
S1234 Clinical Predictors of Fulminant Colitis in Patients With Clostridium difficile Infection
Upload
khangminh22Category
view
1download
0
Fidaxomicin versus vancomycin for clostridium difficile infection: journal
club presentation
Hager ElGeed
Doua AlSaad
BSc Pharm, PharmD Candidates

Why this paper?
1. Recently published paper
2. New medication approved by FDA
3. C. difficile infection is a common complaint in hospital
settings
4. Pharmacists should always be updated in new drugs
approved!
2

Study Summary
Aim
Compare the efficacy and safety of fidaxomicin with those of vancomycin in treating C. difficile infection
Method
Prospective, double-blind, randomized, non-inferiority trial
Fidaxomicin (200 mg twice daily) or vancomycin (125 mg four times daily) orally for 10 days
Primary outcome: rate of clinical cure of C.difficile
Secondary outcomes: recurrence of C.difficile and global cure
3
Study Summary
Results
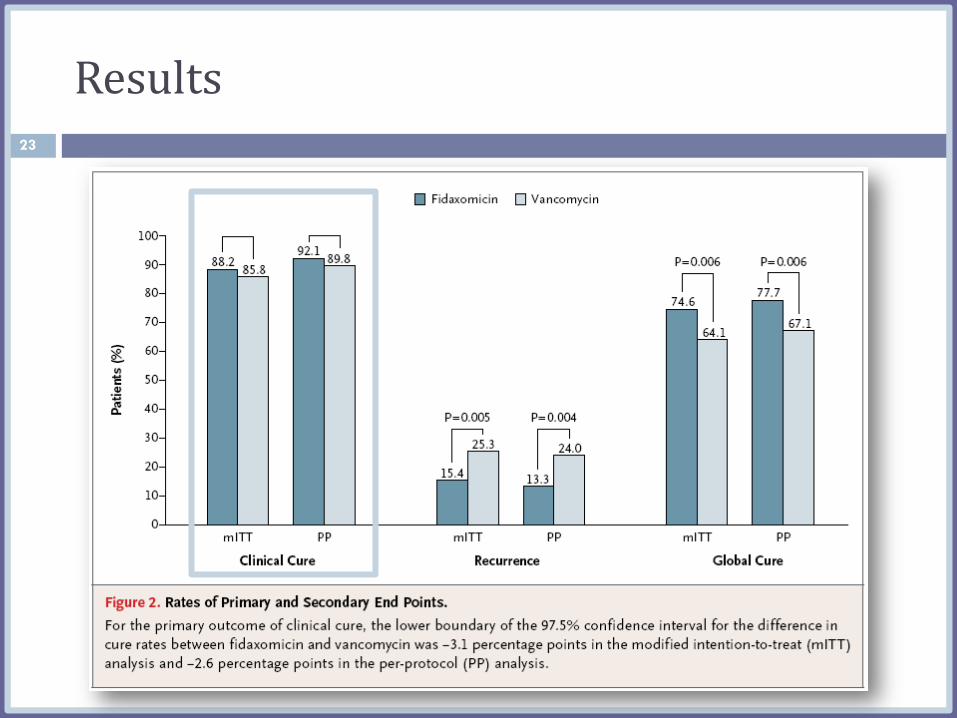
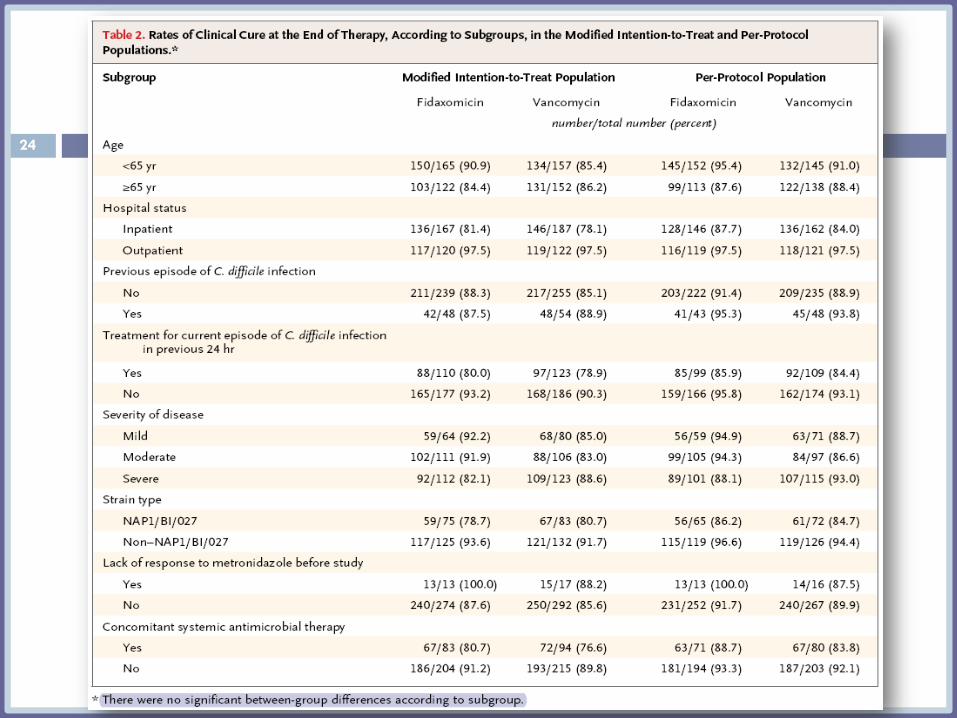
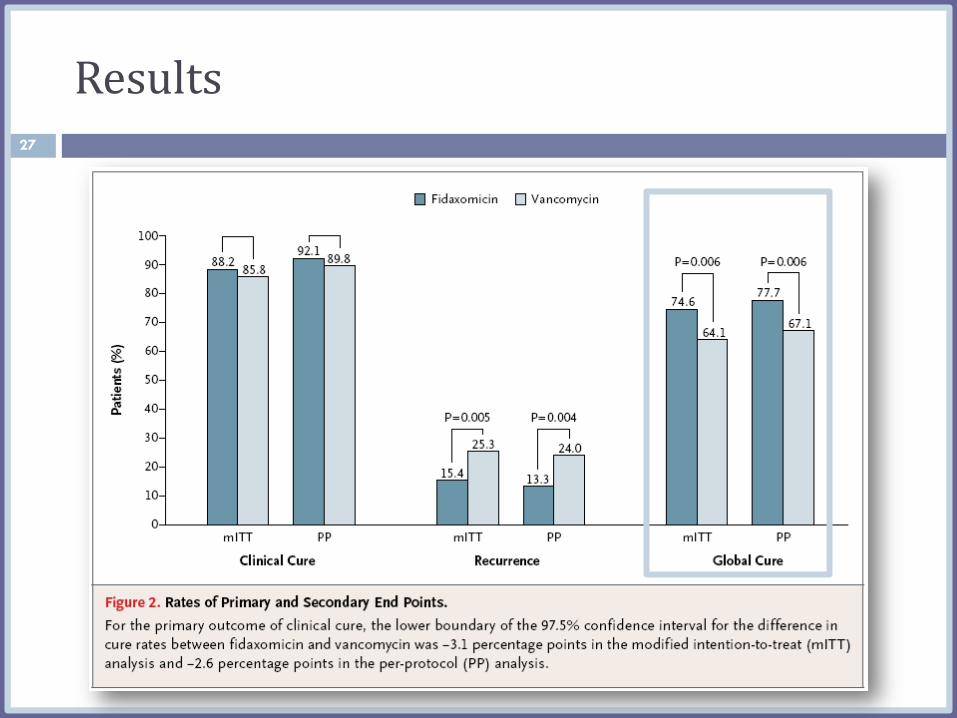
Primary outcome (rate of clinical cure): 88.2% with fidaxomicin and 85.8% with vancomycin (ITT)
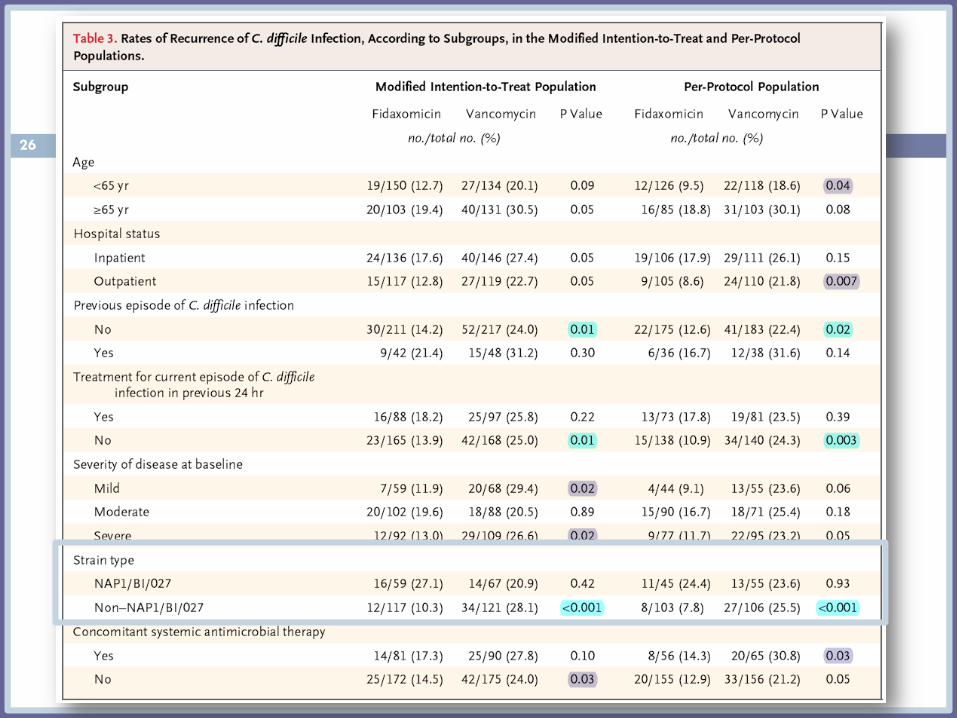
Secondary outcome (recurrence): 15.4% with fidaxomicin vs. 25.3% with vancomycin, P=0.005 (ITT)
Secondary outcome (global cure): 74.6% with fidaxomicin vs 64.1% with vancomycin, P=0.006 (ITT)
Conclusion
The rates of clinical cure after treatment with fidaxomicin were non-inferior to those after treatment with vancomycin
4

About the journal
NEJM is the most widely read, cited, and influential general
medical periodical in the world.
It publishes articles since 1812 in research and key
information at the intersection of biomedical science and
clinical practice.
Peer-reviewed articles
This journal usually has the highest impact factor of the
journals of clinical medicine (53.48 in 2010).
5
Authors 6

Authors 7

Title
Accurate but not adequate
Unbiased
Does not describe the study appropriately: a randomized phase III trial
8

Introduction Current problem
Fidaxomicin and its properties
Previous trial
Rationale
Aim??
9

Introduction
Funnel-like introduction
Sufficient description of the study rationale
Insufficient description of phase II trial
Aim was not clear
10
Methodology
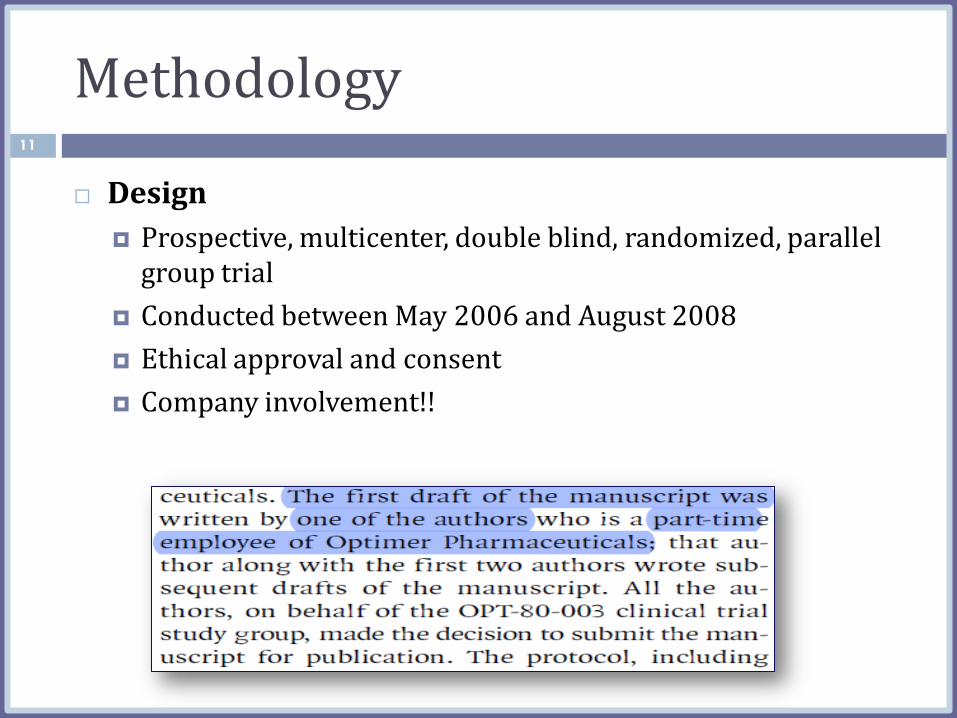
Design
Prospective, multicenter, double blind, randomized, parallel group trial
Conducted between May 2006 and August 2008
Ethical approval and consent
Company involvement!!
11

Methodology
Populations
The study was conducted multiple centers in the US and Canada
12
Inclusion criteria Exclusion criteria
Adults (16 years or older) Life threatening infection
Diagnosed with c. difficile and its toxins in stool specimen
Toxic megacolon
Patients may have received up to 4 doses of metronidazole or vancomycin in 24hrs period before radomization
More than one occurrence of c. difficile infection within 3 months
Previous exposure to fidaxomicin
History of ulcerative colitis or Crohn’s disease

Methodology 13
Randomizations and treatment
An interactive voice-response system and computer generated randomization schedule
Each patient was provided a randomization number and medication kit number
Treatment
200 mg of fidaxomicin every 12 hours with intervening matching doses of placebo
125 mg of vancomycin every 6 hours
Treatment duration: 10 days

Methodology 14
Definitions
Clinical cure:
The resolution of diarrhea (i.e., three or fewer unformed stools for 2 consecutive days), with maintenance of resolution for the duration of therapy and no further requirement
Clinical failure:
The persistence of diarrhea, the need for additional therapy for C. difficile infection, or both.
Global cure:
The resolution of diarrhea without recurrence
Clinical recurrence:
The reappearance of more than three diarrheal stools per 24- hour period within 4 weeks after the cessation of therapy; C. difficile toxins, in stool; and a need for retreatment for C. difficile infection.

Methodology 15
Outcomes:
Efficacy Safety
The primary efficacy end point was the rate of clinical cure
The assessment included a physical examination, electrocardiography, and clinical laboratory testing, including hematologic and biochemical tests and urinalysis.
The secondary efficacy end point was recurrence of C. difficile infection during the 4-week period after the end of the course of therapy and global cure in the modified intention-to-treat and per-protocol populations.
Adverse events were classified according to the terms used in the Medical Dictionary for Regulatory Activities.

Methodology 16
Other outcomes
Statistical analysis
Primary end point
Non-inferiority with margin of -10 points
One-sided with 97.5% CI
Secondary end points
Two-sided tests
Significance level of 0.05
Treatment differences according to age, inpatient vs outpatient status, prior occurrence of C. difficile infection vs no prior, occurrence, disease severity, and strain type
17

Statistical analysis
Secondary end point (cont’)
Severity score (mild, moderate, severe disease)
Time to resolution: Kaplan–Meier method, with a Gehan–Wilcoxon test
Continuous variables: means ±SD
Categorical variables: numbers and percentages
Modified intention-to-treat and per-protocol analysis
Sample size and power??
18
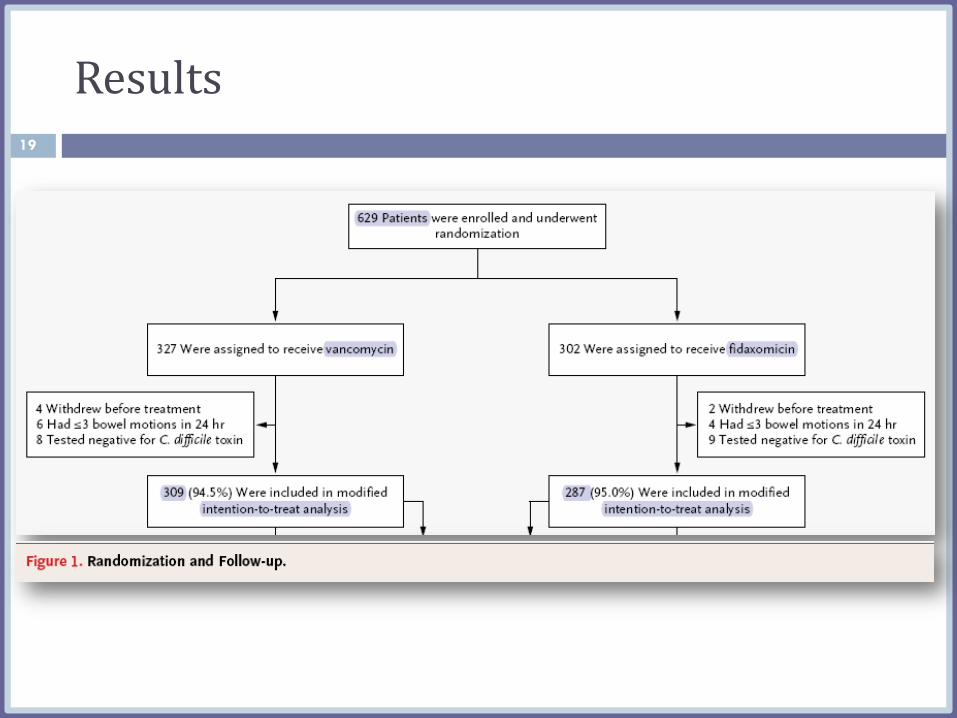
Results 19
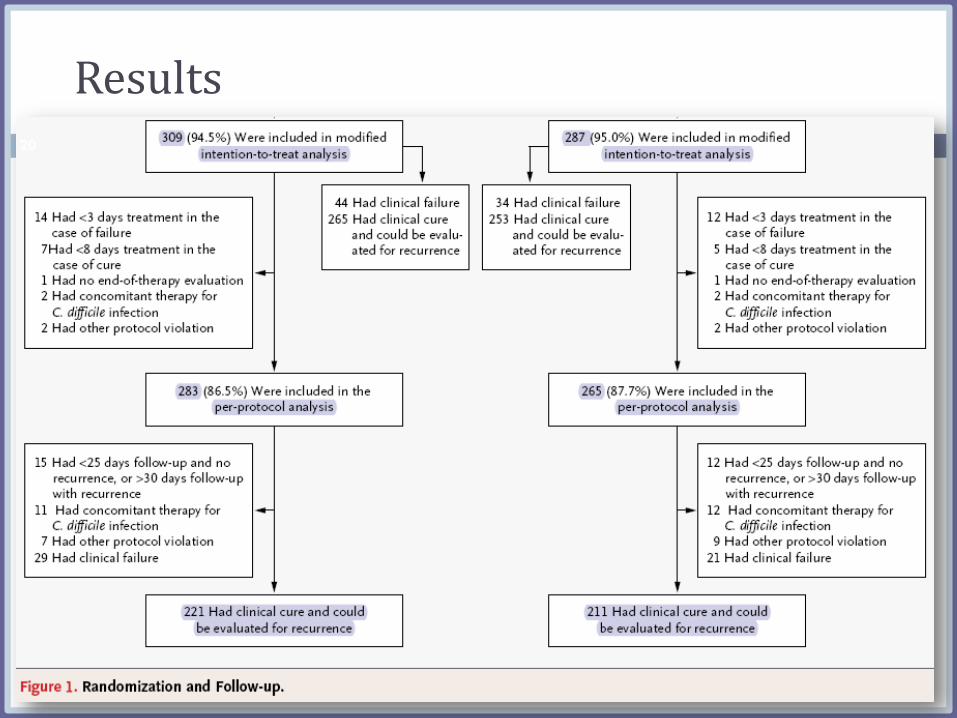
Results 20
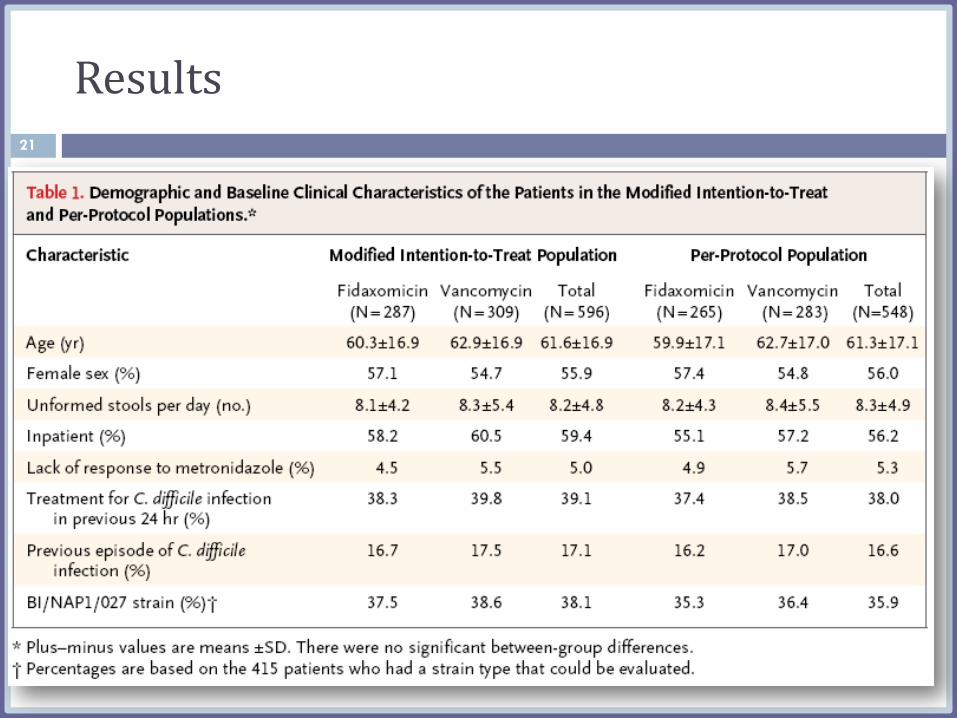
Results 21

Results 22
Results 23
24

Results 25
Results 26
Results 27

Results 28
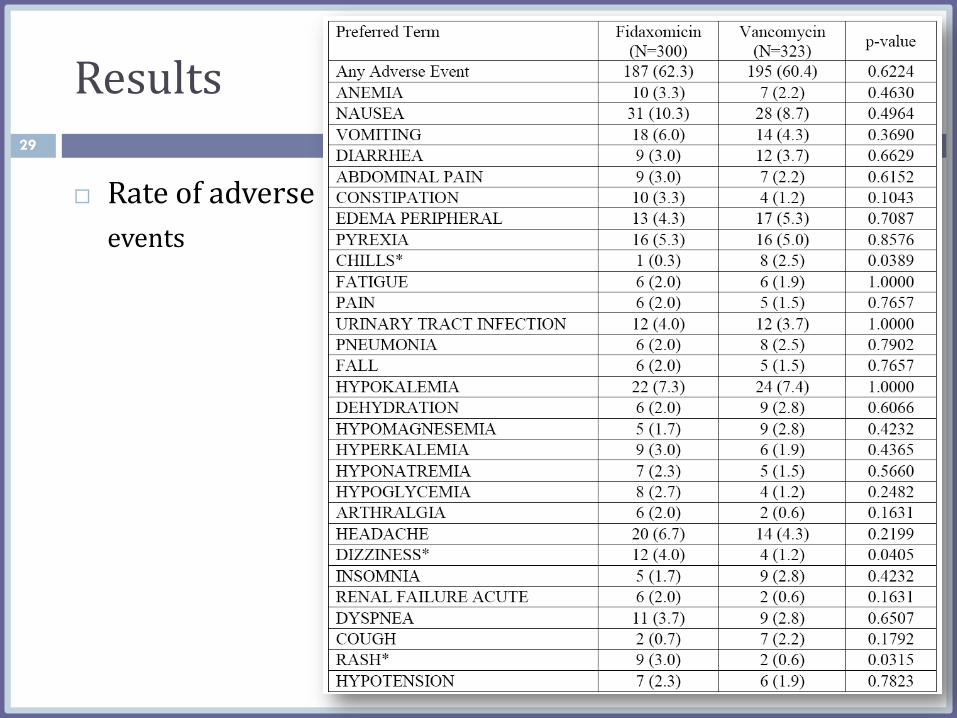
Results
Rate of adverse
events
29

Results
Incidence of
serious adverse
event
30
Results
Microbiological Evaluation
Pharmacokinetic Evaluation
31

Discussion 32

Discussion 33

Discussion 34
Criteria for a good discussion:
1. No any new data in this section
2. Comparing results of the trial to the results of similar previous trials
3. Explanation of any differences found
4. Limitations
5. How the limitations might have affected the results?
Conclusion & External Validity
Comprehensive
Words selection!
No future studies
were suggested
Limited
generalizability
35
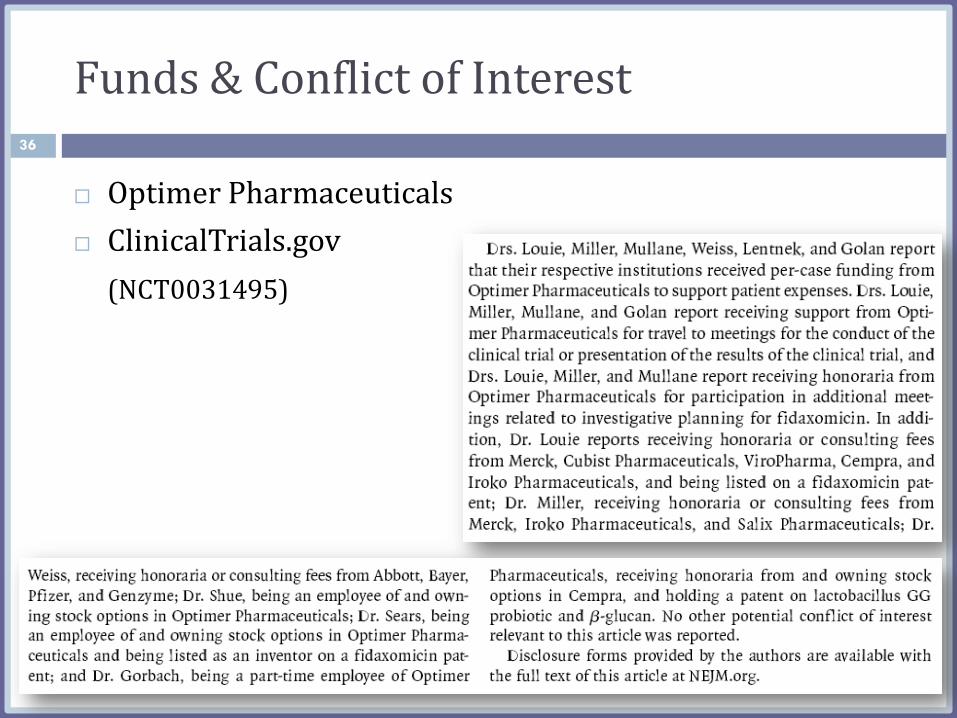
Funds & Conflict of Interest
Optimer Pharmaceuticals
ClinicalTrials.gov
(NCT0031495)
36
References
1986-2010
Authors cited themselves in 5 out of 36 articles
37

Abstract
Well structured
Some important info-
rmation are missed
38

39
Copyright © 2022 FDOKUMEN




















