & Perrier L (2004) Chapter Two: Effectiveness of Pre-licensure Interdisciplinary Education and Post-licensure Collaborative Interventions. In Oandasan I, D'Amour D, Zwarenstein M, Barker K, Purden M, Beaulieau MD, Reeves S,

57
Nasmith L, Bosco C, Ginsburg L & Tregunno D. Interdisciplinary Education for Collaborative, Patient-Centred Practice: Research & Findings Report. Ottawa, ON: Health Canada.
Zwarenstein M, Reeves S &Perrier L (2005). Effectiveness of pre-licensure interprofessional education and post-licensure collaborative interventions. Journal of Interprofessional Care; 19 (Supplement):148-165

58
Appendices Appendix 1: Broad search strategy #1 inter-profession* or interprofession* #2 inter-disciplin* or interdisciplin* #3 inter-occupation* or interoccupation* #4 inter-institution* or interinstitution* #5 inter-agen* or interagen* #6 inter-sector* or intersector* #7 inter-department* or interdepartment* #8 inter-organisation* or interorganisation* #9 inter-organization* or interorganization* #10 interprofessional relations #11 collaborat* or team* #12 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 #13 multi-profession* or multiprofession* #14 multi-disciplin* or multidisciplin* #15 multi-institution* or multiinstitution* #16 multi-occupation* or multioccupation* #17 multi-agen* or multiagen* #18 multi-sector* or multisector* #19 multi-organisation* or multiorganisation* #20 multi-organization* or multiorganization* #21 #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 #22 trans-profession* or transprofession* #23 trans-disciplin* or transdisciplin* #24 trans-institution* or transinstitution* #25 trans-occupation* or transoccupation* #26 trans-agen* or transagen* #27 trans-sector* or transsector* #28 trans-organisation* or transorganisation* #29 trans-organization* or transorganization* #30 #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 #31 educat* or learn* or teach* or train* #32 #12 and #21 and #30 and #31

59
Appendix 2: Focused search strategy 1 *interdisciplinary communication 2 *interprofessional relations 3 *Interdisciplinary Communication 4 *Physician-Nurse Relations 5 *patient care team 6 *multidisciplinary care team 7 *Nutritional Support Team 8 *teamwork 9 *education, interdisciplinary 10 ((nurse? or physician?) adj (collaborat$ or team?)) 11 (collaborative adj practice).tw. (711) 12 (team? adj (approach or learning or performance or work$ or healthcare or intervention or effectiveness)).tw. (5837) 13 ((interdisciplinary or inter-disciplinary) adj (learn$ or educat$ or team? or practice or train$ or course? or intervention? or program? or workshop? or event? or model?)).tw. (2417) 14 ((multidisciplinary or multi-disciplinary) adj (learn$ or educat$ or team? or practice or train$ or course? or intervention? or program? or workshop? or event? or model?)).tw. (5116) 15 ((interprofessional or inter-professional) adj (learn$ or educat$ or team? or practice or train$ or course? or intervention? or program? or workshop? or event? or model?)).tw. (348) 16 ((multiprofessional or multi-professional) adj (learn$ or educat$ or team? or practice or train$ or course? or intervention? or program? or workshop? or event? or model?)).tw. (278) 17 (collaborat$ and (interdisciplinary or inter-disciplinary)).tw. (1468) 18 (collaborat$ and (multidisciplinary or multi-disciplinary)).tw. (1610) 19 (collaborat$ and (interprofessional or inter-professional)).tw. (387) 20 (collaborat$ and (multiprofessional or multi-professional)).tw. (114) 21 or/1-20 (43894) 22 *primary health care/ (25063) 23 *physicians, family/ (7448) 24 *primary nursing care/ (1385) 25 *Community Health Centers/ (3069) 26 *primary nursing/ (2027) 27 *family practice/ (29056) 28 (general adj practitioner).tw. (8593) 29 (family adj physician?).tw. (7506) 30 "primary health care".tw. (10054) 31 (primary adj care).tw. (42202) 32 "integrated health care".tw. (484) 33 "collaborative mental health care".tw. (1) 34 (primary adj nurs$).tw. (1644) 35 (family adj practi$).tw. (7374) 36 "community health cent$".tw. (1250) 37 or/22-36 (104326) 38 21 and 37 (3257) 39 exp sports/ (66005) 40 38 not 39 (3252) 41 limit 40 to english (2866) 42 limit 41 to english language (2866) 43 limit 42 to yr="1999 - 2005" (1251) 44 remove duplicates from 43 (1062) 45 limit 44 to (comment or commentary or editorial or letter or news or newspaper article) [Limit not valid in: Ovid MEDLINE(R),CINAHL; records were retained] (78) 46 44 not 45 (984)