Examination Under Anesthesia for Management of Impalpable Undescended Testis: A Traditional...
7
1 23 World Journal of Surgery Official Journal of the International Society of Surgery/Société Internationale de Chirurgie ISSN 0364-2313 World J Surg DOI 10.1007/s00268-013-1973-1 Examination Under Anesthesia for Management of Impalpable Undescended Testis: A Traditional Technique Revisited Ossama M. Zakaria, Emad Hokkam, Karam E. El Kadi, Waleed H. Al BuAli, Hazem M. Zakaria, Mohamed Y. Daoud, Sameh A. Shehata, et al.
Transcript of Examination Under Anesthesia for Management of Impalpable Undescended Testis: A Traditional...
1 23
World Journal of SurgeryOfficial Journal of the InternationalSociety of Surgery/SociétéInternationale de Chirurgie ISSN 0364-2313 World J SurgDOI 10.1007/s00268-013-1973-1
Examination Under Anesthesia forManagement of Impalpable UndescendedTestis: A Traditional Technique Revisited
Ossama M. Zakaria, Emad Hokkam,Karam E. El Kadi, Waleed H. Al BuAli,Hazem M. Zakaria, Mohamed Y. Daoud,Sameh A. Shehata, et al.
1 23
Your article is protected by copyright and
all rights are held exclusively by Société
Internationale de Chirurgie. This e-offprint is
for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.
Examination Under Anesthesia for Management of ImpalpableUndescended Testis: A Traditional Technique Revisited
Ossama M. Zakaria • Emad Hokkam • Karam E. El Kadi •
Waleed H. Al BuAli • Hazem M. Zakaria • Mohamed Y. Daoud •
Sameh A. Shehata • AbdulRahman S. AlMulhim • Hamed A. AlWadaani
� Societe Internationale de Chirurgie 2013
Abstract
Background Many new tools for management of impal-
pable testes have emerged during the last few years, yet,
not many studies have compared them to the traditional
ways of managing this problem. This work aims to reiterate
the importance of the physical examination under general
anesthesia prior to the surgical procedure in order to decide
the best surgical approach for patients with impalpable
undescended testis, especially in developing countries
where expensive investigations are at premium.
Patients and methods The study included boys who were
treated consecutively and recorded prospectively from
2000 to 2010. Examination under anesthesia (EUA) was
performed during the study period. Those in whom the
testes were palpable underwent the standard orchiopexy
procedure. In those boys where EUA failed to detect the
testes, laparoscopy or extended inguinal exploration was
carried out, and the testes were treated accordingly.
Results On initial clinical evaluation at the outpatient
clinic, 545 boys were recorded to have impalpable testes.
Undescended testis was unilateral in 529 boys and bilateral
in 16 boys. However, on examination under anesthesia only
189 (34.7 %) were impalpable. Among boys in whom the
testes were palpable after EUA, 38 had small-size testes, 18
had normal size, and the remaining 300 boys had a sac or
cord-like structure.
Conclusions Meticulous EUA facilitates the accurate
diagnosis and planning of the surgical approach to patients
with an impalpable testis and should remain part of the
surgeon’s skill set. It is an inexpensive initial evaluation
tool that may help in saving hospital resources, especially
in developing countries.
Introduction
Cryptorchidism is probably the most frequent genital
anomaly encountered in boys, yet this pathology remains
largely unexplained and its long-term prognosis is still
uncertain. Many publications report a single ‘‘best’’
approach to management, and there is ongoing controversy
surrounding the fertility potentials of affected patients after
medical management [1–4].
Approximately 3.5 % of all full-term infants, 30 % of
premature and 100 % of infant with a birth weight of less
than 800 gm have undescended testis [5]. By 3 months of
age, the incidence is reduced to 0.8 %, between 3 months
of age and adulthood the incidence does not change [6, 7].
Thirty percent of undescended testes are bilateral. In 20 %
of cases the testis is impalpable, with 15–20 % of such
nonpalpable testes being absent [4]. Six percent of fathers
with undescended testes also are likely to have children
with the same condition [7, 8].
O. M. Zakaria (&) � W. H. Al BuAli
Division of Pediatric Surgery, Department of Surgery, College of
Medicine, King Faisal University, Riyadh, Kingdom of Saudi
Arabia
e-mail: [email protected]
O. M. Zakaria � E. Hokkam � K. E. El Kadi
Division of Pediatric Surgery, Departments of Surgery, Faculty
of Medicine, Ismailia, Egypt
H. M. Zakaria � M. Y. Daoud � A. S. AlMulhim �H. A. AlWadaani
Department of Surgery, College of Medicine, Dammam
University and KFHU, Al-Khobar, Kingdom of Saudi Arabia
S. A. Shehata
Departments of Surgery, Faculty of Medicine, Alexandria
University, Alexandria, Egypt
123
World J Surg
DOI 10.1007/s00268-013-1973-1
Author's personal copy
The lower the pre-treatment position of the testis, the
better will be the success rate for treatment and also the
fertility potential later on [8]. Medical treatment is effec-
tive only in 10 % [9]. The most effective treatment is
surgery.
However, most surgeons who deal with children with
cryptorchidism have been faced with the dilemma as to the
next step after identification of a nonpalpable testis in the
outpatient visit. They maybe also faced with the question
of what should be the next step when initial inguinal
exploration has not revealed a gonad distal to the internal
inguinal ring. In such instances, the surgeon cannot be sure
whether the testis is truly absent or whether the search was
merely inadequate [10, 11]. Although laparoscopy has
become an important addition to the surgical evaluation
and treatment of males with impalpable testis [10–12]
examination under anaesthesia of patients with impalpable
testes that has been used for decades may reveal a palpable
testis [12].
The present study aimed to reiterate our local experience
in a developing country on the importance of the physical
examination under general anesthesia prior to the surgical
procedure in order to decide the best surgical approach for
patients with impalpable undescended testis.
Patients and methods
This is a retrospective study that included boys who were
treated consecutively and recorded prospectively from
2000 to 2010 in Ismalia, Egypt. All children clinically
diagnosed to have impalpable undescended testes under-
went EUA. Those in whom the testes were palpable
underwent the standard orchiopexy procedure. In those
children where EUA failed to detect the testes, inguinal
exploration or laparoscopy was performed and the testes
were treated accordingly. Intraoperative data on these
patients were collected for age at operation, site or absence
of the testis after EUA, testicular size, associated inguinal
anomalies (vas, epididymis, and processus vaginalis), sur-
gical approach, and the results of surgery.
Examination under anesthesia was performed with the
option of proceeding with the inguinal approach if a testis was
palpated. However, when the testis remained impalpable
laparoscopy or extended inguinal approach was undertaken.
There were no certain criteria for extended inguinal approach
or laparoscopy. However; in the early period of this study most
patients were treated by the extended inguinal approach,
whereas laparoscopy was performed extensively in the late
period of the study. Whenever impalpable under EUA, a
single-stage Fowler-Stephens procedure was the most com-
mon operation in the early period of this study. In the late cases
we performed a two-stage procedure aimed at decreasing the
postoperative testicular atrophy. The finding of a blind-ending
vas deferens, or vas and vessels entering a closed internal ring
resulted in no further surgery, with testicular regression being
the assumed clinical diagnosis. The presence of vas and ves-
sels entering an open internal ring prompted exploration
through a groin approach. The mean follow-up of the second
group ranged from 2 to 36 months for site, size, and function.
We followed a special algorithm for management of the
16 boys with bilateral impalpable testes after clinical
examination. Other associated genital anomalies were
present in one boy with a bifid scrotum and a penoscrotal
hypospadias; this boy underwent chromosomal analysis as
well as magnetic resonance imaging (MRI) that showed the
presence of the testes. Ten boys underwent a human cho-
rionic gonadotropin (HCG) stimulation test to confirm the
presence of testicular tissue after an increase in testoster-
one, follicle stimulating hormone (FSH), and luteinizing
hormone (LH). The remaining 5 boys underwent EUA
followed by diagnostic laparoscopy.
Results
During the study period, 545 patients were recorded with
impalpable testis on routine clinical examination; 529 had
unilateral impalpable cryptorchidism. Among them 300
testes (56.7 %) were left sided and 229 (43.3 %) were right
sided. In addition 16 boys had bilateral undescended testes
(UDT), for a total of 561 impalpable UDT. The boys
ranged in age from 6 to 44 months with mean age of
12 ± 9.5 months (mean ± SD).
However, on examination under anesthesia only 189
patients (34.7 %) had impalpable testes. The testes were
felt in 56 boys; the testes were noted as small sized in
38/56 and of normal size in 18/56 patients; the remaining
300 boys had a sac or cord like structures (Table 1).
Review of the patients’ charts showed that some pre-
operative diagnostic tests were performed in 383 boys
(70.3 %); including ultrasonographic evaluation (US) in
360 boys (66.1 %), computed tomography in 5 boys,
venography in 3 boys, and MRI in one boy (2 %). The
clinically diagnosed impalpable testes did show different
sites on surgical exploration at different age groups.
Table 1 Gonad finding after examination under anesthesia (EUA)
(n = 545)
Palpable 189 (34.7 %)
Impalpable 356 (78.4 %)
Normal-sized testis 18 (3.3 %)
Small-sized testis 38 (7 %)
A sac-like structure 300 (55 %)
World J Surg
123
Author's personal copy
Standard orchiopexy was performed in 56 boys whose
testes were felt at EUA (either normal or small sized). In
the remaining 300 boys with a palpable sac or cord-like
structures, the operative findings showed that the vas def-
erens/epididymis attachment was recorded in 158 testes.
Normal attachment, that is head and tail fusion of the
epididymis with the testis, was noted in 110 testes; 48
testes had abnormal attachment: head attachment only in
17 (5.7 %), tail attachment only in 9 (3 %), complete
detachment of the epididymis in 17 (5.7 %), detached vas
in 3 (1 %), absent vas in 2 (.7 %). Orchiectomy was per-
formed for cases of complete detachment of vas and epi-
didymis (Table 2).
Laparoscopy or the extended inguinal approach was
performed in the 189 boys with impalpable testis after
EUA to ascertain testicular presence and location. Lapa-
roscopy was performed in 76 boys, and the extended
inguinal approach was performed 113 others.
In the laparoscopy group the vas deferens and the
internal spermatic vessel were seen passing through the
internal ring in 52 boys. The inguinal canal was dissected
and then orchiopexy was performed on 40 boys and
orchiectomy was performed on 12 atrophic testes laparo-
scopically. In the remaining 24 boys, the internal spermatic
vessels were found to terminate intraperitoneally with a
blind end and were considered as vanishing testes.
In extended inguinal approach the testes were not found
in the inguinal canal in 75 boys. A retroperitoneal and
intraperitoneal exploration was carried out through the
deep ring. Viable testes were mobilized down to the
scrotum in 59 boys, orchiectomy was carried out on 7
atrophic testes, and nine boys were considered to have
vanishing testes.
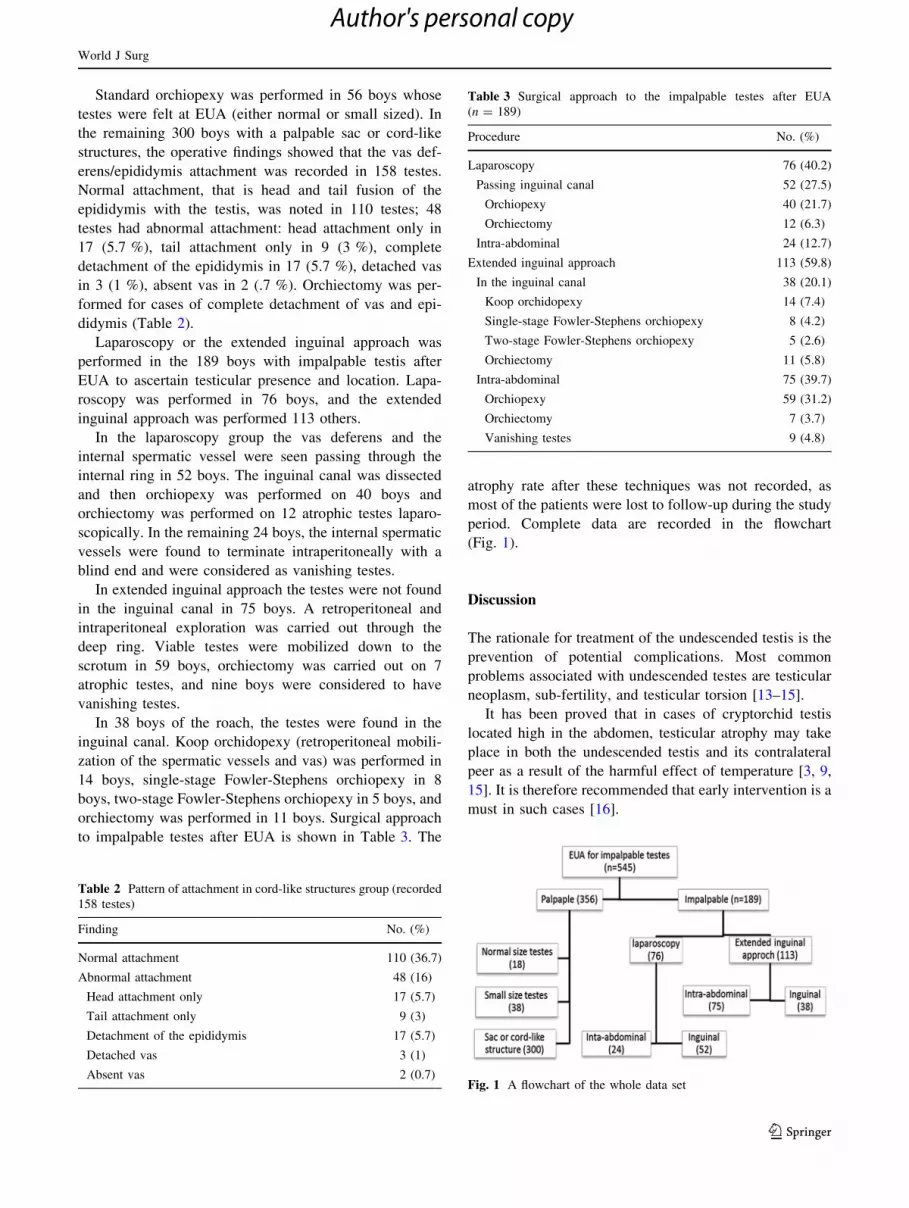
In 38 boys of the roach, the testes were found in the
inguinal canal. Koop orchidopexy (retroperitoneal mobili-
zation of the spermatic vessels and vas) was performed in
14 boys, single-stage Fowler-Stephens orchiopexy in 8
boys, two-stage Fowler-Stephens orchiopexy in 5 boys, and
orchiectomy was performed in 11 boys. Surgical approach
to impalpable testes after EUA is shown in Table 3. The
atrophy rate after these techniques was not recorded, as
most of the patients were lost to follow-up during the study
period. Complete data are recorded in the flowchart
(Fig. 1).
Discussion
The rationale for treatment of the undescended testis is the
prevention of potential complications. Most common
problems associated with undescended testes are testicular
neoplasm, sub-fertility, and testicular torsion [13–15].
It has been proved that in cases of cryptorchid testis
located high in the abdomen, testicular atrophy may take
place in both the undescended testis and its contralateral
peer as a result of the harmful effect of temperature [3, 9,
15]. It is therefore recommended that early intervention is a
must in such cases [16].
Table 2 Pattern of attachment in cord-like structures group (recorded
158 testes)
Finding No. (%)
Normal attachment 110 (36.7)
Abnormal attachment 48 (16)
Head attachment only 17 (5.7)
Tail attachment only 9 (3)
Detachment of the epididymis 17 (5.7)
Detached vas 3 (1)
Absent vas 2 (0.7)
Table 3 Surgical approach to the impalpable testes after EUA
(n = 189)
Procedure No. (%)
Laparoscopy 76 (40.2)
Passing inguinal canal 52 (27.5)
Orchiopexy 40 (21.7)
Orchiectomy 12 (6.3)
Intra-abdominal 24 (12.7)
Extended inguinal approach 113 (59.8)
In the inguinal canal 38 (20.1)
Koop orchidopexy 14 (7.4)
Single-stage Fowler-Stephens orchiopexy 8 (4.2)
Two-stage Fowler-Stephens orchiopexy 5 (2.6)
Orchiectomy 11 (5.8)
Intra-abdominal 75 (39.7)
Orchiopexy 59 (31.2)
Orchiectomy 7 (3.7)
Vanishing testes 9 (4.8)
Fig. 1 A flowchart of the whole data set
World J Surg
123
Author's personal copy
Bevan described the inguinal approach for orchiopexy
100 years ago, which remains the treatment of choice for
palpable undescended testis [17]. However, it is inappro-
priate for an impalpable testis, especially in the intra-
abdominal location, because it results in restricted access
and this has led to a search for another appropriate
approach [13].
The overall accuracy of radiological testing, including
computed tomography, ultrasonography, and magnetic reso-
nance imaging, in localizing a non-palpable testis has been
reported in many studies to be associated with high false
positive and low sensitivity rates [18, 19]. It has been docu-
mented that clinically, physical examination is the most cost
effective tool in the detection of the impalpable testis [19].
Our management of the impalpable testes was EUA
done by a senior staff surgeon to confirm impalpability. If
the testis was palpable, then groin exploration and
orchiopexy was undertaken. However, if no testis was
palpable, laparoscopy per se or the extended inguinal
approach was performed in order to ascertain testicular
presence and location. However, if anorchia was confirmed
during EUA (blind ending vas and vessels), further
exploration was avoided and the boy was considered to
having vanishing testes.
The incidence of true intra-abdominal testis in our series
of impalpable testes was only 21.8 %. In the majority of
patients a testis may be considered impalpable secondary to
a large prepubic fat pad or it may lie within the inguinal
canal and be overlooked, especially when the examination
is conducted by a less experienced junior staff physician.
Therefore, the role of laparoscopy in this group of patients
is controversial [7].
The diagnostic accuracy of laparoscopy for impalpable
testis is well recognized. Yet, in some cases, laparoscopic
findings may be misleading, and a viable gonad may be
missed, with significant medicolegal implications [20, 21].
In recorded data analyzing 107 patients who underwent
laparoscopy for impalpable testis, laparoscopy accurately
determined the location of the gonad in 95 %, and further
intervention was avoided in 15 % by identifying a blind
ending vas and spermatic vessels above the internal
inguinal ring [21].
Increasing experience with the transperitoneal approach
with full mobilization of the testicular vessels and division
of all fibrous bands that restrict their elasticity, gives the
highest chance of successful mobilization into the scrotum
with preservation of the spermatic vessels. It was also the
safest and most effective means of orchiopexy for the true
intra-abdominal testes. Excellent results were also reported
in a systematic review that concluded the pooled estimate
of success rates to be 80 % for single-stage Fowler-Ste-
phens orchiopexy (95 % CI 75–86) and 85 % for two-stage
Fowler-Stephens orchiopexy (95 % CI 81–90). The pooled
odds ratio of the single-stage versus two-stage Fowler-
Stephens orchiopexy was 2.0 (95 % CI 1.1–3.9), favoring
the two-stage procedure. The researchers found no differ-
ence in the success rate between laparoscopic and open
techniques in either single-stage or two-stage Fowler-Ste-
phens orchiopexy [22]. In two patients with atrophic testes,
the histology did not reveal testicular or vasal tissues, so re-
exploration was done.
It can be concluded that clinical diagnosis of impalpable
testis is initially made by examination at the outpatient
department. Heavy patient load and inexperience on the
part of surgeons-in-training may make this assessment
inconclusive. It is therefore recommended that clinical
recognition of impalpable testis should not be considered
absolute in the outpatient department unless the examina-
tion is carried out by an experienced staff member.
Meticulous EUA facilitates safe and accurate planning
of the surgical approach to the patient with impalpable
testis and should remain part of the surgeon’s skills set to
save hospital resources, especially in developing countries,
as it remains an inexpensive initial evaluation.
References
1. Hutson JM, Balic A, Nation T et al (2010) Cryptorchidism.
Semin Pediatr Surg 19:215–224
2. Galifer RB, Kalfa N, Guibal MP (2004) What a hidden testicle
can hide?… or the clinical traps of cryptorchidism. Arch Pediatr
11:350–359
3. Zakaria O, Shono T, Imajima T et al (1998) Fertility and histo-
logical studies in a unilateral cryptorchid rat model during early
and late adulthood. Br J Urol 82:404–407
4. Kumar D, Brimner DN, Brown PW (1989) Fertility after
orchiopexy for cryptorchidism: a new approach to assessment. Br
J Urol 64:516–520
5. Hormann M, Balassy C, Philipp MO et al (2004) Imaging of the
scrotum in children. Eur Radiol 14:974–983
6. Berkowitz GS, Lapinski RH, Dolgin SE et al (1993) Prevalence
and natural history of cryptorchidism. Pediatrics 92:44–49
7. Kirsch AJ, Escala J, Duckett JW et al (1998) Surgical manage-
ment of the nonpalpable testis: the Children’s Hospital of Phil-
adelphia experience. J Urol 159:1340–1343
8. Averous M, Lopez C (2004) Cryptorchidism: the point of view of
a pediatric urologist. Gynecol Obstet Fertil 32:813–817
9. Leung AK, Robson WL (2004) Current status of cryptorchidism.
Adv Pediatr 51:351–377
10. Merry C, Sweeney B, Puri P (1997) The vanishing testis: ana-
tomical and histological findings. Eur Urol 31:65–67
11. Baker LA, Docimo SG, Surer I et al (2001) A multi- institutional
analysis of laparoscopic orchiopexy. Br J Urol 87:484–489
12. Flett ME, Jones PF, Youngson GG (1999) Emerging trends in the
management of the impalpable testis. Br J Surg 86:1280–1283
13. Docimo SG, Silver RI, Cromie W (2000) The undescended testicle:
diagnosis and management. Am Fam Physician 62(2037–2044):
2047–2048
14. Akre O, Pettersson A, Richiardi L (2009) Risk of contralateral
testicular cancer among men with unilaterally undescended testis:
a meta analysis. Int J Cancer 124:687–689
World J Surg
123
Author's personal copy

15. Zakaria O, Shono T, Imajima T et al (1998) Fertility and histo-
logical studies of the contralateral testes in two different intra-
and extra-abdominal rat models of unilateral cryptorchidism. Br J
Urol 82:574–577
16. Zakaria O, Shehata S, Moghazi K et al (2001) Cryptorchidism in
the new millennium: changing attitude of management. Jpn J
Pediatr Surg 37:58–64
17. Bevan AD (1903) The surgical treatment of undescended testi-
cle—a further contribution. JAMA 41:718–724
18. Siemer S, Humke U, Uder M et al (2000) Diagnosis of nonpal-
pable testes in childhood: comparison of magnetic resonance
imaging and laparoscopy in a prospective study. Eur J Pediatr
Surg 10:114–118
19. Hrebinko RL, Bellinger MF (1993) The limited role of imaging
techniques in managing children with undescended testes. J Urol
150:458–460
20. Zaccara A, Spagnoli A, Capitanucci ML et al (2004) Impalpable
testis and laparoscopy: when the gonad is not visualized. JSLS
1:39–42
21. Tennenbaum SY, Lerner SE, McAleer IM et al (1994) Preoper-
ative laparoscopic localization of the nonpalpable testis: a critical
analysis of a 10-year experience. J Urol 151:732–734
22. Elyas R, Guerra LA, Pike J et al (2010) Is staging beneficial for
Fowler-Stephens orchiopexy? A systematic review. J Urol
183:2012–2018
World J Surg
123
Author's personal copy