Essential Revision Notes For MRCP IN Neurology - 1 File ...
129
Essential Revision Notes For MRCP IN Neurology Gehad gamal, MRCP (UK), MD in cardiology Ambassador of European association of cardiovascular imaging in Egypt Registered in Irish Medical Council (IMC)
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Essential Revision Notes For MRCP IN Neurology - 1 File ...

Essential
Revision Notes For MRCP
IN
Neurology
Gehad gamal, MRCP (UK), MD in cardiology
Ambassador of European association of cardiovascular imaging in Egypt
Registered in Irish Medical Council (IMC)


Frontal lobes lesions
• Expressive /Broca's/ non fleunt aphasia: For example, a
person may say something like, "Drive, store. Mom."
meaning to say, "My mom drove me to the store today
• Disinhibition
• Perserveration (frequent actions)
• Primitive reflexs
• Anosmia
• Inability to generate a list

Parietal lobe lesions• Sensory inattention
• Apraxia : the individual has difficulty with the motor planning to perform tasks or movements when asked, provided that the request or command is understood and he/she is willing to perform the task
• Astereognosis (tactile/somatosensory agnosia) , it is connected to tactile sense—that is, touch. Patient finds it difficult to recognize objects by touch based on its texture, size and weight.
• Inferior homonymous quadrantanopia
• Gerstmann's syndrome (lesion of dominant parietal): alexia, acalculia, finger agnosia and right-left disorientation

Temporal lobe lesion• Wernicke's aphasia (Receptive aphasia, fluent aphasia,
or sensory aphasia) , is a type of aphasia in which an individual is unable to understand language in its spoken form. Even though they can speak using grammar, syntax, rate, and intonation, they typically have difficulty expressing themselves meaningfully through speech.
• Superior homonymous quadrantanopia
• Auditory agnosia: there is difficulty distinguishing environmental and non-verbal auditory cues including difficulty distinguishing speech from non-speech sounds even though hearing is usually normal. (EXAMINER: What did you eat for breakfast?...... PATIENT: Breakfast, breakfast, it sounds familiar but it doesn't speak to me )

Occipital lobe lesions
• Homonymous hemianopia
• Cortical blindness
• Visual agnosia


Neurological
examination

INSPECTION MOTOR POWER
SENSATION CEREBELLAR
A home visit is requested by the husband of a 71-year-old woman who is 'off her legs'.
On arriving the patient states that since mid-morning her left arm has felt weak and a degree of facial asymmetry is noted when she smiles.
She is normally fit and well other than a past history of hypertension for which she takes ramipril.
What is the most appropriate action?
• A. Arrange same-day medical admission
• B. Dial 999 for emergency admission
• C. Arrange review at rapid access TIA clinic
• D. Arrange review at rapid access TIA clinic + give aspirin 300 mg
• E. Dial 999 for emergency admission + give aspirin 300 mg

• B. Dial 999 for emergency admission
• This lady is most likely having a stroke, nowadays rightly
recognised as a medical emergency. Aspirin should only
be given once a haemorrhagic stroke has been excluded
• A patient with atrial fibrillation, hypertension and hypercholesterolemia presents with sudden-onset right-sided weakness, hemianopia and aphasia.
• This occurred an hour previously while he was eating his breakfast.
• He is taking aspirin, simvastatin, ramipril and digoxin.
• What action would you recommend?
• CT within the next 4 hours, and transfer to an acute stroke unit
• Immediate CT with a view to iv thrombolysis
• Immediate oral aspirin, then CT as soon as possible
• Immediate CT with a view to heparinisation
• Admission to a stroke unit, with CT in the next 24 hours

• B
• • Therapeutic nihilism is no longer acceptable for stroke
• • Intravenous thrombolysis (0.9 mg/kg iv rtPA (recombinant tissue plasminogen activator) over 1 hour) is now licensed in the UK for acute ischaemic stroke within 4.5 hours
• • Unfortunately, only a subset of patients presents within the time window
• • Both evidence from randomised trials and a Cochrane meta-analysis support this treatment
• • Acute stroke units are similarly supported by randomised trials, and thrombolysis should occur in this setting, but answers A (CT within the next 4 hours, and transfer to an acute stroke unit) and E (Admission to a stroke unit, with CT in the next 24 hours) are not the immediate concerns
• • Aspirin should be administered only after CT, and should be avoided for 24 hours if the patient is thrombolysed
• • Heparin has never been shown in randomised trials to benefit ischaemic stroke, or any ischaemic stroke subtype, in any setting

Stroke: management
NICE also issued stroke guidelines in 2008, although they modified
their guidance with respect to antiplatelet therapy in 2010.
blood glucose, hydration, oxygen saturation and temperature
should be maintained within normal limits
blood pressure should not be lowered in the acute phase unless
there are complications e.g. Hypertensive encephalopathy
aspirin 300mg orally or rectally should be given as soon as
possible if a haemorrhagic stroke has been excluded
with regards to atrial fibrillation, the RCP state: 'anticoagulants
should not be started until brain imaging has excluded haemorrhage
if the cholesterol is > 3.5 mmol/l , start statin

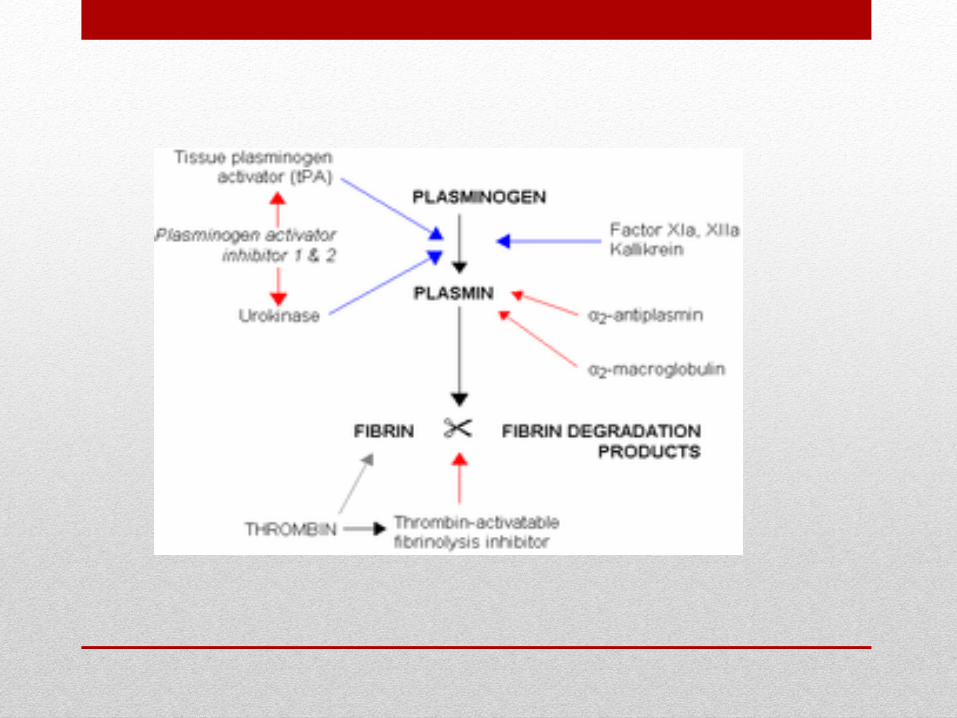
Thrombolysis should only be given if:
It is administered within 4.5 hours of onset of stroke symptoms
• haemorrhage has been definitively excluded (i.e. Imaging has
been performed)
• Alteplase (TPA) is currently recommended by NICE.
Absolute CI
• - Previous intracranial haemorrhage
• - Seizure at onset of stroke
• - Intracranial neoplasm
• - Suspected subarachnoid haemorrhage
• - Stroke or traumatic brain injury in preceding 3 months
• - Lumbar puncture in preceding 7 days
• - Gastrointestinal haemorrhage in preceding 3 weeks
• - Active bleeding
• - Pregnancy
• - Oesophageal varices
• - Uncontrolled hypertension >200/120mmHg

Relative CI
• - Concurrent anticoagulation (INR >1.7)
• - Haemorrhagic diathesis
• - Active diabetic haemorrhagic retinopathy
• - Suspected intracardiac thrombus
• - Major surgery / trauma in preceding 2 weeks
Ischemic Stroke Treatment
TPA, the Gold Standard,
tPA works by dissolving the clot and improving blood flow to the part of the brain being deprived of blood flow. If administered within 3 hours(and up to 4.5 hours in certain eligible patients), tPAmay improve the chances of recovering from a stroke.
Endovascular Procedures
• Another treatment option is an endovascular procedure called mechanical thrombectomy, strongly recommended.
• To remove the brain clot, doctors thread a catheter through an artery in the groin up to the blocked artery in the brain. The stent opens and grabs the clot, allowing doctors to remove the stent with the trapped clot. Special suction tubes may also be used. The procedure should be done within six hours of acute stroke symptoms, and only after a patient receives tPA.

Hemorrhagic Stroke Treatment
Endovascular Procedures
• These procedures are less invasive than surgical treatments, and involve the use of a catheter introduced through a major artery in the leg or arm, then guided to the aneurysm or AVM; it then deposits a mechanical agent, such as a coil, to prevent rupture.
Surgical Treatment
• For strokes caused by a bleed within the brain (hemorrhagic stroke), or by an abnormal tangle of blood vessels (AVM), surgical treatment may be done to stop the bleeding. If the bleed is caused by a ruptured aneurysm (swelling of the vessel that breaks), a metal clip may be placed surgically at the base of the aneurysm to secure it.

Secondary prevention
• NICE also published a technology appraisal in 2010 on the use
of clopidogrel and dipyridamole
• clopidogrel is now recommended by NICE ahead of
combination use of aspirin plus modified release (MR)
dipyridamole in people who have had an ischaemic stroke
• aspirin plus MR dipyridamole is now recommended after an
ischaemic stroke only if clopidogrel is contraindicated or not
tolerated, but treatment is no longer limited to 2 years' duration
• MR dipyridamole alone is recommended after an ischaemic
stroke only if aspirin or clopidogrel are contraindicated or not
tolerated, again with no limit on duration of treatment

With regards to carotid artery endarterectomy:
recommend if patient has suffered stroke or TIA in the
carotid territory and are not severely disabled
should only be considered if carotid stenosis 70- 99%
according ECST (European Carotid Surgery Trial lists)
criteria
or
> 50% according to NASCET (North American Symptomatic Carotid
Endarterectomy Trial)
A 71-year-old man is reviewed following an ischaemic
stroke. He is known to be intolerant of clopidogrel. What is
the most appropriate therapy to help reduce his chance
of having a further stroke?
• A. Aspirin + dipyridamole, Stop dipyridamole after 2
years
• B. Dipyridamole, Stop dipyridamole after 2 years
• C. Aspirin lifelong
• D. Warfarin
• E. Aspirin + dipyridamole lifelong

• E. Aspirin + dipyridamole lifelong
• Stroke management according NICE stroke guidelines in
2008, although they modified their guidance with respect
to antiplatelet therapy in 2010.

A 59-year-old man with no significant past medical history is admitted to hospital following an ischaemic stroke. He presented outside of the thrombolysis window and is treated with aspirin for the first few days. His blood pressure is 130/80 mmHg, fasting glucose is 5.6 mmol/l and fasting cholesterol is 3.9 mmol/l. He makes a good recovery and has regained nearly all of his previous functions upon discharge. Following recent NICE guidelines, which of the following medications should he be taking upon discharge (i.e. after 14 days)?
• A. Aspirin + statin
• B. Aspirin + dipyridamole + statin + ramipril
• C. Clopidogrel + statin
• D. Aspirin + dipyridamole
• E. Aspirin + dipyridamole + statin
• Clopidogrel + statin
• If the cholesterol is > 3.5 mmol/l (135 md/dl )patients
should be commenced on a statin.
• Many physicians will delay treatment until after at least
48 hours due to the risk of haemorrhagic transformation
• Clopidogrel is now recommended by NICE ahead of
combination use of aspirin plus modified release (MR)
dipyridamole in people who have had an ischaemic stroke

A 19-year-old presents as she would like to start a combined
oral contraceptive pill. During the history she states that in
the past she has had migraine with aura. She asks why the
combined oral contraceptive pill is contraindicated. What is
the most appropriate response?
• A. Theoretical risk of ischaemic stroke
• B. Significantly increased risk of ischaemic stroke
• C. Increased frequency of migraines
• D. Migraine is an independent risk factor for venous
thromboembolism
• E. Increased severity of migraines

• B. Significantly increased risk of ischaemic stroke

• Migraine during pregnancy paracetamol 1g is first-line aspirin 300mg or ibuprofen 400mg can be used second-line in the first and second trimester
• Migraine and the combined oral contraceptive (OCP) pill if patients have migraine with aura then the COC is absolutely contraindicated due to an increased risk of stroke (relative risk 8.72)
• Migraine and menstruation many women find that the frequency and severity of migraines increase around the time of menstruation SIGN recommends that women are treated with mefanamic acid or a combination of aspirin, paracetamol and caffeine. Triptans are also recommended in the acute situation
• Migraine and hormone replacement therapy (HRT) safe to prescribe HRT for patients with a history of migraine but it may make migraines worse

• A 69-year-old patient with no previous medical history has been diagnosed with a right-sided lacunar stroke.
• You are now seeing him in the follow-up clinic at 6 weeks, and his hemiplegia is improving. His total cholesterol is 5.5 mmol/l and his blood pressure is 136/78 mmHg.
• He is in sinus rhythm. His blood glucose level is normal.
• He is treated with perindopril for hypertension and aspirin (which he had already been taking prior to the recent stroke)
• What secondary preventive regime should he be taking, on the basis of current randomised evidence?
• Aspirin, statin and diuretic
• Aspirin and statin
• Aspirin and beta blocker
• Clopidogrel and statin
• Aspirin

• D- clopidogril and statin
• • Trials have demonstrated the value of blood pressure
lowering, modification of blood fats and adequate
antiplatelet therapy in secondary prevention of stroke
• • Statins should be started independently of cholesterol
levels as they appear protective even when cholesterol
levels approach the average
• • Dual anti-platelet therapy with aspirin and dipyridamole
therapy for secondary stroke prevention was the treatment
of choice on the basis of the ESPS-2 trial, but this has
now been superceded by NICE guidance which
recommends clopidogrel

A 65-year-old woman presents with new, ongoing speech
disturbance. She is worried that she may have had a stroke.
Which one of the following scoring systems is it most
appropriate to use to evaluate whether she has had a
stroke?
• A. CHADS2 score
• B. ABCD2 score
• C. RCP-RSE score
• D. ROSIER score
• E. CHADS2-VASC score

• D. ROSIER score
• Stroke: assessment Whilst the diagnosis of stroke may
sometimes be obvious in many cases the presenting
symptoms may be vague and accurate assessment
difficult.
• The FAST screening tool (Face/Arms/Speech/Time) is
widely known by the general public following a publicity
campaign. It has a positive predictive value of 78%.
• A variant of FAST called the ROSIER score is useful for
medical professionals. It is validated tool recommended
by the Royal College of Physicians.

ROSIER score

Exclude hypoglycemia first, then assess the following:
• Loss of consciousness or syncope - 1 point
• Seizure activity - 1 point
New, acute onset of:
- asymmetric facial weakness + 1 point
- asymmetric arm weakness + 1 point
- asymmetric leg weakness + 1 point
- speech disturbance +1 point
- visual field defect + 1 point

A stroke is likely if score > 0

Which one of the following statements regarding the
ROSIER score is correct?
• A. It includes assessing the patients visual fields
• B. A total score of 2 makes a diagnosis of stroke unlikely
• C. Patients with a score > 4 are candidates for
thrombolysis
• D. A history of seizure activity adds + 1 points to the
score
• E. It can only be used for symptoms that have resolved
• A. It includes assessing the patients visual fields

A 72-year-old woman with a past history of treated hypertension presents for review. Yesterday she had a 2 hour episode where she couldn't find the right word when speaking. This has never happened before and there were no associated features. Neurological examination is unremarkable and blood pressure was 150/100 mmHg. Her only current medication is amlodipine. What is the most appropriate management?
• A. Aspirin 300mg immediately + specialist review within 2 weeks
• B. Specialist review within 2 weeks
• C. Aspirin 300mg immediately + specialist review within 24 hours
• D. Aspirin 75mg + outpatient CT brain
• E. Specialist review within 24 hours

• C. Aspirin 300mg immediately + specialist review within 24 hours
• This patient has had a transient ischaemic attack (TIA). Her age, blood pressure and duration of symptoms put her in a higher risk category.
• Current guidelines advocate specialist review within 24 hours.
• If a patient's symptoms have not fully resolved then aspirin should be withheld until an haemohorragic stroke has been excluded.
• As this is a transient ischaemic attack (symptoms last less than 24 hours) aspirin should be given as soon as possible.
Transient ischaemic attack
TIA
• NICE issued updated guidelines relating to stroke and transient ischaemic attack (TIA) in 2008.
• They advocated the use of the ABCD2 prognostic score for risk stratifying patients who've had a suspected TIA
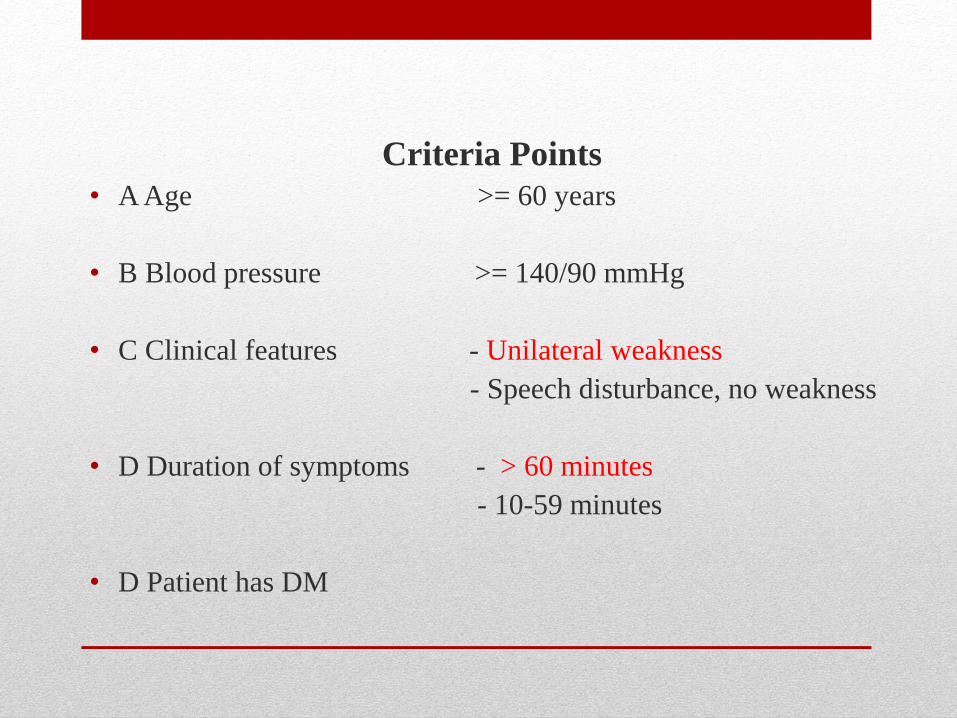
Criteria Points
• A Age >= 60 years
• B Blood pressure >= 140/90 mmHg
• C Clinical features - Unilateral weakness
- Speech disturbance, no weakness
• D Duration of symptoms - > 60 minutes
- 10-59 minutes
• D Patient has DM
People who have had a suspected TIA who are at a higher risk
of stroke (that is, with an ABCD2 score of 4 or above) should
have:
• aspirin (300 mg daily) started immediately specialist
assessment and investigation within 24 hours of onset of
symptoms measures for secondary prevention introduced as
soon as the diagnosis is confirmed, including discussion of
individual risk factors
If the ABCD2 risk score is 3 or below:
• specialist assessment within 1 week of symptom onset,
including decision on brain imaging if vascular territory or
pathology is uncertain, refer for brain imaging
People with crescendo TIAs ???
• People with crescendo TIAs (two or more episodes in a
week) should be treated as being at high risk of stroke,
even though they may have an ABCD2 score of 3 or
below

Antithrombotic therapy
• clopidogrel is recommended first-line (as for patients
who've had a stroke)
• aspirin + dipyridamole should be given to patients who
cannot tolerate clopidogrel
• These recommendations follow the 2012 Royal
College of Physicians National clinical guidelines may
change following the CHANCE study (NEJM 2013),
giving high-risk TIA patients aspirin + clopidogrel for the
first 90 days compared to aspirin alone. 11.7% of aspirin
only patients had a stroke over 90 days compared to 8.2%
of dual antiplatelet patients

With regards to carotid artery endarterectomy:
• recommend if patient has suffered stroke or TIA in the
carotid territory and are not severely disabled , should
only be considered if carotid stenosis > 50%

A 56-year-old man presents to the ER after developing trouble talking after waking up this morning. The symptoms are consistent with expressive dysphasia and lasted about 90 minutes before resolving completely. Neurological examination is unremarkable. A diagnosis of transient ischaemic attack (TIA) is made. His past medical history includes ischaemic heart disease for which he is prescribed aspirin, simvastatin and atenolol. Which one of the following factors is most associated with an increased risk of going on to have a stroke?
• A. History of ischaemic heart disease
• B. History of aspirin use
• C. Duration of this TIA
• D. Expressive dysphasia during this TIA
• E. His age
• C. Duration of this TIA
• This TIA lasted greater than 60 minutes which scores 2 as
part of the ABCD2 prognostic scoring system.
• It is therefore the most significant factor which would
increase his risk of going on to have a stroke.

• A 73-year-old man presents to his GP complaining of a headache and blurring of vision in his right eye lasting for 5 minutes.
• Two days later he developed sudden-onset, left-sided weakness affecting both upper and lower limbs and lasting for 30 minutes. His past medical history includes mild hypertension. He is a non-smoker.
• There are no neurological abnormalities. His blood pressure is 160/90 mmHg, heart rate 88 bpm. There are no audible carotid bruits.
• Which one of the following is the most likely diagnosis?
• Migraine equivalent
• Transient ischaemic attack secondary to carotid artery disease
• Transient ischaemic attack secondary to cardioembolism
• Transient ischaemic attack secondary to small-vessel disease
• Transient ischaemic attack secondary to giant-cell arteritis

• B- Transient ischaemic attack secondary to carotid artery disease
• The patient with headache, visual disturbance and weakness
• • The transient monocular visual disturbance is consistent with the description of amaurosis fugax
• • Characteristically, patients describe a 'curtain coming down' over their vision, but are just as likely to describe blurring or greying
• • Any suggestion that this disturbance is altitudinal (ie has a horizontal cut-off) enhances the possibility that this is a vascular disturbance of the retinal vessels
• • The subsequent left-sided weakness is suggestive of aright cerebral hemisphere transient ischaemic attack
• • The combination of these two strongly points towards a right internal carotid artery stenosis as the source of platelet emboli, although other sources of emboli should be considered
• • However, cardioembolism is unlikely in the absence of either atrial fibrillation or previous cardiac symptoms (of either cardiac ischaemia or cardiac failure)
• • Transient occlusion of a small penetrating vessel could cause the hemiparesis, but not the amaurosis fugax
• • Giant-cell arteritis should always be considered in patients over 60 years of age, but there are no specific features to support the diagnosis, although it is always worthwhile checking the ESR
• • Migraine equivalents (aura-like symptoms without headache) can provide diagnostic difficulties
A 60-year-old man is referred to the rapid access TIA clinic
after experiencing a number of transient episodes of right-
sided weakness. Which one of the following factors is not
part of ABCD2 score used to estimate his risk of future
stroke?
• A. Clinical features
• B. History of diabetes mellitus
• C. Blood pressure
• D. History of aspirin use
• E. Duration of symptoms

• D. History of aspirin use
• NICE issued updated guidelines relating to stroke and
transient ischaemic attack (TIA) in 2008. They advocated
the use of the ABCD2 prognostic score for risk stratifying
patients who've had a suspected TIA:

A 63-year-old female is reviewed in the rapid access transient ischaemic attack clinic. For the past three weeks she has been having episodes of transient loss of vision in the right eye. Carotid ultrasound reveals a 48% stenosis of her right carotid artery and an ECG shows sinus rhythm. She was started on aspirin 300mg od by her own GP after the first episode. What is the most appropriate management of this patient?
• A. Warfarin
• B. Clopidogrel
• C. Carotid endarterectomy
• D. Aspirin
• E. Aspirin and dipyridamole

B- Clopidogril
Antiplatelets
• TIA: clopidogrel
• ischaemic stroke: clopidogrel
• Clopidogrel is recommended first-line (as for patients who've had a stroke)
• aspirin + dipyridamole should be given to patients who cannot tolerate clopidogrel
With regards to carotid artery endarterectomy:
- recommend if patient has suffered stroke or TIA in the carotid territory and are not severely disabled
- should only be considered if carotid stenosis > 50%



• A 51-year-old man underwent aortic valve replacement, which was uncomplicated. Despite his history of alcohol abuse, he was anticoagulated with warfarin.
• After discharge it was noted that he had missed clinic appointments.
• Some 4 months later he was admitted to the Emergency Department with a dense right hemiparesis and moderately severe global dysphasia, unkempt and smelling of alcohol. His INR was 1.4.
• There was a soft diastolic murmur at the left sternal edge and during his admission he developed a fever of 37.9 C.
• Which one of the following is the most likely diagnosis?
• Left-sided intracerebral haemorrhage
• Thromboembolic stroke secondary to bacterial endocarditis
• Left-sided subdural haematoma
• Left, middle cerebral territory, infarction secondary to cardioembolism
• Left hemisphere lacunar stroke
• D- Left, middle cerebral territory, infarction secondary to cardioembolism
• The patient with hemiparesis and moderately severe global aphasia
• The history suggests a large lesion in the left, middle cerebral artery territory involving the cortex
• This rules out the possibility of a lacunar stroke, which is always subcortical
• This may have been the result of a cerebral haemorrhage as he is on warfarin (although at subtherapeutic doses)
• There is no suggestion of head trauma (although this does not exclude it)
• His symptoms are more likely to be the result of cerebral infarction caused by cardiac embolism from the aortic valve
• Bacterial endocarditis needs to be excluded, but fever after stroke is more commonly the result of pneumonia or urinary tract infection which can easily be screened for

• A 57-year-old man presents to the Emergency Department complaining of a clumsy right hand and difficulty speaking.
• His symptoms came on that morning, and were still present 8 hours later. His past medical history includes hypertension and migraines as a young man. He smokes 10 cigarettes per day.
• On examination he was found to have some weakness of the intrinsic hand muscles on his right only.
• Visual fields, speech and sensation were normal. Blood pressure was 180/100 mmHg.
• Which one of the following is the most likely diagnosis?
• Migraine equivalent
• Left pontine microhaemorrhage
• Neck-tongue syndrome
• Left, middle cerebral artery territory, cardioembolic stroke
• Left hemisphere lacunar stroke


• E- Lacunar infarction
• The patient with a clumsy hand and difficulty speaking
• Lacunar infarcts are small deep infarcts with a maximum diameter of 1.5 cm and a volume of 0.2-3.4 cm3
• Lacunar infarcts mainly occur in the basal ganglia, lenticular nucleus and especially the putamin, thalamus and white matter of the internal capsule, pons and centrum semiovale
• • The five classic lacunar syndromes are: pure motor hemiparesis, pure sensory stroke, sensorimotor stroke, ataxic hemiparesis and clumsy-hand dysarthria
• • However in the modern imaging era many more syndromes have been described
• • The history given here is compatible with the dysarthria-clumsy hand syndrome, one of the classic lacunar syndromes, ie subcortical stroke secondary to small-vessel disease
• • The usual site of damage in the dysarthria-clumsy hand syndrome is in the internal capsule or pons
• • However, infarction is more common than a small haemorrhage
• • Both are caused by disease of small perforating arterioles
• • Risk factors include smoking, hypercholesterolemia and hypertension
• • Migraine equivalents (aura-like symptoms without headache) can provide diagnostic difficulties and should always be considered in those with a previous history of migraine, but there is no suggestion of the characteristic slow spread of symptoms in this patient
• • The neck-tongue syndrome consists of pain and paraesthesias in one half of the tongue precipitated by neck movement

• A 69-year-old woman presents with a sudden onset of weakness of her right arm and leg. She is known to be hypertensive.
• There has been no headache, loss of consciousness, visual, speech or sensory symptoms.
• On examination, her blood pressure is 180/90 mmHg, pulse 100 and regular. Heart sounds are normal. There is no carotid bruit. Higher mental function tests are normal. There is no apraxia or neglect. Speech, swallowing and sensation are all normal. There is no visual field defect. There is a mild facial weakness sparing the forehead. The right arm and leg are flaccid and weak. Reflexes and tone are normal. There is a right extensor plantar response.
• What is the most likely cause of this patients symptoms?
• Cardioembolic stroke
• Lacunar stroke
• Right internal carotid artery atheroembolic stroke
• Right internal carotid artery dissection
• Right vertebral artery atheroembolic stroke

• Lacunar infarction
• The patient with sudden onset of weakness of the right arm andleg
• • A sudden onset of focal symptoms and signs strongly suggests stroke
• • The presence of right-sided weakness involving the face, arm and leg, in the absence of sensory loss, language disturbance, hemineglect or visual field defect favours a small deep (lacunar) infarct affecting the corticospinal tract at the level of either the internal capsule or the upper pons
• • The sparing of the forehead, indicating upper motor-neurone facial weakness, favours the former diagnosis
• • The term 'lacune' refers to a small deep infarct resulting from occlusion of a penetrating branch
• • Infarcts occur predominantly in the basal ganglia, internal capsule, thalamus and pons
• • Hypertension and diabetes are the main risk factors
• • Common lacunar strokes include a pure motor hemiparesis, pure hemisensory loss, ataxic hemiparesis and
• dysarthria clumsy-hand syndrome





• A 36-year-old man presents with a 1-day history of left-sided neck pain and right-sided sensorimotor disturbance.
• Shortly after the neck pain had begun, he had noted that his left eyelid was 'drooping', and that he had developed weakness and altered sensation in his right arm and leg.
• He had recently visited a chiropractor for neck pain after a road traffic collision. Examination reveals a left Horner syndrome and weakness and sensory disturbance on the right-hand side with an extensor right plantar.
• What is the most likely clinical diagnosis?
• Carotid artery dissection
• Lateral medullary infarction
• Posterior fossa space-occupying lesion
• Subarachnoid haemorrhage
• Venous sinus thrombosis

• A- The patient with Horner syndrome, weakness andsensory disturbance following a visit to the chiropractor, (CAROTID ARTERY DISSECTION )
• • The constellation of symptoms and signs is best explained by a left carotid artery dissection causing left hemispheric ischaemia, and subsequent right-sided signs
• • Carotid and vertebral artery dissection are reported after chiropractic manipulation and episodes of neck trauma, but are often spontaneous
• • The association of pain in the neck with an ischaemic stroke syndrome should always raise dissection as a possibility
• • Carotid dissection commonly causes Horner syndrome because of the intimate association of sympathetic nerve fibres and the carotid artery
• • There are no posterior circulation symptoms or signs to support a diagnosis of lateral medullary infarction, though this does cause Horner syndrome
• • A posterior fossa lesion would present with progressive rather than sudden-onset symptoms
• • A subarachnoid haemorrhage might present with sudden-onset symptoms, but rarely with focal signs like these and not with Horner syndrome
• • Venous sinus thrombosis might cause right hemiplegia, but does not explain the Horner syndrome and is not usually of sudden onset

• A 23-year-old homeless man is admitted with a history of becoming unwell
after sleeping rough for the last week.
• A few days previously he had complained of feeling rather dizzy and slightly
nauseated. The following day he developed double vision and slurred speech.
His gait became unsteady and he was found collapsed by police officers. He is
brought to the Emergency Department. When asked, he complains of mild pain
situated in the back of his neck. He is drowsy and his speech is very slurred,
but comprehensible.
• On examination of his eye movements, the left eye moves fully but the right eye
does not abduct. He has right-sided facial weakness with sparing of the brow.
In the limbs, he is mildly weak in the left arm and leg. The reflexes in all four
limbs are all very brisk and both plantar responses are extensor. Tests of co-
ordination are reasonably well performed on the bed, but when you get him out
of bed, his gait is very unsteady and he needs to be supported. His chest is
clear and he is apyrexial. The rest of the examination is normal.
What is the most likely diagnosis?
• Vertebral artery dissection
• Drug-induced cerebral arteritis
• Wernicke's encephalopathy
• Tuberculous meningitis
• Right subdural haematoma

• A
• On the face of it he appears to be obtunded, and any of these diagnoses will cause that
• A diagnosis of Wernicke's encephalopathy should be considered in any patient with impaired conscious levels and abnormal eye movements
• However, on closer appraisal of the history, he has a progressive brainstem syndrome, confirmed on neurological examination, which demonstrated impaired consciousness, dysarthria, sixth and seventh cranial nerve palsies, bilateral upper motor neurone signs and ataxia
• This is most likely caused by thrombosis of the vertebral artery after spontaneous dissection (consider the neck pain) which has spread, or embolised, up the basilar artery to occlude the brainstem perforating arteries
• Tuberculous meningitis can also cause a basal meningitis, 'picking off cranial nerves, but he is afebrile with no chest signs therefore making it less likely, but still worth considering
• There is no history of drug abuse, but cocaine can cause cerebral vasculitis with multiple infarcts


• Brown Sequard Syndrome
• Brown Sequard Syndrome
• As a result of the injury to these three main brain pathways the patient will present with three lesions:
• The corticospinal lesion produces spastic paralysis on the same side of the body below the level of the lesion (due to loss of moderation by the UMN).
• At the level of the lesion, there will be flaccid paralysis of the muscles supplied by the nerve of that level (since Lower motor neurons are affected at the level of the lesion).
• The lesion to fasciculus gracilis or fasciculus cuneatus results in ipsilateral loss of vibration and proprioception (position sense) as well as loss of all sensation of fine touch.
• The loss of the spinothalamic tract leads to pain and temperature sensation being lost from the contralateral side beginning one or two segments below the lesion.



• A 62-year-old builder is admitted with a history of collapsing while lifting heavy building blocks. In the Emergency Department he is unable to give a clear history, but his wife says he was previously well. He has smoked all his life and regularly drinks 8-10 pints of beer on a Friday or Saturday night. On examination in the Emergency Department, he was noted to be talking incomprehensibly and to have moderate weakness of his right side.
• On arrival on the ward 3 hours later, he appears awake but is no longer talking at all and responds only to some, but not all, commands. His head and eyes look towards the left. He moves his left arm and leg spontaneously, but even pinching the skin elicits no movement of his right arm or leg. There is no obvious difference in the tone or reflexes in his limbs, but the right plantar response is extensor.
• On general physical examination, you note he is overweight and his blood pressure is 220/120 mmHg.
• The remainder of your examination is normal. Apparently the result of CT head done in the Emergency Department has not been written in his notes.
• What is the most likely diagnosis?
• Left hemisphere intracranial haemorrhage
• Left internal carotid artery occlusion and cerebral infarction
• Posterior fossa haemorrhage with rapid-onset hydrocephalus
• Left hemisphere infarction with subsequent seizures
• Continuing emboli from internal carotid artery stenosis
• A
• • This man has had some form of stroke followed rapidly by deterioration
• • The initial picture, however, is not one of posterior fossa damage
• • The possibility of showers of emboli causing such a picture is extremely unlikely
• • He has clearly suffered from a left hemisphere stroke, and the deterioration is in the same territory, not a different one
• • Seizures may cause temporary deterioration; however, in this case head and eye turning are to the left, which suggests either a right frontal ictal discharge or massive left frontal damage
• • In view of the limb features, the latter is more likely
• • The very rapid progression marginally favours haemorrhage as the diagnosis, but cerebral infarction from left middle cerebral or internal carotid artery occlusion causes a similar syndrome
• • Carotid dissection should also be borne in mind as a possible aetiology if the strike is ischaemic rather than haemorrhagic
• • His risk factors include heavy alcohol intake and hypertension

Extradural (epidural) haematoma
Bleeding into the space between the dura mater and the
skull.
Often results from acceleration-deceleration trauma or a
blow to the side of the head.
The majority of epidural haematomas occur in the temporal
region where skull fractures cause a rupture of the middle
meningeal artery.
Features
features of raised intracranial pressure
some patients may exhibit a lucid interval
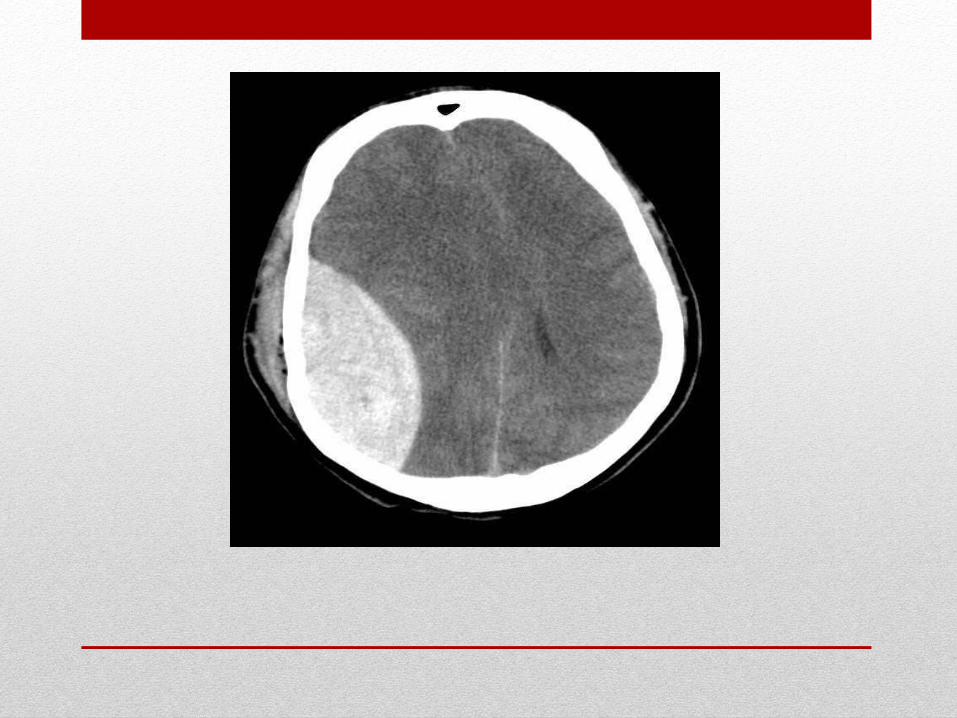

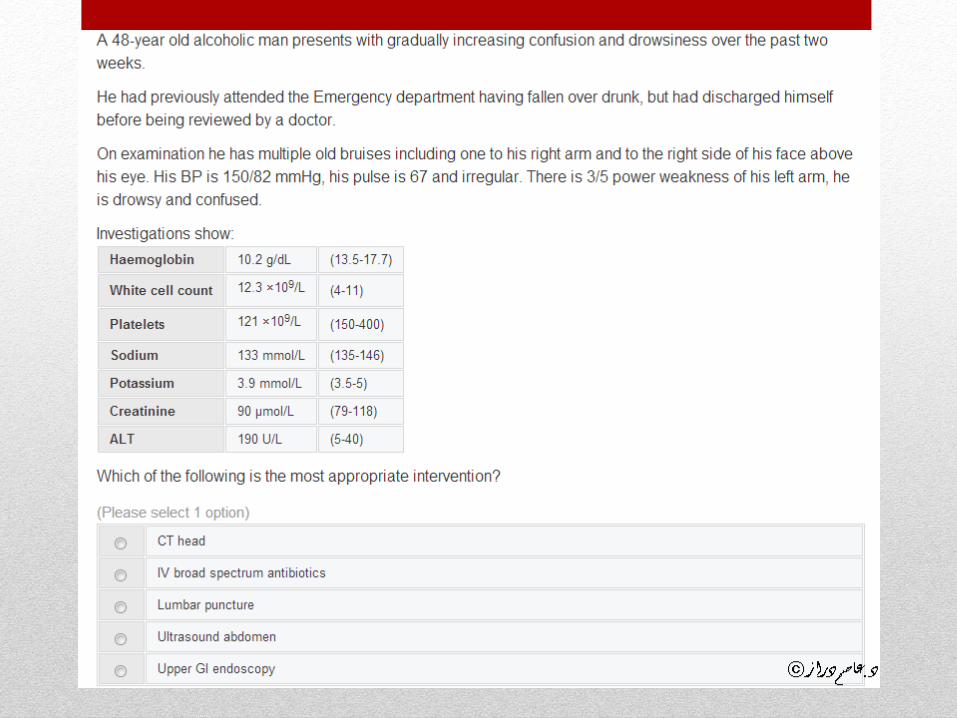
A 73-year-old woman presents with episodic confusion and headaches for the past week. She has a history of alcohol excess and a background of atrial fibrillation and type 2 diabetes mellitus. Her daughter reports that she has been having frequent spells of confusion over the past few days. Last year she was assessed for frequent falls. Her current medications include bisoprolol, metformin and warfarin. Neurological examination is unremarkable and her blood sugar is 6.7 mmol/l. What is the most likely diagnosis?
• A. Korsakoff's syndrome
• B. Wernicke's encephalopathy
• C. Extradural haematoma
• D. Subarachnoid haemorrhage
• E. Subdural haematoma

• E. Subdural haematoma
• Fluctuating confusion/consciousness? - subdural
haematoma
• This patient has a number of risk factors for a subdural
haematoma including old age, alcoholism and
anticoagulation.
• Korsakoff's syndrome and Wernicke's encephalopathy do
not usually cause headaches (ataxia, unconciouse,
ophthalmoplegia)



Subdural haematoma
• Bleeding into the outermost meningeal layer.
• Most commonly occur around the frontal and parietal
lobes.
• Risk factors include old age, alcoholism and
anticoagulation.
• Slower onset of symptoms than a epidural haematoma.

• -most commonly secondary to trauma e.g. old person / alcohol
• -initial injury may be minor and is often forgotten
• -caused by bleeding from damaged bridging veins between
cortex and venous sinuses
C/P
-headache -classically fluctuating conscious level (Fluctuating
consciousness = subdural haemorrhage) -raised ICP

• The combination of falls, alcohol excess, fluctuating
episodes of confusion and focal neurology points
towards a diagnosis of subdural haemorrhage.
• The phrase 'fluctuating conscious level' is common in
questions and should always bring to mind subdural
haemorrhage





• A 69-year-old woman was taken to hospital with a sudden-onset, mild, right hemiparesis and an inability to speak.
• CT scan showed evidence of a recent left hemisphere infarction. She was found to be in atrial fibrillation and was anticoagulated. While in hospital she had a right-sided focal seizure and was treated with phenytoin. She made a good recovery over the next 6 weeks and was discharged home. Phenytoin 300 mg at night was continued, as was warfarin.
• When she was seen in the follow-up clinic 3 months later atrial fibrillation was still present and anticoagulation was continued, but the phenytoin was tailed off to zero. Now, 2 months later, she has been re-admitted having developed a mild right hemiparesis and drowsiness over the previous 10 days.
• On further questioning her husband remembers that she tripped over the rug in the lounge about 10 days earlier. Her INR is 5.1.
What is the most likely cause of her deterioration?
• O Further cardioembolic stroke
• O Concurrent lobar pneumonia
• O Left hemisphere intracerebral haemorrhage
• O Left subdural haematoma
• O Recurrent seizures

• D
• The patient with recurrent mild, right hemiparesis and AF
• The initial story suggests that she suffered a cardioembolicstroke secondary to atrial fibrillation, and that her symptoms were the result of cortical infarction from a left middle cerebral artery branch occlusion
• However, her second admission with gradual onset of symptoms over days is more likely to result from a subdural haematoma secondary to excessive anticoagulation than a recurrent stroke
• Intercurrent infection could also cause deterioration, but not specifically of the right hemiparesis, unless she had made a less than complete recovery, in which case it might appear as though the weakness had got worse
• Recurrent seizures are uncommon, but could cause deterioration if she was in partial status epilepticus

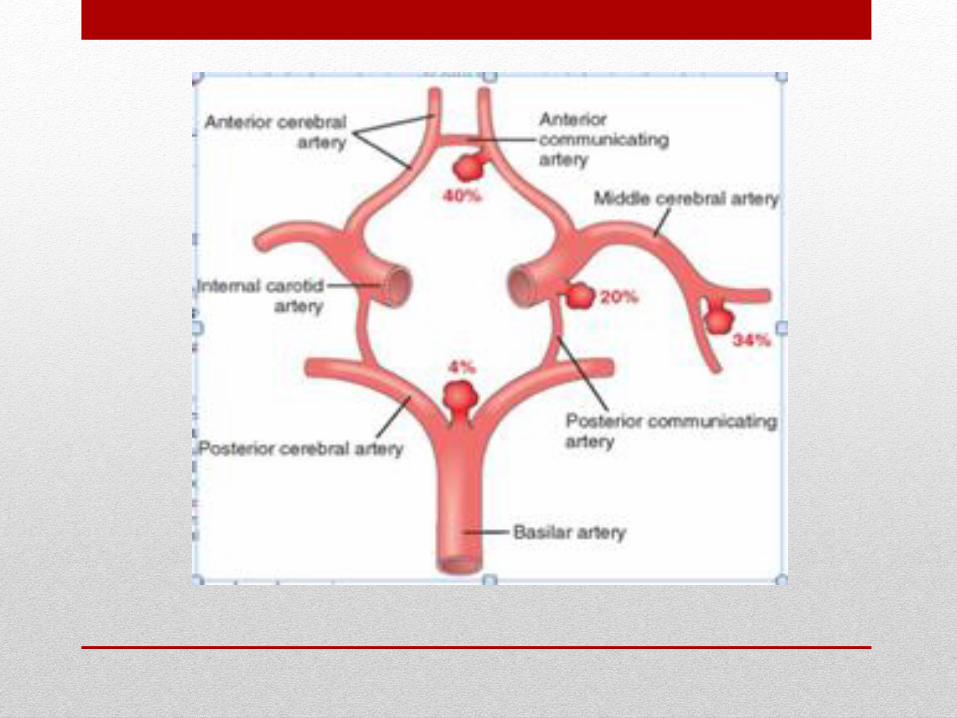
Subarachnoid haemorrhage
Usually occurs spontaneously in the context of a ruptured
cerebral aneurysm but may be seen in association with other
injuries when a patient has sustained a traumatic brain
injury

Causes
• -85% are due to rupture of berry aneurysms (conditions
associated with berry aneurysms include adult polycystic kidney
disease, Ehlers-Danlos syndrome and coarctation of the aorta)
• -AV malformations
• -trauma
• -tumours
Investigations
• - CT: negative in 5%
• - LP: done after 12 hours (allowing time for xanthochromia to
develop)

Complications:
• - Rebleeding (in 30%)
• - Obstructive hydrocephalus (due to blood in ventricles)
• - Vasospasm leading to cerebral ischaemia
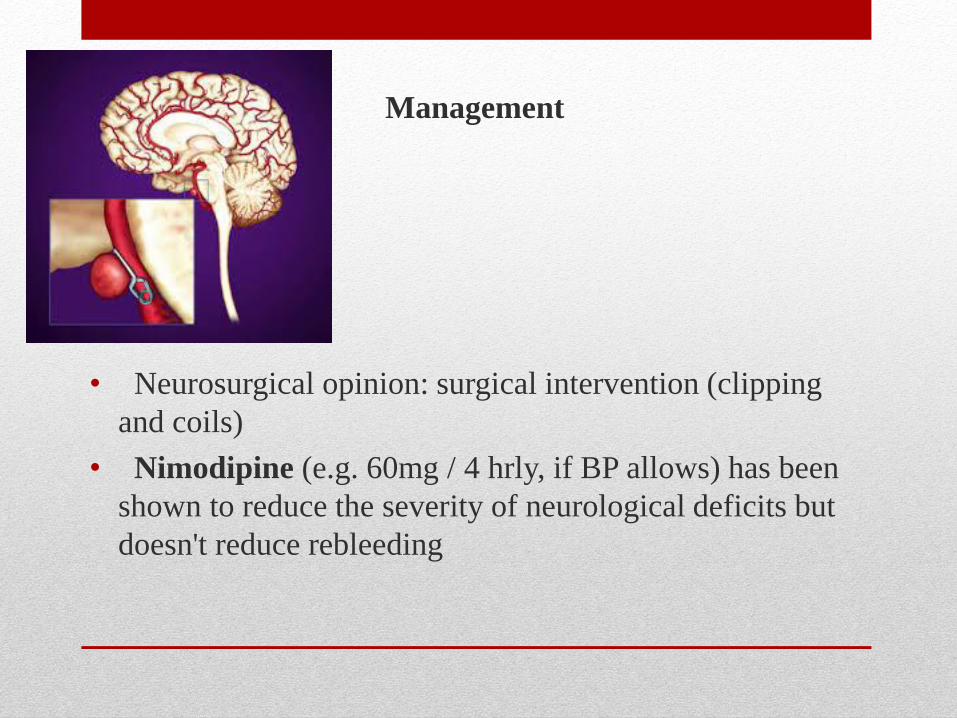
Management
• Neurosurgical opinion: surgical intervention (clipping
and coils)
• Nimodipine (e.g. 60mg / 4 hrly, if BP allows) has been
shown to reduce the severity of neurological deficits but
doesn't reduce rebleeding
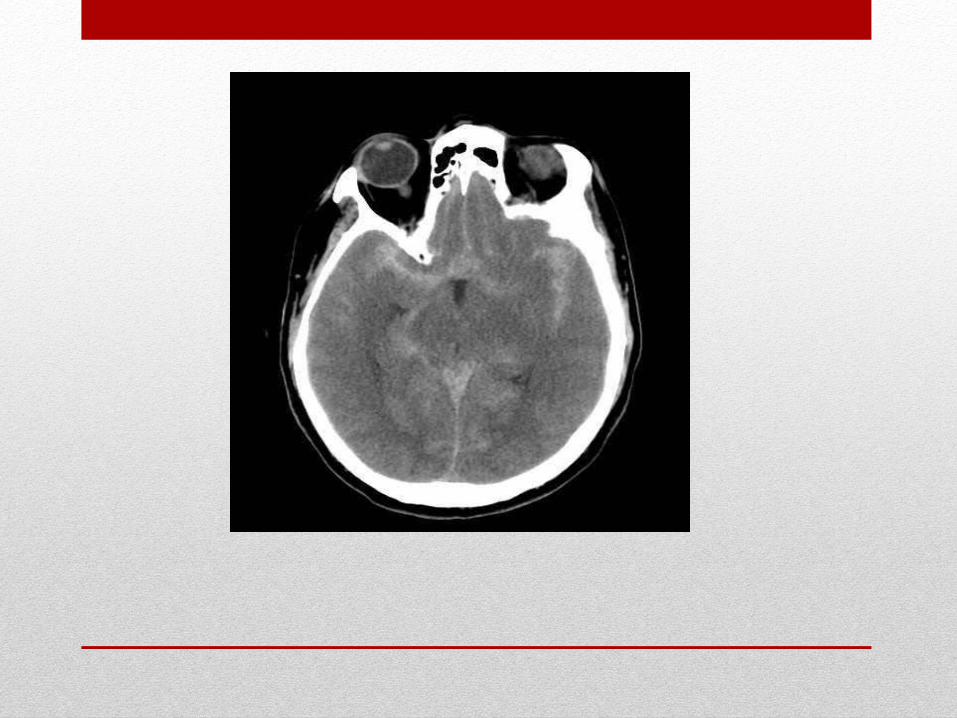
Acute severe headache for DD:
1- Vascular (SAH)
2- Infection
3- Apoplexy
4- Trauma

Spastic paraparesis and
quadreparesis


A- With level
• Cord compression: (trauma, tumour, …..)
• Non cord compression (transverse myelitis e.g. HIV ,
MS, , osteoarthritis of the cervical spine)
• Syringomyelia (dissociative loss)
• Anterior spinal artery occlusion (dissociative loss)

B- Without level
• Demyelination e.g. multiple sclerosis
• Sub-acute combined degeneration
• Friedrich Ataxia
• Syphilis
• Parasagittal meningioma
• Tropical spastic paraparesis
• Hereditary spastic paraplegia
• Motor neuron disease










• A 23-year-old woman is sent to the Emergency Department urgently. She is 36 weeks' pregnant. She describes the sudden onset of right-sided numbness and dysphasia. She initially developed tingling in the right side of her face that spread over a matter of minutes to the right hand. Some 10 minutes later she noticed she was having word-finding difficulty and that her right arm felt clumsy. The whole attack resolved completely within 20-30 minutes. By the time she arrived in the Emergency Department her neurological examination was normal. There is a previous history of headaches and vomiting as a teenager, which varied according to her menstrual cycle.
• Which of the following is the most likely diagnosis?
• Spontaneous dissection of the right internal carotid artery
• Transient ischaemic attack secondary to left hemisphere small-vessel disease
• Hemiplegic migraine
• Partial epileptic seizure
• Cerebral venous thrombosis

• C- migraine equivalent
• The pregnant patient with right-sided numbness and dysphasia
• The presence of a cortical sign such as dysphasia reduces the likelihood of a lacunar transient ischaemic attack
• Both carotid artery dissection (and consequent embolism to the left middle cerebral artery) and cerebral venous thrombosis should be considered
• There is no history of the headache that is common with cerebral venous thrombosis
• • However, the history of a slow march of symptoms and signs suggests migraine aura without headache (migraine equivalent), not transient ischaemic attack
• Pregnancy is associated with an increased incidence of migraine and stroke, especially from eclampsia and cerebral venous thrombosis in the puerperium
• Hemiplegic migraines are also more commonly seen in patients with a previous history of migraine, which may have subsided years previously, or in those with a positive family history of migraine