Gene-asbestos interaction in malignant pleural mesothelioma susceptibility
Upload
independentCategory
view
2download
0
1993;104;399-404Chest S Romero, A Candela, C Martín, L Hernández, C Trigo and J Gil of pleural transudates from exudates.Evaluation of different criteria for the separation
http://chestjournal.chestpubs.org/content/104/2/399
can be found online on the World Wide Web at: The online version of this article, along with updated information and services
) ISSN:0012-3692http://chestjournal.chestpubs.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.reserved. No part of this article or PDF may be reproduced or distributedChest Physicians, 3300 Dundee Road, Northbrook, IL 60062. All rights
ofbeen published monthly since 1935. Copyright1993by the American College is the official journal of the American College of Chest Physicians. It hasChest
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

Objectives: To determine the relative usefulness of differentcriteria for the separation of pleural transudates fromexudates.Design: Prospective evaluation of patients referred forthoracentesis.Setting: Community teaching hospital.Patients: Three hundred fifty-one consecutive patients withpleural effusions referred for thoracentesis. Fifty-four ofthese patients were excluded from the analysis.Measurements: We recorded clinical characteristics and
final diagnosis and measured pleural fluid and serum levelsof total protein, lactate dehydrogenase, and cholesterol. Allpatients included were followed up until final diagnosis.Mean results: Forty-four (15 percent) pleural effusions weretransudates and 253 (85percent) were exudates. The criteriaof Light et al, with a sensitivity of 98 percent and a
specificity of 77 percent for exudates, showed the bestaccuracy (95.2 percent). Moreover, when the cutoff usedfor the criteria of Light et al was modified according to ourown laboratory results, specificity rose to 93 percent withalmost a similar accuracy (94 percent). Protein pleural fluid!serum ratio >0.5 and pleural fluid cholesterol >60 mg/dlshowed equal specificity (91 percent), but the former hadbetter sensitivity for exudates (88 percent vs 81 percent).Conclusions: When the proportion of exudates included is
85 percent or more, as in the present series, the criteria ofLight et al remain the method that offers the highest
accuracy for segregating transudates from exudates..(Chest 1993; 104:399-404)
LCHF=congestiveheartfailureLDH=lactatedehydrogenase
D etermining the cause of a pleural effusion is notalways easy)'2 It frequently requires the use of
different diagnostic techniques, some of which areinvasive and not completely free of morbidity.@@Invasive local procedures, such as pleural biopsy, areindicated only in patients with pleural effusions secondary to pleural abnormalities, in which case theeffusion is usually exudative. Therefore, the first stepin the diagnosis of pleural effusions should he toclassify them as transudates or exudates.56
The criteria established by Light et al@for segregating transudates from exudates have been widely accepted. In their original article, the use of thesecriteria led to the correct classification of the pleuraleffusions tested in 99 percent of the cases. However,several recent reports have shown that the low specificity of the criteria of Light et al may lead tounwarranted invasive interventions in up to 20 to 30percent ofpatients with transudates.7@ This cast somedoubt on the universal applicability of these criteria.Several alternative criteria have been proposed,7'°andsome ofthese, such as cholesterol level, seem to havehigher diagnostic accuracy for identifying transudates.
The main purpose ofthis study is to evaluate a largenumber of patients to compare, prospectively, the
relative usefulness of pleural concentrations of cholesterol to the traditional criteria of Light et a15and theirdifferent individual parameters (pleural lactate dehydrogenase [LDH} concentration, pleural fluid to serum LDH ratio, and pleural fluid to serum proteinratio) for separating exudates from transudates.
MATERI@us AND METHODS
\Ve studied all patients referred to our service for diagnosticthoracentesis from Juno 1986 to October 1989. Patients withpresumedtransudativepleuraleffi@sionswereinformedofthe purelyinvestigational ptII@X)Seof tho exploration. Thoracentesis was performed onl@on those patients who consented. Patients treated withdiuretics ho-fore thoracentesis @verenot ex-lnded.•
After hospital discharge, periodic follow-up wa@maintained forthose patiot@ts with effilsions initially considered to 1w of obscure
origin.The following studieswere performed on all pleural fluid samples:
glucose; protein; I.DH: cholesterol; cell count; differential cellcount; bacterial and fungal culture; a('id-faSt bacilli smear and
culture: and cytology Only the results of the first thoracentesiswere considered. A sample of serum, obtained within 24 h o)fthoracentesis. @vastisod to measure glucose. total protein, cholesterol, and LDII levels. Further studies, including pleural biops)cwere done at the discretion of the primary physician.
Biochemicalparameterswere determined usinga selectivediscrete mllltichannel analyzer (hitachi [email protected] protein o)ncentrations (g/dl) were measured using the hitirot nwthod. Lactatedehvdnogenaselevel (IU) was moasuro-dusing a kinetic UV optimixed standardmethodconformingto the recommendationsof theDeutsche Cesellschaft for Klinische Chemie; the upper normallimit (sern@n)is defined at 46() IU. Clmlesterol le@el(mWdl)wasmeasured using the enzymatic o)lonnletri(' nivthod (cholesteroloxidase-phenol-4 lflhifl( )phenai( )no [C I I(')D-PA P] . high iwrform
ance).
*From the hospital General S.V.S. Universidad de Alicante,Alicante, Spain.
tServieios de Neumologla V Análisis ClInk-os.Manuscript received August 3. 1992; revision accepted January 7.
CHEST I 104 I 2 I AUGUS1 1993 399
Evaluationof DifferentCriteriafor theSeparationof PleuralTransudatesFromExudates* -Santiago Romero, M.D.; Aifredo Candela, M.D.;Concepcion MartIn, M.D.; Luis I-fernández, M.D.; Celia Trigo, M.D.;t andJoan Gil, M.D.
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

CauseNo.%Transudates4414.8Congestive
heartfailure3110.4Livercirrhosis82.7Nephrotic
syndrome51.7Exudates25385.2Malignant
effusions13244.4Parapneunioniceffitsions4916.5Tuberculosis4314.5Pulmonary
emholism186.1Others*113.7Total297100
T
0
:@
E
S..S
Effusions were considered malignant if one of the following
criteria was met: (1) demonstration of malignant cells at cytologicexamination or in a biopsy specimen; or (2) histologically proven
primary malignancywith exclusiono)fanyother causeknown to)beassociatedwith pleural effusions.A pleural effusionwasconsideredto 1@eparapneumonic when there was an acute febrile illness with
purulent sputum and pulmonary infiltrate in the absence of malignancy or diseases causing transudates. Tuberculous pleurisy was
diagnosed with positive culture for Mycobacteriu7n tuberculosis or
pleural biopsyspecimenshowingtypical epithelioid cell granuloma.A diagnosis of pulmonary emtxhis or infarction was made whenthere wasa strongclinical suspicionand a high-probability perfusionscan or abnormal angiogram.
Congestive heart failure (CIIF) was determined by an enlarged
heart , pulmonary venous congestion on radiograph, peripheraledema, responseto)CIIF treatment, and absence of malignancy orpulmonary infiltrates associated with an inflammatory process. Thenephrotic syndrome was diagnosed when the patient had protei
nuria, edema, and hypoalbuminemia. Effusions were considered
secondary to liver cirrhosis when they occured in the absence of
heart failure or malignanc)@The effusions secondary to diseasesthat directly involve pleural
surfaceswere consideredexudatesand the rest were consideredtransudates.
The following criteria for exudates were initially evaluated: thecriteria of Light et al,' pleural fluid to)serum protein ratio >0.5,pleural fluid LDII >307 UIL, pleural fluid to serum LDH ratio>0.6, pleural fluid cholesterol >60 mg/dl, and pleural fluid toserum cholesterol ratio) >0.3. These last two values were appliedafter being established as the best discriminating levels betweentransudatesand exudatesin this series.
Table 1—¿�CauseofPleural Effusions
*Trat,maticor postsurger@@6; pancreatitis,2; temporal arteritis, 2;DressIer'ssyndronie, 1.
Statistical Analysis
The usefulnessof each of the biochemical parameters for identilying exudates was evaluated using Bayesian methods to nieasurethe folloss'ing:sensitivit), TP/(TP + FN); specificit@;TN/(TN + FP);and accurac@@(TP + TN)/(TP + TN + FP + FN) where TP is thenumber of true 1)@siti@'ediagnoses, TN the nuniber of true negativediagnoses,FP the number of falsepositive diagnoses,and FN thenumber offalse negative diagnoses. \Ve lutIst emphasize that becausetransudates and exudates are complementary terms, for a given
analytical parameter, the specificity for exudates correspo)nds to the
sensitivity for transudates. The statistical significance of differences
:::4.?
3.,
3.b@
3,3 .
3.0 I
2@7
2.4
2,1
I.. S
‘¿�.5
I.2
0,@Is...
S., •¿�
‘¿�3
I
0
II
5 E.TI!IS@I•@@:5:
..‘sopF°@
ciIS
I
08
I
T mW@
ZOS
I..S
I@0
I2O
55
E
S.5$
S.
1―••@I55....II.S.
tirSS.S
r'5
ris.
LS
0@
0,$
0-s
0.4
0,2
II
ol0$5
N
N
a
S
PLR@1L ?LUt@'S@AOCLESTEROt REDO PL@M PLUDcHOLSSTSRO( PLBA.I. FLUDp'SOLSILDHR@Jl0 PLBA@LFLUDLDH PLR@ALFLIJ@SNU@ @OT9NSRMIO
FICtIRE 1. Results from 297 patients for pleural fluidlserum cholesterol ratio, pleural fluid cholesterol,pleural fluiidlseri,ni LDII ratio, I)lellral fluid LDII, and pleural fluid/serum pr@teitiratio. T()t(sltranstidates(opencircles)andexudates(solidcircles)areplottedforeachcriterio)n.
400 Criteria for Separation of Pleural Transudates from Exudates (Romero et a!)
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

CriteriaE (%)T(%)Accurac@(%)PF/S
proteins>0.5222/252(88)40/44(91)26212%(89)PFLDH >307lU/L165/252(66)44/44(100)209/296(71)PF/S
LDH>0.6231/249(93)36/44(82)267/293(91)Criteriaof Light etal@245/249(98)34144(77)279/293(95)PF
cholesterol>60mg/dl206/253(81)40/44(91)246/297(83)PF/Scholesterol >0.3222/249(89)30/42(71)252/291(87)
between means was estimated by Student's t test and x2 analysiswith Yates' correction. A p value less than 0.05 was consideredsignificant.
RESULTS
Three hundred fifty-one patients with pleural effusion were evaluated. In 54 patients, despite extensiveevaluation, the cause of the pleural effusion was eitherindeterminate (31 patients) or was due to multiplesuperimposed diseases (23 patients). These patientswere excluded from the study.
The average age of the 297 remaining patients withan effusion of single and known cause was 57 ±18.6years (range, 8 to 95 years); there were 160 men and137 women. Forty-four were defined as having transudates and 253 were identified as having exudates.Among the 44 patients with transudates, 28 (64 percent) were men and 16 (36 percent) were women, withan average age of 68 ±11 years (range , 36 to 86 years).Among the 253 patients with exudates, 132 (52 percent)were men and 121 (48 percent) were women, with aaverage age of 55 ±19 years (range, 8 to 95 years).
The causes of the 297 effusions are shown in Table1. Thirty-one of 44 (70 percent) transudates weresecondary to CHF. One hundred thirty-two of253 (52percent) exudates were considered malignant. Amongthe 132 patients with malignant effusions, 96 (73percent) had pleural cytologic and/or histologic cvidence of malignancy. The two patients with temporalarteritis had their conditions confirmed histologicallywith fl() other cause known to be associated withpleural effusion.
The values for each parameter in all patients studiedare presented graphically in Figure 1.
Ratio ofPleural Fluid Protein to Serum Protein
Using a dividing line of 0.5 to separate transudatesfrom exudates, 262 of 296 patients with pleural effusions were correctly classified (accuracy, 88.5 percent).Four patients with CHF of44 patients with transudateswere falsely classified (specificity, 90.9 percent). Threeof those incorrectly classified had hypoproteinemia.Thirty of 252 exudates were mistakenly classified(sensitivity, 88. 1 percent). Among the misclassifiedexudates, 17 were neoplastic, 9 were parapneumonic,2 were secondary to pulmonary embolism, 1 was
postsurgical, and 1 was tuberculous.
Pleural Fluid LDH
Using 307 IU as a cutoff point for separatingtransudates from exudates, 209 of 296 patients werecorrectly classified (accuracy, 70.6). All 44 patientswith transudates were correctly classified (specificity,100 percent). Eighty-seven of 252 patients with cxii
dates were misclassified using this paralneter (sensitivity, 65.5 percent). Among the exudates falselyclassified as transudates, 48 were neoplastic, 22 wereparapneumonic, 6 were pulmonary embolism, 5 weretuberculous, 3 were posttraumatic, 2 were secondaryto surgery, and 1 was due to temporal arteritis.
Ratio of Pleural Fluid LDH to Serum LDH
Using a dividing line of 0.6, 267 of 293 patientswere correctly classified (accuracy, 91 .1). Among the44 patients with transudates, 8 patients with pleuraleffusions secondary to CHF were incorrectly classified(specificity, 81.8 percent). Eighteen of 249 exudativepleural effusions were misclassified using this parameter (sensitivity, 92.8 percent). The causes of themisclassified exudates were as follows: nine neoplastic,seven parapneumonic, and one each postsurgery andposttraumatic.
The Criteria ofLight et a? (Pleural Fluid to SerumProtein Ratio >0.5, or Pleural Fluid LDH >307 U/L,or Pleural Fluid to Serum LDH Ratio >0.6, forExudates)
Using these criteria for segregating transudates fromexudates, 14 of 293 were misclassified (accuracy, 95percent). All 10 incorrectly classified of the 44 transudates (specificity, 77.3 percent) were secondary toCHF. Among the 249 exudates, 4 were misclassified(sensitivity, 98.4 percent); among these 2 were parapneumonic, and 2 were secondary to breast cancer.
Pleural Fluid Cholesterol
Drawing a dividing line in the concentration ofpleural fluid cholesterol of6O mg/dl, 246 of297 pleuraleffusions were correctly classified (accuracy, 82.8 percent). Four transudates, three secondary to CHF andone secondary to nephrotic syndrome, with choles
Table 2—Transudatesand Exudates Correctly Classified With Each ParameterStudied*
*PF = pleuralfluid;S serum;E exudates;T transudates;LDII lactatedehydrogenase;E (%) sensitivityforexudates;T(%) specificityfor exudates.
CHEST I 104 I 2 I AUGUST,1993 401
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from
DiagnosticCriteriaPF/S-P (%)PF-LDH (%)PF/S-LDH (%)Criteria o)fLight et al@(%)PF-Chol (%)PF/S-Chol(%)Transudates4/44
(9)0/44 (0)8/44 (18)10/44 (23)4/44 (9)12142(29)Neoplastic17/132(13)48/132 (36)9/130 (7)21130 (2)25/132 (19)18/132(14)Parapneuinonic9/49(18)22/48 (46)7/48 (15)2/48 (4)15/49 (37)8/48(17)Tuberculosis1/43
(2)5/43 (12)0/43 (0)0/43 (0)3/43 (7)0/40(0)Others@28(11)12129 (41)2/28 (7)0/28 (0)4129 (14)1/29(3)Total34/296(11)
4—87/296
(29)
NS26/293
(9)
4——--—.---14/293
(5)p<0.05 p<0.001—¿�)(51/297
(17)
,@NS39/291
(13)p<0.01
)s
p<0.01
p<0.05
DiureticsCriteriaWith
(n = 21),mean ±SDWithout
(n = 9),mean ±SDpValuePF-protein(g/dl)2.36±0.862.32±0.65NSPF/S-Protein0.36±0.130.35±0.09NSPF-LDH151.90±51.9126.89±44.02NSPF/S-LDH0.53±0.250.40±0.23NSPF-chol,
m@/dl37.23±14.744.44±19.2NSPF/S-chol0.24±0.110.24±0.11NS
Criteria E (%) T (%) Accuracy (%)
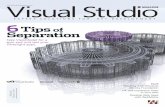
Table 3—NumberofMisclasszfied Pleural Effusions in Each Group Diagnosticfor Every Parameter Studied*
*PF = pleuralfluid;S—¿�serulli;P= pro)teins;Chol -cholesterol;NS notsignificant.
terol levels above that cutoff, were falsely classified(specificity, 90.9 percent). Forty-seven of253 exudateswere incorrectly classified (sensitivity, 81.4 percent).Among these falsely classified exudates, 25 wereneoplastic, 15 were parapneumonic, 3 were tubercubus, and 2 were postsurgical.
Ratio ofPleural Fluid Cholesterol to SerumCholesterol
Using a dividing line of0.3, 252 of291 were correctlyclassified (accuracy, 86.6 percent). Twelve of 42 transudates were misclassified (specificity, 71 .4 percent).Among the transudates incorrectly classified were tenpleural effusio,is due to CHF, one due liver cirrhosis,and one secondary to nephrosis. Twenty-seven of 249exudates were misclassified (sensitivity, 89.2 percent).Eighteen neoplastic, 8 parapneumonic, and 1 postsurgical exudative effusion were mistakenly classified astransudates.
Table 2 indicates the percentage of correctly classifled transudates and exudates and the accuracy of eachcriterion used. Because 10 determinations (0.6 percent) were not received from the laboratory and couldnot be repeated within 24 h of thoracentesis, most ofthe denominators do @iotadd up to 297. For exudates,the criteria of Light et al5 correctly classified 245 of249 patients (98 percent), being the criteria with the
Table 4—Sensitivity and Accuracy ofMod@fiedCriteria oflight et al: Comparison With Classic Criteria ofL.ight et a!
highest sensitivity. The criteria of Light et al alsoshowed the best accuracy (95 percent) of all criteriaused, with a statistically significant difference(p<O.O5). Pleural fluid LDH showed a specificity of100 percent but its sensitivity and accuracy were the
lowest.Table 3 lists the percentages of misclassified pleural
effusions in every diagnostic group for every parameterstudied. It shows that the criteria of Light et al,@withtheir high sensitivity for exudates of any diagnosticorigin, afforded the smallest percentage (5 percent) ofmisclassified pleural effusions.
Looking for new cutoff points that could improvethe discriminating capacity of the criteria of Lightet al,@we found that using the following as new cut-offpoints—0.6for the pleural fluid to serum protein ratio,280 lUlL for LDH pleural fluid concentration, and0.9 for pleural fluid to serum LDH ratio—the accuracyofthe test remained practically unmodified (95 percentto 94 percent) while the specificity rose from 77percent to 93 percent (Table 4).
In Table 5, patients with transudative effusions due
Table 5—Use ofDiuretics in Transudative PleuralEffusions Secondary to CHF: its Effects on Fluid
Chemistry*
Criteria of Light et al' 98 77 95Modified criteriat of 94 93 94
Light et al@
*E = exudates;@ traiisudatcs; E (%) sensitivity for exudates; T(%)= specificityforexudatcs.
tPF/S>0.6 or PF/S-LDH>0.9 or PF-LDH>280 IU fur exudates.
PF=pleural fluid; S=serum; CHF=congestive heart failure;LDII = lactate dehydrogenase; Chol = cholesterol; NS not significant.
402 Criteria for Separation of Pleural Transudates from Exudates (Romero et a!)
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

SourceTotalExcluded, No. (%)IncludedTransudates, No.(%)Light
et al@18333 (18)15047(31)Hammet al@708 (1 1)6231(50)Valdés
et al@28330 (11)25365(26)Presentstudy35154 (15)29744 (15)
to CHF are grouped according to previous therapeuticuse ofdiuretics. One patient was excluded because wecould not ascertain previous use of diuretics. It showsthat the use of diuretics does not significantly changethe mean values of the different parameters used.Among the 21 patients with diuretics, the criteria ofLight et al@correctly classified 14 patients and misclassified 7 patients. The proportion ofpatients receiving long-term diuretics (more than a week) was notsignificantly different between groups.
DISCUSSION
The use of several chemical tests to separate transudates from exudates is recolnmended as a usefulfirst step in determining the cause of a pleural effusion.5'6 In their initial study in 1972, Light et al@usedpleural and serum levels of proteins and LDH toestablish criteria for segregating transudates fromexudates with a sensitivity and specificity both near100 percent. This high diagnostic accuracy together
with a relatively low cost made the criteria of Lightet al the “¿�goldstandard― for initial categorization ofpleural effusions. Recently, however, several prospective studies79 were unable to reproduce the excellentresults obtained by Light et al. In most ofthem, usingthe criteria of Light et al, the sensitivity for exudatesremained high, greater than 95 percent, but thespecificity did not surpass 78 percent. Because thepleural concentration of cholesterol,7'@ albumin,@ andbilirubin'° had shown a high specificity in all thesestudies, these parameters were proposed as alternatives to the classic criteria.
To the best of our knowledge, the present studyincluded more patients than any previous series. Thepercentage of patients excluded due to multiple orunknown diagnosis (15 percent) falls between that ofLight et al5 (18 percent) and Hamm et al7 or Valdéset al@(11 percent). The absence of forced inclusion ofthose patients thought to have transudative pleuraleffusions explains a smaller number of patients withtransudates than in previous series (Table 6). Thoracentesis is not indicated in every patient with heartfailure and pleural effusion unless a comorbid condition is suspected.1113 In the studies by Hamm et al7and Valdéset al,@a high proportion of patients withtransudative pleural effusion were included and among
Table 6—NumberofPleural Effusions Studied, PercentageofExciuded and Percentage of Transudates: Comparison
With Previous Series
them, 94 percent and 88 percent, respectively, weredue to CHF. Since this type of patient usually has avariety of easily discernible features that permit afairly precise diagnosis without resorting to thoracentesis for confirmation, it must be presumed that inmost of them, this diagnostic procedure would not beindicated in routine clinical practice.
From the results ofthe present study, the criteria ofLight et al@appear as the method that offers thehighest accuracy for segregating transudates fromexudates, demonstrating that they are still very effident in classifying pleural effusions.
As in other recent reports,79 while we have foundthese criteria to be the most sensitive for exudates, wewere unable to reproduce the excellent specificityobtained by Light et al.@Ten patients with CHF of the44 transudates included (22.7 percent) were misclassified when using the criteria of Light et al.@However,the use of any alternative criteria, herein assessed,will result in a lower proportion of pleural effusionscorrectly classified.
In clinical settings with a high prevalence of transudates or in cases where patients clinically appear tohave CHF yet have the criteria of Light et a15 thatwould classify them as exudates, the use of alternativecriteria with a better specificity may be indicated.
Using @neof the proposed alternative criteria, thecholesterol level, we found that the specificity washigher than when using the criteria of Light et al.5However, we found that the specificity when using theprotein ratio as a single parameter was identical to theone when using cholesterol level, while sensitivity forexudates was higher. These results do not support theroutine use of cholesterol level for identifying transudates.
Since, according to Light et al,@ three conditionsmust be present for a pleural effusion to be considereda transudate and only one need be present to beconsidered an exudate, one would initially expect alower specificity than sensitivity for exudates. This,however, was not the case in the original study,probably because the cutoff points were carefullychosen. But it did happen in successive studies79 whenthe cutoff points used were those proposed by Lightet al. Given the variability of results from one labora
tory to another, the adoption of cutoff points adaptedto the needs ofone particular laboratory may improvethe specificity of the test without a sensible loss in itscapability to segregate exudates when using “¿�modifiedLight's criteria.― This was the case in our study, andbecause these modified criteria have a silnilar sensitivity and specificity, their use adds another advantage:the absence of any substantial influence of prevalenceon the results.
The treatment of CHF may cause significantchanges in pleural fluid chemistry'4'5 Although the
CHEST I 104 I 2 I AUGUST,1993 403
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

present study was not designed to ascertain theinfluence of diuretics on the protein concentration ofpleural fluids, our results did not show enough evidence to allow us to conclude that these therapeuticagents have a significant influence on the proteinconcentration of transudates due to CHF.
REFERENCES
1 Storey DD, Dines DE, Coles DT Pleural effusion: a diagnosticdilemma. JAMA 1976; 236:2183-86
2 Cunnels JJ. Perplexing pleural effusion. Chest 1978; 74:390-933 Seneff MC, Corwin RW, Gold LII, Irwin RS. Complications
associated with thoracentesis. Chest 1986; 90:97-1004 Ryan CJ, Rodgers RF, Unni KK, Hepper NC. The outcome of
patients with pleural effusion of indeterminate cause at thoracoton)y. Mayo Clin Proc 1981; 56: 145-49
5 Light RW, MacGregor MI, Luchsinger PC, Ball WC. Pleural
effusions: the diagnostic separation o)ftransudates and exudates.Ann Intern Med 1972; 77:507-13
6 Peterman TA, Speicher CE. Evaluating pleural effusions:a twostage laboratory approach. JAMA 1984; 252:1051-53
7 Hamun H, Brohan U, Bohmer R, Missmahl HP Cholesterol in
pleural effusions:a diagnosticaid. Chest 1987; 92:296-3028 ValdésL, Pose A, Suarez J, Gonzalez JR. Sarandeses A, San
JoséE, et al. Cholesterol: a useful parameter for distinguishingbetween pleural exudates and transudates. Chest 1991; 99:1097-
11029 Roth BJ,OMearaTF, Cragun WH. The serum-effusionalbumin
gradient in the evaluation of pleural effusions. Chest 1990;98:546-49
10 Meisel 5, Shamis A, Thaler M, Nussinovicht N, Rosenthal T.Pleural fluid to serum bilirubin concentration ratio for theseparationoftransudates from exudates. Chest 1990; 98:141-44
11 Health and Public Policy Committee, American College ofPhysicians. Diagnostic thoracentesis and pleural biopsy inpleural effusions.Ann Intern Med 1985; 103:799-802
12 Shinto BA, Light RW. Effects of diuresis on the characteristicsof pleural fluid in patients with congestive heart failure. Am JMed 1990; 88:230-34
13 Chakko S. Pleural effusion in congestive heart failure. Chest1990;98:521-22
14 Pillay VKC. Total proteins in serum fluids in cardiac failure. SMr Med J 1965; 39:142-43
15 Chakko 5, Caldwell SH, Sforza PP Treatment of congestiveheart failure: its effect on pleural fluid chemistry. Chest 1989;95:798-802
404 Critenafor Separationof PleuralTransudatesfromExudates(Romeroat a!)
xxv PanamericanCongressThis 25th congress ofthe Union Latinoamericana de Sociedades de Tisiologia y Enfermedades
Respiratonas will be held in Lima, Peru, October 9-12 at the Sheraton Hotel. President of theCongress is Dr. Leonidas Peralta Roncal. The meeting will also be part of the 7th Latin
Amenicais Conference ofthe International Union Against Tuberculosis and Respiratory Disease
as well as the 18th meeting of the Latin American Committee of Tuberculosis Bacteriology.For information, contact:ExcursionesPeruanasSA, Av JosePardo 182 Of503 Miraflores Lima,Peru (51-14-478207;or fax:51-014-451241.
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from

1993;104; 399-404ChestS Romero, A Candela, C Martín, L Hernández, C Trigo and J Gil
exudates.Evaluation of different criteria for the separation of pleural transudates from
July 12, 2011This information is current as of
http://chestjournal.chestpubs.org/content/104/2/399Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/104/2/399#related-urlsThis article has been cited by 17 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtmlonline at: Information about reproducing this article in parts (figures, tables) or in its entirety can be foundPermissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
Reprints
the right of the online article.Receive free e-mail alerts when new articles cite this article. To sign up, select the "Services" link to
Citation Alerts
slide format. See any online figure for directions. articles can be downloaded for teaching purposes in PowerPointCHESTFigures that appear in Images in PowerPoint format
© 1993 American College of Chest Physicians by guest on July 12, 2011chestjournal.chestpubs.orgDownloaded from
Copyright © 2022 FDOKUMEN