Evaluation of the first year of a pilot program in community pharmacy: HIV/AIDS medication therapy...
10
32 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org ABSTRACT BACKGROUND: The advent of combined antiretroviral therapy (ART) has increased treatment effectiveness but created new challenges for patients infected with human immunodeficiency virus (HIV) and for community pharmacists managing patients’ drug therapy. The ability of pharmacist- provided medication therapy management (MTM) services to increase medication adherence, improve health outcomes, and reduce overall medi- cal costs has been demonstrated in community pharmacies for chronic diseases such as diabetes and hypertension. However, the effectiveness of pharmacist-provided MTM services in HIV/acquired immune deficiency syn- drome (AIDS) has not been well studied. In January 2005, a pilot program to evaluate MTM services for patients with HIV/AIDS began in California, allowing 10 HIV/AIDS specialty pharmacies to receive compensation for the MTM services that they provided to HIV/AIDS patients. OBJECTIVES: To examine the first year of the HIV/AIDS pharmacy MTM compensation pilot program, which described and compared pilot and non- pilot pharmacies with respect to (a) patient characteristics; (b) intermedi- ate outcomes including type and number of ART medication regimens used, rates of adherence and excess medication fills for ART, use of contraindi- cated ART regimens, and occurrence of opportunistic infections; and (c) pharmacy and medical costs. METHODS: This was a cohort study examining 2005 Medi-Cal pharmacy and medical claims data for patients with HIV/AIDS who were served by pilot pharmacies versus other pharmacies. The HIV/AIDS patients were Medi-Cal beneficiaries aged 18 years or older as of January 1, 2005, who were continuously enrolled from January 1, 2004, through December 31, 2005, and diagnosed with HIV/AIDS, identified by receipt of at least 1 ART prescription and at least 1 medical claim with a diagnosis (primary or sec- ondary) of HIV/AIDS (ICD-9-CM code 042.0) during both the index period (the year before pilot program implementation, 2004) and the intervention period (the study year, 2005). The only difference in the inclusion criteria for the 2 cohorts was that the pilot pharmacy patients were required to have filled 50% or more of their antiretroviral prescriptions in 2005 at 1 of the 10 pilot pharmacies. Adherence was defined as a medication pos- session ratio (MPR) of 80%-120% and excess medication fills as MPR greater than 120%. Comparisons were made between groups using bivari- ate statistics (Pearson chi-square for categorical variables and t-tests for continuous variables). For comparisons of costs, generalized linear models assuming a gamma distribution and log link function were used; predictor variables for the models included age, gender, race/ethnicity, and dual cov- erage under Medicare. RESULTS: A total of 7,018 HIV/AIDS patients in the Medi-Cal population were identified as meeting the study criteria. Of these, 19.3% (n = 1,353) were pilot pharmacy patients. The demographic profile of pilot pharmacy patients was similar, but not identical, to that of patients receiving medica- tions at other pharmacies. A larger percentage of pilot pharmacy patients were on protease inhibitor-based ART medication regimens (63.8% vs. 54.8%, P< 0.001), remained on a single type of ART therapy throughout the study year (56.8% vs. 34.2%, P< 0.001), and were classified as adher- ent (56.3% vs. 38.1%, P< 0.001), compared with other pharmacy patients. Fewer pilot pharmacy patients used contraindicated regimens (11.6% Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries Jan D. Hirsch, RPh, PhD; Ashley Rosenquist, PharmD; Brookie M. Best, PharmD, MAS; Teresa Ann Miller, PharmD, FCSHP; and Todd P. Gilmer, PhD RESEARCH vs. 16.6%, P< 0.001) or had excess medication fills (19.7% vs. 44.8%, P< 0.001). The rate of opportunistic infections did not differ significantly between groups (28.2% vs. 26.1%, P= 0.121). The total mean (standard error) annual health care cost per patient was 10% higher in pilot phar- macies than in other pharmacies ($40,596 [$889] vs. $36,937 [$479], P= 0.001); driven by use of (a) medications (primarily non-ART medications) and (b) mental health services. Payment from the California Department of Health Care Services for MTM services averaged $1,014 per pilot pharmacy study patient. CONCLUSION: Study findings for the first year of the MTM program sug- gest that the pilot pharmacy patients received more appropriate HIV treatment. The degree to which these differences are affected by self- selection of patients into the pilot pharmacies is unknown. Longer-term outcomes and costs of the pilot program will be examined when data for subsequent years are available. J Manag Care Pharm. 2009;15(1):32-41 Copyright © 2009, Academy of Managed Care Pharmacy. All rights reserved. • The only 2 published studies related to pharmacist-provided MTM services in HIV/AIDS patients both concluded that pharmacist-led interventions had a positive effect on clinical outcomes. However, these studies were small and based in spe- cialized HIV clinics, not community pharmacies. • A chart review study demonstrated improved medication adher- ence (refilling prescriptions on average every 31 vs. 50 days) and a significantly greater reduction in viral load at 6 and 12 months after initiating therapy (both comparisons P <0.05) for patients with HIV/AIDS who attended a pharmacist-led medication adherence clinic (n=80) than for patients not attending. • A prospective study of patients (n=34) attending a pharmacist- managed drug optimization clinic reported significant improve- ment from baseline in CD4+ T-lymphocyte counts (mean [SD] improvement 54 [78] cells per cubic millimeter [mm 3 ], P <0.001) and viral loads (mean reduction 1.02 log 10 copies per milliliter [mL], P =0.004). However, that study lacked a com- parison group. • Larger studies using pharmacy records have demonstrated that improved adherence was correlated with reduced viral load; for example, for each 10% increase in adherence rate, viral load decreased by 0.12 log 10 copies per mL (95% confidence interval [CI] = 0.01-0.23 log 10 copies per mL), and when adherence fell below 95%, the percentage of patients with viral load below 400 copies per mL fell below 60%. What is already known about this subject
Transcript of Evaluation of the first year of a pilot program in community pharmacy: HIV/AIDS medication therapy...
32 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org
ABSTRACT
BACKGROUND: The advent of combined antiretroviral therapy (ART) has increased treatment effectiveness but created new challenges for patients infected with human immunodeficiency virus (HIV) and for community pharmacists managing patients’ drug therapy. The ability of pharmacist-provided medication therapy management (MTM) services to increase medication adherence, improve health outcomes, and reduce overall medi-cal costs has been demonstrated in community pharmacies for chronic diseases such as diabetes and hypertension. However, the effectiveness of pharmacist-provided MTM services in HIV/acquired immune deficiency syn-drome (AIDS) has not been well studied. In January 2005, a pilot program to evaluate MTM services for patients with HIV/AIDS began in California, allowing 10 HIV/AIDS specialty pharmacies to receive compensation for the MTM services that they provided to HIV/AIDS patients.
OBJECTIVES: To examine the first year of the HIV/AIDS pharmacy MTM compensation pilot program, which described and compared pilot and non-pilot pharmacies with respect to (a) patient characteristics; (b) intermedi-ate outcomes including type and number of ART medication regimens used, rates of adherence and excess medication fills for ART, use of contraindi-cated ART regimens, and occurrence of opportunistic infections; and (c) pharmacy and medical costs.
METHODS: This was a cohort study examining 2005 Medi-Cal pharmacy and medical claims data for patients with HIV/AIDS who were served by pilot pharmacies versus other pharmacies. The HIV/AIDS patients were Medi-Cal beneficiaries aged 18 years or older as of January 1, 2005, who were continuously enrolled from January 1, 2004, through December 31, 2005, and diagnosed with HIV/AIDS, identified by receipt of at least 1 ART prescription and at least 1 medical claim with a diagnosis (primary or sec-ondary) of HIV/AIDS (ICD-9-CM code 042.0) during both the index period (the year before pilot program implementation, 2004) and the intervention period (the study year, 2005). The only difference in the inclusion criteria for the 2 cohorts was that the pilot pharmacy patients were required to have filled 50% or more of their antiretroviral prescriptions in 2005 at 1 of the 10 pilot pharmacies. Adherence was defined as a medication pos-session ratio (MPR) of 80%-120% and excess medication fills as MPR greater than 120%. Comparisons were made between groups using bivari-ate statistics (Pearson chi-square for categorical variables and t-tests for continuous variables). For comparisons of costs, generalized linear models assuming a gamma distribution and log link function were used; predictor variables for the models included age, gender, race/ethnicity, and dual cov-erage under Medicare.
RESULTS: A total of 7,018 HIV/AIDS patients in the Medi-Cal population were identified as meeting the study criteria. Of these, 19.3% (n = 1,353) were pilot pharmacy patients. The demographic profile of pilot pharmacy patients was similar, but not identical, to that of patients receiving medica-tions at other pharmacies. A larger percentage of pilot pharmacy patients were on protease inhibitor-based ART medication regimens (63.8% vs. 54.8%, P < 0.001), remained on a single type of ART therapy throughout the study year (56.8% vs. 34.2%, P < 0.001), and were classified as adher-ent (56.3% vs. 38.1%, P < 0.001), compared with other pharmacy patients. Fewer pilot pharmacy patients used contraindicated regimens (11.6%
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
Jan D. Hirsch, RPh, PhD; Ashley Rosenquist, PharmD; Brookie M. Best, PharmD, MAS; Teresa Ann Miller, PharmD, FCSHP; and Todd P. Gilmer, PhD
RESEARCH
vs. 16.6%, P < 0.001) or had excess medication fills (19.7% vs. 44.8%, P < 0.001). The rate of opportunistic infections did not differ significantly between groups (28.2% vs. 26.1%, P = 0.121). The total mean (standard error) annual health care cost per patient was 10% higher in pilot phar-macies than in other pharmacies ($40,596 [$889] vs. $36,937 [$479], P = 0.001); driven by use of (a) medications (primarily non-ART medications) and (b) mental health services. Payment from the California Department of Health Care Services for MTM services averaged $1,014 per pilot pharmacy study patient.
CONCLUSION: Study findings for the first year of the MTM program sug-gest that the pilot pharmacy patients received more appropriate HIV treatment. The degree to which these differences are affected by self-selection of patients into the pilot pharmacies is unknown. Longer-term outcomes and costs of the pilot program will be examined when data for subsequent years are available.
J Manag Care Pharm. 2009;15(1):32-41
Copyright © 2009, Academy of Managed Care Pharmacy. All rights reserved.
• The only 2 published studies related to pharmacist-providedMTM services in HIV/AIDS patients both concluded thatpharmacist-led interventions had a positive effect on clinicaloutcomes.However,thesestudiesweresmallandbasedinspe-cializedHIVclinics,notcommunitypharmacies.
• Achartreviewstudydemonstratedimprovedmedicationadher-ence(refillingprescriptionsonaverageevery31vs.50days)andasignificantlygreaterreductioninviralloadat6and12monthsafterinitiatingtherapy(bothcomparisonsP<0.05)forpatientswith HIV/AIDS who attended a pharmacist-led medicationadherenceclinic(n=80)thanforpatientsnotattending.
• Aprospectivestudyofpatients(n=34)attendingapharmacist-manageddrugoptimizationclinicreportedsignificantimprove-ment from baseline in CD4+ T-lymphocyte counts (mean[SD] improvement 54 [78] cells per cubic millimeter [mm3],P <0.001)andviralloads(meanreduction1.02log10copiespermilliliter [mL],P =0.004).However, that study lacked a com-parisongroup.
• Largerstudiesusingpharmacyrecordshavedemonstratedthatimprovedadherencewascorrelatedwithreducedviralload;forexample, for each 10% increase in adherence rate, viral loaddecreasedby0.12log10copiespermL(95%confidenceinterval[CI]=0.01-0.23log10copiespermL),andwhenadherencefellbelow95%,thepercentageofpatientswithviralloadbelow400copiespermLfellbelow60%.
What is already known about this subject

www.amcp.org Vol. 15, No. 1 January/February 2009 JMCP Journal of Managed Care Pharmacy 33
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
Theadvent of combined antiretroviral therapy (ART) hasincreased treatment effectiveness but created new chal-lenges for patients infected with human immunodefi-
ciency virus (HIV) and for community pharmacistsmanagingpatients’ drug therapy. Combined ART generally consists of 3ormoreHIVdrugstakentogetherfromatleast2ofthe3maindrug classes; protease inhibitors (PI), nonnucleoside reversetranscriptase inhibitors (NNRTI); and nucleoside or nucleotidereverse transcriptase inhibitors (N(t)RTI).1 Because the viruscandevelop resistance against any1drug given alone, at least3ormoredrugs,usuallyfrom2ormoredifferentclasses,mustbeusedat the same time.Treatment regimens containing aPIaretypicallyamongthemostpotentand/ordurableagainstthevirus,butoftenhavetheleasttolerablesideeffects.ComplexARTregimenscontainmultipledrugswithvariousdosingschedules,undesirable side effect profiles, and different storage require-ments for many of the medications.2 Strict adherence to HIVdrugtherapyhasbeenshowntobecrucialtoachievingoptimaltherapeutic outcomes such as reduced viral load, reduction ofdrugresistance,andimprovedsurvival.3-5
The potential of pharmacist-provided medication therapymanagement(MTM)servicestoincreasemedicationadherence,improvehealthoutcomes,andreduceoverallmedicalcostshasbeendemonstratedincommunitypharmaciesforchronicdiseasessuchasdiabetesandhypertension.6,7However,theeffectivenessofpharmacist-providedMTMservicesinHIV/acquiredimmunedeficiencysyndrome(AIDS)hasnotbeenwellstudied.Areviewoftheliteraturefoundonly2studiesthatdescribedthetypeof
MTMservicesprovidedbyapharmacistandassessedoutcomes.BothstudieswereconductedinHIVoutpatientclinics.Thefirst,achartreviewstudy,demonstratedimprovedmedicationadher-ence (refilling prescriptions on average every 31 vs. 50 days,P<0.05)andasignificantlygreaterreductioninviralloadat6and12months (P<0.05)after initiating therapy forpatientsattend-ingapharmacist-ledmedicationadherenceclinicandatleast1educational session from the clinicalpharmacist (n=80) versusthosenotattending(nforcomparisongroupnotreported).8Thesecond,aprospectivestudyofpatients(n=34)whohadanexten-sive history of treatment and attended a pharmacist-manageddrugoptimizationclinic,reportedsignificantimprovementfrombaselineinCD4+T-lymphocytecounts(mean[SD]improvement54[78]cellspercubicmillimeter[mm3];P<0.001)andviralloads(meanreduction1.02log10copiespermilliliter[mL];P=0.004).9 Asignificantdecreaseinthemeandrug-relatedtoxicityscorewasalsoobservedamongpatientsexperiencingdrug-relatedtoxicities(n=25,mean[SD]reductionof1.0[0.8]onthe4-pointRadiationTherapy Oncology Group common toxicity scale, P<0.001).However,thatstudylackedacomparisongroup.
Althoughnot includingaMTMservicescomponent, severalstudies have shown significant correlation between improvedmedication adherence, as measured by pharmacy data, andreduced viral load.10-12 For example, Grossberg et al. reportedthat,foreach10%increaseinadherencerate,viralloaddecreasedby 0.12 log10copiespermL(95%confidenceinterval=0.01-0.23log10copiespermL)andFairleyetal.reportedthat,whenadher-ence fellbelow95%, thepercentageofpatientswithviral loadconsistentlybelow400 copiespermL fell below60%.11,12 It isreasonabletoexpectthattheprovisionofMTMserviceswouldincrease adherence, as it has in other disease states, and thusreduceviralload.However,barrierstothedeliveryofspecializedcounselingservicestoenhanceadherenceinHIV/AIDSpatientsincommunitypharmacysettingshavealsobeenrecognized.Forexample,inastatewidesurveyofpharmacistsinNorthCarolina,59%ofcommunitypharmacistrespondentsindicatedthattheydid not have enough time to provide adherence counseling totheirHIV/AIDSpatients.13
Pilot Program DescriptionIn January 2005, a pilot program to compensate and evaluatecommunity pharmacy-based MTM services for patients withHIV/AIDSbeganinthestateofCalifornia.Thisprogram,underWelfareandInstitutionsCodeSection14199-14199.3,allowed10HIV/AIDSspecialtypharmaciesinthestatetoreceivecompensa-tionfortheMTMservicesthattheyprovidedtoHIV/AIDSMedi-Calpatients.TheCaliforniaDepartmentofHealthCareServices(DHCS) provided pilot pharmacies $9.50 per prescription dis-pensedtoaMedi-Calbeneficiaryforthe3-yeartermofthepilotprogram.TheDHCSselectedthe10pilotpharmaciesbasedonthe requirements of the legislation authorizing the pilot.14 Thefirst 10pharmacies that applied andmet the following criteria
• Toourknowledge,thisisthefirst large-scaleevaluationofanMTMprograminHIV/AIDSpatients.
• AmongMedi-CalpatientsdiagnosedwithHIV/AIDSandusingART, patients of pilot MTM pharmacies (those filling 50%or more of their ART prescriptions at pharmacies that werereimbursedforMTMservices)weremorelikelytouseproteaseinhibitor-based ART medication regimens (63.8% vs. 54.8%,P <0.001) and to remain on a single type of ART regimenthroughout the studyyear (56.8%vs.34.2%,P <0.001), com-paredwithpatientsusingotherpharmacies.
• More pilot pharmacy patients were classified as adherent(56.3%vs.38.1%,P <0.001)andfewerpilotpharmacypatientswereoncontraindicatedregimens(11.6%vs.16.6%,P<0.001),comparedwithotherpharmacypatients.However,therateofopportunistic infections did not differ significantly betweengroups(28.2%vs.26.1%,P =0.121)duringthestudyyear.
• The totalmean [SD] annual health care cost per patientwas10%higher in pilot pharmacies ($40,596 [$889] vs. $36,937[$479],P =0.001);drivenbyuseofmedications(primarilynon-ARTmedications)andmentalhealthservices.
What this study adds

34 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org
were selected: (a) patient population comprising 90% ormoreof persons with HIV/AIDS, (b) had the ability to immediatelyprovidespecializedservicesrenderedbyaqualifiedpharmacistorotherhealthcareprovideroperatingwithinhisorherscopeofpractice, and (c)hadpharmacistsandotherqualifiedhealthcare providers to identify patients who should receive MTMservices.Specializedservicesweredefinedasbeingdistinctfromgeneralizedpatienteducationandinformationactivitiesalreadyrequiredbylawandprovidedforintheprofessionaldispensingfee.Theseservices(a)weretobepatientspecificandindividual-izedservicesprovideddirectlybyapharmacisttothepatientor,inlimitedcircumstances,thepatient’scaregiver,and(b)involvedface-to-face interaction between the patient or caregiver andthepharmacist duringdelivery ofMTM services. Thepossibletypes of MTM services outlined in the legislation were basedon the definition ofMTM services publishedby theAmericanPharmacistsAssociation.15Patientsofpilotpharmacieschosetopatronize pilot pharmacies either through their own selectionprocessand/orbasedonphysicianreferral;thesedecisionsweremadeindependentofthisstudy.
Followinguponpreviousworksuggestingapotentialimpactof pharmacist-providedMTM services on adherence and viralload inHIV/AIDSpatientswhowere treated in thecommunitysetting,8,9theCaliforniaHIV/AIDSpharmacyMTMservicespilotprogramprovidedanopportunitytoinvestigateabroaderrangeof outcomes using a larger sample of patients withHIV/AIDS.TheCalifornia studyexaminedpatients receivingcare atphar-maciesprovidingawiderangeofMTMservicesandcomparedtheiroutcomeswiththoseofsimilarpatientsatotherpharmaciesthroughoutthestate.
Study ObjectivesThepurposeof this studywas toexamine the firstyearof theHIV/AIDSpharmacyMTMservicescompensationpilotprogram.Thestudyusedpharmacyandmedicalclaimsdata todescribeandcomparepatientsfillingprescriptionsatpilot(MTM)versusotherpharmacieswith respect to (a)patientcharacteristics; (b)intermediateoutcomes, includingthenumberandtypeofARTmedicationregimens,ratesofadherenceandexcessivefills,useofcontraindicatedARTregimens,andoccurrenceofopportunisticinfections;and(c)pharmacyandmedicalcosts.
■■ MethodsDescription of the InterventionThe intervention in this study was participation in the DHCScompensation pilot program for MTM services. The programrequired that participating pharmacies be able to immediatelyofferMTMservices; therefore,pharmaciesselectedforthepilotcompensationprogramhadbeenofferinga rangeofMTMser-vices before participating. Although the specific services thateach pilot pharmacy must provide were not defined, all pilotpharmaciesofferedservicesto(a)manageadversedrugreactions
andmedicationsideeffects;(b)evaluatepatientabilitytoadheretomedicationregimens,inconsultationwithphysiciansandcasemanagers;and(c)tailordrugregimenstoaccommodatespecificpatient needs.16 Each pharmacy worked with patients and/ortheirphysiciansaccordingtotheirownpracticenorms,andfur-therdetailswerenotavailabletotheresearchers.
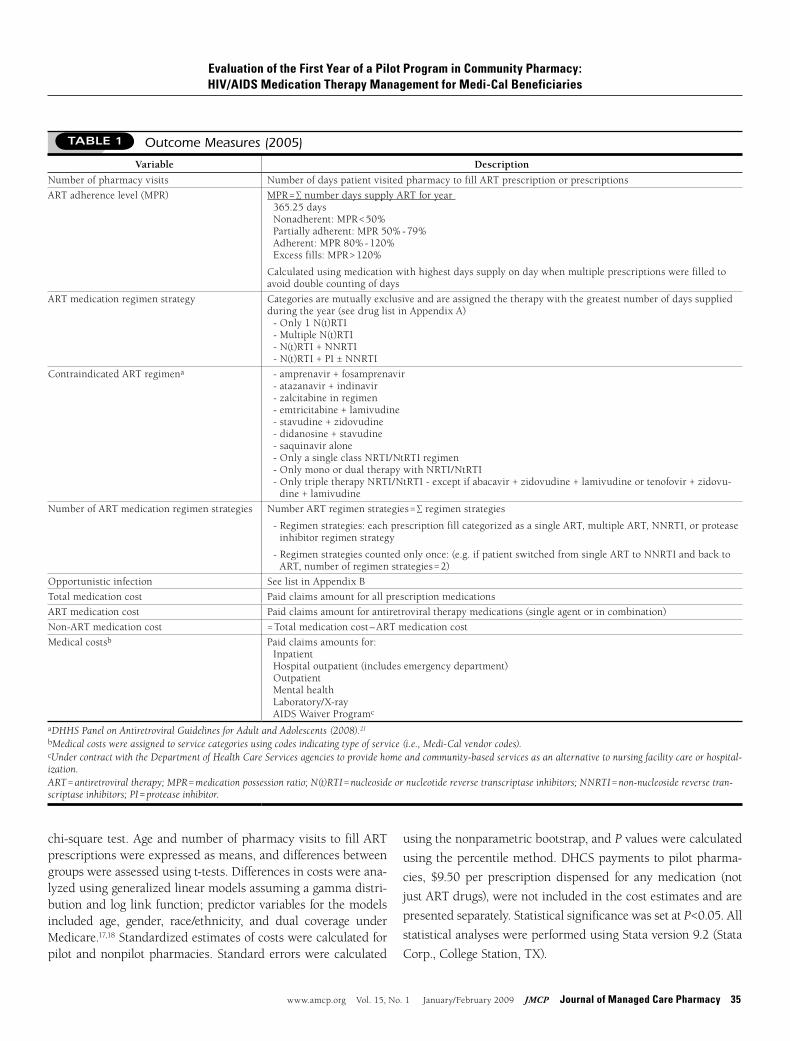
Outcome MeasuresProvision of MTM services in pilot pharmacies was expectedto (a) improve adherence to ART regimens, (b) result inmorerational ART medication strategies (e.g., fewer contraindicatedregimens,fewermedicationchangesperyearwhichcandecreaselikelihoodofdevelopingdrugresistance),(c)decreaseoccurrenceof opportunistic infections, and (d) reduce costs throughmorerationalmedicationusageandreducedneedformedicalservices.Tenoutcomemeasureswereassessed(Table1).
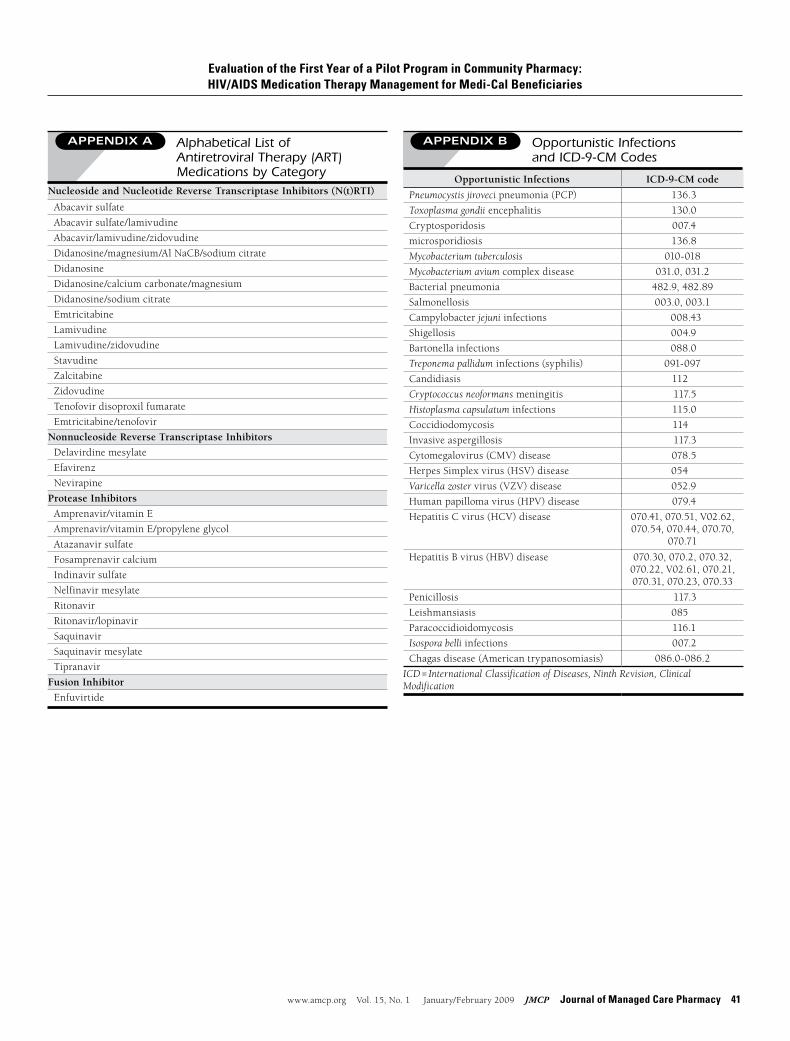
Study Design and Patient SelectionThis was a cohort study examining 2005Medi-Cal pharmacyandmedical claimsdata forpatientswithHIV/AIDS servedbypilotpharmaciesversusotherpharmacies.AllstudyprocedureswereapprovedbytheUniversityofCaliforniaSanDiegoandtheDHCSHumanResearchProtectionPrograms.Thestudygroup,pilotpharmacyHIV/AIDSpatients, consistedofMedi-Cal ben-eficiariesaged18yearsorolderasofJanuary1,2005,whowerecontinuouslyenrolledfromJanuary1,2004,throughDecember31,2005,anddiagnosedwithHIV/AIDS,identifiedbyreceiptofatleast1prescriptionforARTandatleast1medicalclaimwithanHIV/AIDS-relateddiagnosis(primaryorsecondary)International Classification of Diseases, Ninth Revision, Clinical Modification(ICD-9-CM)code042.0duringboththeindexperiod(fromJanuary1throughDecember31,2004)andthestudyperiod(fromJanuary1throughDecember31,2005).TheARTmedicationsareshowninAppendixA.
Patientswereidentifiedaspilotpharmacypatientsiftheyhadfilled50%ormoreoftheirARTprescriptionsin2005at1ofthe10pilotpharmacies.Comparisongrouppatientsmet the sameinclusionandexclusioncriteriaasstudypatients,exceptthattheywerenot identified ashaving filled50%ormore of theirARTprescriptionsin2005at1ofthe10pilotpharmacies.Individualsenrolled in managed care plans were excluded because paidclaims are not generated forMedi-Cal participants enrolled inmanagedcare.
Data Analysis Descriptivestatisticswerecalculatedforallvariables.Frequencydistributions were used to describe categorical variables, andmeans,medians,standarddeviations,andrangeswereusedforcontinuous variables. Gender, dual coverage under Medicare,race/ethnicity,ARTadherenceandARTmedicationcategorywereexpressedaspercentages,anddifferencesbetweengroups(pilotversusotherpharmacypatients)wereassessedusingthePearson
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
www.amcp.org Vol. 15, No. 1 January/February 2009 JMCP Journal of Managed Care Pharmacy 35
chi-squaretest.AgeandnumberofpharmacyvisitstofillARTprescriptionswereexpressedasmeans,anddifferencesbetweengroupswereassessedusingt-tests.Differencesincostswereana-lyzedusinggeneralizedlinearmodelsassumingagammadistri-butionandloglinkfunction;predictorvariablesforthemodelsincluded age, gender, race/ethnicity, and dual coverage underMedicare.17,18Standardizedestimatesofcostswerecalculatedforpilotandnonpilotpharmacies.Standarderrorswerecalculated
usingthenonparametricbootstrap,andPvalueswerecalculated
usingthepercentilemethod.DHCSpaymentstopilotpharma-
cies, $9.50 per prescription dispensed for anymedication (not
justARTdrugs),werenotincludedinthecostestimatesandare
presentedseparately.StatisticalsignificancewassetatP<0.05.All
statisticalanalyseswereperformedusingStataversion9.2(Stata
Corp.,CollegeStation,TX).
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
TABLE 1 Outcome Measures (2005)
Variable Description
Numberofpharmacyvisits NumberofdayspatientvisitedpharmacytofillARTprescriptionorprescriptions
ARTadherencelevel(MPR) MPR=∑numberdayssupplyARTforyear 365.25days Nonadherent:MPR<50% Partiallyadherent:MPR50%-79% Adherent:MPR80%-120% Excessfills:MPR>120%
Calculatedusingmedicationwithhighestdayssupplyondaywhenmultipleprescriptionswerefilledtoavoiddoublecountingofdays
ARTmedicationregimenstrategy Categoriesaremutuallyexclusiveandareassignedthetherapywiththegreatestnumberofdayssuppliedduringtheyear(seedruglistinAppendixA) -Only1N(t)RTI -MultipleN(t)RTI -N(t)RTI+NNRTI -N(t)RTI+PI±NNRTI
ContraindicatedARTregimena -amprenavir+fosamprenavir -atazanavir+indinavir -zalcitabineinregimen -emtricitabine+lamivudine -stavudine+zidovudine -didanosine+stavudine -saquinaviralone -OnlyasingleclassNRTI/NtRTIregimen -OnlymonoordualtherapywithNRTI/NtRTI-OnlytripletherapyNRTI/NtRTI-exceptifabacavir+zidovudine+lamivudineortenofovir+zidovu-
dine+lamivudine
NumberofARTmedicationregimenstrategies NumberARTregimenstrategies=∑regimenstrategies
-Regimenstrategies:eachprescriptionfillcategorizedasasingleART,multipleART,NNRTI,orproteaseinhibitorregimenstrategy
-Regimenstrategiescountedonlyonce:(e.g.ifpatientswitchedfromsingleARTtoNNRTIandbacktoART,numberofregimenstrategies=2)
Opportunisticinfection SeelistinAppendixB
Totalmedicationcost Paidclaimsamountforallprescriptionmedications
ARTmedicationcost Paidclaimsamountforantiretroviraltherapymedications(singleagentorincombination)
Non-ARTmedicationcost =Totalmedicationcost–ARTmedicationcost
Medicalcostsb Paidclaimsamountsfor: Inpatient Hospitaloutpatient(includesemergencydepartment) Outpatient Mentalhealth Laboratory/X-ray AIDSWaiverProgramc
aDHHS Panel on Antiretroviral Guidelines for Adult and Adolescents (2008).21
bMedical costs were assigned to service categories using codes indicating type of service (i.e., Medi-Cal vendor codes).cUnder contract with the Department of Health Care Services agencies to provide home and community-based services as an alternative to nursing facility care or hospital-ization.ART = antiretroviral therapy; MPR = medication possession ratio; N(t)RTI = nucleoside or nucleotide reverse transcriptase inhibitors; NNRTI = non-nucleoside reverse tran-scriptase inhibitors; PI = protease inhibitor.
36 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org
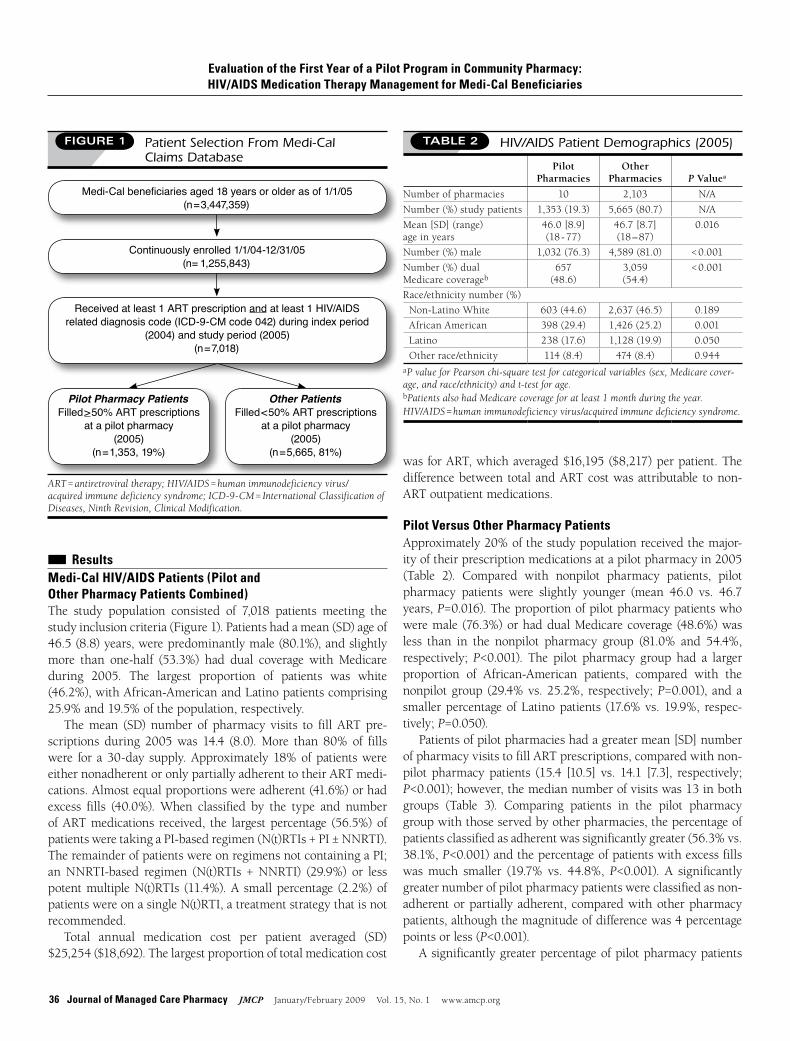
■■ Results Medi-Cal HIV/AIDS Patients (Pilot and Other Pharmacy Patients Combined)The study population consisted of 7,018 patients meeting thestudyinclusioncriteria(Figure1).Patientshadamean(SD)ageof46.5(8.8)years,werepredominantlymale(80.1%),andslightlymore than one-half (53.3%) had dual coverage withMedicareduring 2005. The largest proportion of patients was white(46.2%),withAfrican-AmericanandLatinopatientscomprising25.9%and19.5%ofthepopulation,respectively.
Themean (SD) number of pharmacy visits to fill ARTpre-scriptions during 2005was 14.4 (8.0).More than 80% of fillswere for a30-day supply.Approximately18%ofpatientswereeithernonadherentoronlypartiallyadherenttotheirARTmedi-cations.Almostequalproportionswereadherent(41.6%)orhadexcess fills (40.0%).When classified by the type and numberofARTmedications received, the largestpercentage (56.5%)ofpatientsweretakingaPI-basedregimen(N(t)RTIs+PI±NNRTI).TheremainderofpatientswereonregimensnotcontainingaPI;anNNRTI-based regimen (N(t)RTIs +NNRTI) (29.9%) or lesspotentmultipleN(t)RTIs (11.4%).A smallpercentage (2.2%)ofpatientswereonasingleN(t)RTI,atreatmentstrategythatisnotrecommended.
Total annual medication cost per patient averaged (SD)$25,254($18,692).Thelargestproportionoftotalmedicationcost
wasforART,whichaveraged$16,195($8,217)perpatient.Thedifferencebetween totalandARTcostwasattributable tonon-ARToutpatientmedications.
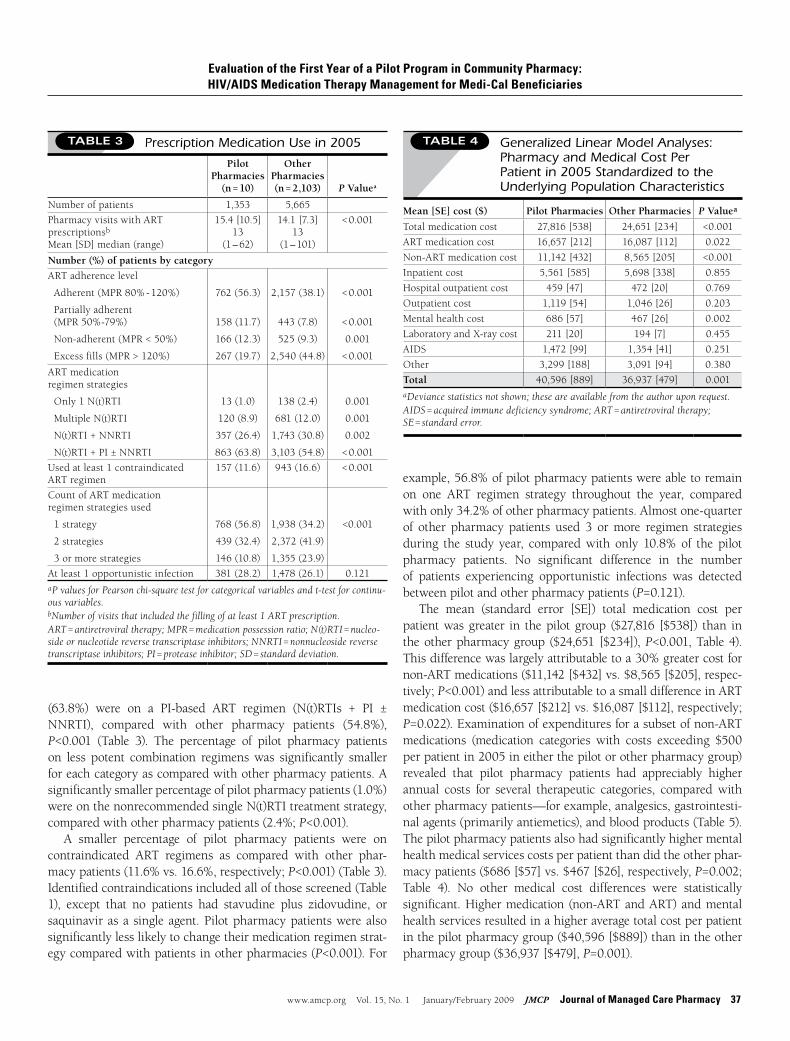
Pilot Versus Other Pharmacy Patients Approximately20%ofthestudypopulationreceivedthemajor-ityoftheirprescriptionmedicationsatapilotpharmacyin2005(Table 2). Compared with nonpilot pharmacy patients, pilotpharmacy patients were slightly younger (mean 46.0 vs. 46.7years,P=0.016).Theproportionofpilotpharmacypatientswhoweremale(76.3%)orhaddualMedicarecoverage(48.6%)wasless than in the nonpilot pharmacy group (81.0% and 54.4%,respectively;P<0.001). The pilot pharmacy group had a largerproportion of African-American patients, compared with thenonpilotgroup(29.4%vs.25.2%, respectively;P=0.001),andasmallerpercentageofLatinopatients (17.6%vs.19.9%, respec-tively;P=0.050).
Patientsofpilotpharmacieshadagreatermean[SD]numberofpharmacyvisitstofillARTprescriptions,comparedwithnon-pilotpharmacypatients (15.4 [10.5] vs. 14.1 [7.3], respectively;P<0.001);however,themediannumberofvisitswas13inbothgroups (Table 3). Comparing patients in the pilot pharmacygroupwiththoseservedbyotherpharmacies,thepercentageofpatientsclassifiedasadherentwassignificantlygreater(56.3%vs.38.1%,P<0.001)andthepercentageofpatientswithexcessfillswasmuch smaller (19.7% vs. 44.8%, P<0.001). A significantlygreaternumberofpilotpharmacypatientswereclassifiedasnon-adherentorpartiallyadherent,comparedwithotherpharmacypatients,althoughthemagnitudeofdifferencewas4percentagepointsorless(P<0.001).
Asignificantlygreaterpercentageofpilotpharmacypatients
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
FIGURE 1 Patient Selection From Medi-Cal Claims Database
ART = antiretroviral therapy; HIV/AIDS = human immunodeficiency virus/acquired immune deficiency syndrome; ICD-9-CM = International Classification of Diseases, Ninth Revision, Clinical Modification.
Medi-Cal beneficiaries aged 18 years or older as of 1/1/05(n = 3,447,359)
Continuously enrolled 1/1/04-12/31/05 (n= 1,255,843)
Pilot Pharmacy PatientsFilled > 50% ART prescriptions
at a pilot pharmacy (2005)
(n = 1,353, 19%)
Other PatientsFilled < 50% ART prescriptions
at a pilot pharmacy (2005)
(n = 5,665, 81%)
Received at least 1 ART prescription and at least 1 HIV/AIDS related diagnosis code (ICD-9-CM code 042) during index period
(2004) and study period (2005)(n = 7,018)
TABLE 2 HIV/AIDS Patient Demographics (2005)
Pilot Pharmacies
Other Pharmacies P Valuea
Numberofpharmacies 10 2,103 N/A
Number(%)studypatients 1,353(19.3) 5,665(80.7) N/A
Mean[SD](range) ageinyears
46.0[8.9] (18-77)
46.7[8.7] (18–87)
0.016
Number(%)male 1,032(76.3) 4,589(81.0) < 0.001
Number(%)dual Medicarecoverageb
657 (48.6)
3,059 (54.4)
< 0.001
Race/ethnicitynumber(%)
Non-LatinoWhite 603(44.6) 2,637(46.5) 0.189
AfricanAmerican 398(29.4) 1,426(25.2) 0.001
Latino 238(17.6) 1,128(19.9) 0.050
Otherrace/ethnicity 114(8.4) 474(8.4) 0.944aP value for Pearson chi-square test for categorical variables (sex, Medicare cover-age, and race/ethnicity) and t-test for age.bPatients also had Medicare coverage for at least 1 month during the year.HIV/AIDS = human immunodeficiency virus/acquired immune deficiency syndrome.
www.amcp.org Vol. 15, No. 1 January/February 2009 JMCP Journal of Managed Care Pharmacy 37
(63.8%) were on a PI-based ART regimen (N(t)RTIs + PI ±NNRTI), compared with other pharmacy patients (54.8%),P<0.001 (Table 3). The percentage of pilot pharmacy patientson less potent combination regimenswas significantly smallerforeachcategoryascomparedwithotherpharmacypatients.Asignificantlysmallerpercentageofpilotpharmacypatients(1.0%)wereonthenonrecommendedsingleN(t)RTItreatmentstrategy,comparedwithotherpharmacypatients(2.4%;P<0.001).
A smaller percentage of pilot pharmacy patients were oncontraindicated ART regimens as compared with other phar-macypatients(11.6%vs.16.6%,respectively;P<0.001)(Table3).Identifiedcontraindicationsincludedallofthosescreened(Table1), except that no patients had stavudine plus zidovudine, orsaquinavir as a singleagent.Pilotpharmacypatientswerealsosignificantlylesslikelytochangetheirmedicationregimenstrat-egycomparedwithpatientsinotherpharmacies(P<0.001).For
example,56.8%ofpilotpharmacypatientswereabletoremainon one ART regimen strategy throughout the year, comparedwithonly34.2%ofotherpharmacypatients.Almostone-quarterof other pharmacy patients used 3 ormore regimen strategiesduring the study year, comparedwith only 10.8%of the pilotpharmacy patients. No significant difference in the numberof patients experiencing opportunistic infections was detectedbetweenpilotandotherpharmacypatients(P=0.121).
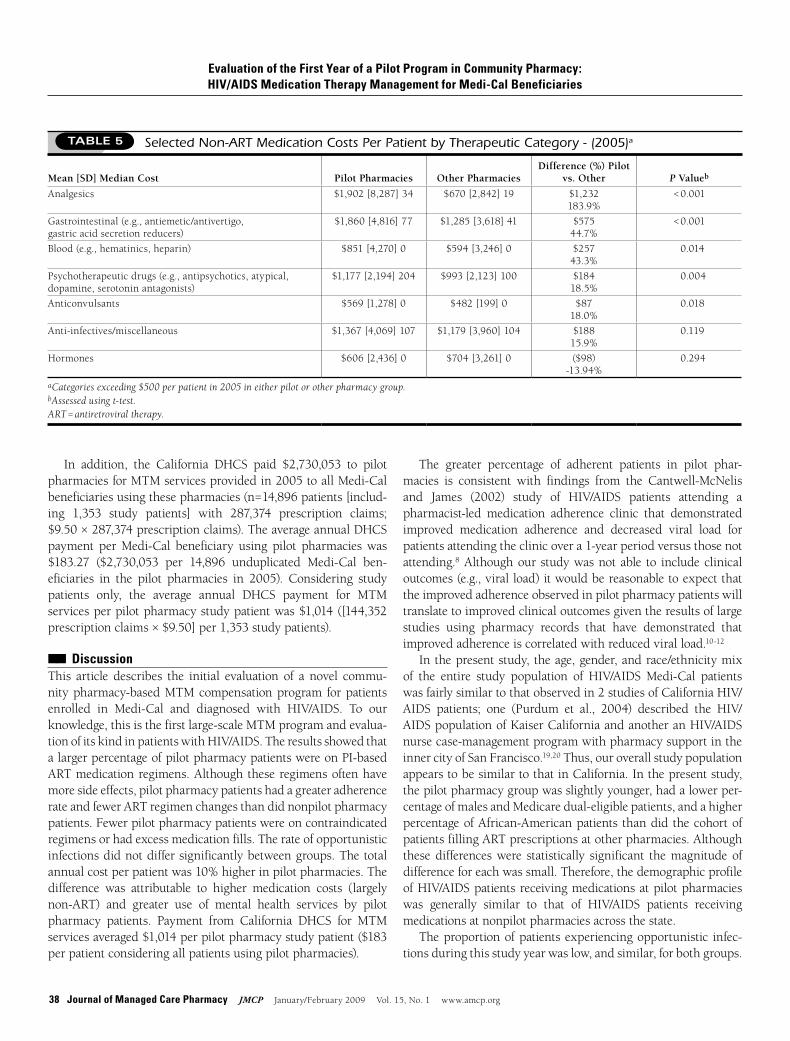
The mean (standard error [SE]) total medication cost perpatientwasgreater in thepilot group ($27,816 [$538]) than intheotherpharmacygroup($24,651[$234]),P<0.001,Table4).Thisdifferencewaslargelyattributabletoa30%greatercostfornon-ARTmedications($11,142[$432]vs.$8,565[$205],respec-tively;P<0.001)andlessattributabletoasmalldifferenceinARTmedicationcost($16,657[$212]vs.$16,087[$112],respectively;P=0.022).Examinationofexpendituresforasubsetofnon-ARTmedications (medication categories with costs exceeding $500perpatientin2005ineitherthepilotorotherpharmacygroup)revealed that pilot pharmacy patients had appreciably higherannual costs for several therapeutic categories, comparedwithotherpharmacypatients—forexample,analgesics,gastrointesti-nalagents(primarilyantiemetics),andbloodproducts(Table5).Thepilotpharmacypatientsalsohadsignificantlyhighermentalhealthmedicalservicescostsperpatientthandidtheotherphar-macypatients($686[$57]vs.$467[$26],respectively,P=0.002;Table 4). No other medical cost differences were statisticallysignificant.Highermedication(non-ARTandART)andmentalhealthservicesresultedinahigheraveragetotalcostperpatientinthepilotpharmacygroup($40,596[$889])thanintheotherpharmacygroup($36,937[$479],P=0.001).
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
TABLE 3 Prescription Medication Use in 2005
Pilot Pharmacies
(n = 10)
Other Pharmacies (n = 2,103) P Valuea
Numberofpatients 1,353 5,665
PharmacyvisitswithART prescriptionsb
Mean[SD]median(range)
15.4[10.5] 13
(1–62)
14.1[7.3] 13
(1–101)
< 0.001
Number (%) of patients by category
ARTadherencelevel
Adherent(MPR80%-120%)
Partiallyadherent (MPR50%-79%)
Non-adherent(MPR<50%)
Excessfills(MPR>120%)
762(56.3)
158(11.7)
166(12.3)
267(19.7)
2,157(38.1)
443(7.8)
525(9.3)
2,540(44.8)
< 0.001
< 0.001
0.001
< 0.001
ARTmedication regimenstrategies
Only1N(t)RTI
MultipleN(t)RTI
N(t)RTI+NNRTI
N(t)RTI+PI±NNRTI
13(1.0)
120(8.9)
357(26.4)
863(63.8)
138(2.4)
681(12.0)
1,743(30.8)
3,103(54.8)
0.001
0.001
0.002
< 0.001
Usedatleast1contraindicated ARTregimen
157(11.6) 943(16.6) < 0.001
CountofARTmedication regimenstrategiesused
1strategy
2strategies
3ormorestrategies
768(56.8)
439(32.4)
146(10.8)
1,938(34.2)
2,372(41.9)
1,355(23.9)
<0.001
Atleast1opportunisticinfection 381(28.2) 1,478(26.1) 0.121aP values for Pearson chi-square test for categorical variables and t-test for continu-ous variables.bNumber of visits that included the filling of at least 1 ART prescription.ART = antiretroviral therapy; MPR = medication possession ratio; N(t)RTI = nucleo-side or nucleotide reverse transcriptase inhibitors; NNRTI = nonnucleoside reverse transcriptase inhibitors; PI = protease inhibitor; SD = standard deviation.
TABLE 4 Generalized Linear Model Analyses: Pharmacy and Medical Cost Per Patient in 2005 Standardized to the Underlying Population Characteristics
Mean [SE] cost ($) Pilot Pharmacies Other Pharmacies P Valuea
Totalmedicationcost 27,816[538] 24,651[234] <0.001
ARTmedicationcost 16,657[212] 16,087[112] 0.022
Non-ARTmedicationcost 11,142[432] 8,565[205] <0.001
Inpatientcost 5,561[585] 5,698[338] 0.855
Hospitaloutpatientcost 459[47] 472[20] 0.769
Outpatientcost 1,119[54] 1,046[26] 0.203
Mentalhealthcost 686[57] 467[26] 0.002
LaboratoryandX-raycost 211[20] 194[7] 0.455
AIDS 1,472[99] 1,354[41] 0.251
Other 3,299[188] 3,091[94] 0.380
Total 40,596[889] 36,937[479] 0.001aDeviance statistics not shown; these are available from the author upon request.AIDS = acquired immune deficiency syndrome; ART = antiretroviral therapy; SE = standard error.
38 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org
The greater percentage of adherent patients in pilot phar-macies is consistent with findings from the Cantwell-McNelisand James (2002) study of HIV/AIDS patients attending apharmacist-led medication adherence clinic that demonstratedimproved medication adherence and decreased viral load forpatientsattendingtheclinicovera1-yearperiodversusthosenotattending.8Althoughour studywasnotable to includeclinicaloutcomes(e.g.,viralload)itwouldbereasonabletoexpectthattheimprovedadherenceobservedinpilotpharmacypatientswilltranslatetoimprovedclinicaloutcomesgiventheresultsoflargestudies using pharmacy records that have demonstrated thatimprovedadherenceiscorrelatedwithreducedviralload.10-12
Inthepresentstudy,theage,gender,andrace/ethnicitymixof the entire study population of HIV/AIDSMedi-Cal patientswasfairlysimilartothatobservedin2studiesofCaliforniaHIV/AIDS patients; one (Purdum et al., 2004) described the HIV/AIDSpopulationofKaiserCaliforniaandanotheranHIV/AIDSnursecase-managementprogramwithpharmacysupportintheinnercityofSanFrancisco.19,20Thus,ouroverallstudypopulationappearstobesimilartothatinCalifornia.Inthepresentstudy,thepilotpharmacygroupwasslightlyyounger,hadalowerper-centageofmalesandMedicaredual-eligiblepatients,andahigherpercentageofAfrican-AmericanpatientsthandidthecohortofpatientsfillingARTprescriptionsatotherpharmacies.Althoughthesedifferenceswere statistically significant themagnitude ofdifferenceforeachwassmall.Therefore,thedemographicprofileofHIV/AIDSpatientsreceivingmedicationsatpilotpharmacieswas generally similar to that of HIV/AIDS patients receivingmedicationsatnonpilotpharmaciesacrossthestate.
Theproportionofpatientsexperiencingopportunistic infec-tionsduringthisstudyyearwaslow,andsimilar,forbothgroups.
In addition, the California DHCS paid $2,730,053 to pilotpharmaciesforMTMservicesprovidedin2005toallMedi-Calbeneficiariesusingthesepharmacies(n=14,896patients[includ-ing 1,353 study patients] with 287,374 prescription claims;$9.50×287,374prescriptionclaims).TheaverageannualDHCSpayment perMedi-Cal beneficiary using pilot pharmacieswas$183.27 ($2,730,053 per 14,896 unduplicated Medi-Cal ben-eficiaries in the pilot pharmacies in 2005). Considering studypatients only, the average annual DHCS payment for MTMservicesperpilotpharmacystudypatientwas$1,014([144,352prescriptionclaims×$9.50]per1,353studypatients).
■■ Discussion This article describes the initial evaluation of a novel commu-nitypharmacy-basedMTMcompensationprogram forpatientsenrolled in Medi-Cal and diagnosed with HIV/AIDS. To ourknowledge,thisisthefirstlarge-scaleMTMprogramandevalua-tionofitskindinpatientswithHIV/AIDS.TheresultsshowedthatalargerpercentageofpilotpharmacypatientswereonPI-basedARTmedicationregimens.Althoughtheseregimensoftenhavemoresideeffects,pilotpharmacypatientshadagreateradherencerateandfewerARTregimenchangesthandidnonpilotpharmacypatients.Fewerpilotpharmacypatientswereoncontraindicatedregimensorhadexcessmedicationfills.Therateofopportunisticinfectionsdidnotdiffersignificantlybetweengroups.Thetotalannualcostperpatientwas10%higherinpilotpharmacies.Thedifference was attributable to higher medication costs (largelynon-ART) and greater use of mental health services by pilotpharmacy patients. Payment from California DHCS for MTMservicesaveraged$1,014perpilotpharmacystudypatient($183perpatientconsideringallpatientsusingpilotpharmacies).
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
TABLE 5 Selected Non-ART Medication Costs Per Patient by Therapeutic Category - (2005)a
Mean [SD] Median Cost Pilot Pharmacies Other PharmaciesDifference (%) Pilot
vs. Other P Valueb
Analgesics $1,902[8,287]34 $670[2,842]19 $1,232 183.9%
< 0.001
Gastrointestinal(e.g.,antiemetic/antivertigo, gastricacidsecretionreducers)
$1,860[4,816]77 $1,285[3,618]41 $575 44.7%
< 0.001
Blood(e.g.,hematinics,heparin) $851[4,270]0 $594[3,246]0 $257 43.3%
0.014
Psychotherapeuticdrugs(e.g.,antipsychotics,atypical, dopamine,serotoninantagonists)
$1,177[2,194]204 $993[2,123]100 $184 18.5%
0.004
Anticonvulsants $569[1,278]0 $482[199]0 $87 18.0%
0.018
Anti-infectives/miscellaneous $1,367[4,069]107 $1,179[3,960]104 $188 15.9%
0.119
Hormones $606[2,436]0 $704[3,261]0 ($98) -13.94%
0.294
aCategories exceeding $500 per patient in 2005 in either pilot or other pharmacy group. bAssessed using t-test.ART = antiretroviral therapy.

www.amcp.org Vol. 15, No. 1 January/February 2009 JMCP Journal of Managed Care Pharmacy 39
Theproportionofpatientswhowerepartiallyadherentornon-adherent inbothgroups is troublesomebecause thesepatientsareatgreaterriskofdevelopingresistancethatcouldaffecttheirlonger-termtherapyoptions.Futureevaluationwillinvestigateifthe rates of opportunistic infections andnonadherence changeduringthesubsequent2yearsofthepilotprogram.
Onefindingdeservesspecialemphasis.Themajorityofpilotpharmacy patients remained on a single type of medicationregimenstrategyfortheyearstudied,comparedwithpatientsofotherpharmacies,whochanged theirmedicationregimentypemoreoften.Even thoughcombinedART treatmenthasproveneffectiveagainstHIV,oneofthekeylimitationsisthatthevirusbecomesresistanttotheavailabledrugs.Themoredrugsandthemoredrugclassesthatapatientisexposedtoincreasesthelikeli-hoodofdevelopingdrugresistance.Patientswhoneedtoswitchregimens often (either due to lack of efficacy or intolerance orinabilitytomanagesideeffects)areessentiallyexhaustingtheirfuturetreatmentoptionsandwillnotremainashealthyor liveaslongaspatientswhoaresuccessfulonasingleregimenforaslongaspossible.Becausethepilotpharmacypatientswereabletouseand stayonapotentPI-based regimenmoreoften thanthe patients filling ART prescriptions at other pharmacies, theexpectation is that the pilot pharmacy patients will maintaintheirhealthandlivelonger.
Theaveragetotalcostperpatientinthepilotpharmacygroupwasapproximately10%greaterthanintheotherpharmacygroup.Medi-Calwastheonlypayerinthestudy;thereforereimburse-mentratesforservicesandproductswereequalbetweengroups(althoughminor variation can occur because of differences inclaim amounts submitted). Thus, differences in expendituresreflecteddifferences inutilizationratesormixofproductsandservices.Thehighercostwasattributabletogreaterutilizationofmedications(largelynon-ART)andmentalhealthservices.
Although statistically significant, the magnitude of dif-ference in average ARTmedication cost per patient betweenpilot and other pharmacies was small, $570 per patient peryear (3.5%). However, pilot-pharmacy patients had a greaternumberofpharmacyvisitstofillprescriptionsandhighertotalmedicationcostduemostlytonon-ARTmedicationusage.Pilotpatientsusedmoreantiemetics,analgesicsandanticonvulsants.ThesemedicationsarecommonlyusedinHIV/AIDSpatientstotreatsideeffectsofARTmedicationssuchasnauseaandpainofperipheralneuropathy.ThisfindingisconsistentwiththatofMarchetal.whoreportedapositiveeffectofpharmacistMTMservices onmedication side effects, expressed in their studyasareduction indrug-related toxicities.9 Inaddition to treat-ingsideeffects,thepilotpharmacypatientsappeartoreceivemoremedicationsforpsychiatriccomorbidities,whichiscon-sistentwiththeincreasedexpendituresonmentalhealthser-vices.Thesefindingssuggestthatthepilotpharmacypatientsmay receive more appropriate HIV treatment and perhapsmore comprehensivemedical access and care for their other
conditions,oftenrelatedtotheirprimarytherapy.There remains a need to determine the ultimate long-term
benefitofpatientsbeingmoreadherentonappropriatecombinedARTregimensandusingmorenon-ARTmedicationsandmentalhealthservicesoverseveralyears.Possiblesavingsinmorecostlyinpatient care will be investigated when data for subsequentyearsofthepilotprogramareavailable.Theselonger-termdataalsowillallowinvestigationofthecost-effectivenessofthe$9.50per prescription payments forMTM services by theCaliforniaDHCS.However,withtheadventofMedicarePartD,thedual-eligible Medicare patients will no longer receive medicationsthroughMedi-Cal and thuswillnotbe available for follow-up.However,theresultsofthispilotmayhelpMedicarePartDplansunderstandthevalueofcommunitypharmacistsprovidingMTMservicestoHIV/AIDSpatients;especiallyMedicareSpecialNeedsPlansfocusingonthispatientpopulation.
LimitationsTheforemost limitationof thisstudy is that it isanevaluationofanongoingprogramandmaybesubjecttoselectionbiasdueto nonrandom assignment of HIV/AIDS patients to pharma-cies. If patients who fill their prescriptions at pilot pharma-cies are different from patients who fill their prescriptions atother pharmacies, then the pilot pharmacy estimated effectwillincludeboththetruepilotprogrameffectandthebaselinedifferential between patients. Although the 2 patient groupsappearedtobesimilarwithregardtoobservablevariables(e.g.,age,gender),nonobservablevariables(e.g.,willingnesstofollowtreatmentprotocols,possiblephysicianreferralofmorecompli-catedpatients topilotpharmacies)maydifferbetweengroupsand affect conclusions. Second, it is possible that someof theother (comparison cohort) pharmacies provided some of thesameservicesasthepilotpharmacies,becauseonlythefirst10pharmaciesmeetingprogramcriteriawereenrolledinthepilotcompensationprogram.
Third,aninherentlimitationtothisanalysisisitsrelianceonMedi-Cal retrospective claimsdata thatdonot include clinicaloutcomessuchasviralloadandCD4counts.
Fourth, our results are relevant to California but may notreflectwhatwouldoccurwithasimilarMTMprograminpatientpopulations with different demographic or disease character-istics. Fifth, comparison of patient outcomes and costs beforeandafterMTMserviceswereinitiatedbypilotpharmacieswasnot possible because the pilot pharmacies providedMTM-likespecialty services for varying amountsof timebefore receivingthe compensation from thepilotprogram.Finally, thiswas ananalysisofonlythefirstyearofthepharmacycompensationpilotprogram.Claimsdatafromsubsequentyearsofthepilotprogramarebeing sought todeterminewhetherobserveddifferences inoutcomesandtreatmentcostscontinuetobeobservedoverthe3-yearperiodofthepilotprogram.
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries

40 Journal of Managed Care Pharmacy JMCP January/February 2009 Vol. 15, No. 1 www.amcp.org
■■ Conclusions Patientsatpilotpharmaciesappeartobenefitfrommorespecial-izedandpatient-specificMTMservicesofferedbypilotpharma-cies.PilotpharmacypatientswereonmorepotentARTregimens,had highermedication adherence rates, fewer excess fills, andfewercontraindicatedregimensthannonpilotpharmacypatients.Importantly,morepilotpharmacypatientsremainedonasingletypeofARTregimenthroughoutthestudyyear,whichdecreasesthe likelihood of developing drug resistance and enhances theabilitytomaintainhealthoveralongerperiodoftime.Totalcostperpatientwas10%higherinpilotpharmacies,withthehighercost attributed tonon-ARTmedications andmentalhealth ser-vices.Longer-termoutcomesandcostsofthepilotprogramwillbeexaminedwhendataforsubsequentyearsareavailable.
DISCLOSURES
PaymenttopharmaciesparticipatinginthepilotprogramforMTMserviceswas fundedbythestateofCalifornia.Therewasnootherexternal fundingforthisresearch.TeresaMillerisemployedbytheCaliforniaDepartmentofHealthCareServicesasSeniorConsultingPharmacist,Medi-CalPharmacyPolicy Branch,CaliforniaDepartment ofHealthCare Services.Her depart-ment has responsibility for implementing the pilotMTM services programsubsequenttotheenactedlegislation.
REFERENCES
1.DHHSPanelonAntiretroviralGuidelinesforAdultandAdolescents—AWorkingGroupoftheOfficeofAIDSResearchAdvisoryCouncil(OARAC).GuidelinesfortheuseofantiretroviralagentsinHIV-1-infectedadultsandadolescents.November3,2008;1-146.Availableat:www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.AccessedDecember2,2008.
2.SafrenSA,OttoMW,WorthJL,etal.TwostrategiestoincreaseadherencetoHIVantiretroviralmedication:Life-Stepsandmedicationmonitoring.Behav Res Ther.2000;39:1151-62.
3.PatersonDL,SwindellsS,MohrJ,etal.Adherencetoproteaseinhibi-tortherapyandoutcomesinpatientswithHIVinfection.Ann Intern Med. 2000;133:21-30.
4.SethiAK,CelentanoDD,GangeSJ,etal.Associationbetweenadherencetoantiretroviraltherapyandhumanimmunodeficiencyvirusdrugresis-tance.Clin Infect Dis.2003;37(8):1112-18.
5.WoodE,HoggRS,YipB,etal.IsthereabaselineCD4cellcountthatprecludesasurvivalresponsetomodernantiretroviraltherapy?AIDS. 2003;17(5):711-20.
6.CranorCW,BuntingBA,ChristensenDB.TheAshevilleProject:long-termoutcomesofacommunitypharmacydiabetescareprogram.J Am Pharm Assoc.2003;43:183-94.
7.McLeanDL,McAlisterFA,JohnsonJA,etal.Arandomizedtrialoftheeffectofcommunitypharmacistandnursecareonimprovingbloodpres-suremanagementinpatientswithdiabetesmellitus. Arch Intern Med. 2008;168(21):2355-61.
8.Cantwell-McNelisK,JamesCW.RoleofclinicalpharmacistinoutpatientHIVclinics.Am J Health Syst Pharm.2002;59:447-52.
9.MarchK,MakM,LouieSG.Effectsofpharmacists’interventionsonpatientoutcomesinanHIVprimarycareclinic.Am J Health Syst Pharm. 2007;64:2574-78.
10.InciardiJF,LeedsAL.Assessingtheutilityofacommunityphar-macyrefillrecordasameasureofadherenceandviralloadresponseinpatientsinfectedwithhumanimmunodeficiencyvirus.Pharmacotherapy. 2005;25:790-96.
11.FairleyCK,PermanaA,ReadTRH.Long-termutilityofmeasuringadherencebyself-reportcomparedwithpharmacyrecordinaroutineclinicsetting.HIV Med.2005;6:366-69.
12.GrossbergR,ZhangY,GrossR.Atime-to-prescription-refillmeasureofantiretroviraladherencepredictedchangesinviralloadinHIV.J Clin Epidemiol.2004;57:1107-10.
13.SmithSR,GolinCE,ReifS.Influenceoftimestressandothervariablesoncounselingbypharmacistsaboutantiretroviralmedications.Am J Health Syst Pharm.2004:61:1120-29.
14.CaliforniaAssemblyBill(AB)1367,Chapter850;Statutesof2004.Availableat:www.info.sen.ca.gov/pub/03-04/bill/asm/ab_1351-1400/ab_1367_bill_20040928_chaptered.pdf.AccessedNovember26,2008.
15.BlumlBM.Definitionofmedicationtherapymanagement:developmentofprofessionwideconsensus. J Am Pharm Assoc.2005;45:566-72.
16.RosenquistA,HirschJD.Developingaprotocolfortheinitialevalua-tionofHIV/AIDSmedicationtherapymanagementservicepilotprograminCalifornia.Posterpresentedat:AmericanCollegeofClinicalPharmacySpringPracticeandResearchForum;April23,2007;Memphis,TN.
17.ManningWG.Theloggeddependentvariable,heteroscedasticity,andtheretransformationproblem. J Health Econ. 1998;17(3):283-95.
18.BloughDK,MaddenCW,HornbrookMC.Modelingriskusinggeneral-izedlinearmodels. J Health Econ. 1999;18(2):153-71.
19.PurdumAG,JohnsonKA,GlobeDR.ComparingtotalhealthcarecostsandtreatmentpatternsofHIVpatientsinamanagedcaresetting. AIDS Care.2004;16:767-80.
20.BambergerJ.ImprovementinbiologicoutcomesfollowinginitiationofacommunitypharmacysupportprogramamongacohortofinnercitypeoplelivingwithHIV.SanFranciscoDepartmentofPublicHealth.December27,2006;1-16.Availableat:www.allionhealthcare.com/downloads/bio_out-comes.pdf.AccessedDecember2,2008.
21.DHHSPanelonAntiretroviralGuidelinesforAdultandAdolescents—AWorkingGroupoftheOfficeofAIDSResearchAdvisoryCouncil(OARAC).GuidelinesfortheuseofantiretroviralagentsinHIV-1-infectedadultsandadolescents.November3,2008;1-146.Availableat:www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf.AppendixTable8,page137.AccessedDecember5,2008.
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
JAN D. HIRSCH, RPh, PhD, is Assistant Professor of Clinical Pharmacy, and BROOKIE M. BEST, PharmD, MAS Clinical Research, is Assistant Clinical Professor of Pharmacy and Pediatrics, at the University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, La Jolla, California. ASHLEY ROSENQUIST, PharmD, is a Pharmacy Resident at the University of North Carolina at Chapel Hill School of Pharmacy. TERESA ANN MILLER, PharmD, FCSHP, is Senior Consulting Pharmacist, Medi-Cal Pharmacy Policy Branch, California Department of Health Care Services, Sacramento, California. TODD P. GILMER, PhD, is Associate Professor, University of California, San Diego, Department of Family and Preventive Medicine, La Jolla, California.
AUTHOR CORRESPONDENCE: Jan D. Hirsch, RPh, PhD, University of California, San Diego, Skaggs School of Pharmacy and Pharmaceutical Sciences, 9500 Gilman Drive, Mail Code 0714, La Jolla, CA 92093-0714. Tel.: 858.822.5562; Fax: 858.822.6857; E-mail:[email protected]
Authors
www.amcp.org Vol. 15, No. 1 January/February 2009 JMCP Journal of Managed Care Pharmacy 41
Evaluation of the First Year of a Pilot Program in Community Pharmacy: HIV/AIDS Medication Therapy Management for Medi-Cal Beneficiaries
Nucleoside and Nucleotide Reverse Transcriptase Inhibitors (N(t)RTI)
Abacavirsulfate
Abacavirsulfate/lamivudine
Abacavir/lamivudine/zidovudine
Didanosine/magnesium/AlNaCB/sodiumcitrate
Didanosine
Didanosine/calciumcarbonate/magnesium
Didanosine/sodiumcitrate
Emtricitabine
Lamivudine
Lamivudine/zidovudine
Stavudine
Zalcitabine
Zidovudine
Tenofovirdisoproxilfumarate
Emtricitabine/tenofovir
Nonnucleoside Reverse Transcriptase Inhibitors
Delavirdinemesylate
Efavirenz
Nevirapine
Protease Inhibitors
Amprenavir/vitaminE
Amprenavir/vitaminE/propyleneglycol
Atazanavirsulfate
Fosamprenavircalcium
Indinavirsulfate
Nelfinavirmesylate
Ritonavir
Ritonavir/lopinavir
Saquinavir
Saquinavirmesylate
Tipranavir
Fusion Inhibitor
Enfuvirtide
APPENDIX A Alphabetical List of Antiretroviral Therapy (ART) Medications by Category
Opportunistic Infections ICD-9-CM code
Pneumocystis jiroveci pneumonia(PCP) 136.3
Toxoplasma gondiiencephalitis 130.0
Cryptosporidosis 007.4
microsporidiosis 136.8
Mycobacterium tuberculosis 010-018
Mycobacterium avium complexdisease 031.0,031.2
Bacterialpneumonia 482.9,482.89
Salmonellosis 003.0,003.1
Campylobacterjejuniinfections 008.43
Shigellosis 004.9
Bartonellainfections 088.0
Treponema palliduminfections(syphilis) 091-097
Candidiasis 112
Cryptococcus neoformansmeningitis 117.5
Histoplasma capsulatuminfections 115.0
Coccidiodomycosis 114
Invasiveaspergillosis 117.3
Cytomegalovirus(CMV)disease 078.5
HerpesSimplexvirus(HSV)disease 054
Varicella zoster virus(VZV)disease 052.9
Humanpapillomavirus(HPV)disease 079.4
HepatitisCvirus(HCV)disease 070.41,070.51,V02.62,070.54,070.44,070.70,
070.71
HepatitisBvirus(HBV)disease 070.30,070.2,070.32,070.22,V02.61,070.21,070.31,070.23,070.33
Penicillosis 117.3
Leishmansiasis 085
Paracoccidioidomycosis 116.1
Isospora belliinfections 007.2
Chagasdisease(Americantrypanosomiasis) 086.0-086.2
ICD = International Classification of Diseases, Ninth Revision, Clinical Modification
APPENDIX B Opportunistic Infections and ICD-9-CM Codes