
Evaluation of amplitude-based sorting algorithm to reduce lung tumor blurring in PET images using 4D...
11
computer methods and programs in biomedicine 87 ( 2 0 0 7 ) 112–122 journal homepage: www.intl.elsevierhealth.com/journals/cmpb Evaluation of amplitude-based sorting algorithm to reduce lung tumor blurring in PET images using 4D NCAT phantom Jiali Wang a,∗ , James Byrne a , Juan Franquiz b , Anthony McGoron a a Department of Biomedical Engineering, Florida International University, 10555 West Flagler Street EC 2610, Miami, FL 33174, USA b Radiological Physics of South Florida, Inc., Miami, FL, USA article info Article history: Received 1 January 2007 Received in revised form 4 May 2007 Accepted 4 May 2007 Keywords: Respiratory gating PET CT Cancer NCAT phantom abstract Purpose: develop and validate a PET sorting algorithm based on the respiratory amplitude to correct for abnormal respiratory cycles. Method and materials: using the 4D NCAT phantom model, 3D PET images were simulated in lung and other structures at different times within a respiratory cycle and noise was added. To validate the amplitude binning algorithm, NCAT phantom was used to simulate one case of five different respiratory periods and another case of five respiratory periods alone with five respiratory amplitudes. Comparison was performed for gated and un-gated images and for the new amplitude binning algorithm with the time binning algorithm by calculating the mean number of counts in the ROI (region of interest). Results: an average of 8.87 ± 5.10% improvement was reported for total 16 tumors with different tumor sizes and different T/B (tumor to background) ratios using the new sorting algorithm. As both the T/B ratio and tumor size decreases, image degradation due to respiration increases. The greater benefit for smaller diameter tumor and lower T/B ratio indicates a potential improvement in detecting more problematic tumors. © 2007 Elsevier Ireland Ltd. All rights reserved. 1. Introduction Lung cancer is one of the most common types of cancers in the United States, with more than 175,000 deaths per year [1]. The early and most probable curable stage of the disease in all histological types is the solitary pulmonary nodule (SPN) [2,3]. Five-year survival for post operation of stage I lung cancer and nodules smaller than 3 cm has been reported to be over 80% [4]. Since the early treatment of a small SPN has a high probability of curability, accurate definition of tumor volume and posi- tion is especially important [5]. Computed tomography (CT) is the most common imaging technique for providing anatom- ical and morphological information of tumors in the body. However, a vast majority of small SPNs appear on CT as inde- terminate tumors [6,7]. Molecular imaging with 18 FDG-PET can provide significantly higher sensitivity (87%) and speci- ∗ Corresponding author. Tel.: +1 305 348 6950. E-mail address: Jiali.Wang@fiu.edu (J. Wang). ficity (91%) than CT (68% and 61%, respectively) in detection and characterization of malignant lung nodules [8–10]. It has become a popular imaging modality for lung cancer diagnosis, staging, and for differentiating tumor recurrence from scar- ring and other benign structures. The advantage of PET has also lead to the proposed use of molecular imaging fused with CT for defining a more accurate delineation of tumor volume. New hybrid PET/CT scanners provide an accurate anatomical framework for molecular imaging and a noise free CT map for more accurate attenuation correction and conse- quently, quantitation of 18 FDG uptake [11]. Even with these advances, only about 15% of SPNs are being detected at an early stage. One major inconvenience of 18 FDG-PET imaging is the relatively long scan time (from 5 to 7 min) compared to the shorter CT collection time (less than 1s), produces PET- CT mis-registration as consequence of the respiratory motion. 0169-2607/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.cmpb.2007.05.004
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Evaluation of amplitude-based sorting algorithm to reduce lung tumor blurring in PET images using 4D...

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls /cmpb
Evaluation of amplitude-based sorting algorithm to reducelung tumor blurring in PET images using 4D NCAT phantom
Jiali Wanga,∗, James Byrnea, Juan Franquizb, Anthony McGorona
a Department of Biomedical Engineering, Florida International University, 10555 West Flagler Street EC 2610, Miami, FL 33174, USAb Radiological Physics of South Florida, Inc., Miami, FL, USA
a r t i c l e i n f o
Article history:
Received 1 January 2007
Received in revised form 4 May 2007
Accepted 4 May 2007
Keywords:
Respiratory gating
PET
a b s t r a c t
Purpose: develop and validate a PET sorting algorithm based on the respiratory amplitude to
correct for abnormal respiratory cycles. Method and materials: using the 4D NCAT phantom
model, 3D PET images were simulated in lung and other structures at different times within
a respiratory cycle and noise was added. To validate the amplitude binning algorithm, NCAT
phantom was used to simulate one case of five different respiratory periods and another
case of five respiratory periods alone with five respiratory amplitudes. Comparison was
performed for gated and un-gated images and for the new amplitude binning algorithm with
the time binning algorithm by calculating the mean number of counts in the ROI (region of
CT
Cancer
NCAT phantom
interest). Results: an average of 8.87 ± 5.10% improvement was reported for total 16 tumors
with different tumor sizes and different T/B (tumor to background) ratios using the new
sorting algorithm. As both the T/B ratio and tumor size decreases, image degradation due
to respiration increases. The greater benefit for smaller diameter tumor and lower T/B ratio
indicates a potential improvement in detecting more problematic tumors.
early stage. One major inconvenience of 18FDG-PET imaging
1. Introduction
Lung cancer is one of the most common types of cancers inthe United States, with more than 175,000 deaths per year [1].The early and most probable curable stage of the disease in allhistological types is the solitary pulmonary nodule (SPN) [2,3].Five-year survival for post operation of stage I lung cancer andnodules smaller than 3 cm has been reported to be over 80% [4].Since the early treatment of a small SPN has a high probabilityof curability, accurate definition of tumor volume and posi-tion is especially important [5]. Computed tomography (CT) isthe most common imaging technique for providing anatom-ical and morphological information of tumors in the body.
However, a vast majority of small SPNs appear on CT as inde-terminate tumors [6,7]. Molecular imaging with 18FDG-PETcan provide significantly higher sensitivity (87%) and speci-∗ Corresponding author. Tel.: +1 305 348 6950.E-mail address: [email protected] (J. Wang).
0169-2607/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights resdoi:10.1016/j.cmpb.2007.05.004
© 2007 Elsevier Ireland Ltd. All rights reserved.
ficity (91%) than CT (68% and 61%, respectively) in detectionand characterization of malignant lung nodules [8–10]. It hasbecome a popular imaging modality for lung cancer diagnosis,staging, and for differentiating tumor recurrence from scar-ring and other benign structures. The advantage of PET hasalso lead to the proposed use of molecular imaging fusedwith CT for defining a more accurate delineation of tumorvolume. New hybrid PET/CT scanners provide an accurateanatomical framework for molecular imaging and a noise freeCT map for more accurate attenuation correction and conse-quently, quantitation of 18FDG uptake [11]. Even with theseadvances, only about 15% of SPNs are being detected at an
is the relatively long scan time (from 5 to 7 min) comparedto the shorter CT collection time (less than 1 s), produces PET-CT mis-registration as consequence of the respiratory motion.
erved.

i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122 113
MP(daamntafs
1
TpSmsttast7sctosotabc
1
Cptu(pbatTcdfnaftaeta
Fig. 1 – One example case: respiration cycles simulated byNCAT phantom, with the same amplitude but differentperiods. Each point on the curves represents the beginningof the collection of PET image following the trigger pulse.The curve in (b) is the normal breath; (a) is a short breathand (c) a longer breath. From (a) to (c), it is clear that if theperiod is not constant, then binning PET images solely
c o m p u t e r m e t h o d s a n d p r o g r a m s
any clinical and research studies have shown that, in 18FDG-ET, respiratory motion degrades the images by reducing SUVstandardized uptake value) and tumor-to-background ratio,istorting the real size, shape and location of the tumornd other structures. These artifacts negatively impact thepplication of 18FDG-PET for the detection of small tumors,onitoring response to treatment and radiation therapy plan-
ing [12–14]. Fluoroscopic studies [15] have demonstrated thathe tumors next to the diaphragm can move with breathing inrange of 30 mm, which is more than four times the 5–6 mm
ull width half-maximum (FWHM) resolution of current PETcanners.
.1. Respiratory gating methods in PET
he gating of PET scans was initially investigated to com-ensate myocardial motion in cardiac PET. Varian Medicalystems (Palo Alto, CA) has developed the real-time positionanagement (RPM) respiratory gating system [16–18]. This
ystem, originally designed for respiratory gating in radiationherapy, has been used by Nehmeh’s group for preliminaryesting and assessment of respiratory gated PET scans. Theyssessed lung motion artifacts in lung cancer and demon-trated more accurate quantitation and definition of PETumors by gating. Anzai Medical (Japan) developed the AZ-73V respiratory gating system which employs a strain gaugeensor to detect the mechanical expansion of the thoracicavity resulting from the respiratory motion. Another gatingechnique was reported recently by the group in the Universityf Texas, M.D. Anderson Cancer Center, which utilize a solid-tate temperature sensor to detect the temperature differencef the air flow in the nostril due to inhalation and expira-ion [19]. These methods have demonstrated the quantitativend qualitative benefits of reducing the blurring of tumorsy taking images at discrete time bins within the respiratoryycle.
.2. Time-based binning algorithm
urrent gating methods are based on the division of the res-iratory cycle into discrete time bins. One limitation of theime-based binning algorithm is image blurring due to irreg-lar respiratory cycles. For example, during a pre-registration
training) period (before scanning), video images of the res-iratory motion sensor are collected while the patient isreathing normally. This training period establishes the char-cteristics that will define a “normal” respiratory cycle (i.e.,he mean amplitude and the mean respiratory cycle period).hen during the PET collection period, the PET/CT cameraan be triggered at a specified time to begin collecting a pre-etermined number of equally spaced PET frames (e.g., eightrames, which is typical). If one or more of the breaths doesot match those pre-defined respiratory cycles (i.e., either themplitude is outside of range, or the period is significantly dif-erent, which can always happen when the patient suddenlyakes a long deep breath or a short breath), then one of two
ctions might be taken: either (1) bin the PET frames into theight respective time bins, which can cause blurring becausehe tumor will not be in the same position for each PET framedded to that bin; or (2) the set of PET frames is discarded,based on time would result in blurring because the tumorsare not in the same position.
which will reduce the overall counts and also result in reducedimage quality.
Fig. 1 shows the respiratory cycles simulated by NCATphantom, and helps explain their respiratory gating processand how a blurring effect can still occur with time-basedbinning algorithm. Fig. 1(b) represents a normal respirationcollected during the “training” period, while Fig. 1(a) repre-sents a breath with a shorter period (higher rate) and Fig. 1(c)a breath that has a longer period. It can be seen that if thePET data are binned according to time, PET data collected dur-ing respiratory cycles represented by (a) and (c) would tend toblur the final image because not all of the positions match thenormal one at the same times in a breath.
1.3. Non-gating methods for respiratory motioncorrection in PET
Several image-based and projection-based algorithms havealso been developed to correct for motion artifacts in PETwithout the need for gating. The advantage of these meth-ods compared to gating is that they are not affected bylow statistical counts and require no additional patient set-
up time. Rahmim has published a comprehensive reviewof motion correction methods in PET [20]. Lamare et al.applied affine transformation to PET data in list mode tocorrect for respiratory motion without the need for gating
s i n
114 c o m p u t e r m e t h o d s a n d p r o g r a m[21]. The advantage is that no additional instrumentation isrequired and it can be applied to correct the motion of otherorgans besides the lungs. Qiao et al. have also successfullyapplied non-rigid motion compensation to list-mode com-puter simulated PET data [22]. While list mode collection isnot generally implemented on clinical cameras, it is proba-bly not a limiting obstacle. Deconvolution has been appliedto reduce lung motion artifact with positive results [23]. Themethod depends on an estimate of patient motion measuredfrom 4D CT images. Generally, deconvolution methods aretheoretically accurate for noise-free data, but they tend toamplify the noise in real PET data. The non-rigid transfor-mation problem continues to be a challenge. To date, suchapproaches are still being developed and have not been imple-mented clinically, compared to gating which is currently beingimplemented.
Nehmeh et al. demonstrated that lung motion can becorrected without using gating by simultaneously imaging aradioactive point-source placed on the patient’s chest [18].This method requires significantly more computation thangating but does not require tracking hardware. It requires anexternal point source and the inherent poor spatial resolutionof PET cannot match the resolution of cameras used for opti-cal motion tracking. The non-gating methods are promisingbecause they need not interfere with the current operation ofthe imaging session, but methods based on external opticaltracking are further in clinical application since they are lesscomputationally intensive. Methods using external markersuffer from the disadvantage that the surrogate signal doesnot directly equate to movement of the tumor. Finally, sincegating methods inherently decrease the image signal-to-noiseratio, they should be combined with some imaging-basedmethods to transform the set of gated images into a singleimage for analysis.
2. Research design and method
2.1. Computer simulation of respiratory motion in PET
Respiratory mechanics has been simulated by the four-dimensional (4D) NURBS-based cardiac-torso (NCAT) phantomdeveloped by Segars and Tsui at the University of NorthCarolina [24]. The 4D NCAT phantom is a well establishedsimulation program and is widely used as a gold standard innuclear medicine imaging research. It can be used to simu-late 18FDG distributions of activity and lung tumors [13]. Manyapplications capable of reading a raw image format can beused to view the phantom images. In this study, amide, a freelyavailable application was used for viewing the phantoms as 2Dslices or as 3D volumes.
2.2. Respiratory amplitude-based sorting method
In order to compensate for the abnormal respiratory cycles, anamplitude gating approach was proposed. Instead of division
of the respiratory cycle in discrete time bins, this new gat-ing method divides respiratory cycles into discrete bins basedon different amplitudes of the cycle, so that each PET framecan be binned correctly based on amplitude rather than time,b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
which will preserve more of the PET frames and thus result inbetter quality PET images.
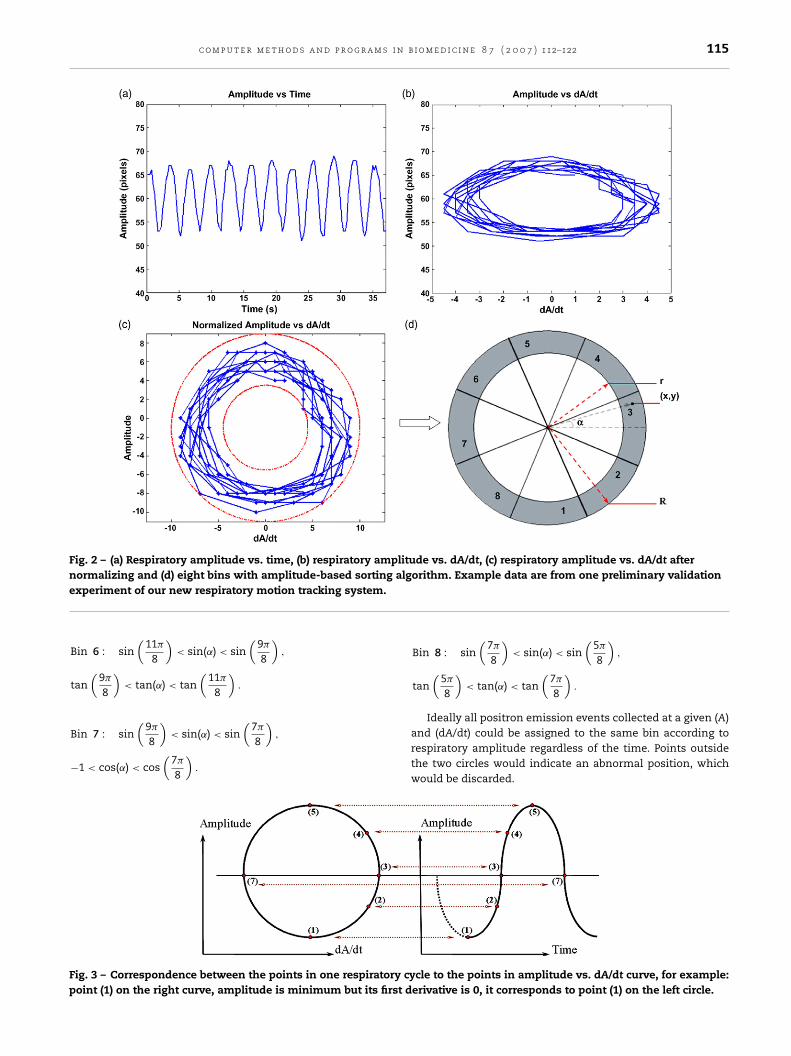
The following is an example protocol: in a clinical set-ting, it would involve coaching patients on their breathingbefore they are scanned, referred to as the training period.After training, data of respiratory motion amplitude (A) withrespect to time (t) is obtained; the first derivative (dA/dt) iscomputed by the forward differences on left and right edges([A(n) − A(n − 1)]/�t) and the central differences on interiorpoints ([A(n) − A(n − 2)]/2�t). Fig. 2(a) shows amplitude as afunction of time, and Fig. 2(b) shows amplitude with respectto its first derivative (dA/dt) (non-normalized). A normalizedplot of amplitude with respect to its first derivative results ina circle for the convenience of our binning, in which data wascentered to the (0,0) point and dA/dt was normalized to thesame scale as amplitude. Fig. 2(c) shows the data in Fig. 2(b)after normalizing, the inner and outer circle radius (r and R)for the range of (A) and dA/dt for idealized curves is deter-mined. The circle of respiratory amplitude (A) with respect todA/dt can be divided into any number of bins. Fig. 2(d) showsideal concentric circles defining the normal respiratory cyclerange determined during the pre-registration training ses-sion divided into eight bins. The PET images could be binnedaccording to respiratory amplitude instead of time (Fig. 3),reducing blur in the final PET image.
Algorithm defining eight bins (here x is the axis of thederivative (dA/dt), y is the axis of the amplitude (A), for ˛, rand R, please refer Fig. 2(d)):
r2 < x2 + y2 < R2, sin(˛) = y√x2 + y2
, cos(˛) = x√x2 + y2
,
tan(˛) = y
x.
Bin 1 : sin(
3�
8
)< sin(˛) < 1, tan
(3�
8
)< tan(˛) or
tan(
5�
8
)> tan(˛).
Bin 2 : sin(
�
8
)< sin(˛) < sin
(3�
8
),
tan(
�
8
)< tan(˛) < tan
(3�
8
).
Bin 3 : sin(
15�
8
)< sin(˛) < sin
(�
8
),
1 > cos(˛) > cos(
�
8
).
Bin 4 : sin(
13�
8
)< sin(˛) < sin
(15�
8
),
tan(
13�
8
)< tan(˛) < tan
(15�
8
).
Bin 5 : −1 < sin(˛) < sin(
13�
8
), tan
(11�
8
)< tan(˛) or
tan(
13�
8
)> tan(˛).
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122 115
Fig. 2 – (a) Respiratory amplitude vs. time, (b) respiratory amplitude vs. dA/dt, (c) respiratory amplitude vs. dA/dt aftern alge
Fp
ormalizing and (d) eight bins with amplitude-based sortingxperiment of our new respiratory motion tracking system.
Bin 6 : sin(
11�
8
)< sin(˛) < sin
(9�
8
),
tan(
9�
8
)< tan(˛) < tan
(11�
8
).
Bin 7 : sin(
9�
8
)< sin(˛) < sin
(7�
8
),
−1 < cos(˛) < cos(
7�
8
).
ig. 3 – Correspondence between the points in one respiratory cyoint (1) on the right curve, amplitude is minimum but its first d
orithm. Example data are from one preliminary validation
Bin 8 : sin(
7�
8
)< sin(˛) < sin
(5�
8
),
tan(
5�
8
)< tan(˛) < tan
(7�
8
).
Ideally all positron emission events collected at a given (A)
and (dA/dt) could be assigned to the same bin according torespiratory amplitude regardless of the time. Points outsidethe two circles would indicate an abnormal position, whichwould be discarded.cle to the points in amplitude vs. dA/dt curve, for example:erivative is 0, it corresponds to point (1) on the left circle.

s i n
116 c o m p u t e r m e t h o d s a n d p r o g r a mBy using the respiratory model of the NCAT 4D phantom,3D phantoms were generated at different times within the res-piratory cycle as volume arrays of 128 × 128 × 128 voxels, withpixel sizes and slice thickness equivalent to those obtained inclinical PET studies. The voxelized phantoms were saved asraw binary images with no header. Each voxel value in an out-put image was stored as a 4 bytes floating point number (LittleEndian). A typical respiratory cycle can be divided into 10, 8or 6 time bins, with equal time intervals. Two sets of respira-tory phantoms were then created for each time bin. The firstcorresponded to a transmission phantom in which only softtissue and lungs were differentiated. The value of the attenu-ation coefficient for lung at 511 keV (0.024 cm−1) was assignedto lung voxels. The rest of the voxels had a value equal to theattenuation coefficient of soft tissue at 511 keV (0.097 cm−1).The second set of phantoms represented the 18FDG distribu-tion in lung and other structures.
2.3. Binning scheme
To compare the amplitude binning algorithm with time bin-ning algorithm, NCAT phantom was used to simulate two
extreme cases. Case 1: one patient with five different respi-ratory periods but the same respiratory amplitude. Case 2:one patient with five different respiratory periods alone withfive different respiratory amplitudes (Fig. 4). We generated 6,Fig. 4 – (a) is case 1 and (b) is case 2. On the left: five different res4.0 s with eight equally spaced time frames, and four different cy4.5 or 5.0 s respiratory period, respectively (abnormal breaths). Othe left but adjusted to the same starting time to show the differ
b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
7, 8, 9 or 10 time-frames of the phantoms over one respira-tory cycle (corresponding to 3.0, 3.5, 4.0, 4.5, 5.0 s respiratoryperiods) and summed the simulation results to mimic clini-cal imaging situations. Images were reconstructed with andwithout respiration motion. Table 1 shows the frame numberin each respiratory cycle and their corresponding bin num-bers with the amplitude binning algorithm. Here all the datapoints in the respiratory cycles were included as the trainingdata. In case 1, the maximum amplitude of diaphragm motionwas 20 mm and the maximum amplitude of AP expansion(anteroposterior diameter of the ribcage) was 12 mm. Theseare normal values for normal tidal breathing [24,25], while incase 2 the parameters used for the maximum amplitude ofdiaphragm motion and the maximum amplitude of AP expan-sion were shown in Table 2.
Comparison was performed for gated and un-gated imagesand for the new amplitude binning algorithm with the timebinning algorithm by calculating the mean number of countsin the same size of ROI. Tumor-to-background ratios pro-grammed into NCAT were 2.5, 5 and 8, and the diameters ofthe simulated tumors were 6, 8.5, 10 and 20 mm. Twelve itera-tions for case 1 and four iterations for case 2 done to validate
the new gating algorithm with NCAT phantom are shown inTable 3. Tumors were placed in the both the right and left lungssimply to show that the results were not influenced by thechoice of lung.piratory cycles, the normal respiratory cycle has a period ofcles with 6, 7, 9 or 10 time frames corresponding to 3.0, 3.5,n the right: the five different respiratory cycles shown inences in the periods.

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b
Table 1 – (a) is for case 1 and (b) is for case 2
Period (s) Frame no.
1 2 3 4 5 6 7 8 9 10
(a) Case 13.0 1 3 4 5 7 83.5 1 3 4 5 6 7 84.0 1 2 3 4 5 6 7 84.5 1 2 3 4 5 6 6 7 85.0 1 2 3 4 5 5 6 7 8 8
(b) Case 23.0 1 2 3 5 7 83.5 1 2 3 4 5 7 84.0 1 2 3 4 5 6 7 84.5 1 2 3 4 5 5 6 7 85.0 1 2 3 4 5 5 5 6 8 8
2
Tp
•••••
The first row in both tables is the frame number in the respiratorycycle and the values in the following rows are their correspondingbin numbers assigned with the amplitude-based sorting algorithm.
.4. Simulation of lung tumors
he parameters of the raw binary file simulated by 4D NCAThantom are as following:
modality: PET/CT
pixel width: 3.125 mmlowest image pixel value: 0 (number of counts)highest image pixel value: 75 (number of counts)rows: 128; columns: 128Table 2 – Parameters used in NCAT phantom for the maximumamplitude of AP expansion for five different respiratory cycles i
Cycle 1 Cycle 2
Period (s) 3.0 3.5AP amplitude (mm) 10 12Diaphragm amplitude (mm) 16.7 20
Table 3 – Iteration table for tumors’ simulations of different tum
Case no. Tumor no. Tumor size (mm)
Case 1
Tumor 1 20Tumor 2 6.0Tumor 3 8.5Tumor 4 10Tumor 5 20Tumor 6 6.0Tumor 7 8.5Tumor 8 10Tumor 9 20Tumor 10 6.0Tumor 11 8.5Tumor 12 10
Case 2
Tumor 13 20Tumor 14 6.0Tumor 15 8.5Tumor 16 10
i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122 117
Lung tumors were simulated assuming a spherical shape.By selecting regions of interest at different slices, the meanand standard deviation (S.D.) of counts could be determinedfor each structure of interest (lesion, lung, soft tissue). Simu-lated phantoms were created by assigning to the voxels v(i) ofeach structure the value:
v(i) = meann
± RND(∗) × S.D.√n
, (1)
where ‘mean’ is the average value of all the counts in eachstructure, S.D. = √
mean, n the number of time bins used tosimulate respiration and RND(*) is a random number withGaussian distribution (mean equal to 0 and standard devia-tion equal to 1). Finally, the blurring effect due to the finiteresolution of PET images was included by the convolution ofeach transaxial slice with a Gaussian filter in which the FWHMof 5 mm in the x and y directions are applied, correspondingto the current resolution of the PET scan. In NCAT phantomdata, the pixel width is 3.125 mm, so the FWHM = 5/3.125 = 1.6pixel. The axial blurring was performed by the convolutionof the images in the axial direction with a one-dimensionalGaussian filter.
3. Result
3.1. Analysis of tumor 1 and tumor 2
As 16 tumors gave us similar results, only detailed results fromtumor 1 and tumor 2 are shown here as examples. The rela-tive activity values (activity values relative to the number of
amplitude of diaphragm motion and the maximumn case 2
Cycle 3 Cycle 4 Cycle 5
4.0 4.5 5.015 18 2025 30 33.3
or sizes and T/B ratios
Tumor/background ratio Tumor position
2.5 Right lung2.5 Right lung2.5 Right lung2.5 Right lung5.0 Right lung5.0 Right lung5.0 Right lung5.0 Right lung8.0 Left lung8.0 Left lung8.0 Left lung8.0 Left lung
2.5 Right lung2.5 Right lung2.5 Right lung2.5 Right lung

118 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
Fig. 5 – (a) Relative activity values for eight bins (tumor 1 in case 1) in four cases: time binning, amplitude binning, withoutve act cas
respiratory motion and without gating and (b) average relatirepresent degradation in three cases compared to the perfec
counts) for eight bins in four cases: time binning, amplitudebinning, without respiratory motion and without gating areshown in Figs. 5(a) and 6(a), where the un-gated case resultsin the lowest value (lowest line), the case without respira-tory motion (perfect case) gives the theoretical value (highestline), and the time binning and amplitudes binning cases aresomewhere between those two lines. In Figs. 5(b) and 6(b),values from different bins were averaged to calculate the per-cent degradation from the perfect case (without respiratorymotion). 3.56% in Fig. 5(b) and 10.42% in Fig. 6(b) are the dif-ferences between two degradations of amplitude gating andtime gating, showing the improvements achieved with thenew amplitude gating algorithm.
3.2. Summary of 16 tumors
The tumor degradation as a function of tumor size is plot-ted in Fig. 7(a)–(c) for case 1 and Fig. 7(d) for case 2. Thezero line is for no degradation (the theoretically optimal per-
formance); subsequent values less than 0% correspond toproportional degradation (potential improvement). It can beseen that as the size of the tumor increases, the degradationdecreases. So the greatest benefit is realized for the small-Fig. 6 – (a) Relative activity values for eight bins (tumor 2 in casefour cases (tumor 2 in case 1).
tivity values in four cases, the percentage values in figuree—without respiration (tumor 1 in case 1).
est tested tumor size. The tumor degradation as a functionof tumor/background ratio for case 1 is plotted in Fig. 8(a)–(d).The zero line is no degradation; subsequent values less than0% correspond to proportional degradation. It can also be seenthat as the tumor to background ratio increases, the degrada-tion decreases. Therefore, greater benefit occurs for smallersize tumor and lower T/B ratio indicating a potential improve-ment in detecting more difficult to detected tumors.
Note that little improvement is gained for large tumorswith high T/B ratios. But these are relatively easy to diag-nose and gating is probably not necessary. The difference ofdegradations between time binning and amplitude binning isexhibited in Fig. 9(a) for case 1 and Fig. 9(b) for case 2. The aver-age improvements were 7.14 ± 3.19% for 12 tumors in case 1,14.07 ± 6.73% for 4 tumors in case 2 and 8.87 ± 5.10% for total 16tumors. As the tumor to background ratio increases, the differ-ence decreases, and as the tumor size increases, the differencedecreases.
4. Discussion
Improving the detectability of a malignant lung tumor in itsinitial stage using 18FDG-PET will impact positively lung can-
1) in four cases and (b) average relative activity values in

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122 119
Fig. 7 – For case 1: (a) percentage degradation in tumor activity (2.5 tumor/background ratio); (b) percentage degradation intumor activity (5.0 T/B ratio); (c) percentage degradation in tumor activity (8.0 T/B ratio). For case 2: (d) percentagedegradation in tumor activity (2.5 T/B ratio). The lowest line is the curve of un-gated tumors compared to ideal tumors( timel al tu
cwpaatittoapibPss
Pfte“dsrip
without respiratory motion). The middle line is the curve ofine is the curve of amplitude gated tumors compared to ide
er patient care. However, because of the long duration ofhole body PET scans, tumor and organ motion due to res-iration can be a major challenge for accurate localizationnd quantification of PET images as the image will be blurrednd the tumor smeared. The long-term goal of this research iso increase the sensitivity and prognostic value of molecularmaging with 18FDG-PET/CT of small lung malignant tumorhat move significantly during respiration, and to improvehe identification and accuracy of 18FDG uptake quantitationf small tumors. The objective of this study was to developnd validate an amplitude-based sorting algorithm and com-are it with time sorting algorithm. Three papers appeared
n 2006 directly comparing amplitude-based gating to phase-ased gating in CT and radiotherapy [26–28] and another inET [29]. The conclusions drawn from the current theoreticaltudy confirms and supports Thorndyke’s experimental PETtudy.
Typical gating methods are based on the division of theET frames into different time bins, which cannot corrector irregular respiratory cycles as demonstrated in Fig. 1. Theime-based binning algorithm for respiratory PET gating gen-rally will discard respiratory periods that are outside of thenormal” range. However, the actual magnitude of allowedeviation from “normal” phase that is used in practice is not
pecified. Even a “real” system must necessarily include someespiratory periods outside the “normal”. Real patient breath-ng can be quite abnormal. Seppenwoolde [30] reported thatatient breathing period averages about 3.6 s with a standardgated tumors compared to ideal tumors and the highestmors.
deviation of about ±0.8 s (about 22% of normal), which is sim-ilar to the range of periods simulated in our study. When“abnormal” imaging frames are discarded, either the countstatistics is decreased leading to greater noise, or the imag-ing session must be prolonged (the latter being what is donein practice). This study is intended to simulate the conditionin which all detected events are utilized. Our goal is to developa method which does not prolong the time patients are inthe imaging camera, because increased procedure times willincrease patient discomfort and the likelihood of movement,and therefore decrease patient throughout and productivity.
This study simulates the cases in which a patient wouldhave difficulty maintaining a steady breathing pattern. Pos-sibly only in such cases will amplitude binning be superior,but even for more “normal” cases it should be as good as timebinning, without added cost with respect to time or materi-als [29]. Also for many gating systems proposed, amplitudebinning will only be practical integrated with a system thataccurately reports amplitude and not just respiratory period. Asystem that does not respond linearly to changes in amplitudelike the thermometer sensor system [8] or the AZ-773V straingauge system may not be suitable for an amplitude binningalgorithm.
From the NCAT simulating result, it can be observed that
in each selected ROI, the relative activity values in fourcases are listed as below: ideal PET images (without res-piratory motion) > amplitude gated PET images > time gatedPET images > un-gated PET images. Here greater value means
120 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
Fig. 8 – For case 1: percentage degradation in tumor activity: (a) is 6 mm tumor; (b) is 8.5 mm tumor; (c) is 10 mm tumor; (d) is20 mm tumor. The lowest line is the curve of un-gated tumors compared to ideal tumors (without respiratory motion), the
eal
middle line is the curve of time gated tumors compared to idtumors compared to ideal tumors.better and more accurate tumor detection. This is what weexpected, in the case without respiratory motion, the exactvalue of the tumor activity was obtained; while with respira-tory motion and without gating, tumor image was degradedand the tumor activity value was reduced; by using the twobinning algorithms, the tumor’s activity value was somewhere
between the two extreme cases, and the amplitude gatingalgorithm demonstrated better results than the time gatingalgorithm. However, implementation of the amplitude binningalgorithm might require list-mode acquisition of PET scanFig. 9 – Difference in degradation (potential improvement) betwefunction of tumor size for different T/B ratios, case 1 on the left a
tumors and the highest line is the curve of amplitude gated
data and require more post-processing time, perhaps run ona pipeline process in near real-time.
It was also found that the accuracy of tumor detection isa function of two factors. One of the factors is the size ofthe tumor. It can be observed from Fig. 7(a)–(d) that as thetumor diameter decreased, the degradation effect of respira-
tory motion blurring on the tumor (potential improvement ofthe detection of the tumor) increases. Thus, tumors smallerthan 10 mm could theoretically be identified, which previouslyhas not been considered feasible with PET. The other factoren amplitude binning and time binning algorithm as and case 2 on the right.

i n b
oitdnr
tdidanrnilob
ohiptaRnwtes
5
IhpciRticfaatas
ptasttch
r
c o m p u t e r m e t h o d s a n d p r o g r a m s
n which the accuracy of tumor detection was seen to depends tumor to background (T/B) ratio (Fig. 8(a)–(d)). The smallerhe T/B ratio the greater the potential improvement of tumoretection. Thus, with binning, especially with amplitude bin-ing, we can theoretically detect the tumors with lower T/Batios.
Another point needs to be addressed here is: the poten-ial improvement achieved might be exaggerated because theata analysis here is one of the worst case scenarios (case 1
s five different periods’ respiratory cycles and case 2 is fiveifferent periods alone with five different amplitudes). Thesere only two particular poor abnormal patient responses. Aormal patient would not be expected to have such abnormalespiratory patterns. They are more likely to have 10 or moreormal breaths with each one or two abnormal breaths. We are
n the process of simulating more general cases. Never-the-ess with the amplitude binning algorithm the quantitationf tumor’s 18FDG uptake will be less susceptible to irregularreathing.
One possible error could occur due to the arbitrary naturef marking the ROI (region of interest) as ROI could includeypoxic or hypo-metabolic regions around the tumor. Even
n the current clinical application, such error cannot be com-letely avoided. In the present study, we tried to minimizehe error by carefully selecting of ROI and accommodatings much of the highest activity region as possible within theOI. Also the effect of photon scatter and attenuation wereot included into the NCAT data, we may be biased becausee know where the tumor is, we did not look at different
umor sites or different tidal volumes, and finally, additionalrror may have resulted from clinical setting errors, etc. Thesehould be considered in the future.
. Conclusion and future work
n this paper, we validated a binning algorithm based on theypothesis that integrating gated PET images at the same res-iratory amplitudes within the respiratory cycle into one binan significantly reduce respiratory motion artifacts, compar-ng this algorithm with current time-base binning algorithm.esults from NCAT phantom simulation demonstrated thathis algorithm was more accurate and reliable in determin-ng the activity value of the tumors. Therefore, it cannot onlyorrect for normal steady respiratory motion, but also corrector variable irregular respiratory and patient motion. It waslso observed that the detection of tumors gets better withmplitude binning algorithm as tumor size decreases or tumoro background (T/B) ratio decreases, so we can improve theccuracy of lung tumor detection by better identification withmaller tumors and with lower T/B ratios.
Future validation work needs to be done using a physicalhantom in the PET/CT machine with the full implementa-ion of the respiratory gating system. Future work will alsossess the new binning algorithm by simulating a real clinicalcanner with SimSET (a Monte Carlo program for emission
omography simulation) incorporated into the NCAT phan-om. Photon scatter and attenuation need to be included in theomputer simulations. Finally the whole system (software andardware) needs to be incorporated into GE/Siemens PET/CTi o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122 121
system and be evaluated using patients, and compared to thestandard clinical practice.
Acknowledgement
This work was supported by a grant from the NIH(R15CA118284-01).
e f e r e n c e s
[1] M.N. Gurcan, B. Sahiner, N. Petrick, H.P. Chan, E.A.Kazerooni, P.N. Cascade, L. Hadjiiski, Lung nodule detectionon thoracic computed tomography images: preliminaryevaluation of a computer-aided diagnosis system, Med.Phys. 29 (2002) 2552–2558.
[2] R.J. Jackman, C.A. Good, O.T. Clagett, L.B. Woolner, Survivalrates in peripheral bronchogenic carcinomas up to fourcentimeters in diameter presenting as solitary pulmonarynodules, J. Thorac. Cardiovasc. Surg. 57 (1969) 1–8.
[3] H. Toomes, A. Delphendahl, H.G. Manke, I. Vogt-Moykopf,The coin lesion of the lung. A review of 955 resected coinlesions, Cancer 51 (1983) 534–537.
[4] N. Martini, M.S. Bains, M.E. Burt, M.F. Zakowski, P.McCormack, V.W. Rusch, R.J. Ginsberg, Incidence of localrecurrence and second primary tumors in resected stage Ilung cancer, J. Thorac. Cardiovasc. Surg. 109 (1995) 120–129.
[5] D.E. Midthun, Solitary pulmonary nodule: time to thinksmall, Curr. Opin. Pulm. Med. 6 (2000) 364–370.
[6] J.J. Erasmus, J.E. Connolly, H.P. McAdams, V.L. Roggli, Solitarypulmonary nodules: part I. Morphologic evaluation fordifferentiation of benign and malignant lesions,Radiographics 20 (2000) 43–58.
[7] M.J. Liptay, Solitary pulmonary nodule: treatment options,Chest 116 (1999) 517S–518S.
[8] S.F. Hain, K.M. Curran, A.D. Beggs, I. Fogelman, M.J.O’Doherty, M.N. Maisey, FDG-PET as a “metabolic biopsy”tool in thoracic lesions with indeterminate biopsy, Eur. J.Nucl. Med. 28 (2001) 1336–1340.
[9] N.A. Dewan, S.D. Reeb, N.C. Gupta, L.S. Gobar, W.J. Scott,PET-FDG imaging and transthoracic needle lung aspirationbiopsy in evaluation of pulmonary lesions. A comparativerisk-benefit analysis, Chest 108 (1995) 441–446.
[10] M.K. Gould, G.A. Lillington, Strategy and cost ininvestigating solitary pulmonary nodules, Thorax 53 (Suppl.2) (1998) S32–S37.
[11] C.B. Caldwell, K. Mah, Y.C. Ung, C.E. Danjoux, J.M. Balogh,S.N. Ganguli, L.E. Ehrlich, Observer variation in contouringgross tumor volume in patients with poorly definednon-small-cell lung tumors on CT: the impact of18FDG-hybrid PET fusion, Int. J. Radiat. Oncol. Biol. Phys. 51(2001) 923–931.
[12] W.P. Segars, B.M. Tsui, Study of the efficacy of respiratorygating in myocardial SPECT with the new 4D NCATphantom, IEEE Trans. Nucl. Sci. 49 (2002) 675–679.
[13] W.P. Segars, B.M. Tsui, A.J.D. Silva, CT-PET image fusion usingthe 4D NCAT phantom with the purpose of attenuationcorrection, IEEE Trans. Nucl. Sci. 3 (2002) 1775–1779.
[14] Z. Zhu, B.M. Tsui, W. Segars, A simulation study of the effectof gating scheme on respiratory motion blurring in FDG lungPET, 49th Annual Meeting of the Society of Nuclear
Medicine, Los Angeles, CA, J. Nucl. Med., 43 (2002), 57.[15] Q.S. Chen, M.S. Weinhous, F.C. Deibel, J.P. Ciezki, R.M.Macklis, Fluoroscopic study of tumor motion due tobreathing: facilitating precise radiation therapy for lungcancer patients, Med. Phys. 28 (2001) 1850–1856.

s i n
122 c o m p u t e r m e t h o d s a n d p r o g r a m[16] S.A. Nehmeh, Y.E. Erdi, C.C. Ling, K.E. Rosenzweig, H.Schoder, S.M. Larson, H.A. Macapinlac, O.D. Squire, J.L.Humm, Effect of respiratory gating on quantifying PETimages of lung cancer, J. Nucl. Med. 43 (2002) 876–881.
[17] S.A. Nehmeh, Y.E. Erdi, C.C. Ling, K.E. Rosenzweig, O.D.Squire, L.E. Braban, E. Ford, K. Sidhu, G.S. Mageras, S.M.Larson, J.L. Humm, Effect of respiratory gating on reducinglung motion artifacts in PET imaging of lung cancer, Med.Phys. 29 (2002) 366–371.
[18] S.A. Nehmeh, Y.E. Erdi, K.E. Rosenzweig, H. Schoder, S.M.Larson, O.D. Squire, J.L. Humm, Reduction of respiratorymotion artifacts in PET imaging of lung cancer byrespiratory correlated dynamic PET: methodology andcomparison with respiratory gated PET, J. Nucl. Med. 44(2003) 1644–1648.
[19] Y. Wang, H. Baghaei, H. Li, Y. Liu, T. Xing, J. Uribe, R. Ramirez,S. Xie, S. Kim, W.-H. Wong, A simple respiration gatingtechnique and its application in high-resolution PETcamera, IEEE Trans. Nucl. Sci. 52 (2005).
[20] A. Rahmim, Advanced motion correction methods in PET,Iran J. Nucl. Med. 13 (2005).
[21] F. Lamare, T. Cresson, J. Savean, C. Cheze Le Rest, A.J. Reader,D. Visvikis, Respiratory motion correction for PET oncologyapplications using affine transformation of list mode data,
Phys. Med. Biol. 52 (2007) 121–140.[22] F. Qiao, J. Clark, T. Pan, O. Mawlawi, Expectationmaximization reconstruction of PET image with non-rigidmotion compensation, Conf. Proc. IEEE Eng. Med. Biol. Soc. 4(2005) 4453–4456.
b i o m e d i c i n e 8 7 ( 2 0 0 7 ) 112–122
[23] I. El Naqa, D.A. Low, J.D. Bradley, M. Vicic, J.O. Deasy,Deblurring of breathing motion artifacts in thoracic PETimages by deconvolution methods, Med. Phys. 33 (2006)3587–3600.
[24] W.P. Segars, Development of a new dynamic NURBS-basedcardiac torso (NCAT) phantom Ph.D. dissertation, TheUniversity of North Carolina, 2001.
[25] W.P. Segars, D.S. Lalush, B.M. Tsui, Modeling respiratorymechanics in the MCAT and spline-based MCAT phantoms,IEEE Trans. Nucl. Sci. 48 (2001).
[26] M.J. Fitzpatrick, G. Starkschall, J.A. Antolak, J. Fu, H. Shukla,P.J. Keall, P. Klahr, R. Mohan, Displacement-based binning oftime-dependent computed tomography image data sets,Med. Phys. 33 (2006) 235–246.
[27] W. Lu, P.J. Parikh, J.P. Hubenschmidt, J.D. Bradley, D.A. Low, Acomparison between amplitude sorting and phase-anglesorting using external respiratory measurement for 4D CT,Med. Phys. 33 (2006) 2964–2974.
[28] N. Wink, C. Panknin, T.D. Solberg, Phase versus amplitudesorting of 4D-CT data, J. Appl. Clin. Med. Phys. 7 (2006) 77–85.
[29] B. Thorndyke, E. Schreibmann, A. Koong, L. Xing, Reducingrespiratory motion artifacts in positron emissiontomography through retrospective stacking, Med. Phys. 33(2006) 2632–2641.
[30] Y. Seppenwoolde, H. Shirato, K. Kitamura, S. Shimizu, M. vanHerk, J.V. Lebesque, K. Miyasaka, Precise and real-timemeasurement of 3D tumor motion in lung due to breathingand heartbeat, measured during radiotherapy, Int. J. Radiat.Oncol. Biol. Phys. 53 (2002) 822–834.




















