Evidenced based management of neonatal hemangiolymphangioma: a case report
70
PRESORT STANDARD U.S. POSTAGE PAID SAN JUAN, PR PERMIT No. 3007
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Evidenced based management of neonatal hemangiolymphangioma: a case report

B LETÍNASOCIACIÓN MÉDICA DE PUERTO RICO
Vol. 100 - Núm 2 - Abril-Junio 2008
PRESORT STANDARD
U.S. POSTAGEPAID
SAN JUAN, PRPERMIT No. 3007


B LETÍNASOCIACIÓN MÉDICA DE PUERTO RICO
Vol. 100 - Núm 2 - Abril - Junio 2008
CONTENIDO
2 JUNTA DE DIRECTORES / JUNTA EDITORA
3 MENSAJE DEL PRESIDENTE Y PORTADA Por: Eduardo Rodríguez Vázquez, MD
7 From the Editorial Desk... Por Humberto Lugo-Vicente, MD
ARTÍCULOS ORIGINALES - ORIGINAL ARTICLES
8 A COMPETENCY-BASED COMMUNICATION SKILLS WORKSHOP SERIES FOR PEDIATRIC RESIDENTS By Débora H. Silva, MD
14 HEMOLYTIC UREMIC SYNDROME IN CHILDREN IN PUERTO RICO: A RARE DISEASE WITH ATYPICAL FEATURES By: Yasmín Pedrogo-Rodríguez, MD, Juan O. Pérez-Rodríguez, MD, Melvin Bonilla-Felix, MD
18 THROMBOCYTOSIS IN ILLICIT DRUGS-EXPOSED NEWBORNS By: Thea Calderón MD, Sonia Medina MD, Inés García MD, Lourdes García MD, Marta Varcárcel MD
21 MANEJO DE LACTANCIA Y AMAMANTAMIENTO: ROL DEL MEDICO RESIDENTE Por: Nerian Ortiz Matos MD, Lourdes García Fragoso MD
24 GENITOANAL FINDINGS IN PUERTO RICAN CHIL- DREN WITH SUSPECTED SEXUAL ABUSE By: Amaris Rivas Carlo MD, Brenda Mirabal MD, MPH
28 LUPUS NEPHRITIS IN PUERTO RICAN CHILDREN AND ADOLESCENTS By: Tami O. Tiamfook MD, Ivonne Arroyo MD, Enid Del Valle MD , Juan O. Pérez-Rodríguez MD, Anarda González MD, and Melvin Bonilla-Félix MD
33 PERCEPTION OF PARENTS REGARDING THEIR CHILDREN’S WEIGHT By: Ilsa J. Nazario Rodriguez MD, Wanda I. Figueroa MD , Jaime Rosado MD, Iris del C. Parrilla MS
39 DO PARENTS KNOW ABOUT THE ADVERSE EF- FECTS OF PASSIVE SMOKING AND THE RELA- TIONSHIP WITH RESPIRATORY ILLNESS ON THEIR CHILDREN? By:Cristina Jiménez-González MD, Vanessa Santini MD, Wanda I. Figueroa Cosme MD, Iris del C. Parilla MS
ARTÍCULOS DE REPASO - REVIEW ARTICLES
47 DEVELOPMENTAL SEX DISORDERS: BRIEF RE VIEW ON CURRENT ETHICAL ASPECTS. By: Francisco Nieves-Rivera, MD and Lilliam González-Pijem, MD
52 DIABETIC KETOACIDOSIS IN PEDIATRICS: MANAGEMENT UPDATE By: Ricardo García-De Jesús MD
REPORTES DE CASOS - CASE REPORTS
57 EVIDENCED BASED MANAGEMENT OF NEONA- TAL HEMANGIOLYMPHANGIOMA: A Case Report. By: Maribel Campos MD, Víctor Ortiz MD, Maria S. Correa MD, Pedro J.Santiago Borrero MD, Ines Garcia MD, Lourdes Garcia MD, Marta Valcárcel
60 PORTADA
62 CME Credits for Vol. 100 Núm 2.
BOLETIN - Asociación Médica de Puerto RicoAve. Fernández Juncos Núm. 1305
P.O.Box 9387 - SANTURCE, Puerto Rico 00908-9387Tel.: (787) 721-6969 - Fax: (787) 724-5208
e-mail: [email protected] site: www.asociacionmedicapr.org
Catalogado en Cumulative Index e Index MedicusListed in Cumulative Index and Index Medicus No. ISSN-
0004-4849Registrado en Latindex -Sistema Regional de Información en Línea para Revistas Científicas de América Latina, el Caribe,
España y Portugal
Diseño Gráfico y Emplanaje realizado por el Departamento de Prensa y Publicidad de la AMPR
E-mail: [email protected]
PORTADA
Dr. Manuel Quevedo BáezÓleo de Miguel Pou, 1955

2 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008
ASOCIACIÓN MÉDICA DE PUERTO RICO - 2008
JUNTA DE DIRECTORES
Eduardo Rodríguez Vázquez, MDPresidente
Ricardo Marrero Santiago, MDPresidente Saliente
Verónica Rodríguez, MDSecretaria
Raúl Casstellanos Bran, MDTesorero
Hilda Ocasio Maldonado, MDVicepresidente AMPR
Rolance Chavier Roper, MDVicepresidente AMPR
Raúl A. Jordán Rivera, MDVicepresidente AMPR
Arturo Arché Matta, MDPresidente Cámara de Delegados
José I. Iglesias, MDVicepresidente Cámara de Delegados
Rafael Fernández FelibertiDelegado Alterno AMA
Eladio Santos Aponte, MDDelegado Alterno AMA
Wanda Vélez Andujar, MDDelegado Alterno AMA
José Gerena DíazPresidente Distrito Este
Gustavo Cedeño Quintero, MDPresidente Distrito NoresteWanda Vélez Andujar, MD
Presidente Distrito SurMildred Arché Matta
Presidente Distrito CentralVerónica Rodríguez, MD
Presidente Consejo de Educación Médica ContinuadaIsmael Toro Grajales, MD
Presidente Consejo Ético-JudicialAlejandro Medina Vilar
Presidente Consejo Relaciones Públicas y Servicios PúblicosJorge Vélez Soto, MD
Presidente Consejo Servicios MédicosEladio Santos Aponte, MD
Presidente Consejo Salud Pública y Bienestar SocialNatalio Debs Elías, MD
Presidente Consejo Política Pública y LegislaciónEmilio Arce Ortiz, MD
Presidente Comité Asesor PresidenteIlia E. Zayas Ortiz, MD
Presidente Instituto Educación Médica
PRESIDENTES
SECCIONES DE ESPECIALIDAD
ANESTESIOLOGÍACarlos Estrada Gutiérrez, MDCIRUGÍA GENERALJosé García Troncoso, MDCIRUGÍA ORTOPÉDICAKenneth Cintrón, MDCIRUGÍA ESTÉTICA Y RECONSTRUCTIVANatalio Debs Elías, MDCIRUGÍA TORÁCICA Y CARDIOVASCULARJosé O’Neill Rivera, MDCIRUGÍA DE MANOJosé Santiago Figueroa. MDDERMATOLOGÍALuis J. Ortiz Espinosa, MDENDOCRINOLOGÍAEladio Santos Aponte, MDMEDICINA DE FAMILIAMarina Almenas, MDMEDICINA FÍSICA Y REHABILITACIÓNMiguel Berríos, MDMEDICINA INTERNARamón A. Suárez VillamilMEDICINA PREVENTIVA Y SALUD PÚBLICARoberto Rosso Quevedo, MDOFTALMOLOGÍAEmilio Arce López, MDOTORRINONARINGOLOGÍACharles JuarbePSIQUIATRÍAPedro Colberg, MDNEUROLOGÍAEdwin Lugo Piazza, MDUROLOGÍAPedro Piquer Merino, MDMEDICINA DE EMERGENCIAPablo Laureano Marti, MD
JUNTA EDITORA
Humberto Lugo Vicente, MDPresidenteLuis Izquierdo Mora, MDMelvin Bonilla Félix, MDCarlos González Oppenheimer, MDEduardo Santiago Delpin, MDFrancisco Joglar Pesquera, MDYocasta Brugal, MDJuan Aranda Ramírez, MDFrancisco J. Muñiz Vázquez, MDWalter Frontera, MDMario. R. García Palmieri, MDRaúl Armstrong Mayoral, MDJosé Ginel Rodríguez, MD

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 3
Vol.: 100 - Núm 2 - Abril - Junio 2008
Mensaje del PresidenteMessage from the President
Por: Eduardo Rodríguez Vázquez, MDPresidente, Asociación Médica de Puerto Rico
La Asociación Médica de Puerto Rico fue fundada en 1902 por el Dr. Manuel Quevedo Báez, en unión a otros distinguidos médicos. Como to-dos los grupos en que median los seres humanos, la Asociación Médica ha atravesado y sobrepasado varias crisis en su historia.
En el último año de su presidencia en la Asociación Médica de Puerto Rico, el sabio cientí-fico Dr. Agustín Sthal (1905-1909) publicó en el periódico La Correspondencia de Puerto Rico el anuncio de su renuncia, “obedeciendo a la indife-rencia completa de los asociados observada desde hace un año y su retraimiento de este centro pro-fesional y científico y conceptuó extinguida la Asociación”. Una de las razones que alegaba para su acción era que nuestro Boletín Científico no se había publicado durante más de un año.
Gracias a la iniciativa de varios médicos, entre ellos el Dr. Pedro Gutiérrez Igaravidez y el Dr. Rafael Vélez López, se llevó a cabo una reunión en Ponce, pudiéndose, entonces, reorgani-zar nuestra Asociación Médica.
De esto resultó el que nos uniéramos, al año siguiente, a la Asociación Médica Americana, por primera vez.
La carta que reproducimos a continuación, escrita por el Dr. Manuel Quevedo Báez y dirigida al Dr. Manuel Pavía Fernández, obedece a otra de las crisis institucionales por las que atravesó la Asociación Médica en la década de 1930.
Me he tomado la libertad de reproducir todo el contenido de la misma para que sirva de mensaje aleccionador a nuestros colegas que as-piran a ser los futuros líderes de esta venerable ins-titución.
Las palabras de nuestro fundador y pri-mer presidente tienen, todavía, gran vigencia en nuestros días.

16 de diciembre de 1935Dr. M. Pavia FernándezSanturce, P.R.
Mi querido y buen amigo: no puedo silen-ciar la satisfacción con que he visto su nombra-miento, surgido con unanimidad de la Asamblea, para la presidencia de la Asociación Médica, du-rante el año próximo. Es motivo justificado para mi la feli-citación que debo darte, bien sentida y franca, por el honor que recibes. Espero que seas, en ese puesto, un conti-nuador feliz del pensamiento original y básico que trajo a la vida esa Asociación y de los empeños puestos en práctica, por cuantos te hemos prece-dido en esa posición de tanta responsabilidad. Sé que arribas a ella en días y momentos difíciles, porque llega, hasta nosotros, a través de todas las distancias, esa ola agria y funesta de los ciegos egoísmos, de irreverencias y de maldades que ha echado a correr, loca, por el mundo. ¡Ojalá no fueran motivos míseros y po-bres los que han sembrado la cizaña en nuestro campo! ¡Ojalá que fueran motivos políticos de honda significación y trascendencia; que obede-cieran a esa política de verdad, de alto sentido moralyconstructivo; laqueenalteceahombresy pue-blos y deja honda huella a su paso por la historia, y no a esa menguada y mezquina que más bien sirve de bochorno y de descrédito a los que la sirven y, de ella, regocijados se nutren! Fuera una fortuna y no pequeña para ti y para cuantos amamos la cordialidad y la unión sincera y fraternal de todas las fuerzas médicas y para cuantos, primero y principalmente, por enci-ma de todo credo u opinión sectarios, nos senti mos puertorriqueños; fortuna grande fuera que,bajo tu presidencia, lograras conjurar esas bo-chornosas diferencias que tanto lastiman al honor y prestigio de nuestra clase médica. Yo así lo espero: primero, por la virtud médica y el patriotismo de nuestros alejados com-pañeros, quienes tienen, siempre, muy hondas sus raíces vinculadas en la Asociación Médica y se-gundo, porque me abona, para esperarlo así, la confianza que tengo en tu probada discreción ybuen juicio y tu buena disposición a mantener in-cólume el espíritu de cordialidad entre la clase.
4 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Si ello no se consiguiese, tendríamos do-lorosamente, que acusarnos todos, de una grave responsabilidad, porque estaríamos haciendo trai-ciónaunodelosmásfirmesexponentesdelacul-tura puertorriqueña y, así, estaríamos culpables, maculando el manto de bien ganado prestigio, que, durante un cuarto y más de siglo, cubrió, con grandes honores, a esta Institución Médica. Las páginas que llenan su historia durante treinta y tres laboriosos y fecundos años, son más que luminosas y brillantes. En ellas se copia todo ese proceso ma-ravilloso de avance, que ha seguido el pensa-miento médico, desenvolviéndose a tono con los progresos médicos, que se realizan en el mundo científico. La medicina que hemos cultivado, nos ha permitido ver como, en fases sucesivas de progreso, hemos ido pasando de las viejas normas de pura intuición, a través de lo objetivo y sintomático, a las formas que, por mediación del microscopio arrancábamos a la “Anatomía Patológica”. Y ya esta en nsus vastos campos explorada, comenza-mos a entrar vislumbrando un campo nuevo pro-metedor de grandes conquistas para la Clínica: el de la Biología. Con estos créditos nuestra gloriosa Asoci-ación tiene un buen crédito conquistado y nuestro deber médico y cívico, como verdaderos puertor-riqueños, es mantenerlo y defenderlo, a toda cos-ta. Está todo eso, de gloria y prestigio, en tus manos y yo me prometo grandes éxitos para tu honor y el de la clase médica. Sinceramente, compañero y amigo
Vol.: 100 - Núm 2 - Abril - Junio 2008
P.S.: Aparte esto, buscar quiero un refugio de honorenestacartaparaponerenélunaflor,queprendieras en el noble pecho de Mimi tu inspira-dora y colaboradora de tus exitos.
¡Ahívalaflor!
Carta del Dr. Manuel Quevedo Báez al Dr. M. Pavía Fernández

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 5
Vol.: 100 - Núm 2 - Abril - Junio 2008
Versión en tamaño real de esta carta puede obtenerse en nuestro web site www.asociacionmedicapr.org en la sección President Desk
Dr. Manuel Quevedo Báez

Copyright © 2008 Daiichi Sankyo, Inc. and Eli Lilly and Company. All Rights Reserved. PG51957 Printed in USA. June 2008.

Vol.: 100 - Núm 2 - Abril - Junio 2008
While we move the golden pages of this journal a little further we have dedicated this sec-ond issue of the Boletin to pediatrics. To the effort of those local scientist who care for the health of newborns, infants and children around our island. Our guest editor for this issue is Dr. Melvin Bon-illa, a pediatric nephrologists and member of the editorial board. He has compiled a fruitful group of interesting original articles, reviews and case report. We have managed to continue with provid-ing 4.0 CME credits awards after reviewing and studying several articles.
Not so long ago, reckon was the 2004, that we had the sad news of losing one of our beloved pediatrician in our community. He was the heart and soul of academics pediatrics within the private practice organizing for eighteen years the Annual Ashford Presbyterian Hospital Pediatric Course. Of course I’m referring to our beloved and friend Dr. Simon Piovanetti.
Two weeks after the idles of March Dr. Piovanetti was born in the rural areas of Sabana Grande. Finishing high school in San German, he did a bachelor degree in science at the University of Puerto Rico. The Second World War caused a personal and academic parenthesis in his life while serving with the 65th battalion of infantry. After serving in the army, he completed his general medicine doctorate and pediatric residency at the Jefferson Medical College in Philadelphia. Mar-ries Provi Keelan Capo and has a daughter, Yvette. Yvette is a renowned pediatrician with a keen in-terest in breast feeding. After finishing the residen-cy years, Simon returns to Puerto Rico where he serves as pediatrician for more than 50 years.
Dr. Piovanetti directed the De-partment of Pediatrics of the Ashford Presbyterian Hospital for more than fifteen years and participat-ed as member of the directive board of the Puerto Rico Medical Association for more than ten years. Since then he wrote four didactic books in Pediat-rics such as: ‘Manual de Pediatría’, ‘Simón Dice’ y las ‘Perlas de Pediatría I and II’.
Patients and family members describe his best assets as the ability to listen and the ability to forgive without resentments. He could transform pain and suffering into happiness and humor in the blink of an eye.
In memorial, this pediatric issue is dedi-cated to the loving character of Dr. Simon Piovan-etti, a great community pediatrician.
From a friend to a friend,
Simón Piovanetti, MD FAAP1920-2004
“Since the opportunity is there I will take advantage of it.”
By: Humberto Lugo-Vicente, MD FACS FAAPEditor-in-chief Boletín Asociación Médica de PR
From the Editorial Desk...
BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 7

8 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008
Artículos Originales - Original Articles
A COMPETENCY-BASED COMMUNICATION SKILLS WORKSHOP SERIES FOR PEDIATRIC RESIDENTSBy: Débora H. Silva, MD
ABSTRACT
Background: The use of advanced communica-tion skills to deal with difficult situations is essen-tial to deliver adequate medical care.
Description: A four-unit competency-based work-shop series was developed for Pediatric Residents. The units are: Communicating Bad News, Commu-nicating in Difficult Physician-Patient Situations, Communicating with Adolescents and Providing Telephone Consultation. The Communicating Bad News unit was fully developed, implemented and pilot tested.
Evaluation: The intervention group performed significantly better (p = 0.001) than the non-inter-vention group in the Pilot Test. Residents found the instructional sessions to be excellent and ef-fective.
Conclusions: A competency-based curriculum is likely to be an effective way to teach the use of ad-vanced communication skills needed in complex situations. In addition to learning the skills, resi-dents are also likely to feel more prepared to deal with the situations they encounter. Both skill and confidence are necessary for the adequate delivery of medical care.
Key words: Communication Skills, Clinical Skills, Giving Bad News
* From the Department of Pediatrics, University of Puerto Rico, School of Medicine Michigan State University Primary Care and Faculty Develop-ment Fellowship.
Address reprints to: Débora H. Silva MD, FAAP, Curriculum Office, U.P.R. School of Medicine P.O. Box 365067 San Juan PR 00936-5067. <[email protected]>
Good doctor-patient communication is es-sential for delivery of adequate medical care (1-9, 20). Effective communication is a core clinical skill and should be taught and evaluated at differ-ent levels in medical education (1, 10-13).
Although most medical schools have established a communication skills curriculum giving emphasis to the medical interview, less attention has been given to teaching advanced communication skills at the residency level (4-5, 16-17).
The Accreditation Council on Graduate Medical Education (ACGME) is requiring evidence of resi-dents’ competence in communication skills since 2003 (13). In addition, by 2010, pediatricians who want to re-certify will need to provide evidence of competency in interpersonal communication skills to the American Board of Pediatrics (14).
Although residency programs are starting to devel-op communication skills curriculums, descriptions are usually narrow in scope, do not address assess-ment of the curriculum, or do not address the use of skills in a more complex context (4, 15, 17-21, 24). Two developers describe their curriculum and include the use of advanced communications skills. Morgan et al. found that residents thought the cur-riculum was valuable and effective, but there was no significant change in communication skills. They argued that residents were already evalu-ated positively in the pre-test, so no change was observed (17). On the other hand, Smith and his colleagues observed that residents trained in com-munication were superior to untrained residents in knowledge, attitudes and interviewing skills (4).
The Pediatric Residency Program at the UPR School of Medicine needs an advanced com-munication skills curriculum. The residency pro-gram is mostly located at a tertiary care center, which serves most of the population in Puerto Rico. In this context, dealing with complex and difficult situations is a common occurrence for residents and they should be adequately prepared.
We conducted a literature review and needs assessment at the residency program and de-veloped a competency-based, advanced communi-cation skills curriculum. The curriculum contains four units: Communicating Bad News, Communi cating in Difficult Physician-Patient Situations,

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 9
Vol.: 100 - Núm 2 - Abril - Junio 2008
Figure 1: Curriculum Structure
Communicating with Adolescents and Answering Telephone Consultations (See Figure1). To begin the assessment of the curriculum, we fully devel-oped, implemented and tested the unit on Commu-nicating Bad News.
METHODSUnit Development Process In able to develop the Communicating Bad News Unit, an extensive literature search was conducted. Also the goals and objectives on com-munication skills of the Residency Program (23) and of the ACGME Competencies were revised (13). Taking all this into consideration, unit ob-jectives, unit content, instructional and evaluation strategies were developed (See Table 1).
Unit Implementation The unit on Communicating Bad News was implemented in March 2004. Two social workers and five standardized patients (SP) were trained to teach, give feedback and evaluate resi-dents’ performance in giving bad news follow-ing the Giving Bad News Checklist based on the SPIKES Protocol for Giving Bad News (26). The first year pediatric residents were divided into an intervention and a non-intervention group by fol-lowing the residency programs’ master program in which some residents are required to attend the teaching activities each month and some are ex-empt. Those residents required to attend the activi-ties during the month of March 2004 comprised the intervention group; those exempt were the con-trols.
Those residents required to attend the activities during the month of March 2004 comprised the in-tervention group; those exempt were the controls. They all signed consent forms to participate in the pilot Objective Structured Clinical Exam (OSCE). Five residents were used as controls in the non-intervention group. Seven residents comprised the intervention group; six completed the training. The intervention group underwent four hours of train-ing.
In session one, residents listened to a lec-ture on how to give bad news according to the Giving Bad News Checklist, viewed a live dem-onstration given by an SP and a faculty member and received the article on the SPIKES Protocol to read (26). In session two, they viewed two vide-otapes of scenarios where bad news was given in an appropriate and an inappropriate manner. Then the residents analyzed the performances shown in the videotapes according to the checklist. In ses-sion three, residents role-played various scenarios in which the physician had to give bad news. Each resident received feedback from a standardized pa-tient (SP). Only two residents also received feed-back from one social worker. They had 15 minutes to complete each role-play and 5 minutes for feed-back. In the last session residents were divided in groups of two and assigned to an SP. Each student had 15 minutes to give bad news to an SP, follow-ing the instructions given to them at the beginning of the interaction. At the completion of the inter-action they received five minutes of feedback from the SP. While one student was giving the bad news to the SP, the other was evaluating the interaction following the checklist.
Residents will use adequate communication skills to deal complex situations
Communicating Bad News
Communicating in Difficult Physician-Patient Situations
Communicating with Adolescents
Providing Telephone Consultations
Giving Dx/Prognosis Taking DNR
Anxious Angry Depressed Denial
Health Maintenance Education

Vol.: 100 - Núm 2 - Abril - Junio 2008
Table 1: Unit Development Table
Unit Objectives Unit Content Instructional Strategies Learner Evaluation
Given a scenario where they have to communicate bad news to a patient/fam-ily (Giving Prognosis, Diagnosis and taking DNR) residents will follow the Giving Bad News Check-list adapted from the SPIKES Protocol for Giving Bad News
1. Article on the SPIKES Protocol for Giving Bad News (26)
2. The Giving Bad News Checklist Based on SPIKES Protocol
3. Examples and criterion for the Giving Bad News Checklist
1. Exp lana t ion : Pre-lecture reading. En-hanced Skills Lecture
2. Demonstration: Live and video dem-onstration following the Giving Bad News Checklist
3. Practice: Role-Playing between resi-dents and practice with simulated patients giv-ing bad news following the Giving Bad News Checklist
Following OSCE for-mat residents will communicate bad news to 2 simulated patients/families fol-lowing the Giving Bad News Check-list adapted from the SPIKES Protocol for Giving Bad News. They will be expected to complete 100% of the major checklist criteria and 80% of the sub-criteria on each encounter
Unit Pilot Test- Evaluation of Learners Three weeks after the four training sessions were completed and after receiving IRB approval, eleven residents, six of the intervention group and five of the non-intervention group, participated in a two station OSCE. During the OSCE they had to give bad news in two different scenarios: announce to the parents the sudden death of their child due to trauma; and give the diagnosis of Down’s syn-drome to the grandparent of a newborn child. Both encounters were evaluated by SPs following the Giving Bad News Checklist. Prior to entering the first station, the intervention group also completed a quiz on knowledge about the SPIKES Protocol.
Evaluation of the Teaching Strategies To evaluate the teaching strategies used in this unit, the residents in the intervention group filled out an evaluation at the end of the four ses-sions. In this questionnaire residents were asked to use a Likert Scale to evaluate the overall effec-tiveness of the sessions in their learning process, and how each of the teaching strategies helped them learn. They were also asked about their con-fidence level in the skill of giving bad news.
Both groups of residents also completed another questionnaire at the end of the OSCE.
By means of open-ended questions, they were as ked their opinion about the OSCE, their perceived preparedness and their confidence level in giving bad news.
RESULTSResults of Pilot Test-Learner Evaluation The intervention’s group average result on the SPIKES Protocol quiz was 93%. The results for the intervention and non-intervention group on the OSCE were compared using the Mann-Whitney Test (Table 2). The intervention group performed significantly better than the non-intervention group on the OSCE (p = 0.001). When evaluating each case separately, the intervention group performed significantly better than the non-intervention group on the sudden death case (p = 0.01), while this difference was marginally significant for the Down’s syndrome case (p = 0.05). Based on an item analysis we noted that the intervention group had one checkpoint in each scenario consistently missing: for the sudden death case they did not ask how the caretaker was feeling; and for the Down’s syndrome case they did not ask about expectations or hopes. On the other hand, the non-intervention group missed a wide variety of checkpoints. The only consistent checkpoints they followed well were giving empathic and validating statements and offering to call for support.
Table 2: Results of Pilot Test
N=11 p = .010 p = .052 p = .001
Sudden Death Case (Mean Checklist Score)
Down’s Syndrome Case (Mean Checklist Score) Overall Score
Intervention N=6Intervention N=5
96 %68 %
91 %78 %
93 %73 %
10 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 11
Results of Teaching Strategies Evaluation The responses of the intervention group in the evaluation of the teaching strategies indicated that they were very satisfied with the curriculum. All of them rated the overall effectiveness of the sessions as excellent. They all strongly agreed or agreed that the article on the SPIKES Protocol, the demonstrations, the role-playing, and the practice with SPs helped them learn. They also strongly agreed or agreed that they received adequate feed-back about their performance and they felt more confident in giving bad news after the sessions. They consistently gave two valuable recommen-dations: to assign more time for each session, and to involve more faculty members.
The questionnaire that the intervention and non-intervention group completed at the end of the OSCE revealed that all the residents in the inter-vention group felt prepared to give the bad news while none in the non-intervention group did. On the other hand, at the time of the OSCE, only two of the six residents in the intervention group felt comfortable giving the bad news; the other four and all the residents in the non-intervention group felt uncomfortable and thought they needed consid-erable practice to improve. All residents agreed a curriculum is necessary to learn these techniques.
DISCUSSION As evidenced by the results, in the pilot test residents in the intervention group performed significantly better than those in the non-interven-tion group when asked to give bad news. The item analysis found that residents in the intervention group did not ask about feelings and hopes. Both gaps are consistent with the usual fears of giving bad news. When someone dies it is hard to ask how the family is feeling because the expected answer is that they are devastated. Further, when we give a diagnosis of a chronic illness, such as Down’s syndrome, we do not want to hear the parents’ hopes because we do not want to destroy them.
More meaningful is the fact that the resi-dents in the intervention group stated they felt pre-pared to give bad news even when they still felt un-comfortable with the situations. At the same time, those in the non-intervention group felt uncomfort-able and ill prepared. A reasonable question would be if physicians can ever feel comfortable giving bad news, irrespective of training. Therefore, feel-ing prepared could arguably be “good enough”.
The didactic component of the curriculum is being implemented in a stepwise manner. At this time all the residents have attended the Commu-nicating Bad News workshops, which have been repeated very two years since 2004. The Unit on Adolescent Communication was offered in 2006.
Vol.: 100 - Núm 2 - Abril - Junio 2008
The Unit on Communicating in Difficult Physician Patient Situations was offered to all second year residents as part of the Residents-as-Teachers Cur-riculum of the Medical School in 2007. The next unit to be developed and implemented will be the Telephone Interview Unit.
For this curriculum to work, faculty must be trained to teach and assess learners in order to achieve consistency in the residents’ performance. Faculty must give reliable feedback throughout the years and among the clinical settings. For this to be achieved, the Faculty Development Program at the University of Puerto Rico School of Medicine has developed a Clinical Educators Curriculum which includes training in Giving Bad News, Dealing with Difficult Physician-Patient Situations and Giving Feedback. All of these topics have been of-fered in a yearly basis since 2006.
The next step will be the development of an OSCE that tests all the clinical skills expected of a pediatrician, since it would be too costly to do one just for communication skills. Meanwhile, evaluation of learners is being done in a monthly manner as part of the usual resident evaluation. The faculty member in charge evaluates and gives feedback on these skills as observed during that month’s rotation.
With the new era of competency assess-ments and the increasing requirements by the gen-eral public and the accreditation agencies, we must teach residents the use of communication skills needed to deal with complex situations. We de-veloped and tested a curriculum to teach advanced communication skills. The results of the pilot test suggest that residents are likely to learn these skills when properly taught in a competency-based man-ner.REFERENCES
1. Association of American Medical Colleges, Report III Contemporary Issues in Medicine: Communication in Medicine. Medical School Objectives Project, October 1999. P.1-23.
2. U.S. Department of Health and Human Services, Healthy People 2010 Conference Edition. January 2000. Vol-ume 1: p.11-3 - 11-21.
3. NYU Macy Initiative on Health Communication, Curriculum. Retrieved August 17, 2003 from the World Wide Web: http://nyumacy.med.nyu.edu
4. Smith, R., et al., The Effectiveness of Intensive Training for Residents in Interviewing A Randomized, Con-trolled Study. Annals of Internal Medicine, 1988. 128 (2): p. 118-126.
5. Kurtz, S., J. Silverman, and J. Draper (1998). Teaching and Learning Communication Skills in Medicine. Radcliffe Medical Press, UK.
6. Meryn, S., Improving doctor-patient communica-tion. BJM, 1998. 316: p. 1922-1930.

12 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008
7. Pfeiffer, C., H. Mandray, A. Ardolino, and F. Willms, The rise and fall of students’ skills in obtaining a medical his-tory. Medical Education, 1998. 32: p. 283-288.
8. Suzuki Laidlaw, T. et. al.,Implementing a commu-nication skills programme in medical school: needs assess-ment and programme change. Medical Education, 2002. 36: p. 115-124.
9. Van Dalen, J., et. al., Teaching and assessing com-munication skills in Maastricht: the first twenty years. Medi-cal Teacher, 2001. 23(3): p. 245-251.
10. Kurtz, S. and J. Silverman, The Calgary-Cambridge Referenced Observation Guides: an aid to defining the cur-riculum and organizing the teaching in communication train-ing programmes. Medical Education, 1996. 30: p. 83-89.
11. Grant, V.J. and S. J. Hawken, What do they think of it now? Medical graduates’ views of earlier training in com-munication skills. Medical Teacher, 2000. 22(3): p. 260-264.
12. Spencer, J. and J. Silverman, Education for commu-nication: much already known, so much more to understand. Medical Education, 2001. 35(3): p. 188-190.
13. ACGME Outcome Project, UPDATE/VERIFY GENERAL COMPETENCIES ASSESSMENT. Retrieved August 17, 2003 from the World Wide Web: http://www.acgme.org
14. Stockman, J. A., P. Miles, and H. P. Ham, The Pro-gram for Maintenance of Certification in Pediatrics. Pediatric Diplomats, Fall 2003. p. 1-5.
15. Dalhousie University, Communication Skills Pro-gram. Retrieved August 17, 2003 from the World Wide Web: http://www.dme.dal.ca/medcomm/program
16. Hulsman, R.L., et.al., Teaching clinically experi-enced physicians communication skills. A review of evalua-tion studies. Medical Education, 1999. 33: p. 655-668.
17. Morgan E. and R. Winter, Teaching Communication Skills: An Essential Part of Residency Training. Archives of Pediatric and Adolescent Medicine, 1996. 150: p. 638-642.
18. Langewitz, W.A., et. al., Improving communication Skills-A Randomized Controlled Behaviorally Oriented Inter-vention Study for Residents in Internal Medicine. American Psychosomatic Society, 1998. 60(3): p. 268-276.
19. Chou, C. and L. Kewchang, Improving Residents’ Interviewing Skills by Group Videotape Review. Academic Medicine, 2002. 77: p. 744.
20. Oh, J., et. al., Retention and Use of Patient-centered Interviewing Skills after Intensive Training. Academic Medi-cine, 2001. 76(6): p. 647-650.
21. Ruiz Morales, R., et. al., Effectiveness of a Clinical Interviewing Training Program for Family Practice Residents: A Randomized Controlled Trial. Family Medicine, 2003. 35(7):p. 489-494.
22. Participants in the Bayer-Fetzer Conference on Physician-Patient Communication in Medical Education,
Essential Elements of Communication in Medical Encoun-ters: The Kalamazoo Consensus Statement. Academic Medi-cine, 2001. 76(4): p. 390-393.
23. General Pediatrics Residency Program, University of Puerto Rico, School of Medicine, Goals and Objectives Manual, 2002. p. 8-12.
24. Roth, C.S., et. al., A communication Assessment and Skill-building Exercise (CASE) for First-year Residents. Academic Medicine, 2002. 77: p. 746-747.
25. Coulehan, J. L. and M. R. Block (2001). “Difficult Feelings in the Medical Interview”. The medical Interview: Mastering Skills for Clinical Practice Fourth Edition. F.A. Davis. p. 208-218.
26. Baile, W. F., et.al. SPIKES-A Six Step Protocol for Delivering Bad News: Application to the Patient with Cancer. The Oncologist, 2000. 5: p. 302-311
27. Vanderkieft, G. K. Breaking Bad News. American Family Physician, 2001. 64(12): p. 1975-1978.
AcknowledgementsThe author would like to thank Dr. Ken Sheets, Dr. Suzanne Kurtz, Dr. Karen Kent and Dr Barbara Korsch for their critical review of the overall curriculum manuscript, submitted as part of the Michigan State University Primary Care and Faculty Development Fellowship at Michigan State University. Spe-cial thanks to Dr. Steve Yelon and John Williamson at Michi-gan State University Primary Care and Faculty Development Fellowship for all the advice and mentorship through out all the steps of the curriculum development and the pilot test im-plementation.
ResumenIntroducción: Saber utilizar destrezas de comunicación avanzadas en situaciones difíciles es un componente esencial de la relación médico-paciente.
Descripción: Con este propósito, se desarrolló un currículo basado en competencias de comunicación avanzada para resi-dentes de Pediatría. El currículo consta de cuatro unidades. La primera unidad, Como Comunicar Malas Noticias, se desarrolló en su totalidad como proyecto piloto. La unidad se implementó utilizando el protocolo de SPIKES para dar malas noticias como base. Los residentes que participaron del grupo de intervención recibieron práctica y retro-insumo en la destreza de ofrecer malas noticias. Al finalizar el piloto, los residentes del grupo de intervención y un grupo control fueron examinados a través de un examen práctico, objetivo y estandarizado utilizando la metodología de Pacientes Estand-arizados.
Evaluación: Se observó que el grupo de intervención ejecutó significativamente mejor que el grupo control en este examen (p<0.001).
Conclusión: En conclusión, un currículo basado en competen-cias parece ser una manera efectiva de enseñar las destrezas de comunicación avanzadas que se necesitan en situaciones difíciles.
Web Site de la Asociación Médica de Puerto Rico
www.asociacionmedicapr.org
Calendario de actividadesPublicaciones on-line
Créditos Educación Médica ContinuadaServicios con PayPal y tarjetas de crédito
Suscripciones on-liney mucho más..


HEMOLYTIC UREMIC SYNDROME IN CHILDREN IN PUERTO RICO:A RARE DISEASE WITH ATYPICAL FEATURESBy:Yasmín Pedrogo-Rodríguez, MD *, Juan O. Pérez-Rodríguez, MD **, Melvin Bonilla-Felix, MD **
Vol.: 100 - Núm 2 - Abril - Junio 2008
* Fom the Department of Pediatrics and ** Section of Pediatric Nephrology, Department of Pediatrics, University of Puerto Rico – Medical Sciences Campus.
Address reprints to: Melvin Bonilla-Félix, MD, Department of Pediatrics, University of Puerto Rico – Medical Sciences Campus. PO Box 365067, San Juan, Puerto Rico 00936-5067. Tel 787-777-3535 x7300. Fax 787-777-3227. [email protected].
ABSTRACT Hemolytic Uremic Syndrome (HUS) con-sists of a triad of acquired hemolytic anemia, throm-bocytopenia, and renal failure that occurs acutely in otherwise healthy individuals. HUS may be di-vided into two broad categories, typical, preceded by a diarrheal prodrome, and atypical. The clinical symptoms of HUS as well as its course, prognosis, and response to treatment appear to be significantly influenced by a number of factors, including age at onset, type and severity of underlying infections, and/or systemic diseases. A retrospective case se-ries review of five patients diagnosed with Hemo-lytic Uremic Syndrome at the Pediatric University Hospital in Puerto Rico between 1997-2007 was performed. The study showed that the incidence of HUS in children in Puerto Rico is lower than other countries. However, the majority of cases have an atypical presentation, which places our patients at higher risk for life-threatening complications.
Index words: hemolytic, uremic, syndrome, pedi-atrics
Hemolytic Uremic Syndrome (HUS) consists of a triad of acquired hemolytic anemia, thrombocytopenia, and renal failure that occurs acutely in otherwise healthy individuals. Since its description in 1955 (1), HUS has been recognized predominantly in children and in this age group is a common cause of acute renal failure. Initially believed to be a renal disorder with secondary he-matologic manifestations, the syndrome should be regarded as a systemic disease. It occurs most com-monly in young children with a mean age of four years old. HUS may be divided into two broad cat-egories, typical, preceded by a diarrheal prodrome, and atypical. The disease most frequently follows an episode of gastroenteritis caused by an entero-hemorrhagic strain of Eschericia coli 0157:H7, (2). Atypical HUS is often insidious in onset, it does not follow a diarrheal illness; and has a high incidence of extrarenal involvement, especially neurologic abnormalities such as focal or general-ized seizures, transient hemiparesis, or even coma (2, 4).
Secondary forms of HUS have been reported fol-lowing use of oral contraceptives, cyclosporine, mitomycin and pyran copolymer. Several reports describe occurrence in more than one member of a family, but the role of genetics factors in predis-position to the disease is unkown. The severity of the renal involvement and the complications, vary from mild renal insufficiency to acute renal failure requiring dialysis and/or plasmapheresis (5).
The incidence of HUS is apparently lower in Puerto Rico than in the United States and other countries. The clinical symptoms of HUS as well as its course, prognosis, and response to treatment appear to be significantly influenced by a number of factors, including age at onset, type and severity of underlying infections, and/or systemic diseases. We herein report the clinical features of the pedi-atric patients diagnosed with HUS at the Pediatric University Hospital between 1997 and 2007.
METHODS A retrospective review of the medical records of five patients diagnosed with Hemolytic Uremic Syndrome at the Pediatric University Hos-pital in Puerto Rico between 1997 and 2007 was performed. All children presented with the clas-sic triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute renal failure. A small group of older children diagnosed during the same period with thrombotic thrombocytopenic purpura due to presence of prominent neurological symp-toms with mild or absent renal disease, were not included in this analysis.
The data collected included the age at presentation of the disease, gender, the presence of sings and symptoms such as diarrhea, bloody stools, anuria, hypertension, neurological fea-tures, the treatment modalities used (dialysis, plas-mapheresis, platelet and pack red blood cell trans-fusions). In addition, important laboratory data such as the urinalysis, estimated glomerular filtra-tion rate (GFR) at presentation and on last evalua-tion were collected. The GFR was calculated using Schwartz formula (6).
14 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 15
Vol.: 100 - Núm 2 - Abril - Junio 2008
These results were compared with the course of illness and survival of patients.
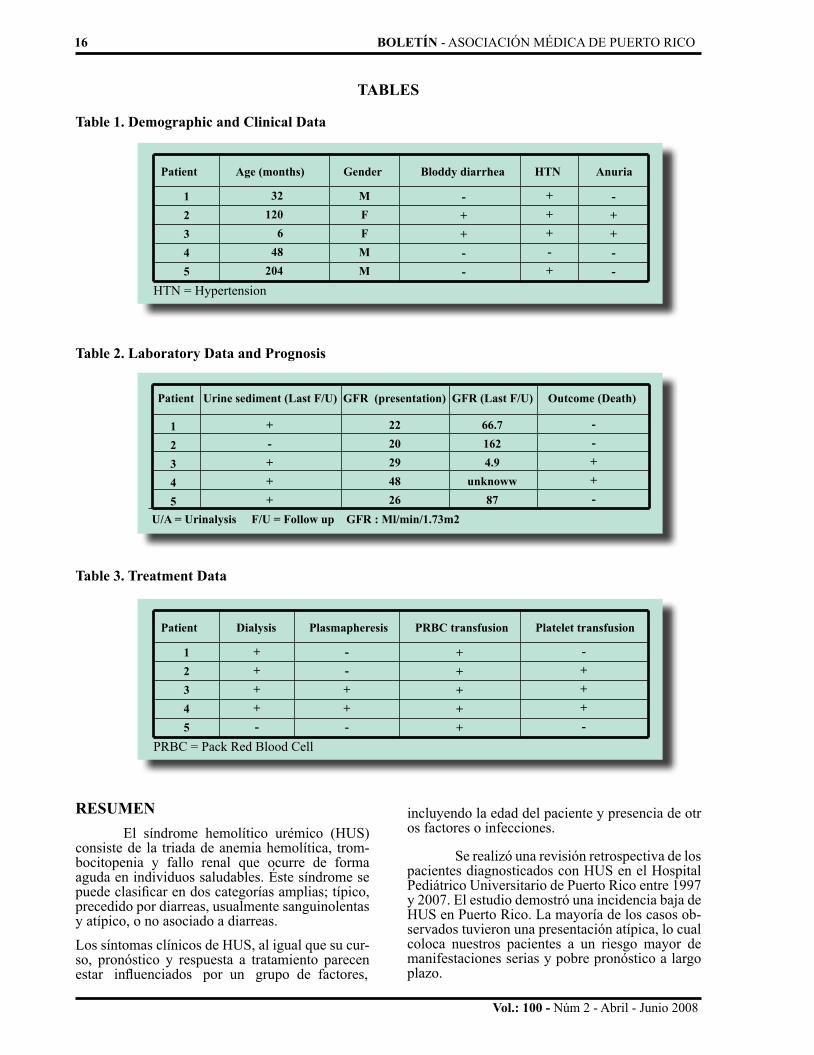
RESULTS The demographic and clinical features are shown on Table 1. There was no significant gen-der predominance. Ages ranged between 6 to 204 months, with a mean age of 82 months. Three out of the five patients presented with diarrhea, two of them with bloody stools (patients 2 and 3). There was no family history of HUS, and no neurologi-cal changes associated with the diagnosis. Also four out of 5 patients had hypertension at presenta-tion. One of them had history of high blood pres-sure since infancy (patient 1) and presented with a hypertensive crisis before developing the classic features of HUS (anemia, thrombocytopenia and acute renal failure symptoms). All the patients pre-sented with hematuria and proteinuria at the time of diagnosis of HUS (Table 2).
At the time of last follow up (2 – 14 months after diagnosis), two of the patients showed no evidence of proteinuria (patients 1 and 2). All the patients had decreased GFR at presentation. Only one patient showed complete resolution of renal disease demonstrated by a normal GFR and uri-nary sediment. Four out of five patients required acute dialysis (Table 3). Three out of five patients required transfusions with red blood cells and platelets. Two of the patients died. Both of them had recurrent episodes of hemolysis and thrombo-cytopenia associated with decreased GFR, requir-ing treatment with plasmapheresis.
DISCUSSION The incidence of HUS in children in Puer-to Rico is lower than other countries. The mean age for HUS in the island (82 months) is similar to other countries (48 months) with higher incidence of the disease. Our report most likely represents most, if not all the cases of HUS in Puerto Rico in the last 10 years. The majority of these cases did not show the typical features of HUS. Only 2 out of 5 had a prodrome of bloody diarrhea. Two out of five patients presented recurrent episodes of hemolysis, thrombocytopenia and renal failure. Both of these patients died during the course of the disease. One of them died from Staphylococcal sepsis, since he had reached end stage renal disease and was receiving peritoneal dialysis. In addition, these two patients received dialysis, plasmapher-esis, platelet and pack red blood cell transfusions due to multiple relapses of the illness, ending in death.
Hemolytic Uremic Syndrome is a rare dis-ease in Puerto Rico. However, the absence of the typical diarrheal prodrome in the majority of our patients, place them in a higher risk category.
This may delay the diagnosis and treatment since it can be confused with other febrile illnesses that are common in the island, such as leptospirosis and dengue fever. Since most of our patients required acute dialysis, early recognition and prompt refer-ral to a Pediatric Tertiary Hospital with dialysis facilities available is important in order to prevent life-threatening complications.
The lower incidence of the disease in Puerto Rico as compared with other countries in the world could result from the cultural preference of most Puerto Ricans to eat well-cooked meat, which decreases the risk of contamination with Eschericia coli. Although we were not able to ob-tain data on the association of E. coli 0157:H7 and HUS in our population, the absence of diarrheal prodrome in three out 5 patients suggests that most of our cases are not associated with E. coli, which might explain the severity of the disease and high mortality rate observed.
In summary, the incidence of HUS in the pediatric population in Puerto Rico is low. Howev-er, because of the absence of a diarrheal prodrome, the disease usually follows an atypical course, re-sulting in significant morbidity and mortality. We believe that all children with the triad of anemia, thrombocytopenia and renal symptoms should be referred immediately to a pediatric tertiary care fa-cility to begin aggressive therapy, including dialy-sis, if necessary.
REFERENCES1. Tarr PI, and, Hickman, Robert: Hemolytic Uremic Syn-drome epidemiology: A population-based study in King County, Washington, 1971 to 1980, Pediatrics July 1987; 80 (1): 41-45.
2. Walters M, Levin M, Smith C, Nokes T, Hardisty R, Dil-lon M, Martin Barrat T: Intravascular platelet activation in the hemolytic uremic syndrome, Advances in Pediatrics Infec-tious Diseases 1989; 4: 51-81.
3. Neill MA, Tarr PI, Clausen CR, Christie DL, Hickman RO: Eschericia coli 0157:H7 as the predominant pathogen asso-ciated with the Hemolytic Uremic Syndrome: A prospective study in the Pacific Northwest, Pediatrics July 1987; 80(1) : 37-40.
4. Remuzzi G, Garella S: HUS and TTP: Variable expression of a single entity, Kidney International 1987; 32: 292-308.
5. Rizzoni G, Claris A, Edefonti A, Facchin P, Franchini F, Gusmano R, Imbasciati E, Pavanello L, Perfumo F, Remuzzi G. Plasma infusion for hemolytic-uremic syndrome in chil-dren: Results of a multicenter controlled trial, J Pediatrics 1988; 112: 284-290.
6. Robertson J, Shilkofski N: The Harriet Lane Handbook, 17th Ed., Pennsylvania, Elsevier Mosby, 2005: 494 – 495.
16 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008
Patient Age (months) Gender Bloddy diarrhea HTN Anuria
Patient Dialysis Plasmapheresis PRBC transfusion Platelet transfusion
TABLES
Table 1. Demographic and Clinical Data
HTN = Hypertension
PRBC = Pack Red Blood Cell
12345
12345
32120
648
204
++++-
MFFMM
--++-
-++--
+++++
+++-+
-++--
-+++-
Table 2. Laboratory Data and Prognosis
Table 3. Treatment Data
Patient Urine sediment (Last F/U) GFR (presentation) GFR (Last F/U) Outcome (Death)
12345
+-+++
2220294826
66.71624.9
unknoww87
--++-
U/A = Urinalysis F/U = Follow up GFR : Ml/min/1.73m2
RESUMEN El síndrome hemolítico urémico (HUS) consiste de la triada de anemia hemolítica, trom-bocitopenia y fallo renal que ocurre de forma aguda en individuos saludables. Éste síndrome se puede clasificar en dos categorías amplias; típico, precedido por diarreas, usualmente sanguinolentas y atípico, o no asociado a diarreas.
Los síntomas clínicos de HUS, al igual que su cur-so, pronóstico y respuesta a tratamiento parecen estar influenciados por un grupo de factores,
incluyendo la edad del paciente y presencia de otr os factores o infecciones.
Se realizó una revisión retrospectiva de los pacientes diagnosticados con HUS en el Hospital Pediátrico Universitario de Puerto Rico entre 1997 y 2007. El estudio demostró una incidencia baja de HUS en Puerto Rico. La mayoría de los casos ob-servados tuvieron una presentación atípica, lo cual coloca nuestros pacientes a un riesgo mayor de manifestaciones serias y pobre pronóstico a largo plazo.


THROMBOCYTOSIS IN ILLICIT DRUGS-EXPOSED NEWBORNSBy: Thea Calderón MD *, Sonia Medina MD *, Inés García MD **, Lourdes García MD **, Marta Varcárcel MD **
Vol.: 100 - Núm 2 - Abril - Junio 2008
* From the Department of Pediatrics, San Juan City Hospital, and ** Section of Neonatology, Department of Pediatrics, U.P.R. School of Medicine, San Juan, Puerto Rico.
Address reprints to: Lourdes García MD, UPR School of Medicine, Department of Pediatrics, Neonatology Section, GPO Box 365067, San Juan, PR 00936-5067. Tel. 787-777-3225, fax 787-758-5307, e-mail [email protected]
ABSTRACT Thrombocytosis in infants exposed in-ute-ro to illicit drugs has been associated to methadone exposure. Although is reported to present in the first two weeks, few studies address its duration and timing of resolution. This study evaluated the presence, duration, and complications of thrombo-cytosis in newborns exposed to illicit drugs. Meth-ods: A retrospective review of medical records of newborns with intrauterine drug exposure ad-mitted to the San Juan City Hospital from 1999 to 2001 was performed. Results: Thirty-one new-borns were included. Eighty-seven percent (87%) presented abstinence syndrome. Of these, 96% presented thrombocytosis. All infants exposed to methadone presented thrombocytosis and 75% of those exposed to heroin and cocaine. Thrombocy-tosis presented at ten days of life with a median resolution at 26 days. Conclusions: In this group of newborns, thrombocytosis was associated to intrauterine exposure to methadone, heroin, and cocaine. Thrombocytosis presented at ten days of life and resolution was seen in three to 4 weeks without complications observed.
Index words: thrombocytosis, illicit-drugs, new-borns
The use of drugs during pregnancy presents consequences to the fetus and neonate. Short and long- term neurobehavioral problems have been documented in infants born to substance-abusing mothers (1). Frequently, these infants are also ex-posed to lack of prenatal care, poor nutrition, and infectious agents. Thrombocytosis in infants with intrauterine exposure to illicit drugs has been re-ported in the literature (2). Most reports associate thrombocytosis to methadone exposure. Thrombo-cytosis is reported to present in the first two weeks of life, but few reports address its duration and tim-ing of resolution. The purpose of this study was to obtain further information on the effects of illicit drugs on newborns along with the natural history of thrombocytosis in this group of patients.
MATERIALS AND METHODS
Medical records of newborns with intrau-terine exposure to illicit drugs, admitted to the San Juan City Hospital during the period of 1999 to 2001 were reviewed. Data gathered included sex, birth weight, and gestational age. Serum platelet counts throughout hospitalization were recorded. Presence of thrombocytosis, duration, and com-plications were recorded. Thrombocytosis was defined as platelet levels higher than or equal to 450,000 x 103/ul for term infants and higher than or equal to 600,000 x 103/ul for preterm infants3. Exclusion criteria included medical conditions as-sociated to thrombocytosis such as infections or inflammation, Down syndrome, congenital adre-nal hyperplasia, and exposure to cephalosporins (3, 4). The study was approved by the Institutional Review Board.
RESULTS
Thirty-one newborns met inclusion crite-ria. Mean gestational age was 36 weeks and mean birth weight 2600 grams. Forty-eight percent (48%) of the newborns were males (17 males, 14 females) and 87% presented positive urine toxicol-ogy.
Eighty-seven percent (87%) of all infants presented drug withdrawal syndrome and all of these infants were treated with paregoric, pheno-barbital or both. Twelve percent (12%) of the term infants were products of mothers that used more than one illicit drug during pregnancy, in compari-son with 54% of the preterm infants (p= 0.0127). The most frequent illicit drug used by mothers was cocaine (40%) followed by multiple drugs (30%), methadone (13.3%), heroin (13.3%), and marihua-na (3.3%).
Ninety-six percent (96%) of patients admit-ted due to drug withdrawal syndrome presented thrombocytosis. Median platelet count in infants with thrombocytosis was 693,000 x 103/ul (range 456,000 x 103 /ul to 1,343,000 x 103/ul).
18 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 19
Increased in platelet count presented ini-tially at ten days of life (range 1-35 days) with a median resolution at 26 days (range 24-49 days). All infants exposed to methadone presented thrombocytosis and 75% of infants exposed to heroin and cocaine. No thrombocytosis was seen in infants exposed to marihuana. Term babies were more likely to present thrombocytosis (88% vs. 57%, p=0.049). Only 4 patients (12.9%) received treatment with aspirin when the platelet count ex-ceeded over 900,000 x 103/ul. None of the babies presented complications associated to the increase in platelet count.
DISCUSSION In neonates, thrombocytosis is defined as an elevated platelet count above 450,000 x 103/ul for term newborns and above 600,000 x 103/ul for preterms (3). The causes of elevated platelet count range from physiologic to vitamin deficien-cies, being the most described cause, “reactive”, from infections or inflammatory processes (5, 6). The mechanism that regulates platelet count in the preterm infant is unknown. It is suggested that the thrombocytosis noted in preterm infants during the first months of life might result from the sizable expansion of blood volume that accompanies rapid weight gain (4).
Platelets originate from megakaryocytes, which form proplatelets in the bone marrow and the lung; this occurs by two megakaryocyte progeni-tors that determine the number of megakaryocytes: the burst-forming unit- megakaryocyte (BFU-MK), which is the more differentiated progenitor, and the colony-forming unit- megakaryocyte (CFU-MK), which is the more differentiated progenitor (3). In the neonate there is increased number of meg-akaryocytes circulating but they are smaller in size in comparison to adult megakaryocytes. It is de-scribed that because larger megakaryocytes gener-ate more platelets than do smaller megakaryocytes, the megakaryocyte of the neonate produces fewer platelets. These megakaryocytes produce small buds called proplatelets, which are then released as platelets.
We observed the presence of significant thrombocytosis seen in babies admitted to our neo-natal service due to exposure to illicit drugs. Upon reviewing medical strategies of intervention with these newborns, we did not find standard protocols for identification and management of thrombo-cytosis in this group of patients. The impact and possible short and long-term consequences of this hematological signs is not well understood. These neonates are not always admitted and studied due to the lack of clinical symptoms associated to the thrombocytosis. In some cases, the babies of illicit drug using mothers are not identified due to the ab-sence of withdrawal signs and the denial of drug use by the mother.
Vol.: 100 - Núm 2 - Abril - Junio 2008
Burstein et al (2) recognized this distur-bance of the hematological system and the compli-cations associated with it in newborns exposed to illicit drugs. He also reported an increase in plate-let-aggregating activity. The complications most commonly reported associated to thrombocytosis include: focal cerebral infarcts, subarachnoid and germinal plate hemorrhages, and consequently neurological degenerations. Nevertheless, even a marked degree of thrombocytosis is rarely associ-ated to complications and nonspecific treatment is usually necessary (5). Most authors do not recom-mend treatment with aggregation inhibitors unless additional risk factors exist such as cyanotic heart disease or immobilization (6).
Newborns with intrauterine drug expo-sure may require pharmacological treatment and the possible effects of these medications should be considered in the analysis of hematological derangements of these newborns. Phenobarbital presents physiologic complications such as meg-aloblastic anemia and hepatic toxicity. Paregoric may cause a decrease in white blood cells and platelets. None of these medications is associated to thrombocytosis.
In this group of newborns, thrombocytosis was associated to intrauterine exposure to metha-done, heroin, and cocaine. Thrombocytosis was seen in 100% of newborns exposed to methadone and in 75% of infants exposed to cocaine and hero-in. No thrombocytosis was seen in infants exposed to marihuana.
Evaluation of the pathogenesis of throm-bocytosis in newborns with intrauterine drug ex-posure is beyond the scope of this study. Increased platelet production mediated by thrombopoietin, redistribution within the circulation, and prolonged platelet survival, have been proposed as possible mechanisms (2). The present analysis provides useful descriptive data to understand the occur-rence and duration of thrombocytosis in these in-fants, which is might represent the first step to de-fine the molecular and biochemical derangements that occur in any mechanism of disease.
REFERENCES1. Bell G, Lau K. Perinatal and neonatal issues of sub-stance abuse. Pediatr Clin North Am 1995;42(2):261-281.
2. Burstein Y, Giardina PJ, Rausen AR, Kandall SR, et al. Thrombocytosis and increased circulating platelets aggregates in newborn infants of polydrug users. J Pediatr 1979;94(6):895-899.
3. Christensen R. Hematologic Problems of the Ne-onate. Philadelphia: WB Saunders; 2000. p. 43-50, 273-281.
4. Sirota L, Bessler H, Weissman Z, Dulitzky F, Djal-detti M. Thrombopoietic activity in preterm newborns and infants. Arch Dis Child 1986;61(6):585-588

Vol.: 100 - Núm 2 - Abril - Junio 2008
5. Chan KW, Kaikov Y, Wadsworth LD. Throm-bocytosis in childhood: A survey of 94 patients. Pediatrics 1989;84(6):1064-1067.
6. Sutor AH. Thrombocytosis in childhood. Semin Thromb Hemost 1995;21(3):330-339.
RESUMENTrombocitosis en infantes expuestos a drogas il-ícitas en útero se ha asociado a exposición a meta-dona aunque son pocos los estudios que evalúan su duración y resolución. Este estudio evaluó la pres-encia, duración y complicaciones de la tromboci-tosis en neonatos expuestos a drogas ilícitas. Mé-todos: Se llevó a cabo una revisión de expedientes médicos de neonatos expuestos a drogas admitidos al Hospital Municipal de San Juan desde 1999-2001. Resultados: Se incluyeron 31 neonatos de los cuales 87% presentaron síndrome de abstinen-cia. De estos, 96% presentaron trombocitosis. To-dos los infantes expuestos a metadona presentaron trombocitosis y 75% de los expuestos a heroína y cocaína. La trombocitosis se presentó a los 10 días con una resolución de 26 días. Conclusiones: En este grupo de neonatos, la trombocitosis se asoció a exposición intrauterina a metadona, heroína y cocaína. La trombocitosis se presentó a los 10 días resolviendo a las 3-4 semanas sin complicaciones.
Jornadas CientíficasClínicas Multifásicas
Conferencias culturalesSeries de Cine
Conciertos
ASOCIACIÓN MÉDICA DEPUERTO RICO
Manténgase informado de las actividadesconsultando la sección Eventos
de nuestro web sitewww.asociacionmedicapr.org
Av. Fernández Juncos 1305 - Santurce - Tel.: (787) 721-6969
20 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 21
MANEJO DE LACTANCIA Y AMAMANTAMIENTO: ROL DEL MEDICO RESIDENTE
Por: Nerian Ortiz Matos MD *, Lourdes García Fragoso MD **
Vol.: 100 - Núm 2 - Abril - Junio 2008
* Departamento de Pediatría, Escuela de Medicina, Universidad de Puerto Rico. ** Sección de Neonatología, Departamento de Pediatría, Escuela de Medicina, Universidad de Puerto Rico. Apoyo: Oficina para el Desarrollo de Destrezas Clínicas y el Programa de Pediatría de Comunidad (HRSA Grant D58HP00413)
Este trabajo ha sido presentado en los siguientes foros: 1. II Congreso Iberoamericano de Neonatología en Porlamar, Venezuela, 30 de junio de 2005. 2. Reunión Asociación Americana de Escuelas de Medicina (AAMC) – Abril 2005. 3. Foro Investigación Recinto de Ciencias Médicas – Marzo 2005. 4. Reunión anual Academia Americana de Pediatria – Octubre 2005.
Correspondencia a: Nerian Ortiz MD, Escuela de Medicina, Universidad de Puerto Rico, Departamento de Pediatría, PO Box 365067 San Juan, PR 00936-5067. Tel. 787-756-4020, Fax 787-777-3227, <[email protected]> ó <[email protected]>
RESUMEN Los médicos están en posición ideal para influenciar la decisión de una mujer sobre la lactancia. Estudios demuestran que los residentes reconocen su rol en promover y apoyar la lactan-cia, pero tienen deficiencias de conocimiento y di-ficultad en aconsejar a madres con problemas de lactancia. El objetivo de este estudio es evaluar la necesidad de un currículo formal sobre lactancia para residentes de Pediatría. Métodos: Participar-on 12 residentes en su primer año de entrenami-ento. Cinco de ellos (casos) recibieron sesiones educativas sobre lactancia. Se le administró una pre-prueba, post-prueba y un examen clínico ob-jetivo estructurado. Resultados: Los participantes de la intervención tuvieron mejor rendimiento en las pruebas administradas y demostraron mejoría en conocimiento sobre manejo de lactancia. Con-clusión: Este estudio demuestra la necesidad de mejorar el conocimiento de los residentes sobre el manejo de la lactancia y su confianza al edu-car a las madres lactantes. Recomendamos la inte-gración de un currículo estructurado de lactancia durante la residencia.
Palabras índices: lactancia, amamantamiento, medico residente
INTRODUCCION La Academia Americana de Pediatría identifica la lactancia como el método ideal de ali-mentación para el infante llevándolo a obtener un crecimiento y desarrollo óptimos (1).
Existen muchos factores que influyen en la decisión de una madre para iniciar y continuar el amamantamiento. Los profesionales de la salud deben estar entrenados para llevar a cabo una pro-moción y manejo adecuado de la lactancia tanto en las unidades de recién nacidos saludables como en las unidades de cuidado crítico.
Los médicos están en una posición ideal para influ-enciar la decisión de una mujer sobre la lactancia ya que ellas los visitan en momentos claves y deci-sivos de la vida del niño.
Estudios han demostrado que los residentes reconocen la importancia de su rol en promover la lactancia y dar apoyo a las madres pero tienen deficiencias de conocimiento y reportan dificultad en aconsejar a madres que presentan problemas con el proceso de lactancia y amamantamiento. Se recomienda el desarrollo de entrenamiento formal en lactancia y amamantamiento en las escuelas de medicina, programas de residencia y a pediatras en la comunidad (1).
El objetivo de este estudio es evaluar la necesidad de un currículo formal y estructurado sobre mane-jo de lactancia y amamantamiento para médicos residentes de Pediatría.
MATERIALES Y METODOS
Doce residentes de primer nivel del Pro-grama de Adiestramiento en Pediatría de la Escue-la de Medicina de la Universidad de Puerto Rico participaron en el estudio. Los residentes llevan a cabo su entrenamiento en el Hospital Pediátrico Universitario y en la Unidad de Recién Nacidos del Hospital Universitario de Adultos. Ambos hos-pitales son instituciones afiliadas a la Escuela de Medicina de la Universidad de Puerto Rico. Estos hospitales sirven mayormente a una población de escasos recursos económicos. Las embarazadas de alto riesgo son referidas para recibir servicios ob-stétricos en el Hospital Universitario de Adultos.
Cinco de los residentes, asignados al azar (casos), recibieron sesiones educativas so-bre manejo de lactancia y amamantamiento en un período de tres meses incluyendo charlas, videos, demostraciones y representación de roles. Los te-mas discutidos se desglosan en la Tabla 1. A todos los participantes se les administró una pre-prueba,
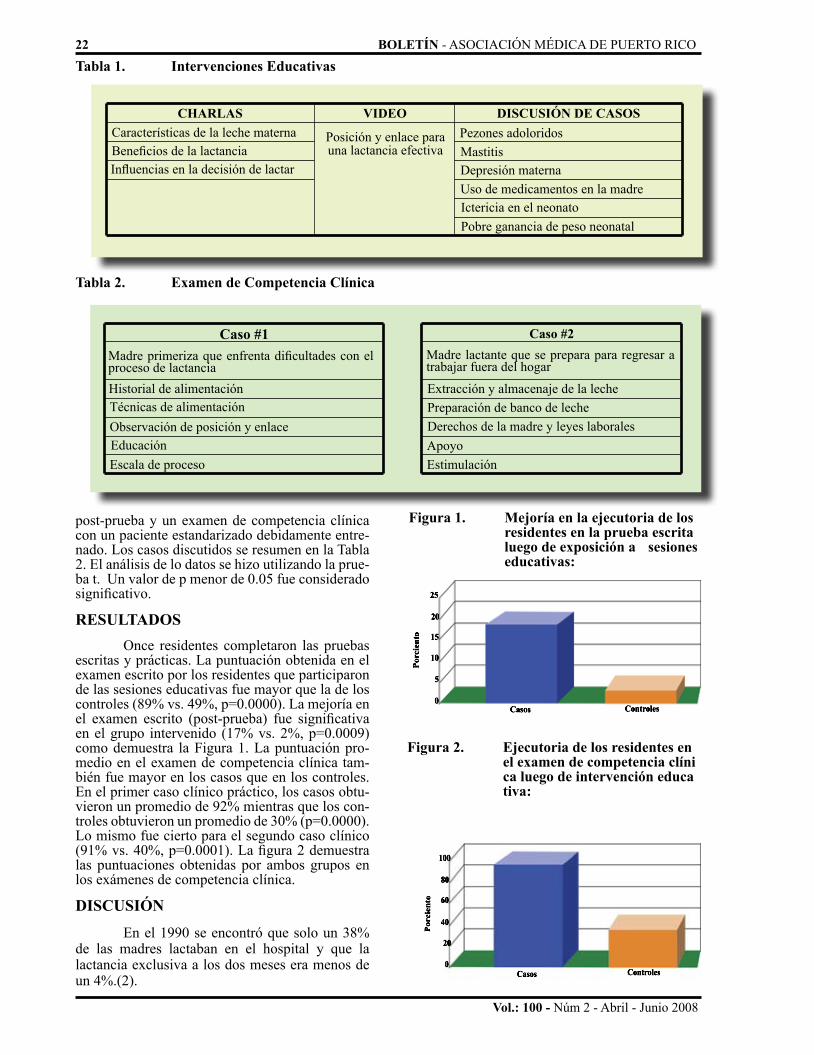
Tabla 1. Intervenciones Educativas
CHARLAS VIDEO DISCUSIÓN DE CASOSCaracterísticas de la leche maternaBeneficios de la lactanciaInfluencias en la decisión de lactar
Posición y enlace para una lactancia efectiva
Pezones adoloridosMastitisDepresión maternaUso de medicamentos en la madreIctericia en el neonatoPobre ganancia de peso neonatal
Tabla 2. Examen de Competencia Clínica
Caso #1 Caso #2Madre primeriza que enfrenta dificultades con el proceso de lactanciaHistorial de alimentaciónTécnicas de alimentaciónObservación de posición y enlaceEducación Escala de proceso
Madre lactante que se prepara para regresar a trabajar fuera del hogar
Extracción y almacenaje de la lechePreparación de banco de lecheDerechos de la madre y leyes laboralesApoyo Estimulación
Porc
ient
o
25
20
15
10
5
0Casos Controles
Figura 1. Mejoría en la ejecutoria de los residentes en la prueba escrita luego de exposición a sesiones educativas:
Por
cien
to
100
80
60
40
20
0Casos Controles
Figura 2. Ejecutoria de los residentes en el examen de competencia clíni ca luego de intervención educa tiva:
post-prueba y un examen de competencia clínica con un paciente estandarizado debidamente entre-nado. Los casos discutidos se resumen en la Tabla 2. El análisis de lo datos se hizo utilizando la prue-ba t. Un valor de p menor de 0.05 fue considerado significativo.
RESULTADOS Once residentes completaron las pruebas escritas y prácticas. La puntuación obtenida en el examen escrito por los residentes que participaron de las sesiones educativas fue mayor que la de los controles (89% vs. 49%, p=0.0000). La mejoría en el examen escrito (post-prueba) fue significativa en el grupo intervenido (17% vs. 2%, p=0.0009) como demuestra la Figura 1. La puntuación pro-medio en el examen de competencia clínica tam-bién fue mayor en los casos que en los controles. En el primer caso clínico práctico, los casos obtu-vieron un promedio de 92% mientras que los con-troles obtuvieron un promedio de 30% (p=0.0000). Lo mismo fue cierto para el segundo caso clínico (91% vs. 40%, p=0.0001). La figura 2 demuestra las puntuaciones obtenidas por ambos grupos en los exámenes de competencia clínica.
DISCUSIÓN
En el 1990 se encontró que solo un 38% de las madres lactaban en el hospital y que la lactancia exclusiva a los dos meses era menos de un 4%.(2).
22 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 23
Vol.: 100 - Núm 2 - Abril - Junio 2008
ABSTRACT Doctors are in an ideal position to influ-ence a woman’s decision about breastfeeding. Studies have shown that residents recognize the importance of their role in promoting and support-ing breastfeeding, but they have knowledge defi-cits and difficulty in advising mothers with lacta-tion problems. The objective of this study is to assess the need of a formal, structured curriculum on breastfeeding for Pediatrics residents. Methods: Participants included twelve residents in their first year of training. Five of them (cases) received edu-cational sessions on breastfeeding. Pre-test, post-test, and an objective struc-tured clinical examination (OSCE) were given to all participants. Results: Residents who par-ticipated in the educational intervention did better than controls in the practical and written tests, and showed improvement in their knowledge about breastfeeding management. Conclusion: This study has shown the need to improve residents’ knowl-edge in breastfeeding management, practices, and confidence when educating breastfeeding mothers. A structured breastfeeding curriculum during the residency is recommended.
Luego de una década, se ha encontrado que el número de madres que lactan ha ido aumentando paulatinamente, no así el número de madres que lacta exclusivamente, pues éste se ha mantenido constante. En Puerto Rico han sido varios los es-fuerzos realizados para promover la lactancia. En el 1995 el Departamento de Salud de Puerto Rico desarrolló una política pública dirigida a promover la lactancia (3). El capítulo de Puerto Rico de la Academia Americana de Pediatría ha trabajado para proteger las prácticas de lactancia y amaman-tamiento (4). Un estudio realizado en el 2000 dem-ostró que solo 62% de las madres lactaba a su bebé al momento de ser dada de alta (5). Meaux reportó la falta de conocimiento en tópicos relacionados a lactancia y muy poca experiencia en el manejo de lactancia entre pediatras en Puerto Rico (6). Re-portes más recientes han demostrado que los médi-cos se encuentran en una posición idónea para me-jorar el número de madres que amamantan. Freed y colegas encontraron que los médicos reconocen la importancia de que se involucren en el proceso de promoción de lactancia pero solo la mitad se clasificó como eficiente en la consejería a las pa-cientes (7). Residentes de Pediatría han reportado que reciben muy poca educación en lactancia, es-pecialmente por medio de técnicas interactivas de enseñanza como representación de roles o interac-ción directa con pacientes en pleno proceso de
amamantamiento y lactancia (6).
En este estudio piloto los residentes de Pediatría demostraron claramente la falta de conocimiento en aspectos relacionados a lactancia y amaman-tamiento. Sin embargo se evidencia la mejoría en la ejecutoria luego de ser expuestos a sesiones educativas formales y estructuradas tanto de tipo pasivas como activas. En las mismas se enfatizan conceptos básicos del manejo de lactancia y ama-mantamiento incluyendo consejería y apoyo a las madres.
La política de lactancia de la Academia Americana de Pediatría hace un llamado a estruc-turar el desarrollo de entrenamiento formal en te-mas de lactancia y amamantamiento en escuelas de medicina, programas de adiestramiento y a pediat-ras en la comunidad (1). Este estudio piloto dem-uestra la necesidad de integrar educación formal de lactancia en el currículo de Pediatría general del programa de adiestramiento. De esta manera se logrará que nuestros residentes de Pediatría, al momento de terminar su entrenamiento, se sientan cómodos promoviendo y apoyando la lactancia ha-biendo recibido educación formal con las herrami-entas necesarias. Así se contribuirá no solo al logro de los objetivos de salud 2010, los cuales tienen como meta que el 75% de las madres lacten en el periodo posparto inmediato y un 50% mantenga la lactancia a los 6 meses de edad, sino también a
la recomendación de la Academia Americana de Pediatría de que todo infante sea lactado exclusi-vamente hasta los seis meses de edad y hasta al año de vida según lo decidan madre e infante
REFERENCIAS1. American Academy of Pediatrics: Breastfeeding and the use of human milk, Pediatrics 2005; 115(2) 496-506.
2. Becerra JE, Smith JC: Breastfeeding patterns in Puerto Rico, Am J Public Health 1990; 80(6): 694-697.
3. Política Pública del Departamento de Salud de Puerto Rico para la Promoción de la Lactancia Materna. 1995. Accessed on 7/18/2003 at www.prlacta.org.
4. Piovannetti Y: Puerto Rico chapter breastfeeding activities, Breastfeeding 2001; 3(1): 15.
5. Parrilla AM, Gorrin JJ: Breastfeeding in Puerto Rico: traditional patterns, national trends and future strate-gies, PR Health Sciences Journal1999; 18(3): 223-228.
6. Meaux L, Davila RR, Aviles J, Parrilla AM: Gyne-cologists-obstetricians and pediatricians: knowledge and ex-perience concerning breastfeeding, PR Health Sciences Jour-nal 1999; 18(3): 251-256.
7. Freed GL, Clark SJ, Lohr JA, Sorenson JR: Pedia-trician involvement in breastfeeding promotion: A national study of residents and practitioners, Pediatrics 1995; 96(3): 490-494.

Vol.: 100 - Núm 2 - Abril - Junio 2008
GENITOANAL FINDINGS IN PUERTO RICAN CHILDREN WITH SUSPECTED SEXUAL ABUSEBy: Amaris Rivas Carlo MD *, Brenda Mirabal MD, MPH *
* From the Department of Pediatrics, U.P.R. School of Medicine, San Juan, Puerto Rico.
Address reprints to: Brenda Mirabal MD, Department of Pediatrics, UPR School of Medicine, PR Health Science Center, San, Juan, PR 00936.
ABSTRACTBackground: Even though the child sexual abuse literature has described and classified the most common genitoanal findings in children evaluated for suspected sexual abuse, there is scarce infor-mation about abused Puerto Rican children. The purpose of this study was to describe the most common genitoanal findings in children referred to the Bio-psychosocial Program for evaluation of suspected sexual abuse between 2003 and 2007.
Methods: A record review of 55 patients was conducted to collect data on genitoanal findings, socio-demographic characteristics and other vari-ables related to the abuse.
Results: Most patients (56.4 %) were between 3-8 years of age. The father was the most com-mon alleged aggressor (25.5%). One third reported anal penetration (34.5%). Most patients (65.5%) had a normal genitoanal exam. A total of 27.3 % had genitoanal findings diagnostic of abuse. The most prevalent risk factors were domestic violence (36.4%) and illicit drug abuse (30.9%).
Conclusion: There was a higher prevalence of di-agnostic findings (27.3%), including anal injuries (14.5%) compared to other studies. Since most children had a normal genitoanal exam, the child’s disclosure is the most important evidence of sex-ual abuse.
Index words: genitoanal, sexual, abuse, children Child sexual abuse is a serious public health problem. Over 78,000 children were esti-mated to be victims of sexual abuse in 2006 in the United States (1). In Puerto Rico, 46,444 children were reported as active cases of child abuse in 2007; of these, 2031 were cases of sexual abuse (2).
Sexual abuse occurs when a child is en-gaged in sexual activities that he or she cannot comprehend, for which he or she is developmen-tally unprepared and cannot give consent, and/or that violate the law or social taboos of society (3). The pediatrician is likely to encounter patients with signs and symptoms suggestive of sexual abuse in his/her practice.
He/she may be the first professional to learn about the situation and be responsible for activating the child protection system. As a mandated reporter (PR Law 177 of 2003) he/she is expected to con-duct a history, physical exam, document the find-ings and report the case to the appropriate authori-ties for investigation and child protection services (4). The pediatrician plays an essential role in the diagnosis and treatment of sexually transmitted diseases, and other physical and mental conditions associated to the situation of sexual abuse. Pediat-ric residencies recognized the need for curriculum changes, and education about child abuse became compulsory for US pediatric residencies in 1997 (3). The evaluation of suspected victims of child sexual abuse, however, often involves detailed in-terviews, collection of forensic evidence, special-ized examination techniques, including colposco-py, and many pediatricians do not feel prepared to conduct such comprehensive medical evaluations. They may prefer to refer these children to physi-cians who have the training and experience.
During the last twenty years, the child sexual abuse literature has contributed to the wealth of knowledge of normal genitoanal findings in children, changes observed with normal devel-opment, normal variants, and changes due to acute and chronic blunt force penetrating trauma (5, 6, 7, 8, 9). In a study by Berenson (5), to describe geni-toanal findings associated with child sexual abuse, positive findings were found in 2.5% of the study population; a hymenal transection, perforation, or a deep notch were found to be definite evidence of sexual abuse or trauma. In a five year prospec-tive study, Heger (6) evaluated 2,384 children with suspected sexual abuse and found that 96.3% had normal medical examinations.
The positive findings described in this study were acute injuries, sexually transmitted diseases, and complete hymenal transections; only 0.04% of patients showed diagnostic anal findings. In a previous study conducted by Adams, (7) to de-scribe examination findings of legally confirmed child sexual abuse, 10% of children were described with diagnostic genital findings, and only 1% pre-sented diagnostic anal findings.
24 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 25
Vol.: 100 - Núm 2 - Abril - Junio 2008
The purpose of this study was to describe genitoanal findings in children who had been re-ferred for suspected child sexual abuse to the Bio-psychosocial Program, of the Department of Pediatrics, U.P.R. School of Medicine in the last five years. The Program, a sub-grantee of the De-partment of Justice’s Victims of Crime funds since 1986, offers interdisciplinary services to child vic-tims of family violence, 0 -17 years old, including social evaluations, abuse-focused psychotherapy, parenting groups and forensic medical exams. The interdisciplinary team also conducts case discus-sions, offers expert testimony and provides emo-tional support to the child victim during the legal process. Cases are referred from the entire island by child protection services, law enforcement, schools, courts, hospital staff and health profes-sionals.
METHODS AND MATERIALS This is a descriptive, retrospective study of children 0 to 17 years of age evaluated for sus-pected sexual abuse at the Bio-psychosocial Pro-gram of the UPR School of Medicine, from 2003 to 2007. A total of three hundred seventeen chil-dren were seen for suspected child sexual abuse during this five year period; systematic randomi-zation was used to select a sample of fifty five pa-tients for chart review. The UPR Medical Sciences Campus Institutional Review Board approved the study. The variables studied were: socio-demo-graphic characteristics, age of the child, type of sexual contact reported, relationship to alleged perpetrator and the genitoanal findings of each pa-tient in the colposcopic exam. The program Statis-tix 8 was used to conduct statistical analyses, such as frequency distributions and chi squares.
RESULTSOur study sample included 33 females and 22 males; 56.4% were in the range of 3-8 years of age, with a mean of 6.3 years. The alleged aggres-sor was a family member in 68.7% of the cases; the father was the most common (25.5%); anoth-er male family member was identified in 43.2% (grandfather, brother or other). No penetration was reported in 16.4%, vaginal penetration (digital or penile) was disclosed in 23.6%, anal penetration (digital or penile) in 34.5%, and oral penetration in 12.7%. Some patients referred more than one type of abuse. In 30.9% of the cases, the type of con-tact was unknown, because the patient did not dis-close, was too young to disclose or abuse was not confirmed (one case). The most prevalent risk fac-tor for child sexual abuse was domestic violence (36.4%), followed by illicit drug abuse (30.9%), (See Table 1).
Most patients (65.5%) had a normal genitoanal exam (See Figure 1). A total of fifteen patients (27.3%) had diagnostic genitoanal findings, which included: healing laceration in the fossa
Figure 1. Genitoanal Findings*
7.30%
27%
65%
Normal Indeterminate Diagnostic
* See classification in Adams JA, Kaplan RA, Starling SP, Me-hta NH, Finkel MA, Botash AS, Kellogg ND, et al. Guide-lines for medical care of children who may have been sexually abused. J Pediatr Adolesc Gynecol. 2007 Jun; 20(3):163-72.
Table 1. Sociodemographic Data of Patients
Total patients: 55
Gender (%)Females Males
60 40Age (%)
0-2 y/o3-8 y/o9/12 y/o≥ 13 y/o
10.956.418.214.5
Aggressor (%)
FatherMale relative
25.5
43.2Type of abuse (%)
No penetrationVaginal penetration
Anal penetrationOral penetration
UnknownRisk factors (%)
Domestic violence
Drug abuse
16.423.634.512.730.9
36.4
30.9
navicularis (16.4%), healing anal laceration (14.5%), partial healing hymenal laceration (3.6%), loss/attenuation of hymen (1.8%). An interesting finding observed in our study was one male patient with penile/scrotal scar. Some patients had more than one diagnostic finding. There were a total of five indeterminate findings in four patients (7.3%): a notch at 9 o’clock, condyloma acuminata in hy-men and fossa navicularis, and two patients with a small ulcer in the anus (Table 2).

Vol.: 100 - Núm 2 - Abril - Junio 2008
In order to identify factors that might help the clinician to predict the likelihood of finding an abnormality in the physical examination, we ana-lyzed a group of variables, including the age of the victim, time since last contact with alleged aggres-sor, and if the child referred vaginal or anal pen-etration. None of the variables studied correlated with findings in the physical examination (Table 3).
There was a higher prevalence of diag-nostic genitoanal findings in this study (27.3%), including anal area (14.5%), when compared to other studies (5-7). Heger described 4% of pa-tients with diagnostic findings, 1 patient (0.04%) presented anal findings (5). In the study by Adams (7), 9% of patients presented with these, and only 1% of anal findings. Berenson (6), described 2% of patients with diagnostic findings; anal findings were not assessed in that study (See Table 4).
DISCUSSION Even though the majority of the children in this study had a normal genitoanal exam, there was a higher prevalence of diagnostic findings (27.3%), compared to other studies (5-7) which report nor-mal findings in more than 95% of children evalu-ated for suspected sexual abuse. This unexpect-edly high prevalence may be related to the small sample size. Eight patients (14.5%) had diagnostic anal findings, which contrasts with 1% of subjects reported by other studies. In this study population, the most common abuse reported (30.9%) was pe-nile anal penetration, contrary to what is reported in the literature and in the local statistics, where fondling and lascivious acts is more prevalent.
The small sample size, delayed reporting, and/or the complex nature of the cases being referred to the Program for expert medical forensic evaluation may have contributed to this finding. One third of these families were involved in illicit drug use, which may place the child at higher risk for more severe abuse.
Cultural practices, beliefs and myths may also help to explain this unexpectedly high rate of anal pen-etration. The myth of defining virginity as an “in-tact” hymen is still common among some Puerto Ricans and other Latinos. The belief that penetra-tion of “other” body orifices may go undetected, may also be a contributing factor. Further studies are recommended, with larger study samples, to determine the prevalence of genitoanal findings, and describe current sexual practices and myths in the Puerto Rican community.
We recognize that our results could be limited by the small sample size, and that study subjects are not representative of all reported sexual abuse cas-es in the island. However, the striking differences observed from previous studies suggest that cul-tural practices and beliefs may have an effect
Table 2. Abnormal findings/injuries on genito anal exam*
Findings (N (%))
IndeterminateDiagnostic*
HymenFossa
Navicularis/ P.Fourchette
Penis/ Scro-tum
Anus
2 (40)3 (14.3)
1 (20)
9 (42.8)
0
1 (4.8)
2 (40)
8 (38.1)
* See classification in Adams JA, Kaplan RA, Starling SP, Me-hta NH, Finkel MA, Botash AS, Kellogg ND, et al. Guide-lines for medical care of children who may have been sexually abused. J Pediatr Adolesc Gynecol. 2007 Jun; 20(3):163-72.
Table 3. Odds ratio and confidence interval of variables analyzed by diagnostic findings.
VariableHistory and Type of Penetration
Time since last contact
Age of patient
Vaginal penetra-tion alone
Anal penetra-tion alone
Odds Ratio 95% CI p value
0.1504, 5.36190.90
1.86
0.90
2
1.04
0.4305, 8.0118
0.1447, 1.6576
0.5322, 7.5162
0.2943, 3.665
NS
NS
NS
NS
NS
Table 4. Comparison of findings in children referred for suspected sexual abuse
Investigator Publication
year
Adams 1994
Berenson 2000
Heger 2002
Rivas 2008
NFemale: Male
236215 : 21
192192 : 0
23841963: 421
5533 : 22
Age (years)Findings (%):NormalIndeterminateDiagnostic:GenitalAnal
< 17 < 8 < 17 ≤ 17
90% 97.5 % 96.3% 65.5%7.3%
9% 2% 4% 12.7%1% Not assessed 0.04% 14.5%
on the prevalence of diagnostic findings in this population. Furthermore, most acute sexual abuse is seen at the hospital’s 24-hour Emergency Room, which explains the low prevalence of acute inju-ries in this study.
26 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 27
Vol.: 100 - Núm 2 - Abril - Junio 2008
RESUMENTrasfondo: Aunque la literatura acerca del abuso sexual en niños ha descrito y clasificado los hallaz-gos genito-anales más comunes en niños evaluados por sospecha de abuso sexual, existe escasa infor-mación acerca de estos hallazgos en niños puertor-riqueños. El propósito de este estudio fue describir los hallazgos genito-anales más comunes en niños referidos al Programa de Bio-sicosocial para eval-uación por sospecha de abuso sexual, desde los años 2003-2007.
Métodos: Se llevó a cabo una revisión de expe-dientes de 55 pacientes para recolectar datos so-bre hallazgos genito-anales, características socio-demográficas y otras variables relacionadas al abuso.
Resultados: La mayoría de los pacientes (56.4%) se encontraban entre las edades de 3-8 años. El alegado agresor fue el padre en la mayoría de los casos (25.5%). Un tercio de los pacientes refirió penetración anal (34.5%). La mayoría de los pa-cientes (65.5%) tuvo un examen genitoanal nor-mal. Un total de 27.3% presentó hallazgos genito-anales diagnósticos de abuso sexual. Los factores de riesgo más prevalentes fueron violencia domés-tica (36.4%) y abuso de drogas ilícitas (30.9%).
Conclusión: Se encontró una mayor prevalencia de hallazgos diagnósticos (27.3%), incluyendo hallazgos anales (14.5%), comparado con otros es-tudios. Dado que la mayoría de los niños tuvo un examen genitoanal normal, la revelación del niño es la evidencia más importante de abuso sexual.
Web Site de la Asociación Médica de Puerto Rico
www.asociacionmedicapr.org
Calendario de actividadesPublicaciones on-line
Créditos Educación Médica ContinuadaServicios con PayPal y tarjetas de crédito
Suscripciones on-liney mucho más..
Serigrafíapor
José Alicea
De venta en la Asociación Médicade Puerto Rico(787) 721-6969
José Alicea nació en 1928 en Ponce, Puerto Rico. Entrenado
como pintor, comenzó su actividad como diseñador gráfico en 1957, bajo la tutoría de Lorenzo Homar. En 1967 fue nombrado Profesor de Imprenta y fundó la Escuela Grá-fica del Instituto de Cultura Puerfica del Instituto de Cultura Puer-
torriqueña.
ACKNOWLEDGMENTSWe would like to thank Dr. Lourdes García, of the UPR Depart-ment of Pediatrics, and Noemí Vázquez, María N. De Jesús, Jenni-fer García and Karim Torres, of the Bio-psychosocial Program of the UPR School of Medicine for their collaboration in this study. The Biopsychosocial Program is a subgrantee of VOCA grant # 2007-VA-GX-0054; 2007-VA-HP-01.
Physicians caring for children should make it a priority to screen for signs and symptoms of sexual abuse, particularly if there are family risk factors such as domestic violence and illicit drug use. Socio-demographic variables do not appear to be associated to the presence of diagnostic find-ings. The evaluation, diagnosis and treatment of children with suspected child sexual abuse should document the history, including a detailed account of the alleged incident/s. Since most of these chil-dren have a normal genitoanal exam, the child’s disclosure is often the most important evidence of sexual abuse.
REFERENCES1. U.S. Department of Health and Human Services, Administration on Children, Youth and Families. Child Maltreatment 2006 (Wash-ington, DC: U.S. Government Printing Office, 2008). Obtained :26 April 2008, http://www.acf.hhs.gov/programs/cb/stats_research/in-dex.htm#can
2. Puerto Rico Family Department, Family and Children’s Administra-tion. Active cases with minors, families and minors involved, yearly evolution. Obtained May 5, 2008. http://www.tendenciaspr.com/Pob-lacion/Tablas_familia/maltrato_de_menores/Casos_activos_2005.htm
3. Kellogg N and the Committee on Child Abuse and Neglect. The Evaluation of Sexual Abuse in Children. Pediatrics. 2005; 116: 506-512.
4. Ley Núm. 177 de 1 de agosto de 2003: Ley para el Bienestar y la Protección Integral de la Niñez, deroga La ley Núm. 342 de 1999: Ley para el amparo de Menores en el Siglo XXI. (P. del S. 2285), 2003, ley 177. Obtained May 5, 2008, http://www.lexjuris.com/LEXLEX/Leyes2001/lex2001177.htm
5. Berenson AB; Chacko MR; Weimann CM; Mishaw CO; Friedrich WN; Grady JJ. A case-control study of anatomic changes resulting from sexual abuse. Am J Obstet Gynecol. 2000; 182: 820-834.
6. Heger A; Ticson L; Velasquez O; Bernier R. Children referred for posible sexual abuse: medical findings in 2384 children. Child Abuse and Neglect. 2002; 26: 645-659.
7. Adams JA; Harper K. Examination findings in legally confirmed child sexual abuse: it’s normal to be normal. Pediatrics 1994; 94:310-317.
8. Adams JA, Kaplan RA, Starling SP, Mehta NH, Finkel MA, Botash AS, Kellogg ND, et al. Guidelines for medical care of children who may have been sexually abused. J Pediatr Adolesc Gynecol. 2007 Jun; 20(3):163-72.
9. Berenson A; Grady J. A longitudinal study of hymenal develop-ment from 3 to 9 of years of age. J Pediatr 2002; 140:600-607.

LUPUS NEPHRITIS IN PUERTO RICAN CHILDREN AND ADOLESCENTSBy: Tami O. Tiamfook MD *, Ivonne Arroyo MD **, Enid Del Valle MD €, Juan O. Pérez-Rodríguez MD ₤, Anarda González MD ‡,and Melvin Bonilla-Félix MD ₤
From * Harvard Medical School, Boston, MA, ** San Juan City Hospital, San Juan, PR, € San Jorge Children’s Hospital, San Juan, PR, ₤ Section of Nephrology, Departments of Pediatrics, UPR School of Medicine, San Juan, PR and ‡ Department of Pathology, University of Puerto Rico, San Juan, PR
Address reprints to: Melvin Bonilla-Felix MD, Department of Pediatrics, University of Puerto Rico-Medical Sciences Campus PO 365067San Juan, PR 00936-5067. Tel: 787-777-3535, ext. 7300 Fax: 787-777-3227. <[email protected]>
ABSTRACT Background: Lupus nephritis is associ-ated with an unfavorable outcome. Its incidence is higher in children. It has been the impression of pediatric nephrologists and rheumatologists in Puerto Rico that the clinical manifestations in Puerto Rican children differ from what has been described in other geographic regions. The po-tential deleterious effects of sun exposure could suggest that Puerto Rican children living in the Is-land are at high risk for severe nephritis. Purpose/Method: To describe the manifestations and iden-tify predictors of patient and renal survival, we re-viewed the medical charts of children diagnosed with lupus nephritis in Puerto Rico between 1987 – 2001. Results: Mesangial glomerulonephritis (Type II) was the most common histopathological lesion observed. We observed a high incidence of nephritis among males, with a male: female ratio of 1:1.9. Conclusions: The presence of type IV ne-phritis and need for acute dialysis at presentation were identified as predictors of poor clinical out-come (development of end stage renal disease or death).
Index words: lupus, nephritis, Puerto Rico, chil-dren
Lupus nephritis (LN), the renal involve-ment in systemic lupus erythematosus (SLE), is associated with an unfavorable outcome. Its inci-dence is higher in children (7, 23) and is second only to infection as the most common cause of death (19). Because of the age of the patients at onset of the disease and the duration of the illness, the pediatric population with LN is at high risk for long-term morbidity and mortality.
The World Health Organization has clas-sified lupus renal disease into five categories (3). Class I is rarely reported whereas, class II devel-ops in about 24% of adult patients, class III in 15%, class IV in 43%, and class V in 15% (1). As in adults, most of the studies in children report that the proliferative lesions (classes III and IV) are the most frequently observed (1, 6, 28). However, more recent reports have suggested that this
pattern might be changing, with an increase in class V lupus nephritis among pediatric patients with SLE (9).
The treatment of lupus nephritis is de-pendent on the histopathology. Often, histology can be predicted based on clinical characteristics. For instance, the degree of renal function at time of biopsy has been recognized as an important pre-dictor of histology (8). Thus, it would be important to study certain populations to describe correla-tions between clinical factors and histopathology in order to predict prognosis and target aggressive therapies to those at higher risk.
In addition, differences in ethnicity may play a key role in the clinical expression of the disease (8). Studies in Asians, African-Caribbeans and African-Americans have shown a higher inci-dence of nephritis in these 3 ethnic groups (9). A higher degree of severity in clinical manifestations associated with higher mortality was reported in a group of Hispanic children from New York, com-prised primarily by Puerto Rican and Caribbean children (22). Studies in Latin American patients have shown that class IV (diffuse proliferative glomerulonephritis), which carries the worst prog-nosis for renal survival, is the most common histo-logical lesion observed (15).
It has been the impression of pediatric nephrologists and rheumatologists in Puerto Rico that the clinical and pathological features of LN in Puerto Rican children differ from what has been described in other geographic regions. In addition to ethnicity, the potential deleterious effects of sun exposure, well documented in SLE (25), would suggest that Puerto Rican children living in the Is-land are at high risk for severe nephritis. Studies in adult Puerto Rican patients with SLE contrast with this view (26).
MATERIALS AND METHODSTo identify predictors of patient and renal survival, we studied the clinical, laboratory and histological characteristics of Puerto Rican children with LN.
28 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Vol.: 100 - Núm 2 - Abril - Junio 2008

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 29
Vol.: 100 - Núm 2 - Abril - Junio 2008
The medical charts of 29 children between the ages of 1 - 18 y/o diagnosed with LN between 1987 and 2001 were retrospectively reviewed. The patients were recruited from three different hospi-tals in San Juan, Puerto Rico, including University Pediatric Hospital, San Jorge Children’s Hospital, and San Juan City Hospital. These three hospitals together provide more than 90% of the pediatric tertiary care in Puerto Rico.
The diagnosis of SLE was established based on the clinical presentation, according to the American Rheumatism Association’s revised clas-sification criteria for lupus and/or laboratory eval-uation consistent with SLE, such as the presence of autoantibodies specific for SLE. Patients were diagnosed with LN if there were manifestations in the urinary sediment (red blood cells and/or red blood cell casts in the urine, proteinuria), and/or abnormal renal function as reflected by an elevated serum creatinine level for age or presence of hy-pertension. Hypertension was defined as systolic and/or diastolic blood pressure value over the 95% for age and height, according to the data published by the Update on the 1987 Task Force Report on high blood pressure in children and adolescents (17).
The renal pathologist performed the histo-logical analysis of renal biopsies, based upon the 1982 classification of the World Health Organiza-tion (5). Biopsies with essentially normal glomeruli or with mild mesangial changes were categorized as class I. Patients with mesangial proliferation or increased mesangial matrix were categorized as class II. Class III was categorized as patients with focal and segmental proliferation of mesangial and endothelial cells, class IV as patients with diffuse proliferation, and class V as patients with membra-nous glomerulonephritis.
There were no patients lost to follow-up. Nephrotic syndrome was defined as having pro-teinuria, hypoalbuminemia, edema, and hypercho-lesterolemia. ESRD was defined as the need for chronic dialysis and/or renal transplantation. GFR was calculated based on height and serum creati-nine, according to Schwartz formula (20).
Data from groups of patients are report-ed as mean ± SE or as percentages. Multivariate analysis was used to determine prognostic factors. Statistical analysis was performed using Fisher’s Exact Test.
RESULTSClinical Features
The mean age at diagnosis of SLE was 11.0 + 3.4 years (mean + standard deviation; range, 2.8-16.8 yr), with a mean age at diagnosis of LN of 11.4 + 3.3 years (range, 2.8-16.8). The average time from diagnosis of SLE to diagnosis of LN was 0.4 + 0.7 year (range, 0-2.0).
Thirty four percent of our patients were males, with a male: female ratio of 1:1.9 (Table 1). Rash was the most common extrarenal manifestation observed in our group of children with nephritis (66%). A total of 6 (20.7%) patients presented with acute renal failure, with 5 of them requiring acute dialysis at the time of presentation.
All the patients were treated with corticos-teroids. At the time of data collection, the patients had been receiving corticosteroids for an average of 4.3 + 3.6 years (range, 0.3-14.3). Cyclophos-phamide had been given to 44.8% of patients and azathioprine to 48%. Two patients had been re-ceiving mycophenolate for less than 6 months.
Table 1. Baseline clinical features
CHARACTERISTICS N %
GENDER
Male 10 34.5
Female 19 65.5
CLINICAL
Fever 10 34.5
Rash 19 65.5
Arthritis 13 44.8
Pleuritis 4 13.8
Pericarditis 2 6.9
Need for Acute Dialysis 6 20.7
Hypertension 10 38.5
Table 2. Baseline laboratory features CHARACTERISTICS N %
Hypocomplementemia 18 78.3
Hematuria 24 82.8
Gross Hematuria 13 44.8
Proteinuria 23 79.3
Nephrotic Syndrome 7 28.0
Hypercholesterolemia 12 41.4
Altered CBC 21 72.4
Altered Liver Function Tests 3 10.3
Decreased GFR
(< 80 ml/min/1.73m2) 6 20.7
Laboratory Features
Hematuria was the most common labora-tory finding at the diagnosis of LN (82.8%), with about half of them showing gross hematuria (Table 2).
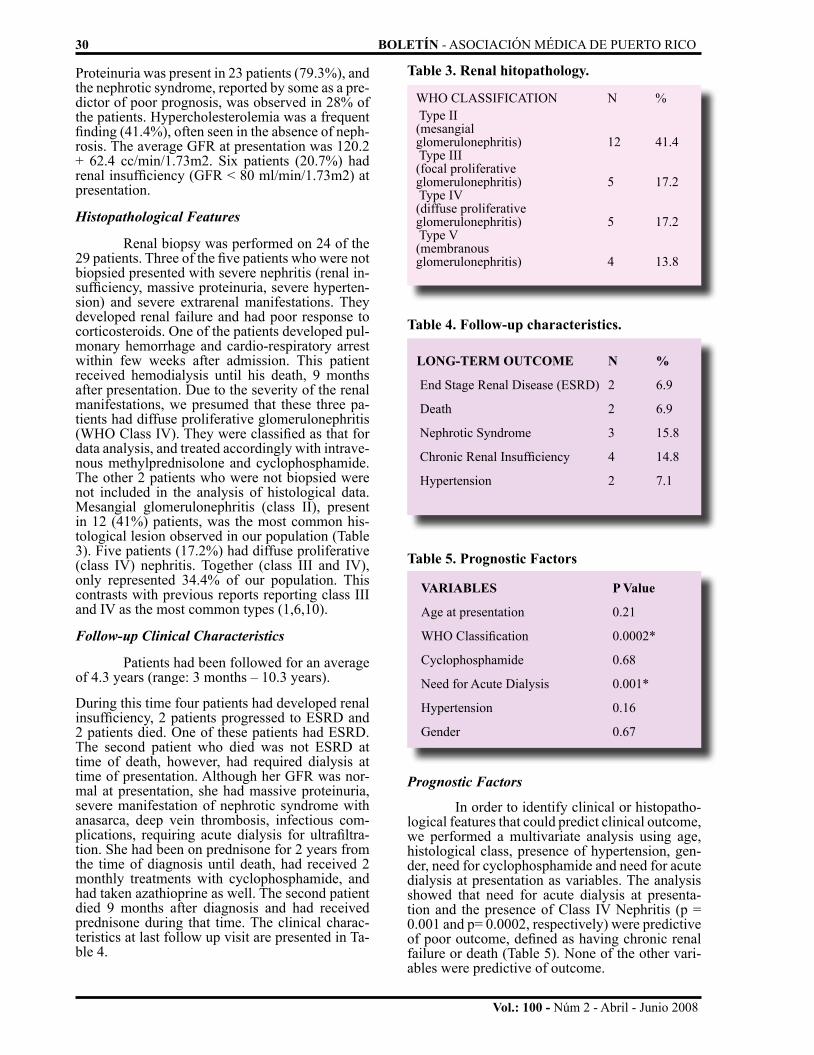
Vol.: 100 - Núm 2 - Abril - Junio 2008
30 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Prognostic Factors
In order to identify clinical or histopatho-logical features that could predict clinical outcome, we performed a multivariate analysis using age, histological class, presence of hypertension, gen-der, need for cyclophosphamide and need for acute dialysis at presentation as variables. The analysis showed that need for acute dialysis at presenta-tion and the presence of Class IV Nephritis (p = 0.001 and p= 0.0002, respectively) were predictive of poor outcome, defined as having chronic renal failure or death (Table 5). None of the other vari-ables were predictive of outcome.
Proteinuria was present in 23 patients (79.3%), and the nephrotic syndrome, reported by some as a pre-dictor of poor prognosis, was observed in 28% of the patients. Hypercholesterolemia was a frequent finding (41.4%), often seen in the absence of neph-rosis. The average GFR at presentation was 120.2 + 62.4 cc/min/1.73m2. Six patients (20.7%) had renal insufficiency (GFR < 80 ml/min/1.73m2) at presentation.
Histopathological Features
Renal biopsy was performed on 24 of the 29 patients. Three of the five patients who were not biopsied presented with severe nephritis (renal in-sufficiency, massive proteinuria, severe hyperten-sion) and severe extrarenal manifestations. They developed renal failure and had poor response to corticosteroids. One of the patients developed pul-monary hemorrhage and cardio-respiratory arrest within few weeks after admission. This patient received hemodialysis until his death, 9 months after presentation. Due to the severity of the renal manifestations, we presumed that these three pa-tients had diffuse proliferative glomerulonephritis (WHO Class IV). They were classified as that for data analysis, and treated accordingly with intrave-nous methylprednisolone and cyclophosphamide. The other 2 patients who were not biopsied were not included in the analysis of histological data. Mesangial glomerulonephritis (class II), present in 12 (41%) patients, was the most common his-tological lesion observed in our population (Table 3). Five patients (17.2%) had diffuse proliferative (class IV) nephritis. Together (class III and IV), only represented 34.4% of our population. This contrasts with previous reports reporting class III and IV as the most common types (1,6,10).
Follow-up Clinical Characteristics
Patients had been followed for an average of 4.3 years (range: 3 months – 10.3 years).
During this time four patients had developed renal insufficiency, 2 patients progressed to ESRD and 2 patients died. One of these patients had ESRD. The second patient who died was not ESRD at time of death, however, had required dialysis at time of presentation. Although her GFR was nor-mal at presentation, she had massive proteinuria, severe manifestation of nephrotic syndrome with anasarca, deep vein thrombosis, infectious com-plications, requiring acute dialysis for ultrafiltra-tion. She had been on prednisone for 2 years from the time of diagnosis until death, had received 2 monthly treatments with cyclophosphamide, and had taken azathioprine as well. The second patient died 9 months after diagnosis and had received prednisone during that time. The clinical charac-teristics at last follow up visit are presented in Ta-ble 4.
Table 3. Renal hitopathology.
WHO CLASSIFICATION N % Type II (mesangialglomerulonephritis) 12 41.4 Type III (focal proliferativeglomerulonephritis) 5 17.2 Type IV (diffuse proliferativeglomerulonephritis) 5 17.2 Type V(membranousglomerulonephritis) 4 13.8
Table 4. Follow-up characteristics.
LONG-TERM OUTCOME N %
End Stage Renal Disease (ESRD) 2 6.9
Death 2 6.9
Nephrotic Syndrome 3 15.8
Chronic Renal Insufficiency 4 14.8
Hypertension 2 7.1
Table 5. Prognostic Factors
VARIABLES P Value
Age at presentation 0.21
WHO Classification 0.0002*
Cyclophosphamide 0.68
Need for Acute Dialysis 0.001*
Hypertension 0.16
Gender 0.67

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 31
Vol.: 100 - Núm 2 - Abril - Junio 2008
typically absence of hypertension or other severe urinary findings (3). The incidence of NS and hy-pertension in our population was not different from the incidence reported in other populations. There-fore, there was not a clear correlation between the histological findings and the initial clinical mani-festations in our patients.
The high incidence of LN among Puerto Rican males is surprising and not previously re-ported for other populations. Males represented thirty five percent of our population with LN, with a male: female ratio of 1:1.9. This is mark-edly elevated when compared with other adult and pediatric populations (18). A report form the North American Pediatric Renal Transplant Cooperative Study describes that 82% of the pediatric patients requiring a kidney transplant for lupus are females (2). A much higher incidence in females, with male: female ratio between 1: 7 to as high as 1: 50 have been reported in adult populations (2,10). Since inheritance seems to play an important role in the pathogenesis of lupus, genetic homogeneity among Puerto Ricans in the Island might have a stronger effect than gender differences (16).
The level of renal function at presentation of LN and the presence of Class IV nephritis are associated with worst prognosis, defined as devel-opment of ESRD or death. This is not a surpris-ing finding. The association of bad prognosis with type IV has been described in children and adults (6, 12-14, 18). The renal function at presentation has been also described as an important prognos-tic factor (6, 14). However, in contrast with other studies in children, we did not find any association between hypertension or complement levels and prognosis (6).
In summary, our study reports important clinical features of LN in Puerto Rican children living in the Island that differ from the classical features describe elsewhere. To our knowledge, the higher frequency of type II nephritis and higher in-cidence in males have never been reported in other populations. The identification of type IV nephritis and need for acute dialysis as predictors of poor clinical outcome indicate that the renal biopsy and degree of renal function at onset serve to identify patients requiring aggressive therapy.
REFERENCES1. Baqi N, Moazami S, Singh A, Ahmad H, Balachandra S, Tejani A. Lupus Nephritis in Children: A longitudinal study of prog-nostic factors and therapy. J Am Soc Nephrol 7: 924-929, 1996.
2. Bartosh SM, Fine RN, Sullivan EK. Outcome after trans-plantation of young patients with systemic lupus erythematosus: a report of the North American pediatric renal transplant cooperative study. Transplantation 72: 973 – 978, 2001.
3. Belmont, Michael. Lupus Nephritis: Treatment Issues. http://cerebel.com/lupus/nephritis.html
4. Bogdanovic R, Nikolic V, Pasic S, Dimitrijevic J, Lipko-vska-Markovic J, Eric-Marinkovic J, Ognjanovic M, Minic A, Stajic
DISCUSSION Our most significant finding is that type II LN (mesangial glomerulonephritis) is the most common histopathological lesion (41.4%) in our group. This contrasts with reports from other stud-ies in children, which report Class IV as the most frequent lesion (4). Tejani had reported several years ago that type IV LN is the most common histological type seen in Hispanic children in New York (22). In addition, the overall prognosis was worst in Hispanic children. Since the population of Hispanic children living in New York is prima-rily comprised by immigrants from the Caribbean (Puerto Rico and Dominican Republic), we were expecting several similarities between Tejani’s data and our population. Nevertheless, the differ-ences observed could be explain by a greater ge-netic homogeneity in Puerto Ricans living in the Island and environmental differences, including weather and sun exposure. In addition, our data represent patients diagnosed after 1990. Tejani’s data was reported in 1983, therefore, patients had been diagnosed in the 1970. Thus, another poten-tial explanation could be a change in histopathol-ogy of LN over time, as reported with other renal diseases (29).
Prior to collecting these data, we had hy-pothesized that since our children live in the tropic under continuous sun exposure, the renal mani-festations of the disease would be more severe in our population. The role of sun exposure has been widely described. In a group of Puerto Ri-can adults with SLE living in the Island Vila et al. reported milder clinical manifestations and lower incidence of LN in patients using photoprotection regularly (25). Although we did not evaluate the use of photoprotection, the finding of milder renal histological lesions in our population, despite con-tinuous sun exposure, at least suggest that living in the tropic is not a risk factor for the presence of type IV nephritis. We cannot explain our findings of milder histological types of LN in our patients based on a referral bias. The hospitals included in the analysis represent the 3 major pediatric tertiary care centers in the Island, which receive the most complex pediatric cases, including the only center with pediatric dialysis services (University Pediat-ric Hospital). Our data is consistent with a report form Vila, who observed that Puerto Rican adults with SLE tend to have milder forms of the disease and lower incidence of LN when compared with other geographical areas (26).
Although type II LN was the predominant histological class observed, clinical manifestations such as hypocomplementemia, hematuria, pro-teinuria, and hematological manifestations were present in the majority (>70%) of our patients. It has been reported that mesangial lupus nephritis is generally accompanied by normal diagnostic find-ings or with a mild degree of hematuria but

Vol.: 100 - Núm 2 - Abril - Junio 2008
32 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Resumen
El desarrollo de nefritis en un paciente con lupus sistémico eritematoso (SLE) se asocia a po-bre pronóstico a largo plazo. Esta complicación se observa con mayor frecuencia en niños que en la población adulta. Por años, los nefrológos y reu-matólogos pediátricos en han tenido la impresión que las manifestaciones de SLE en Puerto Rico varían de lo que se reporta en otras áreas geográfi-cas. Debido al efecto potencial de la continua ex-posición a la luz solar en el Caribe, es posible que la enfermedad se manifieste de forma más severa.
Para describir las manifestaciones de la ne-fritis lúpica en los pacientes pediátricos en Puerto Rico e identificar factores pronósticos, se revisar-on los expedientes de los pacientes diagnósticados con SLE entre 1987 – 2001. La nefritis mesangial (Tipo II) fue la nefritis mas común en nuestra pob-lación. En adición, observamos una incidencia alta en varones con una distribución por género de 1: 1.9 (M : F), lo cual contrasta marcadamente con todos los reportes a nivel mundial. La clasificación histológica de la nefritis (Tipo IV) y la necesidad de diálisis aguda en el momento de la presentación se asociaron a un pronóstico adverso (desarrollo de fallo renal permanente o muerte).
23. Thi Houng DL, Papo T, Bewaufills H, Wechsler B, Bletry O, Baumelou A, Godeau P, Piette JC. Renal involvement in systemic lupus erythematosus: A study of 180 patients from a single center. Medicine 78(3): 148-166, 1999.
24. Vera R, Espinosa G, Pallares L, Ramos-Casals M, Jimenez S, Garcia-Carrasco M, Seisdedos L, Ingelmo M. Systemic Lupus Ery-thematosus (SLE) in childhood: analysis of clinical and immunologi-cal findings in 34 patients and comparison with SLE characteristics in adults. Annals of the Rheumatic Diseases 57(8): 456–459, 1998.
25. Vila LM, Mayor AM, Valentin AH, Rodriguez SI, Reyes ML, Acosta E, Vila S. Association of sunlight exposure and photopro-tection measures with clinical outcome in systemic lupus erythemato-sus Puerto Rican Health Science Journal 18: 89–94, 1999.
26. Vila LM, Mayor AM, Valentin AH, Garcia-Sobera M, Vila S. Clinical and immunological manifestations in 134 Puerto Rican pa-tients with systemic lupus erythematosus. Lupus 8: 279 – 286, 1999.
27. Voulgari PV, Katsimbri P, Alamanos Y, Drosos AA. Gen-der and age differences in systemic lupus erythematosus. A study of 489 Greek patients with a review of the literature. Lupus 11:722 - 729, 2002.
28. Yang L, Chen W, Lin C. Lupus Nephritis in children—A review of 167 patients. Pediatrics 94 (3): 335-340, 1994.
29. Bonilla-Felix M, Parra C, Dajani T, Ferris M, Swinford RD, Portman RJ, Verani R: Changing patterns in the histopathology of idiopathic nephrotic syndrome in children. Kidney Int 55: 1885 – 1890, 1999.
ACKNOWLEDGEMENTSSupported in part by a grant from The Center for Excellence in Aca-demic Medicine, University of Puerto Rico - Medical Sciences Cam-pus.
N. Lupus nephritis in childhood: a review of 53 patients followed at a single center. Pediatr Nephrol 19: 36-44, 2004.
5. Churg J, Sobin LH. Lupus nephritis. In: Renal Diseases. Classification and atlas of glomerular diseases. Tokyo, Igaku Shoin, 127-49, 1982.
6. Emre S, et al. Lupus nephritis in children: prognostic sig-nificance of clinicopathological findings. Nephron 87(2): 118-126, 2001.
7. Font J, Cervera R, Espinosa G, Pallares L, Ramos-Casals M, Jimenez S, Garcia-Carrasco M, Seisdedos L, Ingelmo M. Sys-temic Lupus Erythematosus (SLE) in childhood: analysis of clinical and immunological findings in 34 patients and comparison with SLE characteristics in adults. Annals of the Rheumatic Diseases 57(8): 456–459, 1998.
8. Gomez-Reino J, et al. Survival analysis of 306 Span-ish patients with systemic lupus erythematosus. Arthritis Rheum 37(Suppl): S327, 1994.
9. Sorof JM, Perez MD, Brewer ED, Hawkins EP, Warren RW. Increasing incidence of childhood class V lupus nephritis. J Rheumatol. 1998 Jul;25(7):1413-8.
10. Lopez P, Mozo L, Gutierrez C, Suarez A. Epidemiology of systemic lupus erythematosus in a northern Spanish population: gen-der and age influence on immunological features. Lupus 12(11):860-5, 2003.
11. McCarty DJ, Manzi S, Medsger TA Jr, Ramsey-Goldman R, LaPorte RE, Kwoh CK. Incidence of systemic lupus erythema-tosus. Race and gender differences. Arthritis Rheum 38:1260-70, 1995.
12. McCurdy DK, Lehman TJ, Berstein B, Hanson V, King KK, Nadorra R, Landing BH. Lupus nephritis: prognostic factors in children. Pediatrics 90: 652–653, 1992.
13. Mitjavila F, Pac V, Moga I, Poveda R, Vidaller A, Carrera M, Pujol R. Clinicopathological correlations and prognostic factors in lupus nephritis. Clin Exp Rheumatol 15: 625 – 631, 1997.
14. Mok CC, Ho CT, Chan KW, Lau CS, Wong RW. Outcome and prognostic indicators of diffuse proliferative lupus glomerulone-phritis treated with sequential oral cyclophosphamide and azathio-prine. Arthritis Rheum 46:1003 – 1013, 2002.
15. Molina JF, Drenkard V, Moina J, Cardiel MH, Uribe C, Anaya JM, Gomez LJ, Felipe O, Ramirez LA, Alarcon-Segovia D. Systemic lupus erythematosus in males: A study of 107 Latin Ameri-can patients. Medicine 75(3): 124-130, 1996.
16. Nath SK, Kilpatrick J, Harley JB. Genetics of human sys-temic lupus erythematosus: the emerging picture. Curr Opin Immunol 16: 794 – 800, 2004.
17. National High Blood Pressure Education Program Work-ing Group on Hypertension Control in Children and Adolescents. Update on the 1987 Task Force Report on High Blood Pressure in Children and Adolescents: A Working Group Report from the Nation-al High Blood Pressure Education Program. Pediatrics 98: 649-658, 1996.
18. Ravinal RC, Costa RS, Coimbra TM, Pastorello MT, Coe-lho EB, Dantas M, dos RM. Classes, activity and chronicity indices, and alpha-smooth muscle actin expression as prognostic parameters in lupus nephritis outcome. Lupus 11: 82 – 87, 2002.
19. Rodriguez VE, Gonzalez-Pares EN. Mortality study in Puerto Ricans with systemic lupus erythematosus. Puerto Rican Health Science Journal 19: 335–339, 2000.
20. Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatric Clinics of North America 34:571, 1987.
21. Sorof JM, Samuels J. Ethnicity and recurrence of focal segmental glomerulosclerosis. Pediatric Transplantation. 5(2):69-72, 2001.
22. Tejani A, Nicastri AD, Chen CK, Fikrig S, Gurumurthy K. Lupus nephritis in black and Hispanic children. Am J Dis Child 137: 481 – 483, 1983.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 33
Vol.: 100 - Núm 2 - Abril - Junio 2008
PERCEPTION OF PARENTS REGARDING THEIR CHILDREN’S WEIGHT
By: Ilsa J. Nazario Rodriguez MD *, Wanda I. Figueroa MD *, Jaime Rosado MD *, Iris del C. Parrilla MS *
* From the Department of Pediatrics, Universidad Central del Caribe School of Medicine and Ramon Ruiz Arnau Hospital, Bayamon, PR.
Address reprints to: Ilsa Nazario Rodriguez MD, Department of Pediatrics, Universidad Central del Caribe, School of Medicine, Bayamon, PR.
ABSTRACT Background: The prevalence of over-weight and obesity in 2003 was 63.6% in P.R. and 60.1% in USA. An overweight school-aged child with an obese parent has over 70% chance of being obese in young adulthood. Objectives: To study perceptions of parents about their children’s weight and to determine which factors are associ-ated with parent’s failure to perceive when their children are overweight. Methods: Cross sectional survey, the sample was population of children and their parents, selected by availability, between 4-12 years old in elementary schools (private and public schools), N=234. The instrument was a self-administered questionnaire of 23 questions. SSPS version 10.0 was used for analysis with significance of p < 0.05. Results: 51% of parents perceived themselves overweight while they per-ceived their children in adequate weight (62%), so they don’t get professional help. There’s no signif-icant difference between genders and schools. The study revealed that children’s weight follows the role modeling of their parents (p<0.001). In BMI curve (>85%) showed that 84.3% children have at least one parent with overweight (ow) or obesity (ob) while 15.7% children have no parent with ow/ob (p<0.05). Study showed that 33% of parents do nothing about their children’s weight. Parents con-sider themselves to be responsible for childhood obesity. Conclusions: The majority of the parents does not perceive their children at risk of becom-ing overweight or be overweight, so they do not get help early.
Keywords: perception, body mass index, over-weight, obesity, children
Obesity in children and adolescents rep-resents one of the most frustrating and difficult diseases to manage. Overweight has recently re-ceived considerable attention because of the large increase in its prevalence in the USA over the past two decades, in both adults and children, and be-cause of its consequences for health.1 The World Health Organization defines health as a state of complete physical, mental and social well-being and not merely the absence of disease. It is rec-ognized that obesity, eating disorders, body im-age are all interrelated and need to be addressed in comprehensive ways that do no harm.
Authors recognized in a study of childhood over-weight that early childhood is a critical period in the development of obesity due to the adipose tis-sue rebound. This is the time, usually between ages four and 6, when a child’s adiposity begins to in-crease after a low point in the early years of life.2 The American Academy of Pediatrics recommends yearly calculation of body mass index (BMI), nu-tritional assessment and counseling at every health maintenance visit. The advantage in treating over-weight children at early ages is that they seem to respond to interventions more readily than older children.3 Furthermore, as recent data from the National Center for Health Statistics indicate ap-proximately one in five children in the USA is now overweight. Obesity represents a chronic illness. Therefore, frequent visits, continuous monitoring, and reinforcement will be required for success but will not ensure it.4
In Puerto Rico, 25% of population is obese and 35% is overweight.16 The prevalence of over-weight and obesity in 2003 was 63.6% in P.R. and 60.1% in USA. There is an increase (1996-2002) of 54% in the prevalence of obesity among children of 6-11 years old.12 In Puerto Rico; obesity has massive and sustained increase in publicity though no published papers have reported about the per-ception of parents regarding their children’s obes-ity. There are no studies available about perception of childhood’s obesity in our country. Thus, recog-nition of children who are overweight or at risk for becoming overweight is important so that preven-tion and treatment strategies may be implement-ed early in life.19 Dr. Fontanet, President of the Puerto Rico Pediatric Society stated that 35% of children in Puerto Rico are obese and maybe due to lack of exercise and unbalanced diet.22 Parents and caregivers may not initiate preventive changes unless they first perceive that their child is at risk for some adverse outcome.28
According to Hirschler (2006), the moth-er’s perception of body image and eating behavior of their children is a predictor of overweight.18 The majority of mothers of overweight children (80%) didn’t view them as overweight and these misperceptions were related to education level. Mother’s perceptions about their children’s body image may contribute to obesity in children and

Vol.: 100 - Núm 2 - Abril - Junio 2008
need to be addressed in nutrition education.11 Communities are encouraged to support fitness and physical activity by providing parks, playgrounds, and other facilities that are safe, convenient, ap-pealing and affordable places for children and par-ents to spend time.2
This study aimed to evaluate parent’s fail-ure to perceive their children at risk for overweight or be overweight. An overweight school-aged child with an obese parent has over 70% chance of being obese in young adulthood.
METHOD The study was a cross sectional survey. The sample was population of children with their parents, selected by availability, between 4-12 years old in two elementary schools (one private and one public school) in the urban zone of Baya-mon, Puerto Rico, n=234.
Every child was weighted and measured with portable digital scale and wall’s metric rule in his/her respective school. The instrument was a self-administered questionnaire of 23 questions lasting approximately 10 minutes. The question-naire was administered to parents and their chil-dren in two elementary schools (one private and one public school) in Bayamon. The first eight questions were demographics and the subsequent questions were based in the perception concerning weight of own parents and about their children.
The parent reported her or his own height and weight and provided demographic informa-tion, including child education level (grade) in the questionnaire.
Parent’s perception of their children’s weight was assessed from responses to the ques-tion: “Do you consider your child to be over-weight, underweight, about the right weight or obese?” These responses were compared with the children’s body mass index (BMI) determined from the CDC/NCHS sex and age specific per-centiles for BMI (weight/stature2) calculated from measured values for weight and stature. Children’s BMI values were plotted for sex and age, and val-ues ≥95th percentile were considered overweight, values between 85th and 95th percentile were considered at risk for overweight, values >5th to 84th percentile were considered normal weight and values ≤5th percentile were considered under-weight. Other variables of interest included were each child’s age, sex, and grade level, which care the child, father and mother’s weight and height to calculate BMI.
Data were analyzed using SSPS version 10.0. The significance level was p<0.05. Also were used frequency distributions, chi-square test and correlation analysis.
34 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
RESULTS There were a total of 234 children with their parents, selected by availability, between 4-12 years old in two elementary schools in the ur-ban zone of Bayamon, Puerto Rico. A total of 117 girls and 117 boys were weighted and measured at both elementary schools (Table 1). There were 110 children from public school and 124 children were from private school.
The 51% of parents perceived themselves overweight while they perceived their children in 62% of adequate weight (Figures 2-3). The study revealed that child follows the role modeling of their parents (p<0.001). In child’s BMI curve comparing with parent’s BMI (>85%) showed that 84.3% children have any parent with overweight or obesity while 15.7% of children have no par-ent with overweight/obesity (p<0.05) (Figure 6). There were no significant differences between boys and girls of both types of schools (Figure 7). The comparison of BMI between public and private schools (ages 4-12 years old) showed that 12% of children in public school tend to risk for becoming overweight while 44% of children in the private school tend to the overweight (Figure 8). In the questionnaire, 90% of parents answered that obesity is a health problem while 3% of parents considered that children are healthier if they are fat because they get sick less than slim kids (Figures 10-11).
The 33% of parents did nothing about their children’s weight while 67% of parents did something about it like get nutritionist counseling or evaluation, prepared diet for their children, en-couraged them to exercise, and enrolled the child in sport (Figures 12, 13). Parents considered been responsible for the childhood obesity (Table 3).
DISCUSSION The study highlights an important prob-lem in health promotion. Despite the high rate of overweight risk and overweight among children of 4-12 years old in this study, 33% of parents an-swered in the questionnaire that they did nothing about their children’s obesity while 67% of parents expressed concern that their child was currently overweight. These findings are consistent with the study of Campbell et al. showing equally low rates of concern for child overweight.9 For children currently at overweight risk or be overweight, this was related to the number of overweight parents, so that means that children follow their parental modeling. According to the study of Baughcum et al. only one in five mothers correctly identified their overweight children as overweight.5
Health professionals can help improve recognition of childhood overweight. The charting of child BMI could be encouraged as a part of normal practice, not only to provide an objective
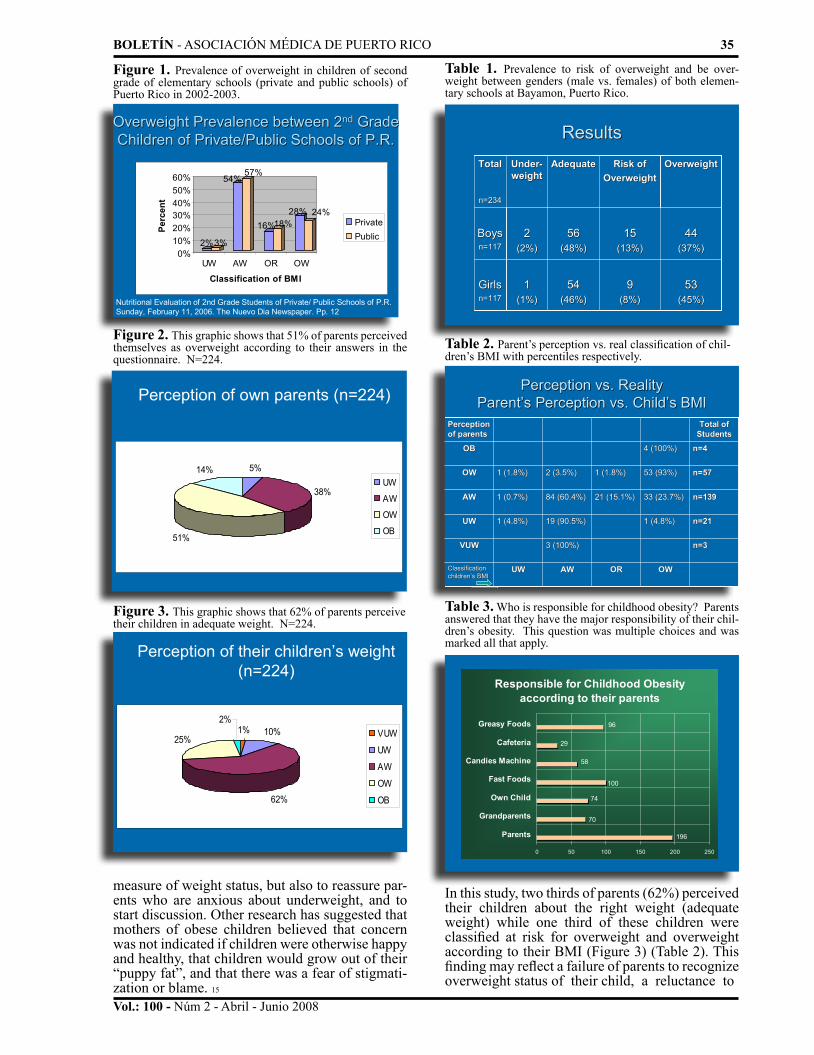
BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 35
Vol.: 100 - Núm 2 - Abril - Junio 2008
Overweight Prevalence between 2Overweight Prevalence between 2ndnd Grade Grade Children of Private/Public Schools of P.R.Children of Private/Public Schools of P.R.
2%3%
54%57%
16%18%28% 24%
0%10%20%30%40%50%60%
Perc
ent
UW AW OR OW
Classification of BMI
PrivatePublic
Nutritional Evaluation of 2nd Grade Students of Private/ Public Schools of P.R. Sunday, February 11, 2006. The Nuevo Dia Newspaper. Pp. 12
Figure 1. Prevalence of overweight in children of second grade of elementary schools (private and public schools) of Puerto Rico in 2002-2003.
Perception of own parents (n=224)
5%
38%
51%
14%UW
AW
OW
OB
Figure 2. This graphic shows that 51% of parents perceived themselves as overweight according to their answers in the questionnaire. N=224.
Perception of their children’s weight (n=224)
1% 10%
62%
25%
2%VUW
UW
AW
OW
OB
Figure 3. This graphic shows that 62% of parents perceive their children in adequate weight. N=224.
Table 1. Prevalence to risk of overweight and be over-weight between genders (male vs. females) of both elemen-tary schools at Bayamon, Puerto Rico.
ResultsResults
5353(45%)(45%)
4444(37%)(37%)
OverweightOverweight
99(8%)(8%)
1515(13%)(13%)
Risk ofRisk ofOverweightOverweight
5454(46%)(46%)
5656(48%)(48%)
AdequateAdequate
11(1%)(1%)
22(2%)(2%)
UnderUnder--weightweight
GirlsGirlsn=117n=117
BoysBoysn=117n=117
TotalTotal
n=234n=234
Table 2. Parent’s perception vs. real classification of chil-dren’s BMI with percentiles respectively.
Perception vs. Reality Perception vs. Reality ParentParent’’s Perception vs. Childs Perception vs. Child’’s BMIs BMI
OWOWORORAWAWUWUWClassification Classification childrenchildren’’s BMIs BMI
n=3n=33 (100%)3 (100%)VUWVUW
n=21n=211 (4.8%)1 (4.8%)19 (90.5%)19 (90.5%)1 (4.8%)1 (4.8%)UWUW
n=139n=13933 (23.7%)33 (23.7%)21 (15.1%)21 (15.1%)84 (60.4%)84 (60.4%)1 (0.7%)1 (0.7%)AWAW
n=57n=5753 (93%)53 (93%)1 (1.8%)1 (1.8%)2 (3.5%)2 (3.5%)1 (1.8%)1 (1.8%)OWOW
n=4n=44 (100%)4 (100%)OBOB
Total of Total of StudentsStudents
Perception Perception of parentsof parents
Table 3. Who is responsible for childhood obesity? Parents answered that they have the major responsibility of their chil-dren’s obesity. This question was multiple choices and was marked all that apply.
Responsible for Childhood Obesity according to their parents
100
29
74
58
96
70
196
0 50 100 150 200 250
Parents
Grandparents
Own Child
Fast Foods
Candies Machine
Cafeteria
Greasy Foods
measure of weight status, but also to reassure par-ents who are anxious about underweight, and to start discussion. Other research has suggested that mothers of obese children believed that concern was not indicated if children were otherwise happy and healthy, that children would grow out of their “puppy fat”, and that there was a fear of stigmati-zation or blame. 15
In this study, two thirds of parents (62%) perceived their children about the right weight (adequate weight) while one third of these children were classified at risk for overweight and overweight according to their BMI (Figure 3) (Table 2). This finding may reflect a failure of parents to recognize overweight status of their child, a reluctance to

Vol.: 100 - Núm 2 - Abril - Junio 2008
36 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
05
101520253035404550
Perc
ent (
%)
UW AW OR OW OBClassification of BMI
BMI Classification
FatherMotherChild
Figure 4. BMI Classification between children’s parents and own child, according to their weight and height. N=234.
Figure 5.Both graphics shows the parental role modeling in their chil-dren. We can see that the child directly compares with their parent’s BMI. N=234.
Do the child follows the role modeling Do the child follows the role modeling of their parents?of their parents?
66.5%
33.5% 31.4%
68.6%
0%10%20%30%40%50%60%70%
0-84% >85%
Child BMI comparing with Father's BMI
UW/AW
OR/OW/OB
64.8%
35.2%
28.9%
71.1%
0%10%20%30%40%50%60%70%80%
0-84% >85%
Child BMI comparing with Mother's BMI
UW/AW
OR/OW/OB
p < 0.001
p < 0.001
Figure 6.Child’s BMI compared with any of their parent with over-weight or obesity, and 84.3% follows their parental modeling. N=234.
Do the child follows the role Do the child follows the role modeling of their parents?modeling of their parents?
25.4%
74.6%
15.7%
84.3%
0%10%20%30%40%50%60%70%80%90%
Perc
ent
0-84% >85%
Child's BMI
No parent withOW/OB
Any parent withOW/OB
p < 0.05
Figure 7. Comparison between male and female genders. N=234.
0
5
10
15
20
25
30
35
40
45
50
Perc
ent (
%)
UW AW OR OWClassification of BMI
Comparison between Genders (234 children)
Boys
Girls
admit that their child is overweight, or a lack of understanding of what “overweight” means. In the current study there were no data available to exam-ine reasons surrounding parent’s misclassification of child overweight status.
Additionally, according to our findings, many parents admitted that they feel responsible about their children’s obesity despite they know in 90% that obesity is a health problem (Figure 10).
In conclusion, the majority of the parents do not perceive their children as overweight or at risk for becoming overweight. Despite people concern about childhood’s obesity in Puerto Rico, most parents surveyed were not concerned about their children’s weight, and many parents did not perceive their overweight children as different from their peers. This may have implications for interventional plans because if their parents did not look for professional help early, thinking that their children were healthy, maybe cause direct negatively impact on their children’s health.
Obesity is easier to prevent than to treat, and prevention focuses in large measure on parent education. In early childhood, education should in-clude proper nutrition, selection of low-fat snacks, good exercise/activity habits, and monitoring of television viewing. Aggressive prevention and intervention in childhood in schools and com-munities are urgently needed.14 Optimally; BMI changes would be discussed with families before the child becomes severely overweight.
To prevent cardiovascular diseases in the adulthood, parents need to involve with their chil-dren in exercises like walking, tennis, swimming, baseball, jogging, dancing among others. Also is very important that parent counsel their child to balanced diet or food.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 37
Vol.: 100 - Núm 2 - Abril - Junio 2008
Figure 8. Comparison of BMI between public and private schools (aged 4-12 years). N=234.
Comparison of BMI between Public and Comparison of BMI between Public and Private Schools (Ages 4Private Schools (Ages 4--12 years)12 years)
0%3%
47% 46%
9% 12%
44% 39%
0%
10%
20%
30%
40%
50%
Perc
ent
UW AW OR OW
BMI Classification
PrivatePublic
Figure 9. Perception of parents regarding to their chil-dren’s weight vs. the reality (BMI classification of children). p<0.001.
Perception vs. Reality Perception vs. Reality ParentParent’’s Perception vs. Childs Perception vs. Child’’s BMIs BMI
140
Parent's perception of their child
OB OW AW UW VUW
No.
Stu
dent
s
160
120
100
80
60
40
20
0
BMI Classification of Child
OW
OR AW
UW
p < 0.001
Figure 10. 90% of parents answered in the questionnaire that obesity is a health problem. N=223.
Obesity is a health problem? (n=223)
90%5.50% 4.50%
0%20%40%60%80%
100%
Per
cent
TRUE FALSE DON’TKNOW
Parent's Answers
Figure 11. 97% of parents answered that children are not healthier if they are fat or chubby because get sick less than slim kids. N=219.
Children are more healthy if they are fat because Children are more healthy if they are fat because they get sick less than slim kids. they get sick less than slim kids. (n=219)(n=219)
3%
97%
0%
20%
40%
60%
80%
100%
Perc
ent
Parent's Answers
TRUEFALSE
Figure 12. 33% of parents did nothing about their chil-dren’s weight (overweight risk or be overweight).
Do parents get some help about Do parents get some help about their childrentheir children’’s weight ?s weight ?
33%
67%
Doing nothing
Do something (Professional help, Diet, Exercise, Sports)
Figure 13. This graphic shows what parents did about their children’s weight. 29% of parents did nothing while 13% get professional help (doctor, nutritionist) and 87% did other things.
Do parents get some help about Do parents get some help about their childrentheir children’’s weight ?s weight ?
29%
13%
25%
33%
17%
12%
0%5%
10%15%20%25%30%35%
Perc
ent
Parent's getting help
Doing Nothing
Professional Help
Diet
Animate toExerciseSports
Other things
REFERENCES1. American Academy of Pediatrics. (2004) Preventing childhood obesity: A national conference focusing on pregnancy, in-fancy and early childhood factors. Pediatrics. 114: Part 2 of 3. Supp. 1139-1173
2. Ariza AJ, Greenberg RS and Unger R. (2004) Childhood overweight: Management approaches in young children. Pediatric Annals. 33(1): 33-38.
3. Barlow SE, and Dietz WH. (1998) Obesity evaluation and treatment: Expert committee recommendations. Pediatrics. 102: 1-11.
4. Batch, JA and Baur, LA. (2005) Management and preven-tion of obesity and it’s complications in children and adolescents. MJA. 182(3): 130-135.
5. Baughcum AE, Chamberlin LA, et al. (2000) Maternal perceptions of overweight preschool children. Pediatrics. 106(6): 1380-1386.

Vol.: 100 - Núm 2 - Abril - Junio 2008
38 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Acknowledgements I gratefully acknowledge the thoughtful comments, cor-rections, and advice of my proctor and mentor Dr. Wanda I. Figueroa, General Pediatrician and Central del Caribe University Researcher. Also I want to thanks to Dr. Jaime Rosado, Pediatric Gastroenterolo-gist at Ramon Ruiz Arnau Hospital, Bayamon, who revised my re-search project. My personal appreciation to Dr. Iris Parrilla and Prof. Mike Velez for support in the statistical analysis of data collected. Thanks to Mrs. Elsa Velez and Mrs. Morales, both Directors of public and private schools respectively in Bayamon, whose facilitated and made possible my investigative project. Also I want to appreciate the collaborative help of Mrs. Carmen Ortiz, Interim Superintendent of Scholar District I of Bayamon. Thanks a lot to Dr. Fermin Sanchez and Dr. Vanessa Santini, my Residency Program’s Director and Pro-gram’s Coordinator respectively, who’s made possible my research presentation at the Annual Puerto Rico Pediatric Convention 2007.
6. Behrman R, Kliegman R and Jonson HB. (2004) Obesity. Nelson Textbook of Pediatrics. 17th Ed: 173-177.
7. Boutelle K, Fulkerson JA et al. (2004) Mother’s percep-tions of their adolescent’s weight status: Are they accurate? Obesity Research. 12(11): 1754-1757.
8. Brener N, Eaton D. et al. (2004) The association between weight perception and BMI among high school students. Obesity Re-search. 12(11): 1866-1874.
9. Campbell M, Williams J, Hampton A & Wake M. (2006) Maternal concern and perceptions of overweight in Australian pre-school-aged children. Medical Journal of Australia. 184(6): 274-277.
10. CDC: Prevalence of overweight among children and ado-lescents: USA 1999-2000. http://www.cdc.gov
11. Contento I, Basch C, Zybert P. (2003) Body image, weight and food choices of latina women and their young children. Journal of Nutrition Education and Behavior. 35: 236-247.
12. Danon M, MD (2006) Obesity: The facts 2006, Endo-crinologist Perspective, Miami Children’s Hospital. Conference at Pediatric Annual Convention.
13. Dennison B, and Boyer PS. (2004) Risk evaluation in pediatric practice: Aids in prevention of childhood overweight. Pedi-atric Annals. 33: 25-30.
14. Dutt S and Ten S. (2007) Complications of obesity in childhood. Pediatric Annals. 36: 96-101.
15. Eckstein KC, Mikhail L, Ariza AJ. (2006) Parent’s percep-tions of their child’s weight and health. Pediatrics. 117(3): 681-690.
16. EFE Agency. (2005) Lupa a los niños obesos. El Nuevo Día Newspaper. Con Salud. March 13, 2005. Pp. 11.
17. Etelson D, Brand D, Patrick P and Shirali A. (2003) Child-hood obesity: Do parents recognize this health risk? Obesity Re-search. 11(11): 1362-1368.
18. Hirschler V. et al. (2006) Como perciben las madres de ninos de jardin de infantes a sus hijos con sobrepeso? Arch. argent. Pediatr. 104(3): 221-226.
19. Hossain N. Obesity, overweight classification and percep-tion among FIU students. http://www.fiu.edu/~health/reports/obesity. Dpt. of Public Health.
20. Jain A, Sherman SN, Chamberlin LA, et al. (2001) Why don’t low-income mothers worry about their preschoolers being over-weight? Pediatrics. 107: 1138-1146.
21. Maynard M, PhD, Galuska D, PhD et al. (2003) Maternal perceptions of weight status of children. Pediatrics. 111(5): 1226-1231.
22. Periódico El Nuevo Día (2007) A combatir la obesidad y la mortalidad infantil. Puerto Rico Hoy. Domingo, 18 de febrero de 2007. Pp. 25.
23. Rodríguez AM. (2006) Evaluación nutricional de los niños de segundo grado de escuela elemental. Overweight and Obesity Na-tional Conference in Paradisus Hotel, P.R. October 18-19, 2006.
24. Rudolf MC, Sahota P. (2000) Increasing Prevalence of Obesity in Primary School Children: Cohort Study. Community Pedi-atrics.
25. The Journal of National Association of State Boards of Education. (2004) The Obesity Epidemic. December 2004. http://www.nasbe.org
26. Weight relatives Division of the Society for Nutrition Education. (2003) Guidelines for Childhood Obesity Prevention Pro-grams: Promoting Healthy Weight in Children. Journal of Nutrition Education and Behavior. 35: 1-4.
27. World Health Organization. Obesity Prevalence Tables. http://www.who
28. Young-Hyman D, Herman LJ, et al. (2000) Care Giver Perception of Children’s Obesity Related Health Risk: A Study of Af-rican American Families. Obesity Research. 8: 241-248
Médico,
Estudiante
de Medicina:
Forma parte de una de las
más antiguas y acreditadas
asociaciones profesionales .
Goza de los beneficios de
pertenecer a la Asociación
Médica de Puerto Rico y
ayúdanos a mejorar la
calidad de vida de nuestrocalidad de vida de nuestro
Pueblo.
Infórmate leyendo las últimaspáginas de este boletín o en la
sección MEMBRESÍAS de nuestroweb site
www.asociacionmedicapr.org

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 39
Vol.: 100 - Núm 2 - Abril - Junio 2008
DO PARENTS KNOW ABOUT THE ADVERSE EFFECTS OF PASSIVE SMOKING AND THE RELATIONSHIP
WITH RESPIRATORY ILLNESS ON THEIR CHILDREN?By:Cristina Jiménez-González MD *, Vanessa Santini MD *, Wanda I. Figueroa Cosme MD *, Iris del C. Parilla MS *
* From the Department of Pediatrics, Universidad Central del Caribe School of Medicine and Ramon Ruiz Arnau Hospital, Bayamon, PR.
Address reprints to: Cristina Jiménez-González MD, Department of Pediatrics, Universidad Central del Caribe, School of Medicine, Bayamon, PR.
ABSTRACT Recent studies still show parental smoke as the number one environmental exposure agent causing asthma in pediatric population. Objective: The purpose of this study is to determine the knowl-edge of parents about the adverse effects of passive smoking and the prevalence of passive smoking in children. Design: Cross sectional study, partici-pants were caregivers of students from first to sixth grade (three private and two public schools) who answered a self-administered survey. Data was analyzed using SPSS. Results: Surveys were col-lected by availability. Total of caregivers was 594, (47% from private and 53% from public school). The total of estimated children in the survey was 1318, and 48.3% in general had recurrent respi-ratory illness. Among caregivers, 12.1% (72) re-ported to be smokers. There were 127 participants who revealed at least 1-3 smokers in their home; these smokers are affecting 167 children who are exposed to secondhand smoke. Among smokers, 16.9% smoked inside the house, 15.5% in their cars and 12.3% smoked in the presence of their children. Participants with higher education had a higher av-erage score on knowledge about adverse effects of smoking (p<.001). Over half of the participants (52%) reported seen anti-smoking promotion on T.V. during previous days. Non-smokers revealed they have seen such promotion recently (p=0.00), but 31% of all participants reported not seen any anti-smoking promotion at all. Conclusions: The prevalence of smokers in our study was 12.1%. We estimated there was more than one smoker in those households where smoking was allowed. There was a higher prevalence of smokers among parents from public schools. There was no significant dif-ference between passive smoker households and non-smoker households for respiratory illness in their children. Pediatricians are giving information to caregivers about active and passive smoking but still, 34% of smokers reported not receiving any information. We need to reinforce the counseling given to caregivers about the adverse effects of smoking has on environmental pollution, and as a cause of other cancers besides lung cancer, recur-rent infections and SIDS.
Keywords: Passive smoking, second hand smok-ing, tobacco smoke, parental smoking
Passive or second hand smoking is defined as the involuntary breathing of other people’s to-bacco smoke. Environmental Tobacco Smoke (ETS) is a complex mixture of more than 4,000 chemical compounds produced by a burning ciga-rette, pipes, or cigars. ETS has been classified by the US Environmental Protection Agency (EPA) as a human lung carcinogen; it is based on the chemical similarity of side stream and mainstream smoke (Cardenas et al, 1997). Tobacco smoke con-tains carcinogens as benzene (related to myeloid leukemia), polycyclic aromatic hydrocarbons, N-nitrous compounds (associated with lung cancer), aryl amines (related to bladder cancer) and carbon monoxide. Also, tobacco smoke is related to na-sal cavity, sinuses, nasopharynx, stomach, liver, kidney and uterine cancers (Vineis et al, 2004). It has been estimated that tobacco smoking is cur-rently responsible for approximately 30 % of all cancer deaths in developed countries, causing 4-5 million deaths per year worldwide. It is projected to increase to 10 million deaths per year by year 2030 (Vineis et.al, 2004). A national survey indi-cated that 43 % of children 2 months to 11 years of age live in homes with at least one smoker in the United States (Pediatrics, 1997).
In children, ETS is associated with otitis media, pharyngitis, sinusitis, lower respiratory in-fections, asthma exacerbations, reduced lung func-tion and Sudden Infant Death Syndrome (Murphy, 2004). Passive smoking is a risk factor for new cases of asthma for children (Murphy 2004, Pedi-atrics 2007). Tobacco smoke produces an adverse physiologic response on the respiratory system; it increases excess mucous production, white blood cells, and permeability of allergens, and decreases the ciliary’s movement, lung elasticity and pre-vents the normal function of the mechanism to re-move the excess mucous. All of these changes pre-dispose for progression of an infection and even lung cancer. Worldwide studies have demonstrated that parental smoking is a major identifiable cause for excess hospitalizations and respiratory infec-tions in children (Peat et.al, 2001, Shiva 2003).
Most smoke exposure occurs at home where responsible adults’ smoking is allowed and 75 % of children who lived with a smoker, are also exposed to smoke outside the house,

Vol.: 100 - Núm 2 - Abril - Junio 2008
inside vehicles, and at grandparent’s house among other expositions (Hopper and Craig 2000, Rapiti 1999).
Cloutier and colleagues (2002) revealed that tobacco smoke was the number one envi-ronmental exposure agent causing asthma among children from 5 to 10 years of age, seeking Medic-aid services in Connecticut. Additionally, the study showed the asthma prevalence was higher among Puerto Ricans.
A survey by Mannino (2002) provided evidence that passive smoking increases asthma severity and is strongly associated with high lev-els of cotinine. Cotinine is a metabolic compound or by product of nicotine that has a half-life of 16 hours. Cotinine is used to measure recent exposure to tobacco smoke and is measured in urine, serum and hair (Vineis 2005, Murphy 2004, and Mannino 2002).
Ramos-Valencia in 2001 estimated that the prevalence of smoking in Puerto Rico is 14.7 %, and about a half million of the population is passive smoker. The study also showed that 7 % of children from 5 to 15 years of age missed at least 1 day per month of school due to asthma (Ramos, 2001). ETS causes an accumulative detrimen-tal lung effect in children when they are exposed both during pregnancy and later after birth (Rizzi, 2004). The children whose mothers had smoked during pregnancy, showed an increase in bronchial reactivity at school age (between 5 to 13 years of age), compared with children whose mothers had not smoked during the entire pregnancy (Landau 2001, Joad 2000, Nuesslein 2002, Henderson 2001, Lux 2000). A review of literature found that thirty studies have demonstrated the undeniable association between exposure to maternal tobacco smoke during the pregnancy and cancer in child-hood (Boffetta et.al 2000).
Children exposed to second hand smok-ing for several hours per day were 3.6 times more likely to develop lung cancer during adulthood than unexposed people (Vineis 2005). Several oth-er studies confirmed that breathing other people’s tobacco smoke causes reactive airway diseases and the lung cancer (Hacksaw 1997, Copas 2000, Nyberg 1998, Brownson 2002, Lee 2000, Reuters 2005, Rapiti 1999).
Due to the overwhelming scientific evi-dence of the adverse health risk for general popu-lation from second hand smoke, Puerto Rico state legislature passed the Law # 40 on August 3, 1993, to prohibit smoking in closed public places ex-cept bars and casinos. On March 2, 2006, Law # 66 emended Law # 40 and prohibited smoking in bars, casinos and private vehicles when there is a minor in a car seat or a minor younger than 13 yrs old (Lexjuris, 2006).The purpose of this study is to: 1) determine the
40 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
knowledge of parents about the adverse effects of passive smoking and its relationship to respiratory illness on children, 2) determine the prevalence of passive smoking in children in a random popula-tion in Bayamón, Puerto Rico, and 3) impact par-ents about the adverse effects of passive smoking. Even though the adverse consequences of second-hand smoking has been publicized and in-formed to the general public, the recent studies still show parental smoking as the number one environ-mental exposure agent causing asthma in pediatric population. There are few studies done in Puerto Rico about adverse effects of passive smoking and its relationship to respiratory illness on children. Our hypothesis is that parents are not well informed of the adverse effects and the con-sequences of second-hand smoking on their chil-dren.
MATERIAL AND METHODS Study Design was a cross sectional sur-vey done between August and December 2006. Participants were caregivers of students from first to sixth grade selected randomly from three private schools: one Catholic, one Luteran and one Laic and two public schools from an Urban Area in Bayamón, Puerto Rico. Permits were ob-tained from the school directors of private schools as well as from the Puerto Rico’s Department of Education. An informed consent was provided to caregivers along with a self-administrable survey that consisted of twenty four questions in Span-ish. Areas covered were status of smoker, places were smoking is allowed, knowledge of adverse of smoking, and demographic data. The estimated time to answer the survey was about fifteen min-utes. The material was distributed by teachers in the students’ notebooks and a reasonable time was given to collect the survey. After all surveys were collected an informative brochure “Children and Second Hand Smoking” in Spanish, published on February 2000 by the Environmental Protection Agency (EPA) was given to all students. VariablesDemographic data: Questionnaires were classified by school system, those answered by caregivers at private schools (system 1) and those answered at public schools (system 2). Relationship of par-ticipant with the child, age of the caregiver, edu-cational level and occupation, number of family members and number of children per household were some of the demographic data asked.Characteristics of smoker: Participants answered if he/she was a smoker and how many years he/she was smoking, number of smokers per household, quantity of cigarettes smoked, place were smoking is allowed (inside/outside house, in the car, near children).
Knowledge about smoking: Participants answered if smoking was a habit, an addiction, as well as,

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 41
Vol.: 100 - Núm 2 - Abril - Junio 2008
its adverse effects related to smoking active, pas-sive or social smoking.
Education about smoking: Participants answered if they have seen anti-smoking promotion and if they gave advice to their children about the side effects of smoking.
Statistical Analysis: The survey was coded and responses were transferred to a Microsoft Excel 2002 spreadsheet. Analyses were performed using Statistical Package for Social Sciences version 10. Data was analyzed by frequencies, cross tabula-tion, Pearson Chi-Square, Fisher’s Exact Test, T-Test and Pearson Correlation. The level of signifi-cance was established at p <0.05.
RESULTS
Demographic Data
A total of 840 questionnaires were handed at three private elementary schools from Bayamón urban area and 279 were returned, for a 33% re-sponse rate. Private school was classified as Sys-tem I.
Two public elementary schools were cho-sen from Bayamón urban area. The total enroll-ment of both schools was 1242 students, and 830 questionnaires were handed and 315 were returned, for a response rate of 38%. Public school was clas-sified as System II. The total of participants on the sample was 594, 47% were from private schools and 53% from public schools (Fig.1).
Informants
Mothers answered 85% (506) of the sur-veys, followed by fathers with 11% (65), grand-mothers 2% (11) and others 0.9% (5) (as guardian, parents, stepfather, aunt and sister, see) (Fig.2). Age of participants ranged from 21-70 years, with a mean age of 37 years old. Regarding employ-ment status, 35.6% of the participants worked for a company, 25% were housewives, 21% had a profession, and 11% worked on their own. Others were government workers (2.7%), retired (1.7%), students (1.7%) and unemployed (0.8%) (Fig. 3). The average school years of the sample was 16 years, 41% of the total informants had a bachelor’s degree (Fig.4).
Figure 2: Percentage of Participants
Figure 3: Percentage of Participants Who Work
Figure 4: Participant Education by System
Figure 5: Diseases in Children among General Population
Figure 1:
The average family size were FOUR mem-bers, the majority of families (47.3%) had 2 chil-dren. The total of estimated children in the survey was 1318. Among the conditions these children presented: 48.3% had respiratory diseases, 17.4%

Vol.: 100 - Núm 2 - Abril - Junio 2008
42 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
had recurrent otitis, 15.5% had recurrent pharyn-gitis, 19.9% had recurrent upper respiratory infec-tions (viral illness), and 7.1% had other diseases not related to smoking (Fig. 5).
Characteristics of smokers
Total prevalence of smokers among par-ticipants was 12% (72) (Fig.6). There was a higher prevalence of smokers in public (14.6%) than pri-vate schools (9.3%) (Fig.7). Of those smokers who reported the number of year they have been smoking (56 out of 72), more than a third (34.8%) had been smoking between 1~10 years. (Fig.8)
Among all the participants 6.7% quit smoking, 17.7% have tried smoking but do not smoke, and 62.1% have never smoked.
There were 127 participants that reported between 1~3 smokers in their home, for a total of 158 smokers (Fig.9).
The majority of smokers (45.1%) smoked half a pack, followed by one pack (25.6%) and 9.8% smoke more than 2 packs a day (Fig. 10).
Among smokers, 34.7% (n=25/72) smoked inside the house versus 83.1% who did not smoke inside their house. Forty six percent of those smokers who smoked inside the house re-vealed smoking 1-2 days; while 22% smoked 7 days, followed by 22% (3-4 days) and 10% for 5-6 days. Other places where they smoked: 88.4% re-vealed smoked outside the house, 15.5% smoked inside the car and 12.3% smoked in presence of their children (Fig.11). In our study 167 children were exposed to second hand smoke. (Fig. 12)
Over all 12.5% cannot quit smoking and 3.8% do not want to quit smoking.
Exposure of pregnant women to passive or active smoking was reported by 12.1% of the participants.
Knowledge of Smoking
There were ten questions on knowledge about the adverse effects of passive smoking. For each participant a score of knowledge about smok-ing was determined based on the proportion of cor-rect answers. “Good knowledge” was established for those participants having at least seven correct answers out of ten. Almost all participants (99.5%) know that smoking is harmful, and 74.6% know about secondhand smoking. Most of the sample (98.1%) knows smoking is harmful to the active as well as passive smoker. Still 43.9% did not con-sider smoking as part of the environmental pollu-tion. Among the diseases related to smoking, 81% of participants know smoking causes respiratory diseases as asthma, bronchitis and emphysema and 79% know about lung cancer (Fig.13).
Figure 6: Prevalence of Smokers in Urban Area in Bayamón
Figure 7: Prevalence of Smokers per System
Figure 8: Number of Years Smoking by Total Smokers
Figure 9: Smokers per Household
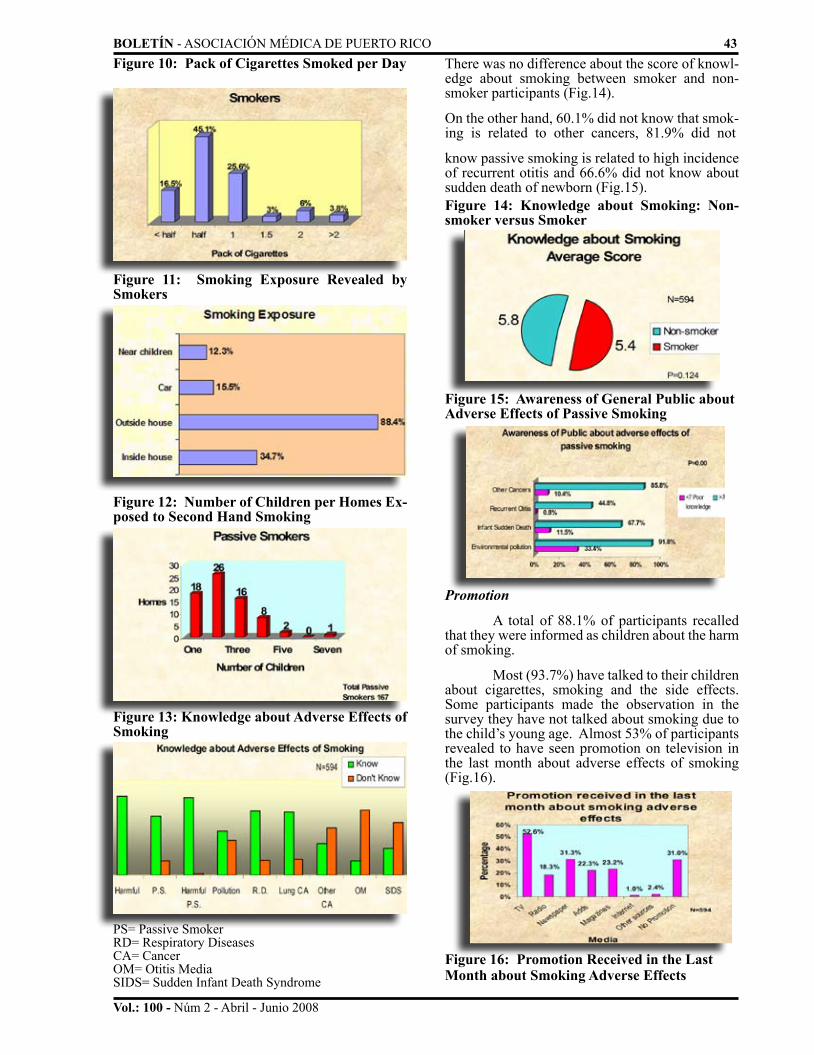
BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 43
Vol.: 100 - Núm 2 - Abril - Junio 2008
There was no difference about the score of knowl-edge about smoking between smoker and non-smoker participants (Fig.14).
On the other hand, 60.1% did not know that smok-ing is related to other cancers, 81.9% did not
know passive smoking is related to high incidence of recurrent otitis and 66.6% did not know about sudden death of newborn (Fig.15).
Figure 10: Pack of Cigarettes Smoked per Day
Figure 11: Smoking Exposure Revealed by Smokers
Figure 12: Number of Children per Homes Ex-posed to Second Hand Smoking
Figure 13: Knowledge about Adverse Effects of Smoking
PS= Passive Smoker RD= Respiratory DiseasesCA= CancerOM= Otitis MediaSIDS= Sudden Infant Death Syndrome
Figure 14: Knowledge about Smoking: Non-smoker versus Smoker
Figure 15: Awareness of General Public about Adverse Effects of Passive Smoking
Promotion
A total of 88.1% of participants recalled that they were informed as children about the harm of smoking.
Most (93.7%) have talked to their children about cigarettes, smoking and the side effects. Some participants made the observation in the survey they have not talked about smoking due to the child’s young age. Almost 53% of participants revealed to have seen promotion on television in the last month about adverse effects of smoking (Fig.16).
Figure 16: Promotion Received in the Last Month about Smoking Adverse Effects

Vol.: 100 - Núm 2 - Abril - Junio 2008
44 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
the Third National Health and Nutrition Exami-nation Survey (1988~1994) that environmental tobacco smoke exposure affects children of all ages, although the exact effects vary between age groups. It is also an important predictor of respira-tory health outcomes in children 4 years and older. In a study done in North Carolina, Sturm and col-leagues (2004) revealed there was a stronger as-sociation between asthma symptoms and passive tobacco smoke than active smoking. In our study, there was no significant difference between pas-sive smokers and non-smoking households for res-piratory illness prevalence (Fig.19 and Table 1). A Swiss study conducted between 1992 and 1993 reported 47% of all children were exposed to ETS, 16% of mothers smoked during pregnancy and children exposed at home to more than 20 ciga-rettes per day were at higher risk for respiratory problems (Hajnal BL et al, 1999).
The participants with a higher education had a higher average score on their knowledge about adverse effects of smoking.
Children learn behaviors done by caregiv-ers and may repeat what they see. A smoker car-egiver is a negative role model for children. We need to reinforce to quit smoking and prevent pas-sive smoking in children.
Among the topics that need to be rein-forced to general population about the adverse ef-fects of passive smoking are: environmental pol-
Most non-smokers revealed that they have seen promotion recently (p=0.000). Among all of the participants, 30% (55% of smokers and 26.5% of non-smokers) informed that a doctor or health pro-fessional has informed them in the past year about side effects of smoking. The rest 70% did not receive any information by a doctor (Fig.17).
With regards to pediatricians, 47% of par-ticipants received verbal, written or both type of orientation by their Pediatrician about smoking and its side effects on their children. On the oth-er hand, 53% did not receive any information by Pediatrician (Fig.18).
DISCUSSION Among all participants, our study revealed a prevalence of smoking of 12.1% in a sample of an urban area in Bayamón. This prevalence is close to the prevalence of the Ramos-Valencia study of 2001, which determined that 14.7% of the popula-tion in Puerto Rico is smoker. There is a higher prevalence of smokers in public than in private school and this is significant (p=0.032). These smokers are affecting 167 children who are passive smokers (estimated percentage of children who are passive smokers, 12.7%) in our study. A National Health and Nutrition Examination Survey done in 1988~1994 revealed that 38% of children were ex-posed to Environmental Tobacco Smoke in their home, and these children had three or more epi-sodes of wheezing , chronic bronchitis, and asth-ma among children from two months to five years old attributable to ETS exposure (Gergen Peter J et al.). Gonzales and colleagues revealed among their population in New Mexico, that 36% of His-panic children (between 2 and 12 years of age) born to U.S. and Mexico Hispanic mothers lived with a smoker household. In our study, most smok-ers revealed they smoke outside the house but still, there is smoking exposure near children (12.3%), inside the house (34.7%) and in the car (15.5%). Also, 46% of those smokers who smoked inside the house revealed smoking 1-2 days per week. It is interesting, those children who are not expose to ETS at home (34%) as reported by Gonzales and colleagues, were exposed to passive smoking when spent time in their grandparent’s house. In our study, three participants wrote in an open ques-tion (how many people smoke in your home?) that their child was not exposed to ETS at home but, there was exposition when divorced father took the child on the weekend, at a grandparent’s house and other relatives’ houses. Hopper and Craig (2000) found that non parental sources of ETS exposure are reported to be common in urban children, so this is another fact we must take in consideration when approaching and performing a complete his-tory taken when addressing a patient especially with asthma or other respiratory diseases.
Mannino and colleagues concluded from
Figure 17: Orientation by Doctor or Health Professional in the Last Year
Figure 18: Orientation given by Pediatrician Revealed by Smoker versus Non-smoker

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 45
Vol.: 100 - Núm 2 - Abril - Junio 2008
The AAP states tobacco-free environment is imperative, because tobacco is major health haz-ard to infants, children, adolescent and their fami-lies.
REFERENCES[1] Cardenas VM, Thun MJ, Austin H, Lally CA, Clark WS, Green-berg RS, Heath CW Jr. Environmental Tobacco Smoke and Lung Cancer Mortality in the American Cancer Society’s Cancer Preven-tion Study II. Cancer Causes Control. July 1997; 8(1):57-64.
[2} Vineis P, Alavanja M, Buffler P, Fontham E, Franceschi S, Gao YT, Gupta PC, Hackshaw A, Matos E, Samet J, Sitas F, Smith J, Stayner L, Straif K, Thun MJ, Wichmann HE, Wu AH, Zaridze D, Peto R, Doll R. Tobacco and Cancer Recent Epidemiological Evi-dence. Journal of the National Cancer Institute. January 21, 2004; 96(2): 99~106.
[3] American Academy of Pediatrics. Committee on Environmental Health. Environmental Tobacco Smoke: A Hazard to Children. Pedi-atrics. April 1997; 99(4):639~642.
[4] Murphy Timothy D, Passive Smoking and Lung Disease. E medi-cine. http://www.emedicine.com/ped/topic2625.htm Last Updated on February 20, 2004. Retrieved June 3, 2004.
[5] Peat JK, Keena V, Harakeh Z, Marks G. Parental Smoking and Respiratory Tract Infection in Children. Paediatric Respir Rev. Sept 2001; 2(3):207~13.
[6] Shiva F, Nasiri M, Sadeghi B, Padyab M. Effects of Passive Smoking on Common Respiratory Symptoms in Young Children. Acta Paediatric. Dec 2003; 92(12):1394~7.
[7] Hopper John A, Craig Kelly A. Environmental Tobacco Smoke Exposure among Urban Children. Pediatrics. October 2000; 106(4) p. e47
[8] Rapiti E, Jindal SK, Gupta D, Boffetta P. Passive Smoking and Lung Cancer in Chandigarh, India. The New Journal of Medicine, Lung Cancer. March 1, 1999; 23(3):183~9.
[9] Cloutier MM, Wakefield DB, Hall CB, Bailit HL. Childhood Asthma in an Urban Community Prevalence, Care System and Treat-ment. Chest 2002; 122:1571~1579.
[10] Mannino DM, Homa DM, Redd SC. Involuntary Smoking and Asthma Severity in Children: Data from the Third National Health and Nutrition Examination Survey. Chest 2002; 122(2): 409~415.
[11] Vineis P, Airoldi L, Veglia L, Olgiati L, Pastorelli R, Autrup H, Dunning A, Garte S, Gormally E, Hainaut P, Malaveille C, Matullo G, Peluso M, Overvad K, Tjonneland A, Clavel-Chapelon F, Boeing H, Krogh V, Palli D, Panico S, Tumino R, Bueno-De- Mesquita B, Peeters P, Berglund G, Hallmans G, Saracci R, Riboli E. Environmen-tal tobacco smoke and risk of respiratory cancer and chronic obstruc-tive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ Online First bmj.com. http://bmj.bmj-journals.com/ doi:10.1136/bmj. 38327.648472.82. Published January 28,2005. Retrieved January 30, 2005.
[12] Ramos Valencia, Gilberto. Estudio Continuo de Salud Para Los Municipios de Puerto Rico Año 2001. http://www.salud.gov.pr/esta-disticas/Estudio%20Continuo.htm. Retrieved June 8, 2004.
[13] Rizzi M, Sergi M, Andreoli A, Pecis M, Bruschi C, Fantulla F. Environmental Tobacco Smoke May Induce Early Lung Disease in Healthy Male Adolescents. CHEST 2004; 125(4):1387~1393.
14] Landau LI. Parental Smoking: Asthma and Wheezing Illness in Infants and Children. Pediatric Respiratory Rev. Sept 2001; 2(3):202~6.
[15] Joad JP. Smoking and Pediatric Respiratory Health. Clin Chest Med. Mar 2000; 21(1):37~46, vii~viii.
[16] Nuesslein TG, Fischer H, Welsing E, Riedel F, Rieger CH. Early Rather Than Recent Exposure to Tobacco Increases Bronchial Reac tivity. Klin Pediatr. Nov~Dec 2001; 214(6):365~70.
[17] Henderson AJ, Sherriff A, Northstone K, Kukla L, Hruba D. Pre-and Postnatal Parental Smoking and Wheeze in Infancy: Cross Cul-tural Differences. Avon study of Parents and Children Study Team.
Figure 19: Recurrent Diseases in Children Ex-posed to Non-smokers versus Smokers
Table 1: Reported Respiratory Diseases in Chil-dren
By Caregivers By Non- By Smokers p value in general Smokers Caregivers (n=594) Caregivers RecurrentRespiratory 48.3% 48.8% 44.4% 0.283 Diseases
Recurrent Otitits 17.4% 17.7% 15.3% 0.376
Recurrent Pharyngitis 15.5 % 16.2% 11.1% 0.176
Upper Respiratory 19.9% 20.6% 15.3% 0.186Diseases
lution, Infant Sudden Death Syndrome, recur-rent otitis and other cancers. Surprisingly, 31% of participants have not seen any anti-smoking pro-motion at all. Participants revealed they received information by pediatricians but, 34% of smokers reported didn’t receive information.
Pediatricians need to continue emphasiz-ing on smoking cessation, counseling, referring and treatment (AAP News, Dec. 2006). Public Schools need public reassurance of environmental pollution, other cancers and SIDS and counseling for smoking cessation due to higher prevalence of smokers in this population. Child health care cli-nicians are in a unique and important position to address parental smoking and the harmful health consequences to their children because of the reg-ular multiple contacts with parents (Winickoff et al, 2005). Winickoff and colleagues presented a Quick Guide to Tobacco Treatment: The 5 A’s for Child Healthcare Clinicians: Ask about tobacco use at visit, advise all tobacco users to quit, asses readiness to quit, assist tobacco users in quitting: (brief counseling, prescription, educational mate-rial), arrange follow up.

Vol.: 100 - Núm 2 - Abril - Junio 2008
46 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
Best D, Weitzman M, Pbert L. State-of-the-Art Intervention for Of-fice- Based Parental Tobacco Control. Pediatrics. 2005; 115(3)750-760.[36] AAP Division of Health Services Research. Pediatricians Cite Barriers to Tobacco Cessation Counseling. AAP News. December 2006; 27(12)17.
Acknowledgments I would like to thank to Dr. Wanda I. Figueroa, Dr. Vanessa Santini, Prof. Iris Parilla and Prof. Mike Vélez for all their guidance and their help including the statistical work. Thanks to all partici-pants in the study for taking time to answer the survey, to all teachers and school nurse for distributing and gathering all the information, to all Directors, and to the Department of Education for all the permits and their interest in this study. Thanks to all Faculty Members and Attending at H.U.R.R.A. Dr. Carmen Sanchez-Bartolomei, Dr. Hay-dee Garcia, Dr. Jesus Balestra and Dr. Fermin Sanchez for all their knowledge and support over the years at the Residency. And last but not least, thanks to my husband Dr. Ben Y. Ju and all my family espe-cially my mom Dr. Jean M. Gonzalez for all the moral support during this work and my training.
European Longitudinal Study of Pregnancy and Childhood. Eur Respir J. Aug 2001; 18(2):323~9.
[18] Lux AL, Henderson AJ, Pocock SJ. Wheeze Associated With Prenatal Tobacco Smoke Exposure: a Prospective, Longitudinal Study. ALSPAC Study Team. Arch Dis Chil. Oct 2000; 83(4):307~12.
[19] Boffetta P, Trédaniel J, Greco A. Risk of Childhood Cancer and Adult Lung Cancer after Childhood Exposure to Passive Smoke; a Meta- Analysis. Environ Health Perspect 2000; 108:73~82.
[20] Stocks J, Dezeteux C. The Effect of Parental Smoking on Lung Function and Development during Infancy. Respirology. Sept 2003; 8(3):266~85.
[21] Hackshae AK, Law MR, Wald NJ, The Accumulated Evidence on Lung Cancer and Environmental Tobacco Smoke. BMJ 1997; 315:980-988.
[22] Copas JB, Shi JQ. Reanalysis of Epidemiological Evidence on Lung Cancer and Passive Smoking. BMJ. February 2000; 320 :(12)417~8.
[23] Nyberg F, Agudo A, Boffetta P,Fortes C, Gonzalez CA, Pershagen G. A European Validation Study of Smoking and Environmental Tobacco Smoke Exposure in Non-smoking Lung Cancer Cases and Controls. Cancer Causes Control. Mar 1998; 9 (2):173~82.
[24] Brownson RC, Alavanja MC, Hock ET, Loy TS. Passive Smok-ing and Lung Cancer in Non-smoking Women. American Journal of Public Health. 2002; 82(11): 1525~1530.
[25] Lee Chien-Hung, Ko Ying-Chin, Goggins William, Huang Jhi-Jhu, Huang Ming-Shyan, Kao Eing-Long, Wang Hwei-Zu. Lifetime Environmental Exposure to Tobacco Smoke and Primary Lung Can-cer of Non-Smoking Taiwanese Women. International Journal of Epi-demiology. 2000; 29:224-231.
[26] Reuters Health Information. Maternal Smoking Linked to Chro-mosomal Instability in Fetal Cells. JAMA 2005; 293:1212~1222, 1264~1265.
[27] Roseby R, Waters E, Polnay A, Campbell R, Webster P, Spencer N. Family and Career Smoking Control Programmers for Reducing Children’s Exposure to Environmental Tobacco Smoke . The Co-chrane Library, Issue 4, 2004. http://www.cochrane.org/ Retrieved January 19, 2005.
[28] Samet JM. A Cohort Study of Active and Passive Smoking in Korea. Johns Hopkins University National Cancer Institute. http://www.cancerportfolio.org/ Retrieved January 30, 2005,
[29] Ley Num. 40 de 3 de agosto de 1993, Ley Num. 66 de 2 de marzo de 2006 www.lexjuris.com Retrieved December 20, 2006.
[30] Gergen PJ, Fowler JA, Maurer KR, Davis WW, Overpeck MD. The Burden of Environmental Tobacco Smoke Exposure on the Res-piratory Health of Children 2 Months through 5 Years of Age in the United States: Third National Health and Nutrition Examination Sur-vey, 1988 to 1994. Pediatrics. 1998; 101: 8 Retrieved on December 29, 2006.
[31] Gonzales M, Malcoe LH, Kegler MC, Espinoza J. Prevalence and Predictors of Home and Automobile Smoking Bans and Child Environmental Tobacco Smoke Exposure: a Cross-Sectional Study of U.S.-and Mexico-Born Hispanic Women with Young Children. BMC Public Health. 2006, 6:265.
[32] Mannino DM, Moorman JE, Kingsley B, Rose D, Repace J. Health Effects Related to Environmental Tobacco Smoke Exposure in Children in the United States: Data From the Third National Health and Nutrition Examination Survey. Arch Pediatri Adolesc Med. Jan 2001; 155(1):36-41.
[33] Sturm JJ, Yeatts K, Loomis D. Effects of Tobacco Smoke Expo-sure on Asthma Prevalence and Medical Care Use in North Carolina Middle School Children. Am J Public Health. 2004; 94:308-313.
[34] Hajnal BL, Braun-Fahrlander C, Grize L, Gassner M, Varonier HS, Vuille JC, Wuthrich B, Sennhauser FH. Effect of Environmen-tal Tobacco Smoke Exposure on Respiratory Symptoms in Children. SCARPOL Team. Swiss Study on Childhood Allergy and Res-piratory Symptoms with Respect to Air Pollution, Climate and Pollen. Schweiz Med Wochenschr. May 1999; 129(19):723-30.
[35] Winickoff JP, Berkowitz AB, Brooks K, Tanski SE, Geller A, Thompson C, Lando HA, Curry S, Muramoto M, Prokhorov AV,
JornadasCientíficas
AMPR
Acreditaciónde Jornadas
Créditoscategoría 1para el TEMEducacióncontinuadacontinuada
2 de agostoPrimera Serie de Seminarios deEducación Continuada para Médicos9:00am a 12:00am 4h/creditsHotel El conquistador - Fajardo
23 de agostoGeriatrics UpdateGeriatrics Update1:00pm a 5:00pm 4h/creditsSede de la AMPR
6 de setiembreCáncer11:30am a 5:00pmSede de la AMPR
27 de setiemb27 de setiembreVaccination Update1:00pm a 5:00pm 4h/creditsSede de la AMPR
4 de octubreMedical Emergencies1:00pm a 5:00 pm 4h/creditsSede de la AMPRSede de la AMPR
1 de noviembreEndocrinology Update1:00pm a 5:00pm 4h/creditsSede de la AMPR
Obtenga la documentación e informaciónen nuestro web site
www.asociacionmedicapr.orgsección Educación
o telefónicamente en la AMPR(787) 721-6969

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 47
Vol.: 100 - Núm 2 - Abril - Junio 2008
Artículos de repaso - Review Articles
DEVELOPMENTAL SEX DISORDERS: BRIEF REVIEW ON CURRENT ETHICAL ASPECTS
By: Francisco Nieves-Rivera, MD and Lilliam González-Pijem, MD *
* From the Section of Pediatric Endocrinology, Department of Pediatrics, U.P.R. School of Medicine, San Juan, Puerto Rico.
Address reprints to Francisco Nieves-Rivera, M. D., Pediatric Endocrinology Section, Department of Pediatrics, University of Puerto Rico School of Medicine, San Juan, Puerto Rico 00936-5067. <[email protected]>
ABSTRACT Among the urgent issues of the current medical ethics is the patient-doctor relationship. The care of patients with disorders of sexual dif-ferentiation (DSD) is an example of this relation-ship and its clinical ethical aspects. For centuries differences in gender have captured our atten-tion. We illustrate examples of DSD patients. The standard of care based on previously accepted hy-pothesis is discussed. Adult population with DSD provided evidence which challenged the way we used to care these individuals. The latter served as an opportunity to revised and develop the current standard of care for individuals with DSD.
The relationship between the suffering person and the ones empowered with the knowl-edge to heal remains as the urgent issue of cur-rent medical ethics. This is portrayed daily in the patient-doctor relationship (6). Disorders of sexual differentiation are not the exception.
For centuries differences in gender have captured our attention. In Genesis 1:27 we have one of the earliest recording on the subject: In the beginning, “God created human beings at his own image, as its own image created them, man and woman…” This would pose an immediate challenge to individuals born unable to fit either definition. It is likely that acquired or congenital problems of sexual differentiation have existed for more than two thousand years: “Because there are eunuchs –unable to have sex— who were born this way…. Mathew 19:12. ”. In our society, sex is as-signed at the time of birth based on the inspection of the external genitalia. Although uncommon, occasionally mother nature challenges us with in-dividuals to whom it is difficult to assign sex at birth because they seem to have ambiguity or an intermediate sex stage of development previously called hermaphrodites or intersex and now referred as developmental sex disorders (DSD).
The relationship between the suffering person and the ones empowered with the knowl-edge to heal remains as the urgent issue of cur-rent medical ethics. This is portrayed daily in the patient-doctor relationship (6).
Disorders of sexual differentiation are not the ex-ception.
For centuries differences in gender have captured our attention. In Genesis 1:27 we have one of the earliest recording on the subject: In the beginning, “God created human beings at his own image, as its own image created them, man and woman…” This would pose an immediate challenge to individuals born unable to fit either definition. It is likely that acquired or congenital problems of sexual differentiation have existed for more than two thousand years: “Because there are eunuchs –unable to have sex— who were born this way…. Mathew 19:12. ”. In our society, sex is as-signed at the time of birth based on the inspection of the external genitalia. Although uncommon, occasionally mother nature challenges us with in-dividuals to whom it is difficult to assign sex at birth because they seem to have ambiguity or an intermediate sex stage of development previously called hermaphrodites or intersex and now referred as developmental sex disorders (DSD).
From the cultural perspective, DSD have been addressed differently ranging from total ac-ceptance to complete rejection. For instance, the Greeks adored DSD, as illustrated by the cult to Hermaphroditus. According to Greek beliefs, Hermes and Aphrodite had a son they named Her-maphroditus. One day Hermaphroditus went for a walk and plunged into a lake to get some relief from the heat. Salmacis, a nymph, immediately fell desperately in love with him. Since the boy rejected her, she hugged him tightly and asked the gods to allow them to stay together forever. Her wish was granted and they stayed together as a single individual with two sexes. The Romans did not share the beliefs of the Greeks and used to kill individuals with DSD. They would let the vultures eat the newborn with DSD by leaving them at the top of a mountain.
Subjects with DSD born with 5 alpha re-ductase deficiency (i.e., the enzyme that catalyzes conversion of testosterone to dehydrotestoster-one), and initially assigned female sex as a rearing gender, have found social acceptance to switch to male gender during pubertal years, when male

Vol.: 100 - Núm 2 - Abril - Junio 2008
48 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
secondary sexual characteristics appear. This is entirely accepted within their community (e.g., Salinas, Dominican Republic) since it is perceive as advantageous situation for labor – more hands would be available to work in the crops for their survival.
During the Middle Ages, DSD were con-sidered God’s punishment to sin. By the Renais-sance, DSD were seen as a curiosity or Mother Nature’s error. In the 18th and 19th centuries, DSD became a subject of scientific interest. But it was not until the 40s and 50s, that the pivotal role played by hormones in sexual differentia-tion gave us a better understanding on the subject. Fine details on the molecular-biological control of sexual differentiation (i.e, gene expression) were described later during the 80s and 90s providing an in depth insight in the intricate signaling system responsible for sexual differentiation (5).
Case Illustration A typical case of DSD is illustrated in the following example. An 18 hour-old newborn is brought for evaluation because of ambiguous geni-talia. Family history was negative for babies born with similar alterations. The external genitalia showed an enlarged genital tubercle (~2 cm) with ventral chordee. There was posterior to anterior fu-sion of labioscrotal folds, with an opening at the base of the genital tubercle. There was a palpable mass in the left inguinal canal that did not resemble gonadal tissue. The right inguinal canal was empty. A pelvic sonogram showed the presence of mülle-rian structures –i.e., uterus, fallopian tubes, and upper vagina. At the end of the first week of life, the baby developed electrolyte derangements i.e., hyponatremia and hyperkalemia. Laboratory stud-ies showed an elevated 17 alpha hydroxyprogester-one serum levels (i.e., compatible with congenital adrenal hyperplasia secondary to 21 hydroxylase deficiency) with barely detectable cortisol. Karyo-type resulted in 46, XX chromosome complement in 100% of the analyzed cells. Congenital adrenal hyperplasia (CAH) was confirmed as the etiology accounting for DSD in this subject.
DISCUSSION Despite over 50 years of experience, the management of DSD secondary to CAH is still a challenge to the medical community.
A newborn female with CAH and DSD requires urgent expert medical attention (2). The ambiguity is highly distressing to the family, therefore, immediate comprehensive evaluation is needed by referral to, or visit by, a pediatric en-docrinologist. An important goal is to ensure that the parents develop a positive relationship toward their child.
A well-organized multidisciplinary team (including specialists in pediatric endocrinology, psychosocial services, pediatric surgery/urology, and genetics) is essential for the diagnosis and management of the infant with DSD. It is important for the coordinator of the team to have experience in the long-term care of newborns with CAH and to provide a consistent message to the parents. The members of the medical team should be cautious and avoid using confounding terminology related to the sex of the newborn. It is, thus, preferable to speak about gonads instead of testes or ovaries while information is being gathered.
In the late 90’s individuals with DSD challenged the scientific community management practices based on the belief that nurture could overcome nature. The standard of care based on this belief plus the paternalistic and secrecy ap-proach were not feel to be appropriate according to the patient’s own experience –i.e., nurture did not override nature. More recently, studies on the biological, psychological, and sociological aspects of gender identity –i.e., the sex with which we psy-chologically identify ourselves and which is usu-ally established by 18 months of age– have ques-tioned the theory of Money where brain can be modified by environment stimuli to adapt to desire rearing sex. Specifically, these studies challenge the concept that the sexual identity of an individual can be totally overcome by the environment (e.g., nurture vs. nature). Perhaps the major limitation of Money’s theory is its lack of follow-up studies and lack of systematic evaluation of individuals with DSD.
An illustration of this was the actual case cited often by Money of the identical twin siblings, known by the pseudonyms of John/Joan (3) born in the 60’s in Canada. By the age of seven months, both began to experience difficulties with voiding secondary to phymosis. At 8 months of age, both twins were taken to a local hospital for a routine circumcision. The electrocautery employed in the procedure in the first twin was apparently mal-functioning and burned John’s penis, causing ir-reversible damage. Several months later, while John/Joan’s parents were watching television, they came across a program in which an expert psy-chologist in DSD from Johns Hopkins was being interviewed. The family called the expert psychol-ogist, Dr. Money, and were immediately scheduled to travel to Baltimore, Maryland.
Dr. John Money was a psychologist born in New Zealand in 1921. He had completed his Ph.D. degree in Harvard at age 25. The topic of his dissertation was gender identity disorders. He became famous worldwide with the theory that it would be possible to modify gender identity early in life irrespective of genetic sex, by providing the desired sex rearing environment. In fact, the case of John/Joan gave him a worldwide reputation as an expert in the field.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 49
Vol.: 100 - Núm 2 - Abril - Junio 2008
Money realized the great opportunity to test his hypothesis upon the evaluation of the affected twin. Thus, female sex reassignment for John was recommended. John lived as Joan for his (her) first 14 years of life. As Joan (John) grew up she be-came isolated, having few friends. Money was still convinced that sexual identity could be completely modified by manipulating the environment. How-ever, in spite of environmental manipulations such as dressing as a girl and having long hair, Joan (formerly John) showed constantly male behavior, e.g., playing with cars. She was constantly reject-ed by her peers since her behavior was perceived as unusual. By the time she reached adolescence, Joan felt attracted to females. After years of re-ceiving psychotherapy sessions, Joan’s therapists recognized the need to tell the actual facts of her infancy. Finally, her father explained to her the ac-cident experienced when she was 8 months of age, opening a new chapter in Joan’s life. This would be followed by re-assuming a male gender iden-tity which was always present although in a hidden way.
Concomitantly, new reports challenging the validity of John Money’s theory on gender identity began to appear while former Joan began a new life. John required testosterone hormonal re-placement; because of orchiopexies he had earlier in life, plus several surgical interventions to im-prove the appearance of the phallus. He had a fam-ily of his own by marrying a woman with children. Unfortunately, John committed suicide at age 38.
Fausto Sterling, an embryologist from Brown University, has rejected the concept that human beings come solely with two sexes and two genders. In other words, sexual organs encompass a spectrum that ranges from a penis and scrotum to a clitoris and vagina. This is true when speaking solely on the ontogeny of the anatomic homolo-gous sexual structures (Table 1).
Emphasis was placed on the capacity to function as a male, i.e., void standing up and hav-ing a phallus that would likely respond to testoster-one or could be successfully surgically repaired. It was believed that the brain was malleable enough so as to easily adjust to the sex and gender identity assigned. As time went by, this position was chal-lenged by groups of affected individuals such as the “Intersex Society of North America” and the “Androgen Insensitivity Support Group” (8). The former group’s founder was born as a genetic male with incomplete virilization. Although his parents’ initial decision was to raise him as a boy, at age 1 ½ they were so worried about the appearance of the external genitalia that they decided to raise him as a girl. He underwent several surgical interventions to obtain an external appearance of the genitalia that would resemble the assigned sex, i.e., removal of the genital tubercle. At 19 she discovered her true DSD identity, i.e., 46, XY male pseudoher-maphrodite. She felt horrified and angry, and this gave her the determination to become activist and speak up gathering other similarly affected individ-uals under the Intersex Society of North America support group. The organization has already con-tacted approximately 400 individuals with similar situations. More recently, The American Academy of Pediatrics and the Lawson Wilkins Pediatric Endocrine Society have become sensitive to spe-cific concerns brought up by these groups.
Recent studies suggest that chromosomes may have an influence in the sexual behavior of some individuals independent of the hormonal milieu. This, in turn, speaks in favor of the no-tion that prenatal, and possibly postnatal, biologi-cal factors may play a major role in the human, gender specific behavior that cannot be obliterated or even modified by the environment. Dr. Milton Diamond, a psychologist from the University of Hawaii-Manoa, has expressed that we do not come into this world in a completely neutral fashion (4). There seems to be a certain degree of preexisting masculinity or femaleness at the time of birth that goes beyond whatever society might attempt to add. Drs. Keith Sigmundson and Diamond have brought to the scientific community the end results of Money’s experiment –“the thesis that social learning is above the imperatives imposed by bi-ology”. Specifically, Diamond proposes that gen-der identity and sexual orientation are present to a large extent at the time of birth. These are both the result of exposure to hormones and to other ge-netically predetermined influences in the brain and central nervous system. As a consequence, there are limitations in terms of the degree of flexibil-ity an individual has that would enable him/her to cross over from one gender to the other. Although the environment plays a role in assisting the indi-vidual to express his/her maleness or femaleness, Diamond says that nature has the predominant strength in terms of the innermost feelings of the
Table 1. External genitalia embryological homolo-gous
Female structures Embriological structure
Male structure
Clitoris Genital Tubercle GlansLabia majora Labioscrotal folds ScrotumLabia minora Urethral folds Penile shaft
Fallopian tubes, uterus, inner vagina
Mullerian ducts Utricle
Wolfian ductsEpididymus, vas-deferens, seminal vesicles, prostate
From the medical care perspective, in the past it was accepted that secrecy and paternalism were the proper way to deal with DSD.

Vol.: 100 - Núm 2 - Abril - Junio 2008
individual that allow him/her to identify either with a male or female, boy or girl (i.e., gender identity). Diamond and Sigmundson believe that we should continue to assign male or female sex to babies born with intersex, but to limit interven-tions to hair length, clothing, and names (i.e., re-versal aspects). Permanent surgical interventions should be deferred until the patient can articulate the gender with which he/she identifies better.
This position has also been supported by The Harry Benjamin International Gender Dys-phoria Association (7). John/Joan’s case demon-strated that the biological marks left in the psy-chosocial identity cannot be easily erased by the environment . In fact, in somewhat isolated com-munities where babies born with 5 alpha reductase deficiency whose brains are exposed to en-dogenous
testosterone and who are initially raised as girls, accept without hesitation gender change at age twelve when often virilization becomes evident. This is also reassured by the social advantages it gives and in agreement with the gender with which they identify. In terms of biological differ-ences, studies in the mid 80s in Amsterdam identi-fied an area in the hypothalamus that was twice the size in homosexual males compared to heter-osexuals. Dean Hamer reported differences in X chromosome patterns in studies in 1993 and 1995 performed in gay brothers.
However, some studies have supported the capability of a psychosexual development that is congruent with gender even in the presence of DSD such as female psychosexual identity in fe-male pseudohermaprhodites with congenital ad-renal hyperplasia (1). Females with CAH show behavioral masculinization, most pronounced in gender role behavior, less so in sexual orientation, and rarely in gender identity. Currently, there is insufficient evidence to support rearing a 46, XX infant fully virilized (i.e., Prader stage 5) as a male. Whereas studies of women whose surgery was performed 20-30 years ago indicate a range of psychosexual difficulties, there is reason for optimism in that the outcome will be better with current surgical and medical treatment. Decisions concerning sex assignment and associated genital surgery must consider the culture in which a child and her/his family are embedded. The decision about surgery should be made by the parents, to-gether with the clinical team, after complete dis-closure of all relevant clinical information and all available options have been discussed, and after informed consent has been obtained (9). The goals of the surgery are: 1) genital appearance compati-ble with gender; 2) unobstructed urinary emptying without incontinence or infections; and 3) good adult sexual and reproductive function.
Nowadays, the decision regarding an in-
50 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO dividual with intersex ought to be shared with the patient and his/her guardians –e.g., parents–, fol-lowing the contemporary practices in medicine. Physicians should assume that the parents of a newborn with ambiguous genitalia can partici-pate and contribute in the discussion openly and honestly in terms of the available options. Psycho-logical support should be provided to the patient and the relatives at the time of the diagnosis and subsequently, as needed. Counseling should ad-dress areas related to adequate sexual functioning, possible reconstructive surgeries, gender role, and living with a chronic illness. In addition, anxiety, depression, contraception, dyspareunia, or other aspects of sexual dysfunction must be addressed.
In spite of the advances attained in under-standing changes at the molecular biology level re-sponsible for sexual ambiguity in the newborn, the main consideration in the management of these
patients remains the sensitive and compassionate care that ought to be provided by health profes-sionals at all times in their interaction with the par-ents.
The Harry Benjamin International Gender Dysphoria Association published a set of standards of care for gender identity disorders in February 2001. The standards set guidelines based on con-sensus from professionals who care for patients with gender identity disorders.
In summary, physicians and health profes-sionals have witnessed the development of means to better understand the regulation of sexual differ-entiation in the human being. The interplay among the genetic sex, phenotypical expression, and psy-chological gender sex identity in DSD has been reviewed. We have learned that biological factors seem to set limits in the capacity to adapt a new gender identity that nurturing cannot overcome. Ethical aspects pertaining to DSD are discussed. Parents should be encouraged to participate in the decision of sex assignment and provided with the appropriate support.
REFERENCES1. Bomalaski, M.A. (2005). A practical approach to intersex. Urology Nursing, 25(1), 11-18, 23-24.
2. Clayton, P.E., Miller, W.L., Oberfield. S.E., Martin Ritzén, E., Sippell, W.G., Speiser, P.W. (2002). Consensus statement on 21-hydroxylase deficiency from the Lawson Wilkins Pediatric Endocrine Society and The European Society for Paediatric Endocrinology. Journal of Clinical Endocrinology and Metabolism, 87(9), 4048-4053.
3. Colapinto, J., (2001). As nature made him: The boy who was raised as a girl. New York: HarperCollins Publisher, 1-289
4. Diamond, M. (2004). Sex, gender, and identity over the years: a changing perspective. Child Adolescent Psychiatry Clinics of North America, 13, 591-607.
5. Feldman Witchel, S., Lee, P. (2002). Ambiguous Genita-lia In: Pediatric Endocrinology. Sperling, M. (Editor) Saunders, 111-133.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 51
Vol.: 100 - Núm 2 - Abril - Junio 2008
6. Lugo, E. (2001). Relación Médico/Paciente: Encuentro interpersonal ética y espiritualidad, 1-222
7. Meyer, W., Bockting. W.O., Cohen-Kettenis, P., Cole-man, E., DiCeglie, D., Devor. H., Gooren, L., Joris Hage, J., Kirk, S., Kuiper, B., Laub, D., Lawrence, A., Menard, Y., Monstrey, S., Patton, J., Schaefer, L., Webb, A., Christine Wheeler, C. (2001) The Harry Benjamin International Gender Dysphoria Association’s Standards of Care for Gender Identity Disorders, 6th revision.
8. Domurat-Greger, A. 240 pp. Intersex in the Age of Ethics Hagerstown, Md., University Publishing 1999
9. Lee PA, Houk Christopher, Ahmed SF, Hughes IA , et al Consensus Statement on Management of Intersex Disorders. Pediat-rics 2006;118;488-500
AcknowledgementsThe authors would like to thank Professor María L. Collazo for her extensive review of the manuscrip
RESUMEN Entre los temas urgentes de la ética clínica actual está la relación médico-paciente que con-tinúa siendo fundamental. El manejo de pacientes con desórdenes de diferenciación sexual (DSD) representa una instancia de aspectos éticos en la clínica. A través del tiempo DSD ha sido tema de interés colectivo. Se ilustran ejemplos de pa-cientes con DSD. Se discute la hipótesis que sir-vió de base en el manejo aceptado y que posteri-ormente fue desafiada por la evidencia recogida en seguimiento de adultos con DSD. Esto último sir-vió de referencia en la revisión y establecimiento del estándar vigente para el cuidado de pacientes con DSD.
You don’t needanother card.
You need a better one
AsociaciónMédica de PuertoRico MasterCardCredit Card with
WorldPointsRewards
Our members deserve the very best. That’s why we’re pleased to present
the Asociacion Medica de Puerto Rico Platinum Plus MasterCard
credit card with WorldPointsrewards from Bank of America.
This No-Annual-Fee card deliversppremium service, unsurpassed
rewards, a money-savingIntroductory Annual Percentage Rate (APR), and the attention to
security our members expect.
Request your AMPR Platinum Pluscard. Just call tool-free and refer to
Priority Code FACL67
1.866.438.6262or apply on-line from our web site
www.asociacionmedicapr.org
Technology In PhysicianTechnology In Physician
Iniciativa de informática médicade la AMPR
Herramientas informáticas para la me-dicina del nuevo milenio.
Con sulte y forme parte de este empren-dimiento de vanguardia.
www.asociacionmedicapr.orgSeccion Herramientas Clínicas en Internet
Vol.: 100 - Núm 2 - Abril - Junio 2008
DIABETIC KETOACIDOSIS IN PEDIATRICS: MANAGEMENT UPDATEBy: Ricardo García-De Jesús MD *
* From the Pediatric Critical Care Medicine Section, Department of Pediatrics UPR School of Medicine, University Pediatric Hospital
Address reprints to: Ricardo García-De Jesús MD – Department of Pediatrics, UPR School of Medicine, PR Health Science Center, Rio Piedras, P.R. 00936. E-mail < [email protected]>
ABSTRACT The management of diabetic ketoacidosis has remained unchanged for several years. Lately, as more evidence has been available, practice has been modified to simplify the management and avoid complications. For the last twenty years pa-tients admitted to the Pediatric Intensive Care Unit (PICU) at the University Pediatric Hospital, were managed following a protocol where the patient’s volume deficit was calculated based on the de-gree of dehydration (mild, moderate, and severe) and then administered accordingly over 36 hours. Also, we administered an insulin IV bolus (0.1u/kg) prior to starting the insulin drip. Our experi-ence employing this approach in the pediatric pop-ulation had been successful having no morbidity or mortality due to cerebral edema. Nevertheless, new evidence, based on studies and international consensus, suggest changes should be made in the management of DKA. It is the new consensus that patients should be rehydrated over 48 hour period, and that the initial insulin bolus should be avoided. Of course, it needs to be pointed out, that the clini-cal status of each patient is the barometer by which therapy should be tailored. The following informa-tion is the new suggested guideline in the manage-ment of DKA.
Severe diabetic ketoacidosis (DKA) is a life-threatening complication of diabetes mellitus. The frequency of DKA at onset of diabetes corre-lates with the regional incidence of type 1 diabetes and is more common in young children, children without a first-degree relative with type 1 diabetes, and individuals whose families are of lower socio-economic status.1 The mortality rate for DKA in children is around 0.15% to 0.31%.2 Despite the more apparent issues of hypovolemia and acidosis, clinically significant cerebral edema, which occurs in 1% of cases, is the most serious risk to children. Because cerebral edema occurs in the context of DKA, reduction of the incidence of DKA should be a major goal of treating children with diabetes.
Diabetic ketoacidosis is the result of complex met-abolic derangements caused by absolute or relative insulin deficiency resulting in hyperglycemia and
an accumulation of ketone bodies in the blood, with subsequent metabolic acidosis and dehydration. In addition, there are increased levels of counter regulatory hormones (glucagon, catecholamines, glucocorticoids and growth hormone) causing ab-normal metabolism of carbohydrates, proteins and fat. The reported mortality rates in children with DKA are usually low, but once cerebral edema de-velops, death occurs in some 20–25%, and signifi-cant morbidity, including pituitary insufficiency, occurs in 10 - 25% of survivors. Where medical services are less well developed, the risk of dying from DKA is greater, and children may die before receiving treatment. Overall, cerebral edema ac-counts for 60 – 90% of all DKA related deaths in children.
Clinical features of DKA include history of polyuria, polydipsia, polyphagia, and weight loss (especially in the diabetes de novo cases). The child will also have signs and symptoms of dehydration and/or shock: mottled skin, delayed capillary refill, dry mucosa, tachycardia, tachyp-nea (Kussmaul breathing), decreased peripheral pulses, sensory changes, oliguria or anuria. Some patients may also present with nausea, vomiting, and abdominal pain that may mimic an acute ab-domen. Fever, increased leukocyte count with left shift, and nonspecific elevation of serum amylase may also be found.
The biochemical criteria for the diagnosis of DKA include hyperglycemia (blood glucose higher than 200 mg/dL) with acidosis (venous blood pH < 7.3 or serum bicarbonate <15 mmol/L), elevated serum ketones (β-hydroxybutyrate and acetoacetate), and ketonuria.3, 4 Clinical symptoms also may vary from mild to severe. Usually hyperapnea, lethargy, headache, acetone breath and sensorium changes maybe indicative of severity and possible cerebral edema. DKA is generally categorized by the se-verity of the acidosis, with mild DKA defined as a venous pH <7.3 and bicarbonate <15 mmol/l; moderate DKA as a pH <7.2 with a bicarbonate <10 mmol/l; and severe DKA as a pH <7.1 and bicarbonate <5 mmol/l. 3, 4
52 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 53
Vol.: 100 - Núm 2 - Abril - Junio 2008
Once DKA is identified, the objectives of patient management are: correction of dehydra-tion, restoration of blood glucose to near normal levels, correction of acidosis and reversion of ke-tosis. Also attention should be given to identify and treat precipitating events and to individualize treatment depending on patient’s age and severity while avoiding therapeutic complications. These considerations and recommendations are in agree-ment with those recently endorsed by the Lawson Wilkins Pediatric Endocrine Society (LWPES), European Society for Pediatric Endocrinology (ESPE), and the International Society for Pediatric and Adolescent Diabetes (ISPAD).5, 6
During the initial emergency assessment and evaluation, the clinician should take the fol-lowing steps:
Perform a clinical evaluation to establish the • diagnosis and determine its cause (while care-fully looking for evidence of infection).
Weight the patient and measure height or • length. Determine body surface area. (see Fig-ure 1)
Assess the patient’s degree of dehydration.•
Assess level of consciousness.•
At the same time, several supportive meas-ures should be undertaken:
Secure the airway and empty the stomach by • continuous nasogastric suction to prevent pul-monary aspiration in the unconscious or se-verely obtunded patient.
Give antibiotics to febrile patients after obtain-• ing appropriate cultures of body fluids.
Provide supplementary oxygen to patients • with severe circulatory impairment or shock.
Bladder catheterization, if a child is uncon-• scious or unable to void on demand (e.g., in-fants and ill young children).
Consider placing a heparin-locked peripheral • intravenous catheter for convenient and pain-less repetitive blood sampling.
A cardiac monitor should be used for continu-• ous electrocardiographic monitoring.
Use a flow chart to record a patient’s clinical • and laboratory data, including vital signs (e.g., heart rate, respiratory rate, blood pressure, level of consciousness [Glasgow coma scale]), details of fluid and electrolyte therapy, amount of administered insulin, and urine output.
Place an intravenous line (or intaosseous, if • necessary) for fluid resuscitation and manage-ment. Preferentially two access sites.
After initial evaluation and assessment obtain blood sample for laboratory measurement of:
serum or plasma glucose; •
electrolytes (basic metabolic panel (BMP) or • Renal Profile with magnesium)
venous (arterial only in critically ill patient) • pH; pCO2; pO2;
complete blood count (CBC);•
HbA1c•
Perform a urinalysis for ketones.•
If there is evidence of infection, obtain appro-• priate specimens for culture (blood, urine, and throat).
If laboratory measurement of serum potassium • is delayed, perform an electrocardiogram for baseline evaluation of potassium status;
Dextrostick every hour from the moment of • admission
Once initial stabilization is performed, the child should receive care in a unit that has:
Experienced nursing staff trained in written • guidelines for DKA management and appro-priate monitoring in children.
Access to laboratories for frequent and timely • evaluation of biochemical variables.
A specialist with training and expertise in the • management of DKA should direct inpatient management.
Children with severe DKA (long duration of • symptoms, compromised circulation, or de-pressed level of consciousness) or those who are at increased risk for cerebral edema (e.g., <5 years of age, low pCO2, high urea nitrogen) should be considered for immediate treatment in a pediatric intensive care unit (PICU).
Hydration The patient should receive maintenance intravenous fluids (IVF’s) plus the deficit correc-tion.
A commonly used formula is the Mosteller for-mula, published in 1987: Metric (area in square meters from weight in kilograms and height in cen-timeters):
Figure 1.

Vol.: 100 - Núm 2 - Abril - Junio 2008
54 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
The objectives of fluid and electrolyte replacement therapy are restoration of circulating volume, so-dium replacement, intra and extra cellular water deficit correction and restoration of glomerular fil-tration to enhance renal clearance of glucose and ketones. Avoid excessive rates of fluid adminis-tration so as not to exacerbate the risk of cerebral edema.5, 6, 7
Administer a Fluid Bolus of an isotonic solution (0.9NSS or Ringer’s Lactate) at 10-20ml/kg over 1 hour. In the presence of decompensated shock consider more rapid infusion rate, and even repeat the dose if necessary. Voiding usually im-plies that vascular space has been expanded. Re-member, try to obtain two IV access to facilitate patient management. Once this initial fluid bolus has been given, subsequent fluid management should be given with a solution that has a tonicity of 0.45% saline or more (0.9% saline or Ringer’s lactate) with added potassium. To ensure proper hydration, total fluid rate must remain constant; this will minimize rapid changes in serum osmo-larity, which may be associated to cerebral ede-ma.8
The rate of intravenous fluid (IVF’s) ad-ministration should be calculated to rehydrate a patient at an even rate over 48 hours.
Calculate total fluid to be administered at • 3000ml/m2/day for the next 48 hrs. Subtrac-tion of the initial fluid bolus is NOT neces-sary.
Add dextrose 5% to IVF’s when glucose falls • to 250mg/dL.
Potassium replacement therapy will be re-• quired regardless of the serum potassium concentration; start replacing potassium after initial volume expansion, presence of voiding and concurrent with starting insulin therapy. However, if the patient is hypokalemic, start potassium replacement immediately after ini-tial volume expansion and before starting in-sulin therapy. If the patient is hyperkalemic, defer potassium replacement therapy until urine output is documented. If immediate se-rum potassium measurements are unavailable, an electrocardiogram may help to determine whether the child has hyper- or hypokalemia. Add the amount of potassium sufficient to maintain serum potassium levels in the normal range. Usually 20-30 mEq/L KCL.
Serum phosphate levels should be monitored, • and severe hypophosphatemia (<1mg/dL) should be treated with potassium phosphate while carefully monitoring serum calcium concentrations to avoid phosphate-induced hypocalcemia.
This occurrence generally can be avoided if • potassium phosphate concentration in the in-travenous fluid does not exceed 20 mEq/L.
Remember to re-evaluate the patient frequent-• ly and chart intake and output closely.
Insulin therapy All patients must receive insulin. Insulin is essential for restoring blood glucose to normal and suppressing lipolysis and ketogenesis. Rehy-dration alone decreases the blood glucose concen-tration but does not reverse ketoacidosis. Start an insulin infusion after the patient has received ini-tial volume expansion. Do not give insulin load-ing dose. Insulin should be given as a continuous infusion (See Figure 2). The infusion rate should be at 0.1 unit/Kg/hr. The serum glucose should fall approximately at 50-100 mg/dL/hr.
Infusion rate should remain between 0.05 - 0.1 U/kg/h until resolution of ketoacidosis (pH > 7.30 and bicarbonate > 15 mmol/L or closure of the anion gap). However, even if the blood glucose concentration is normal or near to normal, intra-venous insulin therapy should not be discontinued until ketoacidosis has resolved. To prevent the de-velopment of hypoglycemia, dextrose should be added to the intravenous fluid when the plasma glucose has fallen to approximately 250 mg/dL.
When ketoacidosis has resolved and the change to subcutaneous insulin is planned, the first subcutaneous injection should be given at an ap-propriate interval before stopping the insulin in-fusion to allow sufficient time for the subcutane-ously injected insulin begin to be absorbed. The starting dose of subcutaneous insulin in new-onset patients recovering from DKA is based on a total daily dose (TDD) of insulin of 0.75 U/kg/day in prepubertal children, and 1 U/kg/day in pubertal patients.4,7,8 This should be discussed with the endocrinology service by consultation. After pa-tient starts to tolerate diet, the dextrose should be removed from IVF’s, and depending on the rehy-dration status IVF’s may be decreased.
During the management of the patient with DKA the following clinical and biochemical monitoring should be performed:
Insulin drip may be prepared as follows:
a. 100 units regular insulin diluted in 100 ml normal saline; (1 unit=1ml)
b. 50 units regular insulin in 500 ml 0.9NSS (0.1 unit= 1ml)
Figure 2.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 55
Vol.: 100 - Núm 2 - Abril - Junio 2008
Formulas
Corrected Sodium:
Measured Serum Na+* {1.6 mEq Na+ * (Serum glucose – 150 mg/dL) / 100}
Serum Osmolarity:
(N=285-295 mOsm/L)
(2 X Serum Na+) K+ + (Serum glucose / 18) + (BUN / 2.8)
Figure 3.
Initially serum sodium can be factitiously de-creased. It is important to calculate the true so-dium levels (See Figure 3). If the patient is hyper-natremic, then fluid replacement should be even more gradual to avoid rapid changes in osmolar-ity. Occasionally after patients acidosis has been resolving, it may re-appear or persist. It may be due to inadequate hydration, discontinuation of insulin infusion or hyperchloremic metabolic aci-dosis. The last one is usually secondary to the pro-longed use on normal saline solution (NSS), and it resolves without treatment. If persistent, you may need to decrease the amount of NSS administered, changing IVF’s temporarily to Ringer’s lactate.
Always watch for complications of therapy, like inadequate rehydration, hypoglycemia, hypokale-mia, and cerebral edema.
Once diet is initiated, calories may be cal-culated as shown in Figure 4. Total calories must be divided as 55% carbohydrates, 30% fat, and 15% proteins. The diet should be given in six feed-ings: breakfast (20% total calories), morning snack (10%), lunch (20%), evening snack (10%), dinner (20%) and night snack (10%).
All patients on DKA should always be consulted to the pediatric endocrinology service. The patient and parents will need orientation and training to deal with the newly diagnosed diabe-tes.
Figure 4.Max. 2500 kcal/ day, unless recommended by dieti-
tian or endocrinologist
Initially, plasma glucose should be measured • hourly.
Serum glucose, serum electrolytes (and calcu-• lated sodium), urinalysis (ketones), pH, pCO2, TCO2, anion gap, calcium and phosphorus levels should be measured every 4 hours for the first 8 hours and then every 6 hours until they are normal.
All data must be recorded carefully on a flow • sheet.
In all patients, continuous cardiovascular and • respiratory monitoring should be performed.
Close Intake and output should be followed • every hour.
Close neurological monitoring should be doc-• umented on the initial 48 hours of manage-ment.
Cerebral edema should be ruled out in cas-es of sudden and severe headaches, changes in the level of consciousness, combativeness, disorienta-tion, changes in vital signs and/or changes in the pupillary reaction.8,9 Re-evaluation of the ABC’s, fundoscopic examination and emergency head CT should be rapidly performed. If brain edema is the cause of patient’s signs and symptoms administer 0.25- 0.5 gm/Kg mannitol 25% or 3ml/Kg 3%NSS over 20 minutes to control brain swelling. Rapid sequence intubation should be considered if pa-tient’s neurological status continues deteriorating or doesn’t improve with the osmolar therapy
It is important to remember that even severe acidosis is reversible by fluid and insulin replace-ment. Insulin stops further synthesis of ketoacids and promotes ketone use. The metabolism of ke-toanions results in the regeneration of bicarbonate and correction of acidemia. Treatment of hypovo-lemia improves tissue perfusion and restores renal function, which increases the excretion of organic acids and reverses any lactic acidosis, which may account for up to 25% of the acidemia. There is no data to support the routine use of bicarbonate in the management of DKA.
Age Calories Kcal/day Weight (Kg) CaloriesKcal/Kg
First year 1000
Each year after 100
<10 100
10-20 50
20> 20

Vol.: 100 - Núm 2 - Abril - Junio 2008
Dunger DB. Pediatrics; 113(2): e133-40 01-FEB-2004.7. Diabetes Mellitus, Type 1, e-Medicine. William H Lamb, MD, FRCP, FRCPCH, Clinical Lecturer, Department of Child Health, The General Hospital, Bishop Auckland, UK. Article Last Updated: Oct 19, 20078. Berrios, F. Diabetic Ketoacidosis: recognition and management. Pediatric Critical care Newsletter. Vol. 3 Num. 1 Jul-Sep 2001.9. Glaser N, Barnett P, McCaslin I, et al. Risk factors for cerebral edema in children with diabetic ketoacidosis: the Pediatric Emergency Medicine Collaborative Research Com-mittee of the American Academy of Pediatrics. N Engl J Med 2001;344:264–9
ResumenEl manejo de cetoacidosis diabética (CD) a per-manecido sin cambiar por varios años. Última-mente, según más evidencia ha estado disponible, se ha modificado la práctica para simplificar la terapia y evitar complicaciones. Por los pasados diez años, los pacientes admitidos a la unidad de cuidado intensivo pediátrica (UCI) en el Hospital Pediátrico de la Universidad de Puerto Rico, fuer-on manejados usando un protocolo donde el défi-cit del volumen del paciente era calculado basado en el grado de deshidratación (leve, moderado, y severo) y re-hidratado agresivamente sobre 36 ho-ras. También, administrábamos un bolo de la in-sulina intravenosa (0.1u/kg) antes de comenzar el goteo de la insulina. Nuestra experiencia, que em-pleaba este acercamiento en la población pediátri-ca, había sido acertada no teniendo ninguna mor-talidad secundario a edema cerebral. Sin embargo, la nueva evidencia, basada en estudios y consenso internacional, sugiere que cambios sean realizados al manejo de CD. Las nuevas tendencias sugieren que los pacientes deben ser rehidratados sobre un período de 48 horas, y que el bolo inicial de la in-sulina debe ser evitado. Por supuesto, necesita ser precisado, que el estado clínico de cada paciente es el barómetro por el cual la terapia debe ser adapta-da. El siguiente artículo repasa el manejo de CD basado en las nuevas sugerencias.
56 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO In the case of the known diabetic with an episode of DKA, the patient and the family will also need a multidisciplinary evaluation and inter-vention to asses the reasons that precipitated the event and educate them in manners to avoid this serious complication. In addition the diabetic pa-tient will need a multidisciplinary evaluation that includes, but is not limited to: dietitian, social worker, ophthalmologist, dentist, psychologist, and diabetes specialist nurse. In summary, DKA is a life-threatening complication of insulin dependent diabetes melli-tus which carry a significant morbidity and mortal-ity for the pediatric population. Adequate identi-fication, evaluation and management of DKA are essential for the successful recovery of the patient. Although our past experience in treating DKA us-ing a more rapid hydration protocol had been un-eventful, we are presenting the new protocol to be employed following evidence-based recommenda-tions by the Pediatric Endocrine Society consensus statement among others. The recommendations are easier to follow, and try to ensure the lowest complications. Always remember, that the clinical status of each patient is the barometer by which therapy should be tailored. REFERENCES1. Curtis JR, To T, Muirhead S, et al. Recent trends in hospitalization for diabetic ketoacidosis in Ontario children. Diabetes Care 2002;25:1591–6.2. Pinkey JH, Bingley PJ, Sawtell PA, et al. Presenta-tion and progress of childhood diabetes mellitus: a prospec-tive population-based study: The Bart’s-Oxford study group. Diabetologia 1994;37:70– 4.3. Diabetes Care. 2005;28(1):186-212.4. Diabetes Care, Volume 29, Num. 5, MAY 20065. Wolfsdorf J. Diabetic ketoacidosis. Pediatr Diabe-tes ; 8(1): 28-43 01-FEB-2007 6. European Society for Paediatric Endocrinology/Lawson Wilkins Pediatric Endocrine Society consensus state-ment on diabetic ketoacidosis in children and adolescents.
Clínicas de SaludMultifásicas
Un servicio gratuitopara la comunidad
Todos los meses en diferentesMunicipios
Asociación Médica de Puerto RicoAuspicia:
Infórmese en la seccion Eventos de nuestro web site o llamando al (787) 721-6969
Invitamos a nuestros medicos, enferrmeras y voluntarios a participar en esteservicio desinteresado a la Comunidad

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 57
Vol.: 100 - Núm 2 - Abril - Junio 2008
Reporte de Casos - Case Reports
EVIDENCED BASED MANAGEMENT OF NEONATAL HEMANGIOLYMPHANGIOMA:
A Case Report.By: Maribel Campos MD *, Víctor Ortiz MD **, Maria S. Correa MD ‡, Pedro J.Santiago Borrero MD ₤,
Ines Garcia MD *, Lourdes Garcia MD, Marta Valcárcel *
* From the Section of Neonatology, Department of Pediatrics, UPR School of Medicine, ** Department of Surgery University Pediatric Hospital, ‡ Department of Pathology, UPR School of Medicine, and ₤ Section of Hematology-Oncology, Department of Pediatrics UPR School of Medicine.
Address Reprints to: Maribel Campos MD, UPR School of Medicine, Department of Pediatrics, Neonatology Section, P.O. Box 365067, San Juan, PR 00936-5067. Tel. 787-777-3225, Fax 787-758-5307, [email protected].
ABSTRACTHemangiolymphangioma is a mixed vascular mal-formation that is detected in the prenatal period by sonography. Five cases of prenatal diagnosis have been reported that have resulted in termination of pregnancy (two) or aggressive versus purely surgi-cal post-natal management. We present the case of an infant with pre-natal diagnosis of a multicystic intra-abdominal mass that received surgical man-agement followed by conservative treatment.
INDEX WORDS: Antenatal diagnosis, hemangiol-ymphangioma, ultrasonography, fetus.
CASE REPORTThis is a baby boy with a prenatal diagnosis of a cystic abdominal lesion in the left flank. At 32 weeks of gestation age (GA), intrauterine drain-age of the mass was performed for treatment and diagnostic purposes, due to evidence of severe ab-dominal distention. Cyst aspirate revealed blood stained fluid. The plan was to allow the pregnancy to continue towards term. At 34 weeks GA, the patient was re-evaluated and obstetric sonogram revealed mass enlargement due to fluid re-accu-mulation. Elective cesarean section performed at 34.6 weeks GA, due to findings on 34-week sono-gram. At birth, he presented respiratory difficulty requiring assisted ventilation. APGAR score was six & 7 at 1 and 5 minutes, respectively. KUB per-formed on admission revealed displacement of the umbilical venous and arterial catheter (Figure 1). Abdominal sonogram revealed a large cystic mass in the left flank without visualization of the left kidney. Abdominal CT confirmed the extension of the cystic mass with displacement of the pre-vertebral vessels and a small left kidney located anteriorly within the mass. At 24 hours of age, a surgical team including both members of Pediatric Surgery and Pediatric Urology Service performed an exploratory celiotomy. The Pediatric Surgeon excised the mass in total including the left kidney, adrenal gland and a portion of the diaphragm (Fig-ure 2).
The surgeon observed invasion of the pre-verte-bral vessels. The entire complex mass including the kidney and the adrenal was fixed in formalin and sent to Pathology.
Figure 1. Note the displacement of the umbilical catheters and bowel
Figure 2. Mass during surgery.

Vol.: 100 - Núm 2 - Abril - Junio 2008
58 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
On macroscopic examination, the speci-men consisted of an irregular soft tissue mass that measured 8.0 x 6.0 x 1.5 cm, and weighed 41.0 gm. Upon sectioning, the kidney and the adrenal gland were adhered to an edematous multicystic soft tis-sue mass located at the hilar region of the kidney and extending beyond the adrenal gland. The cysts ranged in size from 0.5 to 3.0 cm in greatest diam-eter. Most were empty but the largest ones con-tained a dark tan fluid. The internal lining was tan and trabeculated. The kidney measured 5 x 3 x 1.5 cm and weighed 16 gm. Upon sectioning, it pre-sented well demarcation between the cortex and the medulla. The cortex measured 0.2 to 0.3 cm in thickness. The pyelocaliceal system appeared to be unremarkable. The adrenal gland measured 3 x 2 x 1 cm and weighed 2 gm. Externally and on section, it was grossly unremarkable.
Microscopic examination of the mass re-vealed a vascular malformation composed of large vascular channels with blood content admixed with lymphatic channels; hence our pathologic designa-tion of hemangiolymphangioma (Figures 3, 4). In some areas, these vascular channels had a calcified lining and no endothelium at all. Few vessels were larger with a thicker wall. The kidney and the ad-renal gland were histologically normal.
On the postoperative period, the patient developed severe pulmonary hypertension and recurrent pneumothoraces. He suffered a com-plicated neonatal course that included episodes of hypoxemia that required treatment with High Frequency Oxilatory Ventilation (HFOV) and Mil-rinone. After extubation, the patient continued to be oxygen dependent, requiring treatment with diuretics. Following stabilization, follow up radio-graphic studies were performed that showed recur-rence of the cystic lesion with extension from sub-diaphragmatic area to the pelvis. Although the use of interferon 2a and sclerosing agents are effective in some cases3, we decided to manage the patient conservatively with close follow up; and consider its use at a later stage. Follow up ultrasounds re-vealed persistence of a cystic mass with a vascu-lar component (Figure 5). He is now 15 months old and has continued gaining weight, tolerating feedings with minimal respiratory findings. He is not requiring oxygen supplementation. Based on the latest radiographic findings, the location of the mass, and the patient’s clinical status; it was de-cided to continue conservative management of the mass.
DISCUSSIONPrenatal diagnosis of hemangiolymphangioma has been proven to be possible by current sonographic technology.1-5 Intrauterine identification of such a complex mass aids in the obstetric management, especially in the delivery. In the previously report-ed case of intra-abdominal presentation, it led to termination of pregnancy, because it was
considered to have extensive fetal involvement. We received an infant with a large intra-abdominal cystic mass diagnosed at 32 weeks GA. Differential diagnosis of the mass included meconium pseudocyst, mesenteric cyst status post hemorrhage or infection, lymphangioma and a renal cystic mass with secondary hemorrhage or infection. We assessed the final diagnosis of the mass when histopathologic evaluation was completed. As reported by Tseng et al, hemangiolymphangioma should be suspected in any fetus that presents with a multilocular mass with both cystic and solid components and a propensity for rapid growth and invasion into adjacent structures.4
Figure 3. Note dilated vascular channels with blood con-tent and unremarkable endothelium. H & E, 100X.
Figure 4. Note vessels devoid of blood; instead contained lymph. H & E, 40X.
Figure 5. Flow diagram within the mass.

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 59
Vol.: 100 - Núm 2 - Abril - Junio 2008
Detection of blood flow signals by Doppler can also aid in the diagnosis. Although our patient pre-sented many of these characteristics, the inability to visualize the left kidney suggested that the mass was of renal origin. Pre-natal evaluation in this case lead to the delivery of the infant in a tertiary center and involvement of both pediatric surgery and urology services in his initial management that was limited to mass resection. Involvement of the major vessels precluded complete mass excision that lead to mass recurrence after an uphill neona-tal course.
Although surgical excision is reported as the method of management for hemangiolym-phangioma, 9-12 incomplete resection carries the risk of recurrence. In intra-abdominal lymphangi-omas, resection followed by marsupialization of the remaining tissue is recommended.12 In the case of a mixed lesion such as a hemangiolymphangioma; this could lead to uncontrollable bleeding, as it is difficult to distinguish from a hemorrhagic lym-phangiomatous cyst and the vascular component of the mass.
Review of the existing literature revealed the use of interferon 2 a and sclerotherapy with OK 432 to be effective in the management of he-mangiolymphangioma; but aggressive manage-ment was not proven to be effective in other cases and the use of interferon 2 a has been associated to significant side effects in infants. Izquierdo et al., reported a case of a 4 year old with intra-abdomi-nal hemangiolymphangioma treated with steroids without improvement that resulted in death due to massive hemorrhage associated to Kasabach-Merritt coagulopathy.6 Of the other cases reported in the literature, those were a total excision of the mass was accomplished presented the best prog-nosis.4,7,8,13,14 This finding and the possibility of spontaneous regression, guided our decision to manage the patient conservatively with close fol-low up.
This case represents the possibility that these patients are able to thrive even in the pres-ence of a large invasive mass due to its capacity of spontaneous regression.
REFERENCES1. Shah KD, Chevernak FA, Marchevsky AM, Rosenberg JC and Berkowitz, RL. Fetal giant hemangiolymphangioma: report of a case. Am J Perinatol. 1987 Jul;4(3):212-4.
2. Giacalone PL, Boulot P, Marty M, Deschamps F, Laf-fargue F, Viala JL: Fetal hemangiolymphangioma: a case report. Fetal Diag Ther. 1993 Sep-Oct;8(5):338-40.
3. Senoh D, Hanaoka U, Tanaka Y, Tanaka H, Hayashi K, Yanagihara T and Hata T. Antenatal ultrasonographic features of fetal giant hemangiolymphangioma.
4. Tseng JJ, Chow MM and Ho ES. Fetal axillary hemangi-olymphangioma with secondary intralesional bleeding: serial ultra-sound findings. Ultrasound Obstet Gynecol. 2002 Apr;19(4):403-6.
5. Miño Mora M, López Pedrera, MC, Povedano Cañizares, B, etal: Antenatal diagnosis of a cervical hemangiolymphangioma. Prog Diag Prenat. 2002;14(3):136-39.
6. Izquierdo Ramírez J, Angulo Hernández O, Arias y Arias J and Farfan Canto JM: Hemangiolymphangioma of the abdominal cavity complicated with consumption coagulopathy. Bol Med Hosp Infant Mex. 1975 Mar-Apr;32(2):277-85.
7. Morán Penco JM, Borella F, Garibaldi L, Toma P, Dodero P. Hepatic hemangiolymphangioma in an infant. An Esp Pediatr. 1983 Nov;19(5):411-3.
8. Chadna, S, Bhatnagar V, Mitra, DK and Upadhyaya P: Hemangiolymphangioma of the Urinary bladder in a child. J Pediatr Surg. 1987 Nov;22(11):1051-2.
9. Aston SJ, Beasley RW and Thorne CHM. Grabb and Smith’s Plastic Surgery, Fifth Ed, Lippincott-Raven, 1997: 191-203.
10. Mulliken JB and Glowaski J. Hemangiomas and vascular malformations in infants and children: A classification based on en-dothelial characteristic. Plast Reconstruct Surg. 1982;69:412-20.
11. Oldham KT, Colombani PM and Foglia RP. Surgery of Infants and Children Scientific principles and practice, Lippincott-Raven Publishers, 1997: 1727-1742.
12. Stringel G. Pediatric Surgery, Third Ed, Saunders. 2000: 965-983.
13. Vitalta J and Mascaro JM. Hemangiolymphangioma of the tongue treated by transfixion technique. J Dermatol Surg Oncol. 1985 Feb;11(2):168-70.
14. Zacharia TT, Ittoop A, Perumpillichira JJ and Chavham G. Sonographic appearance of a congenital parotid gland hemangiol-ymphangioma simulating malignancy in an infant. J Clin Ultrasound. 2003 Nov-Dec;3(19):493-6.
RESUMEN
El hemangiolinfangioma es una malformación vascular mixta que se puede detectar prenatal-mente por medio de sonografía. De los cinco casos reportados que han diagnosticados intraútero, dos han resultado en terminación del embarazo y tres en tratamiento agresivo versus manejo puramente quirúrgico. Le presentamos el caso de un infante con historial de una masa multi-cística intra-ab-dominal que fue diagnosticada prenatalmente y se trató quirúrgicamente seguido por manejo conser-vador.
La AsociaciónMédica en acción...
Visita nuestro Web Site yentérate de las múltiples
actividades y serviciosque realiza tu Asociación
www.asociacionmedicapr.org
Vol.: 100 - Núm 2 - Abril - Junio 2008
Portada
Manuel Quevedo Báez, MDPor Eduardo Rodríguez Vázquez, MDPresidente de la Asociación Médica de Puerto Rico
“Siempre, en la historia humana, la juventud ha sido la de impulsos generosos, la que ha sen-tido más los anhelos de avance de progreso. Sin titubear ni temer, en su afán de ir hacia adelante aún rompiendo con normas de viejo establecidas. Sólo así es que puede realizarse el progreso en to-dos los órdenes”
Manuel Quevedo Báez, MD
El Dr. Manuel Quevedo Báez nació en el año 1865 en el pueblo de Sabana Grande locali-zado en el sur de la isla de Puerto Rico. Sus padres fueron Domingo Quevedo y Carmen Báez. En su pueblo natal cursó los primeros grados y al igual que otras familias acomodadas de la época fue en-viado a continuar sus estudios de bachillerato en el Colegio de la Congregación de los Padres Je-suitas localizado en Santurce. Este Colegio había sido fundado en el 1858, en el antiguo Seminario Conciliar de San Idelfonso en el Viejo San Juan y trasladado a Santurce posteriormente al año 1886, debido a problemas con las Autoridades Guber-namentales de Puerto Rico, los Jesuitas tuvieron que cerrar el Colegio de Santurce, trasladando el mismo, a la ciudad de Quito, en Ecuador.
El joven Quevedo terminó sus estudios de bachillerato ese mismo año del 1886 en el Insti-tuto Civil de Segunda Enseñanza, localizado en el mismo edificio que albergaba el Colegio de los Jesuitas (este edificio está localizado en la parada 19 de la Avenida Ponce de León en Santurce y es hoy ocupado por el Departamento de Salud del Es-tado Libre Asociado de Puerto Rico.)
Tanto el Colegio como el Instituto con-taron entre sus alumnos con un sinnúmero de jóvenes, luego estudiantes de medicina y médicos, que después se distinguirían en diferentes áreas de la cultura, la ciencia y la política de nuestro país; entre estos figuraban: Antonio Fernández Vega, Manuel Quevedo Báez, Cayetano Coll y Toste, Manuel Guzmán Rodríguez, Manuel Martínez Roselló, José Luis Padilla Otero, Ángel Franco, José Marxuach, Francisco Del Valle Atiles, Ga-briel Ferrer Hernández, Rafael Del Valle Rodrí-guez, Gabriel Villarronga, Pedro Hernández, José De Jesús Tysol, entre otros.
En esa misma época fundó, siendo su di-rector, el periódico El Palenque de la Juventud, en unión de otros jóvenes estudiantes. En esta gestión participaron, entre otros, Luis Sánchez Morales, Mariano Auril y Pedro de Angelis.
Es alrededor de esta época que parte rumbo a España a iniciar sus estudios de medicina. Sus inclinaciones literarias no fueron ininterrum-pidas durante los años que cursó sus estudios en la facultad de medicina de Madrid.
En el año del 1894 finalizó su ca-rrera de médico obteniendo el grado de doctor en medicina y cirugía. Luego de su regreso a Puerto Rico y revalidar su titulo de médico, practicó la medicina en varios pueblos de la isla como Utuado, Mayagüez y Barceloneta, establ-eciéndose, finalmente, en San Juan. En esos años se unió al grupo de los liberales que perseguían el ideal autonomista.
Luego de la Guerra Hispanoamericana in-gresa en las filas del Partido Republicano que di-rigía su colega, el Dr. José Celso Barbosa. Es con el inicio del siglo XX que hace realidad su sueño, colaborando en la fundación de un organismo que albergara a los médicos de Puerto Rico. El 21 de septiembre de 1902 el Dr. Quevedo Báez, en unión a los doctores Ramón Ruiz Arnau, José E. Saldaña, Manuel Figueroa, J.M. Amadeo, Rafael Vélez López, José N. Carbonell, Manuel Fernández Na-cer y otros visionarios, celebran la Asamblea Cons-tituyente de la Asociación Médica de Puerto Rico. En ese año el Dr. Manuel Quevedo Báez es electo primer Presidente de la Asociación Médica de Puerto Rico. Durante su presidencia (1902-1904) funda, en 1903, el Boletín de la Asociación Médica de Puerto Rico, siendo su primer editor el Dr. Ramón Ruiz Arnau. Contribuye en la organización de una Junta de Reválida, siendo su Secretario de 1903 a 1931. Durante esos primeros años mantiene una columna en el Boletín, la que llamó “Nuestras Capacidades Médicas”. En la misma uno de los personajes al que rinde homenaje, a pesar de haber sido su adversario político, fue al Dr. Ramón E-meterio Betances. Como médico durante esas dé-cadas, fue el que publicó más artículos sobre asun-tos pediátricos, totalizando cinco (5). Dirigió en el 1905 la Revista del Ateneo, además de contribuir en diversas revistas y periódicos como El Puerto Rico Ilustrado, El Mundo, El Boletín Mercantil, Plumas Amigas y otras.
60 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 61
Vol.: 100 - Núm 2 - Abril - Junio 2008
Fue el Presidente del Ateneo Puerto-rriqueño del 1912 a 1914, fundador y presidente de la Academia de Medicina Puertorriqueña, Sin-dico de la Universidad de Puerto Rico, Profesor y Presidente del Instituto Universitario José de Die-go, Fundador de la Academia Antillana de la Len-gua y Conferenciante en la Escuela de Medicina Tropical. Son algunas de las múltiples posiciones que ocupó durante su vida. Le hizo honor otro an-tiguo alumno del Colegio, el historiador y médico Cayetano Coll y Toste, preparando el voluminoso trabajo sobre la Historia de la Medicina y Cirugía de Puerto Rico, en dos (2) tomos, publicados en 1946 y 1949, respectivamente, por la Asociación Médica de Puerto Rico.
Como decía el Dr. Salvador Alana Soto y cito: “El Dr. Quevedo Báez fue uno de los más fecundos y fáciles prosistas que ha producido la clase medica del país”.
En resumen, nuestro primer presidente, el Dr. Quevedo Báez se formó emulando al hombre del renacimiento, convirtiéndose al final de sus días en uno de ellos: conocimiento todo y pleni-tud.
ReferenciasDr. S. Arana-Soto - Catálogo de Médicos de PR de Siglos Pasados - Año 1966 - Pag. 345
Antonio López de Santa Ana, S.I. - Los Jesuitas en Puerto Rico de 1858 a 1886 - Contribución a la Historia General de la Educación en Puerto Rico.
Asociación Médica de Puerto Rico - Memorias 1902-1989
Asociación Médica de Puerto Rico - Prensa Médica - Año 14 , Núm. 2 - Los primeros cien años de la Asociación Médica de Puerto Rico - Trasfondo histórico - Pag. 7
Asociación Médica de Puerto Rico - Boletín - Vol 95, Núm 1 - Enero-Febrero 2003 - Eduardo Rodriguez Vázquez, MD - Apuntes para la Historia de la Pediatría en Puerto Rico - Pág. 42
Norberto Lugo Negron - Un precursor sabaneño: Doctor Manuel Quevedo Báez - Asociación Médica de Puerto Rico - Año 2002
Dr. S. Arana-Soto - Diccionario de Médicos Puertorriqueños - Año 1963 - Pag. 48
El Dr. Manuel Quevedo Báez en dos etapas diferentes de su lucha por el en-grandecimiento de la clase médica y los principios sagrados de la profesión.

Vol.: 100 - Núm 2 - Abril - Junio 2008
62 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
CME Credits Vol.100 No 02, 2008
Instructions:To obtain CME four (4) credits AMA 1, you should read and study the following articles and be able to answer the questions correctly. After answering the questions below fill in your personal informa-tion, cut and send with a check for $20.00 payable to: Asociacion Medica de Puerto Rico.
From article:
“THROMBOCYTOSIS IN ILLICIT DRUGS-EXPOSED NEWBORNS”
Thea Calderón MD, et al.
1. The main causes of thrombocytosis in newborns are:
A) infection and inflammation
B) Down syndrome
C) exposure to cephalosporin and illicit drugs
D) all of the above
E) none of the above
2. The most common cause of thrombocytosis in neonates is:
A) infection or inflammatory process exposure
B) exposure to methadone during pregnancy
C) vitamin deficiencies
D) all of the above
E) none of the above
3. The illicit drug most frequently associated with thrombocytosis in the newborn is:
A) heroin
B) cocaine
C) methadone
D) marihuana
E) thinner
From article:
‘PERCEPTION OF PARENTS REGARDING THEIR CHILDREN’S WEIGHT’
Nazario Rodriguez IJ, et al.
4. Most parents perceive their child has an ade-quate weight, when he is overweight due to:
A) a failure of parents to recognize overweight status of their child
B) a reluctance to admit that their child is over-weight
C) a lack of understanding of what “overweight” means
D) all of the above
E) none of the above
5. In early childhood education to prevent obesity includes:
A) proper nutrition with selection of low-fat snacks
B) good exercise/activity habits
C) monitoring of television viewing
D) all of the above
E) a and b
From Article:
‘DEVELOPMENTAL SEX DISORDERS: BRIEF REVIEW ON CURRENT ETHICAL ASPECTS’
Nieves-Rivera et al.
6. Match accordingly the internal genitalia embry-ogenesis homologous:
A) clitoris ___ penile shaft
B) labia majora ___ glans
C) labia minora ___ scrotum
7. Chose the best answer: Among the urgent issues of the current medical ethics are:

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 63
Vol.: 100 - Núm 2 - Abril - Junio 2008
A) the doctor – hospital relationshipB) the hospital staff administration relationshipC) the patient – doctor relationshipD) all of the aboveE) none of the above
8. The goals of surgery in cases of developmental sex disorders (DSD) are:A) genital appearance compatible with gonadsB) unobstructed urinary emptying without inconti-nence or infectionsC) good adult sexual and reproductive functionD) all of the aboveE) none of the above
From the article:“DIABETIC KETOACIDOSIS IN PEDIAT-RICS: MANAGEMENT UPDATE”Ricardo García-De Jesús MD
9. Diabetic ketoacidosis is characterized by:A) hyperglycemia and vomiting. B) moderate dehydration, metabolic acidosis, hy-perglycemia and ketonuria.C) vomiting, fever and hyperglycemiaD) high mortality rate even with adequate manage-ment.E) hyperkalemia, hypoglycemia and hyponatrem-ia. 10. Initial management of DKA includes all Ex-cept: A) fluid bolus B) blood glucose level C) arterial or venous blood gas D) regular insulin IV bolus E) serum electrolytes
11. A 5 y/o boy with DKA and a weight of 20kg has received 20ml/kg fluid bolus, and has already voided. He is started on insulin drip at 0.1unit/kg/hr. His dxt is 315. Which fluid regimen should we start?A) 0.9NSS/D5W + 20mEq/Lt KCL at 3000mL/M2/day
B) 0.9NSS/D5W + 40mEq/Lt KCL at 1800mL/M2/day C) 0.33NSS + 20mEq/Lt KCL at 3000mL/M2/dayD) 0.45NSS + 20mEq/Lt KCL at 3000mL/M2/dayE) 0.45NSS/D5W + 20mEq/Lt KCL at 1500mL/M2/day
12. The most feared complication of diabetic ke-toacidosis is:A) hypernatremiaB) water intoxicationC) brain edemaD) hyperglycemiaE) hyperkalemia
ANSWERS1- (A) (B) (C) (D) (E)2- (A) (B) (C) (D) (E)3- (A) (B) (C) (D) (E)4- (A) (B) (C) (D) (E)5- (A) (B) (C) (D) (E)6- (A)_______ (B)_______ (C) ________7- (A) (B) (C) (D) (E)8- (A) (B) (C) (D) (E)9- (A) (B) (C) (D) (E)10- (A) (B) (C) (D) (E)11- (A) (B) (C) (D) (E)12- (A) (B) (C) (D) (E)
Fill in the following information:Name __________________________________Licence No. _____________Postal Adress_____________________________________________________________________Telephone _____________Fax _______________Cut along the dotted lines, or print from our web site (Scc. Educación), and send answers with check for $20.00 payable to:
Asociacion Medica de Puerto RicoPO Box 9387
San Juan, PR 00908-9387
Web sitewww.asociacionmedicapr.org
Vol.: 100 - Núm 2 - Abril - Junio 2008

Vol.: 100 - Núm 2 - Abril - Junio 2008
64 BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO
OFICINAS ADMINISTRATIVAS SUBSCRIPCIONES Y ANUNCIOS
Asociación Médica de Puerto Rico• Ave. Fernández juncos Núm. 1305 • PO Box 9387 • SANTURCE, Puerto Rico 00908-9387
• Tel 787-721-6969 • Fax: 787- 724-5208 • Email: [email protected] EN BOLETIN Y WEB SITE
[email protected] Site: www.asociacionmedicapr.org
Publicación mensual - $40.00 anuales.
El “Boletín” se distribuye a todos los socios de la Aso-ciación Médica de Puerto Rico como parte de su cuota anual.
Todo anuncio que se publique en el Boletín de la Asoci-ación Médica de Puerto Rico deberá cumplir con las nor-mas establecidas por la Asociación Médica de Puerto Rico y la Asociación Médica Americana.
La Asociación Médica de Puerto Rico no se hace responsa-ble por los productos o servicios anunciados.
La publicación de los mismos no necesariamente implica el endoso de la Asociación Médica de Puerto Rico.
Todo anuncio para ser publicado debe reunir las normas establecidas por la publicación. Todo material debe entre-garse listo para la imprenta y con sesenta días de anteriori-dad a su publicación.
La AMPR no se hará responsable por material y/o artículos que no cumplan con estos requisitos.
Todo artículo recibido y/o publicado está sujeto a las nor-mas y reglamentos de la Asociación Médica de Puerto Rico. Ningún artículo que haya sido previamente publi-cado será aceptado para esta publicación. La Asociación Médica de Puerto Rico
no se hace responsable por las opiniones expresadas o puntos de vista vertidos por los autores, a menos que esta opinión esté claramente expresada y/o definida dentro del contexto del artículo.
Todos los derechos reservados. El Boletín está totalmente protegido por la ley de derechos del autor y ninguna per-sona o entidad puede reproducir total o parcialmente el ma-terial que aparezca publicado sin el permiso escrito de los autores.
“Boletín / Asociación Médica de Puerto Rico” is published monthly for $40.00 per year by:
Asociación Médica de Puerto RicoPO. Box 9387 San Juan, Puerto Rico 00908-9387
1305 Fernández Juncos Ave.Email: [email protected]
"POSTMASTER"
Send address changes to:
Boletín / Asociación Médica de Puerto Rico
1305 Fernández Juncos Ave. P.O. Box 9387
San Juan, Puerto Rico 00908-9387
18 de mayoClínicas Multifásicas Municipio de Aibonito9:00am a 2:00pm
31 de mayoCínicas MultifásicasHIMA San Pablo - Bayamón9:00am a 2:00pm7 de junioÇlínicas MultifásicasSanturce - Sede de la AMPR9:00am a 2:00pm11 de junioHuracanes, cambio climático y la epidemia del cólera en Puerto Rico 1855-1856Dr. Bernard Christenson7:00pmSede de la AMPR18 de junioCine - Dr. Bailey AshfordPresenta: Dr. Norman MaldonadoSede de la AMPR7:00pm
21 de junioCurso CPRSede de la AMPR1:00pm a 5:00pm
27 de junioConcierto lirico APTEL7:00 pmSede de la AMPR
8 de julio105 años del Boletin de la AMPRy nuevo web site7:00 pmSede de la AMPR
16 de julioConferencia: La Generación del 1930en la Ciencia PuertorriqueñaDr. José G Rigau Pérez7:00 pmSede de la AMPR
2 de agostoClínica Multifásica & Centro Unidode Detallistas9:00am a 12:00 amHotel El Conquistador - Fajardo
2 de agostoClínica de Salud MultifásicaMunicipio de Trujillo Alto - Oficina de Servicios al Ciudadano.9:00am a 2:00pmFarmacia Caney - Bo. Las Cuevas
6 de agostoCine: Los muchachos de ParisDr. Justino del Valle7:00pmSede de la AMPR13 de agostoMédicos inmigrantes siglo XIX PonceDra. Ivette Pérez Vega7:00pmSede de la AMPR15-17 de agosto54th Convención del Distrito Este AMPREmbassy Suite Hotel Dorado del Mar23 agostoJornada Científica Geriatrics update1:00 pm a 5:00 pm - 4 hs. créditosSede de la AMPR30 de agostoClínicas MultifásicasMunicipio de CaguasAntiguo CDT9:00 am a 2:00 pm
6 de setiembreJornada Científica Cáncer11:30 am a 5:00 pmSede de la AMPR
10 de setiembreDr. Agustín StahlDr. Eduardo Rodríguez Vázquez7:00pmSede de la AMPR13 de setiembreClínica MultifásicaMunicipio Mayagüez9:00 am a 2:00 pm
27 de setiembreJornada Científica Vaccination update1:00pm a 5:00 pm - 4hs. créditosSede de la AMPR
4 de octubreJornada Científica Medical Emergencies1:00 pm a 5:00 pmSede de la AMPR
1 de noviembreJornada Científica Endocrinology update1:00 pm a 5:00 pmSede de la AMPR
Calendario de actividades de la AMPRTodas las actividades pueden ser corroboradas en nuestro web site

BOLETÍN - ASOCIACIÓN MÉDICA DE PUERTO RICO 65
Vol.: 100 - Núm 2 - Abril - Junio 2008
Asociación Médica de Puerto RicoP.O. Box 9387
SAN JUAN, PR 00908-9387Teléfono (787) 721-6969
SOLICITUD DE INGRESONombre y apellidos (una letra de molde por casillero, deje un casillero vacío en los espacios)
Categoría de socio ACTIVO ACTIVO NO-RESIDENTE INTERNO-RESIDENTE ACTIVO ESPECIAL AFILIADO ESTUDIANTE
Sociedad Médica Distrito Cuota $ PayPal transacción #
A la Junta de Directores:Por la presente solicito ser admitido como socio de la Asociación Médica de Puerto Rico, para lo cual someto la siguiente informa-ción:Dirección Postal:
Ciudad
Ciudad
Estado
Estado
Codigo postal
Codigo postal
País
País
( ) -
( ) -
( ) - ( ) -
Teléfono
Teléfono
Dirección Oficina:
Horarios de Oficina Lunes Martes Miércoles Jueves Viernes Sábados
De:a:
AMPMAMPM
De:a:
AMPMAMPM
De:a:
AMPMAMPM
De:a:
AMPMAMPM
De:a:
AMPMAMPM
De:a:
AMPMAMPM
Marque los quec o r r e s p o n d a
Telefono celular Fax
Email@
Seguro Social # (opcional) Estado civilFecha de nacimiento
Ciudad y pais CiudadaníaDIA MES AÑO
Licencia # Especialidad Año de Graduación Escuela de Medicina
Nombre del padre Nombre de la madre Nombre del conyuge
Interno residente Afiliado EstudianteEntrenamiento
DIA MES AÑO
DesdeHasta
DIA MES AÑO
DesdeHasta DIA MES AÑO
Fecha de graduación
Escuela de Medicina
Por favor responda las siguientes preguntas:Ha sido convicto por alguna felonía en los últimos 5 años?Ha sido su licencia para practicar la medicina limitada, suspendida o revocada, en cualquier jurisdicción, en los últimos 5 años?Ha sido usted objeto de cualquier acción disciplinaria por cualquier Sociedad Médica o Junta de Hospital en los últimos 5 años?
Sí No
Si ha contestado en afirmativa a cualquiera de estas preguntas, por favor añada una explicación completa en hoja aparte.
Entiendo que la convicción de una felonía o la limitación, suspensión o revocación de la licencia para practicar la medicina o acción disciplinaria por cualquier Sociedad Médica o Junta de Hospital podrá, después de justo aviso y audiencia, resultar en la censura, suspensión o expulsión de un socio activo o afiliado.
Certifico que la información arriba brindada es cierta y completa.
FIRMA DEL SOLICITANTE____de ____________________________de________
USTED PUEDE OBTENER ESTE FORMULARIO, INSTRUCCIONES PARA MEMBRESÍA Y PAGO CON TARJETA DE CRÉDITO O PAYPAL EN NUESTRO WEB SITE www.asociacionmedicapr.org

Vol.: 100 - Núm 2 - Abril - Junio 2008
• Instrucciones para los Autores*El “Boletín” acepta para su publicación artículos relativos a medicina y cirugía y las ciencias afines. ¡Igualmente acepta artículos especiales y correspondencia que pudiera ser de interés general para la profesión médica. Se urge a los autores se esfuercen en perseguir claridad, brevedad, e ir a lo pertinente en sus manuscritos, no importa el tema o formato del manuscrito.El artículo, si se aceptara, será con la condición de que se publicara únicamente en la revista. Para facilitar la labor de revisión de la junta Editora y la del impresor, se requiere de los autores que sigan las siguientes instrucciones:• ManuscritoEl manuscrito completo, incluyendo las leyendas y referencias deberán estar escritos en maquinilla a doble espacio; por un sólo lado de cada página, en TRIPLICADO y con amplio margen (ARTÍCULO DEBERÁ SER ACOMPAÑADO POR UN “CD”). En página separada deberá incluirse lo siguiente: título, nombre de autor(es) y su grado (ej.: MD, FACP), ciudad donde se hizo el trabajo, el hospital o institución académica, patrocinadores del estudio, y si un artículo ha sido leído en alguna reunión o congreso, así debe hacerse constar como una nota al calce.El manuscrito debe comenzar con una breve introducción en la cual se especifique el propósito del mismo. Las secciones principales (como por ejemplo: materiales y métodos) deben identificarse con un encabezamiento en letras mayúsculas.Artículos referentes a resultados de estudios clínicos o investigaciones de laboratorio deben organizarse bajo los siguientes encabezamientos: introducción, Materiales y Métodos, Resultados, Discusión, Resumen (en español e inglés), Reconocimiento y Referencias.Artículos referentes a estudios de casos aislados deben organizarse en la siguiente forma: Introducción, Materiales y Métodos si es aplicable,Observaciones del Caso, Discusión, Resumen (en español e inglés), Reconocimientos y Referencias.• NomenclaturaDeben usarse los nombres genéricos de los medicamentos. Podrán usarse también los nombres comerciales, entre paréntesis, si así se desea se usará con preferencia el sistema métrico de pesos y medidas.• TablasLas tablas deben aparecer en hojas separadas. Estas deben incluir el título, y el número de la tabla debe estar en romano. Los símbolos de unidades deben limitarse al encabezamiento de las columnas. Se deben omitir líneas verticales en la tabla. Se usará en las tablas el mismo idioma en el cual está escrito el artículo. Deben limitarse las tablas a solo aquellas que contribuyan al mejor entendimiento del manuscrito.• IlustracionesLas fotografías y microfotografías se someterán como copias en papel de lustre, sin montar o en transparencias. En el reverso de la figura debe aparecer el número de la figura (arábigo) y el autor. Debe indicarse la parte superior de la ilustración.• ResumenUn abstracto no mayor de 150 palabras debe acompañar los manuscritos. Debe incluir los puntos principales que ilustren la substancia del artículo y la exposición del problema, métodos, resultados y conclusiones.• ReferenciasLas referencias deben ir numeradas sucesivamente de acuerdo a su aparición en el texto. Los números deben aparecer en paréntesis al nivel de la línea u oración. Al final de cada artículo las referencias deben aparecer en el orden numérico en que se citan en el texto. Deben utilizarse solamente las abreviaturas para títulos de revistas científicas según indicadas en el “Cumulative Index Medicus" que publica la Asociación Médica Americana.Las referencias deben seguir el patrón que se describe a continuación.1. Para artículos de revistas: Apellido(s) e iniciales del nombre del autor(es), título del artículo, nombre de la revista, año, volumen, páginas. Por ejemplo: Villavicencio R: Soplos inocentes en pediatría, Bol Asoc Méd P Rico 198 1; 73: 479-87. Si hay más de 7 autores, incluir los primeros 3 y añadir et al.2. Para citación de libros donde el autor(es) del capítulo citado es a su vez el (los) editor(es): Apellido(s) e iniciales del autor(es), título del libro, número de edición, ciudad, casa editora, año y página. Por ejemplo: Keith JD, Rowe RD, Vlad P: Heart disease in infancy and childhood, 3d. Ed., New York, MacMillan, 1978: 7893. Para citación de libros donde el editor(es) no es el autor(es) del capítulo citado se añade el autor(es) del capítulo y el título del mismo. Por ejemplo: Olley PM: Cardiac arrythmias; In: Keith ID, Rowe RD, Vlad P Eds. Heart disease in infancy and childhood,3d Ed., New York, MacMillan, 1978: 275-301• Cartas al EditorSe publicarán a discreción de la Junta Editora. Deben estar escritas en maquinilla a doble espacio, no deben ser mayores de 500 palabras, ni incluir más de cinco referencias.(ARTÍCULO DEBERÁ SER ACOMPAÑADO POR UN “CD”)* Estas “Instrucciones para los Autores` son de acuerdo a las normas establecidas por el Comité Internacional de Editores de Revistas Médicas en sus `Requisitos Uniformes para Manuscritos Sometidos a Revistas Bio-Médicas".
B LETÍNASOCIACIÓN MÉDICA DE PUERTO RICO
• Instructions to Authors*The “Buletín” will accept for publication contributions relating to the various areas of medicine, surgery and allied medical sciences. Special articles and correspondence on subjects of general interest to physicians will also be accepted. All material is accepted with the understanding that is to be published solely in this journal.All authors are urged to seek clarity, brevity, and pertinence in the manuscripts regardless of subject or format.In order to facilitate review of the article by the Editorial Board and the work of the printer, the authors must conform with the following instructions:• ManuscriptsThe entire manuscript, including legends and references should be typewritten double spaced in TRIPLICATE with ample margins (ARTICLES SHOULD BE ACCOMPANIED WITH A ”CD”). A separate title page should include the following: title, authors and their degrees (e.g. MD, FACP), city where the work was done, hospital or academic institutions, acknowledgments of financial sponsors, and if the paper has been at a meeting the place and date should be given.The manuscripts should start with a brief introductory paragraph or paragraphs which should state its purpose. The main sections (for example, Materials and Methods) should be identified by heading in capital letters.Articles reporting the results of clinical studies or laboratory investigation should be organized under the following headings: Introduction, Materials and Methods, Result if indicated, Discussion, Summary in English and Spanish, Acknowledgments if any, and References.• NomenclatureGeneric names of drugs should be used; trade names my also be given in parenthesis, if desired, metric units of measurement should be used preferentially.• TablesThese should be typed on separate sheets with the title and table number (Roman) centered. Symbol for units should be confined lo the column headings. Vertical lines should be omitted. The language used in the tables must be the same as that of the article. Include only those tables which will enhance the understanding of the article. They should supplement, not duplicate the text.• IllustrationsPhotographs and photomicrographs should be submitted as glossy prints (unmounted) or slides. They should be labeled in the back with the name of the authors and figure number (Arabic) and the top should be indicated. Legend to the figures should be typed on separate
sheet.• SummaryAn abstract not longer than 150 words should accompany all articles. It must include the main points that present the core of the article and the exposition of the problem, method, results, and conclusions.• ReferencesThese should be numbered serially as they appear in the text. The number should be enclosed in parenthesis on the line or writing and not as superscript, numbers. At the end of the article references should be listed in the numerical order in which they are first cited in the text. The titles of journals should be abbreviated according to the style used in the "Cumulative Index Medicus" published by the American Medical Association. The correct forms of references are as given below:1. For periodicals: Surname and initials of author(s), title of article, name of journal, year, volume, pages. For example: Villavicencio R.: Soplos inocentes en pediatría. Bol Asoc Med P Rico 198 1; 73: 479 87. If there are more than 7 authors list only 3 and add et al.2. For books when the authors of the cited chapter is at the same time the editor: Surname and initials of author(s), title, edition, city, publishing house, ~ear and page. For example: Keith JD, Rowe RD, Vlad P: Heart disease in infancy and childhood, 3d Ed., New York, MacMillan, 1978: 7893. For chapter in book when the author of the chapter is not one of the Olley PM: Cardiac arrythmias: In: Keith JD, Rowe RD, Vlad P. Eds. Heart disease in infancy and childhood, 3d Ed. New York, MacMillan, 1978, 275-301• Letters to the EditorWill be published at the discretion of the Editorial Board. They should be typewritten double-spaced, should not exceed 500 words nor more than five references.ARTICLES SHOULD BE ACCOMPANIED WITH A "CD" *The above 'Instructions to Authors" are according to the format required by the international Committee of Medical Journal Editors in its “Uniform Requirements for Manuscripts Submitted to Biomedical Journals”.