
IMPROVED ROUTH-PADÉ APPROXIMANTS USING VECTOR EVALUATED GENETIC ALGORITHM TO UNSTABLE SYSTEMS
Upload
independentCategory
view
0download
0
Establishment of a High Sensitivity Plasma Assay forHuman Pentraxin3 as a Marker for Unstable
Angina PectorisKenji Inoue, Akira Sugiyama, Patrick C. Reid, Yukio Ito, Katsumi Miyauchi, Sei Mukai, Mina Sagara,
Kyoko Miyamoto, Hirokazu Satoh, Isao Kohno, Takeshi Kurata, Hiroshi Ota, Alberto Mantovani,Takao Hamakubo, Hiroyuki Daida, Tatsuhiko Kodama
Objective—Plasma pentraxin 3 (PTX3) levels are increased in patients with acute myocardial infarction, yet itsinvolvement in unstable angina pectoris (UAP) remains unclear. To critically evaluate the role of PTX3 in UAP, asensitive and precise measurement of PTX3 concentration is needed.
Methods and Results—We established a high sensitive plasma ELISA assay system for the detection of PTX3 usingmonoclonal antibodies. The lower limit of detection of our ELISA was 0.1 ng/mL, sensitivity far greater than the currentcommercially available kit. Plasma samples were obtained from 162 consecutive patients treated for hypertension,hyperlipidemia, diabetes mellitus, or cardiovascular disease at a physician’s office. PTX3 was not associated with anyknown coronary risk factors. Additionally, we collected plasma samples from 252 consecutive subjects admitted to auniversity hospital for coronary artery assessment by coronary angiography. PTX3 was significantly increased inpatients in whom coronary intervention was performed. We further analyzed the plasma level of PTX3 in 52 patientswith effort angina (EAP) and 16 patients with UAP. Compared with the control group, PTX3 were significantly higherin the UAP group.
Conclusions—The levels of plasma PTX3 were increased in patients with arterial inflammation, especially UAP. ThisPTX3 detection system will be useful for the prediction of UAP. (Arterioscler Thromb Vasc Biol. 2007;27:161-167.)
Key Words: PTX3 � hs-CRP � atherosclerosis � inflammation � acute coronary syndrome
Inflammatory mediators are intimately associated with thecascade of events leading to atherosclerotic plaque initia-
tion, development, and rupture.1 This recognition has led tothe evaluation of several markers of inflammation as potentialtools for cardiovascular risk prediction. Among the mostactively studied biomarkers is high sensitivity C-reactiveprotein (hs-CRP). The association between moderately ele-vated hs-CRP levels and an increased risk for development ofcardiovascular events is well established.2
CRP and serum amyloid P component (SAP) are wellknown members of the pentraxin family of proteins. Pentrax-ins are conserved in evolution from Limulus Polyphemus toman. CRP and SAP are referred to as classical short pentrax-ins and are acute phase proteins produced in the liver inresponse to inflammatory mediators. Measurement of CRP isroutinely used for diagnosis and monitoring of diverse in-flammatory and infectious diseases, whereas SAP is a usefulprobe to identify amyloid deposits.3–6 Their main inducer is
interleukin (IL)-6. PTX3 is the first identified long pentraxin,consisting of a C-terminal pentraxin module coupled with anunrelated N-terminal domain.7,8 PTX3 is structurally relatedbut distinct from classic pentraxins. It differs from the classicshort pentraxins in terms of gene organization and localiza-tion, ligand recognition, producing cells, and inducingsignals.
PTX3 is made in response to primary proinflammatorysignals (bacterial products, IL-1, and tumor necrosis factor[TNF], but not IL-6) by diverse cell types, predominantlymacrophages and vascular endothelial cells,9–12 but not liver.Due to the fact that PTX3 is produced from vascularendothelial cells and macrophages, instead of from the liver,PTX3 levels may more directly reflect the inflammatorystatus of the vasculature. Given the similarities and differ-ences between PTX3 and CRP, it is important to assess theusefulness of PTX3 as a novel diagnostic tool for acutecoronary syndrome. An initial study in acute myocardial
Original received May 27, 2006; final version accepted September 3, 2006.From the Laboratory for Systems Biology and Medicine (K.I., P.C.R., T.H., T.K.), Research Center for Advanced Science and Technology, The
University of Tokyo, Japan; the Department of Cardiology (K.I.), Juntendo University Nerima Hospital, Tokyo, Japan; the Perseus Proteomics Inc (A.S.,P.C.R., Y.I., M.S., K.M., H.S., I.K.), Tokyo, Japan; the Department of Cardiology (K.M., T.K., H.O., H.D.), Juntendo University School of Medicine,Tokyo, Japan; the Shin Yokohama Cardiovascular Clinic (S.M.), Kanagawa, Japan; and the Istituto Clinico Humanitas (A.M.), Italy.
K.I. and A.S. contributed equally to this study.Correspondence to Tatsuhiko Kodama, Laboratory for Systems Biology and Medicine, Research Center for Advanced Science and Technology, The
University of Tokyo, 4-6-1, Komaba, Meguro, Tokyo, 153-8904, Japan. E-mail [email protected]© 2006 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org DOI: 10.1161/01.ATV.0000252126.48375.d5
161 by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from

infarction yielded encouraging results,13 and interestingly, itwas also PTX3 that we identified as being suppressed bystatin treatment in human umbilical vein endothelial cells bycDNA microarray analysis.14
In the present study we report the development of a highsensitivity ELISA system for plasma detection of humanPTX3 using two different monoclonal antibodies. Using thissystem we investigated plasma levels of PTX3 as a role ofpredictive biomarker in patients with different severities ofatherosclerotic disease.
Methods
ReagentsBuffers and solutions used in the ELISA were as follows: PTX3recombinant protein for calibration curve; immobilization of anti-body on plates buffer of 150 mmol/L NaCl saline; blocking buffer of1% casein in 10 mmol/L phosphate buffer saline (PBS), pH7.4;calibrator dilution buffer of PBS containing 2% bovine serumalbumin, 0.2% MICROSIDE III (Anresco Laboratories); sampledilution buffer of PBS, 0.2% MICROSIDE III; enzyme conjugatedantibody dilution buffer of Gardian (Pierce Biotechnology Inc)containing 0.1% casein TBS (Pierce Biotechnology Inc), 0.2%MICROSIDE III; washing solution of 0.05% Tween-20 in PBS;substrate solution of TMB (ScyTeK Laboratories Inc); and stopsolution (ScyTeK Laboratories Inc). Commercial PTX3 detectionsystem; anti human PTX3 rat monoclonal antibody; MNB4(ALEXIS Corporation), biotin conjugated anti Human PTX3 rabbitpolyclonal antibody (ALEXIS Corporation).
AntigensRecombinant human PTX3 was expressed in Chinese hamster ovary(CHO) cells as either his-tagged recombinant PTX3 (rPTX3) or asnative non-tagged PTX3 and subsequently purified by means ofHiTrap chelating Nickel column (GE Healthcare Bio-Science Corp)or ion exchange HiPrep 16/10 Q XL Column (GE HealthcareBio-Science Corp), respectively, as previously described.10 Polymer-ization of the purified PTX3 recombinant protein was analyzed by3% to 8% Tris-Acetate gradient gel SDS-PAGE and SYPRO RubyProtein Gel Stain (Invitrogen Corporation).
Monoclonal AntibodiesPTX3-deficient mice15 were immunized with intraperitoneal injec-tions of PTX3 in Freund adjuvant (DIFCO, BD) over a period of 4weeks at 2-week intervals. Fusion of spleen cells from immunizedmouse with mouse myeloma cells, NS-1, was performed in a ratio of10:1 as previously described16. Antibody screening was performedby direct enzyme linked immunosorbent assay (ELISA) method.Monoclonal antibodies were purified from ascites using a HiTrapProtein G HP Column (GE Healthcare Bio-Science Corp). Isotypedetermination was carried out using an ImmunoPure MonoclonalAntibody Isotyping kit II (Pierce Biotechnology Inc) according tomanufacturer’s instructions.
Preparation of Antibody Coated PlatesMonoclonal antibody PPMX0104 was digested by pepsin intoF(ab�)2 as previously described17. The digested PPMX0104 (100 �Lof a 5 �g/mL solution in saline) was coated on a microtiter plate,MaxiSope (Nalge Nunc) at 4°C overnight. After aspirating andwashing with washing buffer 5 times, the wells were then blockedwith 1% casein in PBS, pH7.4 at 4°C overnight. The plate wasaspirated and washed again and the wells were then coated with 150�L/well of Immunoassay Stabilizer (Advanced Biotechnologies Inc)at 4°C overnight. After which the reagent was discarded and the platewas dried in a desiccation chamber overnight.
Preparation of Anti-PTX3 DetectionAntibody-Enzyme ConjugatesOne monoclonal antibody (PPMX0105) was digested by pepsin intoa F(ab�)2 as previously described17 and conjugated with horseradishperoxidase (HRP) according to the manufacturer’s instructions(Peroxidase labeling Kit-SH kit, Dojindo Laboratories).
Assay ProcedureIn the typical assay procedure, all incubations were performed atroom temperature. Sample dilution (100 �L) was added to the wellsof the antibody-coated microtiter plates. Each calibrator or plasmasamples (10 �L) were added to the wells and incubated for 1 hourwith shaking (first reaction). After the wells were aspirated andwashed 5 times with washing buffer (400 �L), Fab’-enzyme conju-gate (100 �L) were added to the wells and incubated for 1 hour withshaking (second reaction). The wells were aspirated and washedagain, and then substrate solution (100 �L) was added to each well.After 30 minutes of incubation (enzyme reaction), stop solution (100�L) was added, and the absorbance at 450 nm was measured with amicroplate reader system (Towa Labo). Experiments were performedin duplicate except where noted otherwise.
Preparation and Sandwich ELISA ofCommercially Available PTX3 Detection SystemCommercially available sandwich ELISA for PTX3 was purchasedfrom ALEXIS Corporation (ALEXIS Corporation). Preparation ofplates and sandwich ELISA were performed according to manufac-tures instruction.
Clinical Testing: Population A (Collected FromShin-Yokohama Cardiovascular Clinic)From January 2006 to April 2006, we measured plasma PTX3 levelsin 162 consecutive subjects (unbiased consecutive clinic visitors; agerange: 32 to 80 years; 105 men and 57 women) who are treated forhypertension, hyperlipidemia, diabetes mellitus, or cardiovasculardisease or come to the clinic for the purpose of an annual healthcheck. We collected baseline data on: body mass index, bloodpressure, and history of smoking. We defined prevalent hyperten-sion, diabetes mellitus, or hypercholesterolemia as follows: hyper-tension, the mean of 2 systolic blood pressure measurements of�140 mm Hg and/or diastolic pressure �90 mm Hg, or the use ofantihypertensive agents; Diabetes mellitus, a hemoglobin A1C levelof �5.9%, and/or a history of or current pharmacological treatmentfor diabetes; Hypercholesterolemia, a total cholesterol level of �220mg/dL, and/or a history of or current pharmacological treatment forhypercholesterolemia.
Patient Examination
Brachial-Artery Pulse Wave VelocityAll subjects were evaluated for brachial-artery pulse wave velocity(ba PWV). Ba PWV was measured using a volumeplethysmographicapparatus (Form/ABI, Colin Co Ltd). Details of the methodologywere as described elsewhere.18,19 The subject was examined whileresting in the supine position. Cuffs were wrapped on both brachiaand ankles. Pulse volume waveforms at the brachium and ankle wererecorded using a semiconductor pressure sensor. Ba PWV wasmeasured after at least 5 minutes rest.
Measuring Carotid Intima–Media ThicknessAll patients were evaluated for carotid artery intima–media thick-ness. Trained technicians used high-resolution B-mode ultrasound toscan three arterial segments bilaterally: the distal 1.0-cm straightportion of the common carotid artery, the carotid bifurcation, and theproximal 1.0 cm of the internal carotid artery.20 Trained readersmeasured intima–media thickness according to a standardized pro-tocol, and recorded whether or not they saw an apparent plaque. Foranalysis, we calculated an overall average of the observed meanintima–media carotid thicknesses of the far wall of the six arterialsegments.
162 Arterioscler Thromb Vasc Biol. January 2007
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from
Population B (Collected From JuntendoUniversity Hospital)From January 2006 to July 2006, we recruited 406 consecutivesubjects, 318 men and 88 women (mean age 65.6�10.5 years, range21 to 88) admitted to Juntendo university hospital for assessment ofischemic heart disease by coronary angiography (CAG). We ex-cluded patients who have a chronic inflammation status (arterioscle-rotic obliterans, aortic aneurysm,21 or rheumatoid arthritis22) becausea level of CRP should be increased. We also excluded patients withheart valvular disease because rheumatic fever causes heart valvulardisease. And because it is unclear about PTX3 level in patients withrenal insufficiency or malignant tumor, patients with more than 2.5mg/dL level of creatinine or with malignant disease were excluded.Therefore 250 subjects, 197 men and 53 women (mean age 66.3�9.8years, range 30 to 87), were analyzed. The patients consisted of 52patients with EAP and 16 with UAP. Stable angina was defined astypical angina precipitated by exertion or emotional stress associatedwith electrocardiographic change. UAP was defined as augmentingchest pain with a recent increase in frequency and duration, lastingmore than 15 minutes or occurring at rest or during minimal effort.These symptoms were combined with ST-segment depression andany changes in biochemical markers of myocardial necrosis (CPKand troponin T). At the time of examination, no subjects in bothpopulations exhibited any evidence of ongoing systemic or cardiacinflammatory diseases. All subjects were of Japanese nationality, andgave their informed consent. This study was approved by the ethicalcommittee of the institution.
Laboratory MeasurementsPlasma total cholesterol, high and low-density lipoprotein cholester-ol, fast blood sugar (FBS), hemoglobin A1C, hs-CRP, and plasmaPTX3 levels were measured. In each case, 4 mL of blood was drawnin EDTA vacuum containers for PTX3 measurement, and werefrozen at �20°C until time of assay. Blood samples were obtainedimmediately before coronary angiography after an overnight fast. Inurgent CAG cases, blood samples were drawn at the beginning of theemergency coronary angiographic examination.
Statistical AnalysisThe data were expressed as mean�SD. Differences between twogroups were analyzed by unpaired t test. All probability values weretwo-tailed, and values of less than 0.05 were considered to indicatestatistical significance. Coefficient of variation (CV) equals the SD
divided by the mean value and represents a statistical measure of thedispersion of data points in a data series around the mean, allowingfor the calculation of an intra-assay precision. Recovery referssimply to the % of exogenous PTX3 detected after addition to plasmasamples. All confidence intervals were calculated at the 95% level.
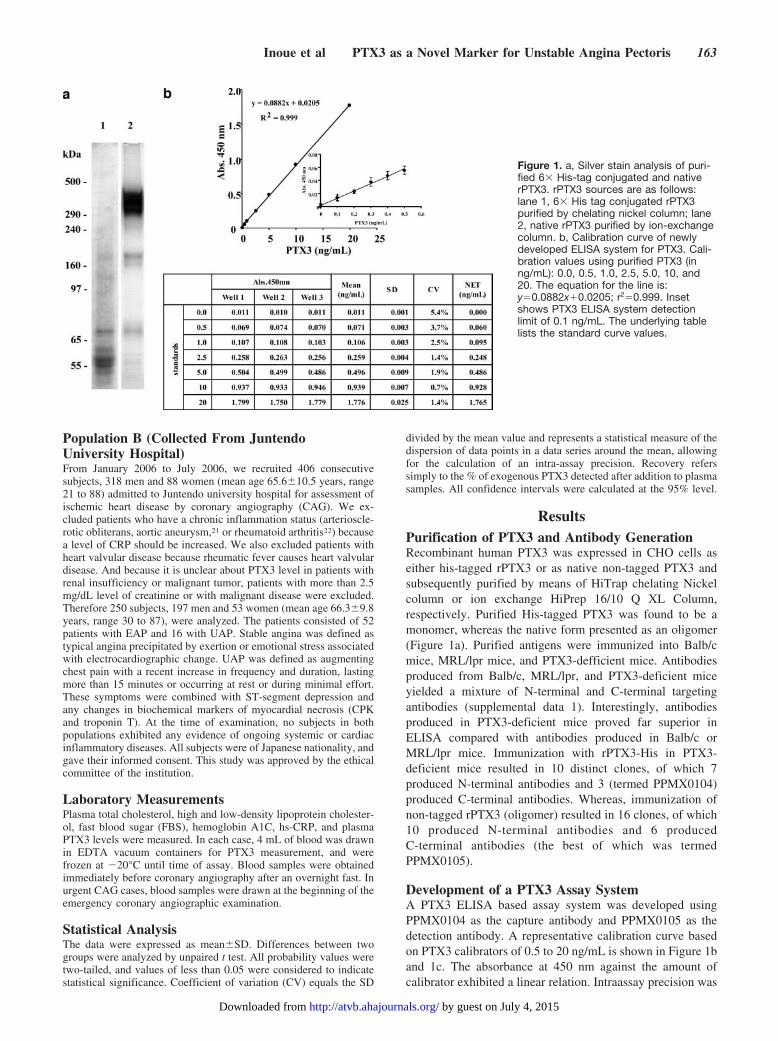
ResultsPurification of PTX3 and Antibody GenerationRecombinant human PTX3 was expressed in CHO cells aseither his-tagged rPTX3 or as native non-tagged PTX3 andsubsequently purified by means of HiTrap chelating Nickelcolumn or ion exchange HiPrep 16/10 Q XL Column,respectively. Purified His-tagged PTX3 was found to be amonomer, whereas the native form presented as an oligomer(Figure 1a). Purified antigens were immunized into Balb/cmice, MRL/lpr mice, and PTX3-defficient mice. Antibodiesproduced from Balb/c, MRL/lpr, and PTX3-deficient miceyielded a mixture of N-terminal and C-terminal targetingantibodies (supplemental data 1). Interestingly, antibodiesproduced in PTX3-deficient mice proved far superior inELISA compared with antibodies produced in Balb/c orMRL/lpr mice. Immunization with rPTX3-His in PTX3-deficient mice resulted in 10 distinct clones, of which 7produced N-terminal antibodies and 3 (termed PPMX0104)produced C-terminal antibodies. Whereas, immunization ofnon-tagged rPTX3 (oligomer) resulted in 16 clones, of which10 produced N-terminal antibodies and 6 producedC-terminal antibodies (the best of which was termedPPMX0105).
Development of a PTX3 Assay SystemA PTX3 ELISA based assay system was developed usingPPMX0104 as the capture antibody and PPMX0105 as thedetection antibody. A representative calibration curve basedon PTX3 calibrators of 0.5 to 20 ng/mL is shown in Figure 1band 1c. The absorbance at 450 nm against the amount ofcalibrator exhibited a linear relation. Intraassay precision was
Figure 1. a, Silver stain analysis of puri-fied 6� His-tag conjugated and nativerPTX3. rPTX3 sources are as follows:lane 1, 6� His tag conjugated rPTX3purified by chelating nickel column; lane2, native rPTX3 purified by ion-exchangecolumn. b, Calibration curve of newlydeveloped ELISA system for PTX3. Cali-bration values using purified PTX3 (inng/mL): 0.0, 0.5, 1.0, 2.5, 5.0, 10, and20. The equation for the line is:y�0.0882x�0.0205; r2�0.999. Insetshows PTX3 ELISA system detectionlimit of 0.1 ng/mL. The underlying tablelists the standard curve values.
Inoue et al PTX3 as a Novel Marker for Unstable Angina Pectoris 163
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from

investigated through the analysis in multiplicate (n�5) of 6different plasma samples, resulting in a coefficient of varia-tion (CV) �4.1% at all PTX3 concentrations tested. Themean�SD concentrations measured (and CV) were as fol-lows: sample 1, 15.91�0.13 ng/mL (0.8%); sample 2,7.17�0.10 (1.3%); sample 3, 9.70�0.30 ng/mL (3.0%);sample 4, 0.95�0.02 (1.6%); sample 5, 0.85�0.03 (4.1%);sample 6, 0.67�0.02 (2.9%) (Table S1 in supplemental data2). Interassay precision was investigated though the analysisof 3 independently performed experiments resulting in a CV�4.3% at all PTX3 concentrations tested. The mean�SDconcentrations measured (and CV) were as follows: sample 1,15.95�0.66 ng/mL (4.1%); sample 2, 7.21�0.22 (3.1%);sample 3, 9.70�0.42 ng/mL (4.3%); sample 4, 0.95�0.02(2.2%); sample 5, 0.87�0.03 (4.0%); sample 6, 0.66�0.01(1.8%) (Table S2 in supplemental data 2).
Analytical Recovery and Assay LinearityRecovery of exogenously added PTX3 from plasma samplesranged from 89.8% to 108.6% respectively (Table 1). Dilu-tion curves of plasma samples showed good linearity (sup-plemental data 3).
Assay Specificity and Cross ReactivityHemoglobin (up to 500 mg/dL), bilirubin (up to 20 mg/L),and chyle (up to 2000 U as Formazine) had no effect on thepresent ELISA. The cross-reactivity with CRP and SAP was�0.7%. In regards to PTX3 stability, PTX3 concentrations inwhole blood remained relatively unchanged for 8 hours at25°C with the use of EDTA plasma.
Comparison to Commercially Available PTX3Assay KitTo examine the efficacy of our detection system, we com-pared our newly developed ELISA system to a commerciallyavailable ELISA system (Table 1). Whereas our kit relies onmonoclonal antibodies as both the capture and detectionantibodies, the commercial ELISA uses a rat monoclonalantibody as the capture antibody and a rabbit polyclonal asthe detection antibody. The commercial kit relies on a 3 stepassay system to detect PTX3 from EDTA plasma at a rangeof 0.25 to 12 ng/mL. Our assay system relies on a 2 stepsystem to detect PTX3 from EDTA plasma at a range of 0.1to 20 ng/mL. Analysis of patient samples using both kitsrevealed a 0 to 4.3% CV for our assay kit and a 4% to 30%
CV for the commercially available kit. In addition, weobserved a recovery rate of 97.2% in our assay systemcompared with an 80% recovery rate in the commerciallyavailable kit.
Patients for the Clinical Study
Diagnostic Testing of Clinical Samples, Normal Rangeof PTX3Before analysis of plasma PTX3 level in patients withatherosclerosis, we measured PTX3 plasma concentration in56-healthy volunteers to determine a normal range. Theirmean age was 40.1�12.1 years, and % male was 59.2%.PTX3 averaged 1.98 ng/mL (95% CI: 1.68 to 2.28).
Diagnostic Testing of Clinical Samples, Independence ofPTX3 From Established Risk FactorsHs-CRP has been known to vary with many conditions, eg,smoking, obesity, age, and diabetes, and it is associated withthe metabolic syndrome, which is strongly linked to aproinflammatory state.23 Therefore we analyzed whetherplasma PTX3 levels were affected by another coronary riskfactor or not. The clinical characteristics of population A arelisted in Table 2. 10.8% of patients were current or formersmokers, 28.4% had diabetes mellitus, 30.2% had hyperlip-idemia, and 46.9% had hypertension. 38.9% of patients
TABLE 1. Comparison of Specs Between a Newly Developed Kit and aCommercially Available Kit
Our PTX3 ELISA System Commercially Available Kit
Capture antibody mouse monoclonal antibody rat monoclonal antibody
Detect antibody mouse monoclonal antibody rabbit polyclonal antibody
Assay steps 2 steps 3 steps
Assay sample EDTA plasma EDTA plasma
Range 0.10 to 20 ng/mL 0.25 to 12 ng/mL
Detection limit 0.10 ng/mL not texted
CV% for samples 0 to 4.3% (n�6) 4 to 30% (n�3)
Recover ratio average 97.2% (89.8 to 108.6%) average 80% (70 to 95%)
TABLE 2. Characteristics of Patients FromShin-Yokohama Cardiovascular Clinic
Characteristic (n�162)
Age, y 63.2�10.8
Males sex, n (%) 105 (64.8)
Diabetes, n (%) 46 (28.4)
Smoker, n (%) 28 (10.8)
Hypercholesterolemia, n (%) 49 (30.2)
Hypertension, n (%) 76 (46.9)
Systolic blood pressure, mm Hg 127.5�11.5
Diastolic blood pressure, mm Hg 69.8�11.5
Body mass index, � 24.2 kg/m2 63 (38.9)
BaPWV, �14.0 m/s 131 (80.9)
IMT, �1 mm 72 (44.4)
Abnormal stress ECG 0
Average (95% CI)
Plasma PTX3, ng/mL 2.19 (2.02 to 2.32)
164 Arterioscler Thromb Vasc Biol. January 2007
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from
showed a BMI of more than 24.2kg/m2. There were twonotable features of population A. First, 80.9% of subjectsshowed a high value of ba PWV. Yamashina et al havereported a ba PWV cutoff value of 14.0 m/s for screeningsubjects at risk of developing cardiovascular diseases in thegeneral population.24 Second, all of the patients’ conditionswere stable. No one had any symptom of chest discomfort orshowed abnormal stress electrocardiograms. In population A,plasma levels of PTX 3 were within the normal range, 2.19ng/mL (95% CI: 2.02 to 2.32). We classified subjects with baPWV values of more than 14.0m/sec as a relative high riskgroup for atherosclerotic disease, and examined their plasmaPTX 3 levels. Table 3 shows that PTX3 levels were indepen-dent of total cholesterol, HDL cholesterol, hemoglobin A1C,smoking status, gender, or obesity, and additionally did notvary with such conditions.
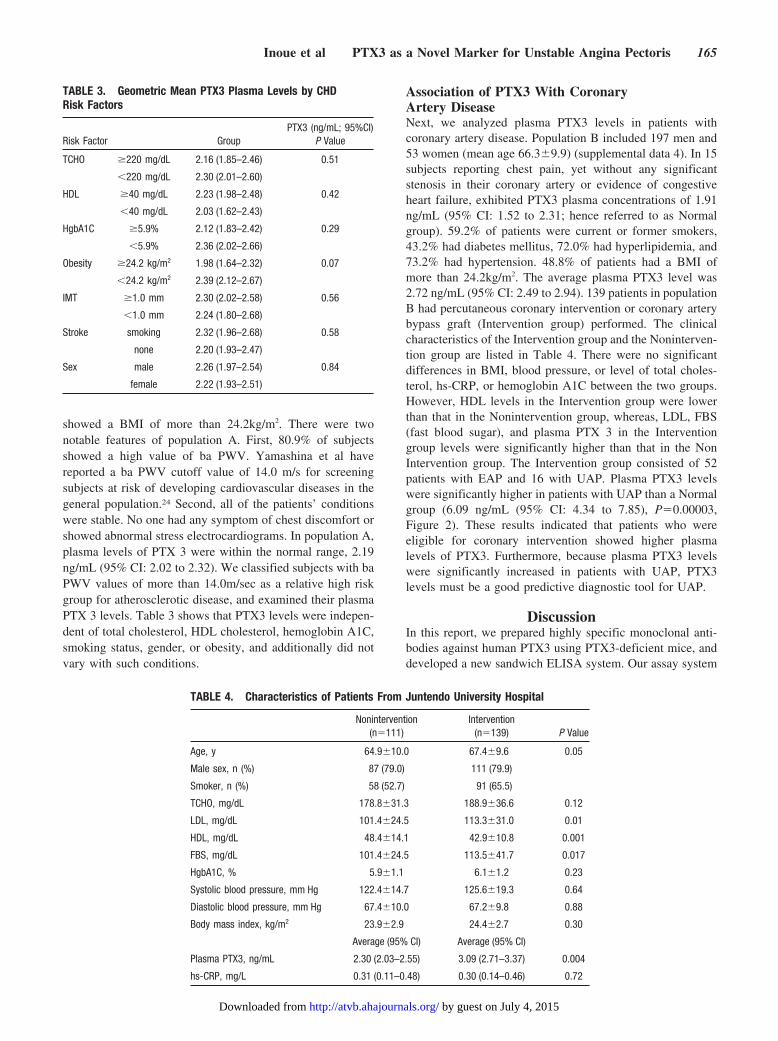
Association of PTX3 With CoronaryArtery DiseaseNext, we analyzed plasma PTX3 levels in patients withcoronary artery disease. Population B included 197 men and53 women (mean age 66.3�9.9) (supplemental data 4). In 15subjects reporting chest pain, yet without any significantstenosis in their coronary artery or evidence of congestiveheart failure, exhibited PTX3 plasma concentrations of 1.91ng/mL (95% CI: 1.52 to 2.31; hence referred to as Normalgroup). 59.2% of patients were current or former smokers,43.2% had diabetes mellitus, 72.0% had hyperlipidemia, and73.2% had hypertension. 48.8% of patients had a BMI ofmore than 24.2kg/m2. The average plasma PTX3 level was2.72 ng/mL (95% CI: 2.49 to 2.94). 139 patients in populationB had percutaneous coronary intervention or coronary arterybypass graft (Intervention group) performed. The clinicalcharacteristics of the Intervention group and the Noninterven-tion group are listed in Table 4. There were no significantdifferences in BMI, blood pressure, or level of total choles-terol, hs-CRP, or hemoglobin A1C between the two groups.However, HDL levels in the Intervention group were lowerthan that in the Nonintervention group, whereas, LDL, FBS(fast blood sugar), and plasma PTX 3 in the Interventiongroup levels were significantly higher than that in the NonIntervention group. The Intervention group consisted of 52patients with EAP and 16 with UAP. Plasma PTX3 levelswere significantly higher in patients with UAP than a Normalgroup (6.09 ng/mL (95% CI: 4.34 to 7.85), P�0.00003,Figure 2). These results indicated that patients who wereeligible for coronary intervention showed higher plasmalevels of PTX3. Furthermore, because plasma PTX3 levelswere significantly increased in patients with UAP, PTX3levels must be a good predictive diagnostic tool for UAP.
DiscussionIn this report, we prepared highly specific monoclonal anti-bodies against human PTX3 using PTX3-deficient mice, anddeveloped a new sandwich ELISA system. Our assay system
TABLE 3. Geometric Mean PTX3 Plasma Levels by CHDRisk Factors
Risk Factor GroupPTX3 (ng/mL; 95%CI)
P Value
TCHO �220 mg/dL 2.16 (1.85–2.46) 0.51
�220 mg/dL 2.30 (2.01–2.60)
HDL �40 mg/dL 2.23 (1.98–2.48) 0.42
�40 mg/dL 2.03 (1.62–2.43)
HgbA1C �5.9% 2.12 (1.83–2.42) 0.29
�5.9% 2.36 (2.02–2.66)
Obesity �24.2 kg/m2 1.98 (1.64–2.32) 0.07
�24.2 kg/m2 2.39 (2.12–2.67)
IMT �1.0 mm 2.30 (2.02–2.58) 0.56
�1.0 mm 2.24 (1.80–2.68)
Stroke smoking 2.32 (1.96–2.68) 0.58
none 2.20 (1.93–2.47)
Sex male 2.26 (1.97–2.54) 0.84
female 2.22 (1.93–2.51)
TABLE 4. Characteristics of Patients From Juntendo University Hospital
Nonintervention(n�111)
Intervention(n�139) P Value
Age, y 64.9�10.0 67.4�9.6 0.05
Male sex, n (%) 87 (79.0) 111 (79.9)
Smoker, n (%) 58 (52.7) 91 (65.5)
TCHO, mg/dL 178.8�31.3 188.9�36.6 0.12
LDL, mg/dL 101.4�24.5 113.3�31.0 0.01
HDL, mg/dL 48.4�14.1 42.9�10.8 0.001
FBS, mg/dL 101.4�24.5 113.5�41.7 0.017
HgbA1C, % 5.9�1.1 6.1�1.2 0.23
Systolic blood pressure, mm Hg 122.4�14.7 125.6�19.3 0.64
Diastolic blood pressure, mm Hg 67.4�10.0 67.2�9.8 0.88
Body mass index, kg/m2 23.9�2.9 24.4�2.7 0.30
Average (95% CI) Average (95% CI)
Plasma PTX3, ng/mL 2.30 (2.03–2.55) 3.09 (2.71–3.37) 0.004
hs-CRP, mg/L 0.31 (0.11–0.48) 0.30 (0.14–0.46) 0.72
Inoue et al PTX3 as a Novel Marker for Unstable Angina Pectoris 165
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from

can detect PTX3 from plasma at concentrations as low as 0.1ng/mL, whereas the lowest detectable concentration of com-mercially available kits is 0.25 ng/mL. Plasma PTX3 levels inhealthy volunteers showed around 1.98 ng/mL. Using thissystem, we measured plasma PTX3 level in two populationsof patients, described as population A and B. Plasma PTX3levels in population A were around 2.19 ng/mL, whereaslevels were around 3.04 ng/mL in patients who were eligiblefor coronary intervention. In patients with UAP, the level ofplasma PTX3 was further elevated, to more than three times(around 6.20 ng/mL) those of normal patients.
These results indicate that PTX3 may be a good predictivemarker for acute coronary syndrome (ACS). The incidenceand potential severity of an ACS makes timely diagnosis andappropriate treatment essential for minimizing morbidity andmortality. Every year in the United States, �2.5 millionpatients are admitted to a hospital with an ACS, two thirds ofwhom are eventually diagnosed with UAP or non–ST-elevation MI.24 Atherosclerotic lesions, composed primarilyof a lipid-rich core and a fibrous cap, develop in virtually allmajor arteries. Autopsy and intravascular ultrasound (IVUS)studies have confirmed the presence of coronary arterioscle-rosis lesions in the majority of asymptomatic individualsorder than 20 to 30 years of age.
Why some plaques rupture and others do not is not entirelyunderstood, although plaques that are prone to rupture sharecertain characteristics. The presence of large, eccentric lipidcores and a large percentage of inflammatory macrophagesare common findings in fissured or rupture plaques. The roleof inflammatory cells and mediators in the degradation andweakening of the protective fibrous cap has recently beenrecognized as a critical component in the pathogenesis ofACS. The majority of lesions rupture at the site of greatestmechanical stress, often the shoulder of lesions where thefibrous cap is adjacent to normal intima, which is also oftenthe site of greatest inflammatory activity.
To make a diagnosis of ACS, biochemical markers and theresting ECG are key components for the proper assessment ofa patient with a suspected ACS. The biochemical markers ofmyocardial necrosis, predominately CPK, as well as troponinT, are also essential in the diagnosis and prognosis of patientswith ACS. Because cardiac troponins are not detected in theblood of healthy individuals and are cardiac specific, they are
sensitive and specific for myocardial necrosis. But becauseUAP does not have any cardiac necrosis theoretically, neitherCPK nor troponin T levels are elevated. Furthermore somestudies have suggested that 5 to 10% of patients with chestpain and exhibiting a normal ECG will subsequently bediagnosed with unstable angina.25 Therefore, there exists aneed to establish an assay system to predict UAP.
PTX3 is an interesting molecule because it was suppressedby statin mostly in endothelial cells, as revealed by gene chipanalysis. And, although PTX 3 is in the same family withCRP, its expression pattern is more tissue specific, especiallyin light of the fact that it is expressed in cells of atheroscle-rotic lesions, like EC, smooth muscle cells, macrophages, andmost recently, in neutrophils. Additionally, in coronary arteryat sites distal from the plaque lesion, PTX3 levels weresignificantly elevated compared with proximal sites, suggest-ing that PTX3 originates from the atherosclerotic plaqueitself, and reflects active atherosclerosis. Therefore, PTX 3 isrecognized as the vascular CRP.
Despite the recent recommendations of the Center for DiseaseControl and the American Heart Association, critical review ofthe accumulating evidence now suggests that CRP is a relativelypoor predictor that does not contribute usefully in this regard.Because elevated CRP levels are intimately linked to conven-tional CHD risk factors, it would seemingly be less valuable toclinicians. In our study hs-CRP level did not increase in eitherthe EAP or the UAP group (UAP group: hs CRP, 0.48�0.79mg/L; EAP group: hs CRP, 0.41�1.07 mg/L; P�0.83).
Understanding of the inflammatory cascade allows theconsideration of a number of inflammatory markers aspotentially useful predictors of prevalent or incident coronaryartery disease (CAD). In 1998, the American Heart Associ-ation convened Prevention Conference V to discuss strategiesfor the measurement of markers of inflammation.26 Thisconference concluded that the most reliable marker to detectacute coronary syndrome must satisfy following criteria: (1)the ability to standardize the assay; (2) independence fromestablished risk factors; (3) association with CAD incidence;(4) the presence of population norms to guide interpretationof results; (5) ability to improve the overall prediction beyondthat of traditional risk factors.
Our analysis suggests that PTX3 represents an exceptionalbiomarker fitting all of these criteria. (1) The ability tostandardize the assay: To establish a high sensitivity ELISAsystem for PTX3, we used different mouse monoclonalantibodies against human PTX3 for capture and signal. Oursystem could measure plasma PTX3 more stably and pre-cisely, and in a manner more specific with less backgroundthan commercially available kits. (2) Independence fromestablished risk factors: Table 3 clearly shows that PTX3 is anindependent factor from established risk factors, unlike CRP.Even the cross-reactivity with CRP or SAP was less than0.7%. (3) Association with CAD incidence: Even in patientswith atherosclerotic lesions receiving treatment (so calledinactivated inflammatory status) like in population A, plasmaPTX3 levels were within normal ranges. But once coronaryarteries became eligible for coronary intervention (so called,activated inflammatory status), plasma PTX3 levels in-creased. These results suggested that this ELISA system
Figure 2. Plasma concentrations of PTX3 among Normal, EAP,and UAP patients. The concentrations of PTX3 expressed asmean�SD.
166 Arterioscler Thromb Vasc Biol. January 2007
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from

represents an ideal tool to predict ACS. (4) The presence ofpopulation norms to guide interpretation of results: From54-volunteer subjects, we determined a normal range ofPTX3 of around 1.98 ng/mL (95% CI: 1.68 to 2.28). (5)Ability to improve the overall prediction beyond that oftraditional risk factors: Currently, we are performing longterm follow-up studies of PTX3 levels in patients receivingtreatment, such as statin or aspirin, needed to fully appreciatethe overall predictive value of PTX3.
A potential limitation to the present study warrants con-sideration. We evaluated the predictable utility of PTX3 in apopulation of patients exclusively with UAP. But becausebecause of the fact that we collected 251 consecutive subjectswho had an indication for coronary angiography, only 16patients could be diagnosed with unstable angina. In general,unstable angina occurs in �6 of every 10 000 people.25
Larger studies are warranted in light of these results.In summary, we developed a highly sensitive ELISA
system for human PTX3 in plasma using monoclonal anti-bodies. Both intra- and interassay imprecision values wereless than 4.1% and 4.3%, respectively. The lower limit ofdetection of this ELISA was 0.1 ng/mL. The dilution curvesof plasma showed good linearity, and the recovery was97.2%. These attributes are far superior to those of acommercially available kit. We found that patients who wereeligible for coronary intervention exhibited high concentra-tions of plasma PTX3, especially in patients with UAP,exhibiting PTX3 levels three times higher than the normalrange. This ELISA system provides a unique tool to assistphysicians in predicting patients with UAP.
AcknowledgmentsThe authors thank Satoko Hamada, Megumi Chujo, Akiko Sawada,Hiroko Iwanari, Aya Sakamoto, and Keiko Katsumi fortechnical support.
Sources of FundingThis study was supported by the Program of Fundamental Studies inHealth Sciences of the NIBIO, NEDO, and by the Fund for Scienceand Technology from The Ministry of Education, Culture, Sports,Science and Technology in Japan.
DisclosuresNone.
References1. Lusis AJ. Atherosclerosis. Nature. 2000;407:233–241.2. Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive
protein and low-density lipoprotein cholesterol levels in the prediction of firstcardiovascular events. N Engl J Med. 2002;347:1557–1565.
3. Pepys MB, Baltz ML. Acute phase proteins with special reference toC-reactive protein and related proteins (pentraxins) and serum amyloid Aprotein. Adv Immunol. 1983;34:141–212.
4. Gewurz H, Zhang XH, Lint TF. Structure and function of the pentraxins.Curr Opin Immunol. 1995;7:54–64.
5. Steel DM, Whitehead AS. The major acute phase reactants: C-reactiveprotein, serum amyloid P component and serum amyloid A protein.Immunol Today. 1994;15:81–88.
6. Baumann H, Gauldie J. The acute phase response. Immunol Today.1994;15:74–80.
7. Breviario F, d’Aniello EM, Golay J, Peri G, Bottazzi B, Bairoch A, SacconeS, Marzella R, Predazzi V, Rocchi M. Interleukin-1-inducible genes inendothelial cells. Cloning of a new gene related to C-reactive protein andserum amyloid P component. J Biol Chem. 1992;267:22190–22197.
8. Lee GW, Lee TH, Vilcek J. TSG-14, a tumor necrosis factor- andIL-1-inducible protein, is a novel member of the pentaxin family of acutephase proteins. J Immunol. 1993;150:1804–1812.
9. Lee GW, Goodman AR, Lee TH, Vilcek J. Relationship of TSG-14protein to the pentraxin family of major acute phase proteins. J Immunol.1994;153:3700–3707.
10. Bottazzi B, Vouret-Craviari V, Bastone A, De Gioia L, Matteucci C, PeriG, Spreafico F, Pausa M, D’Ettorre C, Gianazza E, Tagliabue A, SalmonaM, Tedesco F, Introna M, Mantovani A. Multimer formation and ligandrecognition by the long pentraxin PTX3. Similarities and differences withthe short pentraxins C-reactive protein and serum amyloid P component.J Biol Chem. 1997;272:32817–32823.
11. Introna M, Alles VV, Castellano M, Picardi G, De Gioia L, Bottazzai B,Peri G, Breviario F, Salmona M, De Gregorio L, Dragani TA, SrinivasanN, Blundell TL, Hamilton TA, Mantovani A. Cloning of mouse ptx3, anew member of the pentraxin gene family expressed at extrahepatic sites.Blood. 1996;87:1862–1872.
12. Basile A, Sica A, d’Aniello E, Breviario F, Garrido G, Castellano M,Mantovani A, Introna M. Characterization of the promoter for the humanlong pentraxin PTX3. Role of NF-kappaB in tumor necrosis factor-alphaand interleukin-1beta regulation. J Biol Chem. 1997;272:8172–8178.
13. Peri G, Introna M, Corradi D, Iacuitti G, Signorini S, Avanzini F, PizzettiF, Maggioni AP, Moccetti T, Metra M, Cas LD, Ghezzi P, Sipe JD, ReG, Olivetti G, Mantovani A, Latini R. PTX3, A prototypical long pen-traxin, is an early indicator of acute myocardial infarction in humans.Circulation. 2000;102:636–641.
14. Morikawa S, Takabe W, Mataki C, Kanke T, Itoh T, Wada Y, Izumi A,Saito Y, Hamakubo T, Kodama T. The effect of statins on mRNA levelsof genes related to inflammation, coagulation, and vascular constriction inHUVEC. Human umbilical vein endothelial cells. J Atheroscler Thromb.2002;9:178–183.
15. Garlanda C, Hirsch E, Bozza S, Salustri A, De Acetis M, Nota R,Maccagno A, Riva F, Bottazzi B, Peri G, Doni A, Vago L, Botto M, DeSantis R, Carminati P, Siracusa G, Altruda F, Vecchi A, Romani L,Mantovani A. Non-redundant role of the long pentraxin PTX3 in anti-fungal innate immune response. Nature. 2002;420:182–186.
16. Kohler G, Milstein C. Continuous cultures of fused cells secretingantibody of predefined specificity. Nature. 1975;256:495–497.
17. Parham P. On the fragmentation of monoclonal IgG1, IgG2a, and IgG2bfrom BALB/c mice. J Immunol. 1983;131:2895–2902.
18. Yamashina A, Tomiyama H, Takeda K, Tsuda H, Arai T, Hirose K, KojiY, Hori S, Yamamoto Y. Validity, reproducibility, and clinical signif-icance of noninvasive brachial-ankle pulse wave velocity measurement.Hypertens Res. 2002;25:359–364.
19. Tomiyama H, Yamashina A, Arai T, Hirose K, Koji Y, Chikamori T, HoriS, Yamamoto Y, Doba N, Hinohara S. Influences of age and gender onresults of noninvasive brachial-ankle pulse wave velocity measurement–asurvey of 12517 subjects. Atherosclerosis. 2003;166:303–309.
20. Bond M, Barnes R, Riley WA, Wilmoth SK, Chambless LE, Howard G,Owens B. High-resolution B-mode ultrasound scanning methods in theAtherosclerosis Risk in Communities Study (ARIC). The ARIC StudyGroup. J Neuroimaging. 1991;1:68–73.
21. Norman P, Spencer CA, Lawrence-Brown MM, Jamrozik B. C-ReactiveProtein Levels and the Expansion of Screen-Detected Abdominal AorticAneurysms in Men. Circulation. 2004;110:862–866.
22. Fazzini F, Peri G, Doni A, Dell’Antonio G, Dal Cin E, Bozzolo E,D’Auria F, Praderio L, Ciboddo G, Sabbadini MG, Manfredi AA, Man-tovani A, Querini PR. PTX3 in small-vessel vasculitides: an independentindicator of disease activity produced at sites of inflammation. ArthritisRheum. 2001;44:2841–2850.
23. Grundy SM, Hansen B, Smith SC Jr, Cleeman JI, Kahn RA. Clinicalmanagement of metabolic syndrome: report of the Am Heart Association/National Heart, Lung, and Blood Institute/Am Diabetes Association con-ference on scientific issues related to management. Arterioscler ThrombVasc Biol. 2004;24:e19–e24.
24. Yamashina A, Tomiyama H, Arai T, Hirose K, Koji Y, Hirayama Y,Yamamoto Y, Hori S. Brachial-ankle pulse wave velocity as a marker ofatherosclerotic vascular damage and cardiovascular risk. Hypertens Res.2003;26:615–622.
25. Braunwald E. Heart Disease, a Text Book of Cardiovascular Medicine(fourth edition). Elseveir; Philadelphia, Pa; 2004: 1243–1273.
26. Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO 3rd,Criqui M, Fadl YY, Fortmann SP, Hong Y, Myers GL, Rifai N, Smith SCJr, Taubert K, Tracy RP, Vinicor F. Markers of inflammation and car-diovascular disease: application to clinical and public health practice: Astatement for healthcare professionals from the Centers for DiseaseControl and Prevention and the Am Heart Association. Circulation.2003;107:499–511.
Inoue et al PTX3 as a Novel Marker for Unstable Angina Pectoris 167
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from

Supplemental Data 1. Relation of immunized mice and antibody epitopes
Animals Antigen Antibodies Clone Epitope
Balb/C mice rPTX3-His (E.coli) Monoclonal 2 N-terminal(2)
Balb/C mice rPTX3-His (CHO) Monoclonal 20 N-terminal(4), C-terminal(16)
MRL/lpr mice rPTX3-His (CHO) Monoclonal 9 N-terminal(2), C-terminal(7)
PTX3-KO mice rPTX3-His (CHO) Monoclonal 10 N-terminal(7), C-terminal(3)*
N-terminal(10), C-terminal(6)**PTX3-KO mice rPTX3 (CHO) Monoclonal 16
* PPMX0104 is included ** PPMX0105 is included

Supplemental Data 2
1.8%0.01 0.660.640.670.6664.0%0.03 0.870.870.910.8452.2%0.02 0.950.930.970.9444.3%0.42 9.709.3810.179.5433.1%0.22 7.217.137.467.0424.1%0.66 15.9515.7616.6815.411
3rd2nd1st CV SDMean
(ng/mL)Experiments
Sample No.
Table S2. Inter assay of our PTX3 system
2.9%0.02 0.670.680.660.690.660.6464.1%0.03 0.850.870.830.890.820.8151.6%0.02 0.950.970.940.940.940.9343.0%0.30 9.709.799.769.189.919.8531.3%0.10 7.177.137.147.307.057.2220.8%0.13 15.9115.8415.7615.9816.1015.881
CV SDMean(ng/mL)Well 5Well 4Well 3Well 2Well 1Sample No.
Table S1. Intra assay of our PTX3 system

Supplemental Data 3
0
2
4
6
8
10
12
14
16
18
0 0.2 0.4 0.6 0.8 1 1.2
Dilution
PTX
3 (n
g/m
L)
H2M2P3P2P1

Supplemental Data 4.Characteristics of Patients from University of Juntendo Hospital
Characteristic (N=250)Age-yr 66.3 ± 9.9Male sex -no. (%) 197 (78.8)Smoker- no. (%) 148 (59.2)Diabetes -no.(%) 108 (43.2)Hypercholesterolemia -no.(%) 180 (72.0)Hypertension -no.(%) 183 (73.2)Systolic blood pressure-mmHg 125.1 ± 17.7Diastolic blood pressure-mmHg 67.4 ± 10.0Body Mass Index (≧24.2kg/m2) 122 (48.8)
Ave. (95%CI)Plasma PTX3 (ng/mL) 2.72 (2.49-2.94)hs CRP (mg/L) 0.32 (0.09-0.56)

Mantovani, Takao Hamakubo, Hiroyuki Daida and Tatsuhiko KodamaSagara, Kyoko Miyamoto, Hirokazu Satoh, Isao Kohno, Takeshi Kurata, Hiroshi Ota, Alberto Kenji Inoue, Akira Sugiyama, Patrick C. Reid, Yukio Ito, Katsumi Miyauchi, Sei Mukai, Mina
Unstable Angina PectorisEstablishment of a High Sensitivity Plasma Assay for Human Pentraxin3 as a Marker for
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2006 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.0000252126.48375.d52006;
2007;27:161-167; originally published online November 9,Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/27/1/161World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2006/11/08/01.ATV.0000252126.48375.d5.DC1.htmlData Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 4, 2015http://atvb.ahajournals.org/Downloaded from
Copyright © 2022 FDOKUMEN




















