
Evidence based topical treatments for tinea cruris and tinea corporis: A summary of a Cochrane...
26
SYSTEMATIC REVIEW BJD British Journal of Dermatology Evidence-based topical treatments for tinea cruris and tinea corporis: a summary of a Cochrane systematic review E.J. van Zuuren, 1 Z. Fedorowicz 2 and M. El-Gohary 3 1 Department of Dermatology, B1-Q, Leiden University Medical Centre, PO Box 9600, 2300 RC, Leiden, The Netherlands 2 Bahrain Branch, The Cochrane Collaboration, Awali, Bahrain 3 Primary Care and Population Sciences, Faculty of Medicine, Aldermoor Health Centre, University of Southampton, Southampton, U.K. Correspondence Esther J. van Zuuren. E-mail [email protected] Accepted for publication 23 September 2014 Funding sources None. Conflicts of interest None declared. This paper is based on a Cochrane review published in Issue 8, August 2014 of The Cochrane Library (see http://www.CochraneLibrary.net for further information). Cochrane reviews are regularly updated as new evidence emerges and in response to comments and criticisms. The Cochrane Library should be consulted for the most recent version of this review. DOI 10.1111/bjd.13441 Summary Tinea cruris and tinea corporis are common fungal infections. Most can be trea- ted with a variety of topical antifungals. This review aimed to assess the evidence for the effectiveness and safety of topical treatments for tinea cruris and tinea corporis. Searches included the Cochrane Skin Group Specialised Register, CEN- TRAL in The Cochrane Library, Medline, Embase, LILACS and ongoing trials reg- istries (August 2013). One hundred and twenty-nine randomized controlled trials (RCTs) with 18 086 participants evaluated a range of interventions – mostly azoles. Pooling of data for several outcomes was only possible for two individual treatments. In five studies, terbinafine showed a statistically significant higher clinical cure rate compared with placebo [risk ratio (RR) 4 51, 95% confi- dence interval (CI) 3 10–6 56]. Data for mycological cure could not be pooled owing to substantial heterogeneity. Across three studies, mycological cure rates favoured naftifine (1%) compared with placebo (RR 2 38, 95% CI 1 80–3 14) but the quality of the evidence was low. Combinations of azoles with corticoster- oids were slightly more effective than azoles for clinical cure, but there was no statistically significant difference with regard to mycological cure. Sixty-five stud- ies were assessed as ‘unclear’ and 64 as being at ‘high risk’ of bias; many were over 20 years old, and most were poorly designed and inadequately reported. Although most active interventions showed sufficient therapeutic effect, this review highlights the need for further, high-quality, adequately powered RCTs to evaluate the effects of these interventions, which can ultimately provide reliable evidence to inform clinical decision making. What’s already known about this topic? • Tinea cruris and tinea corporis are common fungal infections of the skin. • A range of treatment options is available but it is unclear which is the most effec- tive. What does this study add? • All included treatments appeared to be effective but most comparisons, except for terbinafine and naftifine, were only evaluated in single studies. • Owing to limitations in study design and reporting, the quality of the evidence was graded low to very low. Tinea cruris and tinea corporis are dermatological conditions frequently seen by general practitioners and dermatologists. Tinea corporis (ringworm) refers to dermatophytosis of the trunk occurring mainly in children and adolescents, while tinea cruris (jock itch) affects the groin and is most frequently seen in adult men. 1,2 © 2014 British Association of Dermatologists 616 British Journal of Dermatology (2015) 172, pp616–641
Transcript of Evidence based topical treatments for tinea cruris and tinea corporis: A summary of a Cochrane...
SYSTEMATIC REVIEWBJD
British Journal of Dermatology
Evidence-based topical treatments for tinea cruris and tineacorporis: a summary of a Cochrane systematic reviewE.J. van Zuuren,1 Z. Fedorowicz2 and M. El-Gohary3
1Department of Dermatology, B1-Q, Leiden University Medical Centre, PO Box 9600, 2300 RC, Leiden, The Netherlands2Bahrain Branch, The Cochrane Collaboration, Awali, Bahrain3Primary Care and Population Sciences, Faculty of Medicine, Aldermoor Health Centre, University of Southampton, Southampton, U.K.
Correspondence
Esther J. van Zuuren.
E-mail [email protected]
Accepted for publication
23 September 2014
Funding sourcesNone.
Conflicts of interest
None declared.
This paper is based on a Cochrane review published
in Issue 8, August 2014 of The Cochrane Library
(see http://www.CochraneLibrary.net for further
information).
Cochrane reviews are regularly updated as new
evidence emerges and in response to comments and
criticisms. The Cochrane Library should be
consulted for the most recent version of this
review.
DOI 10.1111/bjd.13441
Summary
Tinea cruris and tinea corporis are common fungal infections. Most can be trea-ted with a variety of topical antifungals. This review aimed to assess the evidencefor the effectiveness and safety of topical treatments for tinea cruris and tineacorporis. Searches included the Cochrane Skin Group Specialised Register, CEN-TRAL in The Cochrane Library, Medline, Embase, LILACS and ongoing trials reg-istries (August 2013). One hundred and twenty-nine randomized controlledtrials (RCTs) with 18 086 participants evaluated a range of interventions –mostly azoles. Pooling of data for several outcomes was only possible for twoindividual treatments. In five studies, terbinafine showed a statistically significanthigher clinical cure rate compared with placebo [risk ratio (RR) 4�51, 95% confi-dence interval (CI) 3�10–6�56]. Data for mycological cure could not be pooledowing to substantial heterogeneity. Across three studies, mycological cure ratesfavoured naftifine (1%) compared with placebo (RR 2�38, 95% CI 1�80–3�14)but the quality of the evidence was low. Combinations of azoles with corticoster-oids were slightly more effective than azoles for clinical cure, but there was nostatistically significant difference with regard to mycological cure. Sixty-five stud-ies were assessed as ‘unclear’ and 64 as being at ‘high risk’ of bias; many wereover 20 years old, and most were poorly designed and inadequately reported.Although most active interventions showed sufficient therapeutic effect, thisreview highlights the need for further, high-quality, adequately powered RCTs toevaluate the effects of these interventions, which can ultimately provide reliableevidence to inform clinical decision making.
What’s already known about this topic?
• Tinea cruris and tinea corporis are common fungal infections of the skin.
• A range of treatment options is available but it is unclear which is the most effec-
tive.
What does this study add?
• All included treatments appeared to be effective but most comparisons, except for
terbinafine and naftifine, were only evaluated in single studies.
• Owing to limitations in study design and reporting, the quality of the evidence
was graded low to very low.
Tinea cruris and tinea corporis are dermatological conditions
frequently seen by general practitioners and dermatologists.
Tinea corporis (ringworm) refers to dermatophytosis of the
trunk occurring mainly in children and adolescents, while
tinea cruris (jock itch) affects the groin and is most frequently
seen in adult men.1,2
© 2014 British Association of Dermatologists616 British Journal of Dermatology (2015) 172, pp616–641

Clinical diagnosis based on history and appearance should
be supported by microscopy and/or culture to rule out other
diagnoses, for example eczema, erythrasma, intertrigo, psoria-
sis and contact dermatitis. Most infections can be cured with
topical treatments, whereas immunocompromised hosts or
very extensive and severe infections might require additional
oral treatment.1,2 Different groups of antifungals are available,
which include azoles, allylamines, benzylamines, hydroxy
pyridones and thiocarbamates, but it is uncertain which are
the most effective. Furthermore, general practitioners tend to
prescribe preferentially topical corticosteroid and antifungal
combination treatments, but it remains unclear if the benefits
of these combination therapies exceed those of topical antifun-
gals used as monotherapy.1–4
This is a summary of a Cochrane systematic review that was
conducted to evaluate the effects of different topical antifungal
treatments in people with tinea corporis and tinea cruris.1
Materials and methods
A systematic review of randomized controlled trials (RCTs)
was conducted according to a previously published protocol.1
Search strategies
We searched in 10 electronic databases and trial registers up
to August 2013 for eligible trials (Table 1). Earlier issues of
the journal Mycoses (1957–1990) had to be hand-searched
(M.E.-G), whereas studies from later issues were more readily
accessible as they were identified in the MEDLINE search. The
bibliographies of all included studies were also checked for
further references to relevant trials.
No language restrictions were imposed, and several studies
had to be translated prior to assessment. Two of the authors
(E.J.v.Z. and Z.F.) independently screened the titles and
abstracts for eligible RCTs.
Inclusion criteria
RCTs that compared any topical regimen, either used alone or
in combination with other therapies, for tinea cruris or tinea
corporis were included. Dermatophyte infection must have
been confirmed by microscopy and/or culture, and people
with a mix of infections (e.g. additional tinea pedis) were
included. Trials including photodynamic treatment were
excluded.
Outcome measures
The two primary outcomes were (i) rate of mycological cure
(negative mycological testing) and (ii) clinical cure (resolution
of sign and symptoms). Secondary outcomes were relapse and
recurrence; adverse events; duration of treatment and partici-
pant-judged cure.
Data extraction and synthesis
Study details and data were independently extracted and sum-
marized using a structured and pilot-tested data extraction
form, and any disagreements over data entry were resolved by
discussion. Using the Cochrane Collaboration’s domain-based
evaluation tool as described in Chapter 8, Section 8�5, of theCochrane Handbook for Systematic Reviews of Interventions, two authors
(E.J.v.Z. and Z.F.) independently assessed the risk of bias in
the included studies.5 If data were missing from trials, we
attempted, wherever possible, to contact the trial investigators
or sponsors of these studies to provide missing data or to clar-
ify study details. However, as most of these studies were more
than 10 years old we were not always successful in obtaining
these.
Dichotomous outcome data were reported as risk ratios
(RR) with their associated 95% confidence intervals (CI). In
accordance with Chapter 9 of the Cochrane Handbook for Systematic
Reviews of Interventions, using a random-effects model and only if
heterogeneity, as measured by the I2 statistic, was < 50%, data
were combined from individual studies into a meta-analysis.5
We reported heterogeneity as important if it was at least mod-
erate-to-substantial (I² > 50%).5 Most of the treatment
comparisons were presented as a narrative synthesis.
Results
Description of the included studies
The results of the literature search are shown in Figure 1. Of
the 364 references identified from the searches, 129 studies
Table 1 Electronic databases and trial registers searched
Electronic databases Trial registers
The Cochrane Skin Group Specialised Register ISRCTN registry (www.controlled-trials.com)
The Cochrane Central Register of Controlled Trials The U.S. National Institutes of Health ongoing trials register (www.clinicaltrials.gov)Medline The Australian and New Zealand Clinical Trials Registry (www.anzctr.org.au)
Embase The World Health Organization International Clinical Trials Registry Platform(www.who.int/trialsearch)
LILACS Cochrane Skin Group: Ongoing Skin Trials Register (www.nottingham.ac.uk/ongoingskintrials)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 617

met our inclusion criteria.6–134 However, 63 of these con-
tained no usable or retrievable data owing mainly to the
unavailability of separate data for the different tinea infections
(Table S1; see Supporting Information).72–134 The characteris-
tics of the remaining 66 studies are summarized in Table 2.6–71
Of the 129 included studies, 27 had a placebo arm as control,
98 had an active control arm and four studies included both.
The interventions comprised different groups of antifungals,
such as azoles (the majority), allylamines, benzylamines,
hydroxy pyridones, thiocarbamates and other topical antifun-
gals. Study duration was generally between 2 and 4 weeks.
Our primary outcomes and reports of adverse events were
addressed in most trials; however, duration of treatment,
participant-assessed cure and relapse were hardly or inade-
quately addressed.
Risk of bias of included studies
Each of the studies was assessed for risk of bias, and this was
reported for the individual domains (Fig. S1; see Supporting
Information). A risk of bias summary is presented in Figure 2.
The assessments of overall risk of bias indicated that 64 of the
129 studies were categorized as being at ‘high risk of bias’
(plausible bias that seriously weakens confidence in the
results) because one or more domains received a judgement
of ‘high risk’. The remaining studies (n = 65) were rated as
having an ‘unclear risk of bias’ (plausible bias that raises some
doubt about the result). Almost half (n = 63) of the 129
included studies contained no retrievable or usable data; in
the 66 that provided data, 35 were categorized as being at
‘high risk of bias’ and 31 as having an ‘unclear risk of bias’,
indicating that a judgement of high risk of bias was not spe-
cifically associated with having ‘no retrievable or usable data’.
Effects of interventions
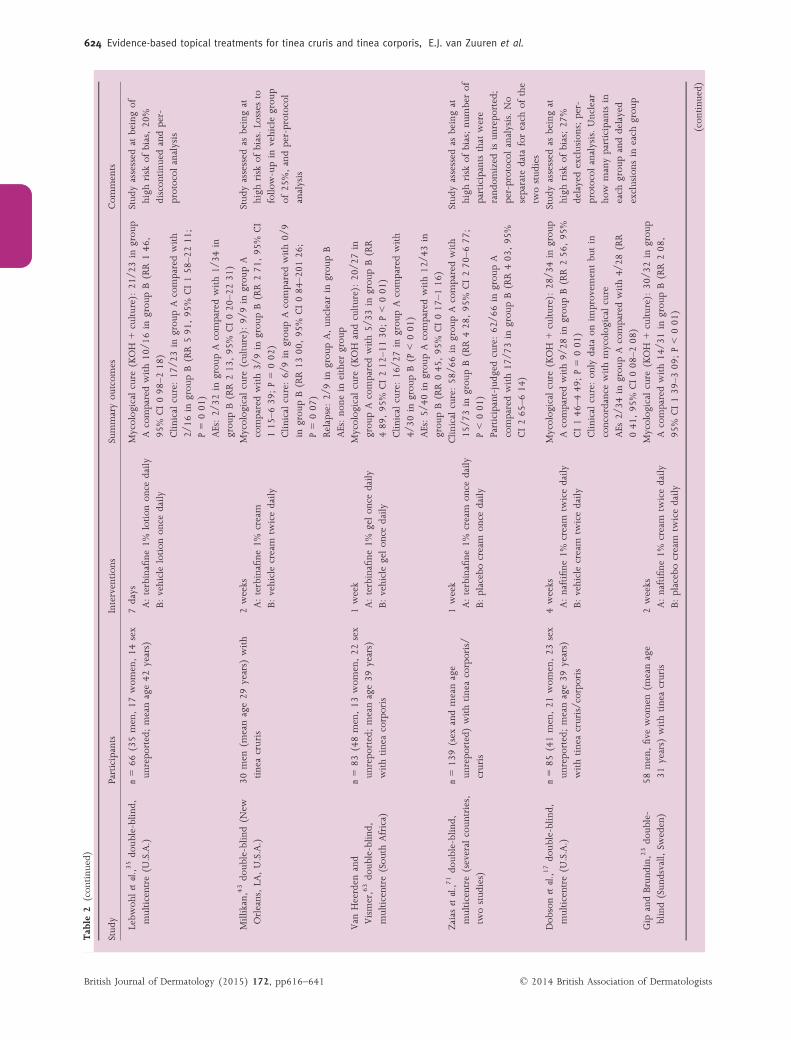
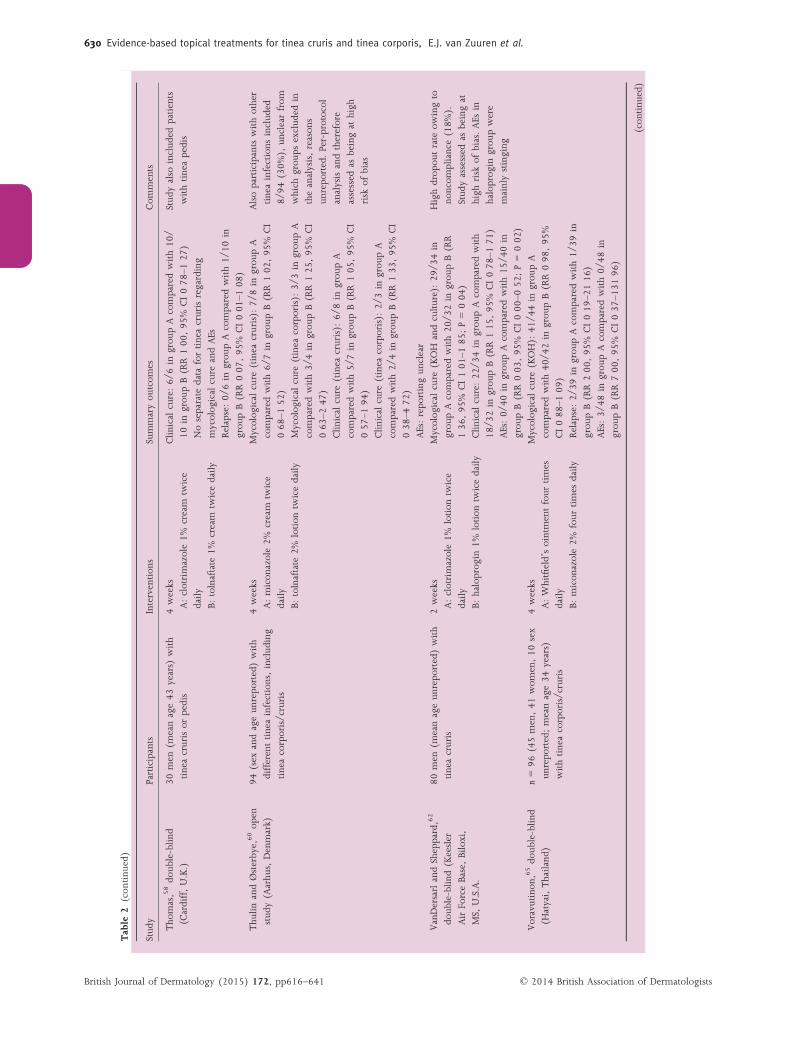
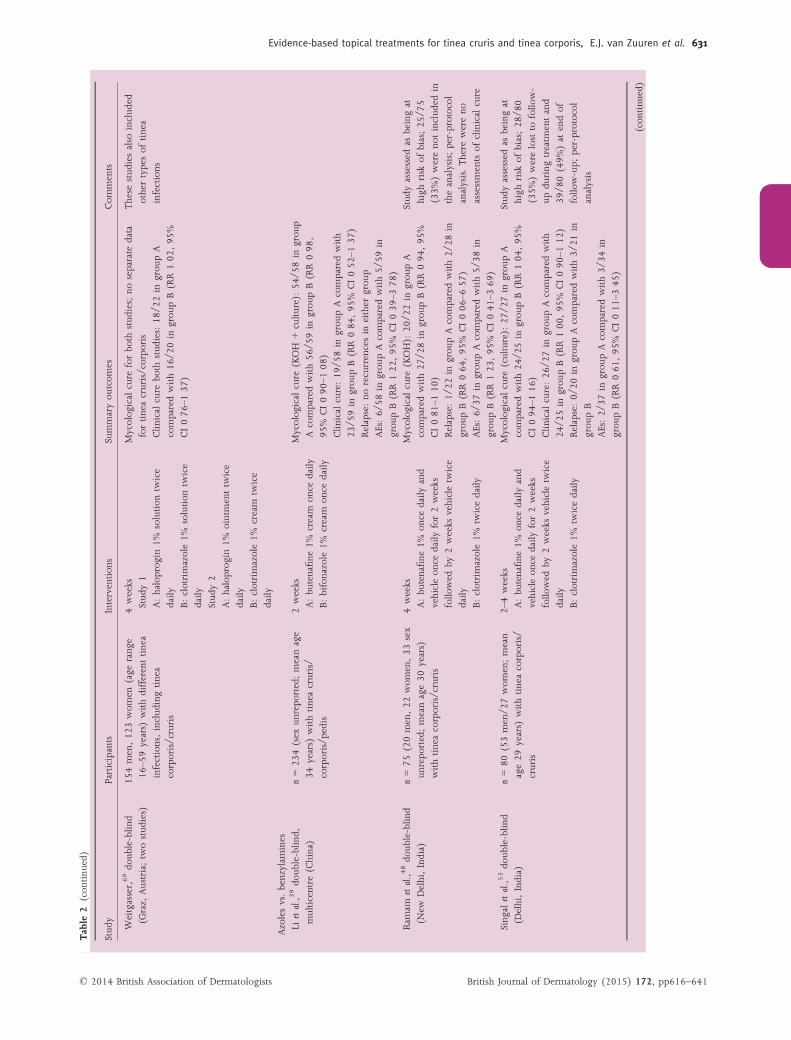
A summary of the key results is provided in Table 2. In view
of the large variety of interventions, pooling was only possible
for several outcomes from just two comparisons: terbinafine
vs. placebo and naftifine 1% vs. placebo. For the comparison
of terbinafine vs. placebo, data for mycological cure are
reported in Table 2; however, in view of the considerable
degree of heterogeneity for this specific outcome, the data
could not be pooled (I2 = 76%). The results are presented in
a Grading Recommendations Assessment, Development and
Evaluation summary of findings table (see Table 3).135 Pooled
data on adverse events showed there were slightly fewer
adverse events in the terbinafine group, and that these were
generally mild, consisting of pruritus and dermatitis (see
Table 3).
For the comparison of naftifine 1% vs. placebo, data from
three studies could be pooled for mycological cure. In the
naftifine group, 83 of 95 patients were considered cured com-
pared with 33 of 92 in the placebo group (RR 2�38, 95% CI
1�80–3�14; P < 0�01). There was no statistically significant
difference in the number of adverse events between the inter-
ventions, with three of 99 occurring in the naftifine group
and seven of 96 in the placebo group (RR 0�44, 95% CI
0�13–1�57).Very limited pooling of outcomes data was possible for
studies that compared azoles with allylamines, or azoles with
combinations of azoles/moderate potent corticosteroid or
azoles vs. benzylamines, and azoles vs. placebo.
With regard to mycological cure there was no apparent dif-
ference in effectiveness between azoles and allylamines (data
not pooled; in view of considerable heterogeneity,
I2 = 75%),9,27,28,30,32,67 except for one study in which allyl-
amines were shown to be more effective.66 Additionally, the
279 recordsidentified through databasesearching(5 duplicates).
364 Records
7 in ‘ongoingstudies’
Total = 44
12 in ‘studiesawaitingclassification’
1 (Banerjee 2012)was a furtherreport of(Banerjee 2011)providingadditional data
24 Full-text articlesexcluded: 15CCTs, 2 caseseries, 5 nocomparator, 2 didnot meet inclusioncriteria
191 Recordsexcluded
173 Full-textarticles assessed for eligibility
129 Studiesincluded inqualitativesynthesis
26 studiesincluded inquantitativesynthesis(meta-analysis)
364 Recordsscreened
87 additionalrecords identifiedthrough othersources(4 duplicates) = 83
Total 274 + 7ongoingstudies = 281
Fig 1. Search results. CCT, controlled clinical trial.
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
618 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2Characteristics
ofinclud
edrand
omized
controlledtrials(RCTs)andsummaryof
results
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Azoles
Azolesvs.placebo
Bagatell,
6do
uble-blin
d(U
.S.A.;
nomoreinform
ation)
33men,four
wom
en(m
eanage
42years)
withtineacorporis/cruris
3weeks
A:bifonazole
1%cream
once
daily
B:vehicleon
cedaily
Mycologicalcure
(KOH):
grou
pA17
/19compared
with10
/14in
grou
pB(RR1�2
5,95
%CI0�8
7–1�8
1)
Mycologicalcure
(culture):
RR1�3
9,95
%CI0�9
9–1
�95Clin
icalcure:grou
pA17
/19comparedwith13
/
14in
grou
pB(RR1�02
,95
%CI0�8
5–1�2
2)NoAEs
wererepo
rted
Stud
yassessed
tobe
athigh
risk
ofbias
owingto
drop
outsin
vehiclegrou
p
andper-protocol
analysis
Bifonazole
isno
tmore
effectivethan
vehiclein
this
stud
y
Miura
etal.,4
4
doub
le-blin
d,multicentre
(Japan)
389men,26
6wom
en(age
rang
e9
–70years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
2weeks
A:econ
azole1%
cream
twicedaily
B:clotrimazole1%
cream
twice
daily
C:placebocream
twicedaily
Mycologicalcure
(tinea
cruris):
28/3
4in
grou
pA
comparedwith30
/34in
grou
pBand10
/37in
grou
pC
Mycologicalcure
(tinea
corporis):
32/3
4in
grou
p
Acomparedwith28
/31in
grou
pBand12
/29in
grou
pC
Clin
icalcure
(tinea
cruris):
26/4
3in
grou
pA
comparedwith30
/34in
grou
pBand11
/40in
grou
pC
Clin
icalcure
(tinea
corporis):
26/4
1in
grou
pA
comparedwith28
/39in
grou
pBand8/
45in
grou
pC
AEs:n=2in
grou
pAcomparedwithn=3in
grou
pBandn=6in
grou
pC
Thisstud
yalso
compares
differentazoles
(see
section
below)
Spiekerm
annandYou
ng,55
doub
le-blin
d,multicentre
(U.S.A.,tw
ostud
ies)
n=13
61(sex
andageun
repo
rted)
withdifferenttineainfections,
includ
ingtineacorporis/cruris
4weeks
Stud
y1:
A:clotrimazole1%
solution
twice
daily
B:vehicletw
icedaily
Stud
y2
A:clotrimazole1%
cream
twice
daily
Vehicle
twicedaily
Mycologicalcure
ofthecombinedstud
ies(KOH):
103/
111in
grou
pAcomparedwith42
/102
in
grou
pB(RR2�2
5,95
%CI1�7
8–2�8
6)Nodata
onclinicalcure
Stud
yassessed
tobe
athigh
risk
ofbias:high
drop
out
rate
(33%
),un
clearfrom
which
grou
ps,reason
s
unrepo
rted;per-protocol
analysis
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 619

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Tanenbaum
etal.,5
7do
uble-
blind(Colom
bia,
twostud
ies)
117men
(meanage29
years)
with
tineacorporis/cruris
3weeks
Stud
y1
A:sulcon
azole1%
cream
once
daily,vehicleon
cedaily
B:clotrimazole1%
cream
twice
daily
Stud
y2
A:sulcon
azole1%
cream
twice
daily
B:vehicletw
icedaily
Stud
y1:
Mycologicalcure
(KOH
andculture):allpatients
inbo
thgrou
pswerecuredafter3weeks
of
treatm
ent
Clin
icalcure:allpatientsin
both
grou
pswere
cured
AEs:0/
30in
grou
pA,4/
27in
grou
pB(RR0�1
0,
95%
CI0�0
1–1�7
8)Stud
y2:
Mycologicalcure
(KOH):
26/2
6in
grou
pA
comparedwith10
/23in
grou
pB(RR2�2
4,95
%CI1�4
2–3�5
4;P<0�0
1)
Clin
icalcure:25
/26in
grou
pAcomparedwith
2/26
ingrou
pB(RR12
�50,95
%CI3�2
9–47
�44;
P<0�0
1)AEs:0/
28in
grou
pAcomparedwith5/
29in
grou
pB(RR0�0
9,95
%CI0�0
1–1�6
3)
Resultsof
cultu
rewere
similar(study
2)Firststud
yalso
compares
differentazoles
(section
below)
Com
parisons
ofdifferentazoles
Banerjee
etal.7(Kolkata,India)
85men,65
wom
en(m
eanage
31years)
withtineacorporis
4weeks
A:am
orolfine
0�25%
cream
twice
daily
B:clotrimazole1%
cream
twice
daily
C:flucon
azole0�5
%geltw
icedaily
Mycologicalcure:grou
pA30
/38comparedwith
32/4
2in
grou
pB(RR1�0
4,95
%CI0�8
2–1�3
1)
Clin
icalcure:grou
pA35
/38comparedwith40
/42
ingrou
pC(RR1�0
6,95
%CI0�9
3–1�1
9)
AEs:on
eparticipantin
grou
pBrepo
rted
increased
erythemaat
theapplicationsite
Participant-judged
cure:grou
pA34
/38compared
with38
/42in
grou
pB(RR0�9
9,95
%CI0�8
5–1�1
5)Mycologicalcure:grou
pB32
/42comparedwith
33/4
1in
grou
pC(RR0�9
5,95
%CI0�7
5–1�1
9)Clin
icalcure:grou
pB40
/42comparedwith37
/
41in
grou
pC(RR1�0
6,95
%CI0�9
3–1�1
9)AEs:on
eparticipantin
each
grou
prepo
rted
increasederythemaat
theapplicationsite
Participant-judged
cure:grou
pB38
/42compared
with36
/41in
grou
pC(RR1�0
3,95
%CI0�8
9–1�2
0)
DataforAvs.Cno
trepo
rted
buttherewas
nostatistically
sign
ificant
difference
betw
eenthetw
otreatm
ent
armsforanyou
tcom
eThisstud
yalso
compared
azoles
withanothertopical
antifung
al(see
correspo
ndingsection
below)
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
620 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Clayton
andKnigh
t,11
doub
le-blin
d(Lon
don,
U.K.)
n=13
6[74men,44
wom
en(sex
ofrestun
clear);agerang
e5–
62years)
withdifferenttinea
infections,includ
ingtineacorporis
4weeks
A:micon
azole2%
cream
twice
daily
B:clotrimazole1%
cream
twice
daily
Mycologicalcure
(culture):
grou
pA14
/15
comparedwith10
/11in
grou
pB(RR1�0
3,95
%
CI0�8
2–1�2
9)Clin
icalcure:no
separate
data
fortineacorporis/
cruris
Relapse:grou
pA=1,
grou
pB=2
AEs:no
separate
data
fortineacorporis/cruris
Stud
yat
high
risk
ofbias;of
thetotalinclud
edat
week
8,56
/136
(41%
)lostto
follo
w-up
Per-protocol
analysis
Clerico
andRibuffo,13
doub
le-blin
d(Rom
e,Italy)
Three
men,37
wom
en(age
rang
e7
–74years)
withdifferenttinea
infections,includ
ingtineacorporis
30days
A:fenticon
azole2%
cream
twice
daily
B:micon
azole2%
cream
twice
daily
Mycologicalcure:insufficientseparate
data
were
repo
rted
forthethreeparticipantswithtinea
corporis
Clin
icalcure:1/
1in
grou
pAcomparedwith2/
3in
grou
pB
NoAEs
wererepo
rted
ineither
grou
p
Onlyon
eparticipantwith
tineacrurisin
grou
pAand
threewithtineacorporisin
grou
pBinclud
ed
Kalisetal.,3
3do
uble-blin
d,
multicentre
(France)
n=79
(sex
andageun
repo
rted)
withtineacruris
2–3weeks
A:oxicon
azole1%
once
daily
B:ketoconazole
2%on
cedaily
Mycologicalcure
andclinicalcure
werecombined:
35/3
6in
grou
pAcomparedwith26
/30in
grou
pB(RR1�12
,95
%CI0�9
–61�3
0)
AEs:0/
42in
grou
pAcomparedwith9/
37in
grou
pB(RR0�0
5,95
%CI0�0
0–0�7
7;P=0�0
8)
AEs
inketoconazole
grou
p
consistedmainlyof
irritant
derm
atitis(n
=3)
and
contactderm
atitis(n
=3)
Sharmaetal.,5
0do
uble-blin
d,
multicentre
(Ind
ia)
217men,43
wom
en(m
eanage
37years)
withtineacorporis/cruris
2weeks
A:sertacon
azole2%
cream
twice
daily
B:micon
azole2%
cream
twice
daily
Mycologicalcure
(culture):
76/1
22in
grou
pA
comparedwith57
/128
ingrou
pB(R
1�40,
95%
CI1�1
0–1�7
7;P=0�0
1)
Clin
icalcure
rateswereidentical
AEs:5/
128in
grou
pAcomparedwith9/
132in
grou
pB(RR0�5
3,95
%CI0�1
8–1�5
4)Sivayathornand
Piam
phon
gsant,54do
uble-
blind(Bangkok,
Thailand
)
n=14
0(70men/3
1wom
en/3
9
sexun
repo
rted;meanage
27years)
withtineacorporis/cruris
2weeks
A:Whitfield’sointmentthreetimes
daily
B:tolnaftate
2%ointmentthree
times
daily
C:clotrimazole1%
cream
three
times
daily
D:micon
azole2%
cream
three
times
daily
Mycologicalcure:6/
28in
grou
pAcomparedwith
12/1
9in
grou
pB,
16/2
7in
grou
pCand21
/27
ingrou
pD
Clin
icalcure:14
/28in
grou
pAcomparedwith
14/1
9in
grou
pB,
21/2
7in
grou
pCand22
/27
ingrou
pD
AEs:no
nein
anygrou
p
Stud
yassessed
tobe
athigh
risk
ofbias;39
/140
(28%
)no
tinclud
edin
theanalysis
Per-protocol
analysis
Thisstud
yalso
compares
othertopicalantifung
als
(see
correspo
ndingsection)
Tho
mas
andEvans,59
investigator-
blind(W
ales,U.K.)
106men
(meanage43
years)
with
tineacrurisor
pedis
4weeks
A:bifonazole
1%gelon
cedaily
B:sulcon
azole1%
twicedaily
Mycologicalandclinicalcure:1/
1in
grou
pA
comparedwith1/
1in
grou
pB
Relapse:no
tin
grou
pAandtheon
ein
grou
pB
failedto
attend
NoAEs
Onlyon
epatientwithtinea
crurisin
each
grou
p
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 621

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
VanderPloegandDe
Villez,61(San
Anton
io,TX,
U.S.A.)
48men
and29
wom
en(m
eanage
42years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
4weeks
A:tiocon
azole1%
cream
twice
daily
B:micon
azole2%
twicedaily
Mycologicalcure
(KOH
andculture):9/
10in
grou
pAcomparedwith6/
6in
grou
pB(RR
0�93,
95%
CI0�6
8–1�2
7)
Noseparate
data
forclinicalcure
AEs:no
separate
data
fortineacruris/corpo
ris
Participantswithothertinea
infections
includ
ed
Venaetal.,6
4
investigator-blin
d(Bari,Italy)
24men,sixwom
en(m
eanage16
–78
years)
withtineacruris
2weeks
A:bifonazole
1%cream
once
daily
B:micon
azole2%
cream
twice
daily
Mycologicalcure
(KOH
andculture):30
/30sites
treatedwithbifonazole,23
/30sitestreatedwith
micon
azole
Clin
icalcure,allsiteswerehealed
Norecurrences,no
AEs
Thiswas
awithin-participant
stud
y,participantswereno
t
blindedandthestud
ywas
assessed
asbeingat
high
risk
ofbias
Com
parisons
ofsameazolewithdifferentdo
sing
regimens
delPalacioetal.,1
5do
uble-
blind(M
adrid,
Spain)
n=60
(38men/2
2wom
en;mean
age45
years)
withtineacruris/
corporis
6weeks
A:eberconazole
1%cream
once
daily
B:eberconazole
1%cream
twice
daily
C:eberconazole
2%cream
once
daily
D:eberconazole
1%cream
twice
daily
Mycologicalcure
(KOH):
100%
inallgrou
ps
Mycologicalcure
(culture):
10/1
5grou
pA,12
/13
grou
pB,
11/1
3grou
pC,10
/14grou
pD
Clin
icalcure:10
/15in
grou
pA,12
/15in
grou
pB,
8/15
ingrou
pC,8/
15in
grou
pD
Relapse:n=3(unclear
inwhich
grou
ps)
AEs:0/
15grou
pA,2/
15grou
pB,
2/15
grou
p
C,2/
15grou
pD
The
data
werecombinedfor
mycologicalcure
(KOH
+cultu
re)to
allow
a
comparisonbetw
eenon
ce-
andtw
ice-daily
regimens.
Thisshow
edno
difference
betw
eengrou
ps(RR0�9
2,
95%
CI0�7
0–1�2
2)
Ram
elet
andWalker-Nasir,49
doub
le-blin
d,multicentre
(Switzerland)
95men,43
wom
en(m
eanage
38years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
7–60
days
A:oxicon
azole1%
cream
once
daily
+placebocream
once
daily
B:oxicon
azole1%
cream
twice
daily
Clin
icalcure
(tinea
cruris):
19/1
9in
grou
pA
comparedwith22
/23in
grou
pB(RR1�0
4,95
%
CI0�9
2–1�1
8)Clin
icalcure
(tinea
corporis):
9/13
ingrou
pA
comparedwith8/
10in
grou
pB(RR0�8
7,95
%CI0�5
4–1�3
9)
AEs:no
separate
data
fortineacruris/corpo
ris
Other
tineainfections
includ
ed.Dataon
mycologicalcure
couldno
tbe
extractedfrom
therepo
rt
ason
lythecure
ratesfor
each
organism
were
provided
andno
tforeach
site
ofinfection
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
622 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Allylamines
Allylamines
vs.placebo
Budimuljaetal.,1
0do
uble-
blind,
twocentres(Ind
onesia)
n=12
0(53men,64
wom
en,sex
ofrestun
clear;meanage
35�5
years)
withtineacruris/
corporis
7days
A:terbinafine
1%cream
once
daily
B:placeboon
cedaily
Mycologicalcure
(KOH
+culture):grou
pA53
/57
comparedwith11
/60in
grou
pB(RR5�0
7,95
%
CI2�9
6–8�6
9)Clin
icalcure:themeanclinicalsign
sand
symptom
sscorein
grou
pAwas
1comparedwith
ascoreof
6in
grou
pB
Relapse:no
relapsein
either
grou
p
One
AE(dermatitis)was
repo
rted
ingrou
pAand
eigh
tin
grou
pB(nodetails)
Participant-judged
cure:grou
pA48
/56compared
with9/
58in
grou
pB(RR5�5
2,95
%CI3�0
0–10
�22)
Each
symptom
(e.g.itch,
pustules)measuredon
a
four-point
scale,
0=no
nexistent,3=severe.
Each
symptom
scorewas
addedup
foreach
participantandthemean
scoreused.Scores
of0–
1wou
ldhave
torepresent
very
mild
disease,
althou
ghitisim
possible
toqu
antify
exactlyho
wmanypeop
lewou
ldbe
cured
Cordero
etal.,1
4
doub
le-blin
d,multicentre
(U.S.A.,Dom
inican
Repub
licGuatemalaandPanama)
n=74
(36men,29
wom
en,nine
sexun
repo
rted;agerang
e5–
76years)
withtineacruris/corpo
ris
1week
A:terbinafine
1%cream
once
daily
B:placeboon
cedaily
Mycologicalcure
(KOH
+culture):grou
pA27
/29
comparedwith5/
16in
grou
pB(RR2�9
8,95
%
CI1�4
3–6�2
0)Clin
icalcure:totalsign
sandsymptom
sscore
redu
cedfrom
7�8to
1�0in
grou
pAcompared
with7�6
to4�1
ingrou
pB
AEs:grou
pA=0,
grou
pB=1
Stud
yat
high
risk
ofbias.
Missing
data
at2-week
follo
w-up:
grou
pA7/
36(19%
);22
/34(58%
)in
grou
pB.
Per-protocol
analysis
Evansetal.,1
8do
uble-blin
d
(U.K.)
22men,nine
wom
en(m
eanage
39years)
withtineacruris/corpo
ris
1week
A:terbinafine
1%cream
once
daily
B:vehiclecream
once
daily
Mycologicalcure
(KOH
+culture):12
/14in
grou
p
Acomparedwith9/
17in
grou
pB(RR1�6
2,95
%CI0�9
9–2�6
6)
Clin
icalcure:meansign
sandsymptom
sscorewas
just<2in
grou
pA,suggesting
minim
alevidence
ofdiseasecomparedwithascoreof
>4in
grou
pB AEs:no
neGreer
andJolly,24do
uble-blin
d
(U.S.A.)
23men
withtineacruris(m
eanage
38years)
2weeks
A:terbinafine
1%cream
twicedaily
B:vehiclecream
twicedaily
Mycologicalcure
(KOH
+culture):9/
9in
grou
pA
comparedwith2/
11in
grou
pB(RR4�5
6,95
%CI1�5
0–13
�87;P=0�0
1)
Clin
icalcure:7/
9in
grou
pAcomparedwith2/
11in
grou
pB(RR4�2
8,95
%CI1�1
6–15
�72;
P=0�0
3)AEs:0/
11in
grou
pAcomparedwith1/
12in
grou
pB
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 623
Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Lebw
ohletal.,3
5do
uble-blin
d,multicentre
(U.S.A.)
n=66
(35men,17
wom
en,14
sex
unrepo
rted;meanage42
years)
7days
A:terbinafine
1%lotion
once
daily
B:vehiclelotion
once
daily
Mycologicalcure
(KOH
+culture):21
/23in
grou
pAcomparedwith10
/16in
grou
pB(RR1�4
6,
95%
CI0�9
8–2�1
8)Clin
icalcure:17
/23in
grou
pAcomparedwith
2/16
ingrou
pB(RR5�9
1,95
%CI1�5
8–22
�11;
P=0�0
1)
AEs:2/
32in
grou
pAcomparedwith1/
34in
grou
pB(RR2�1
3,95
%CI0�2
0–22
�31)
Stud
yassessed
atbeingof
high
risk
ofbias,20
%
discon
tinu
edandper-
protocol
analysis
Millikan,43do
uble-blin
d(N
ewOrleans,LA
,U.S.A.)
30men
(meanage29
years)
with
tineacruris
2weeks
A:terbinafine
1%cream
B:vehiclecream
twicedaily
Mycologicalcure
(culture):
9/9in
grou
pA
comparedwith3/
9in
grou
pB(RR2�7
1,95
%CI
1�15–
6�39;
P=0�0
2)Clin
icalcure:6/
9in
grou
pAcomparedwith0/
9
ingrou
pB(RR13
�00,95
%CI0�8
4–20
1�26;
P=0�0
7)
Relapse:2/
9in
grou
pA,un
clearin
grou
pB
AEs:no
nein
either
grou
p
Stud
yassessed
asbeingat
high
risk
ofbias.Losses
to
follo
w-upin
vehiclegrou
pof
25%,andper-protocol
analysis
Van
Heerden
and
Vismer,63do
uble-blin
d,
multicentre
(Sou
thAfrica)
n=83
(48men,13
wom
en,22
sex
unrepo
rted;meanage39
years)
withtineacorporis
1week
A:terbinafine
1%gelon
cedaily
B:vehiclegelon
cedaily
Mycologicalcure
(KOH
andculture):20
/27in
grou
pAcomparedwith5/
33in
grou
pB(RR
4�89,
95%
CI2�1
2–11
�30;P<0�0
1)Clin
icalcure:16
/27in
grou
pAcomparedwith
4/30
ingrou
pB(P
<0�0
1)AEs:5/
40in
grou
pAcomparedwith12
/43in
grou
pB(RR0�4
5,95
%CI0�1
7–1�1
6)Zaiasetal.,7
1do
uble-blin
d,
multicentre
(severalcoun
tries,
twostud
ies)
n=13
9(sex
andmeanage
unrepo
rted)withtineacorporis/
cruris
1week
A:terbinafine
1%cream
once
daily
B:placebocream
once
daily
Clin
icalcure:58
/66in
grou
pAcomparedwith
15/7
3in
grou
pB(RR4�2
8,95
%CI2�7
0–6�7
7;P<0�0
1)
Participant-judged
cure:62
/66in
grou
pA
comparedwith17
/73in
grou
pB(RR4�0
3,95
%CI2�6
5–6�1
4)
Stud
yassessed
asbeingat
high
risk
ofbias;nu
mberof
participantsthat
were
rand
omized
isun
repo
rted;
per-protocol
analysis.No
separate
data
foreach
ofthe
twostud
ies
Dob
sonetal.,1
7do
uble-blin
d,
multicentre
(U.S.A.)
n=85
(41men,21
wom
en,23
sex
unrepo
rted;meanage39
years)
withtineacruris/corpo
ris
4weeks
A:naftifine
1%cream
twicedaily
B:vehiclecream
twicedaily
Mycologicalcure
(KOH
+culture):28
/34in
grou
p
Acomparedwith9/
28in
grou
pB(RR2�5
6,95
%CI1�4
6–4�4
9;P=0�0
1)
Clin
icalcure:on
lydata
onim
provem
entbu
tin
concordancewithmycologicalcure
AEs
2/34
ingrou
pAcomparedwith4/
28(RR
0�41,
95%
CI0�0
8–2�0
8)
Stud
yassessed
asbeingat
high
risk
ofbias;27
%delayedexclusions;per-
protocol
analysis.Unclear
how
manyparticipantsin
each
grou
panddelayed
exclusions
ineach
grou
p
Gip
andBrun
din,
23do
uble-
blind(Sun
dsvall,
Sweden)
58men,five
wom
en(m
eanage
31years)
withtineacruris
2weeks
A:naftifine
1%cream
twicedaily
B:placebocream
twicedaily
Mycologicalcure
(KOH
+culture):30
/32in
grou
pAcomparedwith14
/31in
grou
pB(RR2�0
8,
95%
CI1�3
9–3�0
9;P<0�0
1)
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
624 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Jordon
etal.,3
1do
uble-blin
d,
multicentre
(U.S.A.)
57men,13
wom
en(m
eanage
40�6
years)
withtineacruris/
corporis
4weeks
A:naftifine
1%cream
once
daily
B:vehiclecream
once
daily
Mycologicalcure:25
/29in
grou
pAcompared
with10
/33in
grou
pB(RR2�3
8,95
%CI1�6
6–
4�87;
P<0�0
1)
AEs:no
nein
grou
pA,tw
oin
grou
pB
Parish
etal.,4
7do
uble-blin
d,
multicentre
(U.S.A.)
282men,52
wom
en(m
eanage
47years)
withtineacruris
2weeks
A:naftifine
2%cream
once
daily
B:vehiclecream
once
daily
Mycologicalcure
(KOH
andculture):50
/75
participantsin
grou
pAcomparedwith8/
71in
grou
pB(RR5�9
2,95
%CI3�0
2–11
�59;
P<0�0
1).
Clin
icalcure:53
/75in
grou
pAcomparedwith
3/71
ingrou
pB(RR16
�72,95
%CI5�4
7–51
�10;
P<0�0
1)
AEs:7/
166in
grou
pAcomparedwith4/
168in
grou
pB(RR1�7
7,95
%CI0�5
3–5�9
4)Com
parisons
withsameallylaminewithdifferentdo
sing
regimens
Evansetal.,2
0do
uble-blin
d,multicentre
(U.K.)
16men,five
wom
en(m
eanage
37years)
withtineacruris/corpo
ris
1week
A:terbinafine
1%cream
once
daily
for1day,
placebosubsequent
6days
B:terbinafine
1%cream
once
daily
for3days,placebosubsequent
4days
C:terbinafine
1%cream
once
daily
for5days,placebosubsequent
2days
D:terbinafine
1%cream
once
daily
for7days
Mycologicalcure:4/
4in
grou
pAcomparedwith
2/4in
grou
pB,
1/2in
grou
pCand4/
4in
grou
pD
Clin
icalcure:4/
4in
grou
pAcomparedwith1/
4
ingrou
pB,
1/2in
grou
pCand3/
4in
grou
pD
Relapse:on
lyin
grou
pA(n
=1)
AEs:no
ne
Stud
yassessed
asbeingat
high
risk
ofbias;34
%
delayedexclusions;per-
protocol
analysis
Azolesvs.allylamines
Azolesvs.terbinafine
Budimulja,9
doub
le-blin
d,multicentre
(Ind
onesia)
100men,85
wom
en(age
rang
e18
–64years)
withtineacruris
3weeks
A:terbinafine
cream
1%on
cedaily
for1weekand2weeks
placebo
B:bifonazole
cream
1%applied
once
daily
Mycologicalcure
(KOH):
grou
pA87
/89compared
with83
/86in
grou
pB(RR1�0
1,95
%CI0�9
6–
1�07)
Mycologicalcure
(culture):
RR1�0
0,95
%CI0�9
6
–1�05
Clin
icalcure:grou
pA88
/89comparedwith82
/
86in
grou
pB(RR1�0
4,95
%CI0�9
8–1�0
9)One
AEwas
repo
rted
ingrou
pA(con
tact
derm
atitis)
Inbo
thgrou
psthere
appeared
tobe
anu
mberof
mycologicalrelapses
atweek8,
althou
ghitwas
not
possible
toconfi
rmthe
precisenu
mberin
view
of
thedrop
outsoccurring
betw
eenweeks
3and8
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 625

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Jerajani
etal.,3
0op
enstud
y,
multicentre
(Ind
ia)
54men,29
wom
en(age
rang
e28
–33
years)
withtineacruris/corpo
ris
2–4weeks
A:sertacon
azole2%
cream
twice
daily
B:terbinafine
1%cream
once
daily
C:lulicon
azole1%
cream
once
daily
Mycologicalcure:20
/20in
grou
pAcompared
with22
/22in
grou
pBand20
/20in
grou
pC
Clin
icalcure:20
/20in
grou
pAcomparedwith
19/2
2in
grou
pBand20
/20in
grou
pC
Norelapsein
anygrou
p
Stud
yassessed
asbeingat
high
risk
ofbias,25
%drop
outsandper-protocol
analysis
Wangetal.,6
6do
uble-blin
d
(Beijin
g,China)
121men,89
wom
en(m
eanage
35years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
2–5weeks
A:terbinafine
1%po
wdertw
ice
daily
B:micon
azole2%
twicedaily
Mycologicalcure
(KOH):
26/2
6in
grou
pA
comparedwith9/
10in
grou
pBand23
/24(RR
1�04,
95%
CI0�9
3–1�1
7)and10
0%cure
intinea
corporis:4/
4in
grou
pAand5/
5grou
pB
Clin
icalcure:15
/26in
grou
pAcomparedwith
13/2
4in
grou
pBand27
/30(RR1�0
7,95
%CI
0�65–
1�75)
Intineacorporis:0/
4in
grou
pAvs.1/
5in
grou
pB
Noseparate
data
forAEs
Azolesvs.naftifine
Haroo
netal.,2
8op
enstud
y(Lahore,
Pakistan)
n=42
(30men,threewom
en,nine
sexun
repo
rted;agerang
e
19–7
0years)
withtineacruris
4weeks
A:naftifine
1%cream
once
daily
B:tiocon
azole1%
cream
twice
daily
Mycologicalcure
(KOH):
15/1
5in
grou
pA
comparedwith18
/18in
grou
pB
Clin
icalcure:after4weeks,theestimated
mean
scorewas
0�25in
grou
pAand0�2
1in
grou
pB
(0=no
symptom
s,1=mild
symptom
sup
to3=severe)
Relapse:no
nein
either
grou
p
Stud
yassessed
asbeingat
high
risk
ofbias;21
%
drop
outs;andper-protocol
analysis
Kagaw
a,32do
uble-blin
d
(Tokyo,Japan)
n=39
3(231
men,14
8wom
en,14
sexun
repo
rted;meanage
42years)
withtineacruris/
corporis/p
edis
2weeks
A:naftifine
1%cream
twicedaily
B:clotrimazole1%
cream
twice
daily
Mycologicalcure
(tinea
cruris):
44/5
1in
grou
pA
comparedwith42
/55in
grou
pB(RR1�1
3,95
%CI0�9
4–1�3
6)
Mycologicalcure
(tinea
corporis):
46/5
6in
grou
p
Acomparedwith46
/62in
grou
pB(RR1�1
1,95
%CI0�9
1–1�3
4)
Clin
icalcure
(tinea
cruris):
44/5
1in
grou
pA
comparedwith40
/55in
grou
pB(RR1�1
9,95
%
CI0�9
8–1�4
4)Clin
icalcure
(tinea
corporis):
46/5
6in
grou
pA
comparedwith44
/62in
grou
pB(RR1�1
6,95
%CI0�9
5–1�4
1)
Noseparate
data
onAEs
are
repo
rted
forparticipants
withtineacrurisandtinea
corporis
Betw
een15
%and20
%per
grou
pno
tinclud
edin
the
analysis;wejudged
thisas
beingat
high
risk
ofbias
Millikan
etal.,4
2do
uble-blin
d,multicentre
(U.S.A.)
n=12
6(78men,26
wom
en,22
sexun
repo
rted;meanage
42years)
withtineacruris/
corporis/p
edis
4weeks
A:naftifine
1%cream
twicedaily
B:econ
azole1%
cream
twicedaily
Com
binedmycologicalandclinicalcure:as
mean
sum
ofclinicalscore,
notas
cure.
AEs:2/
64in
grou
pAcomparedwith8/
62in
grou
pB(RR0�24
,95
%CI0�0
5–1�1
0;P=0�0
7)
Stud
yassessed
asbeingat
high
risk
ofbias;17
�5%missing
outcom
edata;per-
protocol
analysis
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
626 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Top
icalantifung
alscombinedwithtopicalcorticosteroids
Azolesvs.corticosteroid
andazolecombination
Evansetal.,1
9do
uble-blin
d,multicentre
(U.K.)
75men,37
wom
en(age
rang
e12
–81
years)
withtineacruris/corpo
ris
4weeks
A:naftifine
1%cream
twicedaily
B:clotrimazole
1%+hydrocortisone
1%cream
twicedaily
Mycologicalcure
(KOH
+cultu
re):
13/1
5in
grou
pAcomparedwith8/
10in
grou
pB(RR1�0
8,95
%
CI0�7
5–1�5
7)Clin
icalcure:meantotalclinicalsymptom
scores
wererepo
rted
butno
actualcure
rates
AEs:no
separate
data
forparticipantswithtinea
corporis/cruris
Katzetal.,3
4do
uble-blin
d,
multicentre
(U.S.A.)
241men
and90
wom
en(m
eanage
40years)
withtineacruris/corpo
ris
2weeks
A:clotrimazole
1%+betamethasone
diprop
ionate
0�05%
cream
twicedaily
B:clotrimazole1%
cream
twice
daily
C:Betamethasone
diprop
ionate
0�05%
cream
twicedaily
Mycologicalcure
(tinea
cruris):
39/6
0in
grou
pA
comparedwith34
/51in
grou
pBand4/
48in
grou
pC
Mycologicalcure
(tinea
corporis):
32/5
1in
grou
pAcomparedwith25
/49in
grou
pBand12
/38in
grou
pC
Clin
icalcure:no
data
onactualclinicalcure
were
provided
intherepo
rt
AEs:2/
112in
grou
pAcomparedwith3/
113in
grou
pBand9/
106in
grou
pC
AEs
consistedof
mild
-to-
mod
erateparaesthesia
and
skin
erup
tion
Lietal.,3
8do
uble-blin
d,multicentre
(China)
n=13
5(sex
unrepo
rted,meanage
33years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
2–3weeks
A:econ
azole1%
+triamcino
lone
aceton
ide0�1
%cream
twicedaily
B:econ
azole1%
ointmenttw
ice
daily
Mycologicalcure
(KOH
+cultu
re):
39/4
1in
grou
pAcomparedwith37
/41in
grou
pB(RR1�0
5,
95%
CI0�9
3–1�1
9)Clin
icalcure:23
/43in
grou
pAcomparedwith
25/4
2in
grou
pB(RR0�9
0,95
%CI0�6
2–1�3
1)AEs:no
seriou
sside-effectsin
either
grou
p
Pariseretal.,4
6investigator-
blind,
multicentre
(U.S.A.)
n=26
0(sex
andageun
repo
rted)
withtineacruris
2weeks
A:clotrimazole
1%+betamethasone
diprop
ionate
0�05%
cream
twicedaily
B:ketoconazole
2%cream
twice
daily
Mycologicalcure
(KOH
+cultu
re):
81/9
9in
grou
pAcomparedwith81
/99in
grou
pB(RR1�0
3,
95%
CI0�9
0–1�1
7)Clin
icalcure:65
/93in
grou
pAcomparedwith
44/9
9in
grou
pB(RR1�5
7,95
%CI1�2
2–2�0
3;P<0�0
1)
AEs:10
/128
ingrou
pAcomparedwith14
/131
ingrou
pB(RR0�7
3,95
%CI0�3
4–1�5
9)
Totalof
62/2
60(24%
)no
tinclud
edin
efficacy
analysis,
puttingstud
yat
high
risk
ofbias
Shen
etal.,5
1do
uble-blin
d(Shang
hai,China)
69(51men,12
wom
en,sixsex
unrepo
rted;meanage36
years)
withtineacorporis/cruris
3weeks
A:micon
azole2%
cream
twice
daily
B:econ
azole1%
+triamcino
lone
acetate0�1
%cream
twicedaily
Mycologicalcure
(culture):
22/2
3in
grou
pA
comparedwith17
/19in
grou
pB(RR1�0
7,95
%
CI0�9
0–1�2
8)Clin
icalcure:22
/32in
grou
pAcomparedwith
27/3
1in
grou
pB(RR0�7
9,95
%CI0�6
0–1�0
3)AEs:1/
35in
grou
pAcomparedwith1/
34in
grou
pB(RR0�9
7,95
%CI0�0
6–14
�91)
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 627

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
SuandPan,
56do
uble-blin
d
(China)
150men
aged
16–6
3yearswith
tineacruris
2weeks
A:econ
azole1%
+triamcino
lone
acetate0�1
%cream
twicedaily
B:micon
azole2%
+clob
etasol
0�5%
cream
twicedaily
Mycologicalcure
(KOH):
74/7
5in
grou
pA
comparedwith63
/75in
grou
pB(RR1�17
,95
%CI1�0
6–1�3
0;P<0�0
1)
Clin
icalcure:66
/75in
grou
pAcomparedwith
47/7
5in
grou
pB(RR1�4
0,95
%CI1�1
6–1�7
0;
P<0�0
1)Wangetal.,6
8do
uble-blin
d,
multicentre
(China)
n=16
2(120
men,19
wom
en,23
sexun
repo
rted;meanage
40years)
withtineacorporisor
tineapedis
2weeks
A:econ
azole1%
+triamcino
lone
aceton
ide0�1
%cream
twicedaily
B:econ
azole1%
cream
twicedaily
Mycologicalcure
(KOH
+cultu
re):
30/3
3in
grou
p
Acomparedwith31
/35in
grou
pB(RR1�0
3,95
%CI0�8
7–1�2
1)
Clin
icalcure:29
/33in
grou
pAcomparedwith
21/3
5in
grou
pB(RR1�4
6,95
%CI1�0
9–1�9
7;
P=0�0
1)AEs:no
separate
data
Stud
yalso
includ
edpatients
withtineapedis
Wortzel,70do
uble-blin
d,multicentre
(U.S.A.)
270(sex
andmeanageun
repo
rted)
withtineacruris
2weeks
A:clotrimazole1%
cream
twice
daily
B:betamethasone
diprop
ionate
cream
twicedaily
C:Com
bination
ofAandBtw
ice
daily
Mycologicalcure
(KOH
andcultu
re):
13/1
5in
grou
pAcomparedwith15
/15in
grou
pBand6/
15in
grou
pC
Clin
icalcure:15
/15in
grou
pAcomparedwith
3/15
ingrou
pBand2/
15in
grou
pC
AEs:on
ein
grou
pB(burning
andstinging
)
Multicentre
trialbu
tthe
repo
rton
lyinclud
eddata
for45
/47participantsfrom
onecentre
Other
topicalantifung
als
Azolescomparedwithothertopicalantifung
als
Bogaertetal.,8
doub
le-blin
d,multicentre
(Dom
inican
Repub
lic,Guatemalaand
U.S.A.;tw
ostud
ies)
Stud
y1,
n=13
9andstud
y2,
n=90
withtineacruris/corpo
ris
Age
andsexun
clearin
both
stud
ies
4weeks
Stud
y1
A:ciclop
irox
olam
ine1%
cream
twicedaily
B:vehicletw
icedaily
stud
yII
A:ciclop
irox
olam
ine1%
cream
twicedaily
B:clotrimazole1%
cream
twice
daily
Stud
y1Mycologicalcure
(KOH):
grou
pA57
/70
comparedwith31
/69in
grou
pB(RR1�81
,95
%
CI1�3
6–2�4
1;P<0�0
1)Mycologicalcure
(culture):
RR1�8
1,95
%CI1�3
6
–2�41
;P<0�0
1Clin
icalcure:grou
pA50
/70comparedwith12
/
69in
grou
pB(RR4�1
1,95
%CI2�4
1–7
�01;
P<0�0
1)
One
AEin
vehiclegrou
p(burning
)Stud
y2Mycologicalcure
(KOH):
grou
pA33
/40
comparedwith43
/50in
grou
pB(RR0�96
,95
%CI0�8
0–1�1
5)
Mycologicalcure
(culture):
RR1�0
1,95
%CI0�8
5–1
�19Clin
icalcure:grou
pA28
/40comparedwith34
/50
ingrou
pB(RR1�0
3,95
%CI0�7
8–1
�36)
One
AEin
each
grou
p(burning
,stinging
)
The
effect
ofthevehicleon
mycologicalcure
rateswas
greaterthan
wou
ldno
rmally
beexpected
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
628 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Clayton
etal.,1
2do
uble-blin
d(Lon
don,
U.K.)
n=13
6(74men,44
wom
en,rest
unclear;agerang
e5–
62years)
withdifferenttineainfections,
includ
ingtineacorporis
4weeks
A:micon
azole2%
cream
twice
daily
B:clotrimazole1%
cream
once
daily
Mycologicalcure
(culture):
grou
pA14
/15
comparedwith10
/11in
grou
pB(RR1�0
3,95
%
CI0�8
2–1�2
9)Clin
icalcure:no
separate
data
fortineacorporis/
cruris
Relapse
(n):
grou
pA=1,
grou
pB=2
AEs:no
separate
data
fortineacorporis/cruris
Stud
yat
high
risk
ofbias;of
thetotalinclud
edat
week
8,56
/136
(41%
)lostto
follo
w-up.
Per-protocol
analysis
Guillano
andAlabado
,26
doub
le-blin
d(D
avao,Philipp
ines)
26men,14
wom
en(m
eanage
32years)
withtineacruris/corpo
ris
3weeks
A:kakawate/madre
decacao(50%
)ointmentGliricidiasepticum
twice
daily
B:micon
azole2%
ointmenttw
ice
daily
Mycologicalcure:5/
12in
grou
pAcomparedwith
11/1
8in
grou
pB(RR0�6
8,95
%CI0�3
2–1�4
6)Clin
icalcure:no
exactdata
wereprovided.‘Global
respon
seassessmentim
proved
inbo
thtreatm
ent
grou
ps(reportedP<0�0
1)’
AEs:5/
15in
grou
pAcomparedwith1/
18in
grou
pBun
clearho
wmanyparticipantshad>1
AE
Participant-judged
cure:micon
azoleismore
effectivethan
kakawate(P
=0�0
1as
repo
rted
inthearticle)
Adverse
eventsin
grou
pA
(erythem
a,stinging
,oedema,
itchinessand
burning)
andin
grou
pB
(transient
erythema)
Hantschke
and
Reichenberger,27do
uble-
blind(Essen,Germany)
20men,10
wom
en(age
rang
e9–
81years)
Upto
clinicalcure,maxim
um12
weeks
A:clotrimazole1%
cream
twice
daily
B:tolnaftate
1%cream
twicedaily
C:naftifine
1%cream
twicedaily
Mycologicalcure:3/
3in
grou
pA,3/
3in
grou
pB,
5/5in
grou
pC
Clin
icalcure:Com
parablebu
tdelayed
Relapse:grou
pA=1andgrou
pC=1
AEs:0in
grou
pA,1/
5in
grou
pB,
1/3in
grou
pC(‘abu
rningsensation’)
Treatmentwas
continued
untilclinicalcure
was
achieved
Sevenparticipantswith
tineacorporiswere
includ
ed,sixwithtinea
cruris;other
derm
atom
ycoses
werealso
includ
edMachado
-Pinto
andLabo
rne4
1
(Brazil)
13men,15
wom
en(age
rang
e
10–7
0years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
6weeks
A:oxicon
azole1%
cream
twice
daily
B:tolnaftate
1%cream
twicedaily
Mycologicalcure
(tinea
cruris):
4/4in
grou
pA
comparedwith4/
5in
grou
pB(RR1�2
0,95
%CI
0�72–
1�39)
Mycologicalcure
(tinea
corporis):
6/6in
grou
pA
comparedwith4/
4in
grou
pB(RR1�0
0,95
%CI
0�70–
1�43)
Clin
icalcure:identicalto
theabovemycological
cure
AEs:no
separate
data
fortineacruris/corpo
ris
Thisstud
yno
ton
lyinclud
ed
participantswithtinea
crurisandcorporis,bu
talso
includ
edparticipantswith
tineapedisandtinea
manuu
m
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 629
Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Tho
mas,58do
uble-blin
d
(Cardiff,U.K.)
30men
(meanage43
years)
with
tineacrurisor
pedis
4weeks
A:clotrimazole1%
cream
twice
daily
B:tolnaftate
1%cream
twicedaily
Clin
icalcure:6/
6in
grou
pAcomparedwith10
/
10in
grou
pB(RR1�0
0,95
%CI0�7
8–1�2
7)Noseparate
data
fortineacrurisregarding
mycologicalcure
andAEs
Relapse:0/
6in
grou
pAcomparedwith1/
10in
grou
pB(RR0�0
7,95
%CI0�0
1–1�0
8)
Stud
yalso
includ
edpatients
withtineapedis
Thu
linandØsterbye,60op
en
stud
y(Aarhu
s,Denmark)
94(sex
andageun
repo
rted)with
differenttineainfections,includ
ing
tineacorporis/cruris
4weeks
A:micon
azole2%
cream
twice
daily
B:tolnaftate
2%lotion
twicedaily
Mycologicalcure
(tinea
cruris):
7/8in
grou
pA
comparedwith6/
7in
grou
pB(RR1�0
2,95
%CI
0�68–
1�52)
Mycologicalcure
(tinea
corporis):
3/3in
grou
pA
comparedwith3/
4in
grou
pB(RR1�2
5,95
%CI
0�63–
2�47)
Clin
icalcure
(tinea
cruris):
6/8in
grou
pA
comparedwith5/
7in
grou
pB(RR1�0
5,95
%CI
0�57–
1�94)
Clin
icalcure
(tinea
corporis):
2/3in
grou
pA
comparedwith2/
4in
grou
pB(RR1�3
3,95
%CI
0�38–
4�72)
AEs:repo
rtingun
clear
Alsoparticipantswithother
tineainfections
includ
ed8/
94(30%
),un
clearfrom
which
grou
psexclud
edin
theanalysis,reason
s
unrepo
rted.Per-protocol
analysisandtherefore
assessed
asbeingat
high
risk
ofbias
VanDersarlandSheppard,62
doub
le-blin
d(Keesler
AirForceBase,Biloxi,
MS,
U.S.A.
80men
(meanageun
repo
rted)with
tineacruris
2weeks
A:clotrimazole1%
lotion
twice
daily
B:haloprogin
1%lotion
twicedaily
Mycologicalcure
(KOH
andcultu
re):
29/3
4in
grou
pAcomparedwith20
/32in
grou
pB(RR
1�36,
95%
CI1�0
1–1�8
5;P=0�0
4)Clin
icalcure:22
/34in
grou
pAcomparedwith
18/3
2in
grou
pB(RR1�1
5,95
%CI0�7
8–1�7
1)AEs:0/
40in
grou
pAcomparedwith15
/40in
grou
pB(RR0�0
3,95
%CI0�0
0–0�5
2;P=0�0
2)
Highdrop
outrate
owingto
noncom
pliance(18%
).
Stud
yassessed
asbeingat
high
risk
ofbias.AEs
in
haloprogin
grou
pwere
mainlystinging
Voravutinon
,65do
uble-blin
d
(Hatyai,Thailand
)
n=96
(45men,41
wom
en,10
sex
unrepo
rted;meanage34
years)
withtineacorporis/cruris
4weeks
A:Whitfield’sointmentfour
times
daily
B:micon
azole2%
four
times
daily
Mycologicalcure
(KOH):
41/4
4in
grou
pA
comparedwith40
/42in
grou
pB(RR0�9
8,95
%CI0�8
8–1�0
9)
Relapse:2/
39in
grou
pAcomparedwith1/
39in
grou
pB(RR2�0
0,95
%CI0�1
9–21
�16)
AEs:3/
48in
grou
pAcomparedwith0/
48in
grou
pB(RR7�0
0,95
%CI0�3
7–13
1�96)
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
630 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.
Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Weitgasser,69do
uble-blin
d(G
raz,
Austria;tw
ostud
ies)
154men,12
3wom
en(age
rang
e16
–59years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
4weeks
Stud
y1
A:haloprogin
1%solution
twice
daily
B:clotrimazole1%
solution
twice
daily
Stud
y2
A:haloprogin
1%ointmenttw
ice
daily
B:clotrimazole1%
cream
twice
daily
Mycologicalcure
forbo
thstud
ies;no
separate
data
fortineacruris/corpo
ris
Clin
icalcure
both
stud
ies:18
/22in
grou
pA
comparedwith16
/20in
grou
pB(RR1�0
2,95
%
CI0�7
6–1�3
7)
These
stud
iesalso
includ
edothertypesof
tinea
infections
Azolesvs.benzylam
ines
Lietal.,3
9do
uble-blin
d,multicentre
(China)
n=23
4(sex
unrepo
rted;meanage
34years)
withtineacruris/
corporis/p
edis
2weeks
A:bu
tenafine
1%cream
once
daily
B:bifonazole
1%cream
once
daily
Mycologicalcure
(KOH
+cultu
re):
54/5
8in
grou
pAcomparedwith56
/59in
grou
pB(RR0�9
8,
95%
CI0�9
0–1�0
8)Clin
icalcure:19
/58in
grou
pAcomparedwith
23/5
9in
grou
pB(RR0�8
4,95
%CI0�5
2–1�3
7)
Relapse:no
recurrencesin
either
grou
pAEs:6/
58in
grou
pAcomparedwith5/
59in
grou
pB(RR1�2
2,95
%CI0�3
9–3�7
8)Ram
ametal.,4
8do
uble-blin
d
(New
Delhi,India)
n=75
(20men,22
wom
en,33
sex
unrepo
rted;meanage30
years)
withtineacorporis/cruris
4weeks
A:bu
tenafine
1%on
cedaily
and
vehicleon
cedaily
for2weeks
follo
wed
by2weeks
vehicletw
ice
daily
B:clotrimazole1%
twicedaily
Mycologicalcure
(KOH):
20/2
2in
grou
pA
comparedwith27
/28in
grou
pB(RR0�9
4,95
%CI0�8
1–1�1
0)
Relapse:1/
22in
grou
pAcomparedwith2/
28in
grou
pB(RR0�6
4,95
%CI0�0
6–6�5
7)
AEs:6/
37in
grou
pAcomparedwith5/
38in
grou
pB(RR1�2
3,95
%CI0�4
1–3�6
9)
Stud
yassessed
asbeingat
high
risk
ofbias;25
/75
(33%
)wereno
tinclud
edin
theanalysis;per-protocol
analysis.There
wereno
assessmentsof
clinicalcure
Sing
aletal.,5
3do
uble-blin
d(D
elhi,India)
n=80
(53men/2
7wom
en;mean
age29
years)
withtineacorporis/
cruris
2–4weeks
A:bu
tenafine
1%on
cedaily
and
vehicleon
cedaily
for2weeks
follo
wed
by2weeks
vehicletw
ice
daily
B:clotrimazole1%
twicedaily
Mycologicalcure
(culture):
27/2
7in
grou
pA
comparedwith24
/25in
grou
pB(RR1�0
4,95
%
CI0�9
4–1�1
6)Clin
icalcure:26
/27in
grou
pAcomparedwith
24/2
5in
grou
pB(RR1�0
0,95
%CI0�9
0–1�1
2)Relapse:0/
20in
grou
pAcomparedwith3/
21in
grou
pB
AEs:2/
37in
grou
pAcomparedwith3/
34in
grou
pB(RR0�6
1,95
%CI0�1
1–3�4
5)
Stud
yassessed
asbeingat
high
risk
ofbias;28
/80
(35%
)werelostto
follo
w-
updu
ring
treatm
entand
39/8
0(49%
)at
endof
follo
w-up;
per-protocol
analysis
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 631

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Other
topicalantifung
alscomparisons
Dinkelaetal.,1
6do
uble-blin
d,tw
oprim
aryscho
ols
(Tanzania)
124men,12
0wom
en(age
rang
e6–
19years)
differenttinea
infections,includ
ingtineacorporis
2mon
ths
A:triclosansoap
once
daily
B:plainsoap
once
daily
Mycologicalcure
(KOH):
6/7grou
pAcompared
with3/
7in
grou
pB(RR2�0
0,95
%CI0�8
1–4�9
6)
Clin
icalcure:no
precisedata
couldbe
extracted
forparticipantswithon
lytineacorporis
Missing
outcom
edata
45/
224(20%
)combinedwith
per-protocol
analysisjudged
asbeingat
ahigh
risk
ofbias
Fanetal.,2
1do
uble-blin
dRCT
(Guang
zhou
,China)
n=18
3(77men,93
wom
en,13
sexun
repo
rted;agerang
e15
–68
years)
withtineacrurisor
vulvovaginalcand
idiasis
3weeks
A:xianglianlotion
wash+xiangliancream
once
daily
B:po
tassium
perm
anganate
wash+clotrimazole3%
cream
twicedaily
Mycologicalcure
(KOH
+culture):42
/52in
grou
pAcomparedwith27
/45in
grou
pB(RR0�8
4,
95%
CI0�7
2–0�9
7;P=0�0
3)Clin
icalcure:no
separate
data
(datacombined
withmycologicalcure)
FanandYang,
22do
uble-blin
d,multicentre
(China)
n=85
(58men/2
7wom
en;mean
age37
years)
withtineacruris/
corporis
4weeks
A:xianglianlotion
wash+xiangliancream
once
daily
B:po
tassium
perm
anganate
wash+clotrimazole3%
cream
twicedaily
Mycologicalcure
(KOH
+culture)
oftinea
corporis:14
/15in
grou
pAcomparedwith2/
4
ingrou
pB(RR1�8
7,95
%CI0�6
9–5�0
2)Mycologicalcure
(KOH
+culture)
oftineacruris:
10/3
5in
grou
pAcomparedwith4/
12in
grou
pB(RR3�2
1,95
%CI0�3
3–2�2
3)
Clin
icalcure
tineacorporis:11
/15in
grou
pA
comparedwith2/
4in
grou
pB(RR1�4
7,95
%CI
0�53–
4�09)
Clin
icalcure
tineacruris:10
/35in
grou
pA
comparedwith4/
12in
grou
pB(RR0�8
6,95
%CI0�3
3–2�2
3)
Relapse
tineacruris:threein
grou
pA,grou
pB
notrepo
rted
Relapse
tineacorporis:0in
grou
pA;grou
pBno
trepo
rted
Greer
etal.,2
5do
uble-blin
d,multicentre
(U.S.A.)
n=91
(sex
andmeanage
unrepo
rted)withtineacorporis
2weeks
A:bu
tenafin
e1%
cream
once
daily
B:vehicleon
cedaily
Mycologicalcure
(KOH
+culture):37
/42in
grou
pAcomparedwith10
/36in
grou
pB(RR3�1
7,
95%
CI1�8
5–5�4
3;P<0�0
1)Clin
icalcure:24
/42in
grou
pAcomparedwith
9/36
ingrou
pB(RR2�2
9,95
%CI1�2
3–4�2
6;P=0�0
1)
AEs:no
neParticipant-judged
improvem
ent:39
/42in
grou
p
Acomparedwith10
/36(RR3�3
4,95
%CI1�9
6–5�7
0;P<0�0
1)
(con
tinu
ed)
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
632 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Holti,29do
uble-blin
d
(New
castle,U.K.)
n=14
(sex
andageun
repo
rted)
withdifferenttineainfections,
includ
ingtineacorporis
8weeks
A:Whitfield’sointmenton
cedaily
B:pecilocinon
ceaday
Mycologicalcure:on
lyforgrou
pB(2/2
)
Clin
icalcure:on
lyforgrou
pB(2/2
)Norelapsein
either
grou
p
Twoparticipantswithtinea
corporis(the
remaind
erof
patientsin
thisstud
ywere
diagno
sedwithtineapedis)
Ledezm
aetal.,3
6(Venezuela)
60men
(meanage20
years)
with
tineacorporis
1week
A:ajoene
0�6%
geltw
icedaily
B:terbinafine
1%cream
twicedaily
Mycologicalcure
(KOH
+culture):19
/25in
grou
p
Acomparedwith13
/17in
grou
pB(RR0�9
9,95
%CI0�7
0–1�4
0)
Clin
icalcure:no
tassessed
only
clinicalscore
Relapse:1/
19in
grou
pAcomparedwith1/
13in
grou
pB
Stud
yassessed
asbeingat
high
risk
ofbias.High
numberof
drop
outs(30%
).
Twiceas
manydrop
outsin
theterbinafine
grou
p.Per-
protocol
analysis
Lesher
etal.,3
7do
uble-blin
d,
multicentre
(U.S.A.)
n=93
(75men,on
ewom
an,17
sexun
repo
rted;meanage
37years)
withtineacruris
2weeks
A:bu
tenafin
e1%
cream
once
daily
B:vehiclecream
once
daily
Mycologicalcure
(KOH
+culture):29
/37in
grou
p
Acomparedwith4/
38in
grou
pB(RR7�4
5,95
%CI2�2
0–19
�11;P<0�0
1)
Clin
icalcure:23
/37in
grou
pAcomparedwith
6/38
ingrou
pB(RR3�9
4,95
%CI1�8
1–8�5
5;
P<0�0
1)
Relapse:no
nein
either
grou
p.AEs:on
ein
thebu
tenafin
egrou
p(burning
)
Participant-judged
cure:25
/37in
grou
pA
comparedwith9/
39in
grou
pB(RR2�9
3,95
%
CI1�5
8–5�4
2;P<0�0
1)
Participant-judged
cure
increasedat
6weeks
after
treatm
ent–even
morein
favour
ofbu
tenafine
MacasaetandPert,40do
uble-
blind(M
anila,Philipp
ines)
33men,20
wom
en(m
eanage
30years)
withtineacorporis
2weeks
A:griseofulvin
1%solution
once
daily
B:vehiclesolution
once
daily
Mycologicalcure
(culture):
21/2
6in
grou
pA
comparedwith3/
27in
grou
pB(RR7�2
7,95
%CI2�4
6–21
�47;P<0�0
1)
Clin
icalcure:19
/26in
grou
pAcomparedwith
2/27
ingrou
pB(RR9�8
7,95
%CI2�5
5–38
�20;
P<0�0
1)AEs:1/
26in
grou
pAcomparedwith3/
27in
grou
pB(RR0�3
5,95
%CI0�0
4–3�1
2)Oladele
etal.,4
5do
uble-blin
d
(Nigeria)
33men
(age
rang
e20
–60years)
withdifferentskin
infections,
includ
ingtineacorporis/cruris
4weeks
A:Senn
aAlata
soap
twicedaily
B:placebosoap
twicedaily
Clin
icalcure:5/
5in
grou
pAcomparedwith0/
1
ingrou
pB
Durationof
treatm
entun
tilcure:ittook
4weeks
forthefive
participantsin
grou
pAto
becured
Onlysixparticipantshad
tineacorporisandmatched
ourinclusioncriteria;five
werein
theSenn
aAlata
soap
grou
pandon
ein
the
placebosoap
grou
p
(con
tinu
ed)
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 633

data for clinical cure could not be pooled owing to substantial
heterogeneity, but did confirm no difference in effectiveness
between the groups, and the same held true for the number
of adverse events (Table S2; see Supporting Information).
In the comparison of azoles vs. azoles in combination with
corticosteroids there was no difference in mycological cure
between the two treatment arms. In the azole-only group 245
of 313 participants were cured based on negative mycology
compared with 248 of 312 in the azole combined with
moderate potent corticosteroids group (RR 0�99, 95% CI
0�93–1�05).34,38,46,51,68,70 However, based on four stud-
ies,46,51,68,70 the combined treatment appeared to be more
effective with respect to clinical cure than azole monotherapy
(RR 0�67, 95% CI 0�53–0�84; P < 0�01). The number of
adverse events was similar in both groups (RR 1�36, 95% CI
0�68–2�69) (Table S3; see Supporting Informa-
tion).34,38,46,51,70
As in the former comparisons, based on mycological cure
rate, there was no difference in effectiveness between azoles
and benzylamines from three pooled studies: 107 of 112 in
the azole group compared with 101 of 107 in the benzylam-
ines group (RR 1�01, 95% CI 0�94–1�07).38,48,53 Although
the data could not be pooled for clinical cure (significant het-
erogeneity), these results were in concordance with the data
on mycological cure rates. Rates of adverse events were com-
parable for both treatment arms (RR 0�85, 95% CI 0�41–1�76)(Table S4; see Supporting Information).
The final comparison in the review evaluated azoles vs. pla-
cebo,6,44,55,57 but pooling of data was not possible in view of
considerable heterogeneity between the studies, albeit with
the exception of adverse events. With the exception of one
study, mycological and clinical cure rates favoured azoles
(Table S5; see Supporting Information).6
Discussion
One hundred and twenty-nine studies with 18 086 partici-
pants were included in the review; many of the studies were
more than 20 years old.1 Most studies demonstrated some evi-
dence to support the effectiveness and safety of currently used
or prescribed topical antifungal therapies for tinea cruris and
tinea corporis. Only data for some outcomes from studies
comparing terbinafine vs. placebo and naftifine vs. placebo
could be pooled, although the quality of the evidence was
considered to be low. Several studies compared frequency of
application; for those studies that compared once- vs. twice-
daily application there was no statistically significant difference
in any of the outcomes while taking into account that once-
daily application might be expected to lead to improved com-
pliance. Pooling of different classes of antifungals was possible
for topical azoles, benzylamines and allylamines, as well as
azoles combined with corticosteroids. All of the antifungals
appeared to be effective, but this was based on low- to very
low-quality evidence as most studies were assessed as having
an ‘unclear’ to ‘high’ risk of bias. The combined treatment of
azoles and corticosteroids achieved higher clinical (but not
Table
2(con
tinu
ed)
Stud
yParticipants
Intervention
sSummaryou
tcom
esCom
ments
Shietal.,5
2do
uble-blin
d,
multicentre
(China)
n=12
0(74men,23
wom
en,23
sexun
repo
rted;meanage
27years)
withdifferenttinea
infections,includ
ingtinea
corporis/cruris
2–4weeks
A:tetrandine
2%+ketoconazole
2%cream
twicedaily
B:ketoconazole
2%cream
twice
daily
C:tetrandine
2%cream
twicedaily
Mycologicalcure
(KOH
+culture):14
/16in
grou
p
Acomparedwith7/
15in
grou
pBand0/
12in
grou
pC
Clin
icalcure:12
/16in
grou
pAcomparedwith
5/15
ingrou
pBand0/
12in
grou
pC
Relapse:no
nein
grou
pA,tw
oin
grou
pBand
notapplicable
forgrou
pC
AEs:no
nein
anygrou
p
Stud
yassessed
asbeingat
high
risk
ofbias;19
%were
notinclud
edin
theanalysis
–un
clearfrom
which
grou
ps;per-protocol
analysis
KOH,po
tassium
hydroxidepreparation;
RR,risk
ratio;
CI,confi
denceinterval;AE,
adverseevent.Inconsistencyandincompletenessof
data
repo
rtingin
manyof
theolderstud
iesdidno
tallow
usto
undertakeconfi
dently
anystud
yotherthan
theavailablecase
analysisforefficacy
relatedto
cure,whereas
foradverseeffectswere-analysedandrepo
rted
thedata,whereverpo
ssible,accordingto
the
intention-to-treat
principle.
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
634 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

mycological) cure rates than with azole monotherapy, but the
quality of the evidence was also rated as very low. A possible
explanation for this treatment effect is that the azole compo-
nent was responsible for the mycological cure, while the cor-
ticosteroid component had a greater effect on diminishing the
redness of the inflamed skin. A few included studies provided
contradictory results on the effectiveness of Whitfield’s cream,
bearing in mind that this is still a widely used treatment in
many rural areas in developing countries.
The adverse events reported in all of the studies were con-
sidered to be mild and transient, and were balanced between
treatment arms – whether active or placebo controlled.
The quality of the studies (all studies were assessed as being
at unclear to high risk of bias) was mainly influenced by limi-
tations in study design and imprecision due to low sample
size. An important limitation in trial conduct in several studies
was the postrandomization exclusion of participants based on
subsequent negative mycological culture. In the general prac-
tice setting patients will usually receive initial treatment based
solely on a clinical diagnosis pending the results of potassium
hydroxide preparation or culture. This shortcoming in study
conduct and subsequent reporting and analysis could have
been overcome by the investigators undertaking a primary
analysis according to the intention-to-treat principle, followed
by a secondary analysis of those patients that fulfilled the eligi-
bility criteria of a confirmed diagnosis.
Several literature reviews have been published over the last
10–15 years, which, although lacking a systematic search and
critical appraisal of the literature, were broadly in agreement
with our findings that most topical antifungal treatments are
effective.2,136,137,139 No specific preference for an individual
topical antifungal was expressed, with the exception of two
reviews in which allylamines were recommended as the first-
line treatment, which appears to have been based mainly upon
a recognition of their rapid mode of action and shorter treat-
ment duration.2,138 Combined therapy of an antifungal with a
corticosteroid was suggested in two reviews but more
specifically if the tinea infection was accompanied by severe
inflammation.137,139 This treatment approach is still consid-
ered controversial and subject to debate, and some clinicians
even consider this a form of ‘mistreatment’ and that it might
lead to tinea incognito.136,140 Nondermatologists tend to
prescribe these combined agents far more frequently than
dermatologists, which is reportedly owing to a lesser degree
of accuracy in making the correct diagnosis.141 The adverse
events associated with protracted use of topical corticosteroids
are fairly well recognized, but the overall duration of the
included studies was too short for any assessment and, in any
event, these were not reported.
Three similar systematic reviews have been published on
this topic,142–144 and while we are in broad agreement that
their conclusions reflect the findings, we express a degree of
concern about the methodological rigour of these reviews.145
Applying similar language restrictions, i.e. only including
studies in English, Spanish or Portuguese, would have reduced
the number of included studies in our review by 20%, most
of which were in German. The effect of this form of study
selection and its relevance to language bias and the consequent
gap in evidence is well recognized.146 Although the authors of
these reviews indicated they had used the Cochrane ‘risk of
bias’ tool, these assessments and corresponding judgements
for the different domains of this tool were not reported. The
methodological quality of the studies included in these
reviews was assessed using the Jadad scale, which has well-
recognized and acknowledged limitations, specifically in plac-
ing greater emphasis on the reporting of a trial rather than on
its conduct.145
We examined several other clinical references and sources
for guidelines and systematic reviews, for example Agency for
Healthcare Research and Quality; DynaMed; National Guide-
lines Clearinghouse; National Institute for Health and Clinical
Excellence; Scottish Intercollegiate Guideline Network; U.K.
Database of Uncertainties about the Effects of Treatments; and
UpToDate.147–153 With the exception of DynaMed, the major-
ity of these clinical references either did not address tinea
corporis or tinea cruris, or provided very limited current
information that could aid clinical decision making.148
The inadequate reporting in some of the studies and our
inability to obtain missing trial details from the principal
investigators may have contributed to some bias in the assess-
ment of these studies, but it has been clearly stated in our
review when these conditions occurred. The limited data pro-
vided in these studies did not enable fair and reliable compari-
sons to be made for any one single intervention against
another for a specific outcome, with the exception of terbina-
fine and naftifine.
Fig 2. Risk of bias summary: our judgements
about each risk of bias item for each included
study.
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 635

Table 3 Summary of findings of terbinafine vs. placebo10,14,18,24,43,63,71
Terbinafine 1% cream/gel compared with placebo cream/gel for tinea cruris and tinea corporisPatient or population: patients with tinea cruris and tinea corporisSettings: hospital and primary care clinicsIntervention: terbinafine 1% cream/gelComparison: placebo cream/gel
Outcomes
Illustrative comparative risks(95% CI)a
Relativeeffect(95% CI)
Participants,n(studies, n)
Quality ofthe evidence(GRADE)b Comments
Assumed risk Corresponding riskPlacebocream/gel
Terbinafine 1%cream/gel
Mycological cure:Negative KOH microscopy,culture or both. Treatmentduration 1–2 weeks
See comment See comment Notestimable
330 (7) ⊕⊕⊖⊖Lowc,d
Unexplainedstatisticalheterogeneity; datanot pooled
Clinical cure:resolution of clinical signsand symptoms. Treatmentduration 1–2 weeksFollow-up: 2–4 weeks
Study population RR 4�51(3�1–6�56)
273 (5) ⊕⊕⊖⊖Lowe–g165 per
1000746 per 1000(513–1000)
Moderate133 per1000
600 per 1000(412–872)
Adverse effects:reported by investigatorsand/or participantsFollow-up: 0–8 weeks
Study population RR 0�43(0�2–0�92)
469 (7) ⊕⊝⊝⊝Very lowc,h
Contact dermatitis-type symptoms,no systemicadverseeffects reported
97 per 1000 42 per 1000(19–89)
Moderate29 per 1000 12 per 1000
(6–27)Relapse or recurrence:evidence of clinical ormycological infection inpreviously curedparticipantsFollow-up: 1–8 weeks
See comment See comment Notestimable
168 (3) ⊕⊕⊖⊖Lowi,j
Only Budimulja9
allowed anaccurateassessment ofrelapse – nonewere seen ineithergroup (n = 101)
Participant-judged cure:judgement of treatment as‘good’ or ‘very good’
Study population RR 4�46(3�16–6�31)
253 (2) ⊕⊕⊖⊖Lowk–m198 per
1000885 per 1000(627–1000)
Duration oftreatment untilclinical cure:not assessed
Study population Notestimable
0 (0) Seecomment
Outcome notassessed by studyauthors
See comment See comment
CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development and Evaluation; KOH, potassium hydroxide prepara-
tion; RR, risk ratio;⊕, low risk of bias;⊖, high risk of bias. aThe basis for the assumed risk (e.g. the median control group risk across studies) is
provided as follows. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the inter-
vention (and its 95% CI). bGRADE Working Group grades of evidence: ‘high’ quality – further research is very unlikely to change our confidence
in the estimate of effect; ‘moderate’ quality – further research is likely to have an important impact on our confidence in the estimate of effect
and may change the estimate; ‘low’ quality – further research is very likely to have an important impact on our confidence in the estimate of
effect and is likely to change the estimate; ‘very low’ quality – we are very uncertain about the estimate. cRandom sequence generation, allocation
concealment and blinding at unclear risk of bias across studies, with two studies (Lebwohl et al.35 and Millikan43) judged overall to be at high risk
of bias. In both of these studies, there was a high dropout rate (20–25%) in already underpowered studies. dSubstantial unexplained heterogene-
ity. eThree studies (Lebwohl et al.,35 Millikan43 and Zaias et al.71) judged to be at high risk of bias overall. fSmall sample size – optimal informa-
tion size would be 2790 participants. gAlthough there is a large effect (RR 4�51; in all studies RR > 4�00), there are threats to validity (see risk of
bias). hCI includes the threshold for appreciable benefit and nearly no effect, very low number of events and low sample size (optimal informa-
tion size would be 4238 participants). iMillikan43 judged to be at high risk of bias overall – high dropout rate in an underpowered study;
sequence generation, allocation concealment and blinding judged to be at unclear risk of bias in the remaining studies. jLow number of events
and sample size is lower than optimal information size. kBlinding for both studies judged to be at unclear risk of bias; Zaias et al.71 judged overall
to be at high risk of bias – details on total number of randomized participants not given. lNumber of events < 300; optimal information size
would be 2210 participants. mAlthough there is a large effect (RR > 4), there are threats to validity (see risk of bias).
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
636 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

A major limitation of our review was reflected in our
inability to use some of the data reported in the included
studies. In some this was due to the absence of separate data
for different tinea infections or because of the very limited
data available in abstracts to conference proceedings, which
did not permit adequate data extraction in almost half of the
included studies (n = 63).
In conclusion, most of the commonly used topical antifun-
gal treatments are effective and safe. However, no conclusions
could be drawn regarding the superiority of one class of topi-
cal antifungal over another. Pooled outcome data suggested
that the individual treatments terbinafine and naftifine are
effective, but the evidence was rated as low.
Combined treatments of azoles with a corticosteroid
achieved slightly better clinical cure rates based on very low-
quality evidence, but could be justified for a short duration of
use in the presence of inflammation. In resource-poor coun-
tries some of the more expensive treatments may not be avail-
able to everyone, with the possibility that only Whitfield’s
cream and the older azole creams are treatment options.
As all evidence was based on studies assessed as at an
‘unclear’ to ‘high risk’ of bias, the Cochrane review highlights
the need for high-quality, well-designed, adequately powered
and rigorously reported studies that can ultimately provide
reliable evidence to help inform clinical decision making.
Acknowledgments
We are grateful to Hana Burgess, Liz Doney, Beth Stuart and
Michael Moore for their contribution to the original review.
References
1 El-Gohary M, van Zuuren EJ, Fedorowicz Z et al. Topical antifun-gal treatments for tinea cruris and corporis. Cochrane Database Syst
Rev 2014; 8:CD009992.2 Moriarty B, Hay R, Morris-Jones R. The diagnosis and manage-
ment of tinea. BMJ 2012; 345:e4380.3 Goldstein AO, Goldstein BG. Dermatophyte (Tinea) Infections. Available
at: http://www.uptodate.com/contents/dermatophyte-tinea-infections (last accessed 1 April 2014).
4 Fox GN. 10 derm mistakes you don’t want to make. J Fam Pract2008; 57:162–9.
5 Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Inter-ventions 5.1.0. Available at: www.cochrane-handbook.org (last
accessed 1 April 2014).6 Bagatell FK. A prospective study of bifonazole 1% cream in the
once-daily management of tinea corporis/cruris. Adv Ther 1986;3:294–300.
7 Banerjee M, Ghosh AK, Basak S et al. Comparative evaluation ofeffectivity and safety of topical amorolfine and clotrimazole in
the treatment of tinea corporis. Indian J Dermatol 2011; 56:657–62.8 Bogaert H, Cordero C, Ollague W et al. Multicentre double-blind
clinical trials of ciclopirox olamine cream 1% in the treatment of
tinea corporis and tinea cruris. J Int Med Res 1986; 14:210–16.9 Budimulja U. Terbinafine 1% cream vs. bifonazole 1% cream in
the treatment of tinea cruris. Int J Dermatol 1998; 37:871–3.10 Budimulja U, Bramono K, Urip KS et al. Once daily treatment
with terbinafine 1% cream (Lamisil) for one week is effective in
the treatment of tinea corporis and cruris. A placebo-controlledstudy. Mycoses 2001; 44:300–6.
11 Clayton YM, Knight AG. A clinical double-blind trial of topicalmiconazole and clotrimazole against superficial fungal infections
and erythrasma. Clin Exp Dermatol 1976; 1:225–32.12 Clayton YM, Gange RW, Macdonald DM, Carruthers JA. A clinical
double-blind trial of topical haloprogin and miconazole againstsuperficial fungal infections. Clin Exp Dermatol 1979; 4:65–73.
13 Clerico R, Ribuffo A. Efficacy and tolerance of fenticonazole ver-sus miconazole cream. Int J Clin Pharmacol Res 1987; 7:77–81.
14 Cordero C, de la Rosa I, Espinosa Z et al. Short-term therapy of
tinea cruris/corporis with topical terbinafine. J Dermatol Treat1992; 3 (Suppl. 1):23–4.
15 del Palacio A, Cu�etara S, Rodriguez Noriega A. Topical treatmentof tinea corporis and tinea cruris with eberconazole (WAS 2160)
cream 1% and 2%: a phase II dose-finding pilot study. Mycoses1995; 38:317–24.
16 Dinkela A, Feri�e J, Mbata M et al. Efficacy of triclosan soap againstsuperficial dermatomycoses: a double-blind clinical trial in 224
primary school-children in Kilombero District, Morogoro Region,Tanzania. Int J Dermatol 2007; 46 (Suppl. 2):23–8.
17 Dobson RL, Bagatell FK, Hickman JG et al. Naftifine 1% cream inthe treatment of tinea cruris and tinea corporis. Drug Invest 1993;
3:57–9.18 Evans EGV, Shah JM, Joshipura RC. One-week treatment of tinea
corporis and tinea cruris with terbinafine (Lamisil) 1% cream: Aplacebo-controlled study. J Dermatol Treat 1992; 3:181–4.
19 Evans EG, James IG, Seaman RA, Richardson MD. Does naftifinehave anti-inflammatory properties? A double-blind comparative
study with 1% clotrimazole/1% hydrocortisone in clinically diag-nosed fungal infection of the skin. Br J Dermatol 1993; 129:437–42.
20 Evans EG, Seaman RA, James IG. Short-duration therapy with ter-binafine 1% cream in dermatophyte skin infections. Br J Dermatol
1994; 130:83–7.21 Fan RQ, Liang JH, Lu YZ. Treatment of tinea cruris and candidia-
sis of vulva with external application of Flos Caryopyhlli and Rhi-zoma Coptidis Co. J Guangzhou Univ Trad Chin Med 1991; 8:170–5.
22 Fan RQ, Yang YL. Clinical observation on the effect of XianglianFufang preparation for pityriasis versicolor, tinea corporis and
cruris. Chin J Integr Trad West Med 1994; 14:614–15.23 Gip L, Brundin G. A double-blind, two group multicentre study,
comparing naftifine 1% cream with placebo cream in the treat-ment of tinea cruris. Mykosen 1987; 30 (Suppl. 1):38–41.
24 Greer DL, Jolly HW. Treatment of tinea cruris with topical terbi-
nafine. J Am Acad Dermatol 1990; 23:800–4.25 Greer DL, Weiss J, Rodriguez DA et al. A randomized trial to
assess once-daily topical treatment of tinea corporis with butena-fine, a new antifungal agent. J Am Acad Dermatol 1997; 32:231–5.
26 Guillano GJ, Alabado KLP. A randomized, double-blind, clinicaltrial on the effectiveness and safety of 50% Gliricidia sepium (Ka-
kawate/Madre de Cacao) ointment compared with 2% miconaz-ole ointment in the treatment of tinea corporis and tinea cruris
(a pilot study). J Phil Dermatol Soc 2005; 14:15–22.27 Hantschke D, Reichenberger M. [Double-blind, randomised in
vivo investigations comparing the antifungals clotrimazole,tolnaftate and naftifine]. Mykosen 1980; 23:657–68 (in German).
28 Haroon TS, Hussain I, Aman S, Jahangir M. Randomized, com-parative, study of 1% naftifine cream (once daily) and 1% tioco-
nazole cream (twice daily) in the treatment of tinea cruris.Specialist. Pak J Med Sci 1996; 12:181–4.
29 Holti G. A double blind, controlled trial of Whitfield’s ointmentand Variotin in ringworm infections with a 2 year ‘follow-up’.
Acta Derm Venereol 1970; 50:229–31.
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 637

30 Jerajani HR, Janaki C, Kumar S, Phiske M. Comparative assess-ment of the efficacy and safety of sertaconazole (2%) cream ver-
sus terbinafine (1%) cream versus luliconazole (1%) cream inpatients with dermatophytoses: a pilot study. Indian J Dermatol
2013; 58:34–8.31 Jordon RE, Rapini RP, Rex IH Jr et al. Once-daily naftifine cream
1% in the treatment of tinea cruris and tinea corporis. Int J Derma-tol 1990; 29:441–2.
32 Kagawa S. Comparative clinical trial of naftifine and clotrimazolein tinea pedum, tinea cruris and tinea corporis. Mykosen 1987; 30
(Suppl. 1):63–9.33 Kalis B, Grosshans E, Binet O et al. Oxiconazole cream versus ke-
toconazole cream: a prospective, randomized, double-blind mul-
ticentric study in the treatment of tinea cruris. Ann Dermatol Venereol1996; 123:447–52.
34 Katz HI, Bard J, Cole GW et al. SCH 370 (clotrimazole-betametha-sone dipropionate) cream in patients with tinea cruris or tinea
corporis. Cutis 1984; 34:183–8.35 Lebwohl M, Elewski B, Eisen D, Savin RC. Efficacy and safety of
terbinafine 1% solution in the treatment of interdigital tinea pedisand tinea corporis or tinea cruris. Cutis 2001; 67:261–6.
36 Ledezma E, L�opez JC, Marin P et al. Ajoene in the topical short-term treatment of tinea cruris and tinea corporis in humans. Ran-
domized comparative study with terbinafine. Arzneimittelforschung1999; 49:544–7.
37 Lesher JL, Babel DE, Stewart DM et al. Butenafine 1% cream in thetreatment of tinea cruris: a multicenter, vehicle-controlled, dou-
ble-blind trial. J Am Acad Dermatol 1997; 36:S20–4.38 Li Q, Li M, Jin L et al. Clinical efficacy of compound econazole
cream in treatment of tinea corporis, tinea inguinalis, tineamanus, tinea pedis and its safety. Pharm Care Res 2004; 4:52–4.
39 Li M, Bi ZG, Gu J et al. Clinical study of butenafine hydrochloride1% cream in the treatment of tinea pedis, tinea corporis and tinea
cruris. J Clin Dermatol 2006; 35:471–2.40 Macasaet EN, Pert P. Topical (1%) solution of griseofulvin in the
treatment of tinea corporis. Br J Dermatol 1991; 124:110–11.41 Machado-Pinto J, Laborne MS. The use of oxiconazole 1%
cream in the treatment of dermatophytoses. Folha Med 1987;95:381–4.
42 Millikan LE, Galen WK, Gewirtzman GB et al. Naftifine cream 1%versus econazole cream 1% in the treatment of tinea cruris and
tinea corporis. J Am Acad Dermatol 1988; 18:52–6.43 Millikan LE. Efficacy and tolerability of topical terbinafine in the
treatment of tinea cruris. J Am Acad Dermatol 1990; 23:795–9.44 Miura Y, Onuki M, Takahashi S et al. A double-blind study on
utility of econazole cream in dermatomycosis. Rinsho Hyoka Clin
Eval 1979; 7:83–108.45 Oladele AT, Dairo BA, Elujoba AA, Oyelami AO. Management of
superficial fungal infections with Senna alata (‘alata’) soap: a preli-minary report. Afr J Pharm Pharmacol 2010; 4:98–103.
46 Pariser RJ, Pariser DM, Caro E et al. Clinical and mycologicaleffect of clotrimazole/betamethasone dipropionate cream versus
ketoconazole cream in patients with tinea cruris. J Dermatol Treat1995; 6:173–7.
47 Parish LC, Parish JL, Routh HB et al. A double-blind, randomized,vehicle-controlled study evaluating the efficacy and safety of na-
ftifine 2% cream in tinea cruris. J Drugs Dermatol 2011; 10:1142–7.48 Ramam M, Prasad HR, Manchanda Y et al. Randomised controlled
trial of topical butenafine in tinea cruris and tinea corporis. IndianJ Dermatol Venereol Leprol 2003; 69:154–8.
49 Ramelet AA, Walker-Nasir E. One daily application of oxiconazolecream is sufficient for treating dermatomycoses. Dermatologica
1987; 175:293–5.
50 Sharma A, Saple DG, Surjushe A et al. Efficacy and tolerability ofsertaconazole nitrate 2% cream vs. miconazole in patients with
cutaneous dermatophytosis. Mycoses 2011; 54:217–22.51 Shen WM, Hu YW, Gu HY. Econazole compound cream vs mico-
nazole cream in treating tinea corporis & cruris. Chin J New DrugClin Remedies 2002; 21:143–5.
52 Shi JP, Zhang H, Zhang ZD et al. Synergistic effects of tetrandrineon the antifungal activity of topical ketoconazole cream in the
treatment of dermatophytoses: a clinical trial. Chin J Integr Med2011; 17:499–504.
53 Singal A, Pandhi D, Agrawal S, Das S. Comparative efficacy of
topical 1% butenafine and 1% clotrimazole in tinea cruris andtinea corporis: a randomized, double-blind trial. J Dermatol Treat
2005; 16:331–5.54 Sivayathorn A, Piamphongsant T. Topical antimycotic agents for
the treatment of superficial dermatophytoses in Thailand – a dou-ble-blind study. Mykosen 1979; 22:21–4.
55 Spiekermann PH, Young MD. Clinical evaluation of clotrimazole. Abroad-spectrum antifungal agent. Arch Dermatol 1976; 112:350–2.
56 Su JG, Pan XF. The curative effect observation of compoundmiconazole cream in treating tinea cruris. Chin J Dermatovenereol
2001; 15:357.57 Tanenbaum L, Taplin D, Lavelle C et al. Sulconazole nitrate cream
1 percent for treating tinea cruris and corporis. Cutis 1989;44:344–7.
58 Thomas DJ. A study in industry of clotrimazole cream in tineapedis and tinea cruris. Curr Med Res Opin 1976; 3:630–3.
59 Thomas DJ, Evans A. A study in industry of bifonazole (1% gel)and sulconazole cream in tinea pedis and tinea cruris. In: Advances
in Topical Antifungal Therapy (Hay RJ, ed.) Berlin: Springer-Verlag,1986; 68–75.
60 Thulin H, Østerbye P. Miconazole in the treatment of dermato-mycosis. Mykosen 1975; 18:249–53.
61 Vander Ploeg DE, De Villez RL. A new topical antifungal drug:tioconazole. Int J Dermatol 1984; 23:681–3.
62 VanDersarl JV, Sheppard RH. Clotrimazole vs haloprogin treat-ment of tinea cruris. Arch Dermatol 1977; 113:1233–5.
63 van Heerden JS, Vismer HF. Tinea corporis/cruris: new treatmentoptions. Dermatology 1997; 194 (Suppl. 1):14–18.
64 Vena GA, Barile F, Faravelli M, Angelini G. Efficacy and safety ofbifonazole (BAY h 4502) in patients with pityriasis versicolor
and tinea cruris. Mykosen 1983; 26:415–20.65 Voravutinon V. A randomized comparative study in treatment of
tinea corporis, tinea cruris with Whitfield’s ointment and mico-
nazole cream. Thai J Dermatol 1993; 9:1–10.66 Wang AP, Li ZY, Wang DL et al. The clinical Lamisil cream for
body and tinea cruris. J Clin Dermatol 1995; 24:100–1.67 Wang KY, Li CY, Liang LP. A randomized controlled clinical
study of terbinafine powder versus miconazole for the treatmentof tinea manum/pedis and tinea corporis/cruris. Chin J Clin Phar-
macol 2000; 16:265–8.68 Wang AP, Li RY, Shun QN et al. A double blind randomized con-
trolled clinical trial of econazole-triamcinolone acetonide creamin the treatment of tinea pedis and tinea corporis & cruris. Chin J
Clin Pharmacol 2000; 16:345–9.69 Weitgasser H. Clinical and myocological study of the antifungal
agent haloprogin. Mykosen 1977; 20:15–24.70 Wortzel MH. A double-blind study comparing the superiority of
a combination antifungal (clotrimazole)/steroidal (betamethasonedipropionate) product. Cutis 1982; 30:258–61.
71 Zaias N, Berman B, Cordero CN et al. Efficacy of a 1-week, once-daily regimen of terbinafine 1% cream in the treatment of tinea
cruris and tinea corporis. J Am Acad Dermatol 1993; 29:646–8.
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
638 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

72 Abdul Bari MA. Comparison of superficial mycosis treatmentusing Butenafine and Bifonazole nitrate clinical efficacy. Glob J
Health Sci 2012; 5:150–4.73 Alomar C, Bassas S, Casas M et al. Multi-centre double-blind trial
on the efficacy and safety of sertaconazole 2% cream in compari-son with miconazole 2% cream on patients suffering from cuta-
neous mycoses. Arzneimittelforschung 1992; 42:267–73.74 Altmeyer P, Nolting S, Kuhlwein A et al. Effect of fenticonazole
spray in cutaneous mycosis: a double-blind clinical trial versuscyclopyroxolamine spray. J Int Med Res 1990; 18:61–7.
75 Athow-Frost TA, Freeman K, Mann TA et al. Clinical evaluation of
fenticonazole cream in cutaneous fungal infections: a comparisonwith miconazole cream. Curr Med Res Opin 1986; 10:107–16.
76 Avila JM. Treatment of dermatomycoses with sulconazole 1%nitrate cream or miconazole nitrate 2% cream: a double-blind
comparative study. Curr Ther Res 1985; 38:328–33.77 Bj€ornberg A, Tegner E. Treatment of tinea with miconazole and
miconazole-hydrocortisone. Curr Ther Res 1986; 40:471–4.78 Borelli C, Kl€ovekorn G, Ernst TM et al. Comparative study of 2%
sertaconazole solution and cream formulations in patients withtinea corporis, tinea pedis interdigitalis, or a corresponding cand-
idosis. Am J Clin Dermatol 2007; 8:371–8.79 Califano L, Cannavo SP, Ghittoni S et al. Multicenter open rando-
mised comparative study on efficacy and safety of topical fluco-nazole 0.5% vs econazole lipogel 1% in the treatment of localised
dermatomycoses. G Ital Dermatol Venereol 1999; 134:263–9.80 Clayton YM, Connor BL. Comparison of clotrimazole cream,
Whitfield’s ointment and Nystatin ointment for the topical treat-ment of ringworm infections, pityriasis versicolor, erythrasma
and candidiasis. Br J Dermatol 1973; 89:297–303.81 Clayton YM, Hay RJ, McGibbon DH, Pye RJ. Double blind com-
parison of the efficacy of tioconazole and miconazole for thetreatment of fungal infection of the skin or erythrasma. Clin Exp
Dermatol 1982; 7:543–9.82 Cuc�e LC, Assunc�~ao BF, Medawar LG et al. Tolciclate versus mico-
nazole, a double-blind trial in patients with dermatomycosis. J IntMed Res 1980; 8:144–7.
83 del Palacio-Hernanz A, L�opez-G�omez S, Moreno-Palancar P,Gonz�alez-Lastra F. A clinical double-blind trial comparing amorol-
fine cream 0.5% (RO-14-4767) with bifonazole cream 1% in thetreatment of dermatomycoses. Clin Exp Dermatol 1989; 14:141–4.
84 del Palacio A, Lopez S, Gimeno C et al. A randomized comparativestudy: amorolfine (cream 0.125%, 0.25% and 0.5%) in dermato-
mycoses. J Dermatol Treat 1991; 1:299–303.85 del Palacio A, Gip L, Bergstraesser M, Zaug M. Dose-finding study
of amorolfine cream (0.125%, 0.25% and 0.5%) in the treatment
of dermatomycoses. Clin Exp Dermatol 1992; 17 (Suppl. 1):50–5.86 del Palacio A, Cu�etara S, P�erez A et al. Topical treatment of der-
matophytosis and cutaneous candidosis with flutrimazole 1%cream: double-blind, randomized comparative trial with ketoco-
nazole 2% cream. Mycoses 1999; 42:649–55.87 del Palacio A, Ortiz FJ, P�erez A et al. A double-blind randomized
comparative trial: eberconazole 1% cream versus clotrimazole 1%cream twice daily in Candida and dermatophyte skin infections.
Mycoses 2001; 44:173–80.88 Duweb GA, Hassan KA, Mahmoud GS. Topical terbinafine (Lami-
sil-R) cream versus clotrimazole (Micoter-R) cream in the treat-ment of tinea corporis. Australas J Dermatol 1997; 38 (Suppl.
2):284.89 Effendy I, Friederich HC. Double-blind, randomized comparative
study of naftifine solution (once daily) and clotrimazole solution(twice daily) in the treatment of dermatomycoses. Mykosen 1987;
30 (Suppl. 1):104–11.
90 Finzi A, Fiorini A, Monici Preti P, Mounari M. A double blindevaluation of fenticonazole cream 2% and clotrimazole cream 1%
in dermatomycoses. Mykosen 1986; 29:41–4.91 Fredriksson T. Treatment of dermatomycoses with topical tioco-
nazole and miconazole. Dermatologica 1983; 166 (Suppl. 1):14–19.92 Friederich HC, Haas PJ, Tronnier H, Weidinger G. Comparison of
treatment with naftifine and with a combination of a corticoste-roid and an imidazole derivative. Akt Dermatol 1985; 11:77–80.
93 Fulton JE. Miconazole therapy for endemic fungal disease. ArchDermatol 1975; 111:596–8.
94 Ghaninejad H, Gholami K, Hashemi P et al. Sertaconazole 2%
cream vs. miconazole 2% cream for cutaneous mycoses: a dou-ble-blind clinical trial. Clin Exp Dermatol 2009; 34:e837–9.
95 Gip L, Langen ML. Results of a contralateral comparative studybetween Travocort cream and Travogen cream in inflammatory
and allergic dermatomycoses. Mykosen 1980; 23:79–84.96 Gip L, Forsstr€om S. A double-blind parallel study of sulconazole
nitrate 1% cream compared with miconazole nitrate 2% cream indermatomycoses. Mykosen 1983; 26:231–41.
97 Gip L. Comparison of oxiconazole (Ro-13-8996) and econazolein dermatomycoses. Mykosen 1984; 27:295–302.
98 Gong KM, Shi HJ. The report of 2% ketoconazole for skin ring-worm. Chin J Dermatovenereol 1991; 5:253.
99 Grigoriu D, Grigoriu A. Double-blind comparison of the efficacy,toleration and safety of tioconazole base 1% and econazole nitrate
1% creams in the treatment of patients with fungal infections ofthe skin or erythrasma. Dermatologica 1983; 166 (Suppl. 1):8–13.
100 Hall-Smith P. Dermatomycoses: a brief history of therapy and ini-tial results with clotrimazole. Postgrad Med J 1974; 50 (Suppl.
1):70–2.101 Jung EG, Bisco A, Azzollini E et al. Fenticonazole cream once
daily in dermatomycosis, a double-blind controlled trial versusbifonazole. Dermatologica 1988; 177:104–8.
102 Kashin P, Phyfferoen MC, Gibbs DL. A comparative study of onceversus twice daily treatment of superficial dermatophyte and yeast
infections with tioconazole (1%) cream. J Int Med Res 1985;13:88–95.
103 Katz R, Cahn B. Haloprogin therapy for dermatophyte infections.Arch Dermatol 1972; 106:837–8.
104 Keczkes K, Leighton I, Good CS. Topical treatment of dermato-phytoses and candidoses. Practitioner 1975; 214:412–17.
105 Kokoschka EM, Niebauer G, Mounari M, Monici Preti P. Treat-ment of dermatomycoses with topical fenticonazole and econaz-
ole. Mykosen 1986; 29:45–50.106 Kuhlwein A, Busch T. Tinea inguinalis und tinea pedis: cru-
conazol versus bifonazol in der Lokaltherapie. Therapiewoche 1990;
40:1643–5.107 Lassus A, Forstr€om S, Salo O. A double-blind comparison of sul-
conazole nitrate 1% cream with clotrimazole 1% cream in thetreatment of dermatophytoses. Br J Dermatol 1983; 108:195–8.
108 Lassus A, Forsstr€om S. A double-blind parallel study comparingsulconazole with econazole in the treatment of dermatophytoses.
Mykosen 1984; 27:592–8.109 Lassus A, Nolting KS, Savopoulos C. Comparison of ciclopirox
olamine 1% cream with ciclopirox 1%-hydrocortisone acetate 1%cream in the treatment of inflamed superficial mycoses. Clin Ther
1988; 10:594–9.110 Lebwohl M, Foged EK, Karvonen J et al. Terbinafine (1%) solu-
tion and emulsion gel: two new formulations in one week treat-ment of tinea pedis and tinea corporis/cruris. J Eur Acad Dermatol
Venereol 1998; 11 (Suppl. 2):S237.111 Leiste D, Braun W, Fegeler W et al. A double-blind clinical trial
of fenticonazole (2%) spray versus naftifine (1%) spray in
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 639

patients with cutaneous mycoses. Curr Med Res Opin 1989; 11:567–75.
112 Li R, Liu W, Zeng F, Wang A. Assessment of the efficacy andsafety of amorolfine cream vs. bifonazole cream, in the treatment
of tinea corporis/cruris. J Eur Acad Dermatol Venereol 2003; 17 (Sup-pl. 3):319.
113 Luciani P, Barba A. Double blind comparative study of 1%econazole cream and 1% bifonazole cream in the treatment of
dermatomycoses. G Ital Dermatol Venereol 1988; 123:LIII–LVI.114 McVie DH, Littlewood S, Allen BR et al. Sulconazole versus
clotrimazole in the treatment of dermatophytosis. Clin Exp Dermatol
1986; 11:613–18.115 Meinicke K, Striegel C, Weidinger G. Treatment of dermatomy-
coses with naftifine therapeutic efficacy on application once dailyand twice daily. Mykosen 1987; 30 (Suppl. 1):98–103.
116 Mertens RL, Morias J, Verhamme G. A double-blind studycomparing Daktacort, miconazole and hydrocortisone in inflam-
matory skin infections. Dermatologica 1976; 153:228–35.117 Nolting S, Langen ML. [Are topical corticosteroids advantageous
and justifiable in the treatment of dermatomycoses (Travocortcream and Travogen cream were compared in 100 patients in an
interindividual double-blind trial)]. Mykosen 1980; 23:699–706[in German].
118 Nolting S, Weidinger G. Naftifine in severe dermatomycosis-econazole-controlled therapeutic comparison. Mykosen 1985;
28:69–76.119 Nolting S, Semig G, Friedrich HK et al. Double-blind comparison
of amorolfine and bifonazole in the treatment of dermatomycos-es. Clin Exp Dermatol 1992; 17 (Suppl. 1):56–60.
120 Nu~nez CR. Treatment of dermatomycoses with sulconazolenitrate 1% cream or econazole nitrate 1% cream: a double-blind
comparative study. Adv Ther 1985; 2:112–17.121 Qadripur SA. Double-blind parallel comparison of sulconazole
nitrate, 1% cream and powder, with econazole, 1% cream andpowder, in the treatment of cutaneous dermatophytoses. Curr Ther
Res 1984; 35:753–8.122 Repiso Montero T, L�opez S, Rodr�ıguez C et al. Eberconazole
1% cream is an effective and safe alternative for dermatophyto-sis treatment: multicenter, randomized, double-blind, compara-
tive trial with miconazole 2% cream. Int J Dermatol 2006;45:600–4.
123 Schwarz KJ, Luggen H, Banninger R, Konzelmann M. Tests withPevisone in outpatients: double-blind study including 101
patients. Praxis 1978; 67:1112–16.124 Sehgal VN. Ciclopirox: a new topical pyrodonium antimycotic
agent. A double blind study in superficial dermatomycoses. Br J
Dermatol 1976; 95:83–8.125 Smith EB, David LM, Knox JM. Topical clotrimazole in dermato-
phytosis in a prison environment. Postgrad Med J 1974; 50 (Suppl.1):64–6.
126 Susilo R, Korting HC, Strauss UP, Sertaconazole Study Group.Dermatomycoses of the glabrous skin: a double-blind, rando-
mised, comparative trial of sertaconazole 2% cream once dailyversus vehicle. Clin Drug Invest 2003; 23:387–94.
127 Tanenbaum L, Anderson C, Rosenberg MJ et al. Sulconazolenitrate 1.0 percent cream: a comparison with miconazole in the
treatment of tinea pedis and tinea cruris/corporis. Cutis 1982;30:105–7.
128 Tronnier H. Inflammatory dermatomycoses – comparative studyof naftifine and a combination of a corticosteroid and an imidaz-
ole derivative. Mykosen 1987; 30 (Suppl. 1):78–87.129 Vannini P, Difonzo EM, Cordaro CI et al. New therapeutic
approach in skin mycoses: a comparative trial once versus twice
daily applications of fenticonazole in comparison to miconazole.Mycoses 1988; 31:280–4.
130 Viayna C, �Alvarez D, Domper N et al. Eberconazole 1% cream inthe treatment of dermatophytosis: double-blind, randomised
comparative trial with miconazole 2% cream. J Eur Acad DermatolVenereol 2003; 17 (Suppl. 3):14.
131 Wagner W, Reckers-Czaschka R. Oxiconazole in dermatomycosis– a double-blind, randomized comparison with bifonazole. Myko-
sen 1987; 30:484–92.132 Yim SM, Ko JH, Lee YW et al. Study to compare the efficacy and
safety of fluconazole cream with flutrimazole cream in the treat-
ment of superficial mycosis: a multicentre, randomised, double-blind, phase III trial. Mycoses 2010; 53:522–9.
133 Zarowny DP, Rogers RS, Tindall JP. Evaluation of theeffectiveness of griseofulvin, tolnaftate, and placebo in the topical
therapy of superficial dermatophytoses. J Invest Dermatol 1975;64:268–72.
134 Zaun H, Luszpinski P. Multicenter double-blind contralateralcomparison of naftifin and clotrimazole cream in patients with
dermatophytosis and candidiasis. Zeitschr Hautkr 1984; 59:1209–17.
135 Sch€unemann H, Brozek J, Oxman A (eds), The GRADE WorkingGroup. GRADE Handbook for Grading Quality of Evidence and Strength of Rec-
ommendation Version 3.2. Available at: http://www.cc-ims.net/gra-depro (last accessed 10 August 2014).
136 Gupta AK, Cooper EA, Ryder JE et al. Optimal management offungal infections of the skin, hair, and nails. Am J Clin Dermatol
2004; 5:225–37.137 Havlickova B, Friedrich M. The advantages of topical combination
therapy in the treatment of inflammatory dermatomycoses. Myco-ses 2008; 51 (Suppl. 4):16–26.
138 Nadalo D, Montoya C, Hunter-Smith D. What is the best way totreat tinea cruris? J Fam Pract 2006; 55:256–8.
139 Weinstein A, Berman B. Topical treatment of common superficialtinea infections. Am Fam Physician 2002; 65:2095–102.
140 Alston SJ, Cohen BA, Braun M. Persistent and recurrent tineacorporis in children treated with combination antifungal/cortico-
steroid agents. Pediatrics 2003; 111:201–3.141 Smith ES, Fleischer AB Jr, Feldman SR. Nondermatologists are
more likely than dermatologists to prescribe antifungal/cortico-steroid products: an analysis of office visits for cutaneous fungal
infections, 1990–1994. J Am Acad Dermatol 1998; 39:43–7.142 Rotta I, Sanchez A, Gonc�alves PR et al. Efficacy and safety of topi-
cal antifungals in the treatment of dermatomycosis: a systematic
review. Br J Dermatol 2012; 166:927–33.143 Rotta I, Otuki MF, Sanches AC et al. Efficacy of topical antifungal
drugs in different dermatomycoses: a systematic review withmeta-analysis. Rev Assoc Med Bras 2012; 58:308–18.
144 Rotta I, Ziegelmann PK, Otuki MF et al. Efficacy of topical anti-fungals in the treatment of dermatophytosis: a mixed-treatment
comparison meta-analysis involving 14 treatments. JAMA Dermatol2013; 149:341–9.
145 Fedorowicz Z, van Zuuren EJ. Efficacy of topical antifungals inthe treatment of dermatophytosis: an incomplete meta-analysis.
JAMA Dermatol 2013; 149:1243–4.146 Guyatt GH, Oxman AD, Montori V et al. GRADE guidelines: 5,
rating the quality of evidence – publication bias. J Clin Epidemiol2011; 64:1277–82.
147 U.S. Department of Health and Human Services. Agency forHealthcare Research and Quality. Available at: http://www.ahrq.-
gov/ (last accessed 13 August 2014).148 EBSCO. DynaMed. Available at: https://dynamed.ebscohost.com/
(last accessed 13 August 2014).
© 2014 British Association of DermatologistsBritish Journal of Dermatology (2015) 172, pp616–641
640 Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al.

149 U.S. Department of Health and Human Services. National GuidelinesClearinghouse. Available at: http://www.guideline.gov/ (last
accessed 13 August 2014).150 NICE. National Institute for Health and Clinical Excellence. Avail-
able at: http://www.nice.org.uk/ (last accessed 13 August2014).
151 SIGN. Scottish Intercollegiate Guidelines Network. Available at:http://www.sign.ac.uk/index.html (last accessed 13 August
2014).152 NICE. UK Database of Uncertainties about the Effects of Treatments. Available
at: http://www.library.nhs.uk/duets/ (last accessed 13 August
2014).153 UpToDate�. Smarter Decisions. Better Care. Available at: http://
www.uptodate.com/home (last accessed 13 August 2014).
Supporting Information
Additional Supporting Information may be found in the online
version of this article at the publisher’s website:
Fig S1. Studies was assessed for risk of bias. ⊕, low risk of
bias; ⊖, high risk of bias; (?), unclear risk of bias.
Table S1. Included studies with unusable or irretrievable
data.
Table S2. Summary of findings of azoles compared with al-
lylamines.
Table S3. Summary of findings of azoles compared with az-
oles/moderately potent corticosteroid combinations.
Table S4. Summary of findings of azoles compared with
benzylamines.
Table S5. Summary of findings of azoles compared with
placebo.
© 2014 British Association of Dermatologists British Journal of Dermatology (2015) 172, pp616–641
Evidence-based topical treatments for tinea cruris and tinea corporis, E.J. van Zuuren et al. 641




















