
Evolution of interventional vancomycin trials in light of new antibiotic development in the USA,...
8
International Journal of Antimicrobial Agents 43 (2014) 215–222 Contents lists available at ScienceDirect International Journal of Antimicrobial Agents j o ur nal ho me pag e: http://www.elsevier.com/locate/ijantimicag Review Evolution of interventional vancomycin trials in light of new antibiotic development in the USA, 1999–2012 Tian Yu, Chris Stockmann, Alfred H. Balch, Michael G. Spigarelli, Catherine M.T. Sherwin ∗ Division of Clinical Pharmacology, Department of Pediatrics, University of Utah, Salt Lake City, Utah, USA a r t i c l e i n f o Article history: Received 12 August 2013 Accepted 2 October 2013 Keywords: Vancomycin Clinical trials Antibiotics Drug development a b s t r a c t Use of vancomycin has increased following the emergence of resistant Gram-positive bacterial infections. Investigation into recent vancomycin clinical studies provides insight into the optimal use of vancomycin and the development of novel antibiotics for the treatment of resistant infections. Interventional van- comycin trials registered in ClinicalTrials.gov from January 1999 to December 2012 were identified. Trial trends and characteristics were evaluated in the context of vancomycin use and new antibiotic devel- opment. Overall, 122 interventional vancomycin trials were identified, with a significant increase in the number of registered trials per year (P < 0.001). The top three indications studied were skin and soft-tissue infections (28.7%), Clostridium difficile infections (13.1%) and surgical prophylaxis (12.3%). Trials testing vancomycin as an experimental agent differed from trials using vancomycin as an active comparator. Experimental agent trials commonly investigated new formulations, dosing regimen optimisation and combination therapy, which were less likely to be in phase 2 or 3 (25% vs. 70%; P < 0.001), adopt a ran- domisation procedure (70% vs. 98%; P < 0.001), report results (15% vs. 35%; P = 0.02) or be funded by industry (8% vs. 76%; P < 0.001). Active comparator trials mainly focused on monotherapy, which led to six FDA-approved drug products and ten investigational new drugs in late-phase development. This study demonstrated a significant increase in interventional vancomycin trials and its recent success, which resulted in several novel agents against resistant Gram-positive bacteria. Further studies are warranted to determine how these agents can best be incorporated within clinical practice. © 2013 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved. 1. Introduction Outbreaks of resistant bacterial infections have been identified since the early 1980s, among which meticillin-resistant Staphy- lococcus aureus (MRSA) is now the leading cause of resistant infections in the USA [1]. MRSA accounts for more than 460 000 hospitalisations and 19 000 deaths in US hospitals annually [2,3]. Vancomycin is the first-line treatment for resistant Gram-positive bacterial infections, including MRSA [4–6]. Guidelines developed by the Infectious Diseases Society of America (IDSA) recommend that vancomycin dosing be guided by pharmacokinetic or pharma- codynamic target attainment, thereby optimising clinical efficacy and reducing drug-related toxicity; however, this recommendation was not supported by prospective clinical trials at that time [7]. Moreover, increasing vancomycin use has the potential to result in the emergence of vancomycin-resistant enterococci [8]. The conflu- ence of these factors makes it a public health priority to promote the ∗ Corresponding author. Present address: Clinical Pharmacology & Clinical Trials Office, University of Utah Health Sciences Center, 295 Chipeta Way, Suite 1C310, Salt Lake City, UT 84108, USA. Tel.: +1 801 587 7513; fax: +1 801 585 9410. E-mail address: [email protected] (C.M.T. Sherwin). sustainable use of vancomycin and to develop novel antimicrobial agents [9,10]. ClinicalTrials.gov was developed in response to the Food and Drug Administration Modernization Act (FDAMA) of 1997 to provide public access to information on clinical trials [11,12]. This registry was made available to the public by the National Library of Medicine on behalf of the National Institutes of Health in 2000 [13]. The FDA Amendments Act (FDAAA), enacted in 2007, requires that interventional studies of drugs, biologics or devices in phase 2 through 4 with at least one US site be registered at inception in ClinicalTrials.gov [14,15]. Given the mandatory trial registration requirement, it is now possible to systematically evaluate van- comycin clinical studies utilising the ClinicalTrials.gov registry. Trial trends, characteristics and their implications for antibiotic research and development were examined based on two subsets of interventional vancomycin trials: one subset was the group of tri- als testing vancomycin as an experimental agent, which studied the clinical utility of vancomycin itself; and the other subset was trials using vancomycin, standard-of-care for the specific condition, in the active comparator arm. This study aims to inform the sustain- able use of vancomycin and the development of new antibiotics for the treatment of resistant Gram-positive bacteria for years to come. 0924-8579/$ – see front matter © 2013 Elsevier B.V. and the International Society of Chemotherapy. All rights reserved. http://dx.doi.org/10.1016/j.ijantimicag.2013.10.002
Transcript of Evolution of interventional vancomycin trials in light of new antibiotic development in the USA,...

R
Ea
TD
a
ARA
KVCAD
1
slihVbbtcawMte
OS
0h
International Journal of Antimicrobial Agents 43 (2014) 215–222
Contents lists available at ScienceDirect
International Journal of Antimicrobial Agents
j o ur nal ho me pag e: ht tp : / /www.e lsev ier .com/ locate / i jant imicag
eview
volution of interventional vancomycin trials in light of newntibiotic development in the USA, 1999–2012
ian Yu, Chris Stockmann, Alfred H. Balch, Michael G. Spigarelli, Catherine M.T. Sherwin ∗
ivision of Clinical Pharmacology, Department of Pediatrics, University of Utah, Salt Lake City, Utah, USA
r t i c l e i n f o
rticle history:eceived 12 August 2013ccepted 2 October 2013
eywords:ancomycinlinical trialsntibioticsrug development
a b s t r a c t
Use of vancomycin has increased following the emergence of resistant Gram-positive bacterial infections.Investigation into recent vancomycin clinical studies provides insight into the optimal use of vancomycinand the development of novel antibiotics for the treatment of resistant infections. Interventional van-comycin trials registered in ClinicalTrials.gov from January 1999 to December 2012 were identified. Trialtrends and characteristics were evaluated in the context of vancomycin use and new antibiotic devel-opment. Overall, 122 interventional vancomycin trials were identified, with a significant increase in thenumber of registered trials per year (P < 0.001). The top three indications studied were skin and soft-tissueinfections (28.7%), Clostridium difficile infections (13.1%) and surgical prophylaxis (12.3%). Trials testingvancomycin as an experimental agent differed from trials using vancomycin as an active comparator.Experimental agent trials commonly investigated new formulations, dosing regimen optimisation andcombination therapy, which were less likely to be in phase 2 or 3 (25% vs. 70%; P < 0.001), adopt a ran-
domisation procedure (70% vs. 98%; P < 0.001), report results (15% vs. 35%; P = 0.02) or be funded byindustry (8% vs. 76%; P < 0.001). Active comparator trials mainly focused on monotherapy, which led to sixFDA-approved drug products and ten investigational new drugs in late-phase development. This studydemonstrated a significant increase in interventional vancomycin trials and its recent success, whichresulted in several novel agents against resistant Gram-positive bacteria. Further studies are warrantedto determine how these agents can best be incorporated within clinical practice.lsevie
© 2013 E. Introduction
Outbreaks of resistant bacterial infections have been identifiedince the early 1980s, among which meticillin-resistant Staphy-ococcus aureus (MRSA) is now the leading cause of resistantnfections in the USA [1]. MRSA accounts for more than 460 000ospitalisations and 19 000 deaths in US hospitals annually [2,3].ancomycin is the first-line treatment for resistant Gram-positiveacterial infections, including MRSA [4–6]. Guidelines developedy the Infectious Diseases Society of America (IDSA) recommendhat vancomycin dosing be guided by pharmacokinetic or pharma-odynamic target attainment, thereby optimising clinical efficacynd reducing drug-related toxicity; however, this recommendationas not supported by prospective clinical trials at that time [7].
oreover, increasing vancomycin use has the potential to result inhe emergence of vancomycin-resistant enterococci [8]. The conflu-nce of these factors makes it a public health priority to promote the
∗ Corresponding author. Present address: Clinical Pharmacology & Clinical Trialsffice, University of Utah Health Sciences Center, 295 Chipeta Way, Suite 1C310,alt Lake City, UT 84108, USA. Tel.: +1 801 587 7513; fax: +1 801 585 9410.
E-mail address: [email protected] (C.M.T. Sherwin).
924-8579/$ – see front matter © 2013 Elsevier B.V. and the International Society of Chemttp://dx.doi.org/10.1016/j.ijantimicag.2013.10.002
r B.V. and the International Society of Chemotherapy. All rights reserved.
sustainable use of vancomycin and to develop novel antimicrobialagents [9,10].
ClinicalTrials.gov was developed in response to the Food andDrug Administration Modernization Act (FDAMA) of 1997 toprovide public access to information on clinical trials [11,12]. Thisregistry was made available to the public by the National Libraryof Medicine on behalf of the National Institutes of Health in 2000[13]. The FDA Amendments Act (FDAAA), enacted in 2007, requiresthat interventional studies of drugs, biologics or devices in phase2 through 4 with at least one US site be registered at inceptionin ClinicalTrials.gov [14,15]. Given the mandatory trial registrationrequirement, it is now possible to systematically evaluate van-comycin clinical studies utilising the ClinicalTrials.gov registry.
Trial trends, characteristics and their implications for antibioticresearch and development were examined based on two subsets ofinterventional vancomycin trials: one subset was the group of tri-als testing vancomycin as an experimental agent, which studied theclinical utility of vancomycin itself; and the other subset was trialsusing vancomycin, standard-of-care for the specific condition, in
the active comparator arm. This study aims to inform the sustain-able use of vancomycin and the development of new antibioticsfor the treatment of resistant Gram-positive bacteria for years tocome.otherapy. All rights reserved.

216 T. Yu et al. / International Journal of Antimicrobial Agents 43 (2014) 215–222
F , C) ex( ncom(
2
v
(
tccccetatb
ig. 1. Trends of interventional vancomycin trials in the USA from 1999 to 2012: (AP < 0.05). Note: The new formulation trials are composed of studies evaluating van = 5).
. Methods
The sources listed below were utilised to identify interventionalancomycin trials.
(i) An investigation of the US clinical trial registry(http://www.ClinicalTrials.gov) was performed to obtainvancomycin trials registered from January 1999 to December2012 using the search function of ‘vancomycin’. The data setwas downloaded on 2 January 2013. Trials were individuallyreviewed and interventional trials that used vancomycin asan experimental agent or included vancomycin in the activecomparator arm were included in the analysis.
(ii) Trial results were obtained from ClinicalTrials.gov or througha query of PubMed/Medline (http://www.PubMed.gov) usinga combination of search terms, which included the drug name,registry number, principal investigator name and trial sponsor.All searches were conducted between 2 January 2013 and 28February 2013.
iii) Investigational new drugs were identified in vancomycin inter-ventional trials. Their stage of development or approval statuswas confirmed by accessing the innovator company websitesor the FDA website (http://www.FDA.gov).
Based on the comparator role of vancomycin in each trial,rials that tested vancomycin as the experimental agent werelassified as ‘experimental agent trials’, and trials that used van-omycin in the active comparator arm were referred to as ‘activeomparator trials’. Trends of experimental agent trials and activeomparator trials over the study period were assessed by lin-ar regression. Trials were grouped by disease conditions under
he primary purpose of treatment or prevention. Experimentalgent trials were listed by disease conditions and the formula-ions tested for each condition. Active comparator trials were listedy drug products or candidates according to their FDA approvalperimental agent trials; and (B, D) active comparator trials. * Significant differenceycin gels (n = 2)/powders (n = 2) for topical application and inhalable formulations
status, for which the drug class, mechanism of action, novelty ofthe mechanism, formulation/administration route, and detaileddevelopment or approval status were described. Based on pri-mary outcomes and stated hypotheses, trials were categorised intostudies on monotherapy, combination therapy, dosing regimen orpharmacokinetics/pharmacodynamics. These categories were fur-ther differentiated into those that tested superior, non-inferior oropen hypotheses with respect to the experimental agents.
Trial characteristics, including phase, study design (allocation,intervention model, masking, endpoint classification and primarypurpose), recruitment status, age eligibility, study results and fund-ing resources, were compared between experimental agent trialsand active comparator trials by �2 test or Fisher’s exact test,as appropriate. Paediatric trials were defined as those that onlyenrolled patients aged <18 years as well as those that also includedpatients aged ≥18 years but in which the median age of enrolledpatients was <18 years. Funding sources were divided based uponthe lead sponsor for each trial and were categorised as industry ornon-industry, which included academic and governmental spon-sors. All data were analysed with SAS® v.9.3 (SAS Institute Inc., Cary,NC).
3. Results
A total of 142 vancomycin clinical trials were identified in Clin-icalTrials.gov from January 1999 to December 2012, of which 122(85.9%) were interventional trials and the remainder (14.1%) wereobservational trials. Interventional trials were included for analysisin this study.
3.1. Trends in interventional vancomycin trials
Among the interventional trials, 40 (32.8%) used vancomycin asan experimental agent and 82 (67.2%) included vancomycin as anactive comparator. A significant increasing trend in the number of

T. Yu et al. / International Journal of Antim
Fig. 2. Disease condition distribution of interventional vancomycin trials from 1999tia
r(iis(bst
3t
v(peppvs
iwoaoateiaptccjrct
cca
o 2012. Note: 42.8% of bacteraemia trials investigated catheter-related bloodstreamnfections and 80.0% of pneumonia trials studied hospital-acquired or ventilator-ssociated pneumonia.
egistered trials per year was observed in experimental agent trialsP < 0.001), and a similar trend was identified for trials investigat-ng new formulations (P = 0.016) (Fig. 1A). Active comparator trialsncreased over the study period (P = 0.014); however, there was audden drop in the number of registered trials per year in 2008Fig. 1B). A subanalysis revealed that this sharp decline in the num-er of active comparator trials occurred primarily among studiesponsored by industry sources (Fig. 1C,D). The number of paediatricrials also increased over the study period (Fig. 1A,B).
.2. Research and development in interventional vancomycinrials
The three most commonly studied indications in interventionalancomycin trials included skin and soft-tissue infections (SSTIs)28.7%), Clostridium difficile infections (13.1%), and surgical pro-hylaxis (12.3%) (Fig. 2). The conditions studied varied betweenxperimental agent trials and active comparator trials. A largerroportion of experimental agent trials investigated surgical pro-hylaxis (27.5% vs. 4.9%; P = 0.001), unspecified infections (22.5%s. 1.2%; P < 0.001) and cystic fibrosis (10.0% vs. 0%; P = 0.01), and amaller proportion evaluated SSTIs (5.0% vs. 40.2%; P < 0.001).
The distribution of conditions studied, the route of admin-stration and the stage of clinical development for trials in
hich vancomycin was used as an experimental therapeuticr preventive agent are presented in Table 1. Experimentalgent trials mainly investigated alternative formulations/routesf administration (30.0%), dosing regimen optimisation (27.5%)nd combination therapies (15.0%). Trials for unspecified infec-ions, the most studied topic within treatment trials, primarilyvaluated dosing regimen optimisation and pharmacokinetic stud-es in critically ill patient populations (intensive care, dialysisnd extracorporeal membrane oxygenation). Trials for surgicalrophylaxis, the most researched indication within preventionrials, were primarily studied for preventing infections duringardiothoracic and neurosurgical device implantation surgeries,ardiovascular/spine/thoracic/colorectal surgeries and prostheticoint replacements. New formulations/alternative administrationoutes were commonly studied for many indications, including allystic fibrosis trials and nearly one-half of all surgical prophylaxisrials (Table 1).
Investigational antibacterial compounds identified in activeomparator trials are shown in Table 2. There were six antibioticandidates tested in active comparator trials that received FDApproval for their intended indication(s). Of these, two (telavancin
icrobial Agents 43 (2014) 215–222 217
and ceftaroline fosamil) are newly approved drug products thatwere included in the investigational antibiotics list of the 2009pipeline status report from the IDSA [10]. In addition, there areten investigational new drugs in late phases of clinical devel-opment, among which dalbavancin and oritavancin have movedforward from the last status shown in the ISDA’s 2009 list witheach completed two identical phase 3 trials for the treatmentof acute bacterial skin and skin-structure infections (ABSSSIs).Sodium fusidate plus rifampicin combination for prosthetic jointinfections, and pleuromutilin for ABSSSIs are new additions tothe pre-existing list of investigational new drugs for MRSA treat-ment. Aside from these, four experimental therapies, includingfidaxomicin (approved), surotomycin, LFF571 and faecal transplant,were identified in vancomycin active comparator trials for thetreatment of C.-difficile-associated diarrhoea (CDAD).
Interventional vancomycin trials were further categorised basedon their primary outcomes and stated hypotheses (Table 3). Amongexperimental agent trials, 40% investigated vancomycin monother-apy, 23% investigated vancomycin in combination with othertherapeutic agents, 28% evaluated vancomycin dosing regimensand 10% studied vancomycin pharmacokinetics. Active compara-tor trials were primarily classified as monotherapy trials (88%) anda minority utilised combination therapies (12%). Monotherapy tri-als were less common among experimental agent trials (P < 0.001)(Table 3).
3.3. Characteristics of interventional vancomycin trials
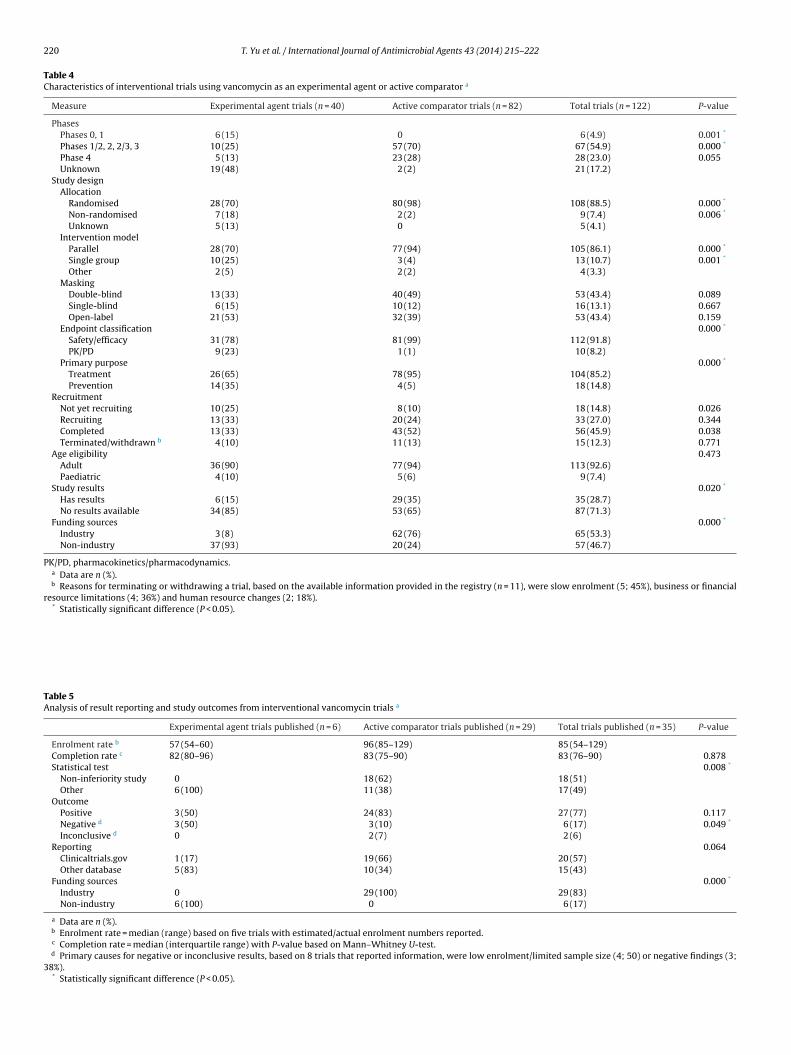
Trial characteristics were compared between experimentalagent trials and active comparator trials (Table 4). There was alower percentage of experimental agent trials in late phases (phases1/2, 2, 2/3 and 3) compared with active comparator trials (25% vs.70%; P < 0.001). Experimental agent trials also differed from activecomparator trials with respect to their study design; a smallerproportion of experimental agent trials were randomised (70% vs.98%; P < 0.001), fewer adopted parallel group assignment (70% vs.94%; P < 0.001) and fewer examined safety/efficacy outcomes (78%vs. 99%; P < 0.001). The primary purpose of the trial also differedbetween experimental agent trials and active comparator trials,with a larger proportion of experimental agent trials registeredwith a primary purpose of prevention (35% vs. 5%; P < 0.001).
Study results were available for 35 interventional vancomycintrials, with an overall reporting rate of 28.7% (Table 5). Experimentalagent trials had a lower probability of reporting results (15% vs. 35%;P = 0.02) and were more likely to be funded by non-industry sourcescompared with active comparator trials (93% vs. 24%; P < 0.001).Among published trials, experimental agent trials were less likely toadopt a non-inferiority design (0% vs. 62%; P = 0.008), which servesas the standard statistical test for drug approval by regulatory agen-cies [21], and were more likely to report negative results thanactive comparator trials (50% vs. 10%; P = 0.049). Published exper-imental agent trials were exclusively sponsored by non-industrysources (100%), whereas published active comparator trials wereexclusively funded by industry sponsors (100%) (P < 0.001).
4. Discussion
The number of interventional vancomycin trials, adopting van-comycin either as an experimental agent or as an active comparator,has increased over the last decade. This was accompanied by anincrease in the number of trials evaluating new formulations and
by an increase in the number of paediatric trials (Fig. 1). Thisoccurred following the rapid spread of MRSA in the USA and maybe attributable to the clinical needs of hospitalists and infectiousdiseases specialists who have few alternative therapeutic agents
218 T. Yu et al. / International Journal of Antimicrobial Agents 43 (2014) 215–222
Table 1Research and development of vancomycin experimental agent trials based on distribution of disease conditions and formulations.
Condition a Formulation/route Status b
Vancomycin experimental agent trial for treatmentUnspecified or multiple infections i.v. • 1 phase 2 dosing regimen on target trough attainment by PK modelling
• 1 dosing regimen on nephrotoxicity under prolonged therapy• 4 dosing regimen on target trough attainment by loading dose (1 paediatric trial and 1 trial incritically ill patients terminated)• 1 PKs in patients on dialysis (+), 1 phase 4 PKs in patients on ECMO• 1 monotherapy on renal organic cation transporters
Cystic fibrosis Inhalable • 1 phase 1, 1 phase 2 monotherapy on AeroVanc inhalation powder• 1 phase 2 combination therapy• 1 phase 1 PKs
Clostridium difficile infections Oral • 1 dosing regimen on extended-time course treatment (withdrawn)• 1 combination therapy for ulcerative colitis
Intracolonic • 1 monotherapy for severe C. difficile colitis (terminated)Skin and soft-tissue infections i.v. • 1 dosing regimen on large-dose, extended-interval administration (–) in outpatients
Topical • 1 phase 2 monotherapy on vancomycin alginate gelBacteraemia i.v. • 1 phase 2 dosing regimen on algorithm-based therapy, 1 dosing regimen on treatment lengthPrimary sclerosing cholangitis Oral • 1 phase 1 monotherapy in paediatric patients, 1 phase 1 monotherapy (+)Ventilator-associated pneumonia Inhalable • 1 phase 2 monotherapy on aerosolised vancomycin (+)Multiple indications i.v. • 1 phase 4 monotherapy on nephrotoxicityRheumatoid arthritis Oral • 1 monotherapy on relation of intestinal bacteria and development of rheumatoid arthritisDiabetes Oral • 1 phase 0 combination therapy on relation of gut microbiota and glucose metabolism
Vancomycin experimental agent trial for preventionSurgical prophylaxis i.v. • 1 phase 3, 1 phase 4 combination therapy for arrhythmia device procedures, 1 phase 4
combination therapy for paediatric cardiovascular surgery, 1 phase 4 combination therapy forvascular surgery (−)• 1 phase 1 PK for neurosurgery• 1 monotherapy for elective thoracic surgery
Topical • 3 monotherapy for spine surgery, neurosurgical device implantation, or coronary artery bypassgraft, 1 phase 1/2 monotherapy on DFA-02 vancomycin-releasing gel for colorectal surgery• 1 combination therapy for joint replacement or spine surgery
Haematological cancer infections i.v. • 1 phase 3 dosing regimen in haematopoietic stem cell transplant patients• 1 phase 3 combination therapy for febrile neutropenia (−)
Dental caries Topical • 1 monotherapy in paediatric patients
i on.asing
ually w
arrpeckctehipha2ari
aasimimpoil
.v., intravenous; PK, pharmacokinetic; ECMO, extracorporeal membrane oxygenatia Trials for treatment or prevention are sorted by each disease condition in decreb + or − indicates positive or negative results, respectively. Target troughs are us
vailable [9]. The overall increase in vancomycin trials was inter-upted by a decline in the number of active comparator trialsegistered in 2008. The decline in industry-sponsored active com-arator trials during this time period coincided temporally with theconomic depression that followed the collapse of the US finan-ial system in 2007–2008 (Fig. 1D) [22]. However, it is also wellnown that a number of factors make antibiotic agents less finan-ially attractive candidates for development than other drug classeshat treat chronic diseases, including short treatment durations,volving bacterial resistance that leads to treatment failure, andesitation to use newly developed antibiotics for fear of develop-
ng resistance, among others [23]. The combination of these factorsaired with the substantial costs associated with drug developmentave led to diminished interest and decreasing investment in newntibiotic agents by major pharmaceutical companies [24,25]. In010–2012, the increasing trend observed in industry-sponsoredctive comparator trials probably reflects renewed interest in theelatively large commercial market due to the severity of MRSAnfections and recovering financial markets [9].
The most effective way to address bacterial resistance is tochieve a balance between developing new antimicrobial agentsnd ensuring the sustainable use of existing therapies [26]. In thistudy, several important avenues were identified for therapeuticnnovations related to vancomycin use, including the develop-
ent of novel formulations, optimisation of dosing regimens andnvestigation of combination therapies (Table 1). Alternative for-
ulations/routes of administration are needed as a minority of
atients cannot tolerate multiple doses of vancomycin treatmentwing to adverse reactions, which may also enable more flexibilityn continuing therapy in the outpatient setting. Current guide-ines suggest that vancomycin be used as the first-line therapyorder according to the number of trials per condition.ithin 10–20 mg/L depending on specific conditions.
for MRSA infections with minimum inhibitory concentrations of≤2 �g/mL; however, suboptimal dosing regimens have been widelycriticised for resulting in treatment failures and adverse clinicaloutcomes [27,28]. This study shows that multiple trials have beenconducted to test the effect of a loading dose on the time requiredto achieve therapeutic concentrations, which is strongly associatedwith improved clinical outcomes. Vancomycin is often combinedwith a second antibiotic for the treatment or prevention of MRSAinfections, especially for surgical prophylaxis. However, there arelimited published data to support this ‘bundled approach’ [29,30].This study shows that several randomised controlled trials arecurrently underway to evaluate the effectiveness of combinationtherapies for the prevention of MRSA surgical site infections.
Vancomycin has already been approved by the FDA and it istherefore unsurprising that experimental agent trials that primarilyfocused on improvements in vancomycin use were less rigorouslydesigned than active comparator trials with regard to randomi-sation procedures, double-blinding and controlled comparisons[31]. This is confirmed in this study in Table 4. Experimentalagent trials mostly remain in early-phase development, in contrastto active comparator trials that are all in late-phase develop-ment. Experimental trials were exclusively funded by non-industrysources, which may serve as the basis for this phenomenon[25].
In a 2009 report, the IDSA identified Enterococcus faecium,S. aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseu-domonas aeruginosa and Enterobacter spp. as the six major
drug-resistant pathogens (‘ESKAPE’) for which drug developmentis of critical public health importance [10]. More recently, C. dif-ficile has been suggested for inclusion as the new ‘C’ in ‘ESCAPE’owing to its prominence as the leading cause of hospital-acquired
T. Yu et al. / International Journal of Antimicrobial Agents 43 (2014) 215–222 219
Table 2Antibacterial compounds identified in vancomycin active comparator trials that received US Food and Drug Administration (FDA) approval or are in advanced (phase 2 or 3)clinical development.
Name (no. of trials) Class (mechanism of action) Novelmechanism a
Formulation/routeStatus b
Compound that received FDA approvalTelavancin (n = 7) Lipoglycopeptide (dual
mechanism of cell-wallsynthesis inhibition andmembrane depolarisation)
Yes i.v. • 2 identical phase 2 (+), 2 identical phase 3 (+) cSSSI• 2 identical phase 3 HAP (+)• 1 phase 2 bacteraemia (+)• FDA approval for cSSSI in 2009 and for HAP in 2013
Fidaxomicin (n = 2) Macrolide (bacterial RNApolymerase inhibitor)
Yes Oral • 2 identical phase 3 CDAD (+)• FDA approval for CDAD in 2011
Ceftaroline fosamil (n = 6) Cephalosporin (cell-wallsynthesis inhibitor)
No i.v. • 2 phase 4 CAP• 1 phase 2/3, 1 phase 3, 2 identical phase 3 (+) cSSSI• FDA approval for CAP and cSSSI in 2010
Tigecycline (n = 2) Glycylcycline (proteinsynthesis inhibitor)
Yes i.v. • 2 phase 3 cSSSI (1 trial +)• FDA approval for cSSSI in 2005
Daptomycin (n = 24) Lipopeptide (cell membranedepolarisation)
Yes i.v. • 2 phase 2 (1 trial +), 1 phase 3, 2 phase 4, 1unknown phase bacteraemia• 1 phase 2 (inconclusive), 4 phase 3 (2 trials +), 7phase 4 (1 trial −) cSSSI• 1 phase 3 (+), 1 phase 4 cSSSI/bacteraemia• 1 phase 2 osteomyelitis (+)• 3 phase 4 surgical prophylaxis• FDA approval for cSSSI and bacteraemia in 2003
Linezolid (n = 6) Oxazolidinone (proteinsynthesis inhibitor)
Yes i.v., oral • 1 phase 4 VAP (−), 1 phase 4 HAP (+)• 1 phase 4 cSSSI (+)• 2 phase 3 CRB (1 trial inconclusive)• 1 phase 3 febrile neutropenia• FDA approval for HAP and cSSSI in 2000
Compound as investigational new drugSodium fusidate plus rifampicin (n = 1) Fusidane/rifamycin
combination (protein synthesisinhibitor)
Yes Oral • 1 phase 2 prosthetic joint infections
Surotomycin (n = 3) Lipopeptide (cell membranedepolarisation)
Yes Oral • 1 phase 2, 2 identical phase 3 CDAD• Granted fast-track status by FDA in 2013
Dalbavancin (n = 3) Lipoglycopeptide (cell-wallsynthesis inhibitor)
No i.v. • 2 identical phase 3 ABSSSI• 1 phase 2 CRB (+)
Oritavancin (n = 2) Glycopeptide (cell-wallsynthesis inhibitor)
No i.v. • 2 identical phase 3 ABSSSI
LFF571 (n = 1) Thiopeptide (protein synthesisinhibitor)
Yes Oral • 1 phase 2 Clostridium difficile infections
Faecal transplant (n = 1) Biological (bacteriacompetition)
Yes Intracolonic • 1 phase 2/3 C. difficile colitis
Pleuromutilin (n = 1) Pleuromutilin (proteinsynthesis inhibitor)
Yes i.v. • 1 phase 2 ABSSSI
Iclaprim (n = 1) Diaminopyrimidine(dihydrofolate reductaseinhibitor)
No i.v. • 1 phase 2 HAP
TD-1792 (n = 1) Glycopeptide–cephalosporinheterodimer (cell-wallsynthesis inhibitor)
Yes i.v. • 1 phase 2 cSSSI (+)
Ceftobiprole medocaril (n = 2) Cephalosporin (cell-wallsynthesis inhibitor)
No i.v. • 2 phase 3 cSSSI (+)
i.v., intravenous; cSSSI, complicated skin and skin-structure infection; HAP, hospital-acquired pneumonia; CDAD, C. difficile-associated diarrhoea; CAP, community-acquiredpneumonia; VAP, ventilator-associated pneumonia; CRB, catheter-related bacteraemia; ABSSSI, acute bacterial skin and skin-structure infection.Note: Trials are sorted in reverse chronological order by the original approval date for FDA-approved drug products or by latest trial registration date for investigational newdrugs.
a Judgment on the novelty of the mechanism is based on Infectious Diseases Society of America (ISDA) reports [10,34] or peer-reviewed journal publications [16–20,37].b + or − indicates positive or negative results, respectively.
Table 3Categories of interventional trials using vancomycin as an experimental agent or active comparator a
Category Experimental agent trials Active comparator trials P-value
Superior Non-inferior Open-ended Total Non-inferior Inferior Total
Monotherapy 8 b 3 5 16 (40) 69 3 72 (88) 0.000*
Combination therapy 6 c 0 3 9 (23) 5 5 d 10 (12) 0.141Dosing regimen 6 3 2 11 (28) 0 0 0 0.000*
PK 0 0 4 4 (10) 0 0 0 0.010*
Total 20 6 14 40 (100) 74 8 82 (100)
PK, pharmacokinetics.a Data are n or n (%).b Seven of eight trials are vancomycin versus placebo or no intervention.c Six of six trials are vancomycin plus control group versus control group or control group plus placebo.d Four of five trials are investigational drug plus vancomycin versus vancomycin or vancomycin plus placebo.* Statistically significant difference (P < 0.05).
220 T. Yu et al. / International Journal of Antimicrobial Agents 43 (2014) 215–222
Table 4Characteristics of interventional trials using vancomycin as an experimental agent or active comparator a
Measure Experimental agent trials (n = 40) Active comparator trials (n = 82) Total trials (n = 122) P-value
PhasesPhases 0, 1 6 (15) 0 6 (4.9) 0.001 *
Phases 1/2, 2, 2/3, 3 10 (25) 57 (70) 67 (54.9) 0.000 *
Phase 4 5 (13) 23 (28) 28 (23.0) 0.055Unknown 19 (48) 2 (2) 21 (17.2)
Study designAllocation
Randomised 28 (70) 80 (98) 108 (88.5) 0.000 *
Non-randomised 7 (18) 2 (2) 9 (7.4) 0.006 *
Unknown 5 (13) 0 5 (4.1)Intervention model
Parallel 28 (70) 77 (94) 105 (86.1) 0.000 *
Single group 10 (25) 3 (4) 13 (10.7) 0.001 *
Other 2 (5) 2 (2) 4 (3.3)Masking
Double-blind 13 (33) 40 (49) 53 (43.4) 0.089Single-blind 6 (15) 10 (12) 16 (13.1) 0.667Open-label 21 (53) 32 (39) 53 (43.4) 0.159
Endpoint classification 0.000 *
Safety/efficacy 31 (78) 81 (99) 112 (91.8)PK/PD 9 (23) 1 (1) 10 (8.2)
Primary purpose 0.000 *
Treatment 26 (65) 78 (95) 104 (85.2)Prevention 14 (35) 4 (5) 18 (14.8)
RecruitmentNot yet recruiting 10 (25) 8 (10) 18 (14.8) 0.026Recruiting 13 (33) 20 (24) 33 (27.0) 0.344Completed 13 (33) 43 (52) 56 (45.9) 0.038Terminated/withdrawn b 4 (10) 11 (13) 15 (12.3) 0.771
Age eligibility 0.473Adult 36 (90) 77 (94) 113 (92.6)Paediatric 4 (10) 5 (6) 9 (7.4)
Study results 0.020 *
Has results 6 (15) 29 (35) 35 (28.7)No results available 34 (85) 53 (65) 87 (71.3)
Funding sources 0.000 *
Industry 3 (8) 62 (76) 65 (53.3)Non-industry 37 (93) 20 (24) 57 (46.7)
PK/PD, pharmacokinetics/pharmacodynamics.a Data are n (%).b Reasons for terminating or withdrawing a trial, based on the available information provided in the registry (n = 11), were slow enrolment (5; 45%), business or financial
resource limitations (4; 36%) and human resource changes (2; 18%).* Statistically significant difference (P < 0.05).
Table 5Analysis of result reporting and study outcomes from interventional vancomycin trials a
Experimental agent trials published (n = 6) Active comparator trials published (n = 29) Total trials published (n = 35) P-value
Enrolment rate b 57 (54–60) 96 (85–129) 85 (54–129)Completion rate c 82 (80–96) 83 (75–90) 83 (76–90) 0.878Statistical test 0.008 *
Non-inferiority study 0 18 (62) 18 (51)Other 6 (100) 11 (38) 17 (49)
OutcomePositive 3 (50) 24 (83) 27 (77) 0.117Negative d 3 (50) 3 (10) 6 (17) 0.049 *
Inconclusive d 0 2 (7) 2 (6)Reporting 0.064
Clinicaltrials.gov 1 (17) 19 (66) 20 (57)Other database 5 (83) 10 (34) 15 (43)
Funding sources 0.000 *
Industry 0 29 (100) 29 (83)Non-industry 6 (100) 0 6 (17)
a Data are n (%).b Enrolment rate = median (range) based on five trials with estimated/actual enrolment numbers reported.c Completion rate = median (interquartile range) with P-value based on Mann–Whitney U-test.d Primary causes for negative or inconclusive results, based on 8 trials that reported information, were low enrolment/limited sample size (4; 50) or negative findings (3;
38%).* Statistically significant difference (P < 0.05).

Antim
icoaiota
rsa3ptsoApp2ctwlaadttsd
taiwcmiac
fsdldmsnwipytat2atldr
s
T. Yu et al. / International Journal of
nfections in the USA [32,33]. This study revealed that most van-omycin active comparator trials were indicated for the treatmentf S. aureus and C. difficile infections (Table 2). Using vancomycins a proxy for the development of antibiotics that feature activ-ty against highly resistant bacteria, this study identified ca. 90%f the systemic antibacterial compounds for Gram-positive infec-ions listed in the 2009 ISDA report [10] and 100% of the recentlypproved drug products featured in the 2013 ISDA update [34].
The development of novel antibiotics for the treatment ofesistant Gram-positive bacterial infections has had several majoruccesses in recent years. For C. difficile infections, fidaxomicin waspproved in 2011, surotomycin was tested in two identical phase
trials, LFF571 was evaluated in a phase 2 trial, and faecal trans-lant was evaluated in a phase 2/3 trial. For S. aureus infections,elavancin and ceftaroline fosamil were approved for complicatedkin and skin-structure infections and pneumonia. Dalbavancin andritavancin were both tested in two identical phase 3 trials forBSSSI. A phase 2 trial is currently underway for sodium fusidatelus rifampicin for prosthetic joint infections or completed forleuromutilin for ABSSSI. Three remaining drugs listed in IDSA’s009 pipeline report (iclaprim, TD-1792 and ceftobiprole medo-aril) have not progressed to later phase trials or been approved byhe FDA for routine clinical use. To meet increasing medical needsithin the context of a dwindling antibiotic pipeline, the ISDA
aunched the ‘10 × ’20 Initiative’ in 2010 to call for the developmentnd regulatory approval of 10 new safe and efficacious systemicntibiotics for ‘ESKAPE’ pathogens by 2020 [35]. Currently, tworugs have been approved and seven candidates are in late-phaseesting; however, to reach the goal of ten new systemic drugs byhe year 2020, substantial investments from the public and privateectors will be required to accelerate the pace of novel antibioticevelopment and approval [34].
There is a clear need for systemically absorbed oral antibioticshat allow intravenous (i.v.) to oral step-down therapy for hospital-cquired infections or initial therapy for community-acquirednfections. Aside from linezolid, sodium fusidate plus rifampicin
as the only alternative regimen identified in vancomycin activeomparator trials that employed an oral formulation for the treat-ent of prosthetic joint infections (Table 2). Pleuromutilin has
ts alternative oral formulation currently under investigation, inddition to the i.v. formulation identified in vancomycin activeomparator trial for the treatment of ABSSSI [36].
A select few novel drug classes have been developed thateature activity against resistant Gram-positive bacteria. In thistudy, fidaxomicin, tigecycline and linezolid are the first approvedrugs of new classes of macrocyclic, glycylcycline and oxazo-
idinone antibiotics, respectively [37–39]. Over 80% of approvedrug products and 60% of investigational drugs function by novelechanisms, including cellular membrane depolarisation, protein
ynthesis inhibition, bacterial competition, or multiple mecha-isms combined (Table 2). However, it must be noted that drugsith novel mechanisms of action do not guarantee improved clin-
cal outcomes. An example can be found in the new non-antibioticolymer tolevamer, which binds and neutralises C. difficile toxinset failed in phase 3 non-inferiority trials versus vancomycin owingo poor tolerability and a high drop-out rate in the experimentalgent arm [40]. It is noteworthy that faecal transplant, an investiga-ional biological therapy that is currently being evaluated in a phase/3 trial for the treatment of CDAD, features a unique mechanism ofction in which C. difficile is displaced from the gastrointestinal tracthrough bacterial competition by directly altering bacterial popu-ation dynamics [41]. Therapies such as this shed light on a wholly
ifferent but potentially effective strategy for managing bacterialesistance in the future.The number of antibacterial compounds that were found to beuperior to vancomycin remains small. Linezolid showed a superior
icrobial Agents 43 (2014) 215–222 221
clinical cure rate compared with vancomycin in a phase 4 compli-cated SSTI trial [42] and a phase 4 hospital-acquired pneumoniatrial [43]; however, no difference in overall or infection-relatedmortality was detected. Dalbavancin exhibited a significantlyhigher clinical cure rate than vancomycin in a phase 2 catheter-related bacteraemia trial; however, only 75 patients were enrolled,which limits the interpretation of the study’s findings [44].
Although the number of interventional vancomycin trials inves-tigating paediatric patients has increased, they account for lessthan one in ten vancomycin trials (Table 4). The Best Pharmaceut-icals for Children Act of 2007 promotes paediatric drug trials inexchange for extended market exclusivity for drug manufacturersin the USA [45]. The Pediatric Research Equity Act of 2007 man-dated the inclusion of drug labelling for paediatric patients [46].Similar legislation in Europe, enacted by the European MedicineAgents, also aims to improve the evidence in the use of paediatricpharmaceuticals by promoting the conduct of clinical trials in pae-diatric populations through a combination of financial incentivesand regulatory requirements [47,48]. However, there is still a largediscrepancy between the burden of paediatric infectious diseasesand the number of vancomycin trials conducted among paediatricpatients [49].
A limitation of this study is that ClinicalTrials.gov does notinclude all clinical studies conducted in the USA. Although Clini-calTrials.gov is the most established and largest trial registry andincludes an estimated 86% of the trials included in the InternationalClinical Trials Registry Platform by the World Health Organiza-tion [50], it did not have complete records for non-interventionalstudies or phase 0–1 trials, as existing US regulatory requirementsdo not mandate their registration. Second, the quality of this trialanalysis depends on the completion and accuracy of trial informa-tion submitted to the registry by the sponsor or their designees[51,52].
In conclusion, the number of interventional vancomycin tri-als registered in the USA increased significantly over the past 14years, as did new formulation trials and paediatric trials. Manytrials used vancomycin as an active comparator, against whichnovel antimicrobial agents were compared for their safety and effi-cacy. These trials led to six FDA-approved new drug products andten investigational new drugs that have been advanced into late-phase development. These new antibiotics are primarily indicatedfor SSTIs, hospital- or community-acquired pneumonia, CDAD andcatheter-related bacteraemia. Further research is needed to deter-mine how to best utilise vancomycin in light of these new additionsto our therapeutic armamentarium.
Funding: Department of Pediatrics, School of Medicine, Univer-sity of Utah (Salt Lake City, UT).
Competing interests: None declared.Ethical approval: Not required.
References
[1] Infectious Diseases Society of America. Bad bugs, no drugs: as antibiotic dis-covery stagnates, a public health crisis brews. Alexandria, VA: IDSA; 2004.
[2] Klein EY, Sun L, Smith DL, Laxminarayan R. The changing epidemiology ofmethicillin-resistant Staphylococcus aureus in the United States: a nationalobservational study. Am J Epidemiol 2013;177:666–74.
[3] Boucher HW, Corey GR. Epidemiology of methicillin-resistant Staphylococcusaureus. Clin Infect Dis 2008;46(Suppl 5):S344–9.
[4] Kirst HA, Thompson DG, Nicas TI. Historical yearly usage of vancomycin.Antimicrob Agents Chemother 1998;42:1303–4.
[5] Moellering Jr RC. Vancomycin: a 50-year reassessment. Clin Infect Dis2006;42(Suppl 1):S3–4.
[6] Levine DP. Vancomycin: a history. Clin Infect Dis 2006;42(Suppl 1):S5–12.
[7] Rybak M, Lomaestro B, Rotschafer JC, Moellering Jr R, Craig W, Billeter M, et al.Therapeutic monitoring of vancomycin in adult patients: a consensus reviewof the American Society of Health-System Pharmacists, the Infectious DiseasesSociety of America, and the Society of Infectious Diseases Pharmacists. Am JHealth Syst Pharm 2009;66:82–98.
2 Antim
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[[
[[
[
[
[
[
[
[
[[[[
[
22 T. Yu et al. / International Journal of
[8] Hamilton CD, Drew R, Janning SW, Latour JK, Hayward S. Excessive use of van-comycin: a successful intervention strategy at an academic medical center.Infect Control Hosp Epidemiol 2000;21:42–5.
[9] Talbot GH, Bradley J, Edwards Jr JE, Gilbert D, Scheld M, Bartlett JG. Bad bugsneed drugs: an update on the development pipeline from the AntimicrobialAvailability Task Force of the Infectious Diseases Society of America. Clin InfectDis 2006;42:657–68.
10] Boucher HW, Talbot GH, Bradley JS, Edwards JE, Gilbert D, Rice LB, et al. Badbugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society ofAmerica. Clin Infect Dis 2009;48:1–12.
11] Horton R, Smith R. Time to register randomised trials. The case is now unan-swerable. BMJ 1999;319:865–6.
12] Tonks A. Registering clinical trials. BMJ 1999;319:1565–8.13] Zarin DA, Tse T, Ide NC. Trial registration at ClinicalTrials.gov between May and
October 2005. N Engl J Med 2005;353:2779–87.14] Food and Drug Administration Amendments Act of 2007.Public Law: 110th
Congress. 2007.15] Zarin DA, Tse T. Medicine. Moving toward transparency of clinical trials. Science
2008;319:1340–2.16] Still JG, Clark K, Degenhardt TP, Scott D, Fernandes P, Gutierrez MJ. Pharma-
cokinetics and safety of single, multiple, and loading doses of fusidic acid inhealthy subjects. Clin Infect Dis 2011;52(Suppl 7):S504–12.
17] Mascio CT, Mortin LI, Howland KT, Van Praagh AD, Zhang S, Arya A, et al.In vitro and in vivo characterization of CB-183,315, a novel lipopeptideantibiotic for treatment of Clostridium difficile. Antimicrob Agents Chemother2012;56:5023–30.
18] Leeds JA, Sachdeva M, Mullin S, Dzink-Fox J, Lamarche MJ. Mechanism of actionof and mechanism of reduced susceptibility to the novel anti-Clostridium diffi-cile compound LFF571. Antimicrob Agents Chemother 2012;56:4463–5.
19] Rohlke F, Stollman N. Fecal microbiota transplantation in relapsing Clostridiumdifficile infection. Therap Adv Gastroenterol 2012;5:403–20.
20] Sader HS, Biedenbach DJ, Paukner S, Ivezic-Schoenfeld Z, Jones RN. Antimi-crobial activity of the investigational pleuromutilin compound BC-3781tested against Gram-positive organisms commonly associated with acutebacterial skin and skin structure infections. Antimicrob Agents Chemother2012;56:1619–23.
21] US Food and Drug Administration. Guidance for industry. Non-inferiority clin-ical trials. Atlanta, GA: FDA; 2010.
22] Bordo MD. An historical perspective on the crisis of 2007–2008. NationalBureau of Economic Research Working Paper; 2008.
23] Projan SJ. Why is big Pharma getting out of antibacterial drug discovery? CurrOpin Microbiol 2003;6:427–30.
24] Spellberg B, Powers JH, Brass EP, Miller LG, Edwards Jr JE. Trends inantimicrobial drug development: implications for the future. Clin Infect Dis2004;38:1279–86.
25] Norrby SR, Nord CE, Finch R; European Society of Clinical Microbiology andInfectious Diseases. Lack of development of new antimicrobial drugs: a poten-tial serious threat to public health. Lancet Infect Dis 2005;5:115–9.
26] Powers JH. Development of drugs for antimicrobial-resistant pathogens. CurrOpin Infect Dis 2003;16:547–51.
27] van Hal SJ, Fowler Jr VG. Is it time to replace vancomycin in the treat-
ment of methicillin-resistant Staphylococcus aureus infections? Clin Infect Dis2013;56:1779–88.28] Gould IM, David MZ, Esposito S, Garau J, Lina G, Mazzei T, et al. New insights intometicillin-resistant Staphylococcus aureus (MRSA) pathogenesis, treatment andresistance. Int J Antimicrob Agents 2012;39:96–104.
[
[
icrobial Agents 43 (2014) 215–222
29] Deresinski S. Vancomycin in combination with other antibiotics for the treat-ment of serious methicillin-resistant Staphylococcus aureus infections. ClinInfect Dis 2009;49:1072–9.
30] Crawford T, Rodvold KA, Solomkin JS. Vancomycin for surgical prophylaxis?Clin Infect Dis 2012;54:1474–9.
31] US Food and Drug Administration. Guidance for industry. Enrichment strategiesfor clinical trials to support approval of human drugs and biological products.Atlanta, GA: FDA; 2012.
32] Elixhauser A, Jhung M. Clostridium difficile-associated disease in U.S. hospitals,1993–2005. Statistical brief #50. Rockville, MD: Healthcare Cost and UtilizationProject (HCUP); 2006.
33] Peterson LR. Bad bugs, no drugs: no ESCAPE revisited. Clin Infect Dis2009;49:992–3.
34] Boucher HW, Talbot GH, Benjamin Jr DK, Bradley J, Guidos RJ, Jones RN, et al.10 × ‘20 progress—development of new drugs active against Gram-negativebacilli: an update from the Infectious Diseases Society of America. Clin InfectDis 2013;56:1685–94.
35] Infectious Diseases Society of America. The 10 × ’20 Initiative: pursuing a globalcommitment to develop 10 new antibacterial drugs by 2020. Clin Infect Dis2010;50:1081–3.
36] BC-3781® [Phase II]. Vienna, Austria: Nabriva Therapeutics; 2013.37] Venugopal AA, Johnson S. Fidaxomicin: a novel macrocyclic antibiotic approved
for treatment of Clostridium difficile infection. Clin Infect Dis 2012;54:568–74.38] Pankey GA, Tigecycline J. Antimicrob Chemother 2005;56:470–80.39] Swaney SM, Aoki H, Ganoza MC, Shinabarger DL. The oxazolidinone line-
zolid inhibits initiation of protein synthesis in bacteria. Antimicrob AgentsChemother 1998;42:3251–5.
40] Berrie C. Tolevamer less effective than standard therapies for C. difficile-associated diarrhea. Medscape Medical News April 24, 2008.
41] Borody TJ, Khoruts A. Fecal microbiota transplantation and emerging applica-tions. Nat Rev Gastroenterol Hepatol 2012;9:88–96.
42] Itani KM, Dryden MS, Bhattacharyya H, Kunkel MJ, Baruch AM, Weigelt JA. Effi-cacy and safety of linezolid versus vancomycin for the treatment of complicatedskin and soft-tissue infections proven to be caused by methicillin-resistantStaphylococcus aureus. Am J Surg 2010;199:804–16.
43] Wunderink RG, Niederman MS, Kollef MH, Shorr AF, Kunkel MJ, Baruch A, et al.Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumo-nia: a randomized, controlled study. Clin Infect Dis 2012;54:621–9.
44] Raad I, Darouiche R, Vazquez J, Lentnek A, Hachem R, Hanna H, et al. Efficacyand safety of weekly dalbavancin therapy for catheter-related bloodstreaminfection caused by Gram-positive pathogens. Clin Infect Dis 2005;40:374–80.
45] Best Pharmaceuticals for Children Act of 2007.Public Law: 110th Congress.2007.
46] Pediatric Research Equity Act of 2007.Public Law: 110th Congress. 2007.47] Regulation (EC) No. 1901/2006. Official Journal of the European Union 2006.48] Regulation (EC) No. 1902/2006. Official Journal of the European Union 2006.49] Bourgeois FT, Murthy S, Pinto C, Olson KL, Ioannidis JP, Mandl KD. Pediatric
versus adult drug trials for conditions with high pediatric disease burden.Pediatrics 2012;130:285–92.
50] Viergever RF, Ghersi D. The quality of registration of clinical trials. PLoS One2011;6:e14701.
51] Mills E, Loke YK, Wu P, Montori VM, Perri D, Moher D, et al. Determiningthe reporting quality of RCTs in clinical pharmacology. Br J Clin Pharmacol2004;58:61–5. Erratum in: Br J Clin Pharmacol 2004;58:102.
52] Zarin DA, Tse T, Williams RJ, Califf RM, Ide NC. The ClinicalTrials.gov resultsdatabase—update and key issues. N Engl J Med 2011;364:852–60.




















